































































































































































































































































































































































































































































































































































































































































































































































































































































































































































































Primary tumor (pT)
- pTX: primary tumor cannot be assessed
- pT0: no evidence of primary tumor
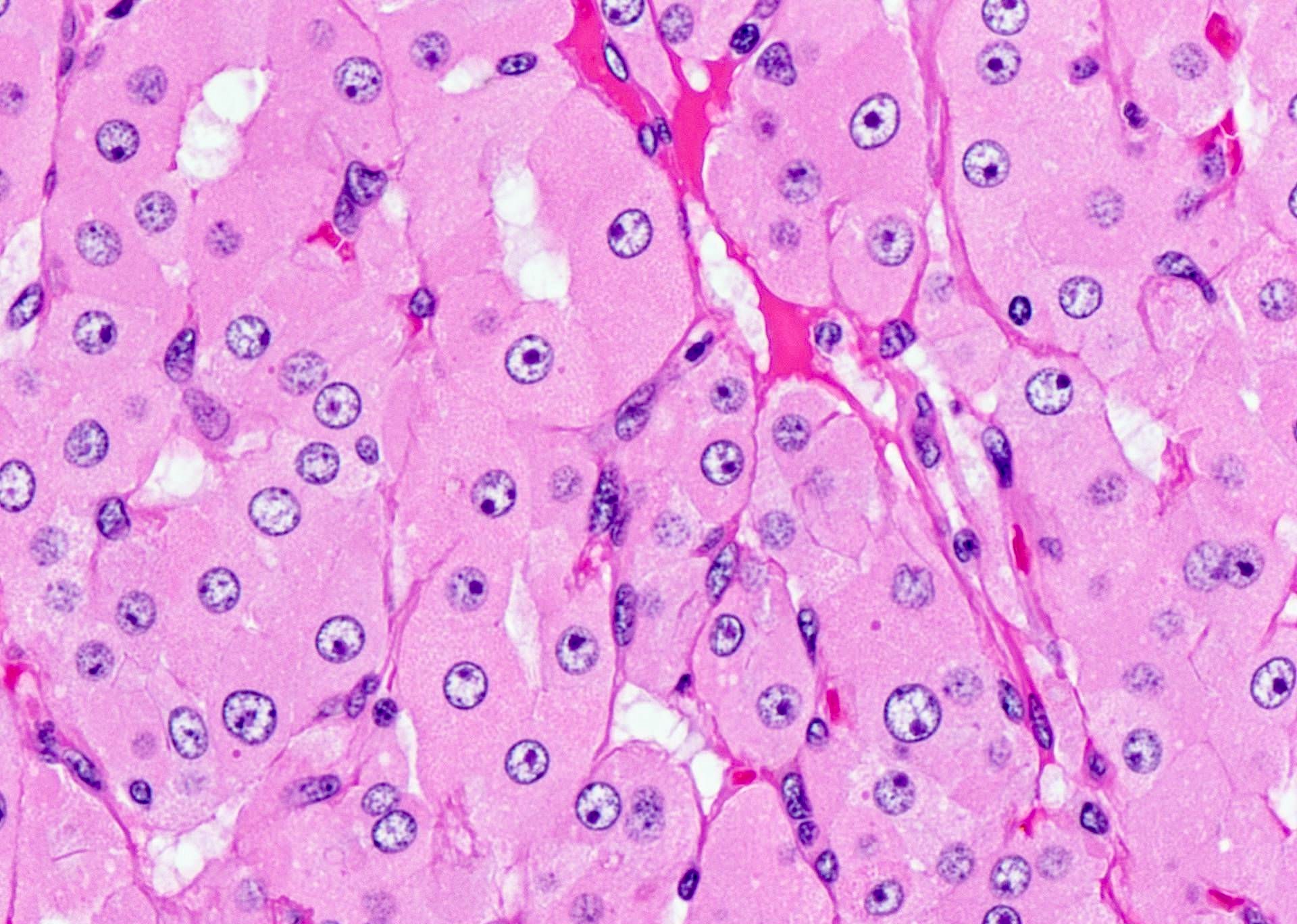
- pTis: atypical parathyroid neoplasm (neoplasm of uncertain malignant potential) (see notes below)
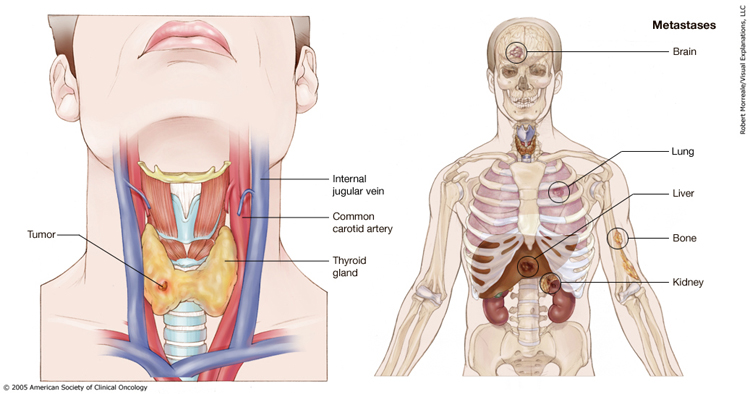
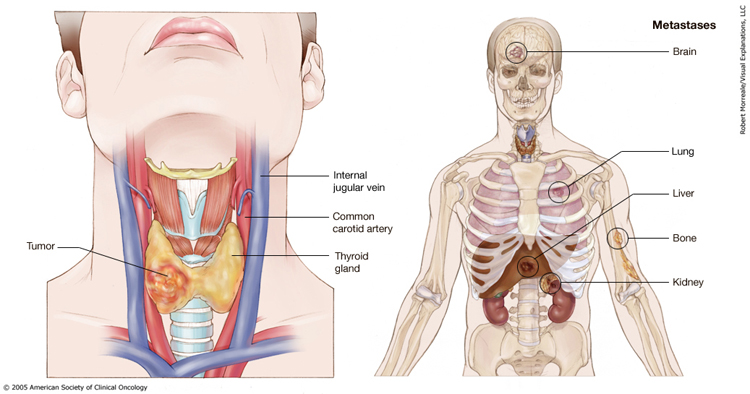
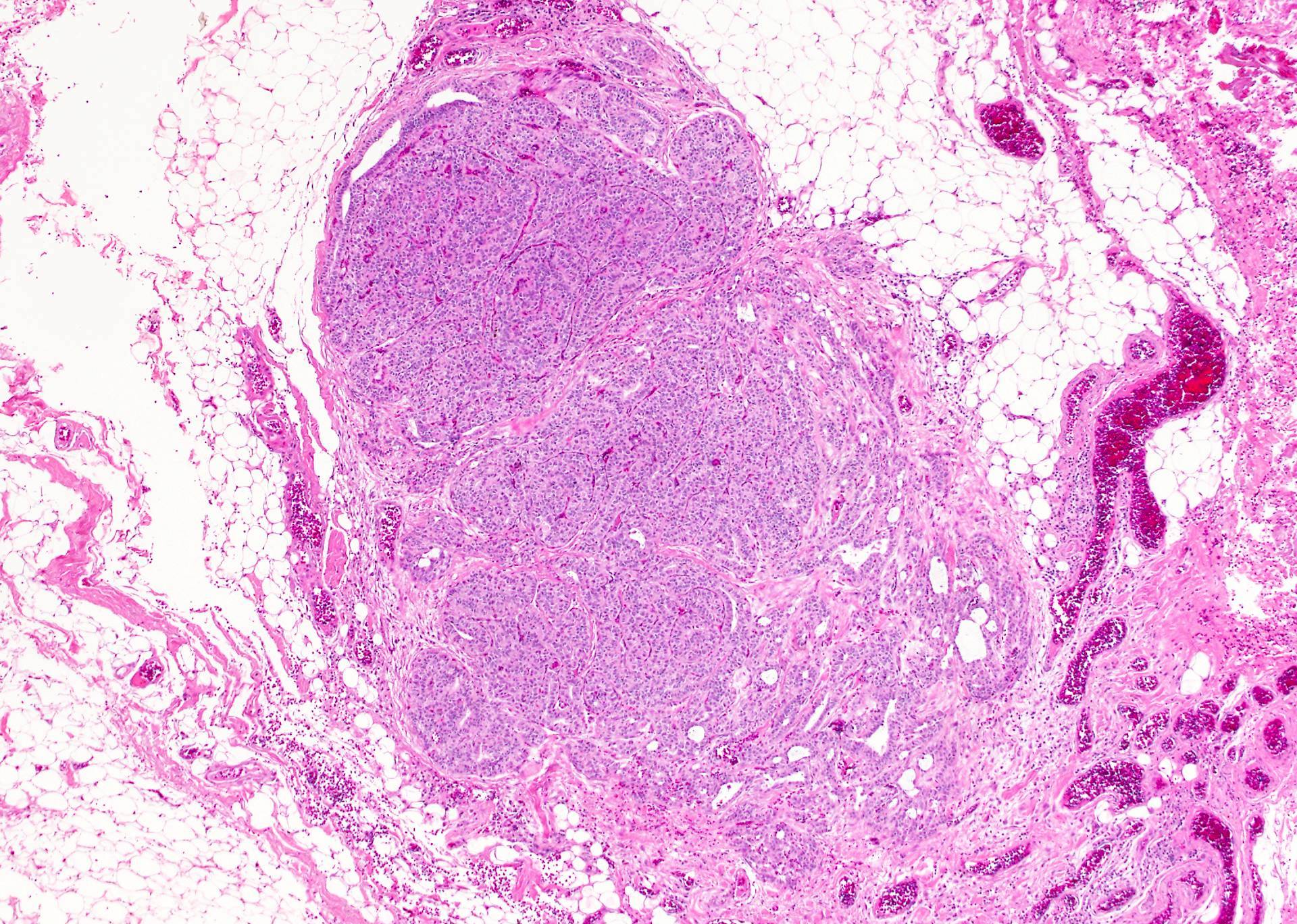
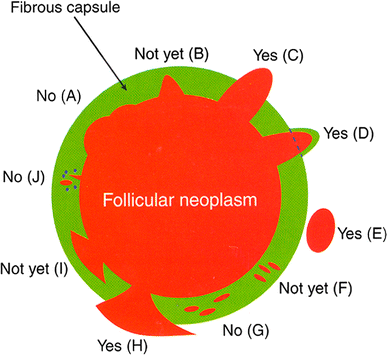
