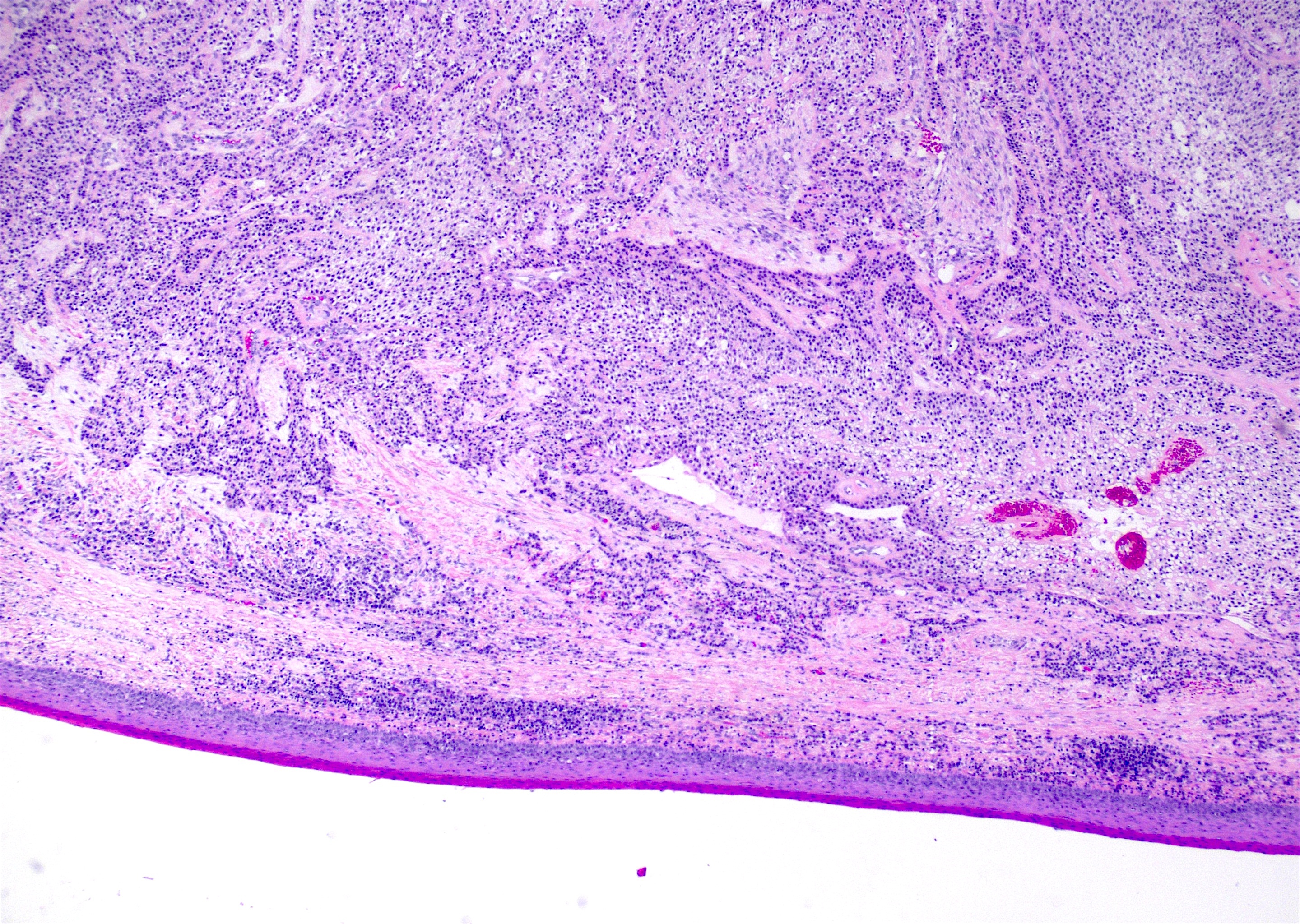
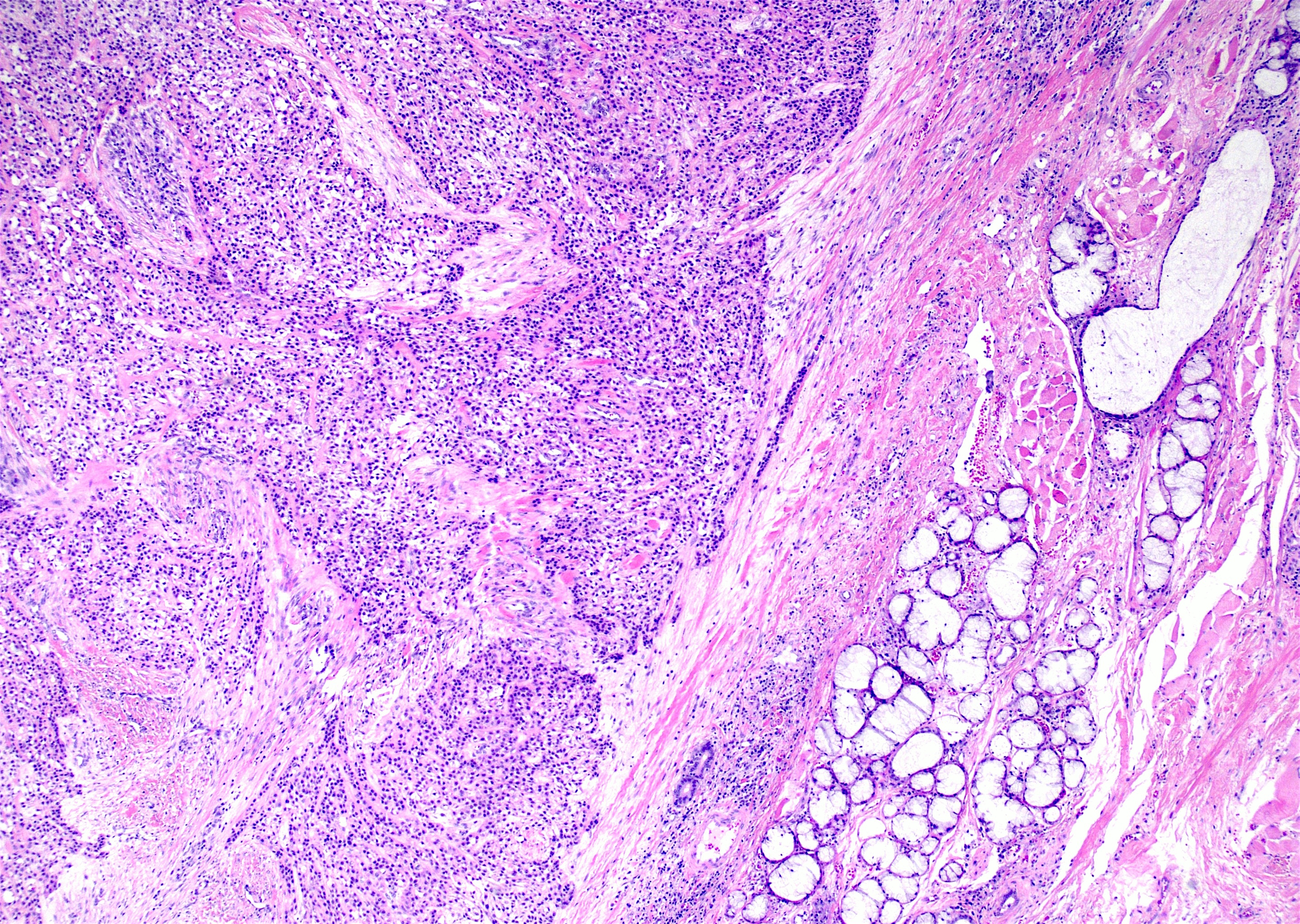
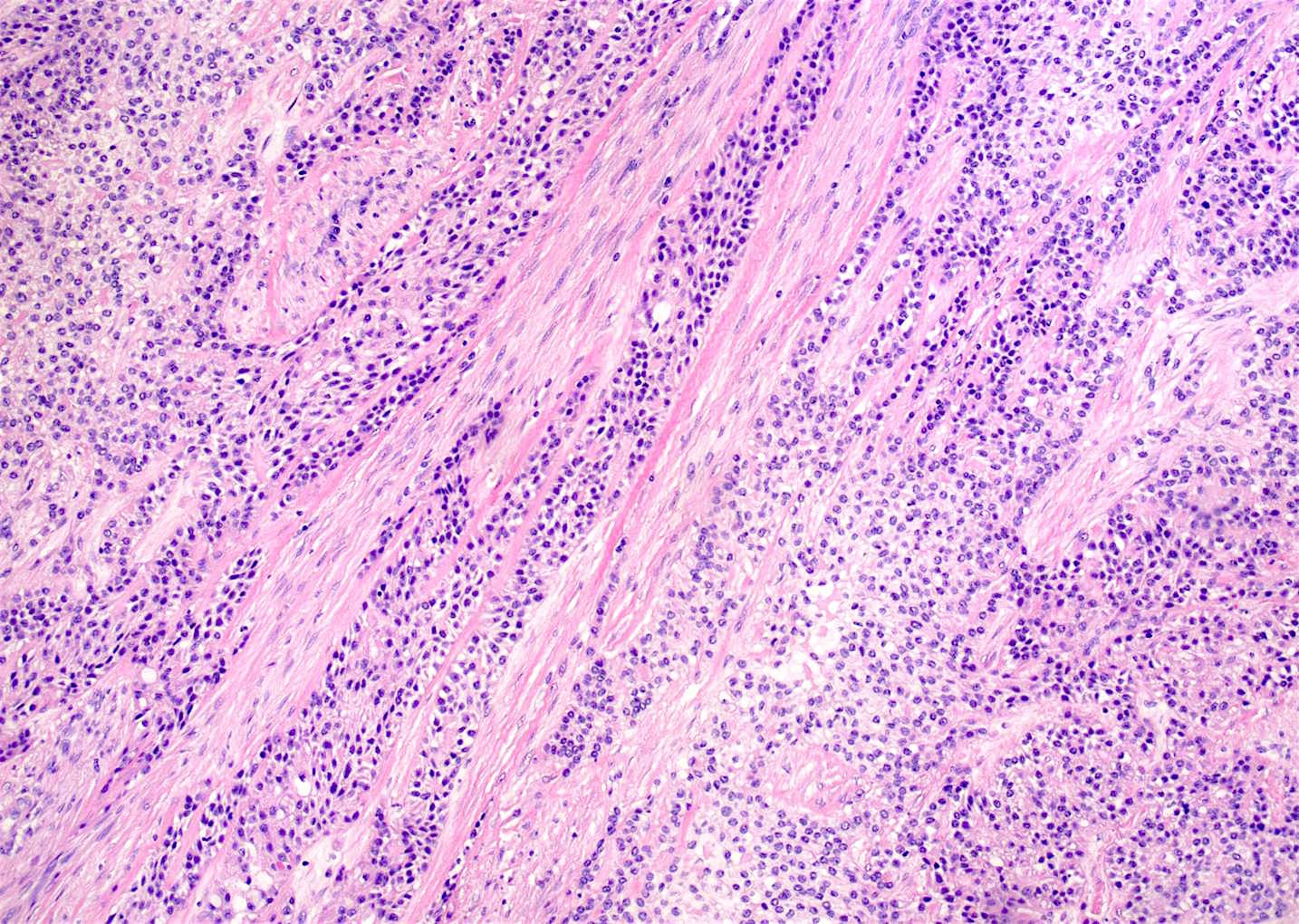
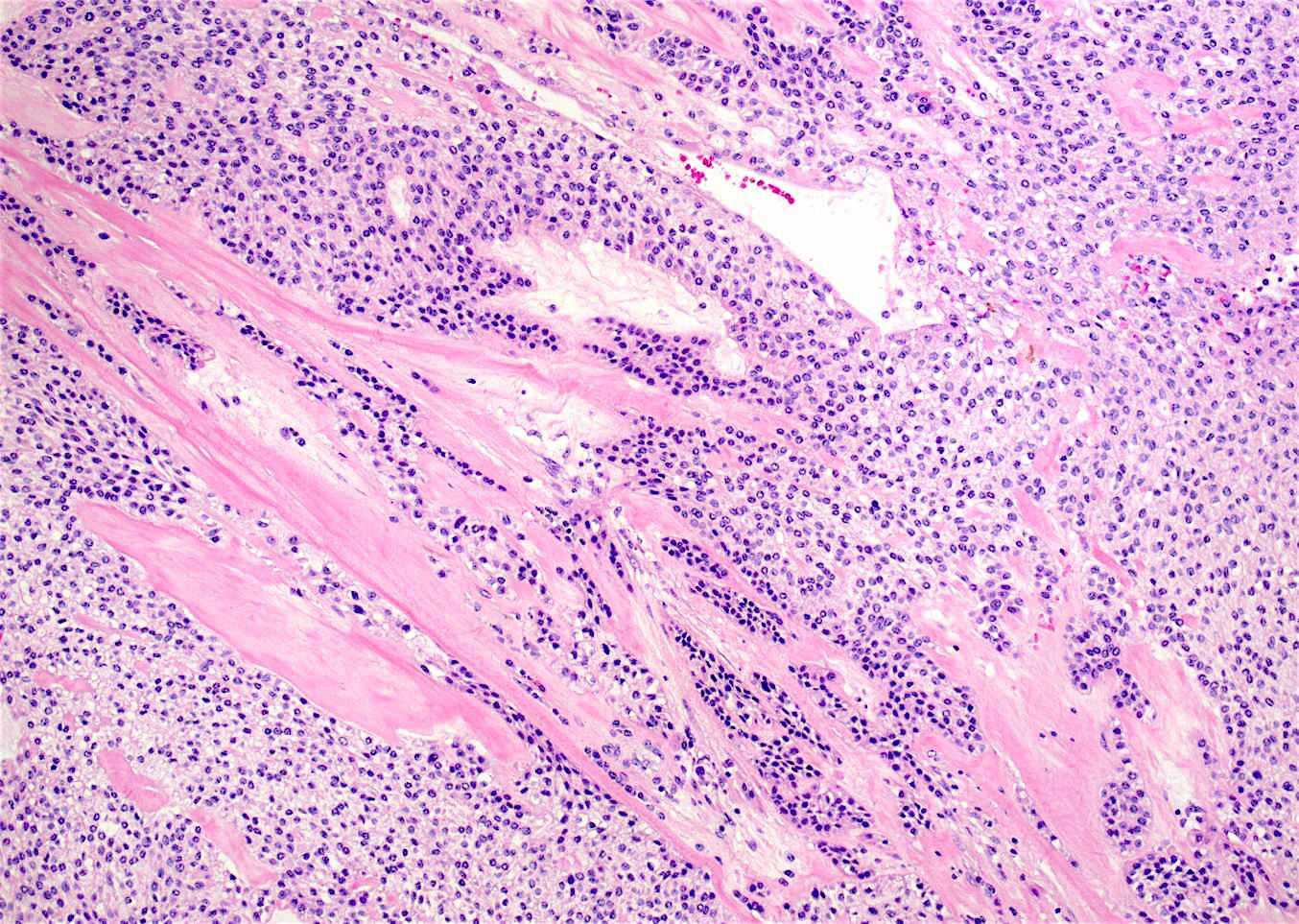
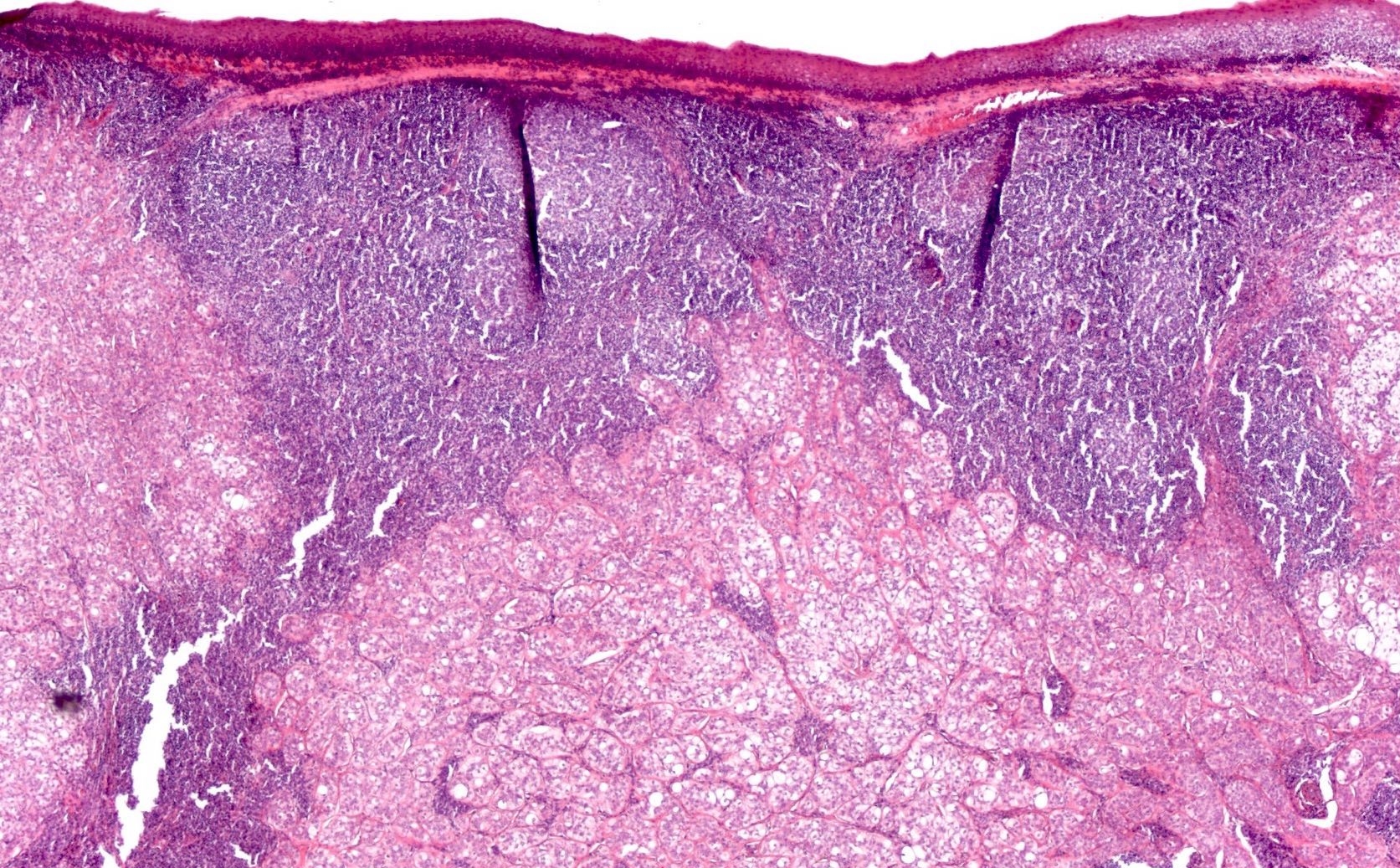
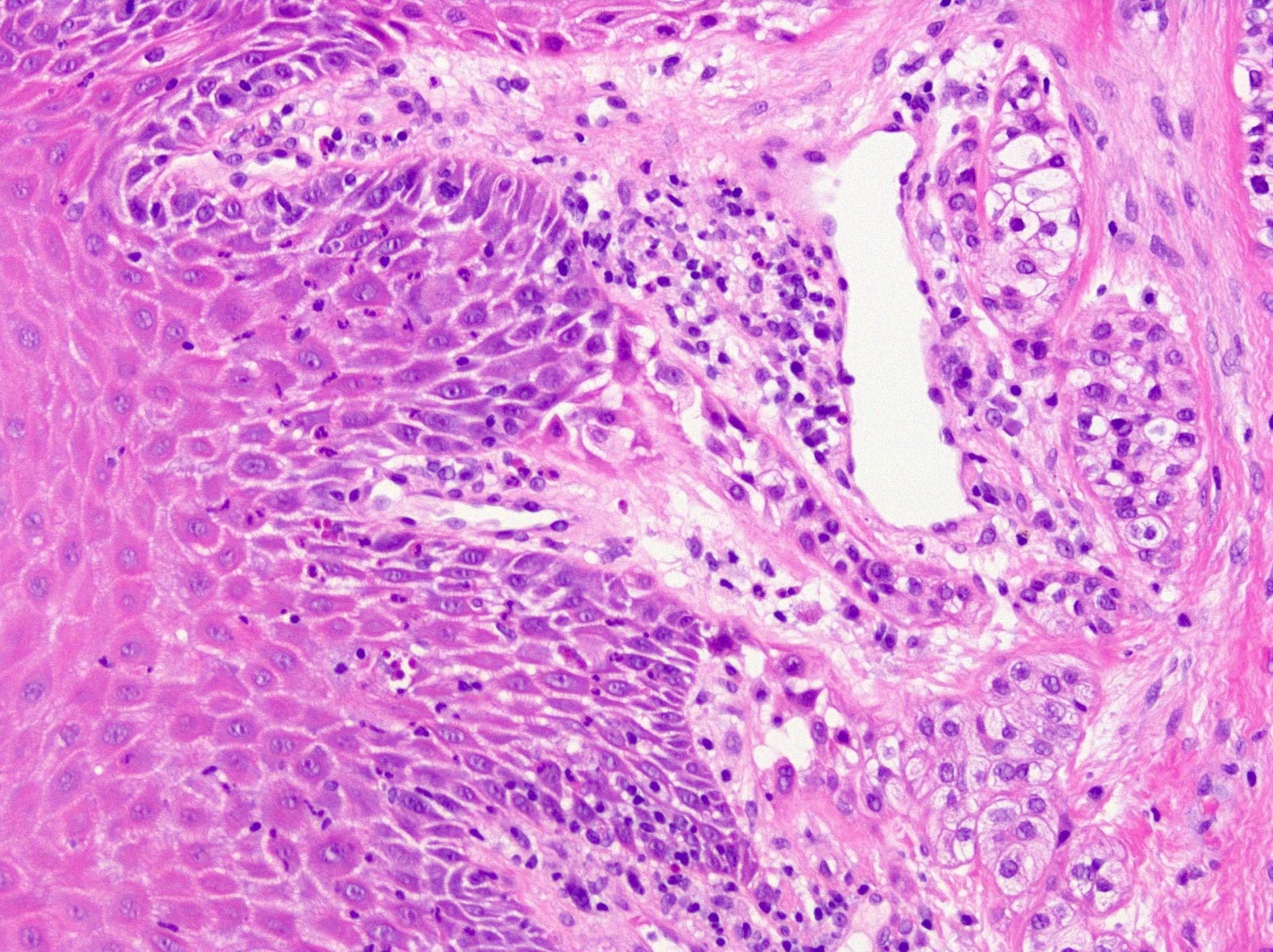
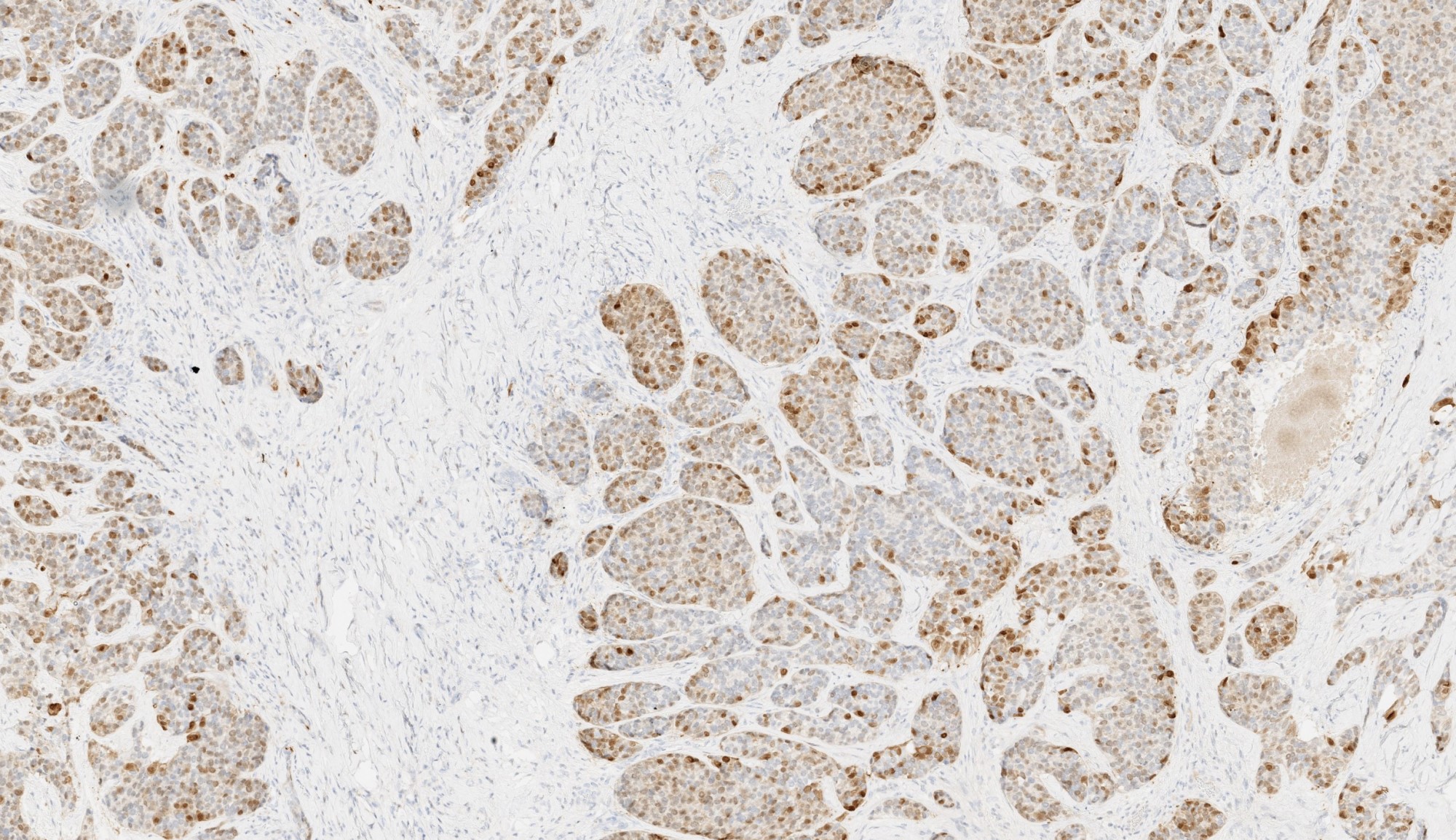
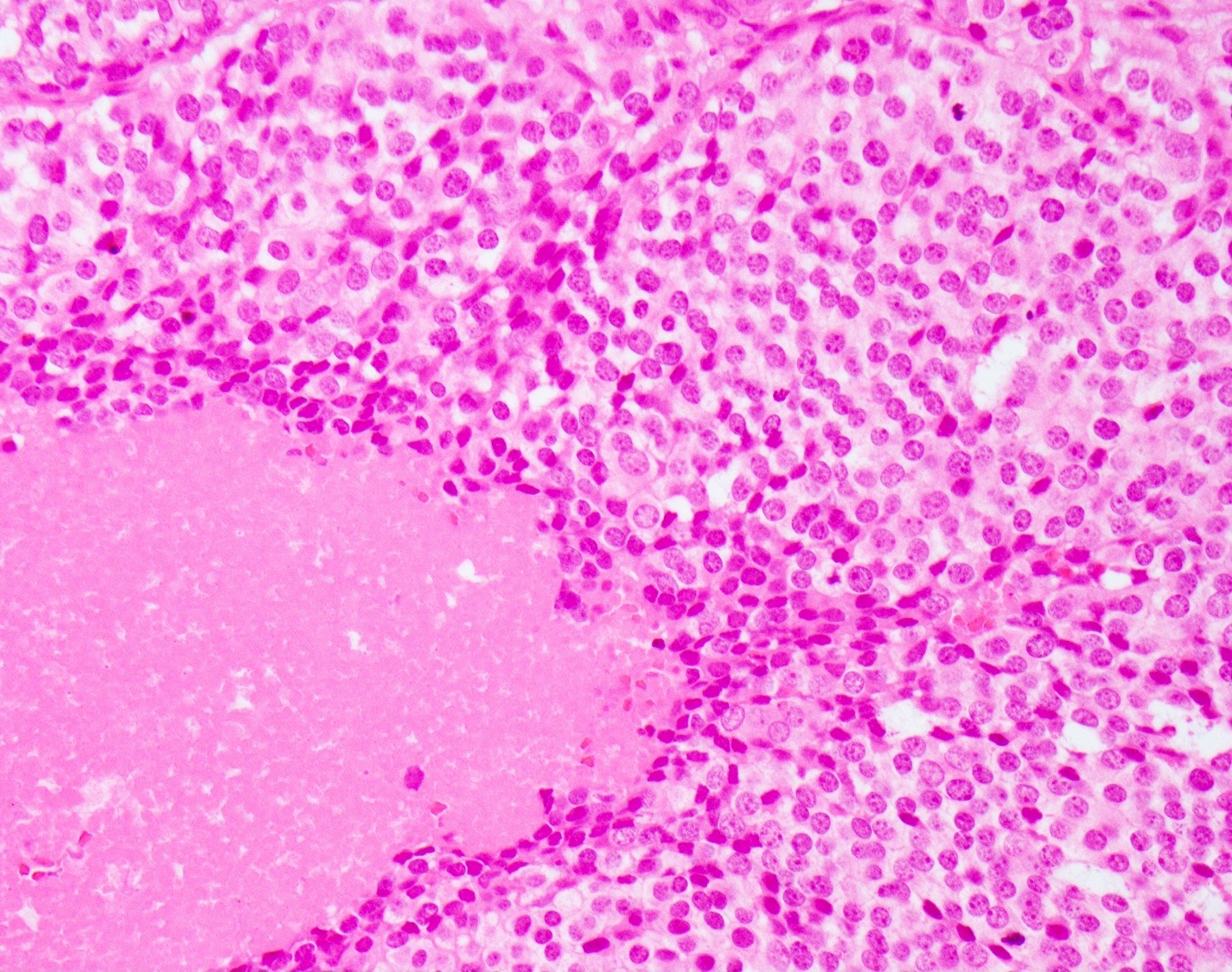
Malignant epithelial neoplasm of the salivary glands characterized by serous acinar cell differentiation (cytoplasmic zymogen granules) in at least some of the neoplastic cells
Essential features
~6 - 8% of all salivary gland neoplasms and 10 - 17% of primary salivary gland malignancies
Parotid gland is the most common site
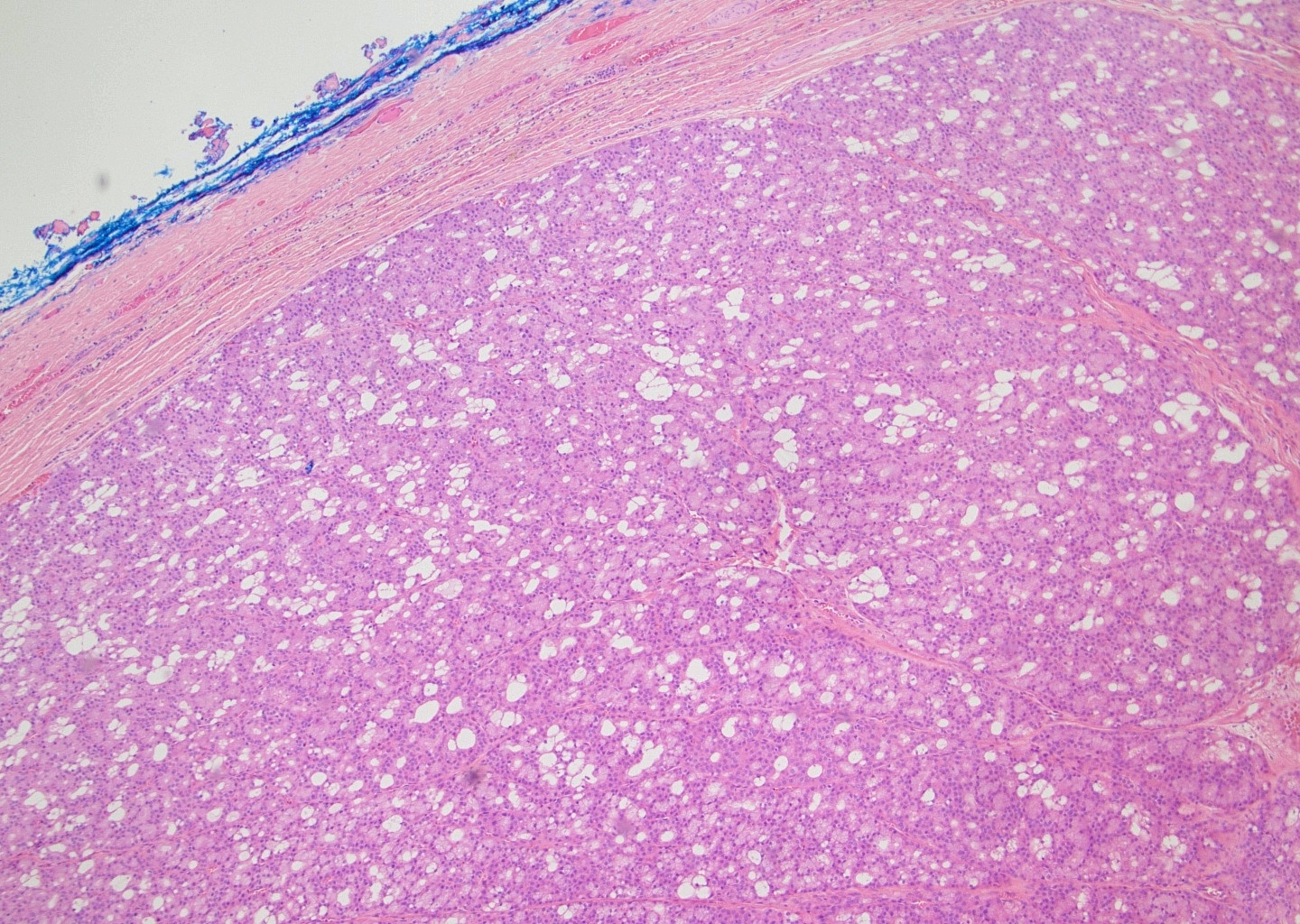
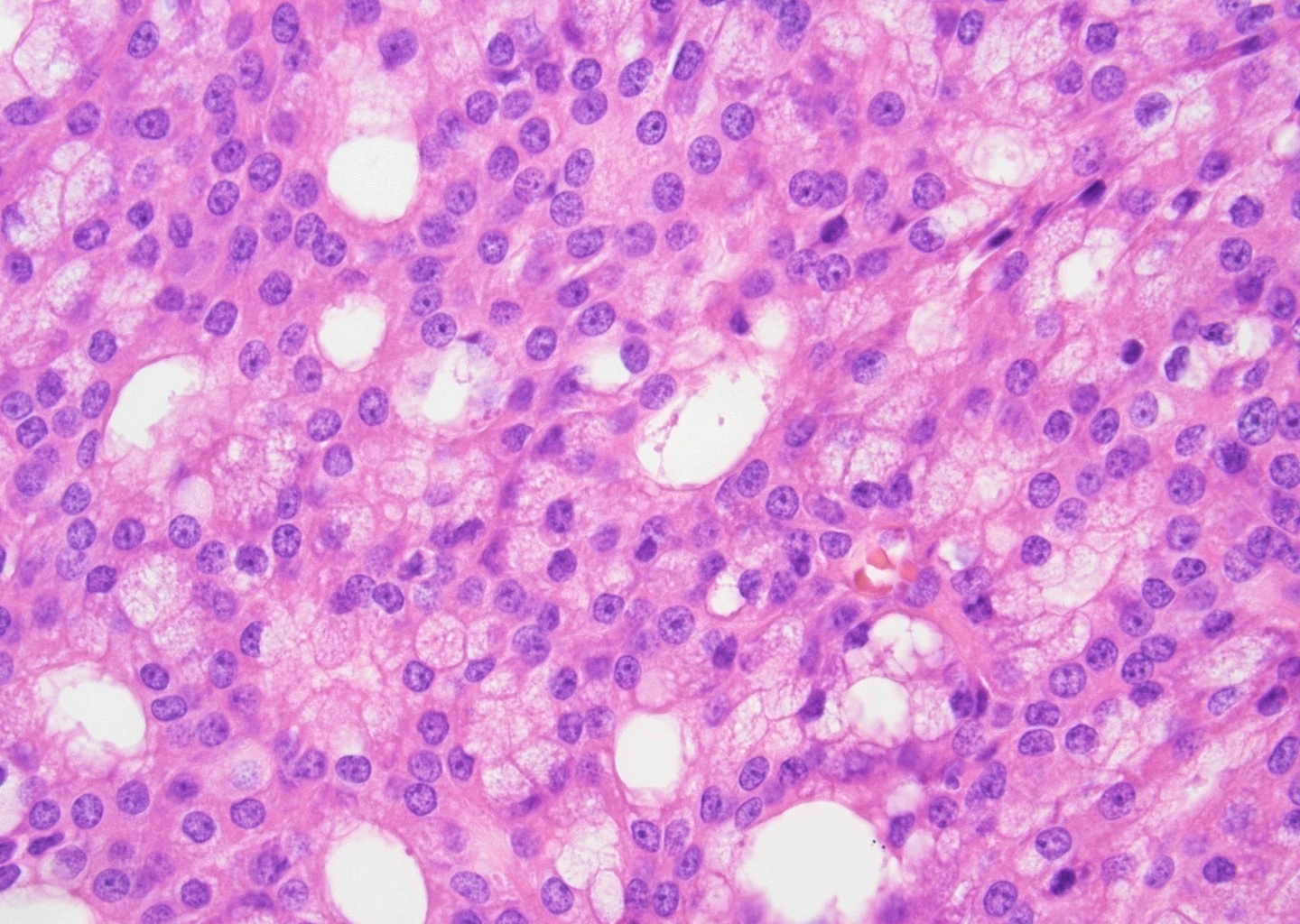
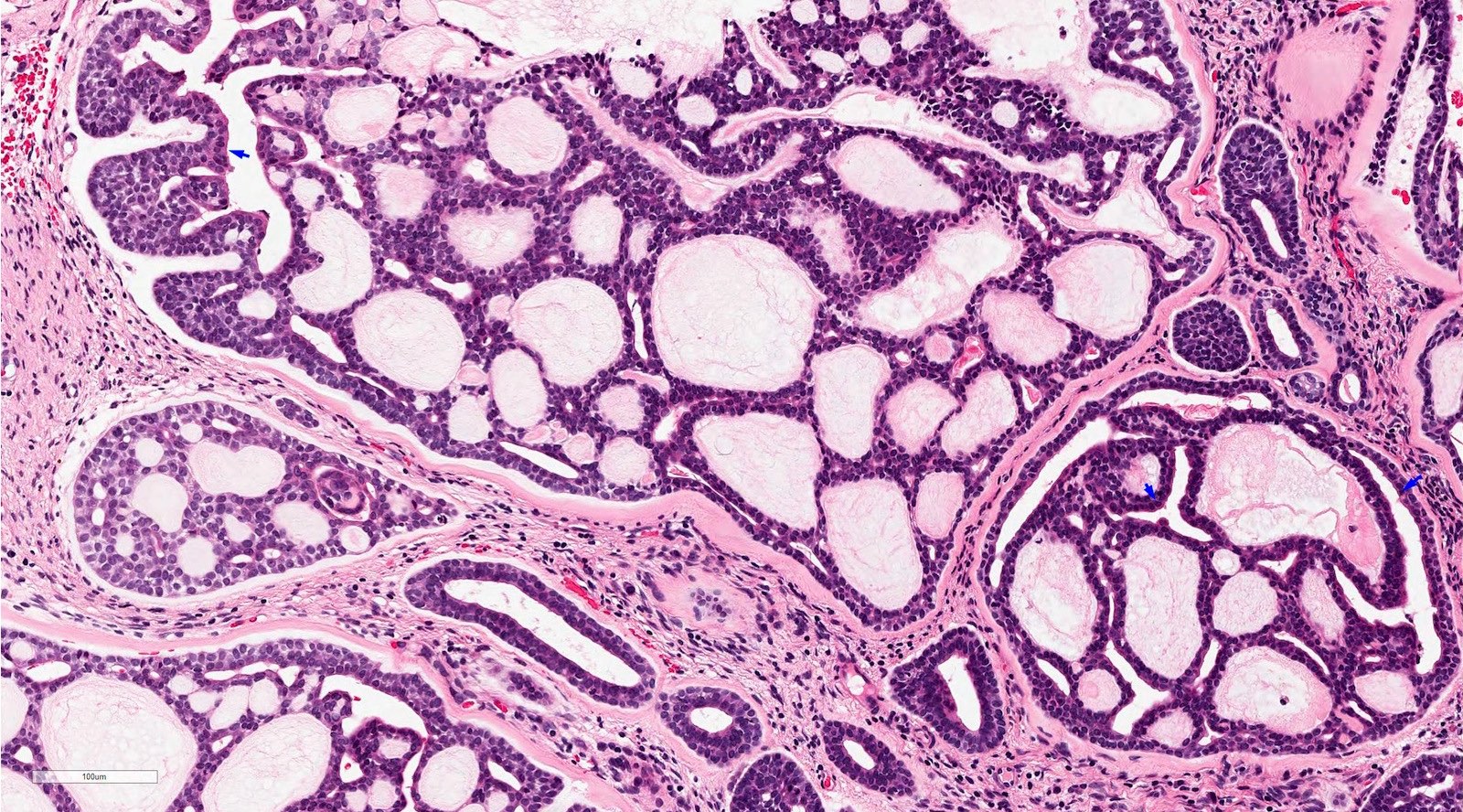
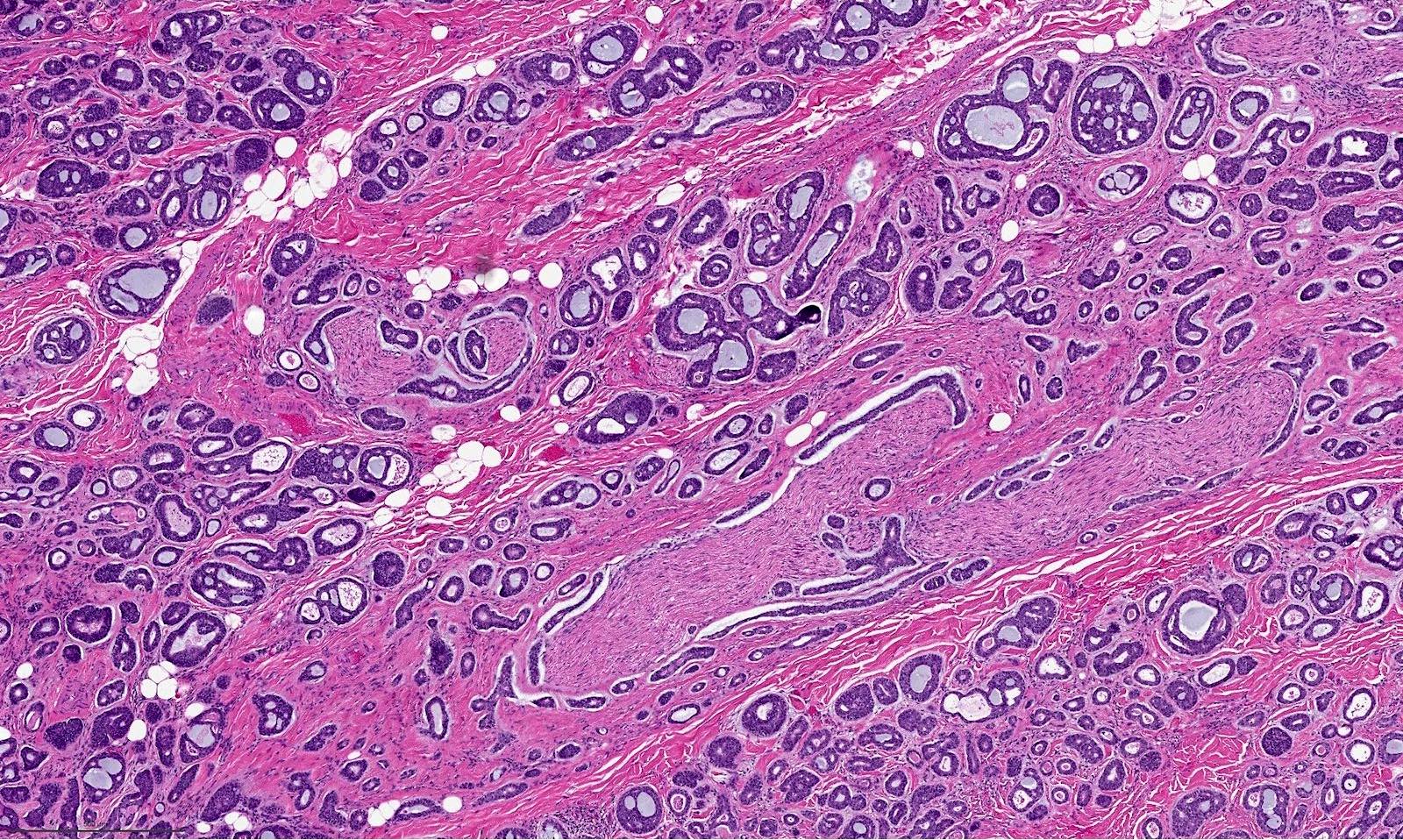
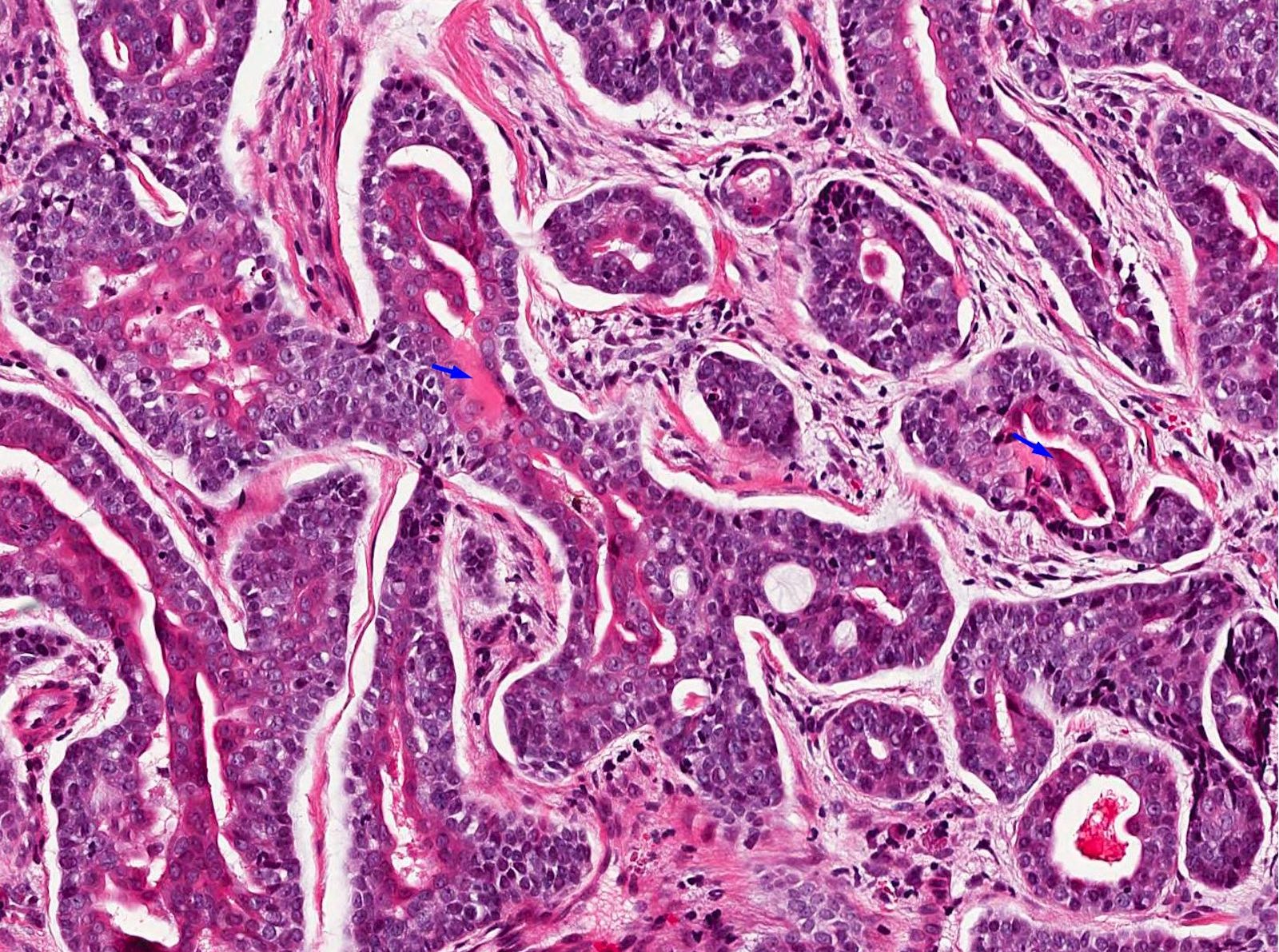
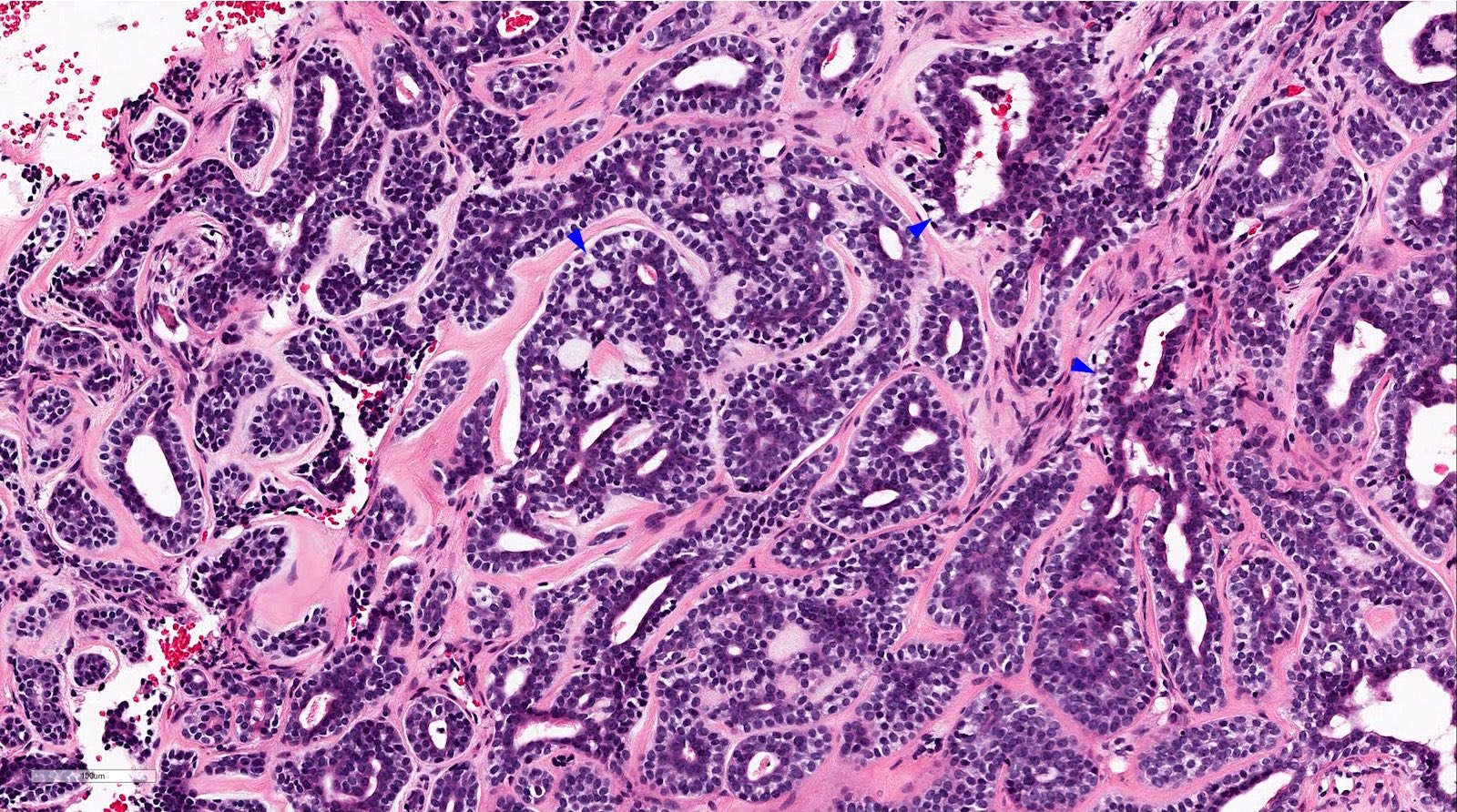
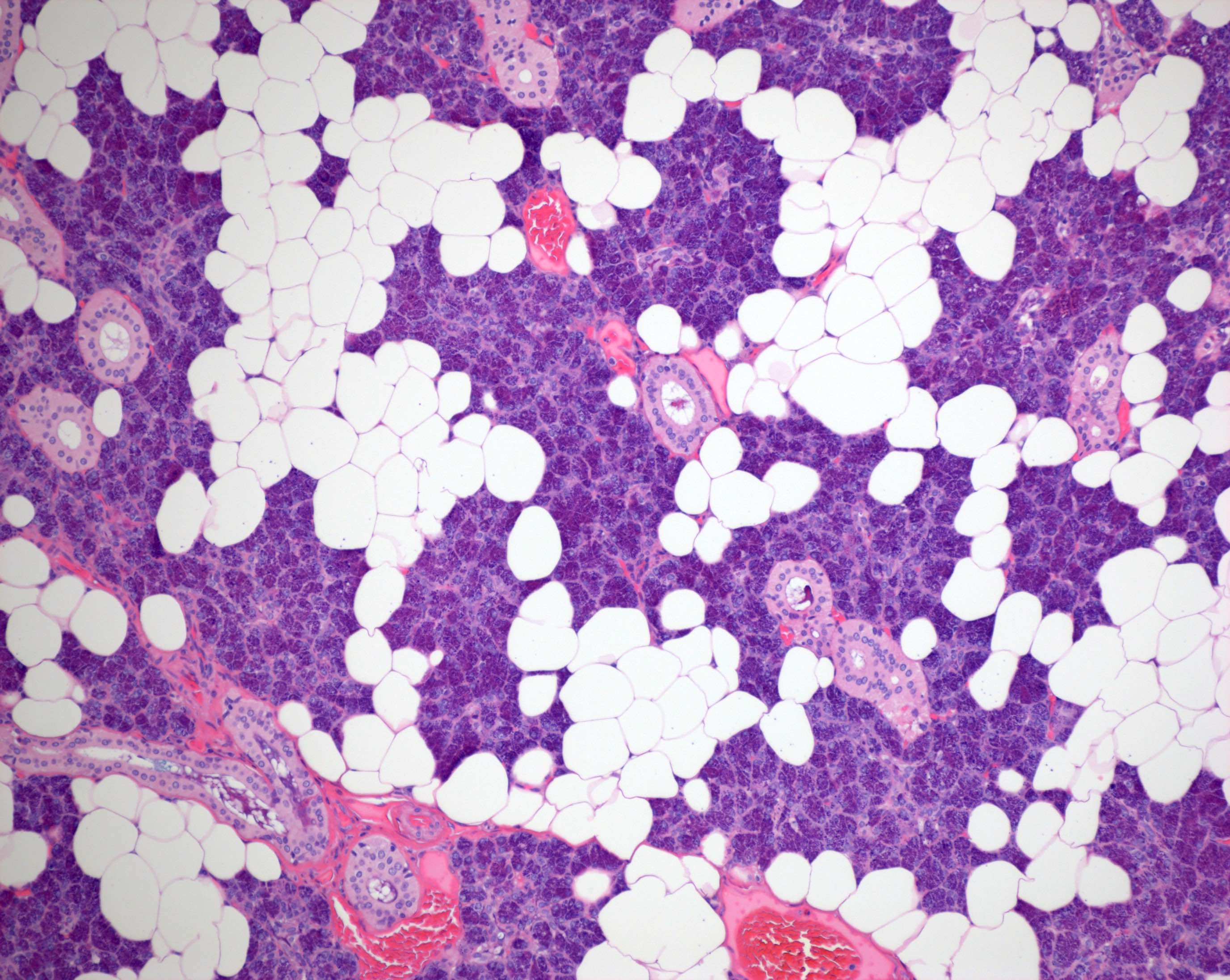
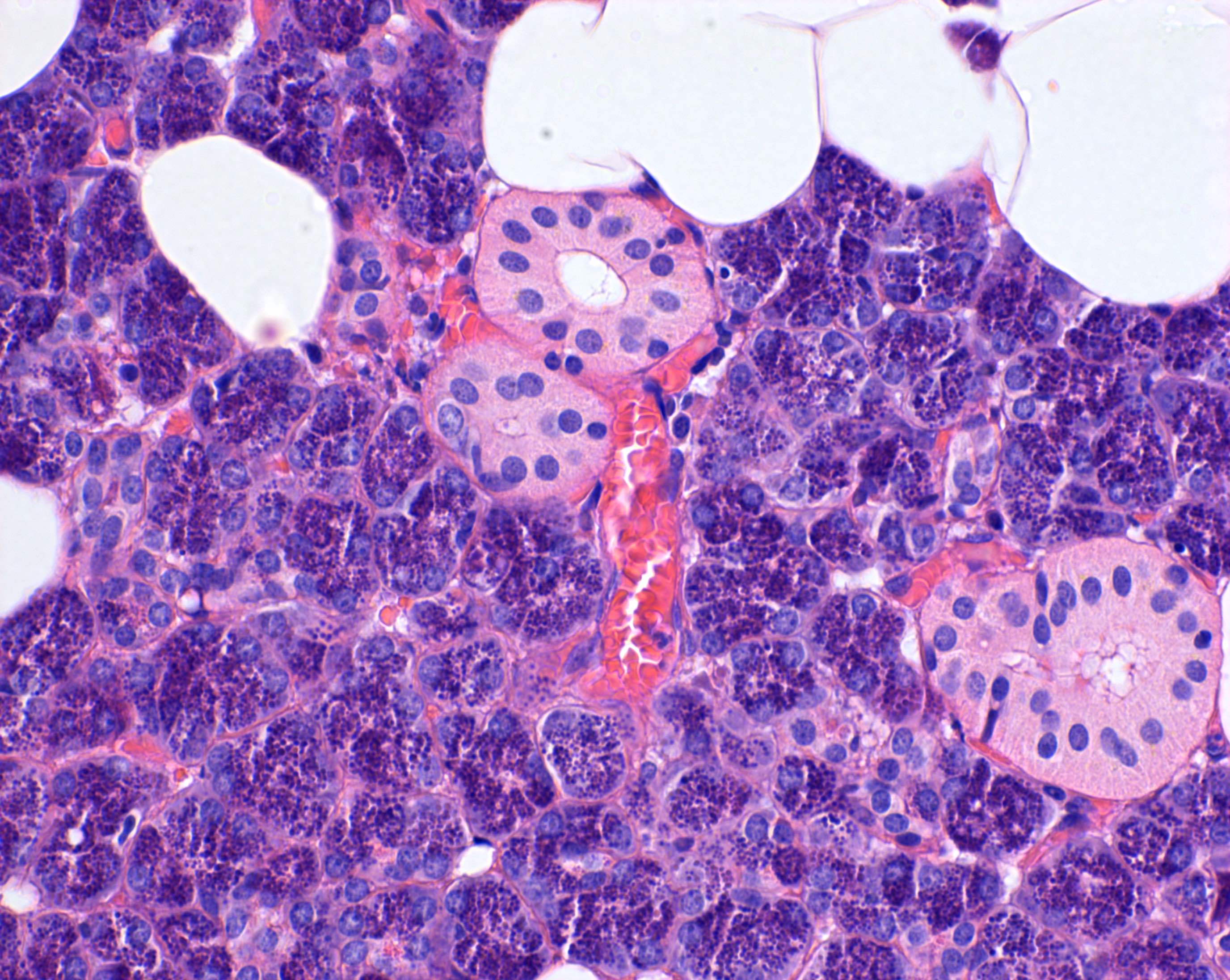
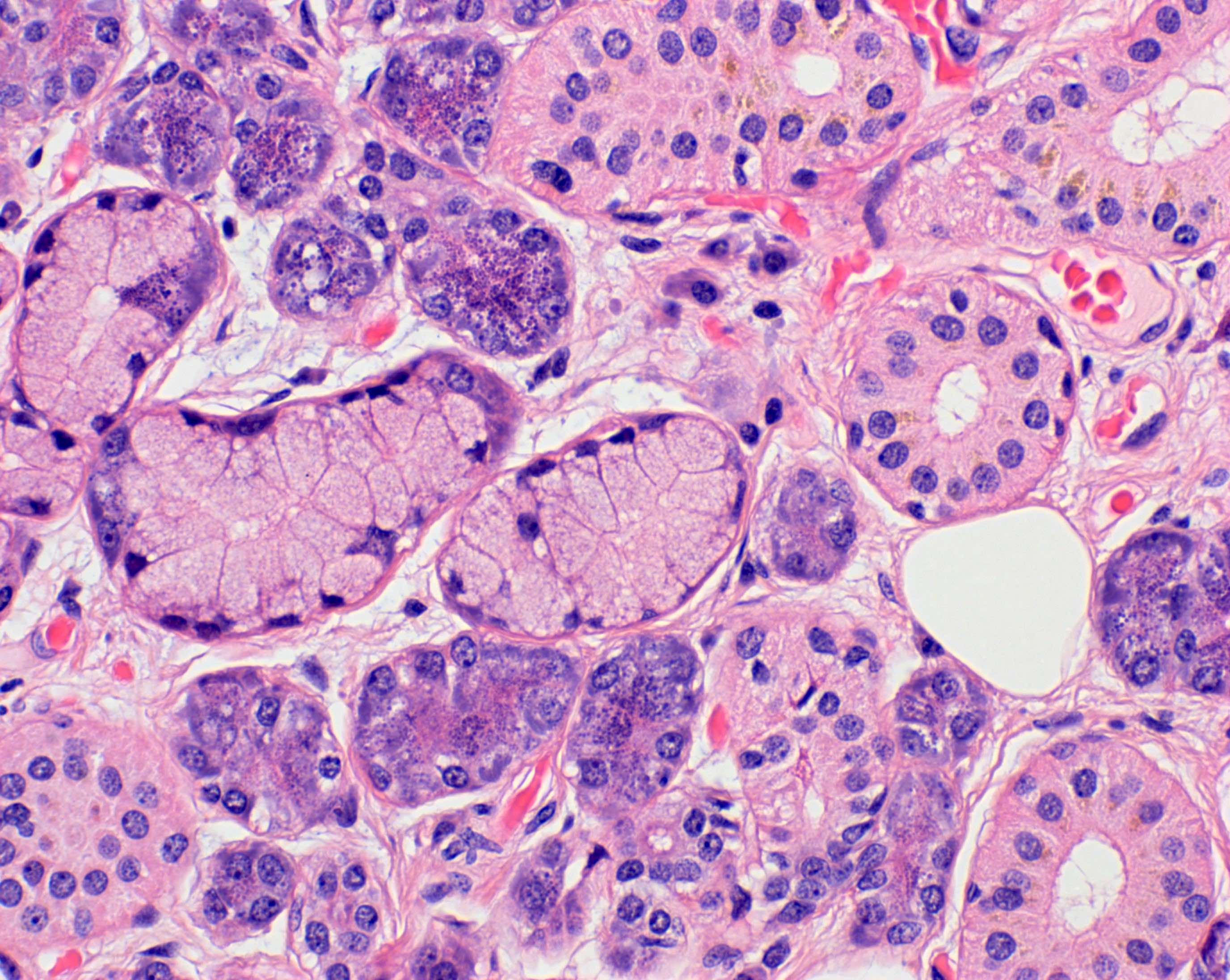
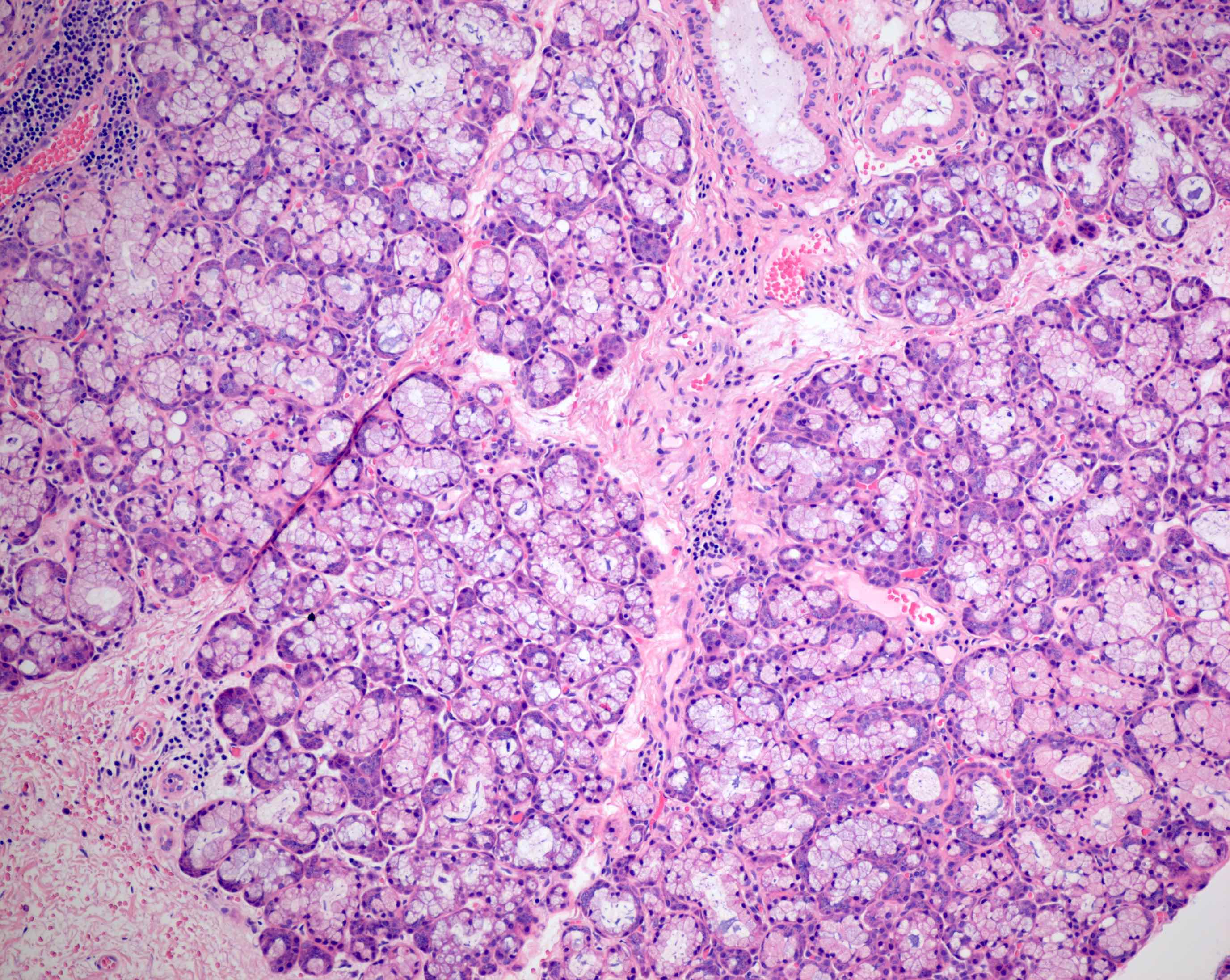
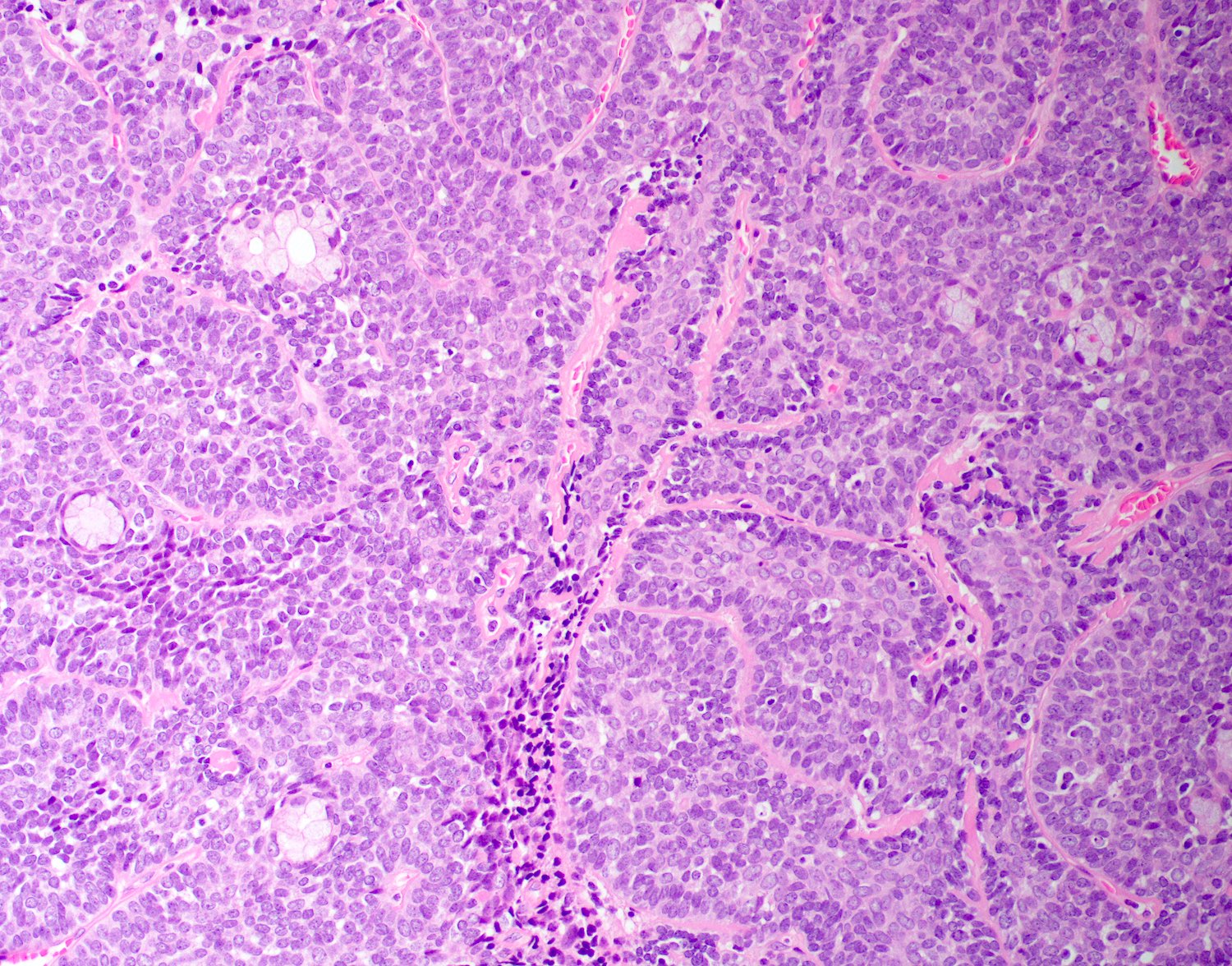
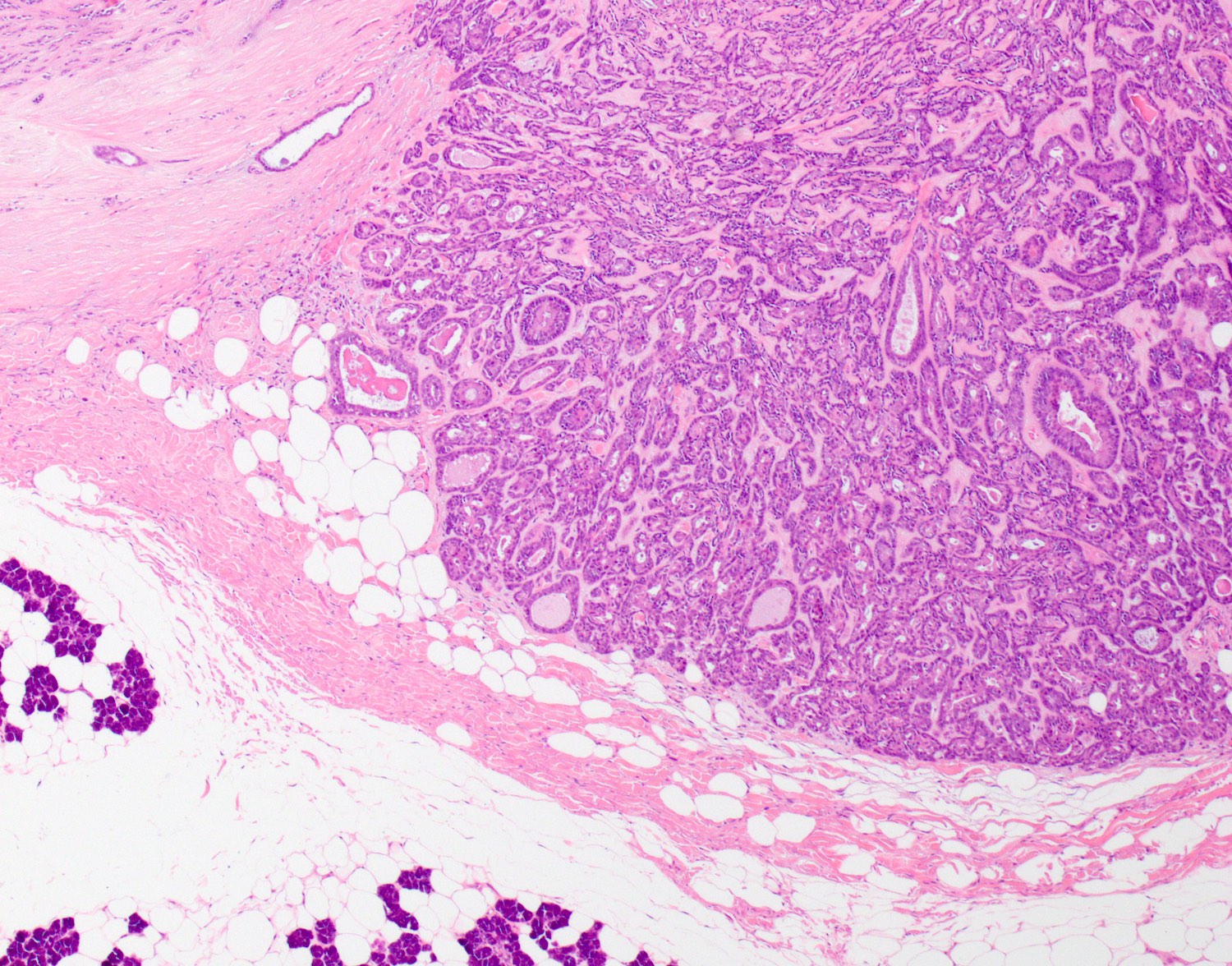
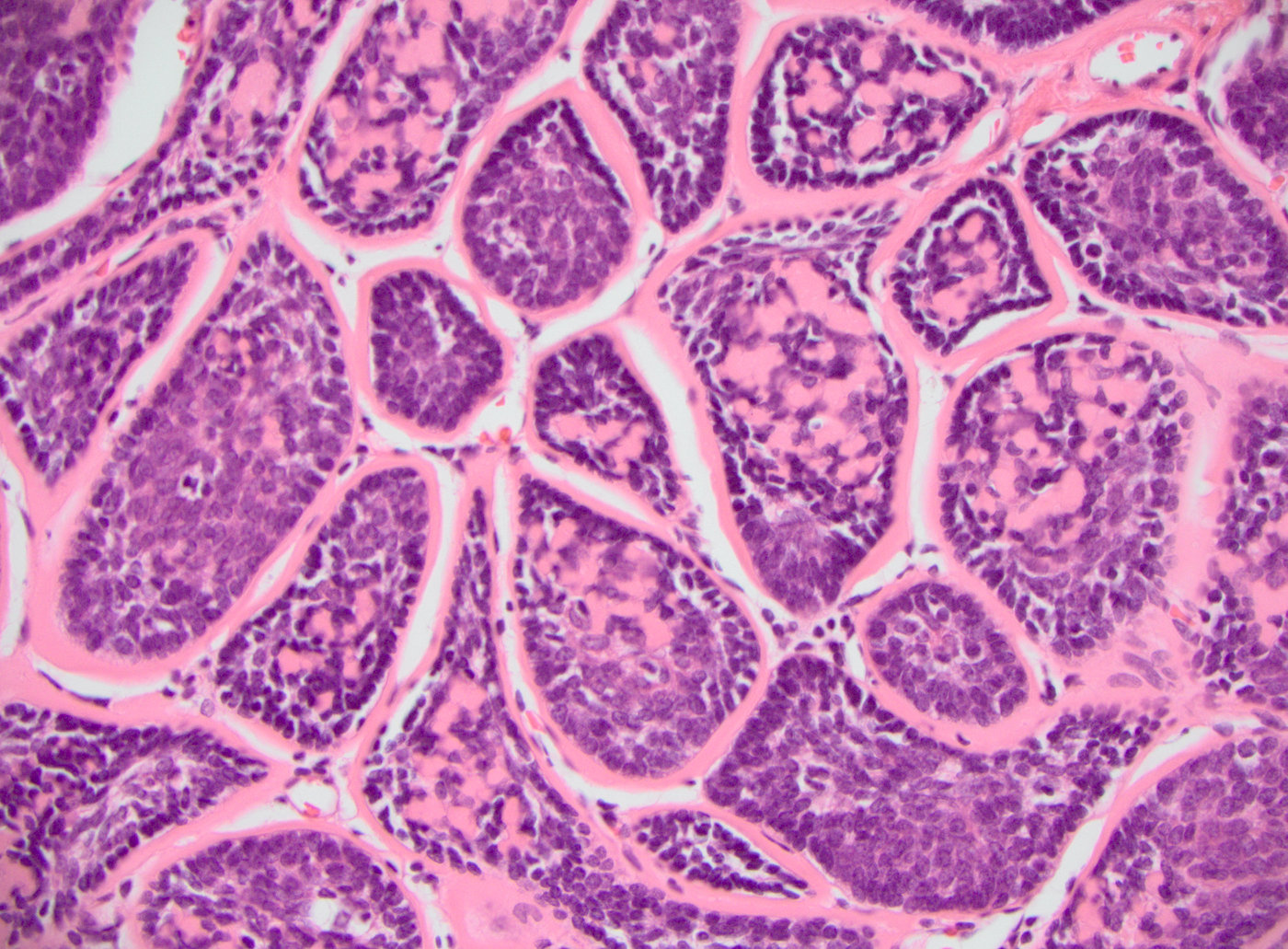
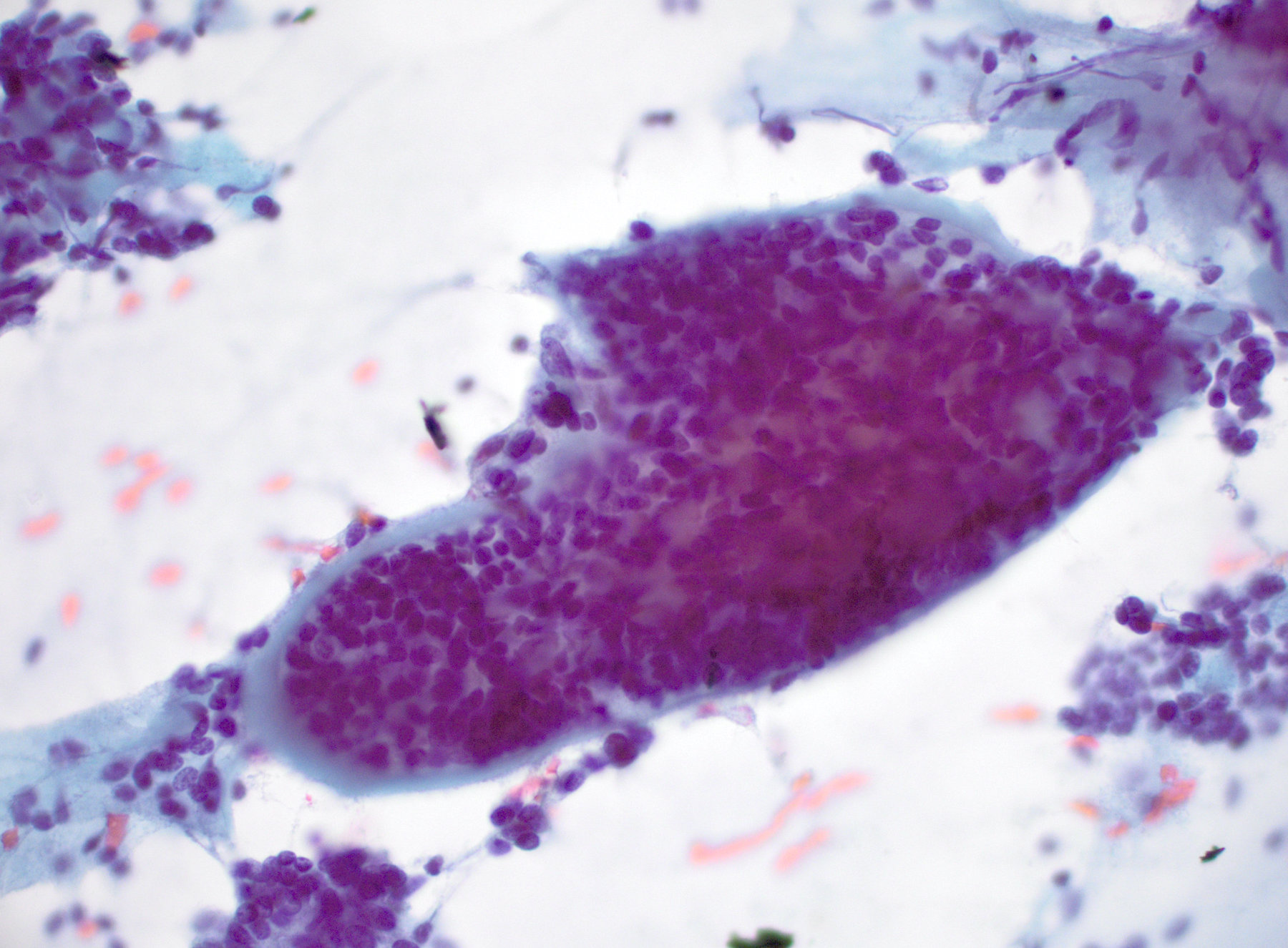
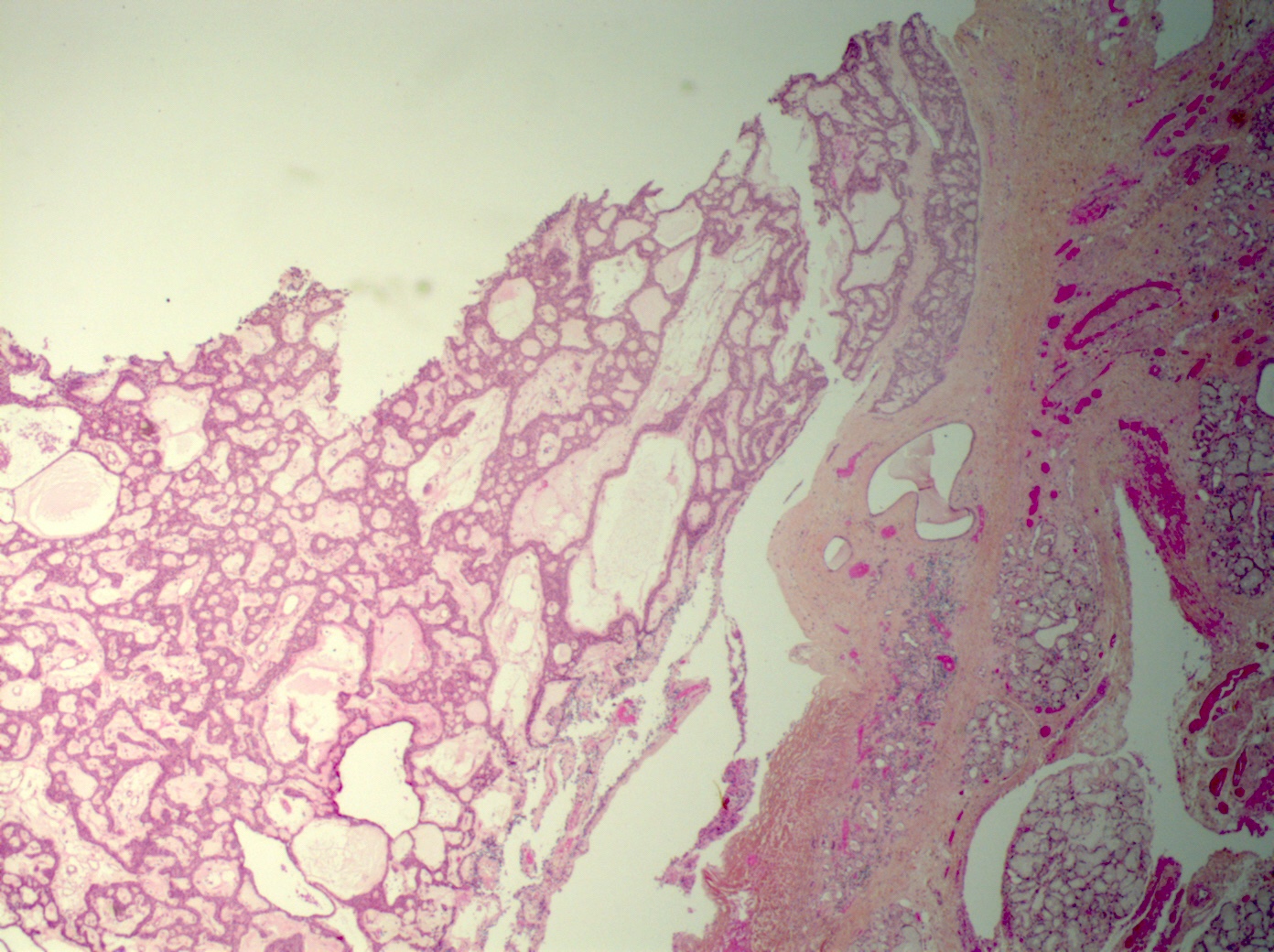
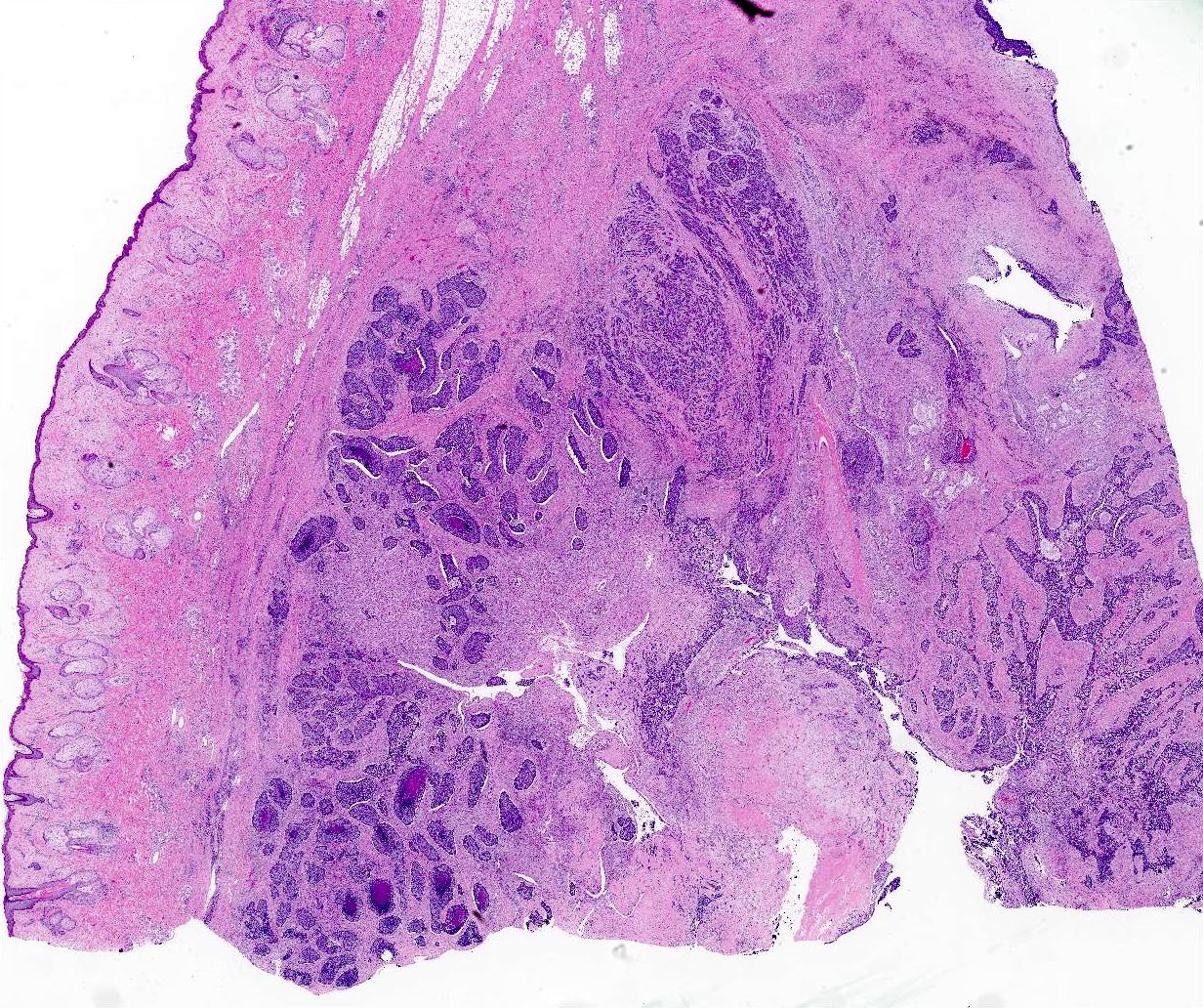
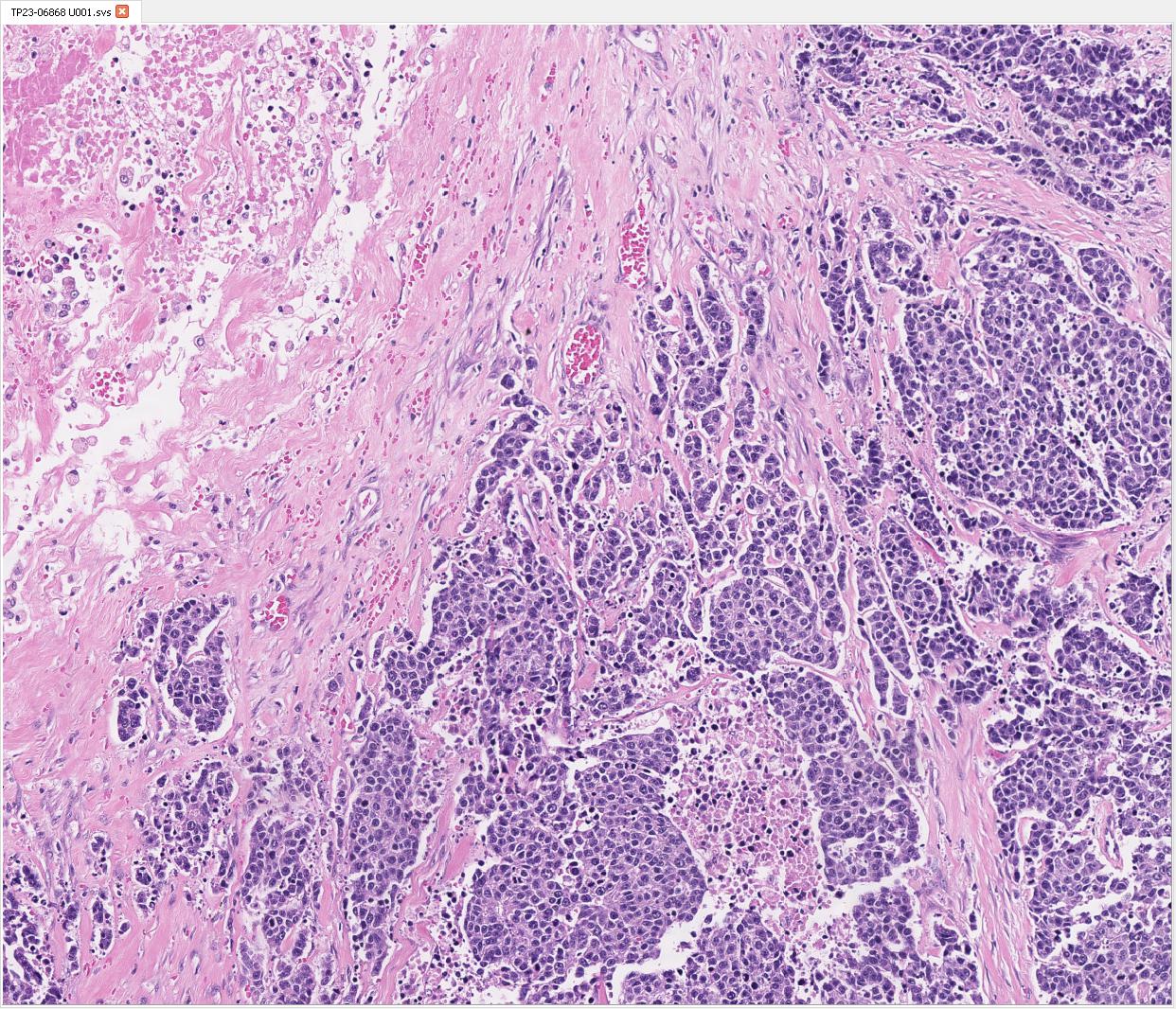
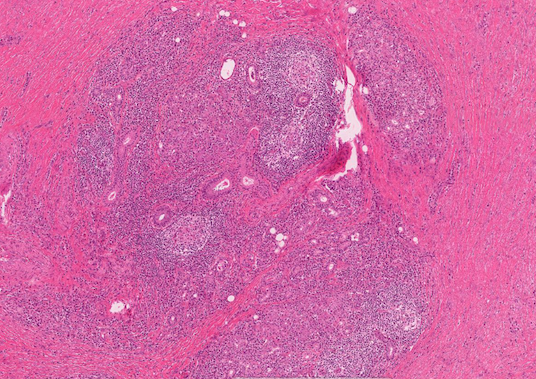
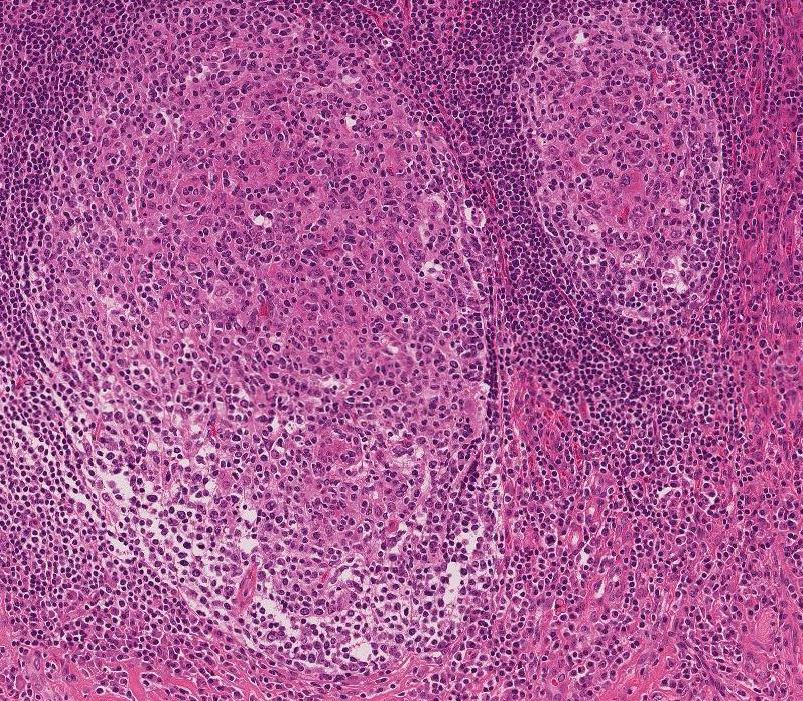
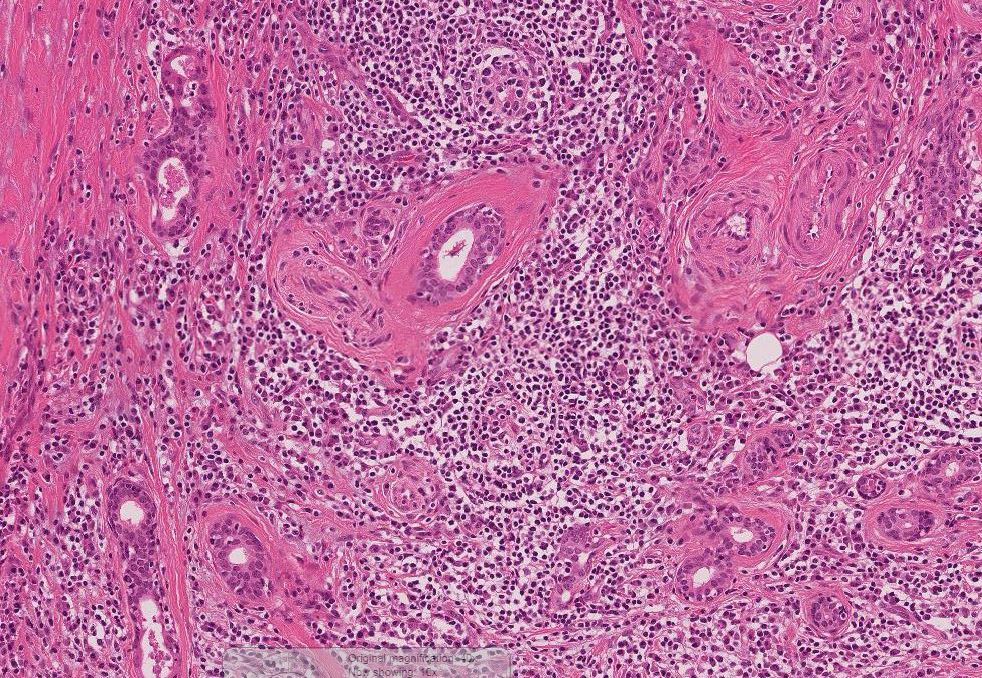
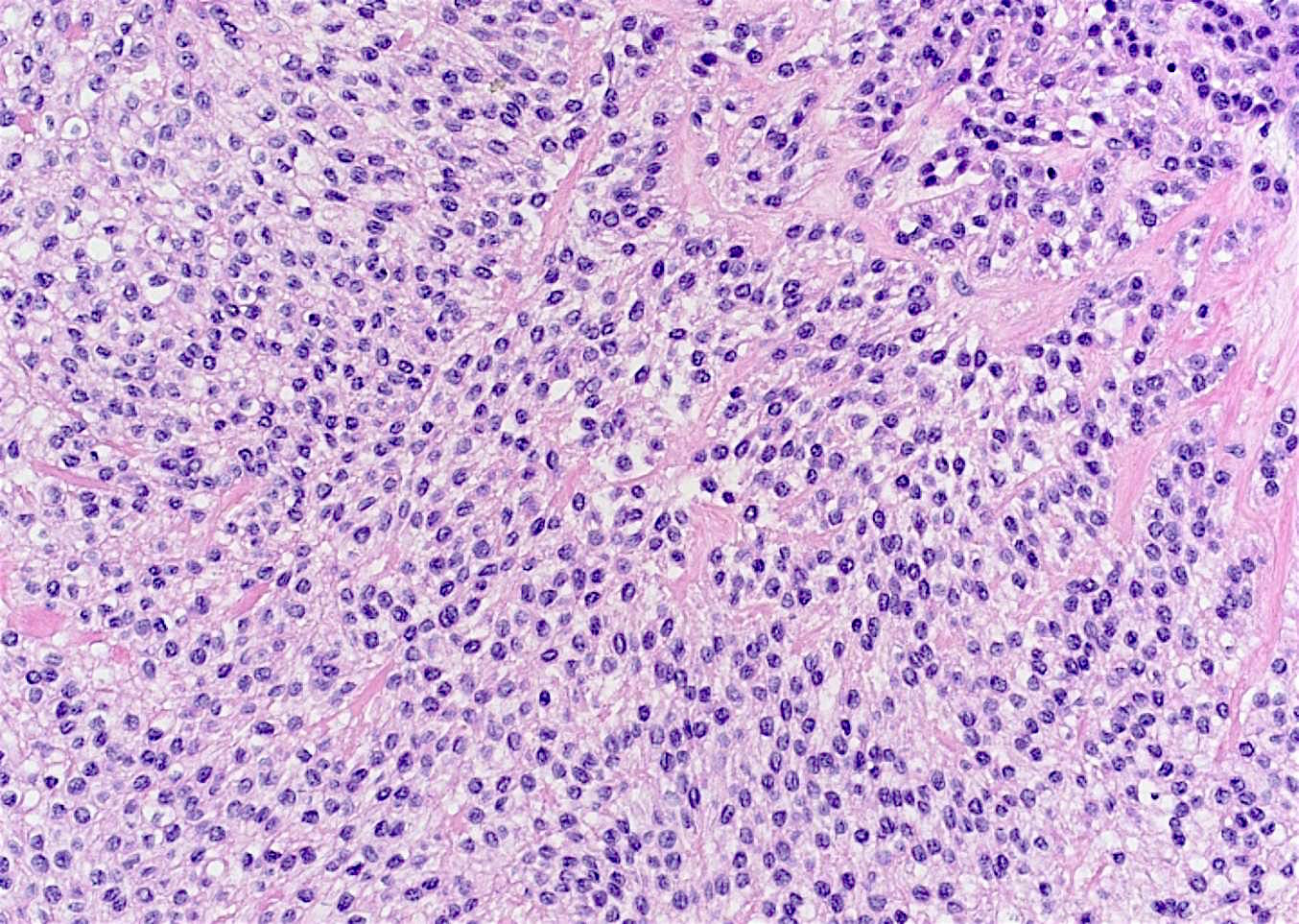
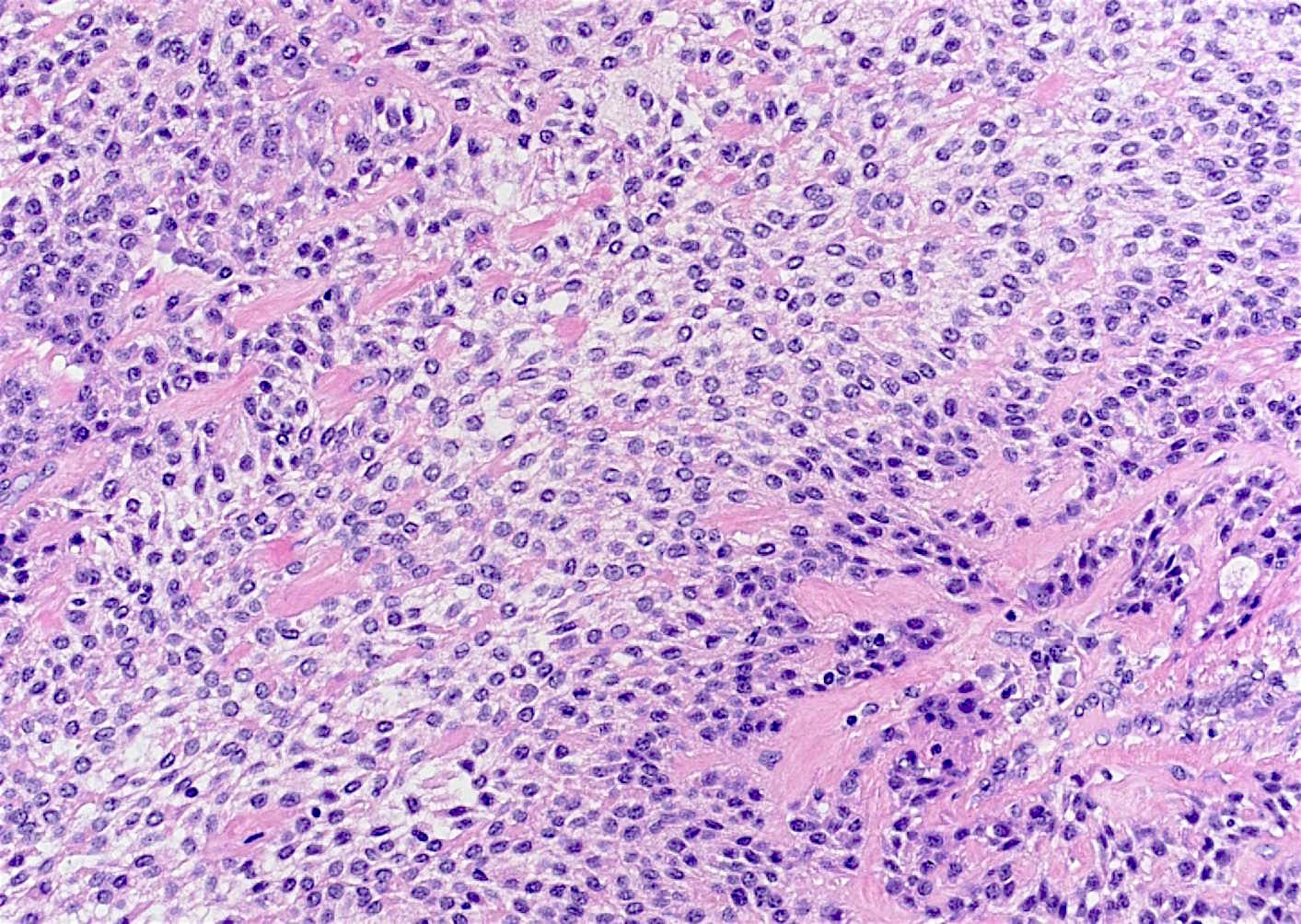
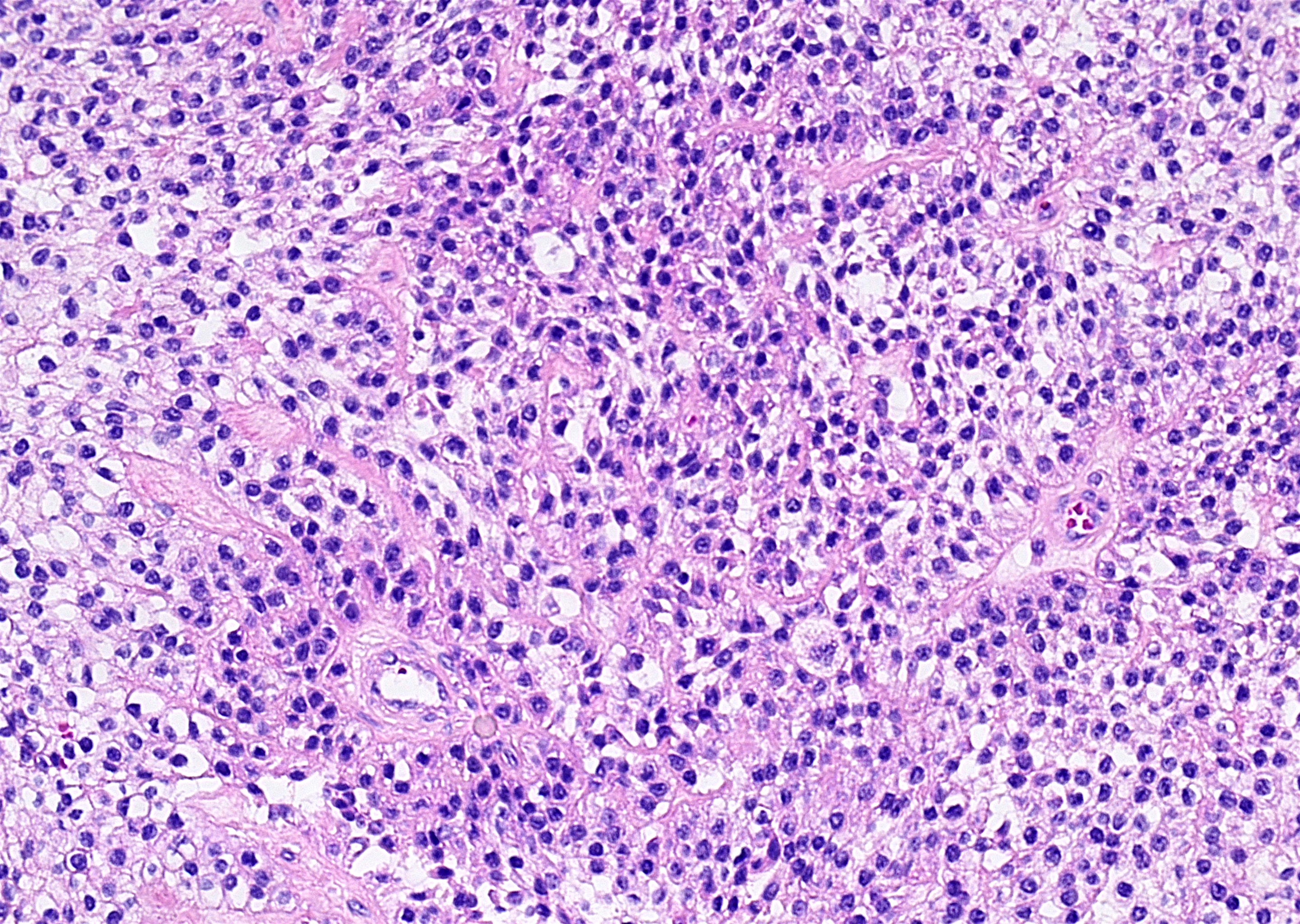
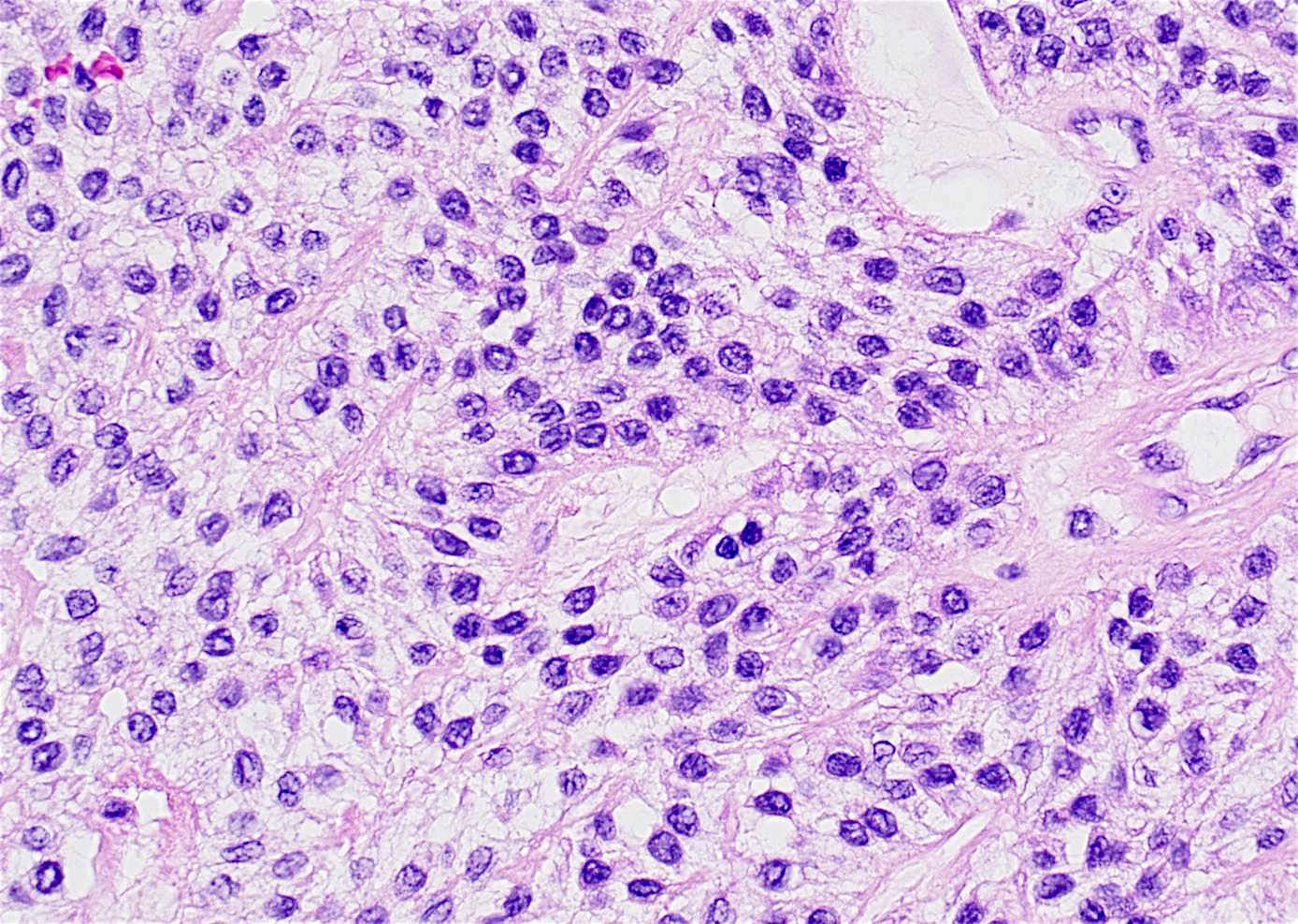
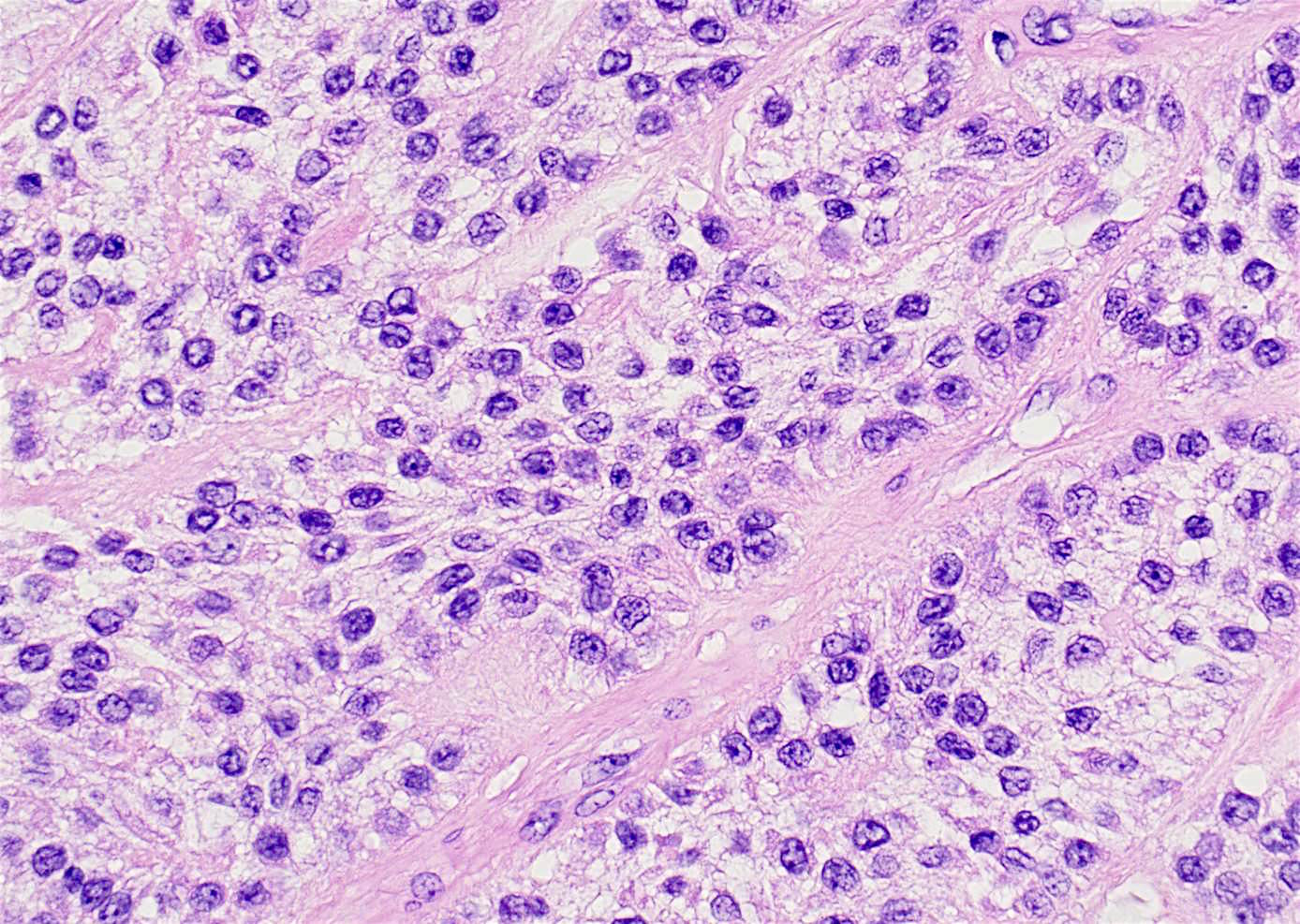
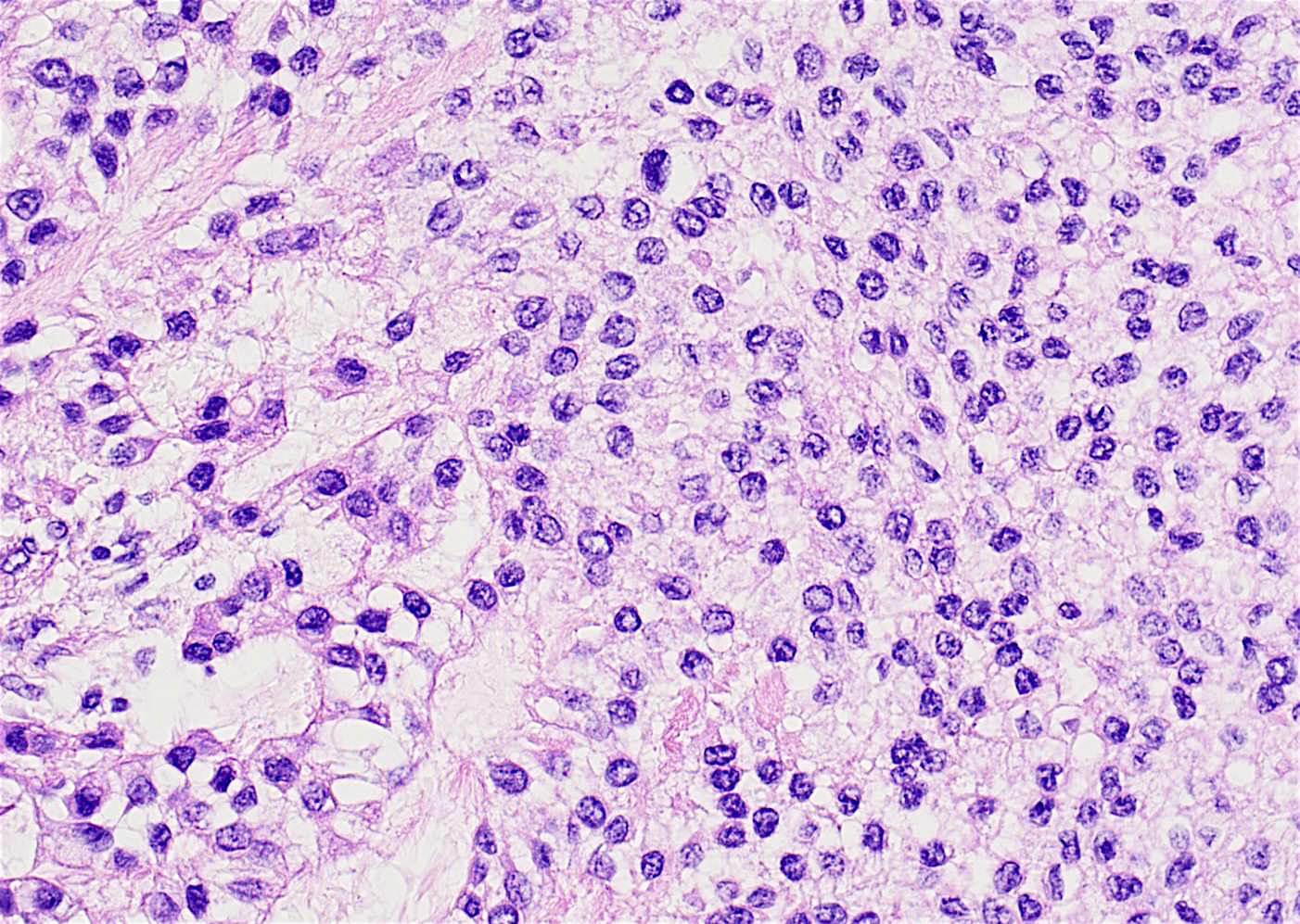
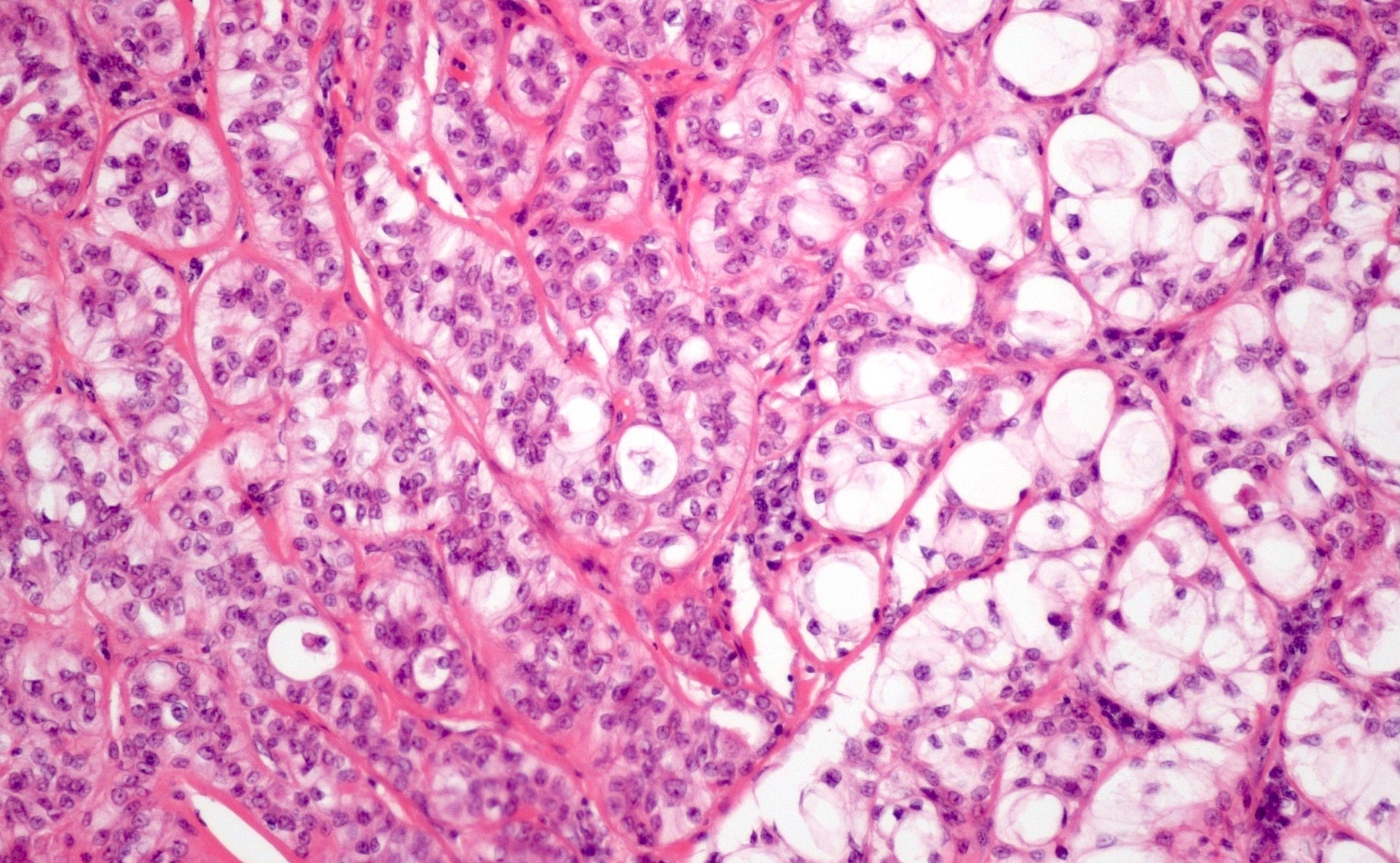
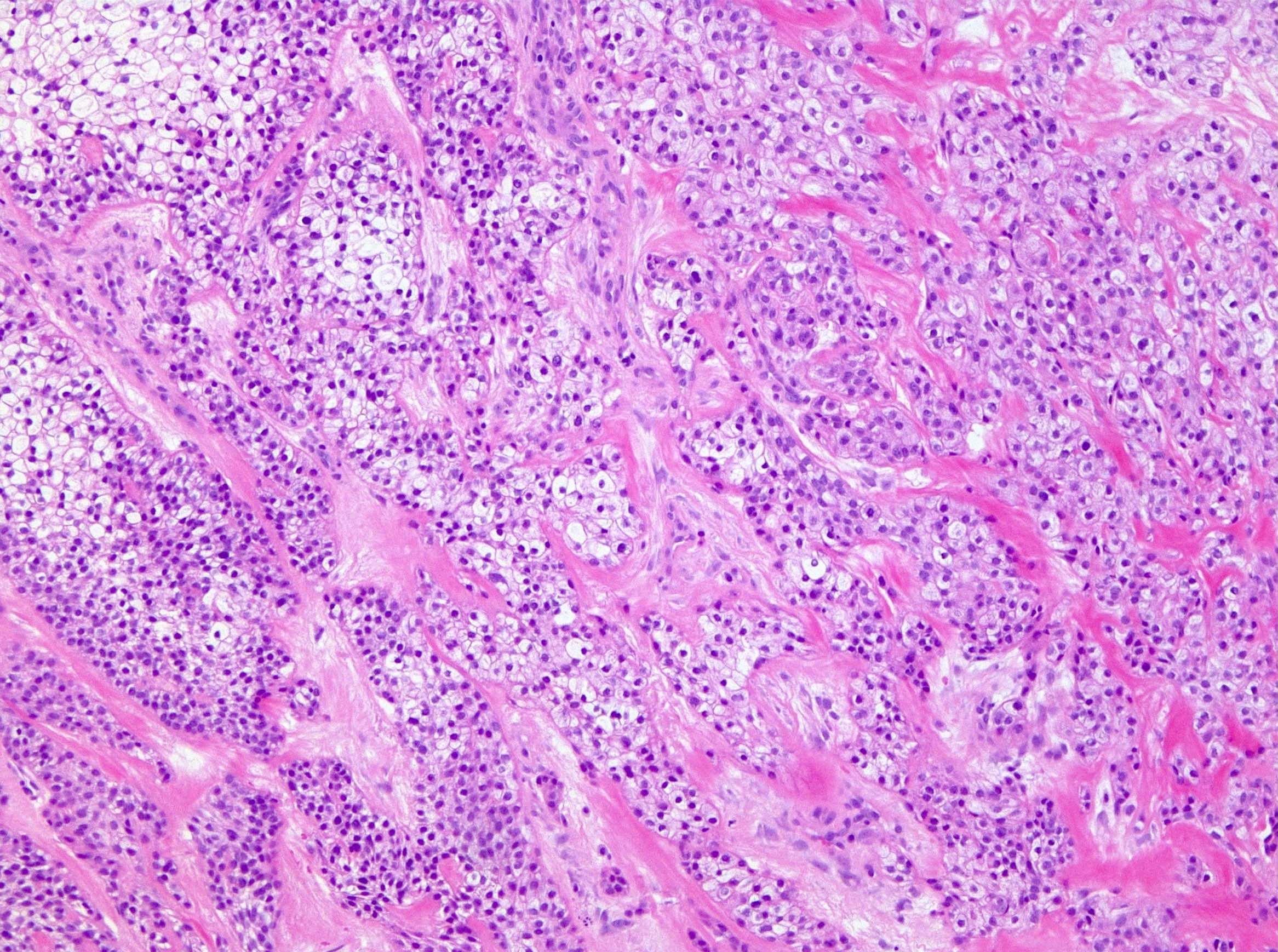
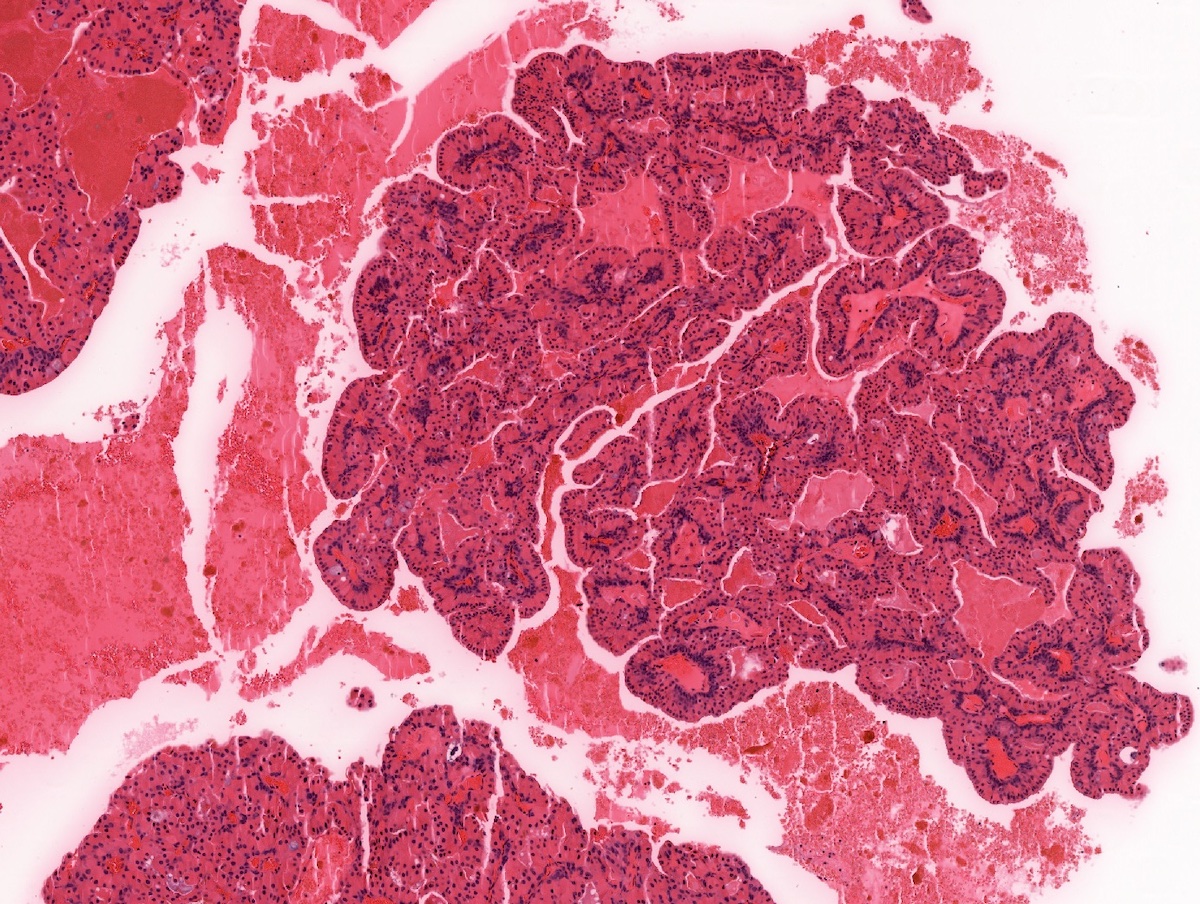
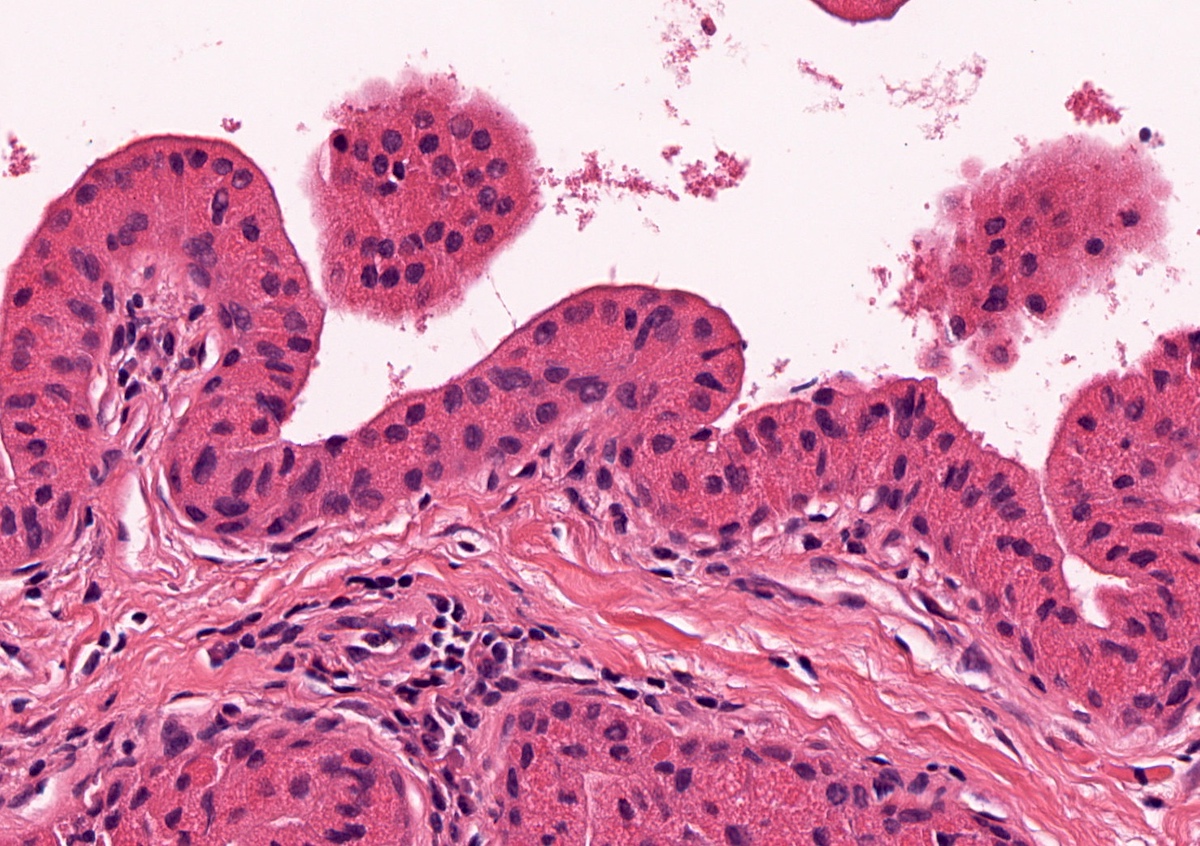
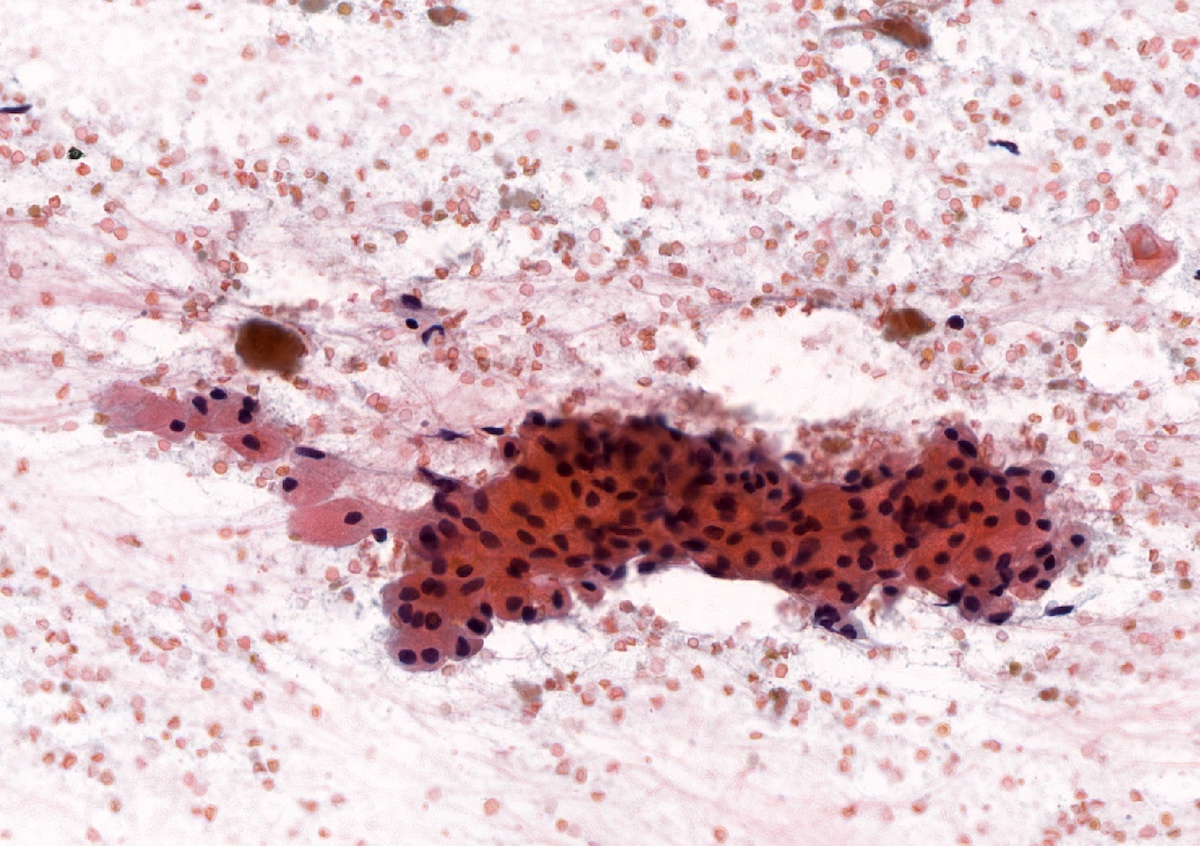
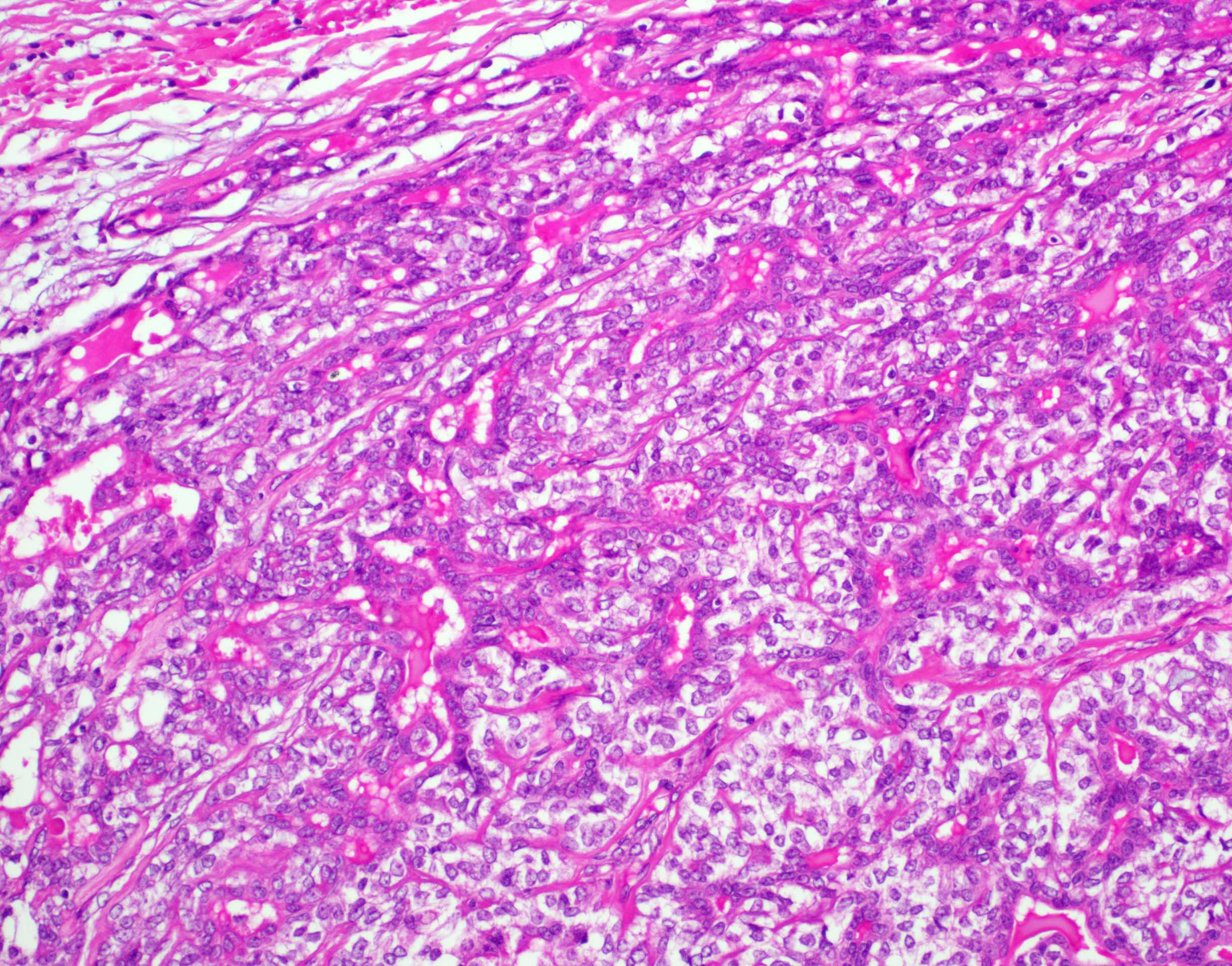
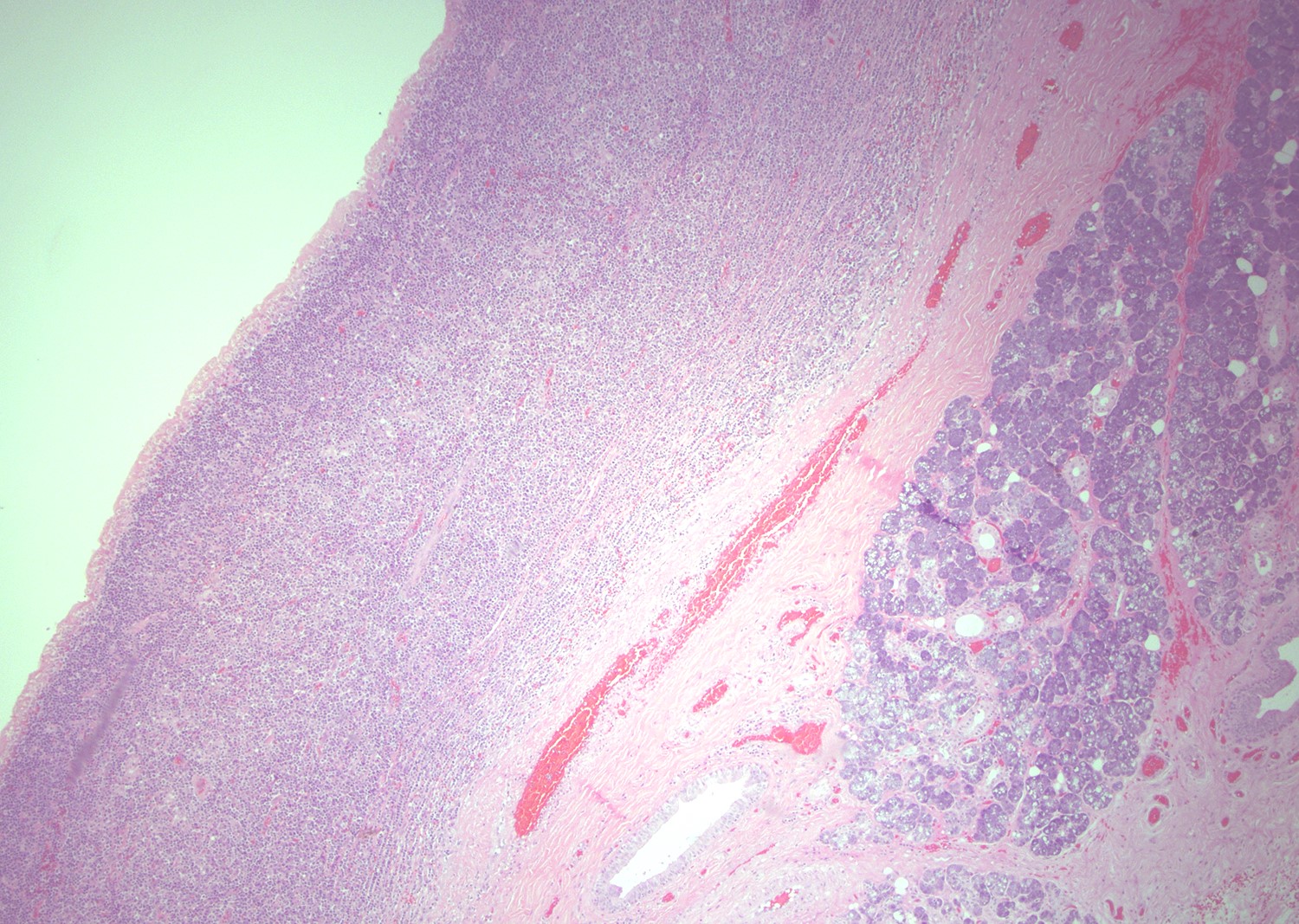
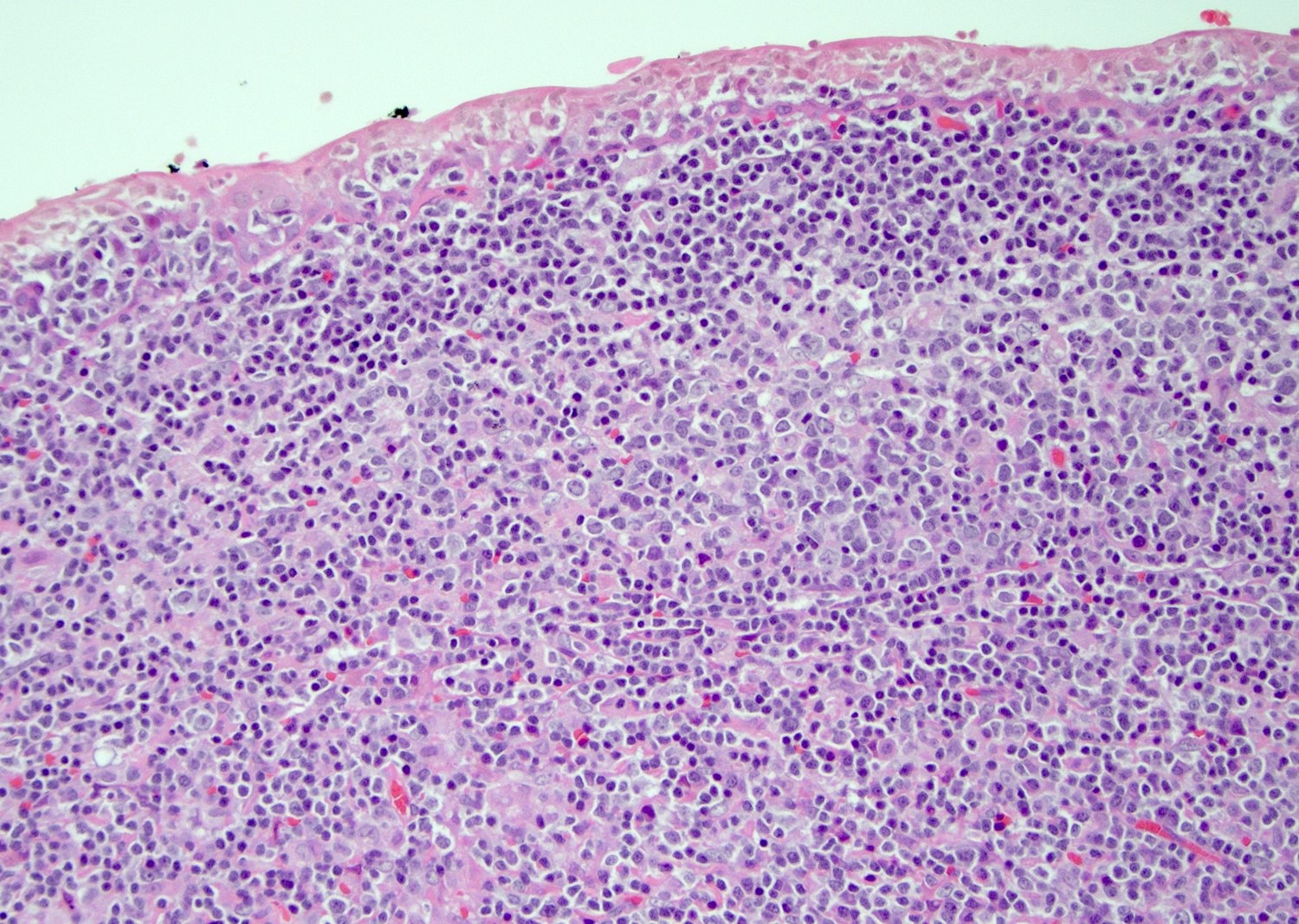
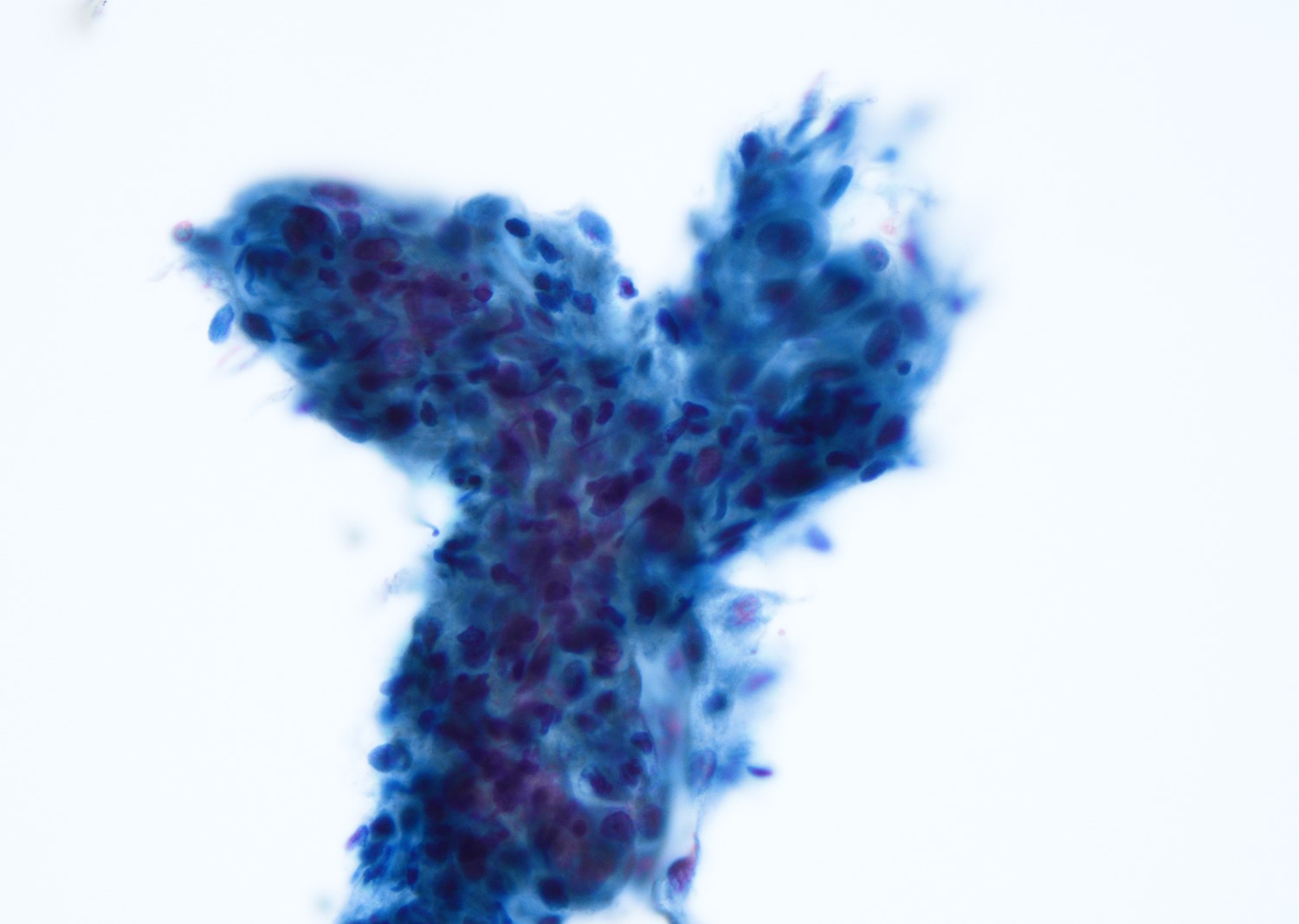
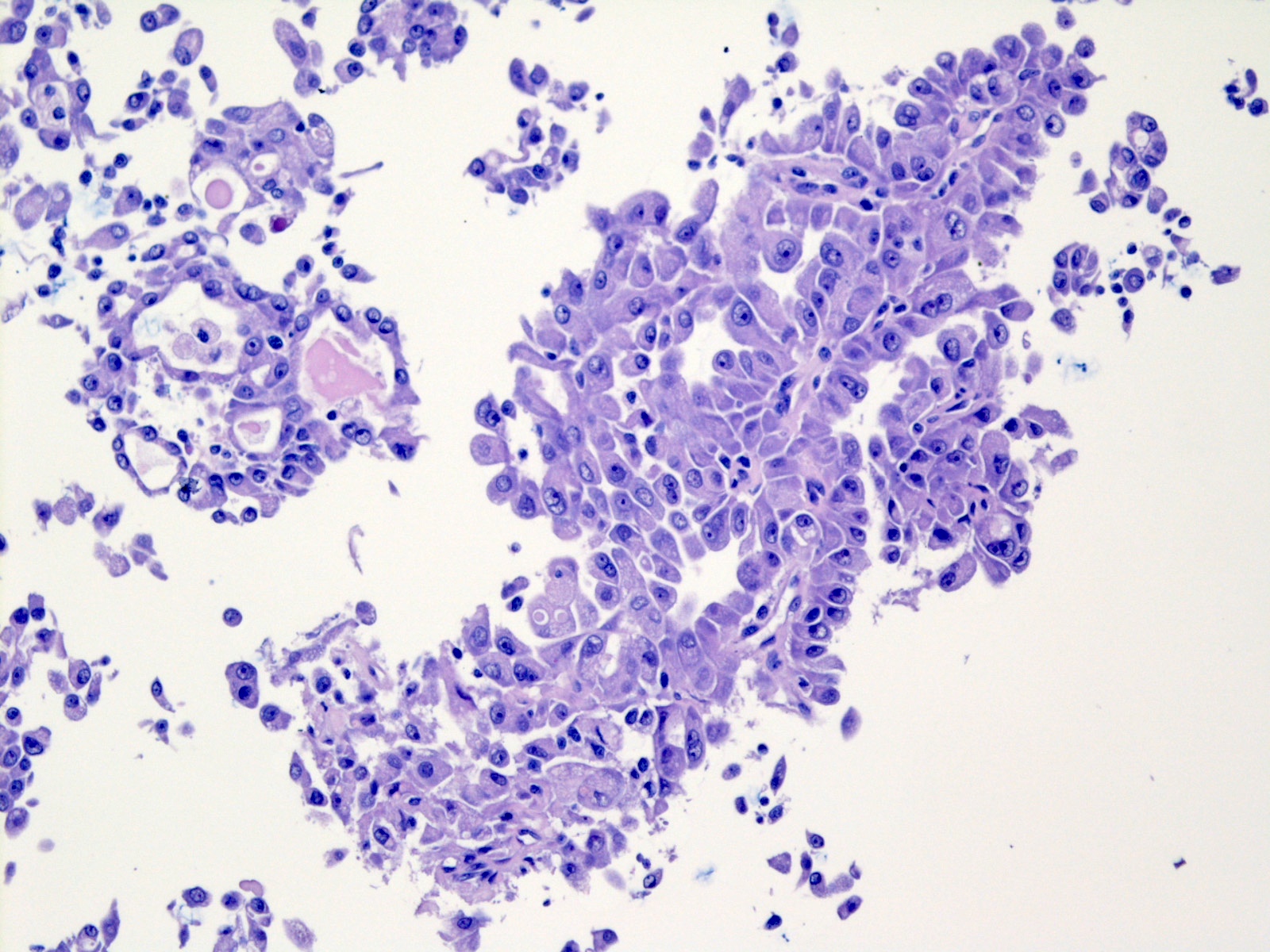
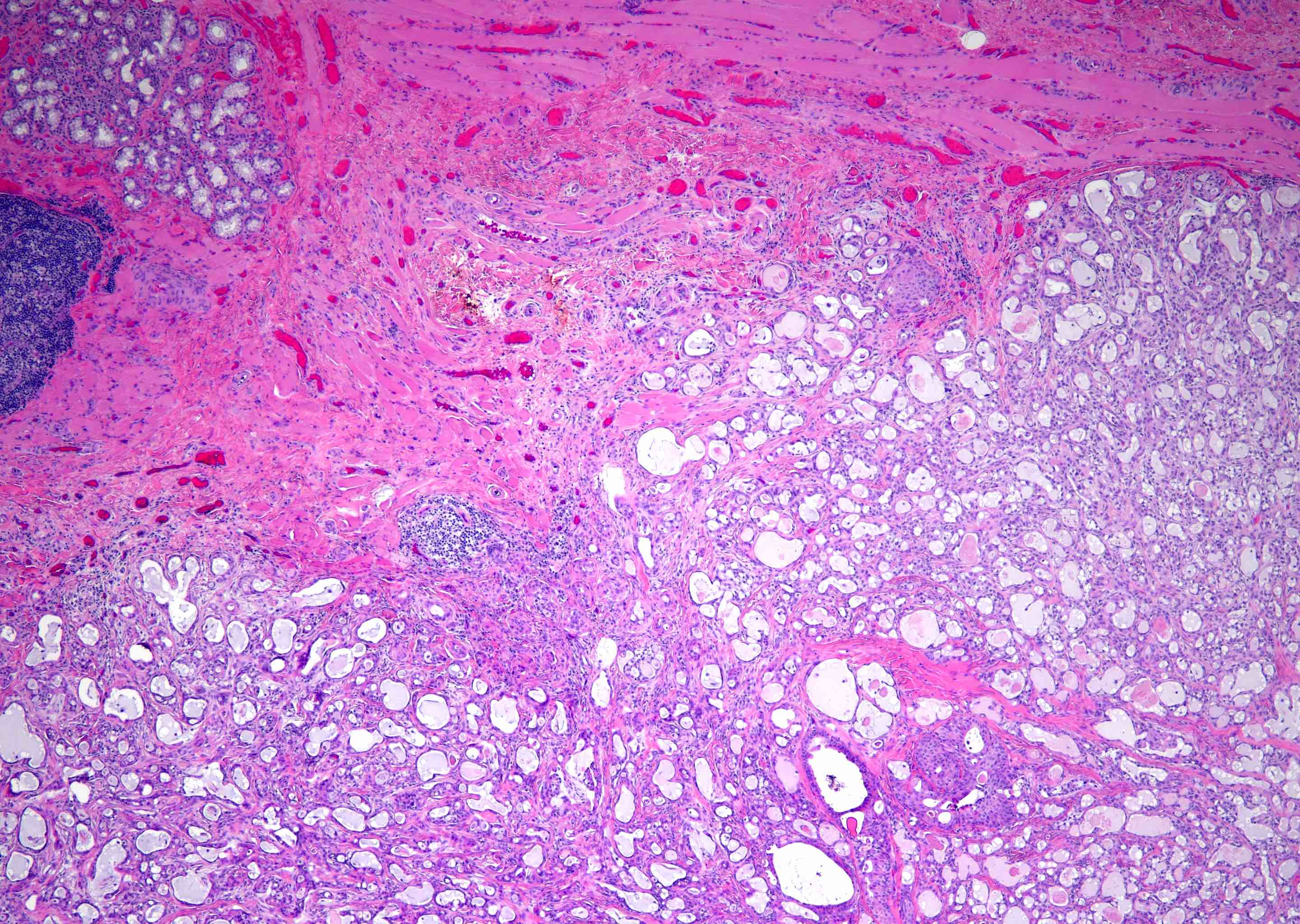
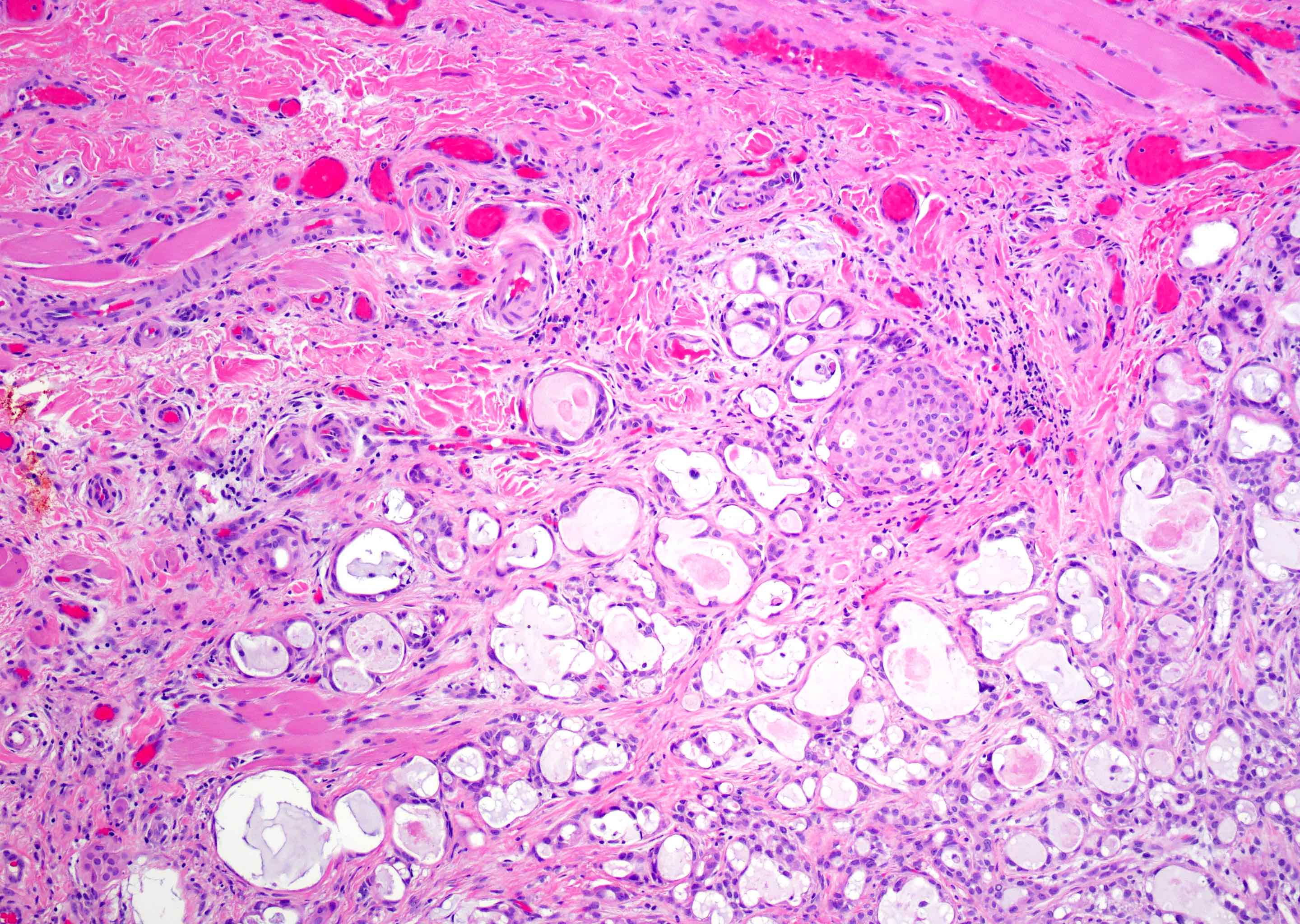
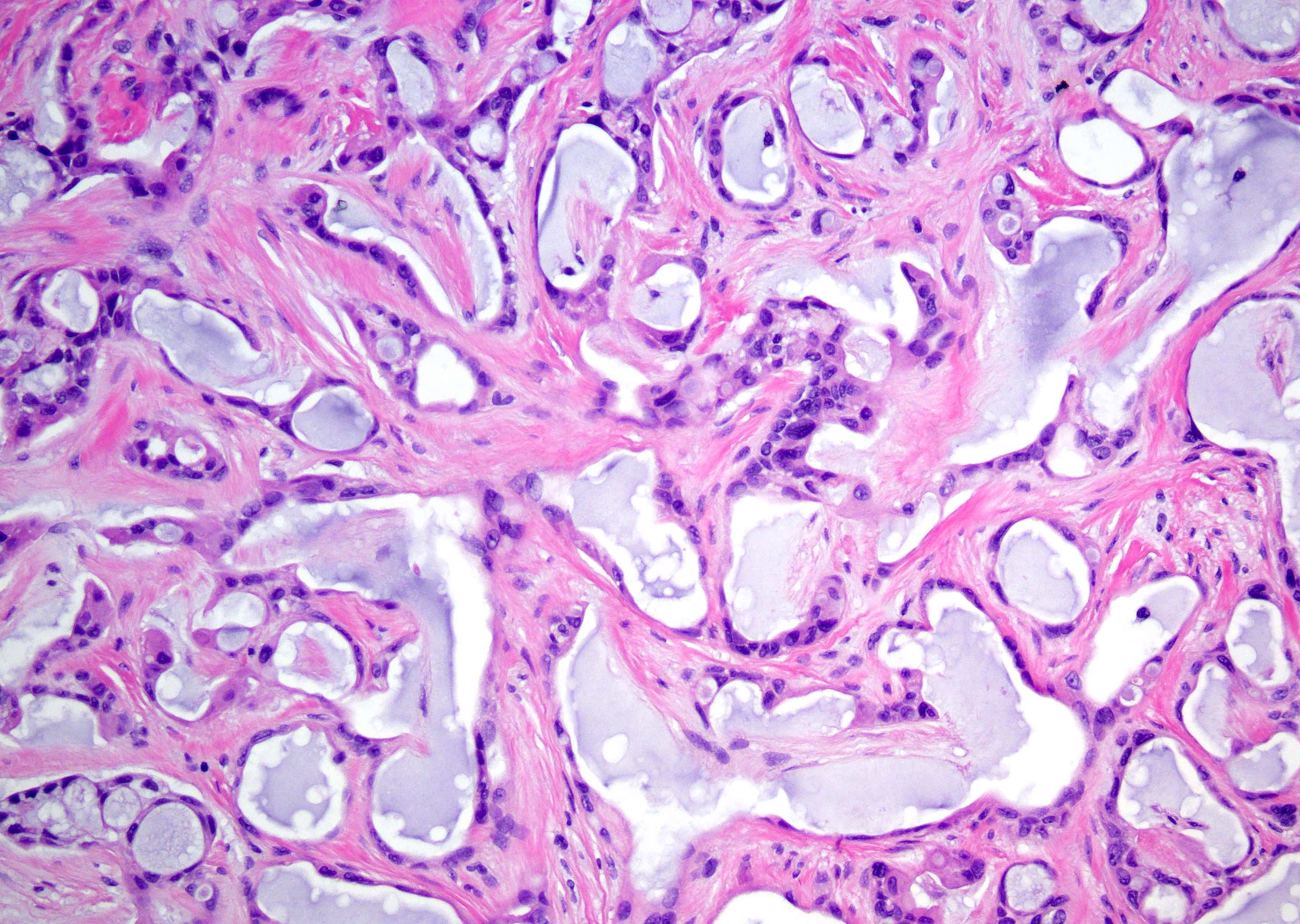
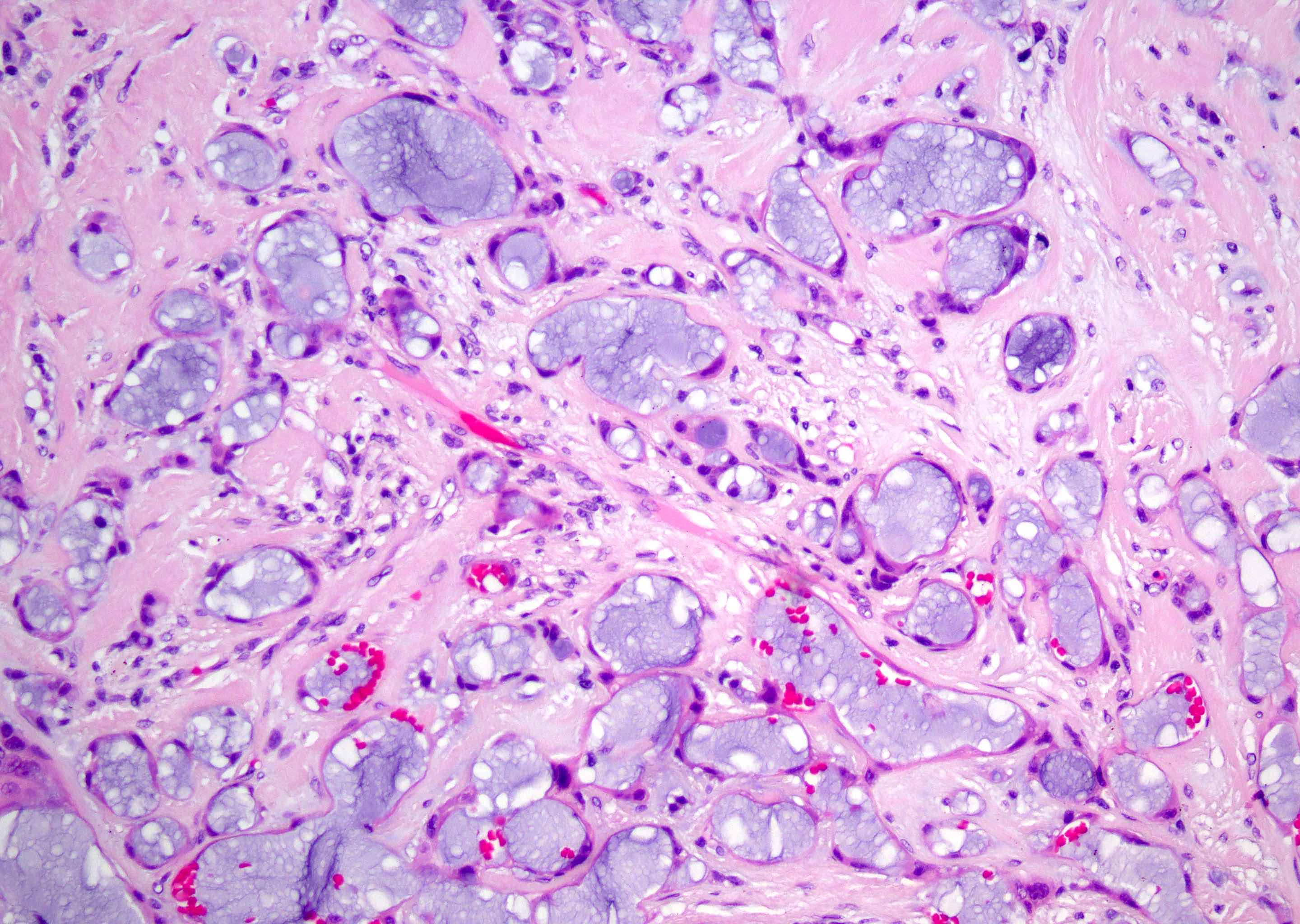
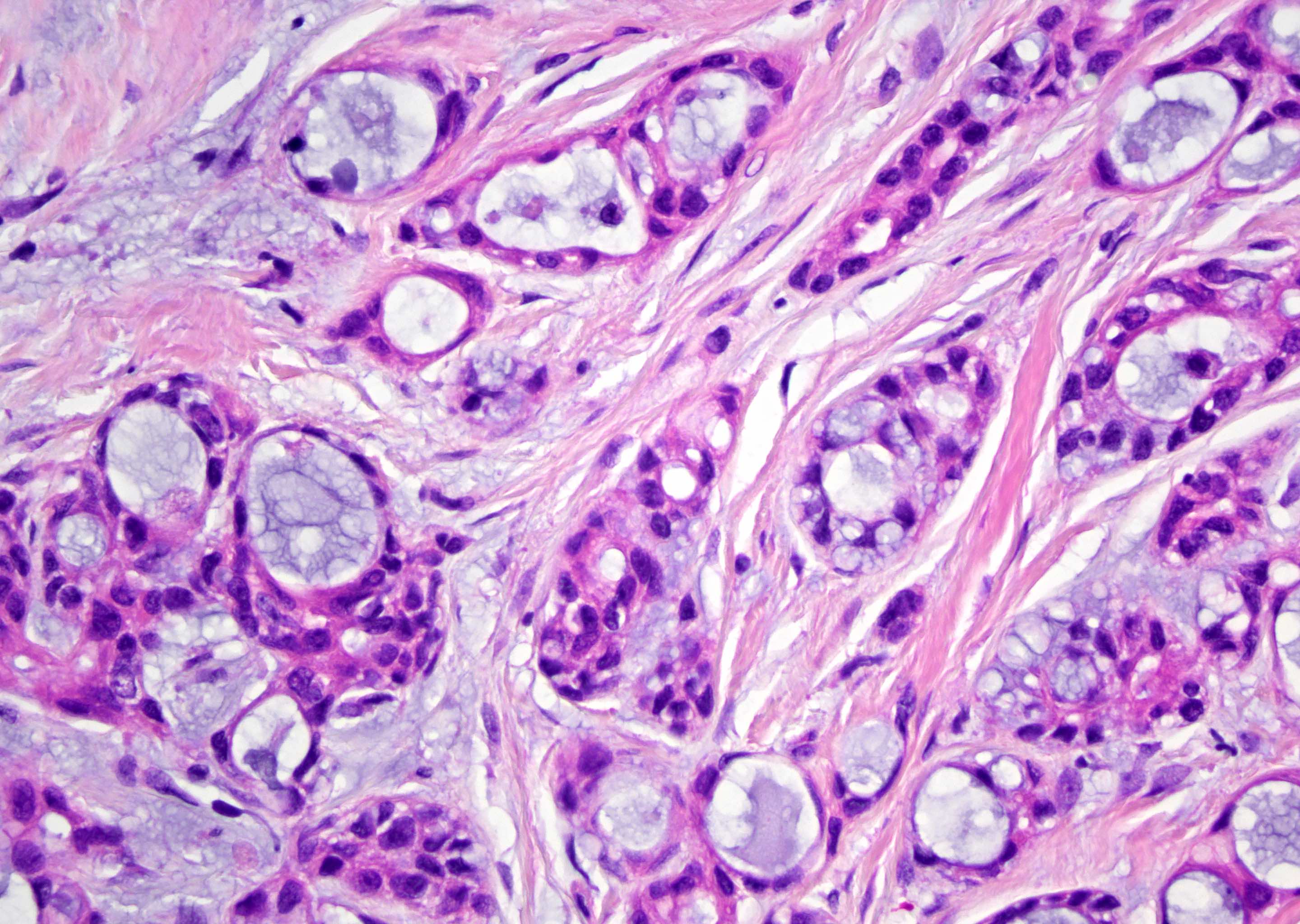
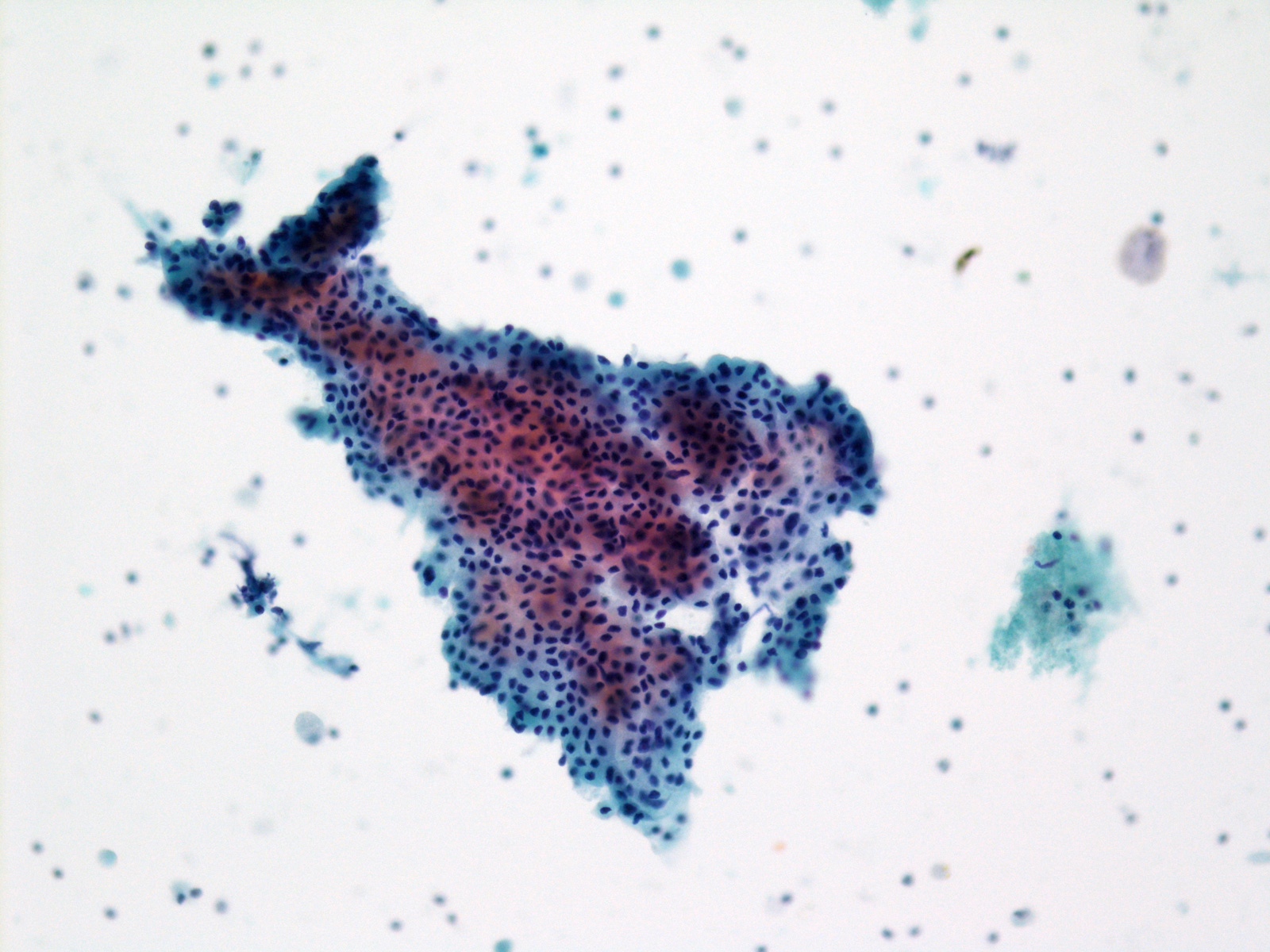
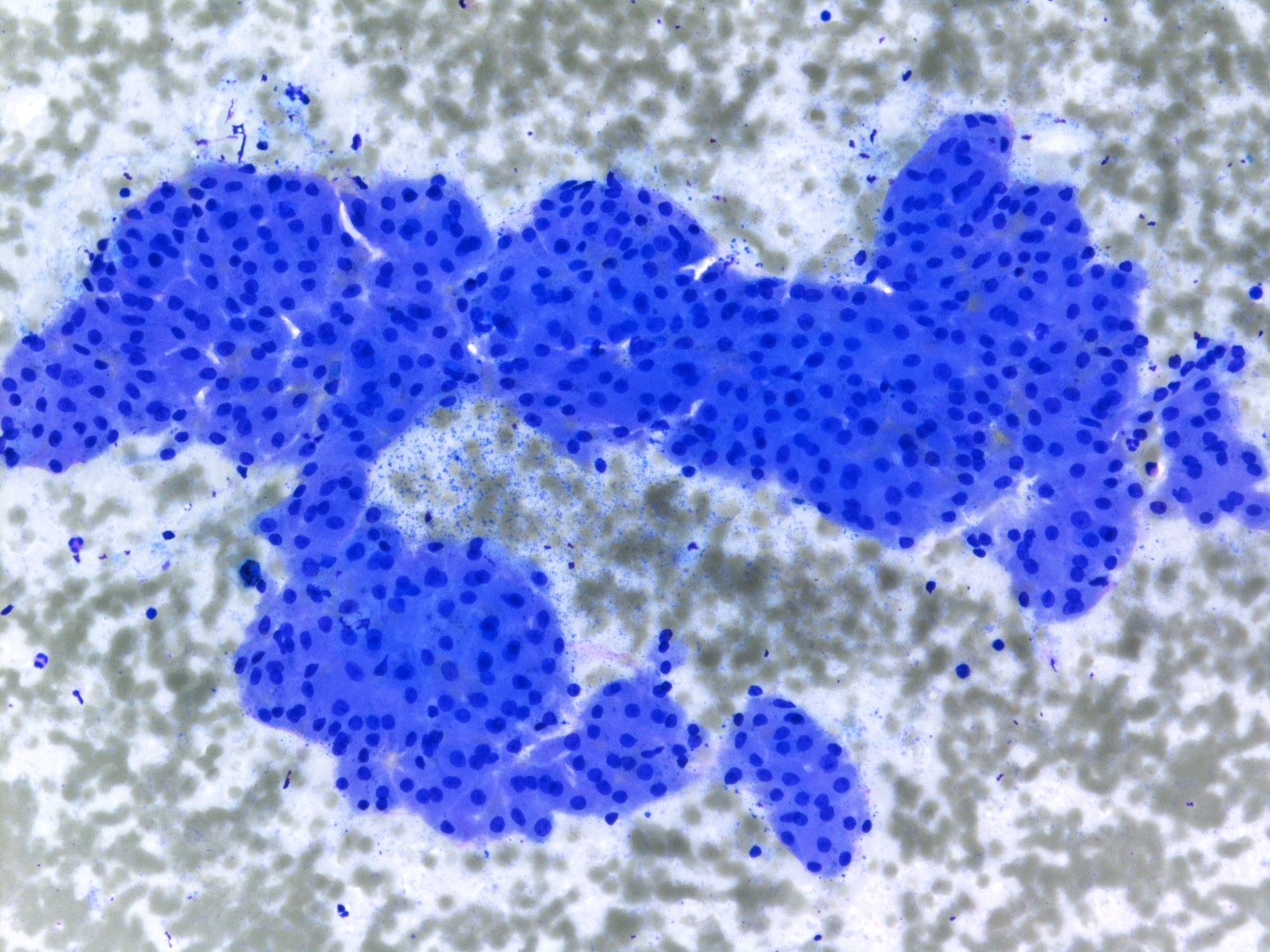
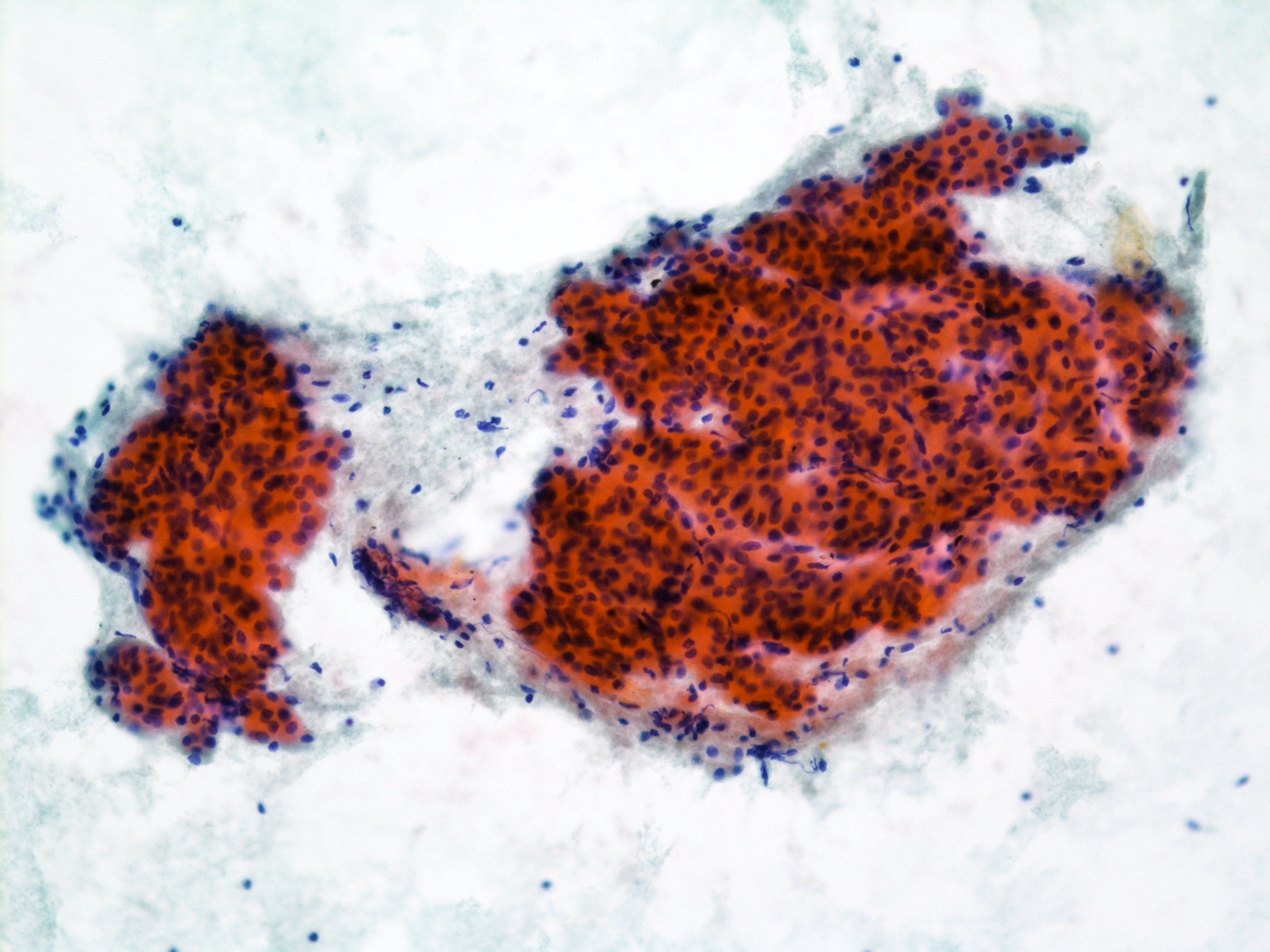
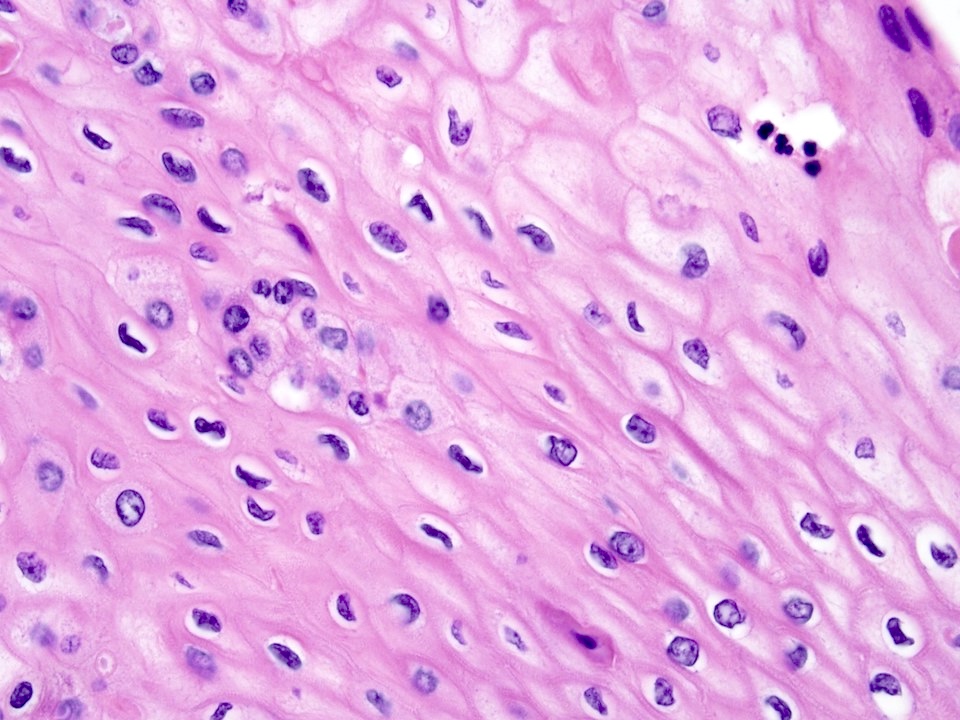
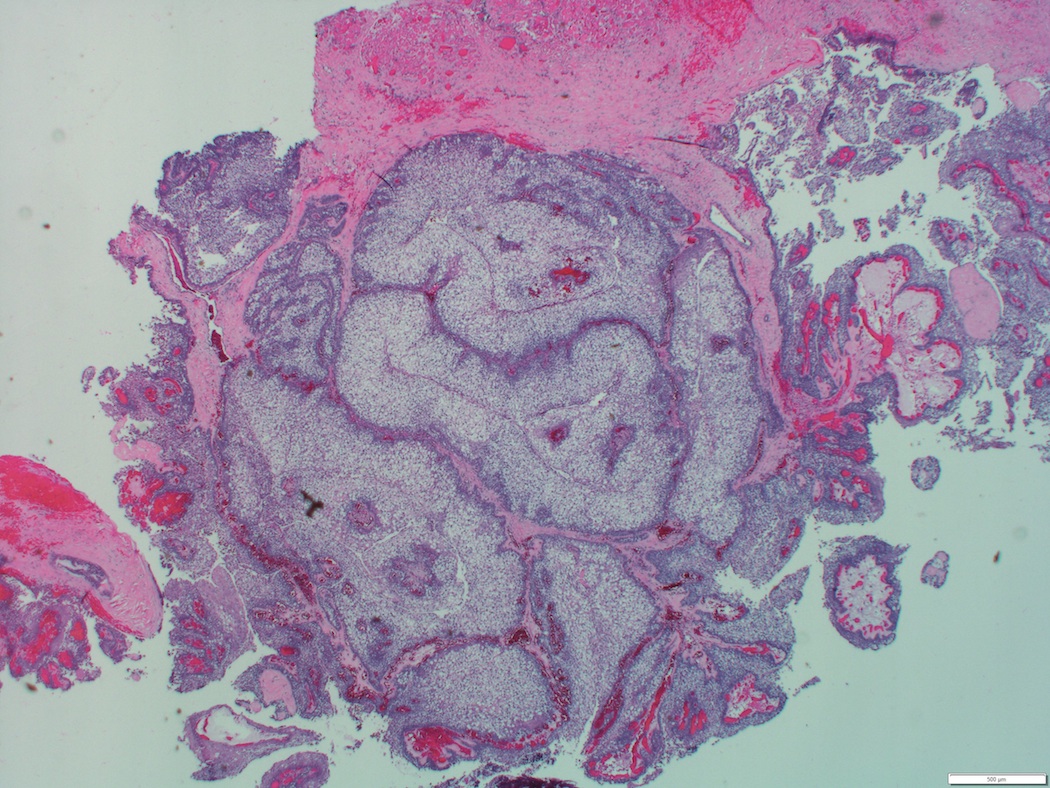
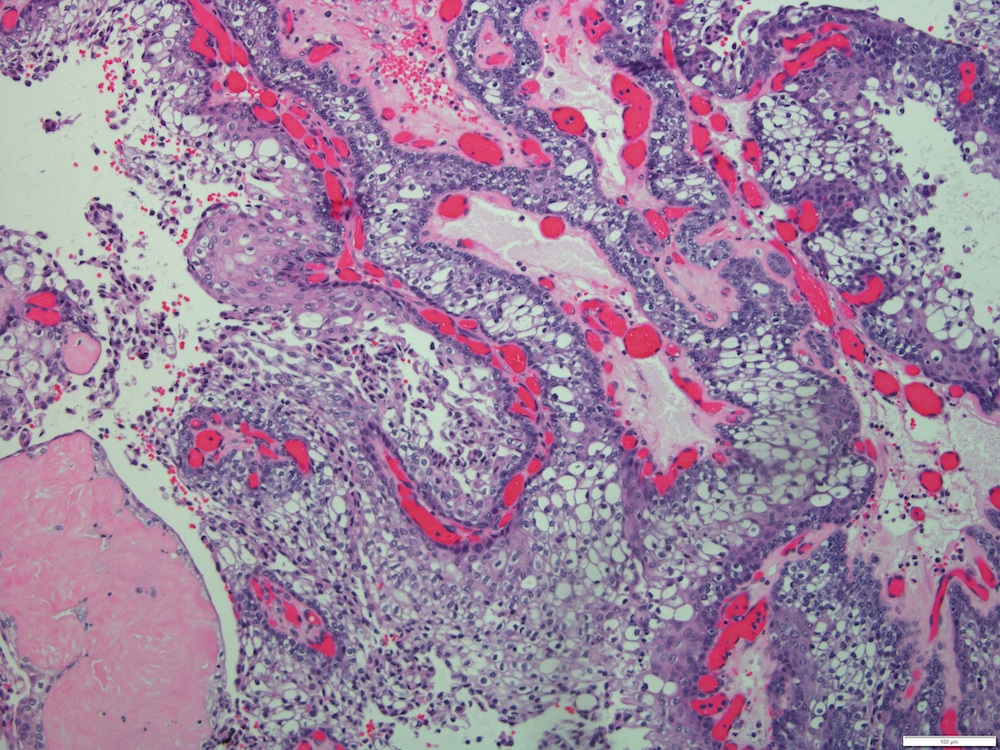
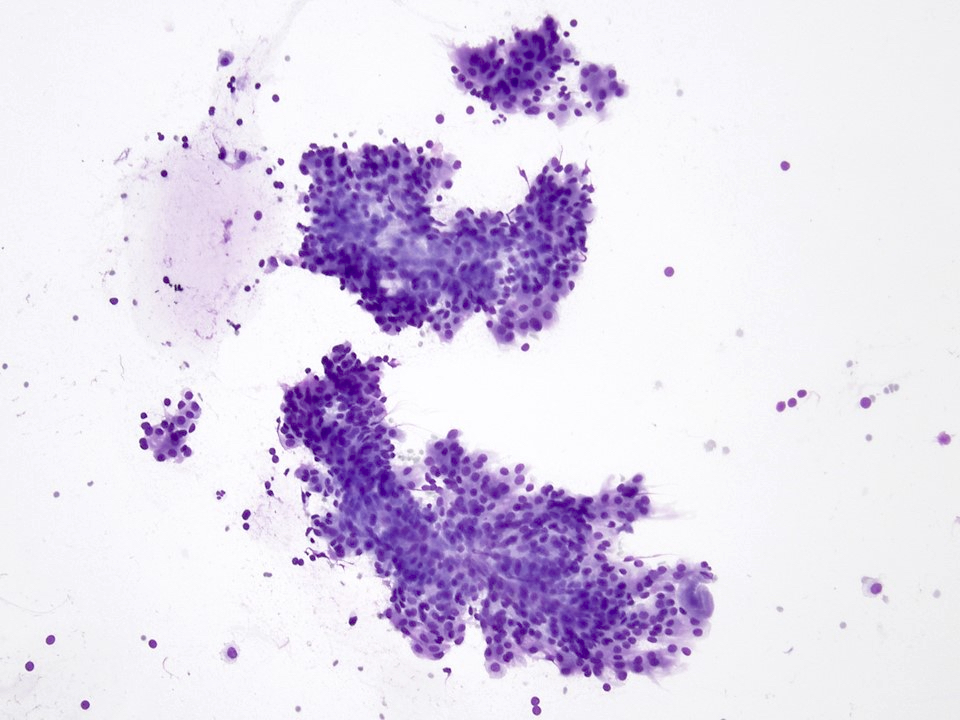
