
Bone & joints
Osteoclastic giant cell rich tumors
Benign
Aneurysmal bone cyst
Authors: Elham Nasri, M.D., John D. Reith, M.D.
Editorial Board Member: Borislav A. Alexiev, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 4 May 2020
Last staff update: 12 October 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Aneurysmal bone cyst
See Review Article: J Pathol Transl Med 2023;57:81

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nasri E, Reith JD. Aneurysmal bone cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneabc.html. Accessed April 1st, 2025.
Definition / general
- Benign, locally destructive multiloculated blood filled cystic lesion of bone
- Classified as an osteoclastic giant cell rich tumor (WHO 2020)
- Primary and secondary forms
- High rate of local recurrence
Essential features
- Imaging: multiloculated lesion with fluid-fluid levels, best appreciated on MRI
- Histology: cyst walls composed of fibroblasts, woven bone and osteoclastic giant cells
- Molecular: rearrangement of USP6 gene (primary form only)
Terminology
- Related term: giant cell lesion of small bones
ICD coding
- ICD-10: M85.50 - aneurysmal bone cyst, unspecified site
Epidemiology
- Rare; 2.5% of all primary bone tumors
- M = F
- In mandible and maxilla, more common in young women
- More common in skeletally immature patients
- Peak incidence in second decade (J Pediatr Orthop B 2004;13:389)
Sites
- Broad skeletal distribution
- Metaphyseal region of long tubular bones, most commonly the femur, tibia and humerus
- Posterior elements of vertebrae
Etiology
- Historically thought to be reactive to underlying vascular events
- Recent molecular data supportive of neoplastic etiology (Genes Chromosomes Cancer 1999;26:265, AJR Am J Roentgenol 1995;164:573)
Clinical features
- Pain and swelling
- Pathologic fracture
- Nerve compression symptoms in cases of vertebral column involvement
- May massively expand the mandible
Diagnosis
- Requires correlation of clinical, radiographic and histologic findings to distinguish primary from secondary aneurysmal bone cyst
- Lack of immunoreactivity for H3G34W (and other histone antibodies) is helpful in excluding giant cell tumor with cystic features
Radiology description
- Xray:
- Eccentric radiolucent lesion with expansile remodeling, involving the metaphysis of long bones
- Finger in the balloon sign possible (Orthop Traumatol Surg Res 2015;101:S119)
- CT scan:
- Well delineated lytic lesion, usually with thin rim of reactive bone
- Fluid-fluid levels occasionally visible
- MRI:
- Multiloculated cyst with characteristic fluid-fluid levels
- Isotope scan:
- Peripheral uptake with central photopenia imparts a donut-like appearances
Radiology images
Contributed by Elham Nasri, M.D.

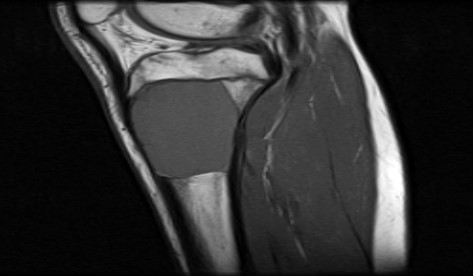
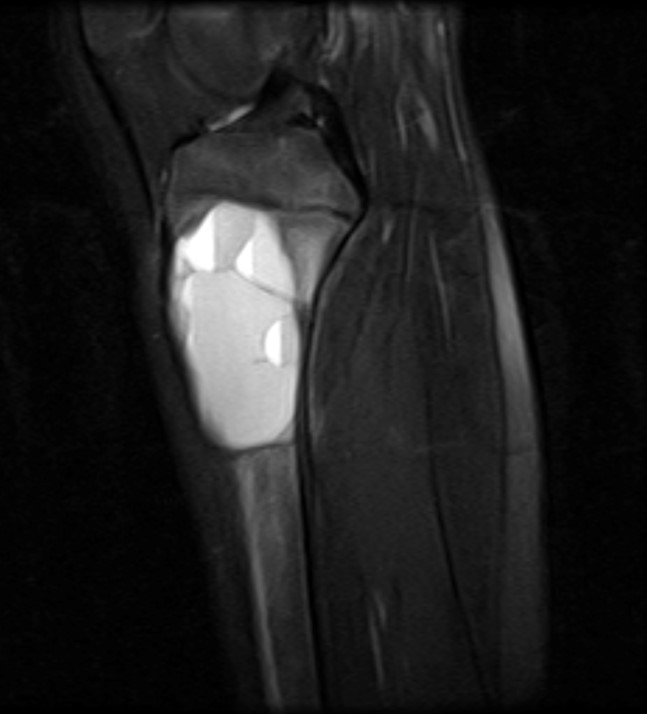
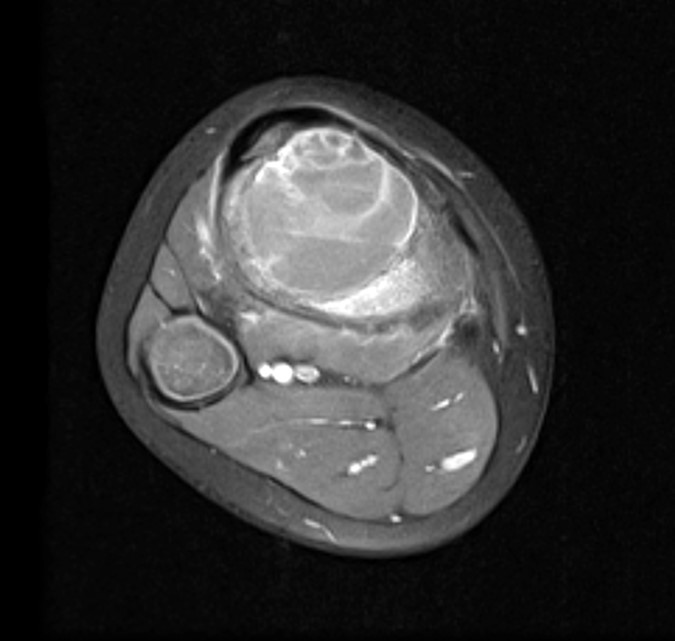
Aneurysmal bone cyst of proximal tibia

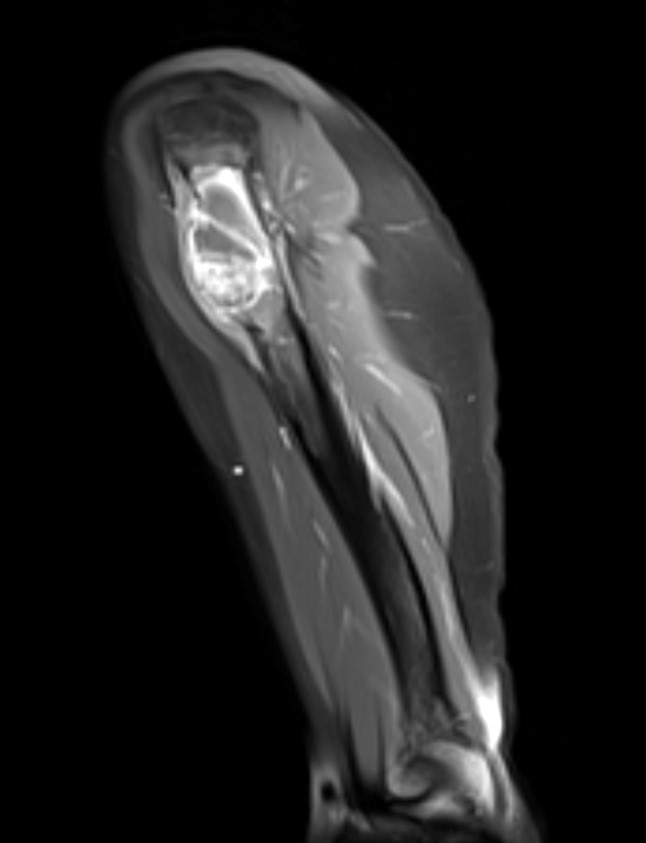
Aneurysmal bone cyst of humerus



Aneurysmal bone cyst of distal tibia


Aneurysmal bone cyst of calcaneus bone
Prognostic factors
- Up to a third have local recurrence (Clin Orthop Relat Res 2008;466:722)
- Rare case reports of metastatic aneurysmal bone cyst (Virchows Arch 2009;455:455)
Case reports
- 7 year old girl with aneurysmal bone cyst in the cervical spine (BMJ Case Rep 2019;12:e231870)
- 12 year old girl with giant aneurysmal bone cyst of the mandible (Natl J Maxillofac Surg 2013;4:107)
- 22 year old man with fracture of an intertrochanteric aneurysmal bone cyst (Cureus 2019;11:e6461)
- 26 year old man with solid variant of aneurysmal bone cyst of the heel (J Med Case Rep 2011;5:145)
- 48 year old woman with metastatic potential of an aneurysmal bone cyst (Virchows Arch 2009;455:455)
Treatment
- Curettage or en bloc resection
- Percutaneous sclerotherapy with doxycycline (Bone Joint J 2020;102-B:186)
- Arterial embolization
- Steroid or calcitonin injection
Clinical images
Images hosted on other servers:

Intraoral tumor
Gross description
- Spongy, multiloculated, hemorrhagic lesion
- Variable size
- Irregular, sharply demarcated borders with thin shell of reactive bone
- Variable amount of solid component
Gross images
Contributed by Elham Nasri, M.D.

