





























































































































































































Primary tumor (pT)
- TX: Tumor cannot be assessed
- T0: No evidence of primary tumor
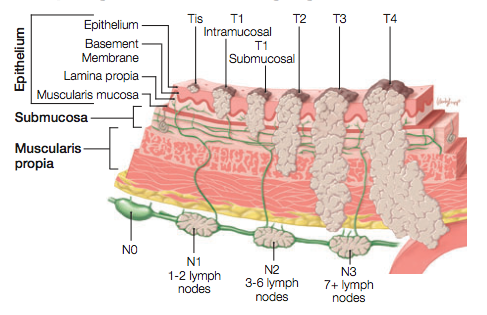
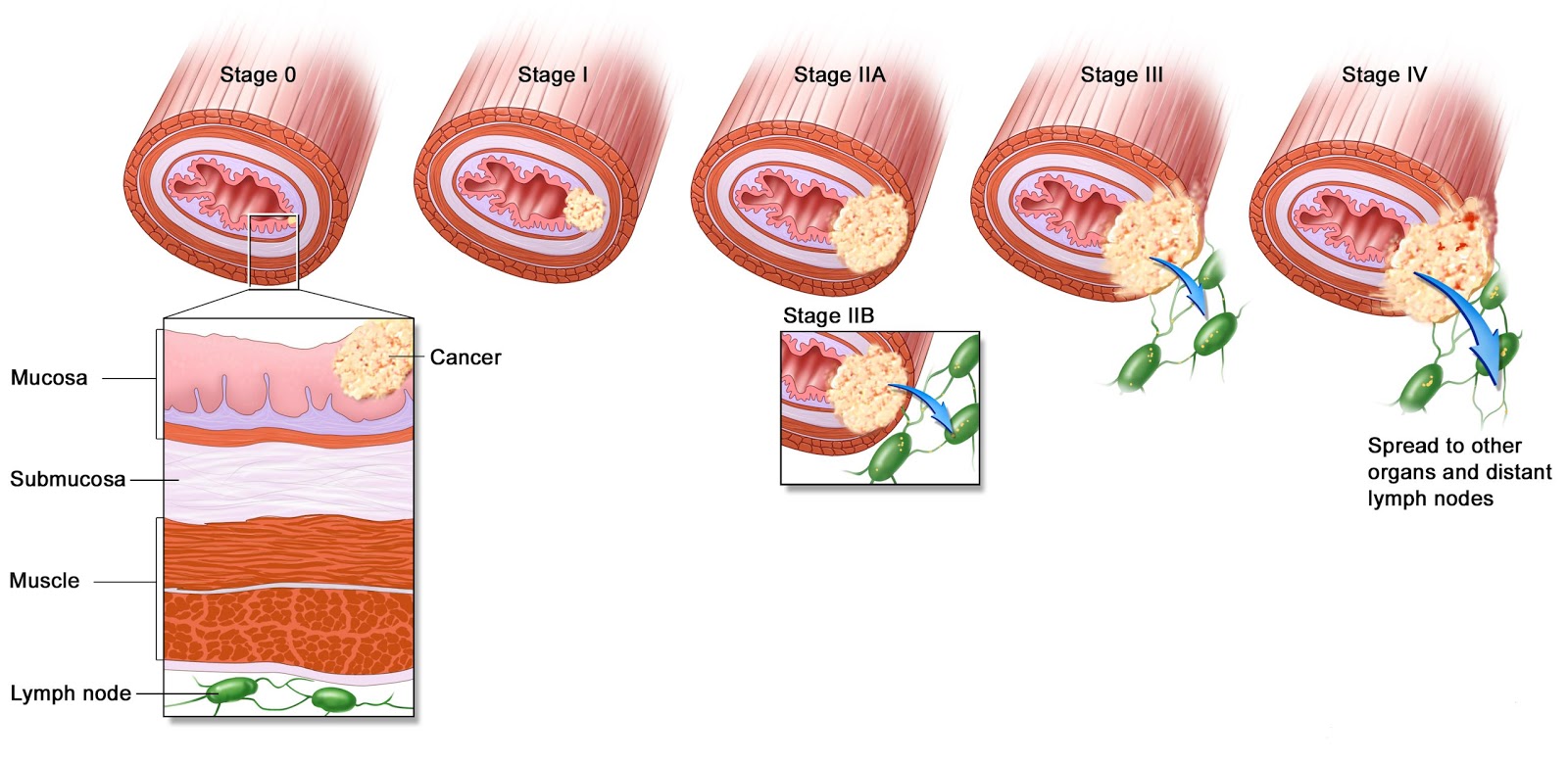
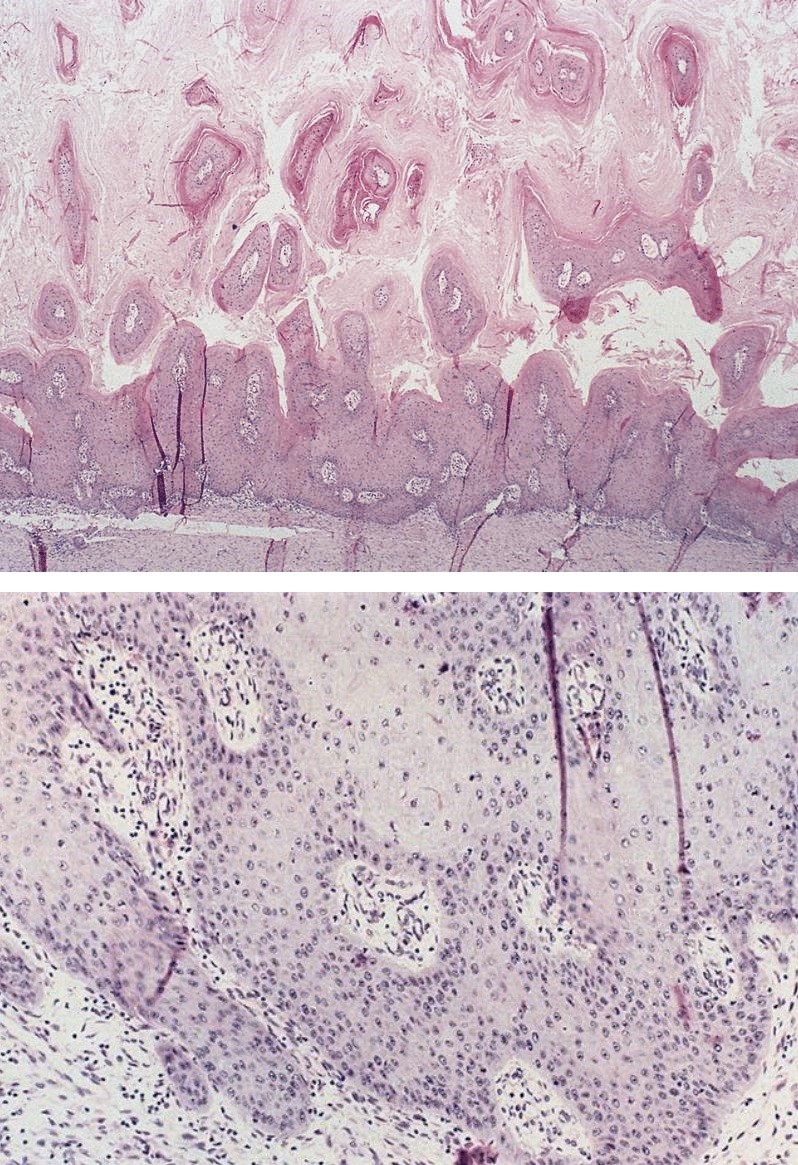
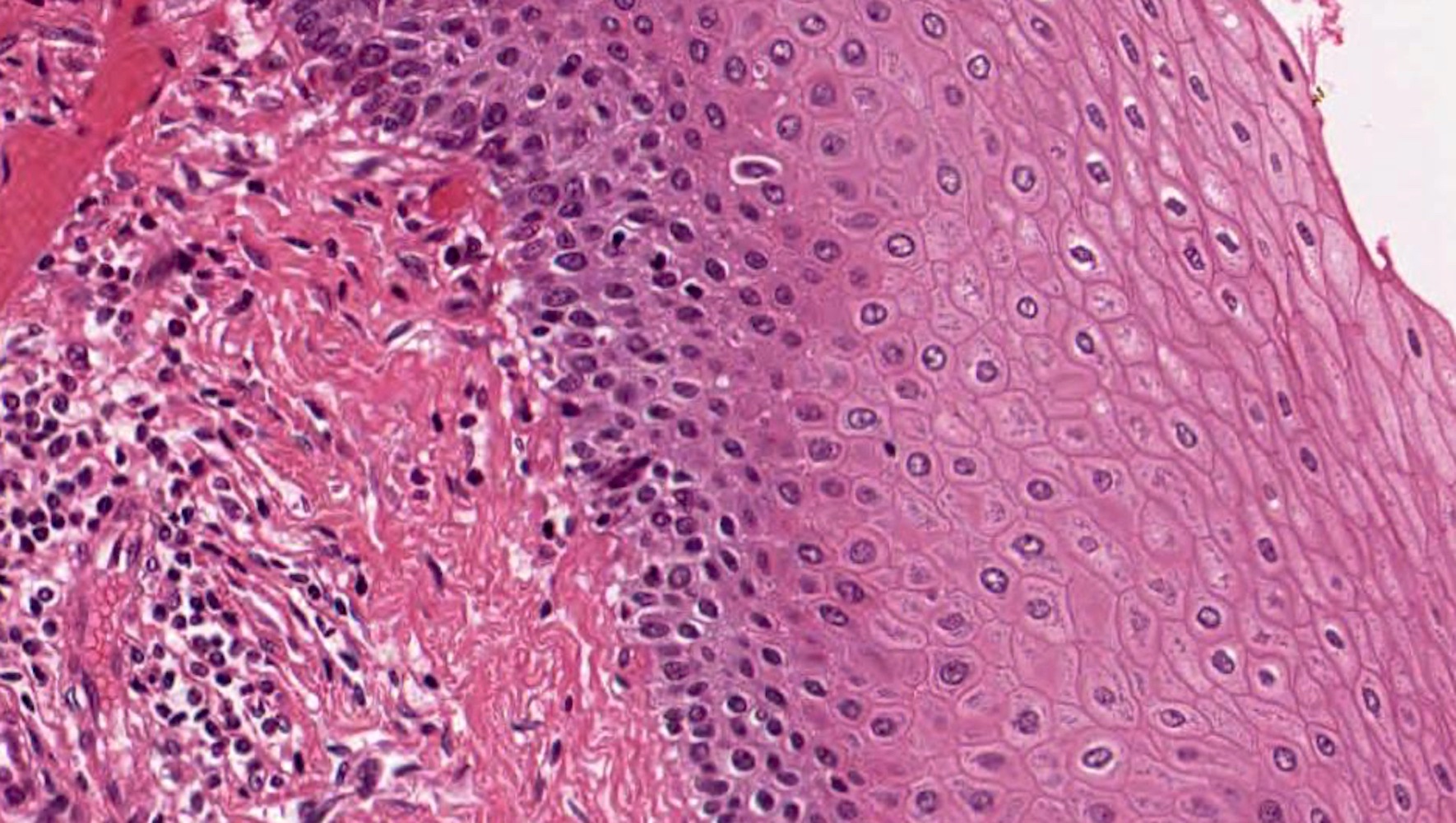
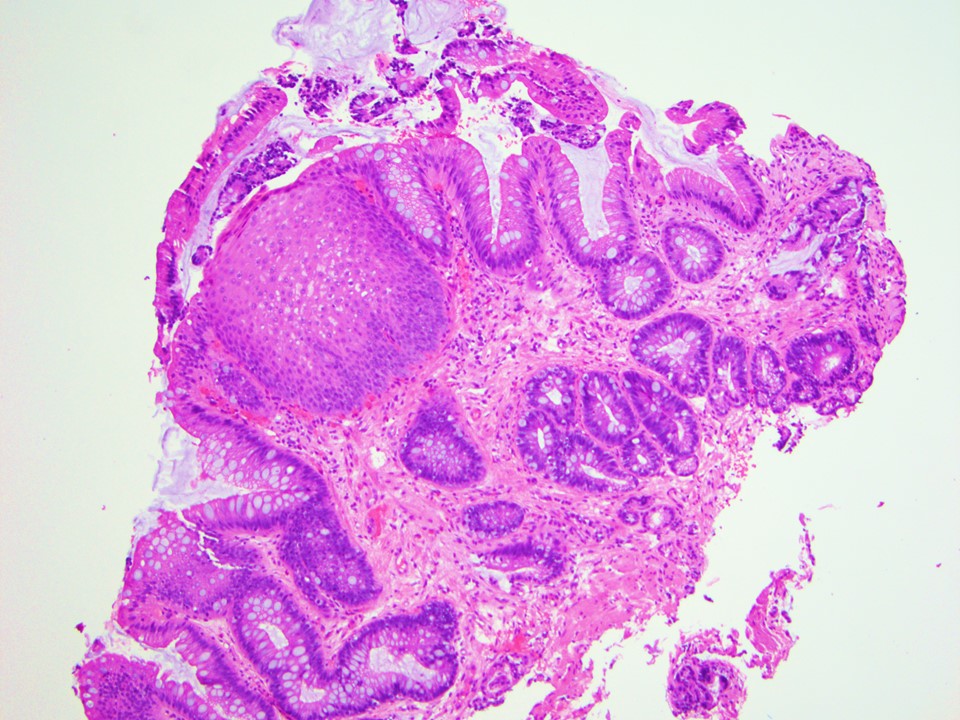
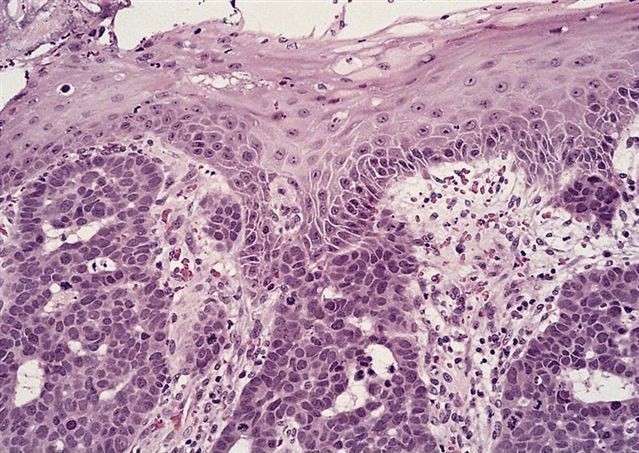
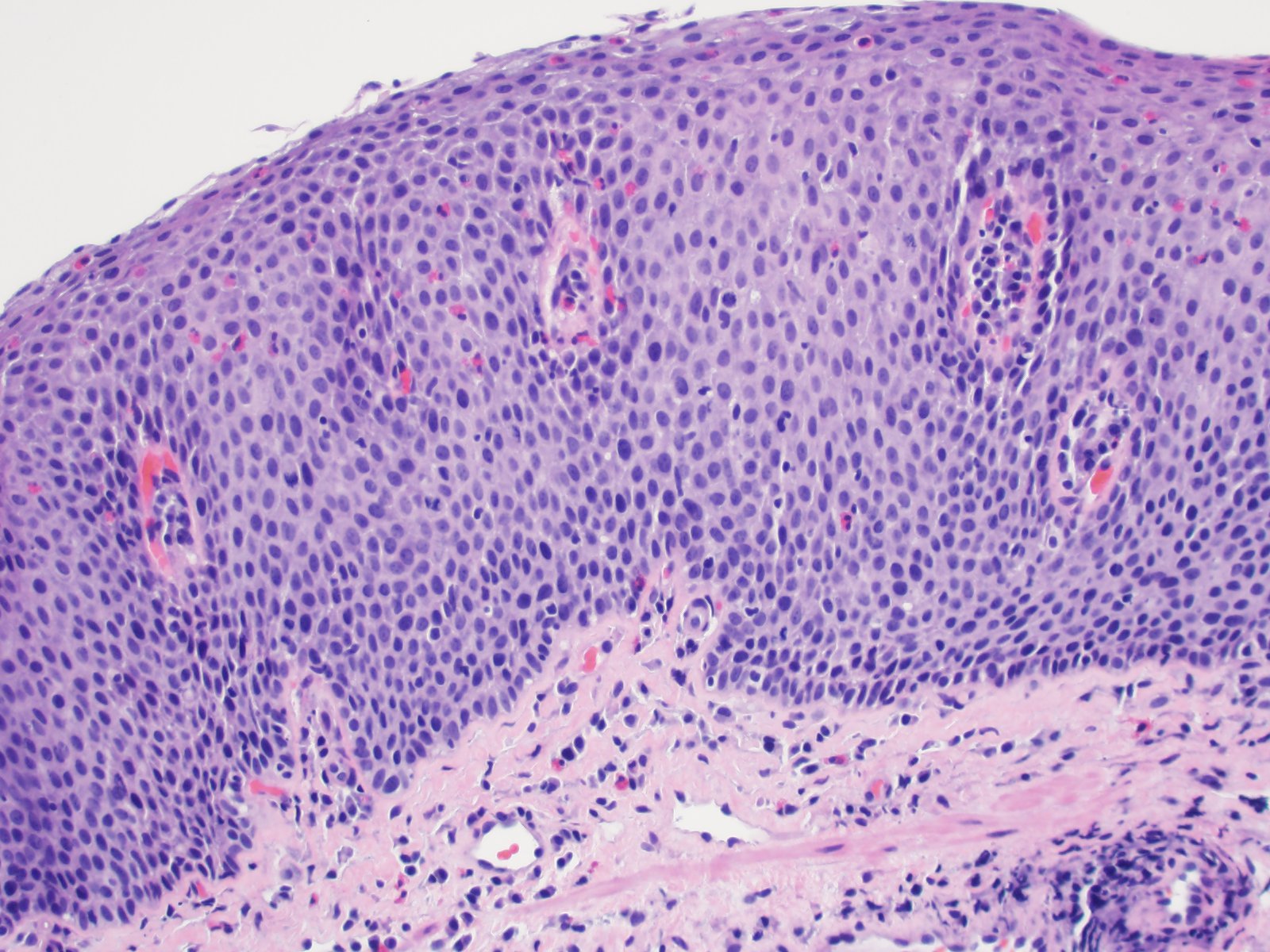
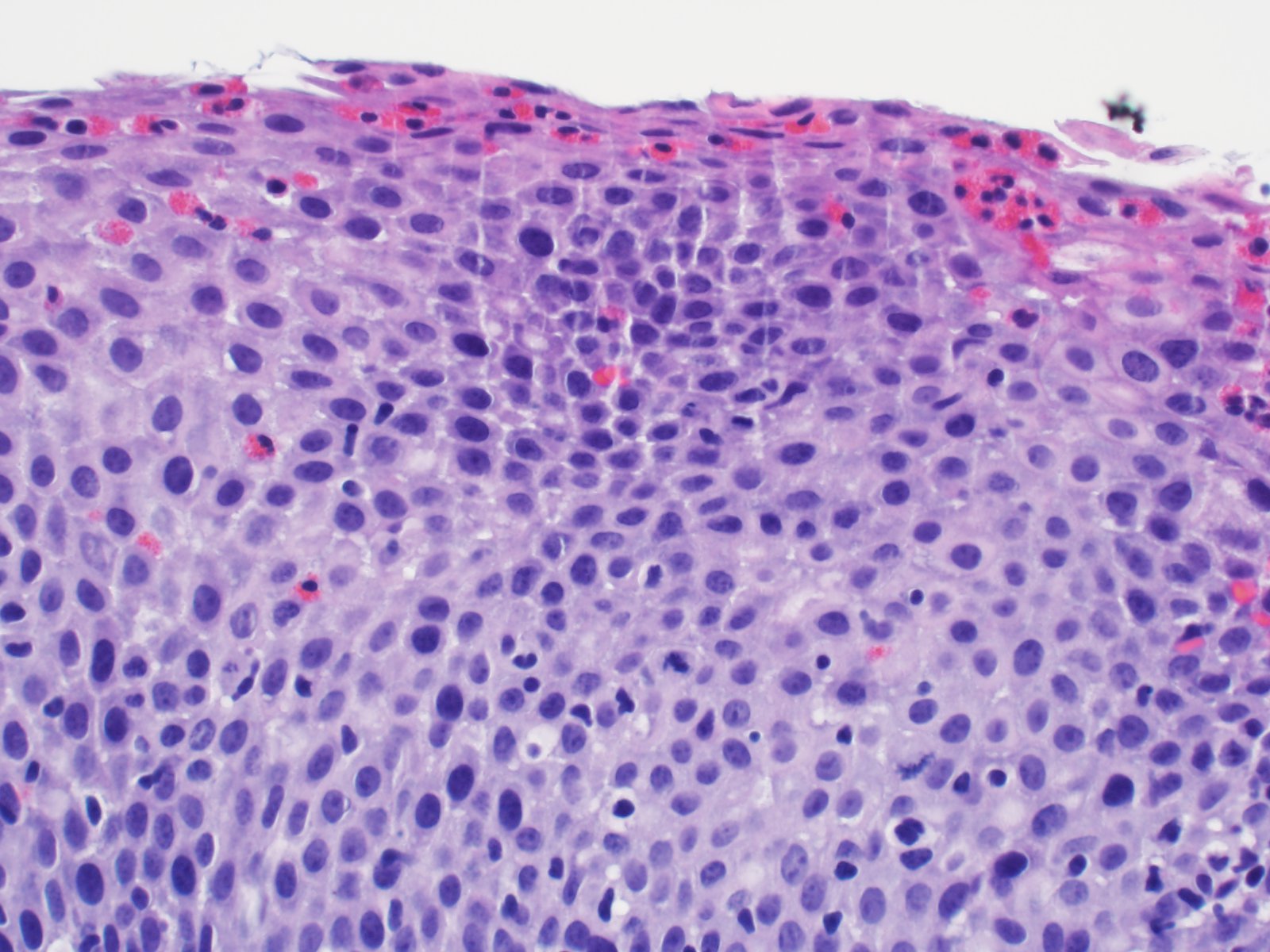
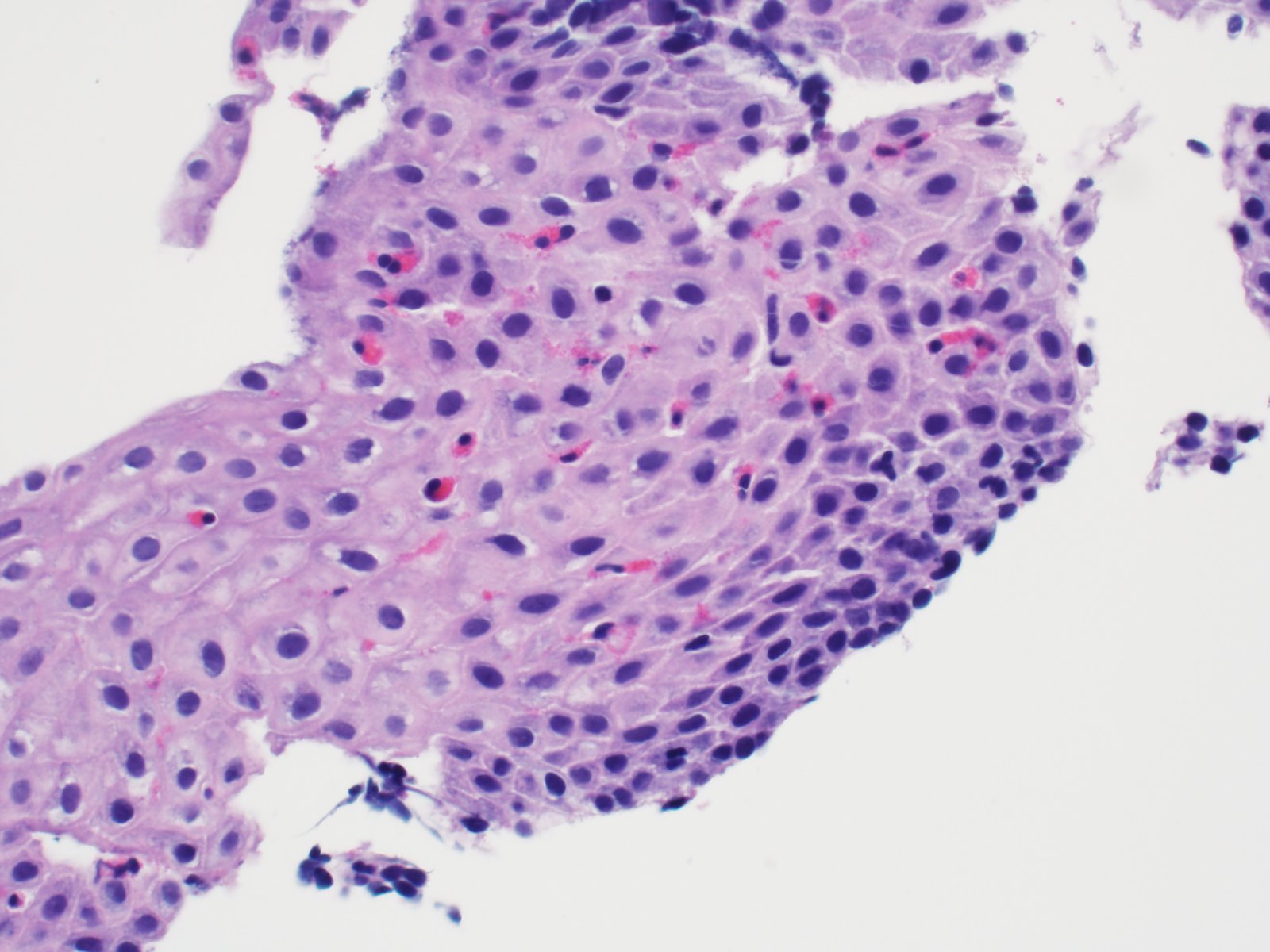