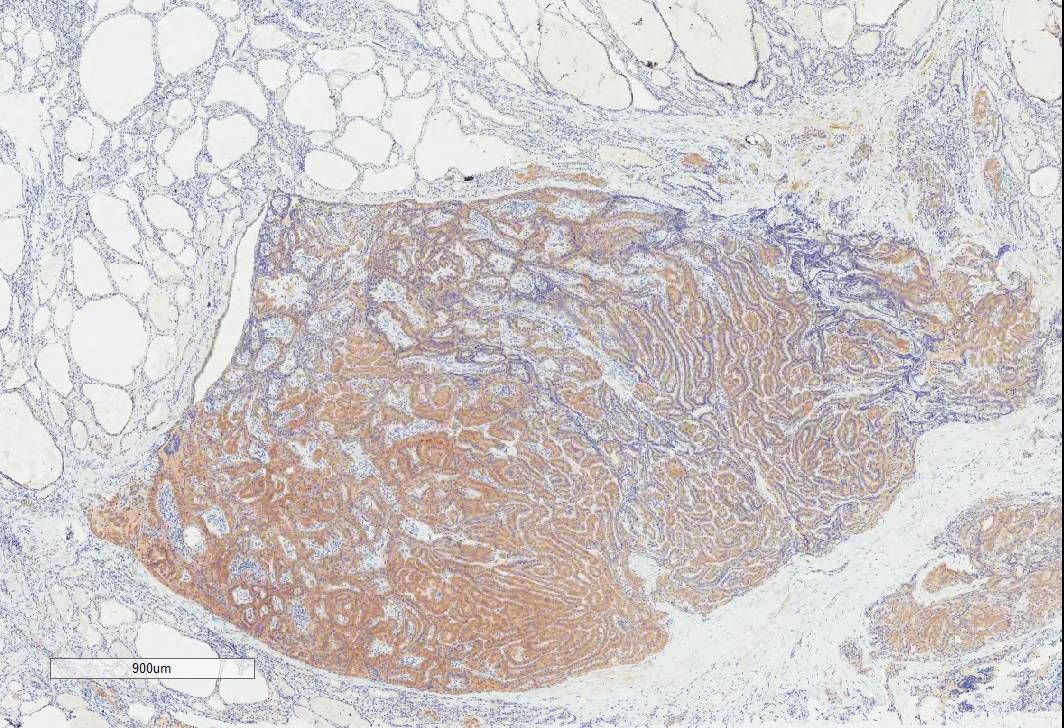
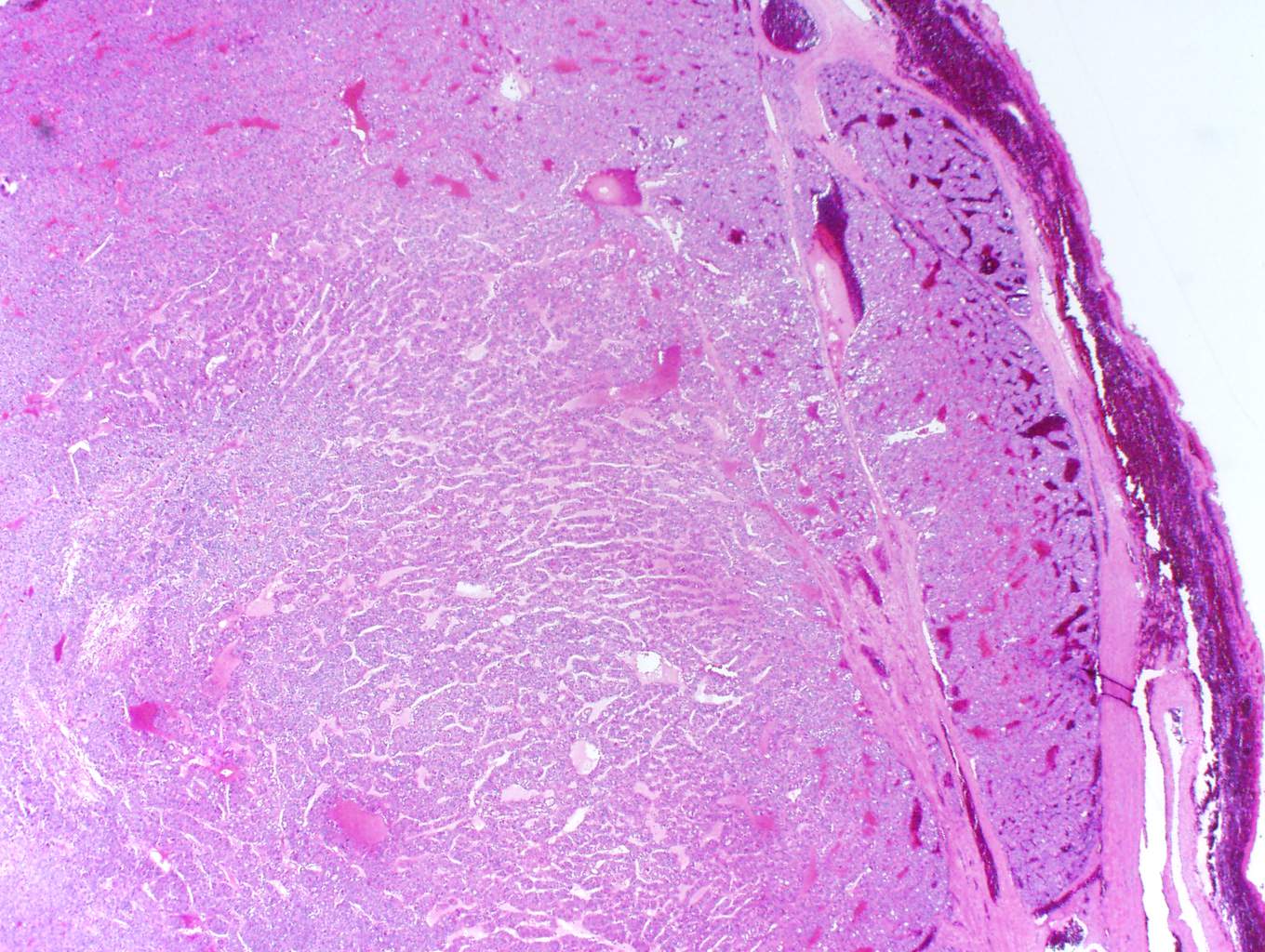
- pT1: localized to the parathyroid gland with extension limited to soft tissue
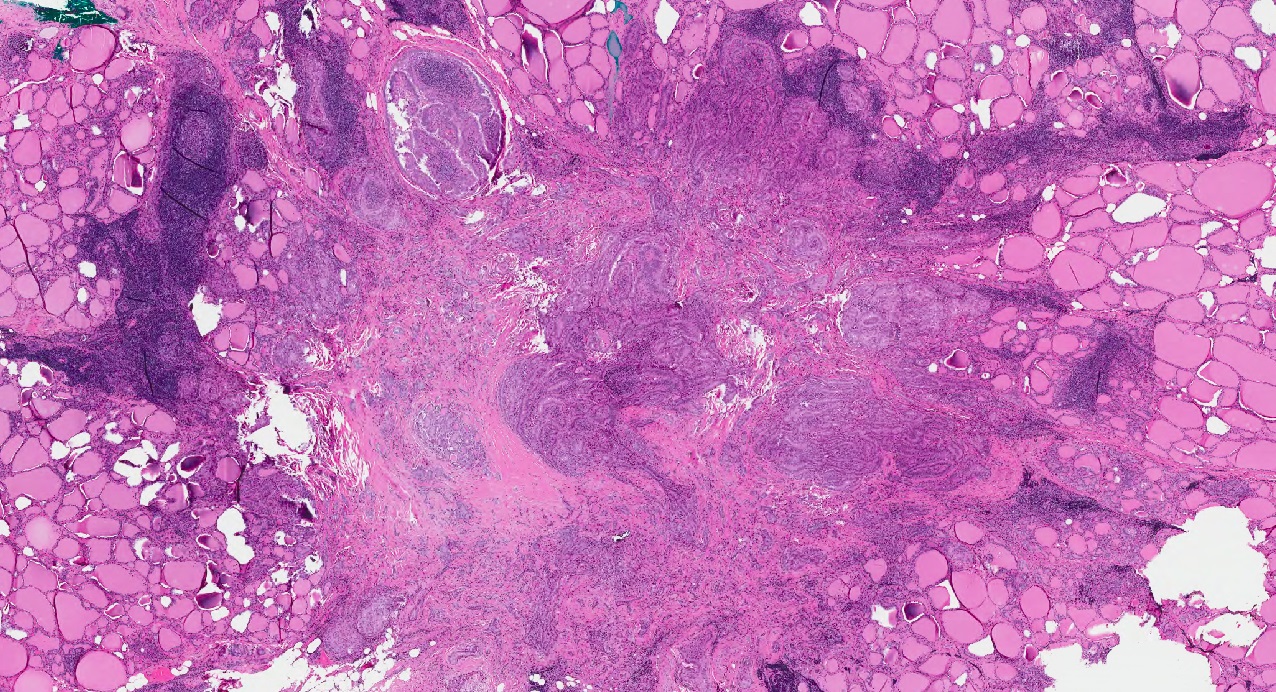
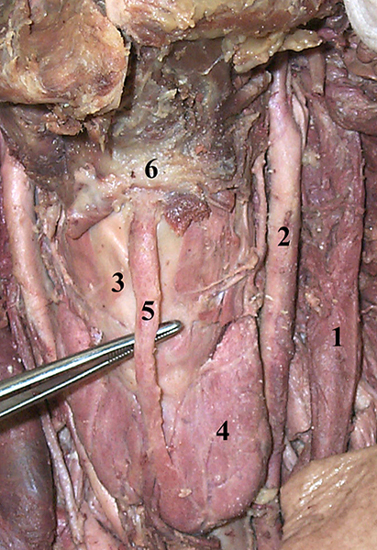
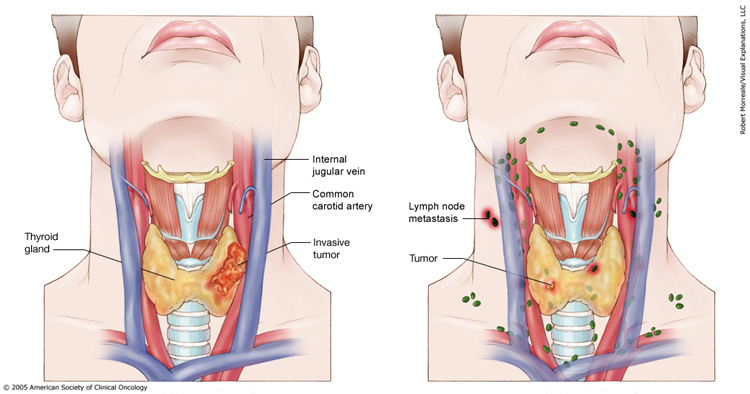
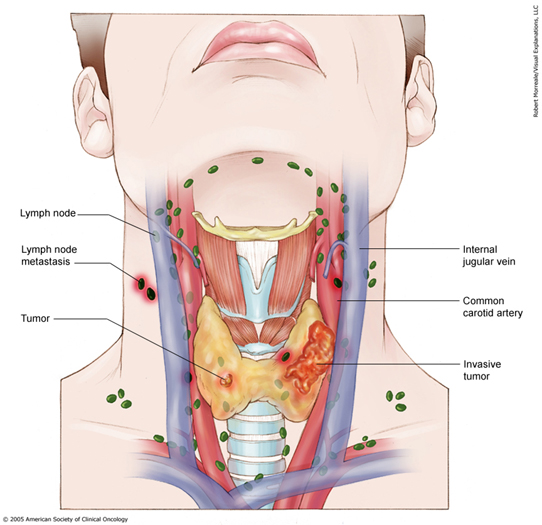
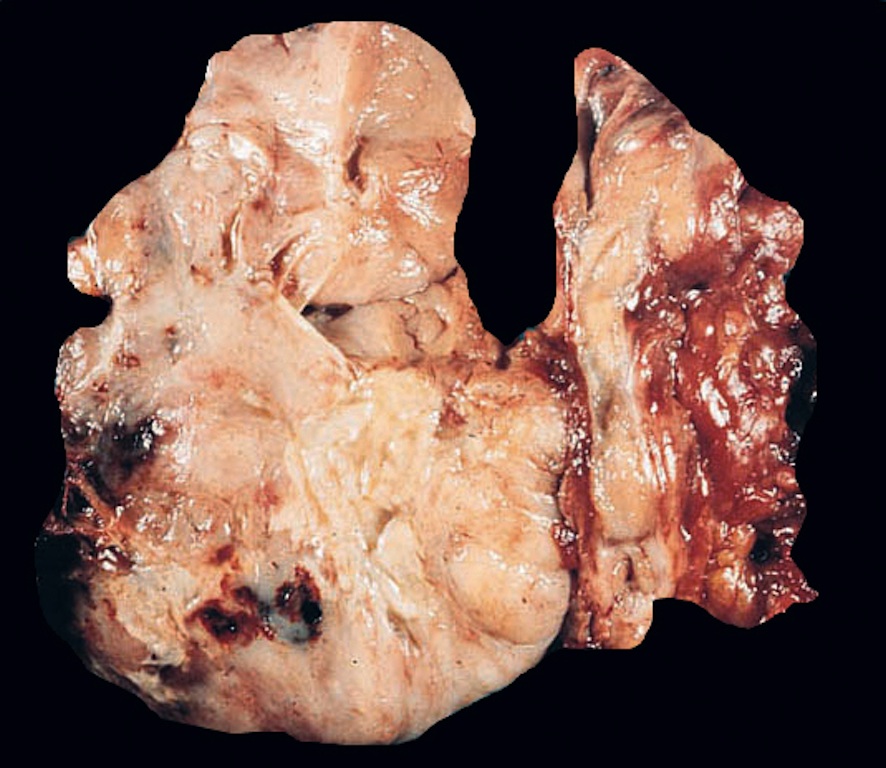
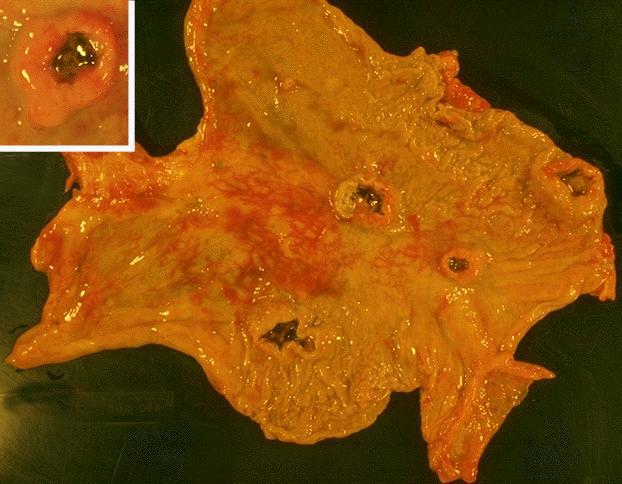
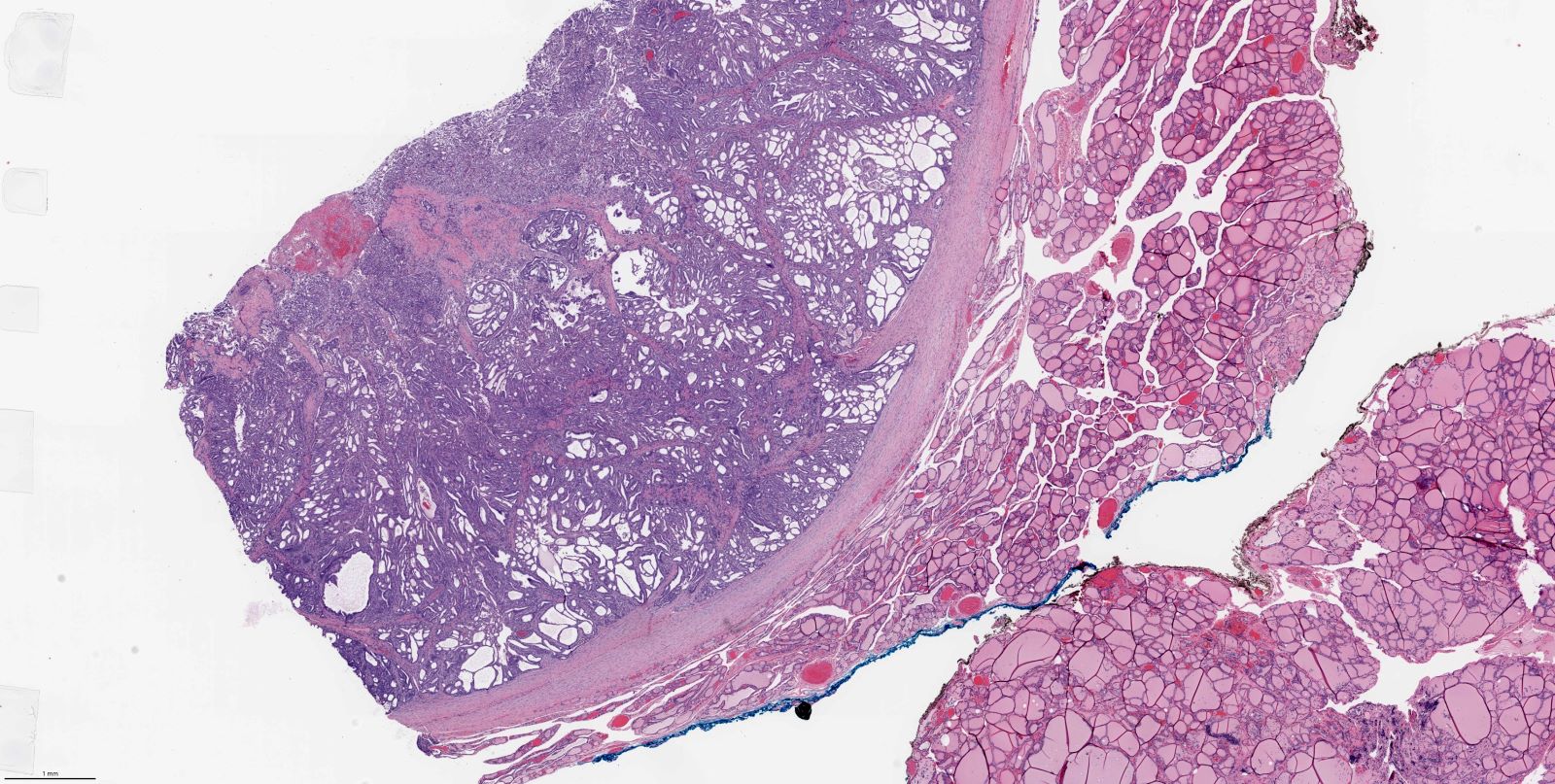
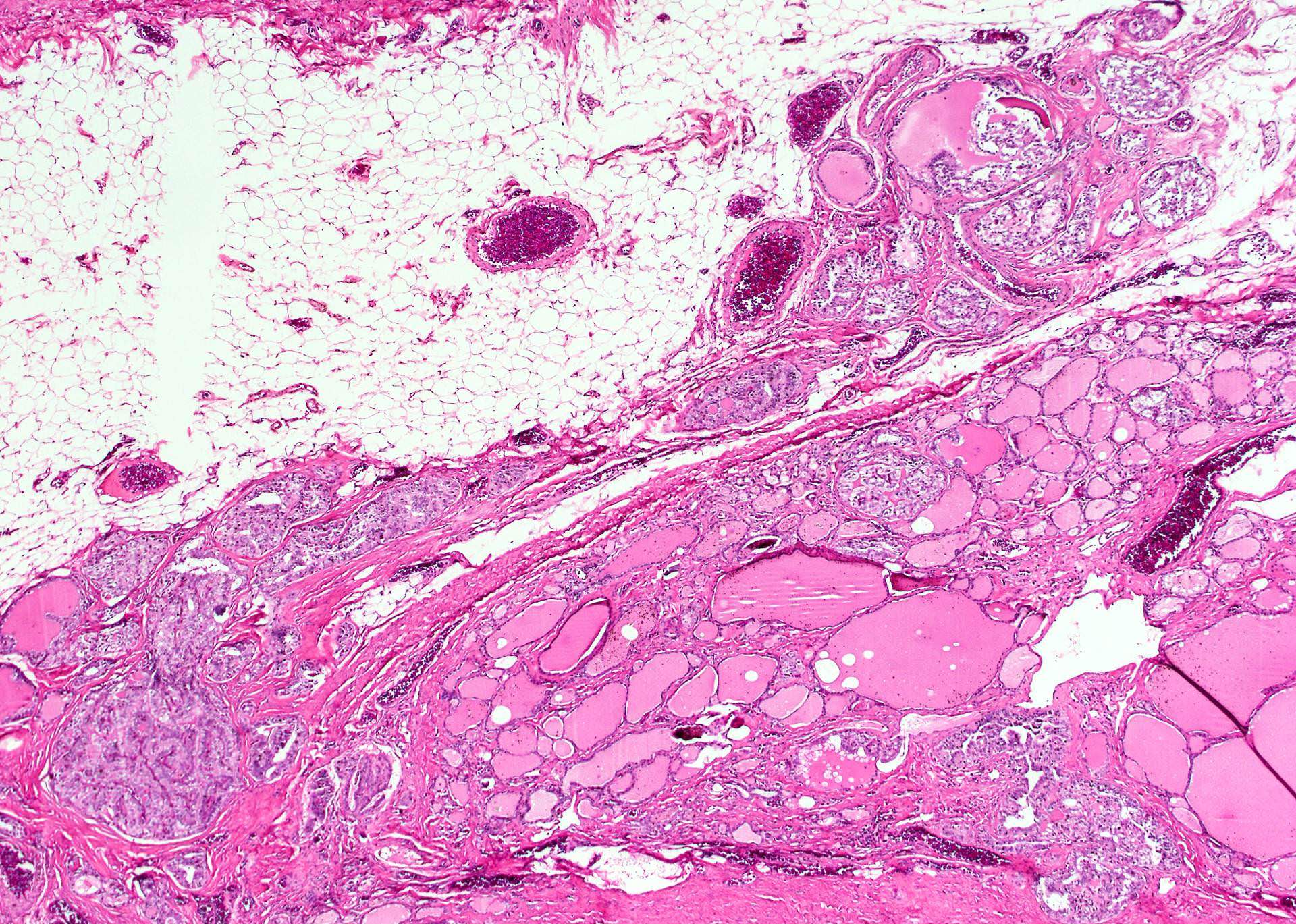
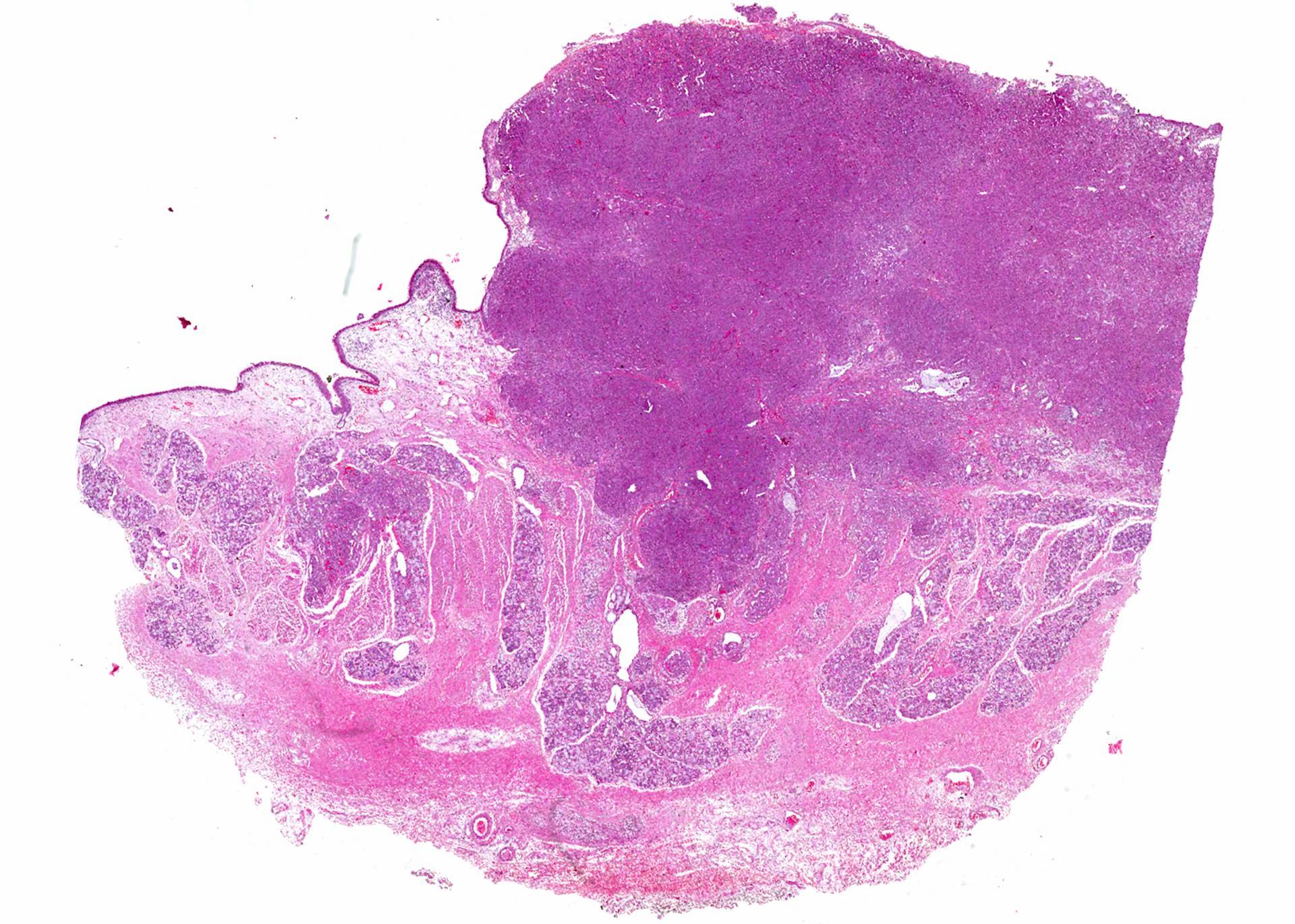
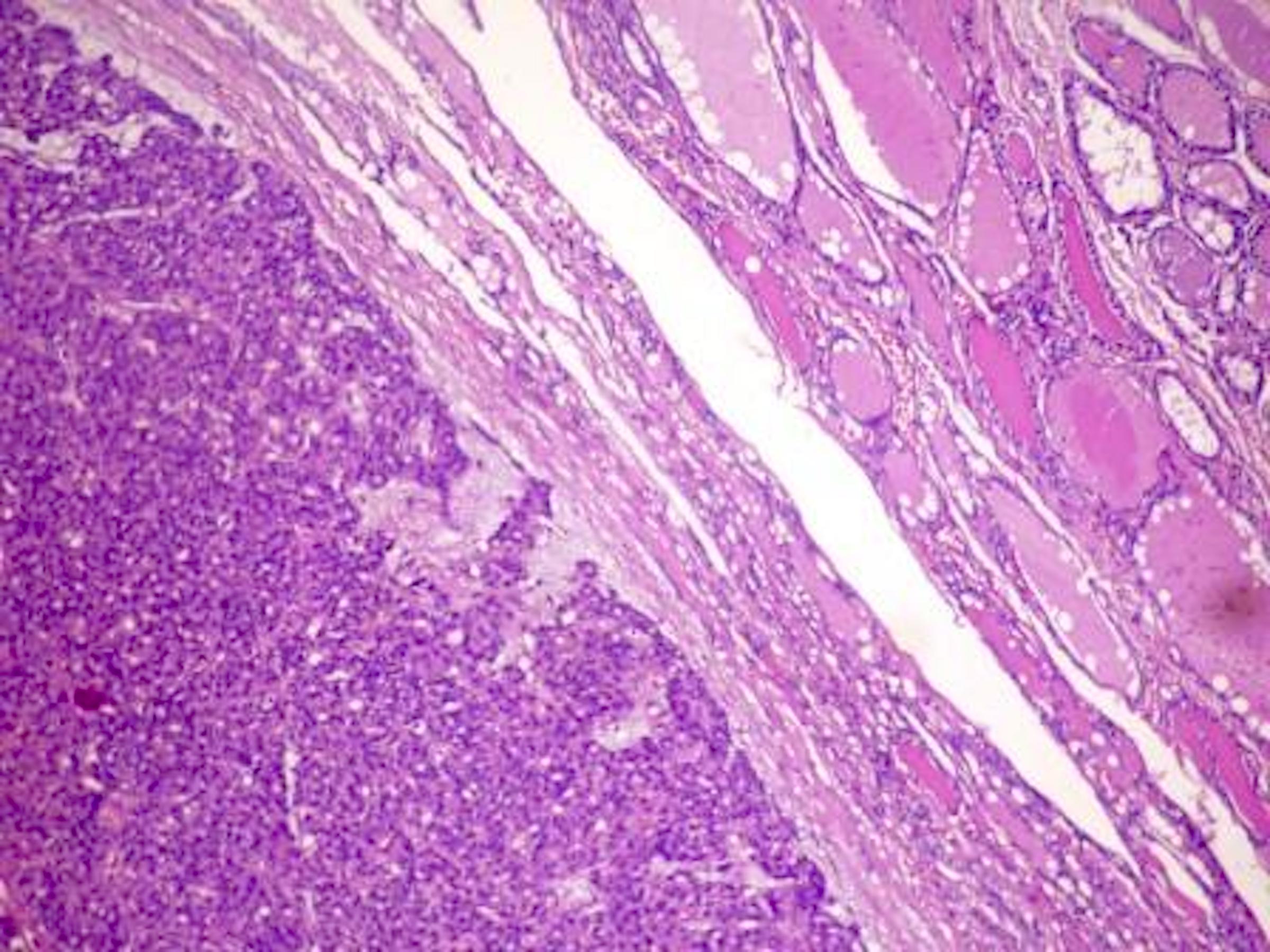
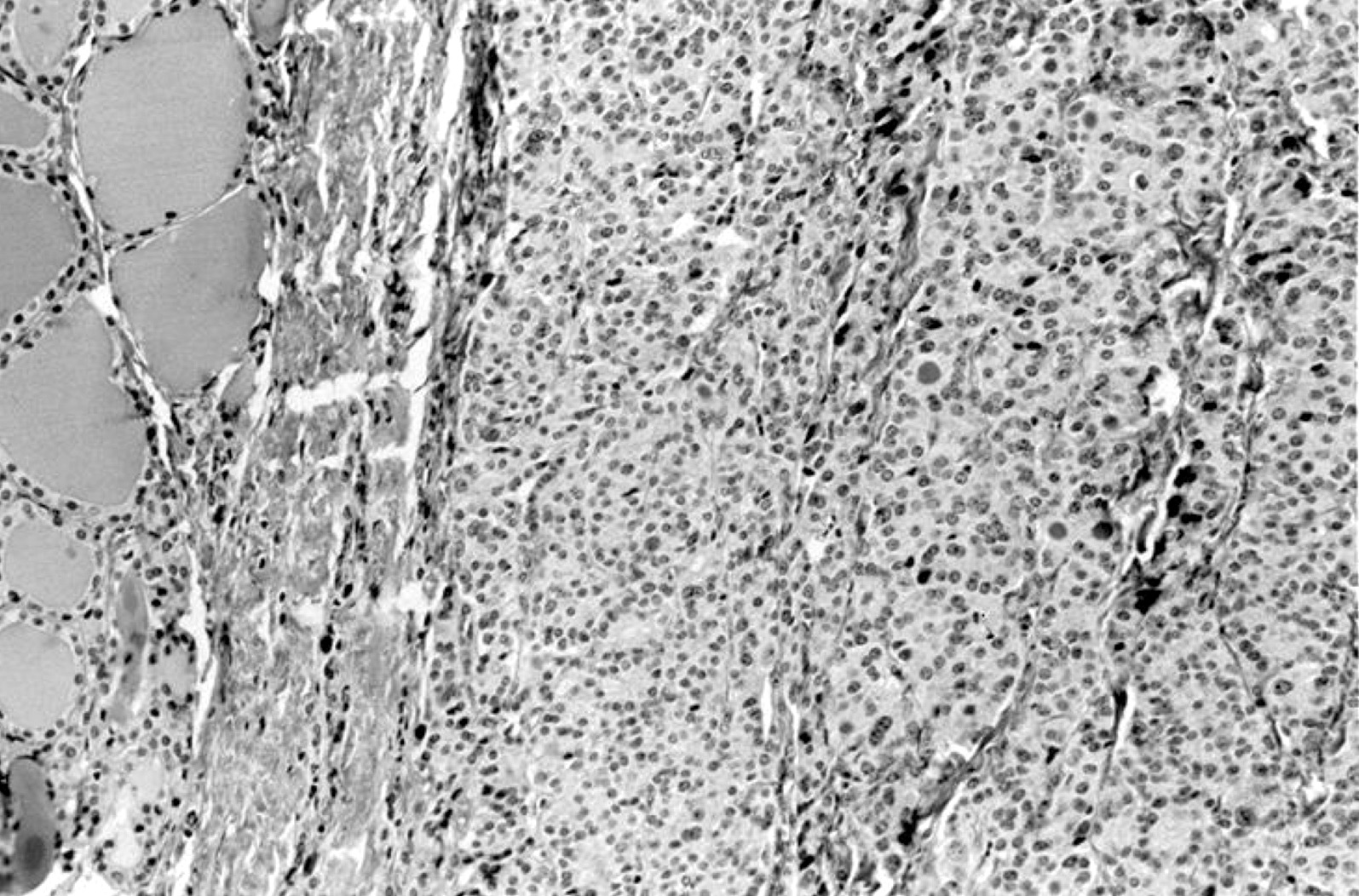
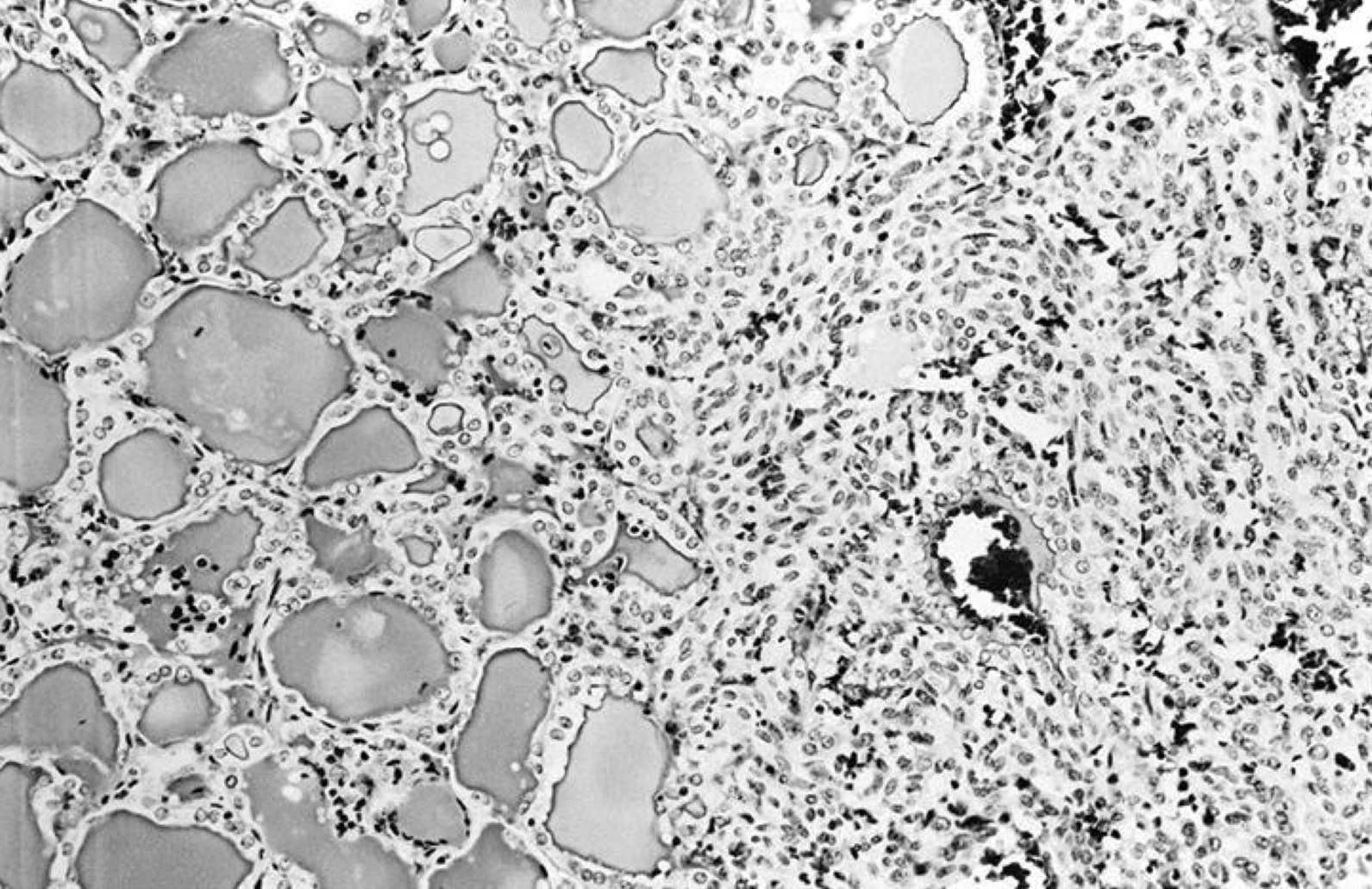
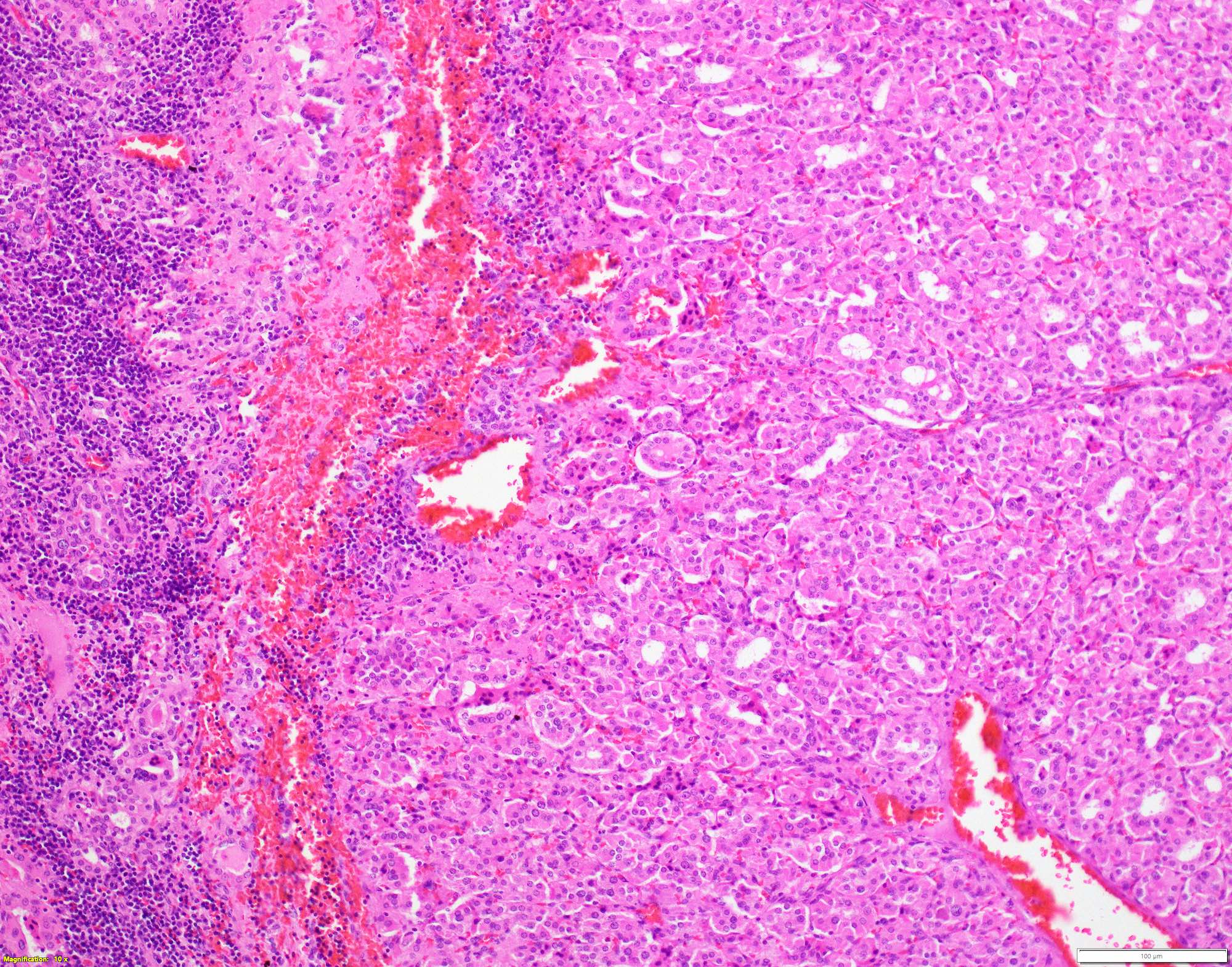
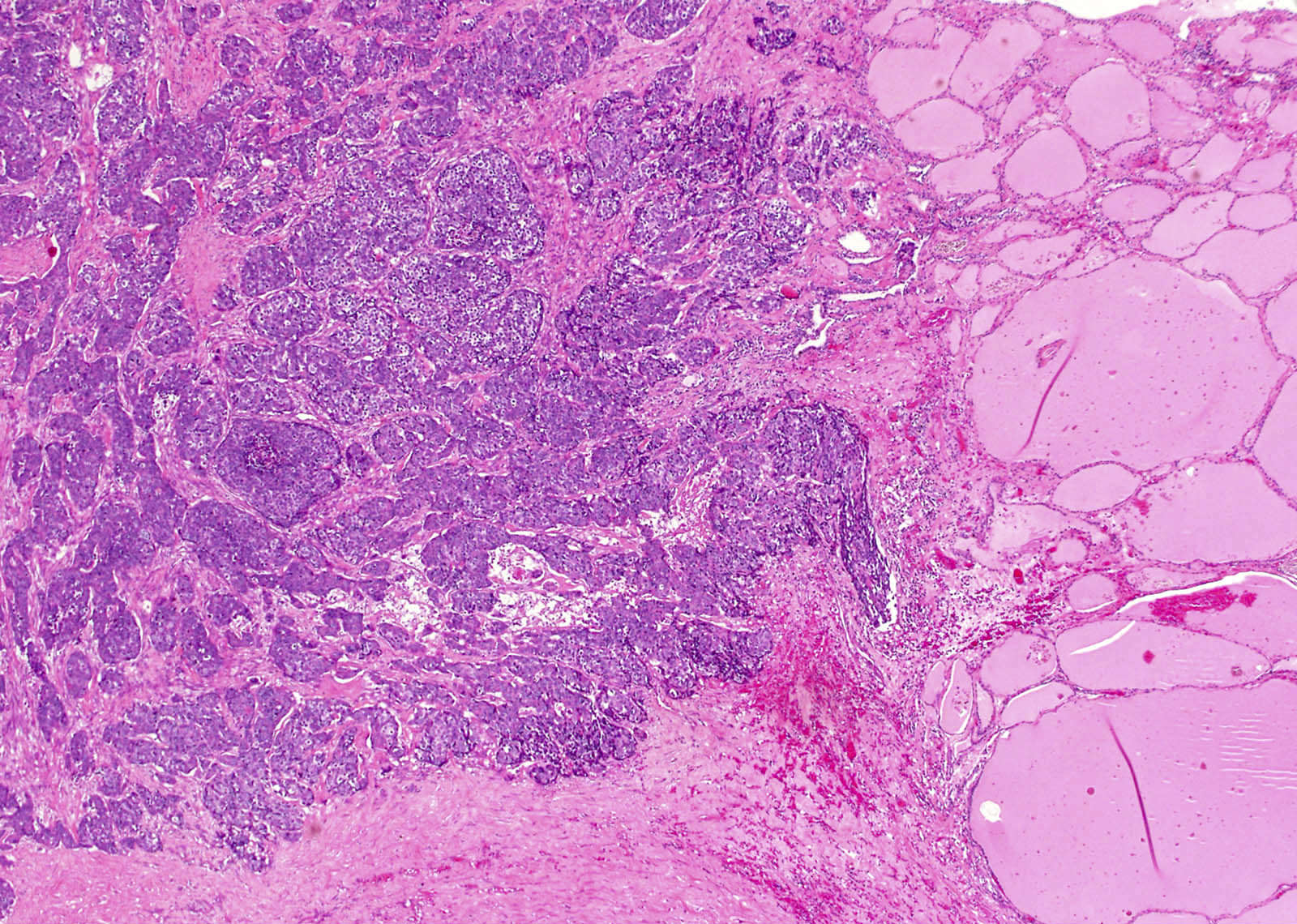
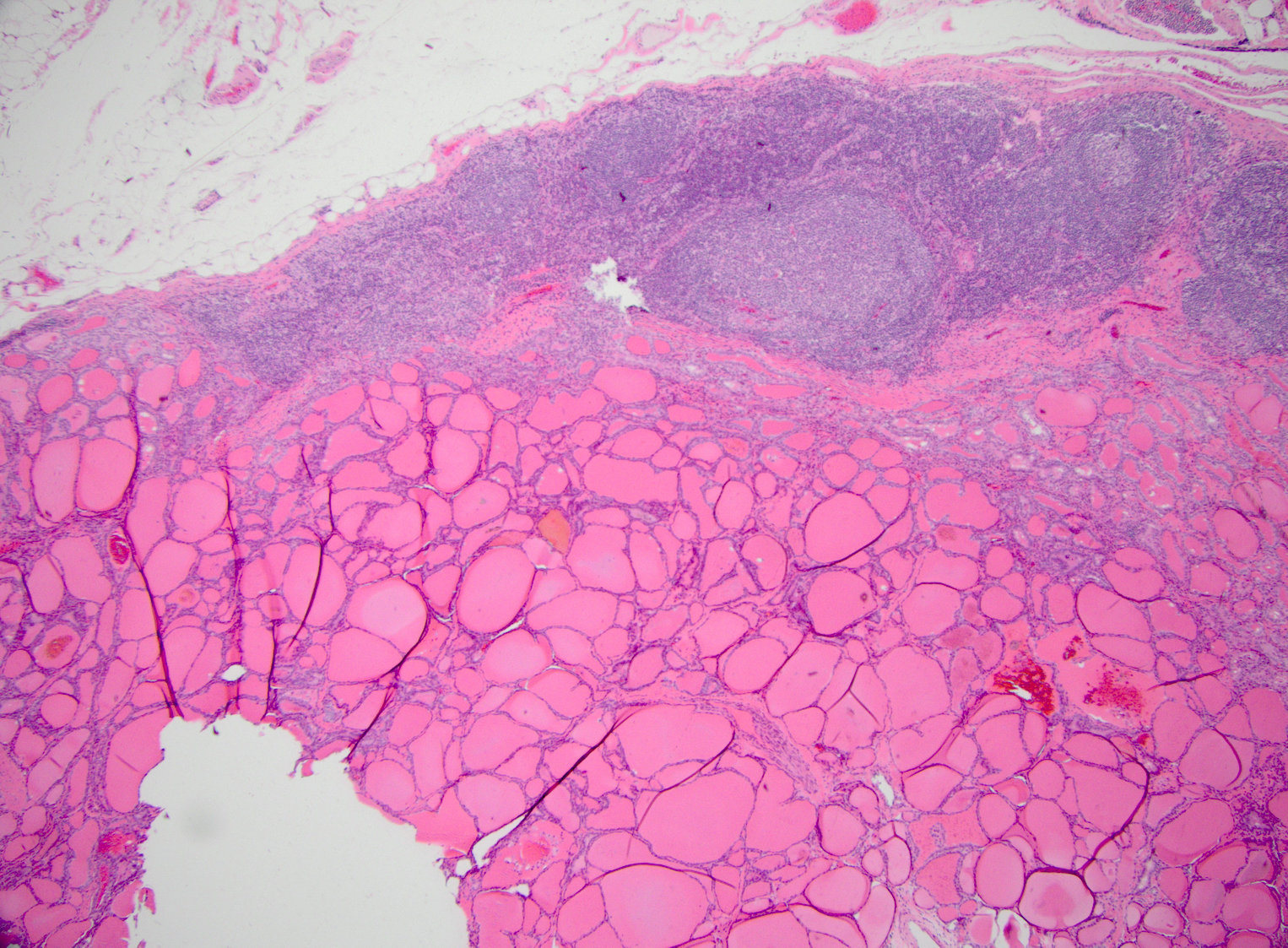
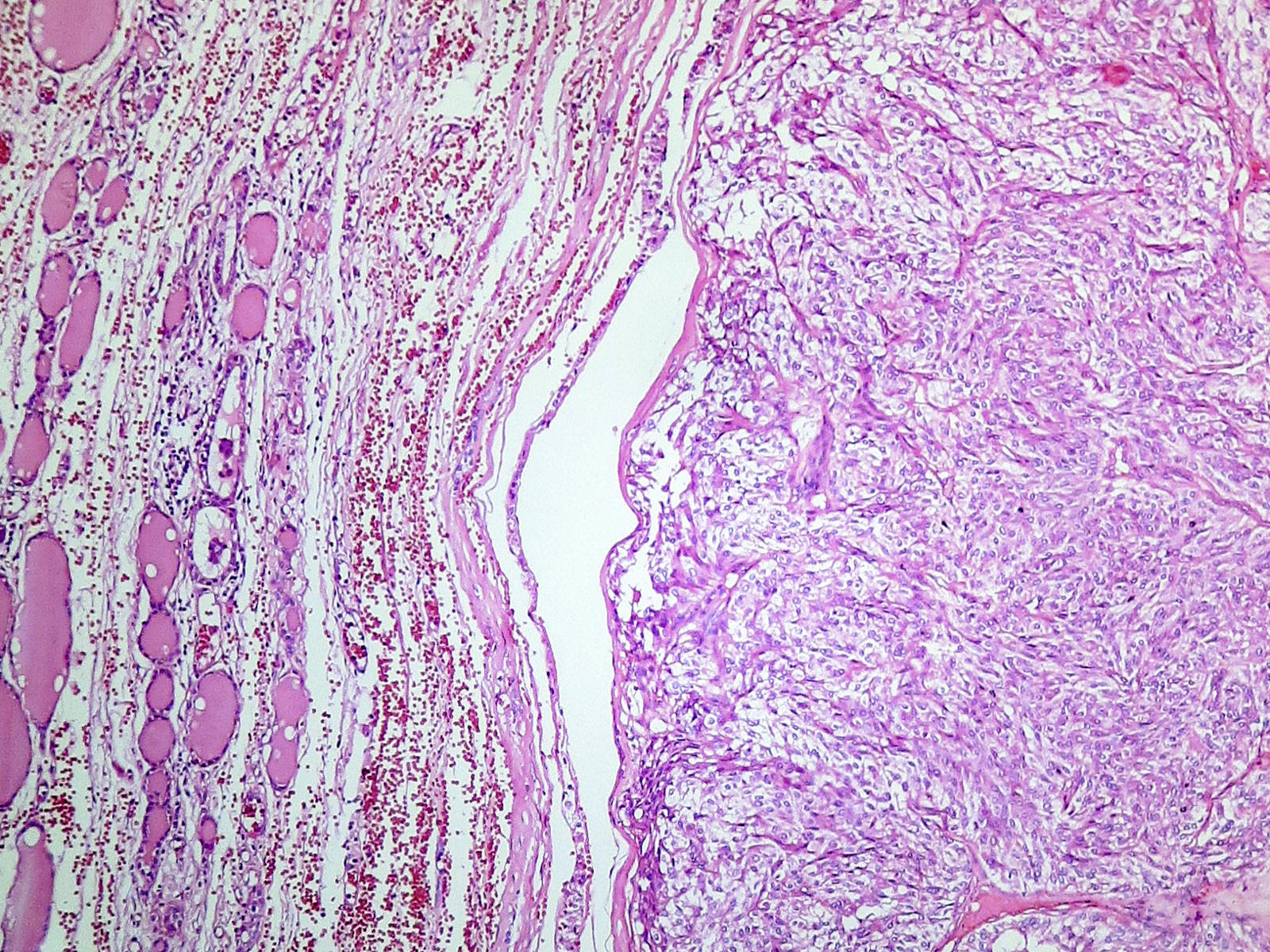
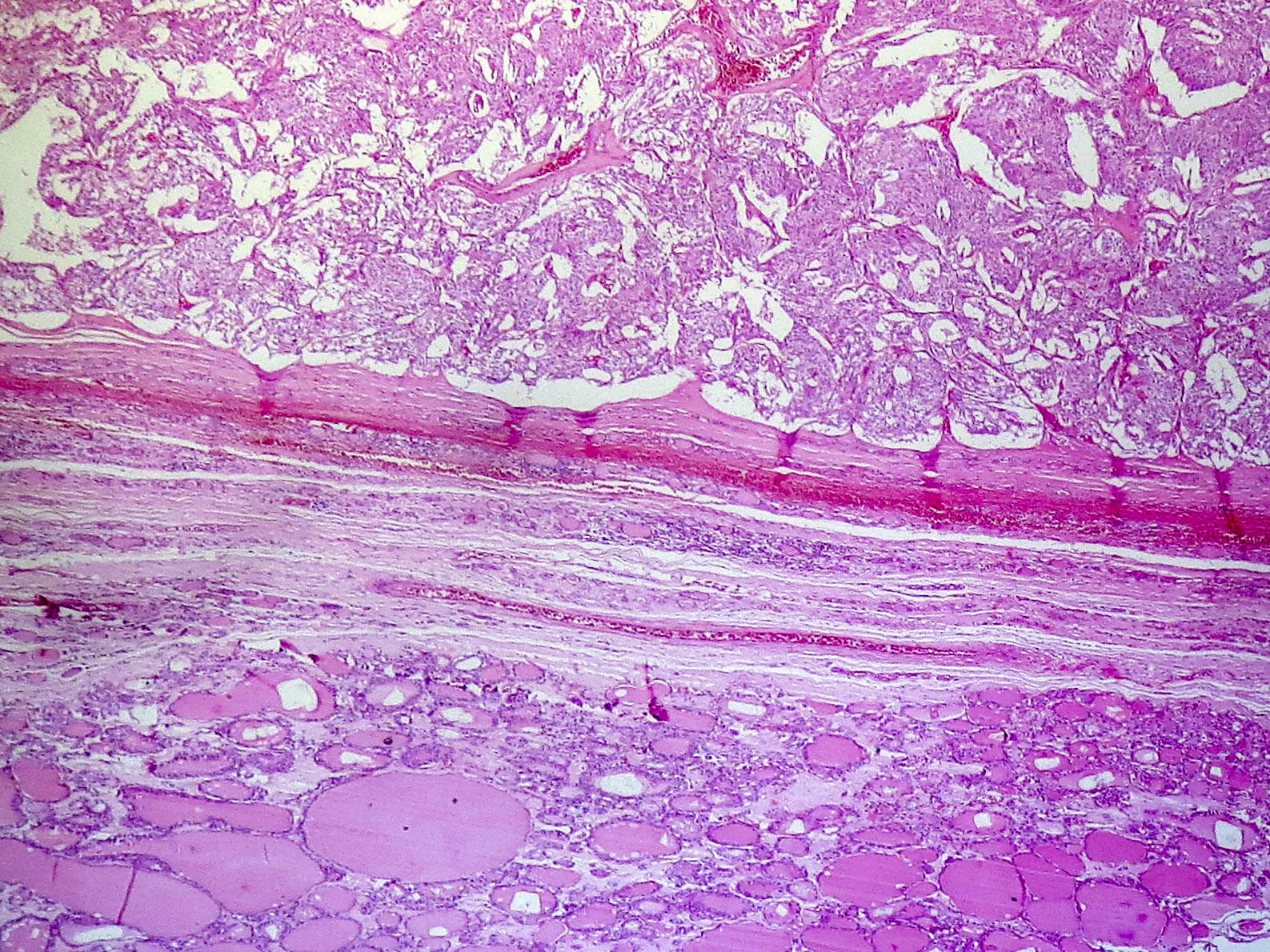
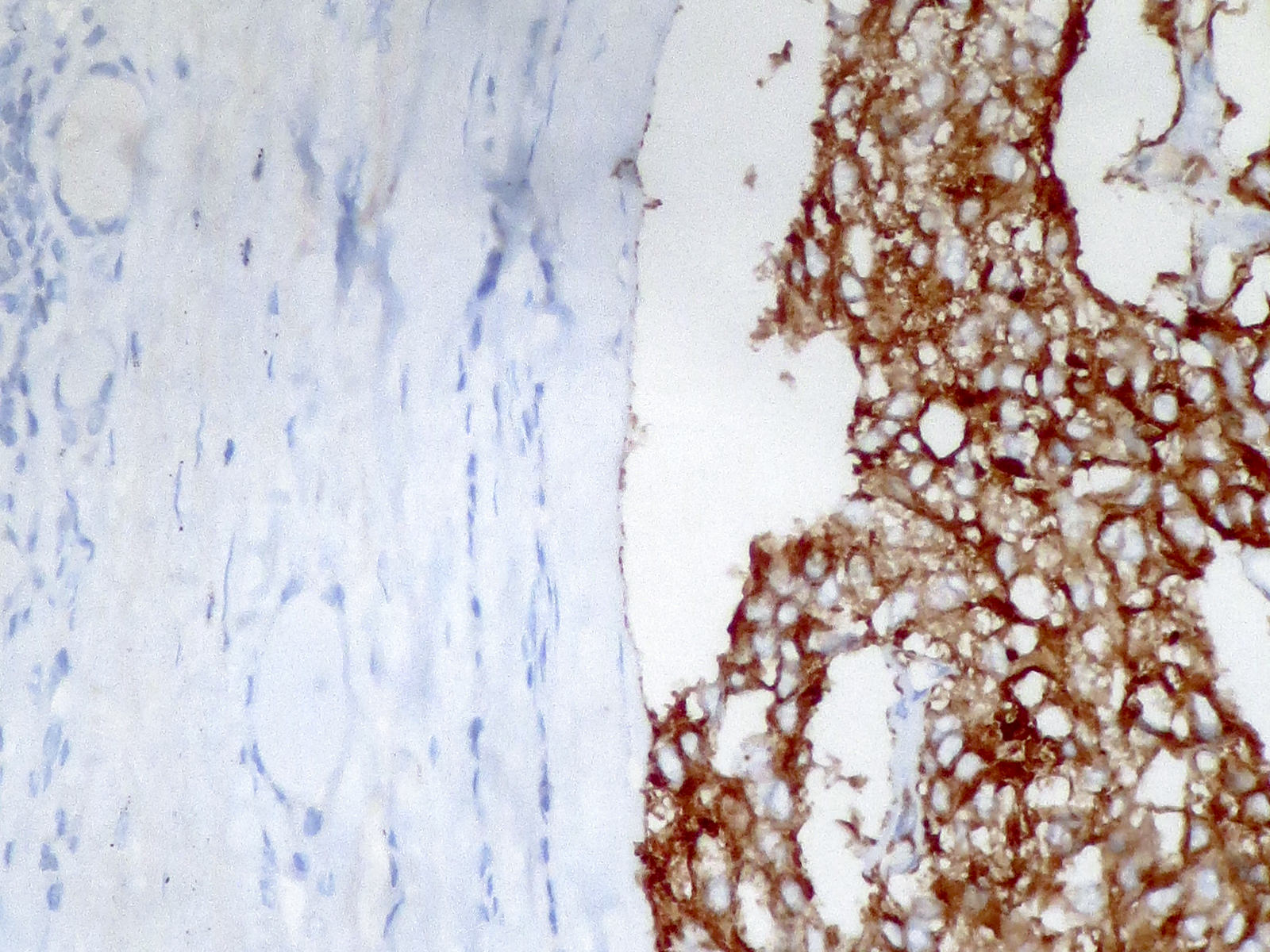
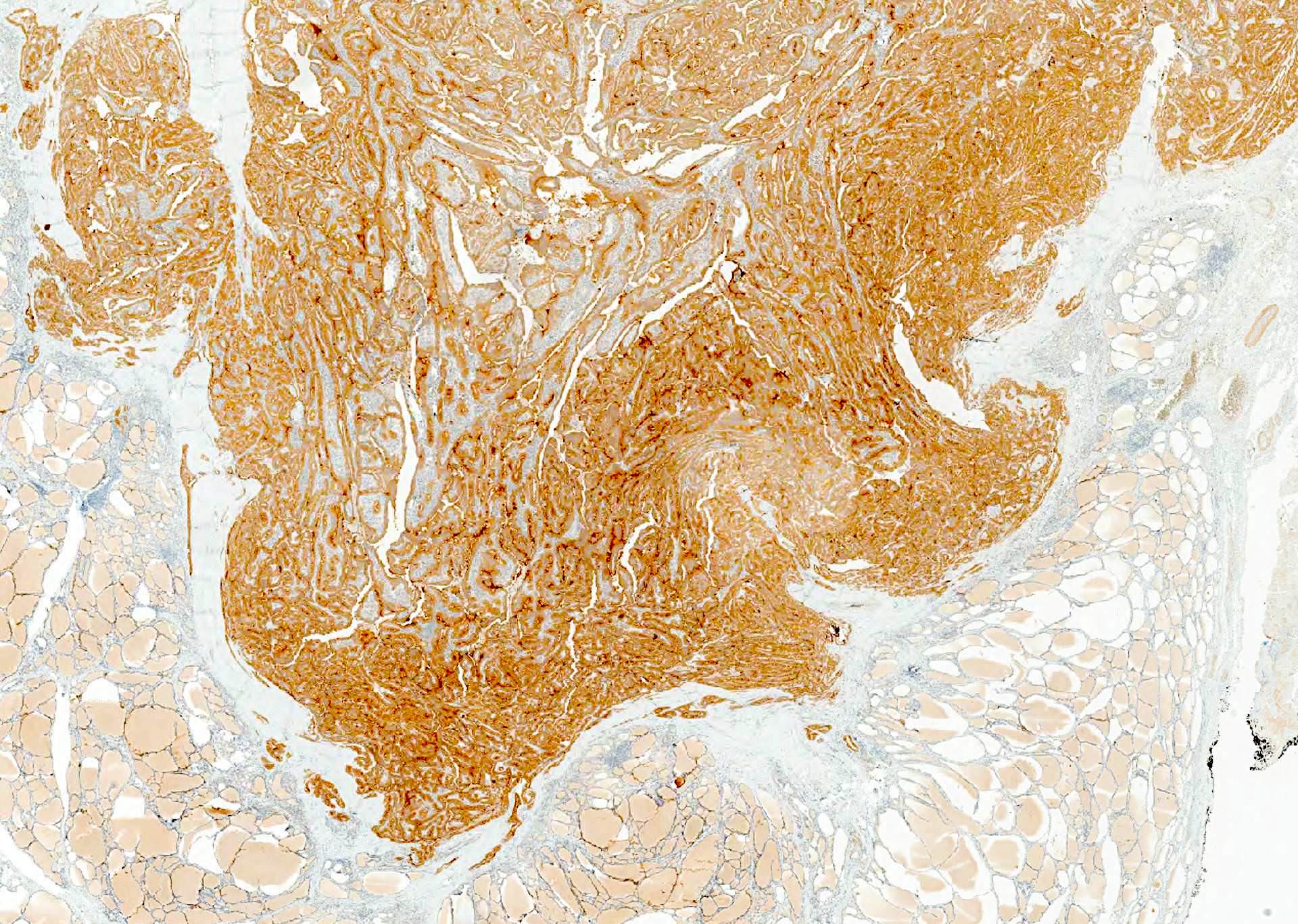
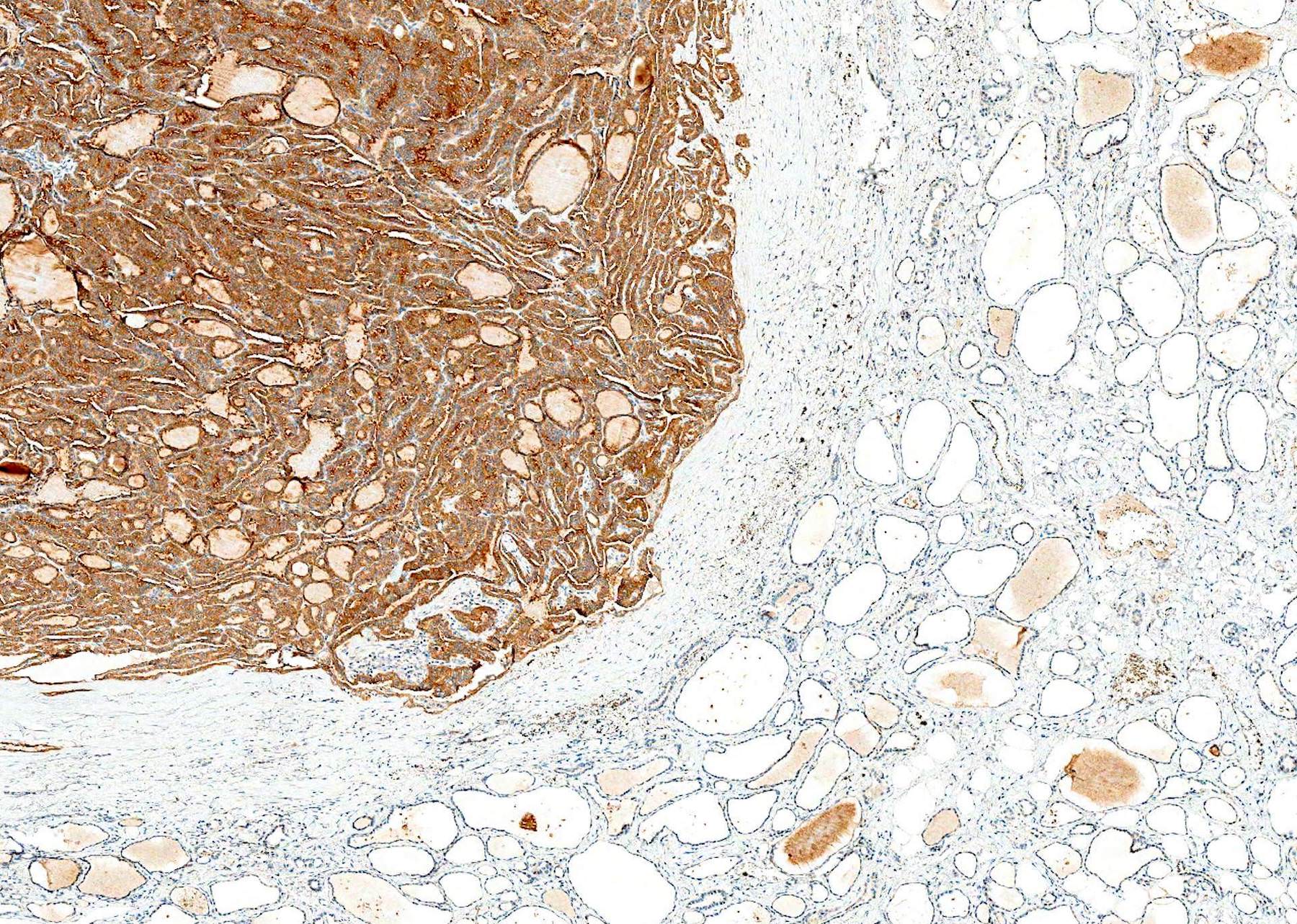
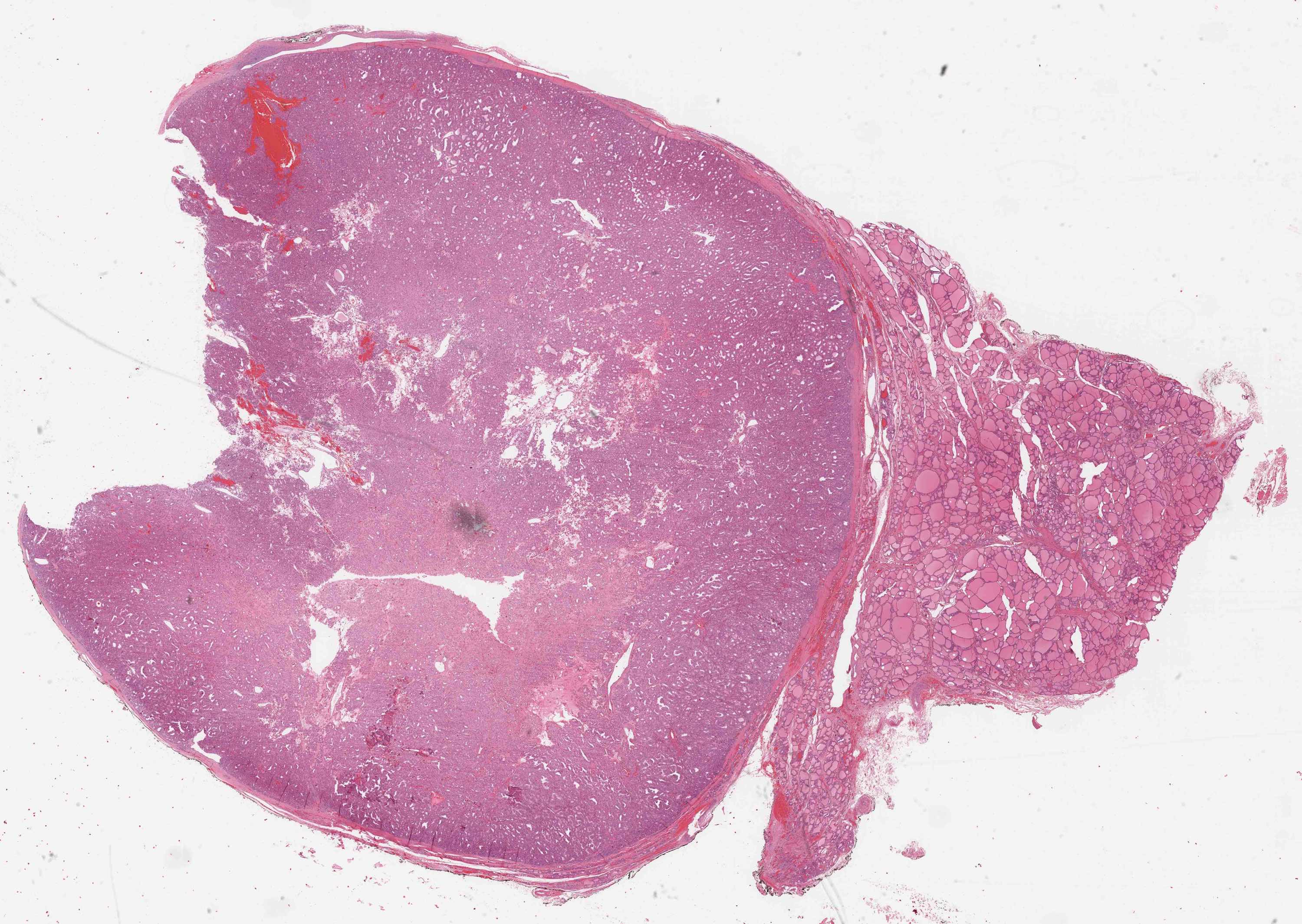
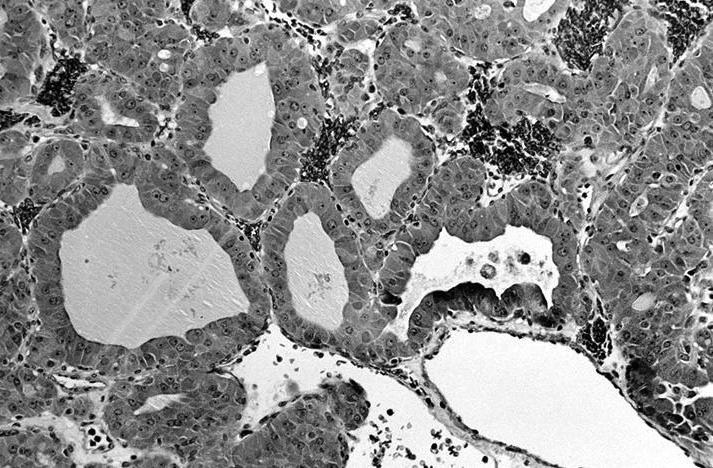
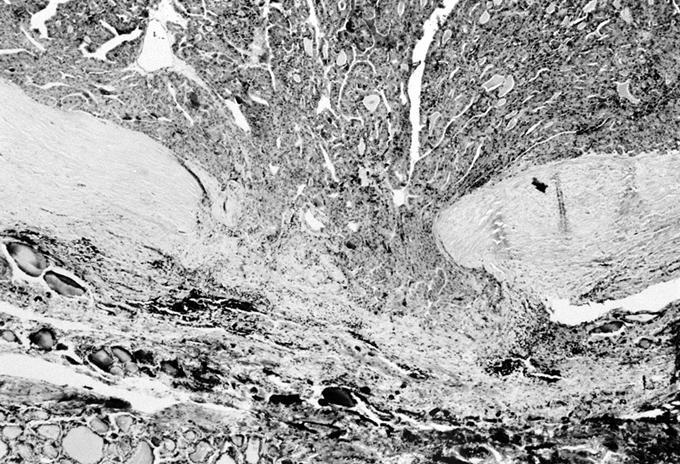
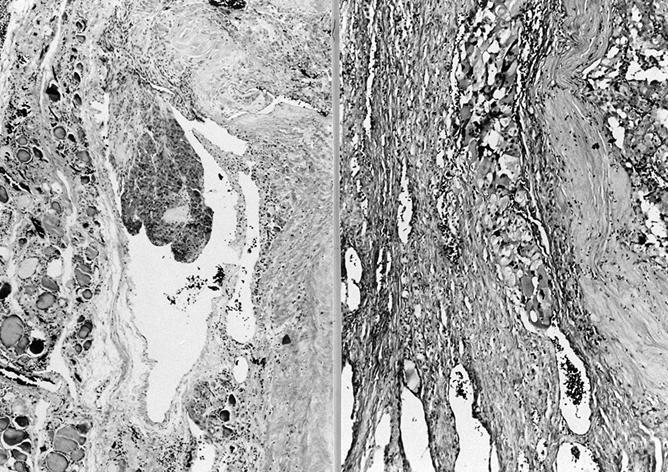
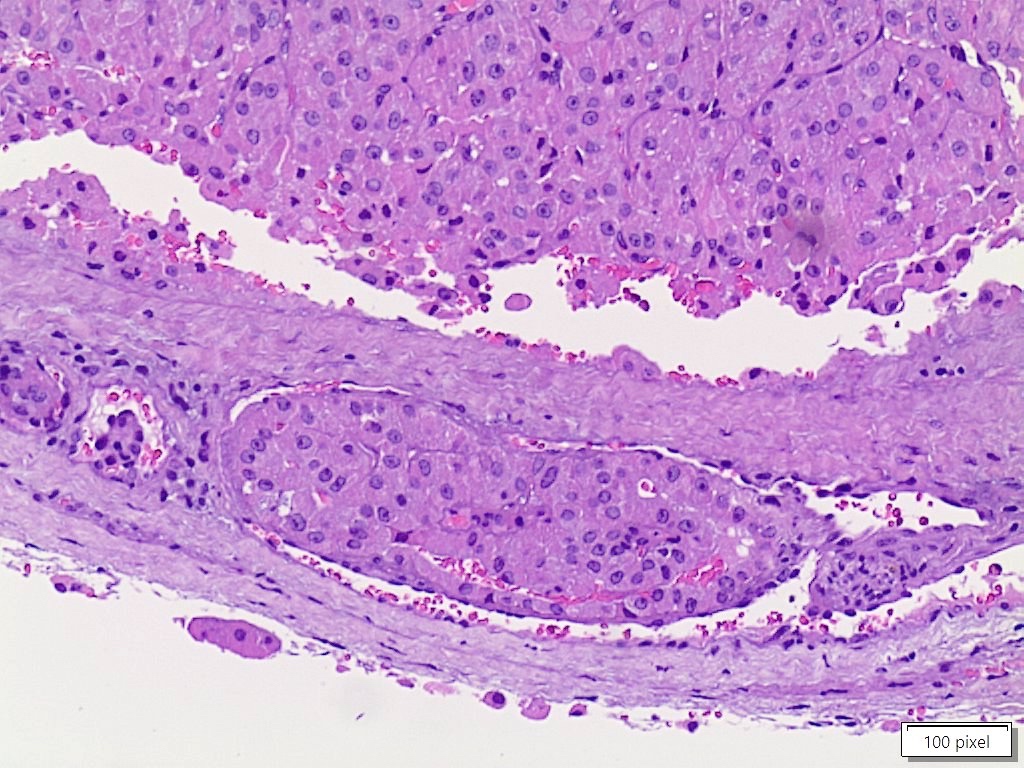
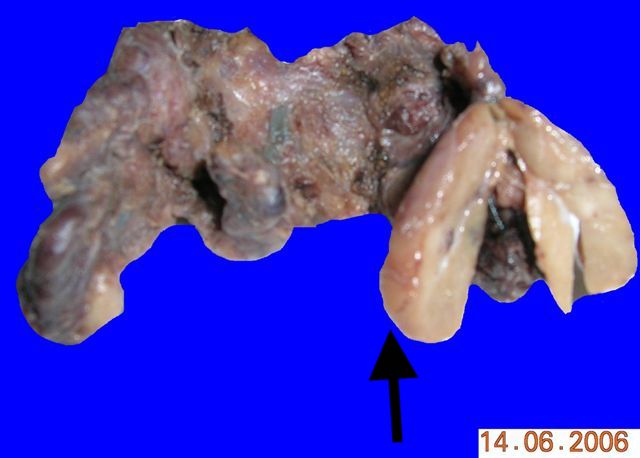
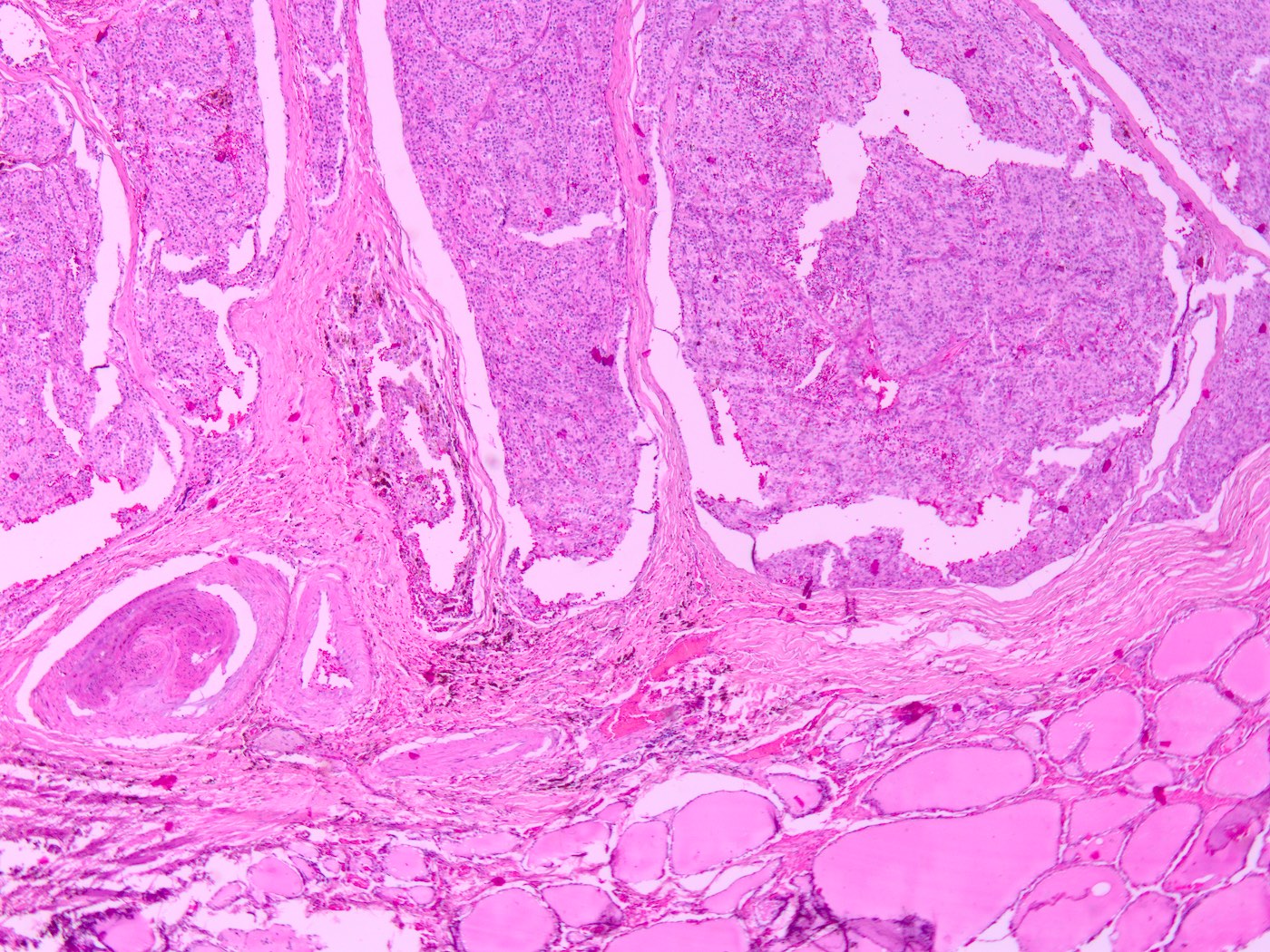
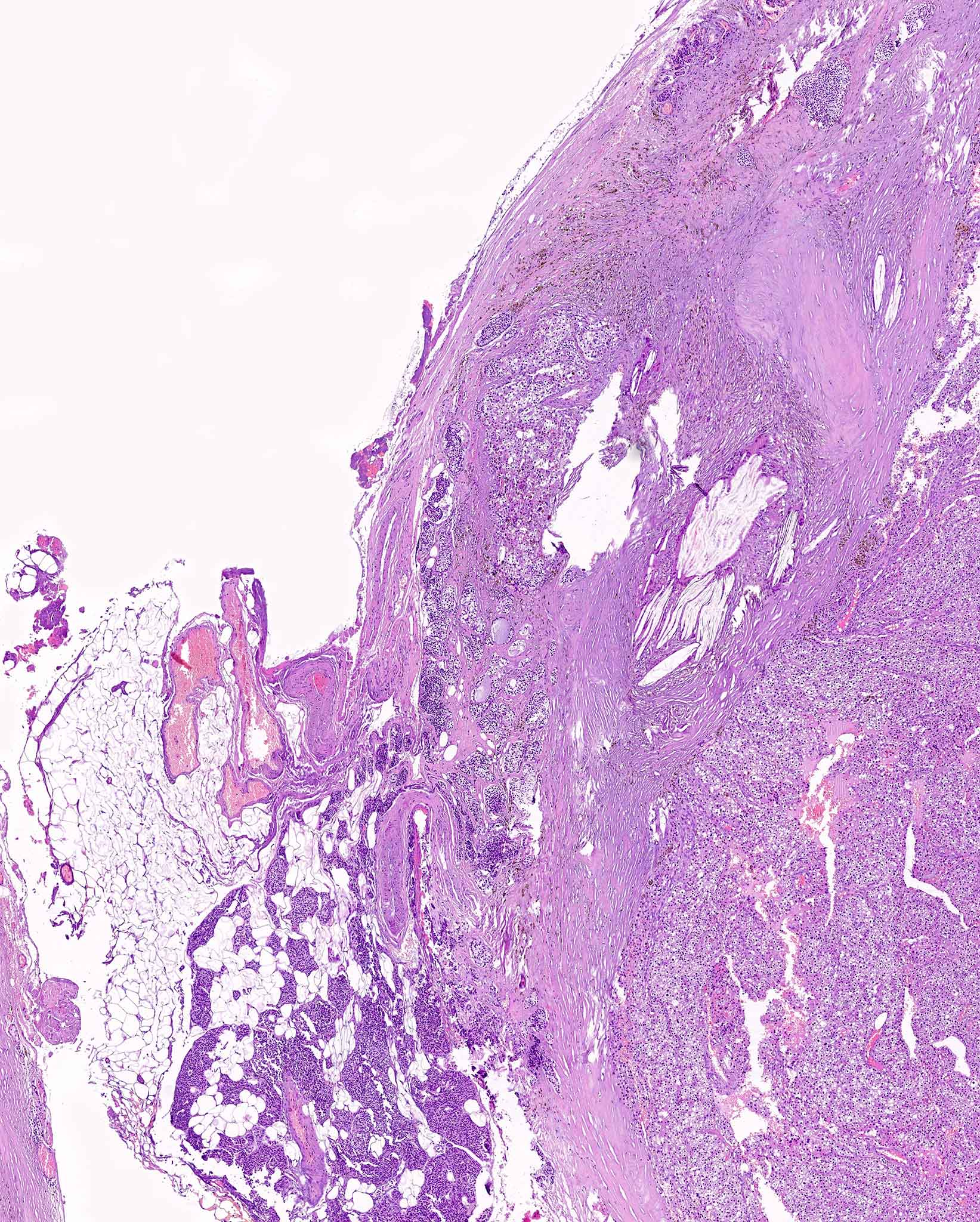
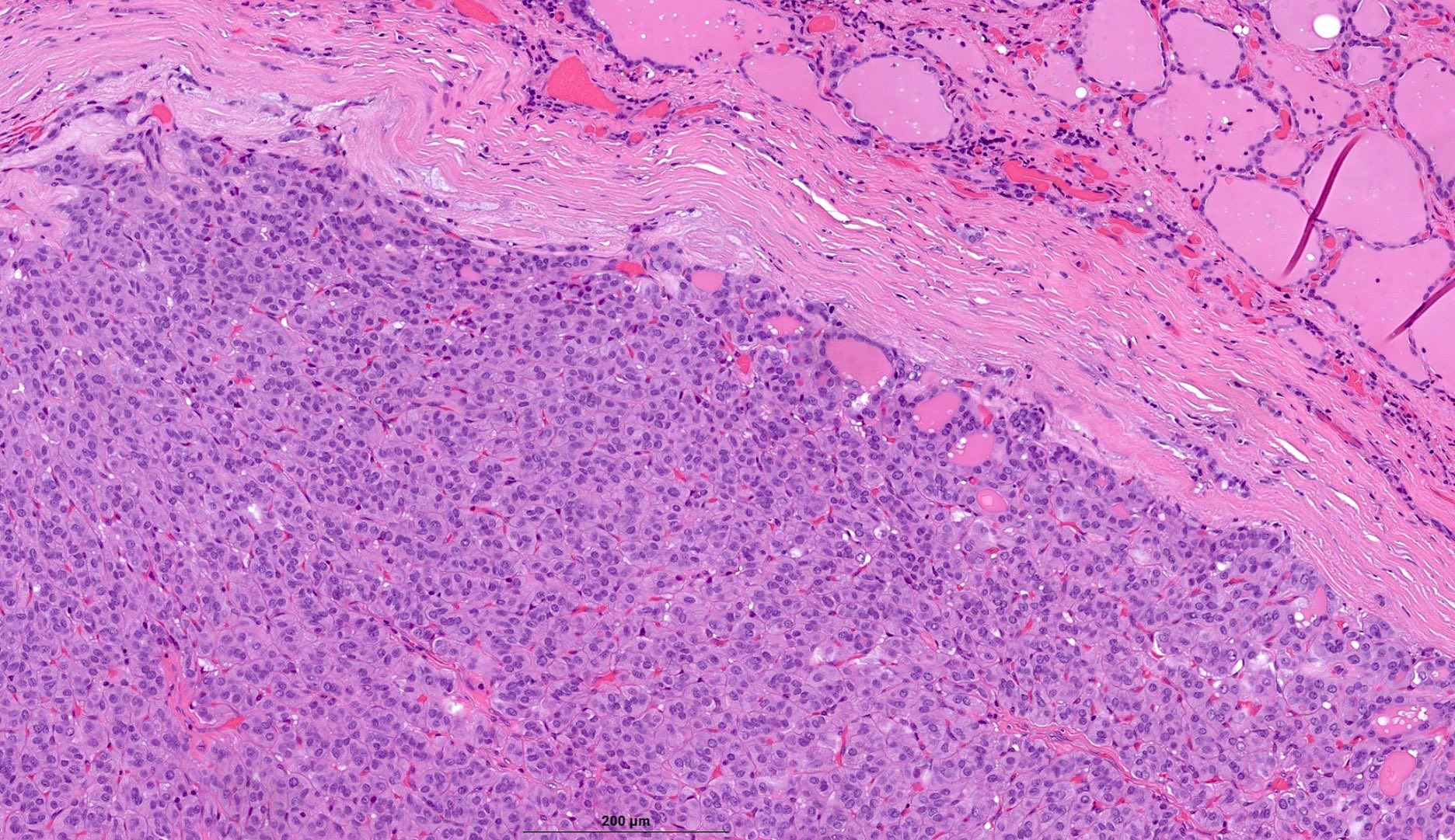
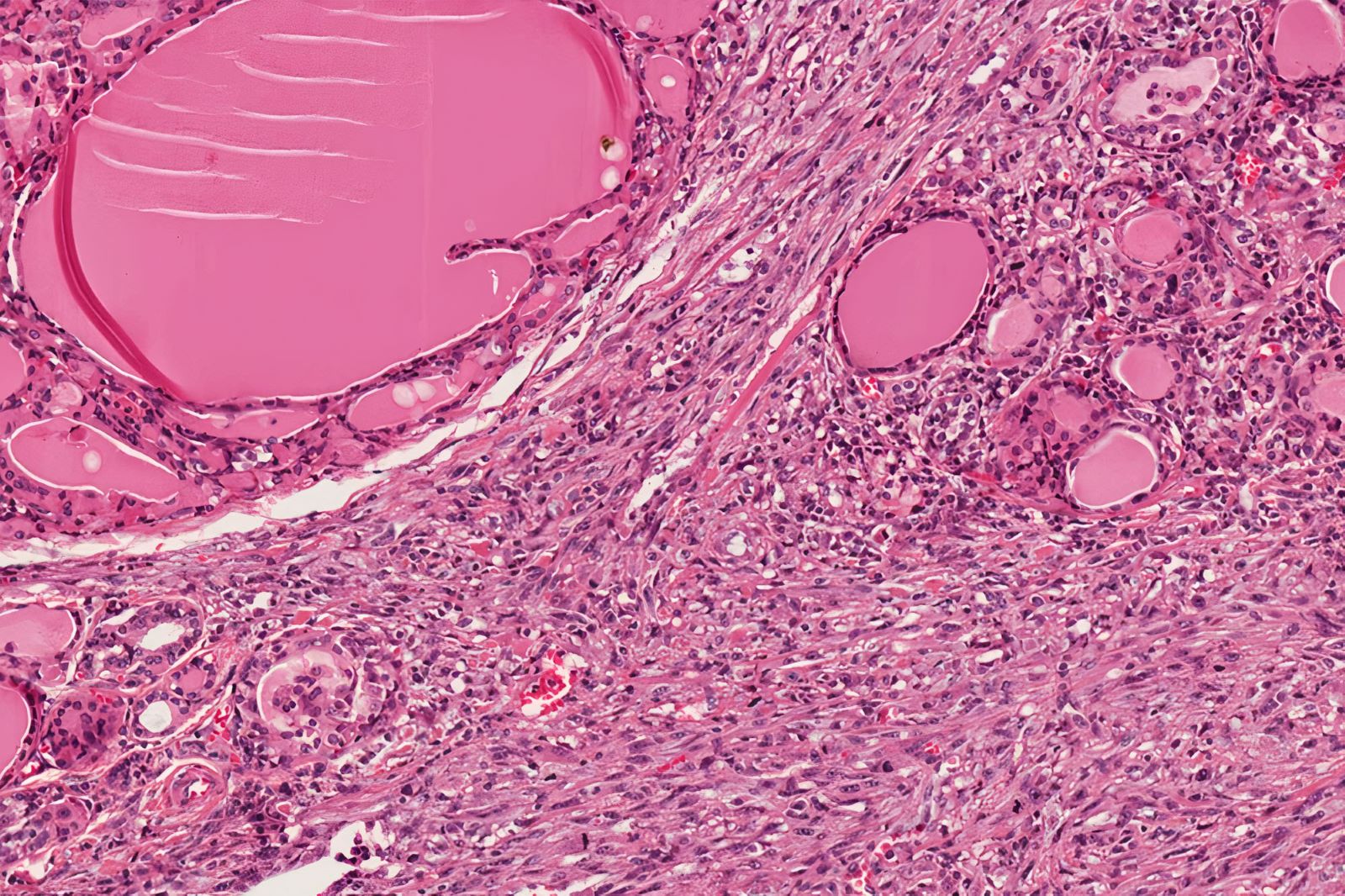