Blood filled cysts
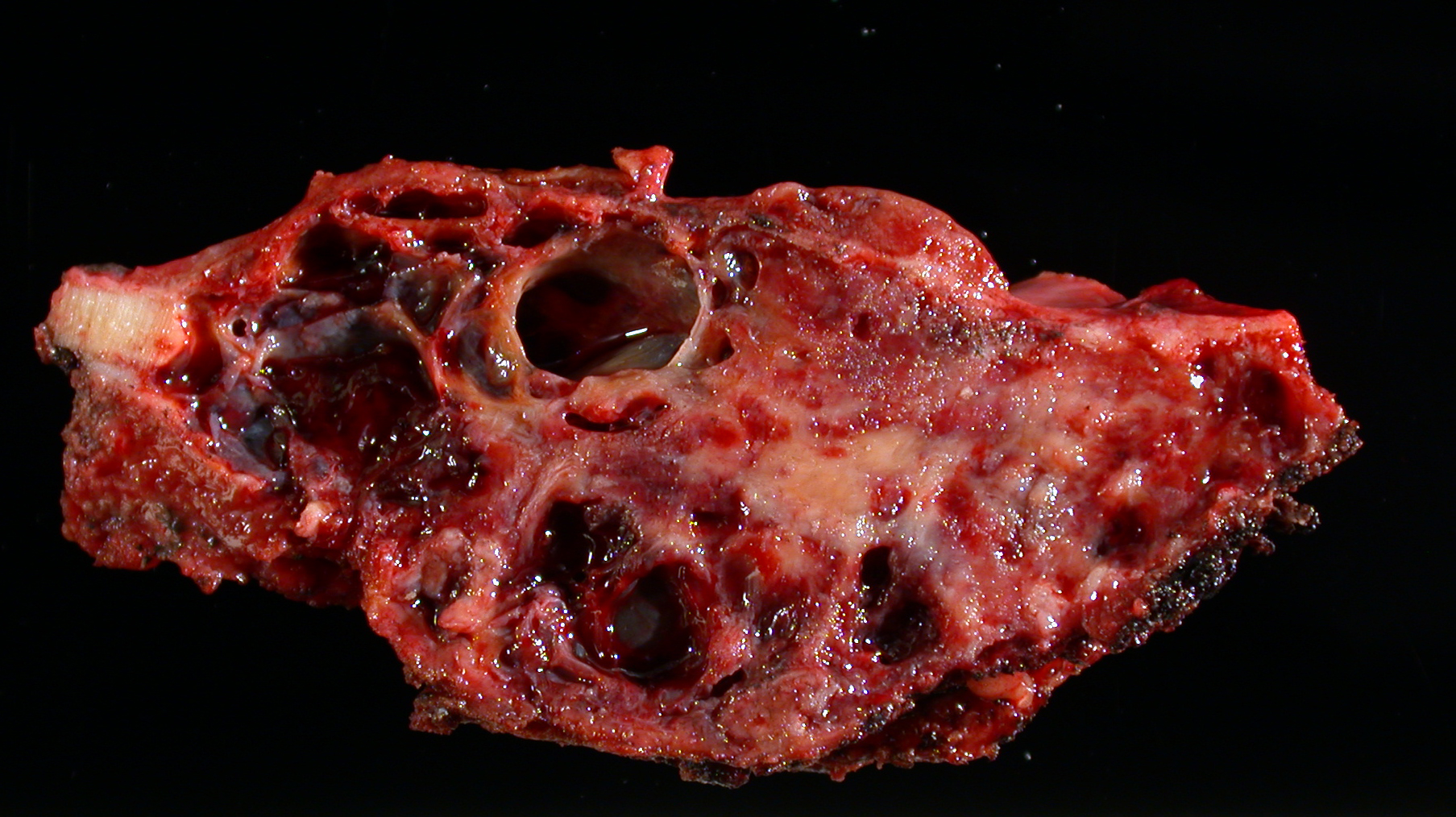
Multiloculated cyst
Frozen section description
- Usually small fragments of cellular septa containing:
- Fibroblast-like stromal cells lacking cytologic atypia
- Osteoclast-like giant cells
- Reactive woven bone