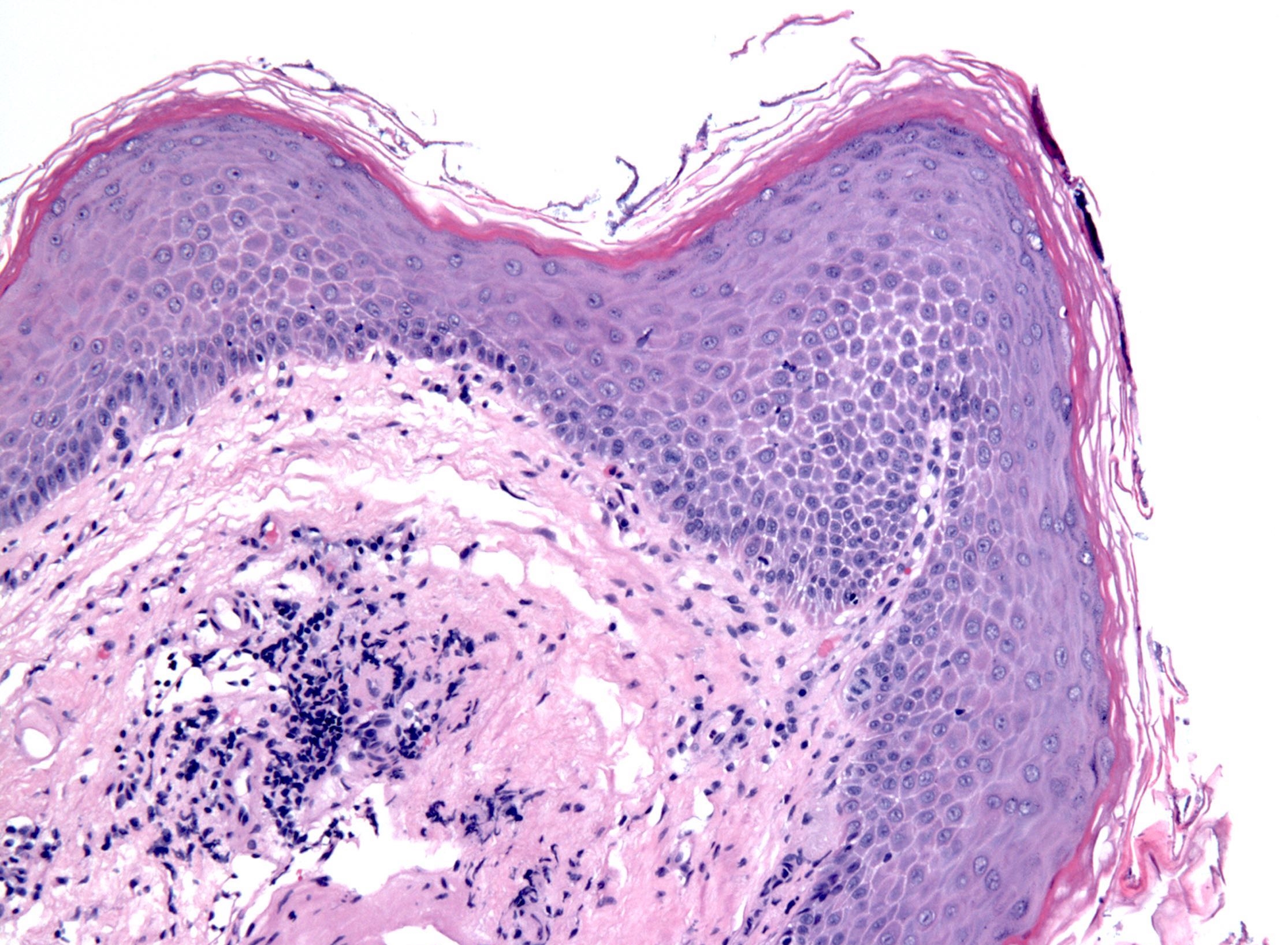
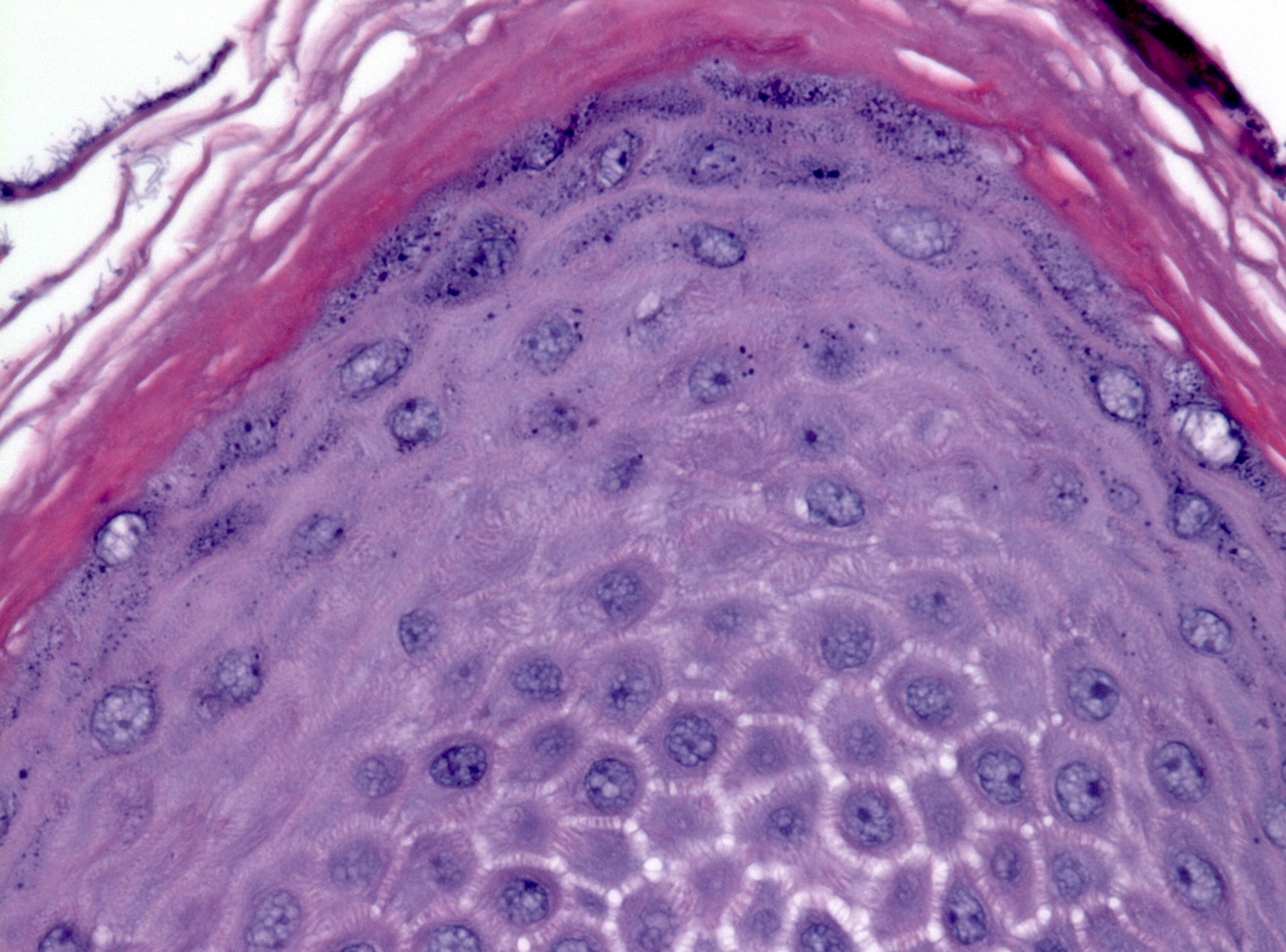
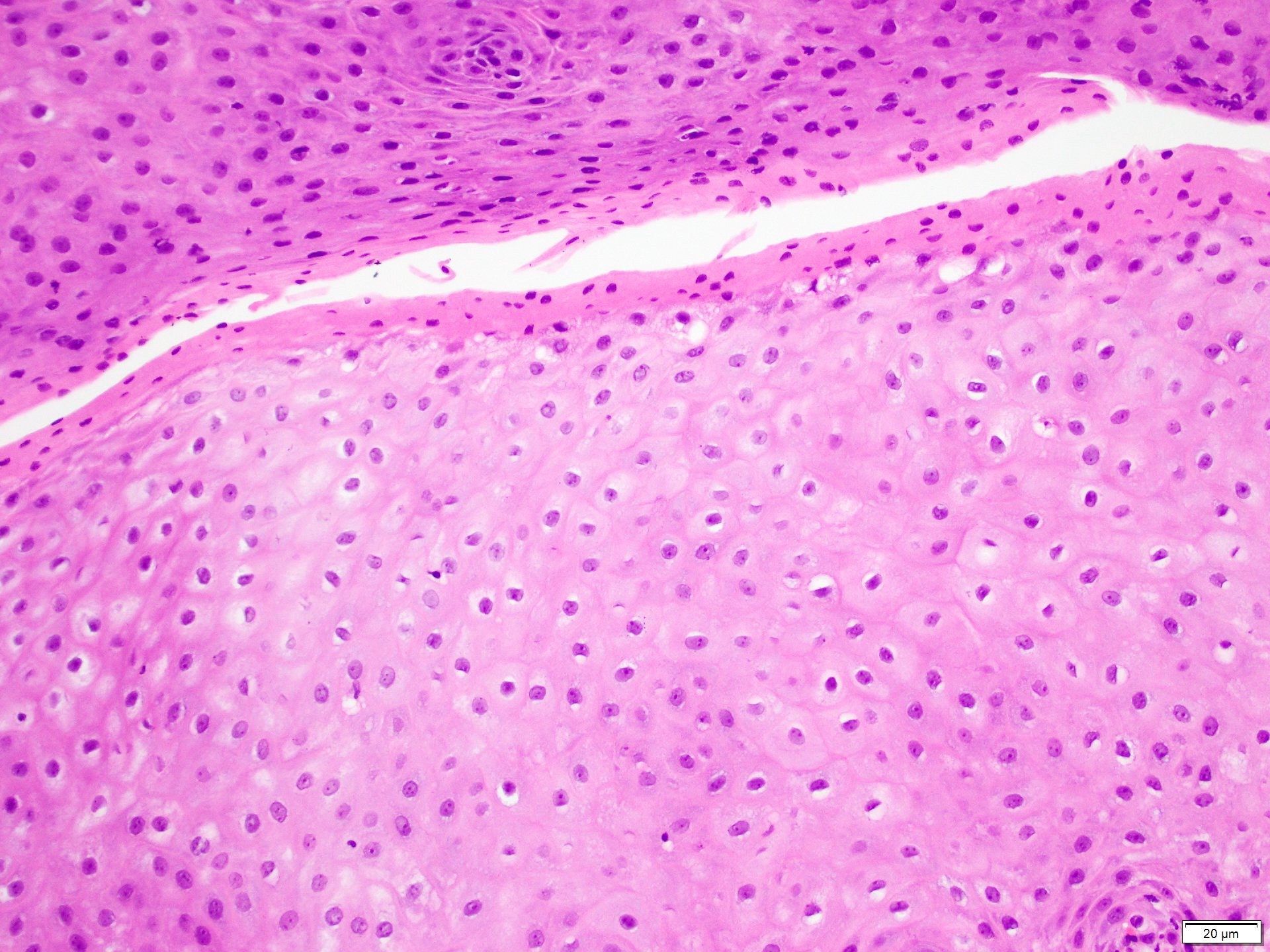
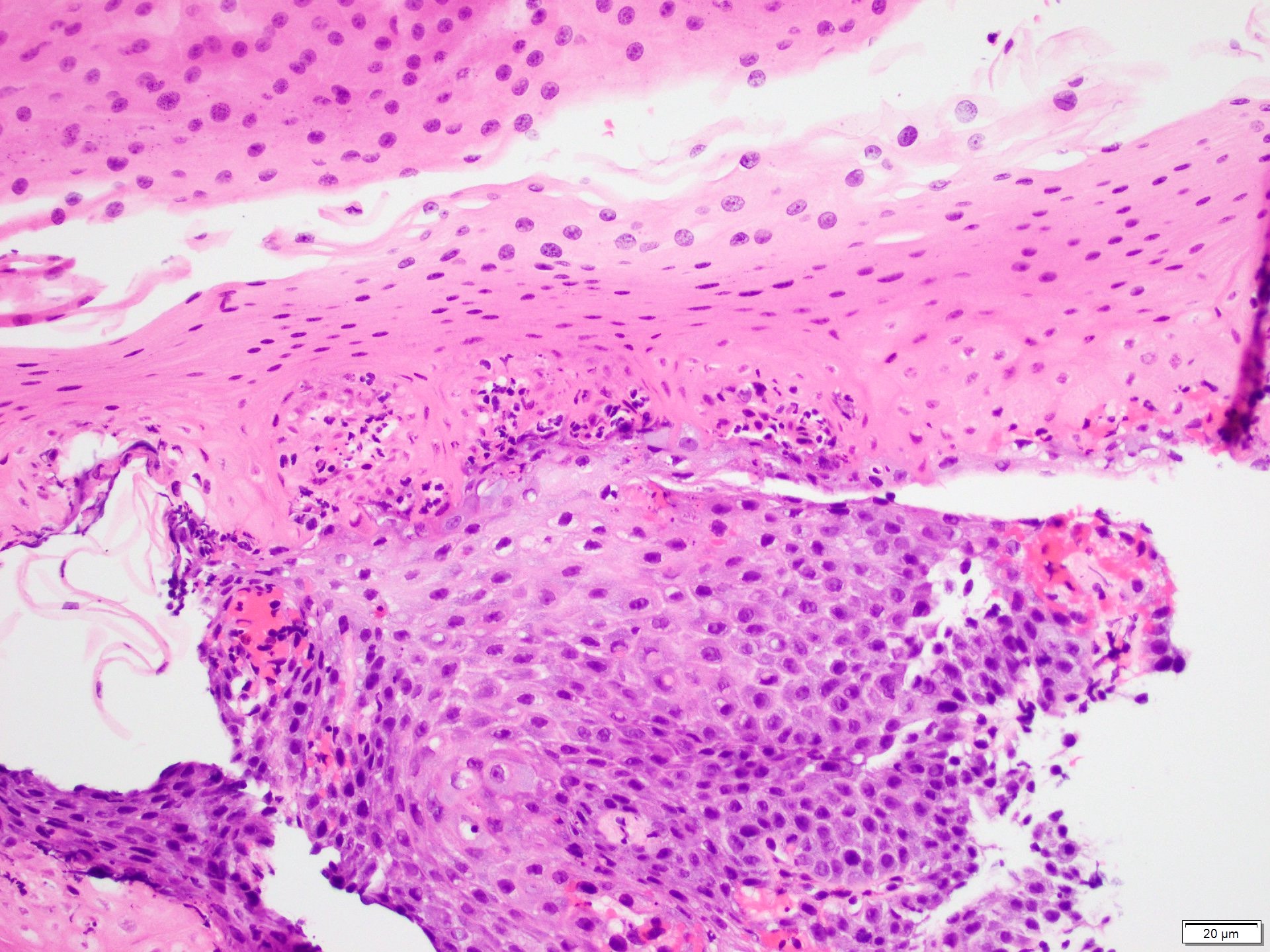
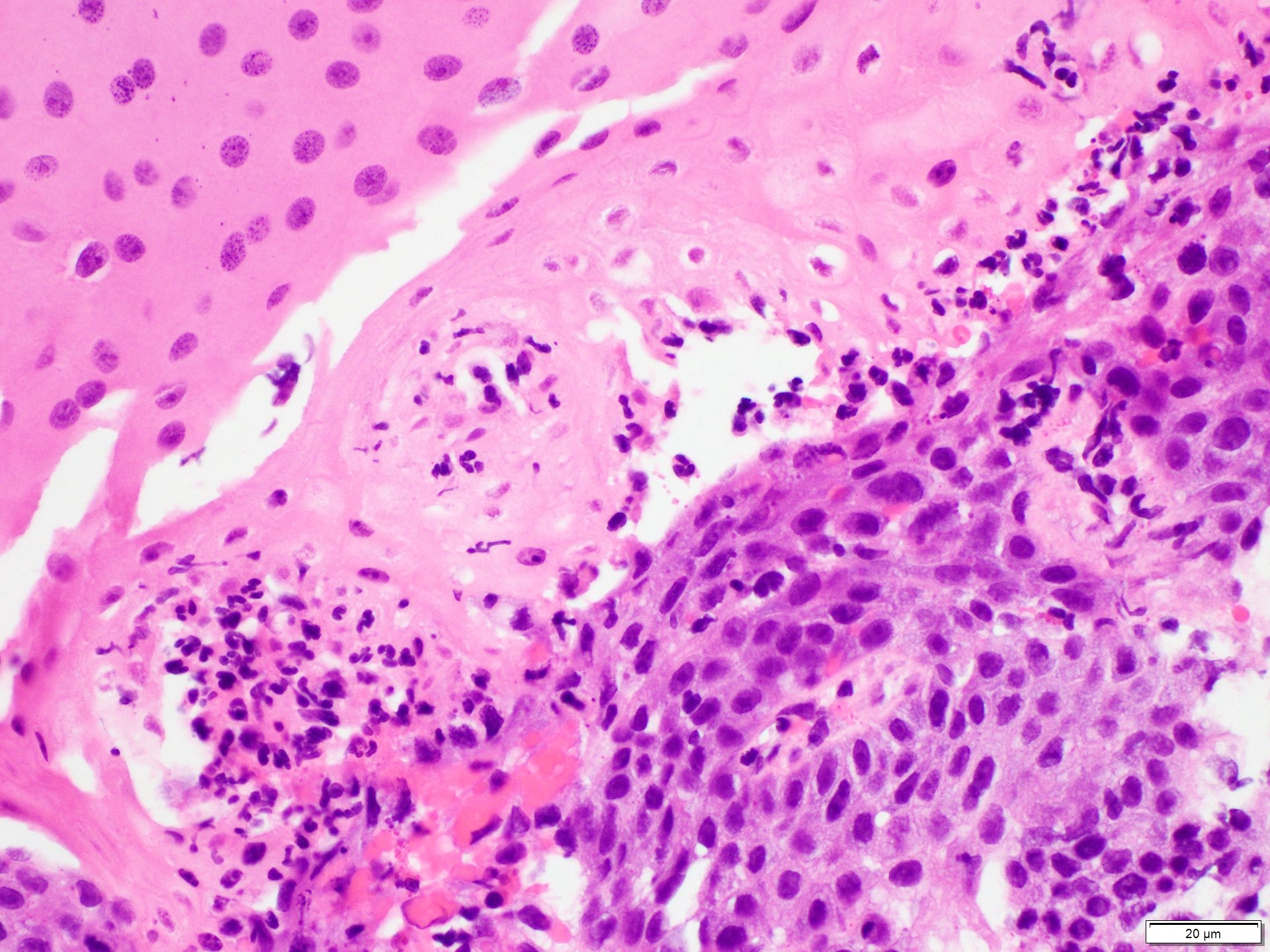
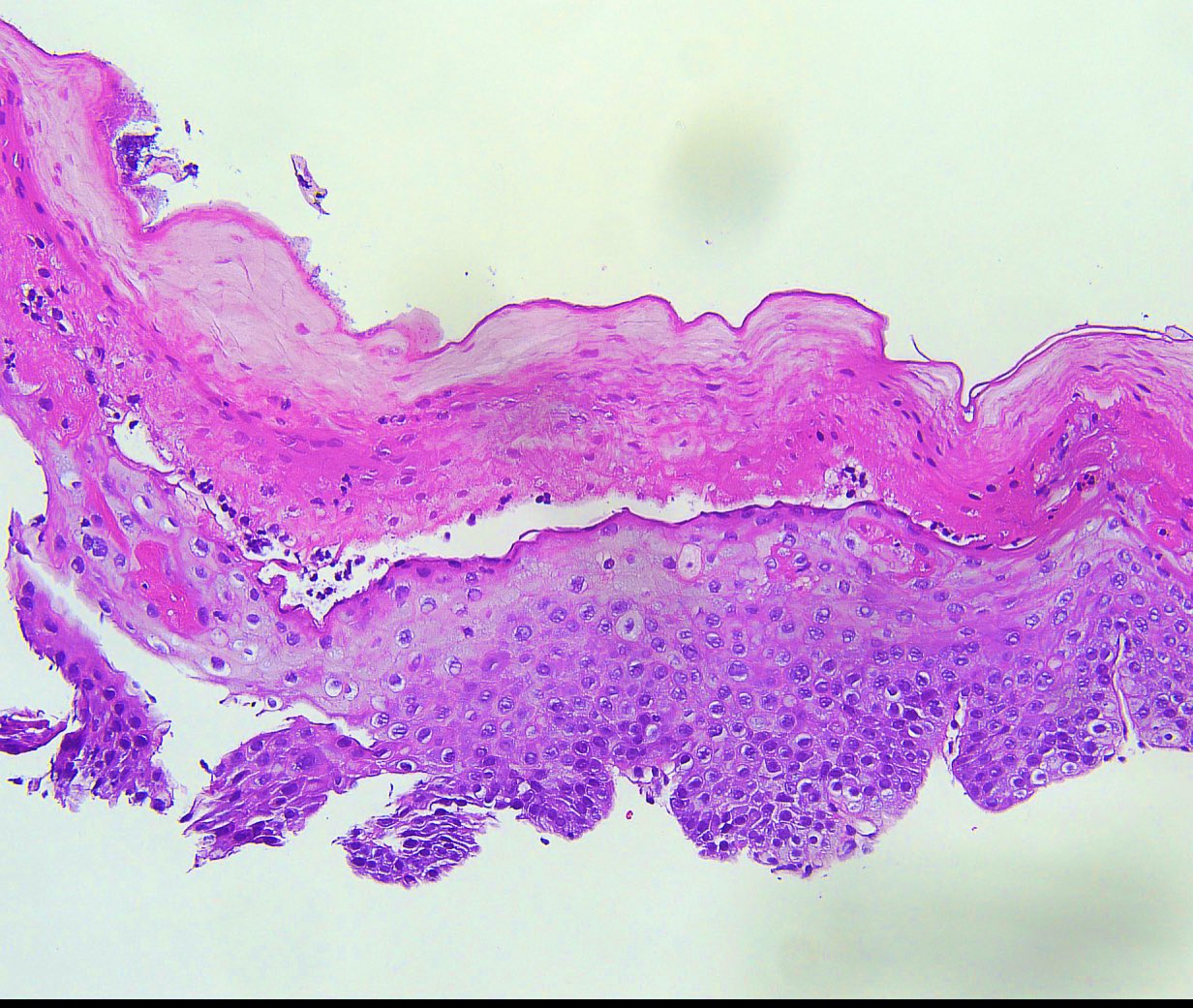
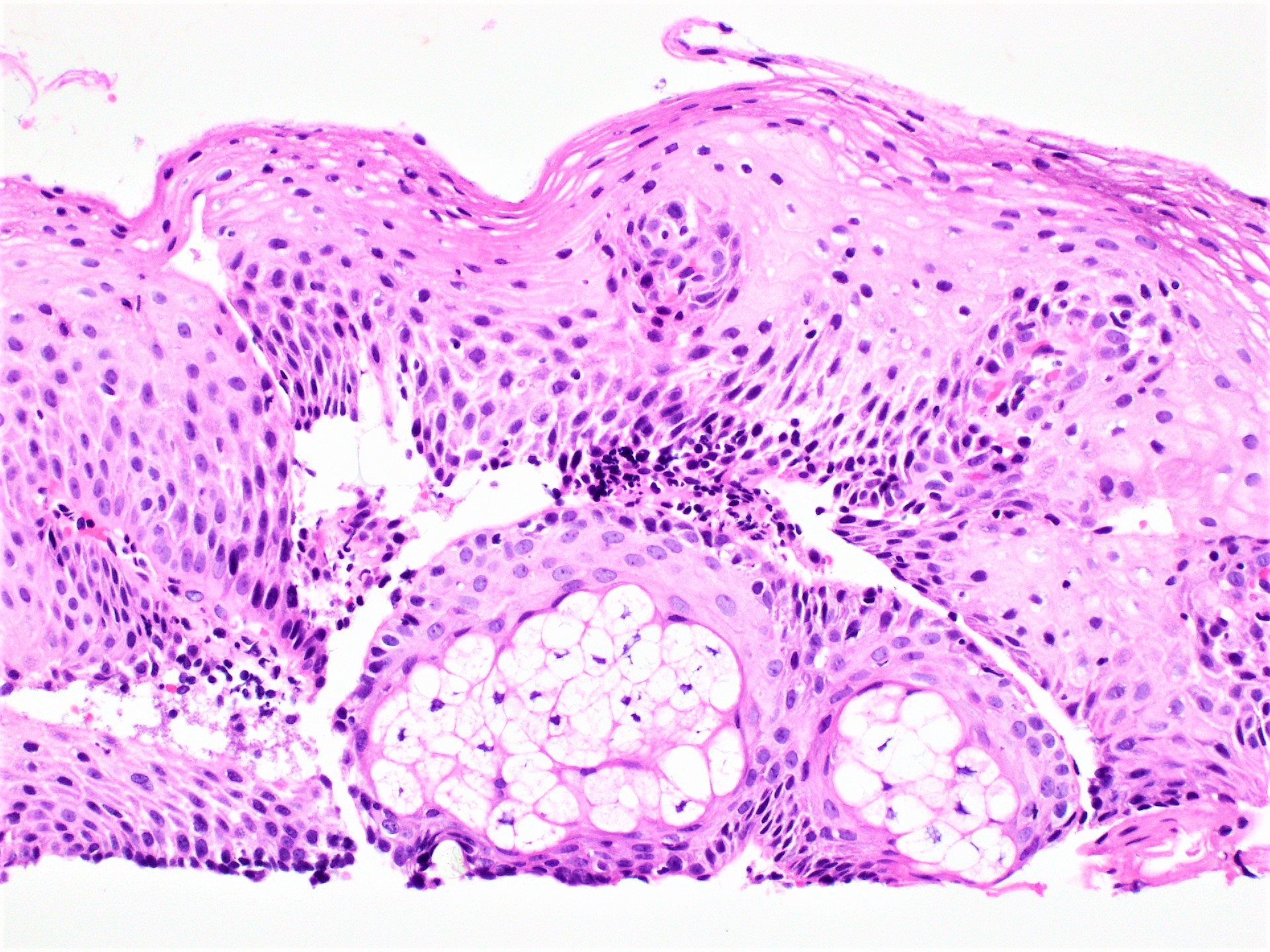
