

Uterus
Carcinoma
Clear cell carcinoma
Editorial Board Member: Jennifer A. Bennett, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 21 April 2020
Last staff update: 9 March 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed search: Clear cell carcinoma uterus


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Huvila J, Gilks CB. Clear cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/uterusclearcell.html. Accessed December 22nd, 2024.
Definition / general
- Tumor of postmenopausal patients that histologically resembles ovarian clear cell carcinoma with clear, oxyphil or hobnail cells
Essential features
- Diagnosed based on characteristic morphology
- Solid architecture more common than papillary
- HNF-1B, napsin A and AMACR positive
- Can be any of the 4 molecular subtypes of endometrial carcinoma but most common is no specific molecular profile (p53, mismatch repair and POLE wild type, estrogen receptor negative)
Terminology
- Also called clear cell adenocarcinoma
ICD coding
Epidemiology
- < 5% of all endometrial carcinomas (Am J Cancer Res 2013;3:70, J Pathol 2017;243:230, Int J Gynecol Cancer 2017;27:1714)
- Usually older, postmenopausal women (Int J Gynecol Cancer 2017;27:1714)
- Rarely associated with Lynch syndrome (Int J Gynecol Pathol 2019;38:S40)
Sites
- Uterus
Pathophysiology
- Heterogeneity of molecular pathogenesis (Histopathology 2015;66:664)
- All 4 molecular subtypes can be seen (p53 abnormal, mismatch repair deficient, POLE mutant and no specific molecular profile) (Histopathology 2015;66:664)
- p53 abnormal (serous-like) are aggressive, similar to other p53 abnormal endometrial carcinomas (Histopathology 2015;66:664)
- Mismatch repair deficient often shows mixed morphology, with clear cell and endometrioid components (J Natl Cancer Inst 2016;108:djv427)
- Only no specific molecular profile (p53, POLE and mismatch repair wild type) fit the classic clinical profile of clear cell carcinoma
Etiology
- Unknown
Clinical features
- Postmenopausal bleeding
- High grade carcinoma confined to the uterus in the majority of cases (Int J Gynecol Cancer 2017;27:1714)
- Associated with an increased risk for thromboembolic events (Int J Gynecol Cancer 2017;27:1714, Am J Cancer Res 2013;3:70)
Diagnosis
- Diagnosis is based on characteristic findings on an endometrial biopsy or curettage, which is typically performed for postmenopausal bleeding
- Abdominal and pelvic imaging can be performed for the purpose of clinical staging
Prognostic factors
- Age and stage are important prognostic factors (Am J Cancer Res 2013;3:70)
- p53 abnormal has worse prognosis (Int J Gynecol Pathol 2019;38:S40)
- Mismatch repair deficient and POLE mutant have more favorable prognosis (J Pathol 2017;243:230)
Case reports
- 66 year old woman with clear cell carcinoma present in endometrial polyps (J Menopausal Med 2016;22:122)
- 73 year old woman with tumor arising from adenomyosis (Int J Gynecol Pathol 2009;28:262)
Treatment
- Total hysterectomy and bilateral salpingo-oophorectomy
- Radiation therapy may be considered
Clinical images
Images hosted on other servers:
Endometrial mass
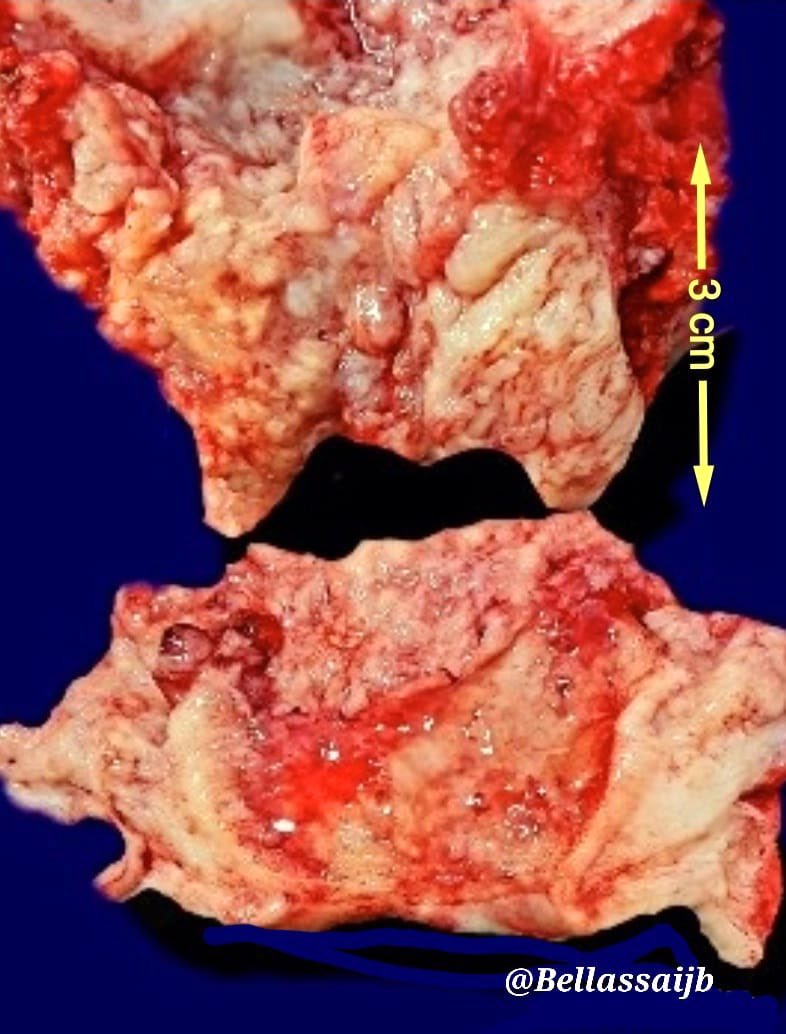
Gross images