- pT2: direct invasion into the thyroid gland
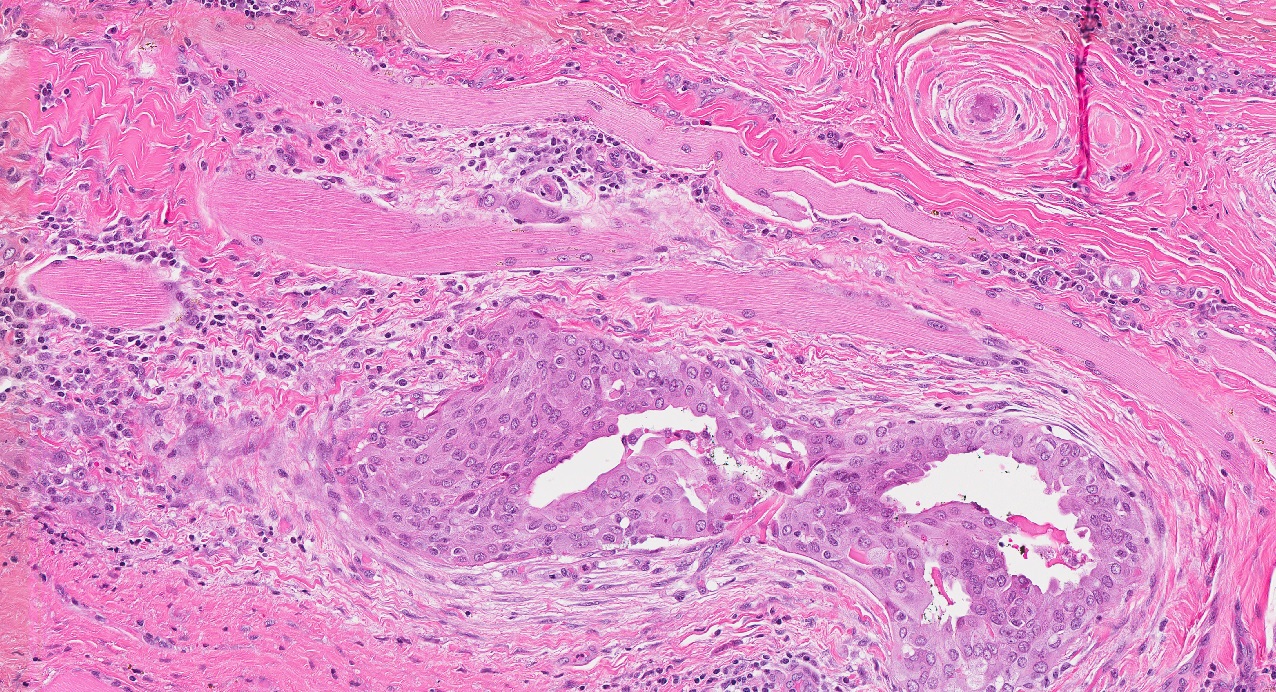
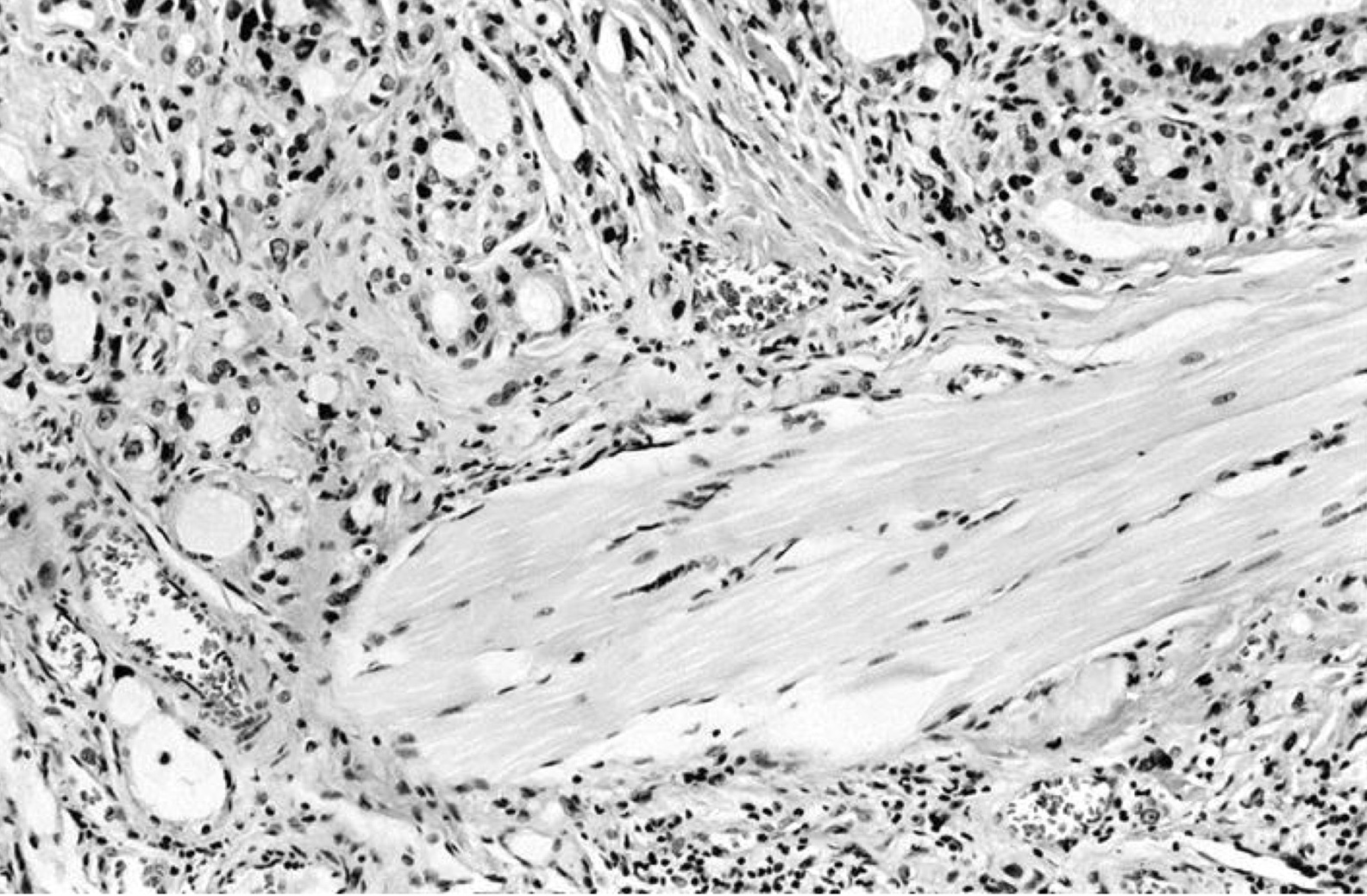
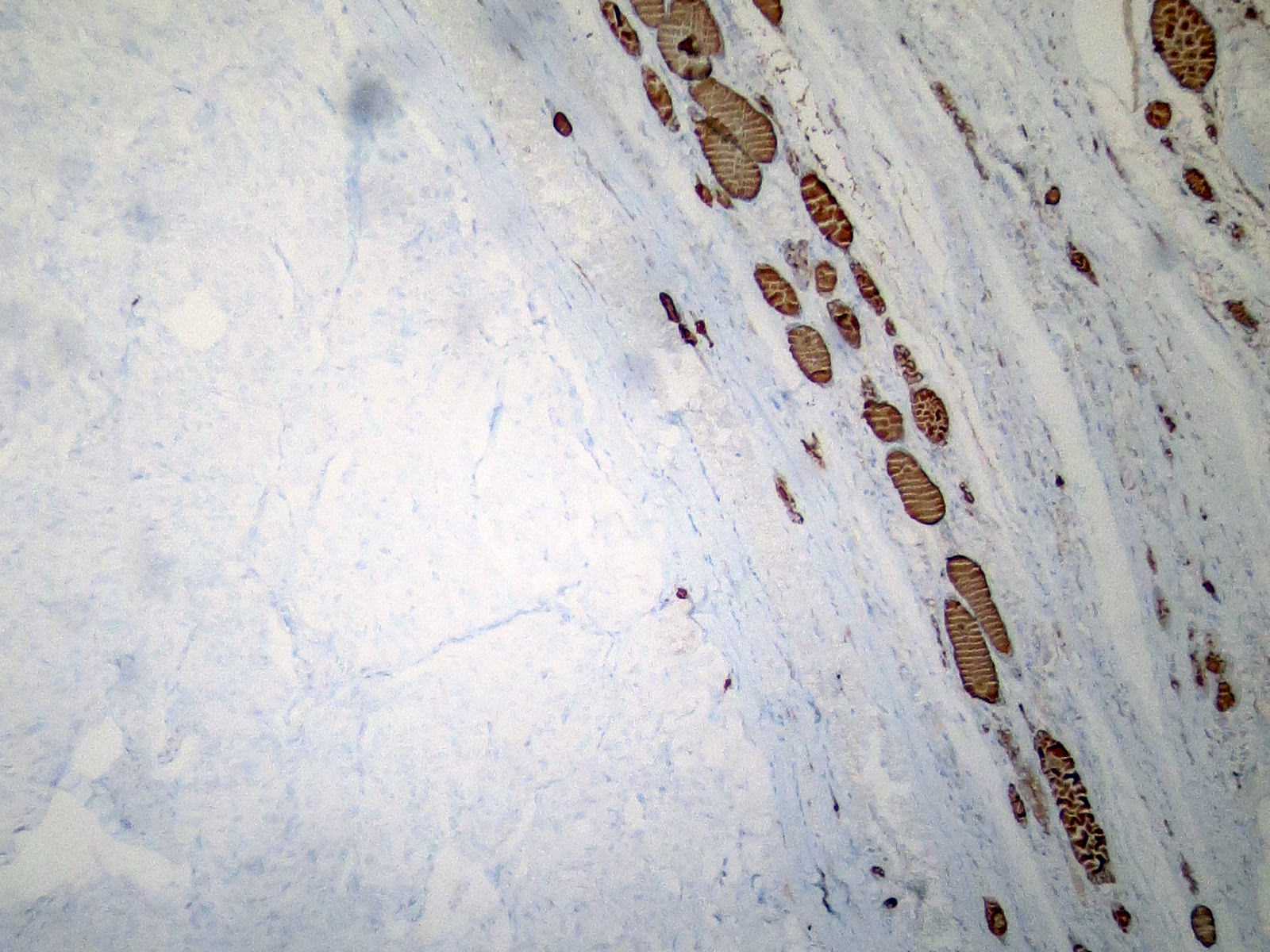
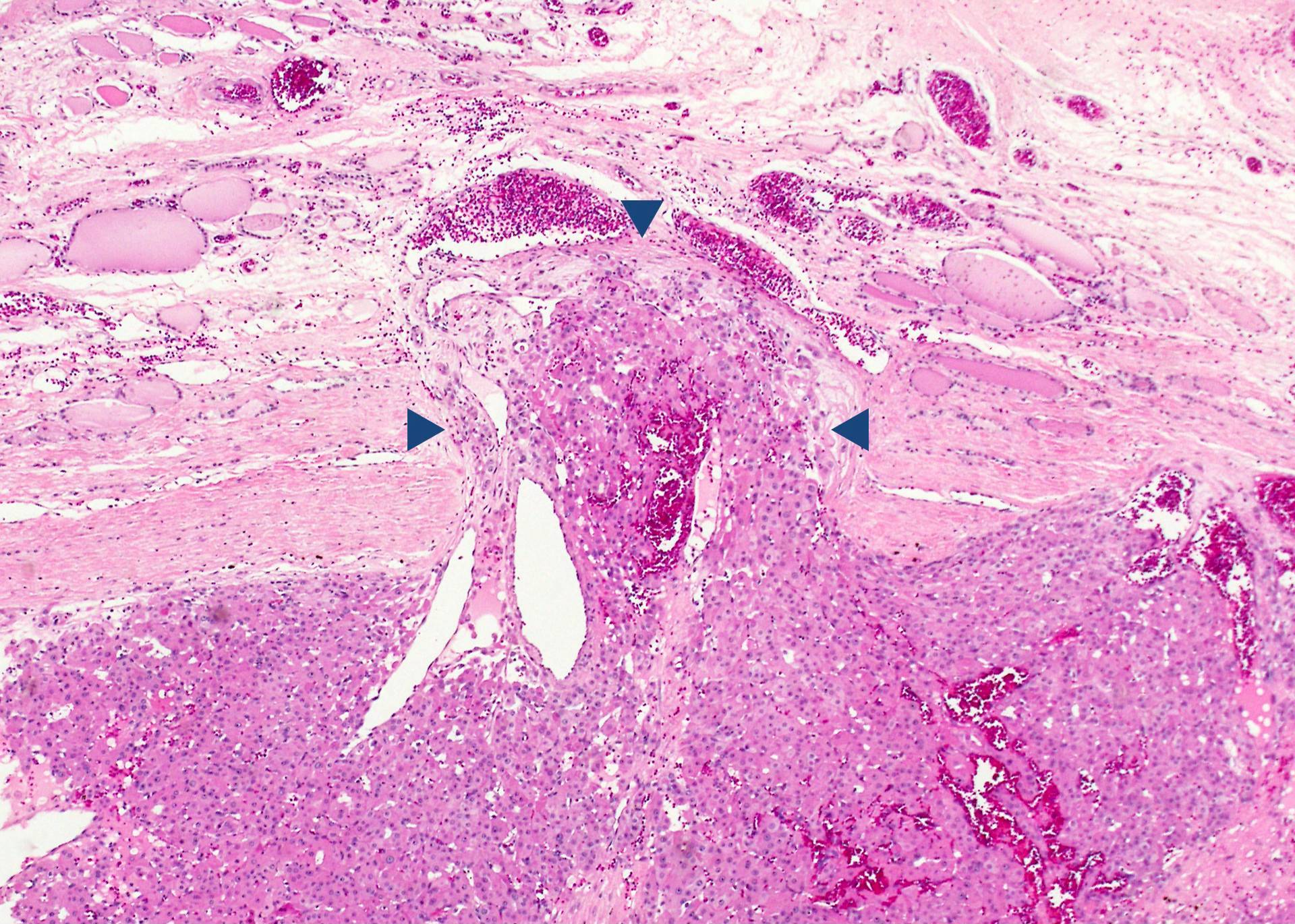
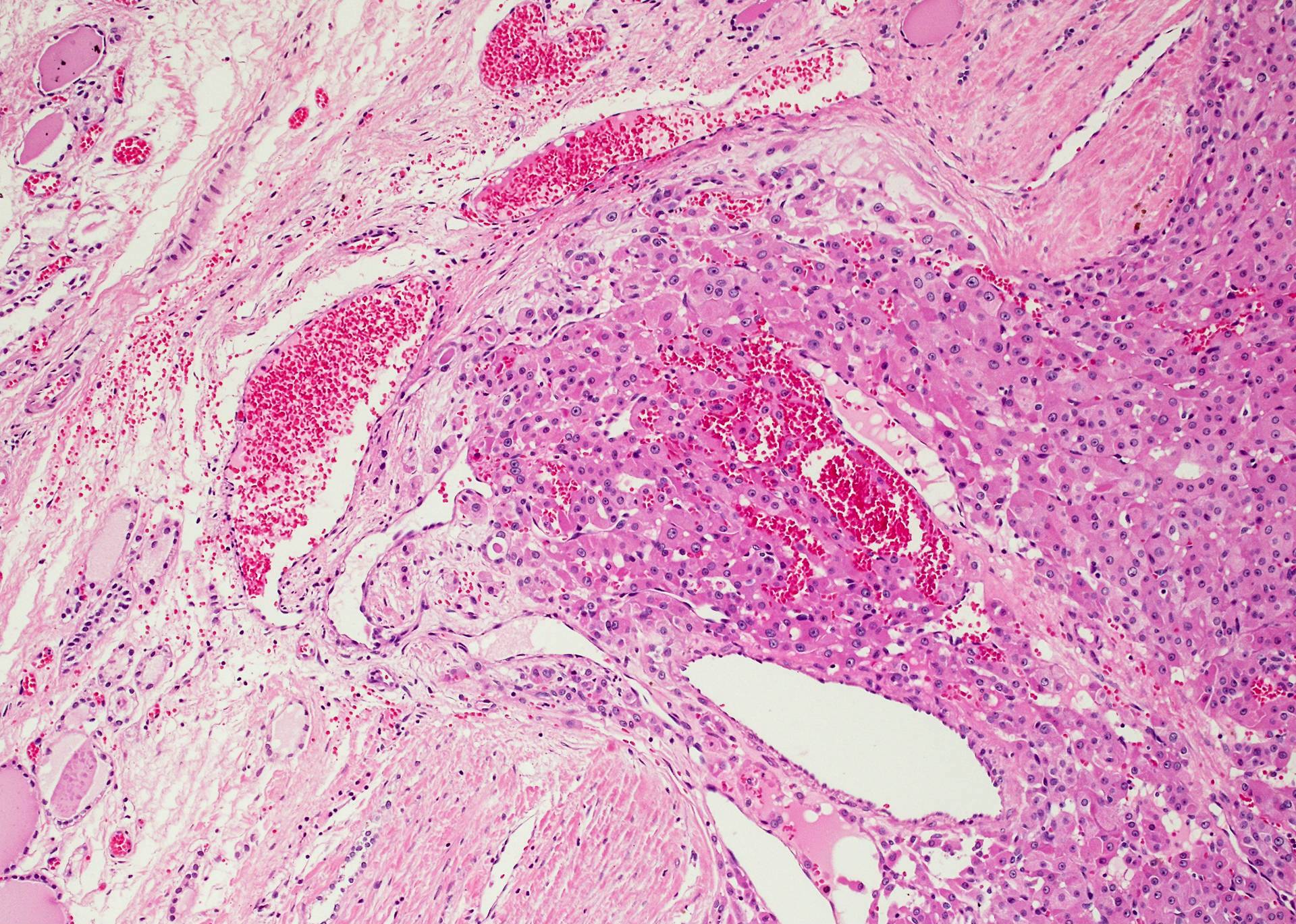
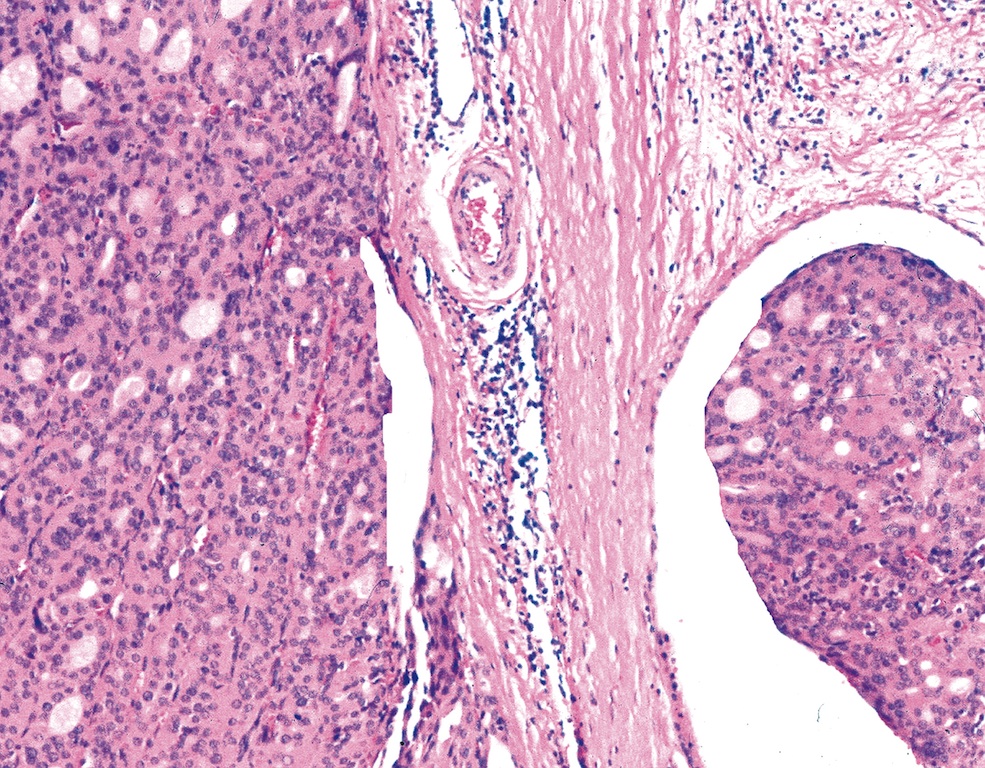
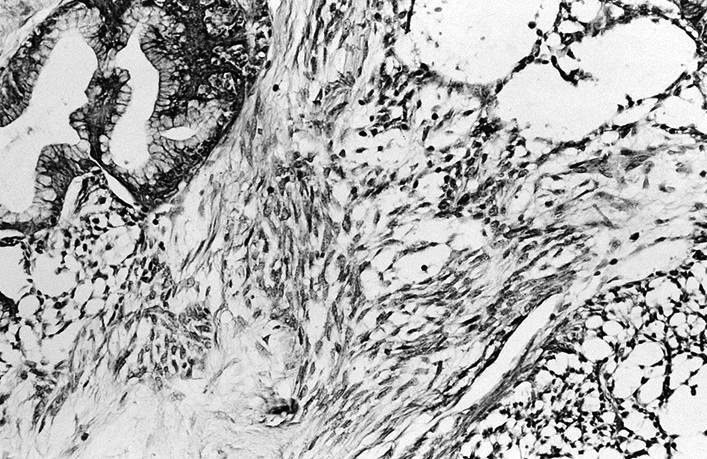
- pT3: direct invasion into recurrent laryngeal nerve, esophagus, trachea, skeletal muscle, adjacent lymph nodes or thymus
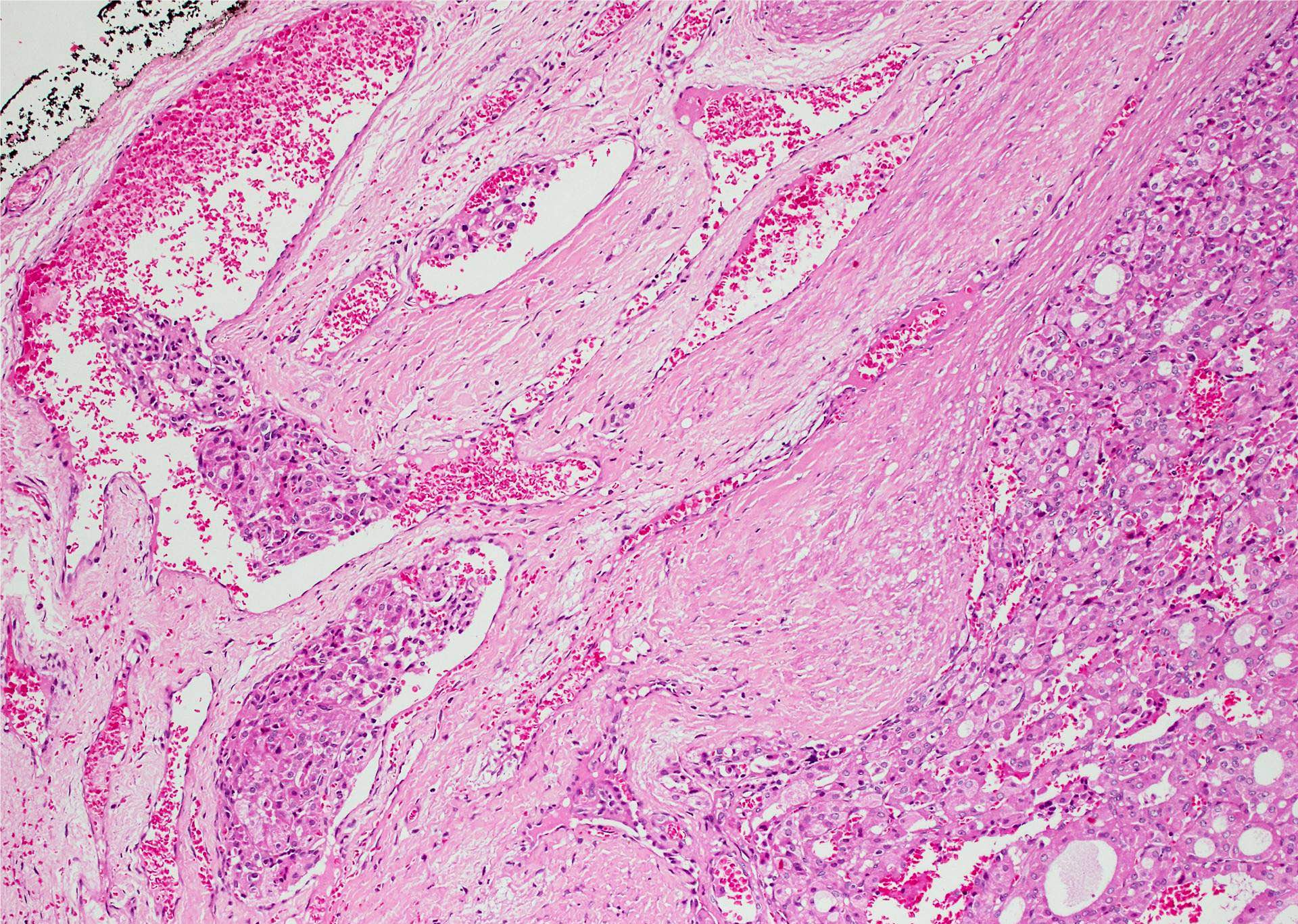
- pT4: direct invasion into major blood vessel or spine
Notes:
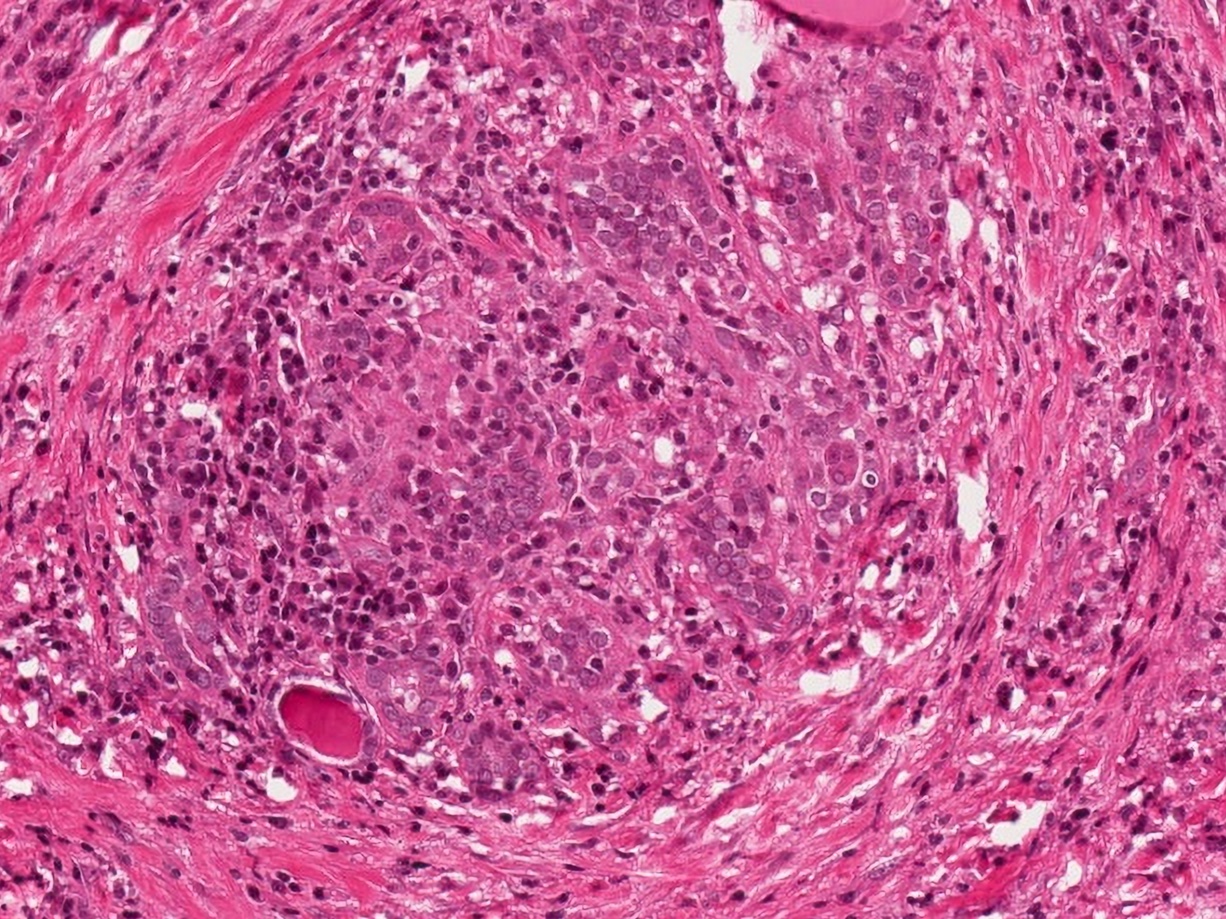
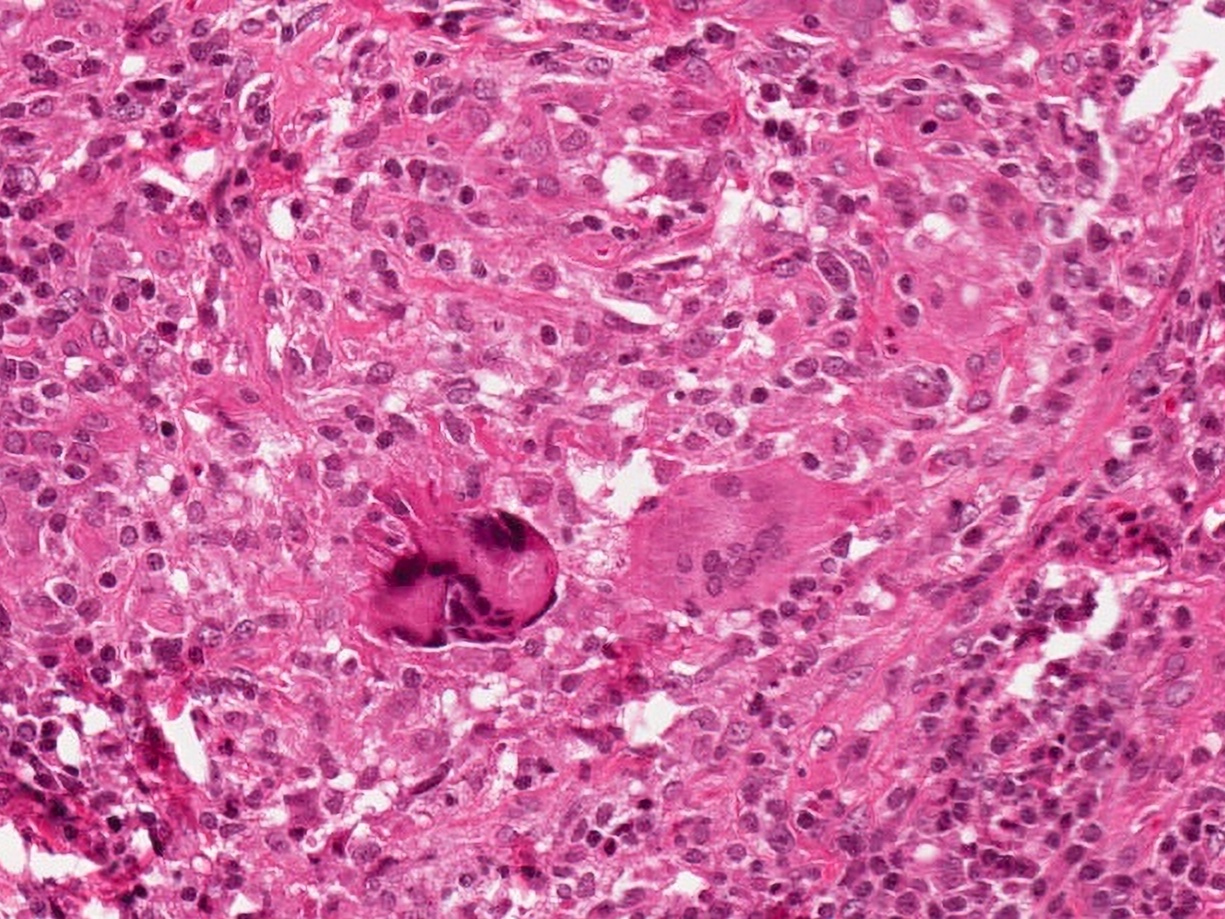
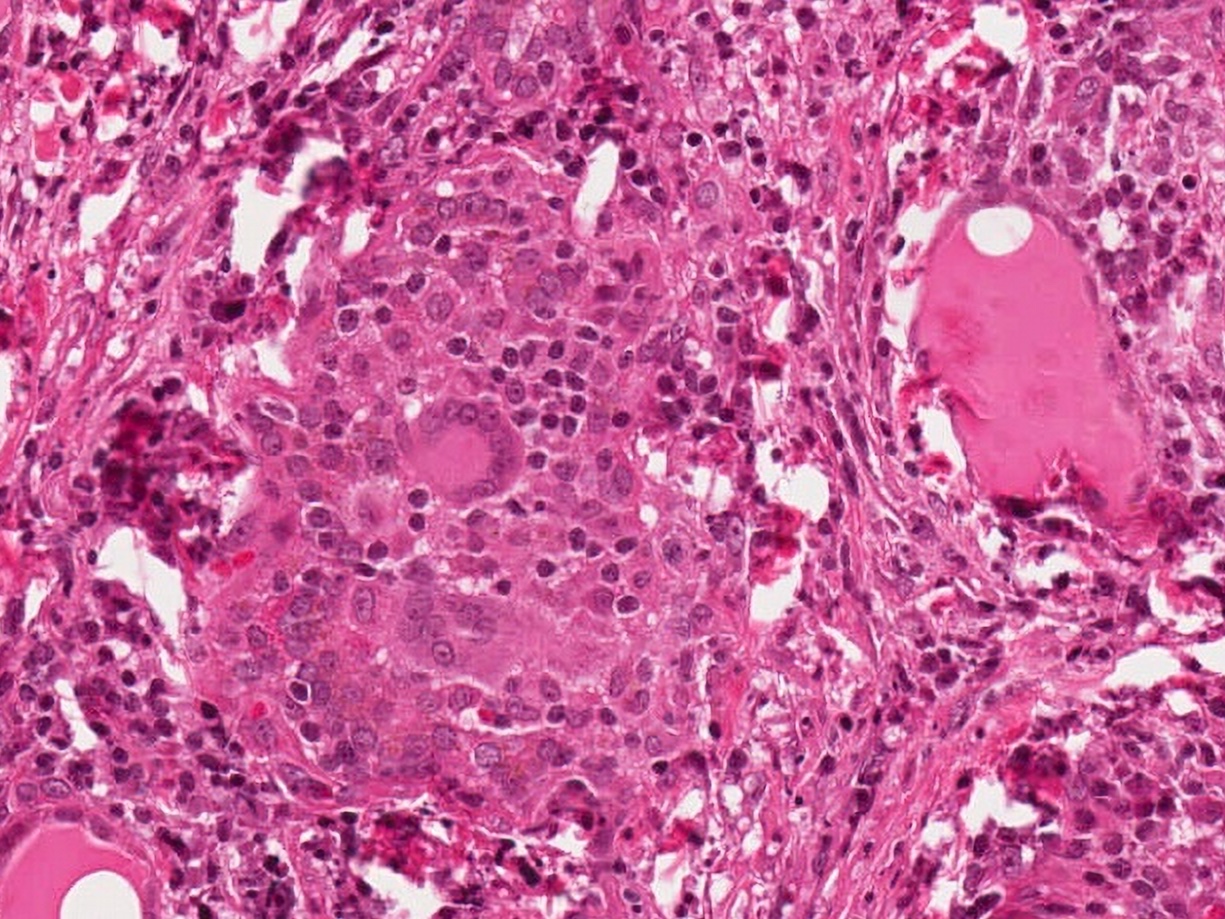
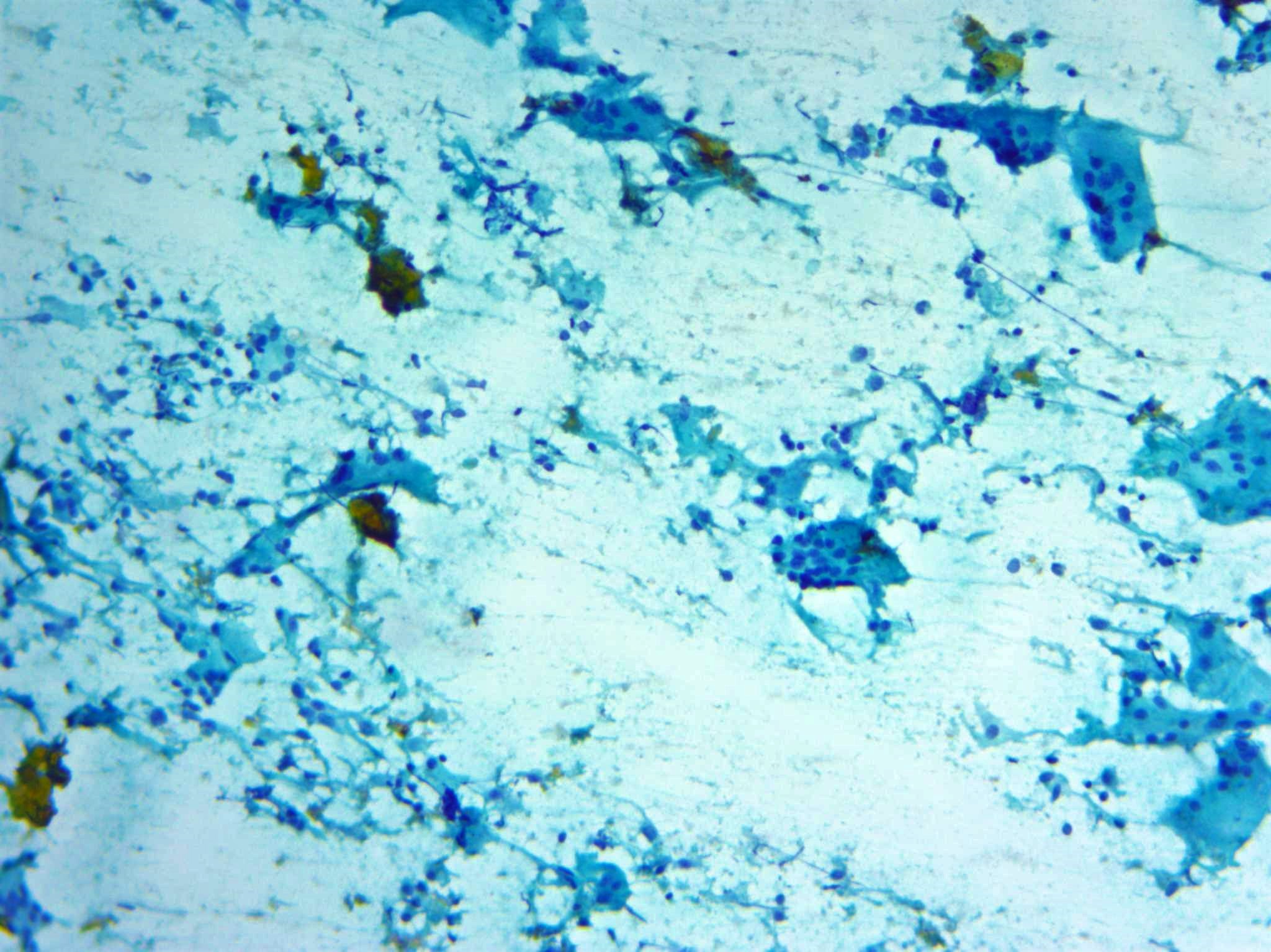
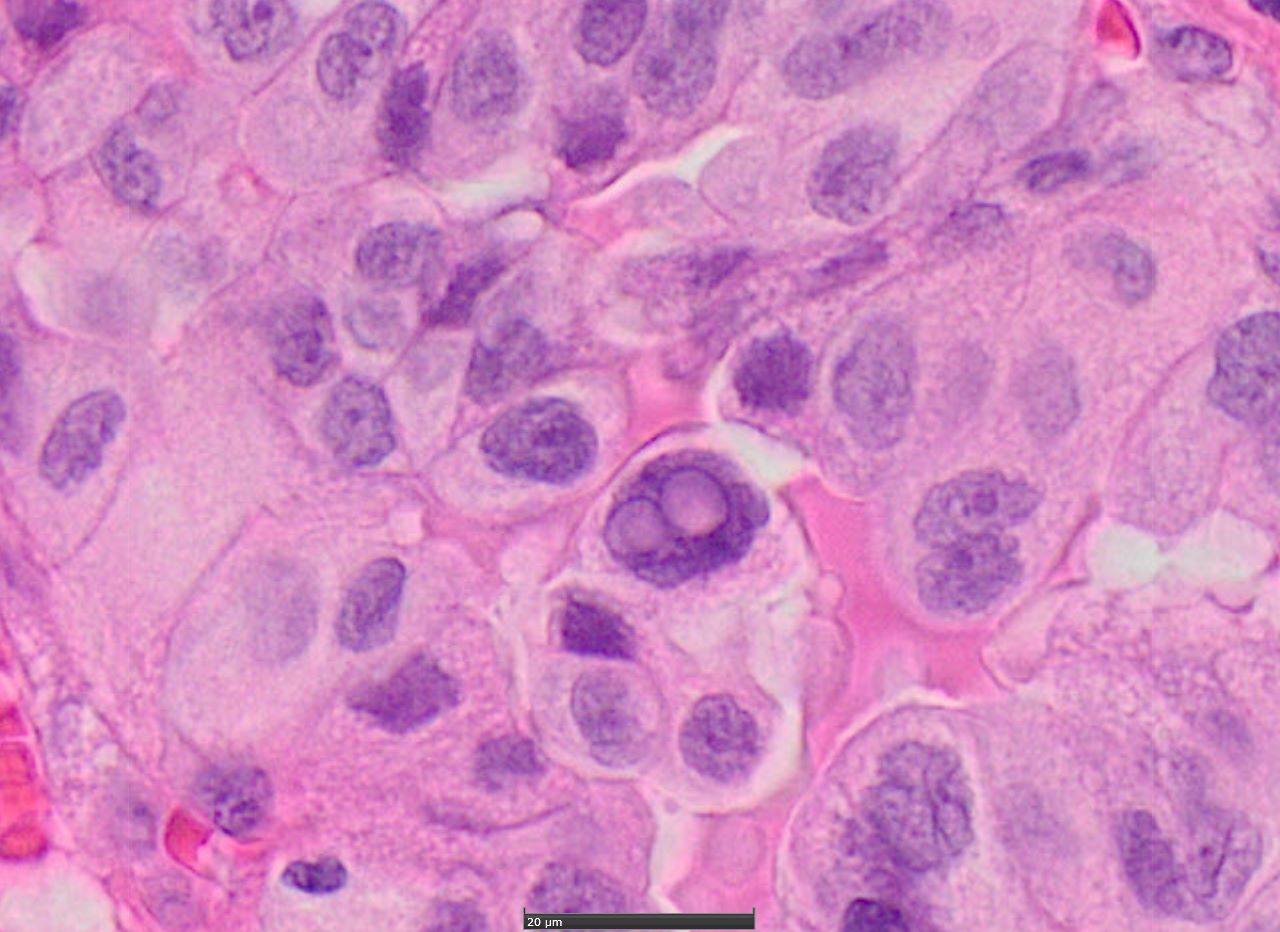
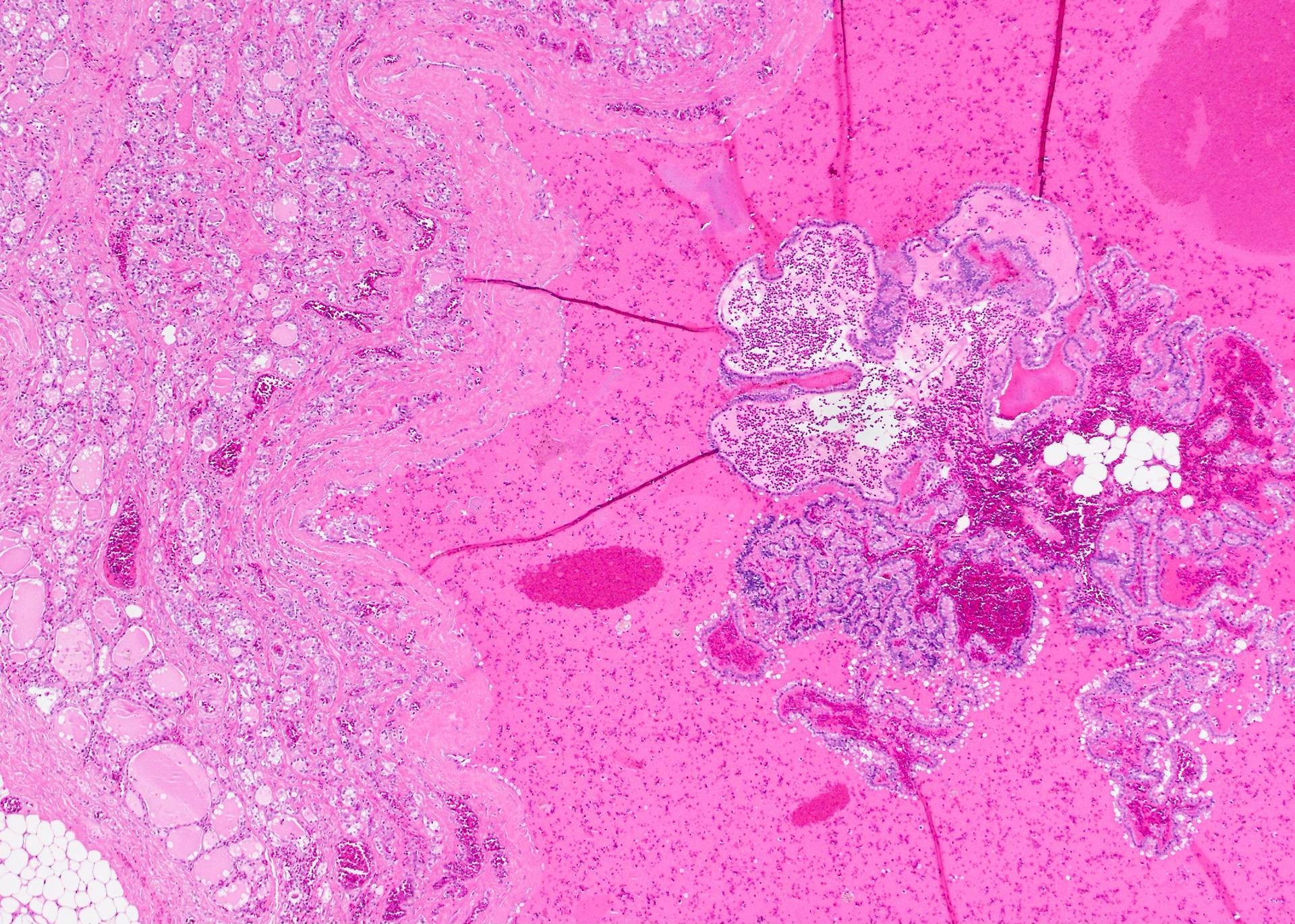
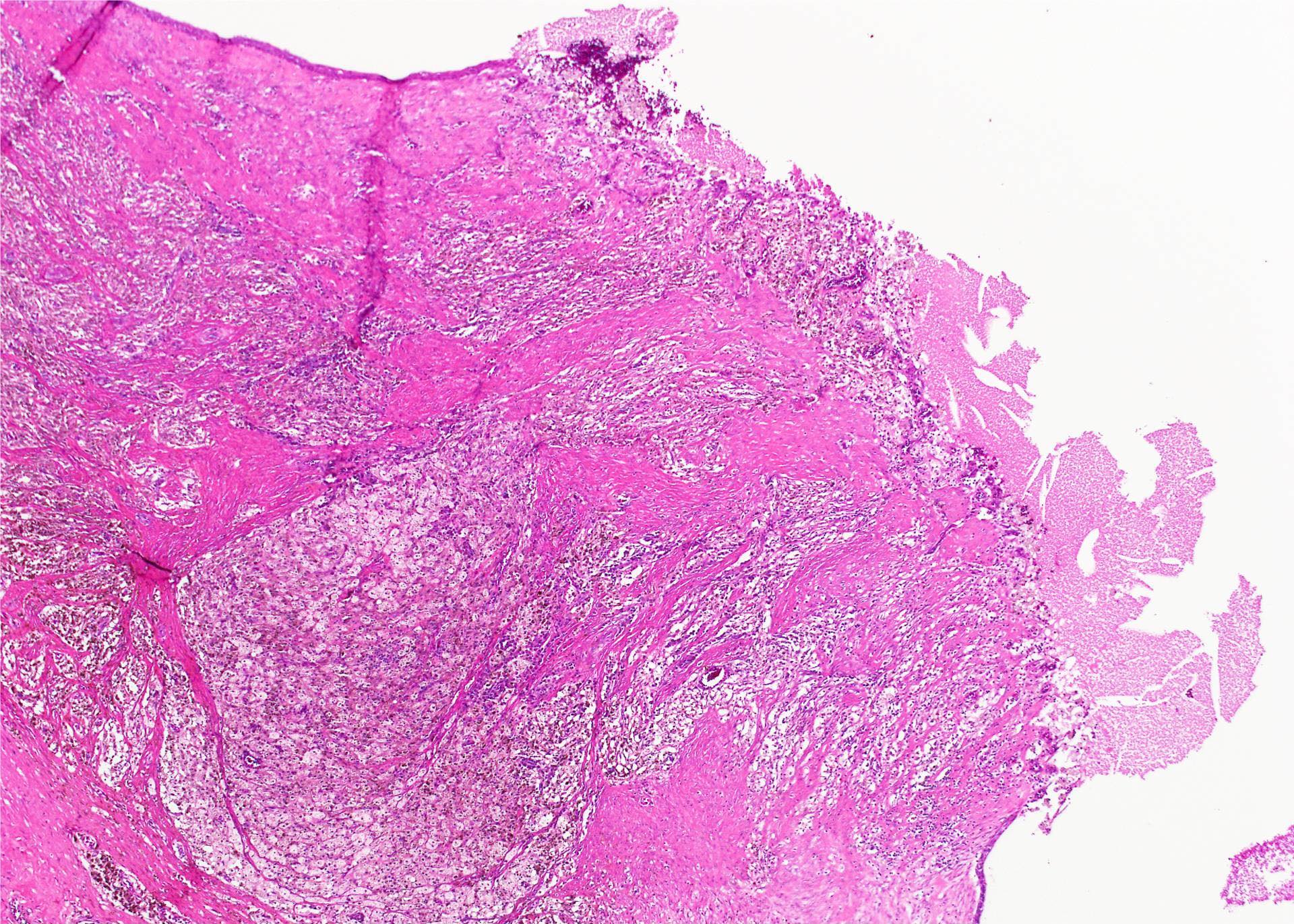
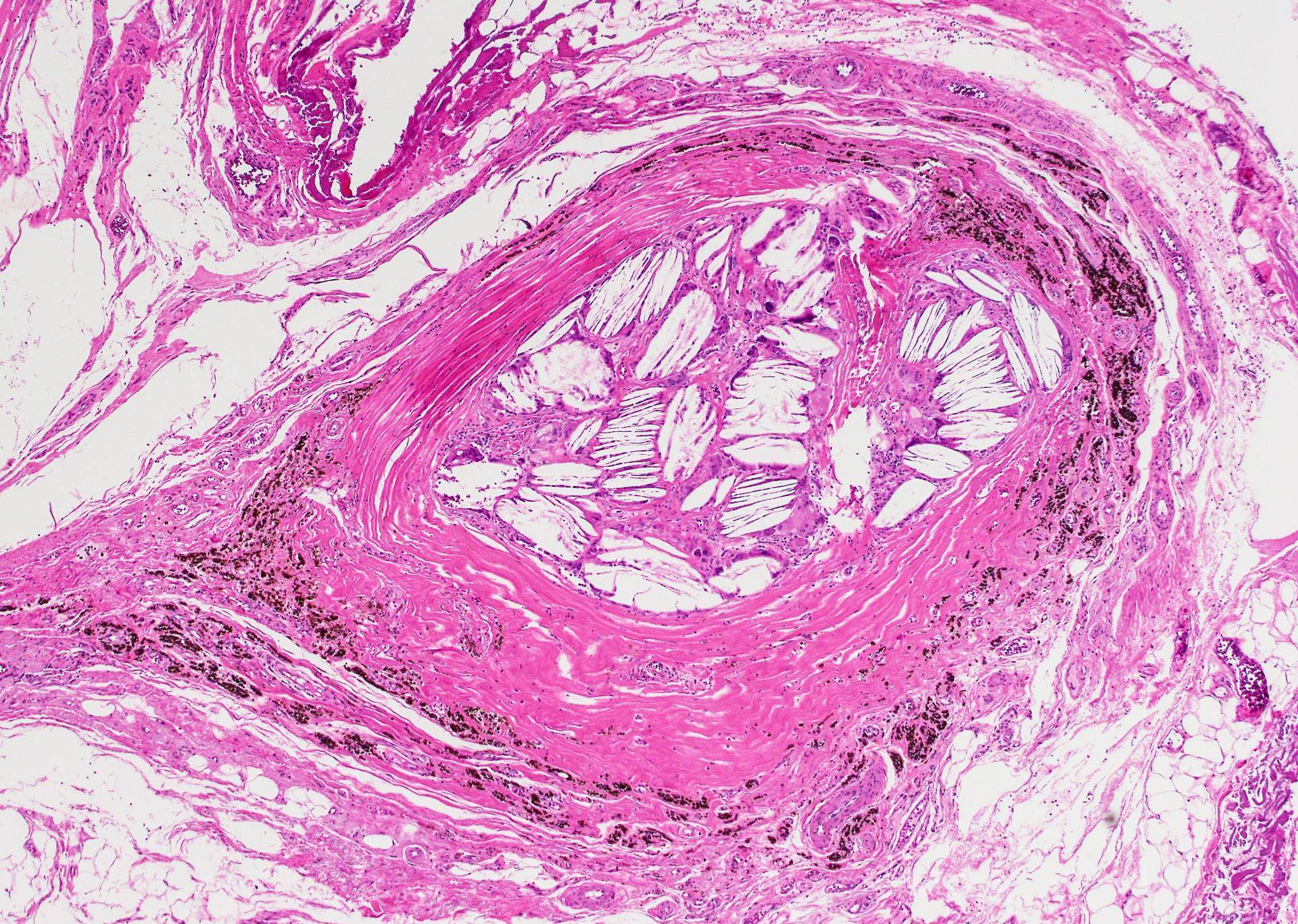
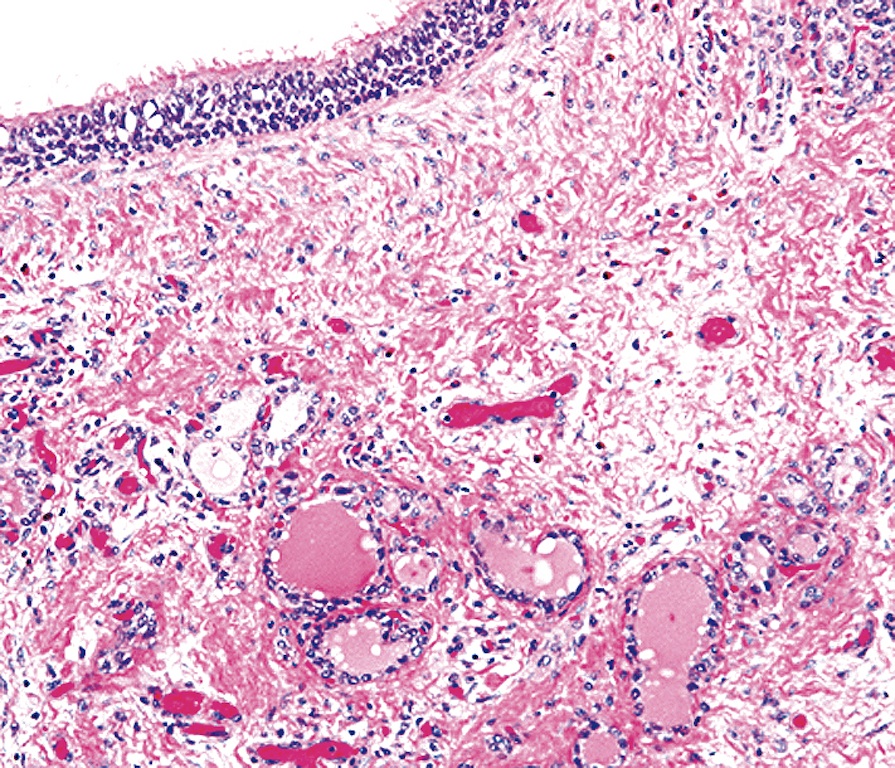
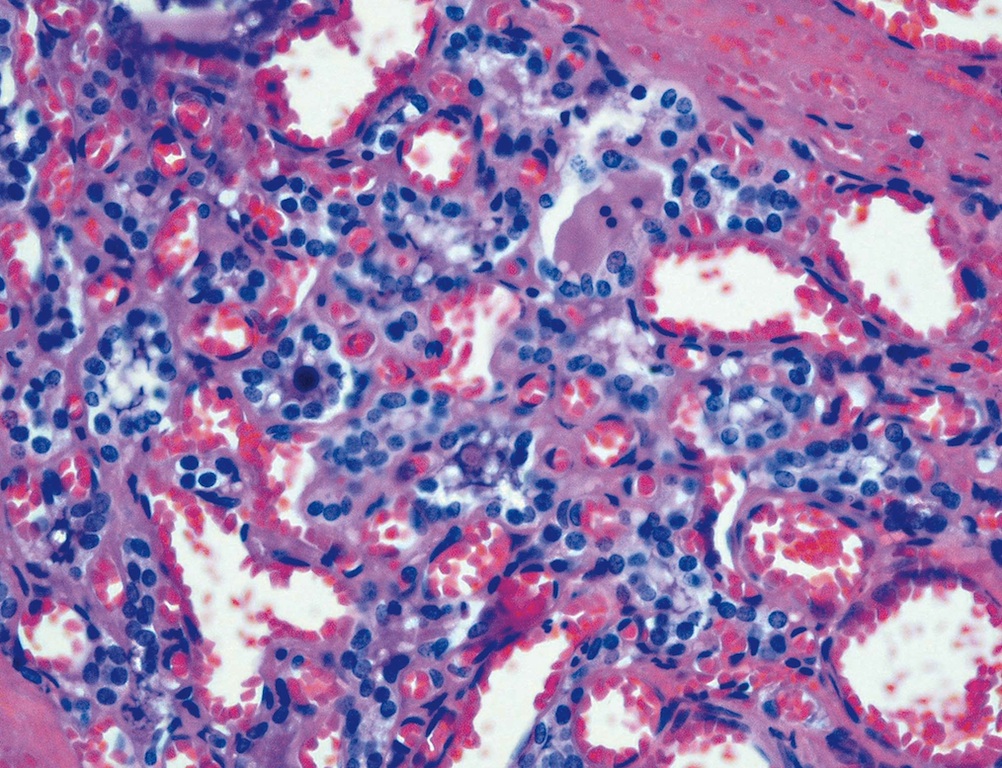
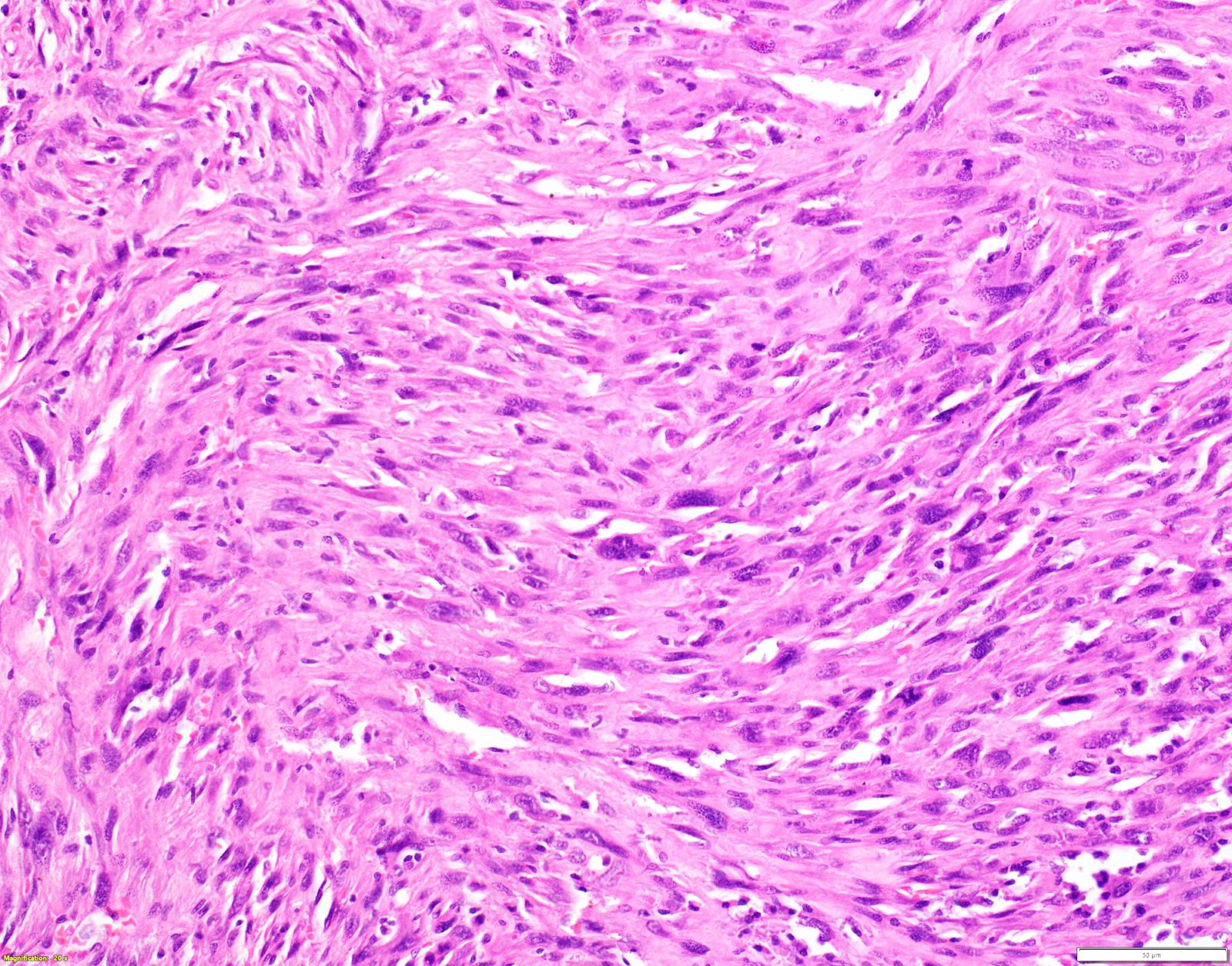
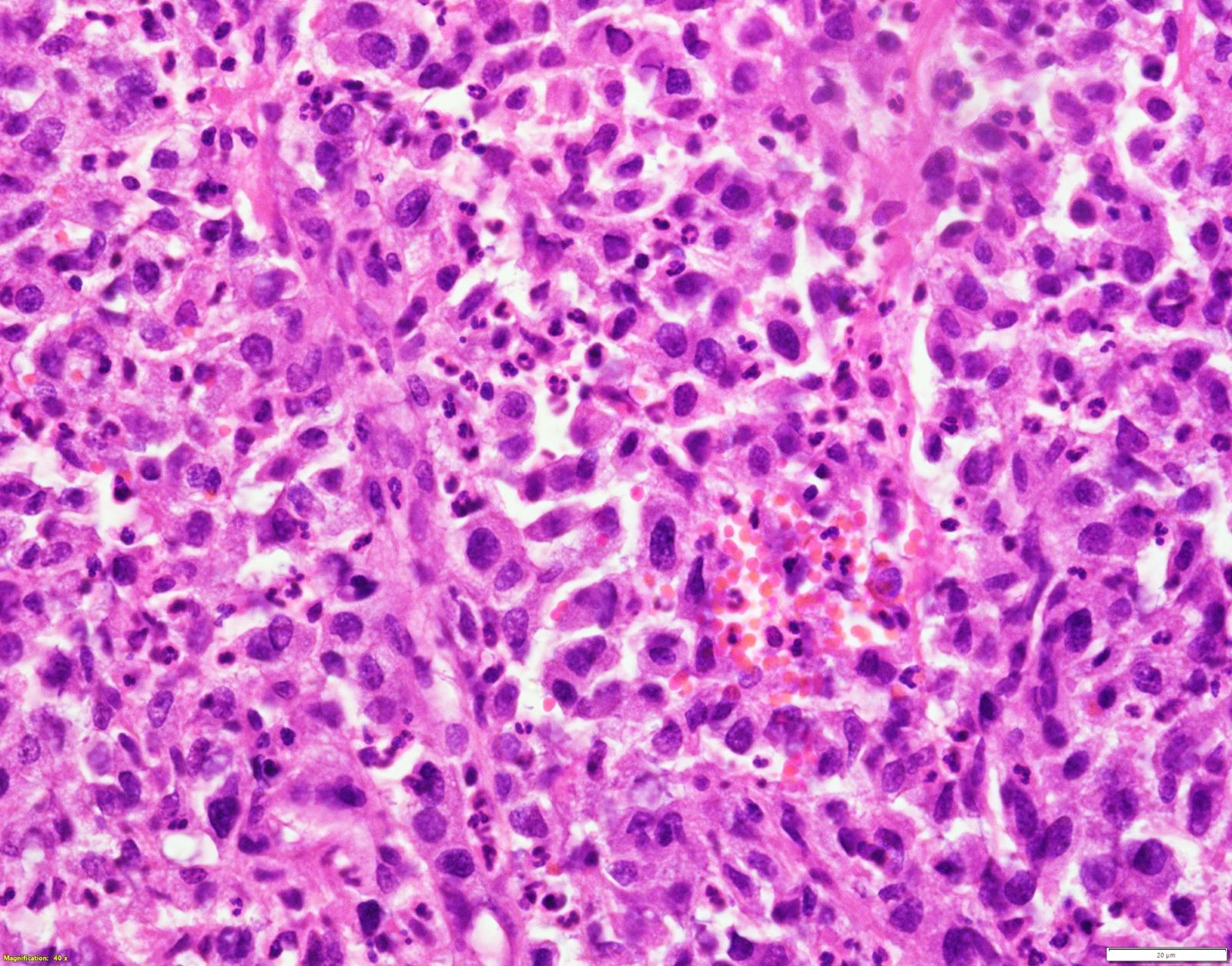
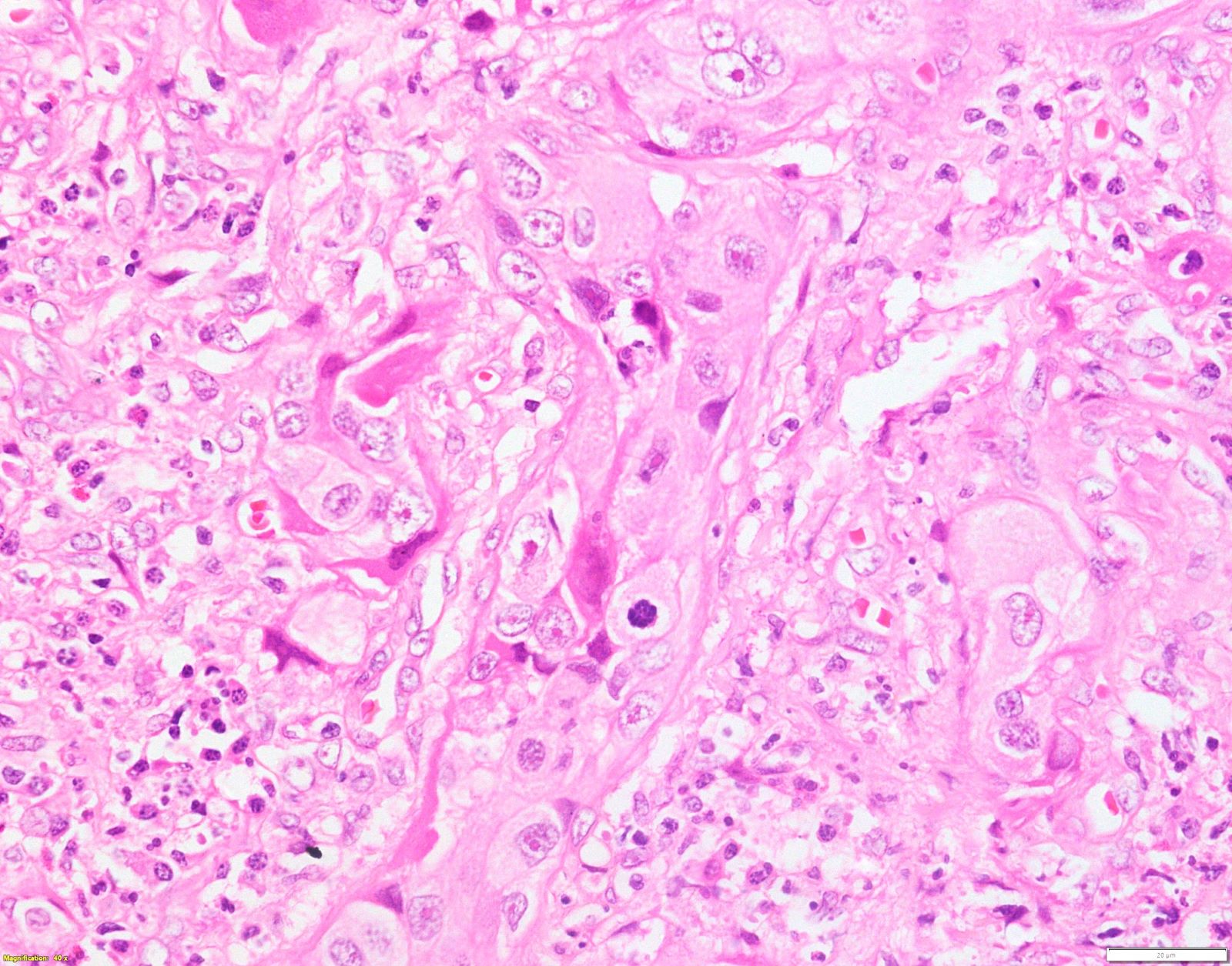
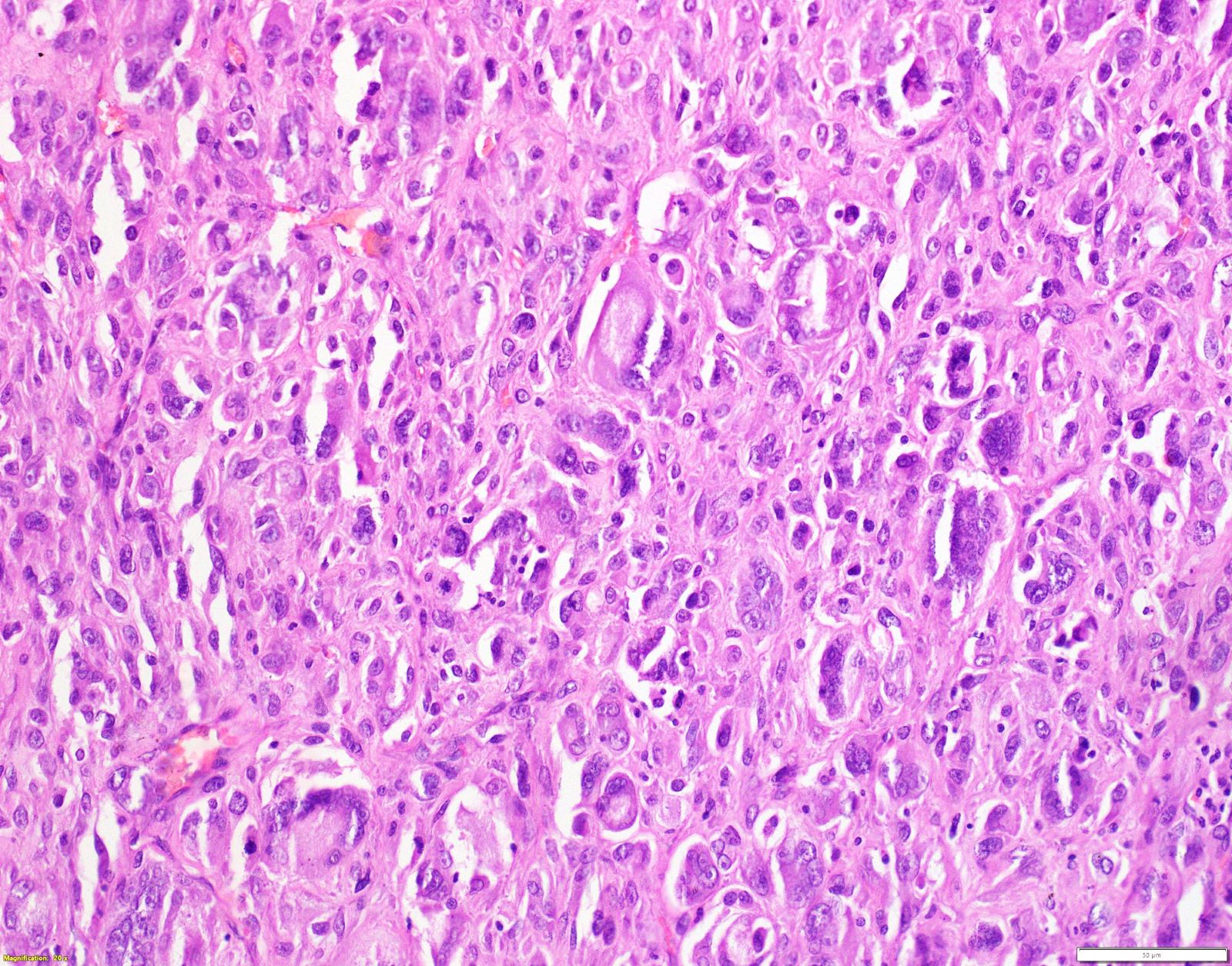
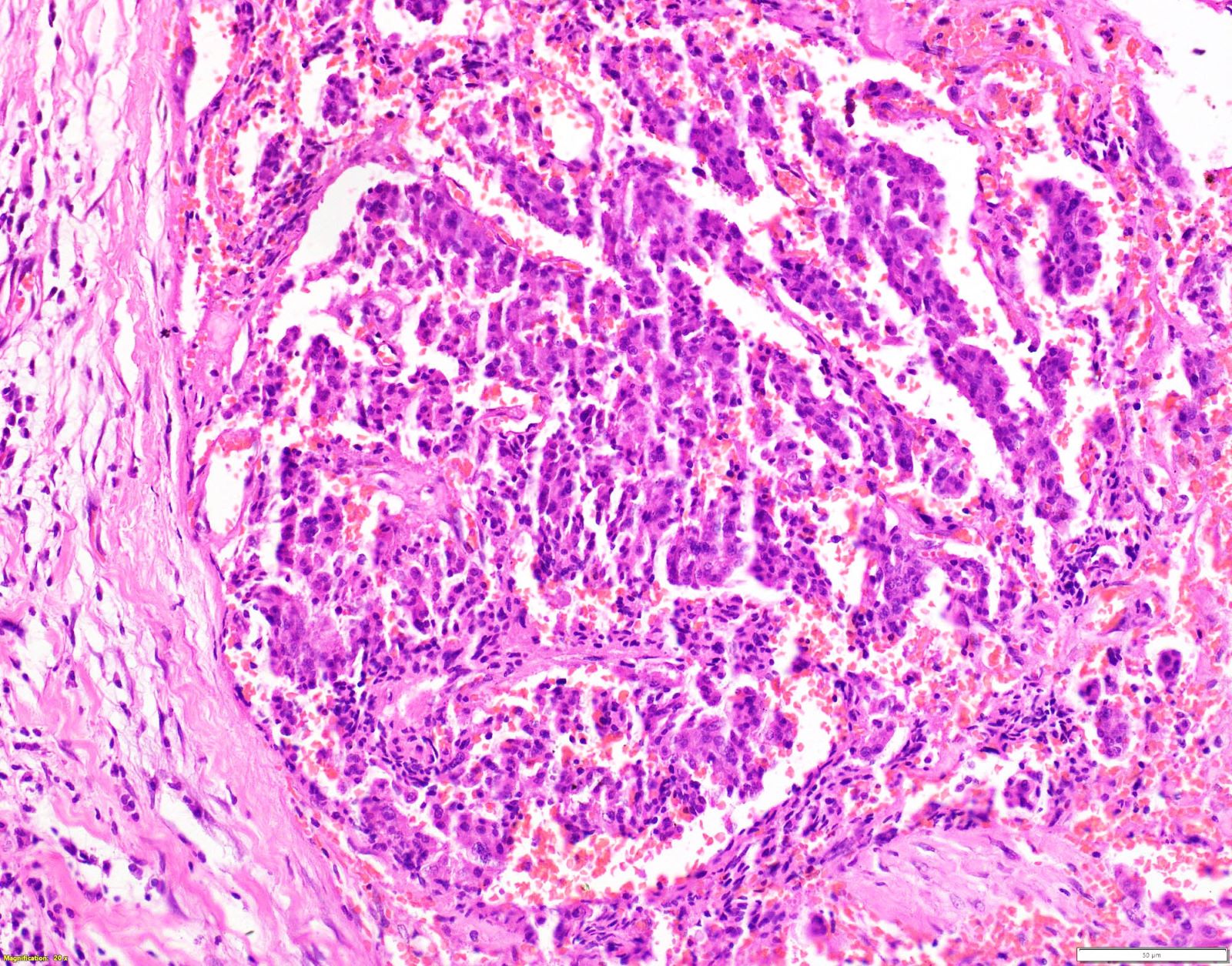
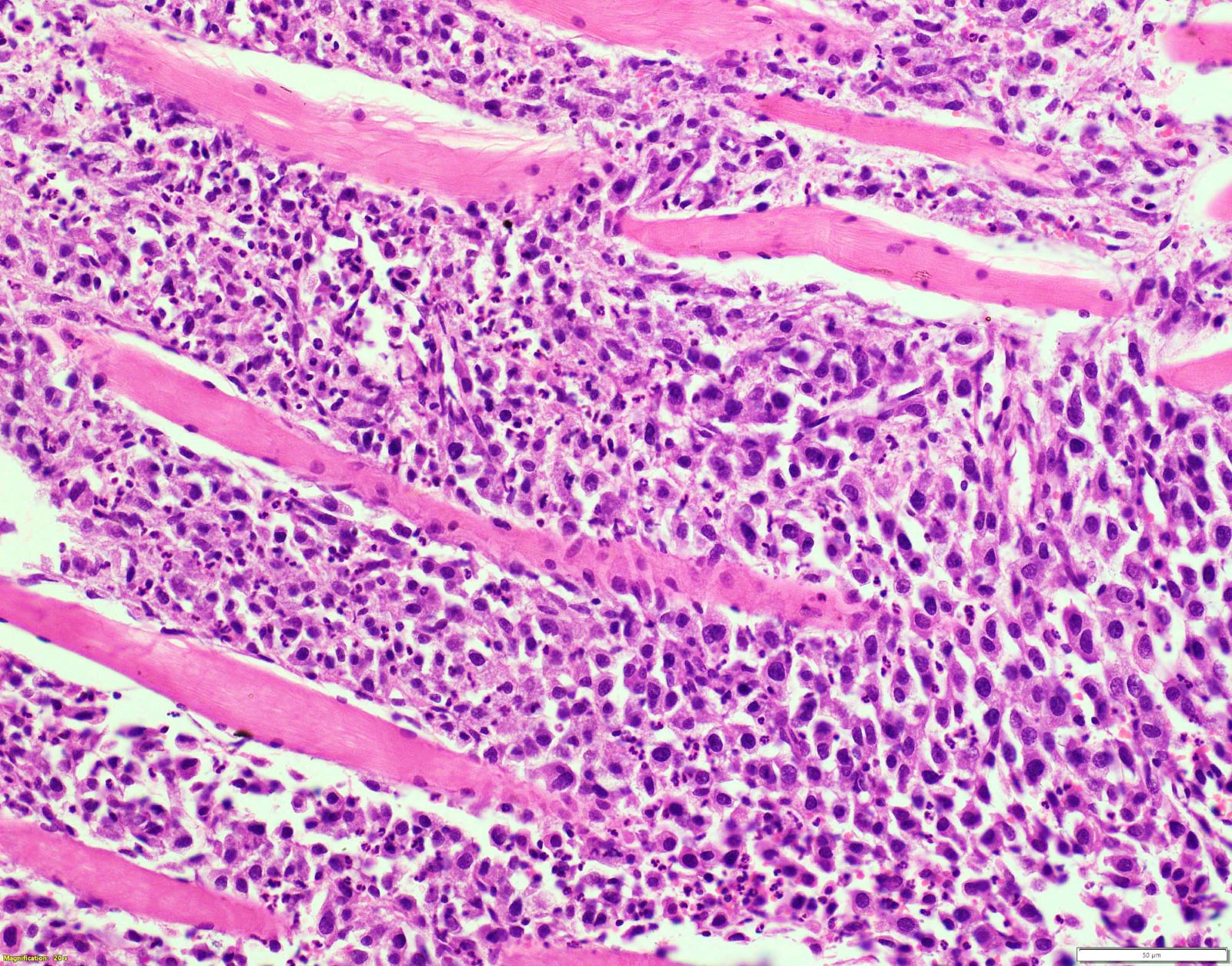
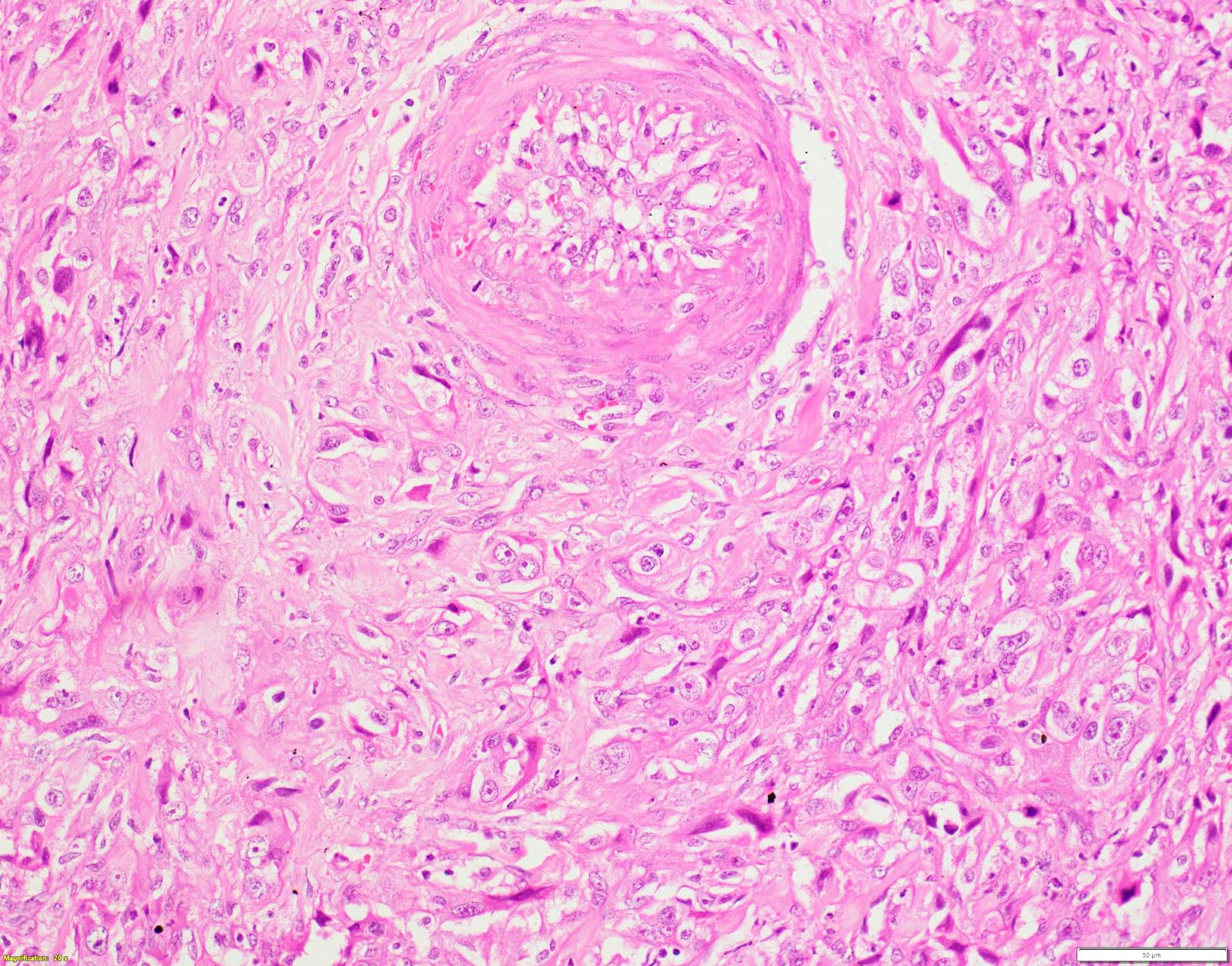
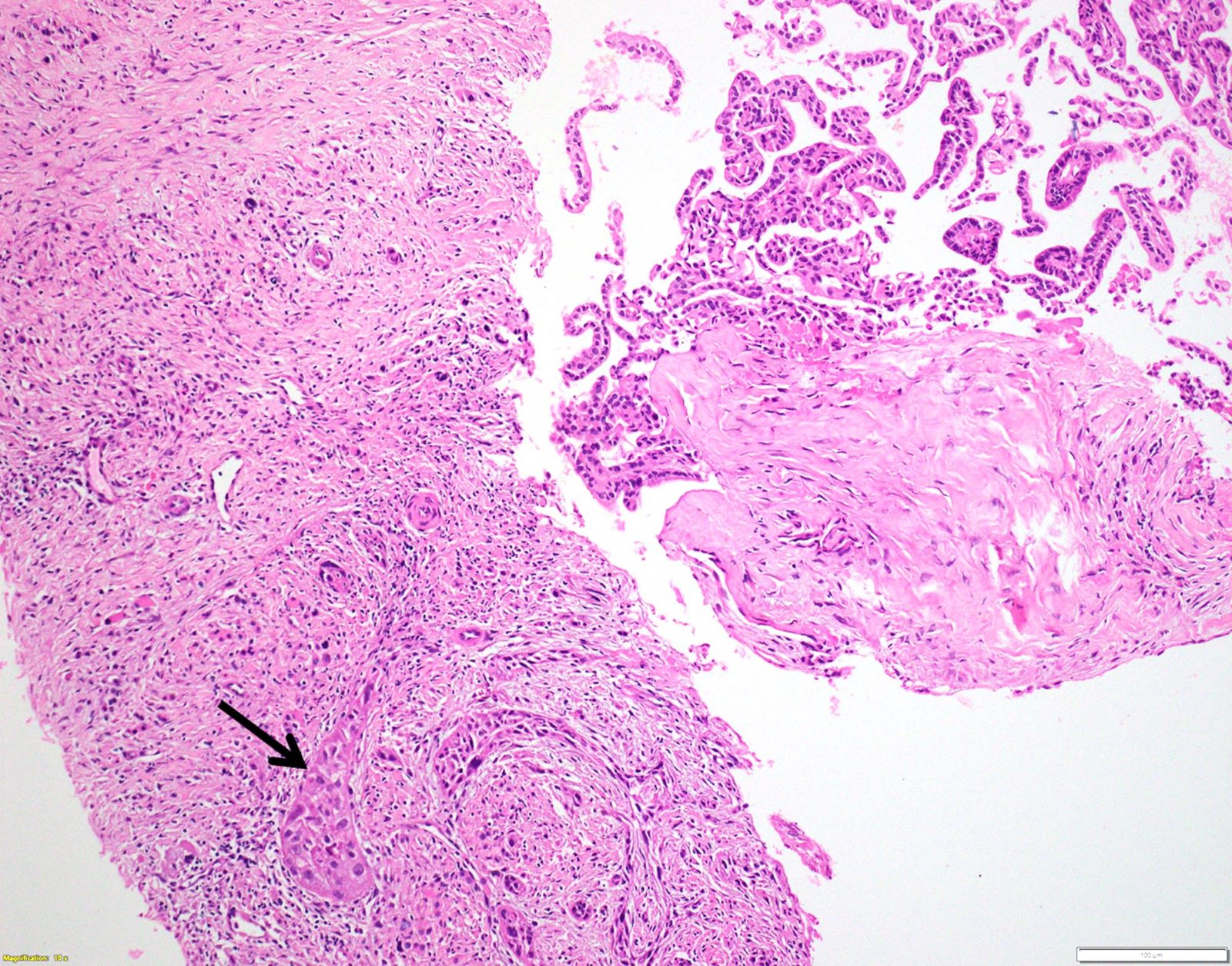
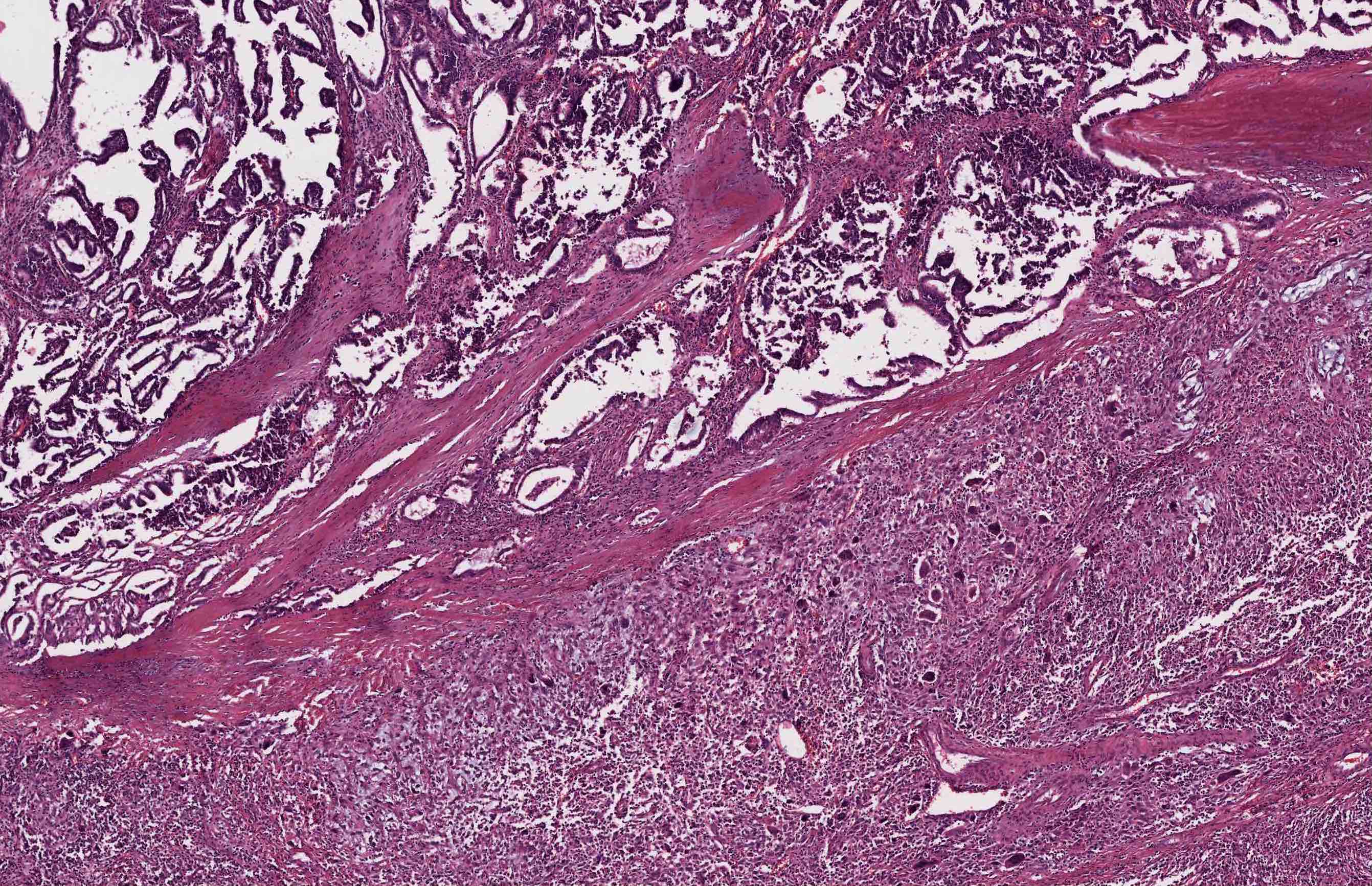