- Mitotic activity typically present, no atypical mitoses
Frozen section images
Contributed by Elham Nasri, M.D.
Cystic spaces and stromal giant cells
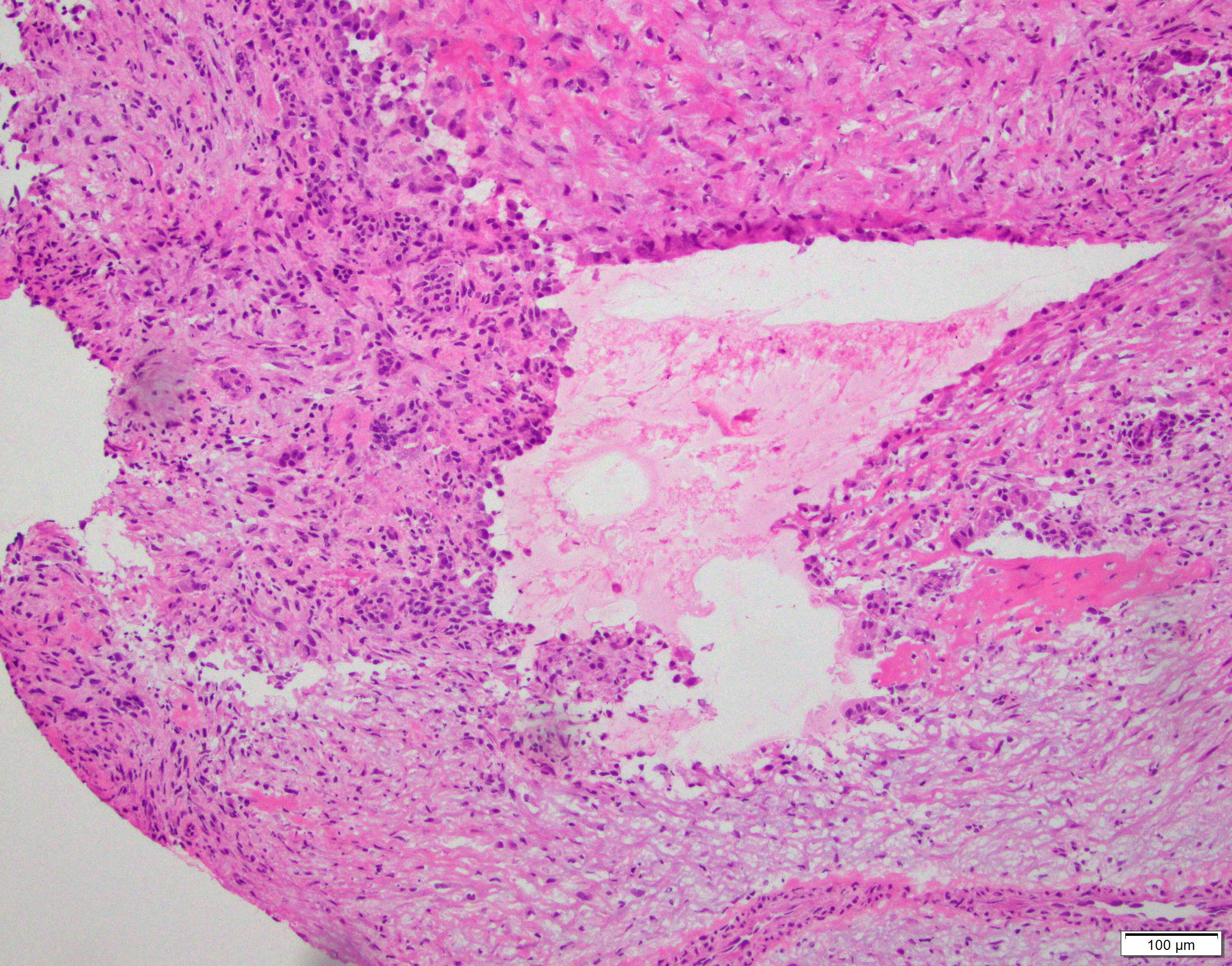
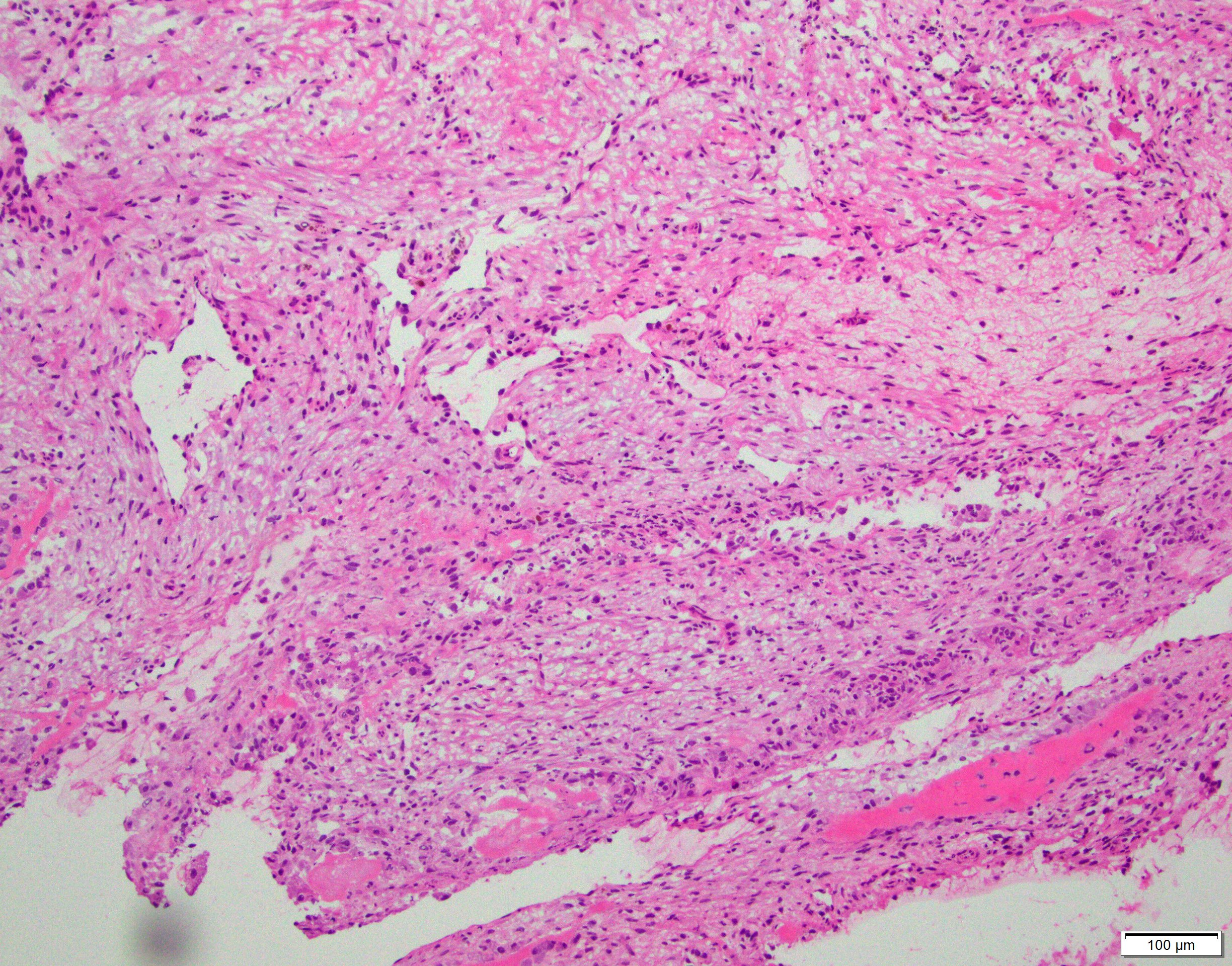
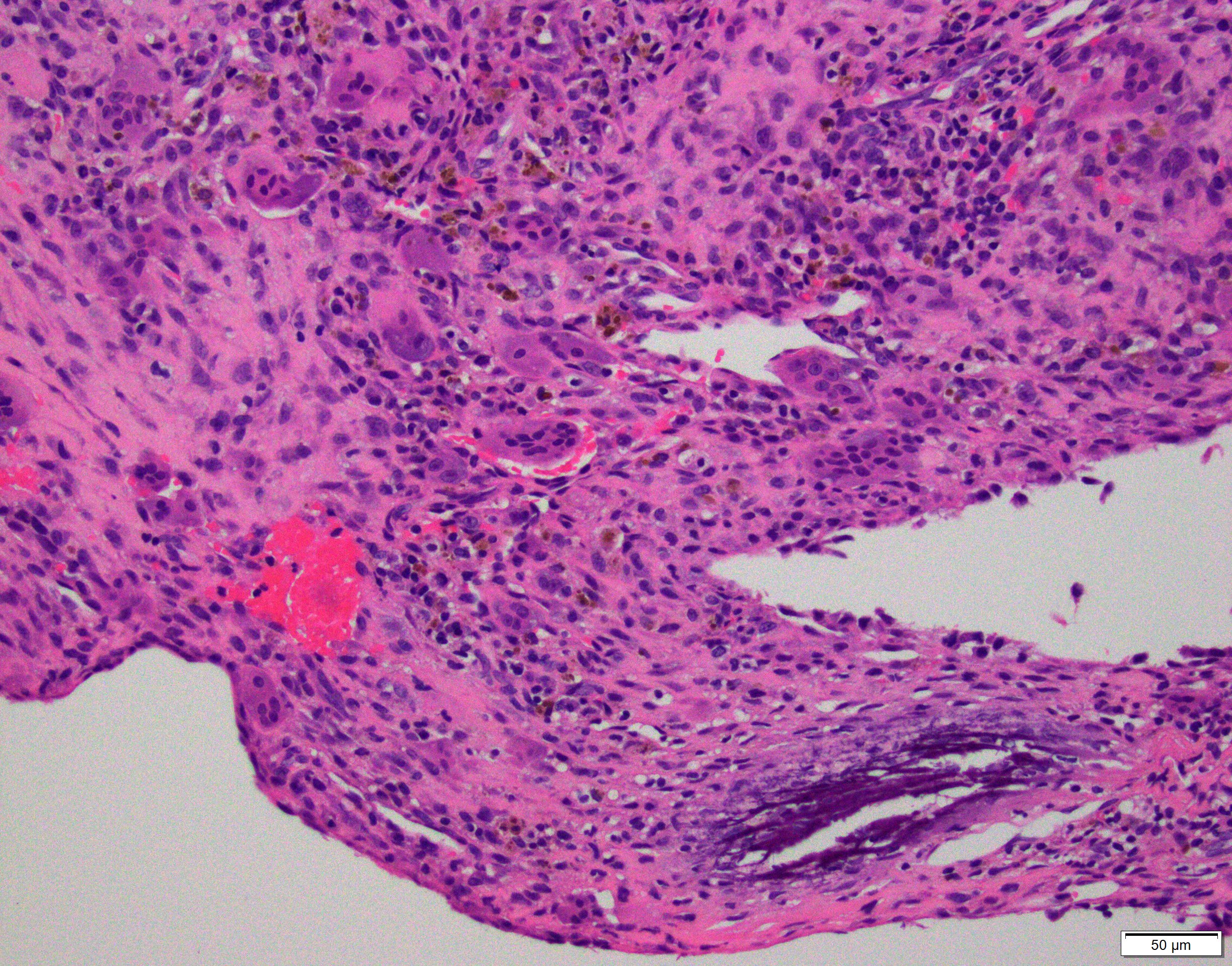
