
Cervix
Mesenchymal / mixed epithelial & mesenchymal tumors
Rhabdomyosarcoma
Authors: Kyle Devins, M.D., Jaclyn Watkins, M.D., M.S.
Editorial Board Member: Carlos Parra-Herran, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 12 October 2021
Last staff update: 25 April 2024
Copyright: 2007-2025, PathologyOutlines.com, Inc.
PubMed Search: Rhabdomyosarcoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Devins K, Watkins J. Rhabdomyosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixrhabdomyosarcoma.html. Accessed April 2nd, 2025.
Definition / general
- Rare sarcoma showing evidence of skeletal muscle differentiation
- Multiple subtypes: embryonal, alveolar and pleomorphic
Essential features
- Most common variant in the gynecologic tract is embryonal, which typically presents as a polypoid vaginal or cervical mass in children and adolescents
- Rhabdomyosarcoma originating in the uterine corpus, fallopian tube or ovary is less common and occurs over a wider age range
- Presence of rhabdomyoblasts, typically expressing MyoD1 or myogenin, is essential for diagnosis
Terminology
- Sarcoma botryoides: refers to the macroscopic appearance of embryonal rhabdomyosarcoma (i.e. polypoid mass resembling a cluster of grapes)
ICD coding
Epidemiology
- Dependent upon subtype and location:
- Embryonal (most common)
- Vagina: most common vaginal cancer in children < 5 years of age
- Uterine cervix: peak incidence 10 - 19 years but may occur in older women
