

Primary tumor (pT)
- TX: primary tumor not assessed
- T0: no evidence of primary tumor
- T1: tumor ≤ 2 cm
- T2: tumor > 2 cm but ≤ 5 cm
- T3: tumor > 5 cm
- T4: tumor of any size invading adjacent organ(s), such as the vagina, urethra or bladder




Classification
of anal
adenocarcinoma

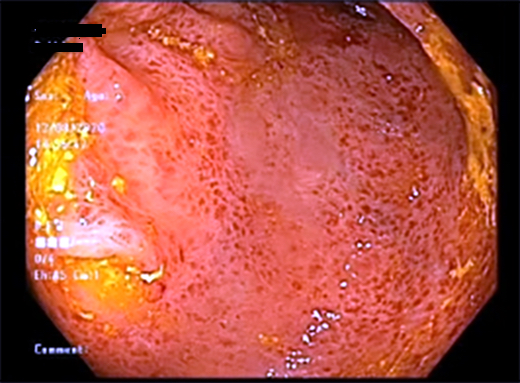
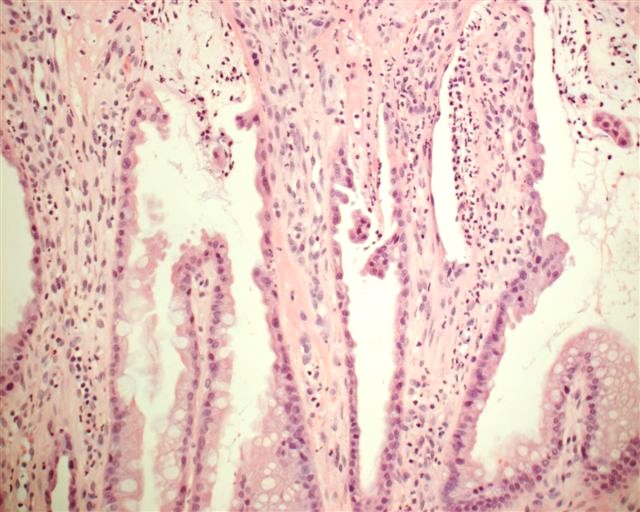
Irregular mucosa and angioectasia

Anal canal cancer
Infiltrating, gland forming
Infiltrating glands
Mucinous and signet ring
Fistula tract associated

Coronal section of rectum and anal canal

Columns of Morgagni and the anal valves

Inner wall of the lower end of the rectum and anus

Median sagittal section of male pelvis

Median sagittal section of female pelvis

Anal / rectal junction and sphincter
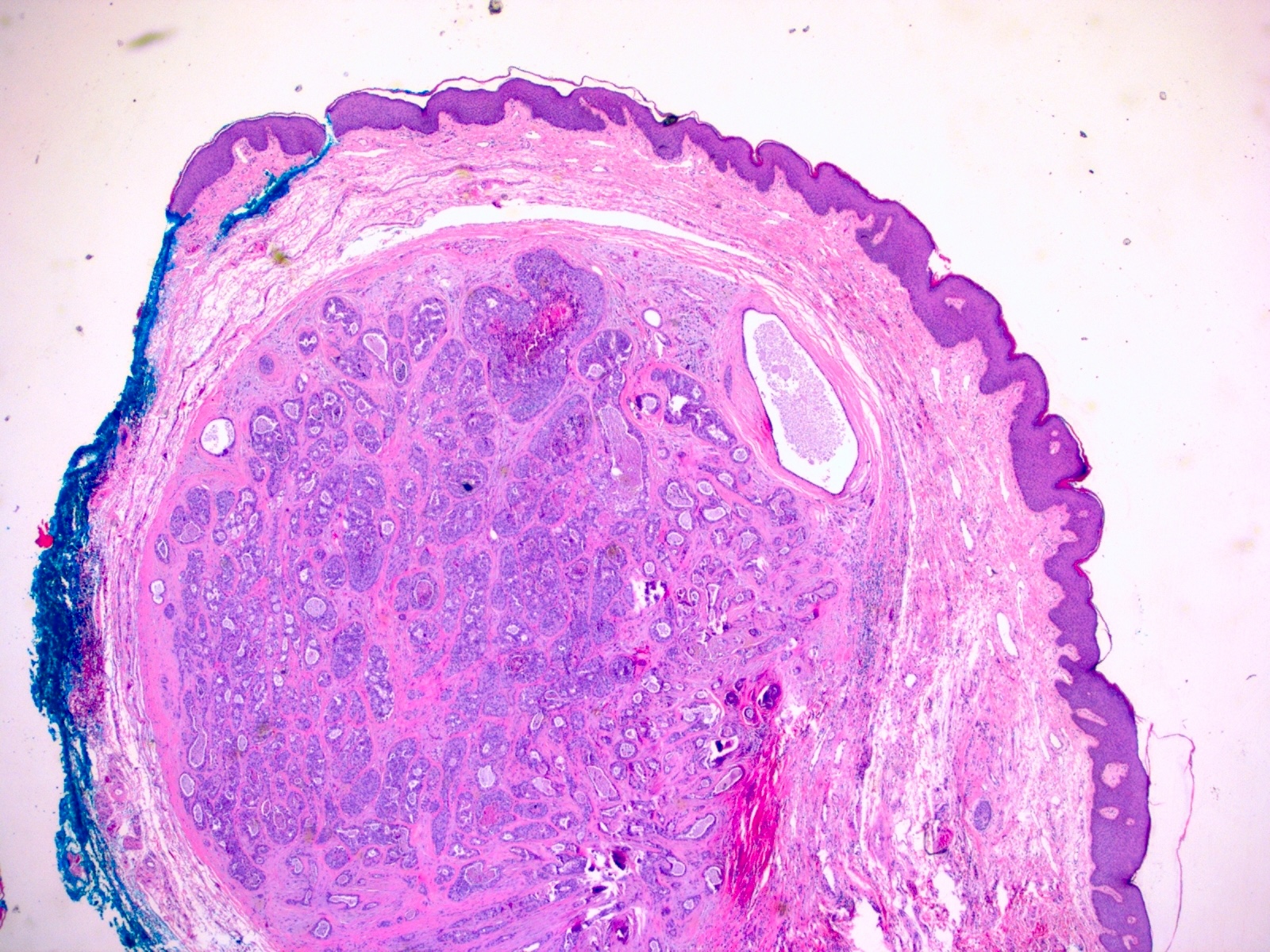
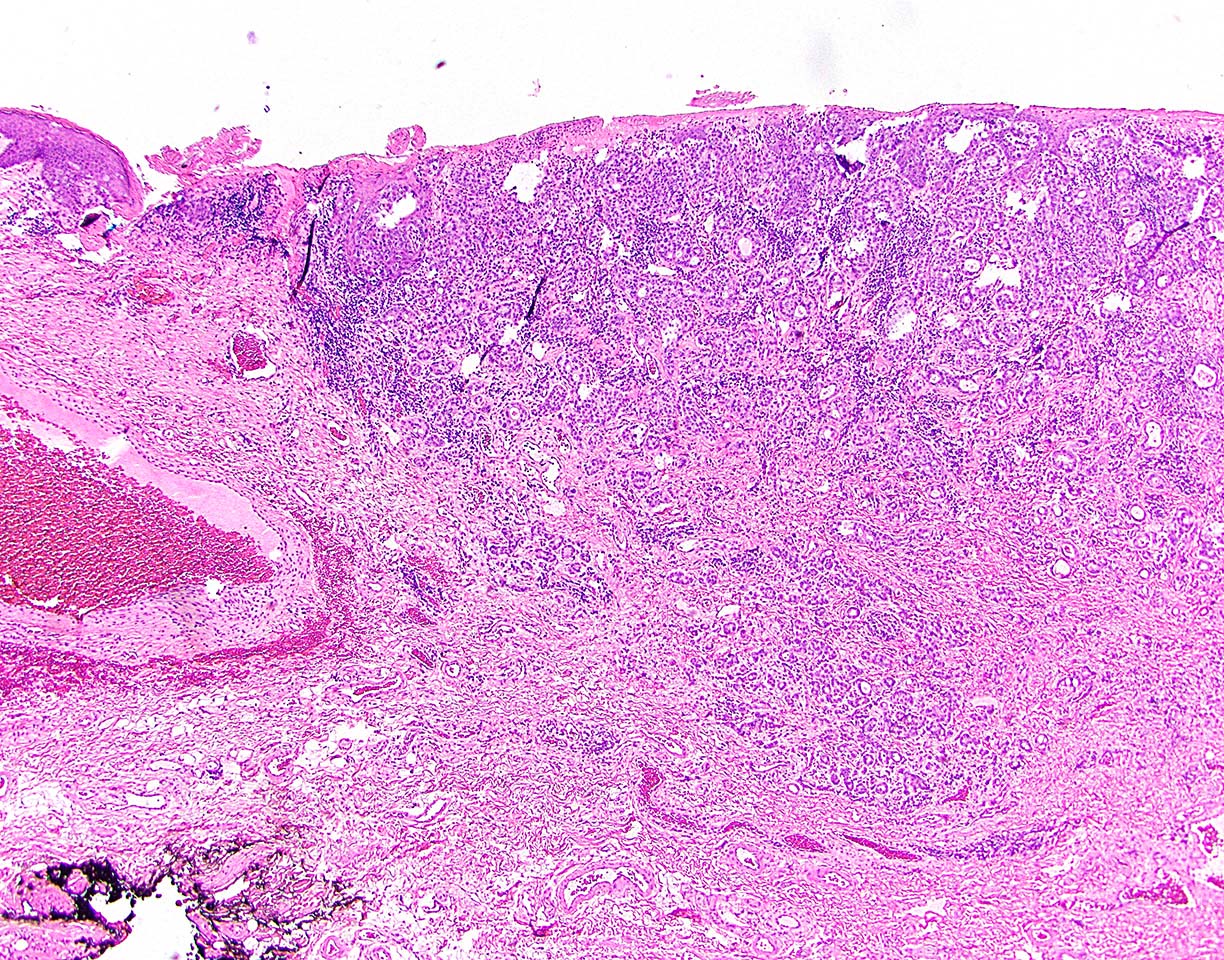
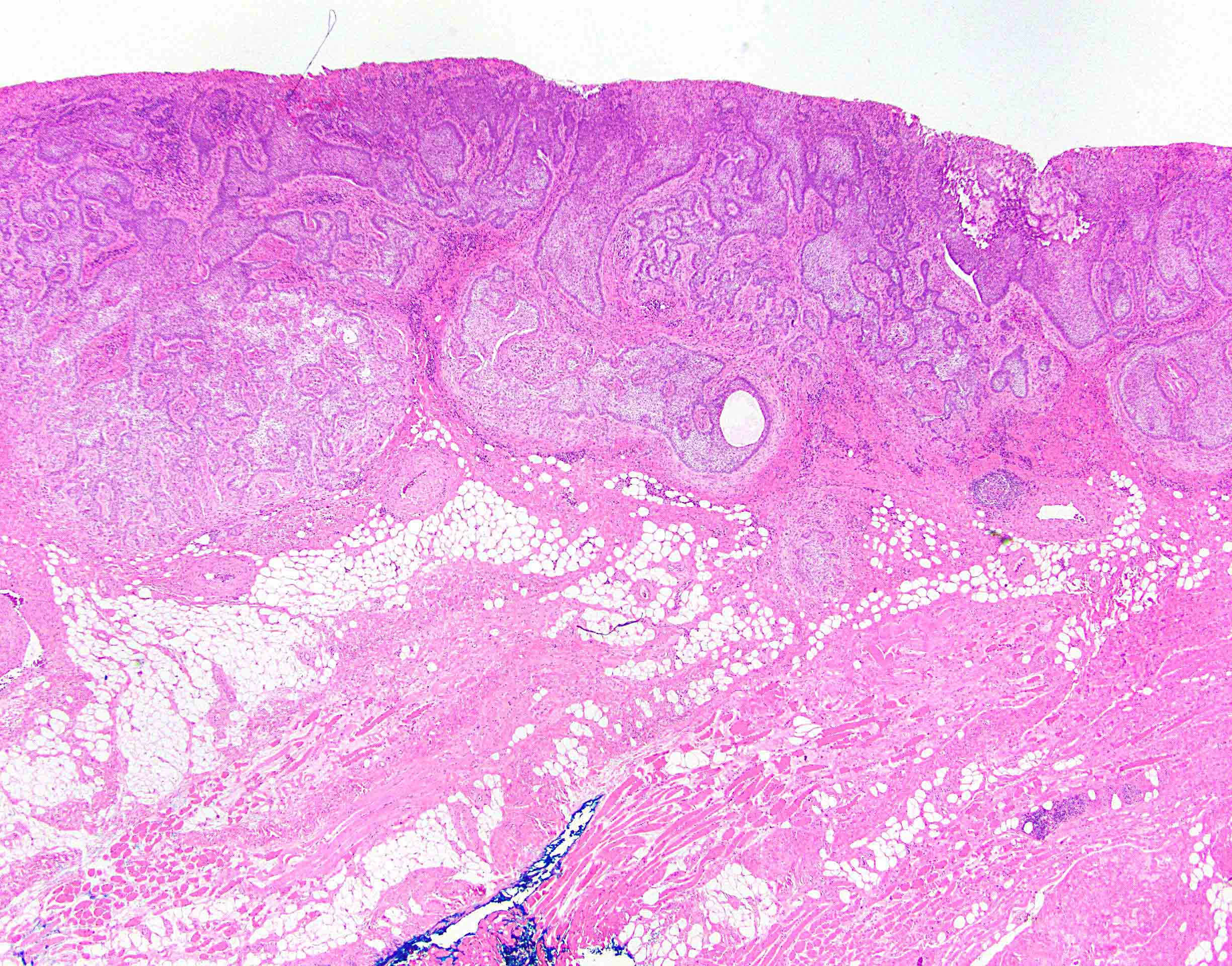
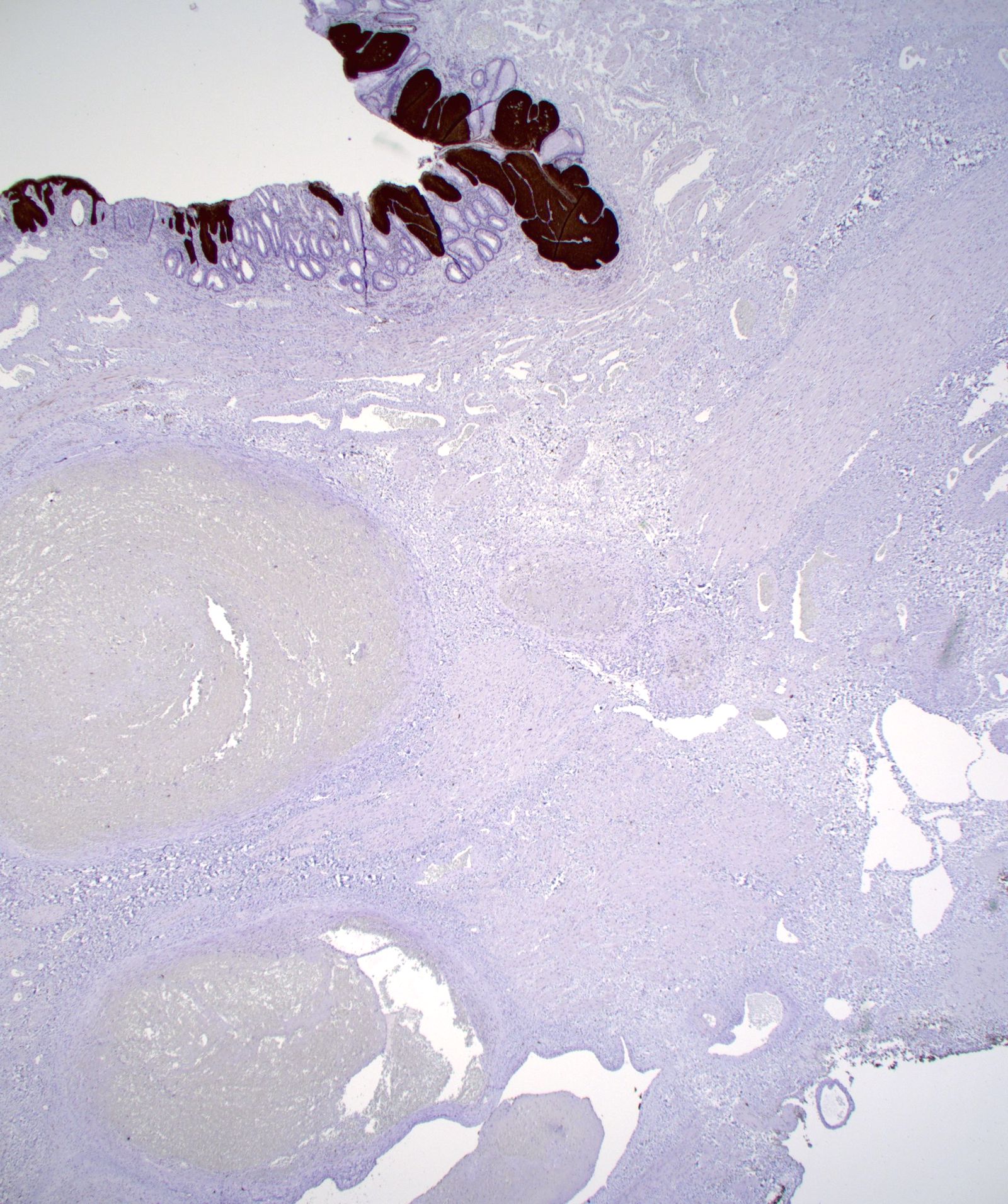
Well circumscribed tumor located deep in perianal dermal tissue
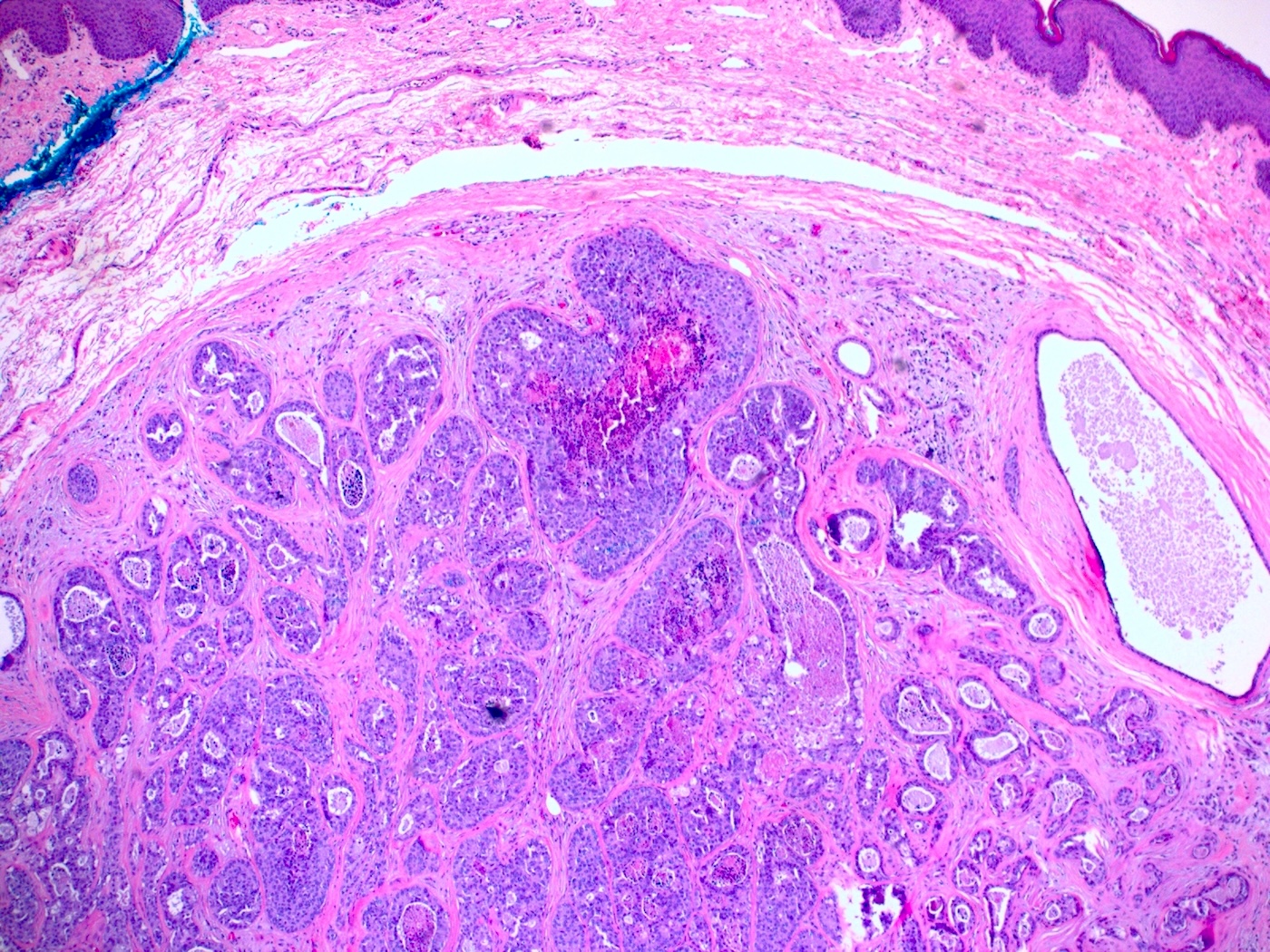
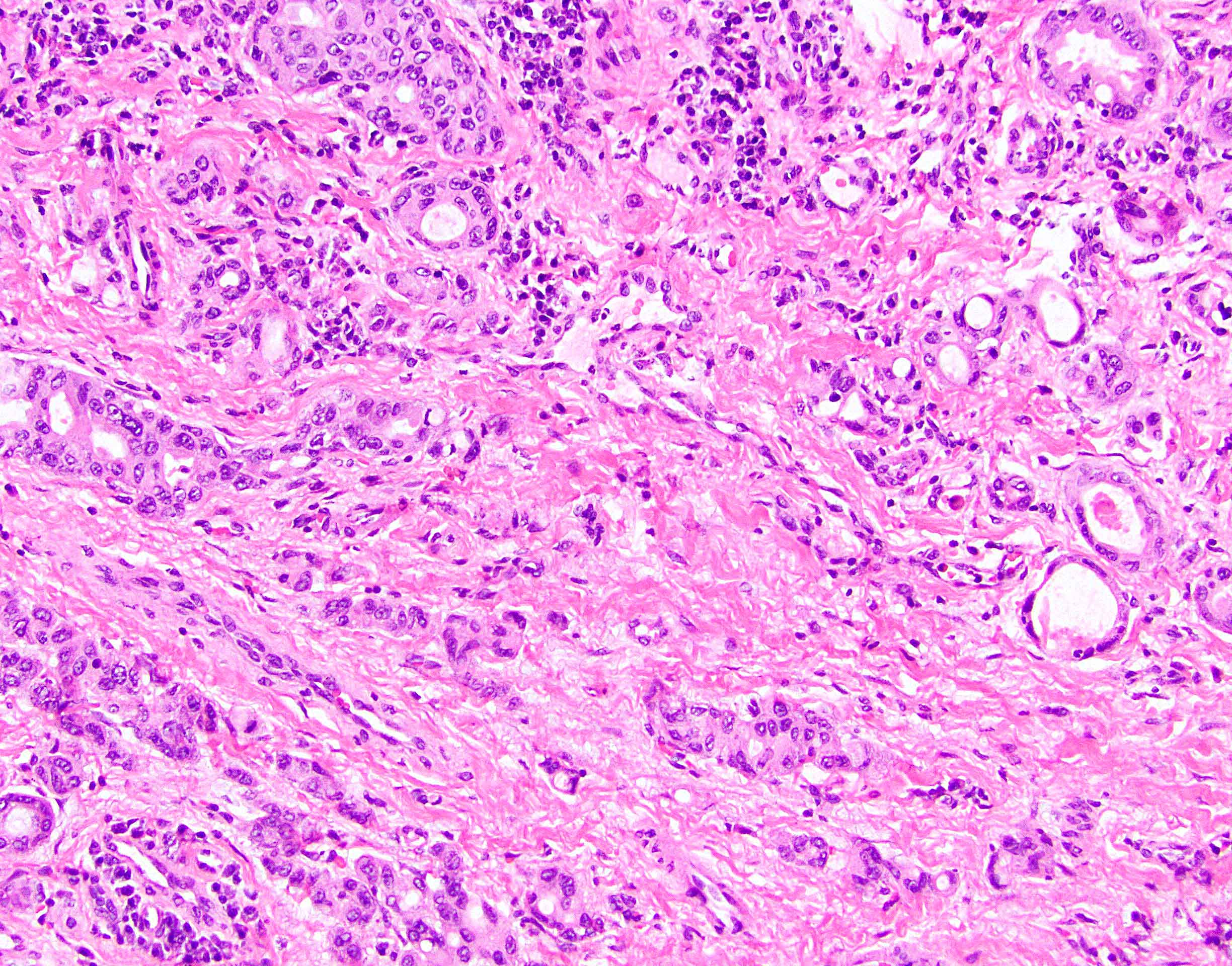
Low high grade components, with comedo necrosis in high grade components
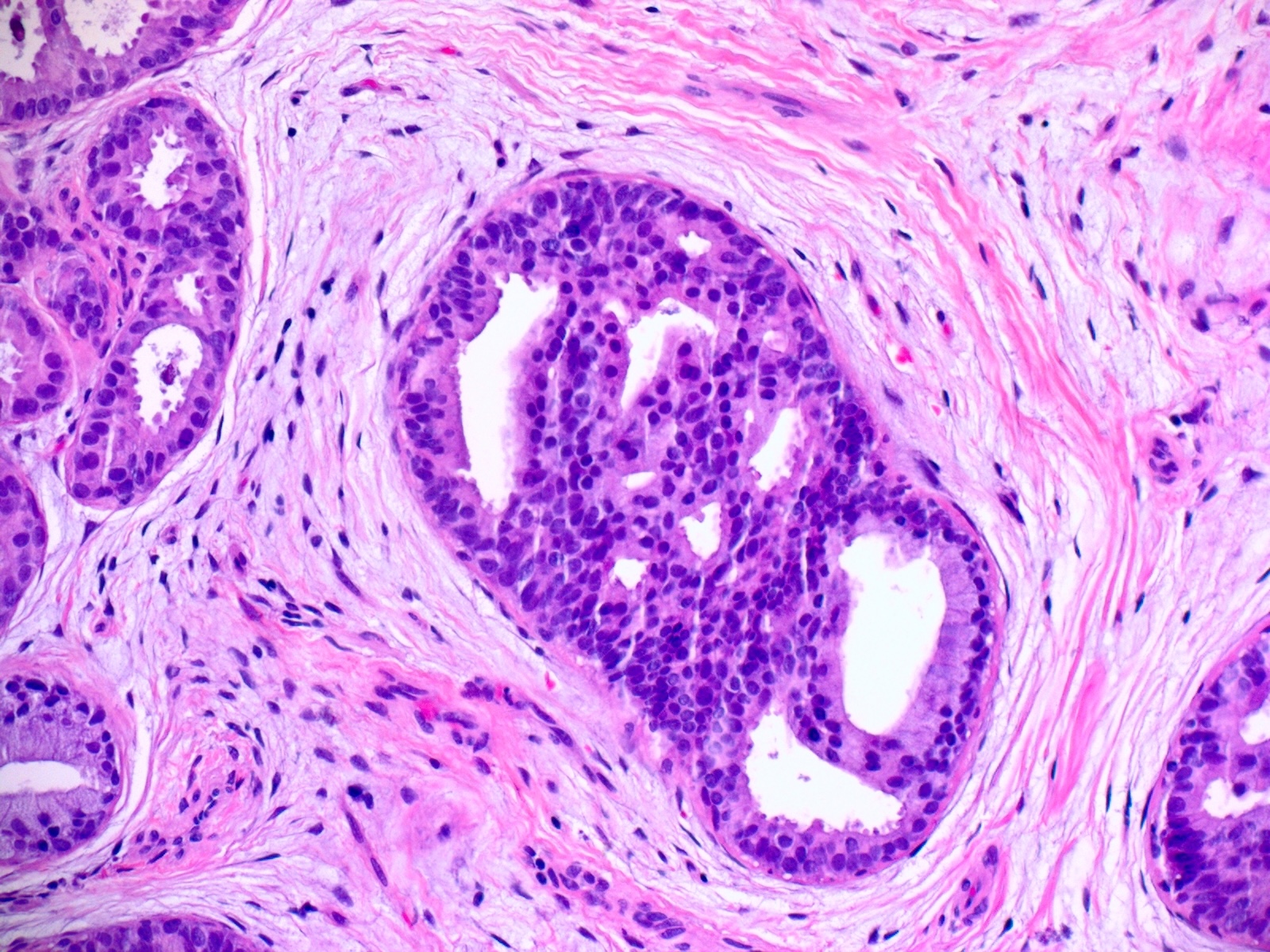
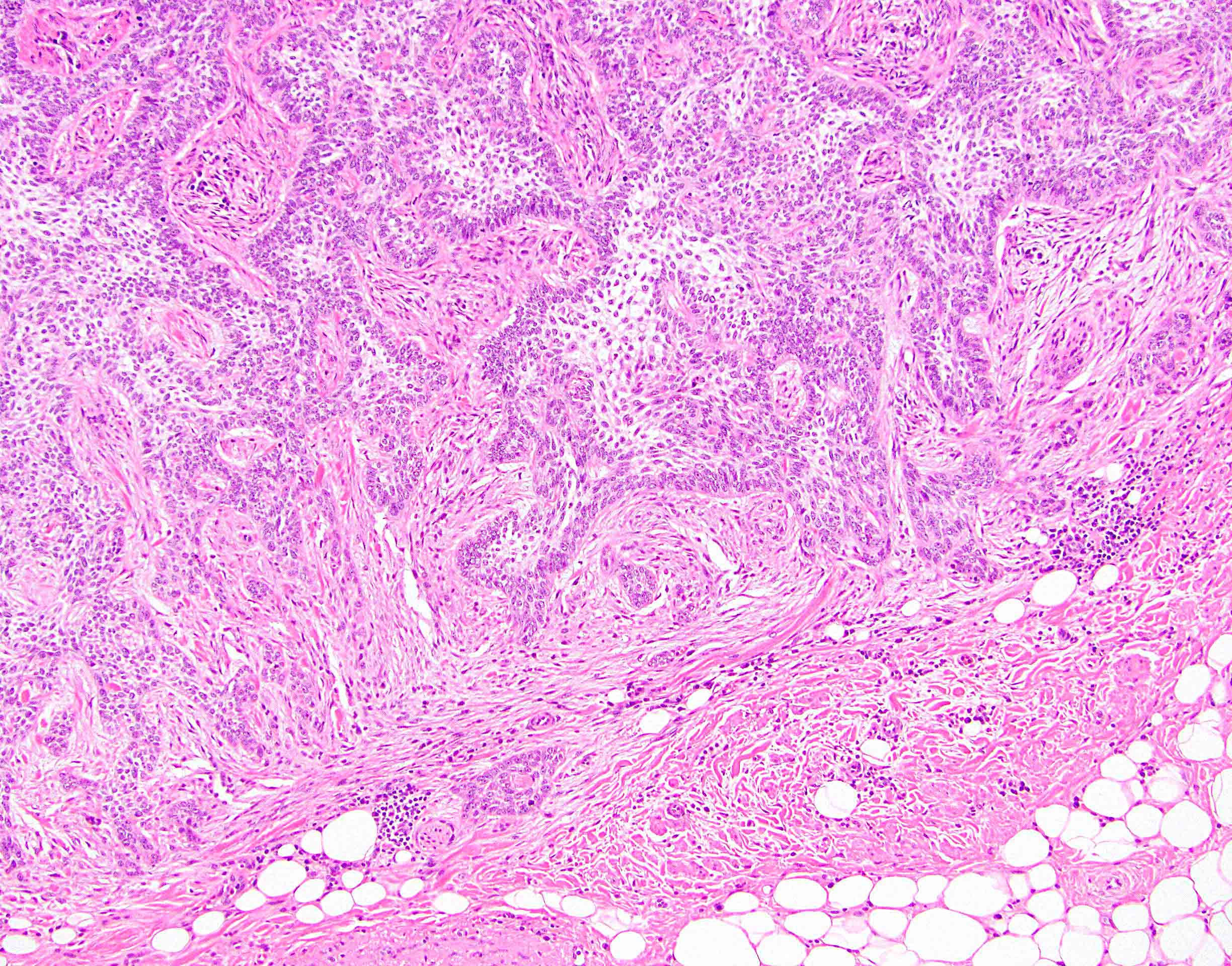
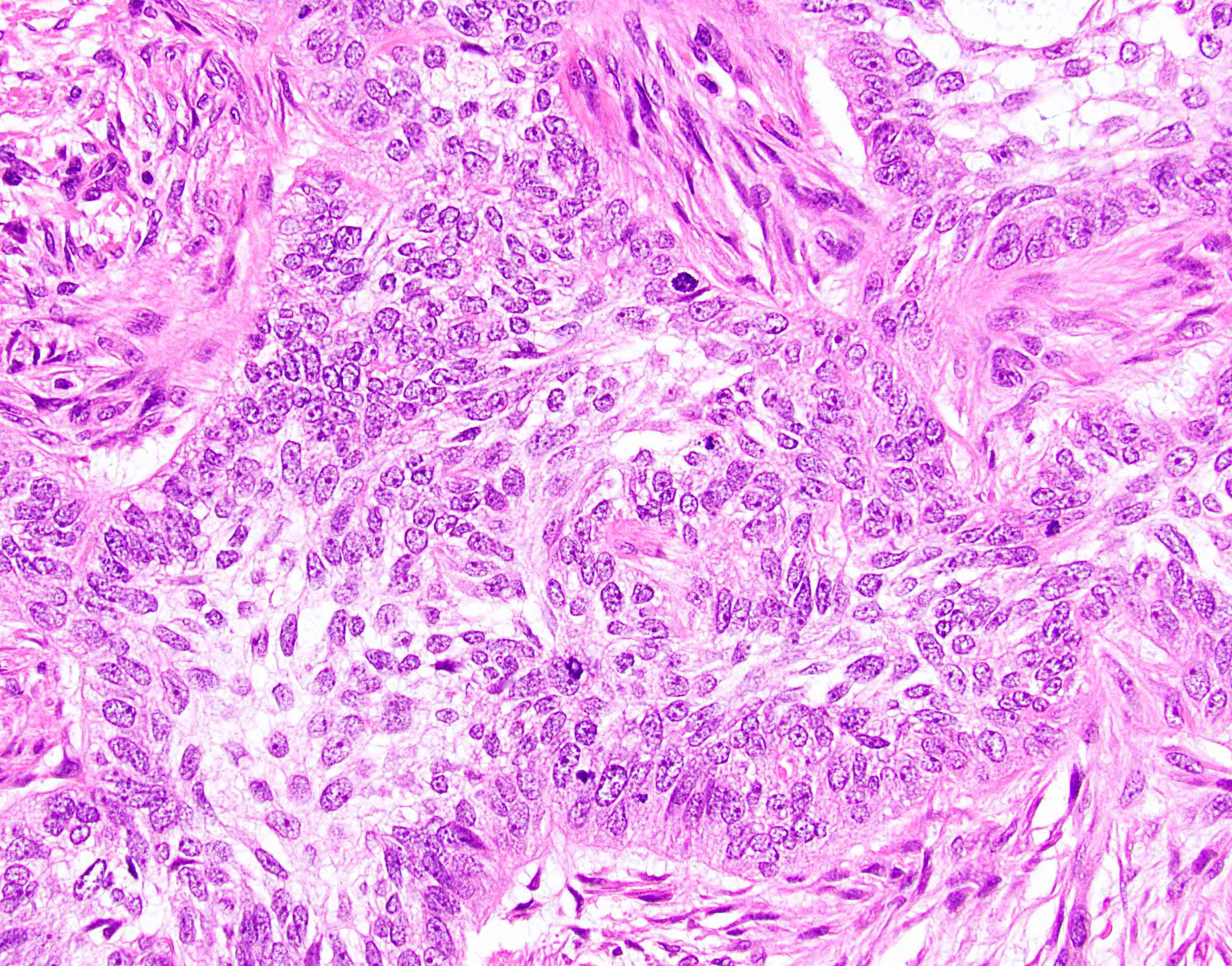
Cribriform architecture, tumor cells with abundant eosinophilic cytoplasm
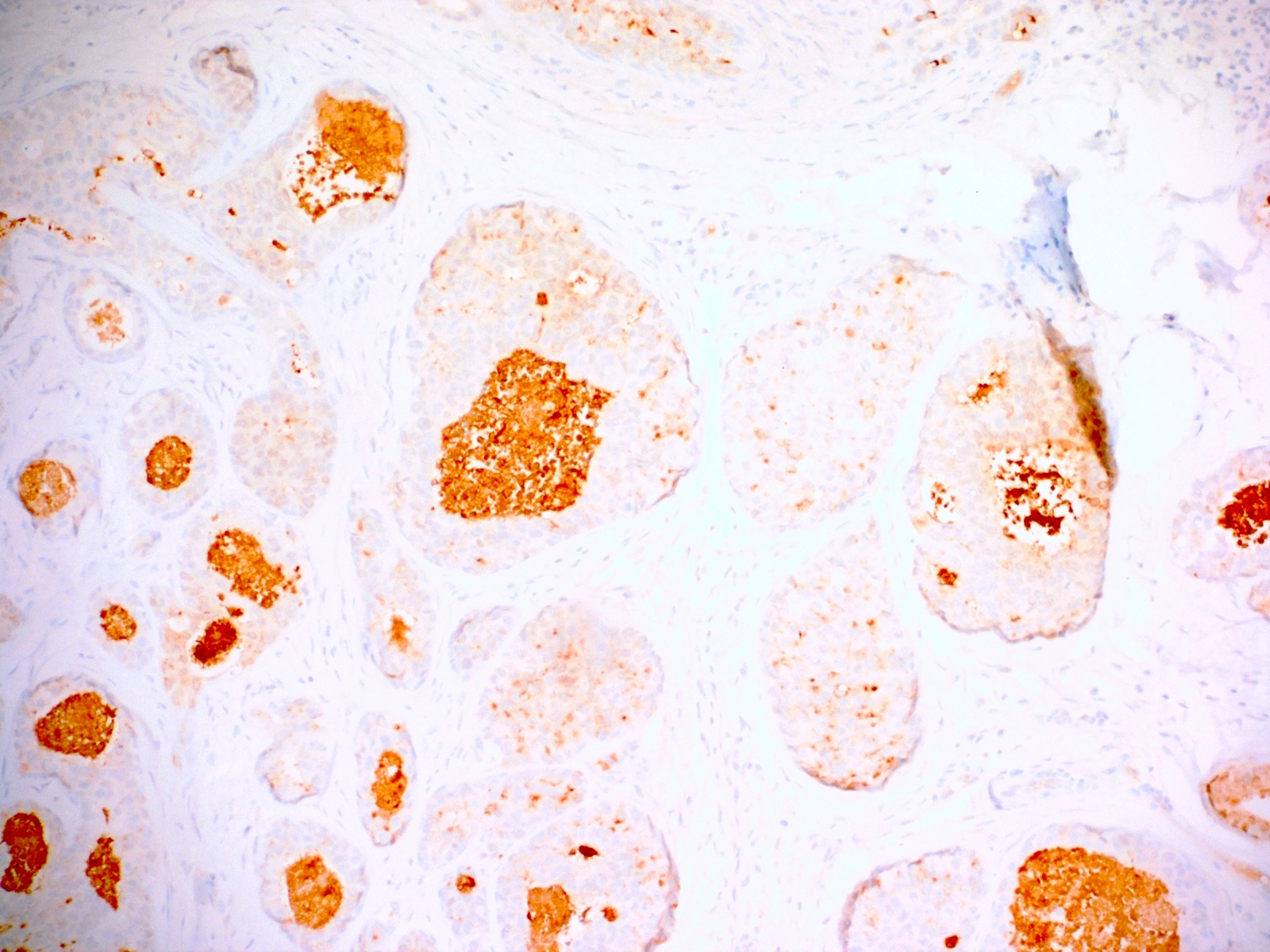
GCDFP-15
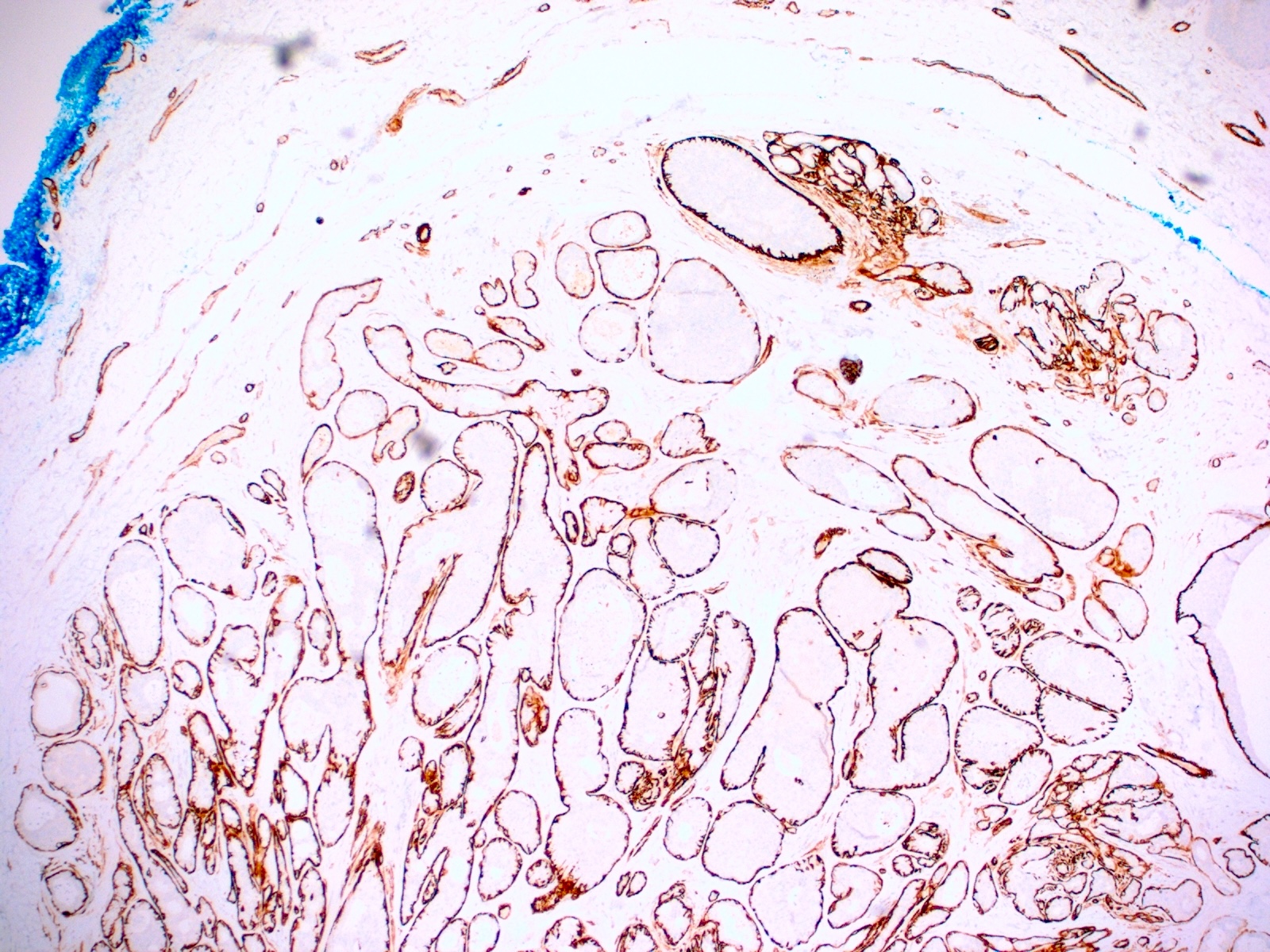
Smooth muscle actin