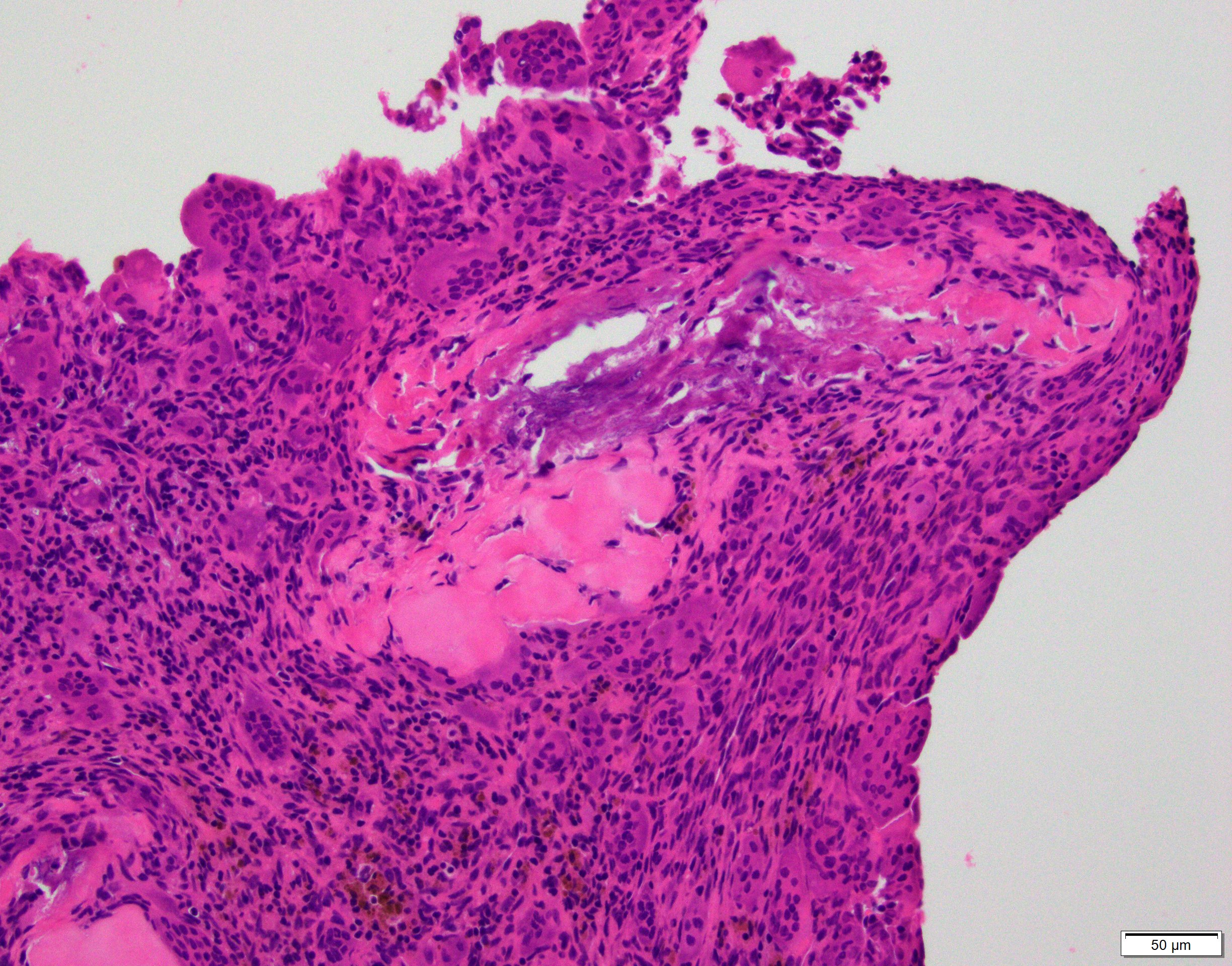
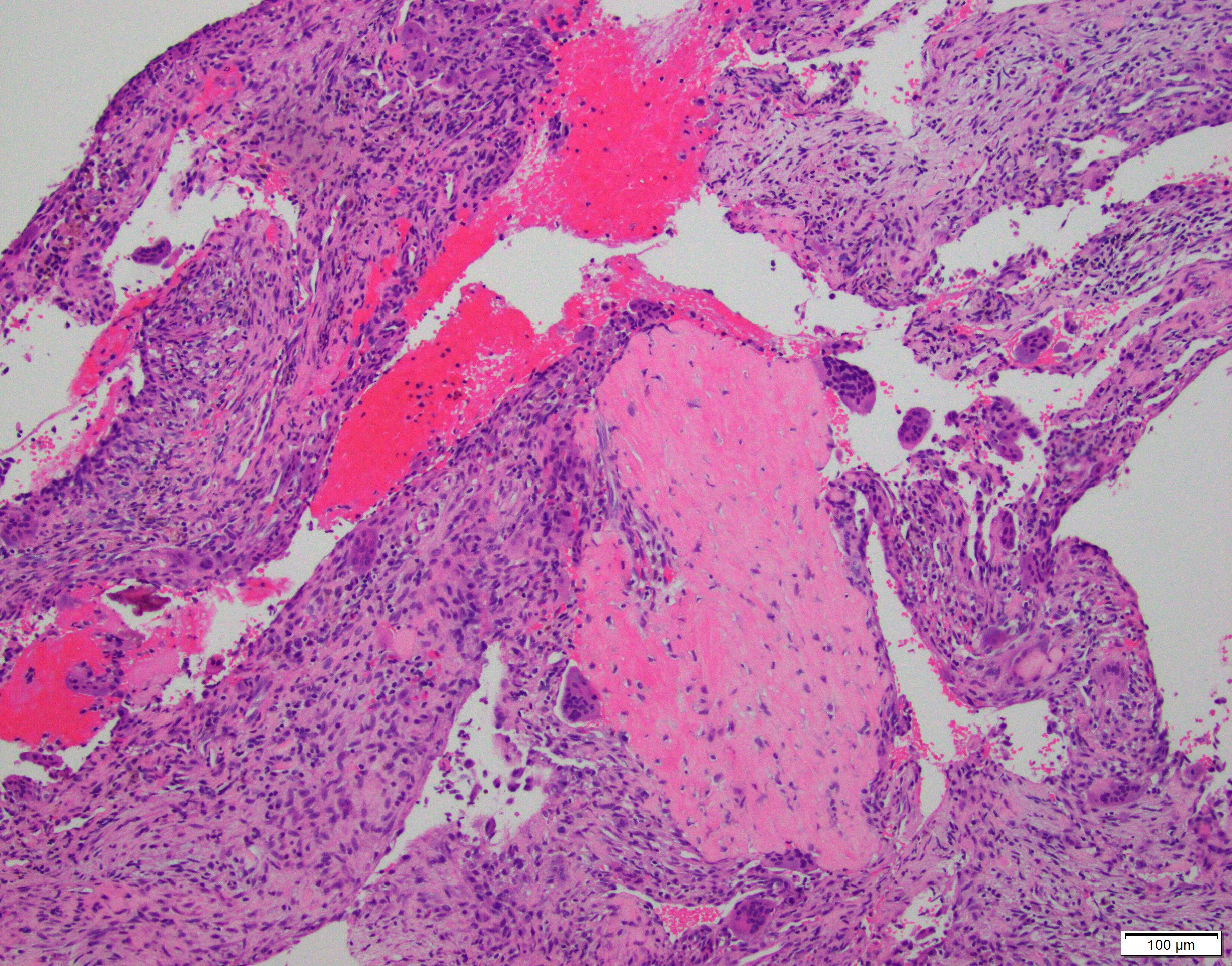
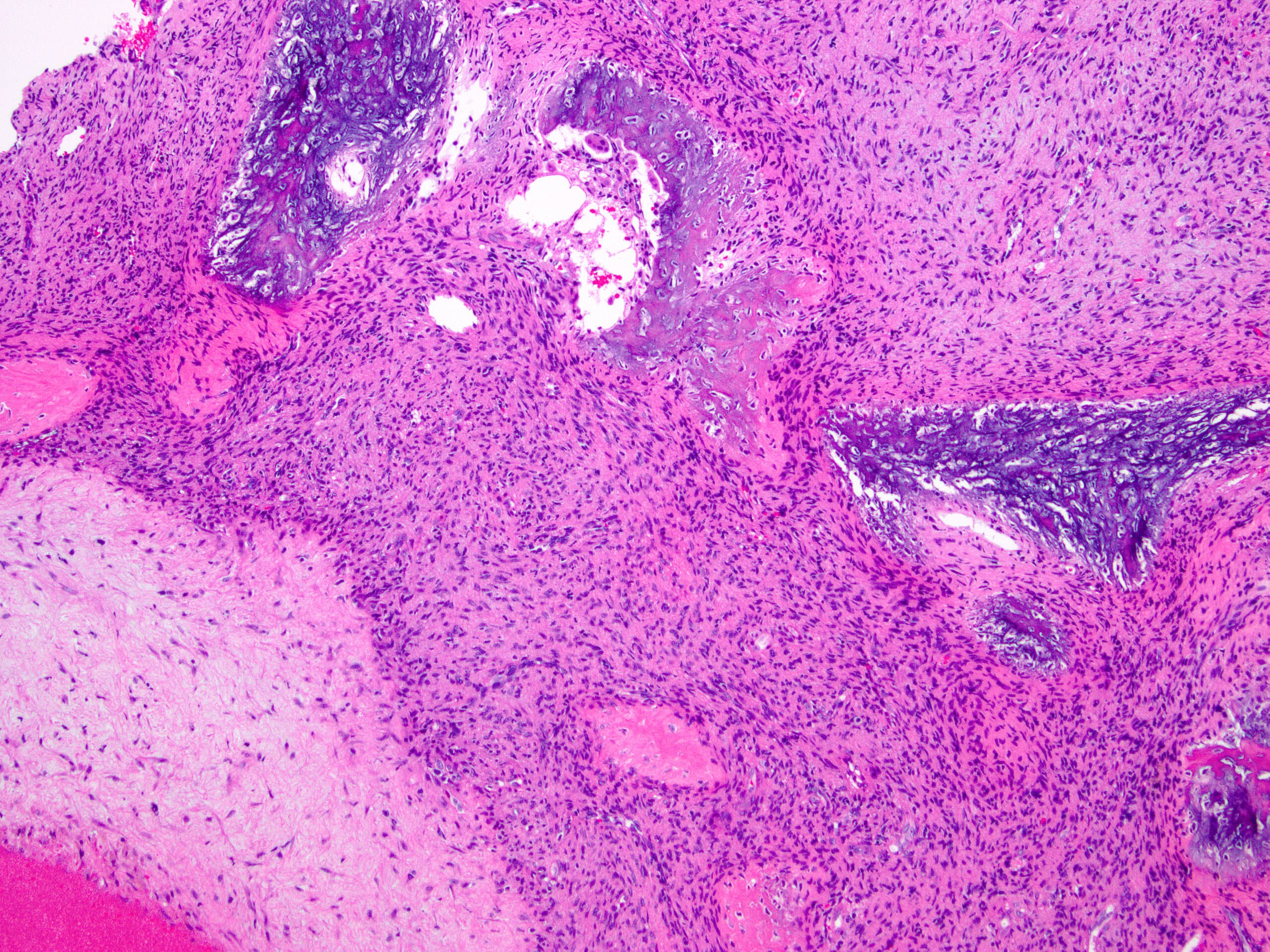
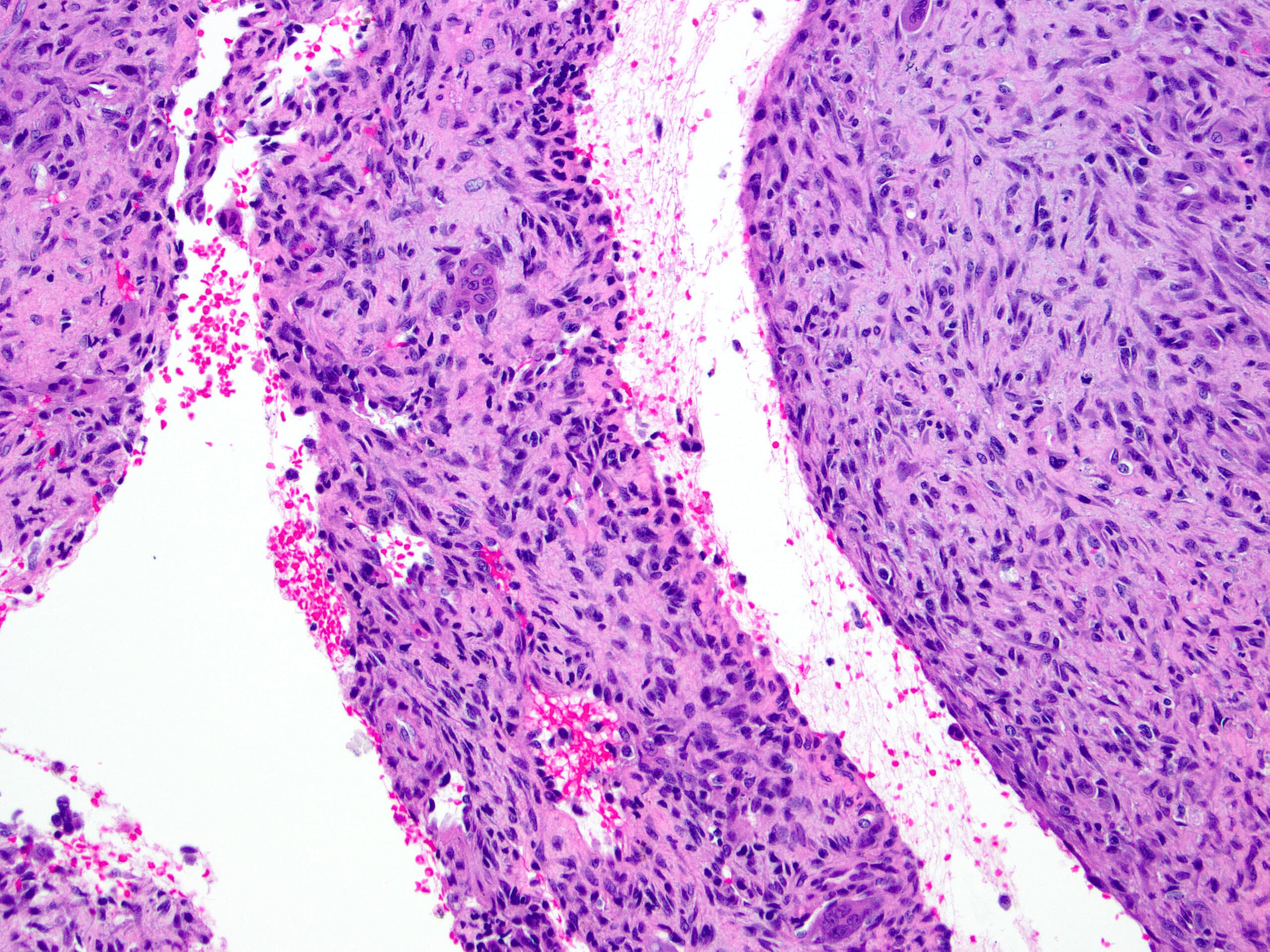
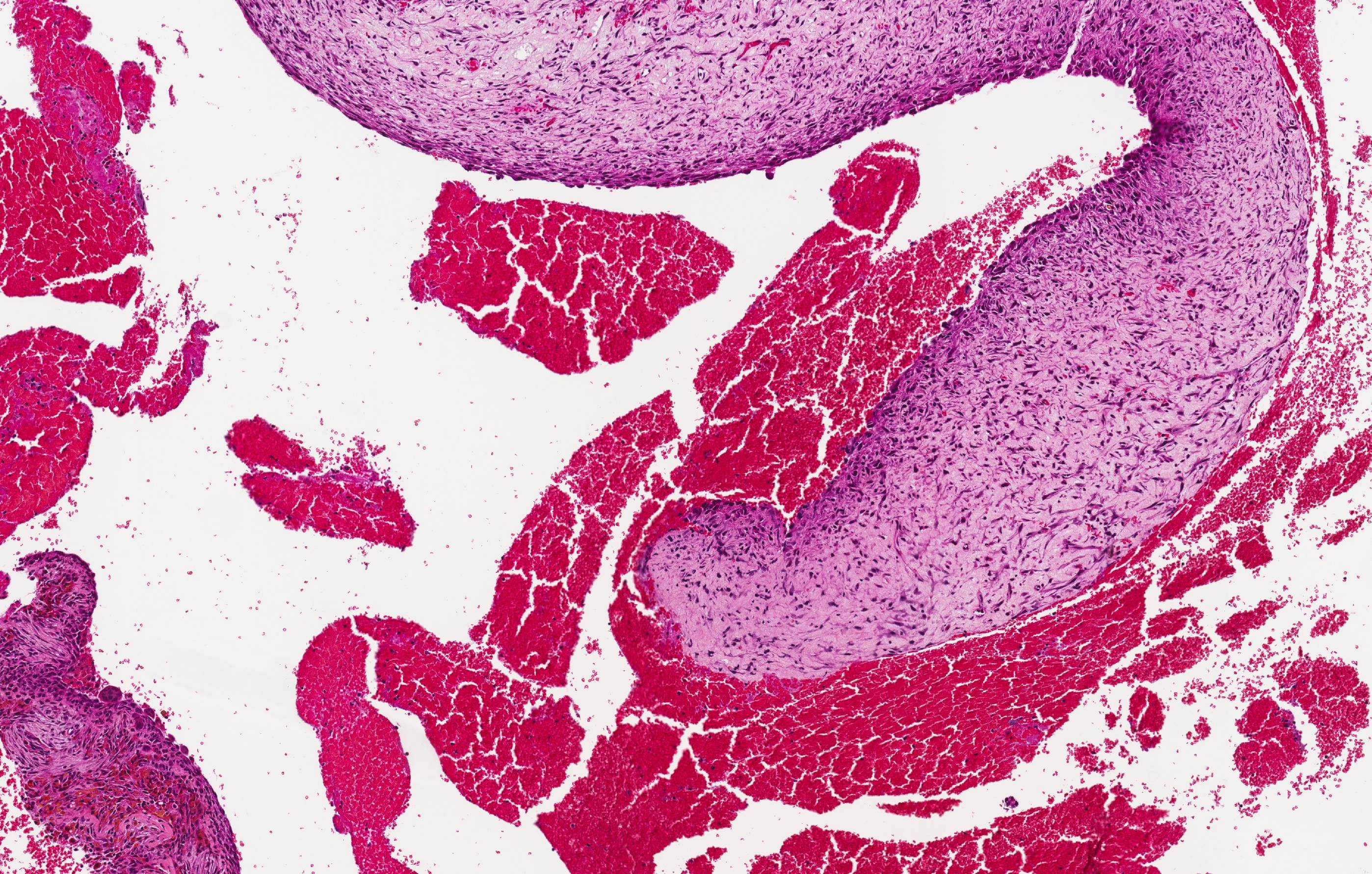
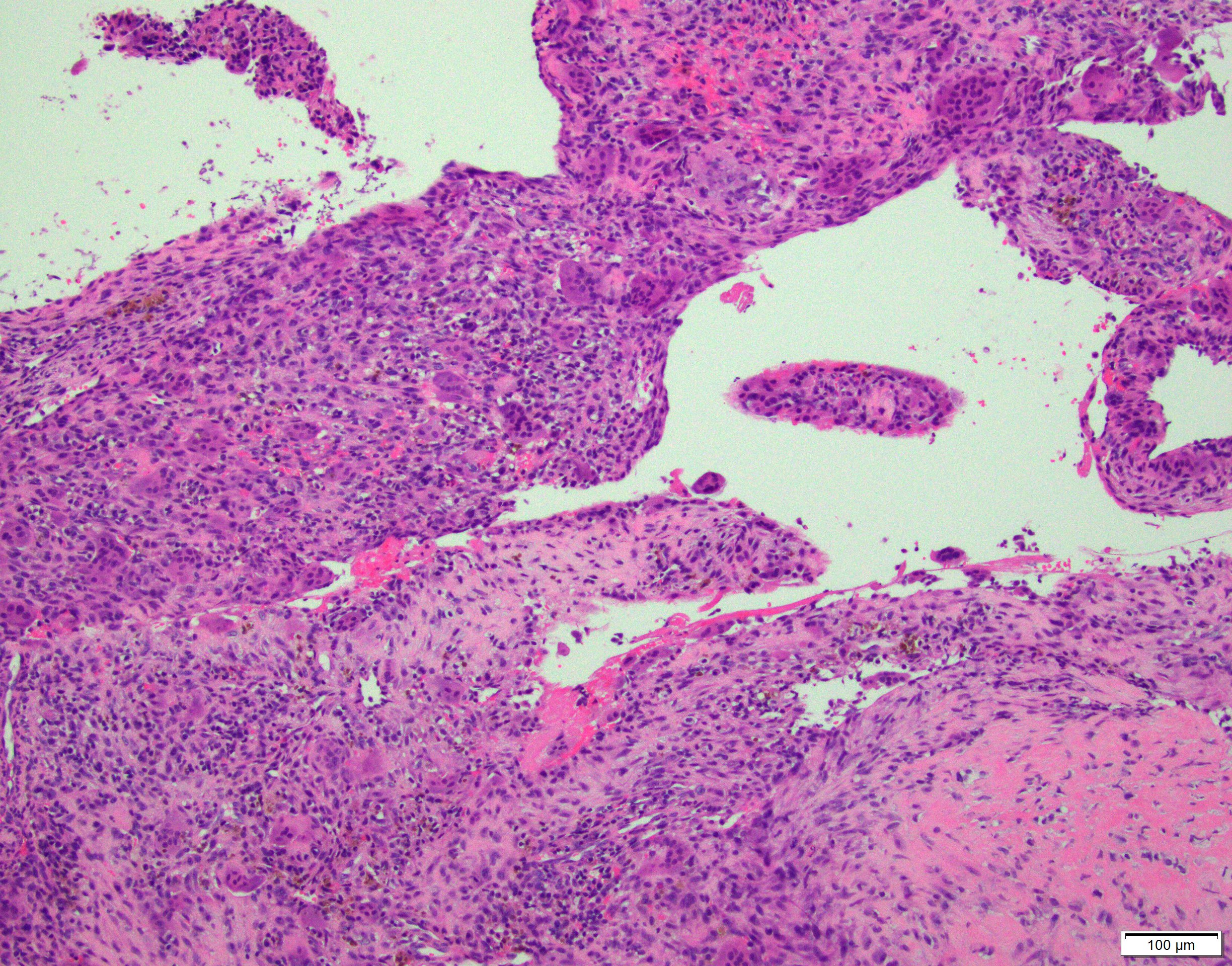
Microscopic (histologic) description
- Multiloculated cystic lesion
- Blood filled cystic spaces separated by cellular septa containing fibroblasts, giant cells and woven bone
- Calcified, basophilic material (blue reticulated chondroid-like material)
- Necrosis not common but mitotic activity is easily identified
- No cytologic atypia (Am J Clin Pathol 2015;143:823)
- Numerous giant cells in connective tissue that line large sinusoidal spaces
Microscopic (histologic) images
Contributed by Elham Nasri, M.D. and Kelly Magliocca, D.D.S., M.P.H.