- Uterine corpus: middle aged and older women
- Alveolar, pleomorphic (rare)
- Wide age range, usually older women
- Embryonal (most common)
- References: Int J Gynecol Cancer 2008;18:190, Gynecol Oncol 1988;29:290, Hum Pathol 2018;74:122
Sites
- Most common: cervix and vagina
- Rarely occurs in the uterine corpus, fallopian tube and ovary
Pathophysiology
- DICER1 alterations are identified in 65 - 95% of embryonal rhabdomyosarcomas of the uterine cervix, with ~50% of these patients harboring germline alterations; conversely, most DICER1 alterations in uterine corpus tumors are somatic (Mod Pathol 2020;33:1207, Mod Pathol 2021 May 20 [Epub ahead of print], Am J Surg Pathol 2020;44:738)
- ~80% of alveolar rhabdomyosarcomas demonstrate recurrent fusions involving FOXO1, most commonly t(2;13)(PAX3-FOXO1) or t(1;13)(PAX7-FOXO1) (Cancer Lett 2008;270:10)
Etiology
- Subset of embryonal rhabdomyosarcomas, particularly of the uterine cervix, occur as a component of DICER1 syndrome with germline DICER1 mutations
Clinical features
- Dependent on tumor location and subtype
- Tumors of the vagina, uterine cervix and corpus may present with vaginal bleeding
- Embryonal rhabdomyosarcomas form a polypoid, grape-like cluster in the vagina and uterus which may protrude from the vagina (Am J Obstet Gynecol 1970;107:484, Gynecol Oncol 1988;29:290)
