



Images hosted on other servers:

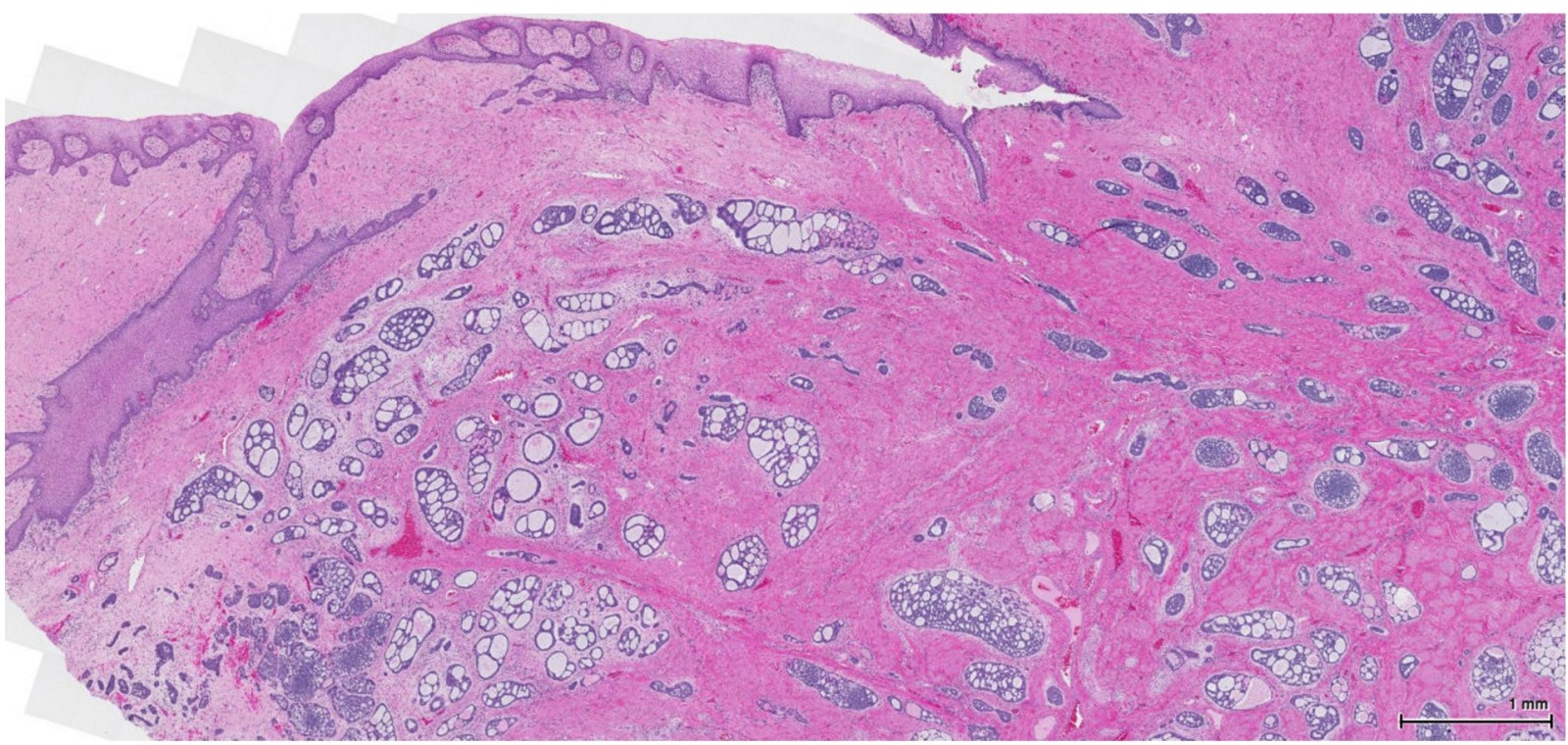
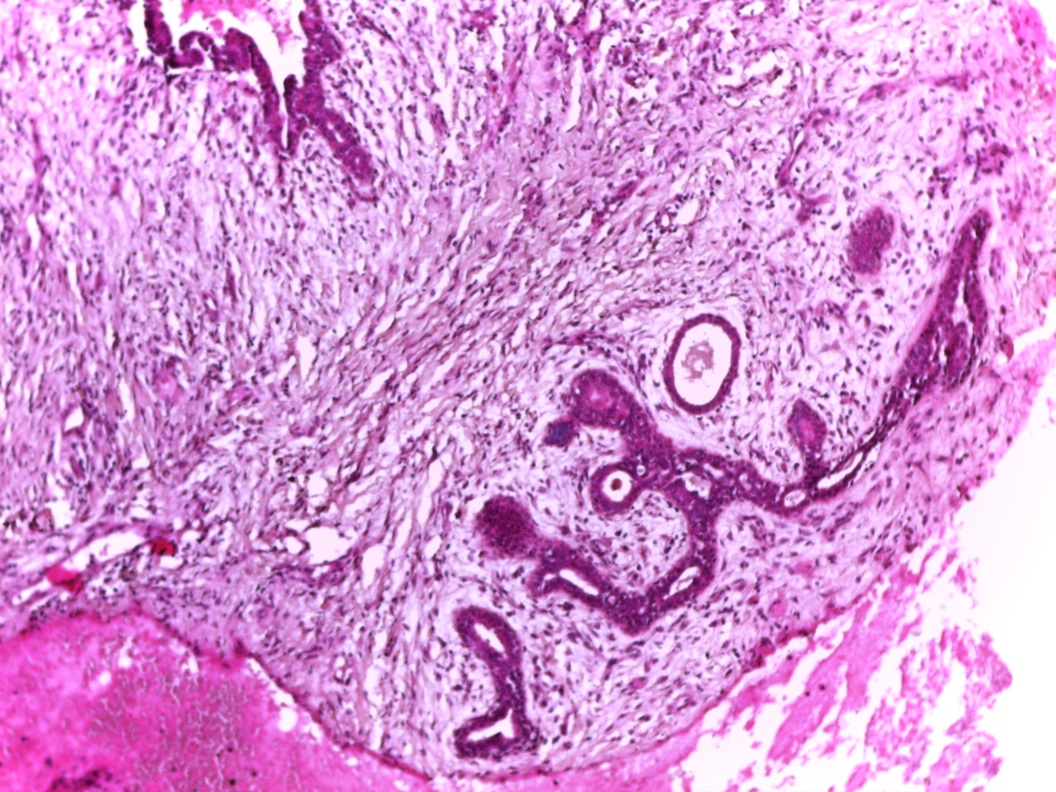
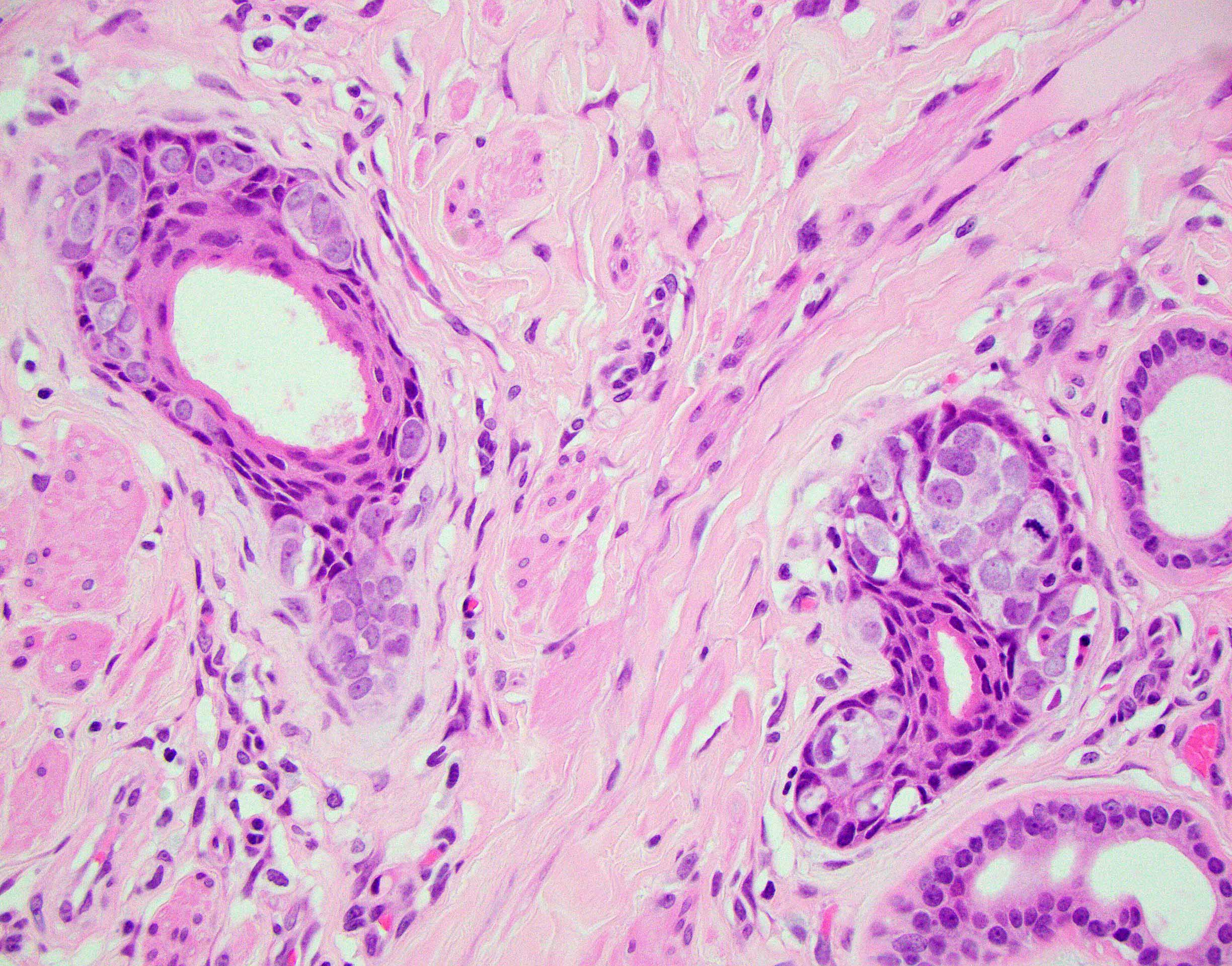
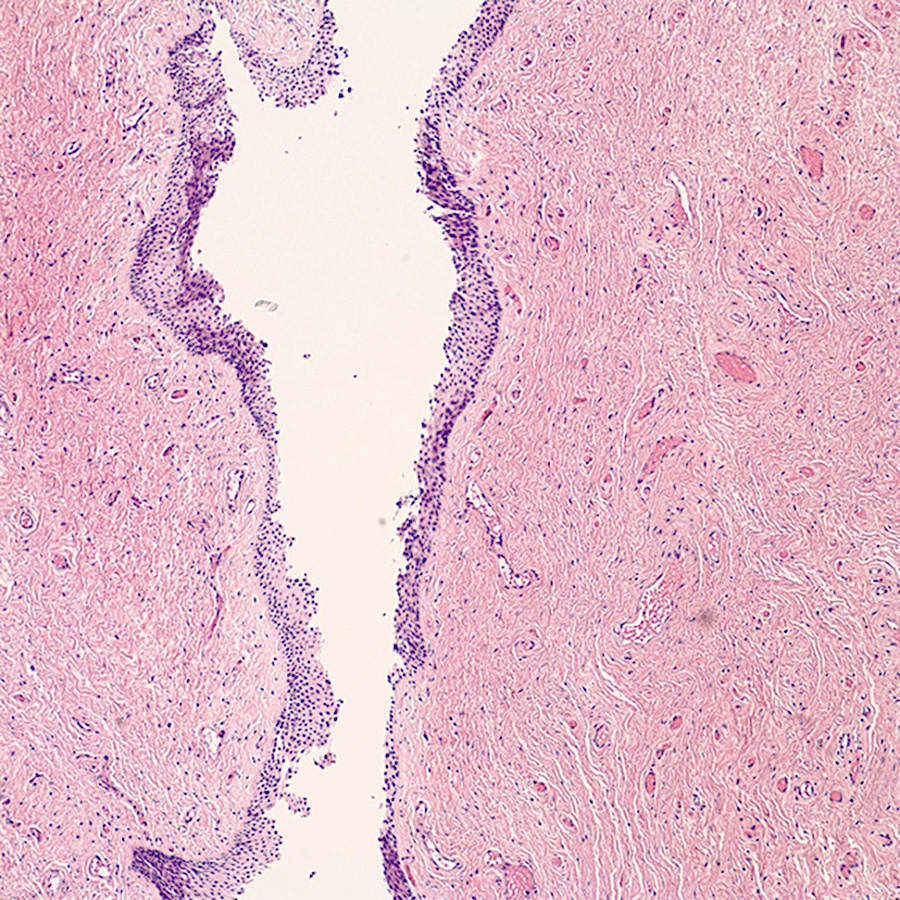
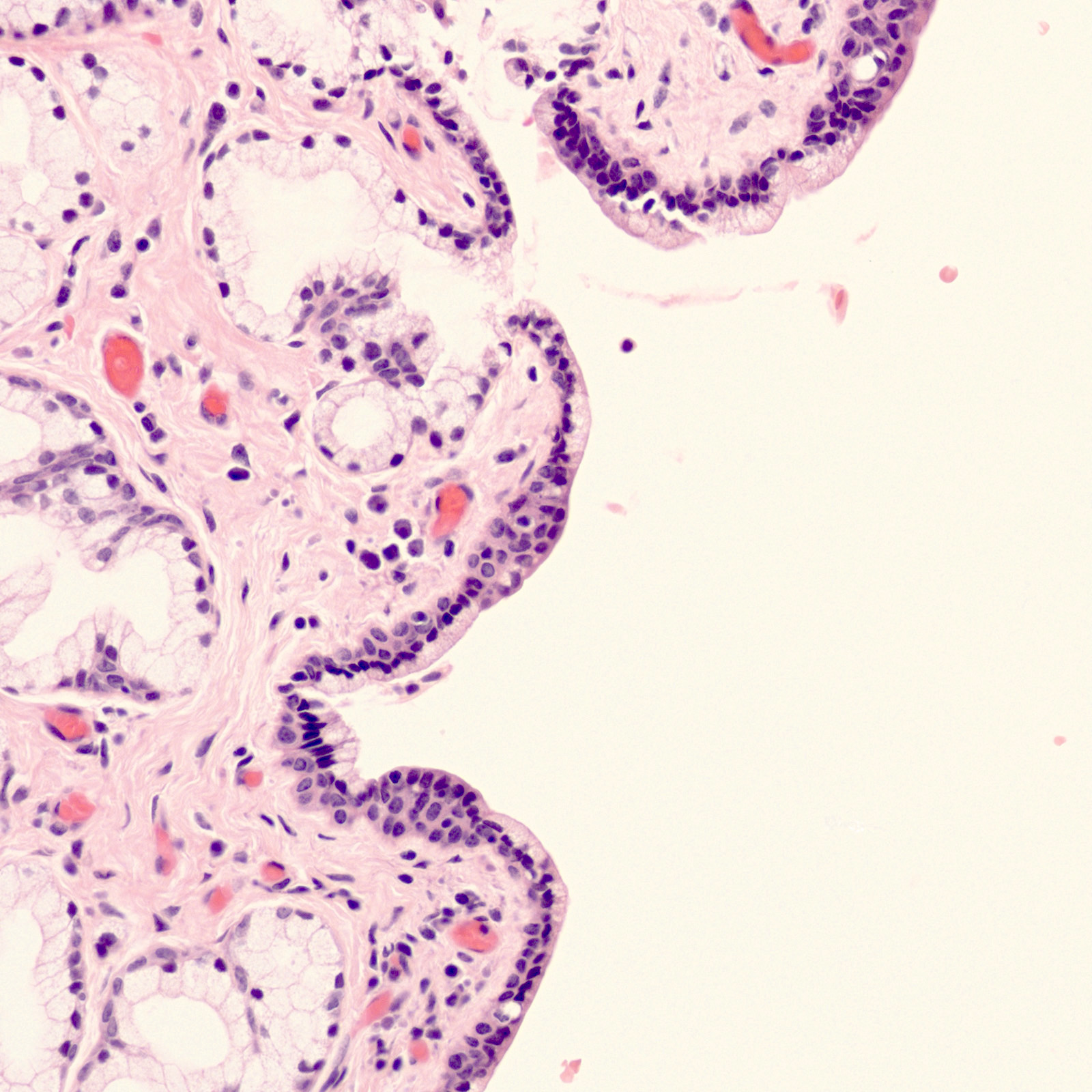
Vaginal adenosis, posterior wall

Vaginal red granular patch
Contributed by Leonel Maldonado, M.D.
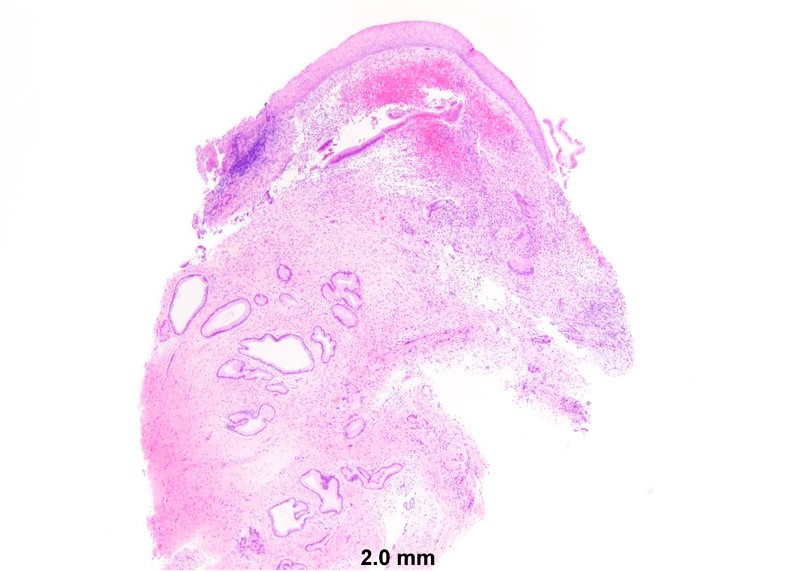
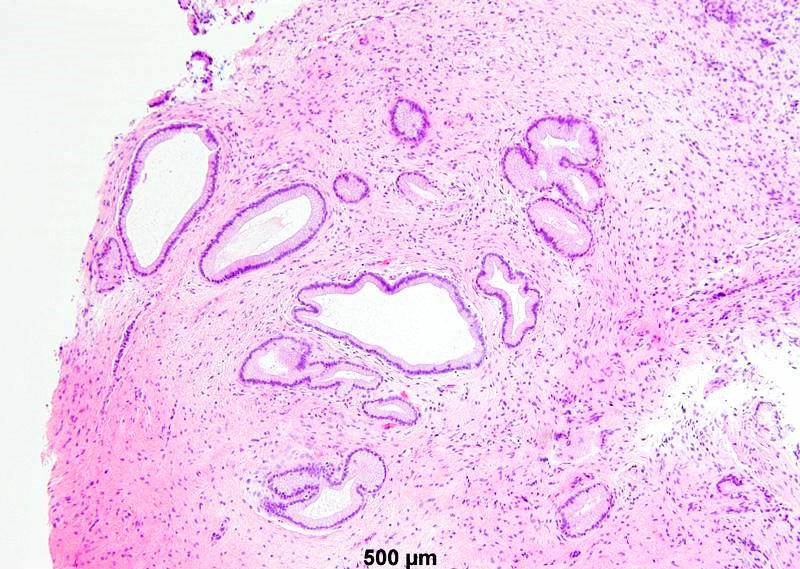
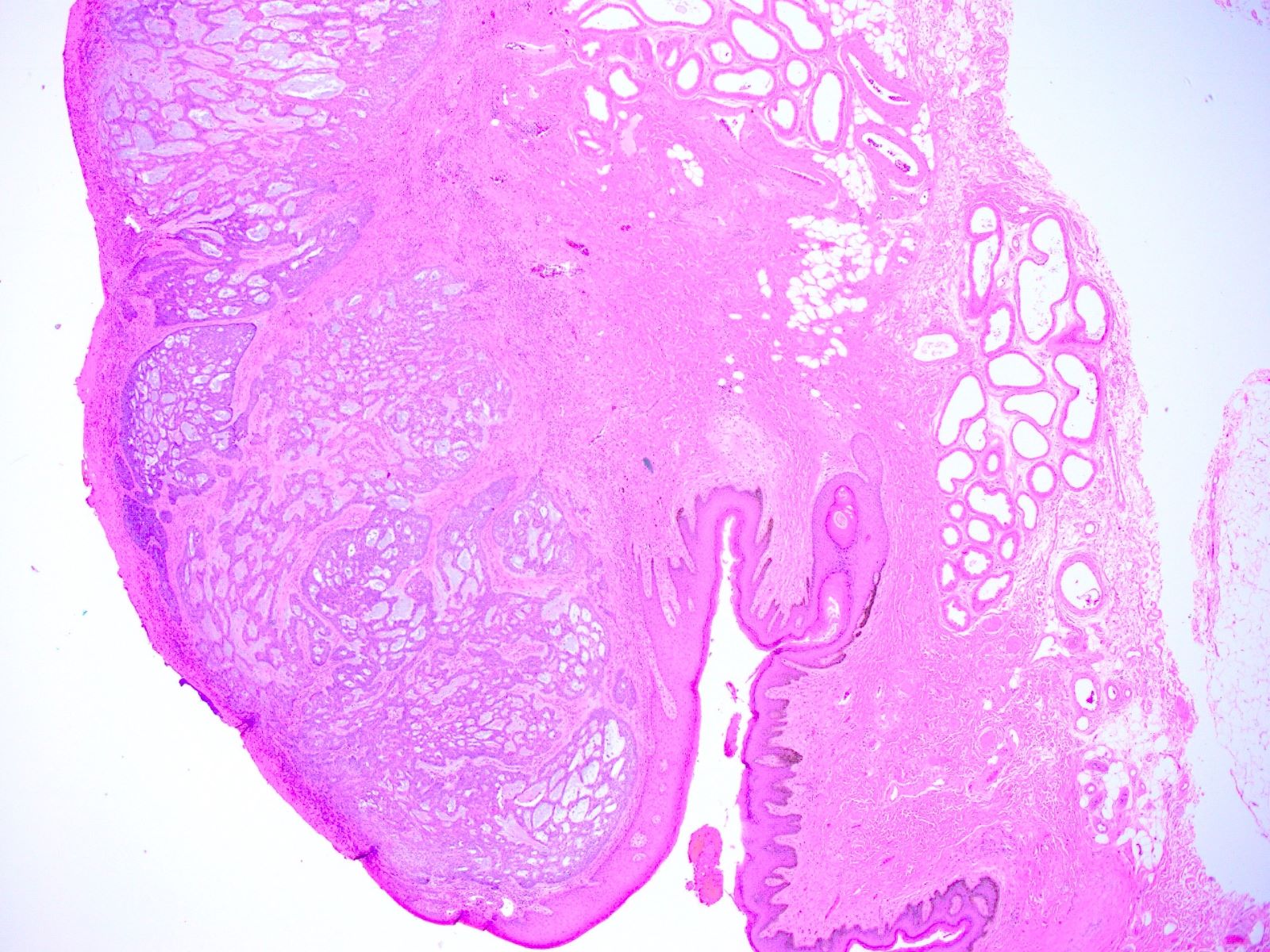
Vaginal wall lesion biopsy

Vaginal wall lesion biopsy
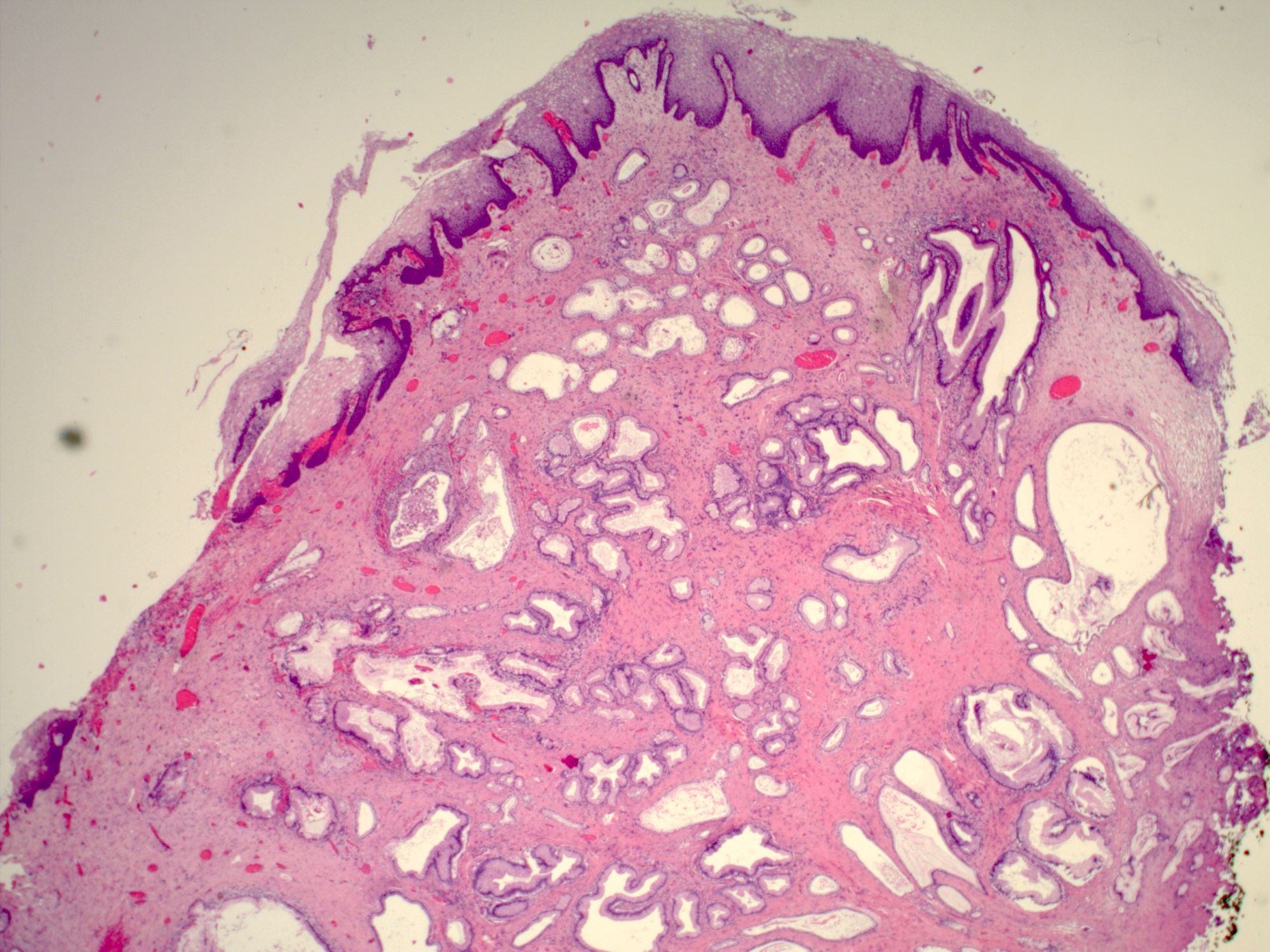
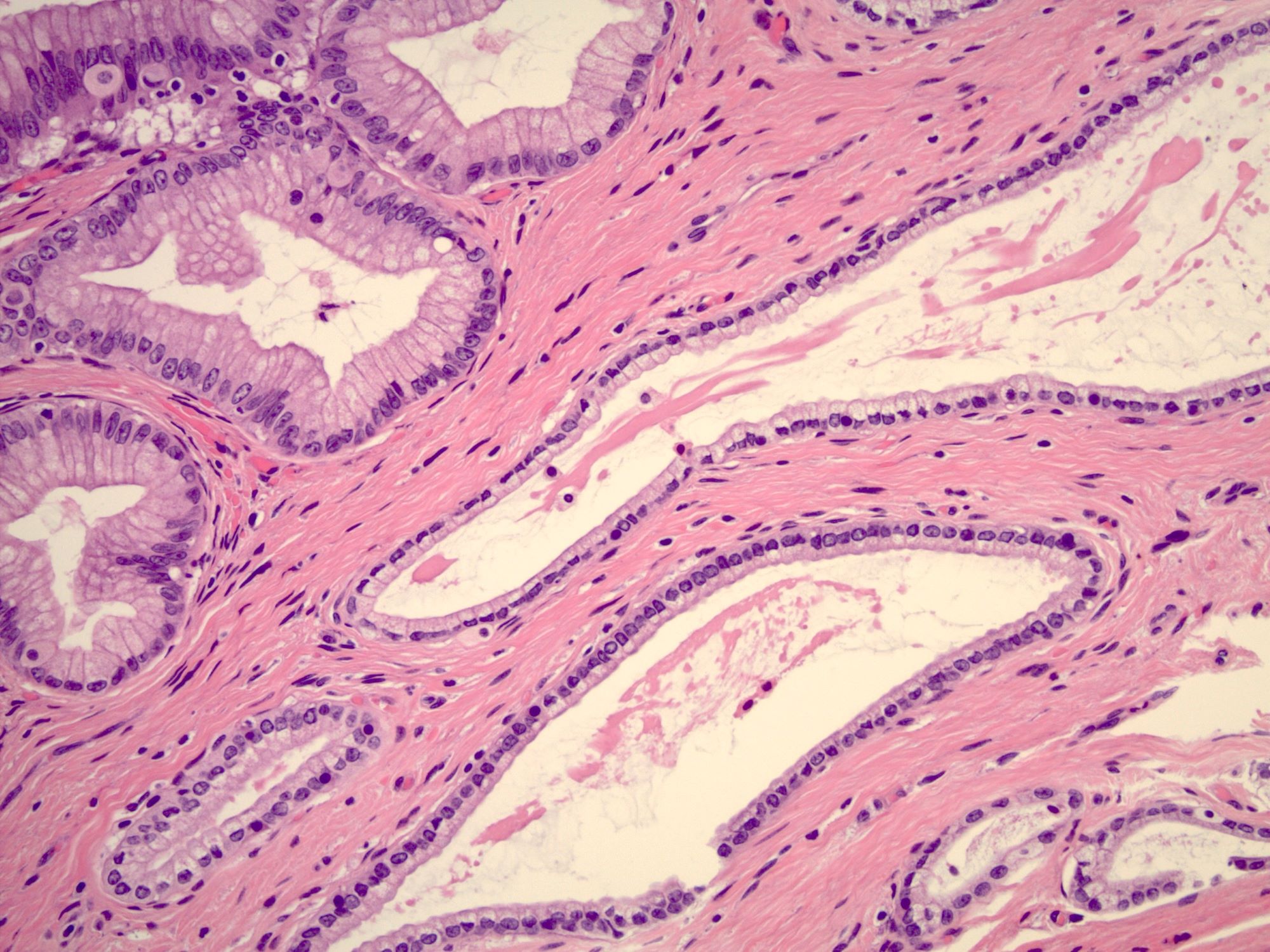
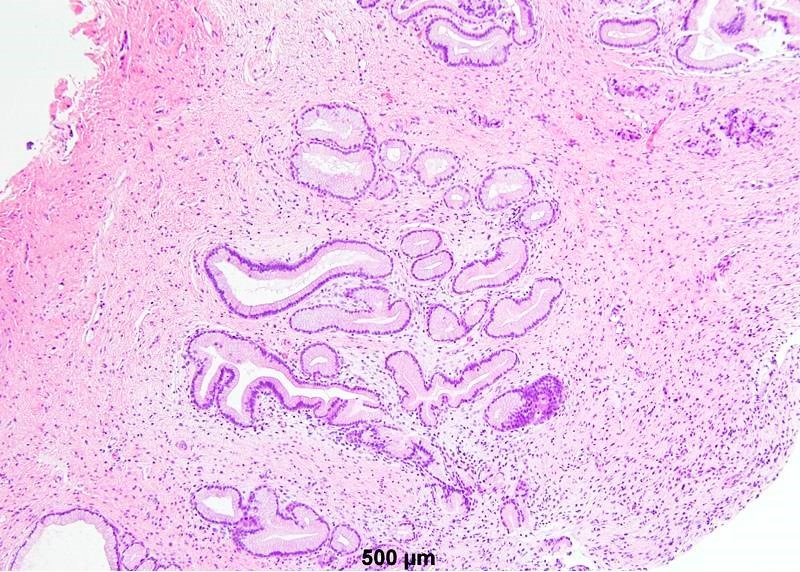
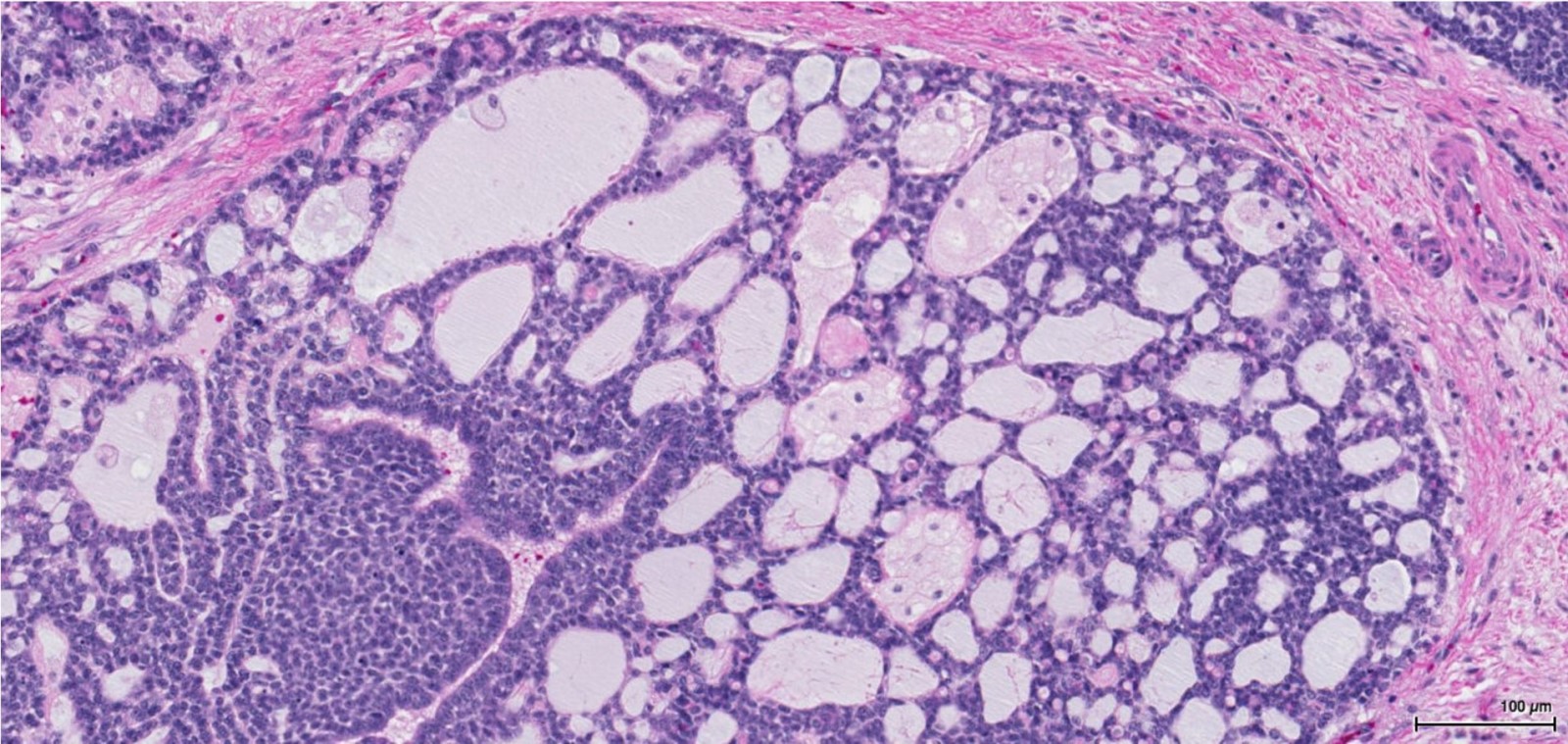
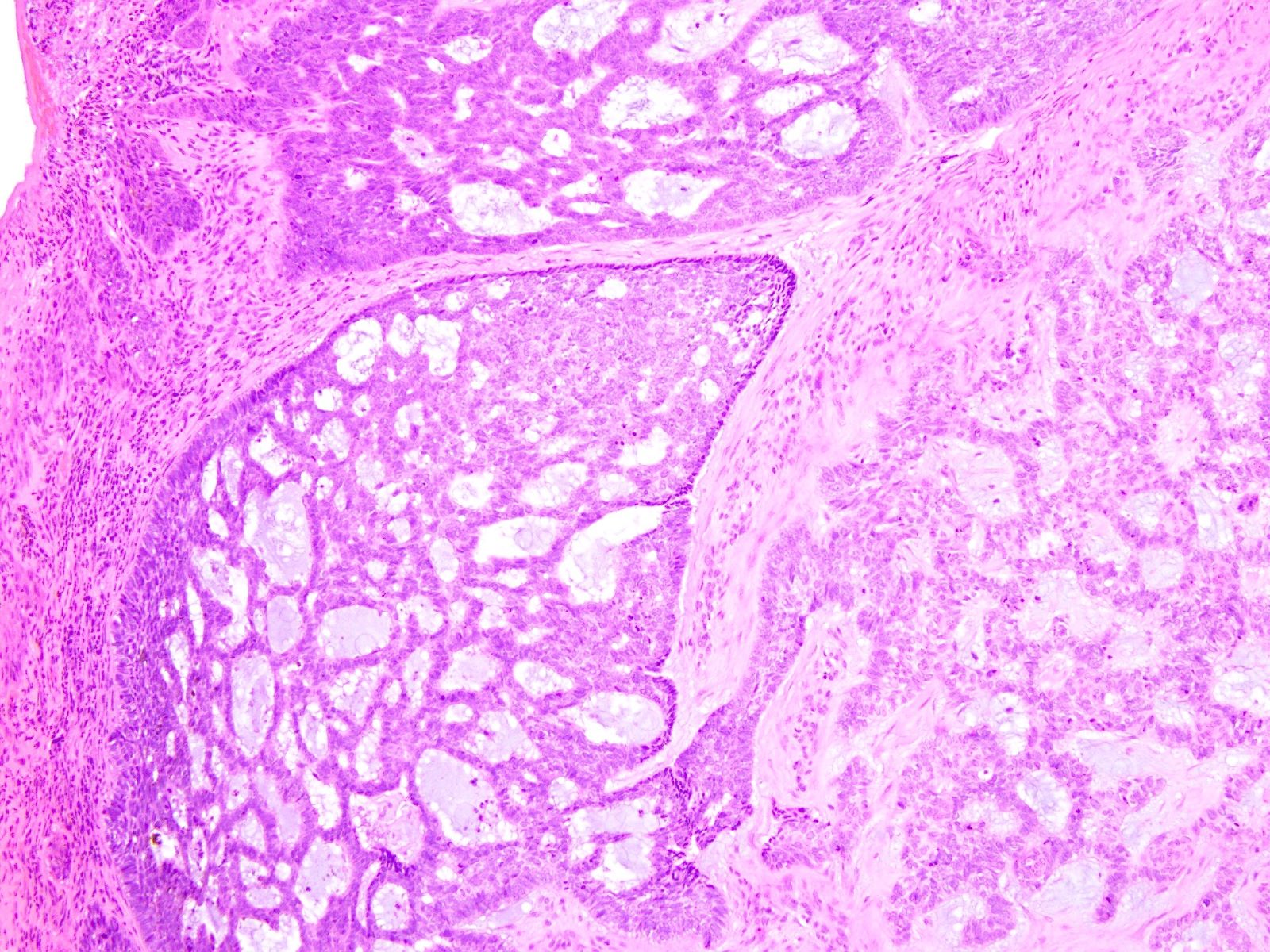
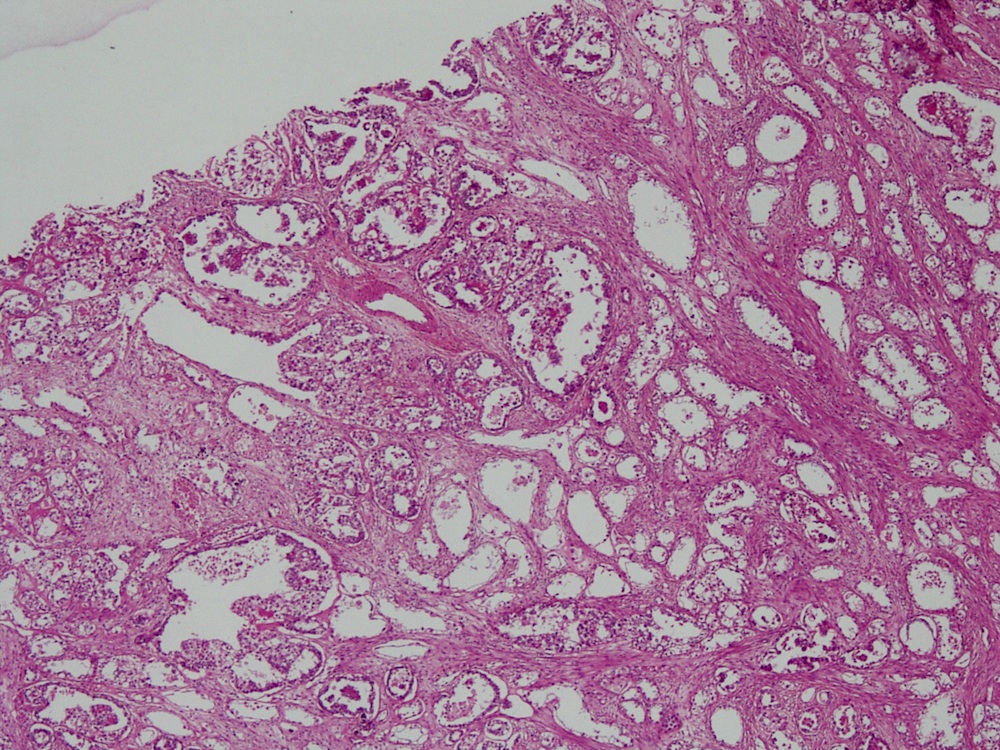
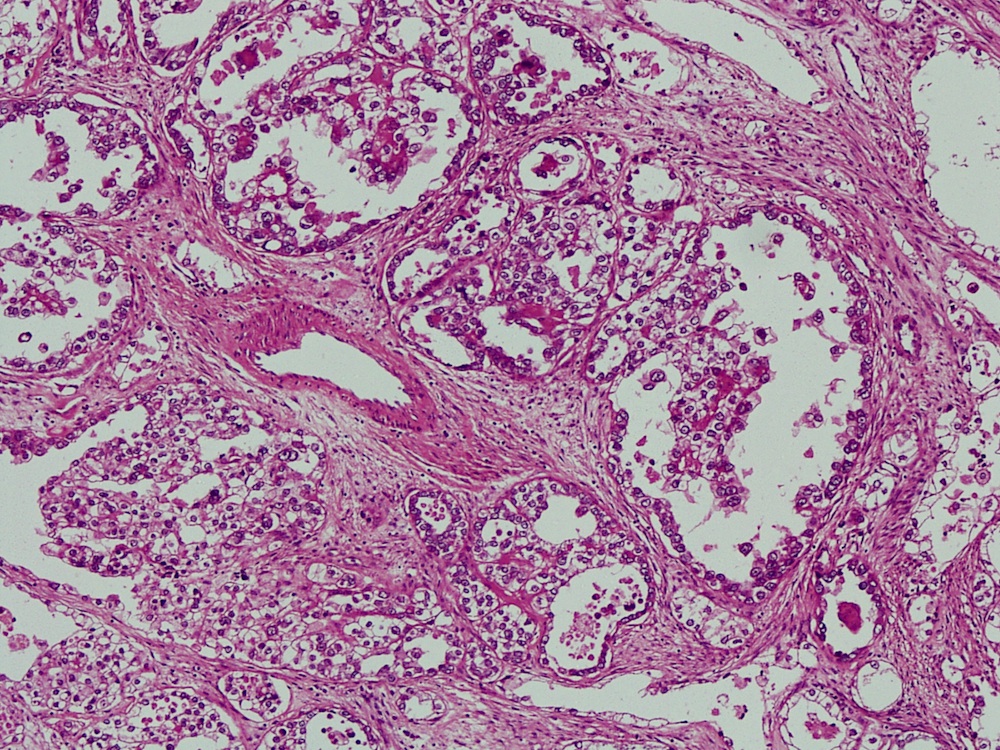
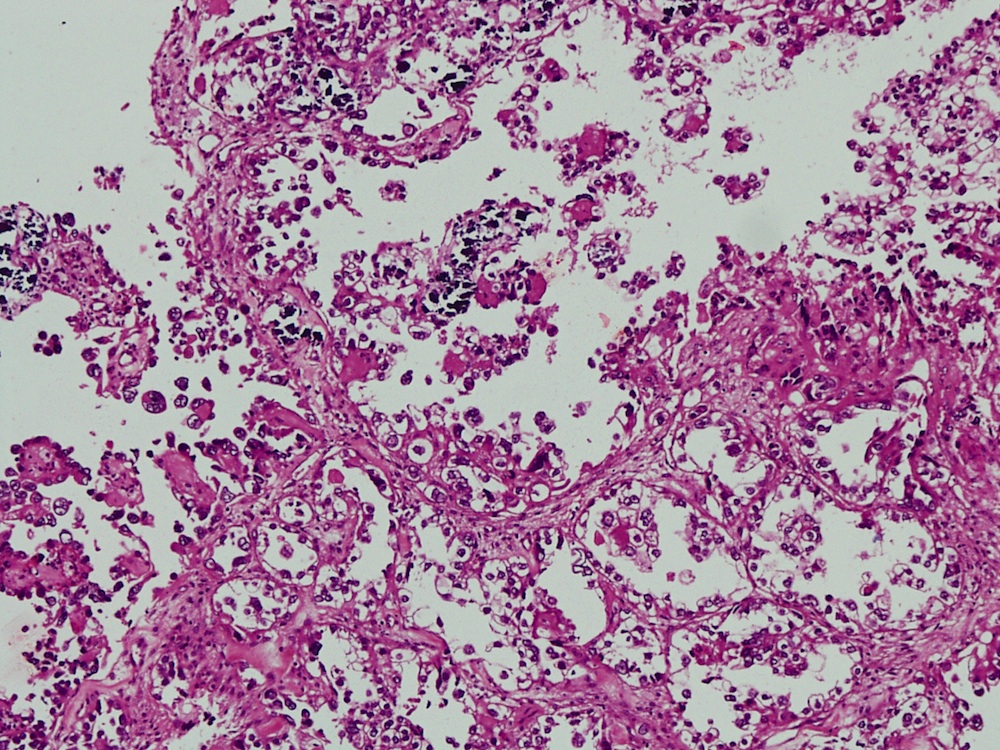
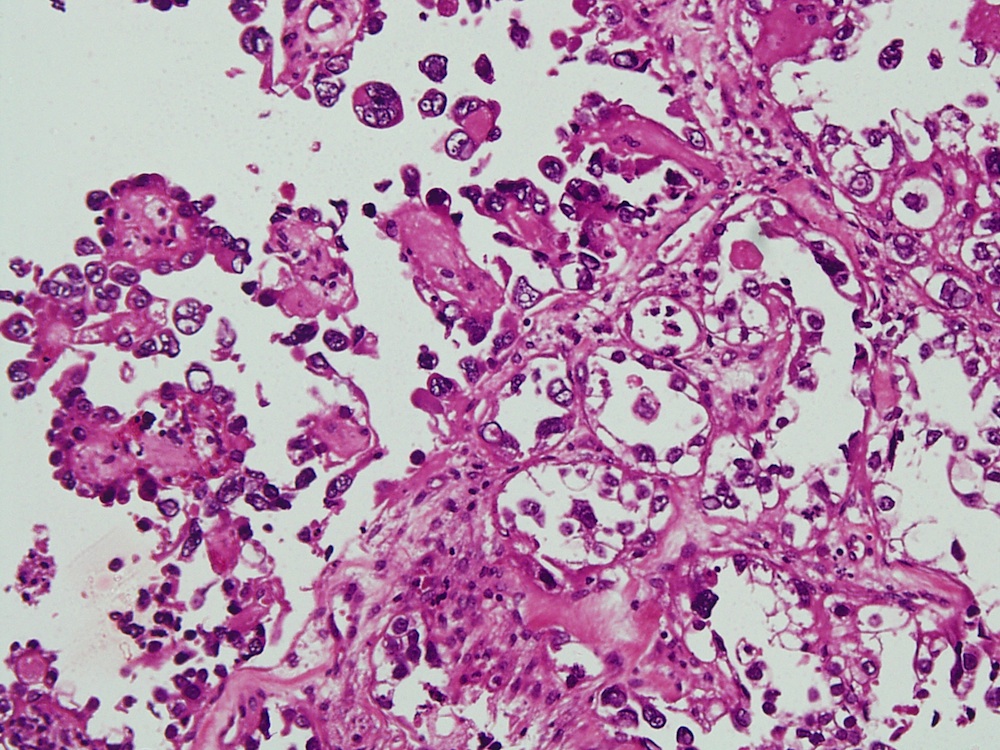
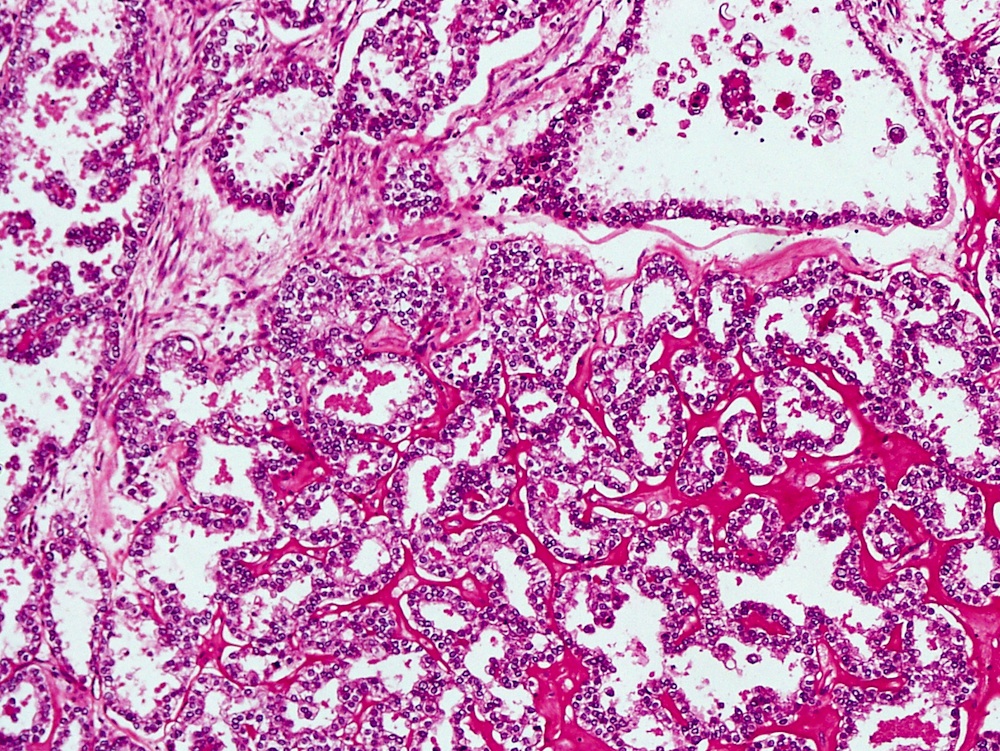
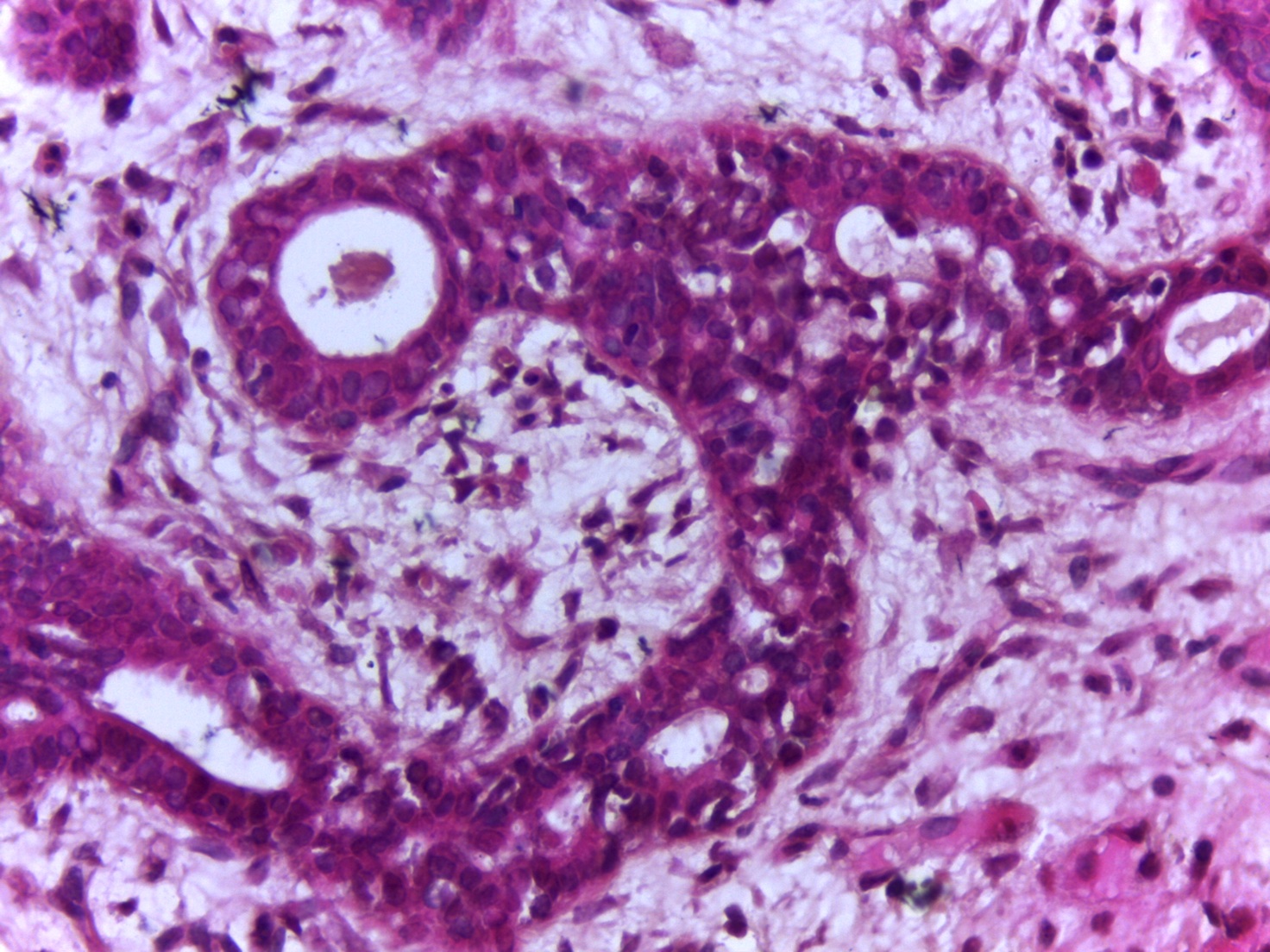
Glands in vaginal mucosa
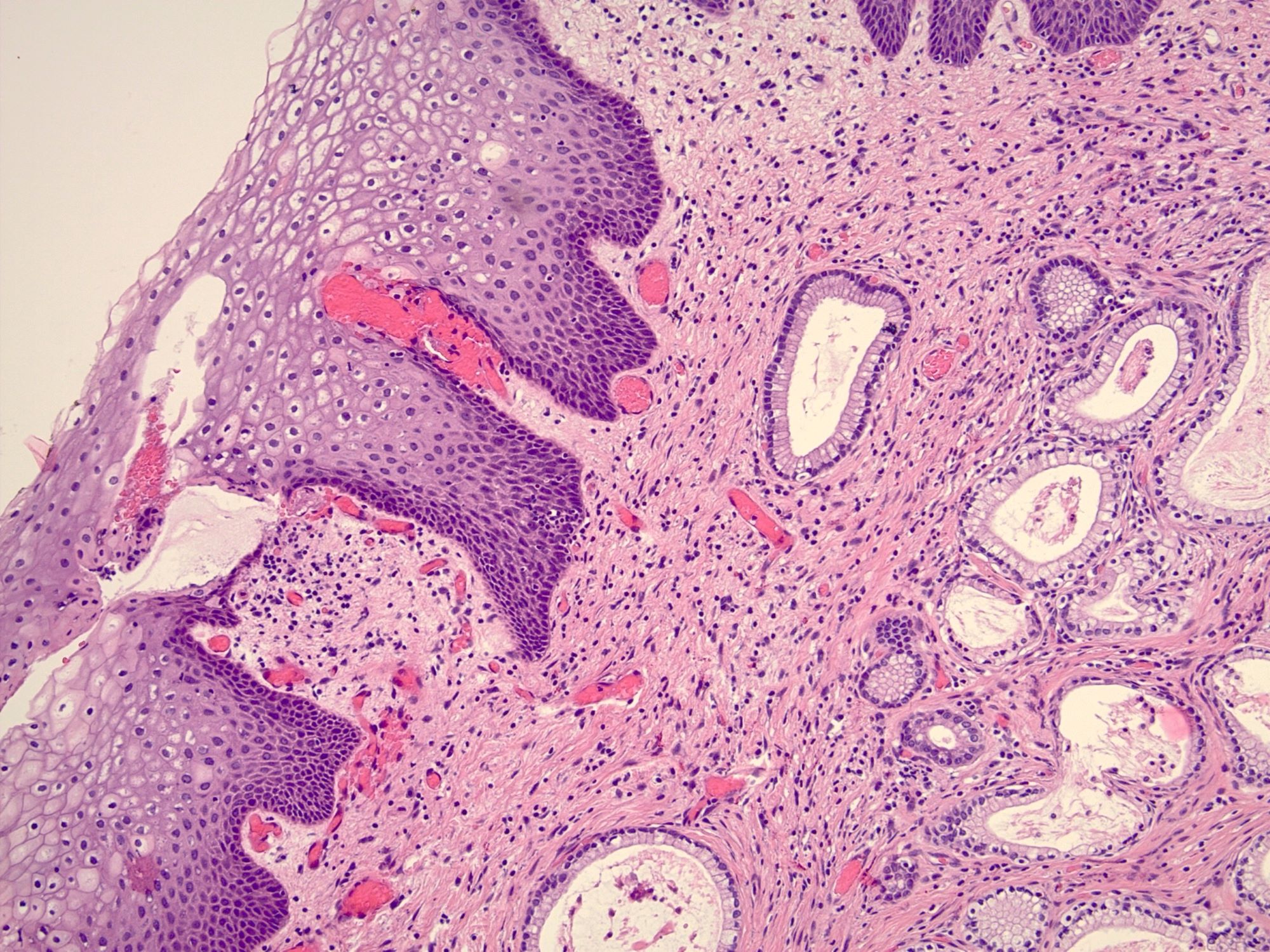
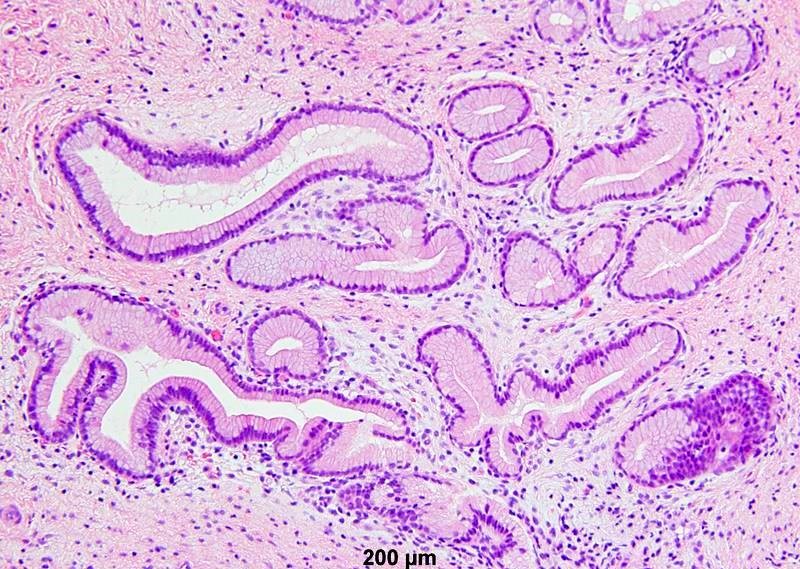
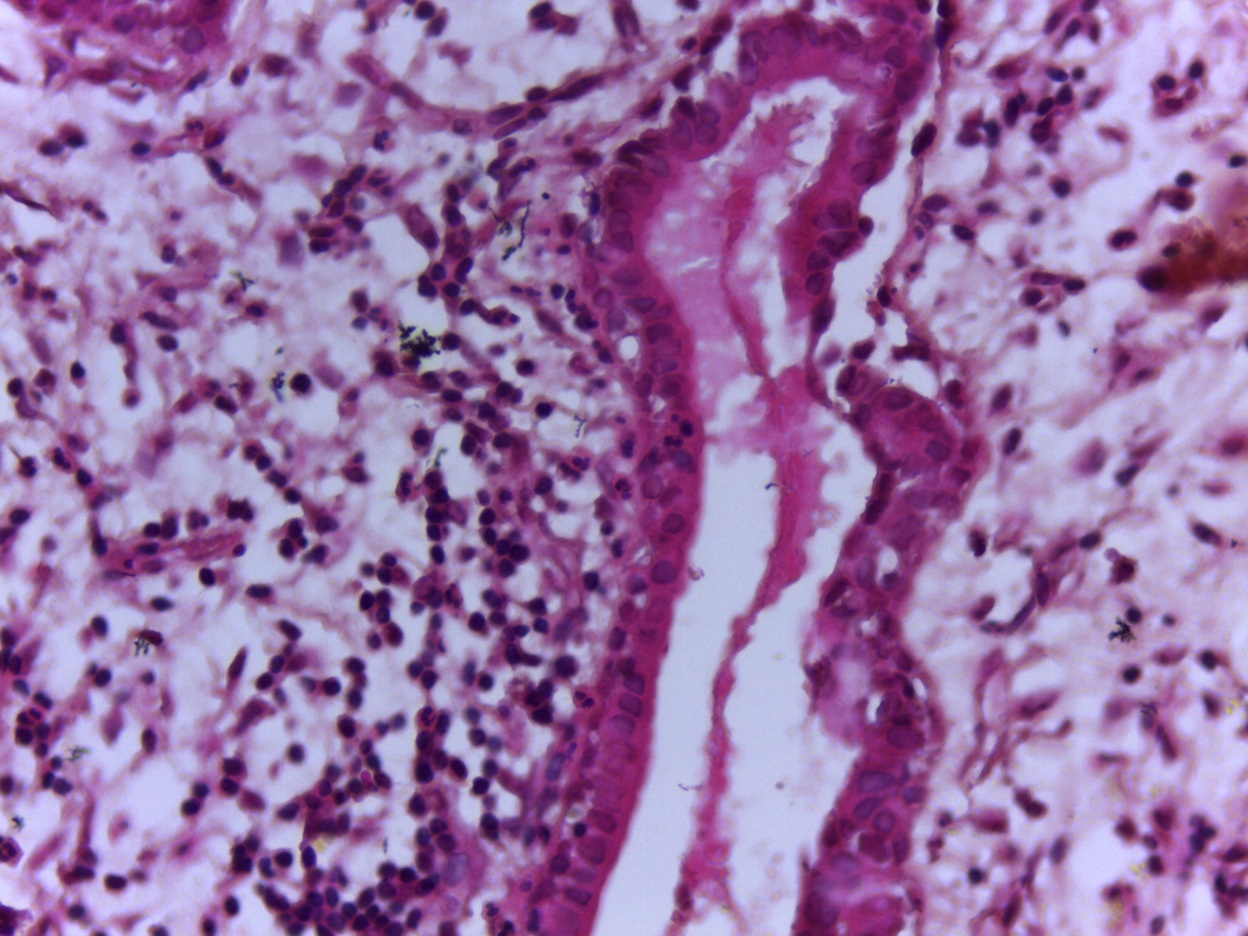
Mucinous glands below epithelium
Contributed by Leonel Maldonado, M.D.
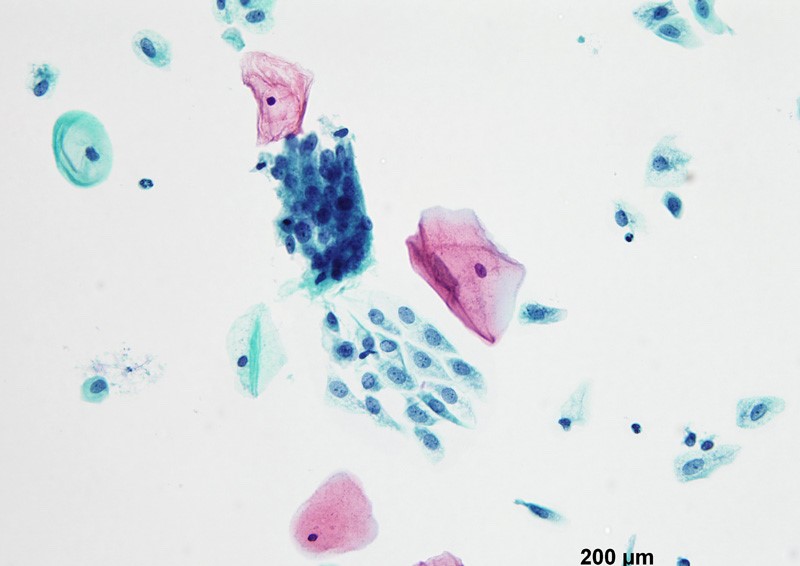
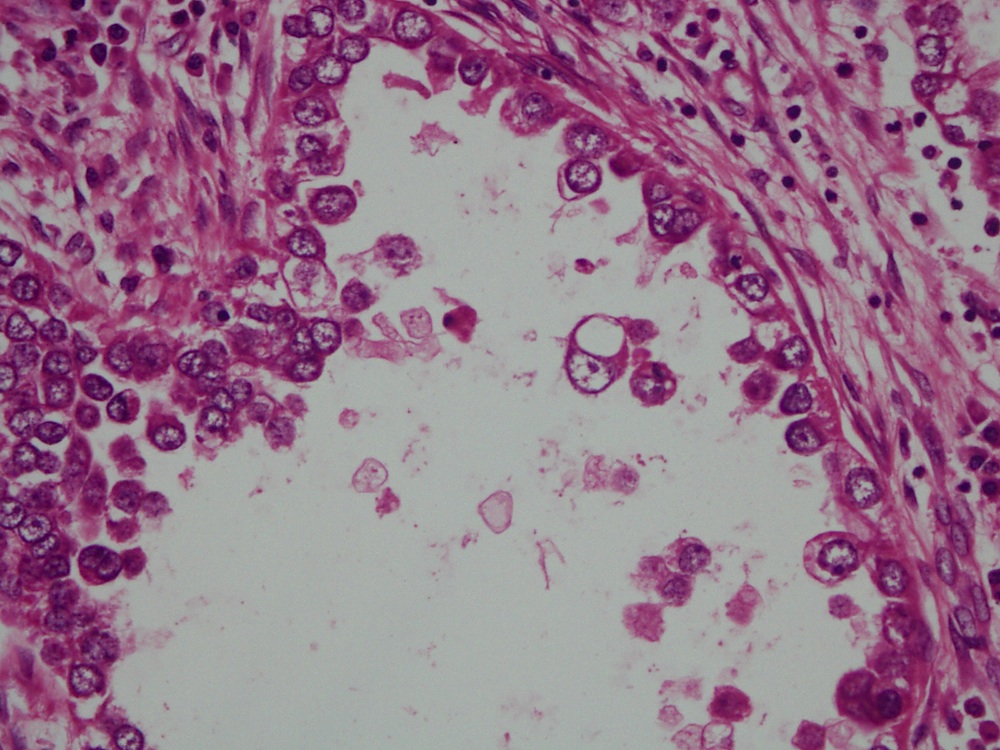
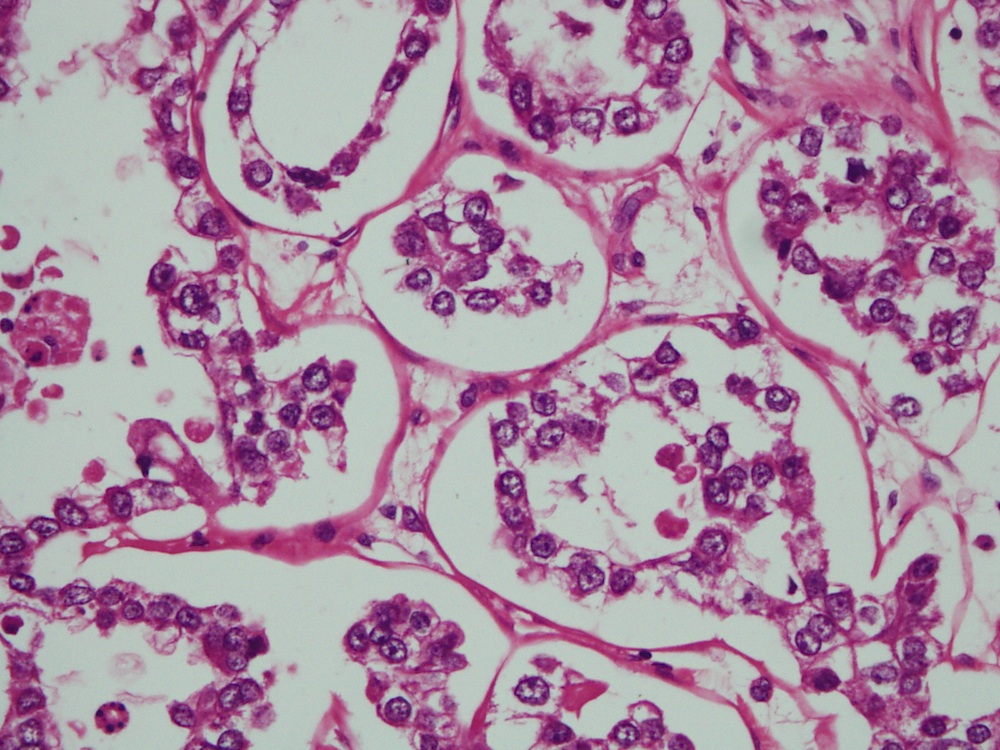
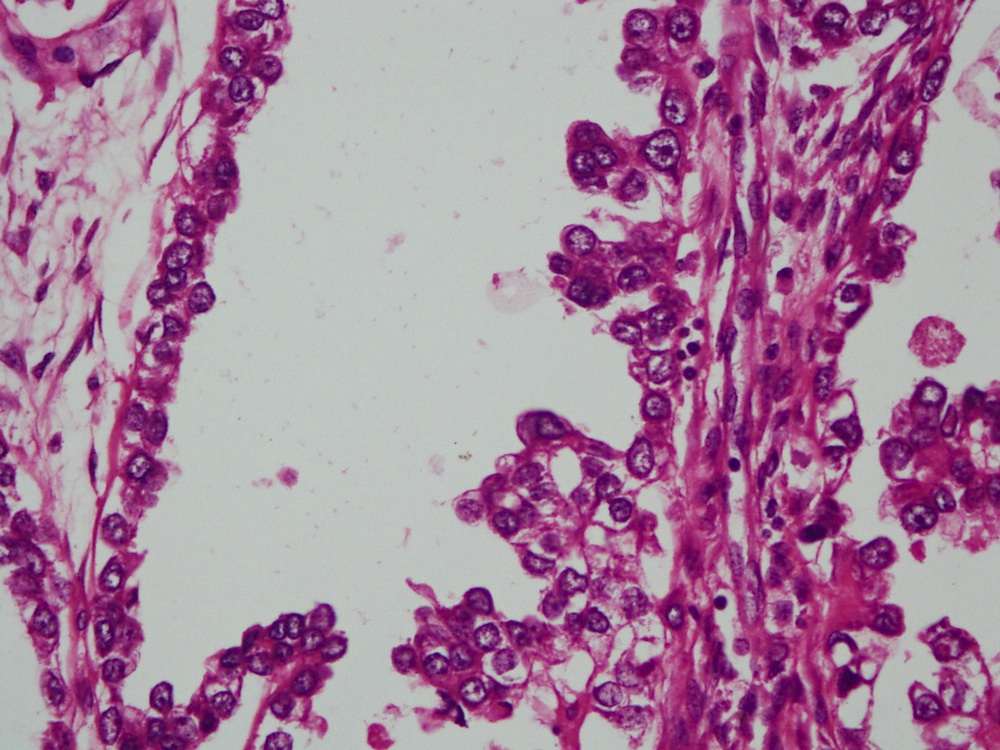
Benign appearing glandular cells
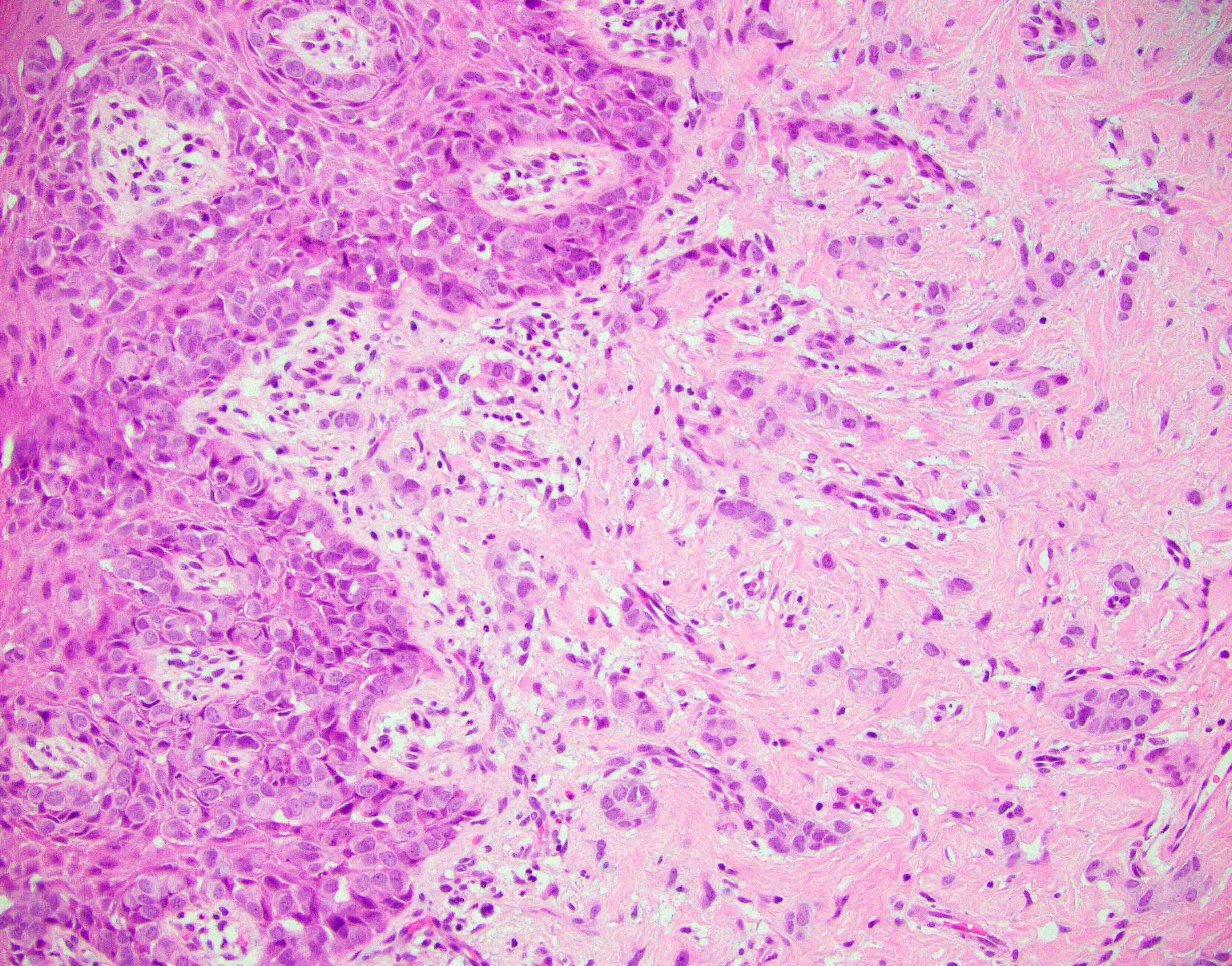
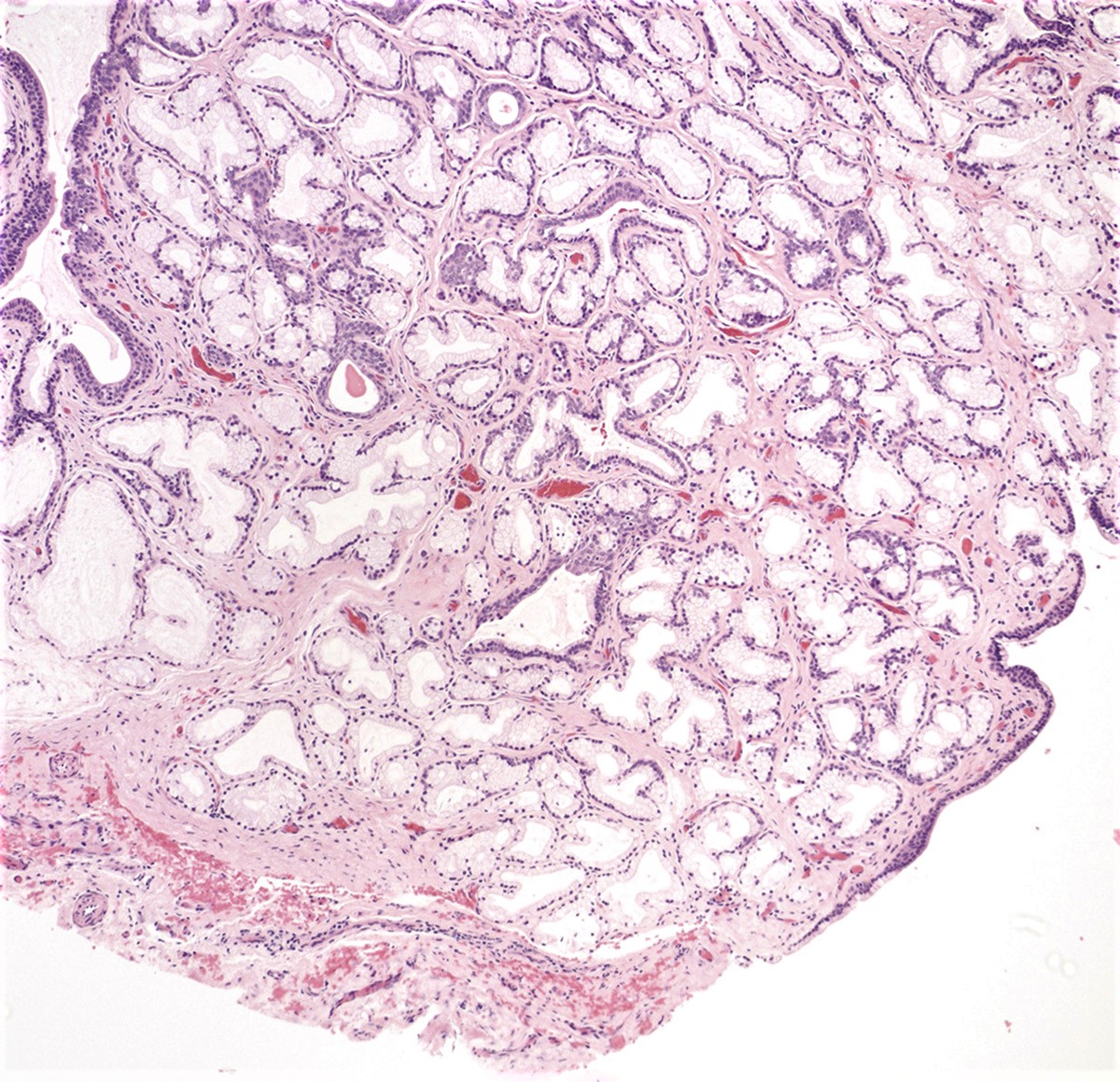
Vaginal adenosis diffuse, rare case
Images hosted on other servers:






