




















.jpg)





























































































































































































































































































































































































%20xray.jpg)

%20xray4.jpg)




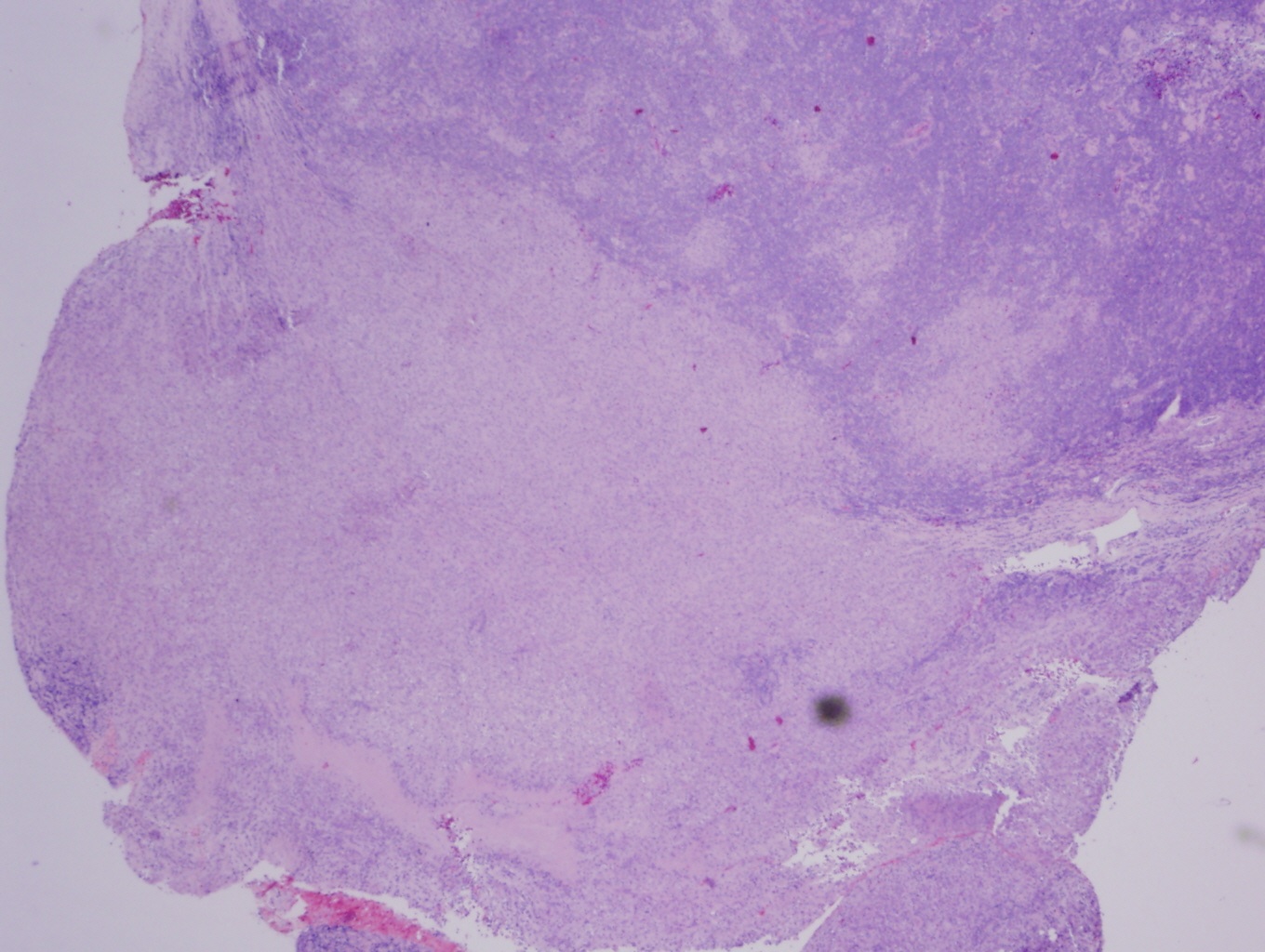
%20gross.jpg)