- Pleomorphic and alveolar rhabdomyosarcomas are more likely to form a solitary mass centered in the myometrium, cervical stroma or ovary (Hum Pathol 2018;74:122, Int J Gynecol Pathol 1998;17:113)
Diagnosis
- Based on morphologic features and the identification of rhabdomyoblasts (by morphology or immunohistochemistry)
- Confirmatory genetic testing can be helpful in select cases
- References: Int J Gynecol Cancer 2008;18:190, Gynecol Oncol 1988;29:290, Hum Pathol 2018;74:122
Radiology description
- Embryonal rhabdomyosarcoma appears as a heterogenous mass, with cystic and solid components on ultrasound; CT demonstrates a similar appearance to that seen on ultrasound (Radiographics 1997;17:919)
Radiology images
Images hosted on other servers:


Vaginal embryonal rhabdomyosarcoma
Prognostic factors
- Overall 5 year survival for all subtypes: 68.4% (Arch Gynecol Obstet 2017;296:327)
- Favorable prognostic factors:
- Embryonal histology (Arch Gynecol Obstet 2017;296:327)
- Young age (Arch Gynecol Obstet 2017;296:327)
- Poor prognostic factors:
- Adult age (Am J Surg Pathol 2007;31:382)
- Alveolar rhabdomyosarcomas with proven FOXO1 fusions
- Alveolar rhabdomyosarcomas without FOXO1 fusions have a prognosis similar to embryonal rhabdomyosarcoma (Pediatr Blood Cancer 2016;63:634)
- Pleomorphic subtype (Cancer Med 2018;7:4023)
- Anaplasia in cases of embryonal rhabdomyosarcoma (Am J Surg Pathol 1993;17:443)
Case reports
- 18 month old girl with an abdominal pelvic mass, vaginal bleeding and a protruding mass in the introitus (J Surg Case Rep 2017;2017:rjx080)