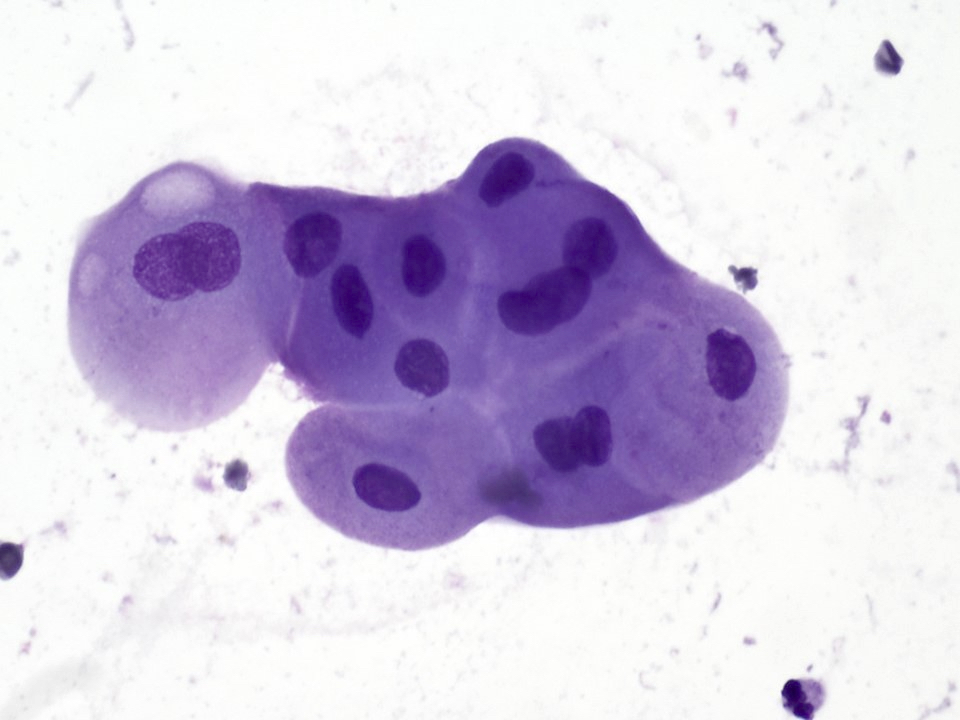
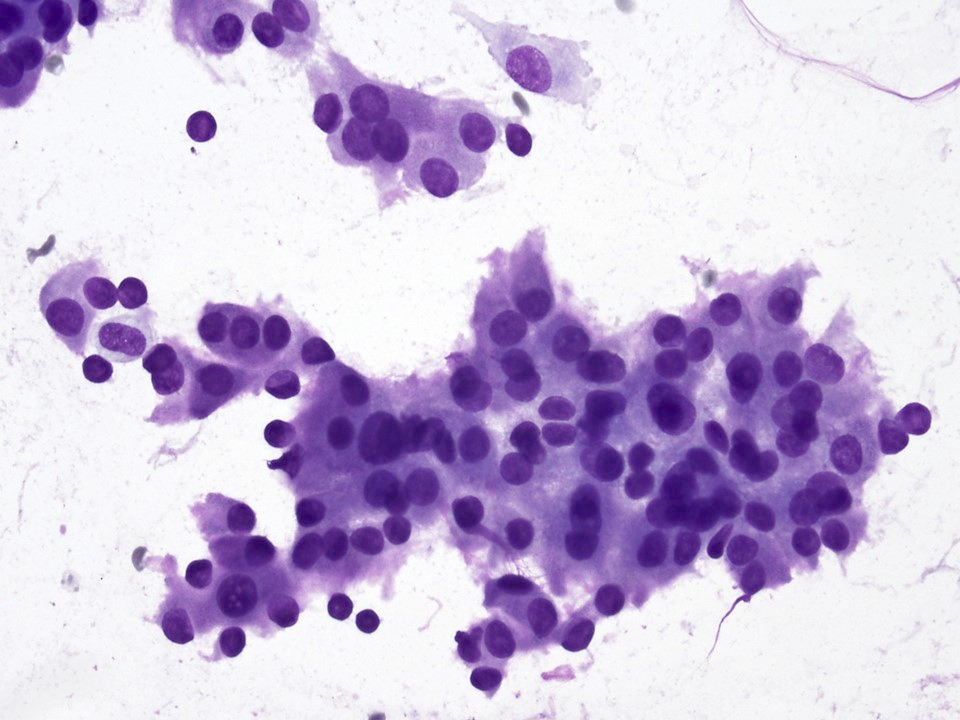
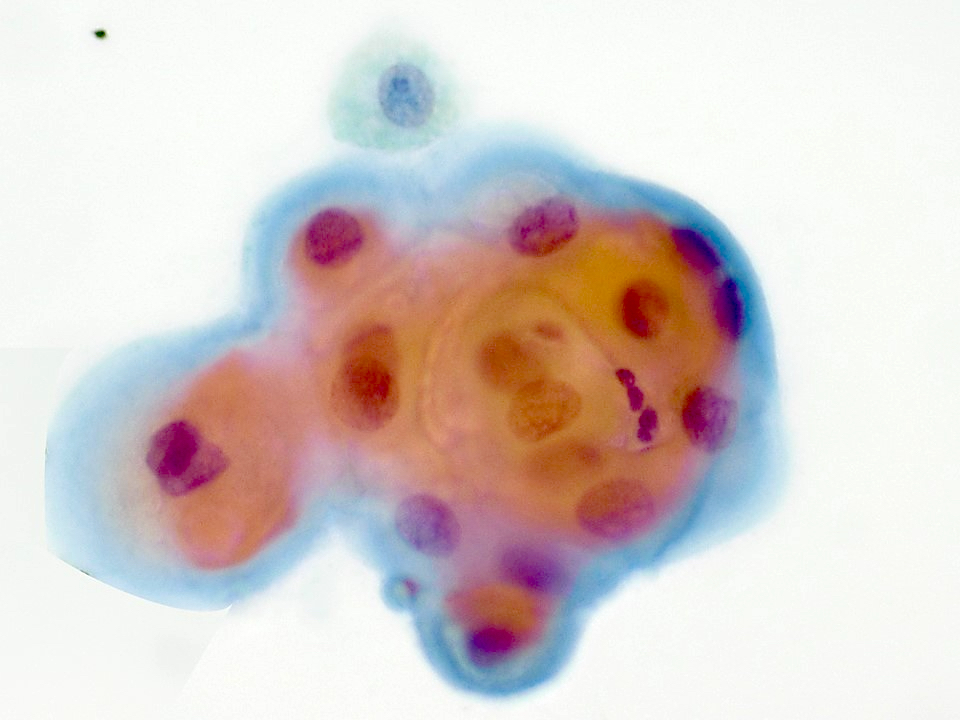
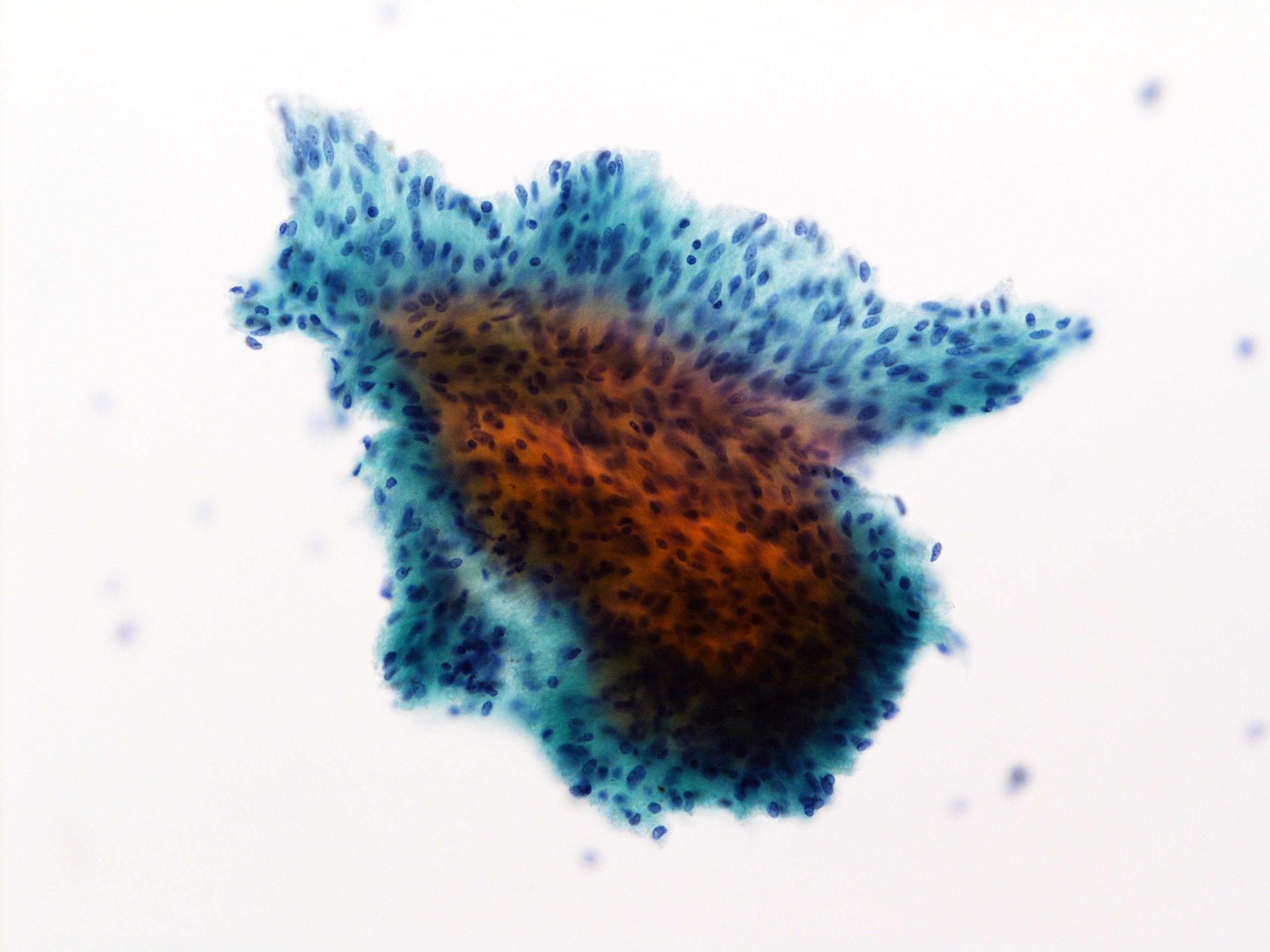
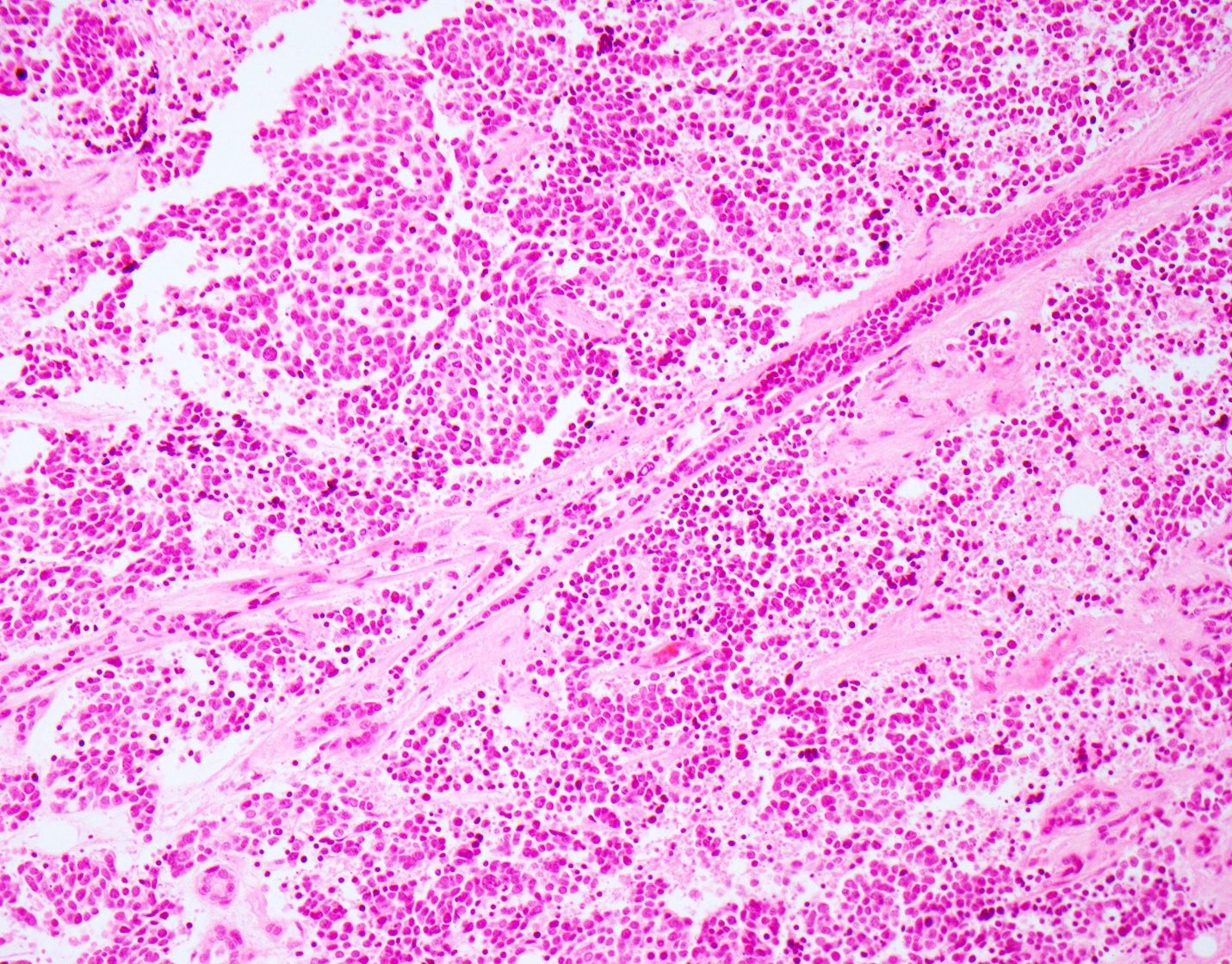
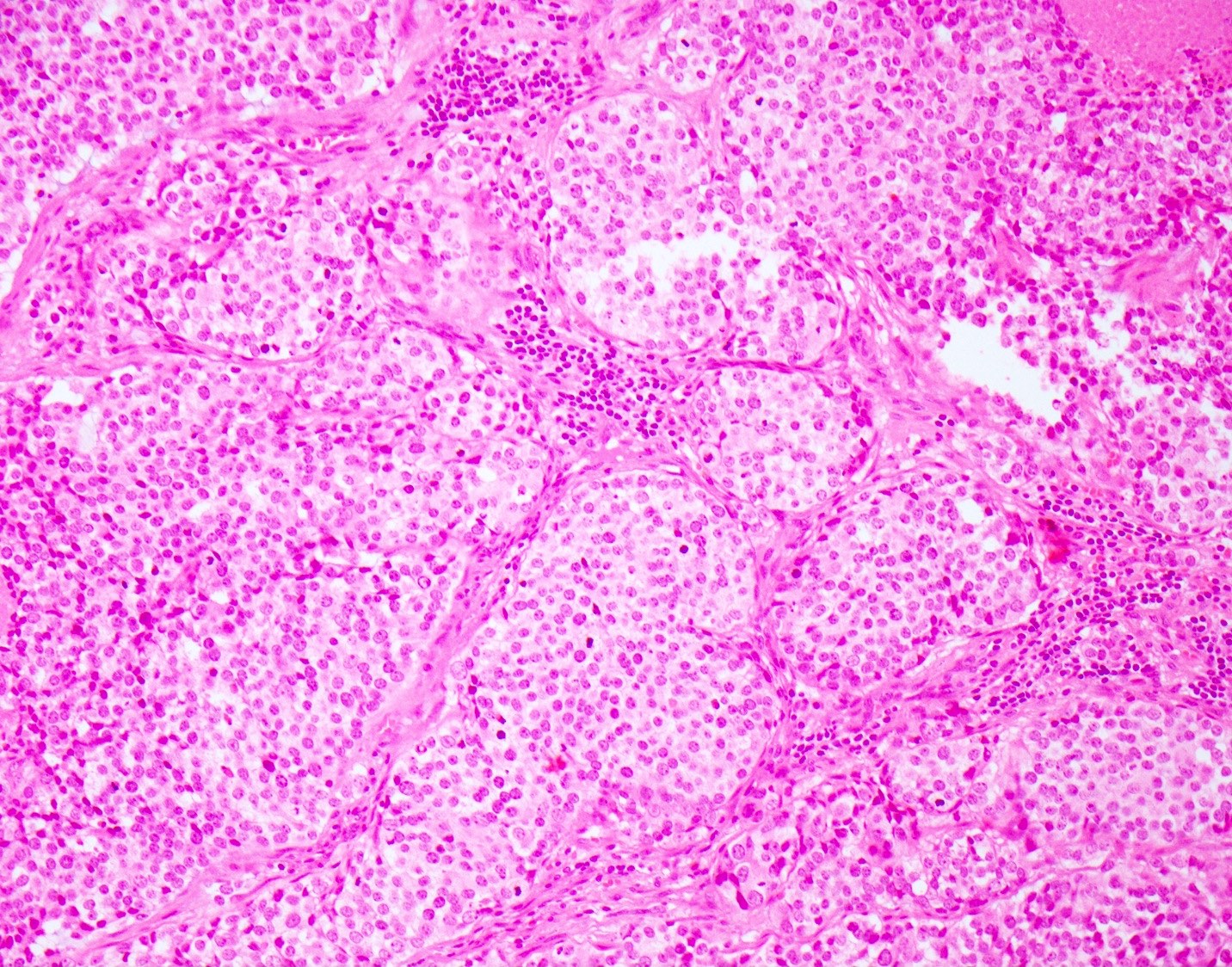
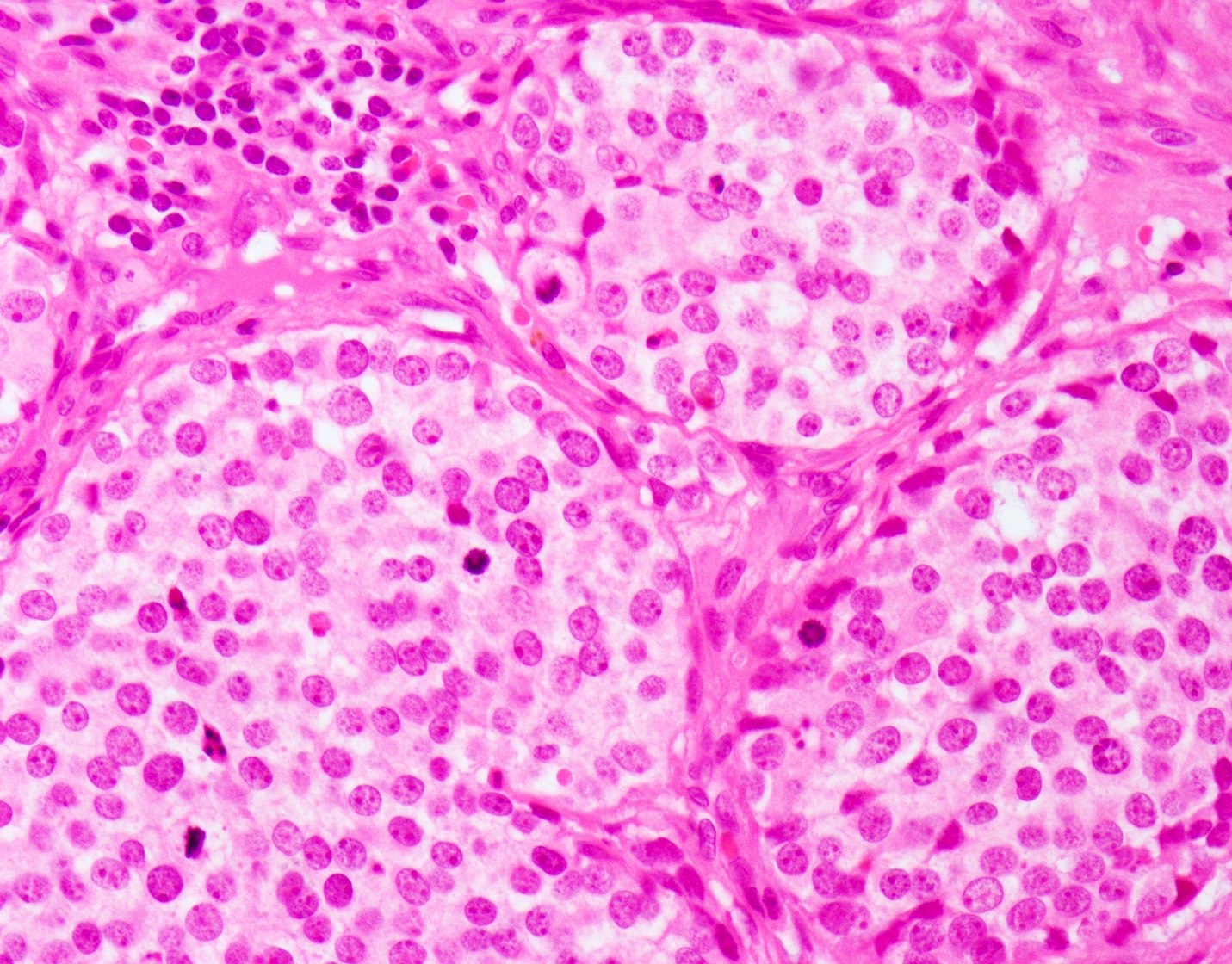
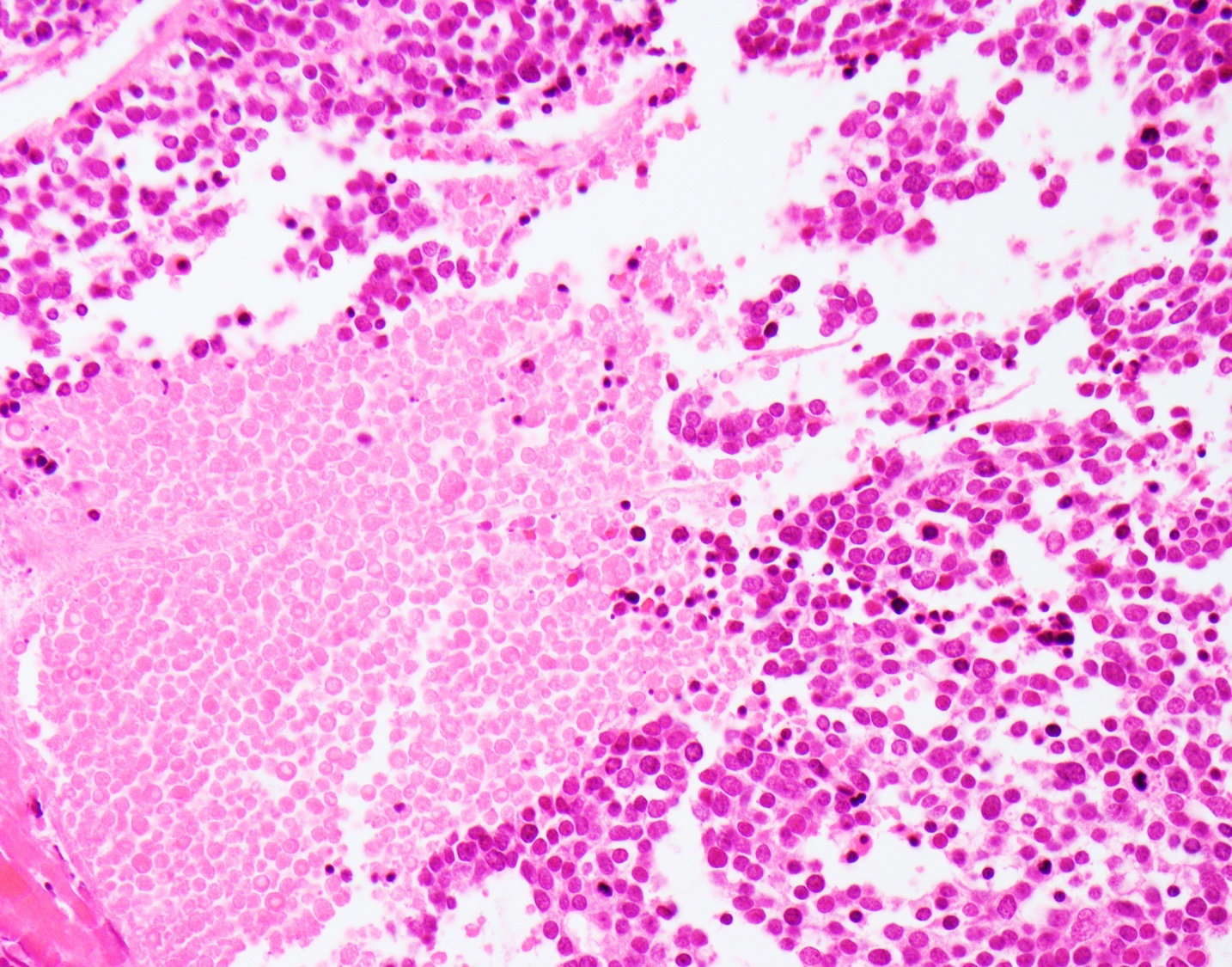
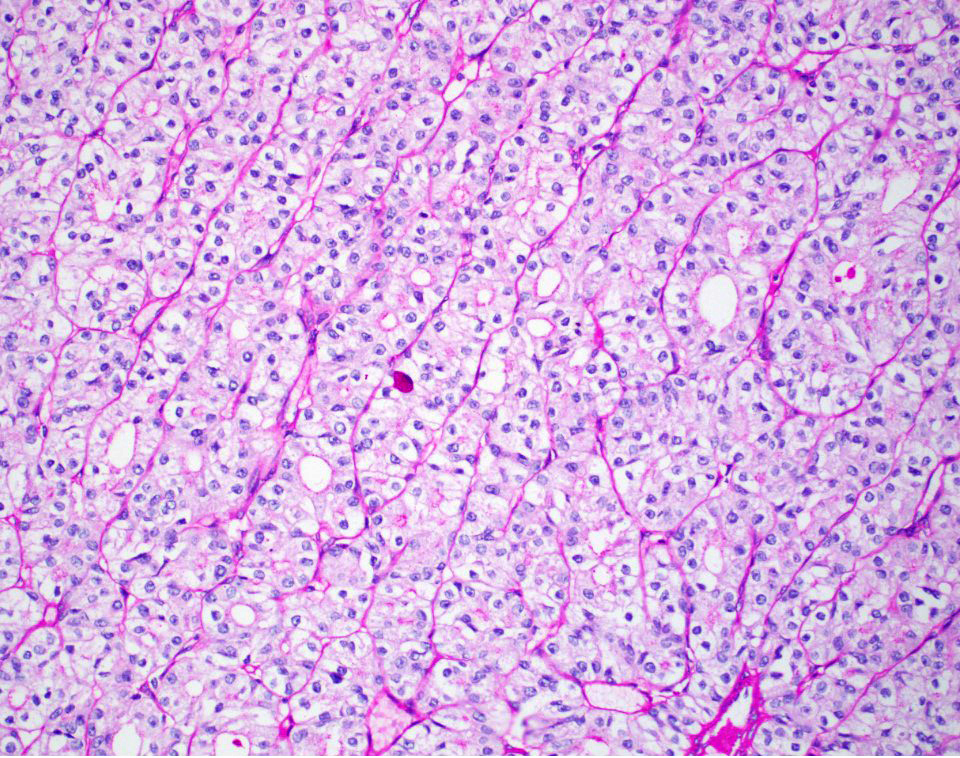
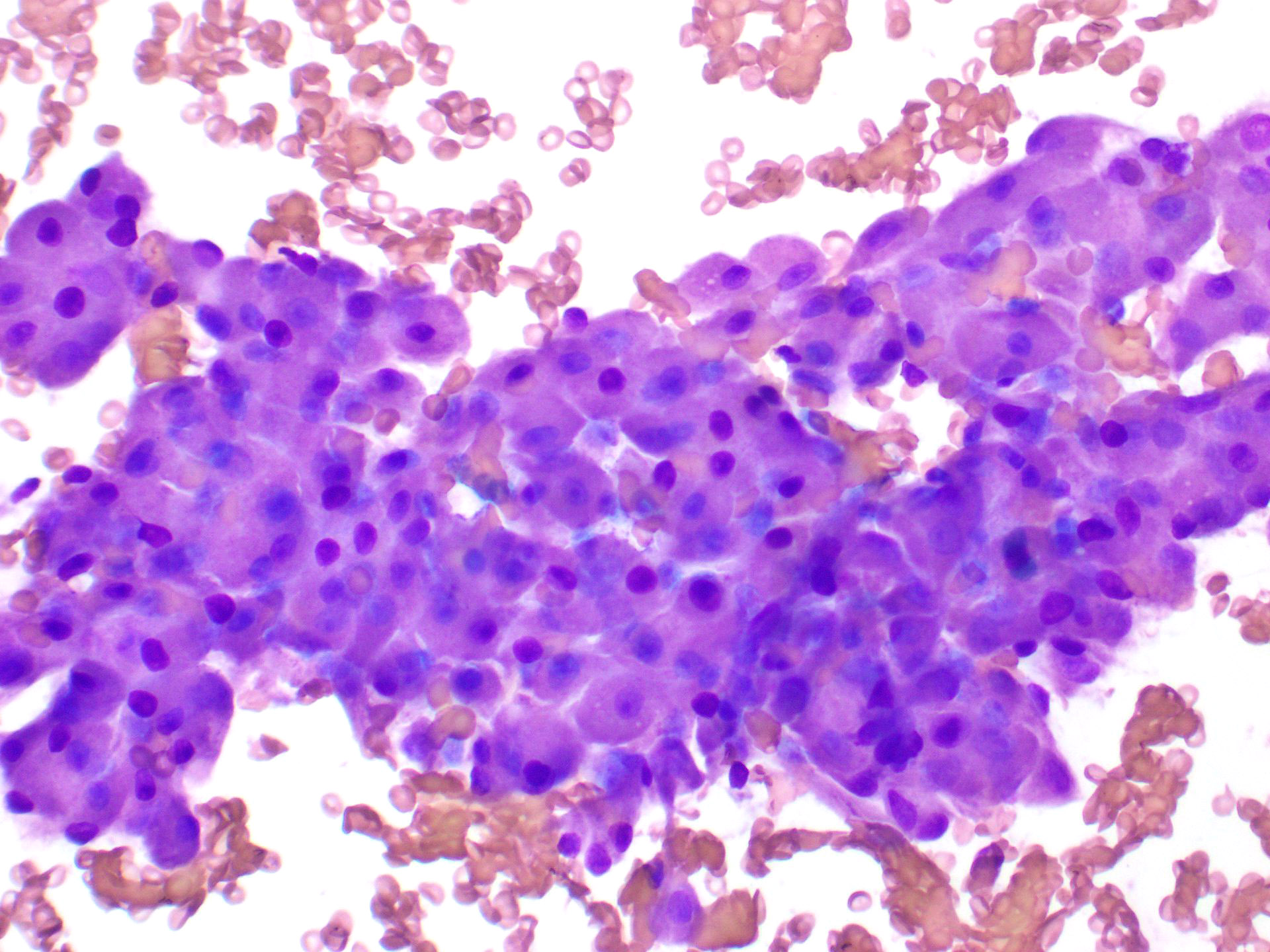
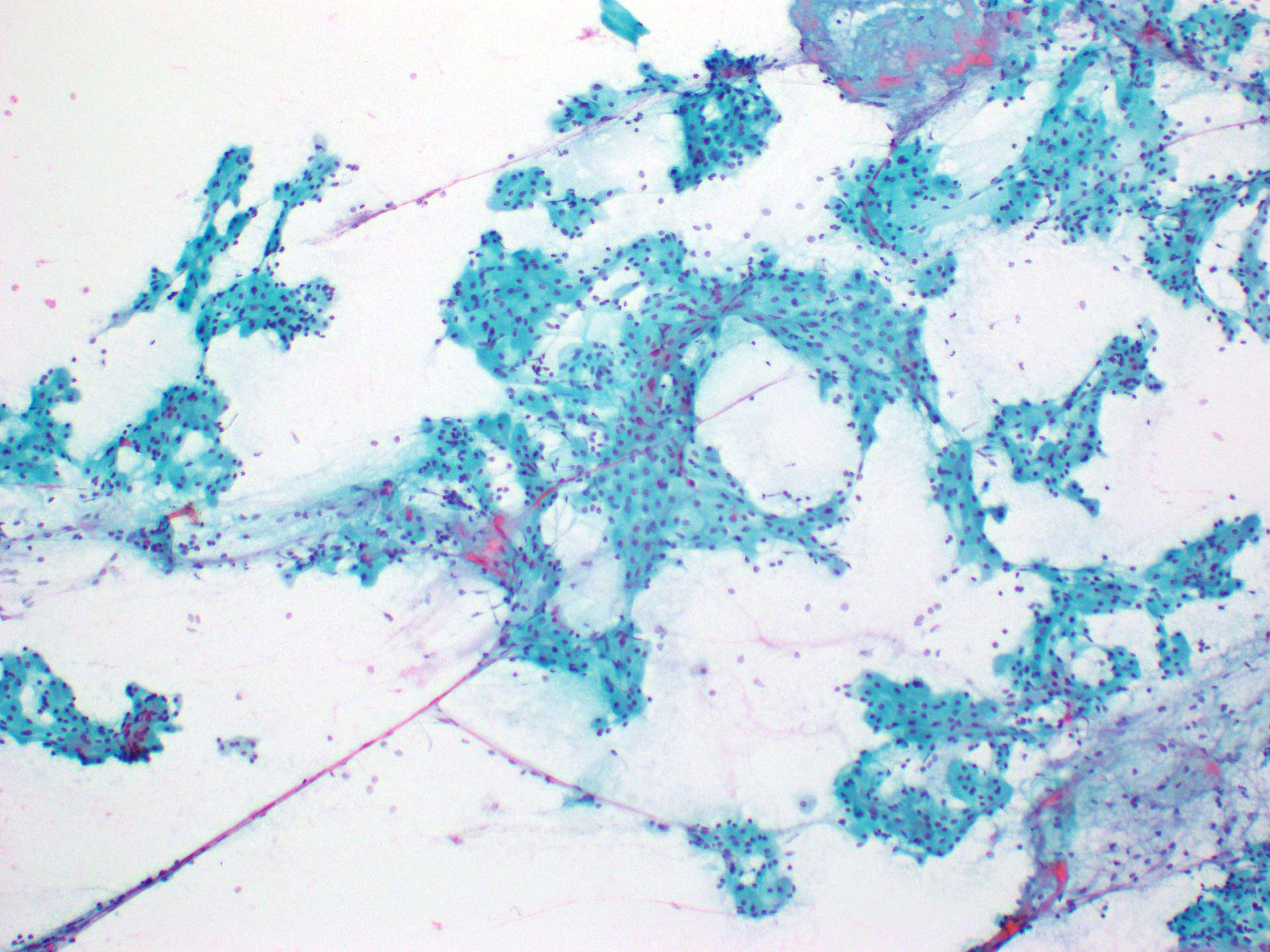
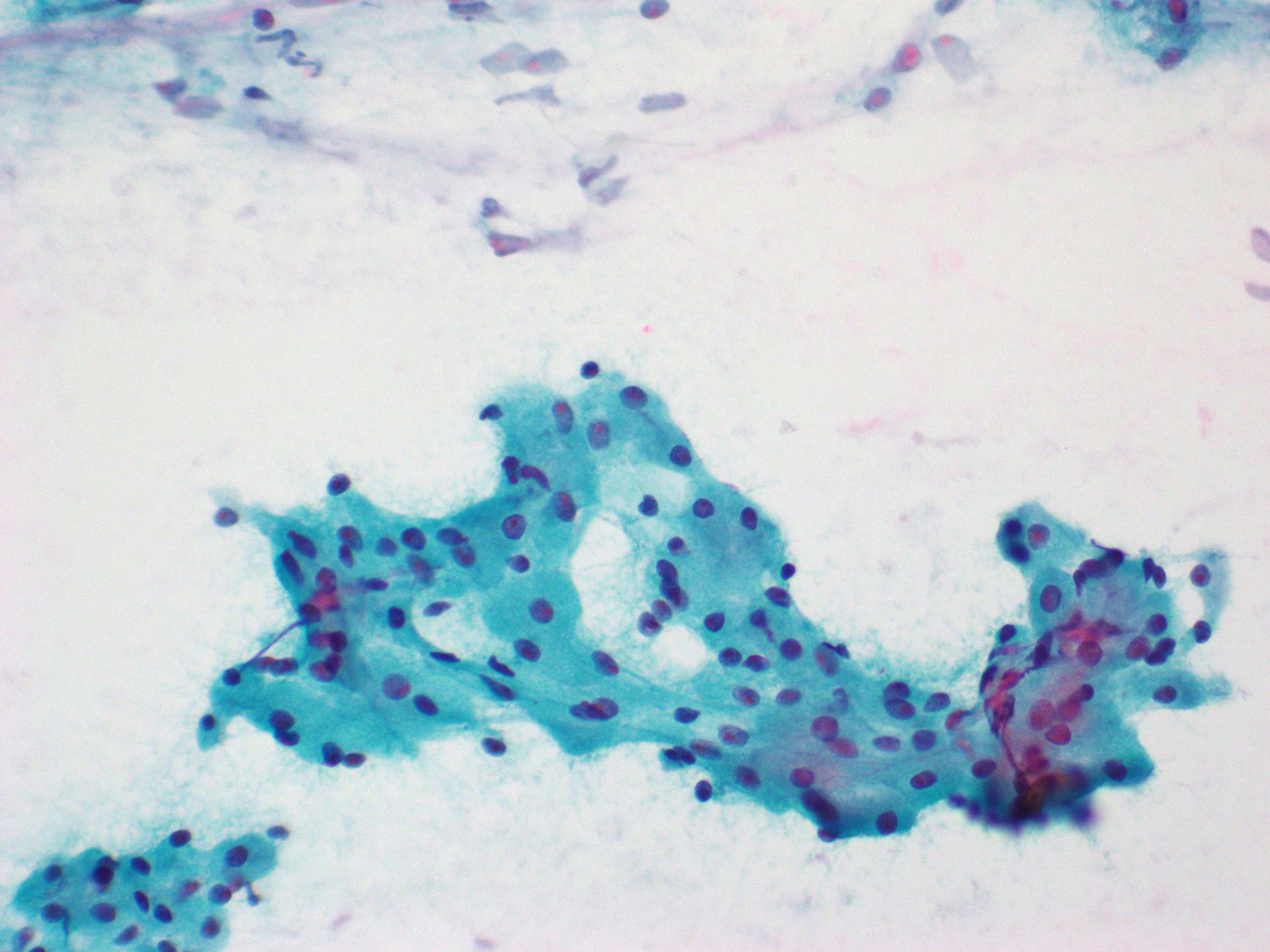
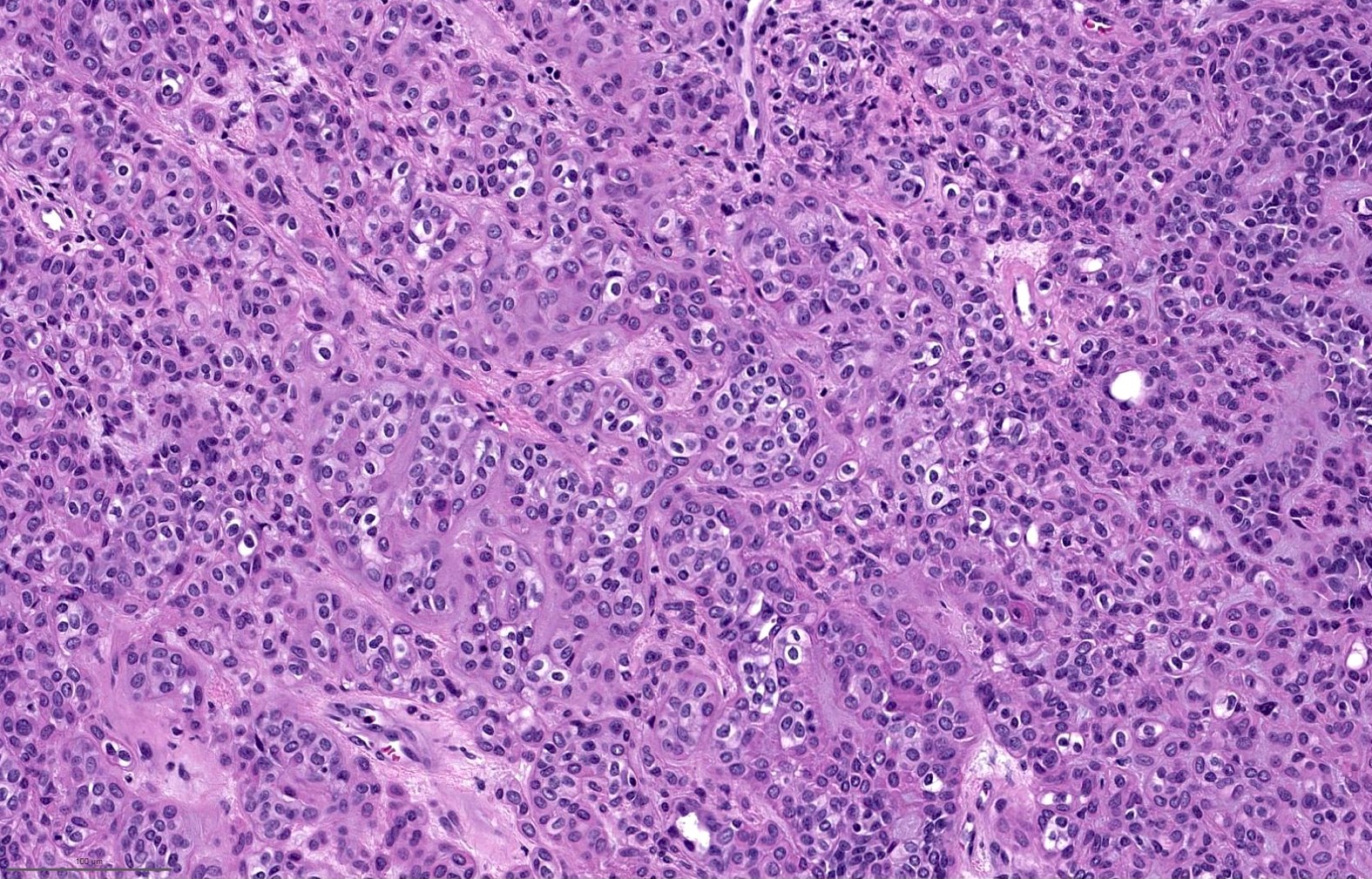
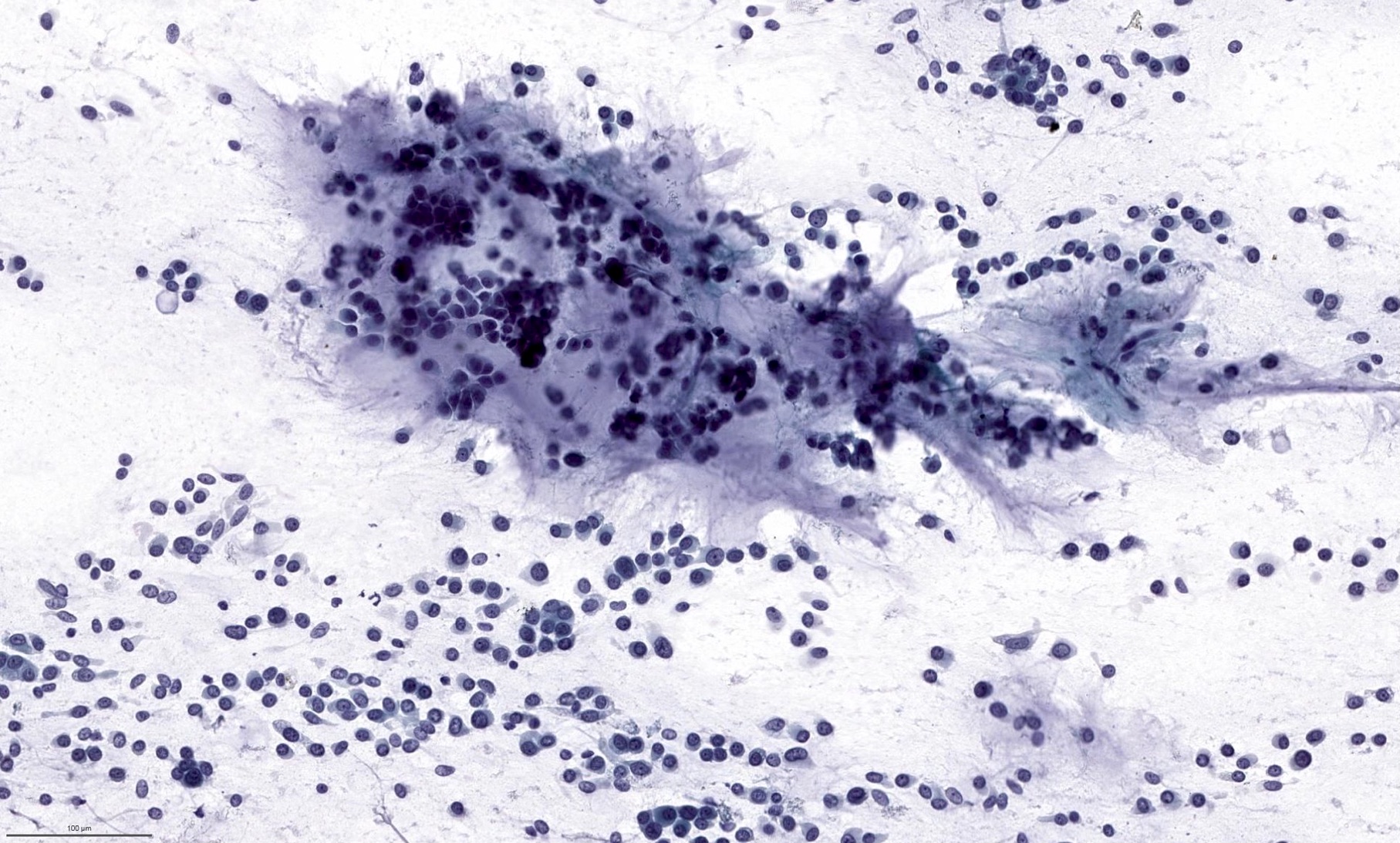
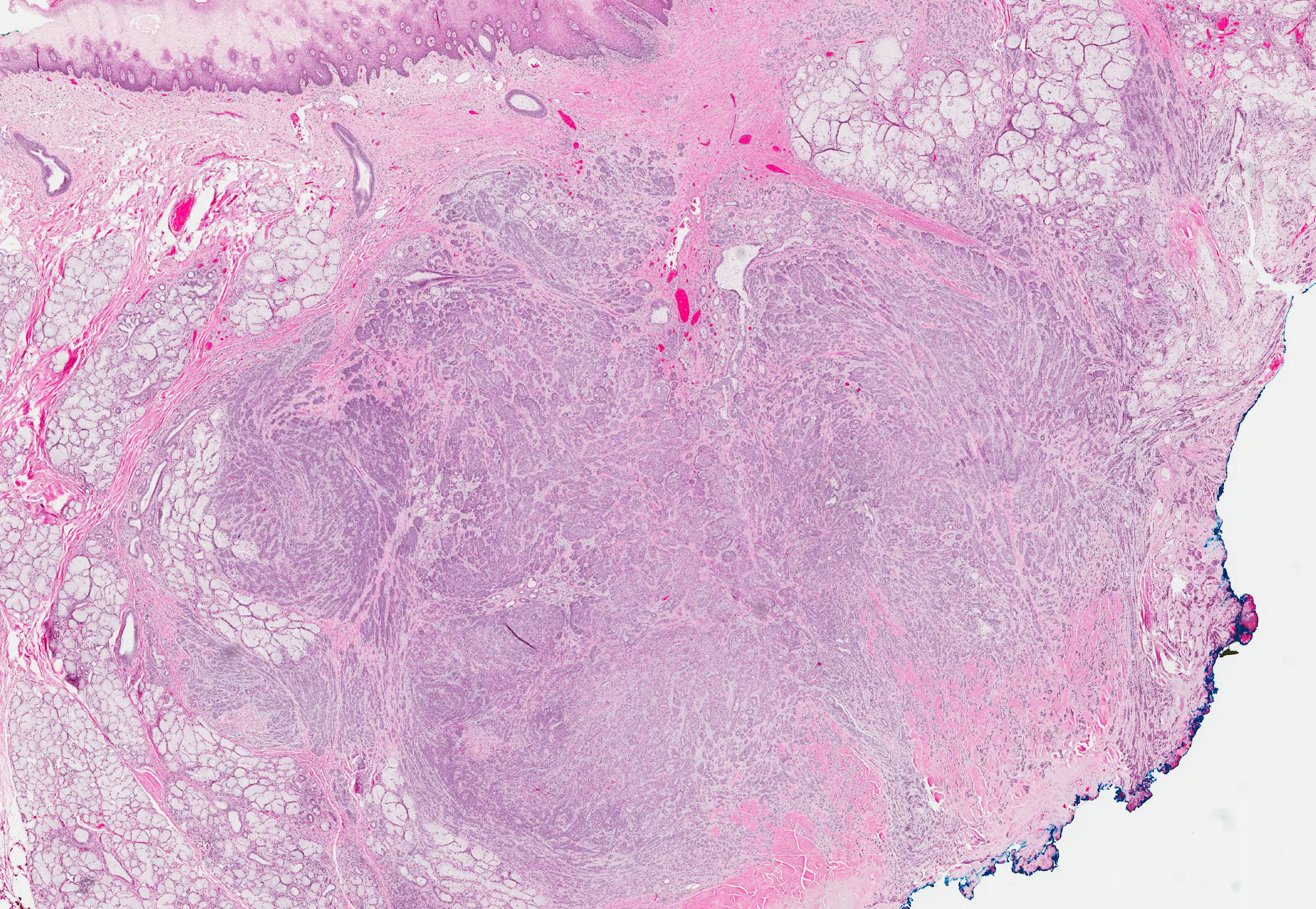
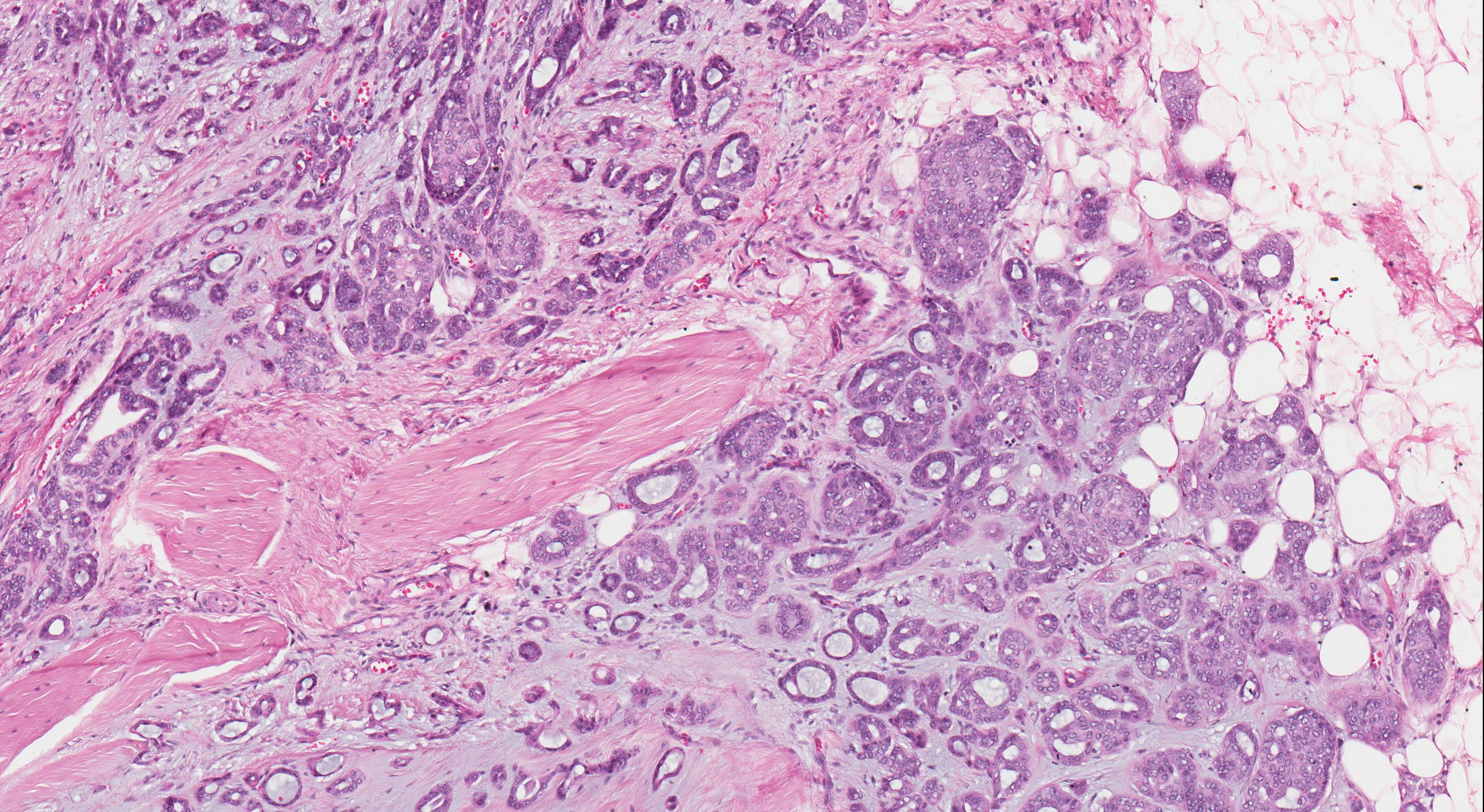
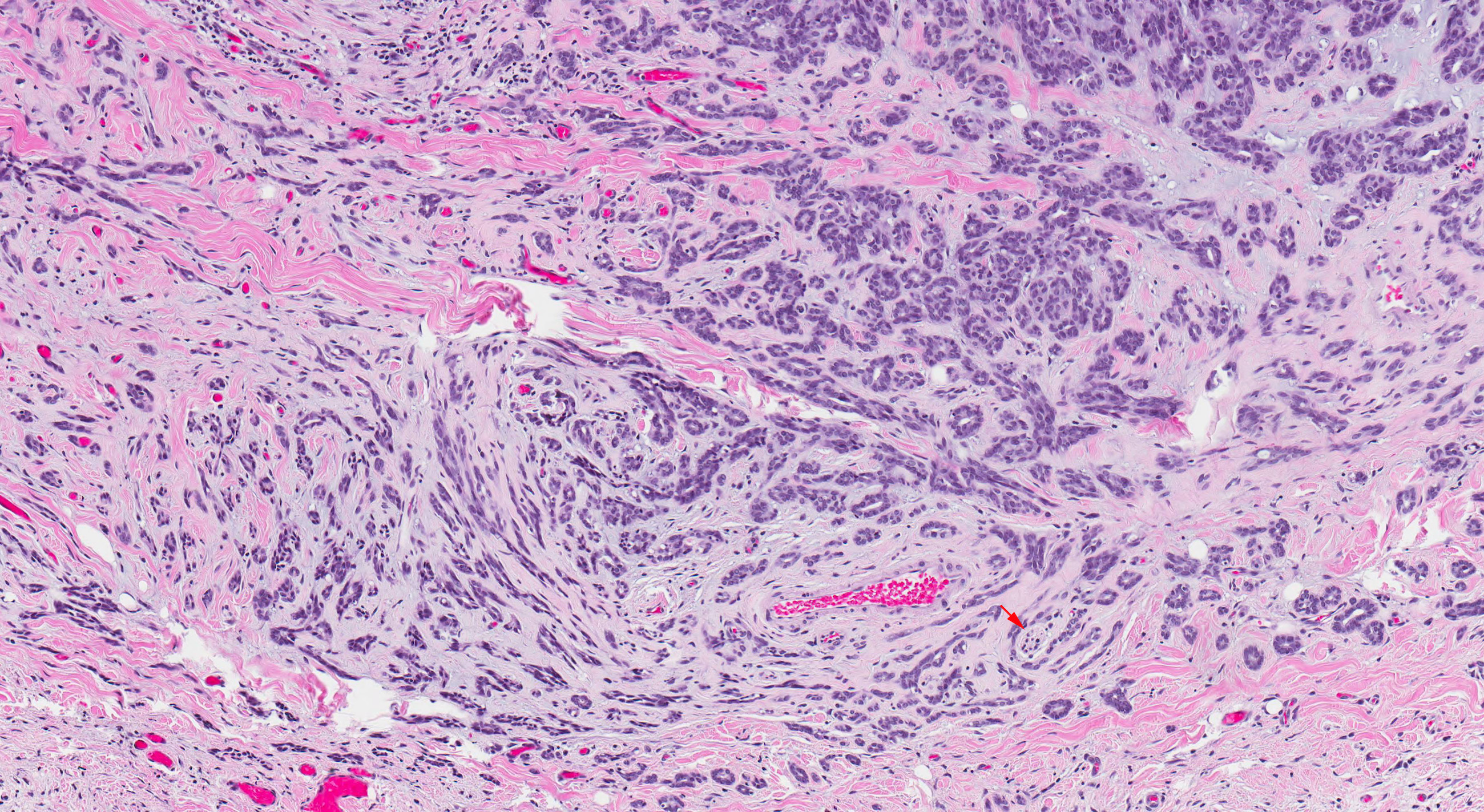
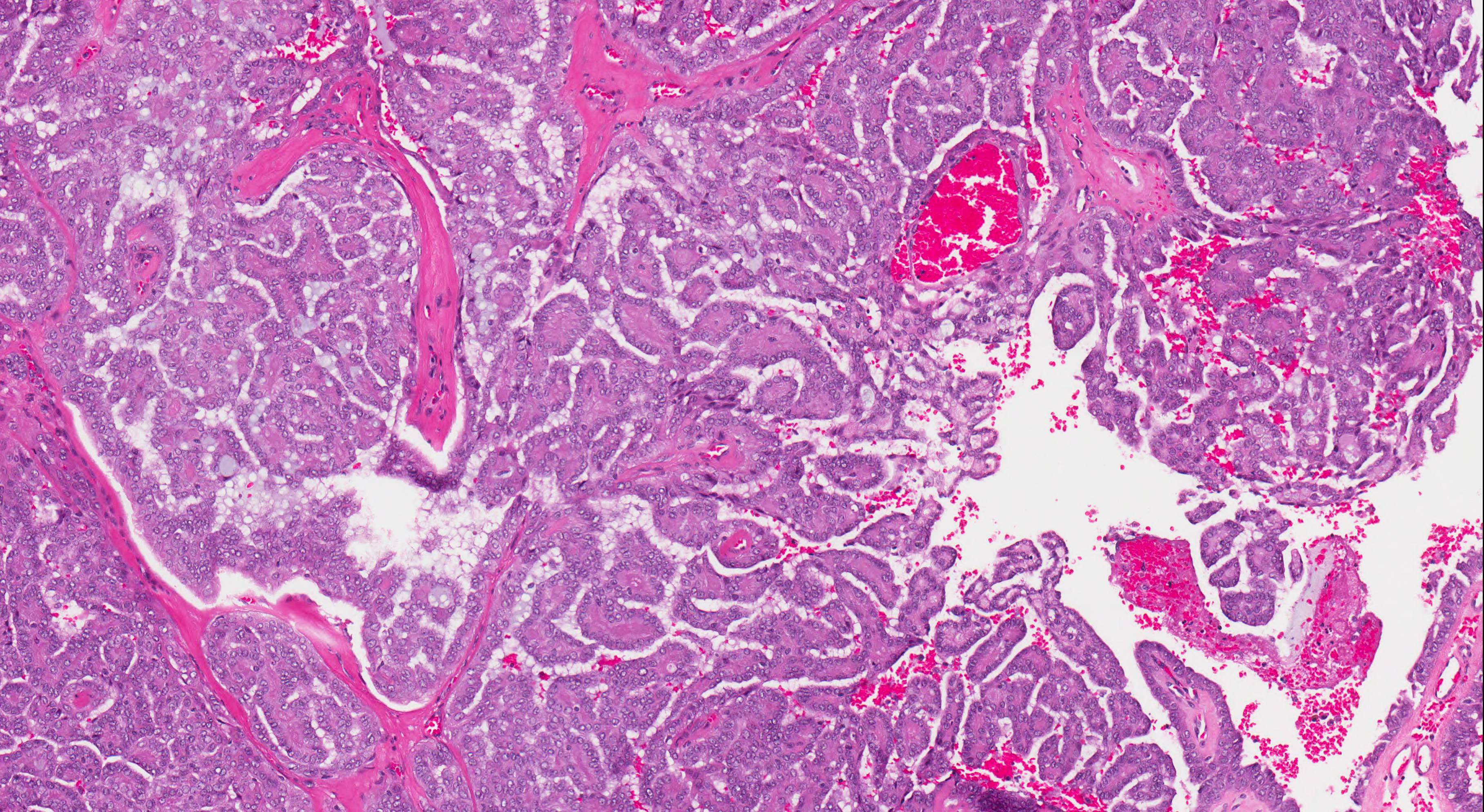
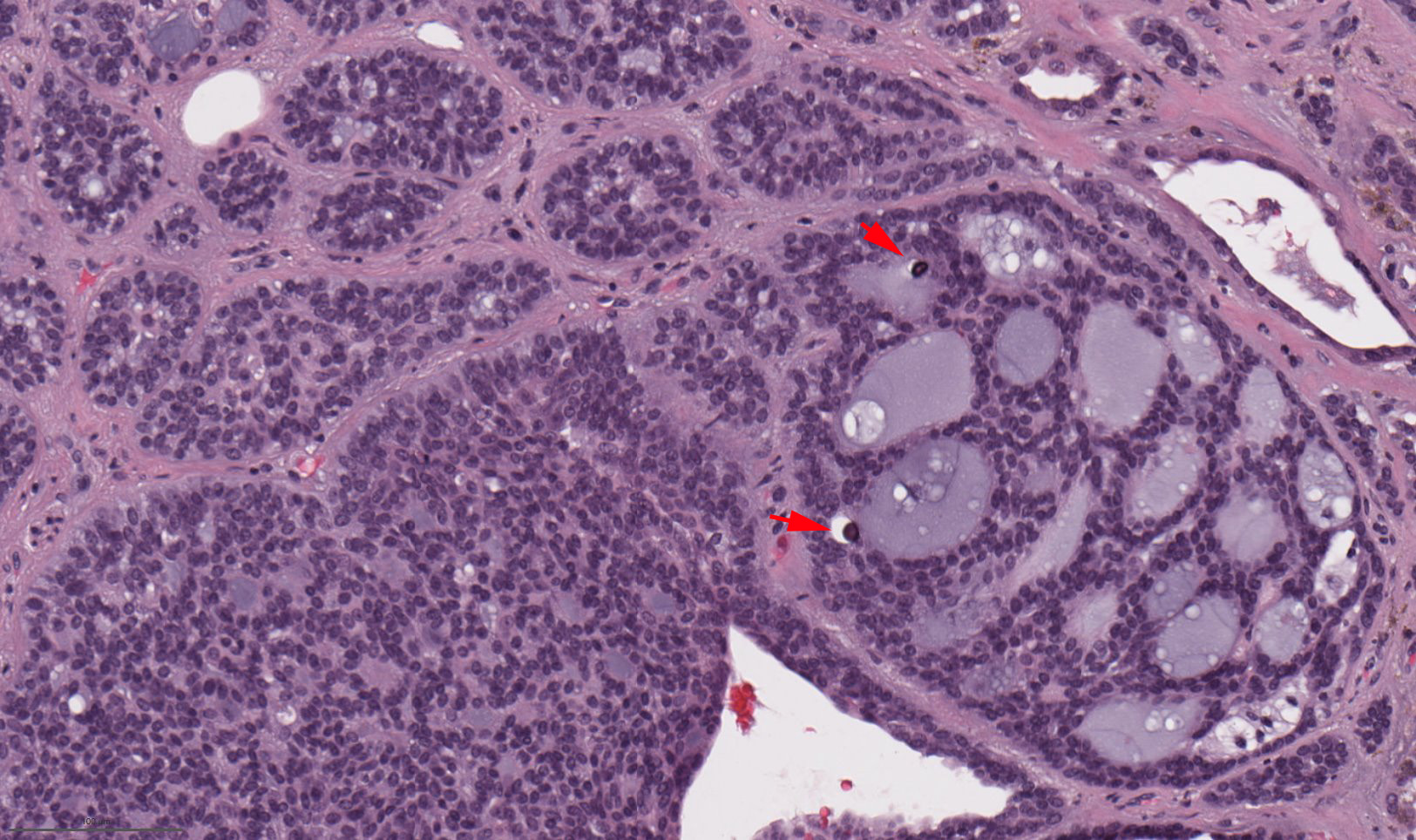
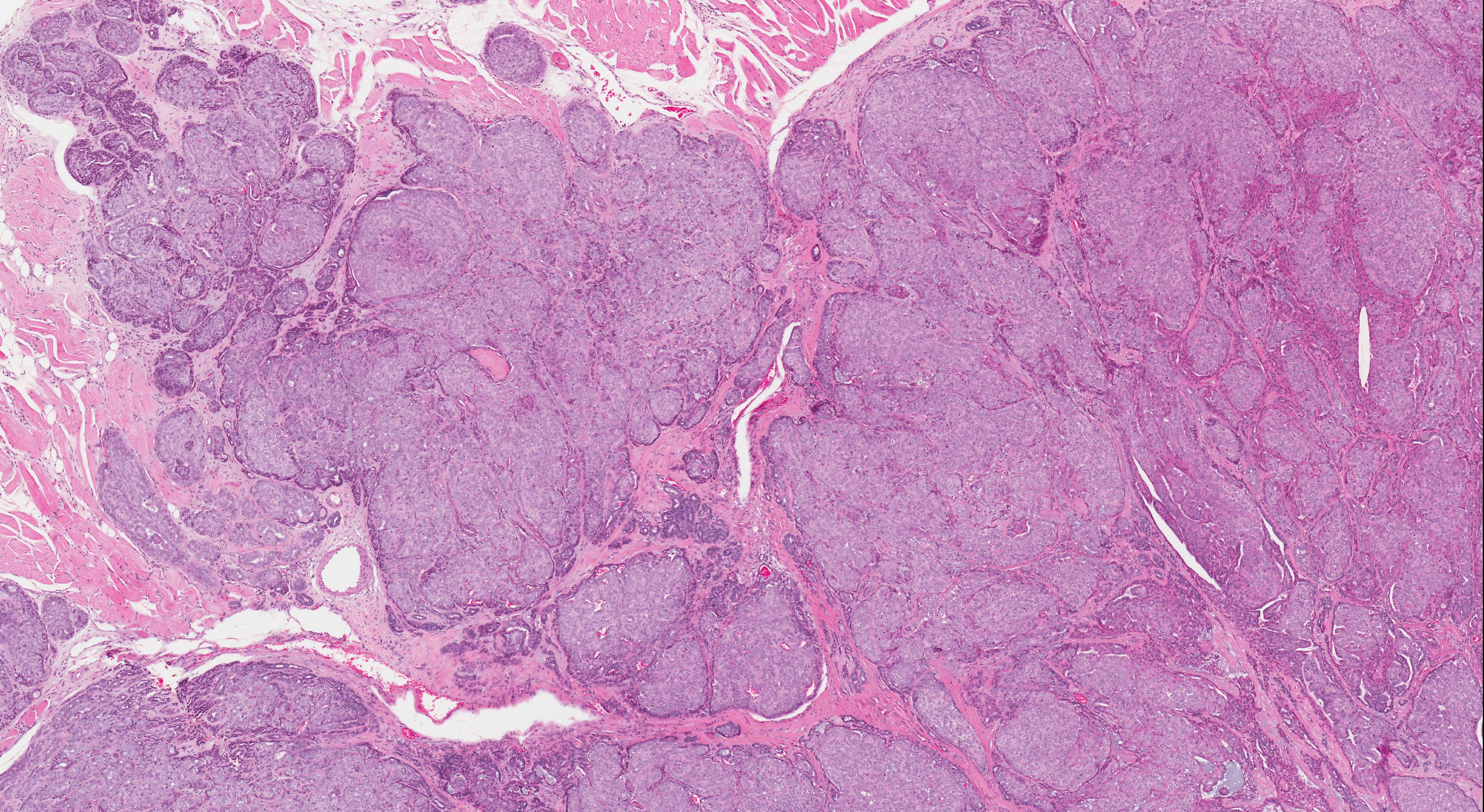
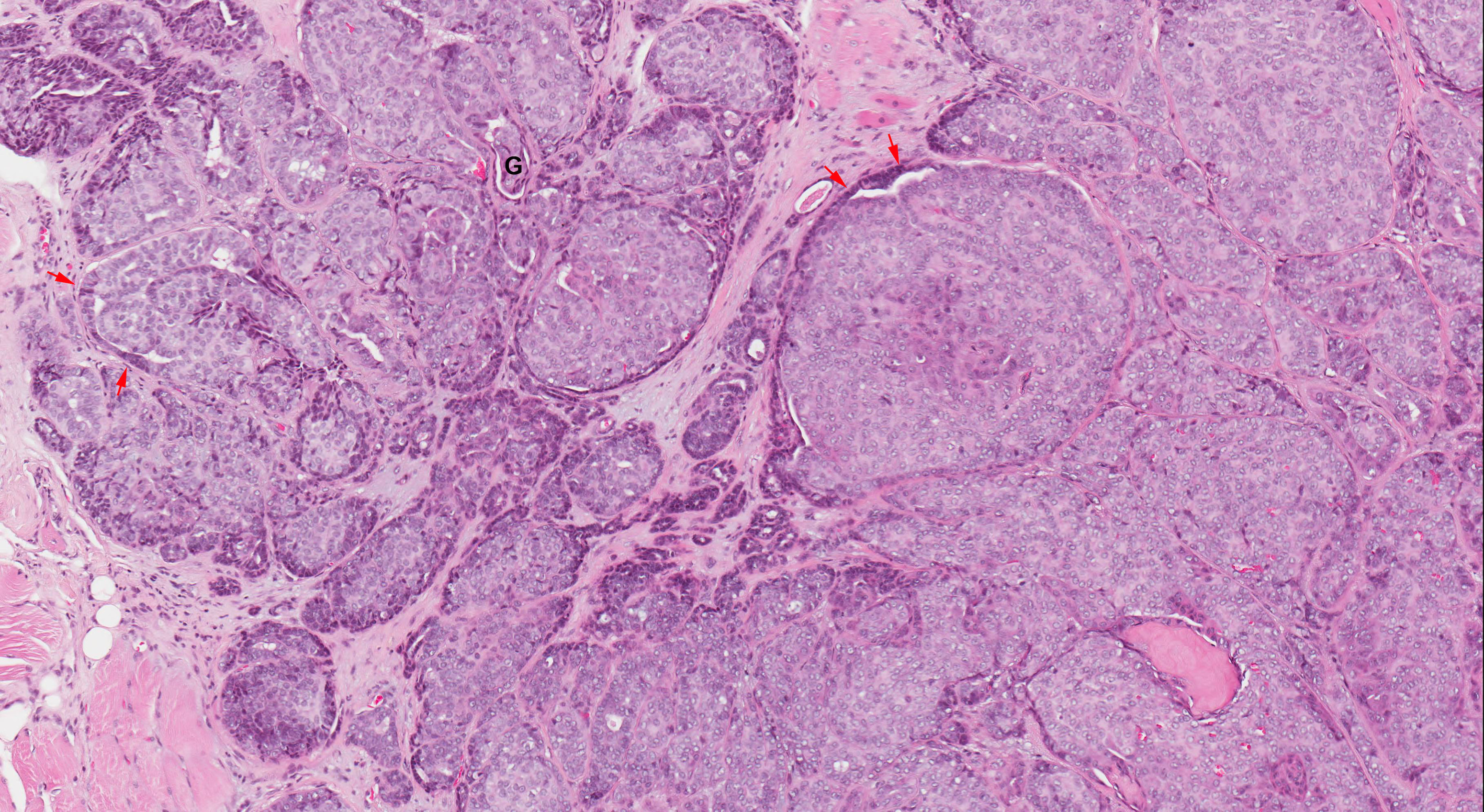
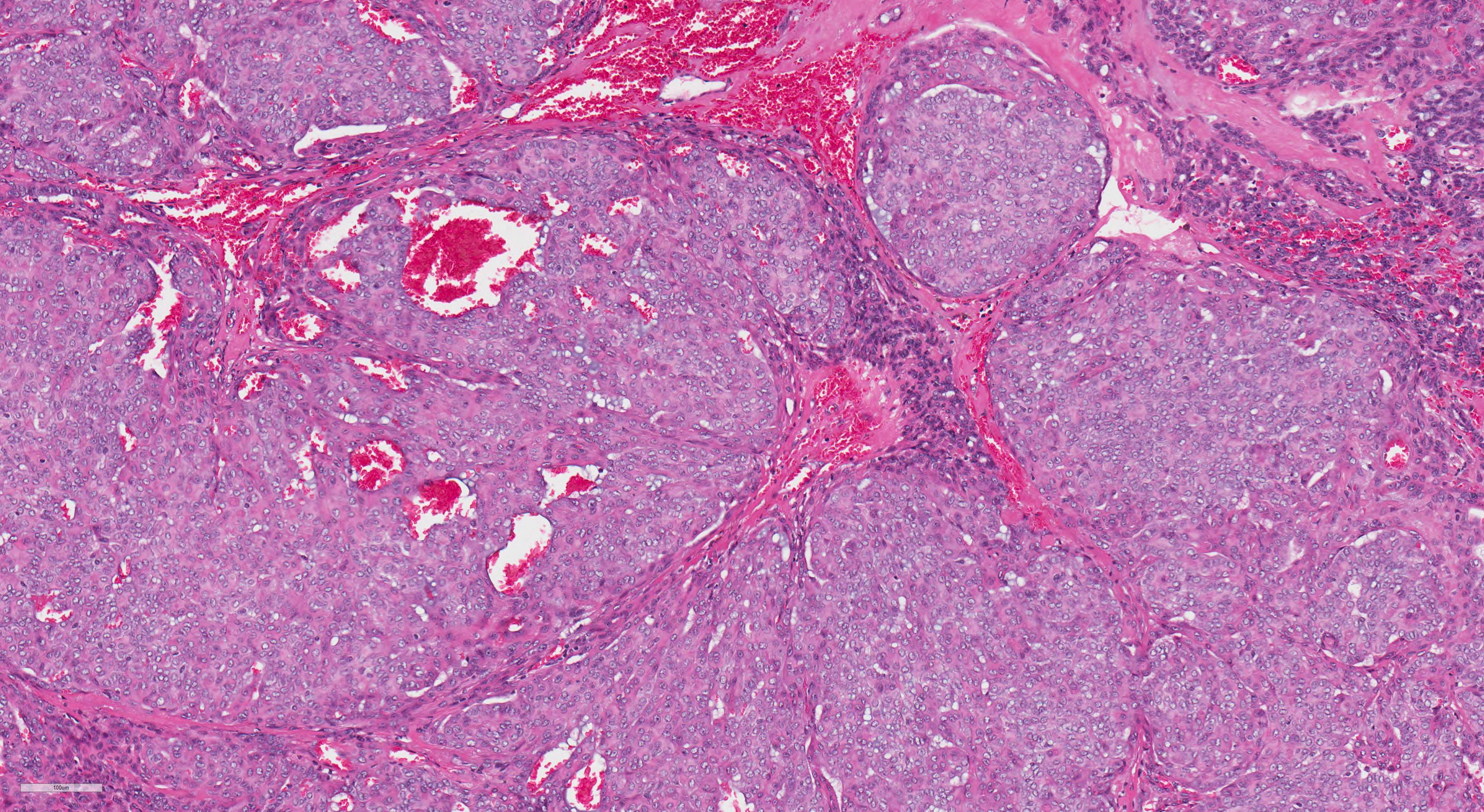
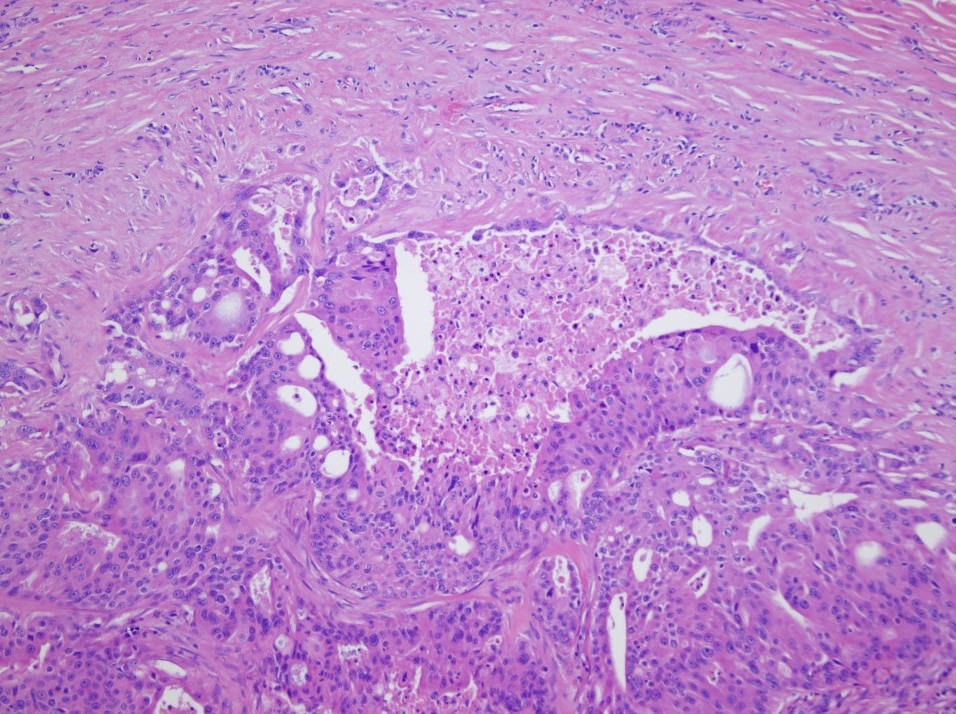
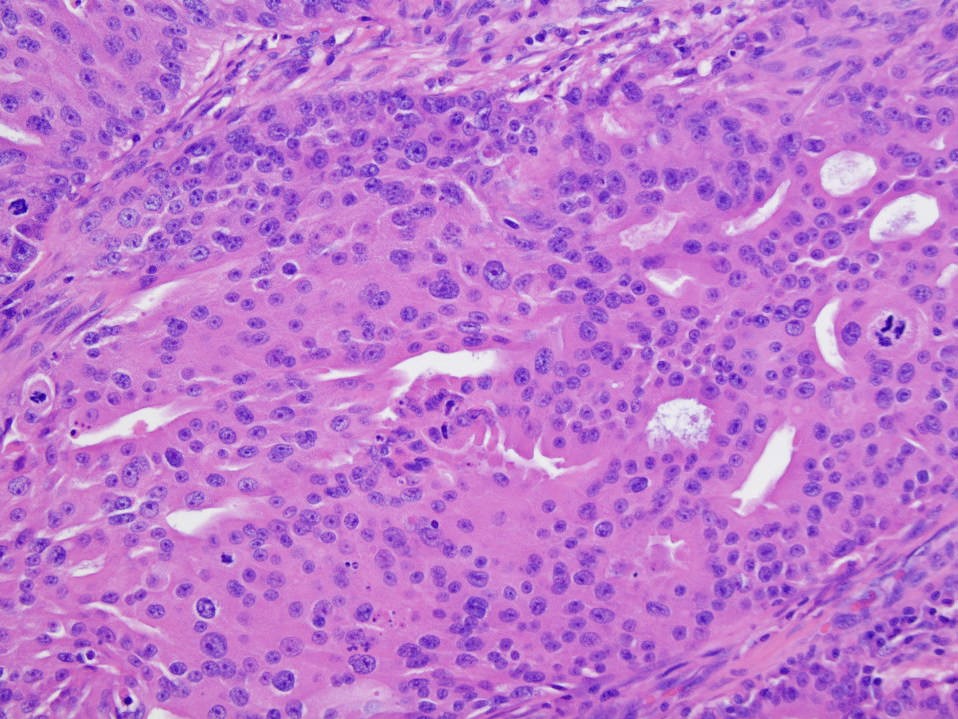
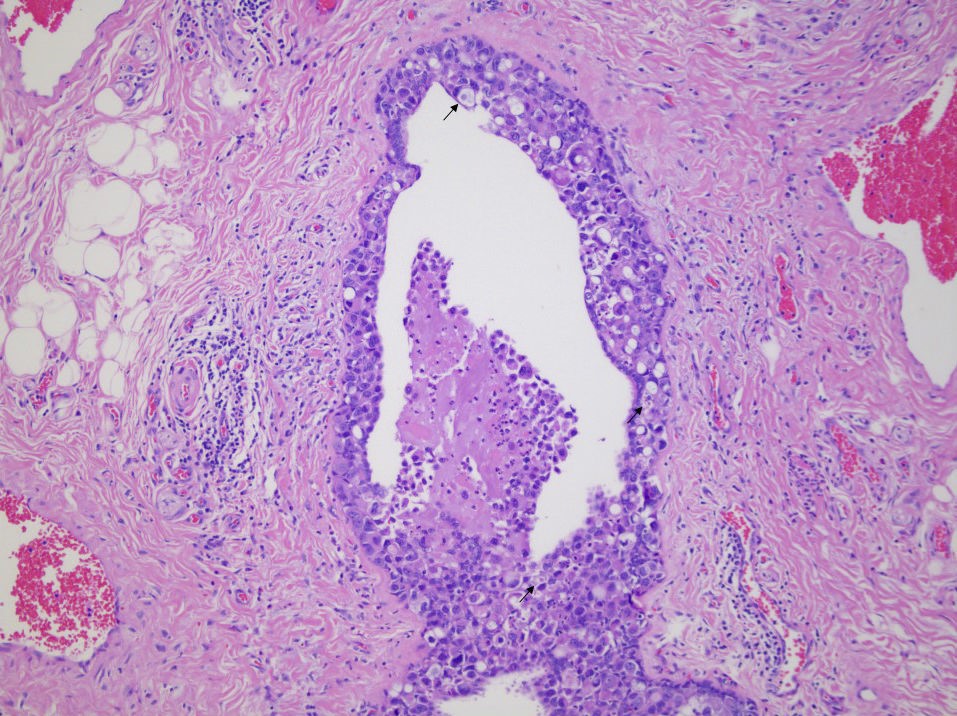
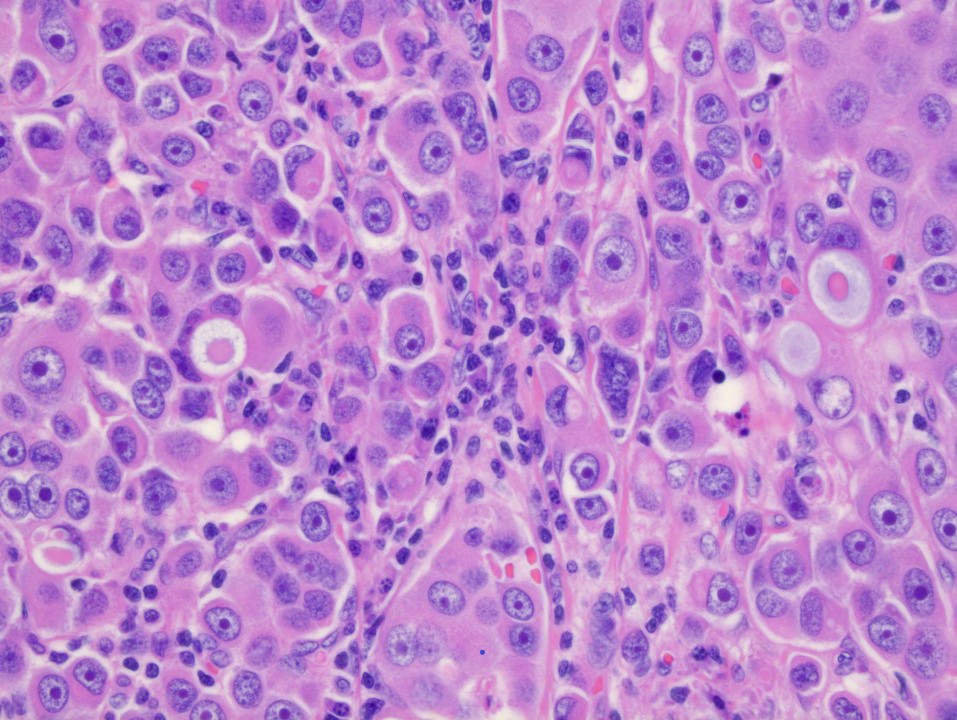
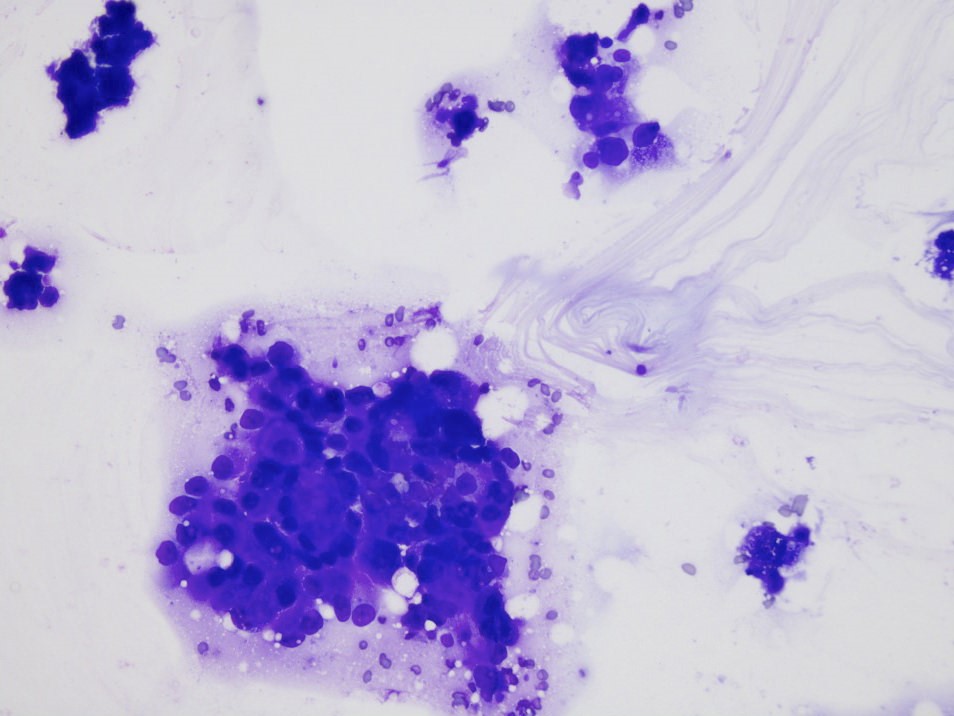
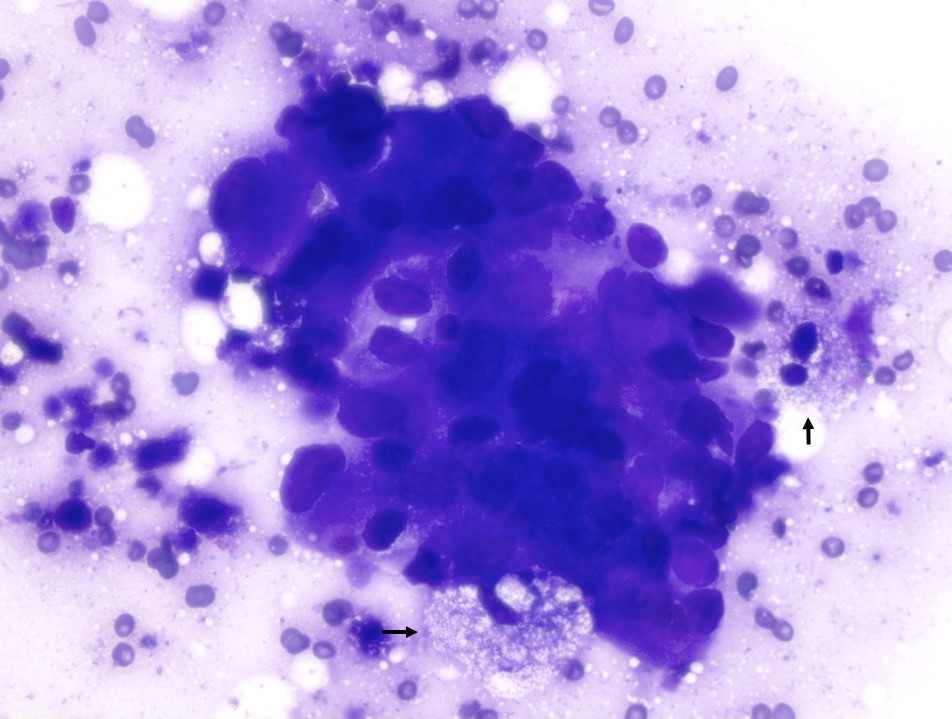
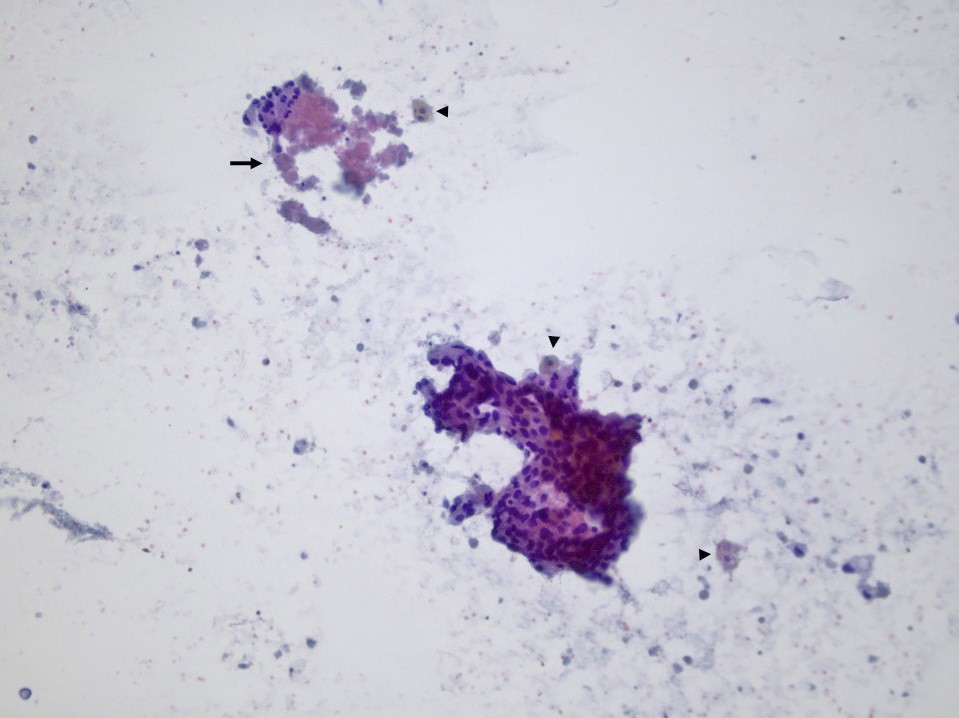
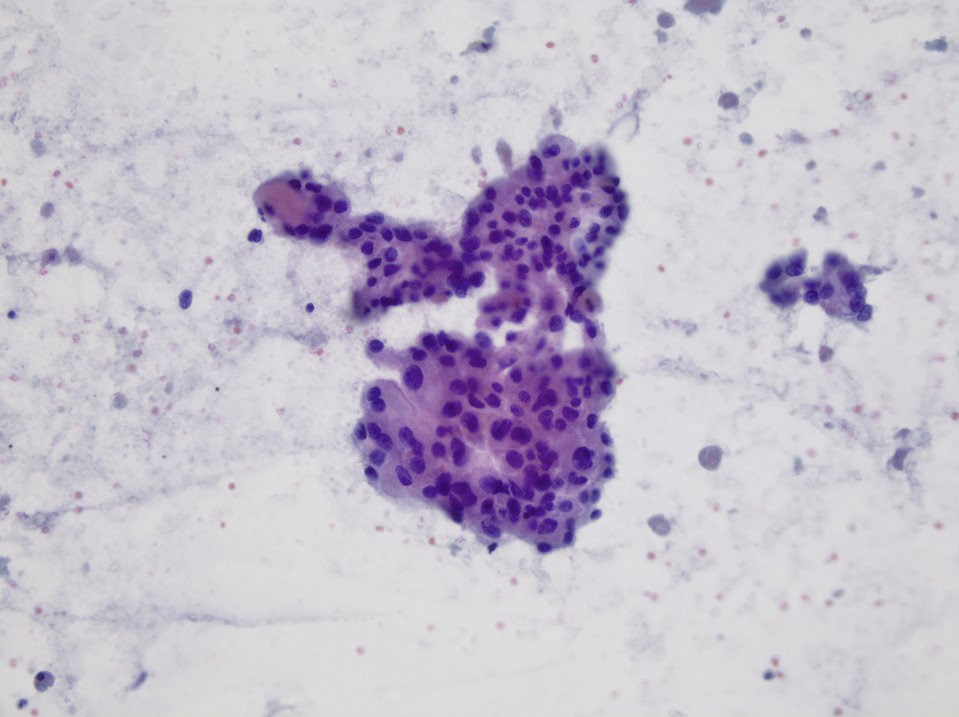
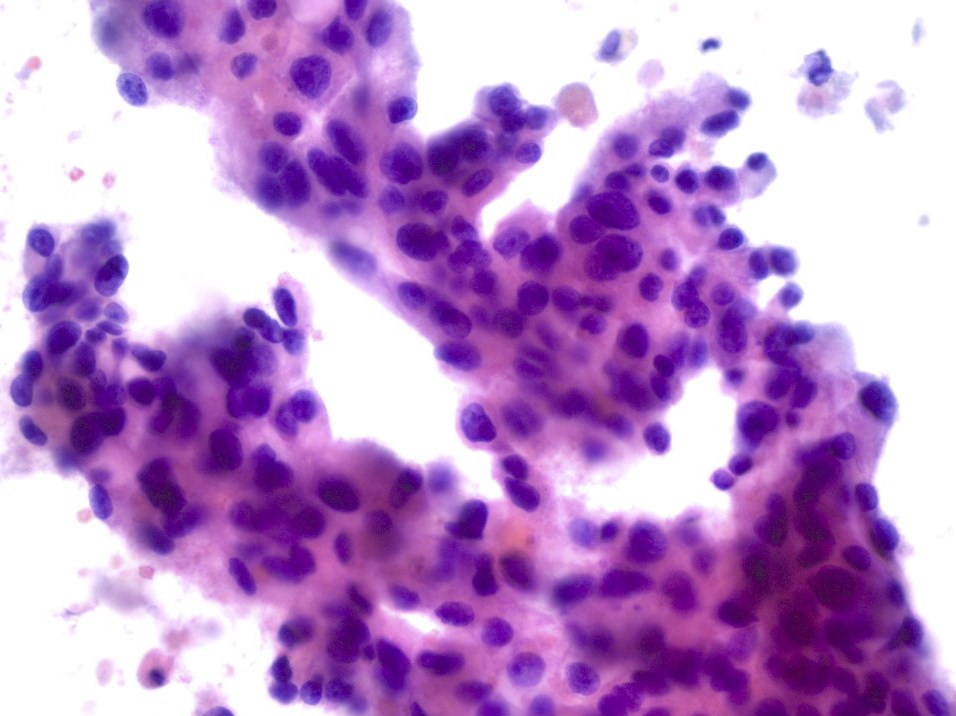
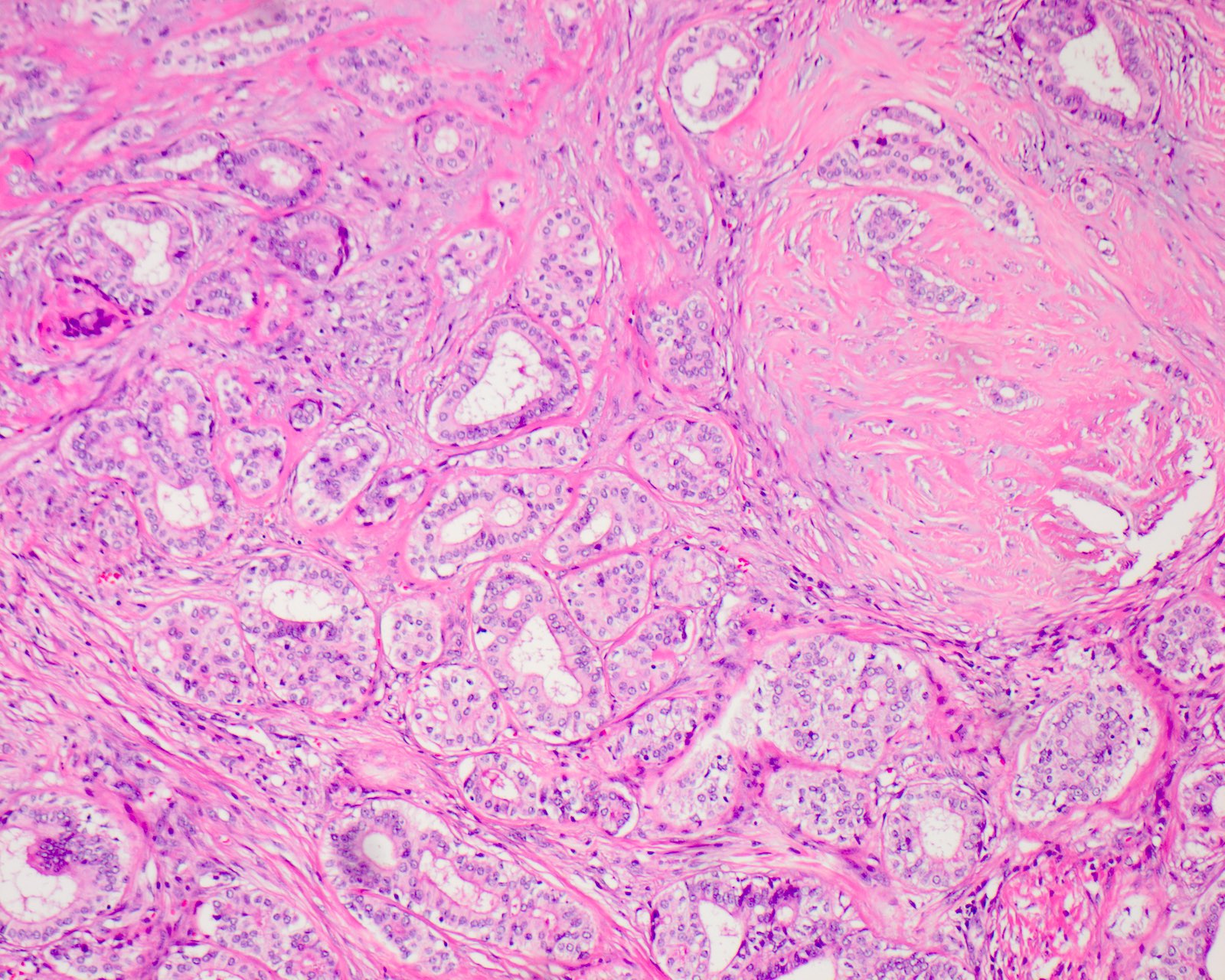
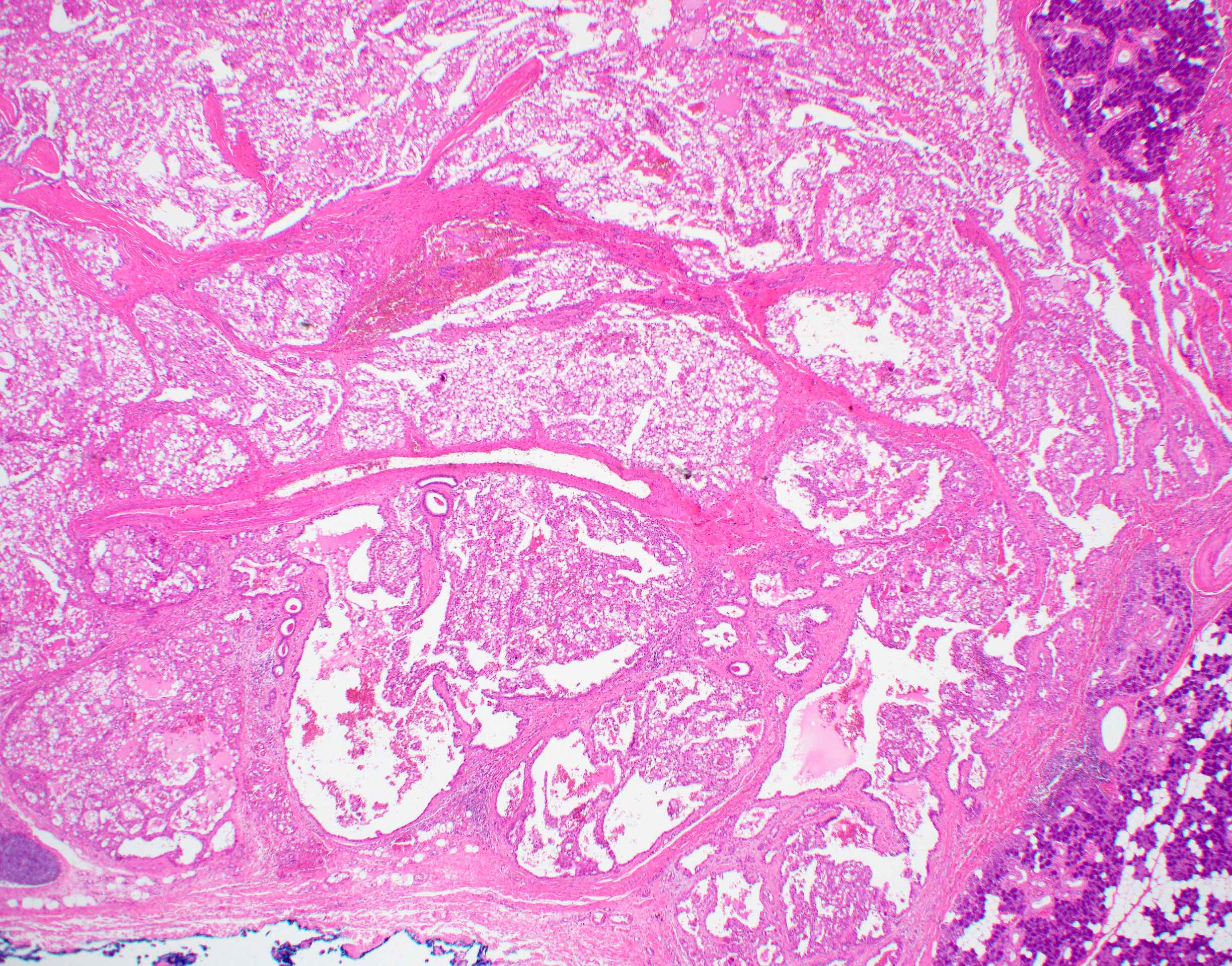
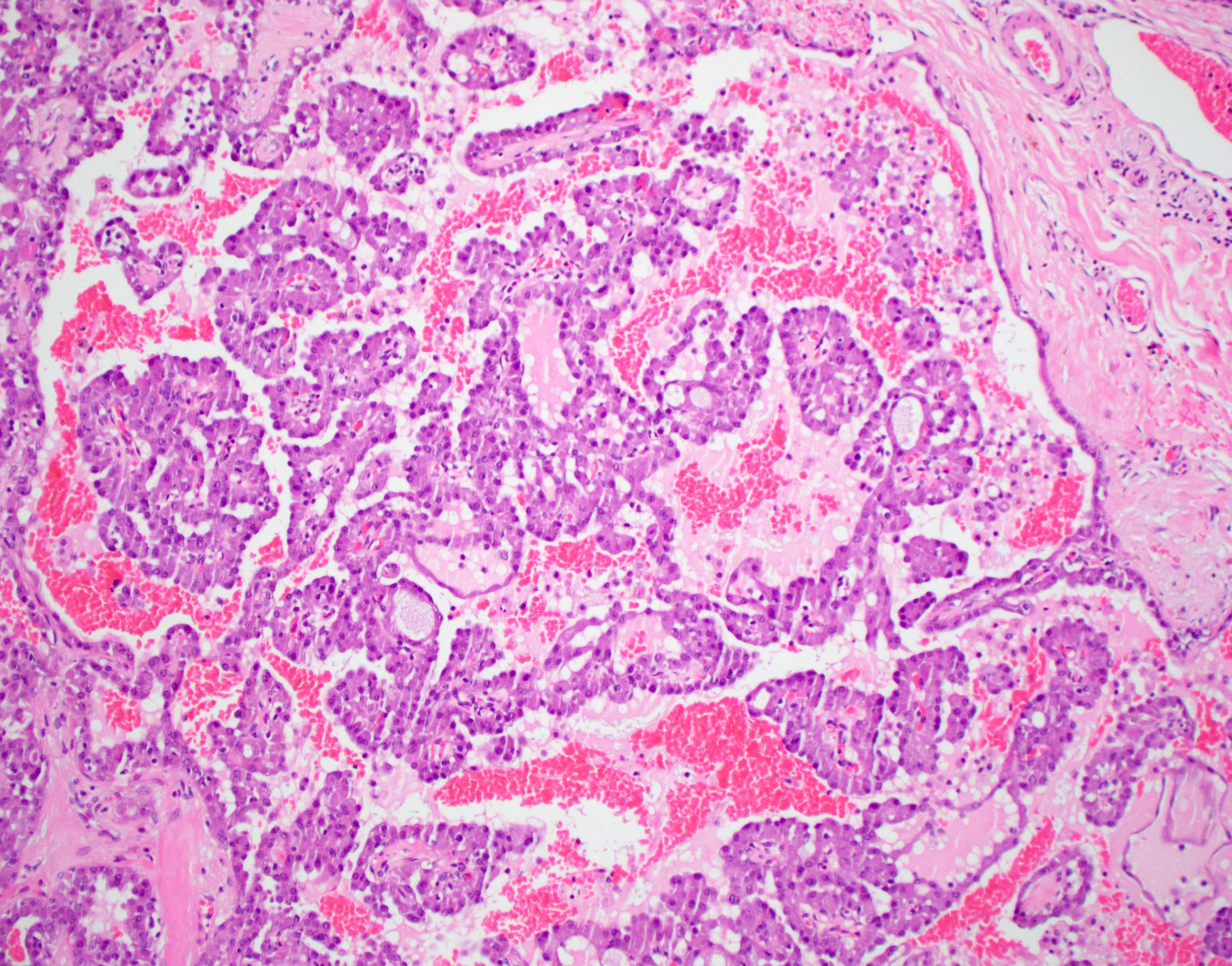
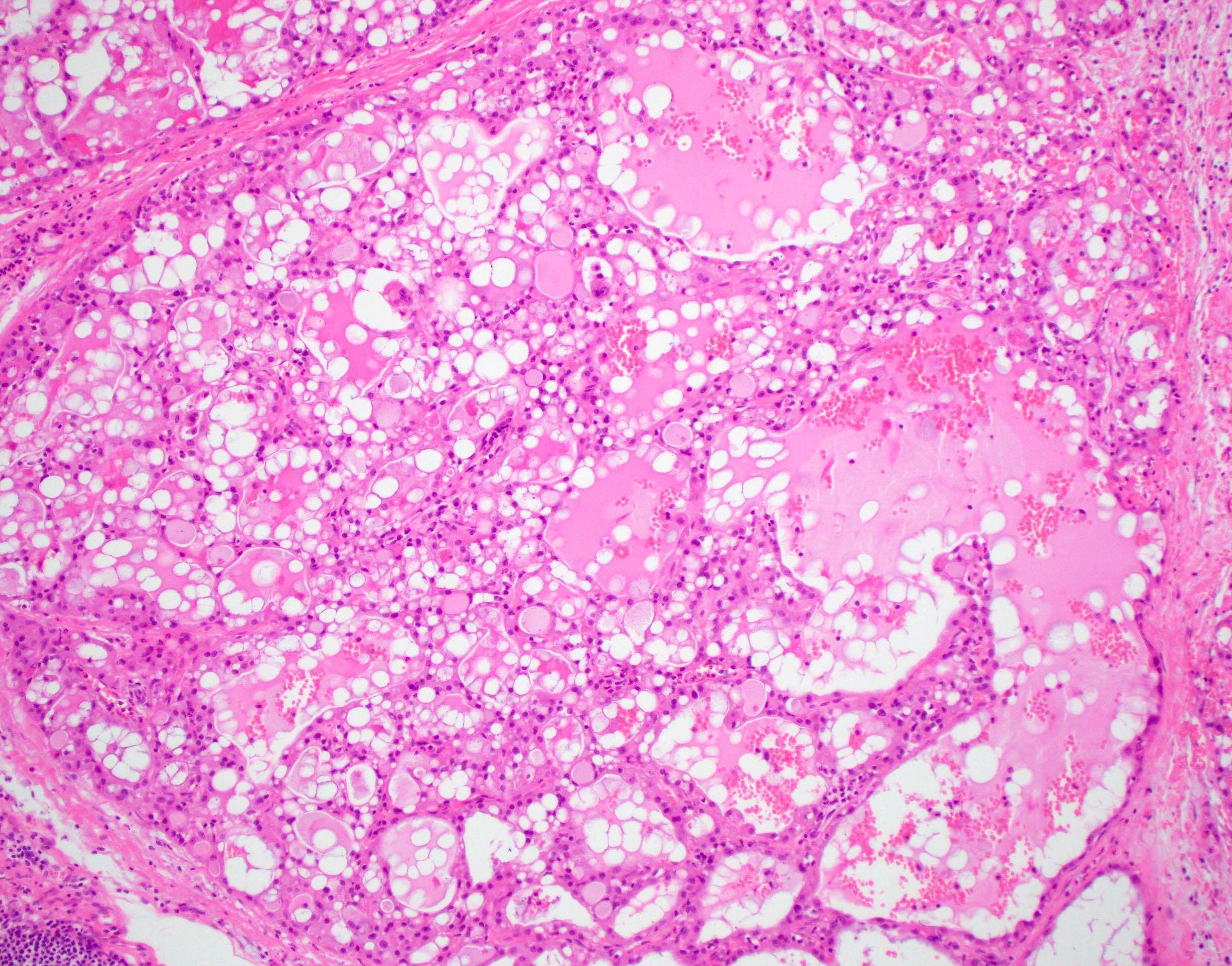
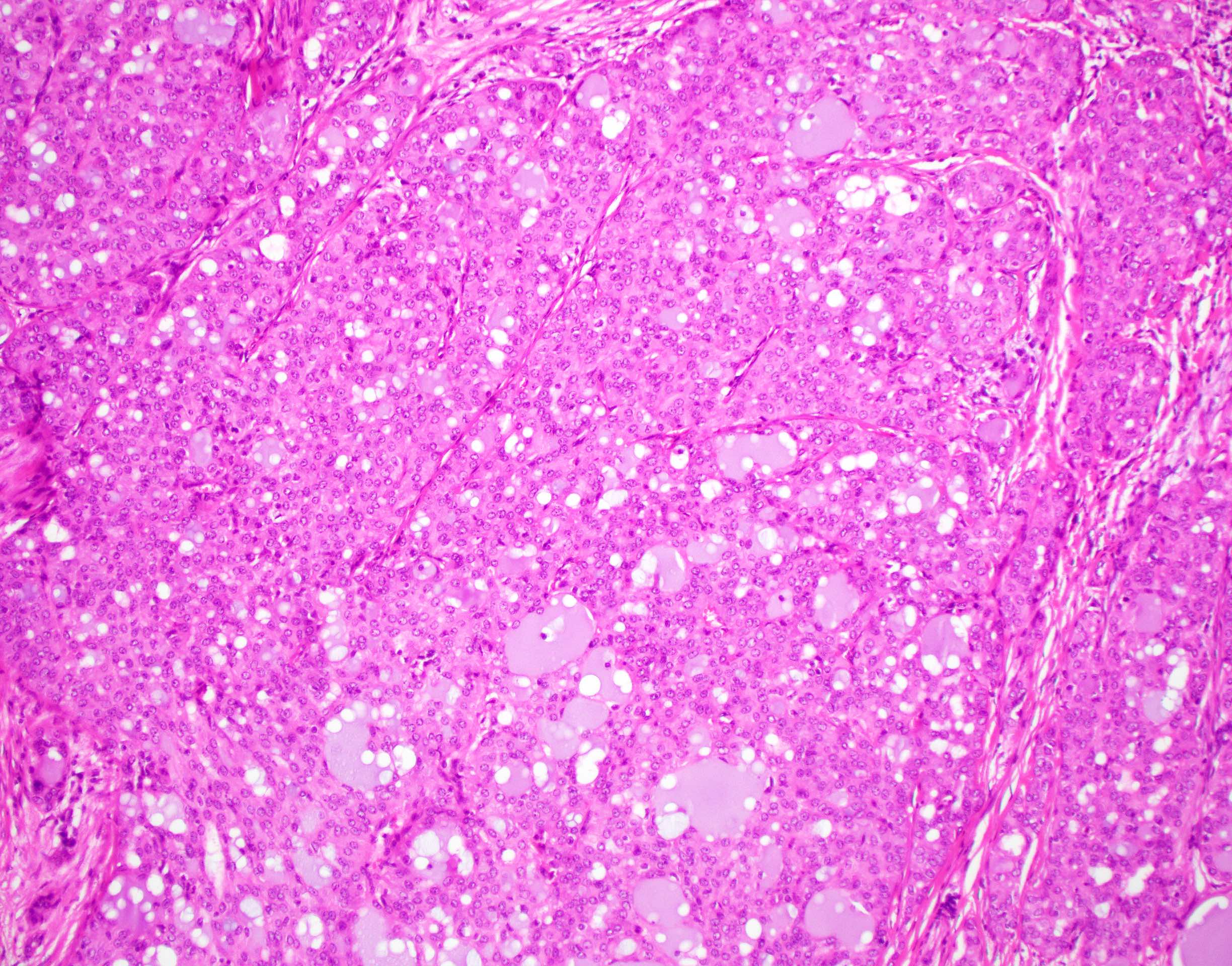
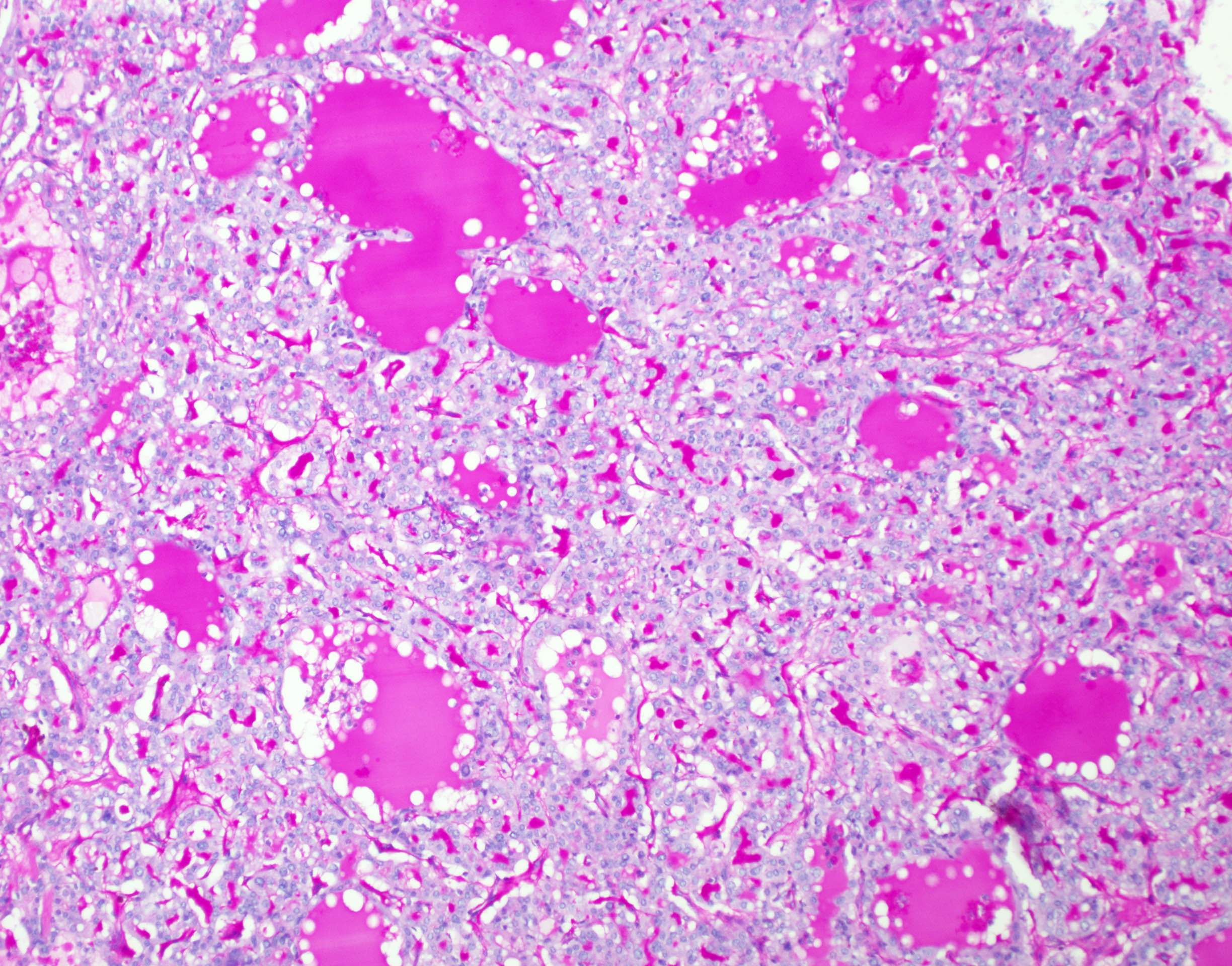
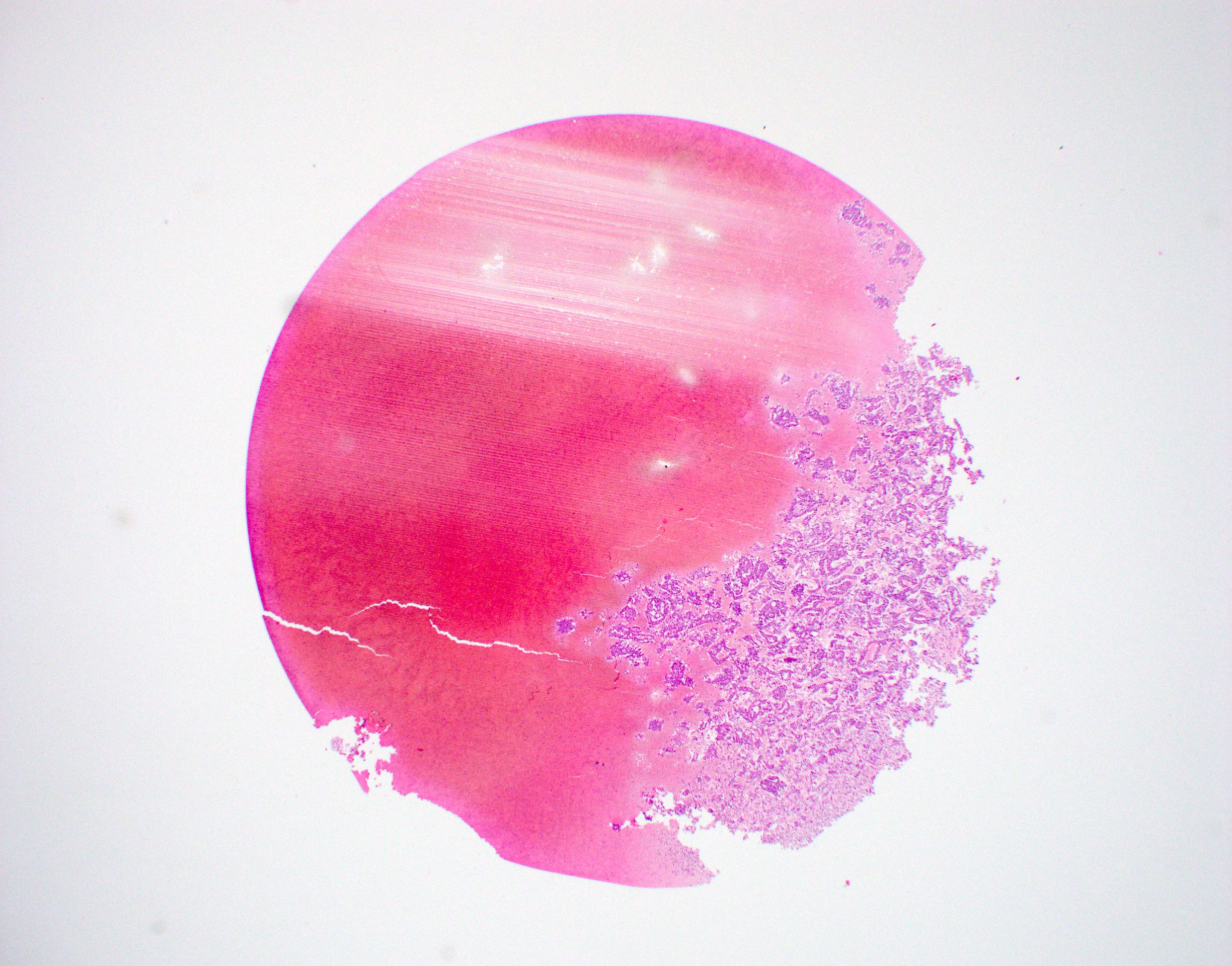
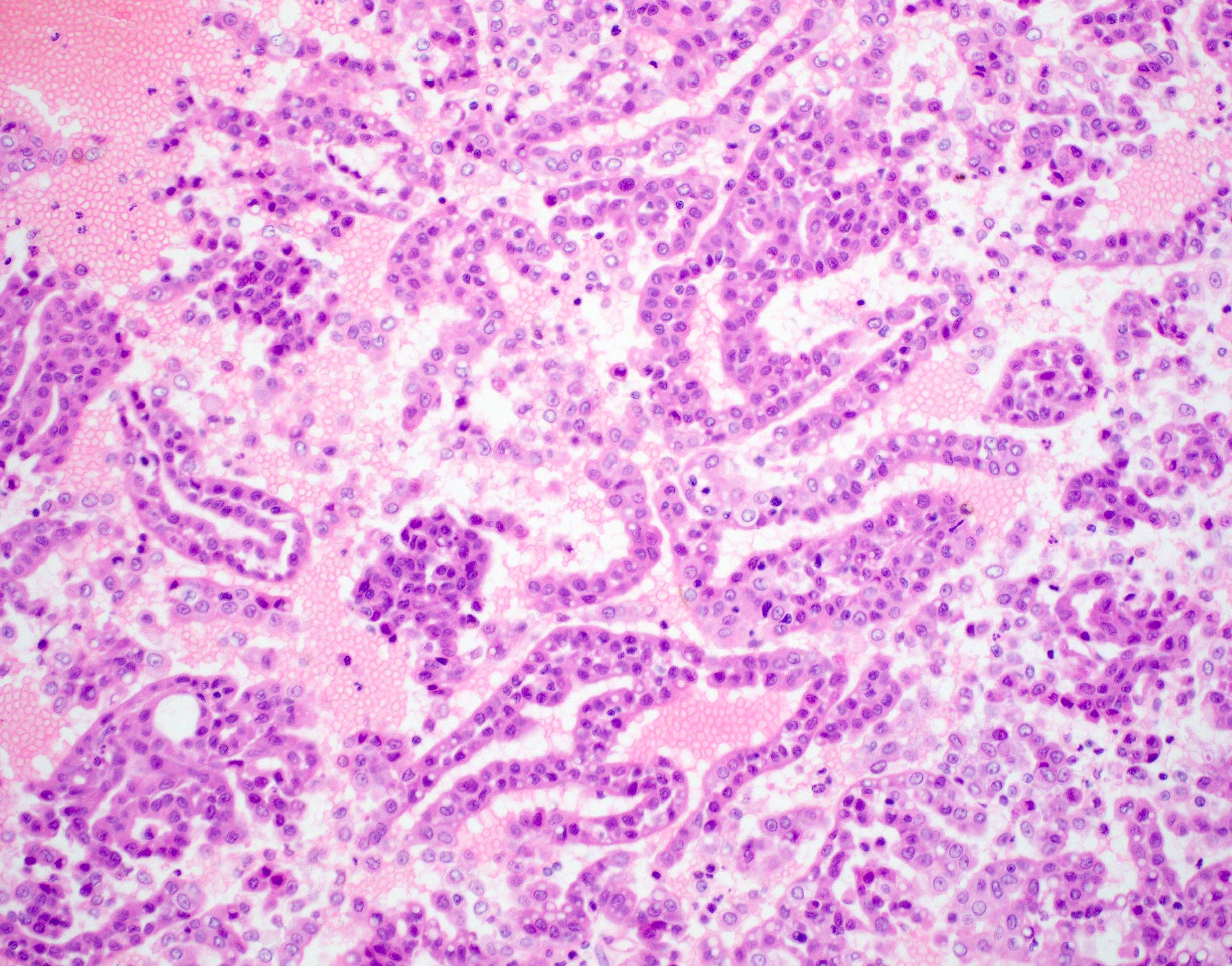
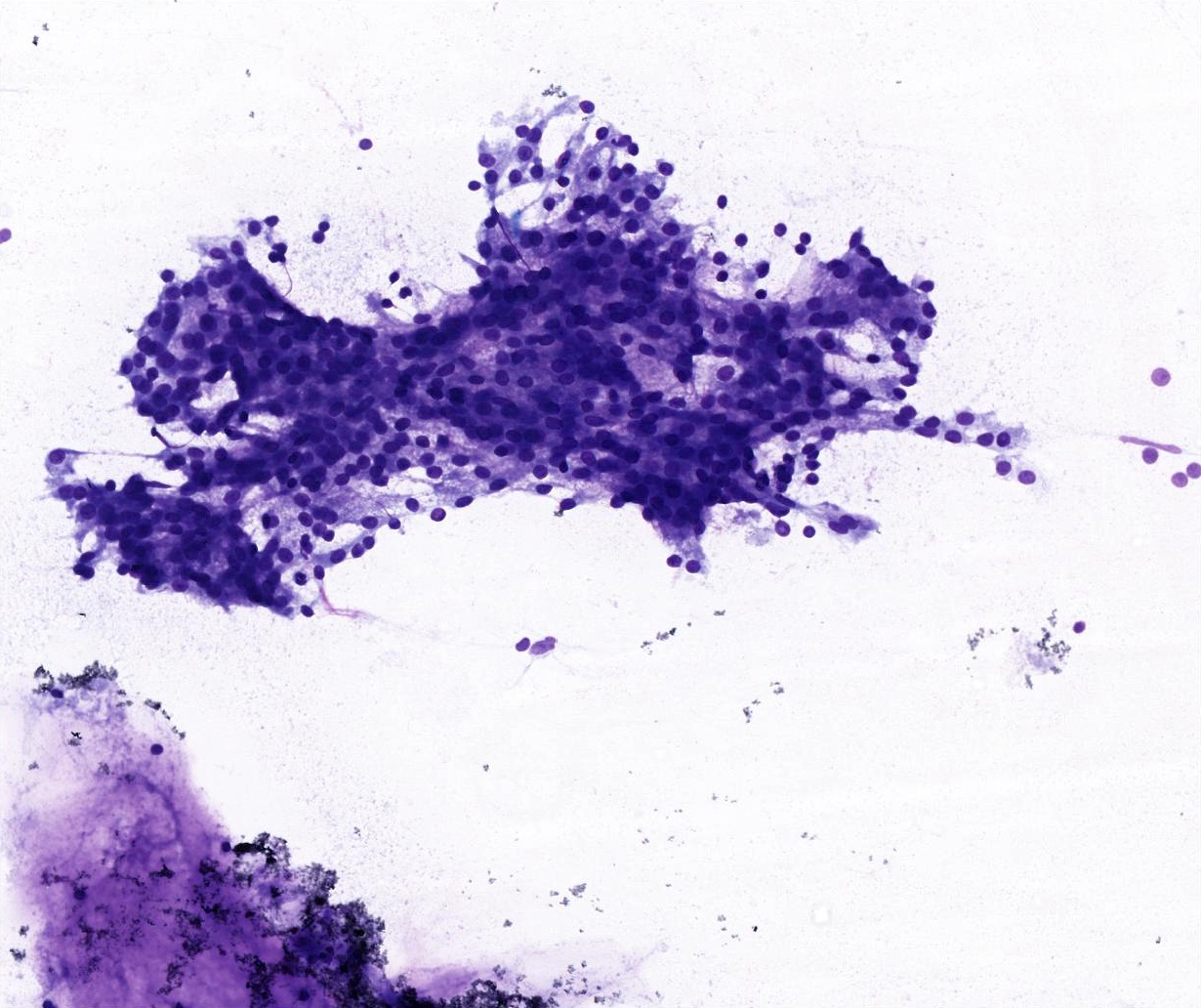
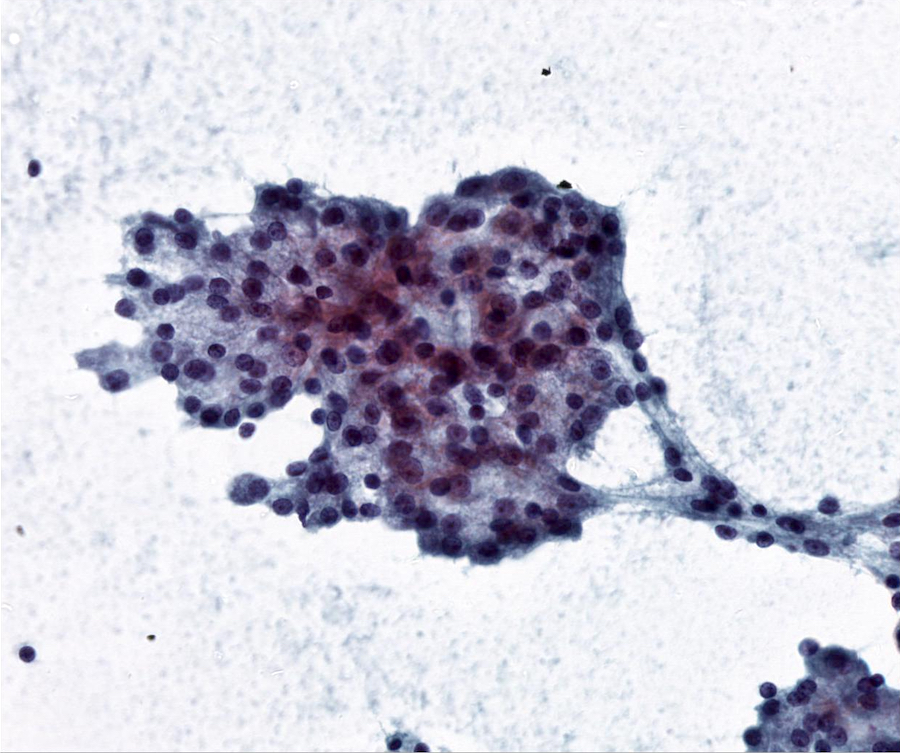
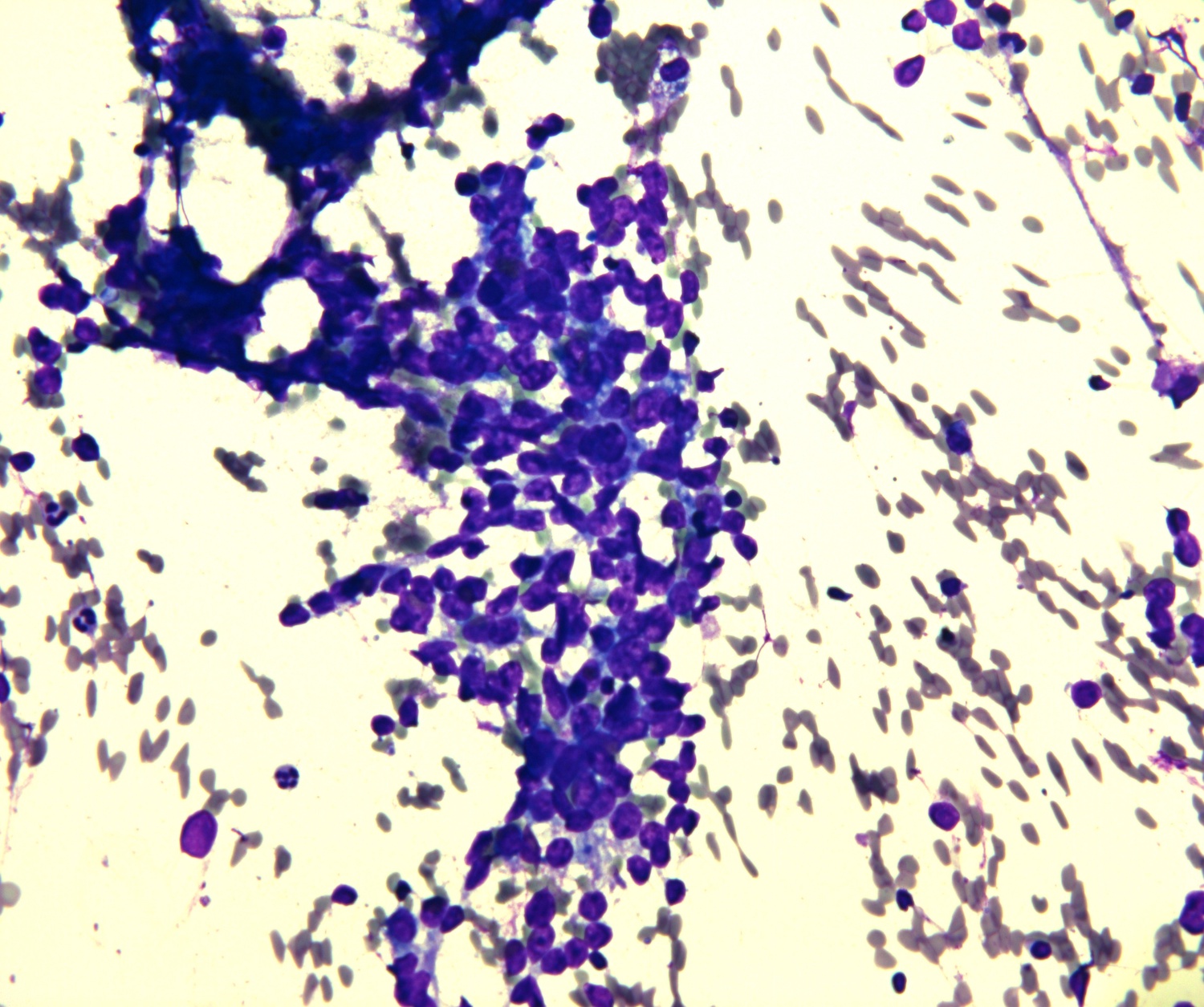
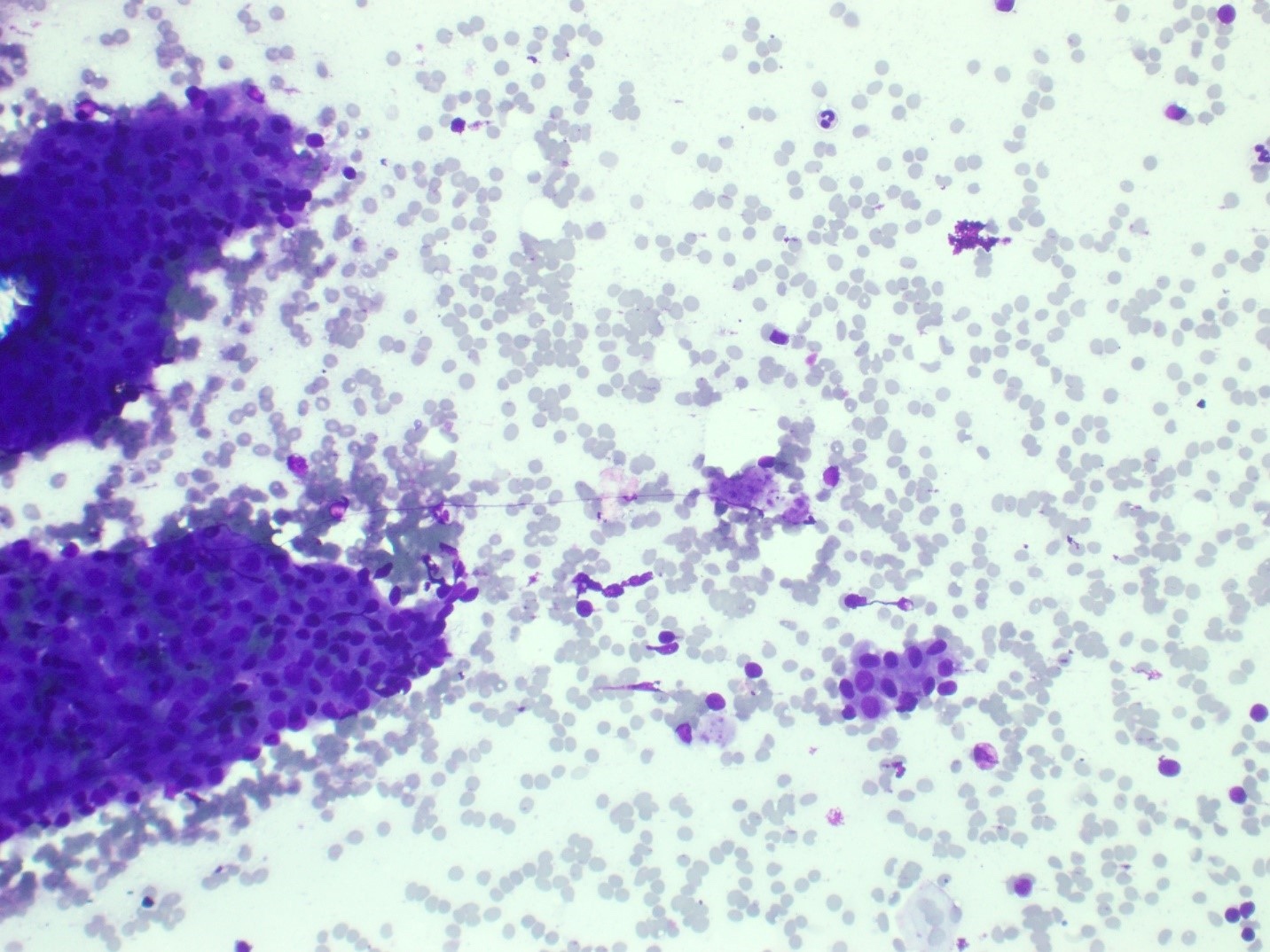
Solid, microcystic, papillary cystic or follicular growth of acinar cells, with granular to vacuolated cytoplasm and eccentric round nuclei with conspicuous nucleoli
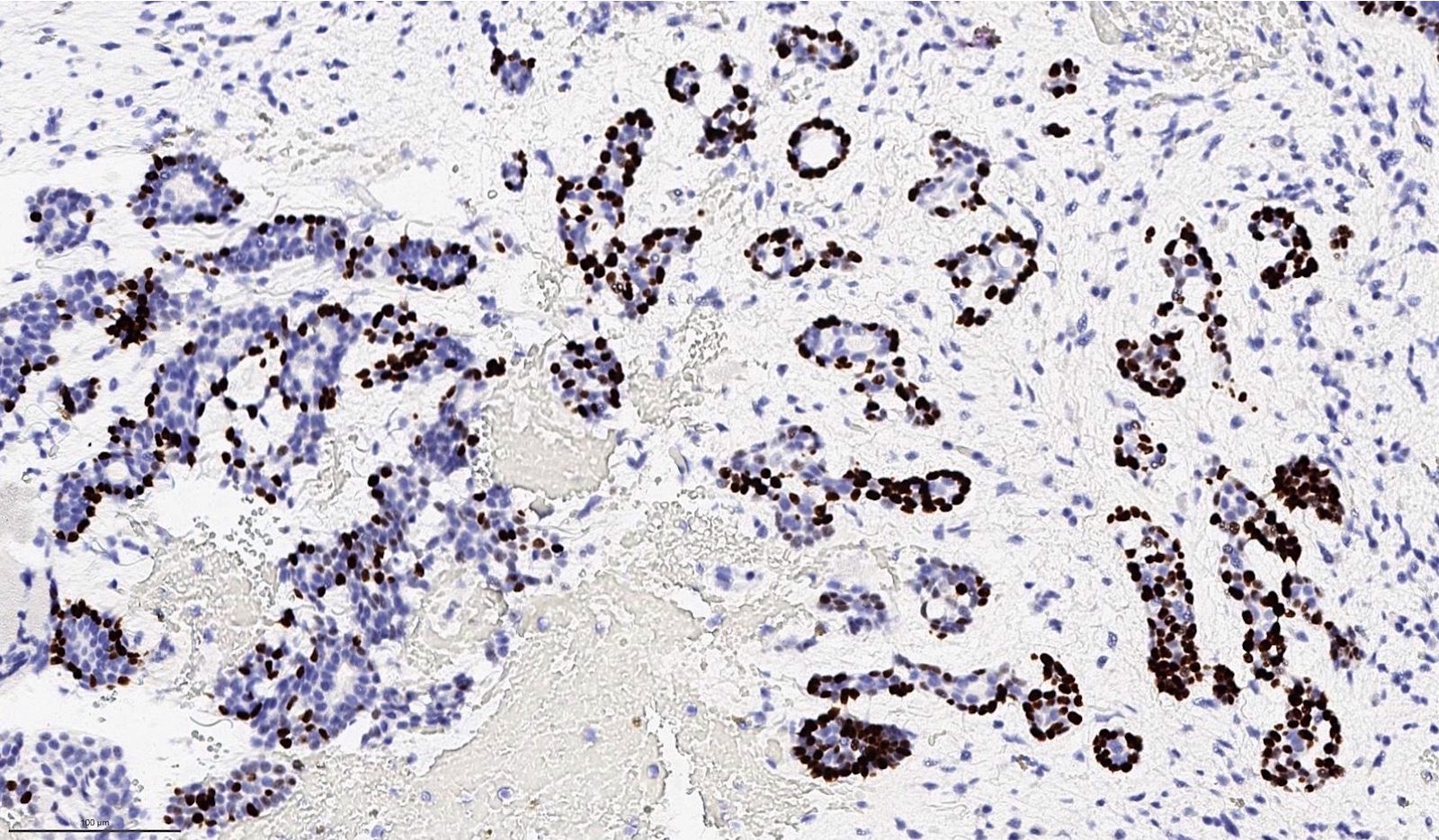
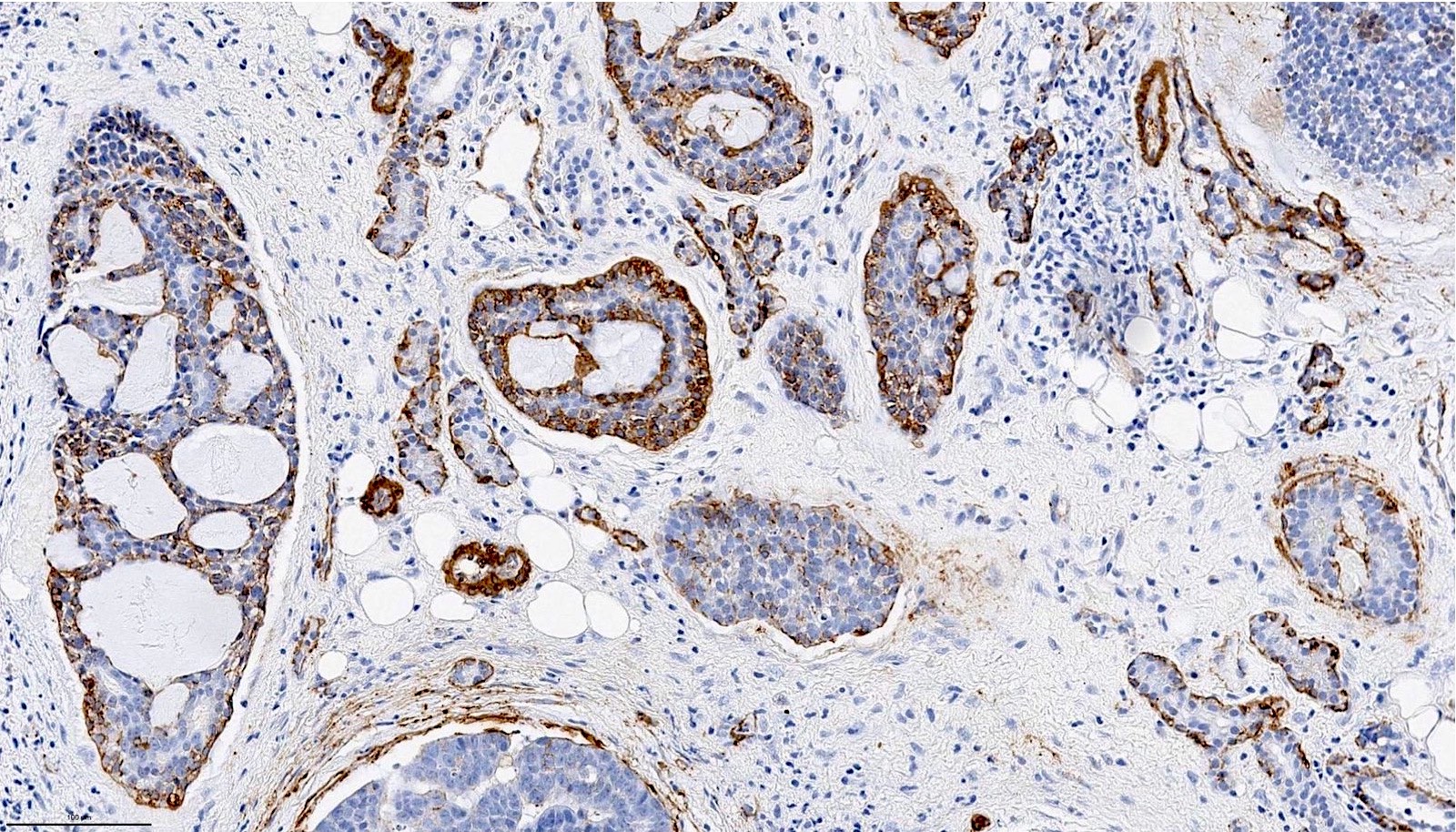
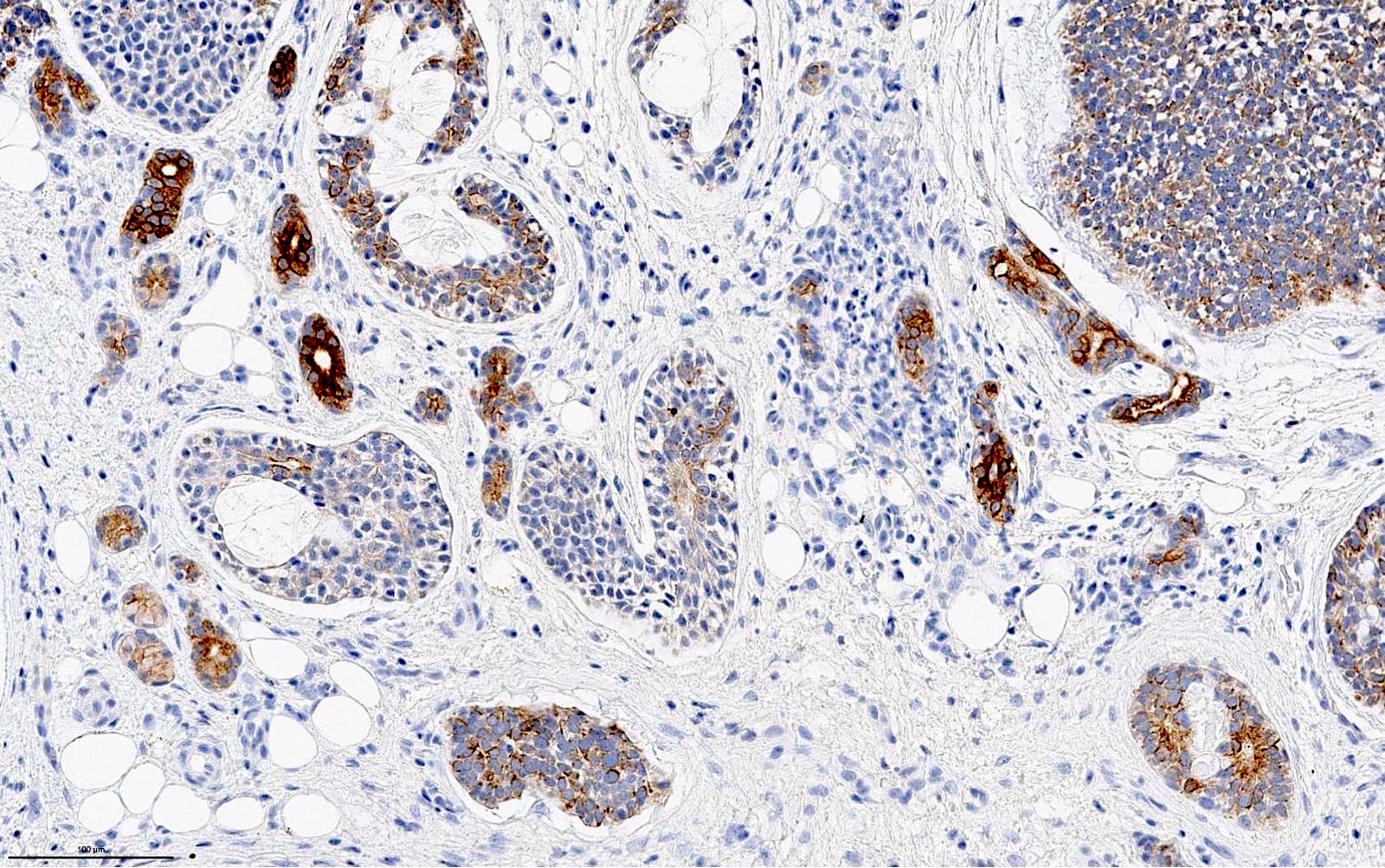
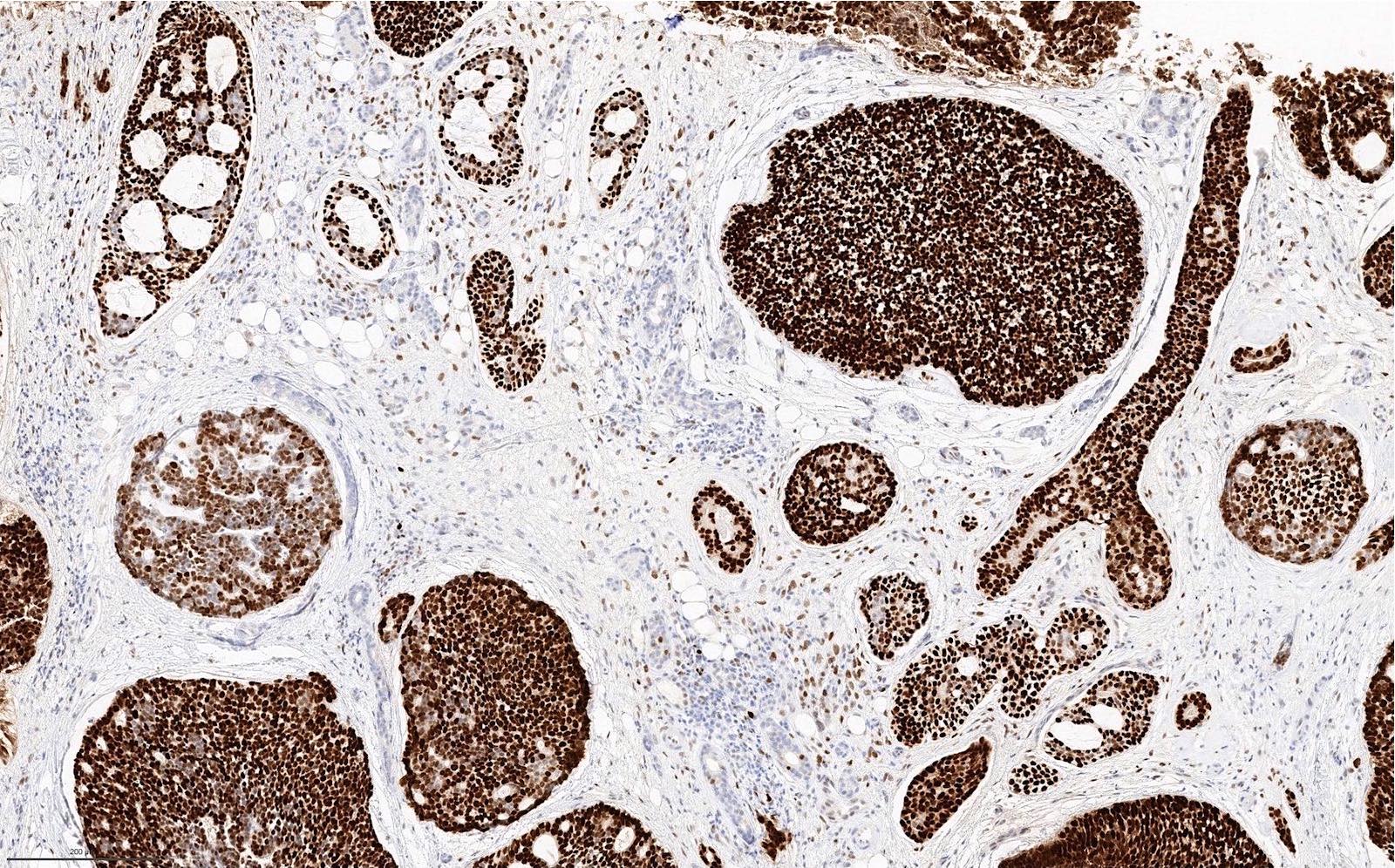
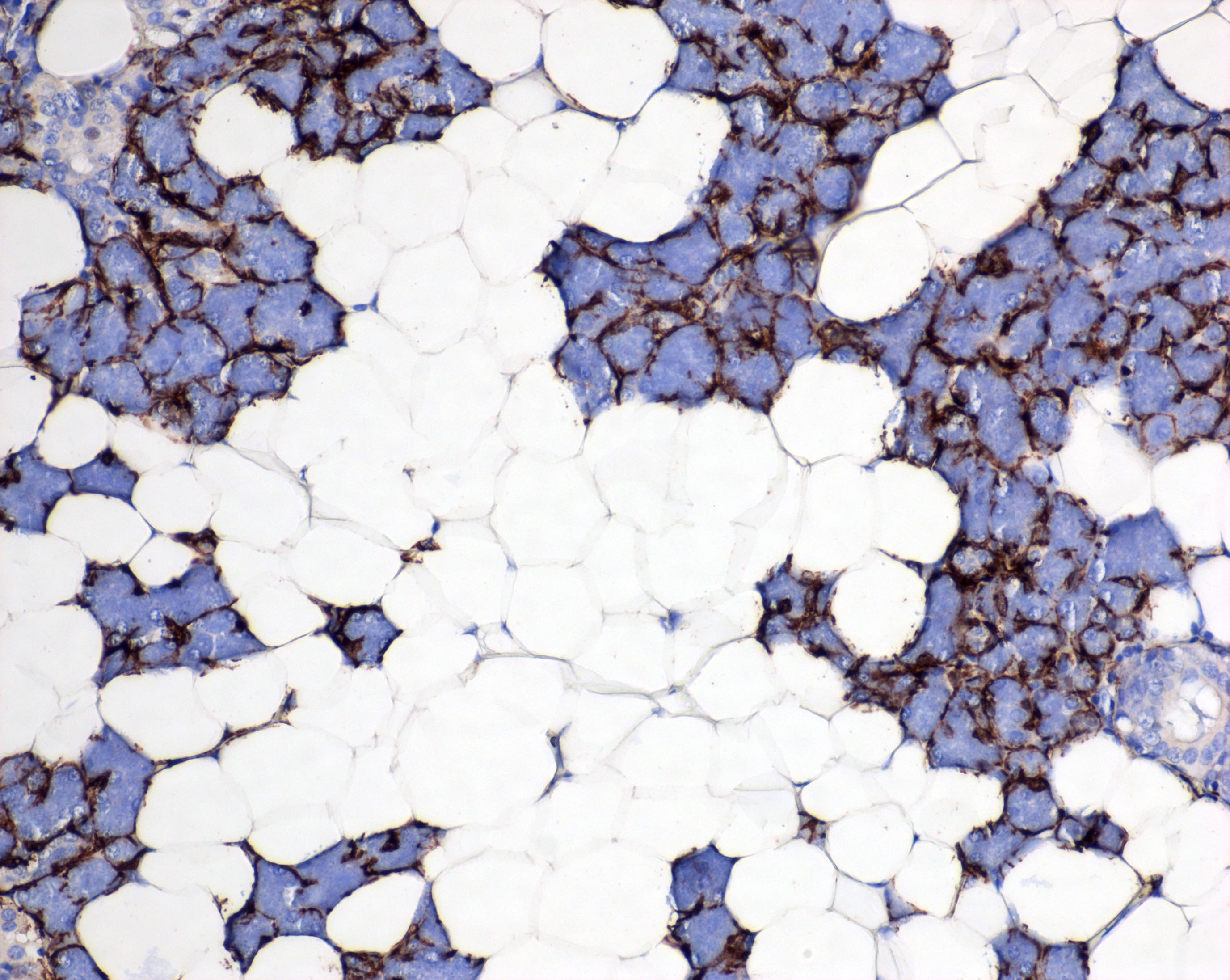
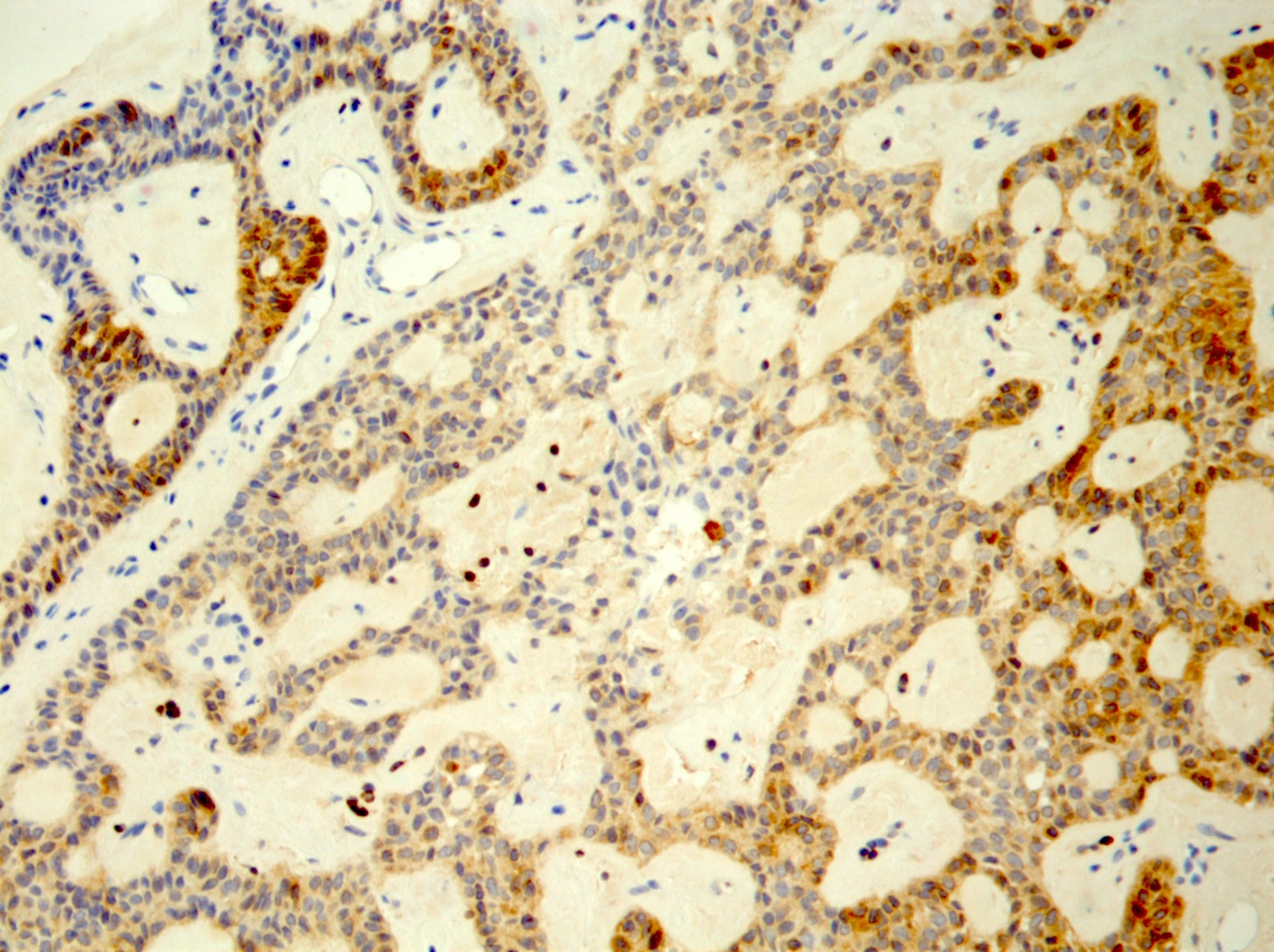
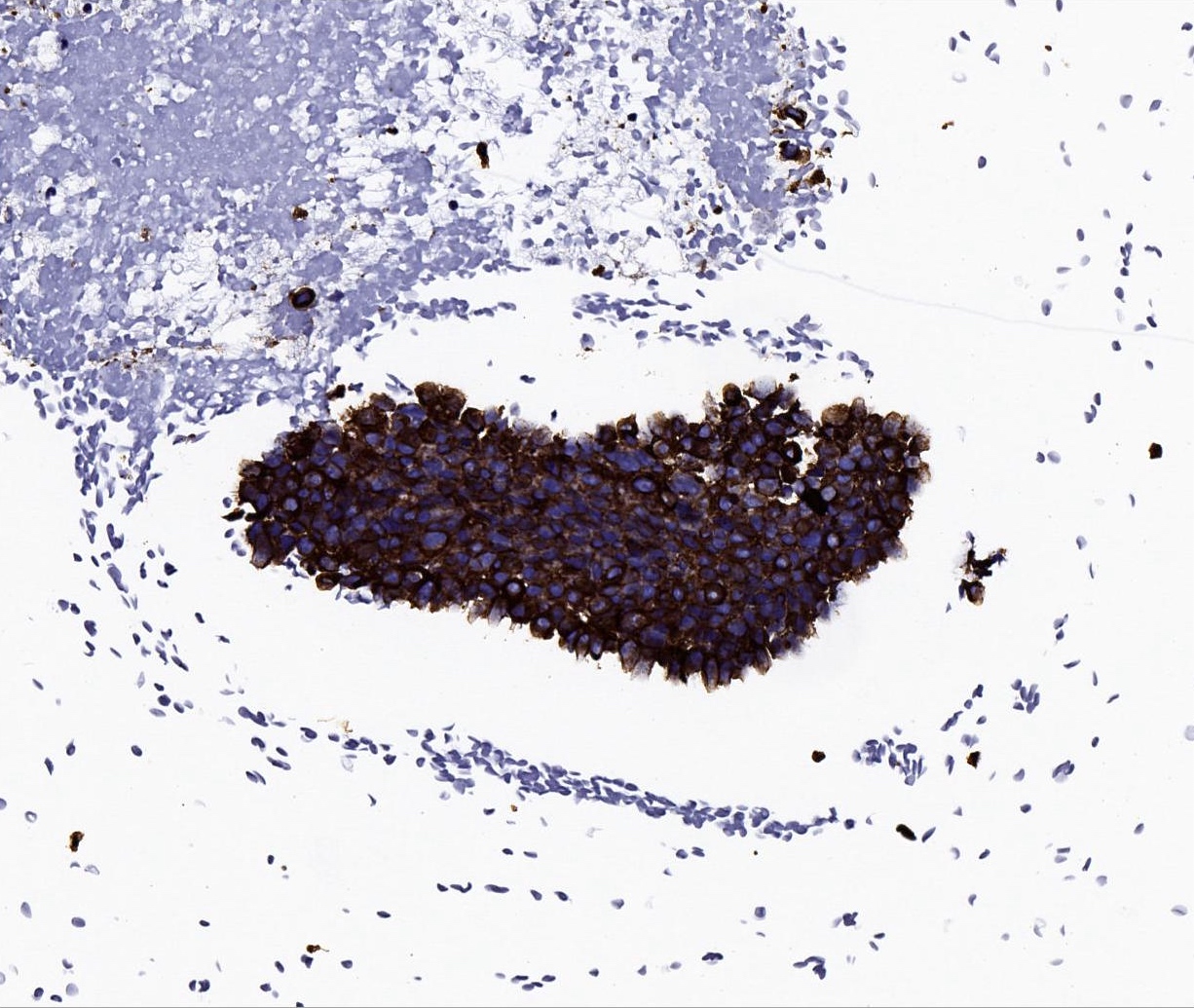
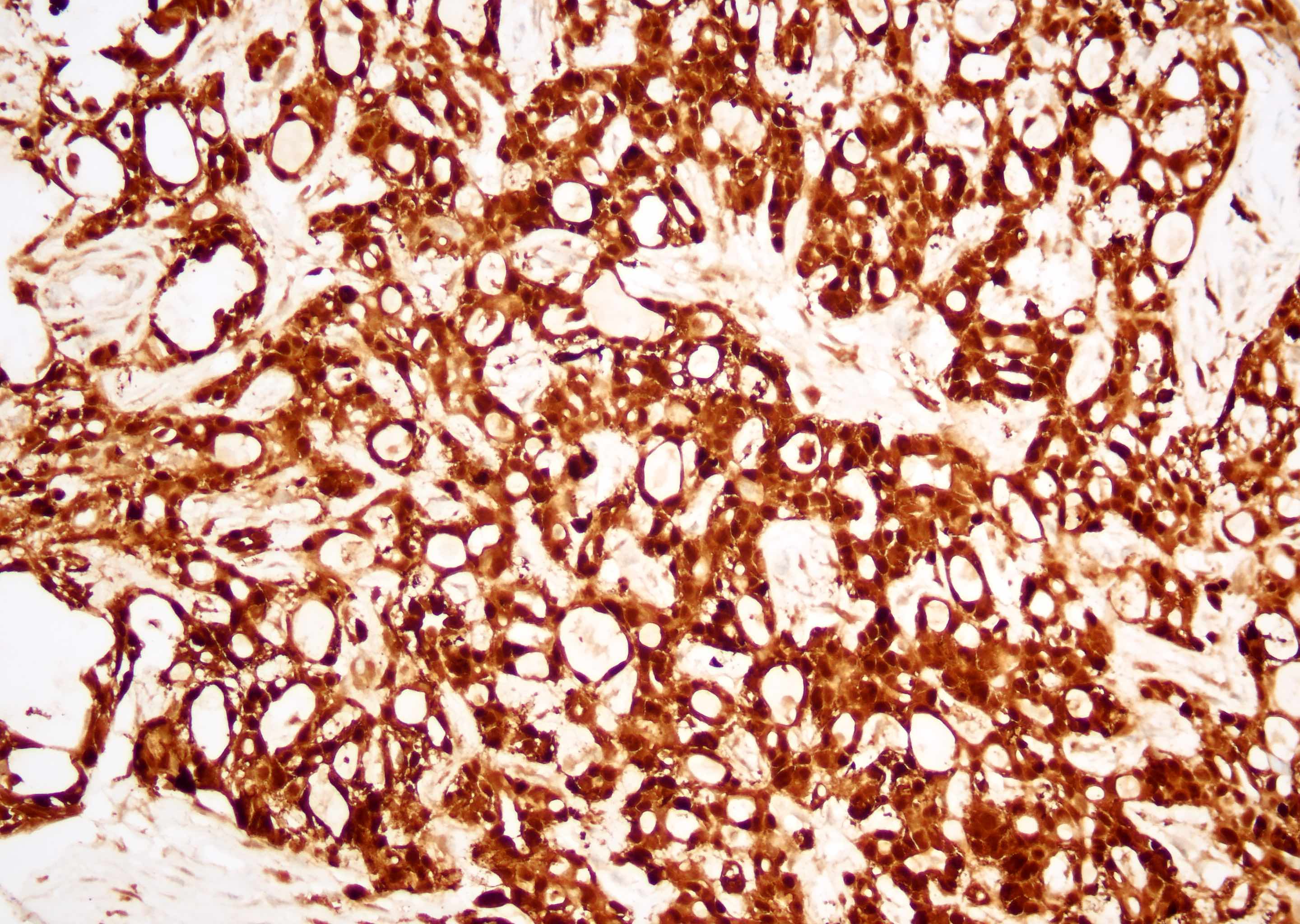
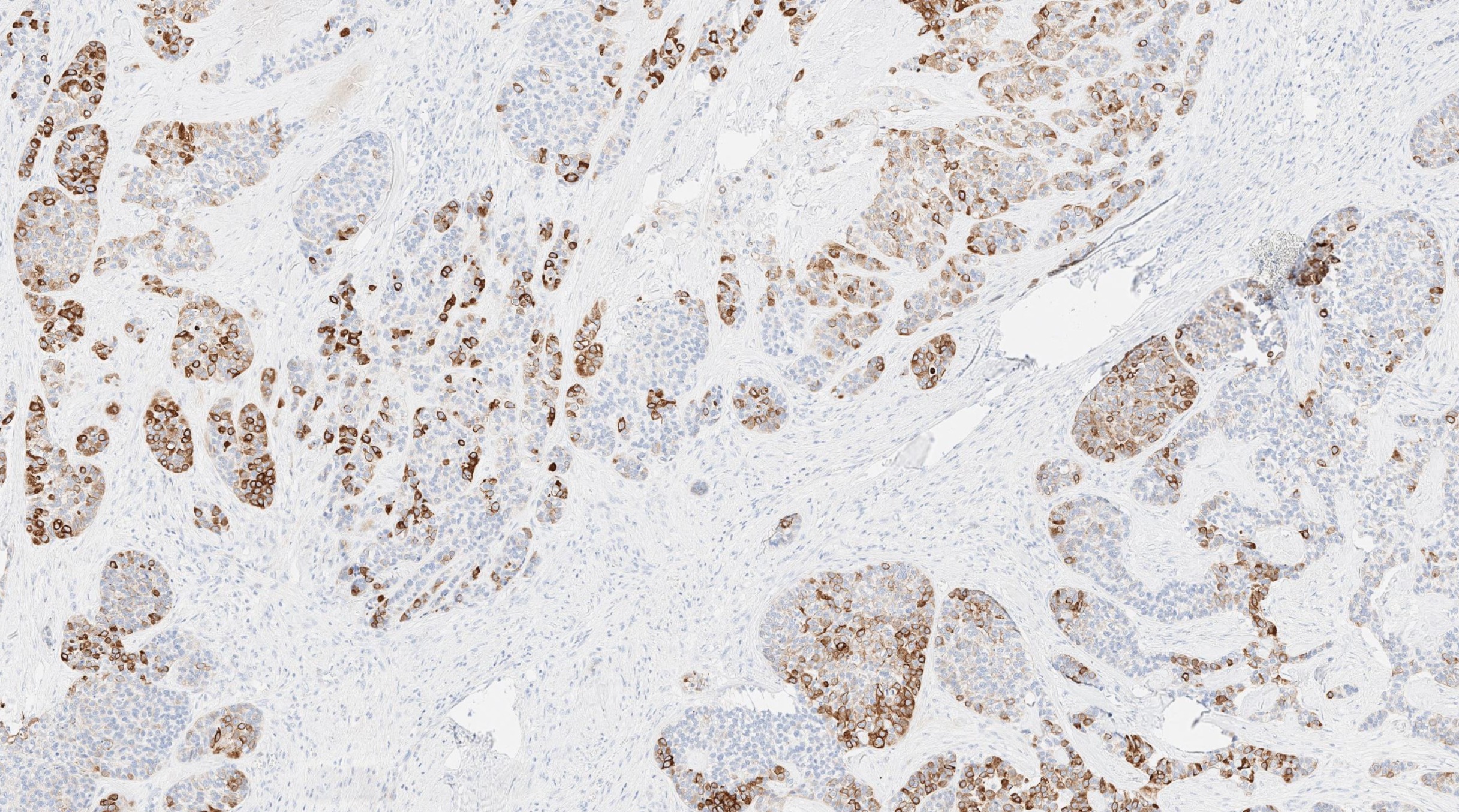
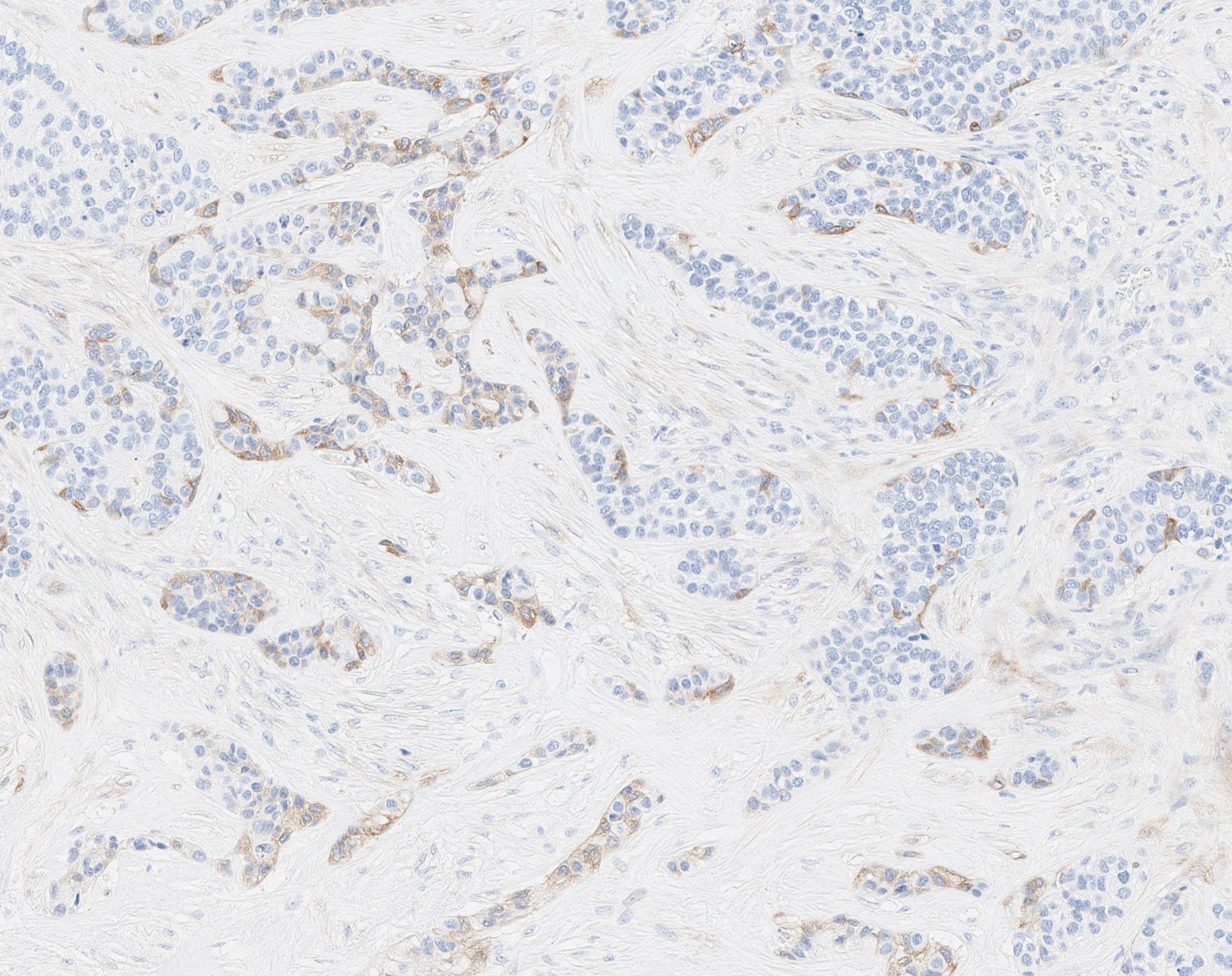
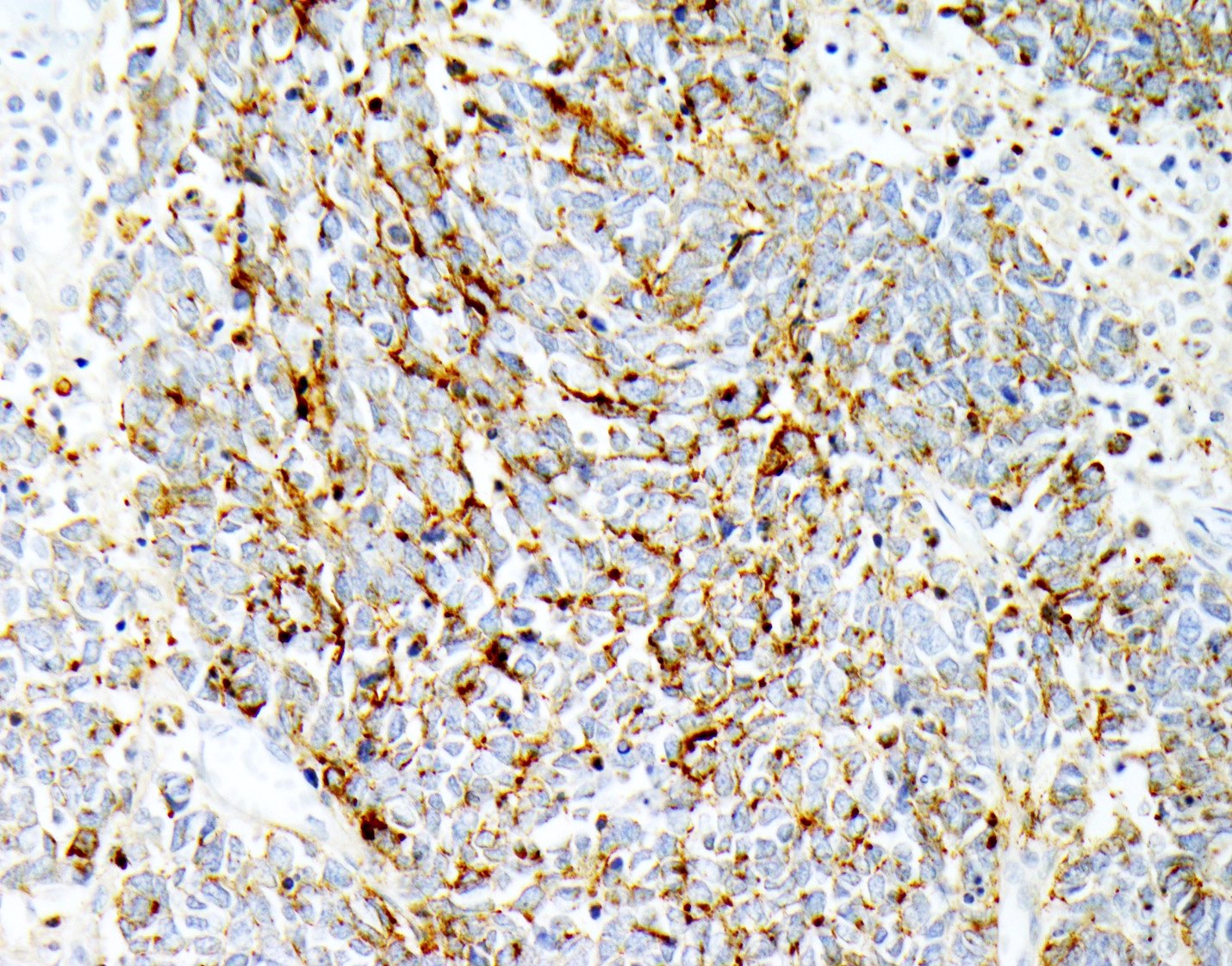
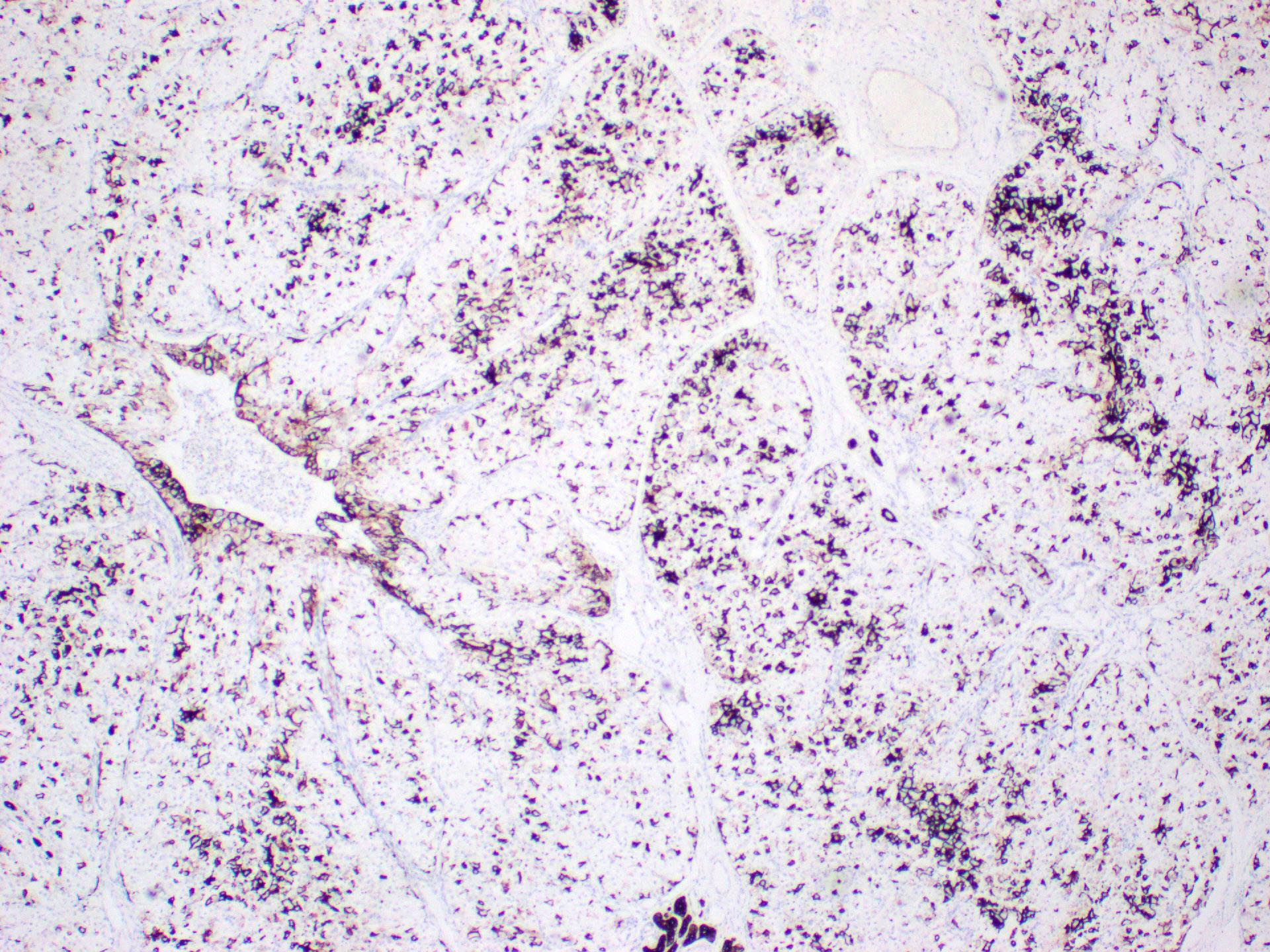
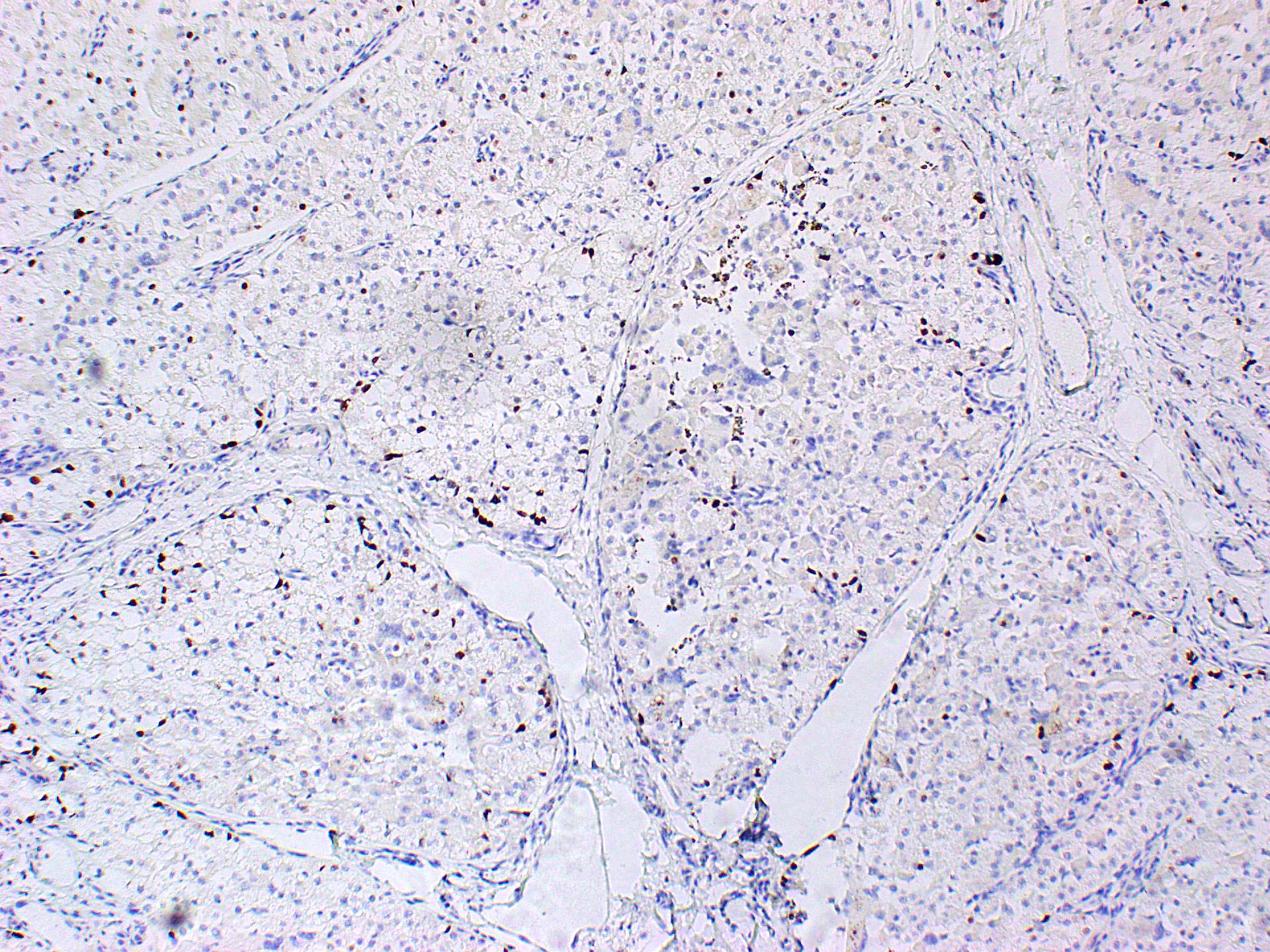
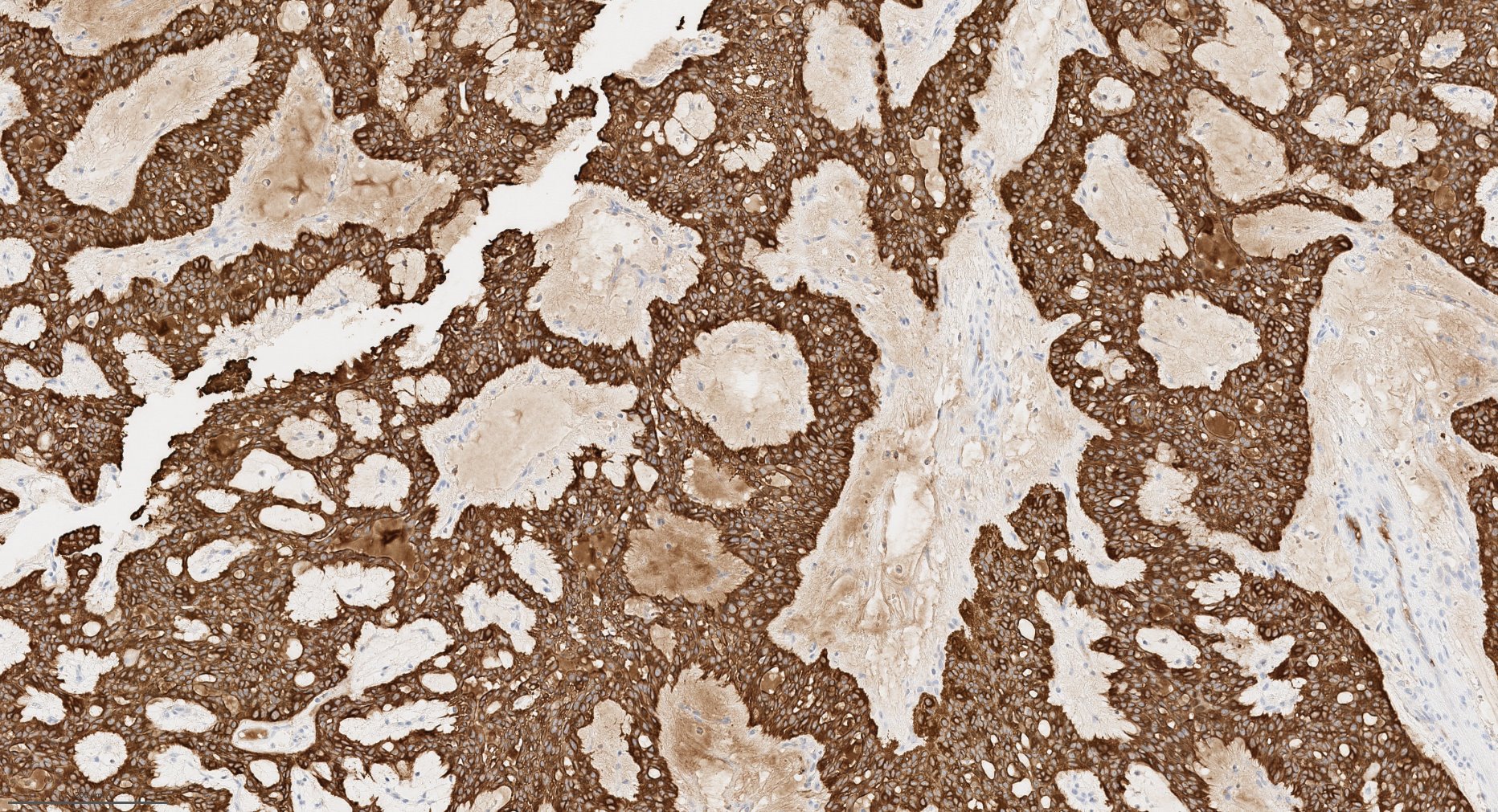
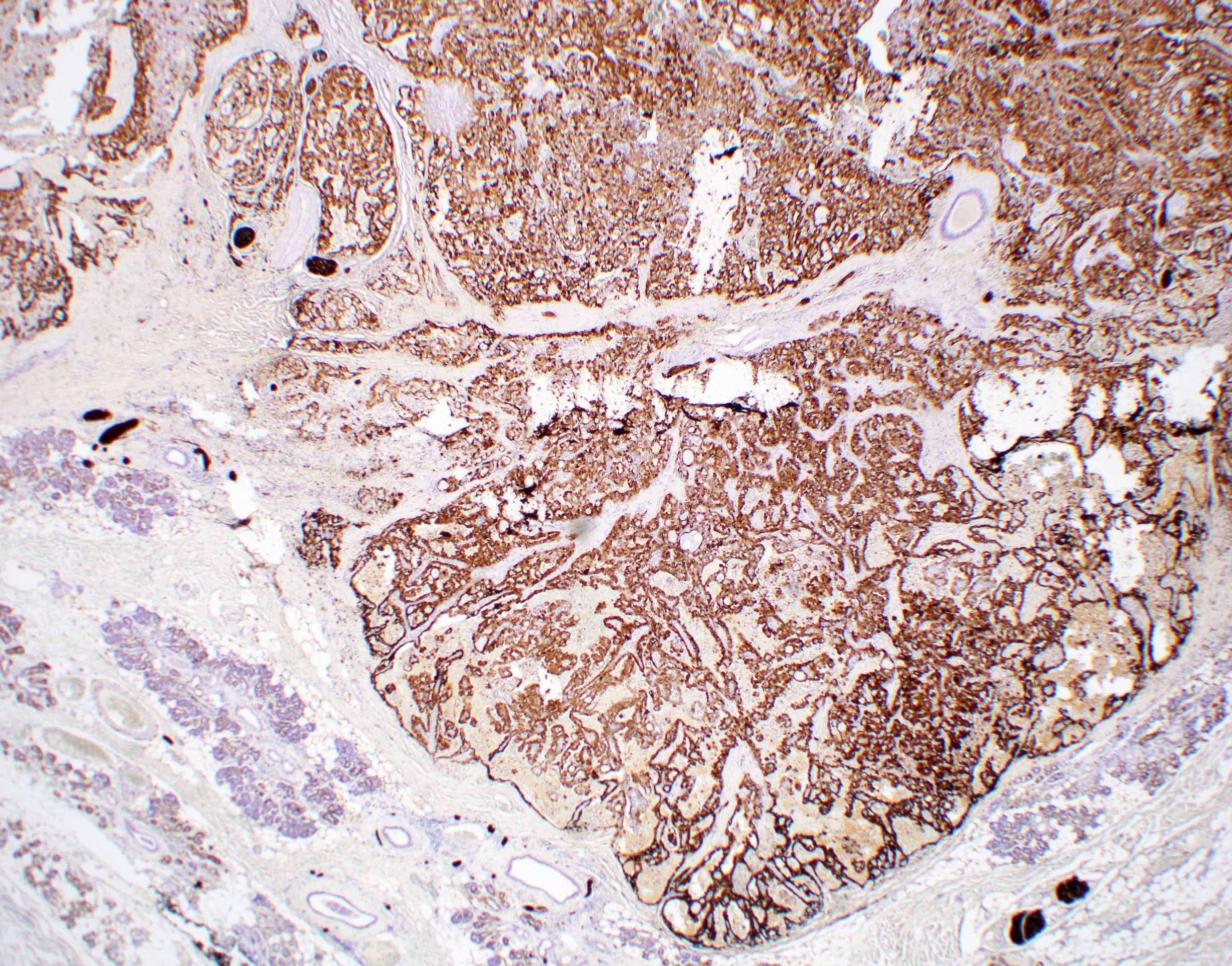
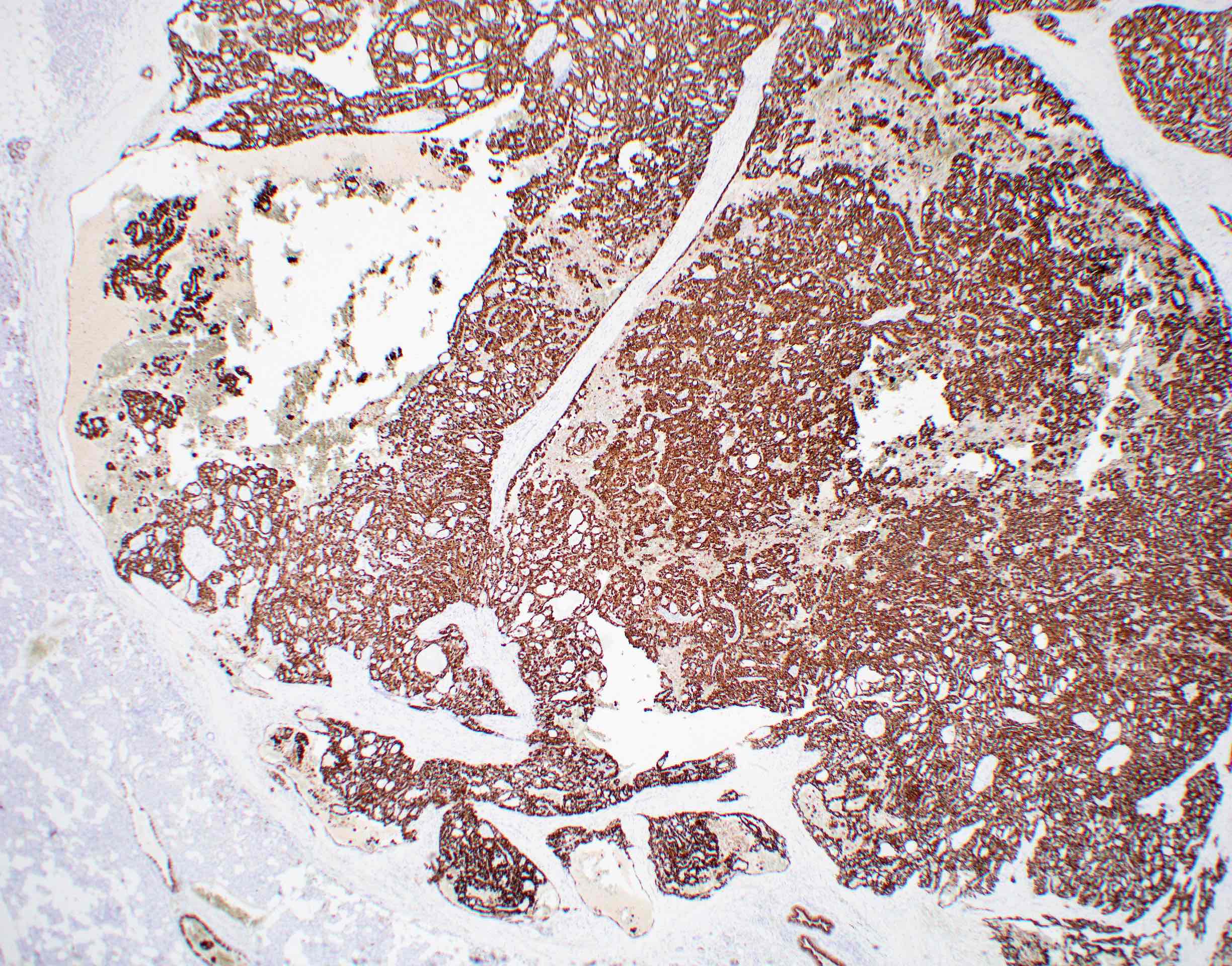
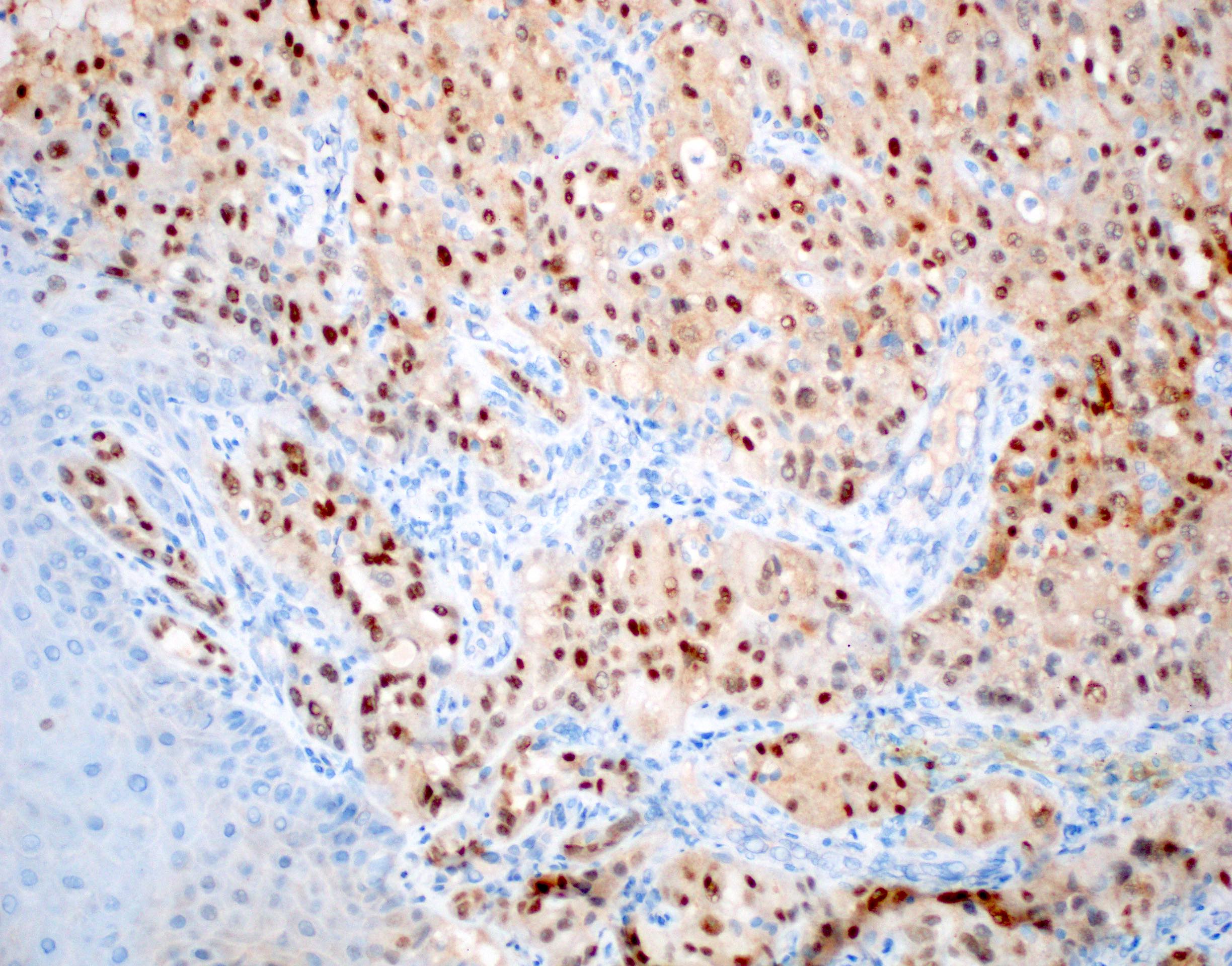