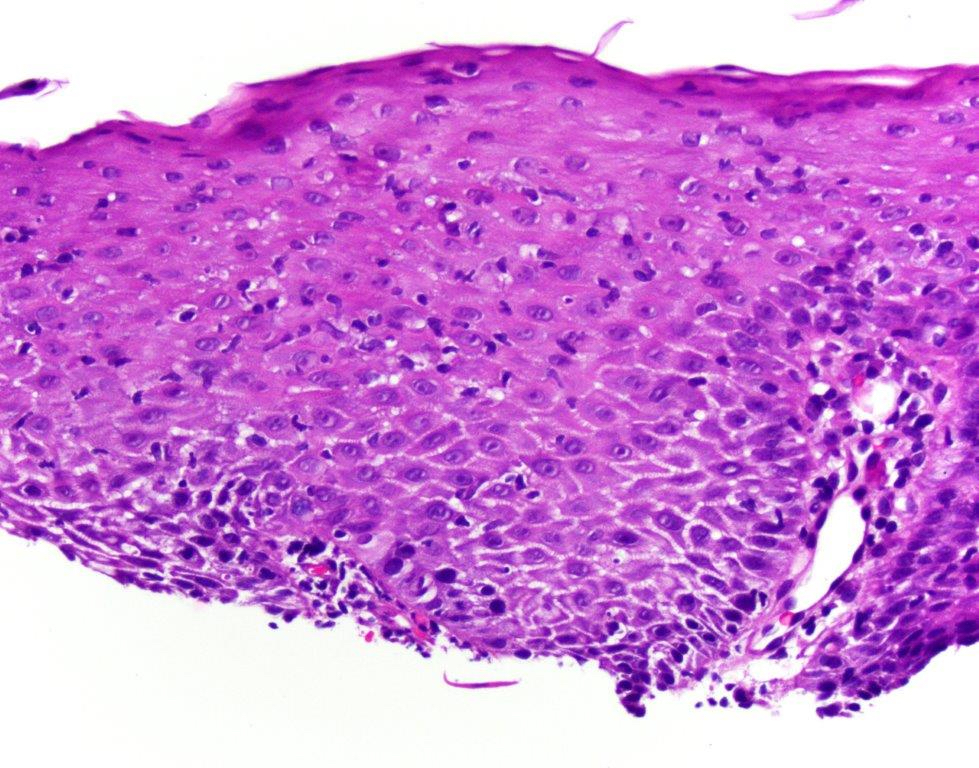
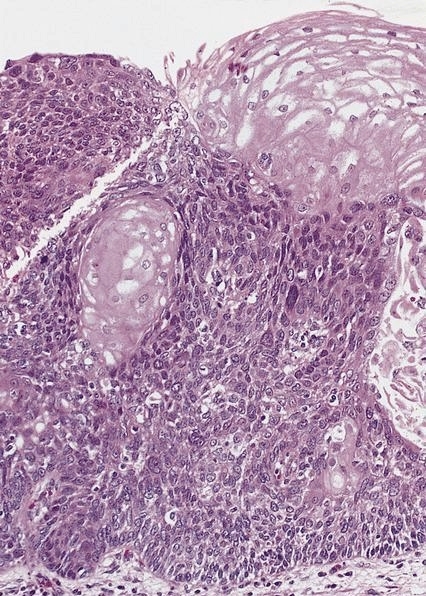
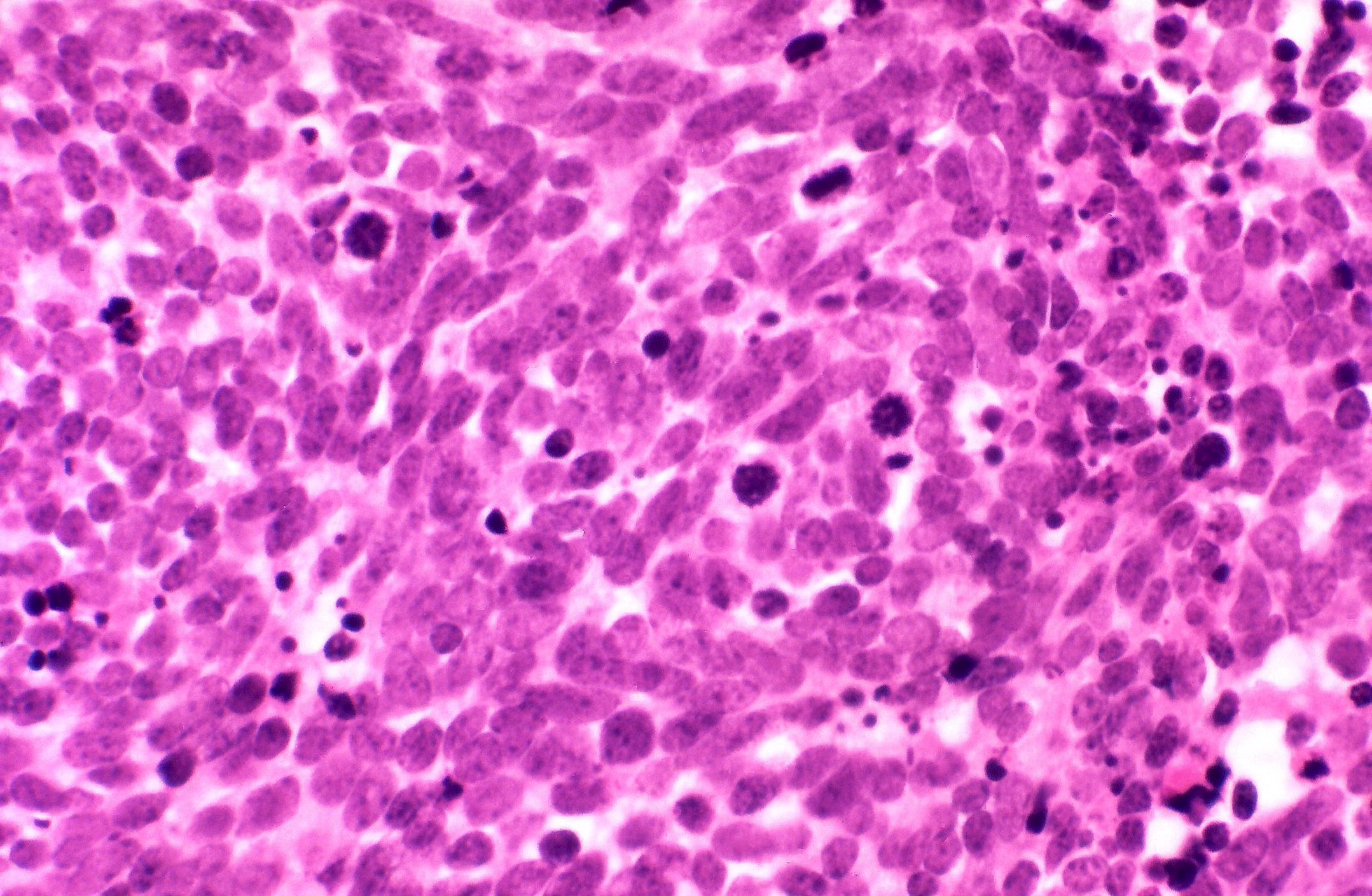
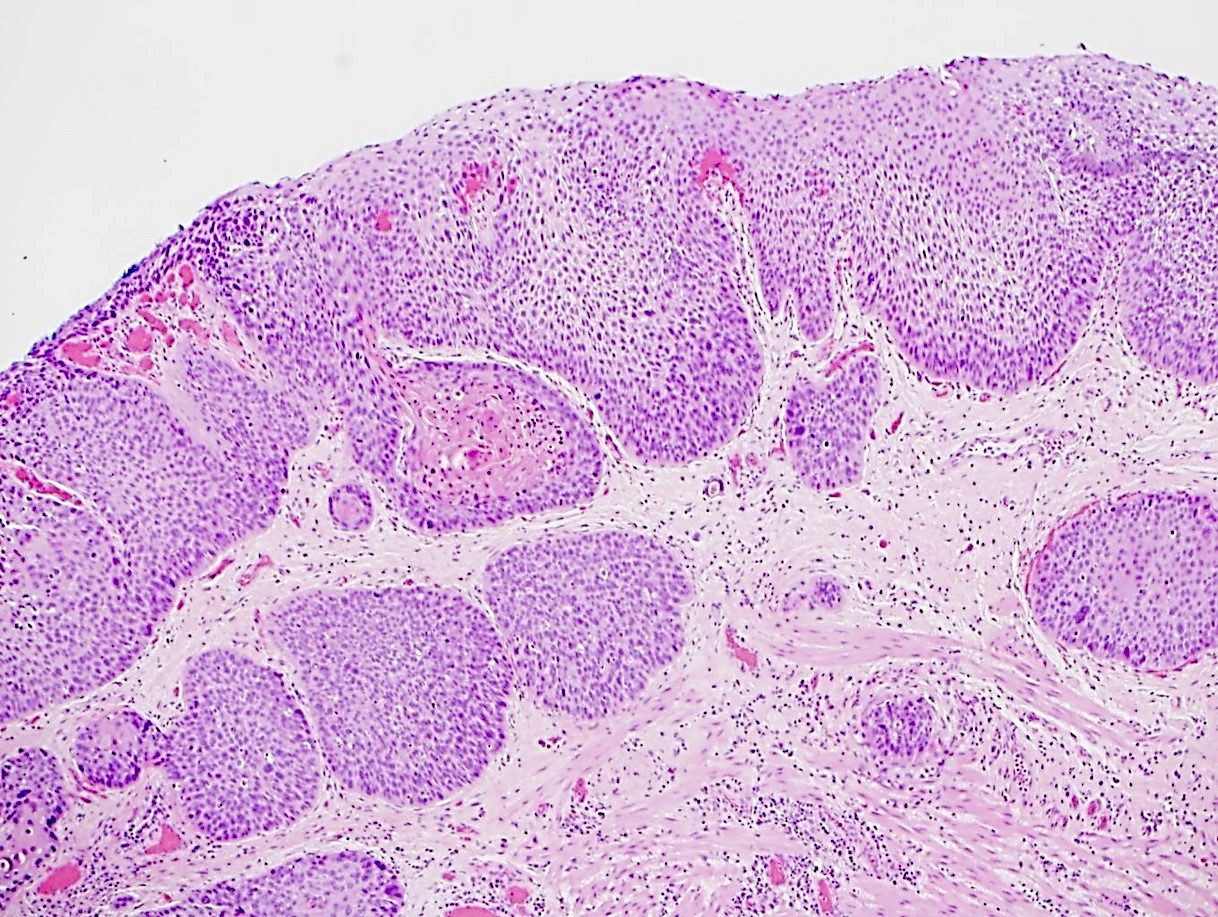
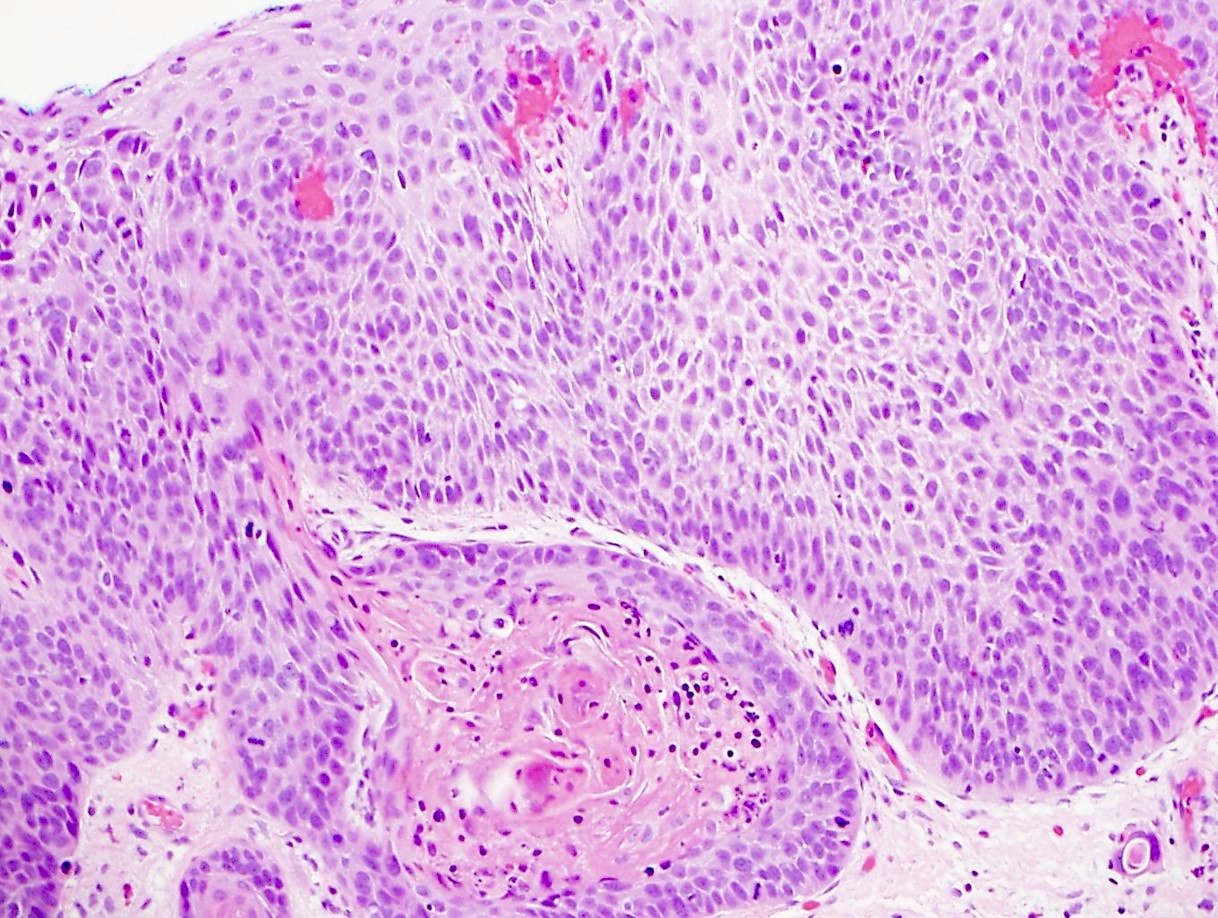
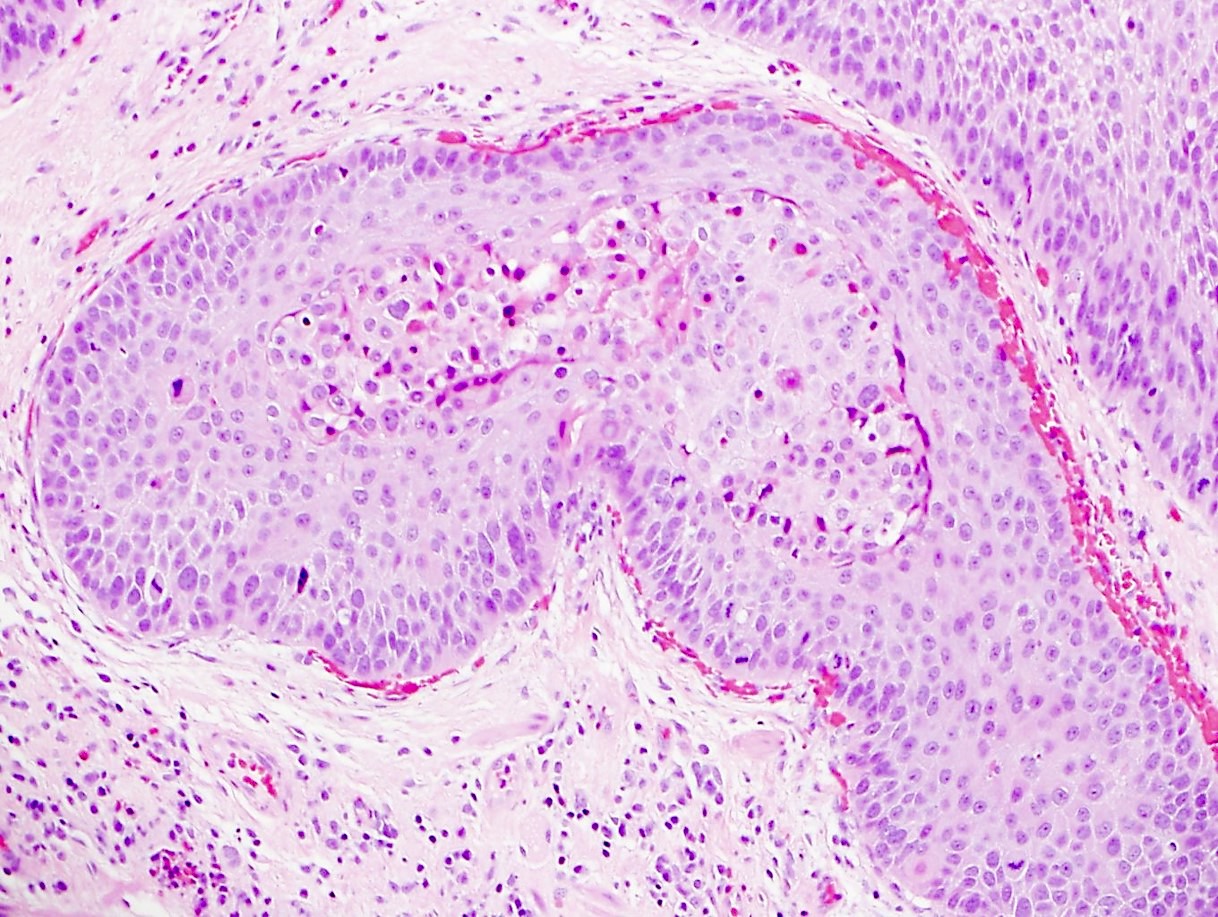
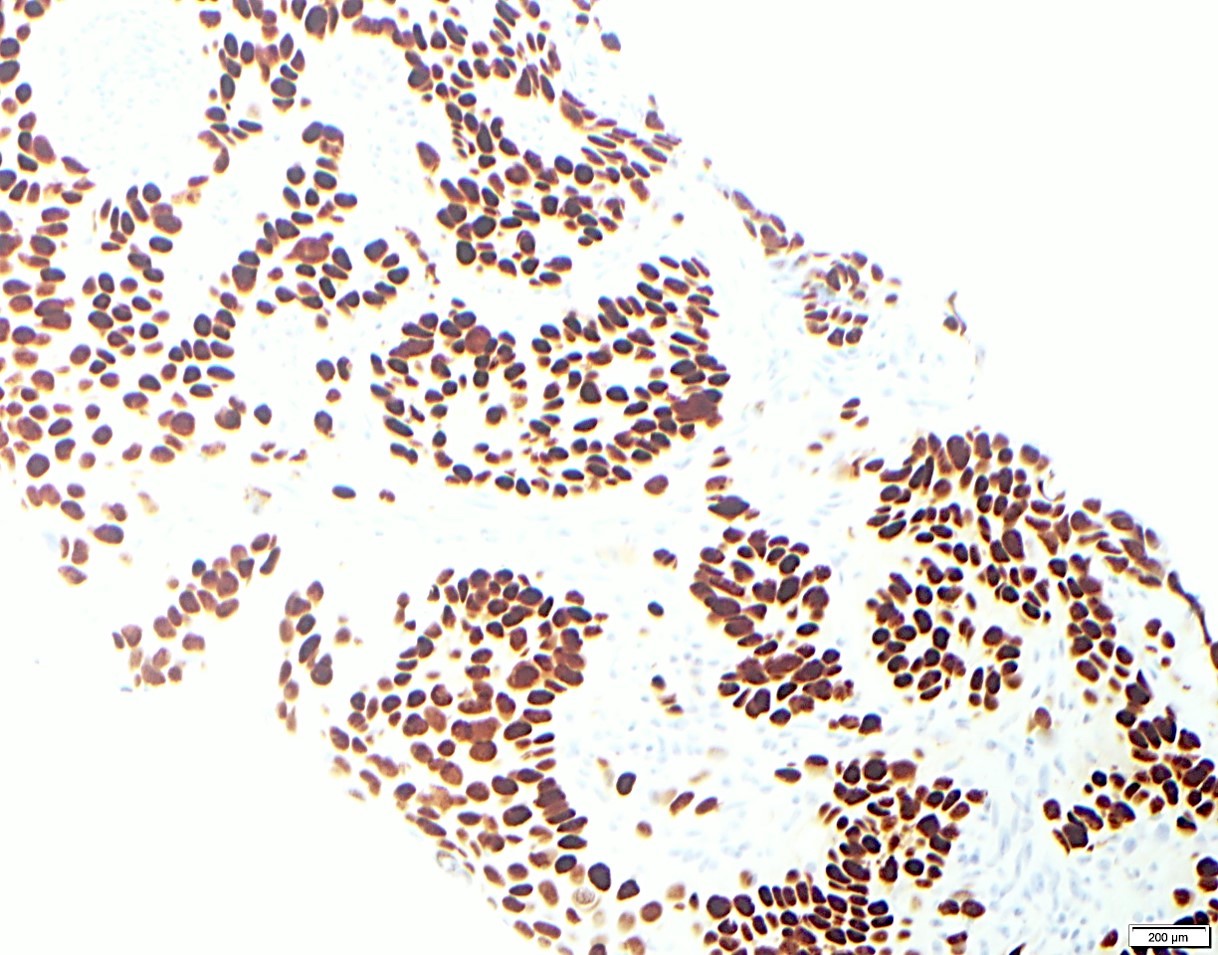
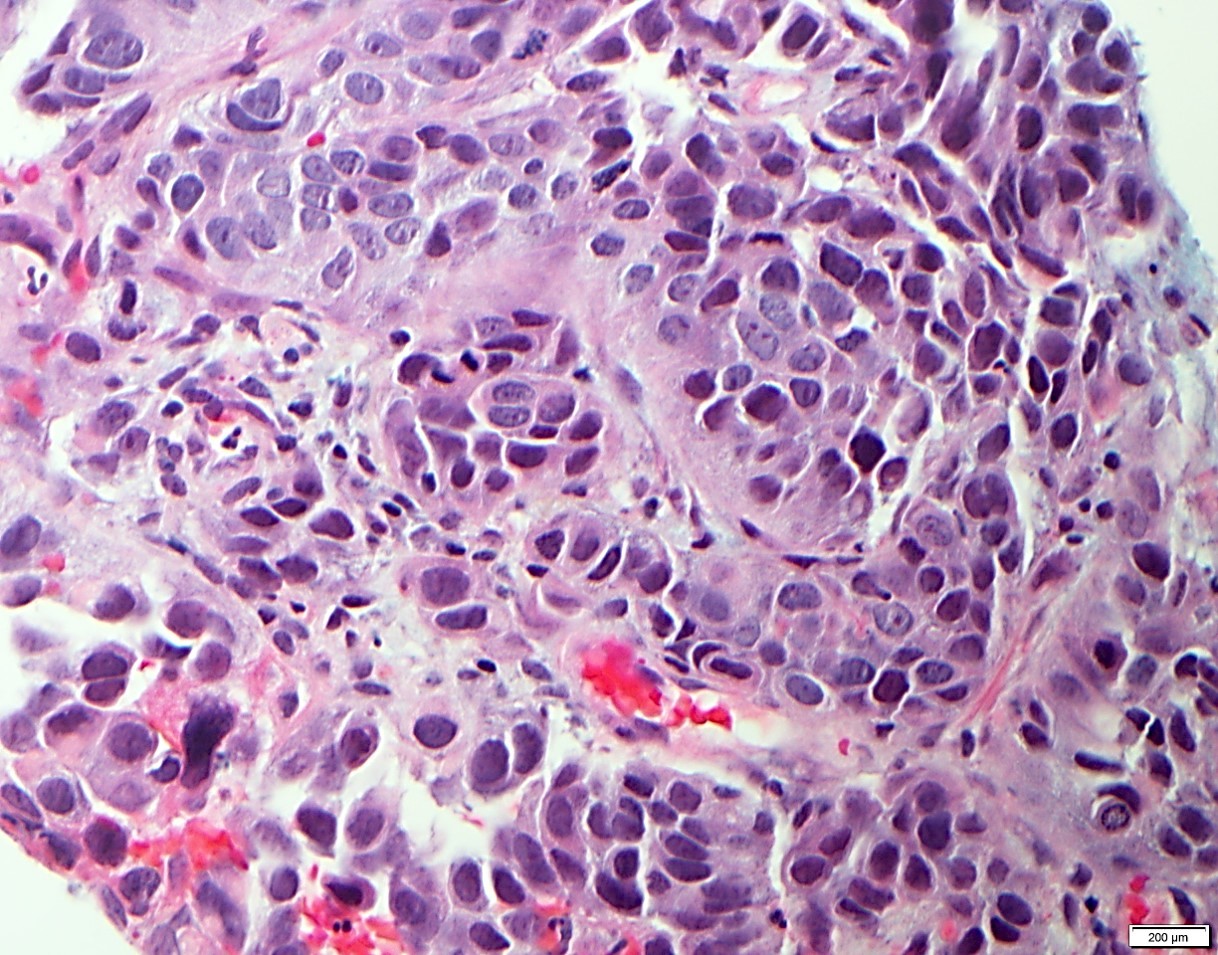