- 10 year old girl with a history of cystic nephroma and 3 week history of vaginal bleeding (J Pediatr Adolesc Gynecol 2020;33:173)
- 24 year old woman with a history of cervical embryonal rhabdomyosarcoma and a synchronous ovarian Sertoli-Leydig cell tumor (Gynecol Oncol Rep 2018;25:94)
- 54 year old postmenopausal woman with abdominal pain and vaginal bleeding (Cureus 2020;12:e9841)
Treatment
- Embryonal rhabdomyosarcoma may be treated with a combination of surgery, chemotherapy and radiation therapy (Int J Gynecol Cancer 2008;18:190)
- Limited data in treating adults, nonembryonal subtypes and noncervicovaginal sites in the female genital tract
- Protocols are typically extrapolated from nongynecologic sites and involve a combination of resection (total hysterectomy and bilateral salpingo-oophorectomy) and chemotherapy with or without radiation (Int J Radiat Oncol Biol Phys 2013;86:58)
Clinical images
Images hosted on other servers:

Cervical embryonal
rhabdomyosarcoma
Gross description
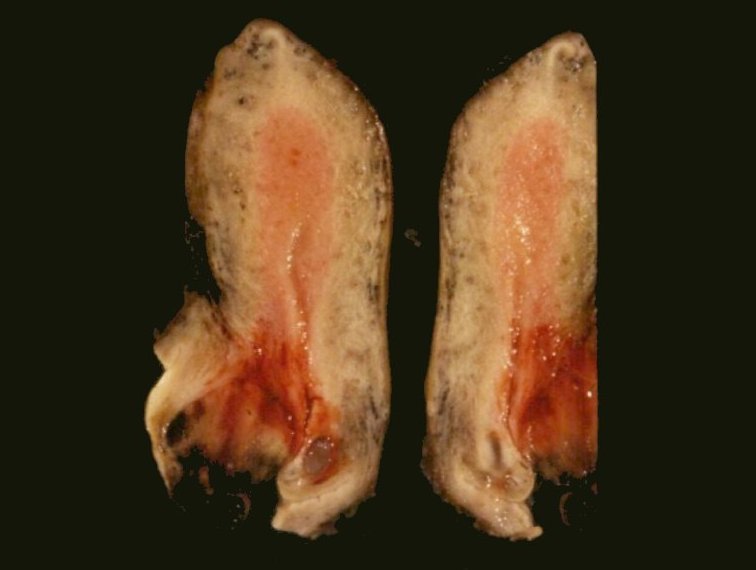
- Botryoid embryonal rhabdomyosarcoma: grape-like polypoid cluster of tan to gray, semitranslucent tissue protruding from the vagina or cervical os
- Uterine rhabdomyosarcoma: myometrially centered tumors with tan-white, fleshy cut surface with hemorrhage and necrosis
- References: Am J Obstet Gynecol 1970;107:484, Gynecol Oncol 1988;29:290
Gross images
Images hosted on other servers:
Gray surface and areas of hemorrhage
Microscopic (histologic) description
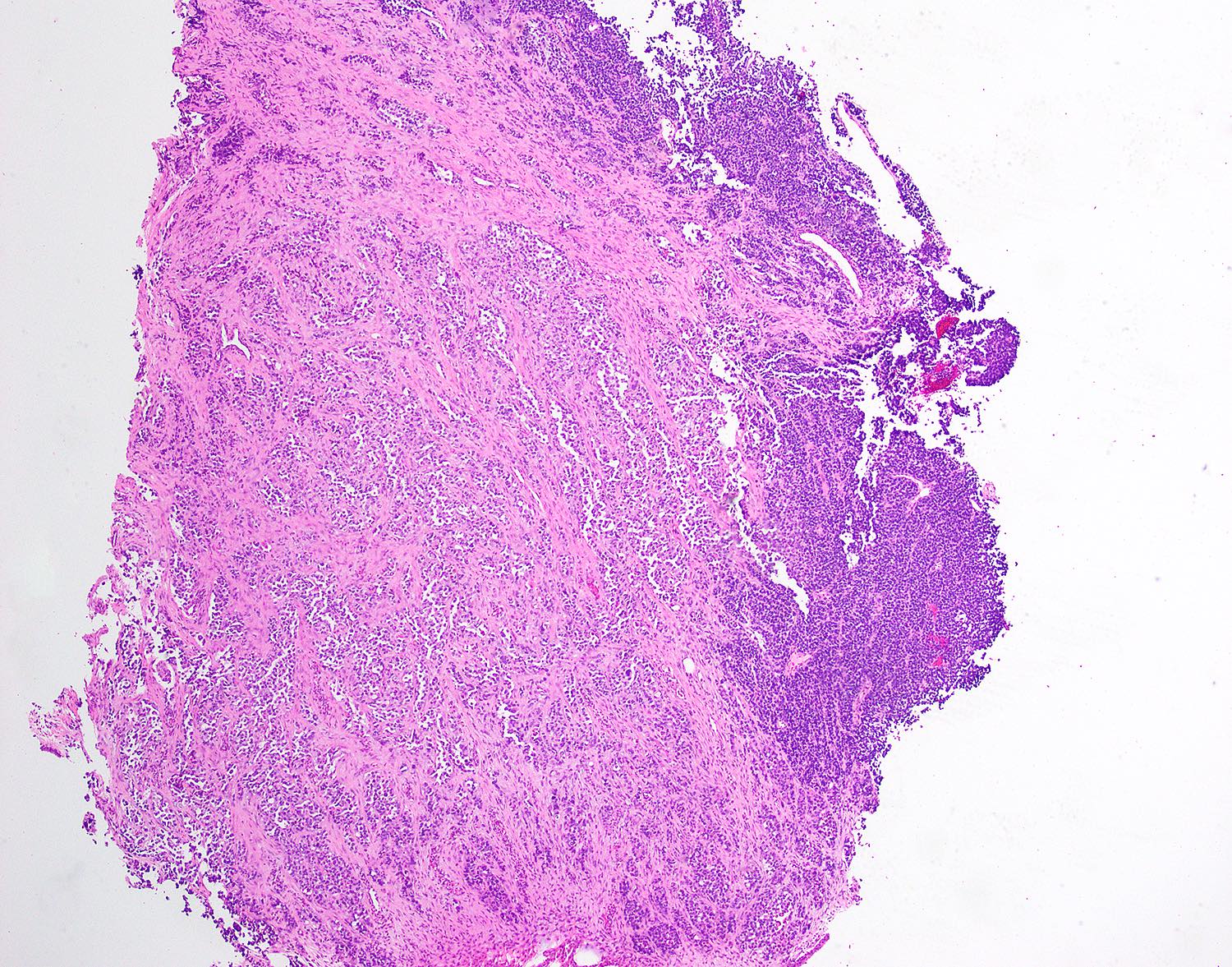
- Embryonal rhabdomyosarcoma (Gynecol Oncol 1988;29:290, Mod Pathol 2012;25:602, Mod Pathol 2021 May 20 [Epub ahead of print])
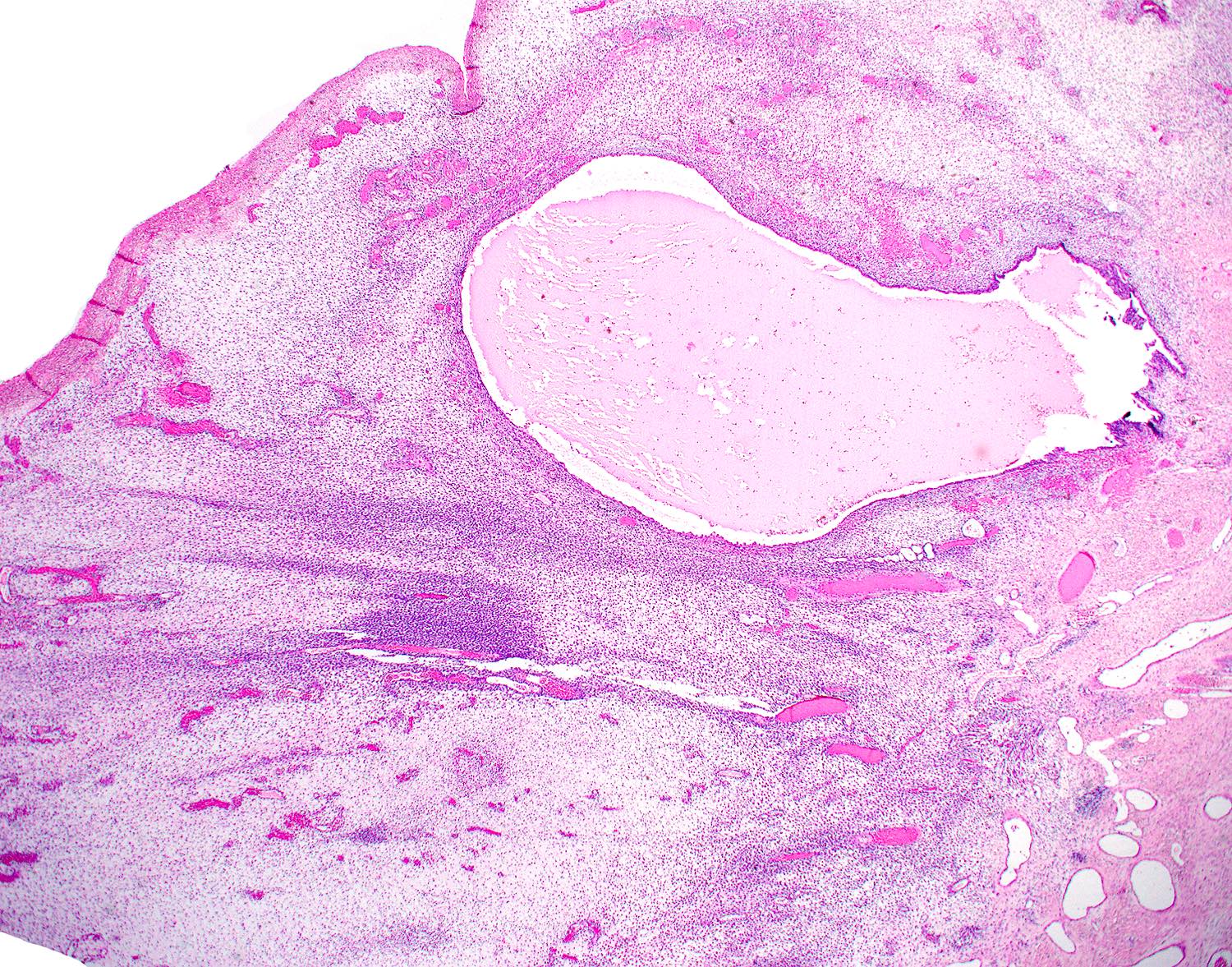
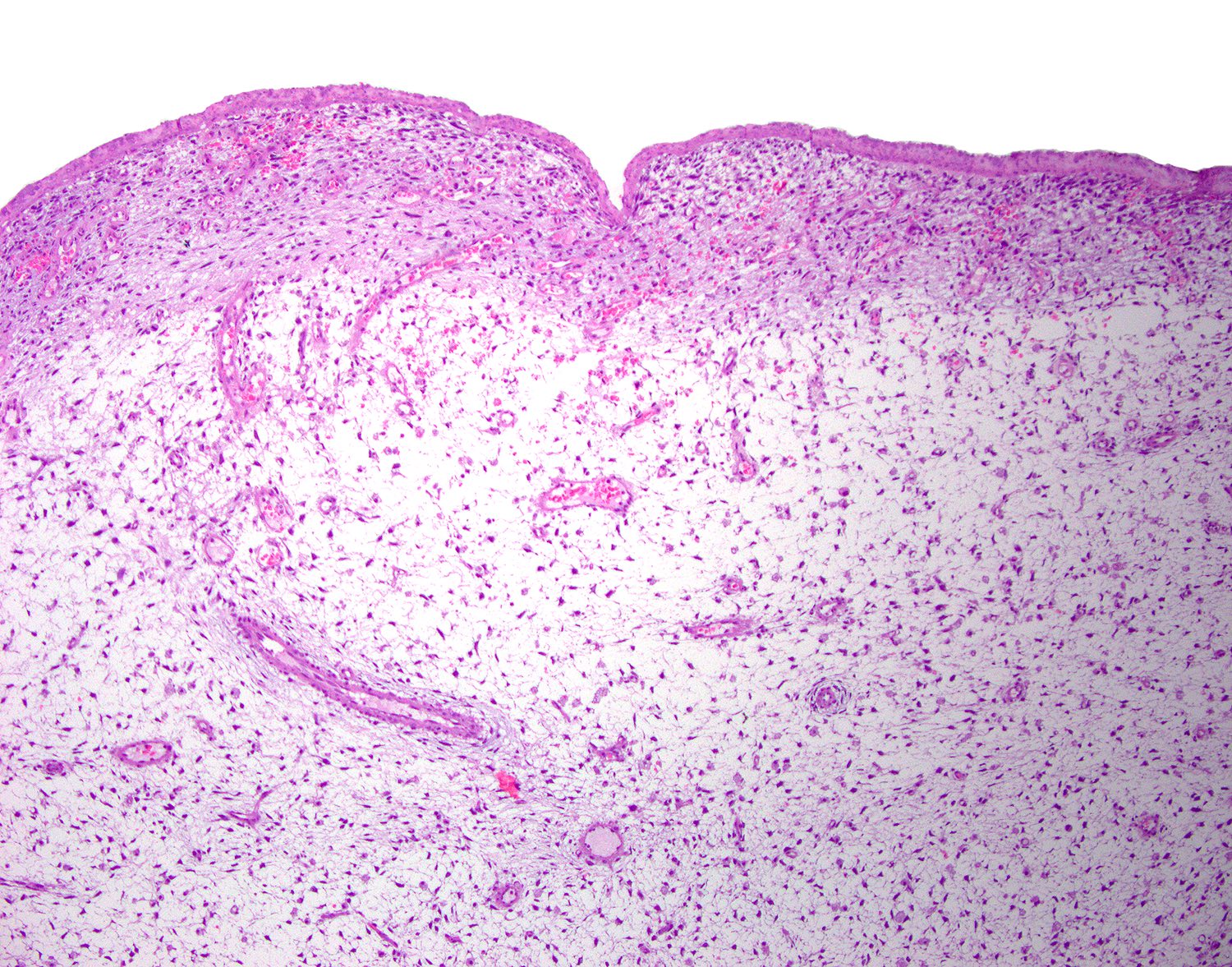
- Alternating hypercellular areas and hypocellular areas with myxoid / edematous (more common) or collagenous (less common) stroma
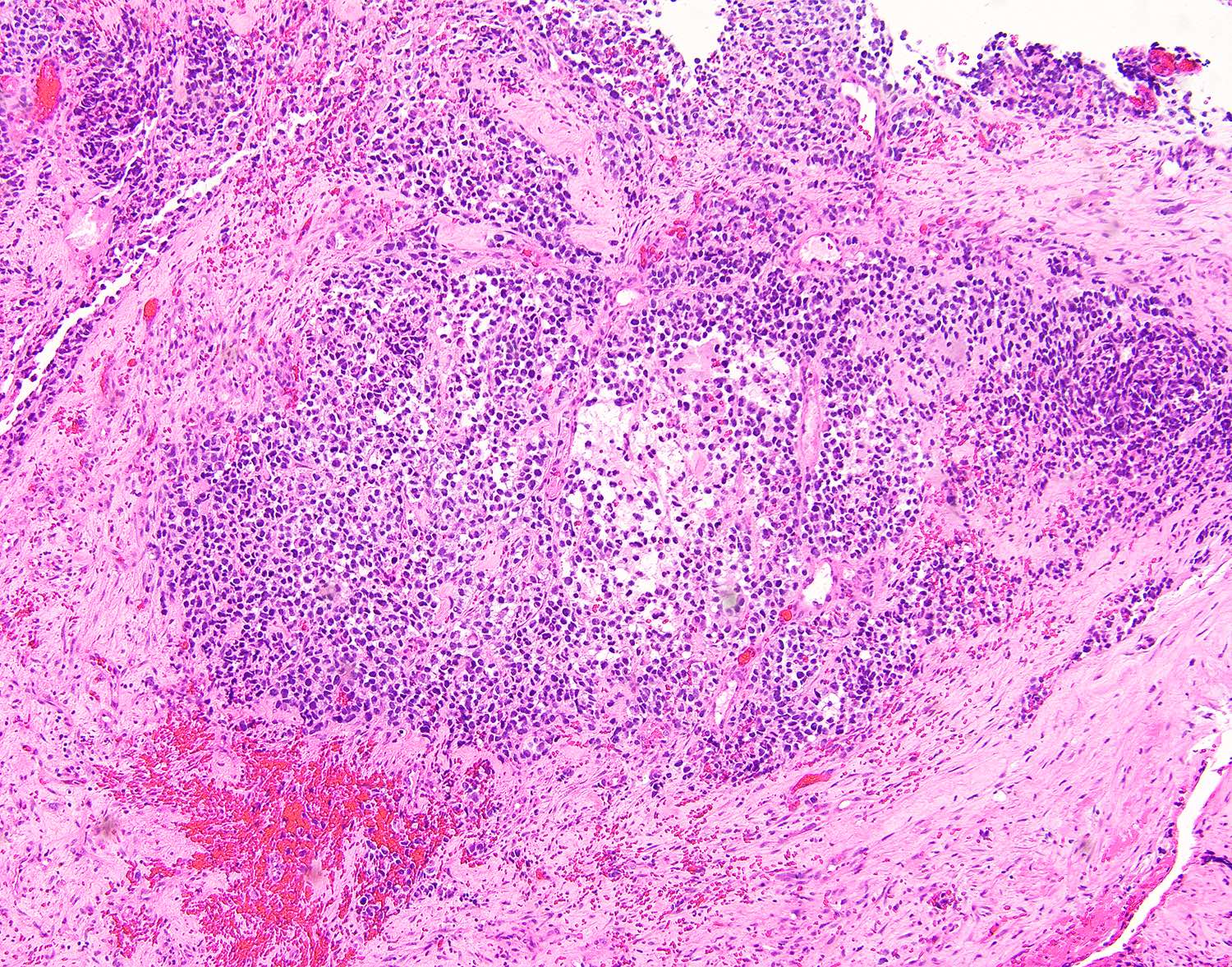
- Densely cellular subepithelial zone (cambium layer) composed of primitive, small cells with hyperchromatic nuclei and mitotic activity
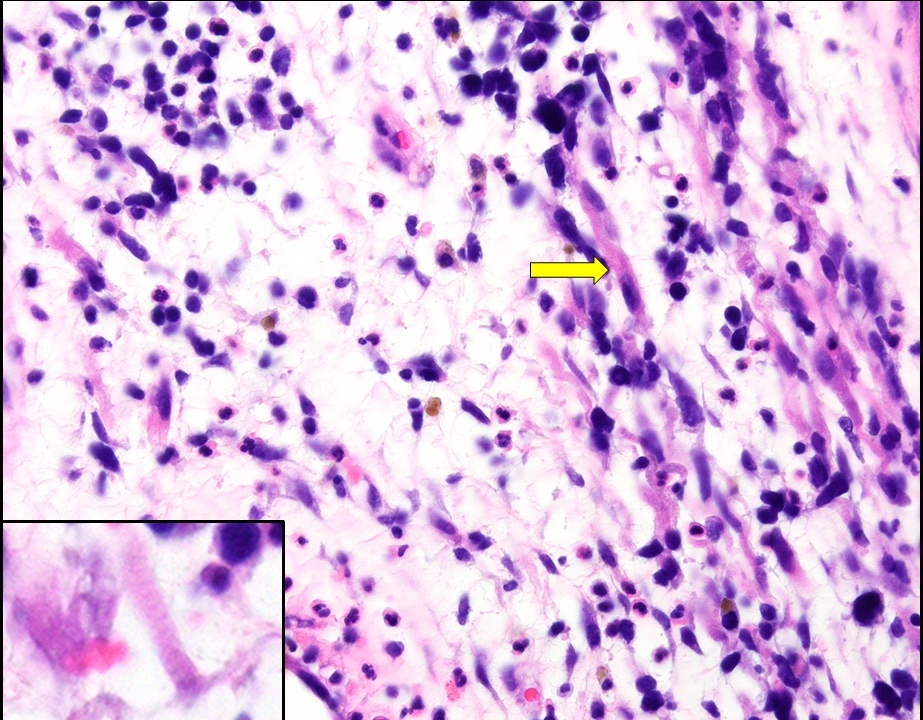
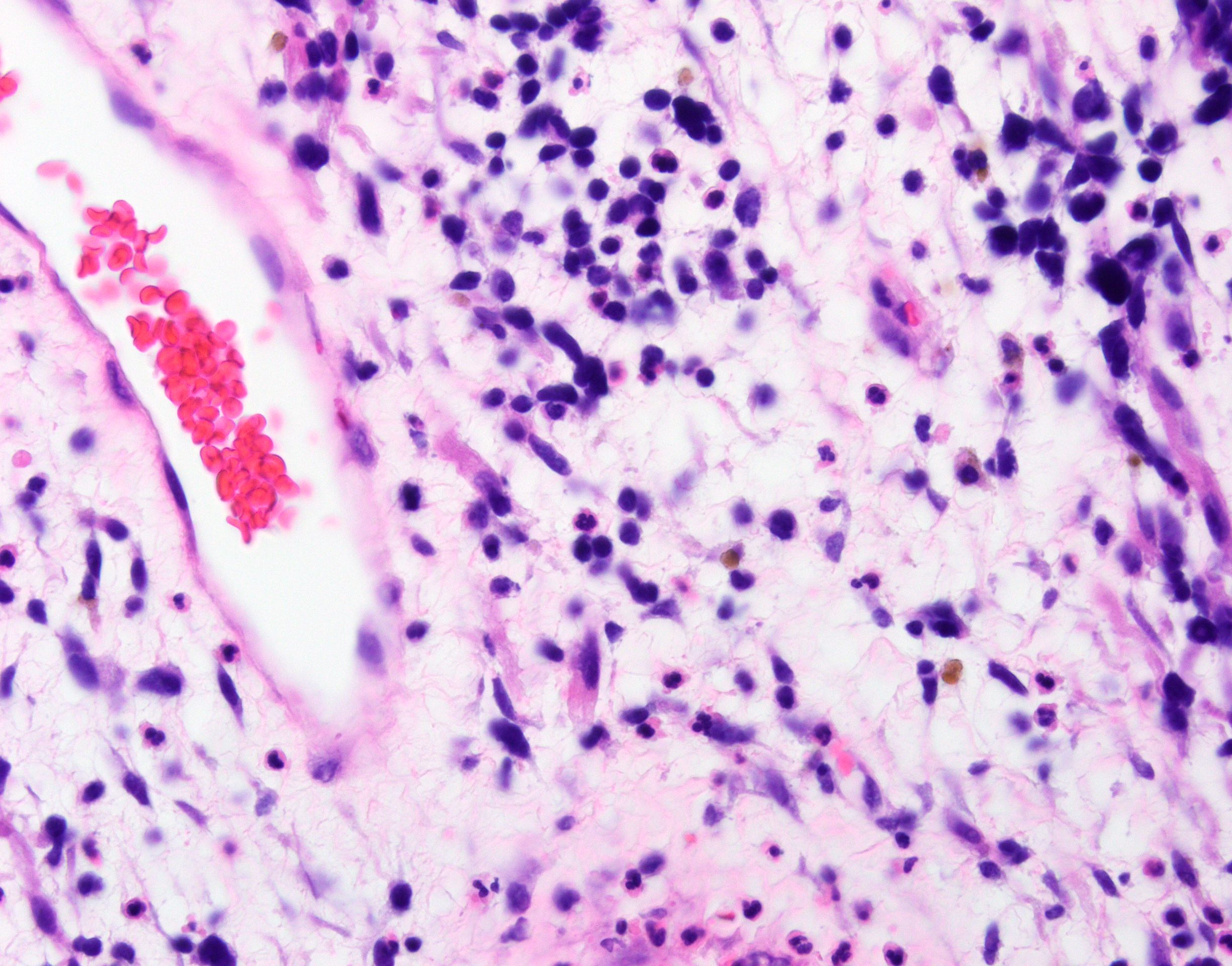
- Rhabdomyoblasts typically seen in hypocellular foci
- Eccentric, dense eosinophilic cytoplasm
- Elongated strap cells (bipolar) or tadpole cells (unipolar) with eosinophilic cytoplasm and cross striations
- Hyaline or fetal type cartilage in ~50% of cases
- Alveolar rhabdomyosarcoma (Hum Pathol 2018;74:122)
- Nests and sheets of primitive small round cells with abundant eosinophilic cytoplasm
- Noncohesive cells floating in empty spaces create characteristic alveolar pattern
- Pleomorphic rhabdomyosarcoma (Hum Pathol 2018;74:122, Int J Gynecol Pathol 2010;29:122)
- Sheet-like growth of pleomorphic round to spindled cells
- Scattered large rhabdomyoblasts
Microscopic (histologic) images
Contributed by Kyle Devins, M.D.