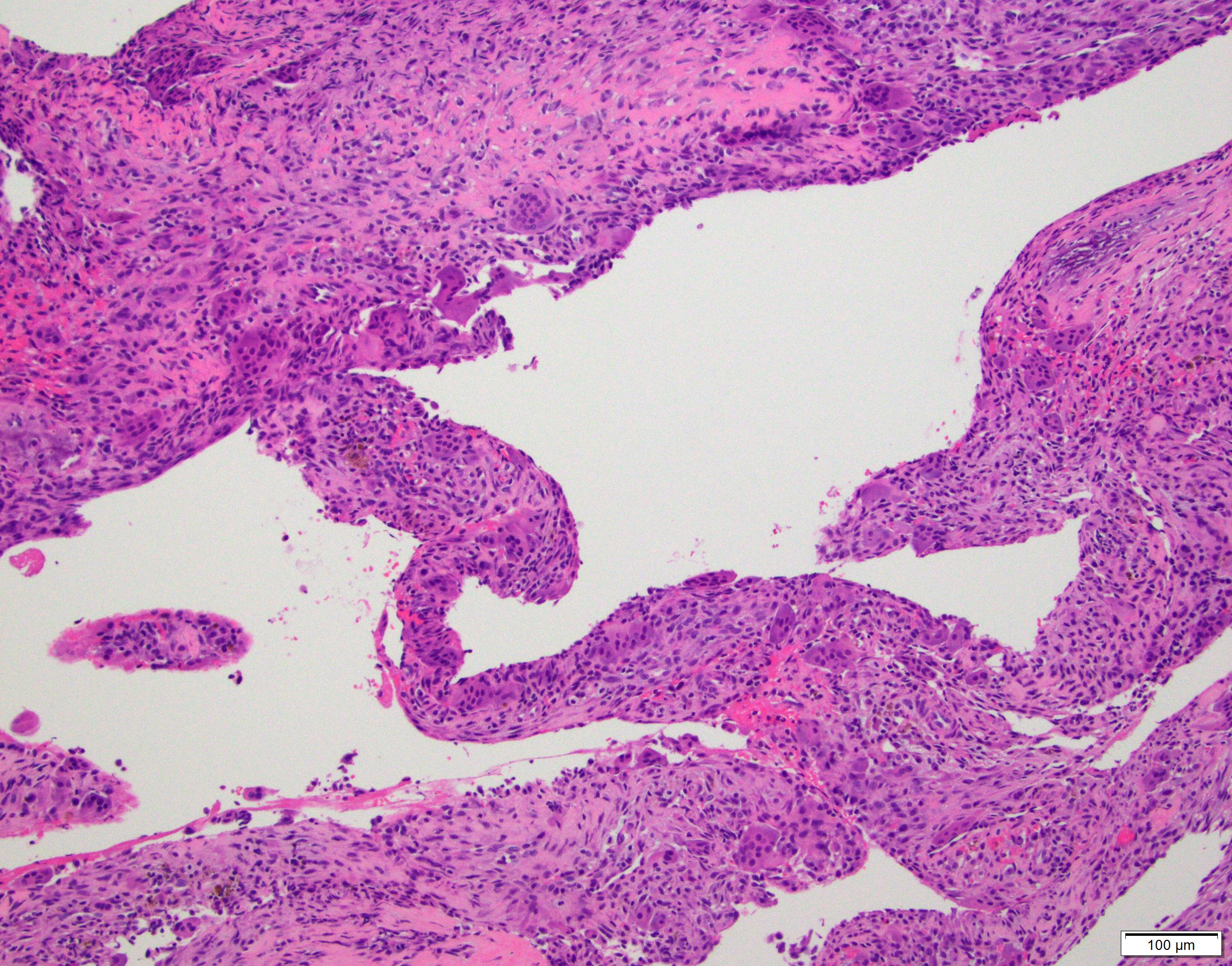
Cysts and giant cells
Blue chondroid like material
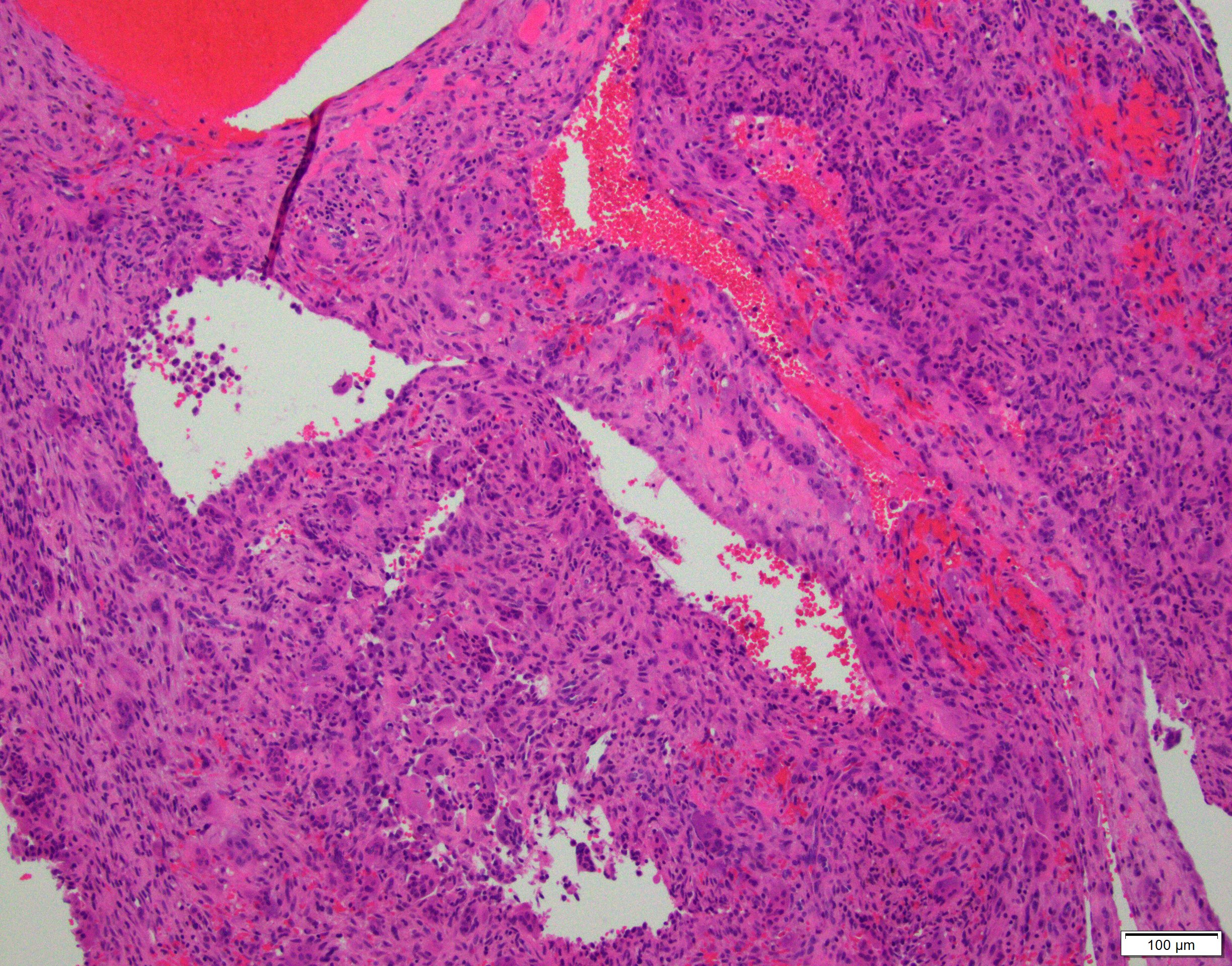
Blood filled cystic spaces
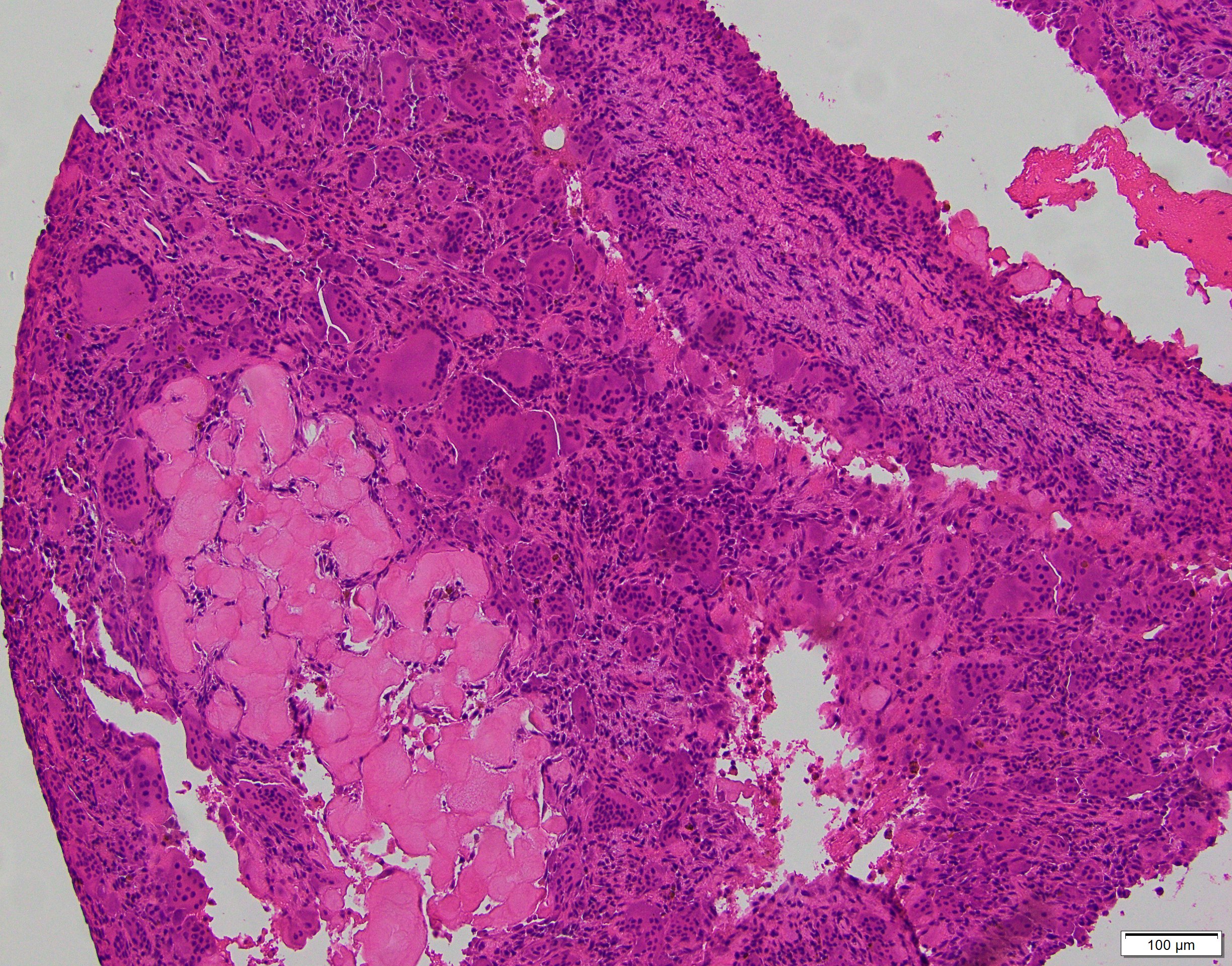
Solid area of cyst wall
Reticulated chondroid-like material
Multiple cystic spaces
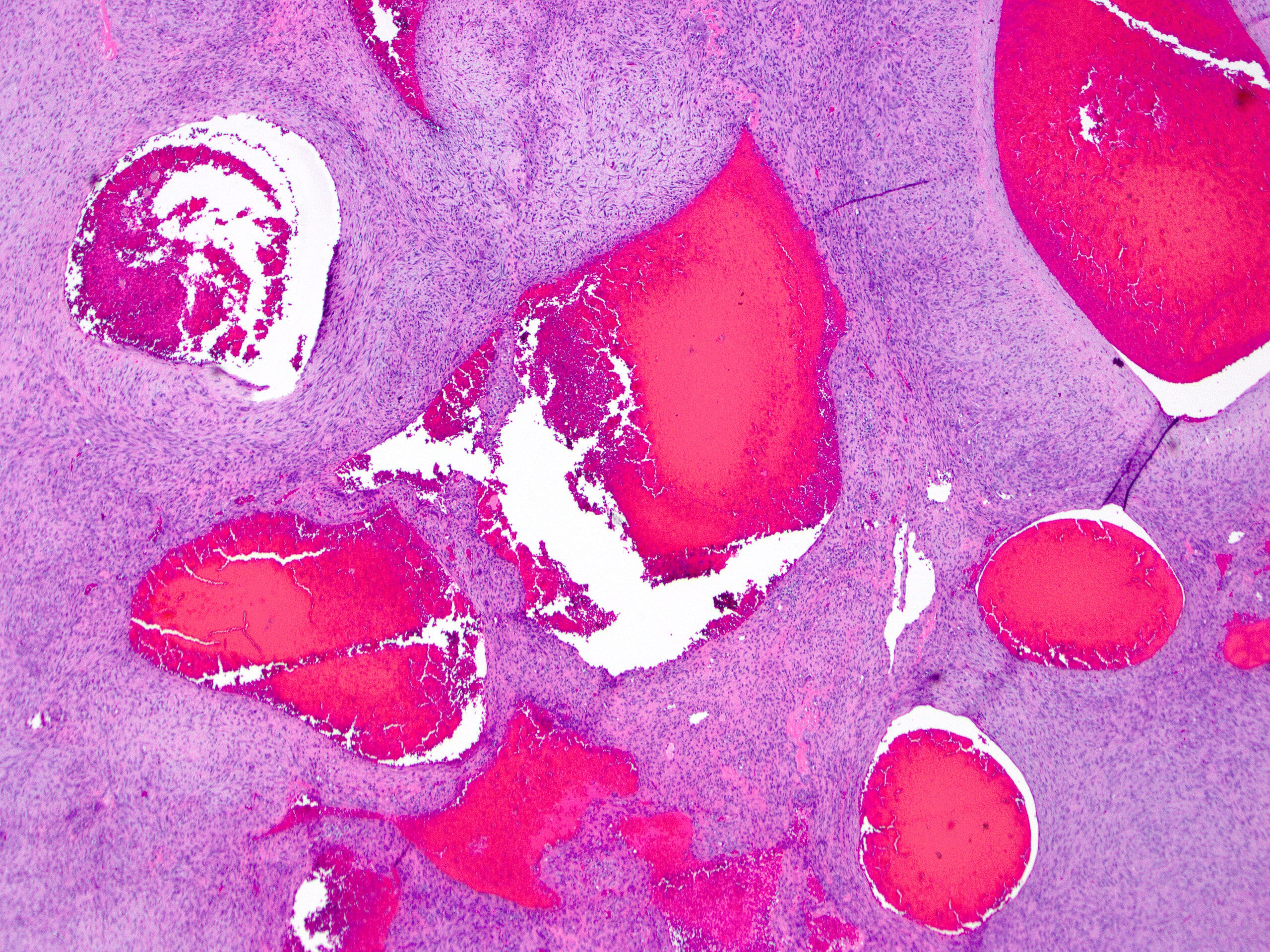
Blood filled cysts
Reticulated chondroid-like material
Cyst wall and giant cells
Aneurysmal bone cyst
Positive stains
- There is no specific immunohistochemical stain for aneurysmal bone cyst
Molecular / cytogenetics description
- Abnormalities of 17p13.2 locus in 63% (Mod Pathol 2004;17:518)
- Fusion of USP6 with:
- CDH11 (most frequent, approximately 30%), TRAP150 (THRAP3), ZNF9 (CNBP), OMD, COL1A1, RUNX2, PAFAH1B1, CTNNB1, SEC31A, E1F1, FOSL2, STAT3, USP9X, ASAP1, FAT1, SAR1A, TNC (Genes Chromosomes Cancer 2017;56:266, Genes Chromosomes Cancer 2019;58:589, Genes Chromosomes Cancer 2020;59:357)
- Fusion of USP6 with:
- Rare case report of unusually aggressive aneurysmal bone cyst with RUNX2-USP6 fusion (Cancer Genet 2017;212:13)
- Rearrangement of USP6 gene can be detected by FISH or fusion panel analysis by next generation sequencing
- Other neoplasms with USP6 gene rearrangement: (Pathologe 2018;39:191)
- Myositis ossificans
- Nodular fasciitis
Sample pathology report
- Mass, distal metaphysis, left tibia, curettage:
- Aneurysmal bone cyst
Differential diagnosis
- Telangiectatic osteosarcoma:
- The most important differential diagnosis
- Similar architecture but contains anaplastic stromal cells
- Frequent atypical mitoses
- No specific diagnostic immunohistochemical stain