Ki67

Perianal basal cell carcinoma
Basal cell carcinoma

Cell clusters

Tumor invading the rectum

Extensive pelvic infiltration of tumor

Pelvic structures infiltrated by tumor

Tumor expands along the endopelvis

Tumor involves the inguinal area

Bulky tumor of vulva and anus

Large exophytic tumor of vulva and perineum
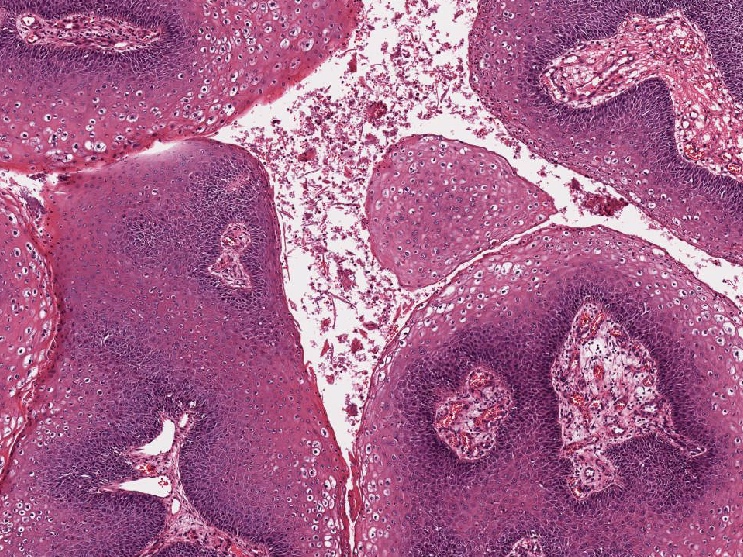
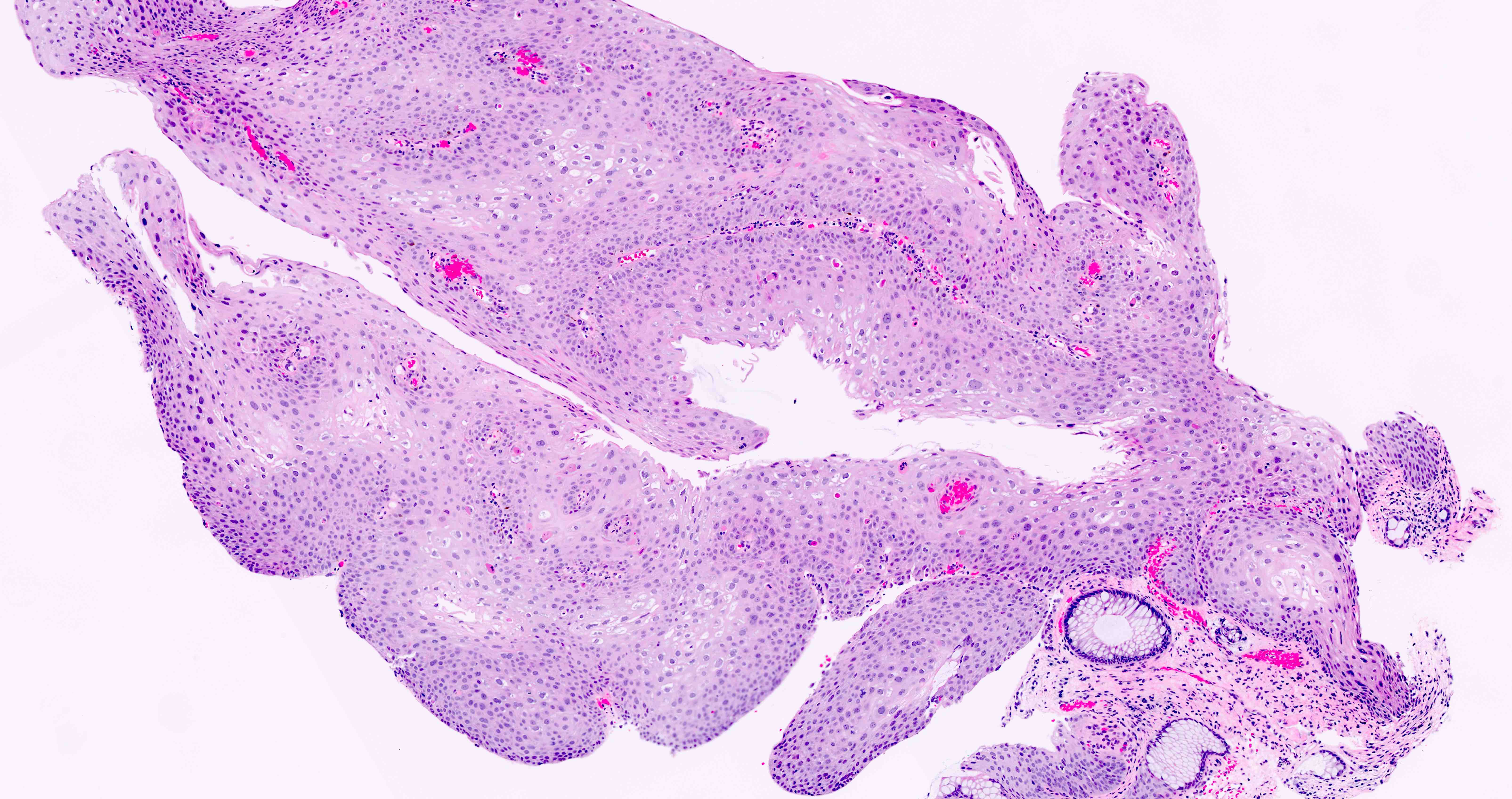
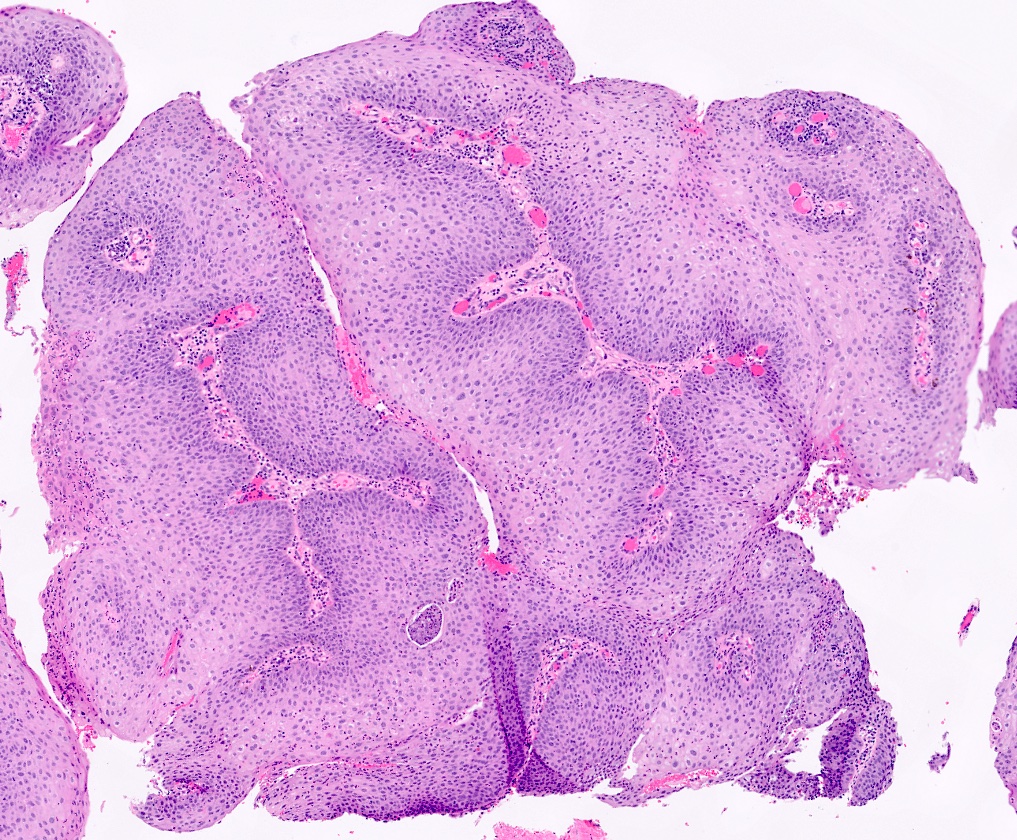
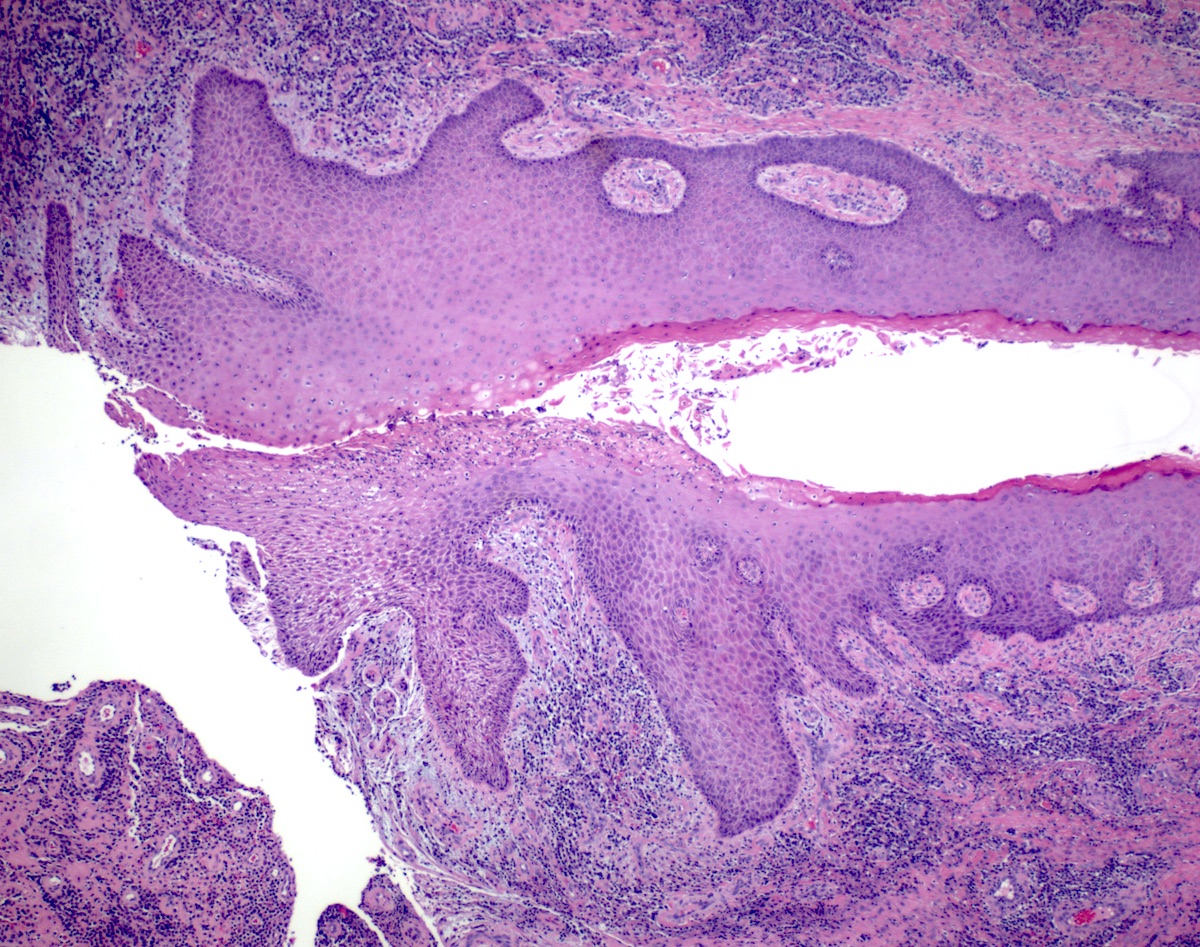
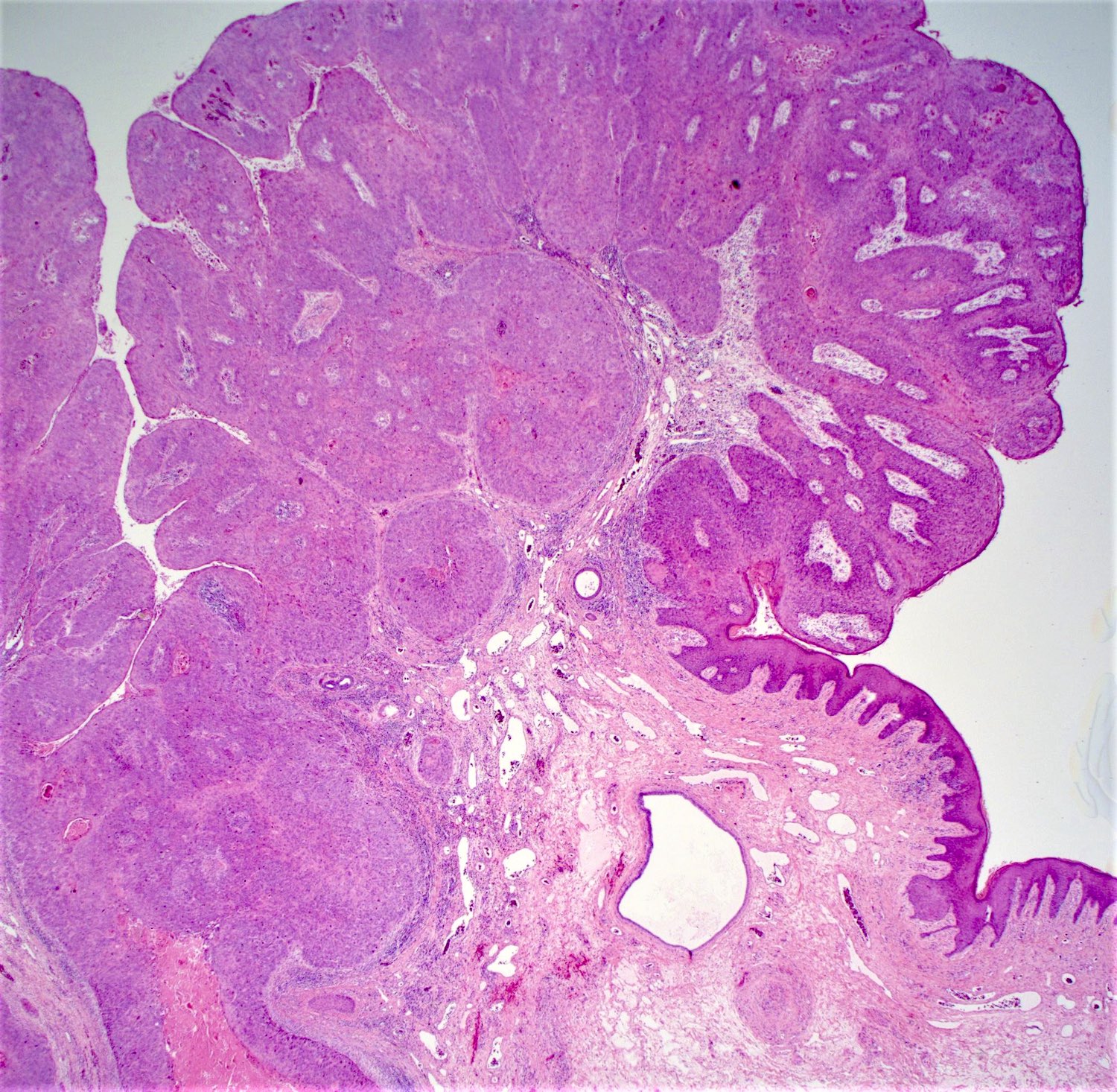
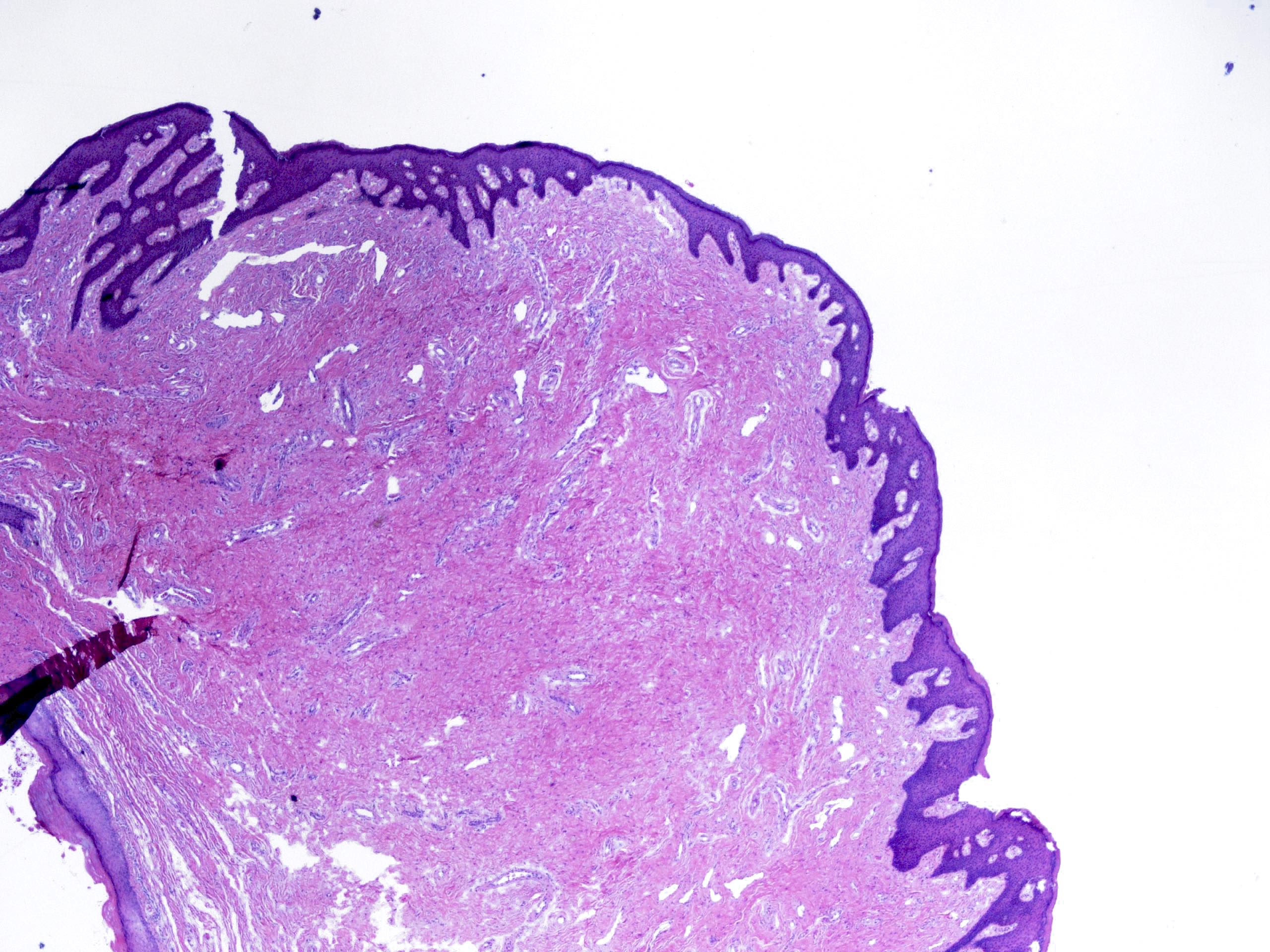
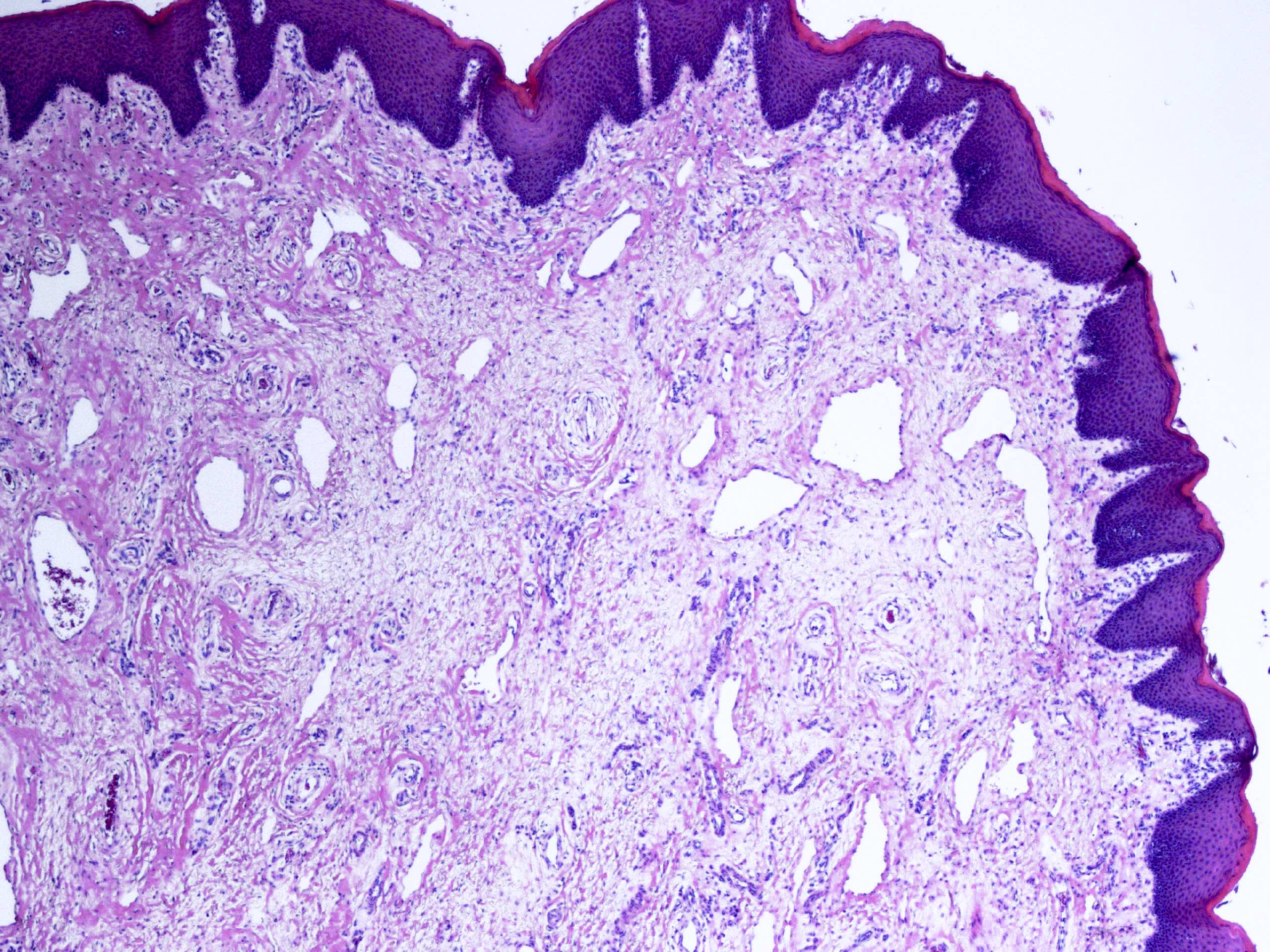
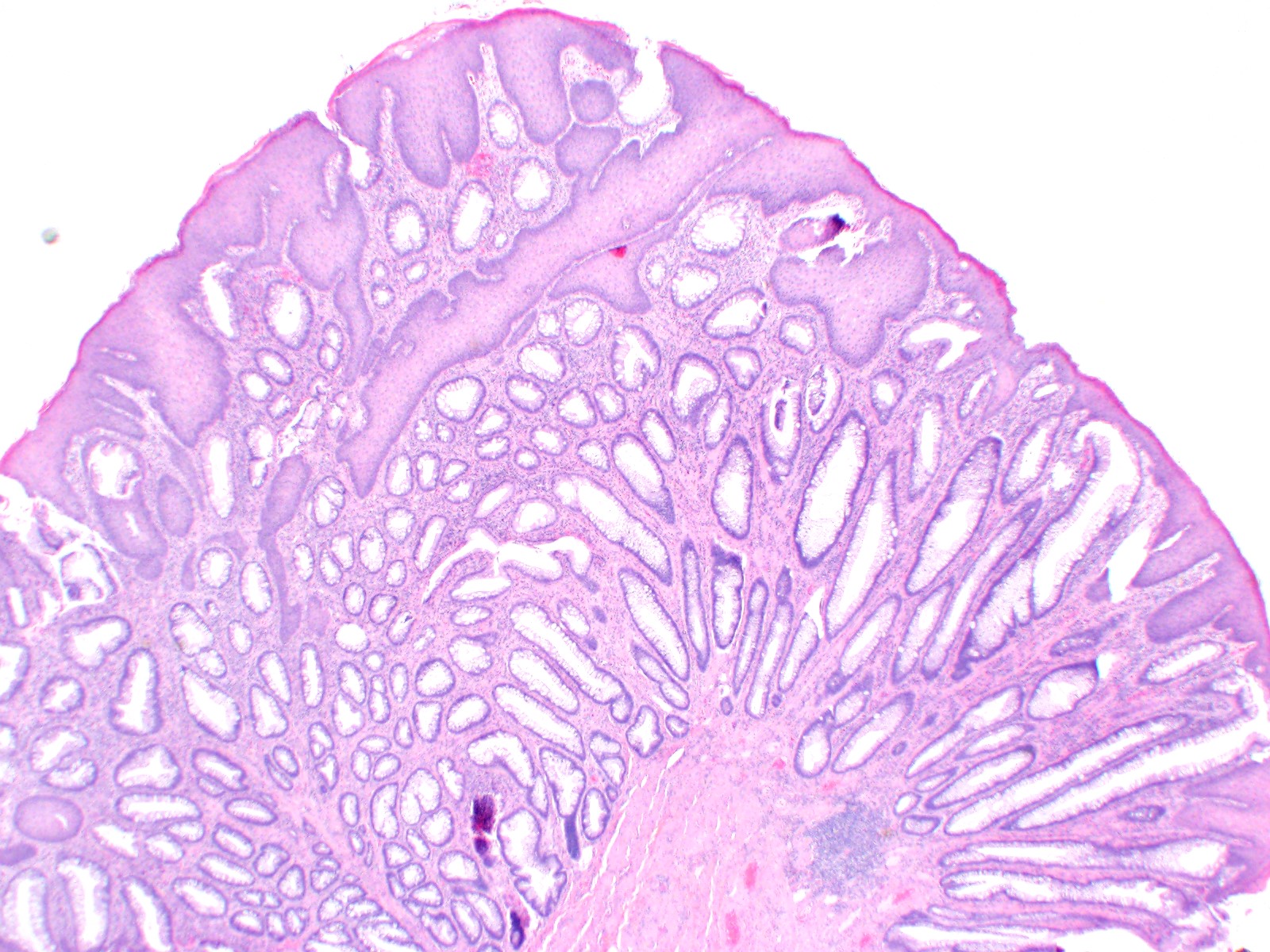
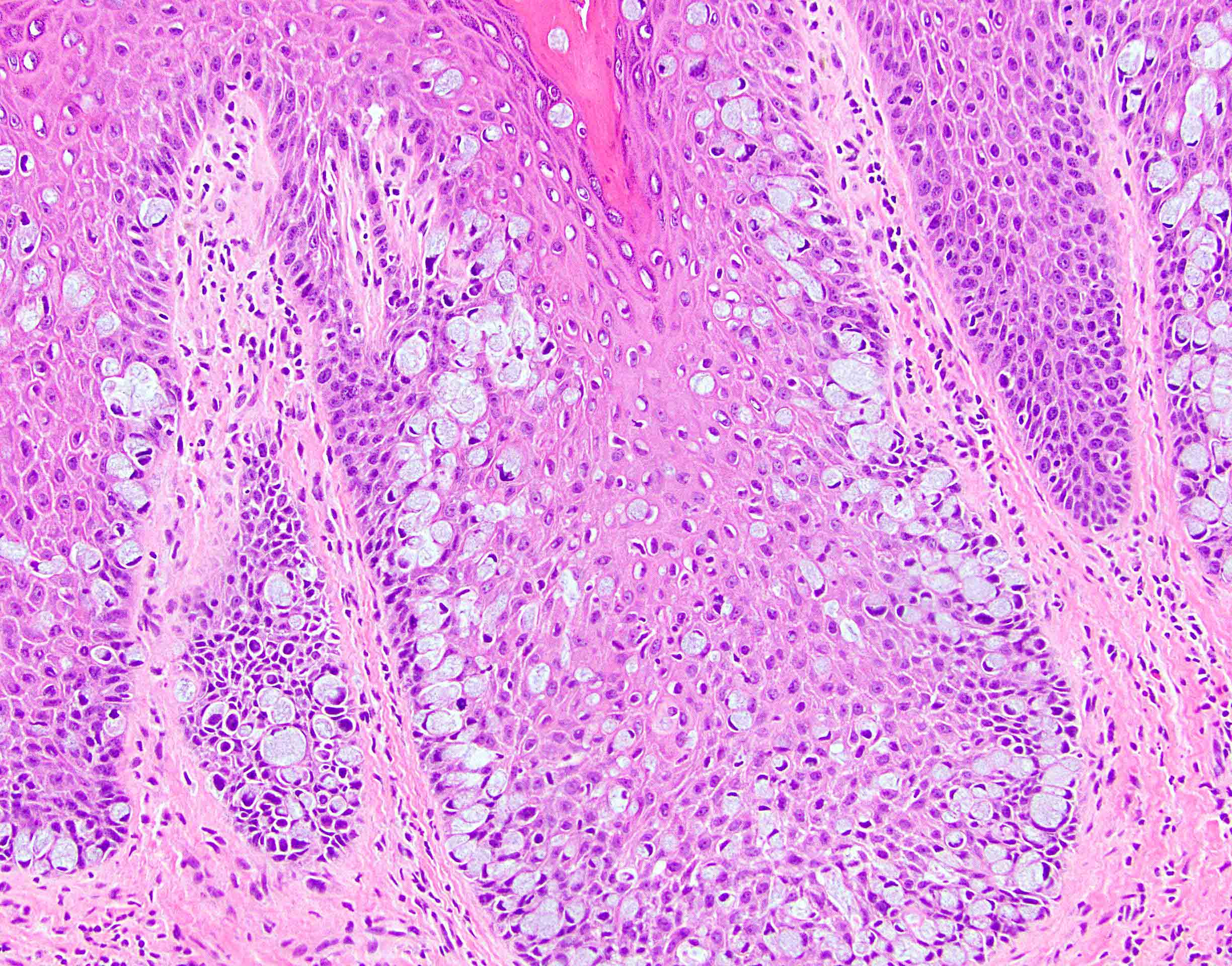
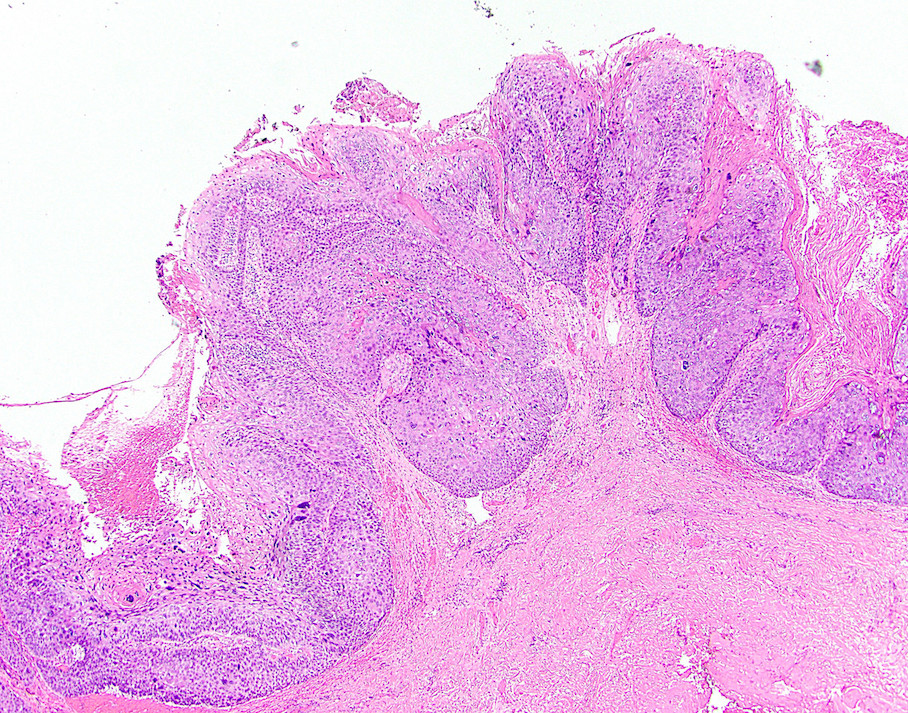
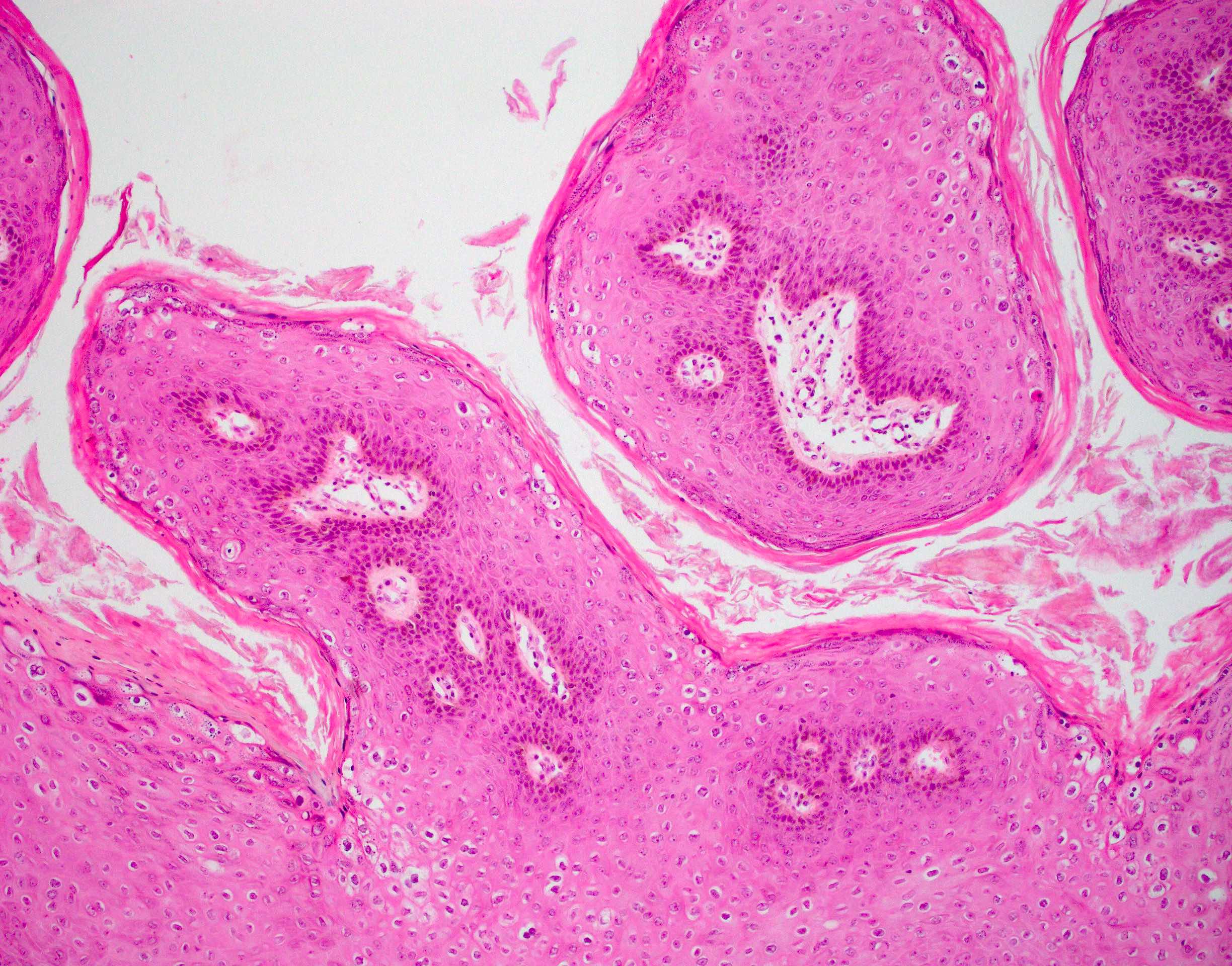
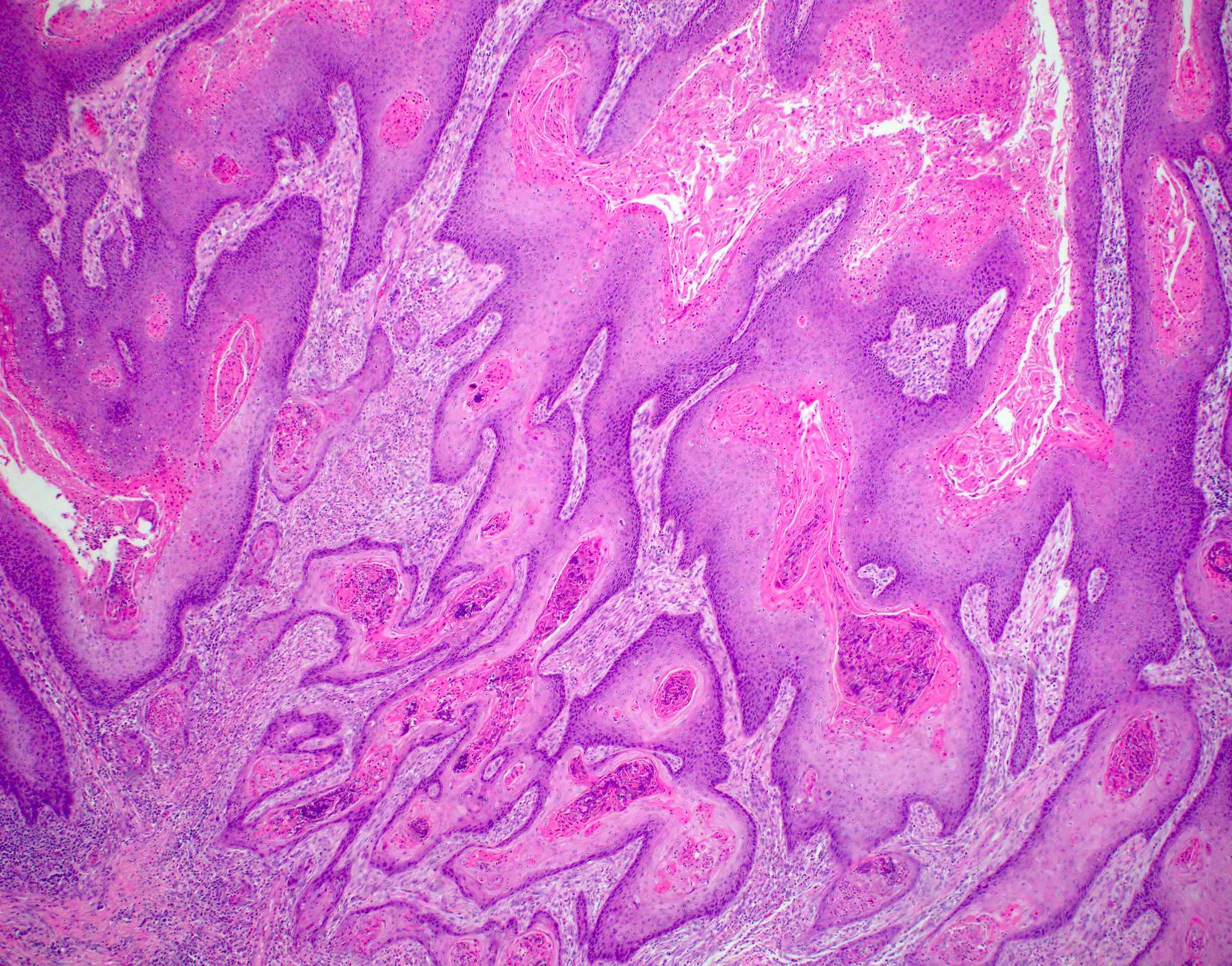
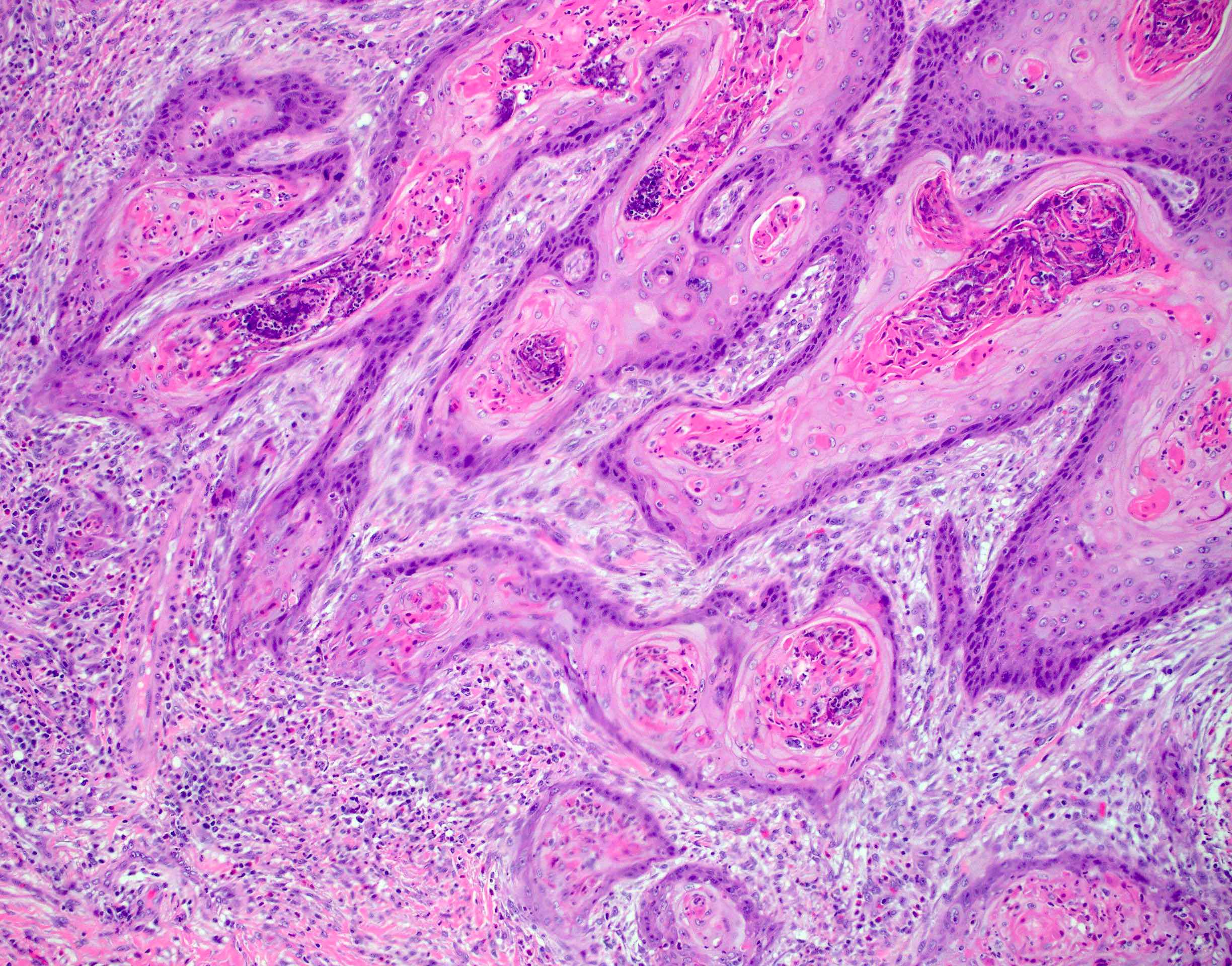
Well formed papillae with fibrovascular cores
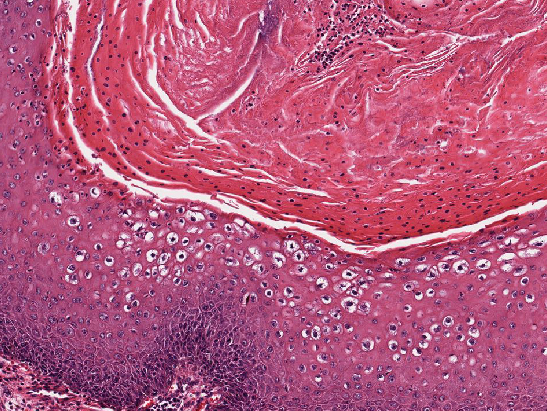
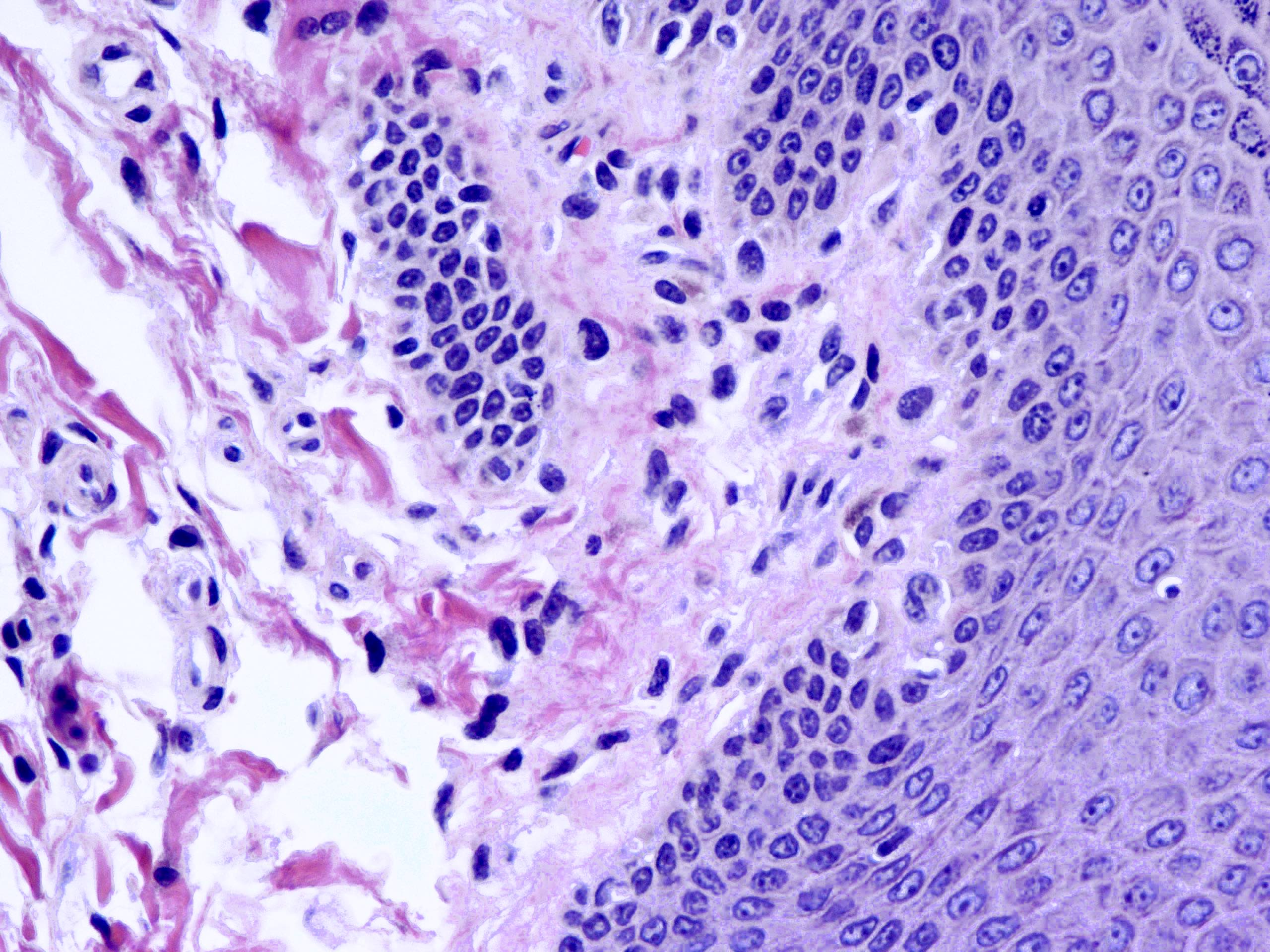
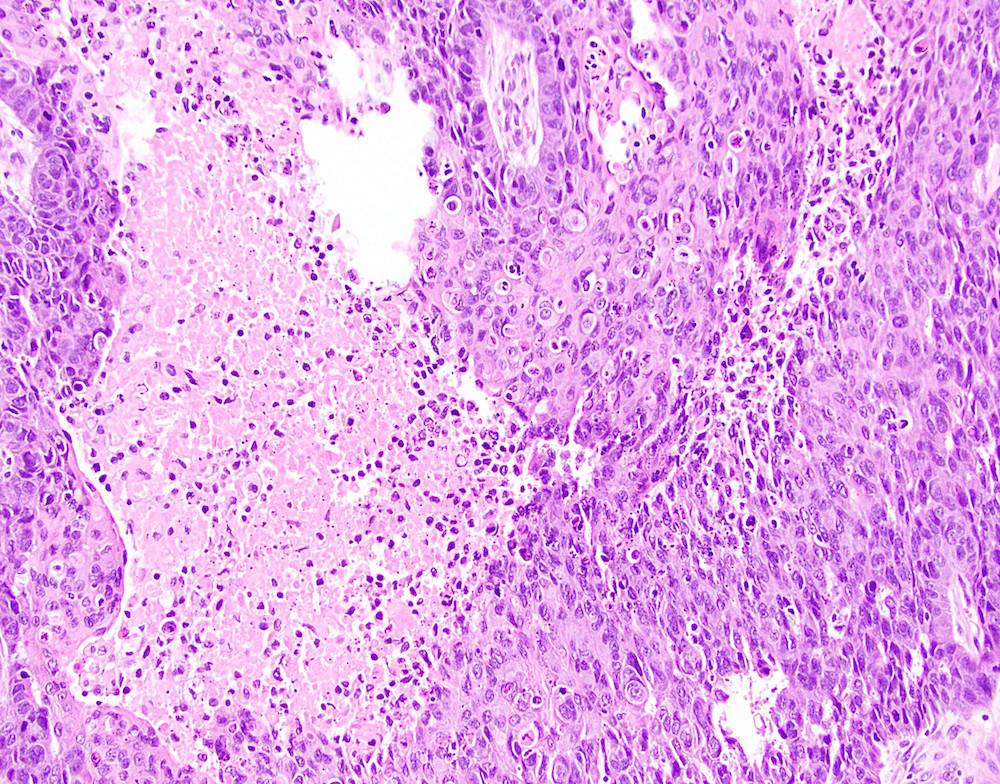
Hyperkeratosis with parakeratosis
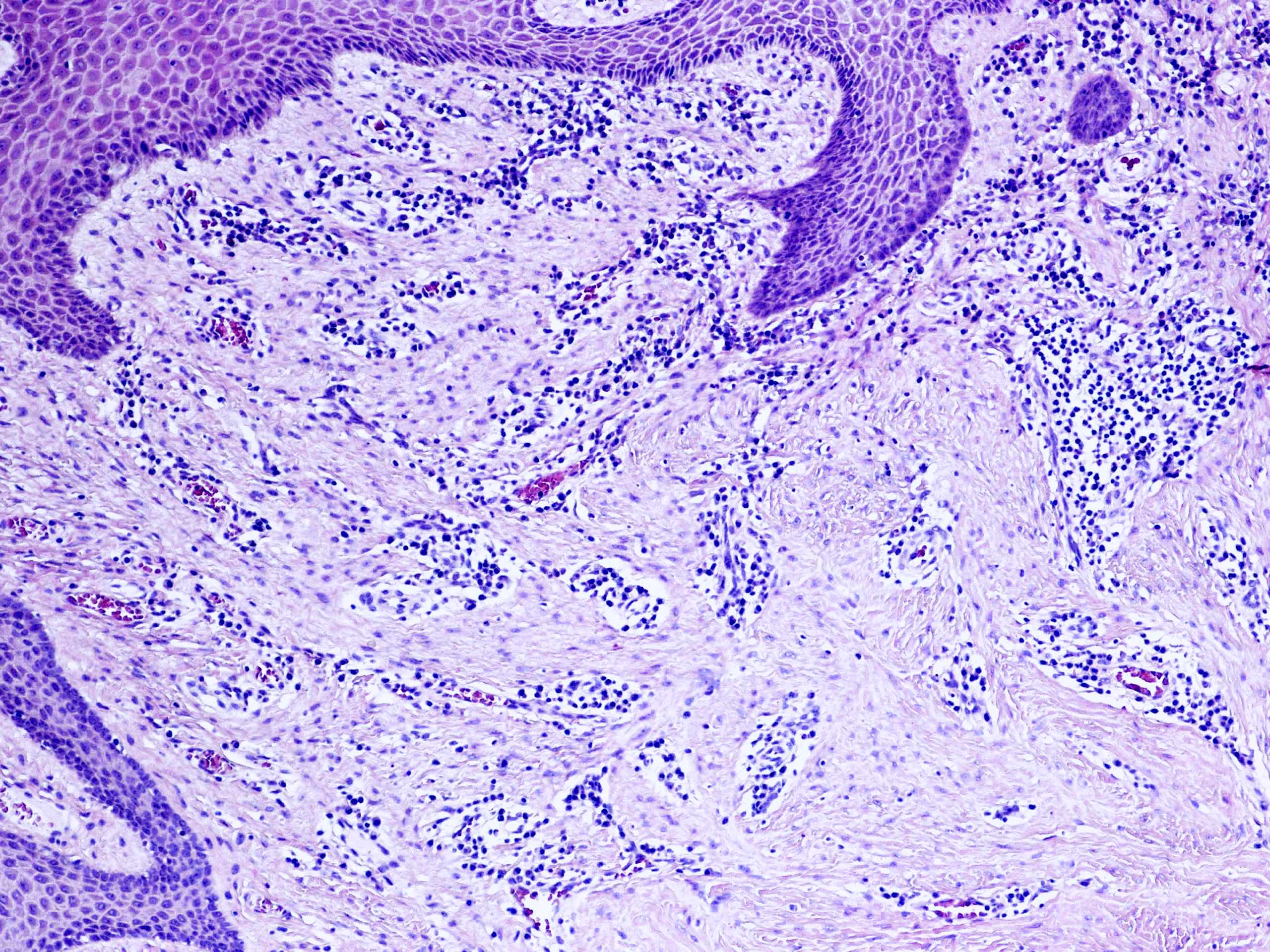
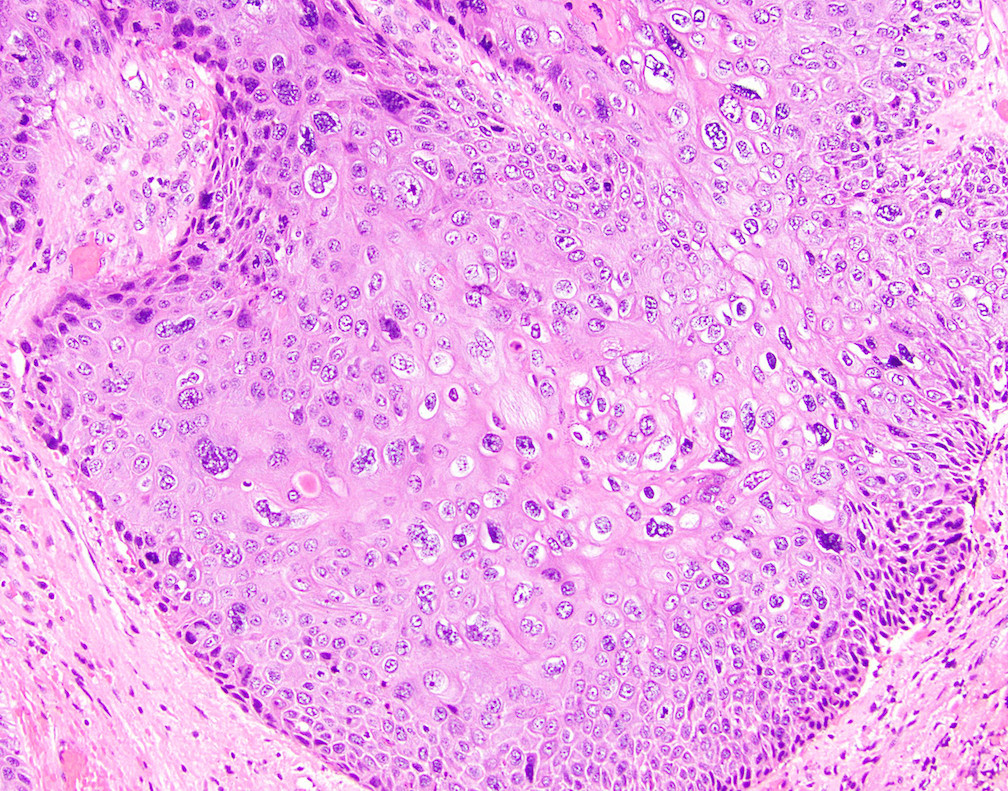
Koilocytes and fungal elements
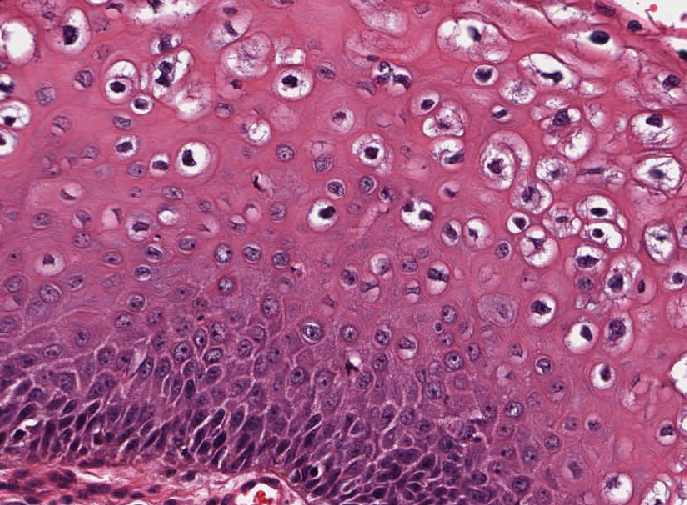
Koilocytes with perinuclear clearing
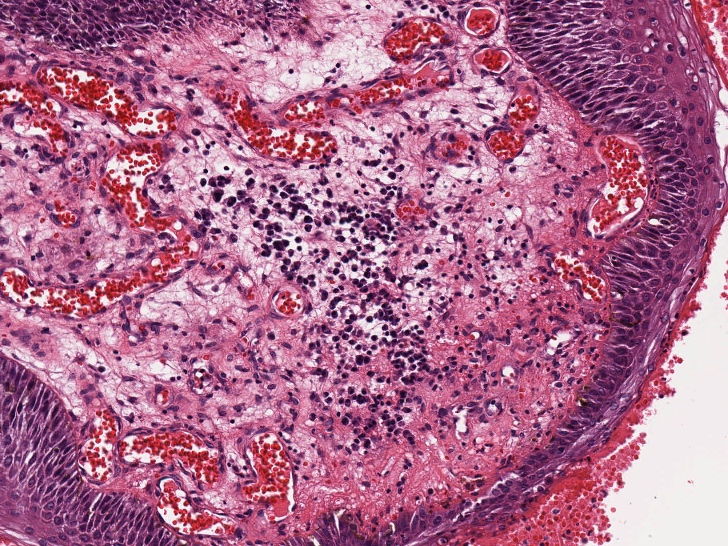
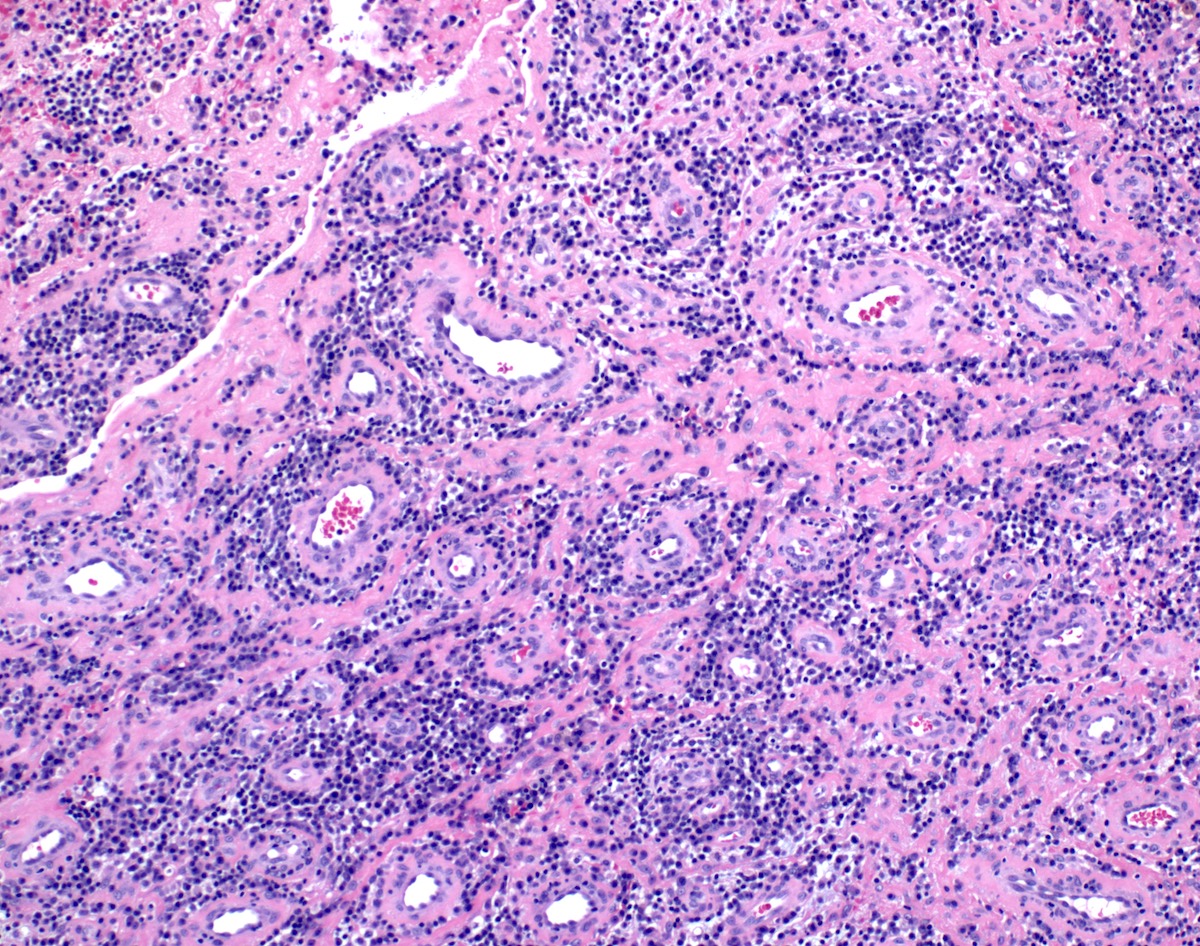
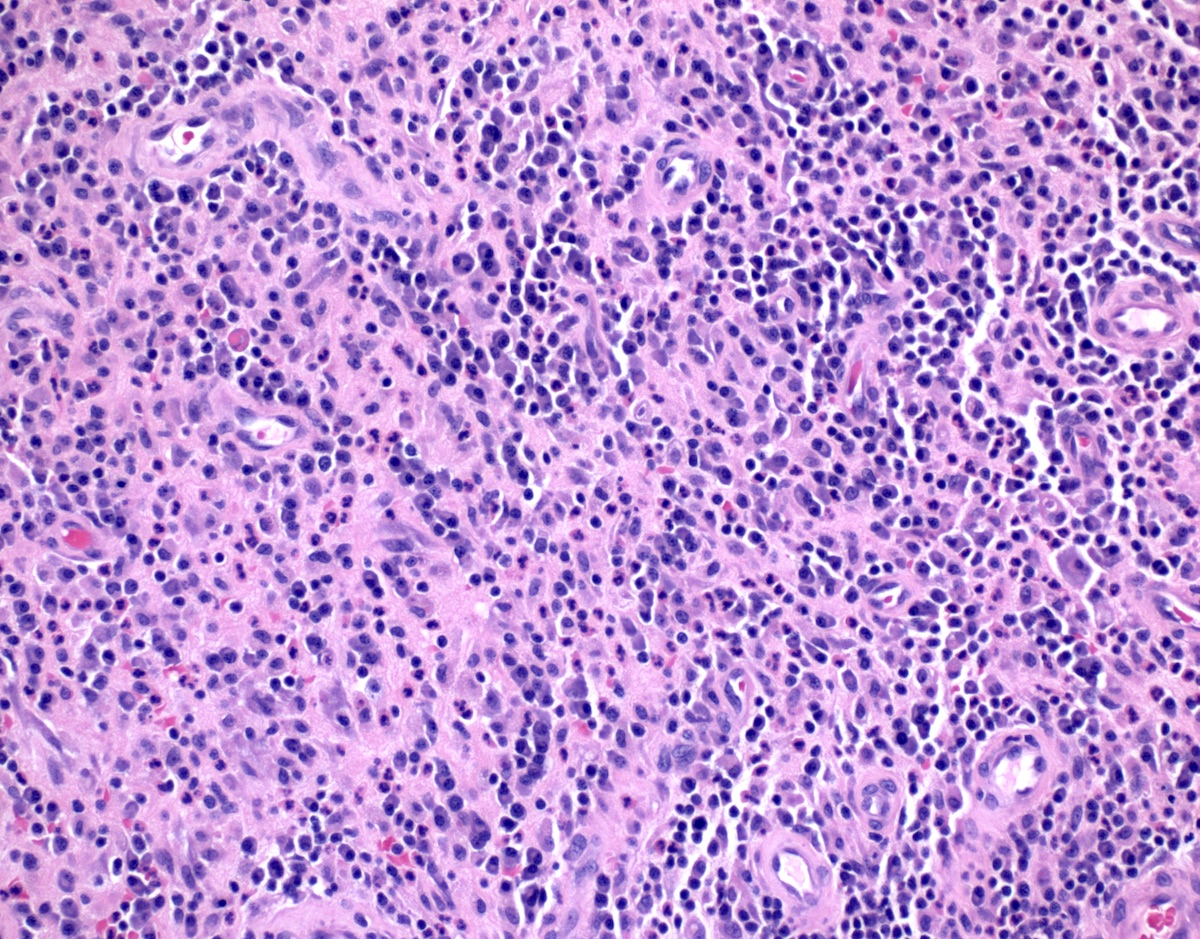
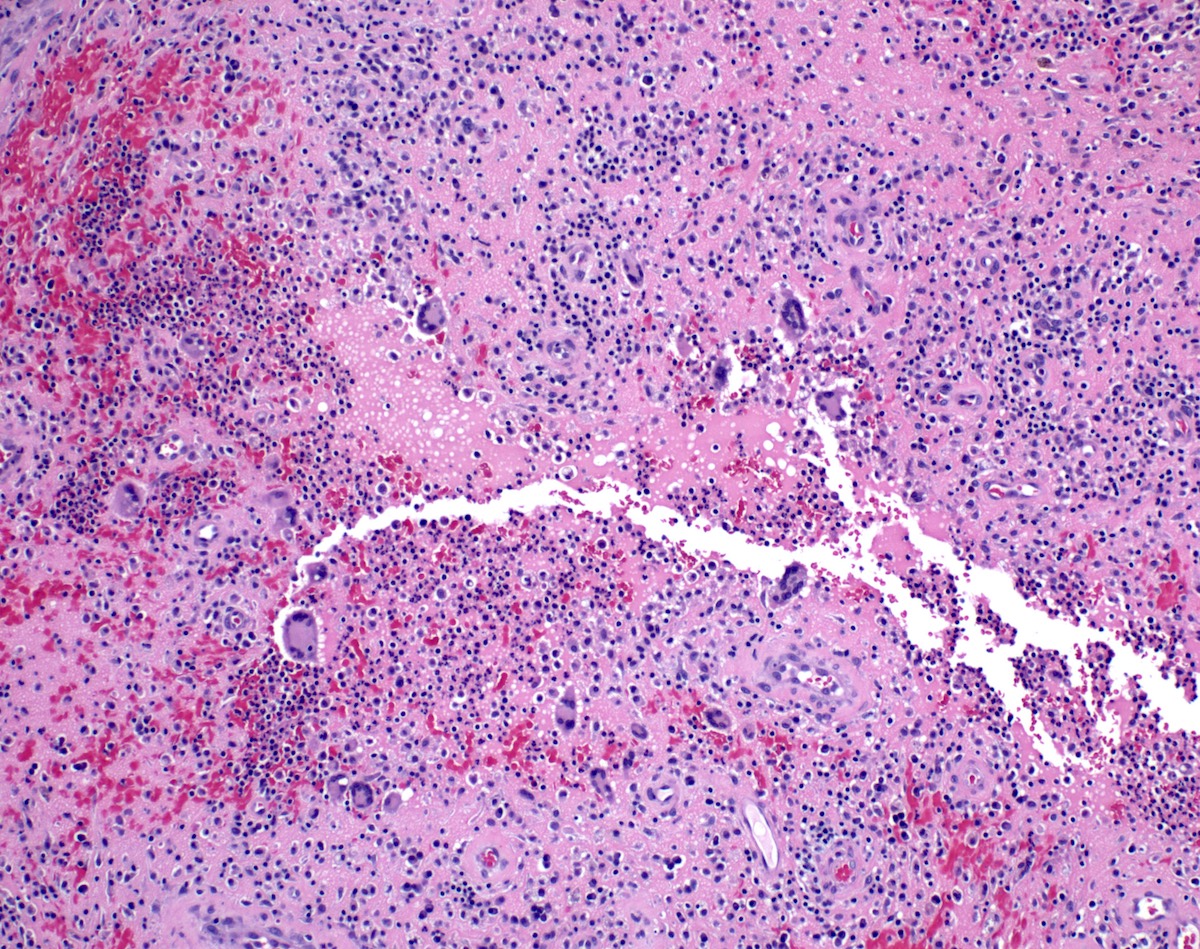
Chronic
inflammation and
vascular changes
in stroma