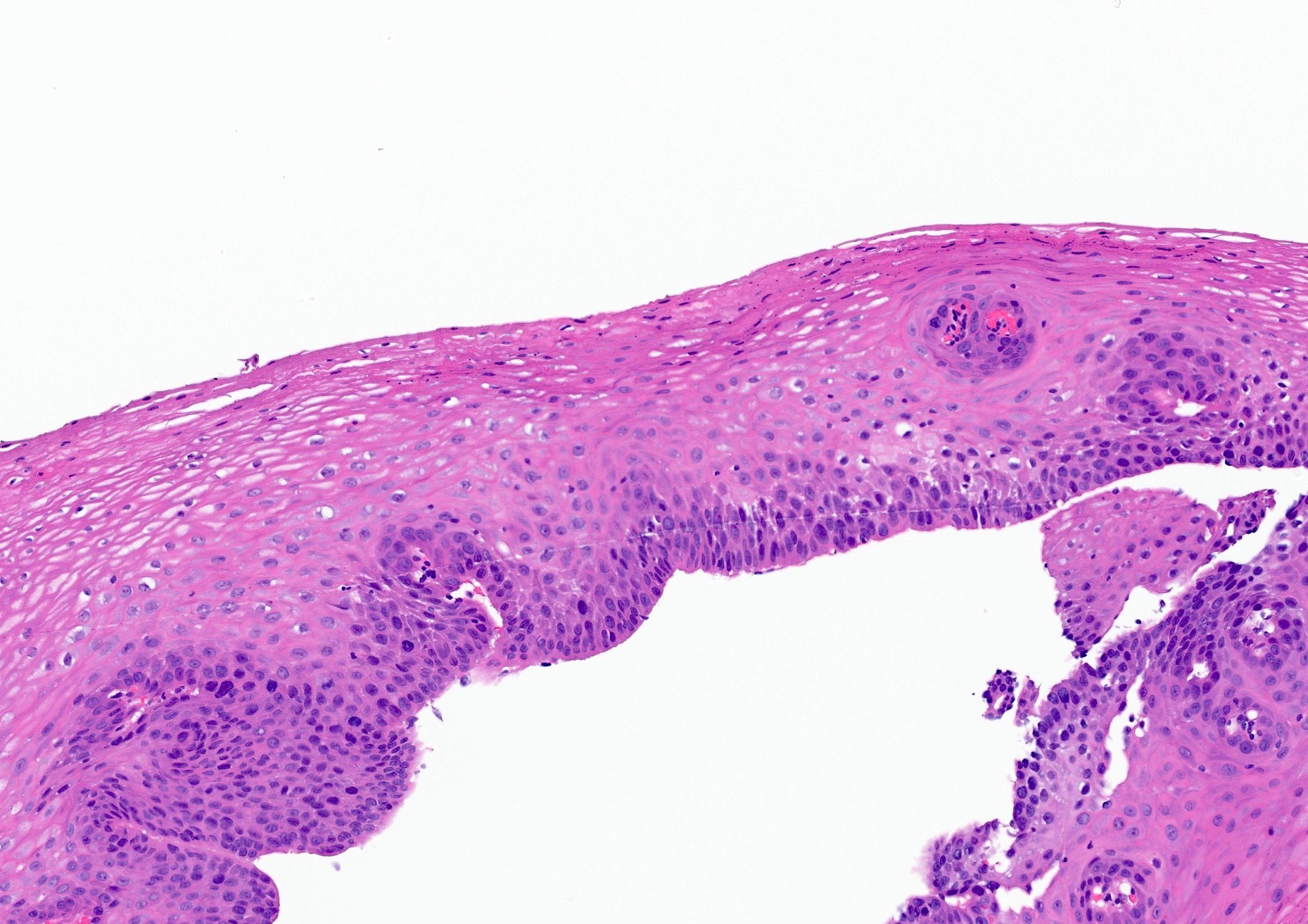
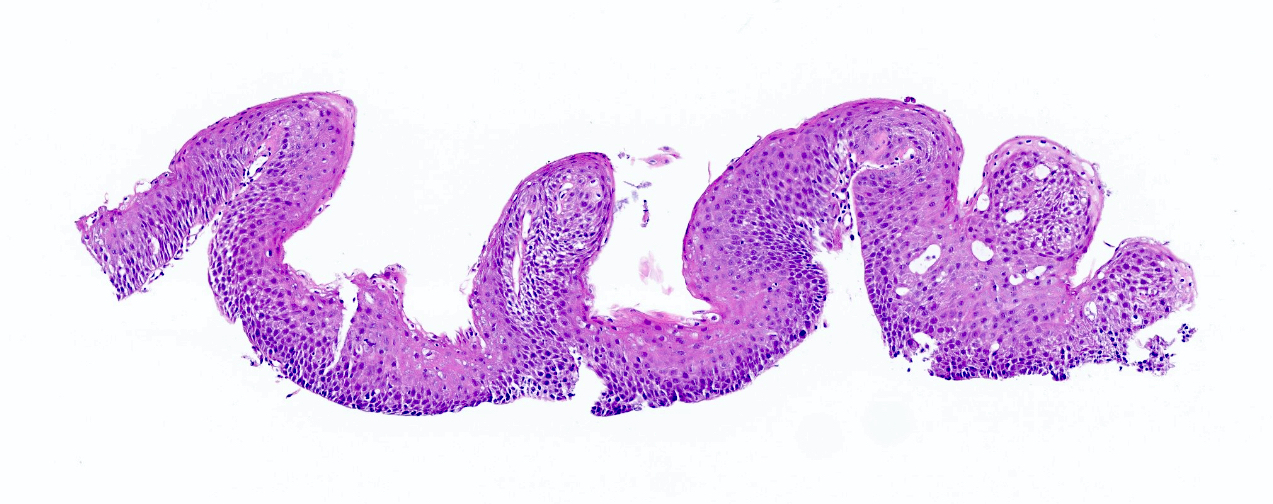
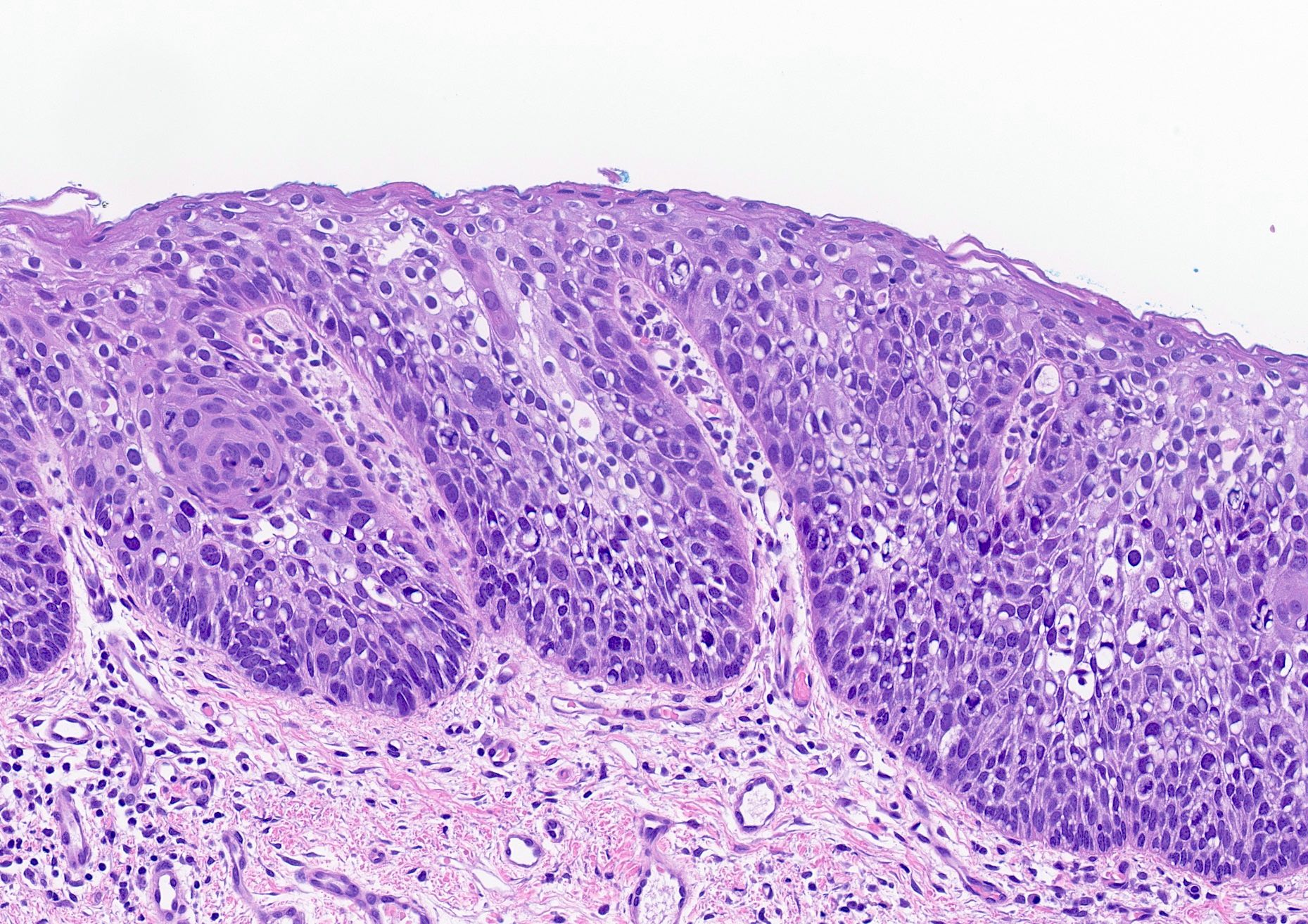
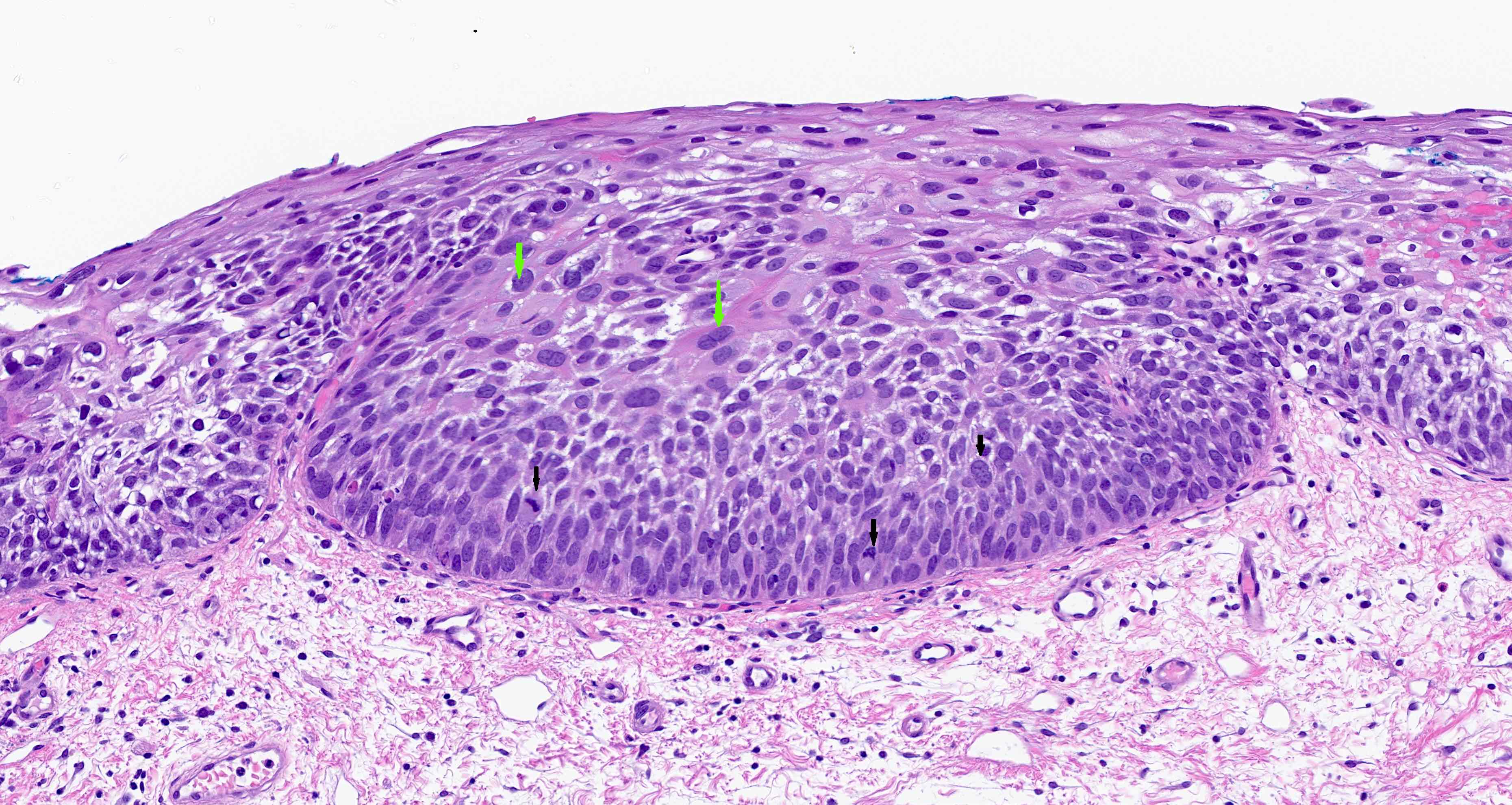
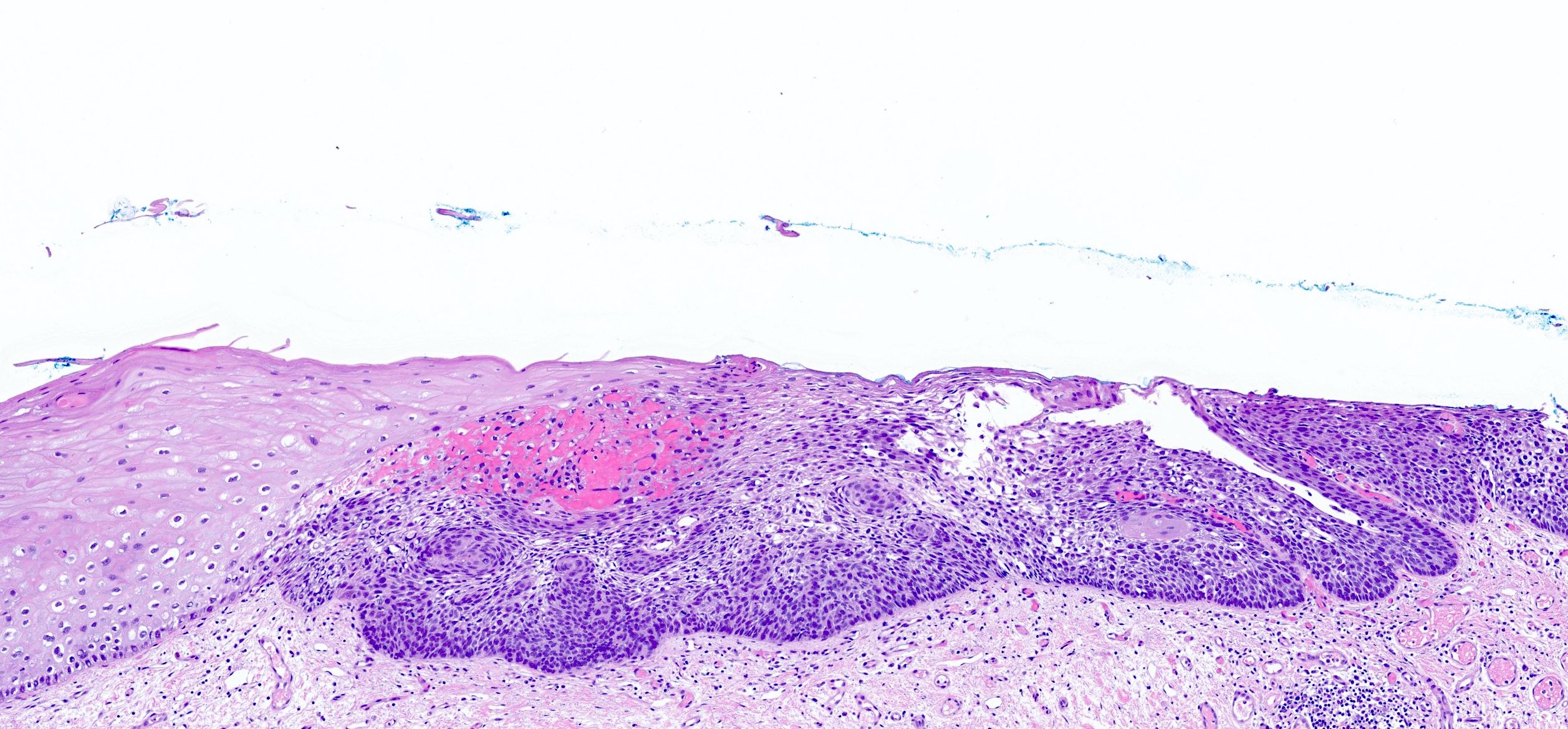
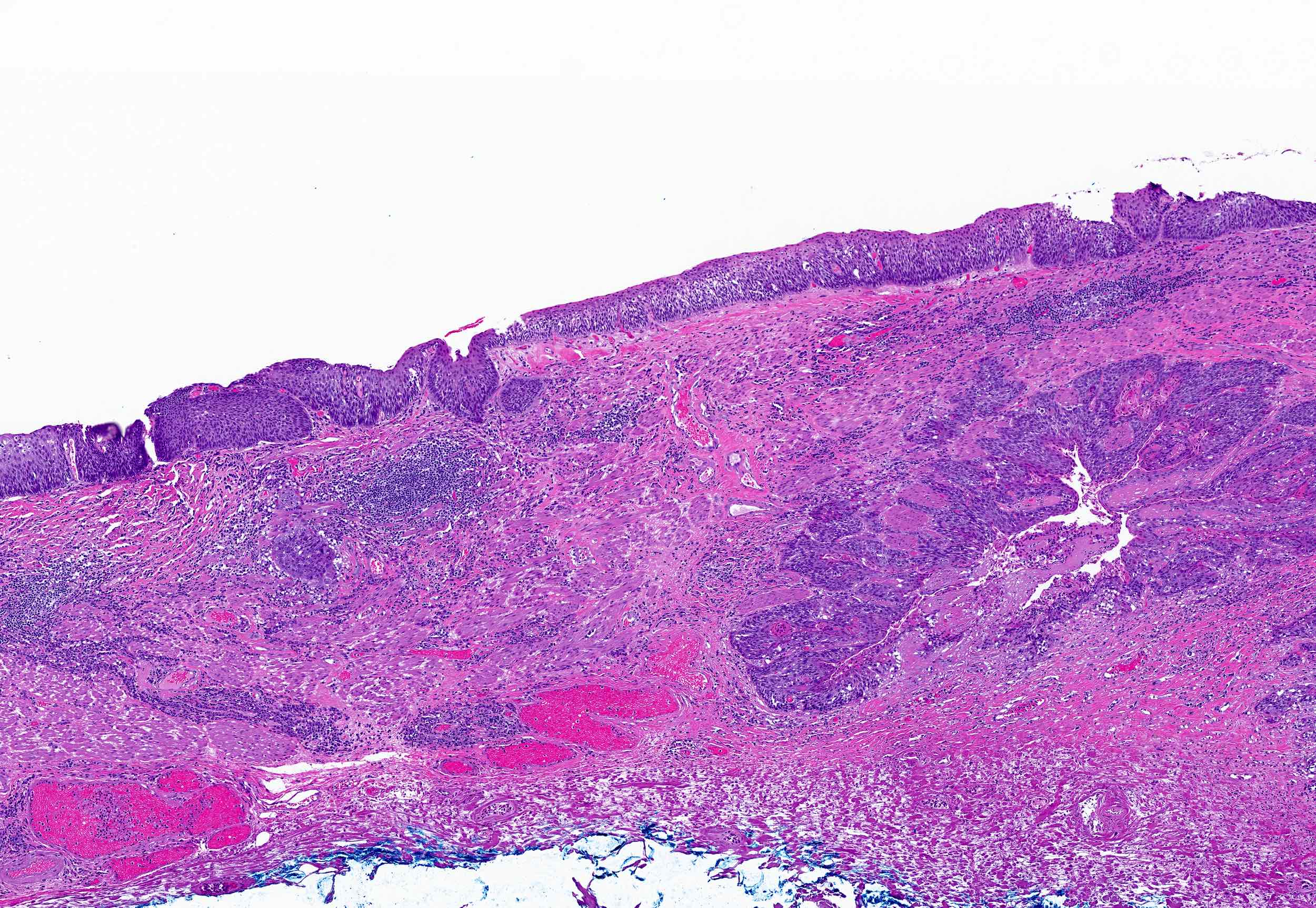
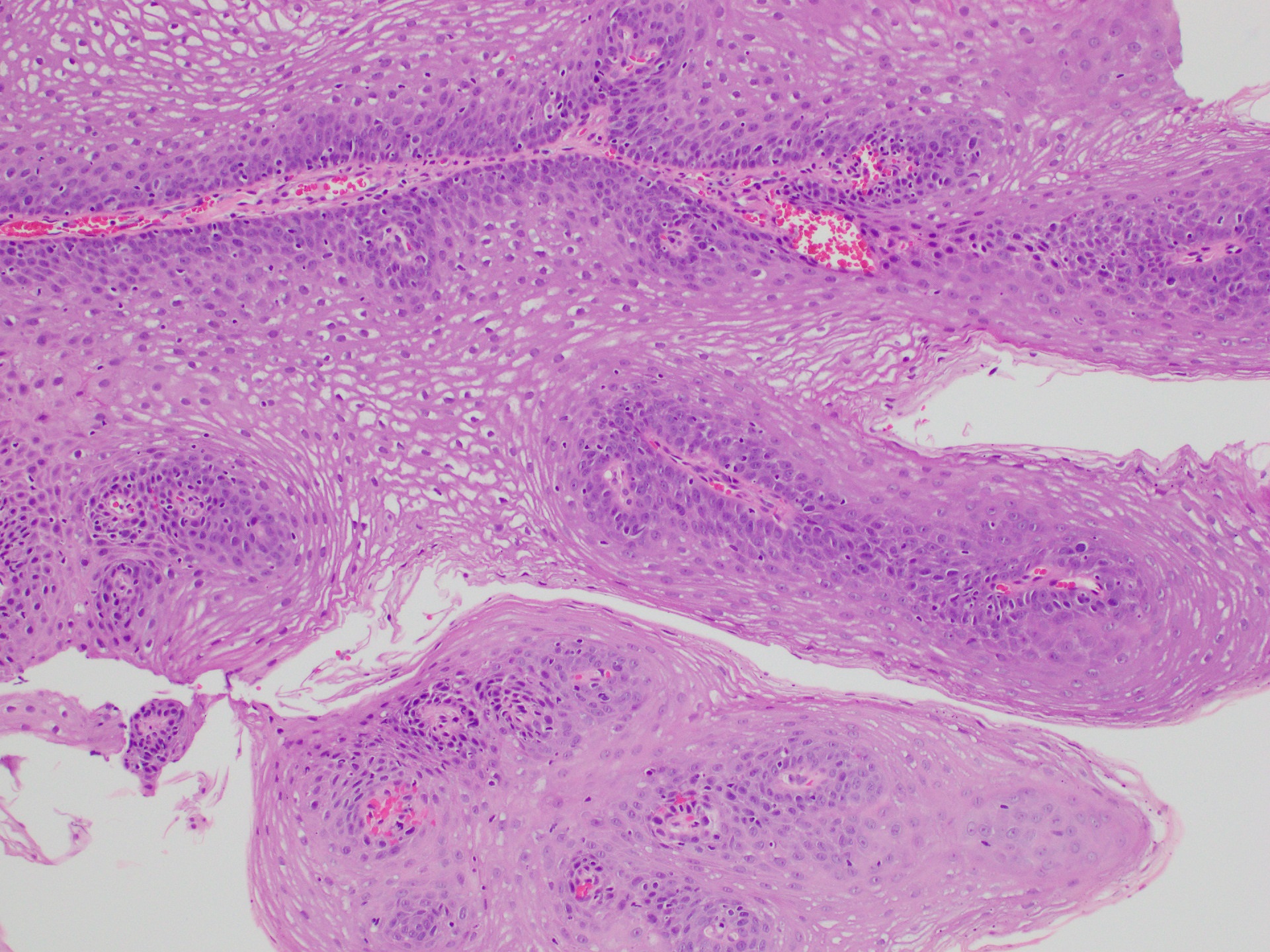