Microscopic (histologic) description
- Diagnosis should be based on the presence of prototypical morphologic (both architectural and cytological) features (Int J Gynecol Pathol 2019;38:S40)
- Cytological features (Am J Cancer Res 2013;3:70, Int J Gynecol Pathol 2019;38:S40)
- Polygonal cells with moderate to abundant clear or eosinophilic cytoplasm
- Hobnail cells and flat cells
- Occasional enlarged irregular nucleoli
- Variable cytological atypia
- Relatively low mitotic index
- High mitotic index or pleomorphic nuclei does not rule out clear cell carcinoma in an otherwise typical tumor
- Occasionally targetoid bodies, eosinophilic globules or psammoma bodies
- Architectural features (Am J Cancer Res 2013;3:70, Int J Gynecol Pathol 2019;38:S40)
- Solid, glandular or papillary architecture or a combination of these
- Stromal hyalinization (uncommon)
- No diffuse nuclear stratification in the papillary areas or diffuse columnar cell changes
Microscopic (histologic) images
Contributed by Jutta Huvila, M.D.
Solid architecture
Glandular architecture
Glandular pattern
Papillary and glandular architecture
Papillary architecture
Hyalinized stroma
Clear cell cytology
Clear and hobnail cells
Oxyphilic cells
Clear and hobnail cells
Targetoid bodies
Psammoma bodies
ER
Napsin A
MSH6
Positive stains
- HNF-1B (67 - 100%) (Histopathology 2015;66:664, Hum Pathol 2007;38:1074)
- Napsin A (56 - 93%) (Am J Surg Pathol 2014;38:189, Int J Gynecol Pathol 2018;37:388)
- AMACR (75 - 88%) (Hum Pathol 2013;44:2814, Hum Pathol 2019;92:10)
- Mismatch repair (MMR) expression (PMS2, MSH2, MSH6, MLH1) is intact in 80 - 90% (J Pathol 2017;243:230, Histopathology 2020;76:336)
- CK7
- p53 (wild type pattern in 67% of cases) (Int J Gynecol Pathol 2019;38:S40, Histopathology 2015;66:664)
Negative stains
- Estrogen receptor, progesterone receptor (most cases negative) (Histopathology 2015;66:664, Int J Gynecol Pathol 2018;37:388)
- CD10 usually negative (Arch Pathol Lab Med 2015;139:39)
Molecular / cytogenetics description
- ~50% are related to p53 abnormal, mismatch repair deficient or POLE mutant
- Remaining cases show occasional KRAS or PIK3CA mutations, without PTEN or TP53 abnormalities (Hum Pathol 2019;92:10)
Sample pathology report
- Endometrium, biopsy:
- Clear cell carcinoma of the endometrium (MMR intact, p53 wild type) (see comment)
- Comment: There is intact expression of mismatch repair proteins (PMS2 and MSH6) and wild type expression of p53, i.e. staining of variable intensity in < 80% of tumor cell nuclei.
Differential diagnosis
- Clear cell carcinoma of ovarian origin:
- Endometrial involvement is presumptive evidence of endometrial primary site
- Endometrial serous carcinoma (Am J Surg Pathol 2013;37:874):
- If p53 abnormal, then serous carcinoma unless completely typical clear cell carcinoma morphology
- Endometrioid endometrial carcinoma with clear cell or secretory change:
- Low grade nuclear features, associated atypical hyperplasia, estrogen receptor positive (strong, diffuse)
- Arias-Stella reaction:
- Younger age, associated pregnancy / progesterone treatment
- Normal glandular architecture
- Low Ki67 labeling index
- Clear cell carcinoma of cervical origin:
- Distinction is based on tumor site; no morphological distinguishing features
- Metastatic renal cell carcinoma, clear cell type:
- History of renal cell carcinoma
- Usually CK7, estrogen receptor and progesterone receptor negative (Arch Pathol Lab Med 2015;139:39)
- Usually positive for CD10 and HNF-1B (Arch Pathol Lab Med 2015;139:39)
Board review style question #1
Which of the following is true about clear cell carcinoma of the endometrium (shown in the image)?
- It is associated with a favorable prognosis
- It is associated with high levels of estrogen exposure (endogenous or exogenous)
- There is molecular heterogeneity
- There is no association with Lynch syndrome
Board review style answer #1
C. There is molecular heterogeneity. Clear cell carcinomas of the endometrium can be associated with mutations in POLE (in which case they have a very favorable prognosis), mismatch repair deficiency (which may be a result of Lynch syndrome), mutations in TP53 (poor prognosis) or none of the above.
Comment Here
Reference: Clear cell carcinoma
Comment Here
Reference: Clear cell carcinoma
Board review style question #2
The immunoprofile of most endometrial clear cell carcinomas includes
- Immunonegativity for AMACR
- Immunopositivity for progesterone receptor
- Immunoreactivity for Napsin A
- Mutant pattern staining for p53
Board review style answer #2
C. Immunoreactivity for napsin A. The immunophenotype of a majority of endometrial clear cell carcinomas is positivity for napsin A and AMACR, negativity for progesterone receptor and wild type staining pattern for p53.
Comment Here
Reference: Clear cell carcinoma
Comment Here
Reference: Clear cell carcinoma