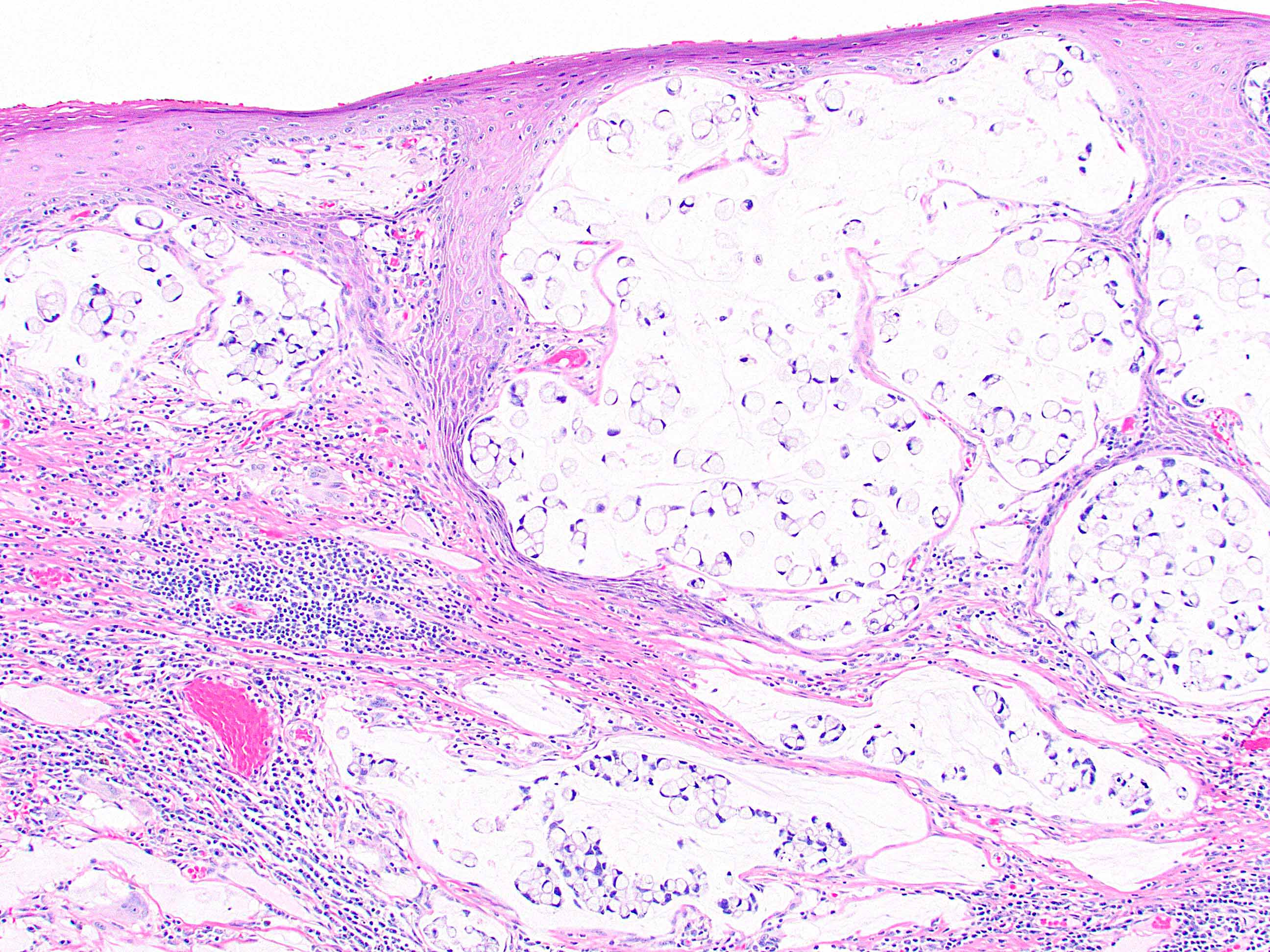
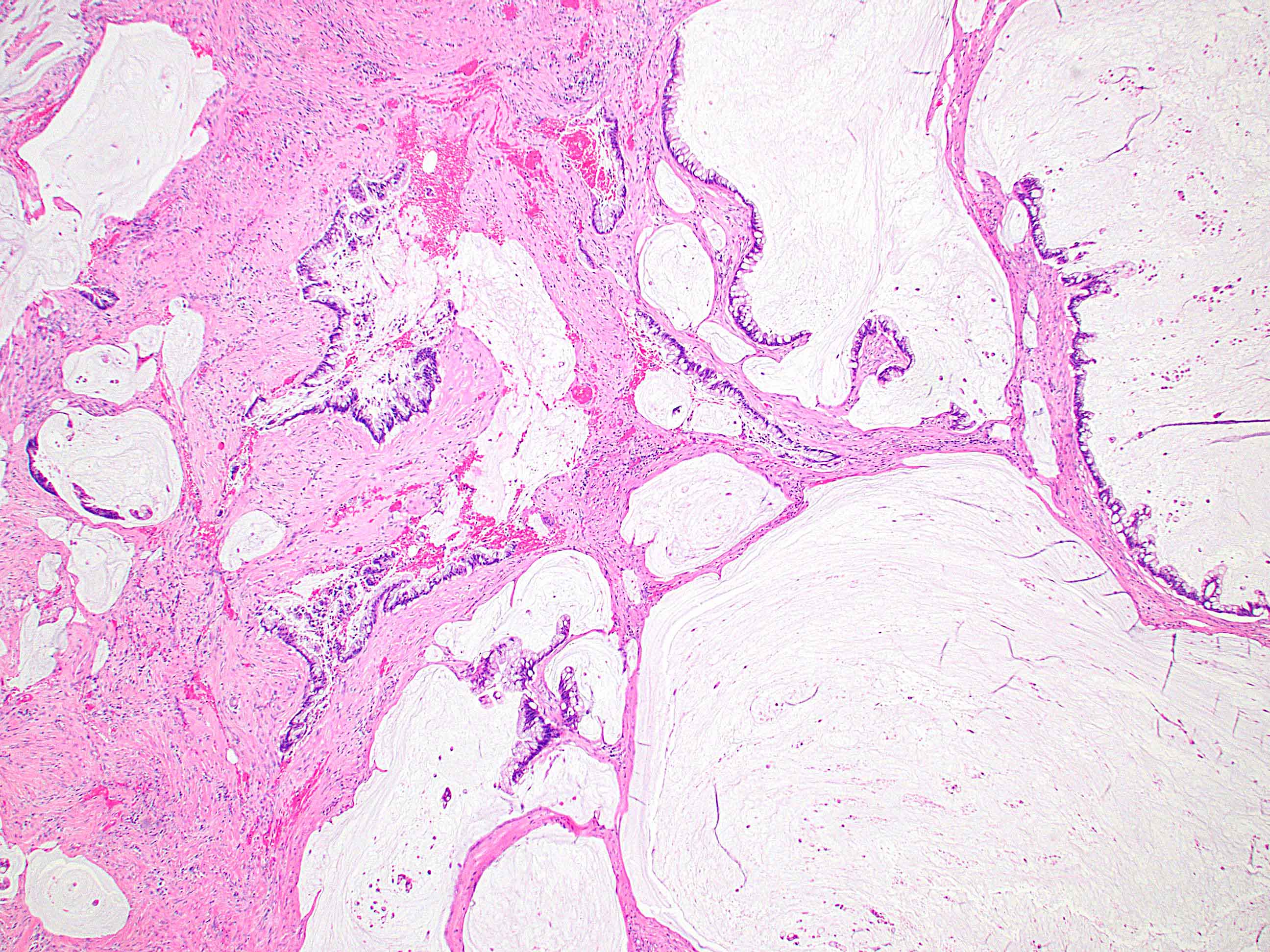
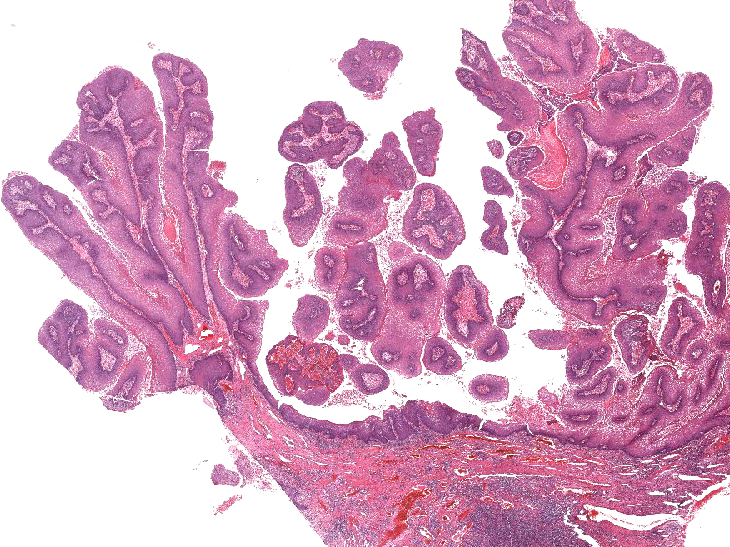
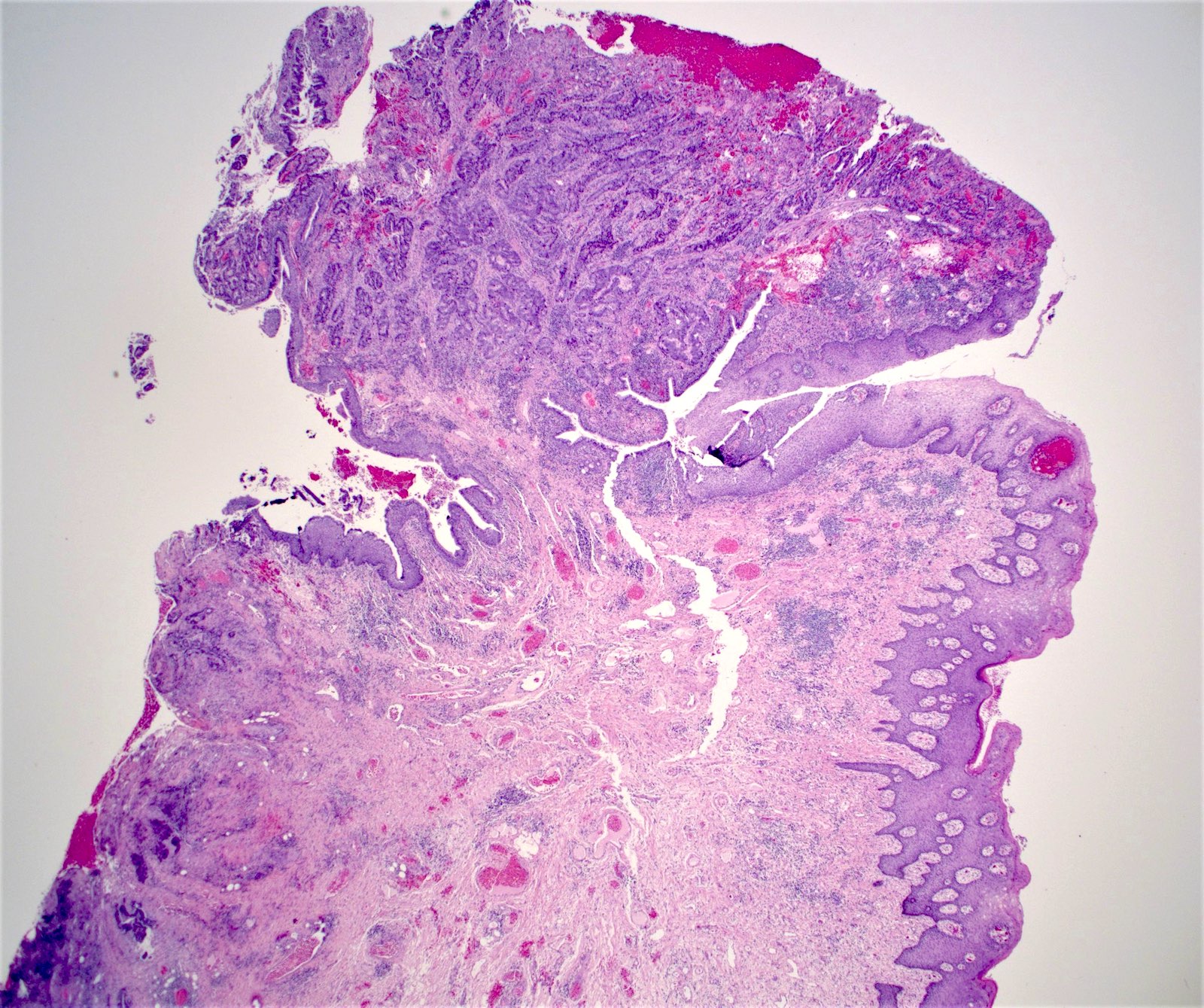
Anal giant condyloma

Buschke-Löwenstein tumor
Giant condyloma
| Tumor summary | Anus |
| Procedure | Complete excision |
| Tumor site | Perianal skin |
| Tumor size | 5 cm |
| Histologic type | Giant condyloma acuminatum |
| Margins | Free, 0.5 cm to radial |
| Extent | Anal canal, below the pectinate line |
| Tumor invasion | Not identified |
| Examined sections | 05 blocks |
| Lymph nodes, # sampled | 10 |
| Lymph nodes, # involved | 0 |
Ancillary study result
| Patchy, 5% of cells Restricted to parabasal layers |
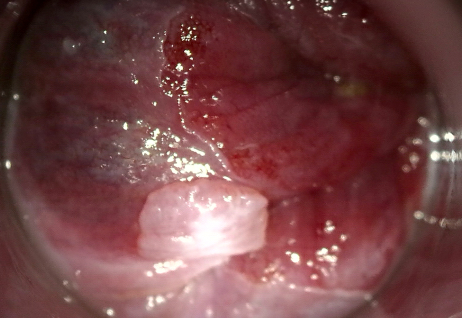

Single warty lesion


Multiple flat lesions

Severe case

Vaginal condyloma
Koilocytosis
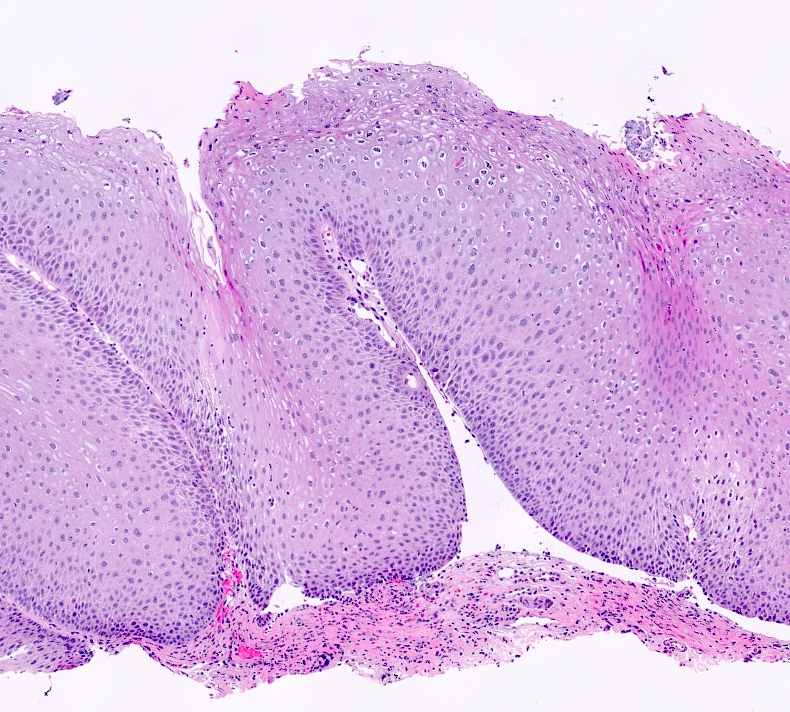
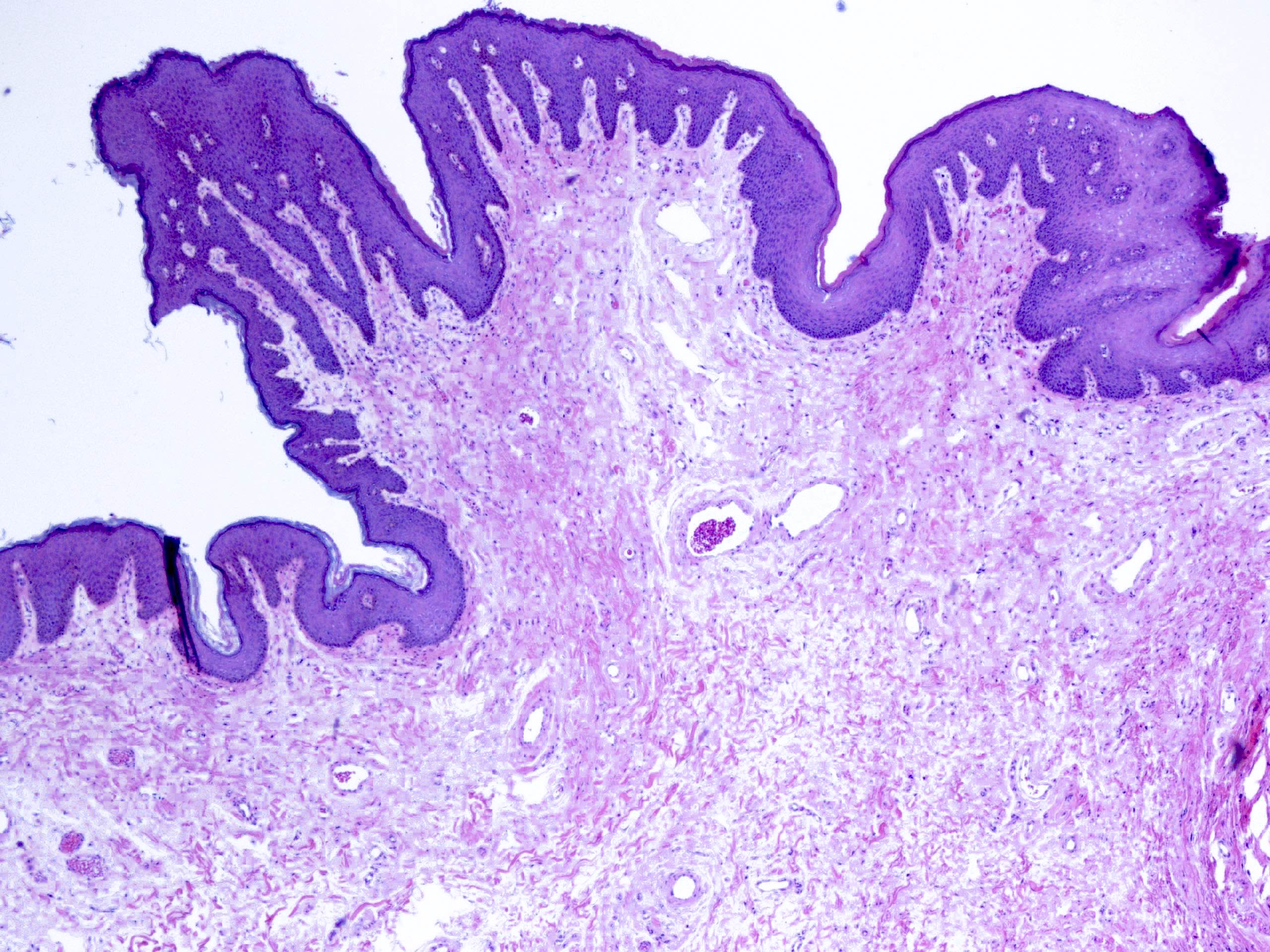
Papillary exophytic squamous epithelium

Hyperplastic squamous epithelium
Papillary exophytic squamous epithelium
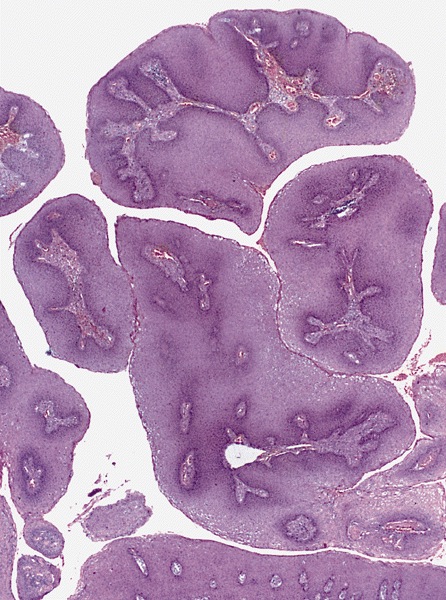
Large papillary structures
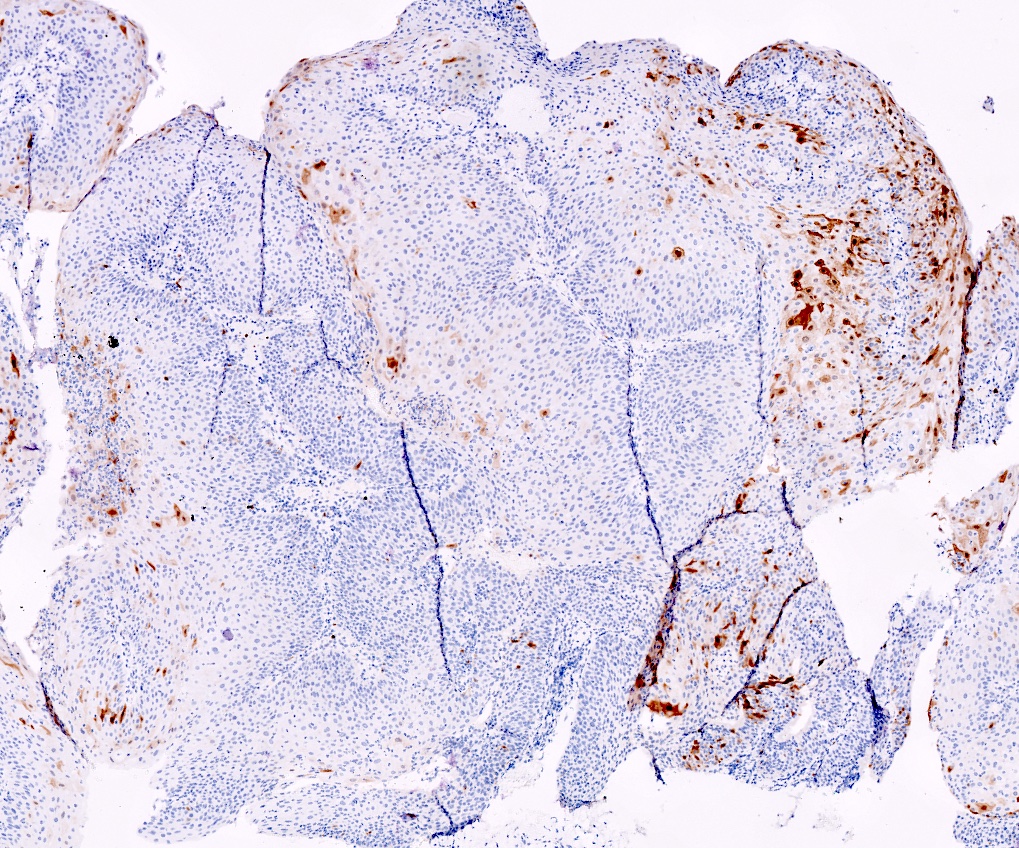
Negative p16 expression (nonblock positivity)


Condyloma acuminatum


LSIL, Pap

Large perianal skin tags

Colon of 39 year old male

Epithelioid cells, giant cells, lymphocytes

Fistula formation

Fistula opening onto perineum

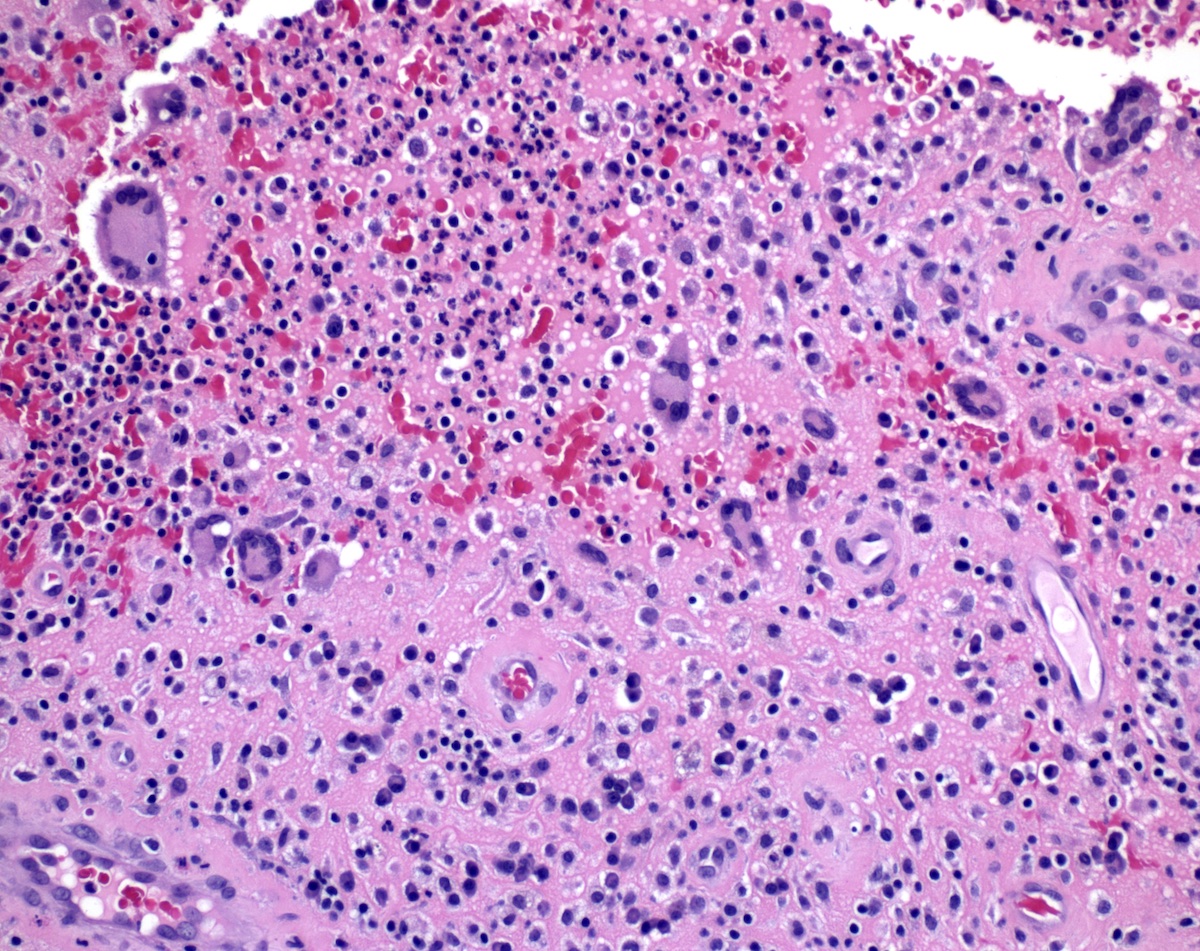
CT findings in a patient with CMV colitis
Diffuse erythema