- Tis: High grade dysplasia, defined as malignant cells confined to the epithelium by the basement membrane
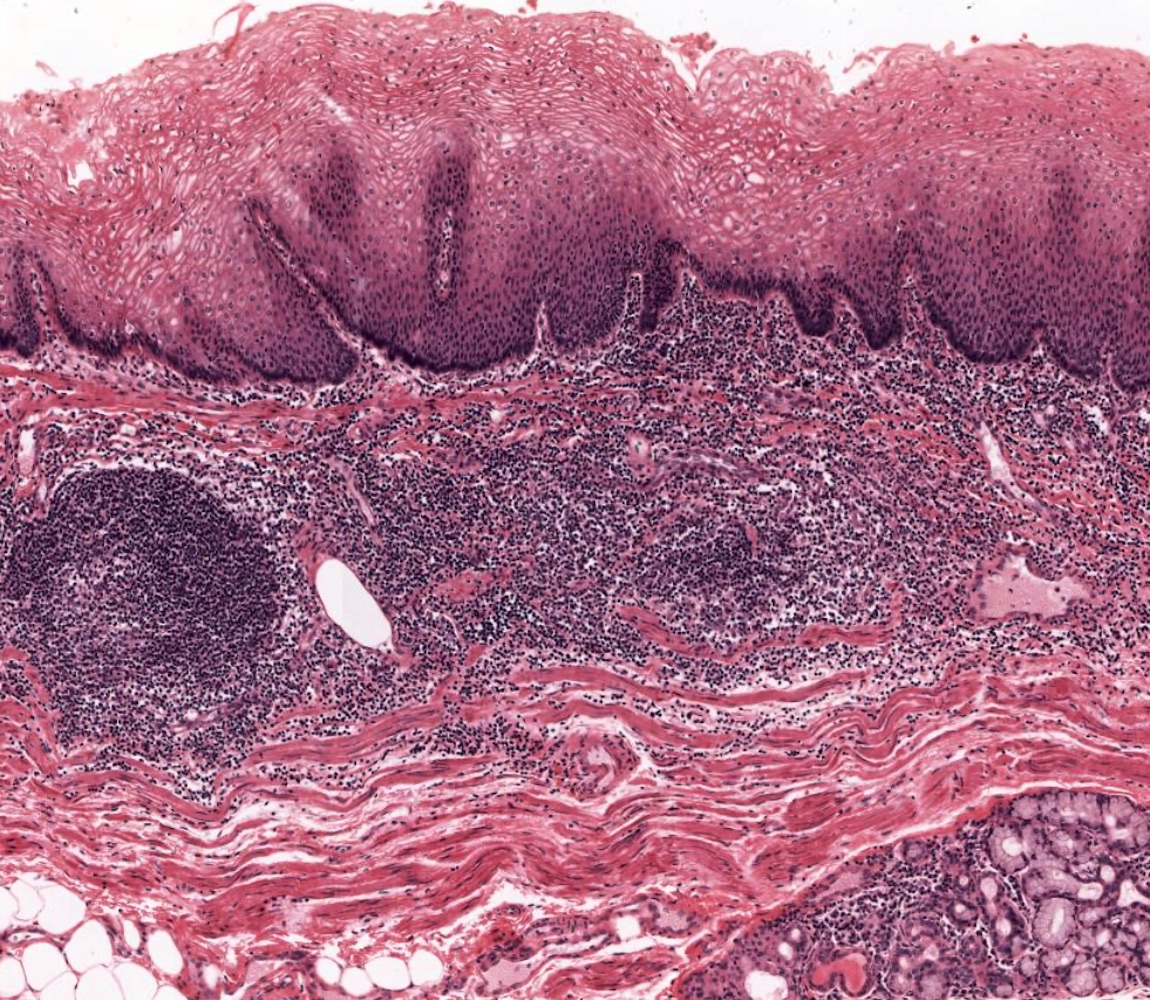
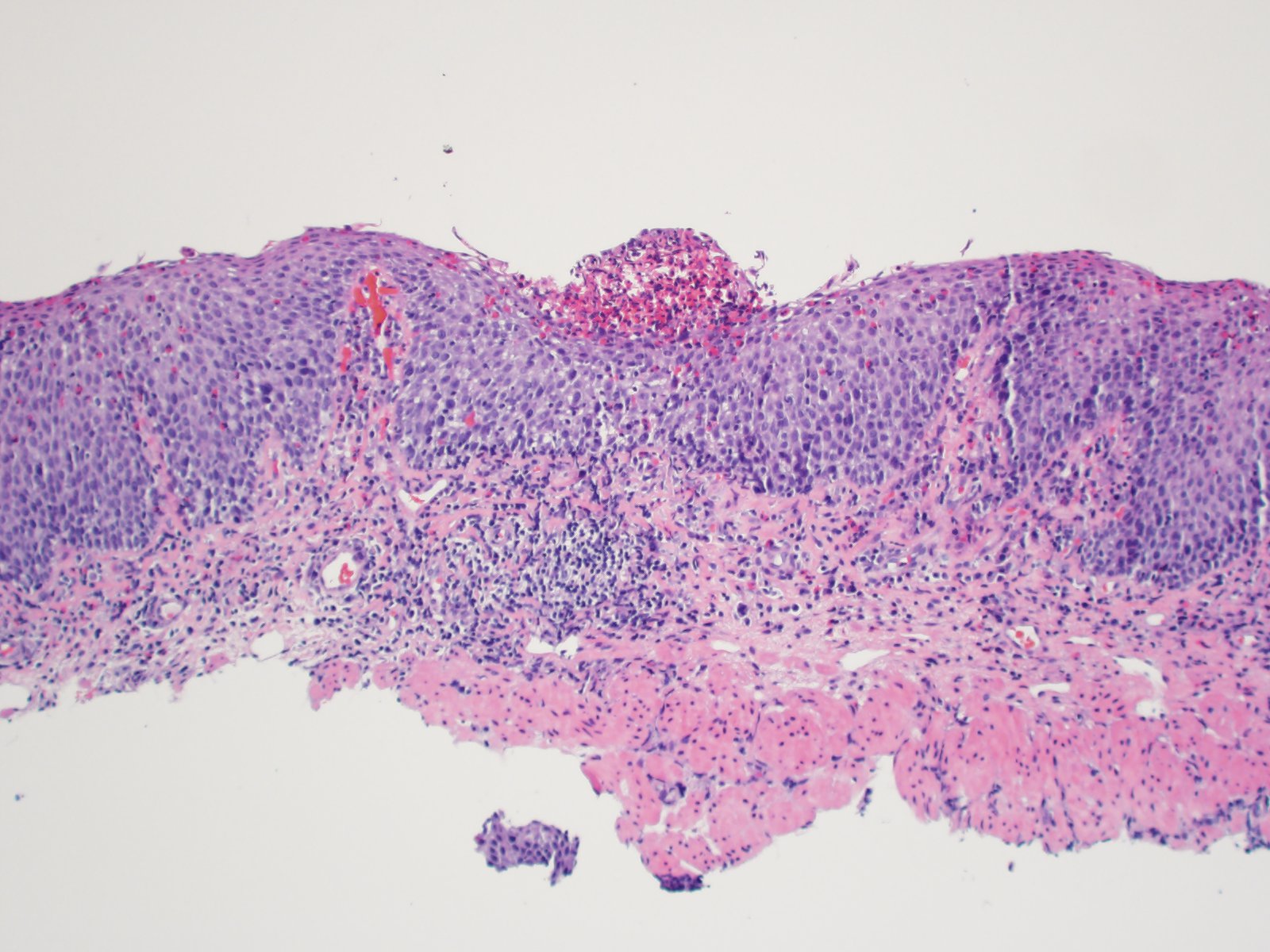
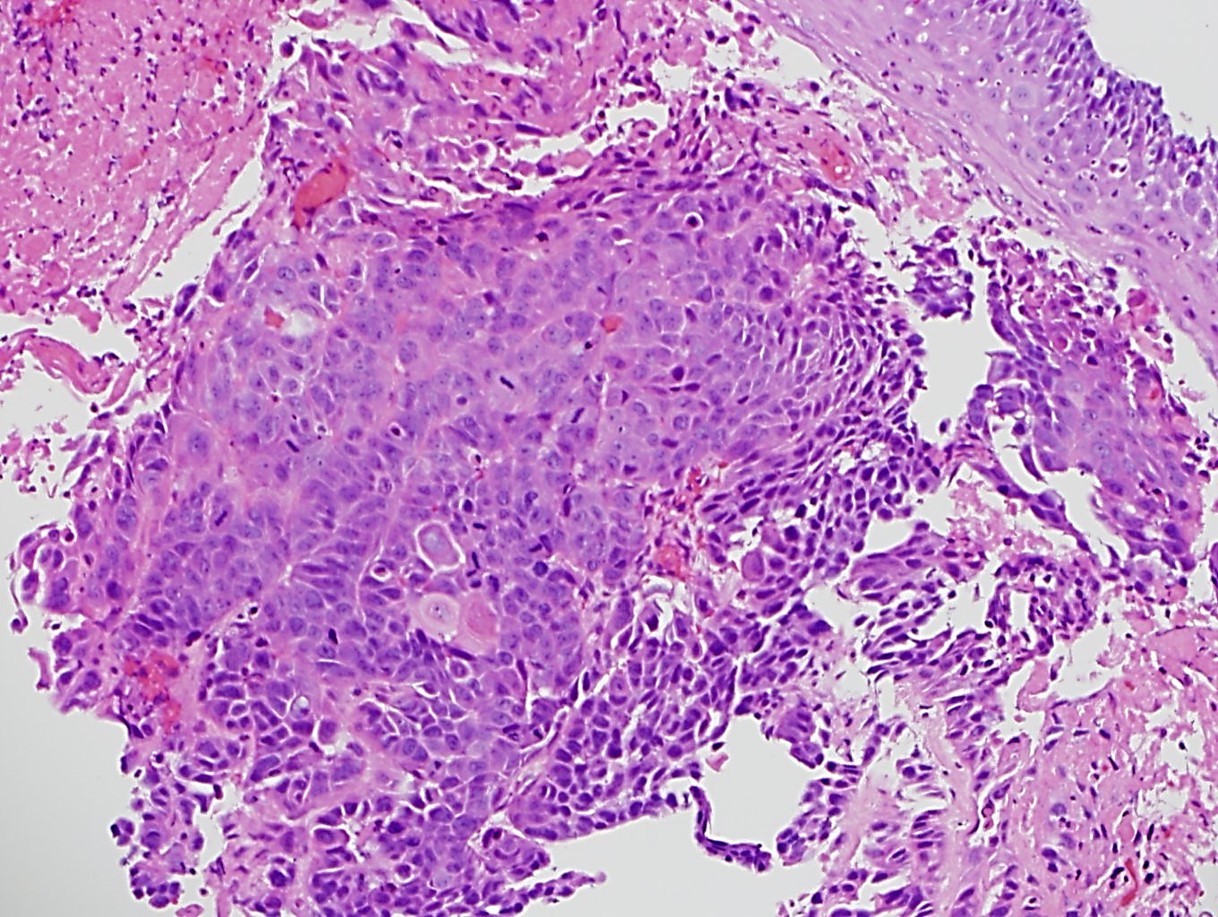
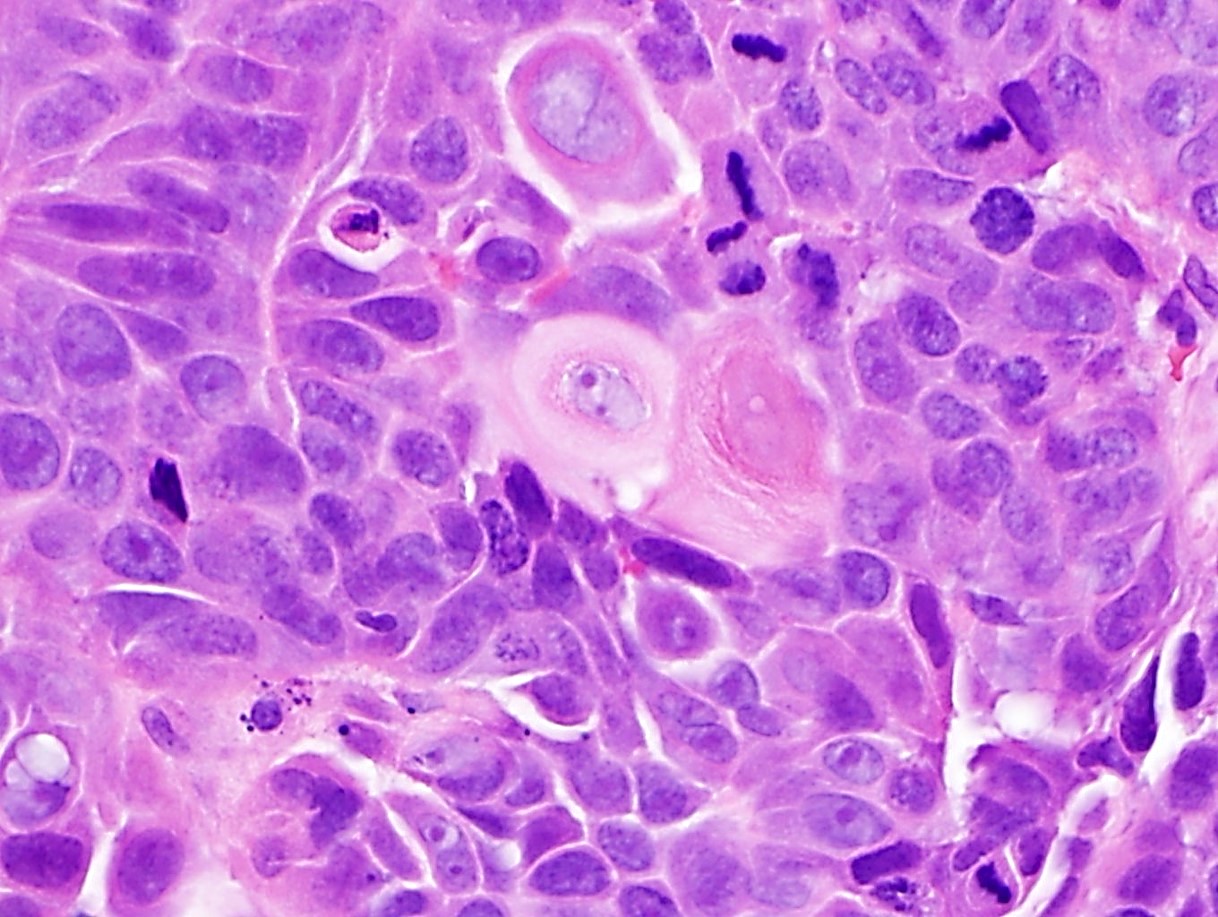
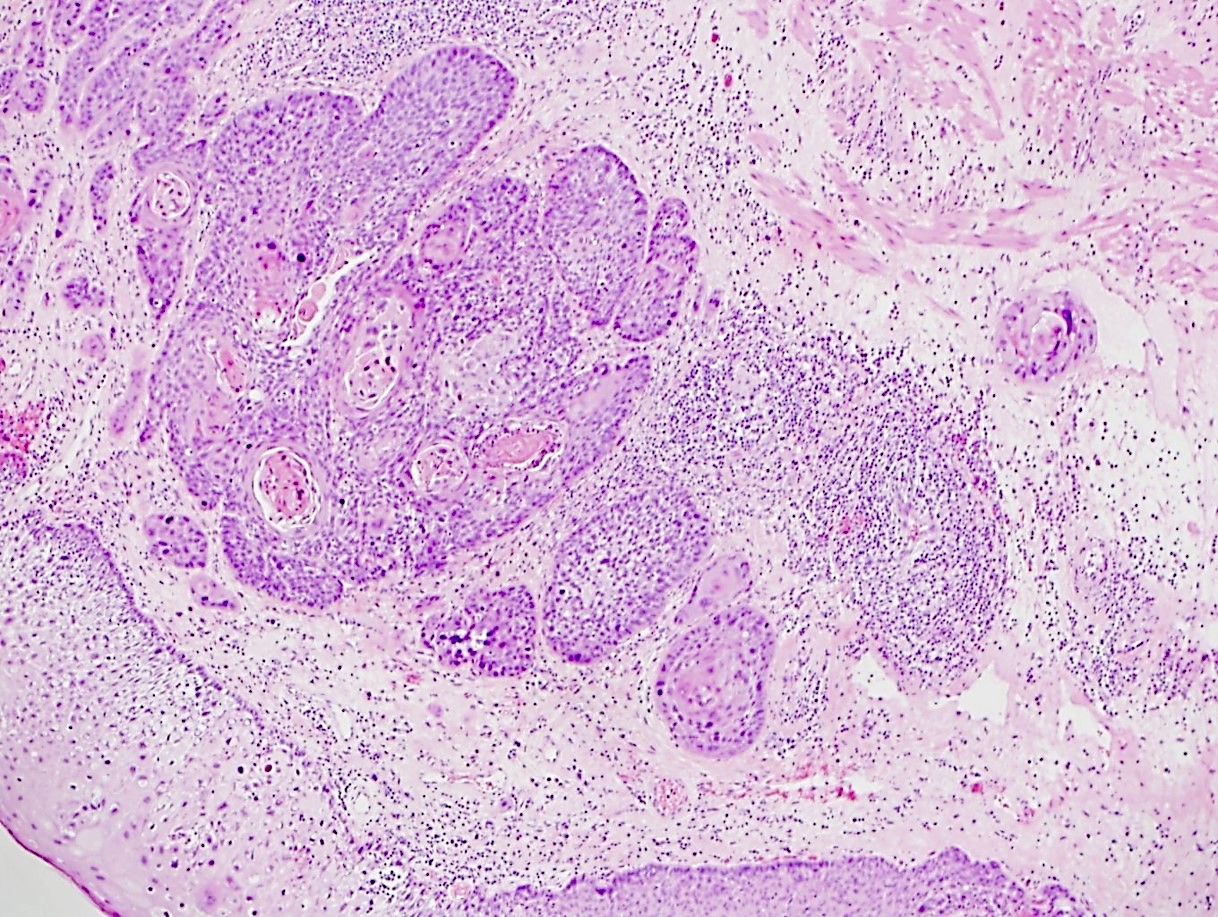