Ultrasound and MRI

MRI

Perineal, MRI
Images hosted on other servers:

Paravaginal, intraoperative

Perineal, intraoperative

Vulvar, preoperative

Vulvar, pre and postoperative
Contributed by @Andrew_Fltv on Twitter
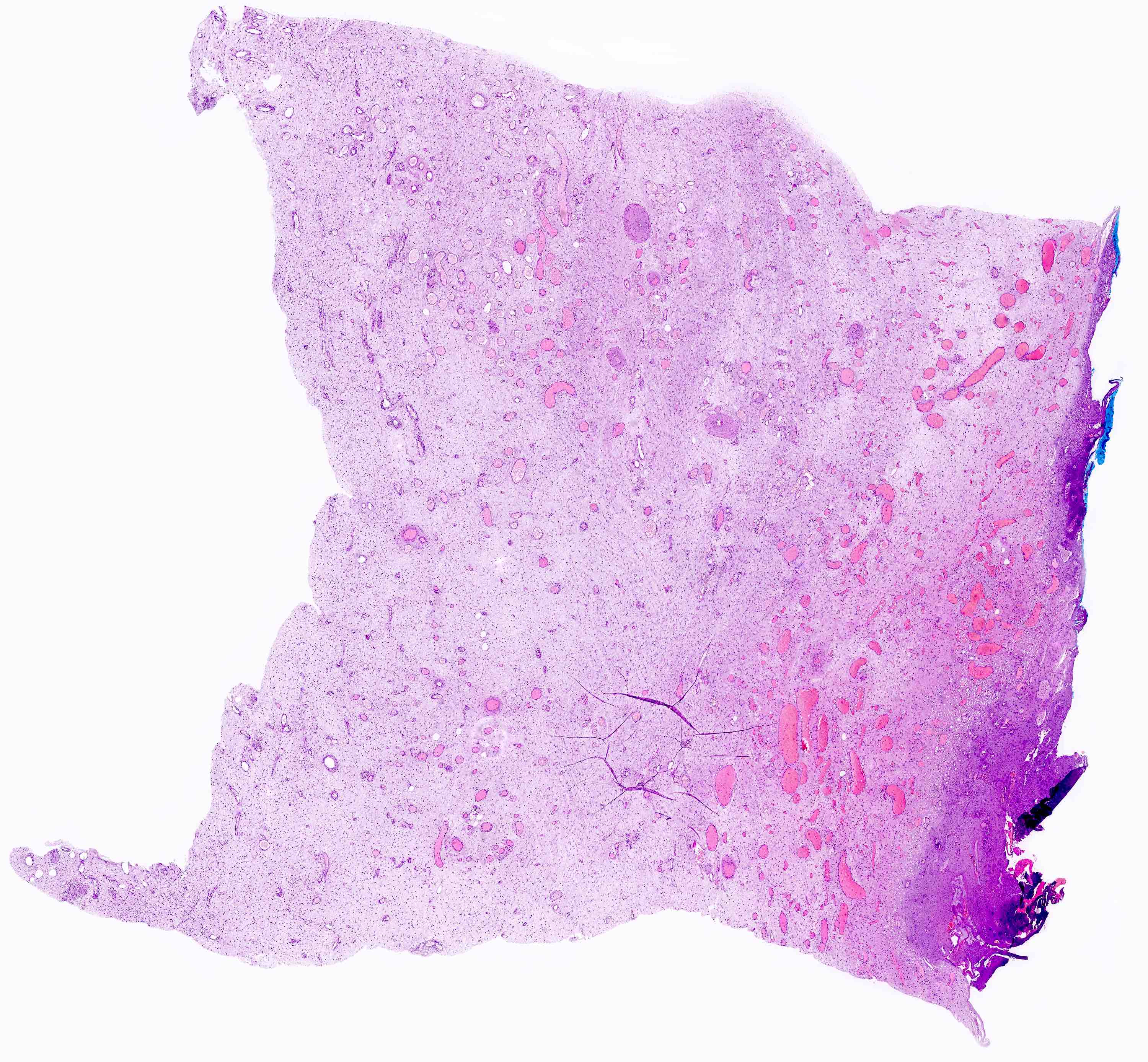
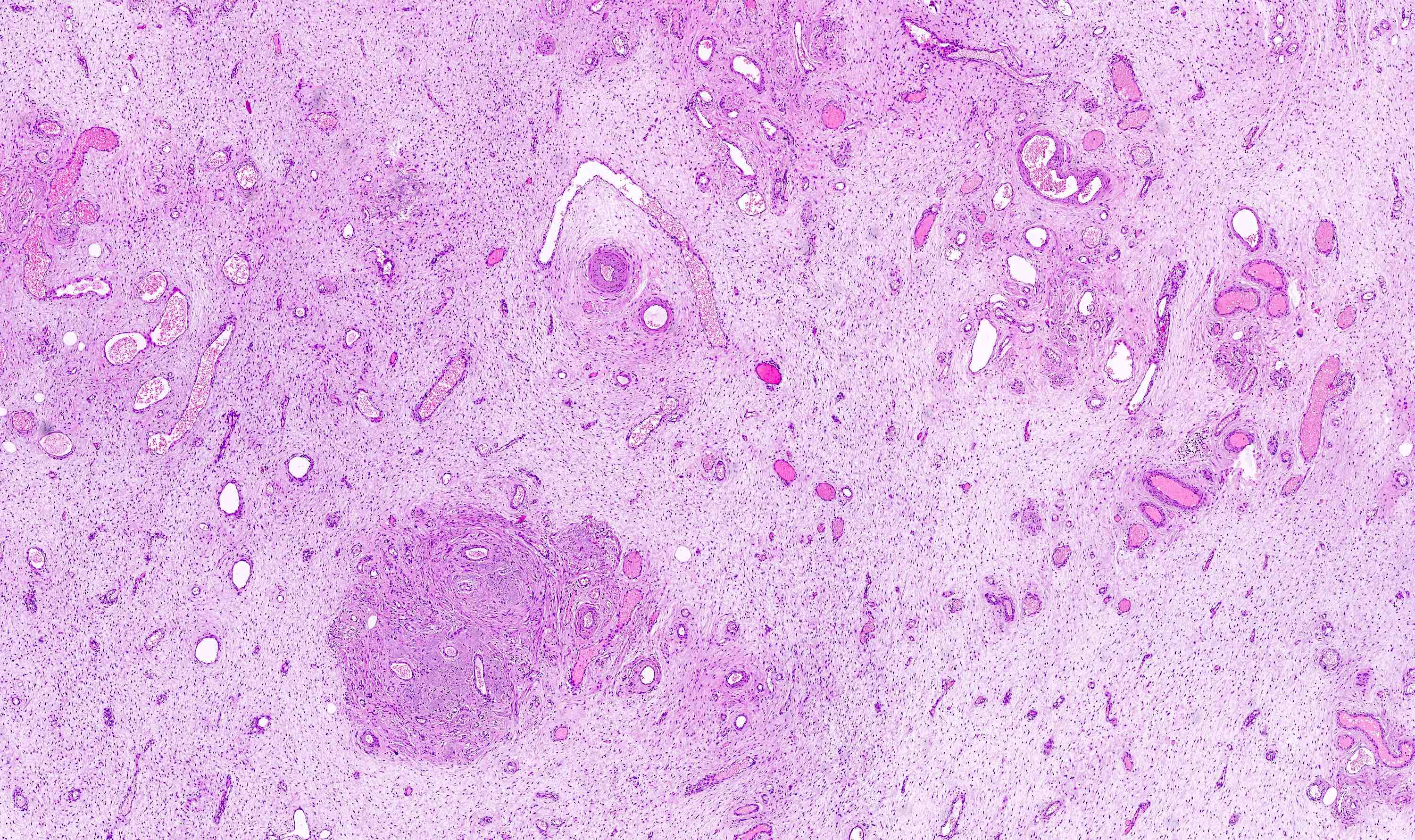
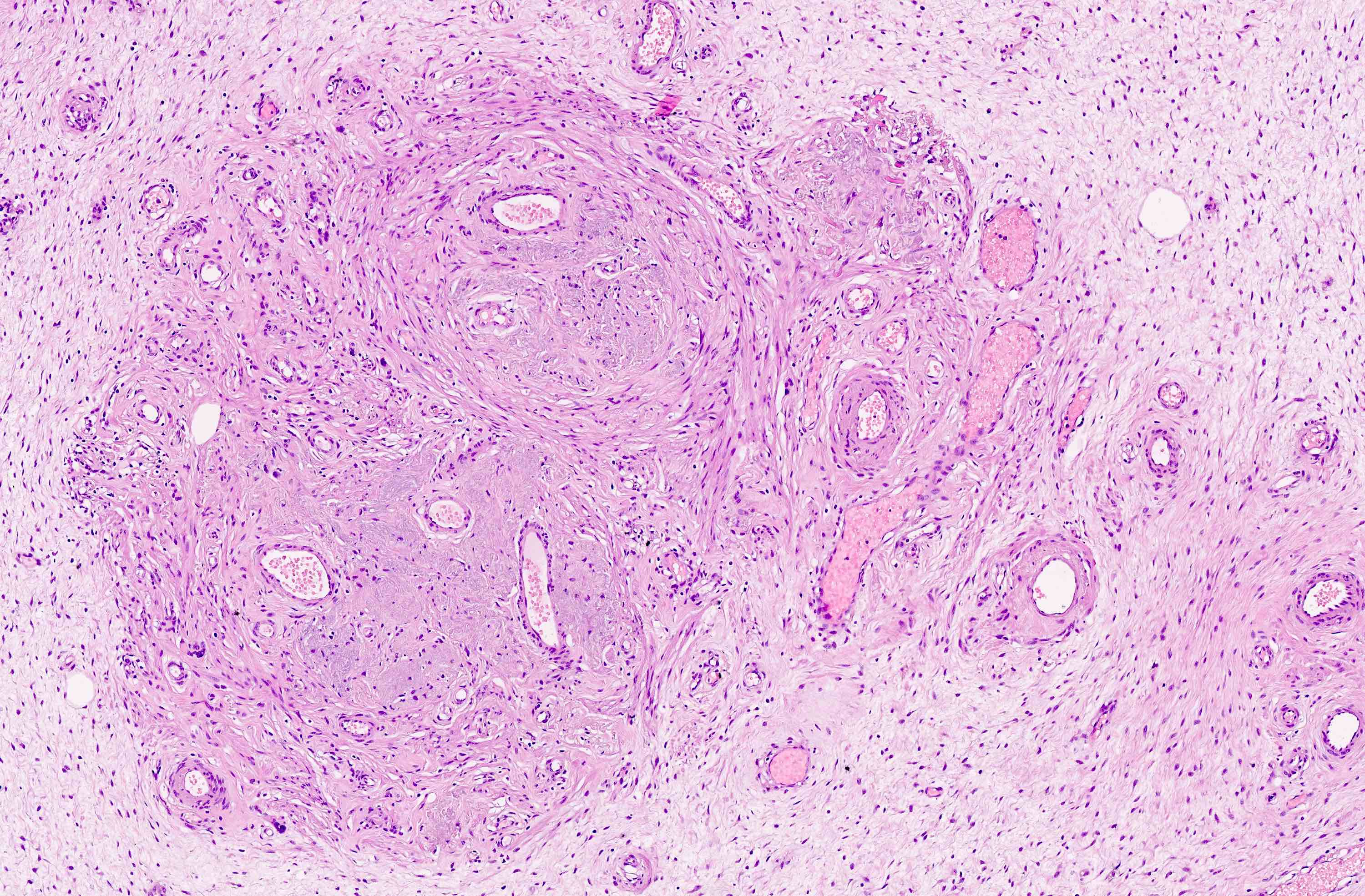
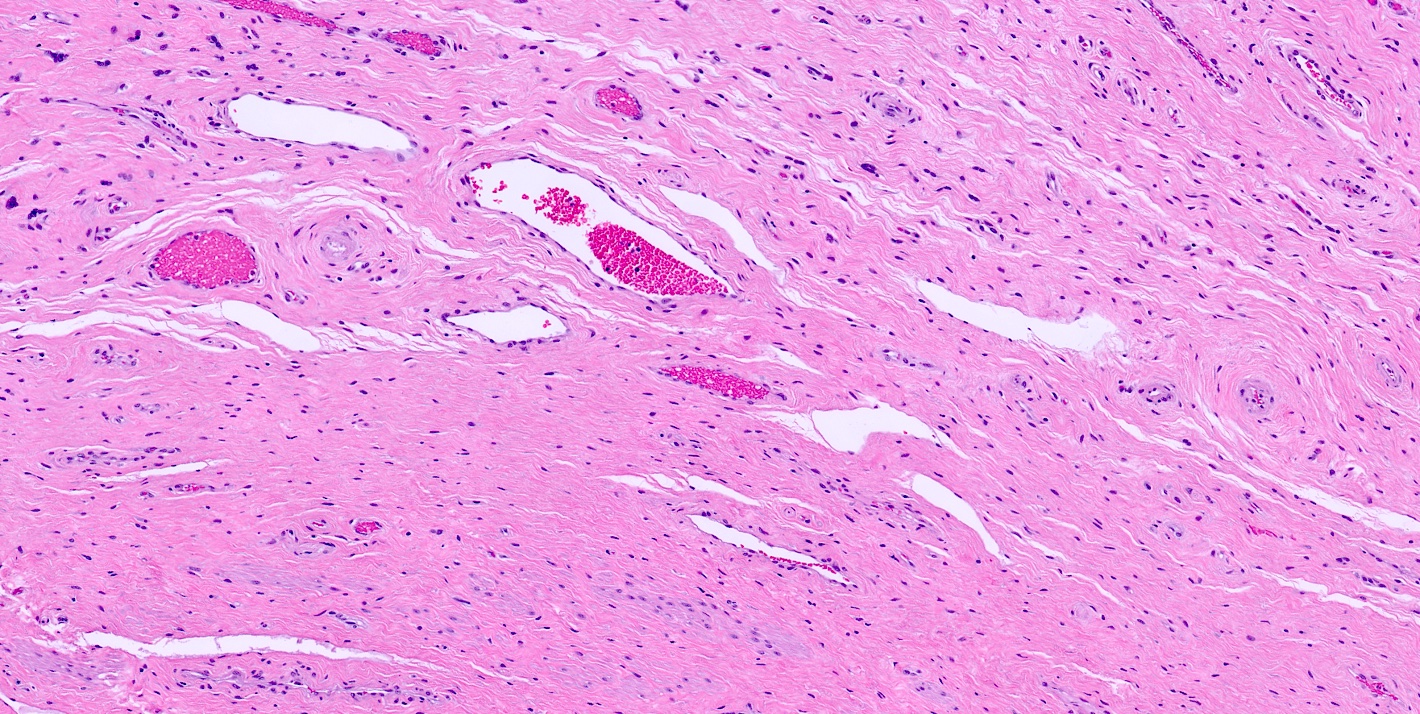
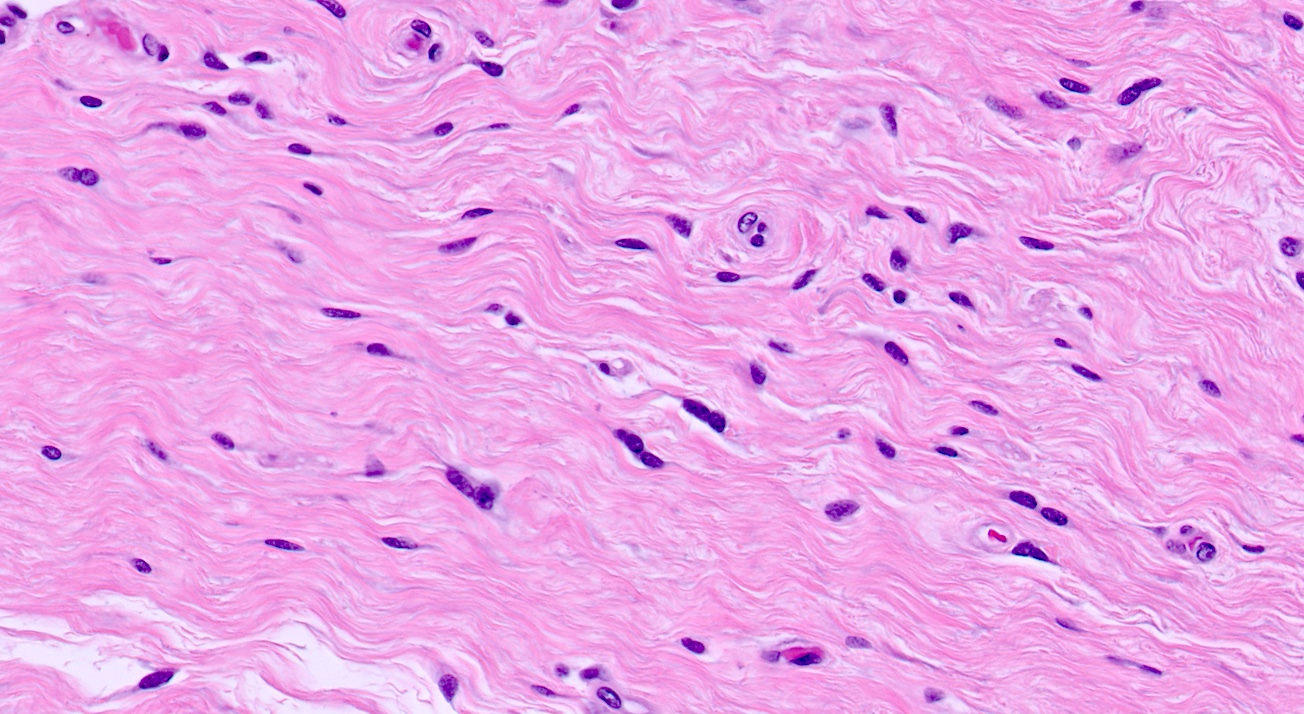
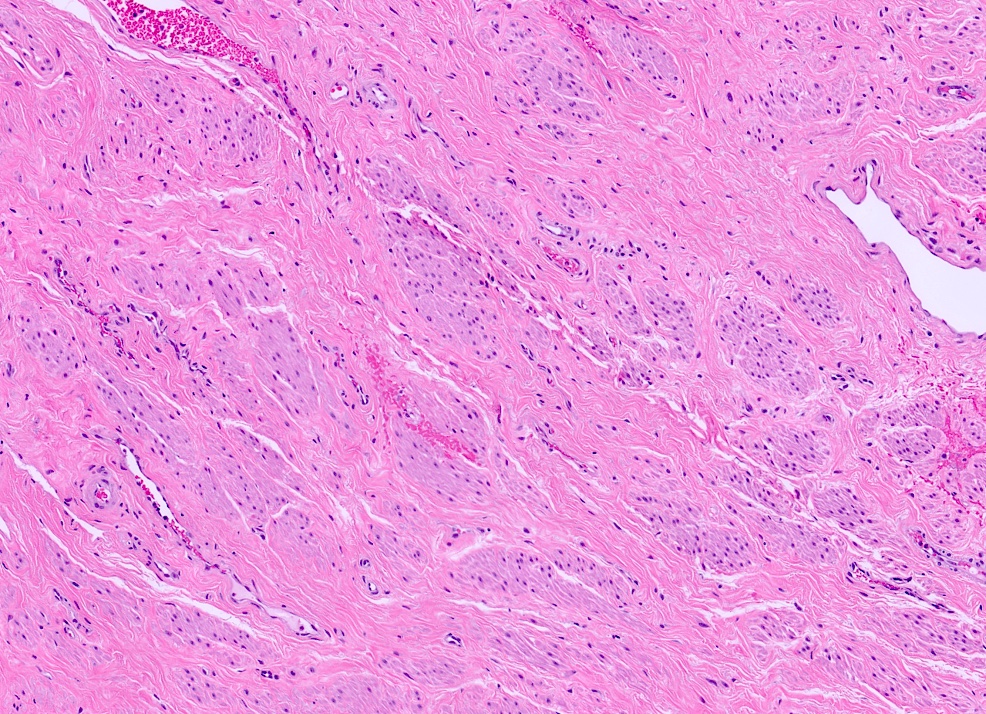
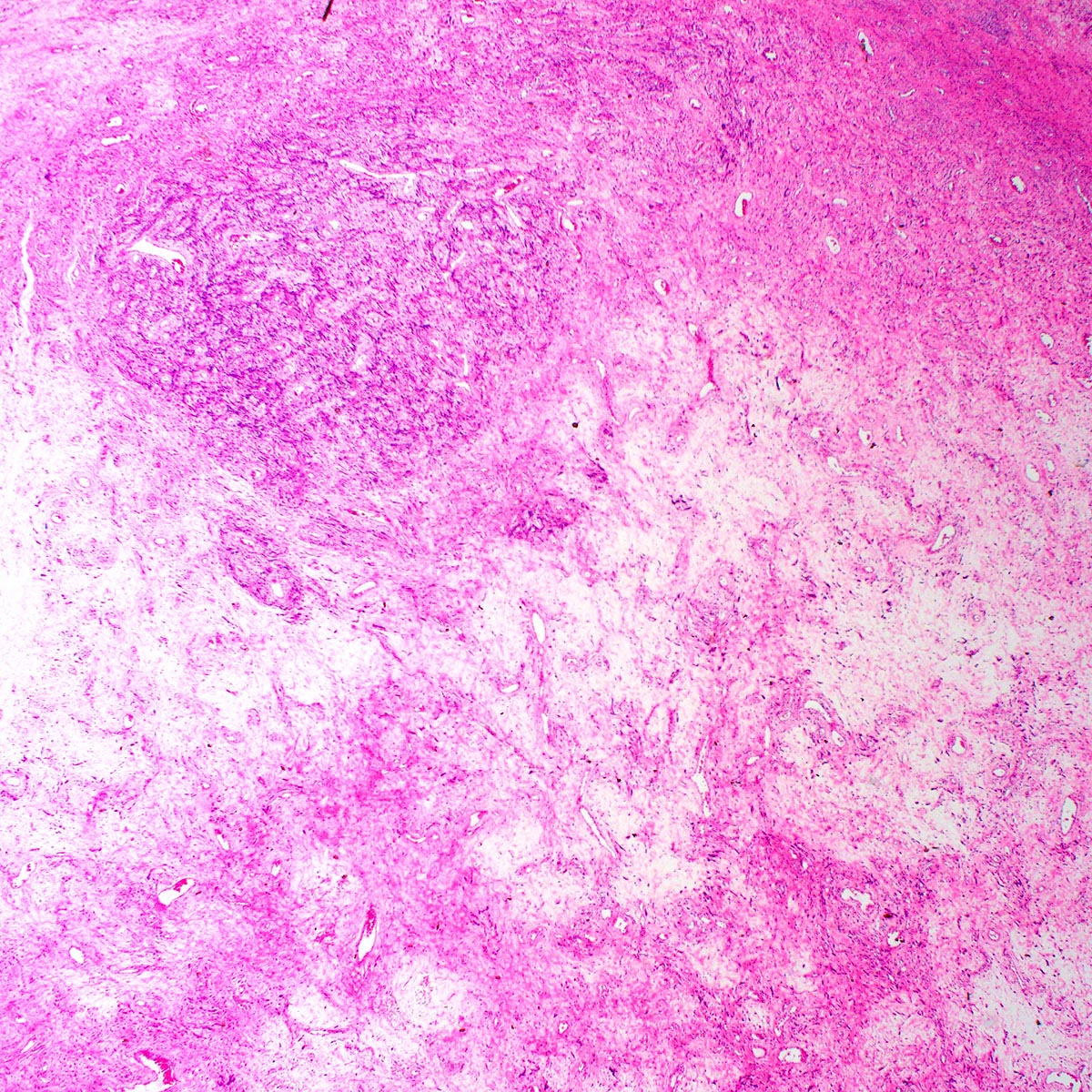
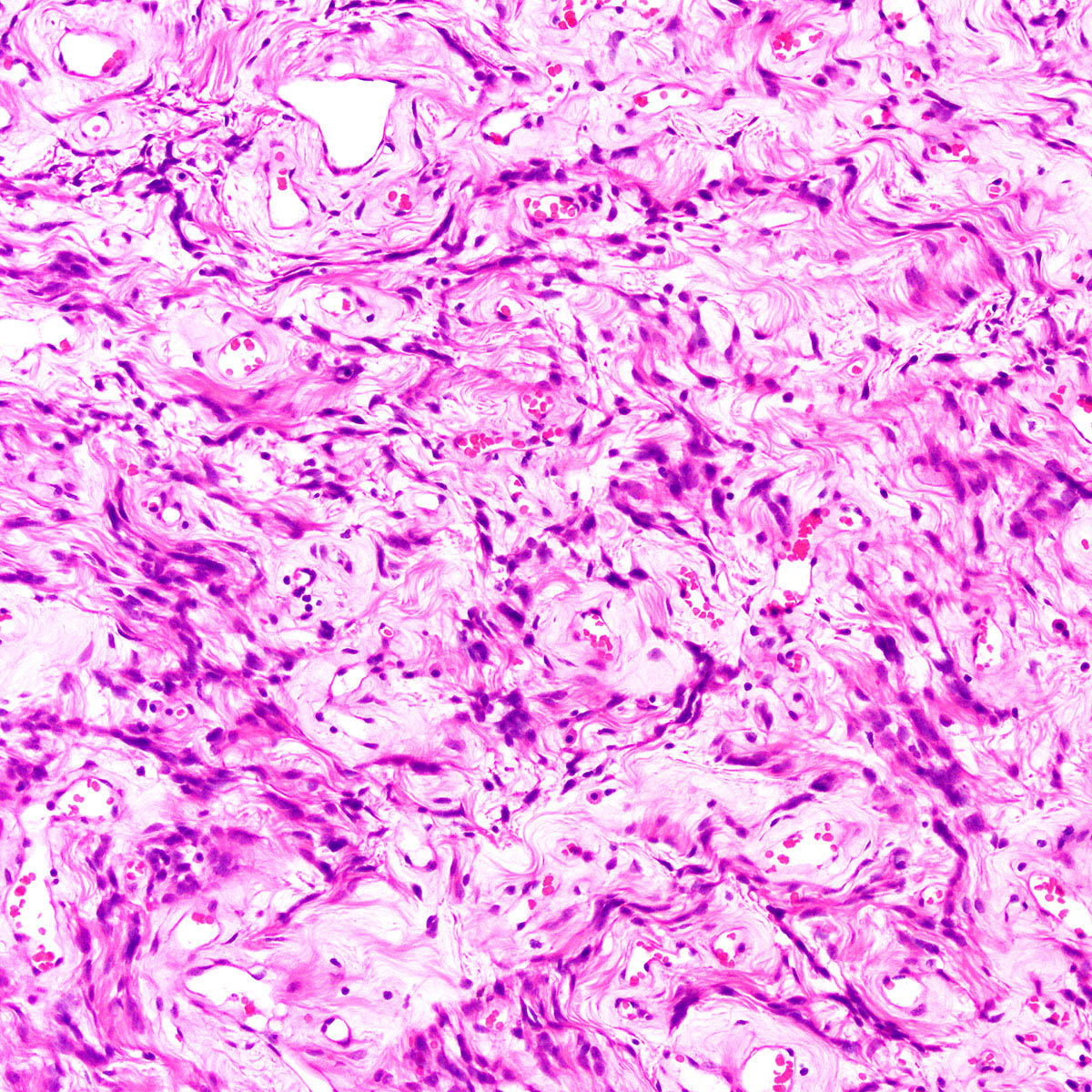
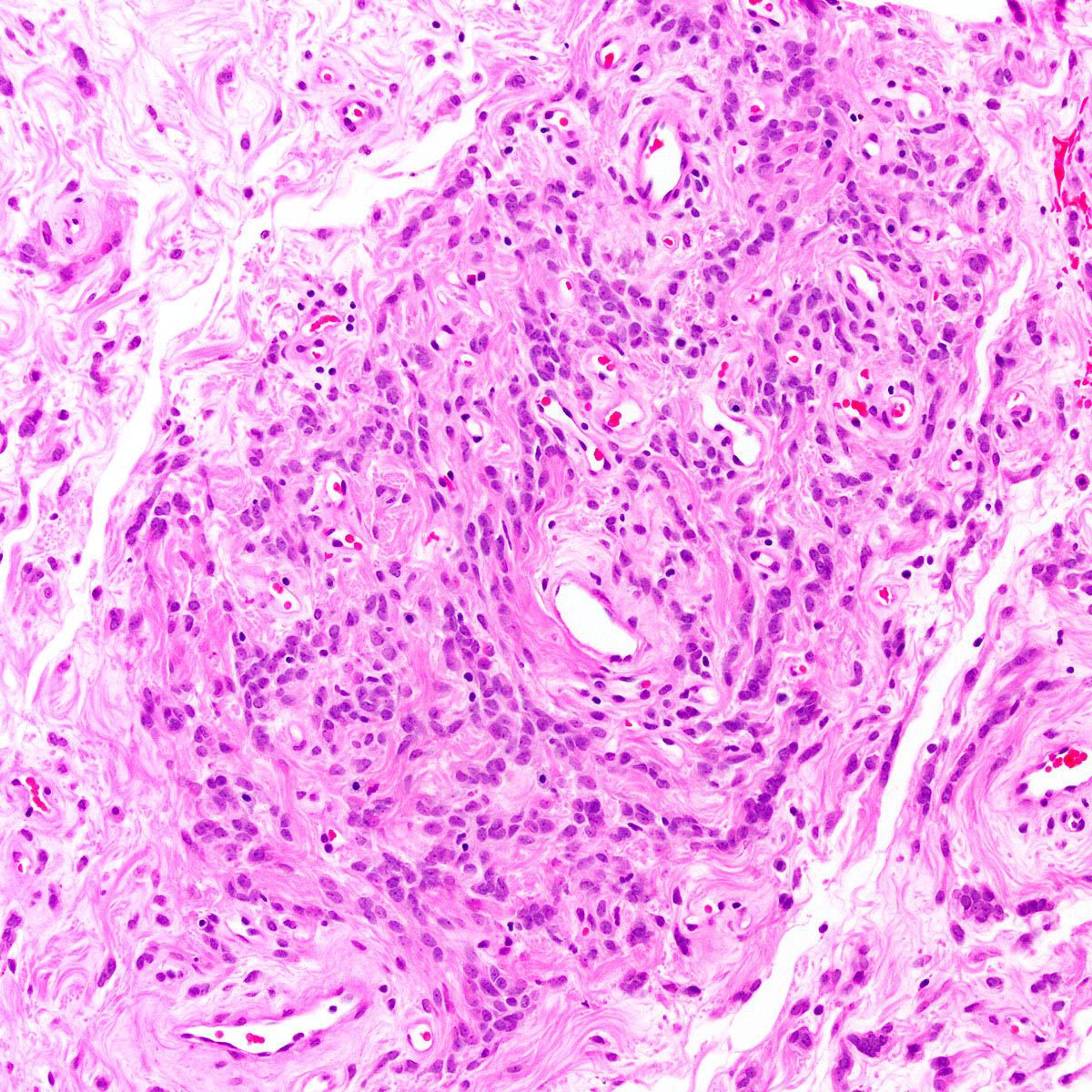
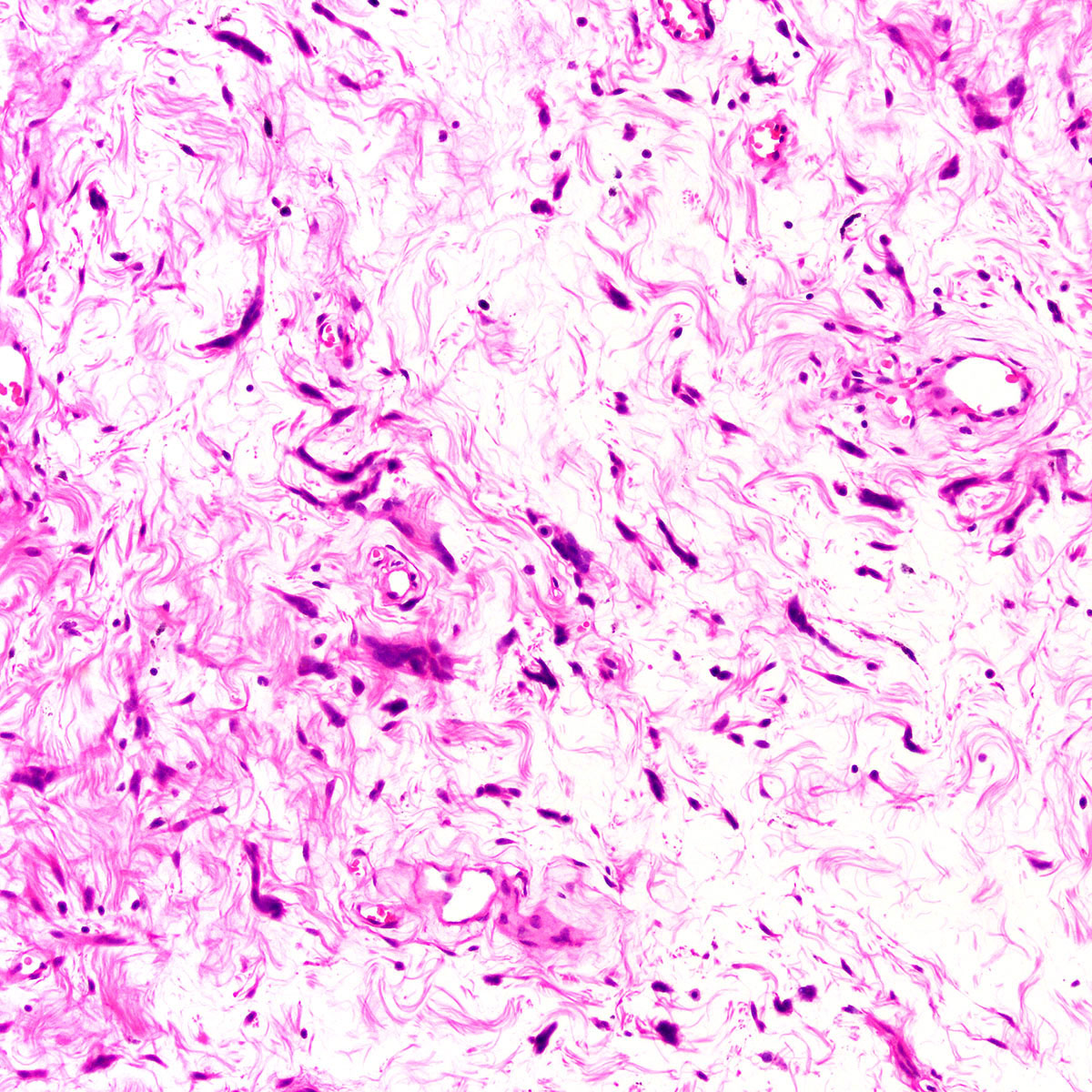
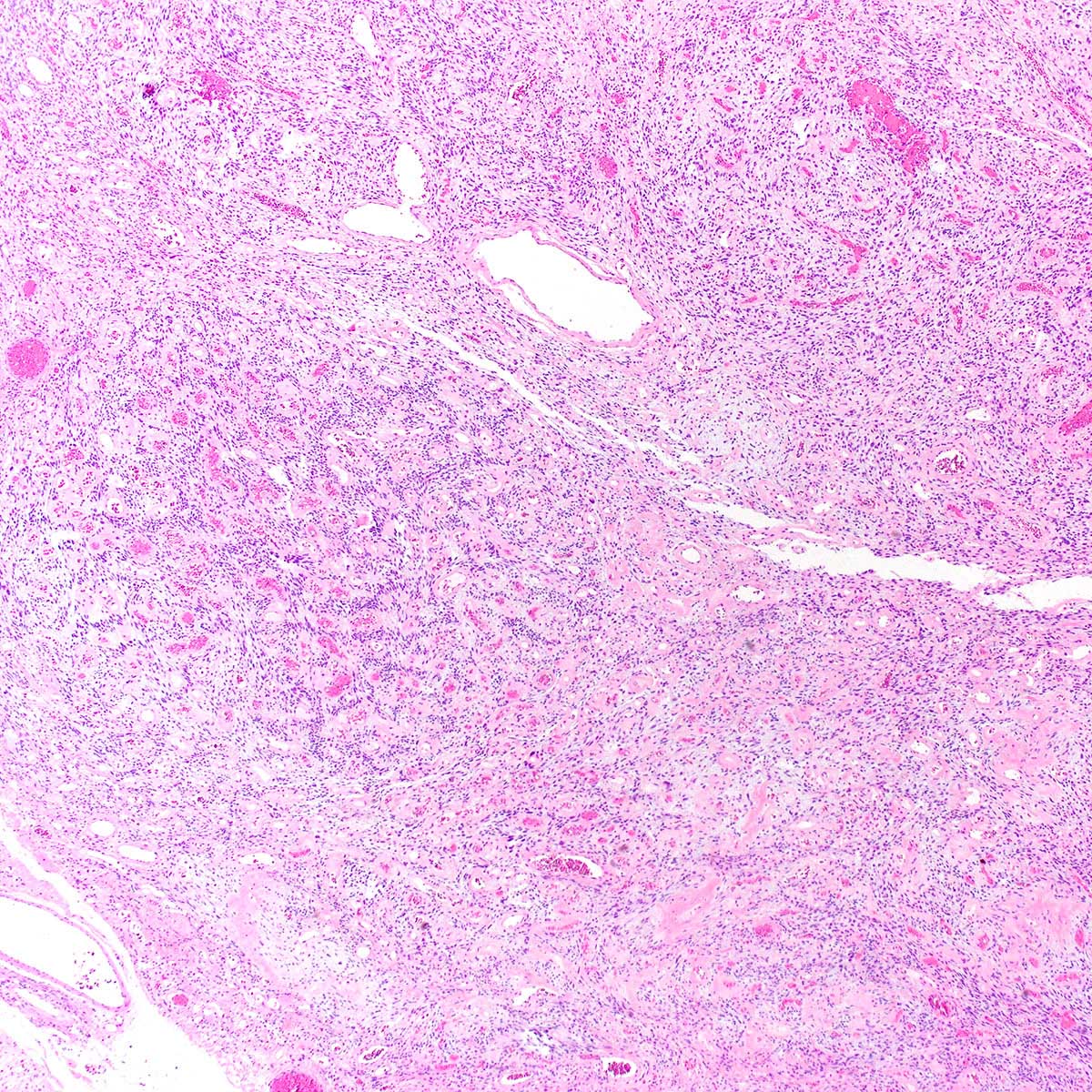
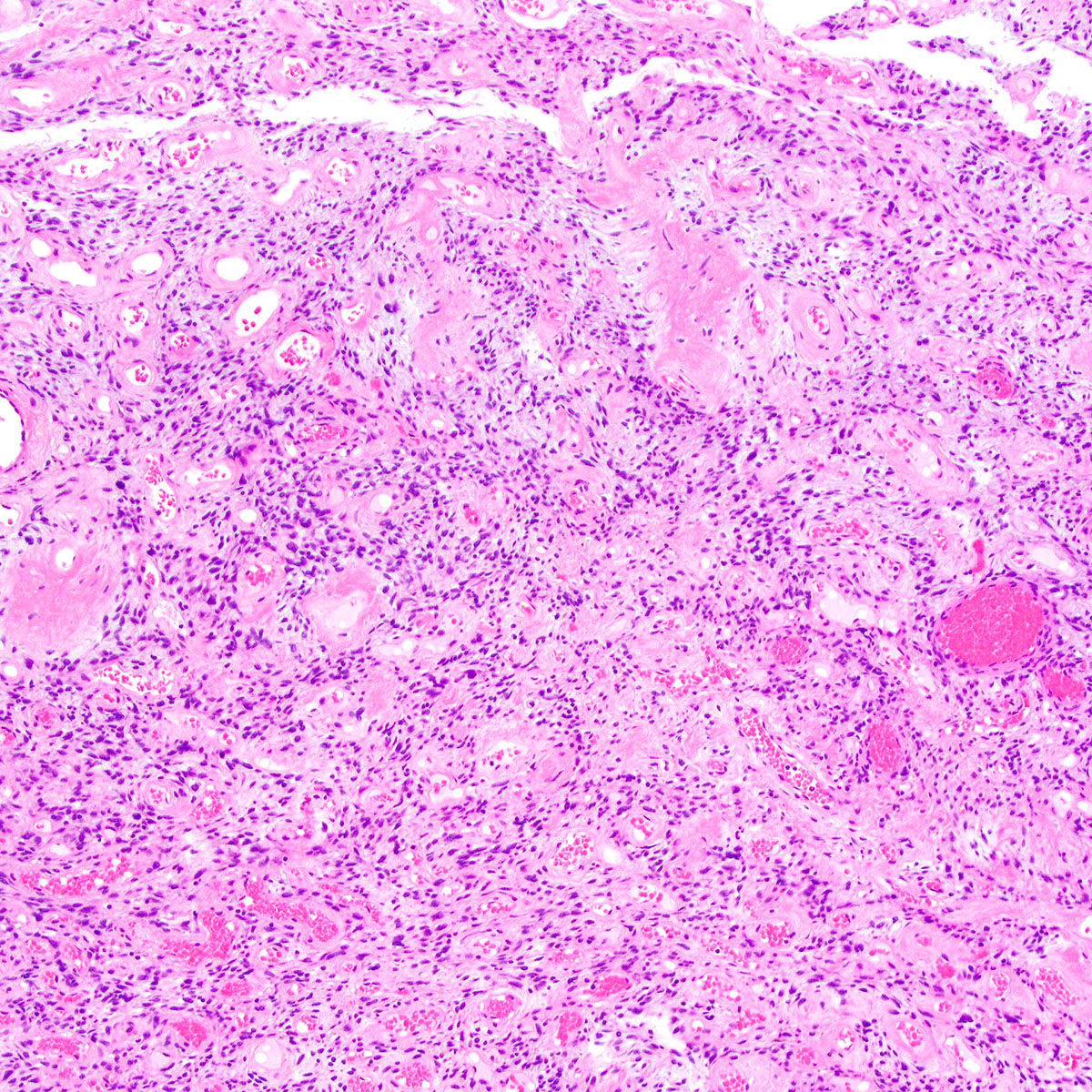
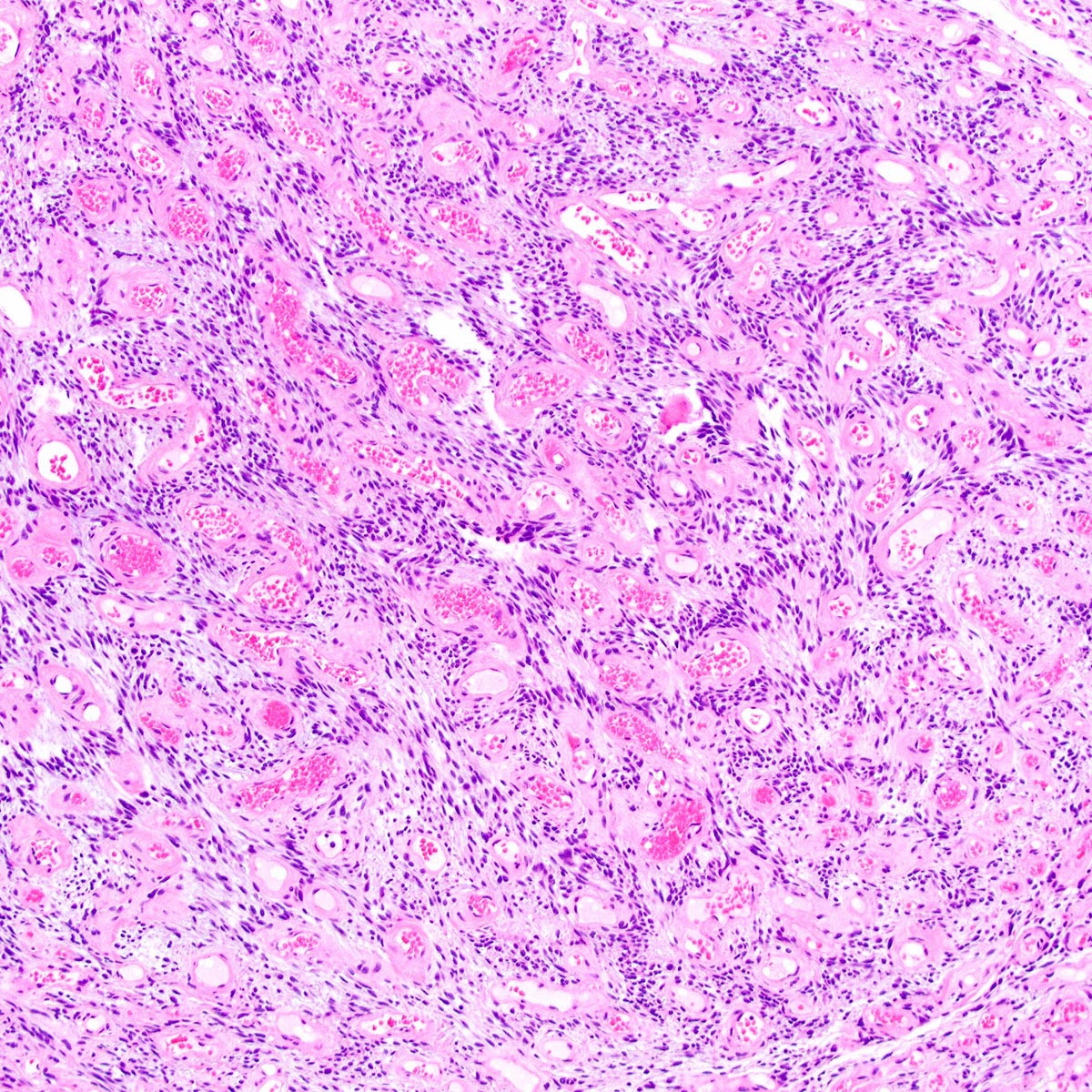
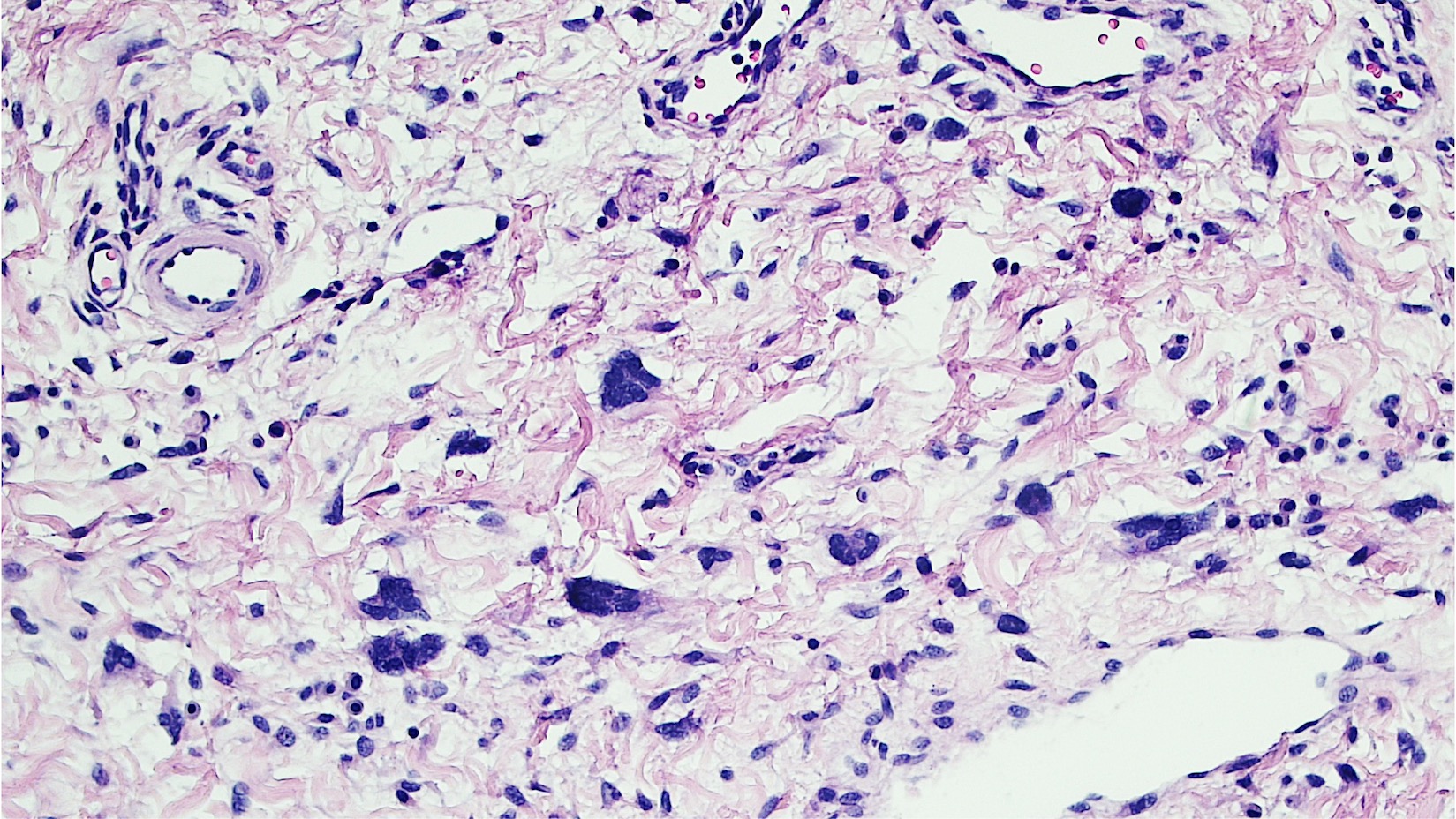
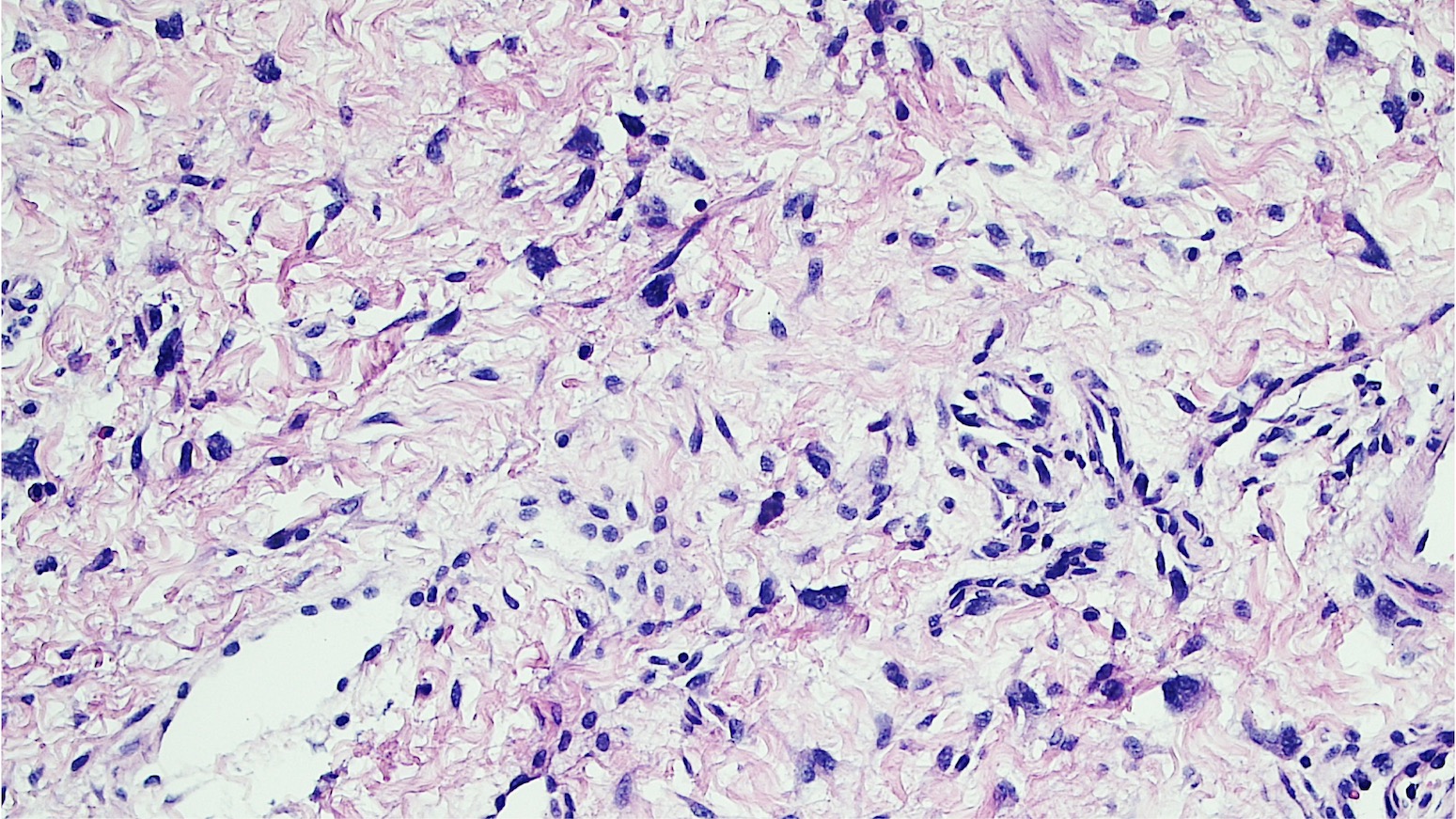
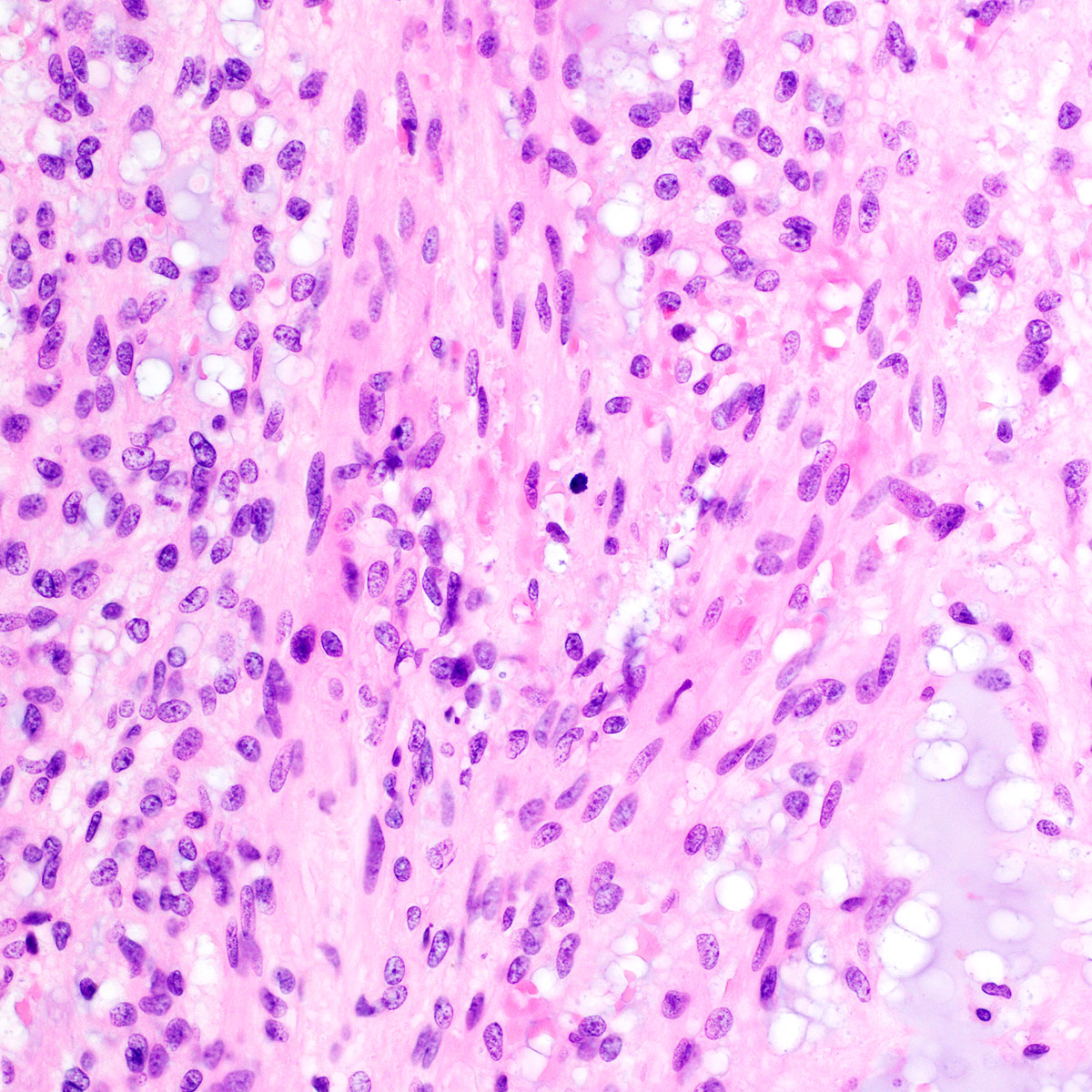
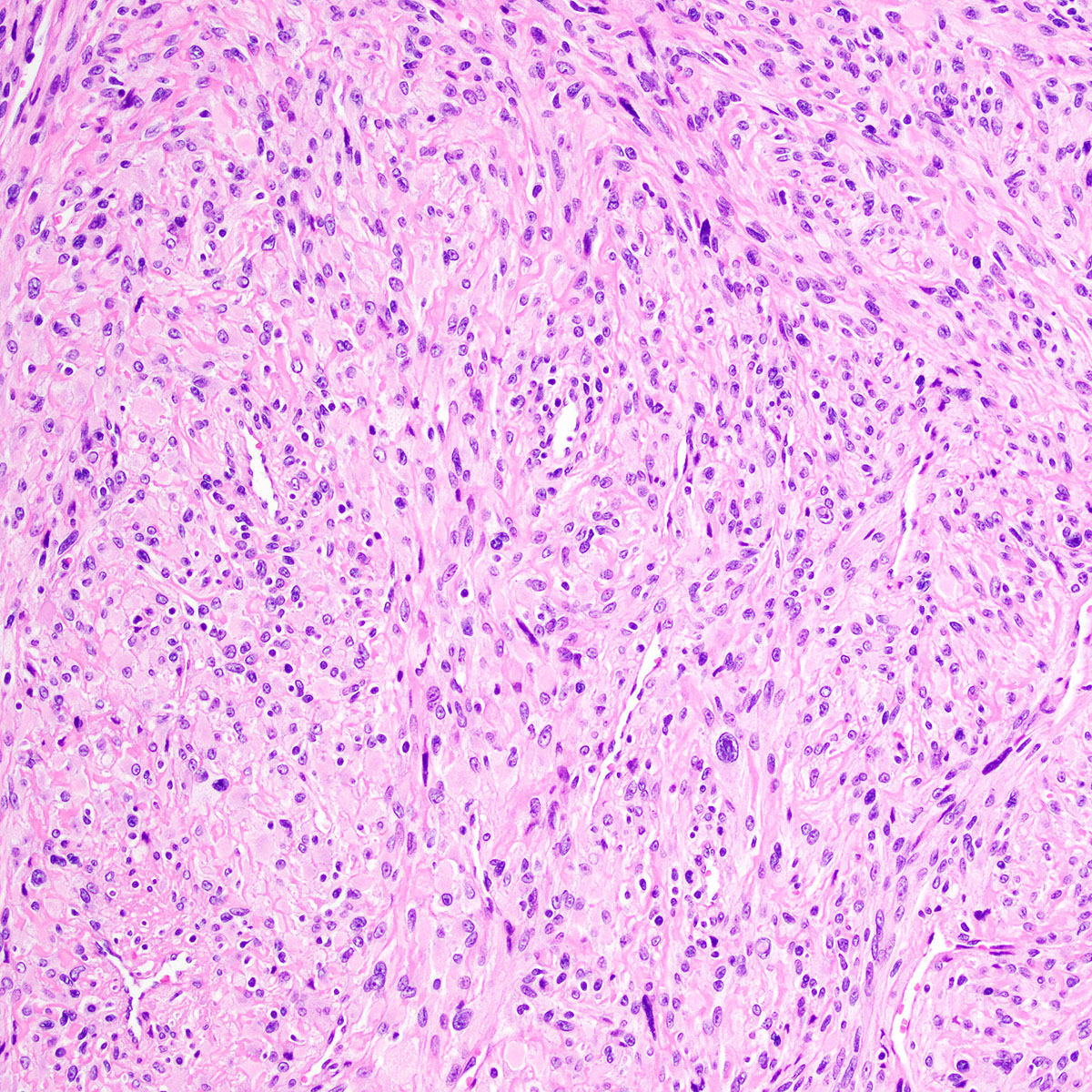
Aggressive angiomyxoma
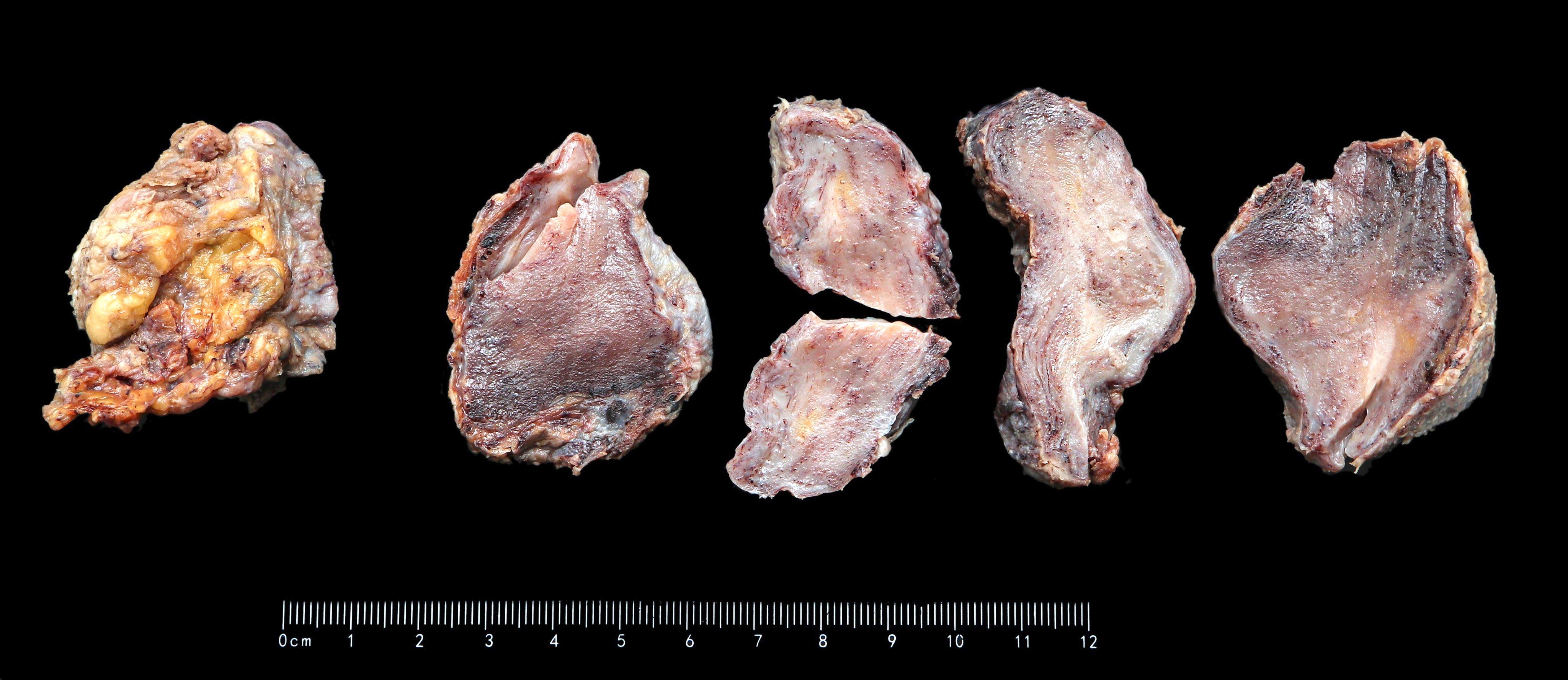
Images hosted on other servers:

Cut surface
Contributed by David B. Chapel, M.D. and @Andrew_Fltv on Twitter
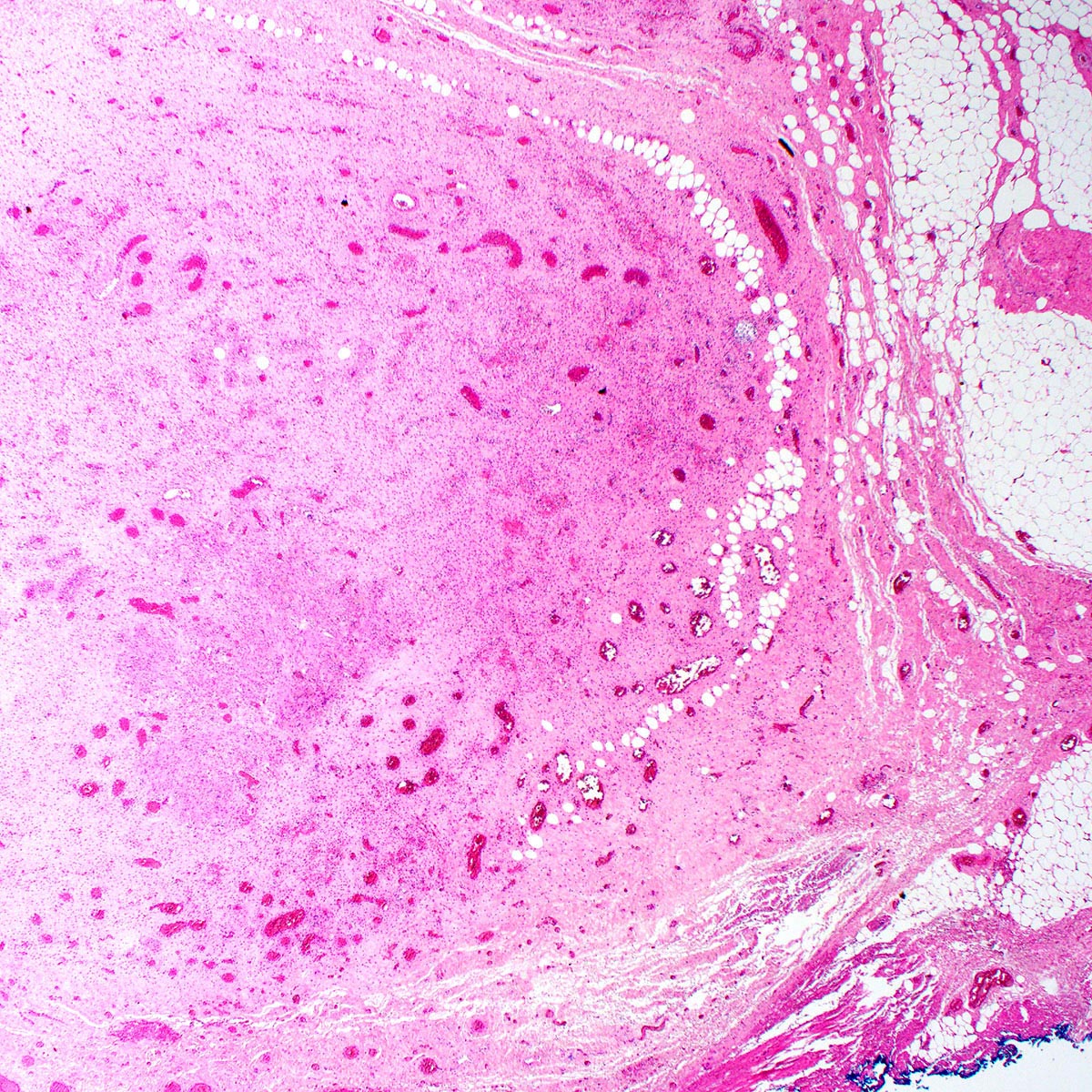
Infiltrative growth
Entrapped adipose tissue
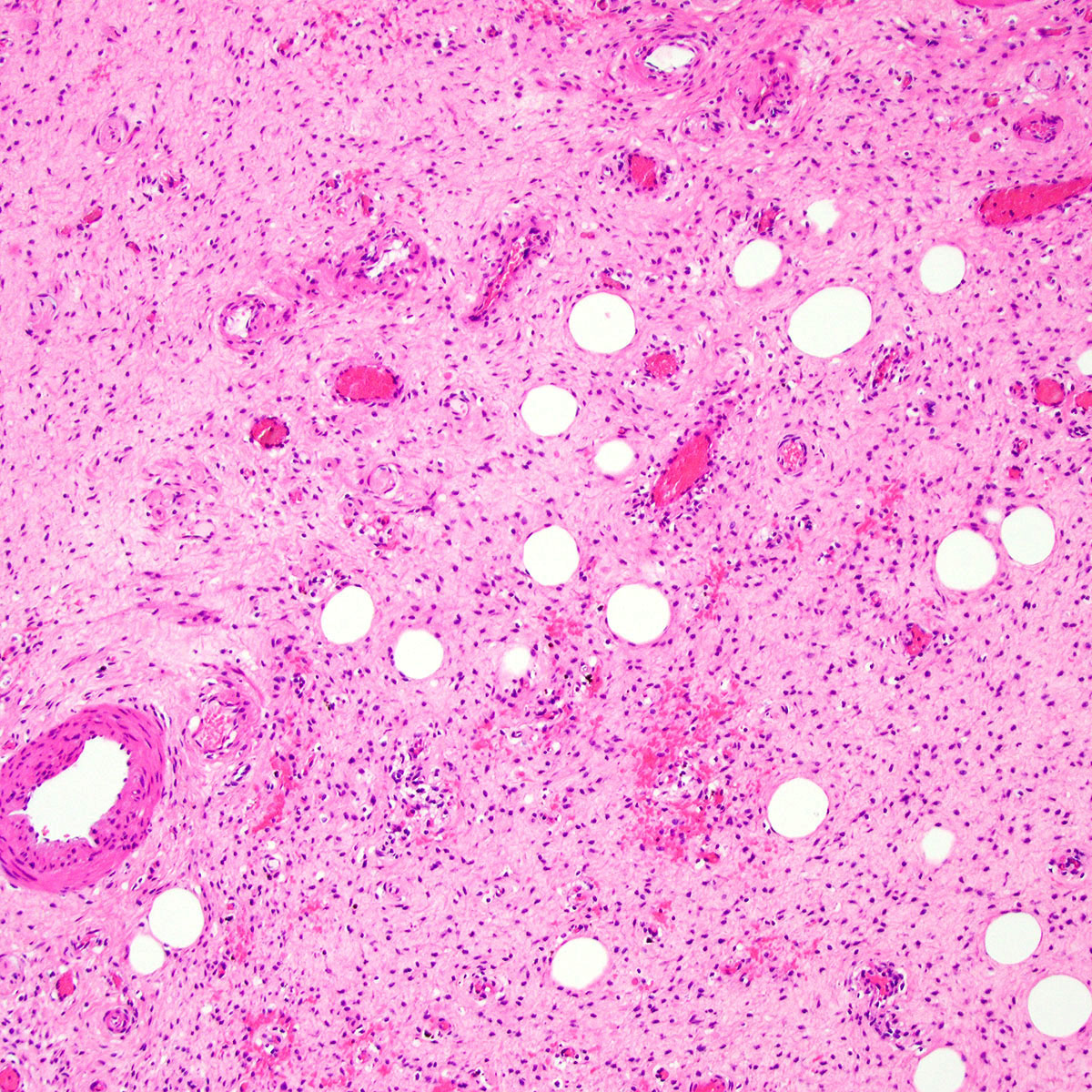
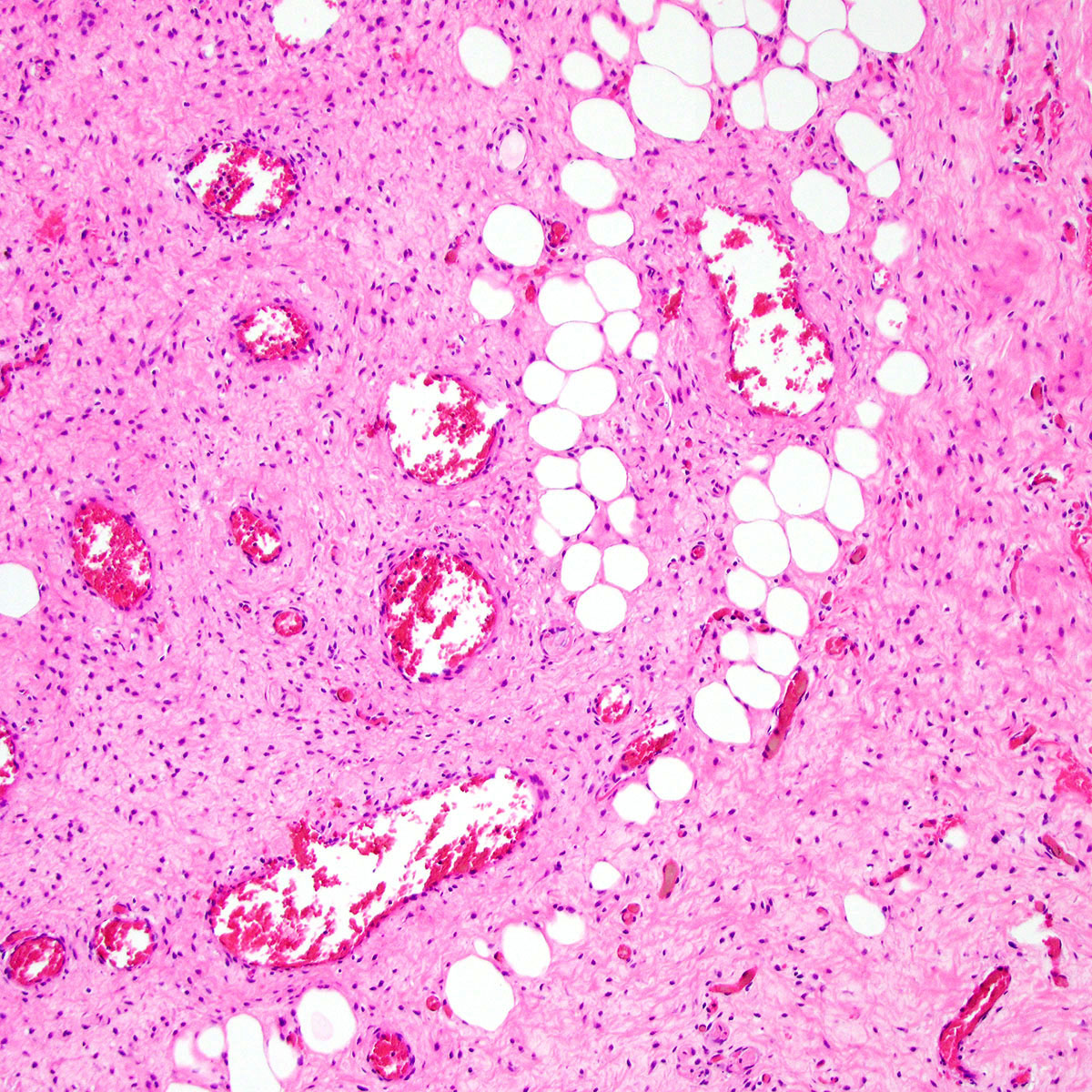
Extravasated red blood cells
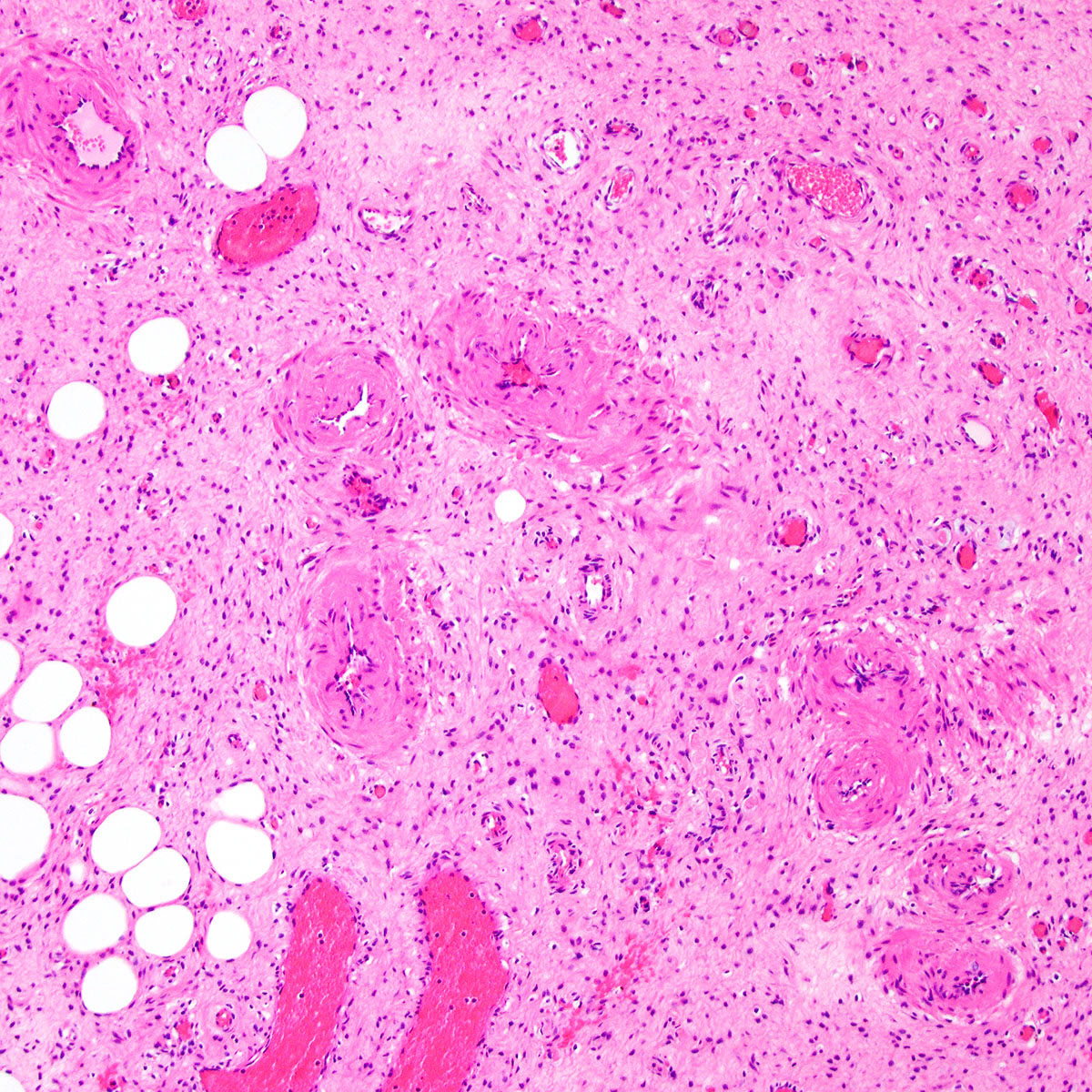
Thick walled vessels
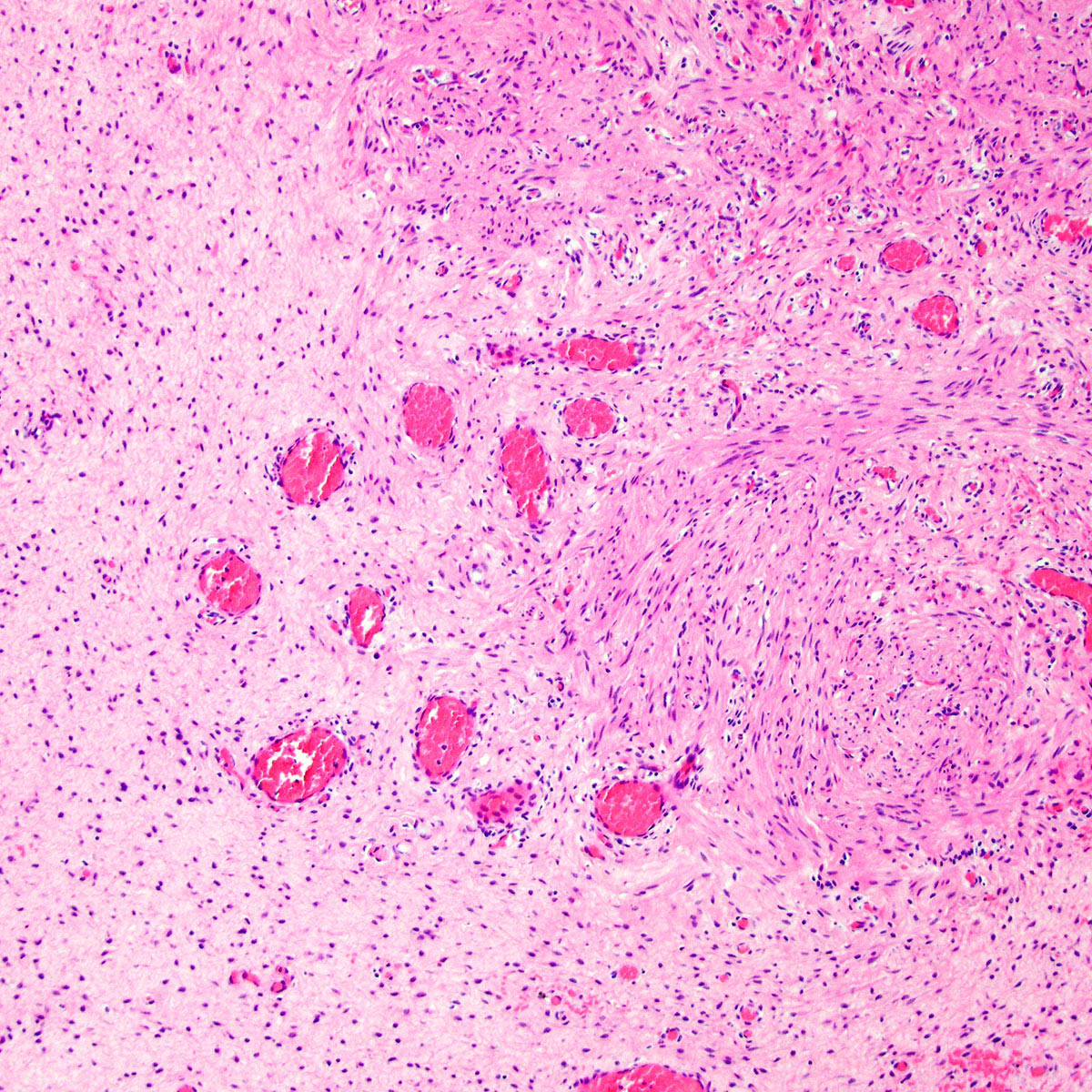
Myoid bundles
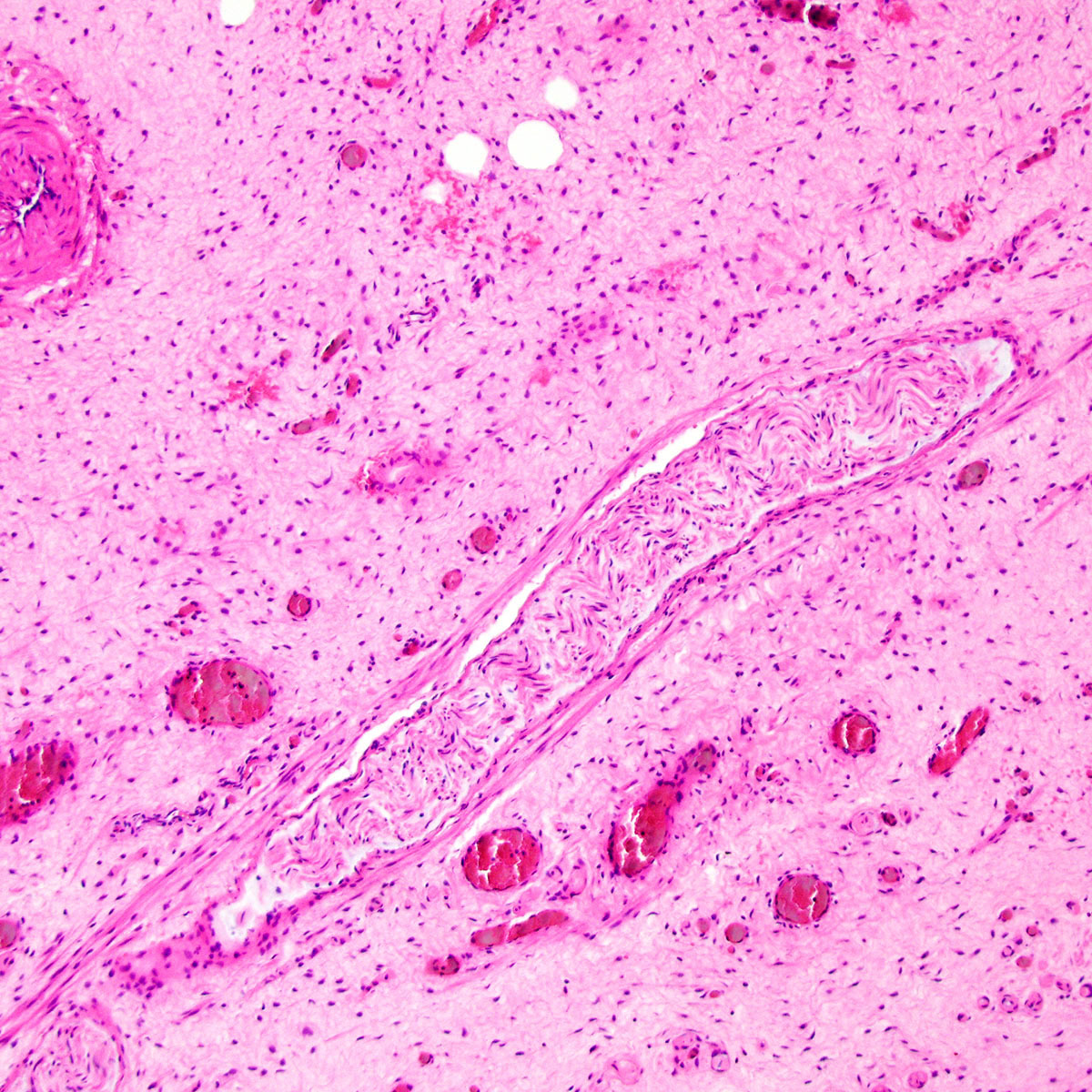
Entrapped nerve
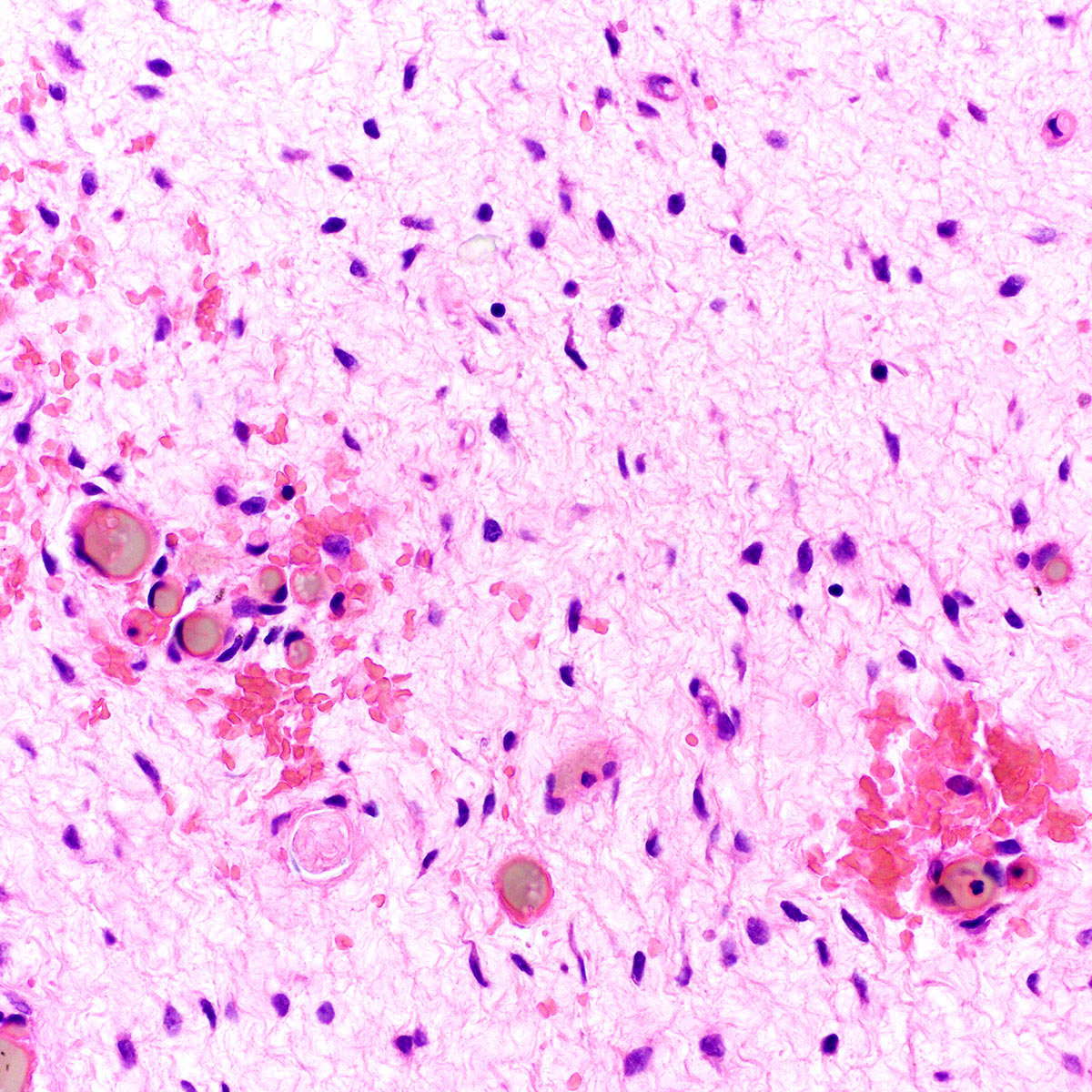
Bland cytology
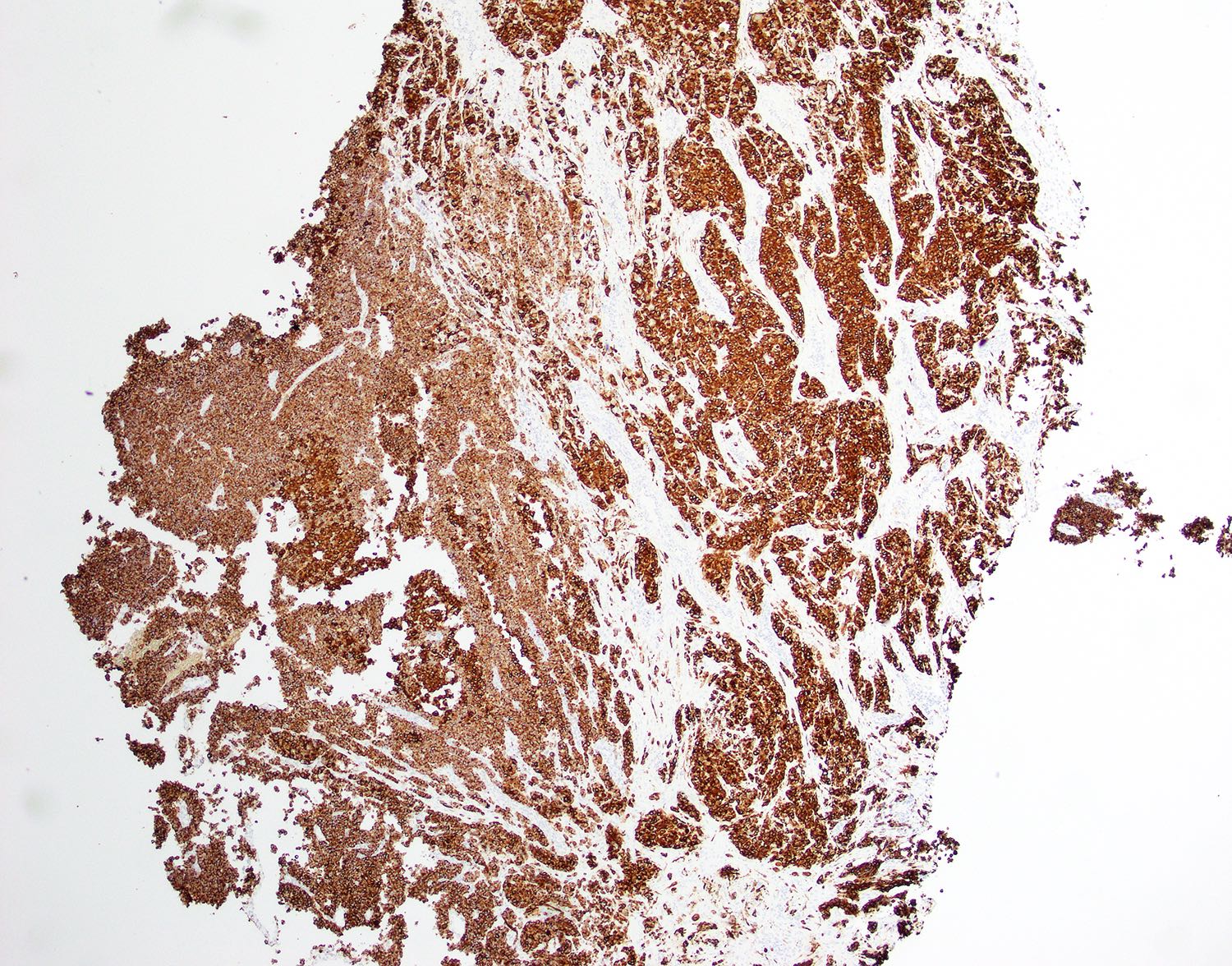
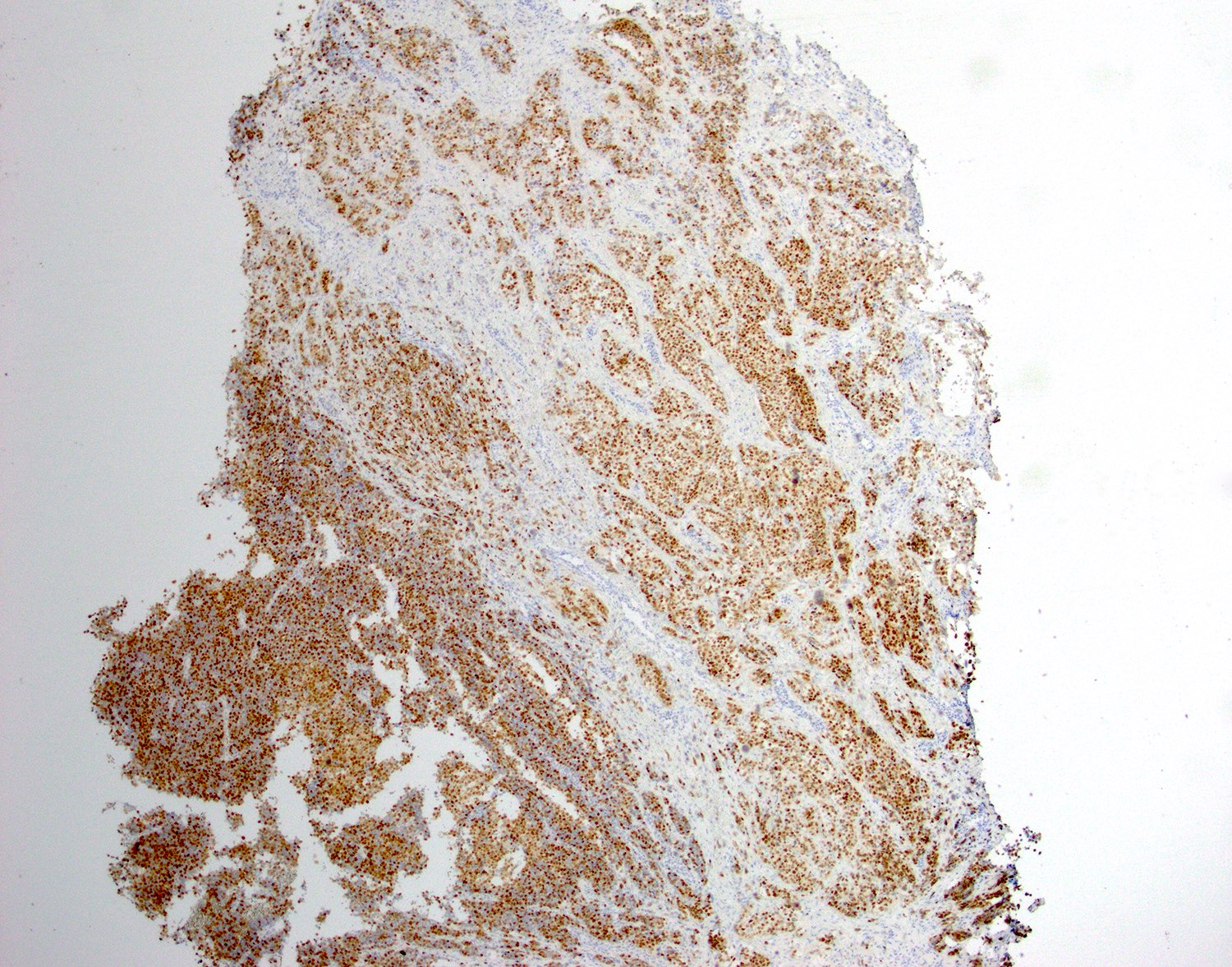
Aggressive angiomyxoma
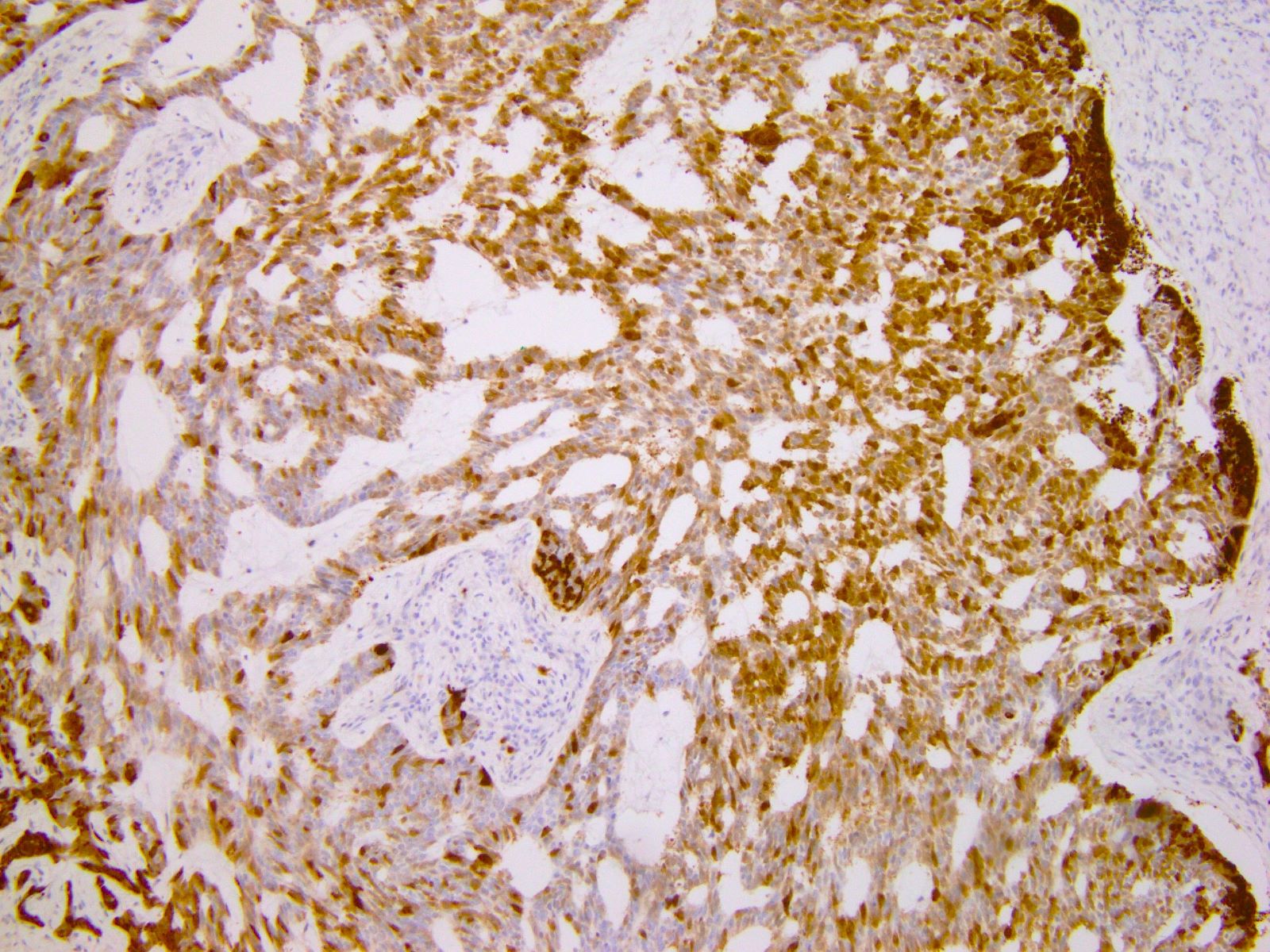
HMGA2
Images hosted on other servers:

FISH, karyotype
Histopathology
Images hosted on other servers:

Lobulated, hypervascular mass originating in the cervix

Well defined mass extending from cervix into vagina
Images hosted on other servers:

Well circumscribed, lobulated mass
Contributed by Katharina Wiedemeyer, M.D. and W. Glenn McCluggage, M.D.

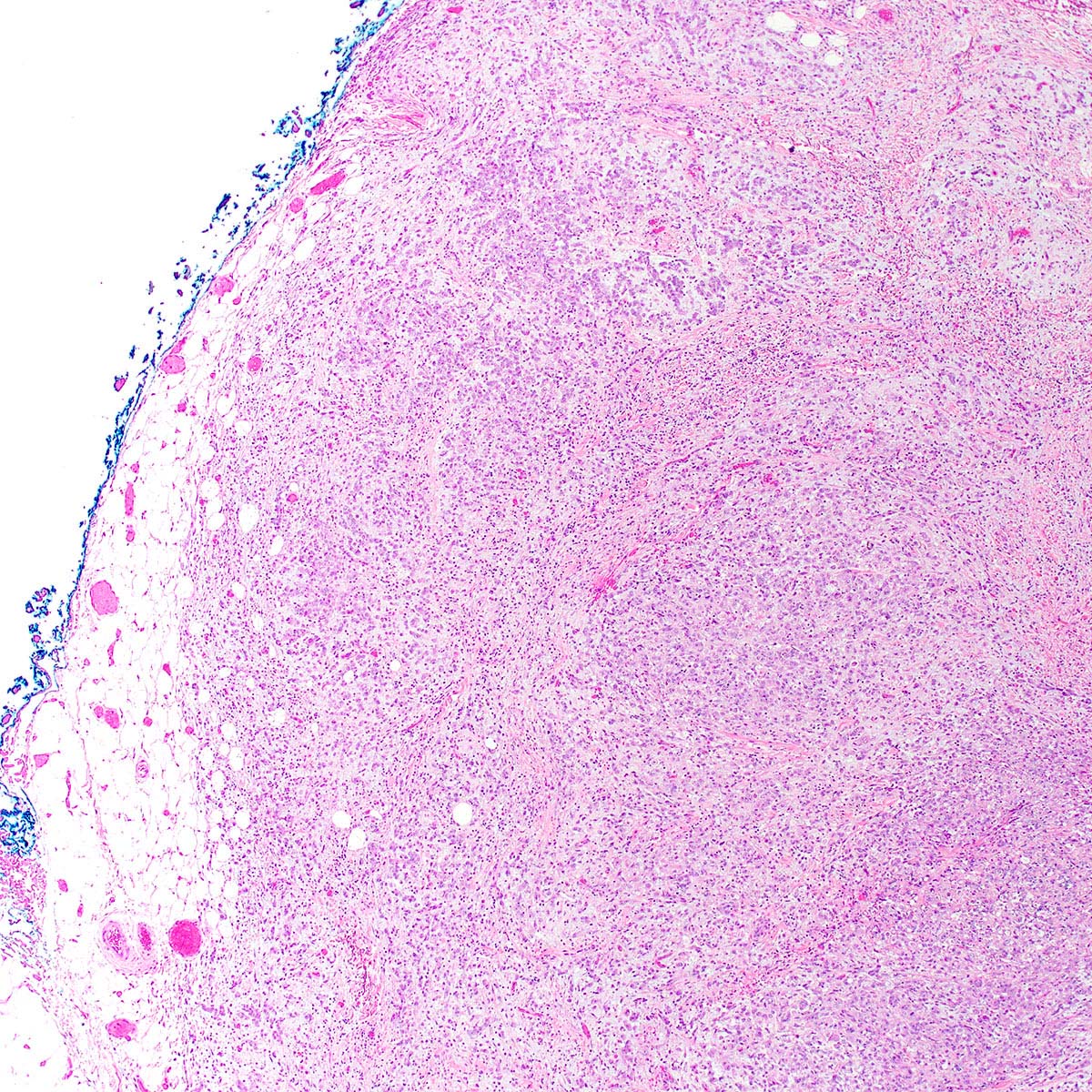
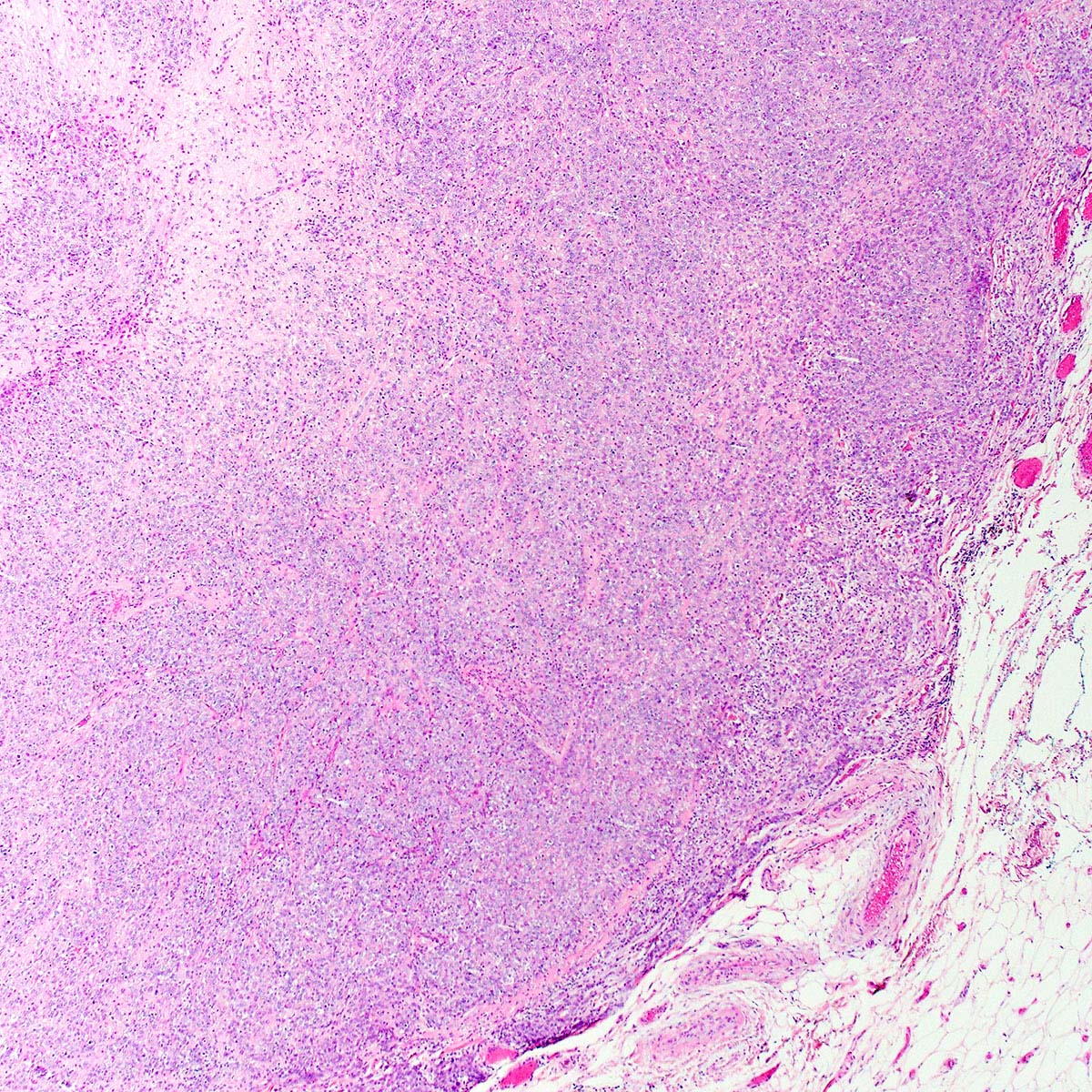
Nested pattern
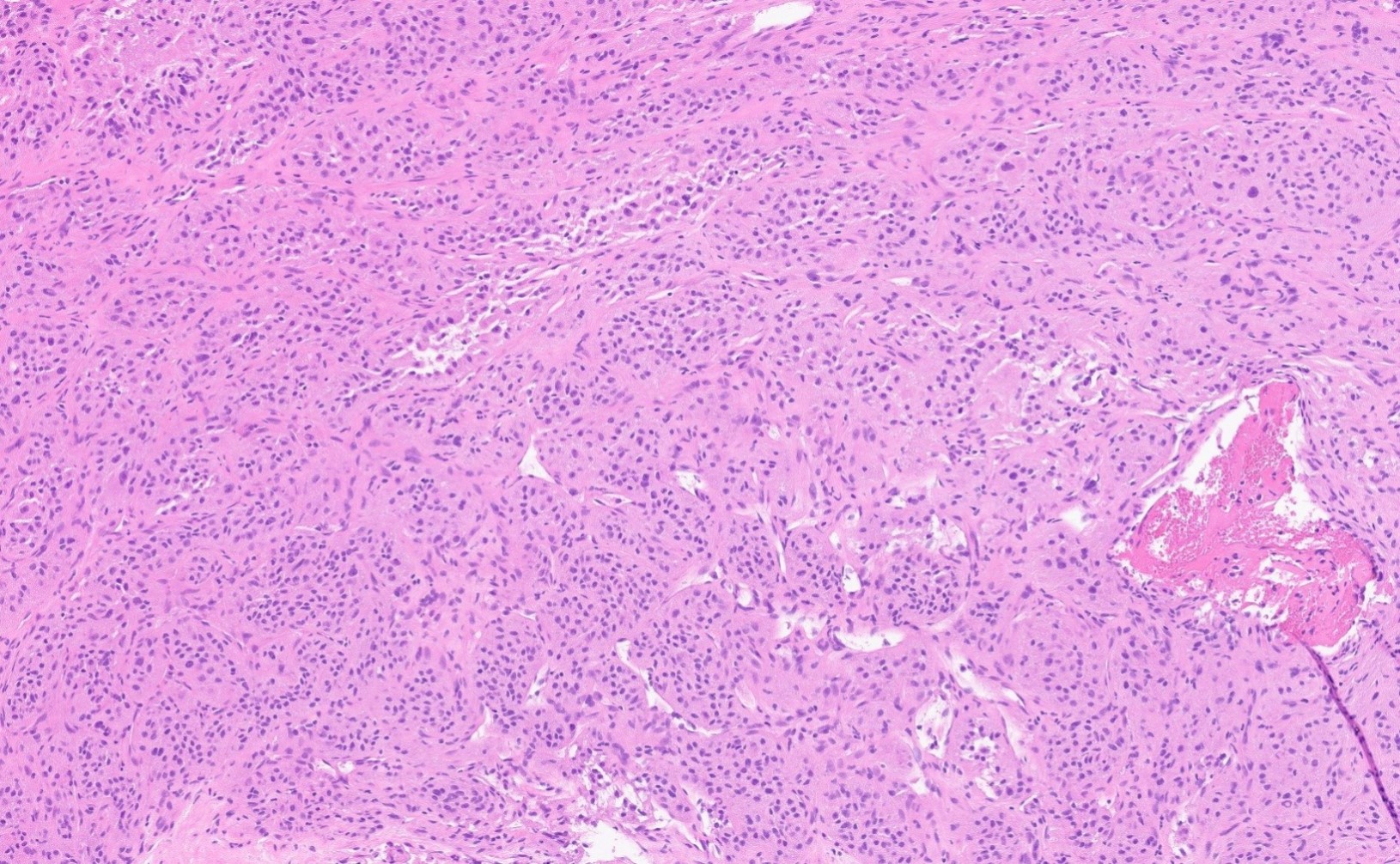
Solid pattern
Vasculature

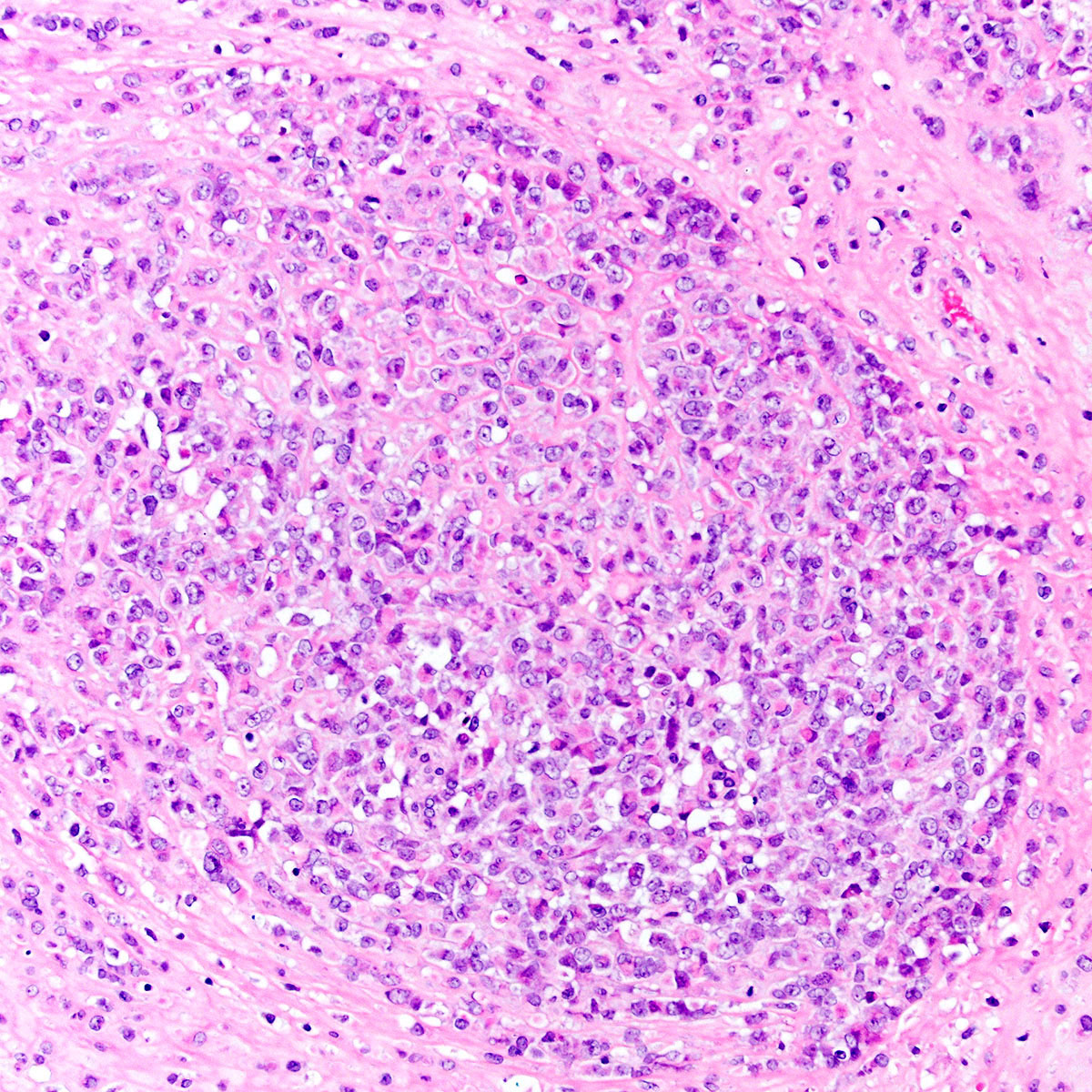
Polygonal cells
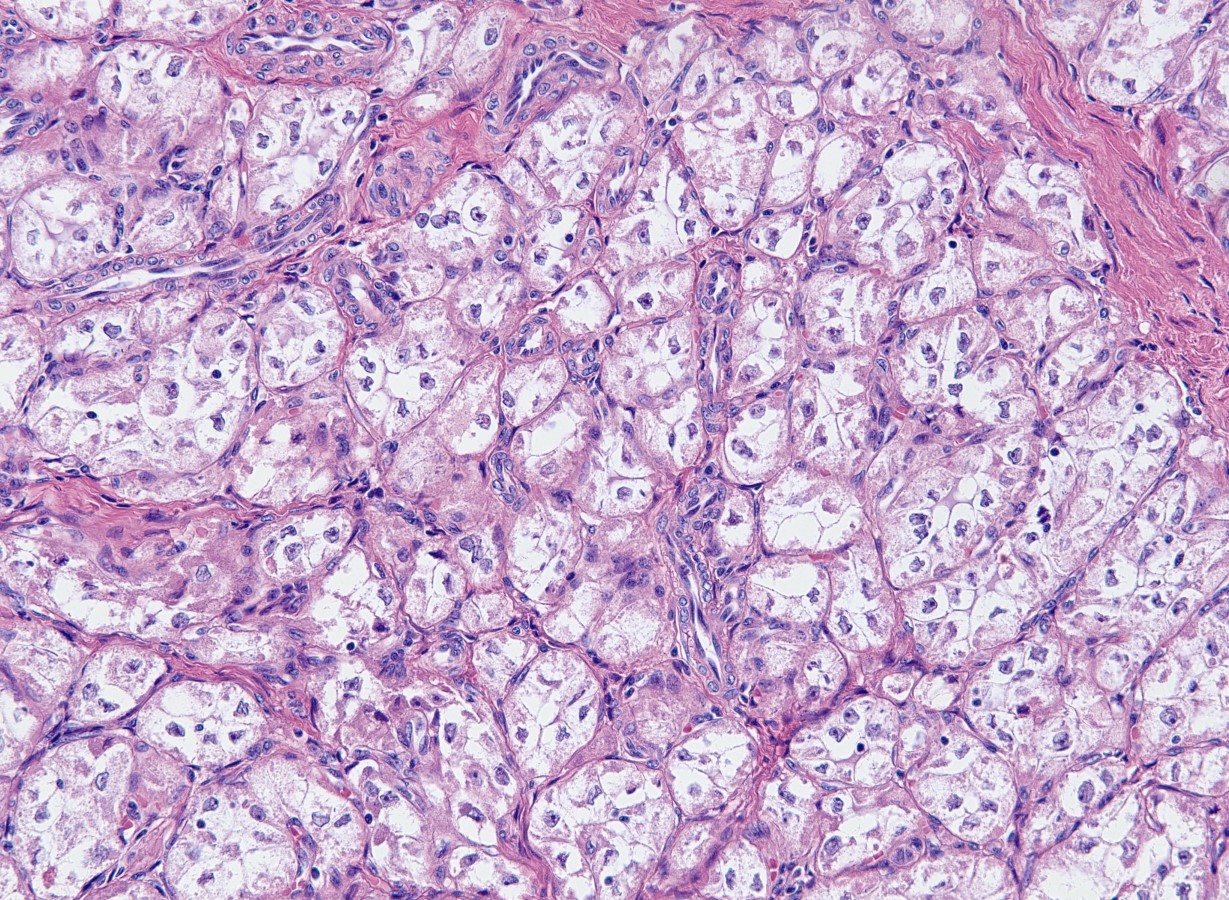
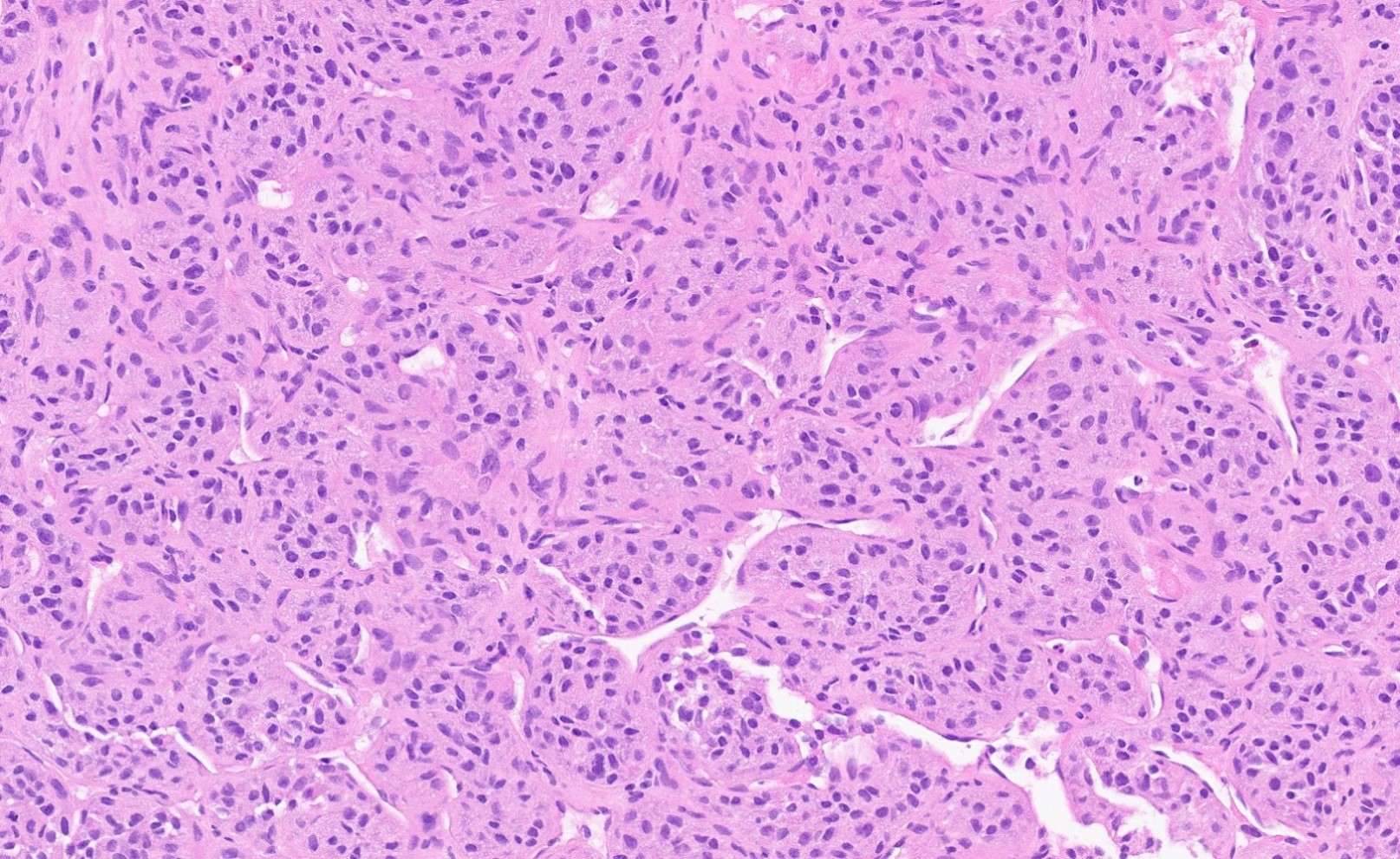
Cells with granular cytoplasm

Cells with monomorphic nuclei and moderate atypia
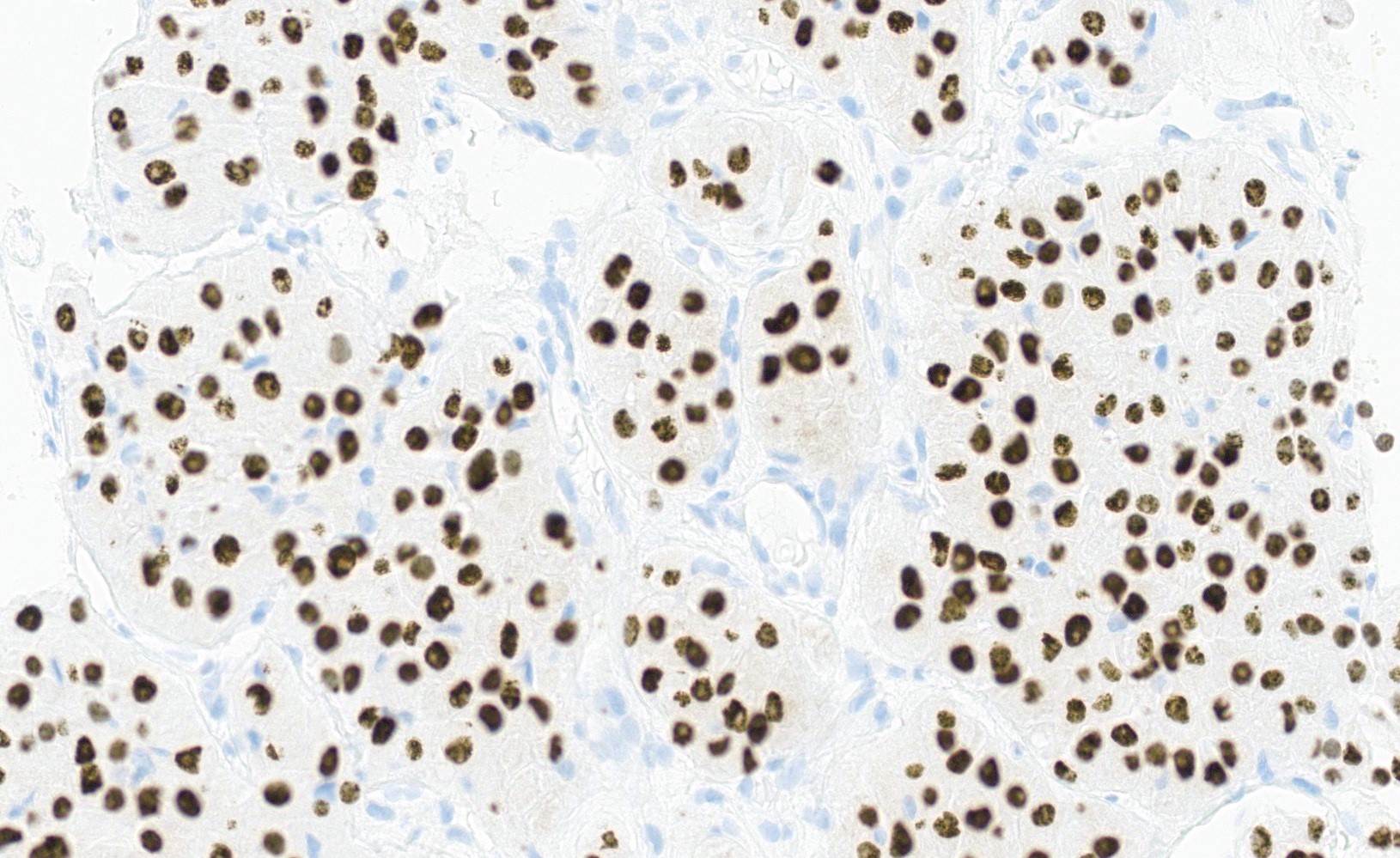
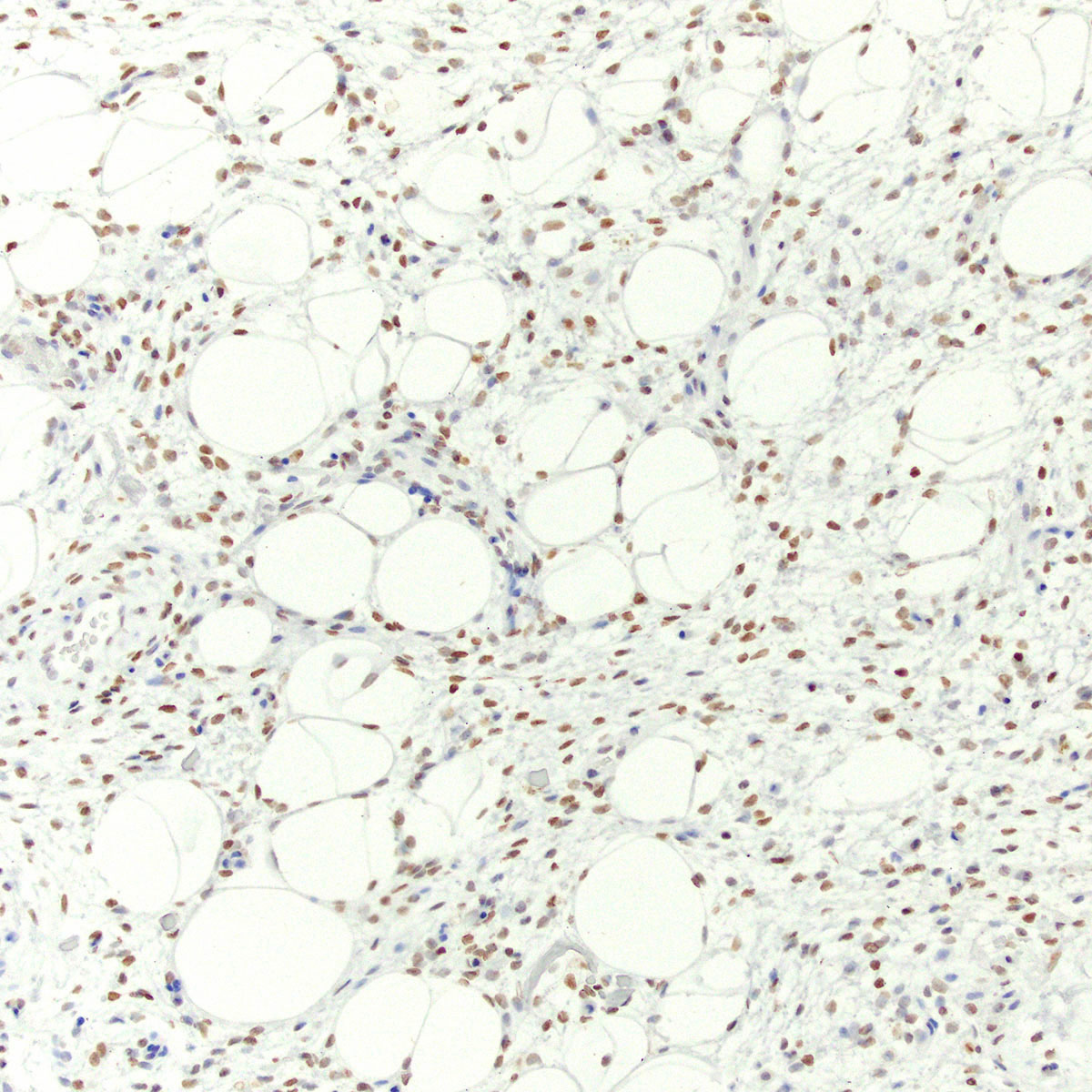
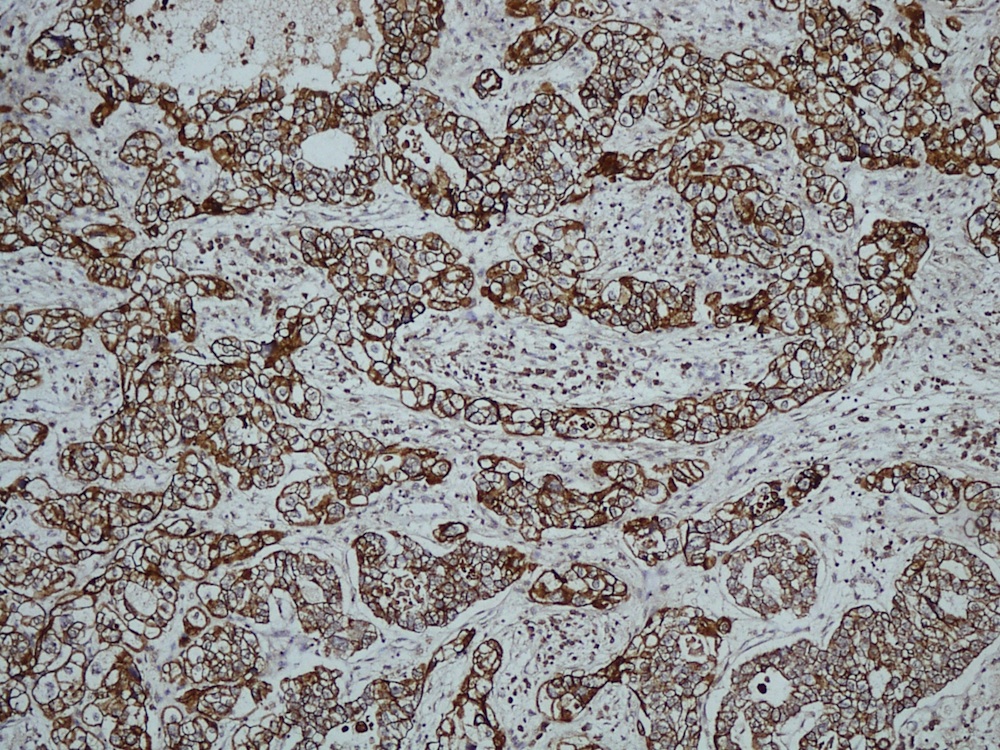
TFE3
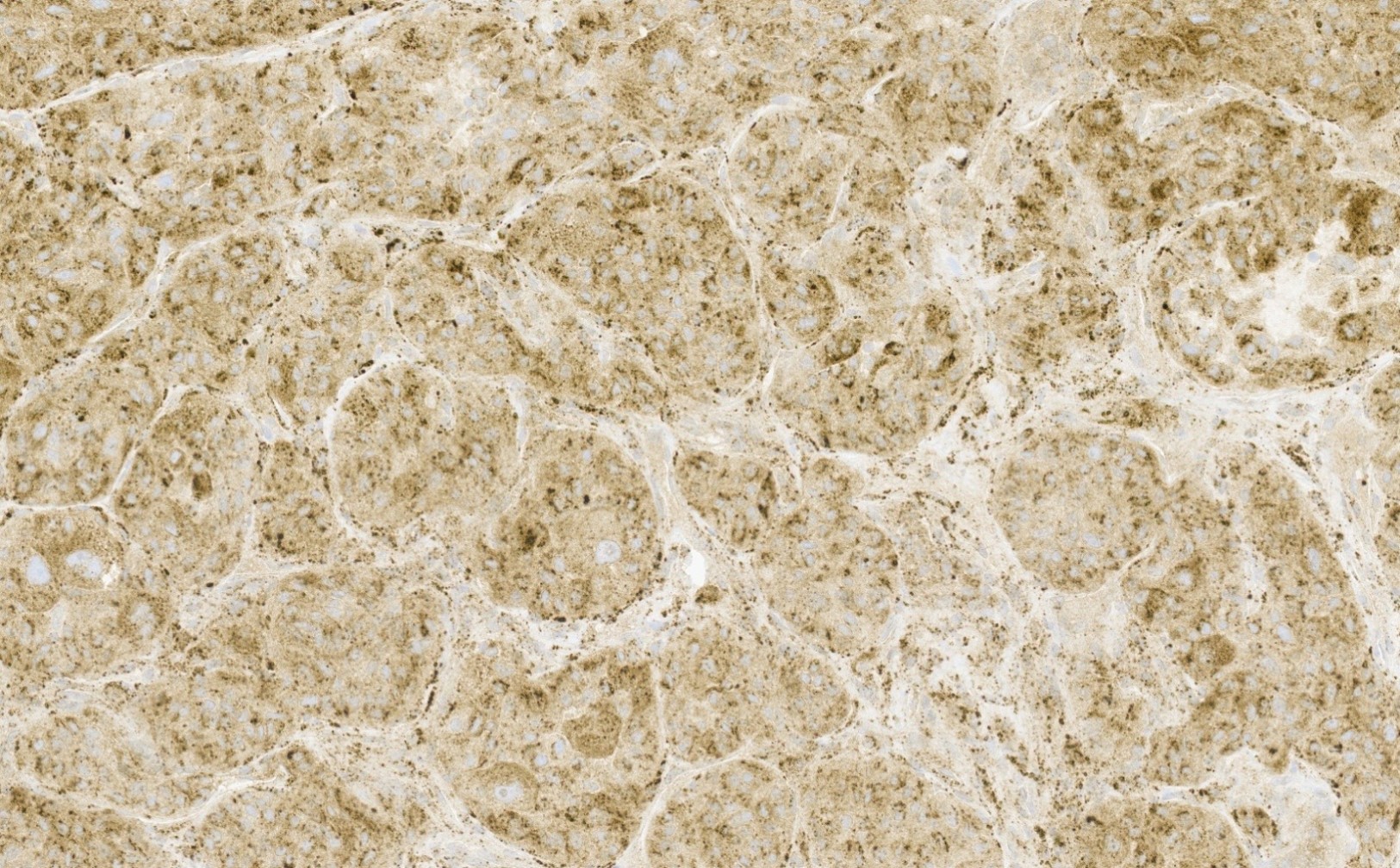
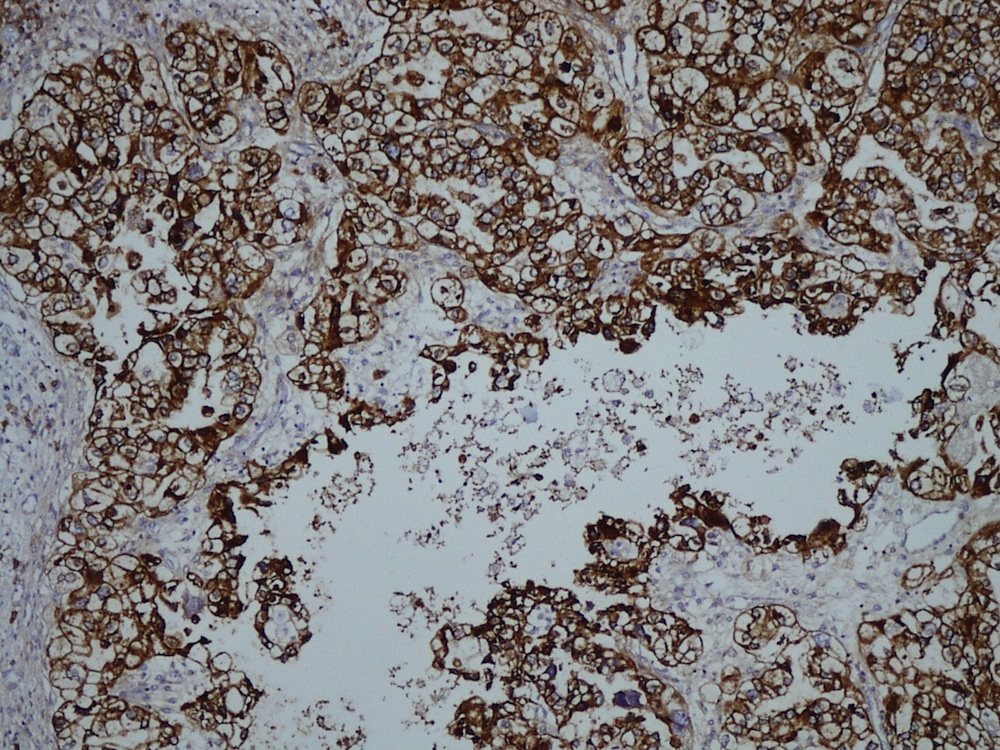
Cathepsin K
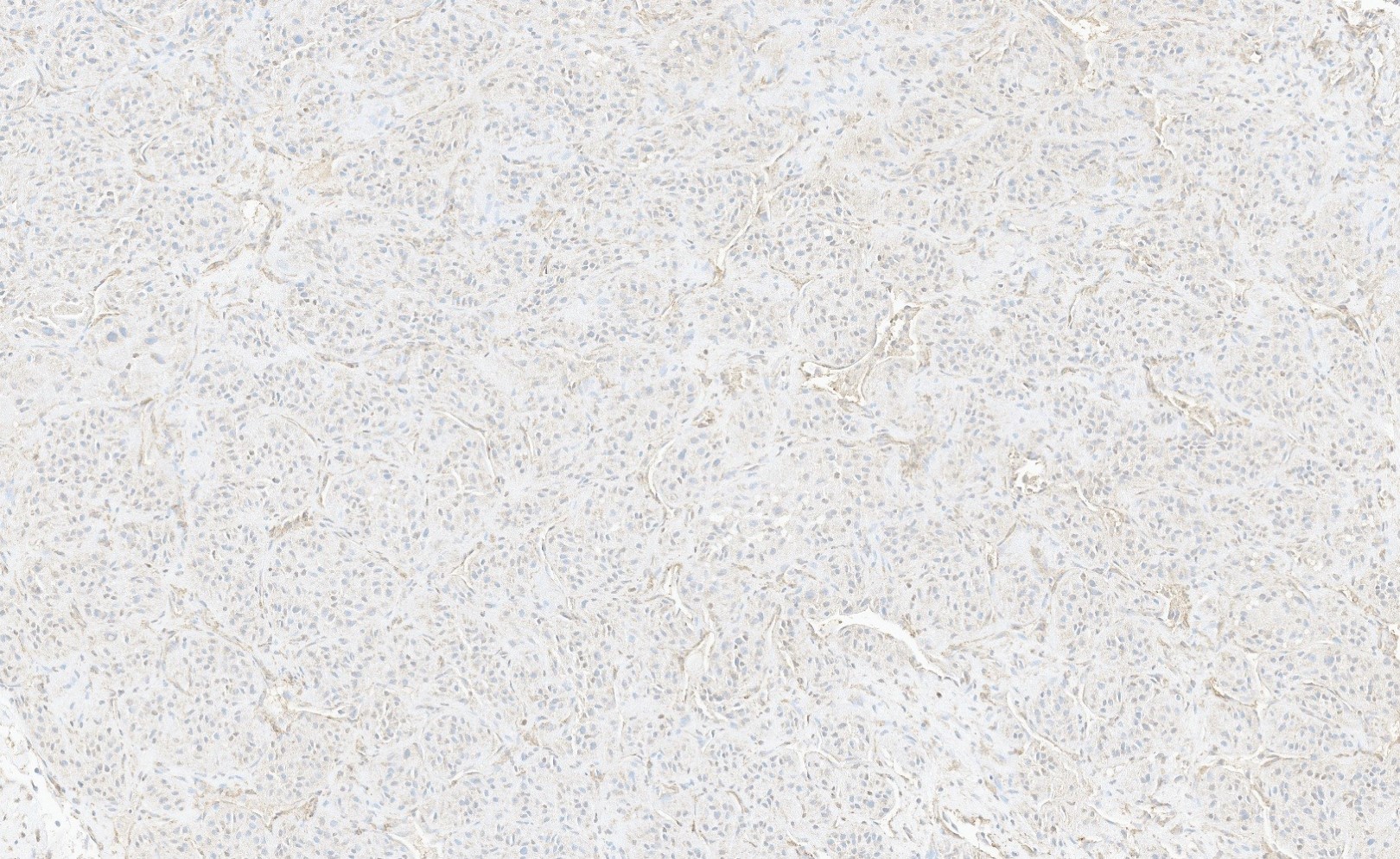
SMA
Images hosted on other servers:

Cytoplasmic electron
dense secretory
granules / rod shaped
crystals
Images hosted on other servers:

ASPL::TFE3 fusion gene in tumor cells
Images hosted on other servers:
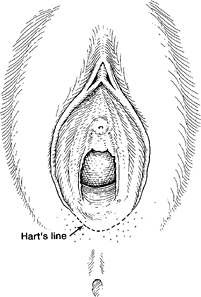
Hart line


Female urethra: embryology and anatomy
Images hosted on other servers:

Labia majora

Vestibule
Contributed by Pooja Srivastava, M.D.
Labia majora overview
Labia minora overview
Vagina overview
Vagina epithelium
Vagina lamina propria
Vagina muscular layer
Normal histology of vagina
Anatomy of female urethra
Histology of female urethra
Images hosted on other servers:


Vaginal ultrasound


Vaginal MRI

Vulvar MRI
Images hosted on other servers:





Intraoperative images
Preoperative image
Images hosted on other servers:

Gross specimen
Contributed by David B. Chapel, M.D.
Alternating cellularity
Spindle cells
Epithelioid cells
Multinucleated cells
Contributed by José Alberto Fonseca Moutinho, M.D.

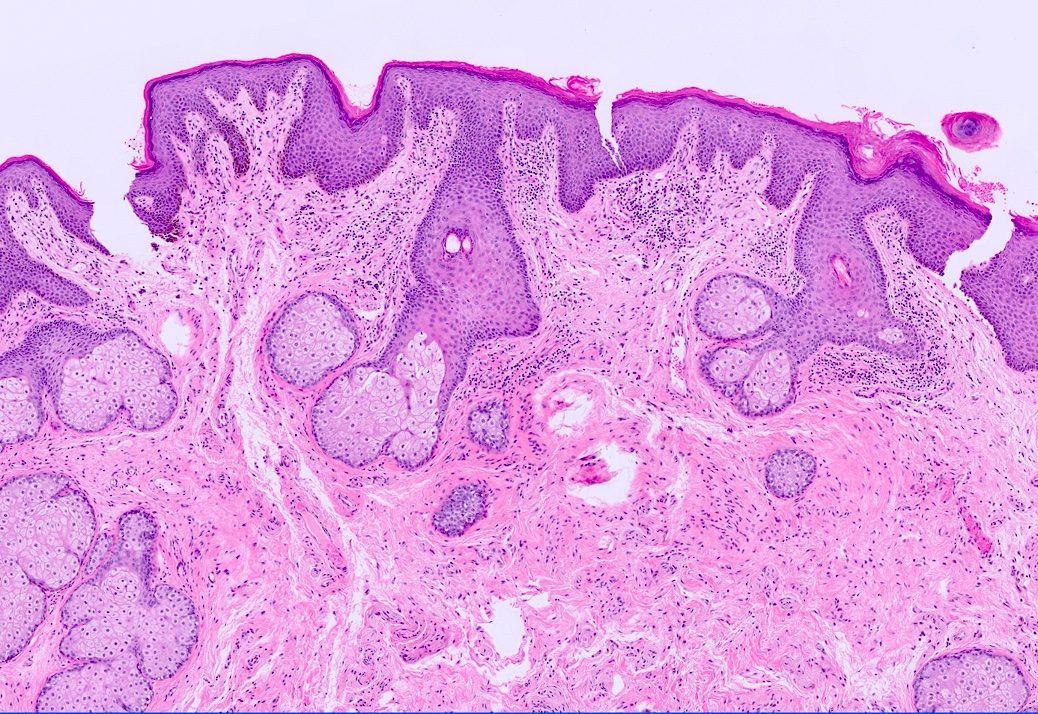
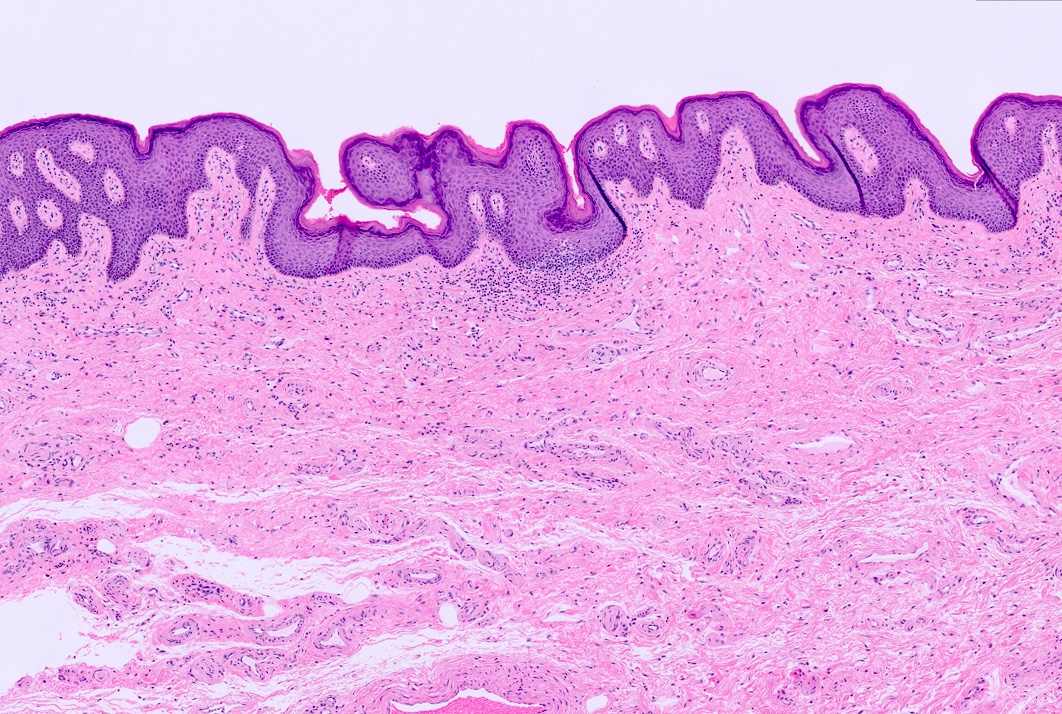
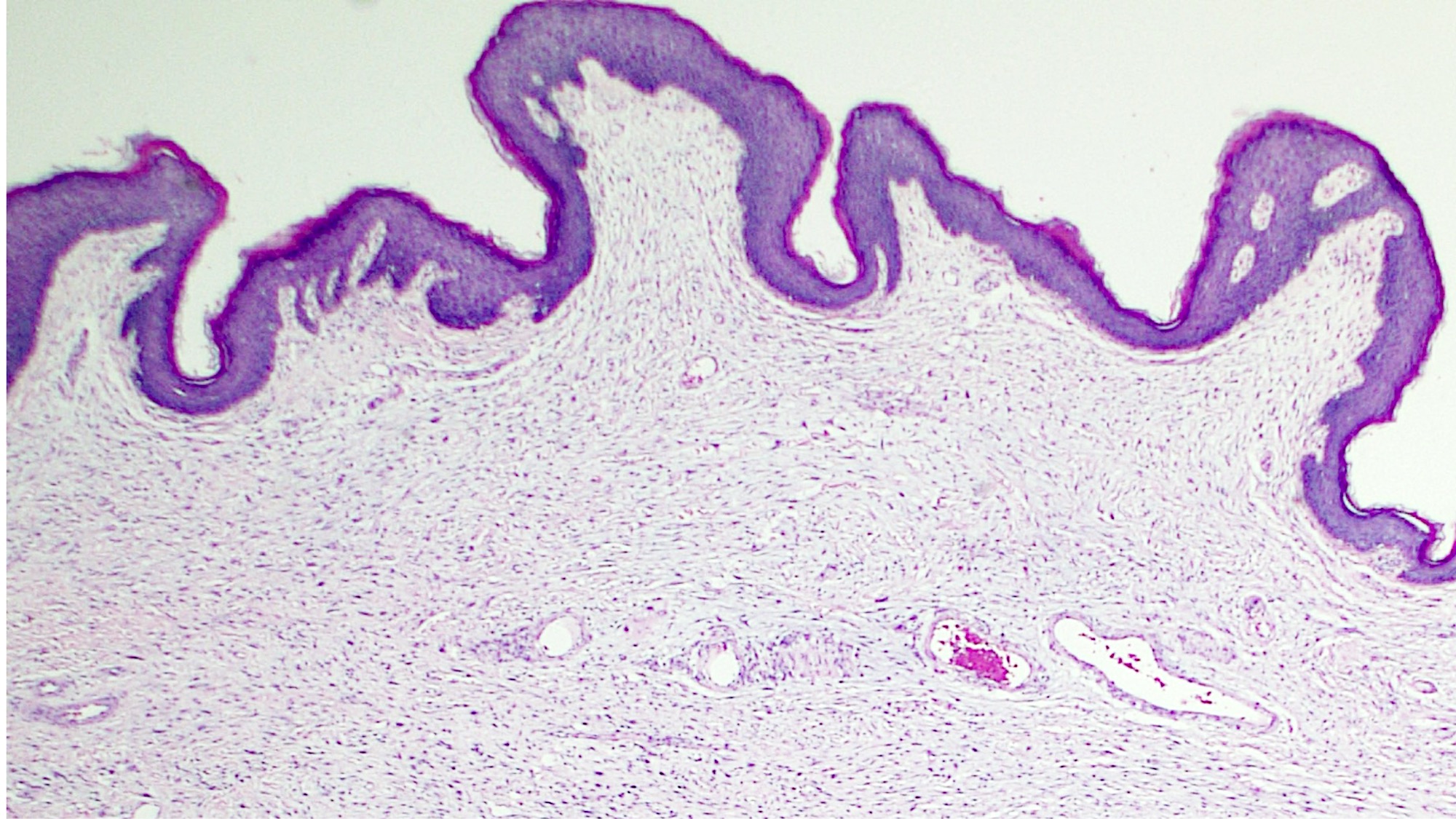
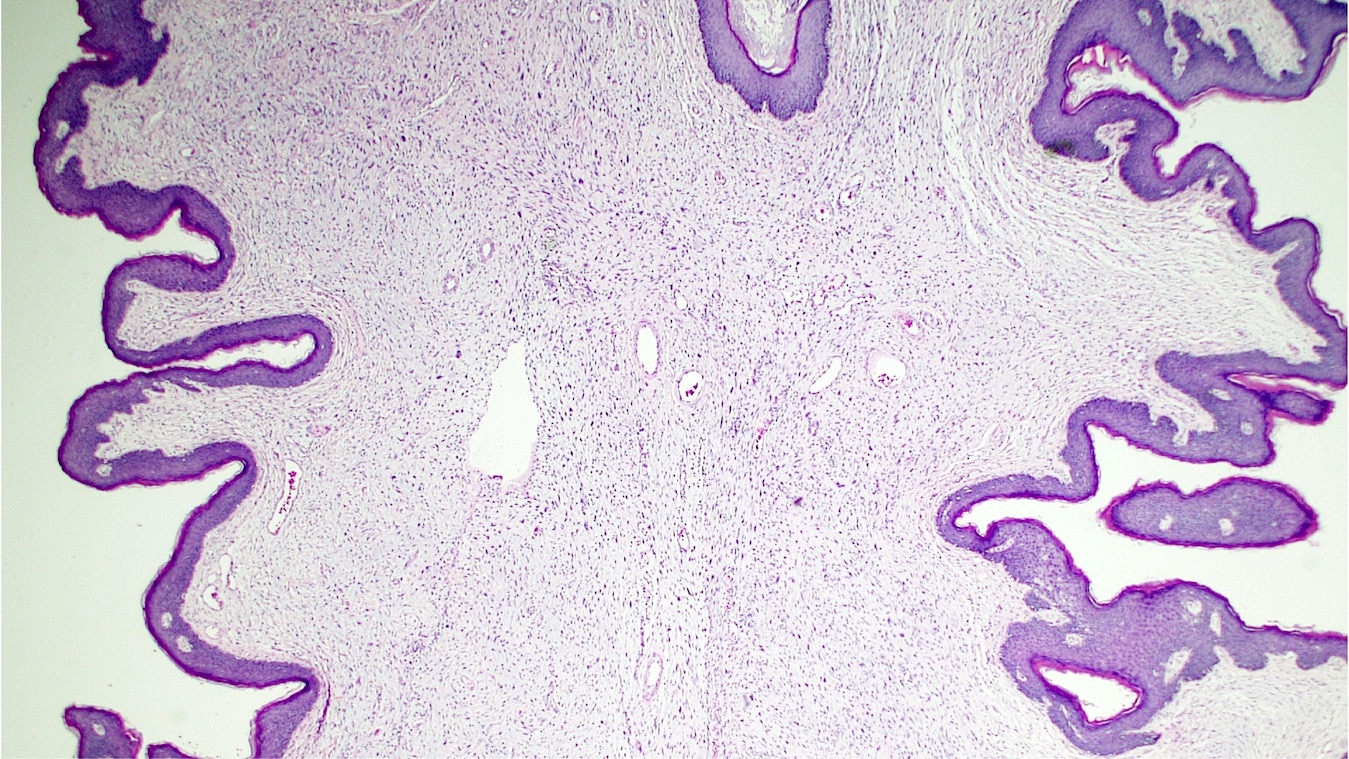
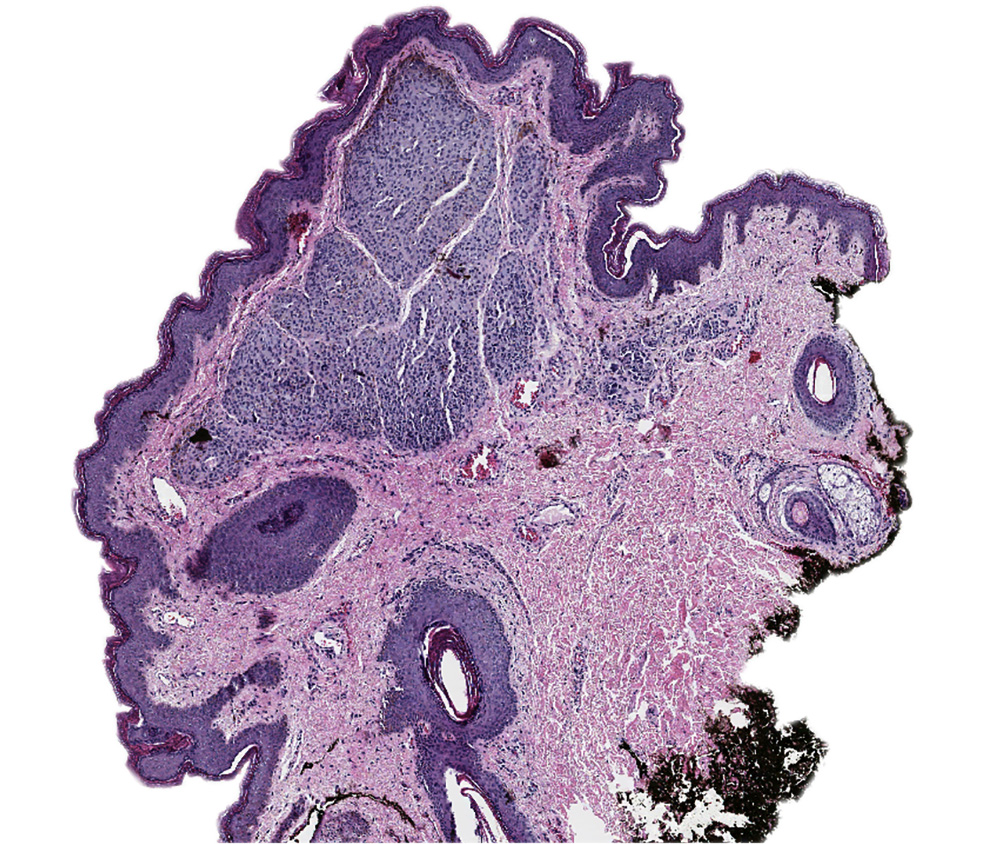
Nevus
Images hosted on other servers:

Irregular dots on the periphery of the lesion

Pigmented lesion
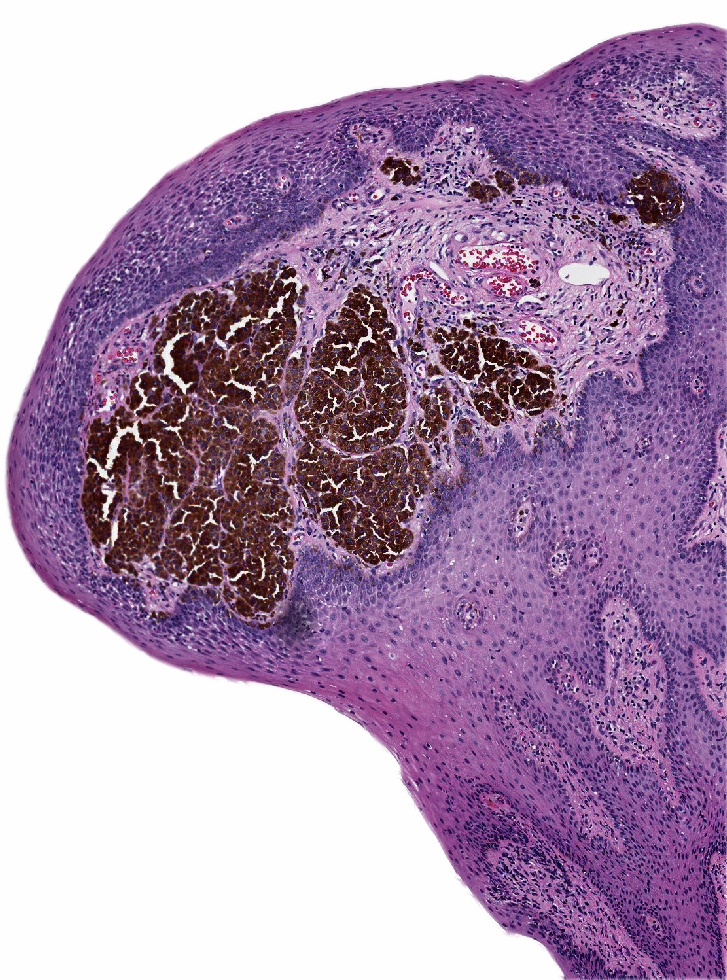
Contributed by Anna Sarah Erem, M.D. and Gulisa Turashvili, M.D., Ph.D.
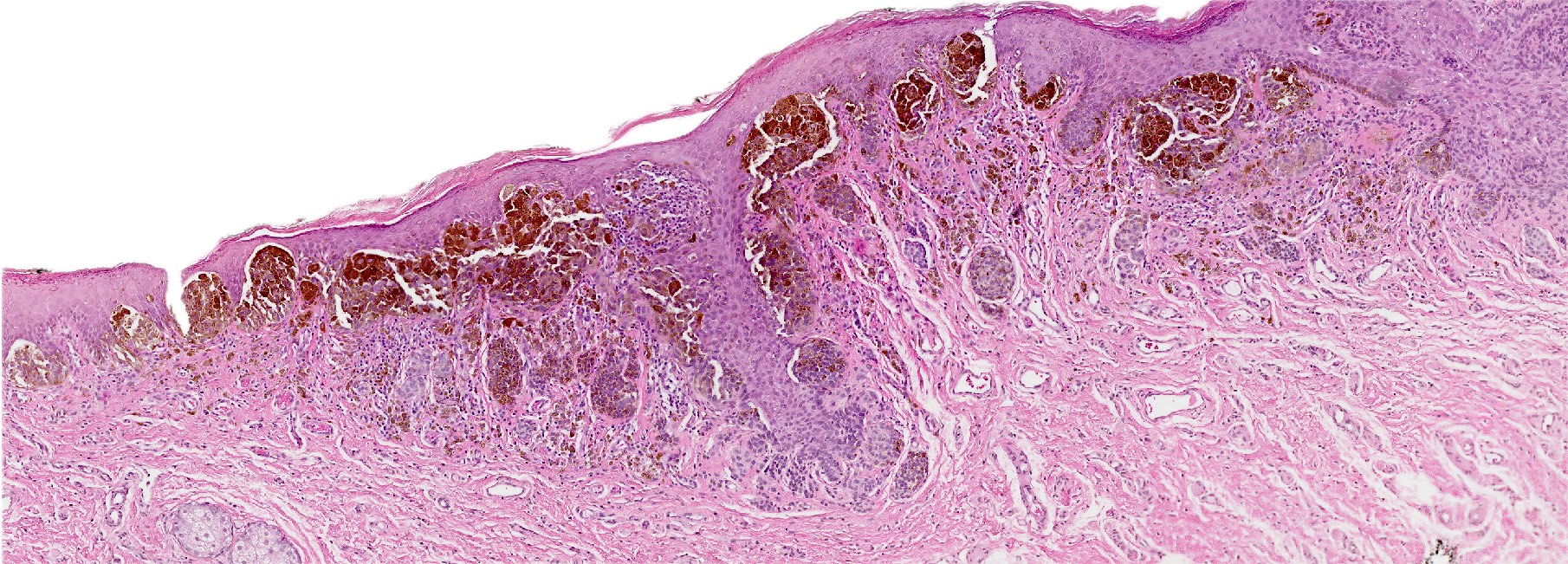
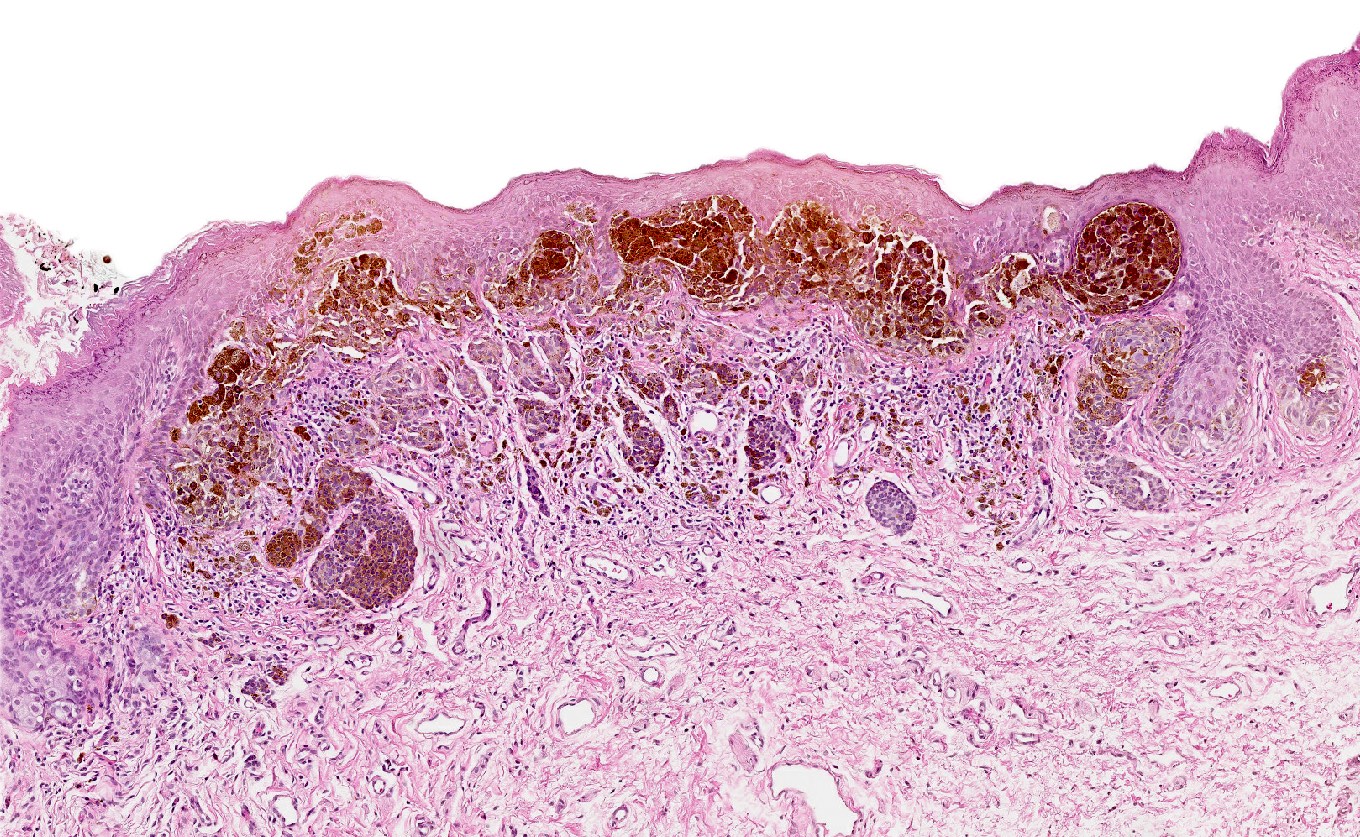
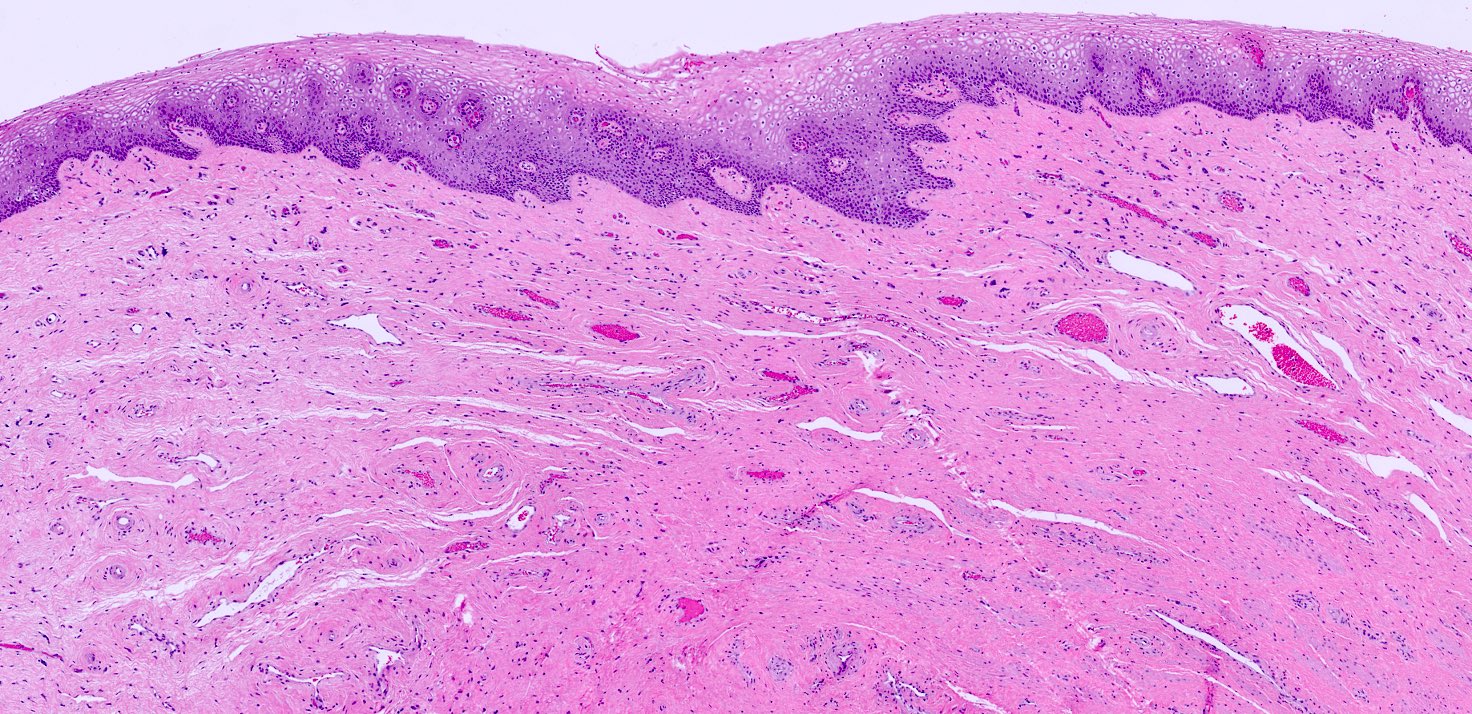
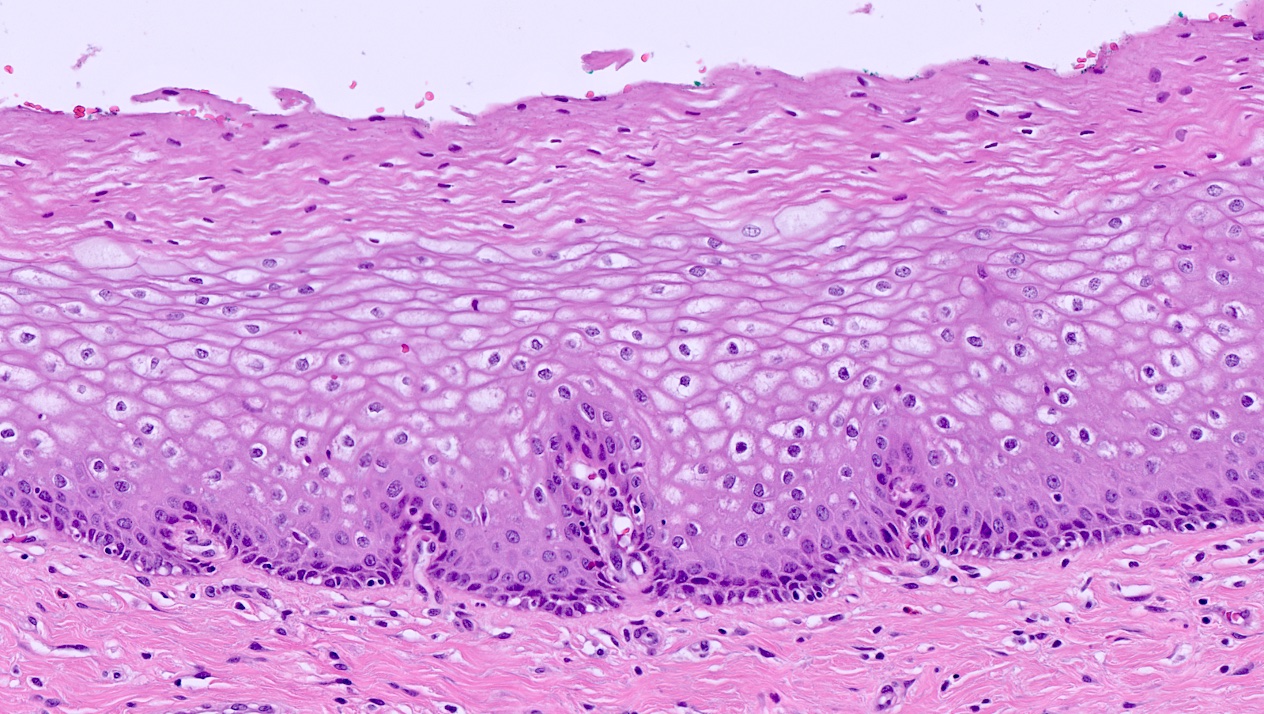
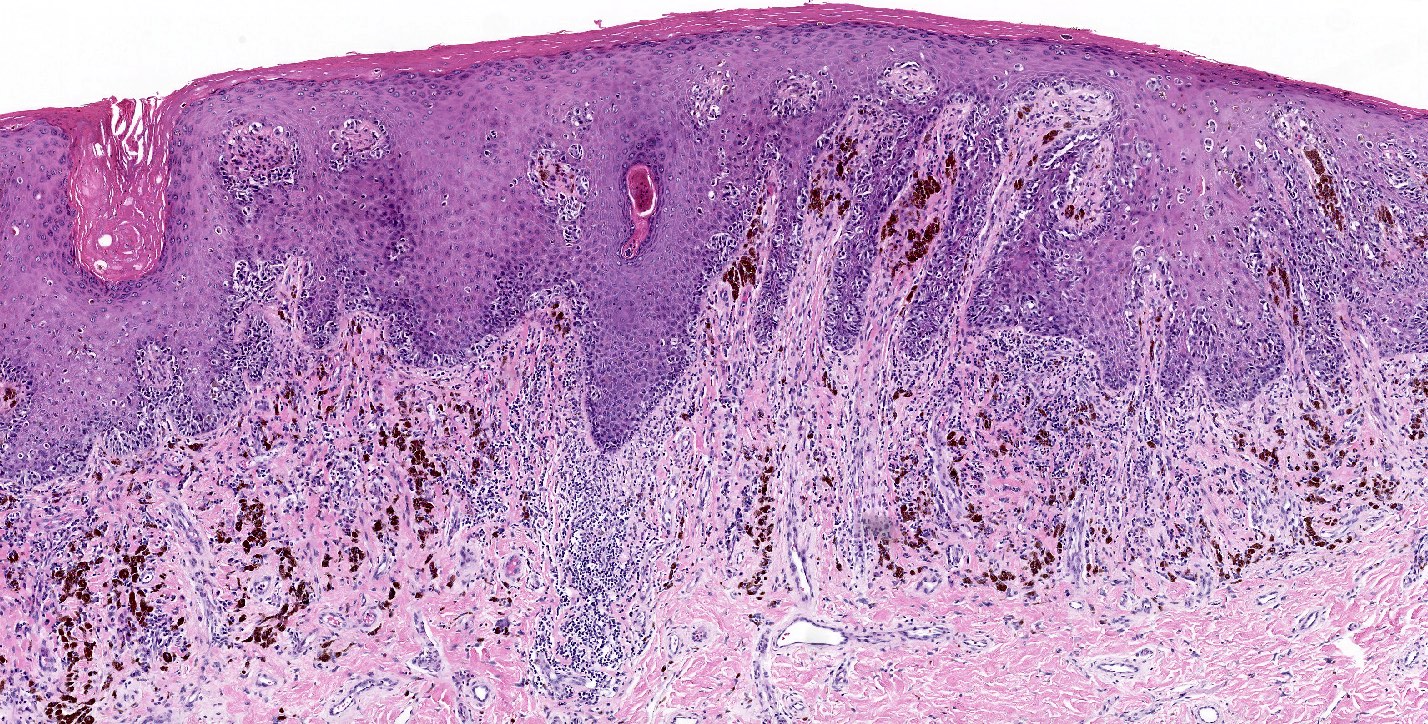
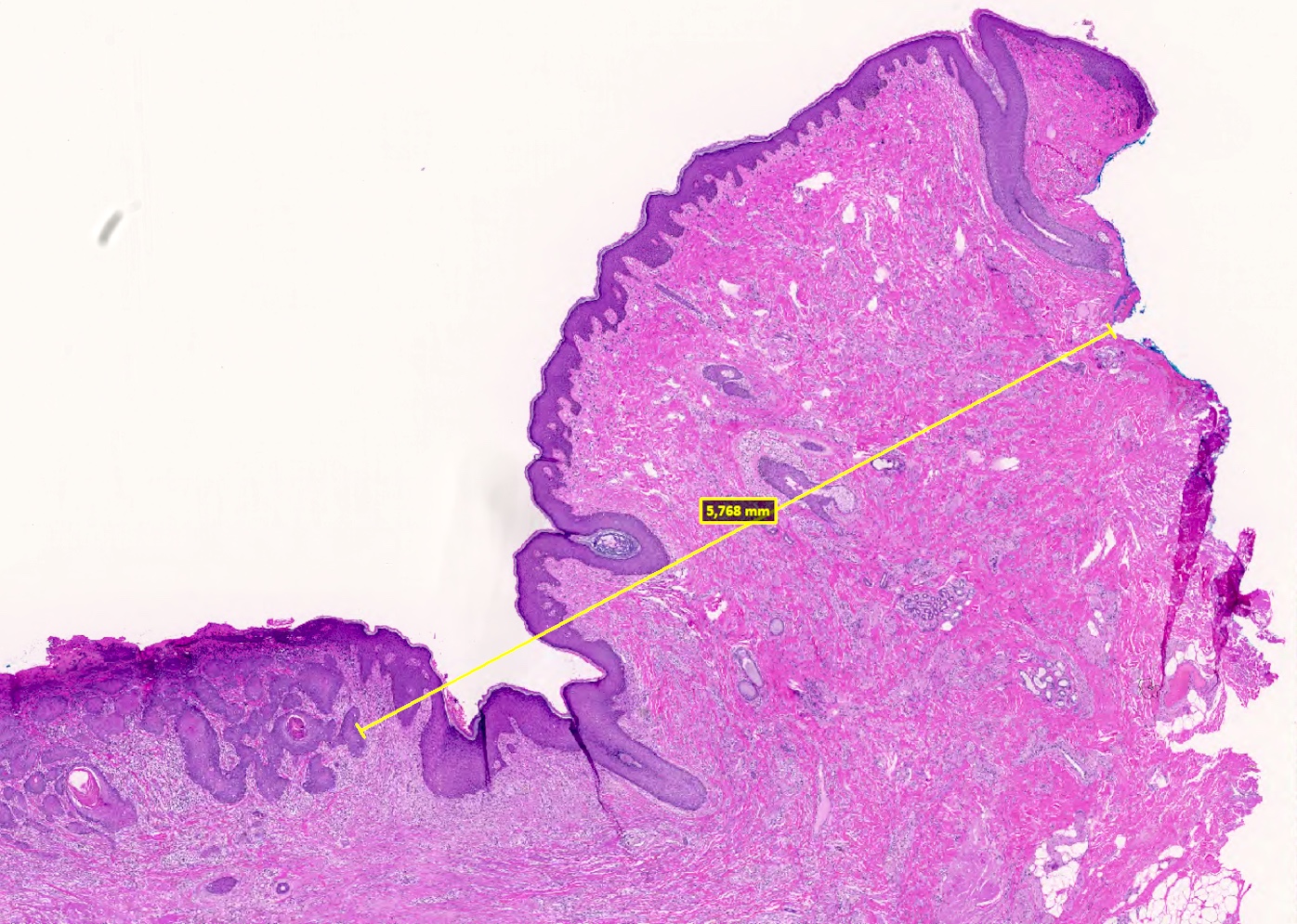
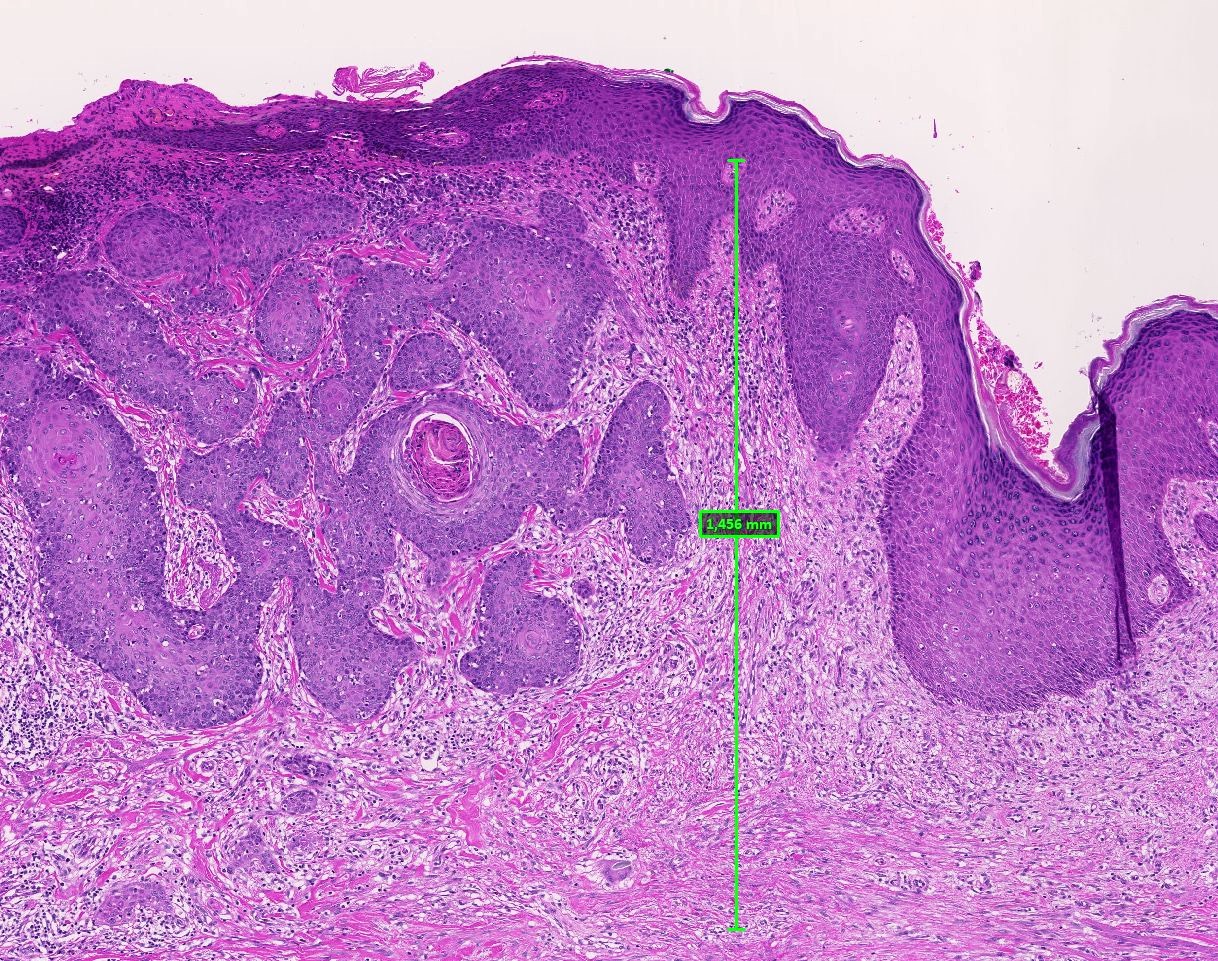
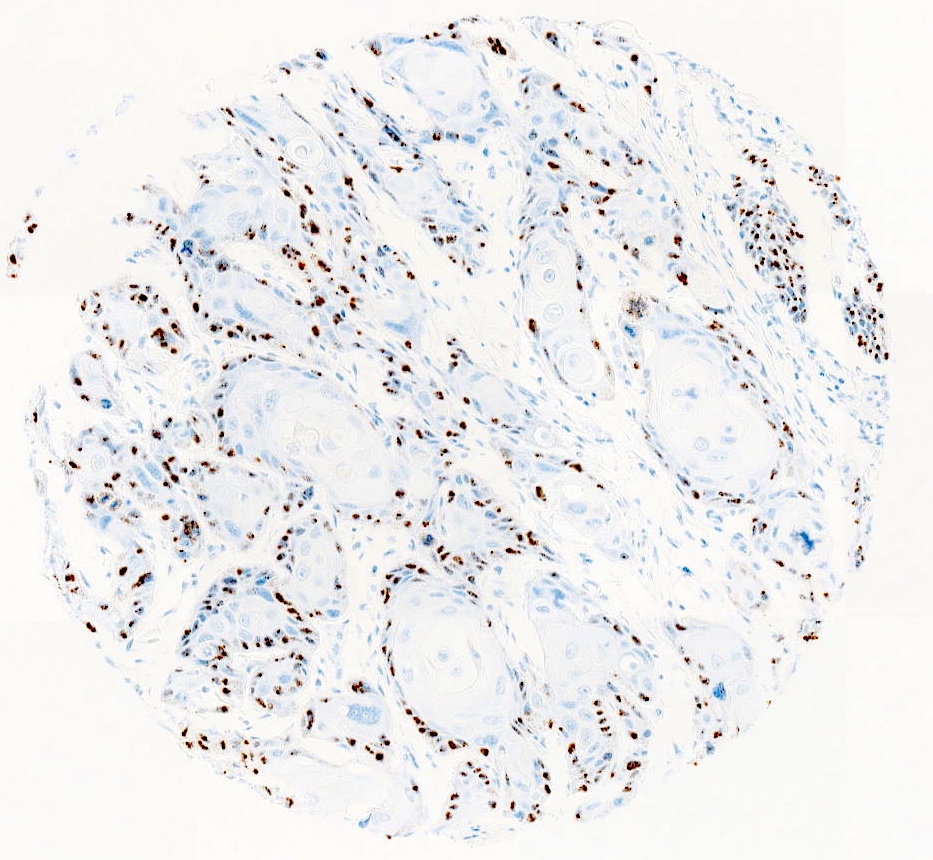
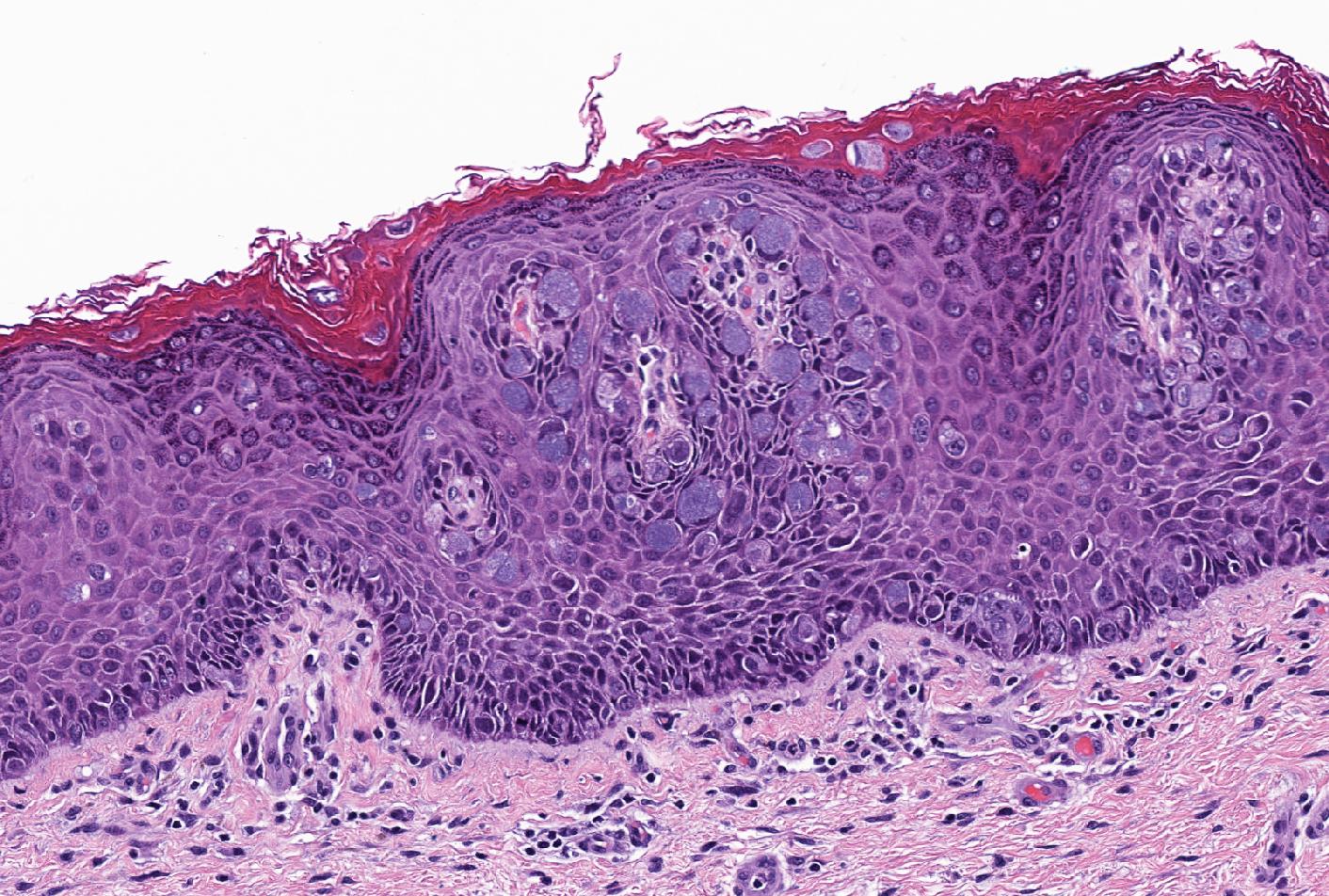
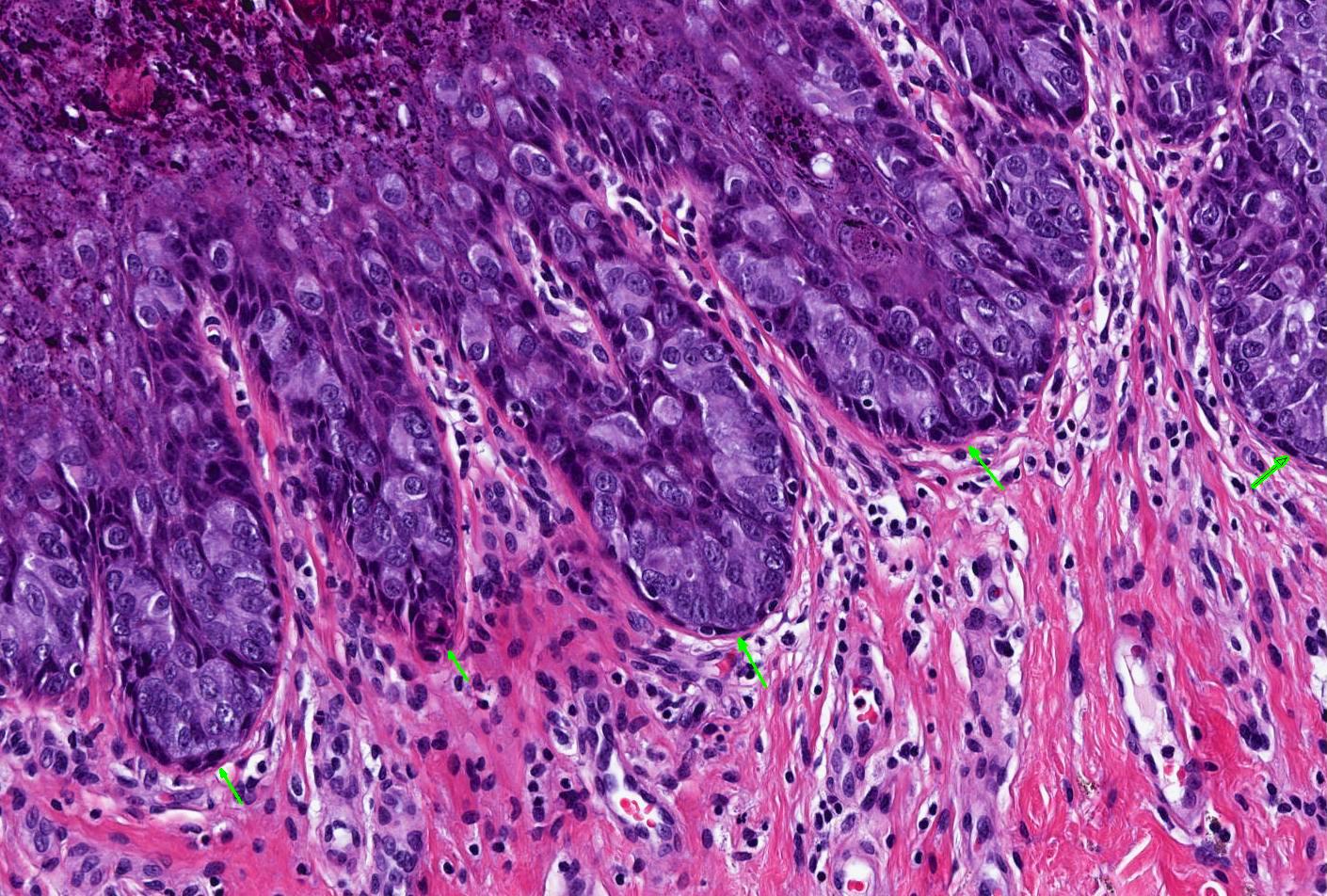
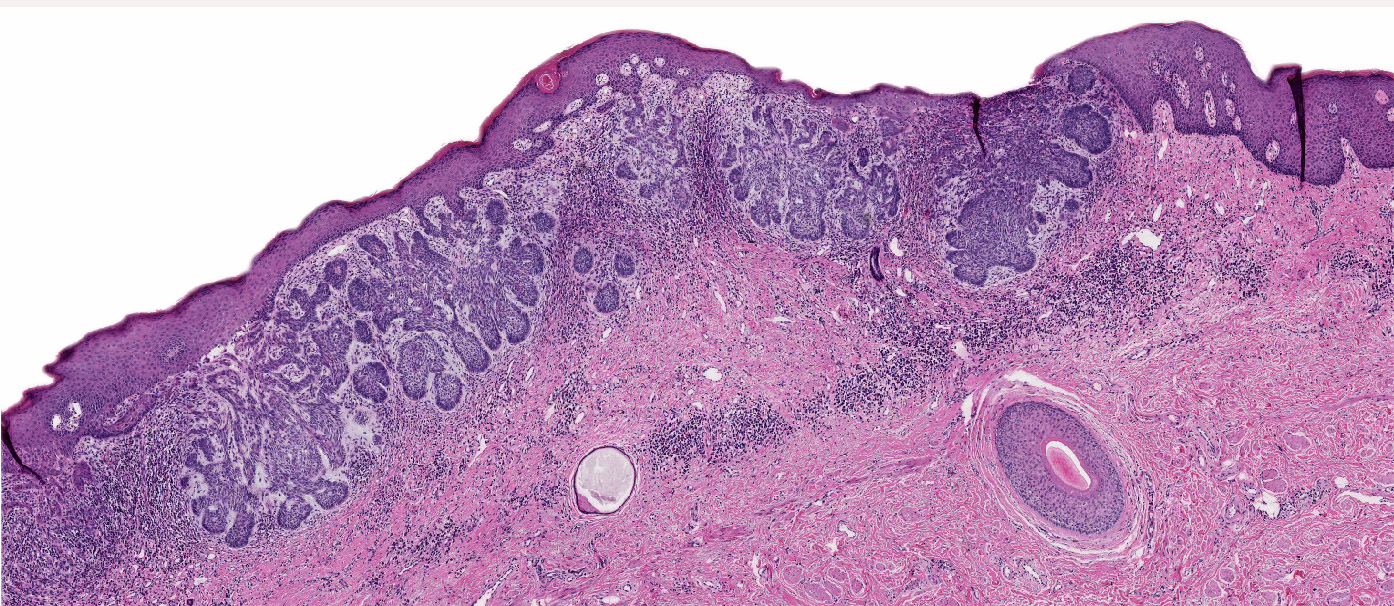
Atypical melanocytic proliferation
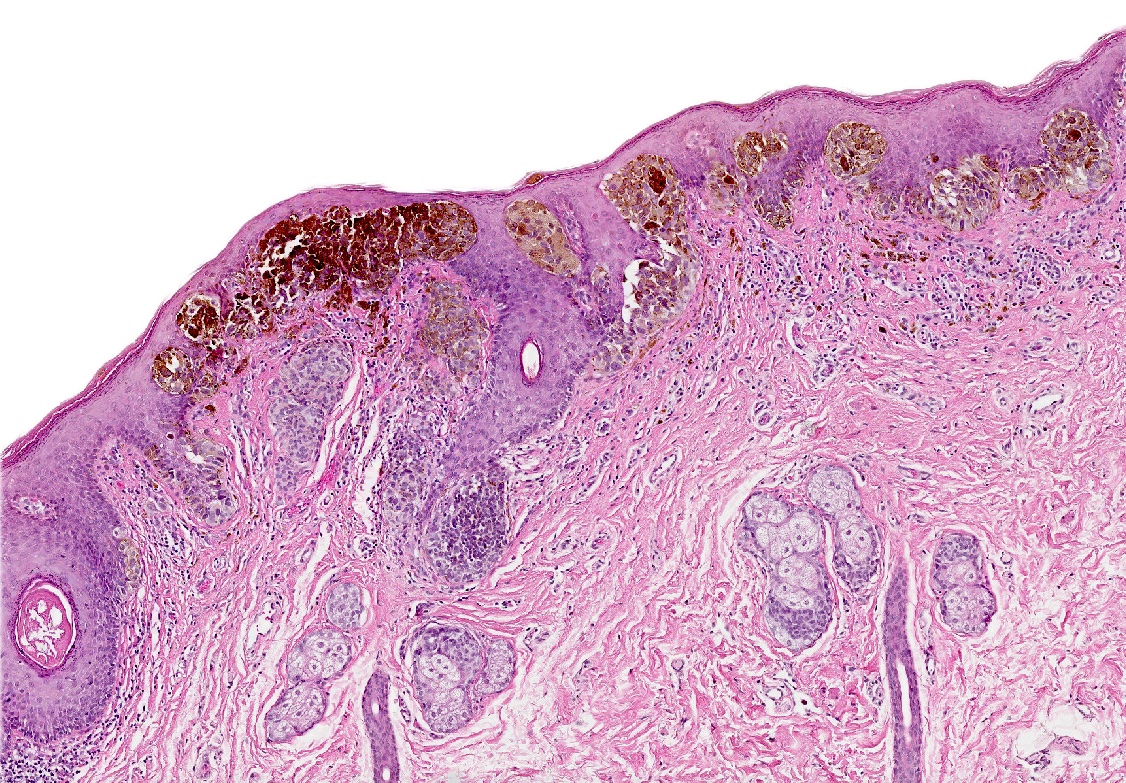
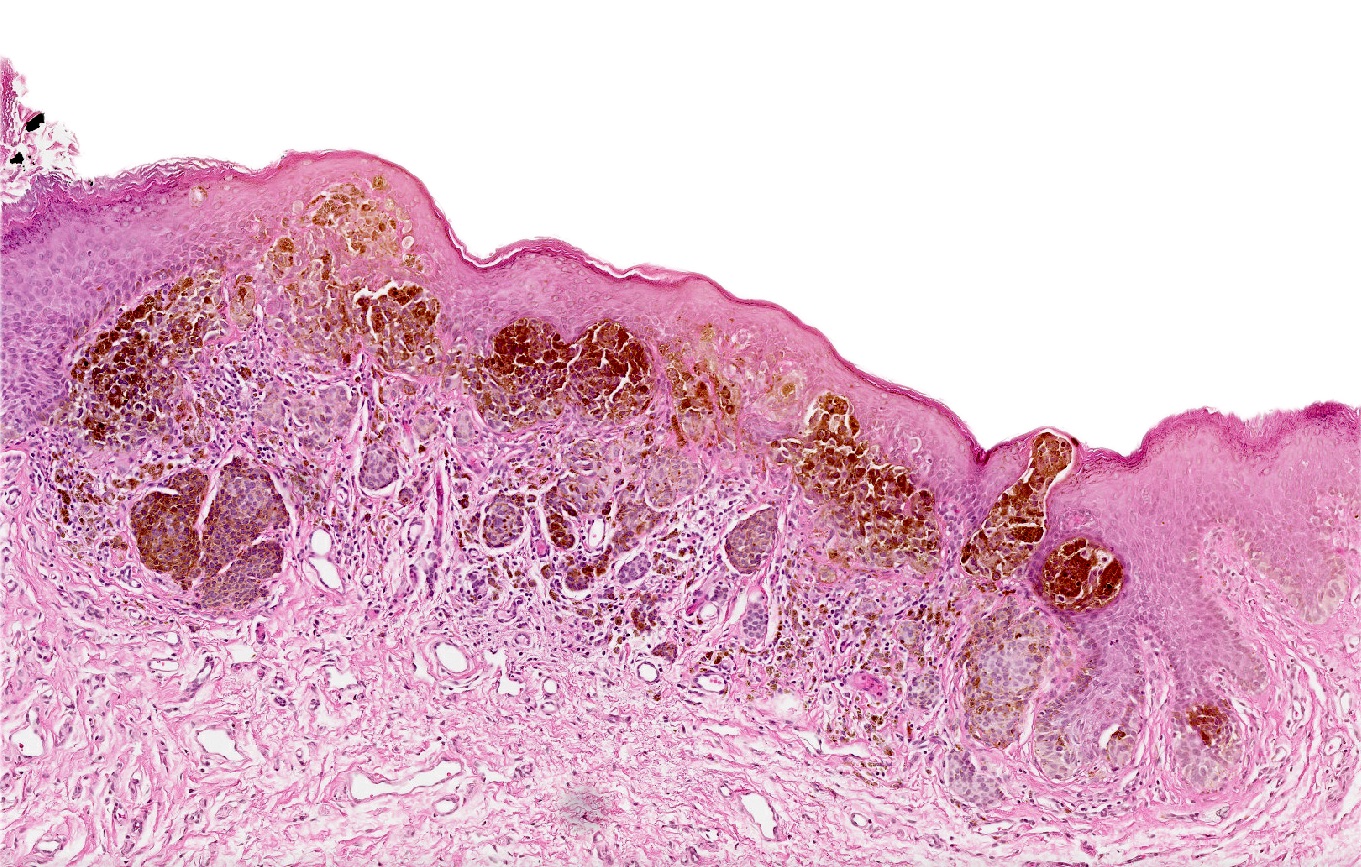
Atypical melanocytic proliferation
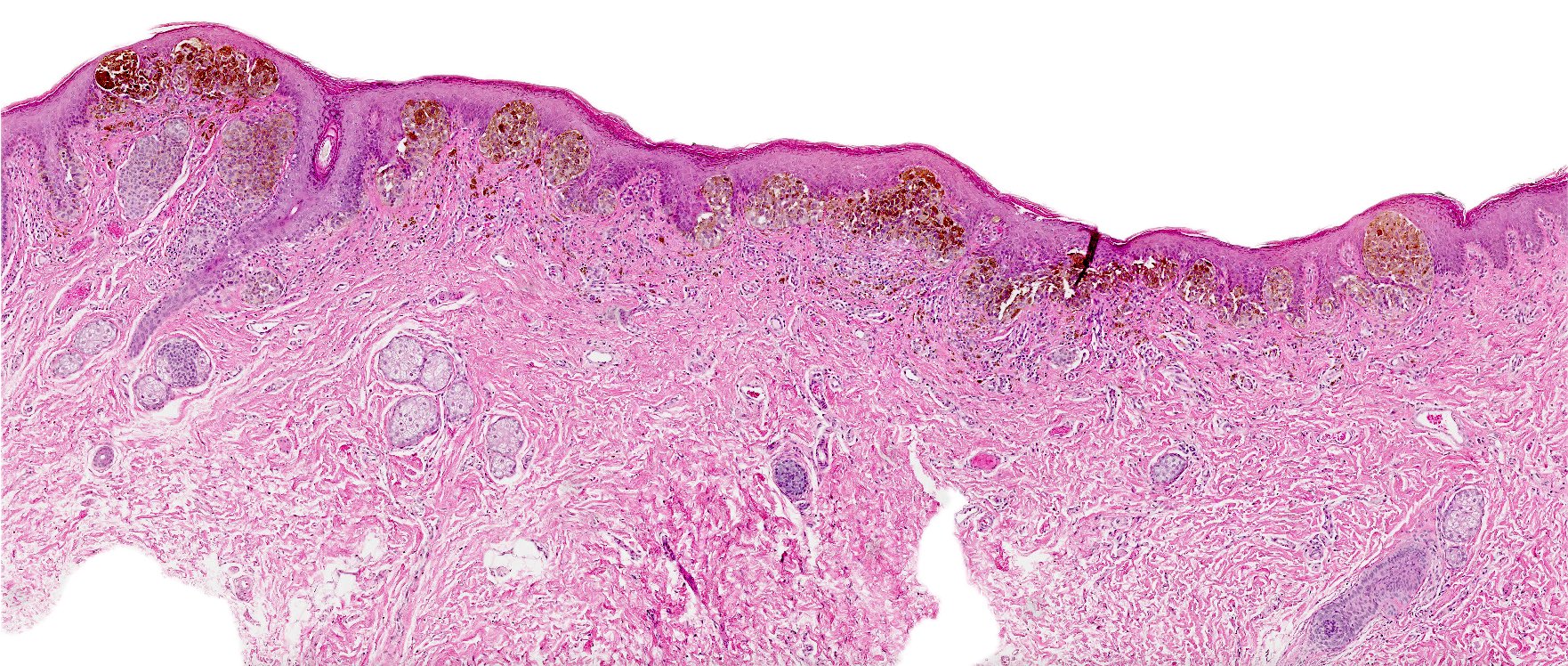
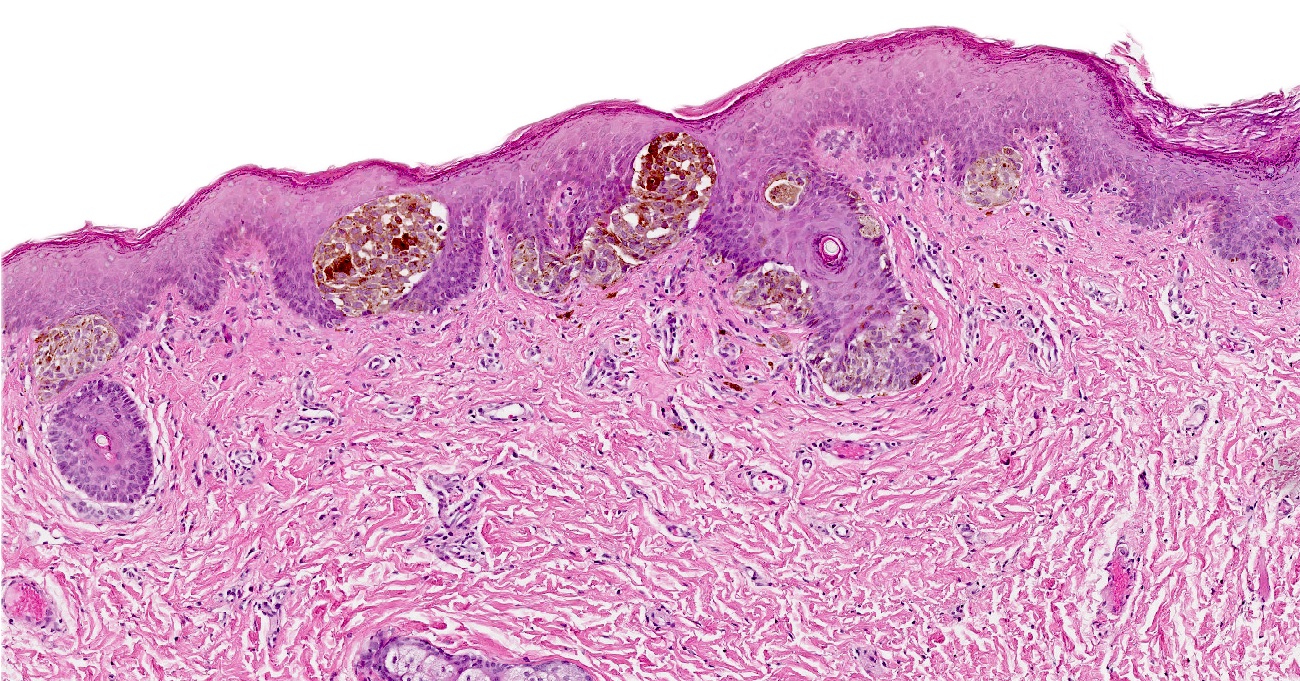
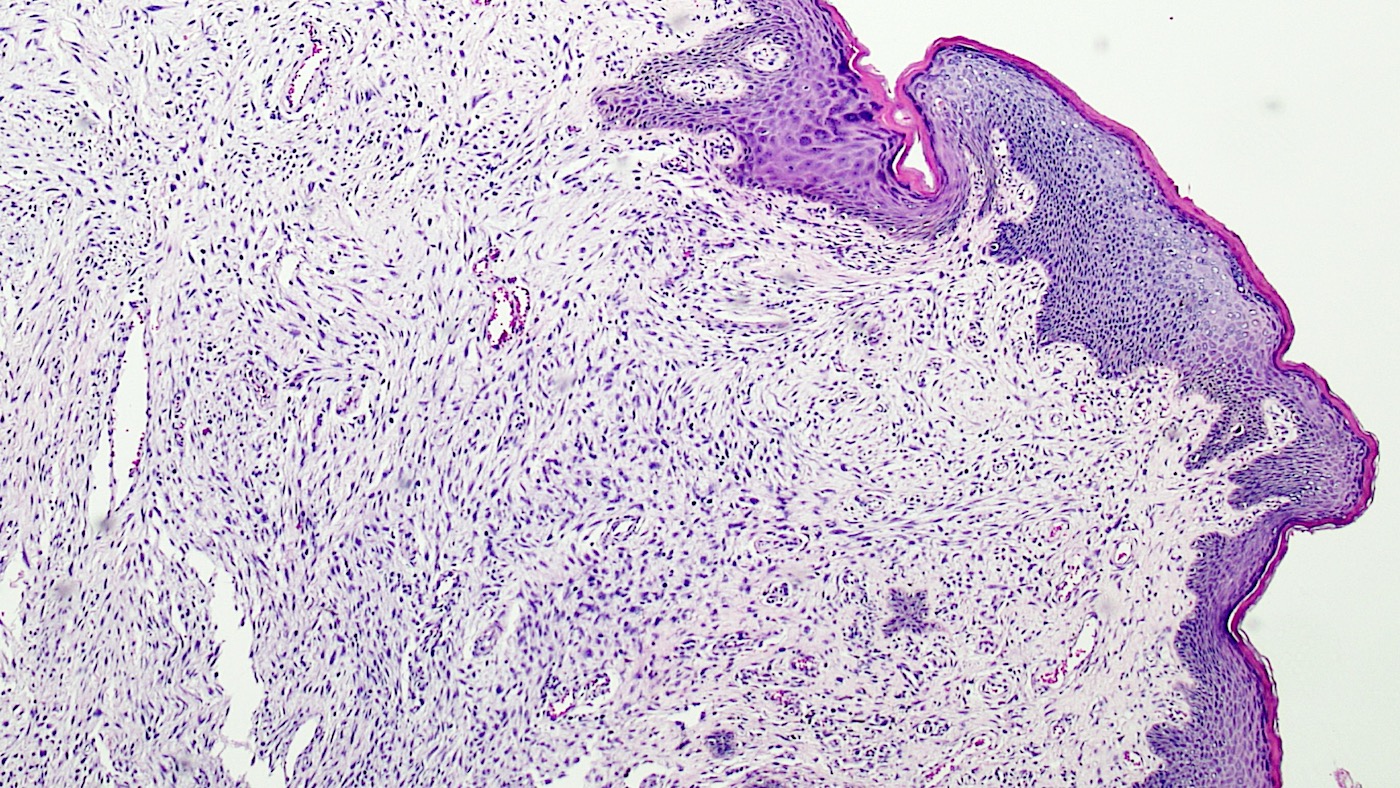
Atypical genital nevi
Atypical nevi and nevi of special sites by Dr. Phillip McKee
Atypical nevi and melanoma by Dr. Steven Wang
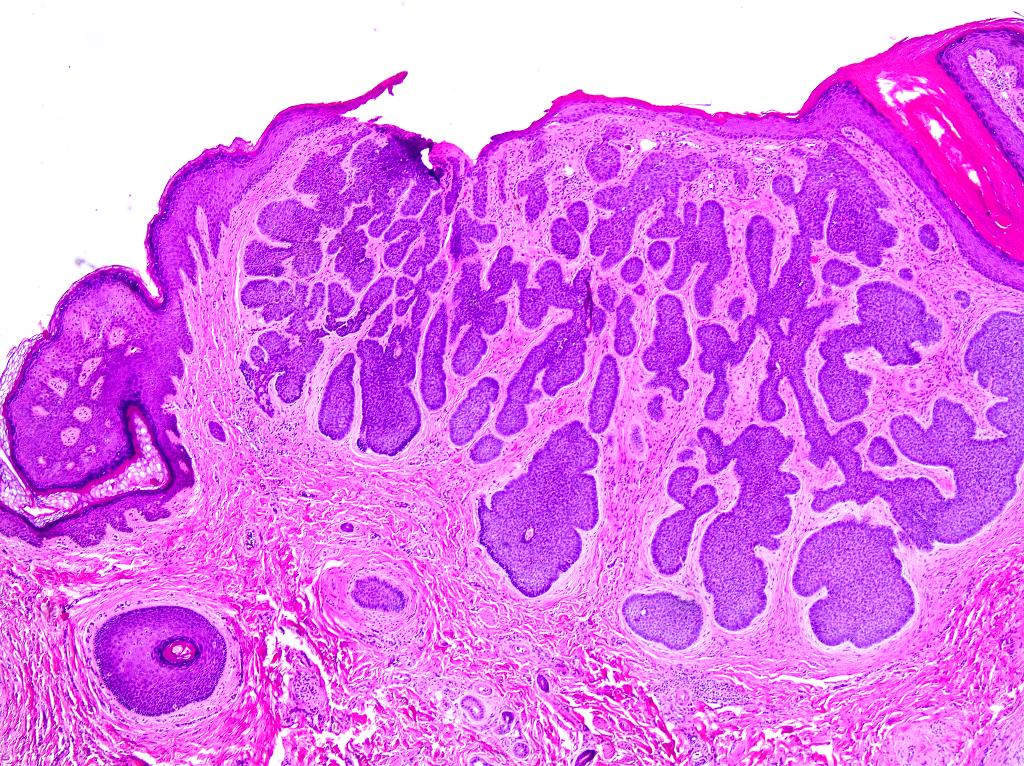
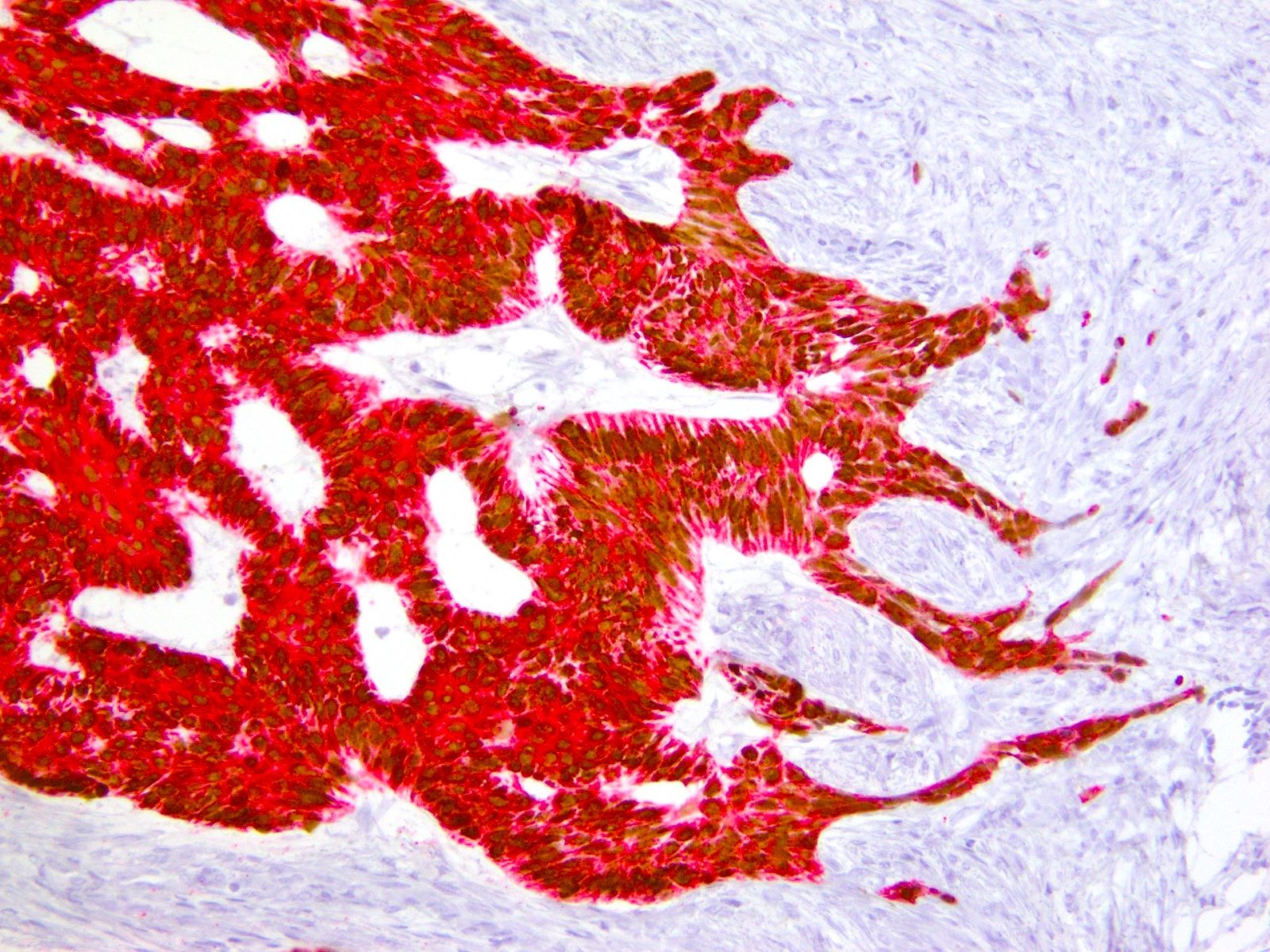
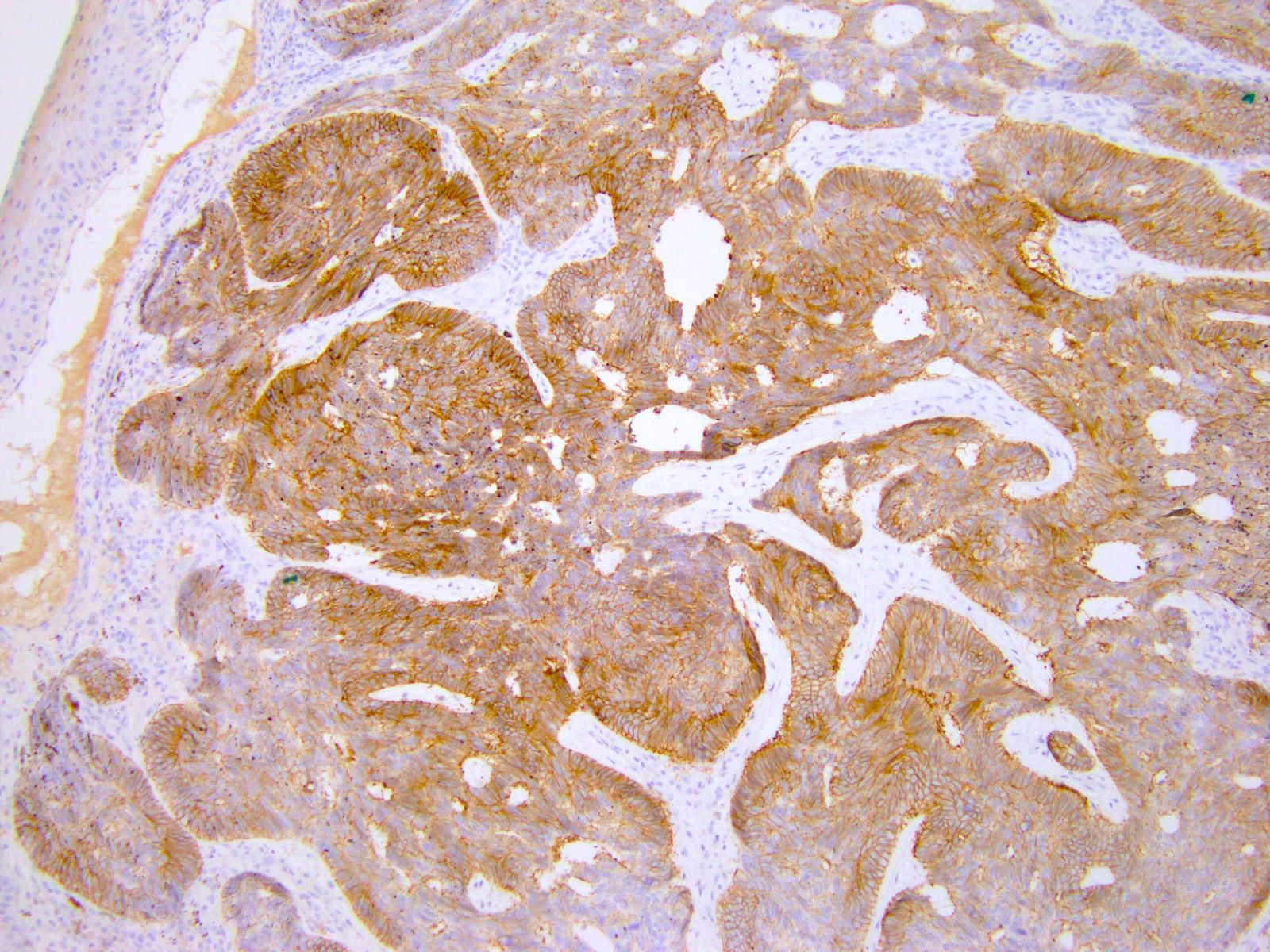
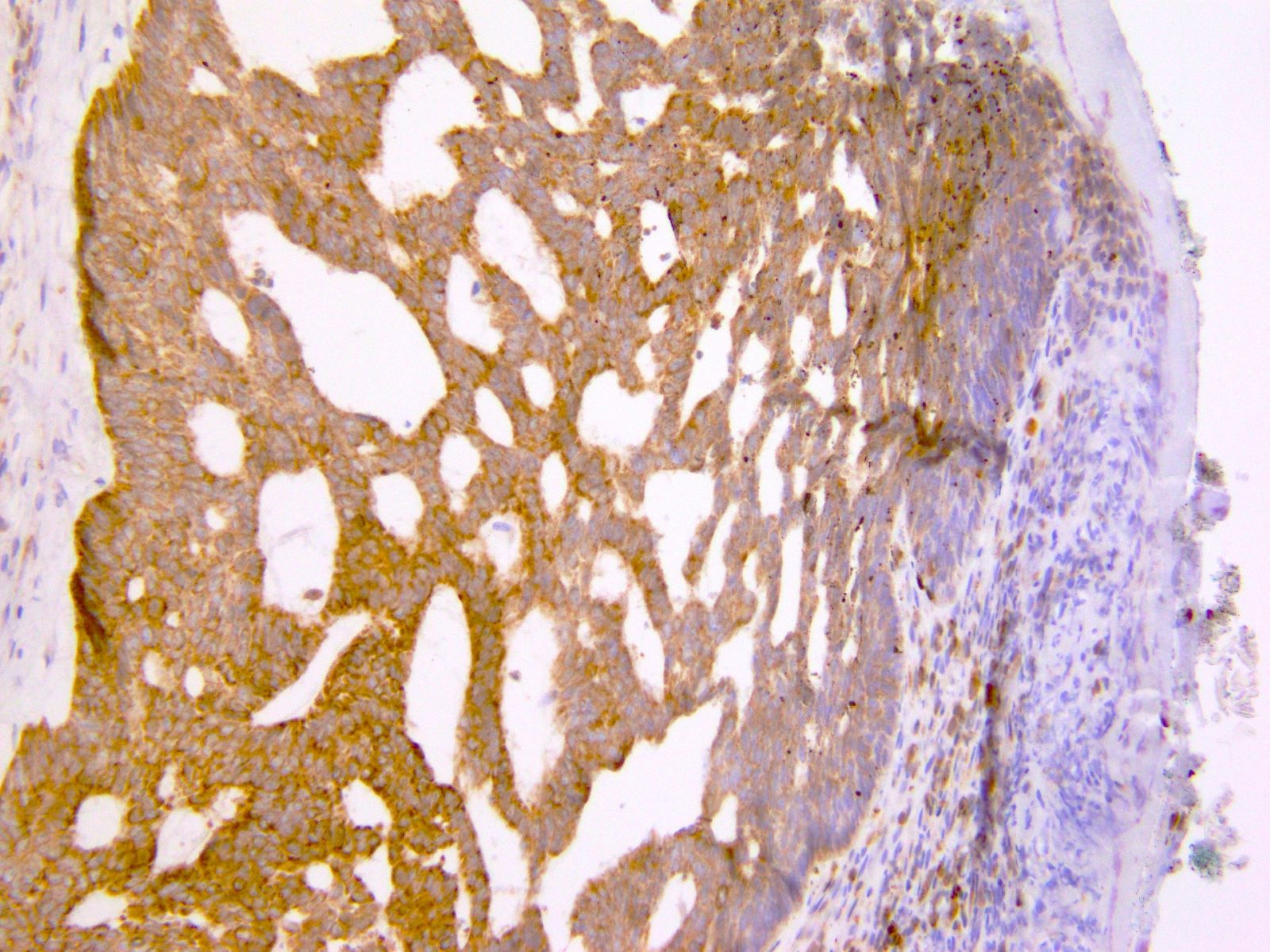
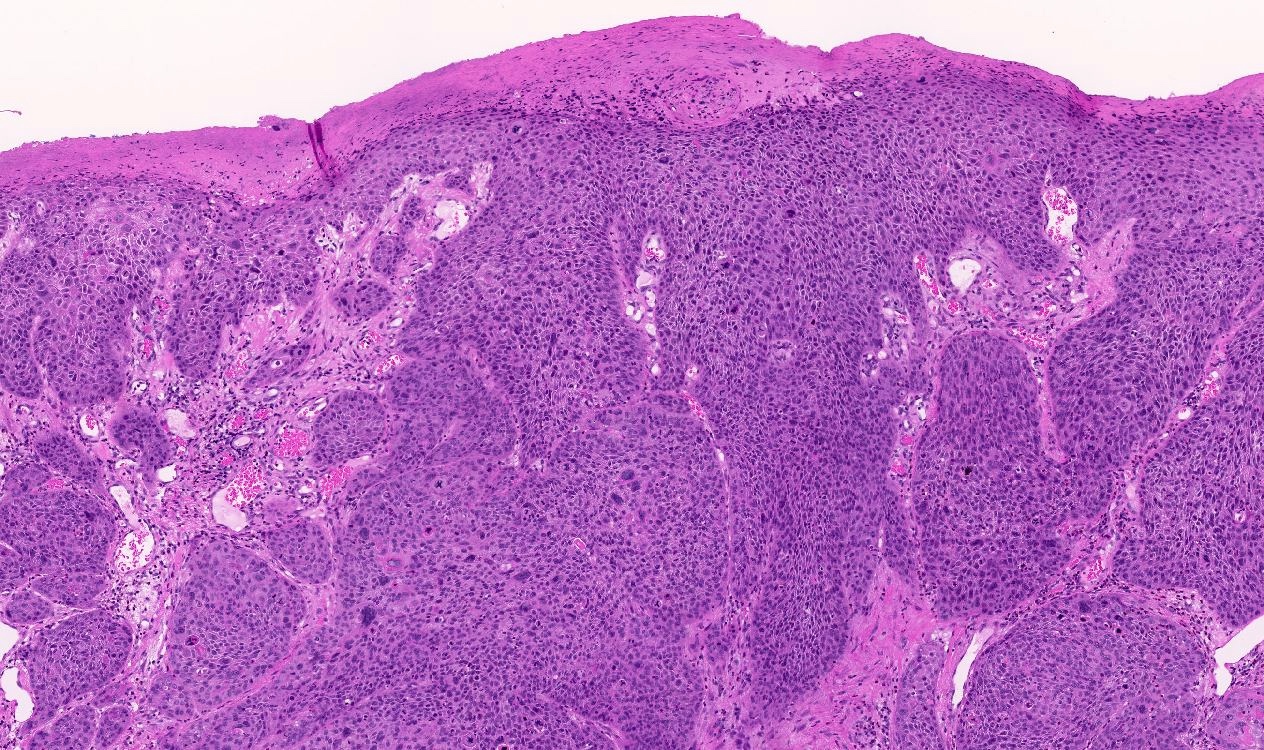
Contributed by Mehrane Nazeran, M.D. and Hugo Horling, M.D.
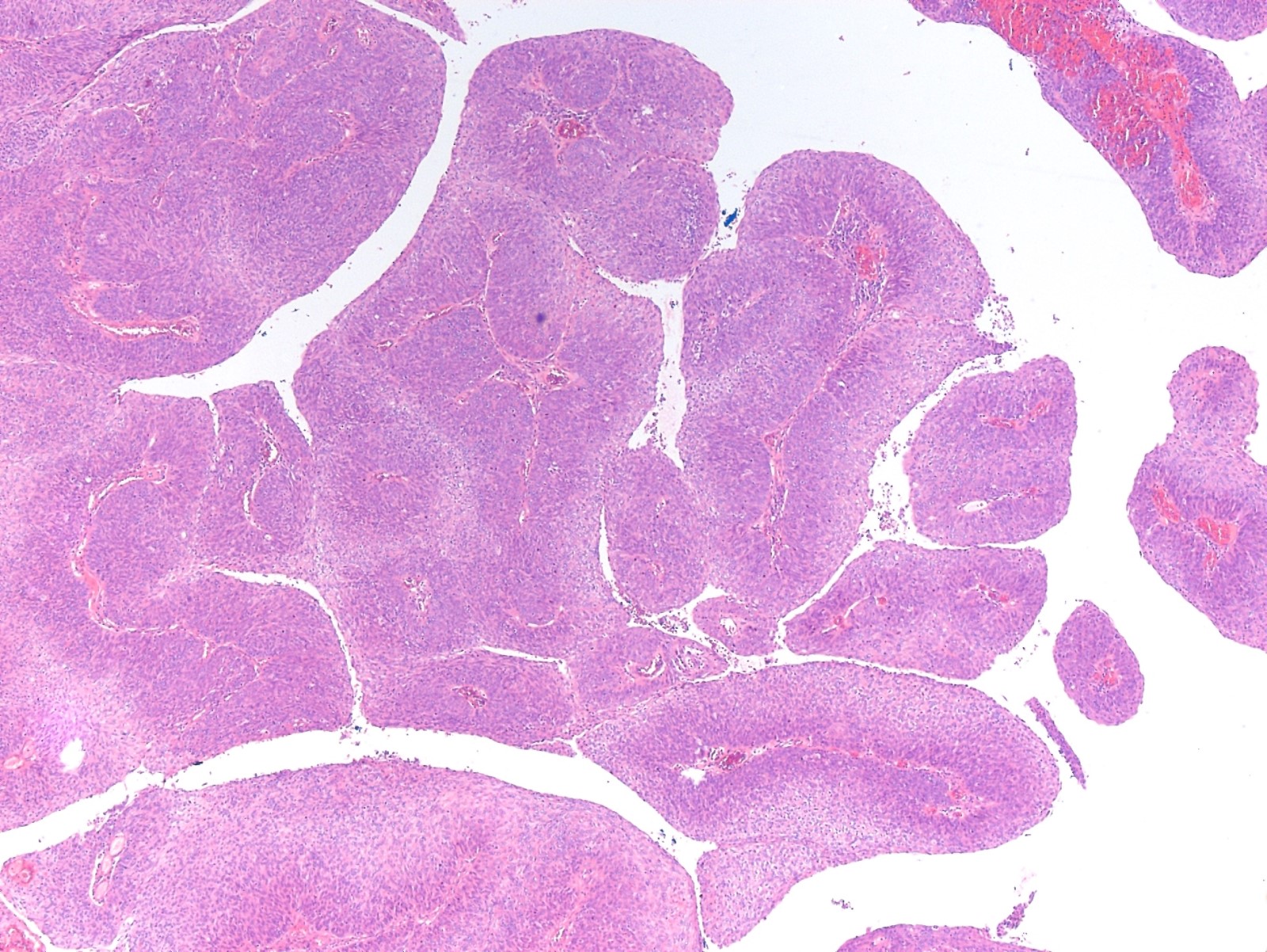
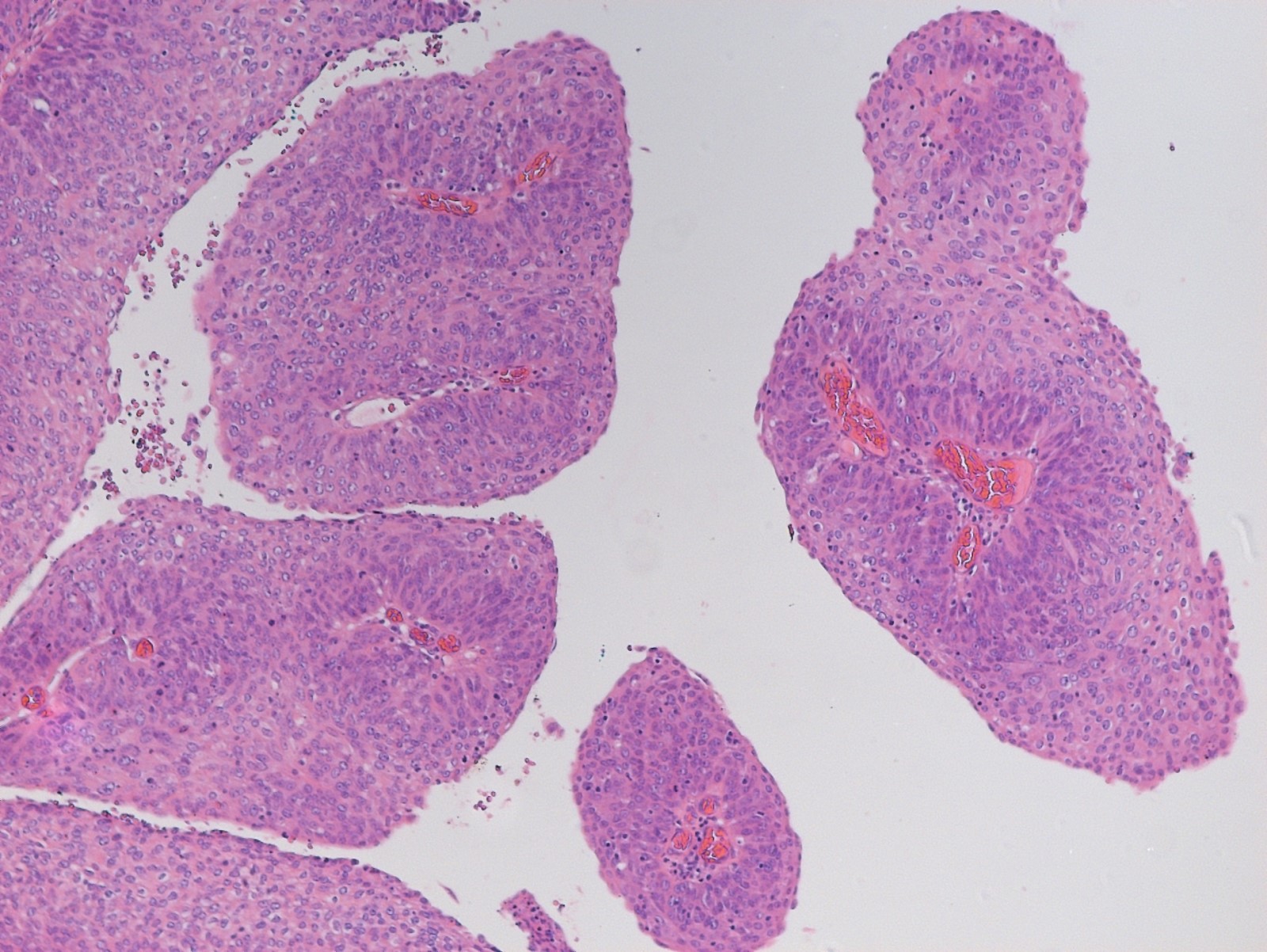
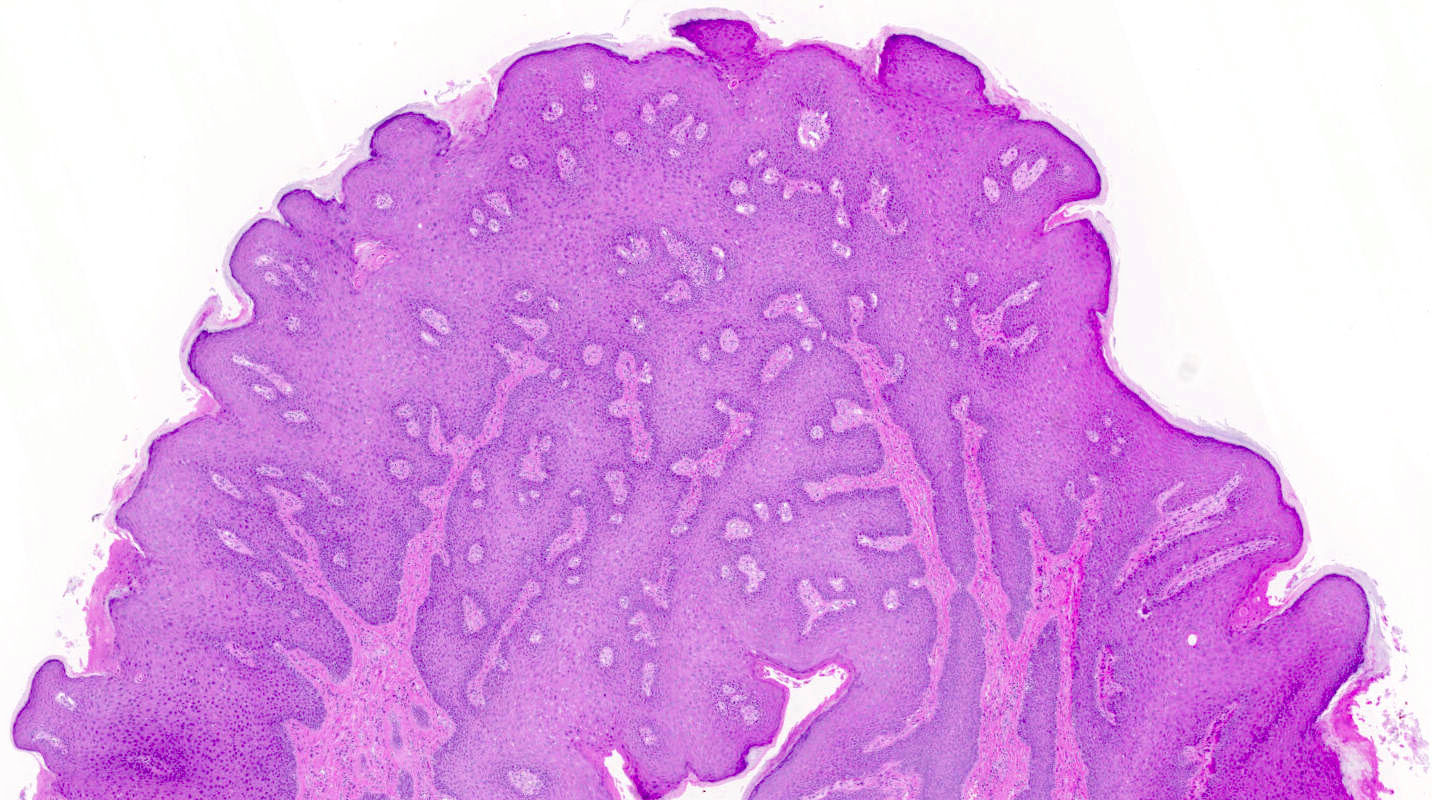
Papillary architecture
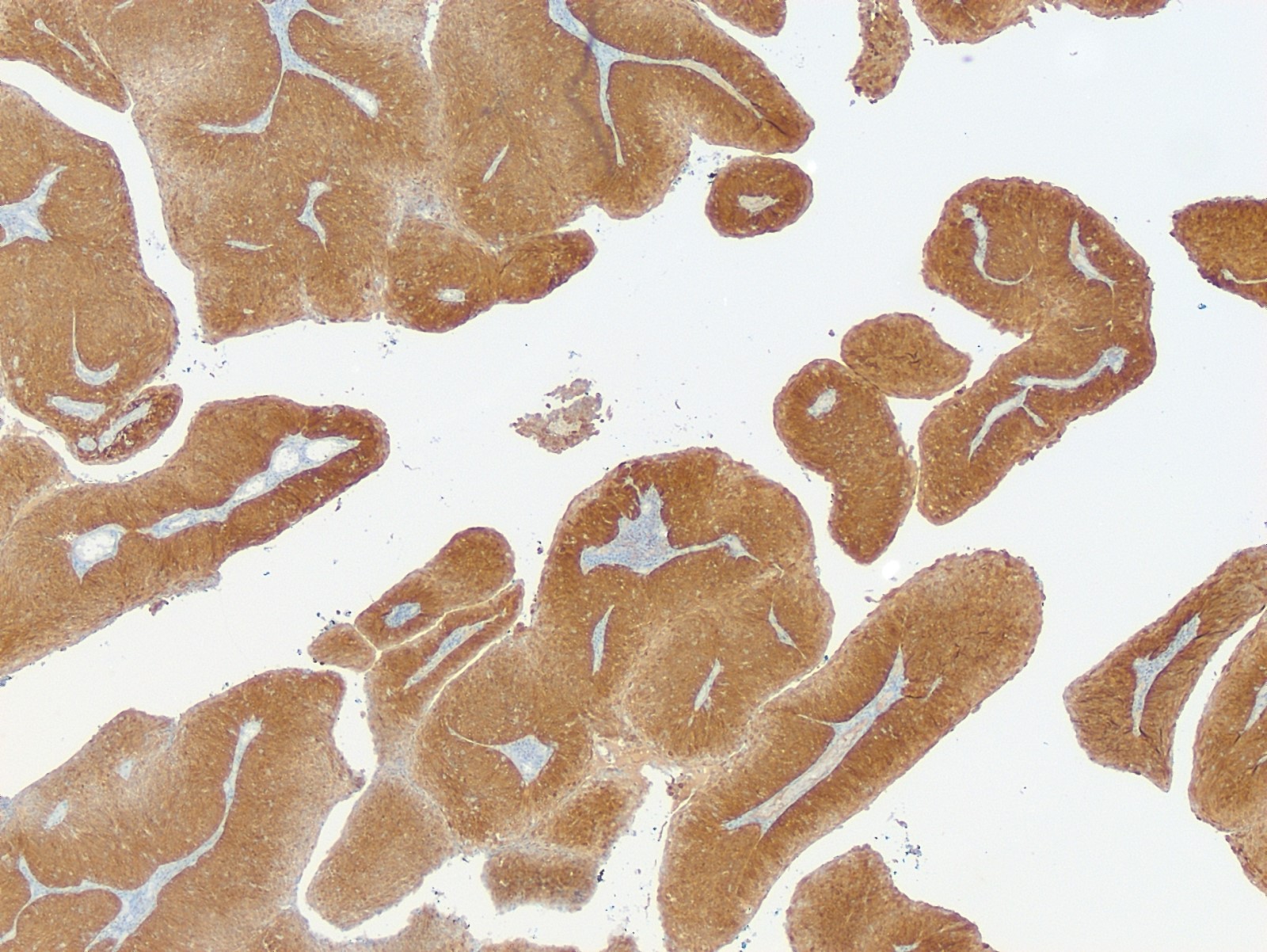
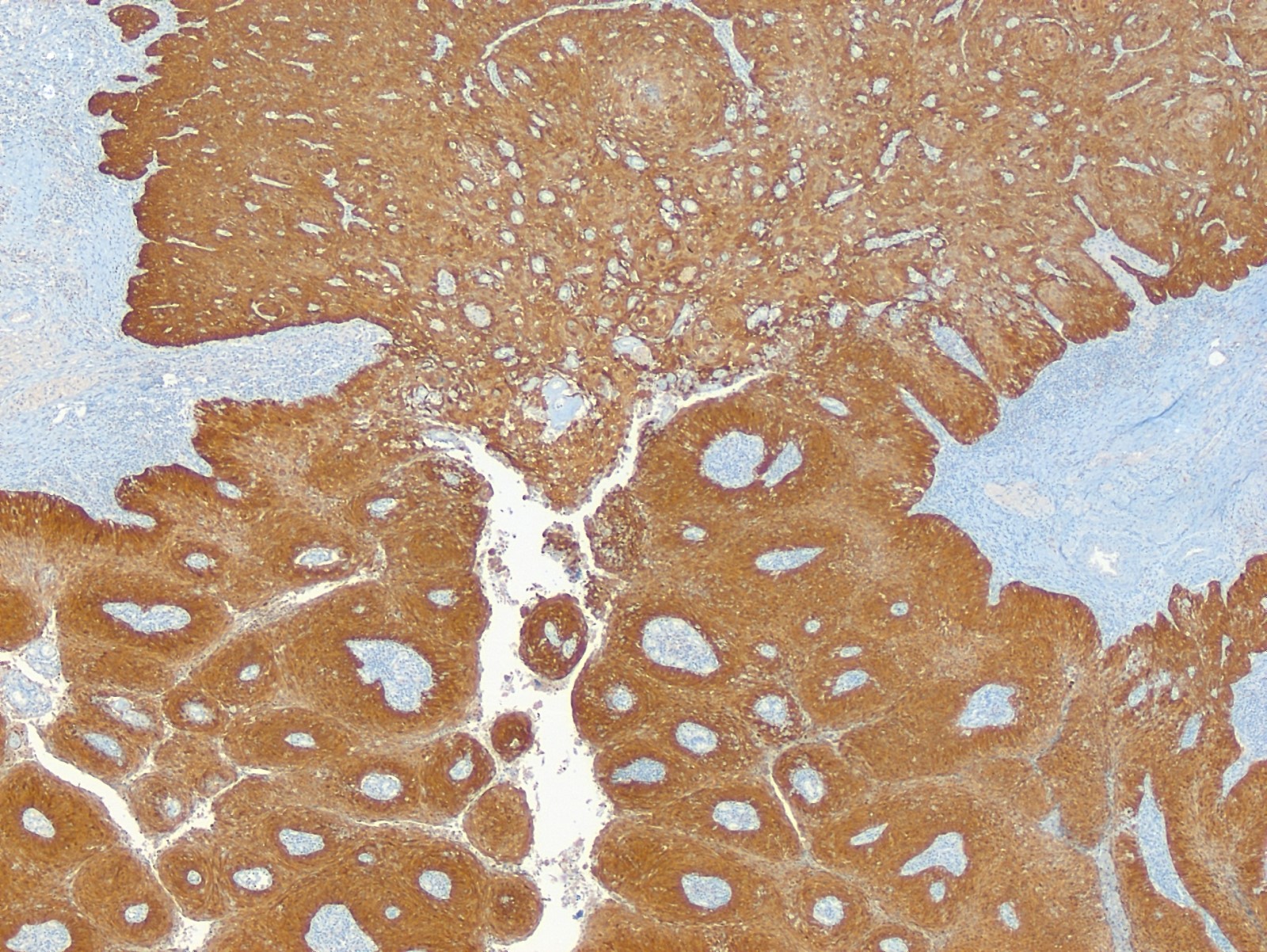
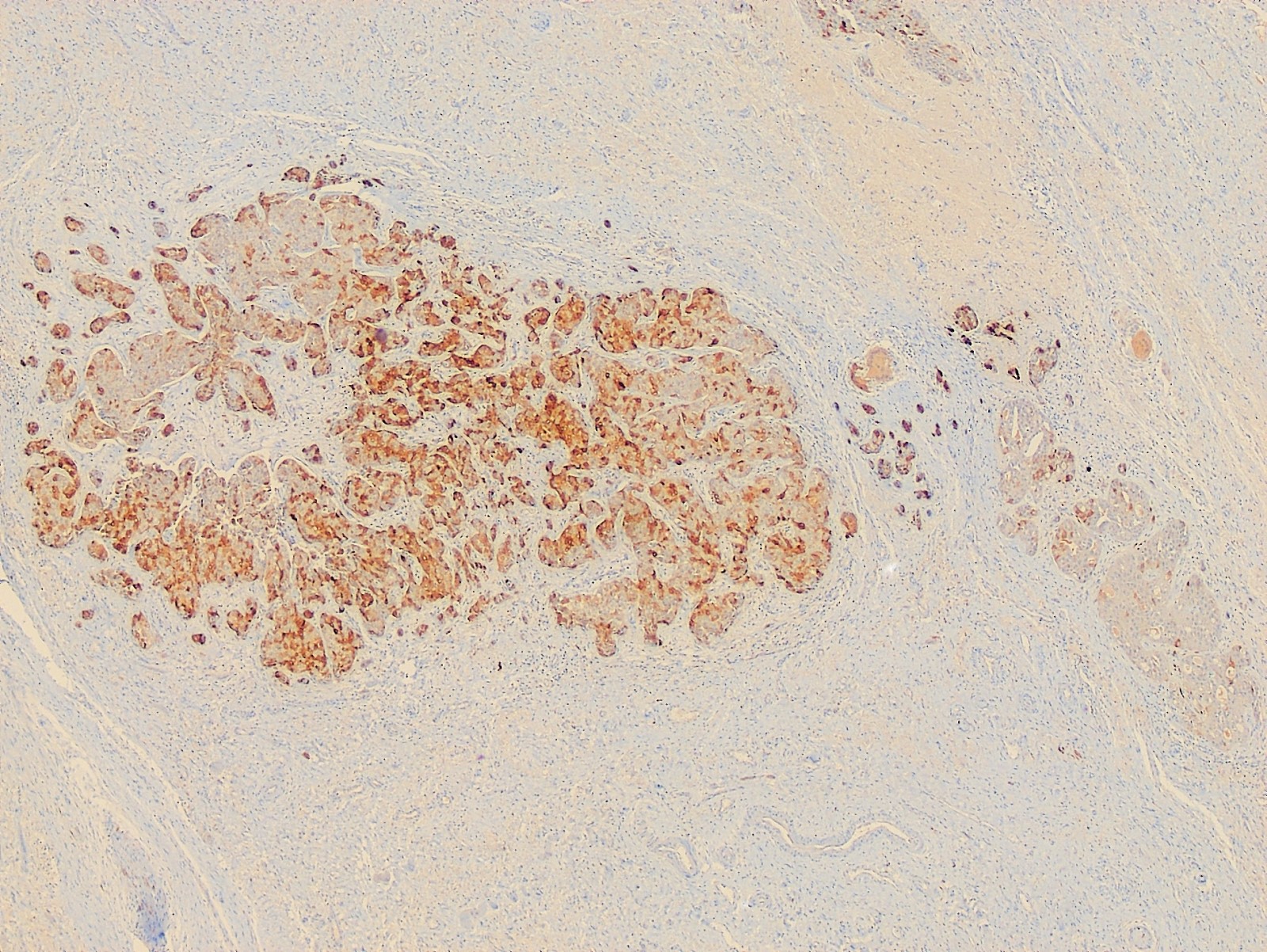
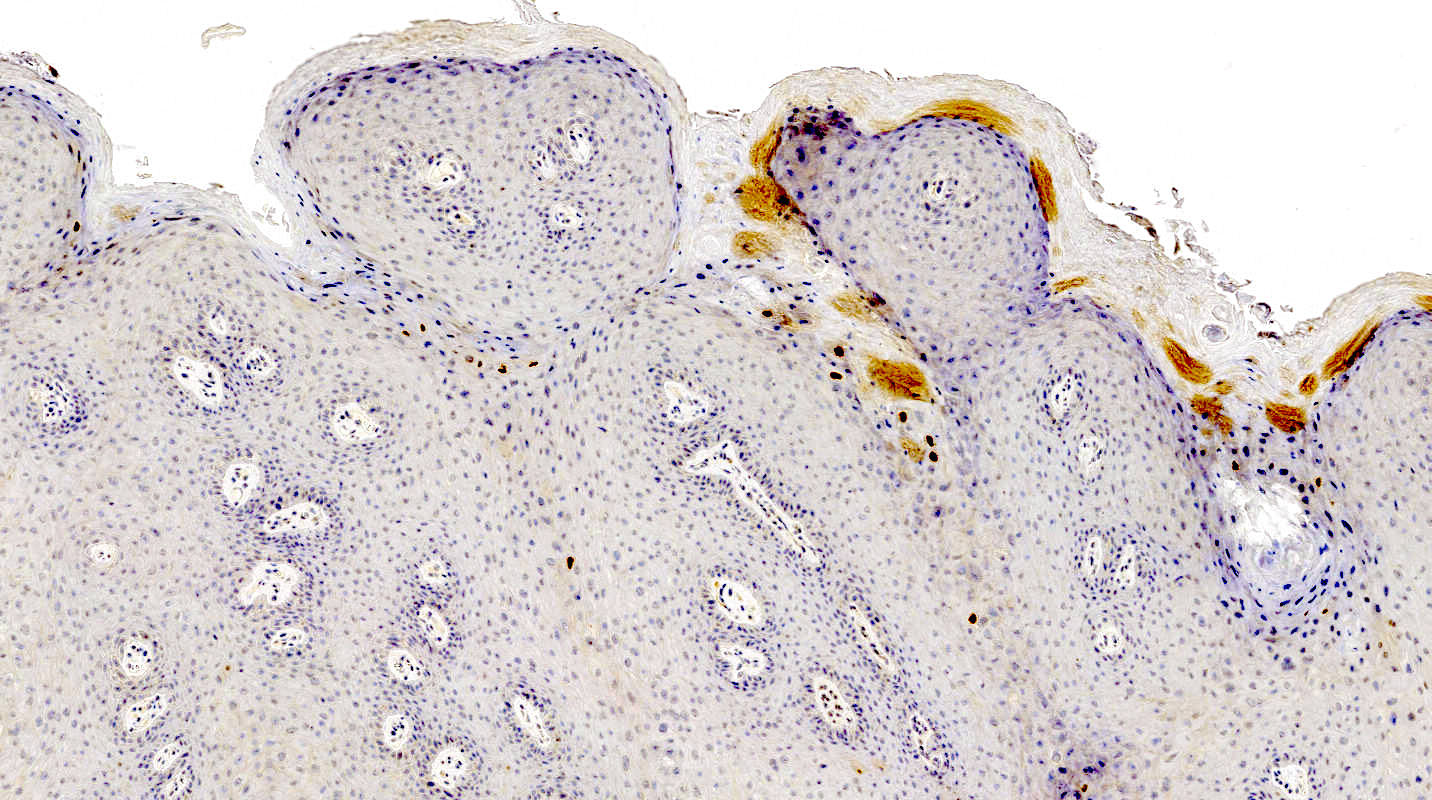
p16
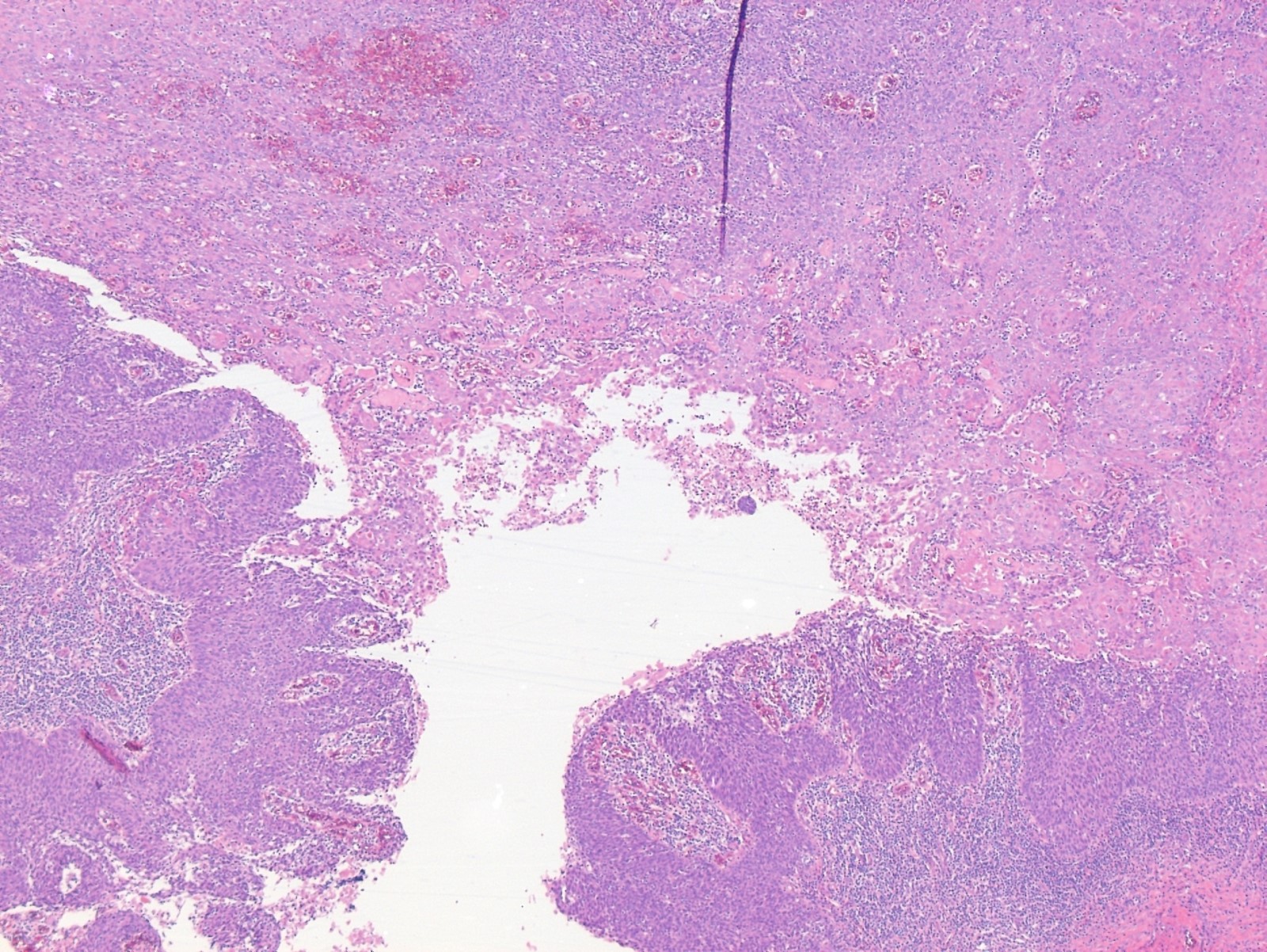
Infiltrating carcinoma
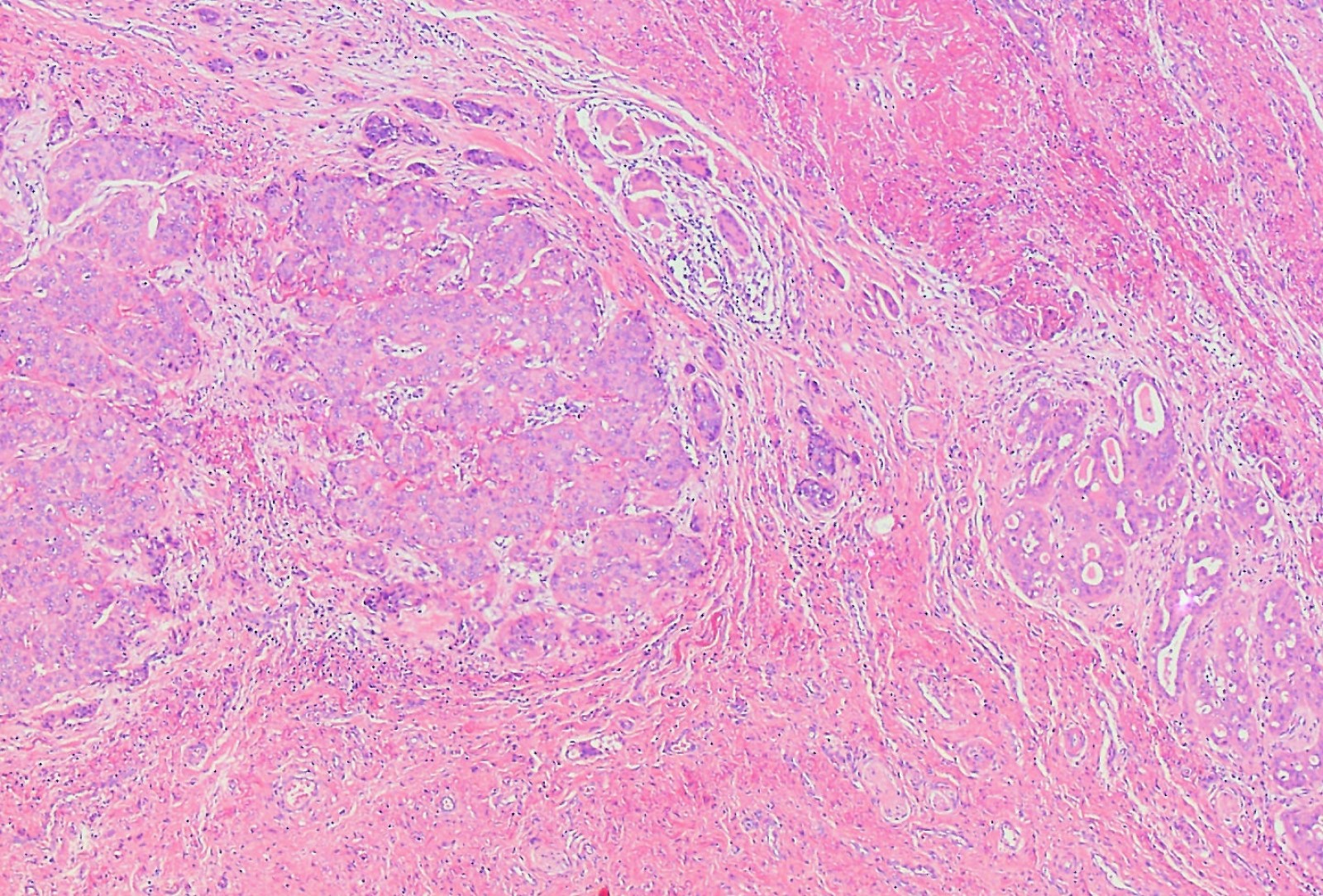
Solid and glandular pattern
Cribriform growth
Glandular pattern
Images hosted on other servers:

Irregularly shaped and ulcerated tumor

Well limited plaque with a pigmented border

Multiple indurated nodules
Contributed by Lucy Ma, M.D. and Priya Nagarajan, M.D., Ph.D.
Nodular growth and cribriform tumor nests
Basaloid cells with mucin production
Retraction artifact
Basaloid lobules with palisading
Cleft formation between basaloid tumor lobules & stroma

Basaloid lobules - conspicuous peripheral nuclear palisade

Cleft formation between basaloid tumor lobules & stroma
p40 - CK5/6 dual stain
BerEP4
BCL2
p16
BCC 101 by Dr. Jerad Gardner
Reporting BCC by Dr. Catriona McKenzie, pathCast
Images hosted on other servers:

Inguinal cellular angiofibroma

Scrotal cellular angiofibroma
Contributed by David B. Chapel, M.D.
Well circumscribed tumor
Hyalinized vessels
Images hosted on other servers:

Karyotype and RB1 FISH

RB1 FISH
Images hosted on other servers:
Fig 1: not involving urethra or clitoris
Fig 2: not originating from cervix
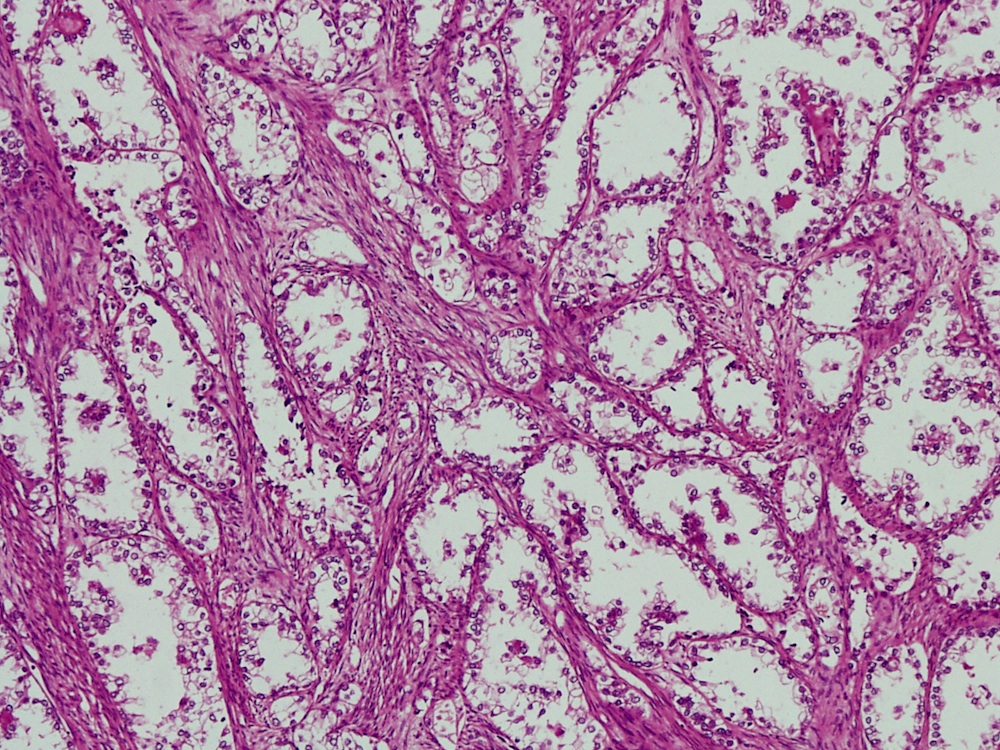
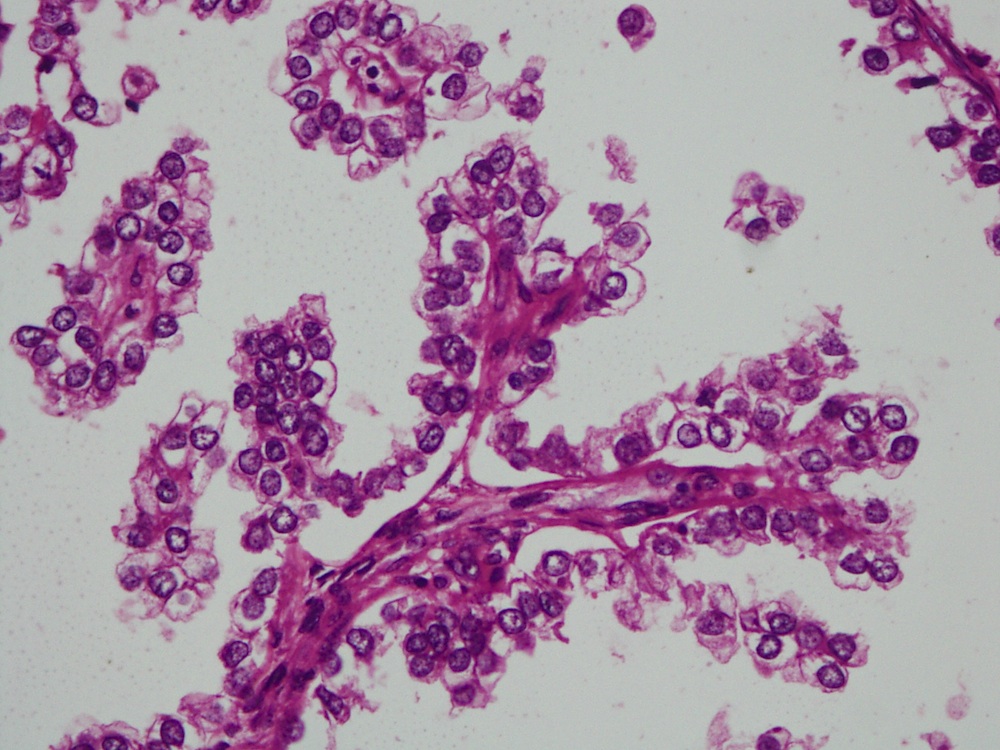
Case #363
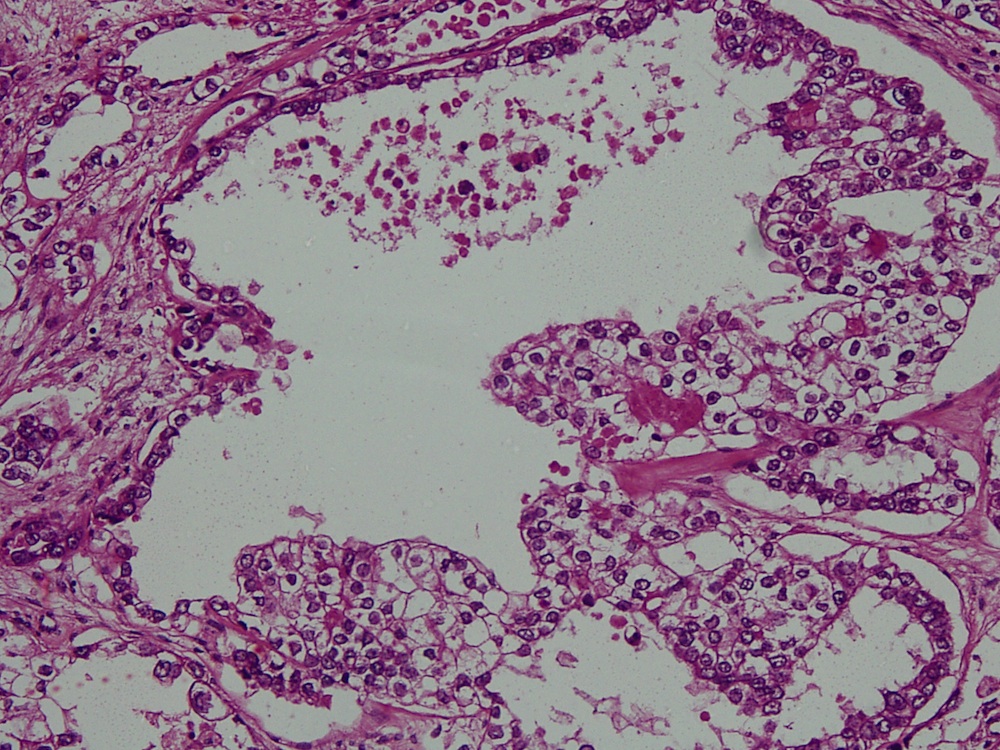


CK7
EMA
Images hosted on other servers:
Fig 3
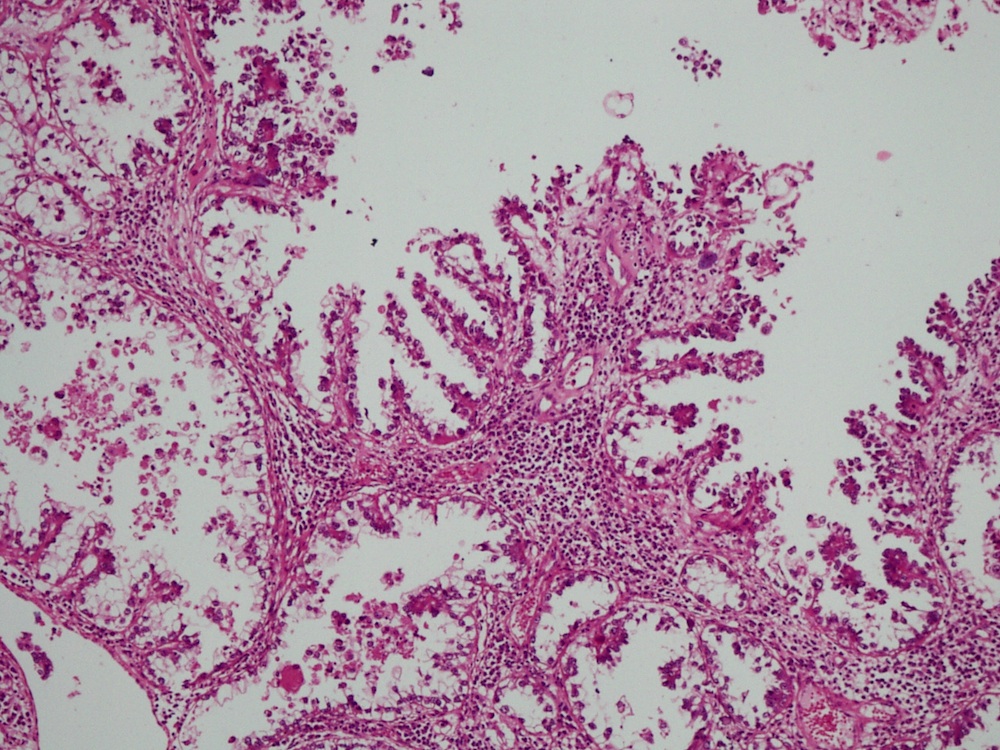
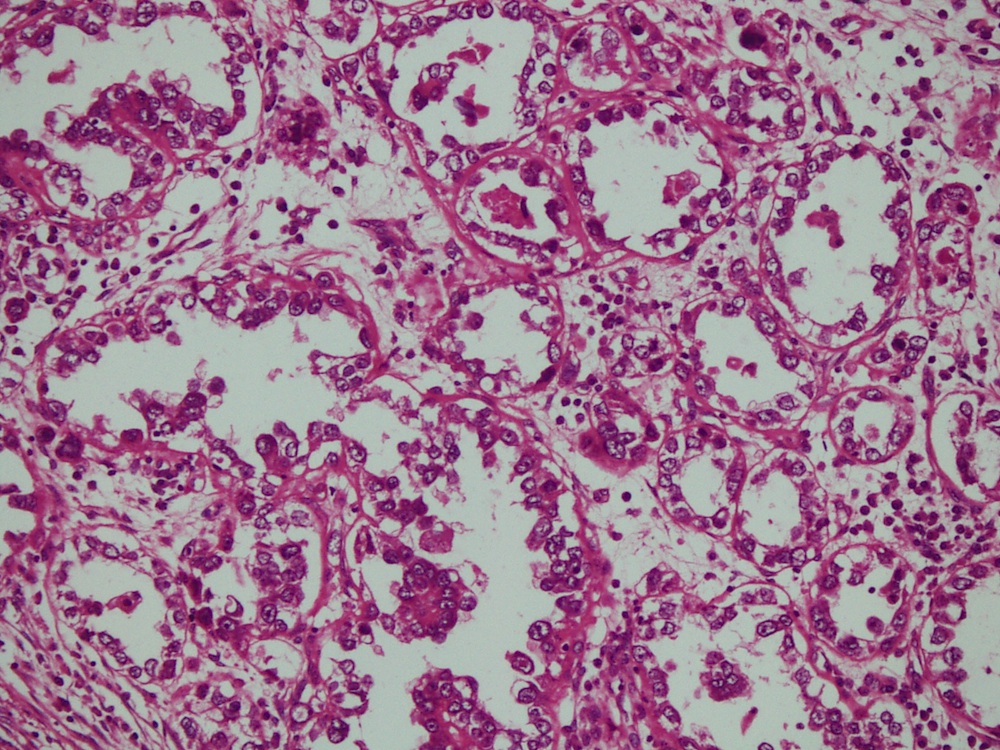
Fig 4: papillae and acini in tubulocystic pattern
Images hosted on other servers:
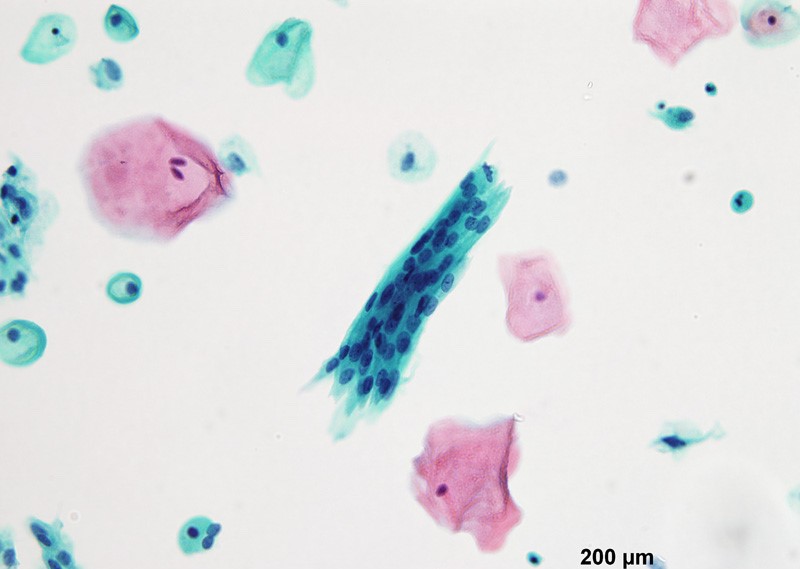
Pap stain
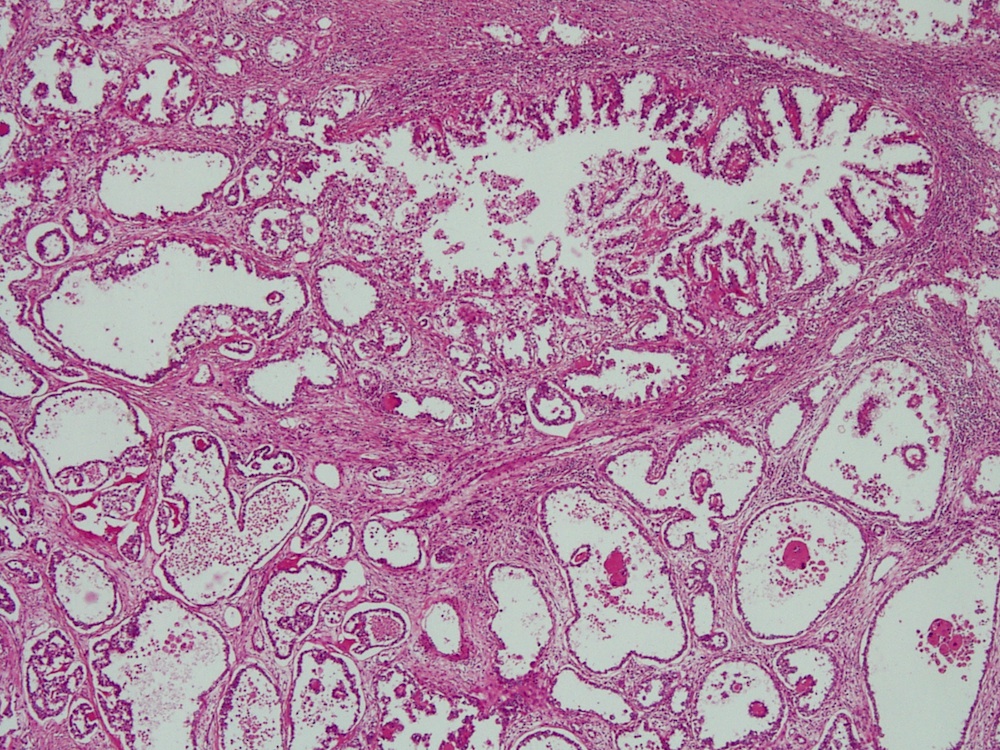
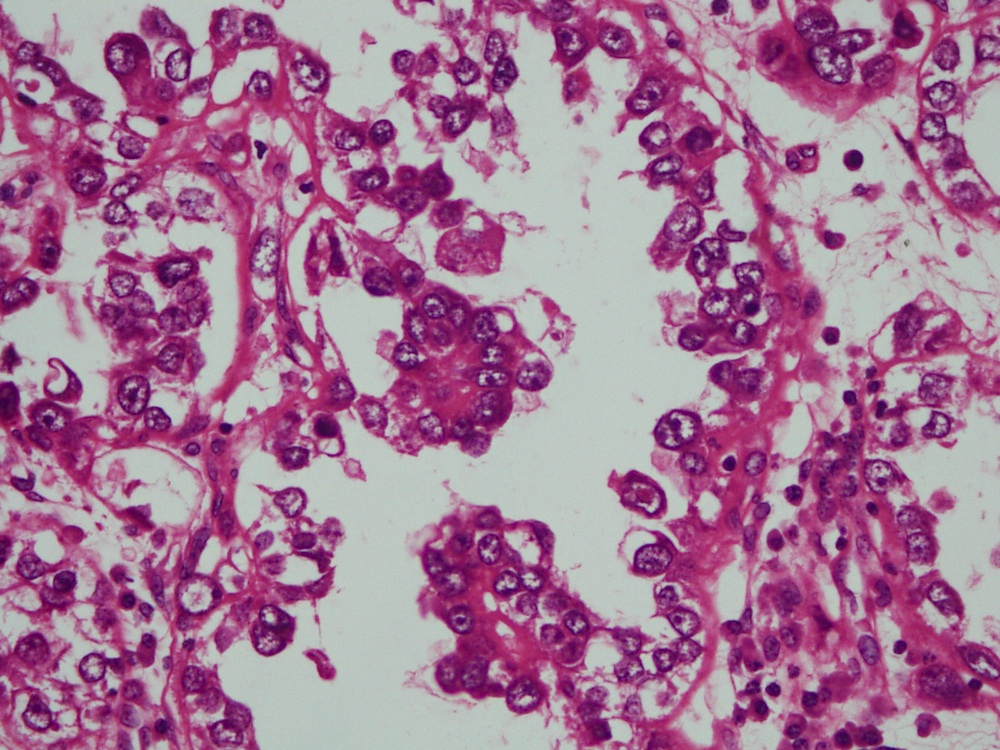
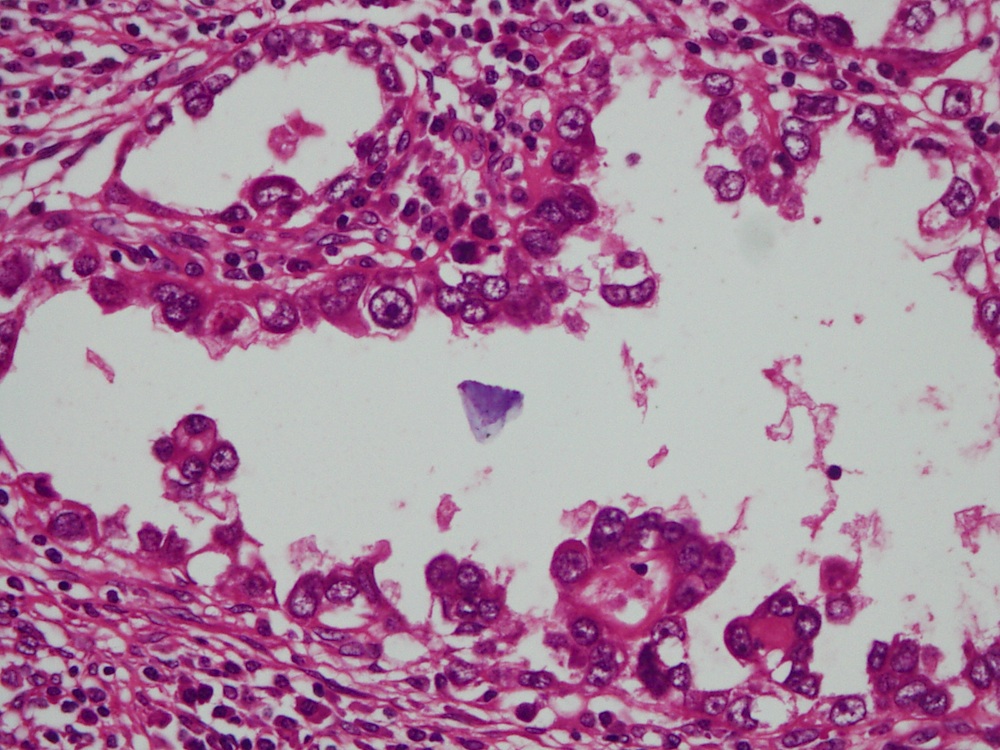
Histopathology vagina - clear cell carcinoma
Contributed by Matthias Choschzick, M.D.
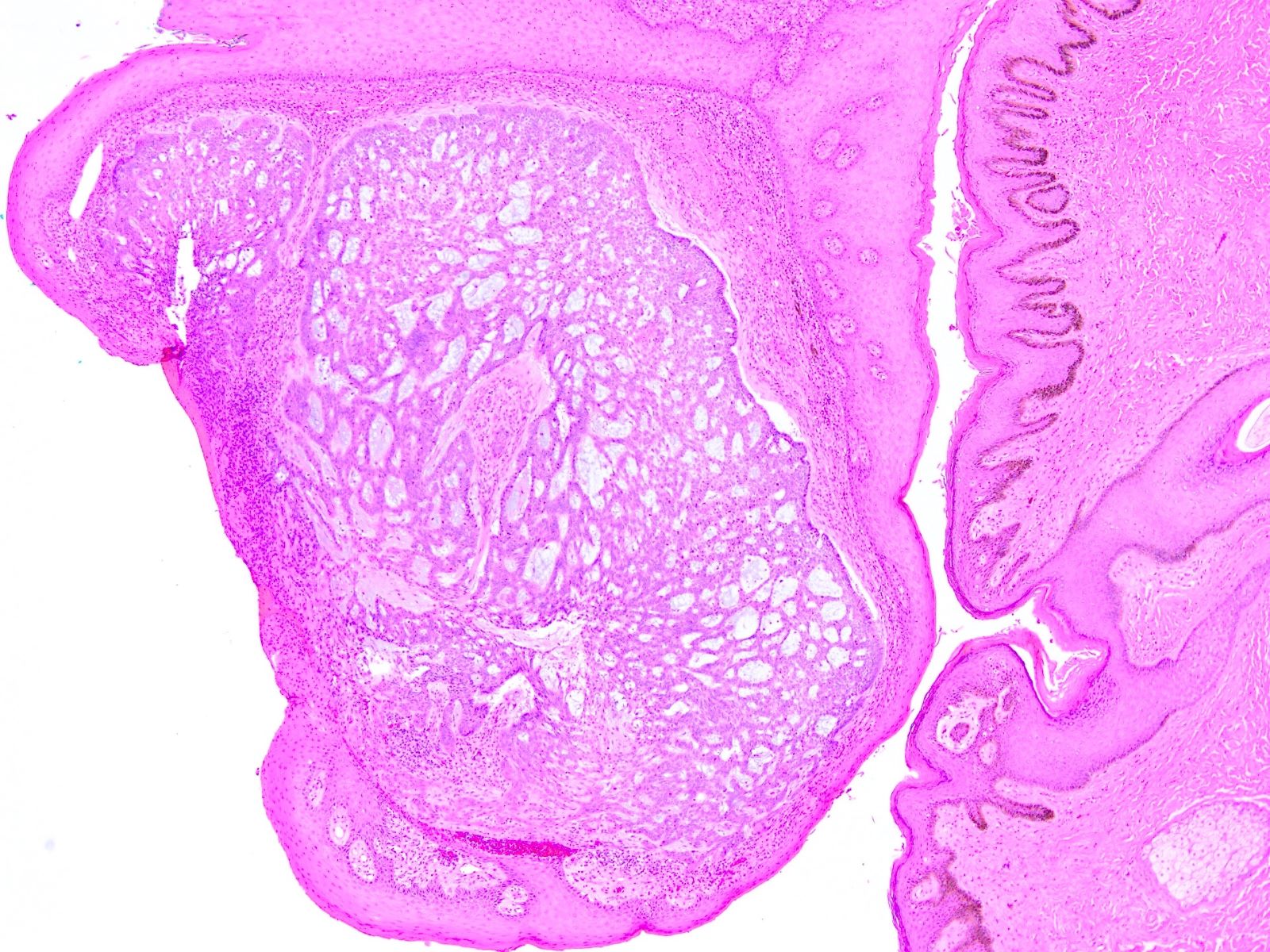
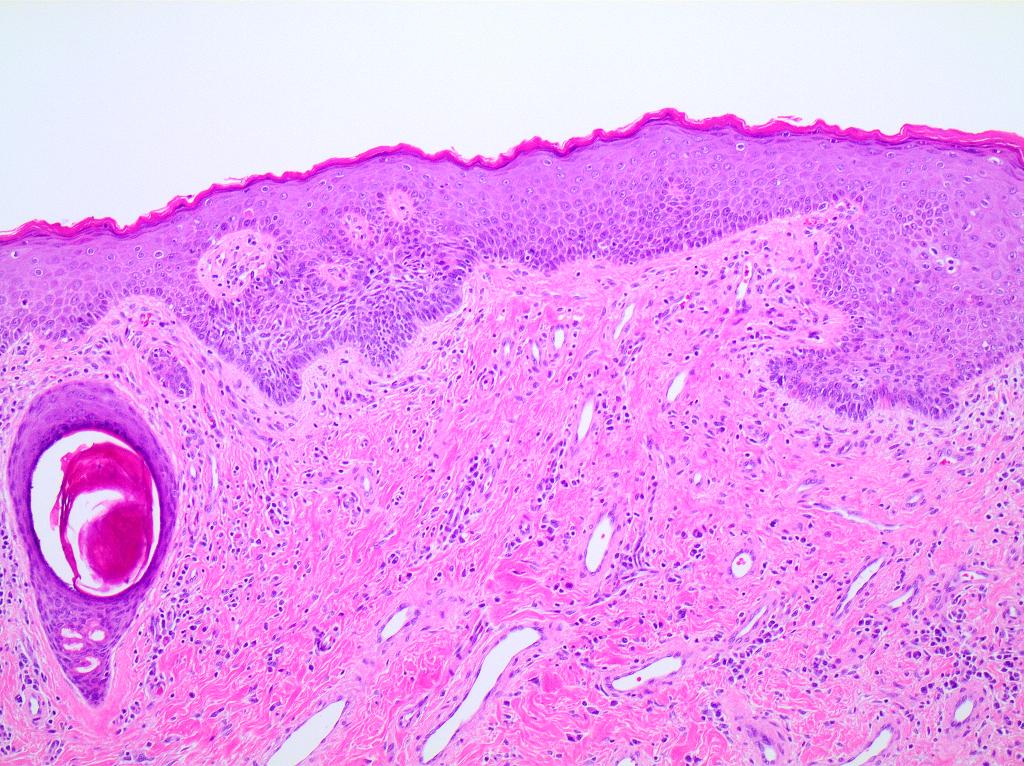
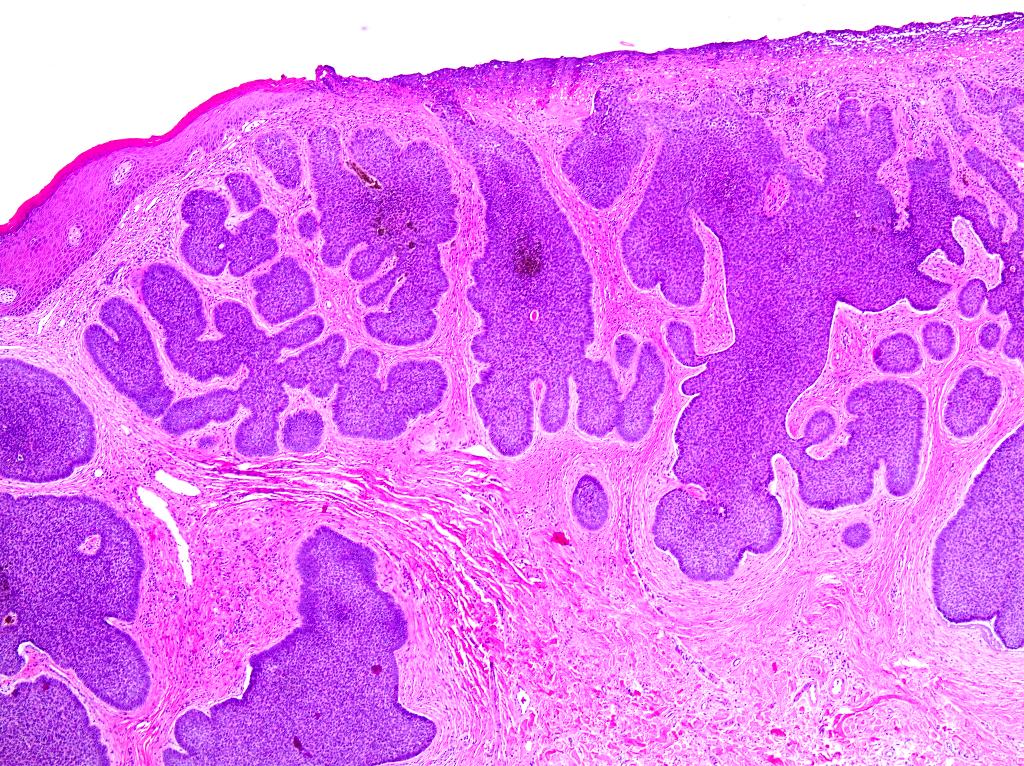
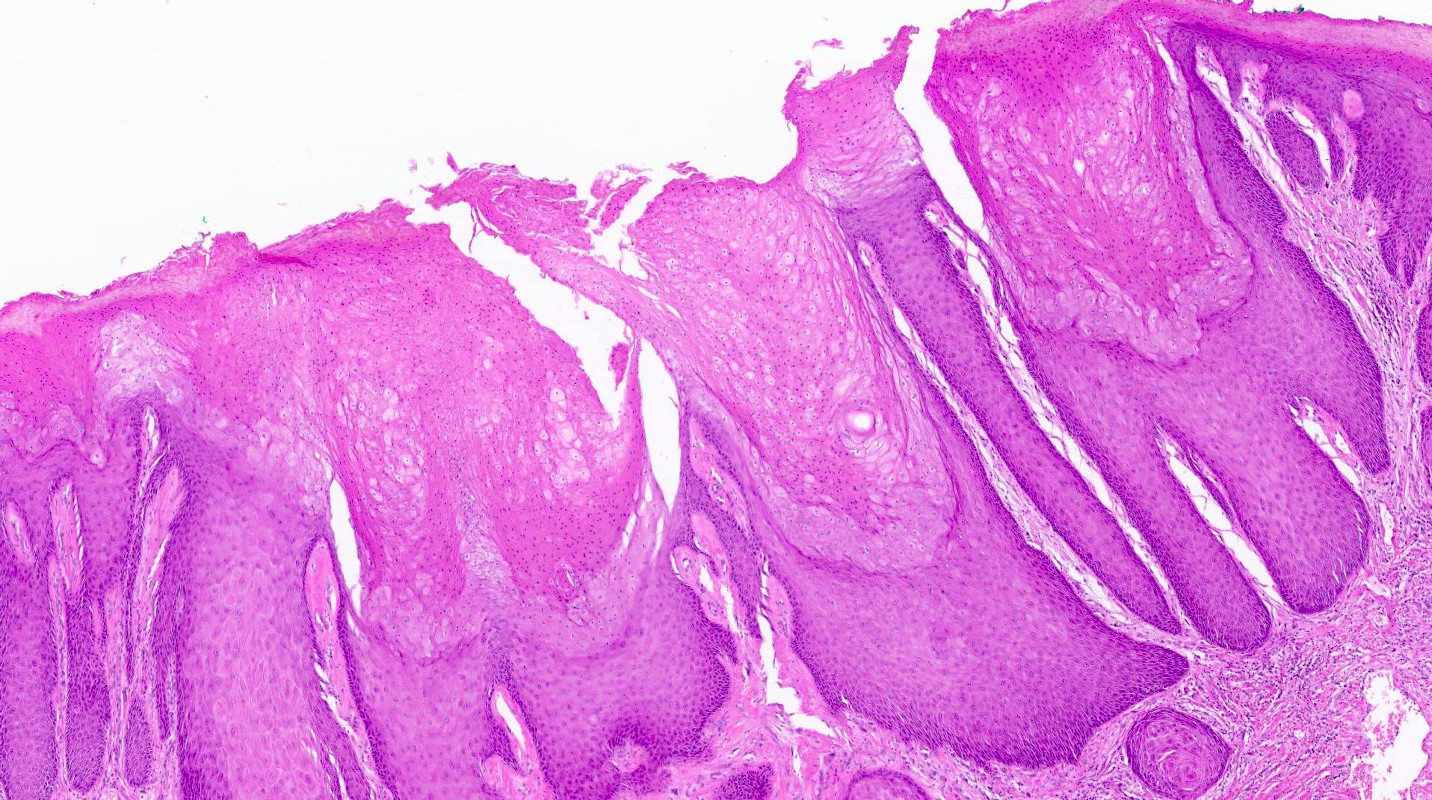
Condyloma acuminatum
Condyloma and HPV
Koilocytosis
Dysplasia
Contributed by José Alberto Fonseca Moutinho, M.D.

Melanocytic lesion
Images hosted on other servers:

Dysplastic nevi defined based on clinical criteria
Contributed by Anna Sarah Erem, M.D. and Gulisa Turashvili, M.D., Ph.D.
Mild cytologic atypia

Shouldering

Nest fusion

Grade 2 cytologic atypia
Melanoma in dysplastic nevi
Dysplastic nevus: 5 minute pathology pearls by Dr. Jerad Gardner
Dysplastic nevi by Prof. Naseem Ahmed
Melanoma arising in a dysplastic nevus by Drs. Philip H. Mckee and Antonina Kalmykova
Histopathology and dermoscopy of severely dysplastic nevus / in situ melanoma by Dr. Sasi Kiran Attili
Dysplastic nevus: fact or fiction by Prof. Cliff Rosendahl
Junctional dysplastic lentiginous nevus by Dr. Ian McColl
Dysplastic nevus by Dr. Sonam Kumar Pruthi
Dysplastic nevus by Audiopedia
Images hosted on other servers:

Endometroid adenocarcinoma
Images hosted on other servers:


MRI, proximal type

Ultrasound, proximal type with lung metastases



CT, proximal type with lung metastases

CT, proximal type with lung metastases
Images hosted on other servers:

Proximal type, preoperative

Proximal type, intraoperative
Images hosted on other servers:

Proximal type,
excision specimen
Contributed by David B. Chapel, M.D. and Priya Nagarajan, M.D., Ph.D.
Infiltrative growth
Sheet-like growth
Atypia
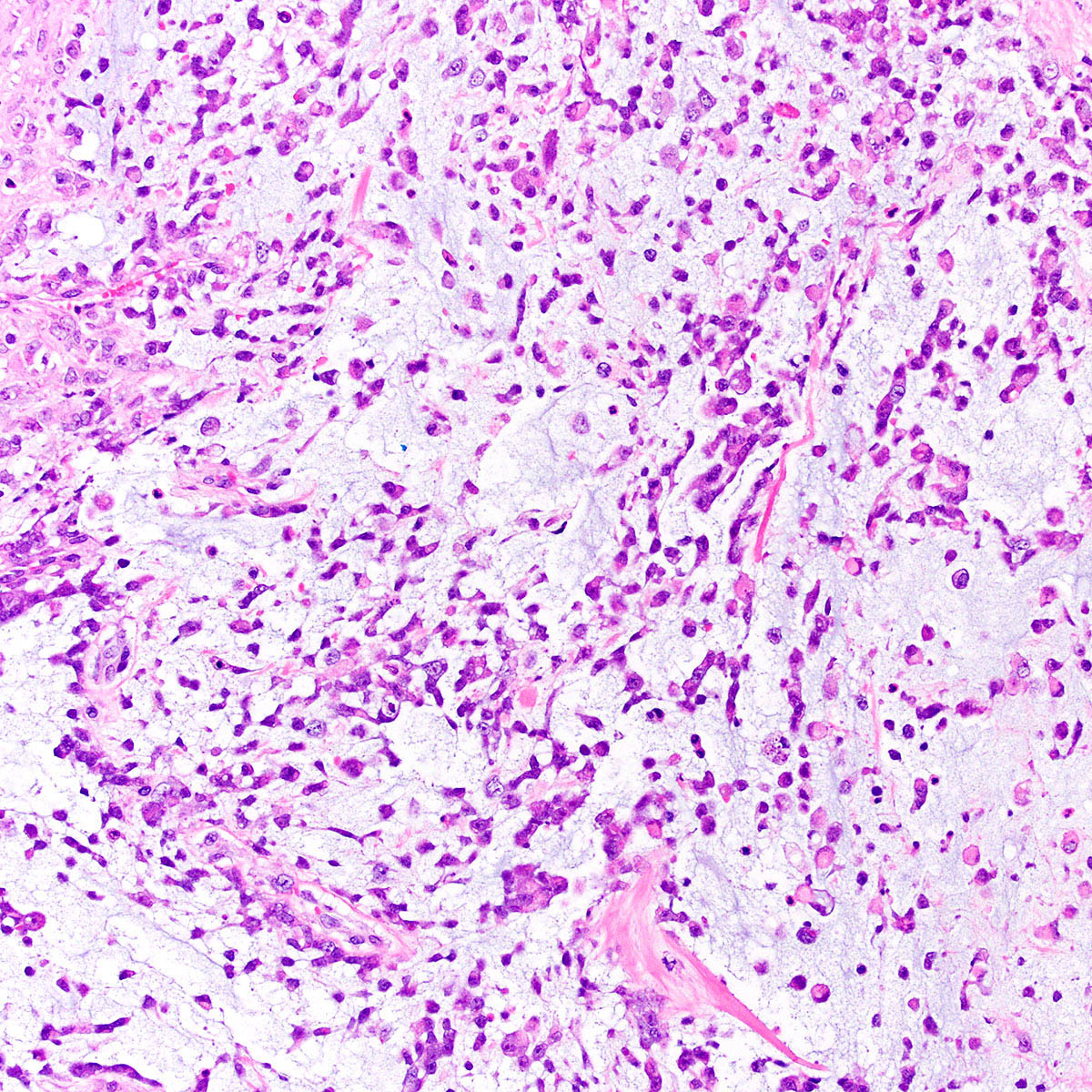
Myxoid stroma
High grade atypia
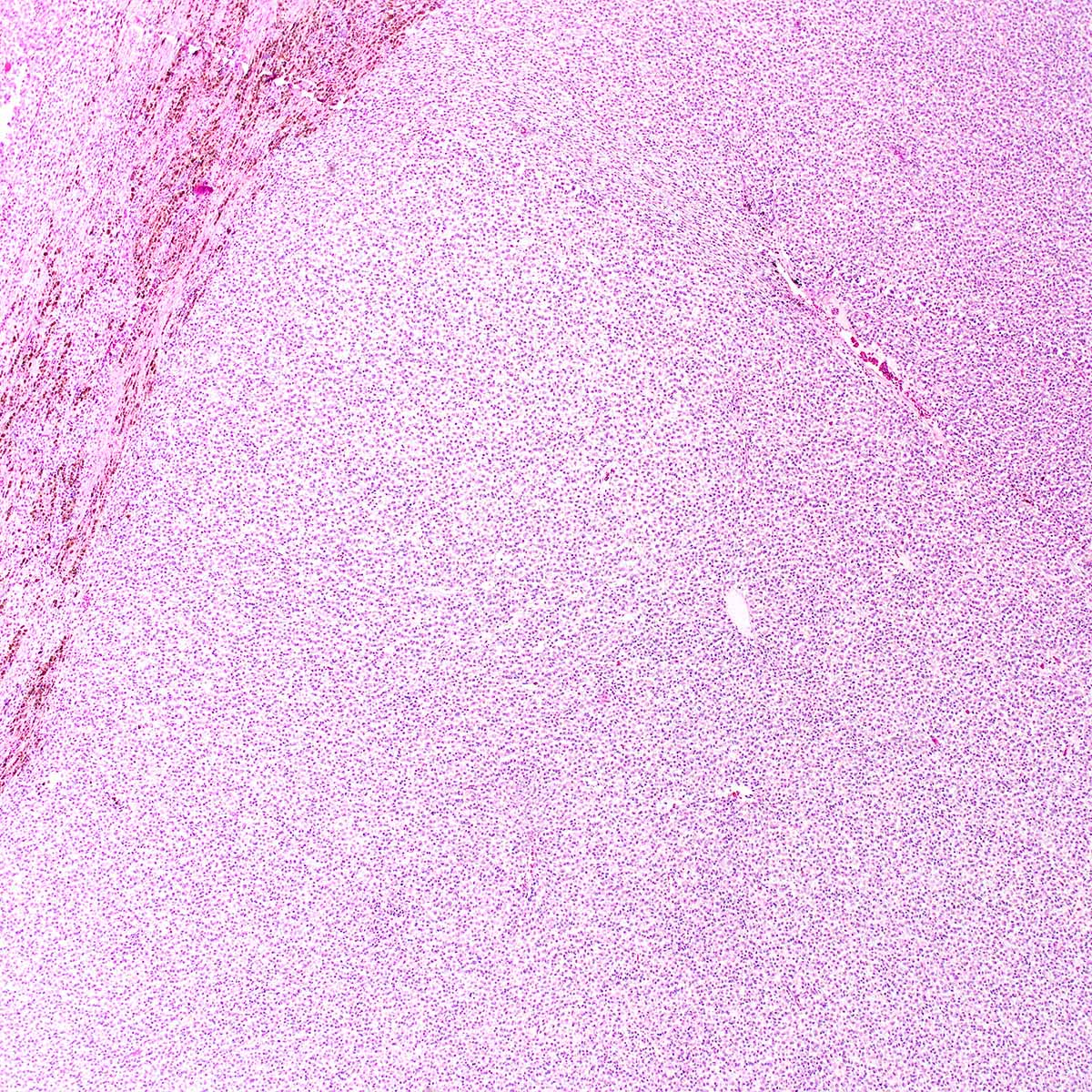
Diffuse growth

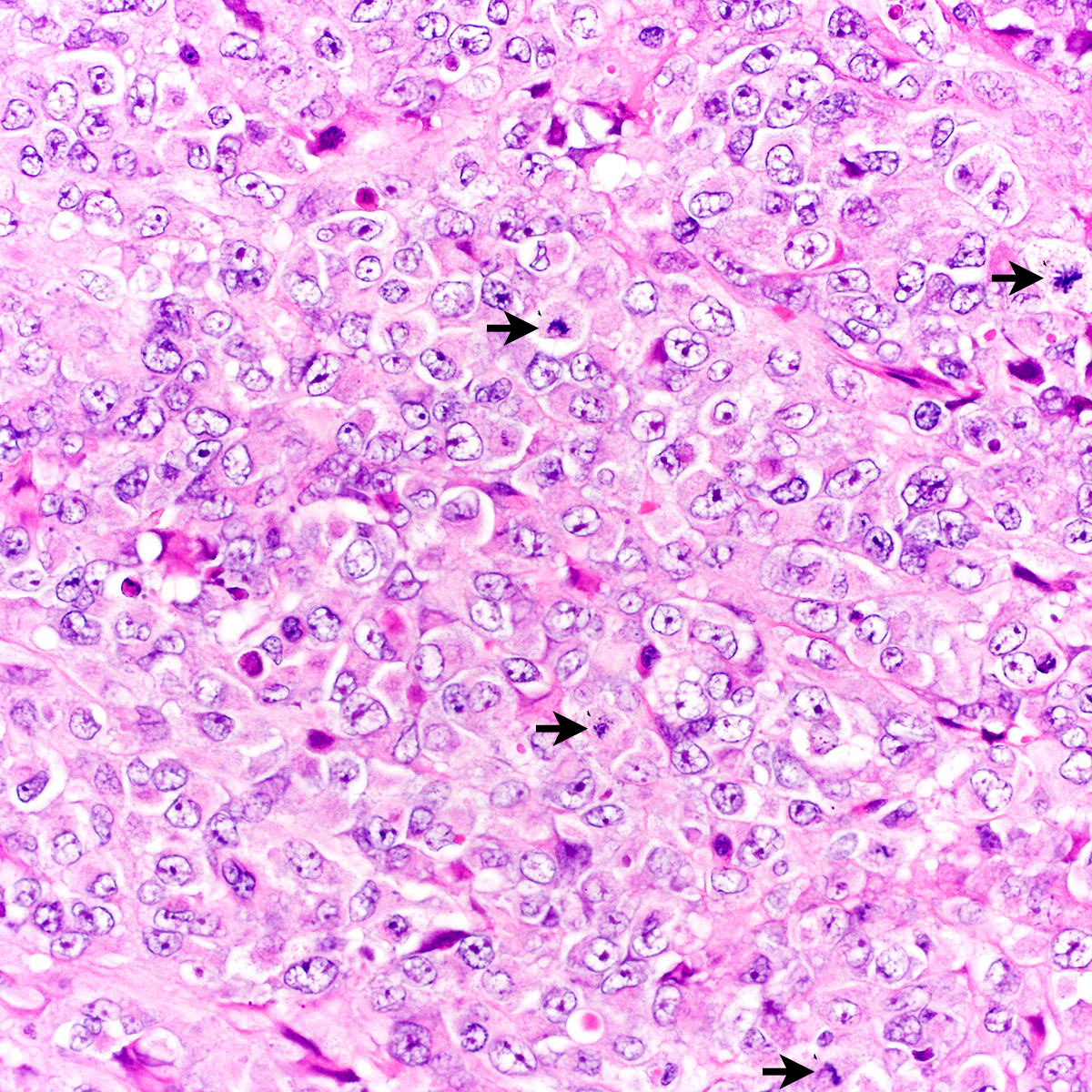
Rhabdoid morphology

Core biopsy

Epithelioid cells
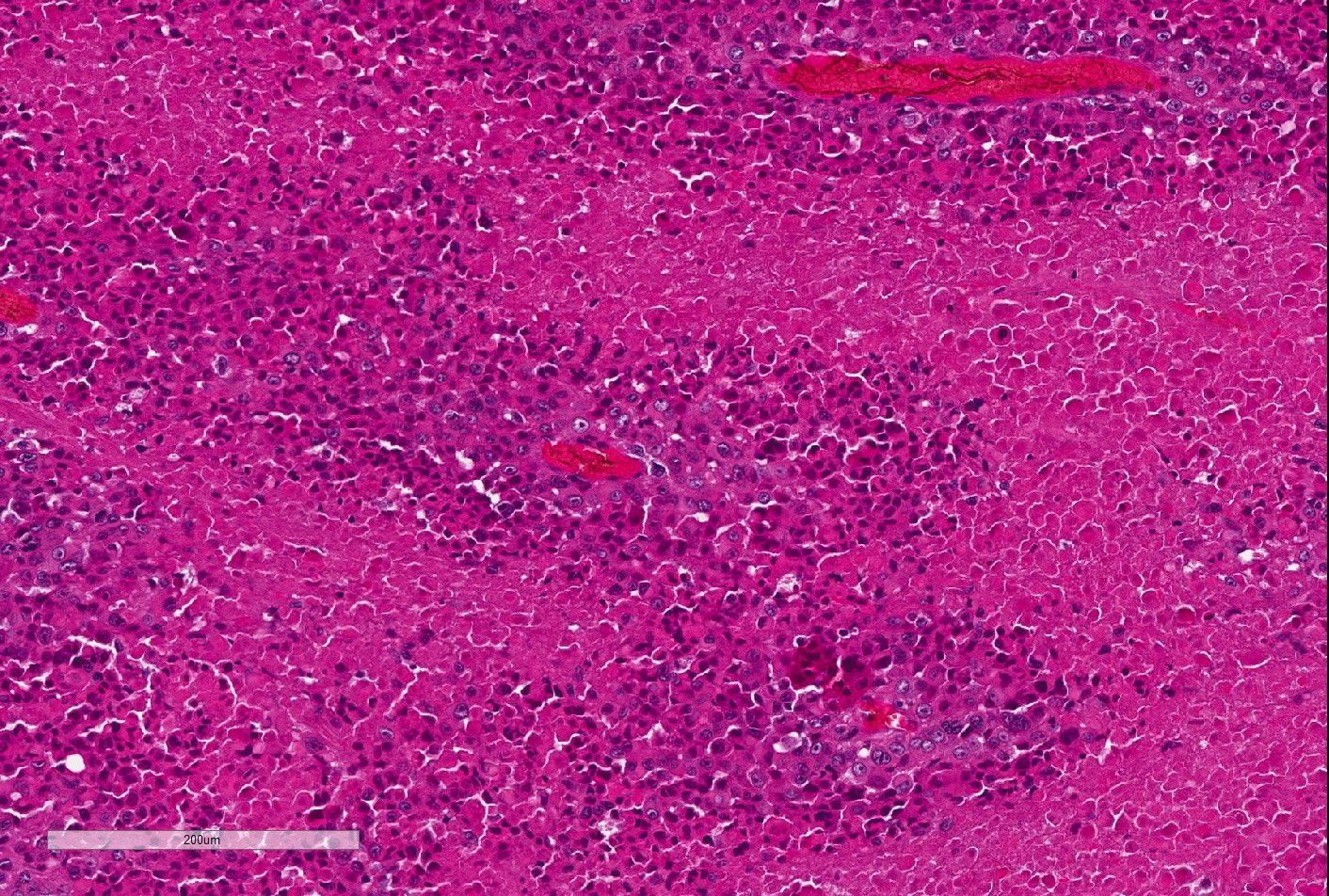
Tumor necrosis
Cytokeratin
Images hosted on other servers:


FISH and aCGH based detection of SMARCB1 deletion
Proximal type epithelioid sarcoma of the groin
Images hosted on other servers:



Labium majora mass

Labium majora polyp
Contributed by Hope Haefner, M.D.