Pseudomembrane
formation
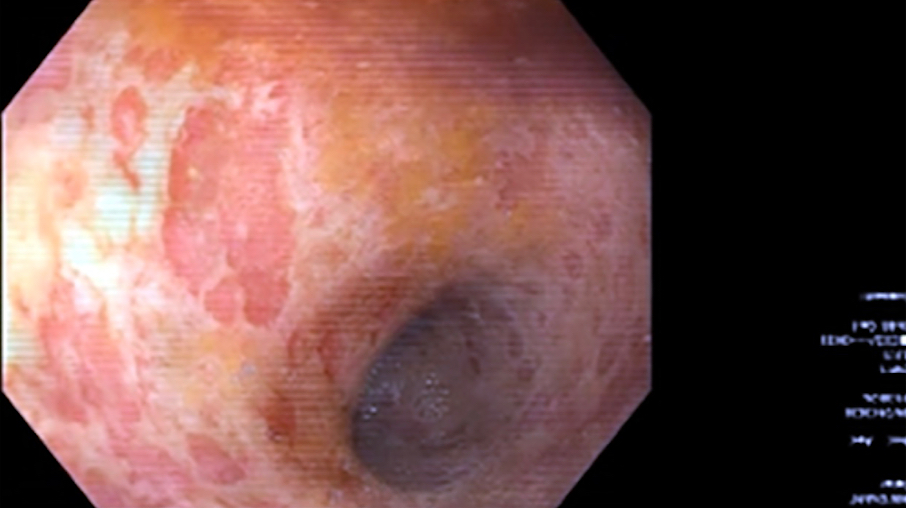
Irregular ulceration, loss of vascular pattern

Diffuse inflammation

Ulcerating mass



Ulceration and erythema

Ulceration secondary to CMV colitis

Terminal ileum

Cecum

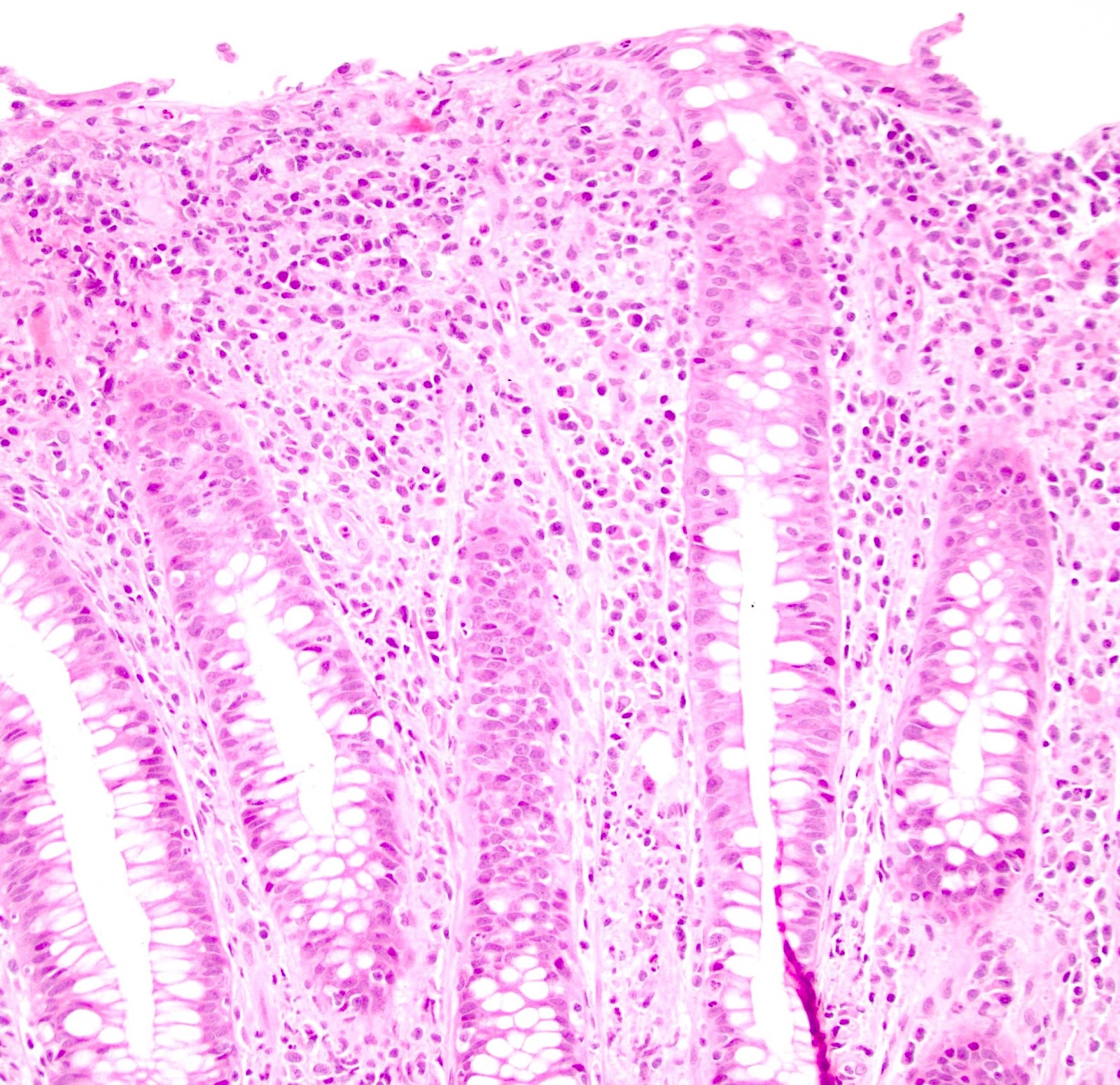
Multiple, small punctate ulcers in the mucosa

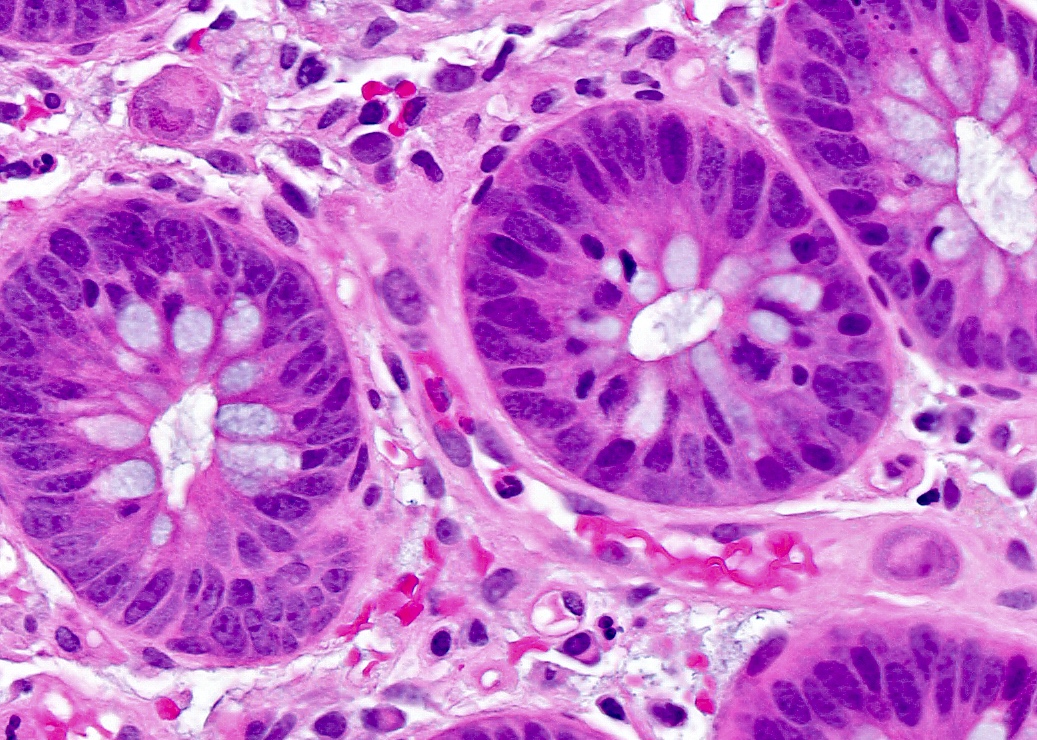
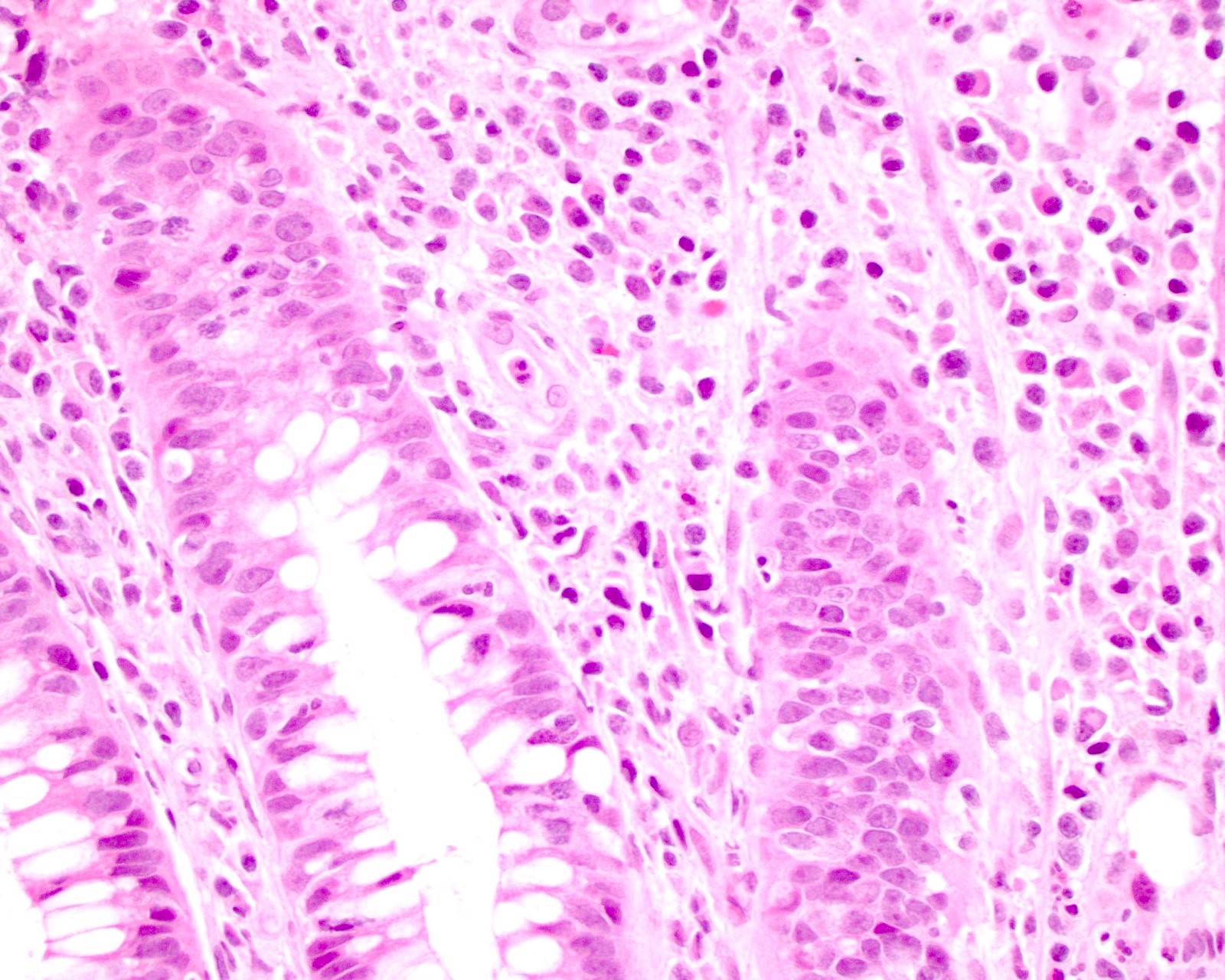
Enlarged cells in colonic lamina propria

Cytomegalic endothelial cells

Owl's eye and coarse red granules
Infected endothelial cells
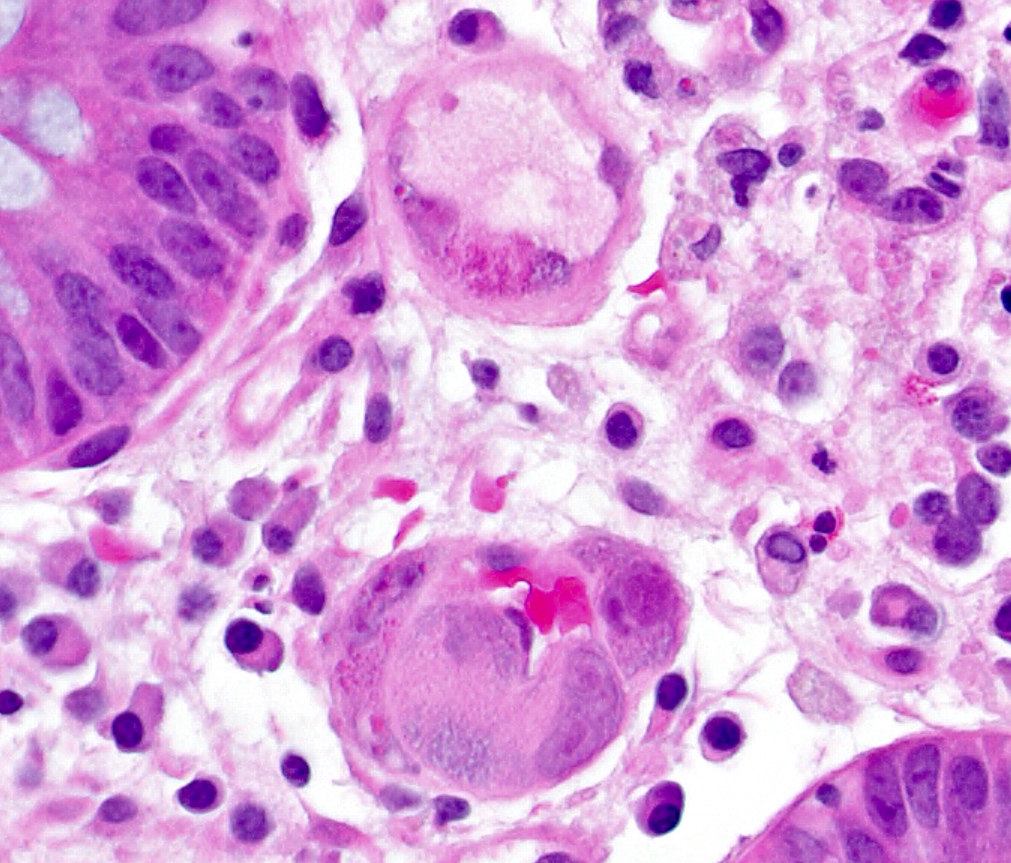
Cytomegalic endothelial cells partially occluding vessel
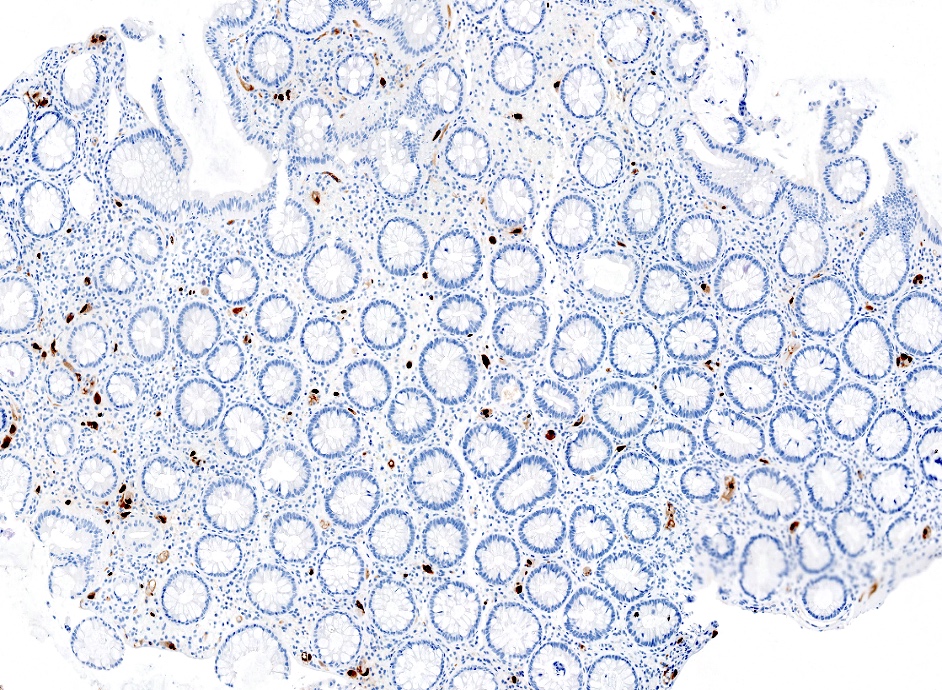
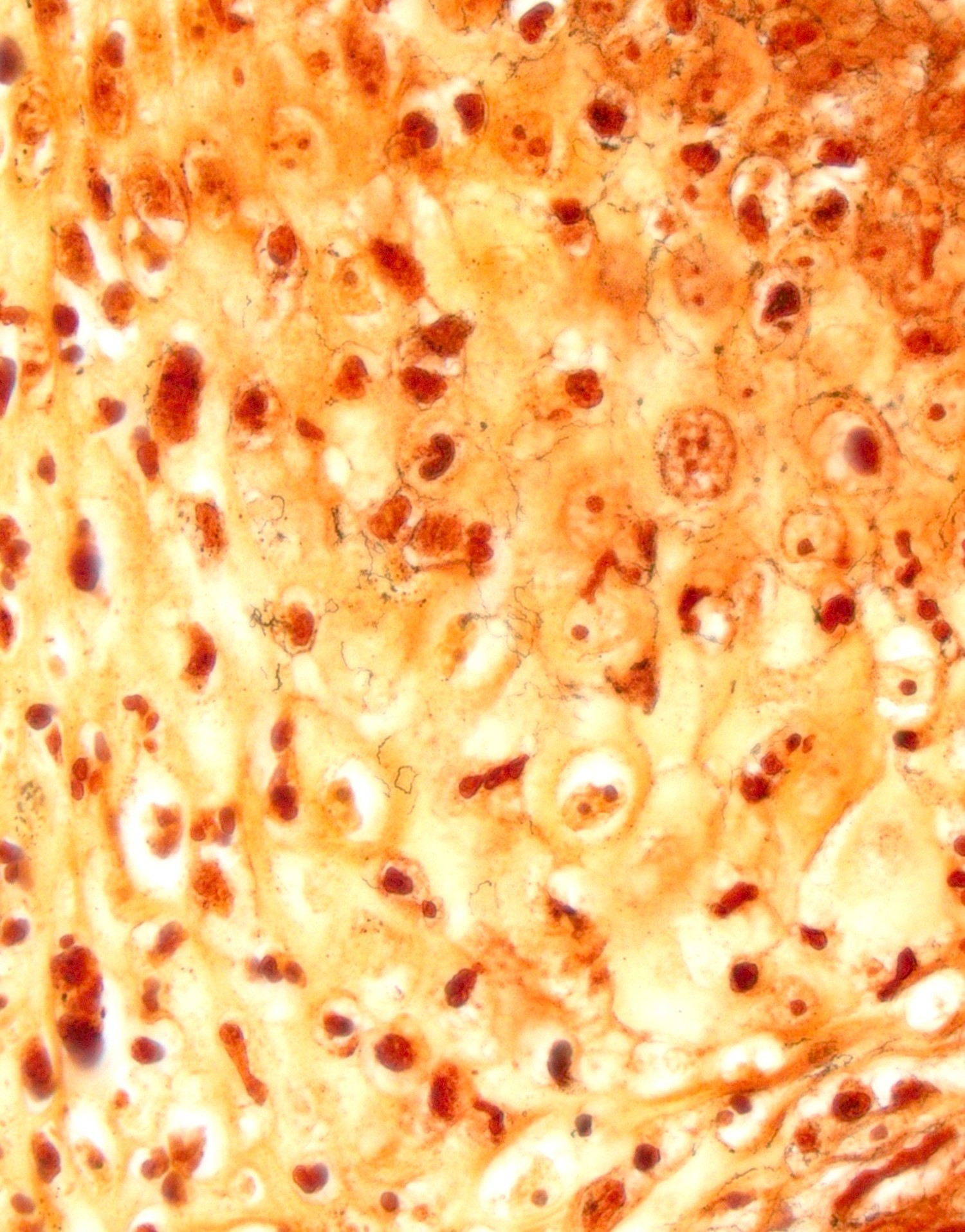
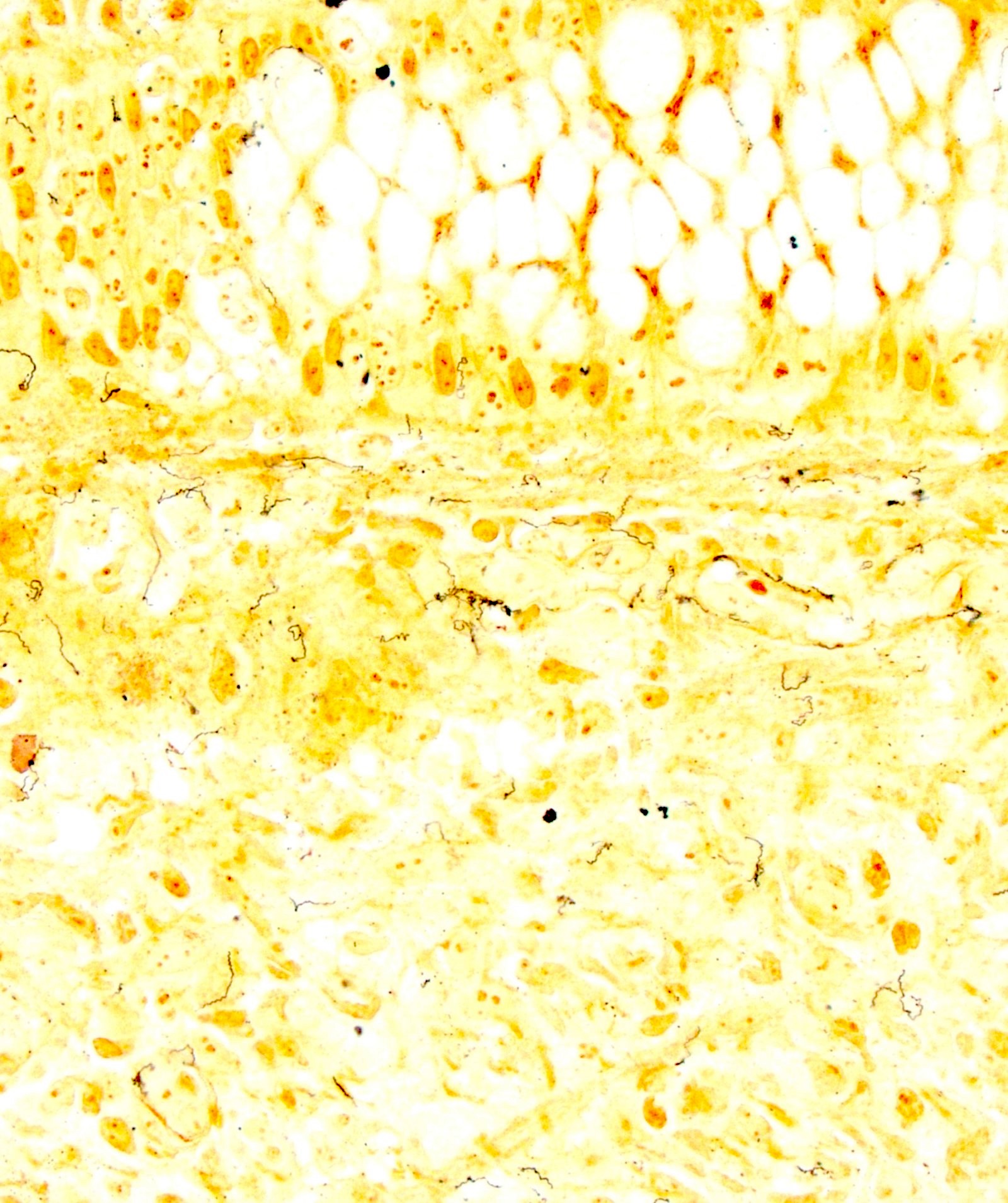
Immunoreactivity with CMV immunostain
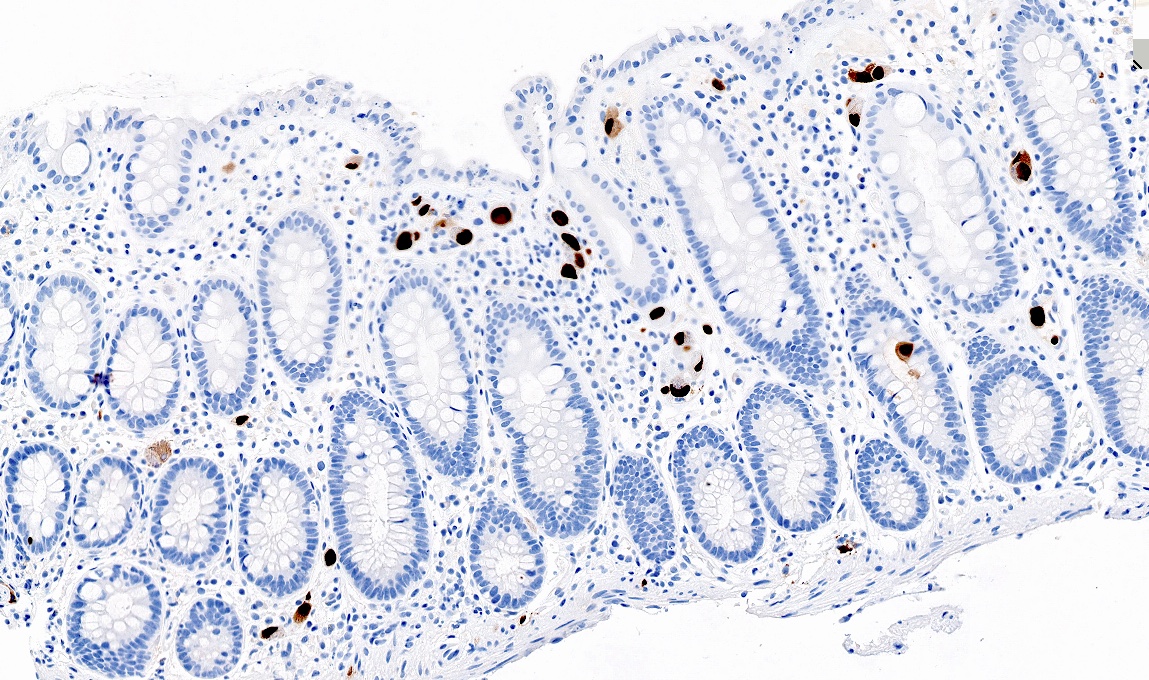
Scattered CMV positive cells
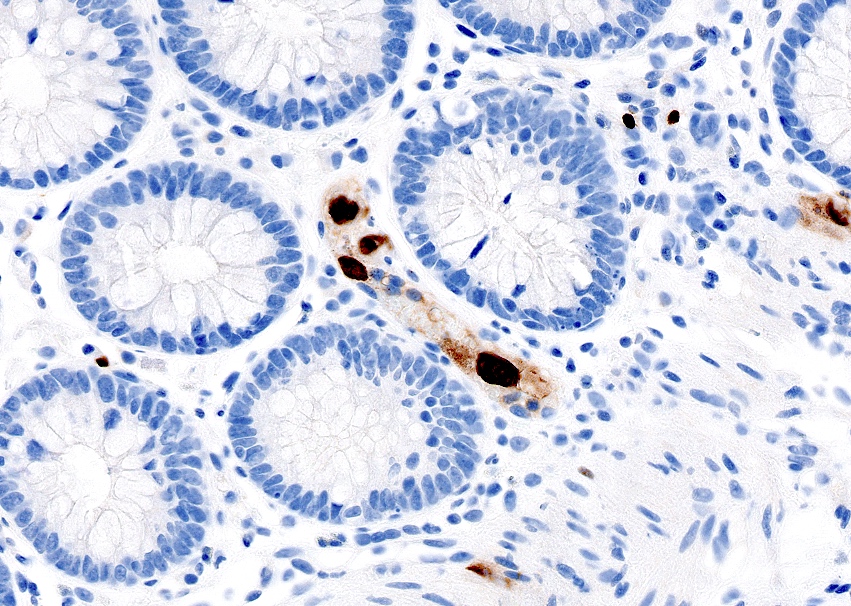
CMV positive endothelial cells
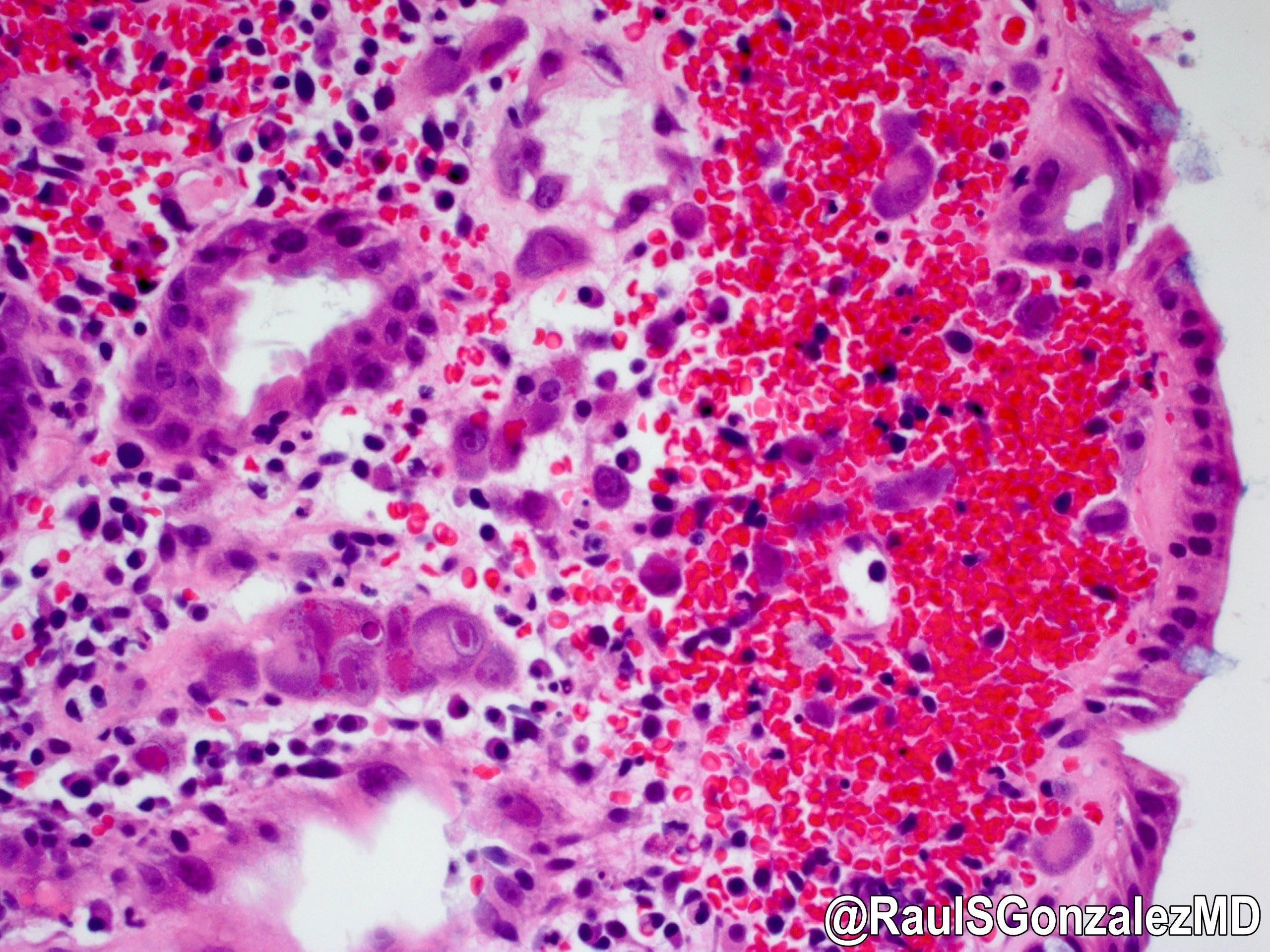
Cytomegalovirus (CMV)
CMV colitis in ulcerative colitis and immunocompromised states
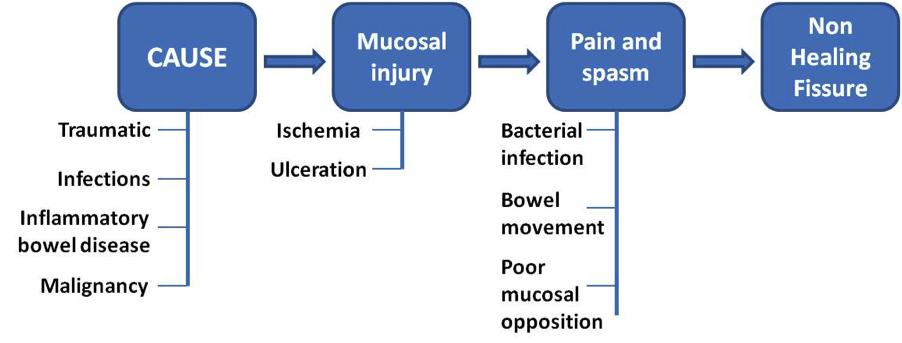
Pathophysiology and progression of anal fissure

Perianal abscesses

Fistulae and ischiorectal abscess

Fistula classification

Endoanal USG

Inflammatory infiltrate

Horseshoe fistula in ano

Multiple fistula tracts
Epithelized anal fistula tract
Granulation tissue with inflammatory cells
Giant cells, in association with granulation tissue
Perianal fistula
Fistula in ano

MRI of perianal mass

Ultrasound of perianal mass

Anal polypoid mass

Perianal cutaneous nodule

Excision of perianal tumor

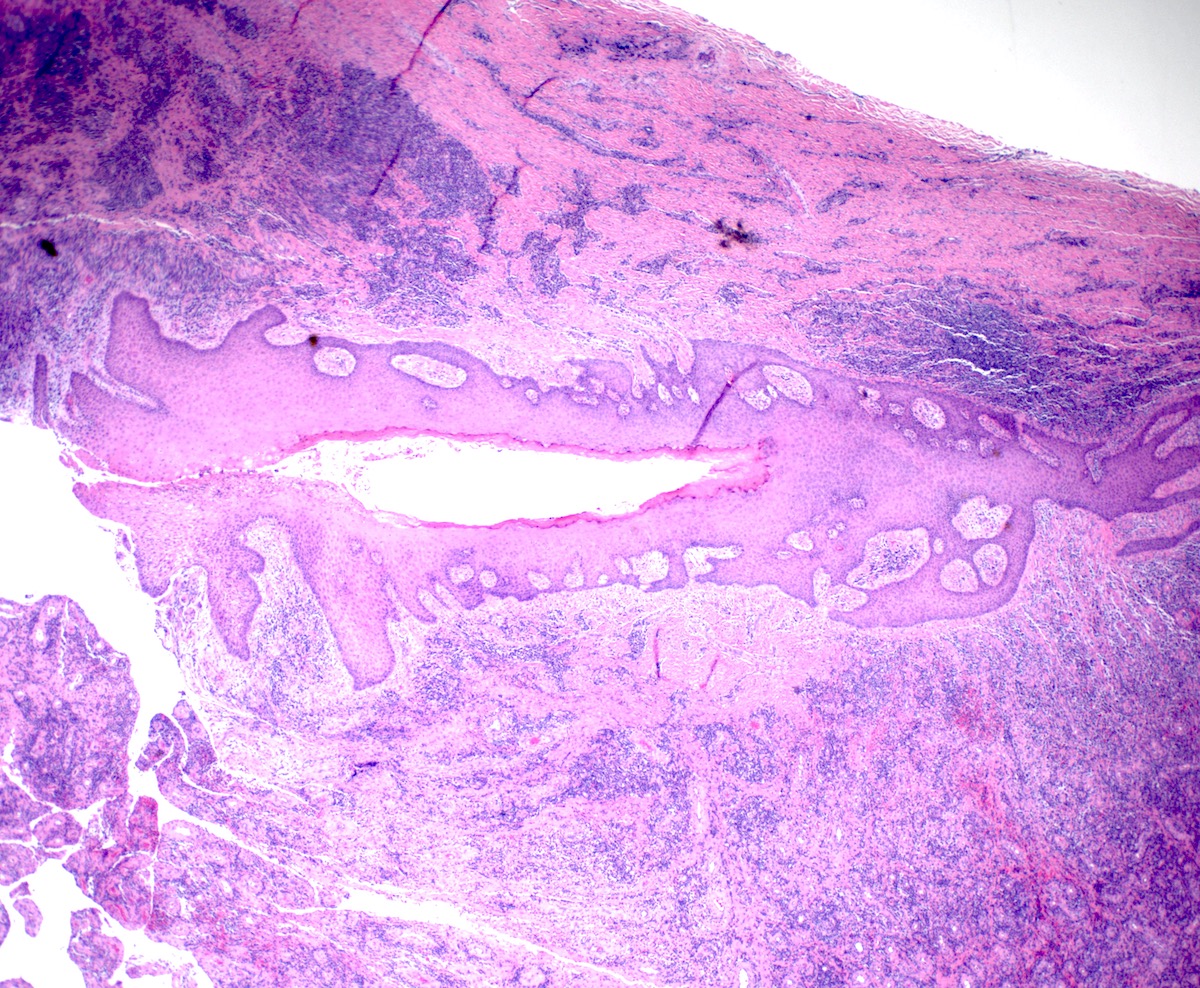
Gastroesophageal junction lesion
Pseudoepitheliomatous
hyperplasia
Phagolysosomes
S100
CD68

Ultrastructural view

Diffuse ulceration

Auto-amputation

Safety pin shaped structures

Epithelioid histiocytes

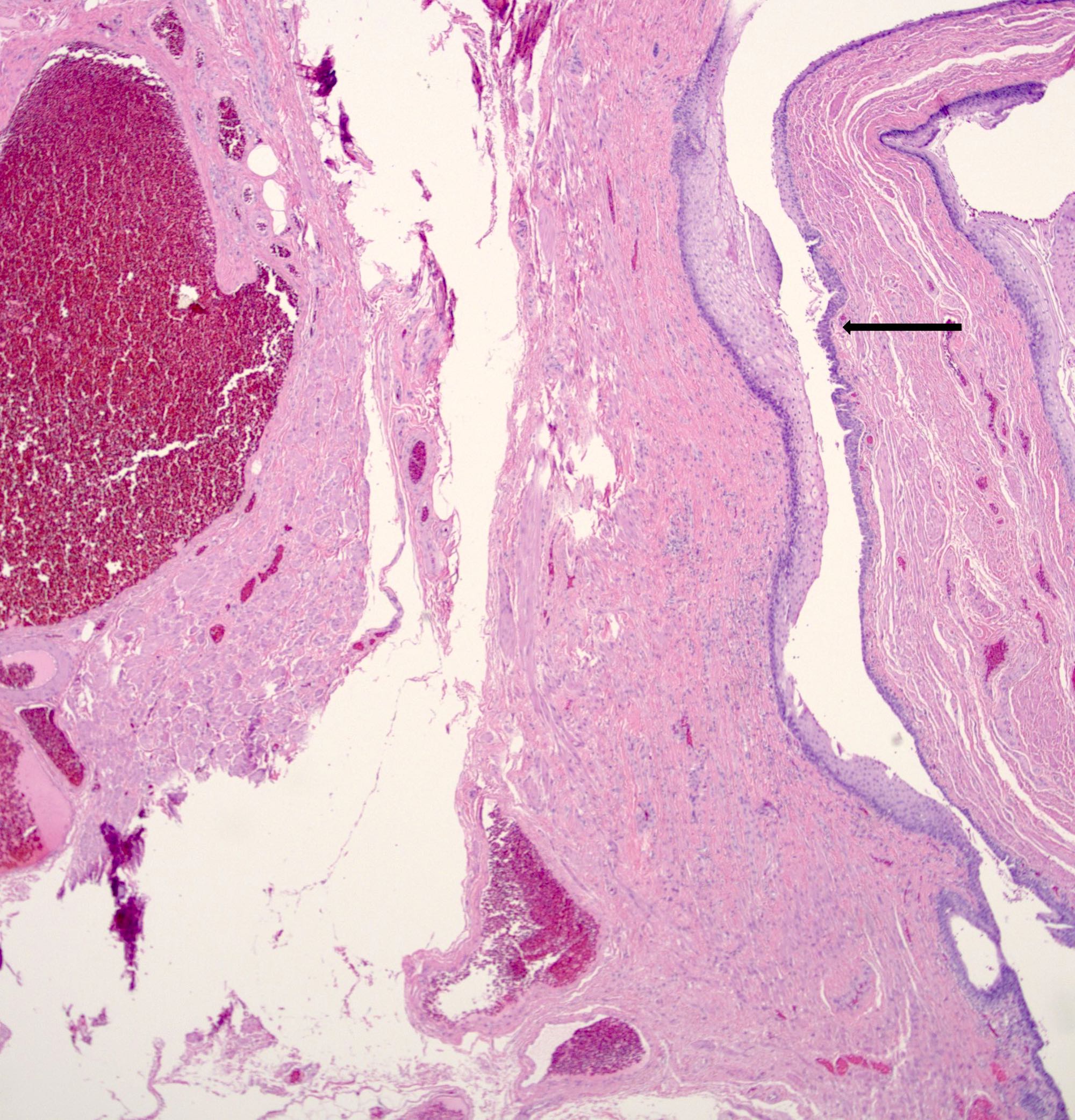
Common sites of major anal and internal hemorrhoids