- T1: Tumor invades the lamina propria, muscularis mucosae or submucosa
- T1a: Tumor invades the lamina propria or muscularis mucosae
- T1b: Tumor invades the submucosa
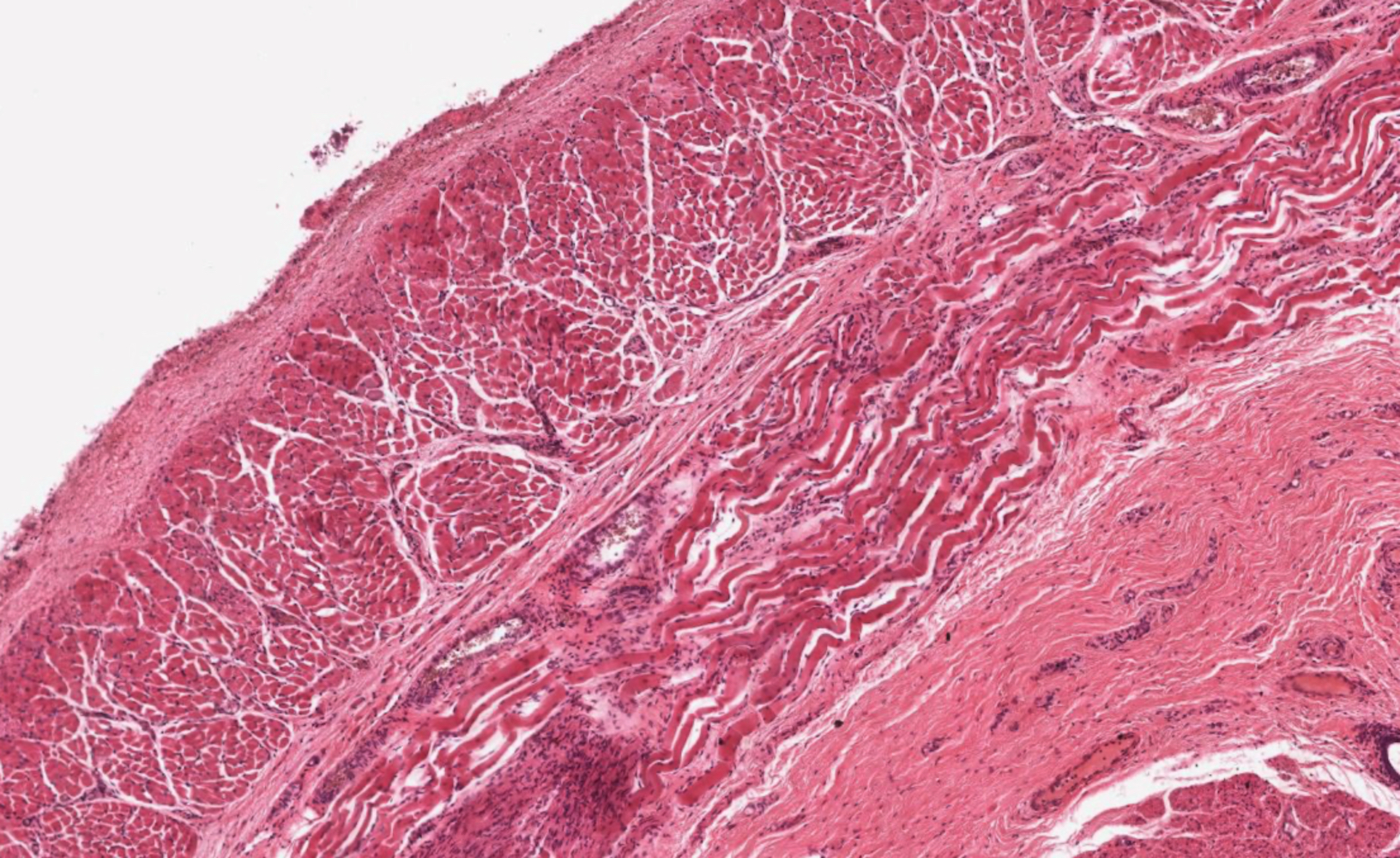
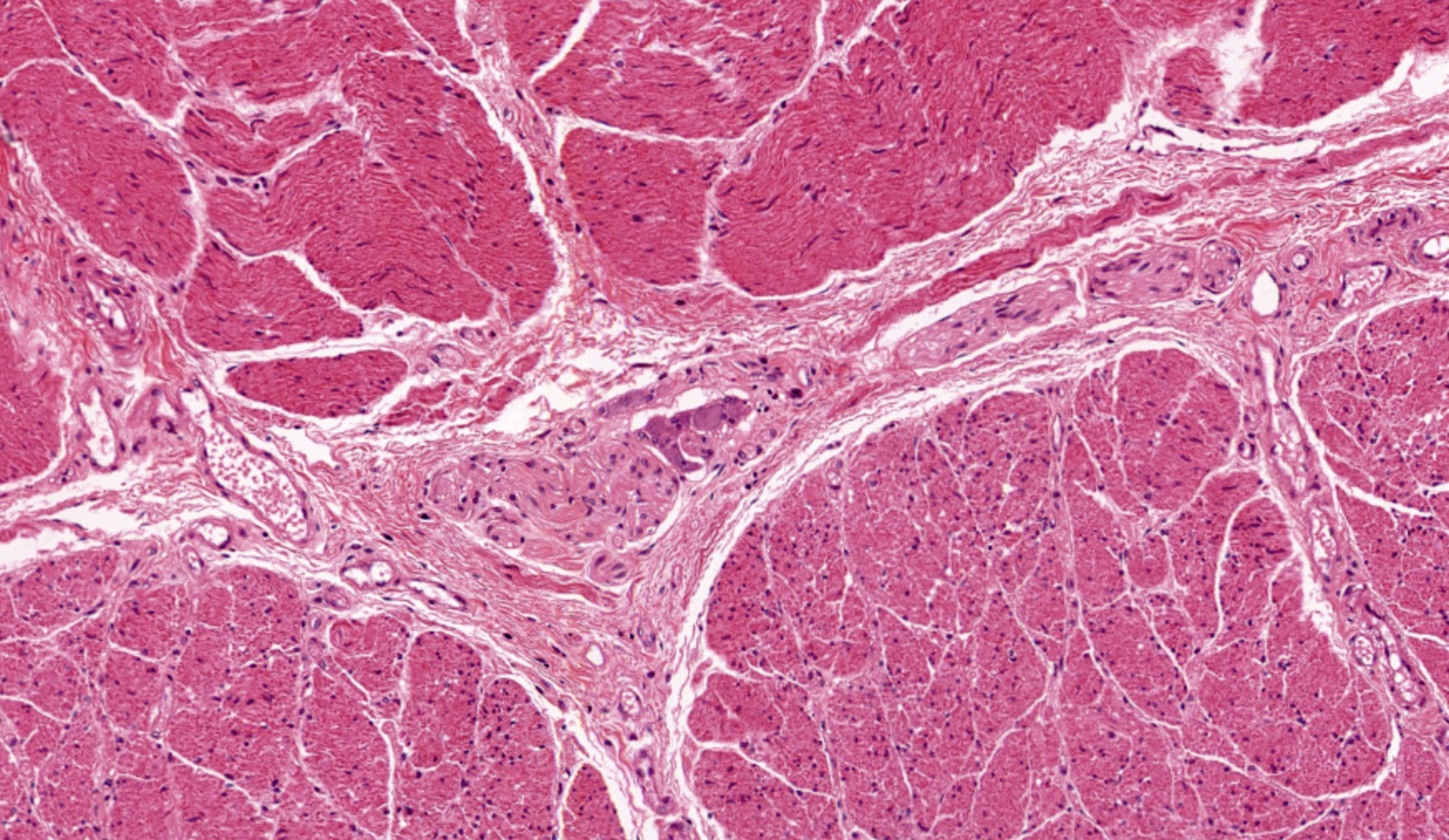
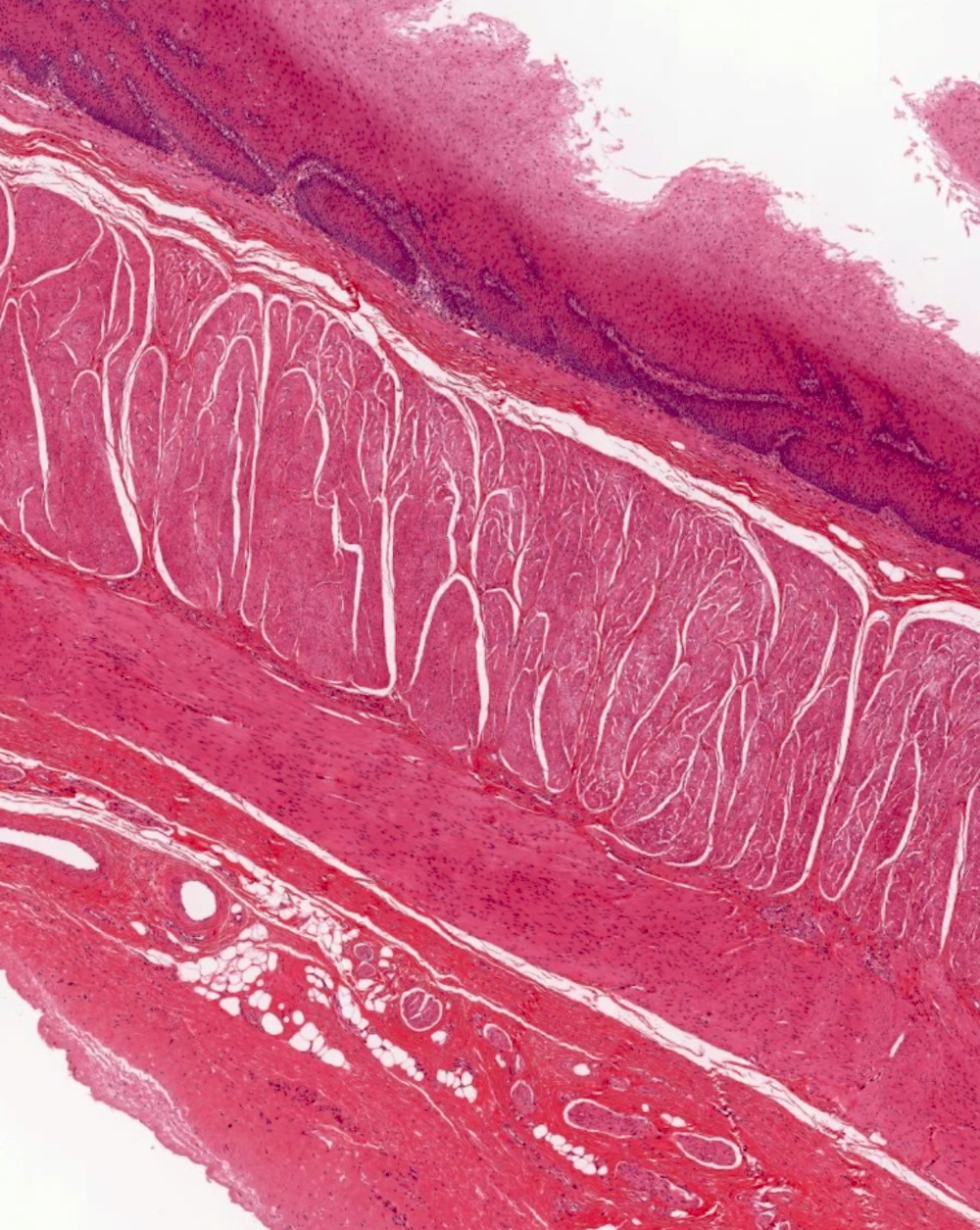
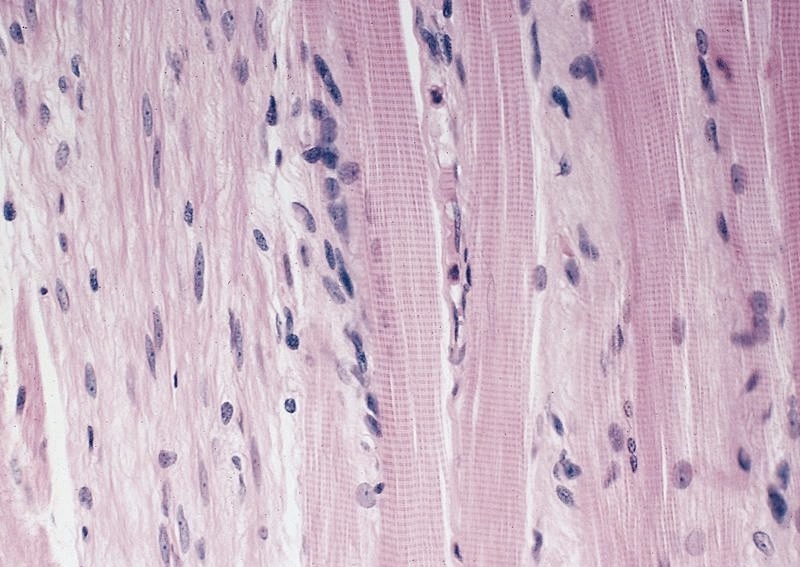