Neoplastic cells positive for pankeratins, DOG1, SOX10 and PASD
Favorable prognosis, with low rates of local recurrence, distant metastasis and high grade transformation
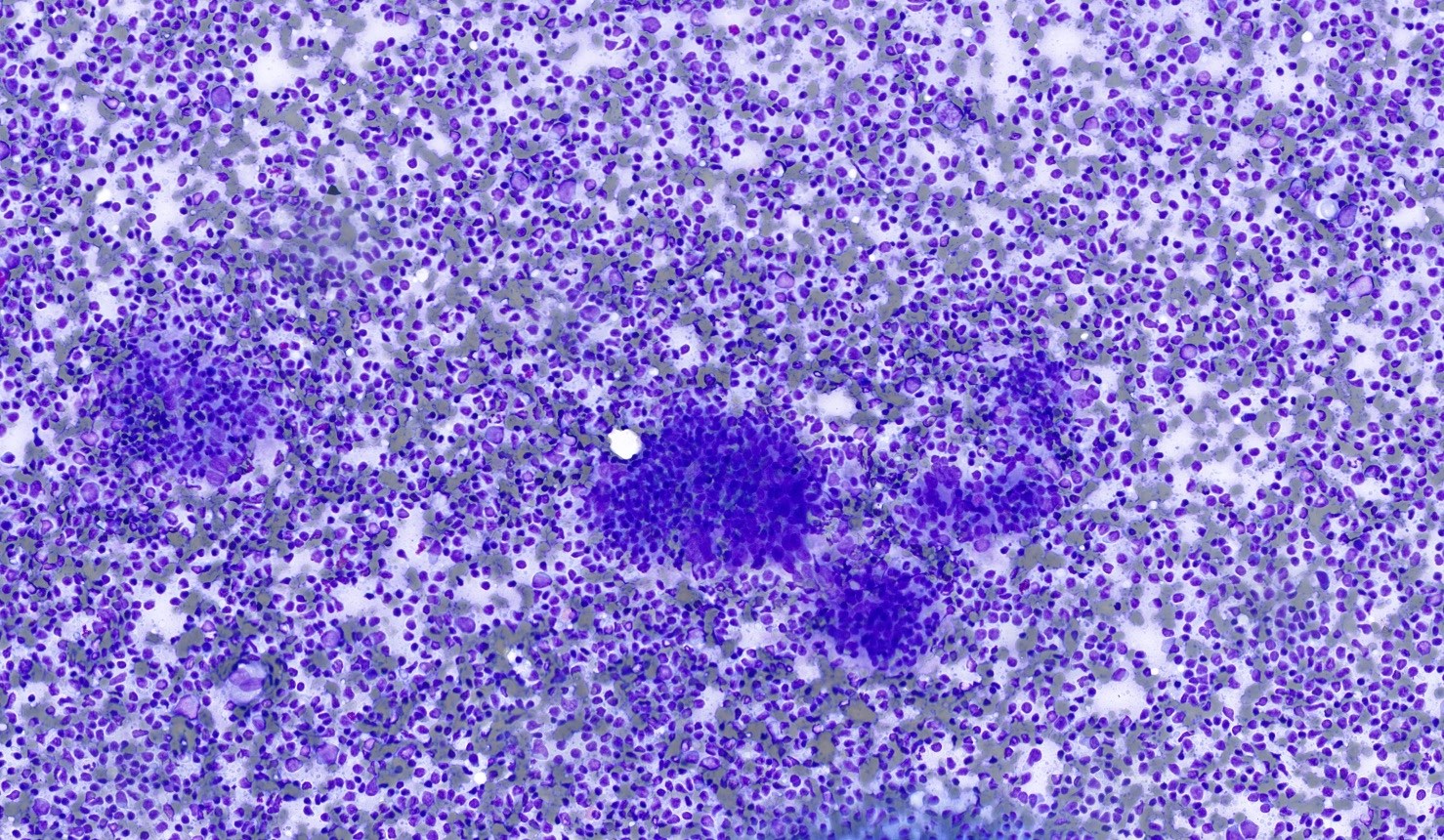
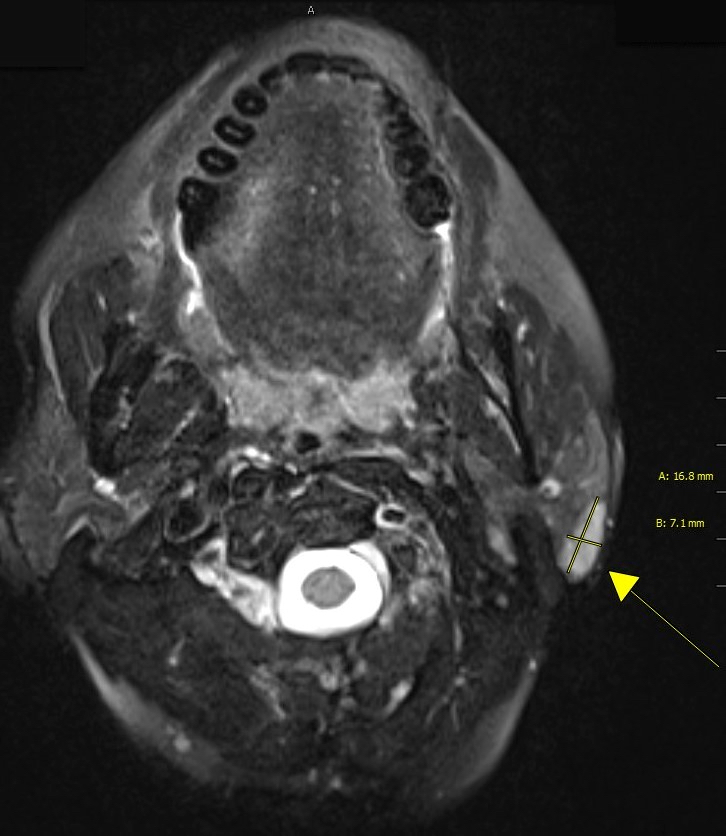
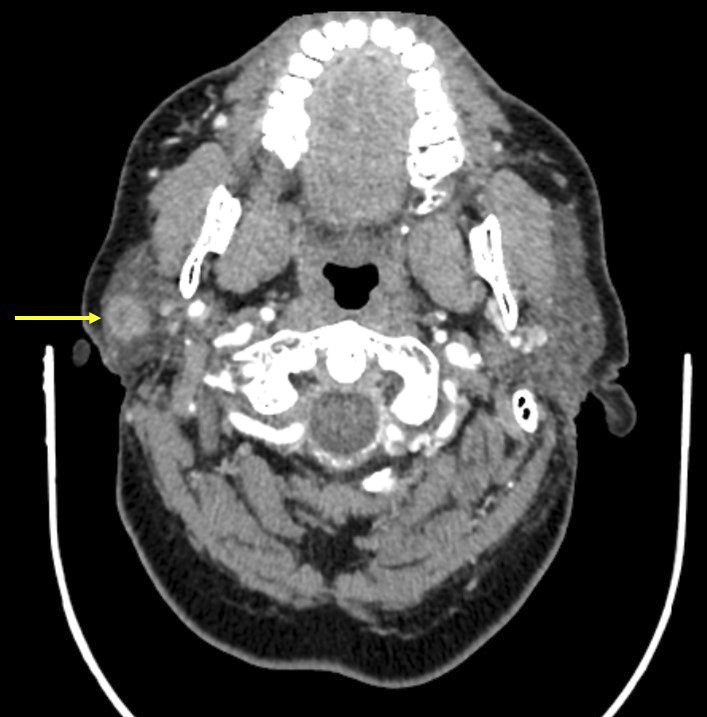
48 year old woman with a 6 month history of a right parotid swelling that rapidly and progressively increased in size (Case Rep Otolaryngol 2017;2017:7296467)
Radiotherapy may be indicated for tumors that metastasize or cannot be completely excised
Systemic therapy may be indicated for high grade tumors, positive margins, advanced stage disease or metastatic tumors
Clinical images
Images hosted on other servers:
1.2 cm upper lip nodule
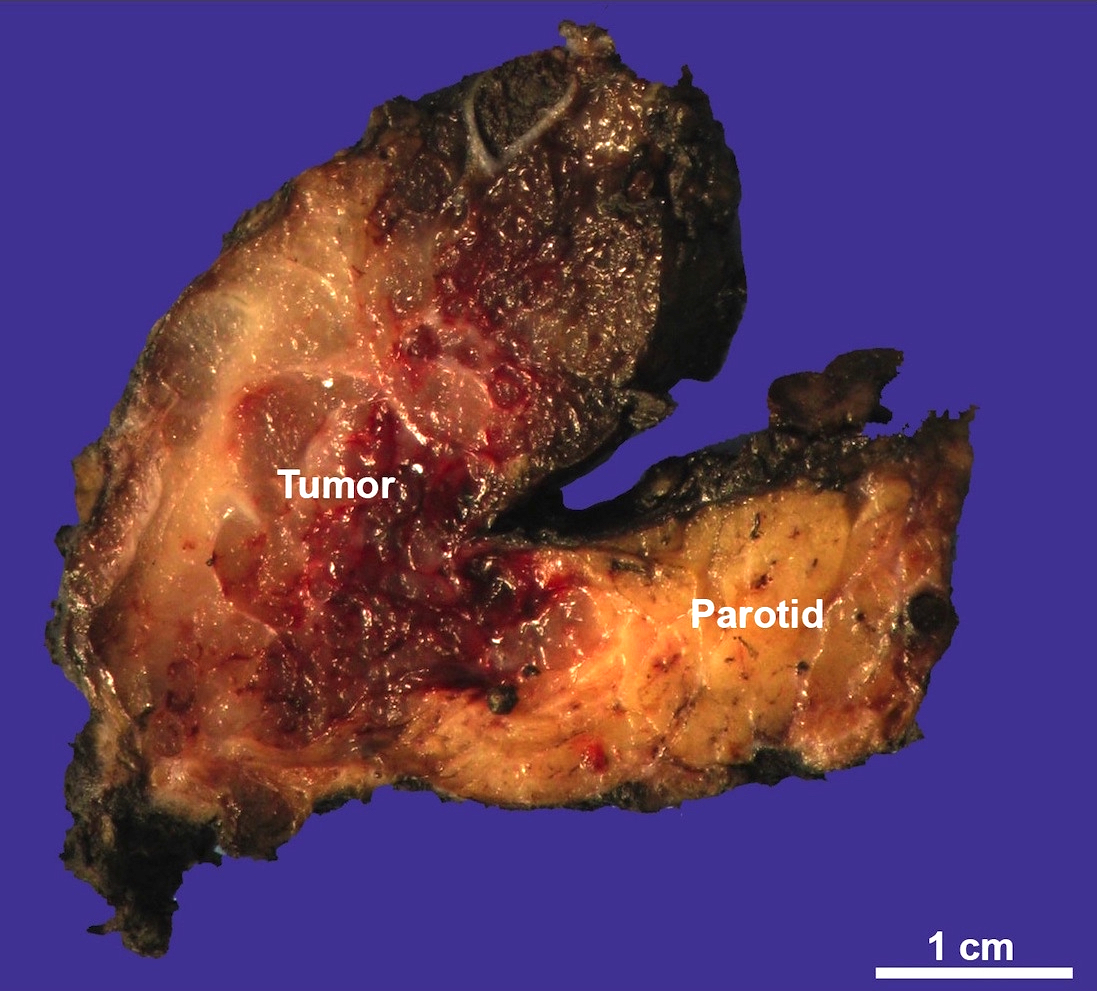
Gross description
Tumor dimensions range from Cancer 1983;52:542)
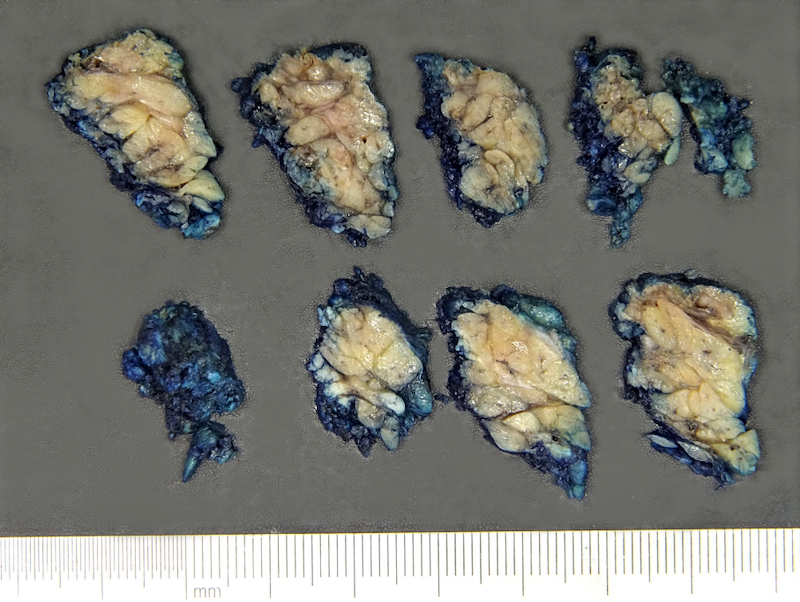
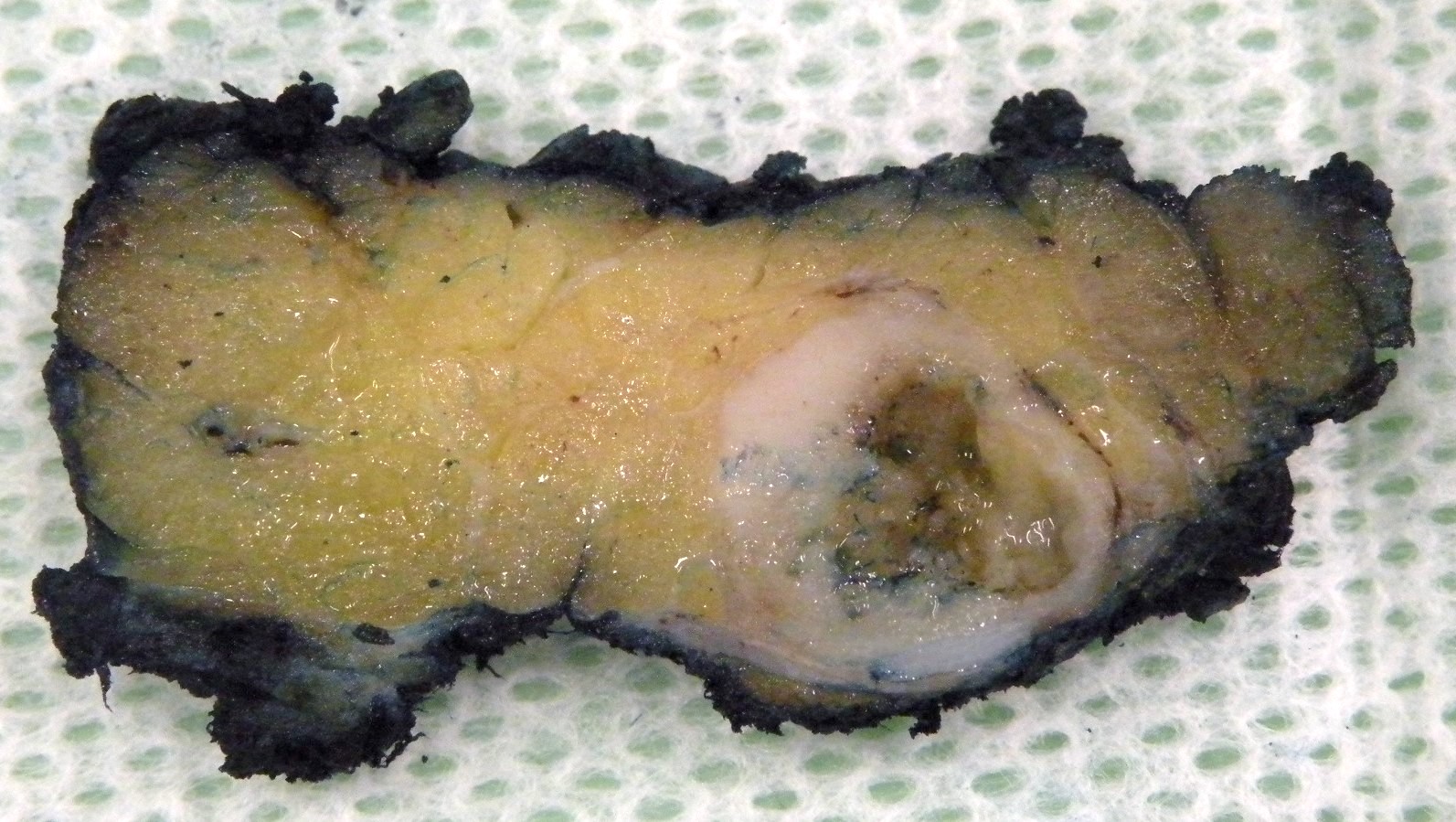
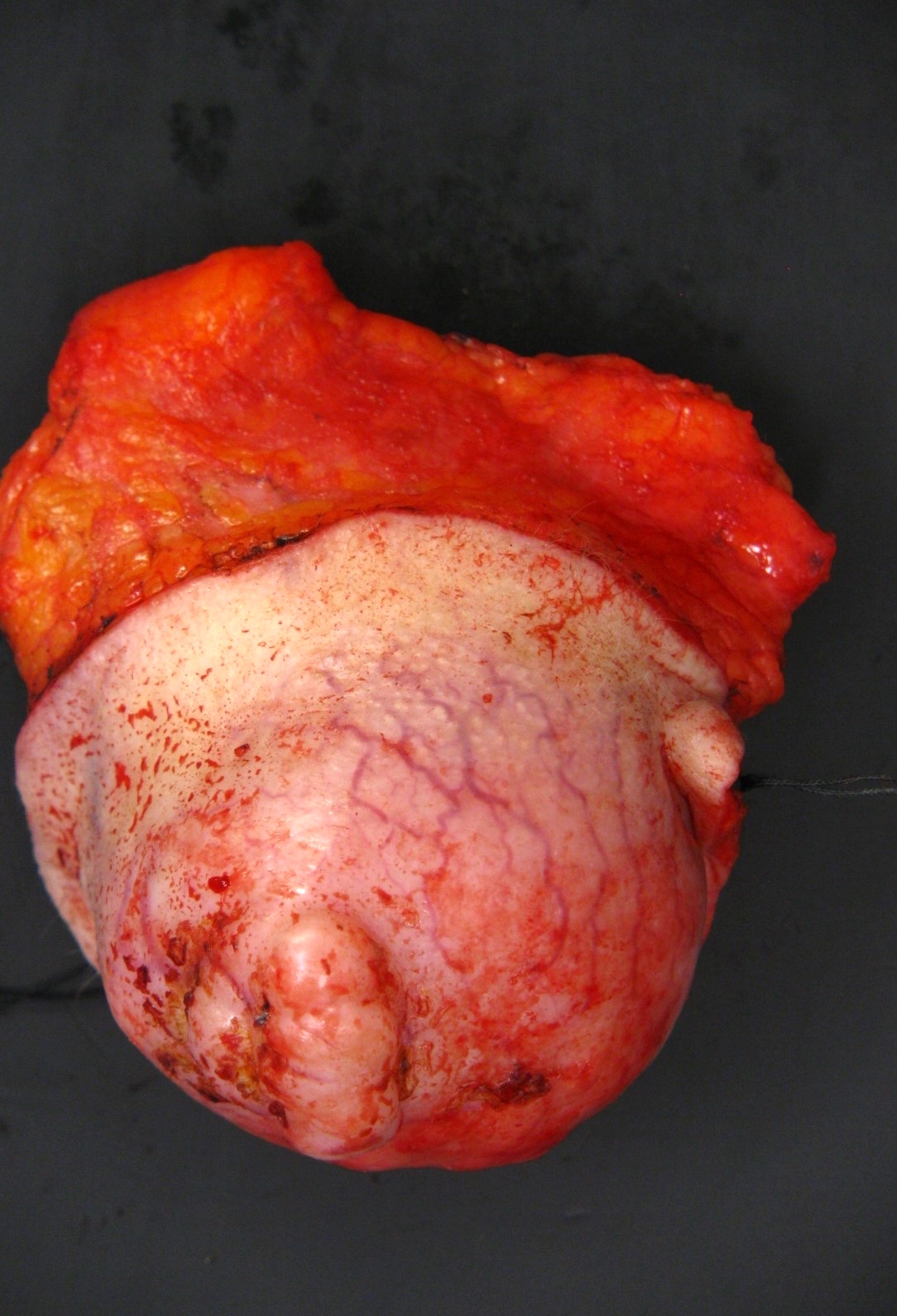
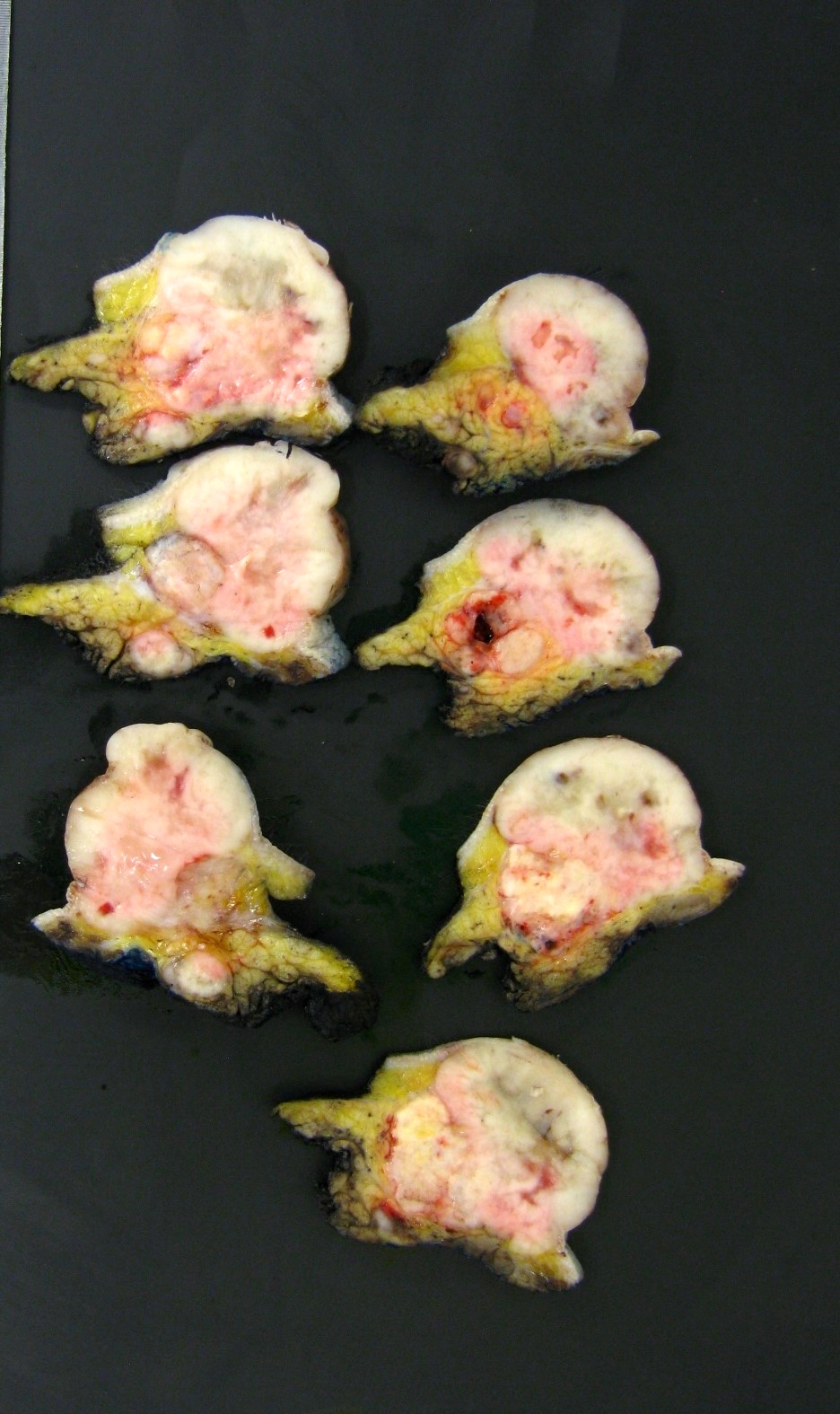
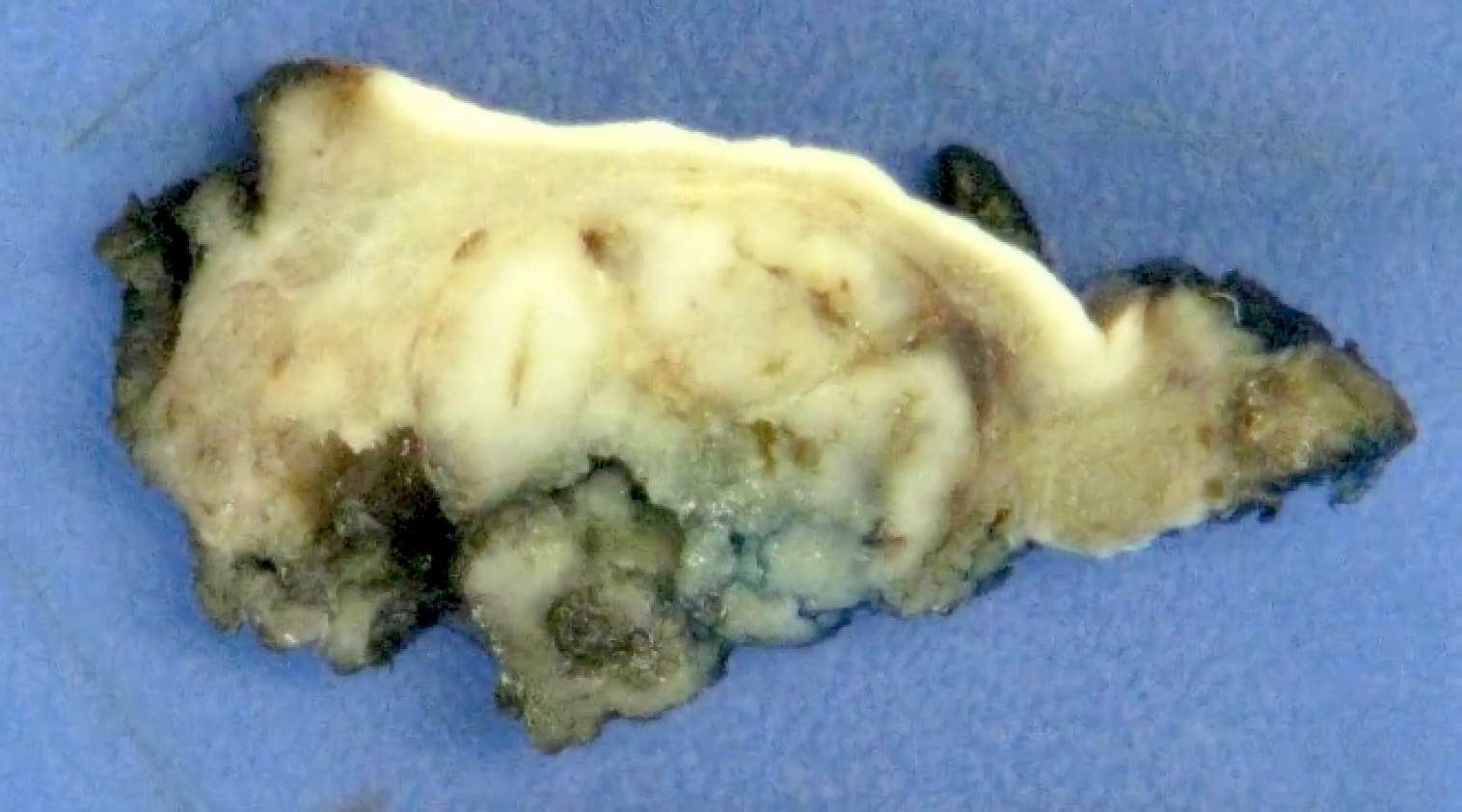
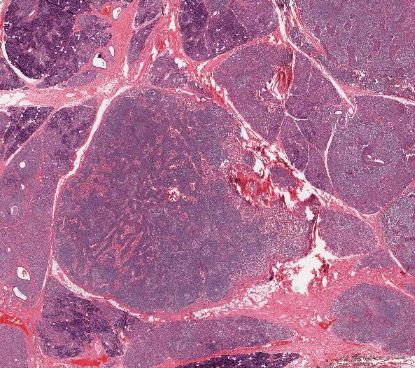
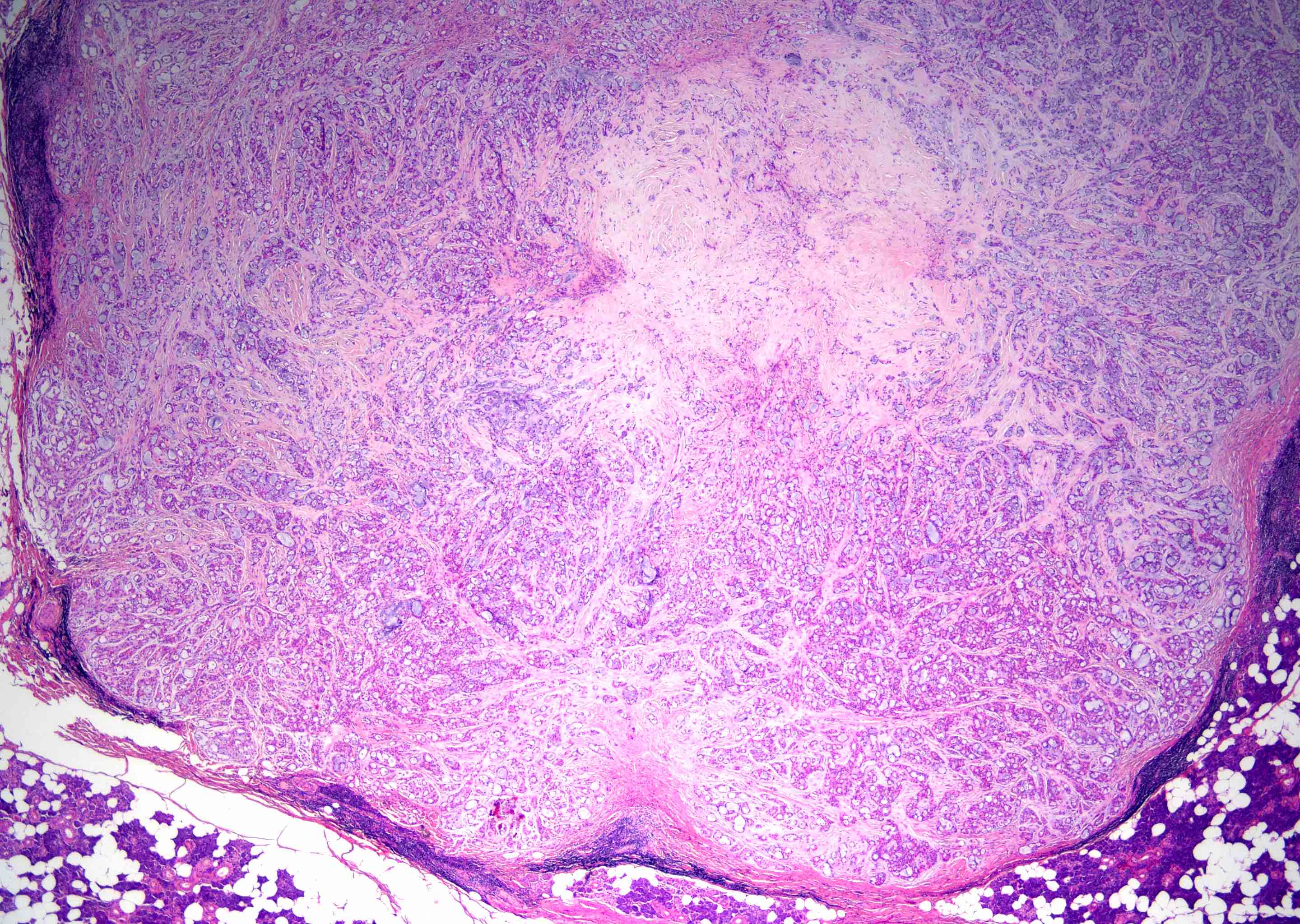
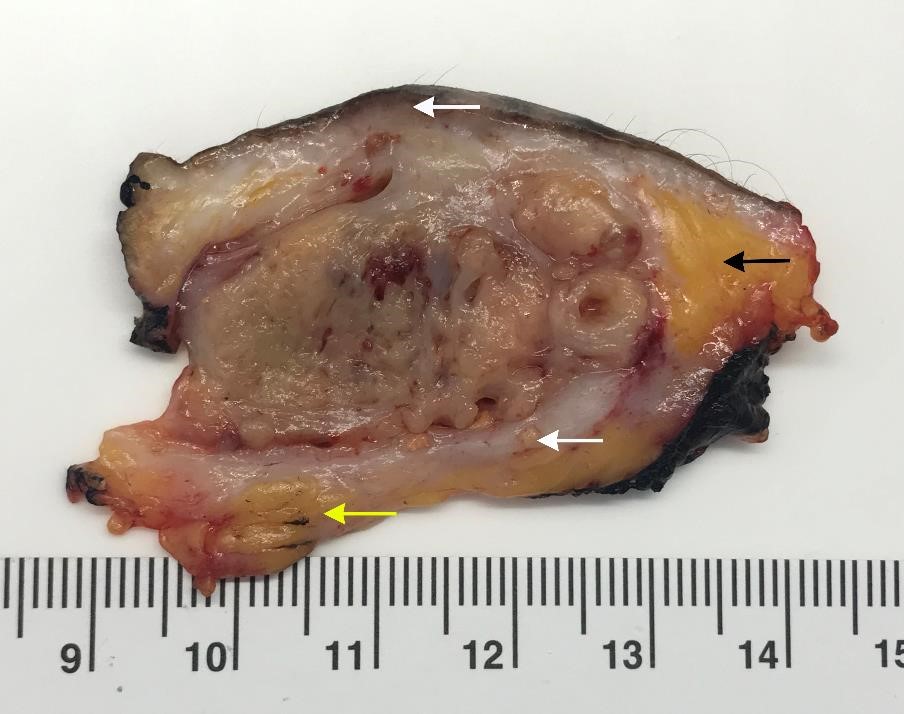
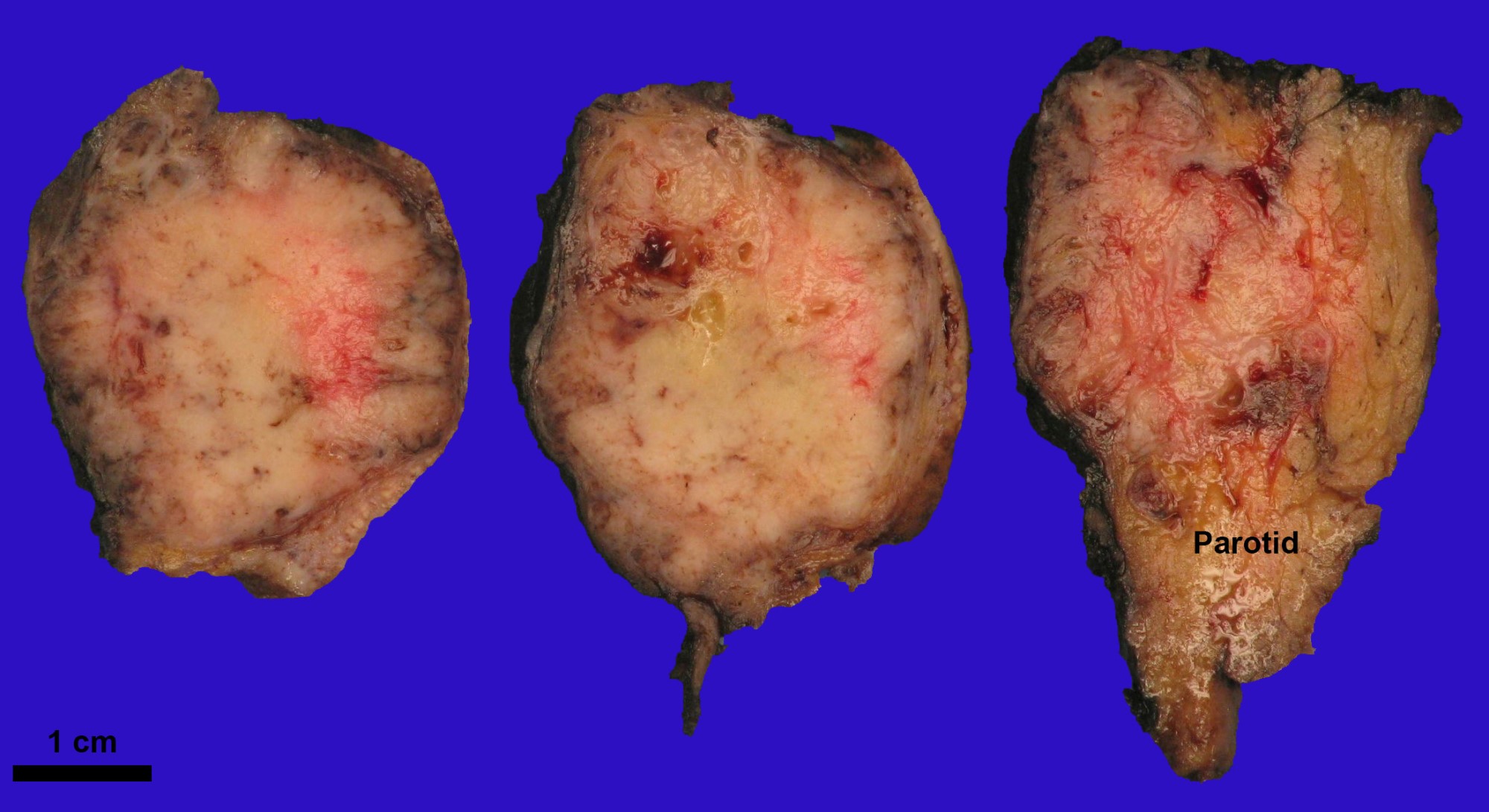
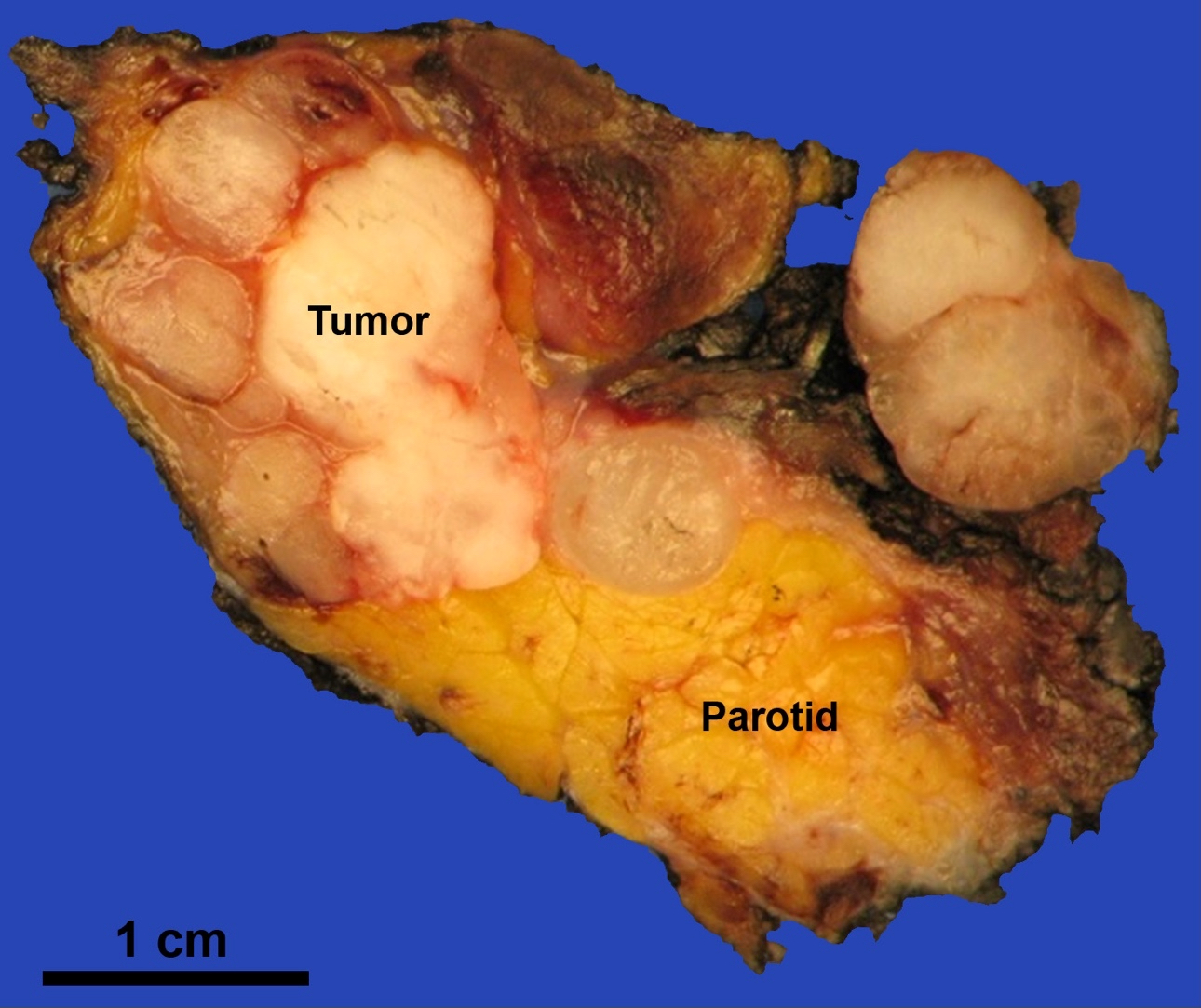
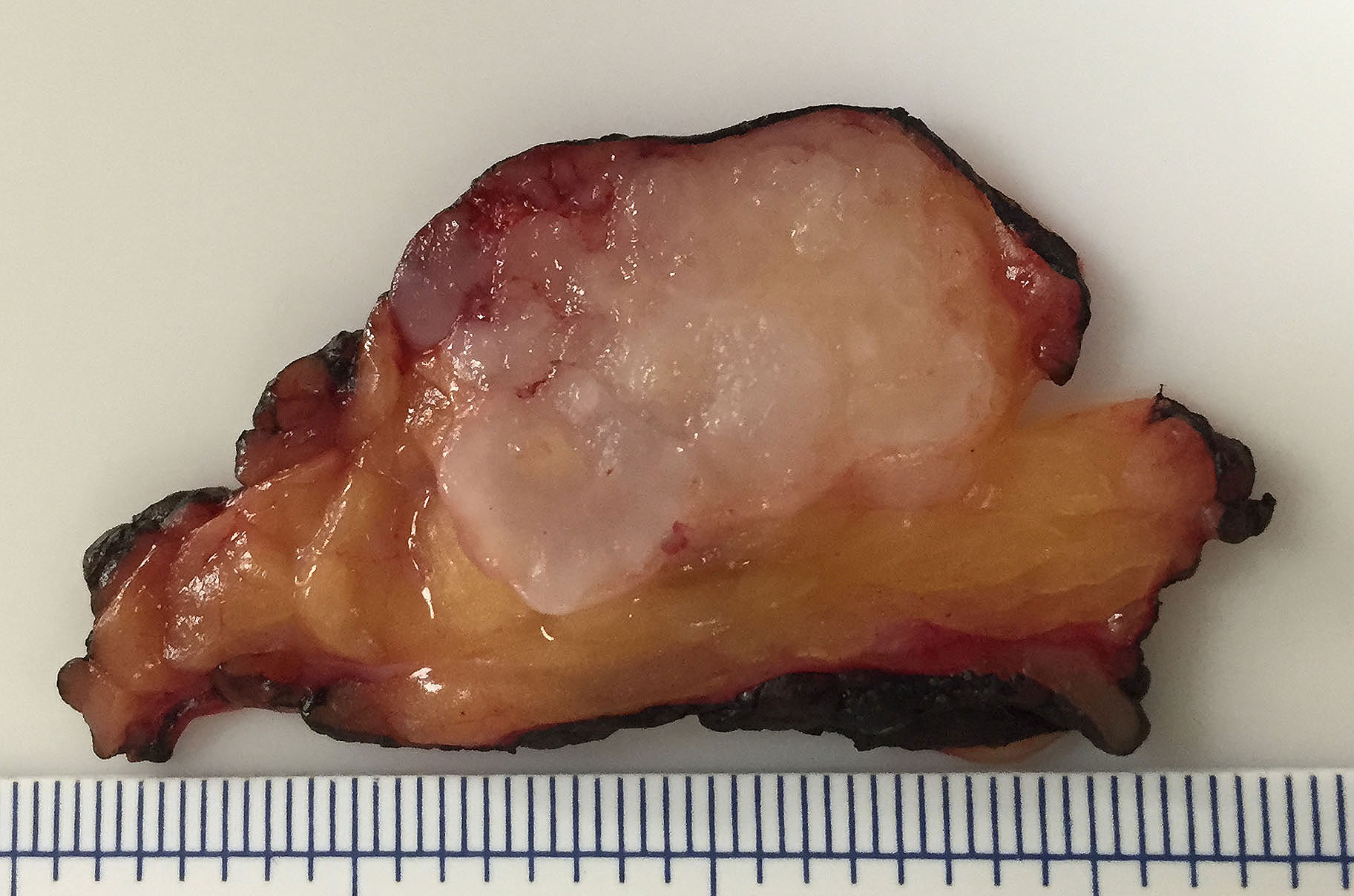
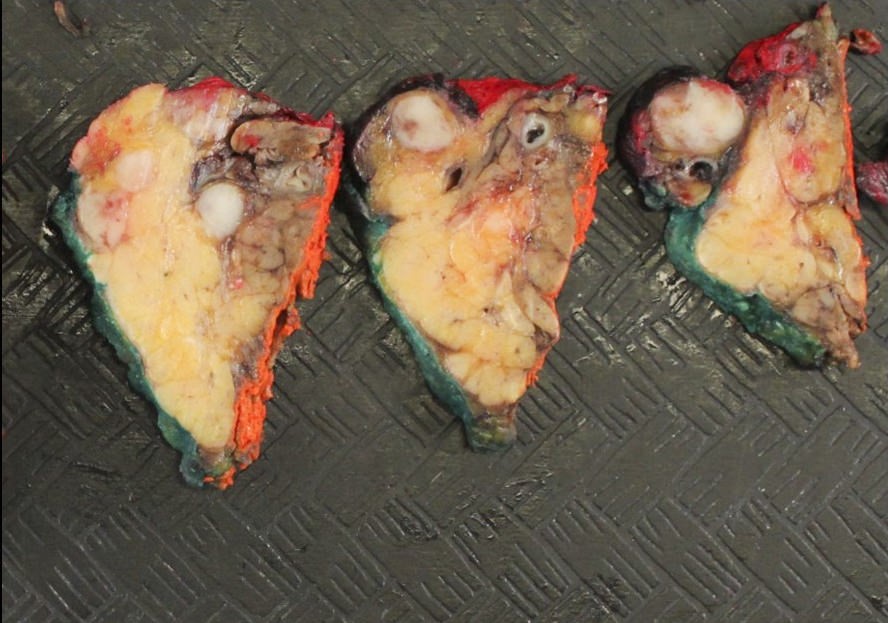
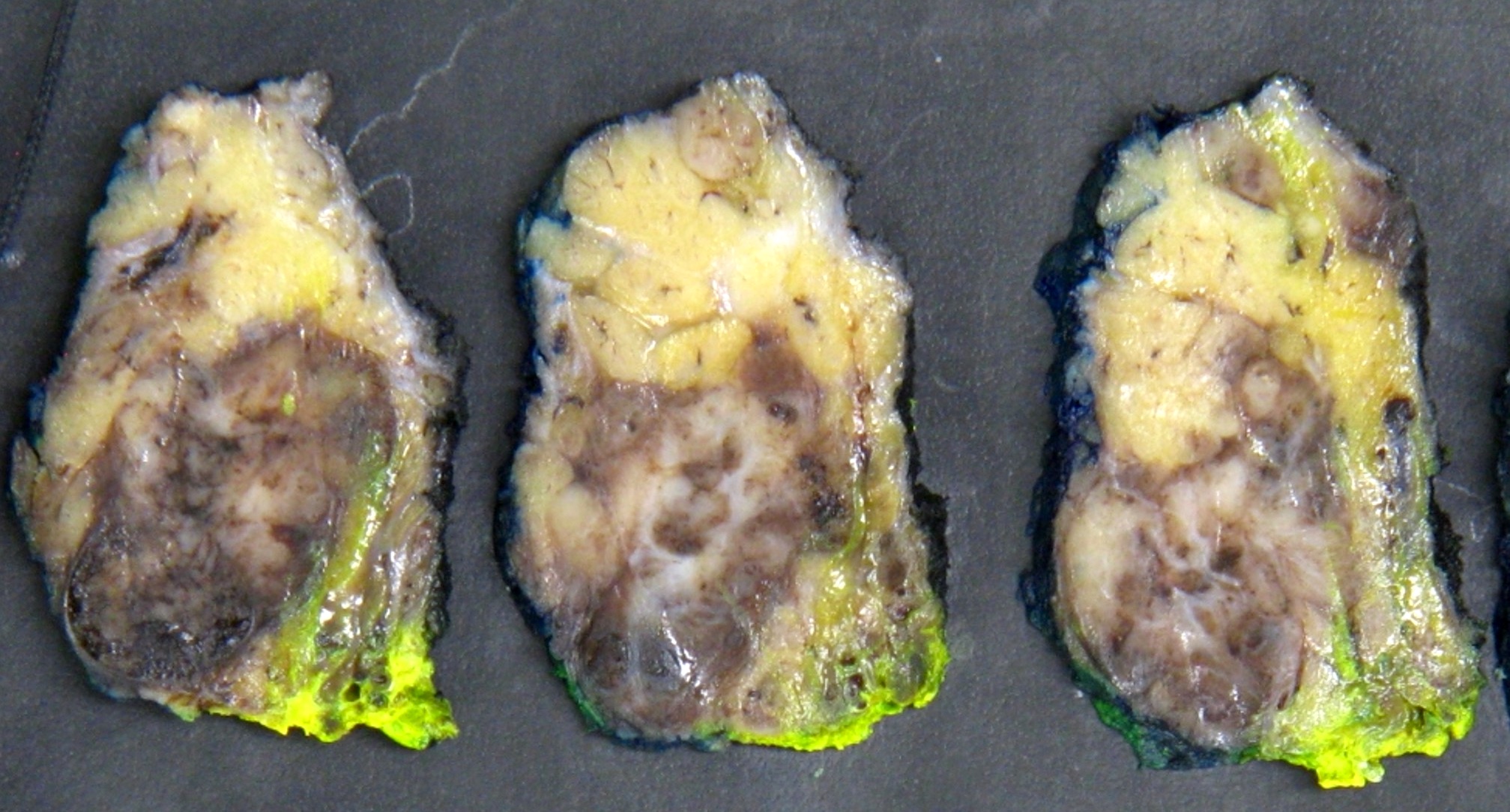
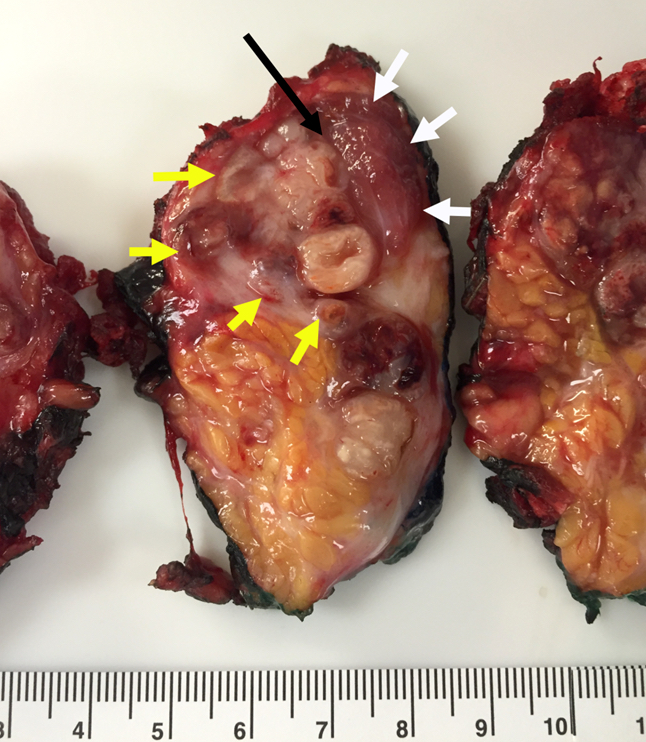
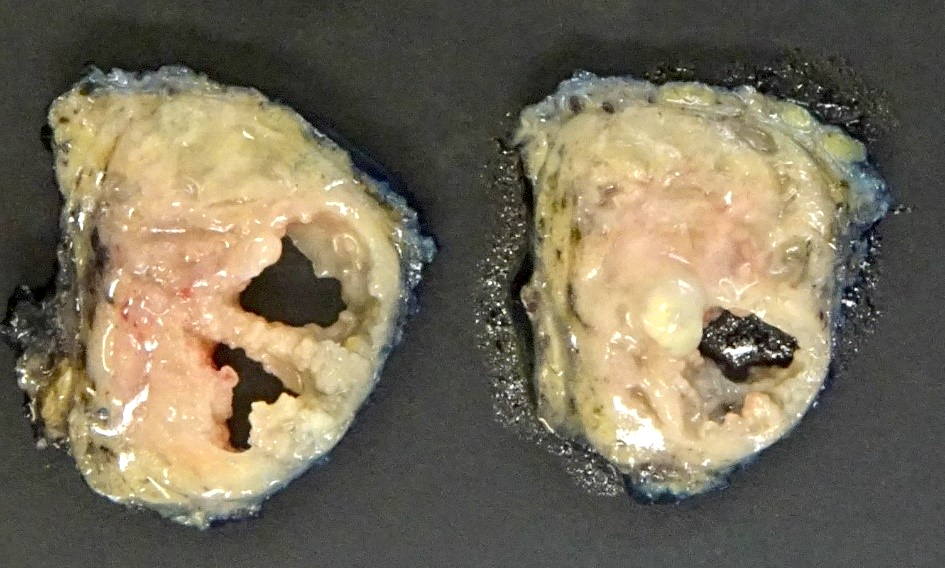
Well circumscribed, soft rubbery, tan-yellow to pink mass with homogeneous cut surface
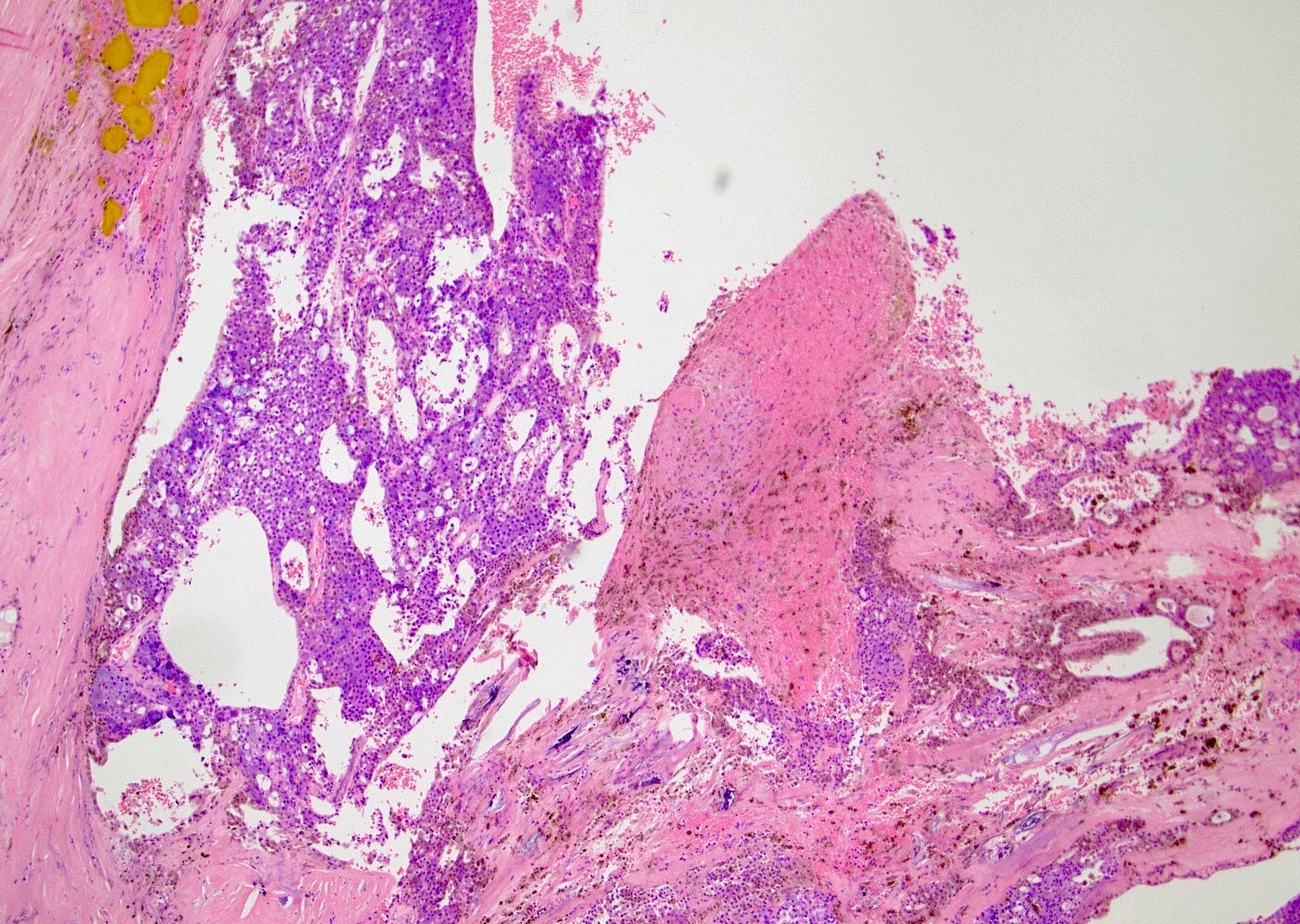
Cystic change and hemorrhage may occur
Gross images
Images hosted on other servers:
Well circumscribed multilobulated mass
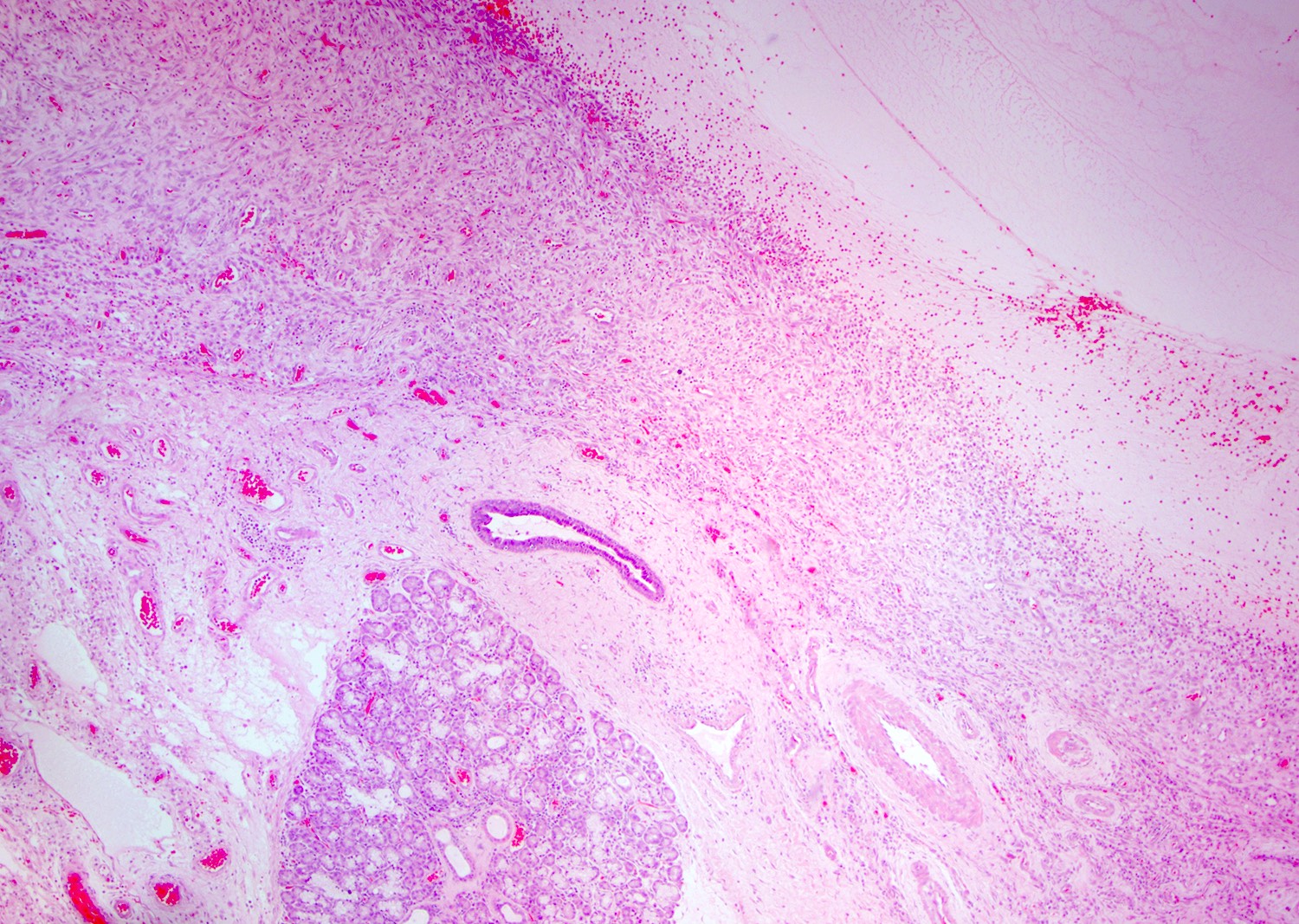
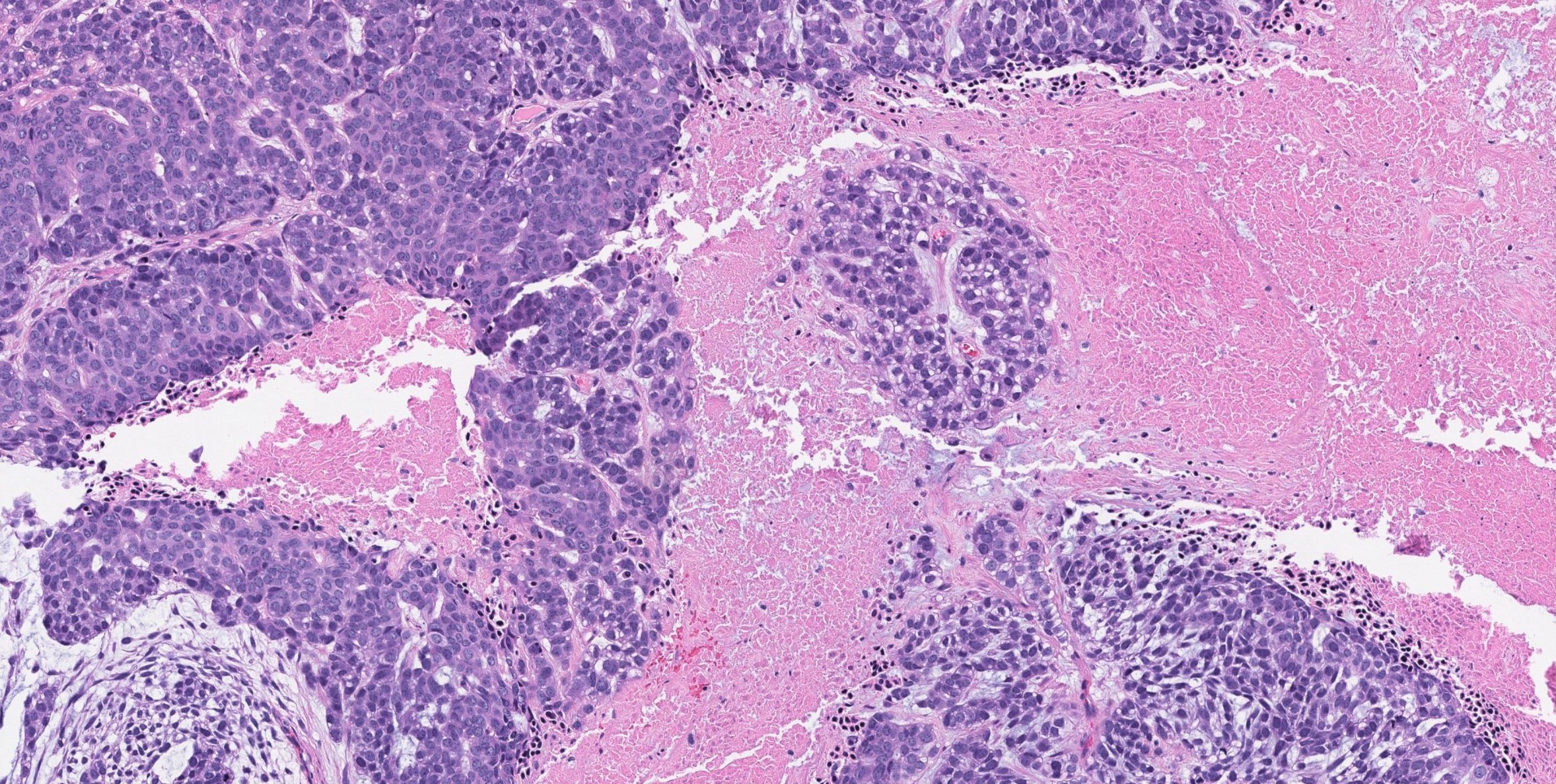
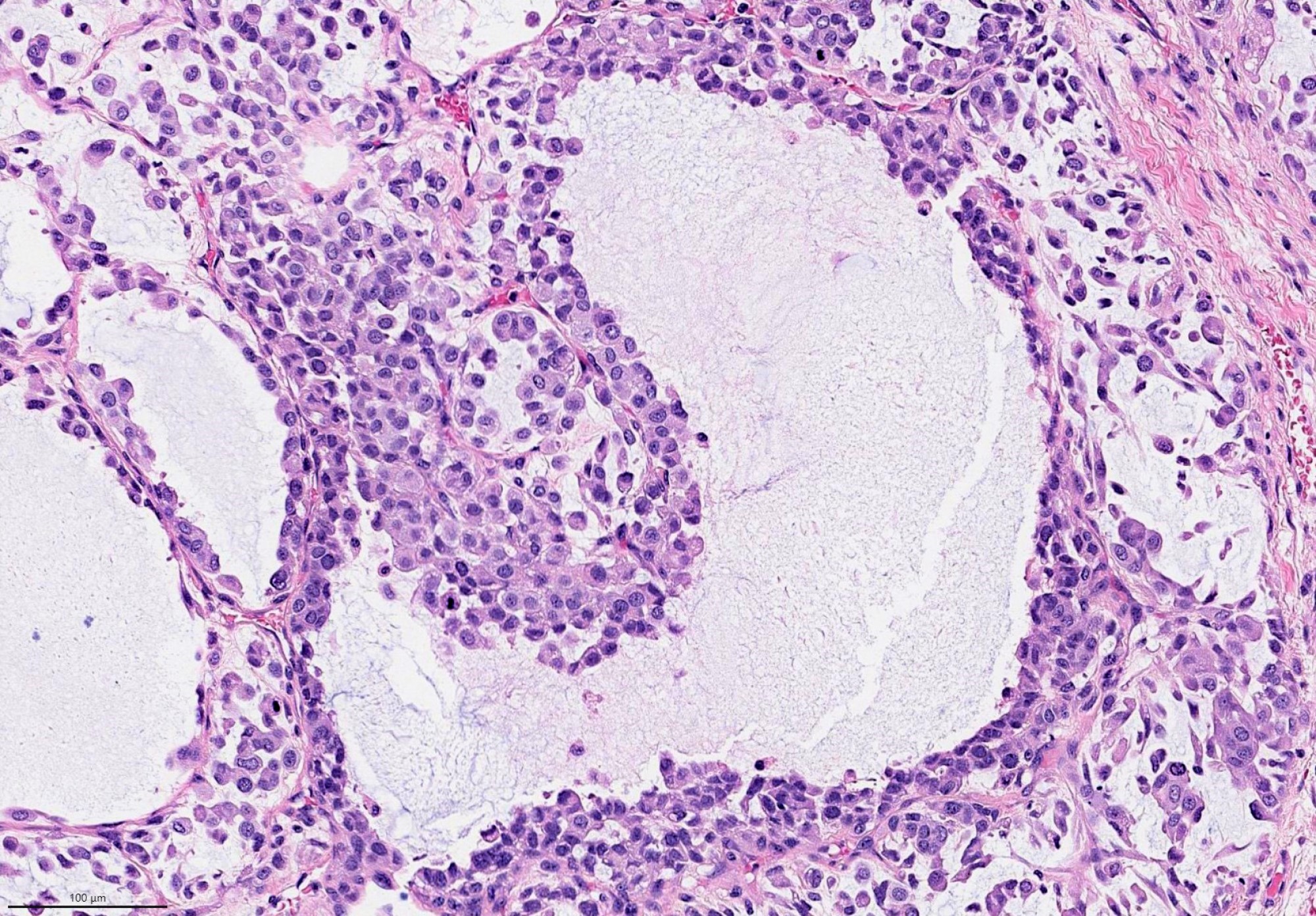
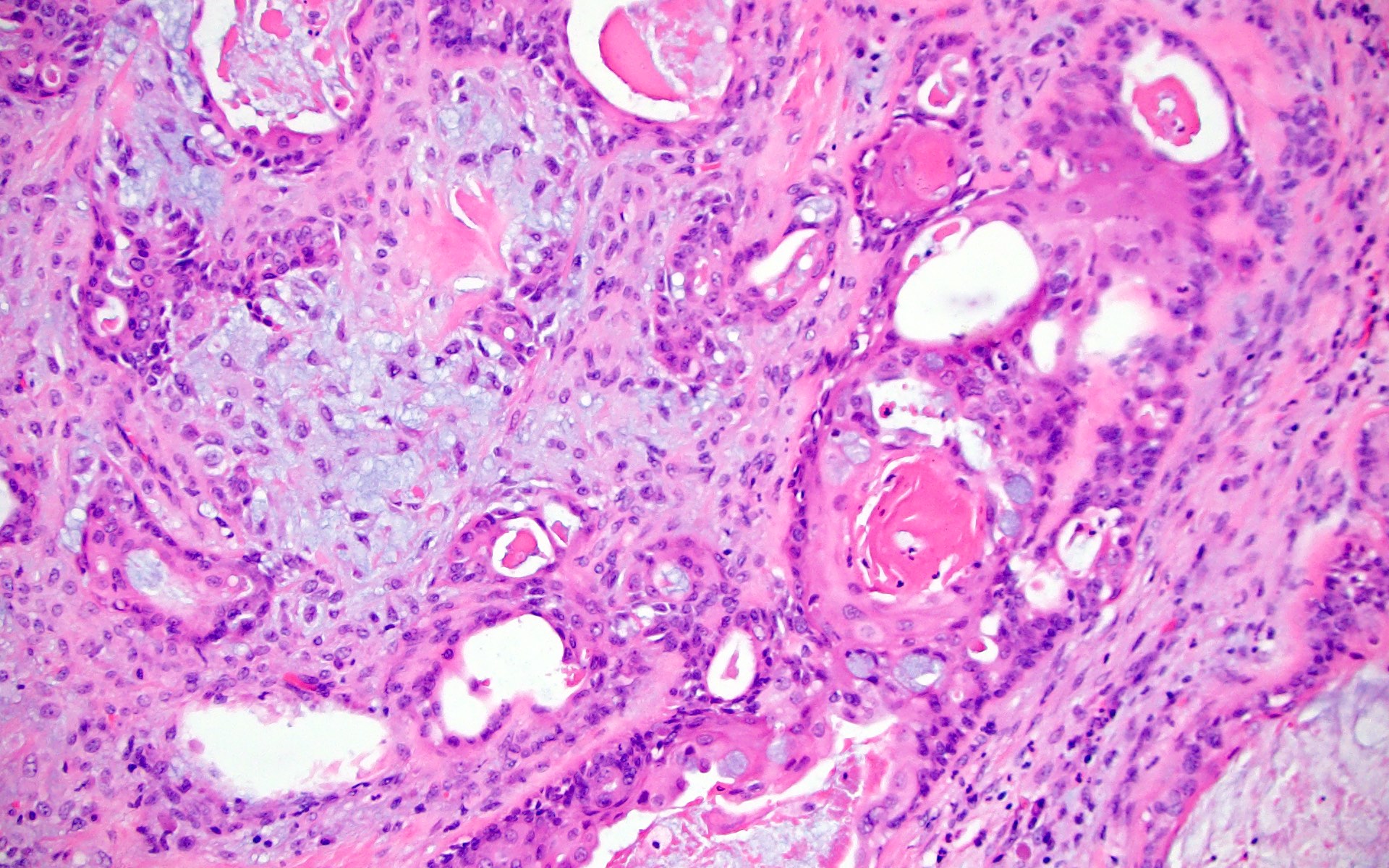
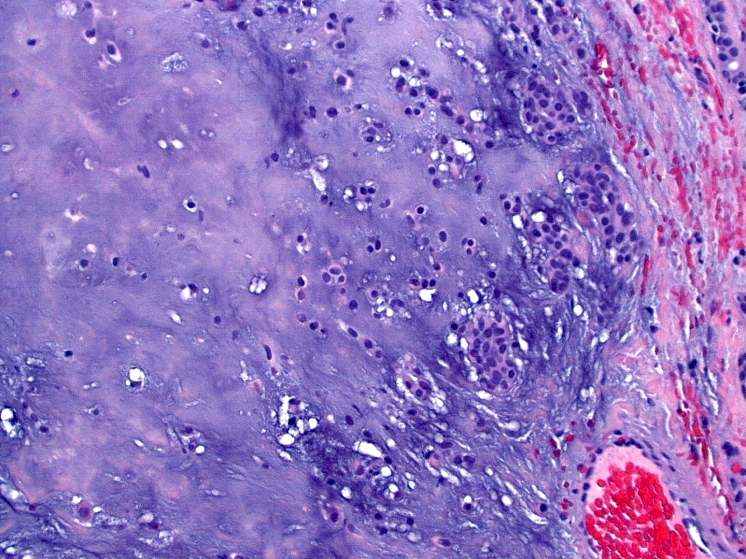
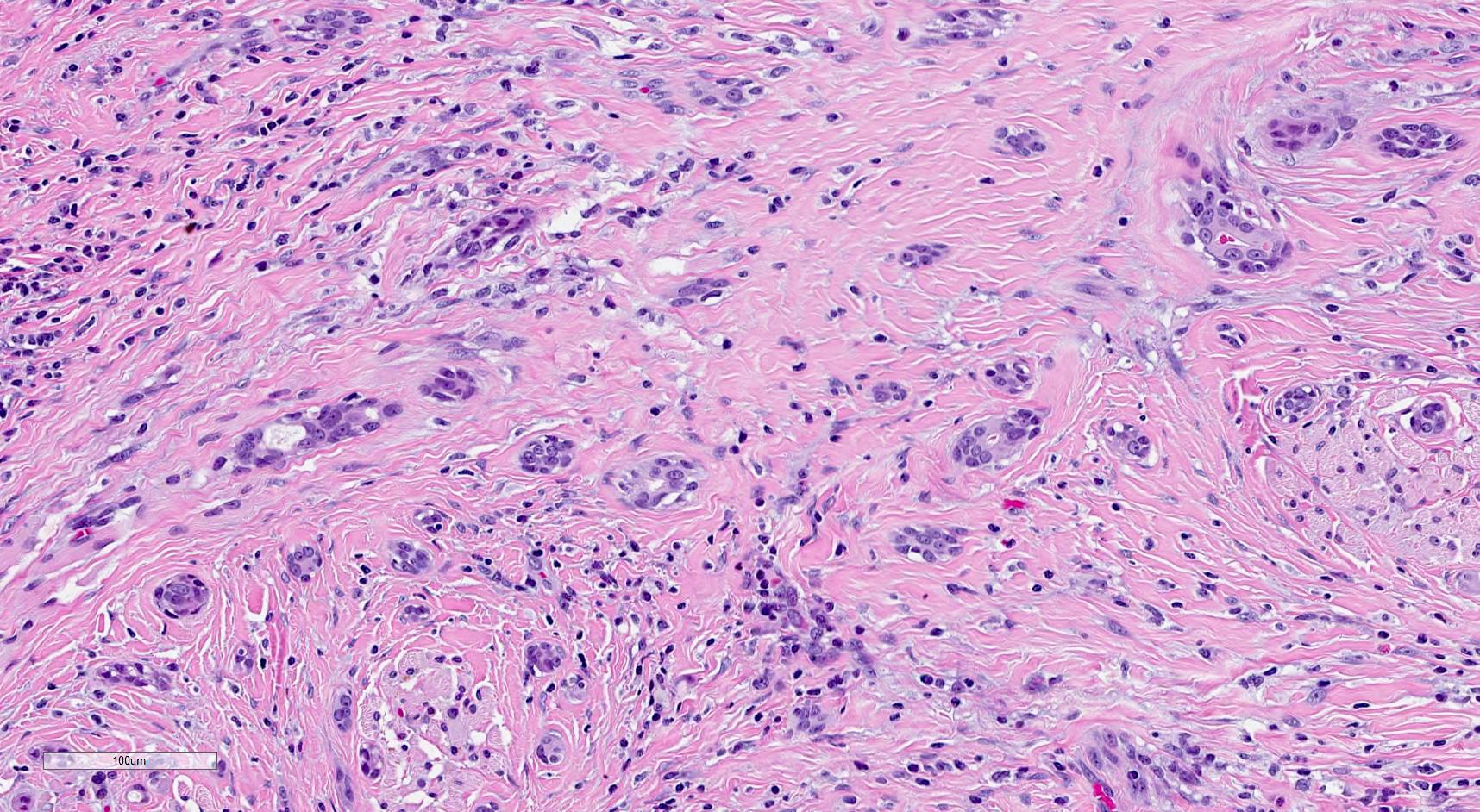
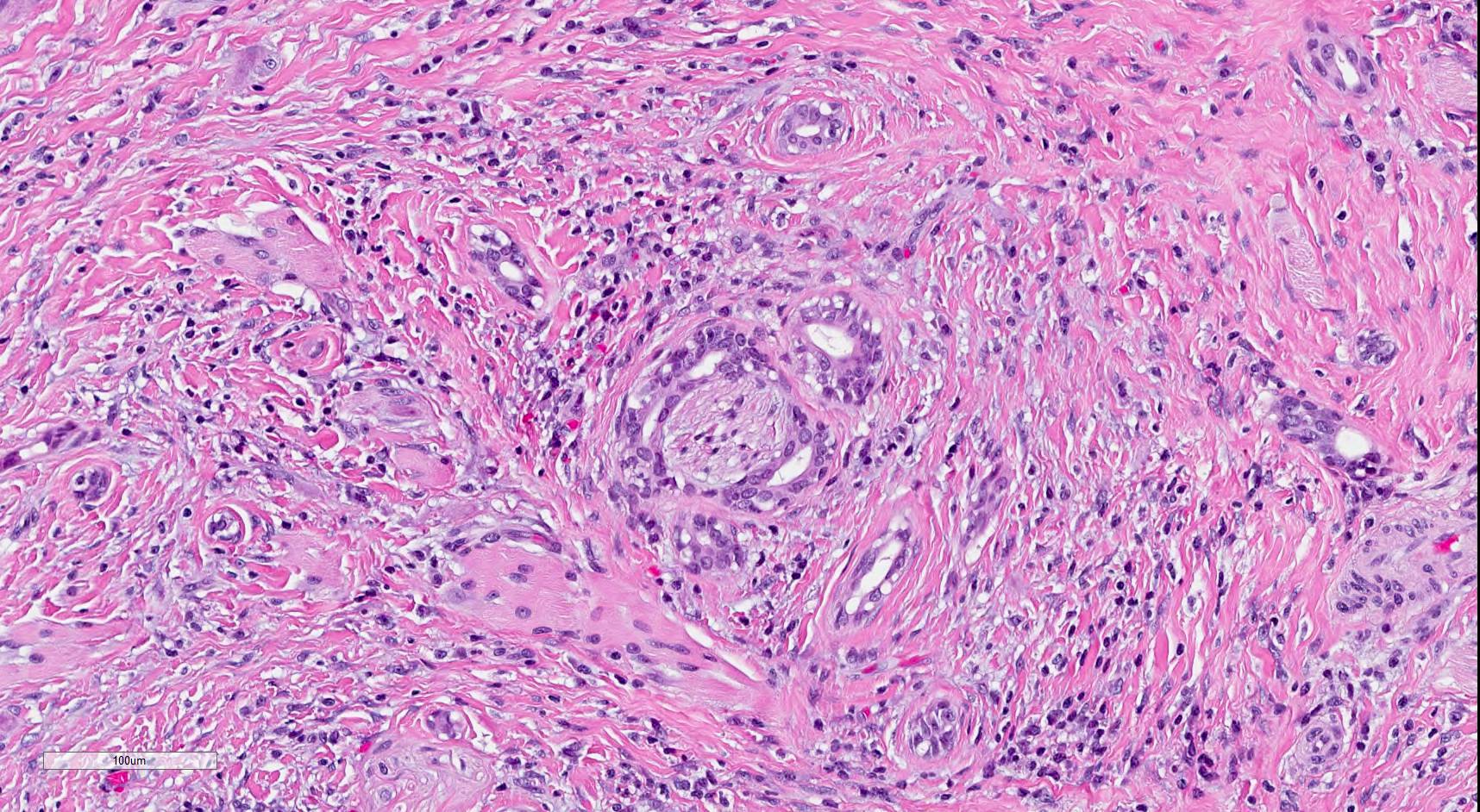
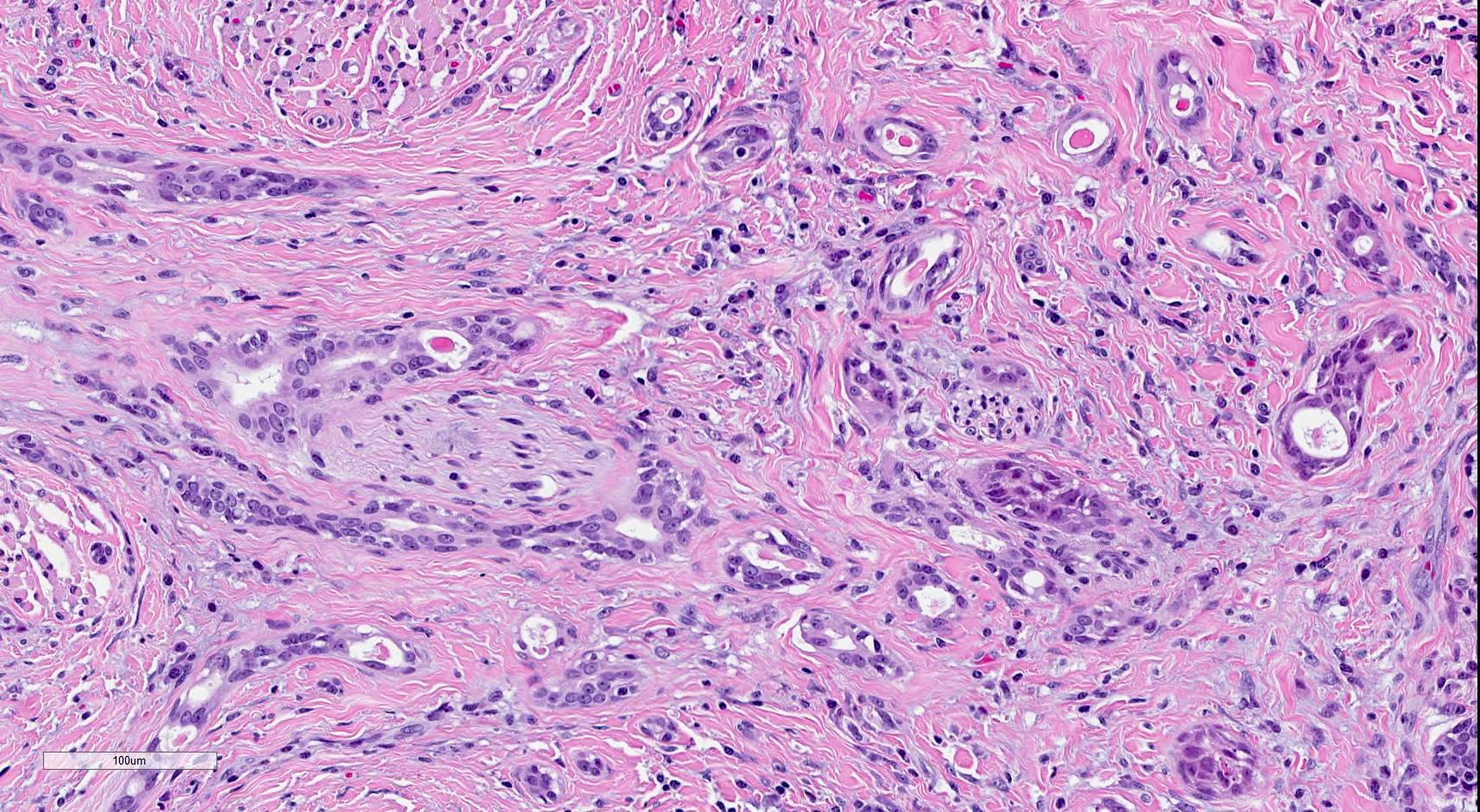
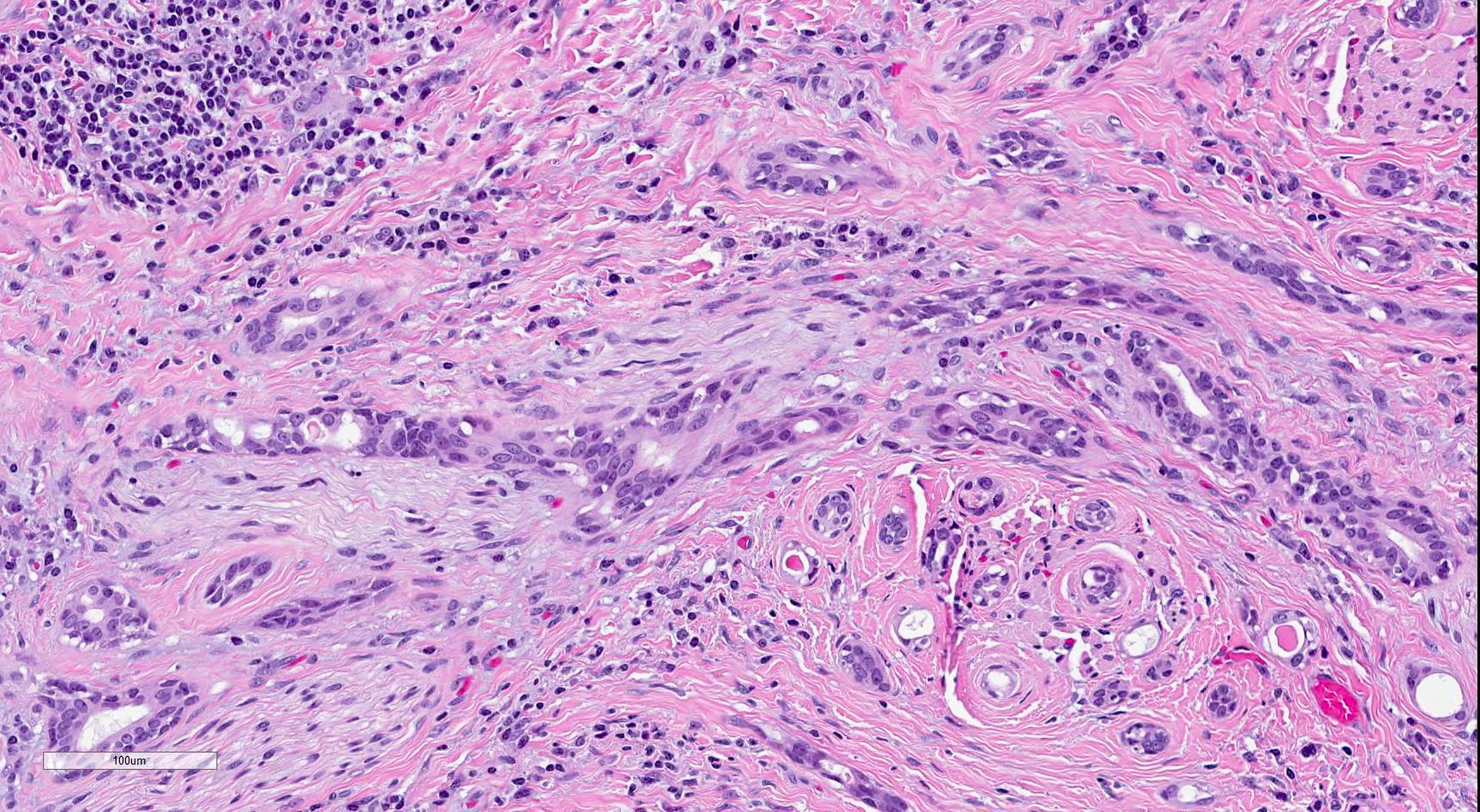
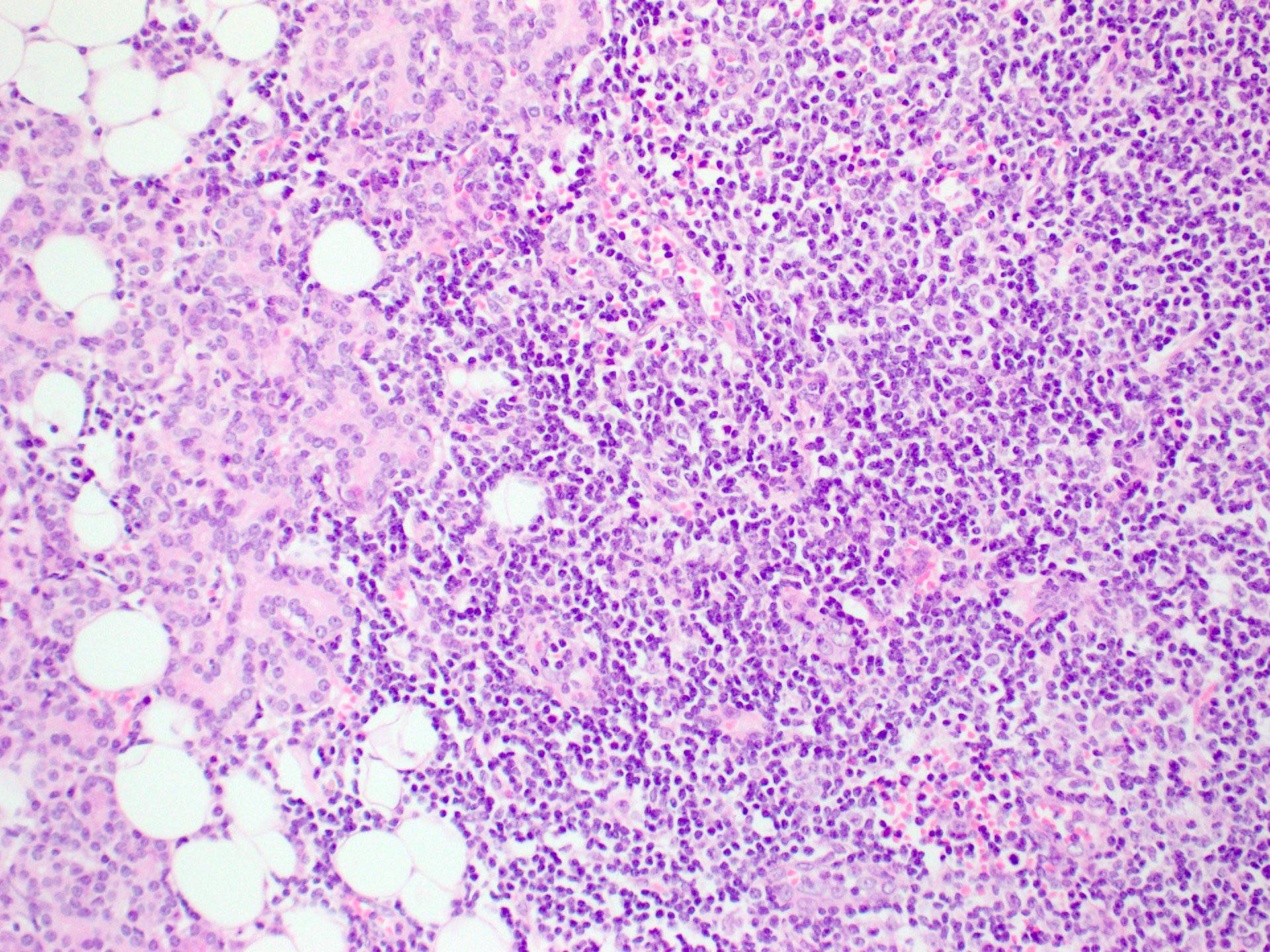
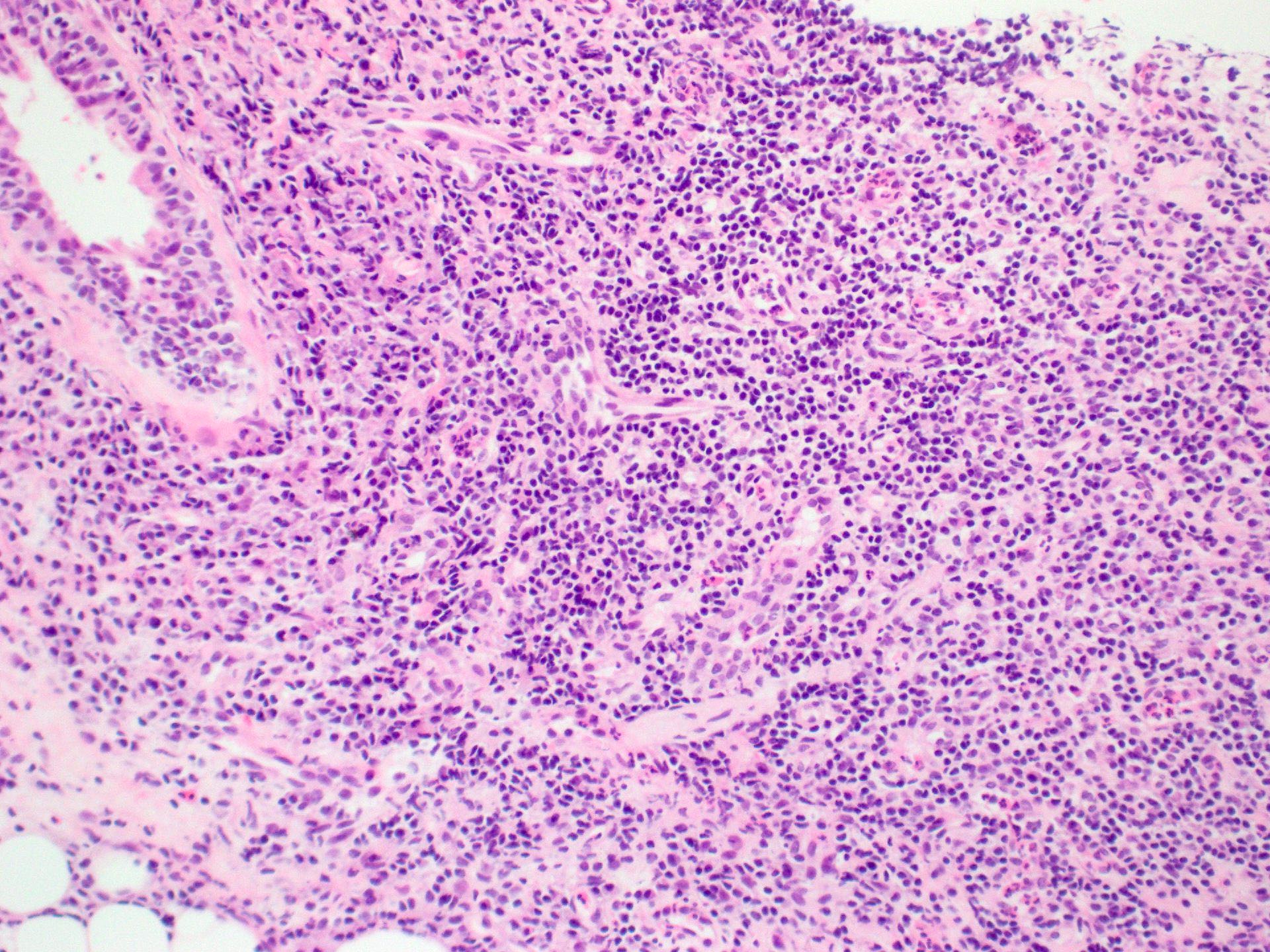
Microscopic (histologic) description
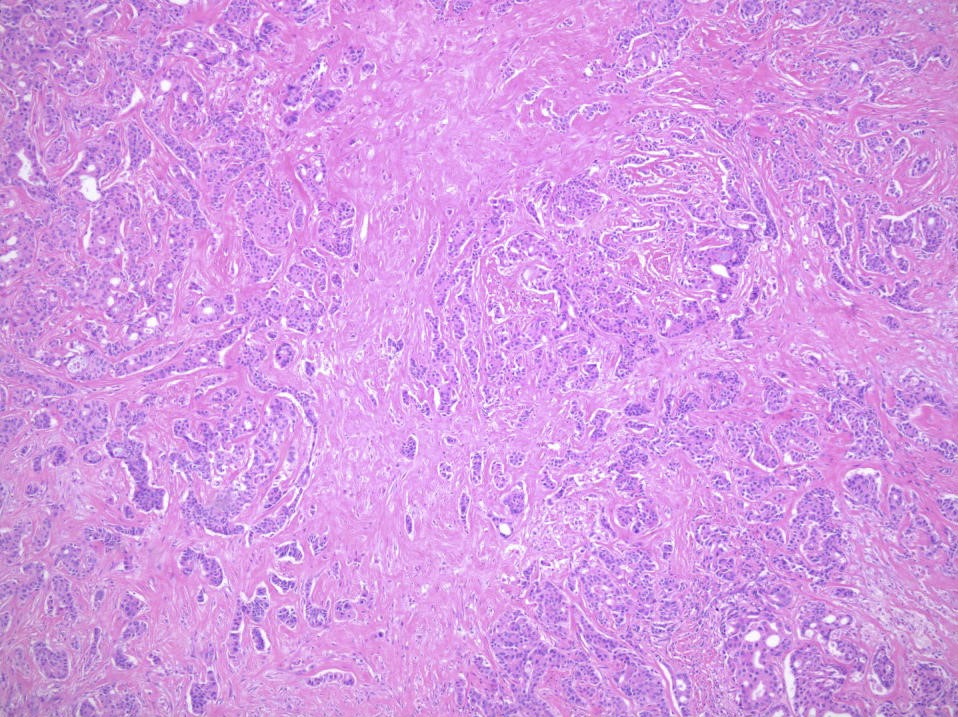
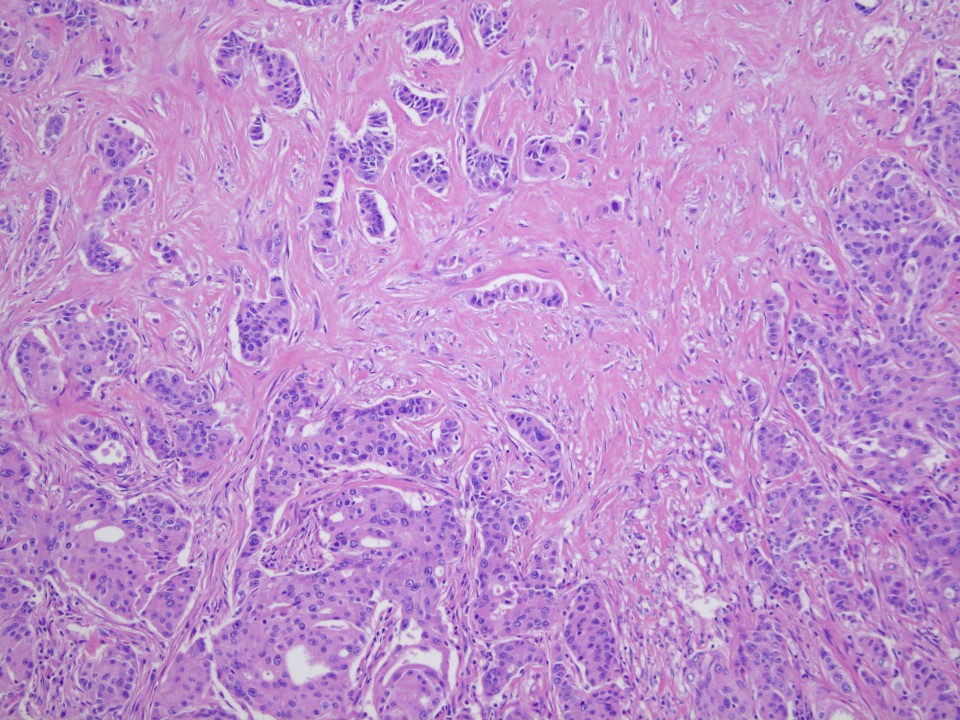
Multiple cell types are noted
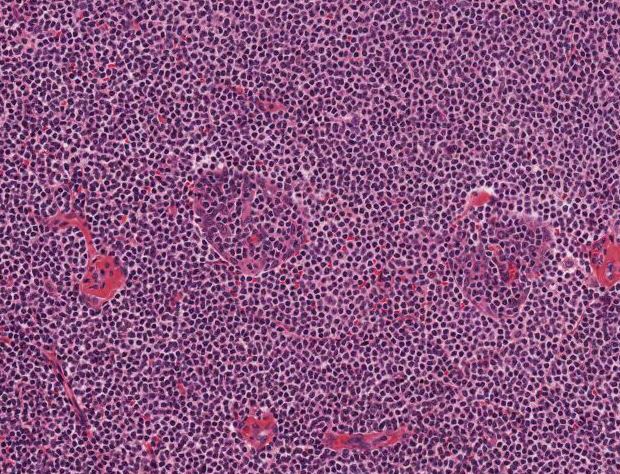
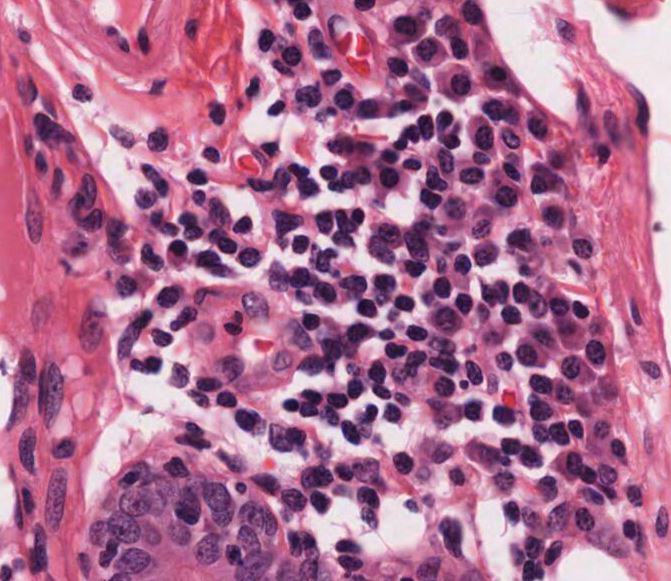
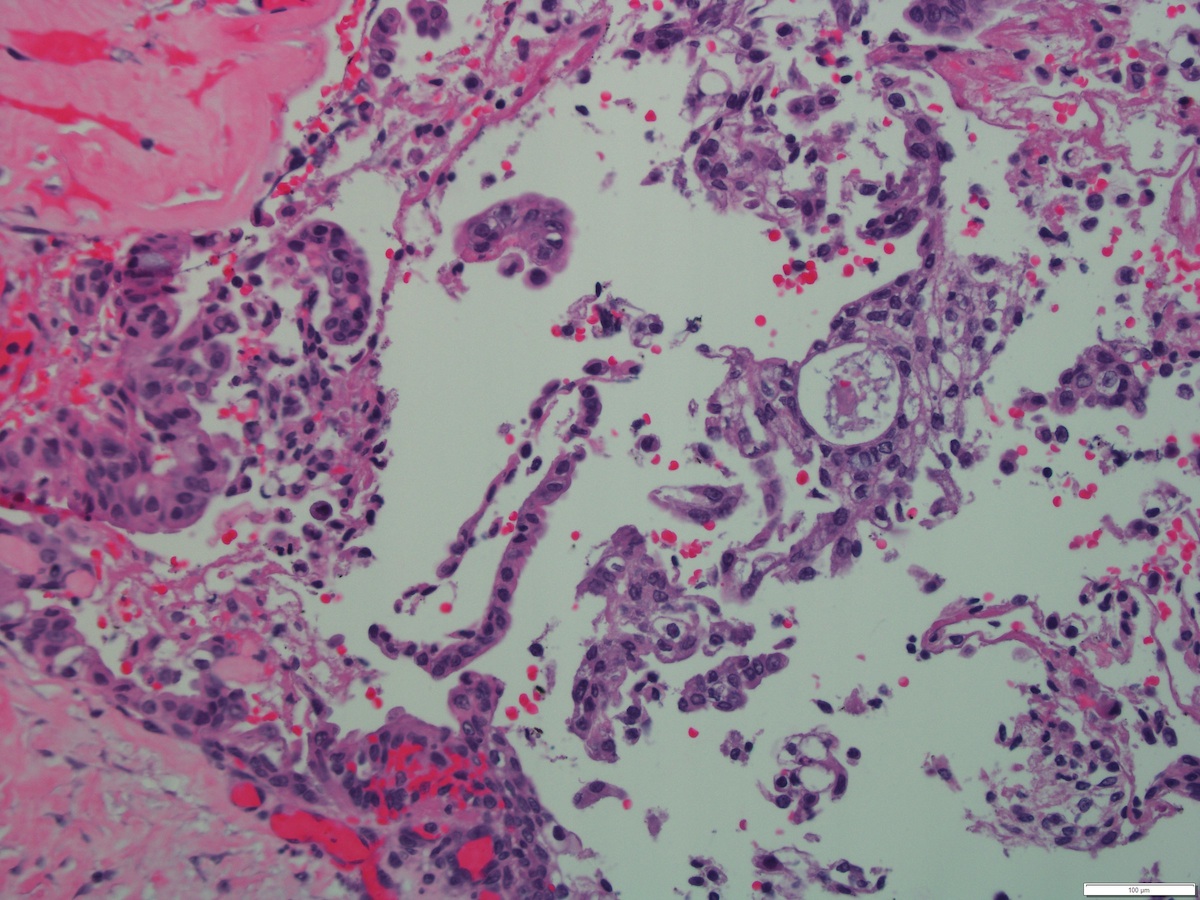
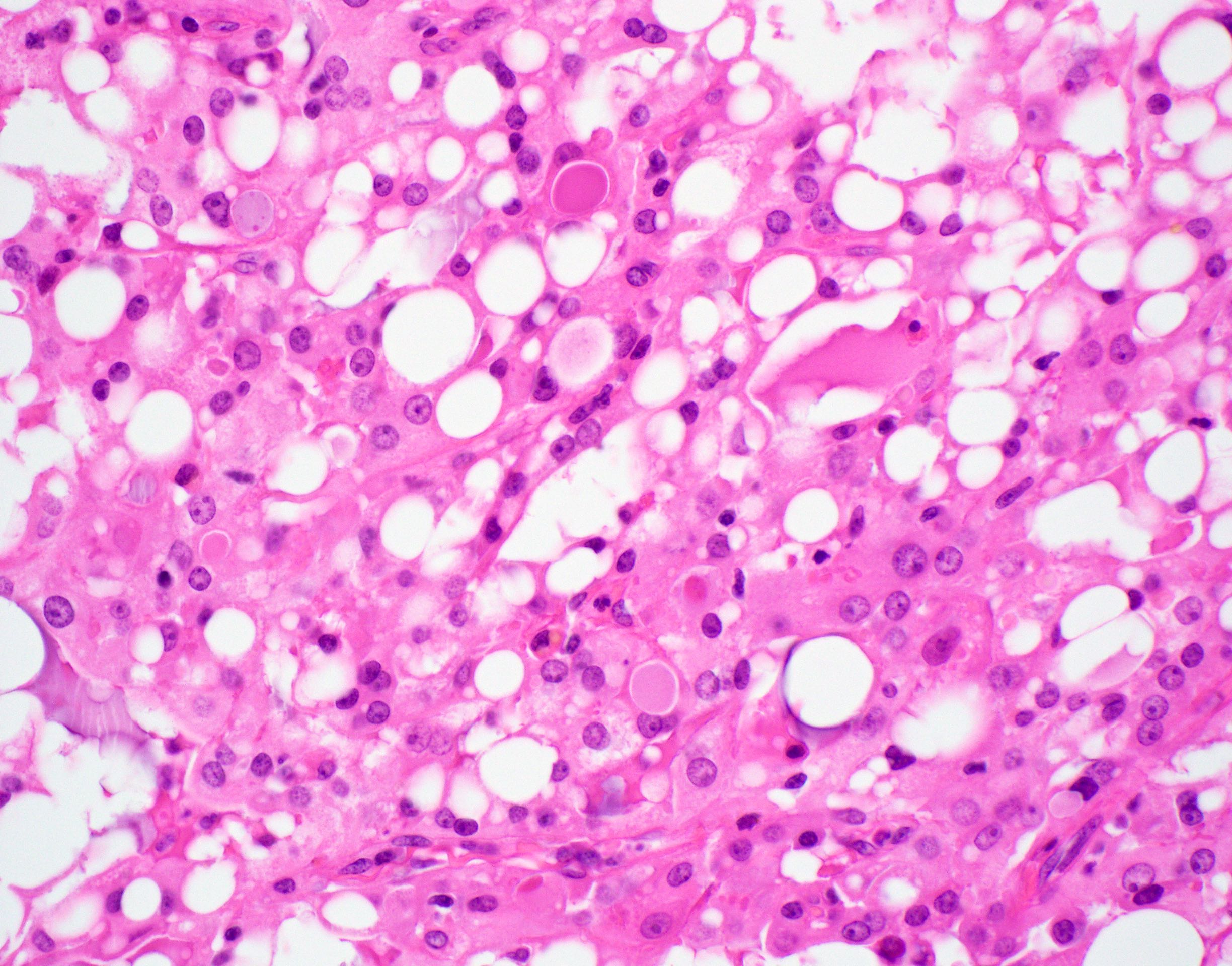
Cell types include serous acinar, intercalated ductal, vacuolated, nonspecific glandular and clear cells
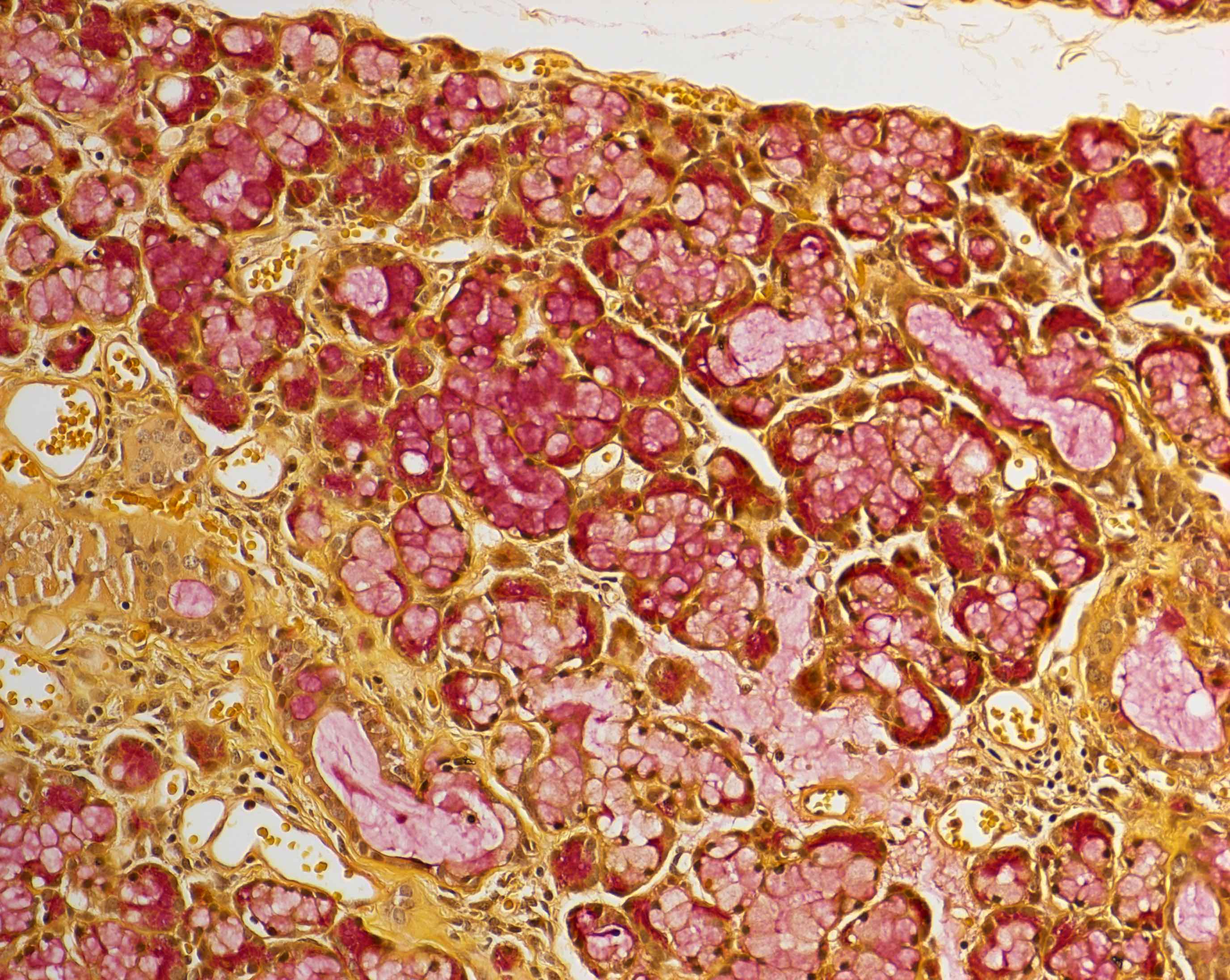