Prominent prolapsed true (internal) hemorrhoids

Hemorrhoids at anorectal junction
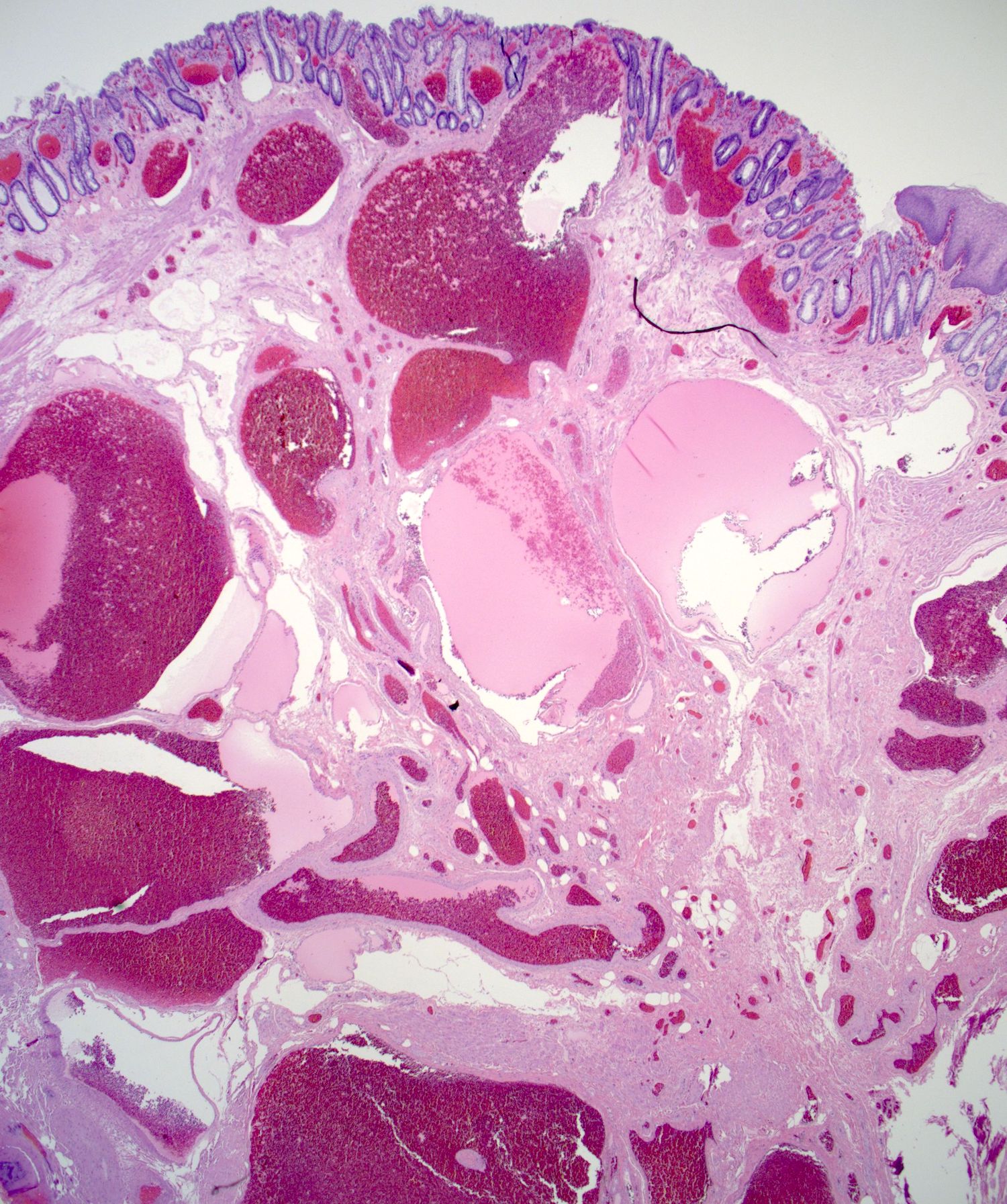
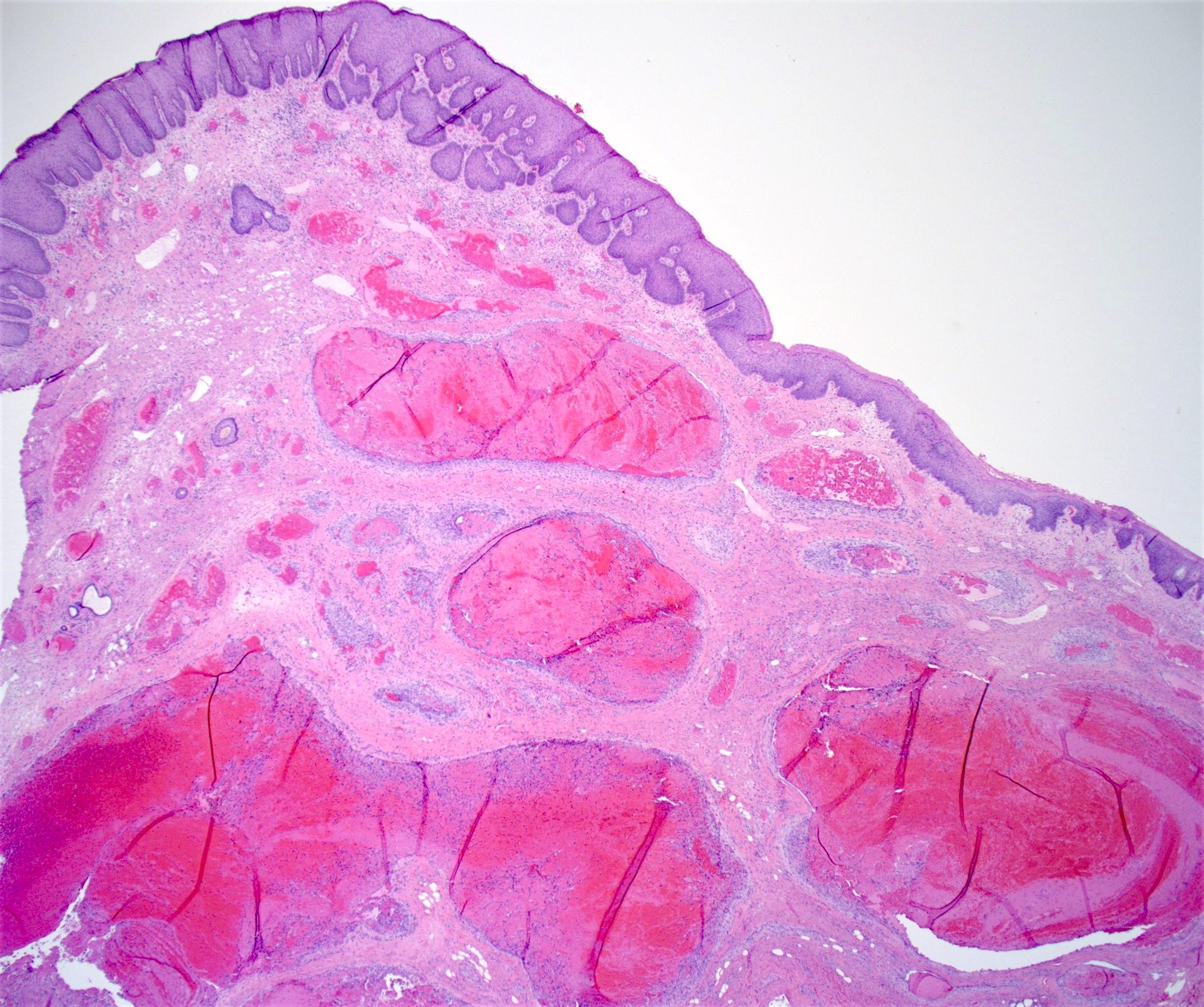
Typical hemorrhoid
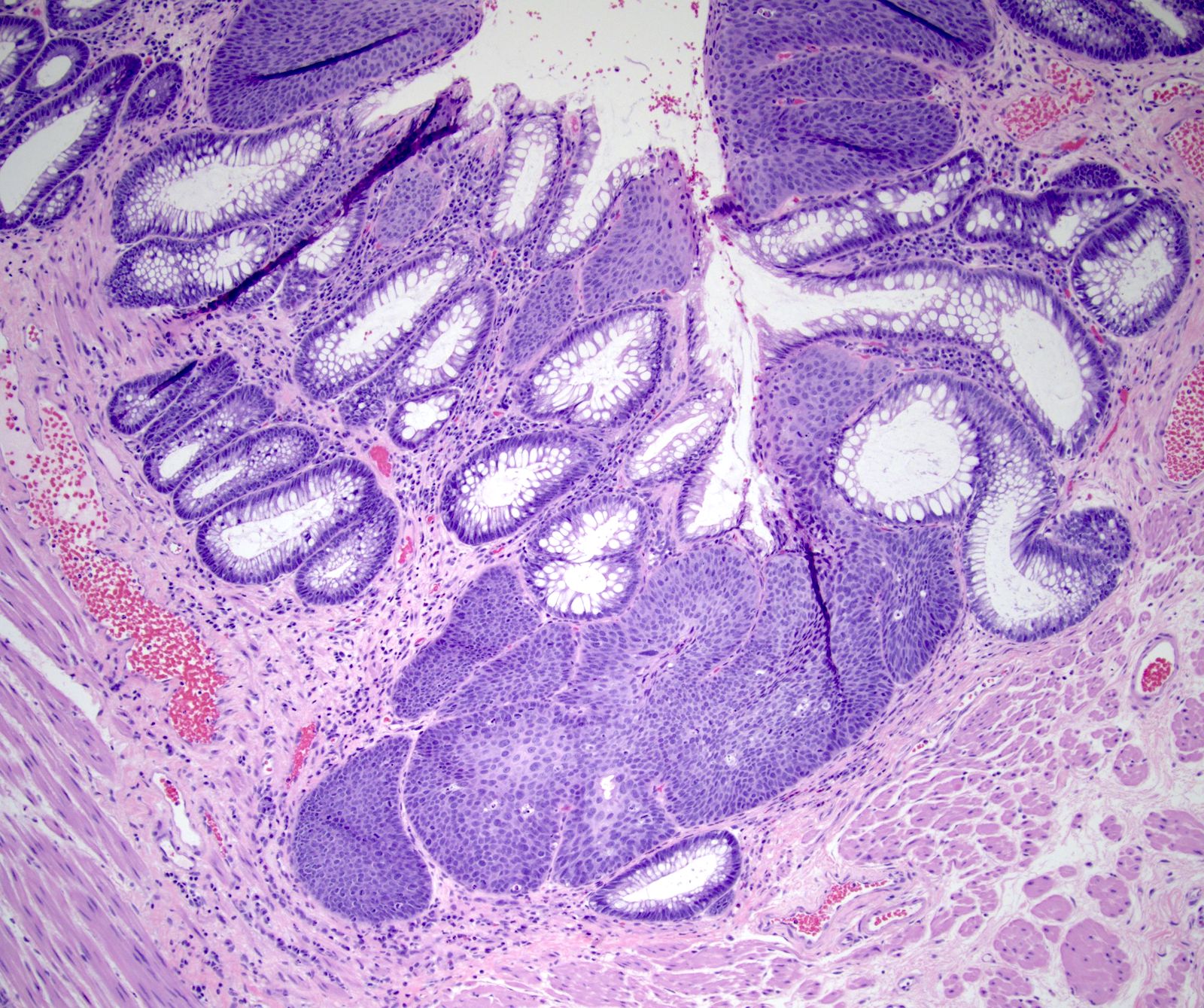
Transitional mucosa
Thrombosed hemorrhoid
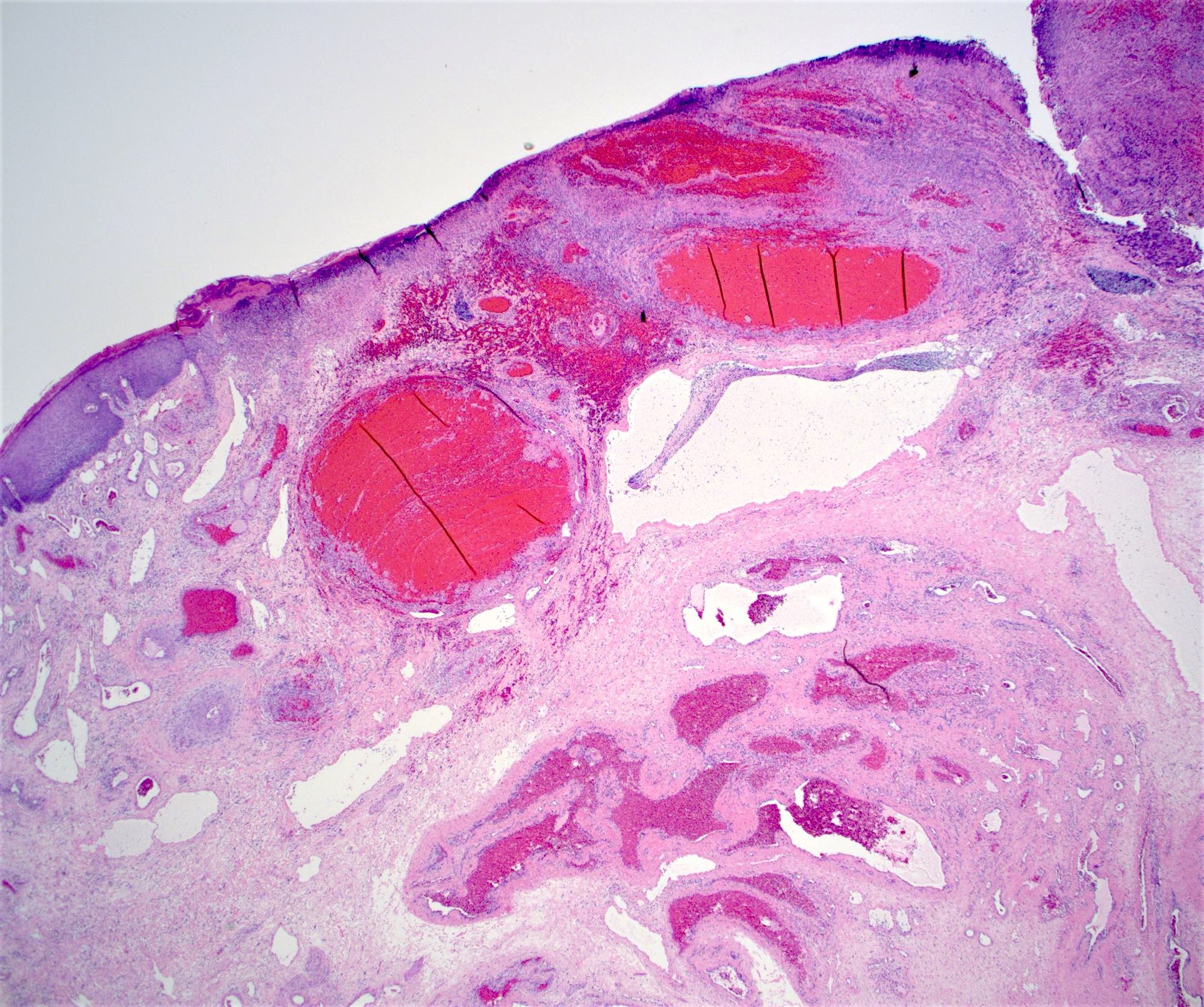
Ulcerated hemorrhoid
AIN3
SCC presenting as hemorrhoids
Colorectal adenocarcinoma presenting as hemorrhoids
Papillary endothelial hyperplasia
Incidental AIN
p16 IHC stain
Histopathology of hemorrhoids
Overview of hemorrhoids

Fistulous tract
Typical features
Thin walled vessels
Chronic inflammation
Atypical stromal cells

Cloacogenic polyps on rectal retroflexion
Squamous and glandular epithelium
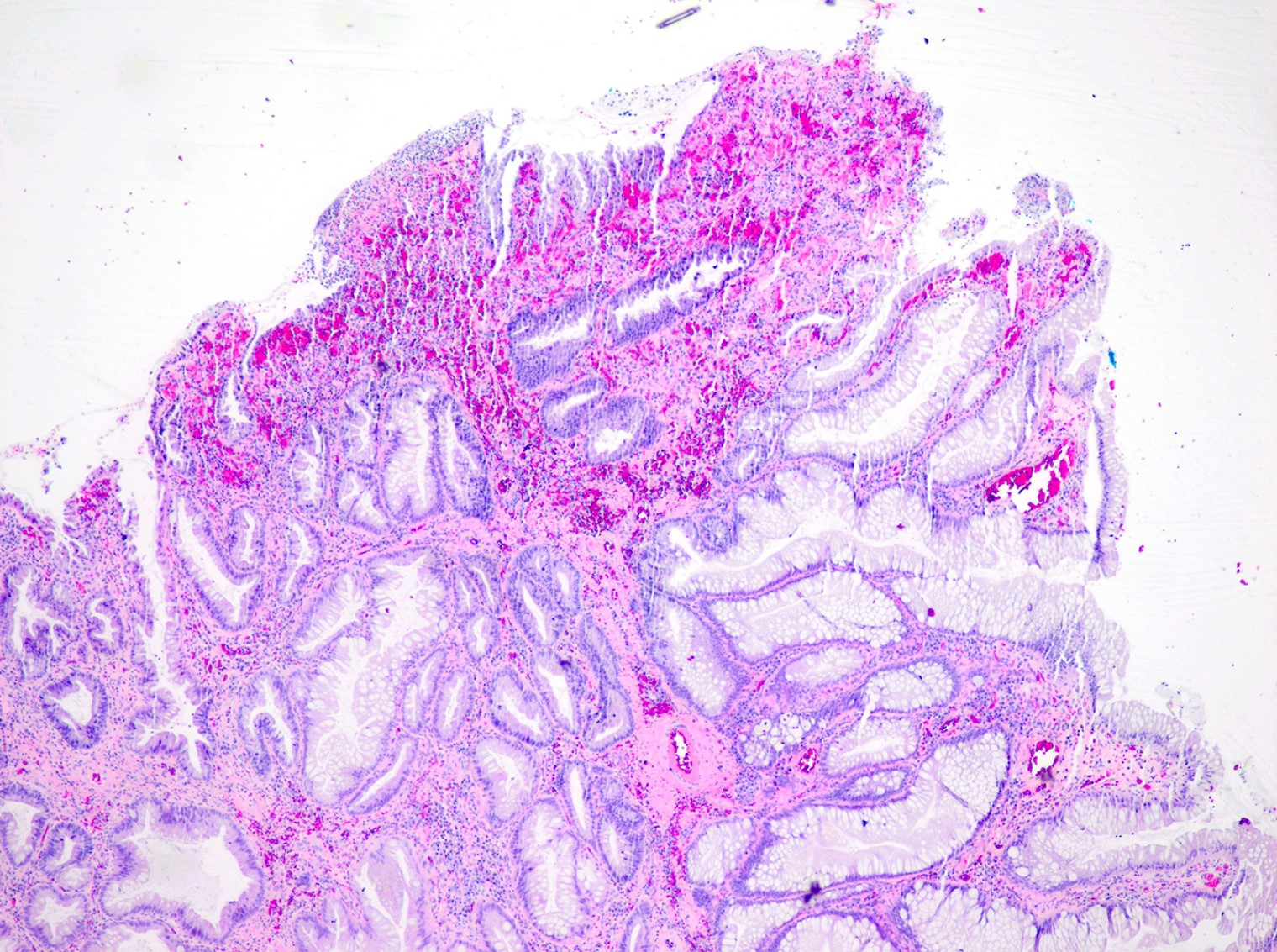
Surface erosion

Mucosal erosion
Regenerative epithelial changes

Groove sign (squamous cell carcinoma, not LGV)

C. trachomatis inclusion bodies (brown)

Anorectal mass (CT of pelvis)

Anorectal mass (MRI)

Anorectal mass (MRI / PET)

Anorectal mass

Prolapsed anal mass

Prolapsed anorectal mass

Polypoid lesion on colonoscopy

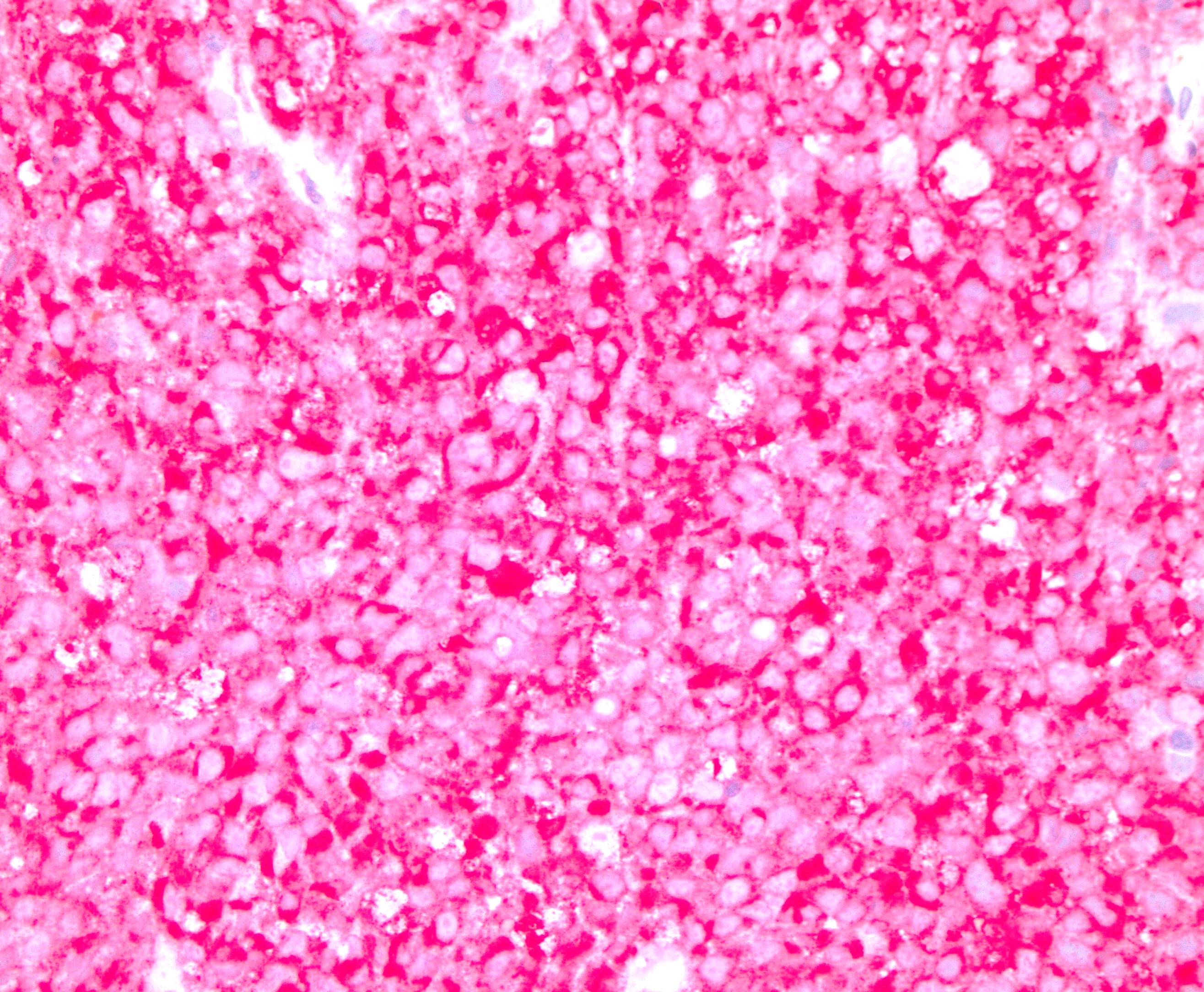
Pigmented anal mass

Anorectal mass
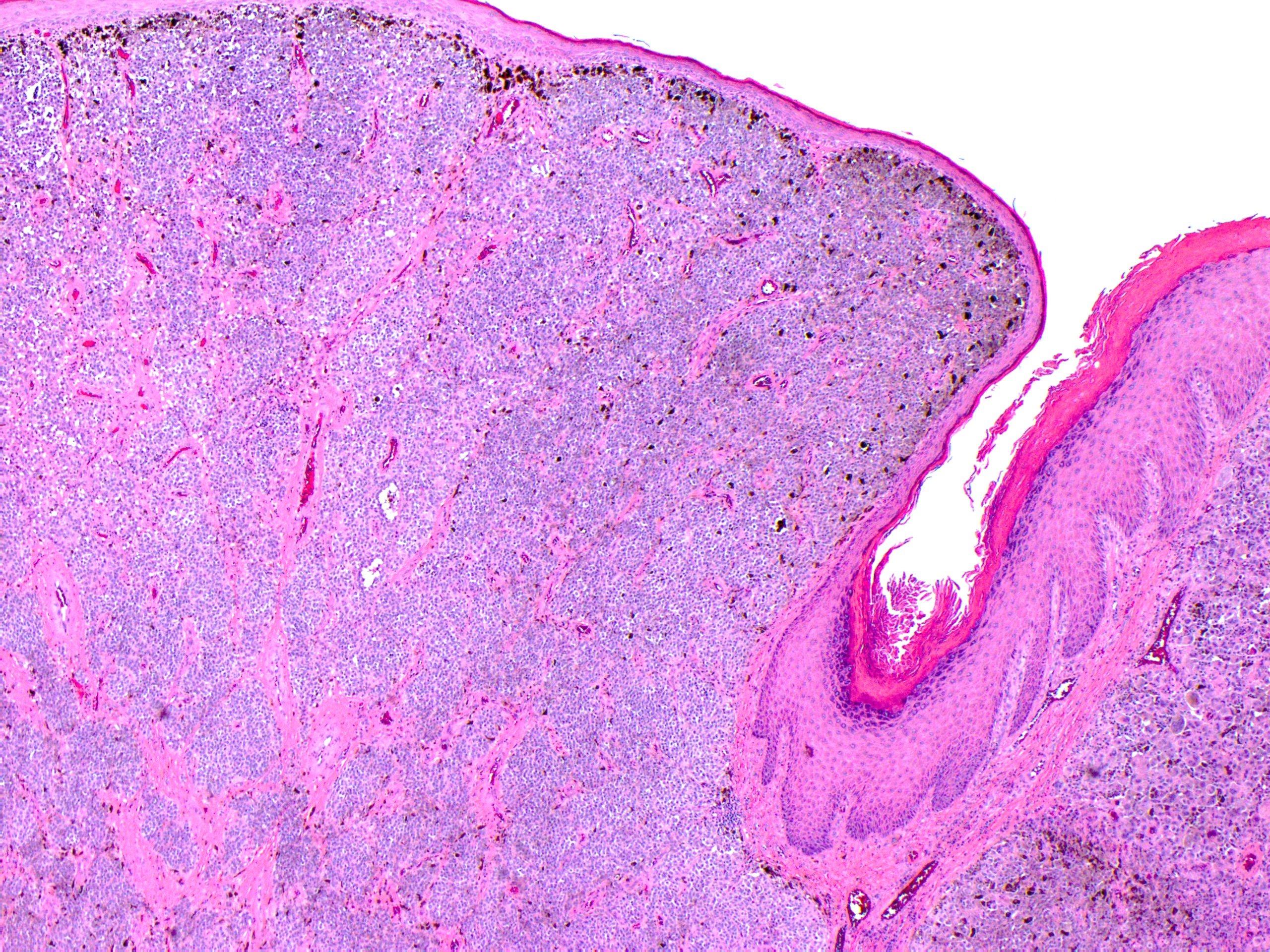
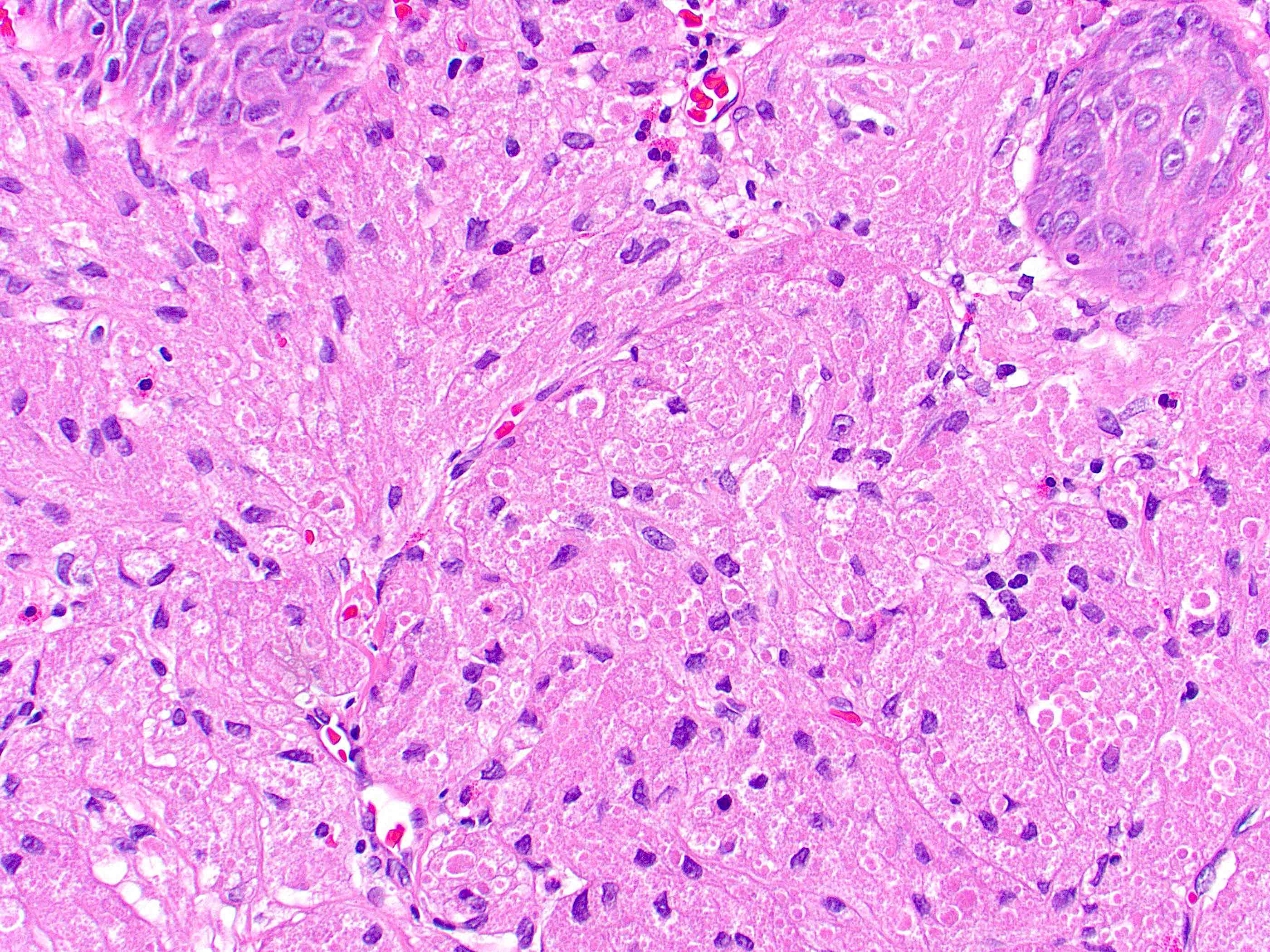
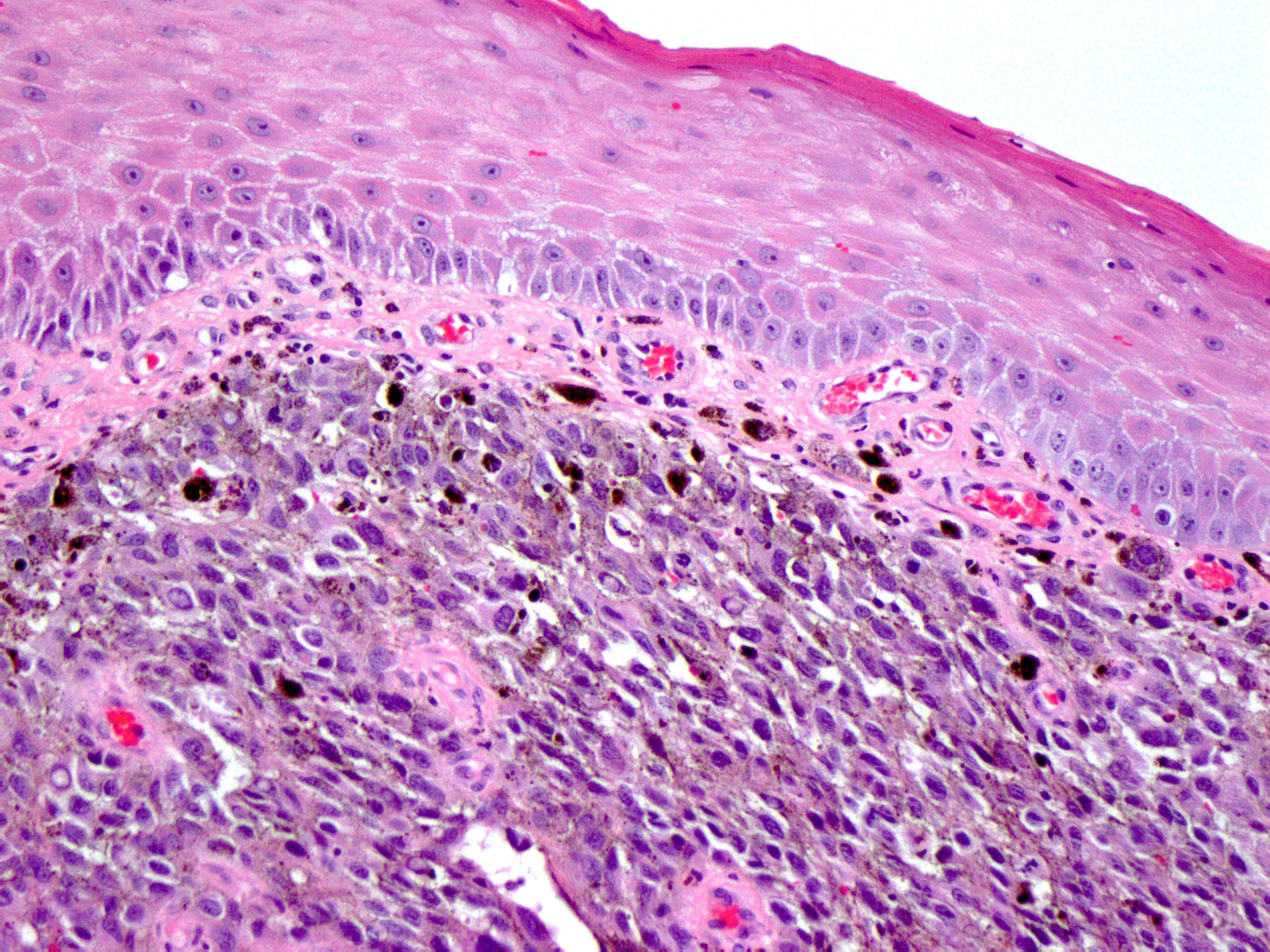
Tumor underlying squamous epithelium
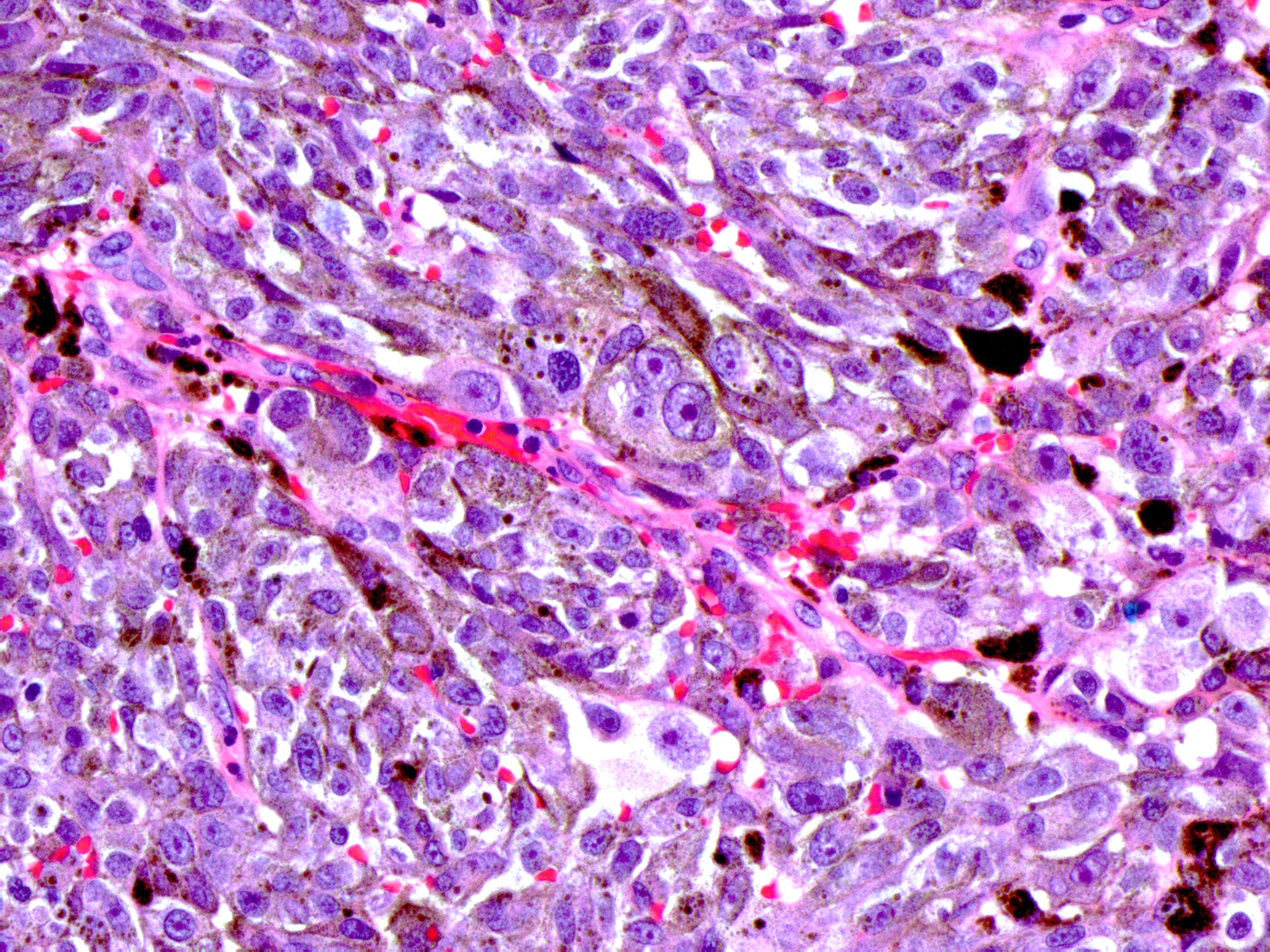
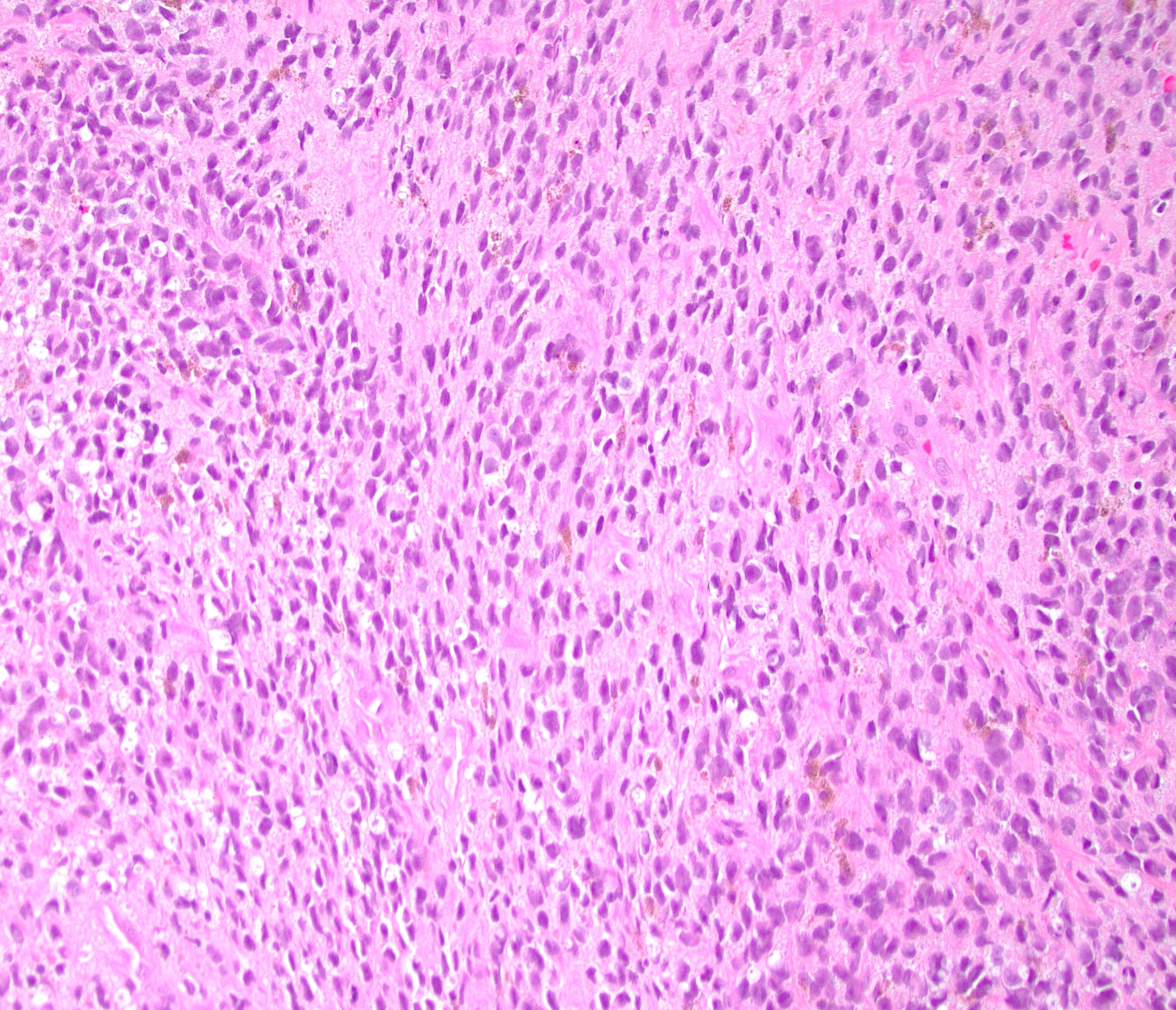
Epithelioid and spindled cells
Malignant cells with pigment
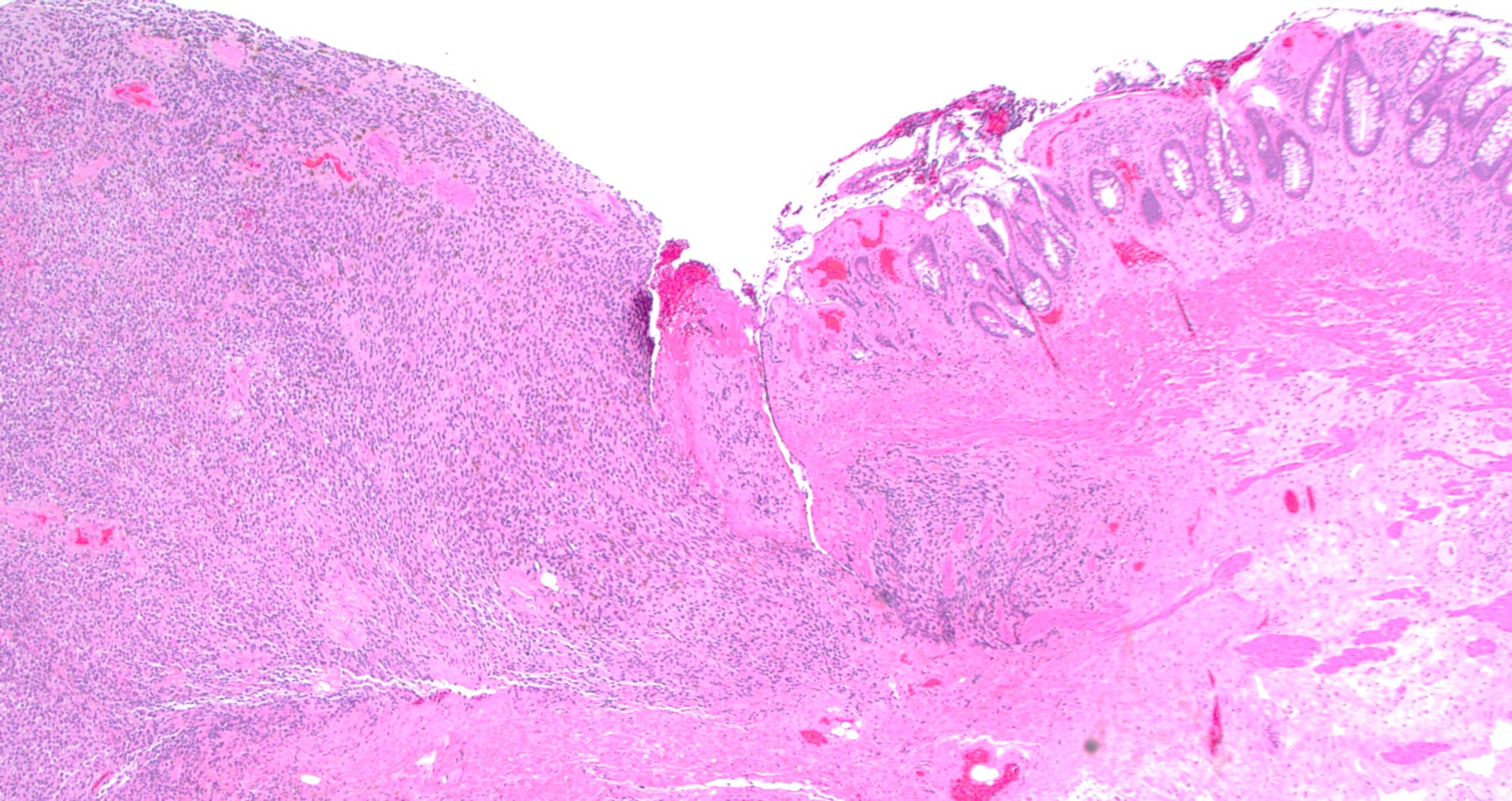
Ulcerated mucosa
Malignant cells with pigment
Large nuclei with prominent nucleoli
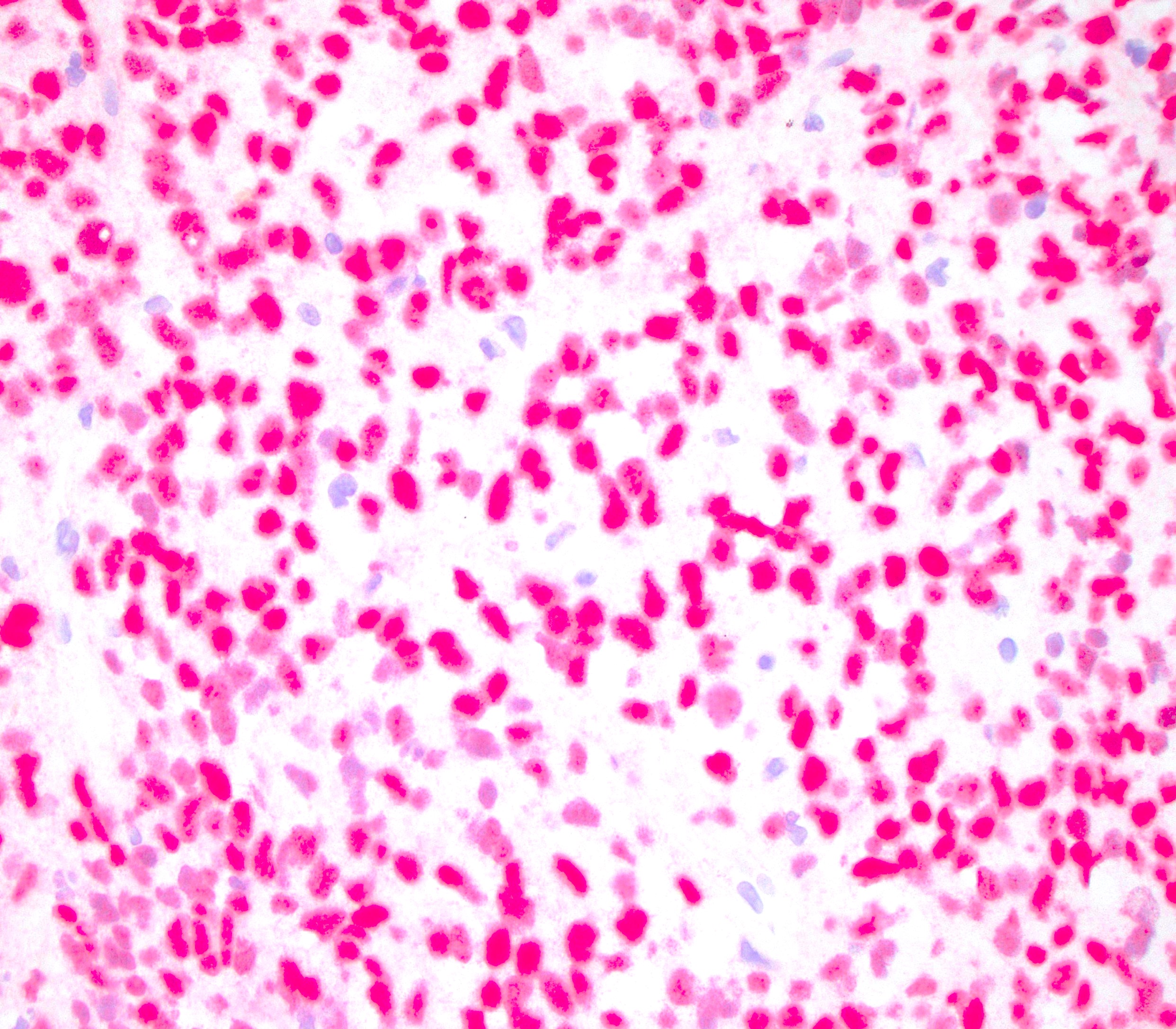
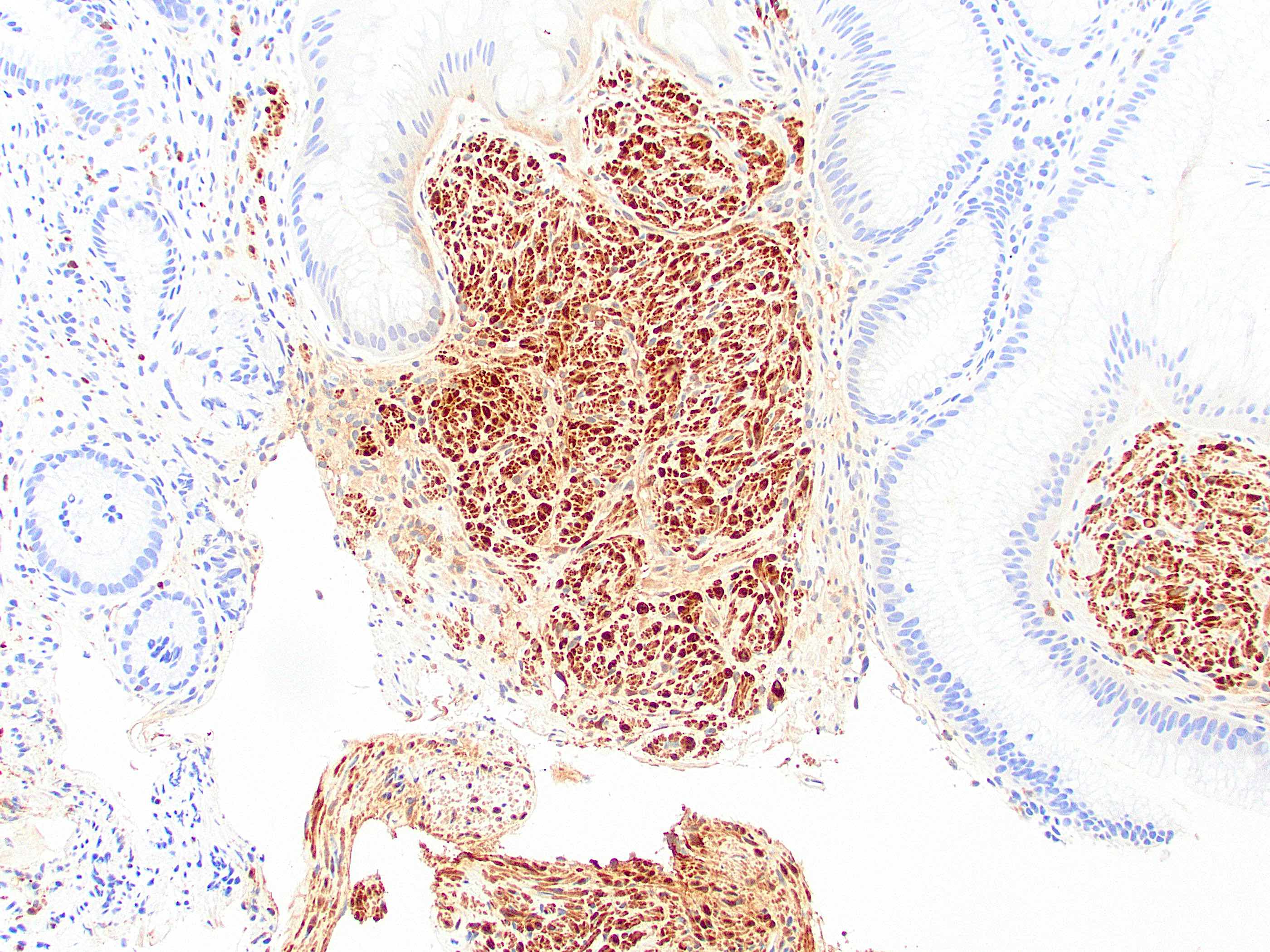
SOX10
MelanA
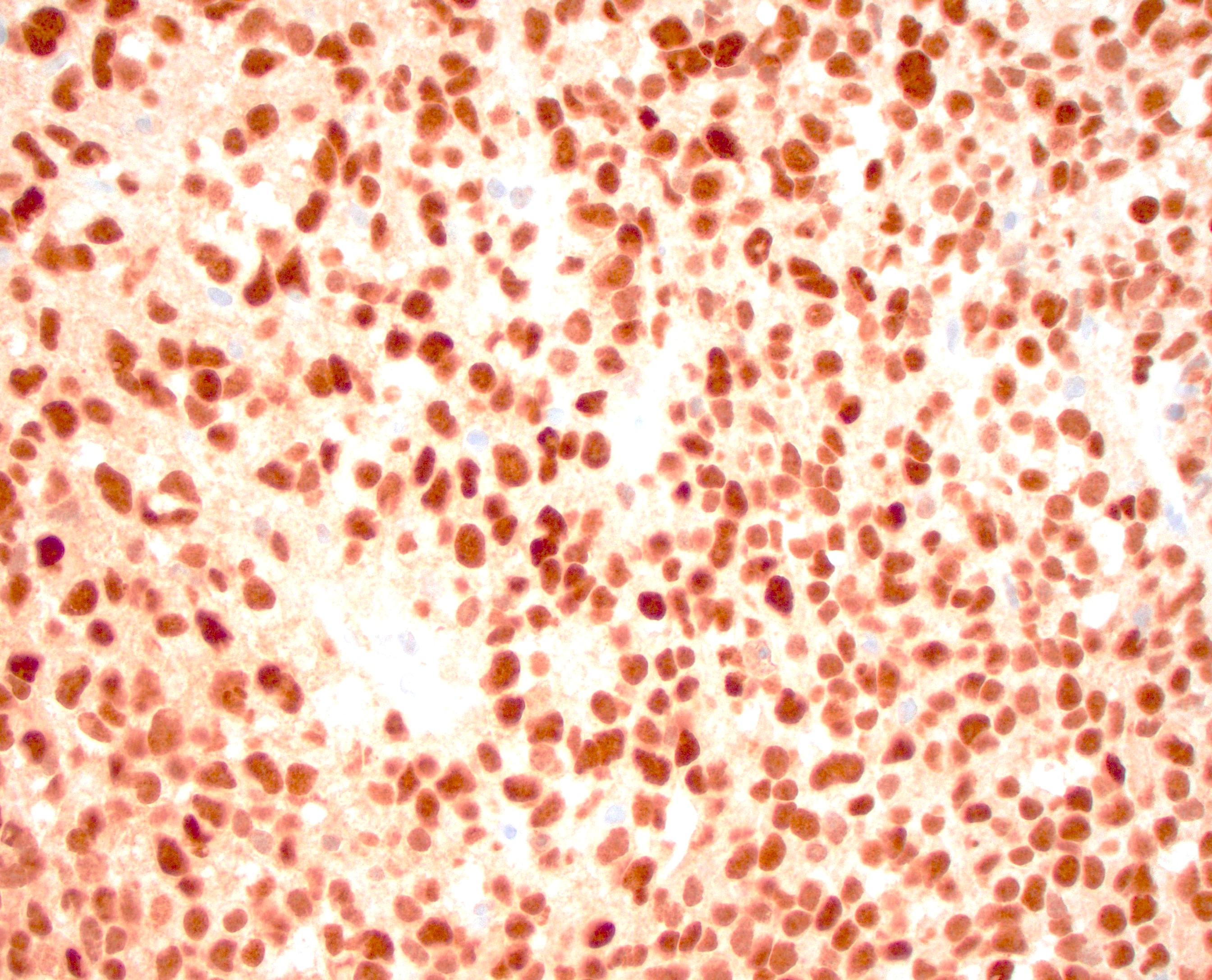
PRAME
 https://pathologyoutlines.com/topic/anusmelanoma.html #pathology #gipath #pathtwitter"
https://pathologyoutlines.com/topic/anusmelanoma.html #pathology #gipath #pathtwitter"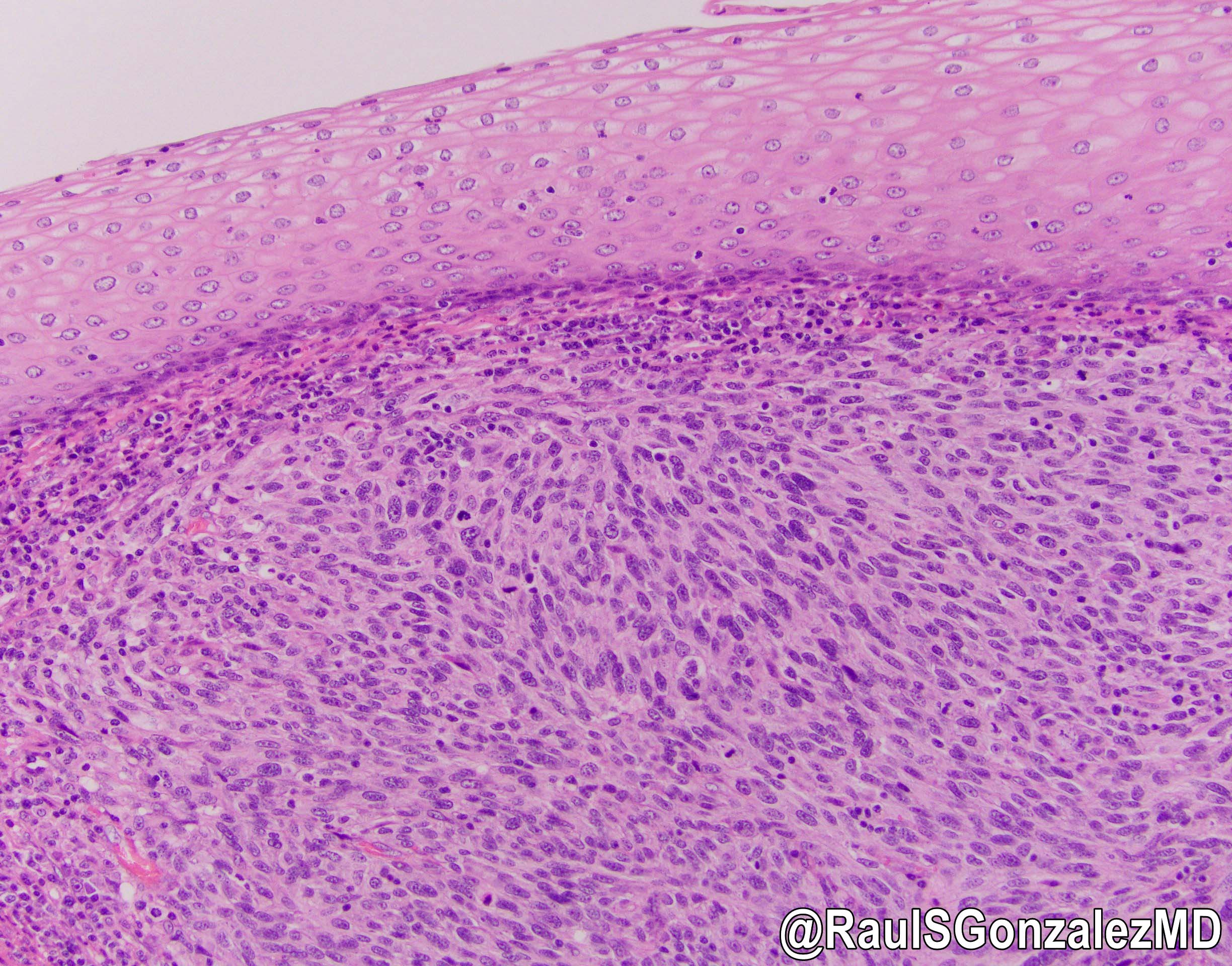 https://pathologyoutlines.com/topic/anusmelanoma.html #pathology #gipath #pathtwitter"
https://pathologyoutlines.com/topic/anusmelanoma.html #pathology #gipath #pathtwitter"
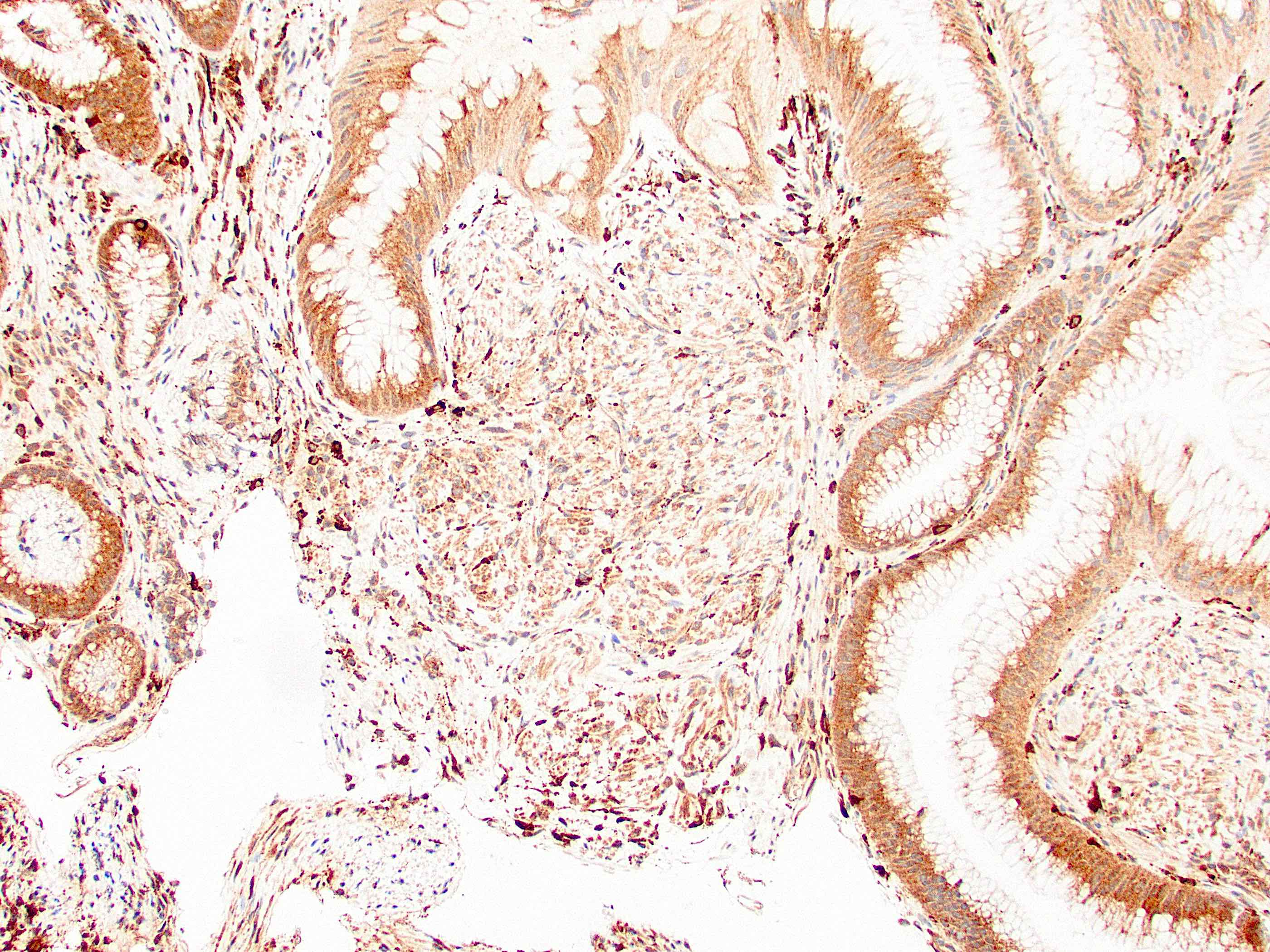
Primary anal melanoma