- T2: Tumor invades the muscularis propria
- T3: Tumor invades adventitia
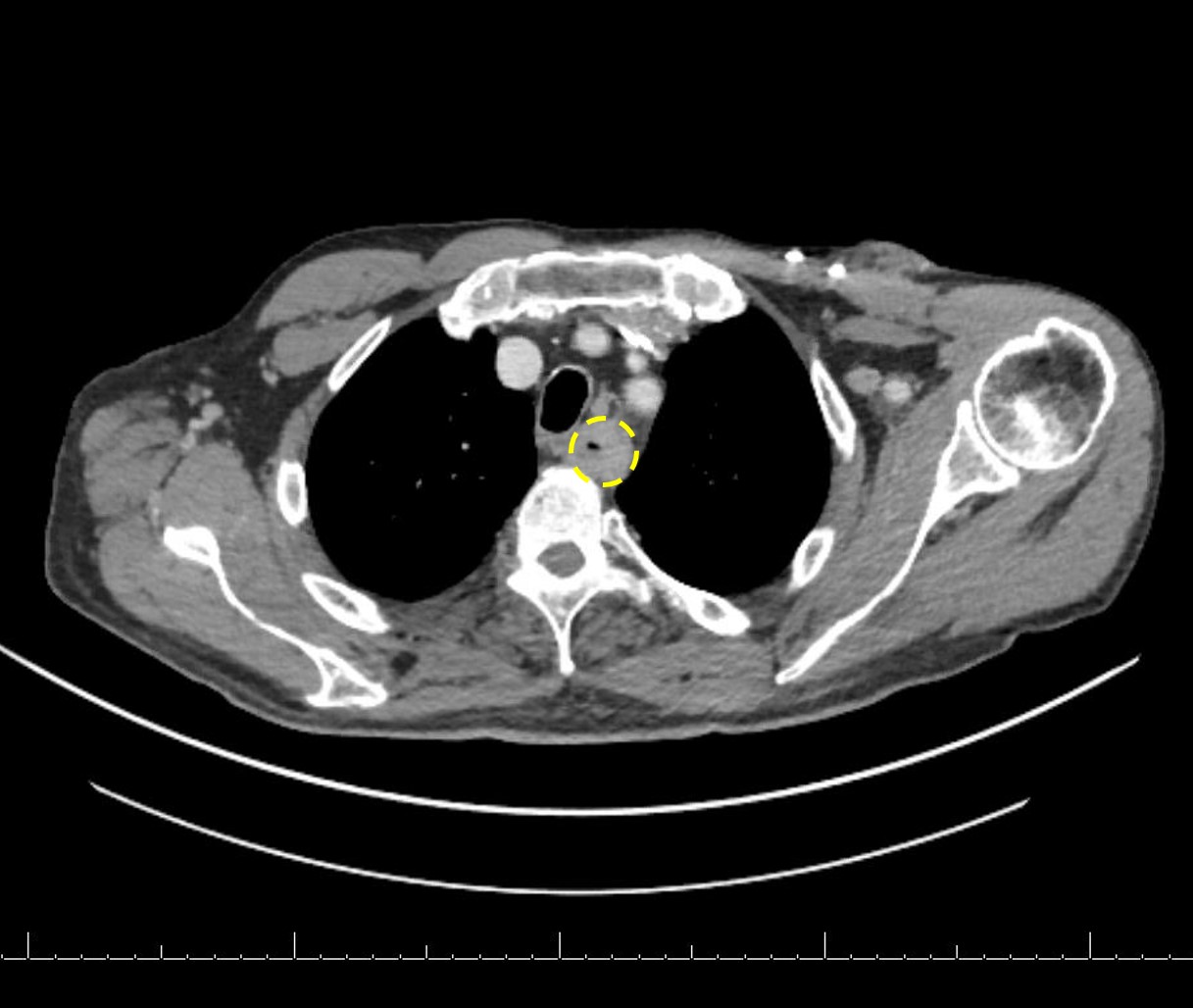
- T4: Tumor invades adjacent structures
- T4a: Tumor invades the pleura, pericardium, azygos vein, diaphragm or peritoneum
- T4b: Tumor invades other adjacent structures, such as the aorta, vertebral body or airway