

Uterus
Nontumor
Adenomyosis / adenomyoma
Author: Irem Onur, M.D.
Editorial Board Member: Ayse Ayhan, M.D., Ph.D.

Last author update: 1 October 2016
Last staff update: 20 February 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Uterine adenomyosis


Table of Contents
Definition / general | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Differential diagnosis | Additional referencesCite this page: Onur I. Adenomyosis / adenomyoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/uterusadenomyosis.html. Accessed December 22nd, 2024.
Definition / general
- A nonneoplastic lesion of myometrial tissue characterized by the presence of endometrial glands and stroma within myometrium (Best Pract Res Clin Obstet Gynaecol 2006;20:511)
- Synonyms: myometrial endometriosis, superficial adenomyosis (1 - 2.5 mm in myometrium), stromal adenomyosis, incomplete adenomyosis, adenomyosis with sparse glands
- Usually an incidental finding in hysterectomy specimens (Int J Gynecol Pathol 1996;15:217)
- May be diffuse or focal
- May be involved by hyperplasia and carcinoma
Terminology
- Adenomyoma: A circumscribed nodular aggregate of benign endometrial glands surrounded by endometrial stroma, with leiomyomatous smooth muscle bordering the endometrial stromal component
ICD coding
- ICD-10: N80.0 - endometriosis of uterus
Epidemiology
- Diagnosed mostly in late reproductive years
- Involves 5 - 70% of surgically removed uteri (wide range due to imprecision of diagnostic criteria)
- Rare in postmenopausal women (except for tamoxifen - associated cases)
- Am J Obstet Gynecol 1958;76:1044, Am J Obstet Gynecol 1962;83:1541, Journal of Minimally Invasive Gynecology 2011;18:428
Risk factors: - Increasing age up to menopause, multiparity, smoking, increased serum estrogen levels (Hum Reprod 2001;16:2418, Acta Obstet Gynecol Scand 2004; 83:699, N Engl J Med 2009;360:268)
- Previous uterine surgery (Obstet Gynecol 2004;104:1034)
- Tamoxifen (J Mol Biol 1976;106:683) (These cases tend to show stromal fibrosis, glandular dilation and various metaplastic changes (Histopathology 2000;37:340)
- Matrix metalloproteinase (MMP) polymorphisms (J Genet 2016;95:611)
Sites
- Frequently in posterior, less commonly in anterior uterine wall
- Rarely in cornua or by cervical os
Pathophysiology
- May result from (a) chronic uterine autotraumatization by physiological mechanical functions and (b) tissue injury and repair (Arch Gynecol Obstet 2015;291:917)
- May be caused by disease of junctional zone (Lancet 1995;346:558)
- Prolactin (Am J Obstet Gynecol 1991;165:232) and immune factors may play a role (Hum Reprod Update 1998;4:312)
Etiology
- Adenomyosis and endometriosis are usually regarded as closely related, but
- Microscopic appearance, and probably their pathogenesis, are somewhat different
- They may occur independently of each other
- Adenomyosis mostly is made up of nonfunctional (basal) endometrium and is frequently connected with the mucosa (vs. endometriosis, composed of functional layers)
- Adenomyosis may represents a unique form of endometrial diverticulosis
- Hypothetical mechanisms include (Crum: Diagnostic Gynecologic and Obstetric Pathology, 2nd Edition, 2011)
- Instillation of endometrium within the myometrium
- In situ metaplasia of pluripotent stem cells retained in myometrium or
- Improper partitioning of the endometrium from the myometrium
- Of note, del(7) (q21.2q31.2), a deletion found in typical leiomyoma, has been found in three cases of adenomyosis, suggesting some pathobiologic overlap between leiomyomata and adenomyosis (Cancer Genet Cytogenet 1995;80:118)
- Definitive distinction between these explanations requires further study
Clinical features
- Nonneoplastic condition presenting with palpably enlarged uterus
- Symptoms are nonspecific: dysmenorrhea, menorrhagia, abnormal uterine bleeding, dyspareunia, chronic pelvic pain associated with the menstrual period and infertility (Eur J Obstet Gynecol Reprod Biol 2009;143:103, N Engl J Med 2010;362:2389)
- Associated with deep infiltrating endometriosis, parity, intense dysmenorrhea and increasing age (Eur J Obstet Gynecol Reprod Biol 2014;181:289)