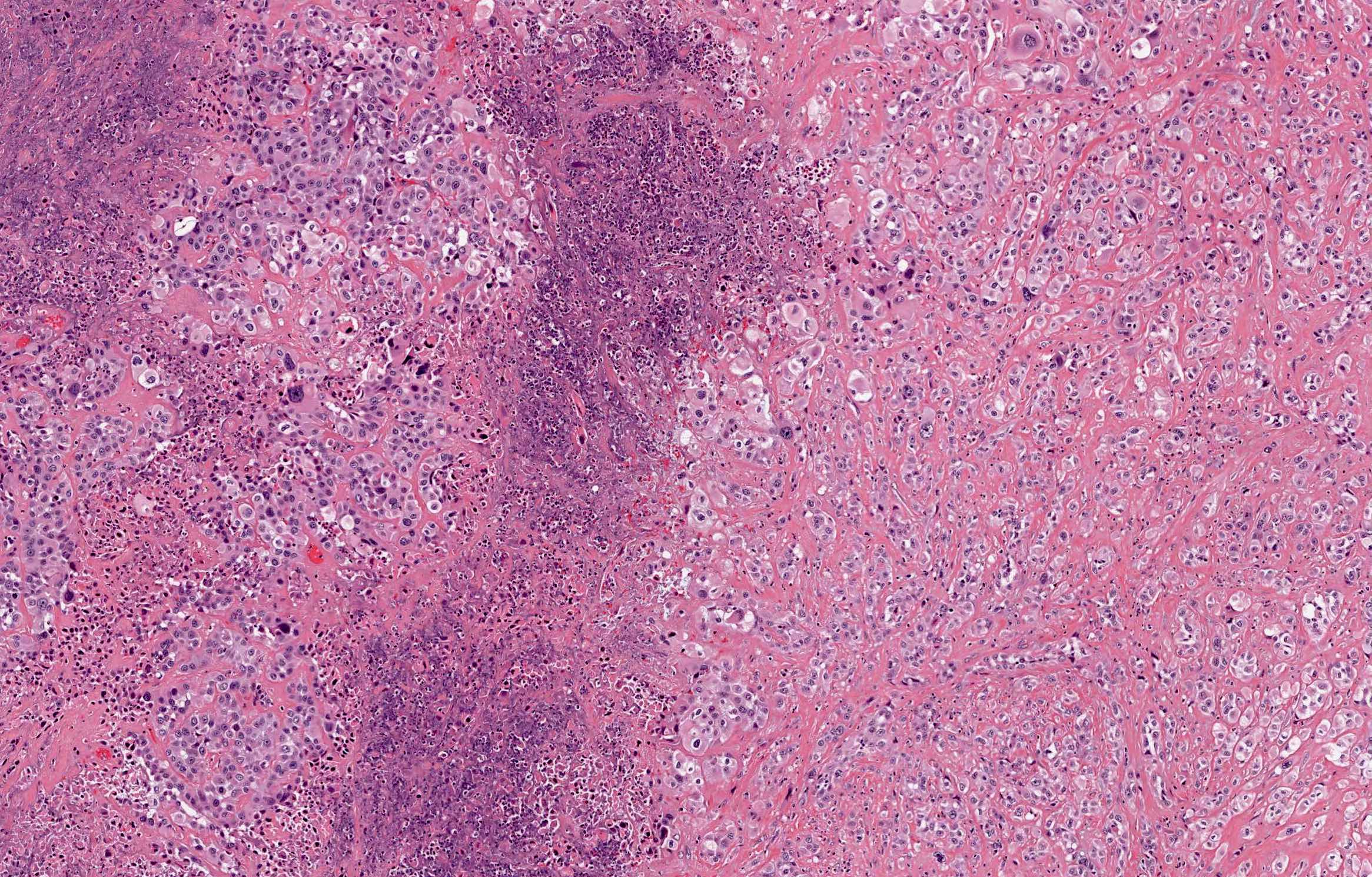
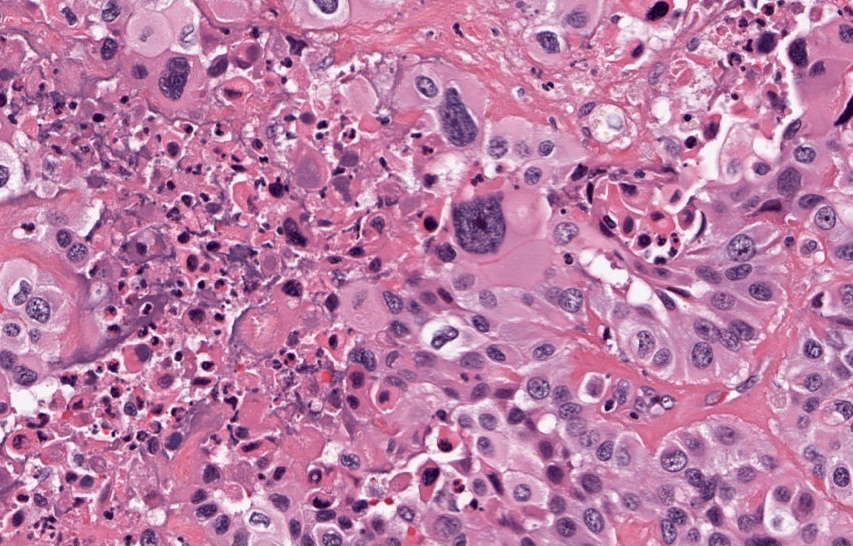
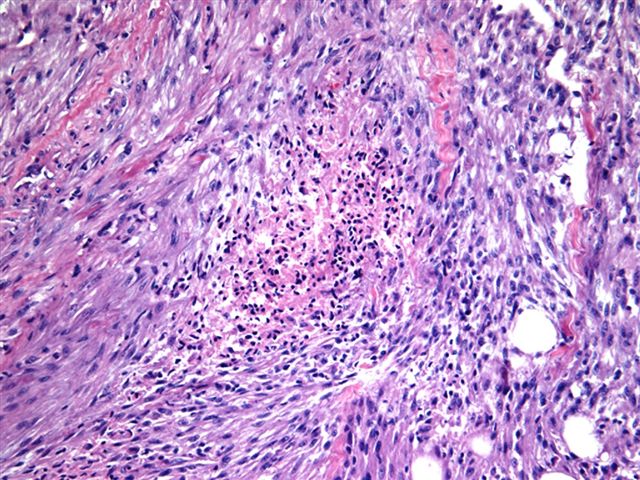
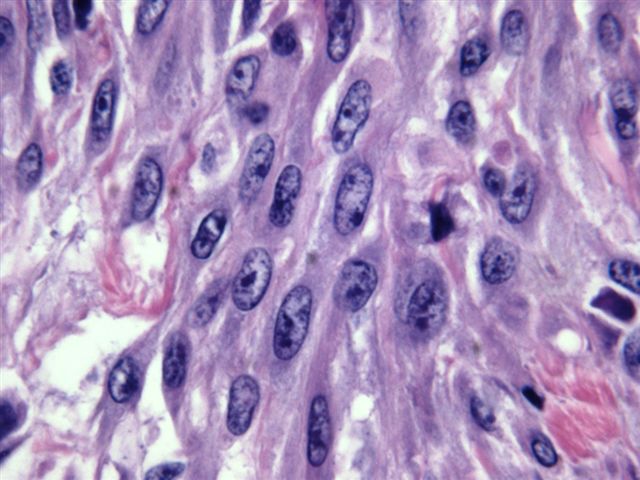
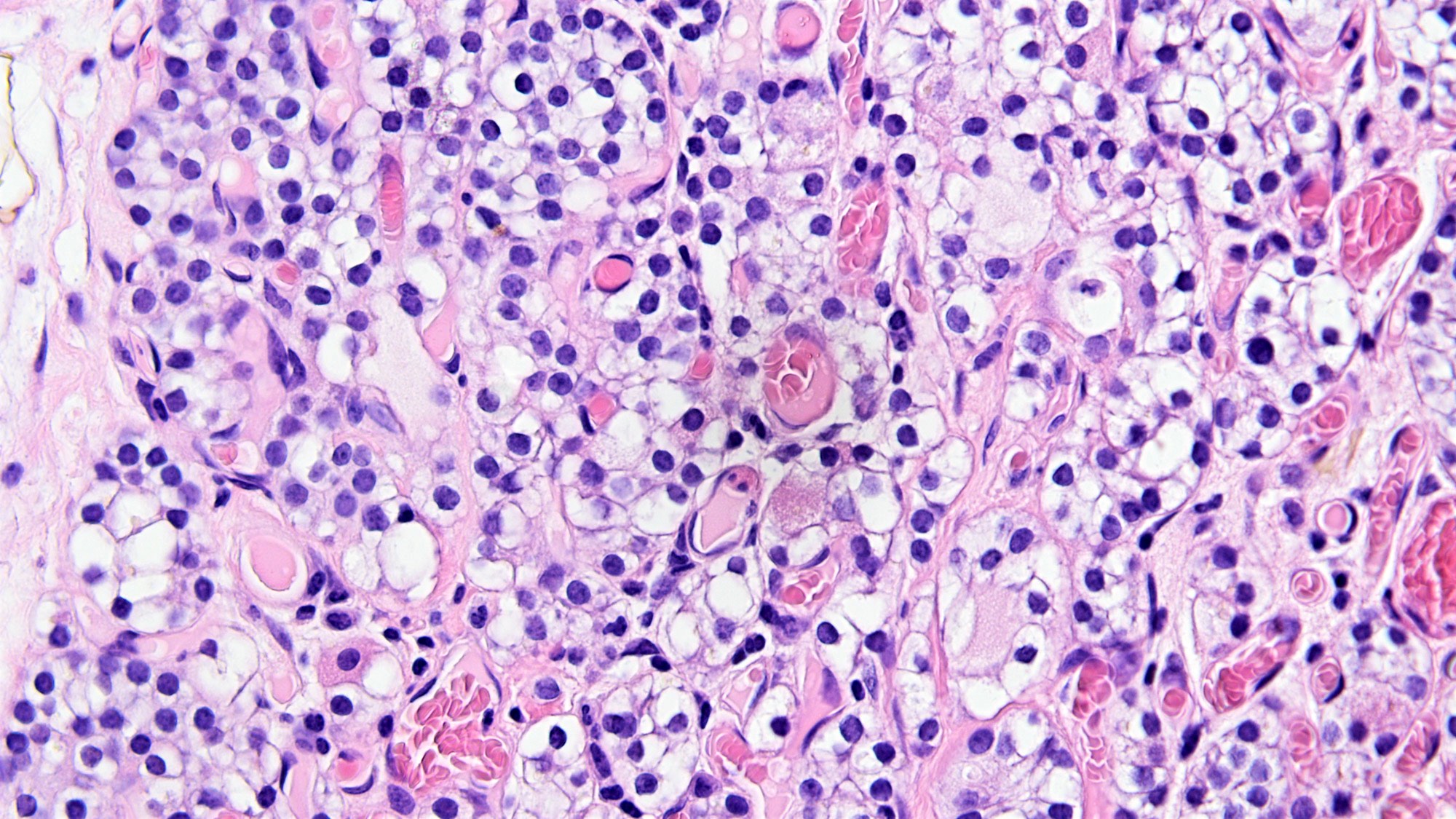
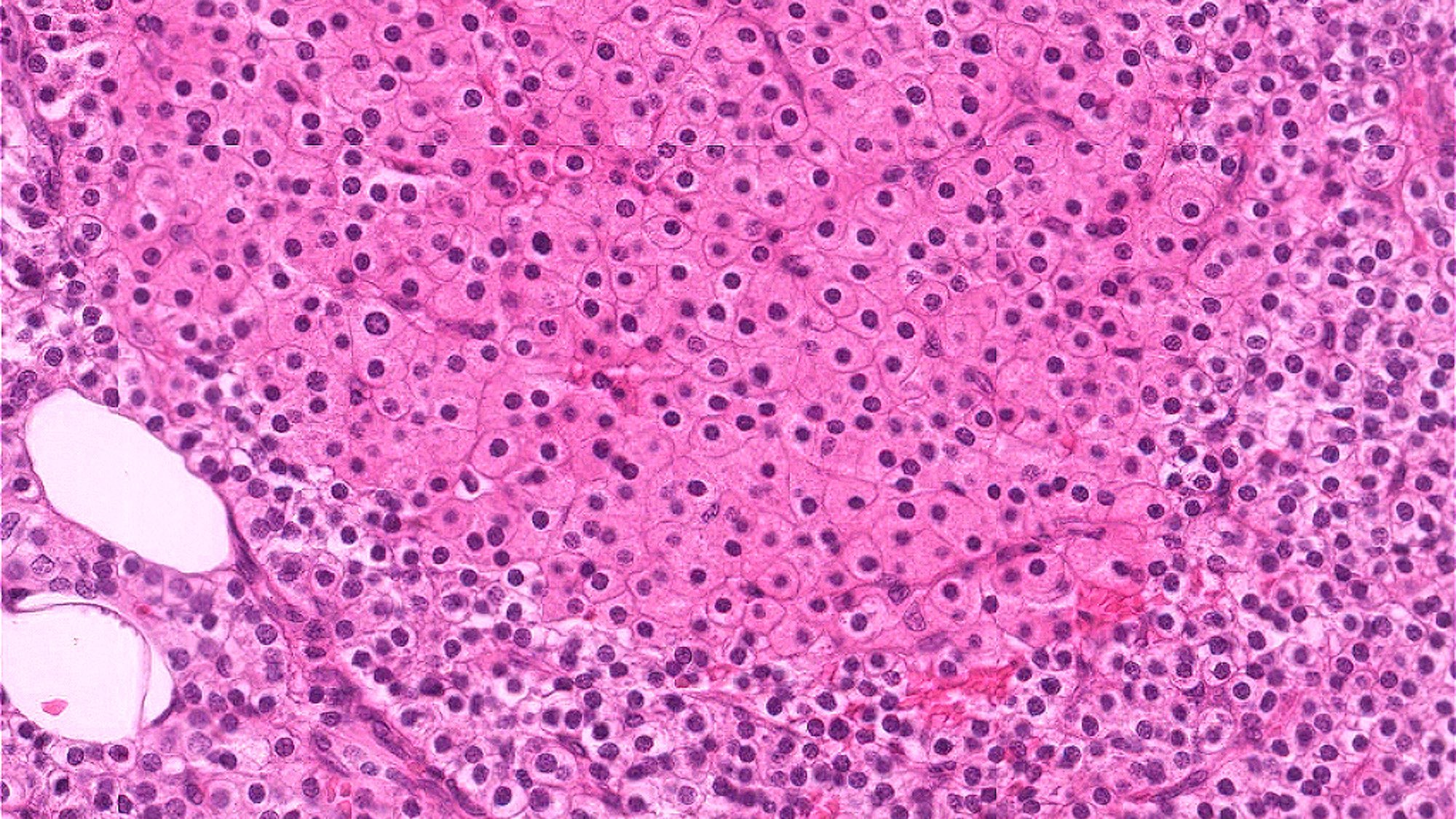
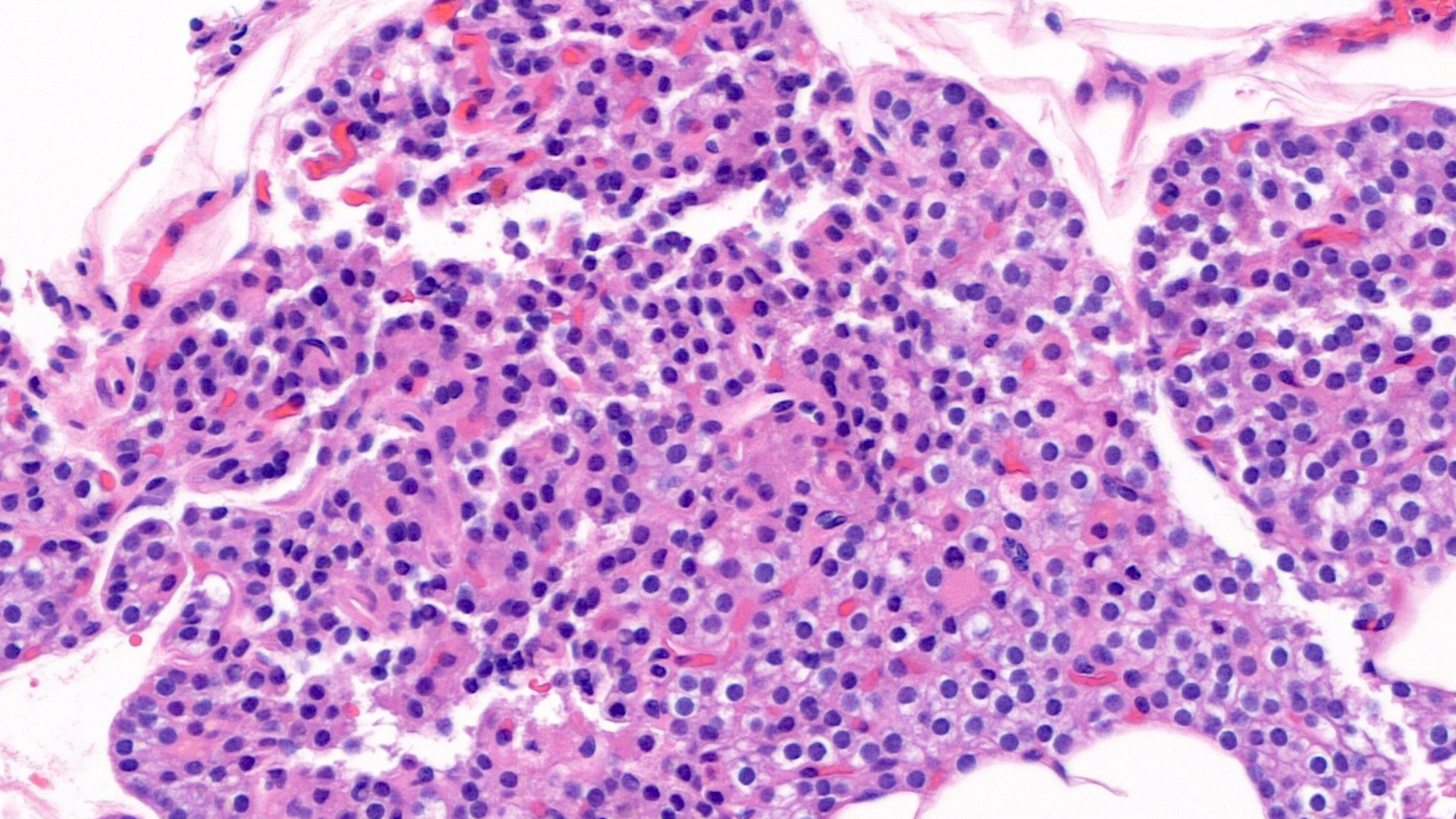
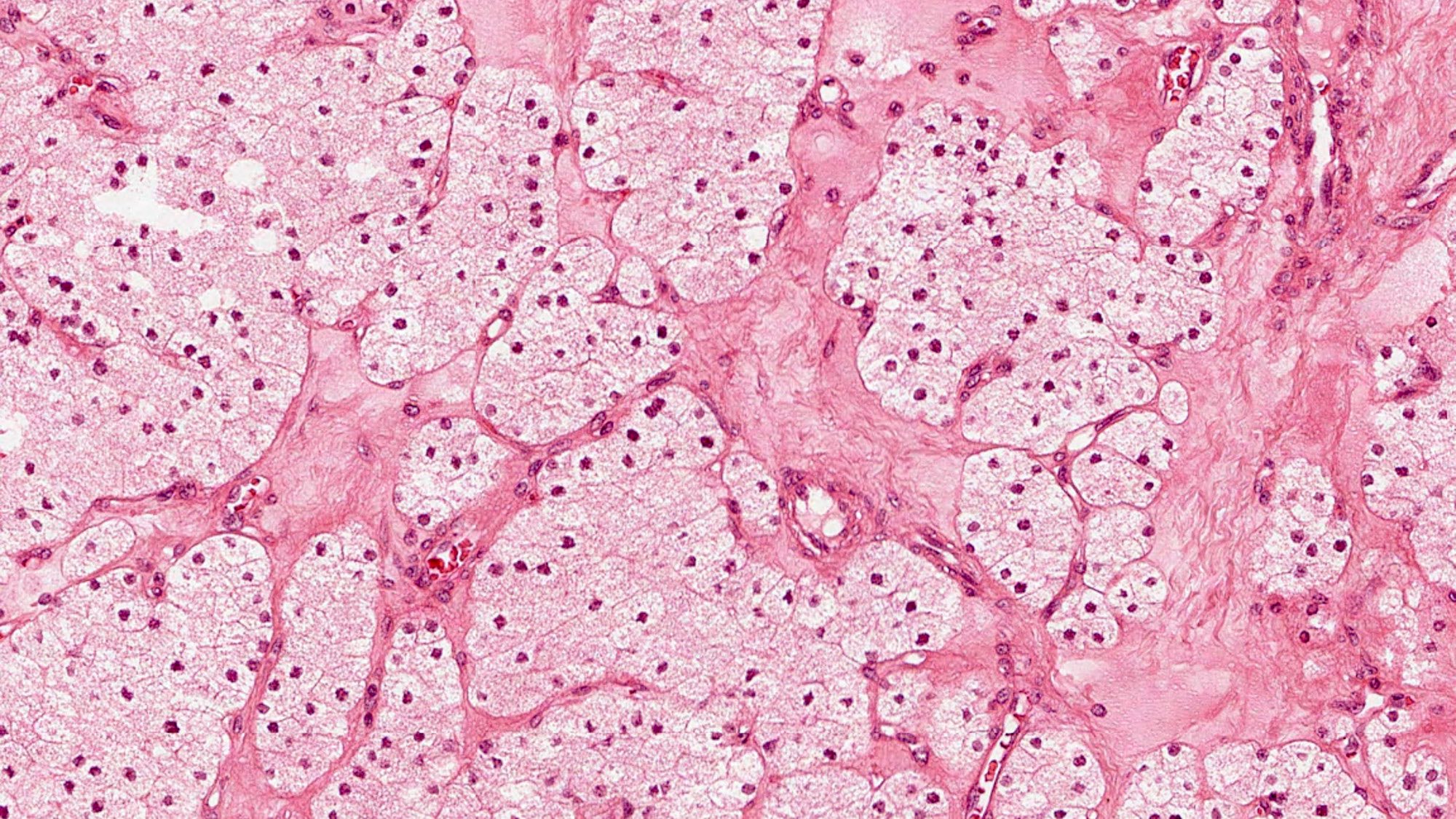
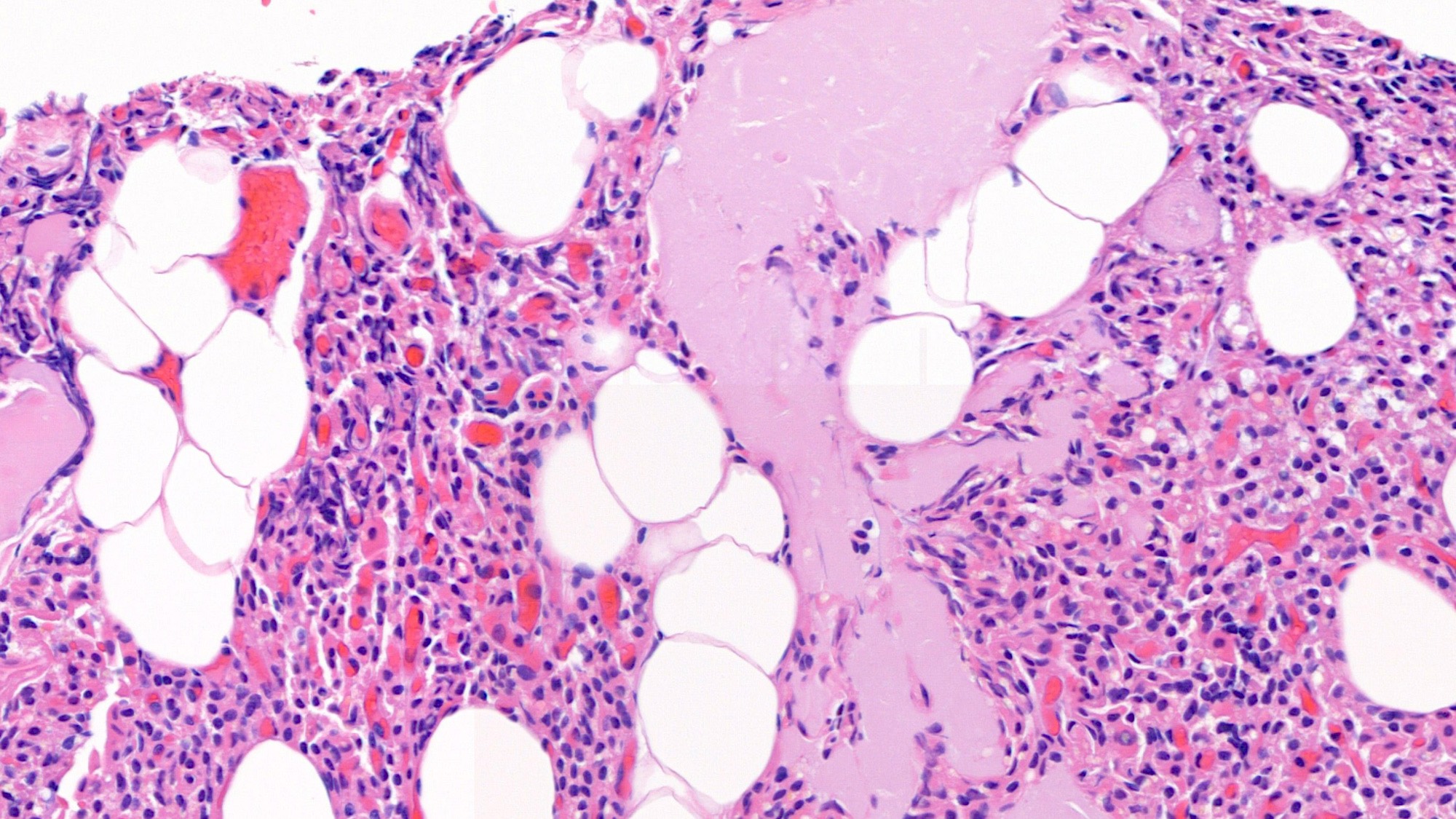
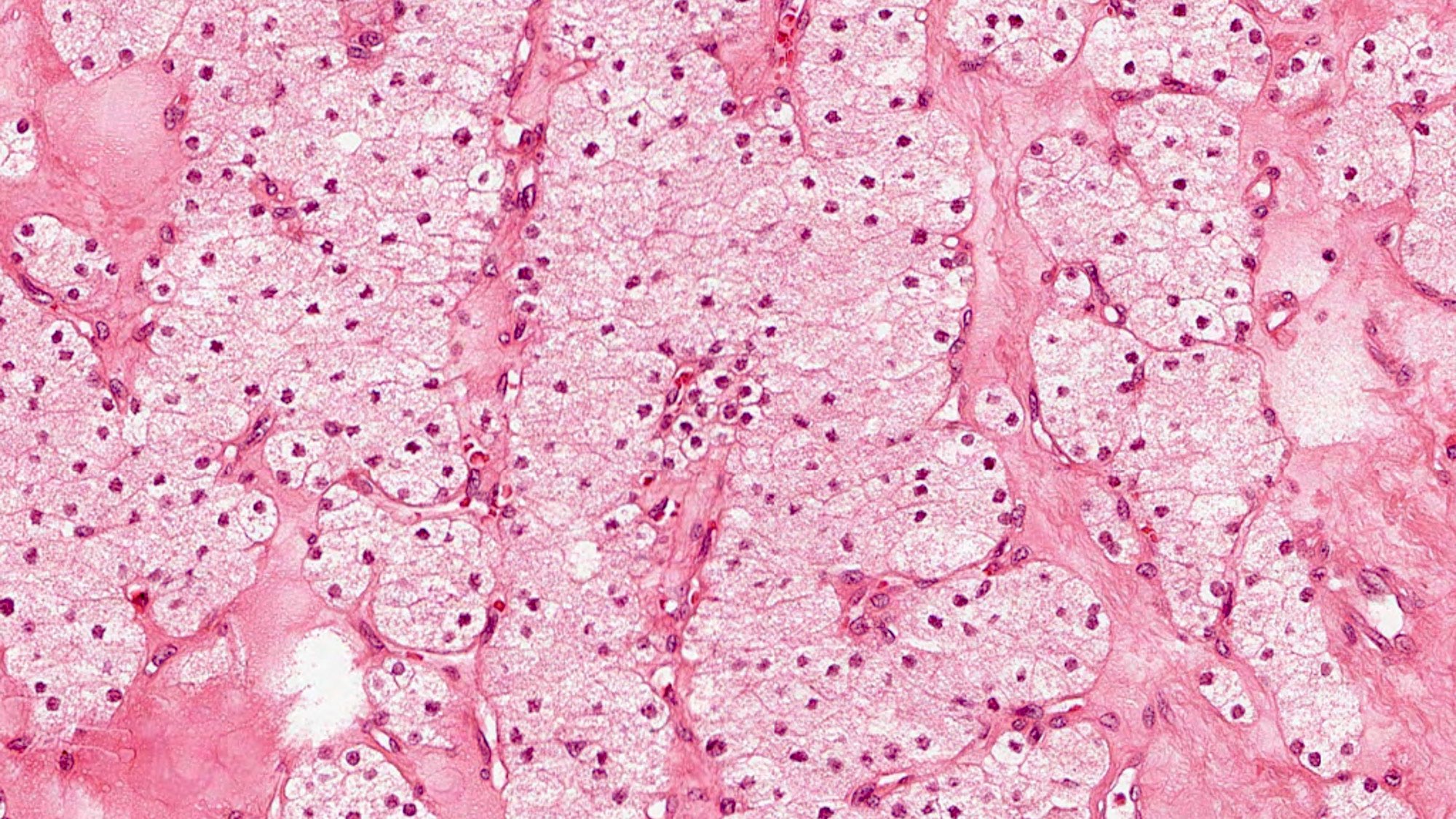
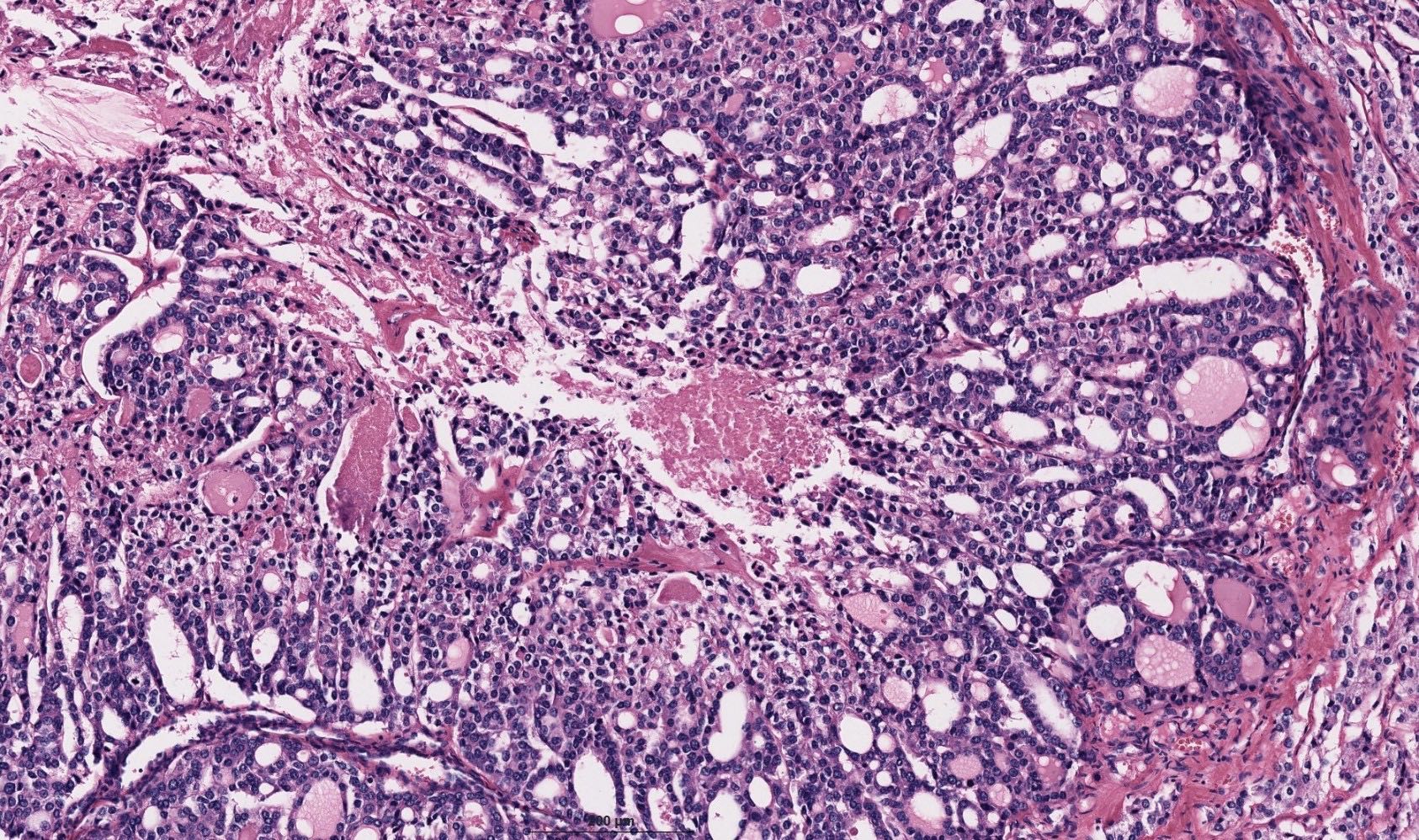
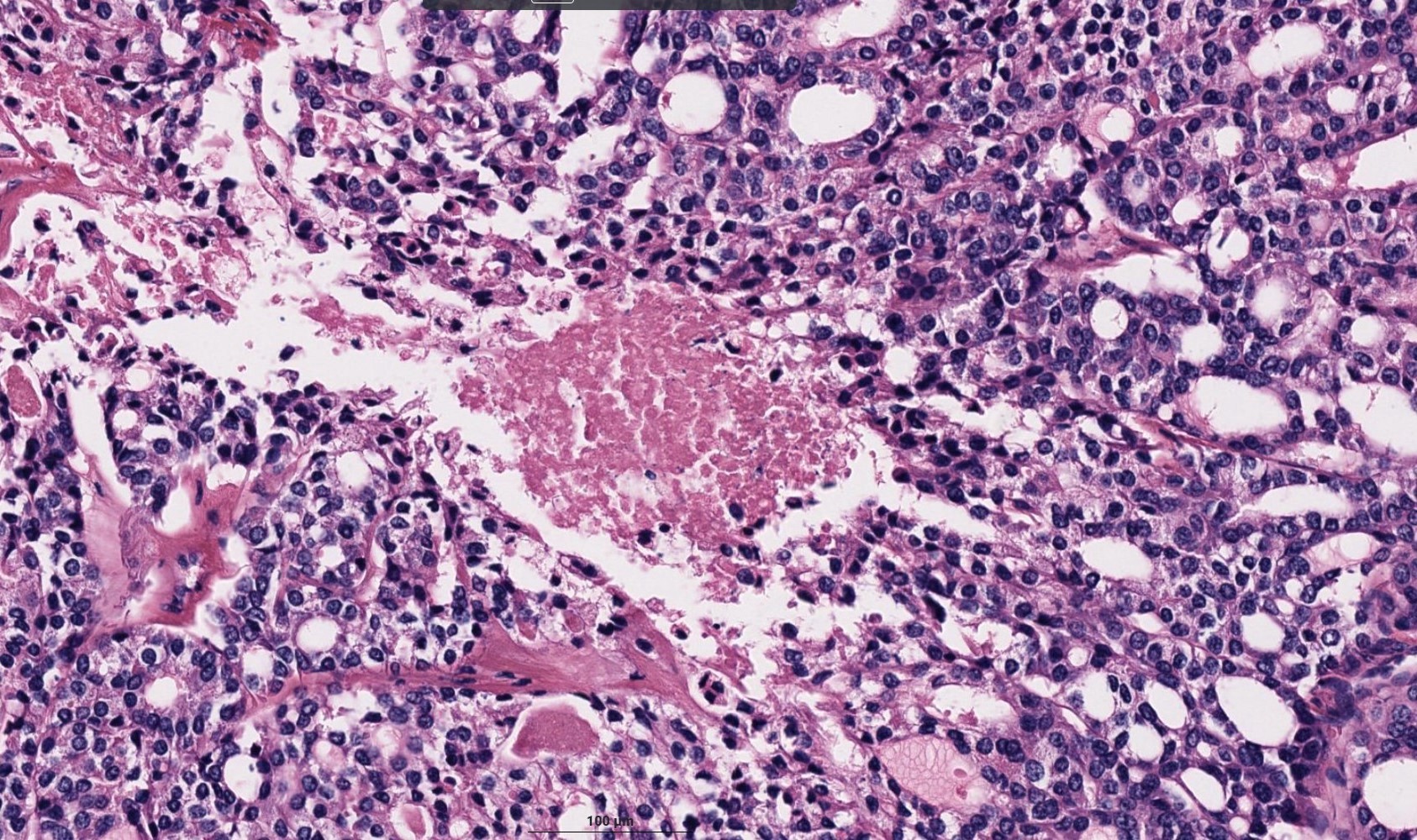
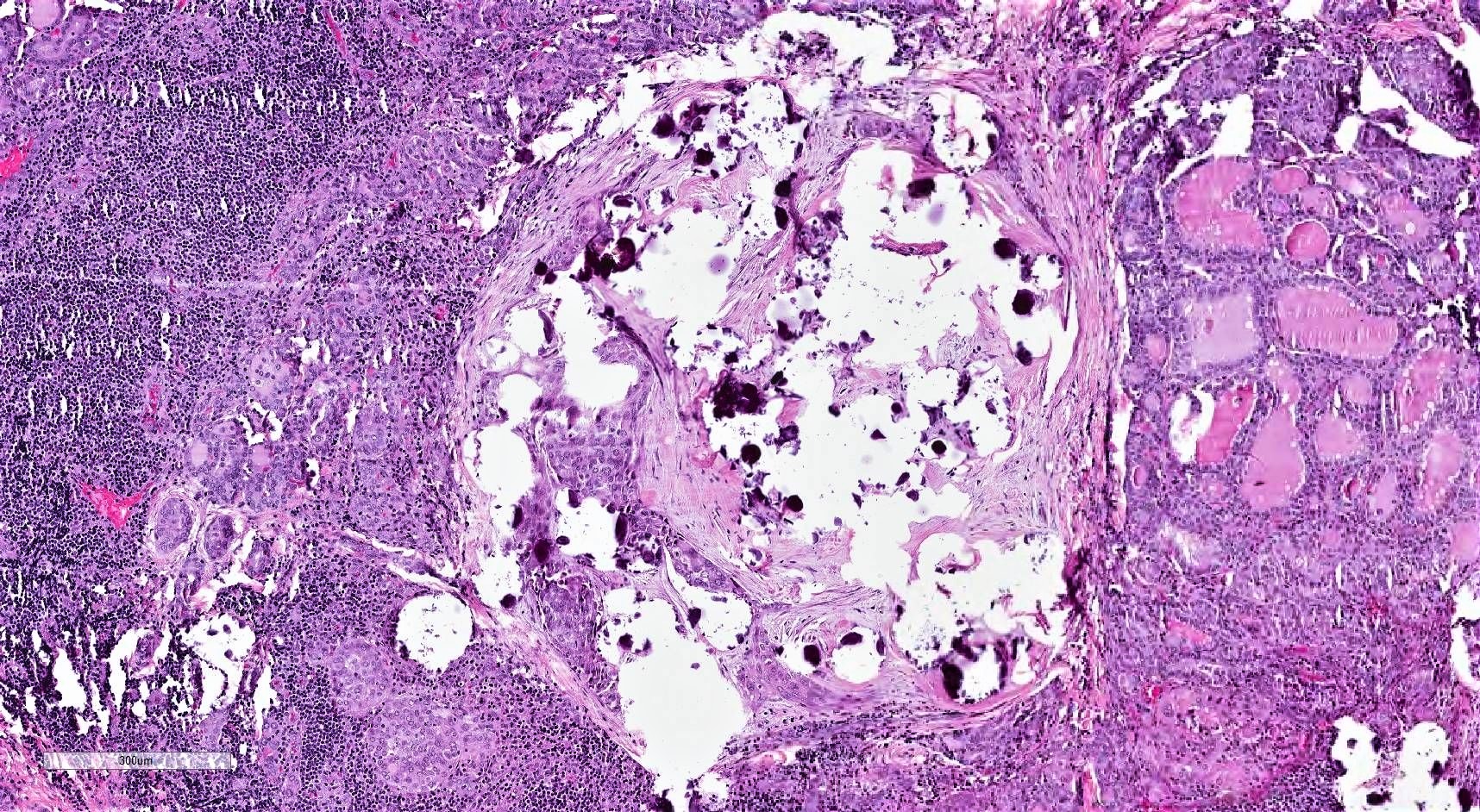
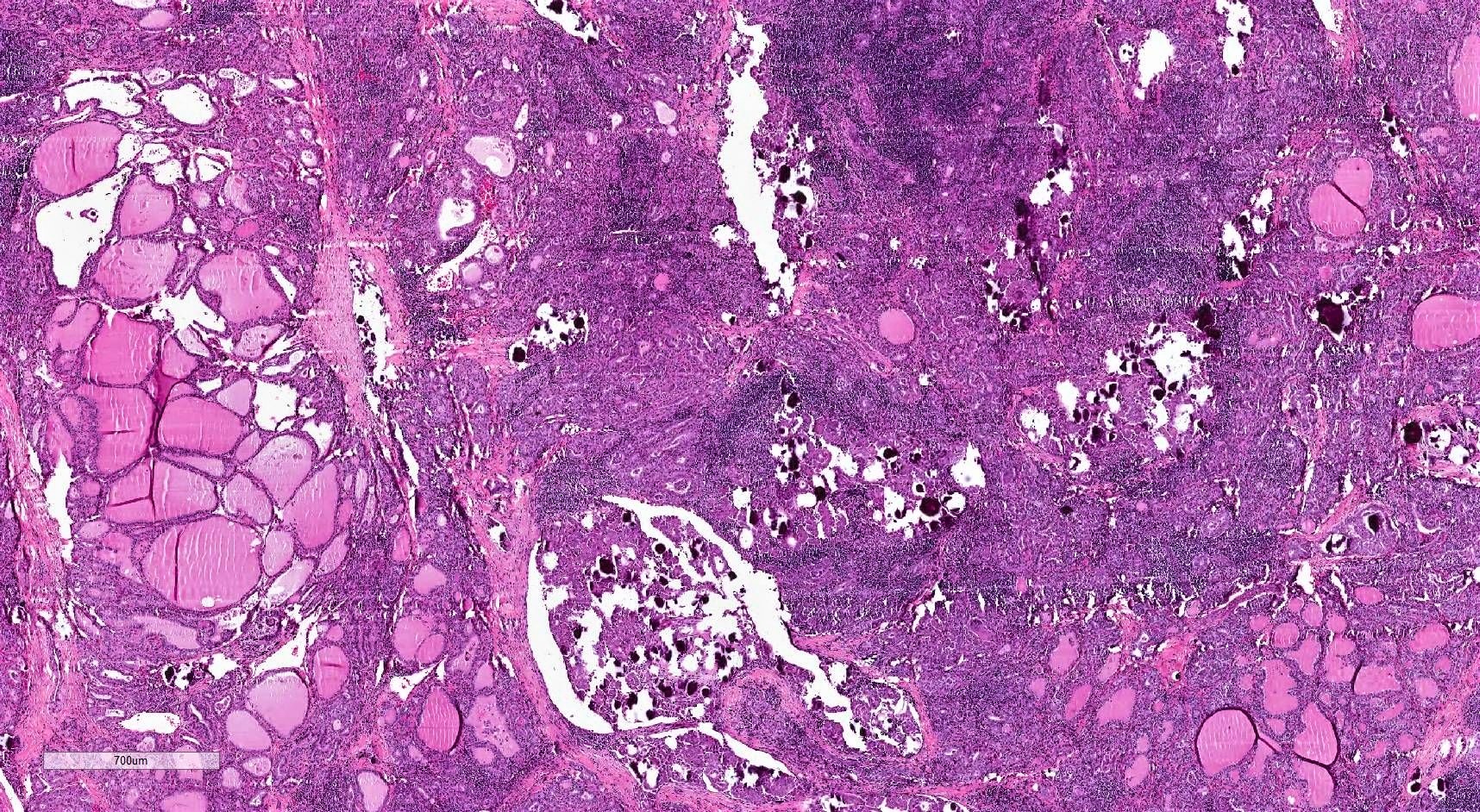
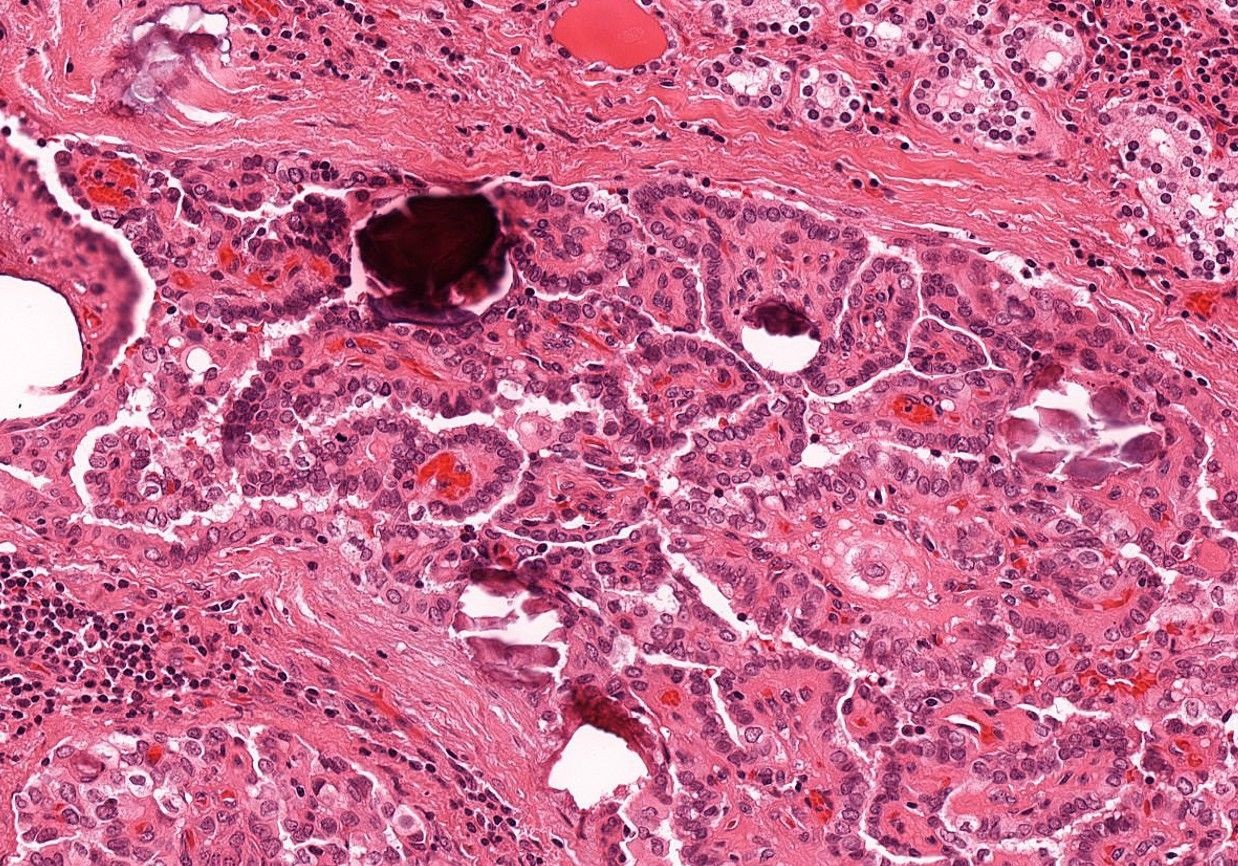
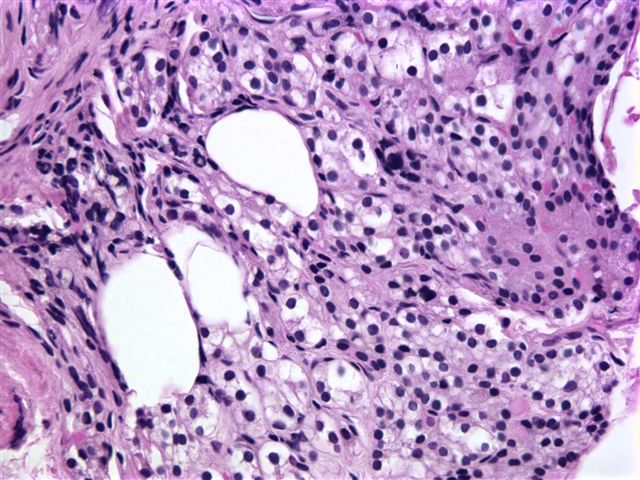
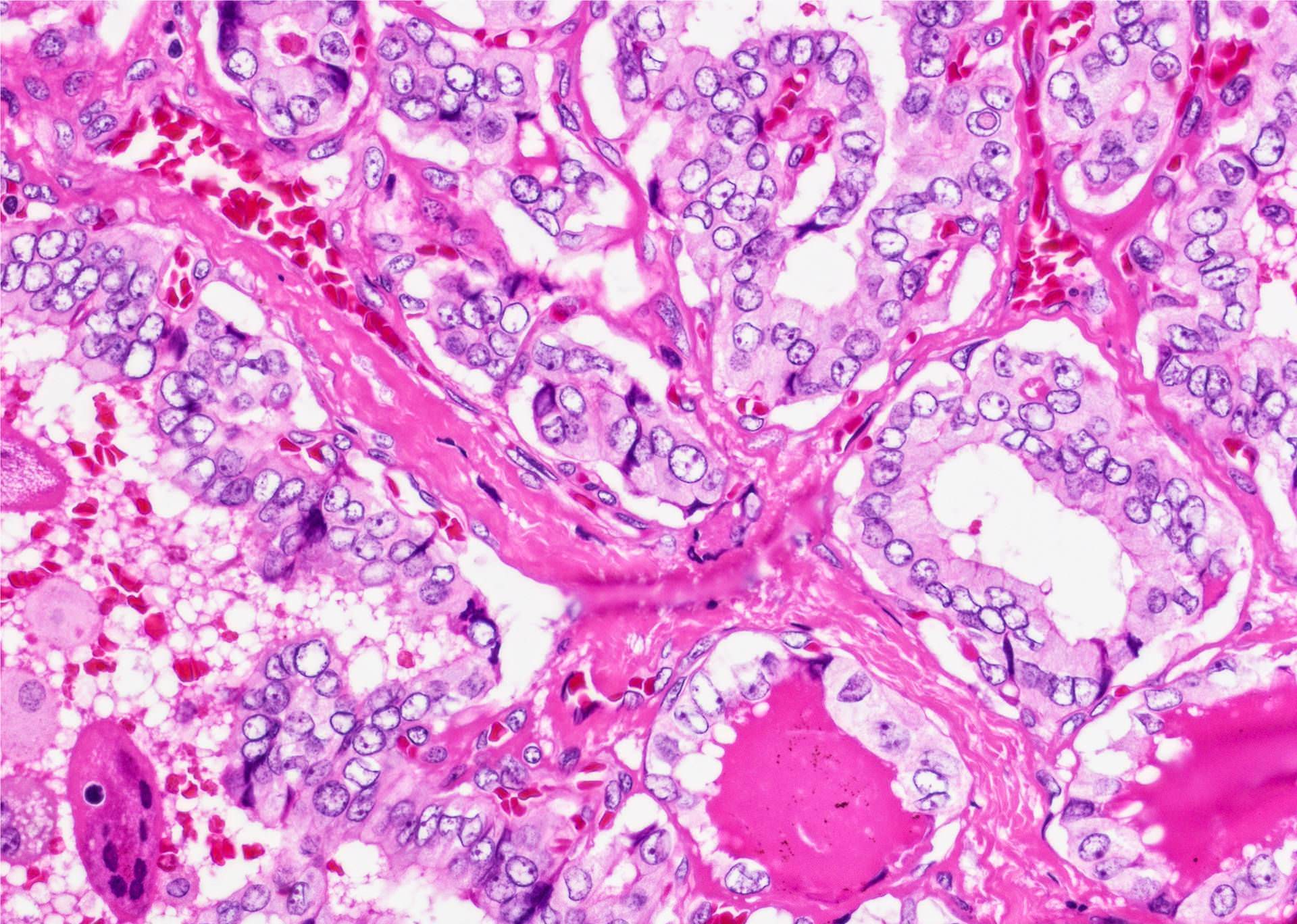
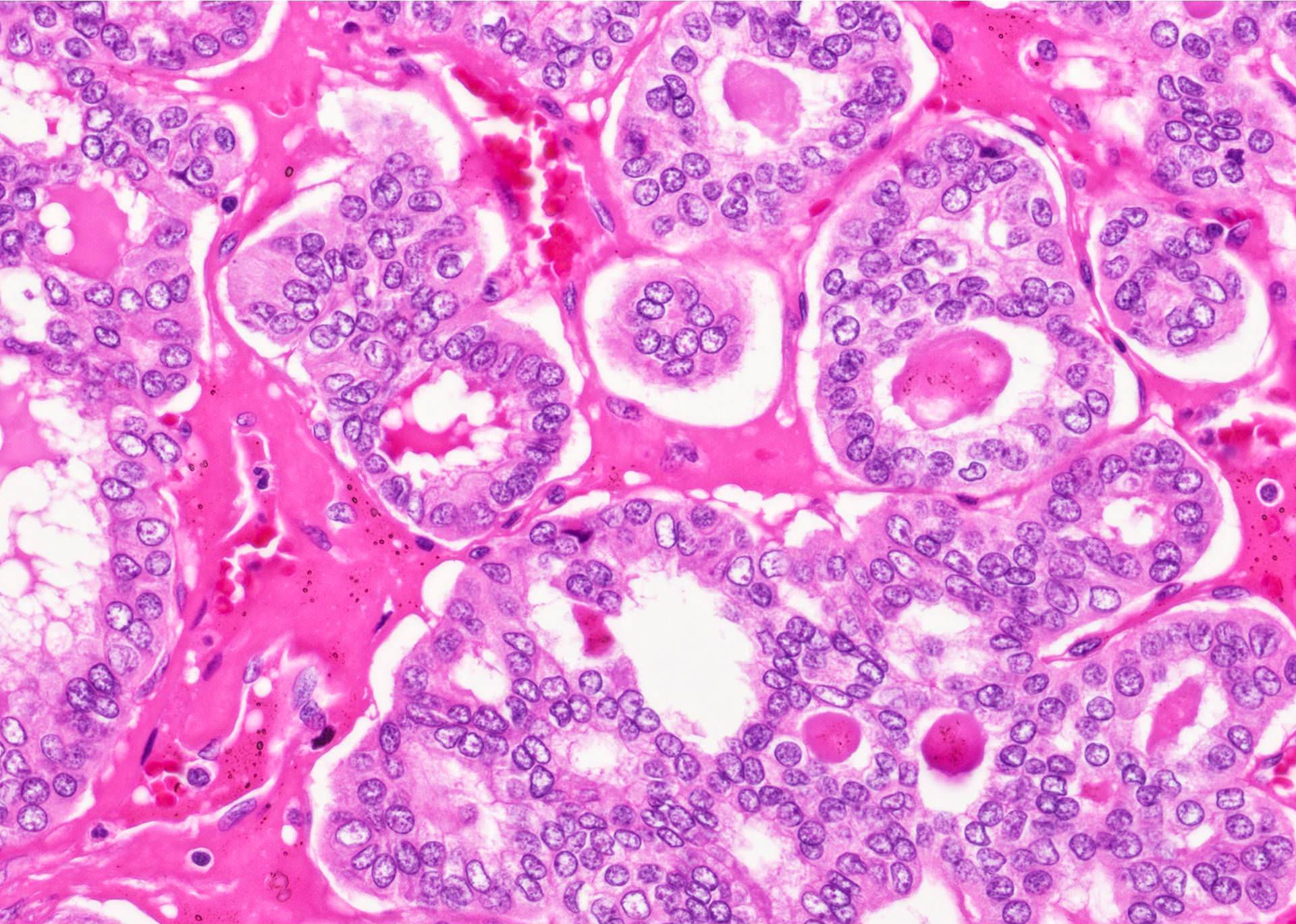
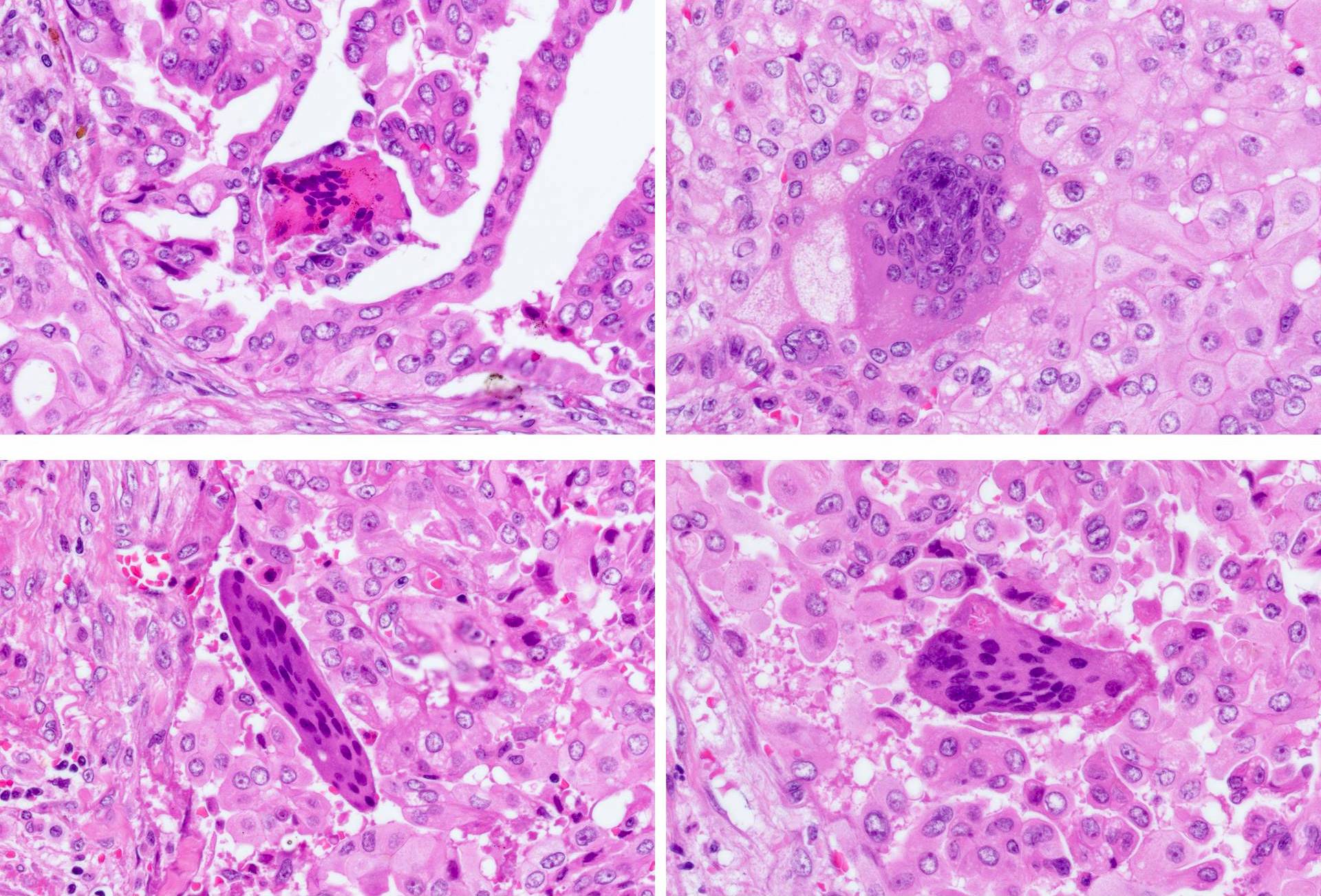
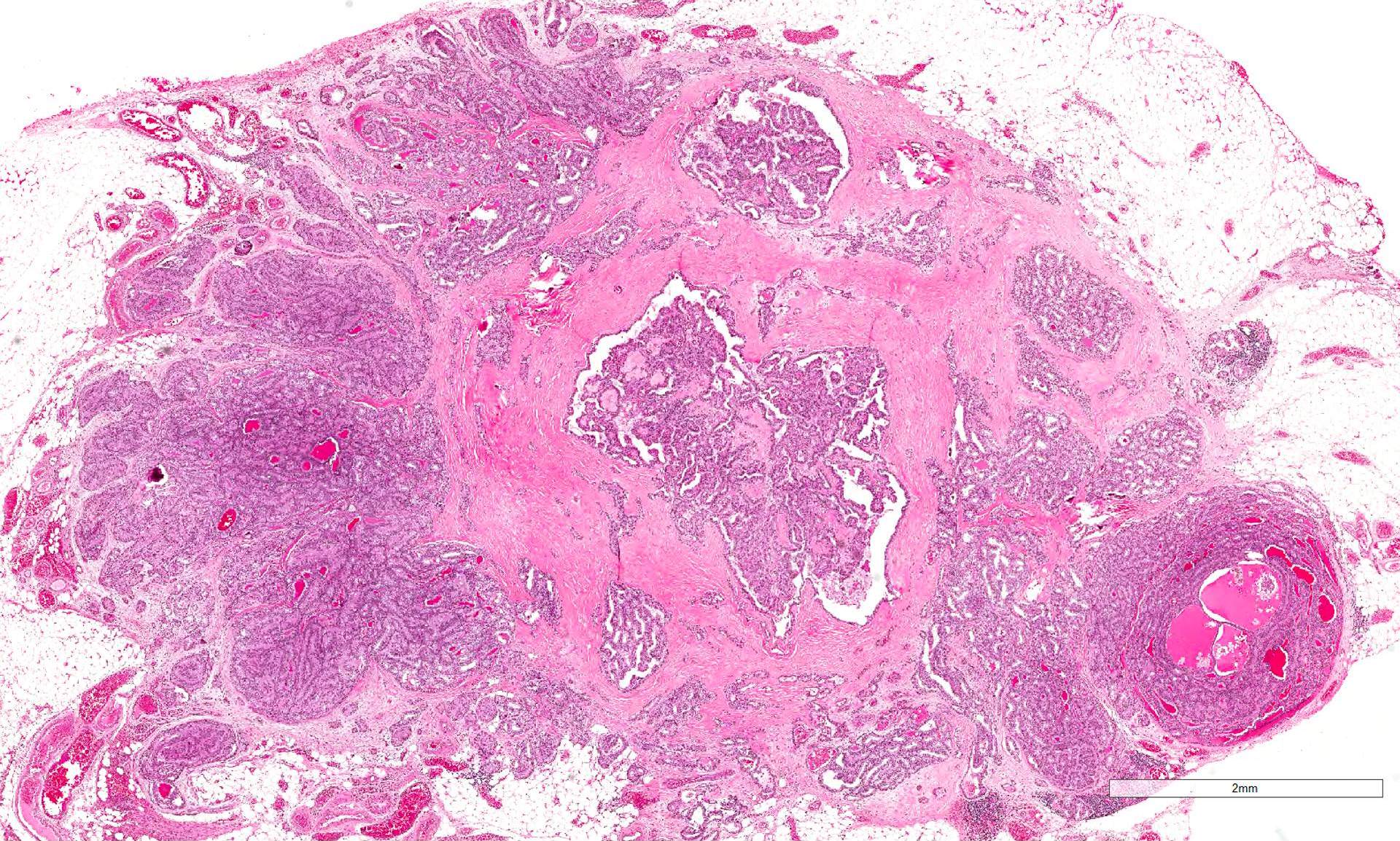
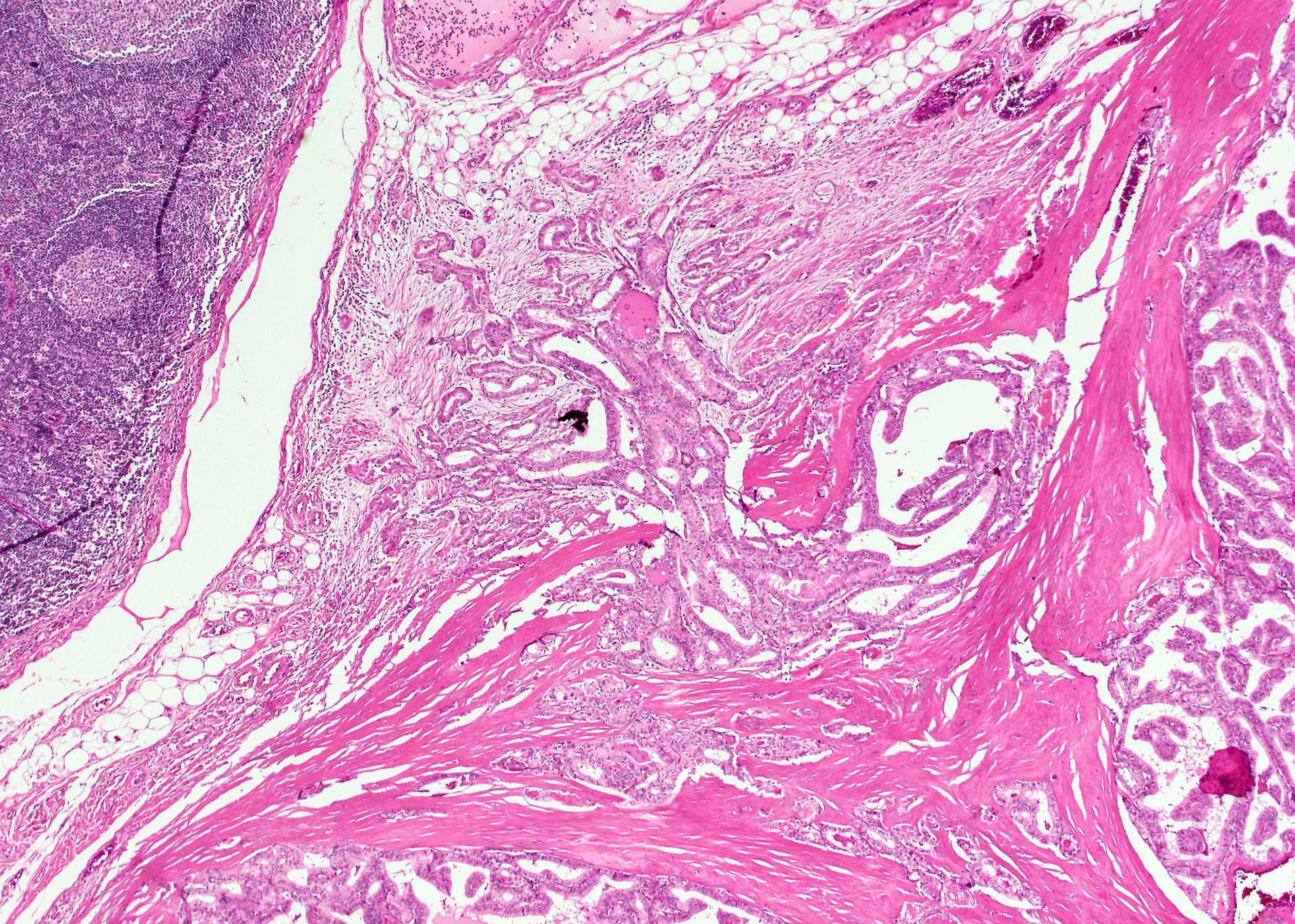
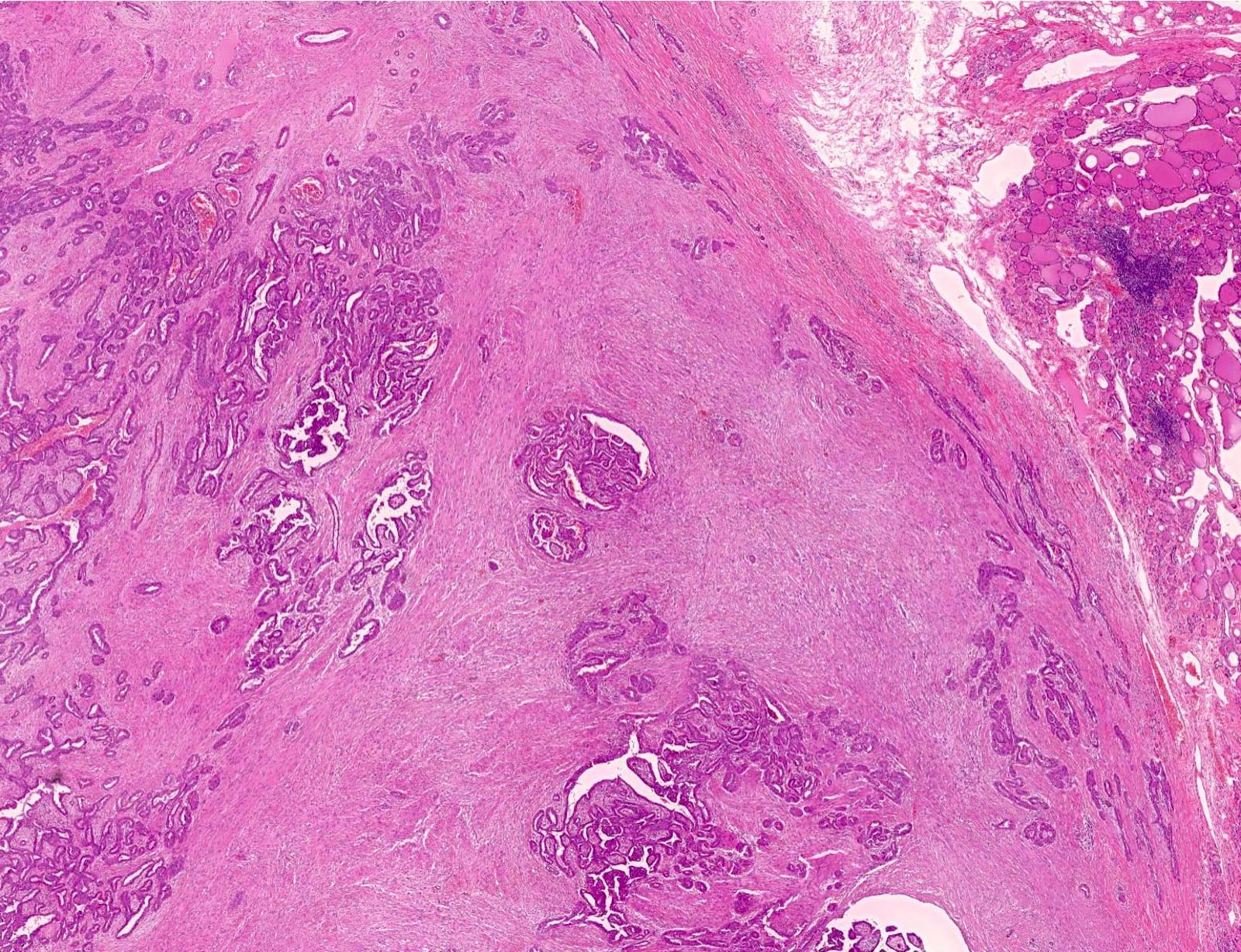
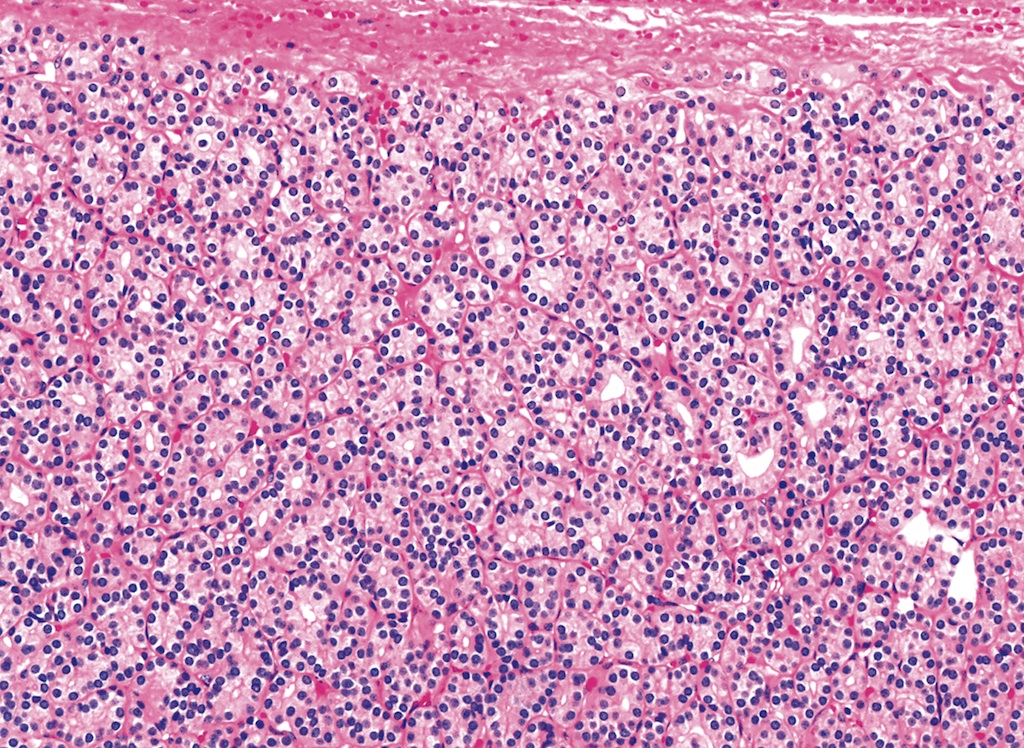
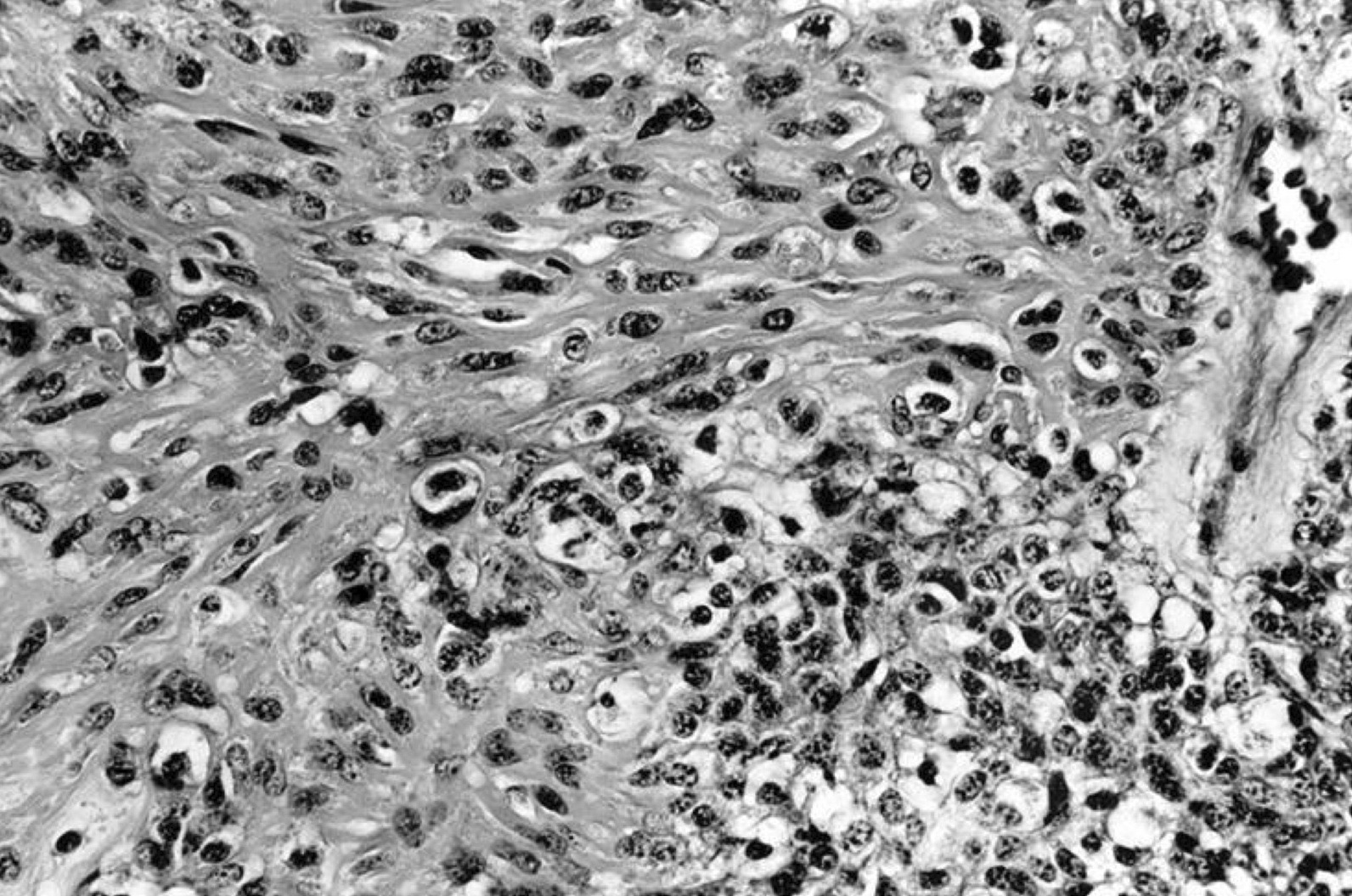
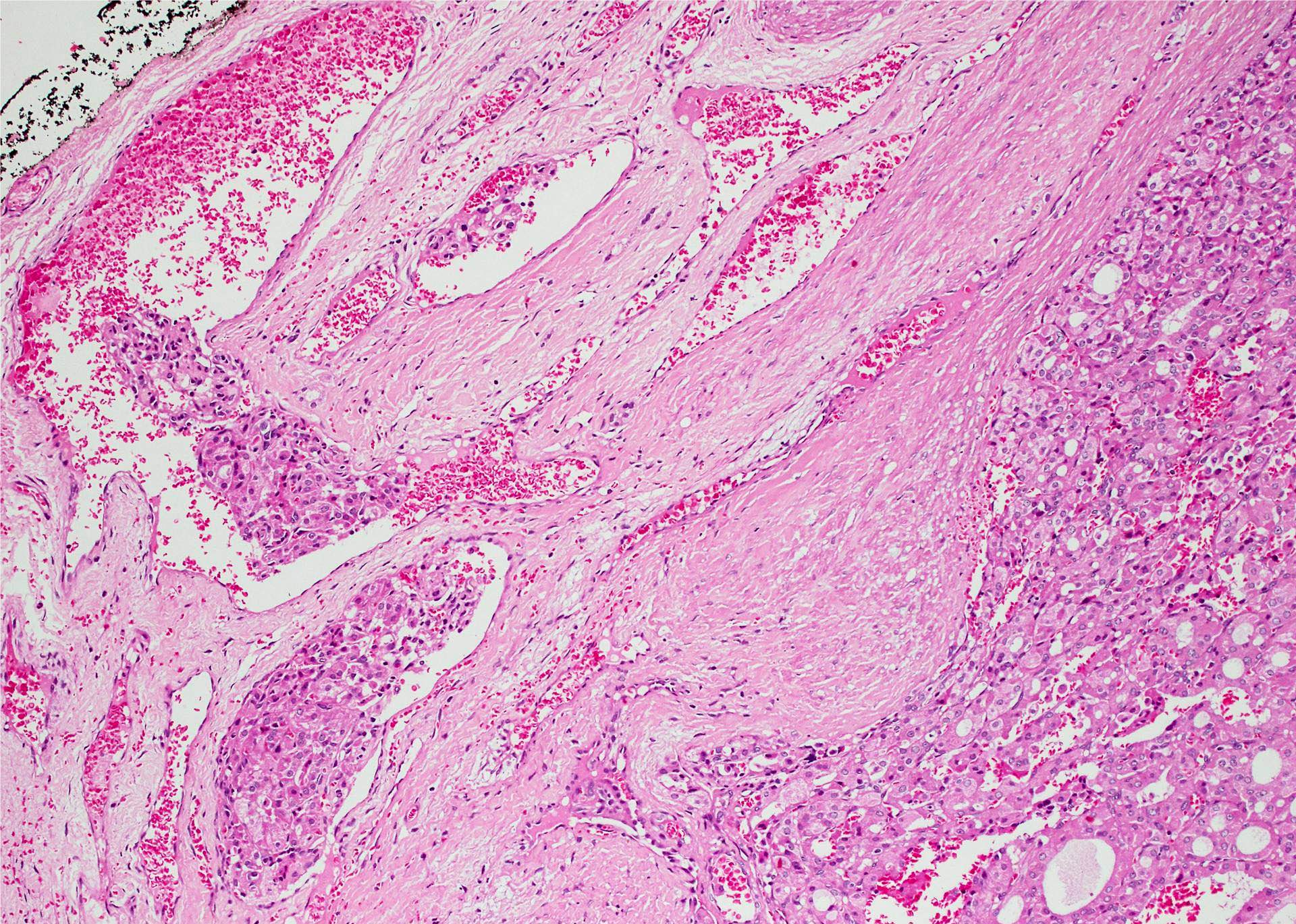
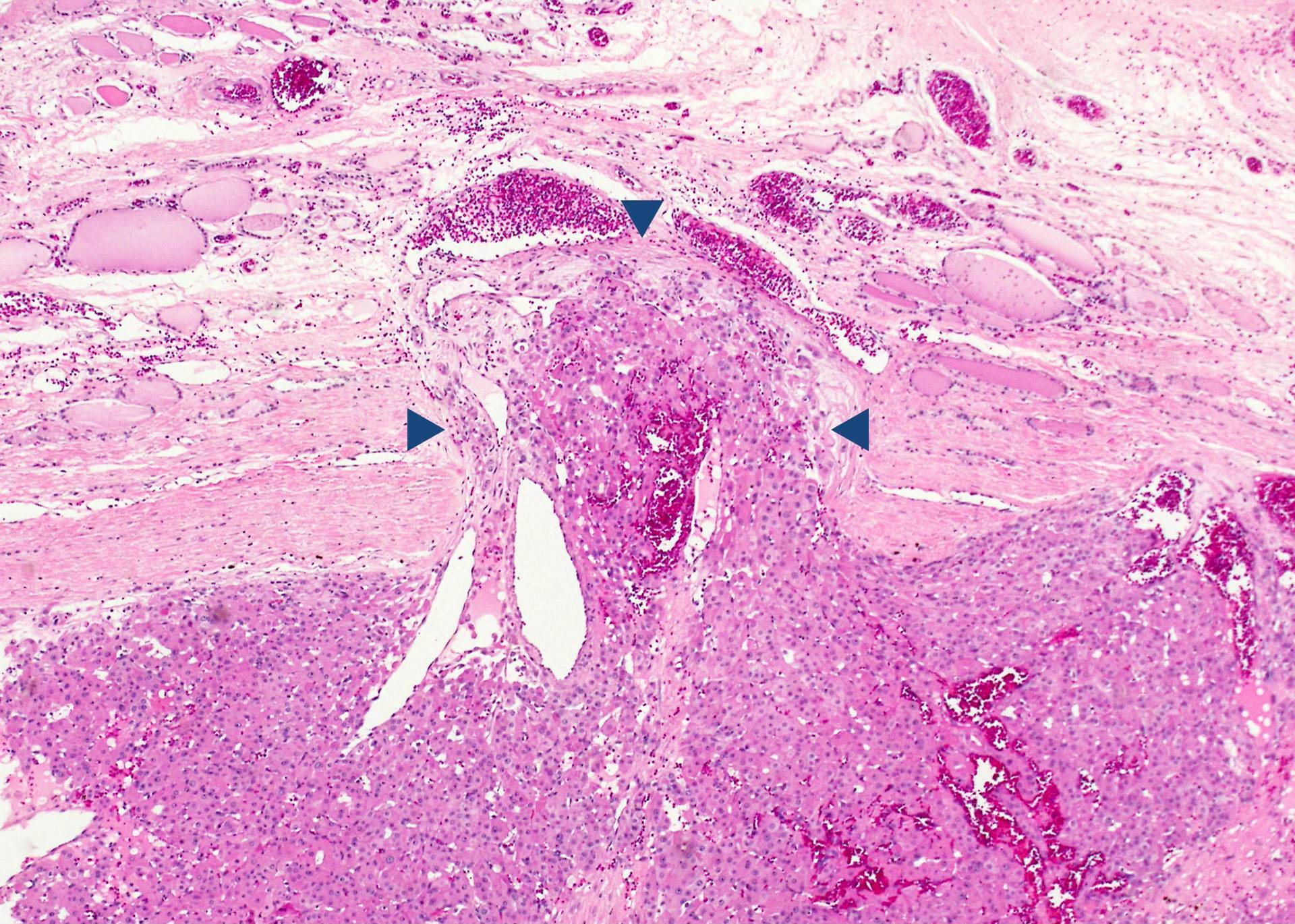
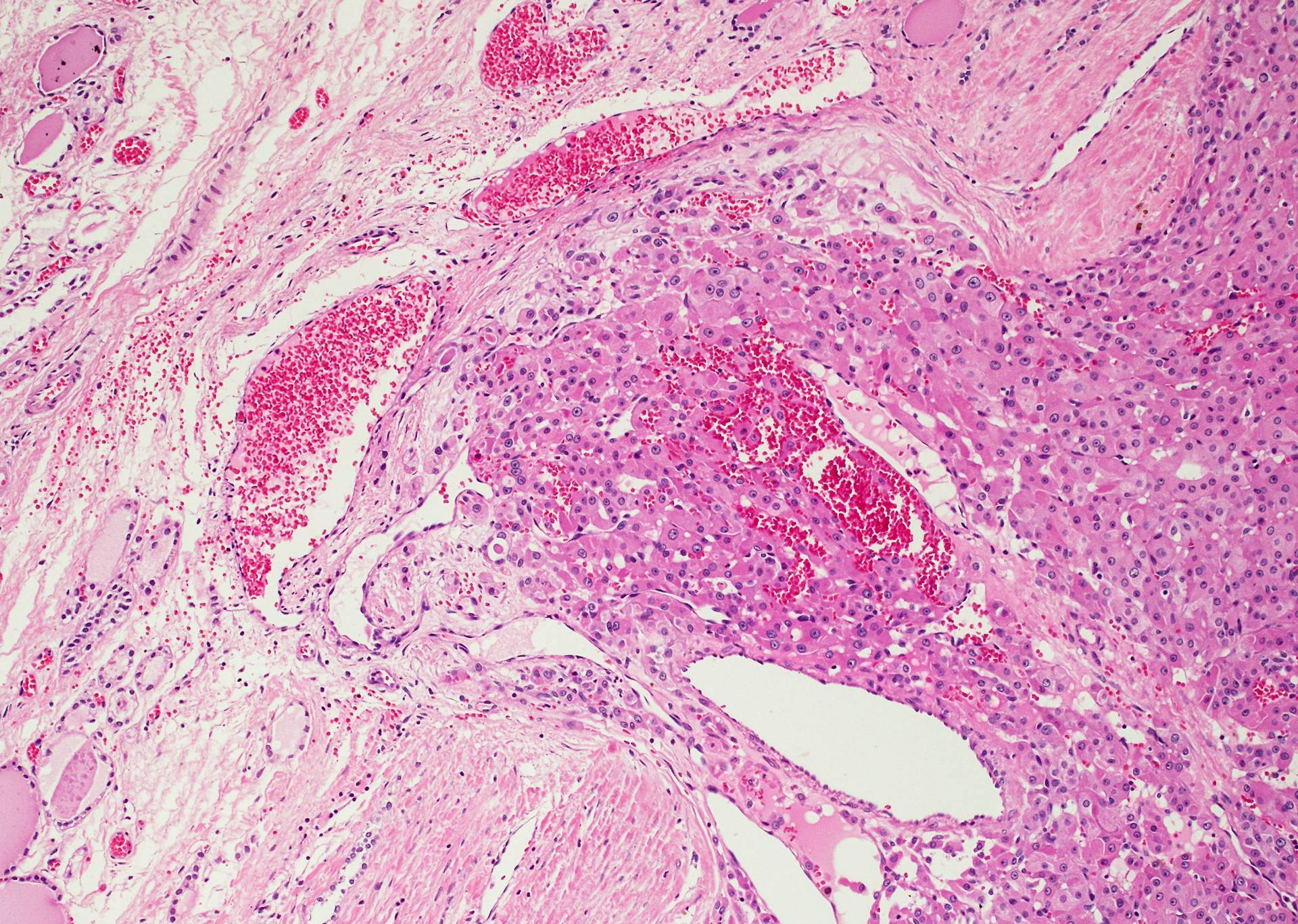
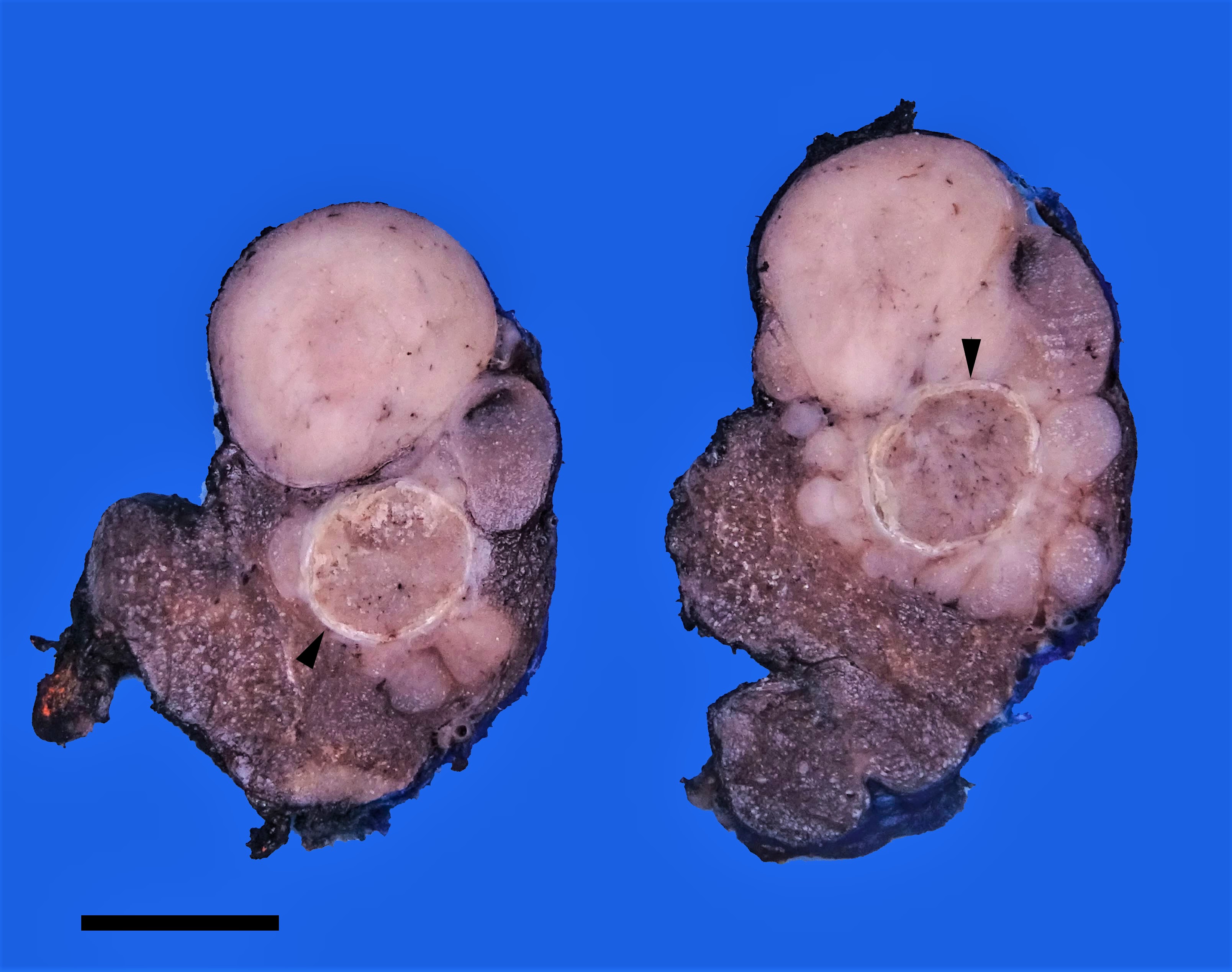
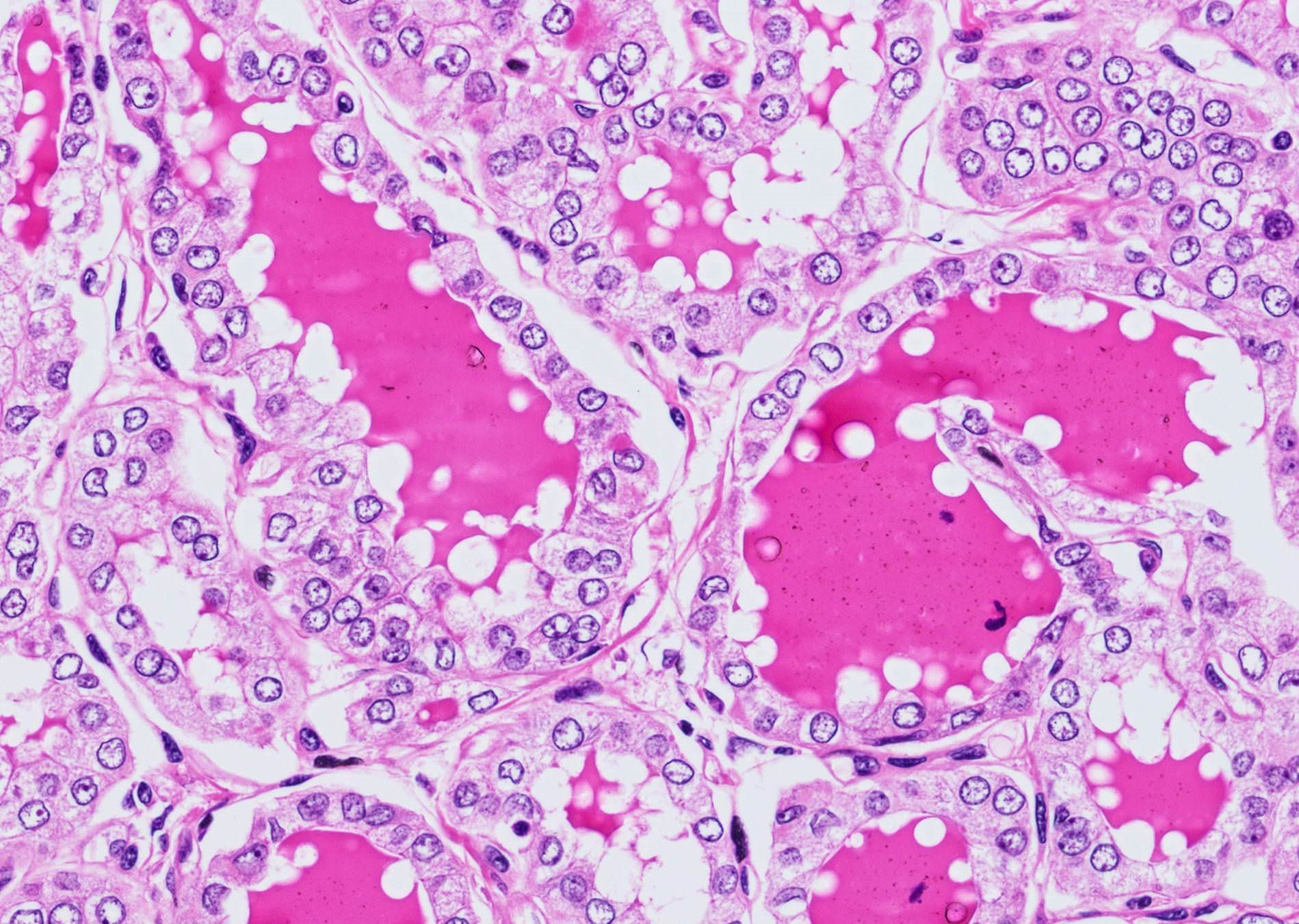
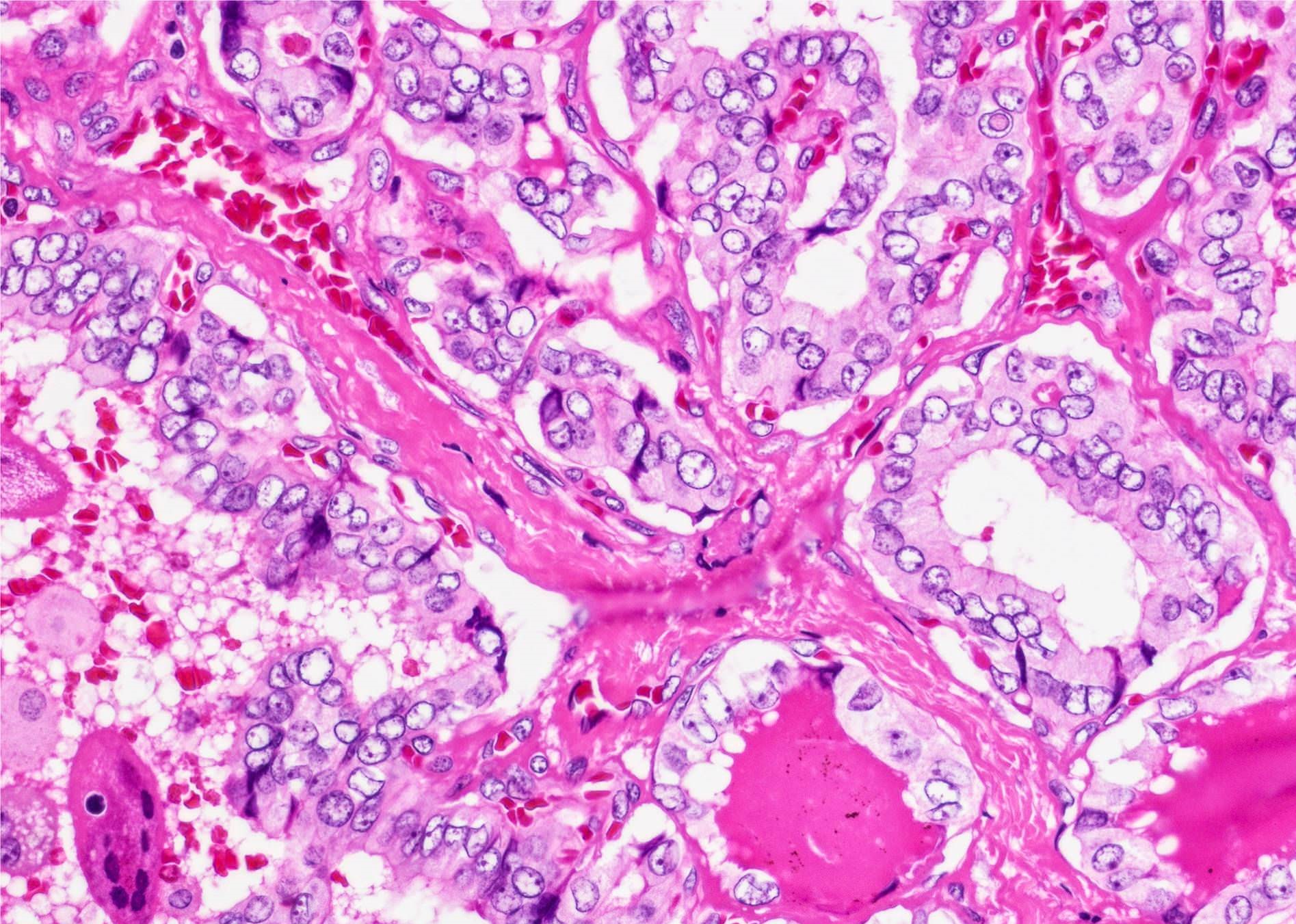
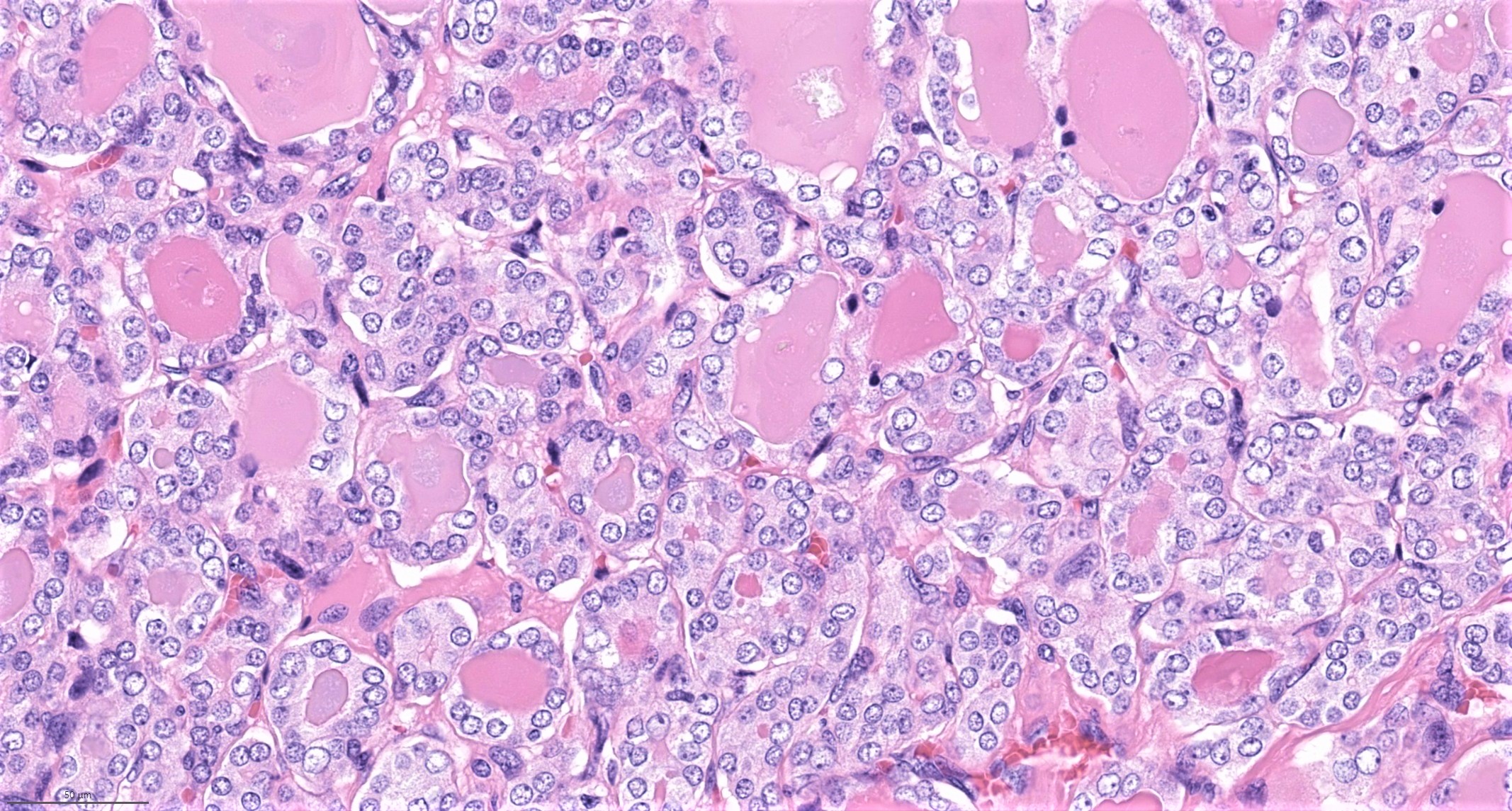
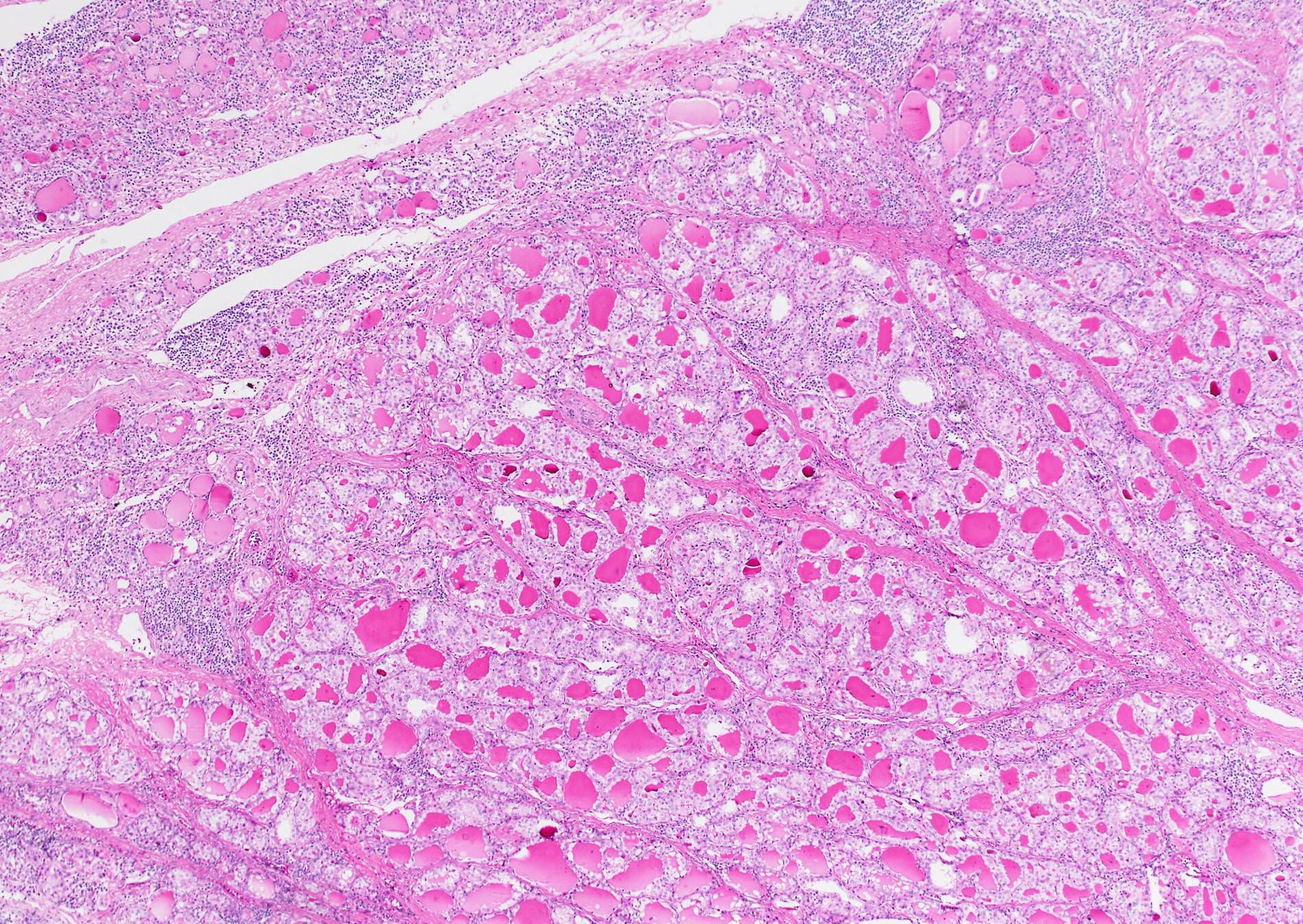
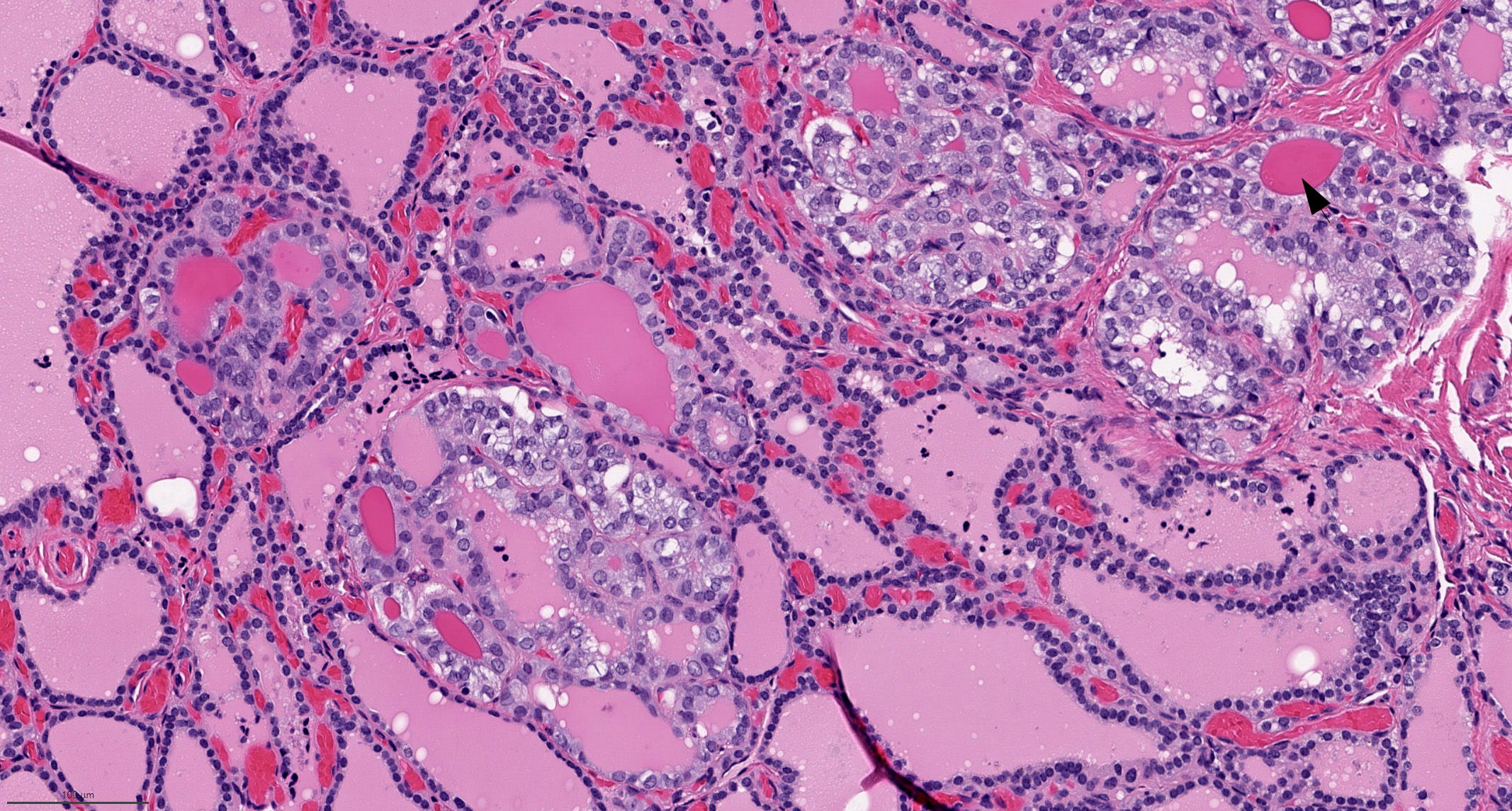
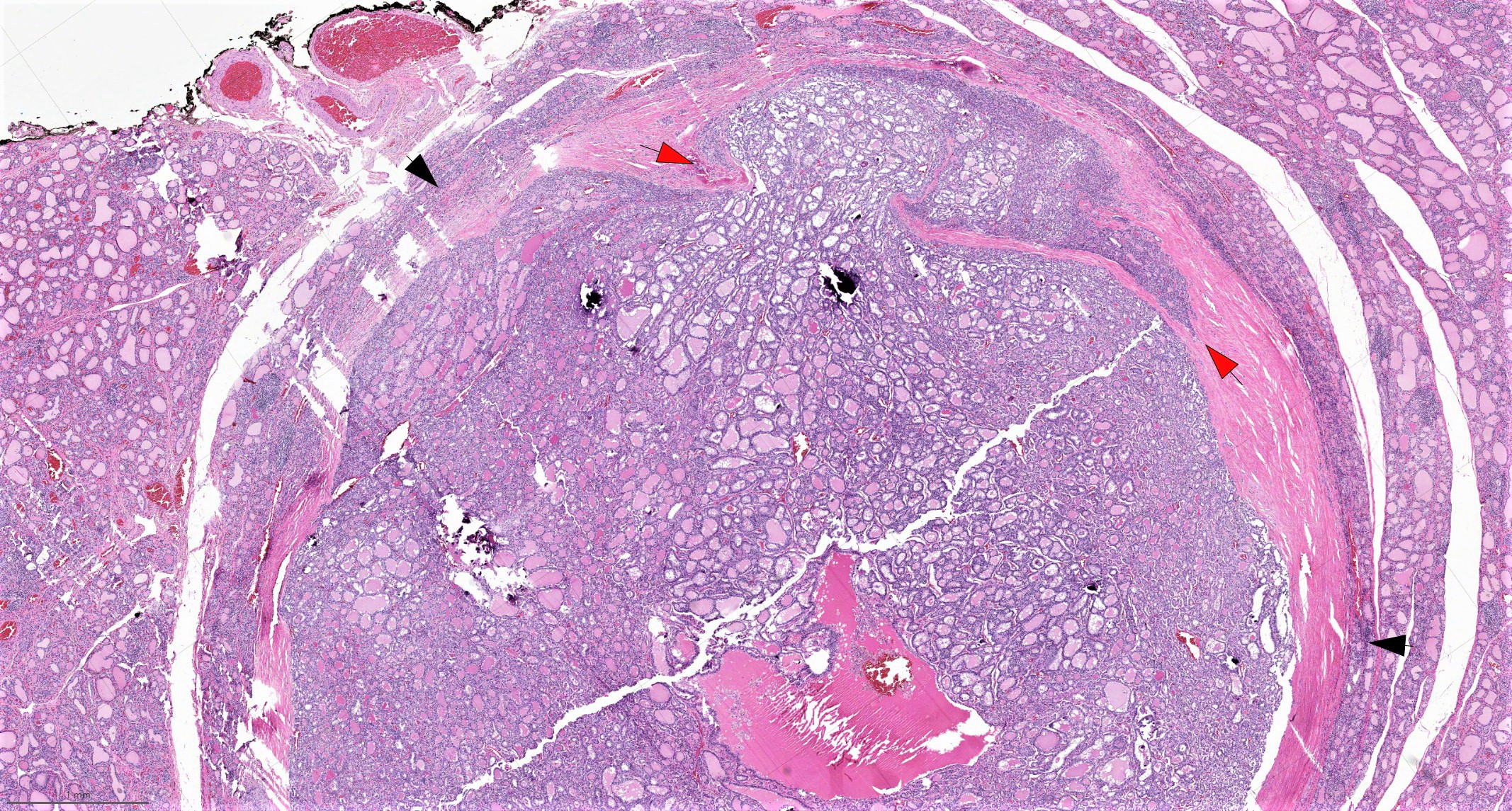