Edematous stroma
Cambium layer
Rhabdomyoblasts
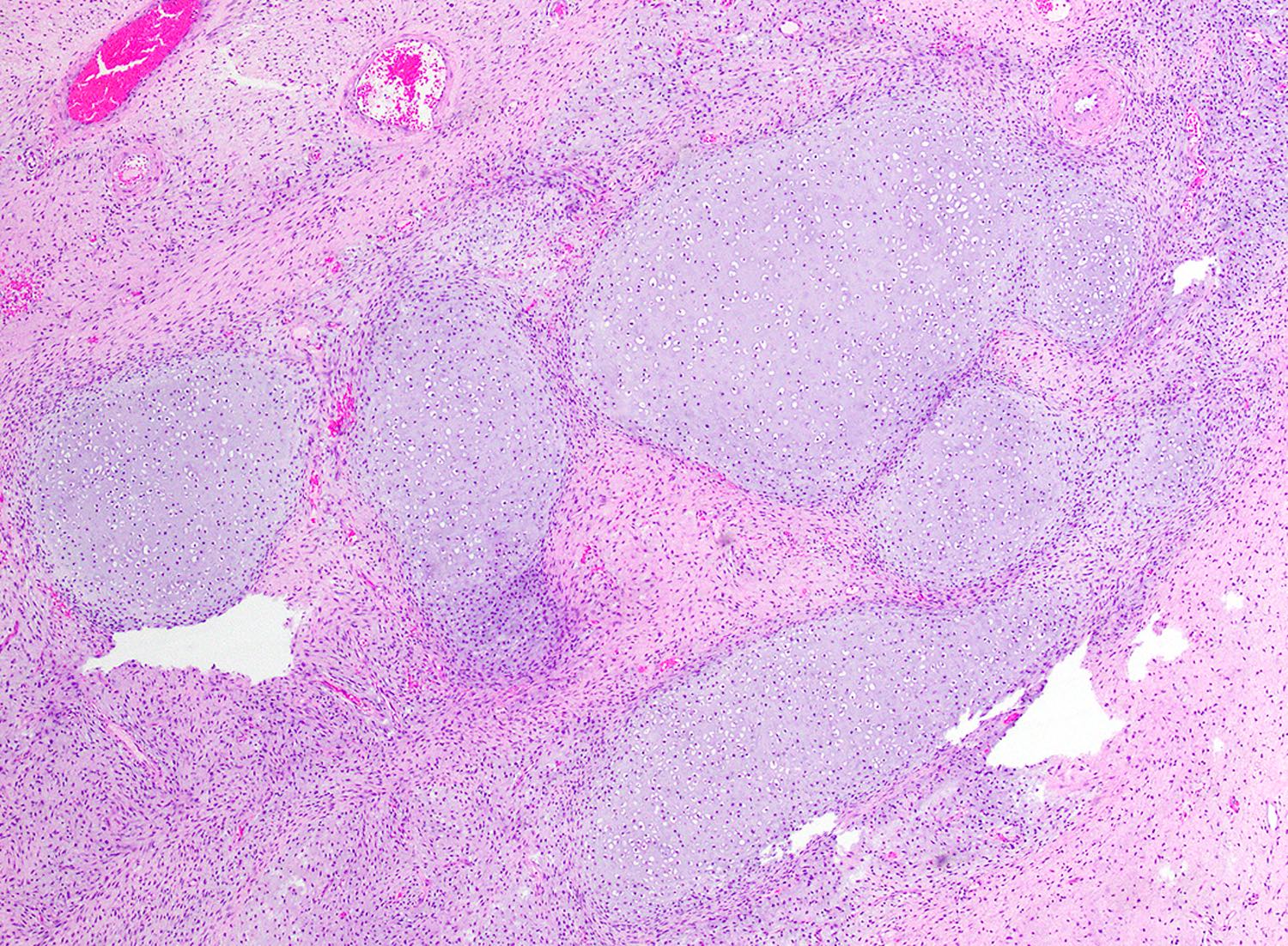
Hyaline cartilage
Nests, sheets and alveolar spaces
Alveolar spaces
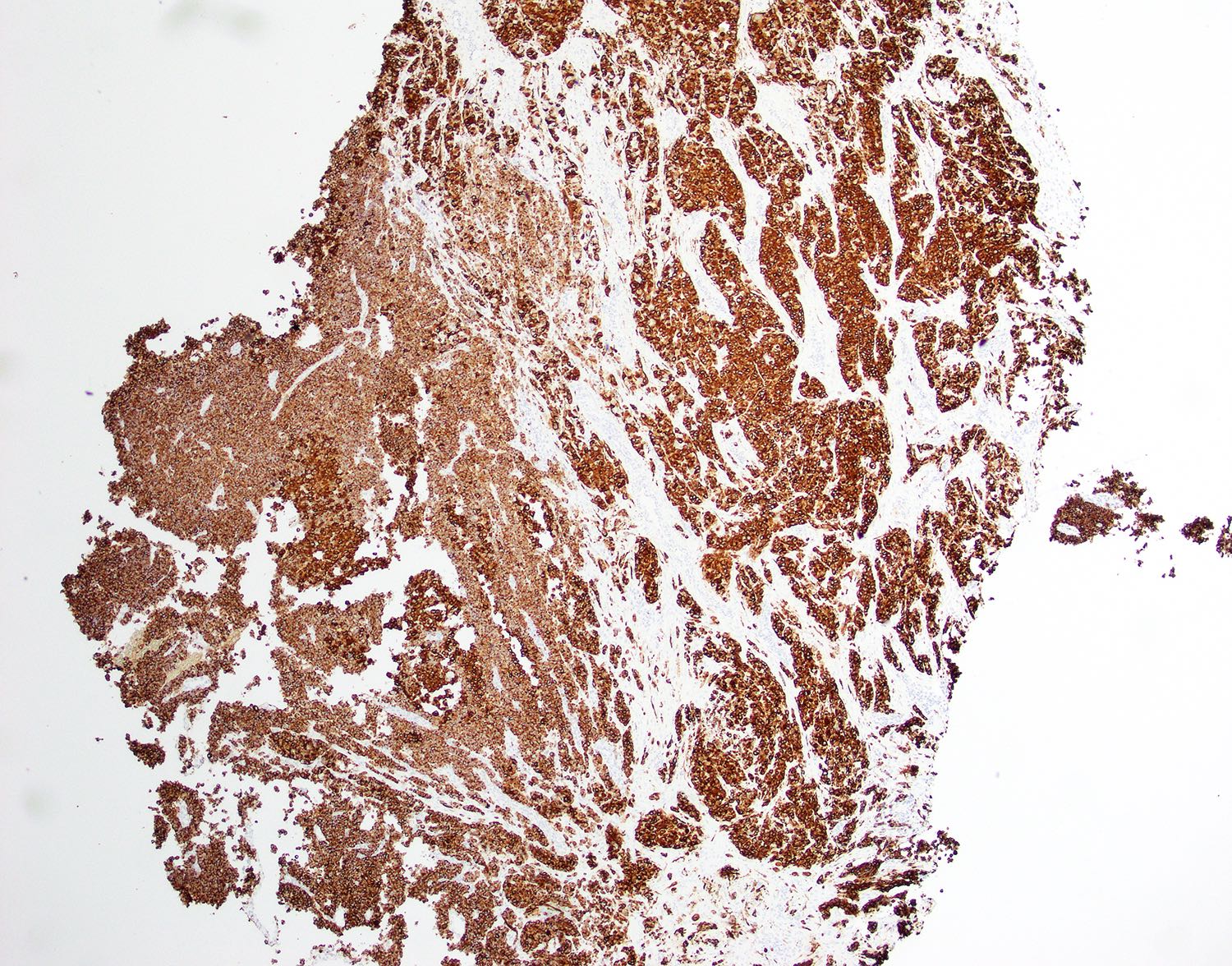
Desmin
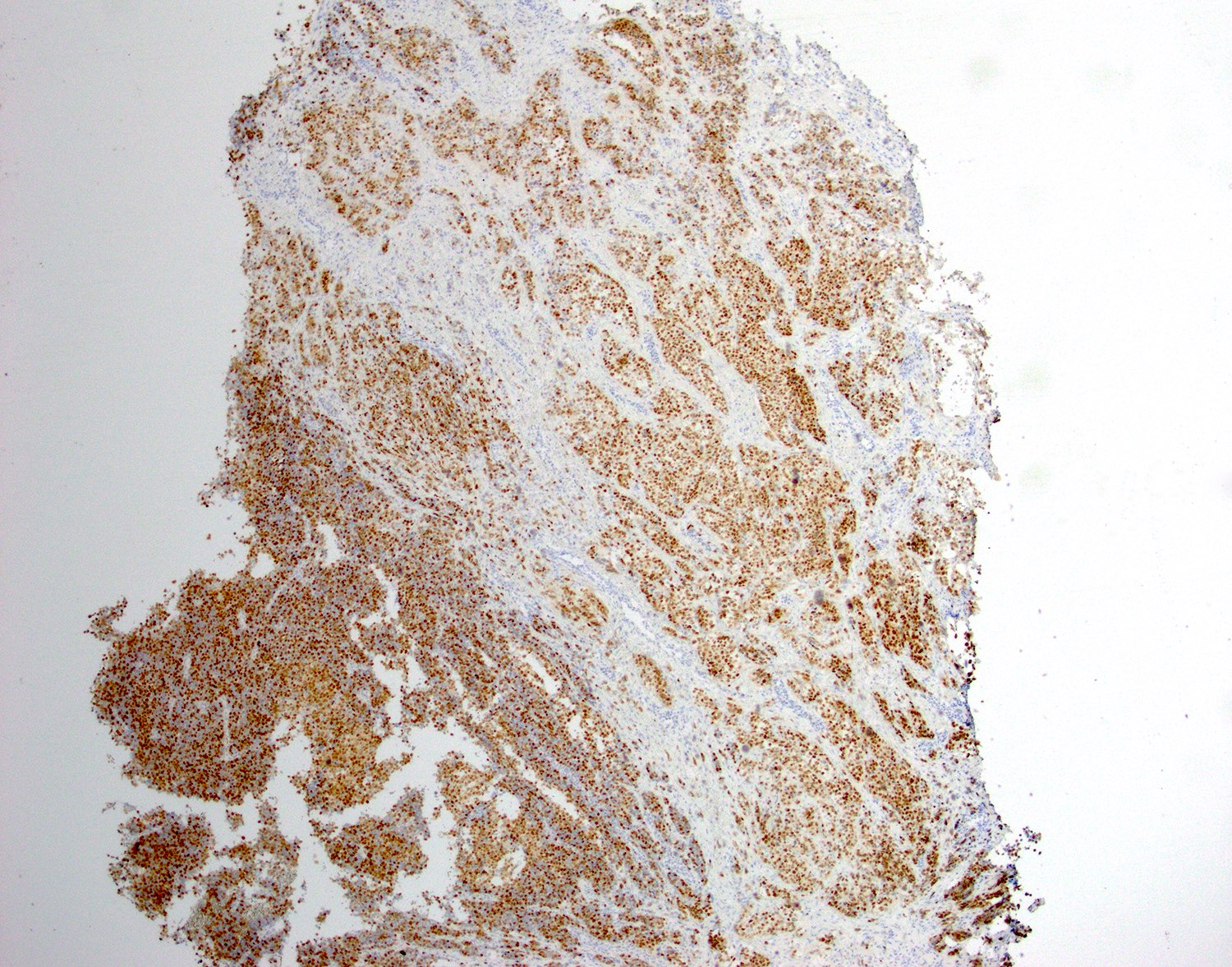
Myogenin
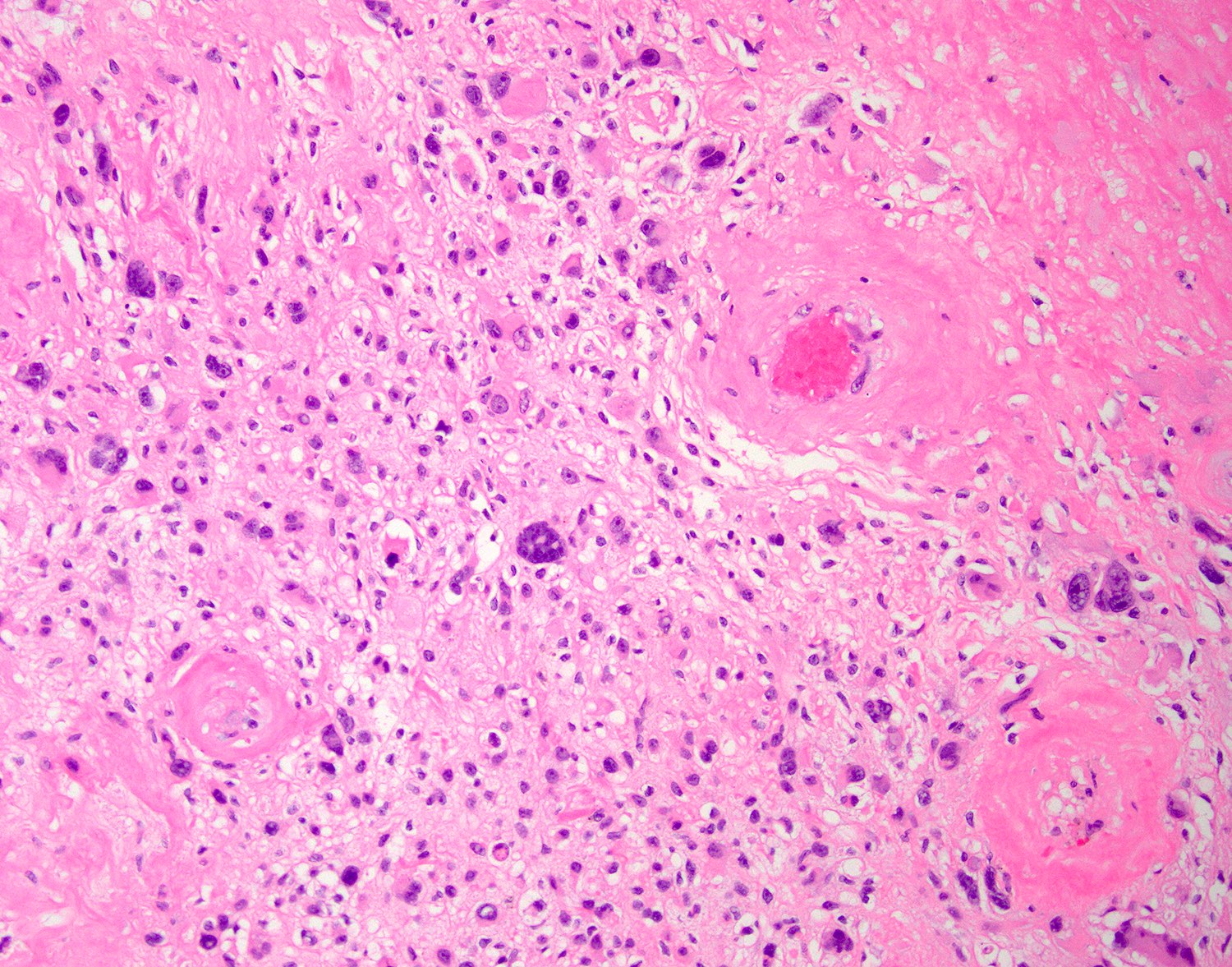
Nuclear pleomorphism
Virtual slides
Images hosted on other servers:

Embryonal rhabdomyosarcoma
Cytology description
- Clusters of atypical hyperchromatic round to ovoid cells (Diagn Pathol 2016;11:3)
- Occasional characteristic unipolar tadpole cells
Cytology images
Images hosted on other servers:

Brushing of
uterine embryonal
rhabdomyosarcoma
Positive stains
- Desmin: diffusely positive in all subtypes
- Myogenin and MyoD1
- High sensitivity and specificity
- Diffuse nuclear staining in alveolar and pleomorphic subtypes
- Typically focal in embryonal
- Myoglobin: less sensitive than myogenin and MyoD1
- Also positive in mature tumors (rhabdomyoma)
- Reference: Am J Surg Pathol 2001;25:1150
Negative stains
- Keratins (rarely may be positive)
- S100
- CD34
- Reference: Am J Surg Pathol 2001;25:1150
Molecular / cytogenetics description
- Embryonal rhabdomyosarcoma
- DICER1 alterations are identified in 65 - 95% of embryonal rhabdomyosarcomas of the uterine cervix, with ~50% of these patients harboring germline alterations; conversely, most DICER1 alterations in uterine corpus tumors are somatic (Mod Pathol 2020;33:1207, Mod Pathol 2021 May 20 [Epub ahead of print], Am J Surg Pathol 2020;44:738)