Vulvar polyp
Images hosted on other servers:


Labia majora mass
Contributed by Albert Alhatem, M.D. and Debra S. Heller, M.D.
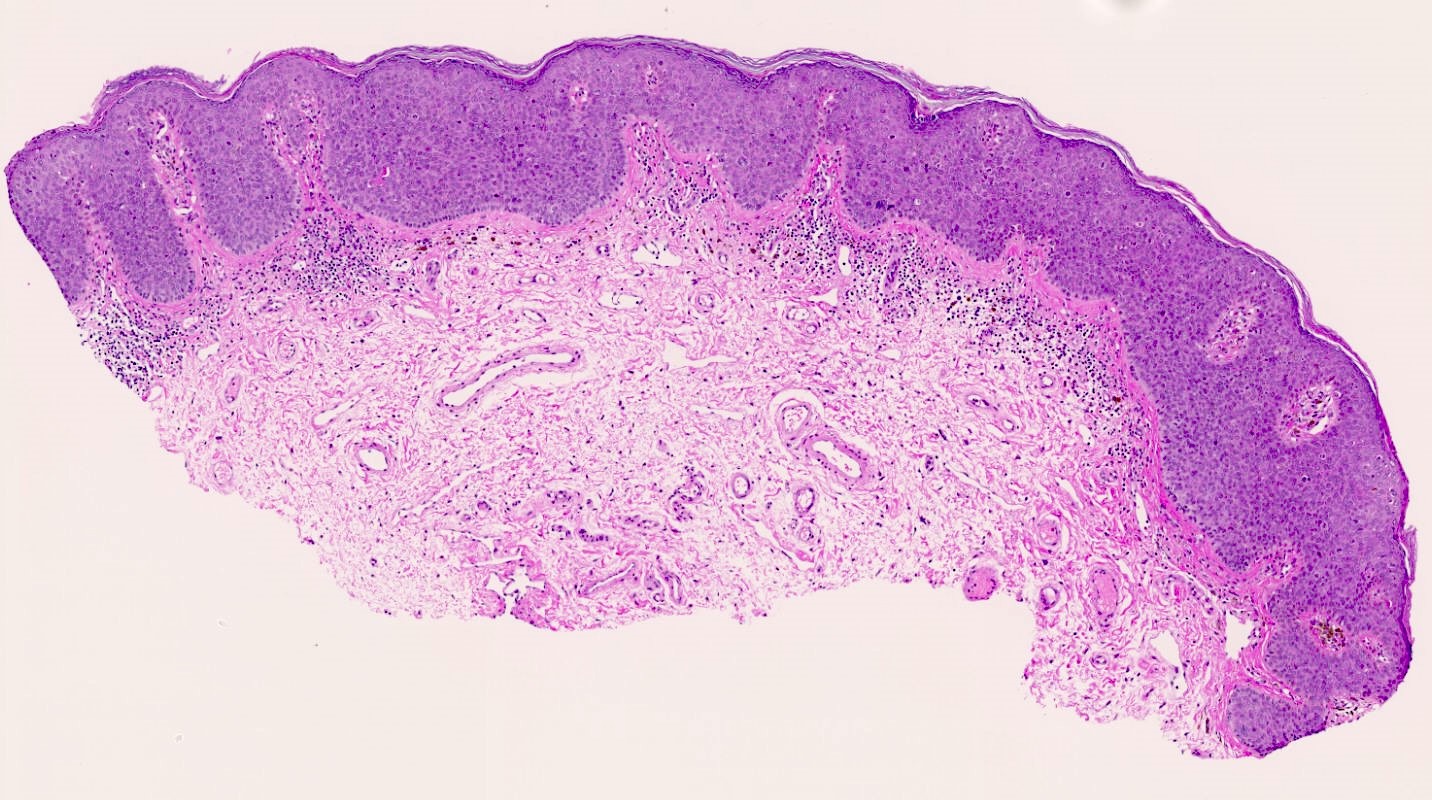
Stroma reaching the epithelium
Hypocellular stromal form
Hypercellular stromal form
Stellate cells
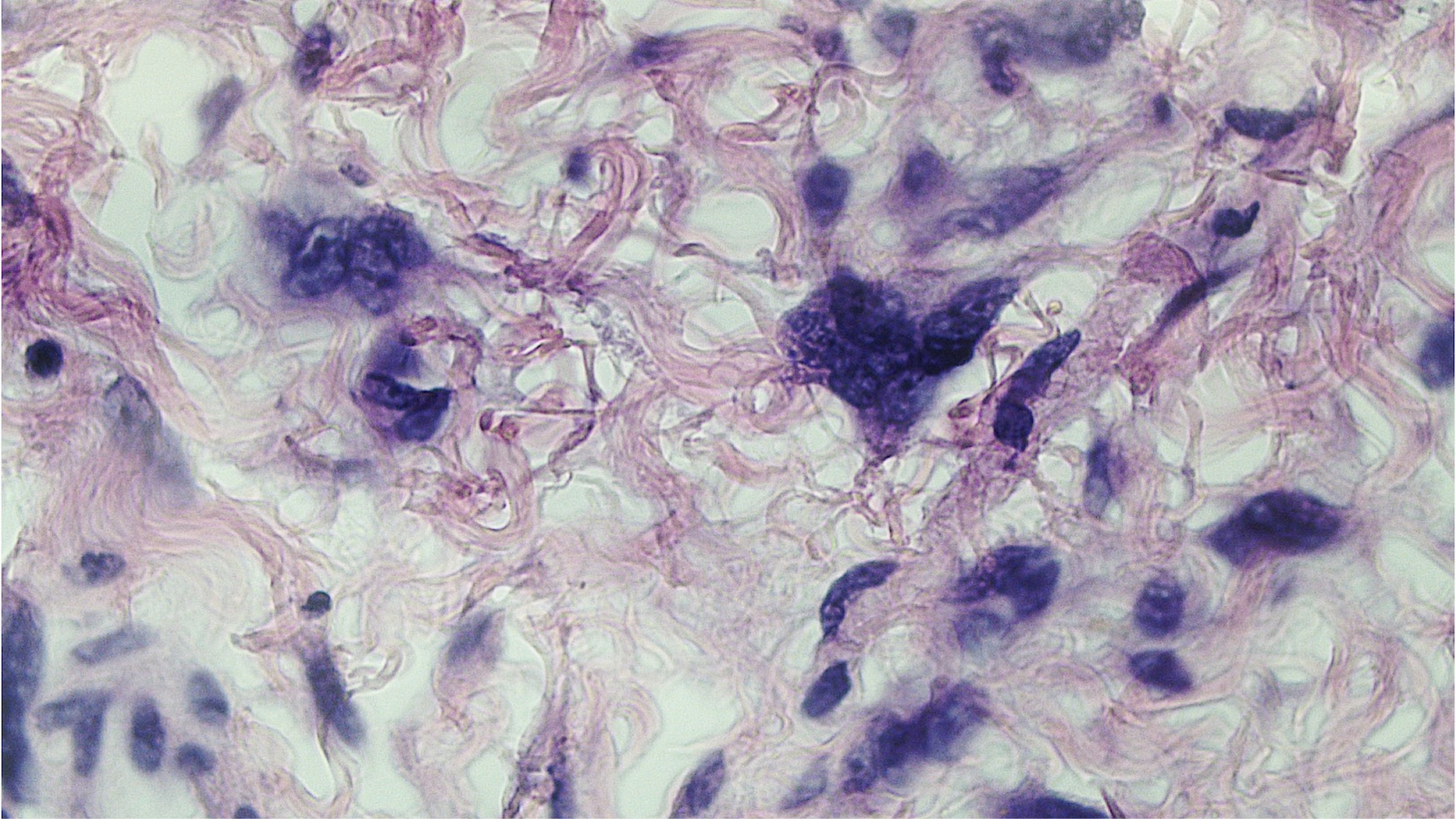
Multinucleated cells
Images hosted on other servers:

White plaque

Ulcerated nodule
Contributed by Matthias Choschzick, M.D.
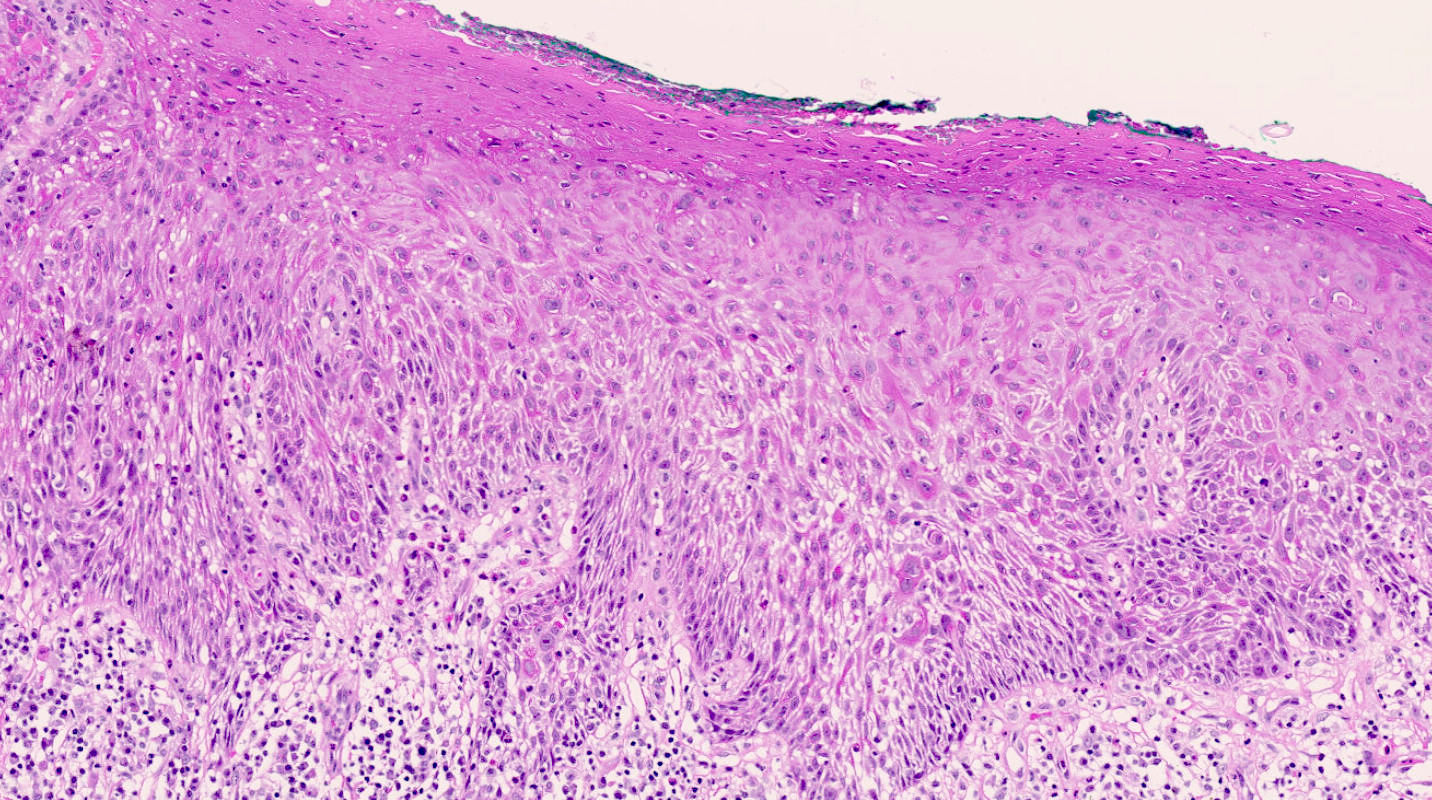
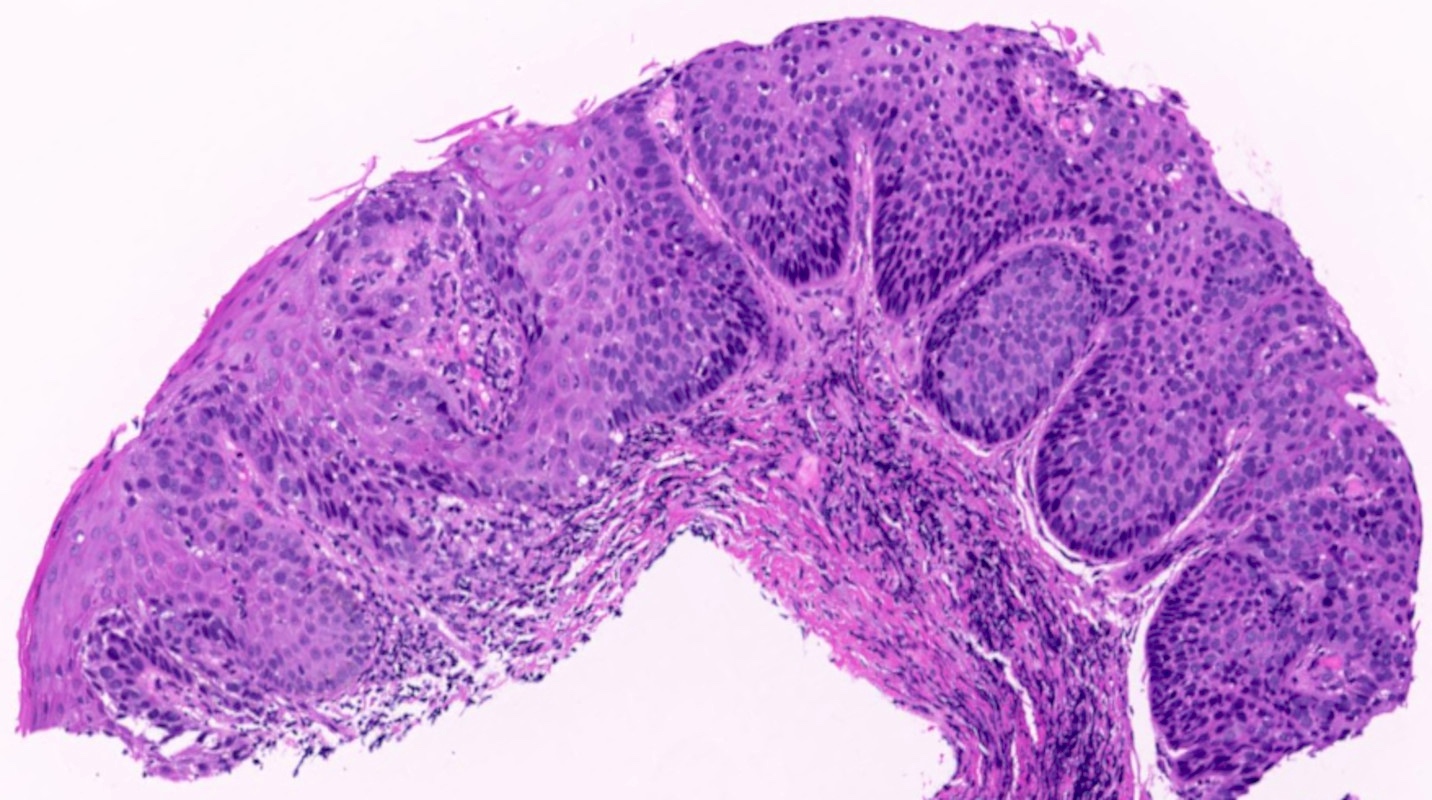
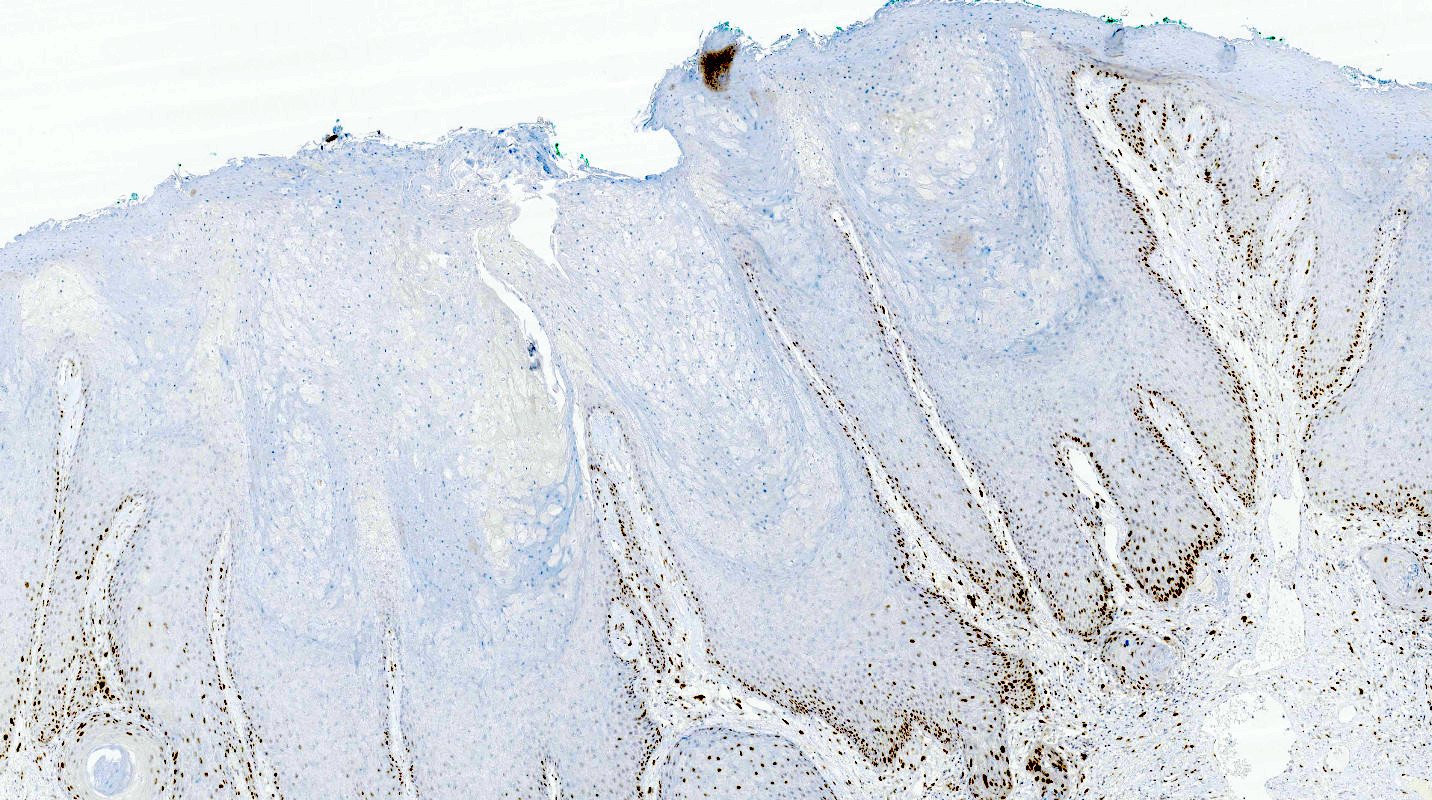
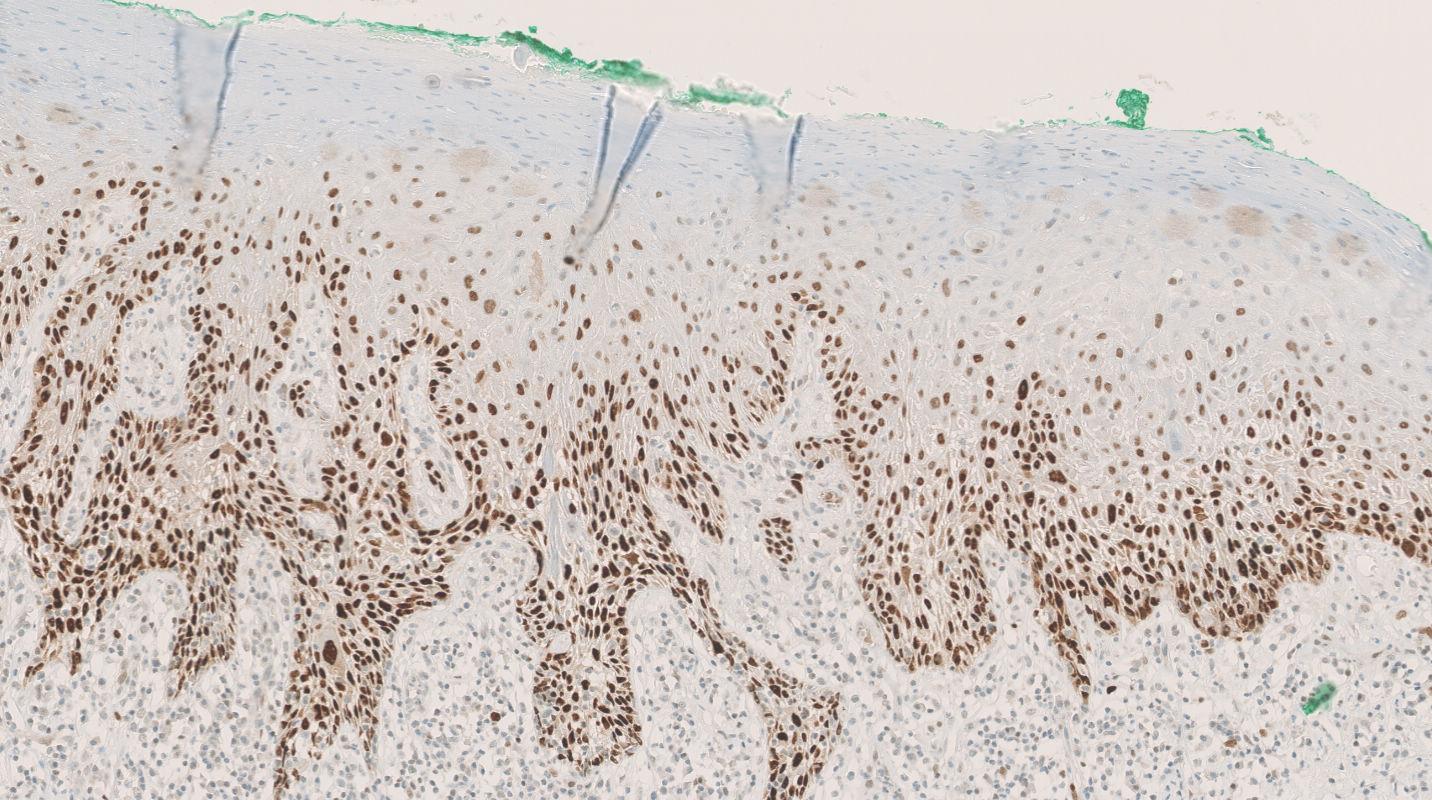
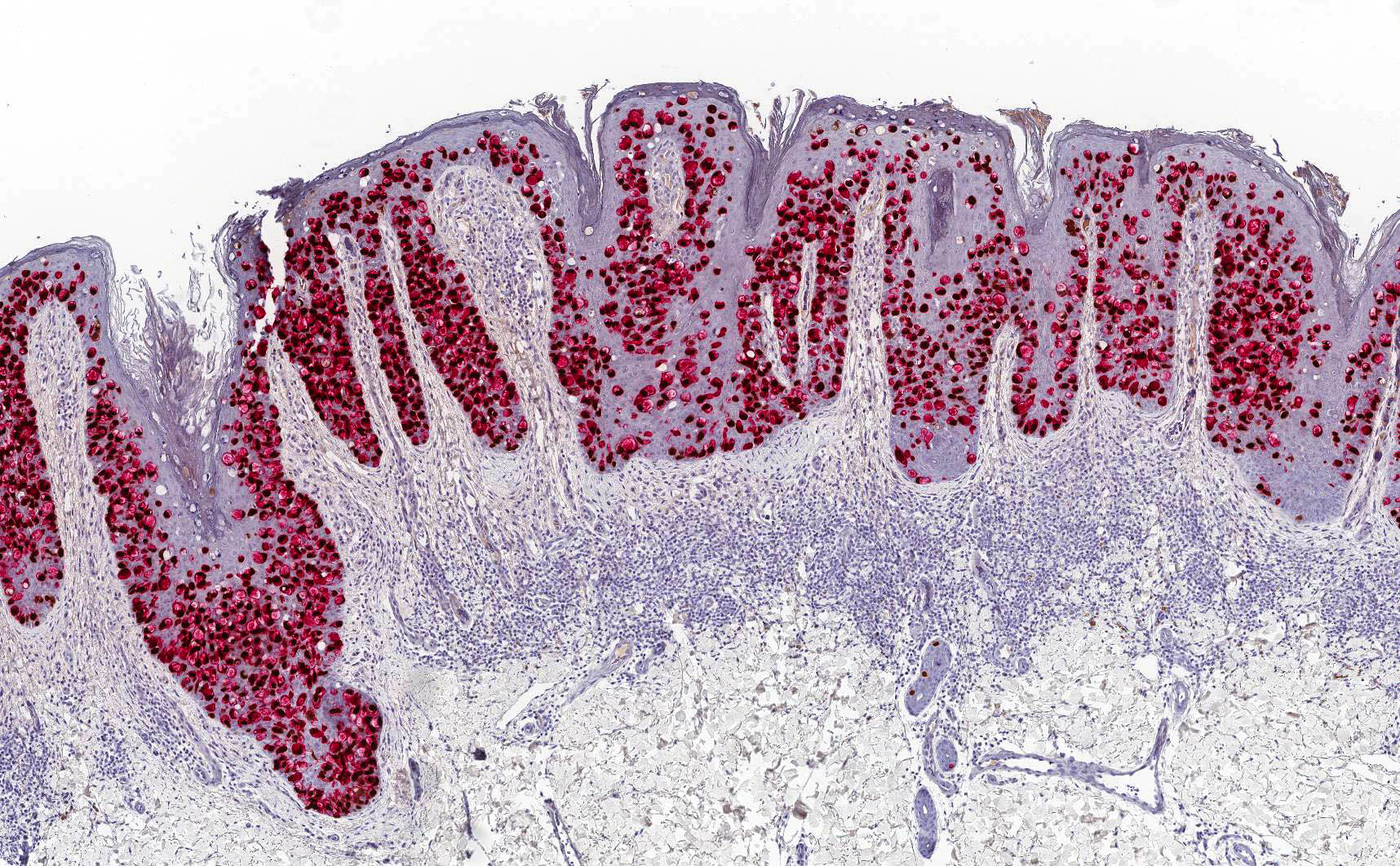
HSIL, basaloid type
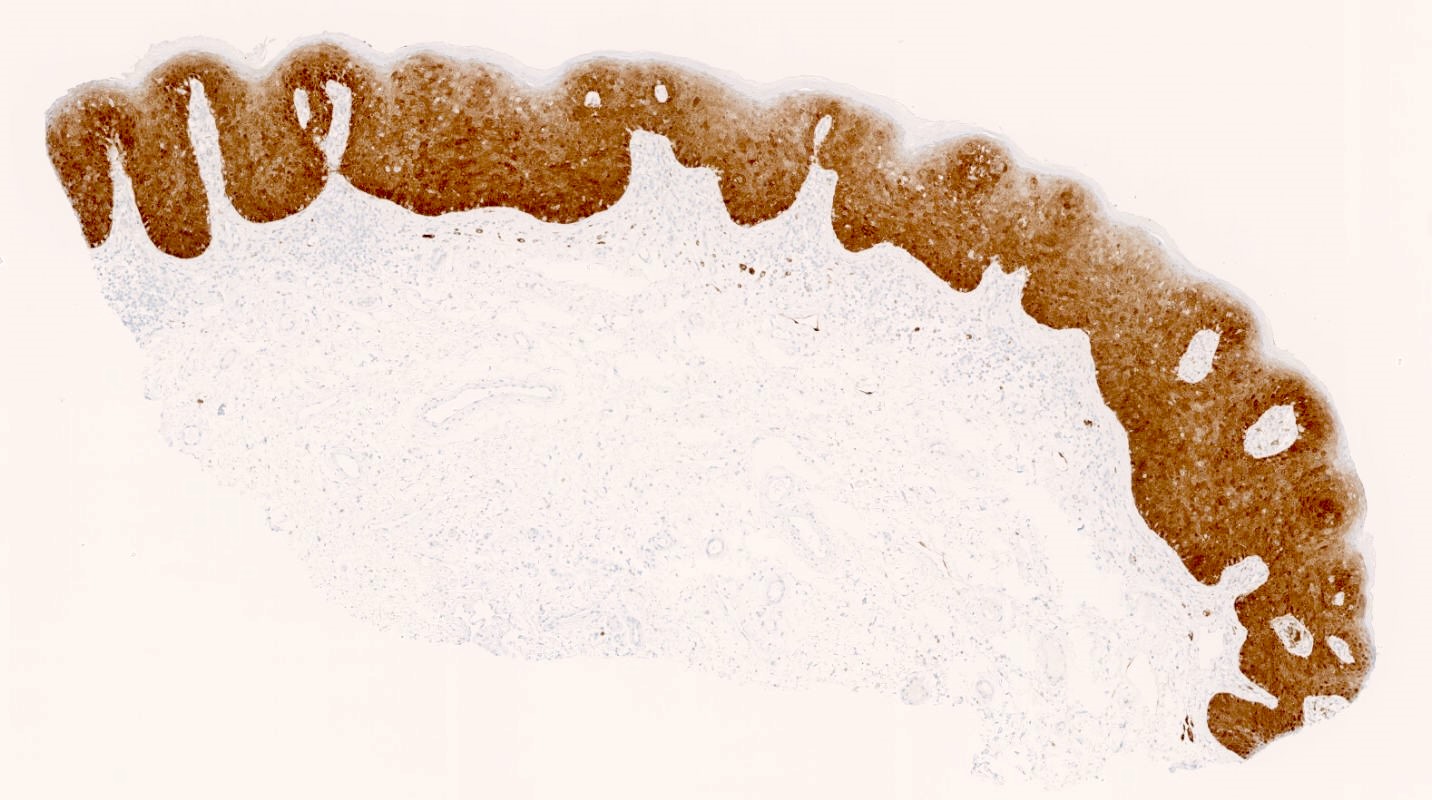
HSIL, p16 block staining

HSIL, increased Ki67
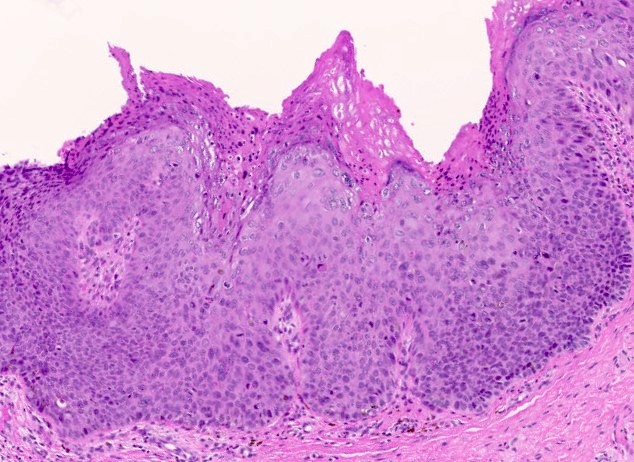
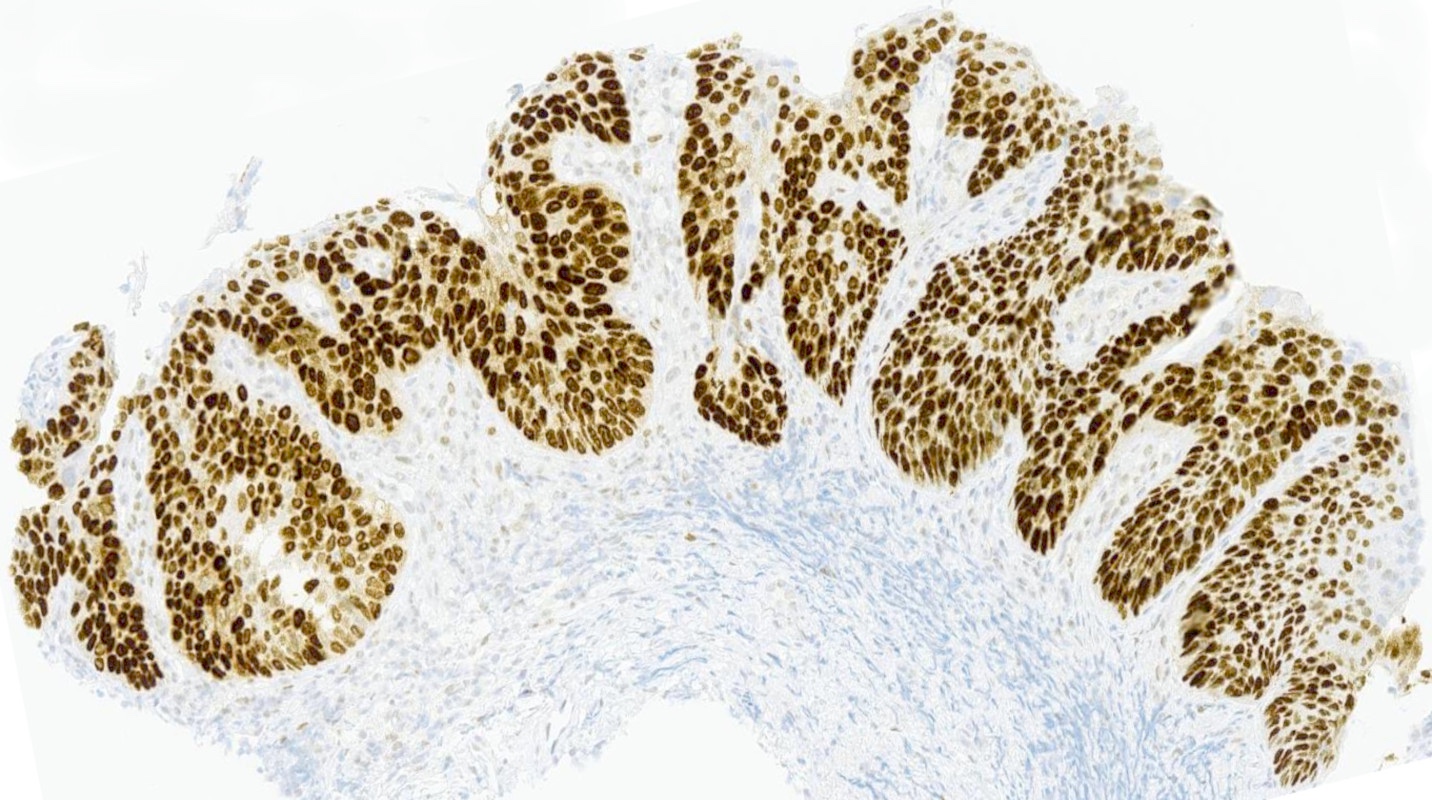
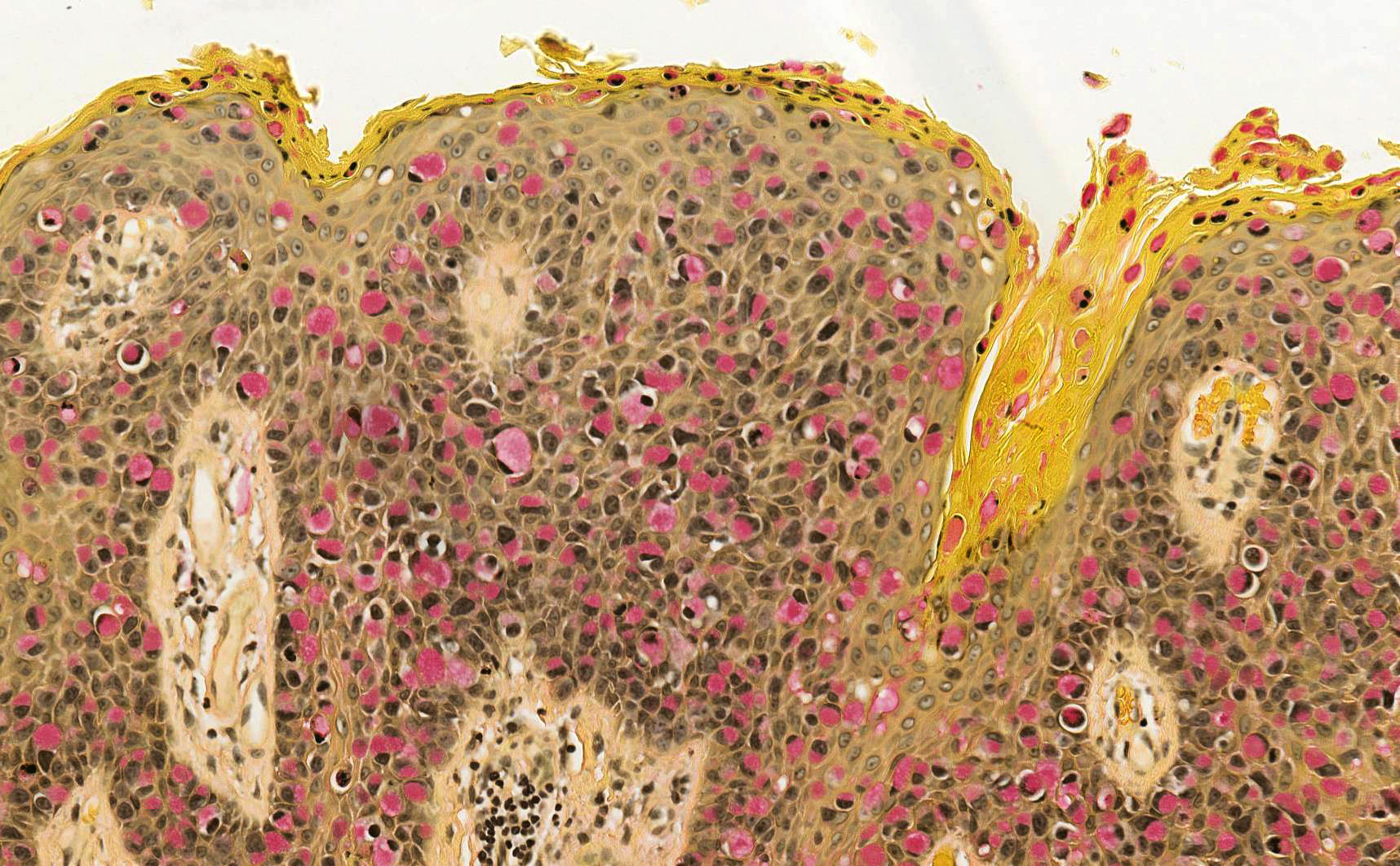
HSIL, warty type
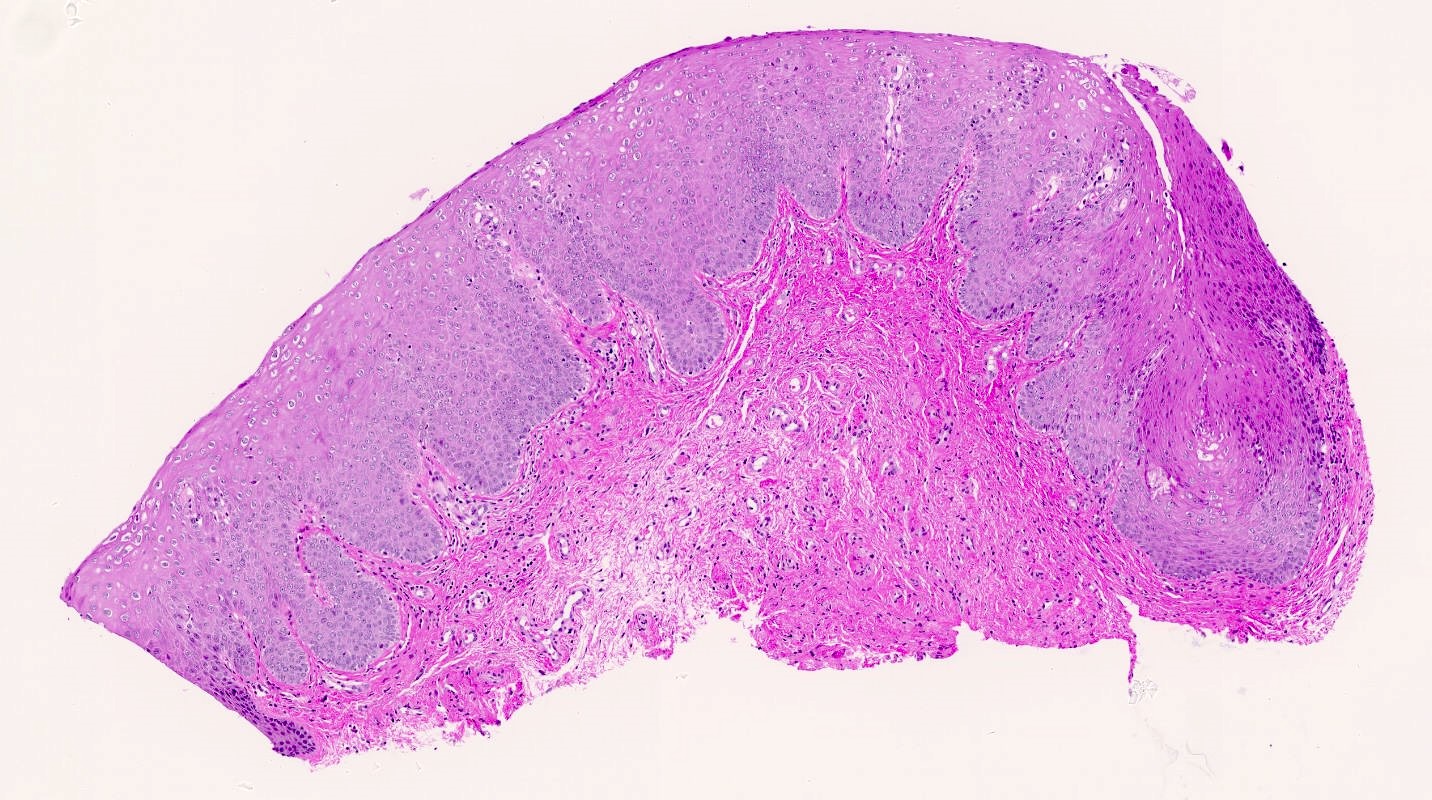
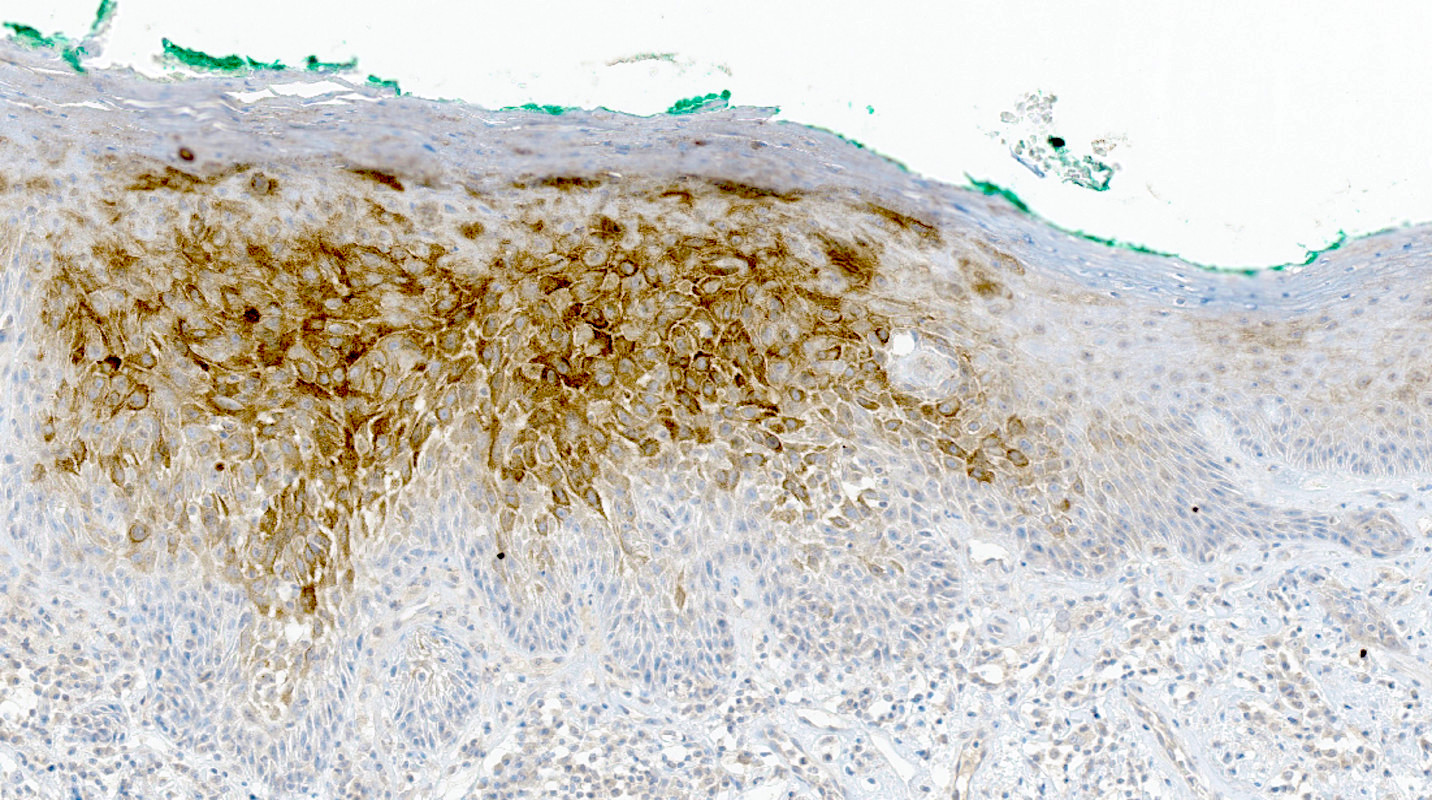
LSIL

LSIL, HPV stain
Contributed by Matthias Choschzick, M.D.
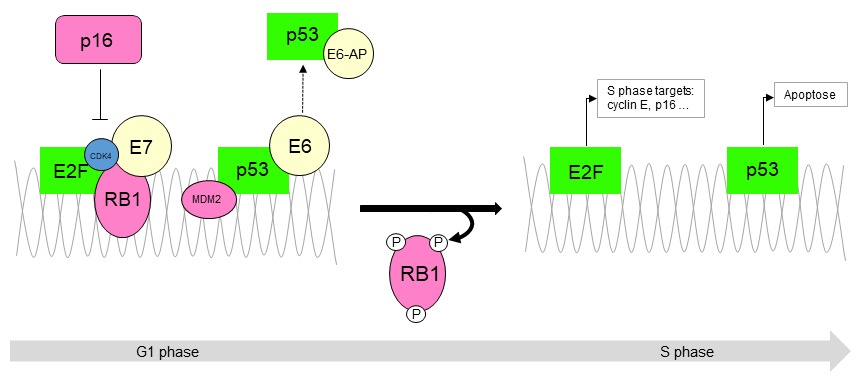
HPV, p16, p53
Images hosted on other servers:

Ulcerative lesion, upper labia minor
Contributed by Matthias Choschzick, M.D.

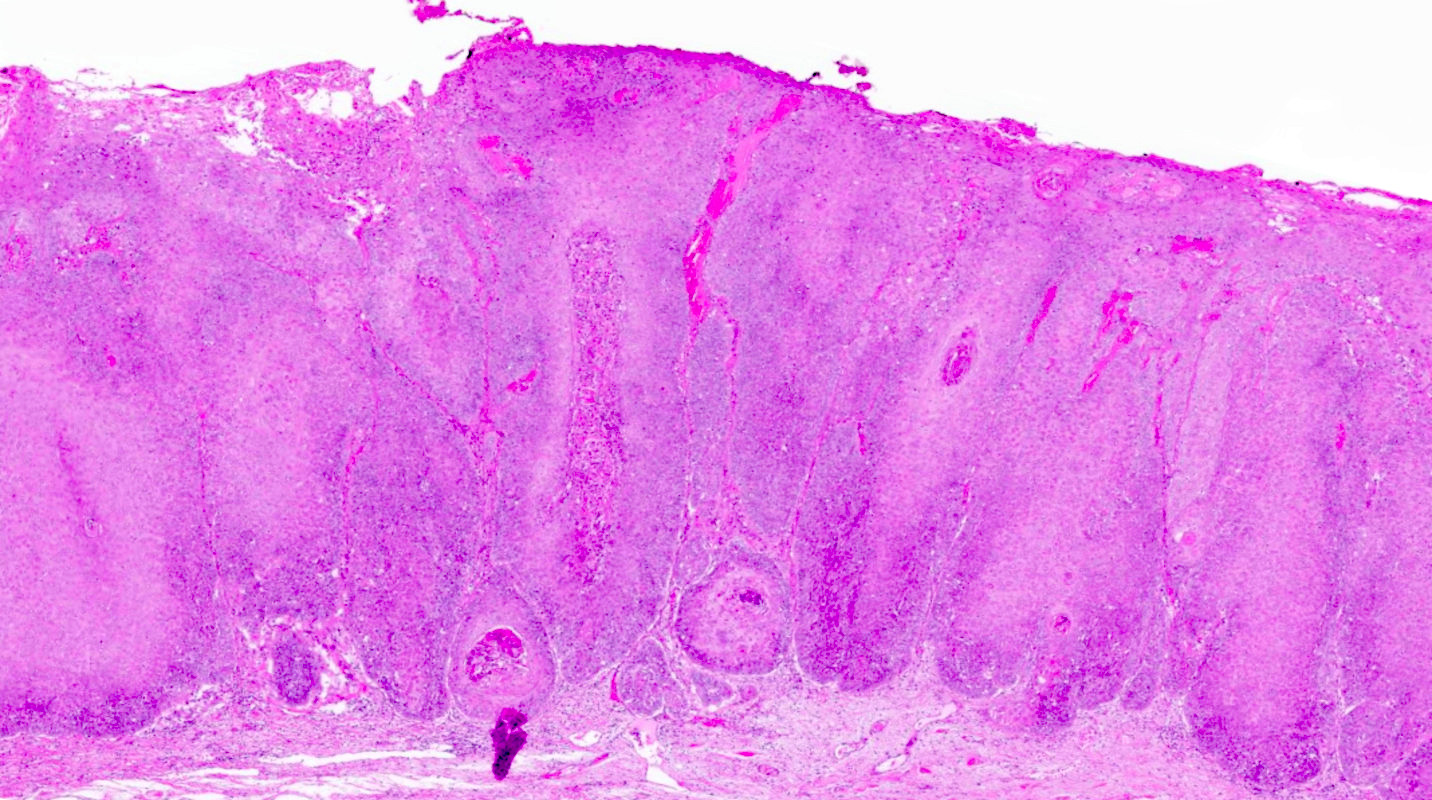
Vulvar carcinoma
Contributed by Matthias Choschzick, M.D.
Nonkeratinizing SCC
Margin
Invasion depth

p16

p53
HPV RNA ISH
Contributed by Matthias Choschzick, M.D.
Basal atypia
Basaloid differentiation
Cell pallor
No atypia

p53 expression
p53 overexpression
CK17
CK17
CK17
Contributed by Matthias Choschzick, M.D.

Keratinizing squamous cells

Clear cells


p53 immunohistochemistry


p53 immunohistochemistry
Table 1: Diagnostic criteria of vulvar erosive lichen planus by the International Society of the Study of Vulvovaginal Disease (ISSVD) (adapted from Br J Dermatol 2013;169:337)
| 3 out of 9 criteria needed for diagnosis |
| Well demarcated erosions or glazed erythema of introitus |
| Wickham striae on surrounding skin |
| Pain or burning |
| Scarring or loss of architecture |
| Vaginal inflammation |
| Involvement of other mucosal surfaces |
| Well defined inflammatory band in superficial connective tissue involving dermoepidermal junction |
| Inflammatory band consists of predominantly lymphocytes |
| Evidence of basal cell layer degeneration (e.g., Civatte bodies, abnormal keratinocytes or basal apoptosis) |
Table 2: Summary of minimum clinicopathologic criteria to diagnose vulvar erosive lichen planus, more specific than those proposed by ISSVD (adapted from J Low Genit Tract Dis 2020;24:317)
| All 5 criteria must be present | |
| Clinical presentation (signs) | Well demarcated glazed red macule or patch located on vestibule, labia minora or vagina* |
| Histopathological correlate | Nonkeratinized squamous epithelium, mucocutaneous junction or adjacent hairless skin |
| Band-like lymphocytic infiltrate abuts the epithelial layer | |
Basal layer with one of the following patterns
| |
| Sclerosis is absent | |
- *Supportive features
- Architectural changes include midline fusion or labia minora, adhesions between affected opposed structures
- Common comorbidities: lichen sclerosis (LS), other types of locations of lichen planus, systemic autoimmune diseases
Table 3: Clinicopathologic features of classic hypertrophic lichen planus (adapted from J Low Genit Tract Dis 2020;24:317)
| Classic lichen planus | Hypertrophic lichen planus | |
| Clinical features | Red, gray-white or purple-brown plaque or papules on hairless or hair bearing skin | Circumferential red plaque over hairless and hair bearing skin of vulva or perianal area |
| Histopathological correlate | ||
| Stratum corneum* | Hyperkeratosis | Marked hyperkeratosis |
| Granular cell layer* | Hypergranulosis | Diffuse and marked hypergranulosis |
| Rete ridge morphology | Mild to moderate acanthosis with irregular rete ridges, often sawtoothed or spiky | Marked acanthosis with deep and irregular rete ridges |
| Basal layer | Apoptotic bodies, squamatization, vacuolar change Lymphocytosis | Apoptotic bodies, squamatization, vacuolar change may be confined to rete tips / basal layer above papillary processes
Lymphocytosis |
| Dermis | Band-like applied lymphocytic infiltrate | |
| Papillary dermal fibrosis | ||
- *May be altered by excoriation, especially in hypertrophic lichen planus
Contributed by M. Luann Racher, M.D.

Bilateral red patch
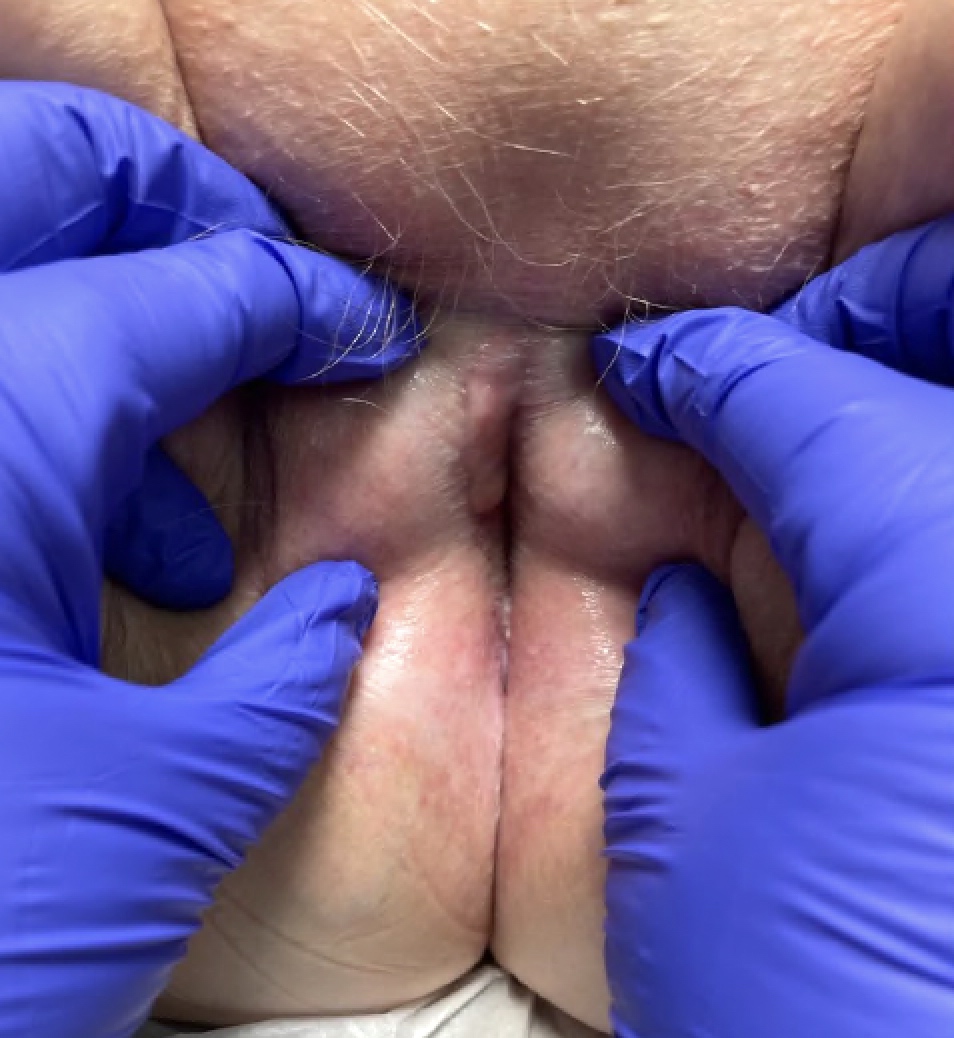
Circumferential red patch

Excoriated erythematous plaque

Excoriated erythematous plaque

Scarring and excoriated plaques
Images hosted on other servers:

Glassy, reticulated, white papules and plaques

Extensive erosion and ulceration
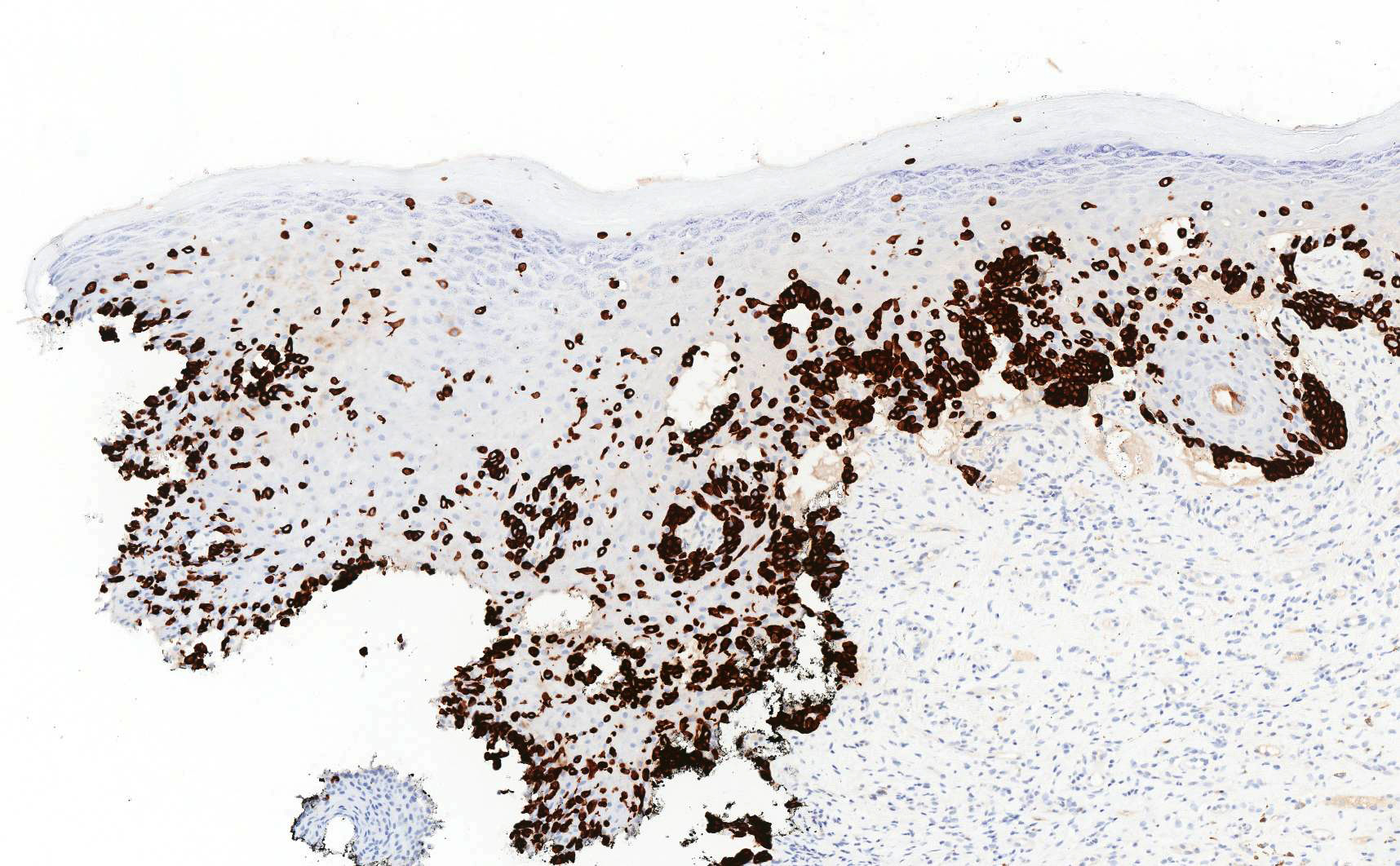
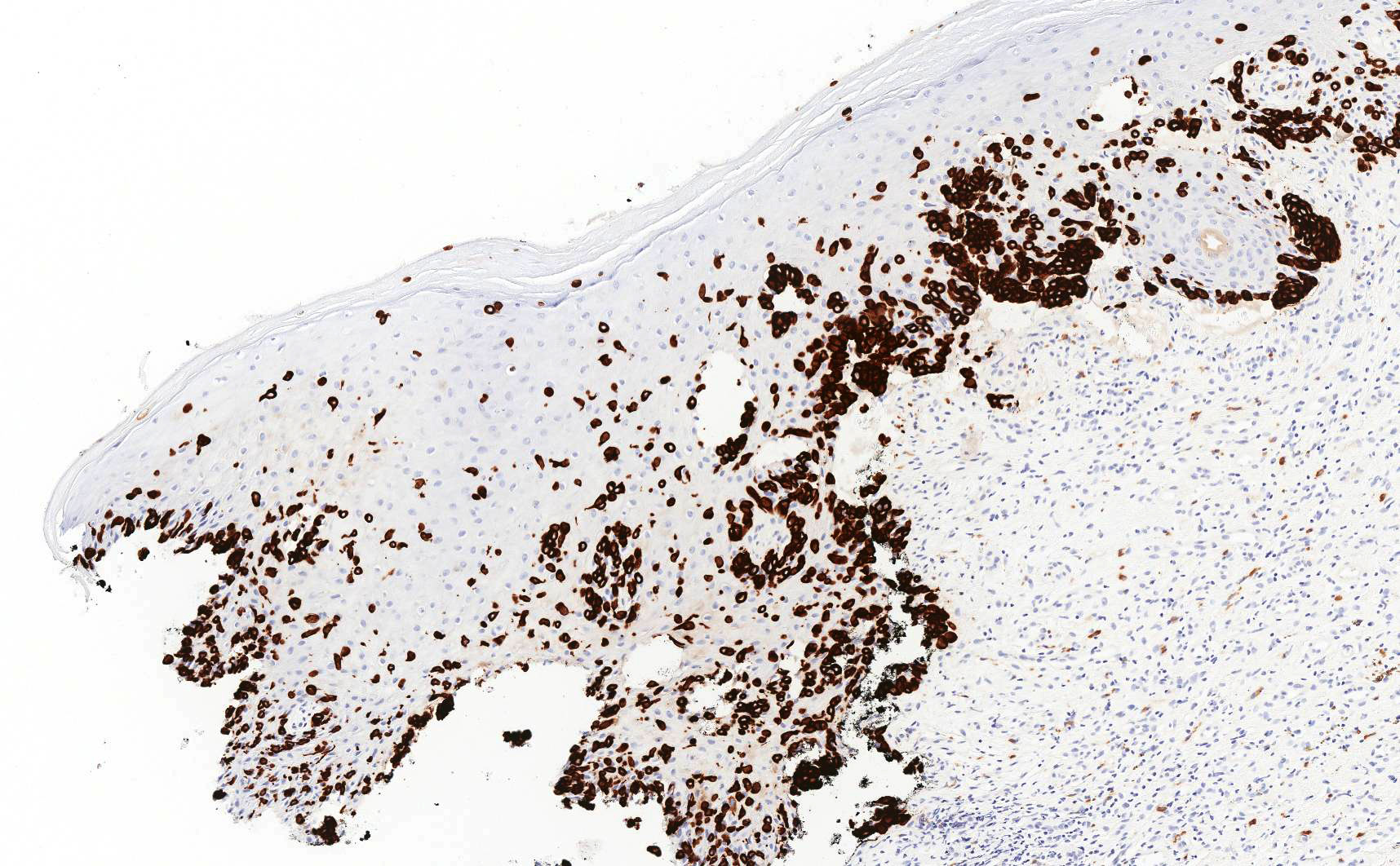
Contributed by Anna Sarah Erem, M.D. and Gulisa Turashvili, M.D., Ph.D.
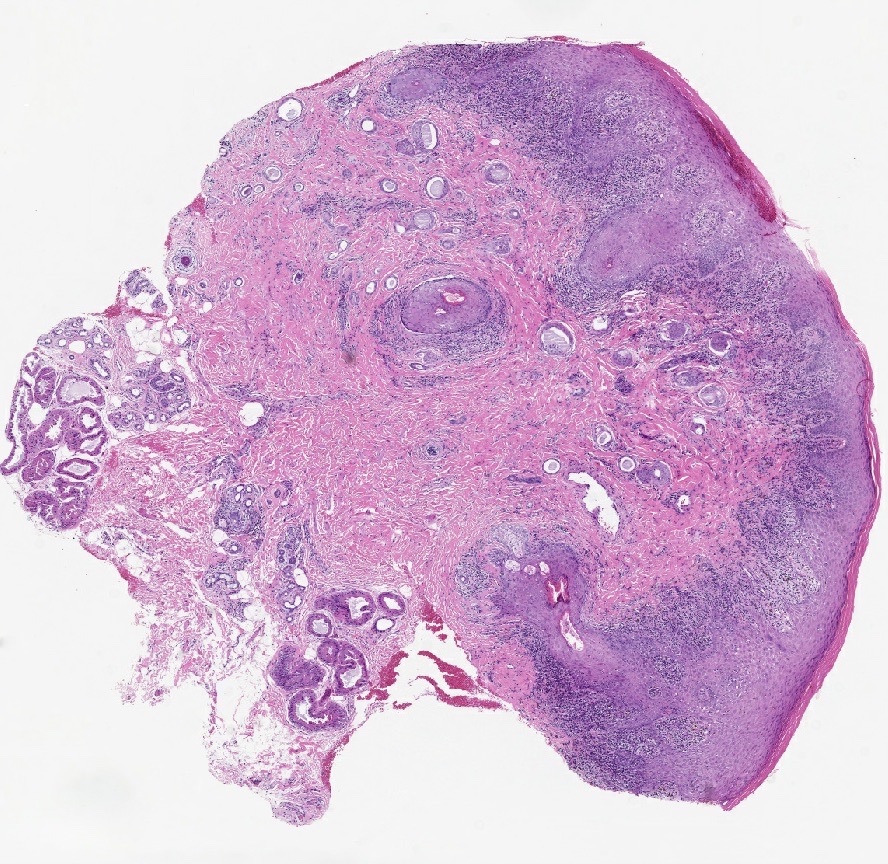
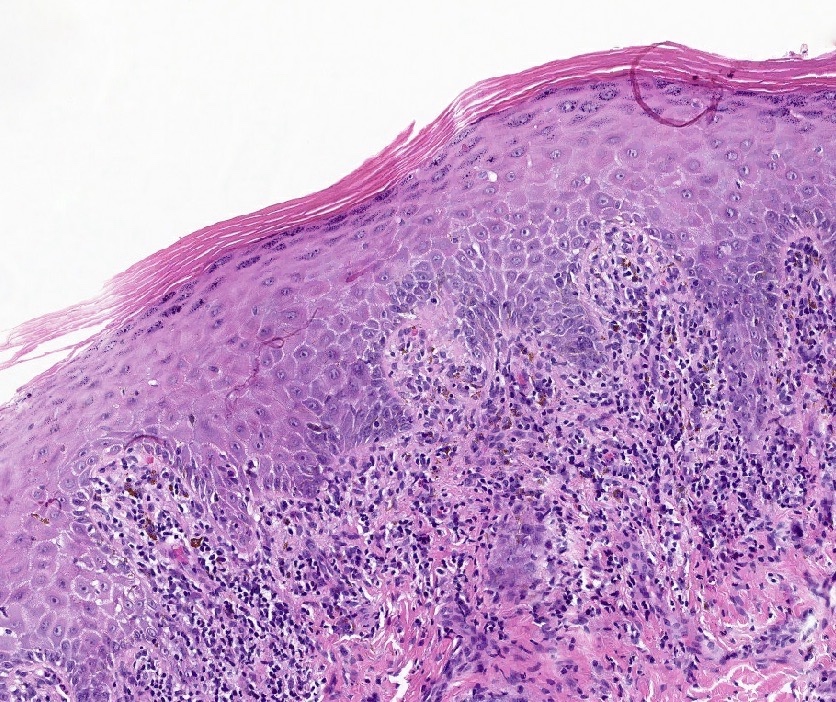
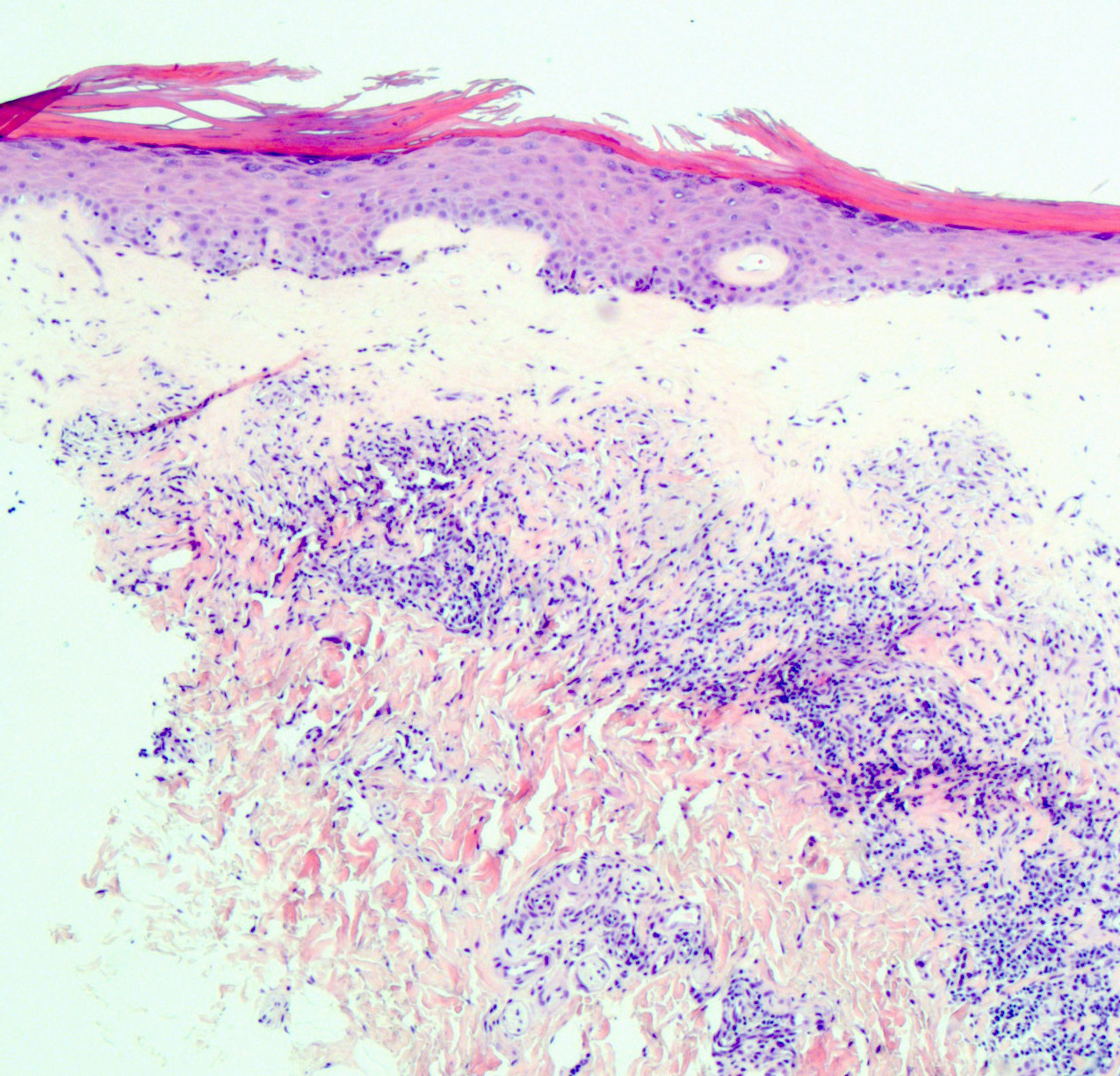
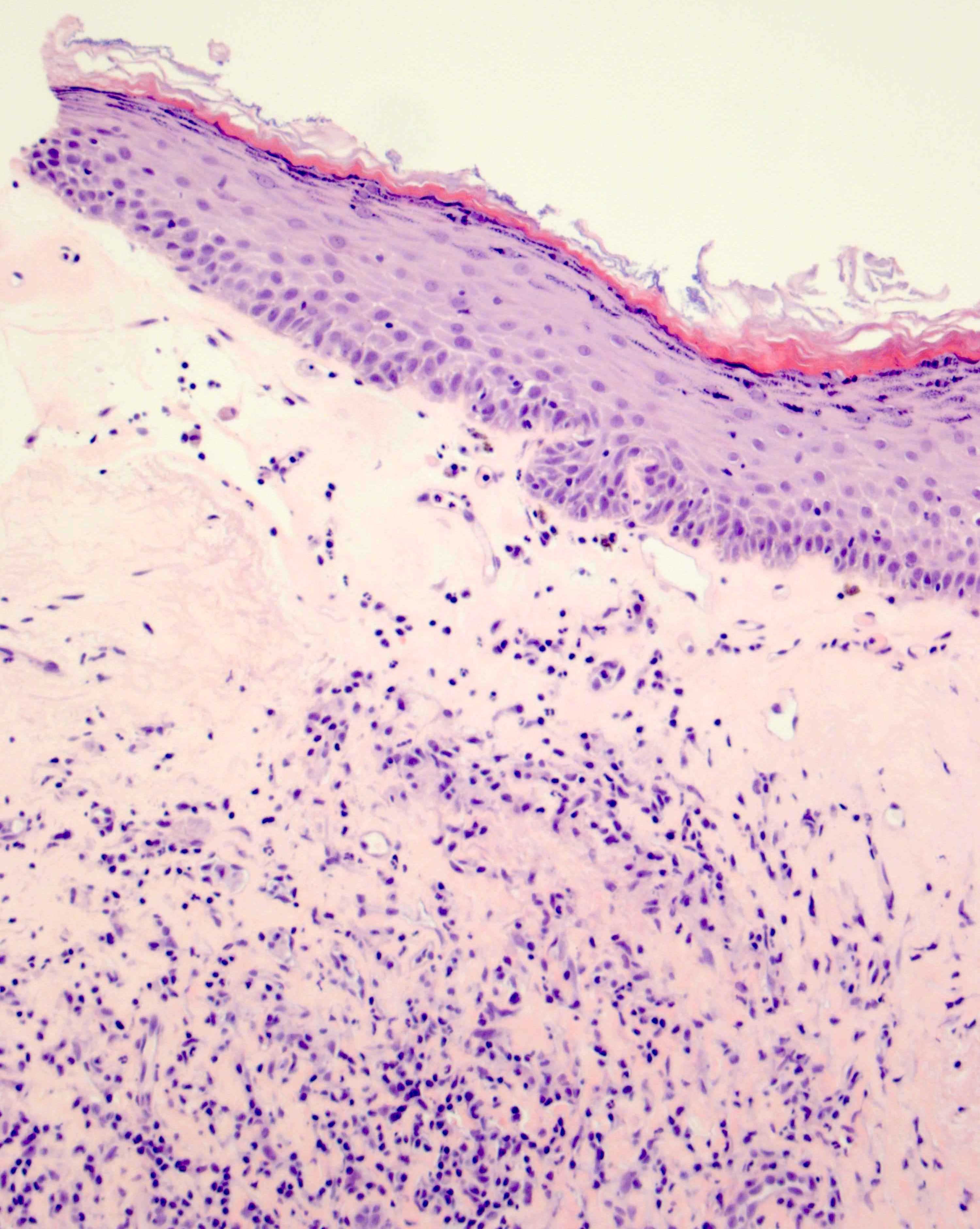
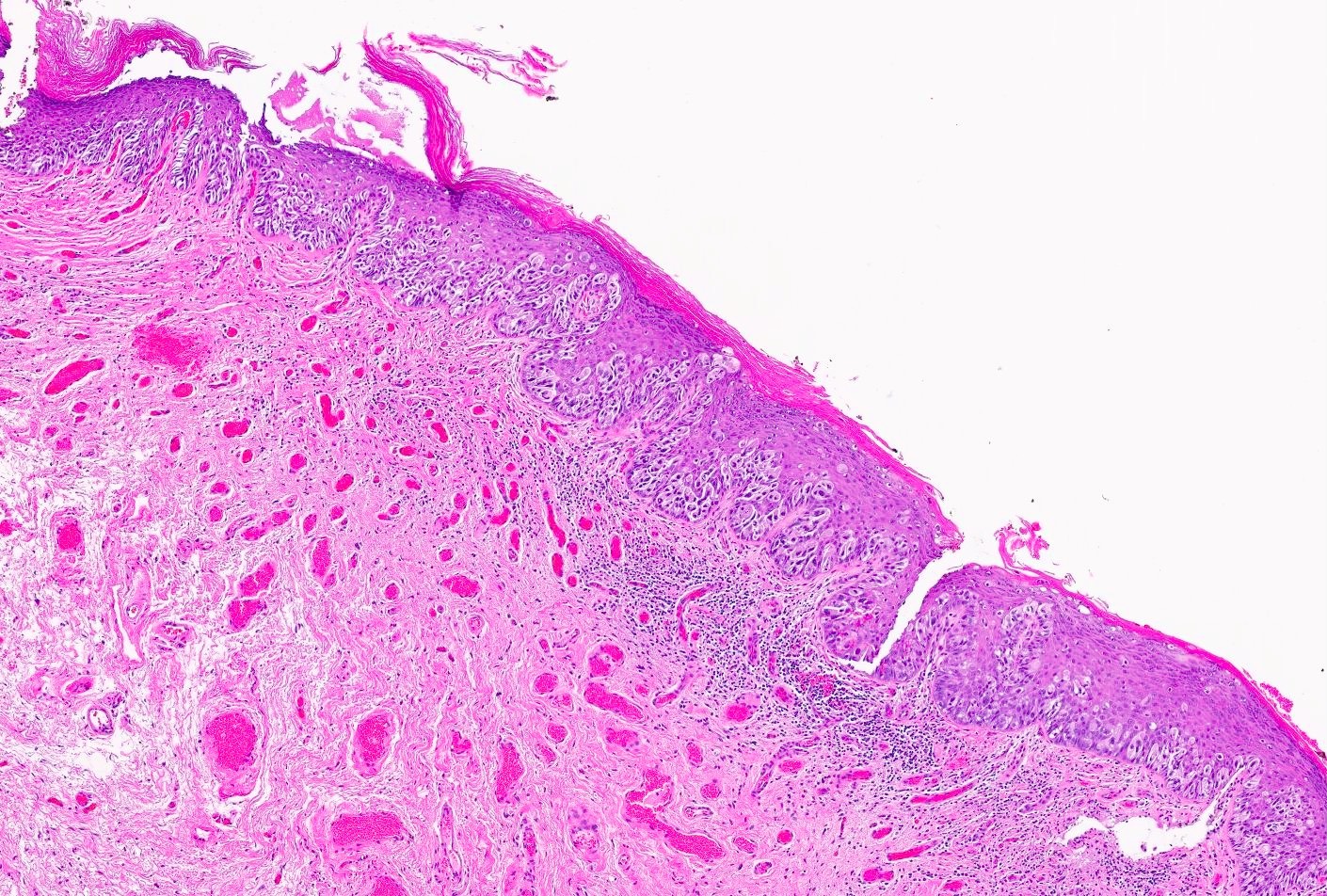
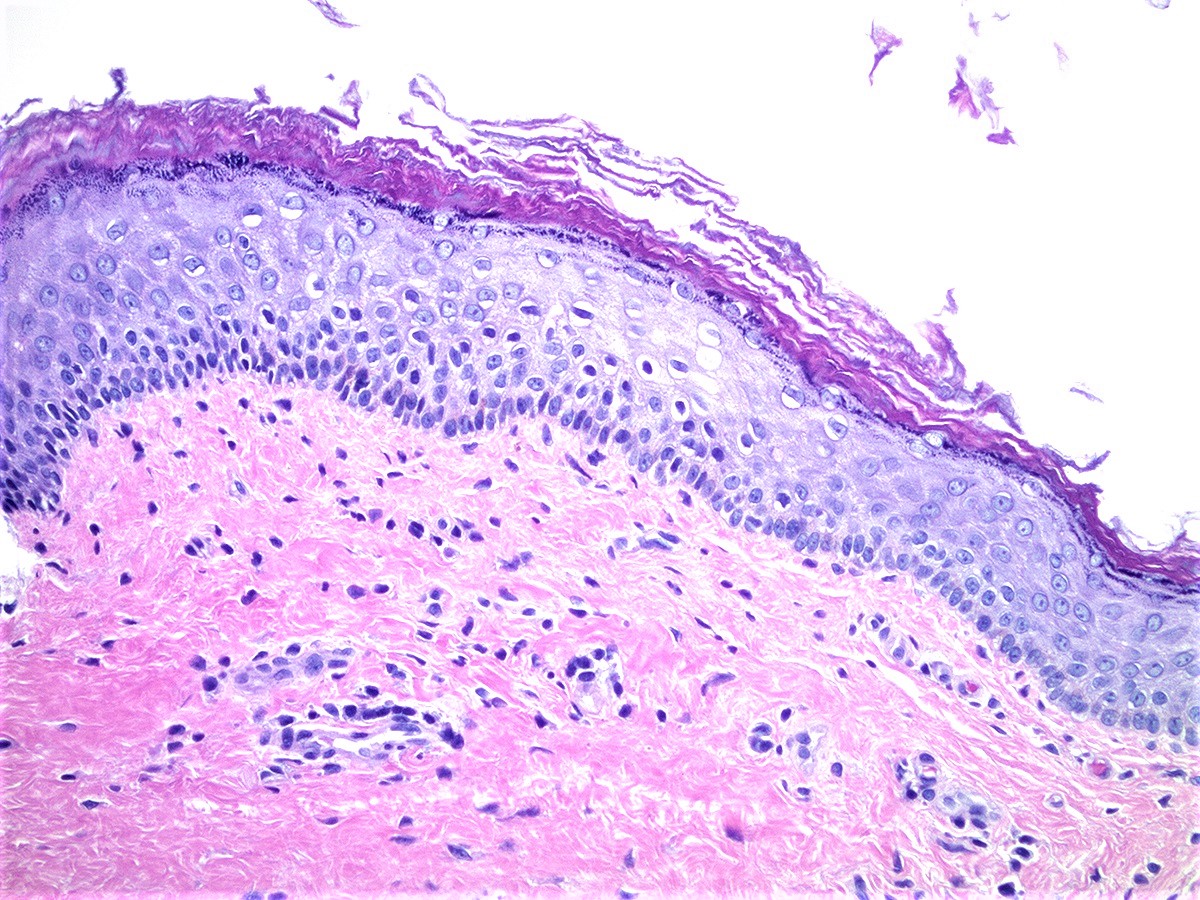
Lichenoid interface dermatitis
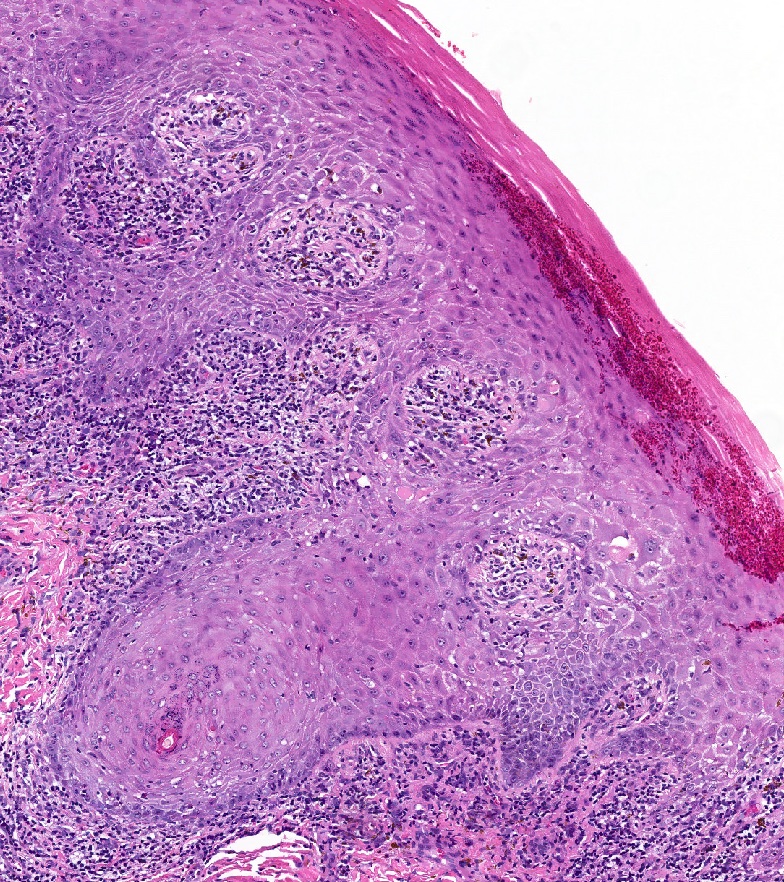
Civatte bodies or colloid bodies
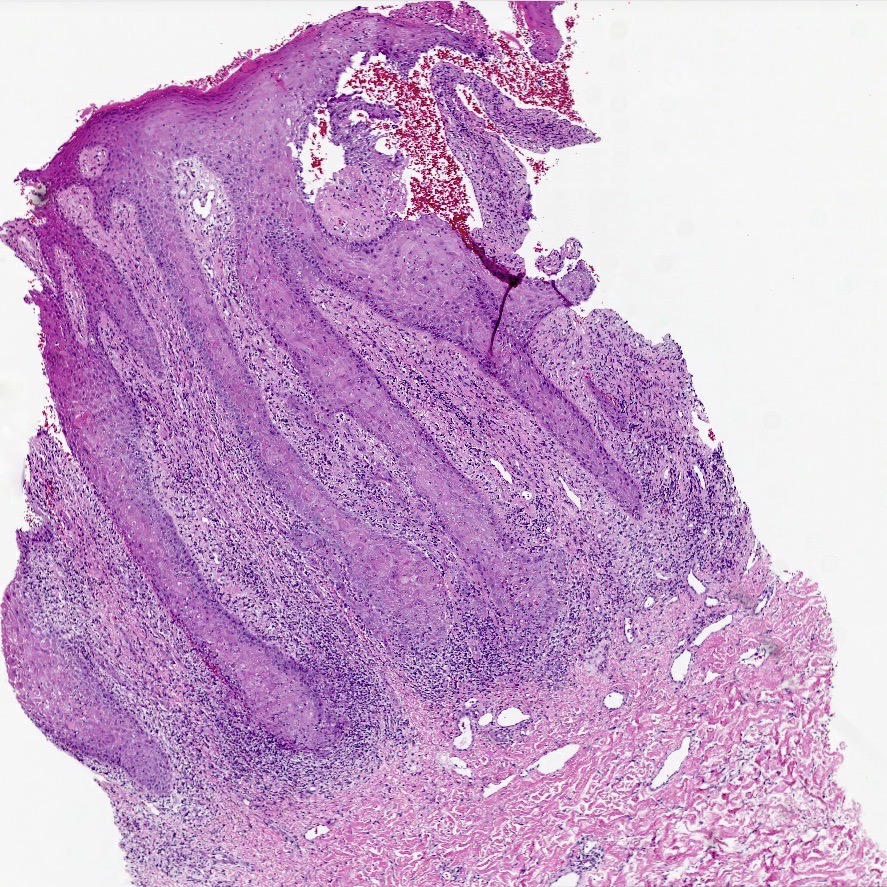
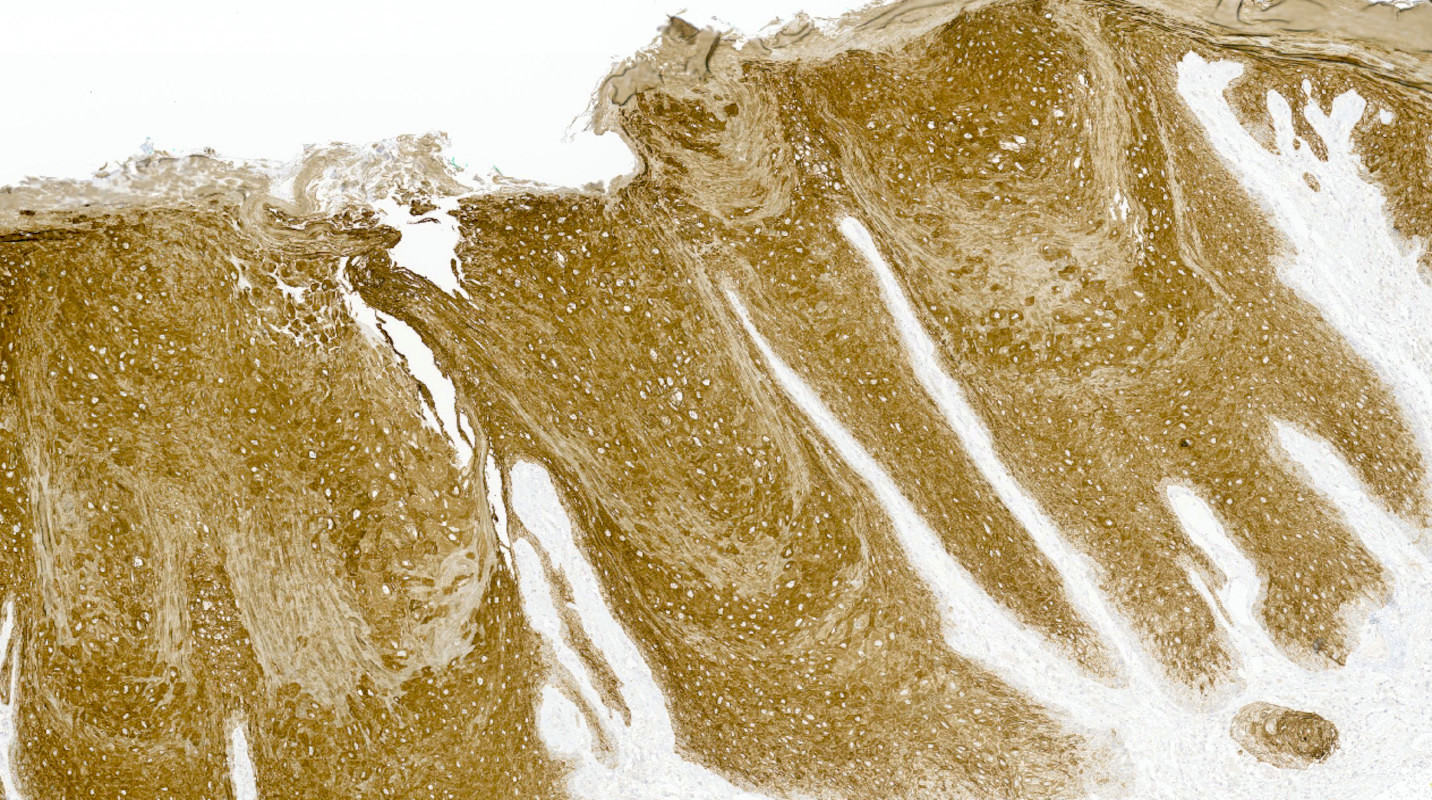
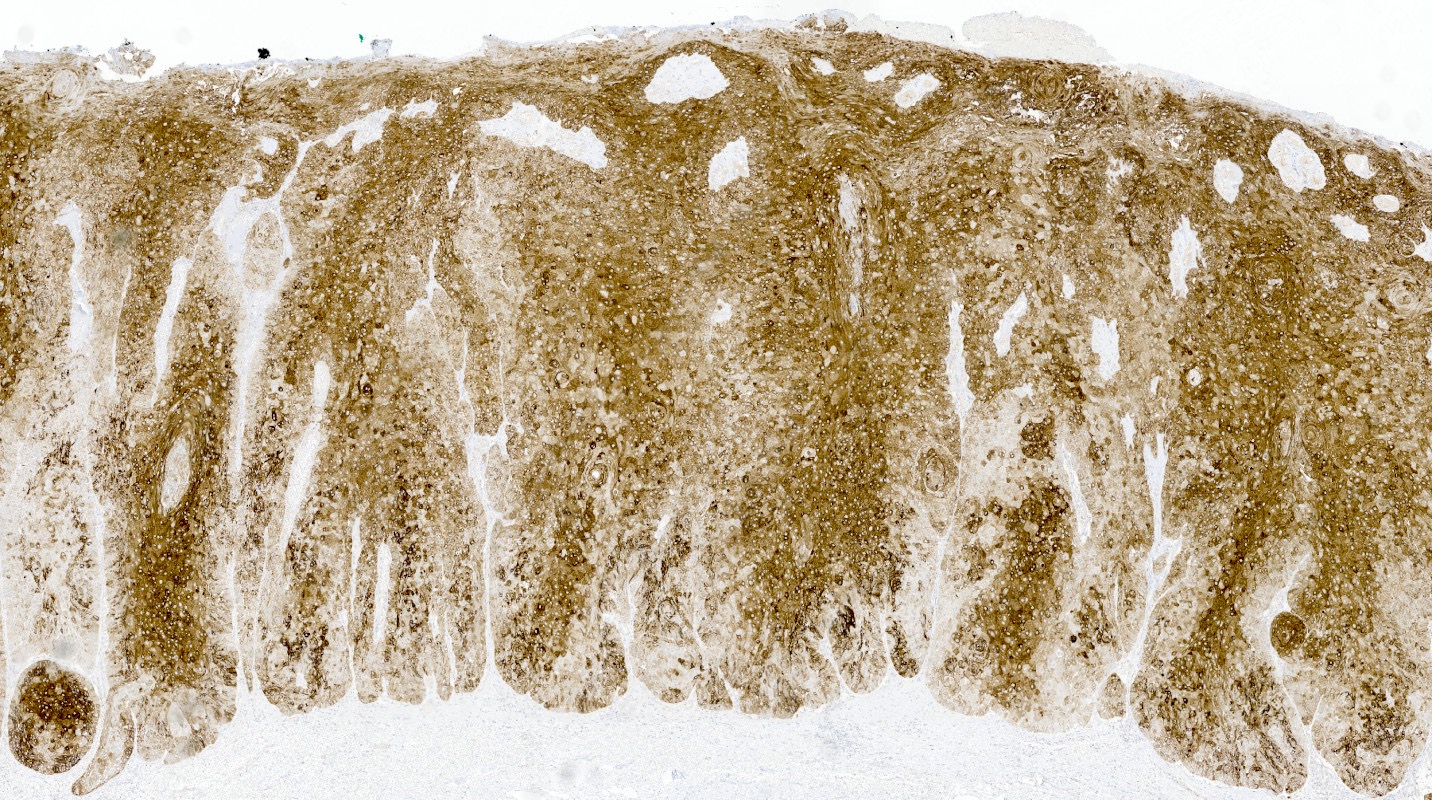
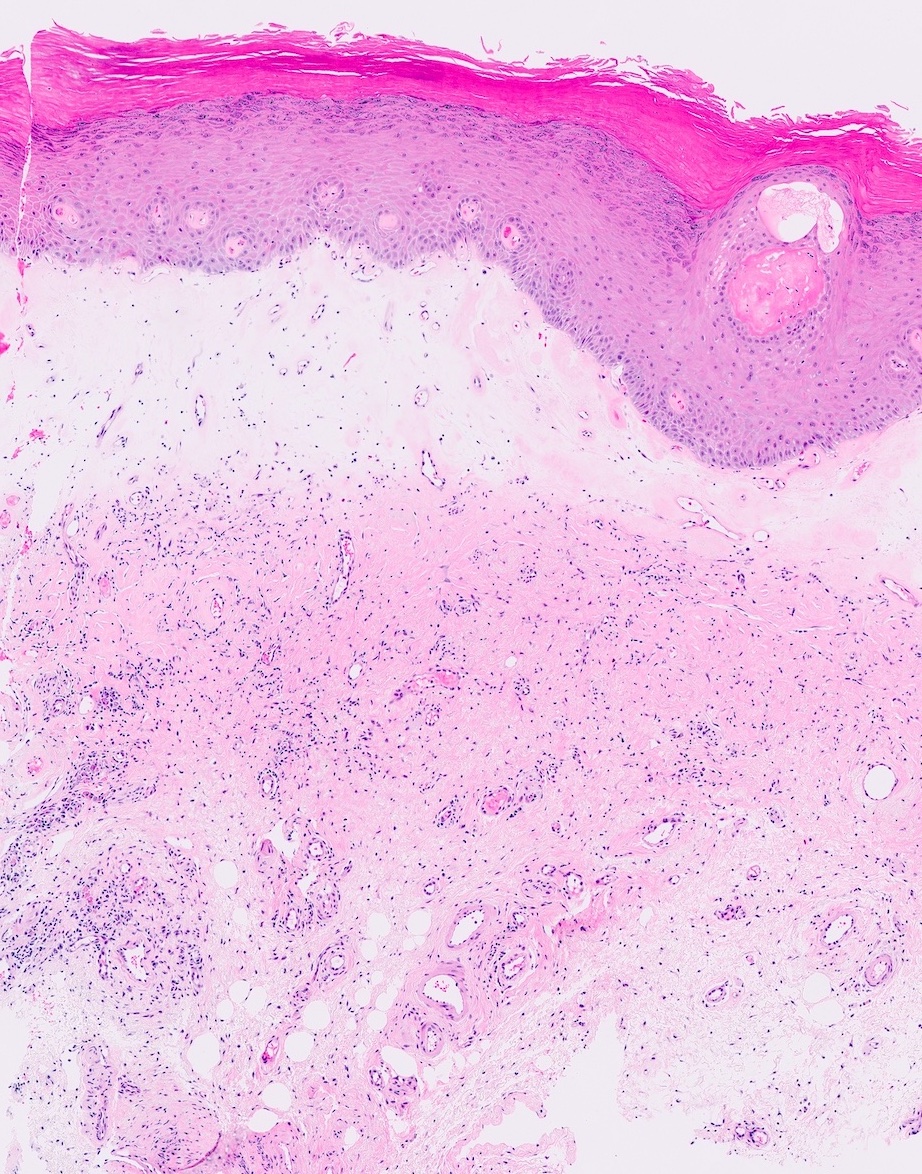
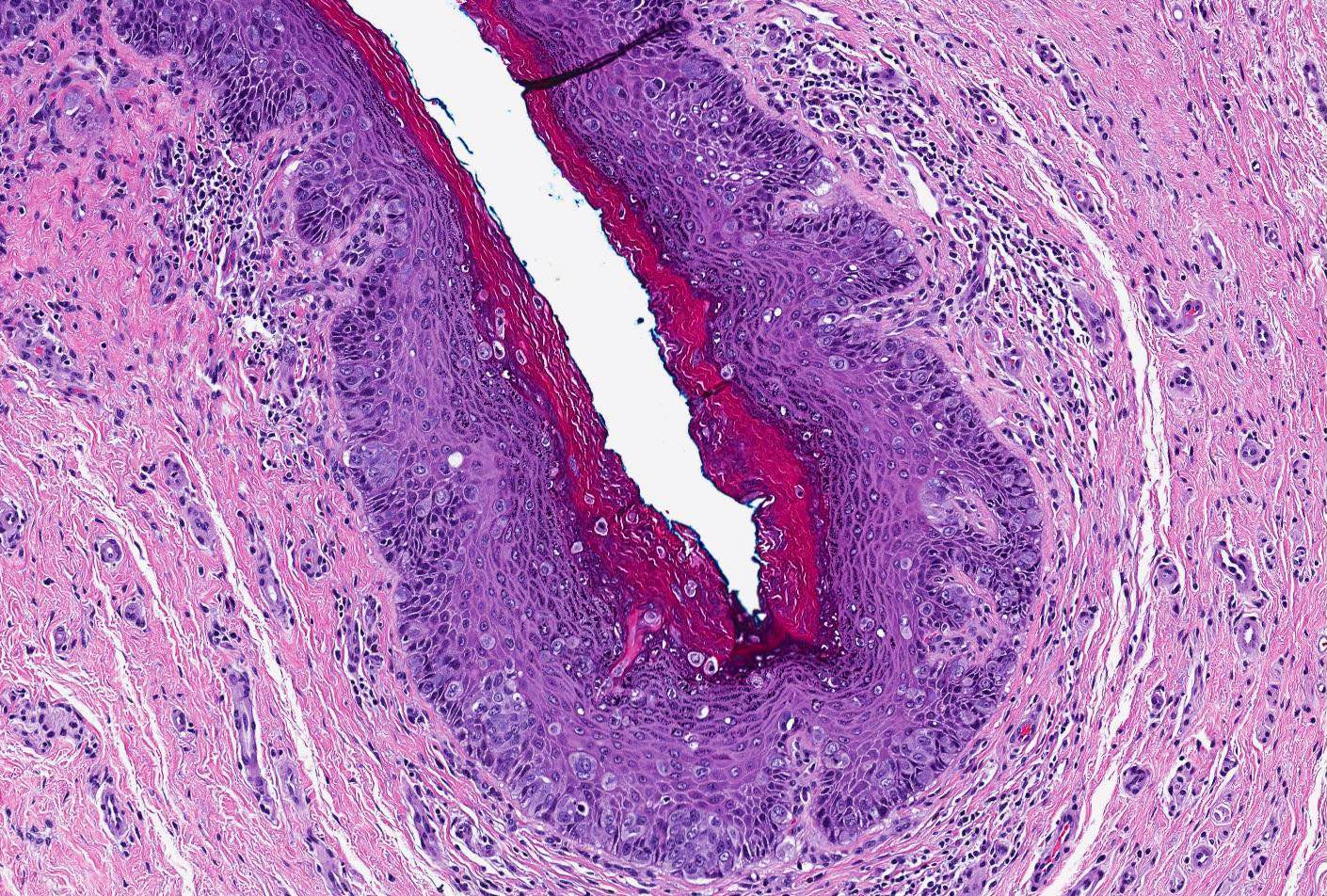
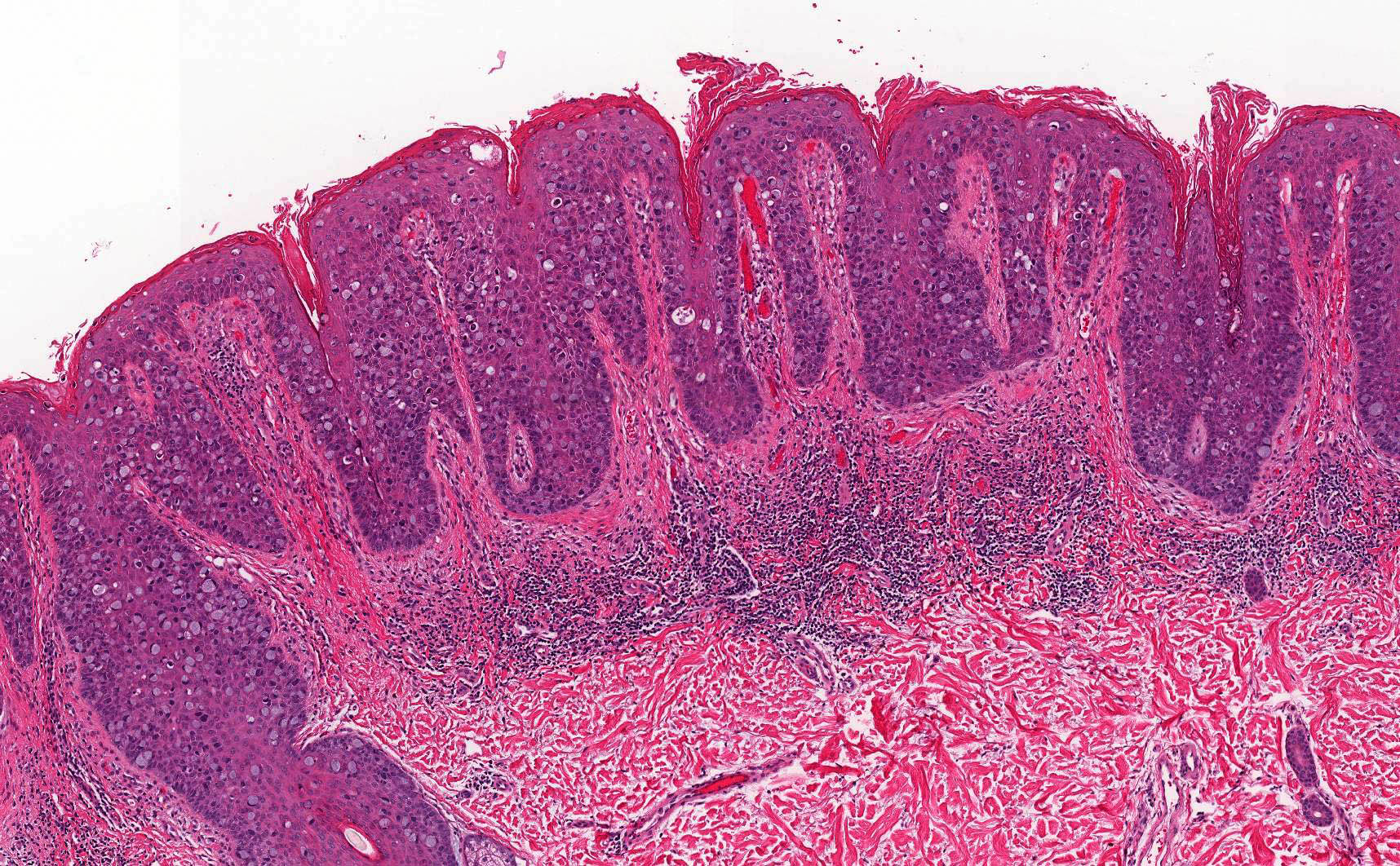
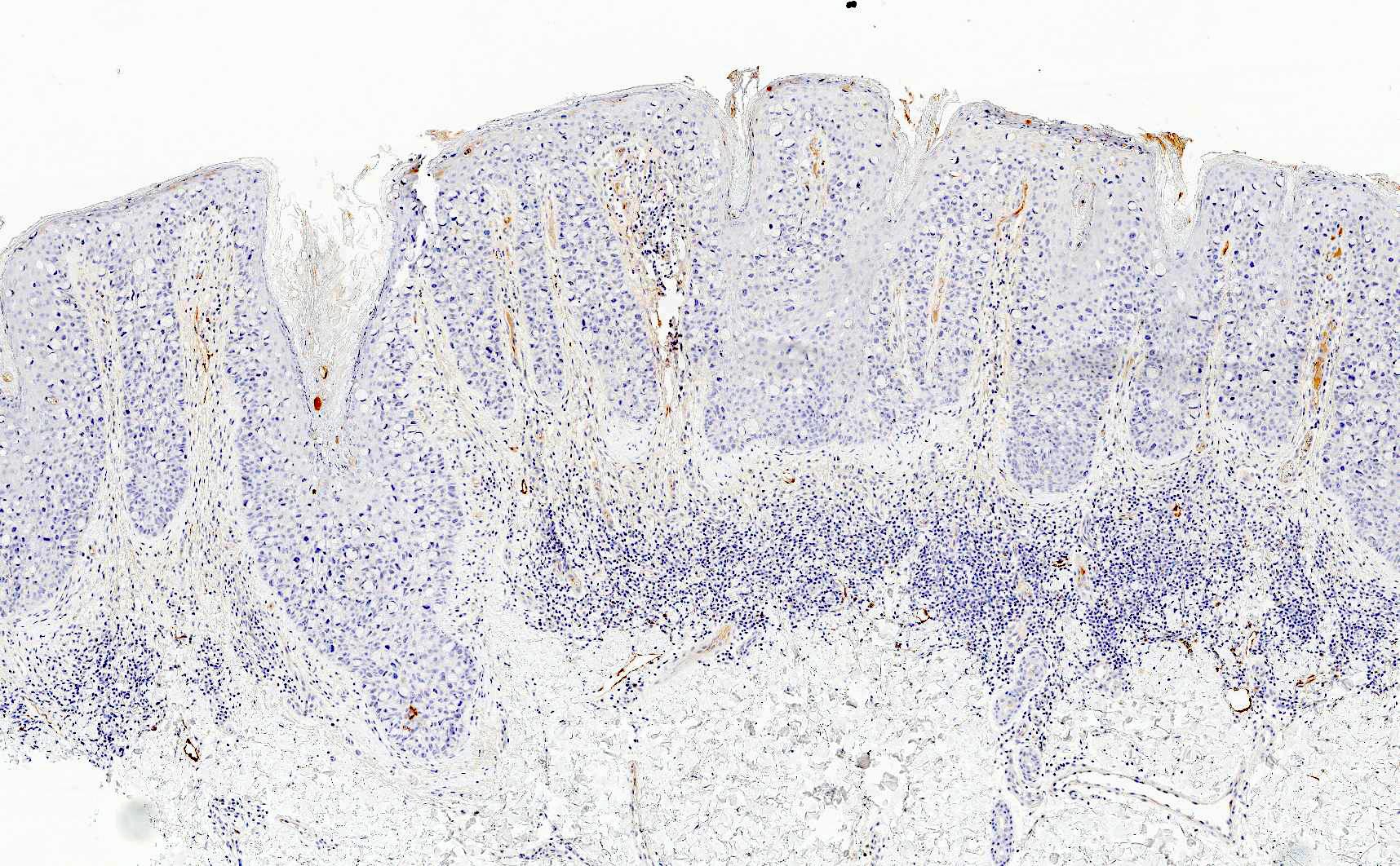
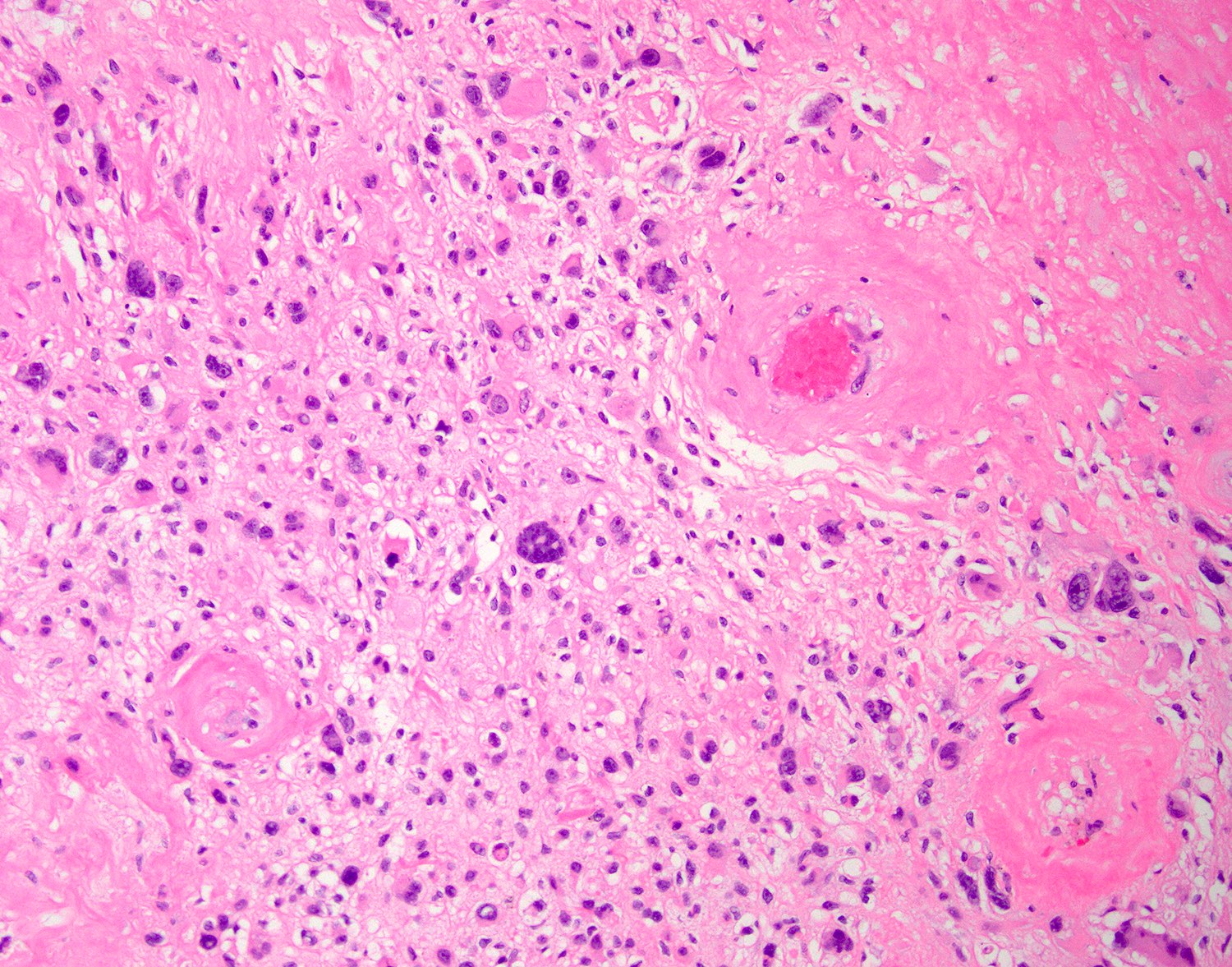
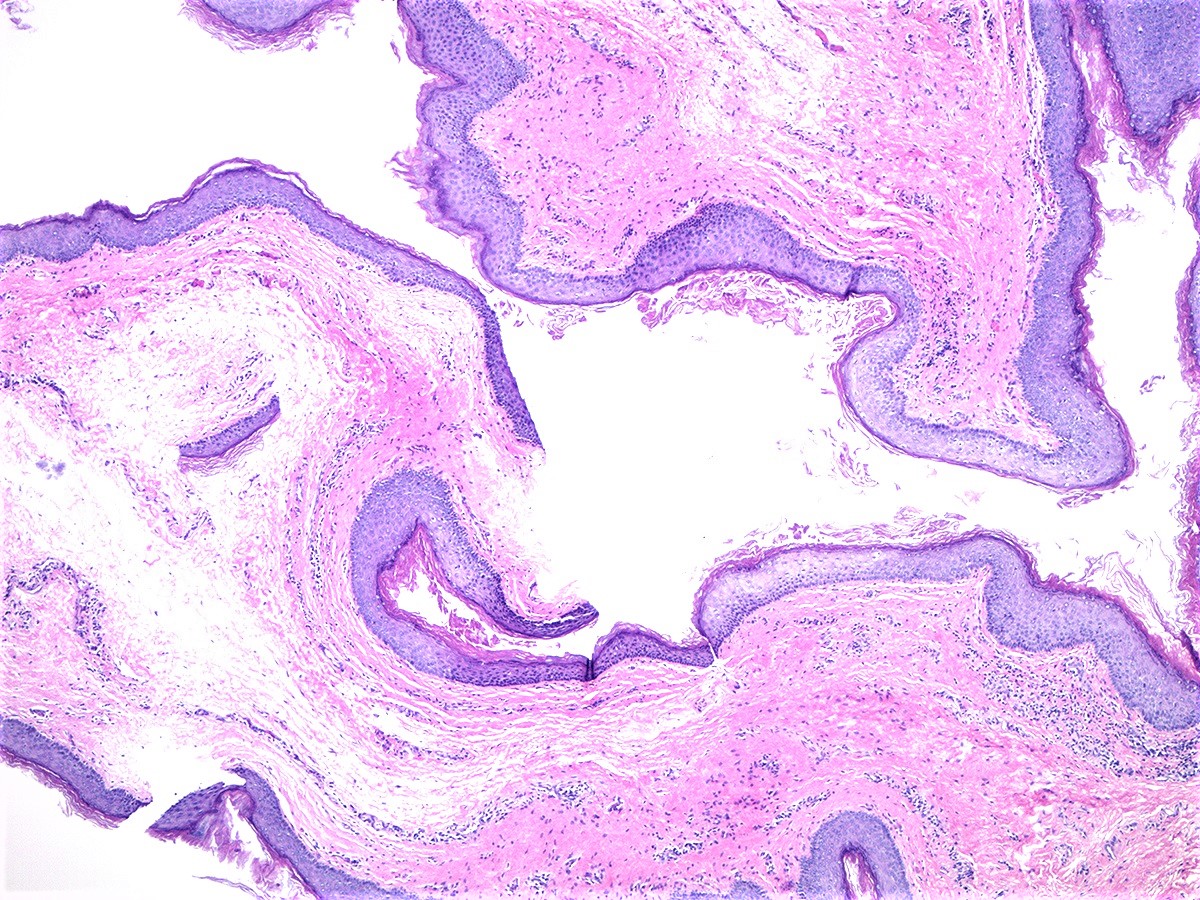
Hypertrophic lichen planus
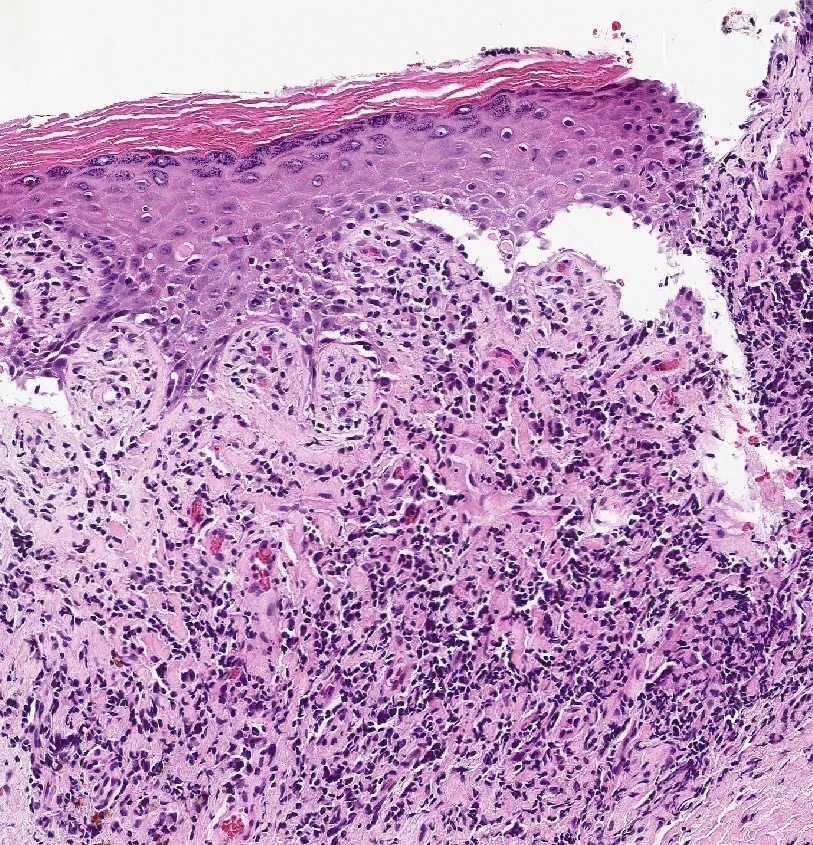
Civatte bodies
and clefting at
dermal epidermal
junction
Hyperkeratosis and hypergranulosis
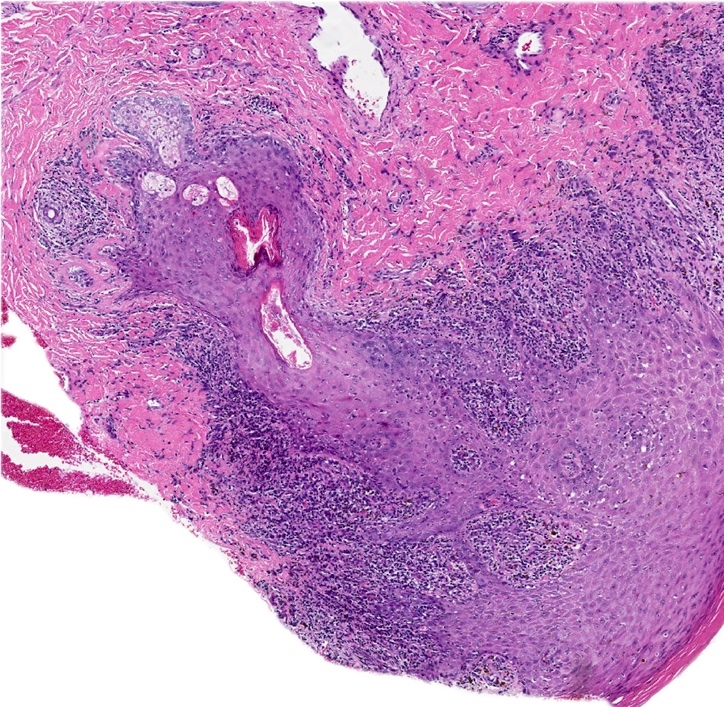
Chronic lichenoid interface dermatitis
Lichen planus & hypertrophic lichen planus
Hypertrophic lichen planus: 5 minute pathology pearls
Lichen planus
Images hosted on other servers:

Cigarette paper appearance

Clitoris becomes buried under clitoral hood
Contributed by Jutta Huvila, M.D., Ph.D.
Typical lichen sclerosis
Sclerotic superficial dermis
Edema

Early lichen sclerosus

Interface change
Introduction to lichen sclerosus
Case #273

Case #273










{kind=link}
Contributed by Anna Sarah Erem, M.D., Gulisa Turashvili, M.D., Ph.D. and José Alberto Fonseca Moutinho, M.D.

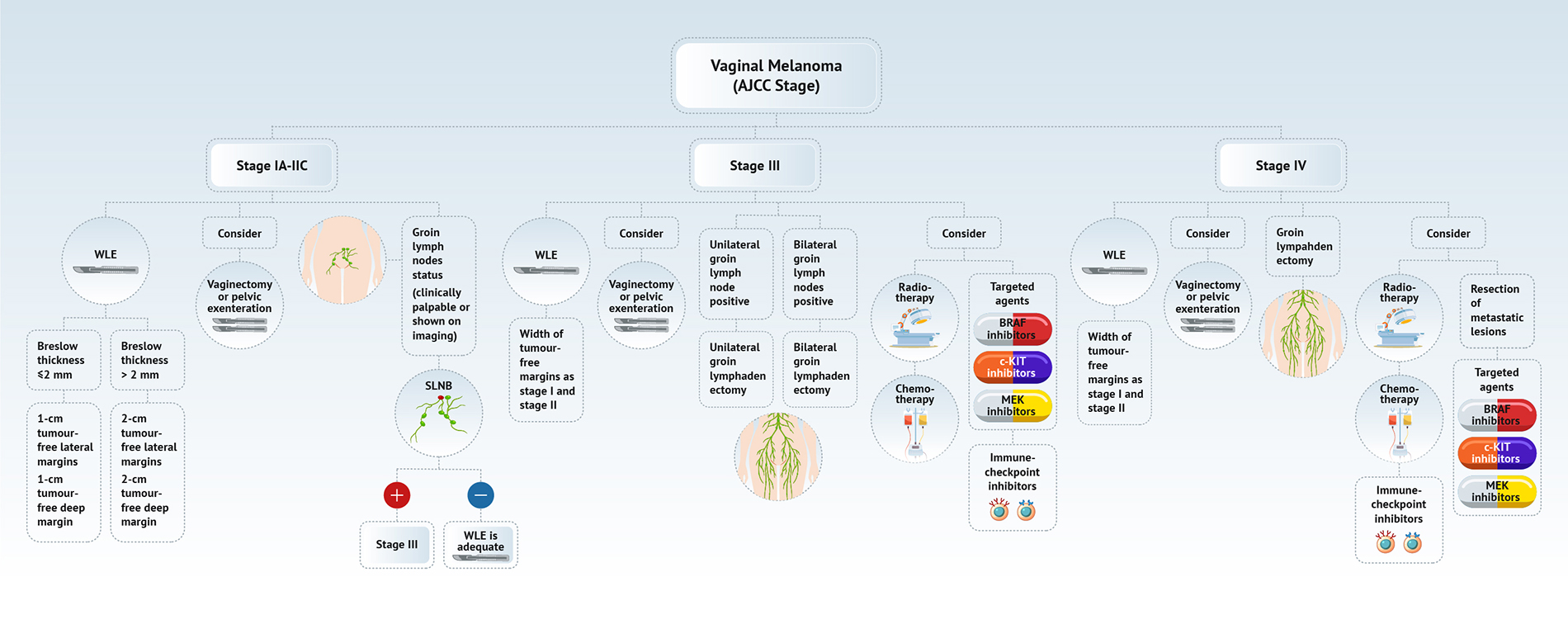
Vulvar melanoma

Vulvovaginal melanoma
Images hosted on other servers:

Nodule and ulcer

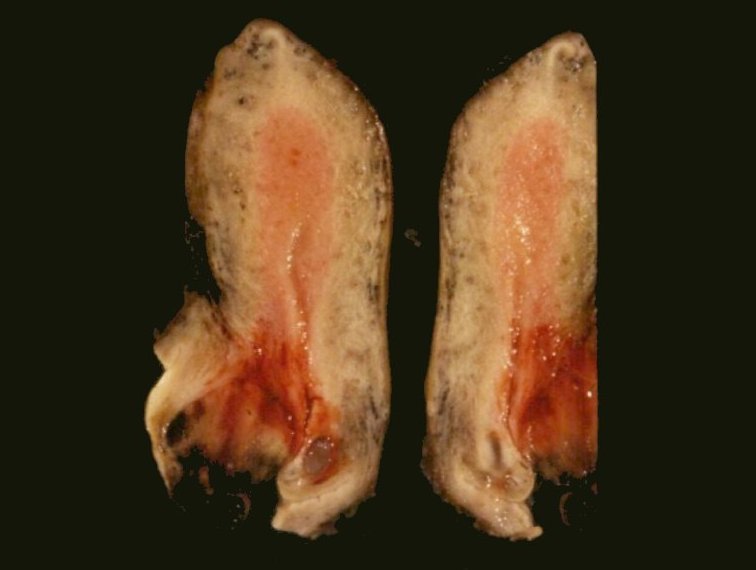
Large friable, gray-white growth

Vulvar melanoma

Nonpigmented primary lesion found in vagina
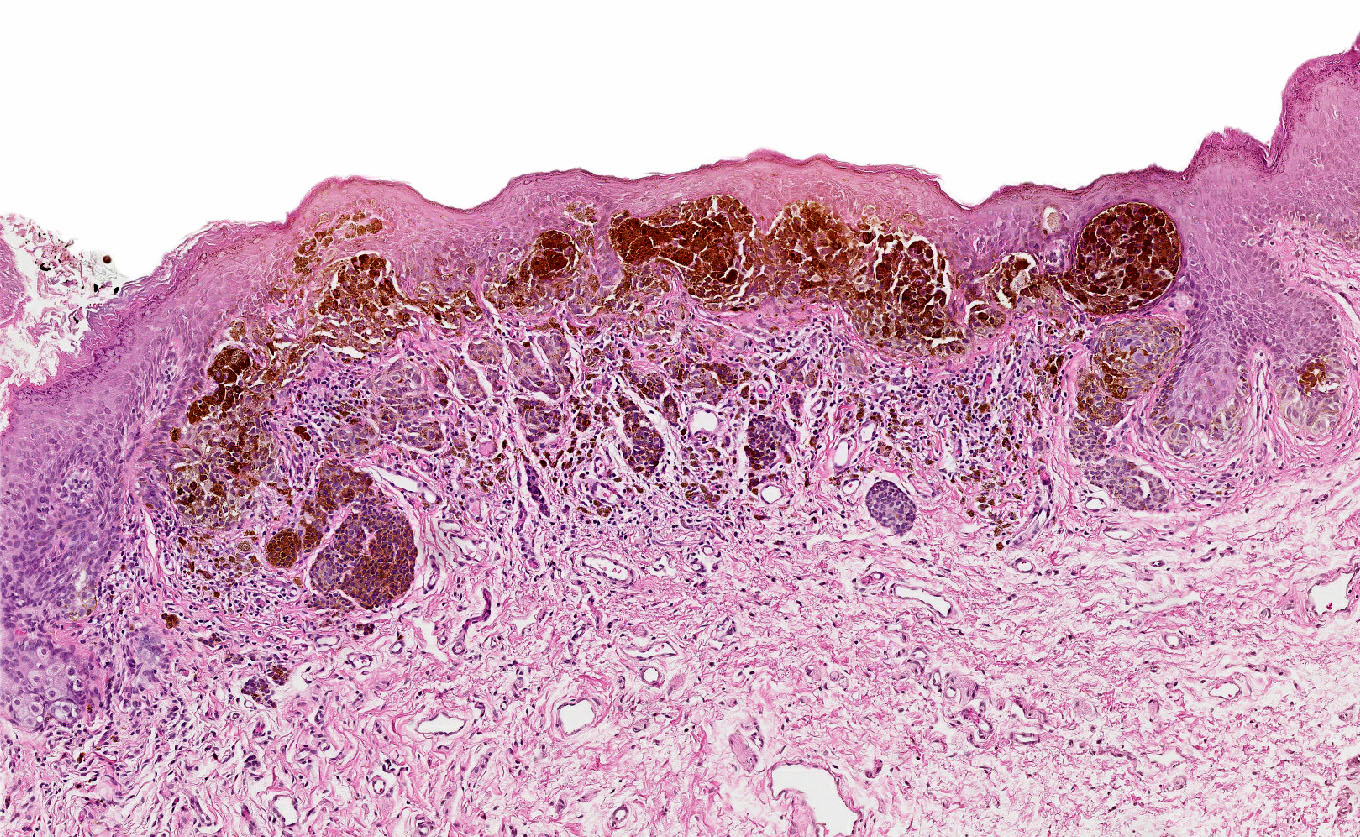
Contributed by Anna Sarah Erem, M.D. and Gulisa Turashvili, M.D., Ph.D.


Vulvectomy for melanoma
Contributed by Anna Sarah Erem, M.D., Gulisa Turashvili, M.D., Ph.D. and Priya Nagarajan, M.D., Ph.D.


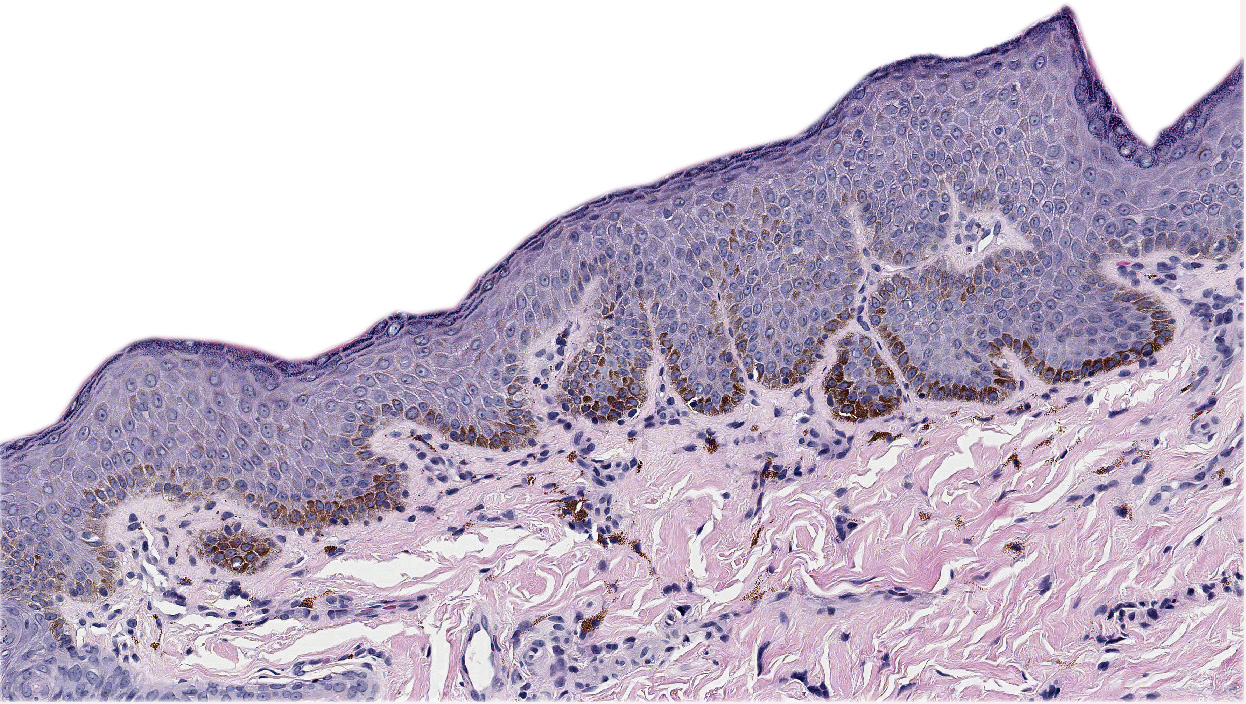
Superficial growth pattern
Melanoma in situ
Melanoma in situ, lentiginous pattern
Vaginal melanoma

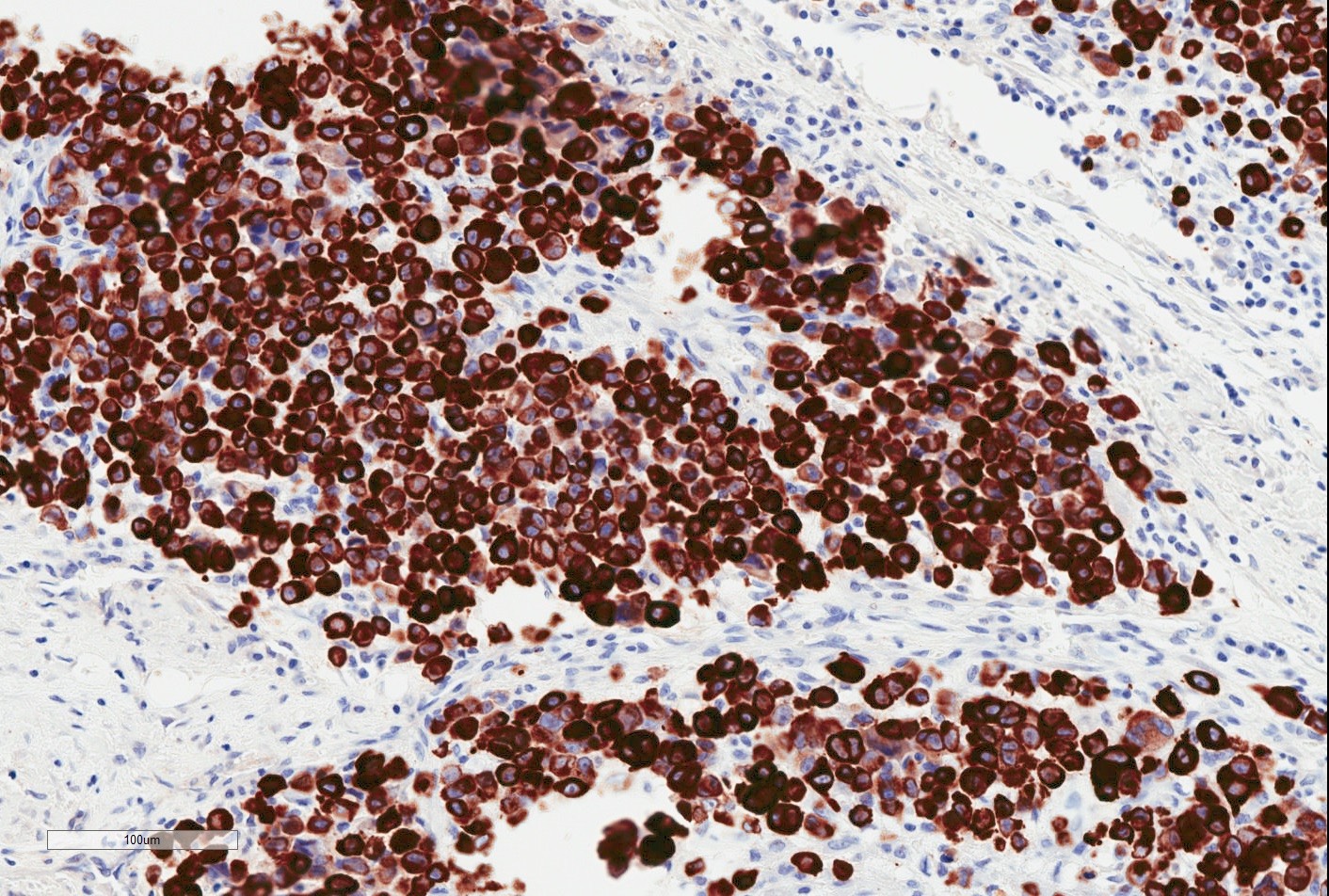
HMB45

Vulvovaginal melanoma
Vulvar melanoma, recurrent

S100

Mucosal vulvar melanoma
MelanA / MART1

Vaginal amelanotic melanoma
Vulvovaginal melanoma
by Dr. Lewis Hassell
Vaginal melanoma radiology
by Dr. Ayushi Gupta
Vaginal melanoma
Images hosted on other servers:

Posterior vaginal wall tumor
Contributed by Brooke Howitt, M.D.
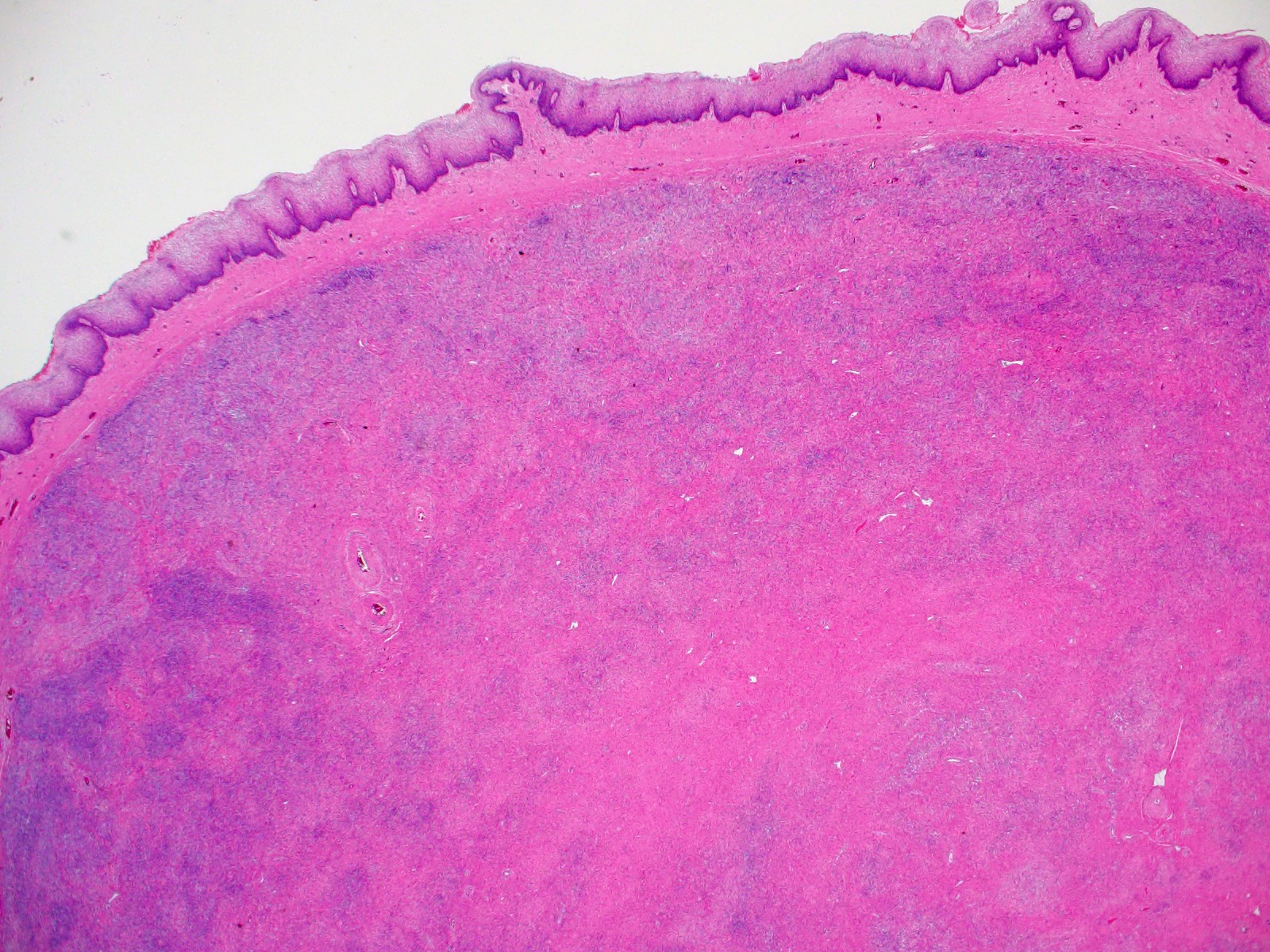
Separation from squamous epithelium
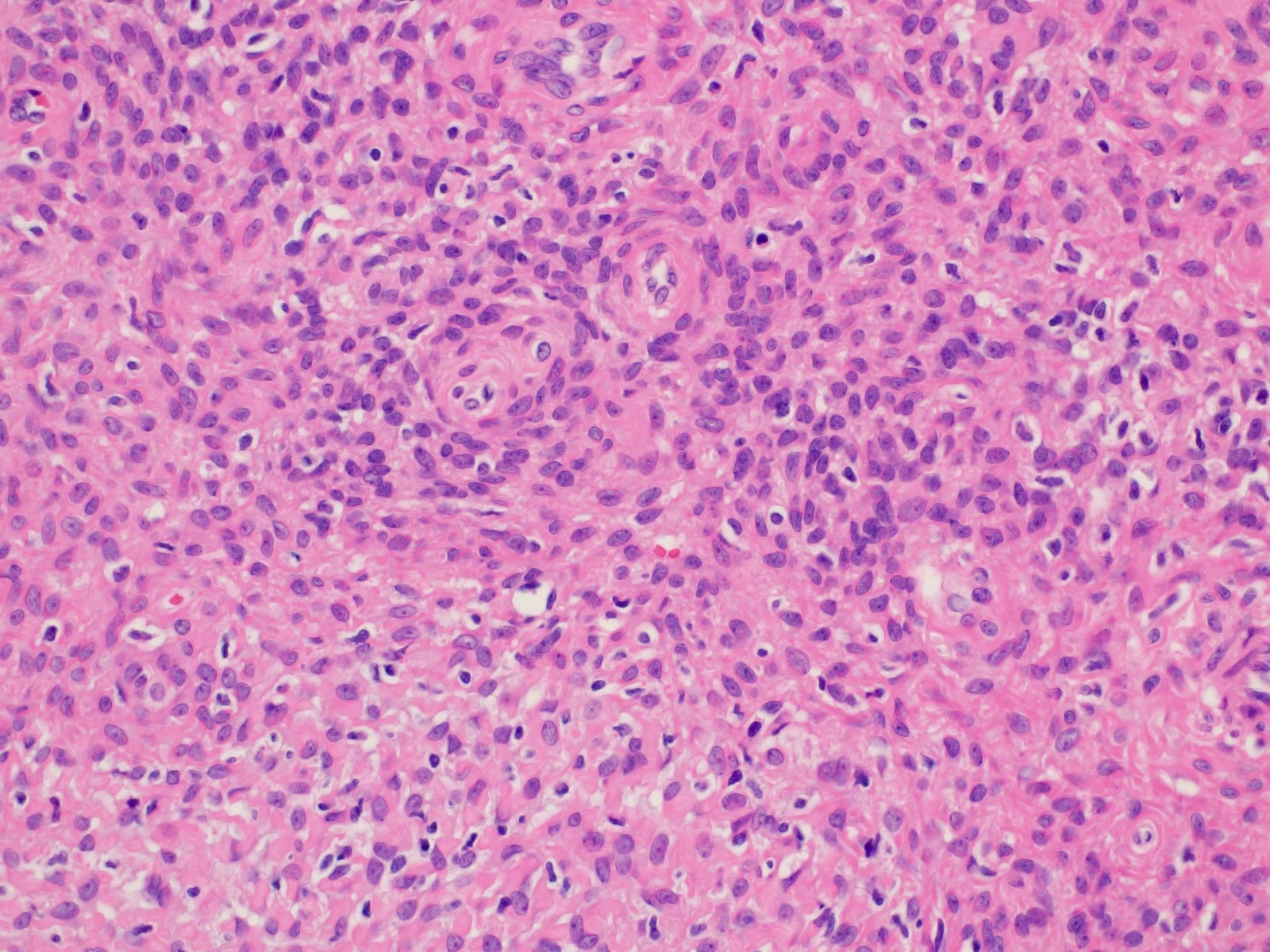
Cytologically bland spindle cells
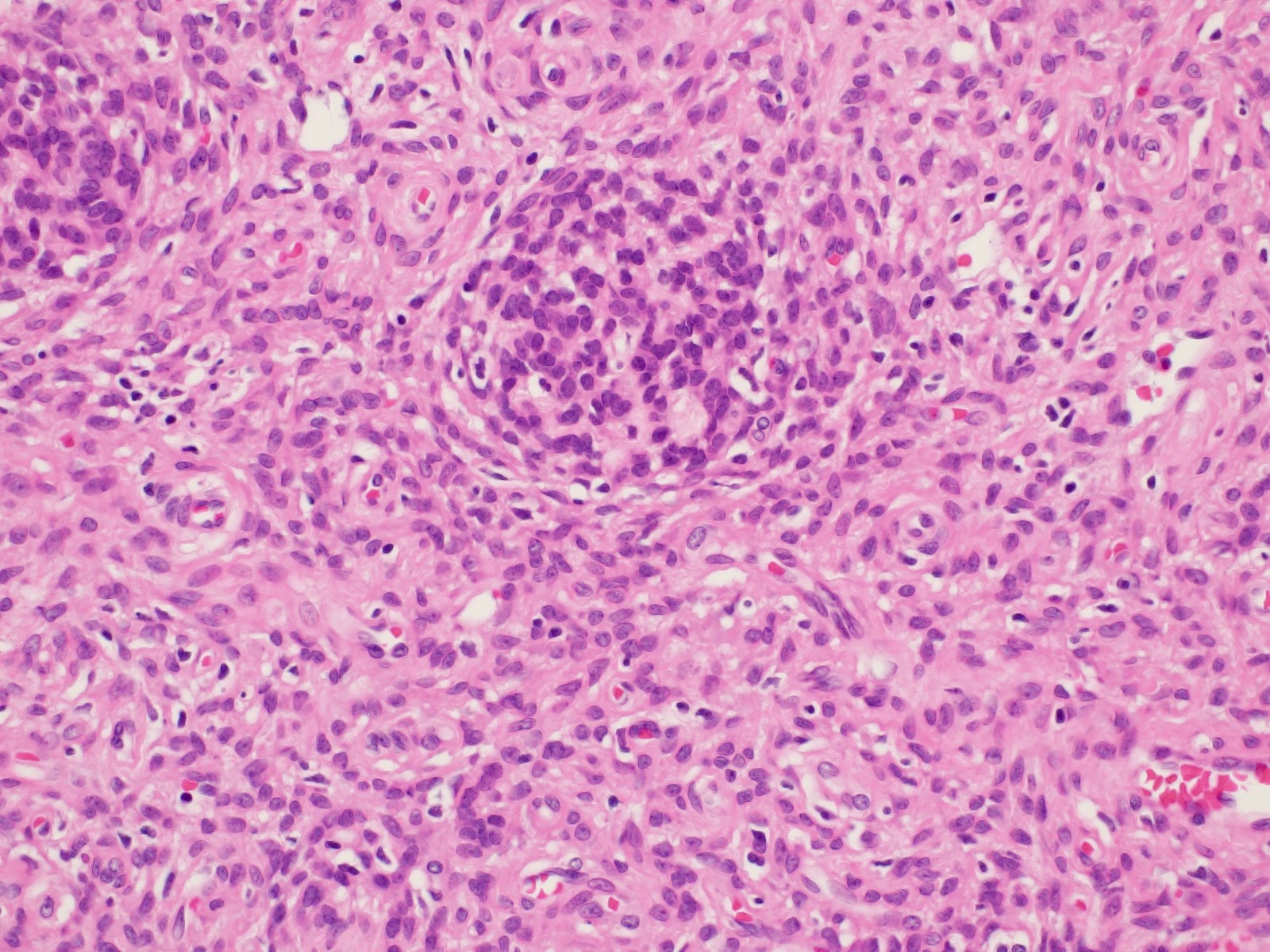
Discrete nests

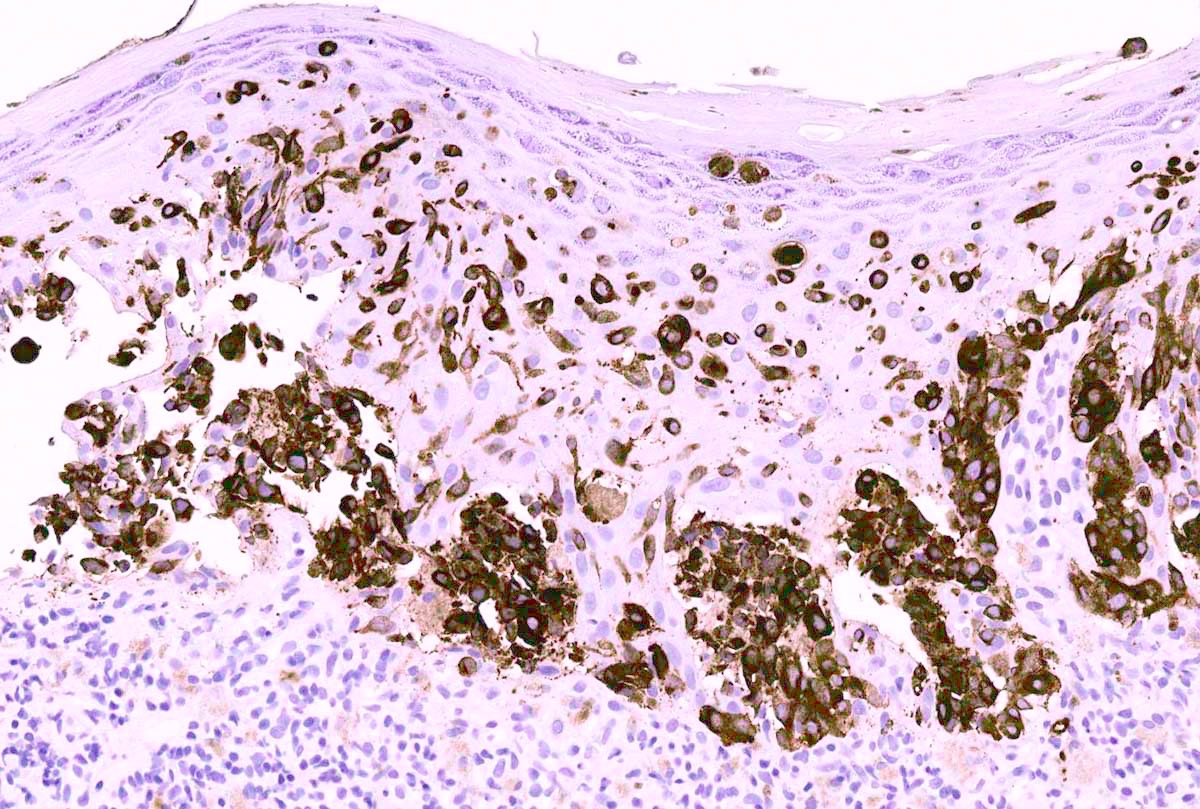
Pancytokeratin
Images hosted on other servers:


Lesion on perineal area

Preoperative

Erythematosquamous
lesion

Before and after treatment

Asymmetrical brown lesion
Contributed by Lucy Ma, M.D.

Plaque-like lesion
Contributed by Priya Nagarajan, M.D., Ph.D. and Lucy Ma, M.D.
Abundant intracytoplasmic mucin

Preservation of basal keratinocytes
Large polygonal cells with pale cytoplasm
Paget cells extending upward as single cells
Adnexal structures
Infiltrating Paget cells
Large invasive nests
Subtle case
Subtle case
Secondary extramammary Paget disease
Mucicarmine positive
Extramammary Paget disease: 5 minute pathology pearls
Paget disease versus melanoma versus squamous cell carcinoma in situ
Table 1: Features distinguishing vulvar nevi, melanosis and melanoma (adapted from J Am Acad Dermatol 2014;71:1241)
| Reassuring features suggestive of a benign process | Concerning features for possible malignancy | |
| Clinical |
|
|
| Dermoscopy |
|
|
| Reflectance confocal microscopy |
|
|
Table 2: Clinical morphology for pigmented vulvar lesions (adapted from Dermatol Ther 2010;23:449)
| Papules and macules | Patches and plaques |
| Pigmented nevi (nevocellular nevi) | Physiologic hyperpigmentation |
| Dysplastic nevi | Postinflammatory hyperpigmentation |
| Malignant melanoma | Vulvar melanosis (vulvar lentiginosis) |
| Anogenital warts | Acanthosis nigricans |
| Vulvar intraepithelial neoplasia | |
| Seborrheic keratosis | |
| Basal cell carcinoma | |
| Angiokeratoma |
Table 3: Genodermatosis syndromes with vulvar melanosis (adapted from J Am Acad Dermatol 2014;71:1241)
| Genodermatosis | Areas affected | Key features | Genetic mutation |
| Peutz-Jeghers syndrome | Oral, perianal and genital area, lips, nostrils, hands, feet | Hamartomatous polyps in the gastrointestinal tract (GIT), breast, ovarian, pancreatic and GIT cancers | STK11 |
| Carney complex | Oral and genital area, lips, eyelids, conjunctiva | Blue nevus, psammomatous melanotic schwannoma, myxomas (usually cardiac), endocrine neoplasms | PRKAR1A |
| Multiple lentigines syndrome (LEOPARD syndrome) | Face, neck, trunk, genital area | Delayed growth, sensorineural deafness, ECG abnormalities, ocular hypertelorism, pulmonic stenosis, abnormal genitalia | PTPN11, RAF1, BRAF |
| Bannayan-Riley-Ruvalcaba syndrome | Face, genital area | Macrocephaly, intellectual and motor deficiencies, joint hyperextensibility, pectus excavatum, scoliosis, intestinal hamartomatous polyposis, lipomas, hemangiomas | PTEN |
| Dowling-Degos syndrome | Axillae, neck, flexural folds, inguinal and genital area | Follicular papules, comedone-like lesions, perioral scar, reticulated hyperpigmentation, hypopigmented or erythematous macules | KRT5 |
Table 4: Clinical and histologic differences between atypical genital nevus and vulvar melanoma
(adapted from Hoang: Melanocytic Lesions - A Case Based Approach, 1st Edition, 2014)
| Proposed diagnosis | Atypical genital nevus of special anatomic site | Vulvar melanoma |
| Age | Premenopausal, young adult | Postmenopausal |
| Size | > 1 cm | |
| Delineation | Well circumscribed | Infiltrative |
| Symmetry | Present | Absent |
| Lateral extension of junctional component | Focal | Present |
| Lentiginous junctional component | Focal | Present |
| Junctional nests | Dyscohesive | Confluent |
| Retraction artefact | Present | Absent |
| Ulceration | Absent or due to trauma | Often present |
| Pagetoid upward spread | Focal, central, inconspicuous | Prominent |
| Cytologic atypia | Superficial, mild - moderate | Deep, moderate to severe |
| Dermal mitosis | Rare and superficial | Conspicuous, atypical, deep |
| Dermal maturation | Present | Absent |
| Melanin pigmentation | Coarse, uniform | Fine, irregular |
| Dermal fibrosis | Broad zone of superficial coarse dermal fibrosis | Regression type |
Contributed by José Alberto Fonseca Moutinho, M.D.