- Tends to regress after menopause (Hum Reprod 2012;27:3432)
- When extensive, it confers a potential risk of infarction and thrombosis and exacerbates menorrhagia via activation of coagulation and fibrinolysis during menstruation (Eur J Obstet Gynecol Reprod Biol 2016;204:99)
Diagnosis
- By histopathologic examination of well oriented hysterectomies
- Essentially should not be diagnosed in curettings or hysteroscopic material
Radiology description
- 2D and 3D transvaginal sonography, sonohysterosalpingography, magnetic resonance imaging and endoscopic techniques (hysteroscopy and laparoscopy) are suggestive (Hum Reprod 2012;27:3432, Eur Rev Med Pharmacol Sci 2015;19:1146)
Prognostic factors
- Benign; excellent prognosis even if not removed
Case reports
- 43 year old pregnant woman with decidualization of uterine adenomyoma (Arch Gynecol Obstet 2015;291:399)
- 49 year old woman with infiltrating adenomyosis of the cervix with features of a low grade stromal sarcoma (Int J Gynecol Pathol 2014;33:253)
- 57 year old woman with endometrioid adenocarcinoma arising from uterine adenomyosis (Case Rep Obstet Gynecol 2014;2014:569295)
- 63 year old woman with adenomyomatous polyp of uterus (Jpn J Clin Oncol 1997;27:350)
- A postmenopausal woman with endometrioid adenocarcinoma arising from uterine adenomyosis (Eur J Gynaecol Oncol 2010;31:719)
Treatment
- Standard management option for women who have completed childbearing is hysterectomy (J Minim Invasive Gynecol 2016;23:164)
- Newer techniques such as laparoscopic radiofrequency thermal ablation are an effective minimally invasive alternative (JSLS 2015 Sep;19:e2015.00071)
- Medical treatment may be considered (Gynecol Endocrinol 2016 Jul 5 [Epub ahead of print])
Gross description
- Often asymmetrically enlarged, globular uterus due to associated myometrial hypertrophy reflected by thickened myometrium (Am J Obstet Gynecol 1962;83:1541, Am J Obstet Gynecol 1962;84:1820)
- Trabeculated cut surface with ill defined hypertrophic swirls of smooth muscle and petechia-like gray foci of endometrium (Am J Obstet Gynecol 1962;83:1541)
- Blood filled cystic spaces may be seen
- Cannot be shelled out
- In elderly women, uterus may appear atrophic
- Mutter: Pathology of the Female Reproductive Tract, 3rd Edition, 2014
Gross images
Contributed by Ayse Ayhan, M.D., Ph.D.
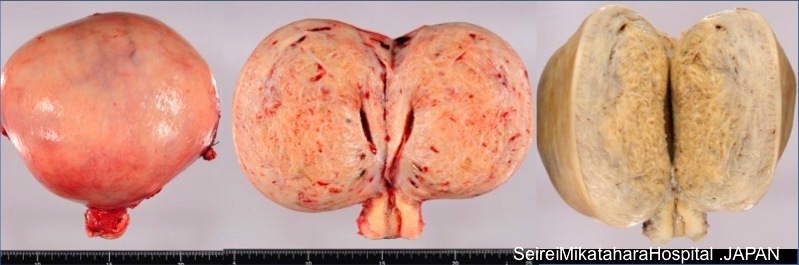
Pre and post-fixed uterus wall

Cut surface of uterus
Images hosted on other servers:

Thickened and spongy myometrium
Microscopic (histologic) description
- Endometrial glands and stroma deep in myometrium
- Depth of penetration of endometrial glands to myometrium is arbitrary
- At least one low power field from endomyometrial junction (which is irregular) or
- 1 to 2.5 mm below basal layer of endometrium
- Or deeper than 25% of overall myometrial thickness
- Often round masses of myometrial smooth muscle proliferation present around endometrial islands
- Glandular tissue usually inactive and of basalis or proliferative type endometrium, but one fourth is functional; hemosiderin is generally absent (Am J Obstet Gynecol 1971;110:275)
- These foci are subject to any disease affecting ortothopic endometrium:
- May show atrophy, metaplasia or decidual change
- May exhibit hyperplasia, atypical hyperplasia / EIN, endometrial carcinoma, endometrial stromal sarcoma, carcinosarcoma (Gynecol Obstet Invest 1999;48:141)
- Microscopic foci may be in vascular spaces resembling endometrial stromal sarcoma (Int J Gynecol Pathol 2010;29:117, Am J Surg Pathol 2013;37:1395, Am J Obstet Gynecol 2012;207:417)
- Stromal adenomyosis (incomplete adenomyosis, adenomyosis with sparse glands) is characterized by lack of glands; it is rare and difficult to diagnose
- References: Robboy: Pathology of the Female Reproductive Tract, 1st Edition, 2001, Reichert: Diagnostic Gynecologic and Obstetric Pathology, 2011, Soslow: Uterine Pathology (Cambridge Illustrated Surgical Pathology), 1st Edition, 2012
Microscopic (histologic) images
Contributed by Ayse Ayhan, M.D., Ph.D.