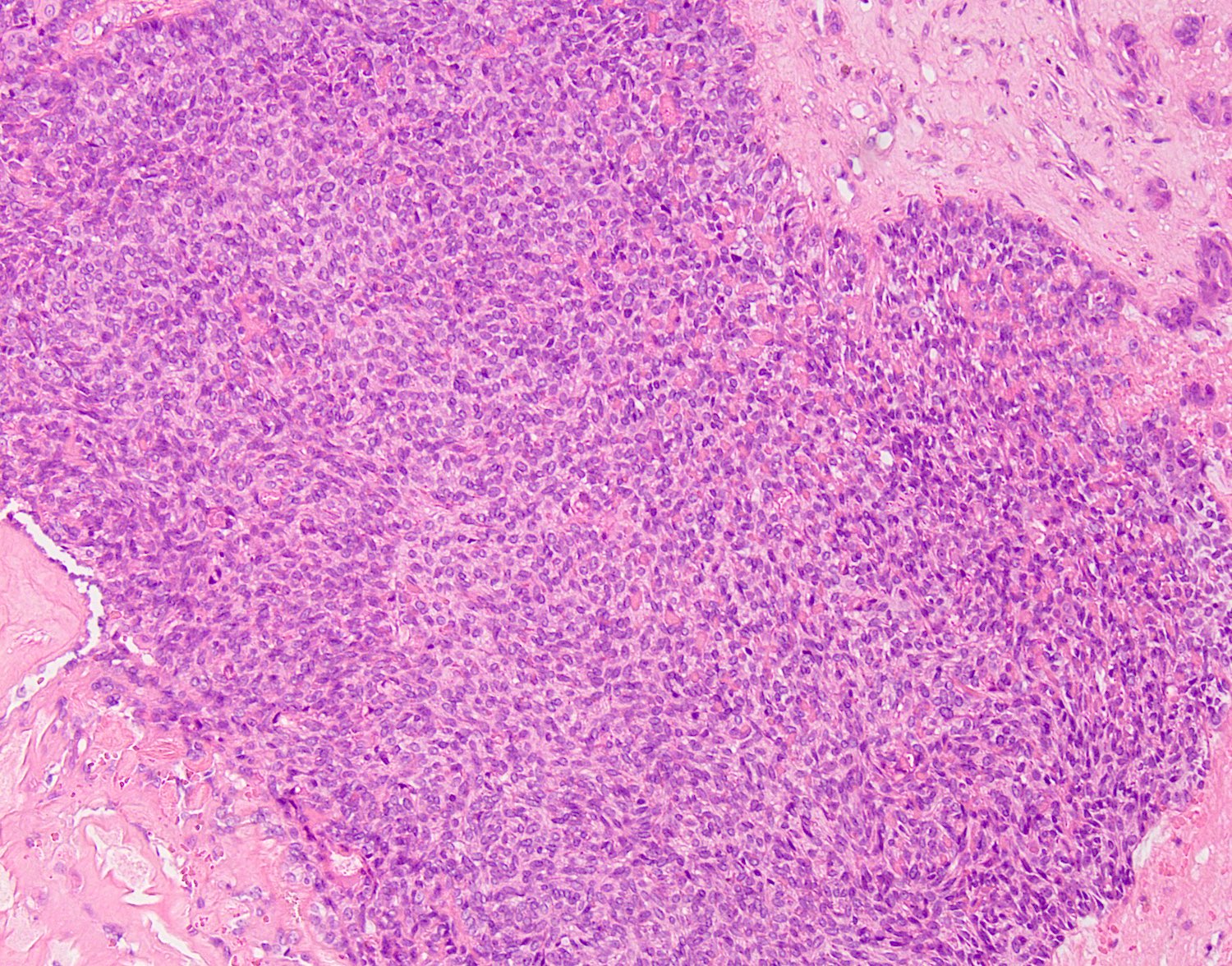
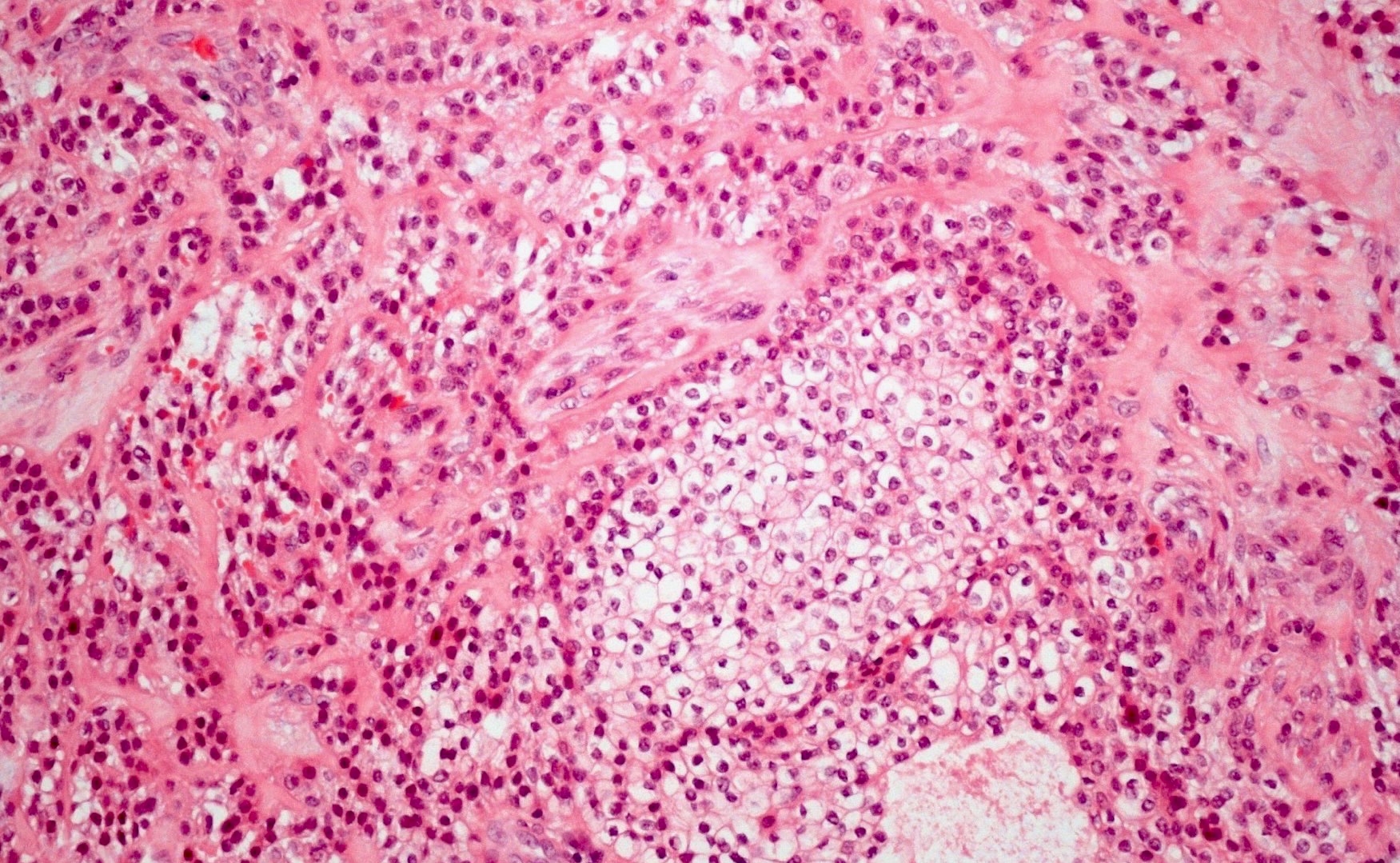
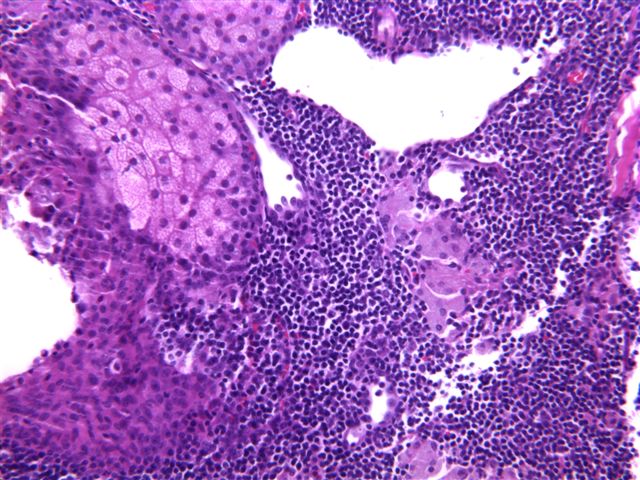
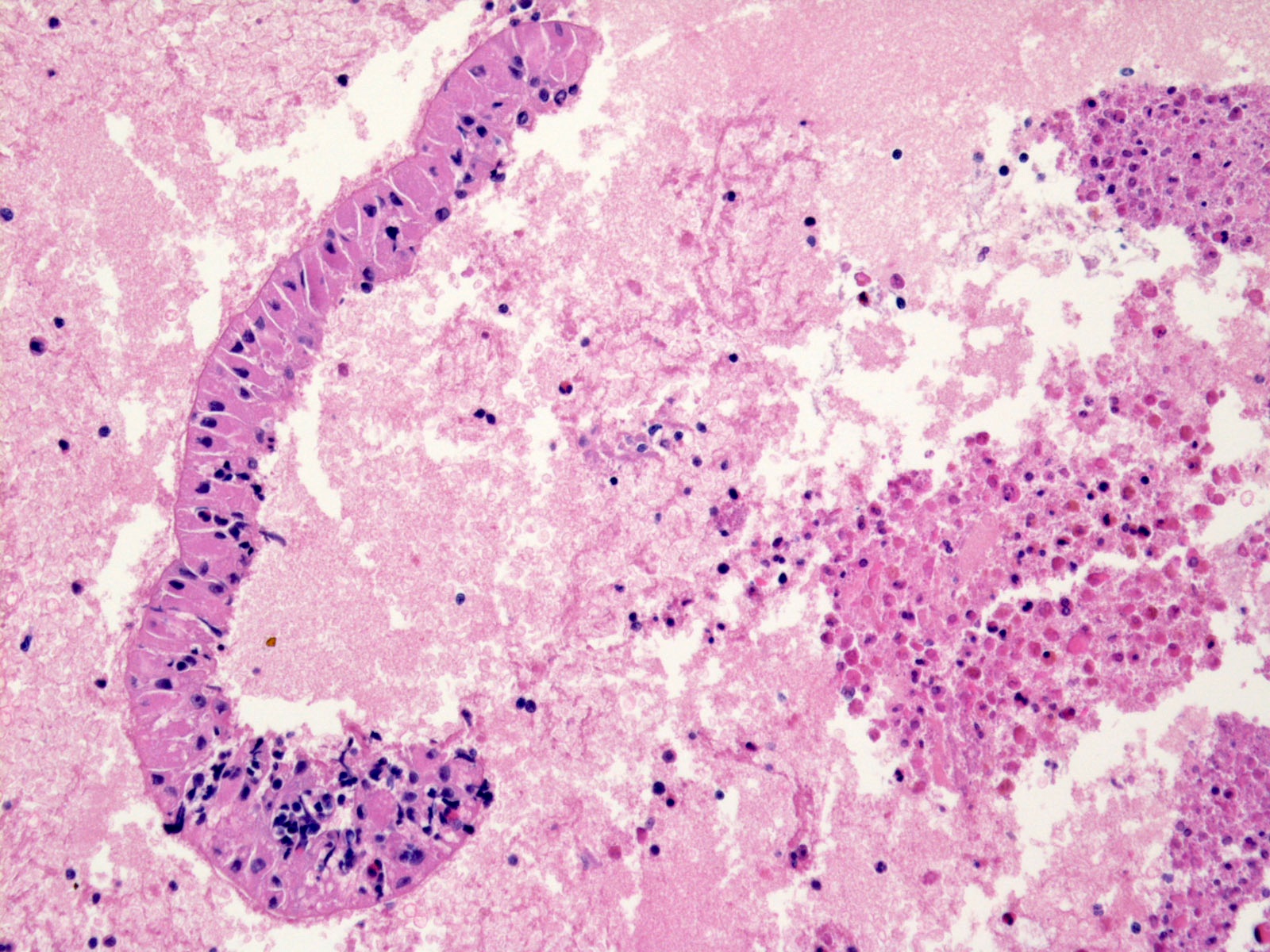
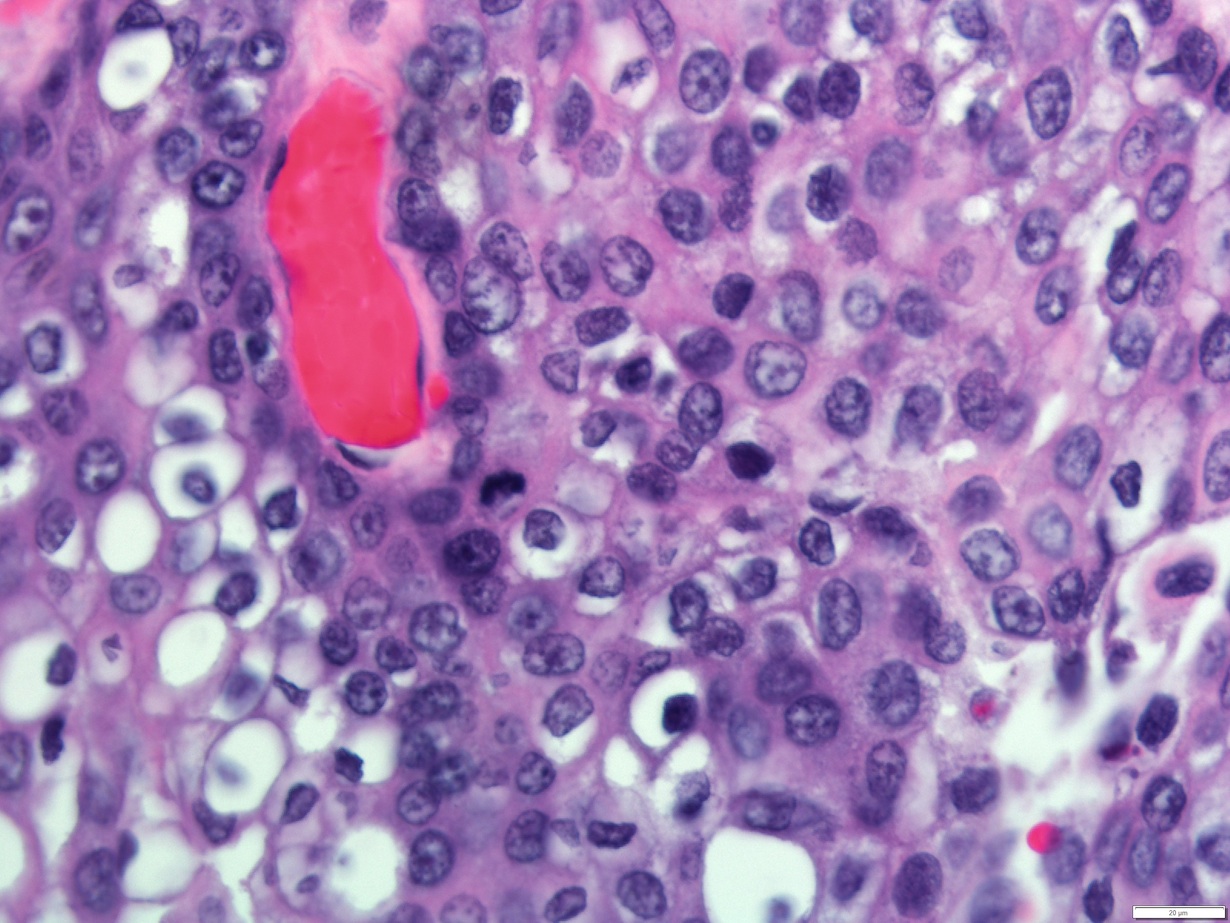
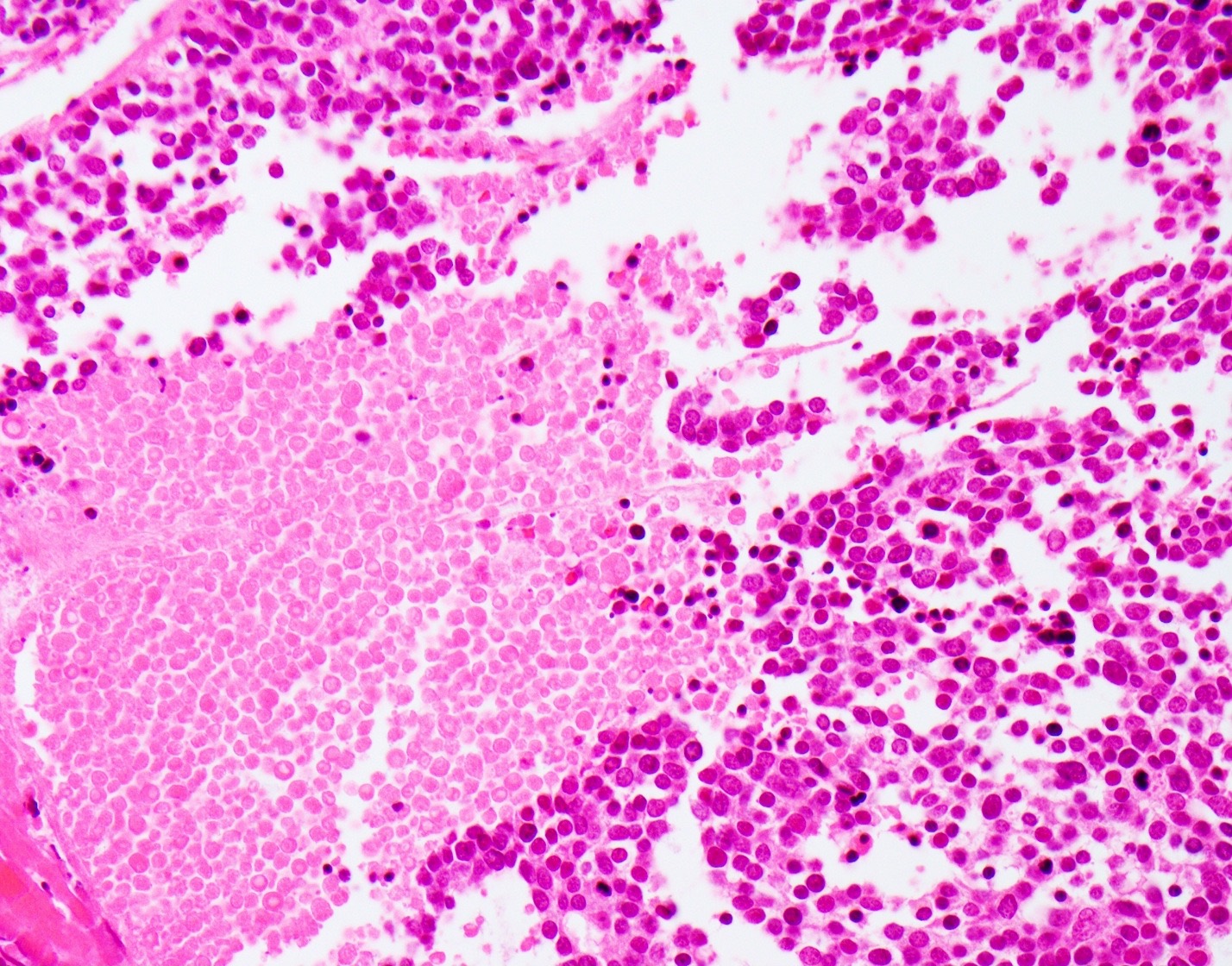
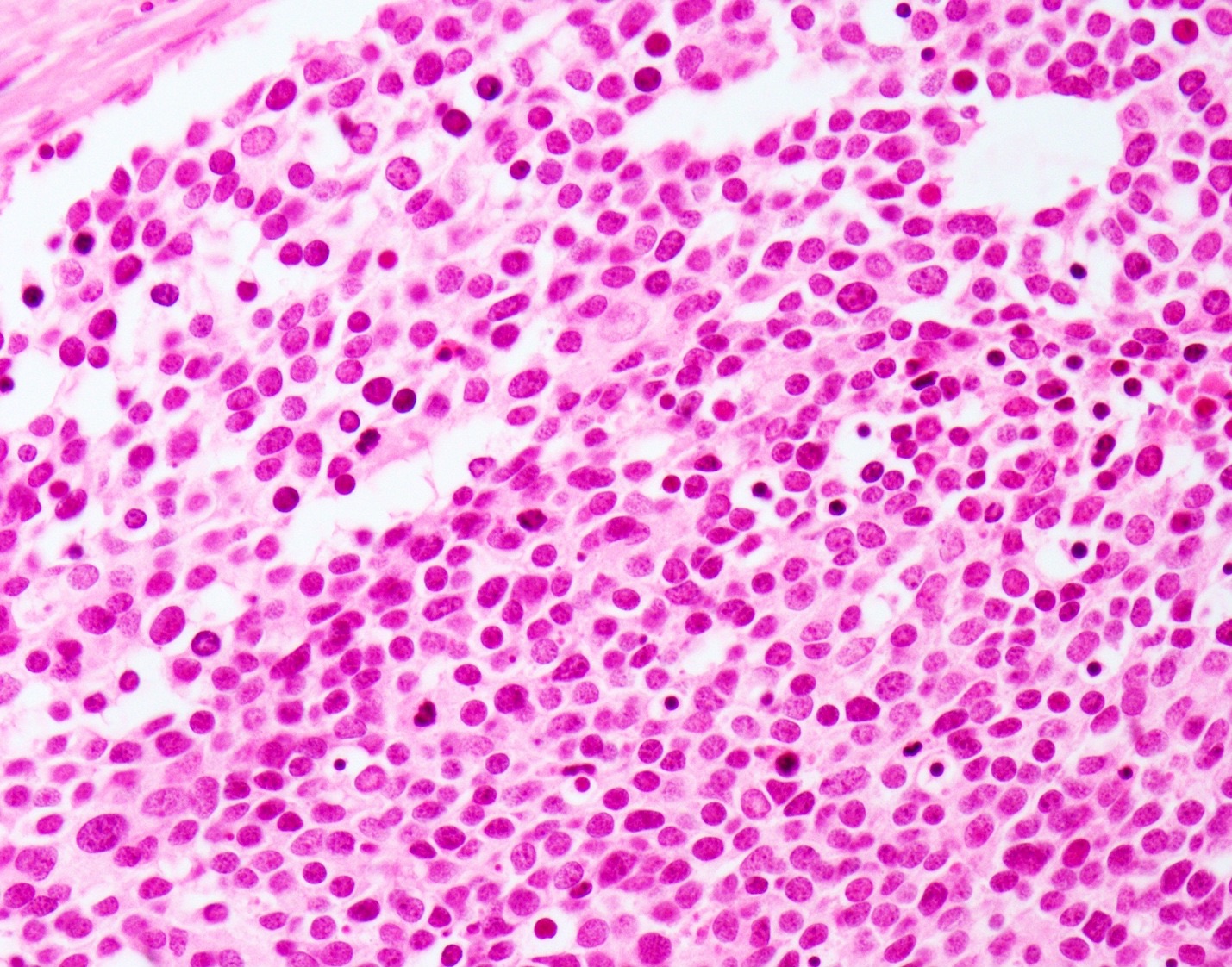
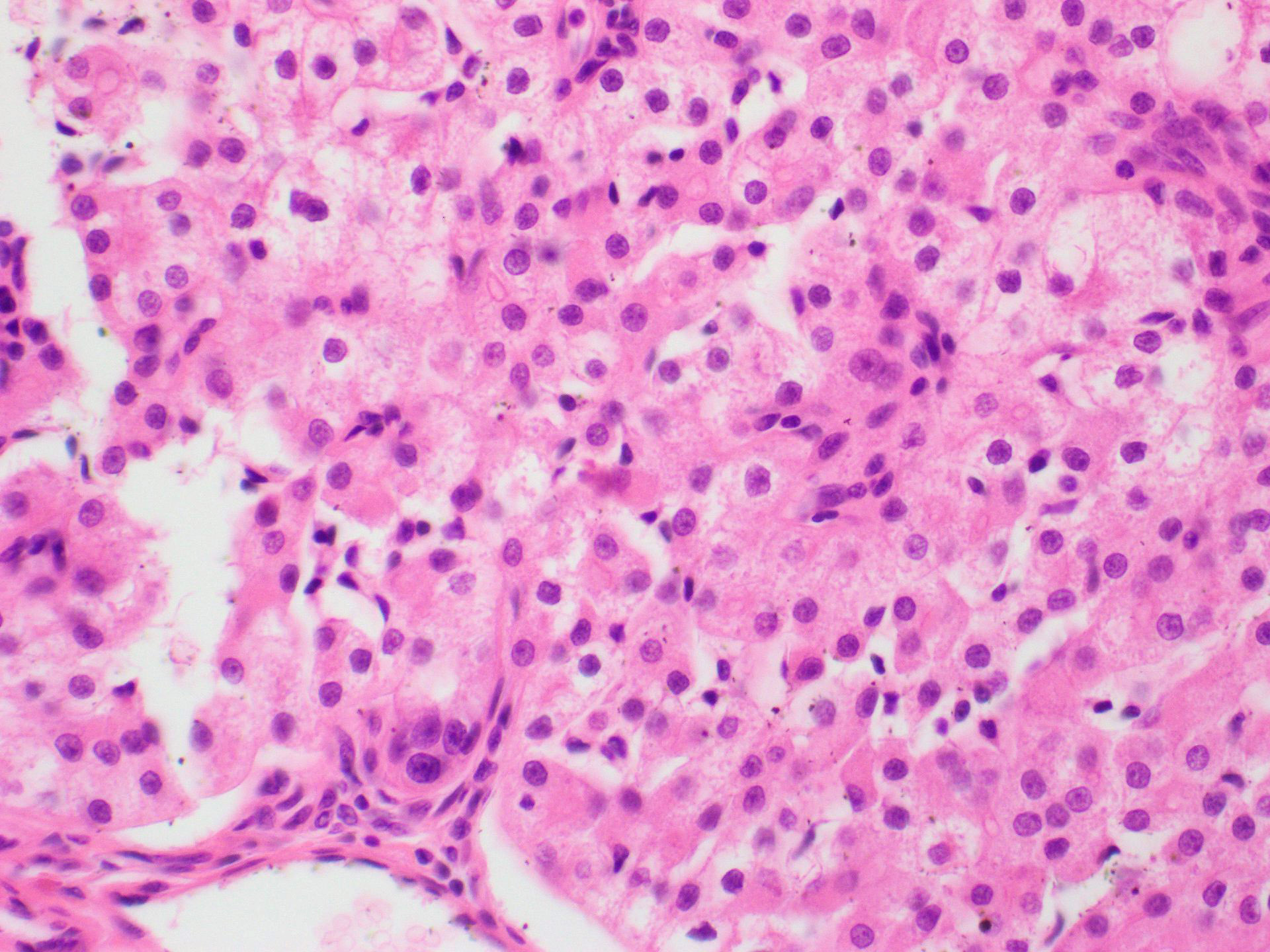
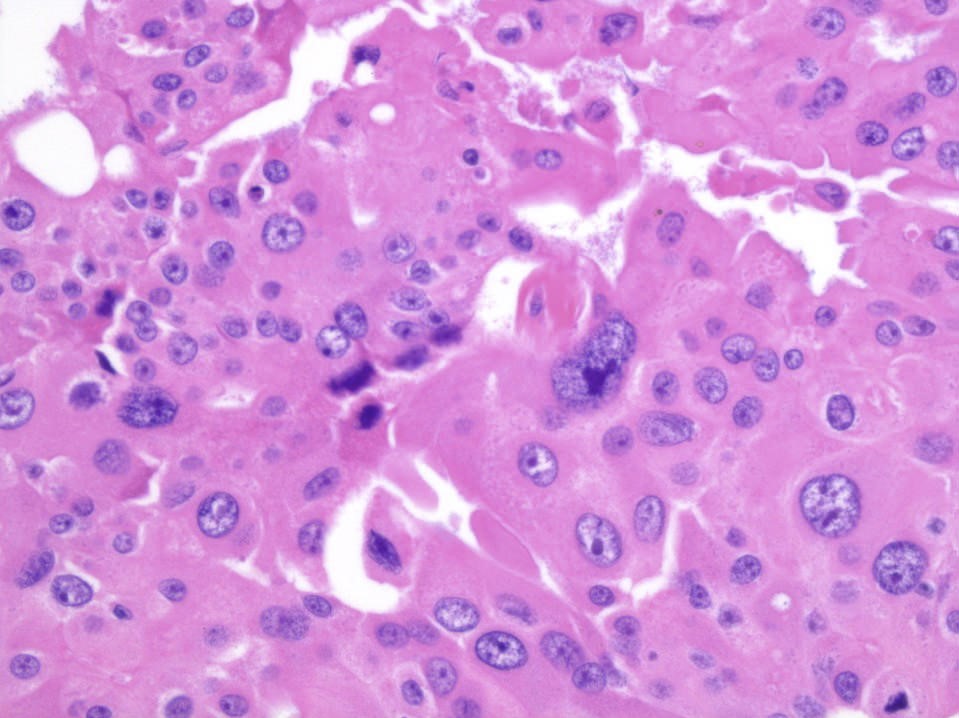
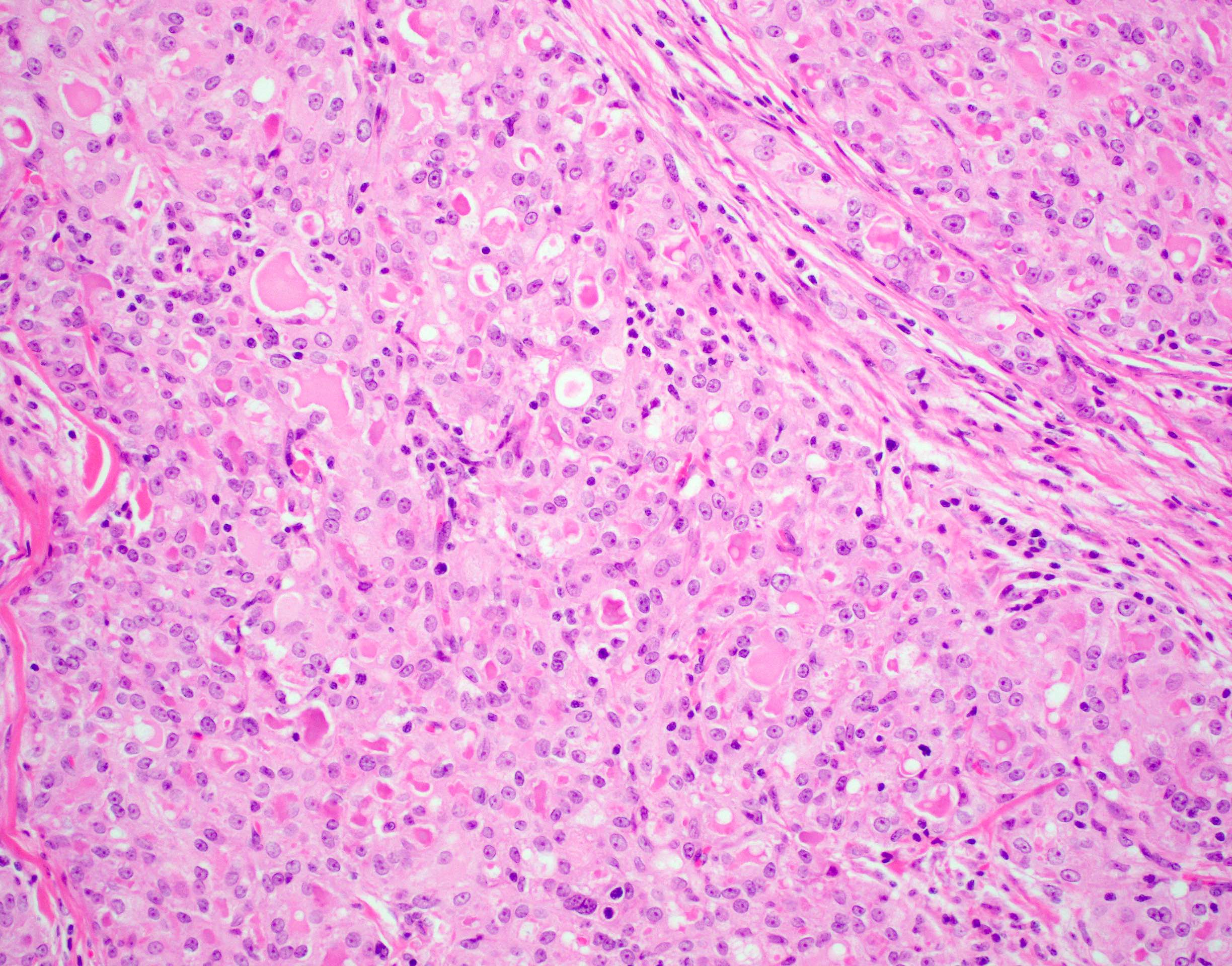
Acinar cells are large and polyhedral, with basophilic granular cytoplasm and eccentric nuclei
Cytoplasmic diastase resistant positive periodic acid-Schiff (PAS) reaction may be focal
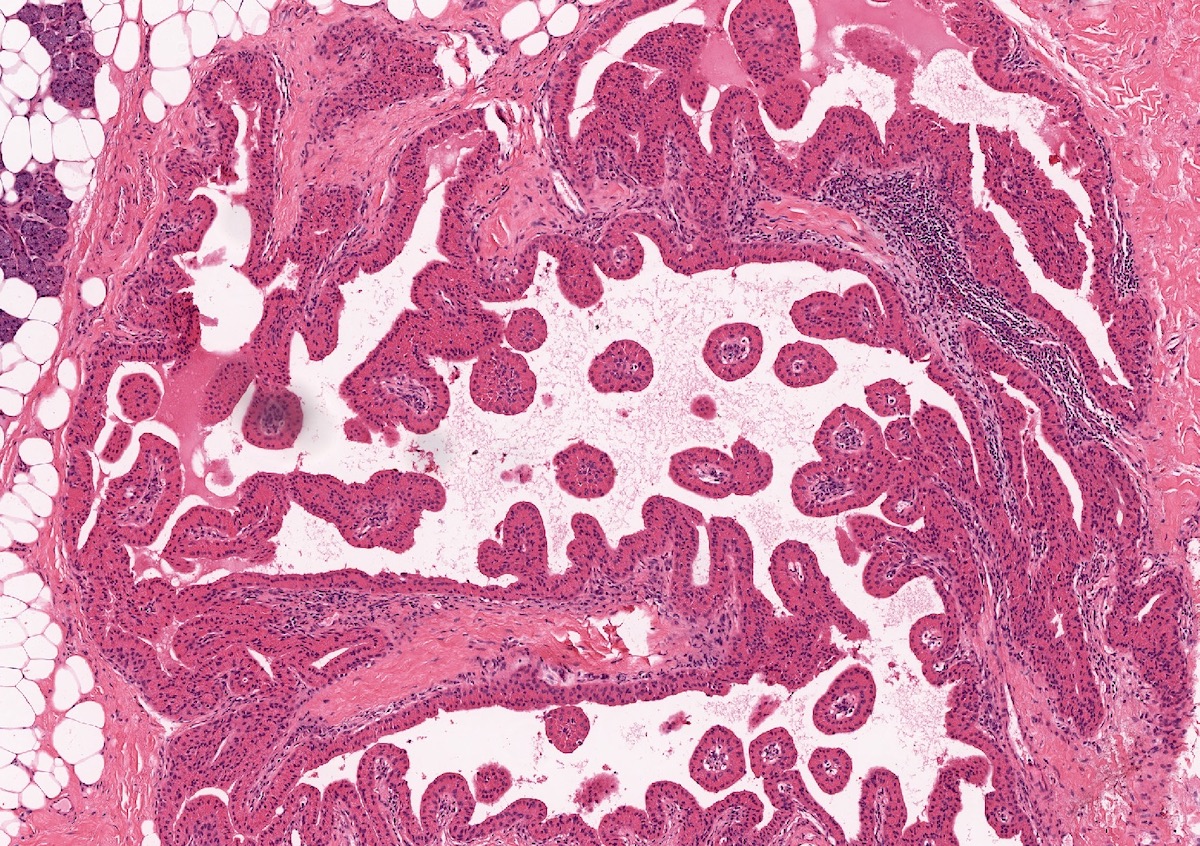
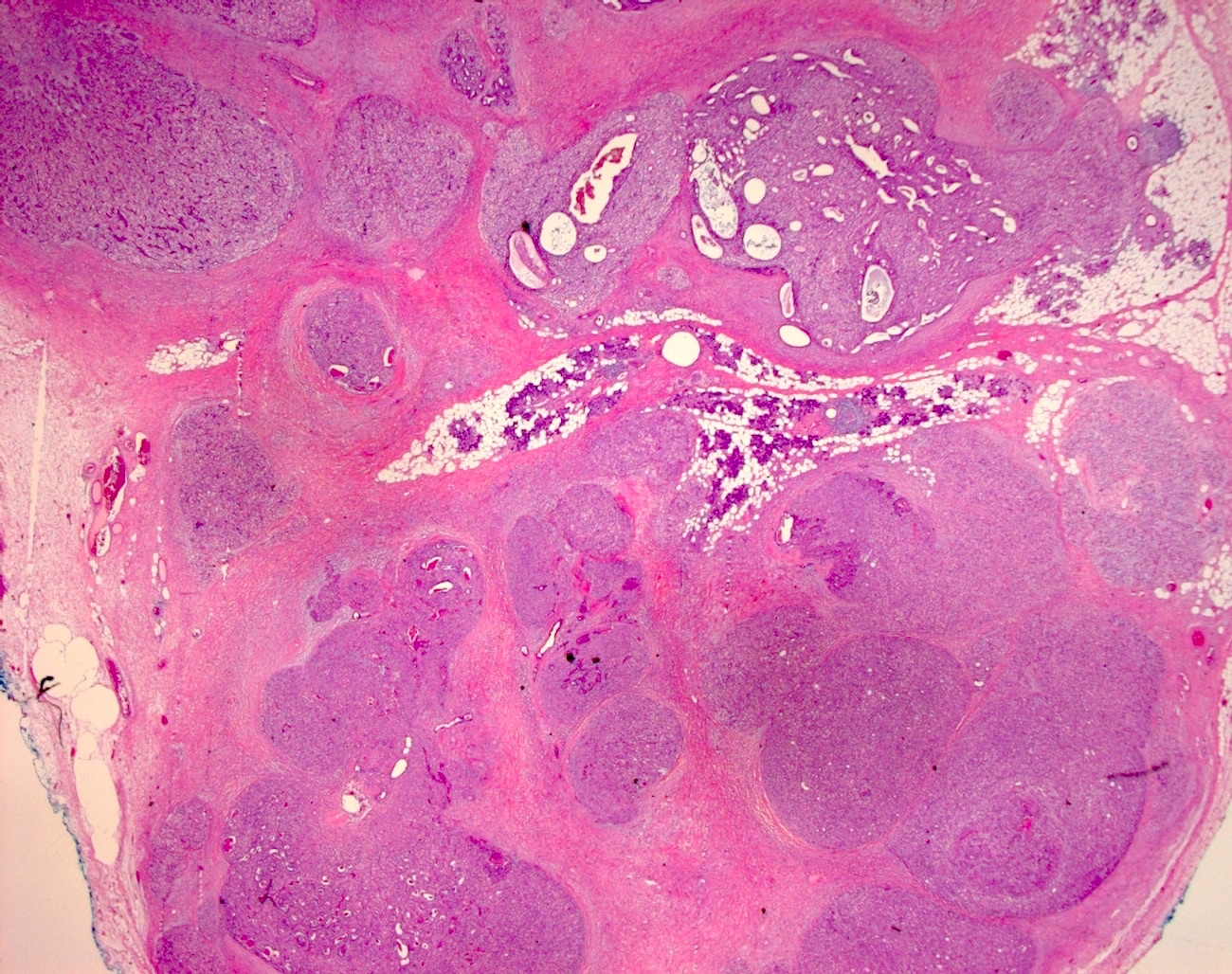
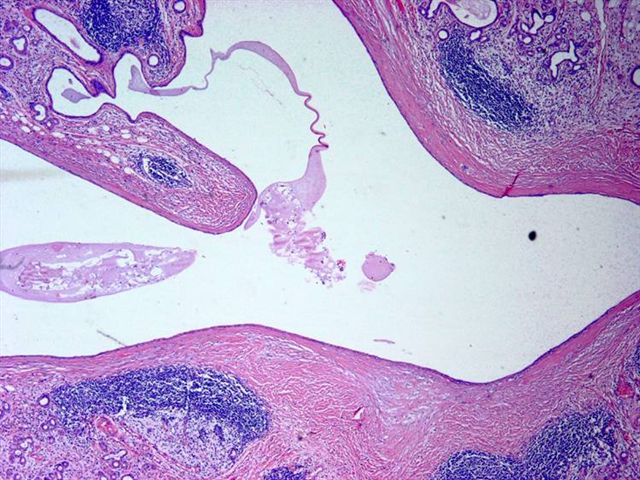
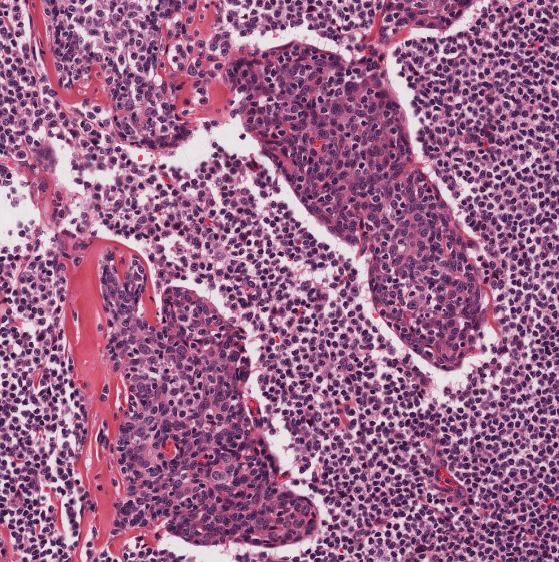
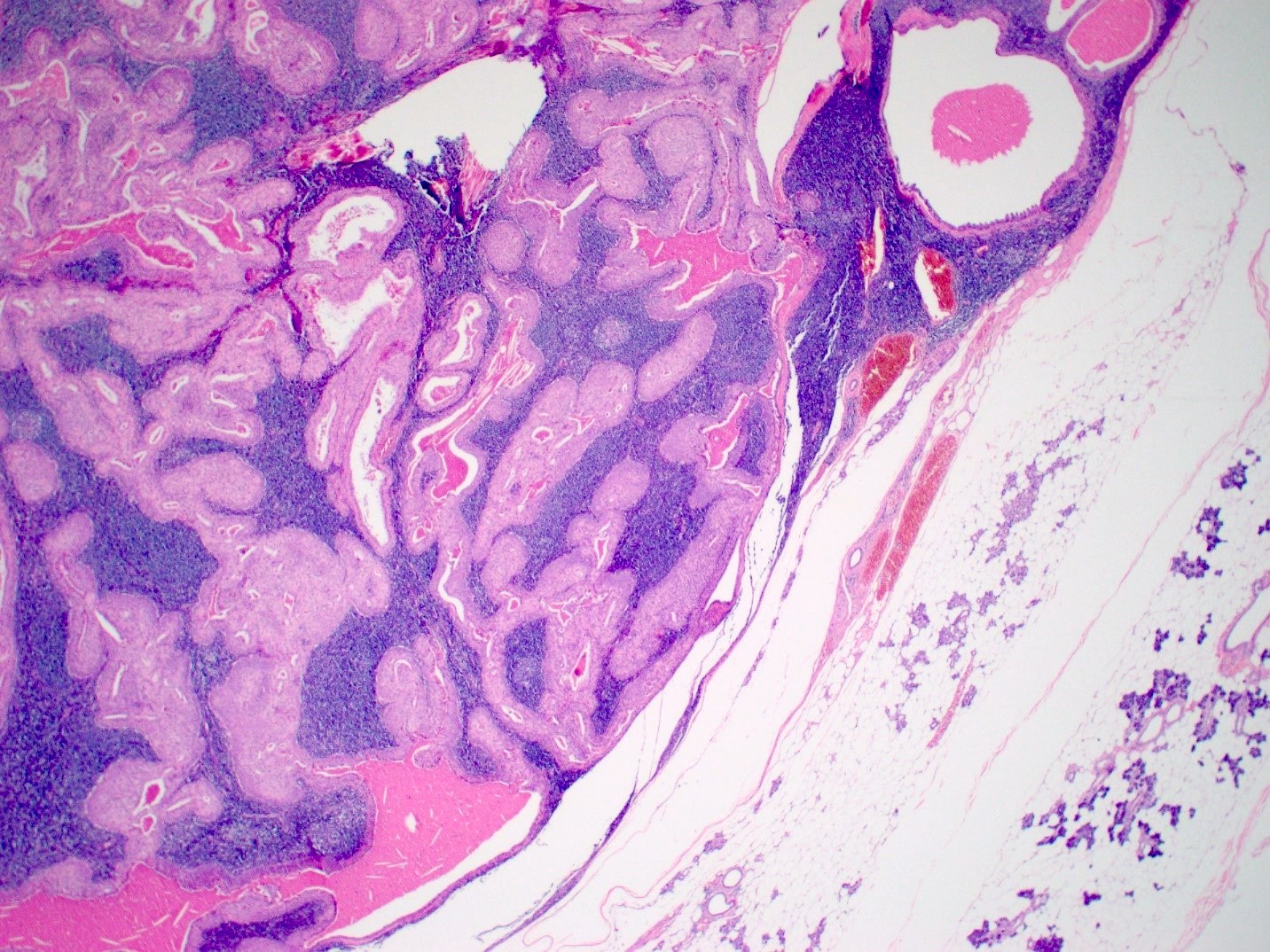
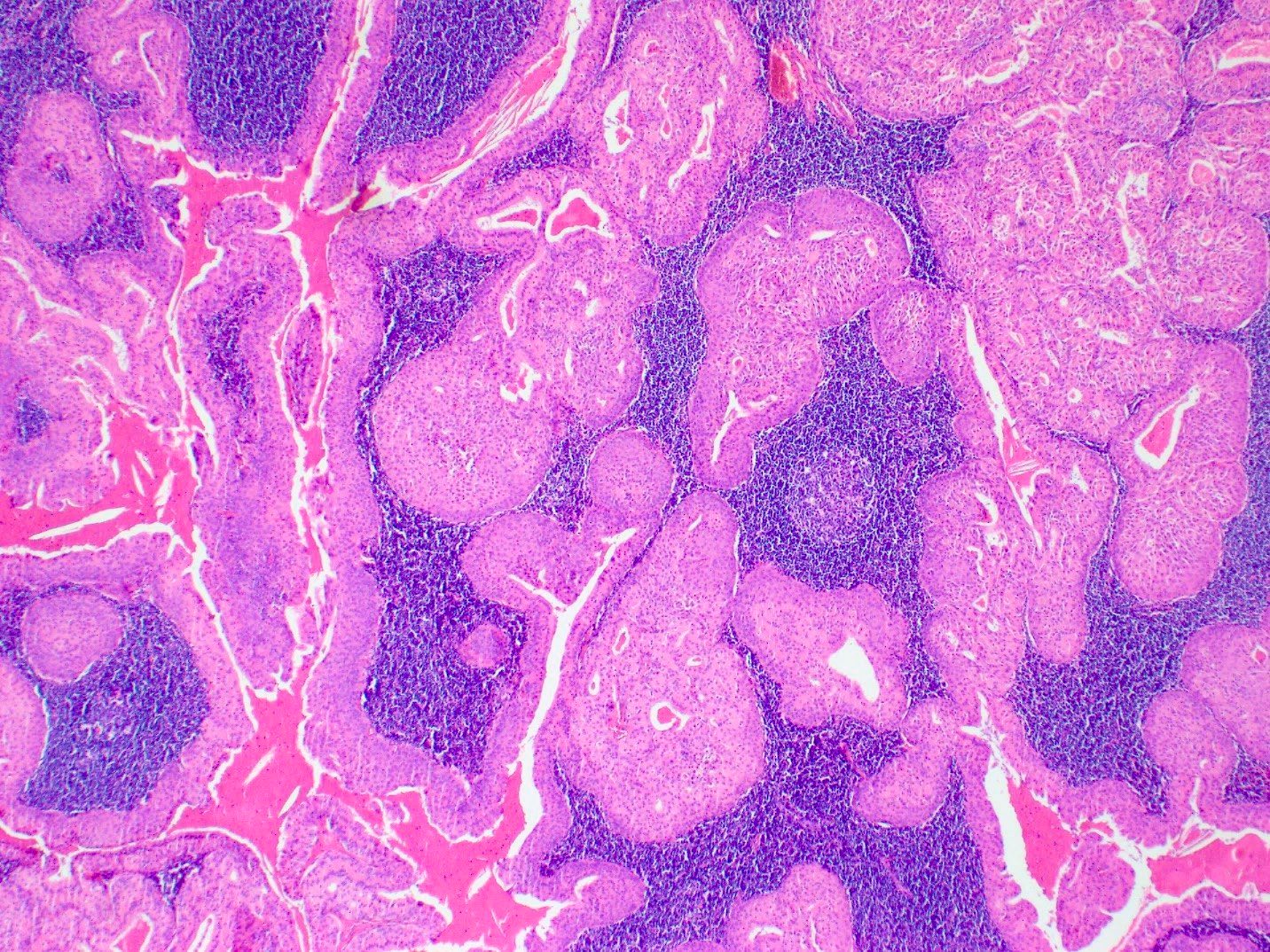
Variety of morphologic patterns, including solid, microcystic, papillary cystic and follicular (Cancer 1983;52:542)
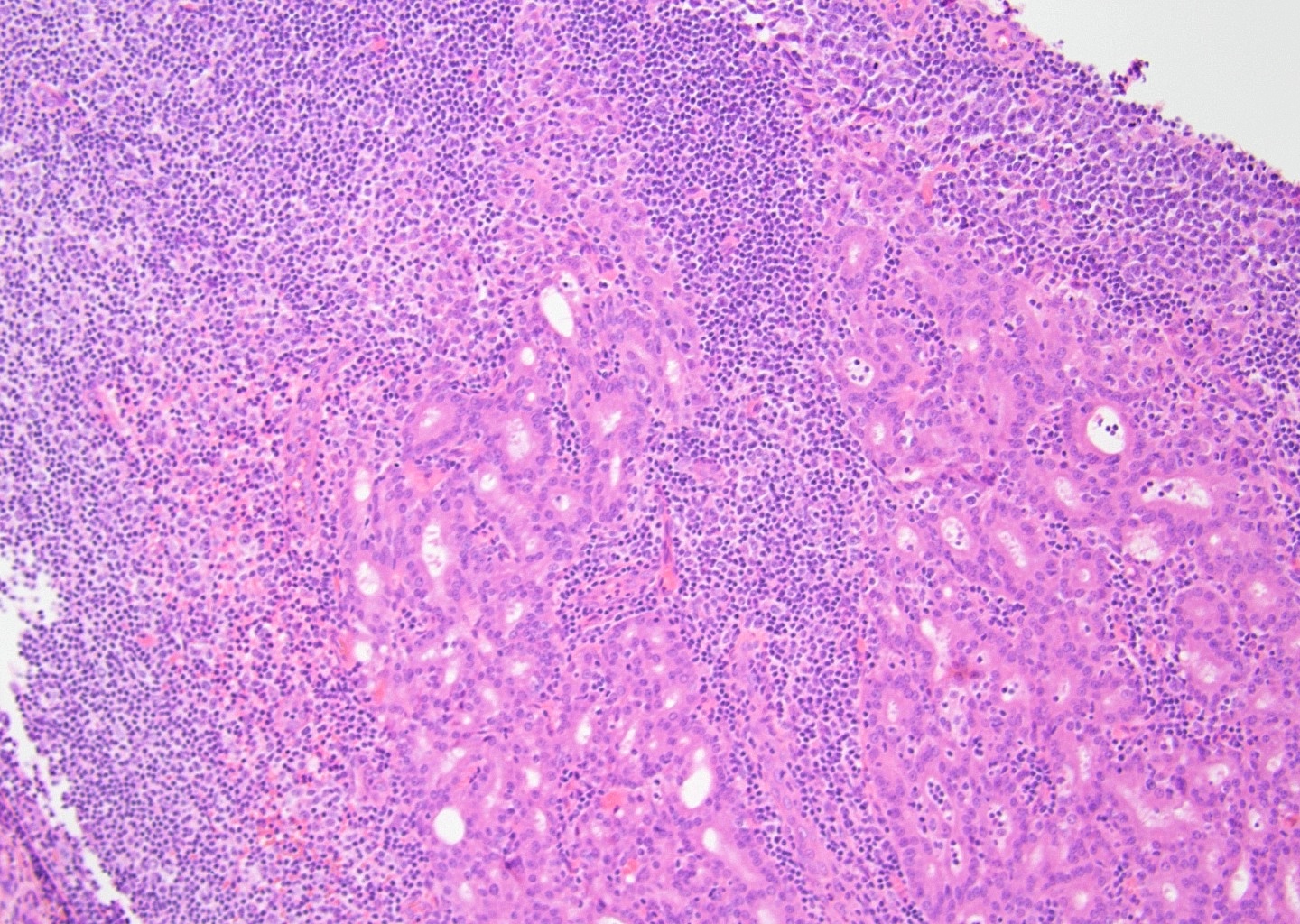
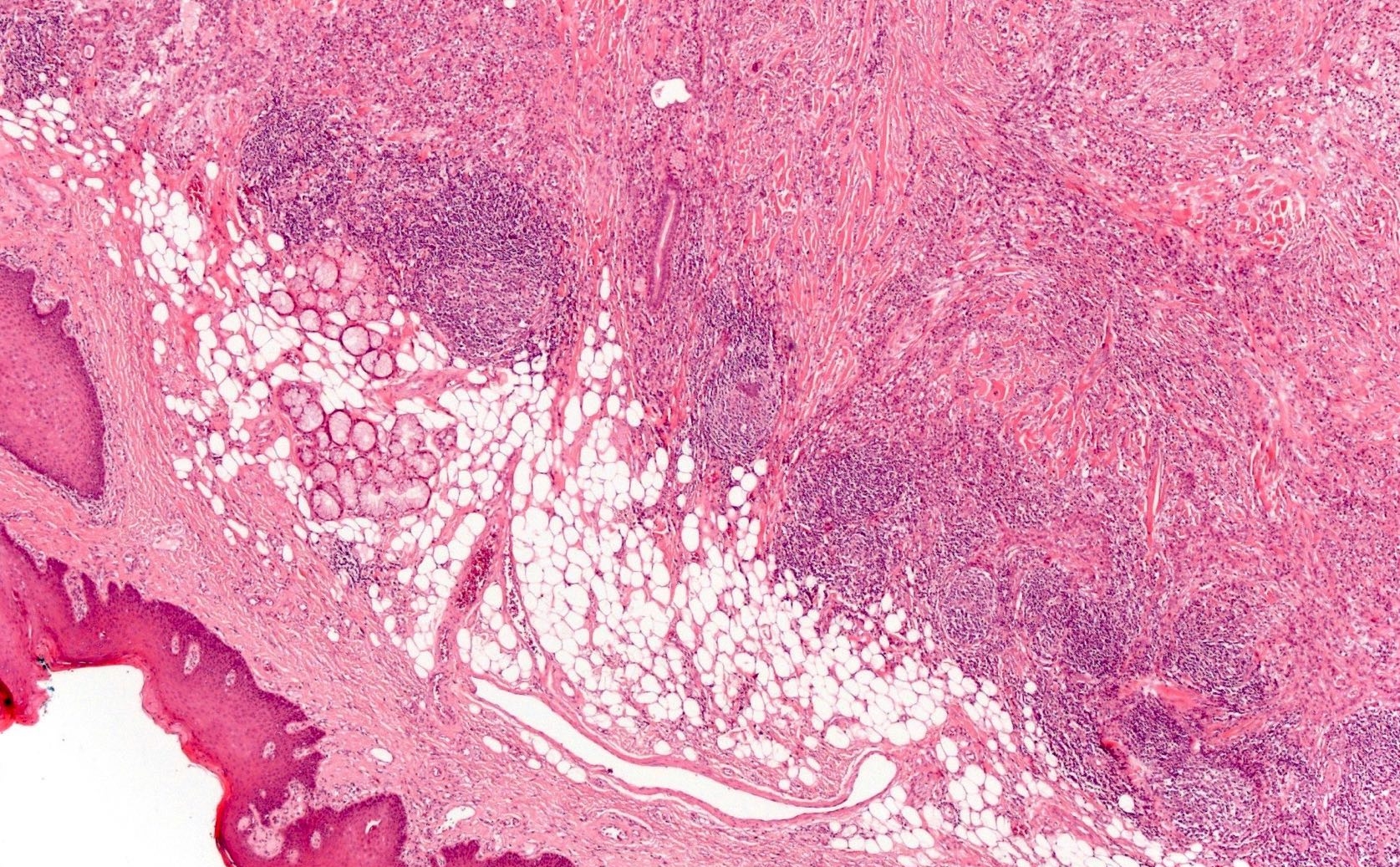
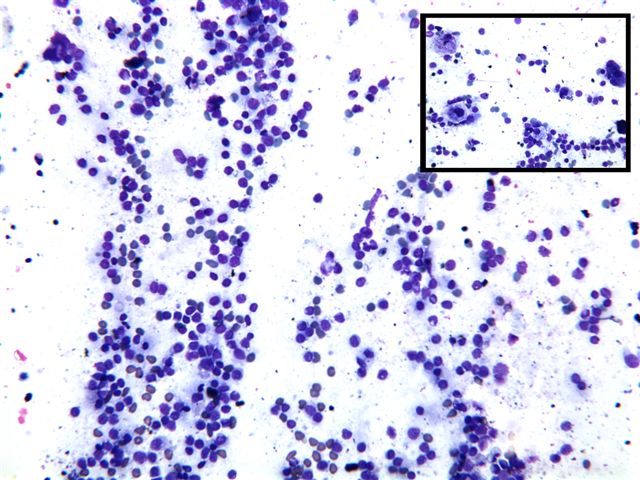
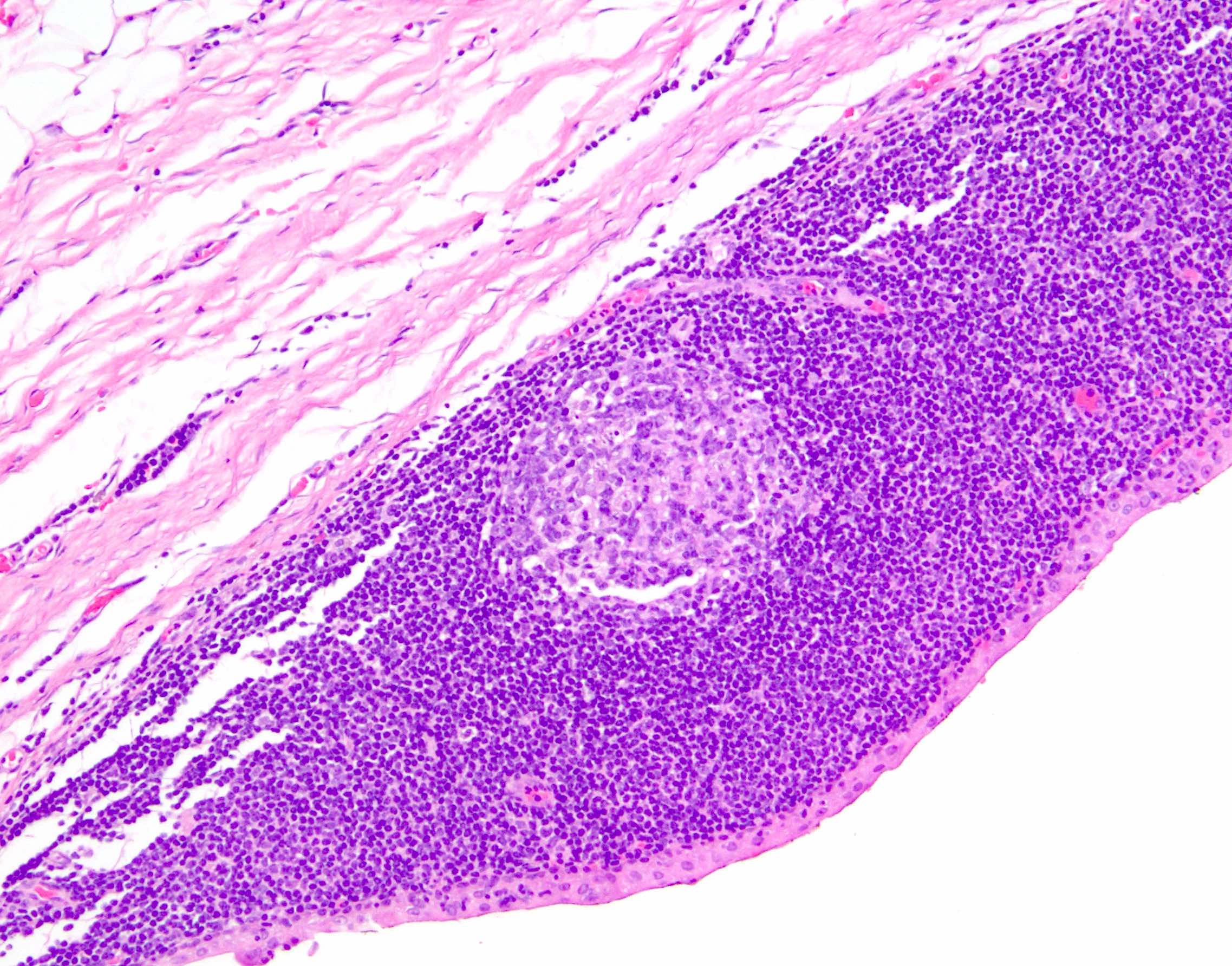
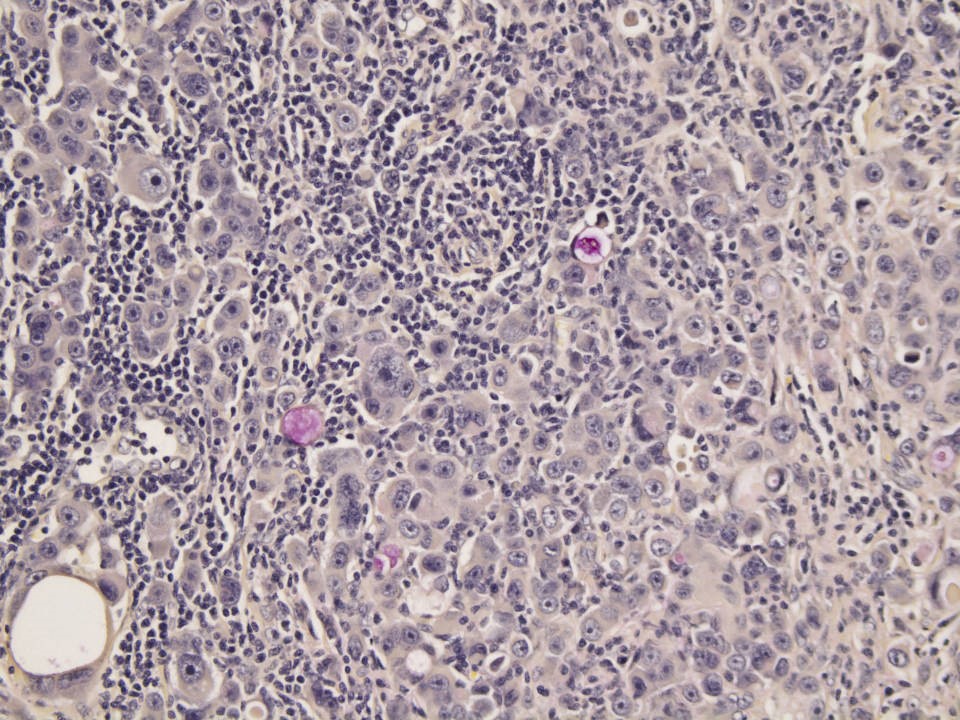
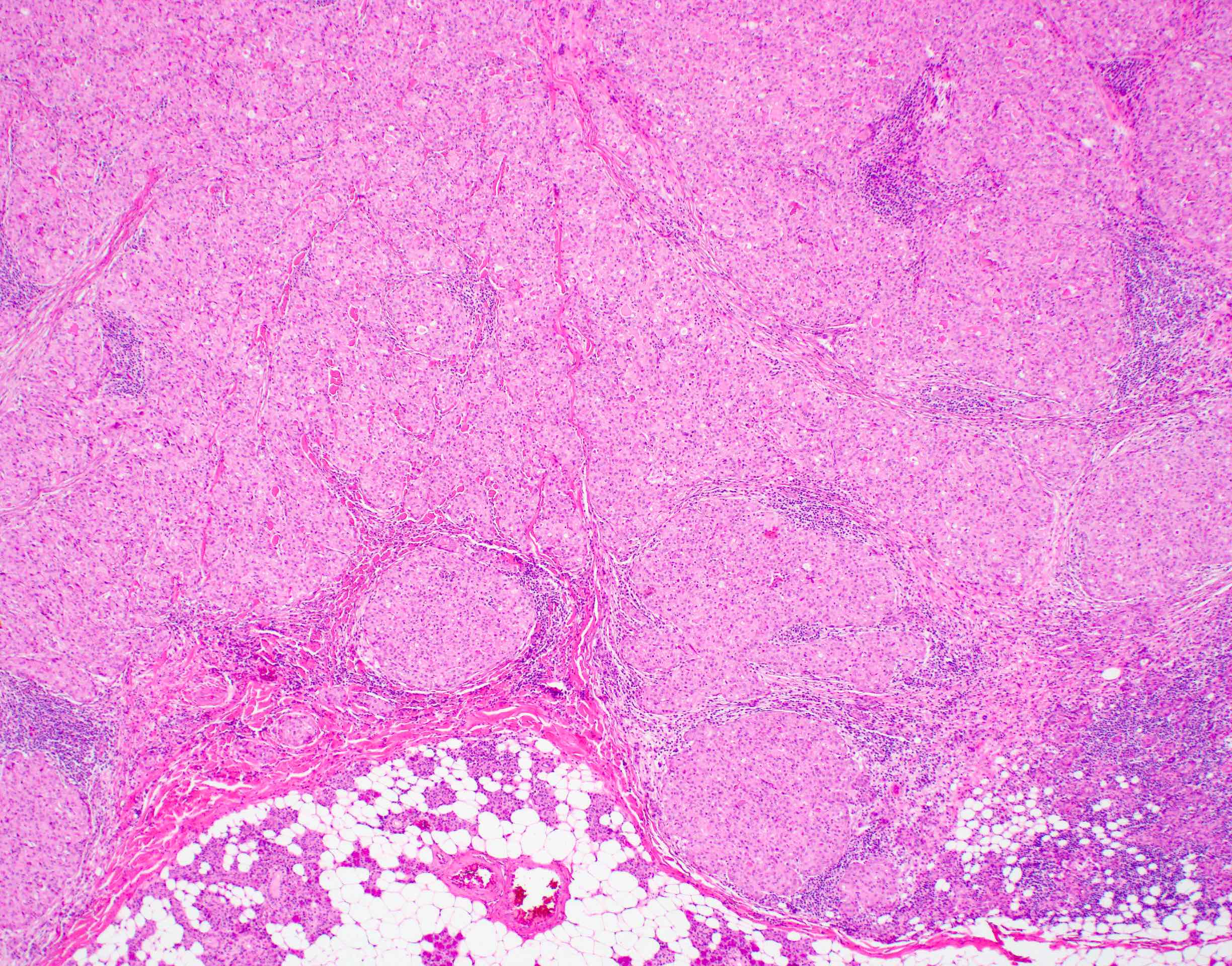
Prominent lymphoid infiltrate may be present (tumor associated lymphoid proliferation varies from randomly scattered, patchy collections of lymphocytes to diffuse, dense infiltrates with well formed follicles throughout the tumor) (Oral Surg Oral Med Oral Pathol 1994;77:19)
Mitosis, necrosis and significant pleomorphism usually absent
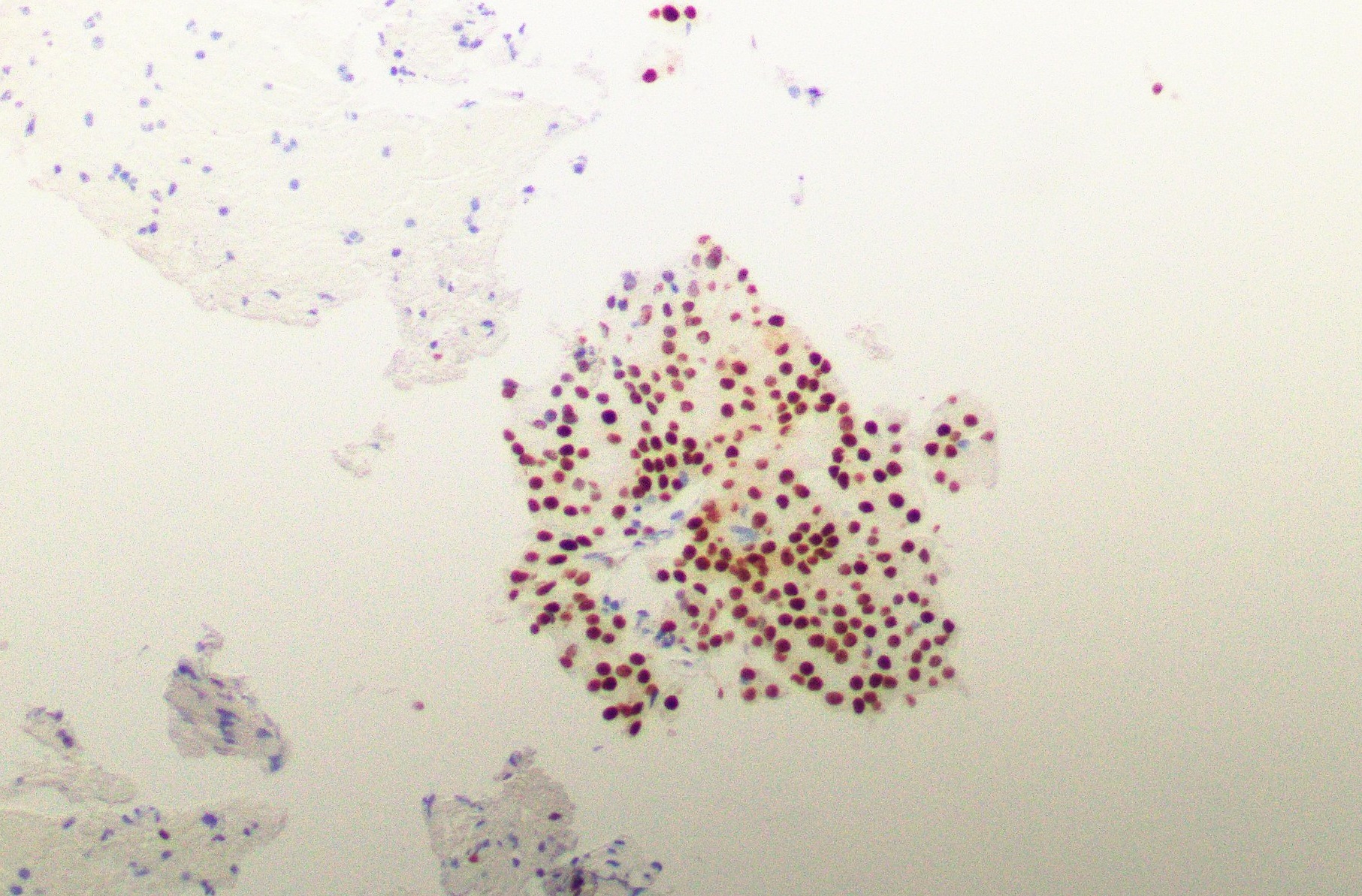
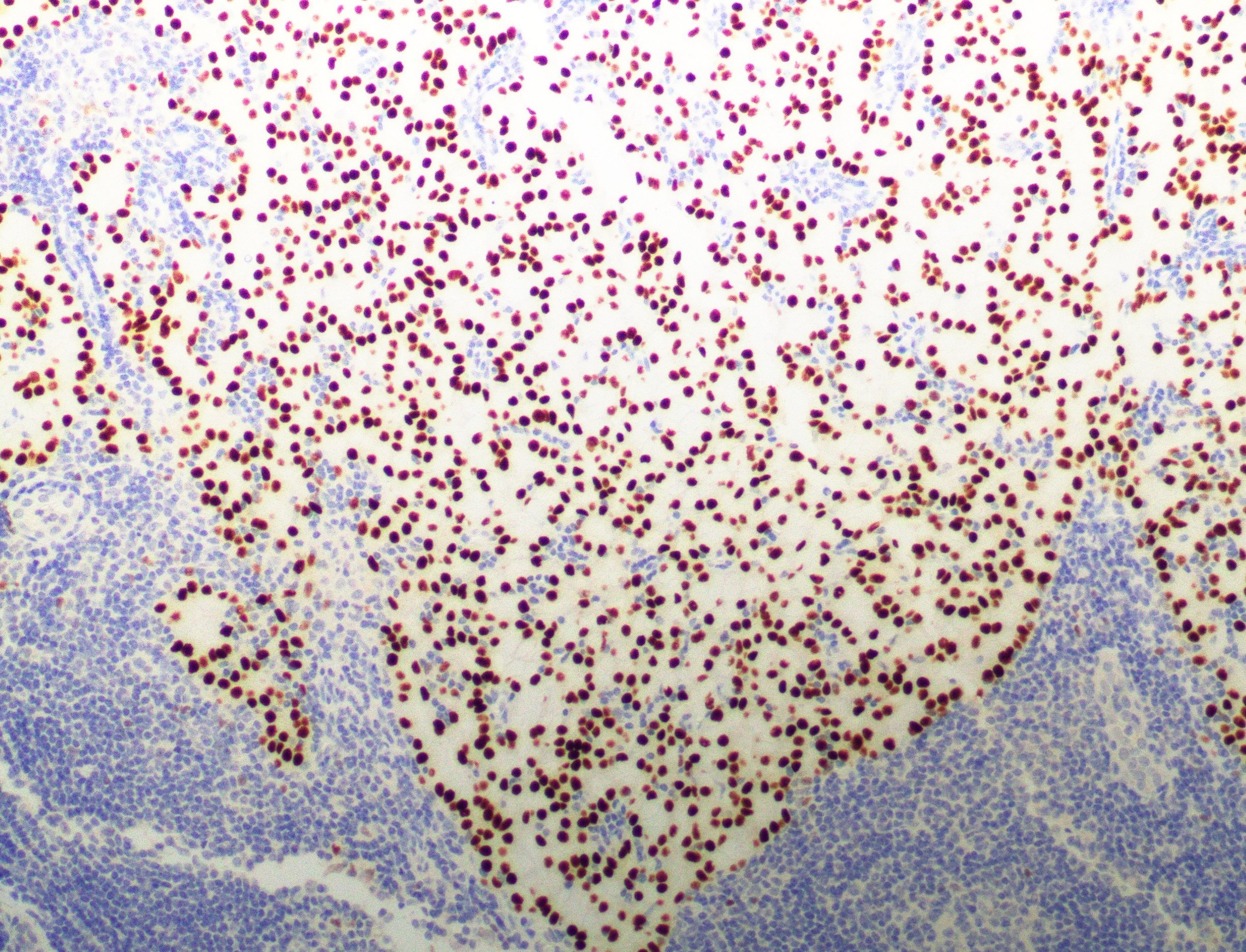
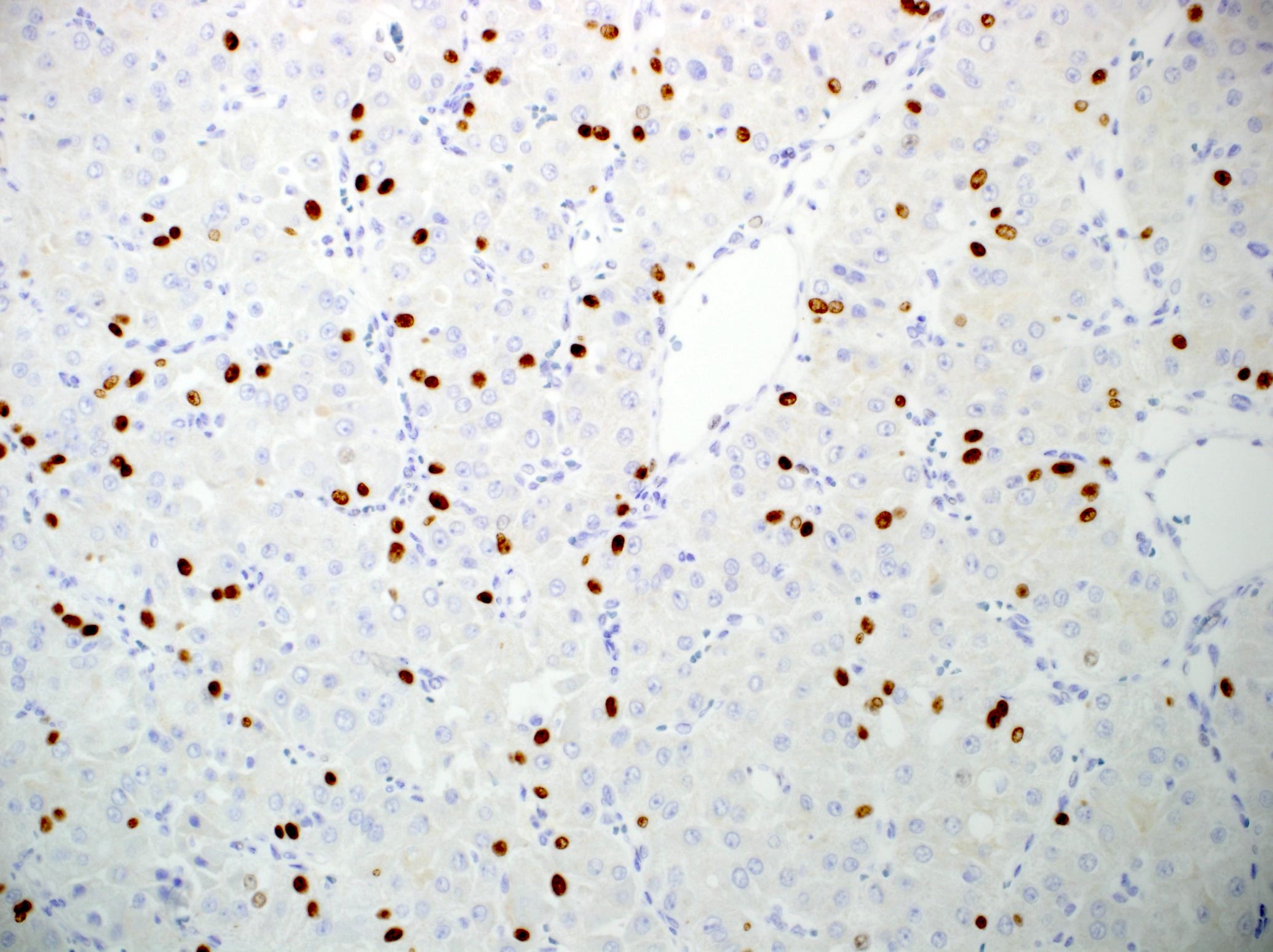
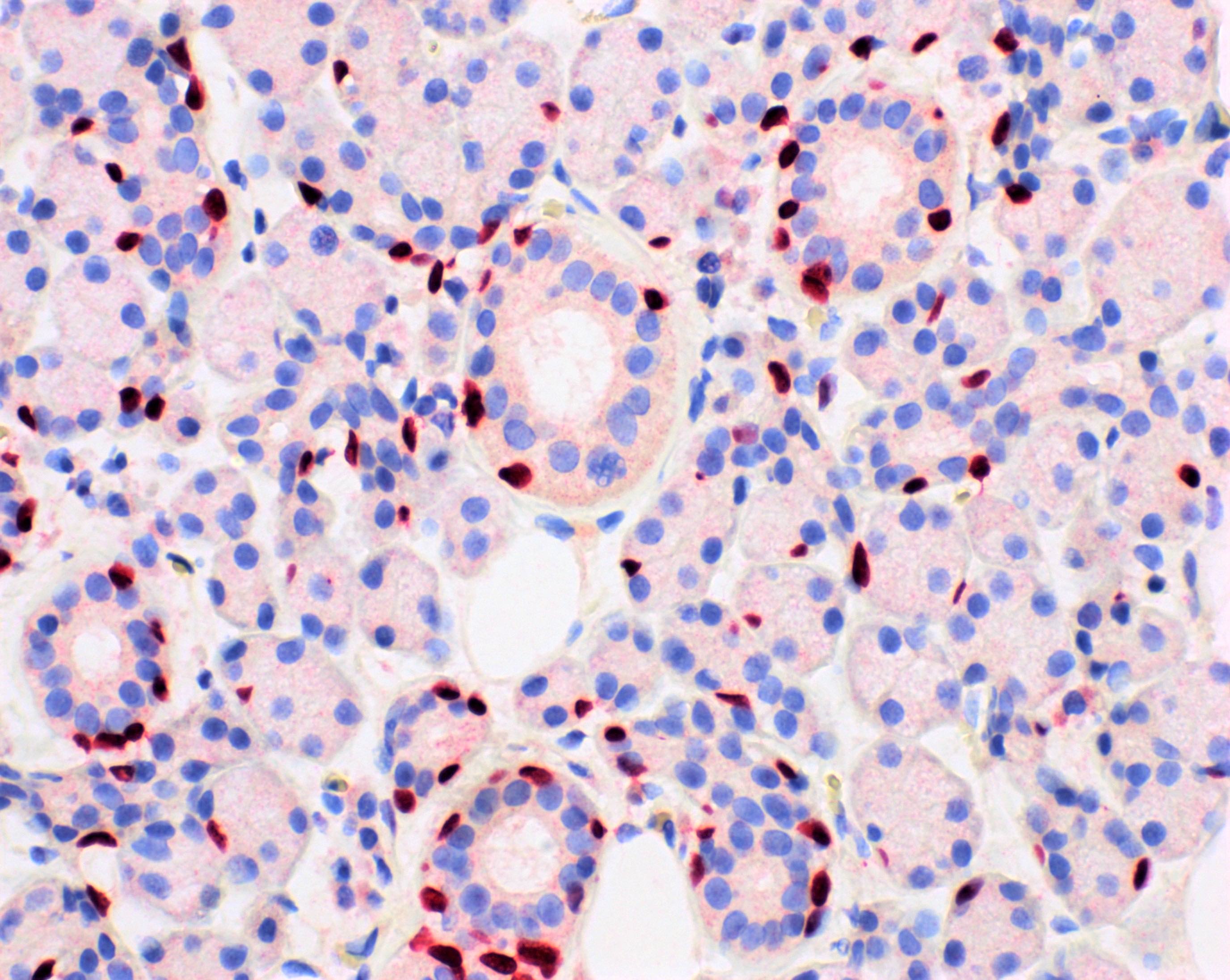
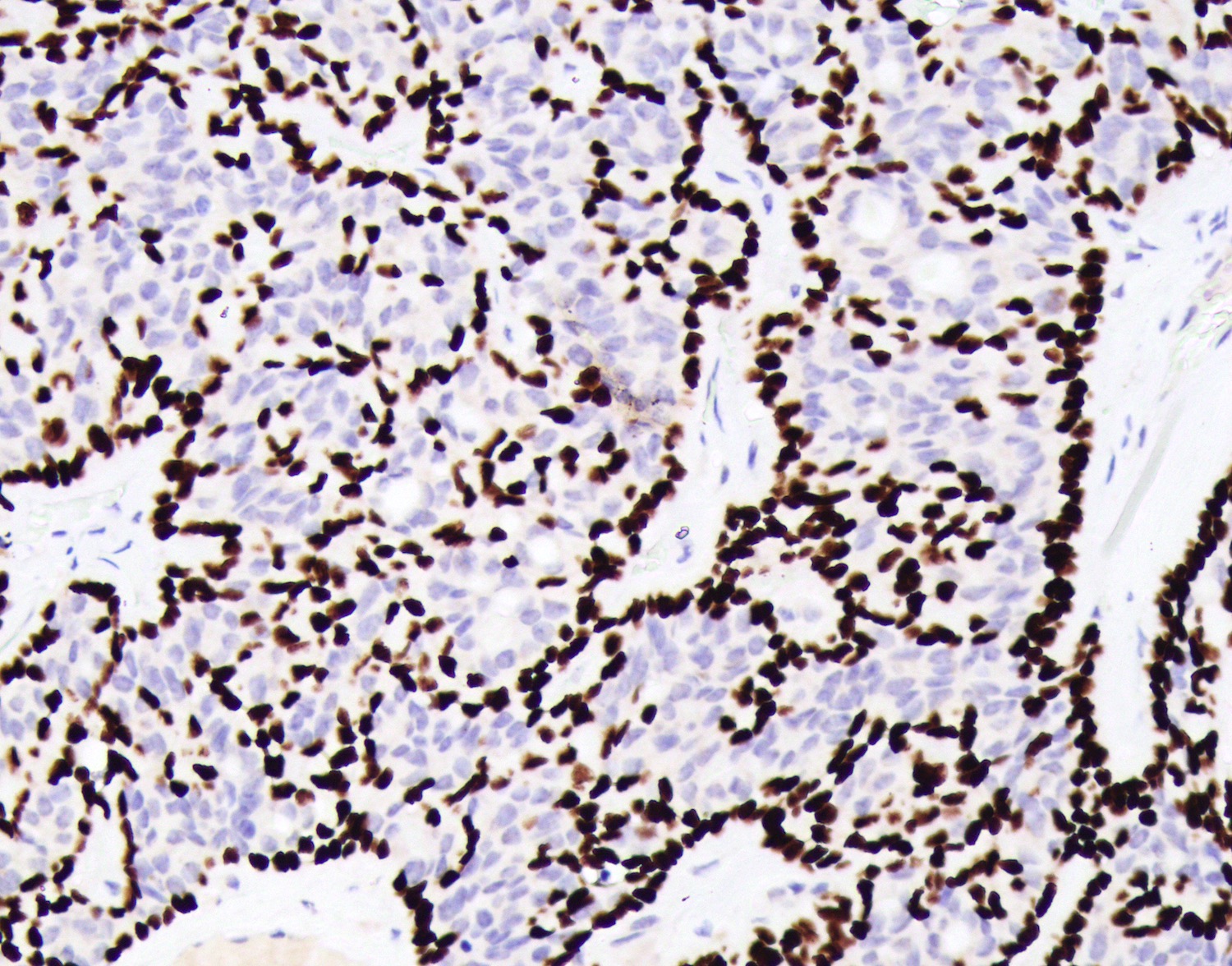
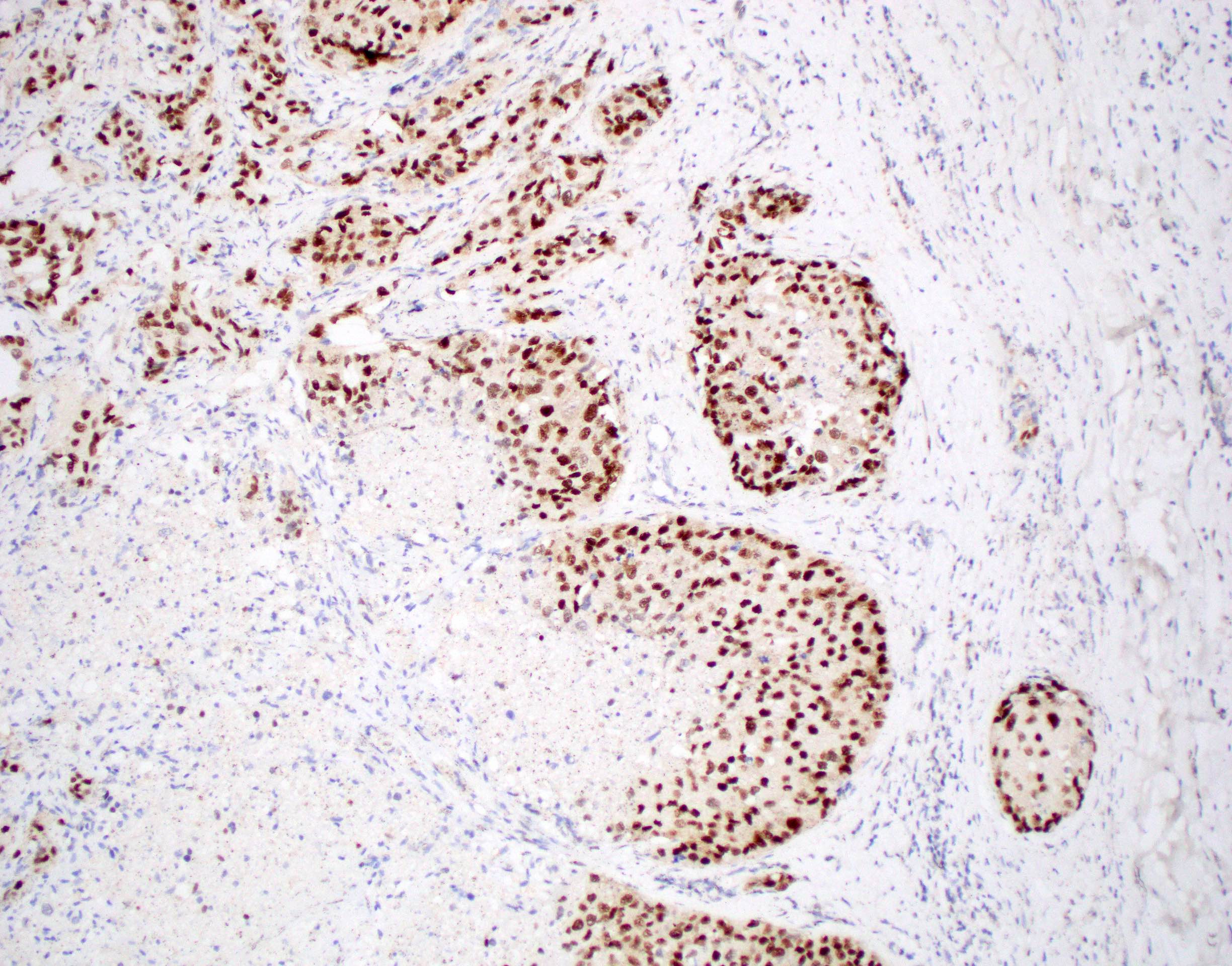
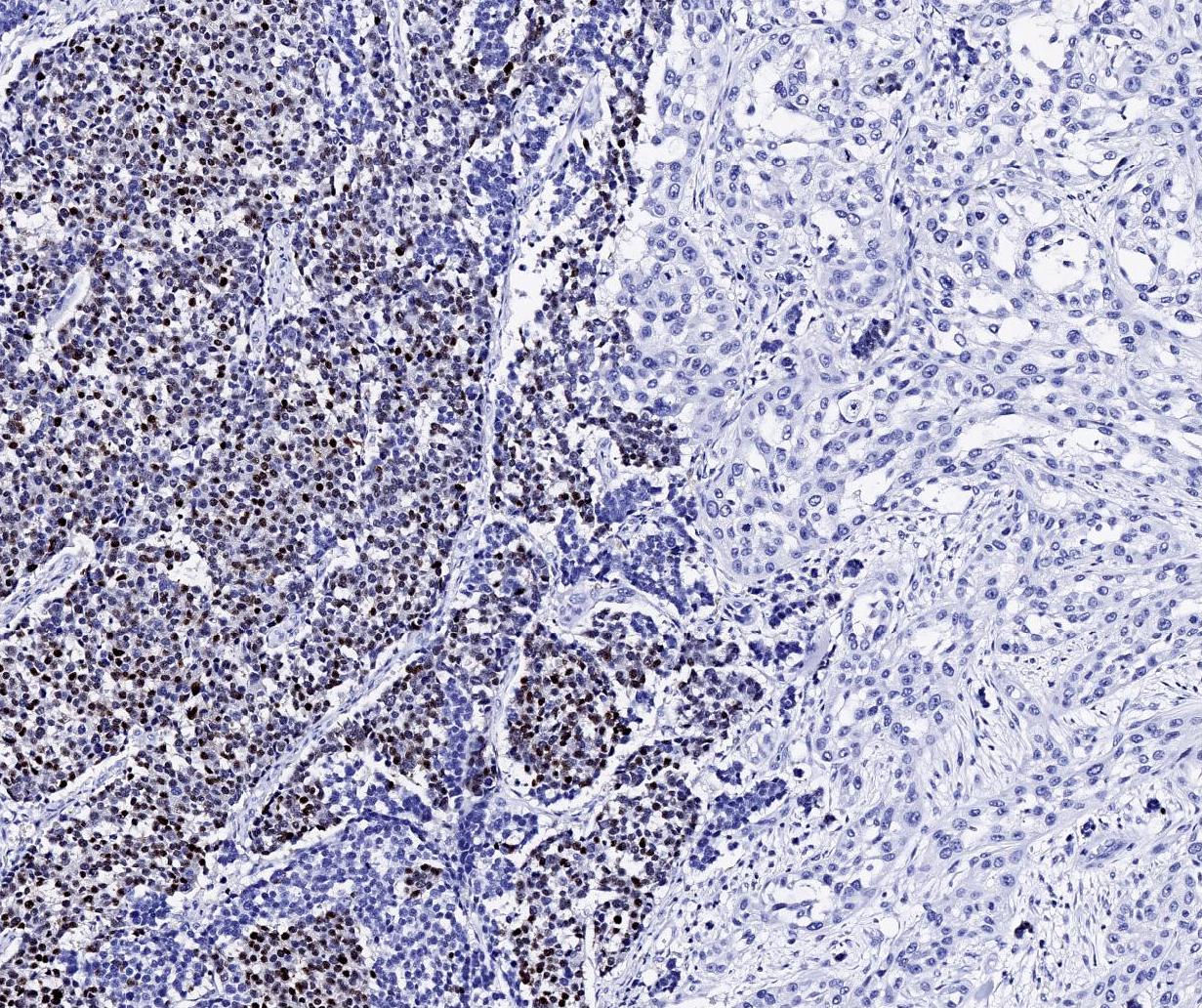
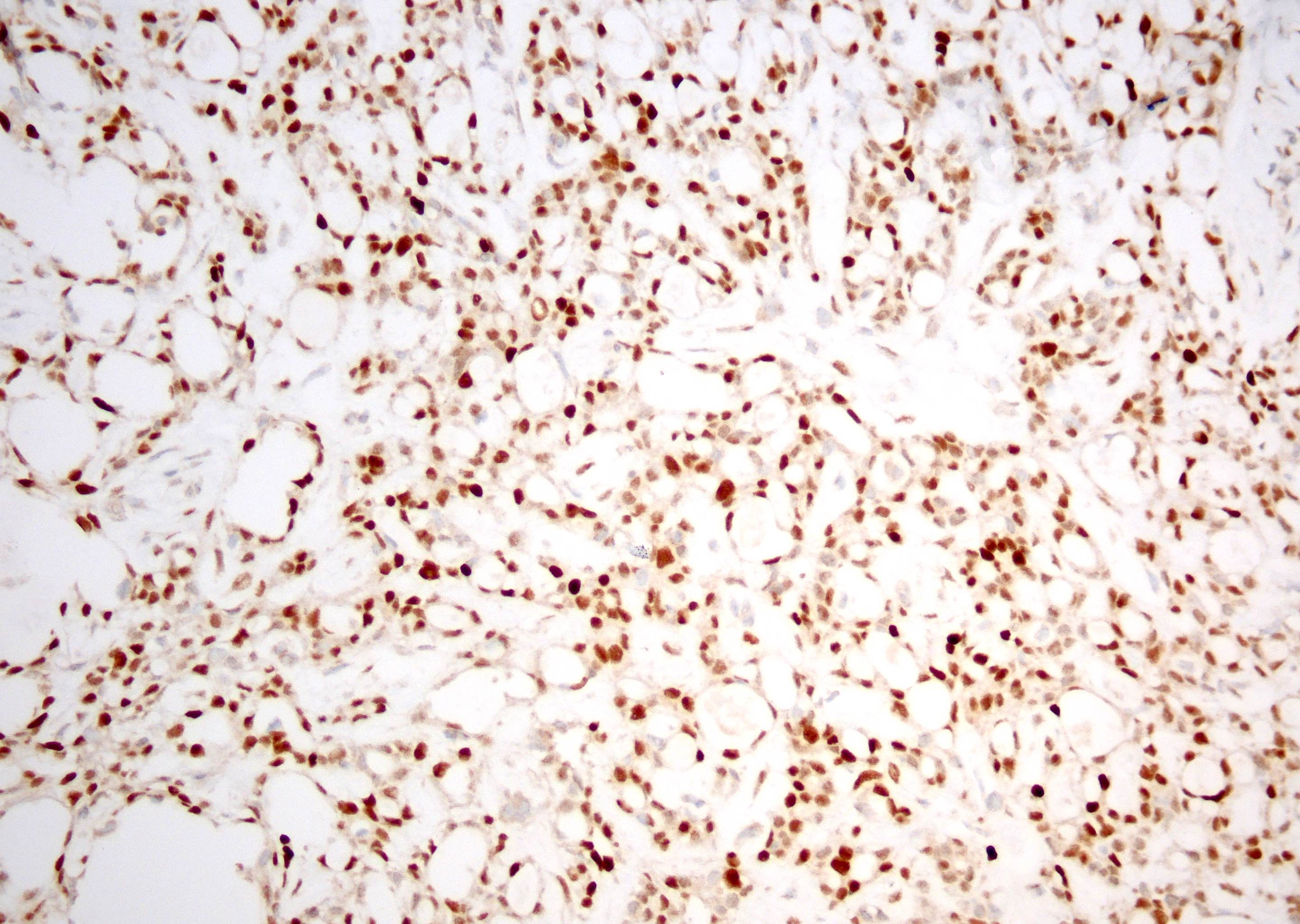
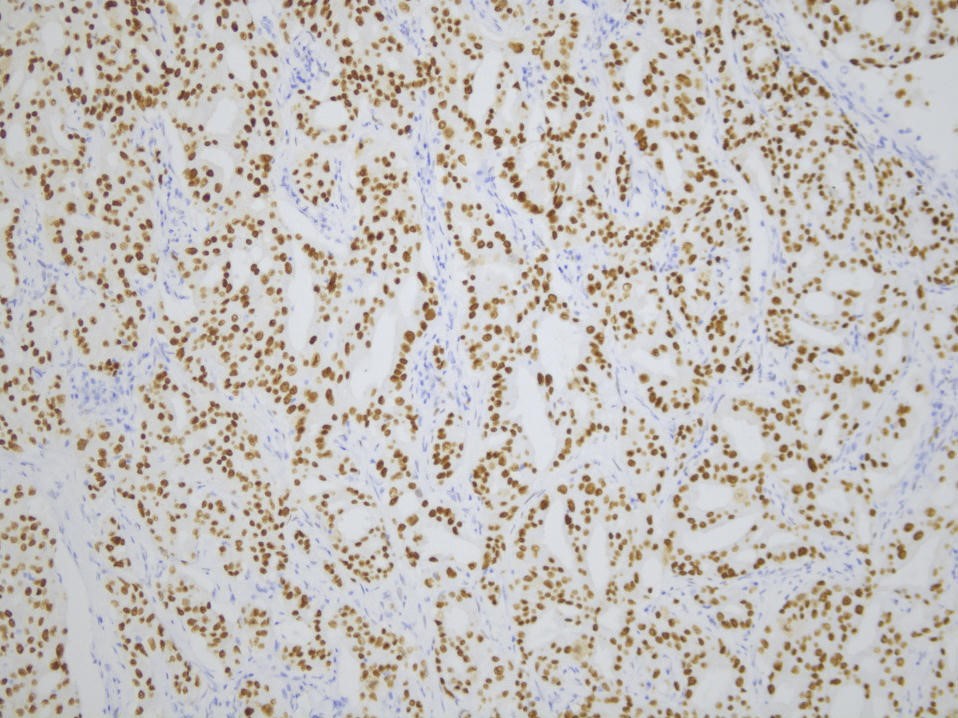
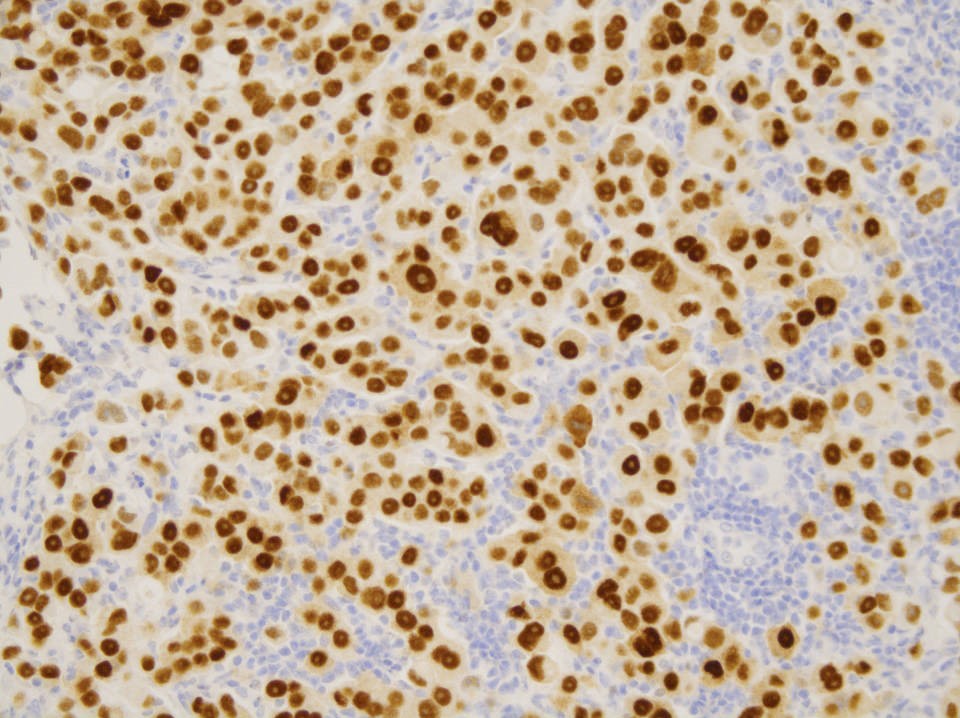
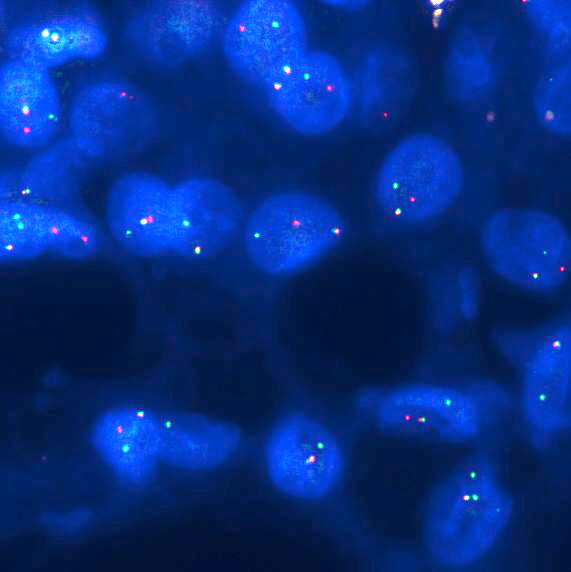
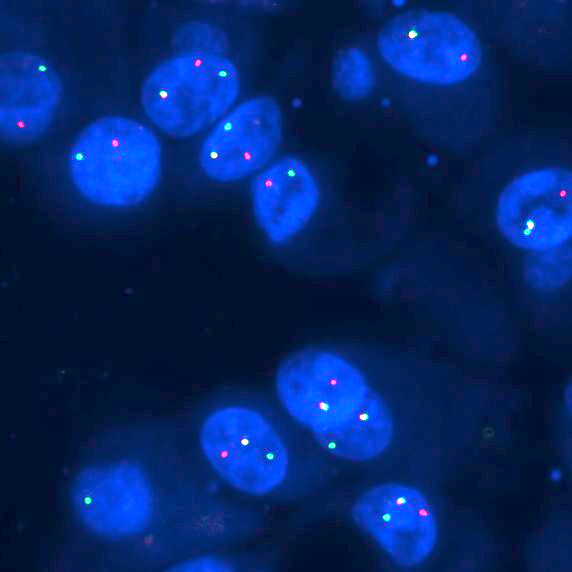
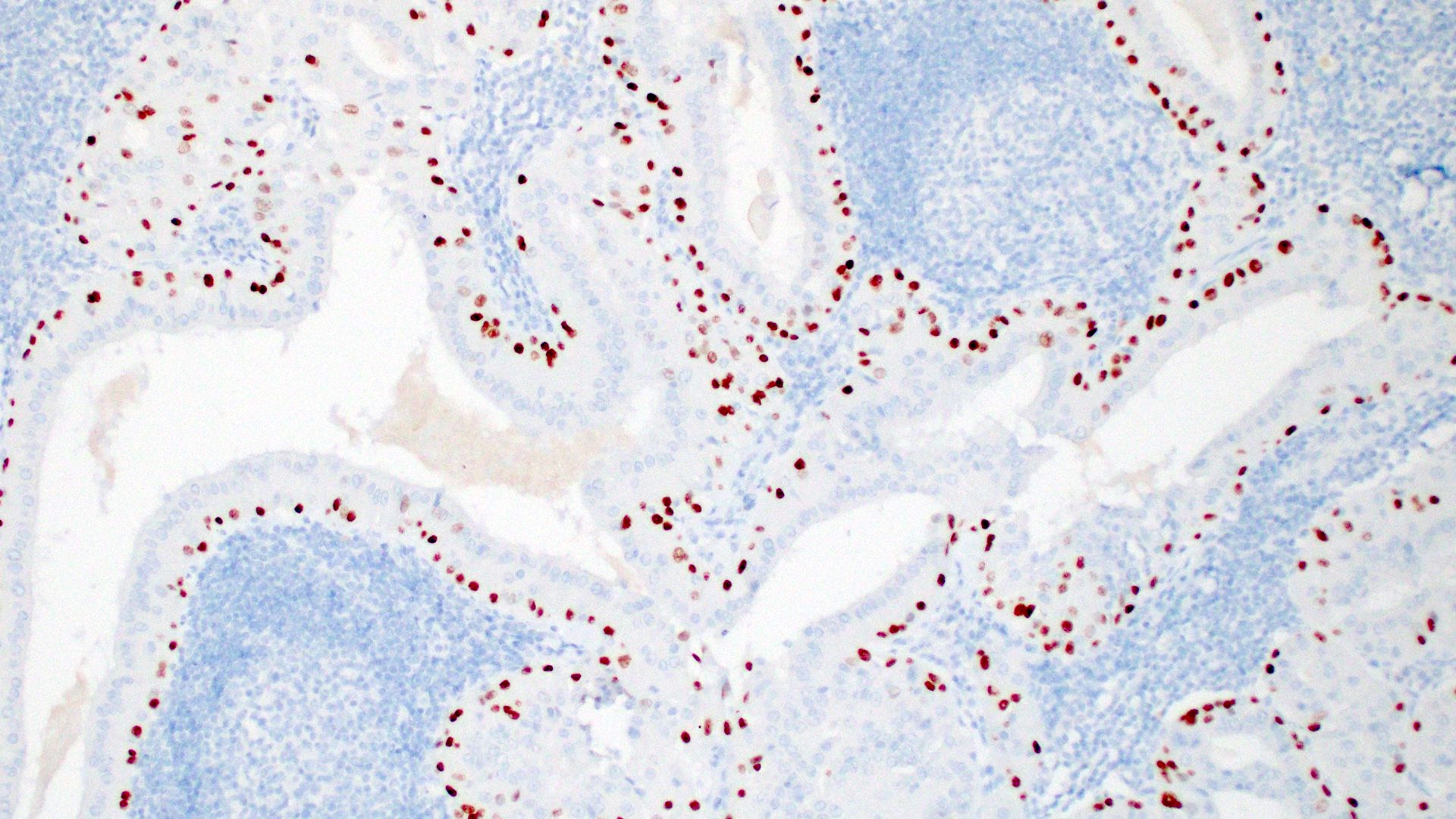
Recurrent (t[4;9][q13;q31]) genomic rearrangement (resulting in translocation of active enhancer regions from the secretory Ca binding phosphoprotein [SCPP] gene cluster to the region upstream of nuclear receptor subfamily 4 group A member 3 [NR4A3], leading to NR4A3 IHC overexpression) (Cancer Cytopathol 2021;129:104)
Loss of function mutations of CDKN2A / CDKN2B gene are associated with high grade histology and distant metastasis (Mod Pathol 2023;36:100150)
Which of the following statements is true regarding acinic cell carcinoma of salivary glands?