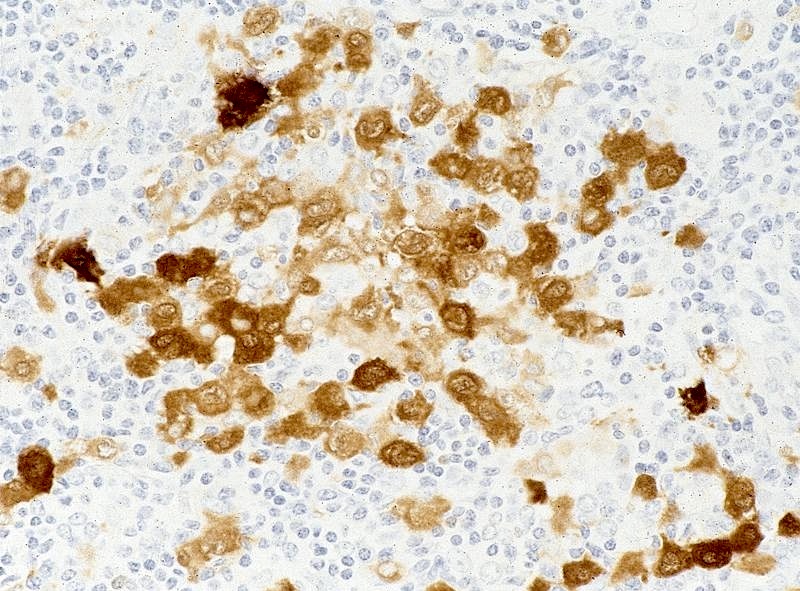
%20keratin%20immunost.jpg)









































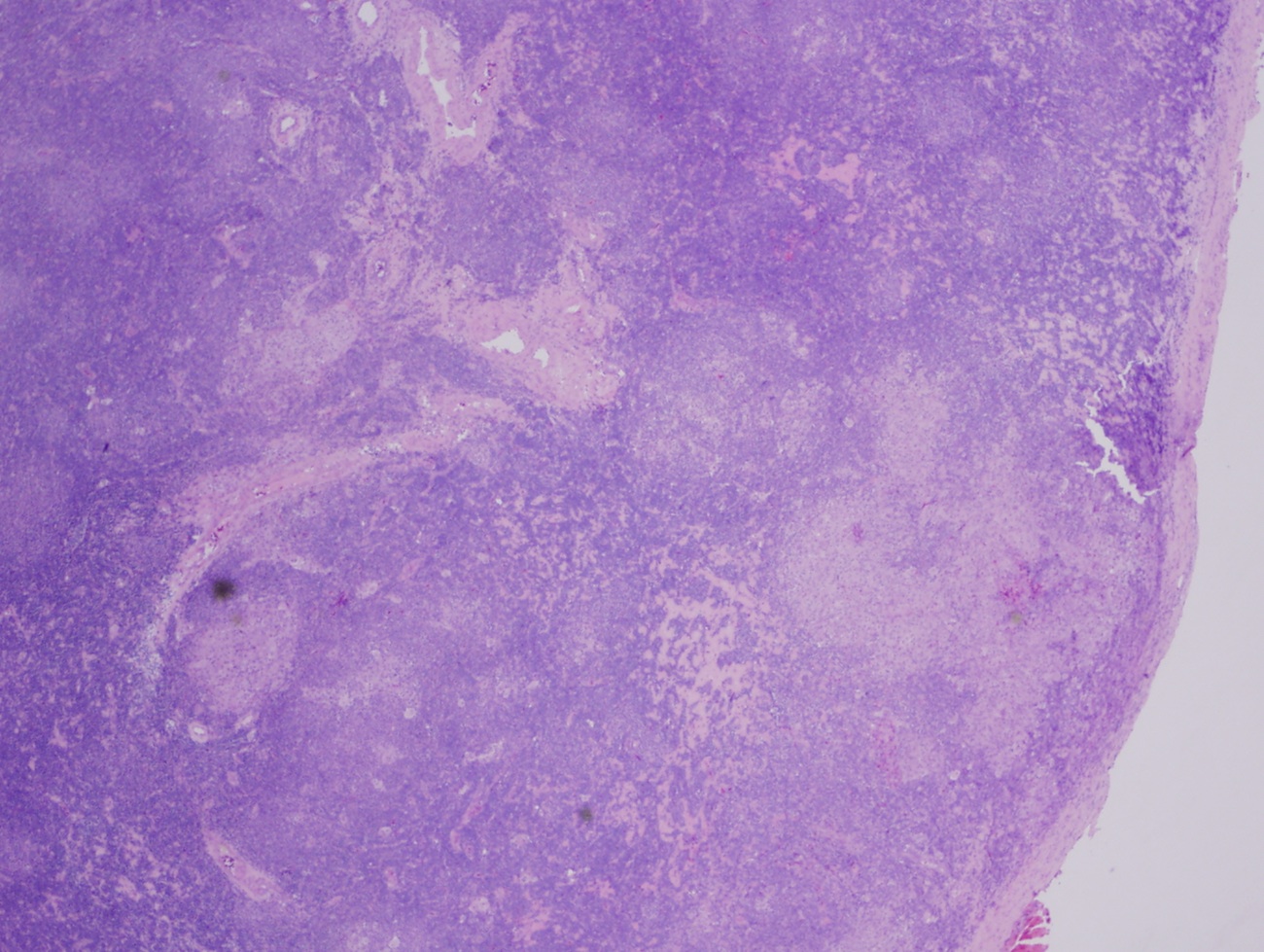
%20type%20gross.jpg)





