- Lacks USP6 gene rearrangement (Med Pregl 2015;68:127)
- Central giant cell granuloma:
- Involve gnathic bones
- Usually solid with no / minimal cystic component (mimics solid aneurysmal bone cyst)
- Lacks USP6 gene rearrangement (J Oral Maxillofac Pathol 2018;22:173)
- Secondary aneurysmal bone cyst:
- Lacks USP6 gene rearrangement
- Extensive sampling is critical to rule out an underlying primary lesion
- More common in:
- Fibrous dysplasia
- Giant cell tumor of bone
- Chondroblastoma
- Osteoblastoma
- Osteosarcoma (Am J Pathol 2004;165:1773)
Additional references
Board review style question #1
- Which of the following lesions does not have characteristic rearrangement of USP6 gene?
- Giant cell tumor of bone with secondary aneurysmal bone cyst
- Myositis ossificans
- Nodular fasciitis
- Primary aneurysmal bone cyst
Board review style answer #1
A. Secondary aneurysmal bone cyst lacks USP6 gene rearrangement.
Comment Here
Reference: Aneurysmal bone cyst (ABC)
Comment Here
Reference: Aneurysmal bone cyst (ABC)
Board review style question #2
- The H&E photo belongs to a well defined multiloculated cystic lesion of proximal tibia of a 17 year old boy. FISH analysis is positive for USP6 gene rearrangement. Which is the correct diagnosis?
- Aneurysmal bone cyst
- Giant cell tumor of bone
- Telangiectatic osteosarcoma
- Unicameral bone cyst
Board review style answer #2
A. Aneurysmal bone cyst. The H&E shows cystic spaces with stromal giant cells. Rearrangement of USP6 gene confirms the diagnosis in the above clinical and radiographic context.
Comment Here
Reference: Aneurysmal bone cyst (ABC)
Comment Here
Reference: Aneurysmal bone cyst (ABC)