Acinic cell carcinoma is a high grade malignant neoplasm
Most commonly occurs in minor salivary glands
Neoplastic cells express DOG1 and SOX10
Younger age at presentation and presence of tumor associated lymphocytes are associated with a poor prognosis
Board review style answer #1
C. Neoplastic cells express DOG1 and SOX10. DOG1 and SOX10 are expressed in benign acinar cells and intercalated duct cells and other salivary gland neoplasms; however, strong diffuse expression of these markers can help distinguish acinic cell carcinoma from other salivary gland neoplasms. Answer A is incorrect because acinic cell carcinoma is considered low intermediate grade malignancy of salivary glands, although high grade transformation may occur. Answer B is incorrect because the majority of cases arise in the parotid gland. Answer D is incorrect because older age at the onset (> 45) and depletion of lymphocytes within the stroma are linked to worse outcomes.
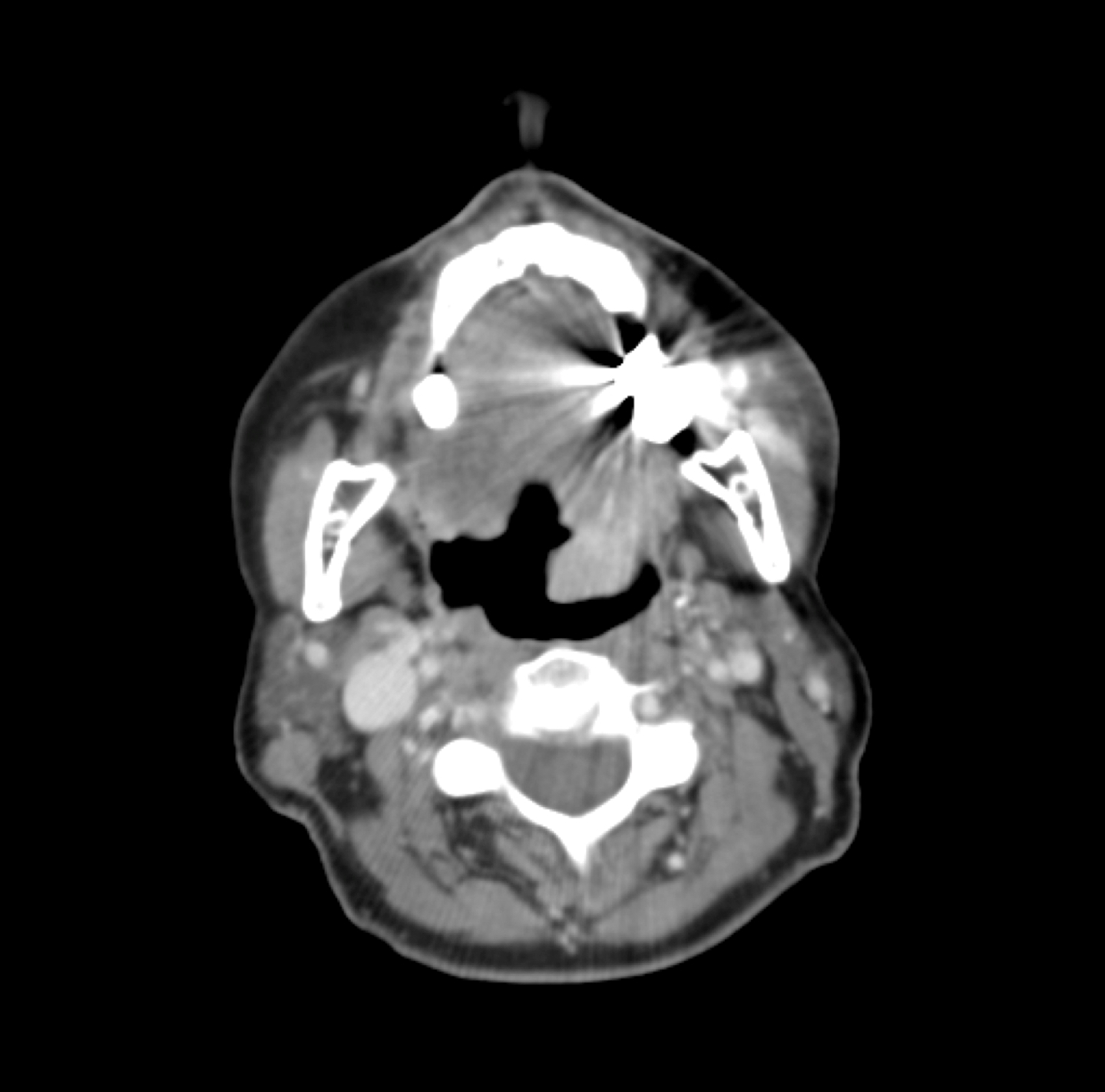
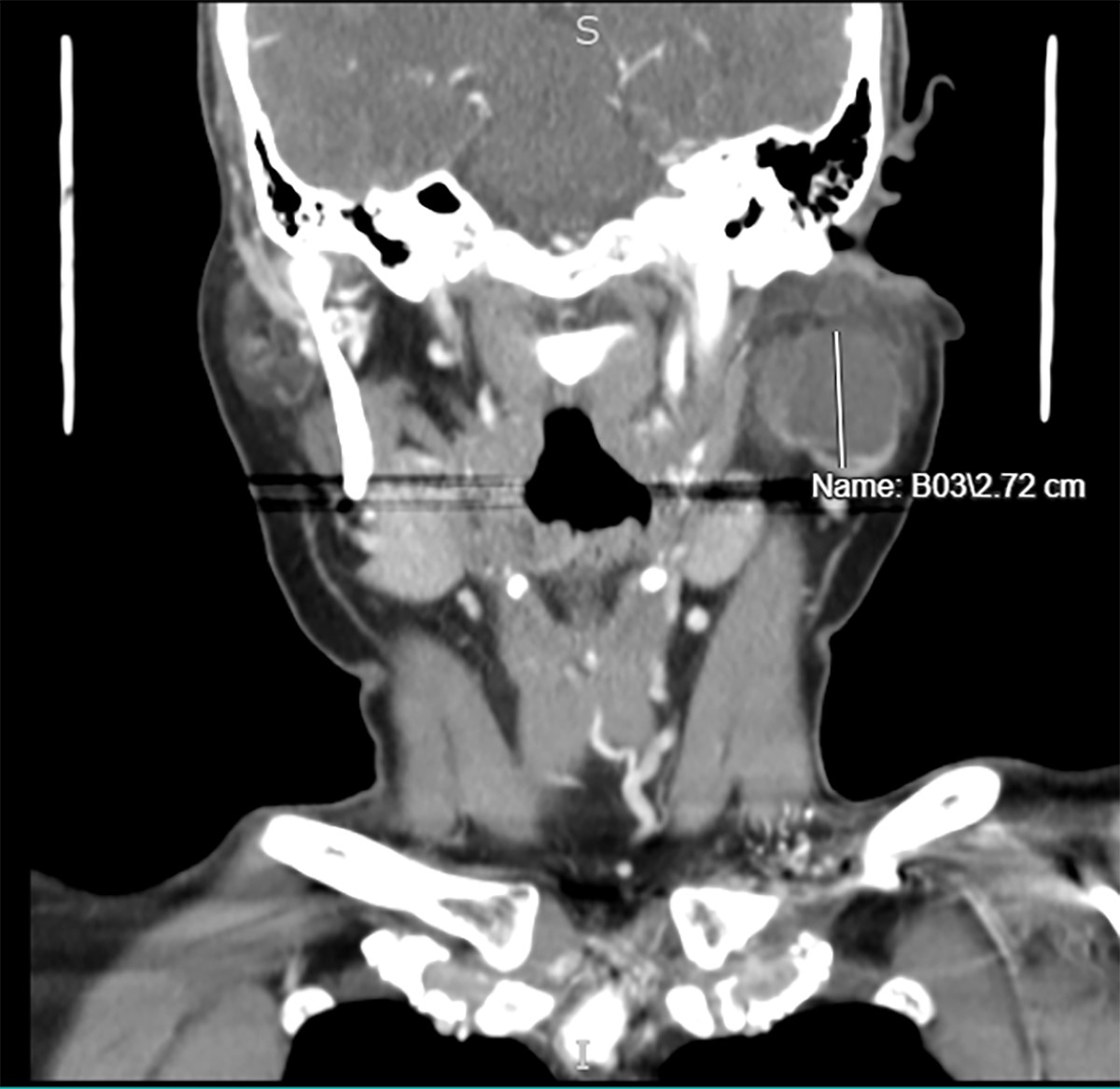
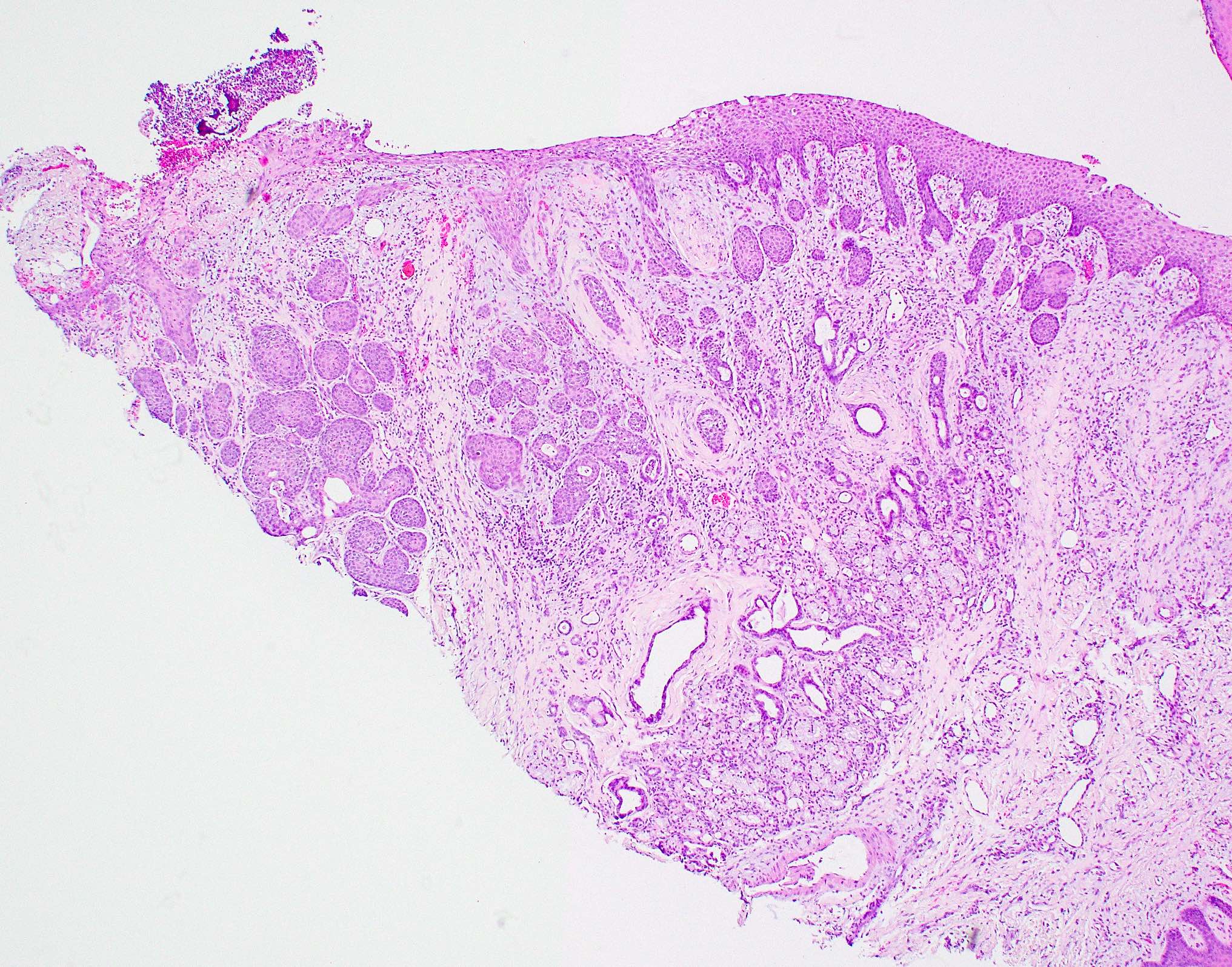
A 51 year old woman presents with a left parotid mass. CT images show a well circumscribed cystic lesion measuring 3 cm. An excisional biopsy is performed (see image above). The neoplastic cells are positive for periodic acid-Schiff with diastase (PASD). Which of the following statements is true regarding this lesion?
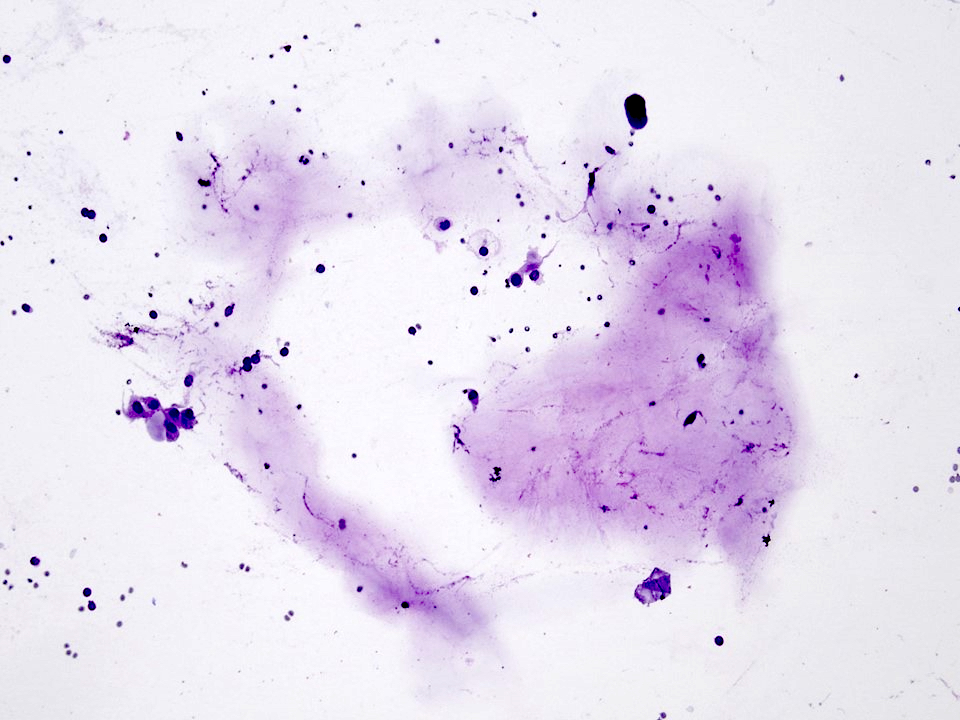
Cytology aspirates of this tumor can show predominance of extracellular mucin
Mitosis, necrosis and significant pleomorphism are usually present
MYB immunohistochemical staining in FNA specimens is useful in the diagnosis of this tumor
Pain and facial nerve dysfunction are uncommon presenting symptoms
Board review style answer #2
D. The most common initial presentation in patients with acinic cell carcinoma is a painless mass without facial nerve involvement. Answer C is incorrect because MYB immunohistochemical staining is useful in the diagnosis of adenoid cystic carcinoma. Answer A is incorrect because the presence of extracellular mucin in aspirates is a feature of mucoepidermoid carcinoma. Answer B is incorrect because acinic cell carcinoma is usually a low grade malignant neoplasm without significant mitosis, necrosis or pleomorphic nuceli.
Invasive tumor, often aggressive, with glandular or ductal differentiation but no features characteristic of other specific types (Arch Pathol Lab Med 2004;128:1385)
Common, 5 - 10% of salivary gland tumors
6 - 10% of salivary gland malignancies, 17% of parotid gland malignancies, 15% of minor salivary gland malignancies
Salivary gland carcinoma, NOS (not otherwise specified) represents a heterogeneous spectrum of carcinomas forming epithelial, ductal or glandular structures; it is a diagnosis of exclusion, specifically exclusive of otherwise defined salivary gland carcinoma entities (Am J Surg Pathol 2021;45:753)
Essential features
Nonspecific heterogeneous spectrum of carcinomas forming epithelial, ductal or glandular structures
Diagnosis of exclusion, specifically exclusive of otherwise defined salivary gland carcinoma entities
2 recognized subtypes: oncocytic adenocarcinoma and intestinal type adenocarcinoma
Oncocytic adenocarcinoma: oncocytic aspect with RA-
Intestinal type adenocarcinoma: intestinal aspect with CDX2+ / CK20+
54 year old man presenting with symptoms of fullness in his tongue, diagnosed as salivary carcinoma, NOS, intestinal type adenocarcinoma (Head Neck Pathol 2017;11:186)
61 year old man presenting with a swelling in the left lower cheek, diagnosed as oncocytic adenocarcinoma of parotid gland (Acta Cytol 2003;47:1099)
66 year old woman with a case of oncocytic adenocarcinoma arising in parotid gland (World J Surg Oncol 2006;4:54)
68 year old woman with previous history of high grade adenocarcinoma of the parotid and metastasis to uterine leiomyoma (Cureus 2020;12:e6789)
In cN0 patients with high grade or in cT3 - T4: elective treatment of the neck with either elective nodal dissection or elective neck irradiation since salivary carcinoma, NOS has a > 20% rate of clinically positive nodal involvement at presentation (Otolaryngol Head Neck Surg 2016;154:121)
In high grade tumors: positive margins, perineural invasion, lymph node metastases, lymphatic or vascular invasion, T3 - T4 tumors or those that are not candidates for surgical resection
Can be considered in cases of tumors with close margins or intermediate grade tumors
Elective neck irradiation in patients with cN0 disease for the following indications: T3 - T4 cancers or high grade malignancies or those that are not candidates for surgical resection
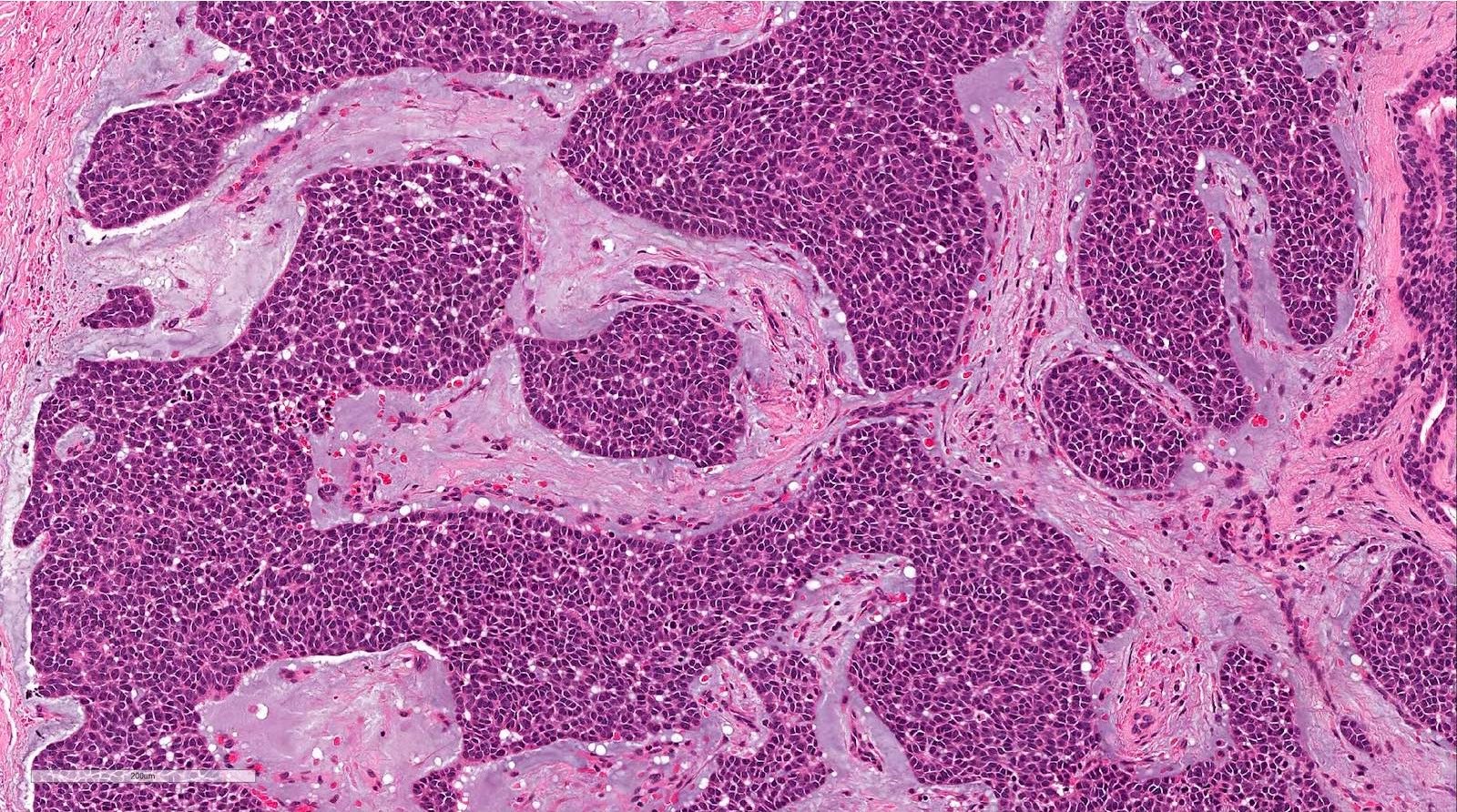
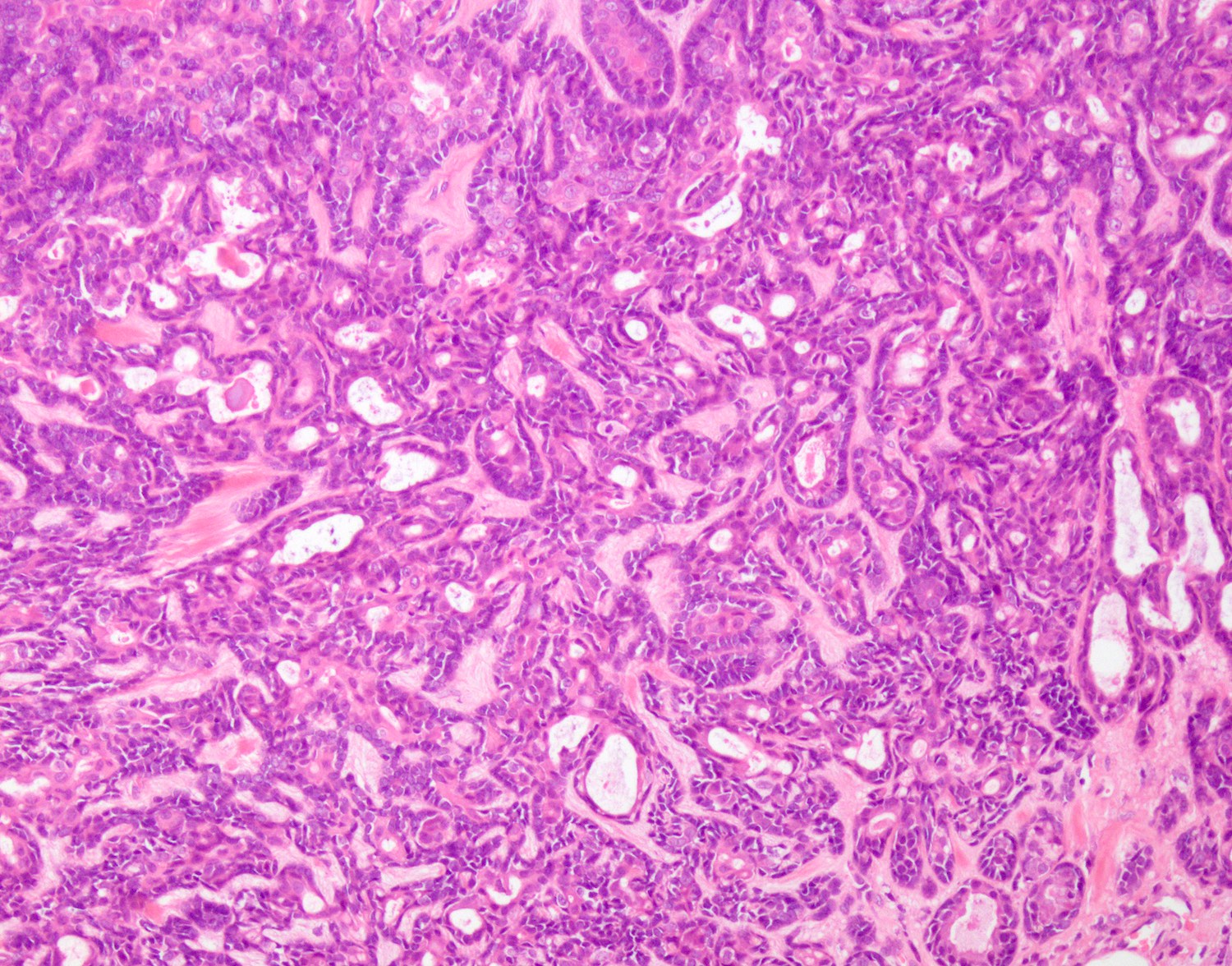
Architectural variety of growth patterns: glandular, papillary, cystic, cribriform, solid, lobular, nest-like, strand-like differentiation and small confluent nests or cords, large islands (Arch Pathol Lab Med 2004;128:1385)
Variety of tumor cells: cuboidal, columnar, polygonal, clear, mucinous, oncocytoid or plasmacytoid (Arch Pathol Lab Med 2004;128:1385)
Parotid oncocytic carcinoma with vascular invasion
Virtual slides
None
Cytology description
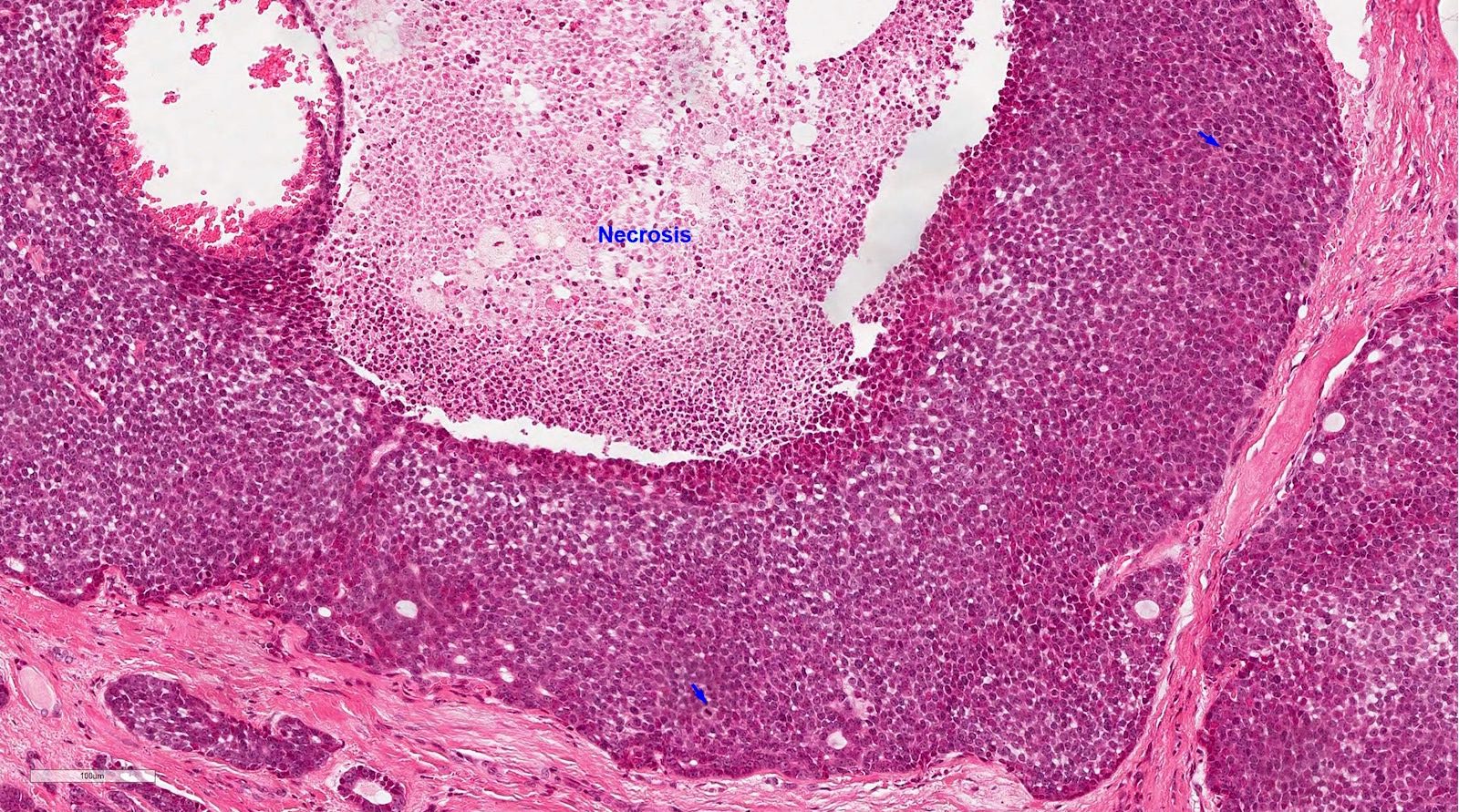
Smears show adenocarcinoma usually with high grade nuclei in a necrotic background and lacking features of other salivary gland carcinomas, resulting in a differential diagnosis of metastases from colon and lung
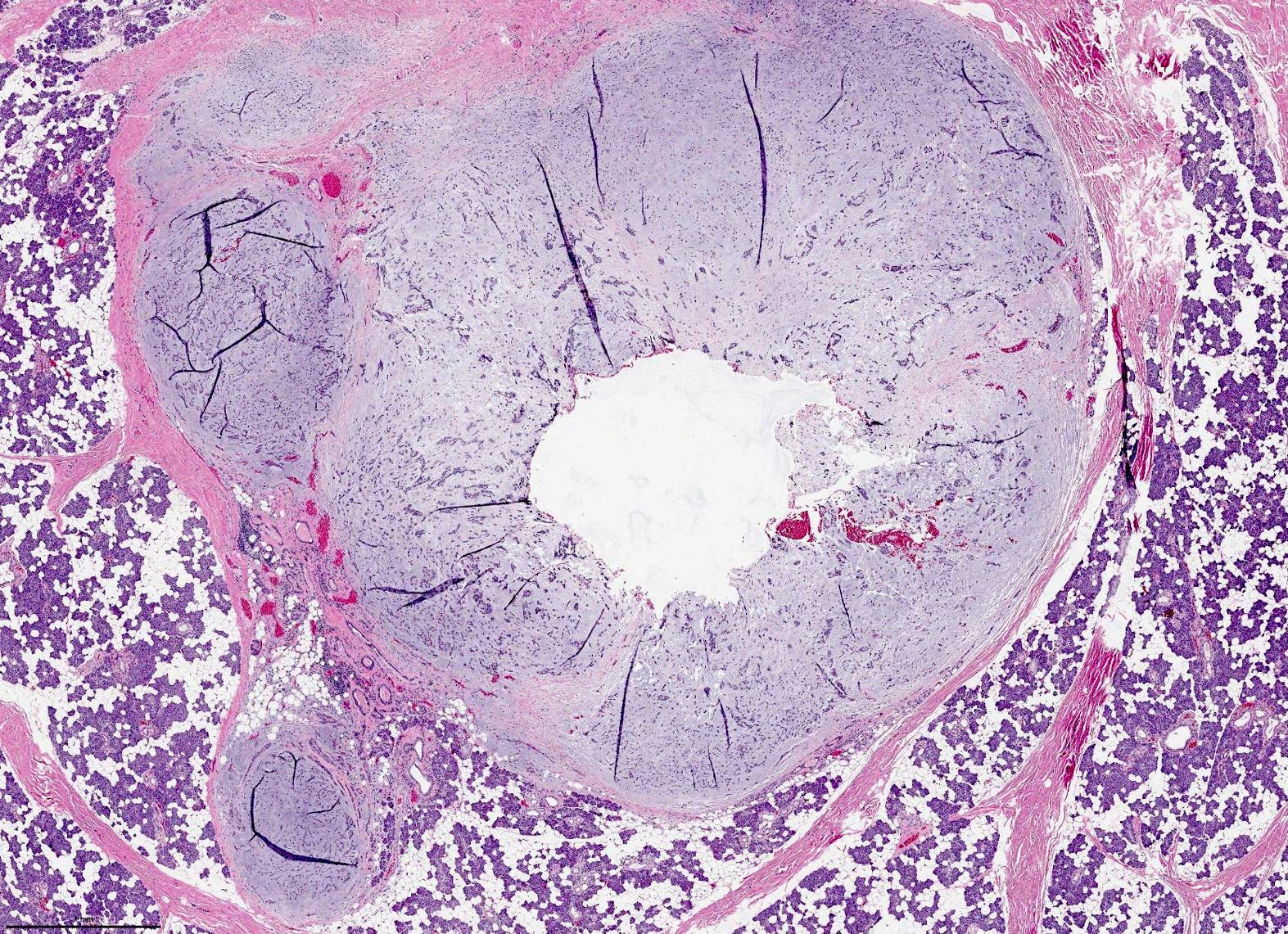
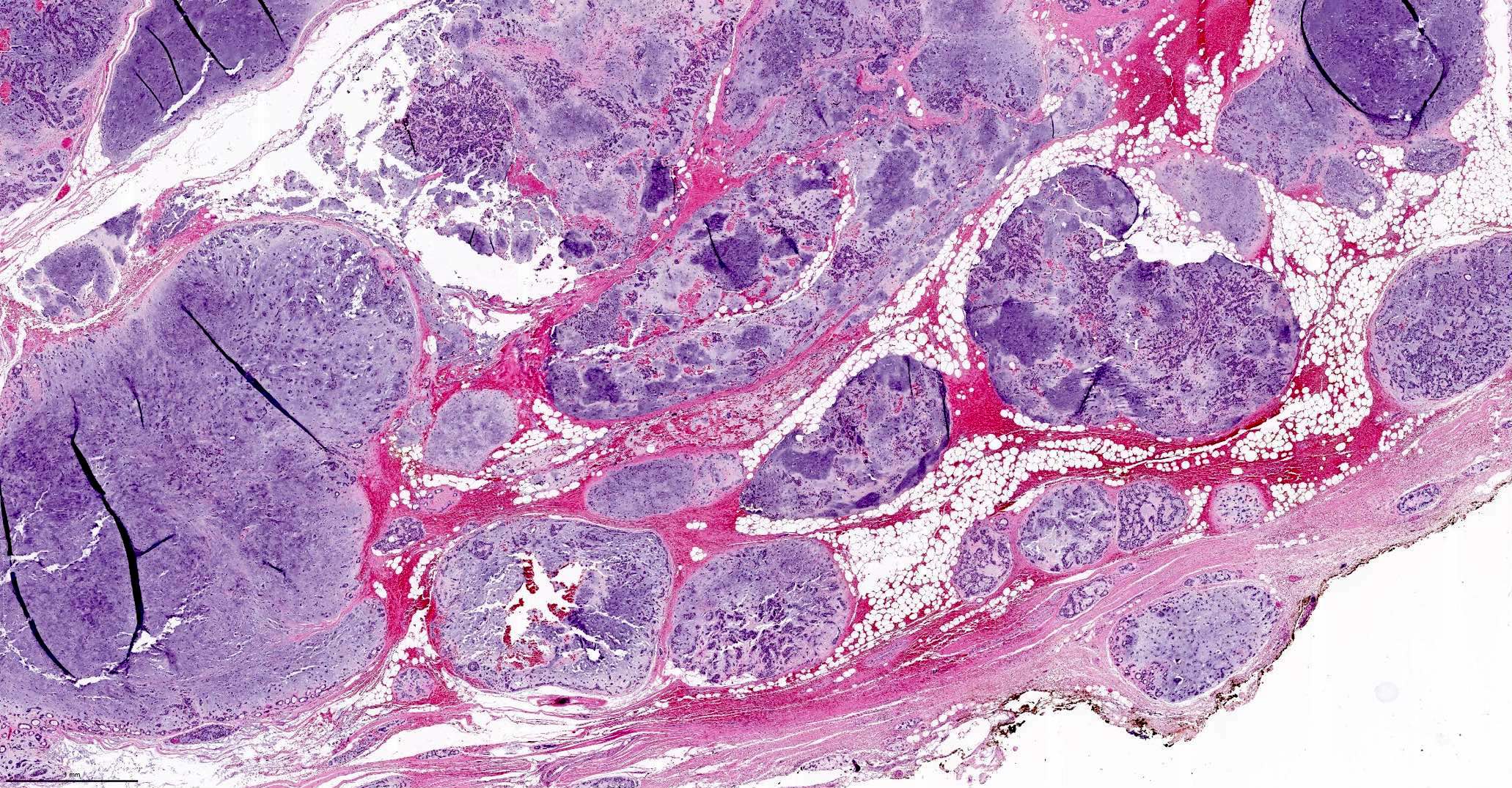
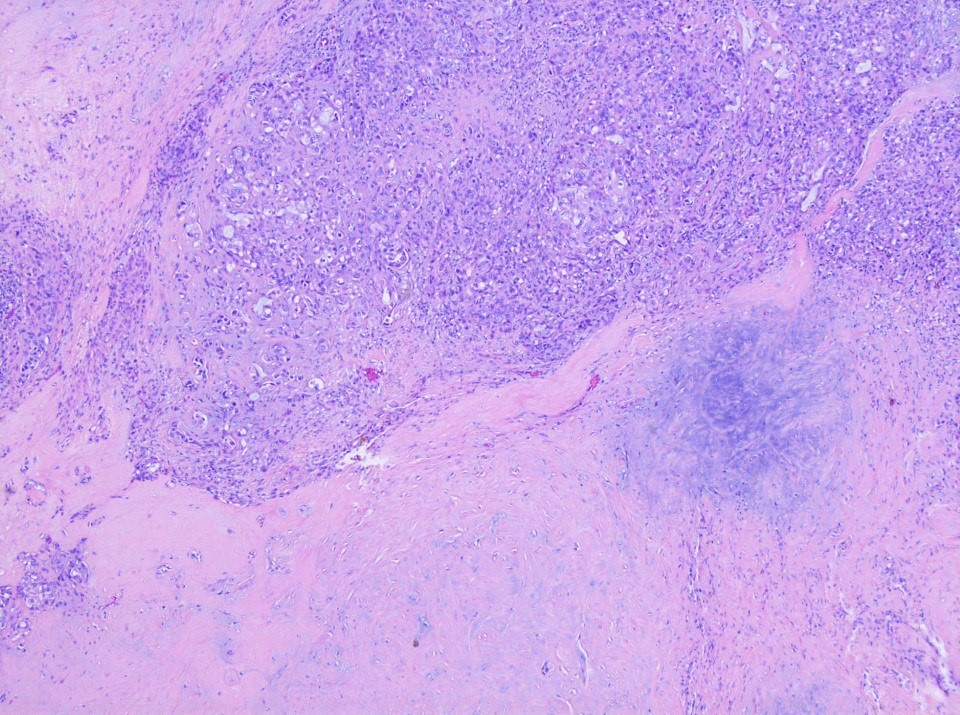
Comment: There is a lobulated and unencapsulated biphasic primary neoplasm. The tumor shows a nodular growth pattern. The tumor is composed of a bilayered arrangement of small to large luminal cells with eosinophilic cytoplasm and outer myoepithelial cells. Immunohistochemically, the inner epithelial cells are positive for AE1 / AE3 and EMA, while the outer myoepithelial layer shows staining for p63, smooth muscle actin and S100. The rest of the staining is negative for CK20, DOG1, AR and PLAG1 / HMGA2. There is no evidence of necrosis or high grade transformation. The molecular analysis is negative for PLAG1, HMGA2, MAML2, PRKD fusions and PRKD1 mutation.
Which of the following statements is true regarding salivary carcinoma, NOS?
It is defined by its peculiar morphological, immunohistochemical and molecular features
It is the most common differential diagnosis of mucoepidermoid carcinoma
Nodal dissection is systematic regardless of the imaging
The oncocytic subtype is the most aggressive
TP53 mutation is never identified
Board review style answer #1
B. It is the most common differential diagnosis of mucoepidermoid carcinoma. Answer C is incorrect because elective nodal dissection is performed if the imaging study identifies lymph nodes suspected of metastasis in low grade carcinoma. Answer D is incorrect because the oncocytic subtype is commonly associated with low grade carcinomas. Answer A is incorrect because the oncocytic subtype is defined by its lack of peculiar morphological, immunohistochemical and molecular features. Answer E is incorrect because TP53 mutation can be identified, along with others such as PI3KCA, NRAS and HRAS.
Which of the following statements is true regarding salivary carcinoma, NOS?
Abundant intracellular or extracellular mucin can be observed
CK20 is not consistently found
Lymph node metastases never occur
The principal differential diagnosis of metastatic colorectal carcinoma must be addressed
This histological subtype is specific for MMR deficiency
Board review style answer #2
D. The principal differential diagnosis of metastatic colorectal carcinoma must be addressed. Answer B is incorrect because CK20, like CDX2, is commonly observed as positive in immunostaining. Answer A is incorrect because only mucinous adenocarcinoma exhibits these features with significant mucinous differentiation, abundant intracellular or extracellular mucin, CK7+ / CK20- and commonly the AKT1 p.E17K mutation. Answer C is incorrect because lymph node metastases can occur. Answer E is incorrect because MMR proficiency is identified, in contrast to the GI tract.
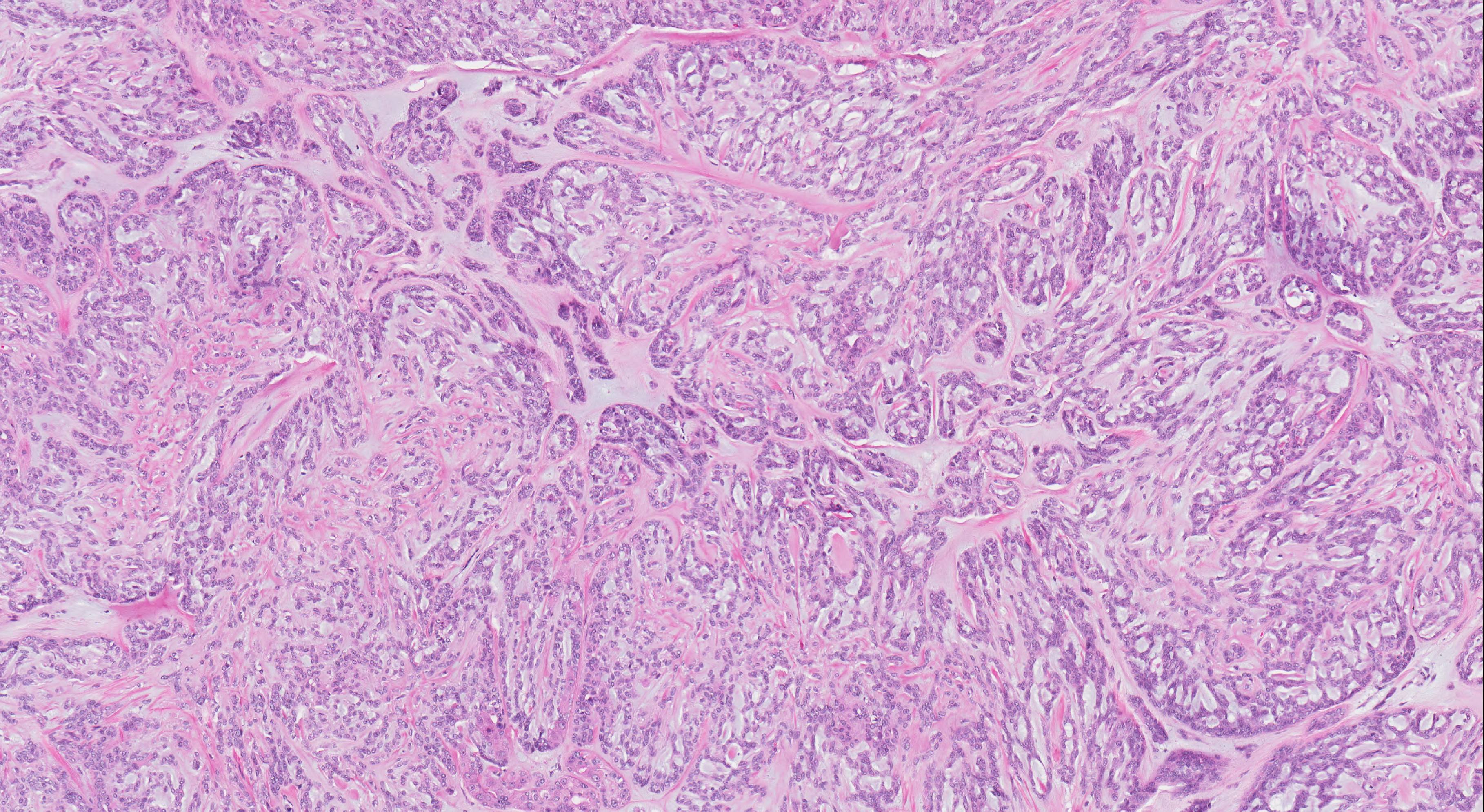
A carcinoma of primary salivary gland or minor salivary gland of upper aerodigestive tract characterized by its biphasic ductal and myoepithelial differentiation, tubular / cribriform / solid architecture (Head Neck 2017;39:456)
May occur in major and minor salivary glands
Among major salivary glands, the most commonly affected site is the parotid gland
Minor salivary glands that may be affected include those of oral cavity, sinonasal tract, nasopharynx, oropharynx and trachea
Essential features
Grows in tubular, cribriform, and/or solid patterns: solid pattern is associated with adverse outcome
60% - 90% carry MYB-NFIB or MYBL1-NFIB fusion
Biphasic tumor showing ductal and myoepithelial differentiation
Diagnosis is based on tissue examination findings of typical histologic features or the presence of fusion involving MYB, MYBL1 or NFIB genes
Radiology images
Images hosted on other servers:
MRI parotid mass
Lung metastases
Prognostic factors
Independent prognostic predictors include AJCC TNM staging, margin status, high mitotic index (defined as ≥ 5 per 10 high power fields) and solid architecture (Am J Surg Pathol 2017;41:1422)
Presence and percentage of solid architecture reflects clinical outcome and should be reported in the pathology report
Other studies show that tumors with higher percentage of solid pattern, defined as 30% or more, are associated with increased risk of recurrence and decreased survival (Cancer 1984;54:1062, Cancer 1978;42:265)
Based on the above data, 2 grading systems have been proposed (table)
Other poor prognostic factors include female sex, older age, sinonasal location, lymphovascular invasion, high grade transformation and intraneural invasion
70 year old woman with soft palate adenoid cystic carcinoma extending to bilateral orbits through perineural spread along cranial nerves (Digit J Ophthalmol 2018;24:1)
Contributed by Bin Xu, M.D., Ph.D. and Kelly Magliocca, D.D.S., M.P.H.
Parotid mass
Cut section turbinate to palate
Frozen section description
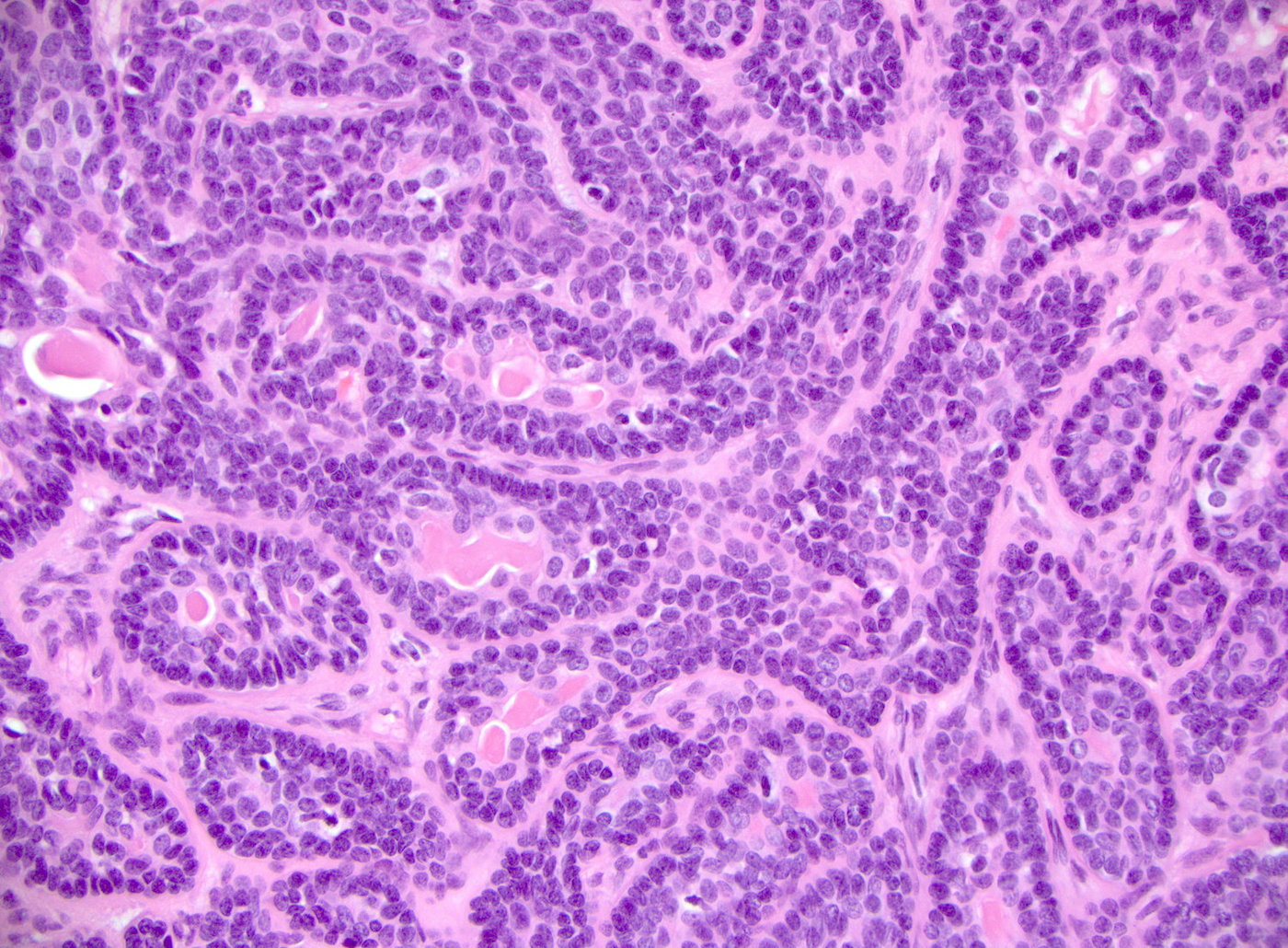
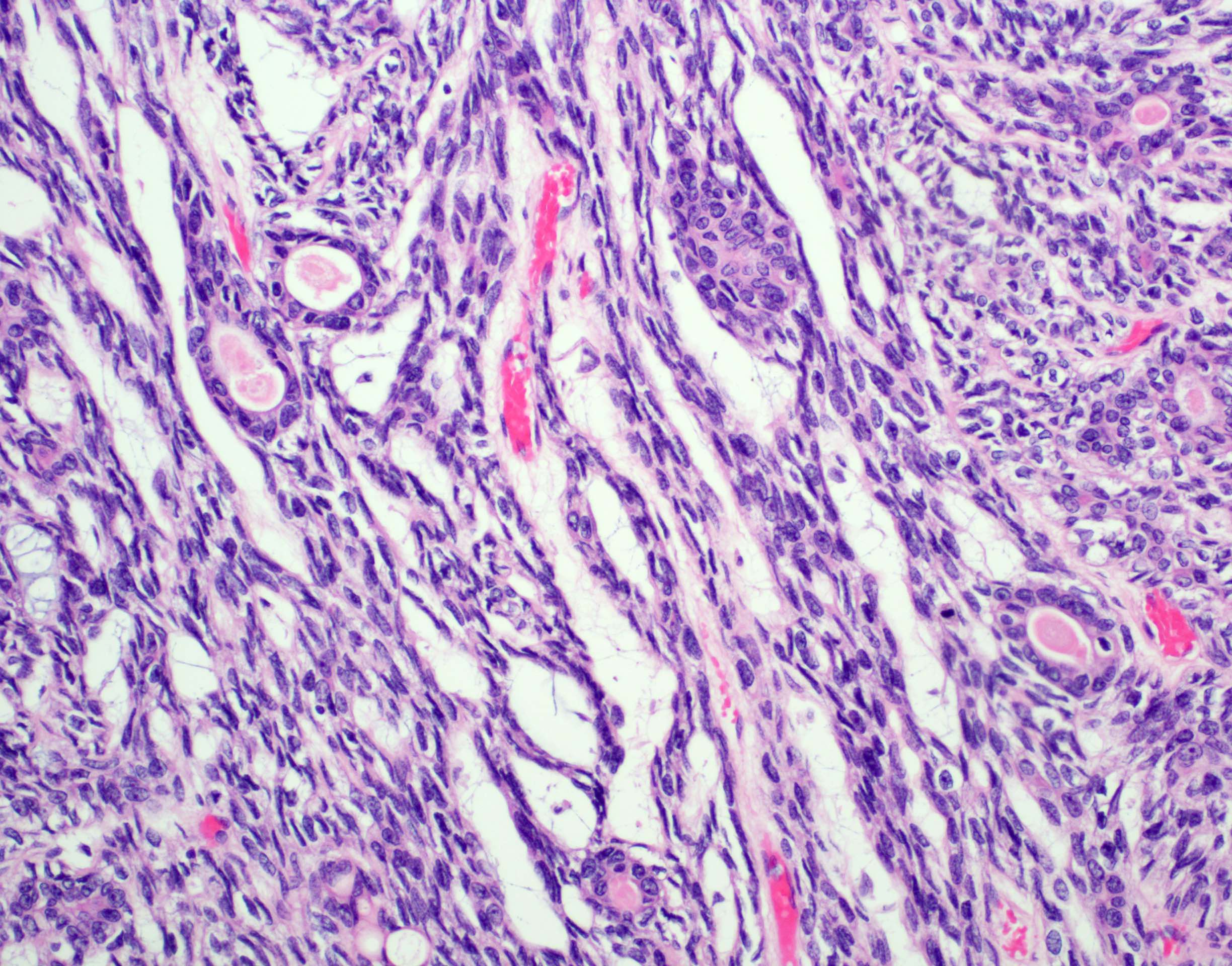
Biphasic pattern of epithelial and myoepithelial cells and the typical tubular / cribriform / solid architecture are useful diagnostic cues
Microscopic (histologic) description
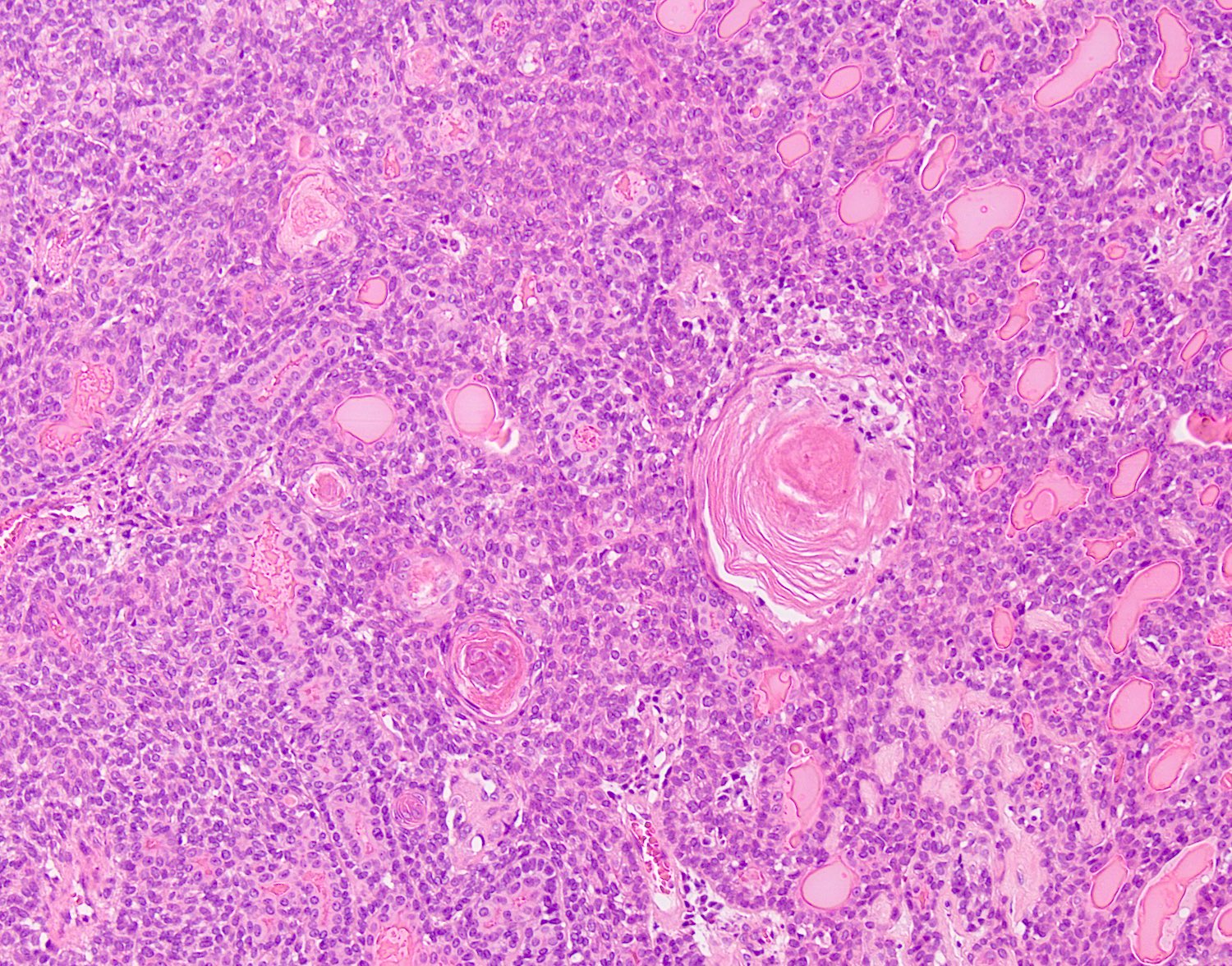
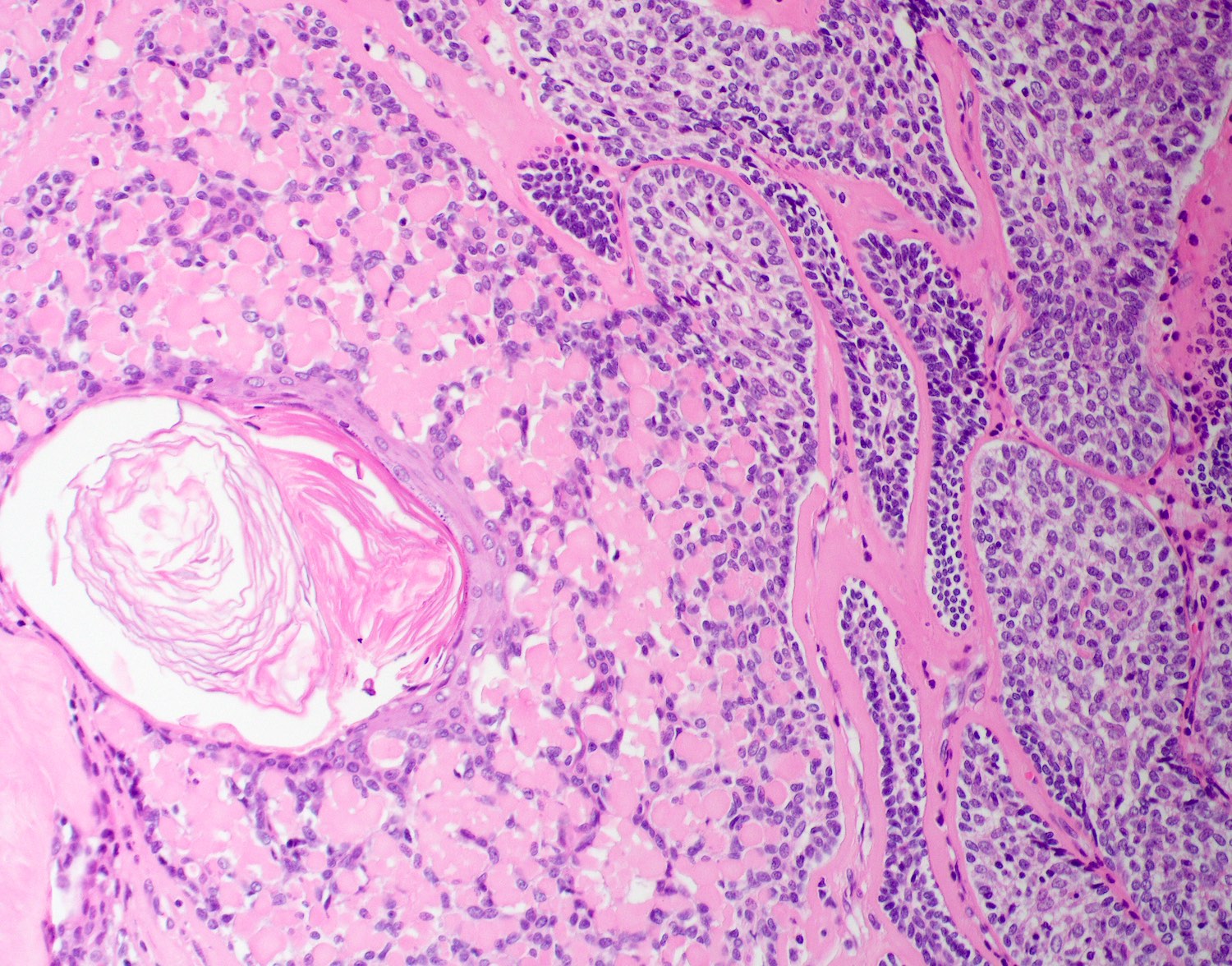
Biphasic salivary gland tumor, composed of ductal and myoepithelial cells
Myoepithelial cells have dark angulated nuclei and scanty cytoplasm, giving a basaloid appearance
Tubular, cribriform and solid architecture
Tubular pattern contains simple tubules composed of inner ductal and outer myoepithelial cells
Cribriform pattern is composed of predominantly myoepithelial cells with myxoid or hyalinized globules
Scattered ductal elements may be seen within the cribriform area
Solid pattern is solid nests composed of sheets of basaloid cells
Perineural invasion is frequent
High grade transformation can be seen in a small number of cases, defined as comedo type tumor necrosis, frequent mitoses (often > 10 per 10 high power fields) and marked nuclear atypia; high grade transformation is associated with high risk of lymph node metastasis, distant metastasis and disease related death (Am J Surg Pathol 2007;31:1683)
Other rare features that may present occasionally include:
Additional mutations involving FGF-IGF-PI3K pathway (in 30%) and chromatin state regulators (e.g. SMARCA2, CREBBP and KDM6A) are reported (Nat Genet 2013;45:791)
Although commonly overexpresses c-KIT by immunohistochemistry, it is not associated with c-KIT mutation
Sample pathology report
Left parotid, parotidectomy:
Adenoid cystic carcinoma, solid, cribriform and tubular pattern (see synoptic report)
Comment: Solid component accounts for 20% of total tumor volume.
Trabecular, tubular and solid growth and usually lacks cribriform growth (adenoid cystic carcinoma lacks trabecular growth)
Prominent peripheral palisading and may contain areas with squamoid eddies
Characterized by mutation of Wnt / beta catenin pathway leading to abnormal nuclear accumulation of beta catenin by immunohistochemistry; lacks fusions involving MYB, NFIB or MYBL1
Basaloid squamous cell carcinoma and HPV+ oropharyngeal squamous cell carcinoma may contain adenoid cystic carcinoma-like areas
Typically shows more pleomorphism, is negative for MYB-NFIB fusion, is diffusely positive for squamous markers (p40, p63 and CK5/6), is negative for myoepithelial markers (S100, calponin and SMA) and may be HPV+
Board review style question #1
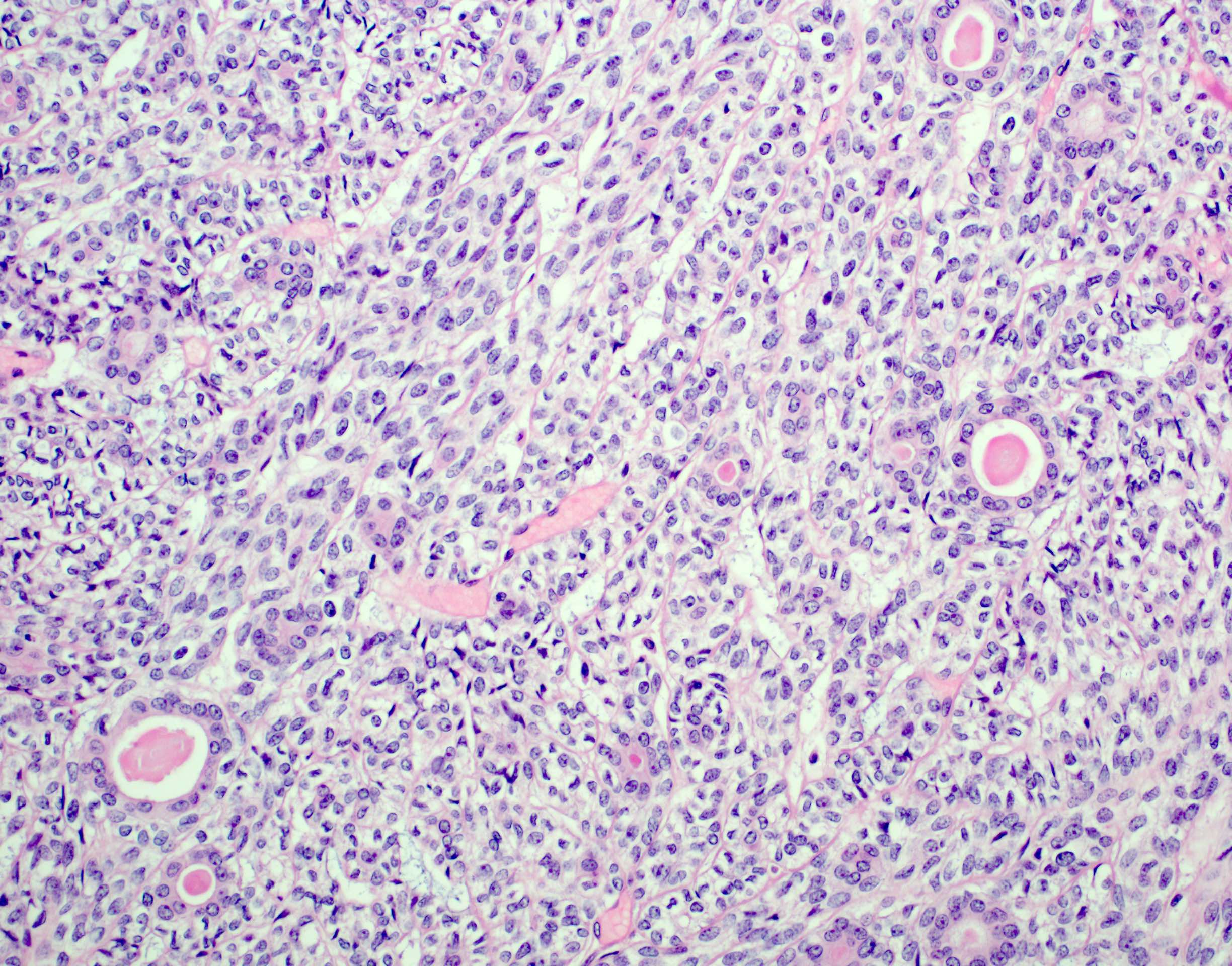
A parotid tumor is resected and the H&E is shown. Which of the following statements is true?
It has an excellent prognosis with 5% risk of recurrence following complete resection of the primary tumor
It is characterized by point mutation involving MYB gene
Solid pattern is associated with adverse clinical outcome
The most common site of this tumor is the parotid gland, followed by submandibular gland
Board review style answer #1
C. Solid pattern is associated with adverse clinical outcome
In addition, there are numerous (600 - 1000) minor salivary glands distributed throughout the submucosa of the upper aerodigestive tract
Essential features
Functional unit of all salivary glands consists of acini and ducts
Acini can be composed predominantly of serous or mucous cells or can be mixed seromucous type
3 main types of ducts are intercalated, striated or interlobular
Myoepithelial cells embrace the secretory unit and are critical for the expulsion of saliva
Saliva has a crucial protective and digestive function within the upper aerodigestive cavity, providing mucosal lubrication, alkaline environment for dental protection, facilitating taste, initiating enzymatic digestion of carbohydrates and contributing to oral immunity
Unique to the parotid gland is the presence of sebaceous glands and intraparenchymal lymph nodes
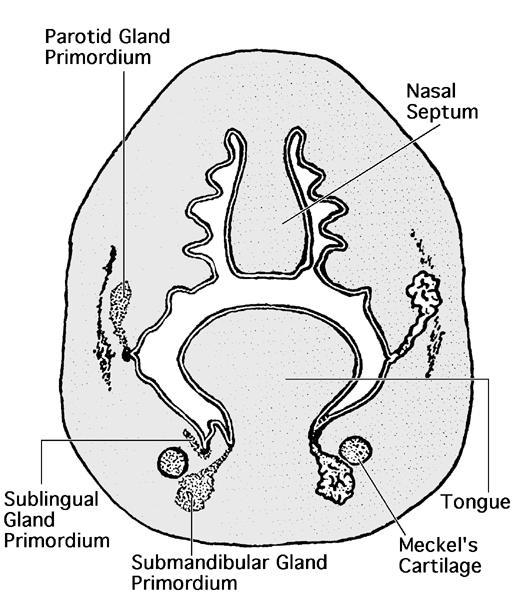
Embryology
Salivary glands are of ectodermal origin
Developmental process begins when preacinar buds invaginate the adjacent mesenchyme, proliferating through cords, which eventually form clefts and produce extensive branching; end result is terminal bulbs, which form the secretory unit (Eur J Mol Clin Med 2020;764)
Parotid anlage appears in the fifth week, followed by the submandibular and sublingual primordia in the sixth and eighth weeks, respectively
Minor salivary glands develop during ninth to twelfth weeks
Connective tissue component of the developing glands progressively lessens with maturation
Capsule of each gland is formed by the surrounding mesenchyme, a process which is delayed for the parotid gland, therefore allowing the integration of parotid buds and lymphoid tissue:
Results in the presence of both intraparotid lymph nodes as well as lymph nodes containing glandular and ductal inclusions
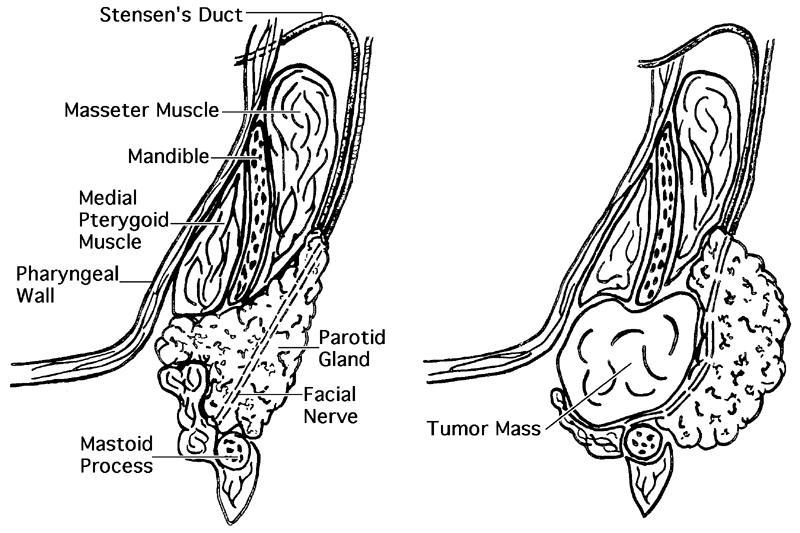
As the parotid gland forms, its embryologic branches intertwine with branches of the facial nerve
Minor salivary glands develop in a similar fashion to the major glands; however, the branching is less extensive and remains located within the submucosa
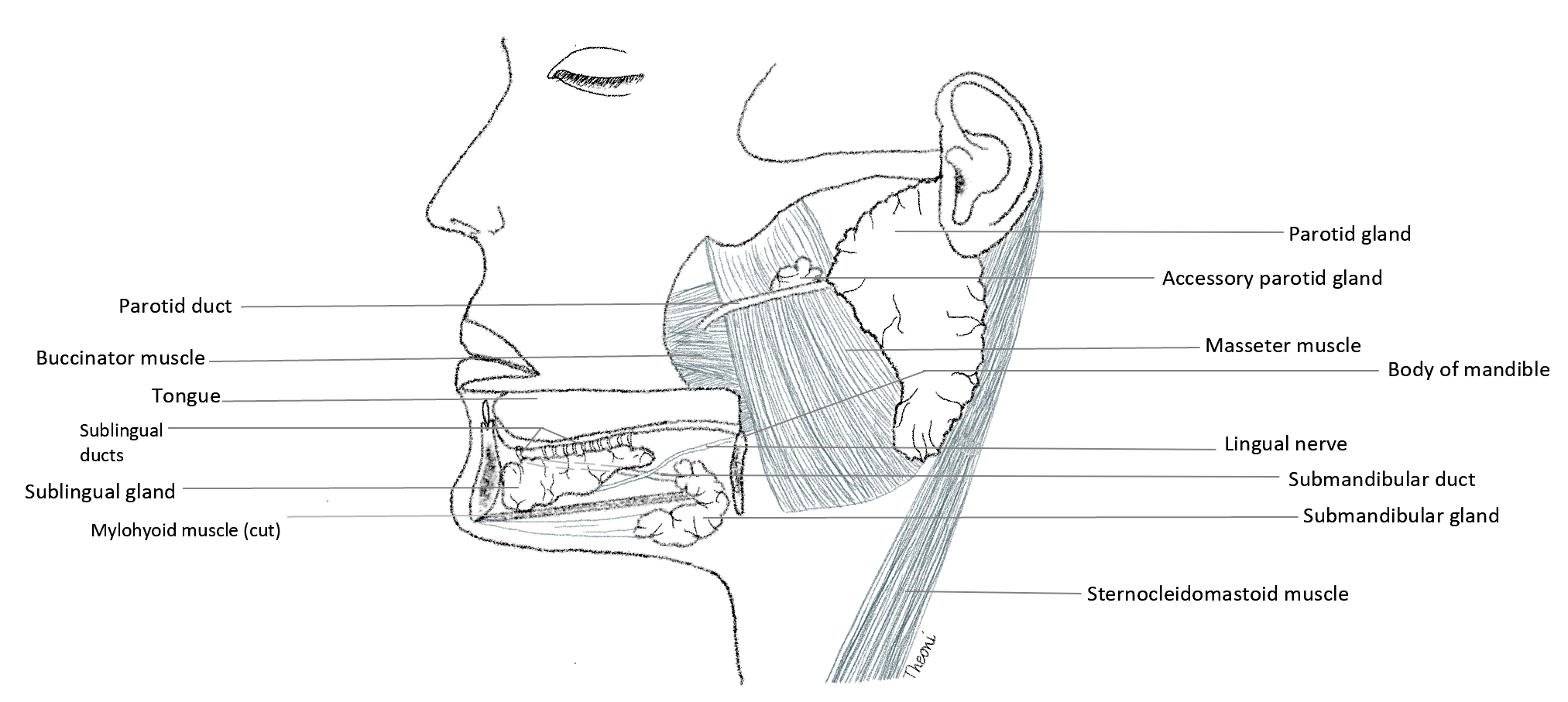
Anatomy
Parotid gland:
Largest of the major salivary glands (weight 15 - 30 g)
Pyramidal shaped and encased in robust parotid fascia, which is a continuation of deep cervical fascia as it travels superiorly
Located in a shallow, preauricular compartment defined by:
Superficially: the superficial musculoaponeurotic system (SMAS) forming parotid fascia and platysma
Inferiorly: the sternocleidomastoid muscle
Medially: the parapharyngeal space
Anteromedially: the mandibular ramus covered by the masseter muscle
Posteriorly: the cartilage of the ear canal and temporal bone
Extracranial trunk of the facial nerve extends from the stylomastoid foramen into the parotid gland and divides into upper and lower division
Branches of the facial nerve traverse the body of the parotid gland to artificially divide the gland into superficial and deep lobes and exit in the form of 5 terminal branches from its anteromedial surface to supply 22 muscles of facial expression
Parotidectomy requires precise dissection of the parotid gland to identify and preserve the integrity of the facial nerve, preventing ipsilateral hemifacial paralysis
Stensen duct (~7 cm) is the main excretory duct of the parotid gland and emerges from the anterior border of the gland to travel horizontally along the superficial surface of the masseter muscle before turning medially to pierce the buccinator muscle and enter the oral cavity adjacent to the second maxillary molar
Accessory parotid tissue, usually adjacent to Stensen duct, can be identified in approximately 20% of individuals (Otolaryngol Clin North Am 2016;49:273)
Clinically important as salivary gland tumors can arise in this location
Submandibular gland:
Second largest of the major salivary glands (weight 7 - 15 g)
Hook shaped around the mylohyoid muscle and enveloped by a capsule continuous with the superficial layer of the deep cervical fascia
Divided into superficial and deep arms
Superficial (largest) portion lies outside the oral cavity below the mylohyoid muscle in the submandibular triangle bound by:
Superficial: platysma
Superior: mandible
Inferior: digastric muscle
Deep portion is formed as the gland curves around the posterior border of the mylohyoid muscle to enter the oral cavity
Wharton duct (~5 cm) is the main excretory duct of the submandibular gland, arises from the deep part of the gland, courses anteriorly and opens onto the sublingual caruncle adjacent to the frenulum of the tongue
Lingual nerve crosses Wharton duct twice lateral to medial and the hypoglossal nerve (CN XII) travels inferior to the duct (Folia Morphol (Warsz) 2018;77:521)
Vertical posterior edge of the submandibular gland and the digastric muscle can be used as a boundary between levels I and II of the neck (Arch Otolaryngol Head Neck Surg 2008;134:536)
Sublingual gland:
Smallest of the major salivary glands (weight 2 - 4 g)
Almond shaped and enveloped by loose connective tissue (no discrete capsule)
Located above the mylohyoid muscle lateral to the submandibular duct and lingual nerve
Fills the medial groove or sublingual fossa of the mandible
Superiorly, the gland creates a mucosal elevation (sublingual fold) on the floor of the oral cavity
There may be multiple minor sublingual ducts, also known as ducts of Rivinus, opening directly onto the crest of the sublingual fold; these may be replaced anteriorly by the major sublingual duct (Bartholin duct), which may connect with the submandibular duct at the sublingual caruncle
Minor salivary glands:
Scattered throughout the oral submucosa, with the exception of the gingiva and anterior hard palate
Not encapsulated and each gland possesses 1 duct draining directly into the oral cavity
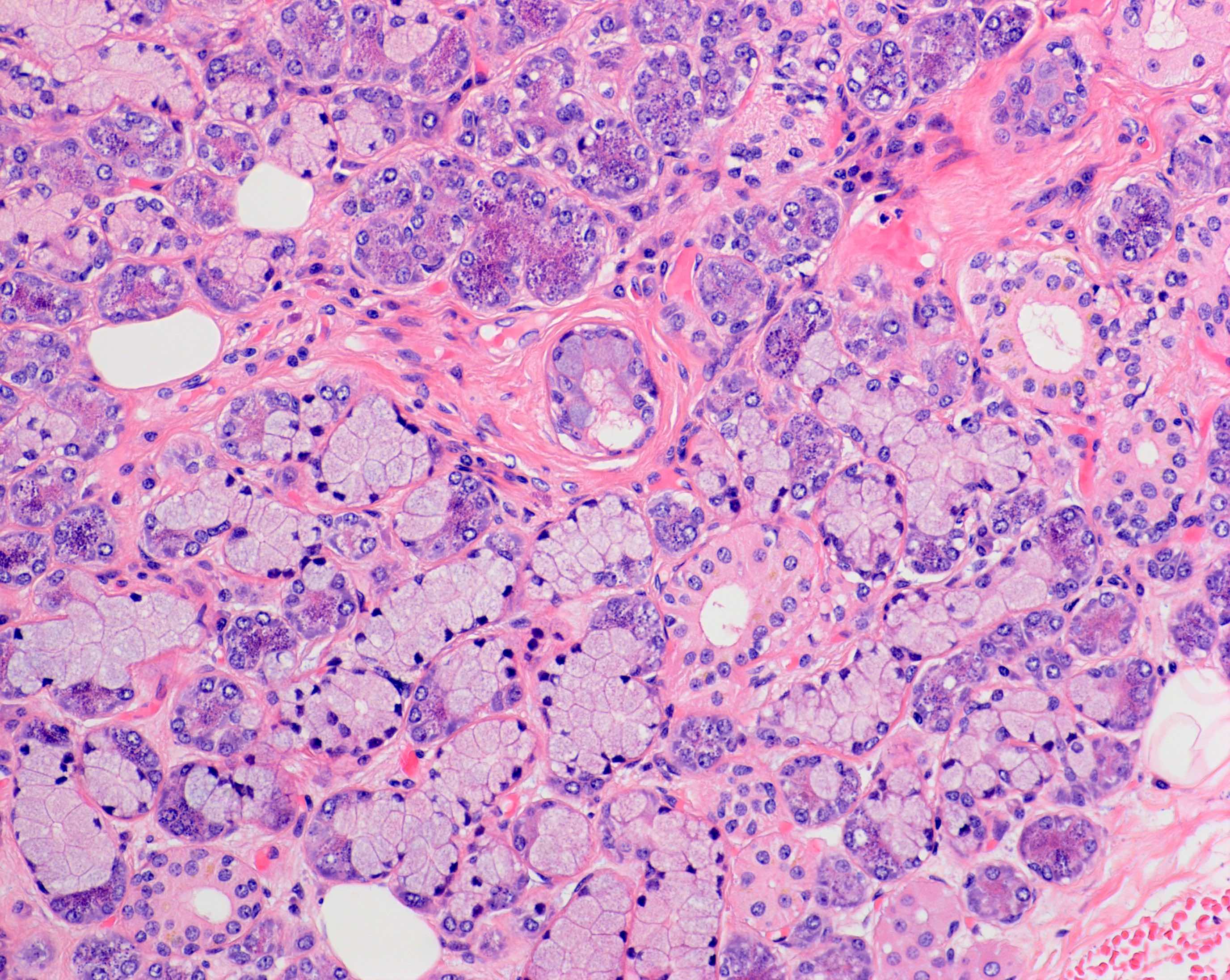
Predominantly mucinous apart from the purely serous von Ebner glands of the dorsal tongue that surround the circumvallate papillae
Vasculature:
Arterial supply
External carotid artery supplies the major salivary glands, coursing superiorly from the carotid bifurcation and providing the facial and lingual arteries that supply the submandibular and sublingual glands
Facial artery is intimately associated with the submandibular gland and is routinely divided above and below the submandibular gland during its removal as there are numerous branches
External carotid artery arrives at the posteromedial surface of the parotid gland, dividing into 2 terminal branches, the superficial temporal artery and maxillary artery, which exit from superior and anteromedial surfaces, respectively
Superficial temporal artery provides the transverse facial artery, which travels anteriorly to supply the parotid gland and parotid duct
Venous outflow
Retromandibular vein is formed in the body of the parotid gland by the union of the superficial temporal and maxillary veins and provides venous return for the gland, descending superficial to the external carotid artery and deep to the facial nerve before eventually joining the external jugular vein
Retromandibular vein is intimately associated with the facial nerve and is used as a surrogate anatomic landmark to determine whether tumors are in the deep or superficial lobe of the parotid gland
Lingual and facial veins drain the submandibular and sublingual glands and flow into the internal jugular vein
Facial vein lies over the submandibular gland and needs to be ligated to access the gland during surgery
Venous anatomy can be variable
Lymphatic drainage
Lymphatic drainage of the parotid gland follows the venous system, draining to a superficial (fascial) and deep (intraparenchymal) group of lymph nodes before flowing into the superior deep cervical nodes
Lymphatic drainage of the submandibular and sublingual glands is received predominantly by the submandibular lymph nodes before progressing to the jugular chain
Innervation:
Both parasympathetic and sympathetic fibers innervate the salivary glands
Parasympathetic syndromes cause salivation
Sympathetic syndromes, anxiety cause dry mouth
Within the oral cavity, parasympathetic innervation to salivary glands is by the facial nerve (VII), branches of which join the maxillary (V2) and mandibular (V3) nerves
Parasympathetic fibers conveyed by the chorda tympani branch of the facial nerve (VII) innervate the submandibular and sublingual glands via the lingual nerve
Chorda tympani nerve unites with the lingual nerve of V3 in the infratemporal fossa before entering the oral cavity to synapse with postganglionic fibers in the submandibular ganglion
Submandibular ganglion is suspended from the lingual nerve and located inferior to the submandibular duct, supplying postganglionic parasympathetic fibers that pass directly to the submandibular and sublingual glands
Branches from lingual nerve to the submandibular gland are ligated during gland excision
Beyond the oral cavity, the parotid gland receives parasympathetic innervation by the auriculotemporal nerve (branch of the mandibular nerve [V3]), a nerve which derives its fibers from the glossopharyngeal nerve (IX) in the infratemporal fossa
Delayed complication of parotid surgery is Frey syndrome, characterized by gustatory sweating
Postganglionic sympathetic fibers branch from the carotid plexus of the external carotid artery and innervate the salivary glands along blood vessels
Physiology
Saliva has a crucial protective and digestive function within the upper aerodigestive cavity, providing mucosal lubrication and dental protection, facilitating taste, initiating enzymatic digestion of carbohydrates and contributing to oral immunity
Saliva synthesizing acinar cells are capable of producing a volume of up to 1.5 L daily, secreted in response to parasympathetic and sympathetic stimulation
Parasympathetic activity favors the production of serous or watery solution
Sympathetic activity triggers protein secretion
Parotid glands are responsible for up to 50% of saliva production upon stimulation (J Med Life 2009;2:303)
Saliva primarily contains the enzymes amylase and lysozyme, IgA and IgG antibodies, inorganic ions and a variable quantity of mucous
Serous and mucous cells of the salivary glands contribute to the composition of saliva and the striated ducts perform critical modification processes, specifically electrolyte reabsorption and secretion
Initially isotonic, saliva becomes a hypotonic, bicarbonate rich solution as it passes through the mitochondria packed striated ducts that facilitate ion transport
Diagrams / tables
Contributed by Theoni Haralabopoulos, M.D. and AFIP
3 major salivary glands (left side)
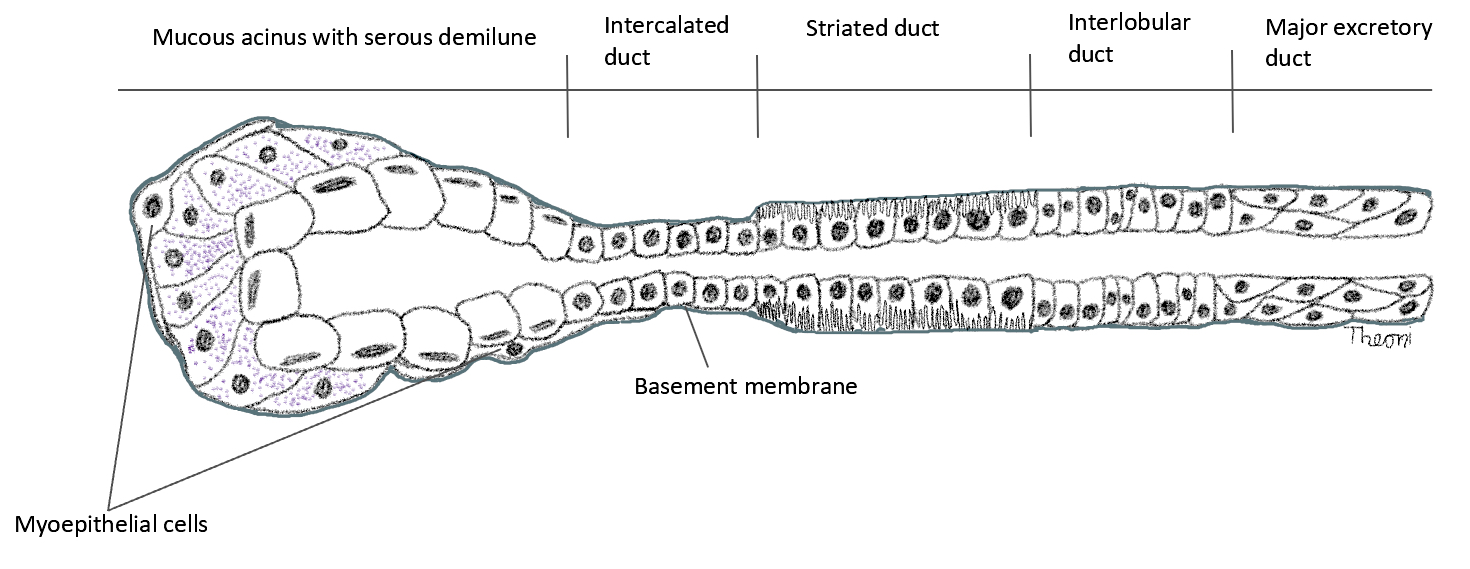
Schematic representation of acinus and ductal system
Embryological development of oral cavity
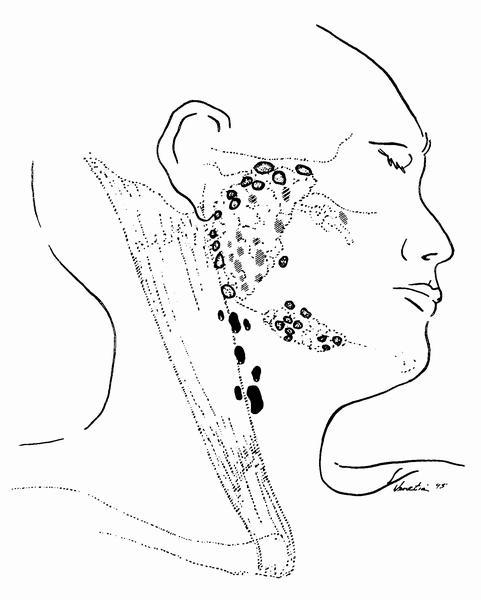
Parotid gland lymph nodes
Horizontal section through parotid gland
Images hosted on other servers:
Overview of major salivary gland anatomy
Clinical implications
Each cellular component can give rise to benign and malignant lesions that may present as swellings, with or without associated discomfort or pain
Salivary gland inflammation (sialadenitis) manifests as lymphoid infiltration and destruction of serous and mucinous acini, leading to pain, swelling and dry mouth; this can be secondary to
Bacterial or viral infection
Autoimmune (e.g., Sjögren syndrome and IgG4 related disease)
Impaction of calculi (sialolithiasis)
Trauma
Irradiation
Dilatation of salivary gland ducts (sialectasis) may be associated with recurrent sialadenitis and typically presents as painful, diffuse parotid gland swelling
Xerostomia following irradiation of the major or minor salivary gland tissues
Neoplasms:
Most (80%) of the salivary gland neoplasms arise in the parotid gland
80% of these are benign; on the other hand, most neoplasms of the sublingual gland are malignant
Primary epithelial
Pleomorphic adenoma, a benign, morphologically diverse tumor, displays both epithelial and myoepithelial derivation
Most common (80%) salivary gland tumor
Typically, the lesion presents as a slow growing, painless and mobile parotid mass (Wiad Lek 2020;73:2339)
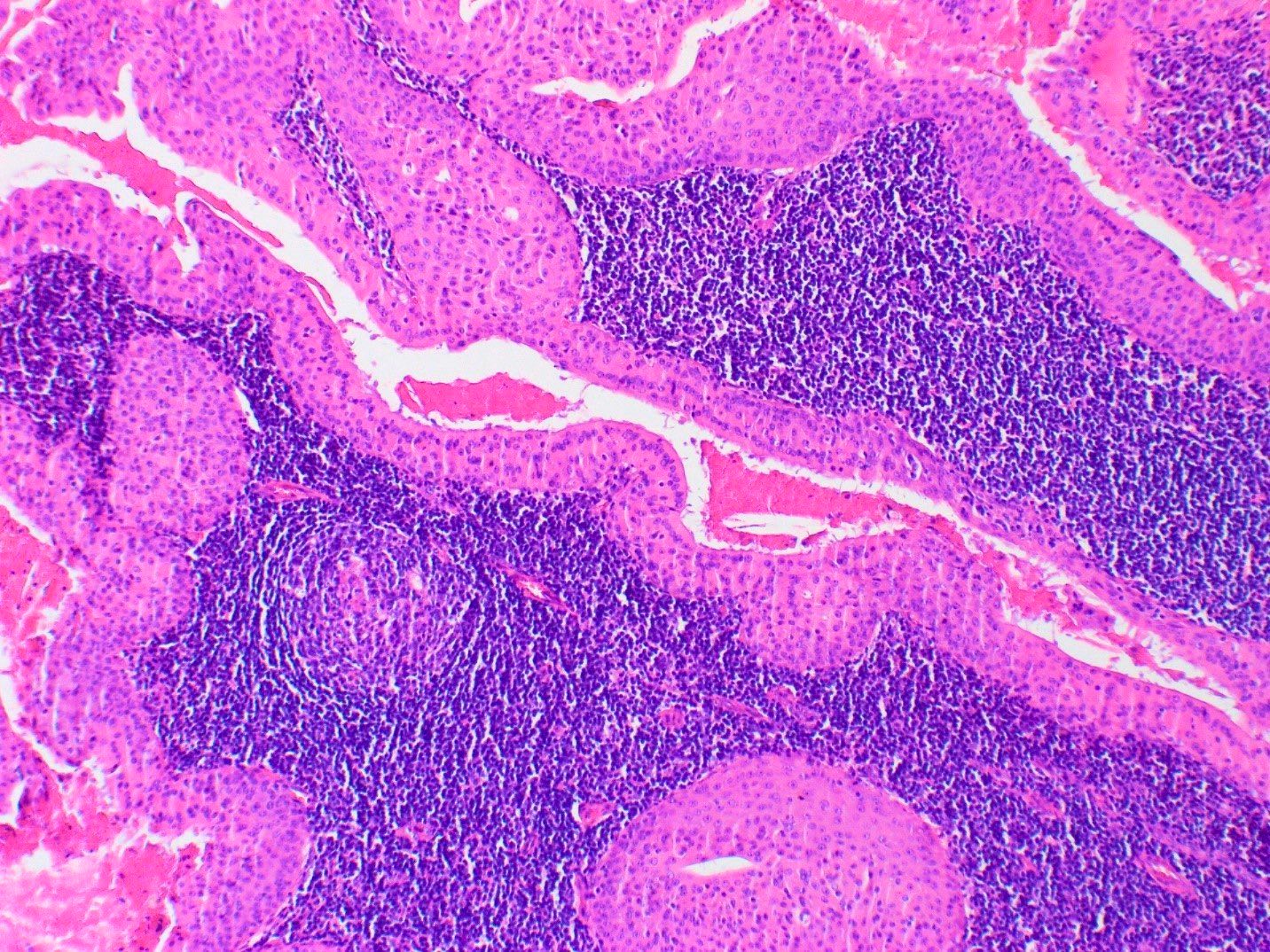
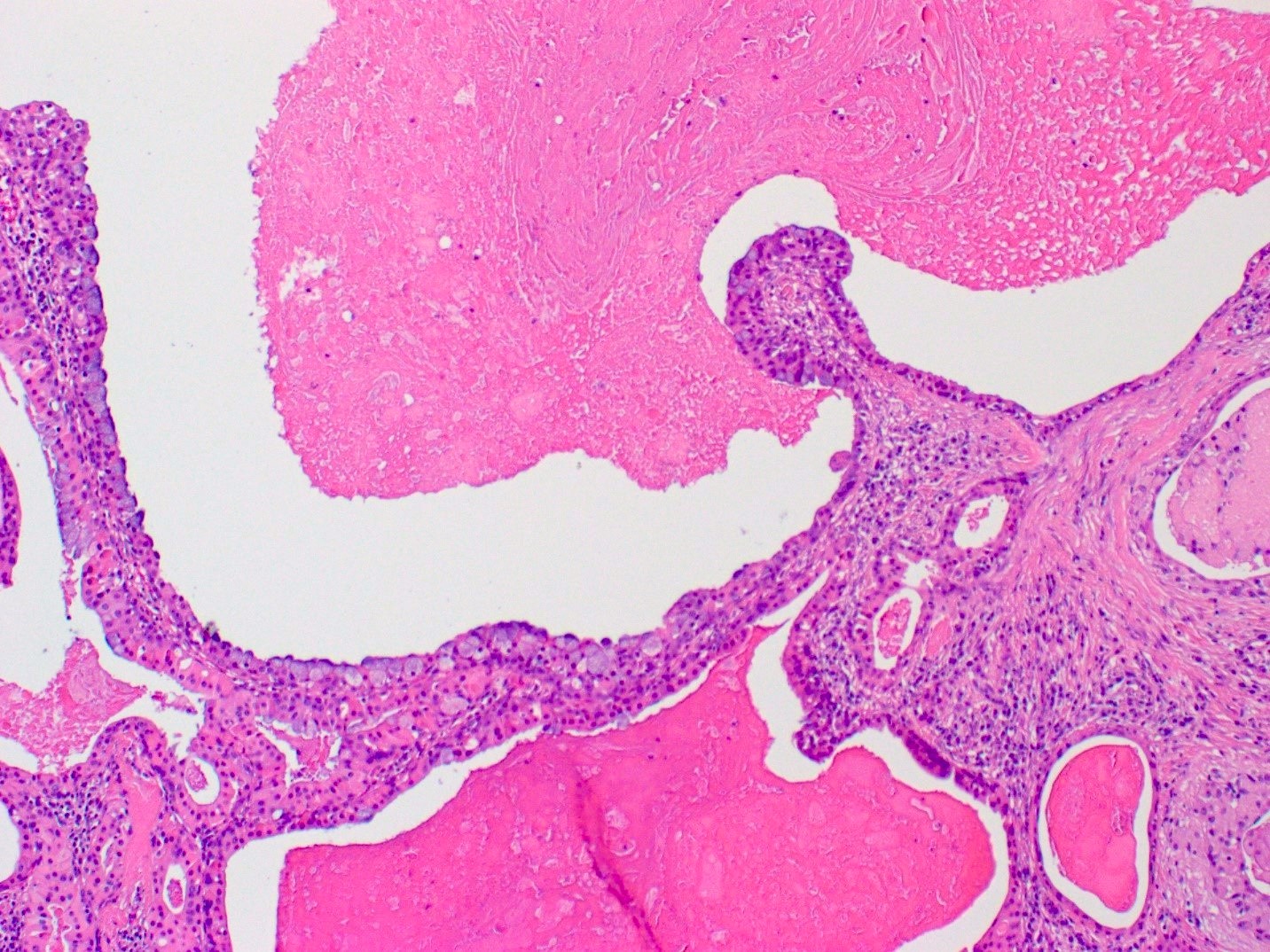
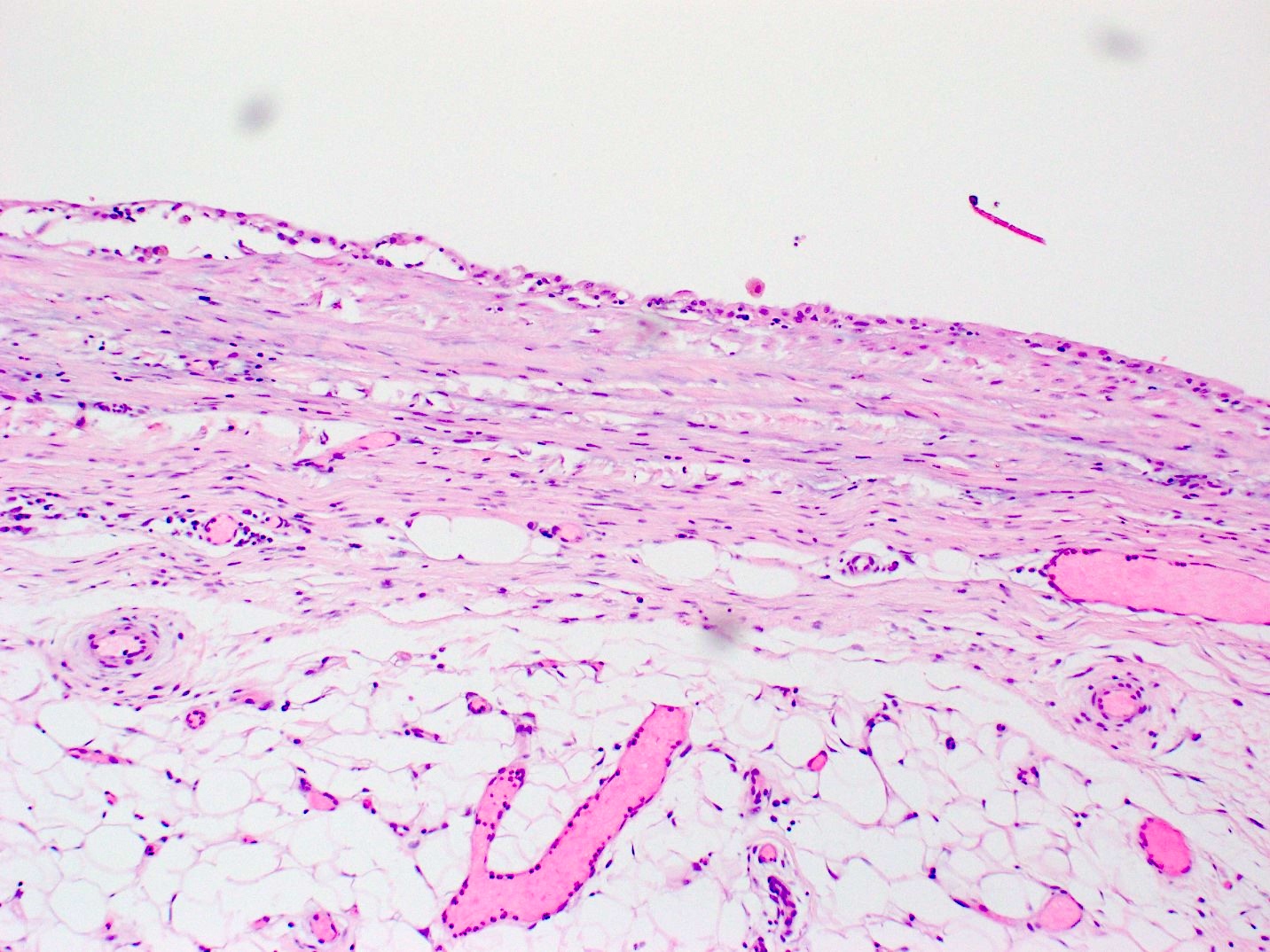
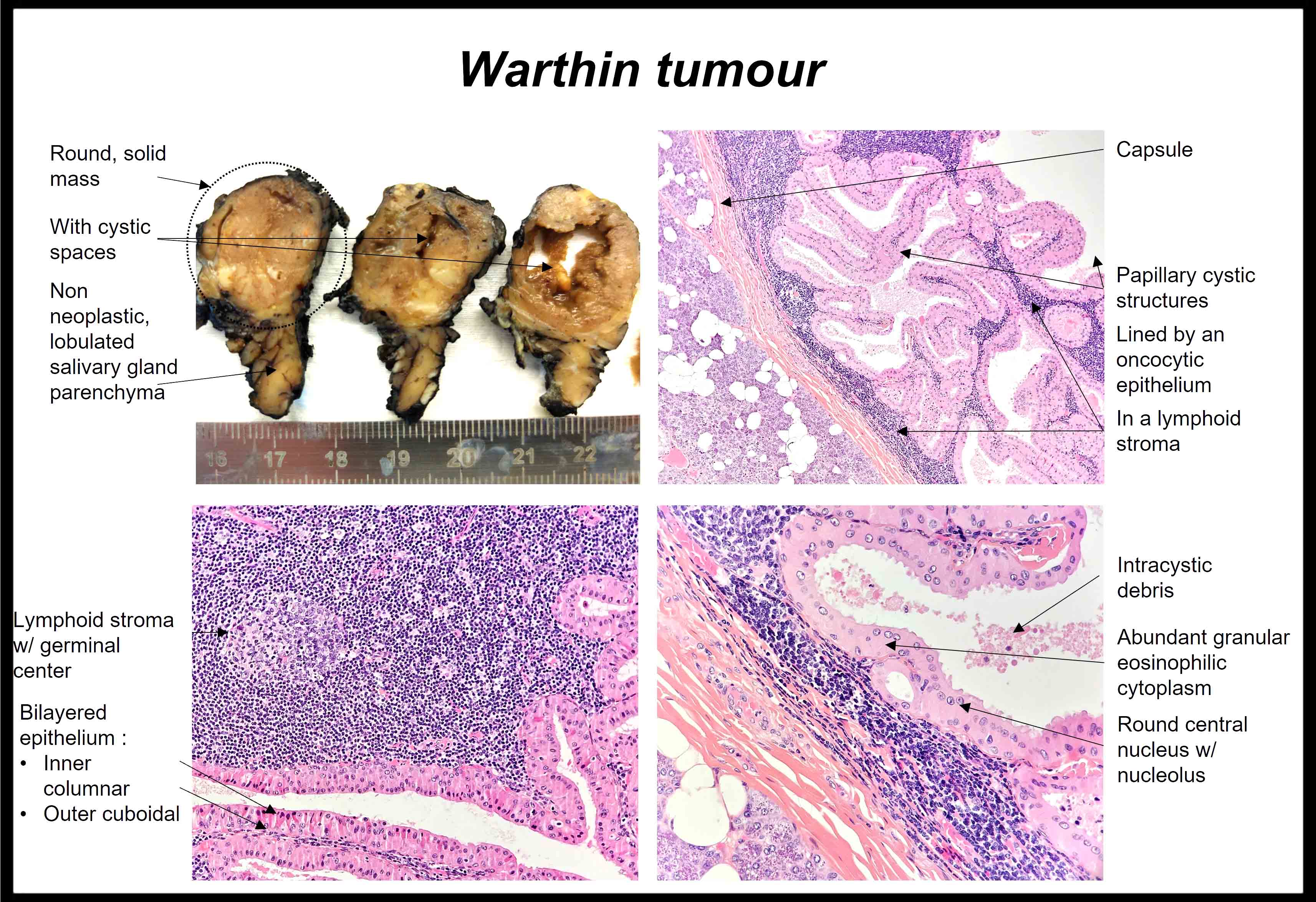
Warthin tumor, the second most frequent benign epithelial neoplasm, originates from heterotrophic salivary ducts present in intra or periparotid lymph nodes
Dual morphological components of a lymphoid stroma and a bilayered, oncocytic epithelium that lines papillary and cystic structures
Oncocytic epithelium rich in mitochondria is derived from the striated ducts
This entity displays male predominance and usually presents as a symptomless, fluctuant parotid lump (J Clin Diagn Res 2014;8:ZD37)
Mitochondria rich oncocytic epithelium can often appear PET avid
Interlobular and intralobular salivary duct epithelium gives rise to the most common salivary gland malignancy, mucoepidermoid carcinoma, comprising mucinous, squamoid and intermediate cells arranged in a solid and cystic architecture
Mucoepidermoid carcinoma predominantly presents as a solitary asymptomatic swelling within the parotid gland; pain and facial paralysis may occasionally occur (Adv Anat Pathol 2006;13:293)
WHO classification system of salivary gland tumors includes nearly 30 other subtypes including adenoid cystic carcinoma, secretory carcinoma, epithelial myoepithelial carcinoma, salivary duct carcinoma and carcinoma ex pleomorphic adenoma
Other neoplasms include lymphomas and metastatic malignancies from the skin and soft tissues of the scalp (squamous cell carcinoma, melanoma, angiosarcoma, pleomorphic dermal sarcoma); these are more likely to occur in the parotid gland due to the presence of native lymph nodes
Malignancies of the parotid gland can involve the facial nerve as the nerve passes through the gland
Minor salivary gland neoplasms generally manifest as submucosal nodules
Cells are periodic acid-Schiff (PAS) reagent positive
Mucous acini
Dominant component in the minor salivary glands of the palate and base of tongue
Round cells filled with mucin and containing a basally located, condensed nucleus
Positive for mucicarmine, alcian blue and PAS with diastase resistance (DPAS)
Mixed seromucous acini
Dominant component in the submandibular (serous predominance) and sublingual (mucous predominance) glands, minor salivary glands of the lip, cheek and anterior tongue
Mucous acini with crescent shaped caps (demilunes) of serous cells
3 main types of ducts are intercalated, striated or interlobular:
Intercalated ducts
Smallest caliber
Emerge from the acinar unit
Lined by a single layer of cuboidal epithelium
Contain reserve cells that regenerate the terminal secretory unit
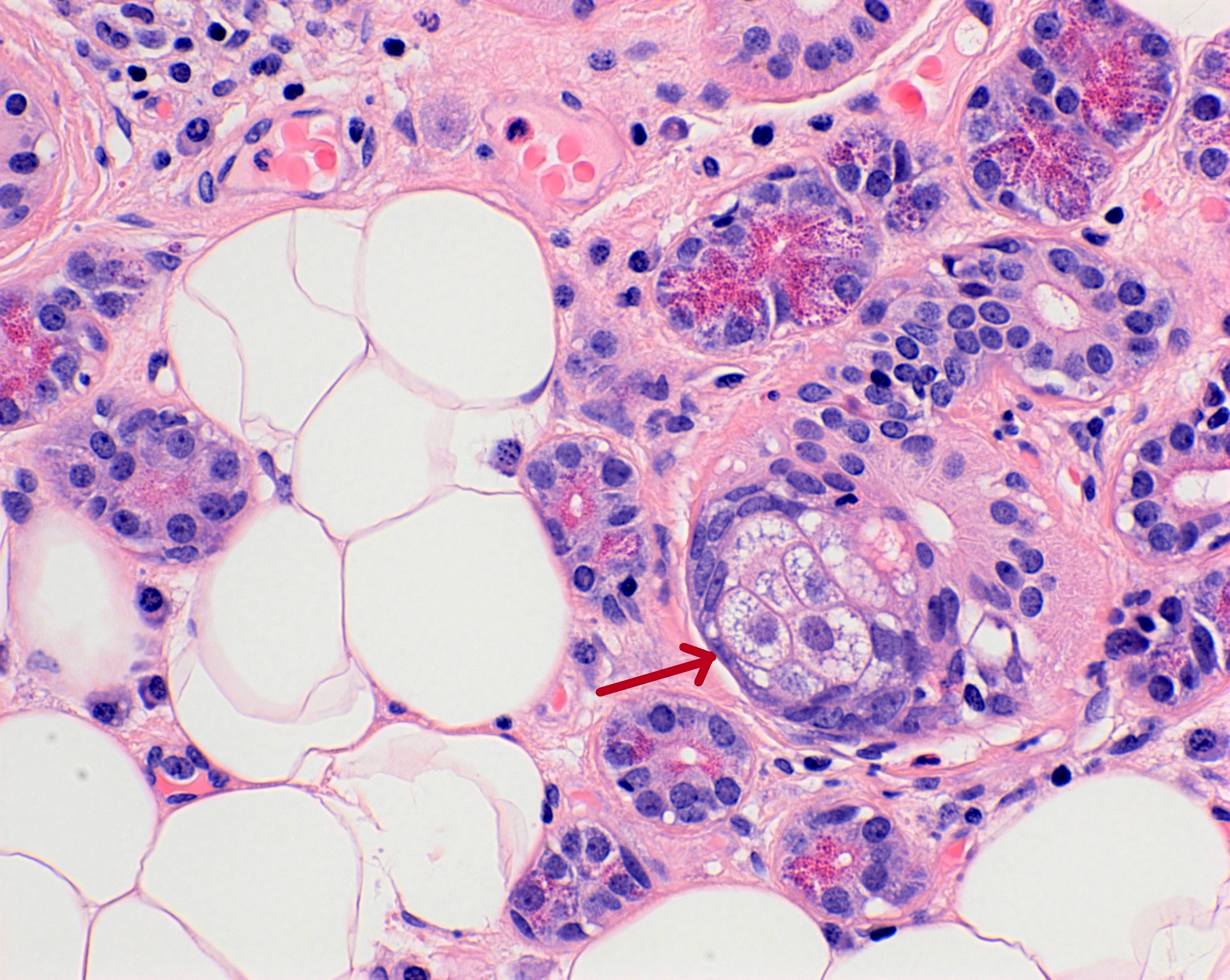
Striated ducts
Proceed from the intercalated ducts
Intralobular
Intermediate caliber between intercalated and interlobular ducts
Lined by columnar epithelium containing basal cytoplasmic striations, formed by rows of mitochondria alternating with folded cell membrane (Anat Rec 2001;264:121)
Contribute to the ionic composition of the saliva
Drain into interlobular ducts
Interlobular ducts
Largest caliber
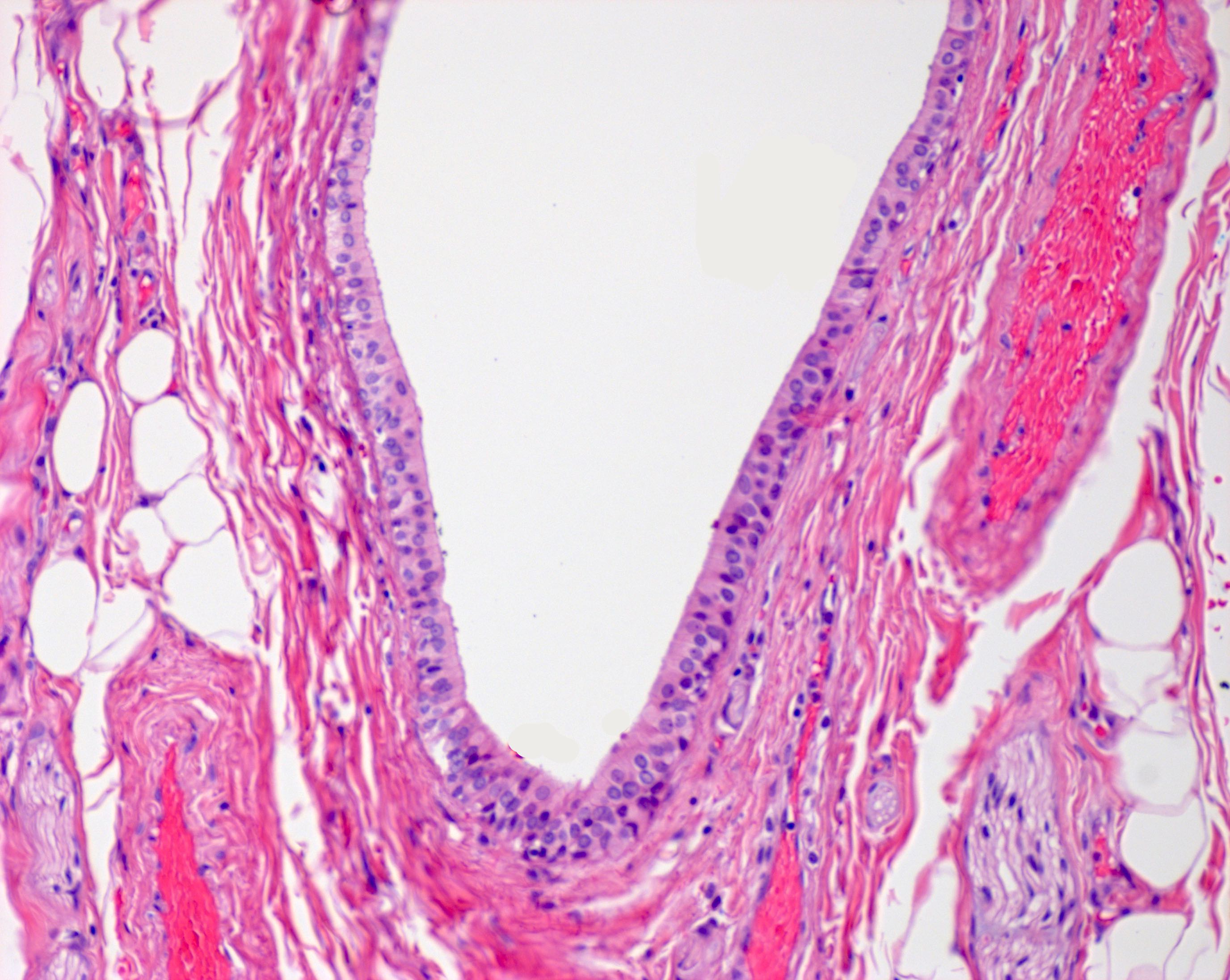
Located within interlobular septa and lined by pseudostratified columnar epithelium
Merge to form the major excretory duct outside the gland, lined distally by nonkeratinized stratified squamous epithelium
Myoepithelial cells are critical for the expulsion of saliva
Contractile myoepithelial cells surround acini, intercalated ducts and striated ducts
Located between epithelial cells and the basement membrane, embracing the secretory unit with long cytoplasmic processes
Generally spindle shaped with blunt ended nuclei and elongated cytoplasmic processes (Microsc Res Tech 1993;26:5)
Normal inclusions within the salivary glands:
Presence of sebaceous glands within the parotid gland is common and are usually found associated with interlobular ducts or may exist as isolated cells within the wall of intercalated or striated ducts (Am J Surg Pathol 1989;13:879)
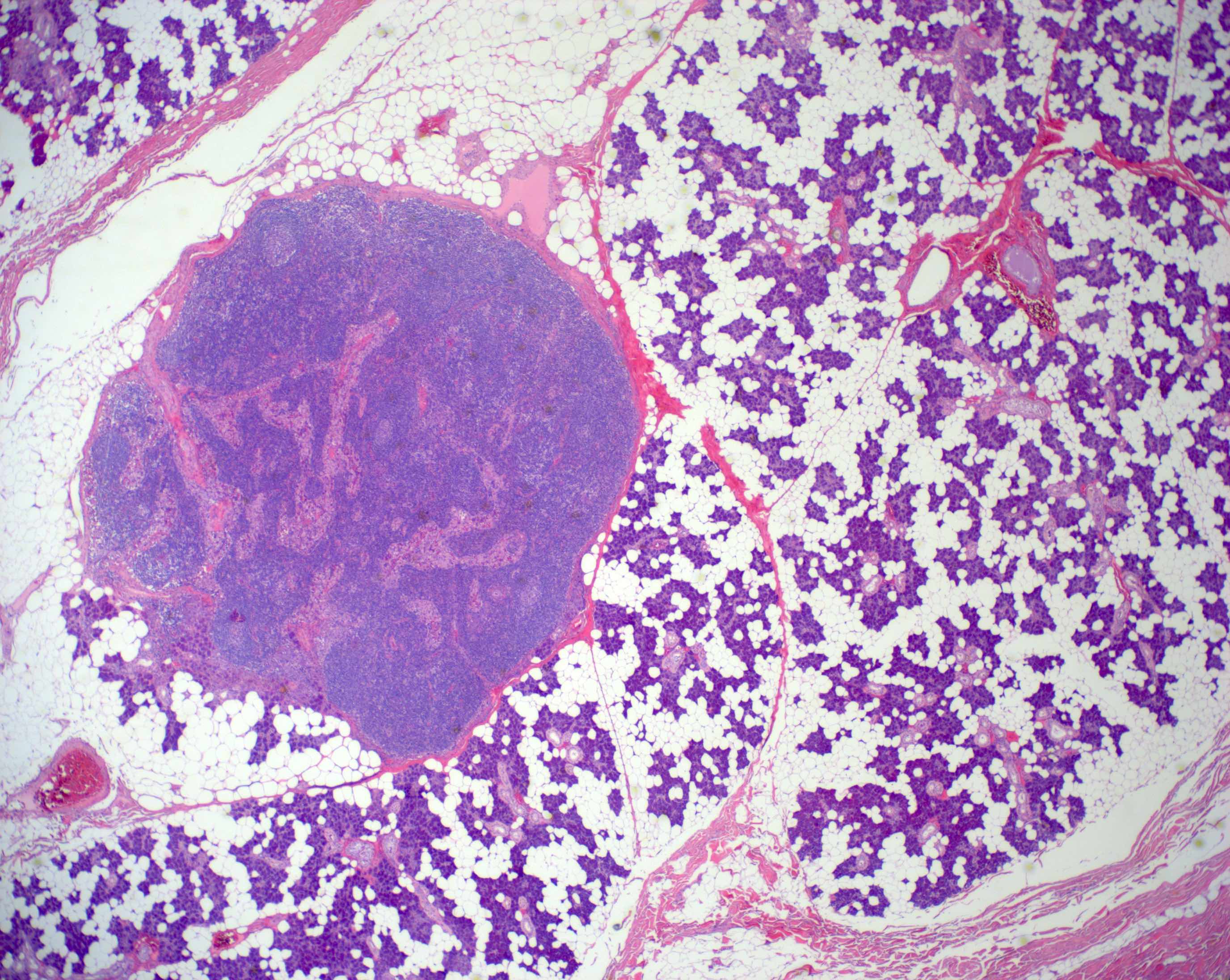
Unique to the parotid gland is the presence of intraparotid lymph nodes, most of which are located superficial to the facial nerve (Br J Plast Surg 1985;38:1)
Often the lymph nodes may lack a well defined capsule and merge with the adjacent salivary gland acini
Which type of salivary duct, pictured above, is responsible for the ion transport that alters the isotonic secretion produced by acinar cells to hypotonic saliva?
Intercalated duct
Interlobular duct
Major excretory duct
Striated duct
Board review style answer #1
D. The striated ducts contain abundant mitochondria to provide the energy for ion transport
Which of the following is true about the parotid gland?
The acini are purely of mucous type
Intraparenchymal lymph nodes may contain glandular inclusions
Wharton duct, the main excretory duct, pierces the masseter muscle to enter the oral cavity
Sebaceous cells may be found within fatty tissue
The facial nerve traverses the superficial surface of the gland
Board review style answer #2
B. Intraparenchymal lymph nodes may contain glandular inclusions. A is incorrect because the acini are purely of serous type in the parotid gland. C is incorrect since the main excretory duct of the parotid gland is Stensen duct, which emerges from the anterior border of the gland, courses horizontally along the masseter muscle and turns medially to pierce the buccinator muscle. D is incorrect because sebaceous cells may exist within the wall of intercalated or striated ducts. E is incorrect because the facial nerve traverses the body of the gland to divide it into superficial and deep lobes.
Occasionally, FNAs with atypical cells which may be otherwise considered nondiagnostic are also included
Essential features
Category is heterogeneous in nature
Differential includes nonneoplastic and neoplastic entities
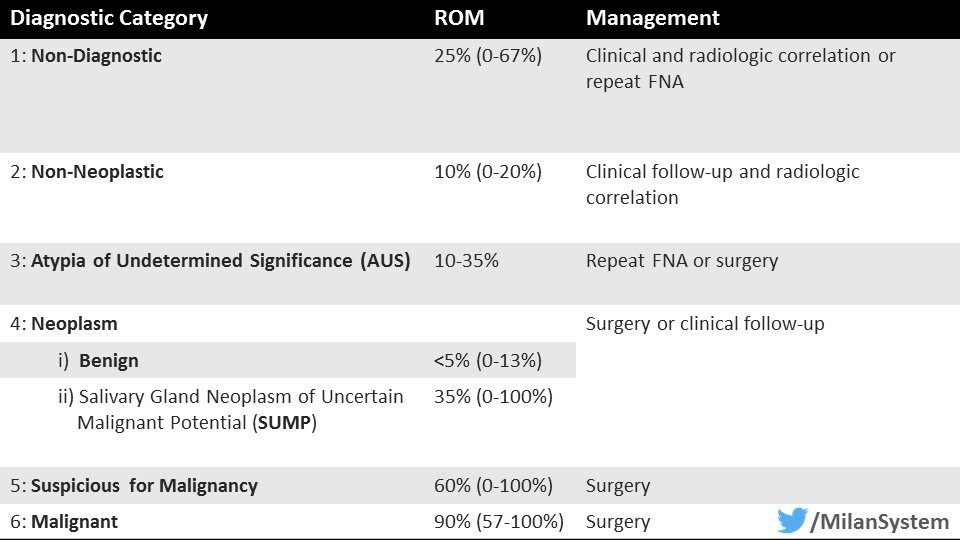
Risk of malignancy is ~20%; the implied risk of malignancy was estimated to be ~20% in the 1st edition of the Milan system but was found to be higher (~30% on average) in subsequent studies with surgical follow up
It is recommended that no more than 10% of FNAs should be interpreted as atypia of undetermined significance
CPT coding
88172 - determination of adequacy of specimen, first pass
88177 - determination of adequacy of specimen, subsequent pass
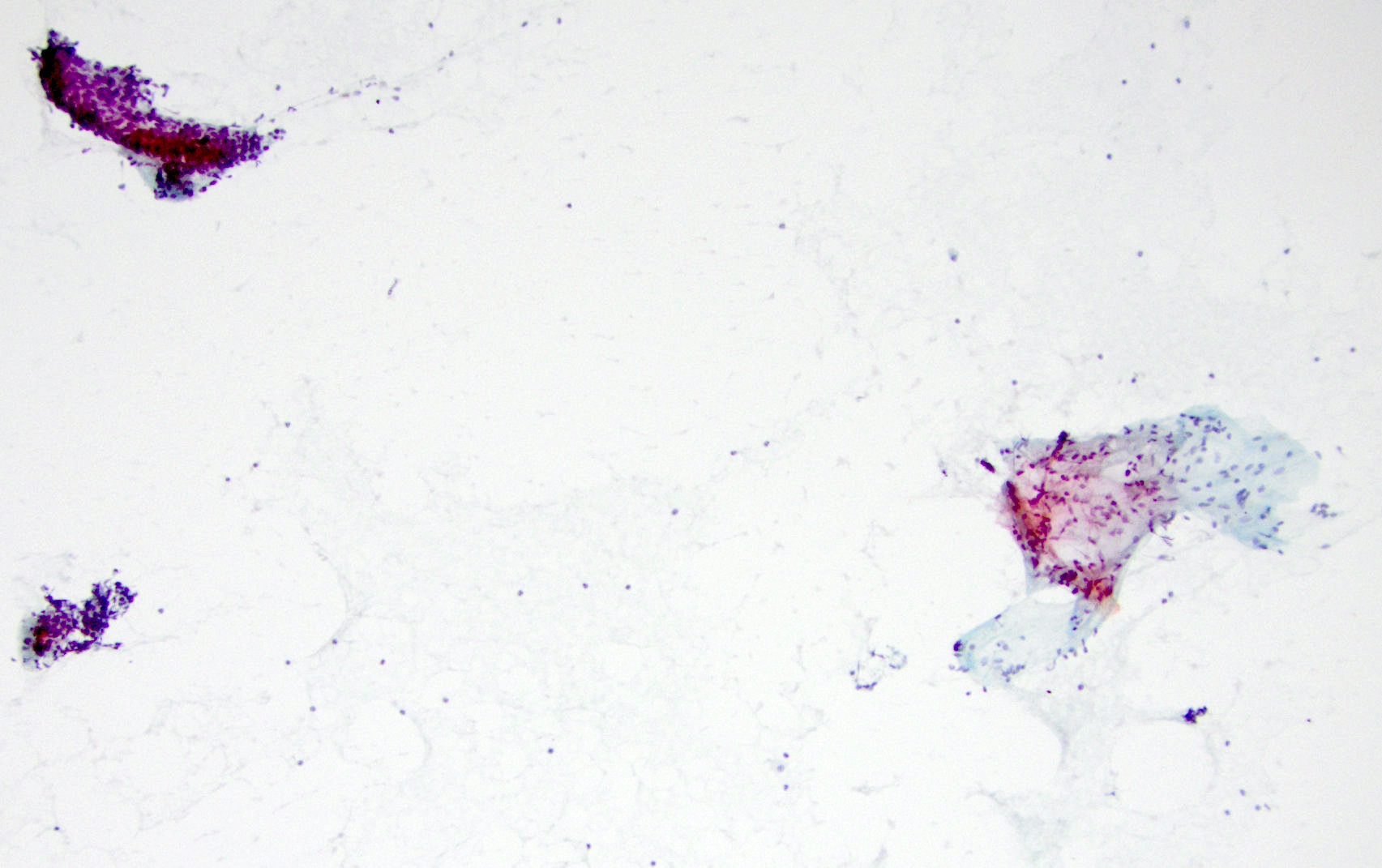
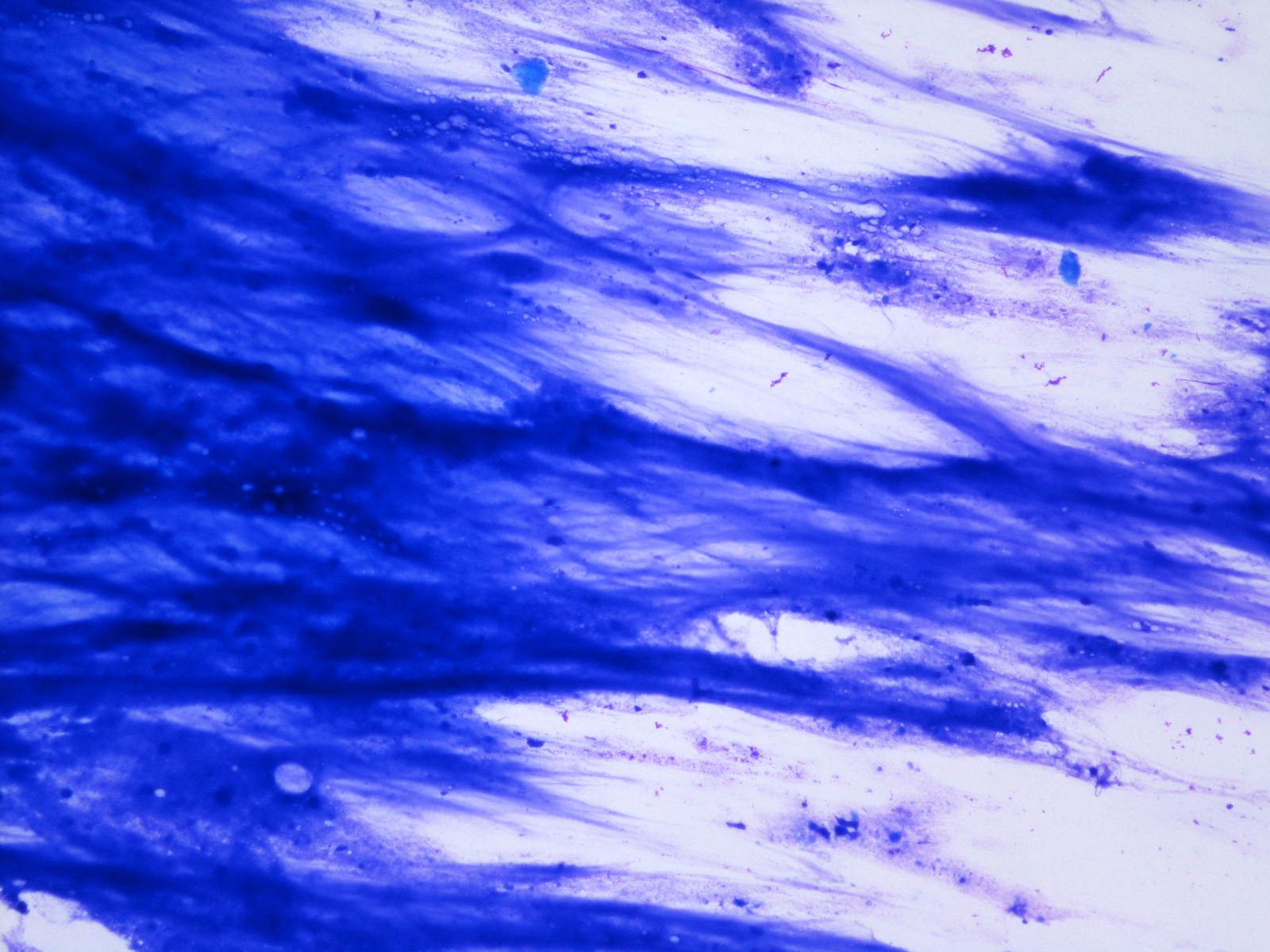
Scant histiocytes in a background of abundant mucin (see comment)
Comment: The specimen is limited by scant cellularity. The differential includes a mucinous cyst, though a low grade mucoepidermoid carcinoma is not entirely excluded. Clinical and radiologic correlation is suggested.
Submandibular, left, fine needle aspiration smears:
Atypia of undetermined significance
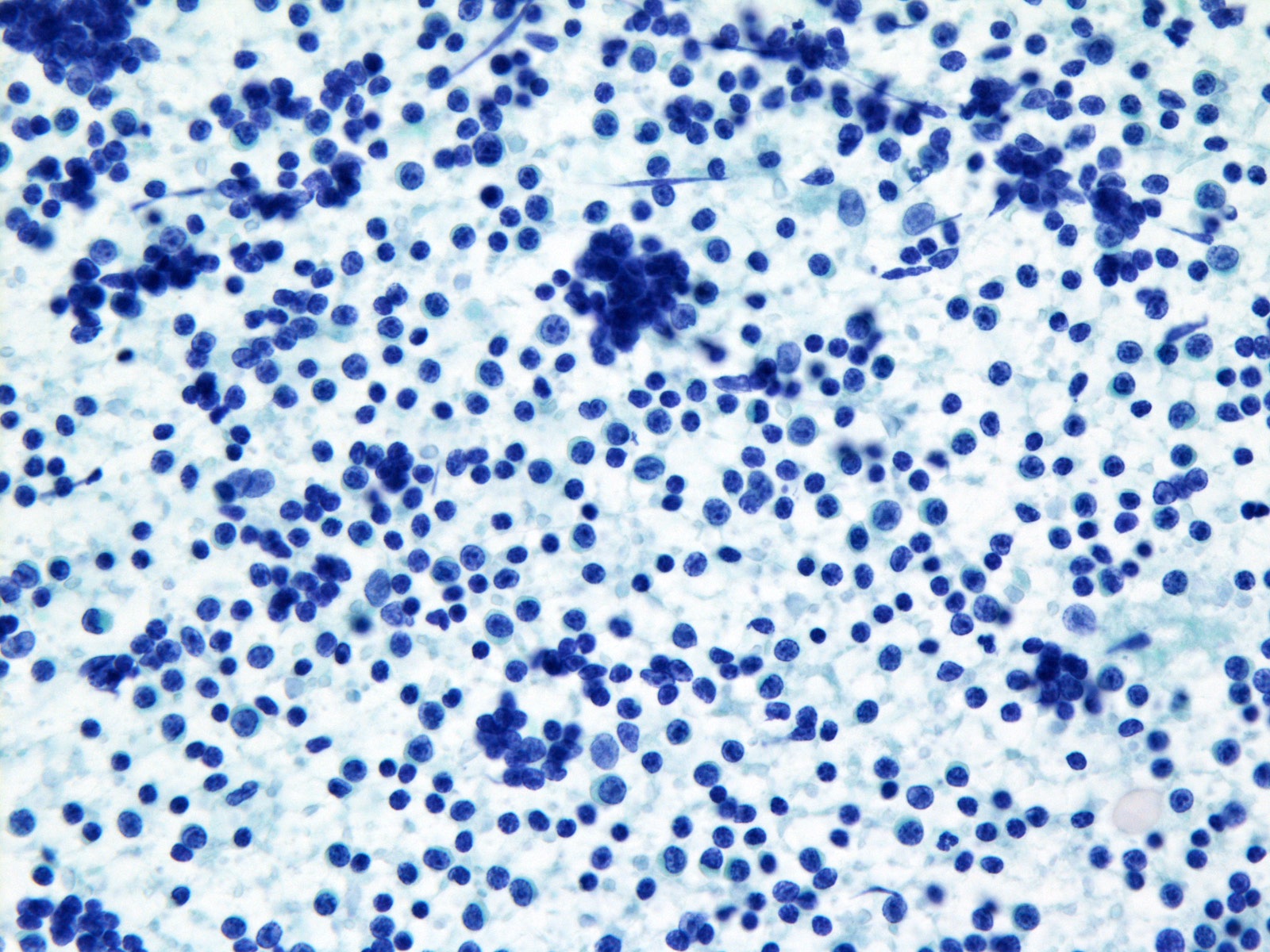
Heterogenous lymphoid elements (see comment)
Comment: Insufficient material was available for flow cytometry. Additional sampling with dedicated material for flow cytometry is suggested if clinical suspicion for a lymphoproliferative disorder persists.
Parotid, right, fine needle aspiration smears:
Atypia of undetermined significance
Rare atypical cells (see comment)
Comment: The specimen is limited by scant cellularity. The differential includes reactive atypia, though a neoplastic process cannot be entirely excluded. Clinical and radiologic correlation is suggested.