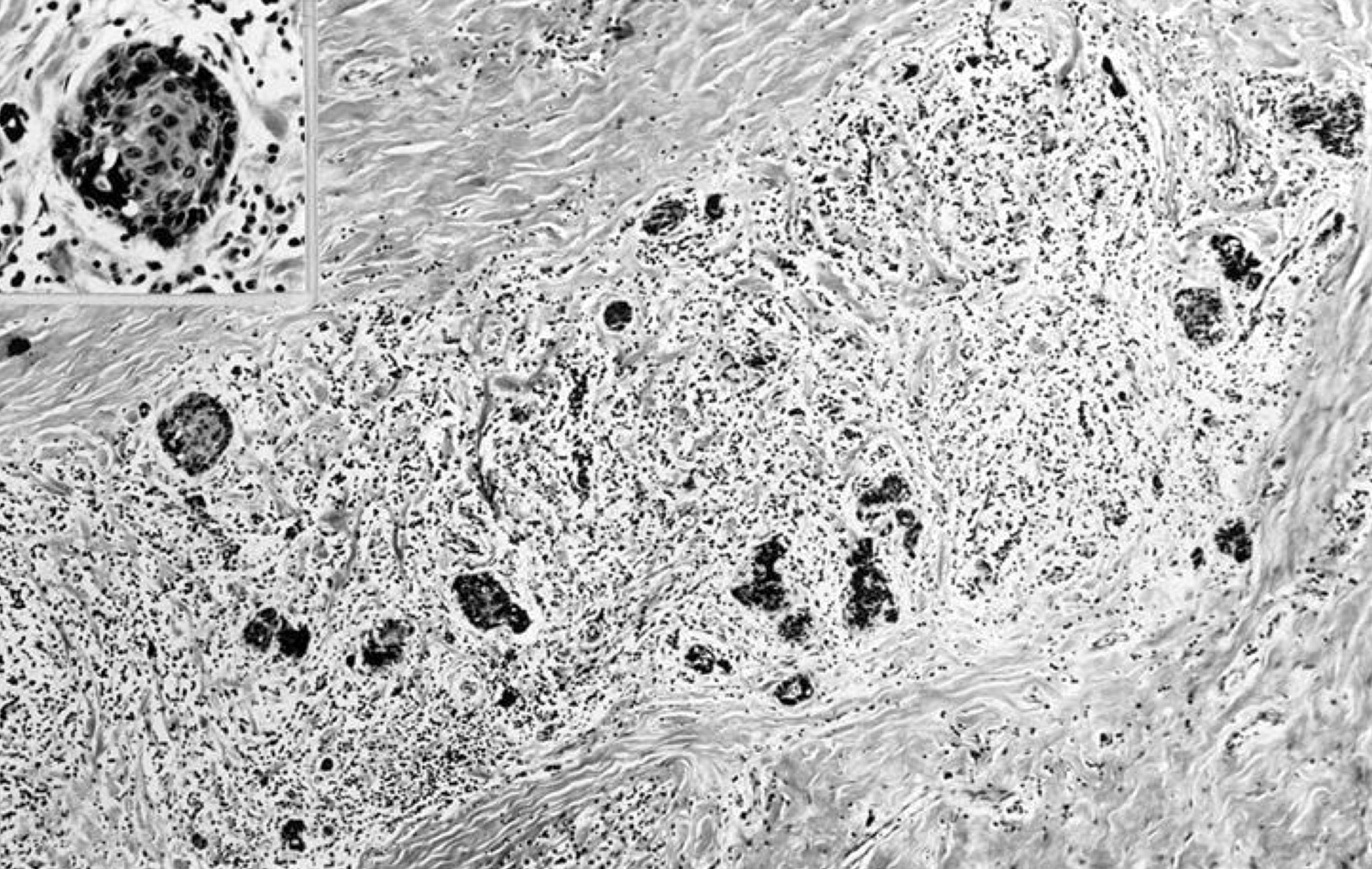
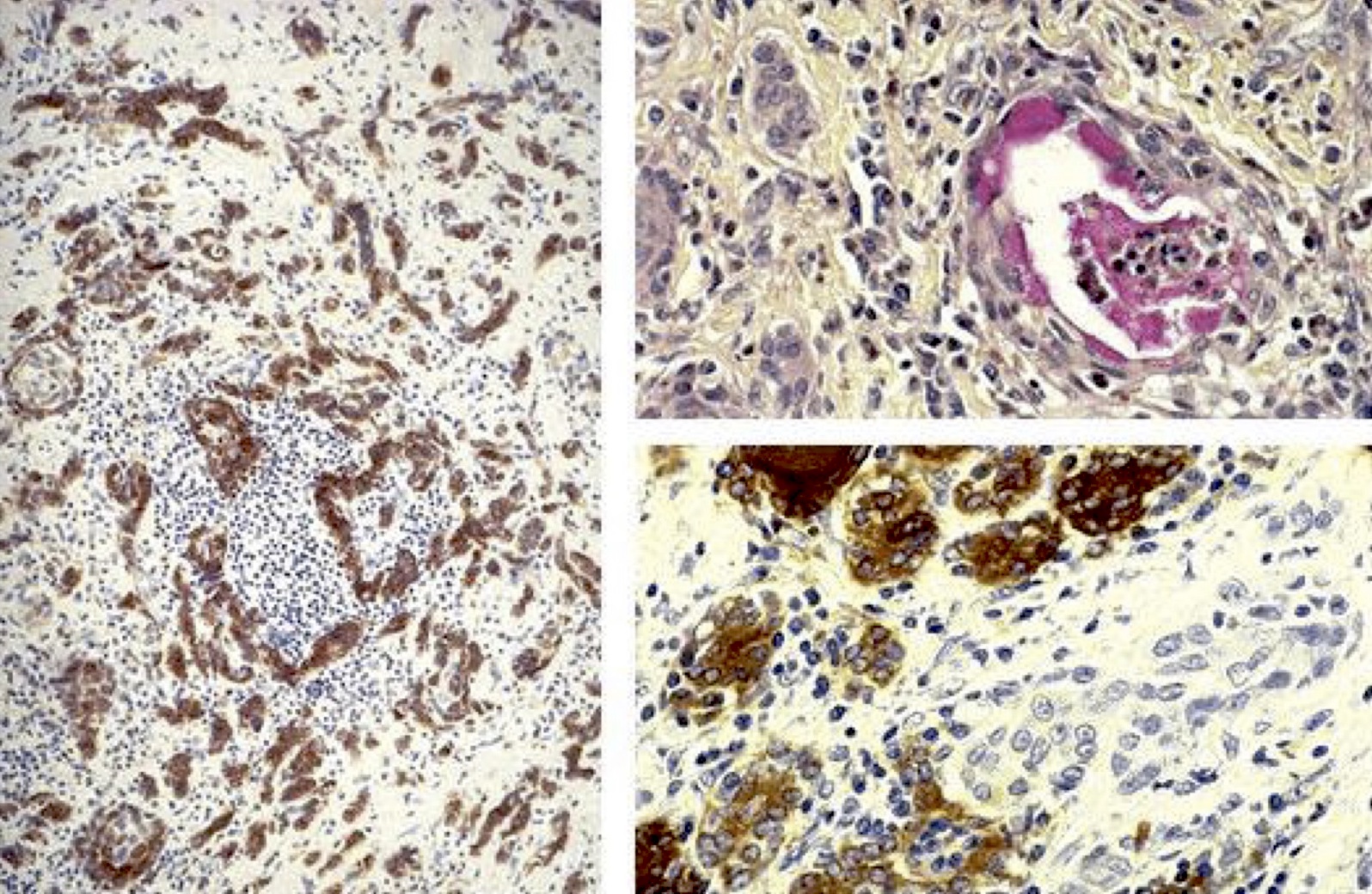
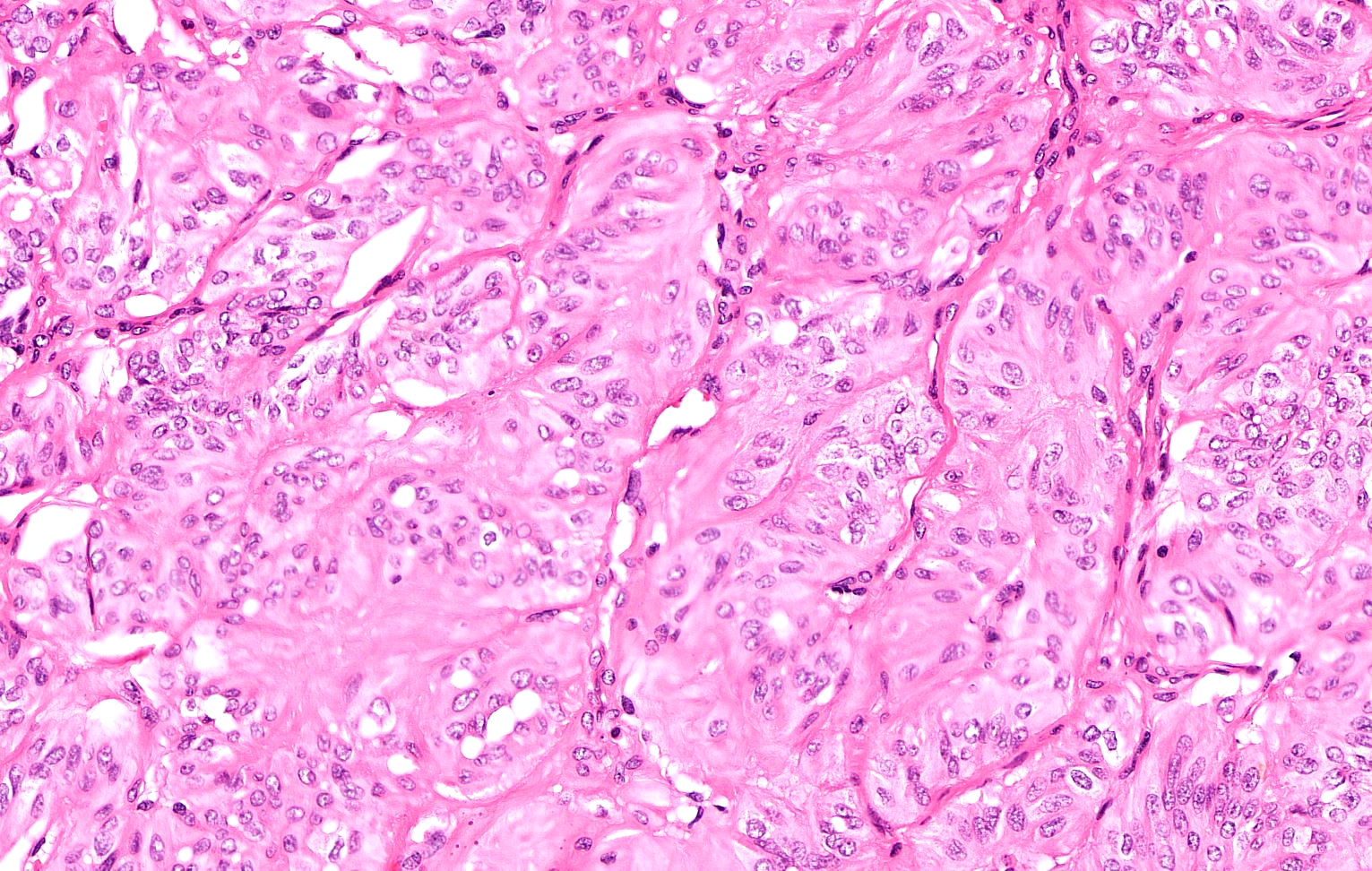
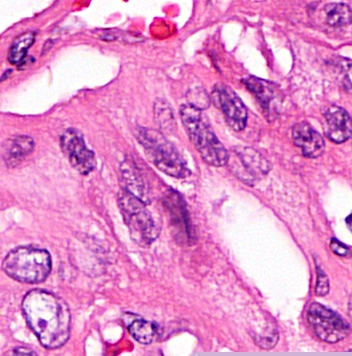
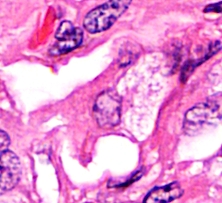
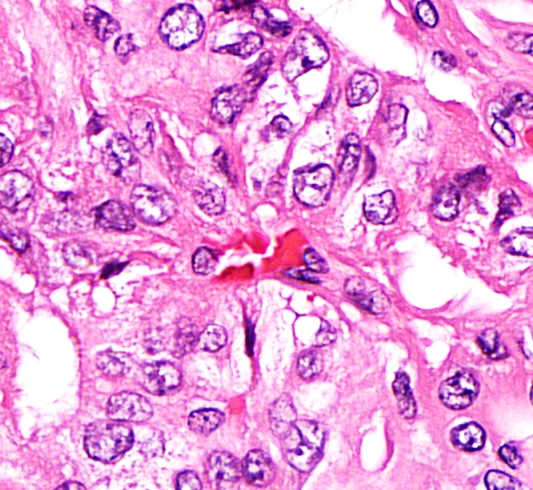
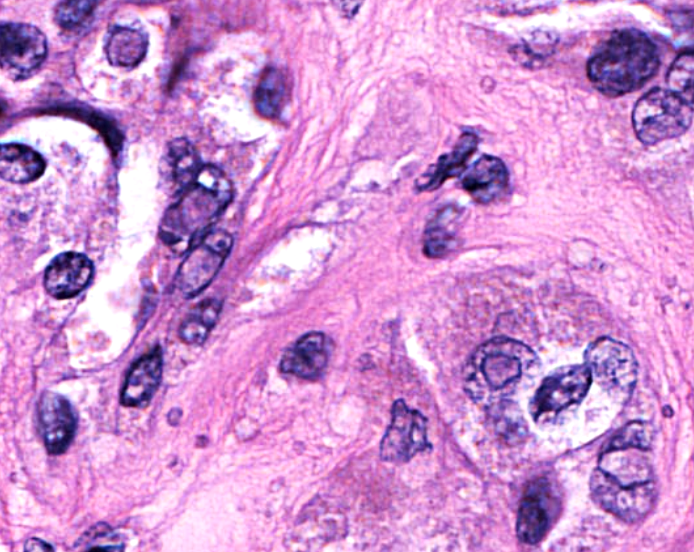
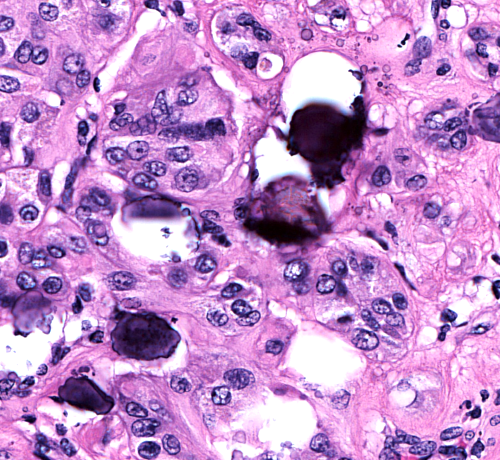
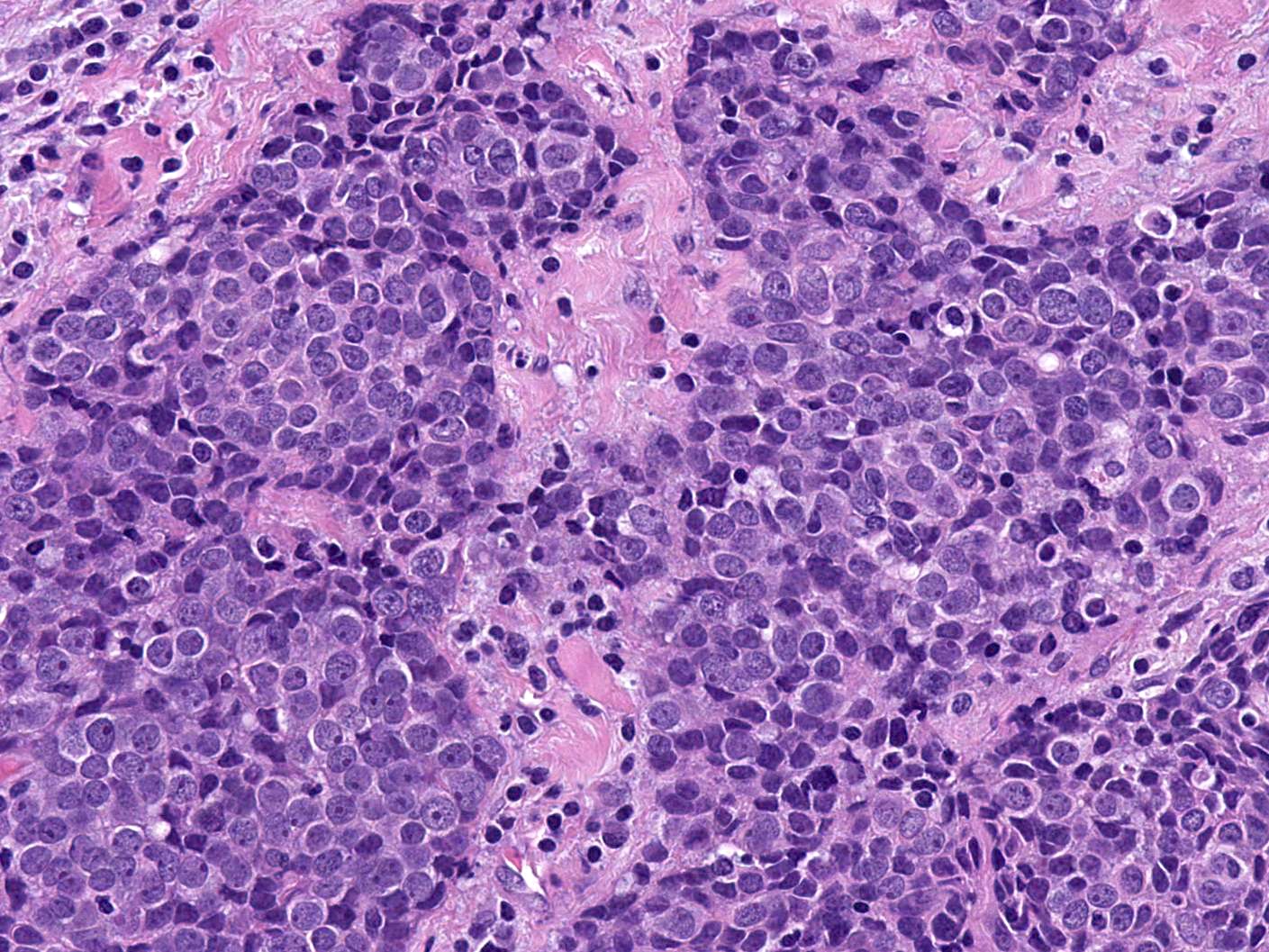
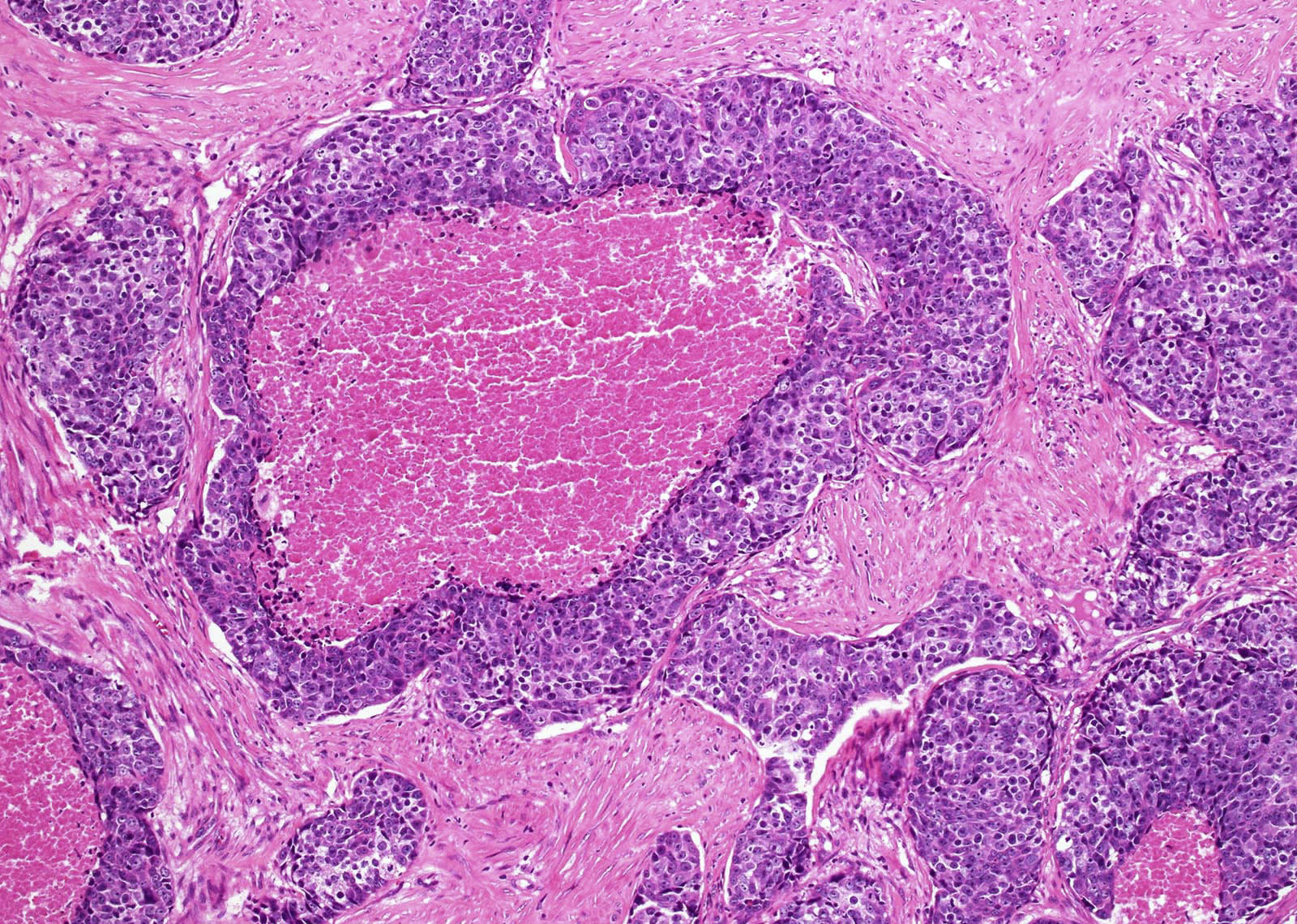
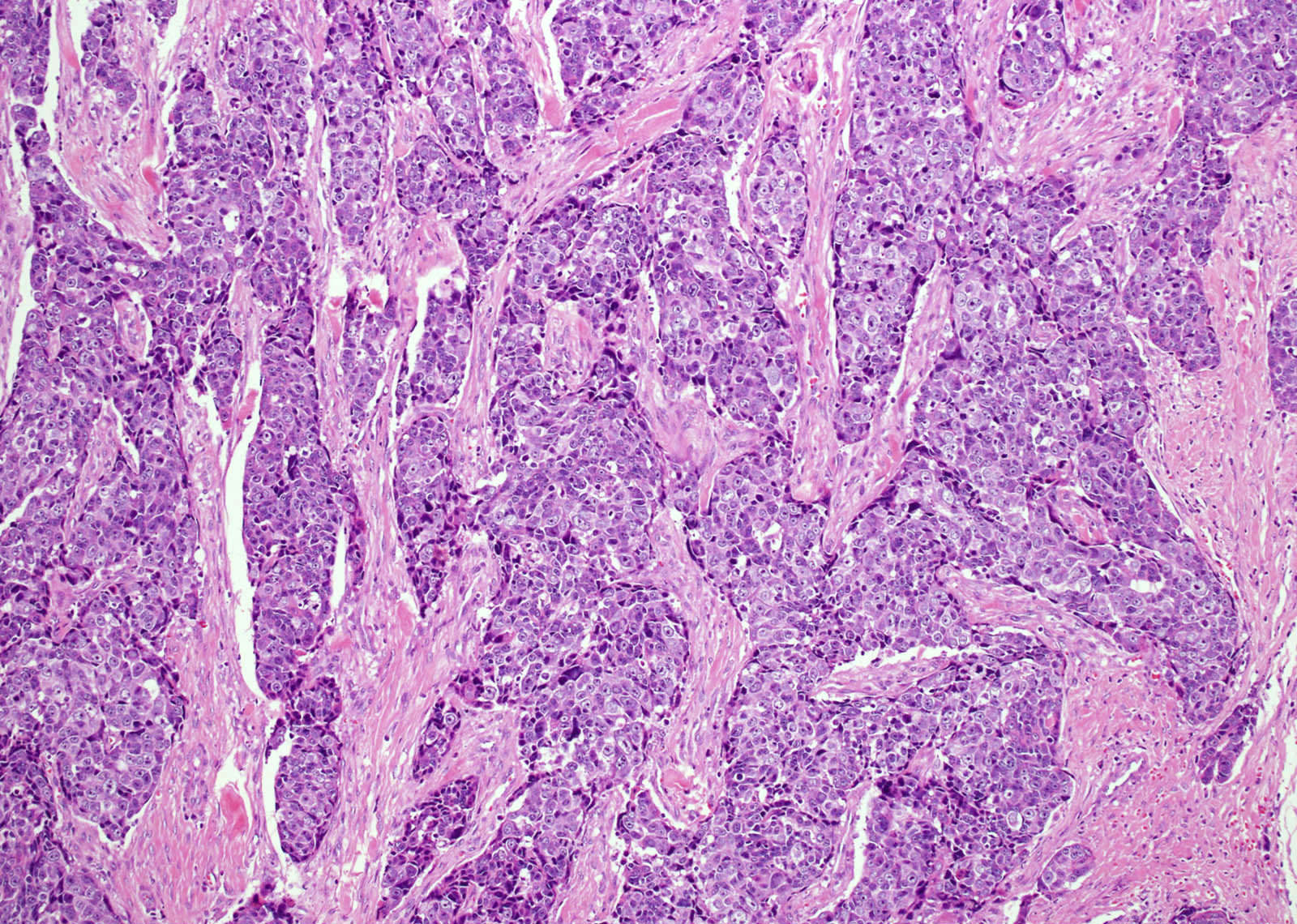
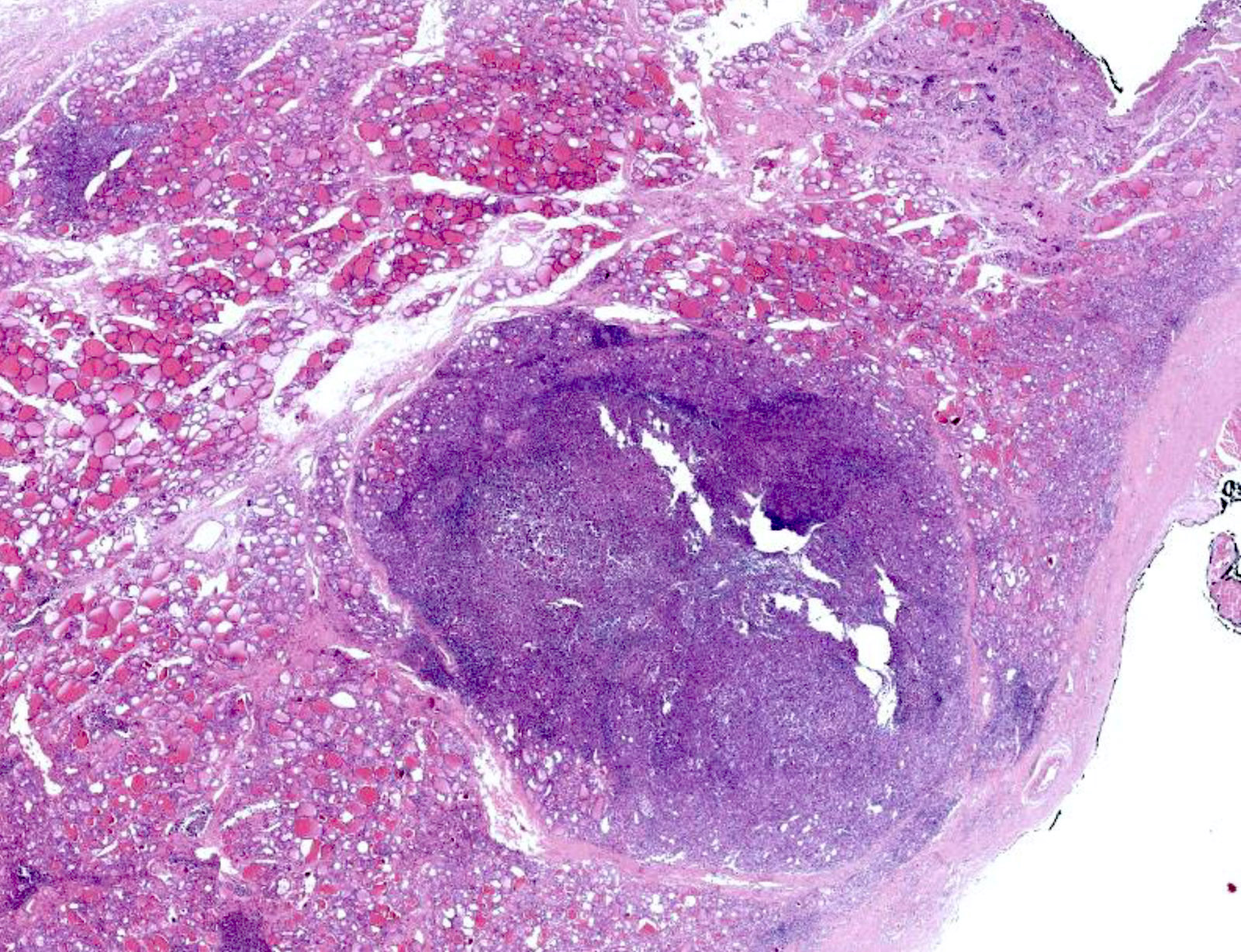
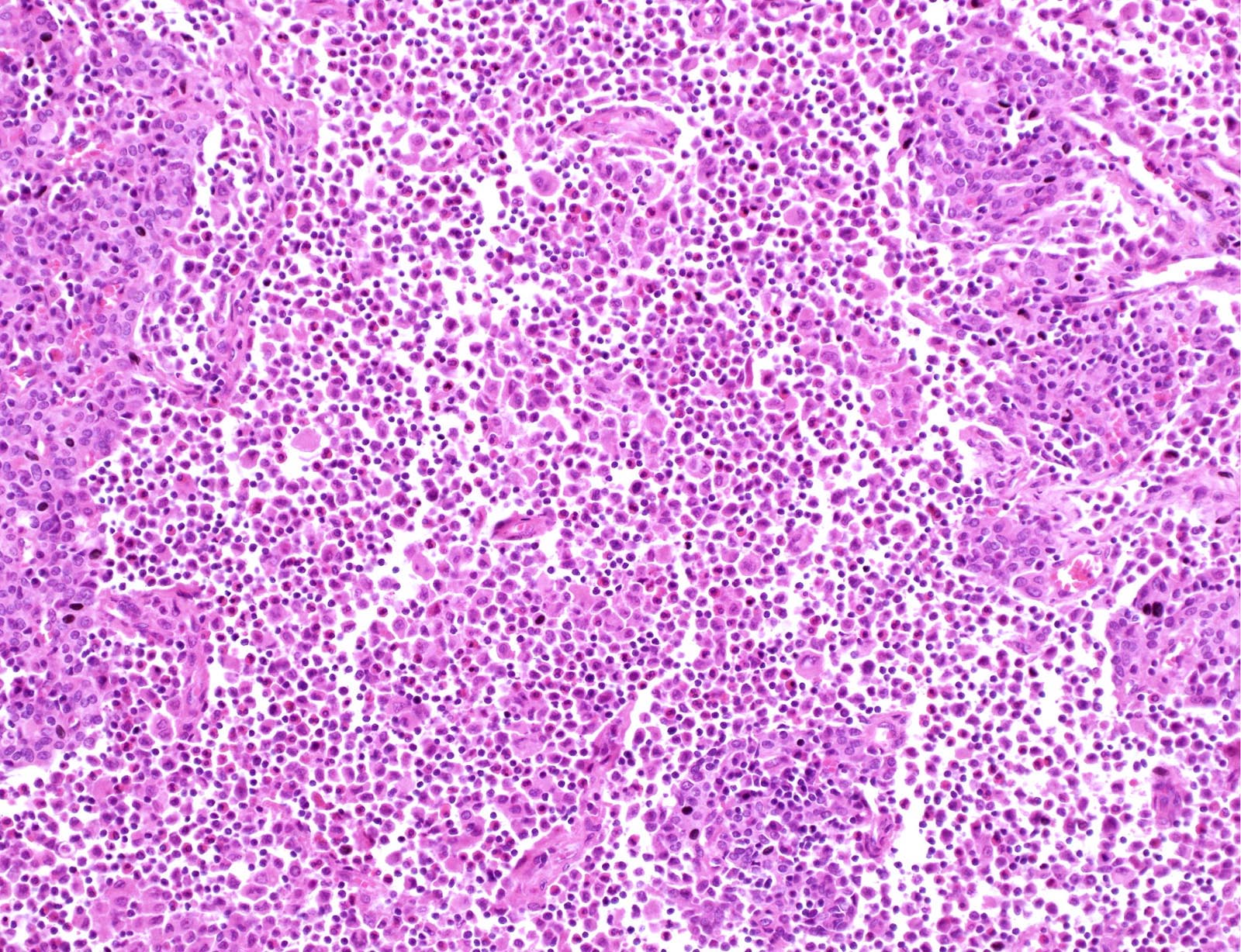
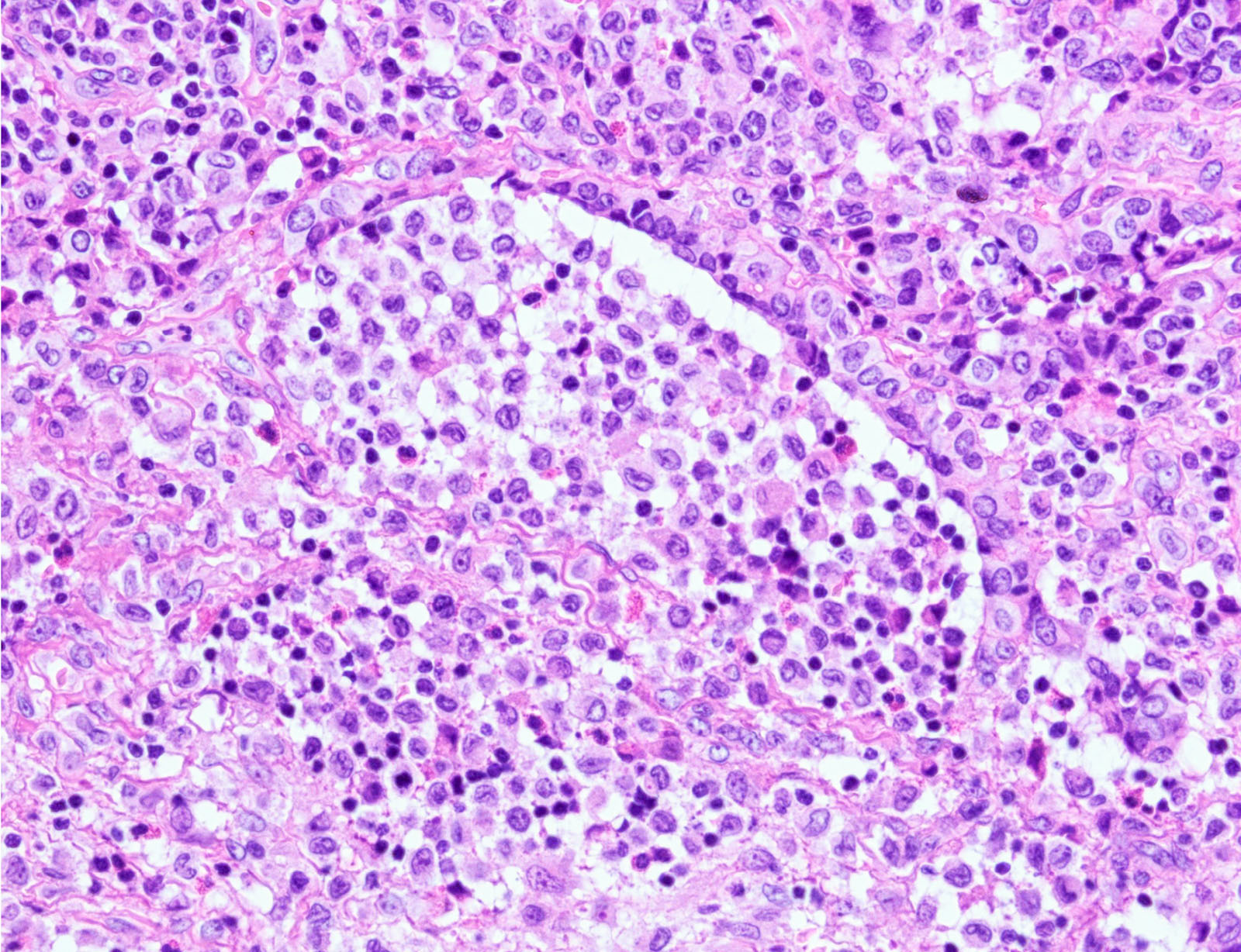
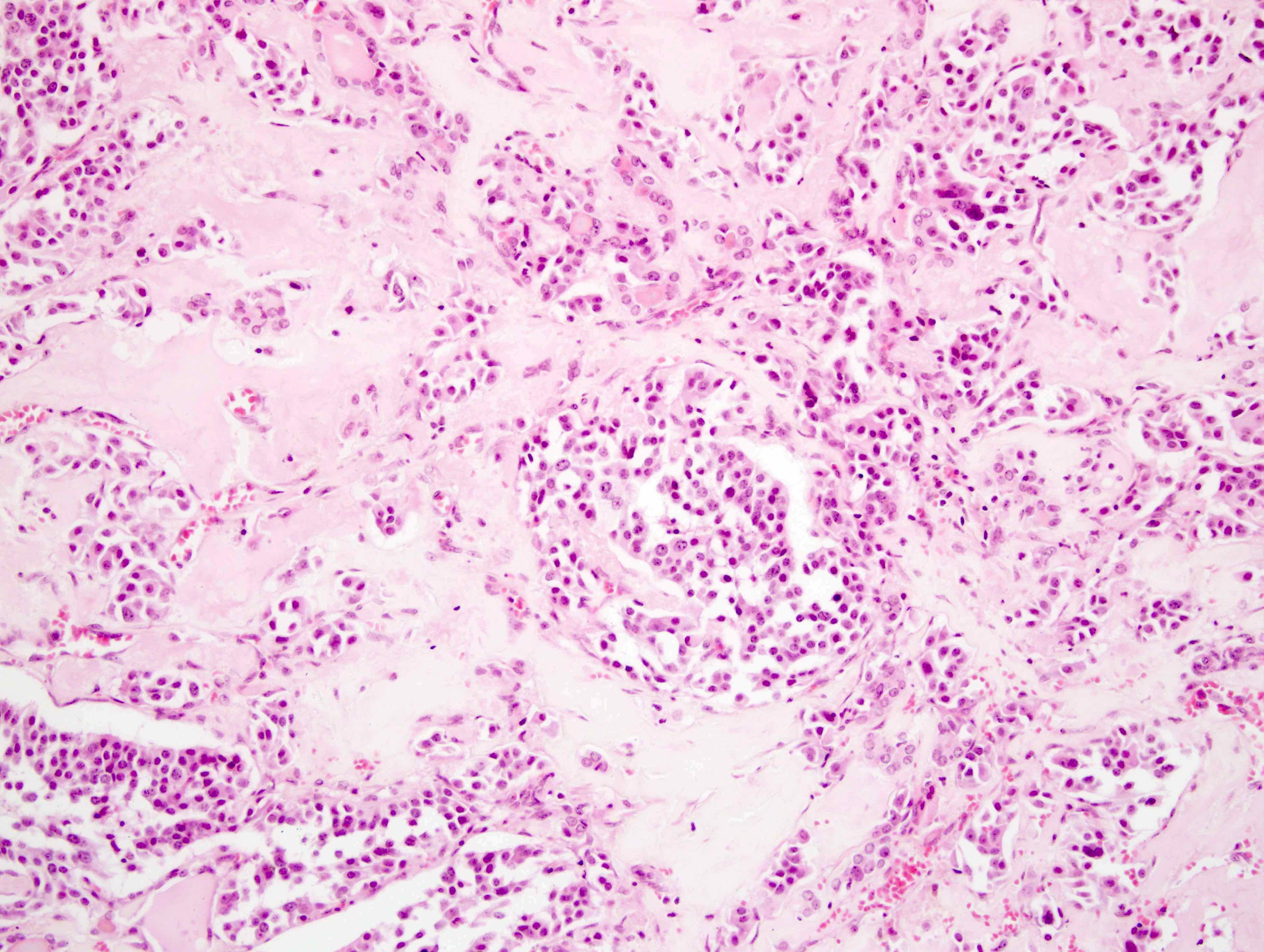
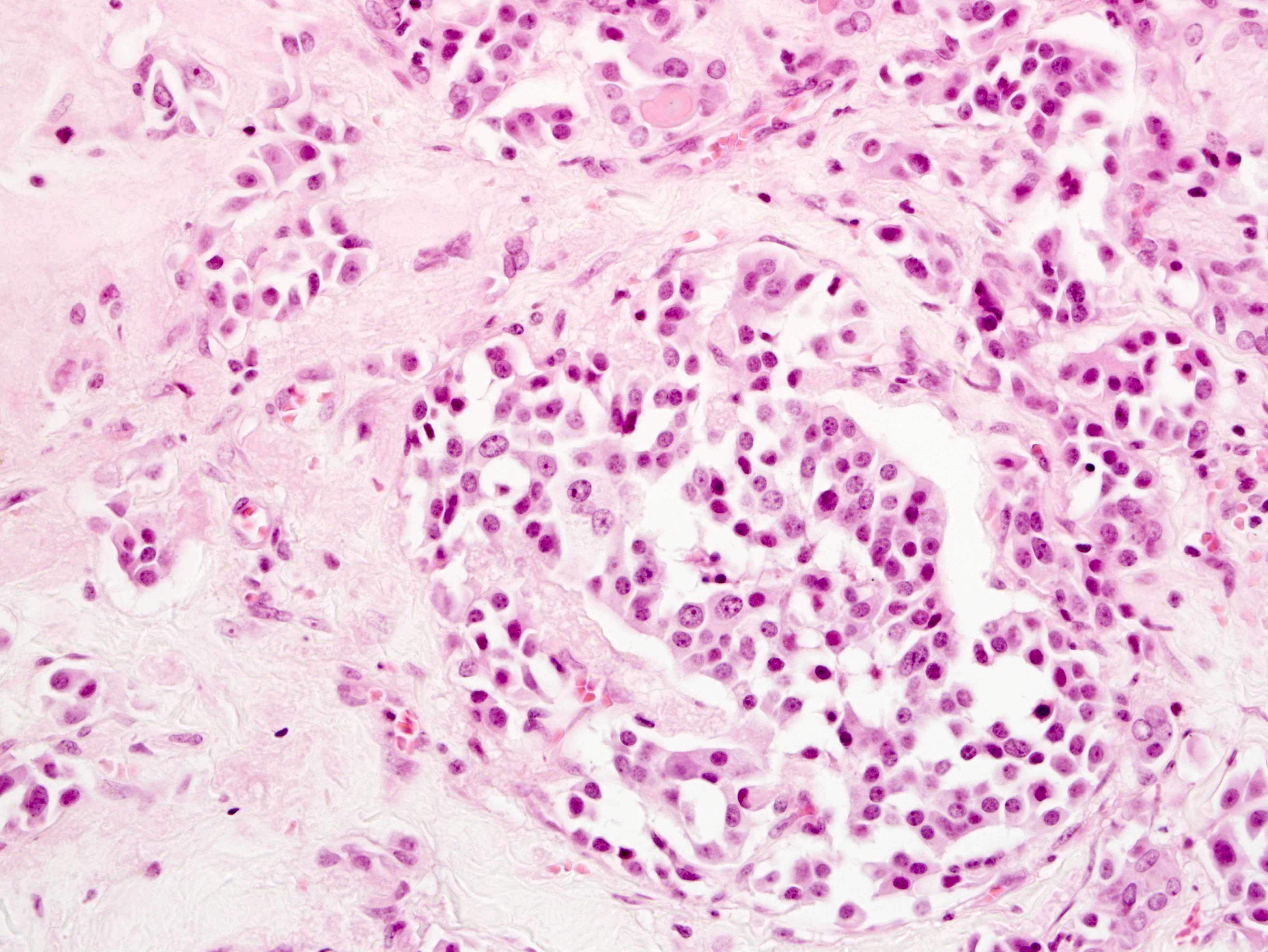
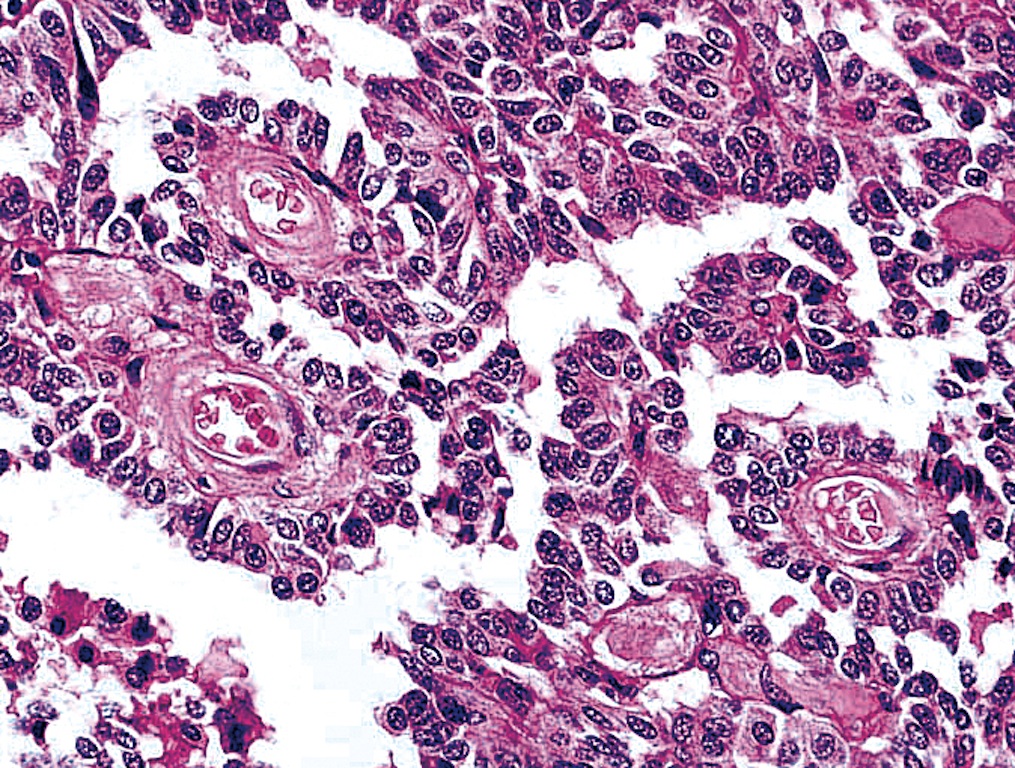
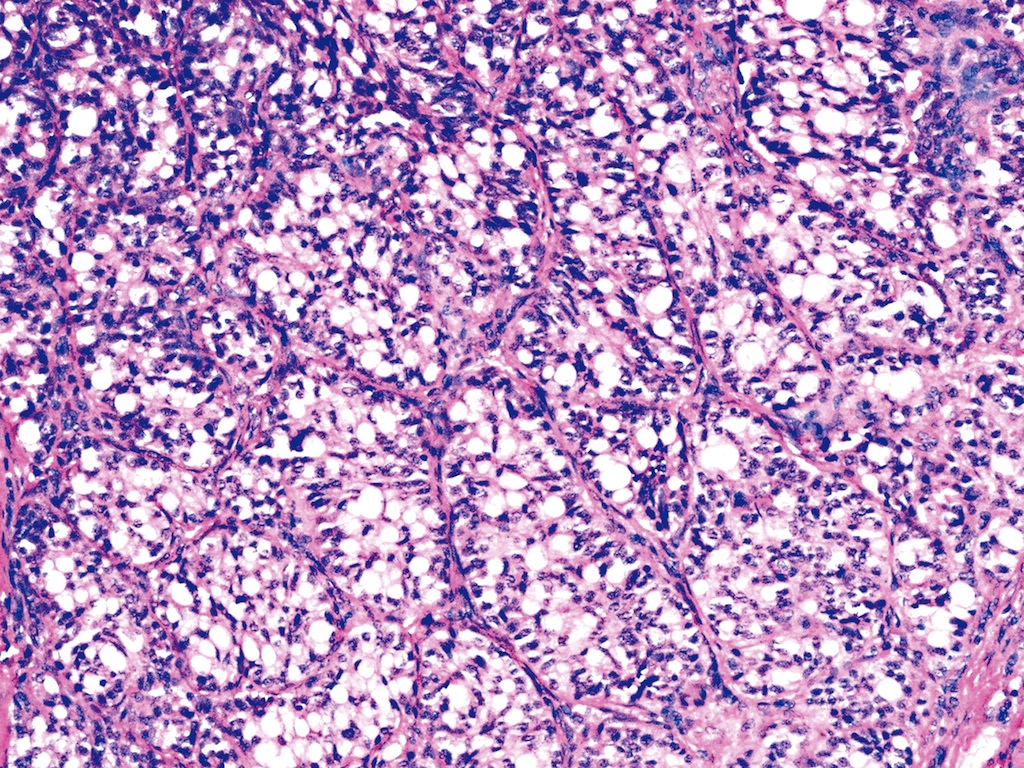
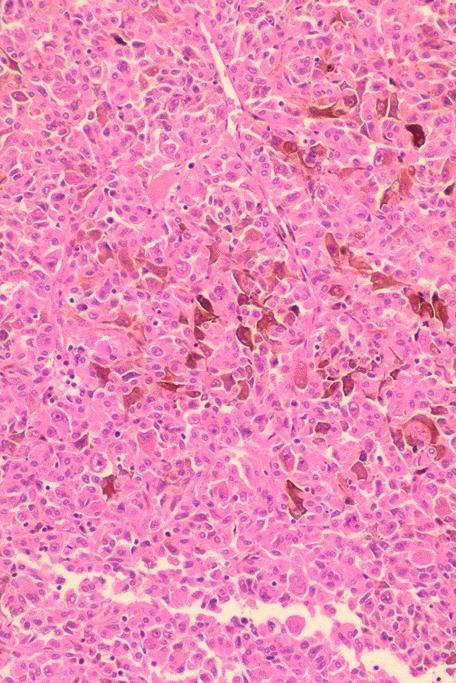
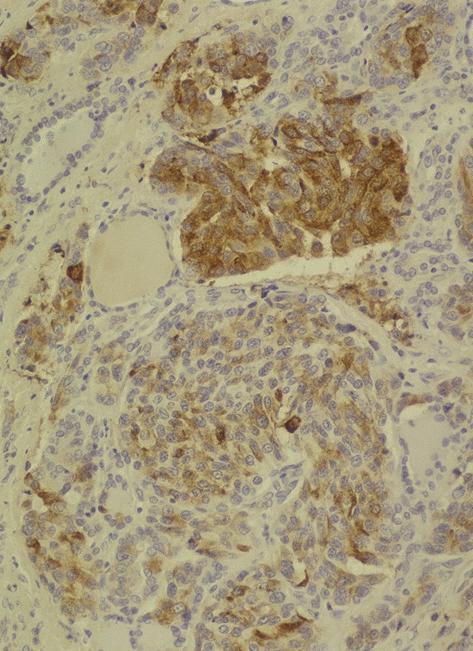
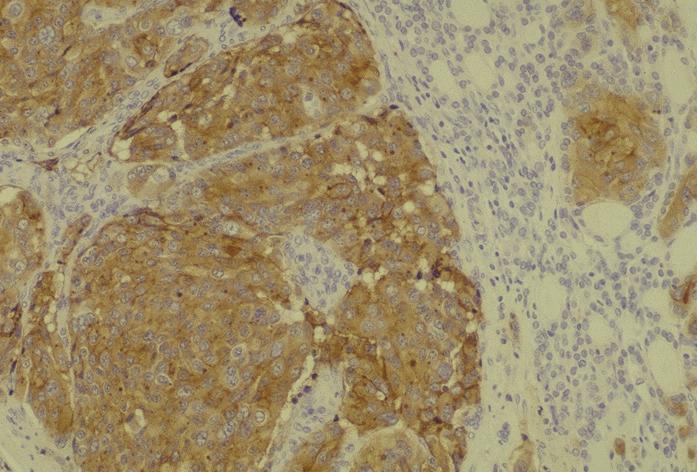
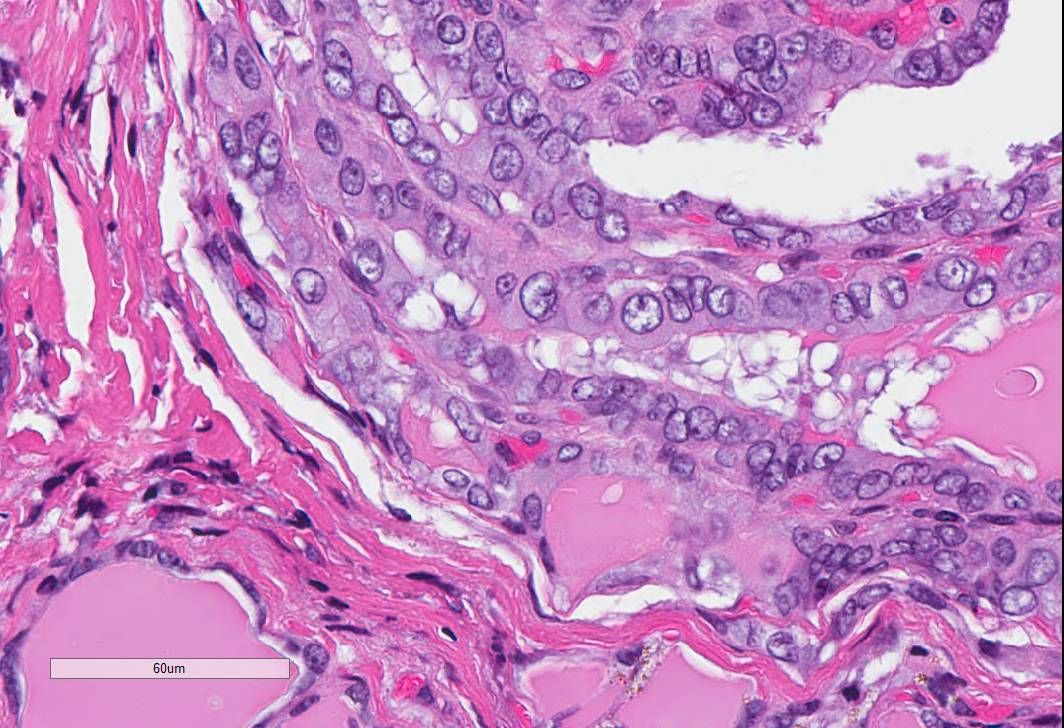
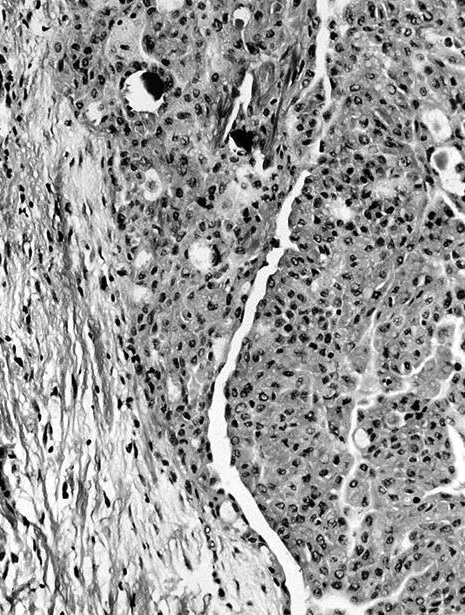
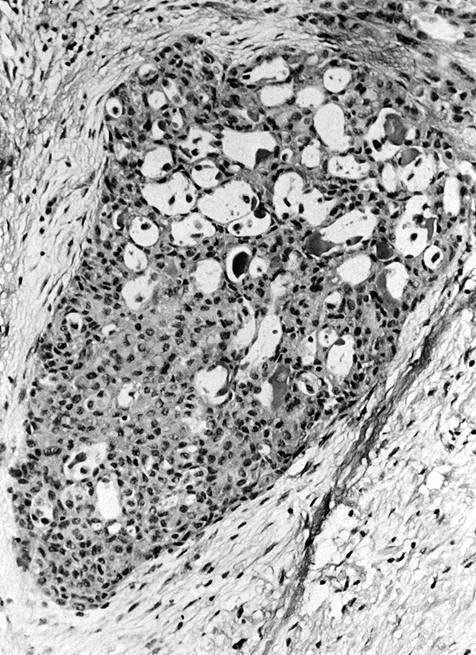
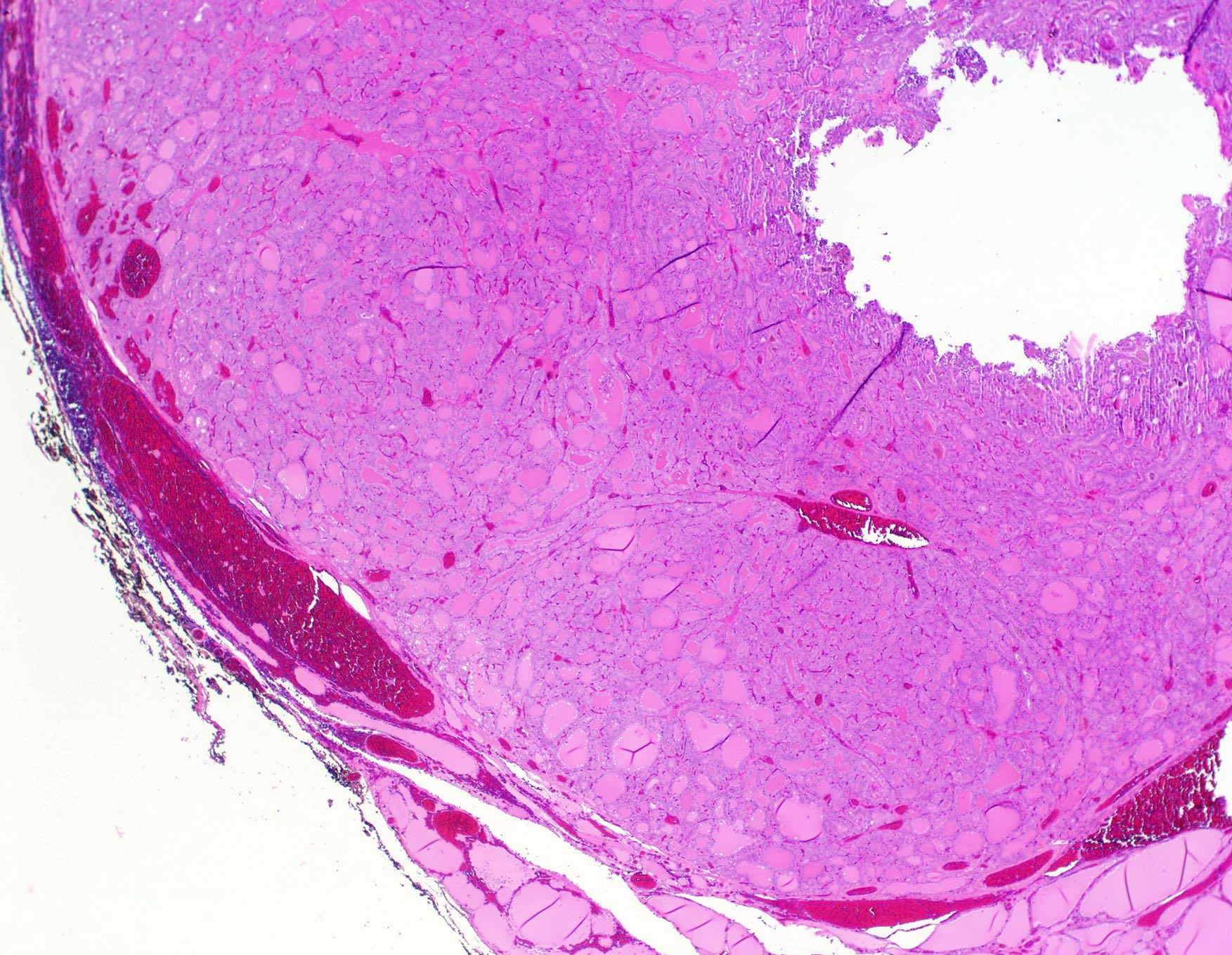
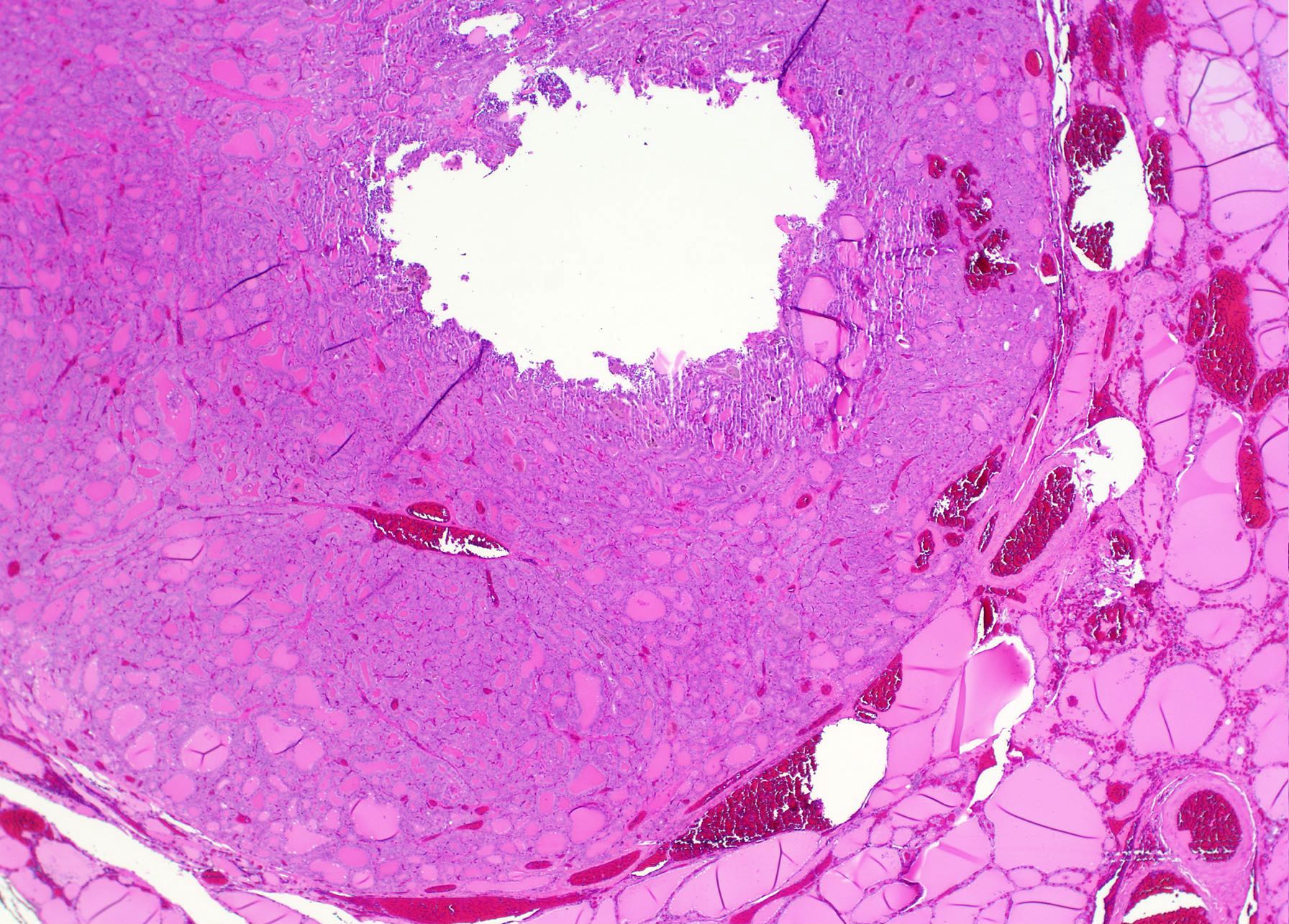
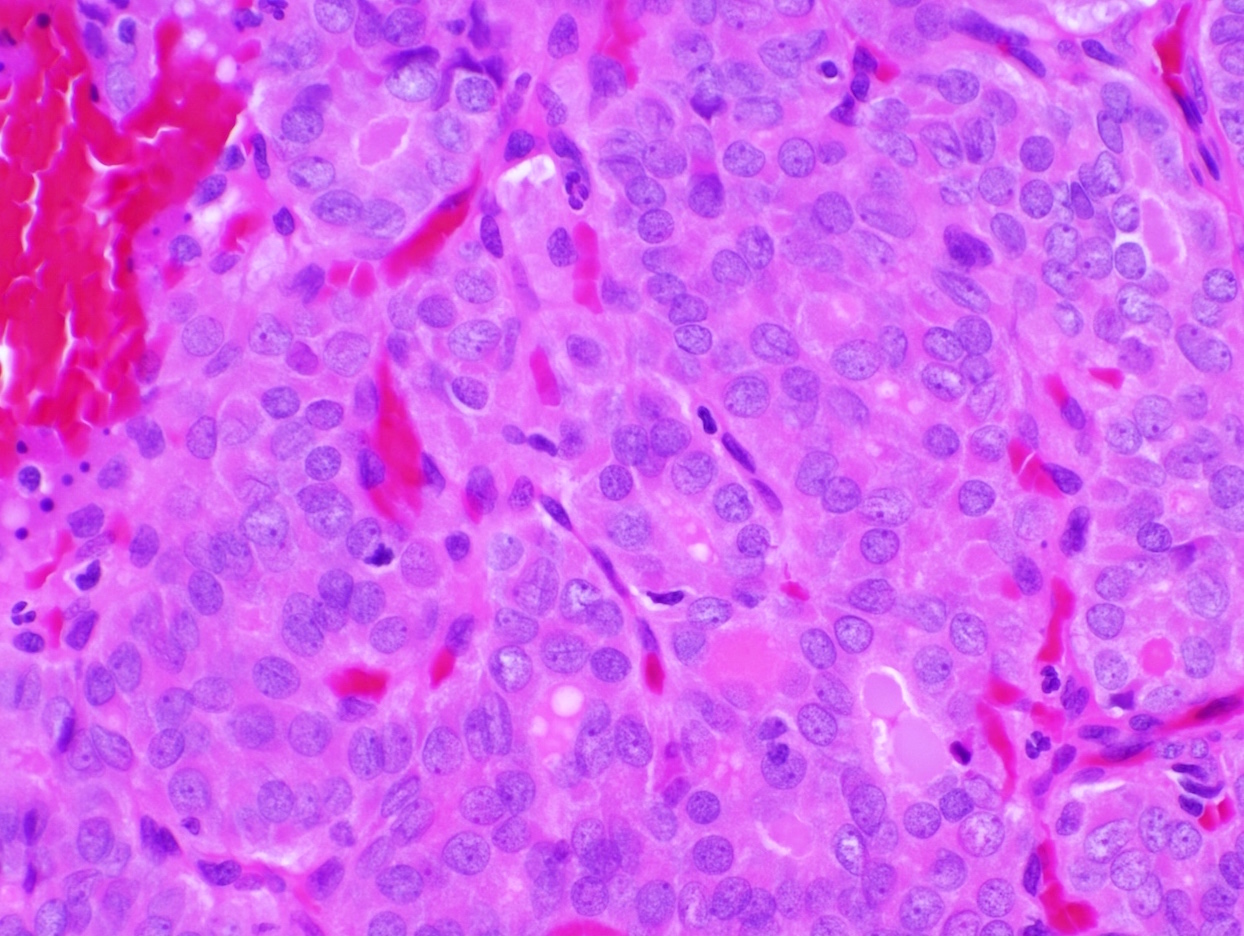
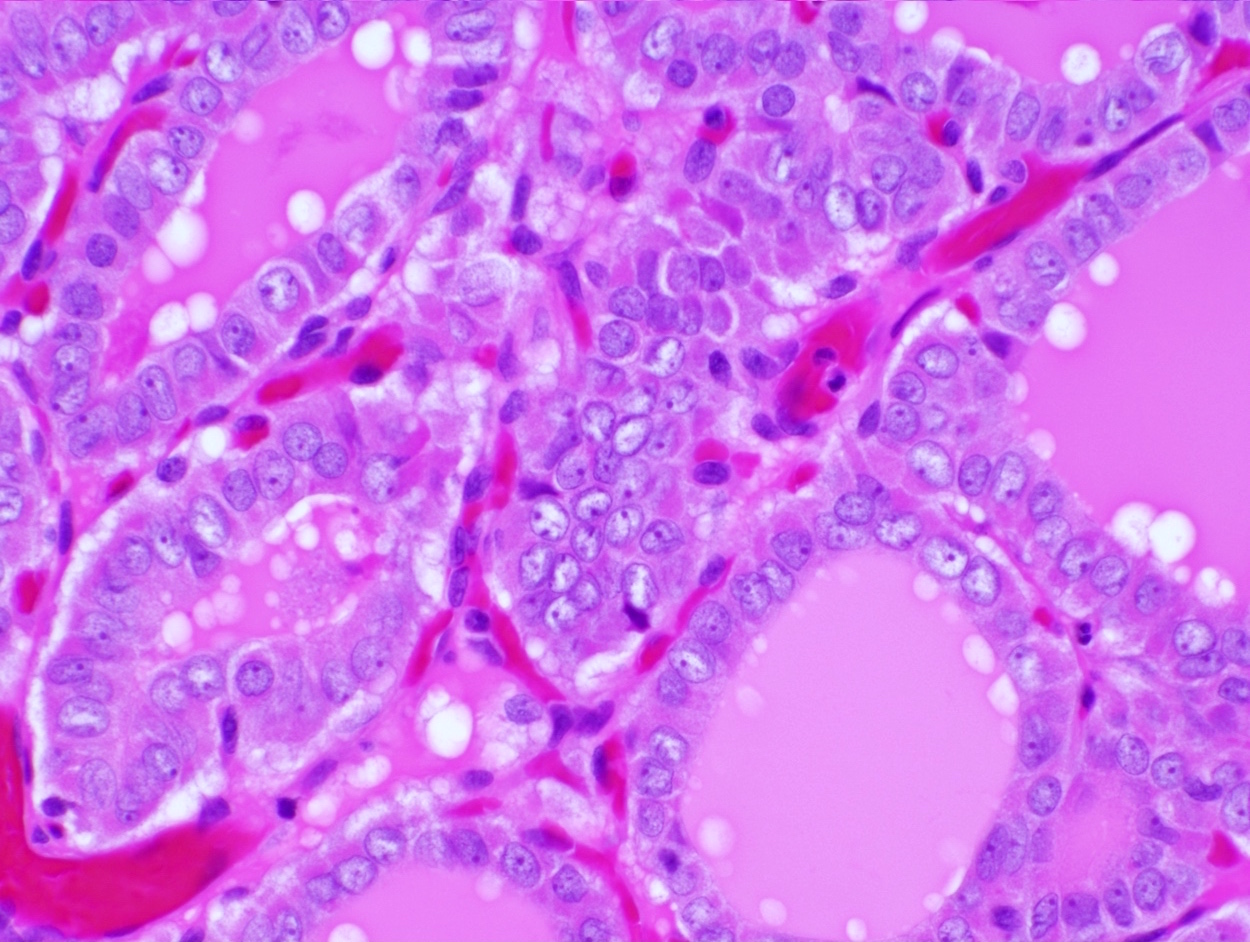
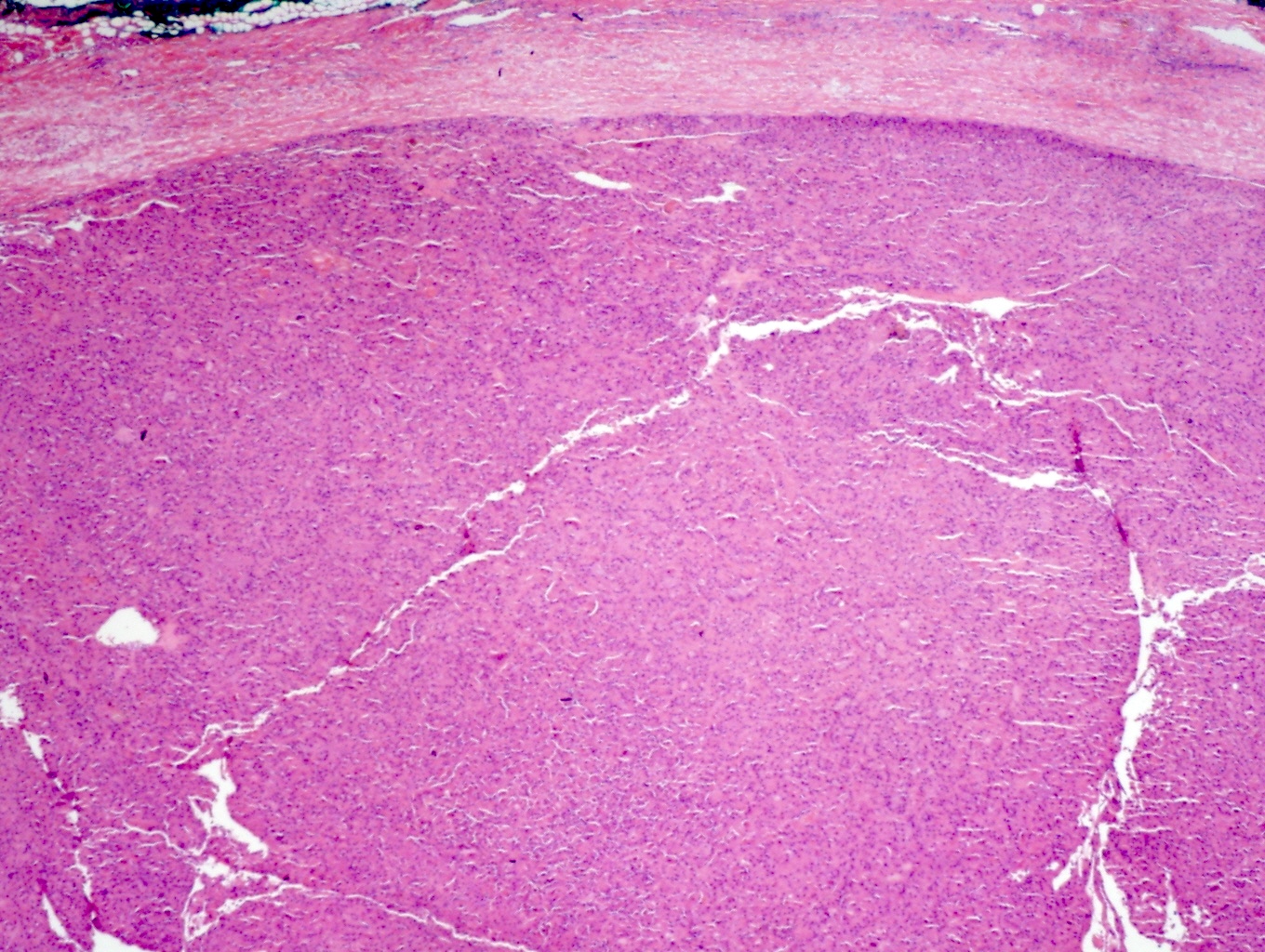
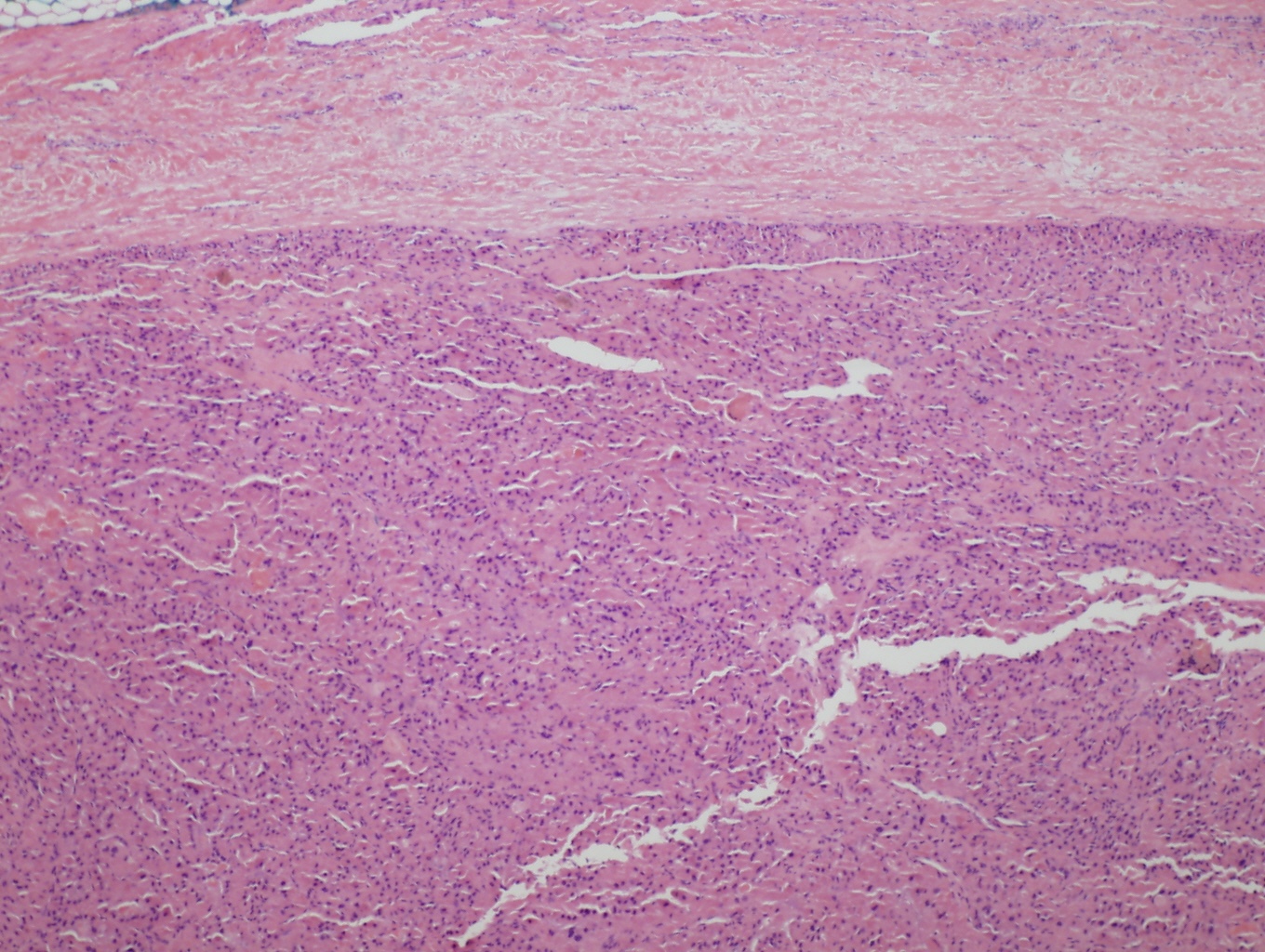
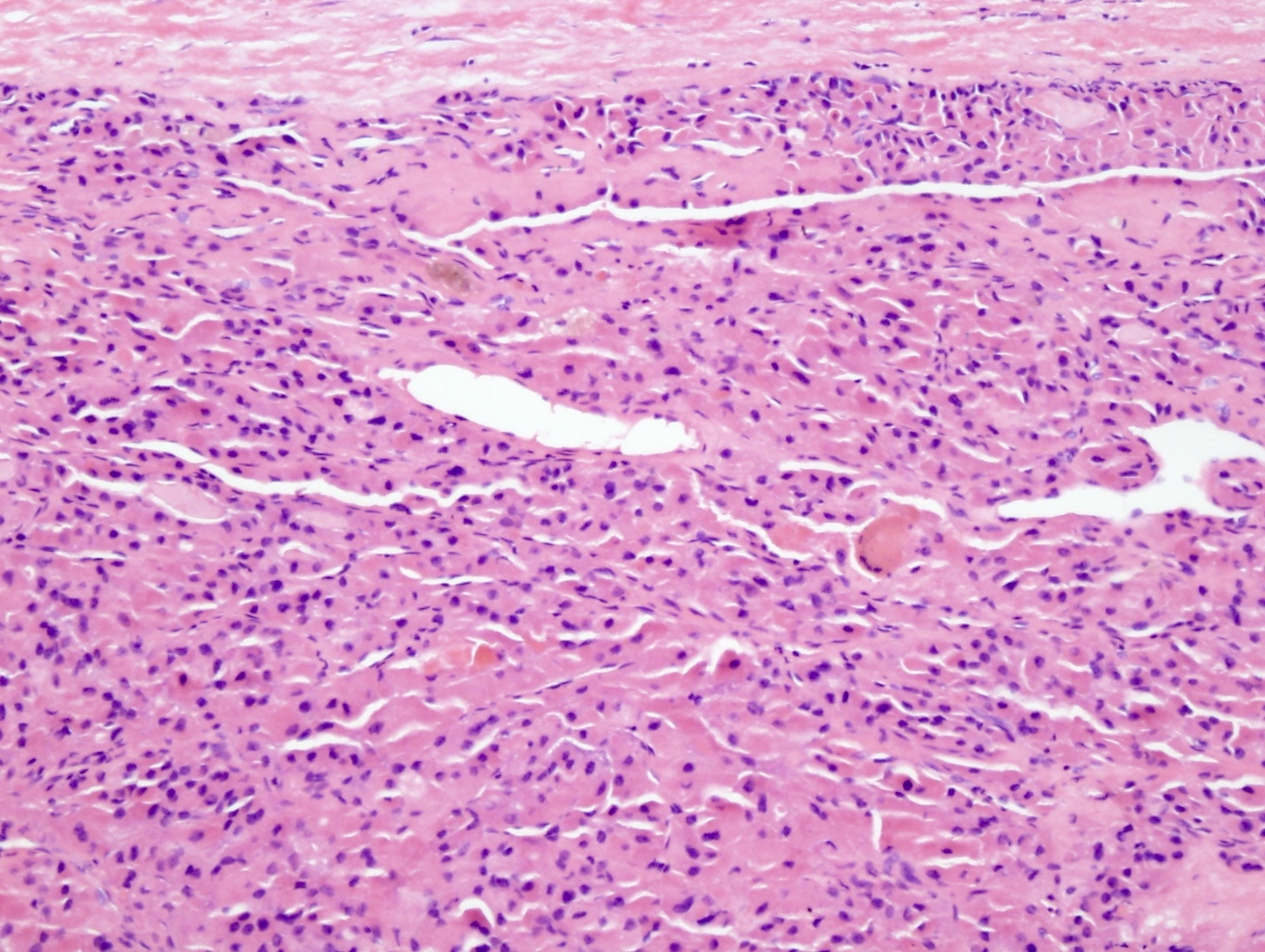
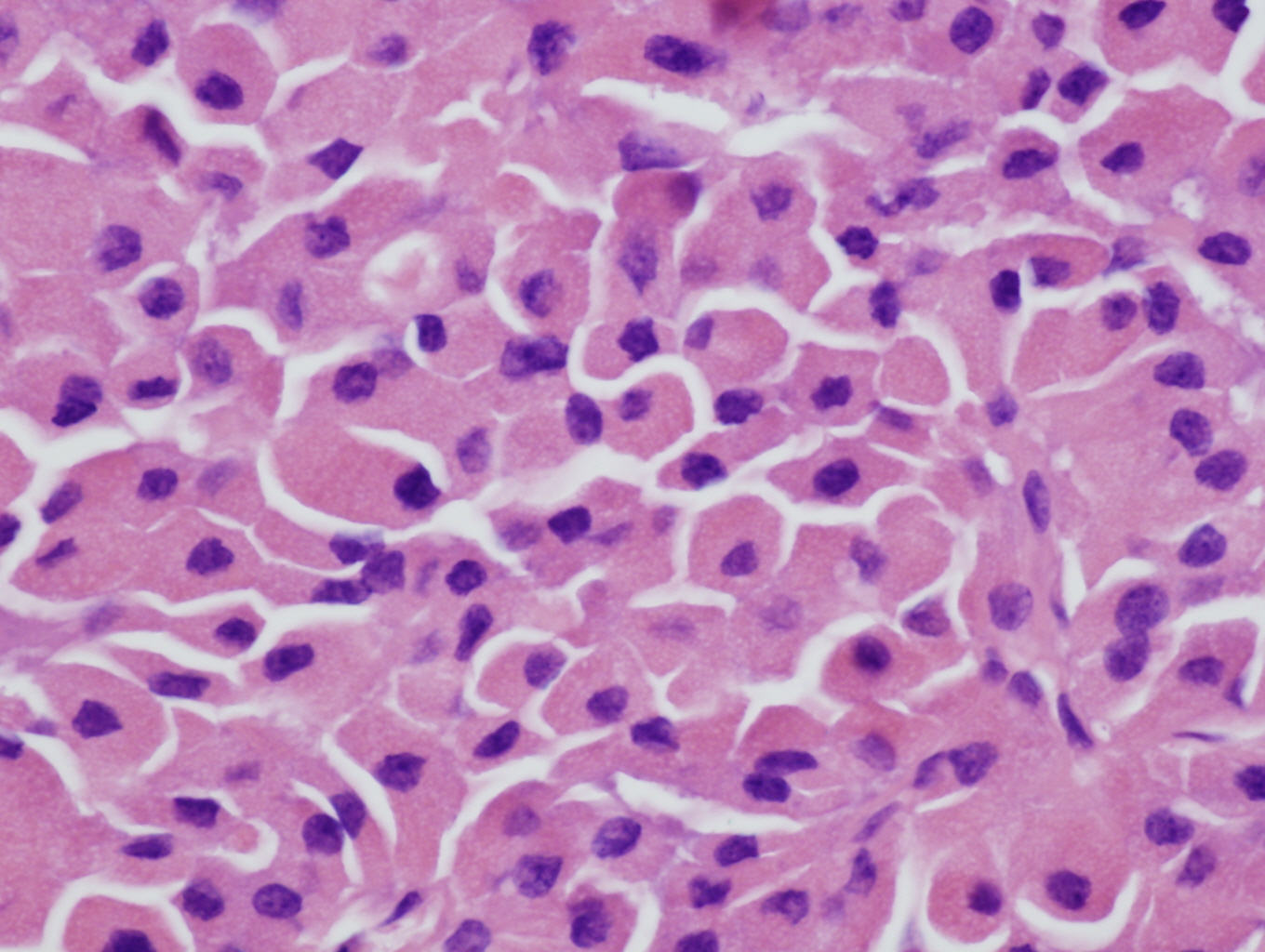
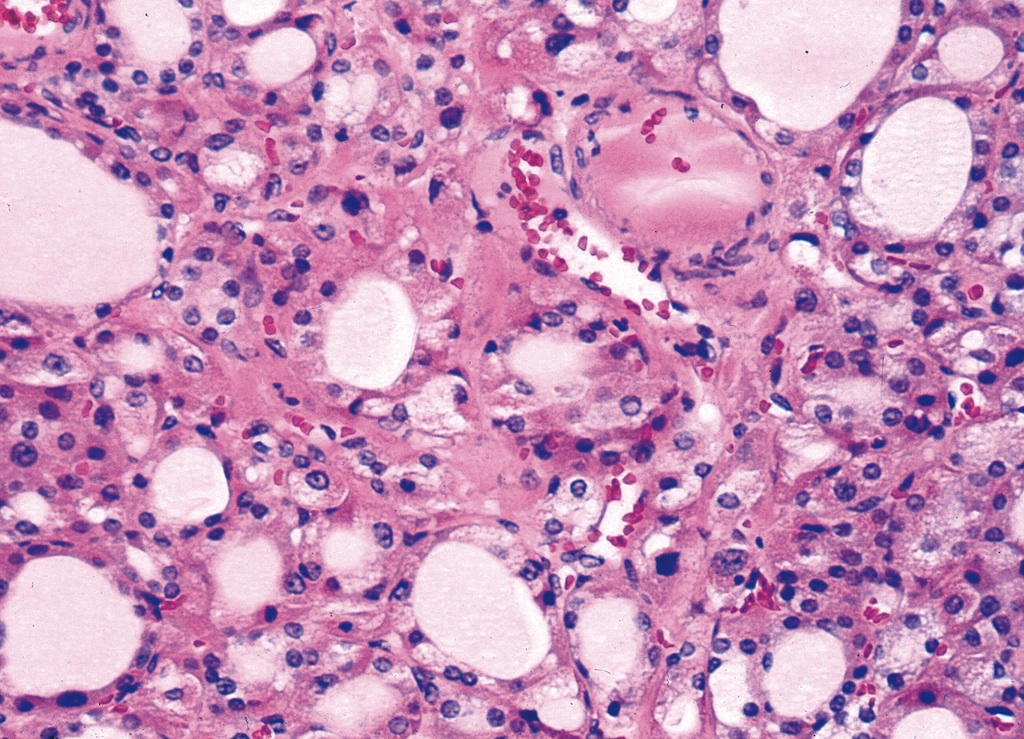