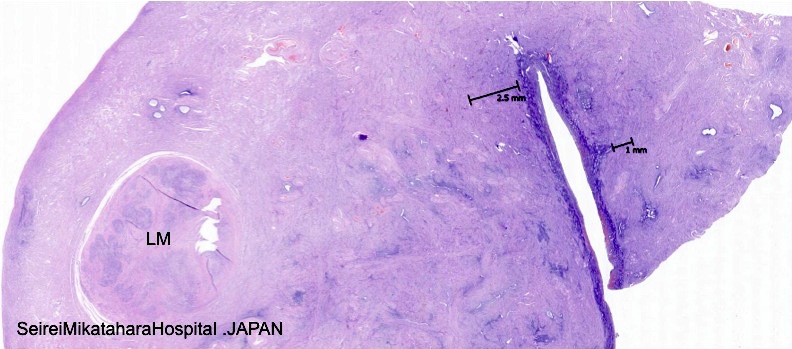
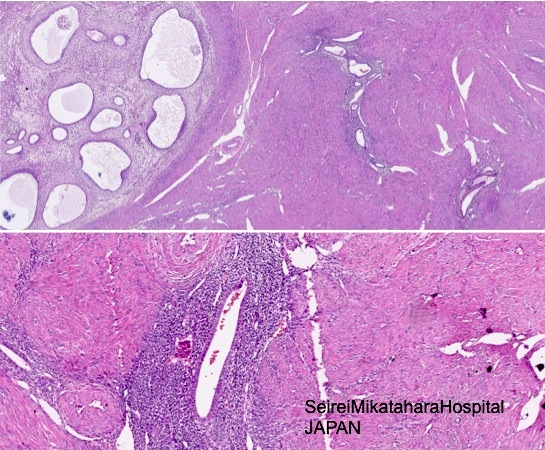
Depth of penetration
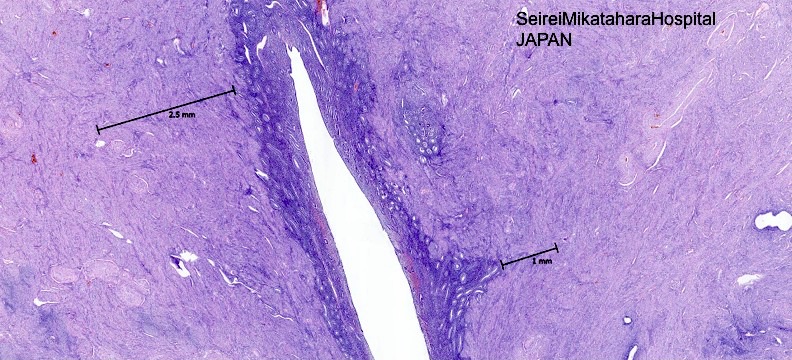
Endomyometrial junction is irregular
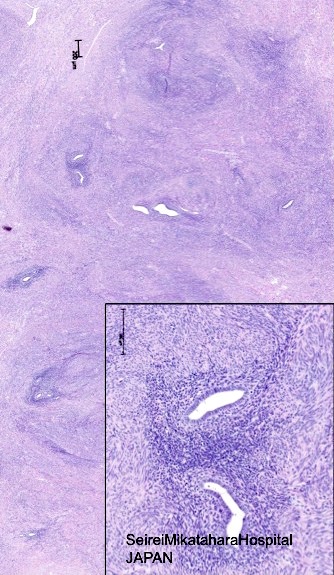
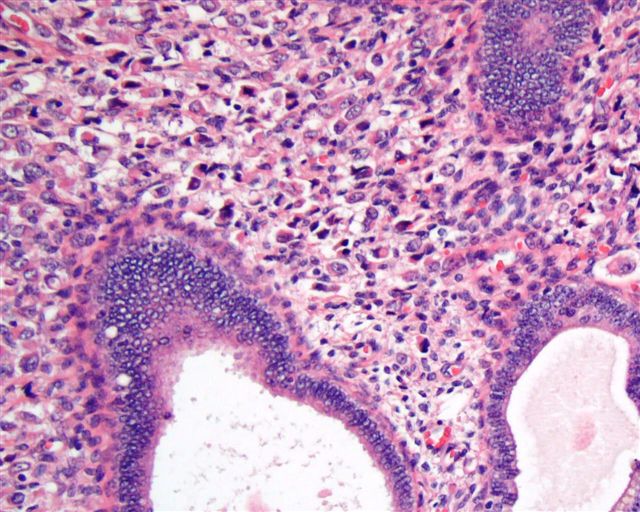
Glandular tissue usually inactive
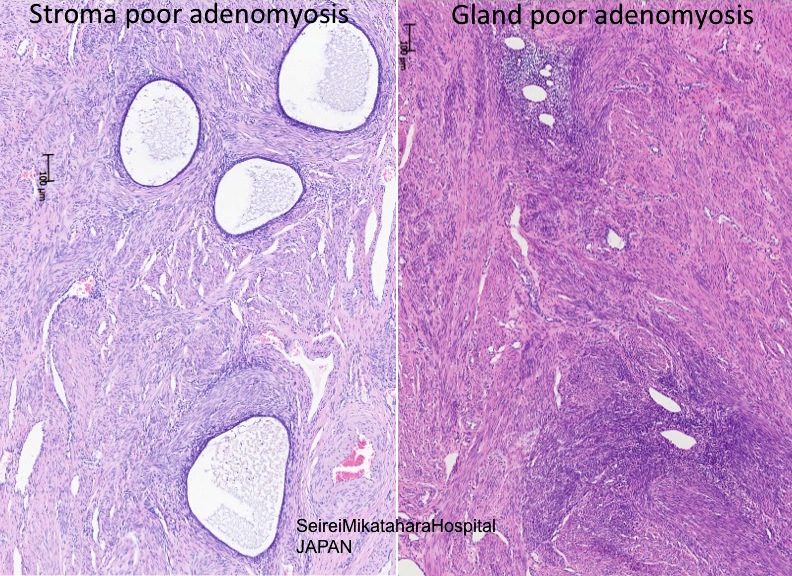
Stroma poor and gland poor
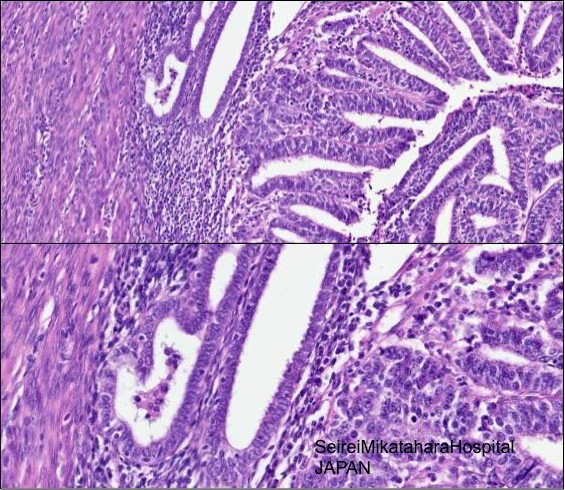
Residual nonneoplastic endometrial glands
Adenosarcoma arising in endometriosis

Various images
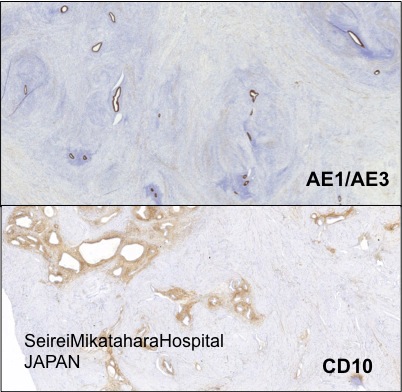
AE1 / AE3 and CD10
Images hosted on other servers:

Endometrial glands and stroma
Positive stains
- CD10 (in endometrial stroma rather than smooth muscle around glands)
- In atrophic adenomyosis CD10 may be weak or focal
- Interferon-inducible transmembrane protein 1 (IFITM1): has superior performance distinguishing endometrial stroma of adenomyosis from mesenchyme surrounding invasive endometrial adenocarcinoma (Am J Clin Pathol 2016;145:486)
Differential diagnosis
- Normal endometrium extension into myometrium (tangential section):
- The diagnosis of adenomyosis depends on the thresholds used by the individual pathologist (Int J Gynecol Pathol 1996;15:217)