Differential diagnosis
Differential diagnosis of lymphocyte rich aspirates includes:
There is no true salivary gland duct epithelial lining and instead this is mimicked by epithelioid macrophages (muciphages) at the periphery of the extravasated mucin
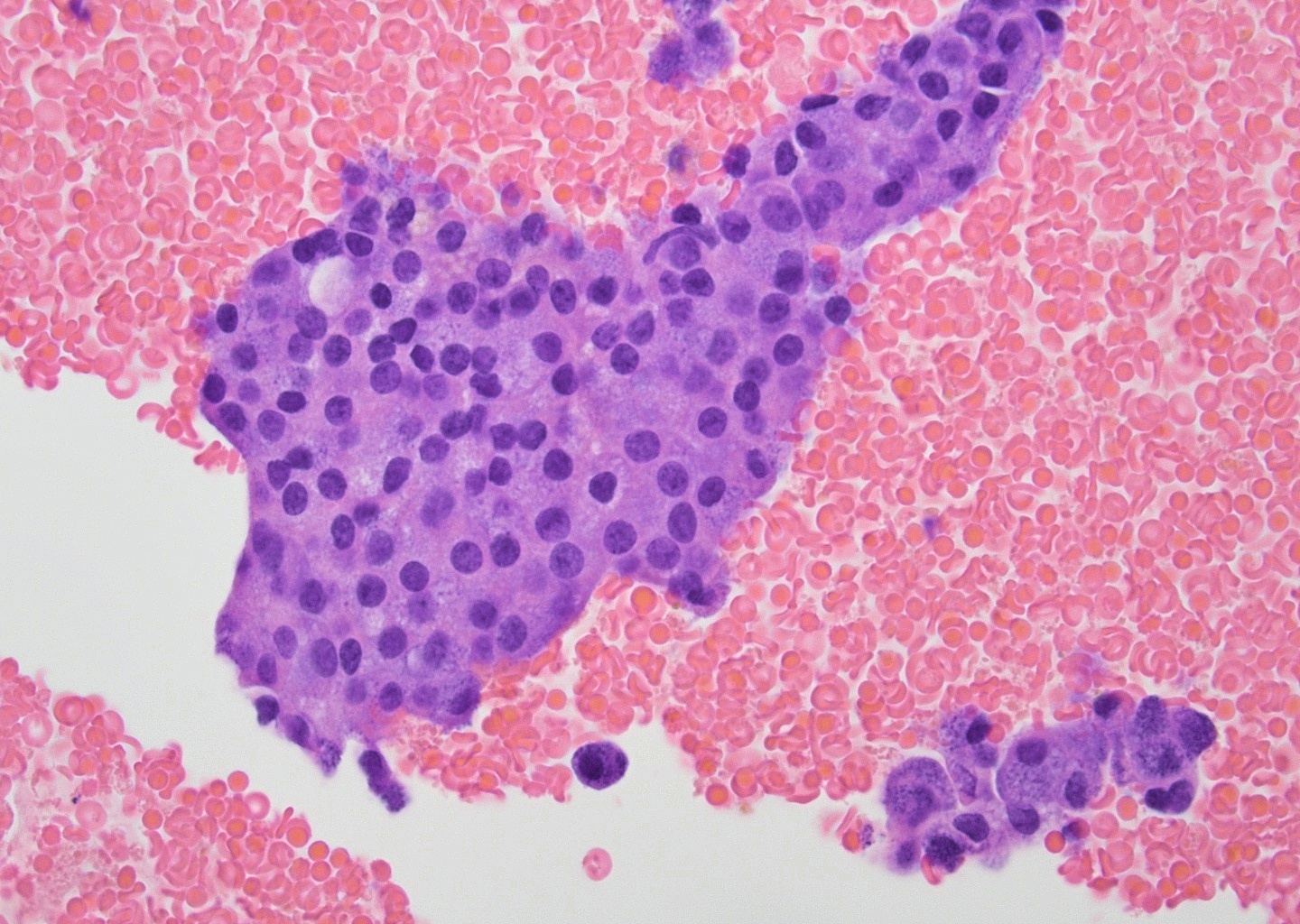
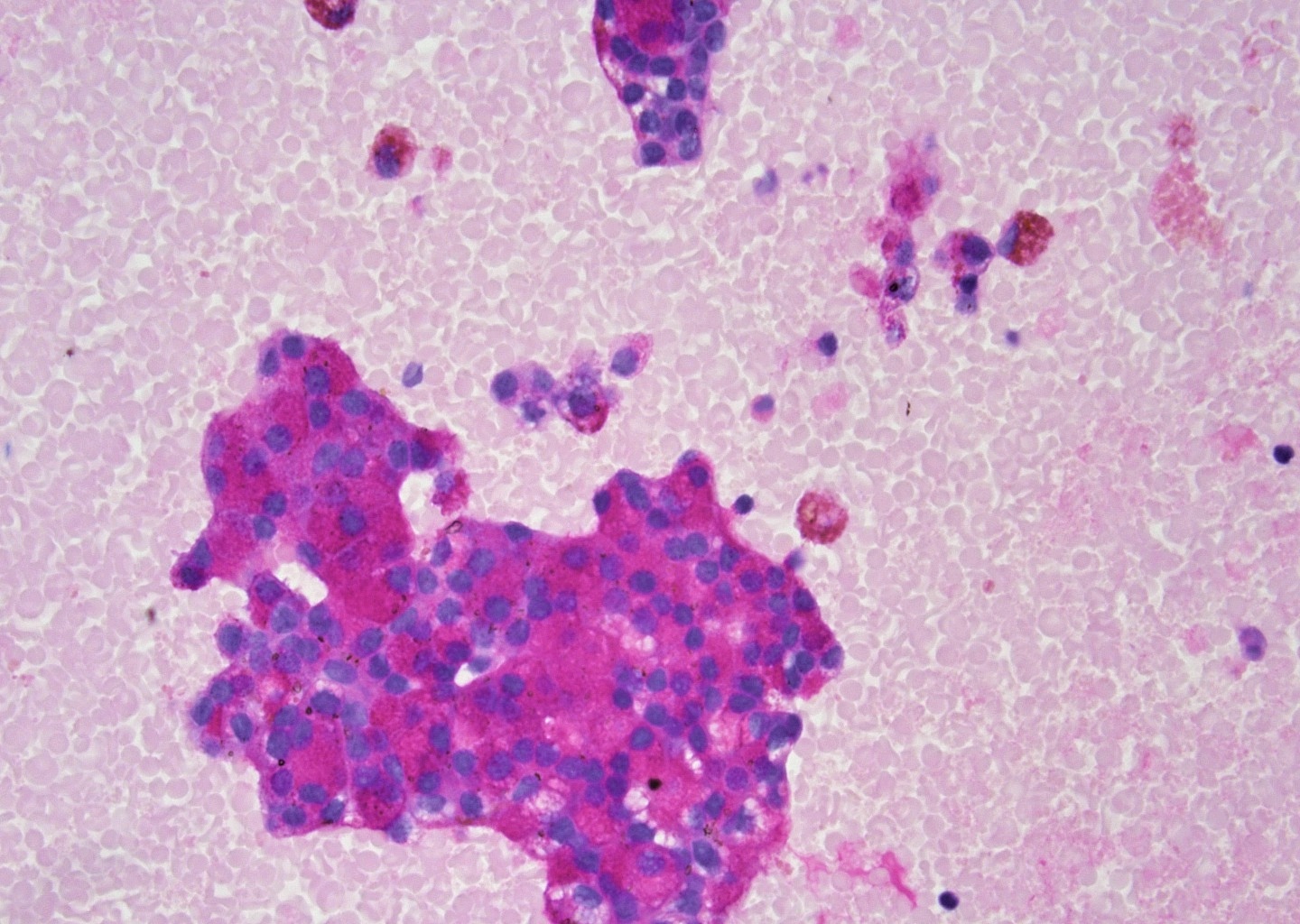
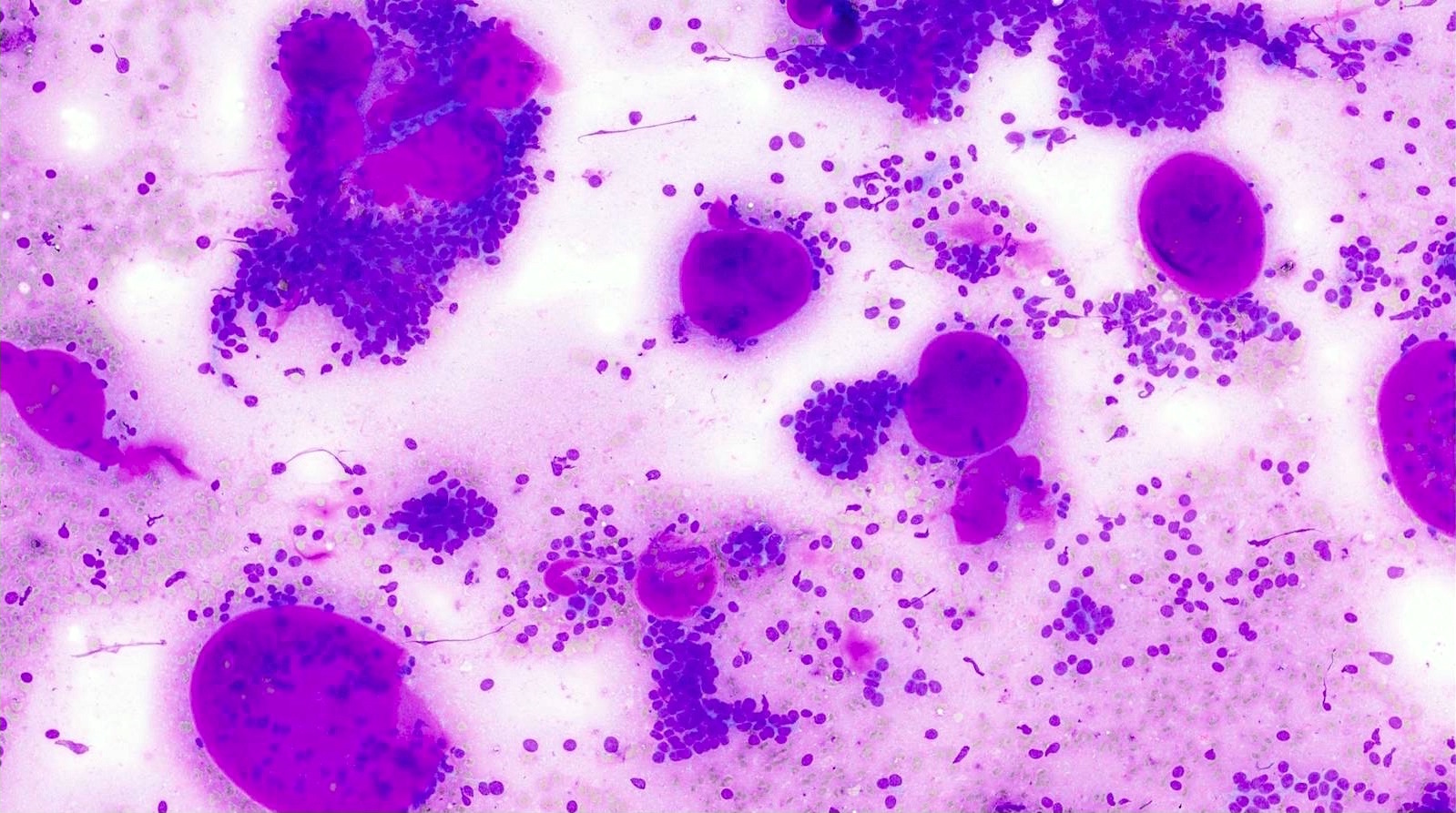
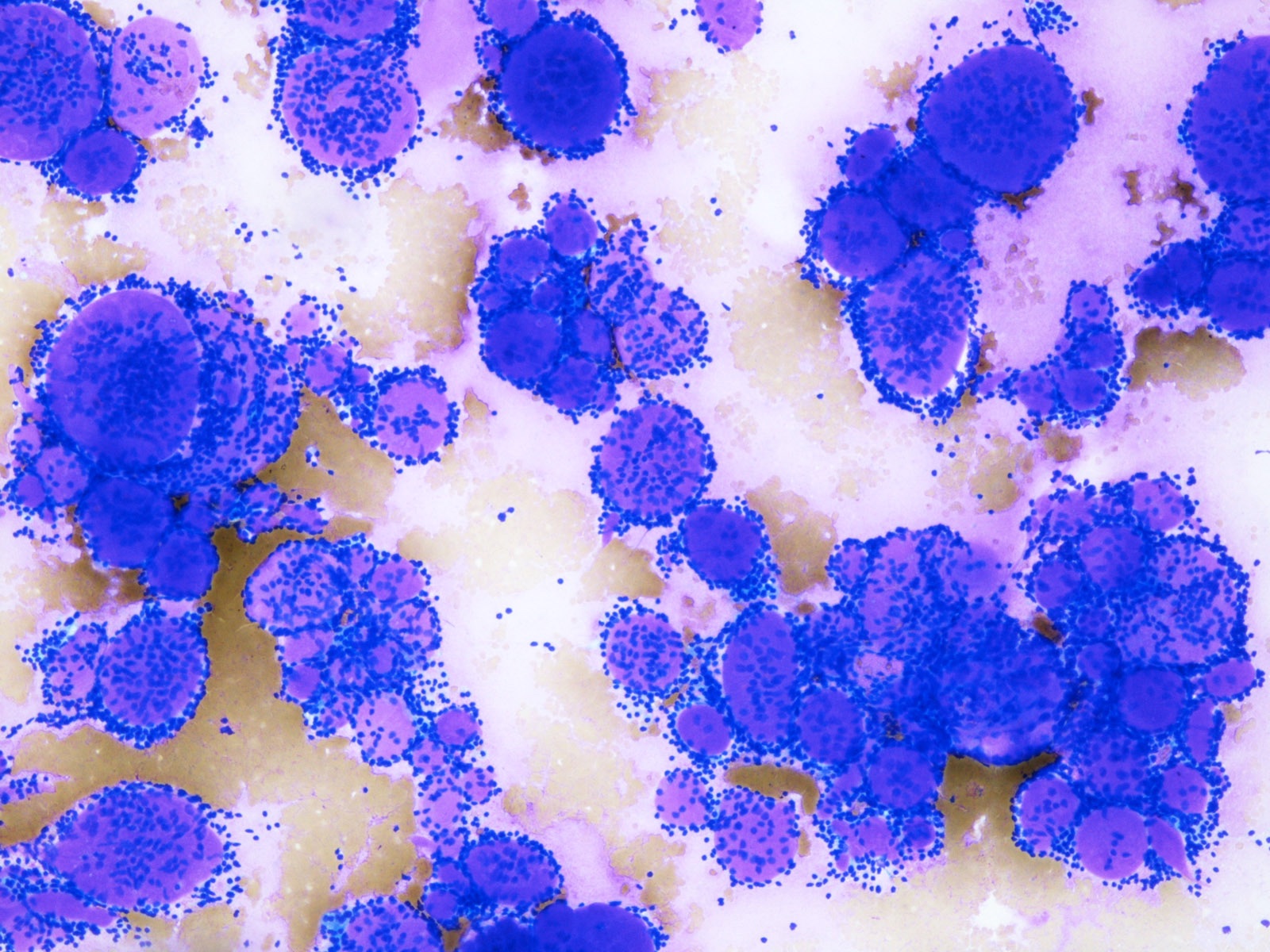
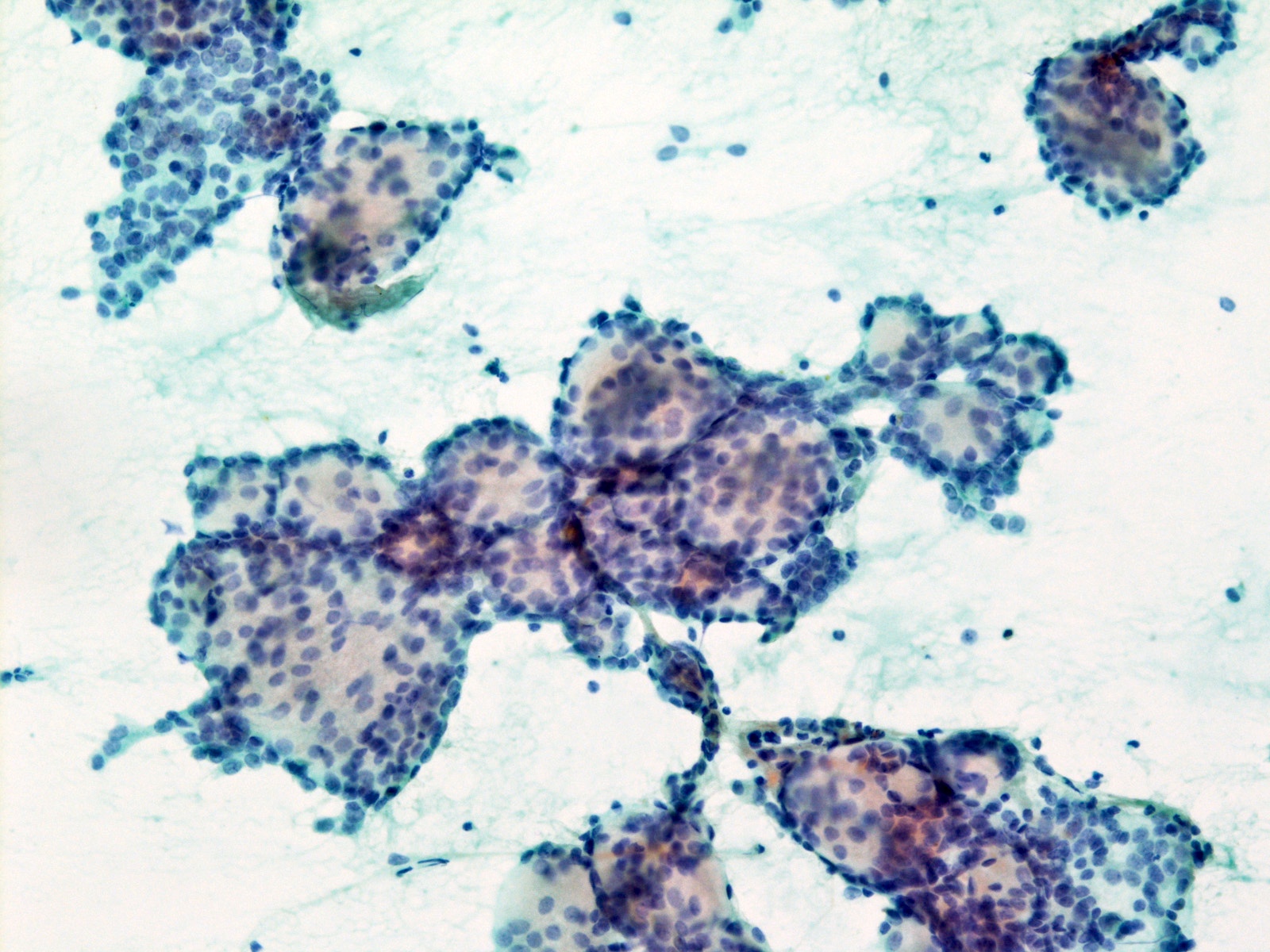
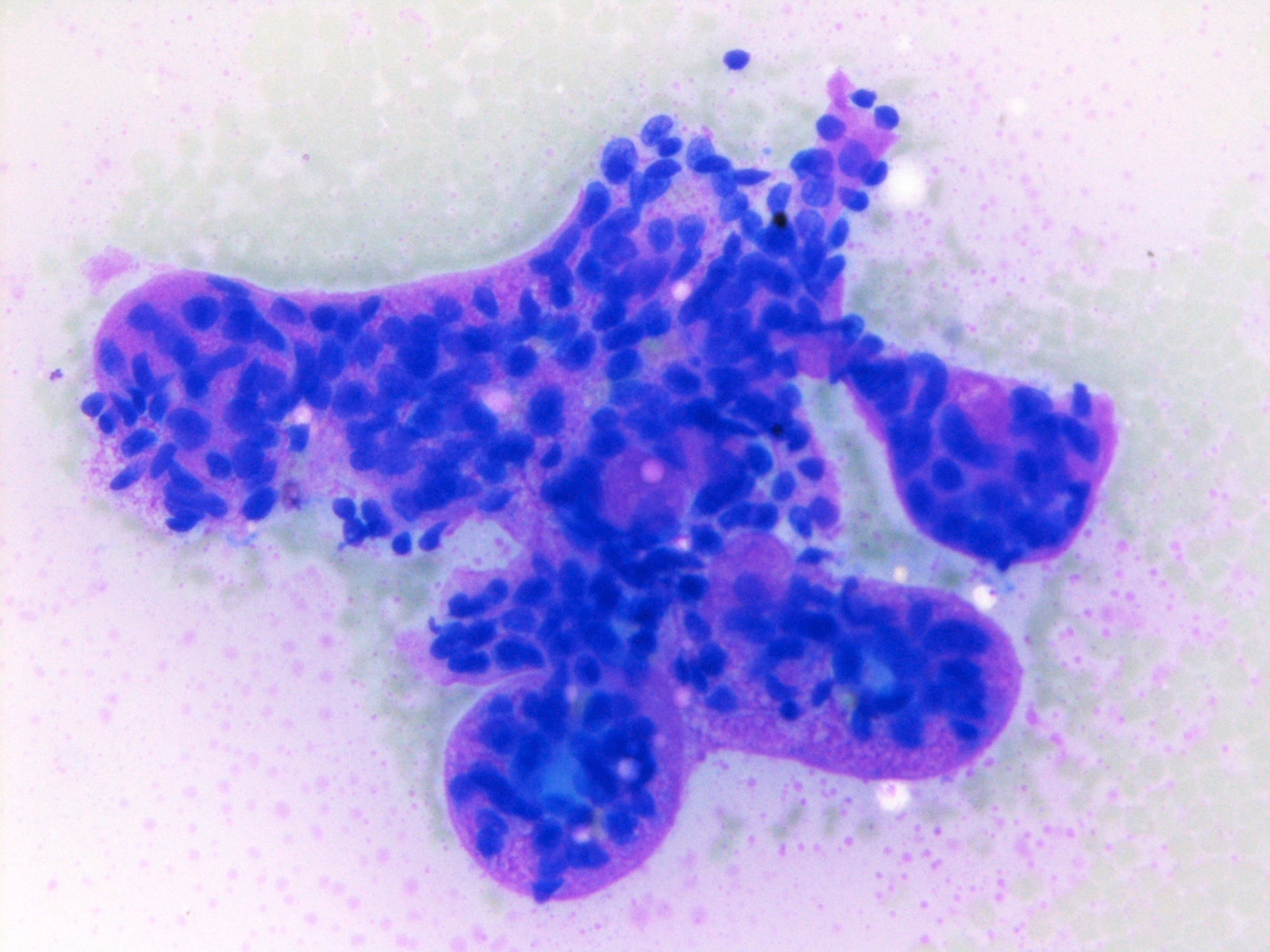
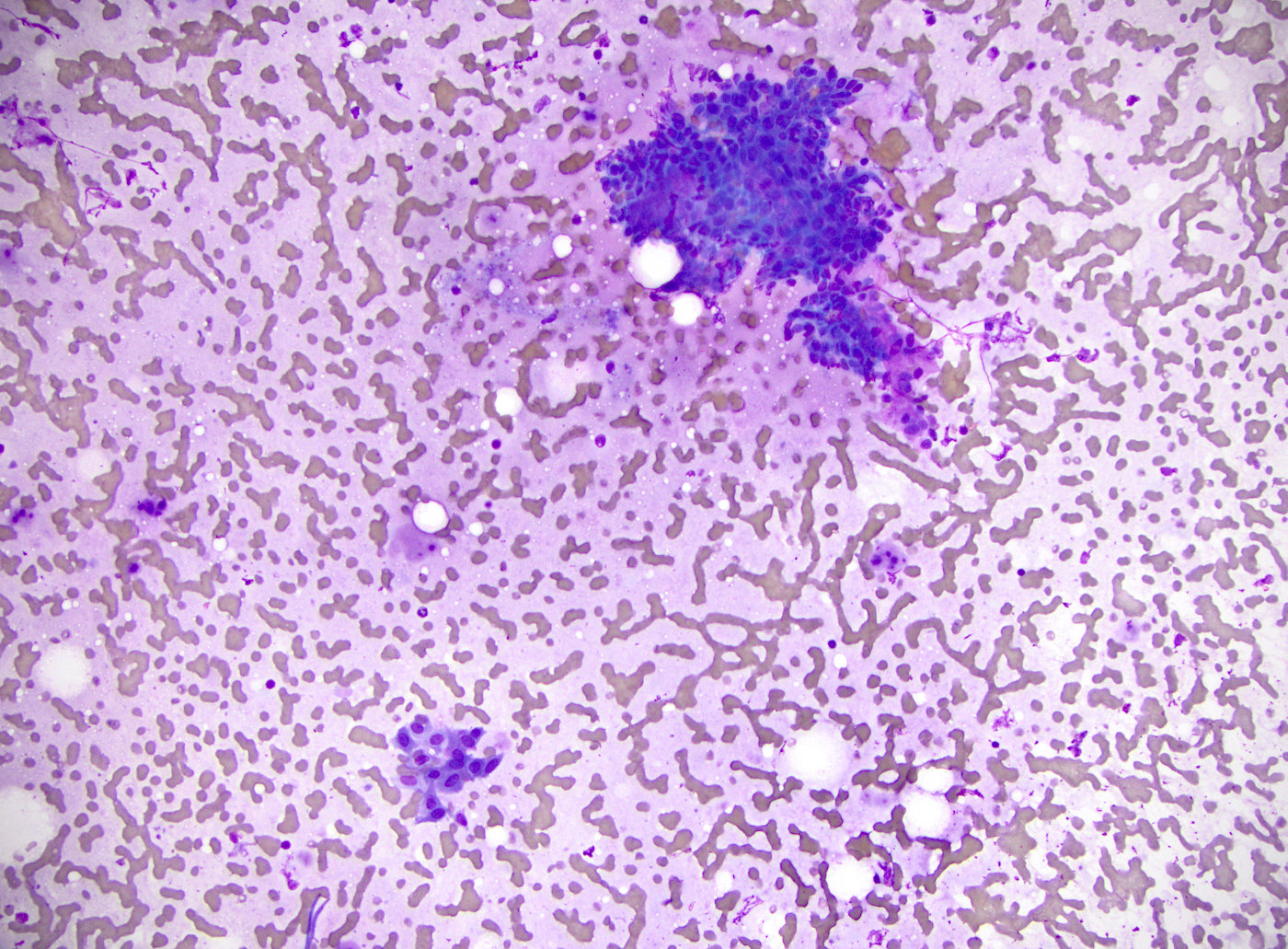
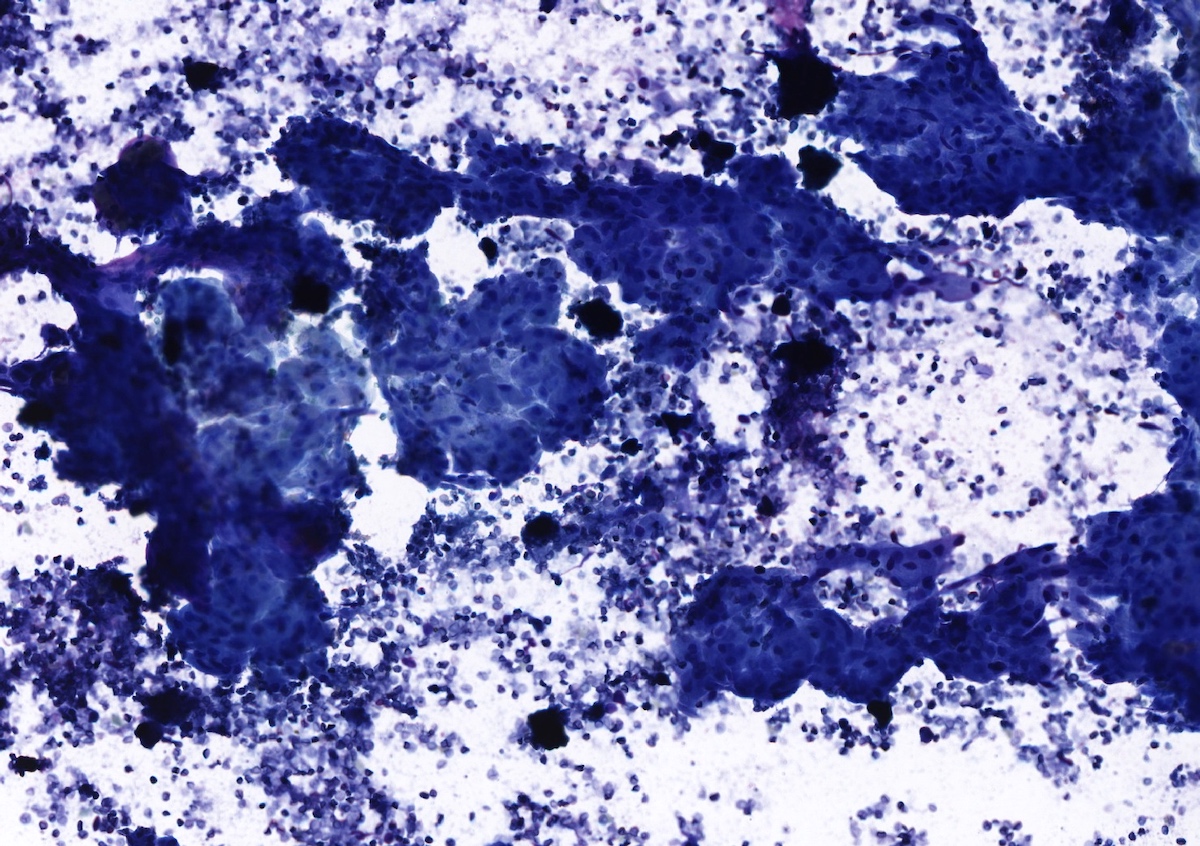
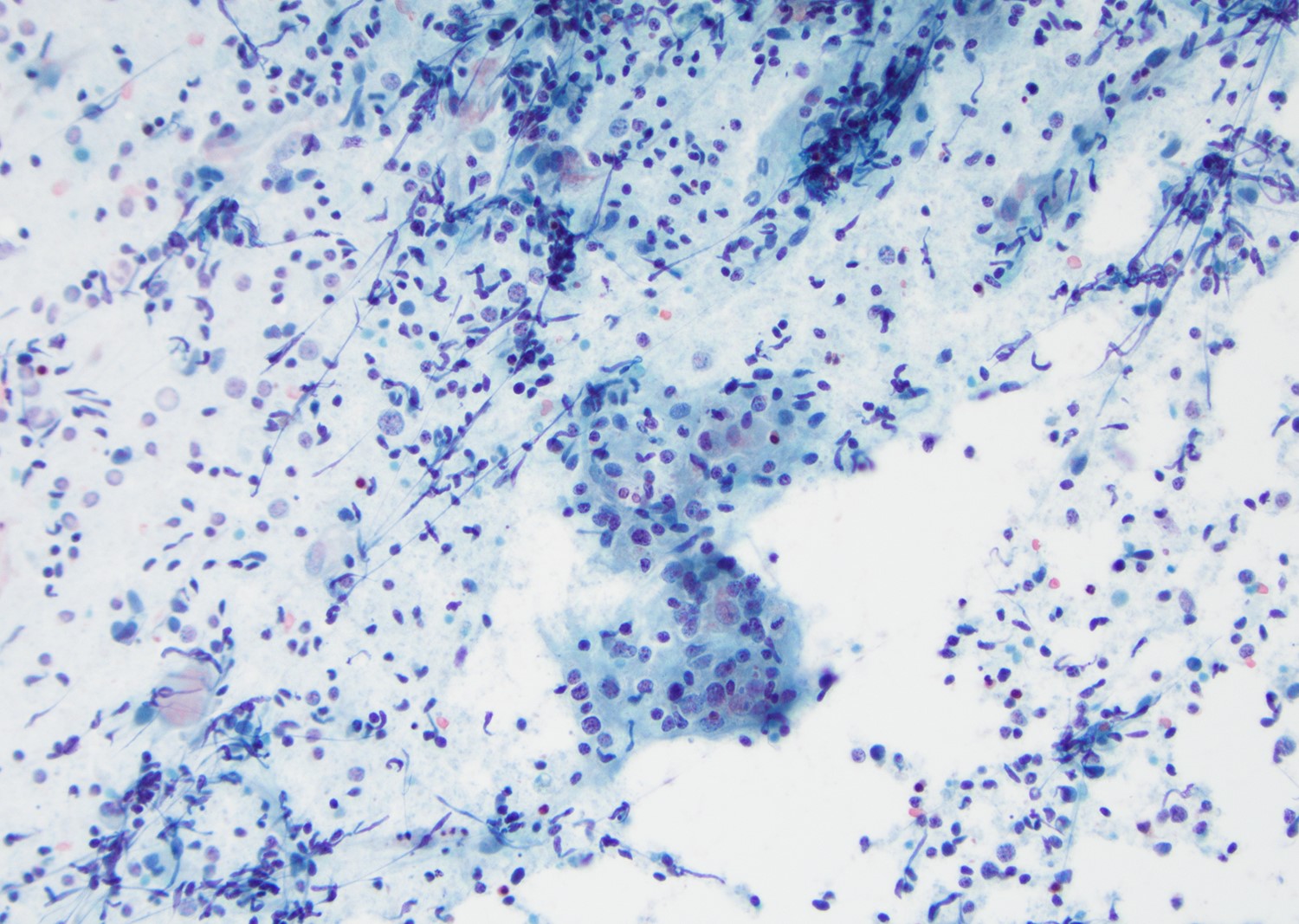
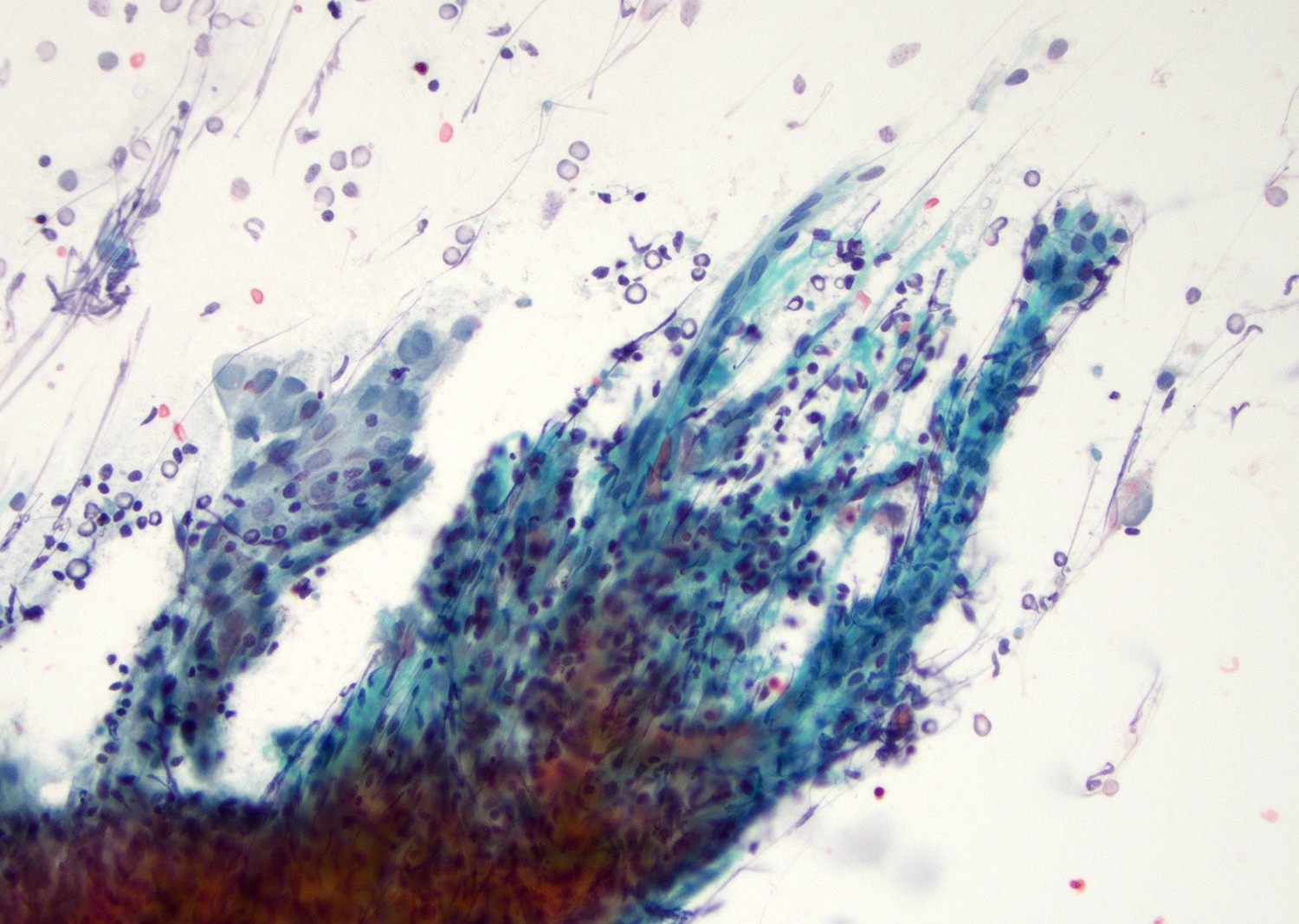
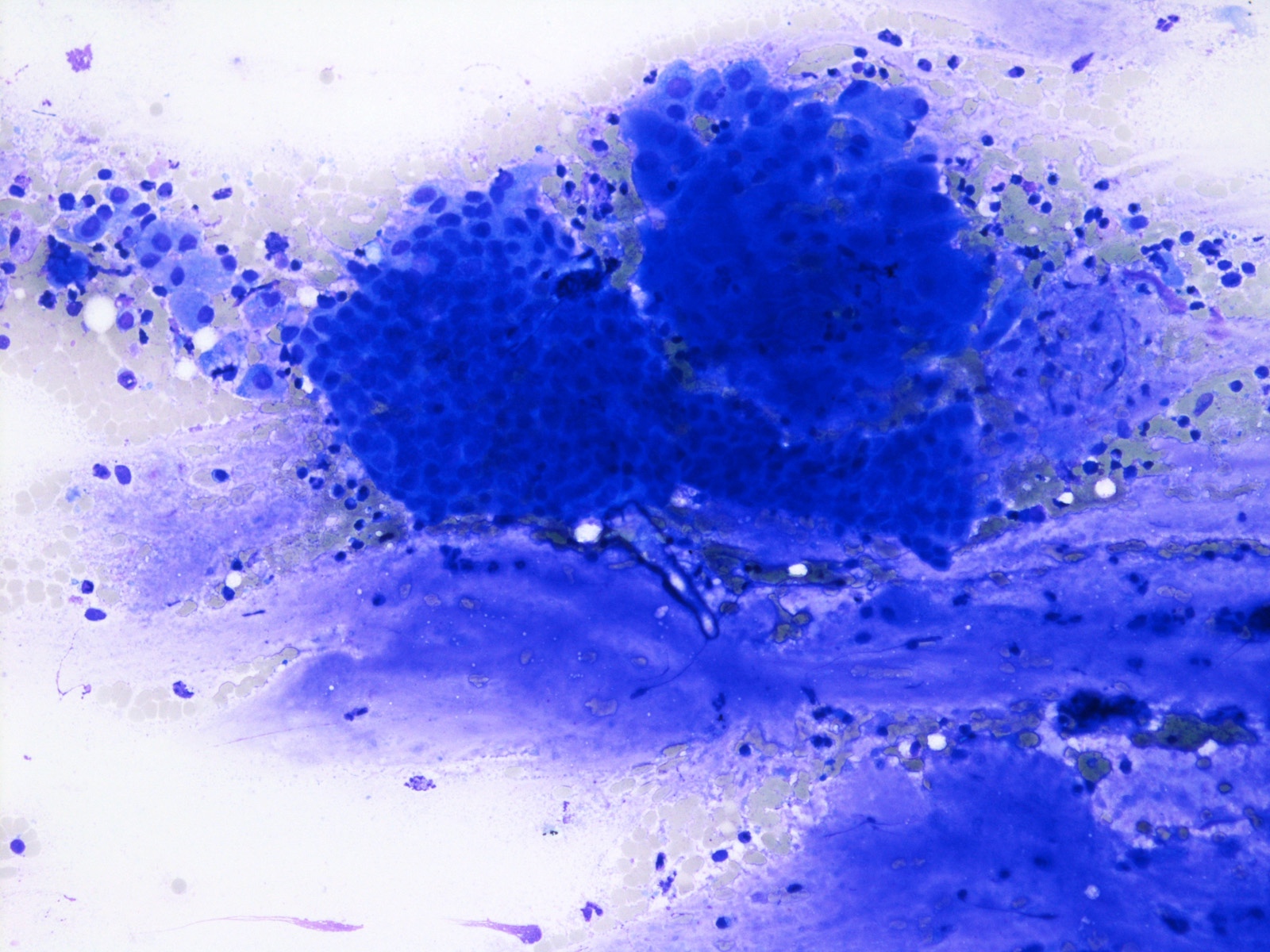
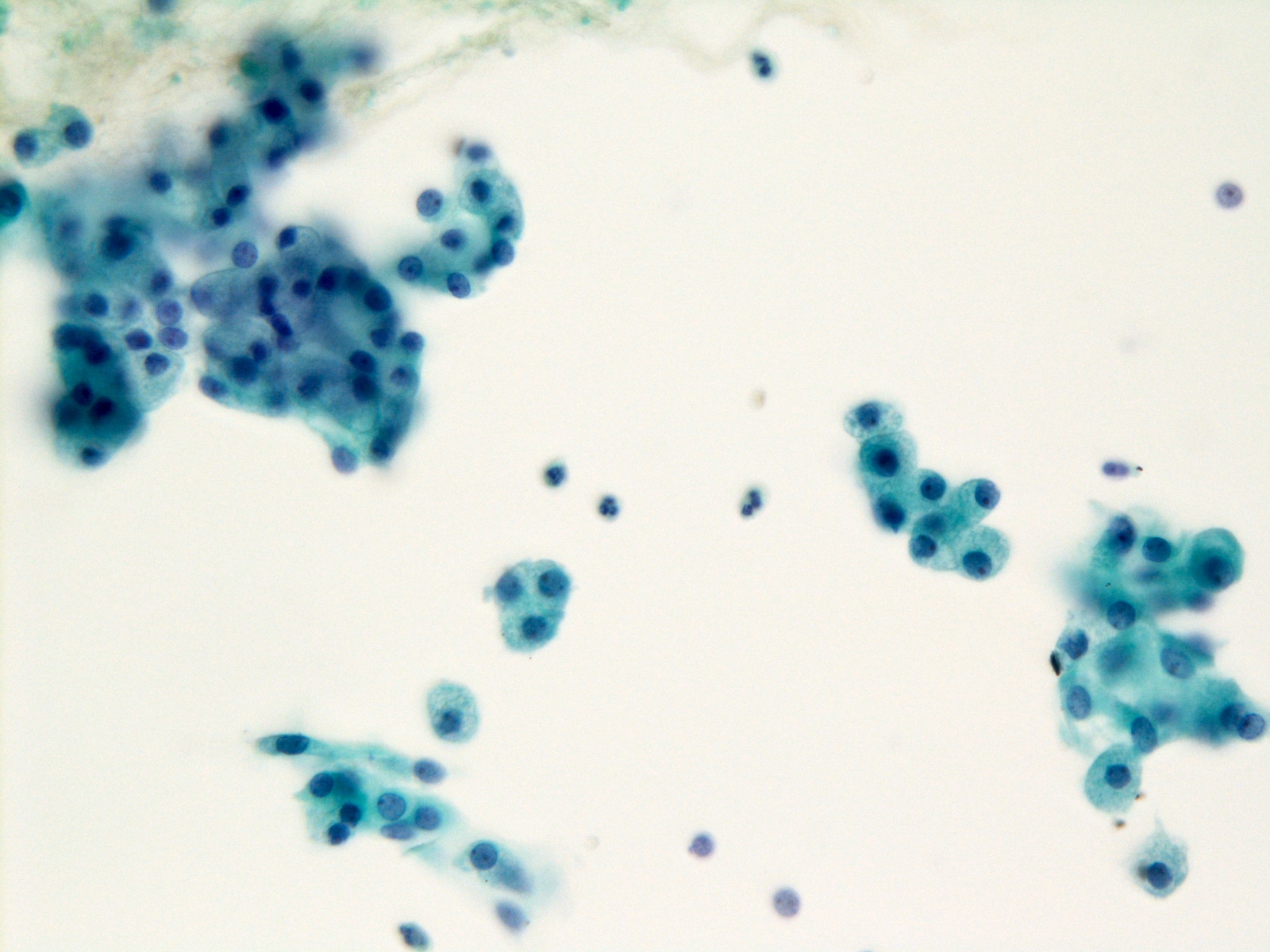
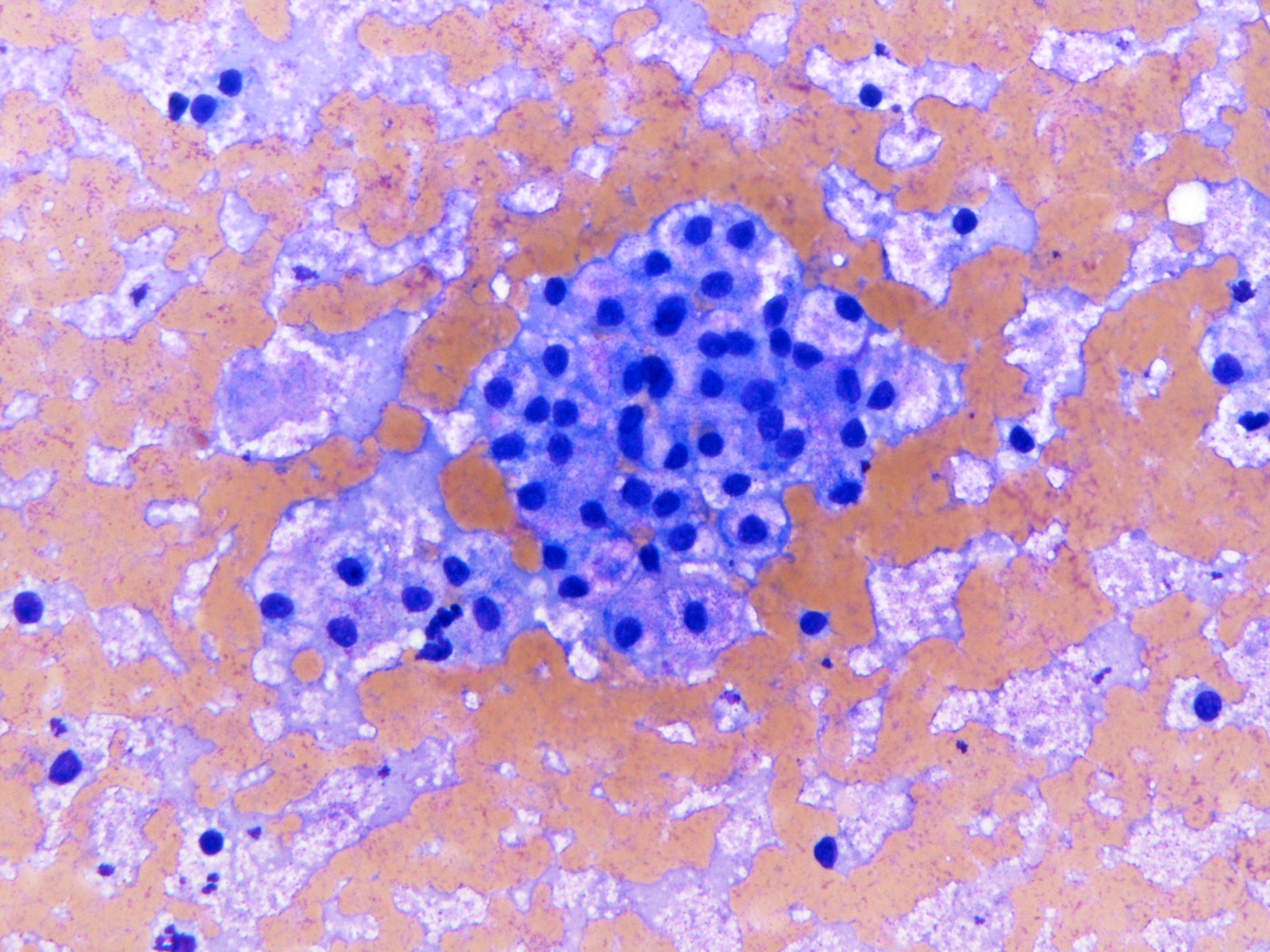
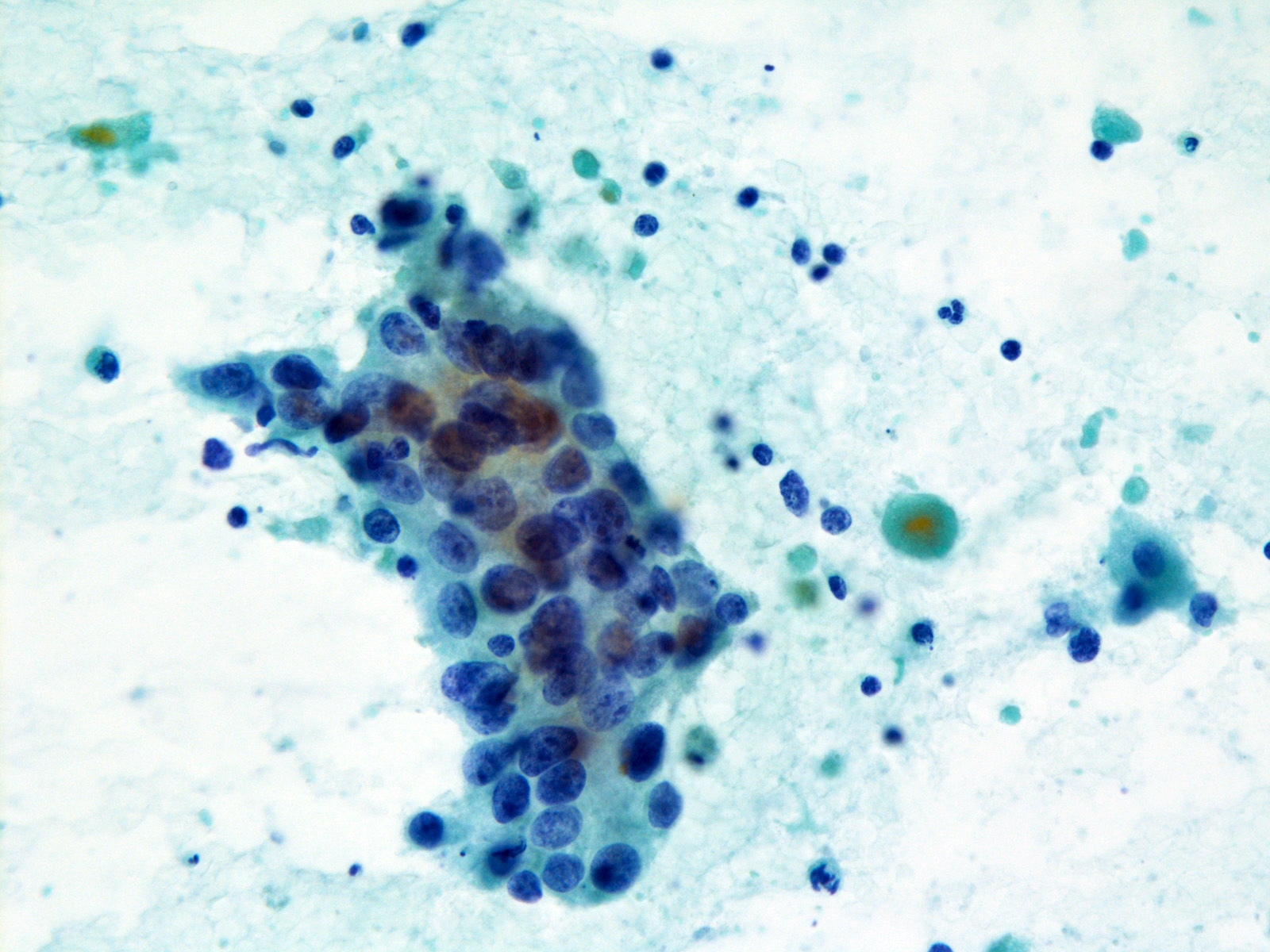
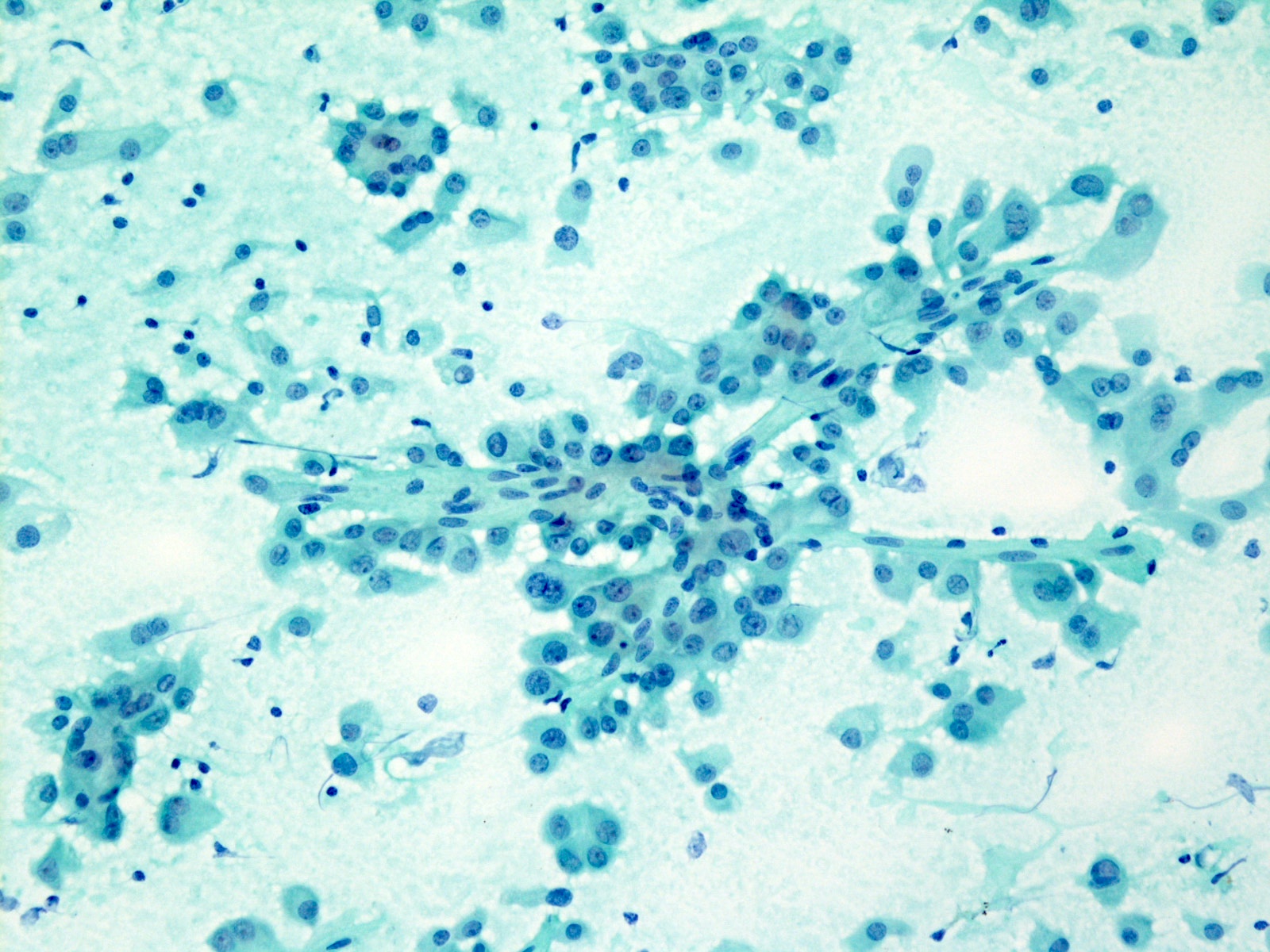
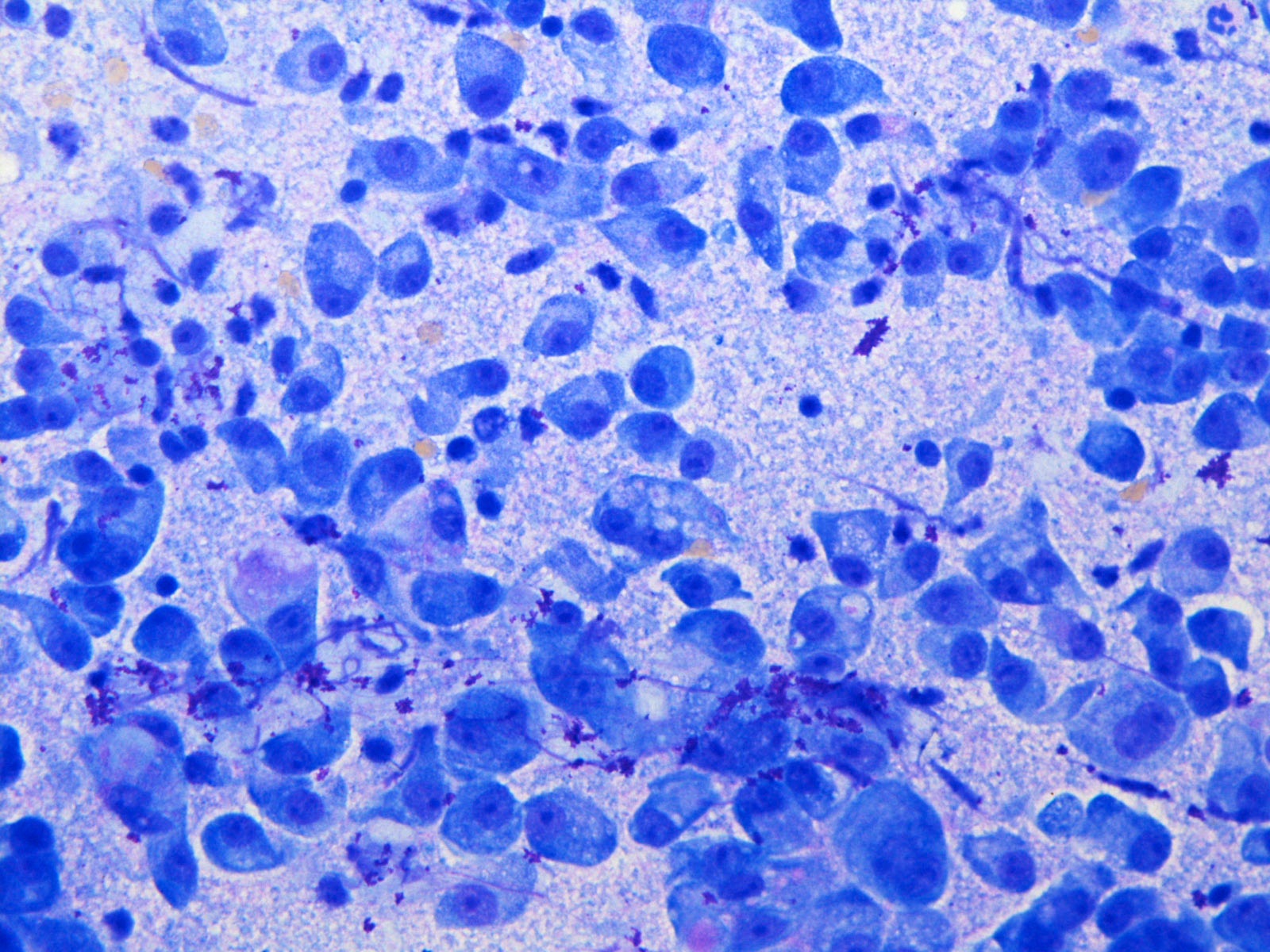
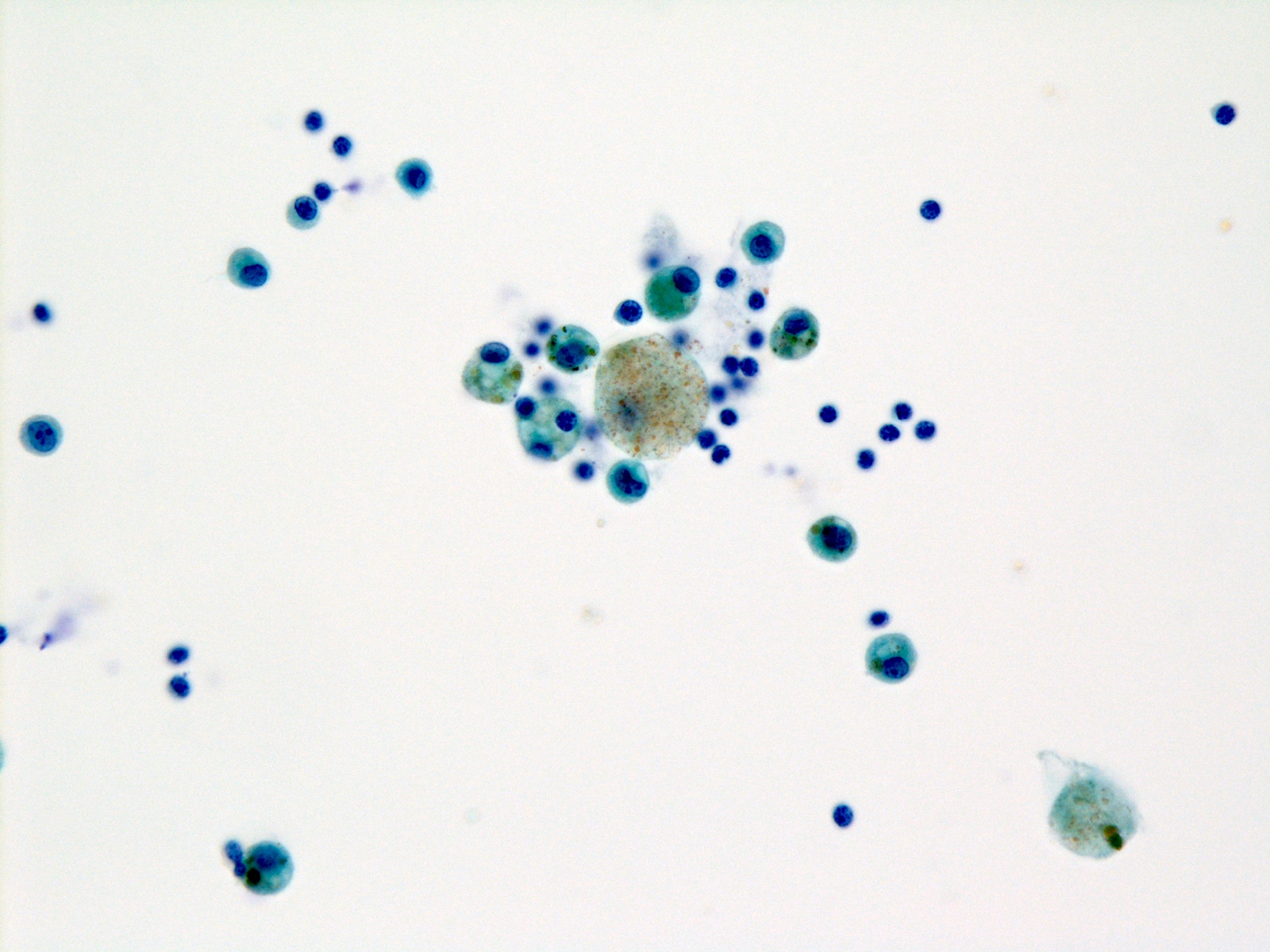
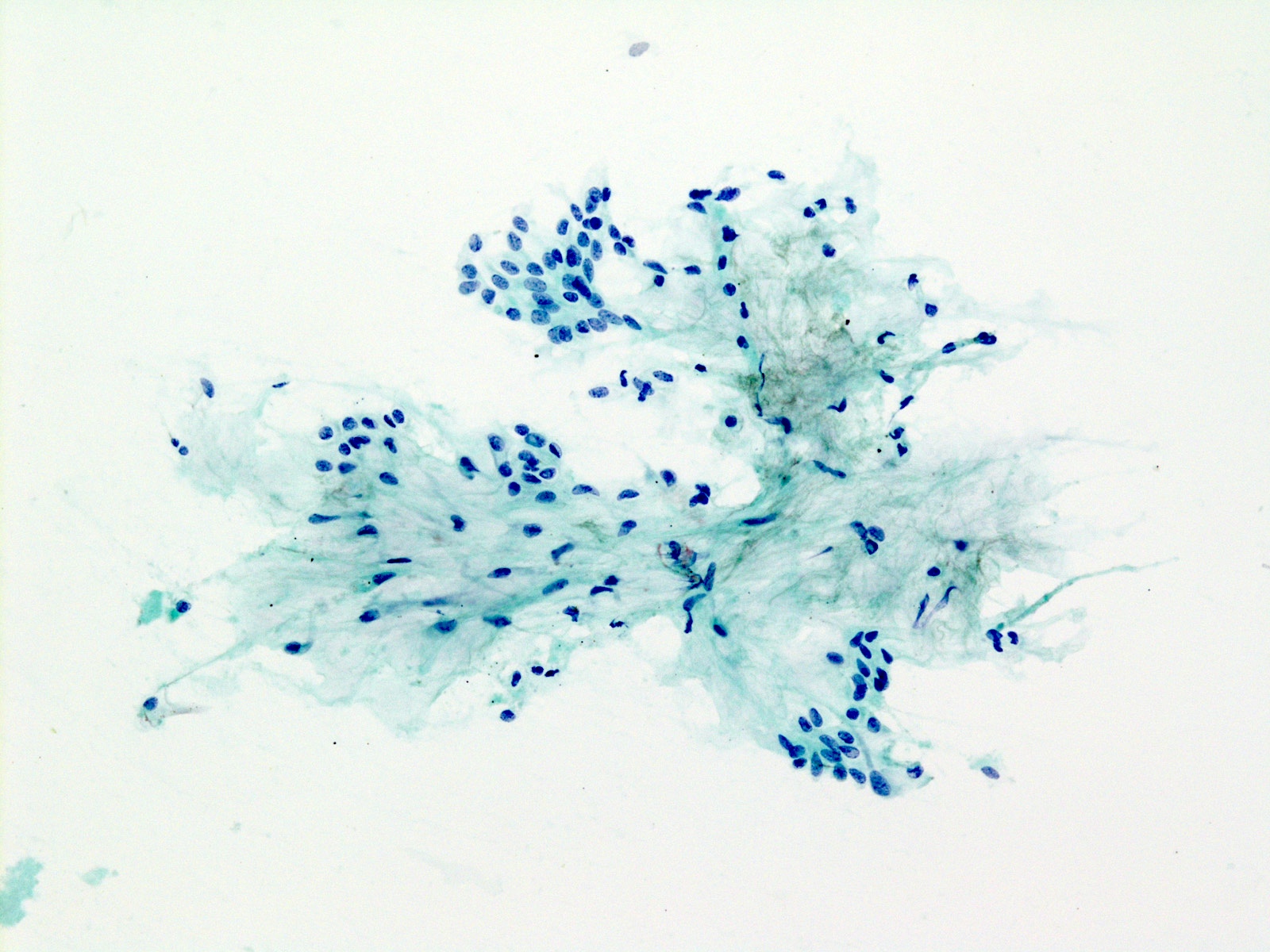
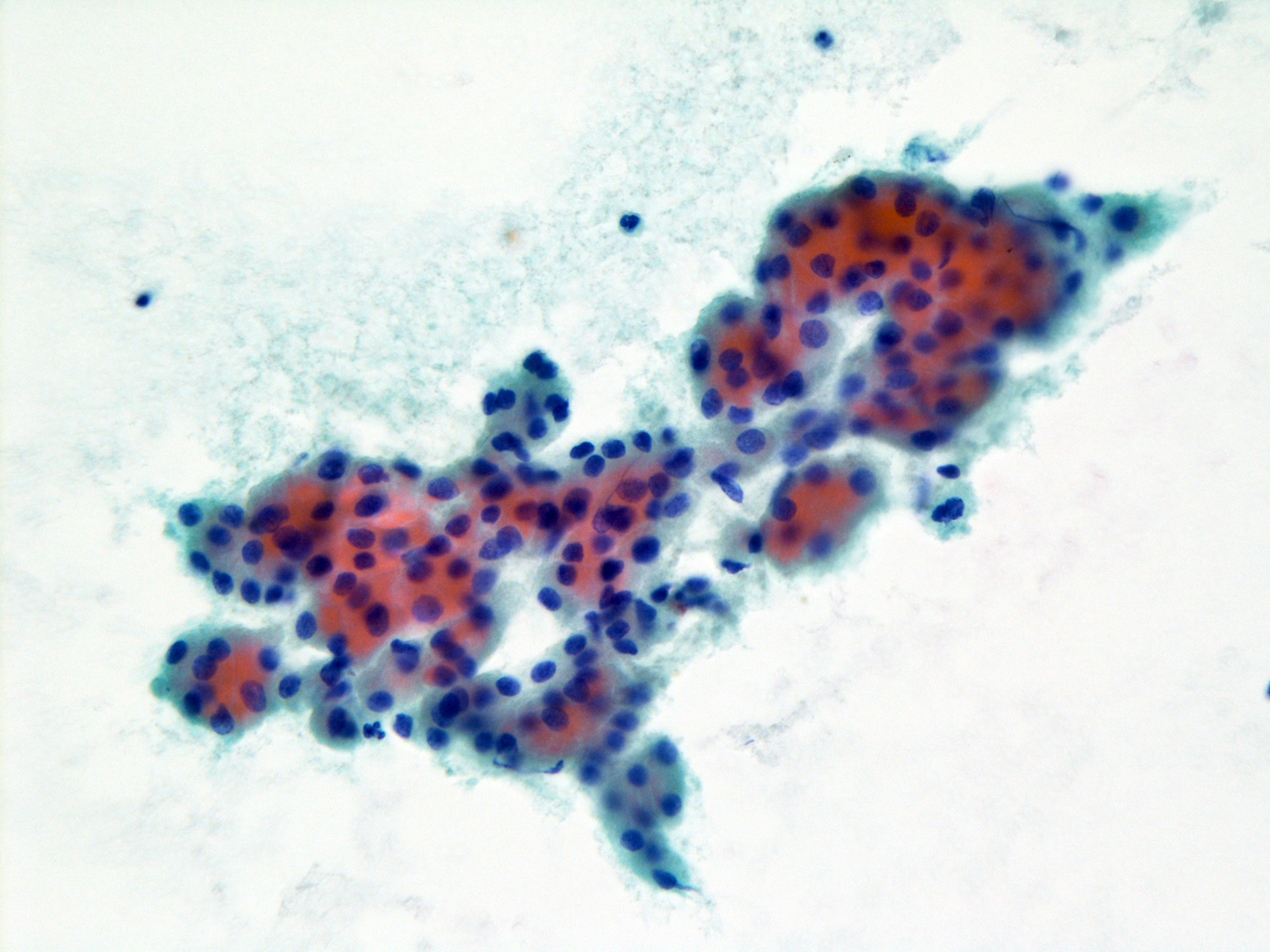
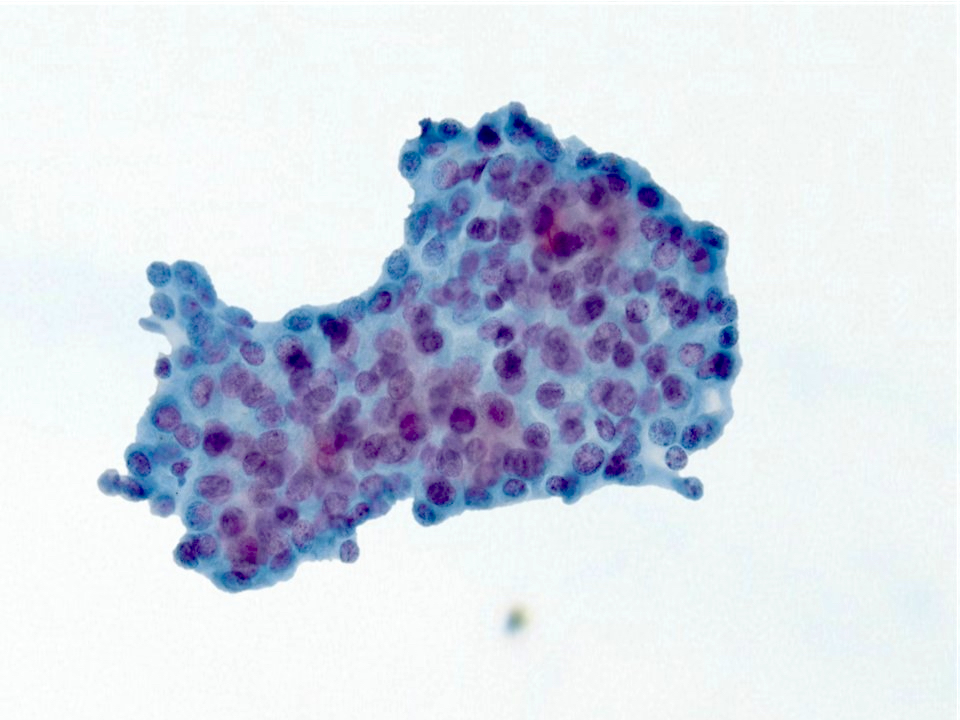
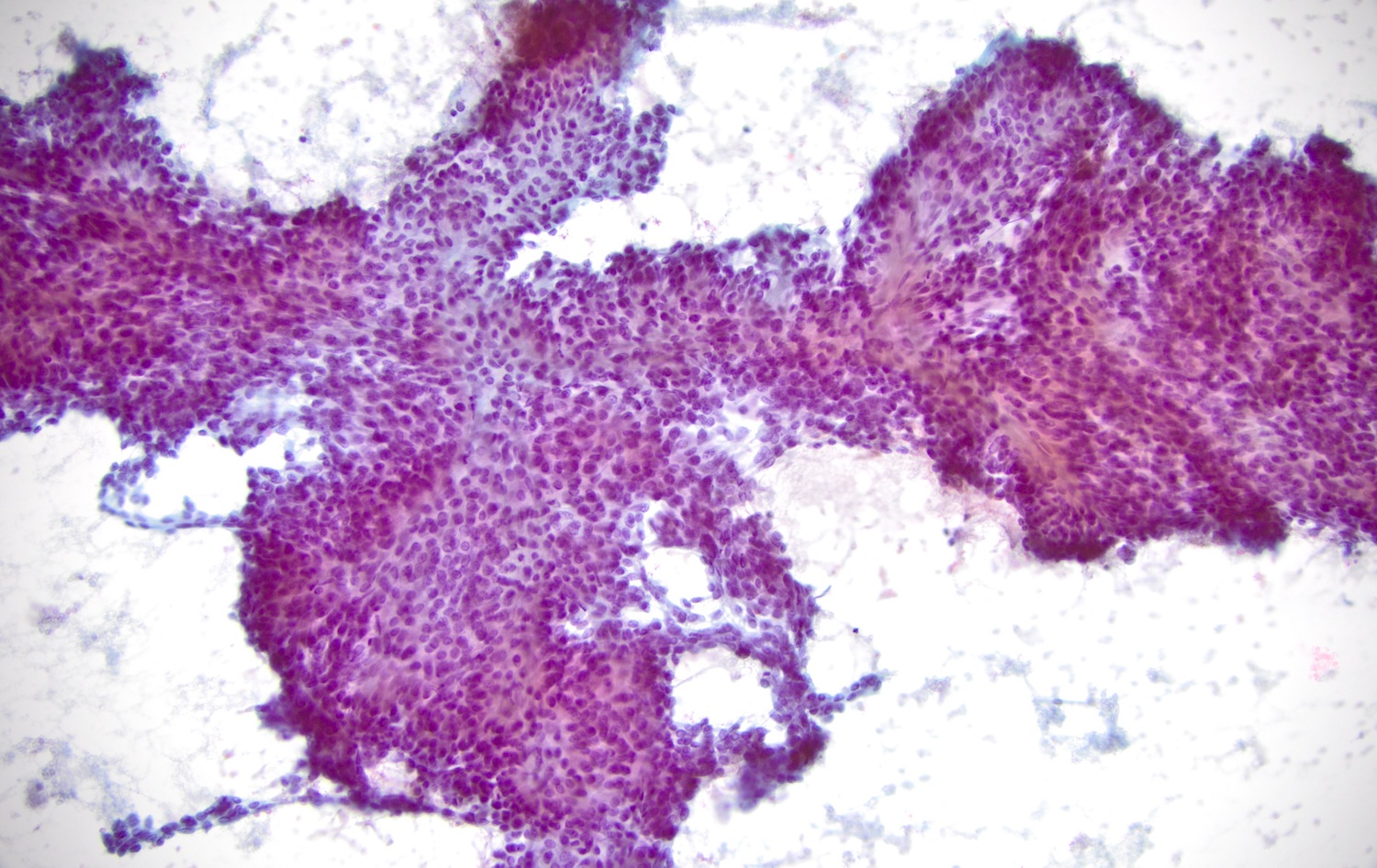
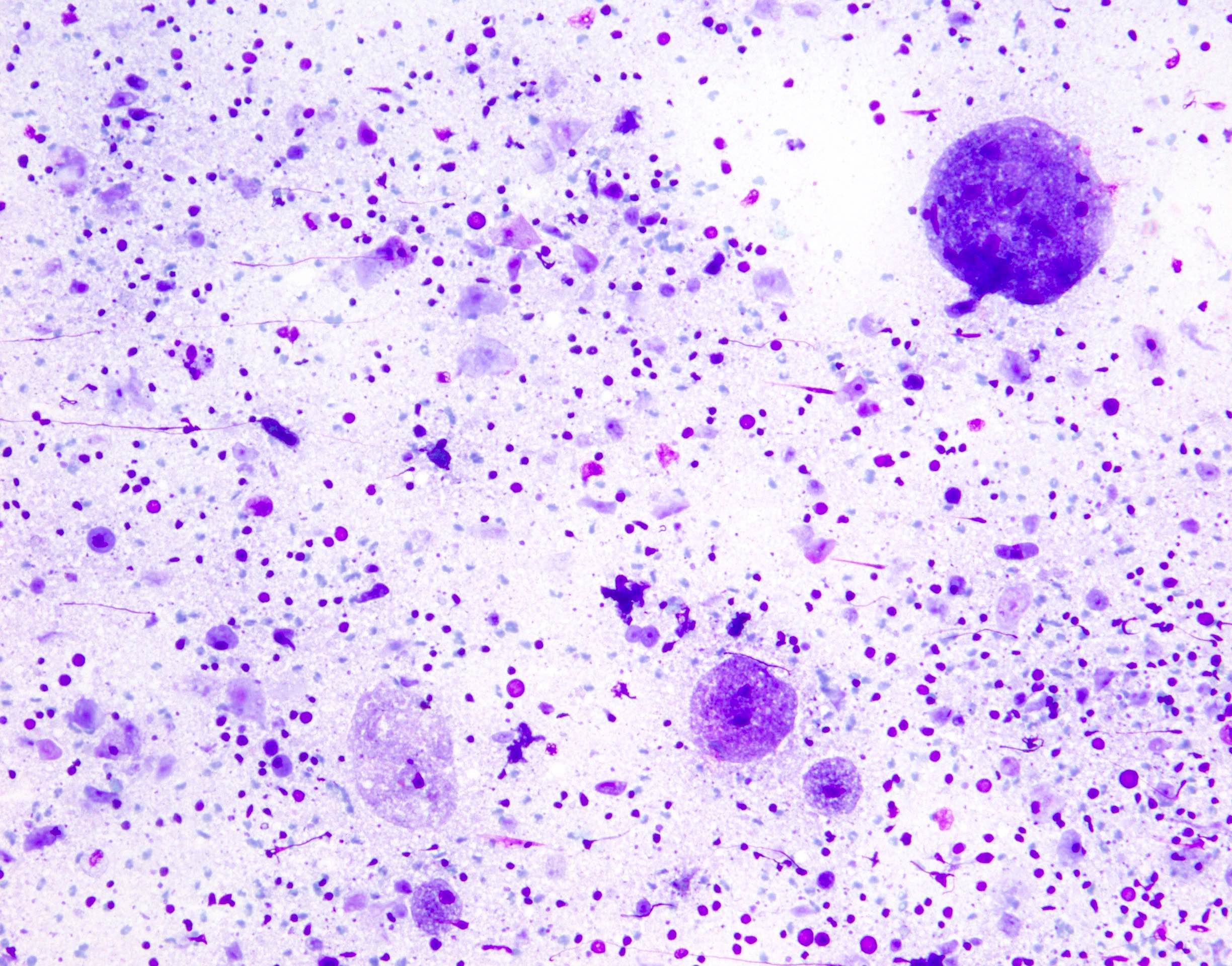
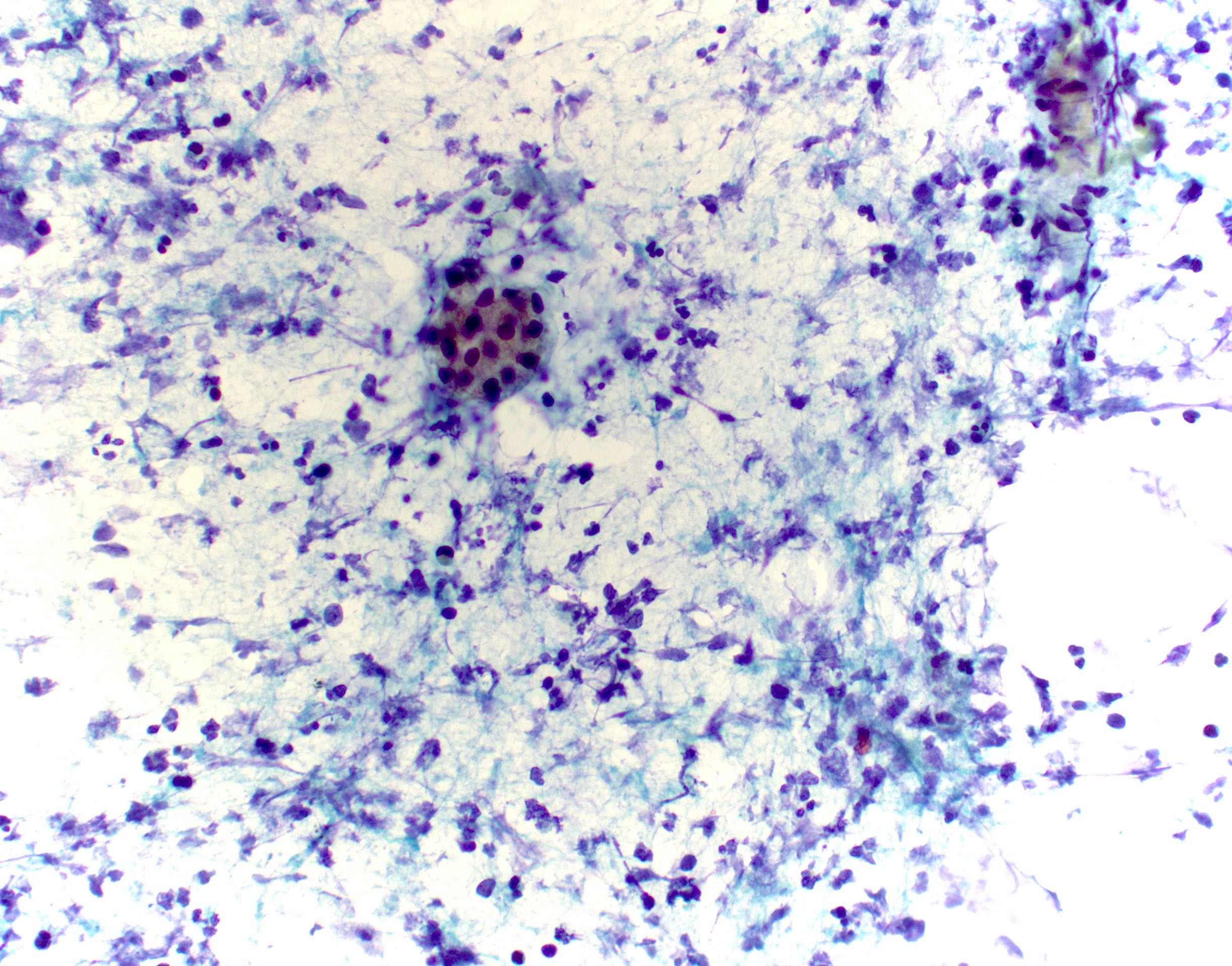
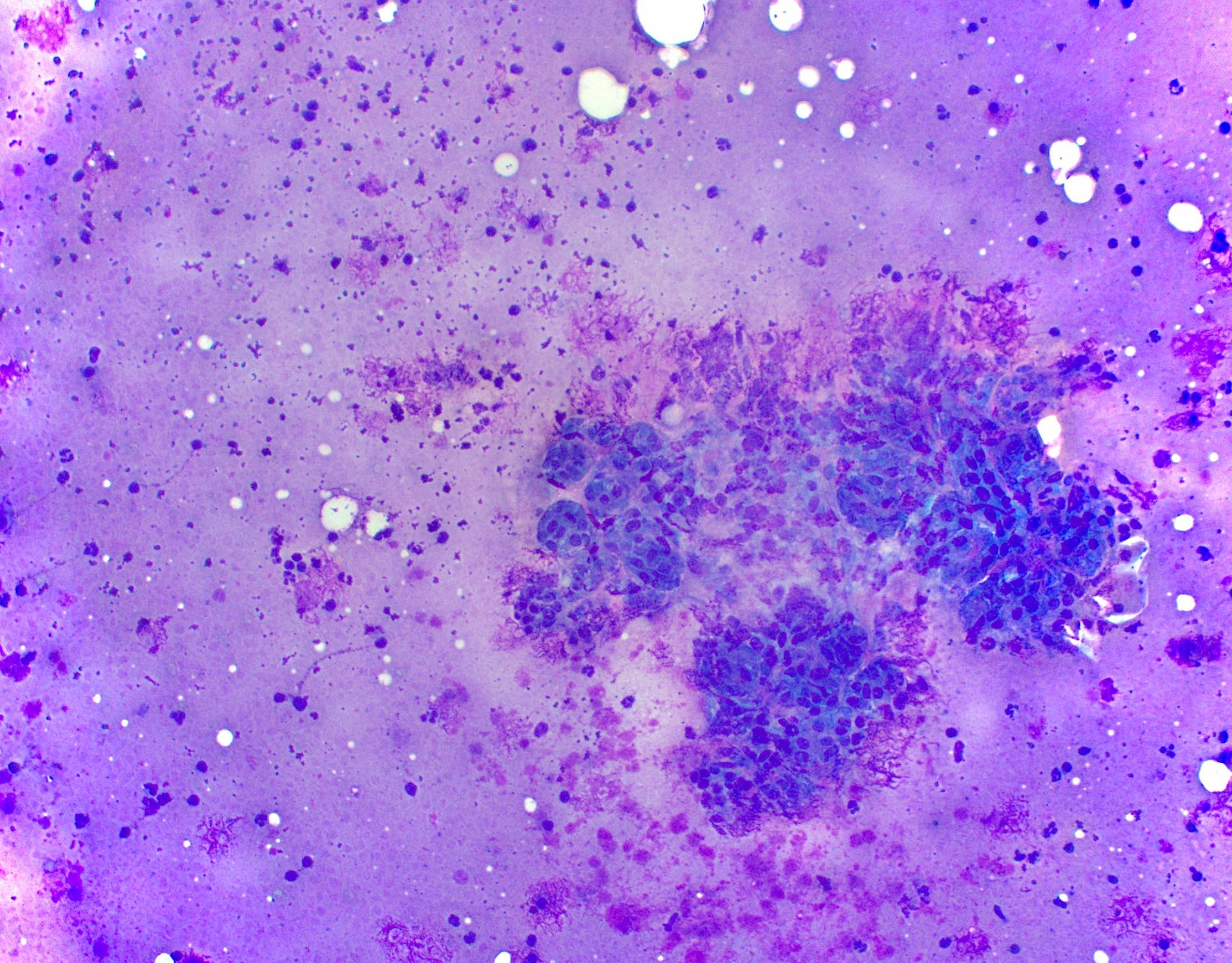
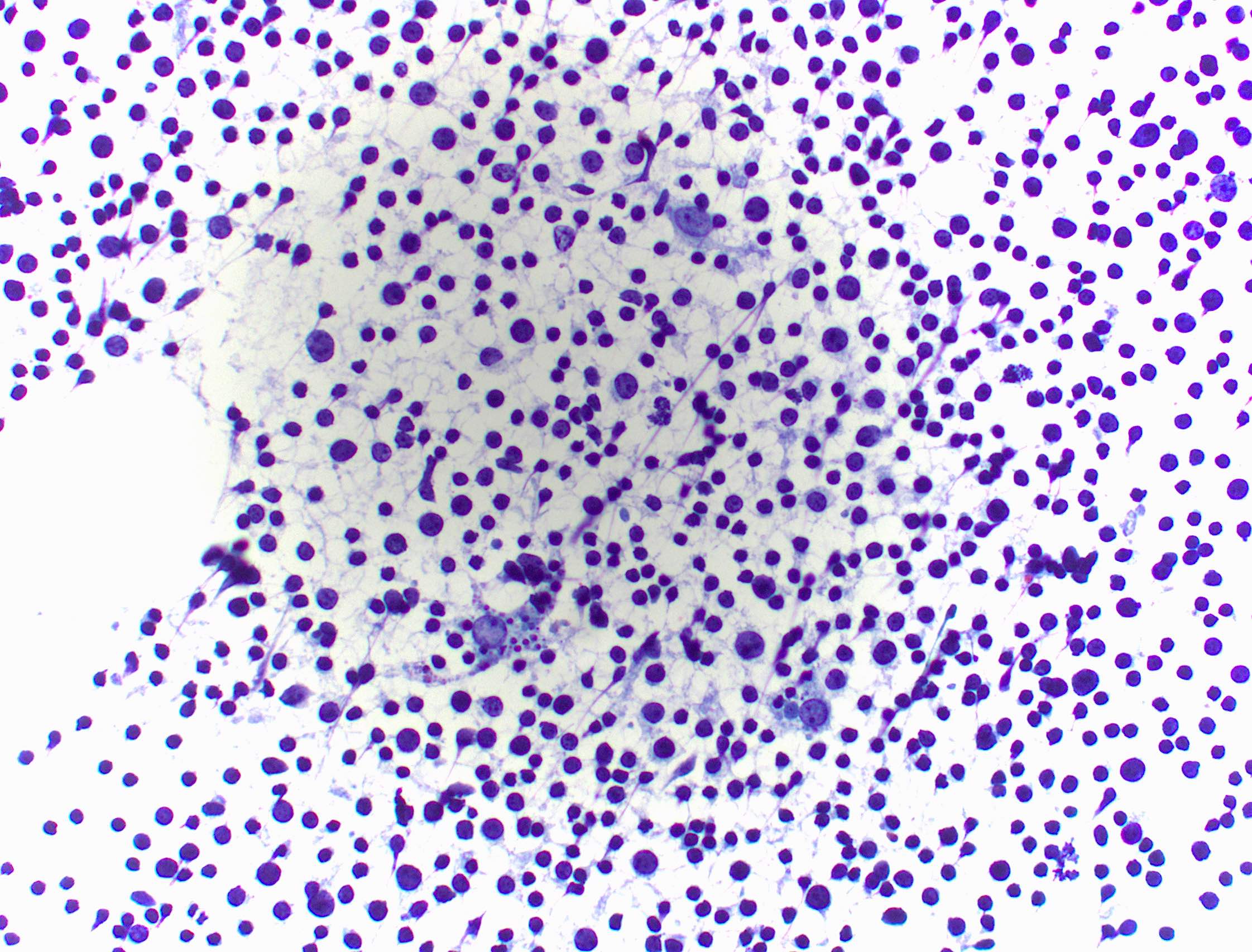
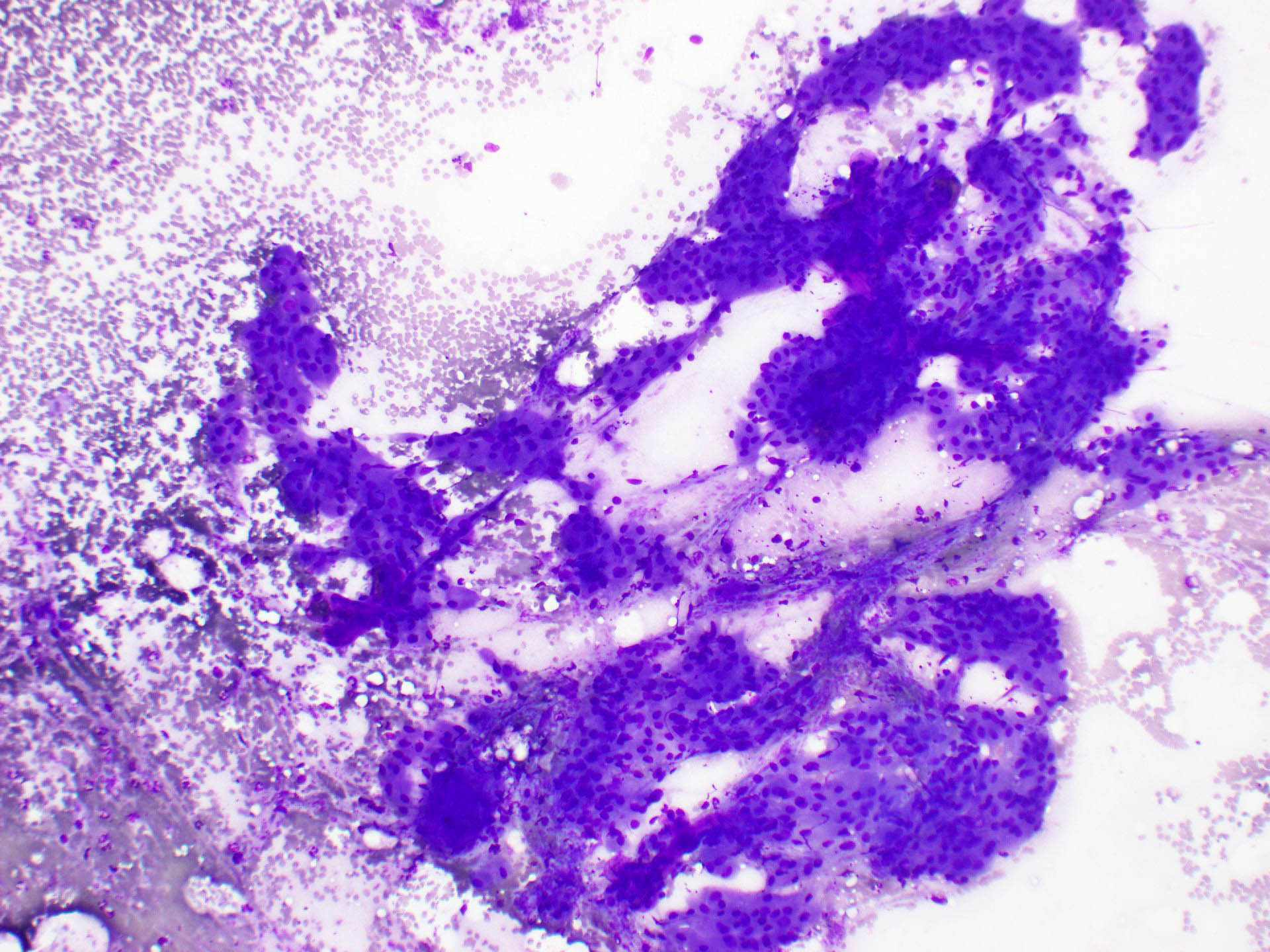
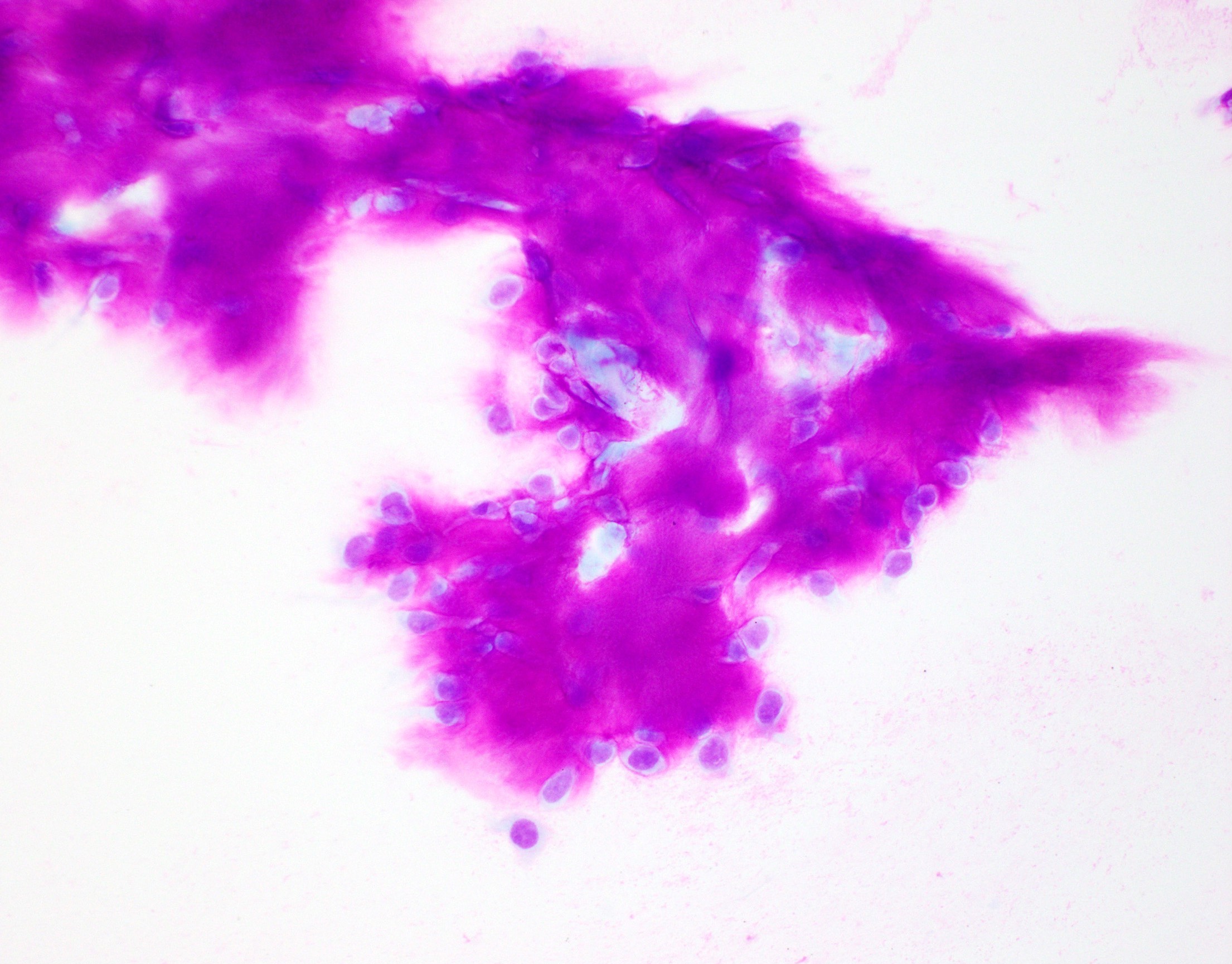
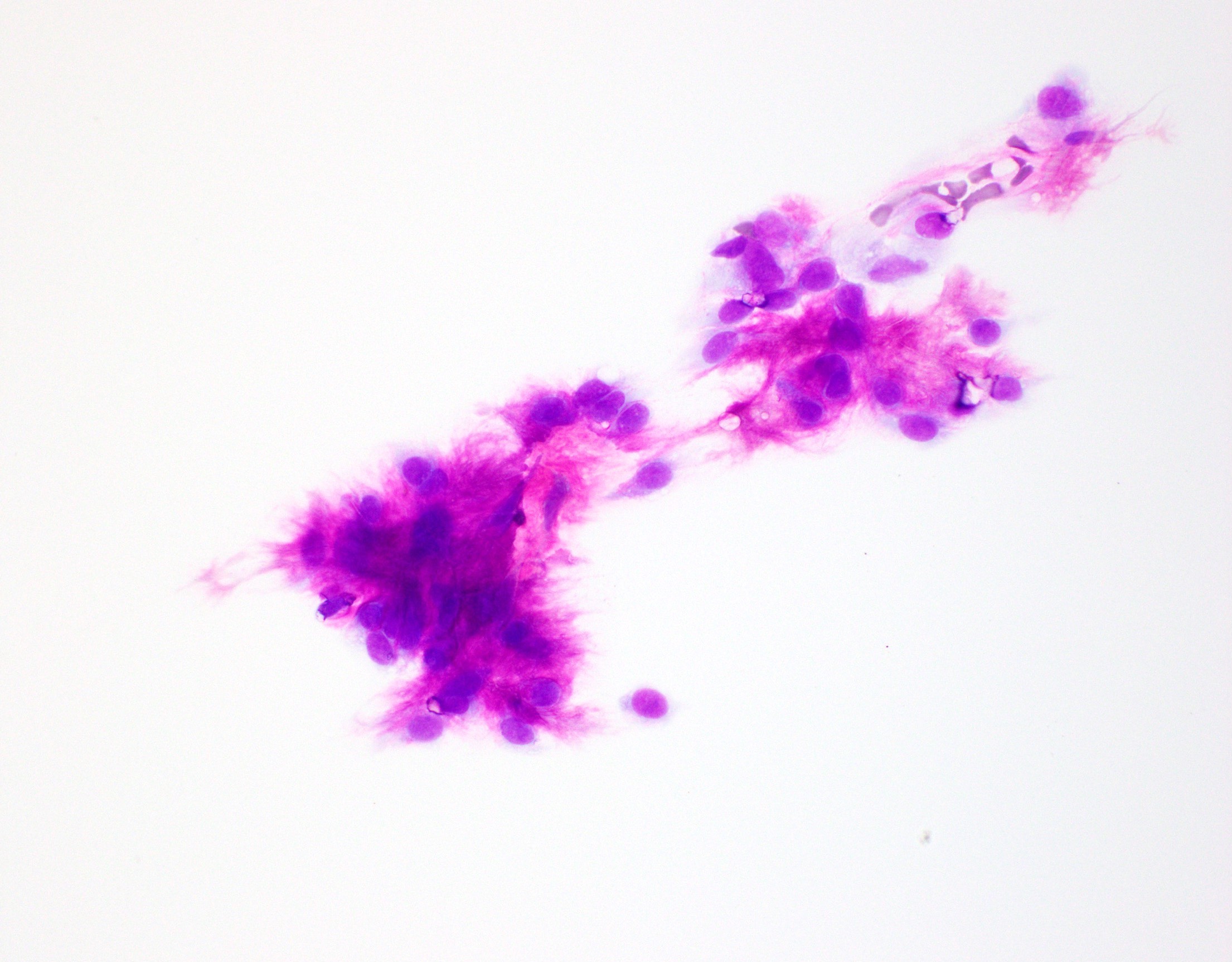
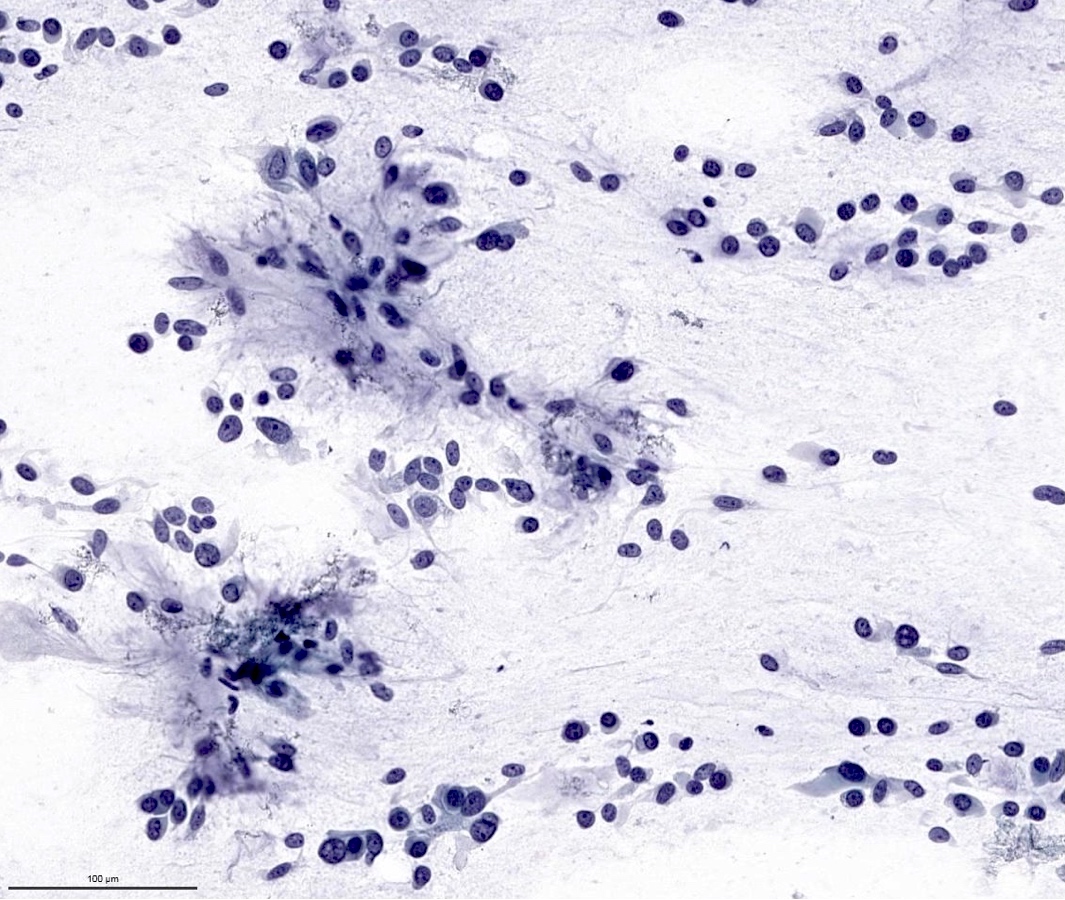
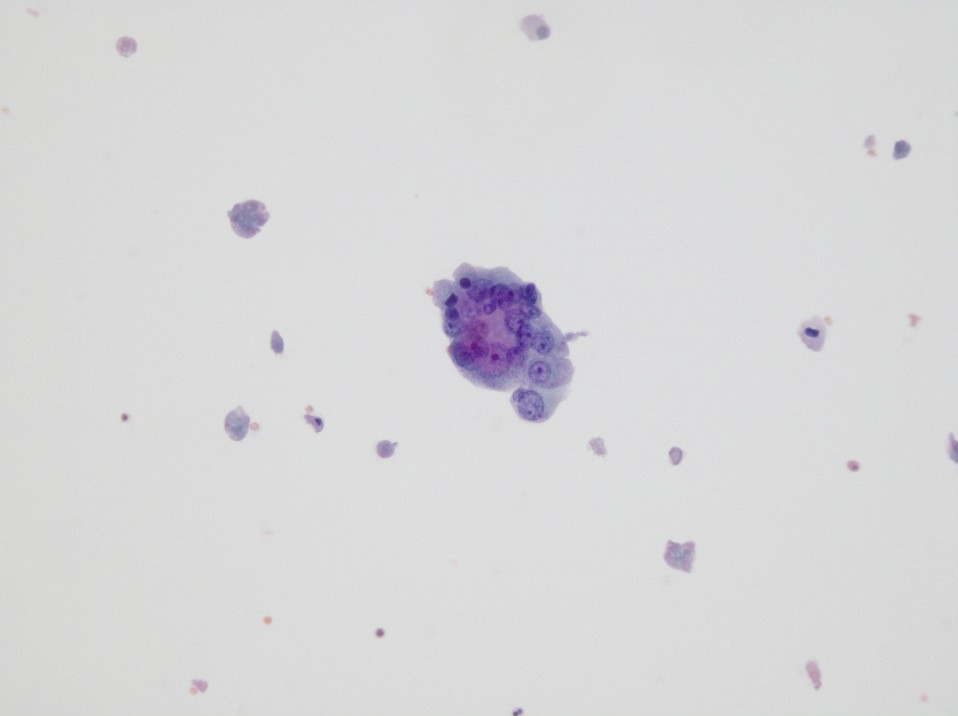
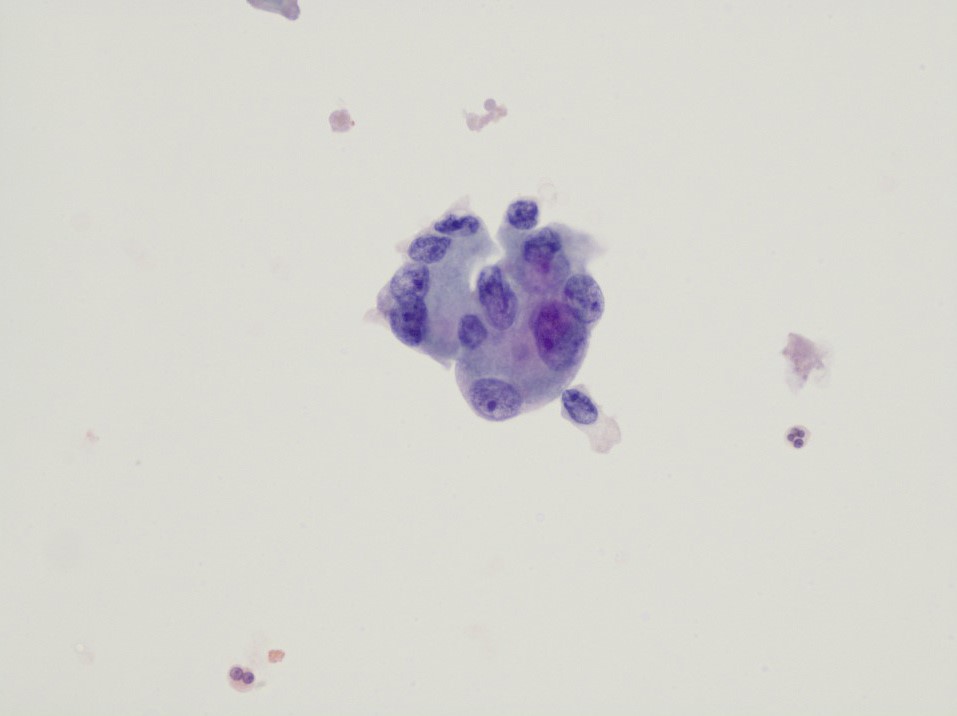
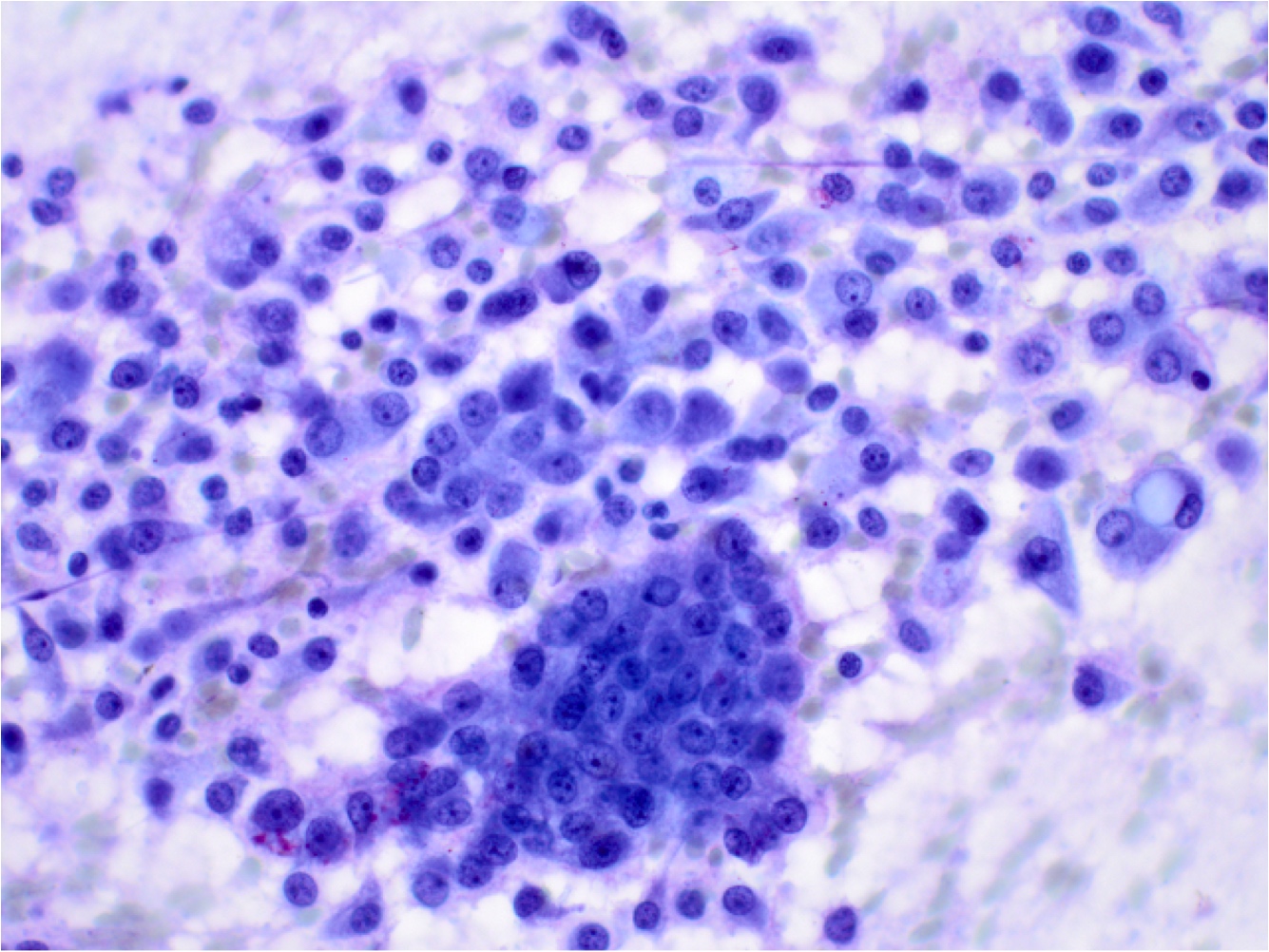
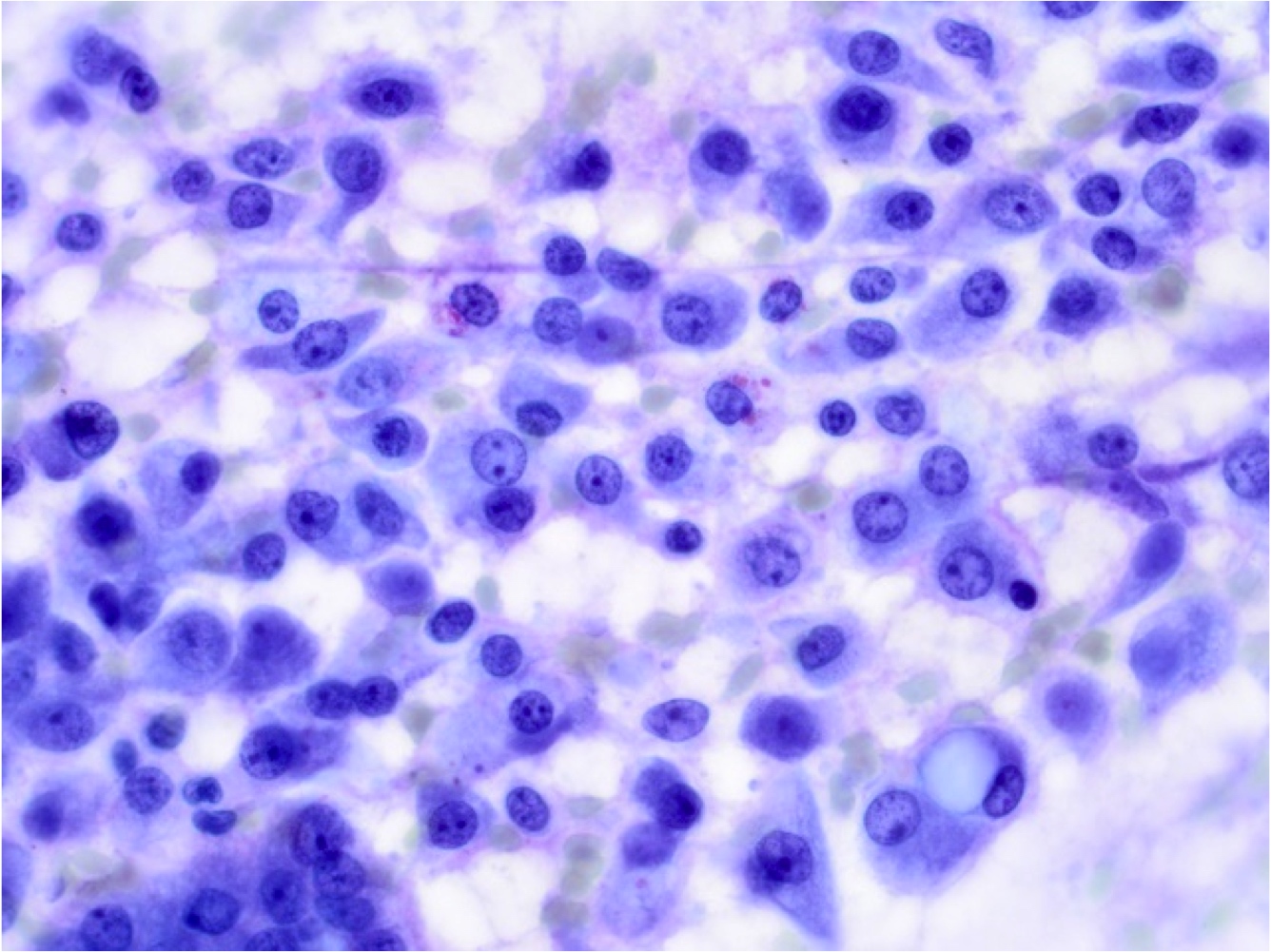
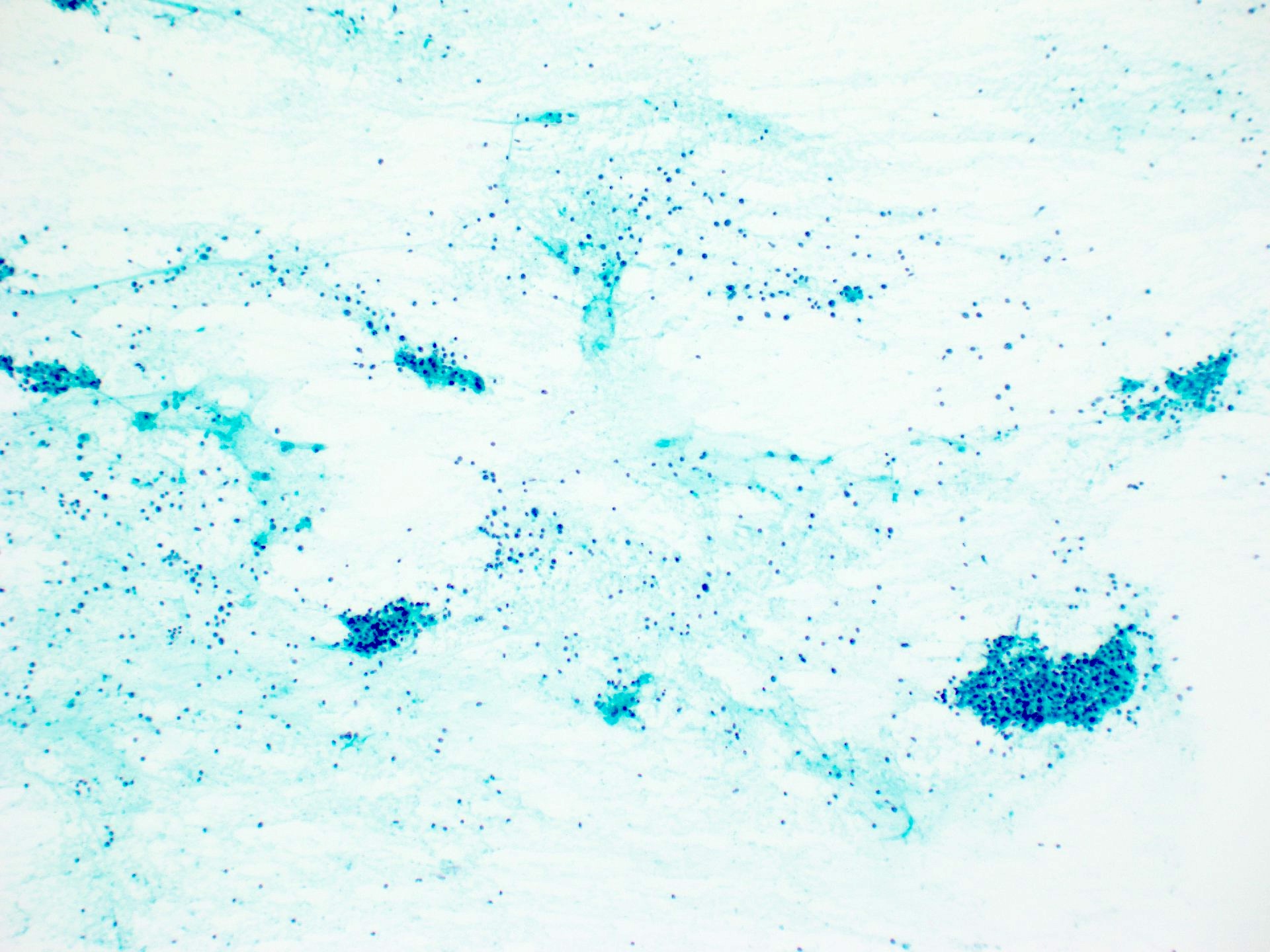
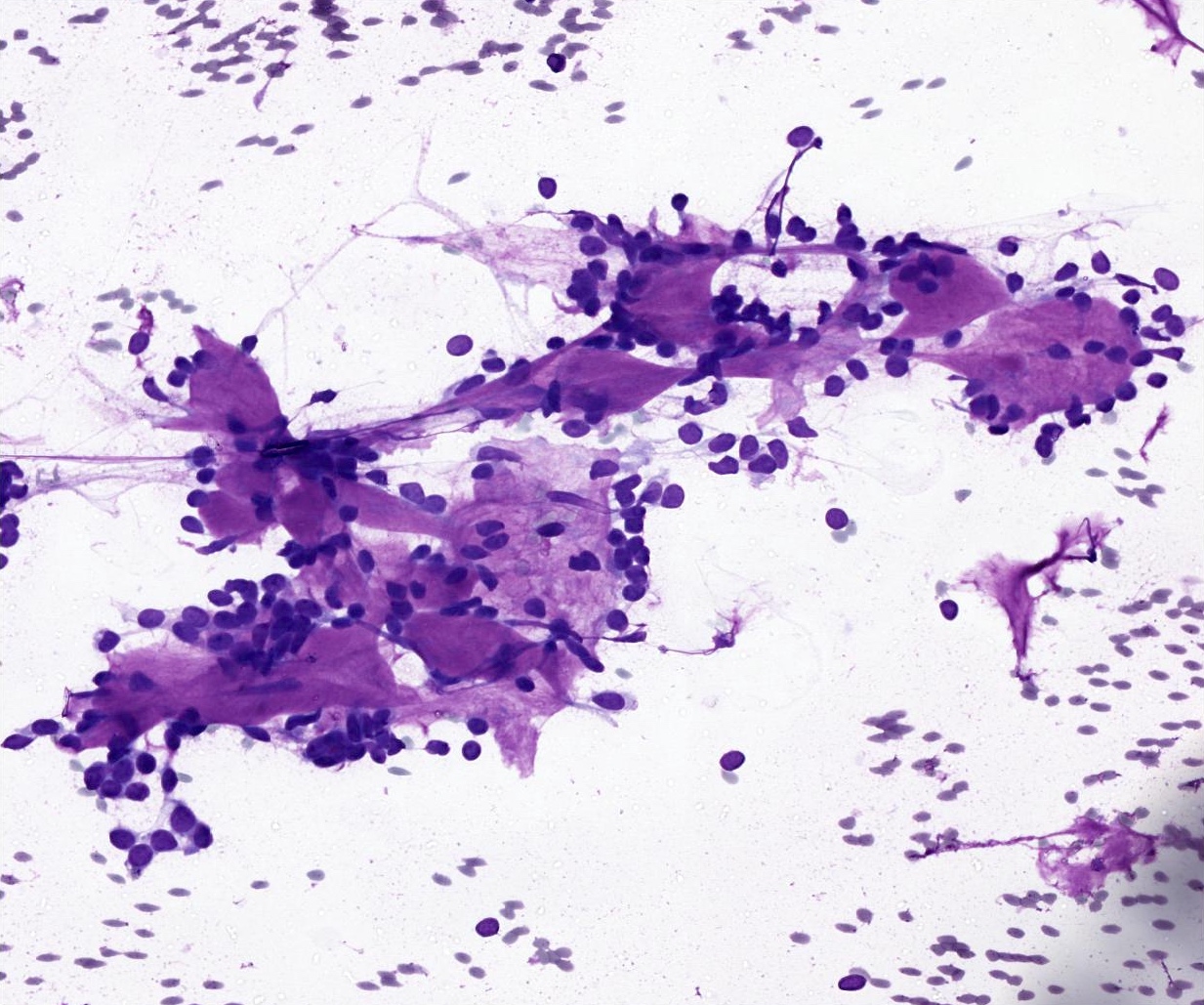
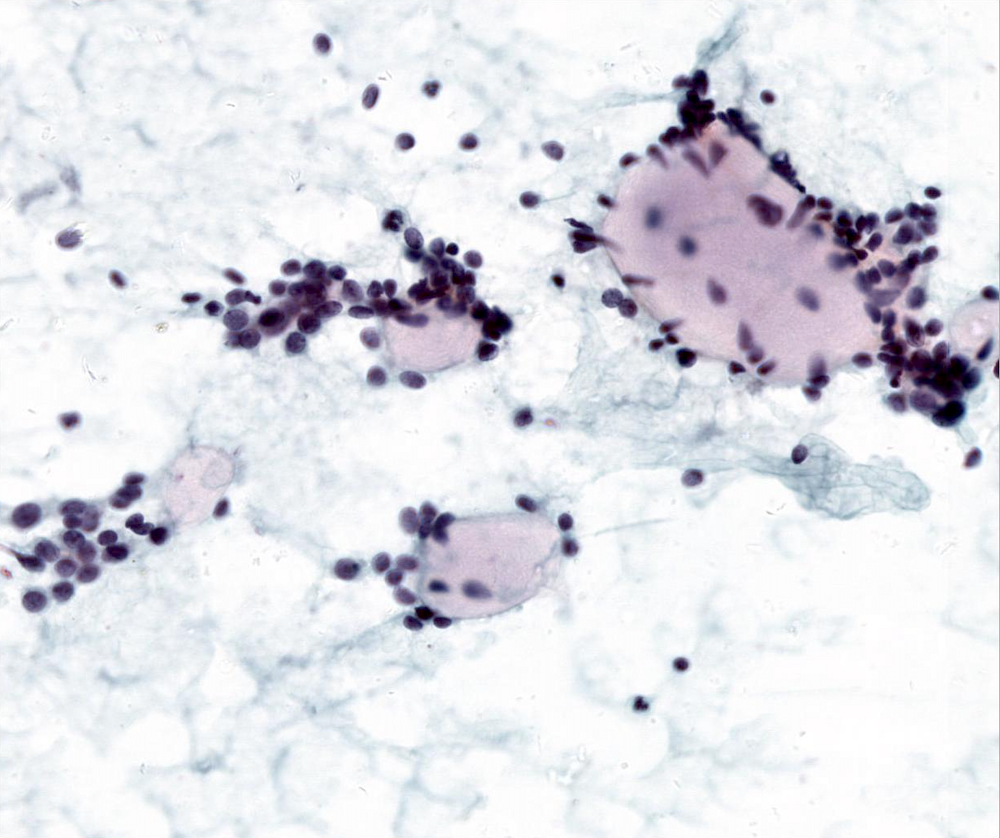
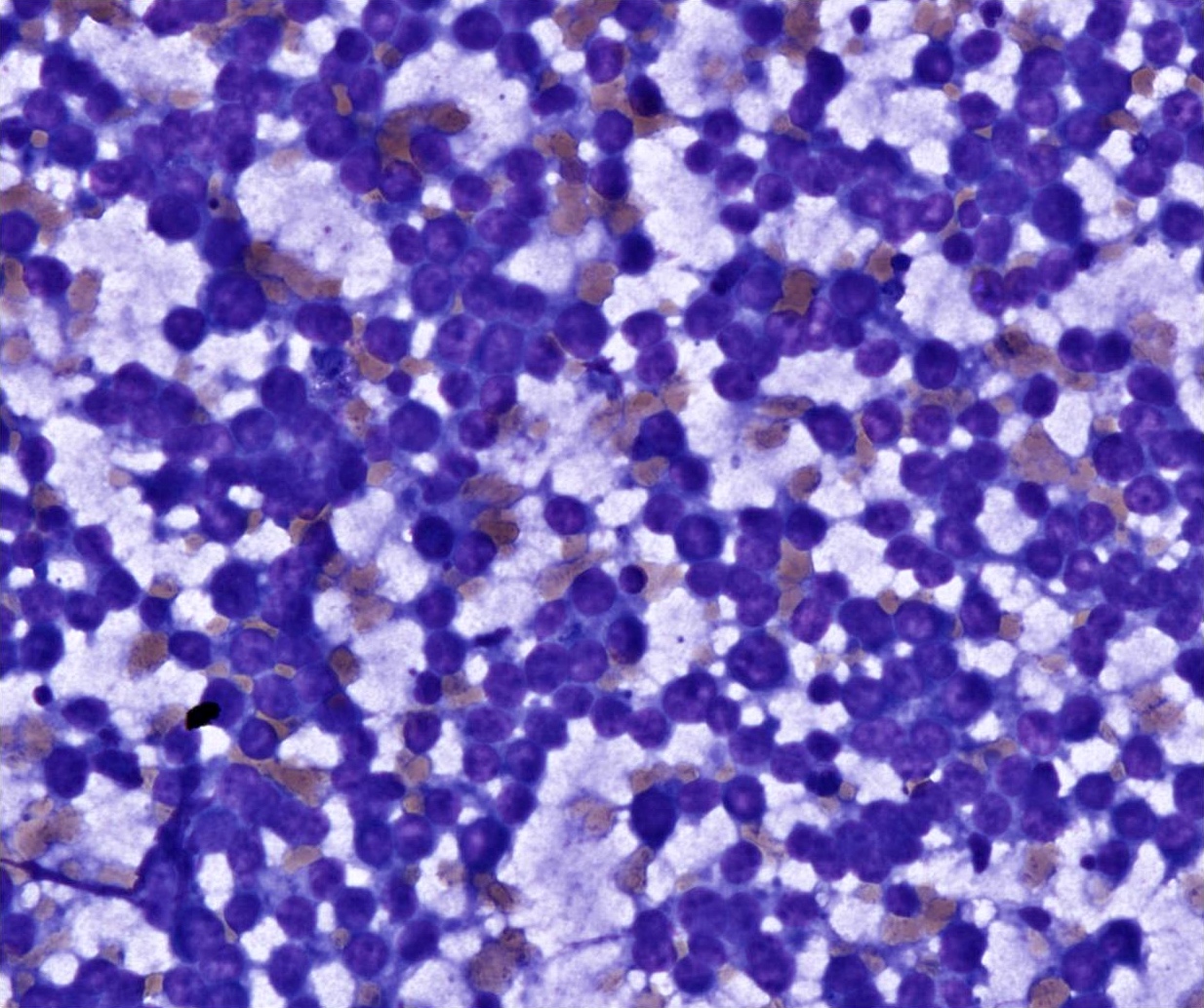
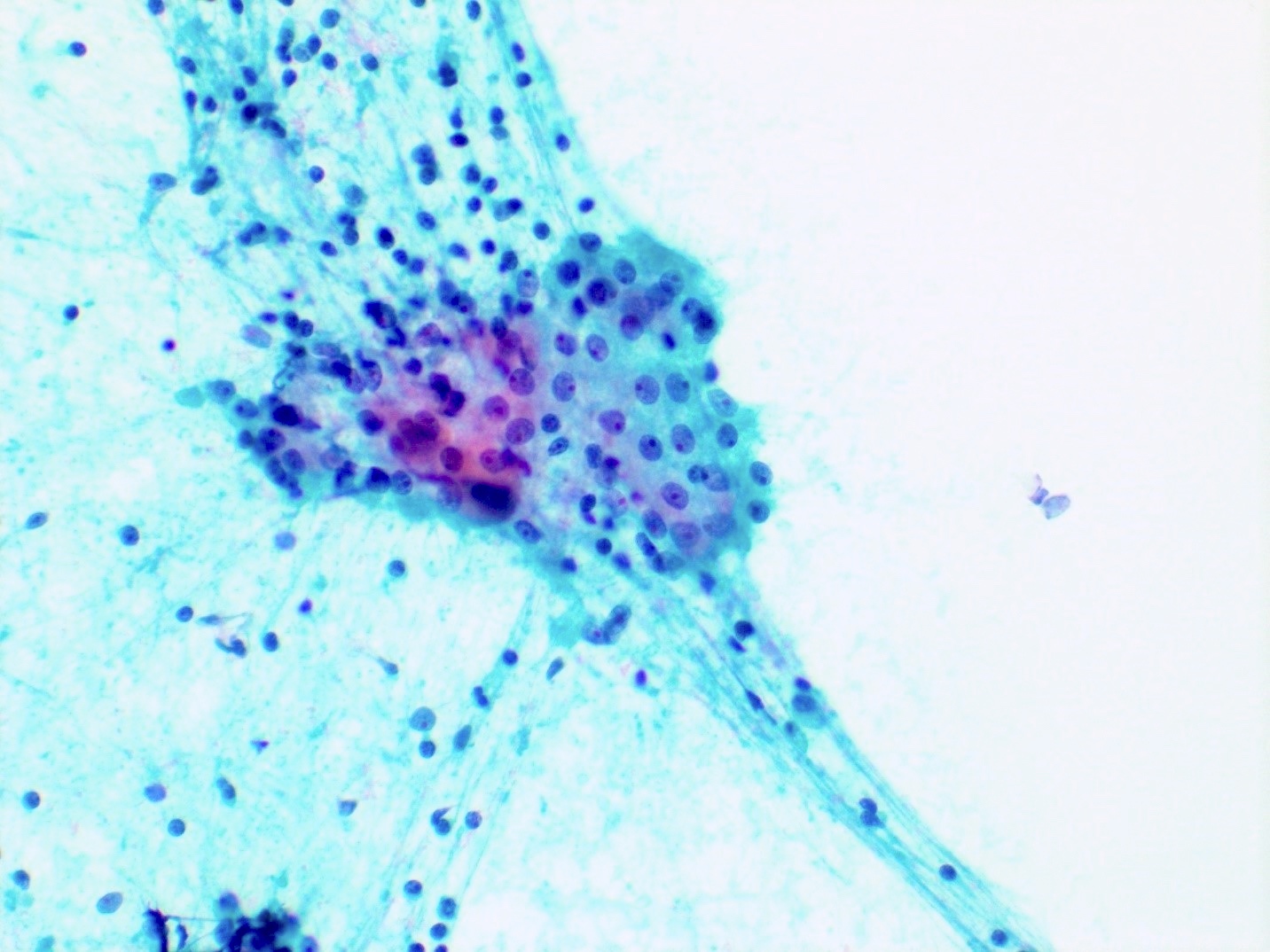
Cohesive clusters or sheets of epithelial cells with variable eosinophilic, granular to vacuolated cytoplasm and uniform nuclei with single nucleoli
Board review style question #1
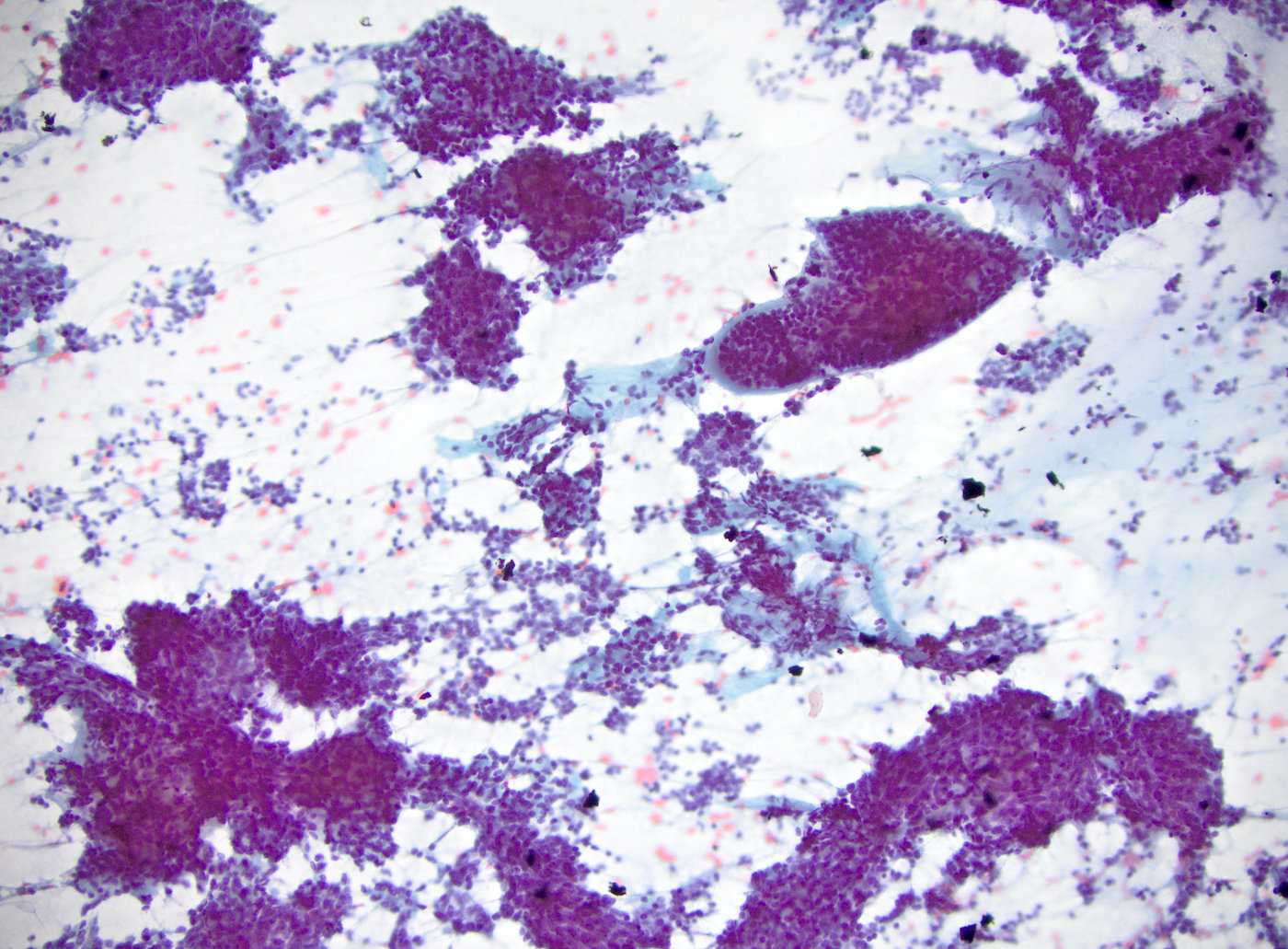
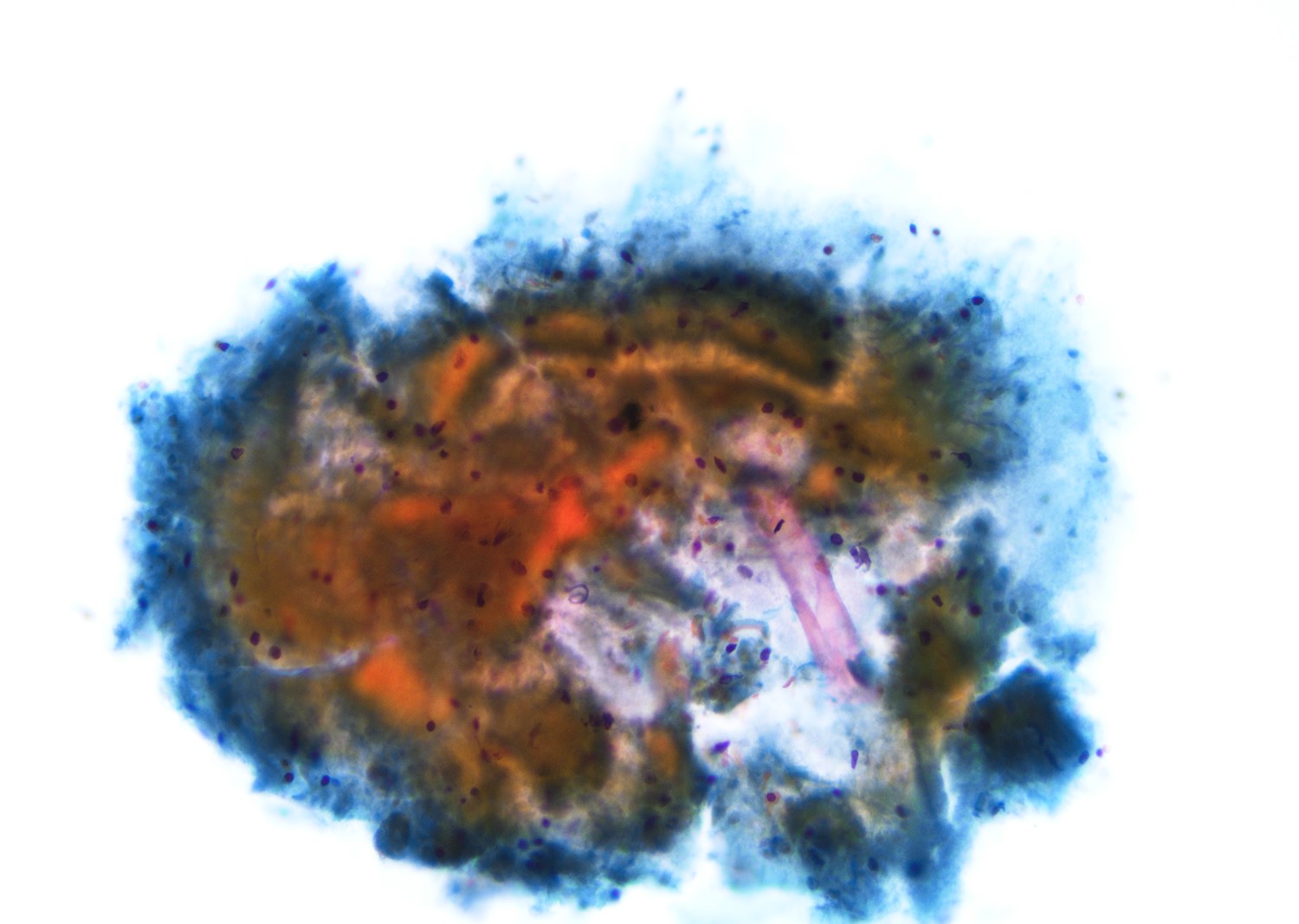
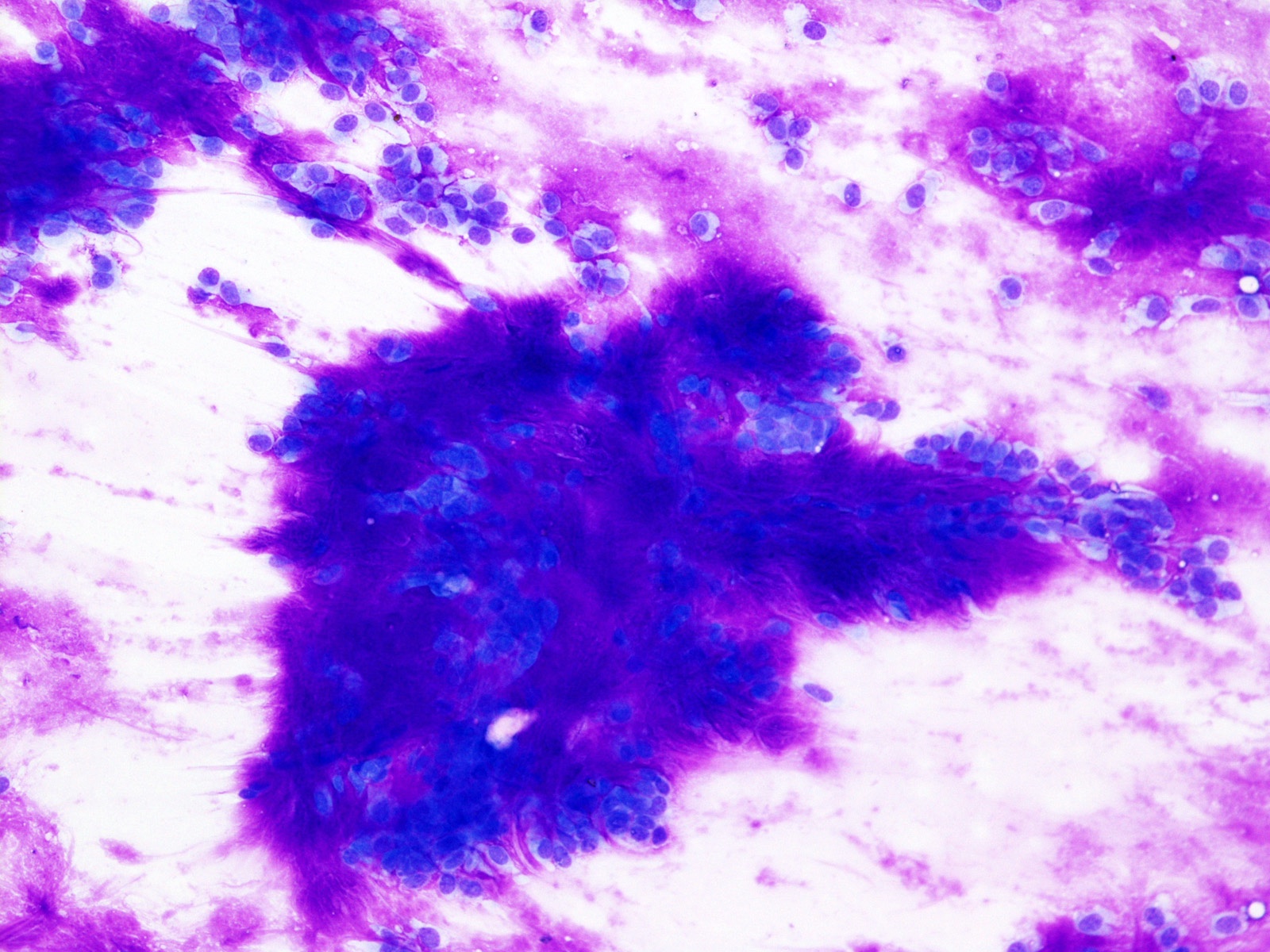
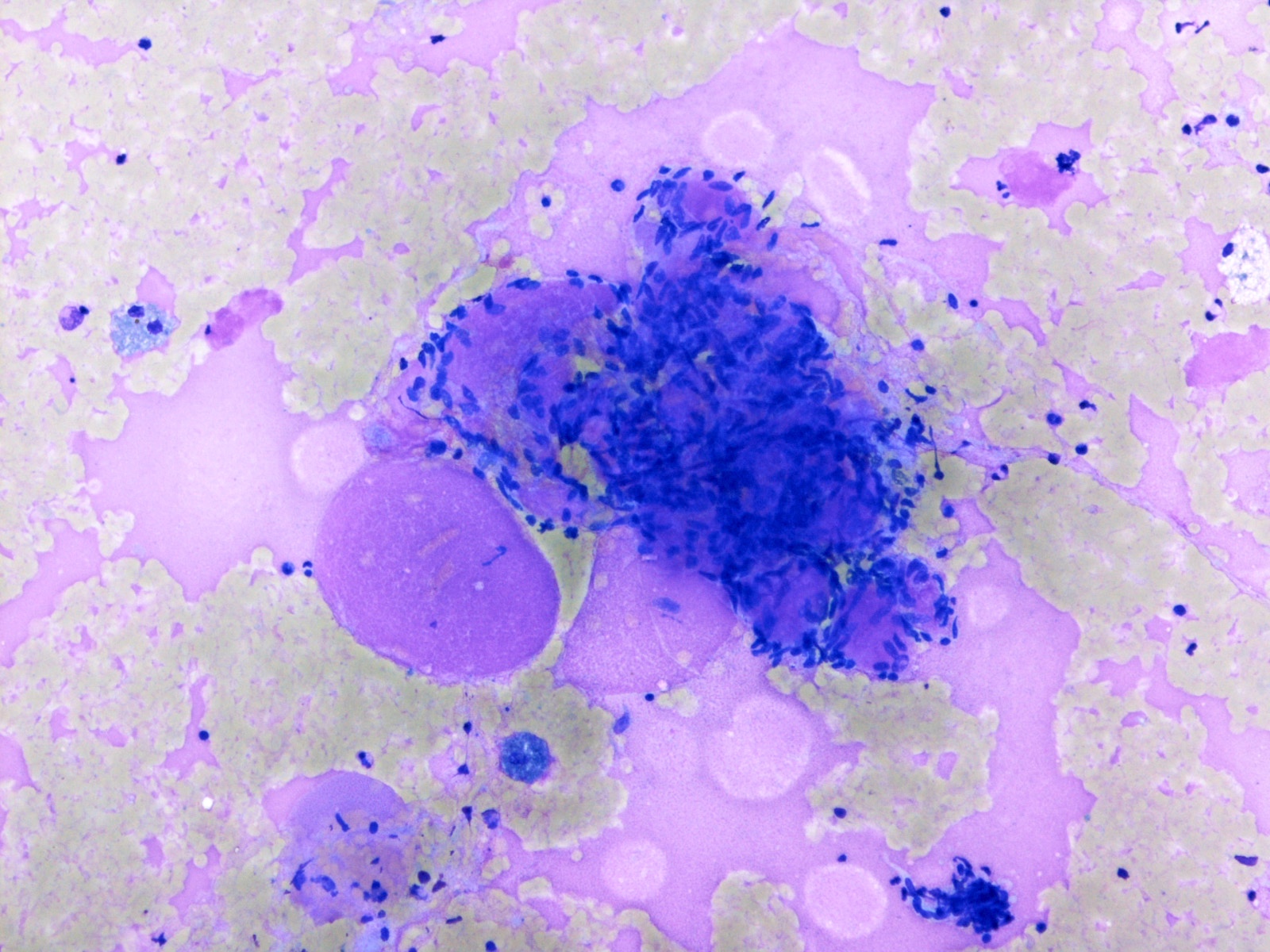
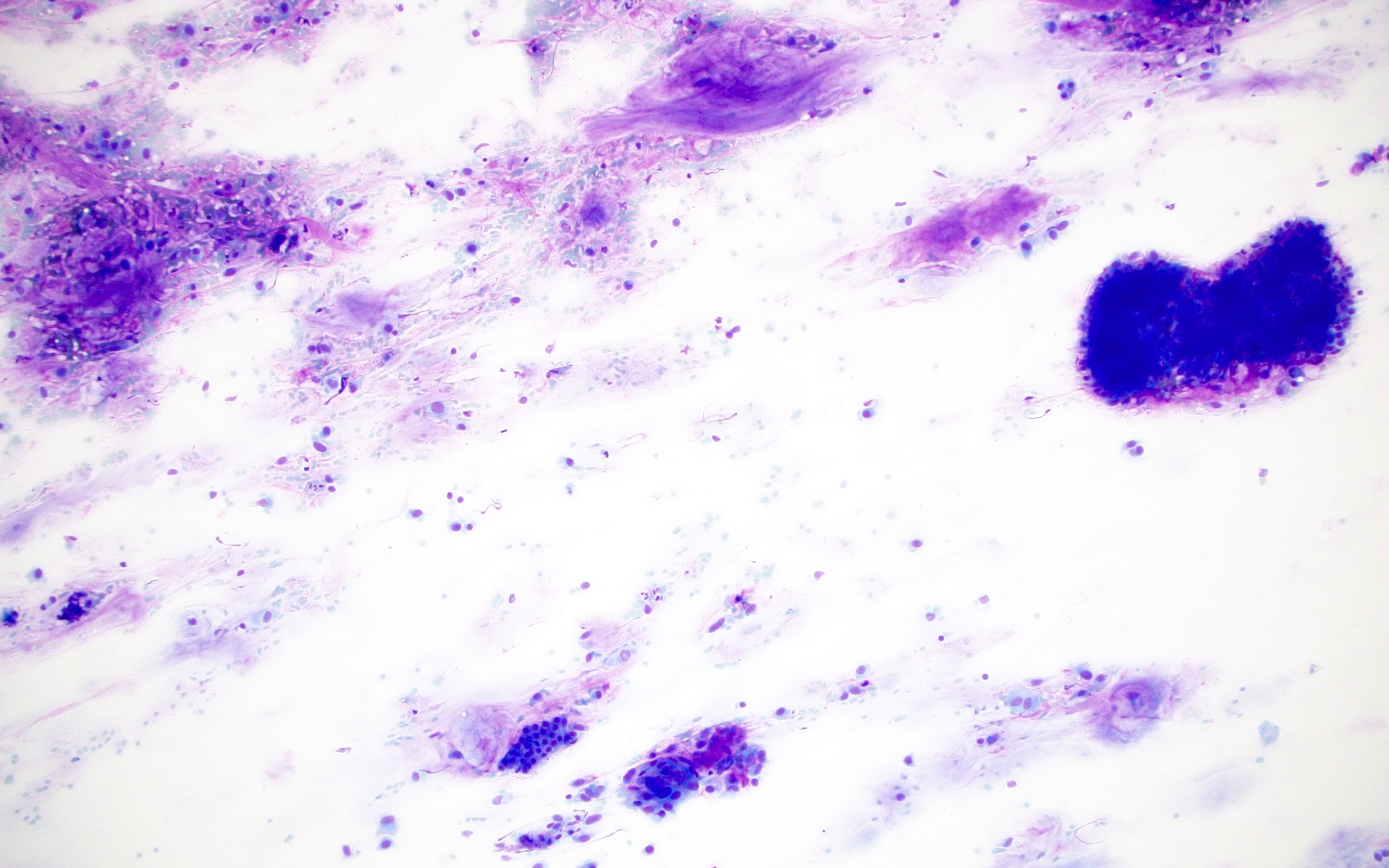
This aspirate smear contains abundant extracellular mucin without epithelial cells. Under which category should this be placed according to the Milan system for reporting salivary gland cytopathology?
Atypia of undetermined significance
Nondiagnostic
Salivary gland neoplasm of uncertain malignant potential
Suspicious for malignancy
Board review style answer #1
A. Atypia of undetermined significance. The image shows abundant extracellular mucin. The differential diagnosis of mucin containing cysts includes mucocele, mucus retention cysts and low grade mucoepidermoid carcinoma. Therefore, atypia of undetermined significance is the correct interpretation on FNA.
What is the implied risk of malignancy on excision if a diagnosis of atypia of undetermined significance is rendered on a fine needle aspiration (FNA) of the parotid?
< 5%
20%
45%
90%
Board review style answer #2
B. 20%. The implied risk of malignancy is ~20% as per the Milan system for reporting salivary gland cytopathology (1st edition 2018), based on a limited number of studies. However, subsequent studies using the Milan system criteria have found the risk of malignancy for a diagnosis of atypia of undetermined significance with surgical follow up to be significantly higher (30% on average) with wide variations across institutions that reflect different types of practices.
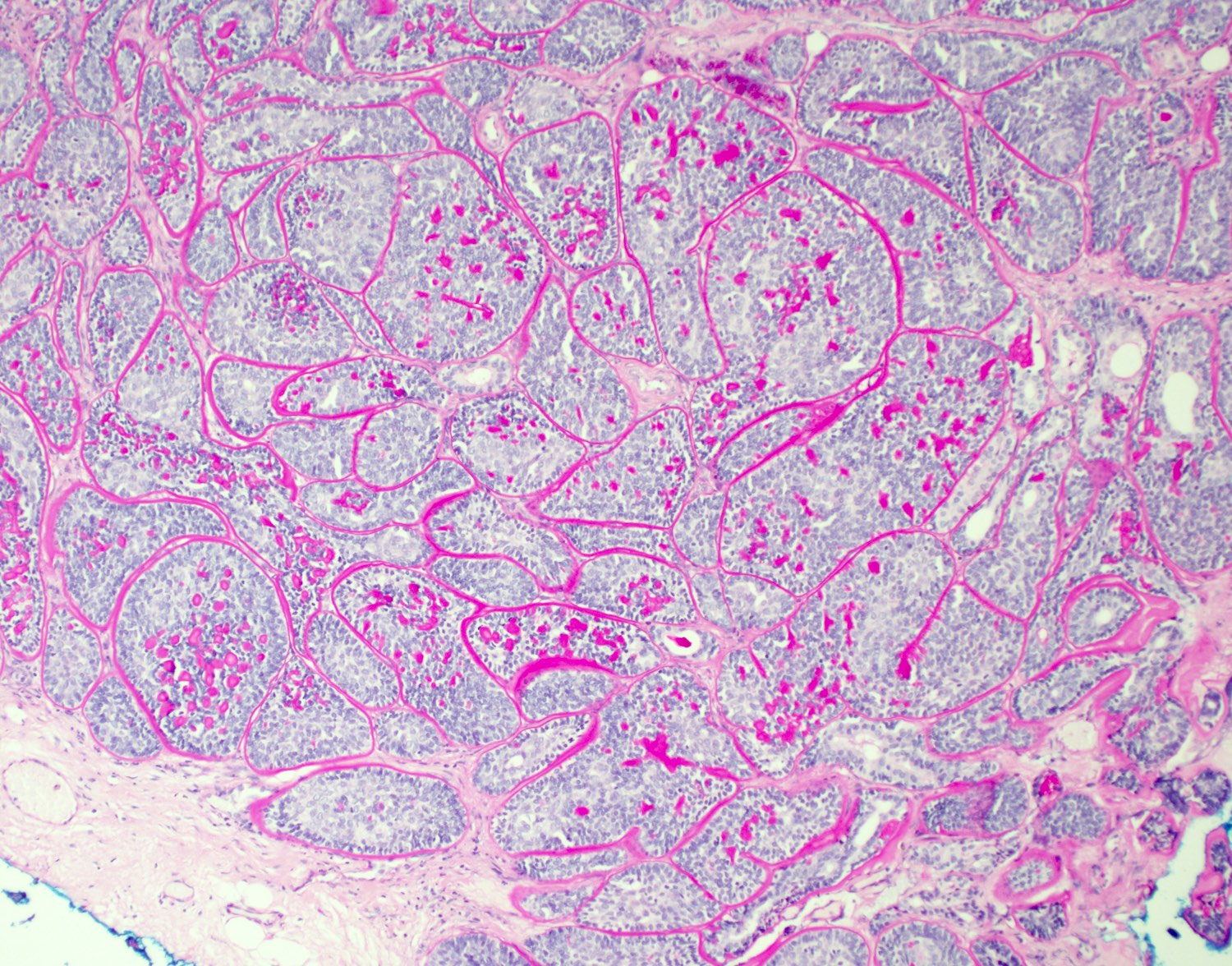
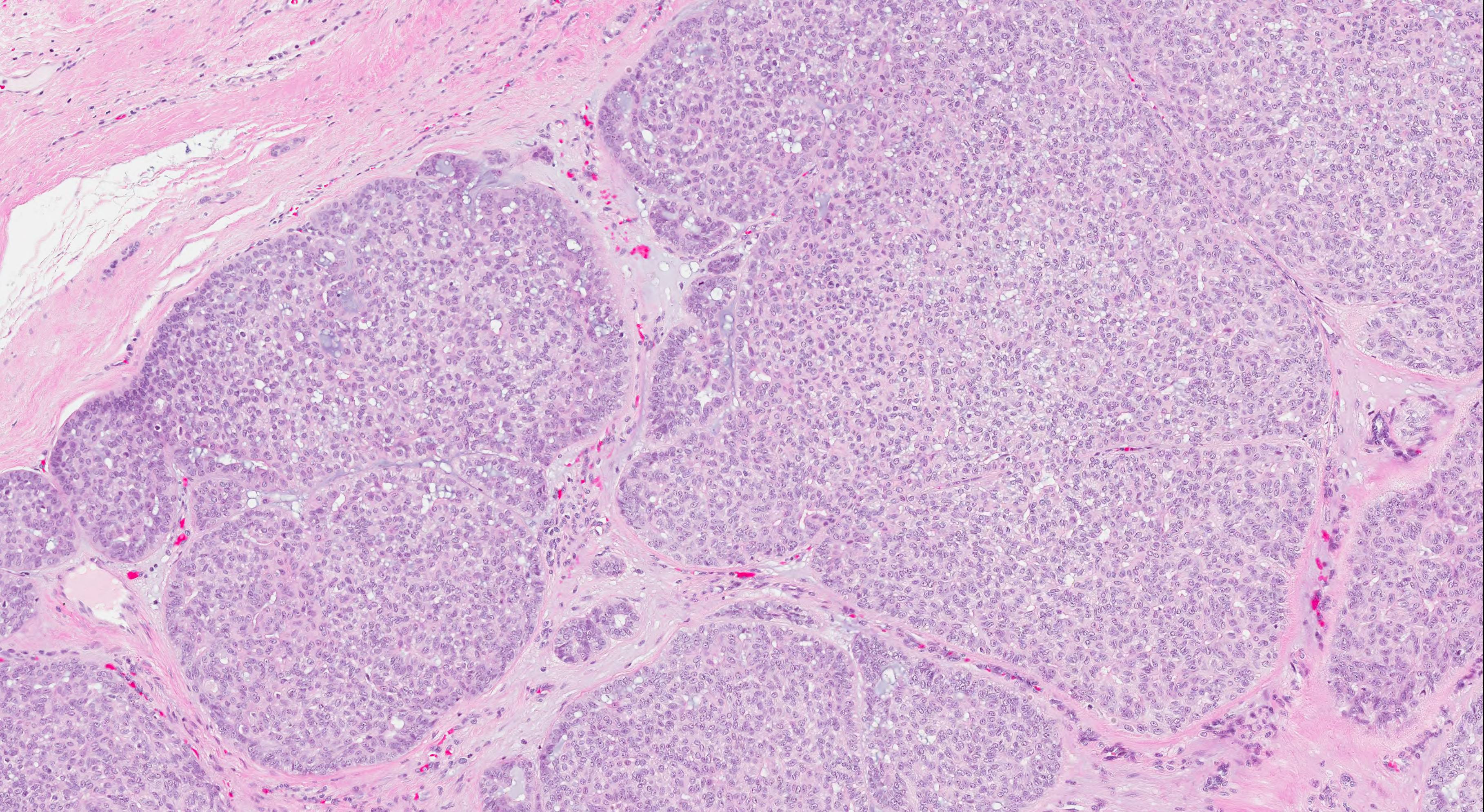
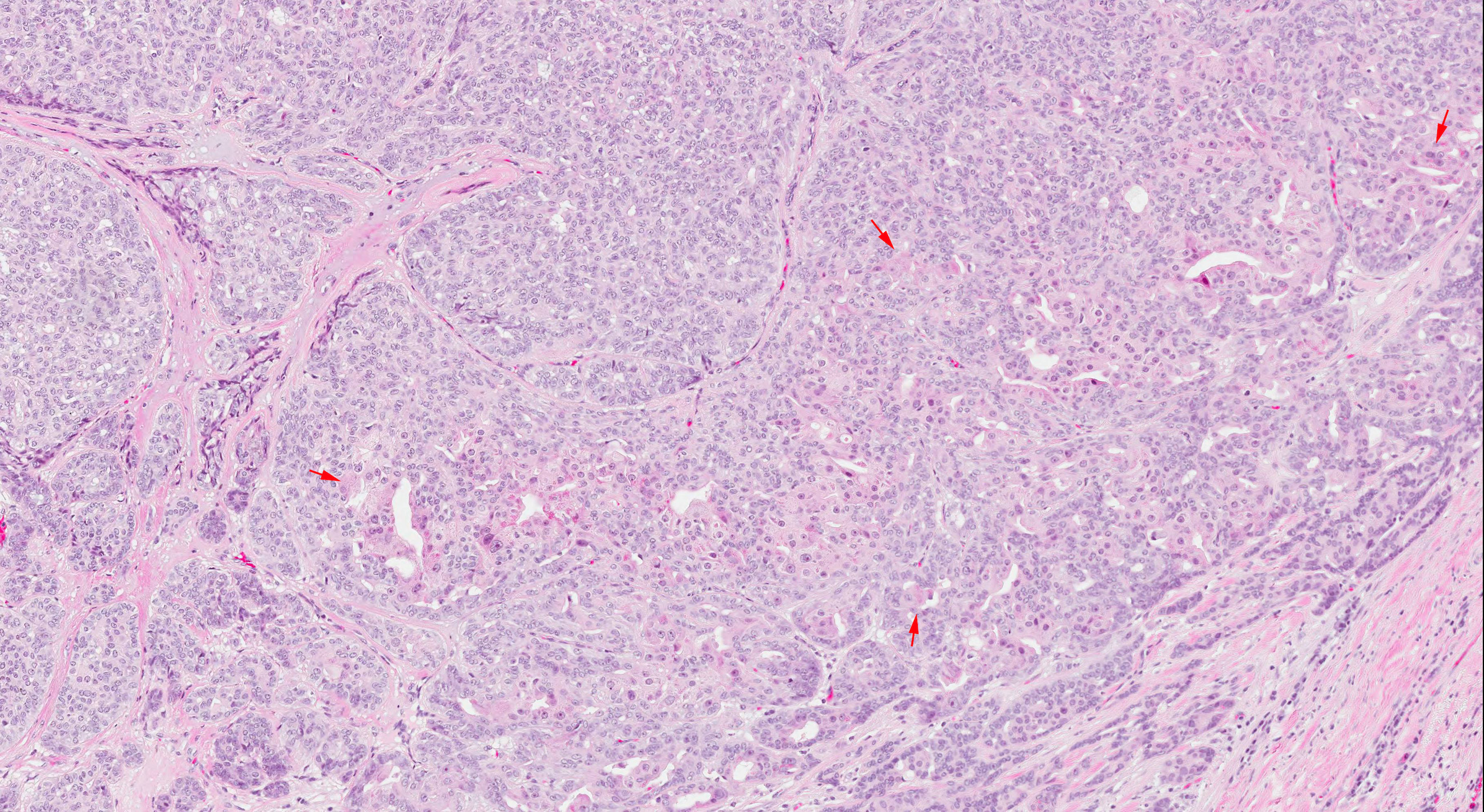
Primary biphasic carcinoma of the salivary glands; composed of basal and ductal cells (Surg Pathol Clin 2021;14:25)
Essential features
Biphasic, low grade malignancy of salivary gland
Parotid is the most common location; rare in other salivary glands and minor salivary gland tissue
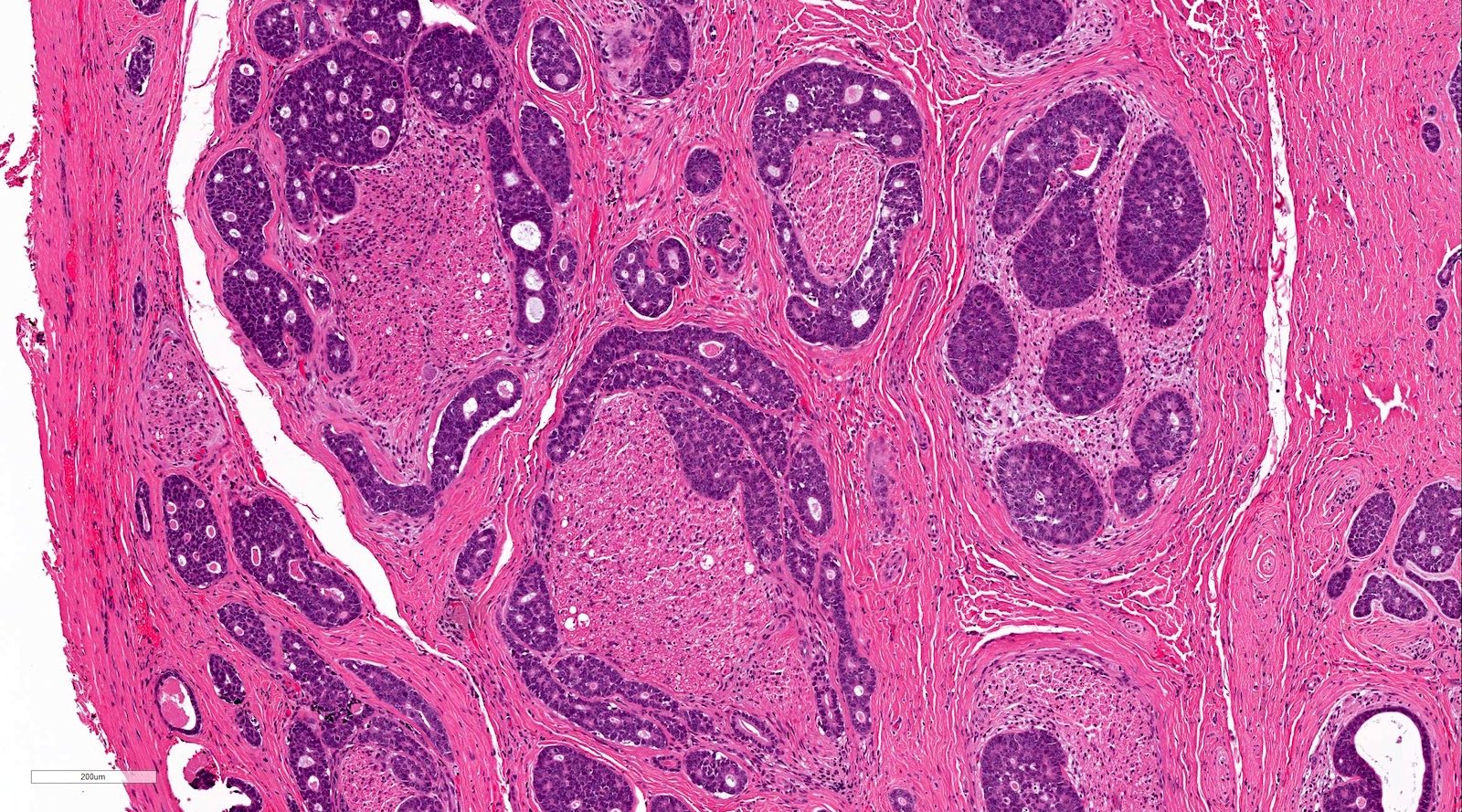
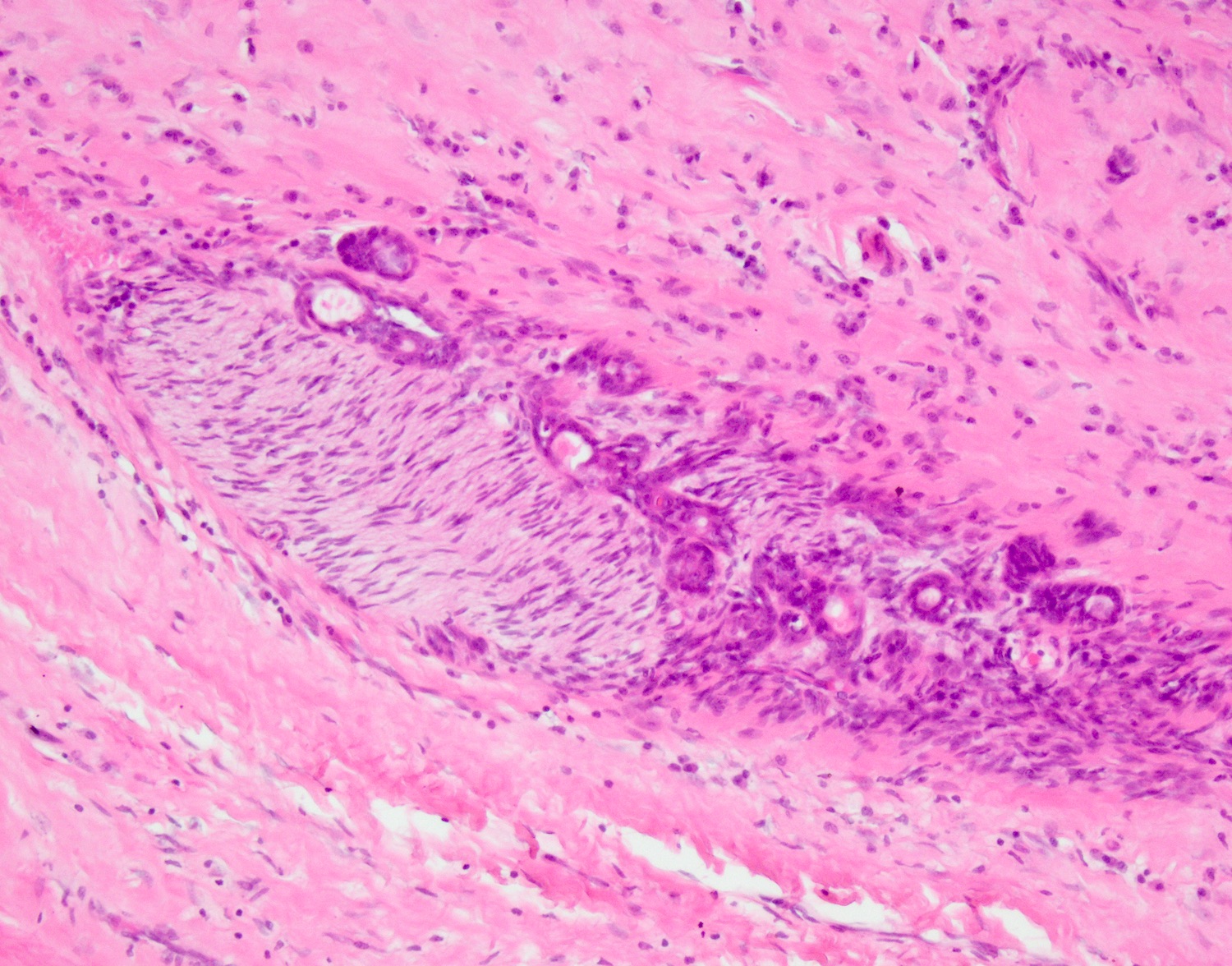
Histologic features similar to basal cell adenoma but with evidence of invasive growth pattern
Diagnosis based on demonstration of a dual cell population of centrally located ductal cells and abluminal basal cells with peripheral palisading of nuclei
Squamous and sebaceous differentiation may be seen
Surgery with clear margins is the mainstay of treatment
Cytologic diagnosis exceedingly difficult due to morphologic overlap with other more common biphasic salivary gland neoplasms, including pleomorphic adenoma and adenoid cystic carcinoma (Diagn Pathol 2013;8:171)
Contributed by Natasha Prosser, B.Sc., M.B.B.S. and Ruta Gupta, M.D.