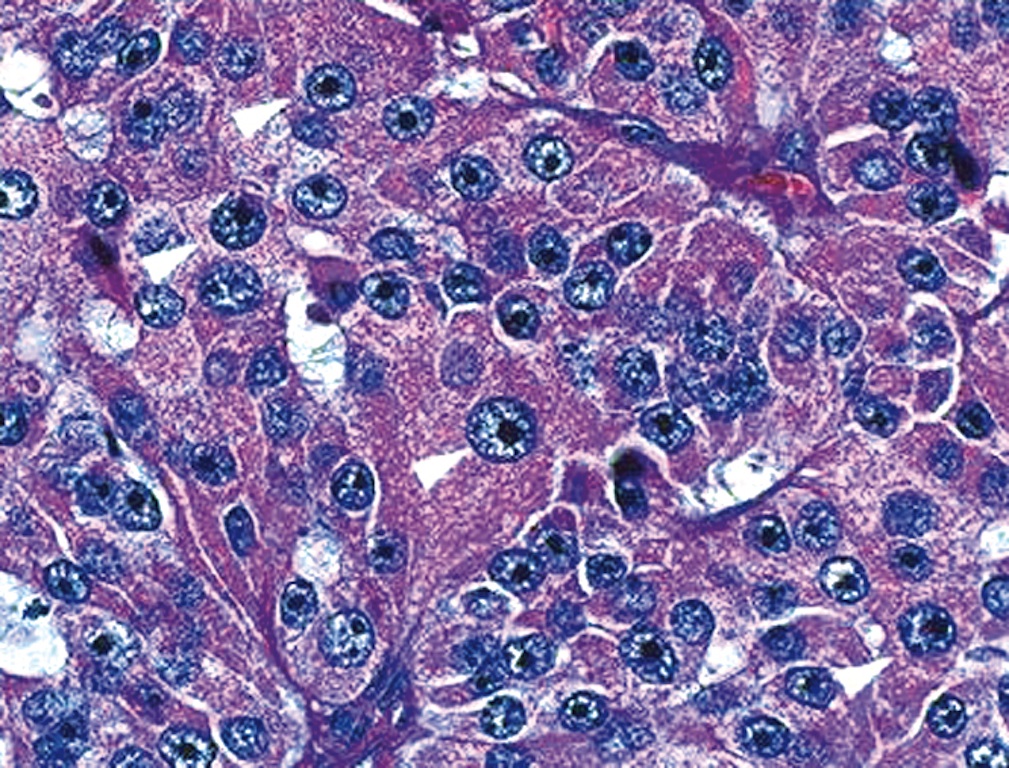
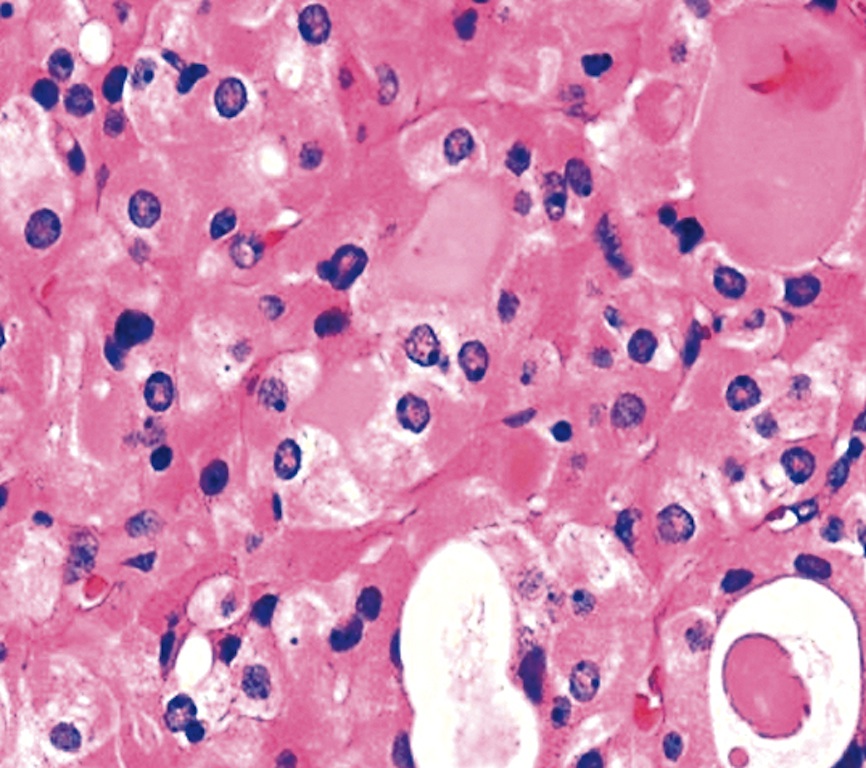
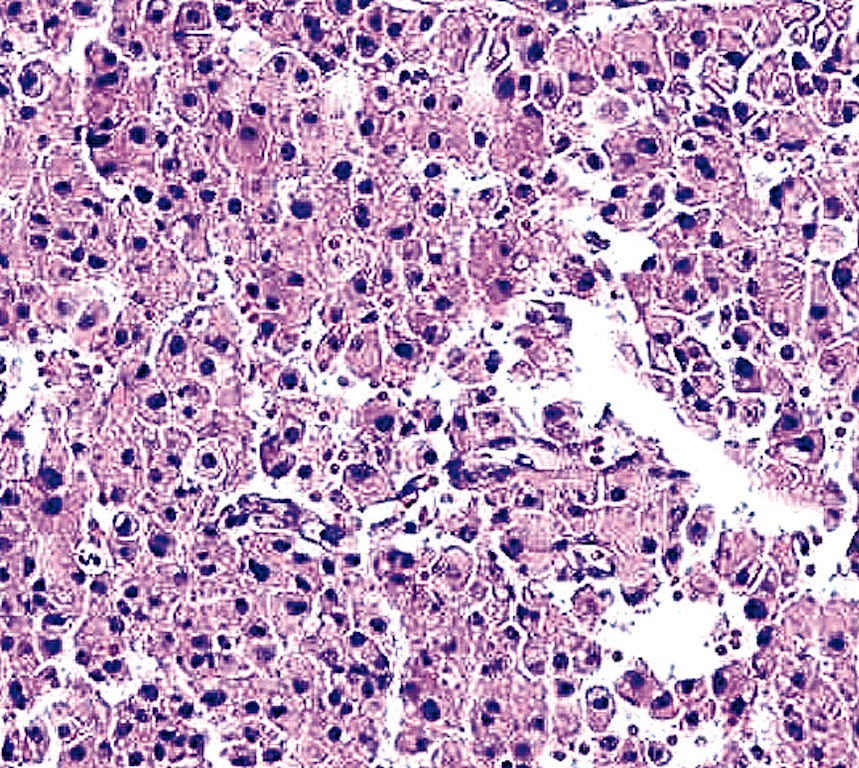
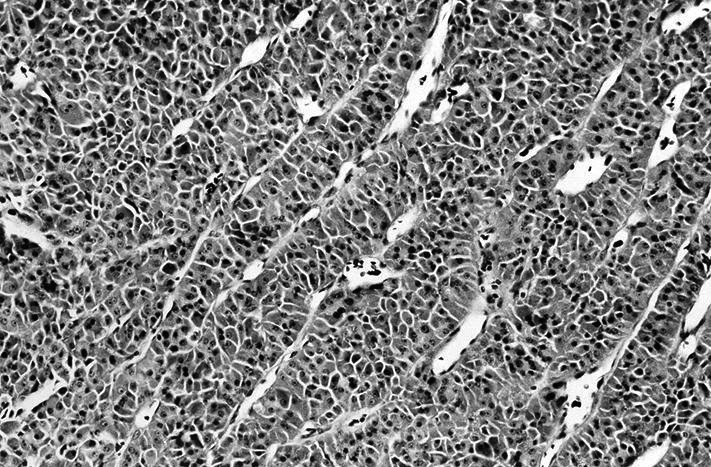
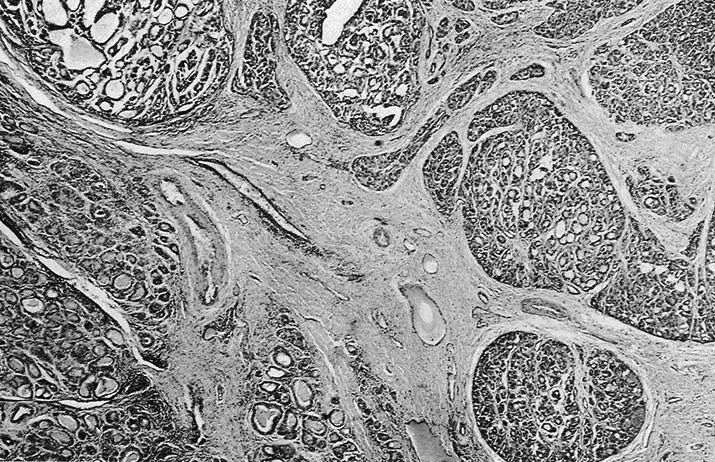
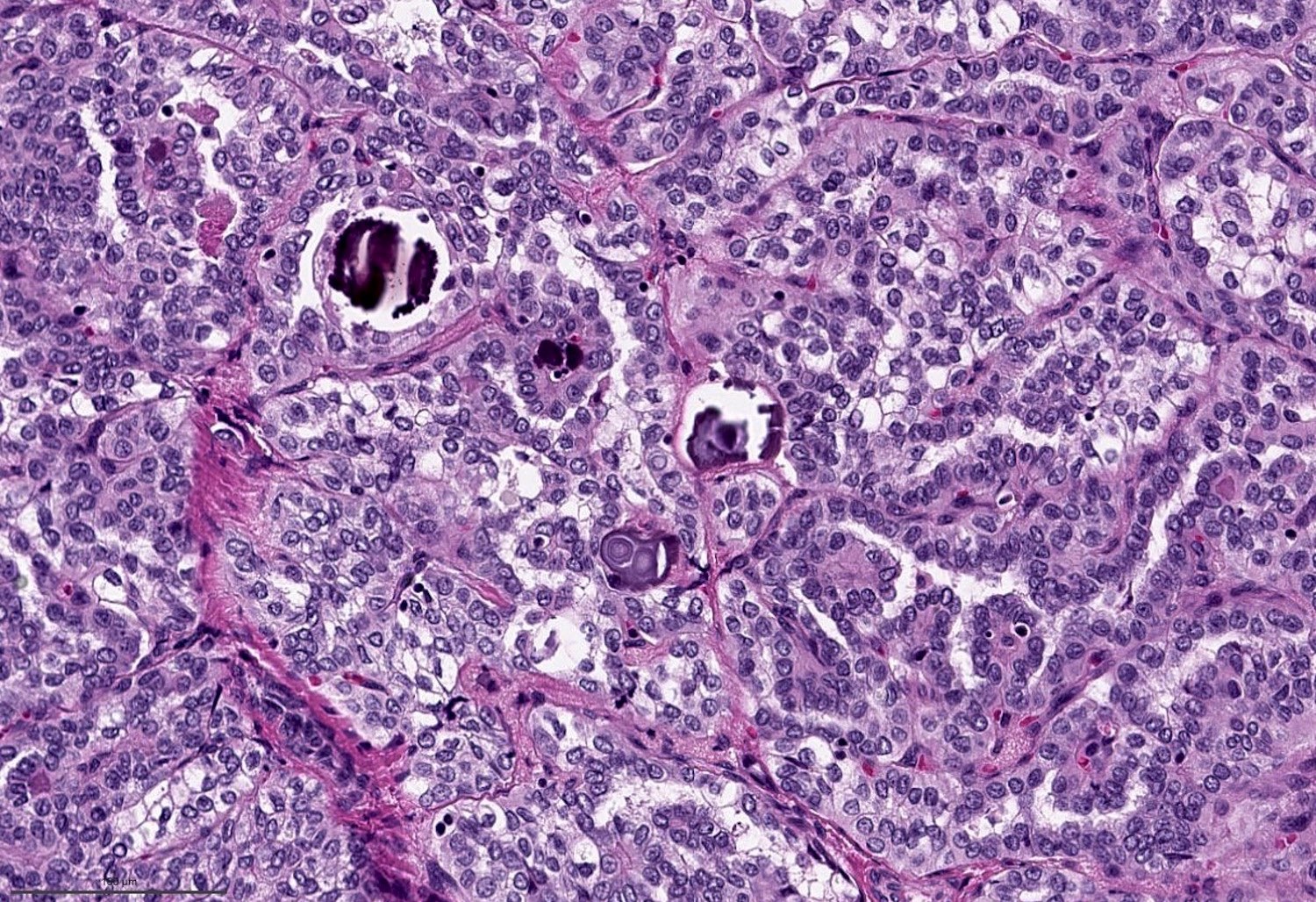
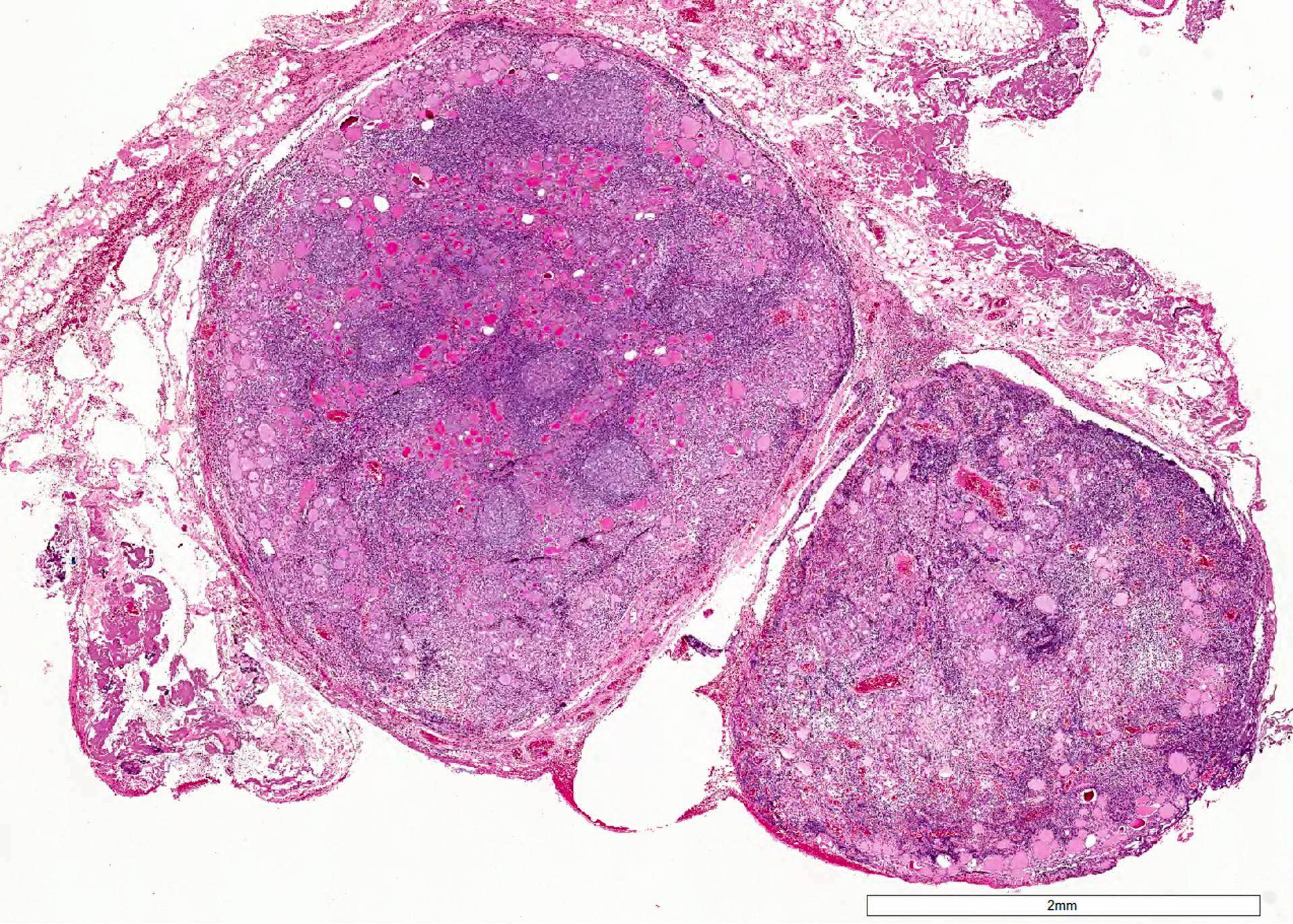
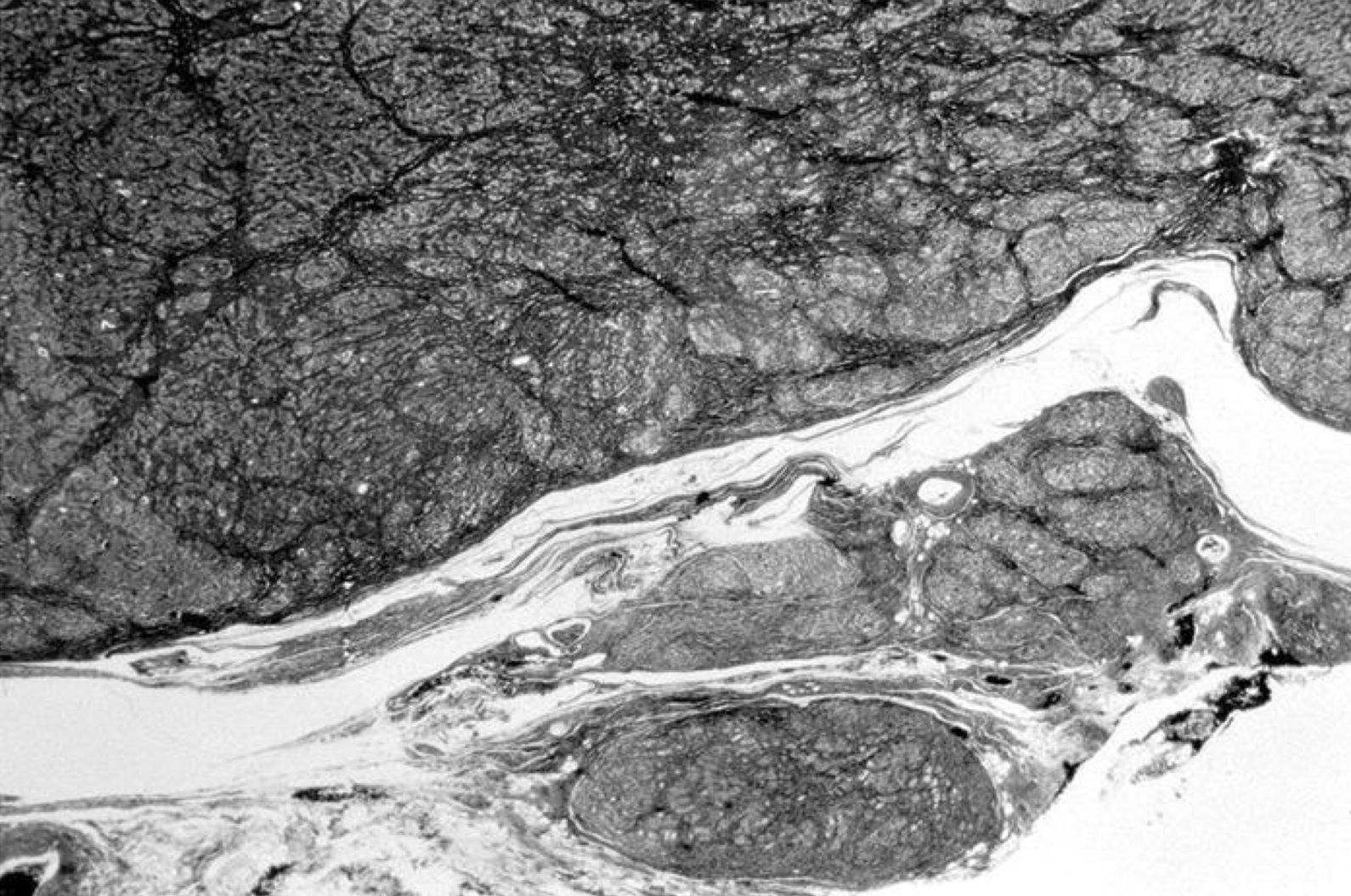
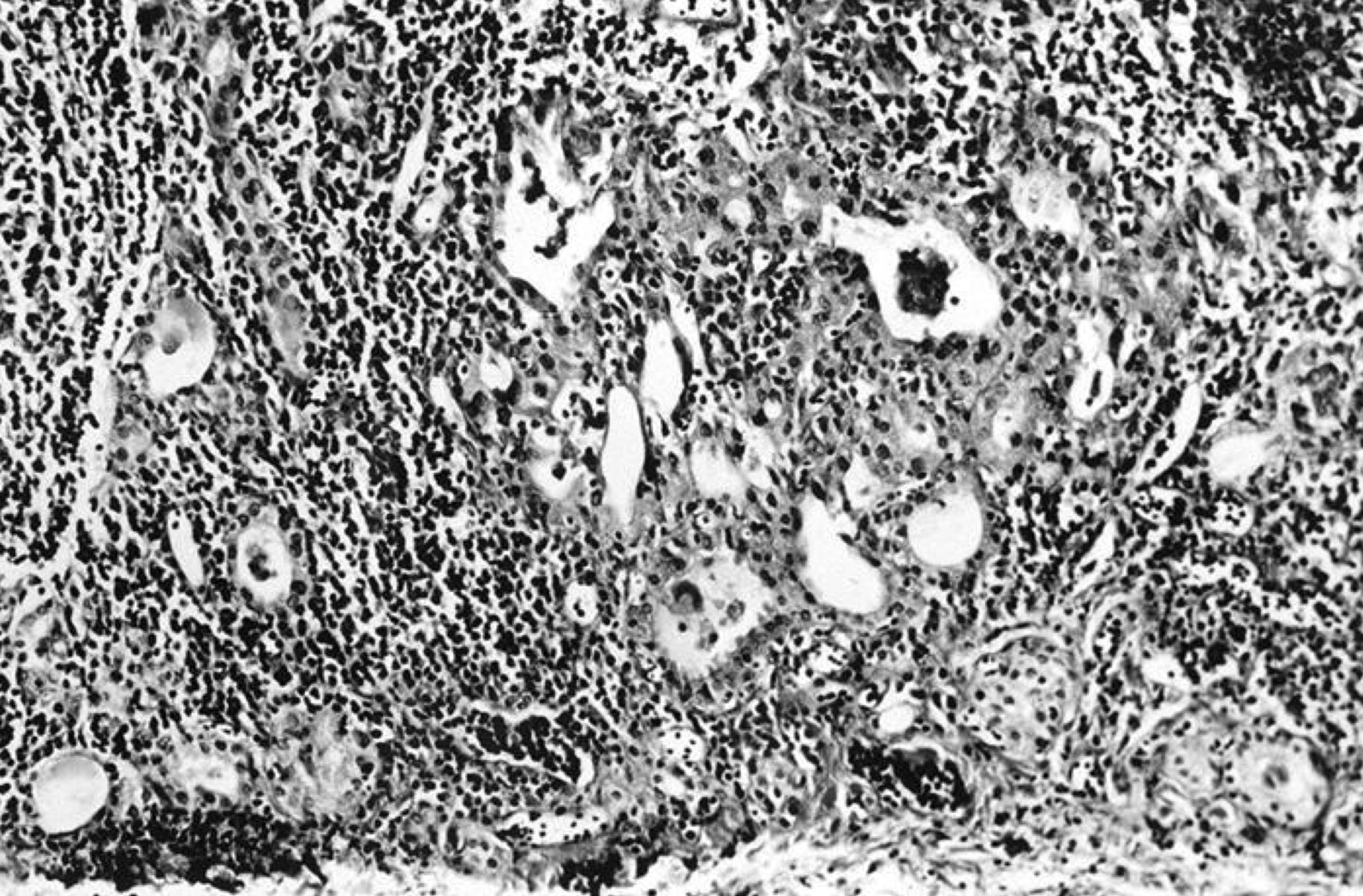
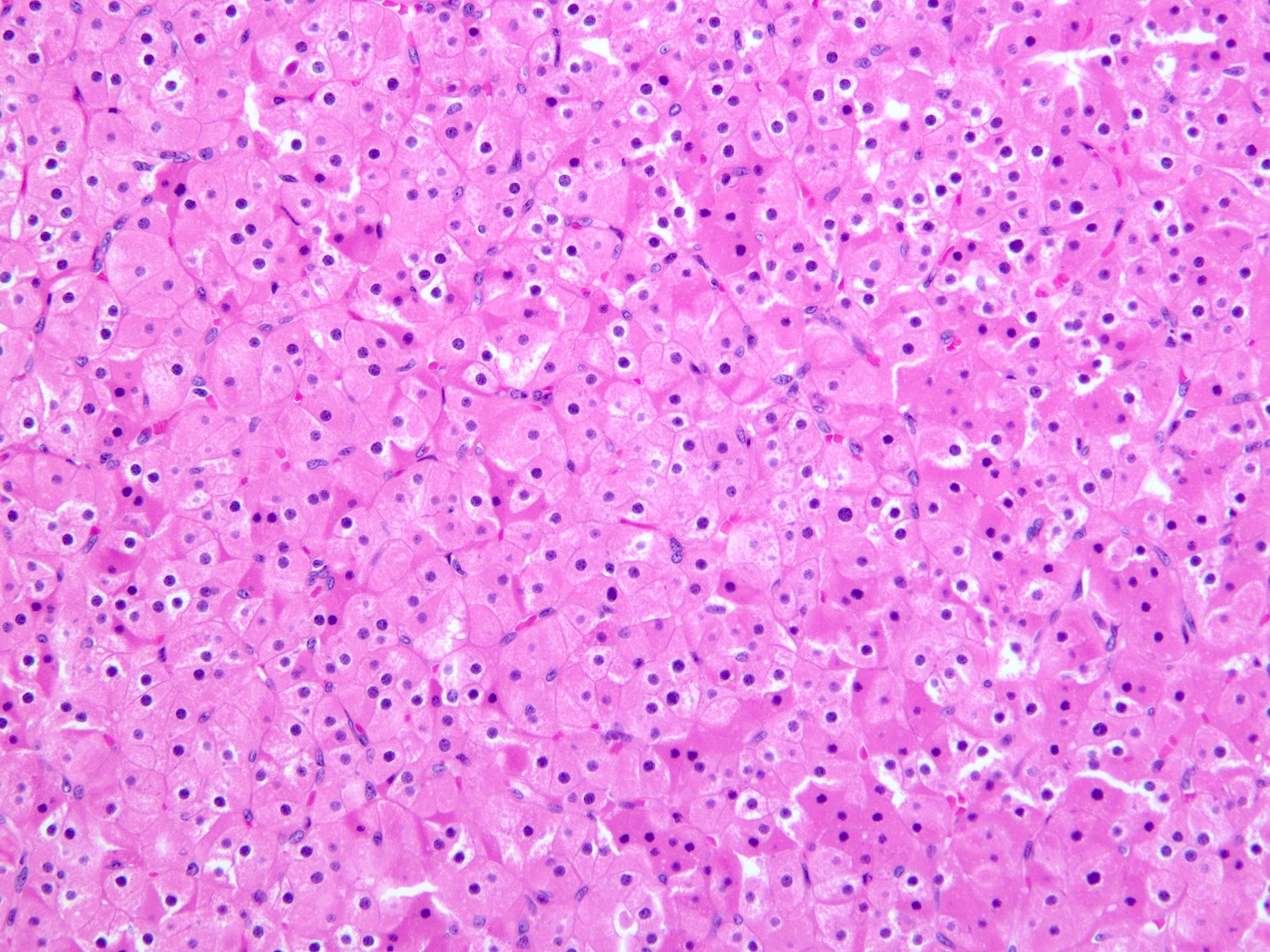
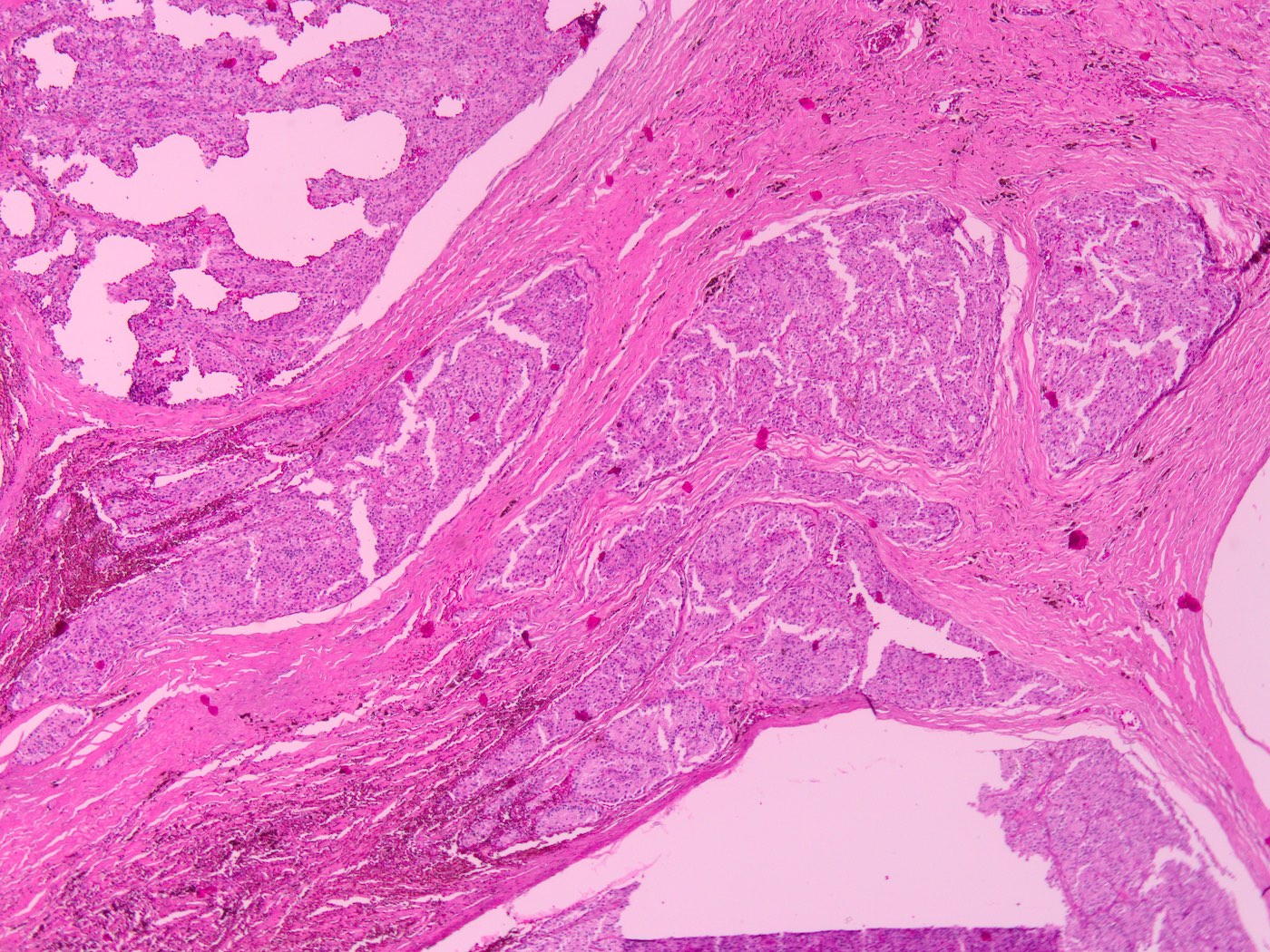
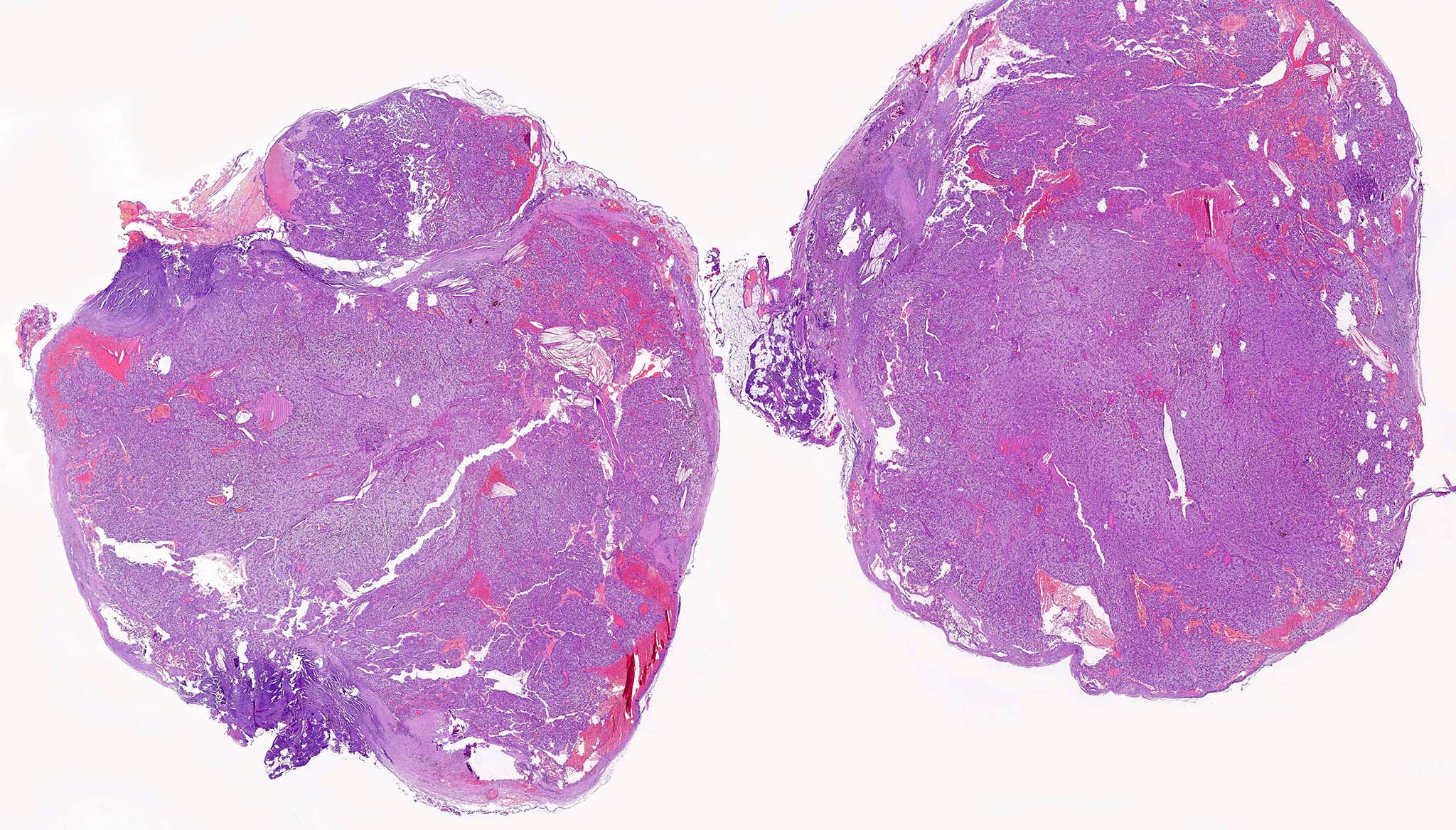
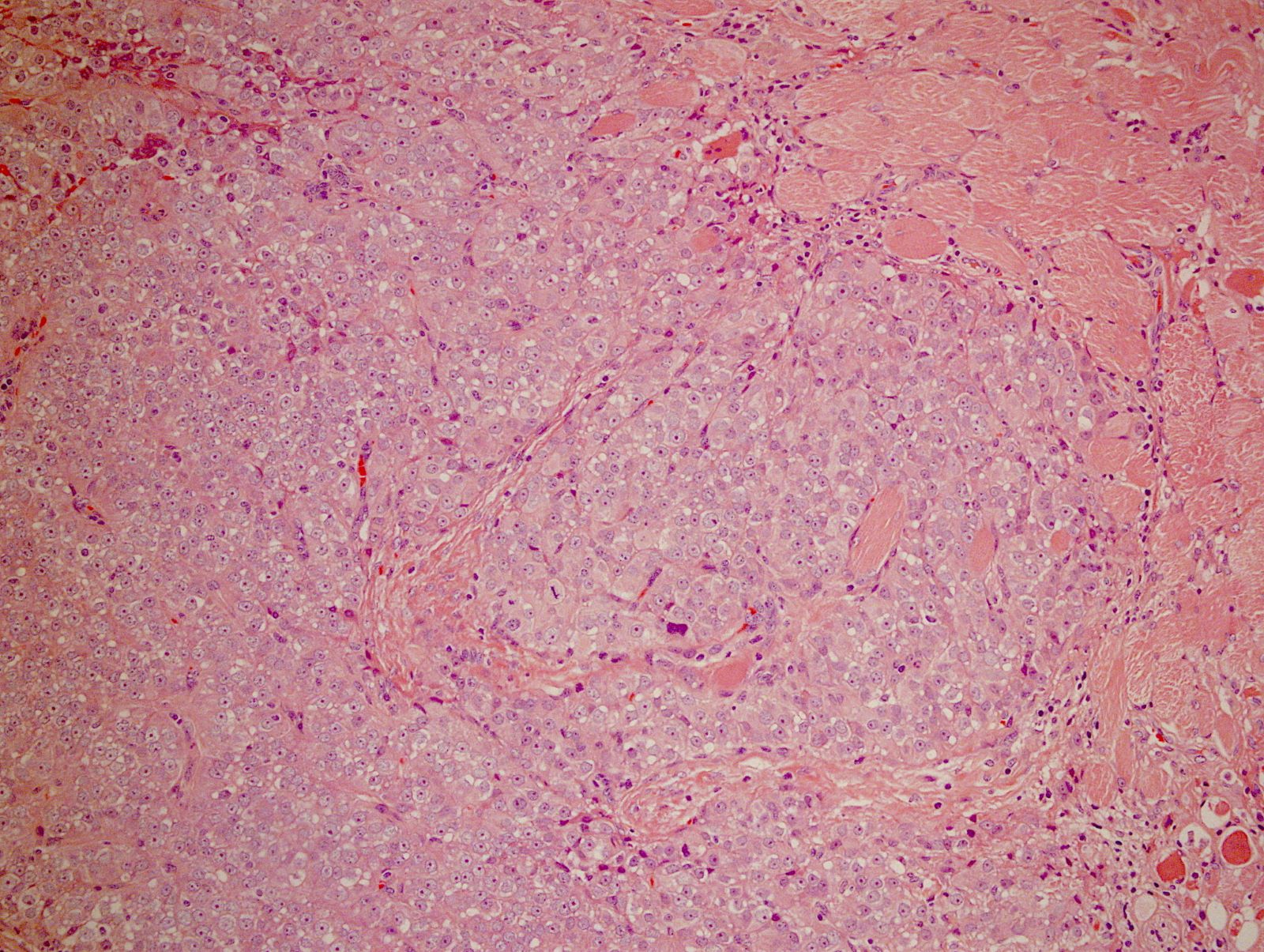
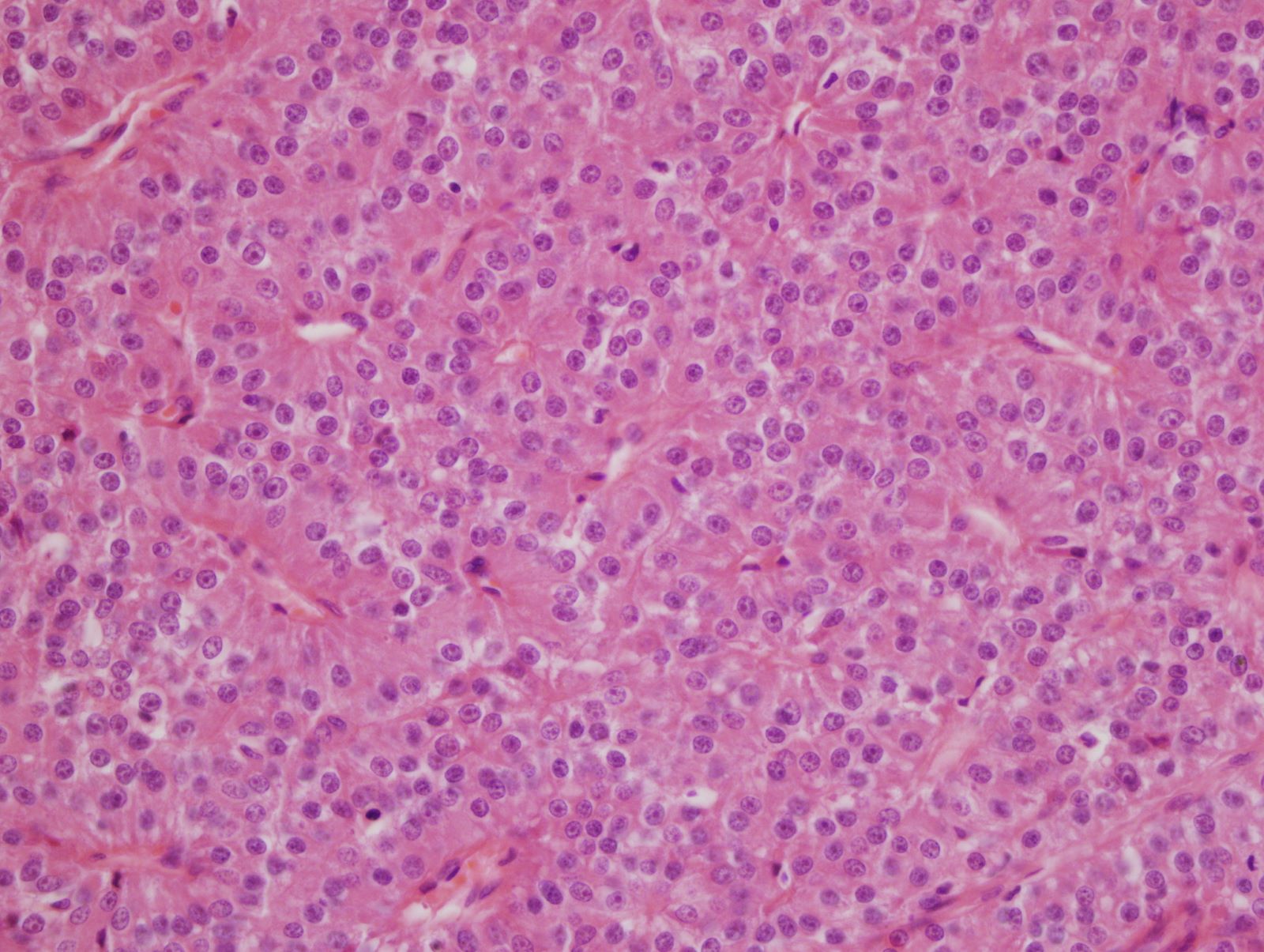
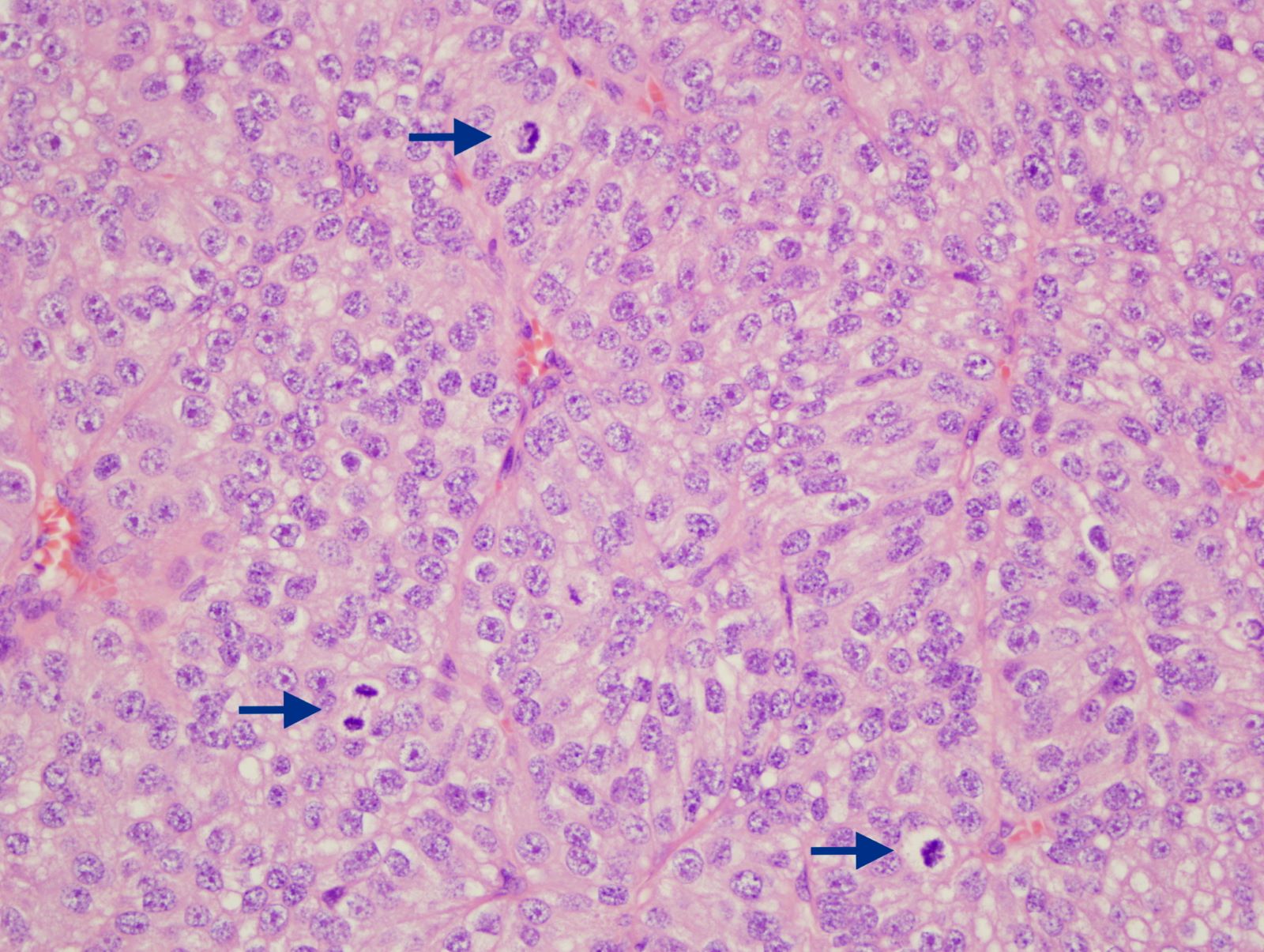
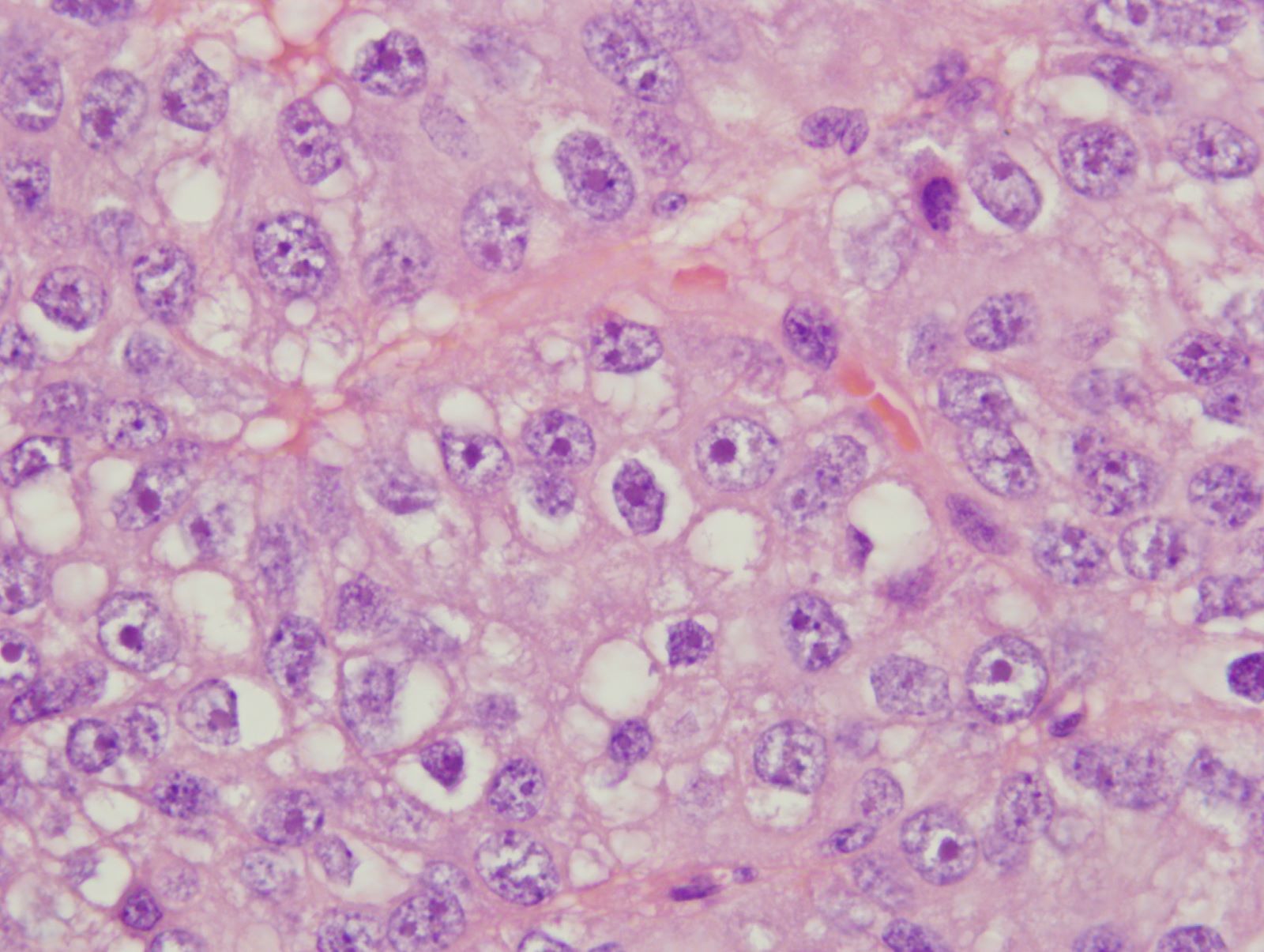
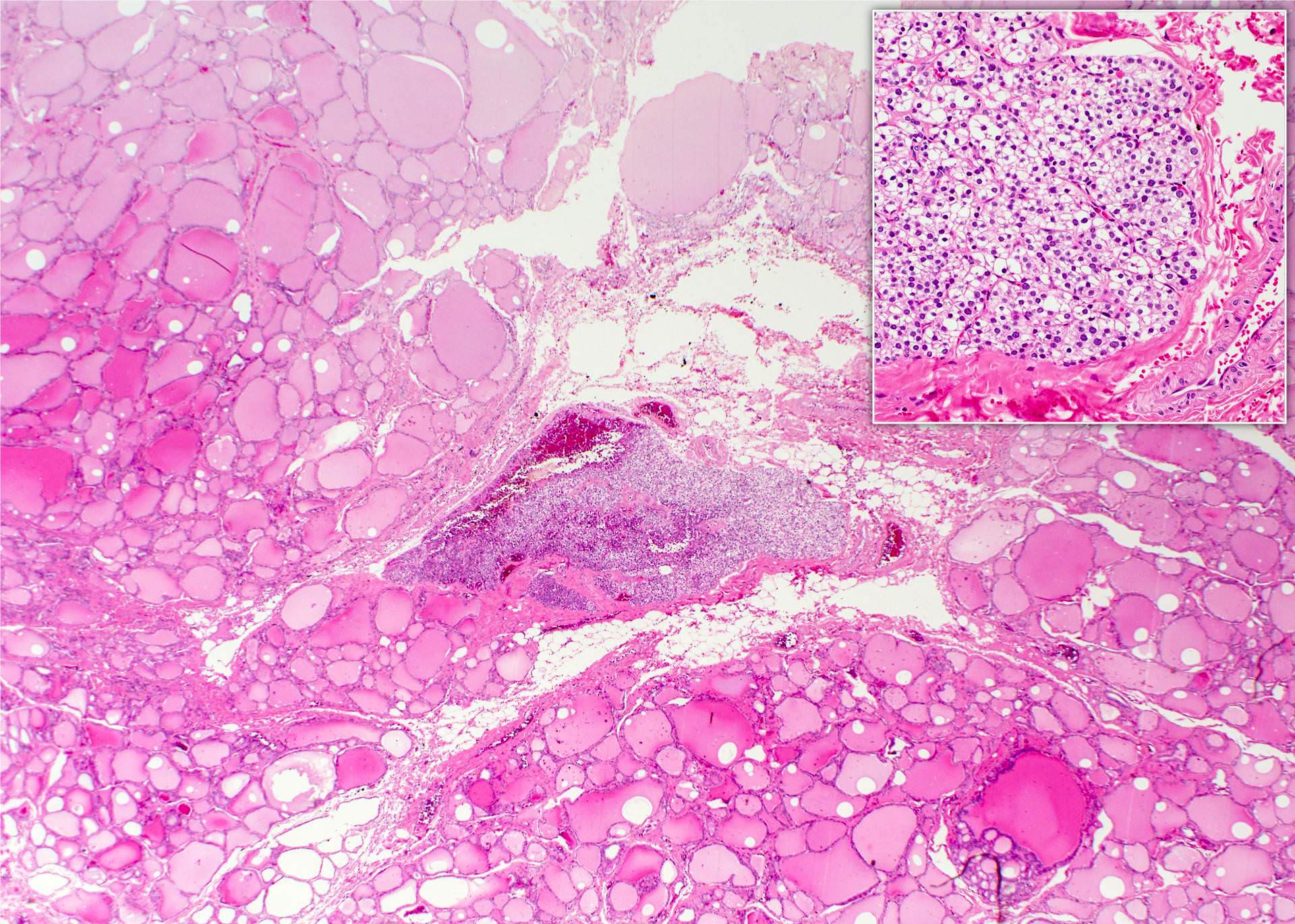
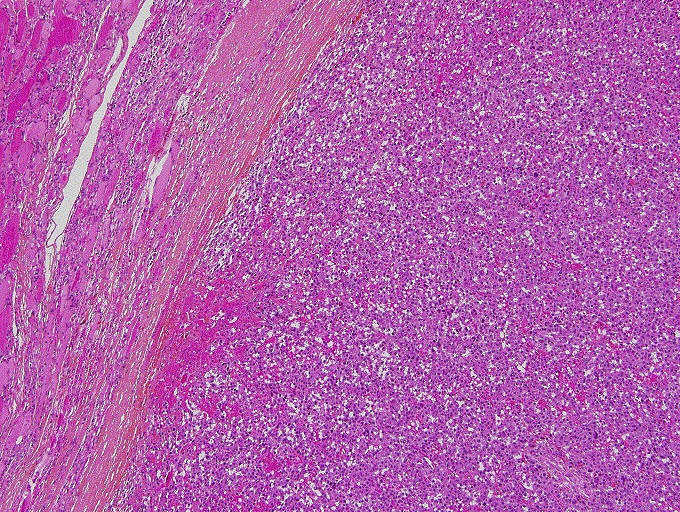
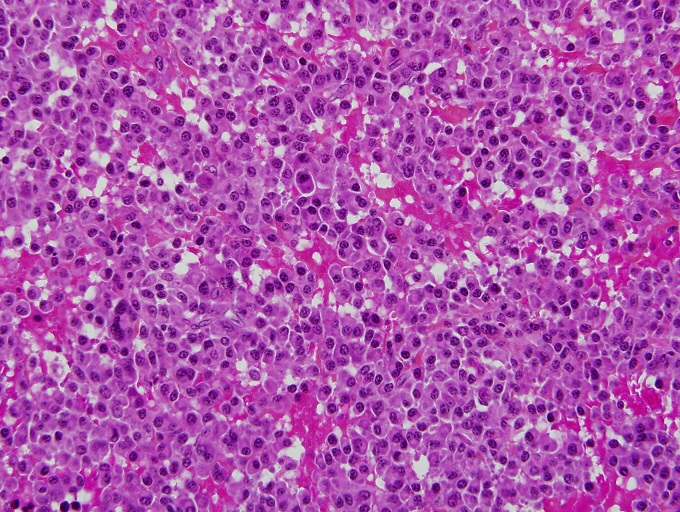
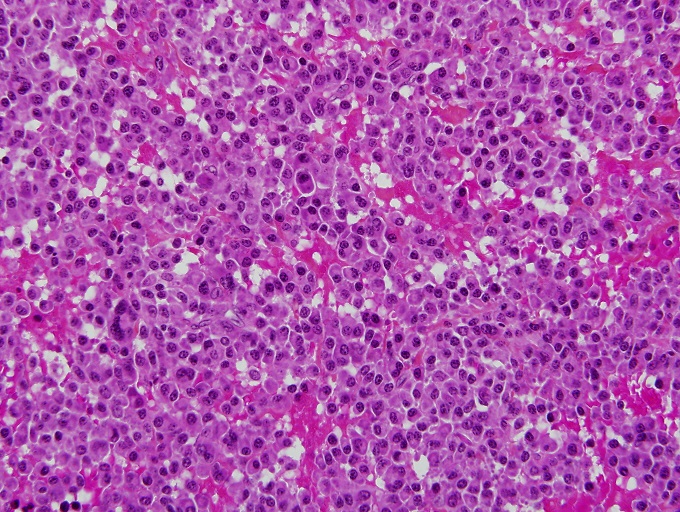
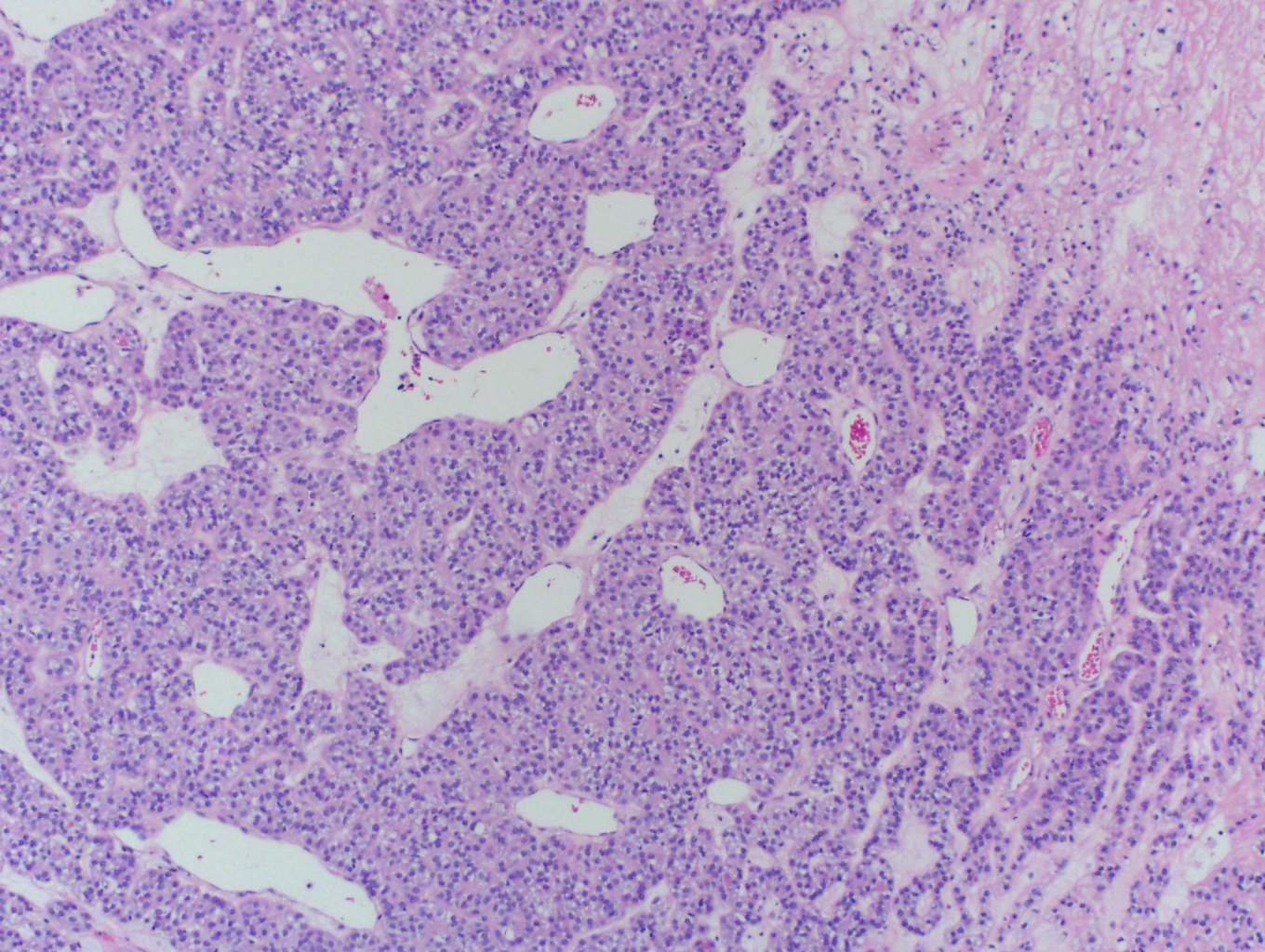
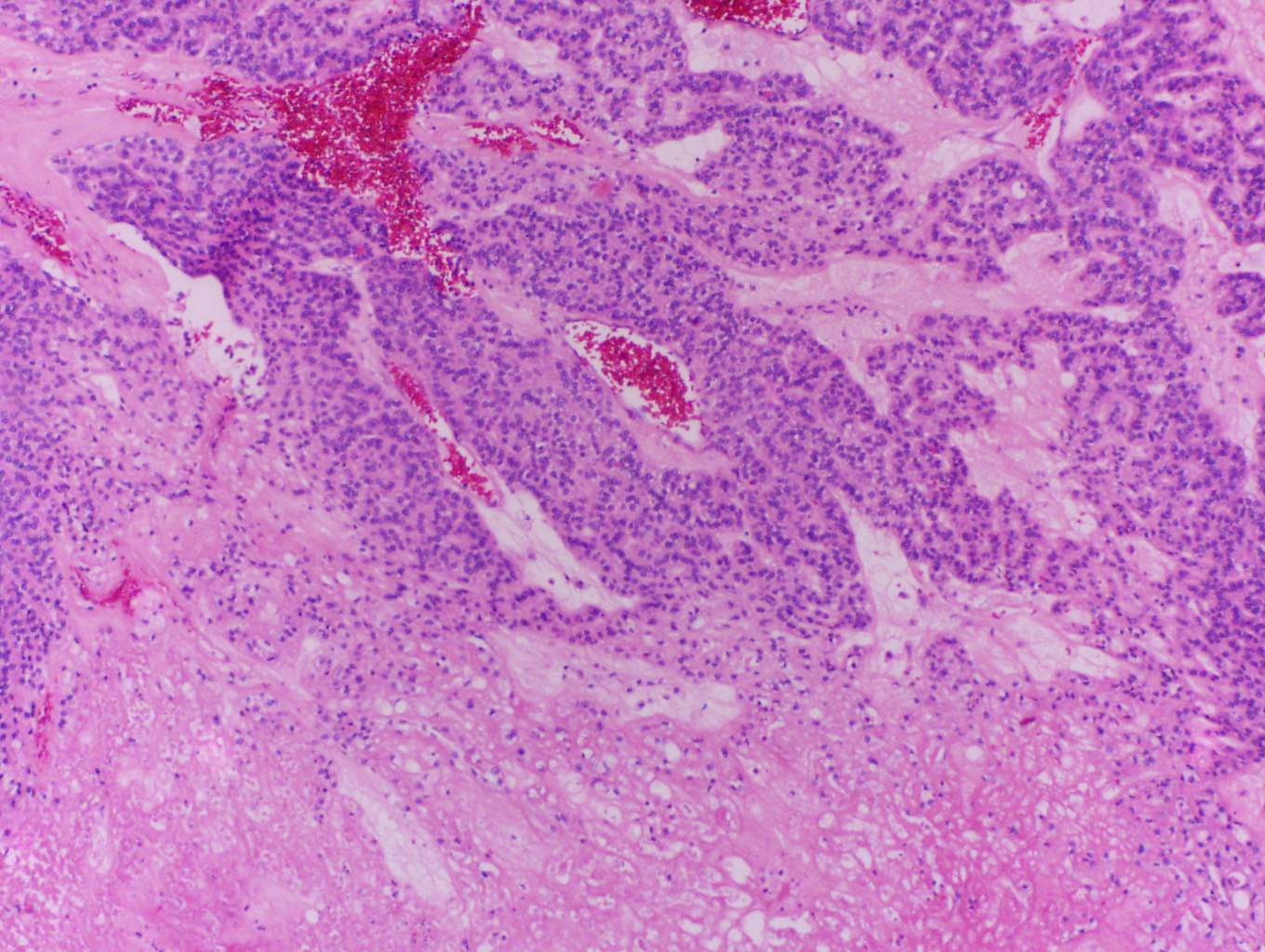
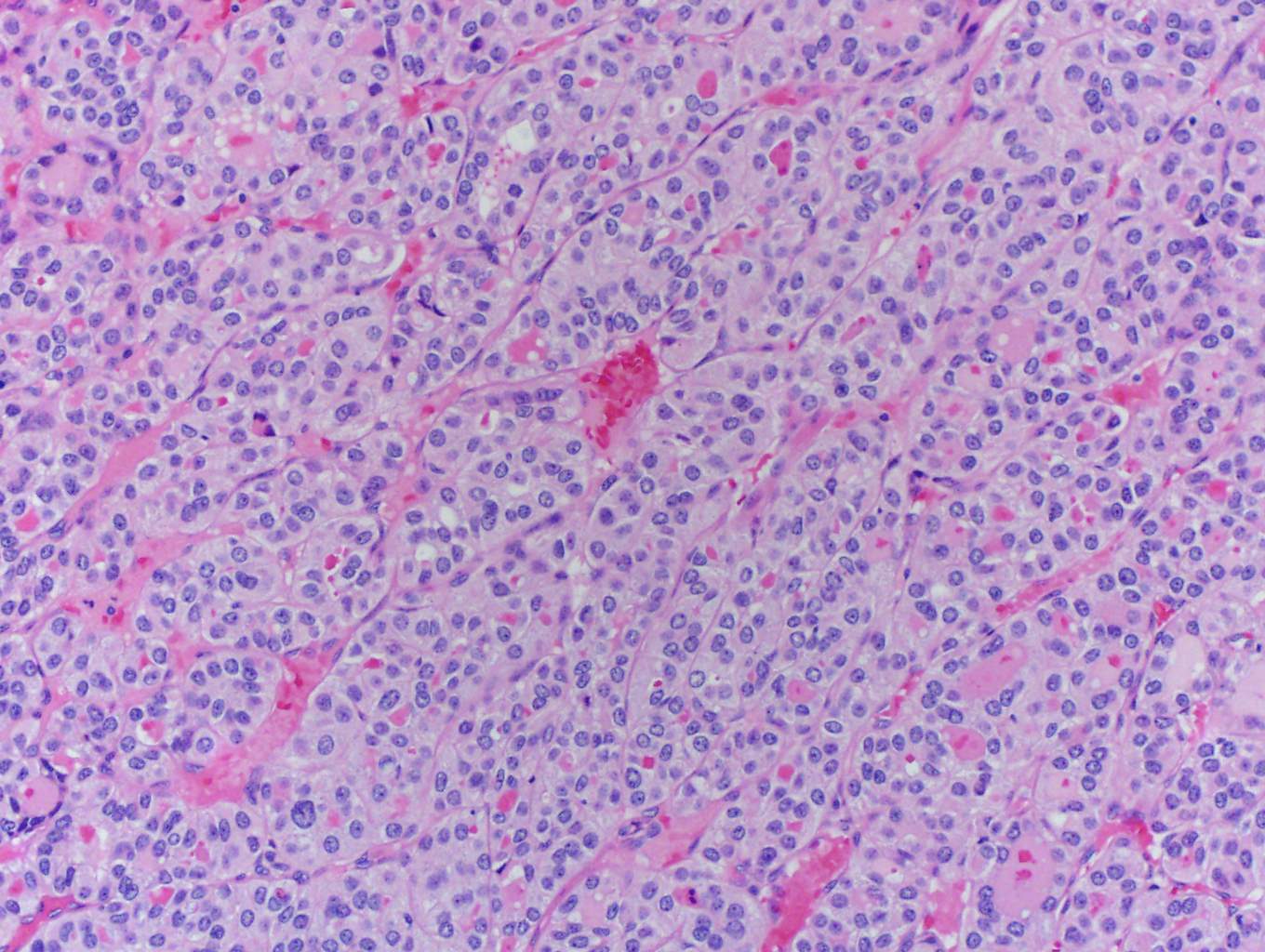
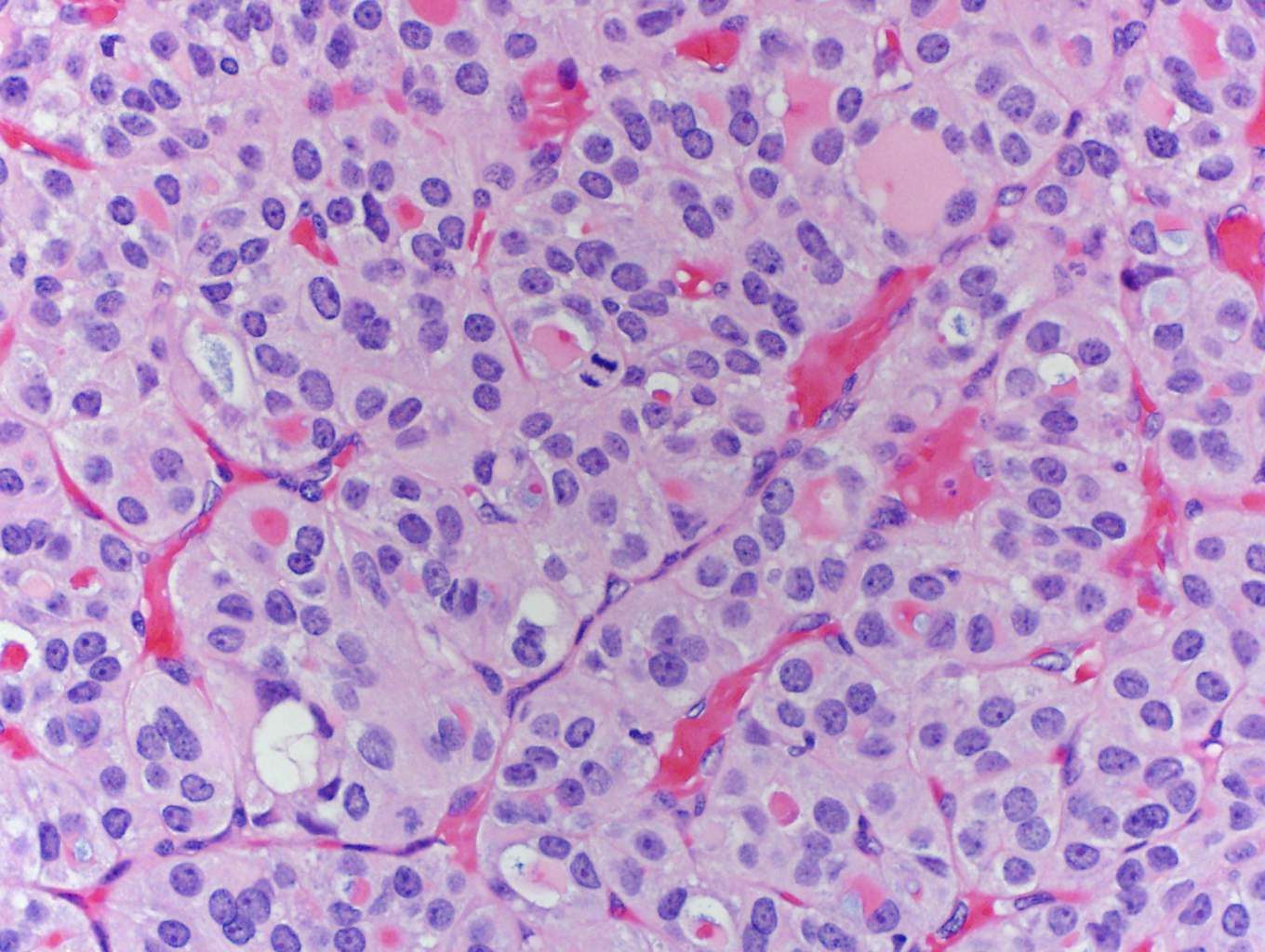
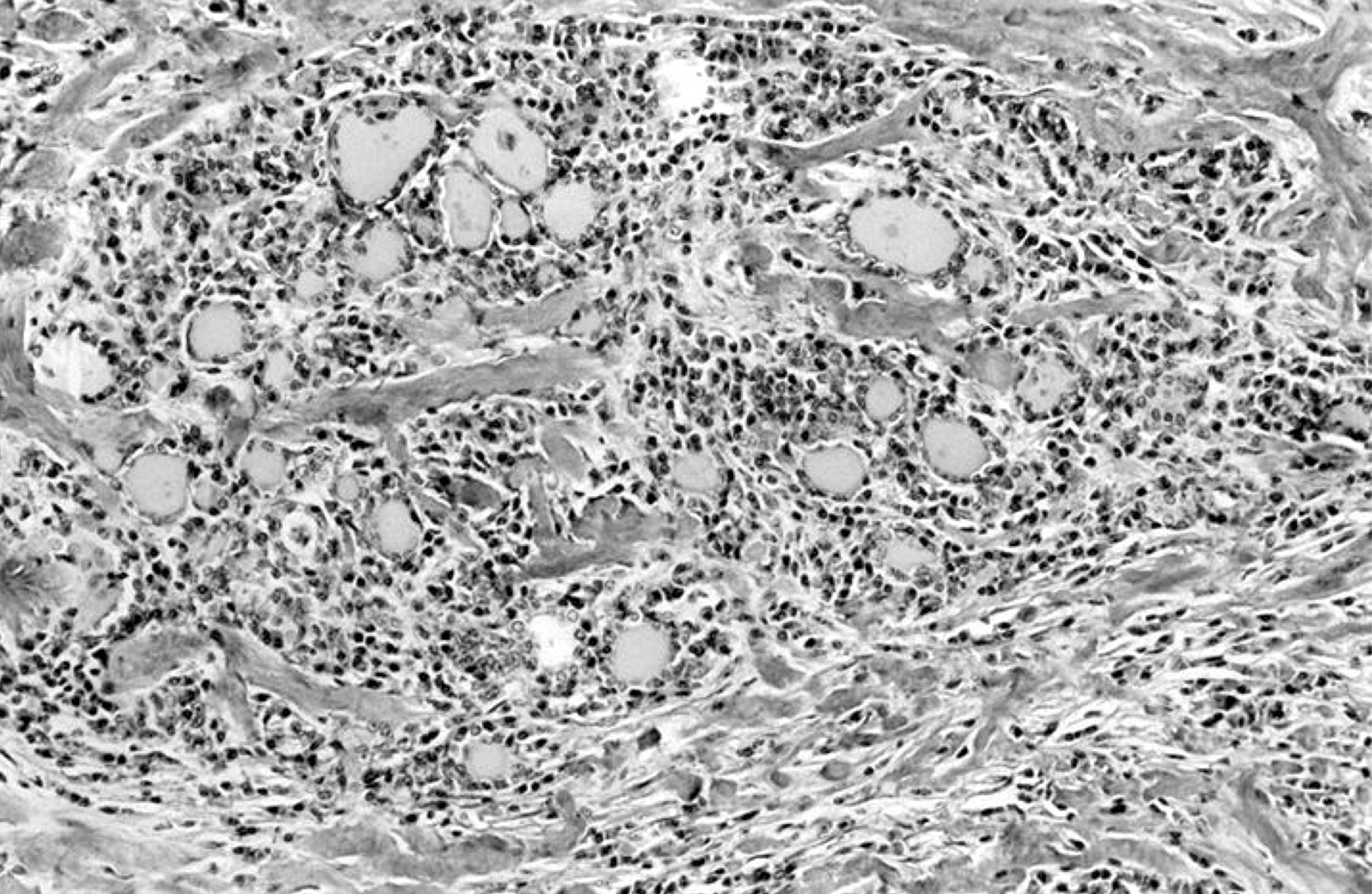
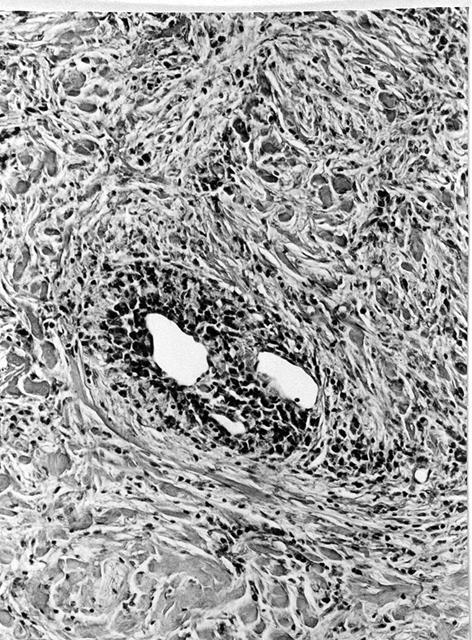
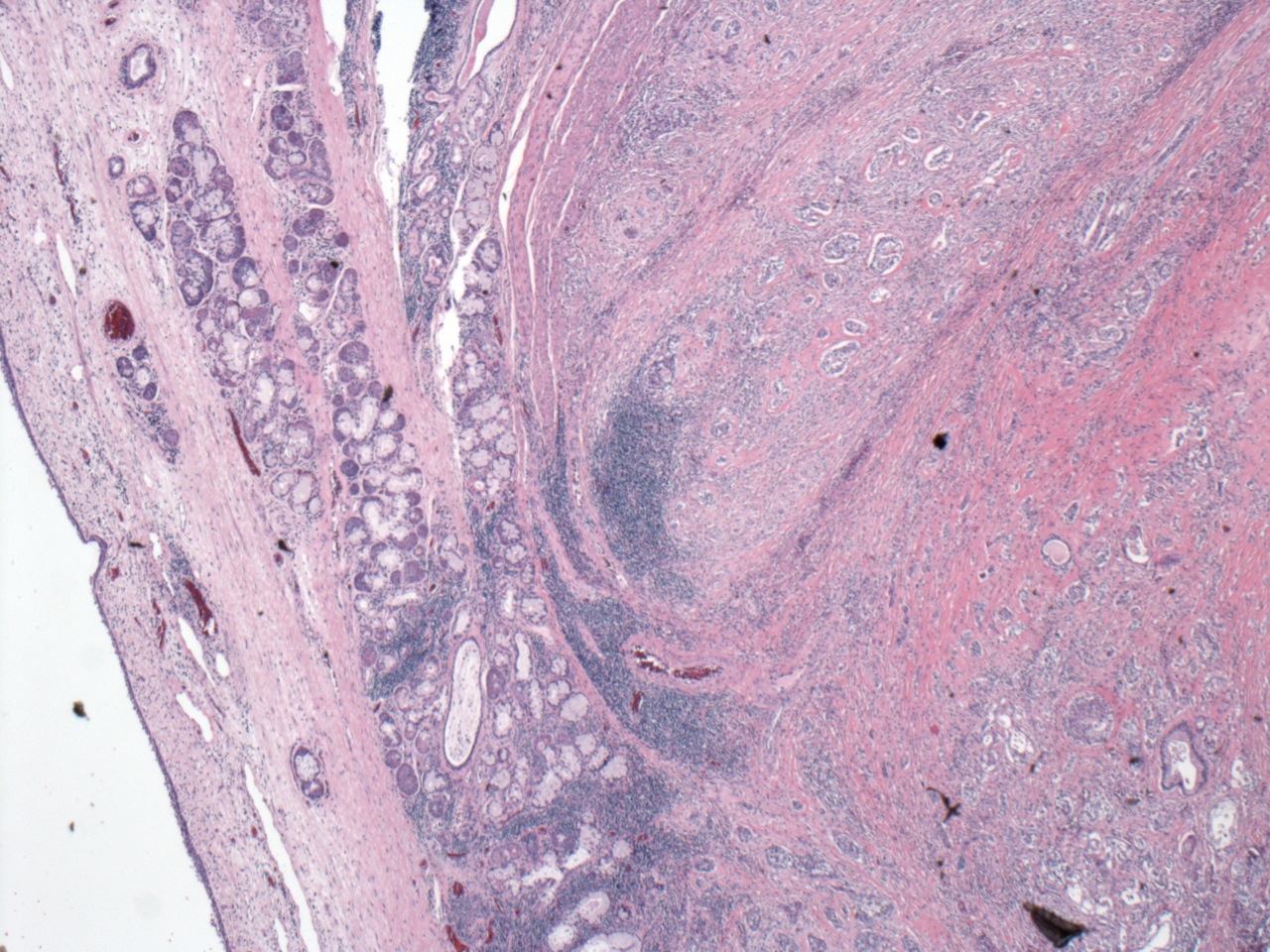
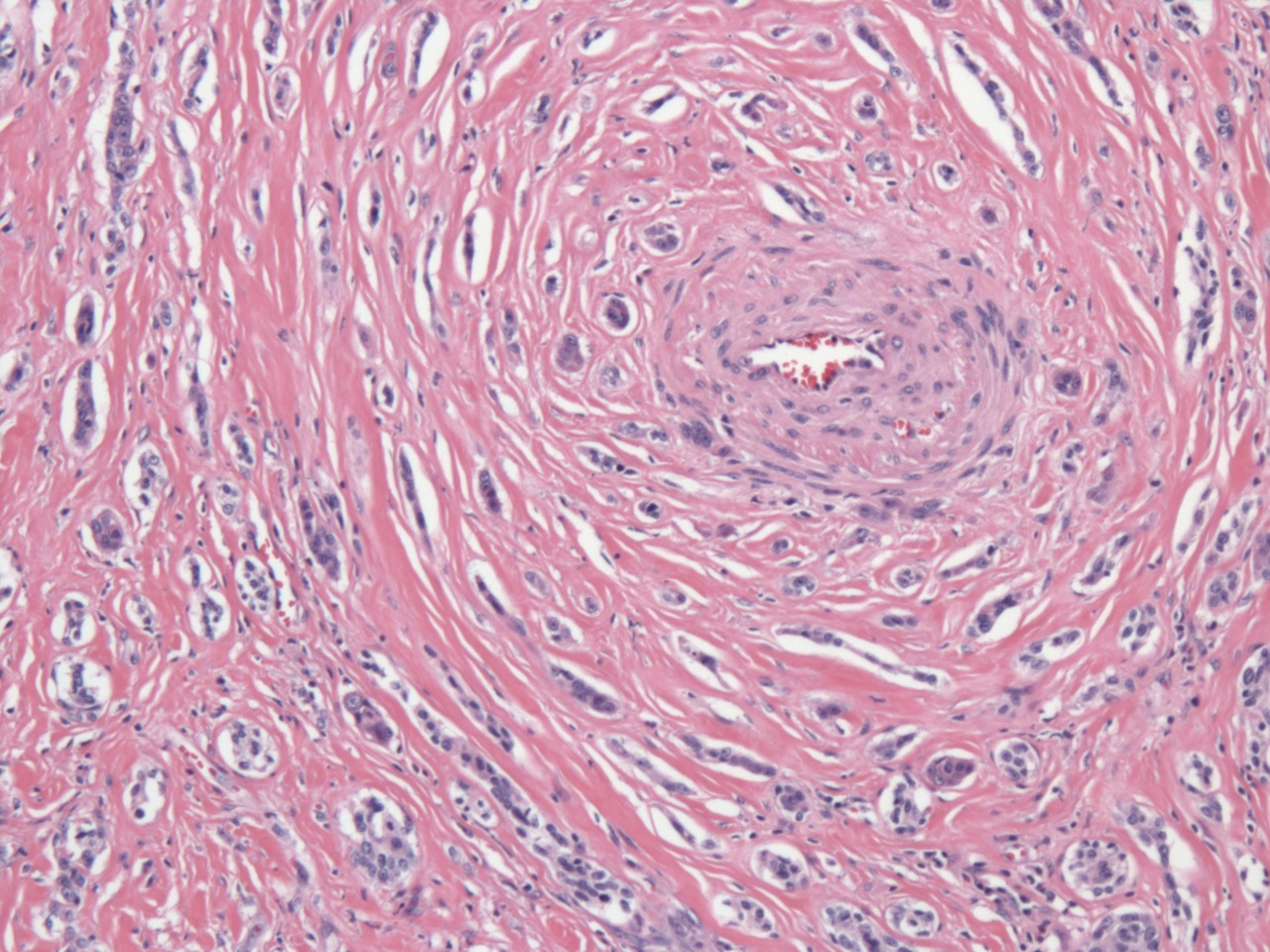
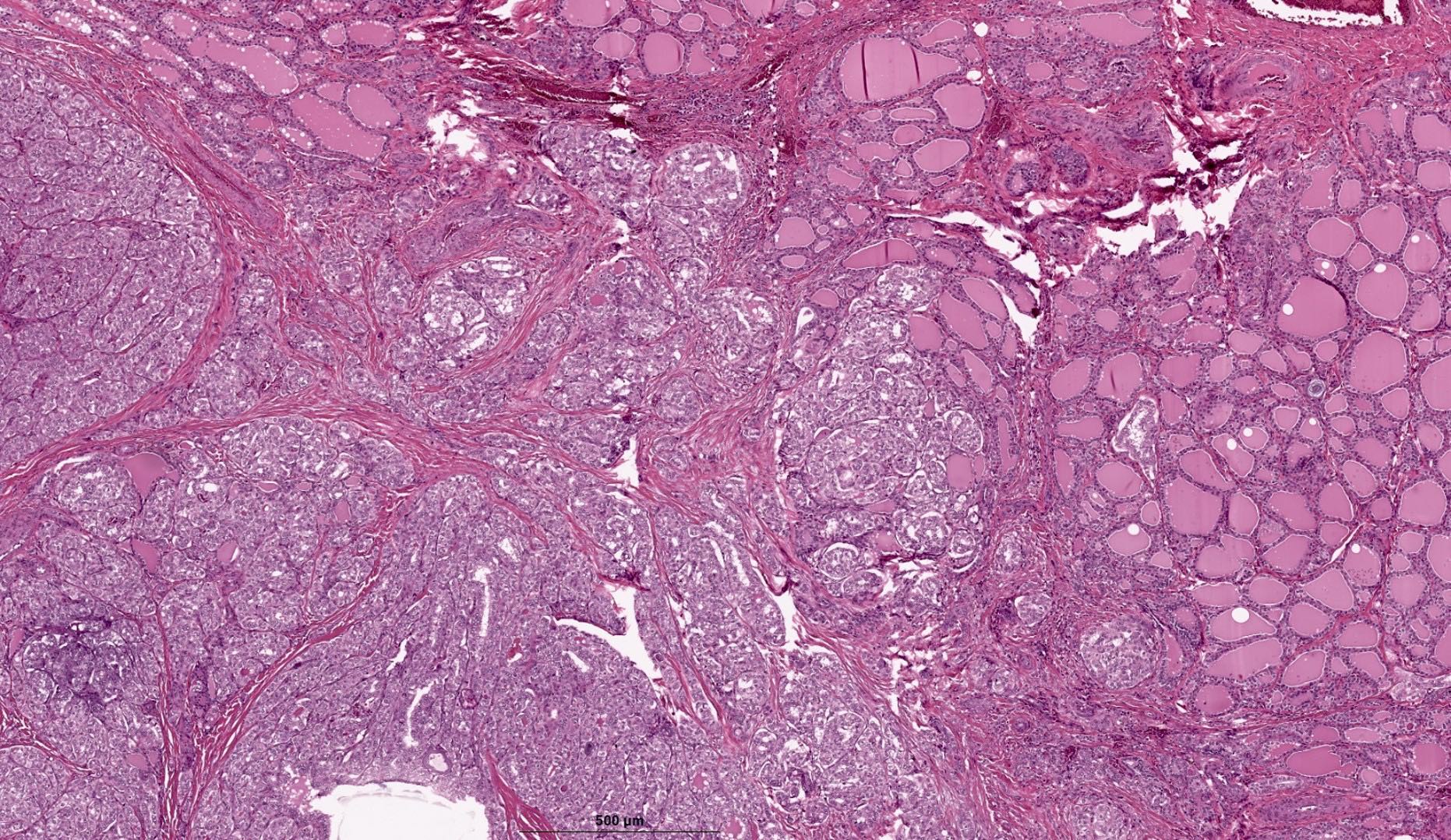
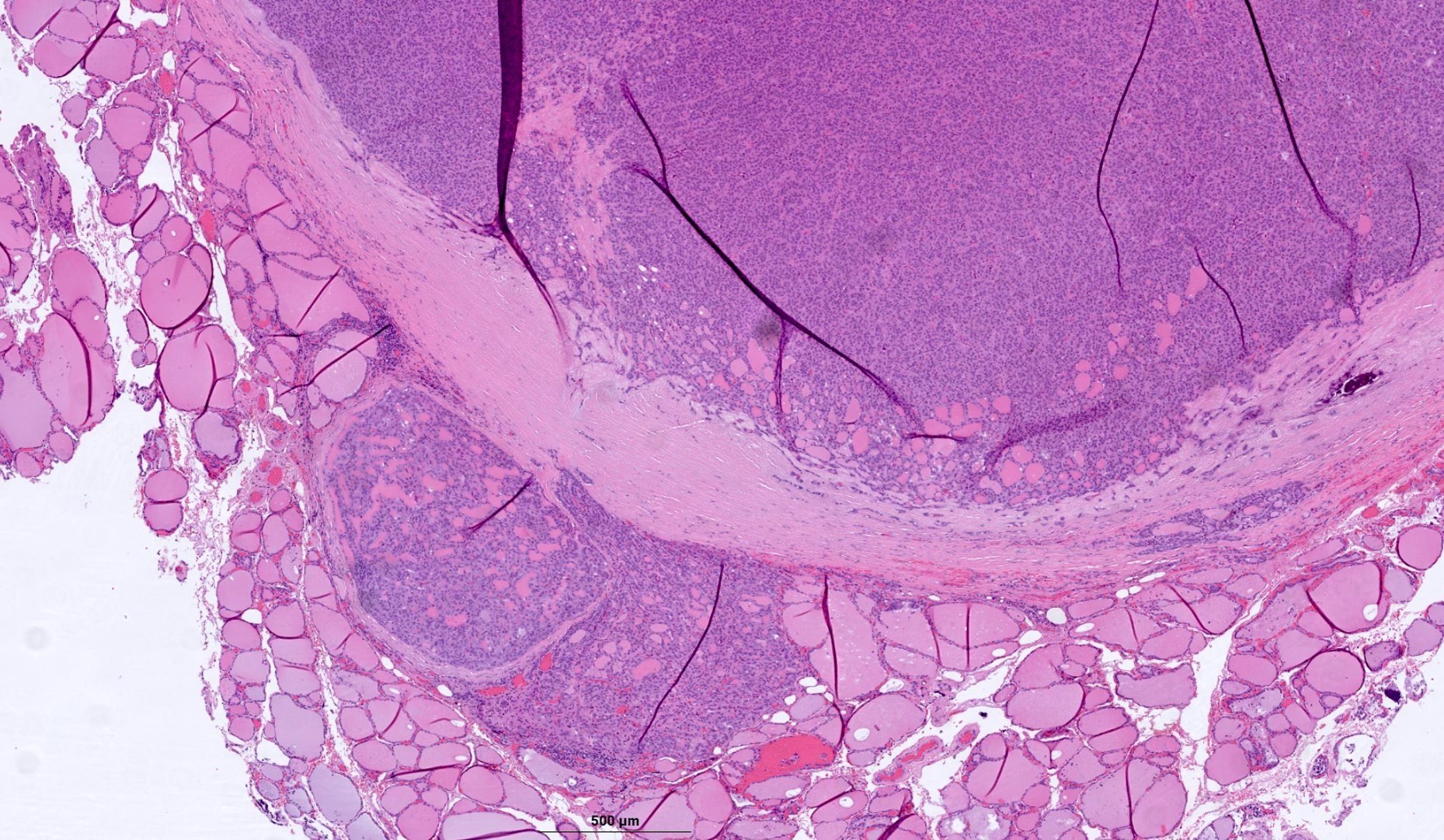
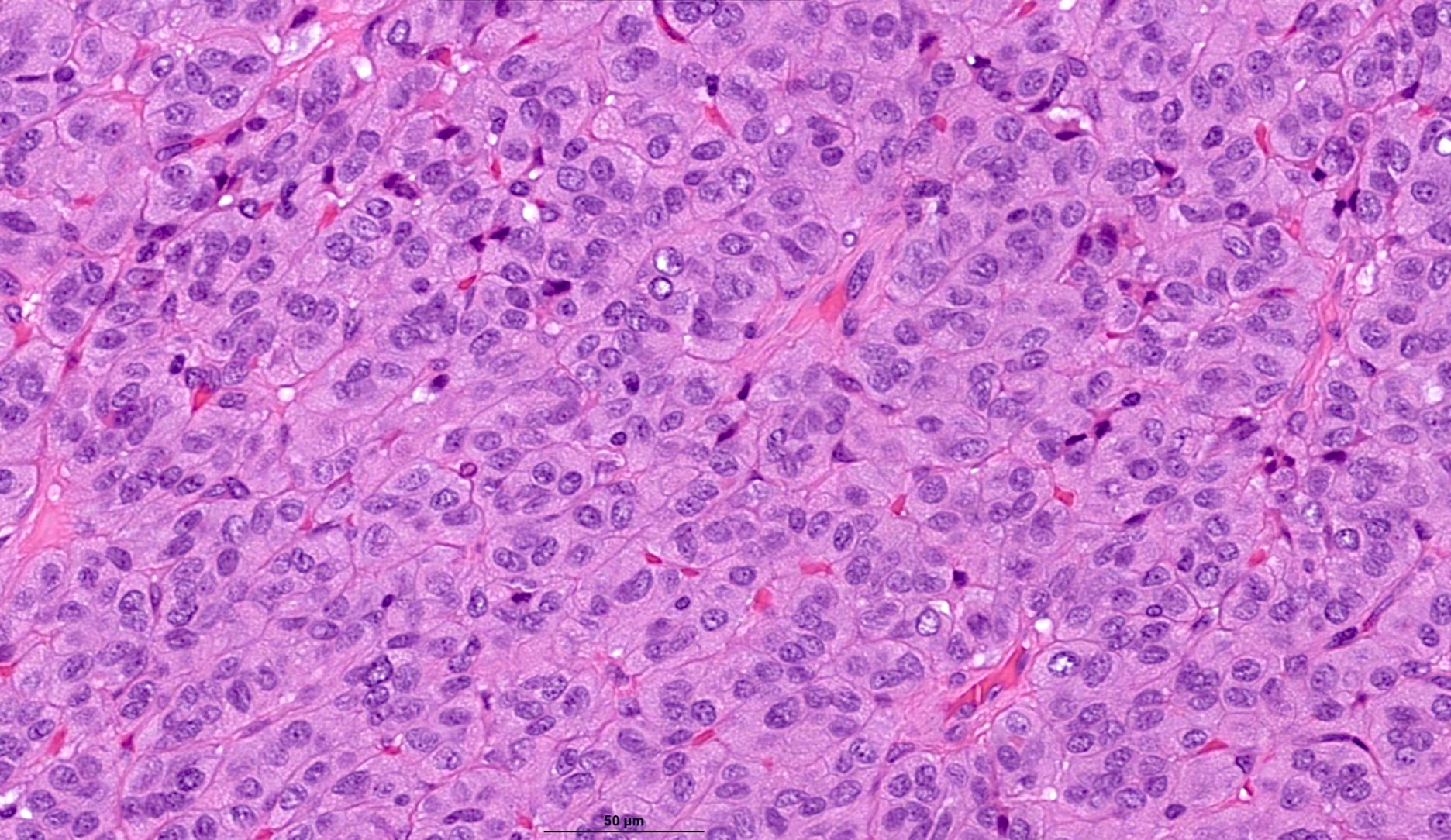
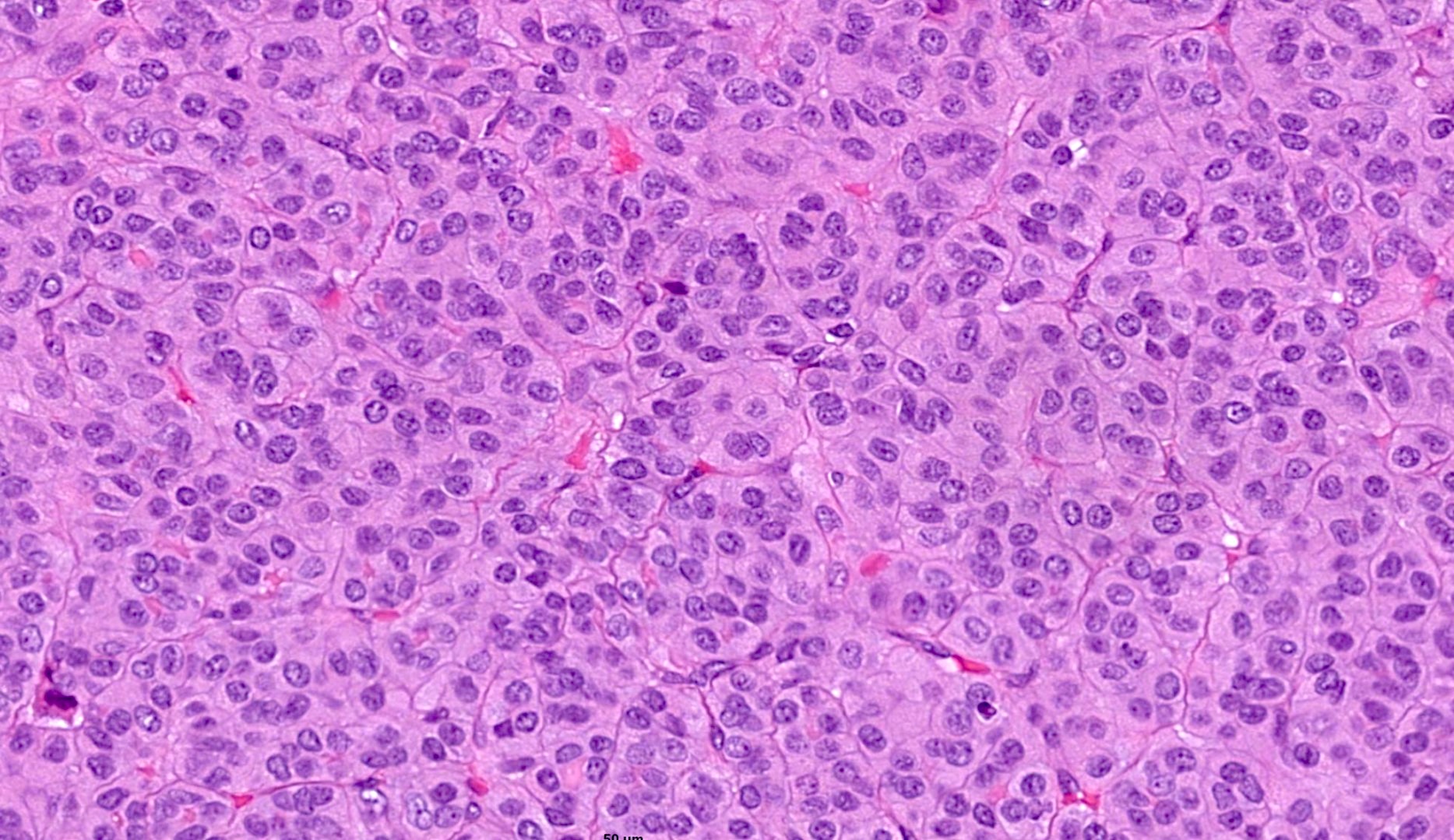
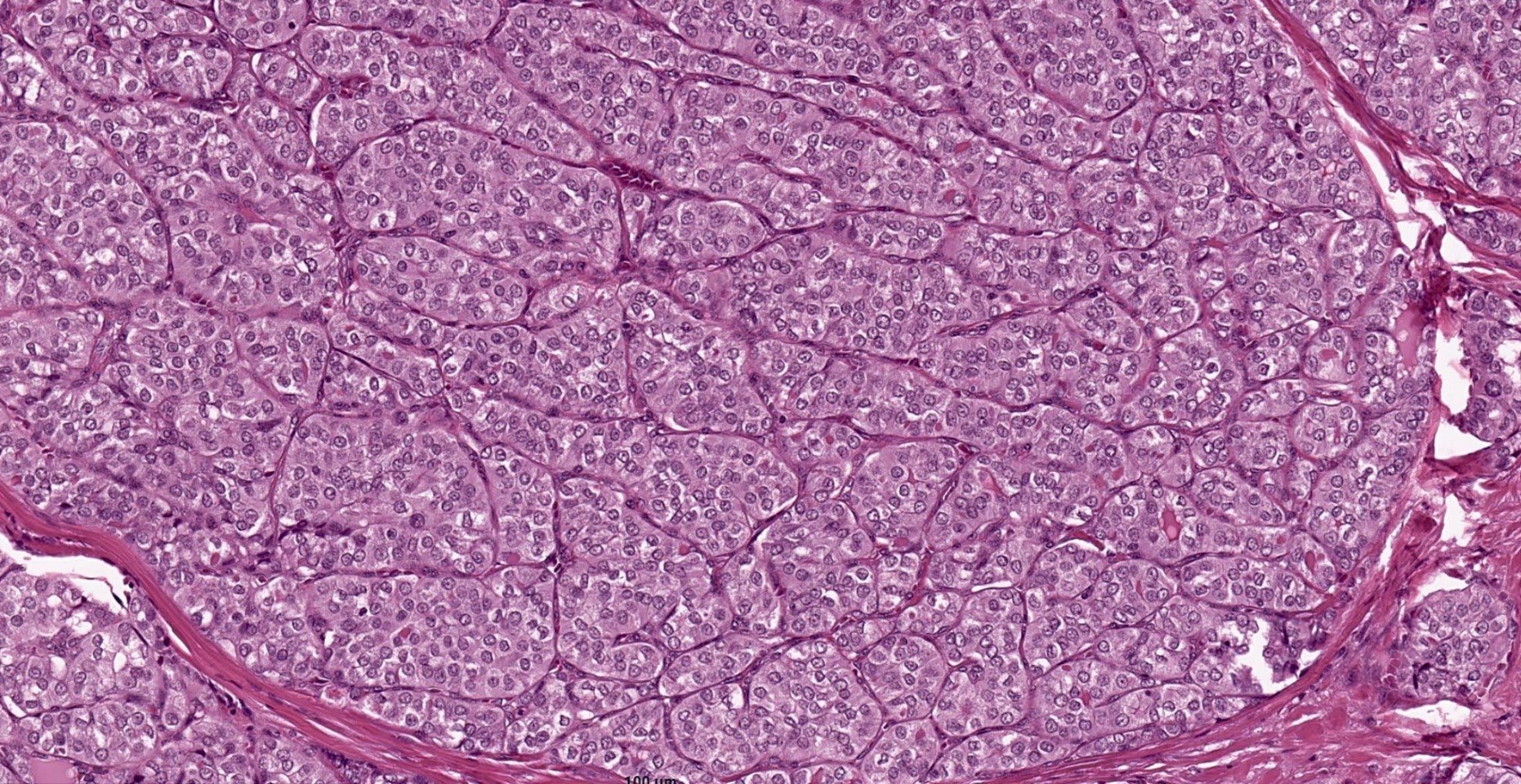
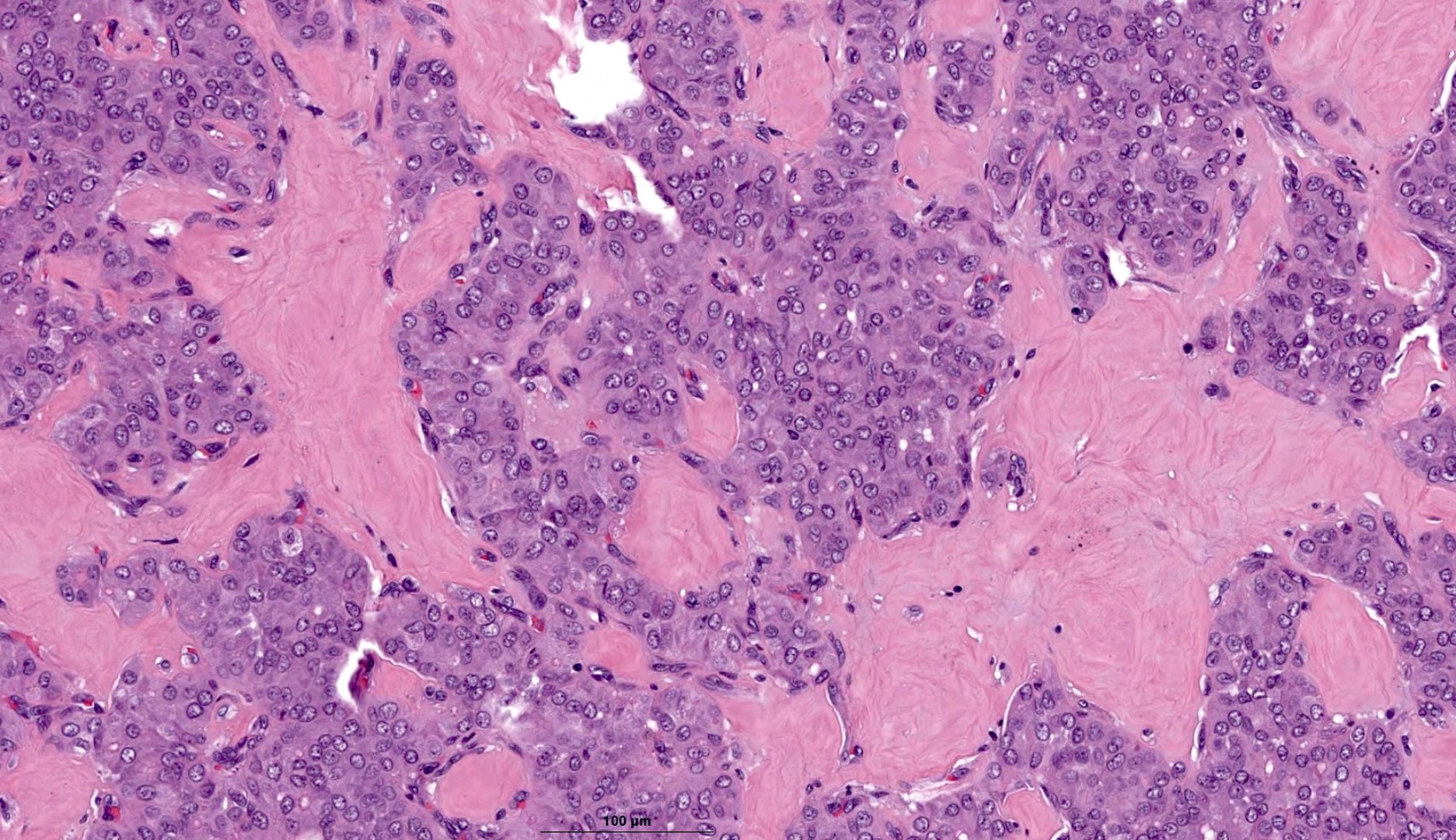