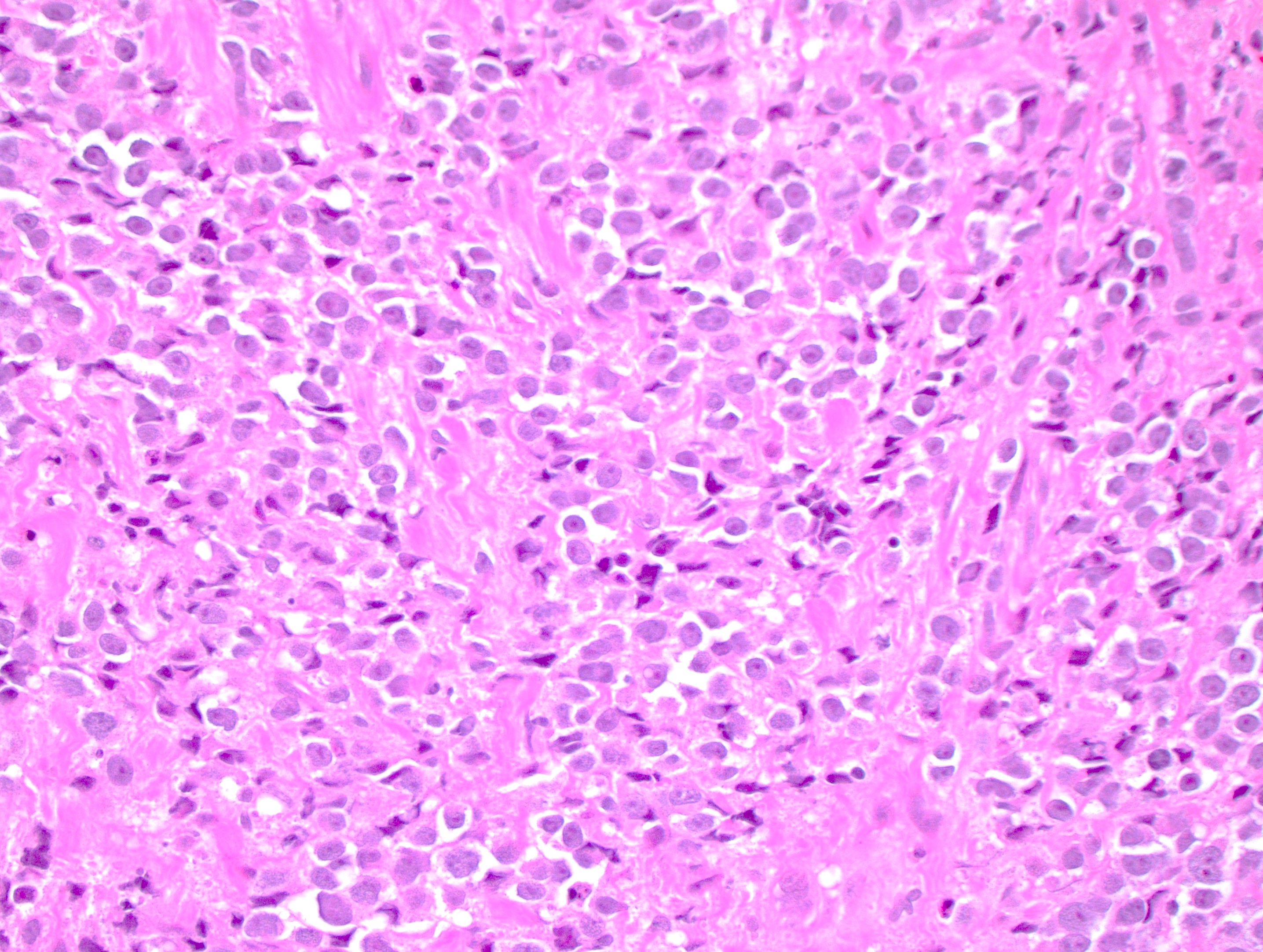
Malignant infiltrative epithelioid cells

MelanA

S100

HMB45

Pankeratin


Metastatic melanoma smears

MRI

PET scan

Metastatic disease
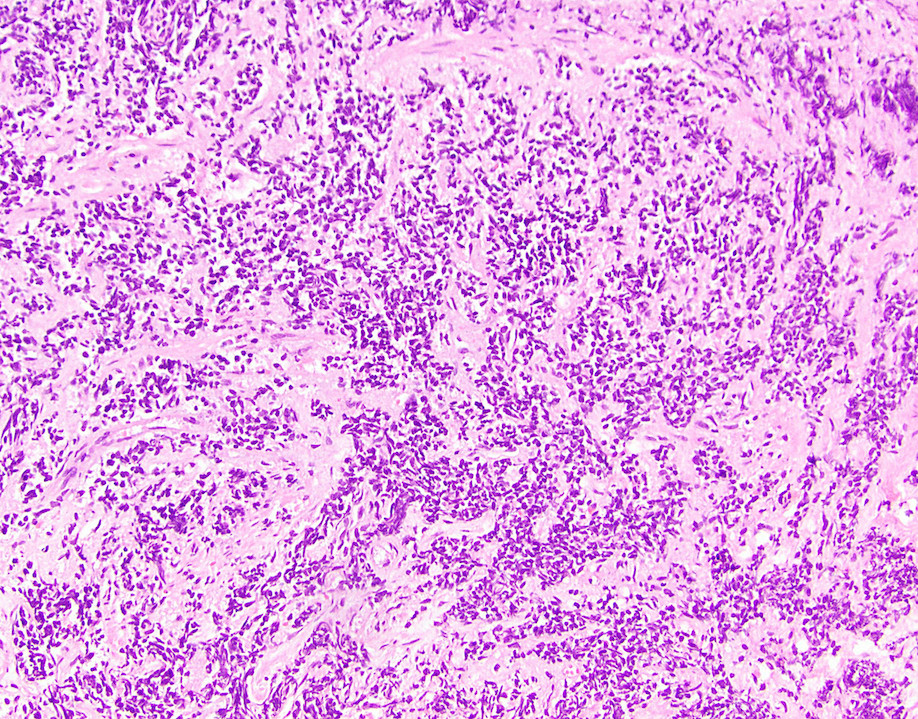
Small cell carcinoma
Large cell carcinoma

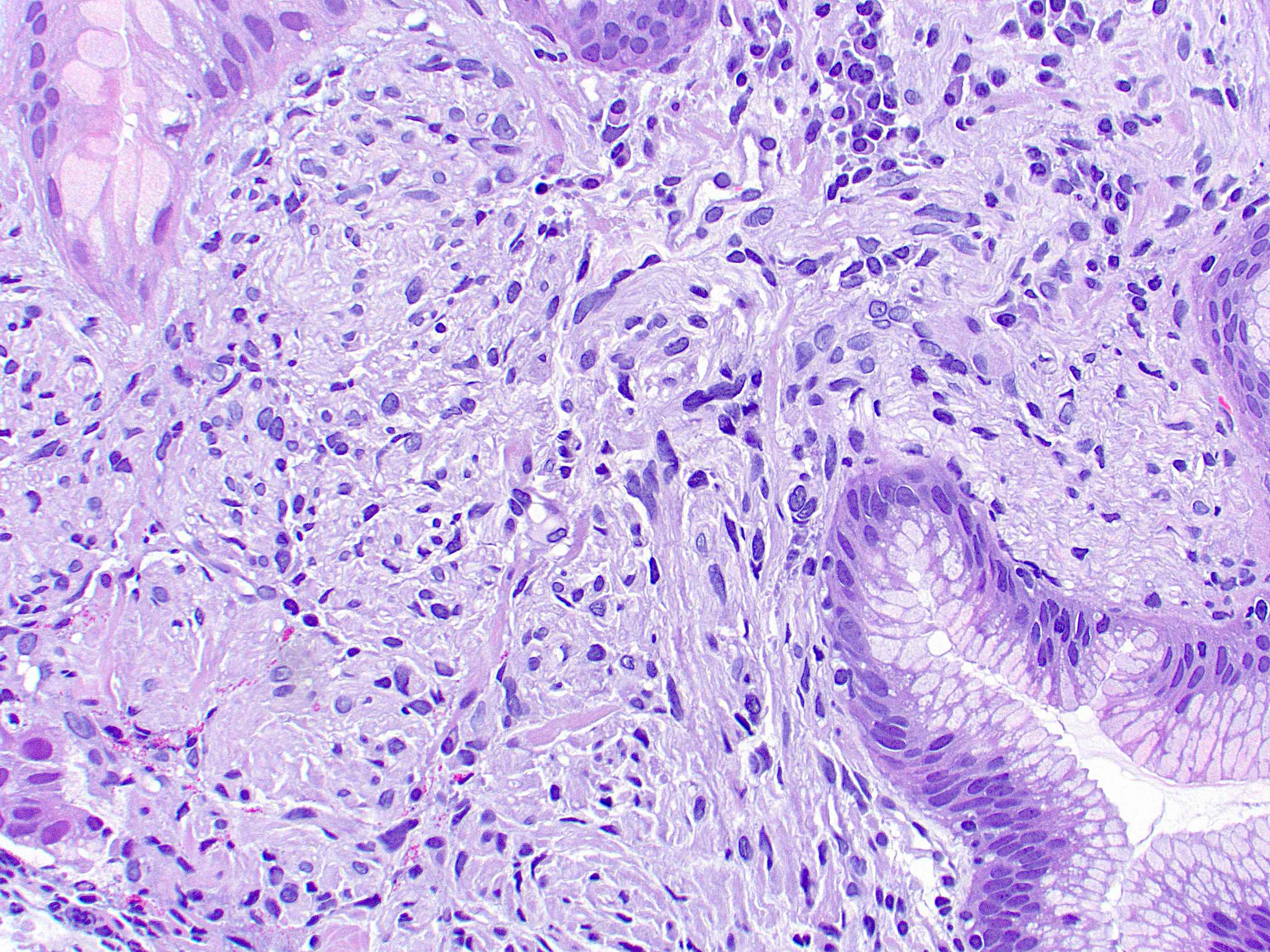
Extensive perianal Paget disease, perineum

Early response

Notable telangiectasia and fibrosis
Visible Paget cells
Prominent intracytoplasmic mucin

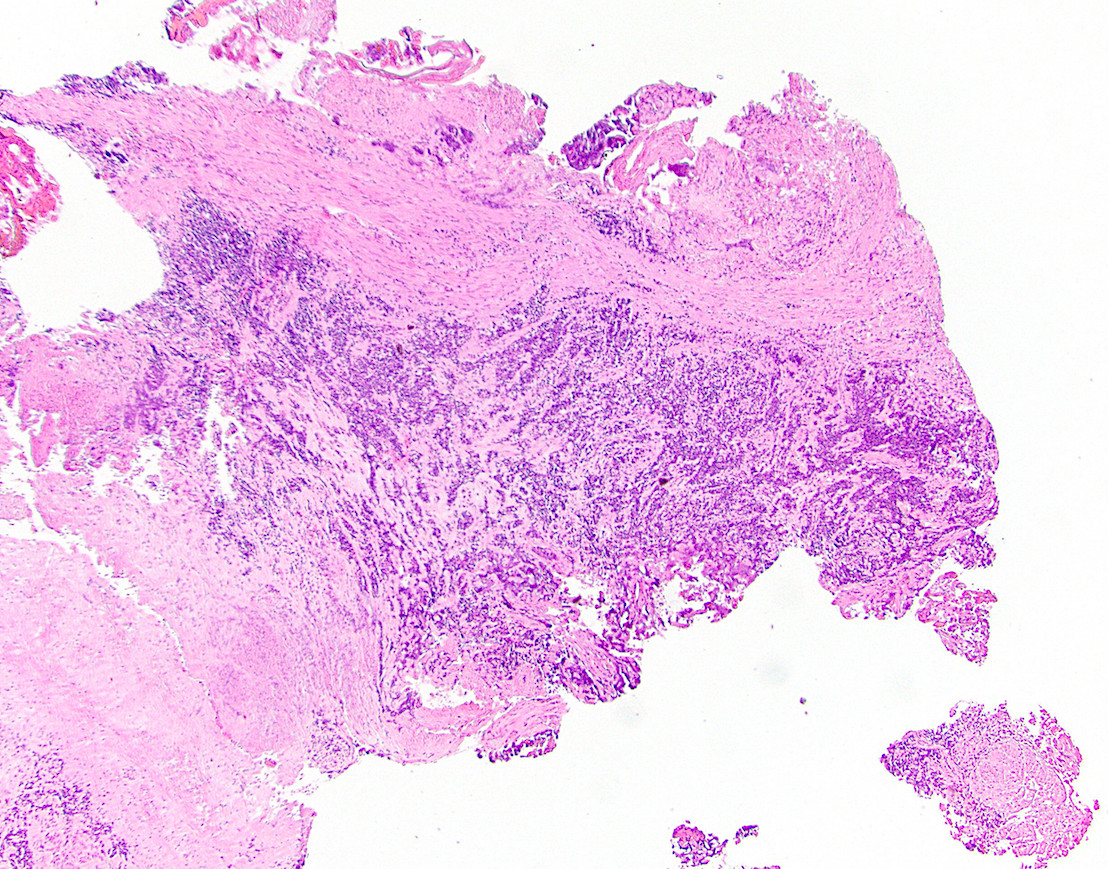
Anorectal tumor

Anal tumor

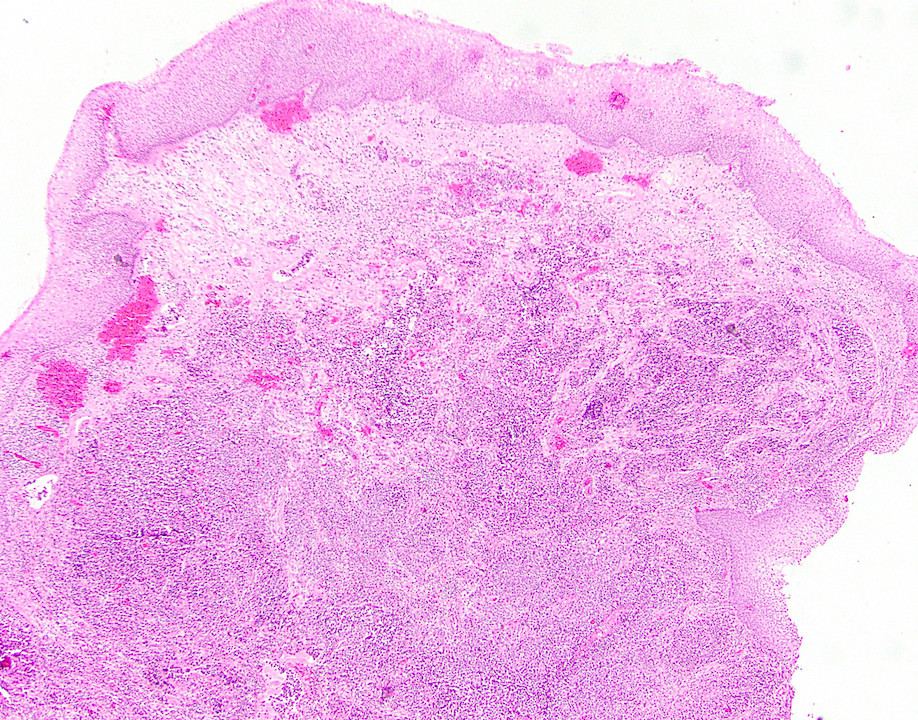
Large exophytic mass
Infiltrating anal mass
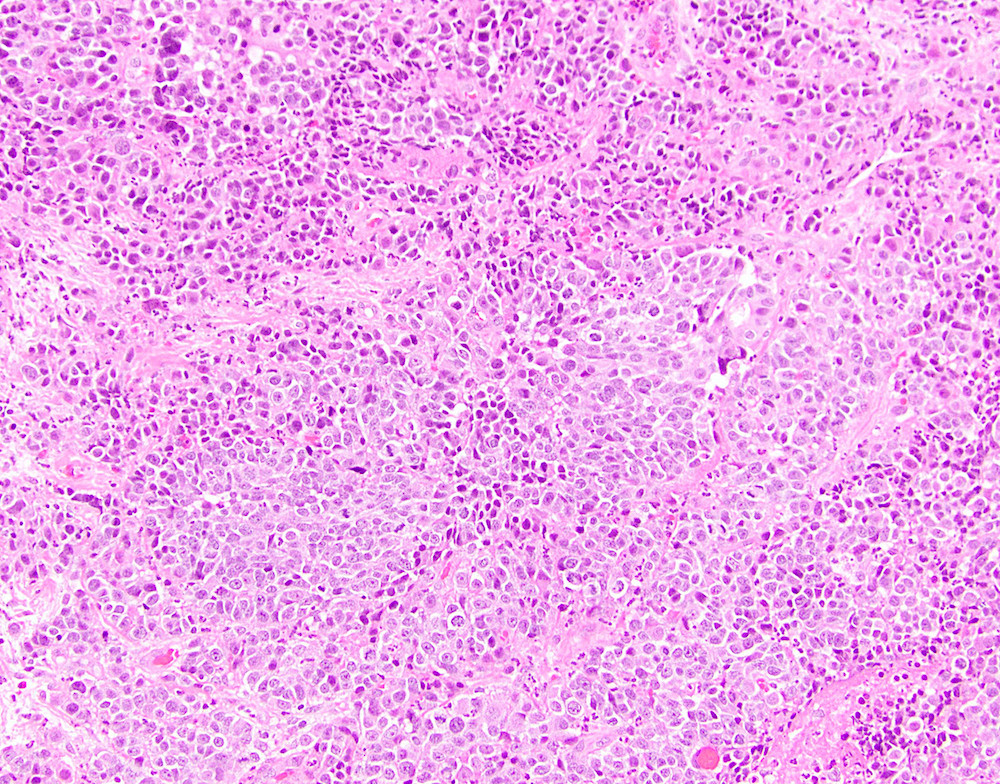
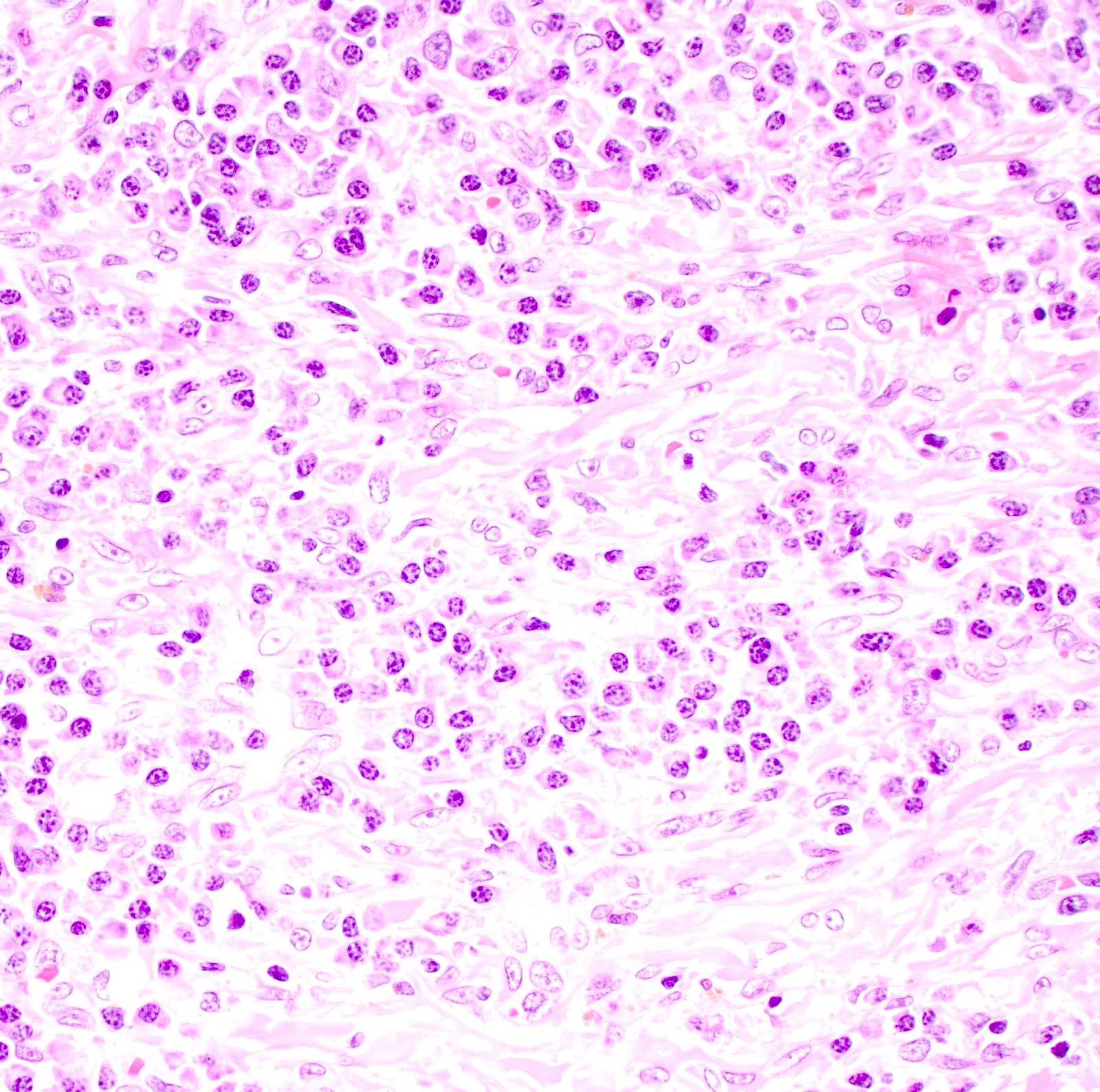
Prominent nuclear atypia
Necrosis
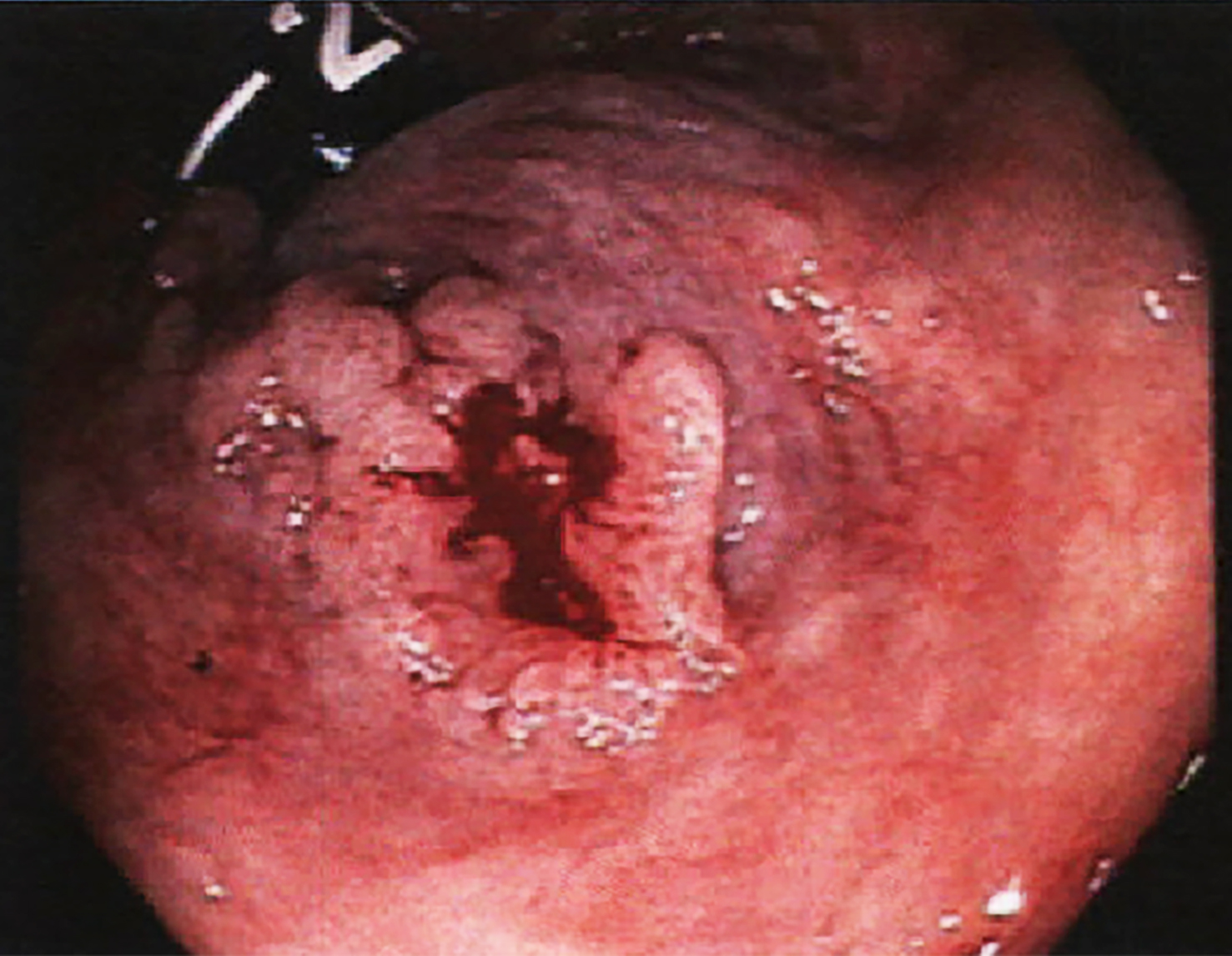
Condyloma acuminatum