Primary tumor (pT)
Categorization for appendicular skeleton, trunk, skull and facial bones:
Categorization for spine:
Note:
Categorization for pelvis:
Note:
- pTX: primary tumor cannot be assessed
- pT0: no evidence of primary tumor
- pT1: tumor ≤ 8 cm in greatest dimension
- pT2: tumor > 8 cm in greatest dimension
- pT3: discontinuous tumors in the primary bone site
Categorization for spine:
- pTX: primary tumor cannot be assessed
- pT0: no evidence of primary tumor
- pT1: tumor confined to one vertebral segment or two adjacent vertebral segments
- pT2: tumor confined to three adjacent vertebral segments
- pT3: tumor confined to four or more adjacent vertebral segments or any nonadjacent vertebral segments
- pT4: extension into the spinal canal or great vessels
- pT4a: extension into the spinal canal
- pT4b: evidence of gross vascular invasion or tumor thrombus in the great vessels
Note:
- Spine segments include right body, left body, right pedicle, left pedicle and posterior element
Categorization for pelvis:
- pTX: primary tumor cannot be assessed
- pT0: no evidence of primary tumor
- pT1: tumor confined to one pelvic segment with no extraosseous extension
- pT1a: tumor ≤ 8 cm in greatest dimension
- pT1b: tumor > 8 cm in greatest dimension
- pT2: tumor confined to one pelvic segment with extraosseous extension or two segments without extraosseous extension
- pT2a: tumor ≤ 8 cm in greatest dimension
- pT2b: tumor > 8 cm in greatest dimension
- pT3: tumor spanning two pelvic segments with extraosseous extension
- pT3a: tumor ≤ 8 cm in greatest dimension
- pT3b: tumor > 8 cm in greatest dimension
- pT4: tumor spanning three pelvic segments or crossing the sacroiliac joint
- pT4a: tumor ≤ 8 cm in greatest dimension
- pT4b: tumor > 8 cm in greatest dimension
Note:
- Pelvic segments include sacrum, iliac wing, pubic rami / symphysis / ischium and acetabulum / periacetabulum






























































%20with.jpg)