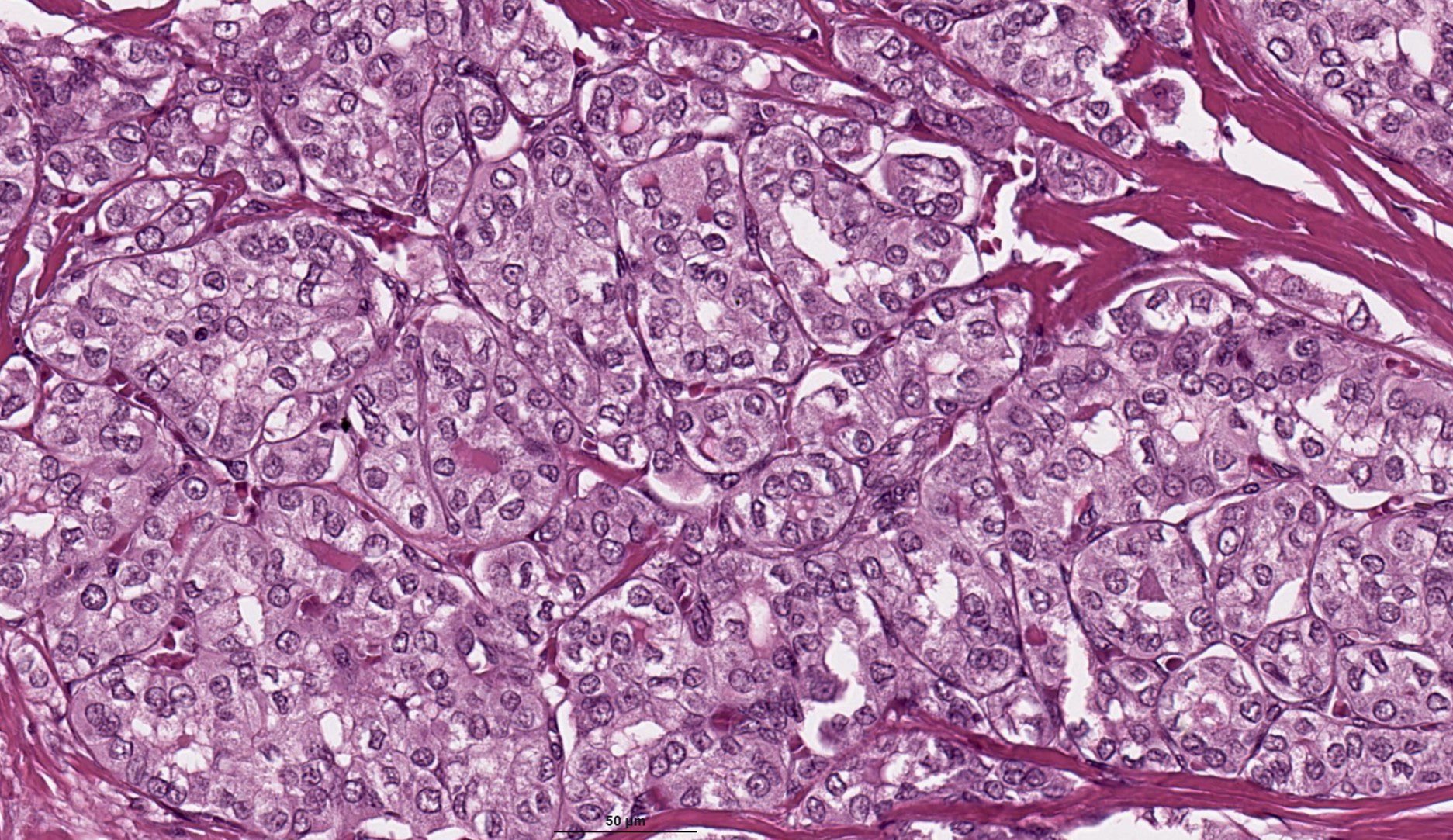
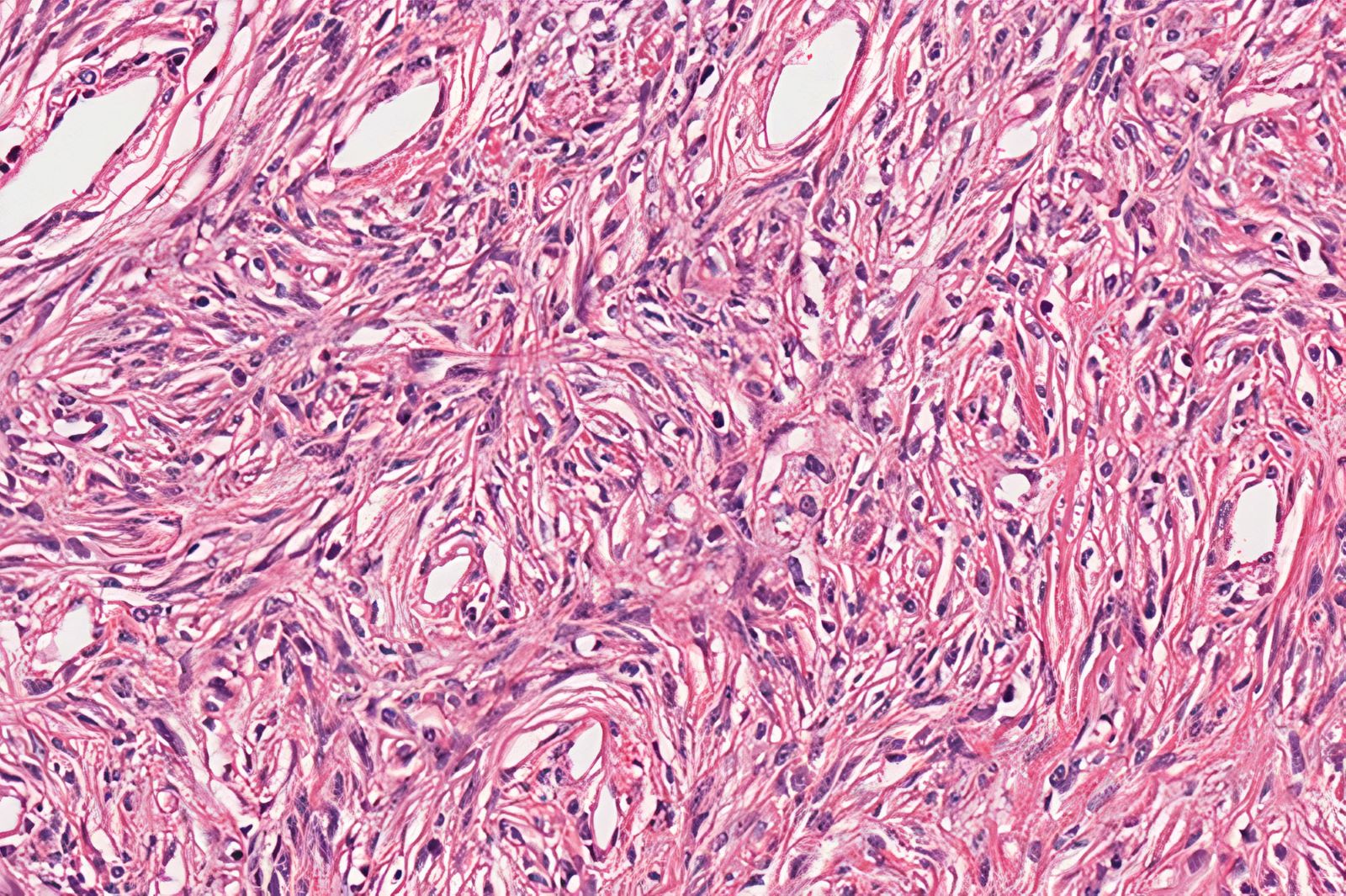
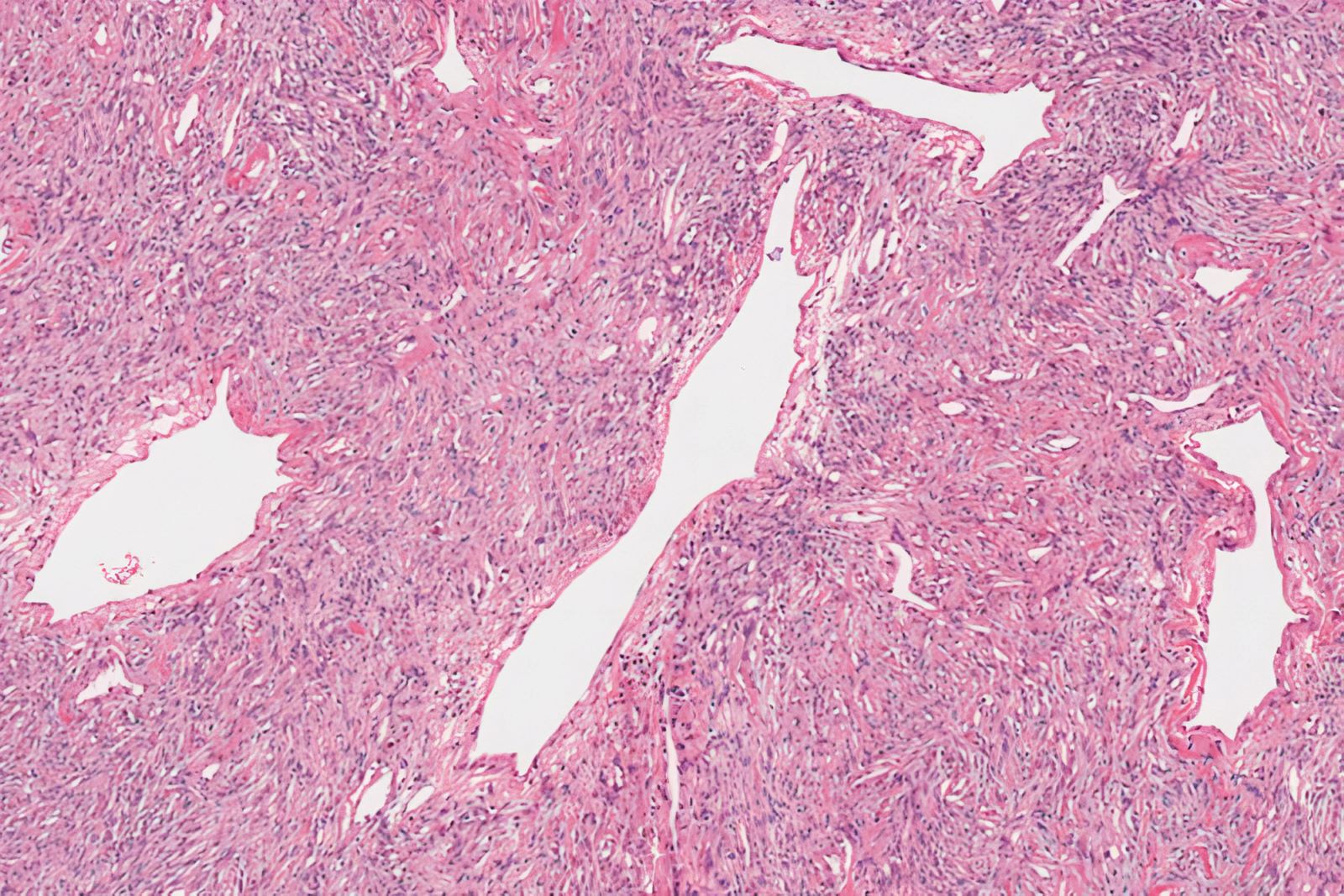
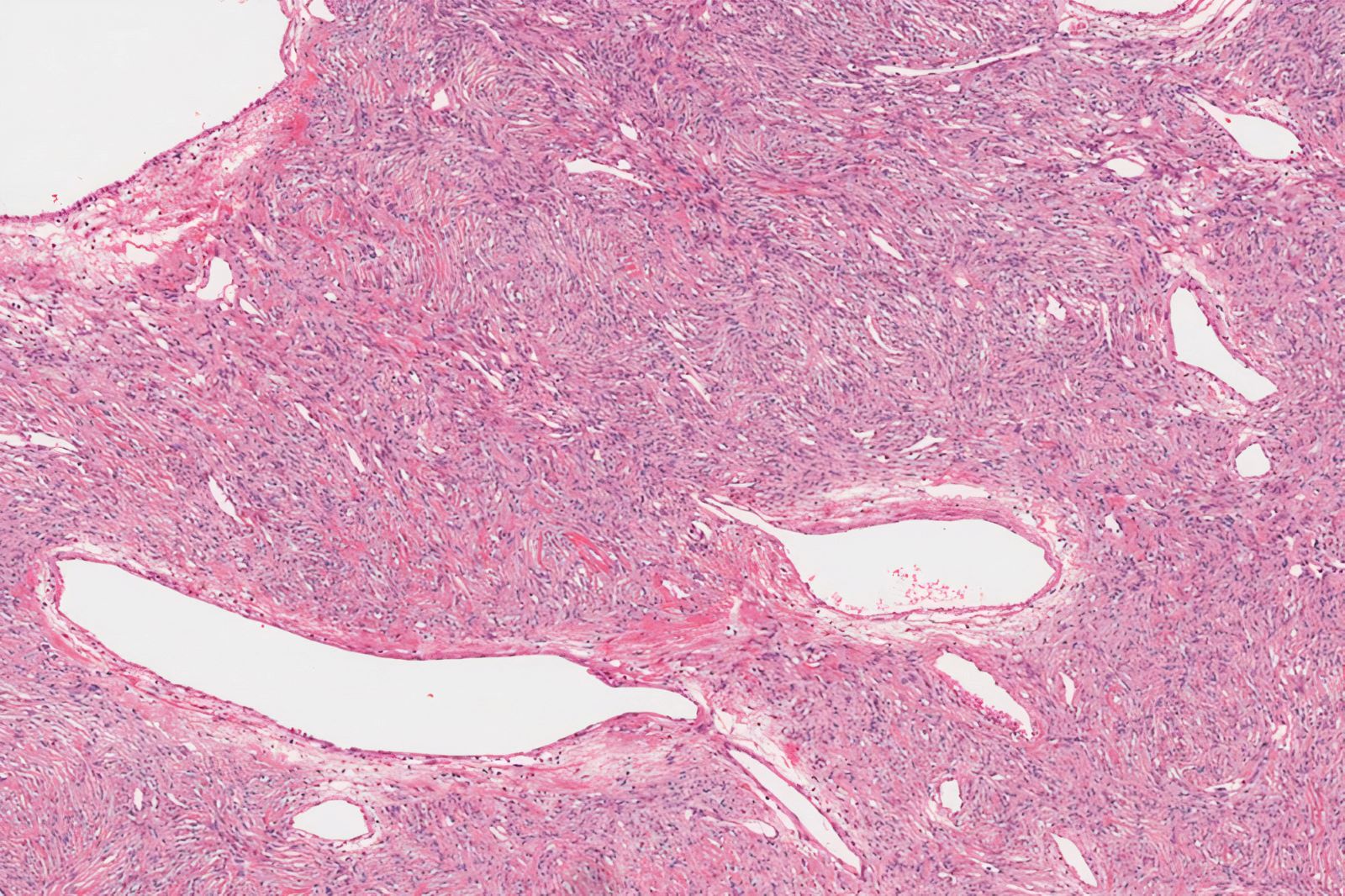
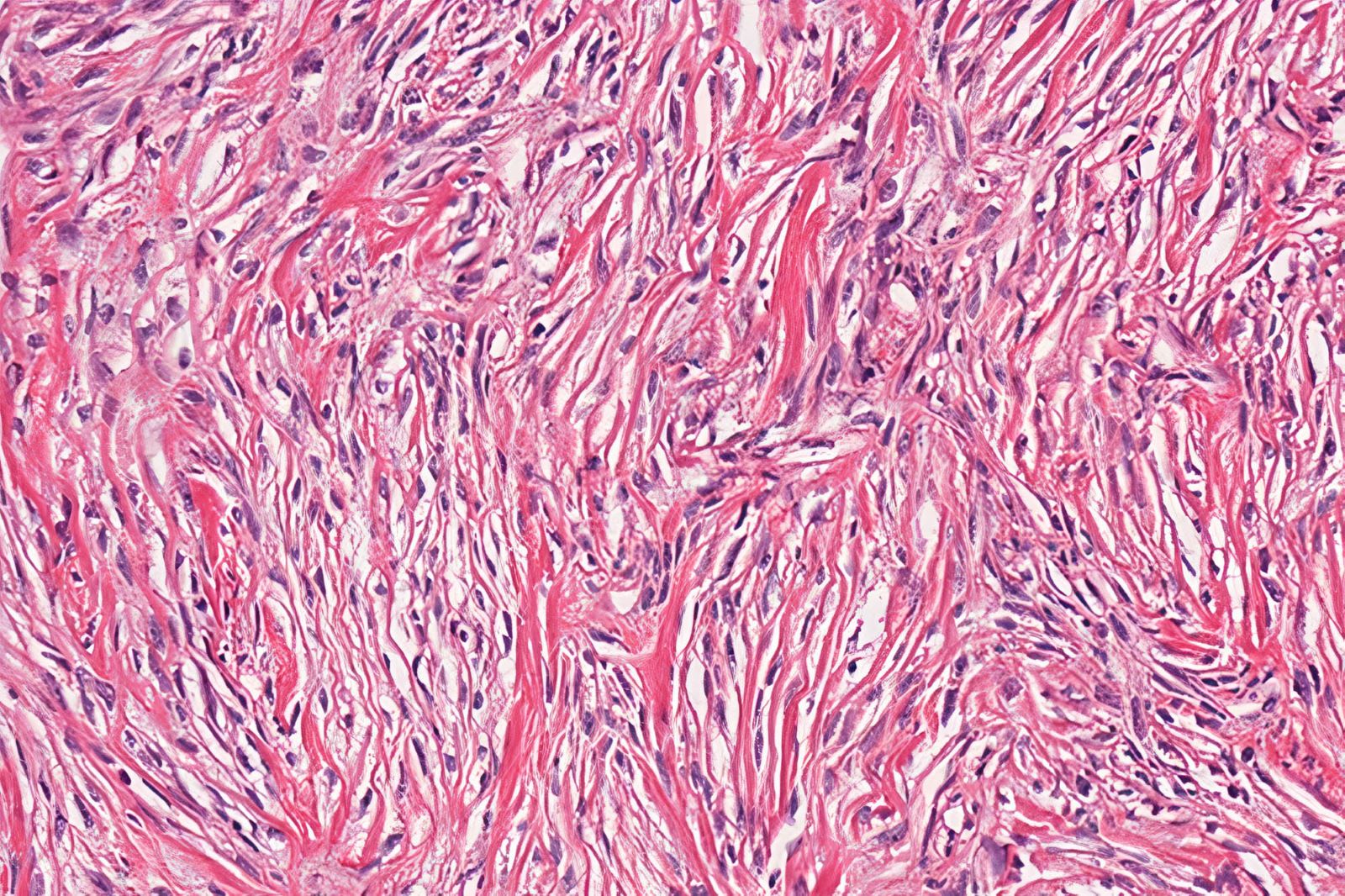
- Atypical parathyroid neoplasm is defined as a tumor that is histologically or clinically worrisome but does not fulfill the more robust criteria (i.e. invasion, metastasis) for carcinoma
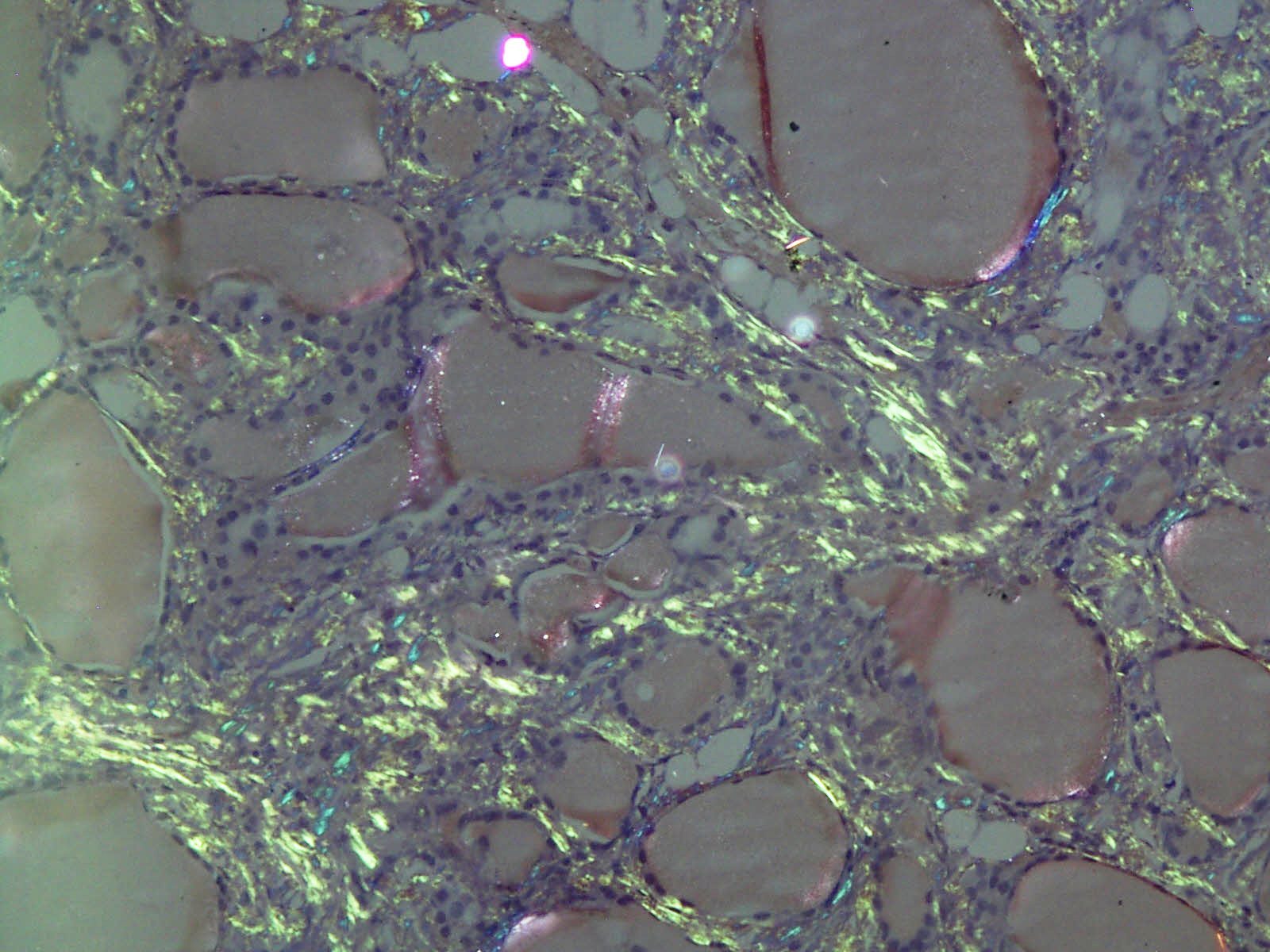
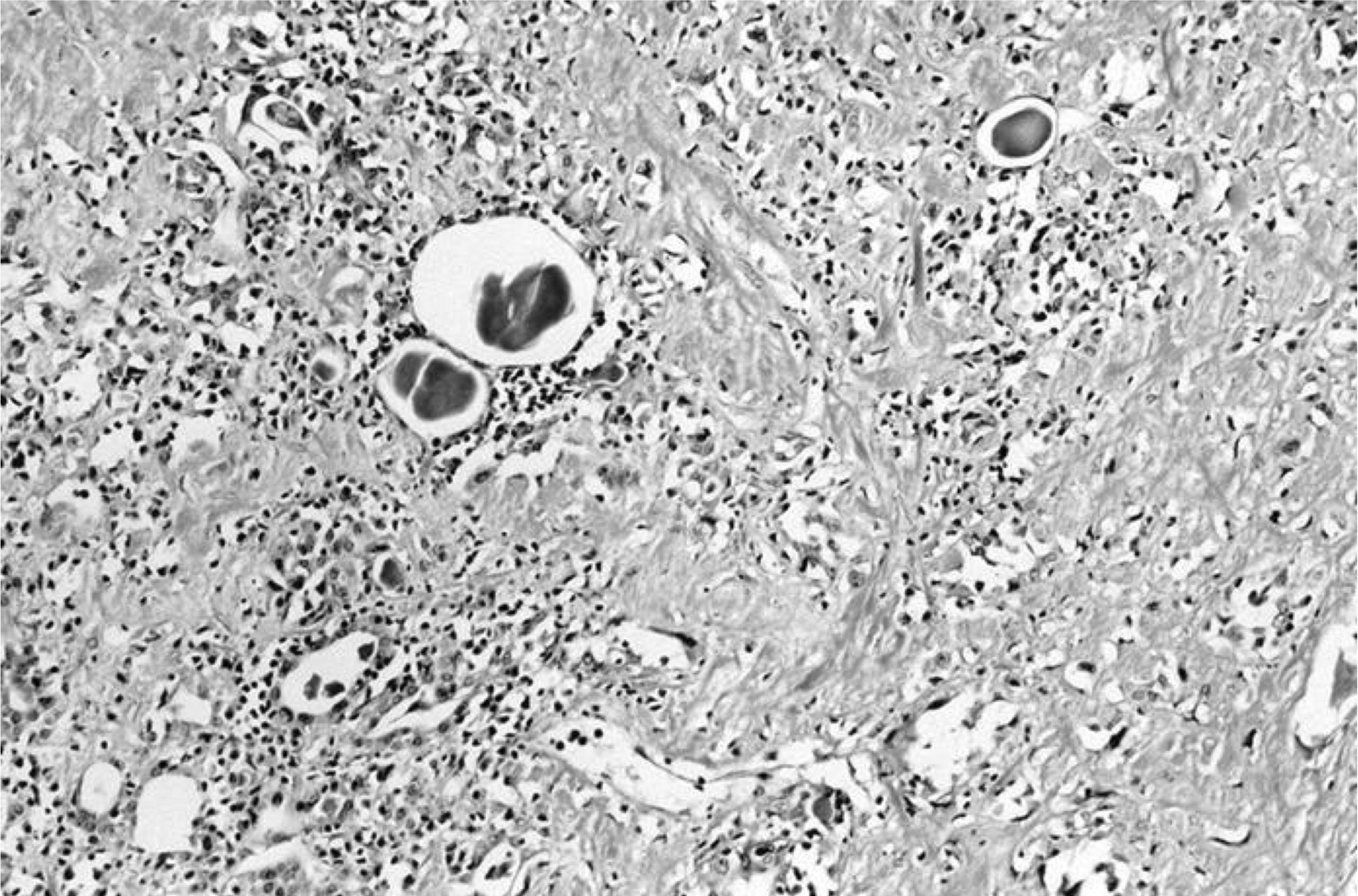
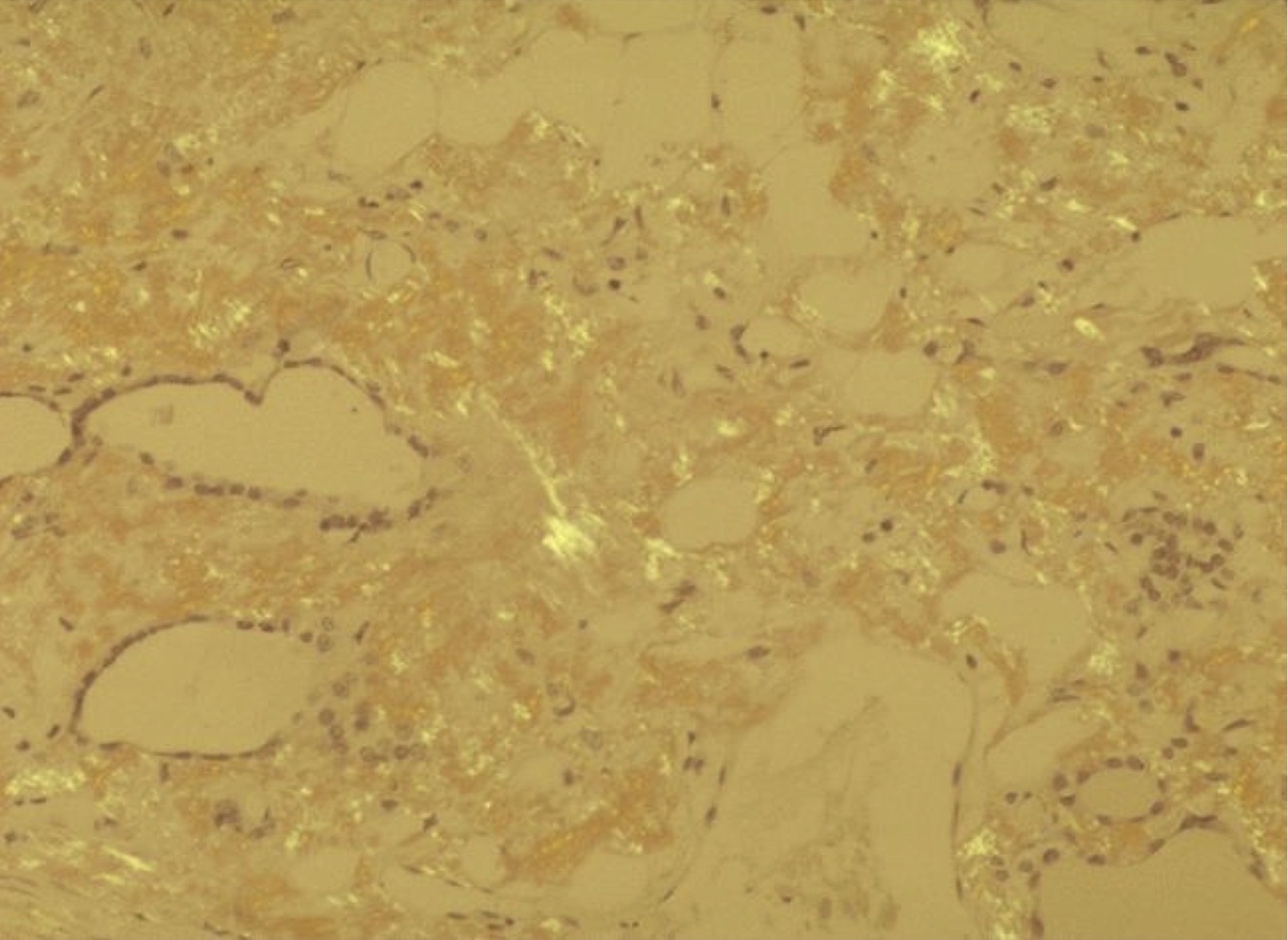
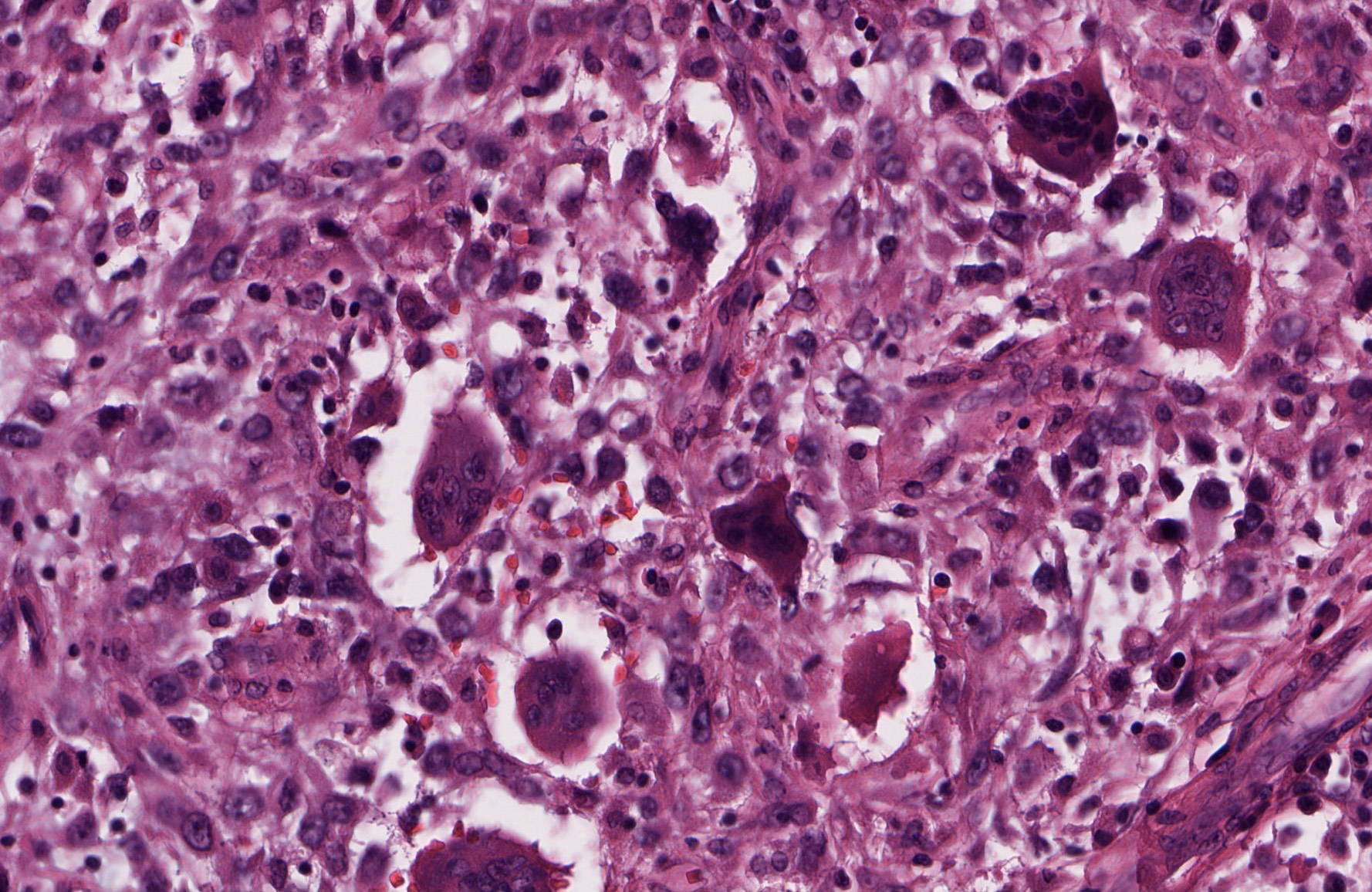
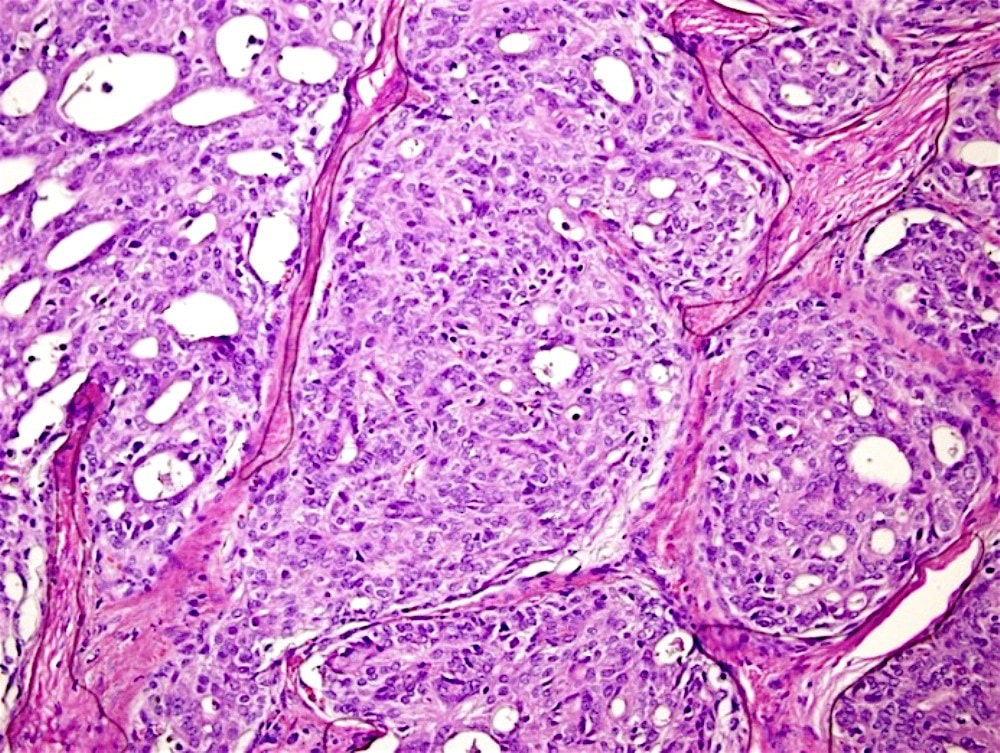
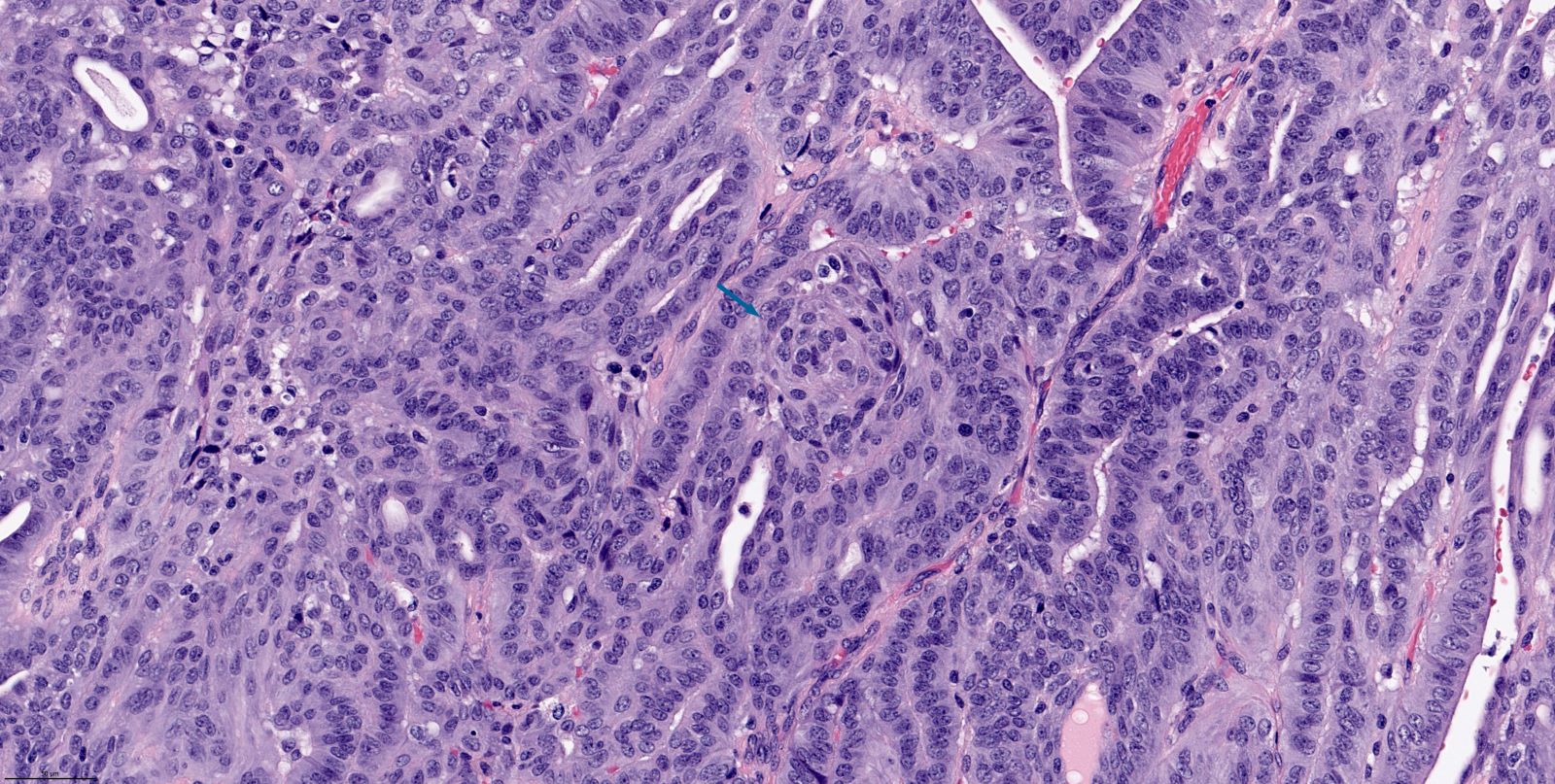
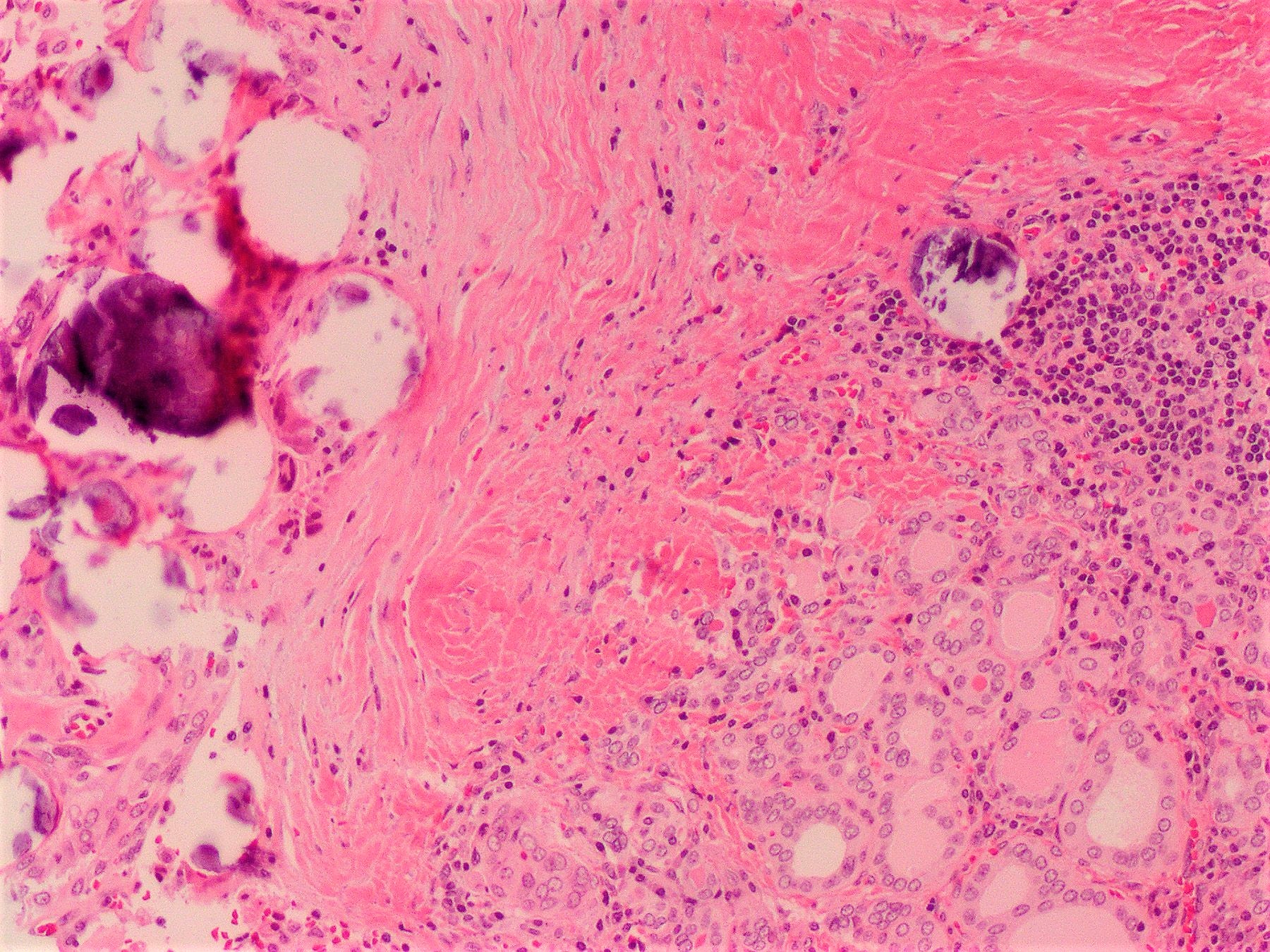
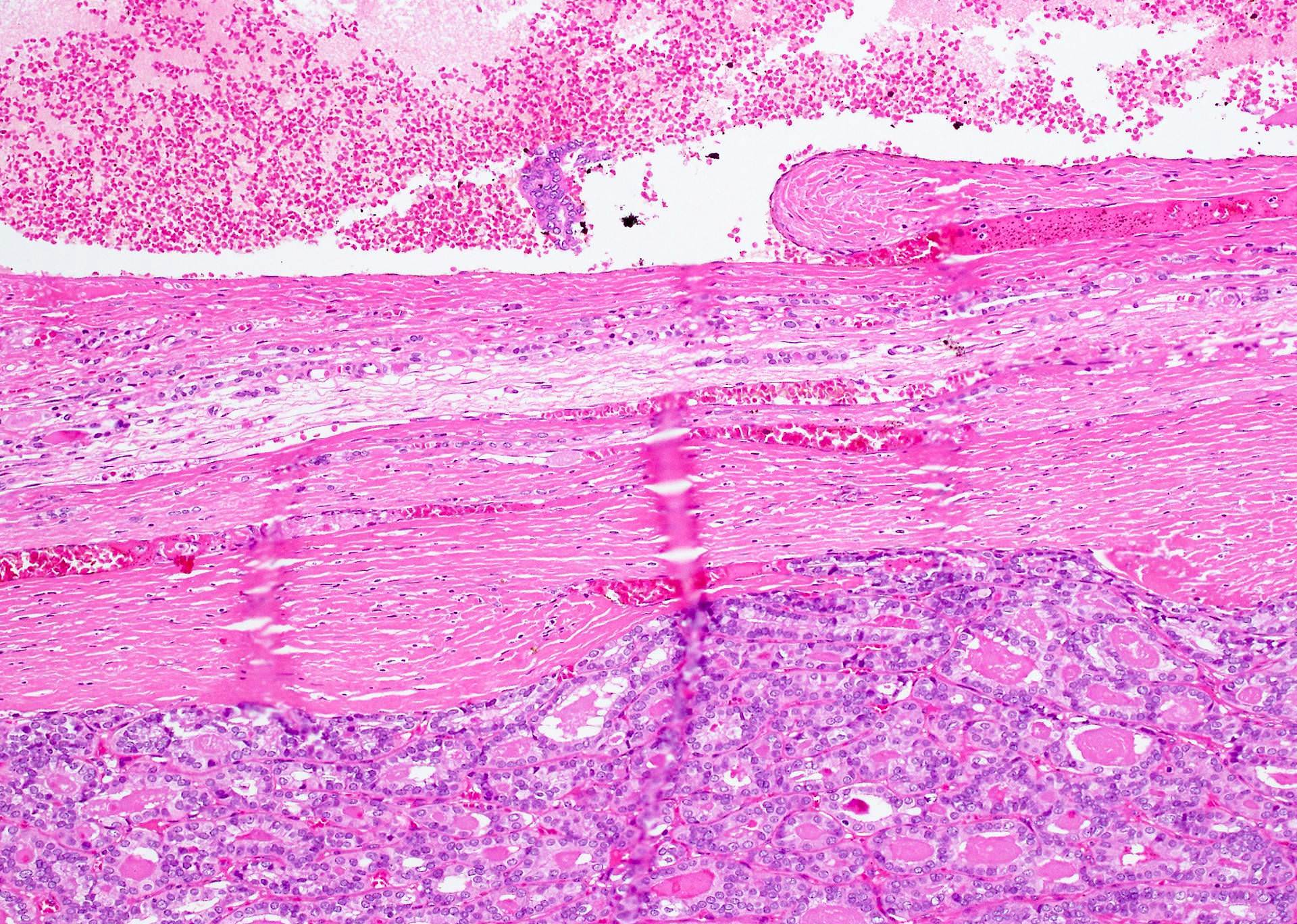
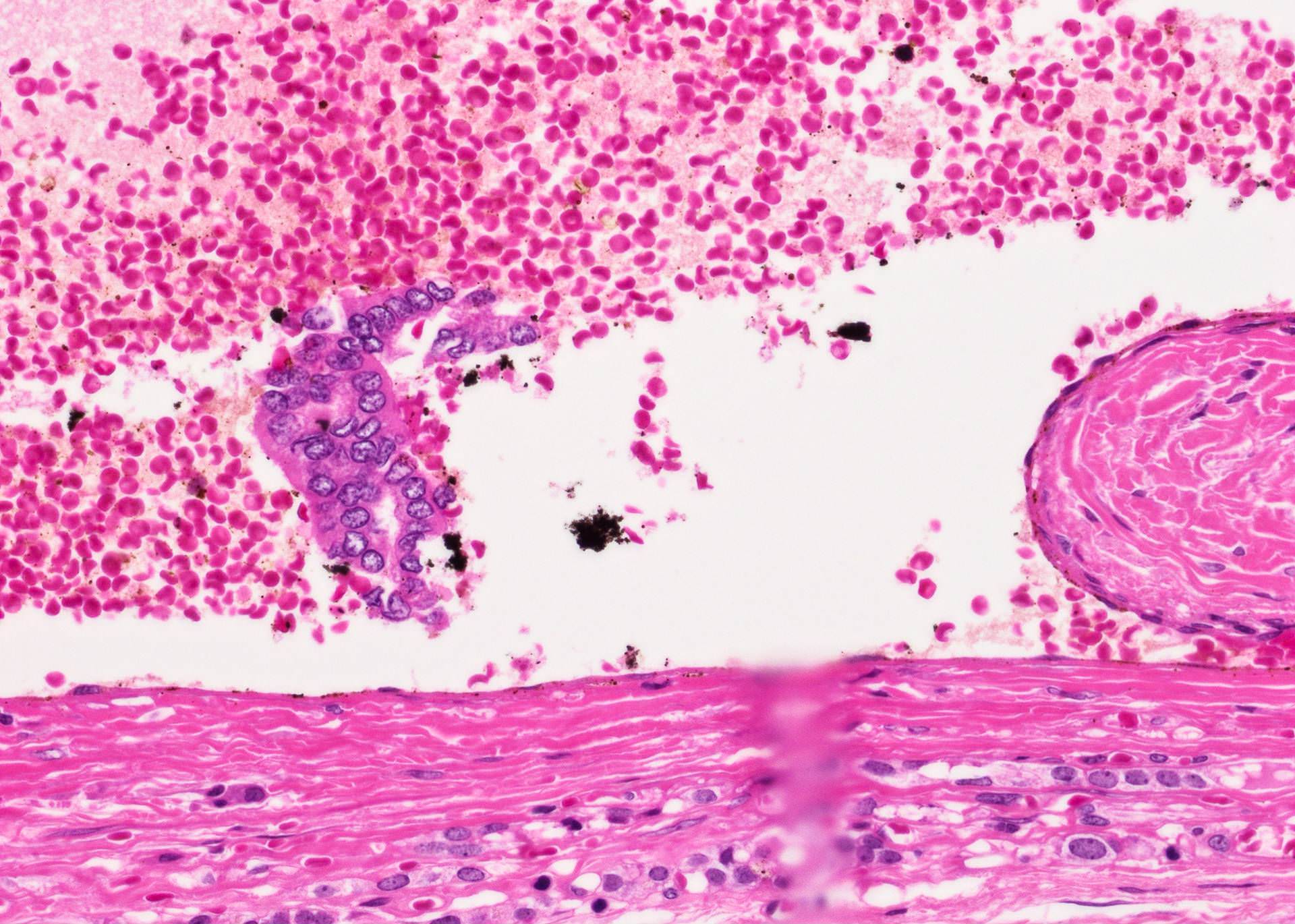
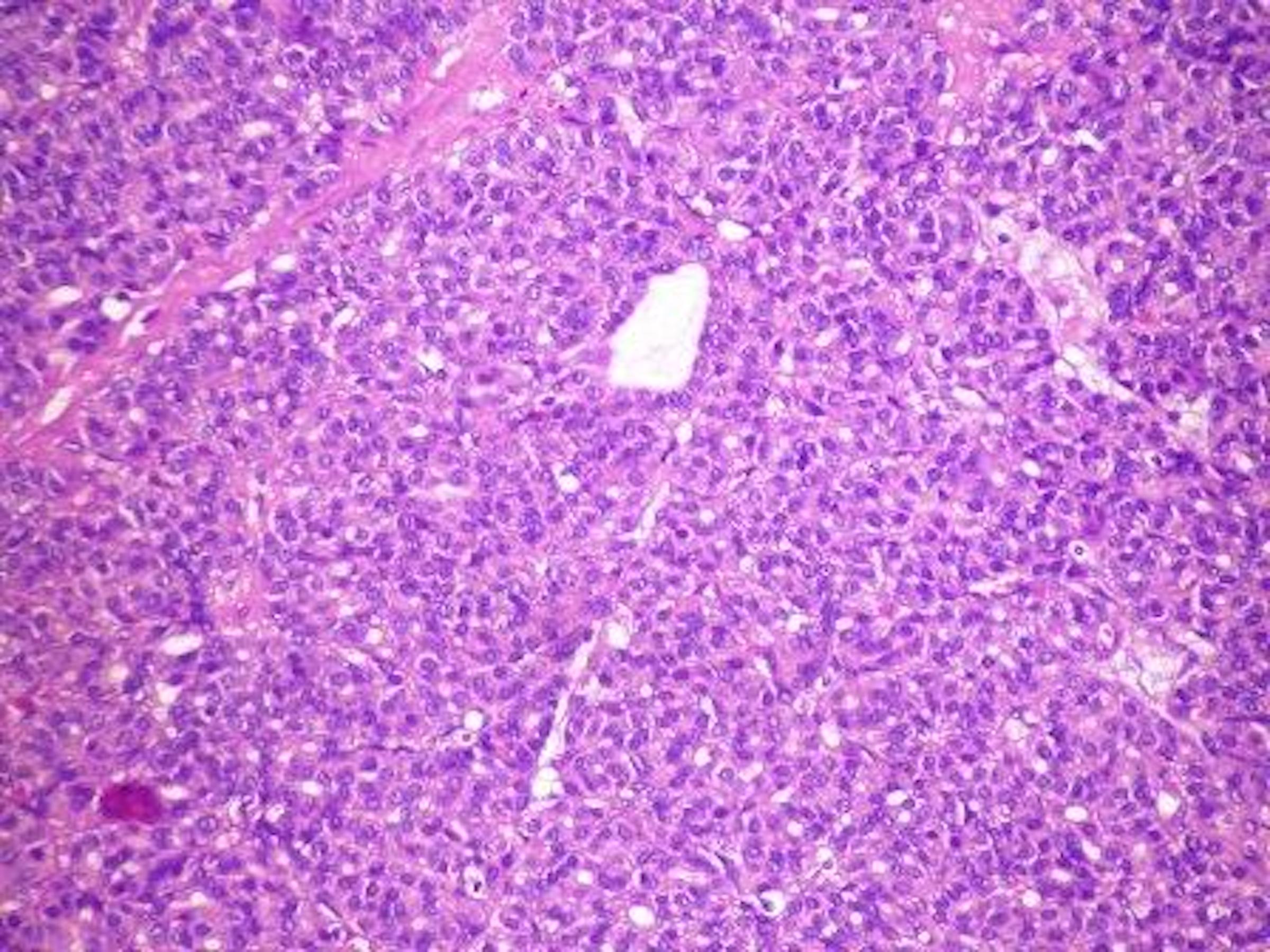
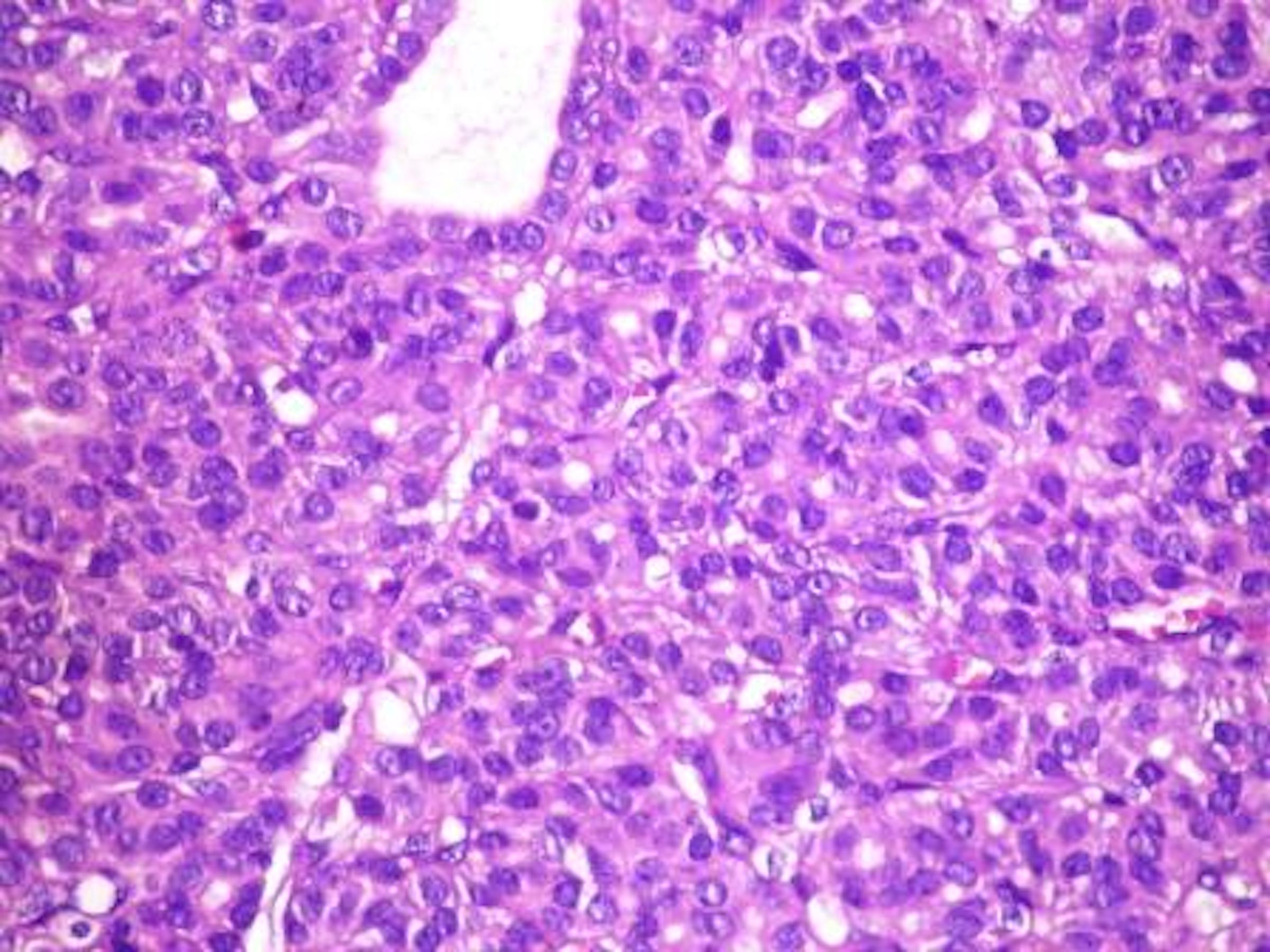
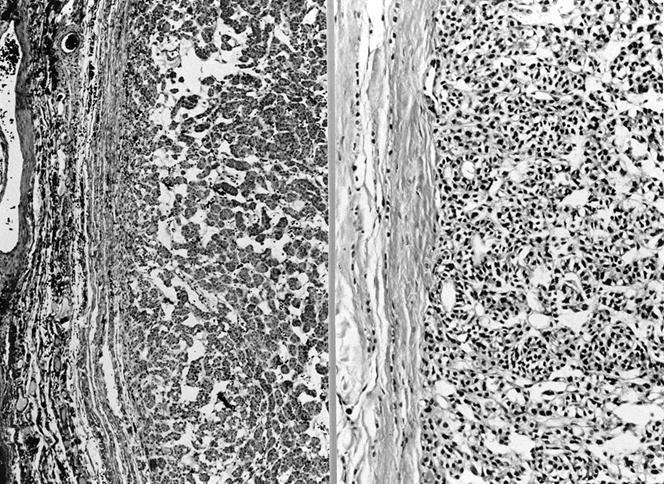
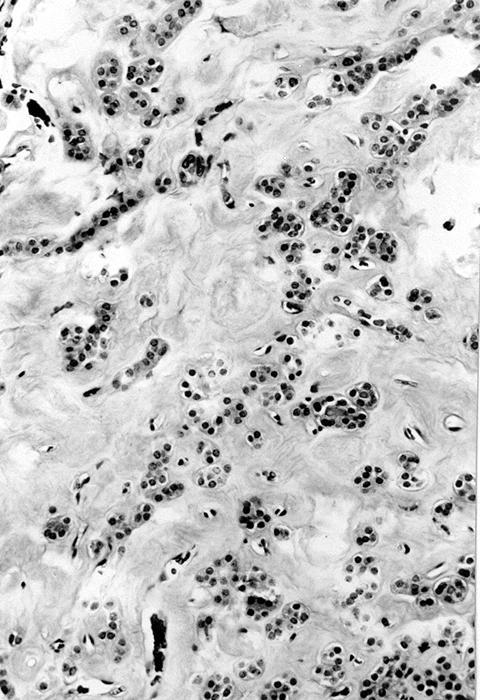
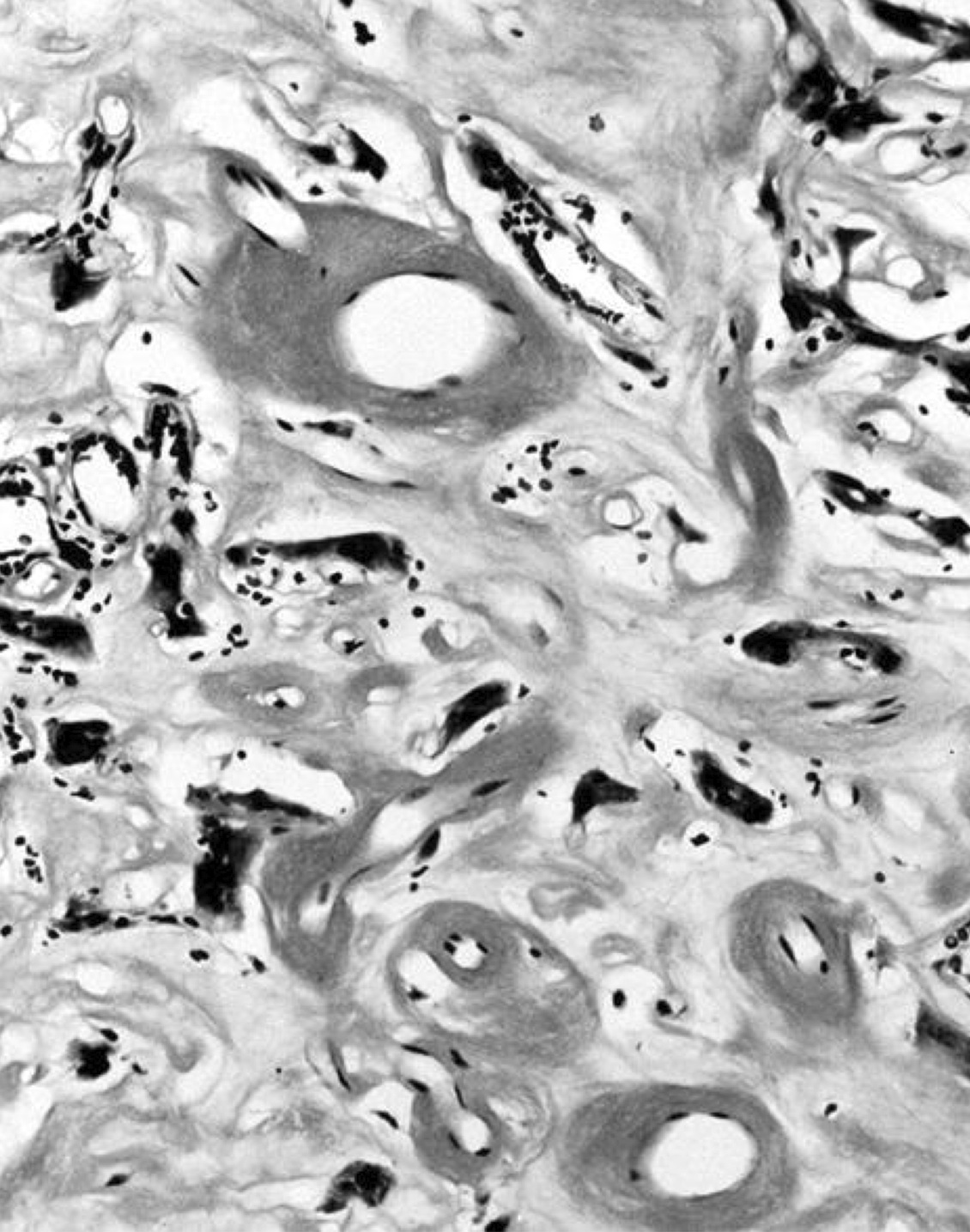
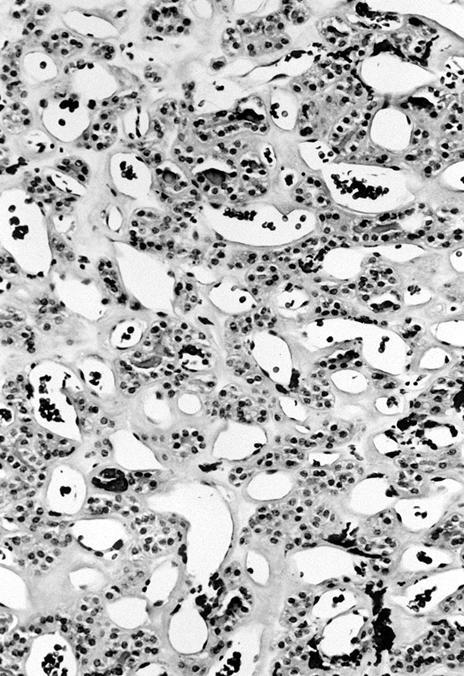
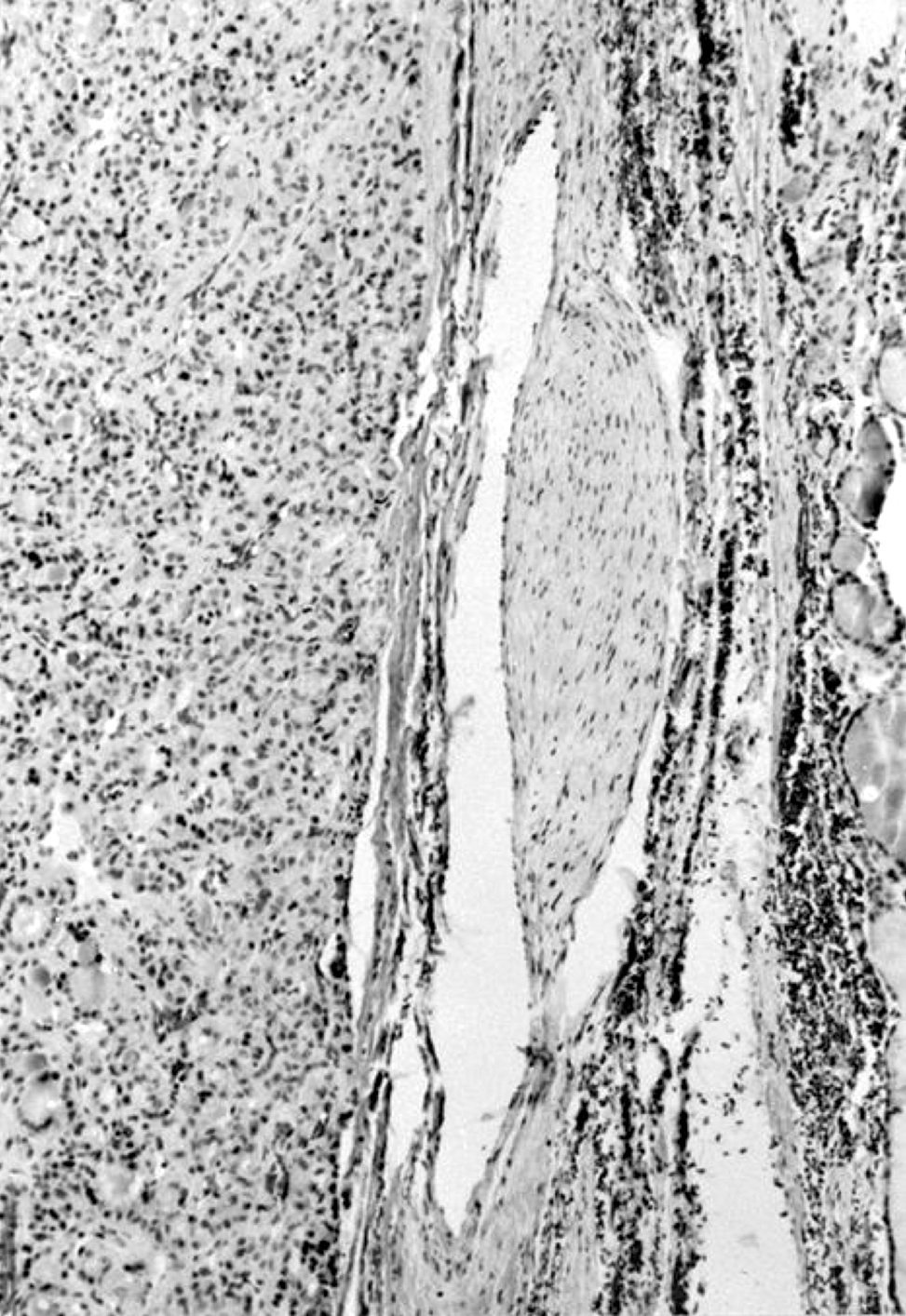
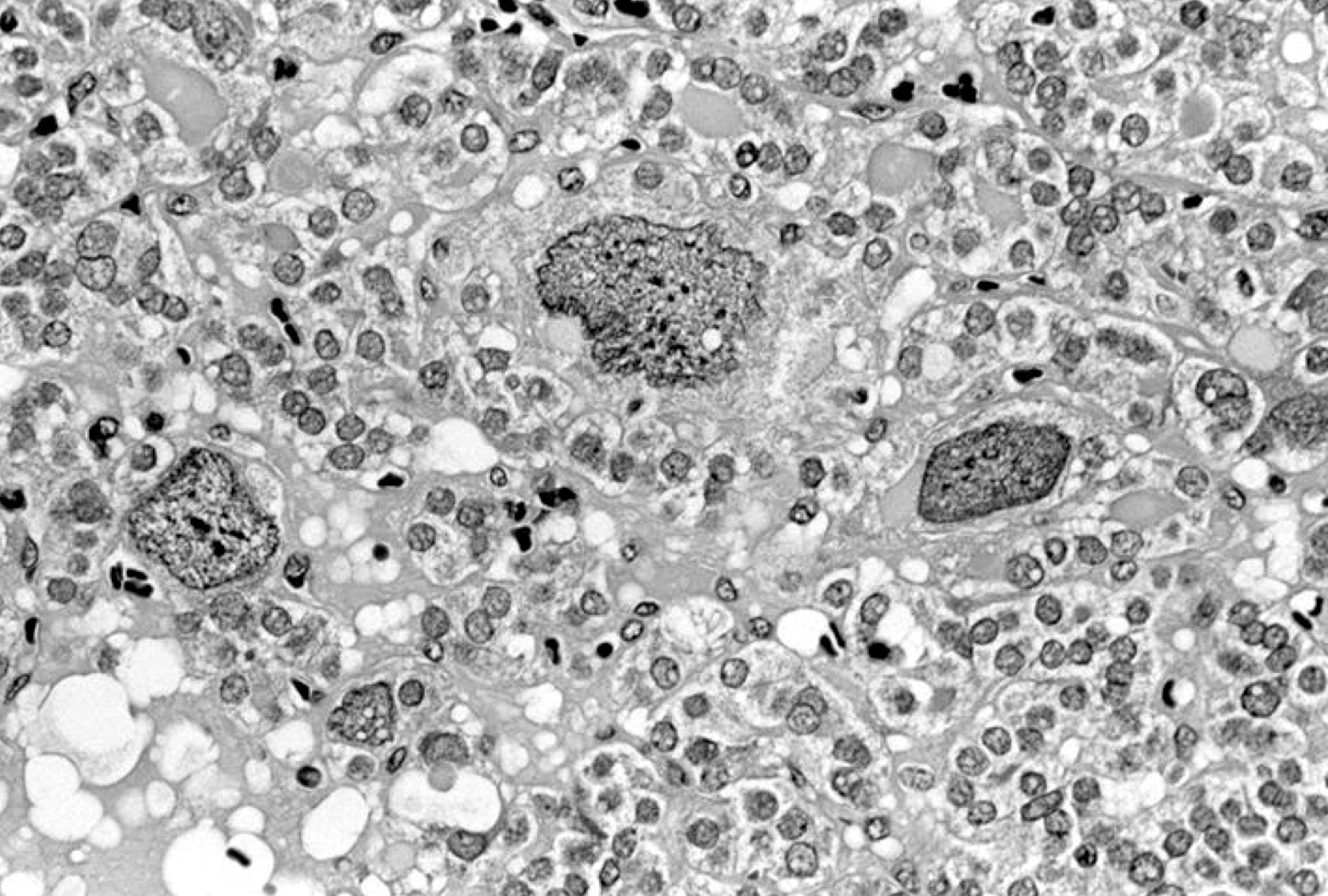
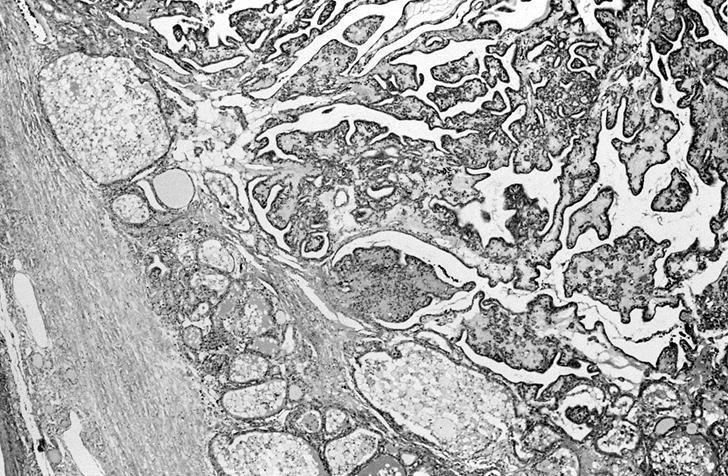
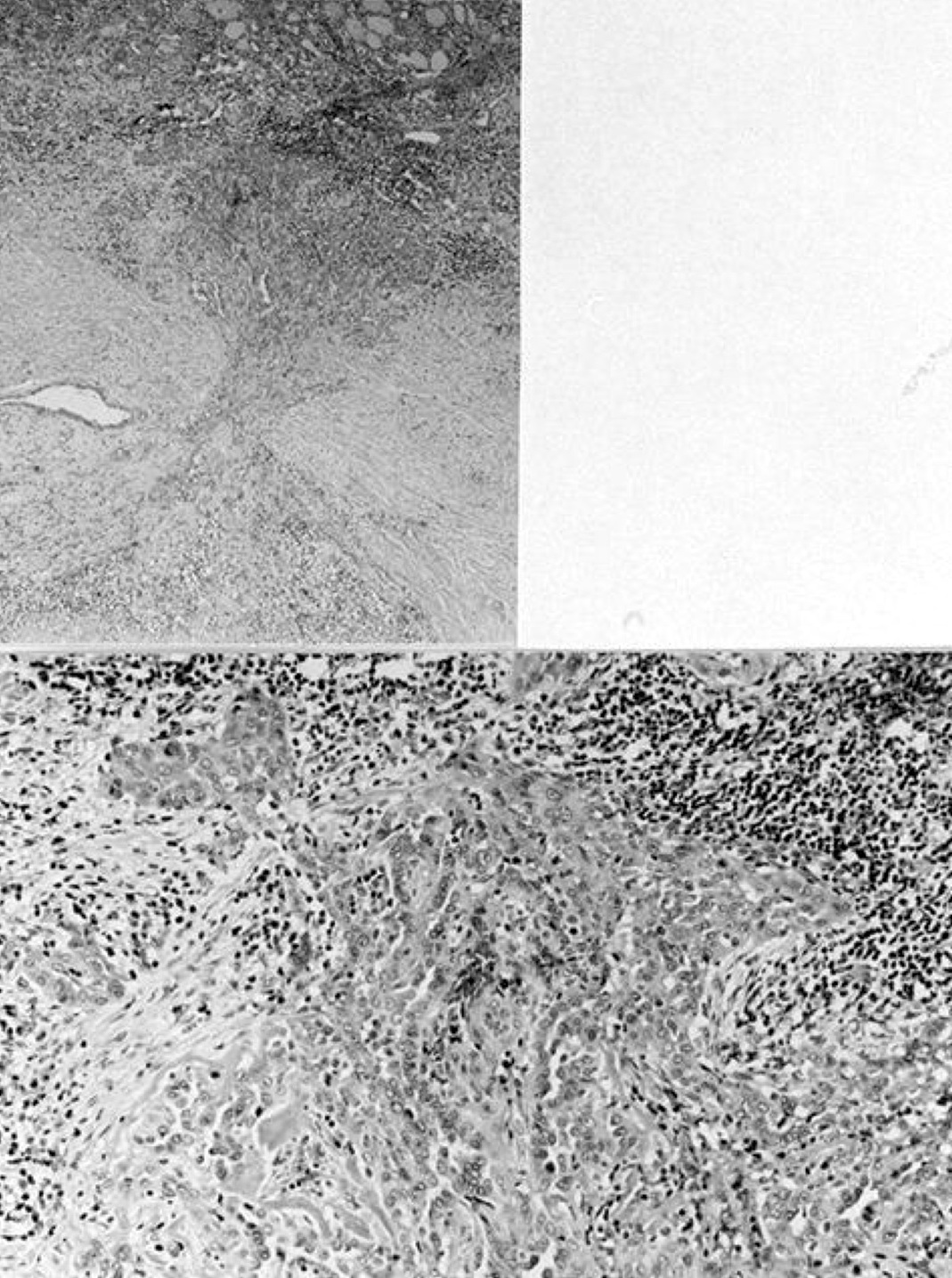
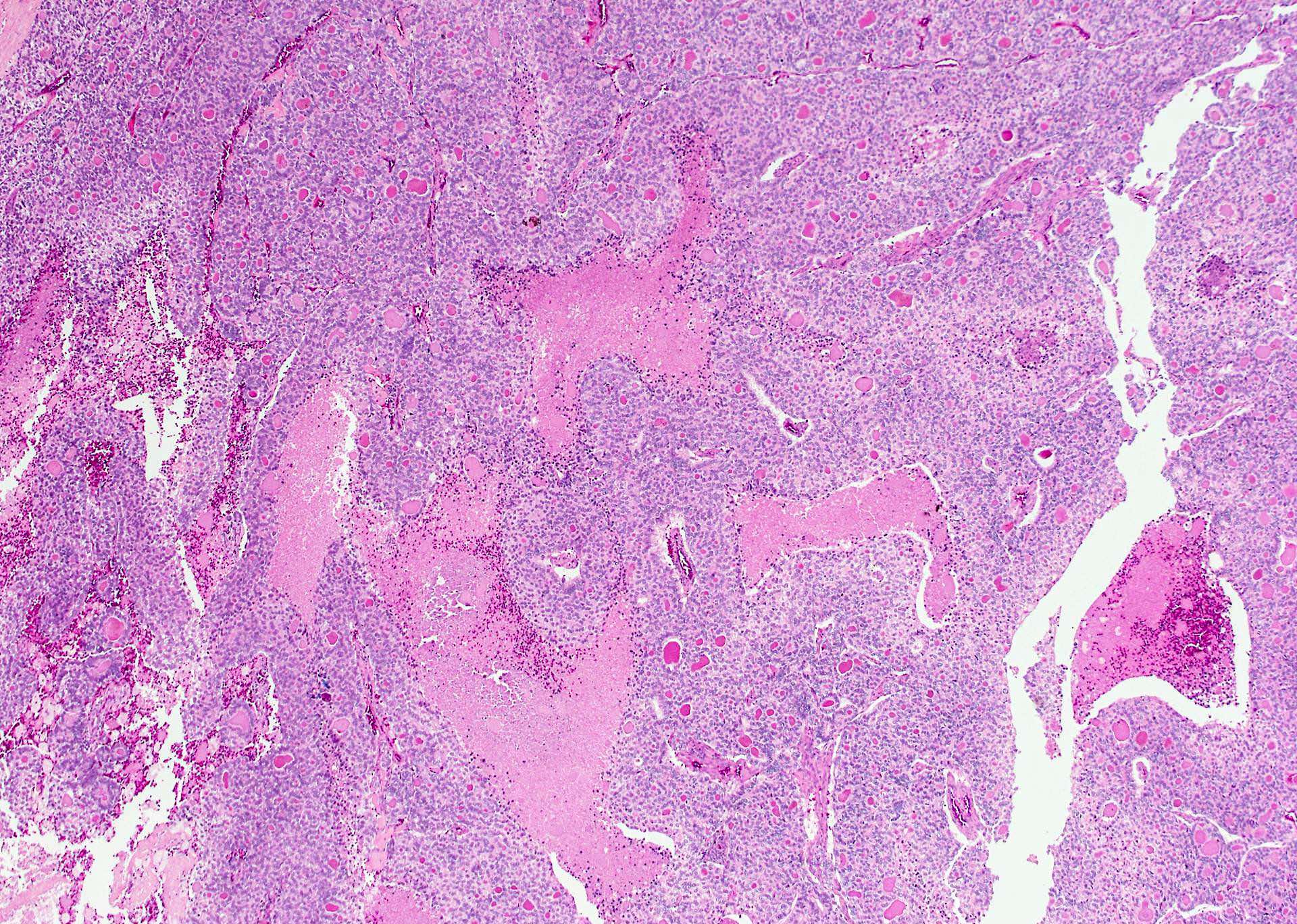
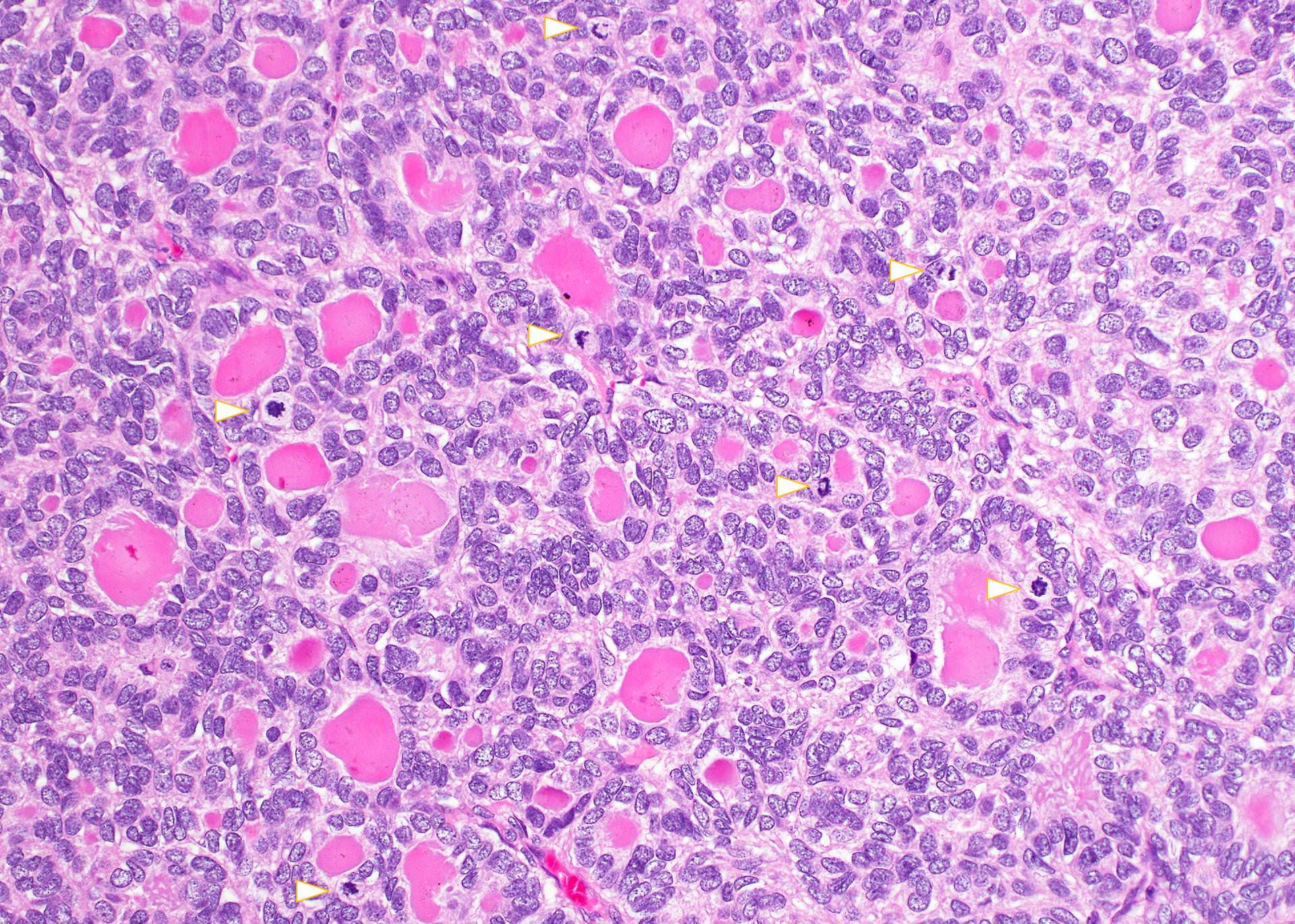
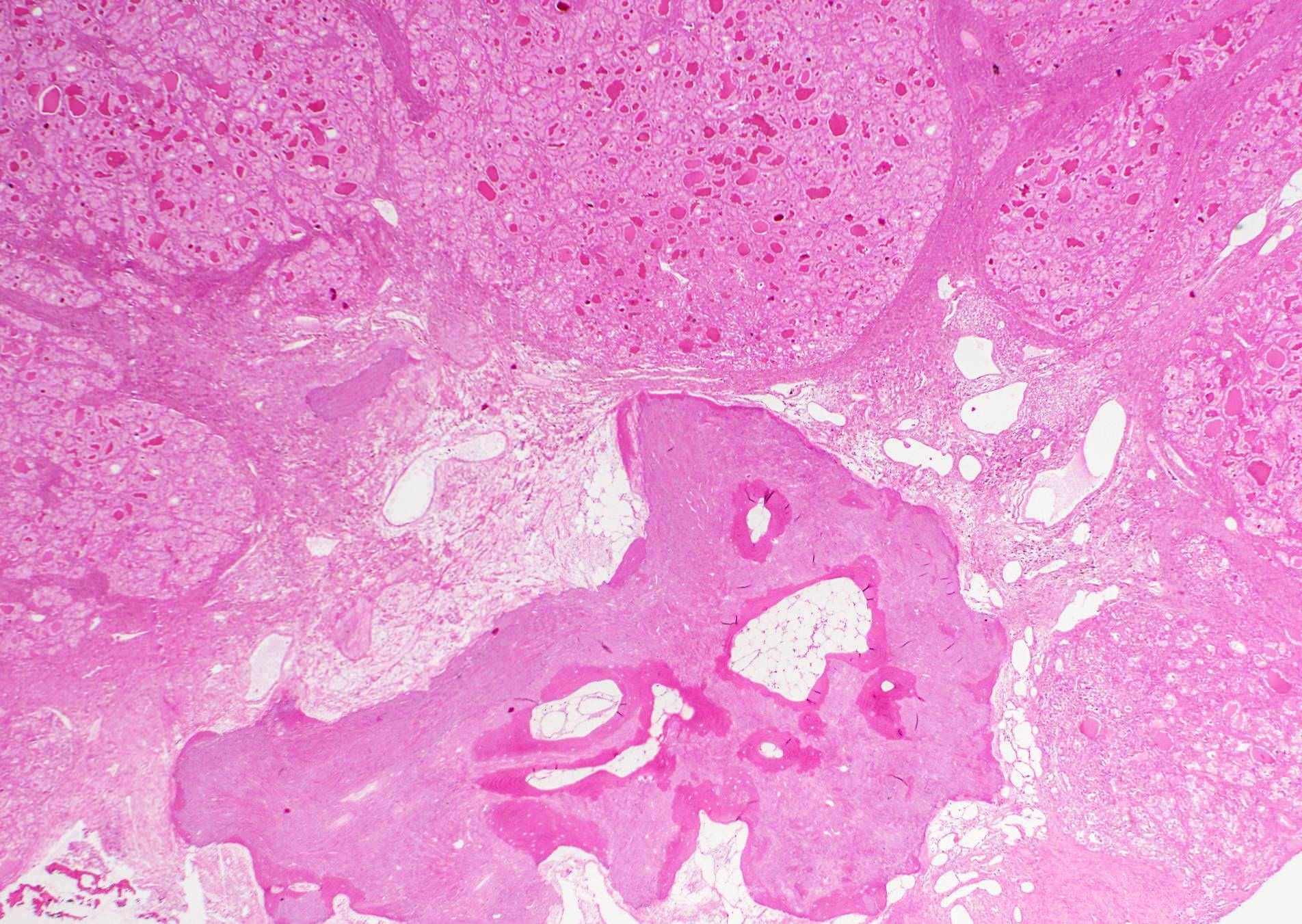
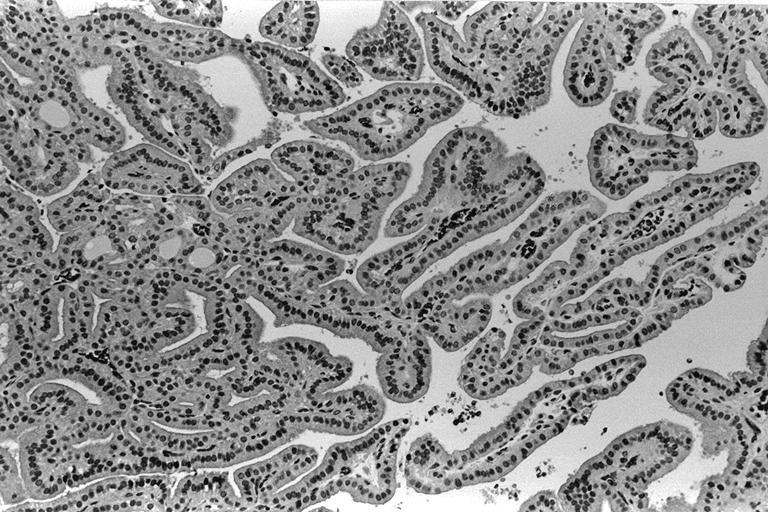