Acanthosis nigricans

Angiokeratoma

Postinflammatory
hyperpigmentation

Melanosis / lentiginosis

Physiologic pigmentation

Pigmented condyloma acuminata

Nevus

Pigmented seborrheic keratosis

Pigmented basal cell carcinoma
Images hosted on other servers:

Hyperpigmented, brownish macules

Angiokeratoma of Fordyce
Contributed by Emory University School of Medicine
Angiokeratoma
Genital melanocytic macule
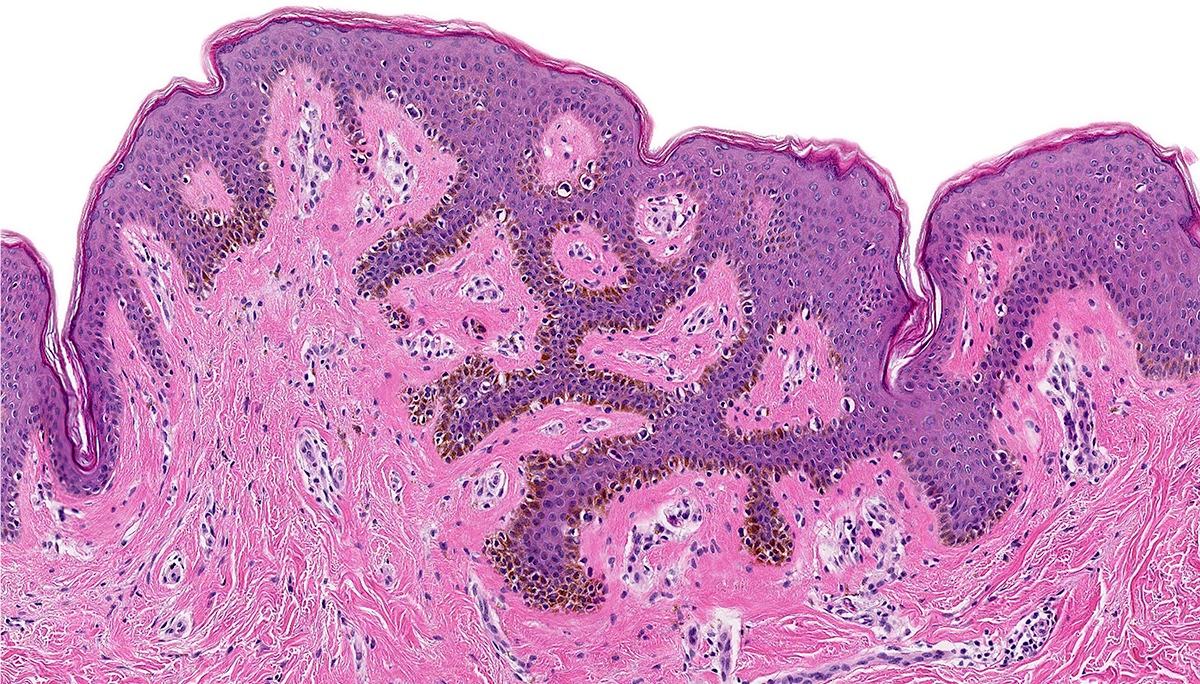
Vulvar compound melanocytic nevus
Compound melanocytic proliferation
Blue nevus, common type
Basal cell carcinoma

Seborrheic keratosis
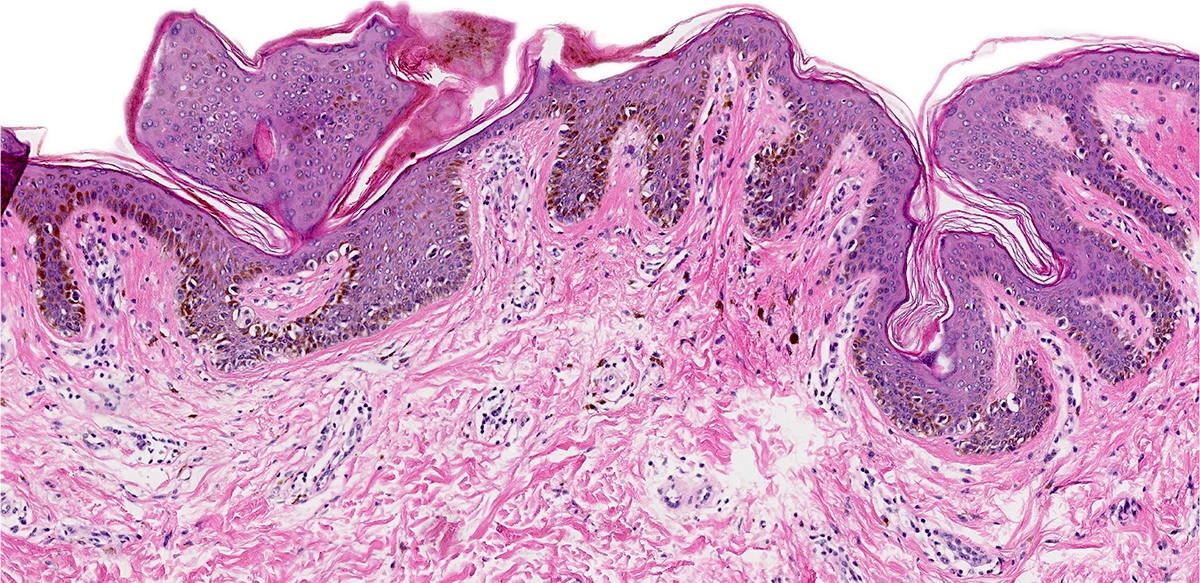
Atypical melanocytic nevus, genital type
Angiokeratoma by Filip Sokol
Angiokeratoma by Pathology mini tutorials
Atypical nevi and nevi of special sites by Dr. Phillip McKee
Images hosted on other servers:


Vaginal embryonal rhabdomyosarcoma
Images hosted on other servers:

Cervical embryonal
rhabdomyosarcoma
Images hosted on other servers:
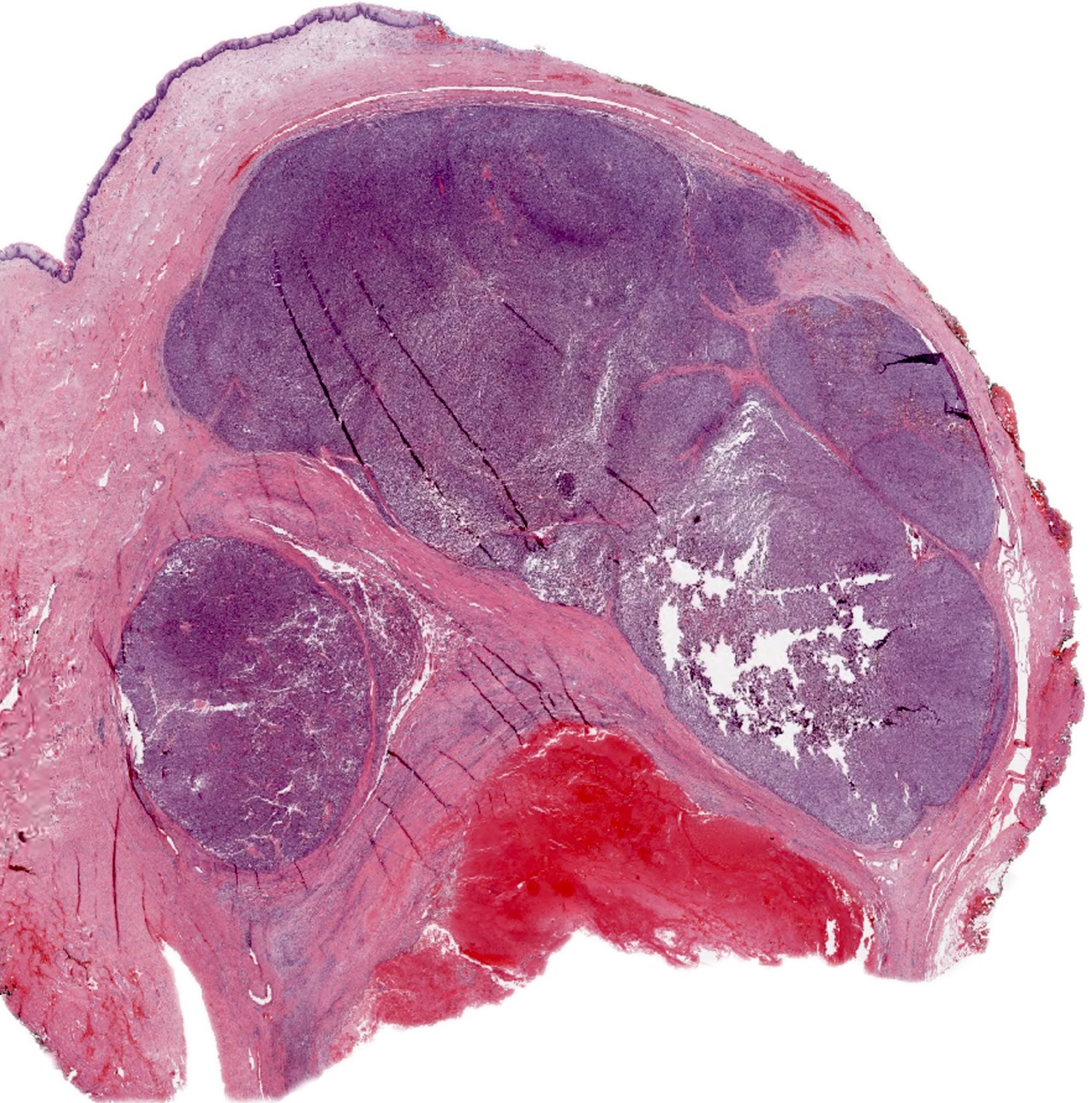
Gray surface and areas of hemorrhage
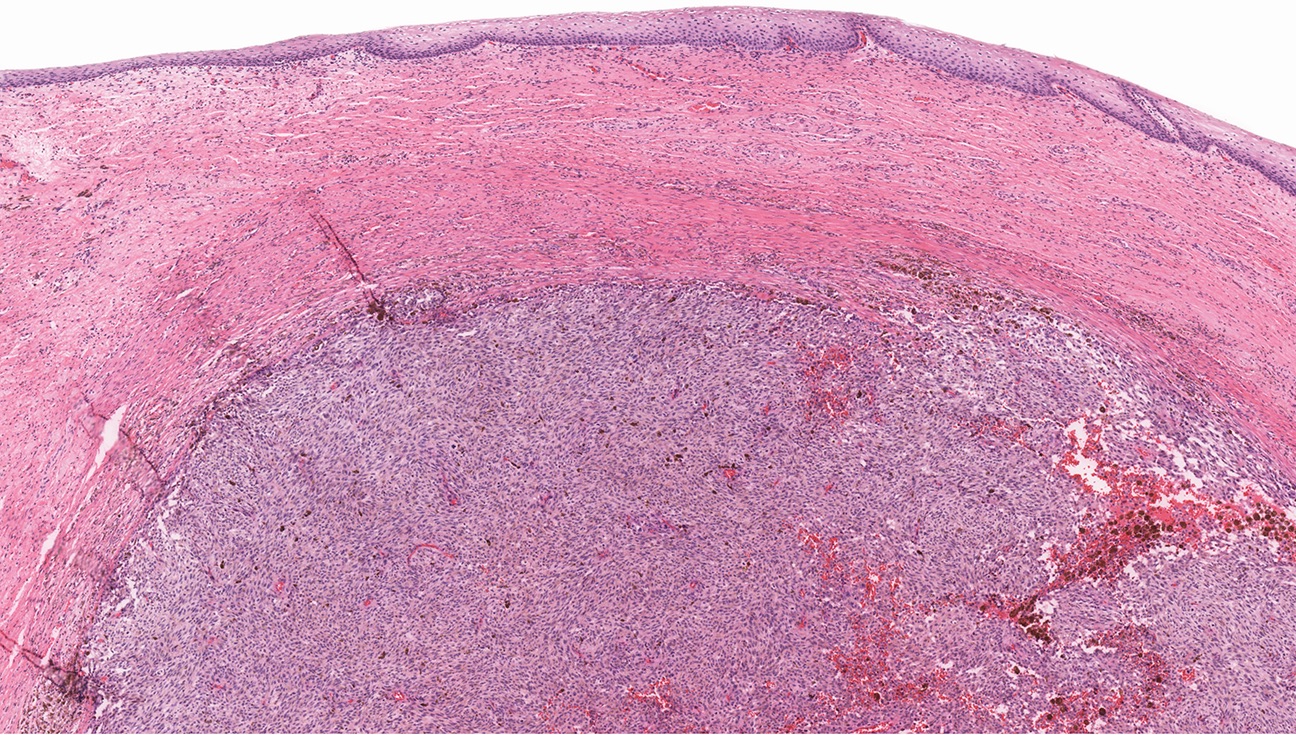
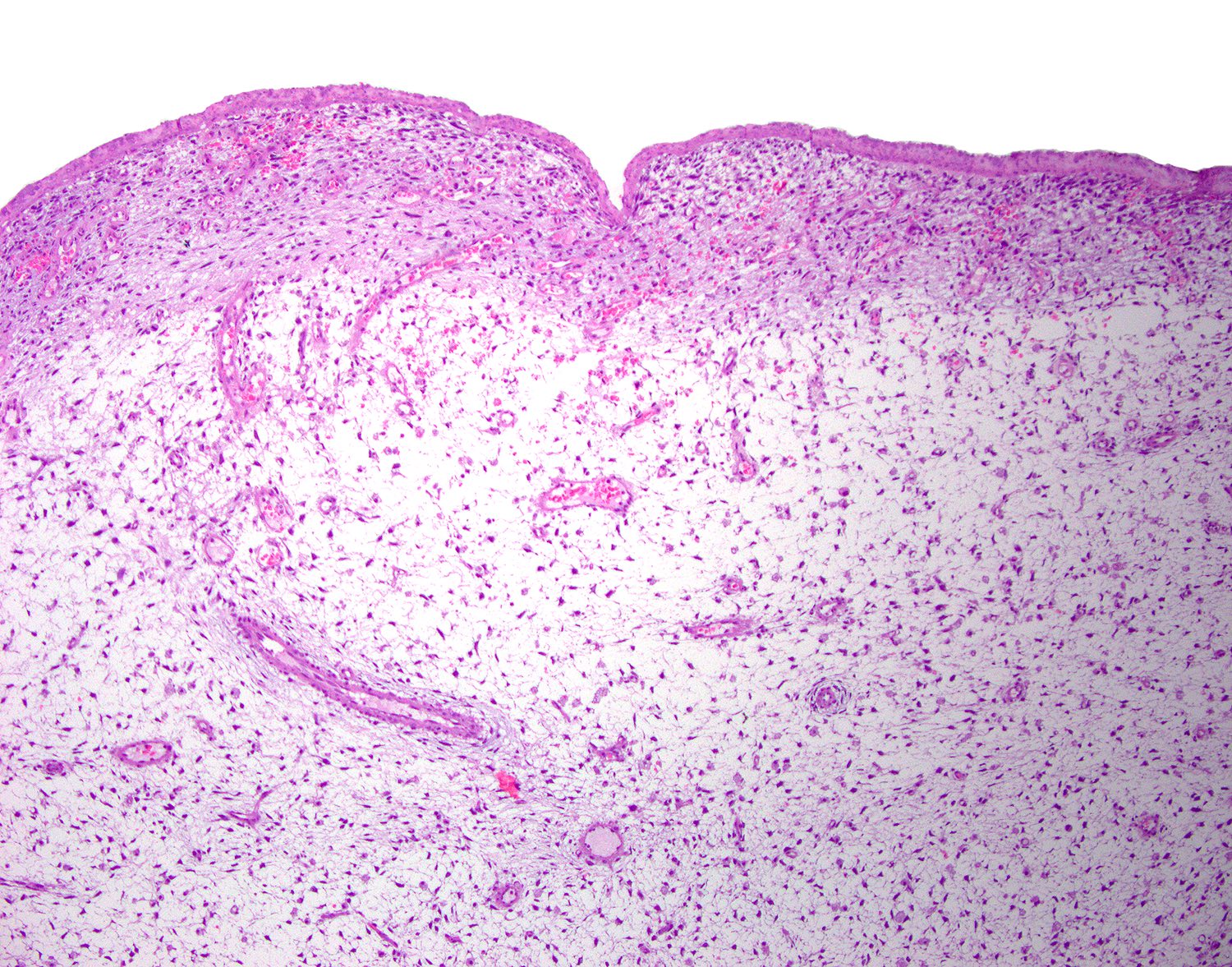
Contributed by Kyle Devins, M.D.
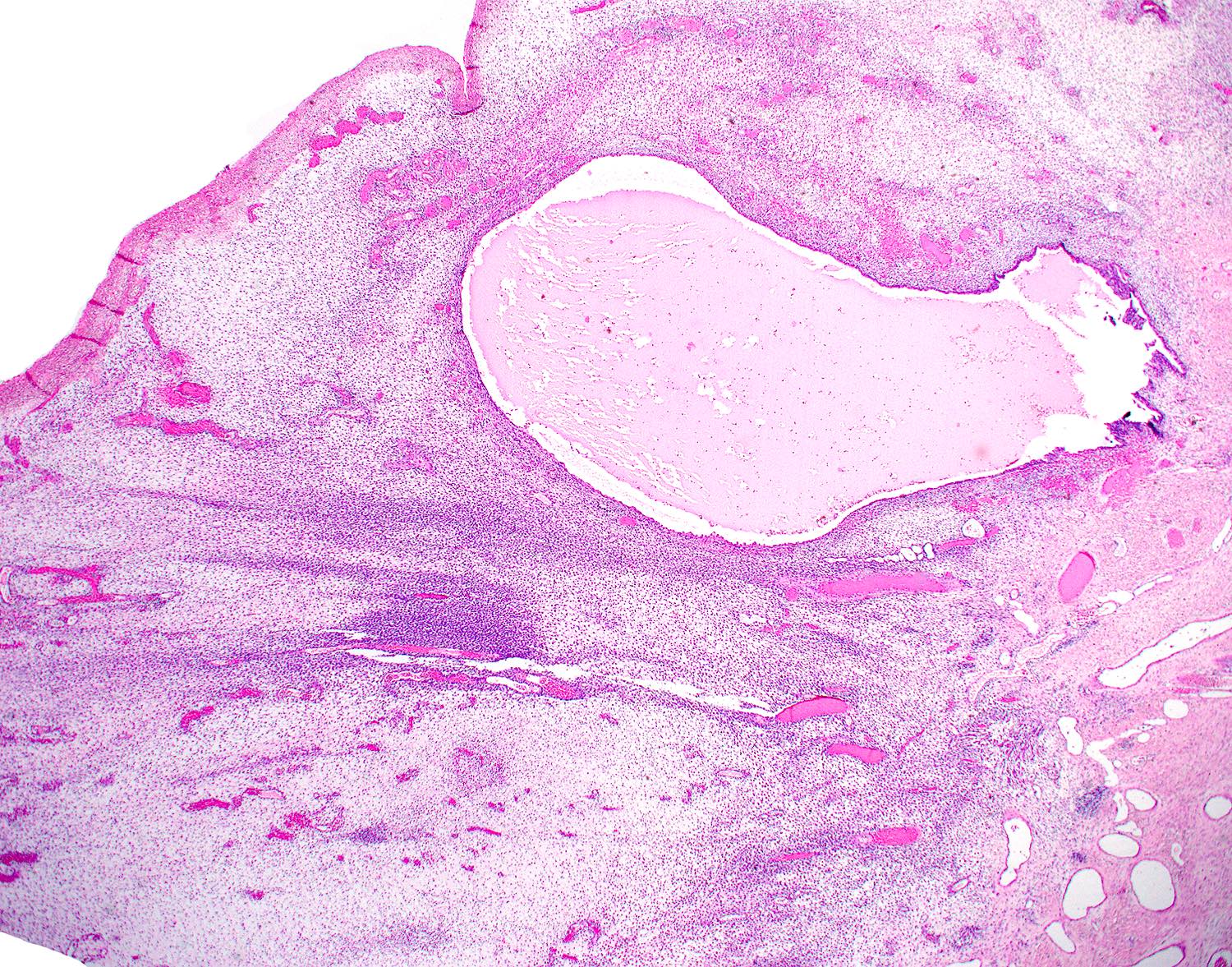
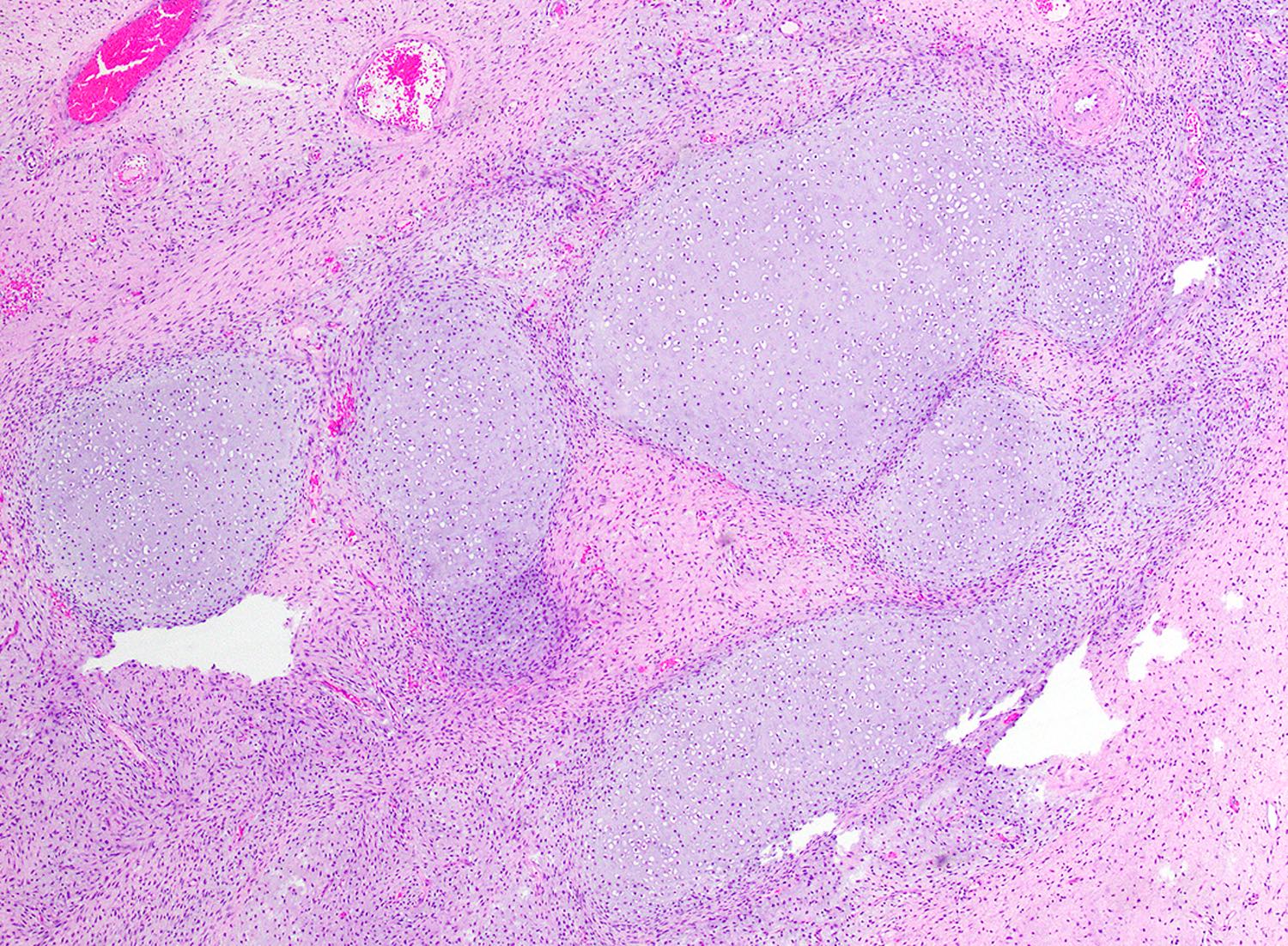
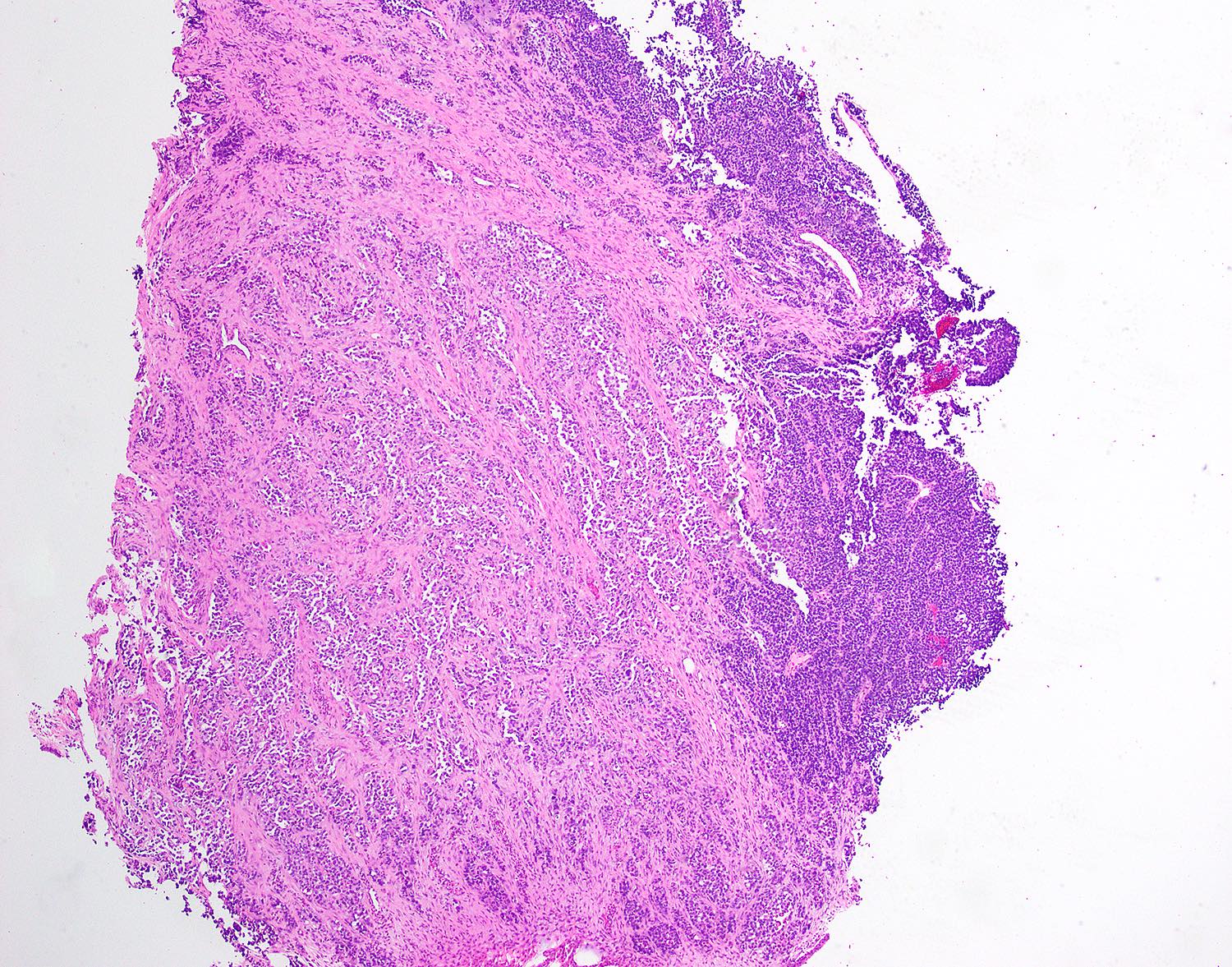
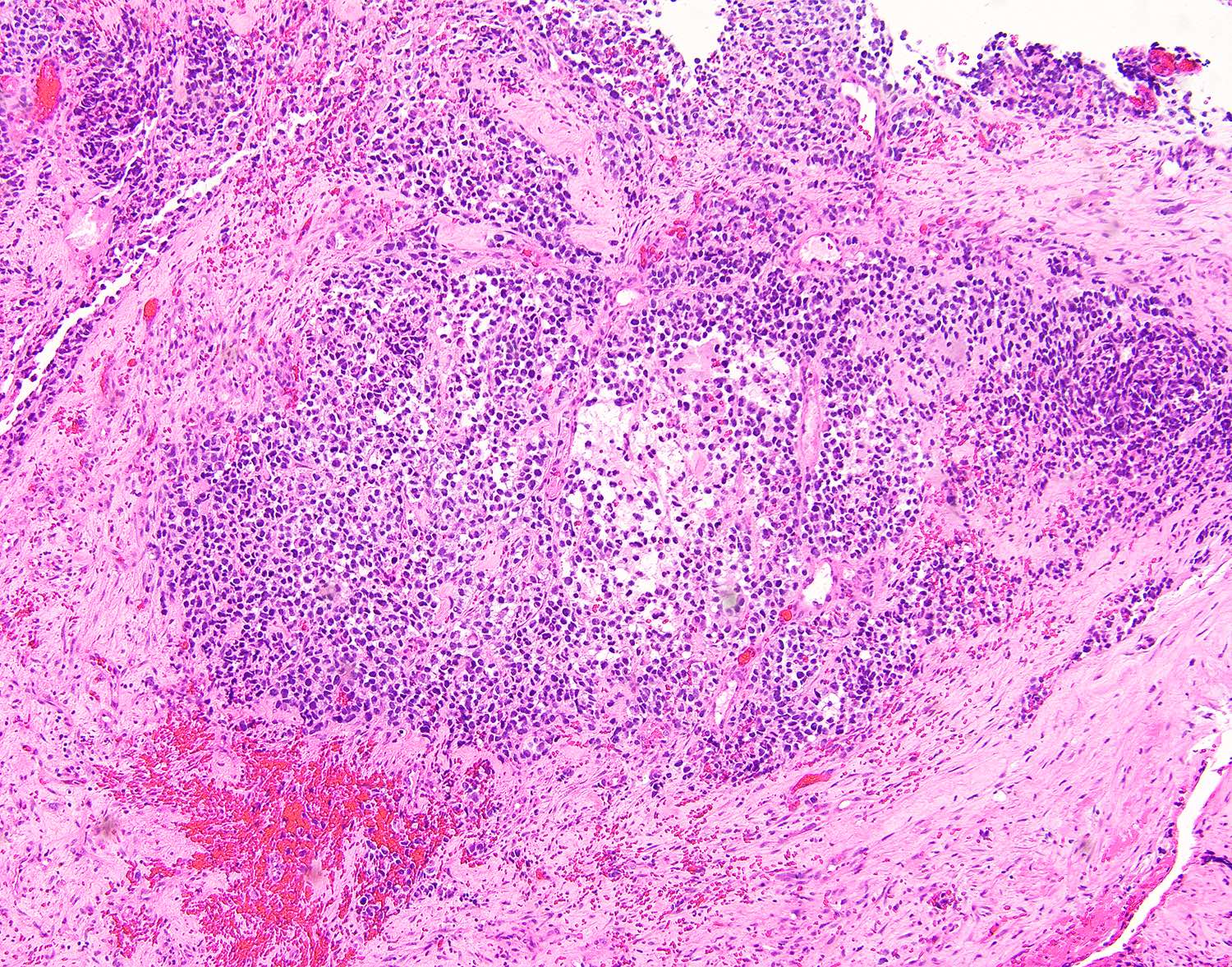
Edematous stroma
Cambium layer
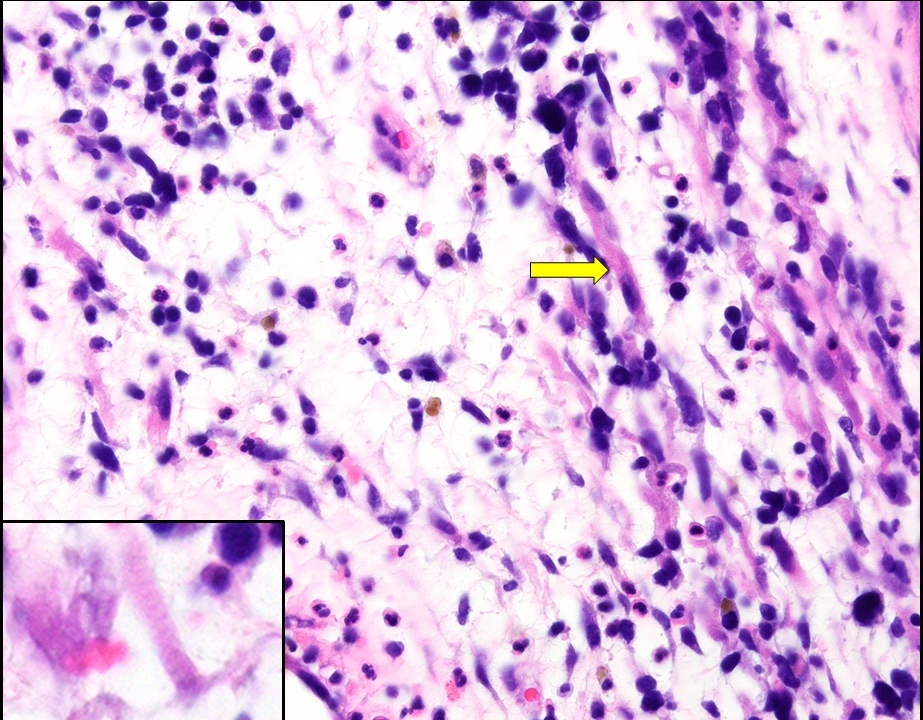
Rhabdomyoblasts
Hyaline cartilage
Nests, sheets and alveolar spaces
Alveolar spaces
Desmin
Myogenin
Nuclear pleomorphism
Images hosted on other servers:

Brushing of
uterine embryonal
rhabdomyosarcoma
Images hosted on other servers:

Vulvar leiomyoma




Vaginal leiomyoma, MRI

Vaginal leiomyoma, MRI and angiography


Vaginal leiomyoma, ultrasound

Vaginal leiomyoma, MRI & CT



Vaginal leiomyosarcoma, MRI
Images hosted on other servers:

Vulvar leiomyoma, preoperative examination

Vulvar leiomyoma, intraoperative

Vulvar leiomyosarcoma, preoperative examination
Vaginal leiomyosarcoma, preoperative examination
Images hosted on other servers:

Vulvar leiomyoma, excision specimen

Vulvar leiomyoma, cut surface

Vaginal leiomyoma, cut surface
Vaginal leiomyosarcoma, gross examination
Contributed by David B. Chapel, M.D.
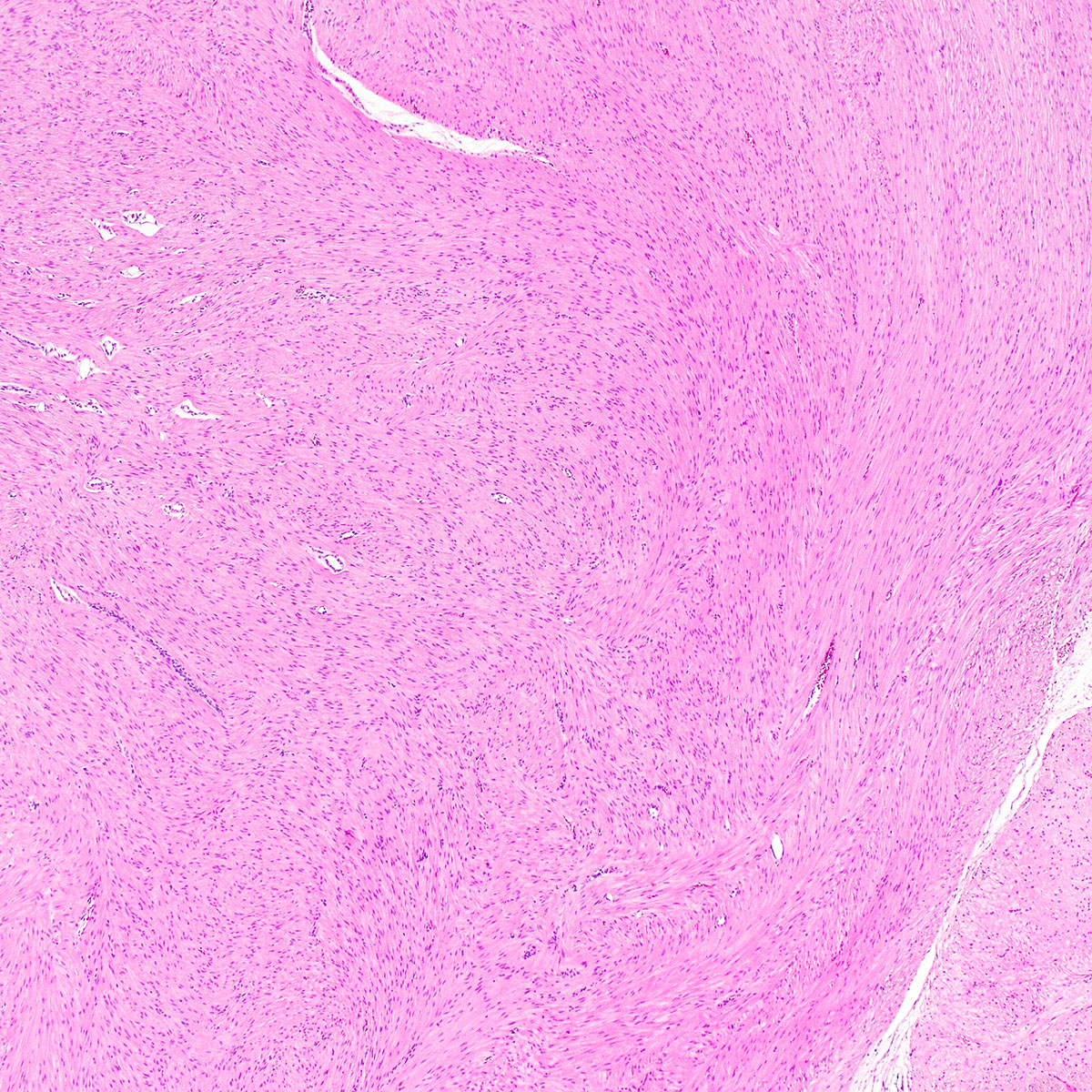
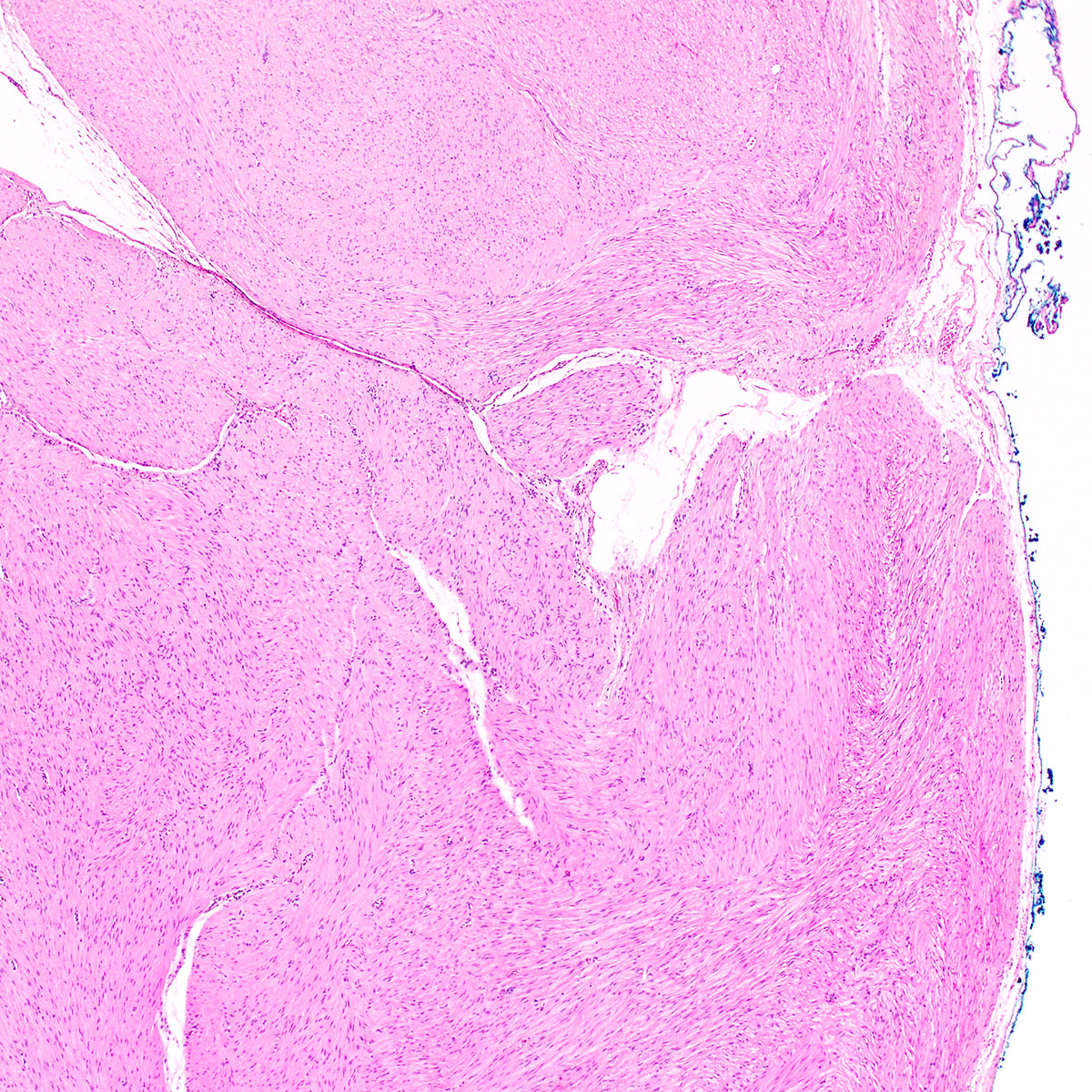
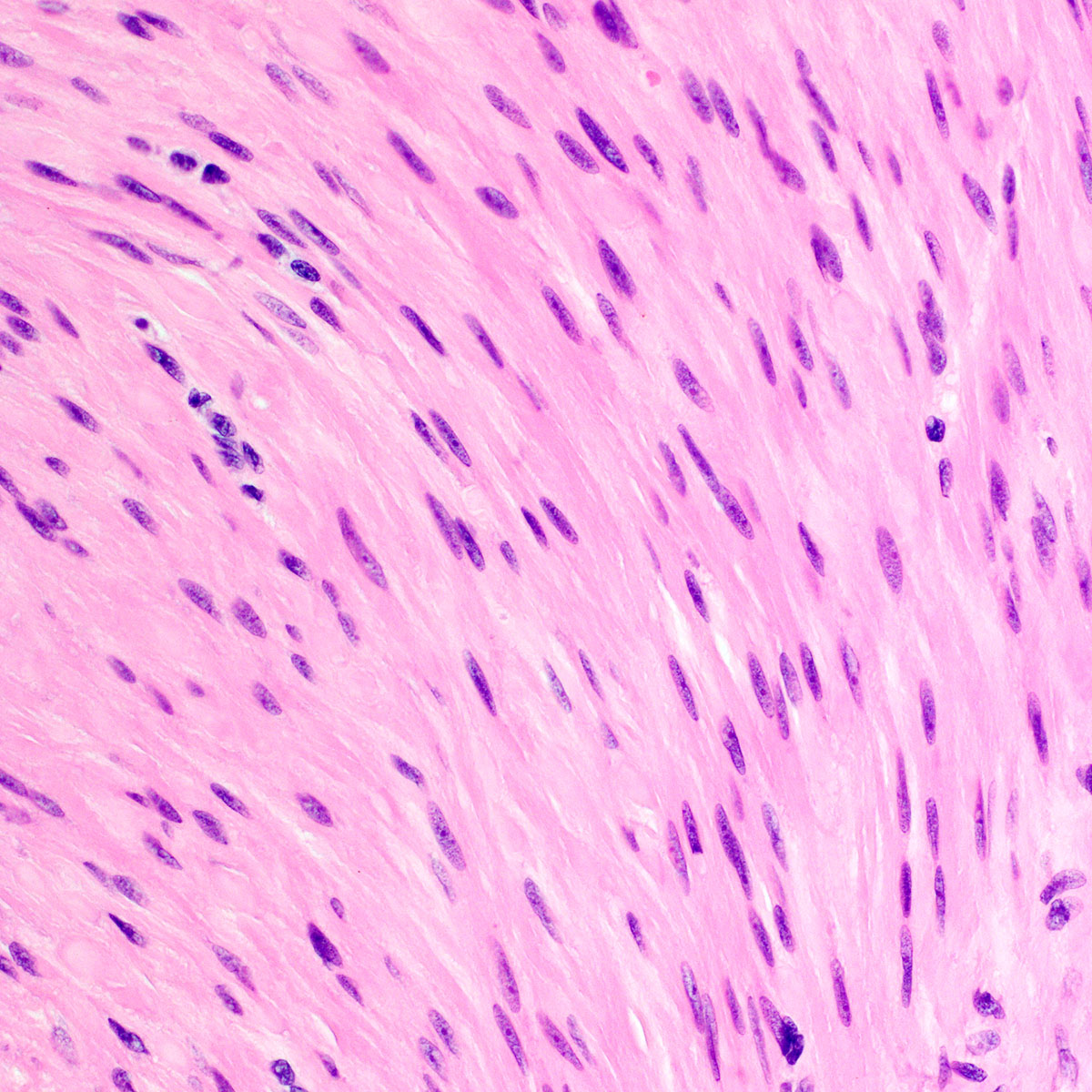
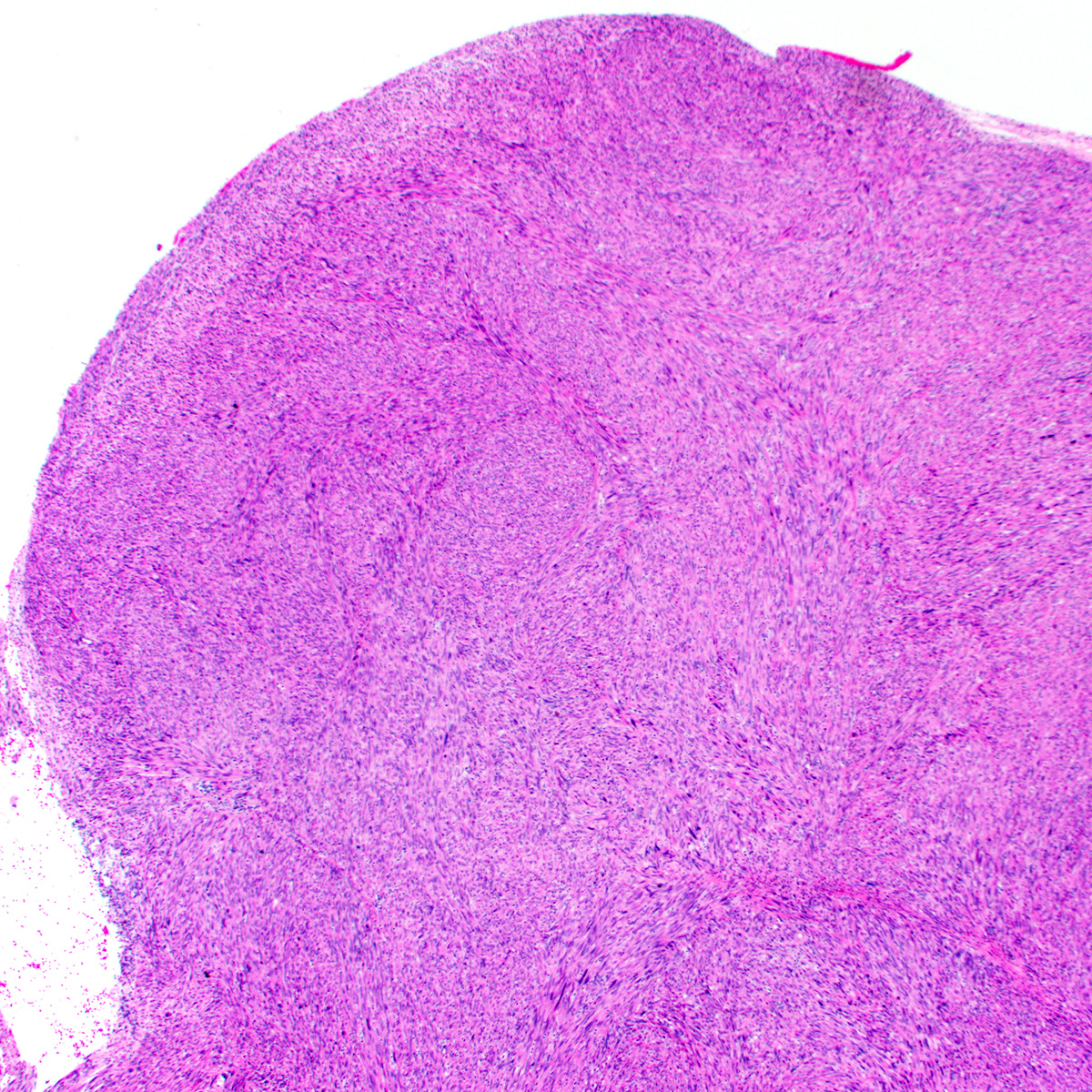
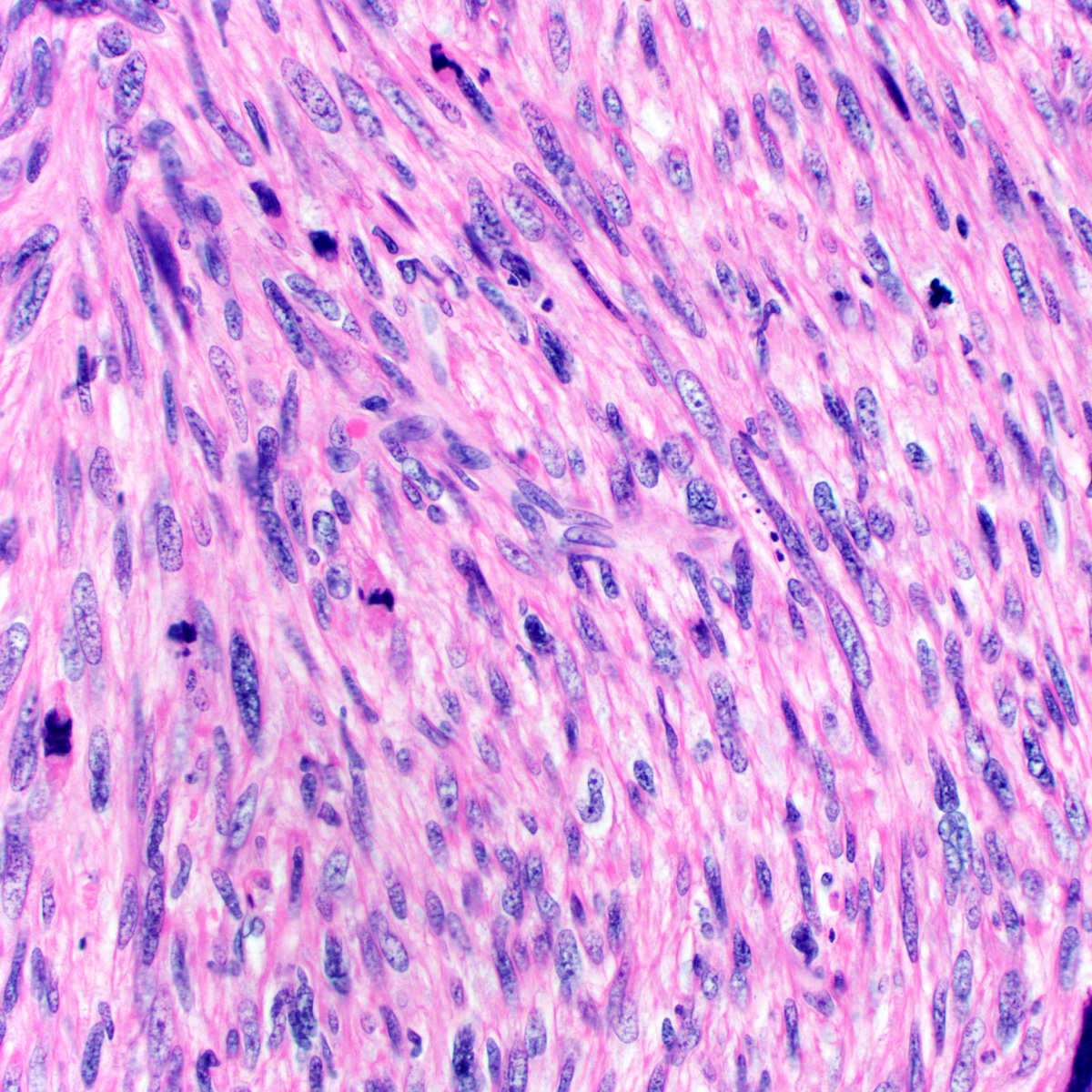
Vulvar leiomyoma
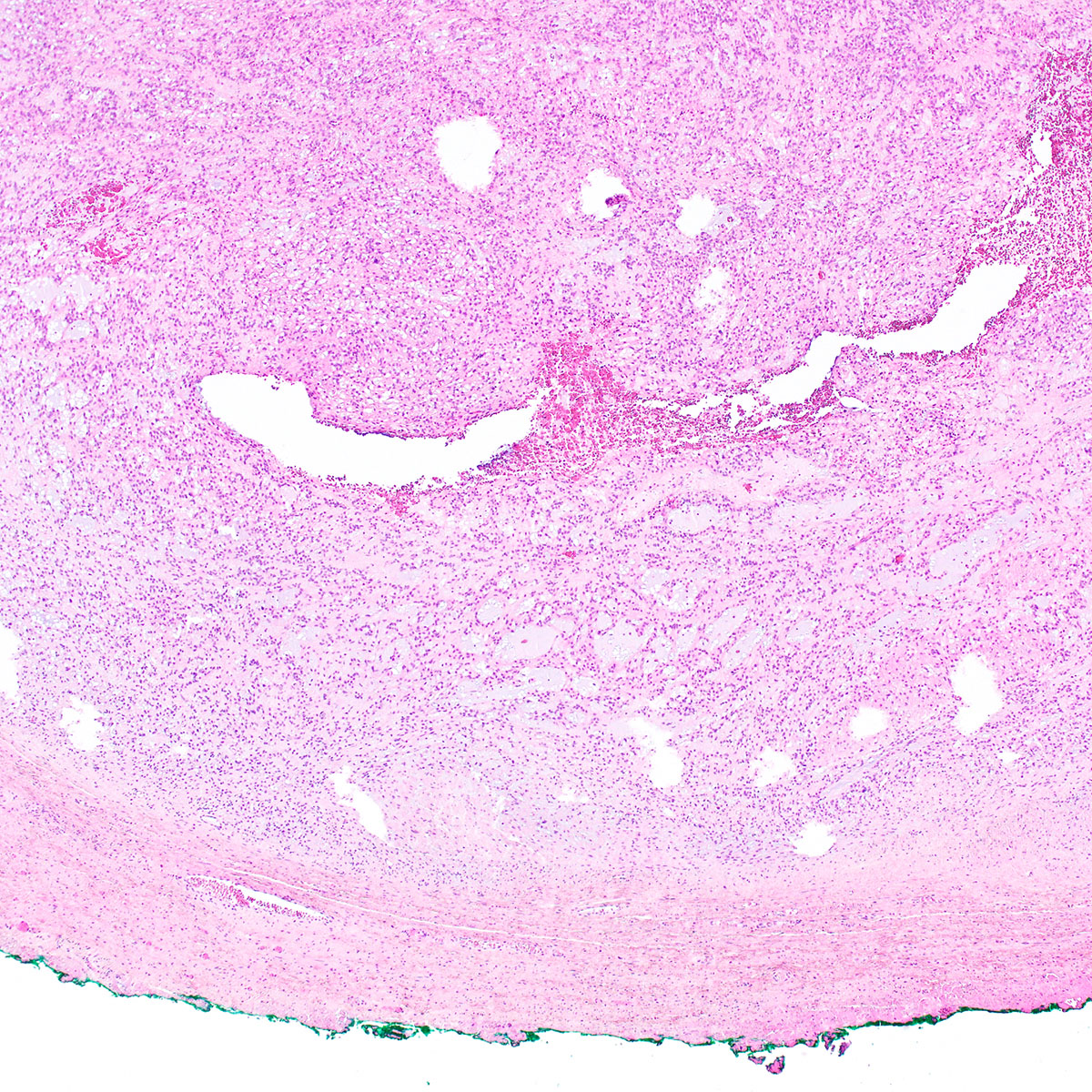
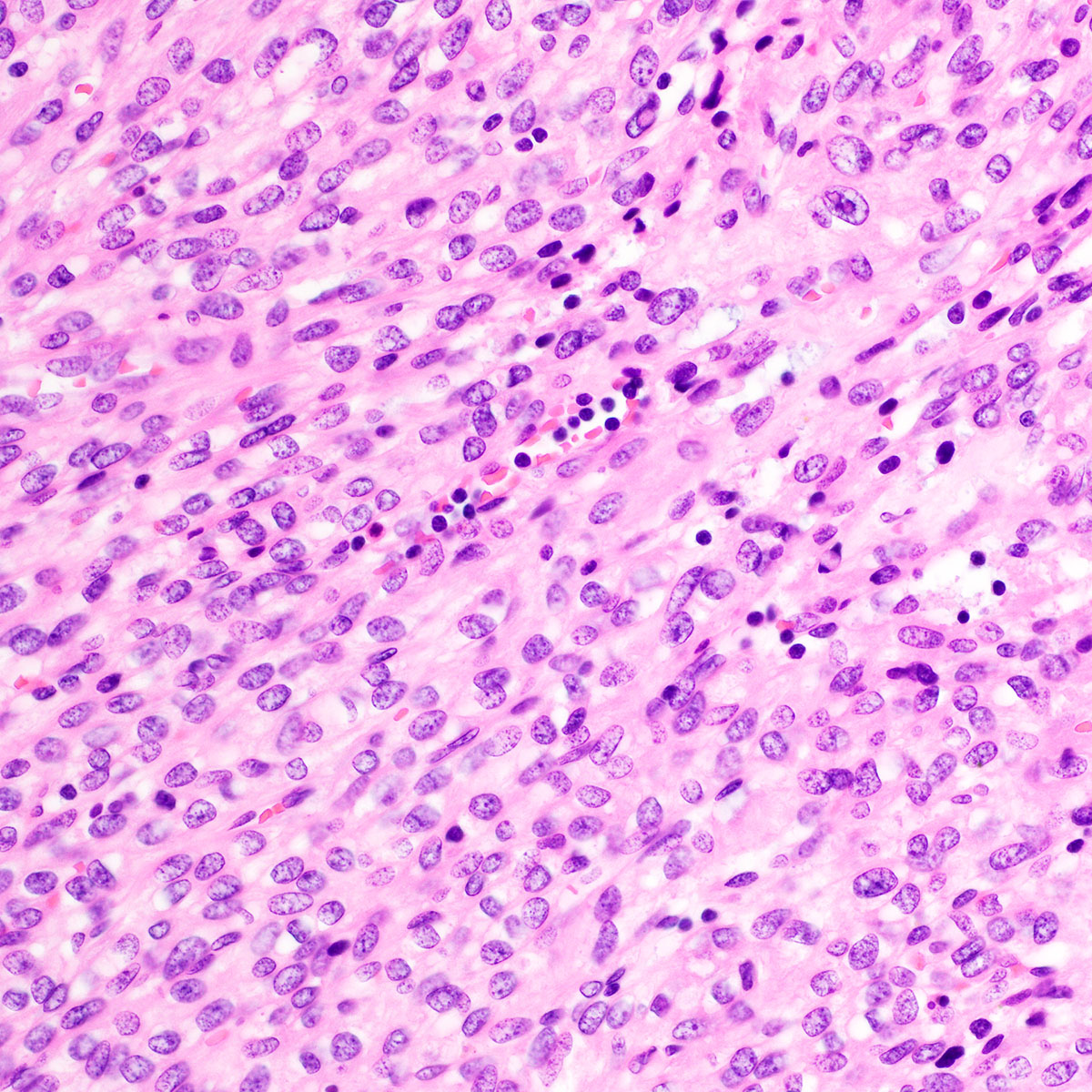
Vulvar leiomyosarcoma
Vulvar STUMP
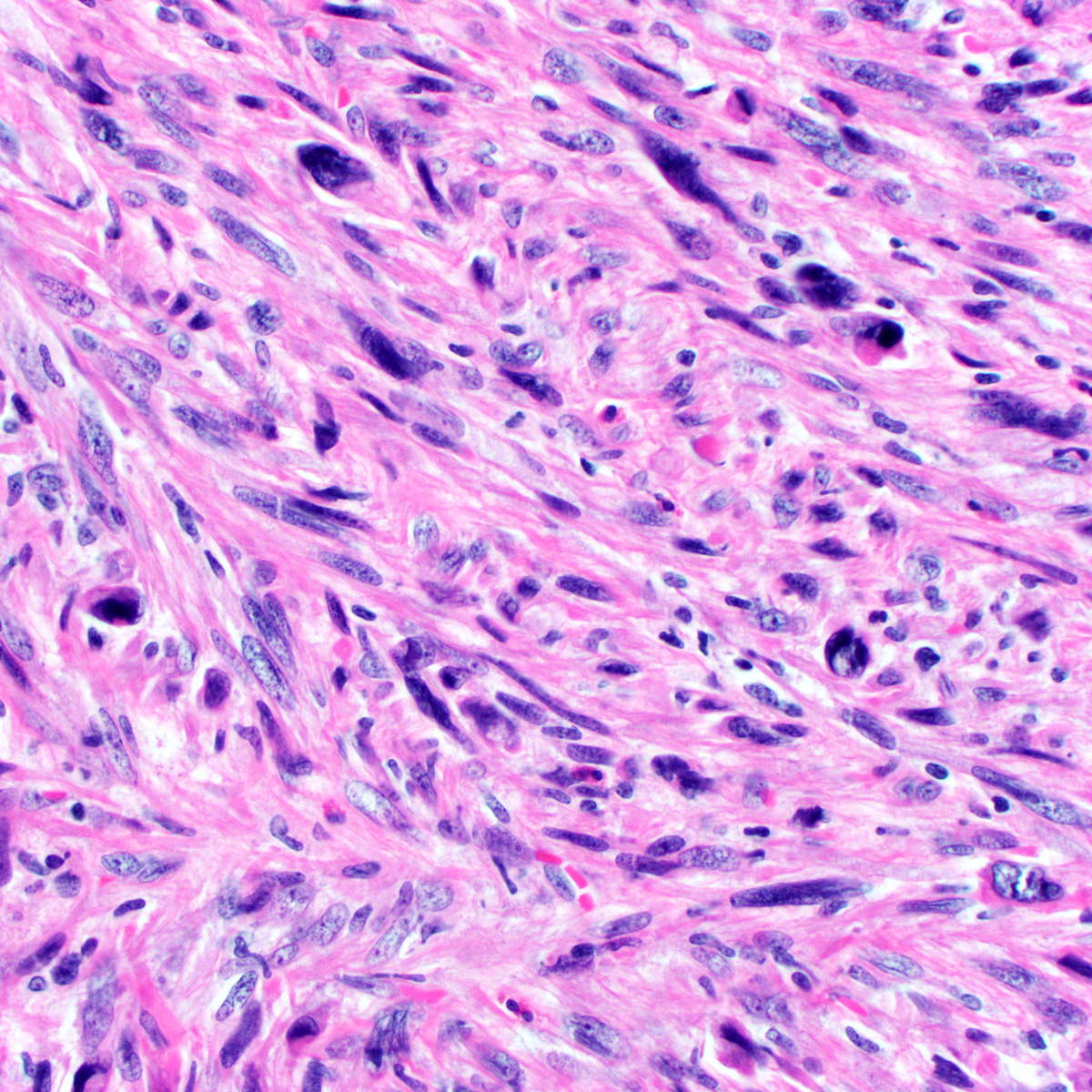
Vaginal leiomyosarcoma
Images hosted on other servers:

Scanning and transmission electron micrographs
Contributed by Shazia Khan, M.D. and Natalia Buza, M.D.


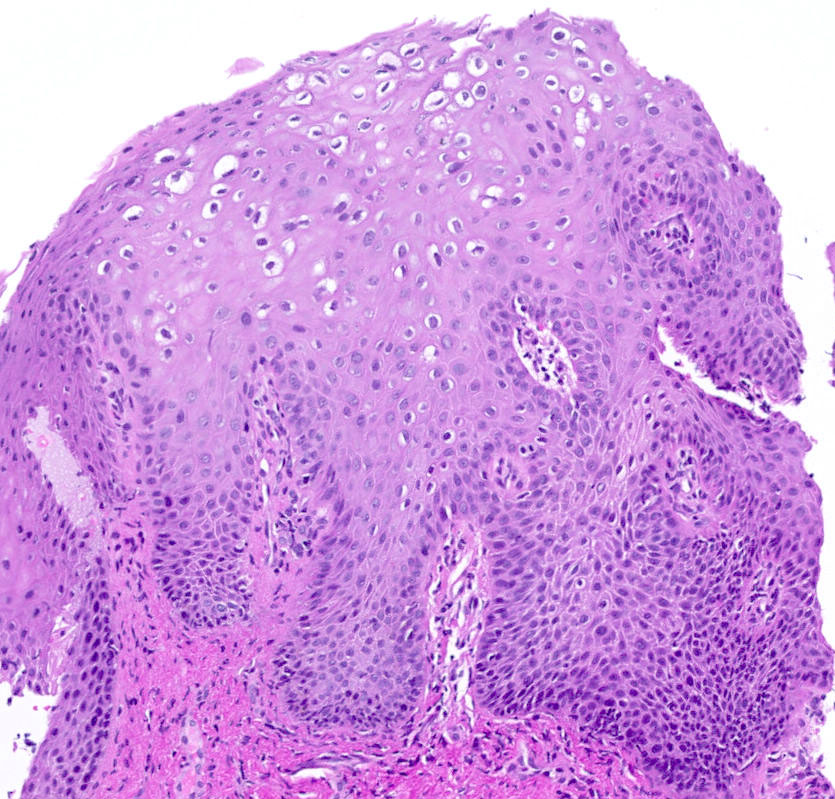
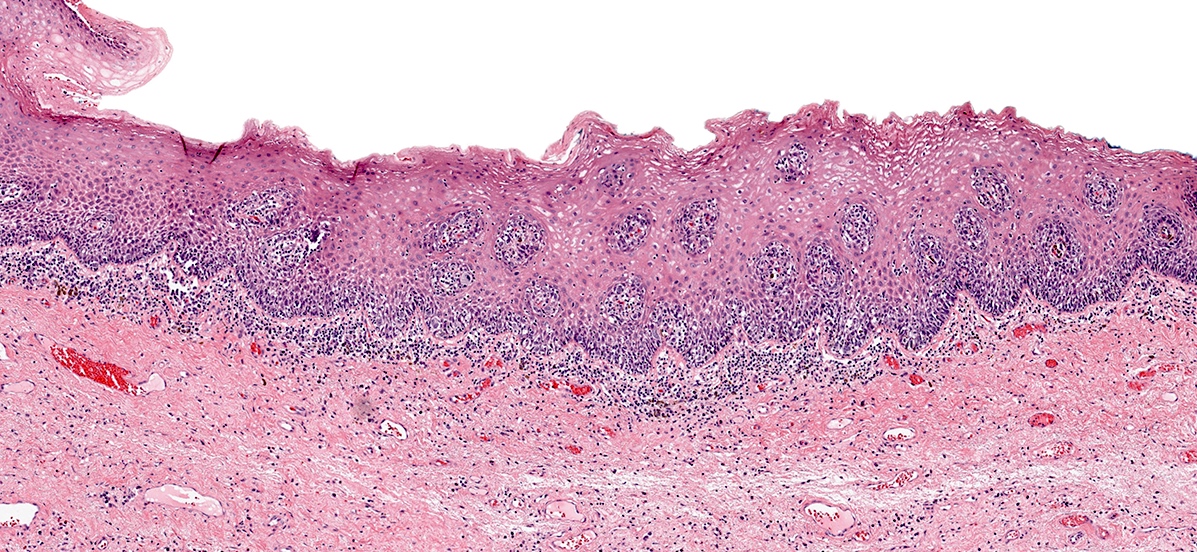
LSIL / VAIN 1

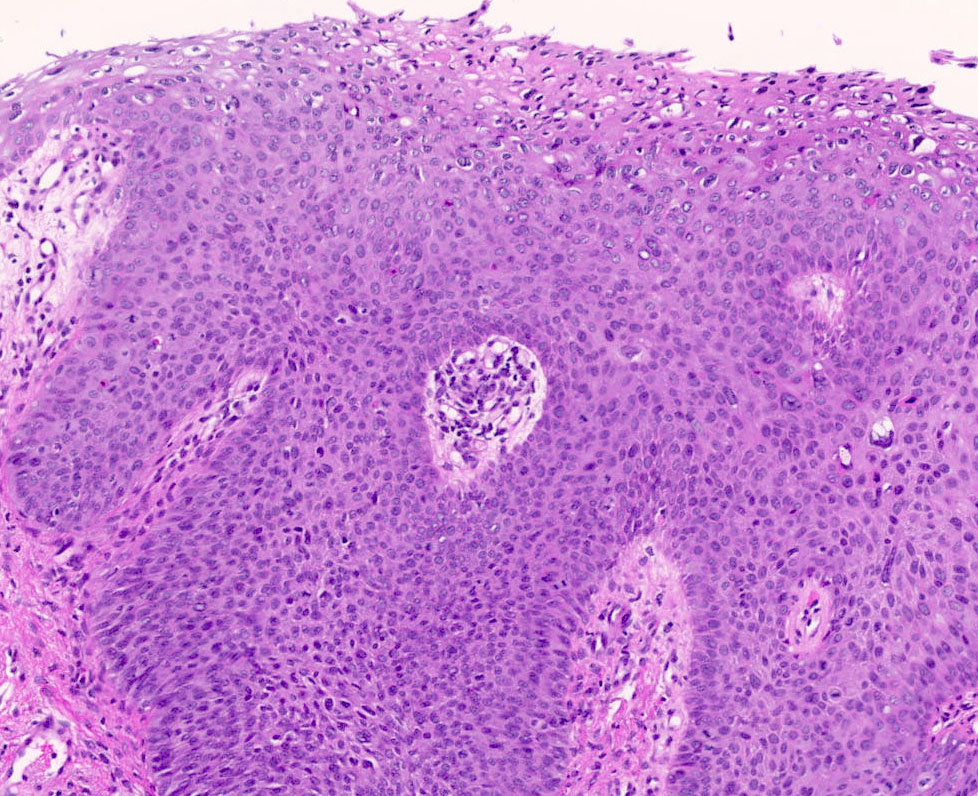
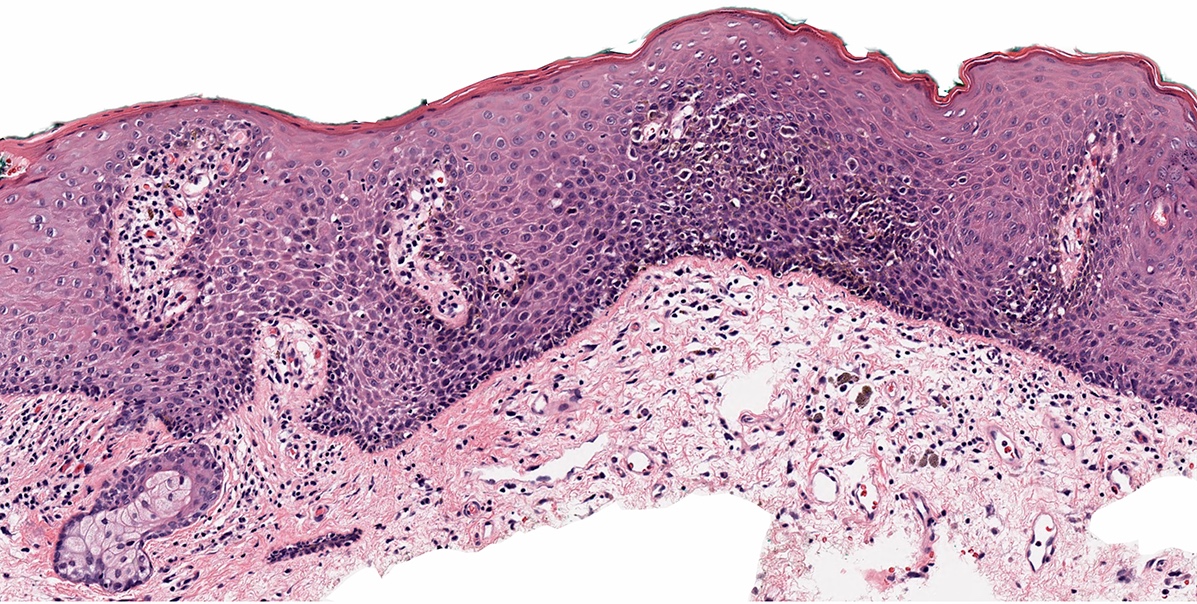
HSIL / VAIN 2

LSIL / VAIN1 (p16 immunostain)

LSIL / VAIN1 (Ki67 immunostain)

HSIL / VAIN 2 (p16 immunostain)

HSIL / VAIN 2 (p53 immunostain)

HSIL / VaIN2 (Ki67 immunostain)
Contributed by Morgan Hrones, M.D. and Natalia Buza, M.D.
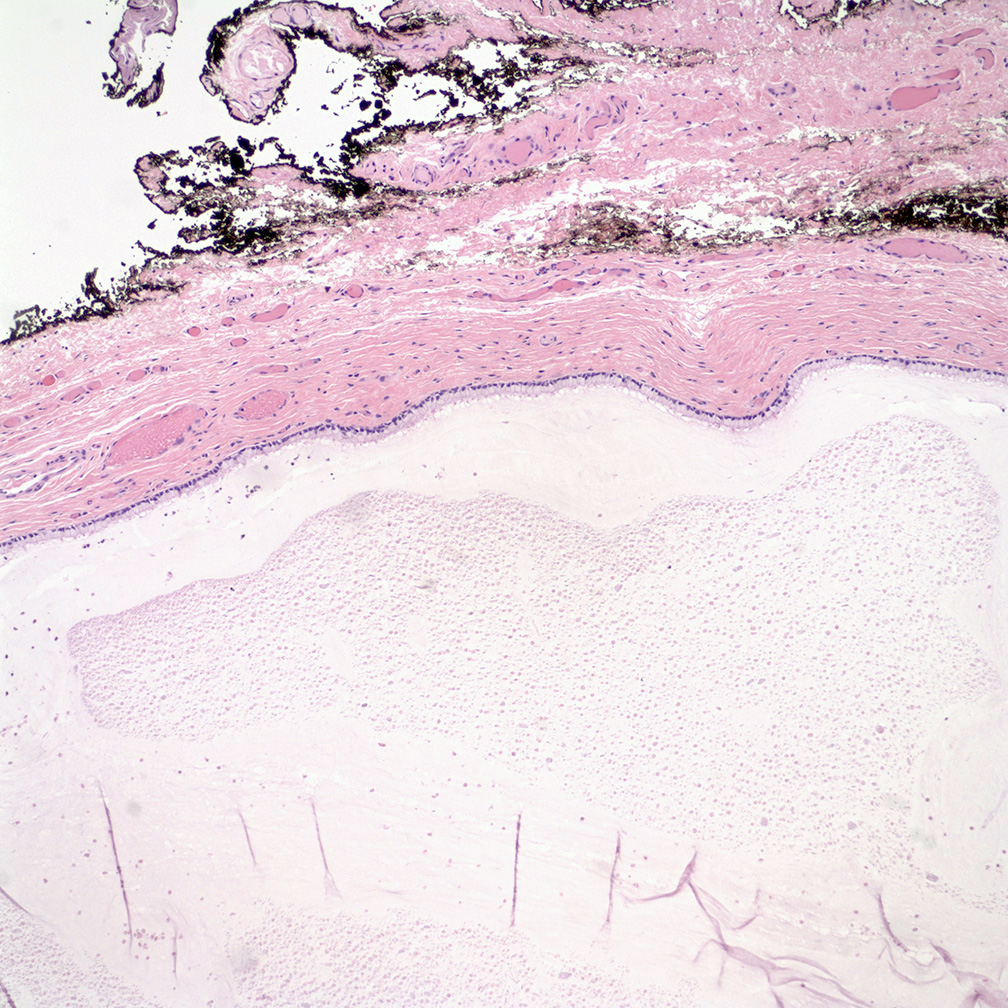
Mucinous cystic lining
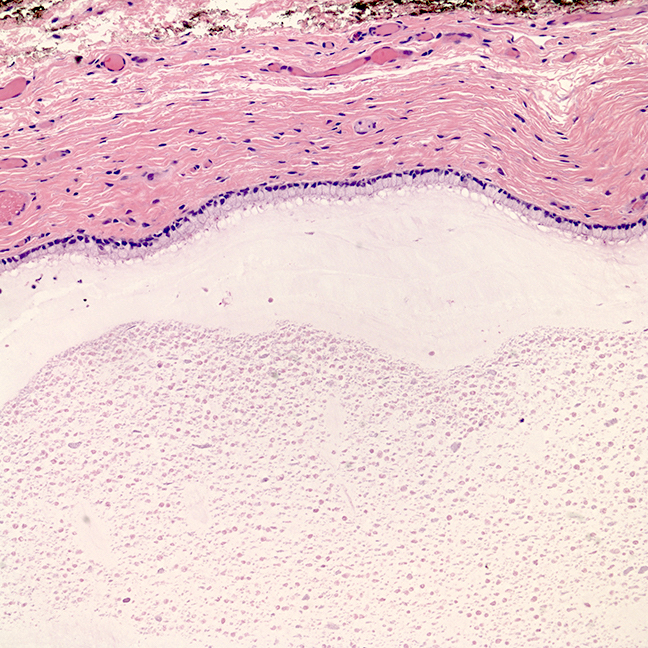
Bland appearing cyst lining
Benign urothelial cyst
Benign urothelial lined cyst
Benign epidermal inclusion cyst
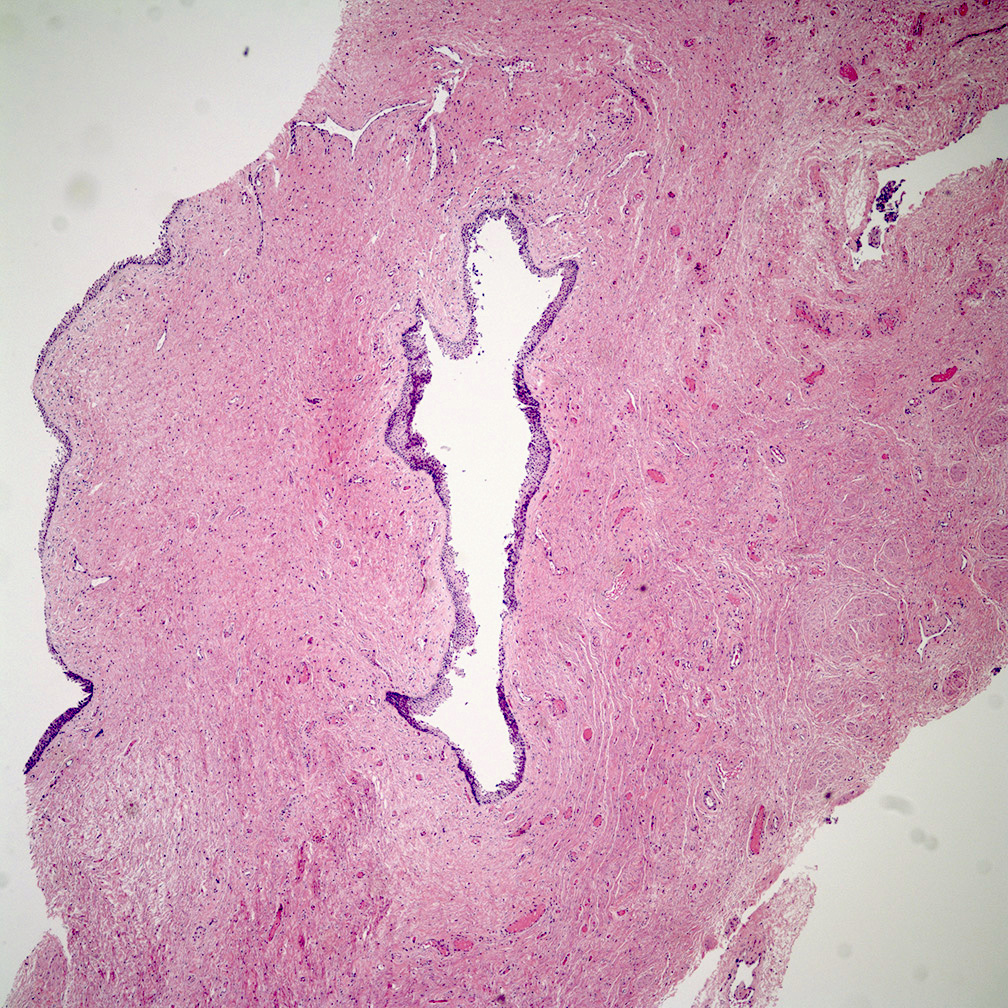
Bartholin cyst with adjacent Bartholin glands
Bartholin cyst
Bartholin gland cyst of the vulva - histopathology
Clement: 2019
Crum: 2017
Crum: 2015
Fadare: 2015
Hoang: 2015
IARC: 2020

Nucci: 2020
Nucci: 2023
Vang: 2023
Find related Pathology books: gynecologic