Anoscopy
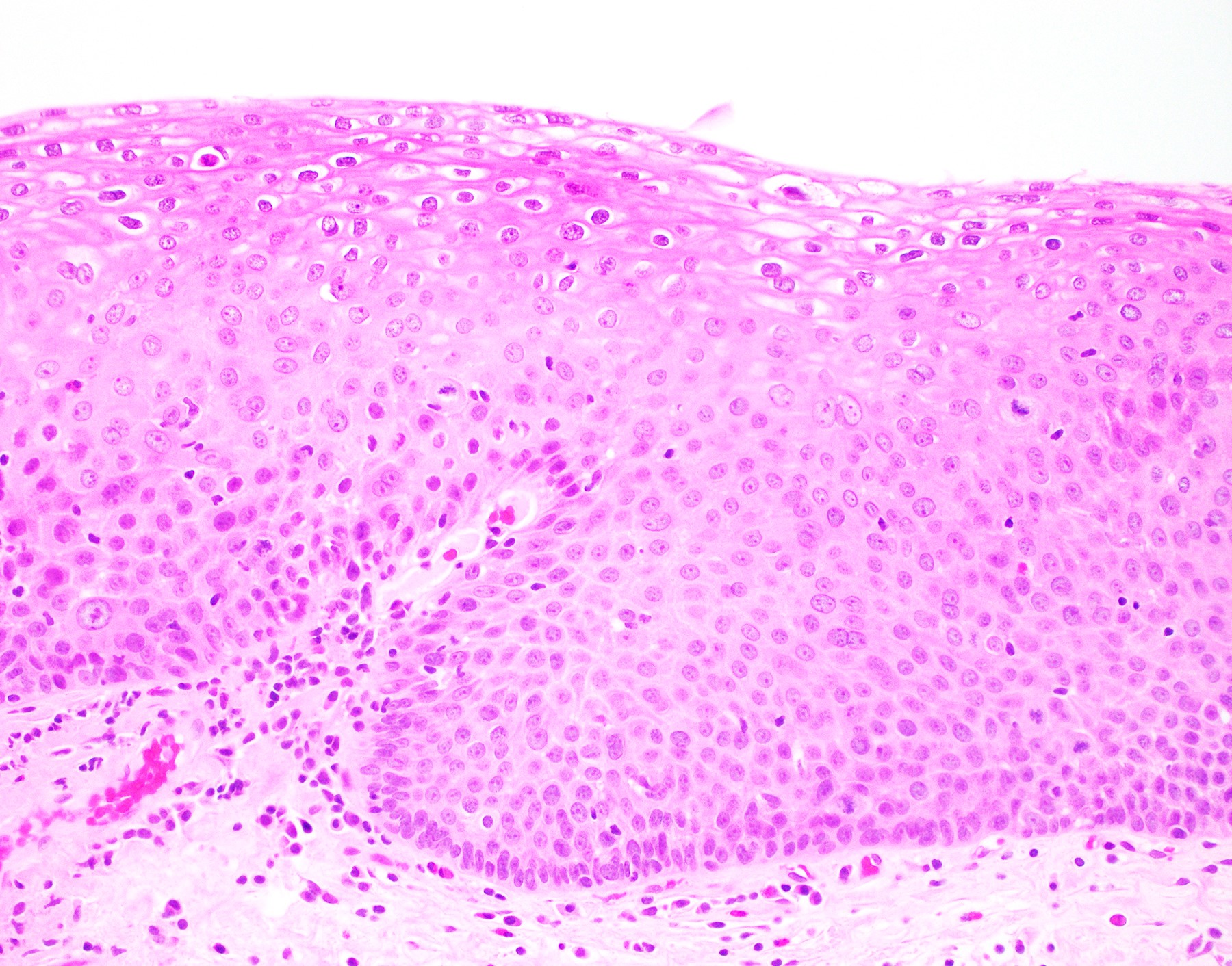
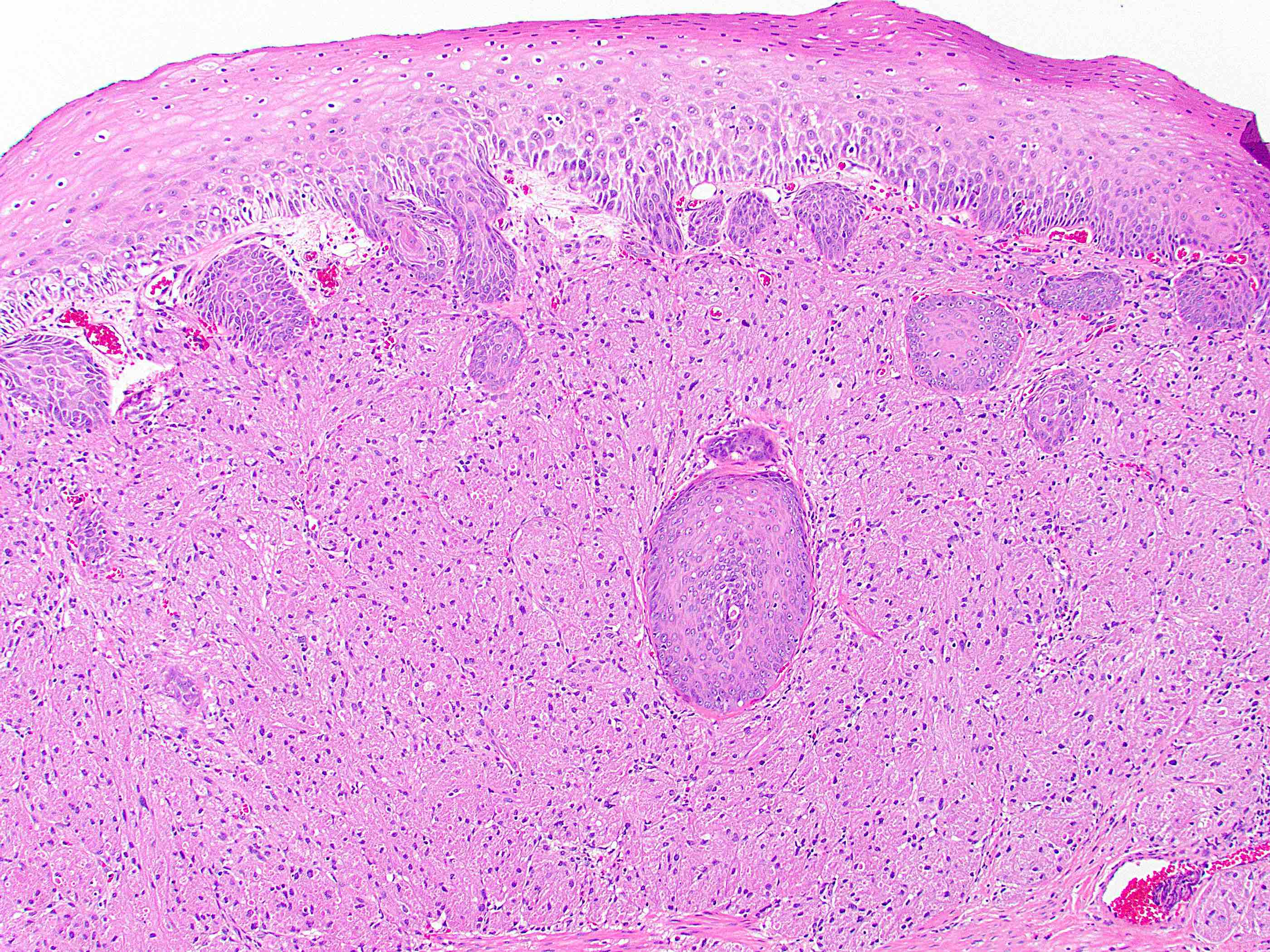
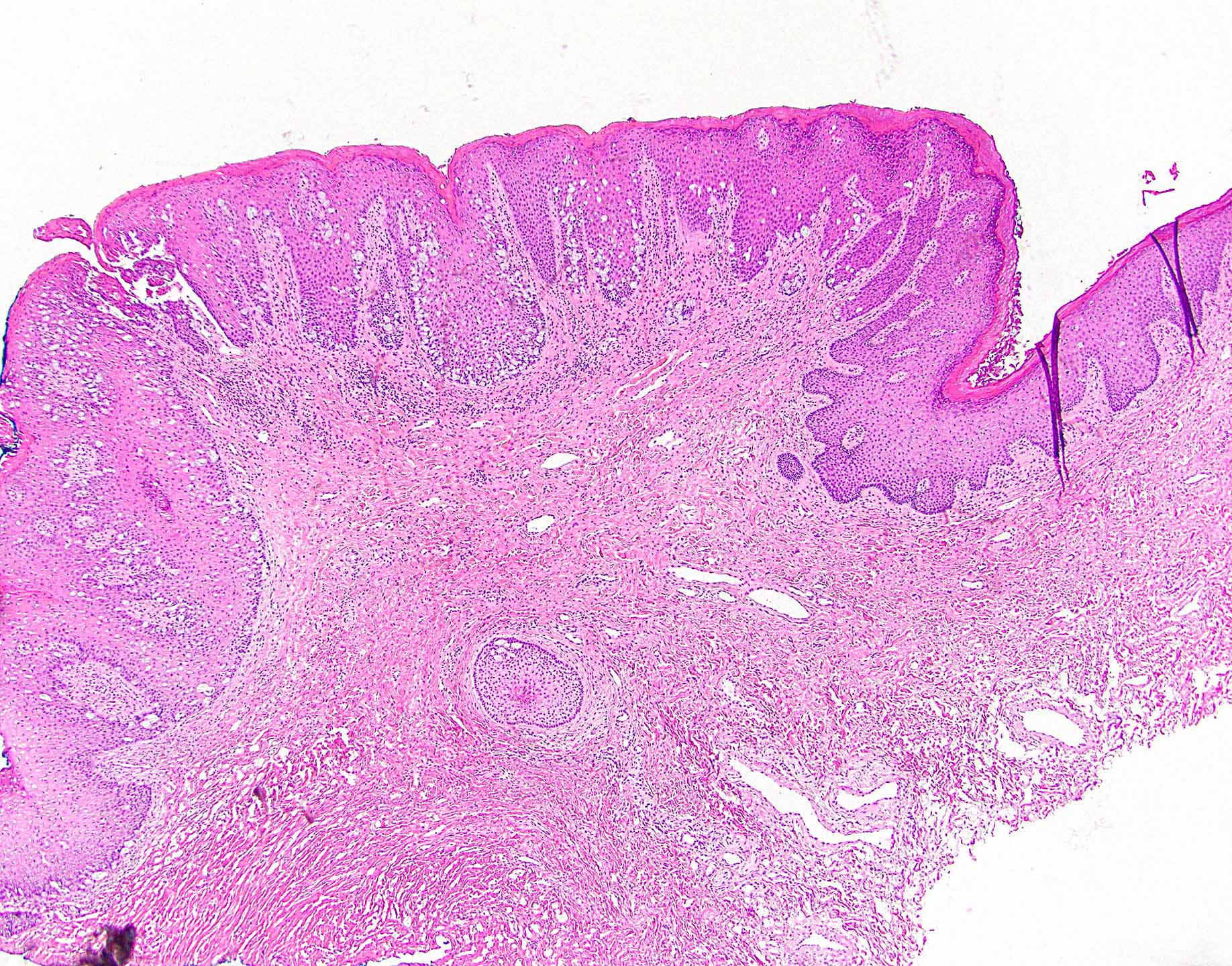
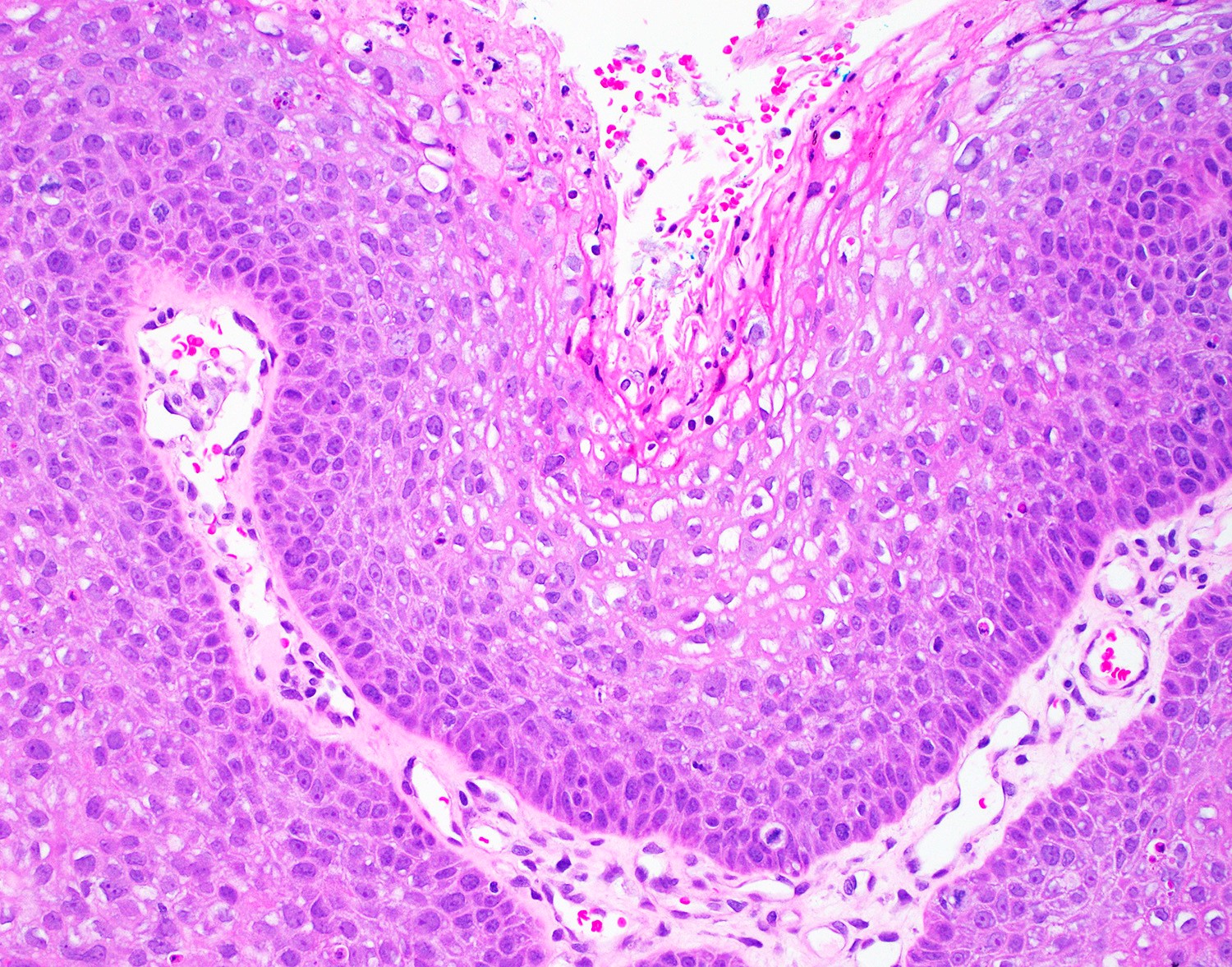
Flat squamous proliferation
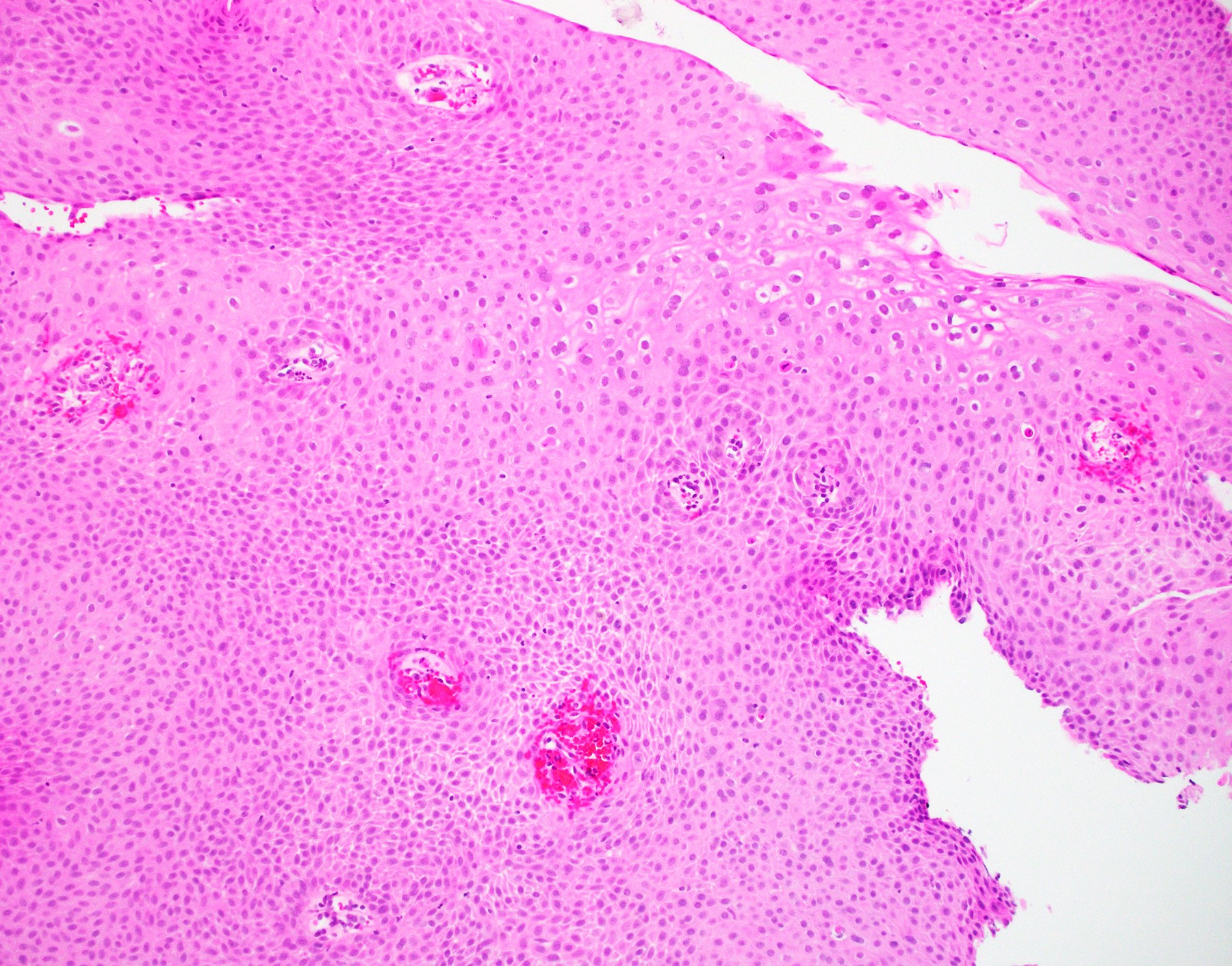
Papillary squamous proliferation

Papillary squamous proliferation, parakeratosis and koilocytosis
Condyloma with invasion
Invasive
squamous cell
carcinoma arising
in condyloma
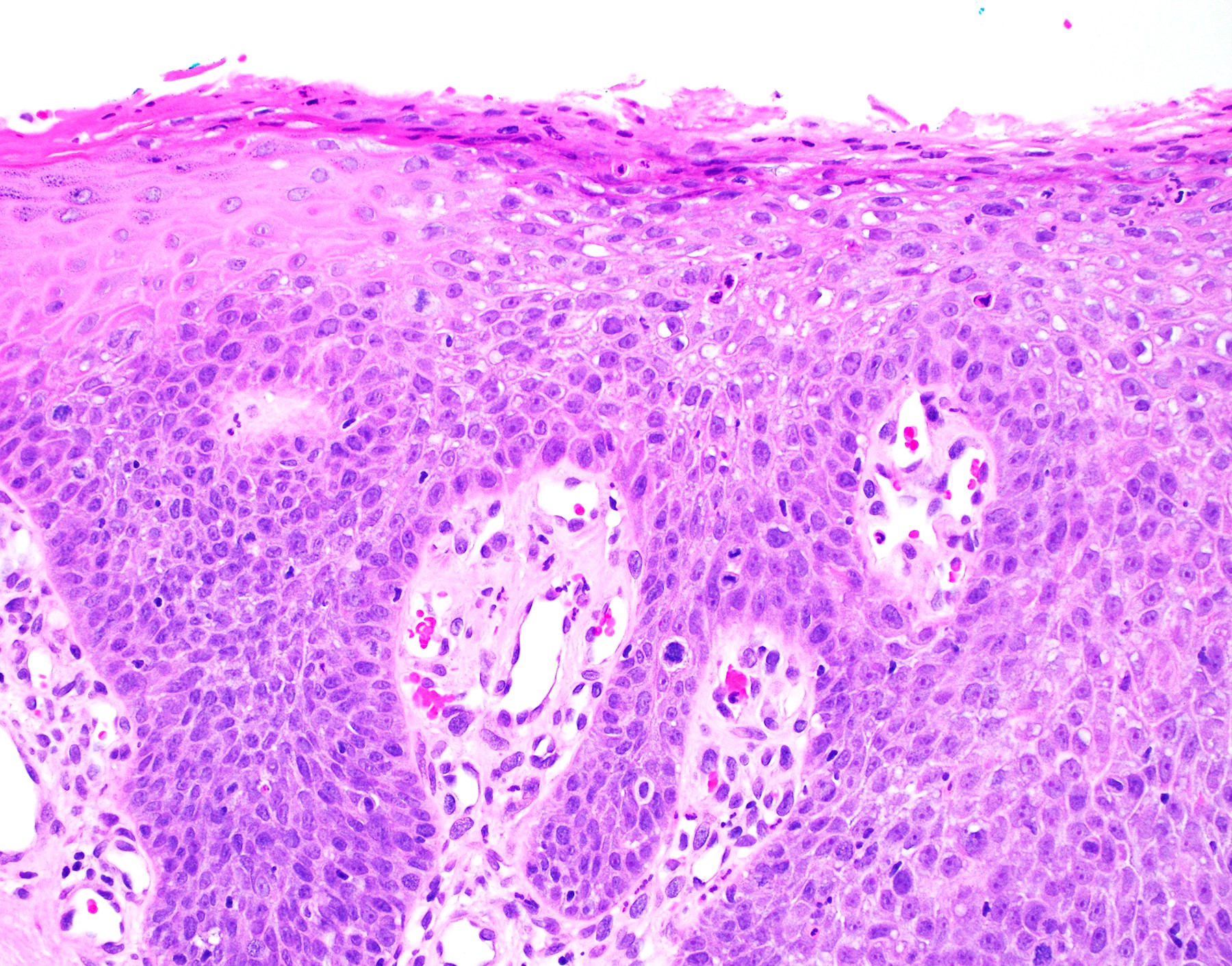
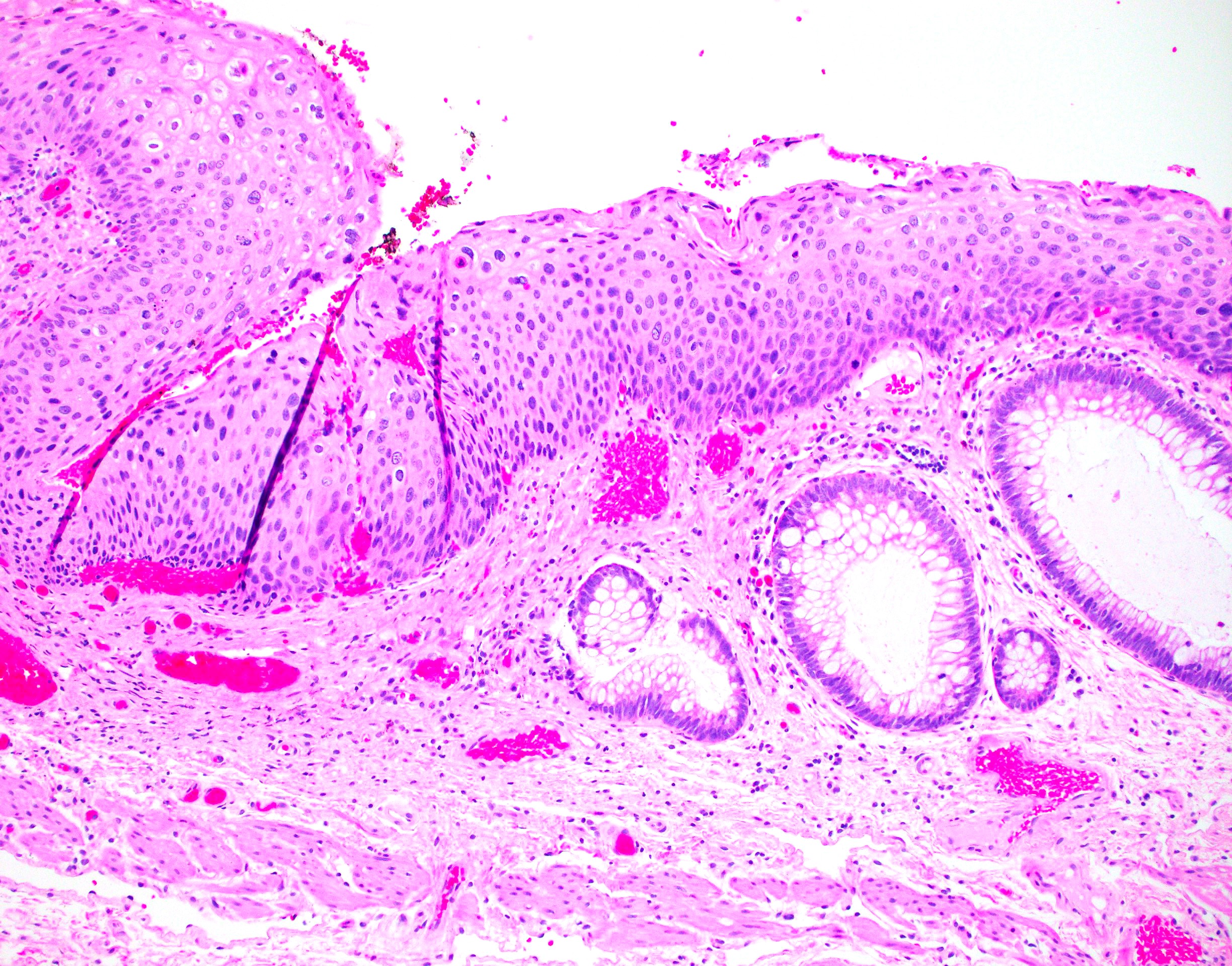
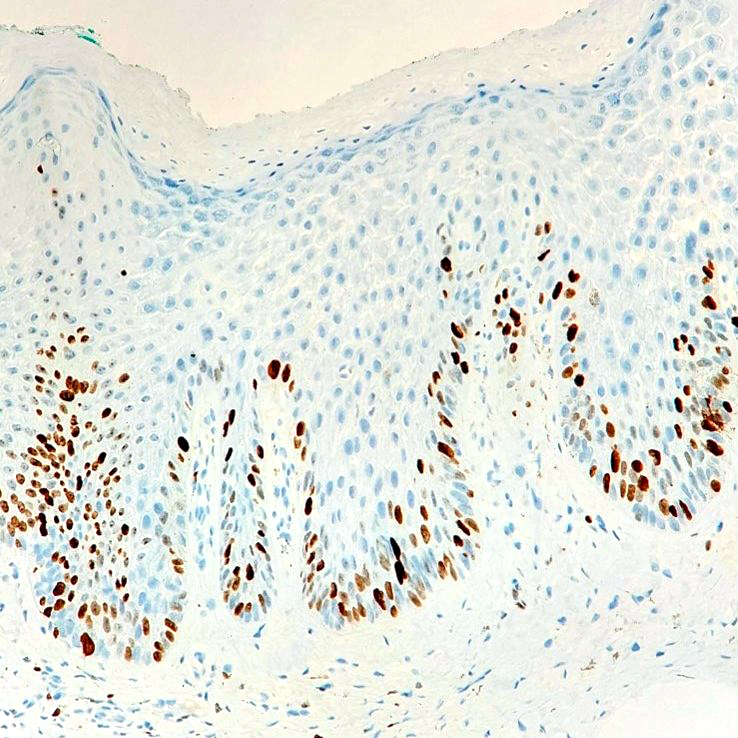
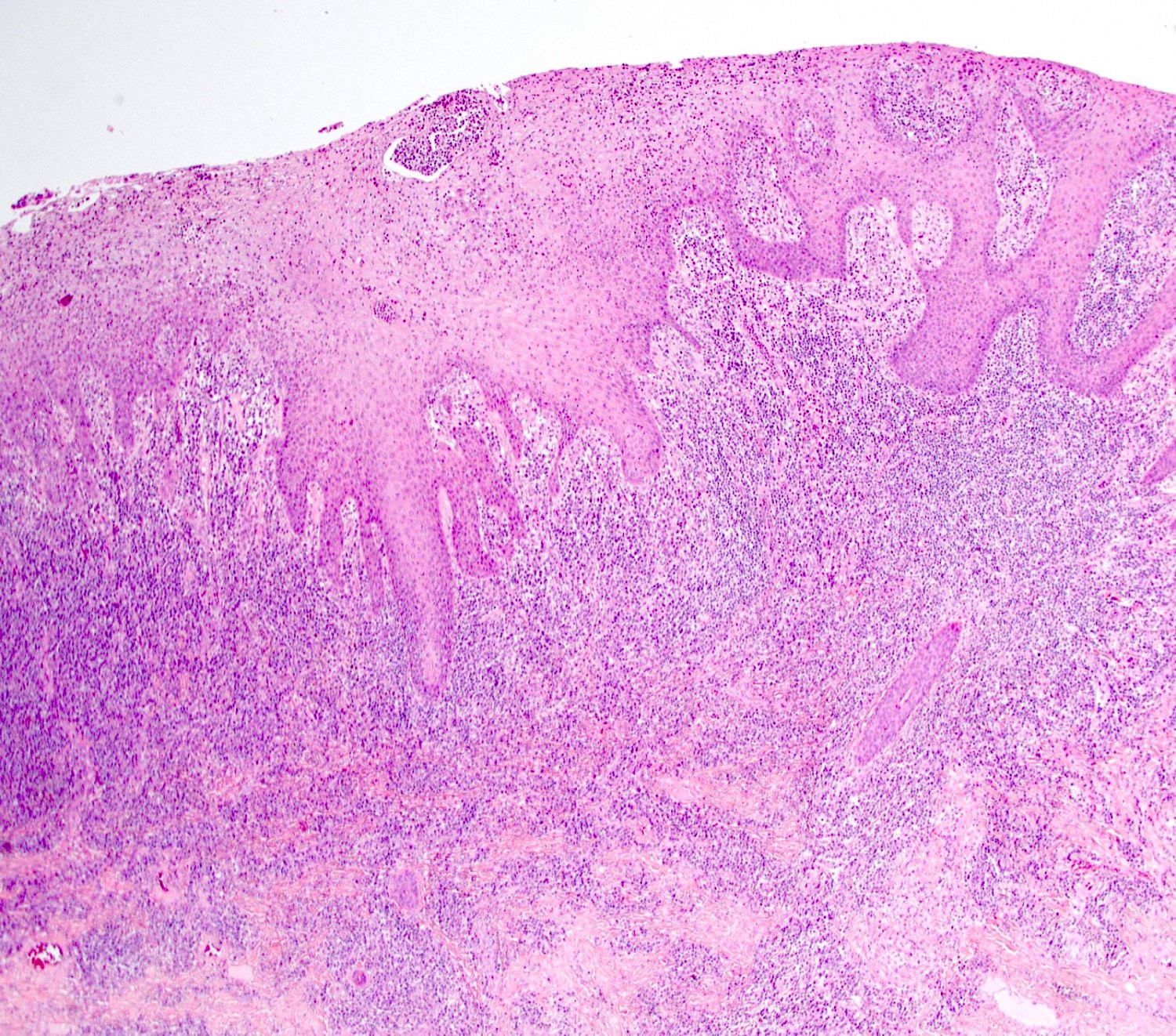
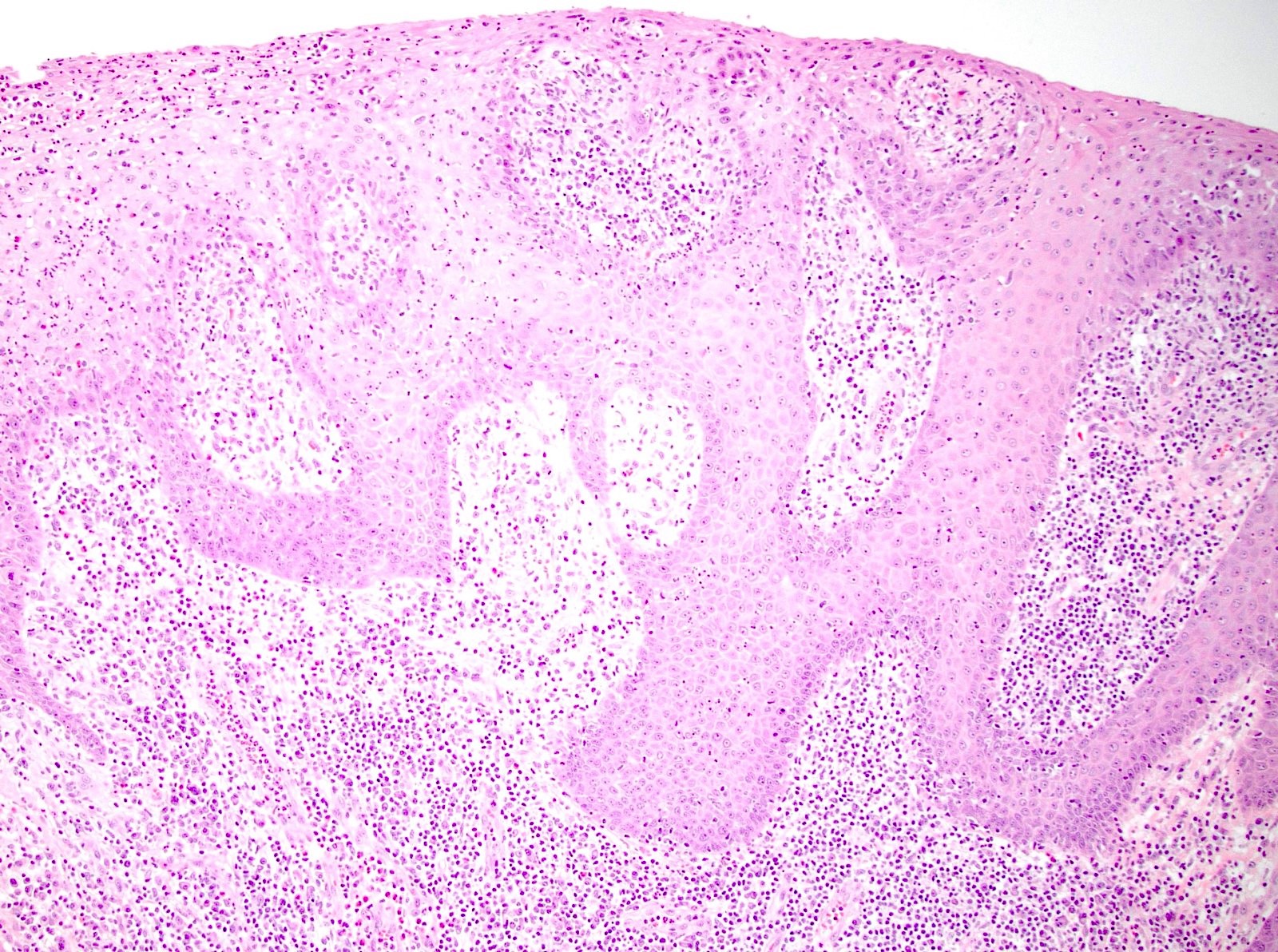
HSIL
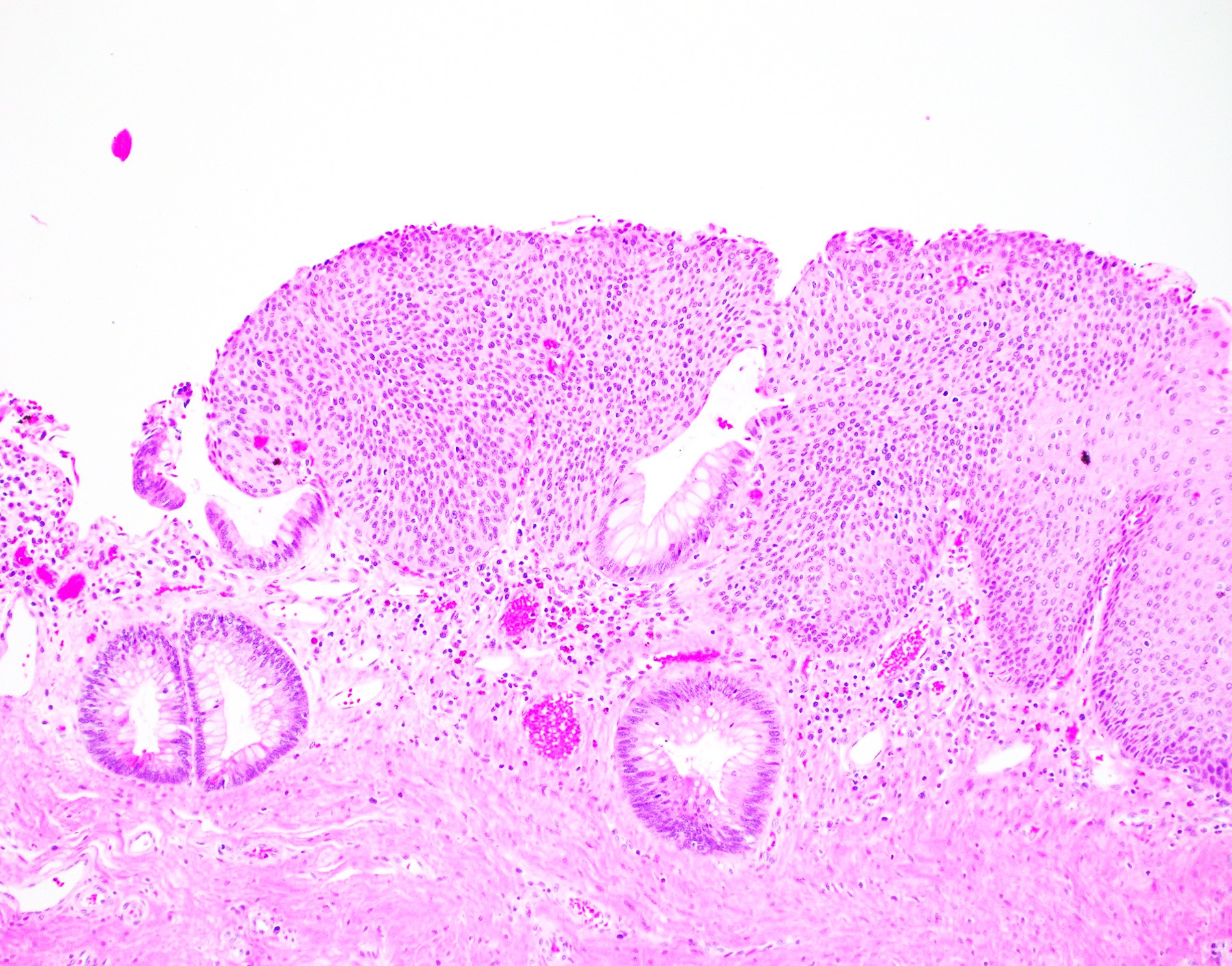
HSIL at the anal transitional zone
Involving a hemorrhoid
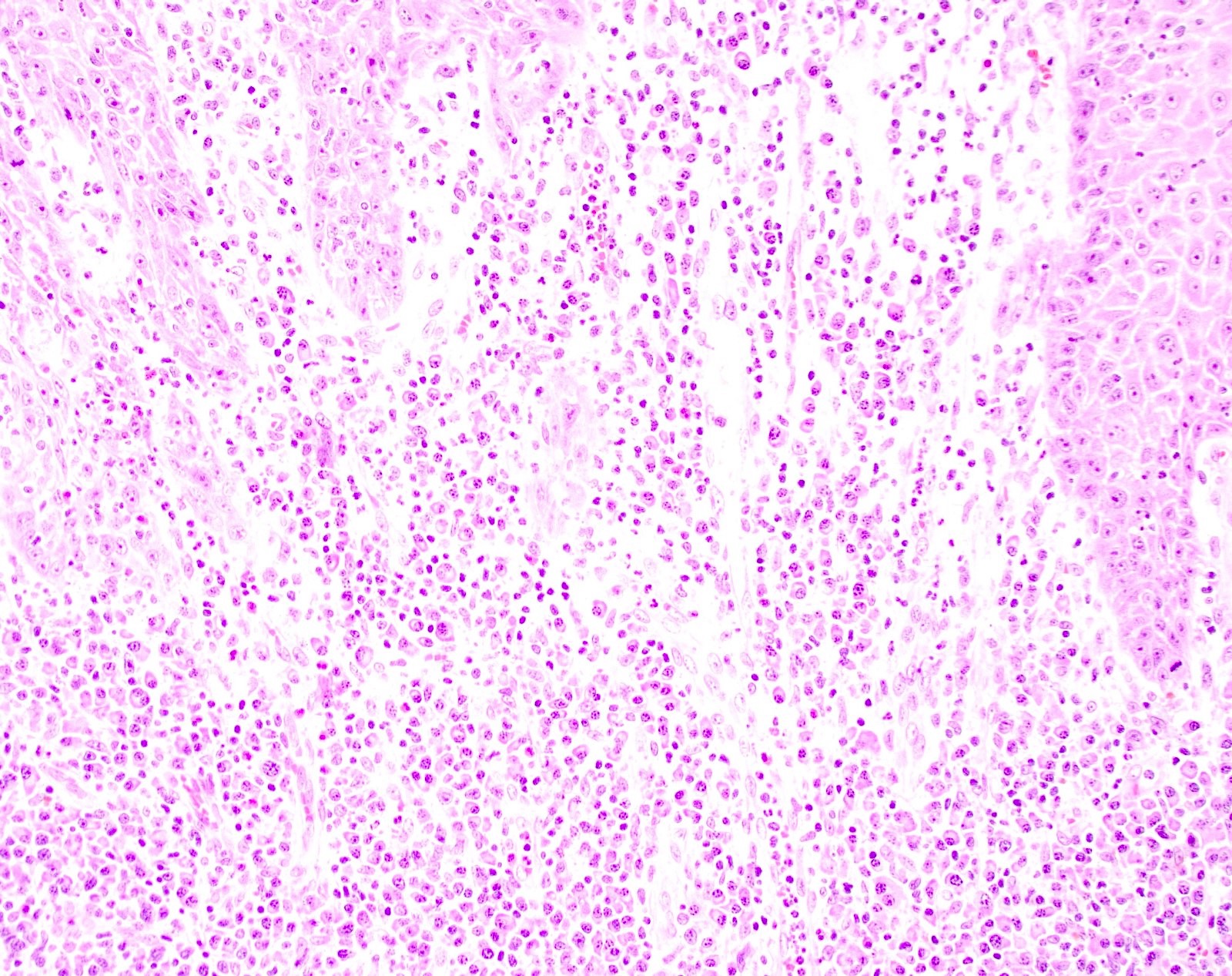
Squamous dysplasia
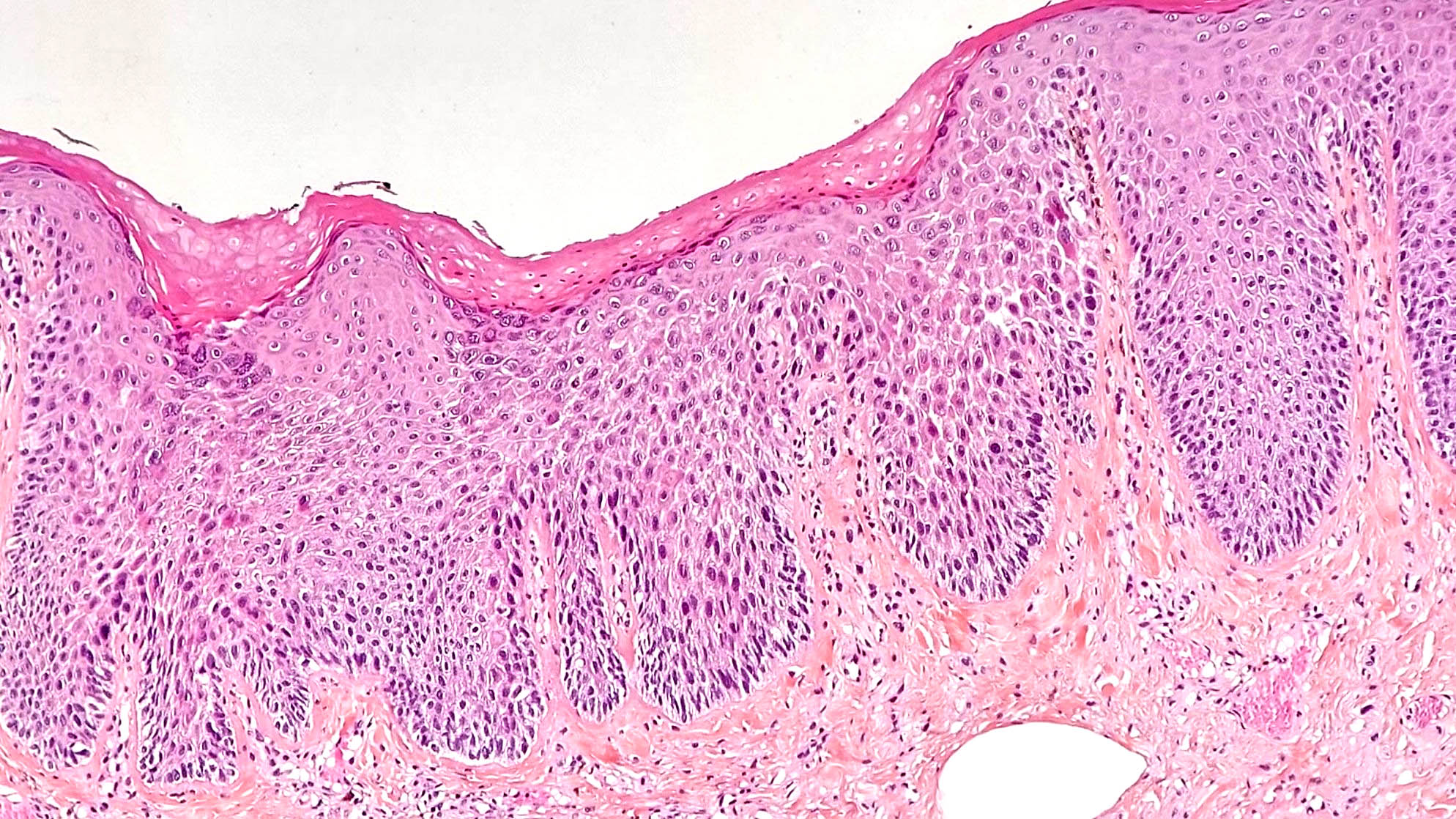
Squamous dysplasia
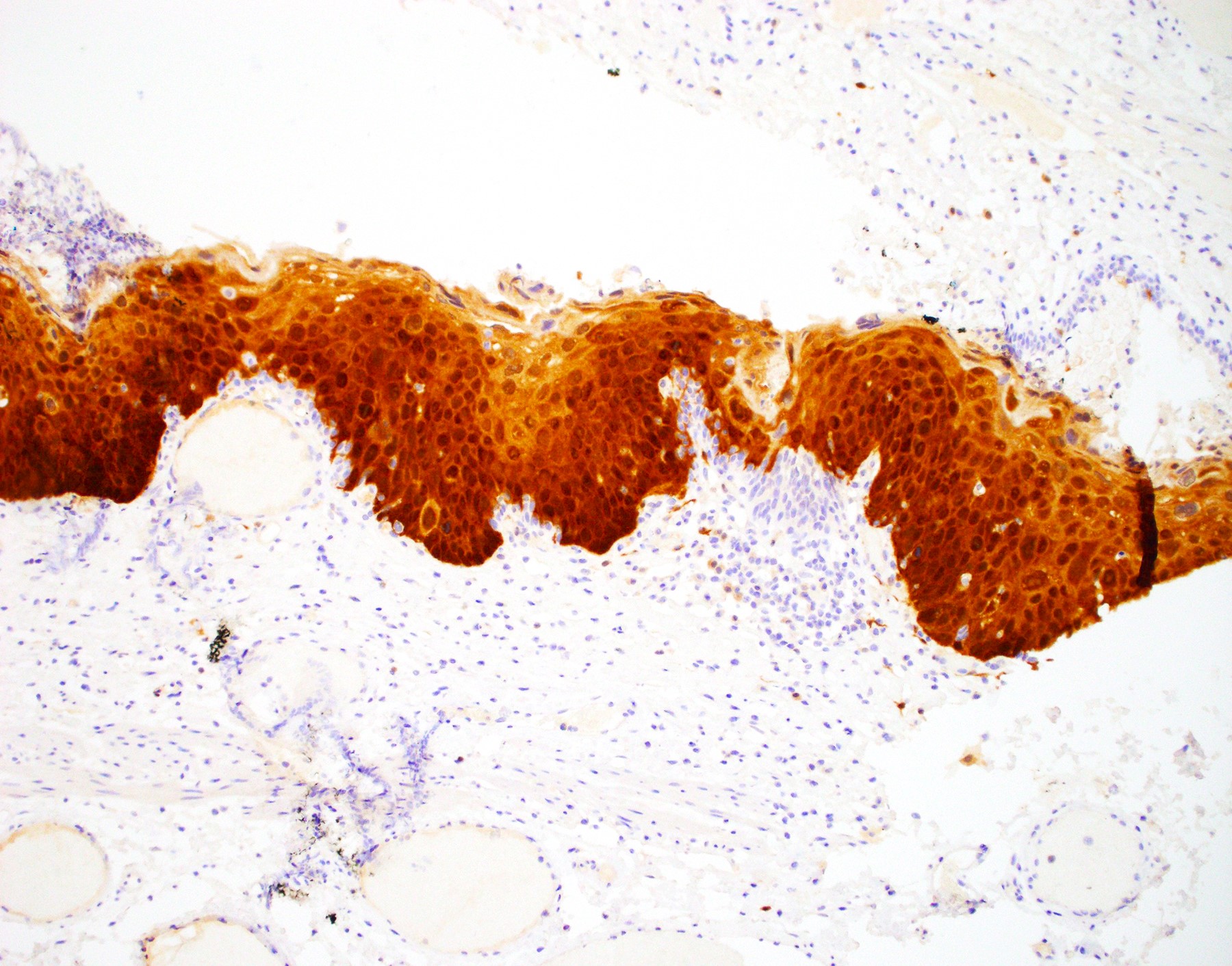
p16 immunohisto-
chemistry
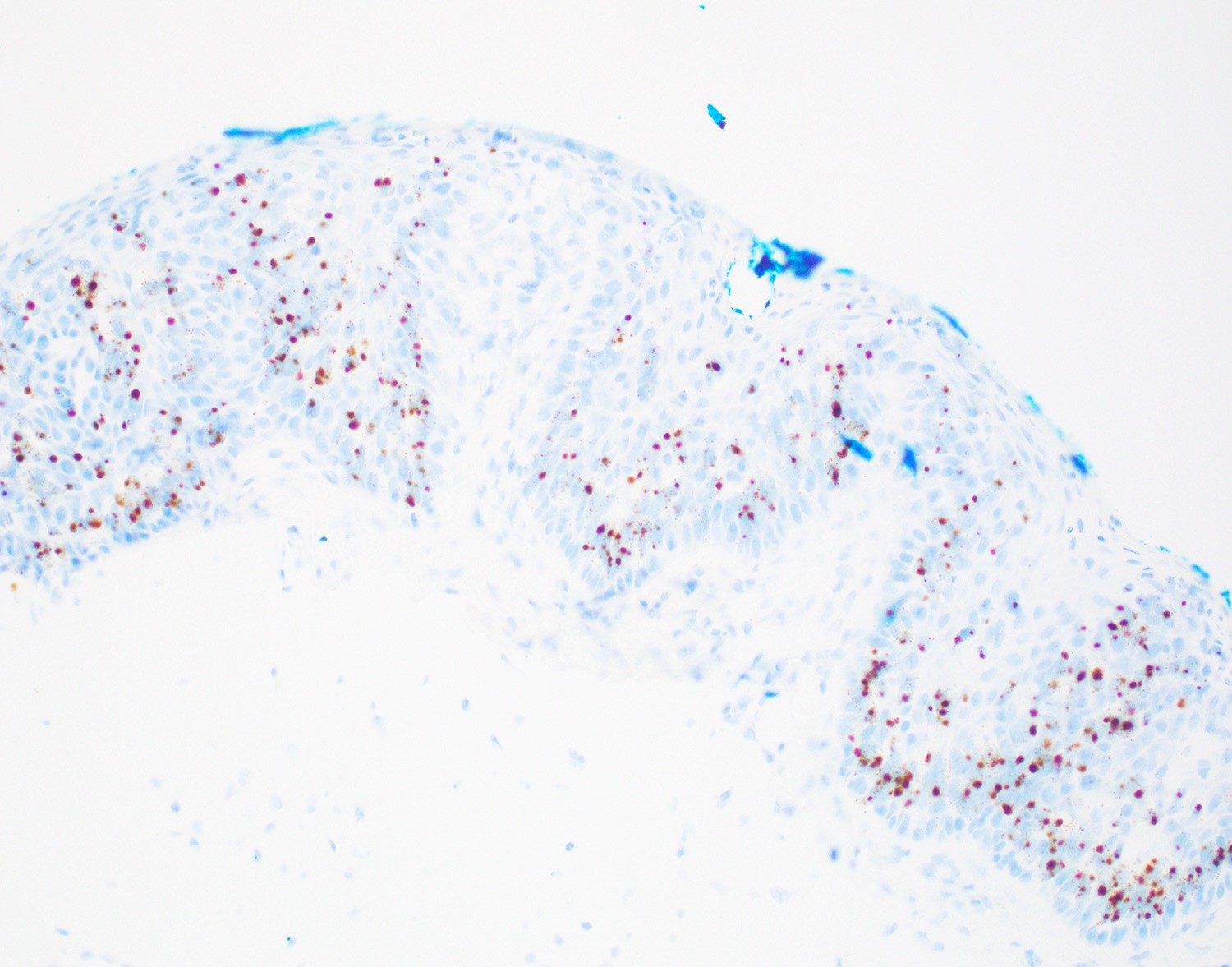
HPV in situ hybridization