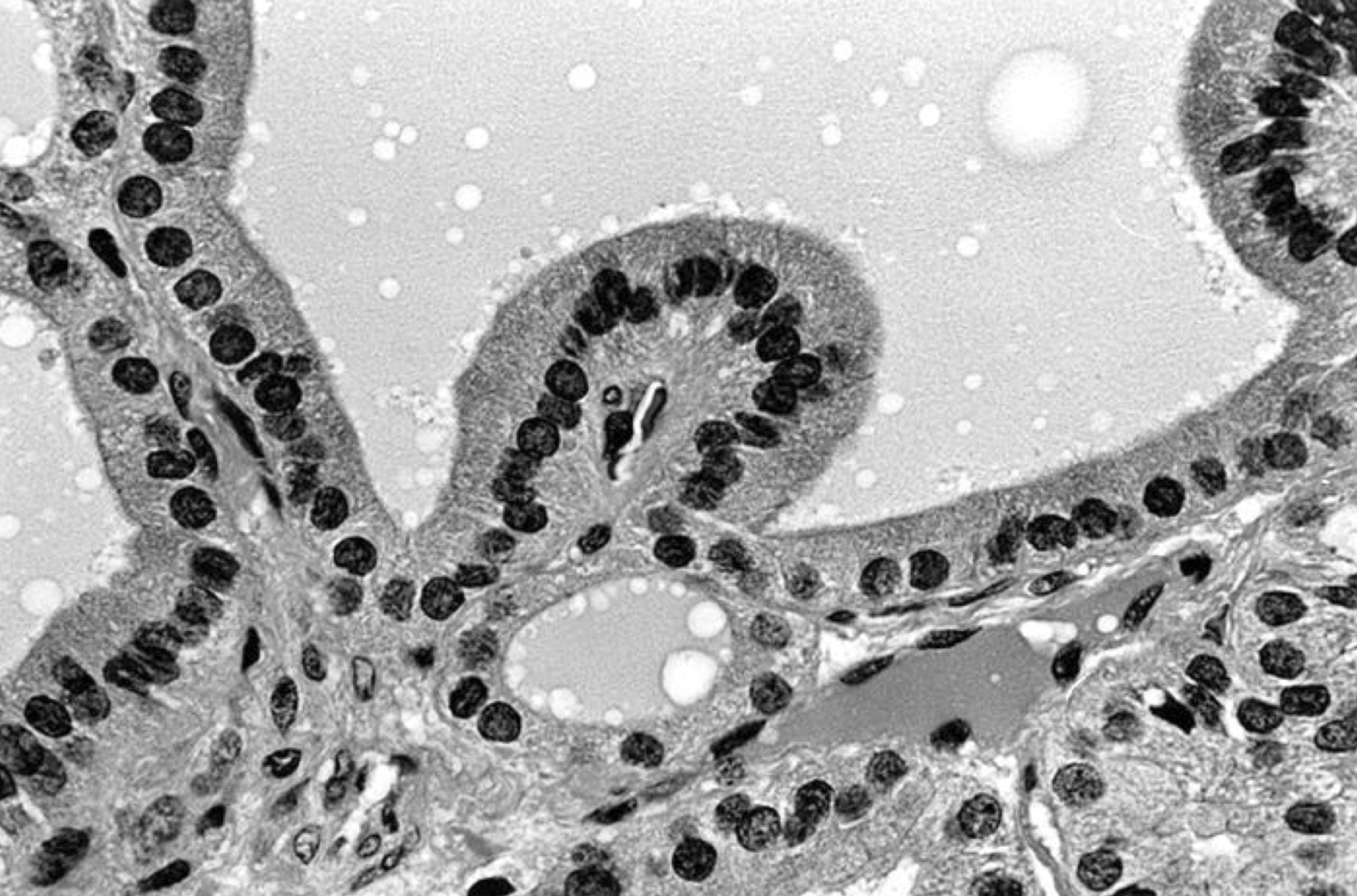
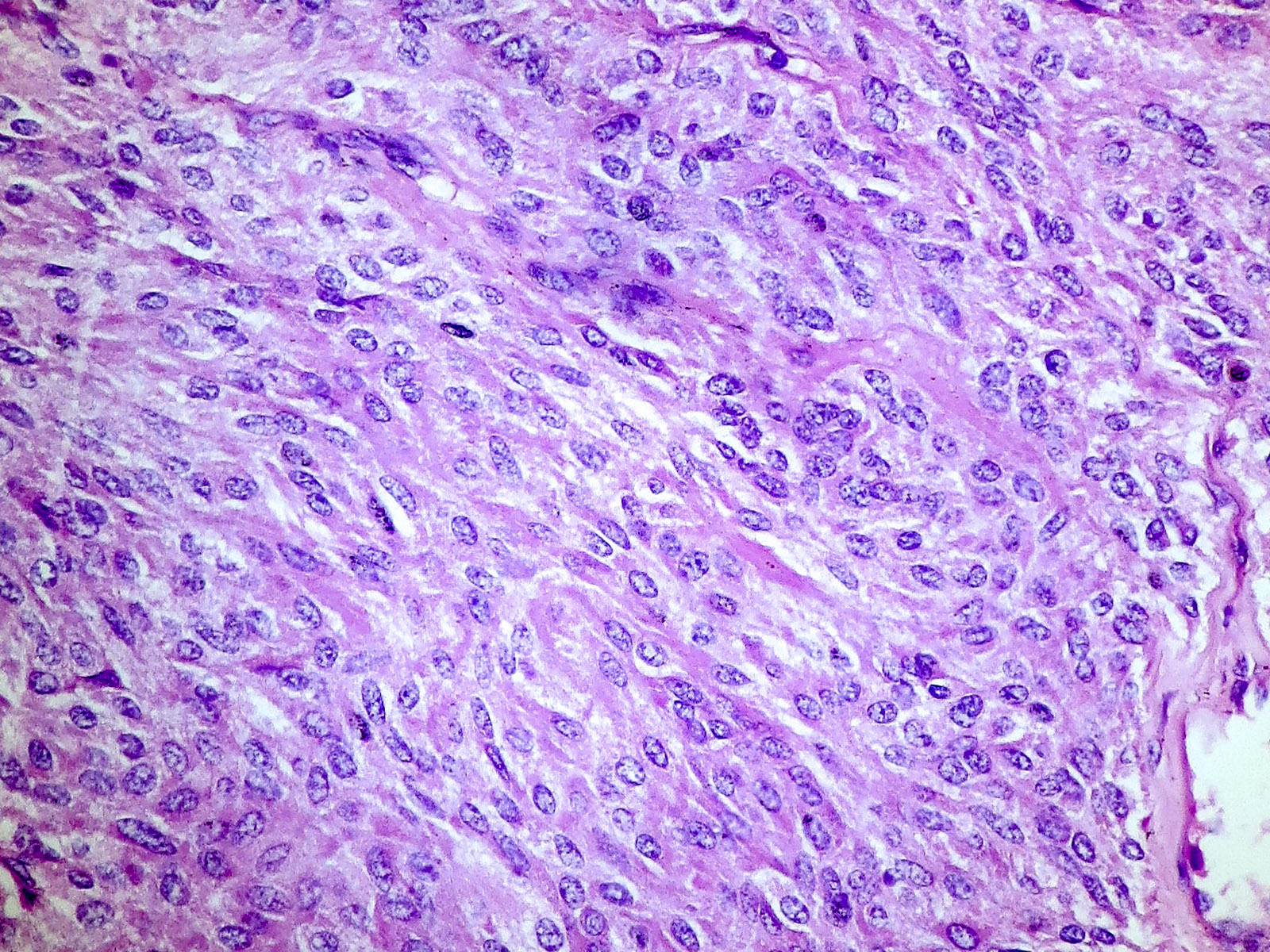
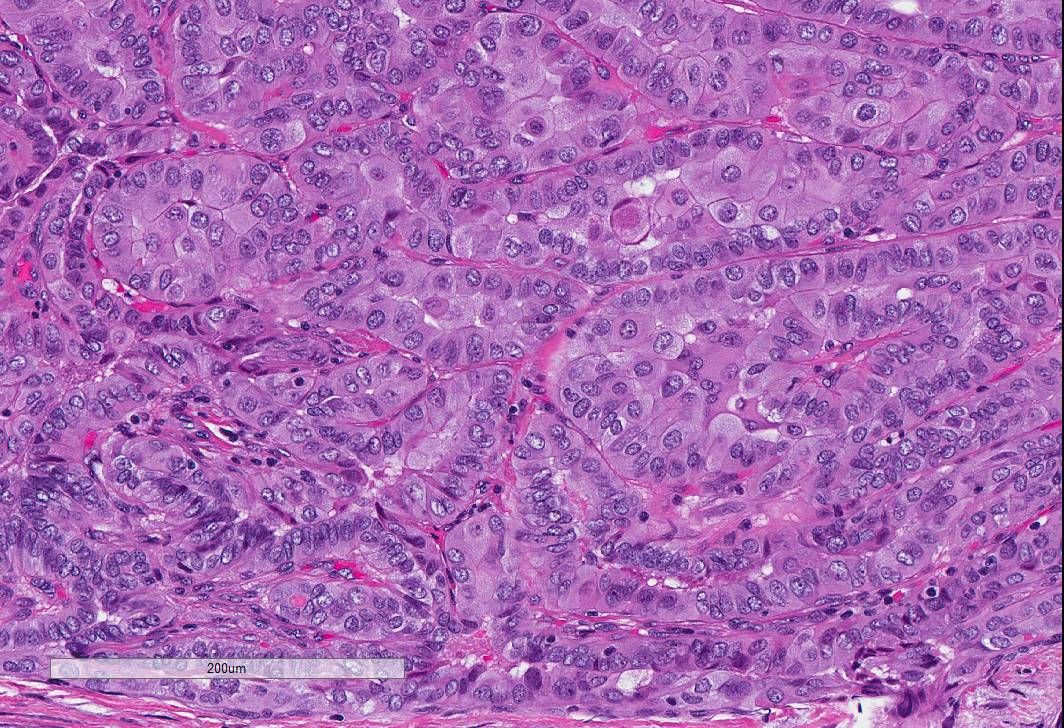
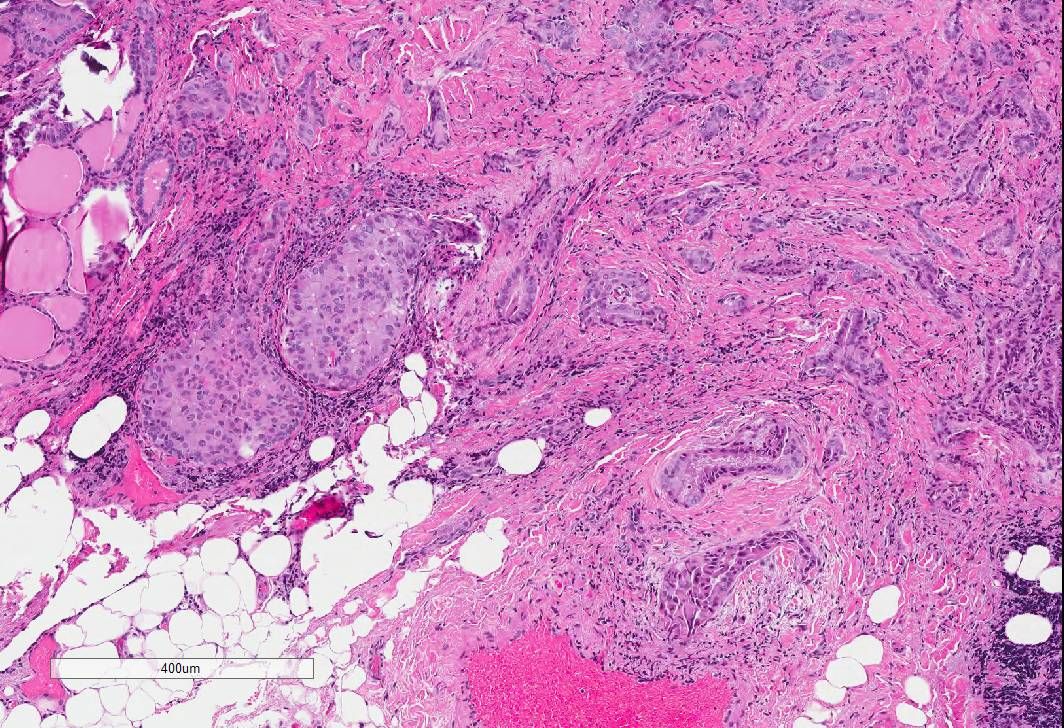
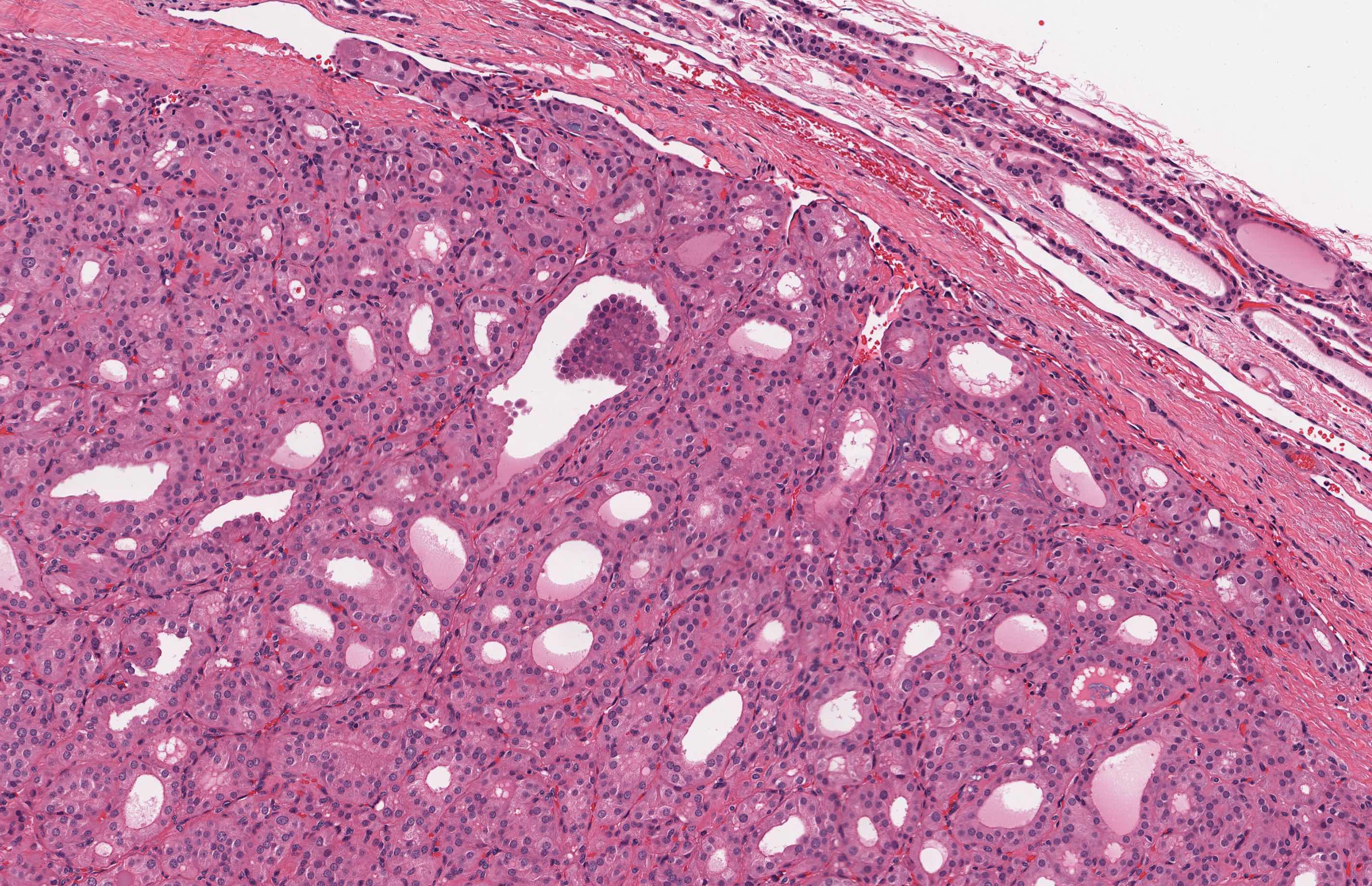
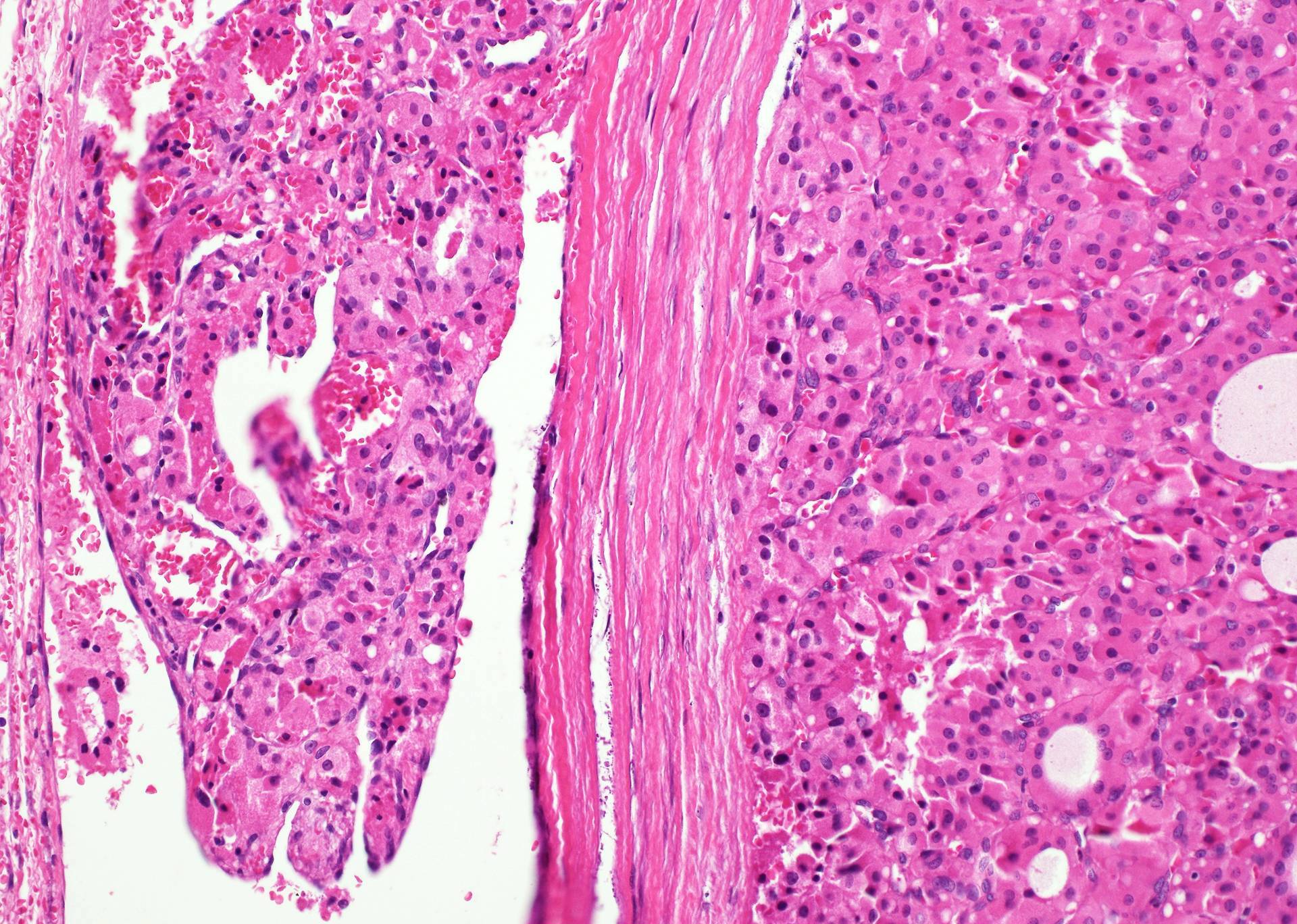
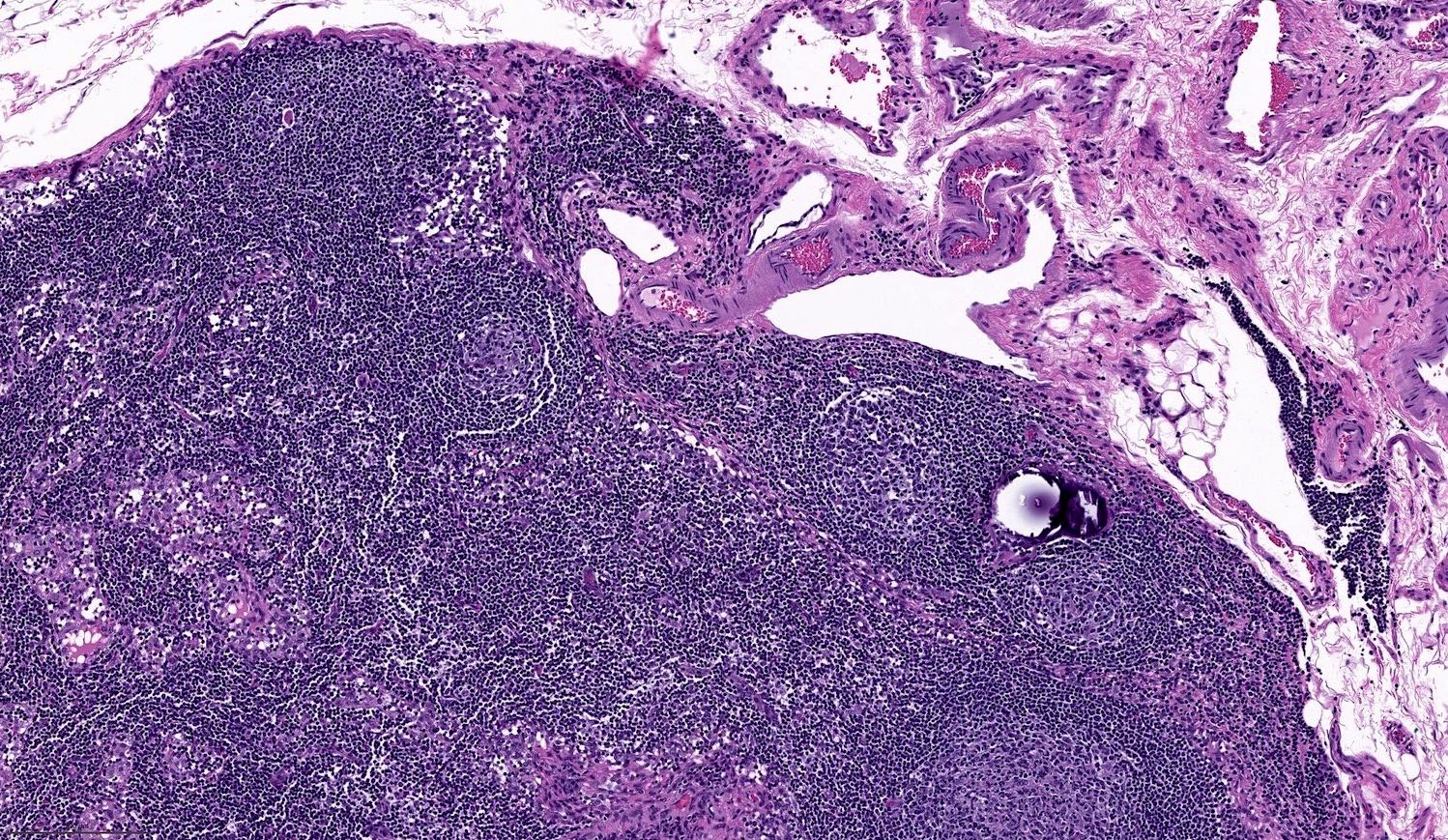
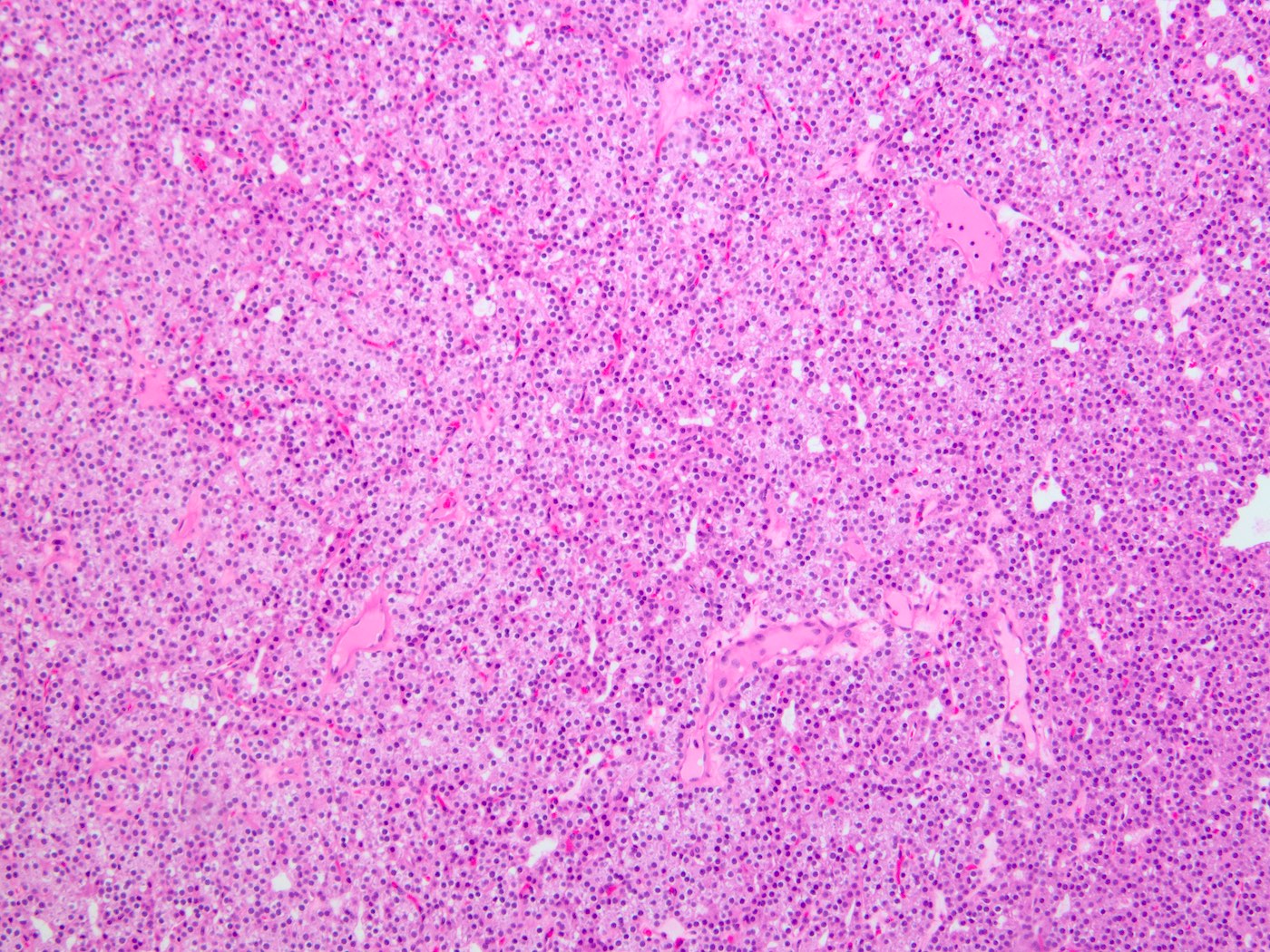
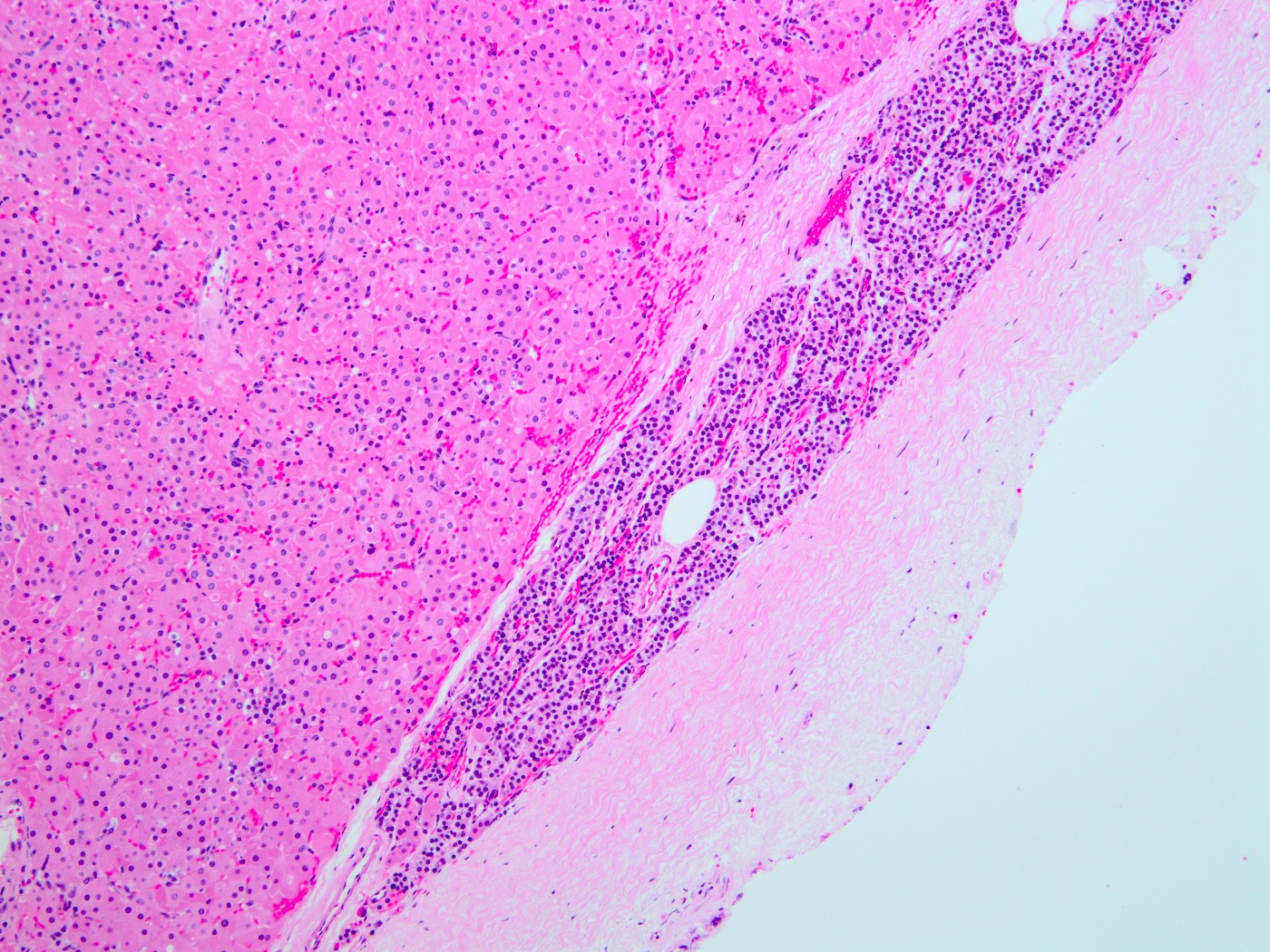
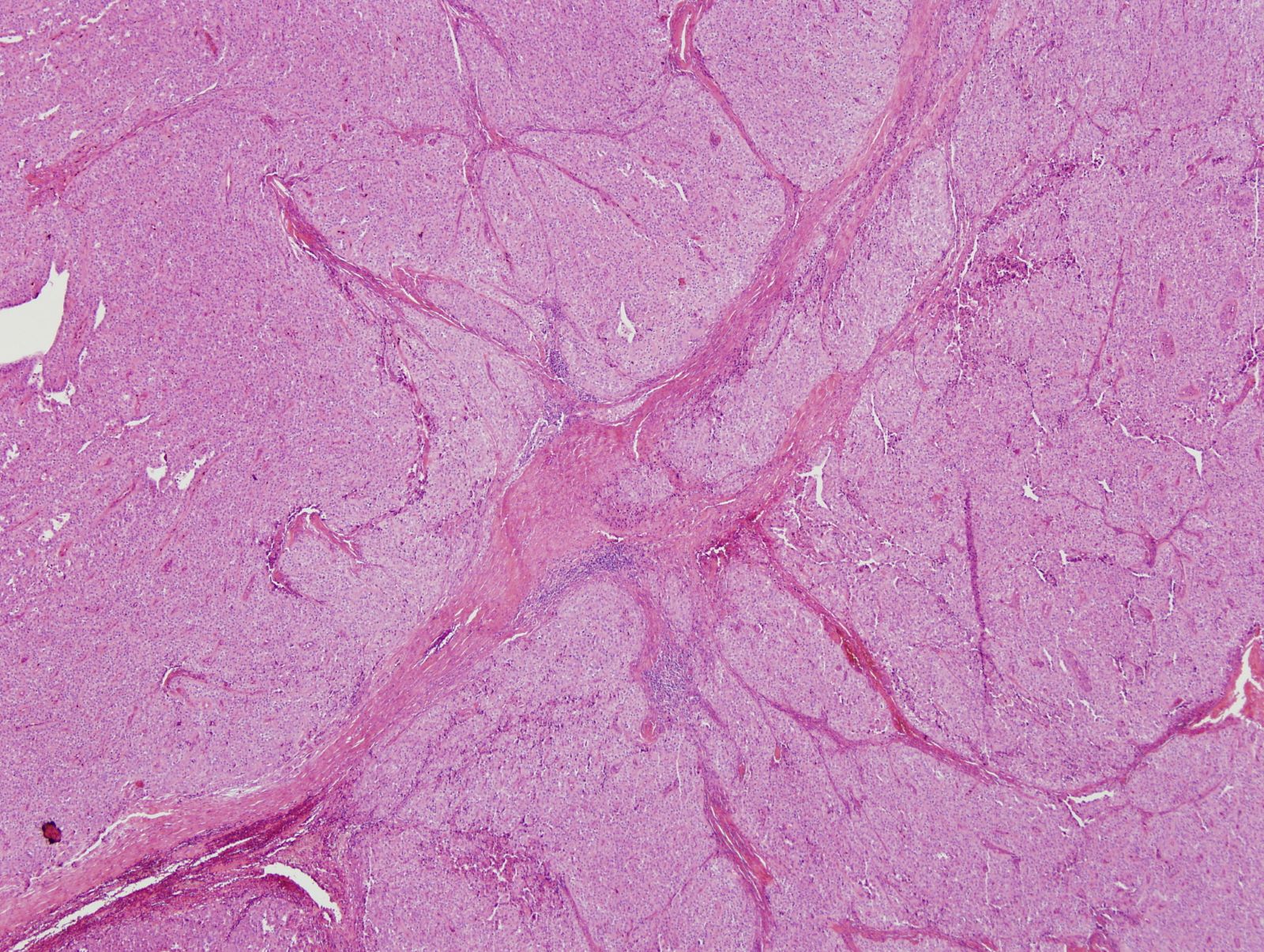
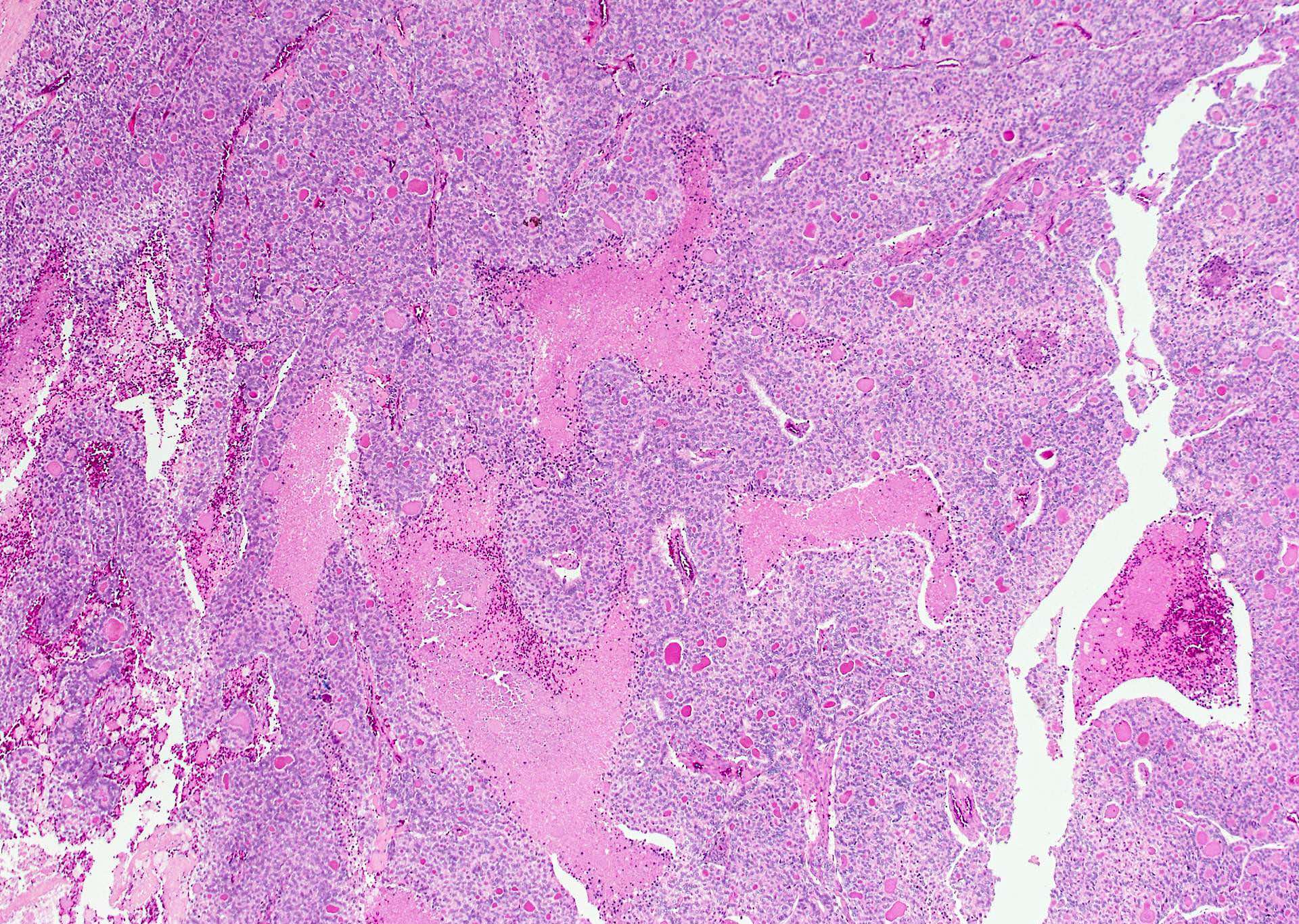
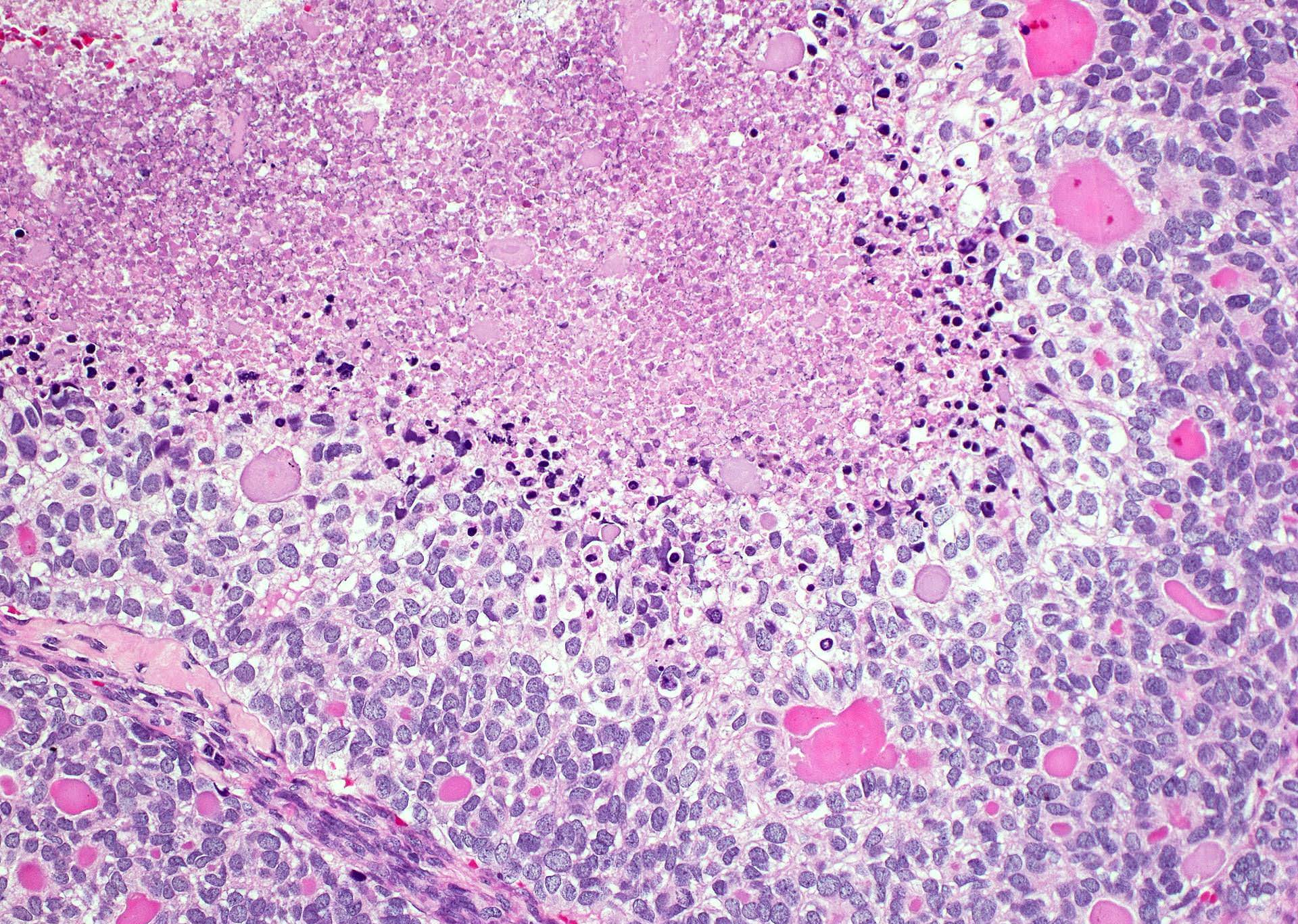
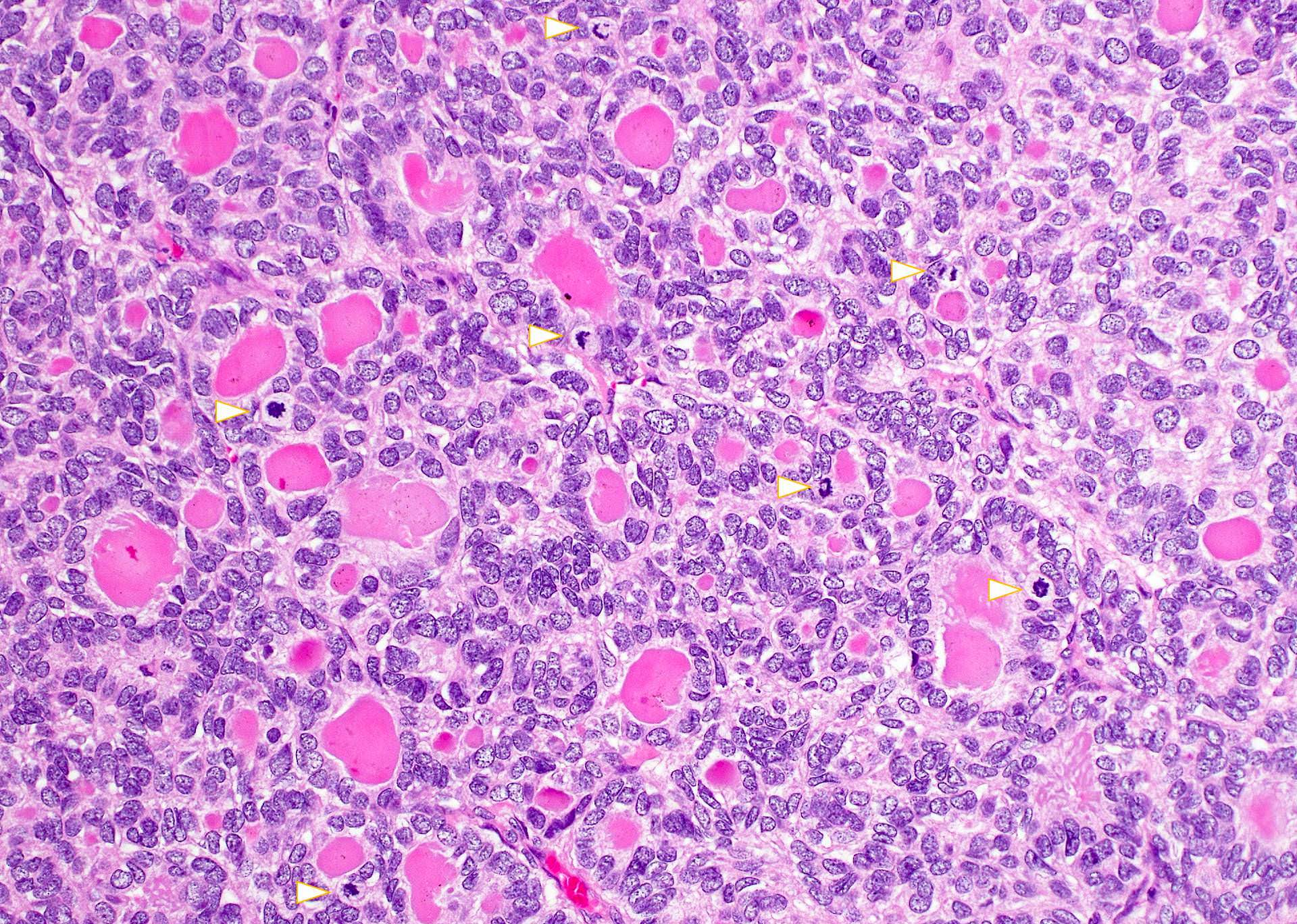
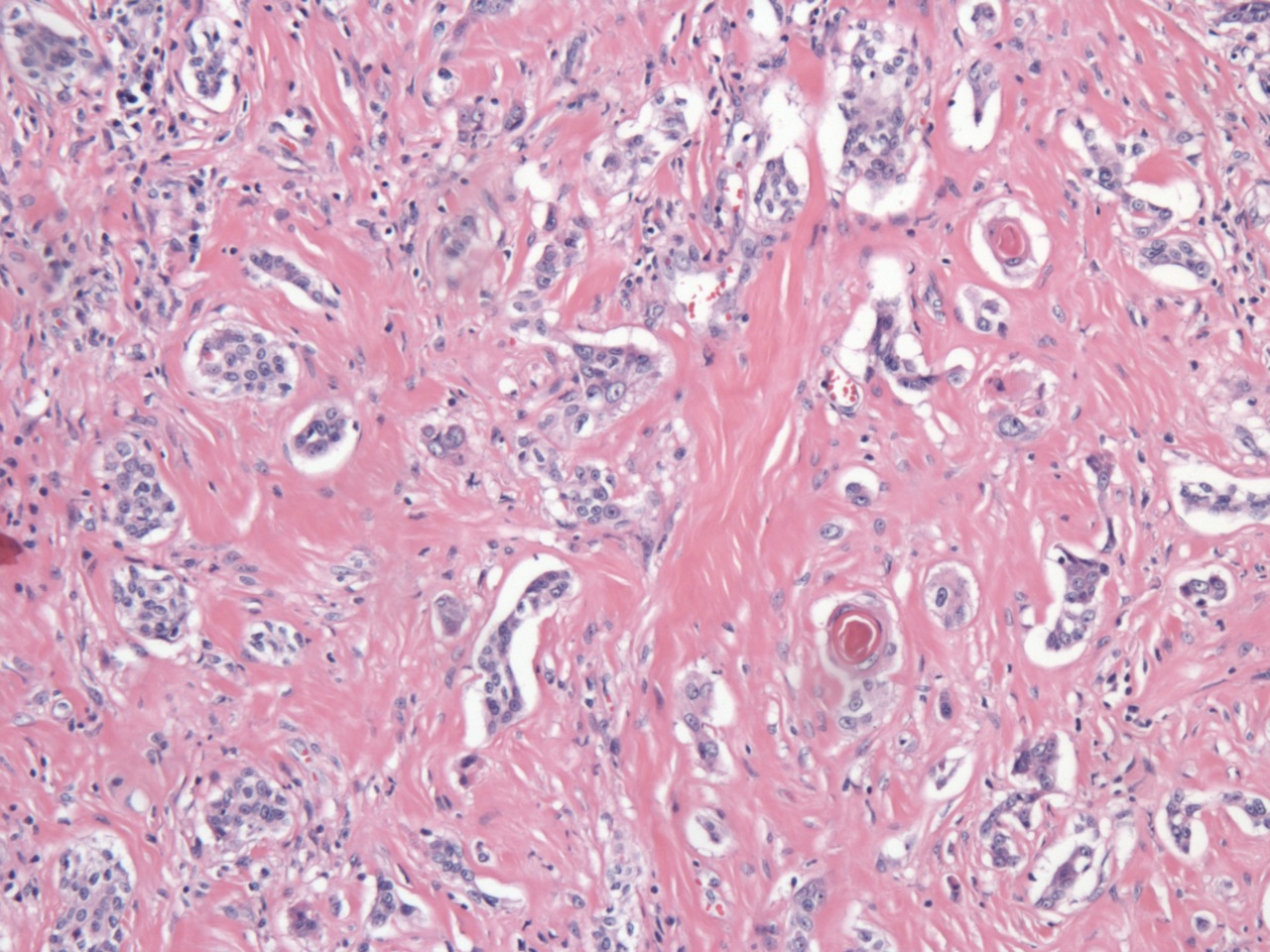
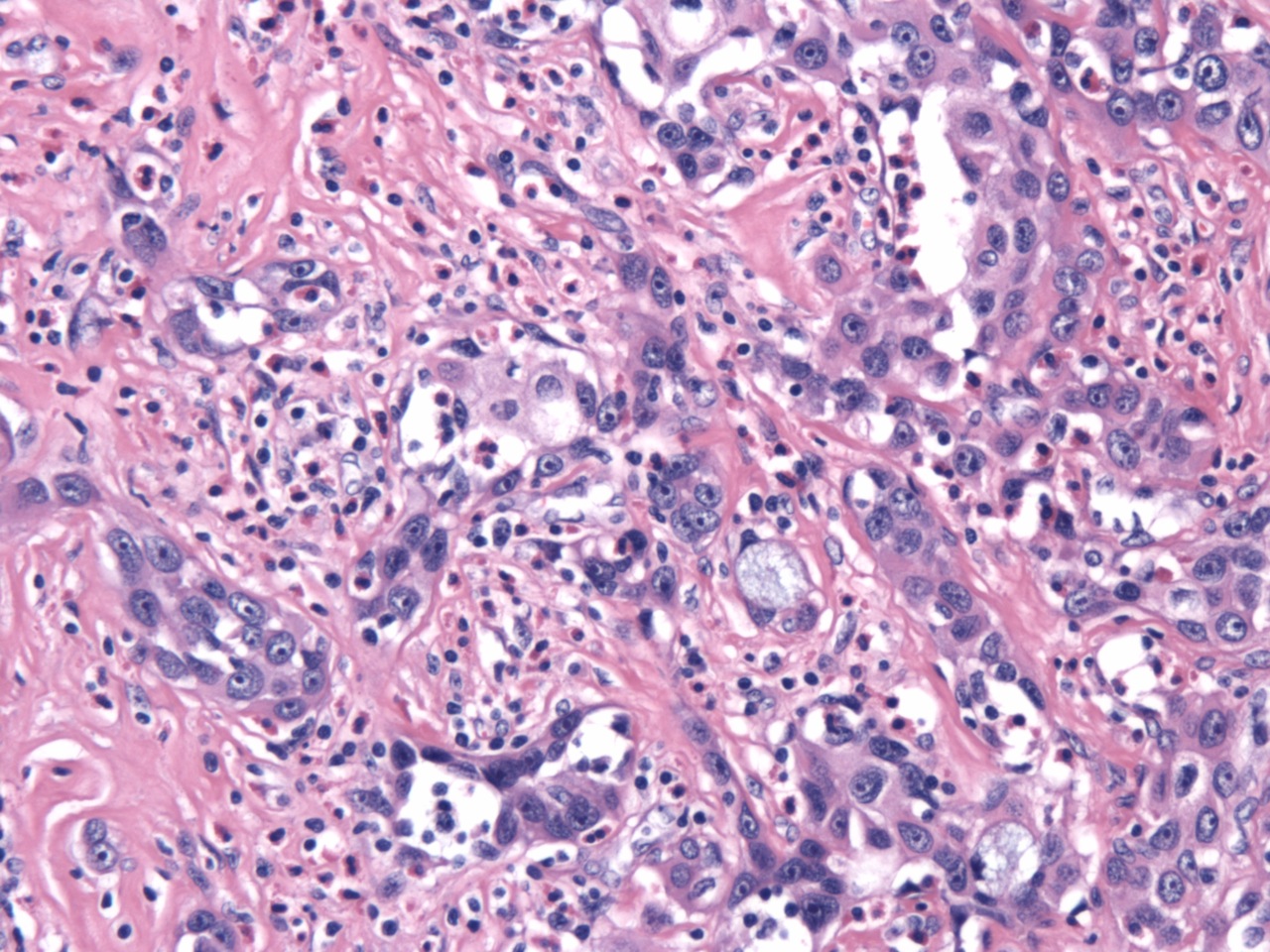
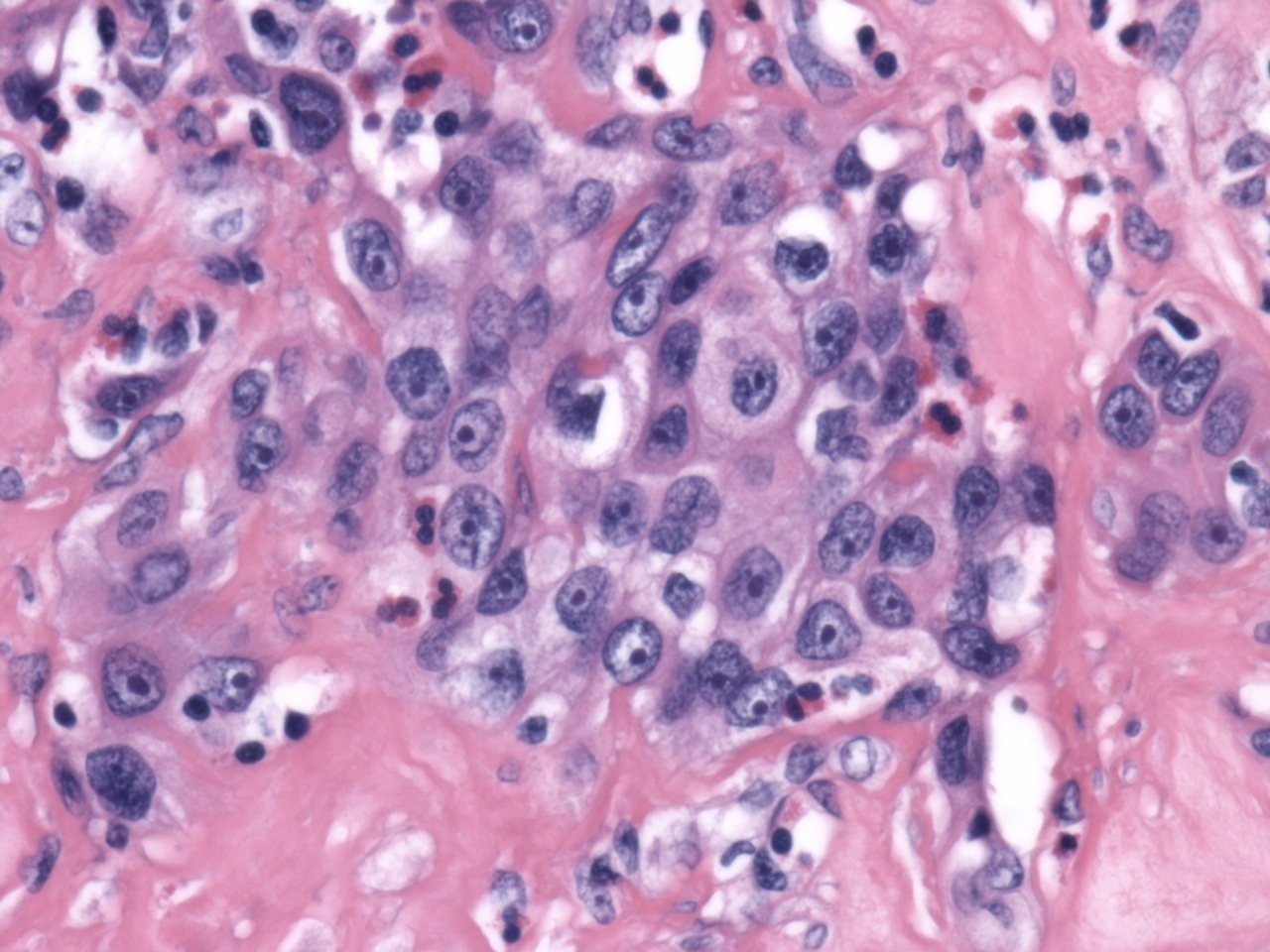
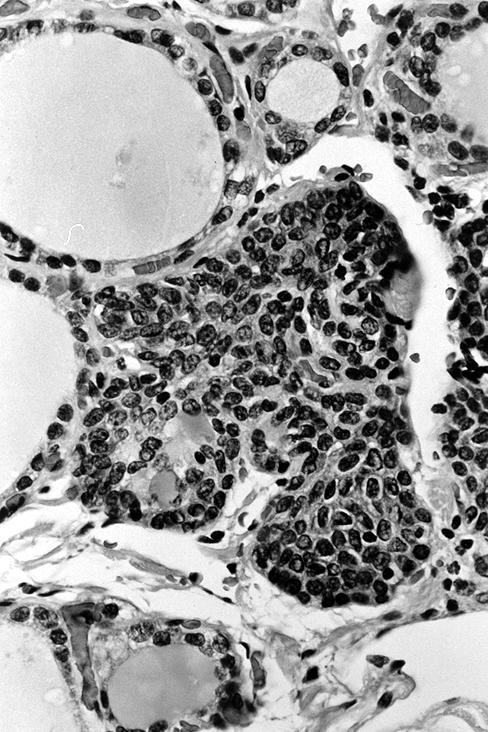
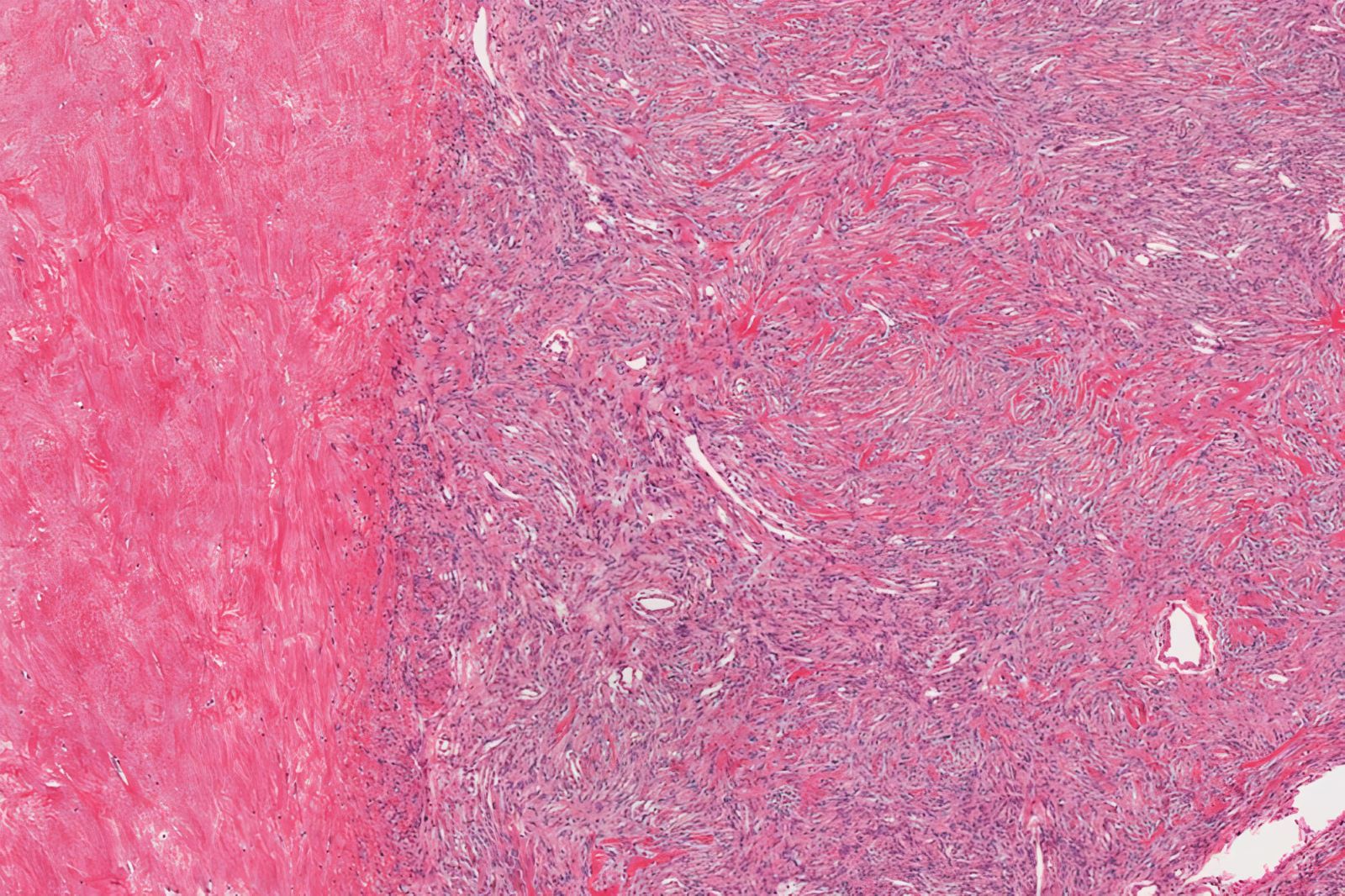
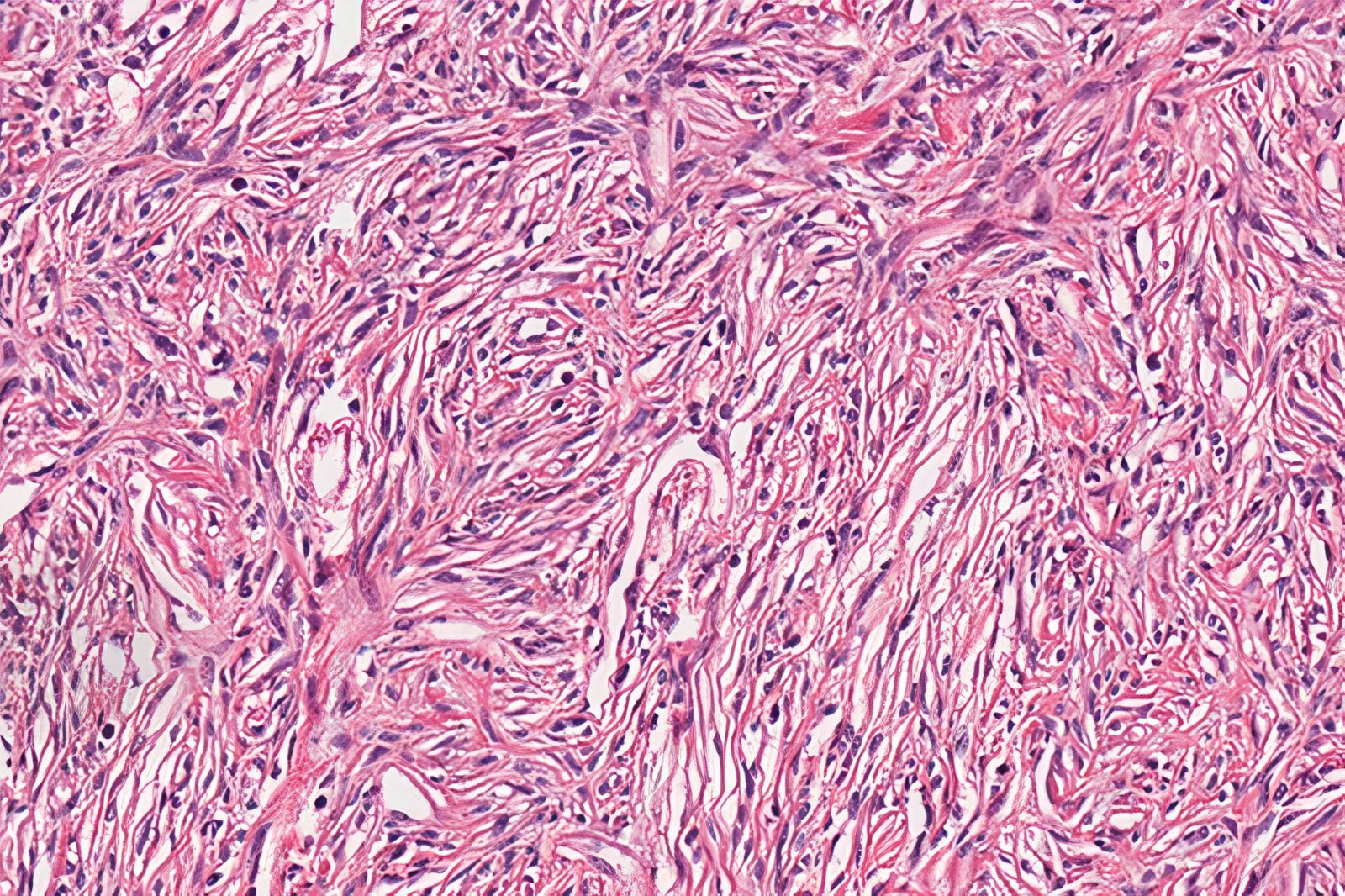
- Generally includes tumors that have 2 or more concerning features, such as fibrous bands, mitotic figures, necrosis, trabecular growth or adherence to surrounding tissues intraoperatively
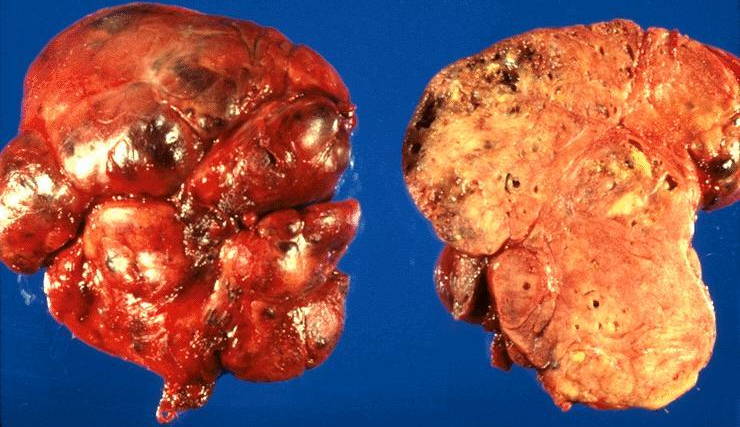
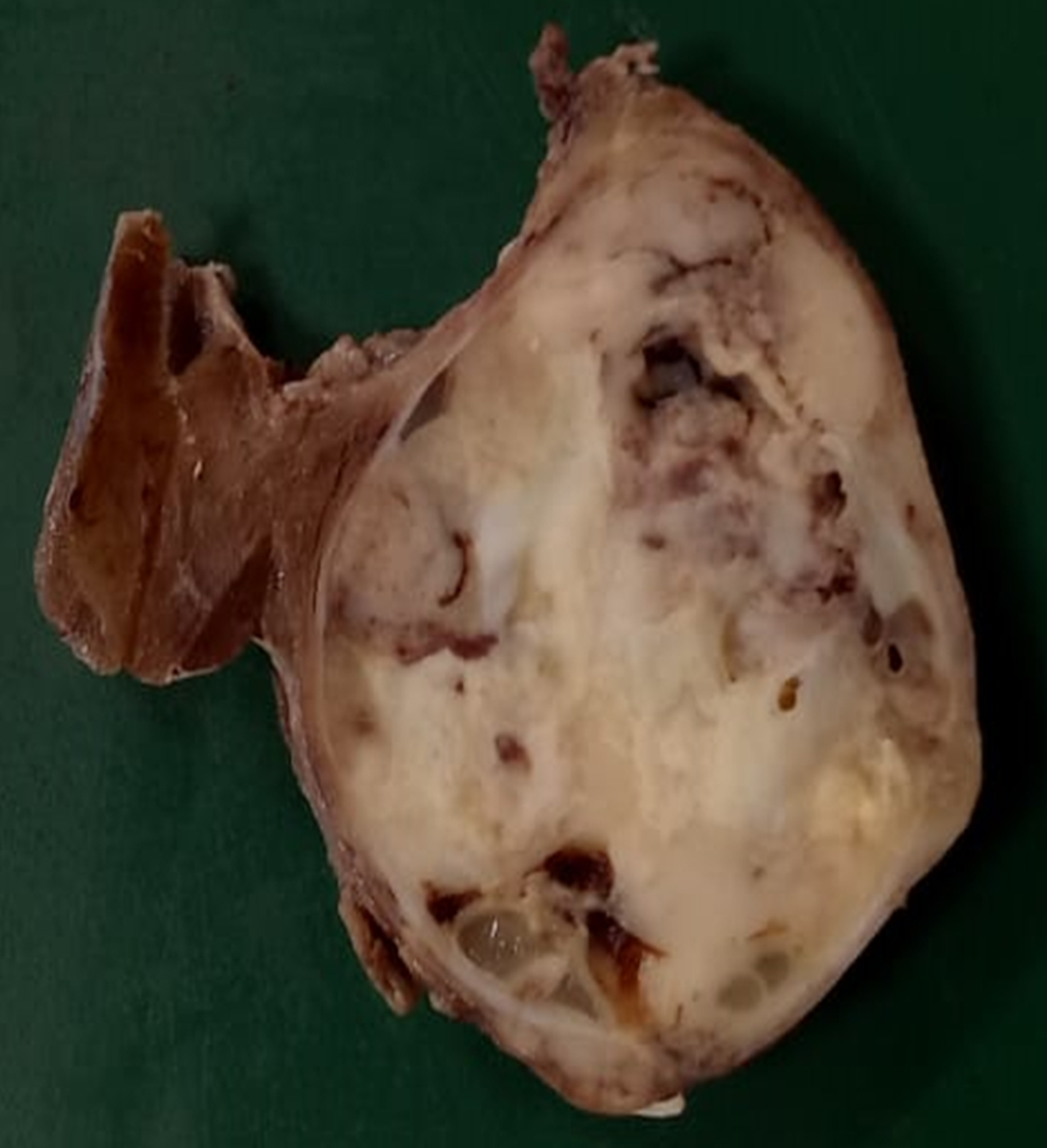
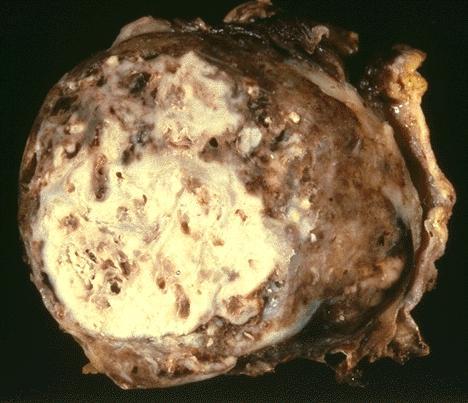
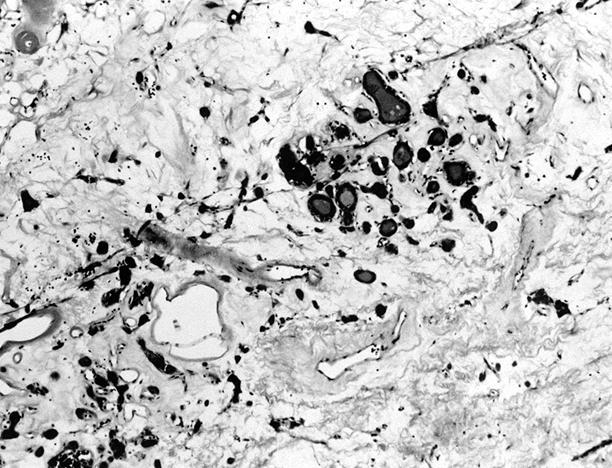
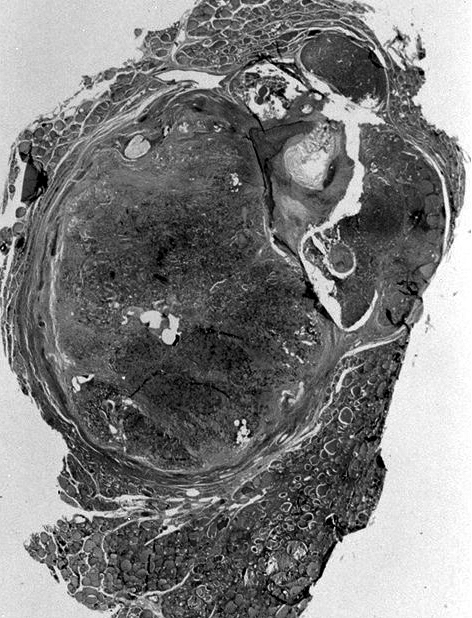
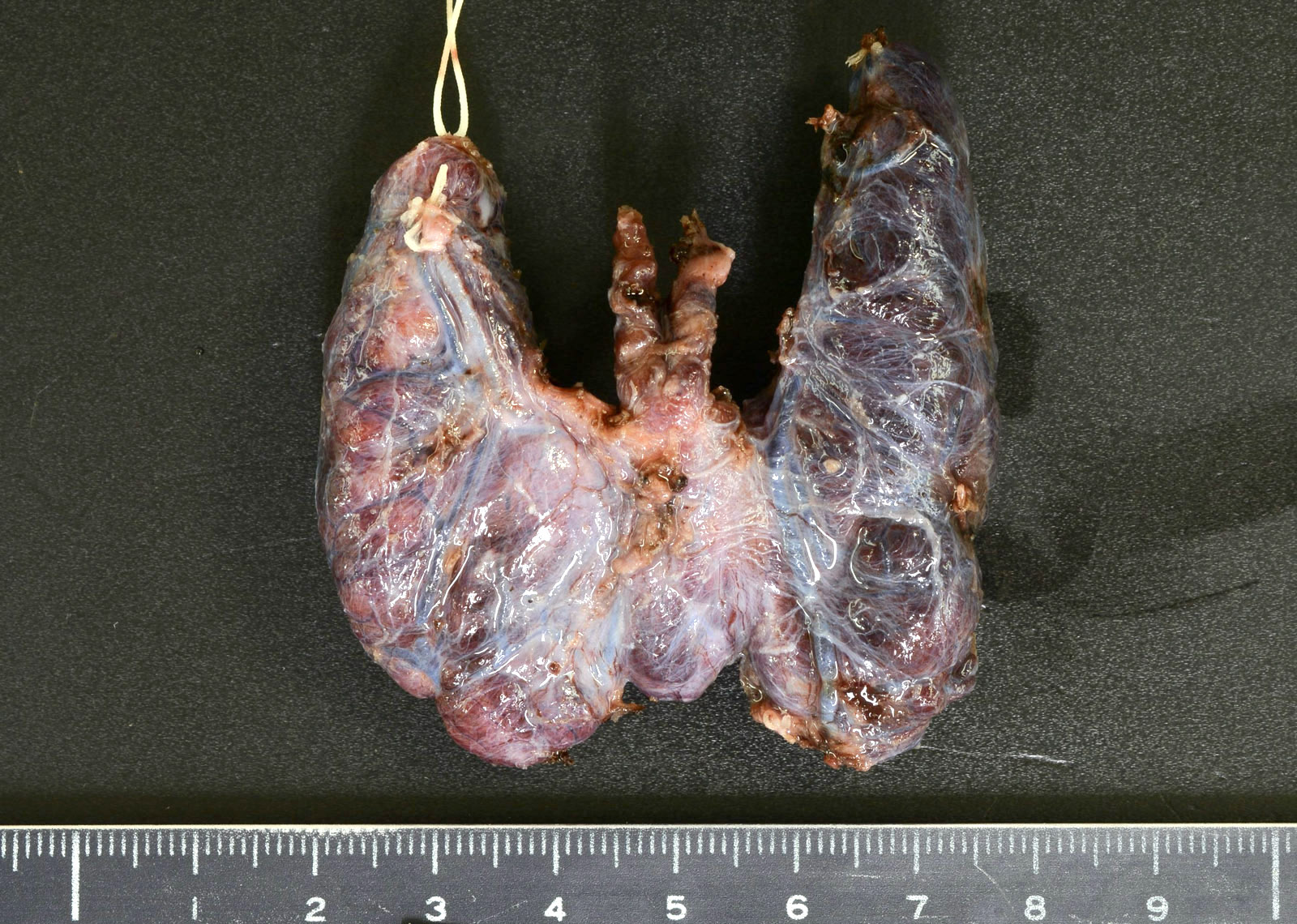
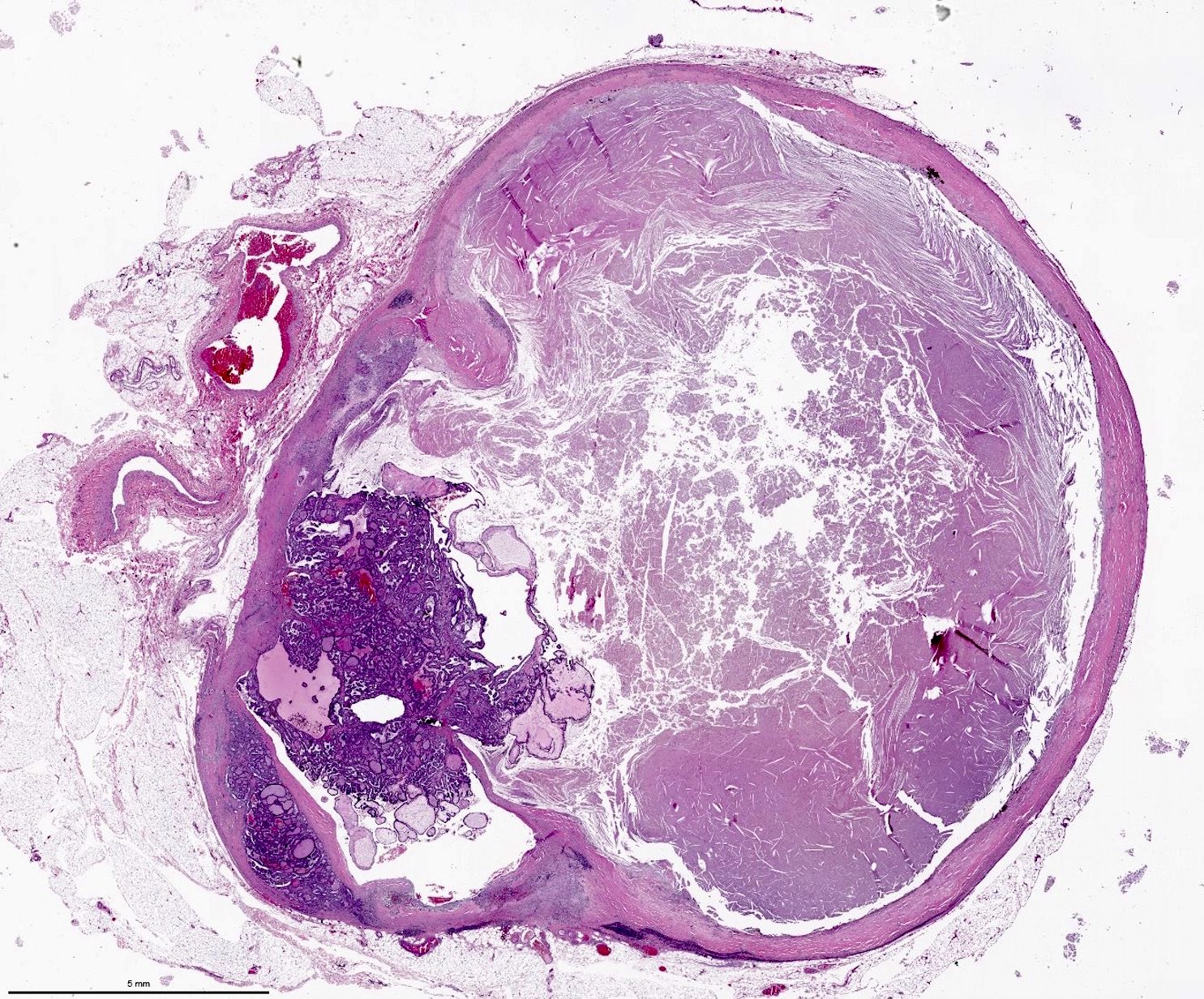
- Usually have a smaller dimension, weight and volume than carcinomas and are less likely to have coagulative tumor necrosis