Peripheral palisading
Biphasic tumor composition
Solid pattern
Tubular and trabecular growth patterns
Membranous pattern
Glandular elements
Squamous morules
Invasion
Perineural invasion
DPAS special stain
Beta catenin IHC
Cytokeratin 7 IHC
p63 IHC
Ki67 IHC
Cytology description
Cytologic diagnosis of basal cell adenocarcinoma is exceedingly difficult as the smears show a dual cell population and are rich in stroma, similar to several biphasic salivary gland neoplasms:
Cellular smears with irregular cohesive cell clusters
Small and intermediate sized basaloid cells with peripheral palisading
Dense, nonfibrillary stroma at the periphery of cell groups
Malignant features with nuclear atypia, mitotic activity or necrosis are rare
Comment: The sections show a partly encapsulated tumor composed of anastomosing tubules and ductules with a prominent hyaline stroma. In most areas, there appears to be a double cell layer, with CK7 positive pale cells surrounded by SMA positive darker cells abutting the hyaline stroma. There is invasion of adipose tissue with an extension close to the parotid gland. No perineural invasion was found. The tumor is 0.8 mm from the nearest inked margin of excision. Mitoses are sparse.
A 70 year old man presents with a slow growing, painless lesion in the parotid. On gross examination, the lesion is well circumscribed, with a cream, partly cystic lesion. Which of the following is correct?
Cytology is helpful in the diagnosis of this lesion
Invasion distinguishes this lesion from its benign counterpart
Molecular features are often used to differentiate this tumor from mimics
This low grade neoplasm frequently metastasizes to the lung
Board review style answer #1
B. Invasion distinguishes this lesion from its benign counterpart. The tumor is a basal cell adenocarcinoma, a rare, indolent malignant counterpart to basal cell adenoma. Evidence of invasion is essential for diagnosis.
Initially included in the group of monomorphic adenoma (unfavored term) along with canalicular adenoma; in 1991, recognized as an independent entity in the second edition of the Salivary Gland Tumors Classification by the WHO
Essential features
Rare benign epithelial tumor of the salivary gland, displaying monomorphic basaloid cells without a myxochondroid component
Terminology
Also called monomorphic adenoma, basaloid salivary gland adenoma
Membranous adenoma also called dermal analogue tumor
Frequent in elderly adults between fifth and seventh decades; uncommon in young adults (J Dent (Shiraz) 2015;16:291)
Female predilection (2:1) except for the membranous type, which bears an equal M:F distribution (J Laryngol Otol 1989;103:756)
Membranous type basal cell adenomas can associate with Brooke-Spiegler syndrome (Eur J Dermatol 2004;14:139)
Sites
> 80% arise in the major salivary glands, mostly parotid gland (mainly in the superficial lobe), followed by the submandibular gland (5%) and 6% in intraoral location with upper lip being the most common site, followed by the buccal mucosa
Pathophysiology
Intercalated duct lineage (IDL) could be precursor; IDL, tubular basal cell adenoma (BCA) and nontubular BCA form a continuum of lesions in which IDLs are related closely to tubular BCA (Histopathology 2014;64:880)
According to some studies, myoepithelial or intercalated duct lineage might be the origin of BCA (J Maxillofac Oral Surg 2010;9:289)
Epithelial tumor cells of pleomorphic adenoma (PA) may form BCA through certain differentiation mechanisms; basal cells of the epithelium of PA possess reserve cell functions, through epithelial - mesenchymal transdifferentiation, forming the predominant basaloid cell population of basal cell adenoma (Auris Nasus Larynx 2006;33:97)
Etiology
Etiology and risk factors for BCA are unknown
Membranous type basal cell adenomas can associate with Brooke-Spiegler syndrome (multiple familial trichoepithelioma) caused by CYLD mutation (Eur J Dermatol 2004;14:139)
Clinical features
Rare, 1 - 2% of epithelial tumors of salivary glands; 2% of benign salivary gland tumors
Solitary or part of turban tumor, Brooke-Spiegler syndrome
Usually adults, 67% female, mean age 58 years
Rarely is congenital and resembles embryoma
Almost all arise in parotid gland, with submandibular gland being a distant second
Usually appears as a firm and mobile, slow growing, asymptomatic mass
Low recurrence rate except for membranous type
Rarely transforms into malignancy; more likely if membranous type (4% malignant transformation)
Membranous type may present as multiple nodules; may coexist with dermal cylindromas or trichoepitheliomas
Diagnosis
Diagnosis is established by the histological study; generally, biopsy is accepted as the most accurate method to obtain the diagnosis, although some authors advocate for fine needle aspiration if physical access to the tumor is available
Radiology description
Nonspecific
Oval to round tumor with smooth distinct margin and high incidence of internal macro or microcysts
Relatively homogenous signal intensity of the solid portion; tumor capsule is low signal intensity on T2 weighted images (Dentomaxillofac Radiol 2010;39:349)
Radiology images
Images hosted on other servers:
Basal cell adenoma in left parotid gland
Basal cell adenoma versus pleomorphic adenoma of the parotid gland
Prognostic factors
Recurrence rate ~ 2% on average; almost nonexistent for the solid and trabecular - tubular variants
Membranous type most commonly associated with recurrence (25 - 37%), likely due to the multicentricity rather than because of true recurrences (Acta Otolaryngol 1998;118:588)
Malignant transformation is more common in the membranous type (4%) than in the other types; total parotidectomy rather than superficial parotidectomy is proposed in the membranous type of BCA (J Oral Maxillofac Pathol 2016;20:142, Acta Otolaryngol 1998;118:588)
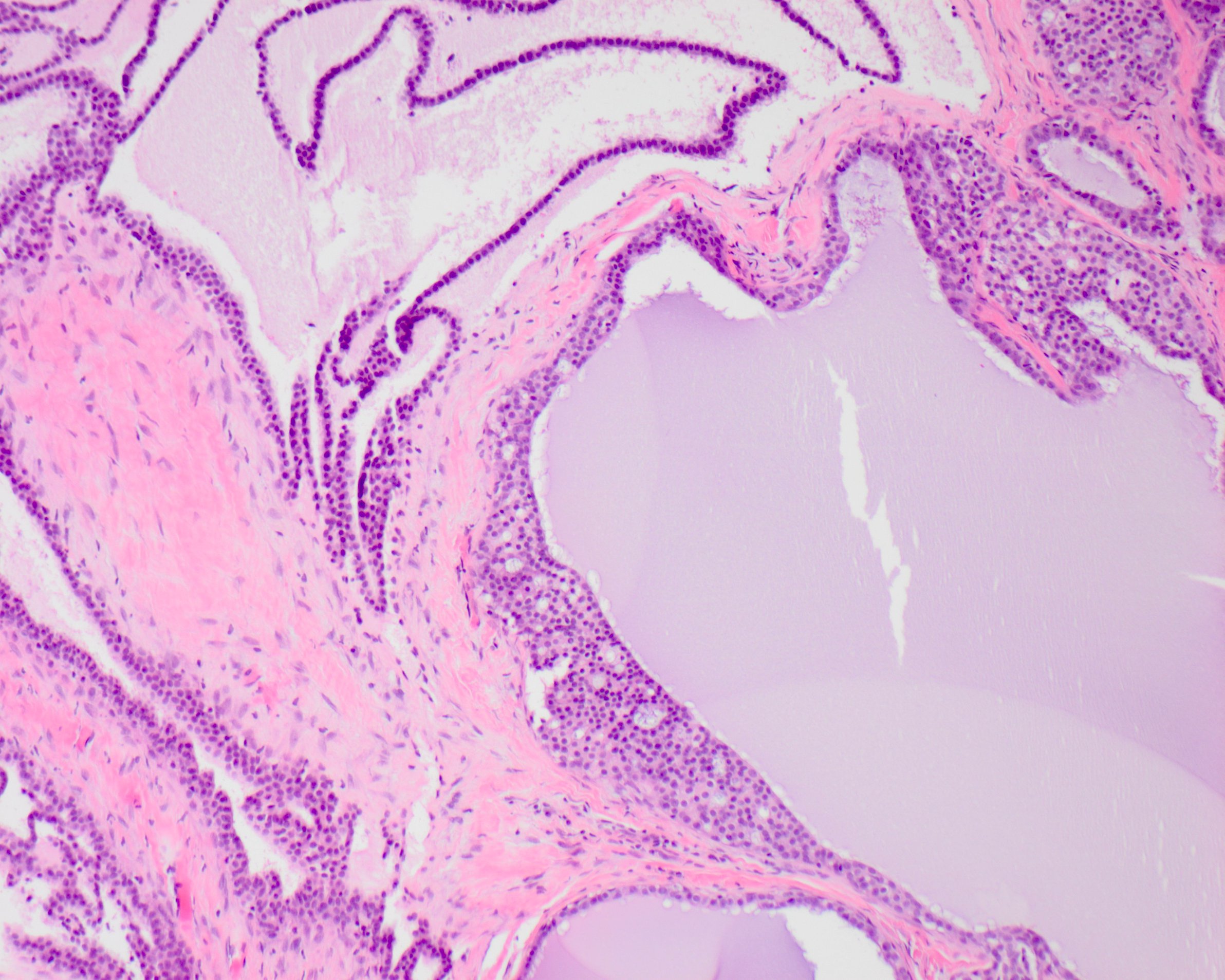
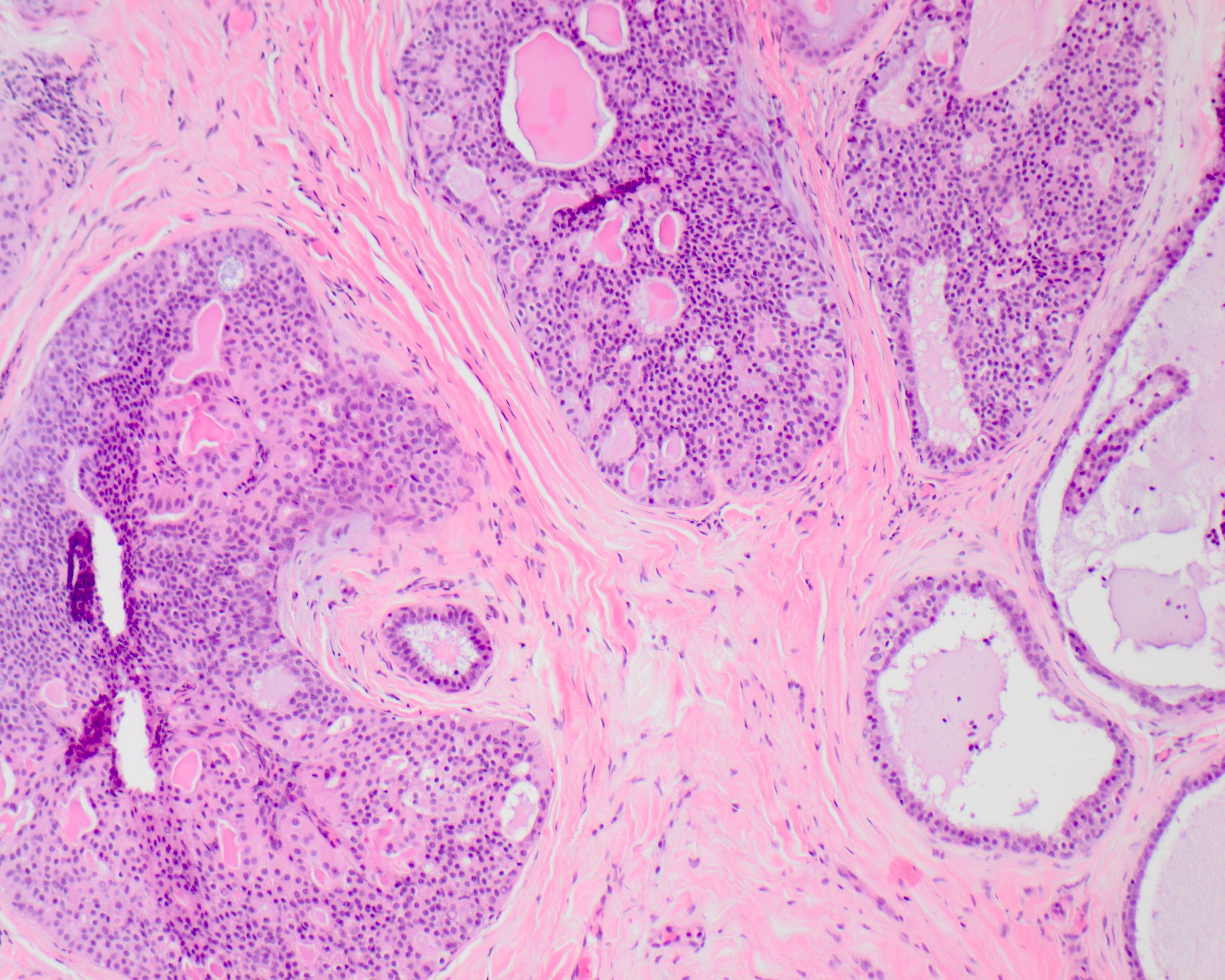
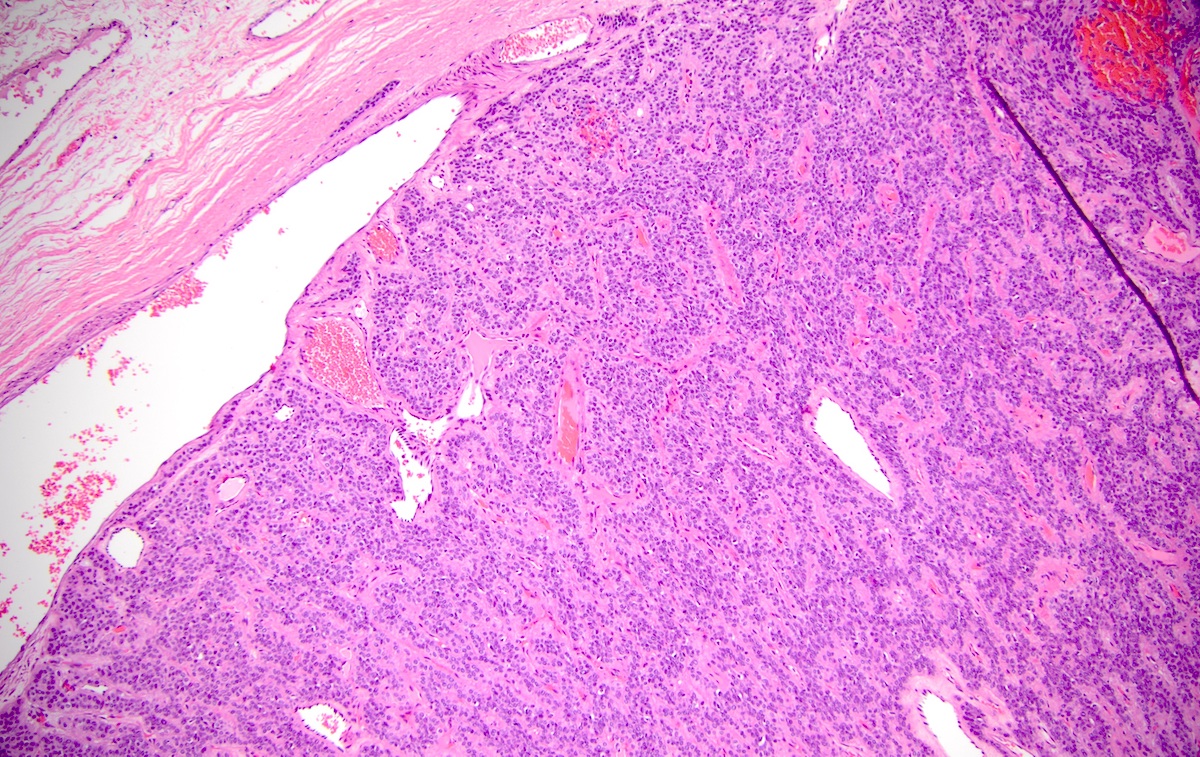
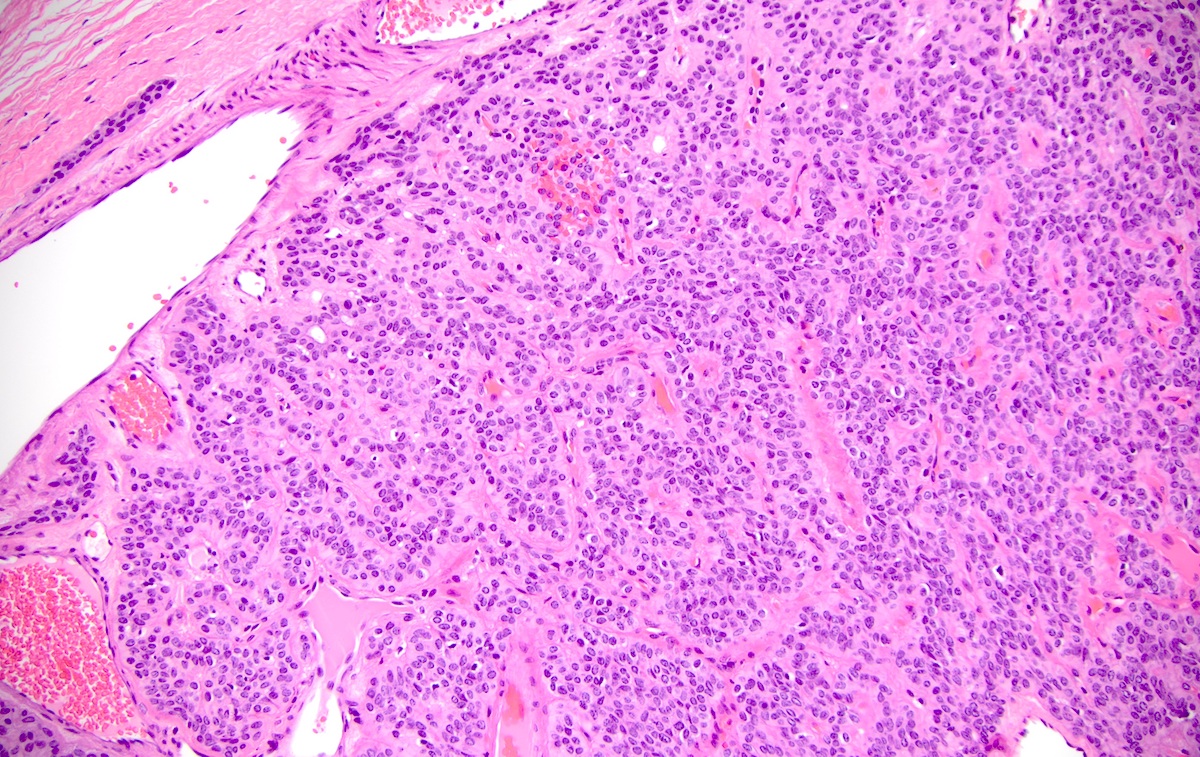
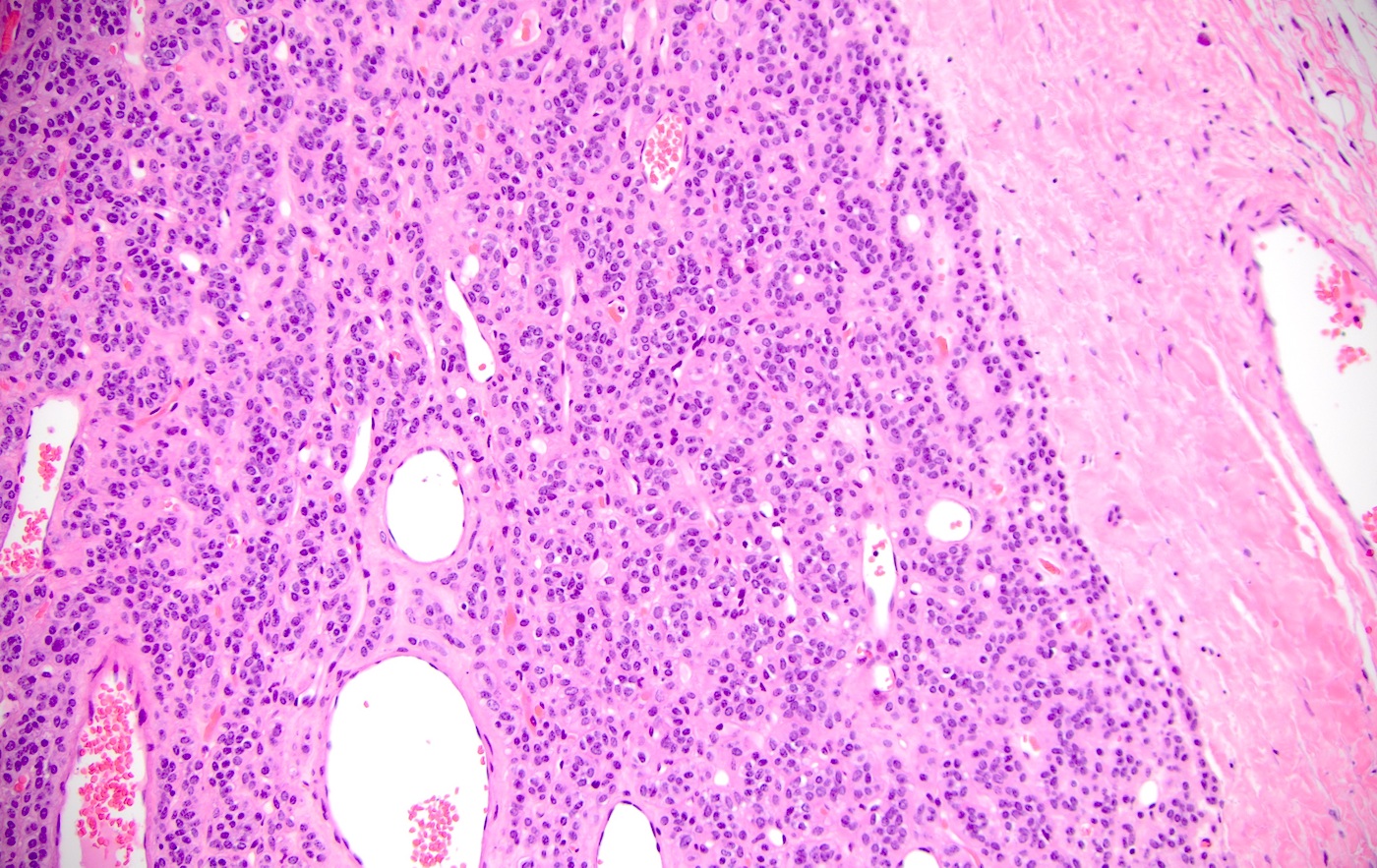
Solid pattern: most common, basaloid cells are present in the form of solid masses which may show peripheral palisading
Trabecular pattern: narrow or broad trabeculae which may get interconnected with each other creating a reticular pattern
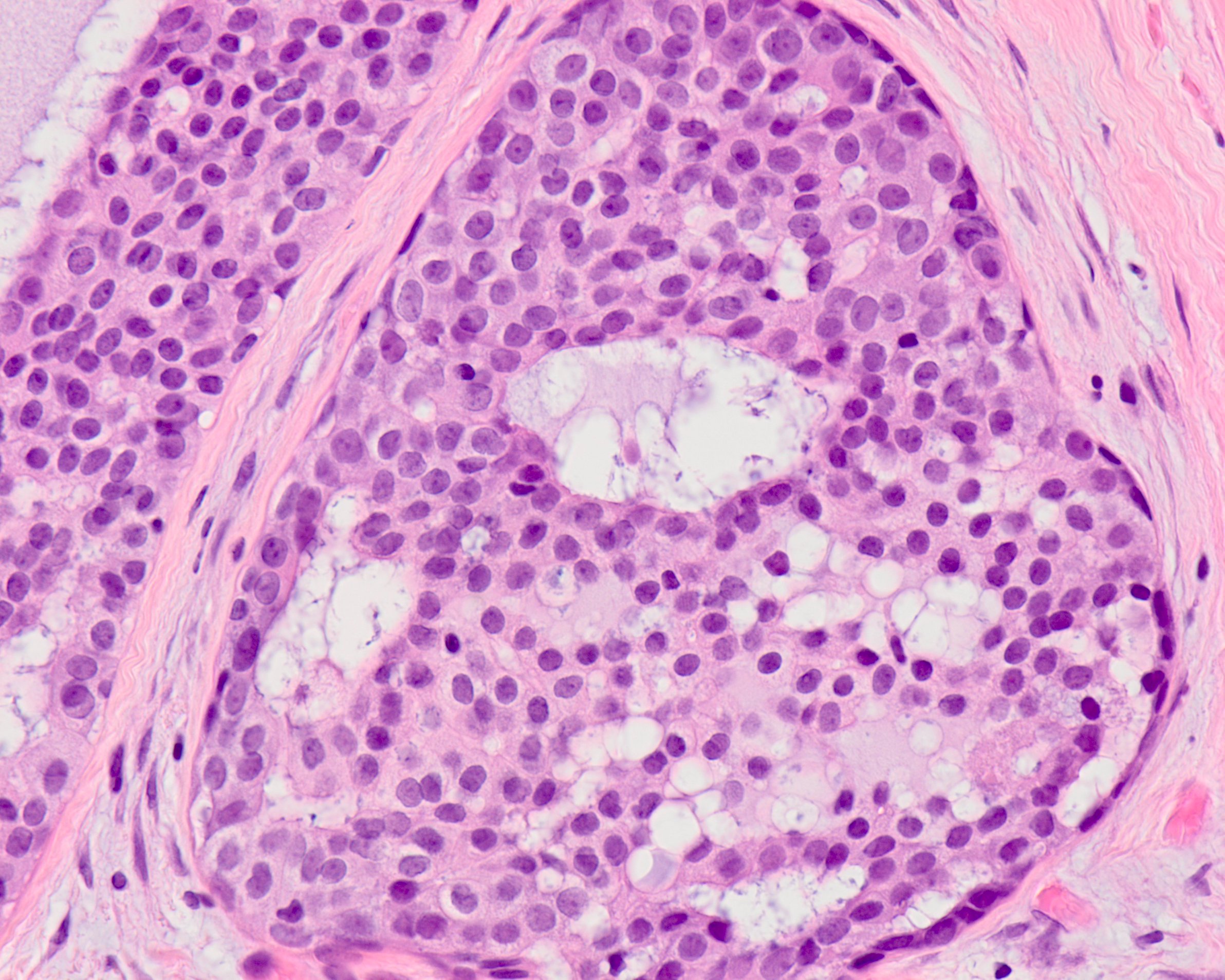
Tubular pattern: numerous tubules consisting of a central lumen and an outer single layer or double layered lining of cuboidal and basaloid cells is seen; the lumen often contains an eosinophilic secretion / mucin which is PAS positive
Membranous types: histologically identical to dermal cylindroma, eosinophilic hyaline membranes separating cell nests; BCA with greater than 50% membranous pattern should be designated as membranous type
Cyst formation is common and can be a main histopathologic feature of basal cell adenoma
Occasionally has acinar cells, squamous whorls or keratinization
No invasion, no perineurial invasion, no chondromyxoid matrix
Chondromyxoid stroma blended with epithelial cells, BCA with prominent myoepithelial derived stroma and stroma in BCA does not blend into the epithelial nests
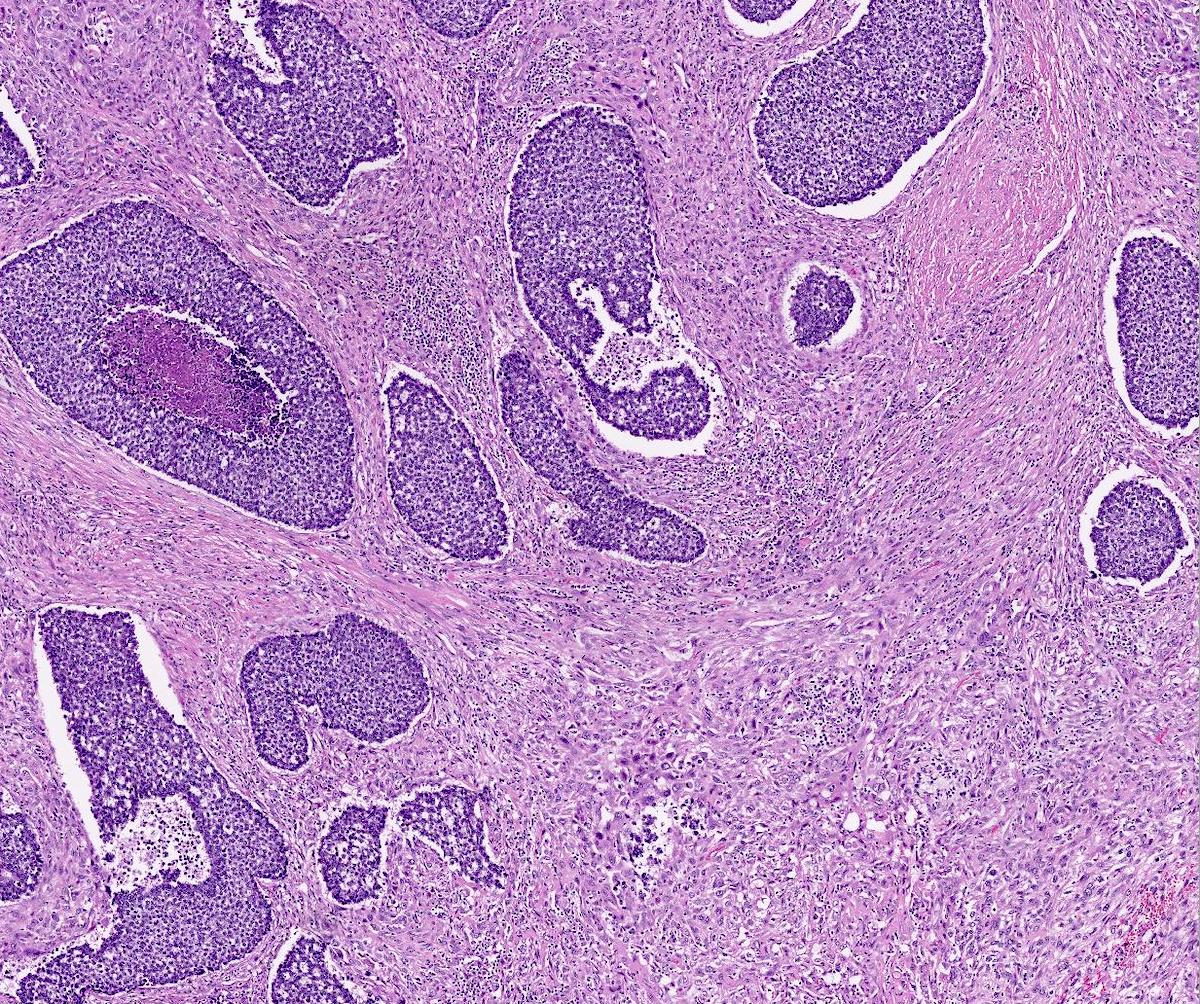
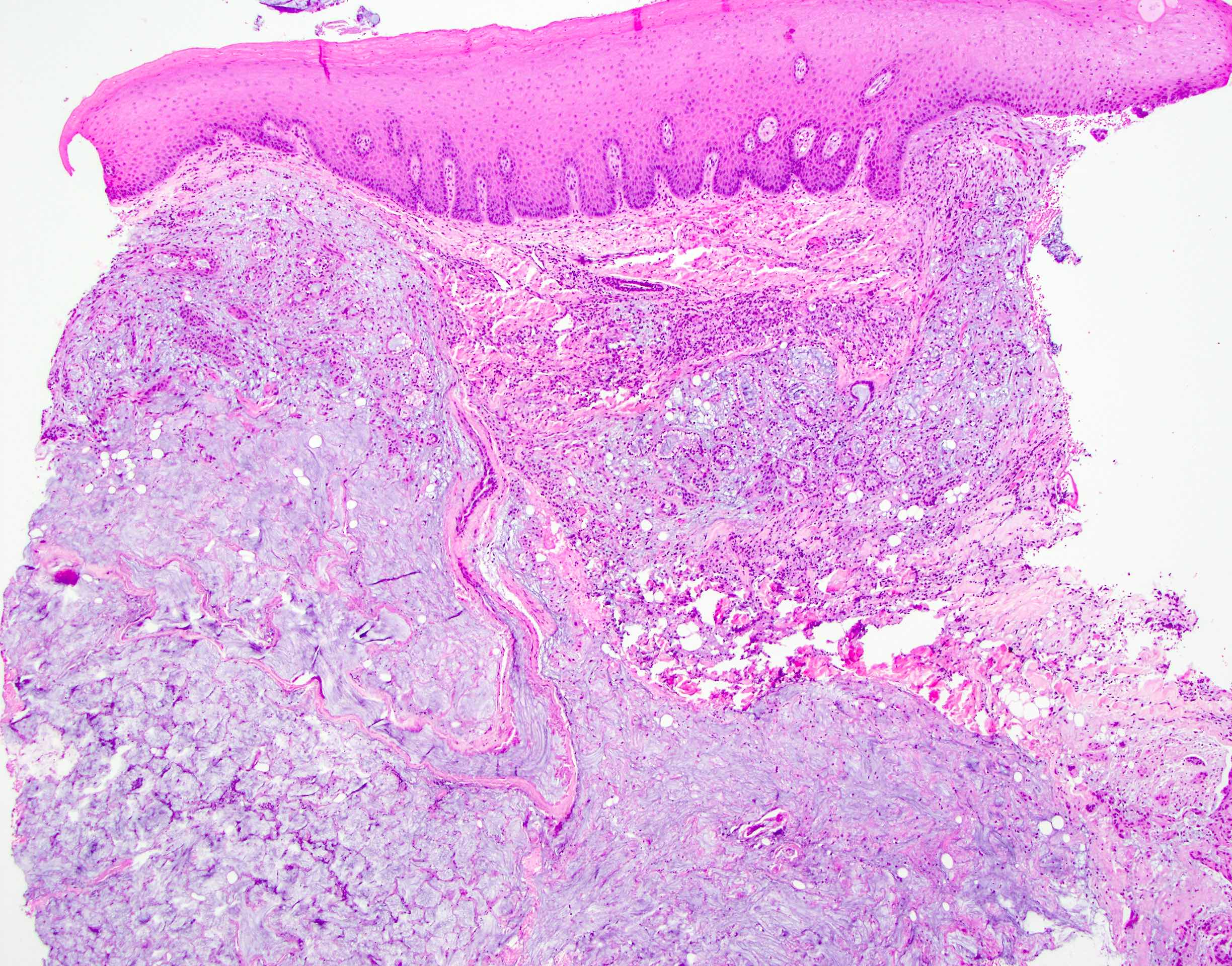
A 56 year old woman presents with a nodule close to the left ear. Imaging reveals a well circumscribed 1.6 cm nodule in parotid gland. Biopsy findings are shown in the picture above. Which of the following statements is true about this entity?
Cystic change is uncommon
Due to the high recurrence rate, total excision is required for all of these neoplasms
It is one of the most common neoplasms in the salivary glands
It occurs more often in younger patients
It can be associated with Brooke-Spiegler syndrome
Board review style answer #1
E. It can be associated with Brooke-Spiegler syndrome. Brooke-Spiegler syndrome is a rare genetic disease characterized as an inherited skin tumor predisposition syndrome presenting with skin appendage tumors (cylindromas, spiradenomas and trichoepitheliomas) and salivary gland tumor. Some patients can have a membranous basal cell adenoma of the salivary gland. It is caused by germline mutations in the CYLD gene (16q12-q13).
Which of the following markers is most useful to differentiate tubular / trabecular predominant basal cell adenoma from pleomorphic adenoma?
Beta catenin
Calponin
CMA
p63
S100
Board review style answer #2
A. Beta catenin. Jo et al. reported that nuclear beta catenin staining can be present in 83% of basal cell adenomas. All adenoid cystic carcinomas (0/20) and pleomorphic adenomas (0/20) were negative. 4 of 5 basal cell adenomas had exon 3 CTNNB1 mutations (Am J Surg Pathol 2016;40:1143).
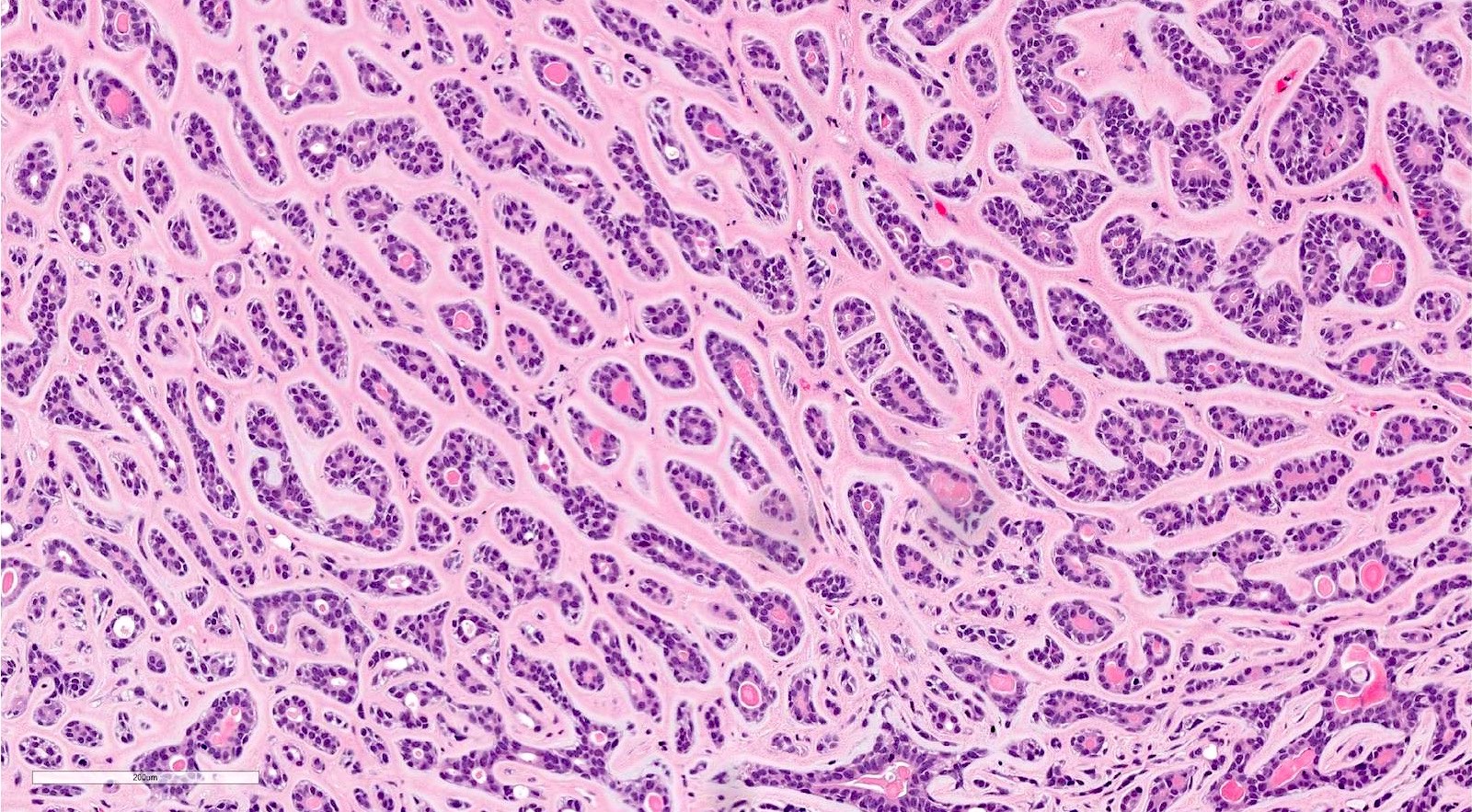
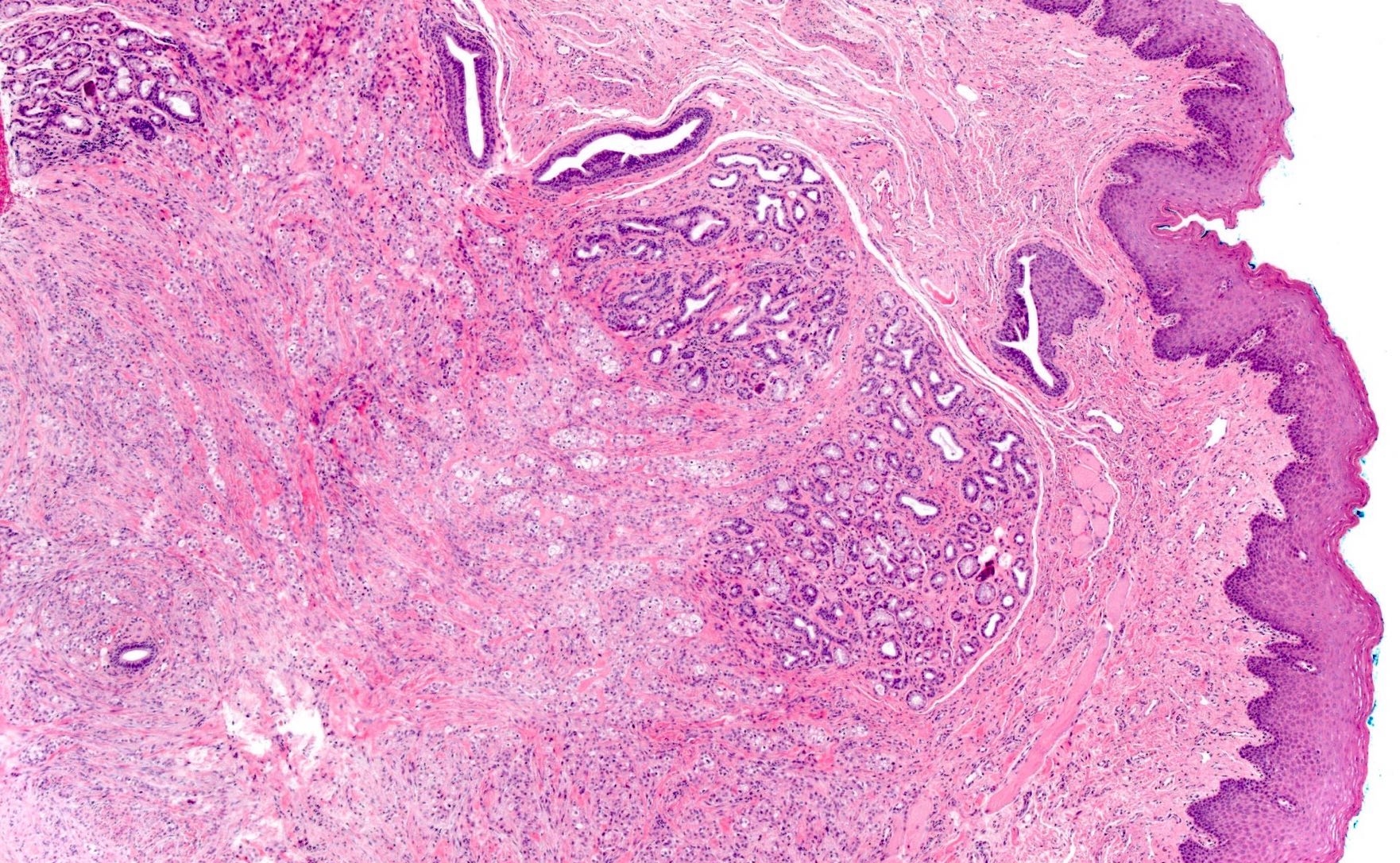
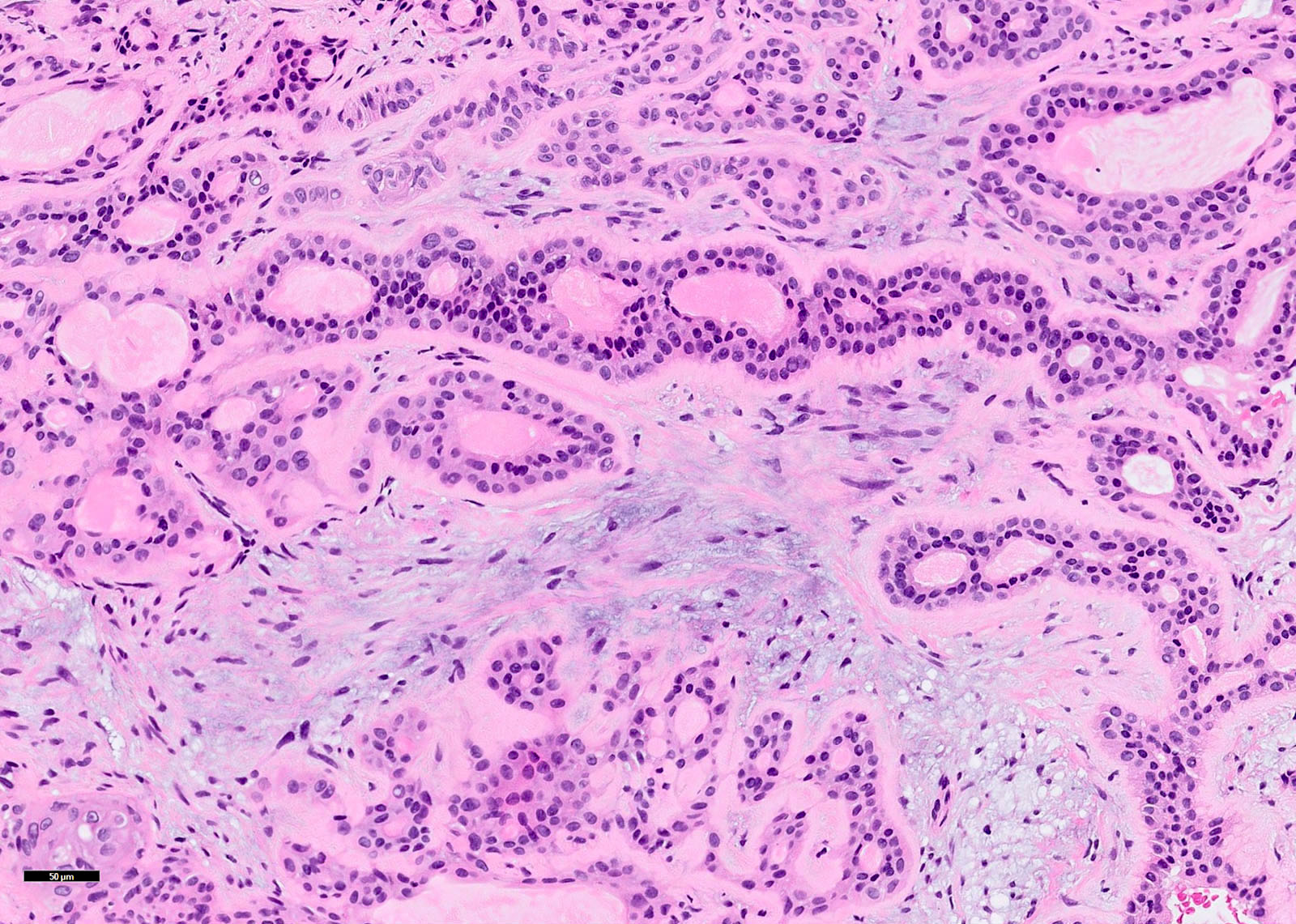
Benign epithelial neoplasm composed of cubocolumnar cells disposed in branching and interconnecting cords and associated with a paucicellular, vascular stroma
Heterogeneous, moderate to strong cytoplasmic WT1 (periphery of ribbon-like structures); in microadenomatous foci, associated with cuboidal cells (Pathol Res Pract 2014;210:726)
2 rows of cells (tall columnar cells surrounding the canalicular lumina and conical cells situated between columnar cells, with direct contact with stromal connective tissue); interdigitating cells
Canalicular lumen: minimum amount of cell debris; no mucoid material
Small number of desmosomes
Ovoid nuclei, moderately prominent nucleoli, patchy condensation of chromatin
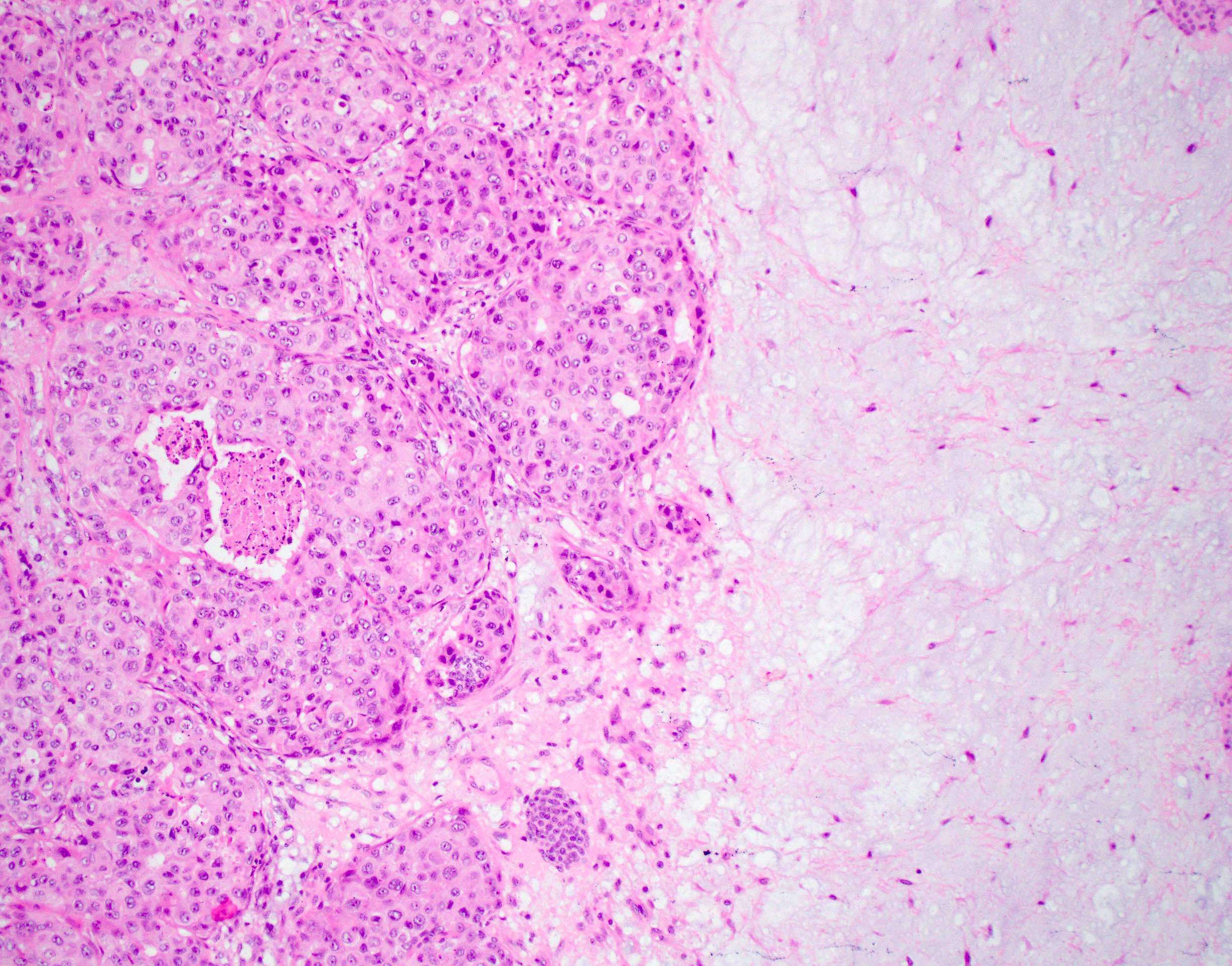
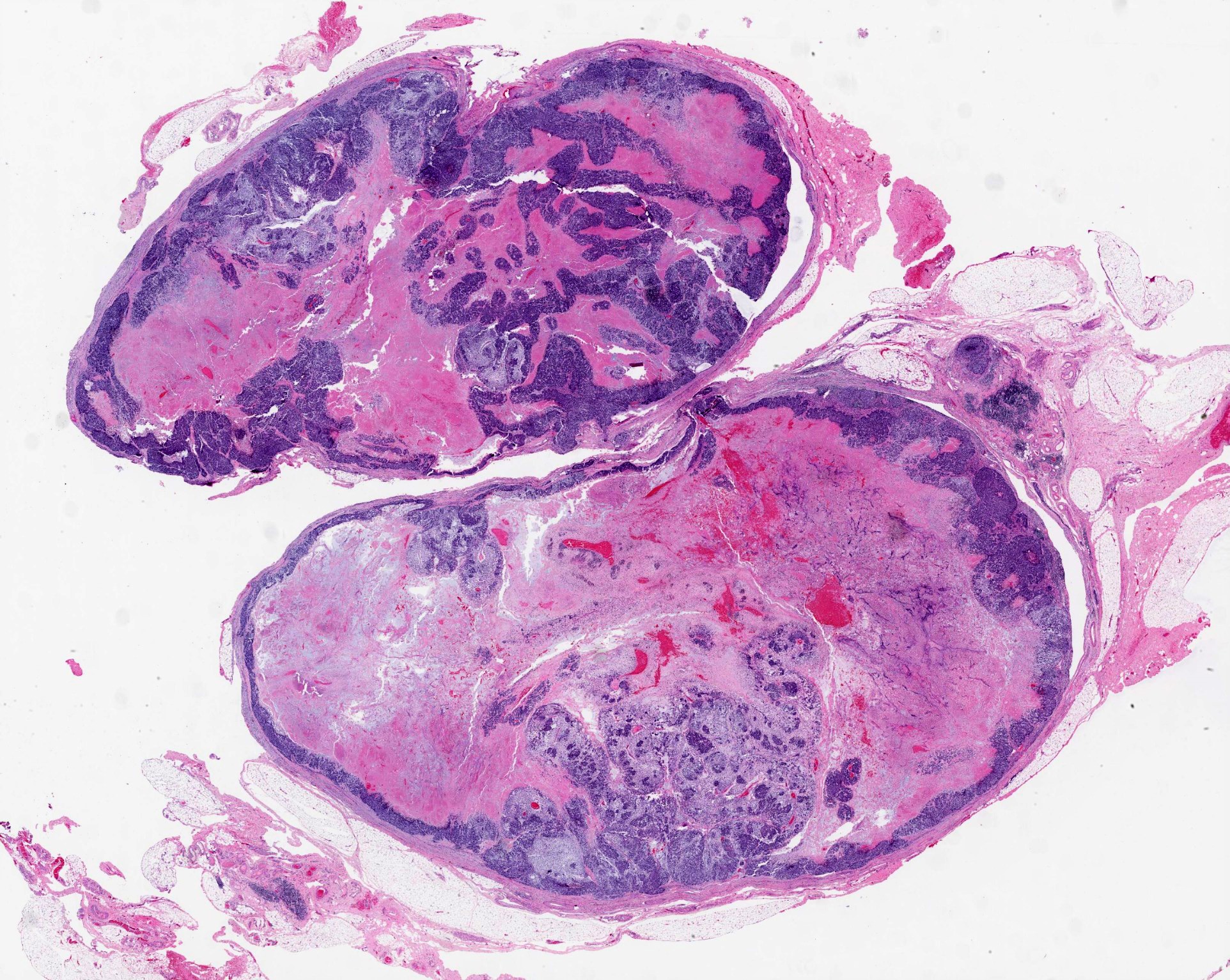
Epithelial or myoepithelial malignancy developing from primary or recurrent pleomorphic adenoma
Essential features
Identification of both malignant and benign components is essential for diagnosis; in cases where the benign component has been obliterated by carcinoma, a history of pleomorphic adenoma at the site must be documented
5% of pleomorphic adenomas undergo malignant transformation, with the highest risk associated with recurrent or longstanding pleomorphic adenoma
Typical clinical presentation is a longstanding palpable mass in the parotid region that has undergone recent rapid growth
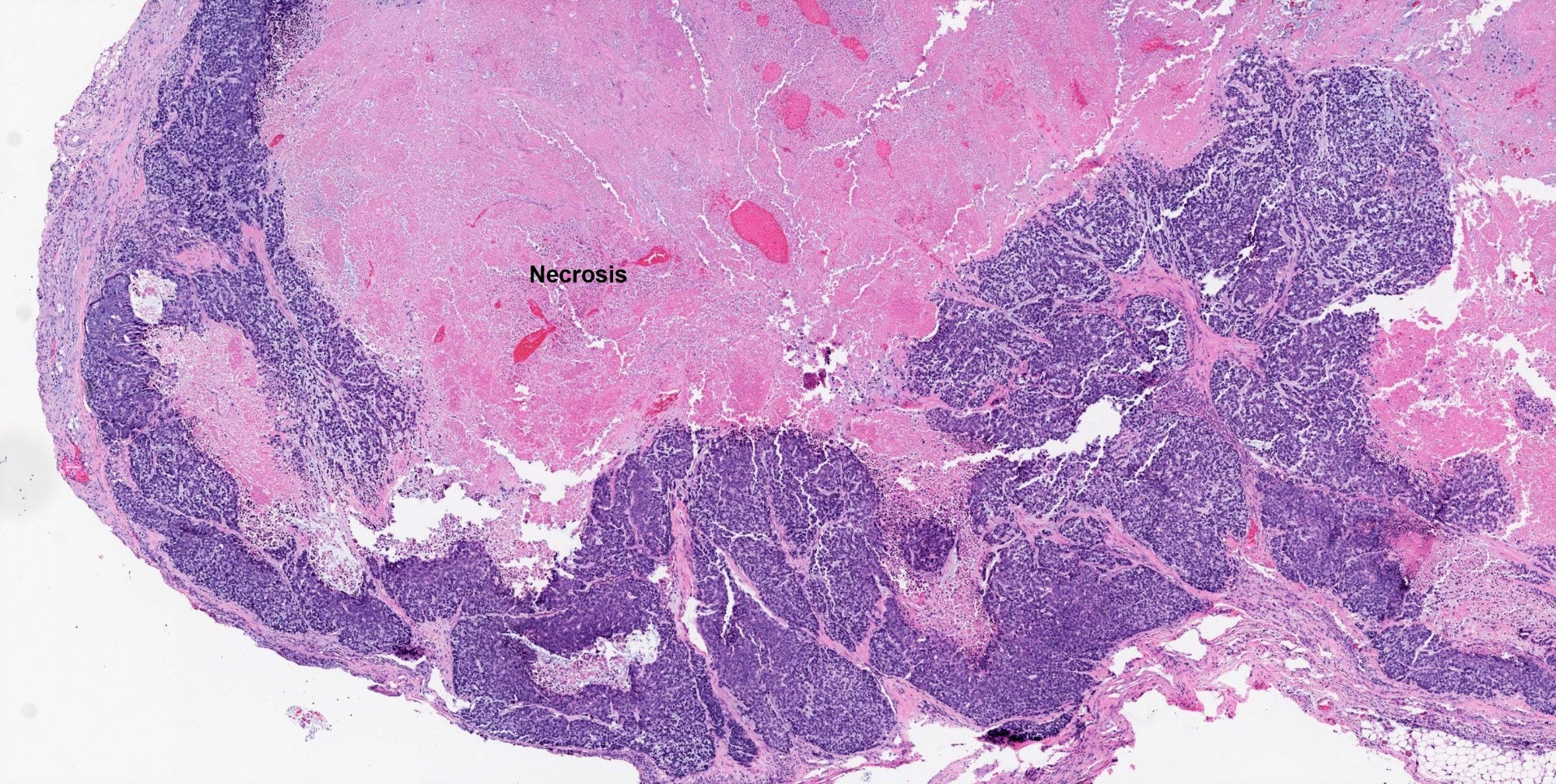
Salivary duct carcinoma and adenocarcinoma NOS are the most frequently encountered malignant components; other malignant components can be myoepithelial carcinoma or epithelial myoepithelial carcinoma
Main predictors of outcome are patient age, tumor diameter, degree of capsule invasion, histological subtype of malignant component and lymph node or distant metastases
Terminology
Malignant mixed tumor (not recommended due to possible confusion with carcinosarcoma)
May present as a sudden increase in size of a preexisting lump, pain or facial paresis / paralysis
Long history of a mass prior to sudden increase in size is common, suggesting that long delays in treatment of pleomorphic adenoma increase the likelihood of malignant transformation (Acta Oncol 2009;48:132)
Advanced cases may present with skin ulceration or dysphagia (Head Neck 2001;23:705)
Diagnosis
Definitive diagnosis rests on microscopic analysis with documentation of both benign pleomorphic adenoma and malignant components
Sudden increase in size of a longstanding pleomorphic adenoma can raise clinical suspicion of carcinoma ex pleomorphic adenoma
Radiology description
MRI is superior to CT as it is most sensitive in detecting malignancy and allows better delineation of tissue planes and infiltrative edges (Head Neck Pathol 2012;6:1)
Characteristic MRI finding is the presence of both encapsulated and invasive components
Encapsulated (pleomorphic adenoma) component:
Shows a variety of signal intensities on MRI, reflecting the variability in architectural and cytomorphologic features (AJNR Am J Neuroradiol 2008;29:865)
Invasive component:
Hemorrhage, necrosis, irregular margin or infiltration of surrounding tissues
Some studies suggest worse outcomes when the malignant component is myoepithelial carcinoma (Hum Pathol 2010;41:927)
Histological grade, invasiveness, lymph node involvement and perineural invasion are associated with distant metastases (World J Surg Oncol 2013;11:180)
Prognosis for carcinoma ex recurrent pleomorphic adenoma is significantly worse than the prognosis for carcinoma ex primary pleomorphic adenoma (Histopathology 2011;59:741)
Successful treatment requires input from a multidisciplinary team (Head Neck 2019;41:269)
Surgical excision with negative surgical margins is the mainstay of treatment
Extent of surgery depends on the size and location of the tumor, status of the adjacent cervical nodal basins and relationship to facial nerve, mandible, ear canal and lateral temporal bone
Myoepithelial cells individually dispersed or in loose clusters
Dense fibrillary metachromatic matrix is the most characteristic finding: appears magenta in Romanowsky type stains
Carcinomatous component:
Pleomorphic, hyperchromatic cells, clumped chromatin, high N/C ratio (Cytojournal 2015;12:7)
Necrotic background
Features specific to the type of carcinoma may be seen (e.g. mucous cells, squamoid cells)
Fine needle aspiration has low sensitivity in the diagnosis of carcinoma ex pleomorphic adenoma, likely due to sampling error (Plast Reconstr Surg 2005;116:1206)
Even when a diagnosis is possible, cannot differentiate between noninvasive and invasive tumors (Cytojournal 2015;12:7)
Carcinomatous component is more likely to be identified on FNA if it is high grade and extensive (Diagn Cytopathol 2020;48:149)
TP53 mutations were detected in 37% of intracapsular carcinoma ex pleomorphic adenoma (Histopathology 2007;51:362)
Copy number gains in 9p and 22q have been detected in carcinoma ex pleomorphic adenoma of lacrimal gland (Ophthalmology 2014;121:1125)
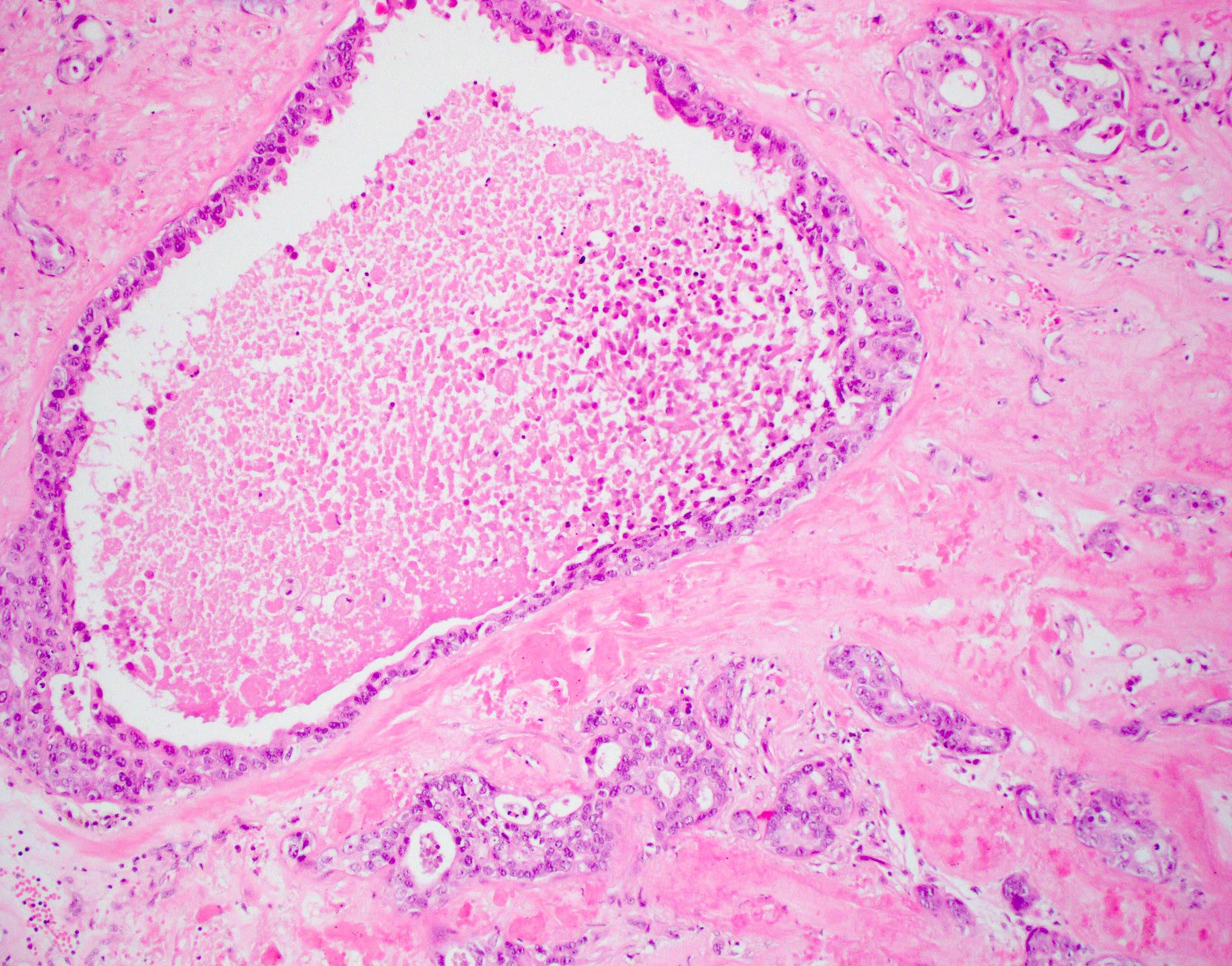
Sample pathology report
Carcinoma ex pleomorphic adenoma (see comment)
Comment: In large areas, the tumor shows a sclerotic nodule. Several infiltrative glands and ducts are seen extending from the periphery of this sclerotic nodule into the adjacent residual salivary gland and attached skeletal muscle. Occasional glands show internal cribriform architecture with Roman bridges and arches and resemble ductal carcinoma in situ of the breast. The glands are lined by cells with an apocrine appearance with apical snouts, moderate eosinophilic cytoplasm and enlarged nuclei with distinctive nucleoli. Mitoses are present. Multiple foci of lymphovascular involvement are present. Perineural involvement is seen. The tumor is present at the margin of resection. In addition, 5/25 lymph nodes in the accompanying neck dissection show metastatic carcinoma. History of a longstanding nodule in the region of the parotid gland with sudden increase in size and new onset facial palsy is noted. The clinical history and the morphologic features support a diagnosis of a carcinoma ex pleomorphic adenoma.
Small protrusions of tumor beyond the tumor capsule, found in up to a quarter of cases and without clinical consequence unless incompletely excised (Laryngoscope 2001;111:2195, Cancer 1998;82:617)
Must not be confused with malignant transformation
De novo carcinoma:
Identification of residual pleomorphic adenoma (or a history of recurrent / incompletely excised pleomorphic adenoma) is essential for diagnosis of carcinoma ex pleomorphic adenoma
PLAG1 and HMGA2 genetic aberrations are seen in carcinoma ex pleomorphic adenoma but not its malignant de novo counterparts (Hum Pathol 2015;46:26)
Regarding carcinoma ex pleomorphic adenoma, which of the following statements is true?
Fine needle aspiration is a highly sensitive technique for the diagnosis of this entity
Malignant transformation is equally likely to occur in a primary pleomorphic adenoma as it is in recurrent pleomorphic adenoma
Not always possible to identify the preexisting pleomorphic adenoma macroscopically
Submandibular gland is the most common site of origin
Board review style answer #1
C. It is sometimes not possible to identify the pleomorphic adenoma macroscopically or even microscopically; this is one of the reasons why thorough sampling is required. This is because the malignant component may overgrow and subsume the benign component. In such circumstances, a history of pleomorphic adenoma, particularly if longstanding or recurrent, is vital for correct diagnosis. Like pleomorphic adenoma, carcinoma ex pleomorphic adenoma arises most commonly in the parotid gland. Recurrent pleomorphic adenoma has a higher risk of malignant transformation than primary pleomorphic adenoma. Fine needle aspiration has low sensitivity in the diagnosis of carcinoma ex pleomorphic adenoma, largely due to sampling error.
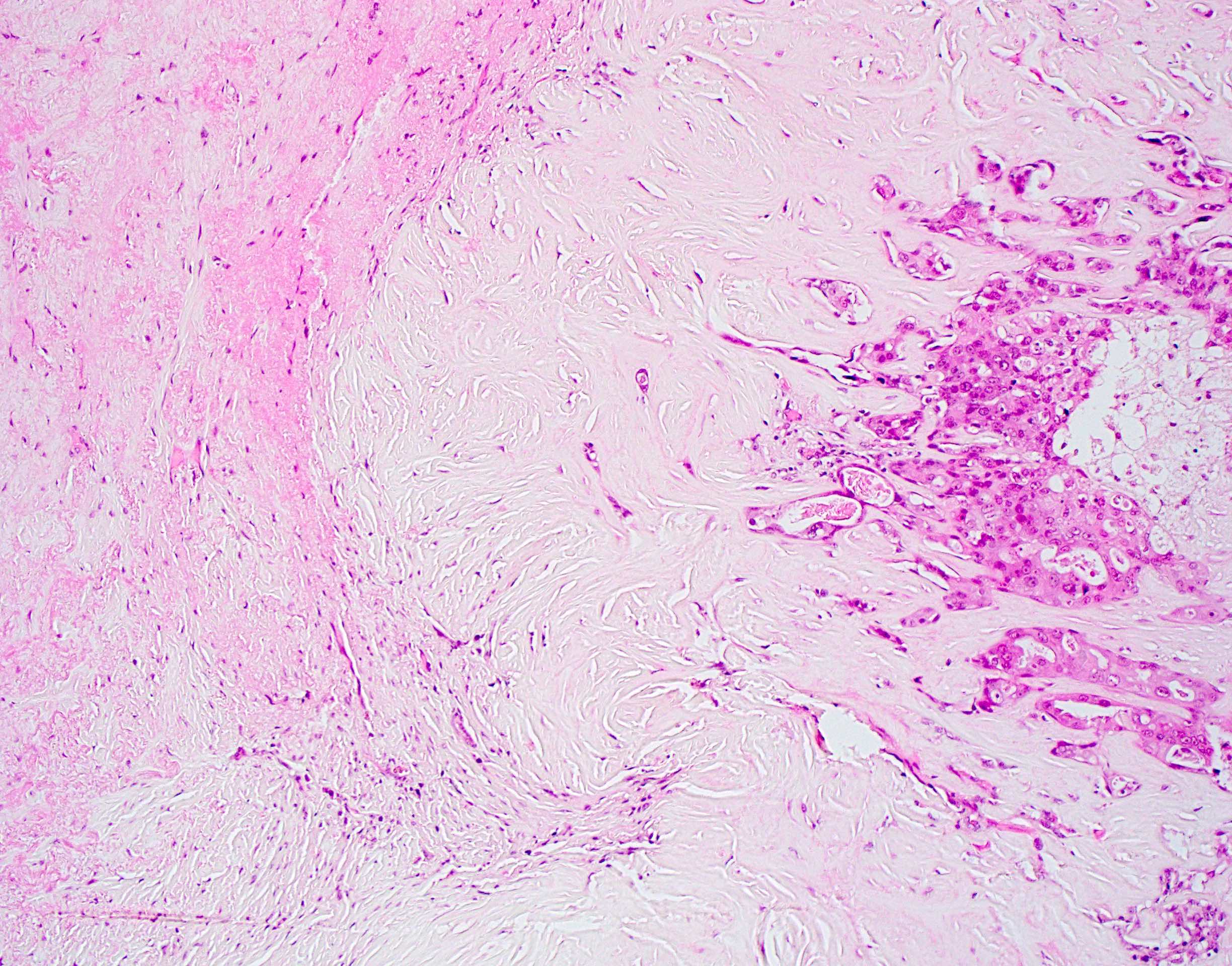
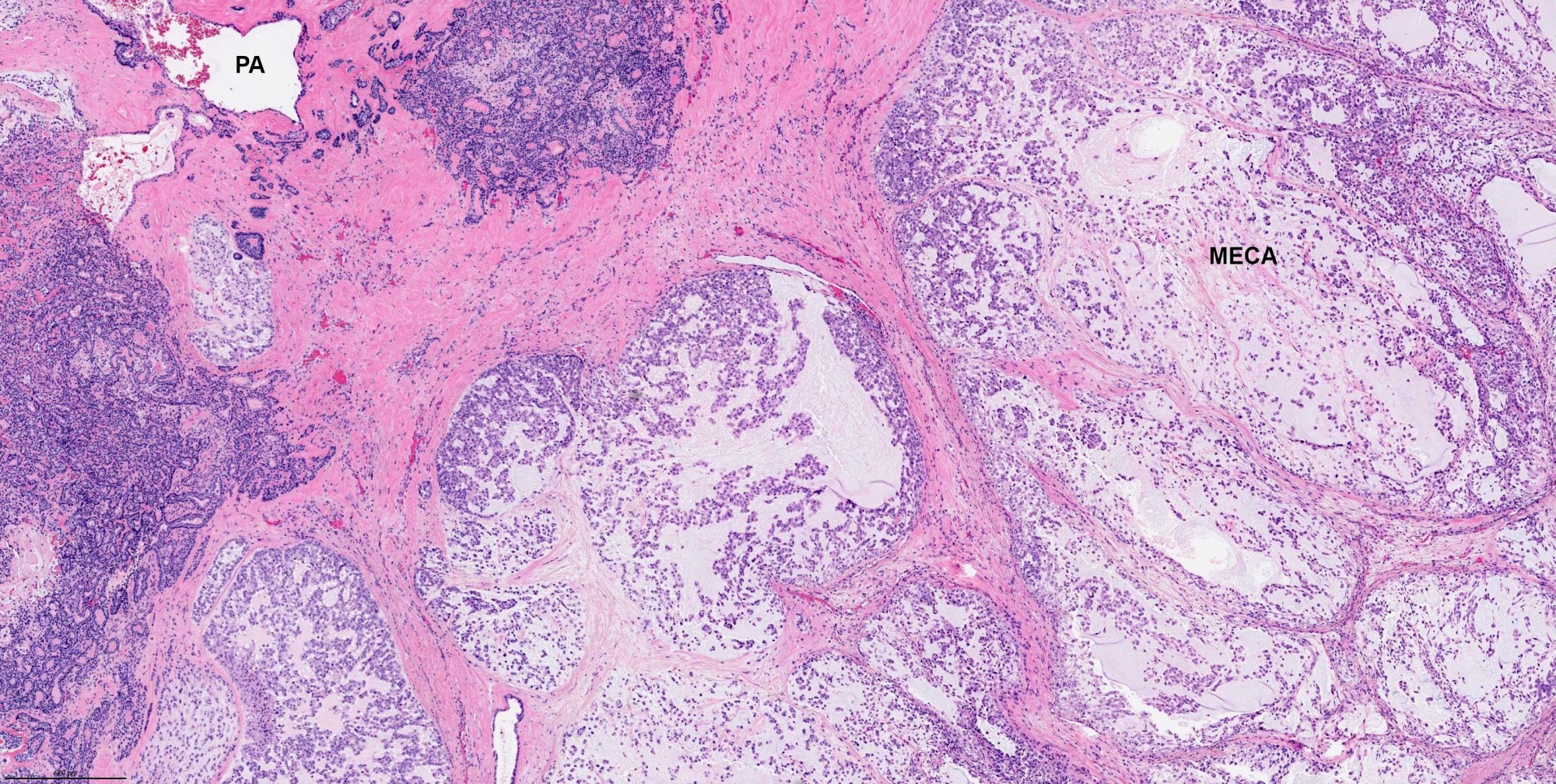
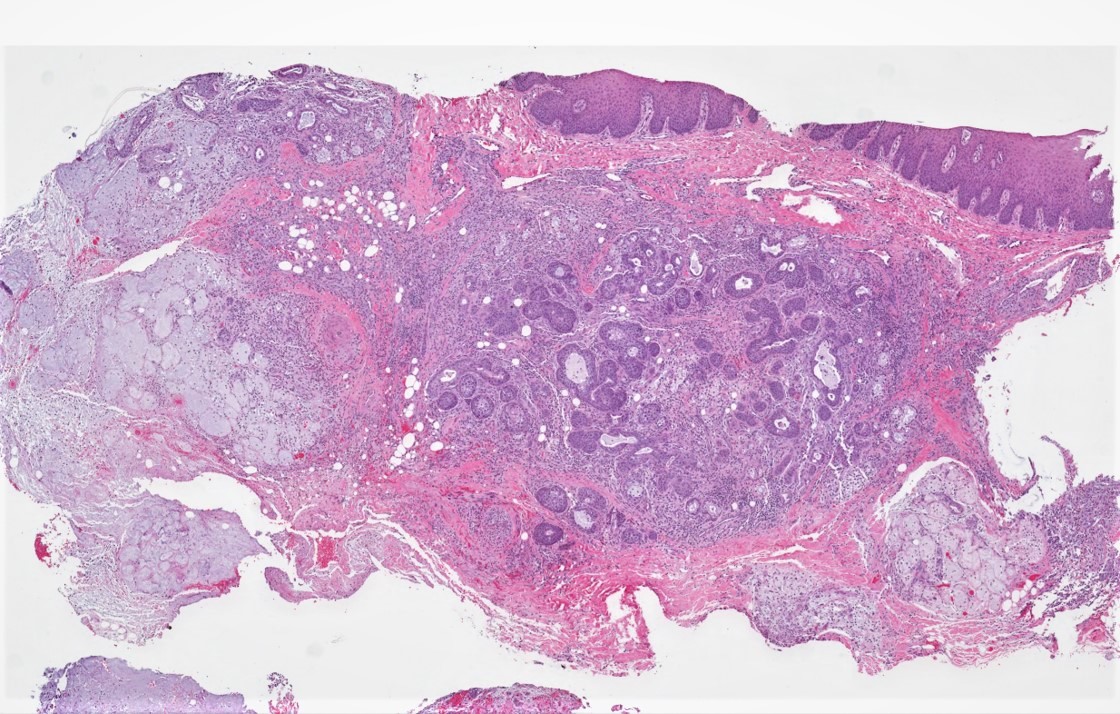
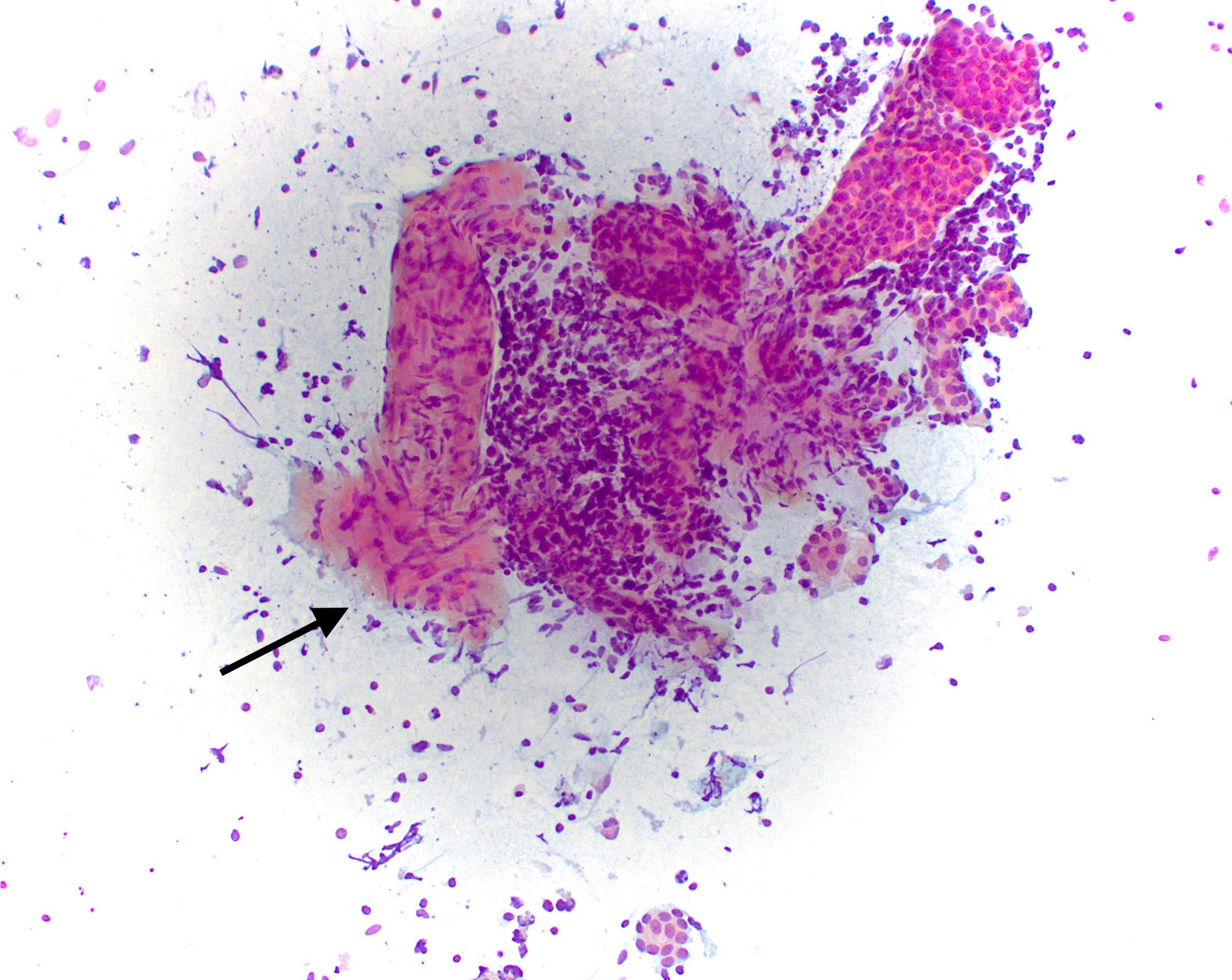
A 57 year old man presents with right facial swelling and paralysis. Following appropriate workup, he undergoes surgical resection of the right facial mass. A representative histological image is provided above. Regarding his diagnosis, which statement is true?
Component on the left is commonly encountered in this entity
Molecular features of the cellular component are completely distinct from those of the paucicellular component
Paucicellular component on the right is irrelevant to the final diagnosis
Presence or absence of a complete capsule around the cellular component does not alter the patient’s prognosis
Board review style answer #2
A. The correct diagnosis is carcinoma ex pleomorphic adenoma. The component on the left is morphologically identical to salivary duct carcinoma, the most common malignant component of carcinoma ex pleomorphic adenoma other than adenocarcinoma NOS. The component on the right is the preexisting pleomorphic adenoma, which is a requirement for diagnosis. PLAG1 and HMGA2 molecular aberrations are encountered in both pleomorphic adenoma and carcinoma ex pleomorphic adenoma. The presence of a tumor capsule is of paramount prognostic significance, as noninvasive or minimally invasive carcinoma ex pleomorphic adenoma is associated with excellent outcomes.
Derivation of the sarcomatous component has been postulated from myoepithelial cells of pleomorphic adenoma and primary carcinomatous components (Histopathology 2023;82:576)
May have a longstanding mass or history of recurrent mass that represents a pleomorphic adenoma (Laryngoscope 2020;130:E335)
Facial pain and paresis (facial nerve palsy)
Otalgia
Dysphagia
Skin ulceration
May have a history of radiation therapy for pleomorphic adenoma
Advanced stage of presentation with lymph node metastasis and distant hematogenous spread (17.2%), mostly to lung and liver; there is a high frequency of local recurrence (Laryngoscope 2020;130:E335, Histopathology 2023;82:576)
Diagnosis
Neck mass that typically leads to imaging studies (computed tomography [CT] / magnetic resonance imaging [MRI]) and fine needle aspiration (FNA)
Definite diagnosis only rendered after surgical resection
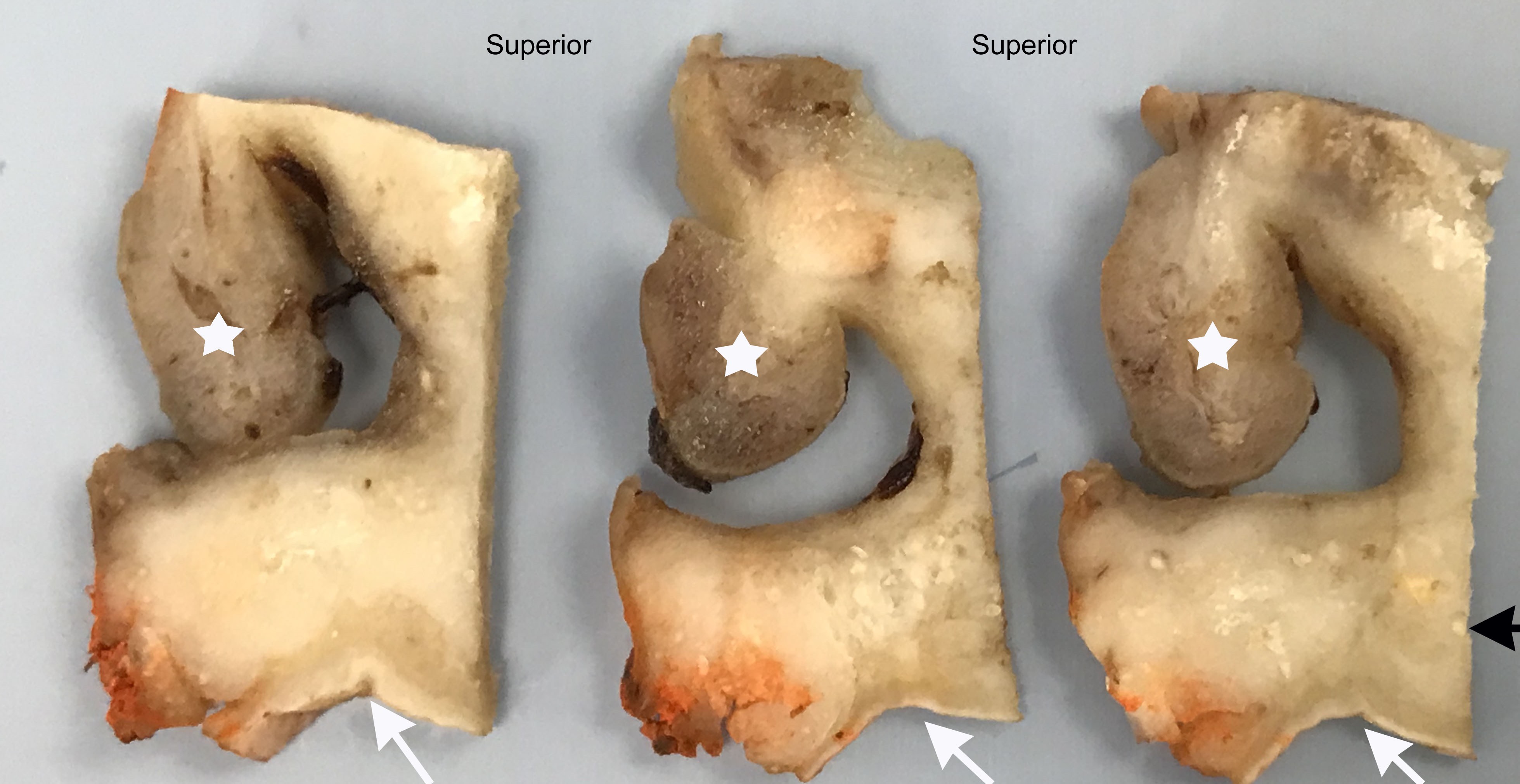
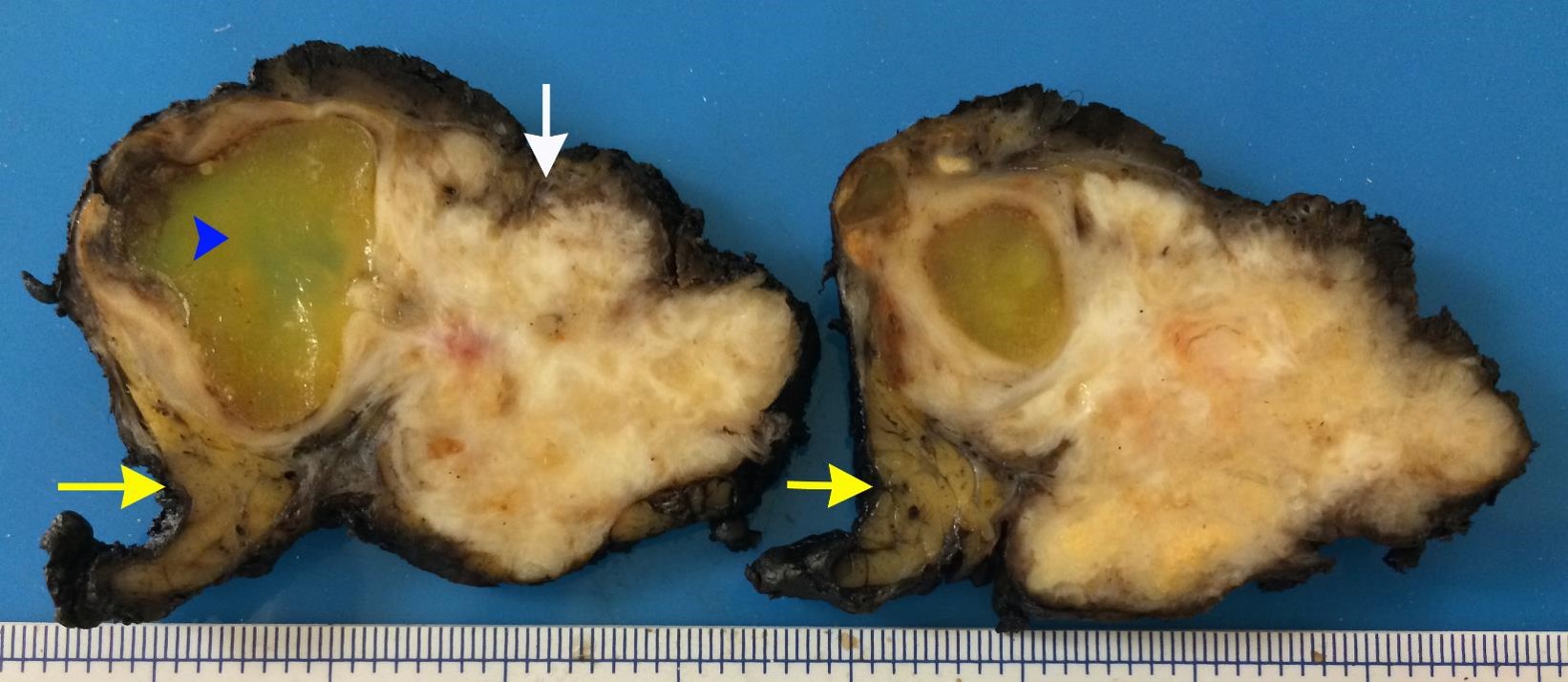
Smaller, often sclerotic nodule may be present that represents a pre-existing pleomorphic adenoma (Histopathology 2023;82:576)
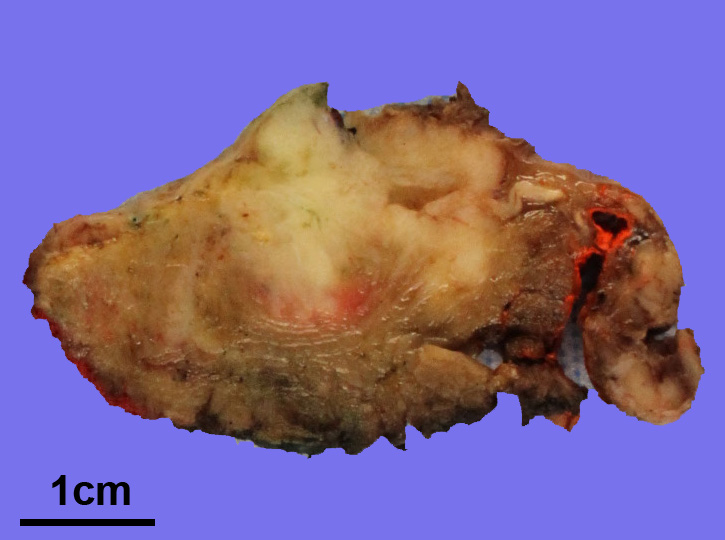
Gross images
Contributed by Alexander Tang, M.B.B.S.
Cut section of tan, fleshy carcinosarcoma
Frozen section description
Diagnosis of high grade carcinoma or raising a possibility of sarcoma component is required from a representative section of the tumor for appropriate surgical management, including defining the extent of resection and the levels of neck dissection required
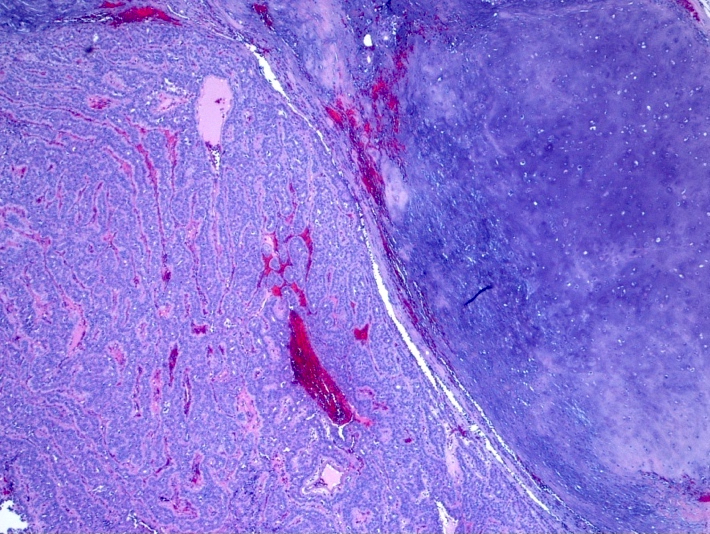
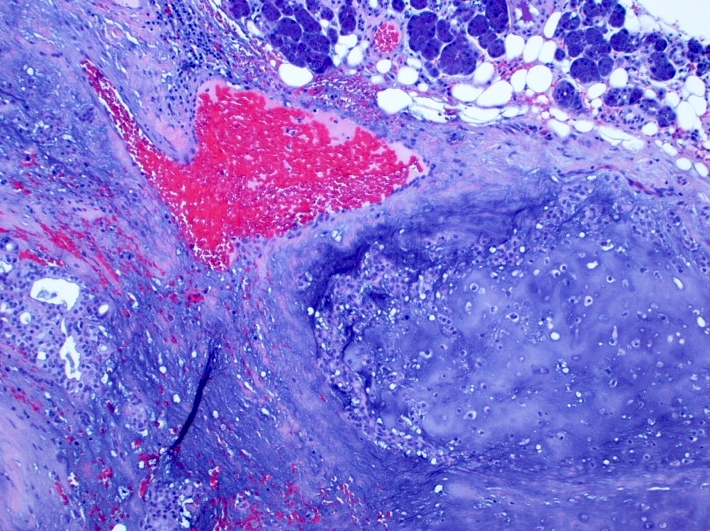
Microscopic (histologic) description
Variable combination of malignant epithelial and sarcomatous tumor components
There may be more than 1 type of carcinoma or sarcoma
Intraductal pathway of tumorigenesis displays intraductal neoplasia, combined with dominant undifferentiated or salivary duct type carcinoma as an epithelial component and with pleomorphic or osteo / chondrosarcoma as a mesenchymal component
Myoepithelial pathway of tumorigenesis displays an absence of intraductal neoplasia and almost obligate combination of myoepithelial carcinoma and chondrosarcomatous differentiation
Sarcomatous components frequently dominate
High grade cytomorphology; mitotic figures and necrosis are frequently seen
PLAG1::CTNNB1, PLAG1::FGFR1, PLAG1::HNRNPA2B1 and HMGA2::WIF1 fusions have been reported (Histopathology 2023;82:576)
Sample pathology report
Left parotid, parotidectomy:
Carcinosarcoma (see comment)
Comment: The biphasic tumor features both malignant epithelial (undifferentiated carcinoma) and sarcomatous (chondrosarcoma) components. Focally, there is a sclerotic area with myoepithelial cells, which could be suggestive of residual pleomorphic adenoma component.
A 68 year old man who has a history of longstanding right parotid mass presented with a rapidly enlarging mass of the right parotid. A radical resection is performed. What is the diagnosis?
Carcinoma ex pleomorphic adenoma
Carcinosarcoma
Pleomorphic adenoma
Spindle cell squamous carcinoma
Board review style answer #1
B. Carcinosarcoma. The slide shows a mixture of undifferentiated carcinoma and spindle / pleomorphic sarcoma components. Along with the history of longstanding right parotid mass, which is typically associated with pleomorphic adenoma, the histological features are consistent with carcinosarcoma. Answer C is incorrect because pleomorphic adenoma does not show carcinoma and sarcoma components. Answer A is incorrect because a sarcomatous component is not present in carcinoma ex pleomorphic adenoma. Answer D is incorrect because although spindle cell squamous carcinoma can exhibit a sarcomatoid appearance, there is a conventional squamous cell component in the form of intraepithelial dysplasia, carcinoma in situ or invasive squamous cell carcinoma. It is also typically not associated with a longstanding parotid mass.
Which of the following statements is true about salivary carcinosarcoma?
It is a low grade indolent salivary gland malignancy
Most common sarcomatous component is chondrosarcoma
No necrosis and hemorrhage is seen
There is no association with pleomorphic adenoma
Board review style answer #2
B. Most common sarcomatous component is chondrosarcoma. The most common sarcomatous component in salivary carcinosarcoma is chondrosarcoma (51.2%). Answer A is incorrect because salivary carcinosarcoma is a high grade salivary gland malignancy. Answer D is incorrect because salivary carcinosarcoma may arise from pre-existing pleomorphic adenoma and may be suggested by the presence of extensive hyalinized stroma. Answer C is incorrect because necrosis and hemorrhage are commonly seen in salivary carcinosarcoma.
30 - 60 year old adults with a higher incidence in males
Sites
Obstructive sialadenitis due to stones mostly affects the submandibular gland (80%) unilaterally without a side predilection (Oral Surg Oral Med Oral Pathol 1972;33:2)
Alkaline pH, increased mucinous and mineral content of its saliva (elevated calcium and phosphate concentrations) predisposes to calculi
Wharton duct runs upward, making saliva flow against gravity and is narrow and tortuous, further contributing to salivary stasis (Mayo Clin Proc 2018;93:266)
Approximately 15% of salivary stones occur within the parotid gland
Sublingual and other minor salivary glands are rarely affected
Pathophysiology
Mechanism is unclear and may be due to:
Multiple intracellular microcalculi which accumulate during secretory inactivity and are excreted into the ducts where they act as a nidus for the eventual formation of a sialolith (Otolaryngol Clin North Am 2009;42:927)
Bacteria or food debris enter the distal submandibular or parotid ducts and act as a nidus for the development of larger calculi (Arch Otolaryngol Head Neck Surg 2001;127:66)
Etiology
Uncertain but possible factors for stone formation include:
Anatomic, affecting saliva formation or flow, such as duct stenosis or inflammation
39 year old woman with a history of migraines presented for evaluation of recurrent left sided submandibular swelling (J Oral Maxillofac Surg 2016;74:2447)
Comment: There is a prominent periductal lymphoplasmacytic infiltrate containing lymphoid aggregates with prominent germinal centers. Some ducts appear ectatic and filled with debris suggestive of a microlith. Others are affected by squamous and mucinous metaplasia. These changes are associated with varying degrees of acinar atrophy and fibrosis.
A 55 year old man presents with a history of intermittent pain and swelling of the submandibular gland after eating. A biopsy with immunostains for IgG4 and IgG was performed and demonstrated a positive plasma cell ratio of 20%. Which of the following is the most likely diagnosis?
Unique malignancy commonly arising in minor salivary glands, usually intraoral
Molecularly defined by expression of EWSR1::ATF1 fusion oncogene or related fusion variants
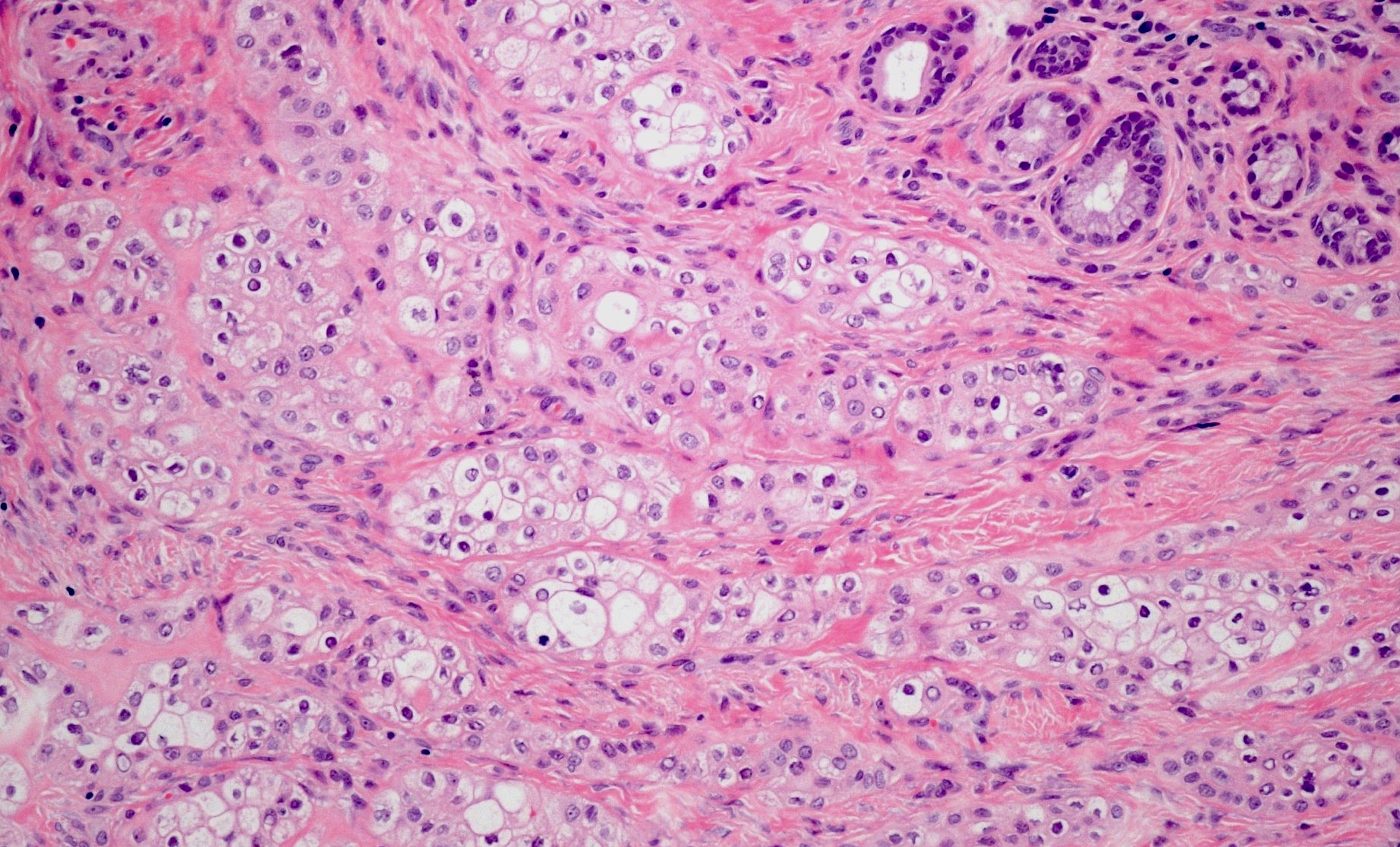
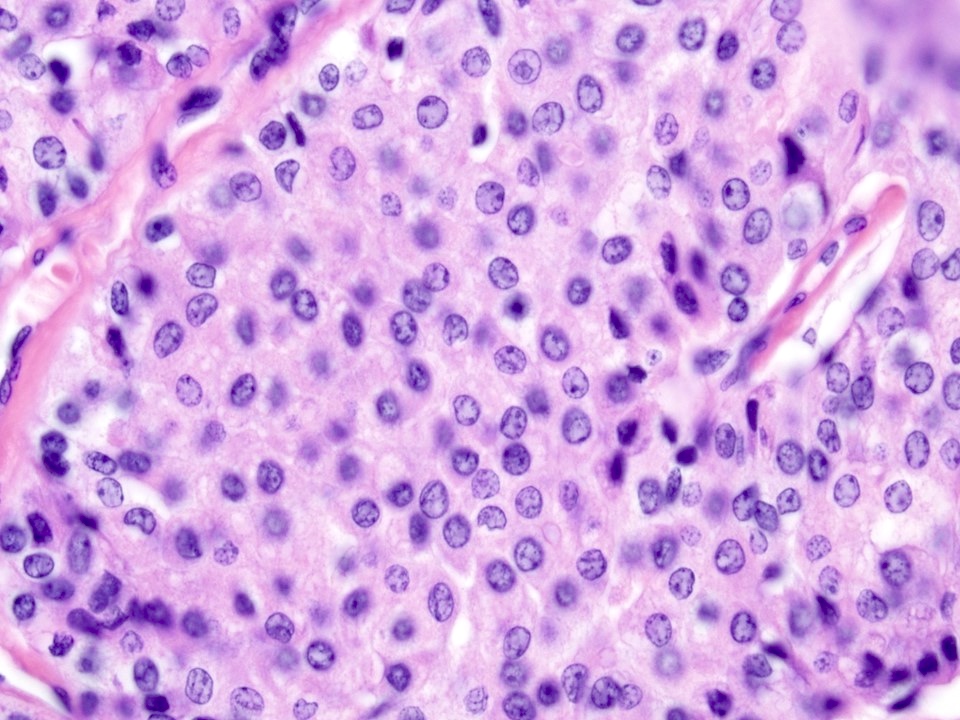
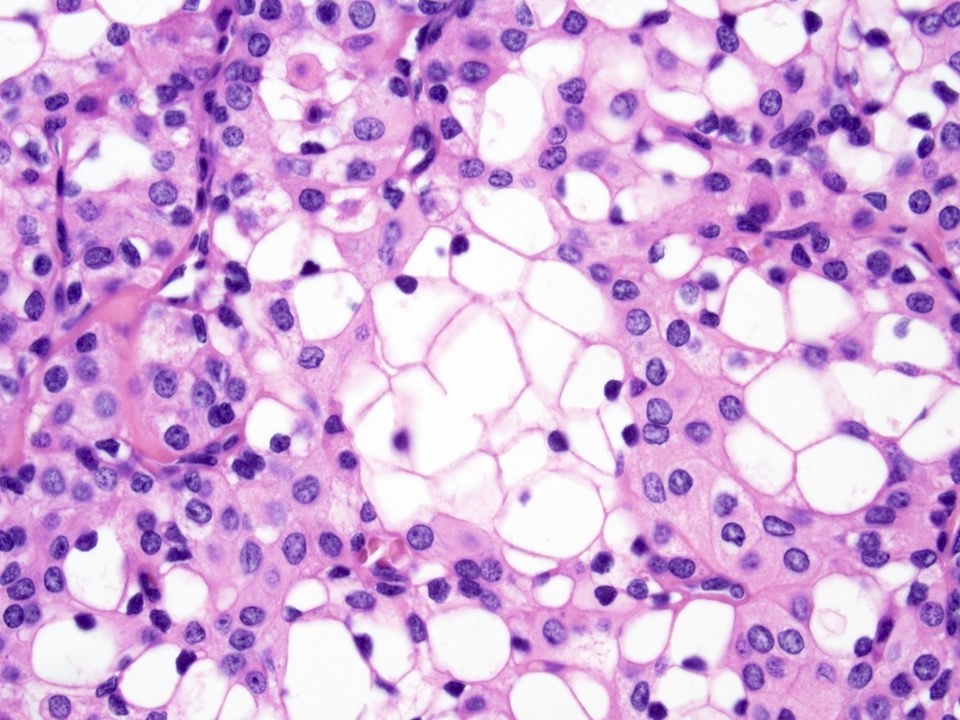
Low grade salivary gland tumor composed of bland monomorphic tumor cells with clear to eosinophilic cytoplasm, arranged in nests, trabeculae and cords in a hyalinized stoma
Essential features
Rare salivary gland neoplasm
Most commonly involves intraoral minor salivary glands (> 80%)
2 stroma types: dense hypocellular hyalinized tissue, juxtaposed to a desmoplastic stroma, is virtually pathognomonic
Molecularly defined by presence of EWSR1 fusion (ATF1 most common partner)
Low grade with few nodal and distant metastases
Terminology
Clear cell carcinoma (2017 WHO)
Clear cell adenocarcinoma (2008 AFIP )
Clear cell carcinoma, not otherwise specified (2005 WHO)
ICD coding
ICD-9: 142.9 - malignant neoplasm of salivary gland, unspecified
ICD-10: C08.9 - malignant neoplasm of major salivary gland, unspecified
Definitive diagnosis may be difficult on histology alone due to its wide range of appearance and both morphologic and immunohistologic overlap with other entities in the differential; thus, FISH analysis for ESWR rearrangements is often necessary
Radiology description
Nonspecific findings, including well demarcated and isointense on T1 weighted, and hyperintense on T2 weighted imaging (AJNR Am J Neuroradiol 2007;28:127)
Radiotherapy, alone or in combination with chemotherapy, may play a role in recurrent disease; however, evidence is weak (Crit Rev Oncol Hematol 2016;102:55)
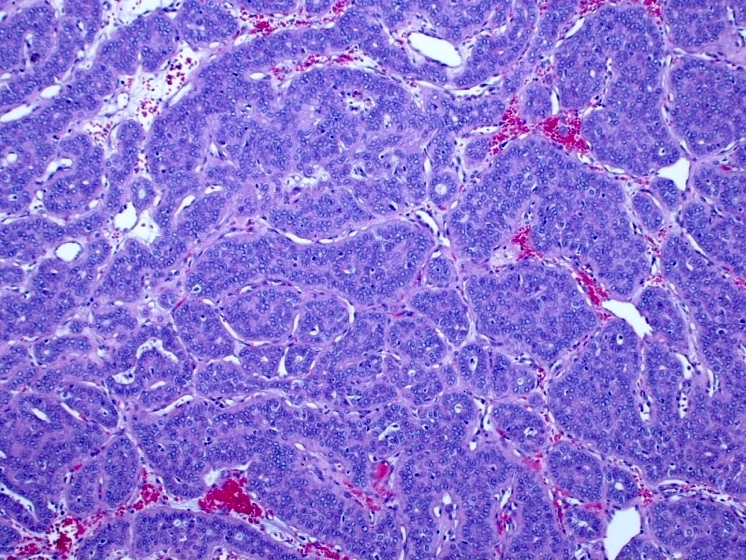
Monomorphic cells with clear or eosinophilic cytoplasm arranged in anastomosing nests, trabeculae or cords (Am J Surg Pathol 1994;18:74)
2 stroma types: dense hypocellular hyalinized tissue, juxtaposed to a desmoplastic stroma that may appear myxoid, is virtually pathognomonic (Head Neck Pathol 2013;7:S20)
Contributed by Pooja Navale, M.D. (Case #483), Tony Ng, M.D., Ph.D. and Erin Chapman, M.D
Circumscribed lesion
Cord-like to trabecular architecture
Hyalinzied stroma
Anastomosing nests
Monotonous cells
Clear to eosinophilic cytoplasm
Bland nuclei
Centrally placed nuclei
Inconspicuous nucleoli
Soft palate mass
Clear cell proliferation
Base of tongue mass
Clear cell and columnar phenotype
Buccal mass
Nests and cords of clear cells
Submucosal tissue
Posterior maxilla submucosal tumor
Islands and cords of tumor cells
p40
PASD
Cytology description
Cohesive clusters of monotonous epithelial cells with abundant clear cytoplasm, uniform round to oval nuclei, granular chromatin, small nucleoli, nuclear grooves and intranuclear cytoplasmic inclusions
Lacks rearrangements with PBX1, ZNF444 and POU5F1, suggesting it is not the salivary gland equivalent of soft tissue myoepithelial tumor (Head Neck Pathol 2013;7:S20)
Sample pathology report
Oropharynx, right base of tongue, complete excision:
Hyalinizing clear cell carcinoma (see comment)
Comment: The carcinoma is composed of cells with abundant clear to variably eosinophilic cytoplasm, which are arranged in long cords, interconnecting trabeculae and nests. Nuclei are centrally placed with inconspicuous nucleoli. The background is remarkable for a myxoid appearing stroma that is sharply demarcated from a hyalinized basement membrane-like material. There is no evidence of necrosis or perineural invasion. Immunohistochemical stains were performed with the following results: cytokeratin and p40 positive; S100, SMA and calponin negative.
A mass from the soft palate of a 54 year old woman is resected. A representative image of the tumor is shown above. Which of the following statements is true regarding this entity?
By definition, it does not contain mucin, making it distinct from mucoepidermoid carcinoma
Microscopically, these are characterized by 2 stroma types: dense hypocellular hyalinized tissue, juxtaposed to a desmoplastic stroma that may appear myxoid; this finding is virtually pathognomonic
Most behave in an aggressive fashion
These carcinomas should be graded according to the 3 tiered system described by Milchgrub
While it can arise from the minor salivary glands, the majority occur in the parotid
Board review style answer #1
B. Microscopically, these are characterized by 2 stroma types: dense hypocellular hyalinized tissue, juxtaposed to a desmoplastic stroma that may appear myxoid; this finding is virtually pathognomonic. Most cases of hyalinizing clear cell carcinoma (HCCC) arise from the intraoral minor salivary glands, commonly those of the base of tongue and soft palate. A minority occur in the major salivary glands. Mucinous differentiation can be seen in up to 50% of cases, ranging from focal dot-like to diffuse. This can make the distinction from mucoepidermoid carcinoma challenging. There is no formal grading system for HCCC (Milchgrub first described HCCC, however). While most tumors are low grade, there are a few cases in the literature with high grade transformation. Finally, HCCC is characterized microscopically by cells with abundant clear to variably eosinophilic cytoplasm, which are arranged in long cords, interconnecting trabeculae and nests. The background is remarkable for 2 stroma types: dense hypocellular hyalinized tissue, juxtaposed to a desmoplastic stroma that may appear myxoid. The latter finding is virtually pathognomonic.
Hyalinizing clear cell carcinoma of salivary gland is most commonly associated with which of the following gene fusions?
CRTC1 (MECT1)::MAML2
ETV6::NTRK3
EWSR1::ATF1
EWSR1::CREM
EWSR1::PBX1
Board review style answer #2
C.EWSR1::ATF1. Greater than 80% of hyalinizing clear cell carcinomas (HCCCs) have EWSR1::ATF1 fusions. Albeit, anchored multiplex polymerase chain reaction has demonstrated a novel variant EWSR1::CREM fusion in a minority of cases. This finding is biologically justified as CREM and ATF1 both belong to the CREB family of transcription factors. Soft tissue myoepithelial tumors (SMET) also harbor EWSR1 rearrangements. The partner genes in these neoplasms include PBX1, ZNF444 and POU5F1, suggesting that HCCC is not the salivary gland equivalent of soft tissue myoepithelial tumor. HCCC can be difficult to discriminate from mucoepidermoid carcinoma (MEC). Both can have mucinous differentiation. The former, however, possesses a characteristic myxoid appearing stroma that is sharply demarcated from a hyalinized basement membrane-like material. MEC predominantly affects the parotid and has a greater tendency for cysts lined by goblet cells rather than a cord-like or anastomosing trabeculae architecture. Lastly, MEC contains MAML2 fusions.
Prominent papillary architecture with oncocytic cells
Microscopic (histologic) description
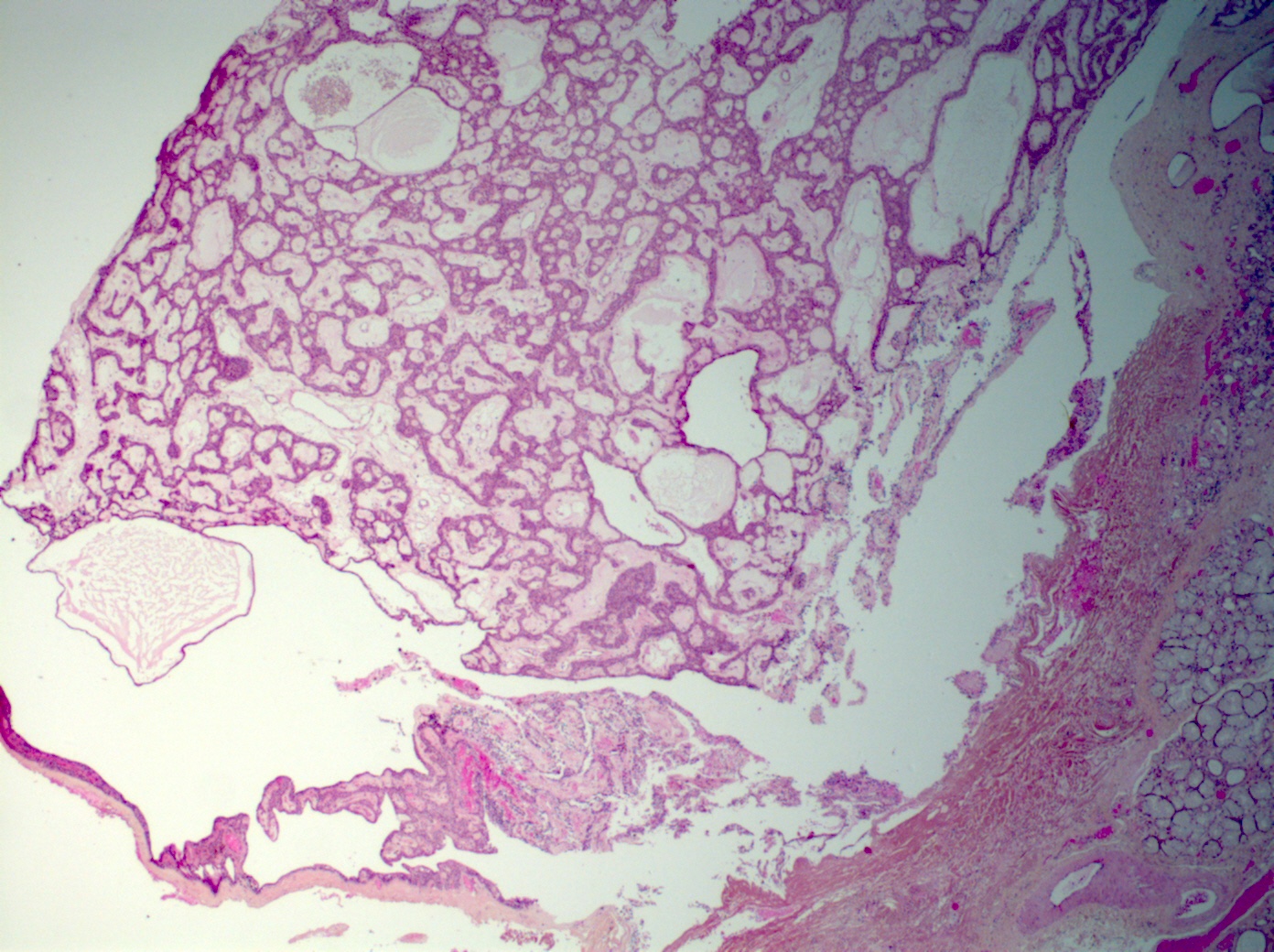
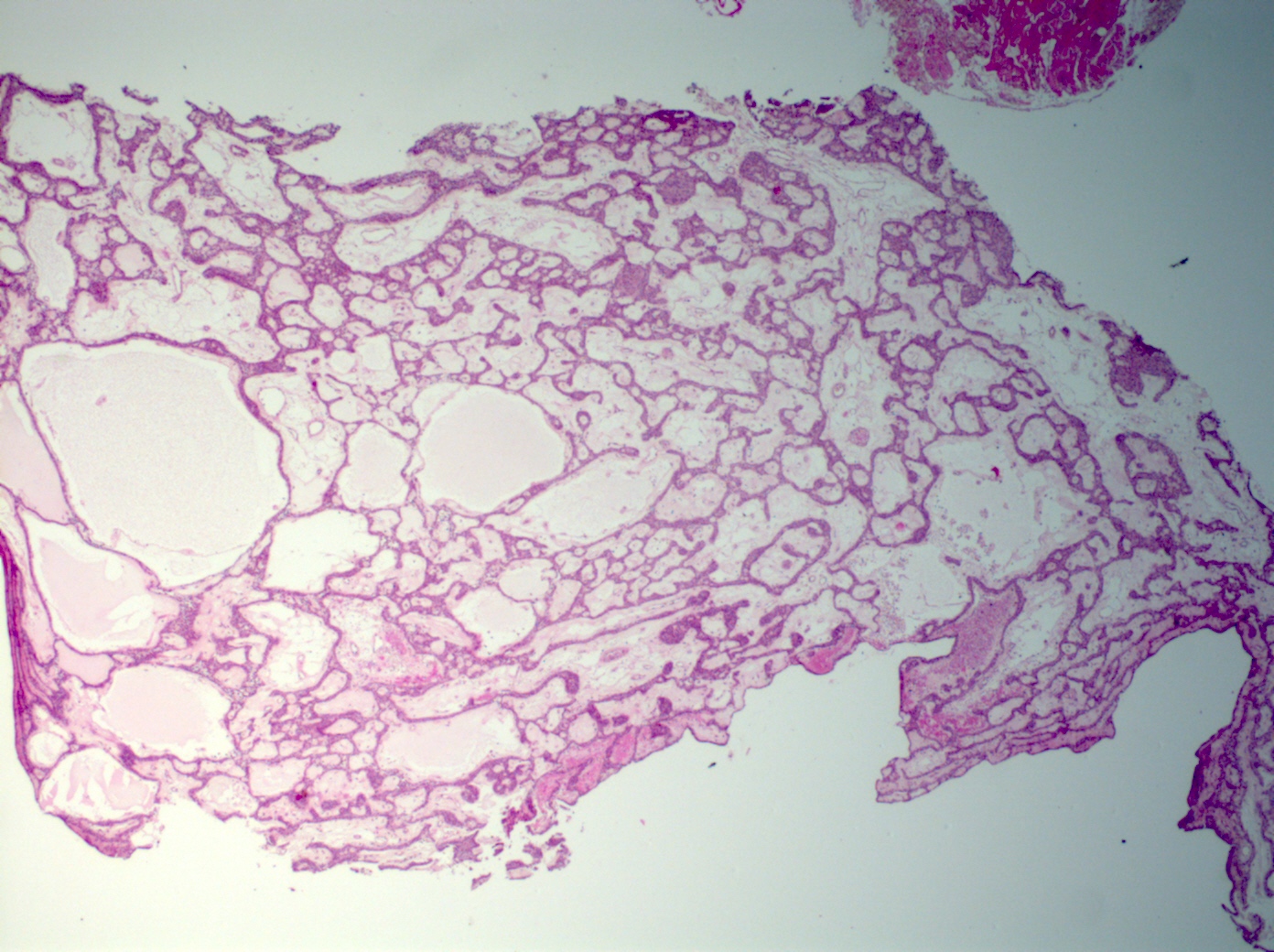
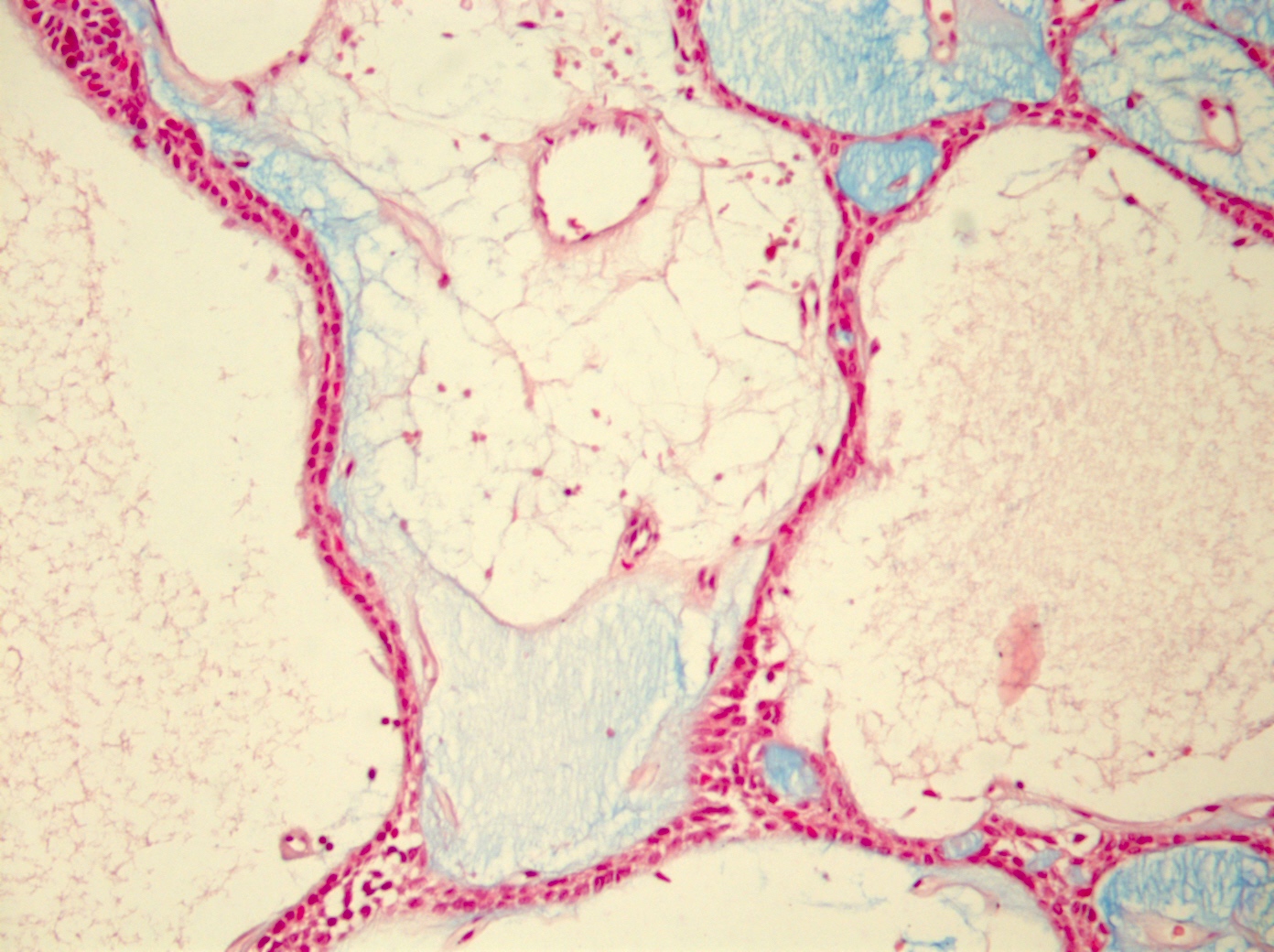
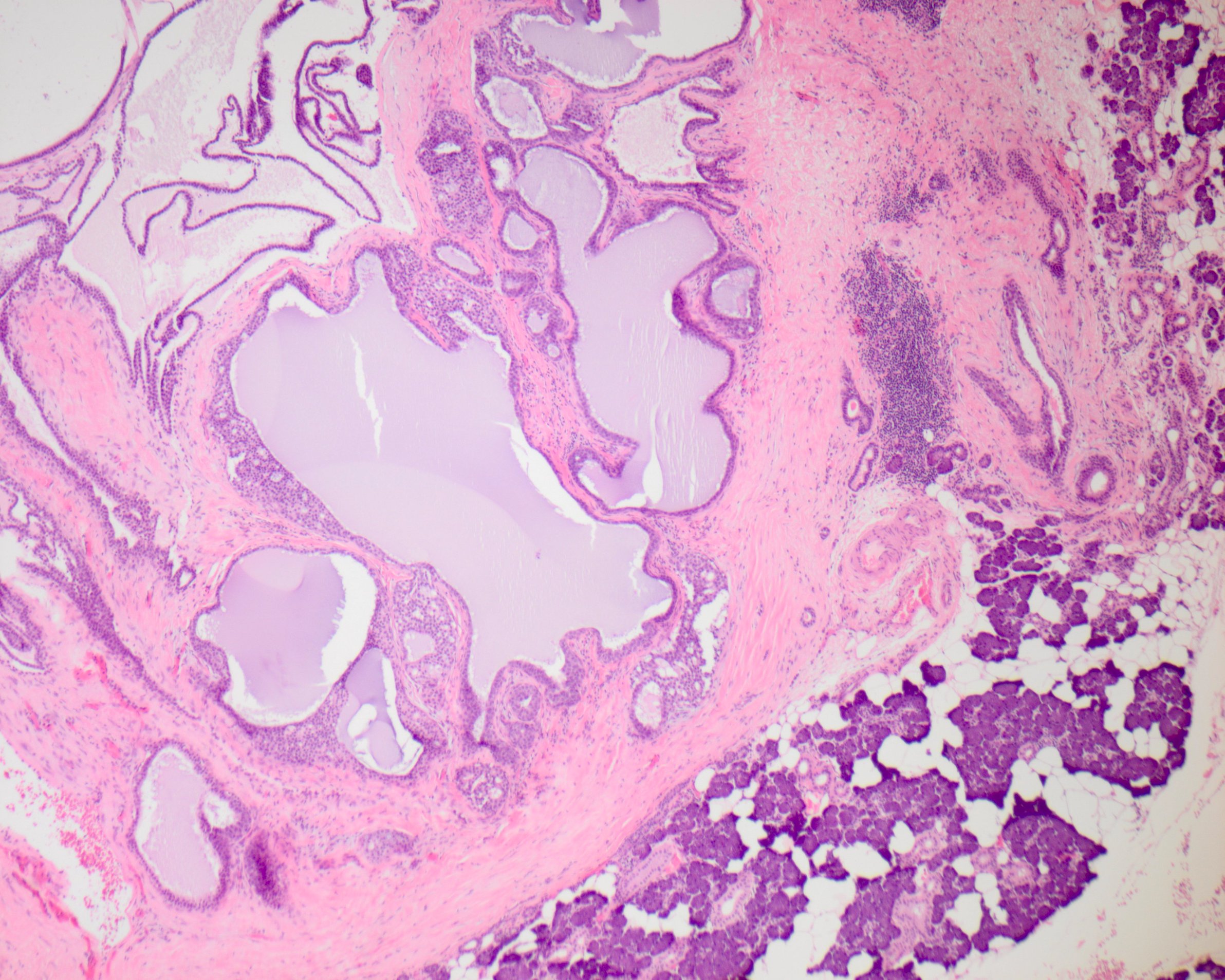
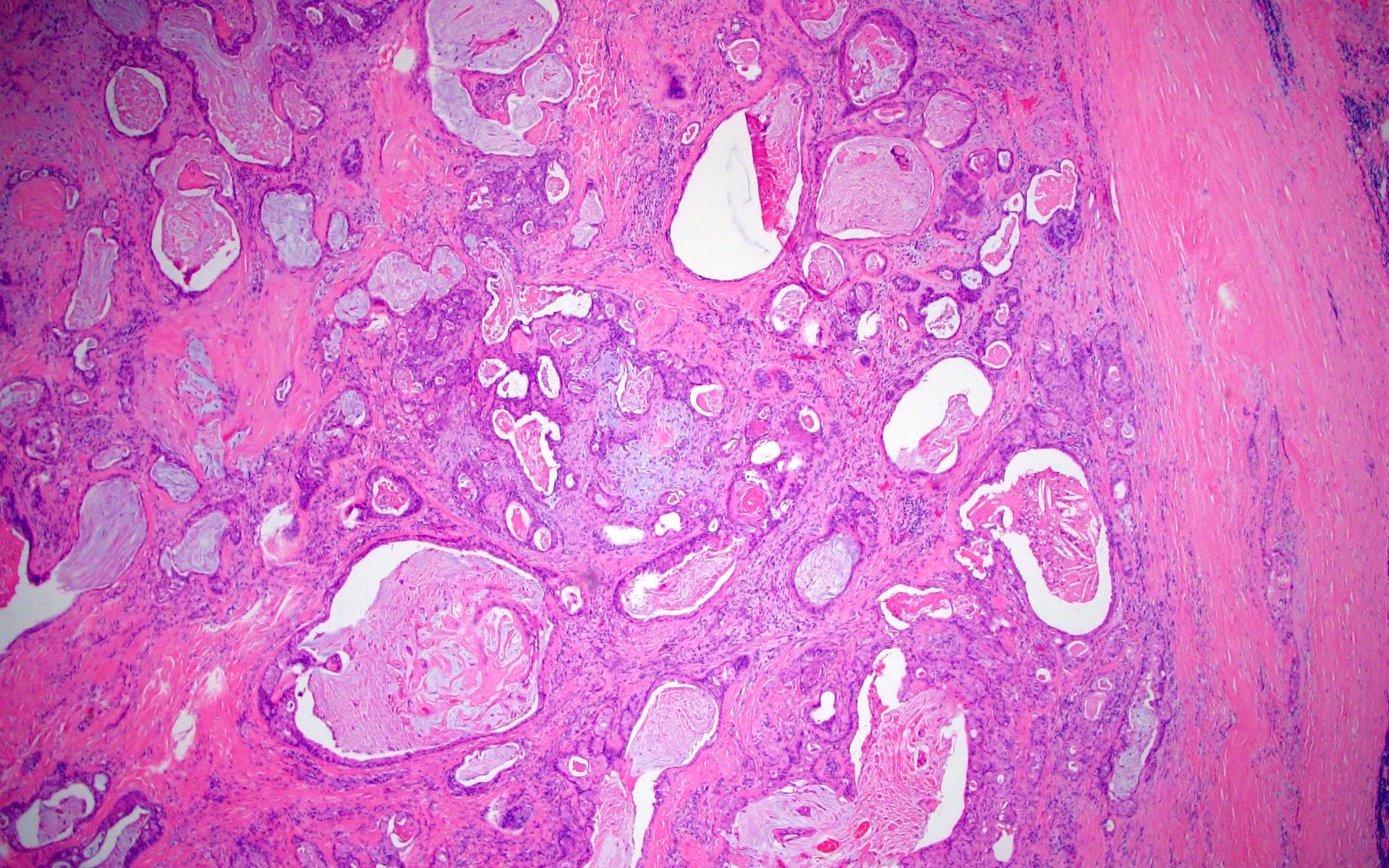
Uni or multiloculated cystic lesion (multiloculated growth is more common)
Well circumscribed, with peripheral entrapment of benign salivary gland tissue
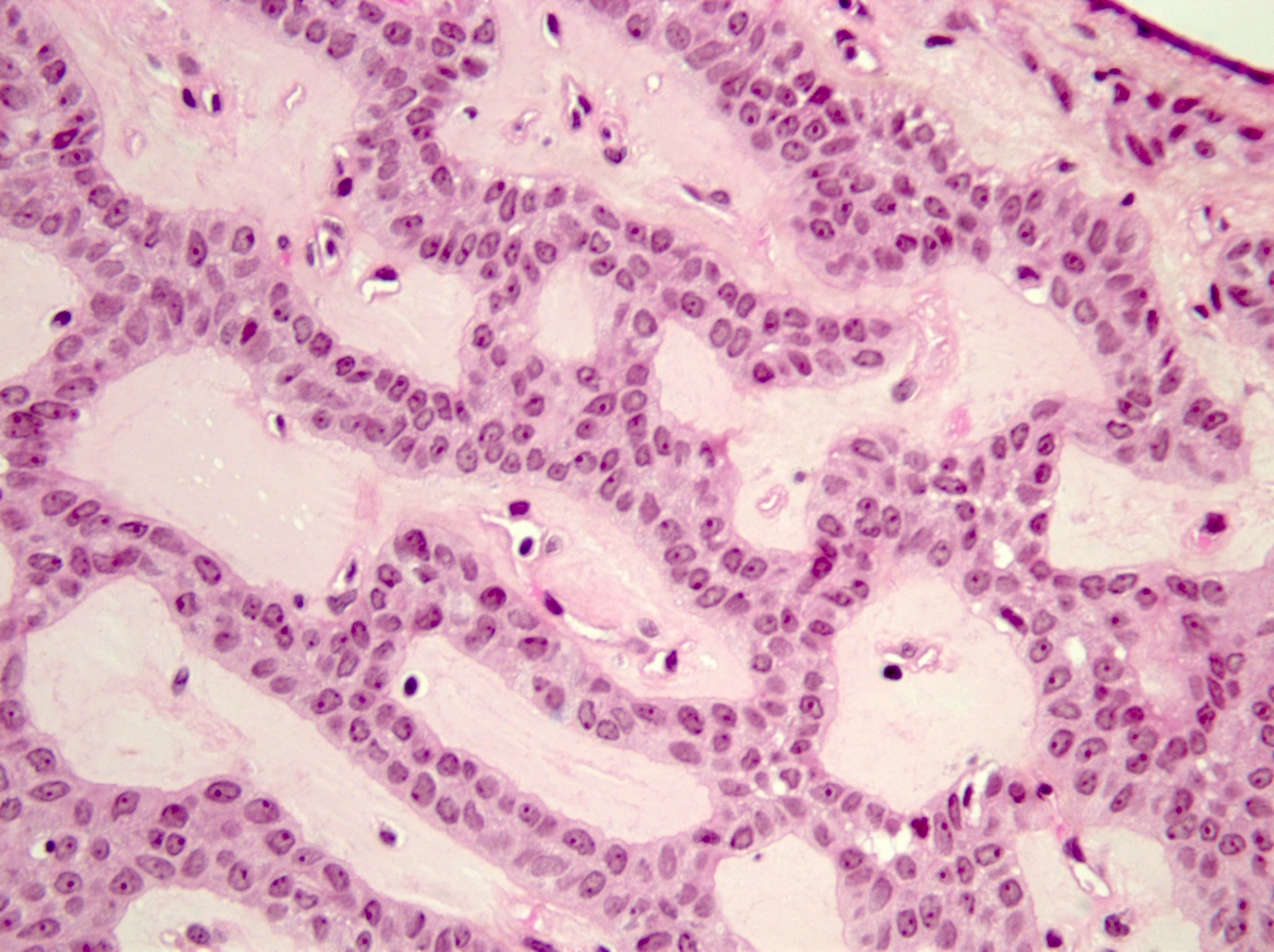
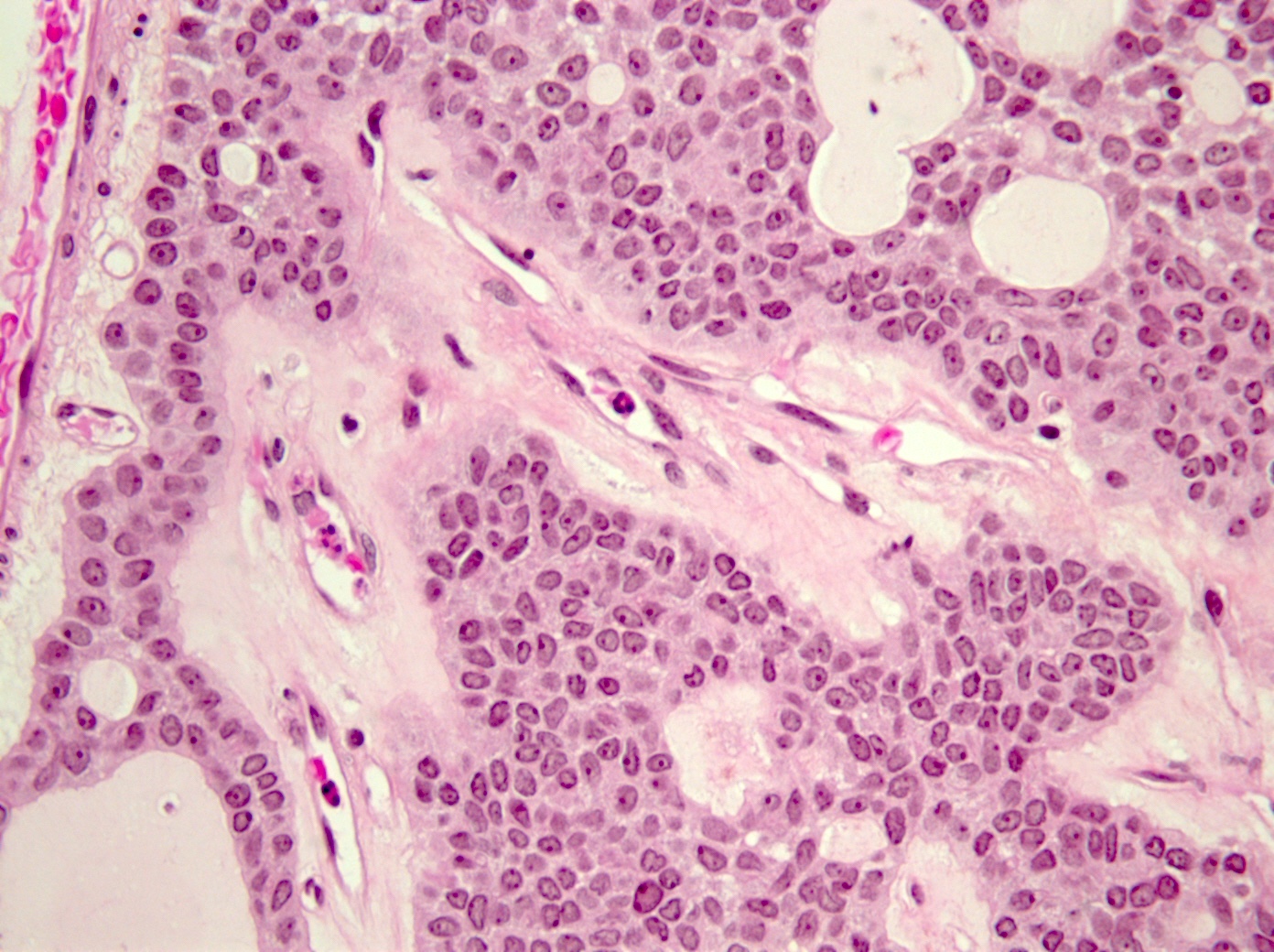
Simple papillary architecture, should not have complex architecture, mitoses or atypia
Lining epithelial cells are commonly a mixture of columnar, cuboidal and oncocytic cells
May also see mucinous, squamous and rarely ciliated cells
Mucinous cystadenoma is rare; lacks architectural and nuclear atypia
Consider unicystic mucoepidermoid carcinoma in the differential diagnosis
Prominent multiloculated / multicystic growth pattern gives a low power appearance of more lumens than epithelial cells
Simple papillary projections and true papillae are common; however, complex papillary tufting should alert the pathologist to other differential diagnoses (e.g. intraductal carcinoma)
Resembles apocrine intraductal carcinoma of the breast with monotonous population of neoplastic cells usually filling the duct space with large nuclei and prominent nucleoli
May have cribriform, micropapillary or solid growth pattern
Reactive extravasation of mucin lined by compressed granulation tissue containing muciphages and inflammatory cells
Not a true cyst with epithelial lining, although adjacent ductal epithelium may be seen
Most commonly found in the lower labial mucosa / buccal mucosa
Board review style question #1
Which of the following FISH tests is useful in ruling out malignancy in equivocal cases of cystadenoma with mucinous metaplasia?
ETV6
EWSR1
MAML2
MYB
PLAG1
Board review style answer #1
C. MAML2 is positive in up to 80% of low grade mucoepidermoid carcinoma. Mucinous metaplasia may occur in cystadenoma. Typically, these cases will lack intermediate cells and infiltrative edges seen in cases of mucoepidermoid carcinoma. However, for equivocal cases, a negative MAML2 FISH analysis can provide additional support to exclude malignancy.
Which immunohistochemical panel would be most useful in supporting the diagnosis of macrocystic secretory carcinoma over that of cystadenoma?
GATA3+, S100+, SOX10+, MUC4+
KIT+, SOX10+, mammaglobin+, MYB+
Mammaglobin+, CK20+
S100-, p63+, P40+
Board review style answer #2
A. A panel type approach is often beneficial in salivary gland tumors. GATA3 is a nuclear stain that is positive in many malignancies, particularly breast and urothelial carcinomas. In the salivary gland, GATA3 stains secretory carcinoma, salivary duct carcinoma and other types of salivary gland neoplasms (Head Neck Pathol 2013;7:311). The addition of S100+, SOX10+ and MUC4+, in addition to mammaglobin+ weighs against cystadenoma and with the correct morphology, supports macrocystic secretory carcinoma. Nuclear stains are generally easier to interpret than cytoplasmic stains, like mammaglobin, due to high background staining. S100 stains most salivary gland neoplasms including secretory carcinoma and is not specific for it. KIT is seen in adenoid cystic carcinoma.