- No smooth muscle hypertrophy around islands of endometrium when normal (Robboy: Pathology of the Female Reproductive Tract, 1st Edition, 2001), glands continuous with endometrium (Gattuso: Differential Diagnosis in Surgical Pathology, 3rd Edition, 2014)
- Adenomyoma: not diffuse, has distinct borders (Fletcher: Diagnostic Histopathology of Tumors, 4th Edition, 2013); smooth muscle is not neoplastic (Nucci: Diagnostic Pathology: Gynecological, 1st Edition, 2014)
- Endometrial stromal sarcoma vs adenomyosis with gland-poor or sparse glandular component: no glandular tissue, invades myometrium in tongues, no muscular hypertrophy, unusual to contain diffuse small regular glands (Am J Clin Pathol 1995;103:218), widespread vascular involvement, forms a definable tumor mass (Robboy: Pathology of the Female Reproductive Tract, 1st Edition, 2001; diagnostic gynecologic and obstetric pathology, Soslow: Uterine Pathology (Cambridge Illustrated Surgical Pathology), 2012)
- Low grade endometrial stromal sarcoma with endometrioid glandular differentiation: endometrium usually involved by neoplastic process, has a dominant stromal component with widely spaced glands, lacks associated myometrial hypertrophy, increased stromal mitotic activity and widespread vascular involvement, periglandular cuffing (Soslow: Uterine Pathology (Cambridge Illustrated Surgical Pathology), 2012, Oncol Lett 2016;11:1213)
- Adenomyosis with atrophic and fibrotic stromal component (scattered glands within myometrium) vs. invasion by a well differentiated endometrioid adenocarcinoma: atrophic glands, absence of a low magnification infiltrative pattern, endometrial stroma strands around some glands, typical adenomyosis elsewhere in uterus, lack of a host reaction to the glands and absence of an associated endometrial adenocarcinoma (Soslow: Uterine Pathology (Cambridge Illustrated Surgical Pathology), 2012)
- Carcinoma involving adenomyosis vs endometrioid carcinoma invading myometrium: lobulated, rounded contours, residual nonneoplastic endometrial glands and / or stroma of adjacent uninvolved adenomyosis, typically compressed at periphery (Nucci: Diagnostic Pathology: Gynecological, 1st Edition, 2014)
- Please note that “adenomyosis like infiltration of endometrial cancer” is an entity describing the pattern of infiltration (Adv Anat Pathol 2013;20:141)
- Adenomatoid tumor: no endometrial stroma, glandular spaces lined by flat cuboidal epithelium, mesothelial origin (Gattuso: Differential Diagnosis in Surgical Pathology, 3rd Edition, 2014)