- Alveolar rhabdomyosarcoma
- Recurrent fusions of FOXO1 gene in ~80%, most commonly t(2;13)(PAX3-FOXO1) or t(1;13)(PAX7-FOXO1) (Cancer Lett 2008;270:10)
- Pleomorphic rhabdomyosarcoma
- Often complex karyotype without consistent genetic abnormality (Cancer Genet Cytogenet 2003;140:73)
Sample pathology report
- Cervix, polypectomy:
- Embryonal rhabdomyosarcoma (see comment)
- Comment: The tumor demonstrates polypoid fragments with myxoid / edematous stroma and scattered aggregates of primitive cells. Clusters of differentiating rhabdomyoblasts with focal cross striations are seen, which are highlighted by an immunohistochemical stain for desmin. There is also focal positivity for myogenin and myoD1, supporting the above diagnosis.
Differential diagnosis
- Müllerian adenosarcoma:
- Most important differential consideration for botryoid embryonal rhabdomyosarcoma due to polypoid architecture and consolidation of stroma underneath epithelium
- Typically shows more abundant epithelial elements with phyllodes-like architecture
- Stromal overgrowth may make epithelial component difficult to identify but extensive sampling often reveals areas of classic adenosarcoma
- Fibroepithelial polyp, especially those with atypical cells:
- Malignant mixed Müllerian tumor (MMMT) with rhabdomyoblastic differentiation:
- Extensive sampling typically reveals the malignant epithelial component
- Undifferentiated endometrial carcinoma / undifferentiated uterine sarcoma:
- Uterine tumor resembling ovarian sex cord tumor:
- ESR1-NCOA2 fusions can show rhabdoid morphology (Am J Surg Pathol 2020;44:1563)
- Sex cord-like morphology may provide clue to diagnosis (corded, retiform, trabeculated)
- SMARCA4 deficient uterine sarcoma:
- Rhabdomyoma:
- Lacks cambium layer and primitive small cells
Additional references
Board review style question #1
Which of the following is true about the pictured tumor?
- Benign entity with minimal chance of recurrence
- Most common presentation is a polypoid mass in the cervix or vagina of children and adolescents
- Most often occurs in the uterus of adult women
- Immunohistochemistry is unhelpful in establishing the correct diagnosis
Board review style answer #1
B. Most common presentation is a polypoid mass in the cervix or vagina of children and adolescents
Comment Here
Reference: Rhabdomyosarcoma
Comment Here
Reference: Rhabdomyosarcoma
Board review style question #2
Which of the following features are associated with poor prognosis in gynecologic rhabdomyosarcoma?
- Age < 10 years at diagnosis
- Embryonal histology
- FOXO1 gene fusion
- Somatic DICER1 mutation
Board review style answer #2