49 year old man with inverted ductal papilloma in buccal mucosa of mandible (Pathol Int 2006;56:457)
70 and 72 year old men with benign sublingual tumor and parotid papilloma with microinvasion and intraparotid lymph node metastases (Arch Pathol Lab Med 2000;124:291)
Treatment
Surgery; does not recur
Microscopic (histologic) description
Intraductal papilloma
Centered in excretory ducts of minor salivary gland
Unicystic lesion lined by apillary proliferation composed of bland cuboidal to columnar epithelial cells with fibrovascular cores
Rarely has intermixed mucinous cells
No cytologic atypia and only rare mitotic figures
Inverted ductal papilloma
Generally has central opening that communicates with surface mucosa
Unencapsulated lesion composed of complex endophytic proliferation of non-keratinizing squamous epithelium which resembles inverted papilloma of nasal cavity
Can have intermixed goblet cells and columnar cells
No cytologic atypia and only rare mitotic figures
Microscopic (histologic) images
Images hosted on other servers:
Upper lip tumor has papillary proliferation of epithelial cells with branching fronds in cystically dilated duct lumen
Cytology description
Compact clusters of papillary monomorphic columnar cells with abundant finely vacuolar cytoplasm; oval nuclei basally located, indistinct nucleol; no squamous cells (Acta Cytol 1999;43:457)
A: secretary granules, rough endoplasmic reticulum, golgi apparatus
and mitochondria; B: microvilli on luminal surface of epithelial cells
appear to be secretory; C: annulate lamellae composed of parallel
arrays of cisternae have small annuli or fenestrae
Uncommon malignant biphasic salivary gland neoplasm composed of luminal ductal cells surrounded by myoepithelial cells
Essential features
Rare primary salivary gland neoplasm
Biphasic neoplasm with a combination of both epithelial and myoepithelial elements
Generally good prognosis; poorer prognosis associated with minor salivary gland location, large tumor (> 4 cm), high proliferation index, margin status, high grade transformation
Rarely presents with facial nerve palsy and lymphadenopathy, may indicate high grade transformation (Medicine (Baltimore) 2017;96:e8988)
Diagnosis
Clinical examination and investigations such as magnetic resonance imaging and fine needle aspiration generally do not provide a definitive preoperative diagnosis
Univariate tumor related predictors of lower disease free survival include margin status, lymphovascular invasion, tumor necrosis, myoepithelial anaplasia (> threefold variation in size, irregular nuclear membranes, coarse chromatin, macronucleoli) (Am J Surg Pathol 2007;31:44)
Multivariate patient related predictors of lower disease free survival include > 80 years at time of diagnosis, worse in African American population, nonsurgical treatment (BMC Ear Nose Throat Disord 2018;18:15)
Poorer prognosis associated with minor salivary gland location, large tumor (> 4 cm), high proliferation index, margin status, high grade transformation (Am J Surg Pathol 2010;34:1258)
Should not be used; a reliable diagnosis of epithelial myoepithelial carcinoma may not be possible on frozen section
Microscopic (histologic) description
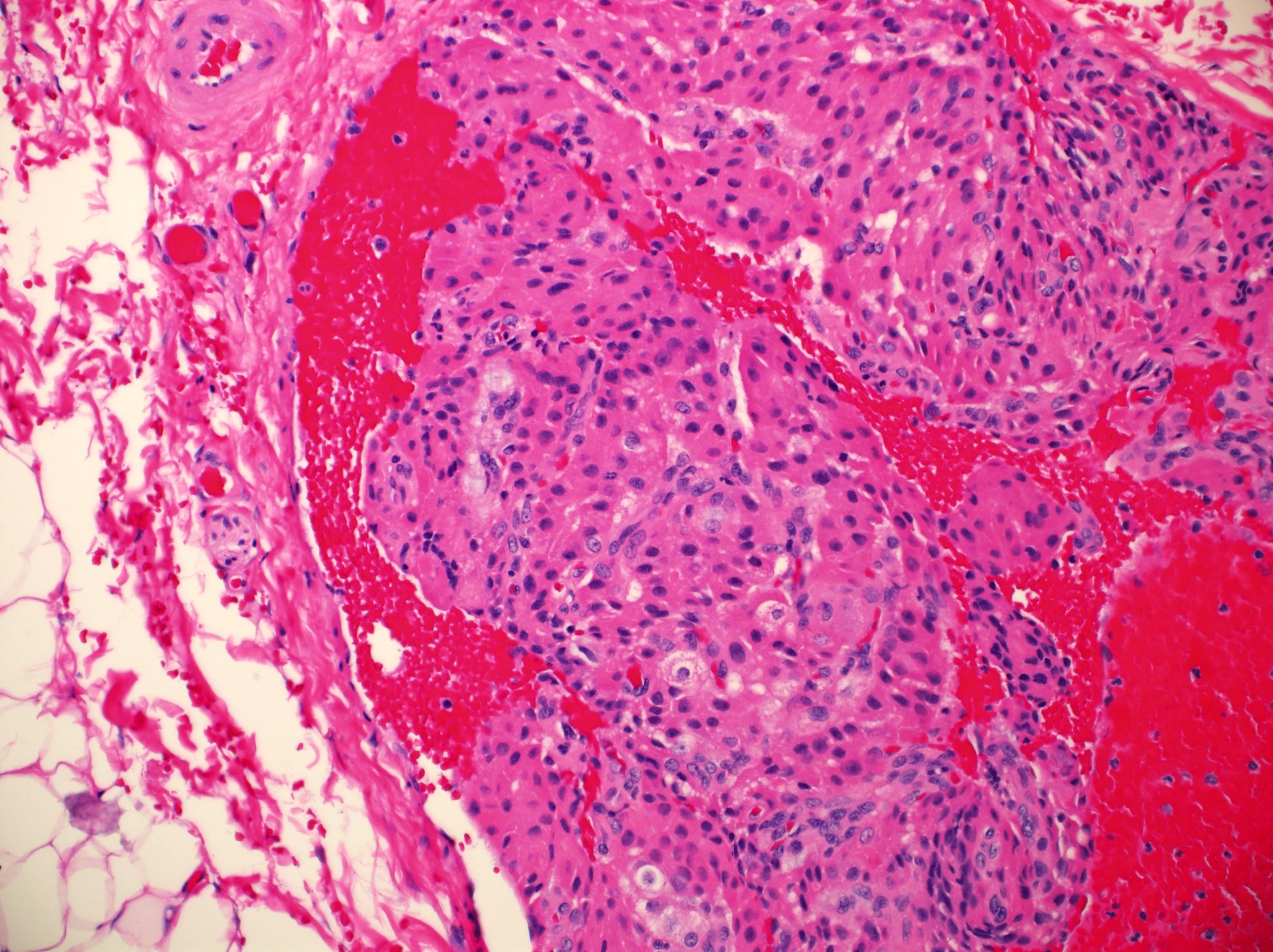
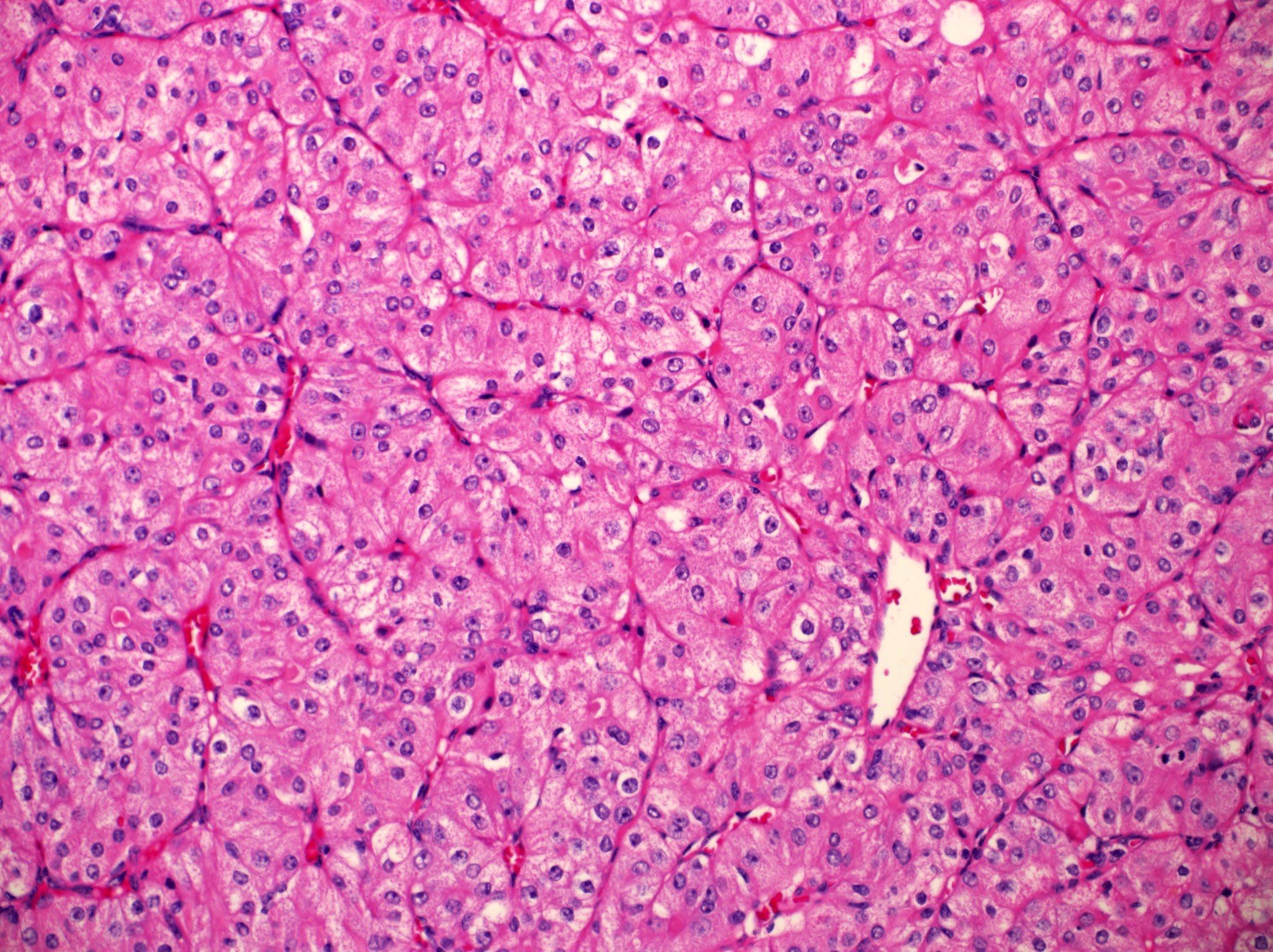
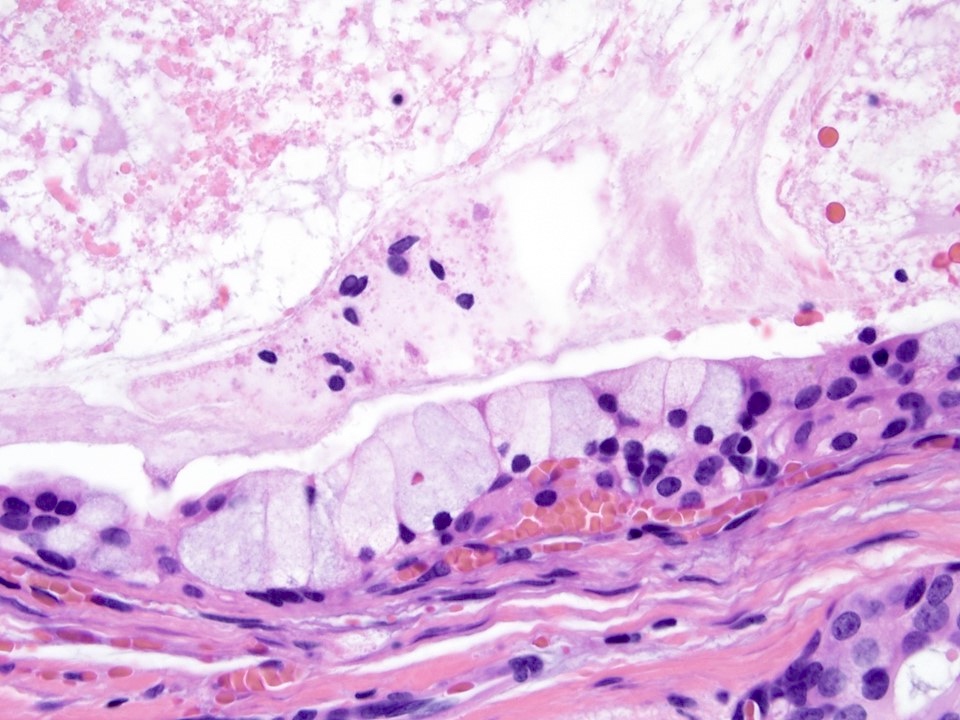
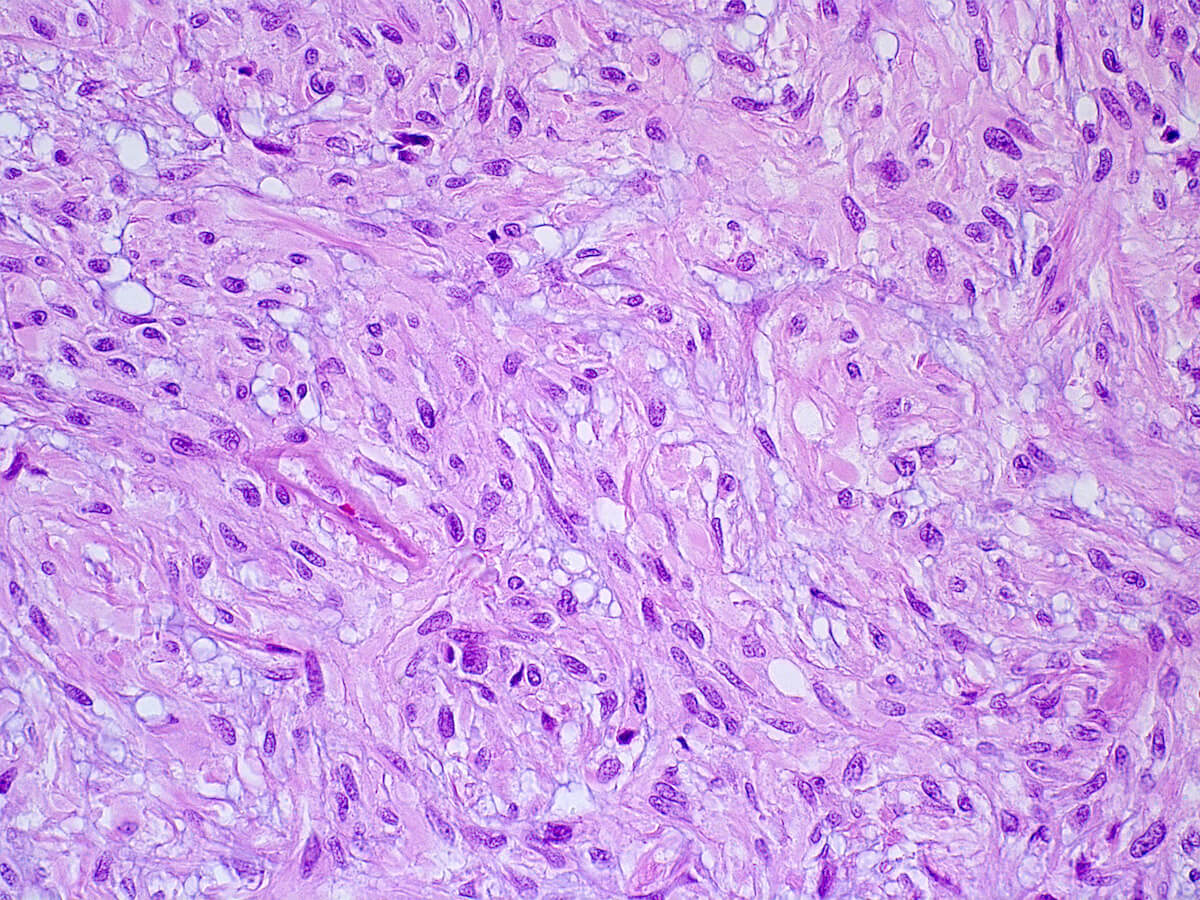
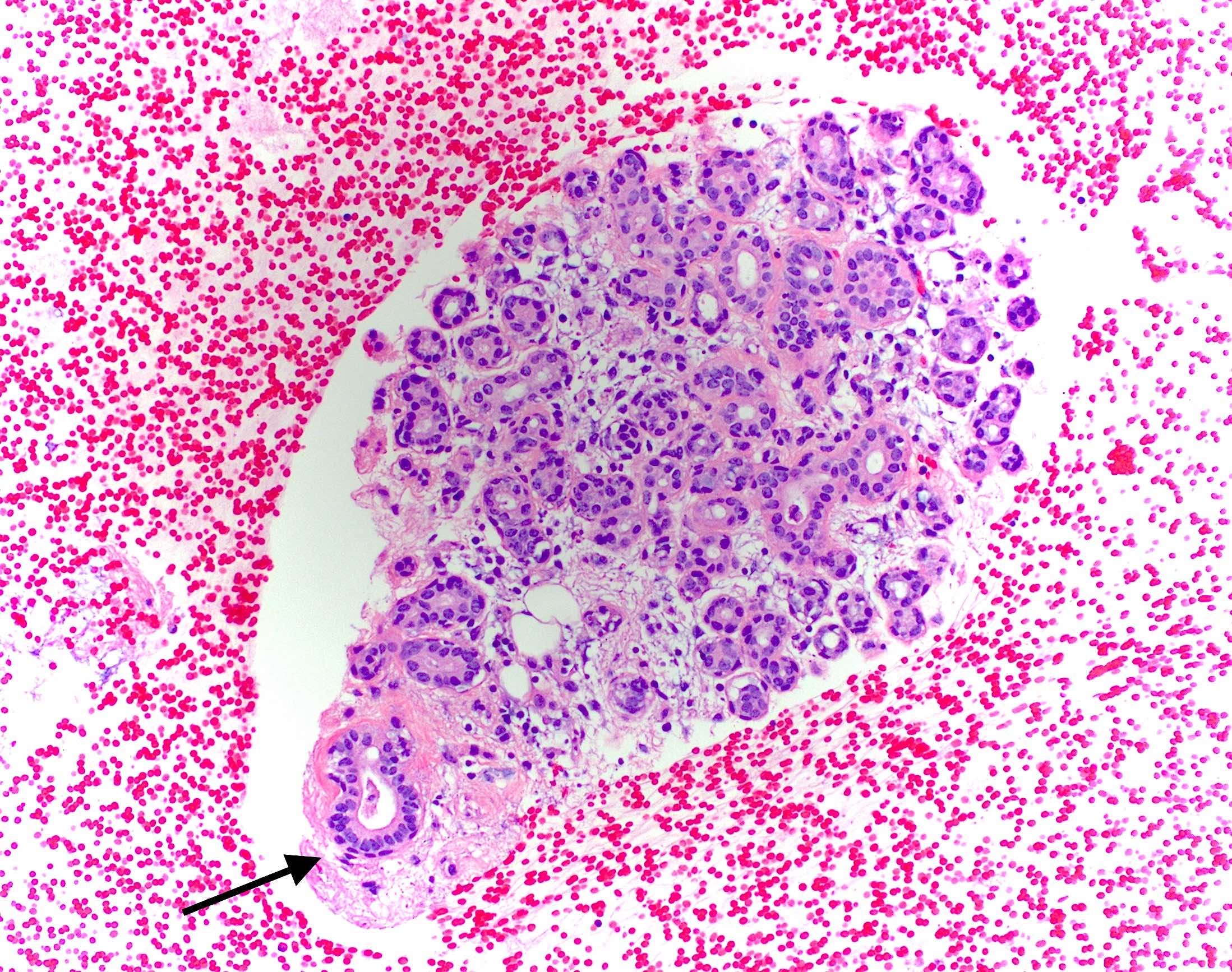
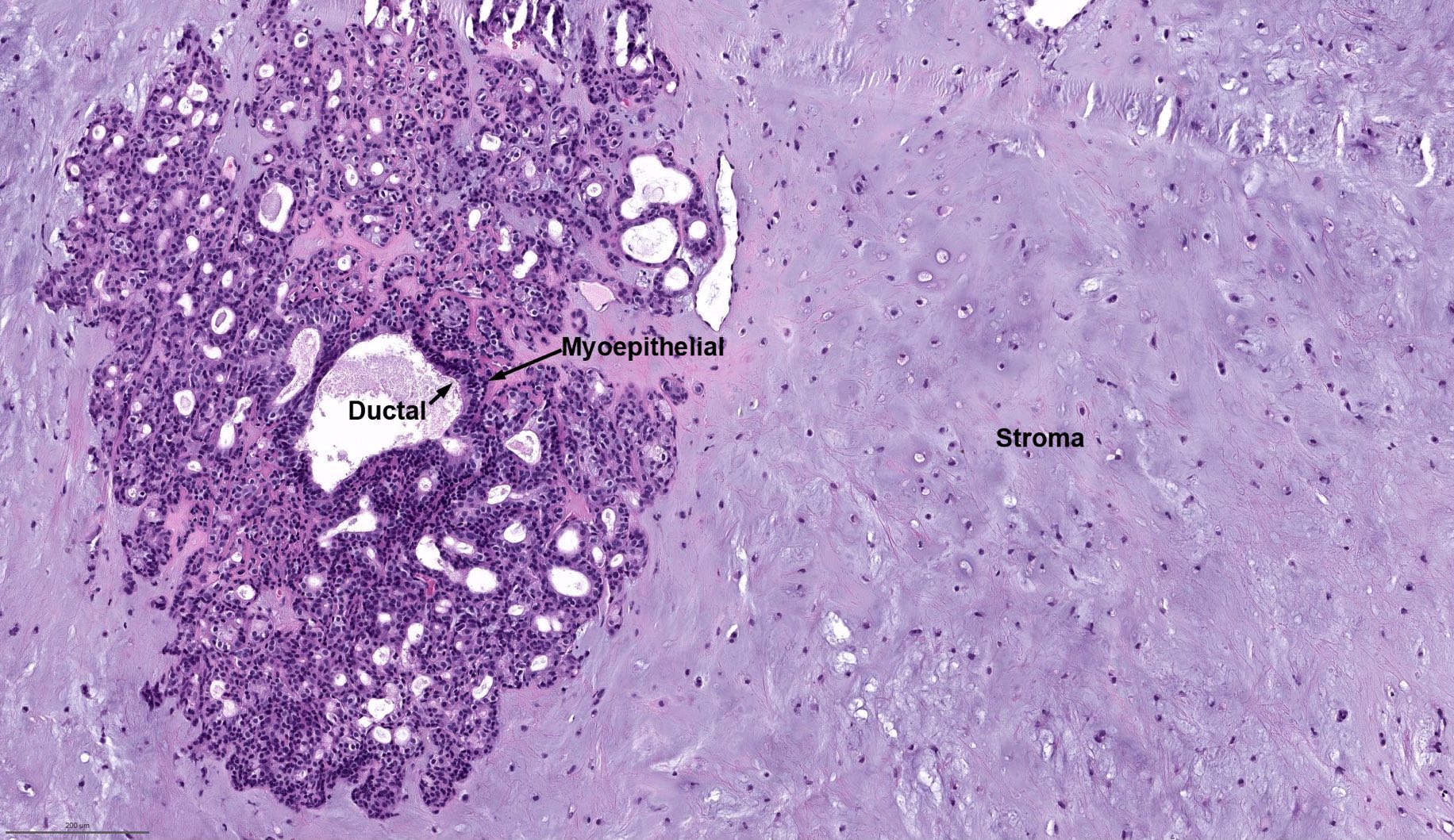
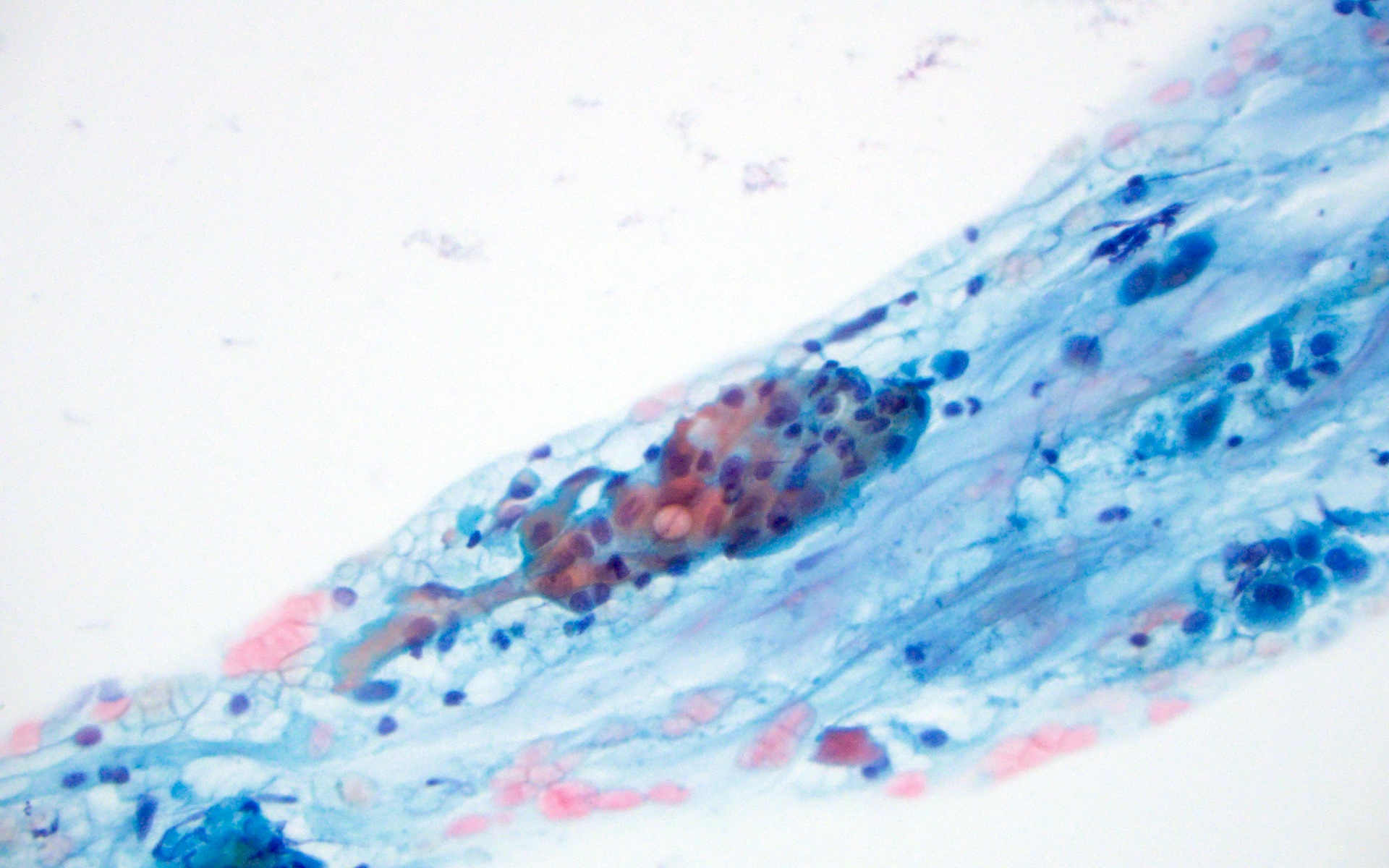
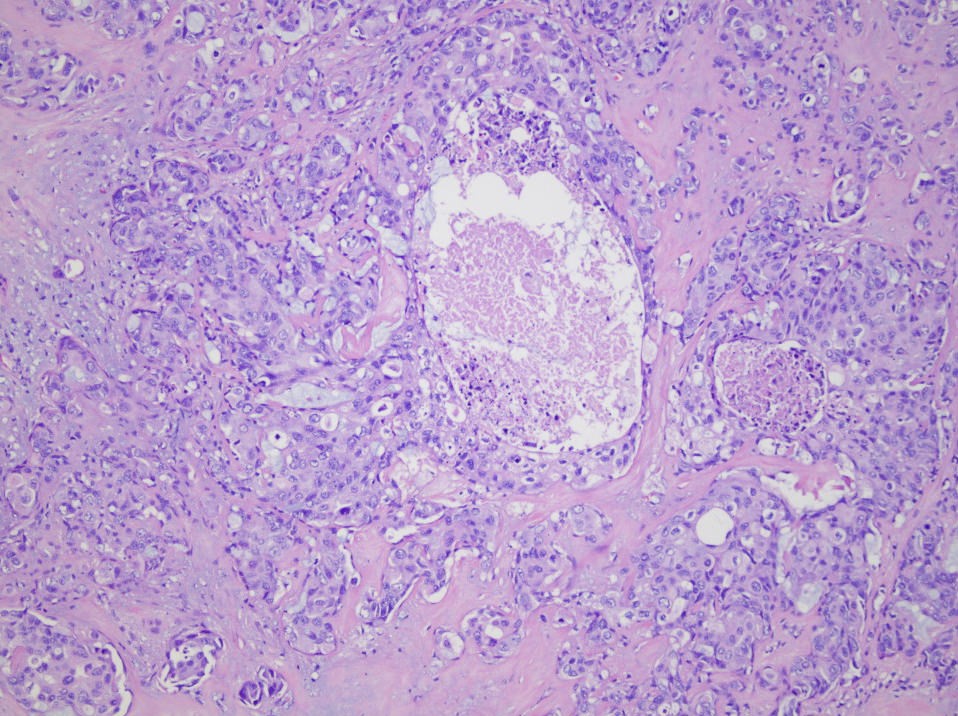
Bilayered arrangement of small luminal cells with eosinophilic cytoplasm and outer myoepithelial cells with clear cytoplasm rich in glycogen (diastase sensitive PAS+)
A few morphologic types may be seen, depending on the proportion of epithelial and myoepithelial cells present
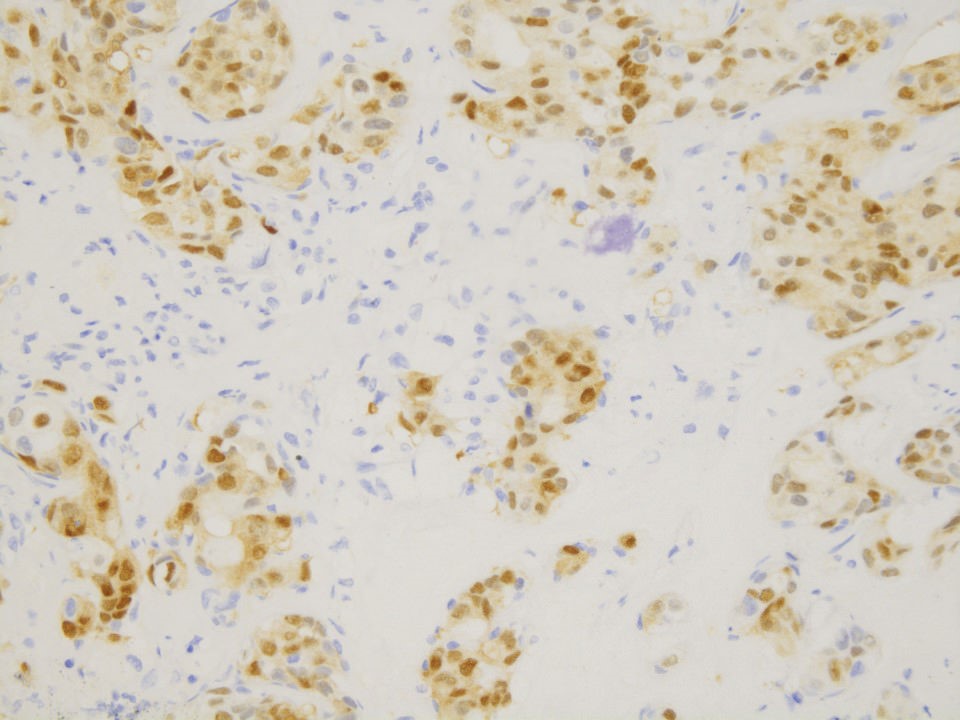
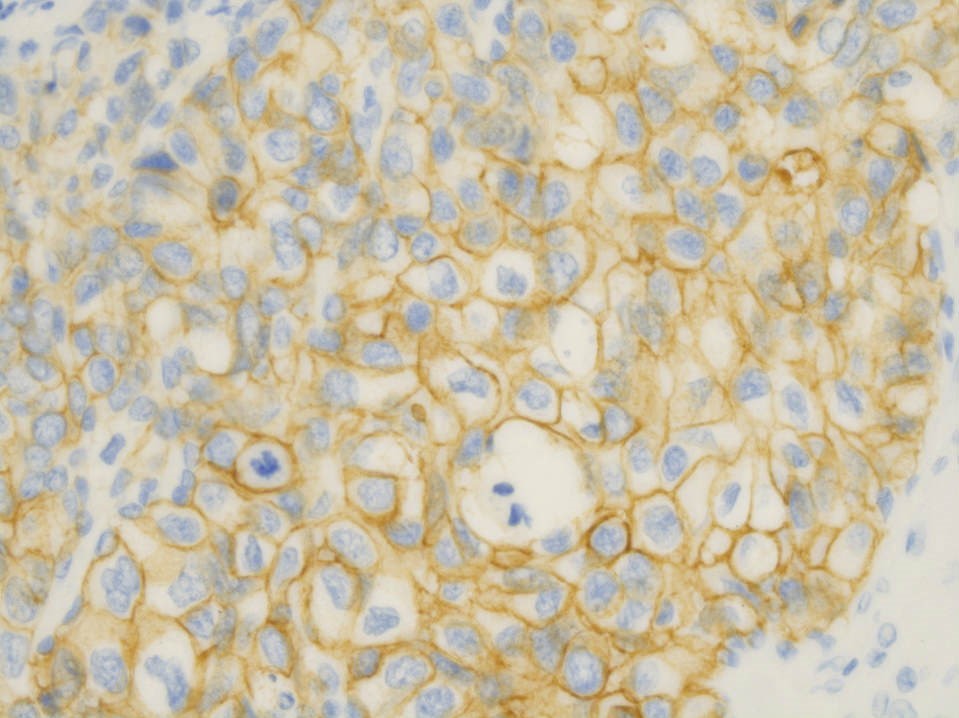
Comment: There is a lobulated and unencapsulated biphasic primary neoplasm. The tumor shows a nodular growth pattern. The tumor is composed of bilayered arrangement of small luminal cells with eosinophilic cytoplasm and outer polygonal clear, rich in glycogen (diastase sensitive PAS+) myoepithelial cells. Immunohistochemically the inner epithelial cells are positive for AE1 / AE3 and EMA, while the outer myoepithelial layer shows staining for p63, smooth muscle actin and S100. There is no evidence of necrosis or high grade transformation.
A 65 year old woman presented with a 3 month history of unilateral cheek lump that recently increased in size. A histologic image of the resection is provided above. What is the most common histological feature associated with this lesion?
Many recent advances in salivary gland molecular alterations
Molecular testing is not generally needed for diagnosis but may be helpful in histologically difficult cases, small biopsies and cytology specimens (Cancer Cytopathol 2018;126:627)
Essential features
Genetic alterations include rearrangements, fusions and amplifications
Trastuzumab given to patients with recurrent or metastatic salivary duct carcinoma that overexpresses HER2 with demonstrated survival benefit (Ther Adv Med Oncol 2022;14:17588359221119538)
This treatment may be supplemented with androgen deprivation therapy if the tumor is androgen receptor positive by immunohistochemistry
Secretory carcinoma may be treated with TRK inhibitors including larotrectinib and entrectinib (Head Neck 2023;45:1315)
NOTCH1 inhibitors for adenoid cystic carcinoma are in the clinical trial phase
MYB acts as coactivator to increase NR4A3 transcription
Promotes proliferation genes such as MYC
Promotes expression of microRNAs that repress expression of tumor suppressor genes
Subset with t(8;9) → MYBL1::NFIB
Activating NOTCH1 mutations (9q34.3)
Notch1 into active fragment, ICN1
ICN1 is transferred into the nucleus and promotes gene transcription of Hes1, c-Myc, interleukin 7 receptor α chain (IL7Rα) and insulin-like growth factor 1 receptor (IGF1R)
Which of the following is characteristic of mucoepidermoid carcinoma and not squamous cell carcinoma?
ETV6 gene rearrangements
EWSR fusions
HER2 amplification
MAML2 gene rearrangements
Board review style answer #1
D.MAML2 gene rearrangements are seen in mucoepidermoid carcinoma but not squamous cell carcinoma. Answer C is incorrect because HER2 amplification is seen in salivary duct carcinoma. Answer B is incorrect because EWSR fusions are seen in clear cell carcinoma. Answer A is incorrect because ETV6 gene rearrangements are seen in secretory carcinoma.
H&E and androgen receptor immunostain are shown. What is the best diagnosis for the parotid tumor?
Mucoepidermoid carcinoma
Salivary duct carcinoma
Secretory carcinoma
Warthin tumor
Board review style answer #2
B. Salivary duct carcinoma. The image shows nuclear androgen receptor positivity, consistent with salivary duct carcinoma. This immunostain is helpful not only for diagnosis but also for treatment. Answers A, C and D are incorrect because they are not characterized by androgen receptor positivity.
Tumor extension (intra or extraglandular), to adjacent structures
Status of resection margins
Vascular invasion
Perineural invasion
Lymph nodes: for each level, number obtained, number involved by tumor, size of largest nodal metastases, presence of extracapsular spread, side, if appropriate - major nerve (e.g. facial) or vessel (e.g. jugular vein), bone, skin involvement
Normal salivary gland tissue at a site where normally not present
Usually in head and neck
Due to abnormal persistence and development of vestigial structures, misplacement of salivary gland rests along embryologic pathways of migration during development or by salivary differentiation from remnants of primitive embryologic structures
Intranodal (periparotid most common) or extranodal
May undergo same pathologic processes as usual salivary gland tissue
Most common neoplasm is Warthin tumor
Intranodal
More common than extranodal
In infants, most nodes within / near parotid gland contain salivary gland tissue, usually in medullary portion of node
Frequent but less common in adults
Usually composed of intercalated and intralobular ducts but also serous type acini and immature ducts
Extranodal
May be high or low in head and neck
High: mandible, mastoid bone, external and middle ear, tonsil, mylohyoid muscle, palatine tonsil, gingiva, pituitary gland, cerebellopontine angle; due to abnormalities in migration of embryonic tissue
Low: related to bronchial pouches in lower neck, thyroid gland or parathyroid gland; most commonly at medial border of right sternocleidomastoid muscle near sternoclavicular joint
Case reports
53 year old woman with cerebellopontine angle solitary fibrous tumor with ectopic salivary gland tissue
(Am J Surg Pathol 2004;28:139)
Presents as painless, bilateral enlargement of lacrimal and salivary glands with mild secretory dysfunction
IgG4 related disease is now recognized as systemic disorder, characterized by high serum IgG4, marked infiltration of IgG4 positive plasma cells and severe fibrosis
Diagnosis depends on histologic appearance, elevated ratio of IgG4/IgG, variable elevated serum IgG4 levels
Submandibular gland biopsy is more useful than labial salivary gland biopsy
Corticosteroids and rituximab (by targeting peripheral CD20 positive plasma cells) appear to be effective for IgG4 related diseases
Terminology
Previously called Mikulicz disease and Mikulicz syndrome, but these terms are considered ambiguous and outdated by some sources
Intercalated duct lesions (IDL) encompass a morphologic spectrum that ranges from intercalated duct hyperplasia (IDH) to intercalated duct adenoma (IDA)
These are benign salivary ductal proliferations resembling bilayered (epithelial and myoepithelial) intercalated ducts
Majority (85%) of IDL arise in the parotid gland, followed by the submandibular gland (11%), with a few found in the oral cavity (4%) (Am J Surg Pathol 2009;33:1322)
Pathophysiology
Adenomas have been shown to harbor hotspot HRAS pathogenic variants, while hyperplasia often has CTNNB1 mutations (Head Neck Pathol 2023;17:393)
Etiology
Unknown
Diagrams / tables
N/A
Clinical features
Smaller intercalated duct lesions are frequently identified incidentally on resection specimens (Am J Surg Pathol 2009;33:1322)
Intercalated duct adenomas can manifest clinically, as they can grow to larger sizes
IDL have been proposed to represent a precursor lesion to other neoplasms; this hypothesis is supported by reports of IDL located next to a morphologically distinct tumor, a phenomenon often referred to as a hybrid tumor
IDL may be present in association with other salivary gland neoplasms, such as basal cell adenoma, epithelial myoepithelial carcinoma, basal cell adenocarcinoma, pleomorphic adenoma, mucoepidermoid carcinoma, Warthin tumor and acinic cell carcinoma (Am J Surg Pathol 2009;33:1322)
IDL have also been reported in the setting of chronic parotitis
Diagnosis
Frequently identified incidentally on surgical resection specimens
WHO essential diagnostic criteria: monotonous proliferation of cuboidal ductal cells surrounded by myoepithelial cells, sometimes with acinic cells
Majority of cases reported are small, unifocal lesions typically measuring 1 - 8 mm; most lesions are Am J Surg Pathol 2009;33:1322)
Diffuse or multifocal lesions have also been reported
Gross images
Images hosted on other servers:
Removed parotid tumor
Frozen section description
Salivary gland biphasic epithelial lesion
Frozen section images
N/A
Microscopic (histologic) description
IDL manifest as a nodular, occasionally multinodular, proliferation of cuboidal ductal cells with attenuated myoepithelial cells, sometimes containing acinic cells (Am J Surg Pathol 2009;33:1322)
IDL are subdivided into adenoma (when discrete, well circumscribed or encapsulated) and hyperplasia (when blending with adjacent acini) (Head Neck Pathol 2023;17:393)
Hybrid patterns can be seen; hybrid pattern includes mixed features of a partially encapsulated adenoma-like lesion admixed with irregular hyperplasia-like areas at 1 or more edges
In each architectural pattern, IDL consist of proliferations of small back to back ducts / tubules lined by eosinophilic to amphophilic ductal cells with small bland nuclei; a myoepithelial layer surrounds all the ducts
Microscopic (histologic) images
Contributed by Manish Mahadeorao Bundele, M.B.B.S., M.D.
Parotid lesion
Circumscribed lesion
Peripheral palisading
Irregular border merging
Bland, bilayered ducts
Monomorphic, bland ductal cells
Beta catenin
CAM 5.2
p63
SOX10
Virtual slides
N/A
Cytology description
Smears show cohesive, large tissue fragments of epithelial cells with high N:C ratios and bland oval nuclei, with admixed thin stromal strands (Head Neck Pathol 2016;10:269)
Immunofluorescence description
N/A
Immunofluorescence images
N/A
Positive stains
Immunohistochemically, IDL resemble the staining pattern of normal intercalated ducts
While not yet clinically relevant, molecular sequencing has identified pathogenic mutations, specifically CTNNB1 in hyperplastic and hybrid IDL type lesions; CTNNB1 mutations are also found in basal cell adenoma / adenocarcinoma
HRAS hotspot mutations have been reported in intercalated duct adenomas, which have also been found in epithelial myoepithelial carcinoma
These genetic findings suggest that IDL are truly neoplastic and demonstrate molecular overlap with basal cell adenoma / adenocarcinoma and epithelial myoepithelial carcinoma (Head Neck Pathol 2023;17:393)
Molecular / cytogenetics images
N/A
Videos
N/A
Sample pathology report
Parotid gland, parotidectomy:
Intercalated duct lesion (see comment)
Sections show a nodular lesion composed of small back to back ducts / tubules lined by a bilayered epithelium, with cuboidal luminal cells and flattened abluminal cells. The lesion peripherally merges into adjacent salivary acini.
On immunohistochemistry, SOX10 is diffusely positive, consistent with intercalated duct phenotype. Immunostain for p40 is positive in abluminal cells. Aberrant nuclear beta catenin is also noted in lesional cells.
Comment: Intercalated duct lesions, including hyperplasia and adenoma, are rather uncommon, benign salivary gland lesions that may be associated with other tumor types and may represent a precursor lesion.
The lesion shown above is incidentally found at the periphery of a parotid basal cell adenoma resection specimen. What is the diagnosis?
Basal cell adenocarcinoma
Intercalated duct adenoma
Intercalated duct hyperplasia
Sclerosing polycystic adenoma
Board review style answer #1
C. Intercalated duct hyperplasia. This lesion features bland bilayered ducts with irregular border and merges with adjacent acini. Awareness of this lesion is important as the presence of it adjacent to basal cell adenoma may be misinterpreted as feature of malignancy; however, answer A is incorrect because typical features of tumoral capsular invasion are required for the diagnosis of basal cell adenocarcinoma. Answer B is incorrect because intercalated duct adenoma is well circumscribed or encapsulated. Answer D is incorrect because typical histological features of sclerosing polycystic adenoma, such as a circumscribed salivary gland neoplasm composed of large acinar cells with brightly eosinophilic intracytoplasmic granules and variable ductal and cystic components, including foamy, vacuolated and apocrine cells, are not seen here.
Incidental microscopic finding (70% incidence) during histologic examination of a salivary gland tumor
Predominates in male patients (3:1) in sixth decade of life
More frequent in parotid compared to submandibular gland (3:1)
Hypothesized to be a precursor lesion of salivary gland tumor, especially epithelial myoepithelial carcinoma
Microscopic (histologic) description
Proliferating ducts admixed with acinar cell complexes
Ducts are frequently lined with single layer of cells; on occasion, may have luminal and abluminal lining cells
Acinar cells are characterized by atrophic changes (loss of zymogen granules, decrease in cell volume) resulting in morphologic resemblance to intercalated ducts
Small cuboidal cells with eosinophilic to amphophilic cytoplasm and small, oval nuclei with dispersed chromatin and inconspicuous nucleoli (Cancer 1996;78:958)
Comment: The neoplasm is well circumscribed and consists of a complex intraductal proliferation of epithelial cells arranged in cribriform and papillary patterns. A p63 immunostain highlights the myoepithelial layer surrounding these intraductal nests. Comprising cells contain abundant granular eosinophilic cytoplasm and nuclei with prominent nucleoli. Mitoses are inconspicuous and necrosis absent. Additional immunohistochemical stains were performed and are positive for androgen receptor (AR), while negative for S100 and SOX10.
Which of the following is true regarding this variant of intraductal carcinoma with the following immunophenotype: S100 and SOX10+; AR-?
It is associated with HRAS and PIK3CA hotspot mutations
It is the most common variant
It is the type most likely to exhibit high grade nuclear features
It is usually GCDFP-15+
Board review style answer #1
B. It is the most common variant
The photomicrograph shows an intraductal proliferation of bland appearing cuboidal cells arranged in cribriform and clinging patterns. Nuclei are small and oval with a dispersed chromatin distribution. Immunohistochemical studies were positive for S100 and SOX10, while negative for AR (androgen receptor) and GCDFP-15. This constellation of findings is characteristic of the intercalated duct-like variant, which is the most common of the variants. It is frequently associated with RET fusions, commonly NCOA4-RET. HRAS and PIK3CA hotspot mutations are usually seen in the apocrine variant, which is the form more likely to exhibit higher grade atypia. It has the following immunophenotype: S100-, SOX10-, AR+ and GCDFP-15+. This staining pattern is similar to that of salivary duct carcinoma, leading to some to believe that apocrine intraductal carcinoma may be a precursor to conventional salivary duct carcinoma.
Which of the following is true regarding intraductal carcinoma?
A diagnosis can be made on core biopsy
Has a marked predilection for women
It is most common in the submandibular gland followed by the parotid
No purely intraductal carcinomas have definitively recurred or distantly metastasized
Board review style answer #2
D. No purely intraductal carcinomas have definitively recurred or distantly metastasized.
Intraductal carcinoma involves the parotid (84.6%), intraparotid lymph nodes (5.1%), accessory parotid gland (2.6%), submandibular gland (2.6%) and minor salivary glands (5.1%). Women and men are almost equally affected, with a female to male ratio of 1.5:1. According to the diagnostic criteria outlined by Cheuk et al., a diagnosis of intraductal carcinoma can be made once an invasive component is excluded. This requires thorough sampling or the demonstration of a myoepithelial layer around the epithelial nest by immunohistochemistry. This is more confidently accomplished on an excisional specimen. When confined by a myoepithelial cell layer, no intraductal (or in situ) carcinomas have definitively recurred or distantly metastasized.
Well circumscribed, resembles lipoma at other sites
Median 2 cm (range, 1 - 4 cm)
Gross images
Case #49
Well circumscribed tumor
Images hosted on other servers:
Parotid sialoangiolipoma
Microscopic (histologic) description
Lipoma: bland appearing adipose tissue; osteolipoma or angiolipoma variants exist
Lipoadenoma: mature adipose cells (> 90% mass) and proliferated glandular tissue (sharply demarcated, duct - acinar units or proliferated glands, may resemble sertoliform tubules), oncocytic change, sebaceous differentiation, squamous metaplasia
Sialolipoma:
Mature adipose tissue mixed with acinar, ductal, basal and myoepithelial cells of normal salivary gland
Also duct ectasia with fibrosis, prominent lymphoid infiltrates with nodular aggregates in stroma, oncocytic changes, sebaceous differentiation
Vascular variant is sialoangiolipoma
Microscopic (histologic) images
Case #49
Acini and dilated ducts
Ducts with fibrosis of wall infiltrated by lymphocytes
Peripheral
lipomatous tissue
with central salivary
gland elements
Lipoma-like areas
Images hosted on other servers:
Lower lip tumor
Submandibular sialoangiolipoma
Parotid sialoangiolipoma
Pleomorphic lipoma with classic floret-like cells
Chondroid lipoma
of lip has chondroid
and lipomatous
features
Oncocytic lipoadenoma of parotid
Spindle cell lipoma of parotid gland
Cytology description
Nonspecific findings (Eur Arch Otorhinolaryngol 2008;265:S47); spindle cell lipomas have bland appearing spindle cells in myxoid background, CD34+ mature fat cells; S100 may be negative
Benign parotid mass with sebaceous features and lymphoid stroma
Parotid gland mass
With synchronous squamous cell carcinoma
Cytology description
Mixed population of large and small lymphocytes, plasma cells and occasional tingible body macrophages
3 dimensional, cohesive aggregates of epithelial cells, often with cytoplasmic vacuoles characteristic of sebaceous differentiation, surrounded by layers of basaloid cells (Acta Cytol 2004;48:551)
Low grade mucoepidermoid carcinoma: epithelial islands, ducts and cysts tend to be haphazardly distributed with variable shapes and sizes; usually infiltration of connective tissue or parenchyma; cells have some atypia, cells are mucin+
Normal sebaceous glands: present in 10% of parotid glands but no mass
Warthin tumor: prominent cysts and lymphoid stroma, cysts have bilayered oncocytic epithelium
Undifferentiated carcinoma common / familial in the Inuit and Chinese; presents as unilateral mass of parotid gland, submandibular gland or minor salivary glands in adults
Clinical features
May be associated with uterine lymphoepithelioma-like carcinoma
Metastases common to regional lymph nodes; distant metastases to liver, lung, bone
Treatment with surgery and radiotherapy; relatively good outcome (Br J Radiol 2006;79:52)
Sporadic lymphoepithelial cyst may result from cystic dilation of ducts within intraparotid or periparotid lymph node or branchial cleft remnants
HIV associated lymphoepithelial cyst likely forms due to hyperplasia of intra-salivary gland lymph nodes and associated ductal obstruction (J Int Assoc Provid AIDS Care 2017;16:120)
Sjögren syndrome associated lymphoepithelial cysts arise secondary to infiltration of B cells into the ductal epithelium and their expansion within the striated ducts and subsequent basal ductal cell hyperplasia (Nat Rev Rheumatol 2021;17:333)
37 year old woman with a history of HIV and Hodgkin lymphoma presented with right sided facial swelling for 4 days; 47 year old man with a history of HIV / AIDS and Mycobacterium avium complex (MAC) infection presented with right sided jaw mass for 2 months (J Int Assoc Provid AIDS Care 2017;16:120)
Treatment
Conservative therapy, with institution of highly active antiretroviral therapy medication in HIV related cases (HIV AIDS (Auckl) 2012;4:81)
Surgical treatment not indicated for HIV associated lymphoepithelial cysts unless there is doubt about the diagnosis or there are cosmetic considerations (Head Neck 2018;40:1073)
Repeated fine needle aspiration and drainage, sclerotherapy, radiotherapy, surgery (Head Neck 2018;40:1073)
Clinical images
Images hosted on other servers:
Diffuse swelling involving the left parotid gland
Gross description
Cystic structure containing a serous clear watery straw colored fluid with smooth and glistening inner lining
Gross images
Images hosted on other servers:
Unilocular cyst with straw colored fluid
Frozen section description
Benign lymphoepithelial cyst
Microscopic (histologic) description
Most cases show a unilocular cyst with a thin stratified squamous lining
Ciliated, cuboidal or columnar epithelial lining is seen in rare cases
Epithelium is surrounded by dense polymorphous lymphoid tissue with germinal centers and sinusoidal spaces
Lymphocytes frequently permeate the epithelial cyst lining cells
Benign lymphoepithelial cyst with reactive follicular hyperplasia
Sample cytopathology report
Parotid, left, fine needle aspiration:
Fragments of squamous epithelium, lymphocytes and cyst content (see comment)
Comment: The differential diagnosis includes benign lymphoepithelial cyst, cystic lymphoid hyperplasia, lymphoepithelial sialadenitis, benign cyst with lymph node sampling or a Warthin tumor.
May be isolated or associated with Sjögren syndrome
Histologically characterized by the lymphoepithelial lesion, which is formed by a proliferation of ductal remnants permeated by lymphocytes (Virchows Arch 1999;434:315)
Essential features
May be isolated or associated with Sjögren syndrome
Usually occurs in women
Affects the parotid (90%) and submandibular gland (10 - 15%) with rare involvement of the minor salivary glands
Histologically characterized by the lymphoepithelial lesion, which is formed by a proliferation of ductal remnants permeated by lymphocytes
Indolent behavior; however, continued observation is mandatory because of an increased risk for lymphoma development (MALT lymphoma)
Terminology
Myoepithelial sialadenitis: a misnomer as ultrastructural and immunohistochemical studies showed that the cells involved are not myoepithelial cells but rather basal epithelial cells (Virchows Arch 1999;434:315)
If the submandibular gland is affected in patients with Sjögren syndrome, the parotid glands are usually also involved
Etiology
Cause of lymphoepithelial sialadenitis unassociated with Sjögren syndrome has not been determined (Chin Med J (Engl) 2015;128:493)
Lymphoepithelial sialadenitis in the setting of Sjögren syndrome is likely multifactorial, with environmental and genetic factors causing an abnormal autoimmune response (Pathol Int 2008;58:465)
Positive serum anti SSA, anti SSB or a positive rheumatoid factor and antinuclear antibody titer of 1:320 are present when associated with Sjögren syndrome (Med Clin North Am 2014;98:1407)
Prognostic factors
Indolent behavior; however, continued observation is mandatory due to increased risk for lymphoma development (MALT lymphoma) (Med Oral Patol Oral Cir Bucal 2007;12:E479)
Case reports
18 year old woman with linear cutaneous lupus erythematosus and submandibular sialadenitis (Clin Exp Dermatol 2001;26:56)
Comment: There is extensive chronic inflammation with plasma cells and lymphocytes containing follicles with germinal centers. The infiltrate effaces the parenchyma, resulting in acinar loss. Residual ducts show hyperplasia of their lining as well as permeation by lymphocytes. These glandular complexes represent the lymphoepithelial lesion.
Clonal monocytoid B cells both within and encircling the lymphoepithelial lesions to form halos and anastomosing cords, which can interconnect the lymphoepithelial lesions (Med Oral Patol Oral Cir Bucal 2007;12:E479)
A 40 year old woman complaining of xerostomia, dry eyes and bilateral salivary gland enlargement undergoes excision of her parotid. After receipt of the pathologic diagnosis, her clinician tells her that she is at increased risk for which of the following?
Burkitt lymphoma
Hodgkin lymphoma
Extranodal marginal zone B cell lymphoma
Anaplastic large cell lymphoma
Board review style answer #1
C. Extranodal marginal zone B cell lymphoma. The patient has lymphoepithelial sialadenitis.
High grade carcinoma: ill defined, infiltrative border, heterogeneous internal signal with cystic change and necrosis (Eur J Radiol 2008;66:419)
Low grade carcinoma: overlapping features with benign salivary gland tumors
Case reports
9 year old girl, 16 year old girl and 45 year old man with secretory carcinoma of the parotid gland, cytologically mimicking mucoepidermoid carcinoma or acinic cell carcinoma (Diagn Cytopathol 2016;44:519)
53 year old women with Warthin-like variant of mucoepidermoid carcinoma of the parotid gland, cytologically mimicking Warthin tumor (Diagn Cytopathol 2017;45:1132)
Second most common (10 - 15%) malignant salivary gland tumor
Sheets or loosely cohesive cells without regular acinar organization
Plump tumor cells with abundant granular to vacuolated cytoplasm, indistinct cell borders and variable zymogen secretory granules best seen on Romanowsky type stain
Minimal nuclear atypia and frequent naked nuclei
Marked nuclear pleomorphism, prominent nucleoli, high nuclear/cytoplasmic ratio, necrotic background and loss of acinic differentiation in high grade transformation (Cancer Cytopathol 2021;129:318)
Due to overlapping cytomorphology among various high grade salivary gland carcinomas or salivary gland tumors with high grade transformation, classification of a specific tumor type might not be the most relevant and diagnosis of high grade carcinoma alone should be sufficient for most of the cases regarding the clinical decision making
Malignant basaloid tumor consisting of epithelial and myoepithelial cells in various histologic configurations, including cribriform, tubular and solid
Uniform basaloid cells with scant cytoplasm, oval to angulated hyperchromatic nuclei and indistinct nucleoli
Various architecture patterns, including microcystic, tubular and syncytial clusters
Characteristic extracellular hyaline globules or cylinders of acellular metachromatic stroma with sharp borders best seen on Romanowsky type stain
Marked nuclear pleomorphism, prominent nucleoli, high nuclear/cytoplasmic ratio and necrotic background in high grade transformation (Cancer Cytopathol 2021;129:318)
Which histological diagnosis most likely corresponds to this cytologic aspirate?
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Secretory carcinoma
Board review style answer #1
C. Mucoepidermoid carcinoma. A fragment of intermediate cells with intermingled mucous cells containing orange colored intracytoplasmic mucin is characteristic for a mucoepidermoid carcinoma.
Which histological diagnosis most likely corresponds to this cytologic aspirate?
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Secretory carcinoma
Board review style answer #2
B. Adenoid cystic carcinoma. Basaloid tumor cells with prominent hyaline globules arranging in cribriform pattern are characteristic for an adenoid cystic carcinoma.
Most common submandibular metastatic tumors are metastatic squamous cell carcinoma from upper aerodigestive tract or skin or melanoma to submandibular lymph nodes
Distant metastases to salivary glands also arise from breast, colon, kidney, lung, prostate
Imaging modalities for workup of salivary gland neoplasms include ultrasonography, computed tomography (CT) and magnetic resonance imaging (MRI) (Otolaryngol Head Neck Surg 2021;164:27)
Histologic diagnosis of minor salivary gland tumors generally utilizes incisional or excisional biopsy
SS18 break apart FISH (assay used in diagnosis of synovial sarcoma) is 93% sensitive for diagnosis (Head Neck Pathol 2021;15:1192)
Molecular / cytogenetics images
Images hosted on other servers:
SS18 rearrangement by FISH
Sample pathology report
Right buccal mucosa, excision:
Microsecretory adenocarcinoma, low grade (1.5 cm) (see comment)
No lymphovascular or perineural invasion is present
Margins are uninvolved
Comment: The tumor consists of a well demarcated but focally infiltrative neoplasm consisting of anastomosing microcysts and cords of epithelioid cells with attenuated eosinophilic cytoplasm, prominent basophilic luminal secretions and scant hyalinized stroma. Immunostains show that the tumor cells are diffusely positive for S100 and p63 but negative for p40. Fluorescence in situ hybridization using SS18 break apart probe demonstrates an SS18 rearrangement. The combined morphological and immunohistochemical features support the diagnosis of microsecretory adenocarcinoma, a recently described low grade salivary gland neoplasm that generally has an excellent prognosis.
A 42 year old woman presents for a routine dental cleaning and a small, firm, painless mass involving the hard palate is discovered. At higher power, the tumor cells are monotonous with hyperchromatic nuclei. They show diffuse positivity for S100 and p63 and are negative for p40. Break apart fluorescence in situ hybridization reveals a rearrangement of SS18. What is the diagnosis?
Microsecretory adenocarcinoma
Polymorphous adenocarcinoma
Sclerosing microcystic adenocarcinoma
Secretory carcinoma
Tubular adenoid cystic carcinoma
Board review style answer #1
A. Microsecretory adenocarcinoma. The image shows a well demarcated mass composed of anastomosing microcysts containing prominent basophilic secretions. Answer B is incorrect because polymorphous adenocarcinoma can show tubular and microcribriform architecture with S100 positivity and discordant p63 and p40 staining; however, polymorphous adenocarcinoma typically shows more infiltrative borders and heterogeneous architecture. Answer C is incorrect because sclerosing microcystic adenocarcinoma can show microcystic architecture but demonstrates an infiltrative growth pattern and biphasic cell populations with a relatively abundant desmoplastic stromal component. Answer D is incorrect because secretory carcinoma demonstrates a microcystic architecture and is positive for S100 but tends to show predominantly eosinophilic secretions and is generally negative for p63. Answer E is incorrrect because tubular adenoid cystic carcinoma often shows some microcystic architecture with basophilic intraluminal secretions but shows widely infiltrative borders and at least focal cribriform architecture. Evidence of SS18 rearrangement is highly specific for microsecretory adenocarcinoma, which has been shown to harbor a unique MEF2C::SS18 fusion.
The Milan System for Reporting Salivary Gland Cytopathology (MSRSGC) was developed by an international consortium of experts and endorsed by the American Society of Cytopathology (ASC) and the International Academy of Cytology (IAC)
The effort started in September 2015 in Milan and the atlas was published in 2018
Aims to standardize reporting terminology in order to replace the conventional, descriptive interpretation for salivary gland fine needle aspirations (FNA) for better communication between clinicians and between institutions
Main outputs useful for clinical decisions and lab quality control are risk of malignancy (ROM) and frequency of each diagnostic category
Essential features
Consists of 6 diagnostic categories:
Nondiagnostic
Nonneoplastic
Atypia of undetermined significance (AUS)
Neoplasm (benign and salivary gland neoplasm of uncertain malignant potential [SUMP])
Conditions better classified as salivary gland neoplasm of uncertain malignant potential (SUMP):
Matrix producing carcinomas with basaloid cells falsely interpreted as pleomorphic or basal cell adenoma (ex: adenoid cystic carcinoma, basal cell adenocarcinoma → SUMP with basaloid features)
Carcinomas with oncocytic / oncocytoid cells or prominent lymphocytic infiltrates falsely interpreted as Warthin tumor or oncocytoma (ex: Warthin-like variant of mucoepidermoid carcinoma, mucoepidermoid carcinoma with lymphoid cuffing, acinic cell carcinoma with / without lymphoid infiltrates, secretory carcinoma → SUMP with oncocytic / oncocytoid features)
Carcinomas with bland myoepithelial-like morphology falsely interpreted as pleomorphic adenoma or myoepithelioma (ex: myoepithelial carcinoma, epithelial myoepithelial carcinoma, secretory carcinoma → SUMP, not otherwise specified, with myoepithelial features)
Basal cell adenoma, myoepithelioma and cystadenoma due to overlapping cytomorphology with other malignant tumors
Basaloid neoplasm (risk of malignancy: 27.6%), salivary gland neoplasm with predominant oncocytic cells (risk of malignancy: 20.0%) (Cancer Cytopathol 2018;126:490)
Oncocytic / squamoid subtype (risk of malignancy: 61.1%), basaloid subtype (risk of malignancy: 40.0%) and myoepithelial subtype (risk of malignancy: 18.8%) (Cancer Cytopathol 2018;126:924)
Basaloid features (risk of malignancy: 38.5%), oncocytic features (risk of malignancy: 7.7%), unspecified features (risk of malignancy: 41%) (Cancer Cytopathol 2019;127:377)
Features that are highly suggestive of but not unequivocal for malignancy
Common SM conditions:
Markedly atypical cells with poor preparation or obscuring factors
Limited cytologic features of a specific malignancy (ex: adenoid cystic carcinoma with limited cellular atypia or hyaline globules, mucoepidermoid carcinoma with limited mucus cells or extracellular mucin, secretory carcinoma with limited cytoplasmic vacuolization or papillary formations)
Suspicious cytologic features in a subset of cells but admixed with predominant features of a benign lesion (ex: carcinoma ex pleomorphic adenoma)
Monomorphic population of small lymphocytes suspicious for a low grade lymphoma
Scant large atypical lymphocytes suspicious for a high grade lymphoma or Hodgkin lymphoma
High grade carcinoma (ex: salivary duct carcinoma, lymphoepithelial carcinoma, tumor with high grade transformation, etc.)
Carcinoma with intermediate or multiple grades (ex: mucoepidermoid carcinoma, adenoid cystic carcinoma, myoepithelial carcinoma, etc.)
Other malignancy: lymphoma, sarcoma, metastasis, etc.
Common false positive conditions:
Pleomorphic or basal cell adenoma with prominent hyaline globules falsely interpreted as adenoid cystic carcinoma → better classified as SUMP with basaloid features
Benign tumor or nonneoplastic lesion with squamous or mucinous metaplasia falsely interpreted as mucoepidermoid carcinoma (ex: pleomorphic adenoma, Warthin tumor, chronic sialadenitis → better classified as AUS or SUMP)
Diagnostic tip:
An attempt should be made to subclassify these aspirates into different grades and specific types of carcinoma if possible
A 62 year old man presents with a 3.6 cm left parotid nodule. The fine needle aspiration shows a cellular smear, which is composed of fragments of bland looking, basaloid cells intermingled with magenta colored hyaline globules. What is the best diagnosis according to the Milan System for Reporting Salivary Gland Cytopathology?
Category IVB: salivary gland neoplasm of uncertain malignant potential, with basaloid features
Category VI: malignant, adenoid cystic carcinoma
Board review style answer #1
C. Category IVB: salivary gland neoplasm of uncertain malignant potential, with basaloid features
Basaloid neoplasms showing overlapping morphology of bland basal cells and acellular metachromatic matrix are better classified as salivary gland neoplasm of uncertain malignant potential, with basaloid features. The final pathology of the same case showed a basal cell adenoma with prominent hyaline globules.
A 39 year old woman presents with multiple submandibular nodules. A 2.3 cm intrasubmandibular gland nodule undergoes ultrasound guided fine needle aspiration. The cytology shows a proliferation of monotonous small lymphocytes and scattered tingible body macrophages. What is the best diagnosis according to the MSRSGC?
Category I: nondiagnostic
Category II: nonneoplastic
Category III: atypia of undetermined significance
Category VI: malignant, lymphoma
Board review style answer #2
C. Category III: atypia of undetermined significance
Bland lymphocytic aspirates showing any evidence of monomorphic population are better classified as atypia of undetermined significance. The subsequent excision of a lymph node adjacent to submandibular gland showed a follicular lymphoma.
Nonneoplastic cyst-like, mucus accumulation of the salivary gland (Acta Cytol 2022;66:359)
Note: this chapter is referring specifically to extravasation type mucoceles; retention type mucoceles are covered under the separate salivary duct cyst chapter
Cyst-like structure surrounded by granulation tissue with no cyst lining epithelium consists of abundant mucin, scattered macrophages and rare inflammatory cells (Otolaryngol Clin North Am 2021;54:543)
Painless, gradually increasing in size, unilateral mass near or within the salivary gland or well defined, dome shaped, fluctuant nodule of buccal mucosa (J Pharm Bioallied Sci 2012;4:S180)
Diagnosis
Pseudocyst with a granulation wall (histology)
Abundant mucin, scattered macrophages and inflammatory cells (cytology)
Tail sign, diagnostic of sublingual ranula, communication between the sublingual and submandibular components of the cystic mass located behind the posterior free edge of the mylohyoid muscle (Am J Otolaryngol 2015;36:114)
Comment: The specimen consists of predominantly mucin and rare macrophages. The differential diagnosis includes mucocele, low grade mucoepidermoid carcinoma, Warthin tumor and less likely, pleomorphic adenoma.
Fine needle aspirate (FNA) of a cystic sublingual mass in a 23 year old woman is shown above. The patient noticed a small bump 2 weeks ago. The aspirated material looks like the image shown. What is the most likely diagnosis?
Mucocele
Mucoepidermoid carcinoma
Squamous cell carcinoma
Warthin tumor
Board review style answer #1
A. Mucocele. Mucocele consists of mucin and scattered macrophages. Answer B is incorrect because there are no atypical epithelial cells or mucin producing cells. Mucoepidermoid carcinoma is more cellular than the above case. Answer C is incorrect because there are no malignant squamous cells. Squamous cell carcinoma consists of malignant squamous cells with variable degree of maturation and intracellular keratin. Anisonucleaosis and pleomorphism are common features of squamous cell carcinoma in cytology specimens. Answer D is incorrect because there are no oncocytes or lymphocytes. Warthin tumor consists of fragments of oncocytes and lymphocytes in a cystic background.
Fine needle aspirate (FNA) of a submandibular gland is shown above. 2 passes were performed and all slides displayed the same cytomorphology. The mass completely disappeared after the aspiration. What is the most correct diagnosis when applying the Milan System for Reporting Salivary Gland Cytology?
Atypia of undetermined significance
Malignant
Nondiagnostic
Nonneoplastic
Board review style answer #2
A. Atypia of undetermined significance. Abundant mucin even without any epithelial cells is considered atypical in the Milan system due to a risk of malignancy and potential overlap with low grade mucoepidermoid carcinoma. Answer C is incorrect because there is abundant mucin in the background. Answer D is incorrect because there is no salivary gland epithelium and there are no salivary gland acini. Answer B is incorrect because there is no epithelial component indicating a malignant process such as acinic cell carcinoma.
4 histologic grading systems (2 quantitative and 2 qualitative)
2 different morphologic quantitative point systems, although histologic grading using any grading system appears to be inconsistent (Am J Surg Pathol 2019;43:885)
Epidermoid cells attached to each other with desmosomes and mucus cells showing mucous globules with stellate mucoid material
(Oral Surg Oral Med Oral Pathol 1979;47:247)
65 year old African American man with a painless hard palate mass metastasizing to lung and spine (Case Rep Pathol 2019;2019:3863270)
Treatment
Surgical resection with negative margin is considered the standard of care
Gross description
Gross appearance is nonspecific
Tumor is often present as an expansile, lobulated to multinodular, beige to white mass, sometimes with ill defined / infiltrative border
Gross images
Contributed by Abeer Salama, M.D. and Bin Xu, M.D., Ph.D.
Lobulated parotid mass
Microscopic (histologic) description
Invasiveness is typically demonstrated as expansile invasive multinodular growth: myoepithelial carcinoma rarely shows infiltration of single cells / small clusters or desmoplastic reaction
Nodules often have a hypocellular center with hyalinized stroma or bland necrosis surrounded by a hypercellular peripheral zone
Tumor necrosis can be seen within the hypercellular central zone of a tumor nodule
Currently, there is no well defined, widely accepted grading system: presence of tumor necrosis is considered by some as a feature of high grade myoepithelial carcinoma (Am J Surg Pathol 2015;39:931)
Composed (near) entirely of myoepithelial cells showing various cytologic features, including clear cell, epithelioid, plasmacytoid or spindle cell morphology
Hyalinized, myxoid or myxochondroid stroma may be seen in myoepithelial carcinoma de novo and ex PA
Common architectural patterns include solid, trabeculae, cords, nests and single cells
Presence of pre-existing / residual pleomorphic adenoma component can be seen in myoepithelial carcinoma ex PA
Microscopic (histologic) images
Contributed by Abeer Salama, M.D. and Bin Xu, M.D., Ph.D.
Multinodular invasive growth
Expansile lobulated growth
Necrotic hypocellular central zone
Myoepithelial carcinoma ex PA
Epithelioid features
Plasmacytoid features
Clear cell features
Spindle cell features
S100 immunostain
CAM5.2 immunostain
Calponin immunostain
Cytology description
Hypercellular specimen composed entirely of myoepithelial cells
Myoepithelial cells shows a mixture of plasmacytoid, epithelioid or spindle morphology arranges as small groups or single cells (Cancer 2002;96:32, Kokyu To Junkan 1985;33:533)
Scant amount of metachromatic stroma, mitotic figures and nuclear pleomorphism may be present
Myoepithelial carcinoma, high grade, 3.5 cm (see comment and synoptic report)
Comment: The tumor shows a mitotic index of 8 per 10 high power fields. Tumor necrosis is noted. Immunohistochemistry studies show that the tumor is positive for S100, calponin and CAM5.2, whereas negative for HMB45. The morphologic and immunohistochemical features are most consistent with myoepithelial carcinoma.
Pleomorphic adenoma can be myoepithelial rich and may contain areas with pure myoepithelial cells
Pleomorphic adenoma may have pseudopod(s) protruding outside of tumor capsule
Difference:
Pleomorphic adenoma lacks the multinodular / lobulated invasive growth of myoepithelial carcinoma and contains areas typical of pleomorphic adenoma with ductal, myoepithelial and stromal component
Both tumors contained one cell type and are positive for S100
Other myoepithelial markers, e.g. calponin and SMA, are typically negative or very focally positive in polymorphous adenocarcinoma
Polymorphous adenocarcinoma shows architectural diversity with single filing, trabecular, cribriform, papillary and solid growth pattern, whereas myoepithelial carcinoma usually has cord and solid architecture
Myxoid stromal component may be seen in polymorphous adenocarcinoma but is usually focal
Myoepithelial tumors arising from salivary glands or soft tissue are indistinguishable on histology and immunohistochemistry level (Head Neck Pathol 2020;14:121)
EWSR1 fusions with POU5F1, PBX1, ZNF444, KLF17 and PBX3 seem restricted to soft tissue myoepithelial tumors (Head Neck Pathol 2020;14:121)
Radiological correlation is essential to determine the site of origin
A parotid tumor is resected from a 46 year old man. The tumor is positive for S100, cytokeratin AE1 / AE3 and calponin, whereas negative for AR. What is the diagnosis?
Adenoid cystic carcinoma
Myoepithelial carcinoma
Pleomorphic adenoma
Salivary duct carcinoma
Board review style answer #1
B. The low power H&E clearly shows invasion, which supports a diagnosis of carcinoma and excludes benign entities, such as pleomorphic adenoma. At high power, the tumor contains one type of tumor cells, which exclude all carcinoma with biphasic patterns (e.g. adenoid cystic carcinoma). The immunohistochemical profile is consistent with myoepithelial phenotype. Therefore, the correct diagnosis is myoepithelial carcinoma.
Which of the following statement about the myoepithelial carcinoma of the salivary gland is true?
It harbors PRKD1 fusion
It has negligible risk of distant metastasis
It is biphasic, composed of epithelial (ductal) and myoepithelial elements
It may arise de novo or ex pleomorphic adenoma
Board review style answer #2
D. Myoepithelial carcinoma contains only one cell type (myoepithelial cells) and does not contain epithelial (ductal) cells. PRKD1 fusion is seen in polymorphous adenocarcinoma / cribriform adenocarcinoma. Myoepithelial carcinoma is relatively aggressive, with approximately 20% risk of distant metastasis. It may arise de novo or ex pleomorphic adenoma.
Rare, benign tumor composed almost exclusively of myoepithelial cells
Essential features
Epithelial component should be less than 5% (some consider even focal epithelial differentiation sufficient to label the tumor as pleomorphic adenoma) (J Oral Maxillofac Pathol 2013;17:257)
Monomorphic histology and rare or absent ductal structures in myoepithelioma differentiate it from pleomorphic adenoma
Myoepithelial cells are contractile cells originating from the ectoderm, found in normal tissues with secretory function that aids in excreting glandular secretions (Ear Nose Throat J 2011;90:E9, Clin Pract 2014;4:628)
Common stem cell with a bidirectional differentiation into epithelial or myoepithelial cell is hypothesized to be the cell of origin; the varied histological types (spindle, plasmacytoid, epithelioid, clear and oncocytic) exhibited by myoepitheliomas can be attributed to the various stages in the differentiation from a cell that has the potential to differentiate into epithelial cells (J Clin Diagn Res 2013;7:1165)
Myoepitheliomas and pleomorphic adenomas are hypothesized to exist along a continuum, with a shared chromosome 12q cytogenetic abnormality (Cancer Genet Cytogenet 1999;113:49)
May contain enhancing nodules and nonenhancing areas of linear bands, slit-like shaped or of cystic configuration
MRI: well circumscribed, lobulated, inhomogeneous enhancement, apparent diffusion coefficient, different from Warthin tumor and similar to pleomorphic adenoma (AJNR Am J Neuroradiol 2009;30:591)
Regular follow up to evaluate for local recurrence
Clinical images
Images hosted on other servers:
Plasmacytoid myoepithelioma of minor salivary glands
Gross description
Up to 5 cm; encapsulated, may have cystic change
Absence of grossly myxoid or chondroid areas
Solid, tan or yellow-tan glistening cut surface
Usually encapsulated in parotid gland and no capsule for those in minor salivary glands (Ear Nose Throat J 2001;80:155)
Frozen section description
Nonspecific, may show atypical cells, usually need to defer to permanent for further characterization
Microscopic (histologic) description
Spindled, epithelioid, plasmacytoid, clear or oncocytic cells; most tumors are composed of a single cell type but combinations may occur (Clin Pract 2014;4:628)
Well circumscribed or encapsulated with a thin capsule
Stroma, when present, may be hyalinized, fibrous, myxoid or mucoid; lipomatous stroma may rarely been seen.
Encapsulation uncommon in minor salivary gland tumors
Architectural pattern: solid (non-myxoid), myxoid, reticular (canalicular-like) or mixed patterns of myoepithelial cells with no ductal differentiation
Mucinous myoepithelioma is rarely reported; contains abundant intracellular mucin material, which may be mistaken for signet ring cell adenocarcinoma of salivary gland with positive myoepithelial markers and should be distinguished from secretory myoepithelial carcinoma (Head Neck Pathol 2013;7:S85)
Microscopic (histologic) images
Contributed by Xiaofeng Zhao, M.D., Ph.D. and Shuanzeng Wei, M.D., Ph.D.
Plasmacytoid variant may be negative for all myoepithelial markers
Electron microscopy description
Composed of a single cell population characterized by numerous cytoplasmic filaments, duplication of basement membrane material and characteristic cytoplasmic appearance of myoepithelial cells (Arch Pathol 1974;98:312, Oral Oncology Extra 2005;41;104)
For palatal myoepitheliomas, encapsulation is not a reliable criterion
High cell proliferative activity (i.e. 7 mitosis instances per 10 high power fields or a Ki67 labeling index > 10%) may indicate malignancy (Cancer 1998;83:1292)
A 46 year old man presents with swelling close to his right ear. Imaging reveals a well circumscribed 1.8 cm nodule in the parotid gland. Biopsy findings are shown in the picture above. Which of the following statements about this tumor is true?
Monomorphic tumor cells and absence of ducts help to differentiate myoepithelioma from pleomorphic adenoma
Mucinous features should rule out this entity
Sometimes the epithelial component can be as high as 30%
This lesion is most common in minor salivary glands of palate
This tumor is completely benign and no malignant transformation has been reported
Board review style answer #1
A. Monomorphic tumor cells and absence of chondromyxoid stroma and ducts help to differentiate myoepithelioma from pleomorphic adenoma. The presence of chondromyxoid stroma is consistent with pleomorphic adenoma rather than myoepithelioma.
Which of the following is correct about myoepithelioma?
Negative for keratin
Negative for nuclear beta catenin
Negative for S100
Negative for SMA and HHF35
Positive for PLAG1 translocation
Board review style answer #2
E. Positive for PLAG1 abnormalities. Detection of PLAG1 rearrangement by cytogenetics or other methods can be helpful. NTF3-PLAG1, FBXO32-PLAG1 and GEM-PLAG1 fusions have been detected in oncocytic myoepithelioma (Ann Diagn Pathol 2017;28:19, Hum Pathol 2020;103:52).
Reactive, self resolving inflammatory condition of the salivary glands that most often affects the palate and is known to mimic malignancy both clinically and histopathologically
Essential features
Classically begins as a swelling that evolves into a crater-like ulceration, which resolves within 3 - 12 weeks
Most commonly affects the palate
Necrosis or disruption of salivary acini with squamous metaplasia of ductal structures
Etiology is thought to be a reaction to trauma or smoking in a setting of vascular compromise / tissue ischemia
Mimics malignancy both clinically and histopathologically
Other sites include buccal mucosa, floor of mouth, nasal cavity, trachea, parotid gland, sublingual gland, submandibular gland, larynx, maxillary sinus, tongue, tonsil and retromolar trigone (Arch Pathol Lab Med 2009;133:692)
Pathophysiology
Unknown pathogenesis; thought to be caused by vascular ischemia that interrupts the blood supply to the underlying salivary glands (Stomatologija 2022;24:56)
Etiology
Smoking / vaping
Trauma, including
Nonspecific mechanical trauma
Trauma from dental procedures or anesthetic, especially with vasoconstrictors
Trauma from an ill fitting denture or orthodontic appliances
Acute onset, erythematous or mucosal colored swelling often precedes development of crater-like ulceration, which measures 1 - 3 cm (Arch Pathol Lab Med 2009;133:692)
Abrupt, rapidly progressing swelling with subsequent formation of a crateriform ulceration and spontaneous healing over a span of 3 - 12 weeks is clinically diagnostic for necrotizing sialometaplasia (NSM); however, the aggressive clinical behavior / appearance may prompt biopsy to rule out malignancy prior to regression (Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114:577)
Close clinical follow up is imperative; if lesional tissue does not heal, biopsy is advised to rule out neoplasia
Diagnostic biopsy or rebiopsy is recommended in nonhealing lesions
Clinical images
Contributed by Douglas Damm, D.D.S., Ashley Clark, D.D.S., Eric Mencarelli, M.D., D.D.S. and Molly Housley Smith, D.M.D.
Palatal ulceration and erythema
Midline palatal ulceration
Bilateral palatal ulcerations
Microscopic (histologic) description
Squamous metaplasia of ductal structures and acini with preservation of the salivary lobular architecture is an essential feature, according to World Health Organization (see WHO classification-oral cavity & oropharynx)
Necrosis / infarction of acini characterized by loss of nuclei and cell borders with or without zones of spilled mucin
Pseudoepitheliomatous hyperplasia with generally bland cytology or keratinocytic regenerative atypia
Reactive, myxocollagenous background stroma
Surface ulceration, granulation tissue and subacute inflammation may be present
Has been conceptualized by 5 histologic stages of development and evolution: infarction, sequestration, ulceration, repair and healing (Int J Oral Surg 1982;11:283)
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H. (Case #497) and Molly Housley Smith, D.M.D.
Metaplasia of residual salivary ducts
Pseudoepitheliomatous hyperplasia
Bland cytology
Spilled mucin
Surface ulceration
Glandular necrosis
Acute inflammation
Healing stage
Positive stains
Immunohistochemistry is often not necessary for diagnosis
Comment: The microscopic sections show ulcerated mucosa with zones of pseudoepitheliomatous hyperplasia without prominent cytologic atypia. Squamous metaplasia of ductal structures with preservation of lobular architecture is appreciated along with necrosis of salivary acini and extravasated mucin. No evidence of a neoplasm is identified upon review of multiple deeper levels. Clinical follow up to ensure complete resolution of the lesional tissue is recommended.
Differential diagnosis
Although the clinical differential diagnosis for an ulceration or swelling on the palate may include a variety of entities (e.g., salivary gland neoplasm, T cell lymphoma, granulomatosis with polyangiitis, deep fungal or bacterial infection), the main histopathological differential diagnosis includes mucoepidermoid carcinoma, squamous cell carcinoma or subacute necrotizing sialadenitis
Exhibits pleomorphism / abnormal mitotic figures, as compared with NSM which often shows pseudoepitheliomatous hyperplasia with bland cytology (Head Neck Pathol 2022;16:54)
Rapid onset of a painful swelling, typically on the palate, which is characterized by necrosis of salivary glands and mixed inflammation but lacks surface ulceration and shows minimal to no squamous metaplasia of ductal epithelium (Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114:577)
Necrotizing sialometaplasia most commonly affects what site?
Minor salivary glands of the lip
Minor salivary glands of the palate
Parotid
Submandibular gland
Board review style answer #1
B. Minor salivary glands of the palate. Although necrotizing sialometaplasia can affect any of the given answer choices, it classically involves the minor salivary glands of the hard palate. Answers A, C and D are incorrect because necrotizing sialometaplasia occurs at these sites less frequently than in the minor salivary glands of the palate.
A patient presents to clinic with severe pain and an ulceration on the hard palate. She states that the lesion began after a dental procedure as a swelling that rapidly progressed to an ulceration over the course of a couple weeks. What is the diagnosis?
Mucoepidermoid carcinoma
Necrotizing sialometaplasia
Squamous cell carcinoma
T cell lymphoma
Board review style answer #2
B. Necrotizing sialometaplasia. The patient presented with the classic clinical history of acute onset of a rapidly progressing lesion on the hard palate, which began as a swelling that subsequently ulcerated. Biopsy revealed large zones of pseudoepitheliomatous hyperplasia, squamous metaplasia of ducts, lack of overt pleomorphism and areas of acinar necrosis and mucin spillage. Answer A (mucoepidermoid carcinoma) is incorrect because the lobular architecture of the gland is preserved and there is no proliferation of cystic spaces or neoplastic goblet cells. Although T cell lymphomas classically may affect the hard palate, answer D is incorrect because the biopsy did not show an atypical lymphoid infiltrate. Answer C (squamous cell carcinoma) is incorrect as the proliferation of squamous epithelium classically forms the pseudoepitheliomatous hyperplasia type pattern and lacks cellular pleomorphism.
Submandibular gland: 10% of all salivary gland tumors, 55 - 60% are benign
Minor salivary glands (including sublingual glands and seromucinous glands of the upper aerodigestive tract): 20% of all salivary gland tumors, 10 - 30% of sublingual gland tumors and 50% of minor salivary gland tumors are benign
Clinical features
Frequency among all the Milan system categories: 30 - 40%
On ultrasound, benign salivary gland tumors are usually well defined and hypoechoic (Eur J Radiol 2008;66:419)
Case reports
12 year old boy with a parotid juvenile sclerosing polycystic adenosis, cytologically mimicking a Warthin tumor (Diagn Cytopathol 2019;47:1208)
41 year old woman with a glandular schwannoma at submandibular region, cytologically mimicking a pleomorphic adenoma (Diagn Cytopathol 2015;43:395)
53 year old women with Warthin-like variant of mucoepidermoid carcinoma of parotid glands, cytologically mimicking a Warthin tumor (Diagn Cytopathol 2017;45:1132)
61 year old man with an epithelioid schwannoma of the facial nerve, cytologically mimicking a parotid pleomorphic adenoma (Diagn Cytopathol 2014;42:58)
70 year old man with a cystic pleomorphic adenoma of parotid gland, cytologically mimicking a mucoepidermoid carcinoma (Diagn Cytopathol 2005;32:229)
78 year old woman with a pleomorphic adenoma at hard palate, showing predominant plasmocytoid myoepithelial cells and cytologically mimicking a poorly differentiated carcinoma (Diagn Cytopathol 2009;37:56)
Mixture of myoepithelial cells, ductal cells and extracellular stroma
Myoepithelial cells are usually the predominant cell type with various cytomorphology, including round, polygonal, plasmacytoid, spindle, etc.
Ductal cells show bland cytologic features with organized honeycombing or ductal arrangement
Extracellular matrix shows characteristic feathery / fibrillary borders and bright magenta color on Romanowsky type stain and gray-green chondromyxoid features on Papanicolaou stain
Warthin tumor: 20 - 30% of all benign salivary gland FNA
Sheets of oncocytes and mixed population of lymphocytes in a characteristic dirty proteinaceous background
Oncocytic sheets show an organized honeycombing or papillary arrangement and are typically cyanophilic at the periphery and bright orange at the center on Papanicolaou stain
Oncocytes show densely granular cytoplasm, centrally located nuclei and small nucleoli
Cellular oncocytic aspirates with very clean background
Oncocytes show abundant finely granular cytoplasm, centrally placed or eccentric nuclei and occasional distinct nucleoli
Cellular arrangement can be irregular sheets, small clusters or single cells
Most FNA of basal cell adenoma, myoepithelioma and cystadenoma should be better classified as salivary gland neoplasm of uncertain malignant potential (SUMP) due to overlapping cytomorphology with other malignant tumors
Other benign mesenchymal neoplasms:
Schwannoma: spindle shaped cells with wavy nuclei and bipolar cytoplasmic processes in syncytium-like fragments
Lipoma: fragments of benign adipocytes with clear cytoplasm and small nuclei
Hemangioma: bloody aspirates with few groups of bland spindle shaped endothelial cells
Low grade carcinomas with oncocytoid features, e.g. acinic cell carcinoma and secretory carcinoma, usually show zymogen granules or secretory globules instead of the mitochondria type fine granules in the cytoplasm
A 45 year old man presented with a 2.8 cm, slow growing mass at left parotid region. He underwent ultrasound guided FNA for evaluation. What is the best diagnosis?
Basal cell adenoma
Oncocytoma
Pleomorphic adenoma
Warthin tumor
Board review style answer #1
C. Pleomorphic adenoma. Magenta colored extracellular matrix with feathery / fibrillary borders and intermingled bland myoepithelial cells are characteristic features of a pleomorphic adenoma.
Which salivary gland tumor below should be reported on FNA as "salivary gland neoplasm of uncertain malignant potential (SUMP)"?
Basal cell adenoma
Oncocytoma
Pleomorphic adenoma
Warthin tumor
Board review style answer #2
A. Basal cell adenoma. Basal cell adenoma shows overlapping morphological features with basal cell adenocarcinoma in FNA. The distinction between these 2 tumors depends on the histological examination to demonstrate tumor invasion. Moreover, pleomorphic adenoma with predominant basal cells and solid / tubular variant of adenoid cystic carcinoma can also cytologically mimic a basal cell adenoma. Therefore, it is recommended to report FNA with basal cell features as SUMP with basaloid features in the Milan system.
Fine needle aspiration (FNA) result with cytomorphologic features diagnostic of a neoplasm but because a specific entity cannot be ascertained, a malignant neoplasm cannot be excluded
SUMP cases that could not be comfortably placed in either basaloid or oncocytic / oncocytoid subcategory
Common scenarios
FNA with focal atypical features in a tumor otherwise favoring a benign neoplasm (e.g., cellular pleomorphic adenoma or pleomorphic adenoma with anisonucleosis that are indefinite for benign)
FNA with a predominance of an unclassified cell type (e.g., plasmacytoid, spindle, mixed, etc.)
Adenoid cystic carcinoma: MYB or MYBL1 rearrangement
Oncocytic / oncocytoid SUMP
Mucoepidermoid carcinoma: MAML2::CRTC1 / 3
Acinic cell carcinoma: NR4A3 rearrangement
Secretory carcinoma: ETV6::NTRK3
Hyalinizing clear cell carcinoma: EWSR1::AFT1
Gene mutation testing (by PCR or NGS)
Basaloid SUMP
Basal cell adenoma: CTNNB1 mutation
Adenoid cystic carcinoma: NOTCH1 mutation in a subset
Polymorphous adenocarcinoma: PRKD1 E710D
Sample pathology report
Parotid gland, right, fine needle aspiration:
Neoplasm: salivary gland neoplasm of uncertain malignant potential (SUMP)
Cellular basaloid neoplasm (see comment)
Comment: The specimen shows monotonous basaloid cells with minimal nuclear atypia and scattered hyaline globules. There are no high grade features, such as mitoses or necrosis. The differential diagnosis includes basal cell adenoma / adenocarcinoma, pleomorphic adenoma and adenoid cystic carcinoma. Suggest correlation with clinical and radiologic findings.
Parotid gland, left, fine needle aspiration:
Neoplasm: salivary gland neoplasm of uncertain malignant potential (SUMP)
Cellular oncocytic / oncocytoid neoplasm (see comment)
Comment: The specimen shows monotonous oncocytic / oncocytoid cells with minimal nuclear atypia in a lymphoplasmacytic background. Scattered mucinous extracellular materials are noted but no mucous cells are present. The differential diagnosis includes Warthin tumor with mucinous metaplasia and low grade mucoepidermoid carcinoma with oncocytic change. Suggest correlation with clinical and radiologic findings.
Basaloid SUMP cases with a purely fibrillary extracellular matrix are compatible with a pleomorphic adenoma and are recommended to be classified as benign neoplasm (category IVA)
A 62 year old man presents with a 3.6 cm left parotid nodule. The fine needle aspiration shows a cellular smear, which is composed of fragments of bland looking, basaloid cells intermingled with magenta colored hyaline globules. What is the best diagnosis according to the Milan System for Reporting Salivary Gland Cytopathology?
Category IVB: salivary gland neoplasm of uncertain malignant potential, with basaloid features
Category VI: malignant, adenoid cystic carcinoma
Board review style answer #1
C. Category IVB: salivary gland neoplasm of uncertain malignant potential, with basaloid features. Basaloid neoplasms showing overlapping morphology of bland basal cells and extracellular nonfibrillary matrix are better classified as salivary gland neoplasm of uncertain malignant potential, with basaloid features. The final pathology of the same case showed a basal cell adenoma with prominent hyaline globules.
A 49 year old woman presents with a 2.5 cm right parotid nodule. Fine needle aspiration cytology is performed and the result is shown in the figure. What would be the most likely diagnosis if the patient receives surgical excision?
Basal cell adenoma
Mucoepidermoid carcinoma
Secretory carcinoma
Warthin tumor
Board review style answer #2
A. Basal cell adenoma. The figure shows a proliferation of basaloid cells admixed with extracellular matrix. It is consistent with the cytologic diagnosis of SUMP with basaloid features. The differential diagnosis includes matrix producing tumors with basaloid cells, such as basal cell adenoma / adenocarcinoma and adenoid cystic carcinoma. Answers B - D are incorrect because Warthin tumor, mucoepidermoid carcinoma and secretory carcinoma are the less likely options since they usually present with neoplastic cells harboring more abundant cytoplasm and often would be interpreted as SUMP with oncocytic / oncocytoid features.
Most common clinical presentation: rapidly growing neck mass
Diagnosis
Fine needle aspiration or core biopsy of mass
Radiology images
Images hosted on other servers:
Parotid mass
Prognostic factors
Unknown
Case reports
48 year old woman with a right cheek mass (small cell carcinoma ex pleomorphic adenoma) (Head Neck Pathol 2012;6:502)
1 patient in a series of 25 acinic cell carcinomas with high grade transformation had small cell carcinoma ex acinic cell carcinoma of the parotid gland (Head Neck Pathol 2016;10:152)
Comment: Histologic sections show a small cell neuroendocrine carcinoma involving the parotid gland. The tumor cells are positive for synaptophysin, chromogranin and cytokeratin 20. TTF1 is negative. Immunohistochemistry for Merkel cell polyomavirus (MCPyV) is also negative. The majority of high grade neuroendocrine carcinomas located in the parotid gland represent metastases, usually from the head and neck skin, rather than primary salivary carcinomas. Correlation with clinical history and physical exam findings is recommended to exclude a metastasis. Even in the absence of an identifiable cutaneous primary, occult metastatic Merkel cell carcinoma is still more likely. Mutational signature analysis from next generation sequencing assays may aid in determining tumor origin as a UV signature would favor a metastasis from a cutaneous primary.
Differential diagnosis
Metastatic neuroendocrine carcinoma:
Parotid gland contains lymph nodes which are a favored site of metastasis from cutaneous head and neck cancer
Clinical history is most useful; however, there may not be an identifiable skin tumor and primary tumor regression also possible (Am J Dermatopathol 2016;38:e154)
Absence of associated low grade salivary tumor (other than Warthin tumor)
Also CK20 positive in perinuclear, dot-like pattern
A 70 year old man presented with an enlarging mass in the left cheek soft tissue. The mass was removed and shows the histology above. The tumor is positive for CK20 (dot-like) and synaptophysin and is negative for CK7. Which of the following features would favor a salivary primary over a metastasis from an occult cutaneous primary tumor?
Rhabdomyoma: may resemble at intraoperative frozen section; positive for skeletal muscle markers; different morphology on permanent section (Arch Pathol Lab Med 1983;107:638)
FNA with insufficient amount of lesional cells to provide an informative interpretation (ideally > 60 lesional cells for adequate evaluation)
Poorly prepared slides with artifacts (e.g., air drying, obscuring blood and poor staining) that preclude the evaluation of the cellular component
Normal nonneoplastic salivary gland elements in the setting of a clinically or radiologically defined mass
Nonmucinous cyst fluid without an epithelial component
Terminology
Nondiagnostic
Nondiagnostic, cystic fluid only for nonmucinous cyst fluid without an epithelial component
Etiology
Palpation guidance without ultrasound, inadequate sampling determined by rapid on site evaluation and lesions with cystic, vascular or diffuse nature are significantly associated with nondiagnostic results (Cancer Cytopathol 2022;130:609)
FNA with Poorly prepared slides with artifacts (e.g., air drying, obscuring blood and poor staining) that preclude the evaluation of the cellular component
Normal nonneoplastic salivary gland elements in the setting of a clinically or radiologically defined mass
Nonmucinous cyst fluid without an epithelial component
Submandibular gland, left, fine needle aspiration:
Nondiagnostic (see comment)
Nonneoplastic benign salivary gland elements only
Comment: The finding of nonneoplastic salivary gland elements only does not explain the presence of a clinically or radiologically defined mass. Repeat fine needle aspiration under radiologic guidance is recommended if clinically indicated.
Parotid gland, left, fine needle aspiration:
Nondiagnostic (see comment)
Comment: Cystic fluid only.
Board review style question #1
A 45 year old woman presents with a 2.8 cm right parotid nodule. Ultrasound demonstrates a well defined nodule with heterogeneous echogenicity. Fine needle aspiration is performed. What is the best diagnosis according to the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC)?
Atypia of undetermined significance
Benign neoplasm, pleomorphic adenoma
Nondiagnostic
Nonneoplastic
Board review style answer #1
C. Nondiagnostic. The presence of normal nonneoplastic salivary gland acinar cells only in the setting of a clinically and radiologically defined mass should be diagnosed as nondiagnostic. The FNA sample is not considered representative of the lesion detected on clinical and radiologic examination. Repeat FNA under radiologic guidance is recommended if clinically indicated.
A 38 year old man presents with a 3.0 cm right parotid mass. Ultrasound demonstrates a mixed solid and cystic tumor. Fine needle aspiration is performed. What is the best diagnosis according to the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC)?
Atypia of undetermined significance, mucinous cystic lesion
Malignant, low grade mucoepidermoid carcinoma
Nondiagnostic, cyst fluid only
Nonneoplastic, compatible with mucocele
Board review style answer #2
A. Atypia of undetermined significance, mucinous cystic lesion. This FNA contains abundant mucin without any epithelial cells. The differential diagnosis includes a benign mucinous cyst; however, a low grade mucoepidermoid carcinoma cannot be excluded. Based on the MSRSGC, the most appropriate diagnosis would be atypia of undetermined significance. Clinical and radiological correlations are needed. Aspiration of a residual mass, if present, may help to achieve a more specific diagnosis.
Sialoliths can be detected using ultrasound (usually the initial examination imaging) or unenhanced computed tomography (Br J Radiol 2003;76:271)
Magnetic resonance sialography or conventional sialography can be performed in case of high suspicion for a nonradiopaque calculus (J Clin Imaging Sci 2018;8:47)
Tumor-like lesions
Some inflammatory conditions can produce salivary gland enlargement with homogeneous enhancement, mimicking neoplasia (e.g., chronic sclerosing sialadenitis) (J Clin Imaging Sci 2018;8:47)
Simple cysts
Round / oval mass with well delineated borders, anechoic center and clear posterior acoustic enhancement
May represent benign entities (reactive lymph nodes, salivary duct cyst, lymphoepithelial cyst) but it is noteworthy that benign and malignant neoplasms may also present standard features of a simple cyst (J Ultrason 2016;16:191)
Intracystic attenuation or signal intensity are due to viscosity or increased protein concentration of the cystic fluid content (Jpn J Radiol 2019;37:627)
HIV associated lymphoepithelial lesion
Numerous entirely cystic, combined cystic and solid or entirely solid lesions, which are typically bilateral (Jpn J Radiol 2019;37:627)
Radiology images
Contributed by Jose Manuel Gutierrez Amezcua, M.D. and Tamar C. Brandler, M.D., M.S.
Deep parotid lobe nodule
Solid and cystic parotid lesion
Parotid solid enhancing lesion
Enlarged periparotid lymph node
Case reports
51 year old woman, 59 year old man, 67 year old woman and 88 year old man with chronic sclerosing sialadenitis (Küttner tumor) misinterpreted as neoplastic in the context of previous head and neck malignancy (Head Neck Pathol 2016;10:389)
Reactive lesion to salivary gland duct obstruction and buildup of salivary contents that results in duct ectasia
Acellular or paucicellular aspirate of benign acinar / ductal cells, background debris containing macrophages (cyst contents), with or without inflammatory cells and amylase crystalloids
Contributed by Jose Manuel Gutierrez Amezcua, M.D., Pascale G. Levine, M.D. and Tamar C. Brandler, M.D., M.S.
Amylase crystalloids
Cyst contents
Cyst with lymphoid and squamous cells
Benign epithelial cells and lymphocytes
Lymphoepithelial cyst excision
Granulomatous sialadenitis
Giant cell
Acute sialadenitis
Chronic sialadenitis
Reactive lymph node
Sample pathology report
Nonneoplastic:
Granulomatous sialadenitis (see comment)
Comment: Smears show predominantly benign salivary gland acinar cells, chronic inflammation, epithelioid histiocytes forming granulomas and scattered multinucleated giant cells. These findings may be related to chronic sialadenitis, duct obstruction or sarcoidosis. Clinical and radiologic correlation is recommended.
Nonneoplastic:
Reactive intraparotid lymph node (see comment)
Comment: Smears show a mixed lymphoid population with a predominance of mature lymphocytes, scattered tingible body macrophages and germinal center fragments (lymphohistiocytic aggregates). Please correlate with concurrent flow cytometry.
Nonneoplastic:
Consistent with salivary duct cyst (see comment)
Comment: Smears show groups of ciliated respiratory type columnar cells, abundant amylase crystals, scattered macrophages, few groups of oncocytic metaplastic cells, benign salivary acinar cells and some background inflammation and debris. No atypia, mucin or malignancy is seen. These cytologic findings are compatible with a nonneoplastic cyst.
Differential diagnosis
Cystic salivary gland lesions:
Interpretation is challenging due to overall low cellularity and not well established diagnostic criteria
Specimens containing nonmucinous cystic fluid only are best classified as nondiagnostic
Specimens containing benign acinar or ductal epithelial components, background debris with macrophages (cyst contents) with or without inflammatory cells and amylase crystals are best classified as nonneoplastic (Cancer Cytopathol 2021;129:214)
Specimens containing abundant mucin with or without epithelial cells are best classified as atypia of undetermined significance (AUS) due to the possibility of underlying mucoepidermoid carcinoma (Head Neck Pathol 2018;12:548)
Lymphoma:
Lymphomas originating from the salivary glands are rare, accounting for ~3% of all malignant tumors which more commonly affect the parotid glands (World J Clin Cases 2020;8:2717)
Risk factors include certain viral infections (HIV, EBV), immunosuppression and autoimmunity, particularly Sjögren syndrome
Usually presents with a unilateral asymptomatic mass that enlarges over a period of time, with or without cervical lymphadenopathy
Whenever non-Hodgkin lymphoma is in the differential, additional passes for flow cytometry evaluation are recommended
Reassuring features of benignity in specimens with abundant lymphoid tissue include:
Mixed, heterogeneous population of mature lymphocytes and background lymphoglandular bodies
Tingible body macrophages
Lymphohistiocytic aggregates (fragments of germinal center)
Board review style question #1
A 40 year old patient undergoes ultrasound guided fine needle aspiration (FNA) of a 2.1 cm cystic lesion in the inferior aspect of the parotid gland. The aspirate smear stained with Diff-Quik is shown above. Which of the following would be the appropriate way to characterize this lesion?
Atypia of undetermined significance
Nondiagnostic
Nonneoplastic
Salivary gland neoplasm of uncertain malignant potential
Major salivary glands: tumor is usually encapsulated and solid
Minor salivary glands: tumor is unencapsulated and less well delineated; cystic change may be present
Gross images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.
Multiple nodules
Well circumscribed nodule
Frozen section description
N/A
Frozen section images
N/A
Microscopic (histologic) description
Generally a well circumscribed nodule; may lack circumscription in the minor salivary glands
Solid sheets, nested, trabecular or ductular architecture; microcysts and macrocysts are rare
Exclusively or predominantly composed of oncocytes and separated by thin fibrovascular septae
Oncocytes are large, polyhedral shaped with distinct cell membranes and abundant granular eosinophilic cytoplasm
Nuclei are centrally located, round, vesicular with prominent nucleoli
Absence of significant nuclear pleomorphism, increased mitoses and necrosis
Absence of infiltrative growth
Psammoma bodies and tyrosine-like crystals may be present
Other cell types that may present in limited quantity within the tumor, especially following a fine needle aspiration: mucous cells, squamous cells or sebaceous cells
Basal cells can be seen at the periphery of the tumor
Clear cell oncocytoma is a histologic variant that consists entirely or predominantly of clear cells
Reasons for clear cytoplasm
Fixation and tissue processing artifact
Accumulated glycogen content that displaces the mitochondria to the periphery of cells
Microscopic (histologic) images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.
Well circumscribed oncocytic tumor
Tumor cells arranged in nests
Oncocytes
Mucous cell within oncocytoma
CK7
p63
Virtual slides
not provided
Cytology description
Smears are usually cellular
Oncocytes (cells with granular eosinophilic cytoplasm) are arranged in sheets, papillary fragments and individual cells
Cytologic atypia is absent to minimal
Absence or very sparse lymphoid component
Distinction of oncocytoma from oncocytosis or another salivary gland lesion with prominent oncocytic metaplasia may not be possible on cytology alone
Cytology images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.
Loosely cohesive tumor cells
Low N:C ratio
Papillary architecture
Dense, finely granular cytoplasm
HTML NOTE: Keep these images?
Contributed by Jen-Fan Hang, M.D.
Cytoplasm of the oncocytes is packed with abundant mitochondria, which are oval or elongated in shape with stacked cristae
Other organelles, such as endoplasmic reticulum and Golgi complex, are sparse
Continuous basement membrane around cell clusters
Electron microscopy images
Images hosted on other servers:
Cytoplasm packed with mitochondria with stacked cristae
Molecular / cytogenetics description
not provided
Molecular / cytogenetics images
not provided
Videos
not provided
Sample pathology report
Left parotidectomy:
Oncocytoma with background multinodular oncocytic hyperplasia (see comment)
Comment: There is a dominant encapsulated oncocytic nodule. The salivary gland parenchyma shows occasional scattered microscopic oncocytic nodules. There is no evidence of malignancy.
Differential diagnosis
Oncocytic metaplasia:
Metaplastic change
No mass forming lesion
Ductal and acinar epithelium transformed into oncocytes due to metaplastic process in aging
Which of the following statements regarding oncocytoma of the salivary gland is true?
The tumor is common in young patients
The tumor is malignant
The tumor is positive for PAX8
The tumor is rare and occurs mostly in the parotid gland
Board review style answer #1
D. The tumor is rare and occurs mostly in the parotid gland. Oncocytoma constitutes about 1 - 2% of salivary gland neoplasms and mostly occurs in the parotid gland, followed by the submandibular gland and minor salivary gland. Answer A is incorrect because this tumor occurs mostly in middle aged to older people. Answer B is incorrect because oncocytoma is benign. Answer C is incorrect because oncocytoma is PAX8 negative, which is useful in differentiating this tumor from metastatic renal cell carcinoma.
Which of the following statements about oncocytic cells in oncocytoma of the salivary gland is true?
Cytology can differentiate oncocytosis from oncocytoma
FISH analysis is positive for MAML2 rearrangement
Oncocytic cells are diffusely positive for p63, p40 and CK5/6
The main organelle in the cytoplasm of oncocytic cells is the mitochondria
Board review style answer #2
D. The main organelle in the cytoplasm of oncocytic cells is the mitochondria. Answer C is incorrect because oncocytic cells are predominantly positive for cytokeratins such as CK7 and EMA but very focally positive for p63, p40 and CK5/6, which is useful in differentiating this tumor from mucoepidermoid carcinoma. Answer A is incorrect because cytology cannot differentiate oncocytosis from oncocytoma. Answer B is incorrect because MAML2 rearrangement is seen in mucoepidermoid carcinoma.
Well circumscribed with fibrous capsule, solid, tan-red-brown, lobulated, often small, may have cystic spaces
Microscopic (histologic) description
Eosinophilic or clear cell (glycogen) with sheets, trabeculae, acini or follicular patterns of monotonous large polygonal cells with well defined cell borders, deeply eosinophilic, granular cytoplasm, small round nuclei
Vascular stroma, may have clear cell change, background of oncocytic nodular hyperplasia, psammoma bodies, tyrosine rich crystals
No mitotic figures, no elastosis
Microscopic (histologic) images
Images hosted on other servers:
Various images
Cytology description
Cellular oncocytic aspirates with very clean background
Oncocytes show abundant finely granular cytoplasm, centrally placed or eccentric nuclei and occasional distinct nucleoli
Cellular arrangement can be irregular sheets, small clusters or single cells
Prior radiation increases the risk of developing pleomorphic adenoma
Clinical features
Slow growing, painless, well circumscribed mass involving salivary gland
Diagnosis
Diagnosis can be rendered on preoperative cytology or biopsy, showing typical metachromatic fibrillary stroma (in cytology) or triphasic growth pattern (on biopsy)
Benign metastasizing mixed tumors
Rare, controversial clinical entity with late metastasis (6 - 52 years) after tumor excision
Benign morphology in original and metastatic tumor
Associated with incomplete pleomorphic adenoma surgery / local recurrence, post cardiac transplant patient / immunosuppression (Mod Pathol 1998;11:1142)
Radiology description
Mass with well defined or bosselated border, hyperintense on T2 MRI
Radiology images
Images hosted on other servers:
MRI parotid tumor
Prognostic factors
Benign tumor: surgical resection with negative margin is considered curative
Enucleation is associated with 15 - 25% risk of local recurrence
Primary tumor: well demarcated, bosselated gray-white myxoid mass
Recurrent tumor: numerous myxoid to fibrotic nodules of various size, giving a shotgun bullet appearance
Gross images
Contributed by Bin Xu, M.D., Ph.D., Kelly Magliocca D.D.S., M.P.H. and Case #392
Primary pleomorphic adenoma
Recurrent pleomorphic adenoma
Pleomorphic adenoma
External surface
Cut surface
Microscopic (histologic) description
Bosselated outer surface, often with tongue-like protrusions (pseudopods)
Typically has 3 components:
Epithelial (ductal) component forming the inner layer of cysts and tubules
Myoepithelial cells as the outer layer of cysts and tubules and scattered within the myxoid stroma
Cytology of myoepithelial cells can be plasmacytoid, spindled, epithelioid, clear or stellate shaped
Stromal component is typically myxoid, chondroid or myxochondroid
It can also be hyalinized or fibrotic
Metaplastic changes may be seen, e.g. adipose metaplasia, osseous metaplasia, squamous metaplasia (sometimes with keratinization), sebaceous metaplasia and mucinous metaplasia
Intravascular permeation has been reported in a small percentage of cases and does not increase the risk of recurrence or distant metastasis
Increased cellularity: so called cellular pleomorphic adenoma
Increased mitotic activity
Myoepithelial rich area or tumor
Microscopic (histologic) images
Contributed by Bin Xu, M.D., Ph.D., Andrey Bychkov, M.D., Ph.D., Shuanzeng (Sam) Wei, M.D., Ph.D. and Case #404
Encapsulated mass
Bosselated interface
Pseudopods
Recurrent pleomorphic adenoma
Triphasic tumor
Clear myoepithelial cells
Plasmacytoid myoepithelial cells
Spindle myoepithelial cells
Squamous and mucinous metaplasia
Adipose and osseous metaplasia
Tyrosine crystals
Biphasic population
Multiple cysts filled with mucin
Squamous and mucinous cells
Pleomorphic adenoma
Myoepithelial cells
Chondroid stroma
Myoepithelial cells
Virtual slides
Contributed by Andrey Bychkov, M.D., Ph.D.
Pleomorphic adenoma
Cytology description
Matrix containing tumor
Typical feature is its unique fibrillary stroma
Mixture of myoepithelial cells, ductal cells and extracellular stroma
Myoepithelial cells are usually the predominant cell type with various cytomorphology, including round, polygonal, plasmacytoid, spindle, etc.
Ductal cells show bland cytologic features with organized honeycombing or ductal arrangement
Extracellular matrix shows characteristic feathery / fibrillary borders and bright magenta color on Romanowsky type stain and gray-green chondromyxoid features on Papanicolaou stain
Cytology images
Contributed by Bin Xu, M.D., Ph.D., Jen-Fan Hang, M.D. and Shuanzeng (Sam) Wei, M.D., Ph.D.
Demonstrates frank evidence of malignancy, e.g. marked nuclear pleomorphism, frank necrosis, invasion beyond pre-existing capsule, perineural or lymphovascular invasion
A 45 year old man presented with a 2.8 cm, slow growing mass at left parotid region. He underwent ultrasound guided FNA for evaluation. What is the best diagnosis?
Basal cell adenoma
Oncocytoma
Pleomorphic adenoma
Warthin tumor
Board review style answer #3
C. Pleomorphic adenoma
Magenta colored extracellular matrix with feathery / fibrillary borders and intermingled bland myoepithelial cells are characteristic features for a pleomorphic adenoma.
Polymorphous adenocarcinoma is an indolent salivary gland carcinoma characterized by cytologic uniformity and architectural diversity, predominantly affecting minor salivary glands, in particular the hard and soft palate
Essential features
Occurs in minor salivary glands predominantly, in particular the palate in approximately 60% of cases
Other possible primary sites are minor salivary glands of upper aerodigestive tract, including oral cavity (e.g. floor of mouth, retromolar trigone, lip and lateral tongue), oropharynx (e.g. base of tongue and tonsil), sinonasal tract and nasopharyx
May occur in major salivary gland, in particular the parotid gland, in less than 5% of cases
Clinical features
Commonly presents with palpable mass
Diagnosis
Typically rendered in biopsy or resection specimens
Radiology description
No specific radiologic findings
CT and MRI are used preoperatively to establish the extent of disease and the presence of bone invasion
The presence of at least 10% of papillary or at least 30% of cribriform architecture is an independent adverse prognostic factor (Am J Surg Pathol 2016;40:1526)
Tumors harboring PRKD1, PRKD2 or PRKD3 fusion incur 50% risk of lymph node metastasis (Mod Pathol 2020;33:65)
Other adverse pathologic prognostic factors reported include larger tumor size, advanced stage, lymphovascular invasion, bone invasion, perineural invasion of large nerve and tumor necrosis (Eur Arch Otorhinolaryngol 2018;275:1681)
Case reports
43 year old Japanese man with palate polymorphous adenocarcinoma with high grade transformation (Head Neck Pathol 2019;13:131)
Neck lymph node dissection may be performed for patients with a diagnosis of cribriform adenocarcinoma or with clinically positive lymph node(s)
Postoperative radiation therapy may be considered on an individual basis, especially for tumors with positive margins or perineurial invasion (Eur Arch Otorhinolaryngol 2018;275:1681)
Typically presents as a submucosal white to beige, firm, lobulated nodule or mass with infiltrative border
Gross images
Contributed by Bin Xu, M.D., Ph.D.
Macroscopic appearance
Microscopic (histologic) description
Diagnostic criteria:
Cytologic uniformity: the tumor is composed entirely of one type of tumor cells characterized by monotonous pale nuclei with marked chromatin clearing resembling that of papillary thyroid carcinoma
Architectural diversity: showing highly variable architectural patterns of different proportions, including single filing arrangement, trabecular, tubular, reticular, papillary, solid and cribriform pattern
Targetoid arrangement and streaming of tumor cells and nests around nerves and vessels are common
First described as a tumor with a high propensity to base of tongue/posterior tongue location and a high risk of nodal metastasis (Histopathology 1999;35:495)
Shares the same cytologic features of optic clearing pale nuclei and immunohistochemistry profile as polymorphous adenocarcinoma
Characterized by lobulated architecture separated by fibrous septa and relatively uniformed solid, cribriform or microcystic architecture
Peripheral palisading, peripheral clefting and glomeruloid structures are common
Microscopic (histologic) images
Contributed by Bin Xu, M.D., Ph.D.
Infiltrative mass
Optical clearing of nuclei
Targetoid arrangement and perineural invasion
Papillary architecture
Cribriform architecture
Reticular pattern
Solid pattern
Oncocytic changes
Cribriform adenocarcinoma of salivary gland
S100
CK7
Virtual slides
Images hosted on other servers:
Polymorphous adenocarcinoma
Cytology description
Given that most tumors are located intraorally, fine needle aspiration cytology is rarely used for the diagnosis
Case reports show that this tumor typically contains uniform tumors cells with ground glass nuclei, scattered nuclear grooves and inconspicuous nucleoli
Cytology images
Images hosted on other servers:
Papanicolaou stain
Positive stains
S100, CK7 and SOX10: diffusely and strongly positive
Risk factors: radiation exposure (atomic bomb survivors, radiation therapy, chemoradiation therapy) with mean latency after low dose radiation exposure of 11 years for malignant tumors and 21 years for benign tumors
Alcohol and tobacco are NOT risk factors except for Warthin tumor (associated with smoking)
Bilateral tumors: Warthin tumor is most common, also pleomorphic adenoma and acinic cell carcinoma
15% of parotid tumors are malignant, 40% elsewhere
Children: pleomorphic adenoma most common but more often malignant; most common malignant tumors are mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma
Regional lymph nodes: nodal metastases usually evident on initial clinical evaluation
Low grade tumors rarely metastasize to regional nodes, high grade tumors often do; nodal involvement tends to be orderly from intraglandular to adjacent nodes to upper and midjugular nodes and occasionally to retropharyngeal nodes
Bilateral nodal involvement is rare
Metastases: usually to lungs
Sites
> 90% arise in parotid gland, 5% in submandibular gland
Deep parotid tumors may present as intraoral masses
Sublingual tumors are rare and may be difficult to distinguish from minor salivary gland primary tumors of anterior floor of mouth
Minor salivary gland tumors usually in hard palate (site with most glandular tissue); may arise in lymph nodes around salivary glands
39 year old man complaining of decreased mobility of lower left eyelid and painless swelling of the left preauricular area (Folia Histochem Cytobiol 2015;53:342)
45 year old man with cytology and followup surgical pathology (J Cytol 2017;34:107)
50 year old patient with progressive facial paralysis and left parotid mass (Mod Pathol 2012;25:919)
Tumors typically have ill defined borders but may appear well circumscribed
Cut surface is heterogeneous and can show gross evidence of necrosis
Regional lymphadenopathy is common
Gross images
Contributed by Jalal B. Jalaly, M.B.B.S., M.S.
Enlarged intraparotid lymph nodes
Frozen section description
Typically not indicated as cytology is usually diagnostic of a high grade malignancy
High grade malignancy with necrosis and cellular pleomorphism
Microscopic (histologic) description
Invasive tumor cells with ample eosinophilic (oncocytic) cytoplasm forming cords, nests and cribriform glands in a desmoplastic stroma
Nuclear cytology is high grade with nuclear pleomorphism
In situ component frequently shows central necrosis
Secondary salivary duct carcinomas show pleomorphic adenoma intimately associated with the malignant component (~40% of salivary duct carcinomas are secondary) (Am J Surg Pathol 2015;39:705)
Clusters of epithelial cells with high grade pleomorphic nuclei and ample cytoplasm
Mitotic figures and apoptotic debris
Immunohistochemical stains can be done on cell block slides to confirm the diagnosis (AR positive) and rule out metastasis / other primary high grade neoplasms of the salivary gland (see
IHC section)
Contributed by Jalal B. Jalaly, M.B.B.S., M.S. and Jen-Fan Hang, M.D.
Diff-Quik
Pap stain
ThinPrep
Prominent nucleoli
Hyperchromasia
Immunofluorescence description
HER2 amplification by FISH analysis may be necessary for 2+ cases by HER2 immunohistochemistry (as defined by the American Society of Clinical Oncology / College of American Pathologists (ASCO / CAP) guidelines for breast cancer) (Arch Pathol Lab Med 2018;142:1364)
Samples are considered to be amplified when the average copy number ratio (HER2 / CEP17) is ≥ 2.0 (Oncotarget 2017;8:59023)
Which of the following immunohistochemical stains is characteristic of salivary duct carcinoma?
Androgen receptor
DOG1
Estrogen receptor
GATA3
SOX10
Board review style answer #1
A. Androgen receptor. Although GATA3 is frequently positive in salivary duct carcinoma, it is also positive in other salivary and nonsalivary gland malignancies. DOG1, SOX10 and estrogen receptor are usually negative.
What percentage of salivary duct carcinomas arise from preexisting pleomorphic adenoma (i.e., carcinoma ex pleomorphic adenoma) as seen in the photomicrograph?
Sclerosing microcystic adenocarcinoma (SMA) is an exceedingly rare tumor of presumed minor salivary gland origin that closely resembles cutaneous microcystic adnexal carcinoma (MAC)
It arises in mucosal sites in the head and neck region
SMA is made up of deeply infiltrative, variably sized bland ducts, tubules, cords and nests that contain a biphasic population of myoepithelial cells and cuboidal cells within an abundant, densely sclerotic stroma (Head Neck Pathol 2019;13:215, Surg Pathol Clin 2021;14:137)
Essential features
Sclerosing microcystic adenocarcinoma (SMA) is a unique and rare tumor of presumed salivary origin in the head and neck region that shows significant morphologic overlap with microcystic adnexal carcinoma (MAC) of the skin (Surg Pathol Clin 2021;14:137, Diagnostics (Basel) 2022;12:1288)
It is composed of a biphasic population of inner cuboidal and outer myoepithelial cells that form highly infiltrative and variably sized ducts, tubules, cords and nests within a dense collagenous stroma; perineural invasion and skeletal muscle involvement is prominent
Myoepithelial cells are often attenuated but are occasionally clear while the cuboidal component is relatively monomorphic with eosinophilic cytoplasm and round nuclei with even chromatin, occasional nucleoli and no increase in mitosis
Although follow up data are limited, patients with SMA have had uniformly good outcomes without locoregional recurrence or distant metastases (Surg Pathol Clin 2021;14:137)
Most commonly arises from minor salivary glands in the intraoral cavity, including the tongue, lip mucosa, floor of mouth and buccal mucosa, as well as the nasopharynx (Surg Pathol Clin 2021;14:137, Head Neck Pathol 2016;10:501)
SMA may show morphologic overlap with cutaneous MAC because normal intraoral minor salivary glands have morphologic and functional overlap with normal eccrine sweat glands
Recently, whole exome sequencing of a single case revealed a moderate tumor mutational burden, a putative loss of function mutation in CDK11B and no molecular overlap with mutations previously identified in MAC, though more work needs to be done (Anticancer Res 2020;40:6375)
Etiology
Like MAC, immunosuppression may play a role in the pathogenesis of SMA (several of the cases described have had a history of immunosuppressive therapy for autoimmune disorders, chemotherapy or radiation)
Both SMA and MAC exhibit an infiltrative growth pattern and a highly aggressive local behavior with perineural invasion that can cause numbness (Hum Pathol Rep 2021;26:300577)
Due to extensive perineural invasion, clear surgical margins may be difficult; patients with positive margins are recommended to undergo adjuvant radiation therapy
Diagnosis
Tumors may be visualized or palpated on the physical exam while imaging, such as CT and MRI, can be utilized to examine the extent of disease
Definitive diagnosis will typically be made on an excisional biopsy specimen
Patients with positive surgical margins are recommended to receive adjuvant radiation therapy
Although follow up data are limited, patients with SMA have had uniformly good outcomes without locoregional recurrence or distant metastases (follow up durations ranging from 21 to 60 months) (Ann Diagn Pathol 2021;54:151806, Surg Pathol Clin 2021;14:137)
73 year old man with a history of nasopharyngeal carcinoma treated with radiotherapy, presented with an ulcerating left tonsillar tumor (Ann Diagn Pathol 2021;54:151806)
5 case series of tumors closely resembling MAC occurring in the mucosal surfaces of the head and neck (Head Neck Pathol 2016;10:501)
Treatment
Wide, local excision with selective neck dissection, though lack of lymph node metastasis in the reported literature may favor against a neck dissection (Hum Pathol Rep 2021;26:300577)
Assessment of surgical margins, especially during intraoperative evaluation, is extremely challenging if not impossible due to the paucicellular and low grade nature of the tumor (Head Neck Pathol 2019;13:215)
Microscopic (histologic) description
SMA has a distinctive low power appearance of a relatively paucicellular tumor with clearly invasive variably sized ducts, tubules, cords and nests within densely sclerotic or desmoplastic stroma
Invasive component is composed of a biphasic population of inner cuboidal and outer myoepithelial cells
Myoepithelial cells are often attenuated and flattened but are occasionally more prominent and clear
Cuboidal cells are relatively monomorphic with eosinophilic cytoplasm and round nuclei with even chromatin, occasional nucleoli and no increase in mitosis
Recently, whole exome sequencing of a single case revealed a moderate tumor mutational burden, a putative loss of function mutation in CDK11B and no molecular overlap with mutations previously identified in MAC (Anticancer Res 2020;40:6375)
However, the molecular landscape of SMA is largely unknown at this point in time
Sample pathology report
Tongue, partial glossectomy:
Sclerosing microcystic adenocarcinoma (2.4 cm), margins uninvolved by carcinoma (see synoptic report and comment)
Comment: Sections show deeply infiltrative nests, cords and tubules of tumor cells embedded in prominent desmoplastic to densely collagenous stroma. The tumor is composed of a biphasic population of peripheral, flattened myoepithelial cells with central, bland cuboidal ductal cells with round nuclei, evenly dispersed chromatin and occasional nucleoli. Significant atypia and necrosis are not identified and mitotic figures are not conspicuous. Lumens of various sizes containing occasional dense, globular eosinophilic secretory material are present. The tumor infiltrated into skeletal muscles and multiple foci of perineural invasion are identified. On immunohistochemistry, the outer myoepithelial population stains positively for p63 and SMA while the inner cuboidal ductal cells stain positively for CK7. This immunohistochemical staining pattern supports the diagnosis.
CD117 is expressed by the luminal cells in virtually all cases of tubular adenoid cystic carcinoma but is consistently negative in SMA (Ann Diagn Pathol 2021;54:151806)
Detection of MYB or MYBL1 rearrangements can also confirm the diagnosis of adenoid cystic carcinoma in 50 - 80% of cases (Surg Pathol Clin 2021;14:137)
Cystic with admixture of intermediate cells, epidermoid cells and scattered mucocytes or nests of mucocytes in varying proportions
Lacks the characteristic sclerotic / hyalinized stroma observed in SMA
One exception is an uncommon eosinophilic variant of MEC with areas of hyalinization
However, this rare variant manifests in major salivary glands, mainly the parotid gland and prominent eosinophilia is not observed in SMA (Diagnostics (Basel) 2022;12:1288)
Detection of MAML2 gene fusions can confirm the diagnosis
Which of the following immunohistochemical staining patterns support a diagnosis of sclerosing microcystic adenocarcinoma?
CK7 in central ductal / epithelial component; p63 in peripheral myoepithelial cell population
p63 in central ductal / epithelial component; CK7 in peripheral myoepithelial cell population
S100 in central ductal / epithelial component; pancytokeratin in peripheral myoepithelial cell population
SMA in central ductal / epithelial component; pancytokeratin in peripheral myoepithelial cell population
Board review style answer #1
A. CK7 in central ductal / epithelial component; p63 in peripheral myoepithelial cell population. The central ductal component showing positivity for pancytokeratin and CK7 and the peripheral myoepithelial cell population expressing smooth muscle actin, S100, p63 and p40 (Surg Pathol Clin 2021;14:137). Answers B - D are incorrect because these are not the immunohistochemical staining patterns for sclerosing microcystic adenocarcinoma.
Sclerosing microcystic adenocarcinoma (SMA) has been seen in association with which of the following?
Alcohol
HPV infection
Immunosuppression
Smoking
Board review style answer #2
C. Immunosuppression. SMA frequently arises in the context of immunosuppression (Anticancer Res 2020;40:6375). Answers A, B and D are incorrect because alcohol, HPV infection and smoking have not been reported as associations with this tumor.
Parotid gland (around 70%), occasional examples in the submandibular glands and oral cavity (Am J Surg Pathol 2017;41:e33)
Pathophysiology
Originally believed to be a reactive, nonneoplastic process resembling fibrocystic changes of the breast but evidence suggests it is likely neoplastic (Head Neck Pathol 2020;14:630)
Demonstration of clonality in 6 cases using the human androgen receptor assay (HUMARA) (Am J Surg Pathol 2006;30:939)
Targeted next generation sequencing demonstrated mutations in genes that are well established to be drivers in human neoplasms (Head Neck Pathol 2020;14:630)
Well circumscribed proliferation of scattered dilated, variably sized ducts lined by hyperplastic epithelium in a vague nodular pattern
Foci of apocrine change
Dense stroma
Because a definitive diagnosis may not be possible at the time of frozen section, a descriptive interpretation such as "sclerotic fibrous material with benign appearing glandular elements" could be rendered (Pathology 2016;48:93)
Comment: Sections show a well demarcated nodule of densely collagenized stroma intermingling among a proliferation of acini and tubules. The latter are lined by cells which vary from vacuolated to foamy to apocrine to mucinous. Some ducts possess a hyperplastic epithelium with atypia reminiscent of ductal carcinoma in situ. Acini are remarkable for prominent eosinophilic intracytoplasmic granules which are highlighted upon PAS stain. No invasive growth is recognized.
A 50 year old woman presents with a slow growing parotid mass. Calponin and p63 immunostains highlighted a subset of the cells. Elsewhere in the lesion, acini containing large, brightly eosinophilic, periodic acid-Schiff positive, intracytoplasmic granules were identified. What is the most likely diagnosis?
Generally indolent clinical course with recurrence rates of < 10% and 10 year overall survival of 95% after macroscopically complete resection (Head Neck 2019;41:1227)
While definite thresholds are not yet described, nuclear pleomorphism, easily identified mitotic activity or presence of comedonecrosis have been described to confer poor prognosis (Int J Clin Exp Pathol 2014;7:9008)
44 year old man with painless buccal mass showing high grade transformation on histology developed pleural metastases within months of diagnosis (Int J Surg Pathol 2017;25:613)
59 year old woman with metastatic high grade secretory carcinoma with ETV6-RET rearrangement (Am J Surg Pathol 2018;42:1121)
74 year old man with cervical lymph node involvement with no evident primary site of disease (Case Rep Oncol 2017;10:192)
Pale eosinophilic colloid-like intraluminal secretions; secretions are periodic acid-Schiff (PAS) reagent positive and diastase resistant (Am J Surg Pathol 2010;34:599)
Tumor cells have eosinophilic or vacuolated cytoplasm and monomorphic round vesicular nuclei with small but distinctive nucleoli
Occasional lymphovascular invasion and perineural invasion are seen (Head Neck 2019;41:1227)
High grade transformation has been reported with a distinct population of tumor cells exhibiting solid or trabecular growth, infiltrative margins, desmoplastic stromal reaction, comedo-like necrosis, nuclear pleomorphism, increased mitotic rate, loss of secretory activity and perineural invasion
Cohesive clusters or sheets of epithelial cells with variable eosinophilic, granular to vacuolated cytoplasm and uniform nuclei with single nucleoli (APMIS 2019;127:491)
GATA3: 100% sensitive; useful to distinguish from histologic mimic acinic cell carcinoma but nonspecific (53%) when the differential diagnoses include a variety of other salivary gland neoplasms (Head Neck Pathol 2013;7:311)
Salivary gland neoplasms characterized by gene fusions
Case presentations of various salivary gland pathologies
Sample pathology report
Left parotid, excision:
Secretory carcinoma (see comment)
Comment: There is a well demarcated but focally infiltrative parotid neoplasm with lobulated growth, macrocystic and microcystic areas. The cysts are lined by relatively monomorphic epithelioid cells with moderate amounts of vacuolated eosinophilic cytoplasm and a central round nucleus with a small but distinctive nucleolus. The microcysts contain colloid-like eosinophilic secretions. Immunohistochemistry shows tumor cells to be positive for S100, MUC4, pan-TRK and GATA3 and negative for DOG1. The combined morphological and immunohistochemical features strongly support the diagnosis of secretory carcinoma, a primary salivary gland malignancy. This is further confirmed by fluorescent in situ hybridization using ETV6 break apart probe demonstrating ETV6 rearrangement. Lymphovascular or perineural involvement is not seen. The tumor is 2 mm from the closest margin of resection.
Secretory carcinoma generally demonstrates indolent behavior. However, it has a propensity to recur unless completely excised. Local lymph node metastasis occurs in up to 22% of patients and distant metastasis, while rare, has been reported in a subset of cases
A 48 year old man has a parotid nodule for 9 - 12 months. Which of the following is true?
It is characterized by PAS diastase resistant cytoplasmic zymogenic granules and immunohistochemically by positivity for DOG1 and S100
It is characterized by PAS diastase resistant cytoplasmic zymogenic granules and immunohistochemically by positivity for ER and PR
It is characterized histologically by PAS diastase resistant intraluminal secretions and immunohistochemically by positivity for androgen receptor and p63
It is characterized histologically by PAS diastase resistant intraluminal secretions and immunohistochemically by positivity for pan-TRK, S100 and mammaglobin
It is generally a highly aggressive malignancy with most patients showing distant solid organ metastases at presentation
Board review style answer #1
D. It is characterized histologically by PAS diastase resistant intraluminal secretions and immunohistochemically by positivity for pan-TRK, S100 and mammaglobin. The image shows a secretory carcinoma with abundant secretions.
A 49 year old woman has a lesion on the floor of the mouth with metastases to lymph nodes. The tumor cells show strong staining with S100 and MUC4. Which of the following genetic changes are likely to be found in this tumor?
ETV6-NTRK3 translocation
HER2 amplification
MAML2-CRTC1 translocation
MYB-NFIB translocation
PLAG1 translocation
Board review style answer #2
A.ETV6-NTRK3 translocation. The image shows a secretory carcinoma with papilliform architecture.
While immunization has reduced the frequency of paramyxovirus (mumps), there were 150 outbreaks and 9,000 cases in the United States between 2015 and 2017 (JAMA 2019;322:1022)
Sites
Both affect the parotid; however, mumps is typically bilateral
Parotid is more prone to acute suppurative sialadenitis because serous saliva is less able to protect against bacterial infection than the mucoid rich content of saliva from the sublingual and submandibular glands (Oral Maxillofac Surg Clin North Am 2009;21:353)
Etiology
Acute suppurative sialadenitis is due to retrograde bacterial contamination from the oral cavity in a setting of impaired salivary flow
Staphylococcus aureus is the most common cause; Streptococcal species and Haemophilus influenza are also common (Ann Surg 1962;156:251)
Patients present with tender enlargement of the salivary glands
Epididymo-orchitis occurs in 20 - 30% of postpubertal males affected by mumps (Am J Hyg 1959;69:91)
Diagnosis
Diagnosis of mumps is made on symptoms and physical exam and is supported by serology or reverse transcription PCR (RT-PCR) (J Virol Methods 2020;277:113817)
Based on clinical examination with culture of purulent discharge
14 year old girl presents with facial swelling after orthodontic treatment (J Orthod 2012;39:314)
50 year old woman develops parotid swelling after endoscopic retrograde cholangiopancreatography (Gastrointest Endosc 2011;74:199)
Treatment
Acute suppurative sialadenitis is managed by antimicrobial therapy based on culture result with surgical drainage if abscess develops
Mumps is self limited
Microscopic (histologic) description
Diagnoses of both acute suppurative and viral sialadenitis are usually reached on clinical grounds, although rarely biopsied
Acute suppurative sialadenitis is associated with edema, hyperemia and acute inflammation
Viral sialadenitis shows diffuse interstitial edema, intense hyperemia and a dense lymphohistiocytic infiltrate (Am J Pathol 1949;25:1105)
Sample pathology report
Parotid, right, biopsy:
Acute suppurative sialadenitis (see comment)
Comment: There is edema, hyperemia, bacteria and increased numbers of neutrophils. Neutrophils surround and infiltrate ducts and focally is associated with duct destruction. If clinically indicated, correlation with culture results would be helpful in directing appropriate antibiotic therapy.
Differential diagnosis
Diagnosis of infectious sialadenitis is usually made clinically and thus microscopic evaluation is rare
Rare benign biphasic tumor with exophytic squamous component and endophytic glandular component
Well differentiated papillary hyperplastic squamous epithelium covering ductal component of cleft-like cystic spaces lined by cuboidal or columnar epithelium with occasional goblet cells
Well circumscribed, round / oval, papillary tumor of mucosal surface
Microscopic (histologic) description
Biphasic, with well differentiated papillary hyperplastic squamous epithelium covering ductal component of cleft-like cystic spaces lined by cuboidal or columnar epithelium with occasional goblet cells
Oncocyte is predominant cell; contains numerous mitochondria, parallel filaments within cell cytoplasm attached by desmosomes (Arch Pathol Lab Med 1986;110:523)
Tight, solid clusters of atypical basaloid cells plus dispersed epithelial and myoepithelial cells with metachromatic magenta hyaline globular material
Characterized by lymphocytic infiltrates of the affected glands with subsequent dysfunction of these glands and the clinical picture of sicca syndrome
Considered primary if not associated with other systemic disease or secondary if it occurs in association with another underlying autoimmune condition (Clin Exp Med 2022;22:9)
Essential features
Chronic autoimmune disorder of uncertain etiology
Characterized by focal lymphocytic sialadenitis with subsequent clinical sequela including keratoconjunctivitis sicca (dry eyes) and xerostomia (dry mouth)
Diagnosed using a combination of subjective and objective measures as determined by the 2016 American College of Rheumatology / European League Against Rheumatism (ACR / EULAR) classification
Salivary gland biopsy findings consistent with diagnosis are focal lymphocytic sialadenitis with a focus score (FS) ≥ 1
Incidence of 6.92 per 100,000 person-years (person-years is defined as the estimate of the actual time at risk in years that all persons contributed to a study) (95% confidence interval, 4.98 - 8.86)
Prevalence of 60.82 cases per 100,000 inhabitants (Europe, South America, Asia) (95% confidence interval, 43.69 - 77.94) (Ann Rheum Dis 2015;74:1983)
Numerous theories have been proposed; however, a consensus has not been established (Immunol Lett 2011;141:1)
Etiology
Etiology is unknown
Likely multifactorial with potential genetic, environmental and hormonal factors suggested; however, no causal associations have been demonstrated (Clin Exp Rheumatol 2022;40:2211)
Primary Sjögren syndrome
90% of patients with high anti-Ro and anti-La antibody titers are HLA DR3 positive (Clin Med (Lond) 2007;7:53)
Secondary Sjögren syndrome
Sjögren syndrome associated with rheumatoid arthritis has a different genetic background (HLA DR4) (Lancet 2005;366:321)
Diagrams / tables
Images hosted on other servers:
ACR / EULAR classification criteria for primary Sjögren syndrome
Score ≥ 4 is compatible with a diagnosis of primary Sjögren syndrome in patients experiencing ocular or oral dryness or with clinical suspicion due to systemic features (Arthritis Rheumatol 2017;69:35)
Factors assessed include
Labial salivary gland biopsy with lymphocytic sialadenitis and focus score ≥ 1 (3 points)
Hypoechogenic areas, hyperechogenic reflections and poorly defined salivary gland borders (J Clin Med 2020;9:2492)
Ultrasound findings may be incorporated in the diagnostic features in the future; however, these require further validation (Clin Exp Rheumatol 2018;36:159)
Radiology images
Images hosted on other servers:
Sialography findings: normal versus Sjögren
Ultrasound findings suggestive of primary Sjögren syndrome
Prognostic factors
High focus score predicts greater decline in unstimulated salivary flow over time (Ann Rheum Dis 2008;67:949)
Overall increased risk of lymphoma with an estimated risk of 5 - 15% of patients (Presse Med 2012;41:e511)
Risk of lymphoma thought to be 40 times greater than the general population (Ann Intern Med 1978;89:888)
Most commonly low grade non-Hodgkin lymphoma, specifically extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma
Features thought to be associated with increased risk of transformation to lymphoma include
High focus score
Particularly focus score ≥ 3 has a positive predictive value of 16% and negative predictive value of 98% for non-Hodgkin lymphoma (Ann Rheum Dis 2014;73:1537)
Detection of ectopic germinal centers, although some studies did not find these a predictive factor for MALT lymphoma (Rheumatology (Oxford) 2013;52:276)
Recommended at least 4 labial salivary glands with a surface area of at least 8 mm2 to allow for adequate assessment and focus scoring (Ann Rheum Dis 2017;76:1161)
Microscopic (histologic) images
Contributed by Alice Ormandy, M.B.B.S., M.P.H. and Salman Marvi, M.D.
Multiple nodular lymphocytic aggregates
Lymphocytic aggregates with germinal centers
Nodular lymphocytic aggregate
Core biopsy parotid
Germinal center
Submandibular gland lymphoid aggregates
Submandibular gland germinal centre
Cytology description
Nonspecific findings
May find benign myoepithelial and ductal epithelial cells interspersed with a lymphocytic infiltrate
Focal lymphocytic sialadenitis with associated mild atrophy of the salivary acini (see comment)
Comment: There is a single nodular lymphocytic aggregate (1 cluster of > 50 lymphocytes per 4 mm2, focus score = 1). There is no germinal center formation and no features to suggest malignancy. The finding of focal chronic sialadenitis with a focus score of 1 is compatible with the diagnosis of Sjögren syndrome in the correct clinical context. Correlation with clinical history, radiology, serology and flow cytometry is recommended.
What features on the salivary gland biopsy shown from a patient with Sjögren syndrome are associated with an increased risk of lymphoma?
Atrophy
Fat infiltration
Fibrosis
Focus score ≥ 3
Board review style answer #1
D. Focus score ≥ 3. A high focus score, particularly ≥ 3, has a positive predictive value of 16% and negative predictive value of 98% for non-Hodgkin lymphoma (Ann Rheum Dis 2014;73:1537). Answers A, B and C are incorrect because fat infiltration and fibrosis are all features that can be present in salivary gland biopsies of patients with Sjögren syndrome; however, they have not been associated with increased risk of lymphoma in these patients.
What is the most common salivary gland lymphoma occurring in patients with primary Sjögren syndrome?
Diffuse large B cell lymphoma
Extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma
Follicular lymphoma
Hodgkin lymphoma
Board review style answer #2
B. Extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma. Answers A and C are incorrect because diffuse large B cell lymphoma and follicular lymphoma have been reported in salivary glands; however, they are not the most common lymphoma in this site. Answer D is incorrect because Hodgkin lymphoma is rare in salivary glands (Rheumatology (Oxford) 2022;61:3818).
True salivary gland primaries of squamous cell carcinoma are very rare; most squamous cell carcinomas are metastases to intraparotid lymph nodes from primaries in oral cavity, upper aerodigestive tract or skin
Squamous cell carcinomas represent 16 - 54% of malignant salivary gland tumors, about 11% of malignant tumors of major salivary glands
Clinical features
Squamous cell carcinomas (primary or secondary) are most frequent parotid malignant tumor (30 - 37%), represent 4% of submandibular gland tumors
Usually men (when considering major salivary gland tumors); also associated with AIDS
May occur in Stensen duct
Rapid painless growth with infiltration of surrounding structures, regardless of origin; may cause acute facial paralysis
Staging of definitive resections for primary salivary gland carcinoma and neuroendocrine carcinoma of the parotid, submandibular or sublingual gland should use this system
On occasion it may be difficult to distinguish a sublingual salivary gland primary with certainty from a salivary gland tumor arising from minor salivary glands in the anterior floor of mouth
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
There are no significant changes to pT classification
Carcinomas for which the pTis designation may be applied include some intracapsular carcinomas ex pleomorphic adenomas and intraductal carcinomas
pN classification now incorporates extranodal extension
Use of the CAP protocol is not required for recurrent tumors or for metastatic tumors that are resected at a different time than the primary tumor
Use of this protocol is also not required for pathology reviews performed at a second institution (i.e. secondary consultation, second opinion or review of outside case at second institution)
pT1: Tumor ≤ 2 cm without extraparenchymal extension
pT2: Tumor > 2 cm but ≤ 4 cm without extraparenchymal extension
pT3: Tumor > 4 cm or tumor with extraparenchymal extension
pT4a: Tumor of any size invading skin, mandible, ear canal or facial nerve
pT4b: Tumor of any size invading skull base or pterygoid plates or encases carotid artery
Notes:
Extraparenchymal extension is clinical or macroscopic evidence of invasion of soft tissues
Microscopic evidence alone does not constitute extraparenchymal extension for classification purposes
Regional lymph nodes (pN)
pNX: Regional lymph nodes cannot be assessed
pN0: No regional lymph node metastasis
pN1: Metastasis in a single ipsilateral lymph node ≤ 3 cm without extranodal extension
pN2a: Single ipsilateral lymph node metastasis ≤ 3 cm with extranodal extension or > 3 cm but ≤ 6 cm without extranodal extension
pN2b: Metastasis in multiple ipsilateral lymph nodes ≤ 6 cm without extranodal extension
pN2c: Metastasis in bilateral or contralateral lymph node(s) ≤ 6 cm without extranodal extension
pN3a: Metastasis in a lymph node > 6 cm without extranodal extension
pN3b: Extranodal extension in a single ipsilateral lymph node > 3 cm or single contralateral node or multiple nodes with metastases, any with extranodal extension
Notes:
A selective neck dissection will include 10+ lymph nodes and a comprehensive neck dissection (radical or modified radical neck dissection) will include 15+ lymph nodes
Negative pathologic examination of a smaller number of nodes still mandates a pN0 designation
Midline nodes are considered ipsilateral nodes
Measurement of tumor metastasis:
Cross sectional diameter of the largest lymph node metastatic deposit (not the lymph node itself) is measured in the gross specimen at the time of macroscopic examination or if necessary, using the histologic slide
Extranodal extension (ENE):
AJCC 8th edition introduces the use of ENE in pN categorization
Must be clearly defined as tumor present within the confines of the lymph node and extending through the lymph node capsule into the surrounding connective tissue, with or without associated stromal reaction
Distant metastasis (pM)
pM0: No distant metastasis
pM1: Distant metastasis
AJCC prognostic stage grouping
Stage 0:
Tis
N0
M0
Stage I:
T1
N0
M0
Stage II:
T2
N0
M0
Stage III:
T3
N0
M0
T0 - 3
N1
M0
Stage IVA:
T4a
N0 - 1
M0
T0 - 4a
N2
M0
Stage IVB:
Any T
N3
M0
T4b
Any N
M0
Stage IVC:
Any T
Any N
M1
Registry data collection variables
Extranodal extension clinical (present versus absent)
Extranodal extension pathological (present versus absent)
Extent of microscopic extranodal extension (distance of extension from the native lymph node capsule to the farthest point of invasion in extranodal tissue)
Perineural invasion
Lymphovascular invasion
p16 / HPV status
Performance status
Tobacco use and pack years
Alcohol use
Depression diagnosis
Histopathologic type
Mucoepidermoid carcinoma
Adenoid cystic carcinoma
Acinic cell carcinoma
Polymorphous adenocarcinoma
(Mammary analogue) secretory carcinoma
Salivary duct carcinoma
Carcinoma ex pleomorphic adenoma
Epithelial myoepithelial carcinoma
(Hyalinizing) clear cell carcinoma
Adenocarcinoma, not otherwise specified
Includes cystadenocarcinoma, intestinal type adenocarcinoma and mucinous adenocarcinoma
Basal cell adenocarcinoma
Carcinosarcoma
Intraductal carcinoma
Lymphoepithelial carcinoma
Myoepithelial carcinoma
Oncocytic carcinoma
Poorly differentiated carcinoma
Large cell neuroendocrine carcinoma
Small cell neuroendocrine carcinoma
Undifferentiated carcinoma
Sebaceous adenocarcinoma
Squamous cell carcinoma
Notes:
In this current classification, sialoblastoma is designated as a tumor of uncertain malignant potential
Metastasizing pleomorphic adenoma has been collapsed under pleomorphic adenoma
Since the biologic behavior of these still overlaps with the other malignant tumors, these can be reported under "other"
Board review style question #1
Regarding the following parotid gland primary salivary gland adenocarcinoma, which of the pT category criteria in the 8th edition AJCC staging guide is satisfied by the examination of this gross resection specimen photograph?
pT1 by depth of invasion
pT2 by tumor size
pT3 by presence of necrosis
pT3 by extraparenchymal extension
Board review style answer #1
D. pT3 by extraparenchymal extension (white arrows point to border of skeletal muscle, yellow arrows point to border of malignancy, black arrow points to tumor invading skeletal muscle)
FNA that shows cytologic features suggestive of malignancy and meets some but not all of the criteria for malignancy
FNA should be subcategorized if possible (e.g., suspicious for a primary salivary gland malignancy, suspicious for metastasis, suspicious for lymphoma)
15 - 35% of parotid gland, 41 - 45% of submandibular and 70 - 90% of sublingual glands tumors are malignant (Head Neck Pathol 2022;16:1043)
In comparison, more than half of minor gland tumors (including palate, tongue, the floor of the mouth, retromolar region and lips) are likely to be malignant (Head Neck Pathol 2022;16:1043)
Clinical features
Frequency among all the Milan system categories: 4%
Risk of malignancy (ROM) is 83% in the 2nd edition of Milan System, with a large study demonstrating a ROM of 83.3% (Cancer Cytopathol 2018;126:94)
Laboratory
For FNAs of suspicious for malignancy (SM), ancillary studies can help to refine the differential diagnosis and place the specimen into a more definitive diagnostic category
Pathologic lymph nodes in the drainage territory of a mass are suggestive of malignancy (Radiographics 2006;26:745)
Cytology description
FNA should be subcategorized if possible (e.g., suspicious for a primary salivary gland malignancy, suspicious for a metastasis, suspicious for lymphoma) (Diagn Cytopathol 2017;45:820)
Significant proportion will be suboptimal samples of a high grade carcinoma
Reasons that a salivary gland FNA leads to an interpretation of suspicious for malignancy include
Presence of markedly atypical cells with poor smear preparation, cell preservation, fixation artifact or obscuring blood or inflammation
Presence of limited cytologic features of a specific type of malignancy
Scant cellularity but presence of markedly atypical or suspicious cytologic features (prominent nucleoli, anisonucleosis, increased N:C ratio, nuclear molding, prominent nuclear pleomorphism, atypical mitoses and coarse chromatin)
Scant sample with features suggestive of a neuroendocrine neoplasm
Scant sample with features suggestive of a metastatic lesion
Many of the aspirates of lymphoma classified as suspicious for malignancy lack sufficient material for ancillary studies; some of the cytomorphologic features suggestive of lymphoma include
Prominent population of large atypical lymphocytes with coarse chromatin and prominent nucleoli, seen in large cell lymphomas
Monomorphic population of small to intermediate sized lymphocytes, seen in follicular lymphoma, mantle cell lymphoma, small lymphocytic lymphoma
Heterogeneous lymphoid population with atypical forms, seen in extranodal marginal zone lymphomas (EMZL), in particular in patients with history of Sjögren syndrome
Cytology images
Contributed by Manish Mahadeorao Bundele, M.B.B.S., M.D. and Rebecca Tian Mei Au, M.B.B.S.
Suspicious for acinic cell carcinoma
Suspicious for adenoid cystic carcinoma
Suspicious for mucoepidermoid carcinoma
Suspicious for large cell lymphoma
Suspicious for metastatic carcinoma
Suspicious for high grade basal cell adenocarcinoma
Sample pathology report
Parotid, right, fine needle aspiration smears:
Satisfactory for evaluation
Suspicious for malignancy
Rare markedly atypical cell clusters, suspicious for high grade carcinoma
Parotid, right, fine needle aspiration smears:
Satisfactory for evaluation
Suspicious for malignancy
Atypical cell clusters in a mucinous background, suspicious for low grade mucoepidermoid carcinoma
Parotid, right, fine needle aspiration smears:
Satisfactory for evaluation
Suspicious for malignancy
Monomorphic population of small lymphoid cells, suspicious for non-Hodgkin lymphoma (see comment)
Comment: Additional tissue sampling either by repeat FNA or other tissue biopsy is recommended for further evaluation with ancillary studies, including flow cytometry.
Parotid, right, fine needle aspiration smears:
Evaluation limited by low yield of well preserved cells
Suspicious for malignancy
Cyst contents with atypical squamous cells with enlarged hyperchromatic nuclei / dyskeratotic cells, suspicious for metastatic keratinizing squamous cell carcinoma
Differential diagnosis
Aspirates with scant cellularity but presence of markedly atypical cells:
Highly cellular with 3 dimensional clusters and single discohesive cells in a dirty / necrotic background and with overtly malignant cytologic features with abundant finely granular cytoplasm, nuclear pleomorphism, prominent nucleoli and frequent mitoses
Wide range of cytomorphologic appearances; classically shows discohesive pleomorphic cells with eccentric nuclei, prominent nucleoli and fine to coarsely granular cytoplasmic melanin pigment
Cellular aspirate with lymphoepithelial lesions (cohesive sheets of ductal cells and small mature lymphocytes percolating through the epithelial sheets)
Mixed population of lymphocytes, dendritic cells and tingible body macrophages with predominance of small mature lymphocytes
Irregular sheets and clusters of large polygonal cells with abundant homogeneous granular cytoplasm, well defined cytoplasmic borders and enlarged, round nuclei with distinct nucleoli
What is the risk of malignancy on excision if a diagnosis of suspicious for malignancy is given on a fine needle aspiration (FNA) of the parotid?
~40%
~60%
> 80%
Board review style answer #1
D. > 80%. The risk of malignancy is 83%, as per the Milan System for Reporting Salivary Gland Cytopathology. Answers A - C are incorrect because the risk on excision is higher than 80% if reported as suspicious for malignancy on FNA.
This is a representative image from a parotid gland fine needle aspiration. On cell block immunostaining, the epithelial cell clusters are positive for GATA3, AR and negative for DOG1, while the spindle cells are positive for p63 and SOX10. What category should this aspirate be placed in according to the Milan System for Reporting Salivary Gland Cytopathology?
Atypia of undetermined significance
Benign neoplasm
Malignant
Suspicious for malignancy
Board review style answer #2
D. Suspicious for malignancy. As mentioned above, on cell block immunostaining the atypical epithelial cell clusters are positive for GATA3, AR and negative for DOG1. These features raise the possibility of carcinoma with oncocytoid / apocrine features, such as salivary duct carcinoma. The background bland spindle myoepithelial cells are positive for p63 and SOX10 suggests a pleomorphic adenoma component. Given the limited cluster of cells with carcinoma morphology and admixed with bland myoepithelial cells, the correct answer is suspicious for malignancy. Answer B is incorrect because atypical cells are seen. Answer A is incorrect because the degree of atypia seen in these few atypical cell clusters is of high grade and is generally beyond this category. Answer C is incorrect because qualitative and quantitative features of atypical cells are insufficient for this category.
Solid areas and multiple cysts with papillary projections are apparent on the cut surface
Gross images
Contributed by Sapna Balgobind, M.B.B.Ch.
Cut surface
Microscopic (histologic) description
Varying proportions of papillary cystic structures lined by bilayered oncocytic epithelial cells and surrounded by a lymphoid stroma including germinal centers
Epithelial component is comprised of inner columnar and outer cuboidal cells
Limited foci of squamous, mucous, ciliated and sebaceous cells can be present
Absent MAML2 fusion (positive in mucoepidermoid carcinoma)
Sample pathology report
Salivary gland, parotidectomy:
Warthin tumor (see comment)
Comment: Sections show a well circumscribed tumor with a papillary architecture. The papillae are lined by bilayered oncocytic epithelial cells with a surrounding lymphoid stroma, containing germinal centers.
A 49 year old man presents with bilateral, slow growing parotid masses. An H&E section of the tumor is pictured above. What is the most likely diagnosis?
Classic Warthin tumor
Lymphoepithelial cyst
Oncocytoma
Warthin-like variant of mucoepidermoid carcinoma
Board review style answer #1
A. Classic Warthin tumor. The photograph shows features of a classic Warthin tumor with papillary structures lined by bilayered oncocytic epithelium. The other entities on the list do not match the entity shown on the H&E photograph provided.