Squamous dysplasia
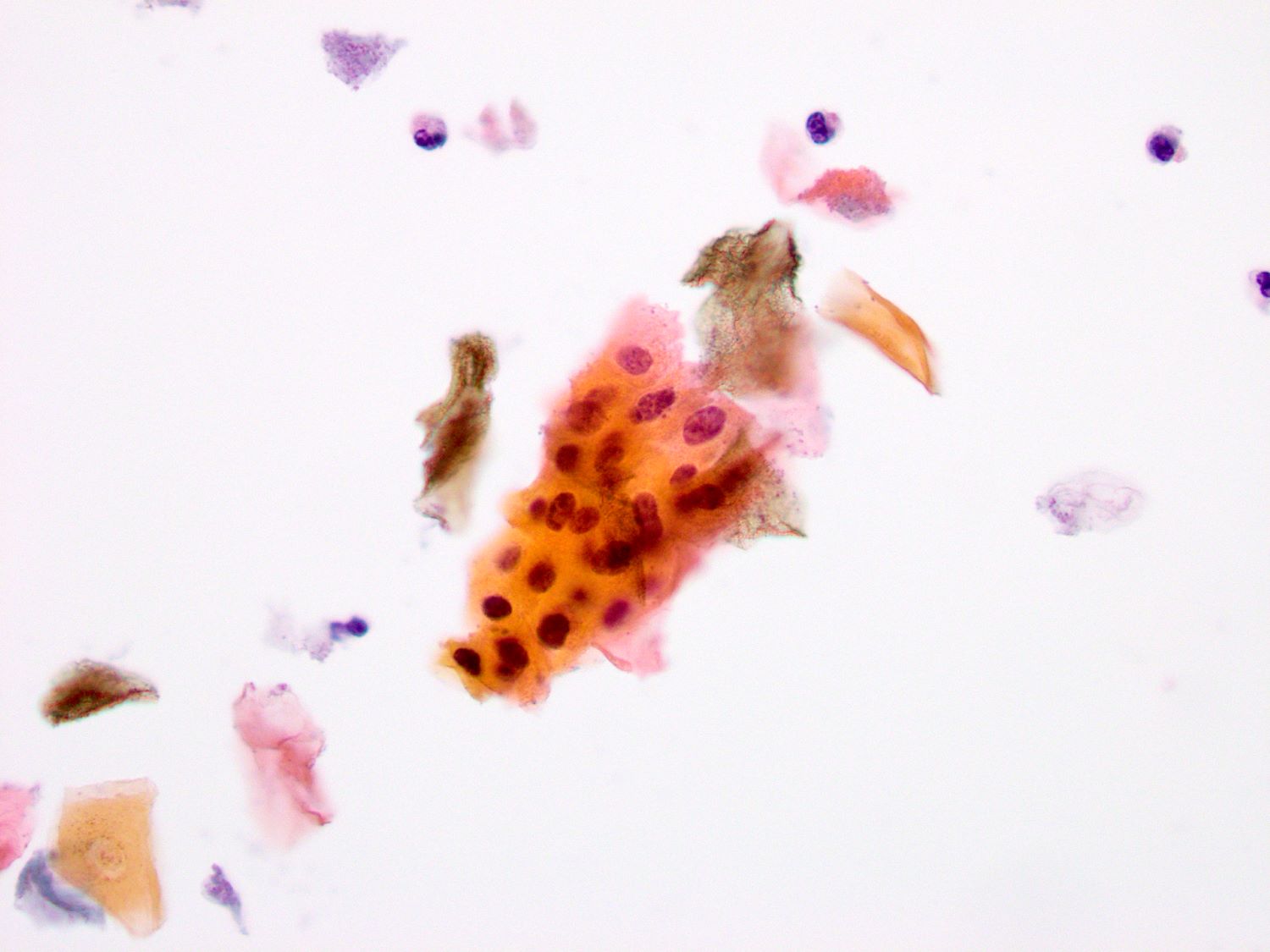
Anal Pap smear
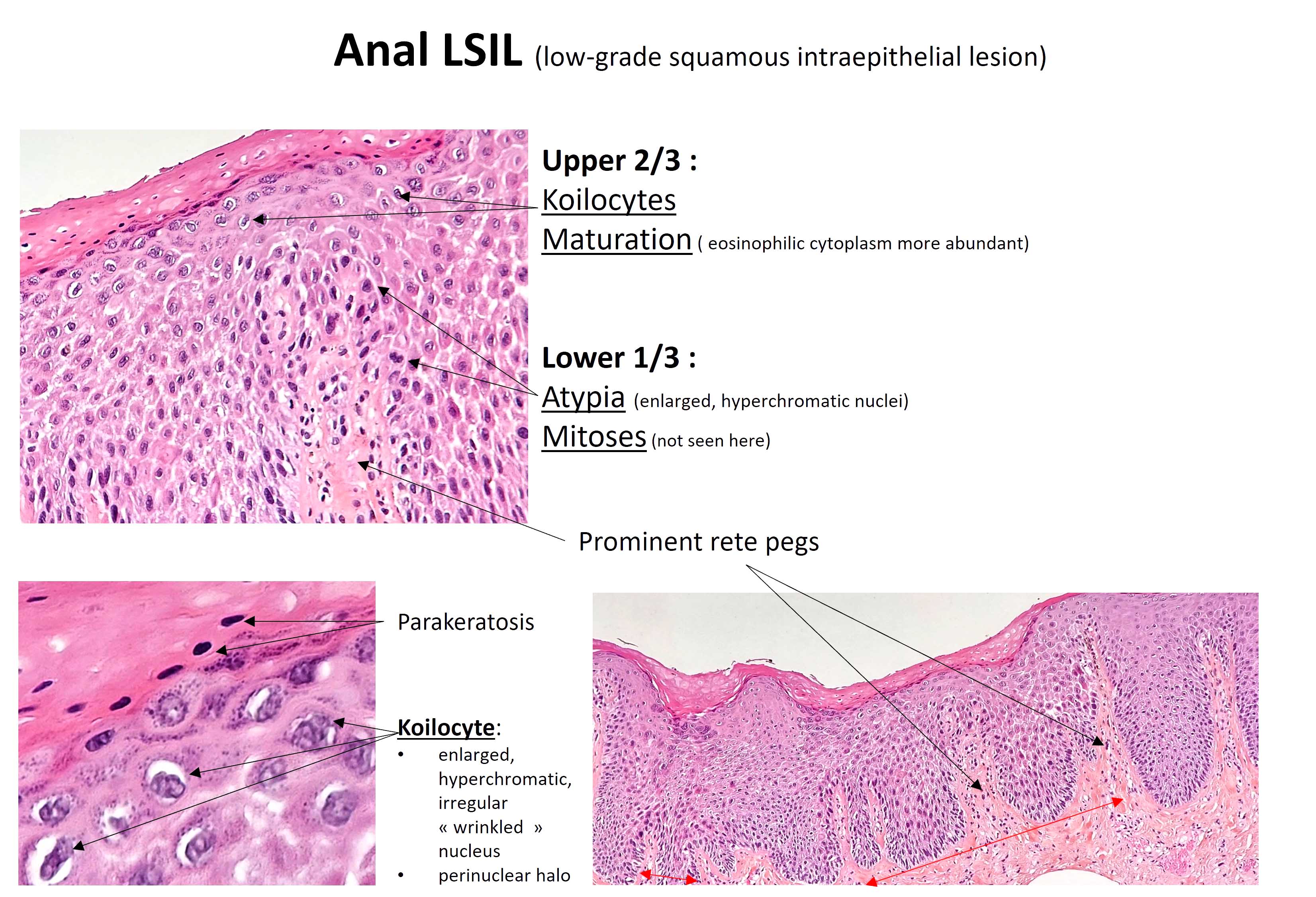
LSIL
| Stage group I: | T1 | N0 | M0 |
| Stage group IIA: | T2 | N0 | M0 |
| Stage group IIB: | T1 - 2 | N1 | M0 |
| Stage group IIIA: | T3 | N0 - N1 | M0 |
| Stage group IIIB: | T4 | N0 | M0 |
| Stage group IIIC: | T4 | N1 | M0 |
| Stage group IV: | any T | any N | M1 |

Multiple perianal lesions

Anorectal ulcerated mass

Exophytic perineal lesions

Condylomata lata
Epithelial hyperplasia and inflammation
Plasma cell infiltrate
Rectal biopsy with inflammation
Silver stain
T. pallidum IHC
Perianal condyloma lata
Syphilis stains and IHC

Retrorectal space

Retrorectal cystic mass

Malignant transformation

Posterior approach view

Intact resection

Mud-like contents

Tailgut cyst adenocarcinoma
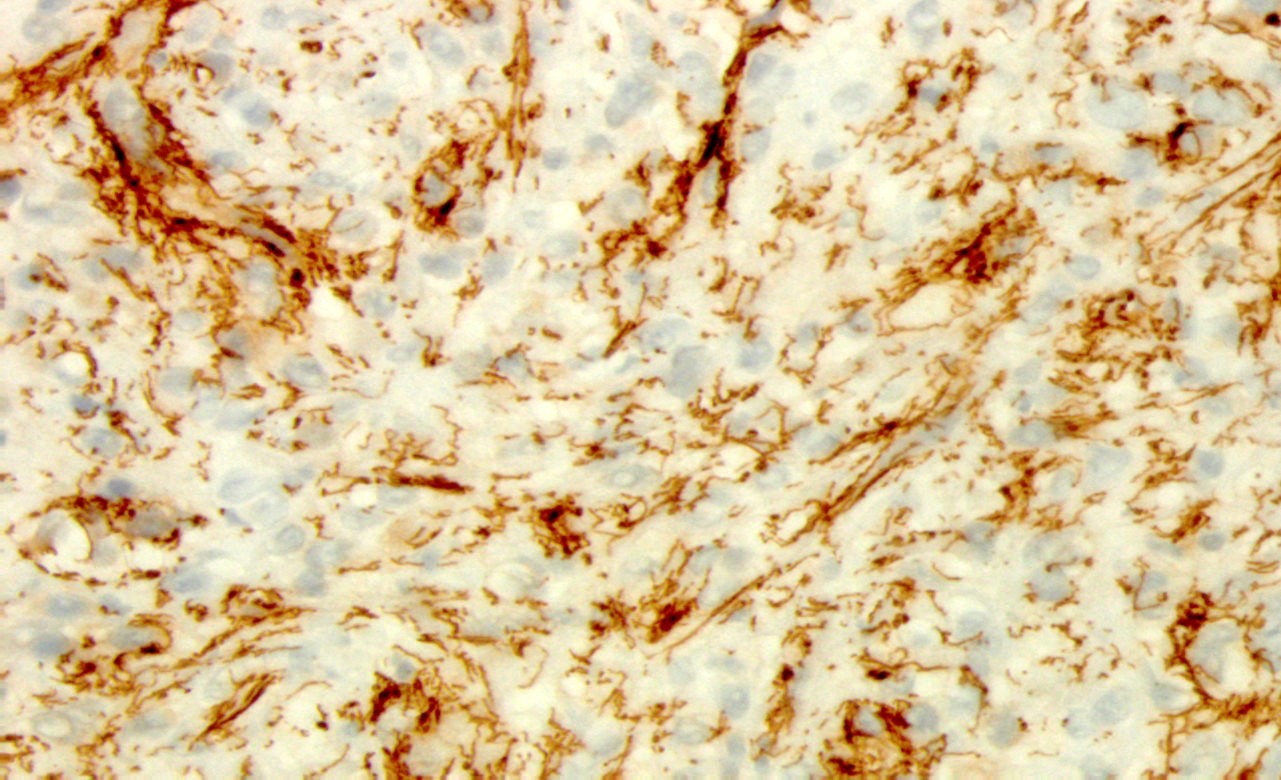
Dense fibroconnective tissue stroma
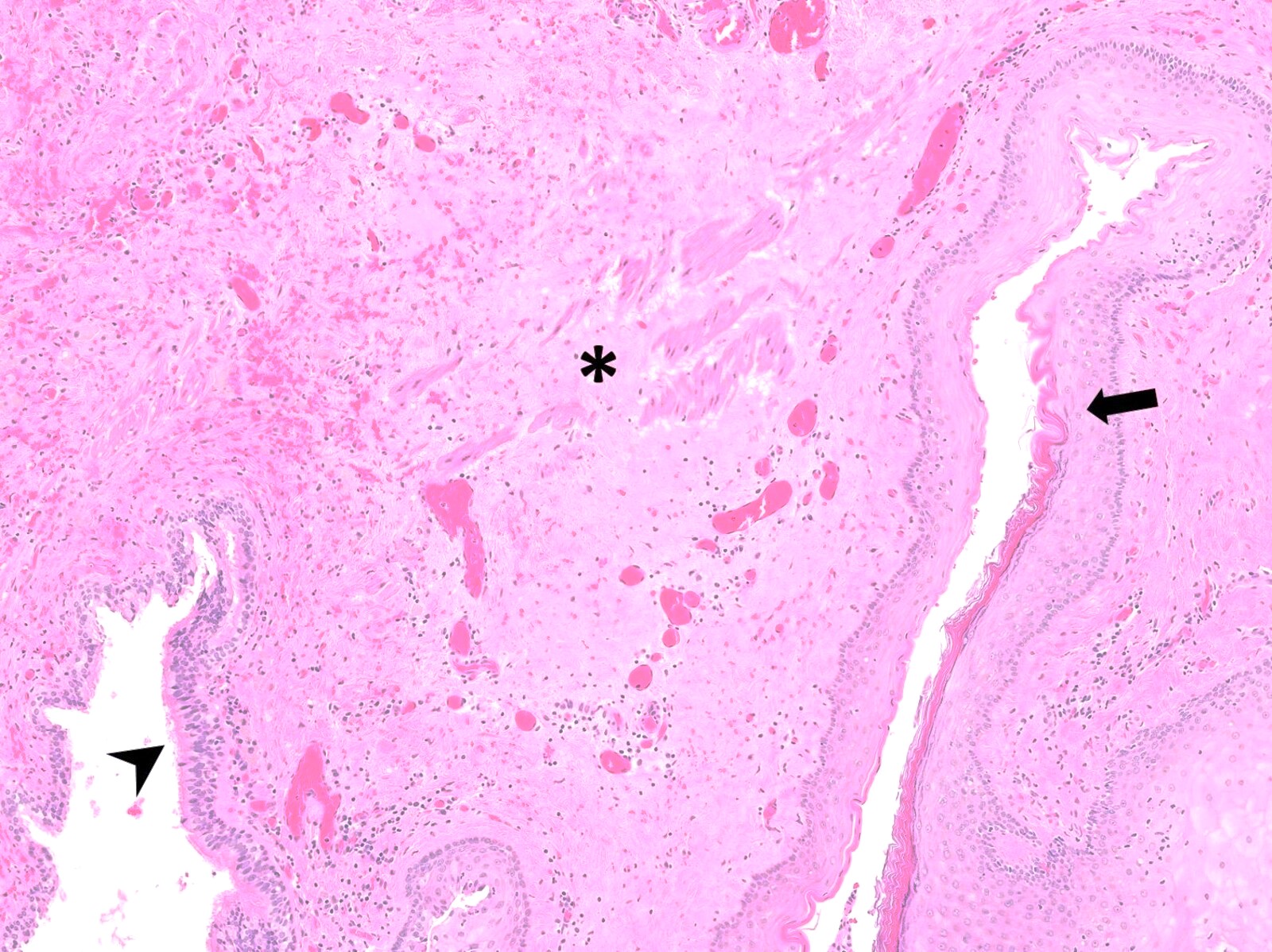
Disorganized smooth muscle
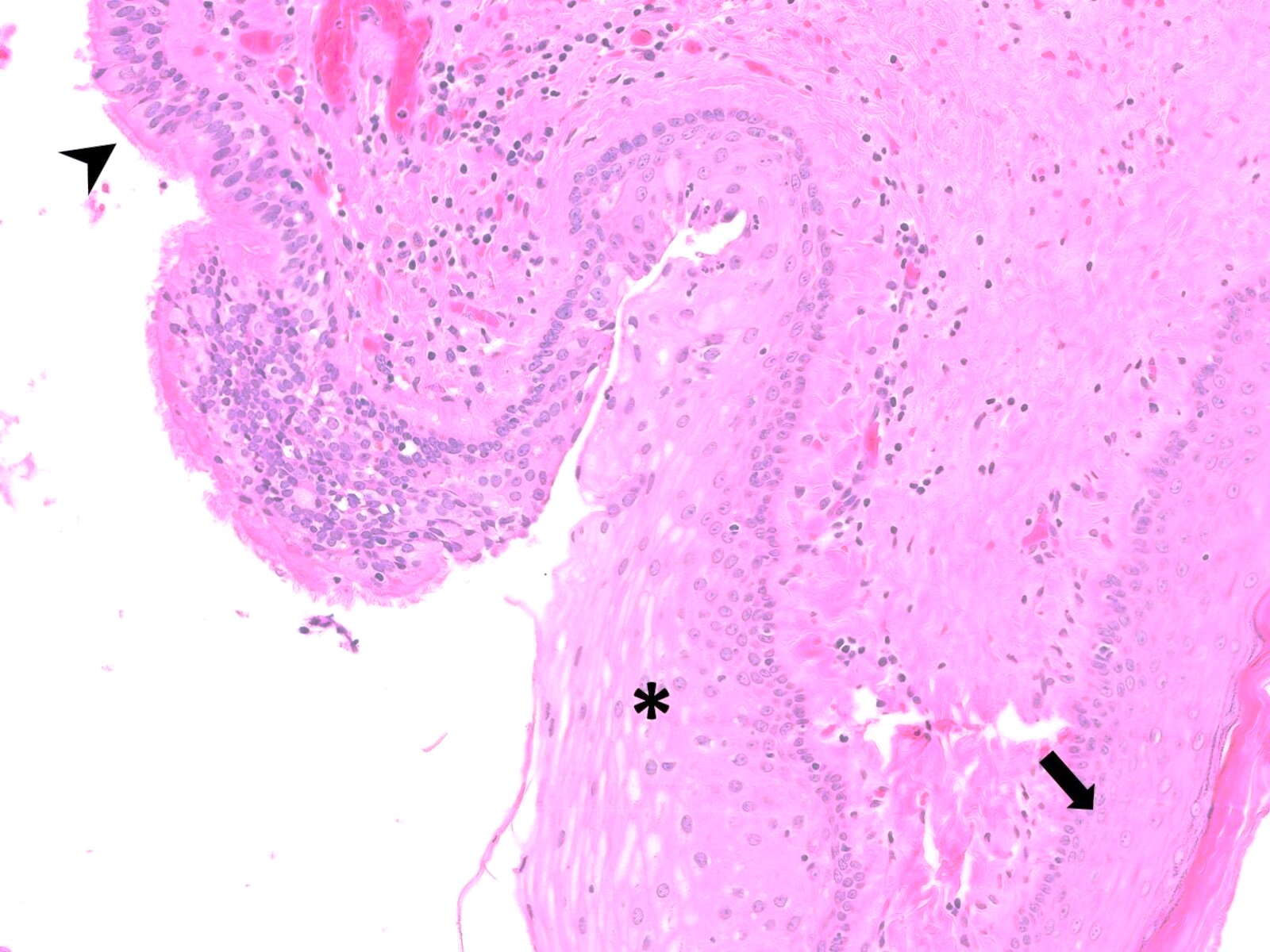
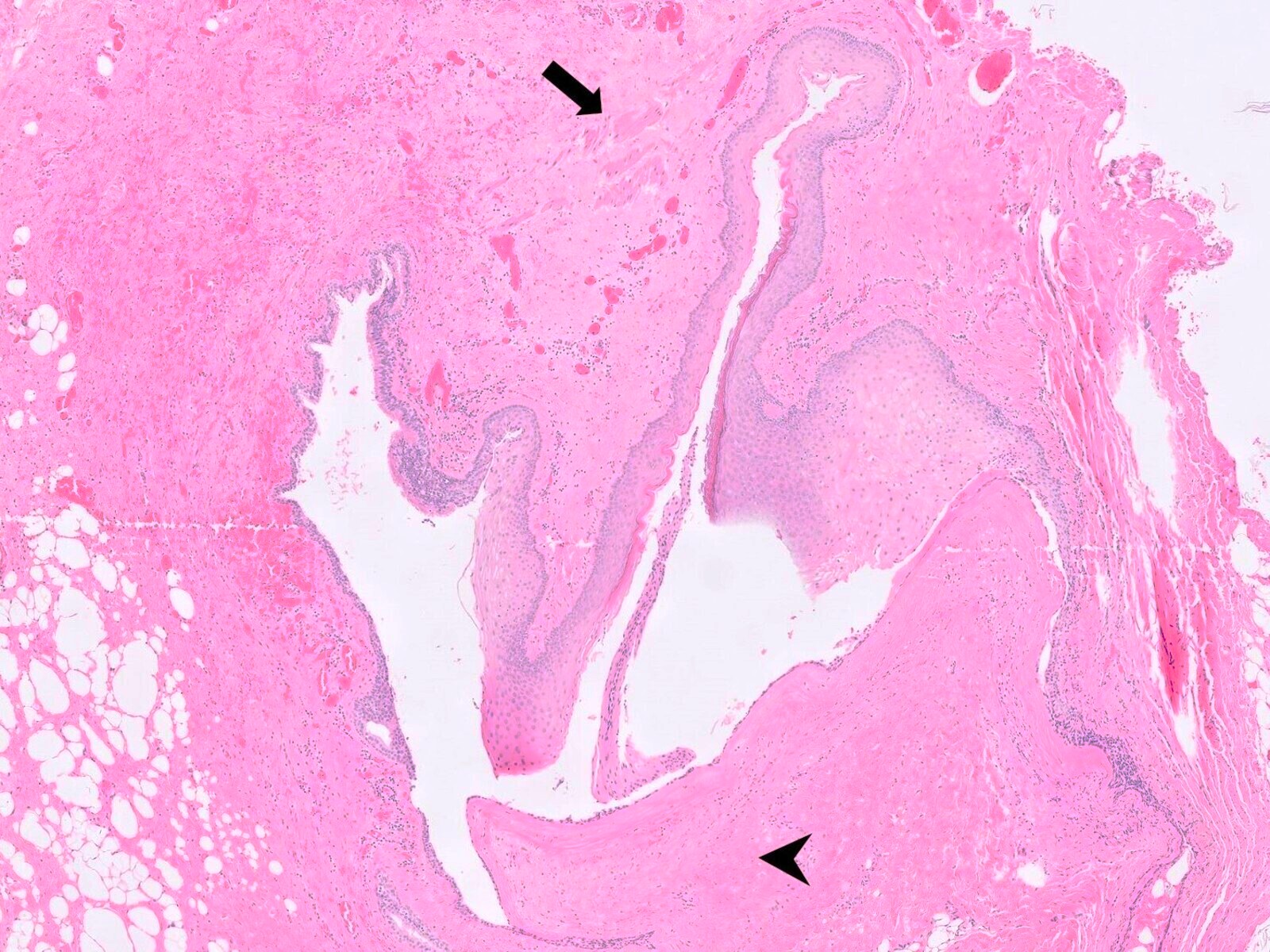
Epithelial linings
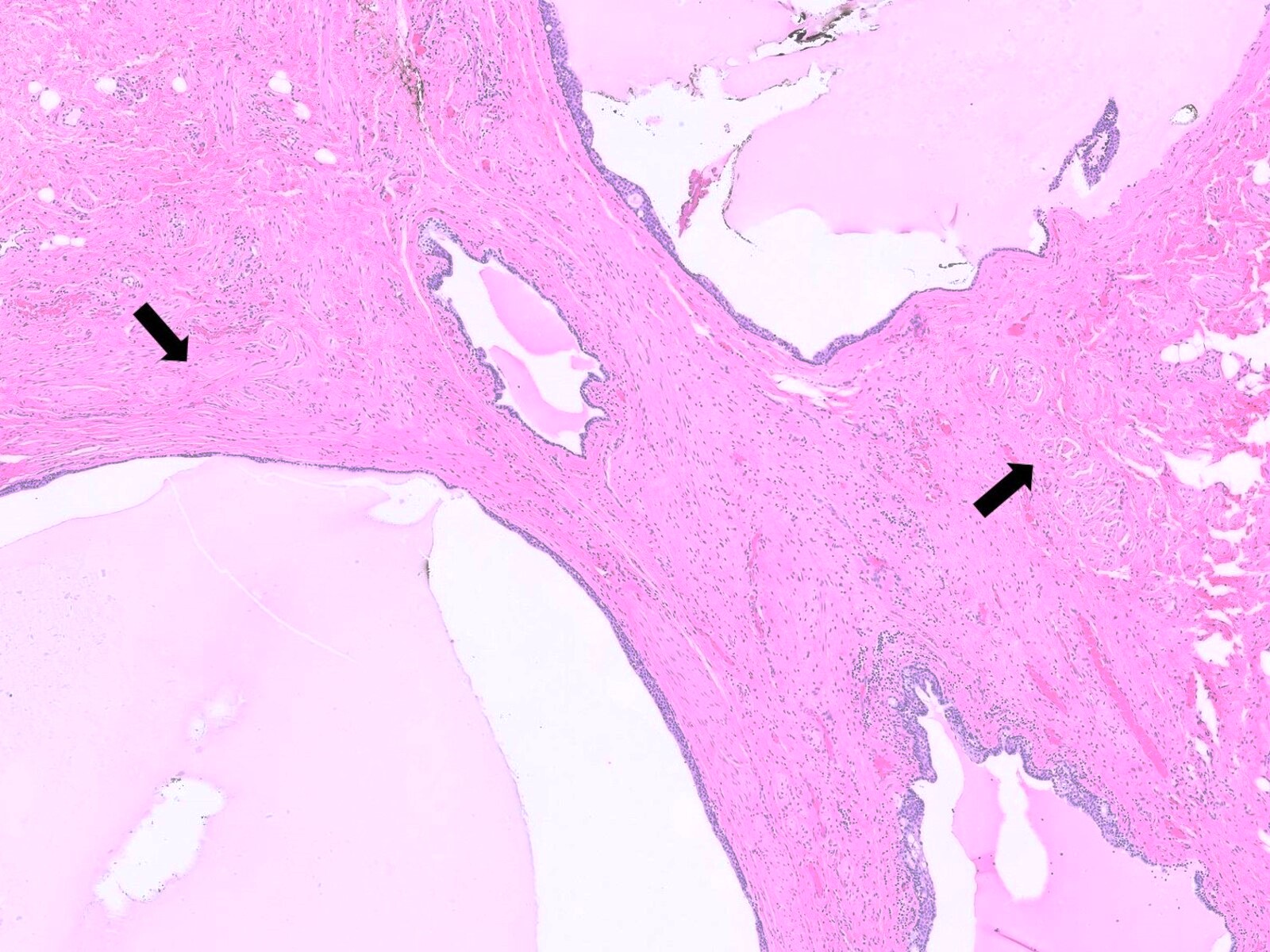
Multiple loculations
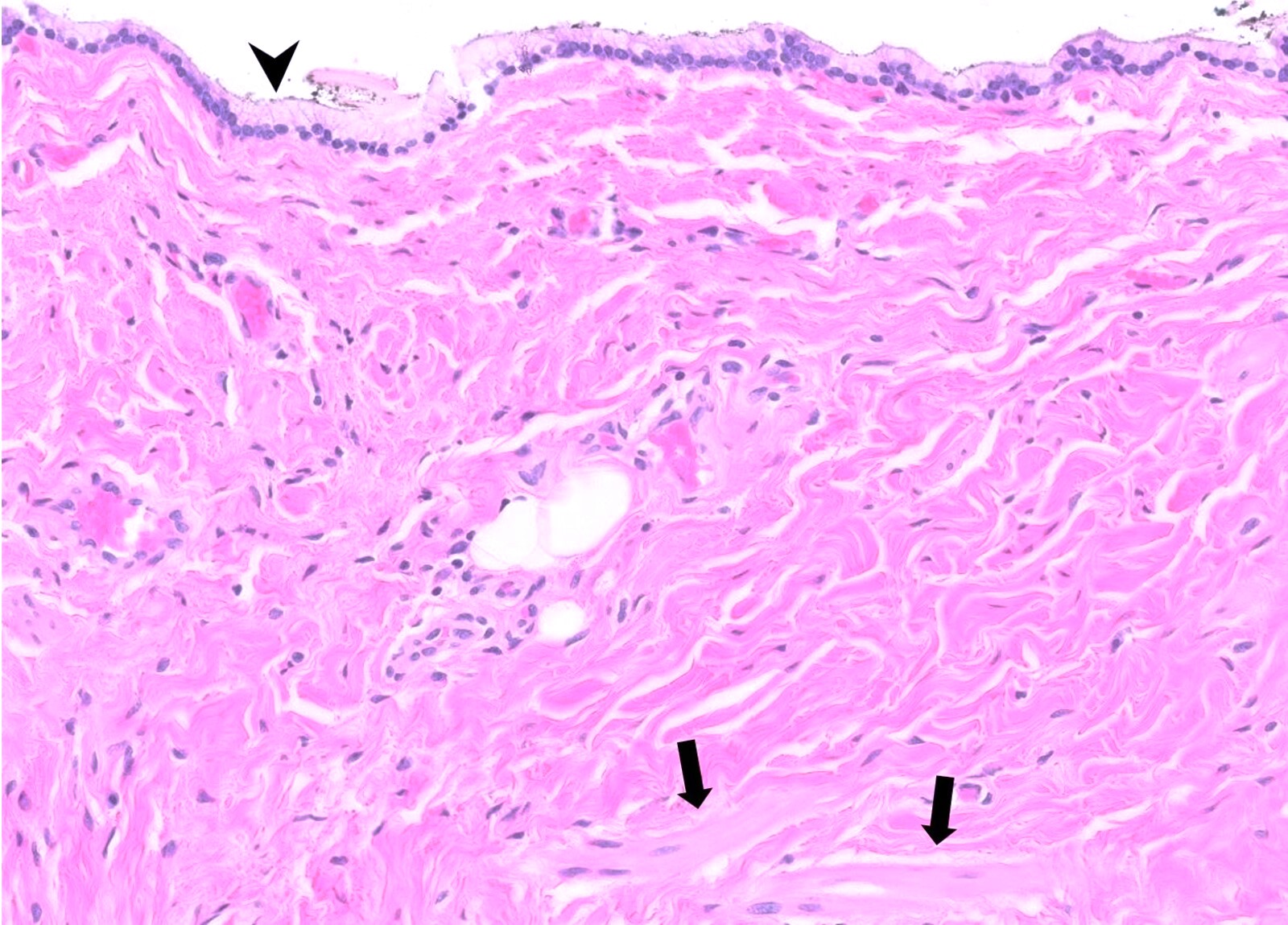
Mucinous columnar epithelium
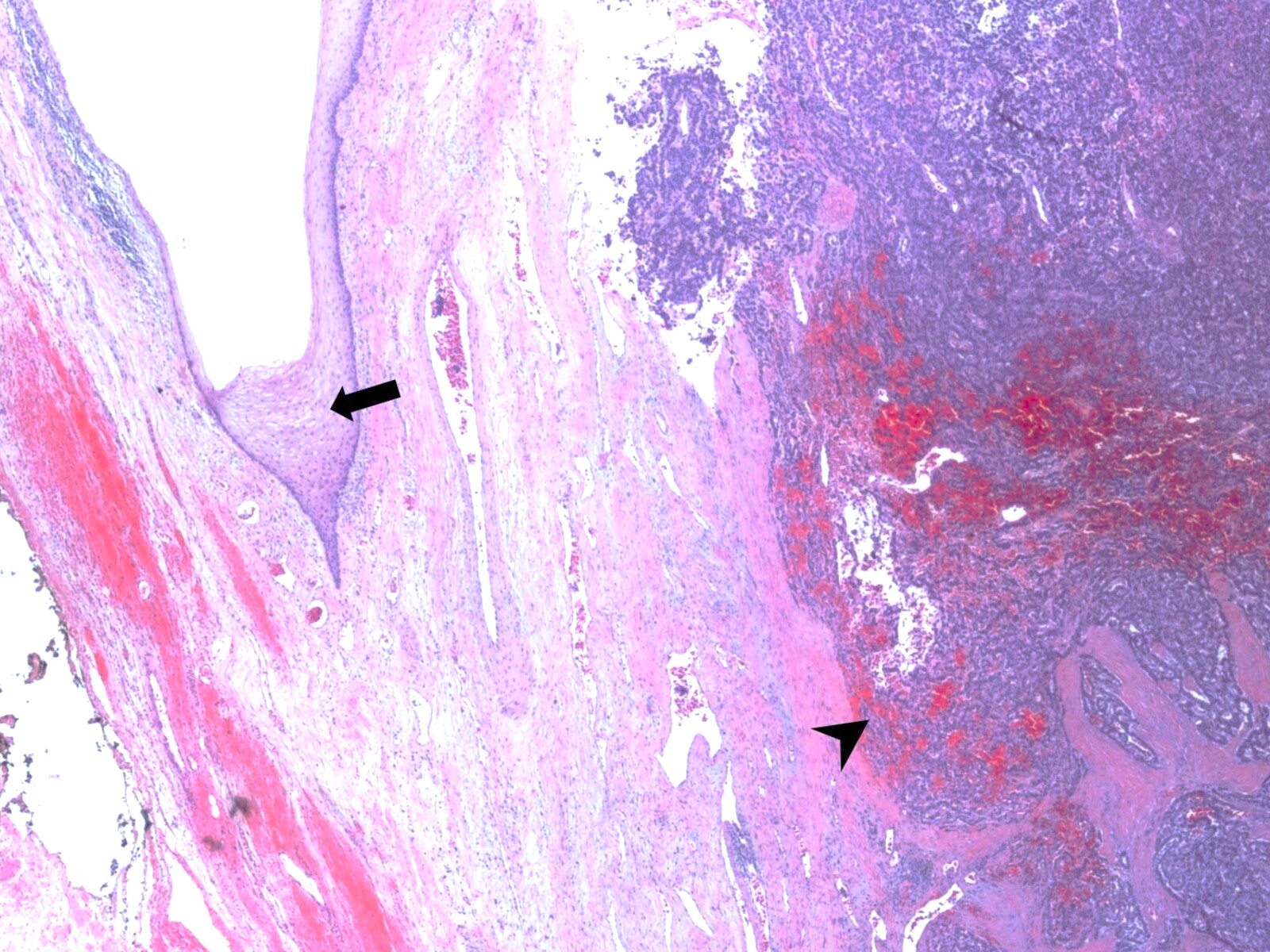
Neoplastic transformation, neuroendocrine tumor
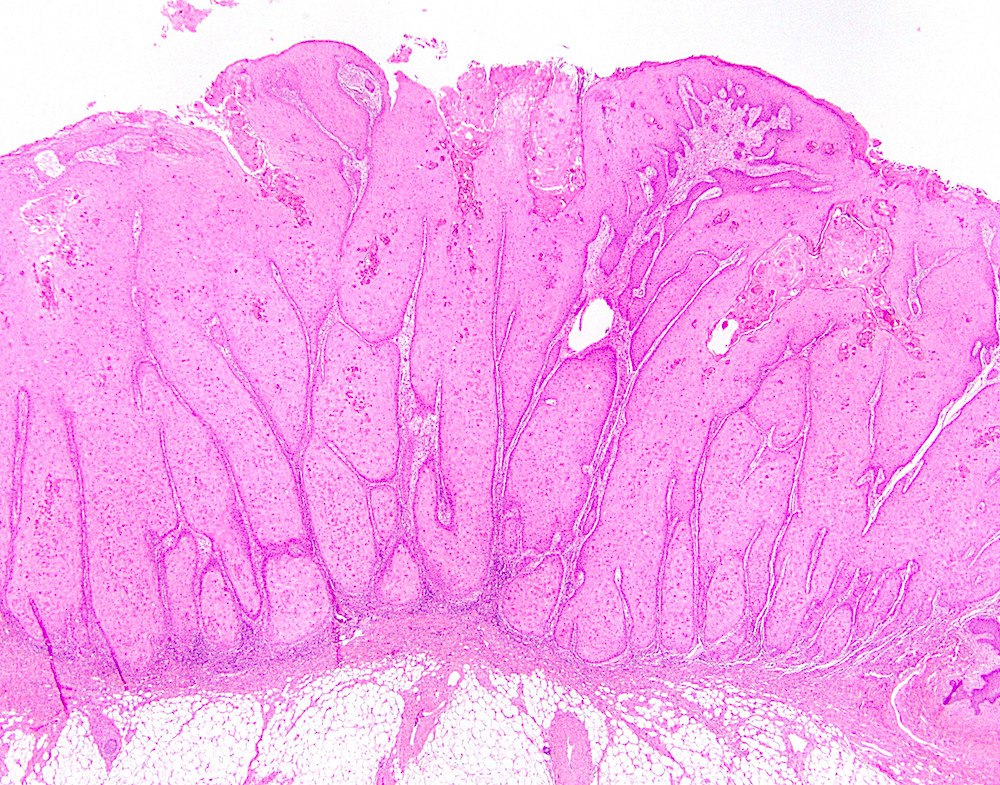
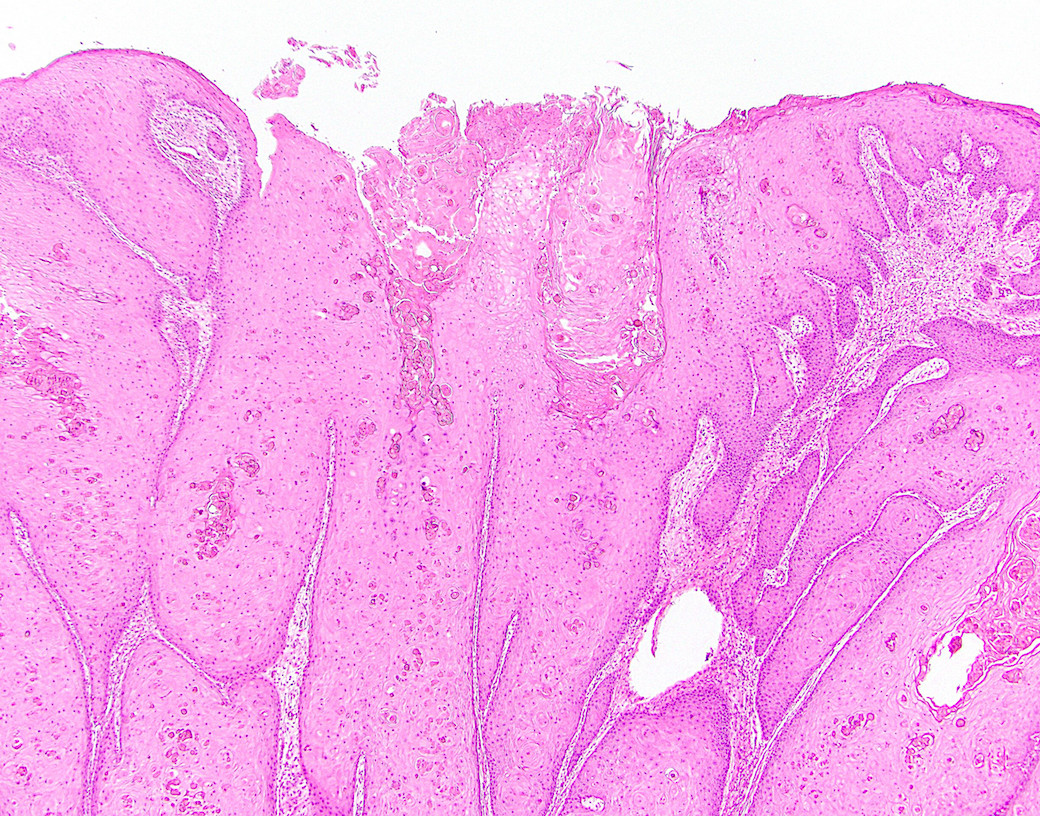
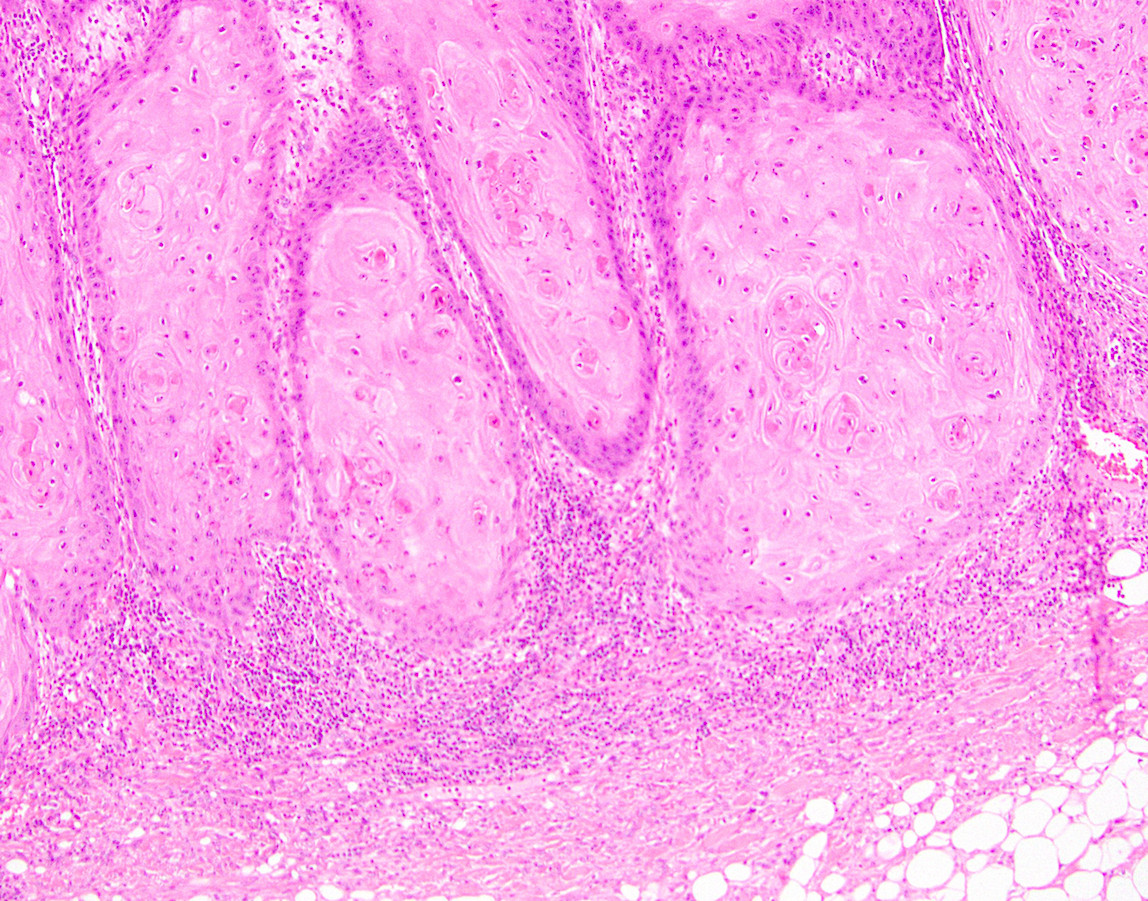
Verrucous carcinoma
Cohen: 2014
Greenson: 2019

IARC: 2019
Lamps: 2015
Montgomery: 2024
Odze: 2022
Srivastava: 2023

Voltaggio: 2024
Yantiss: 2021
Zutshi: 2016

