
Thyroid & parathyroid
Cytology
Fine needle aspiration
Ultrasound
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.


Last author update: 21 March 2023
Last staff update: 21 March 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Ultrasound guided FNA

Table of Contents
Definition / general | Essential features | Terminology | Diagrams / tables | Sonographic features of thyroid nodules and lymph nodes | Reporting systems | Advanced imaging approaches | Clinical features | Radiology description | Radiology images | Case reports | Videos | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jug R, Jiang X. Ultrasound. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidultrasound.html. Accessed April 2nd, 2025.
Definition / general
- Ultrasound is an imaging modality based upon sound waves that has several modes that are helpful to visualize thyroid anatomy and blood flow
- Basic physics principles:
- Ultrasound probe both emits and receives sound waves
- Medical ultrasound: 2 - 20 MHz
- Lower frequencies: better penetration, lower resolution
- Higher frequencies: lower penetration, higher resolution
- B mode (brightness mode):
- 2D black and white image in < 1 mm slice
- Emitted waves are reflected back from the target material relative to the degree of the material's acoustic impedance, which is dependent on density
- Higher density materials generally reflect more and look brighter
- For example, bone is more reflective than soft tissue; thus, bony structures appear brighter on ultrasound images in contrast to darker surrounding tissue
- Doppler mode:
- Measures direction and speed of tissue / blood motion
- M mode (motion mode):
- Pulses are emitted in quick succession and each time, an image is taken; over time, this is analogous to recording a video in ultrasound (used for heart valves)
- References: Arch Pathol Lab Med 2010;134:1541, Radiol Clin North Am 2011;49:417
Essential features
- Ultrasound is an imaging modality based upon sound waves that has several modes that are helpful to visualize thyroid anatomy and blood flow
- Benign thyroid nodules appear small or large with predominant cystic change, fluid filled (as opposed to solid), hyperechoic or honeycomb morphology
- Thyroid nodules suspicious for malignancy are solid, are taller than they are wide, contain microcalcifications and are hypoechoic, with thin capsules or irregular borders and intramodular vascularity
Terminology
- Anechoic: black (e.g., blood, cystic fluid)
- Azimuthal plane: midsagittal plane of transducer; beam used to guide needle in ultrasound guided fine needle aspiration (UGFNA)
- Hyperechoic: brighter than surrounding tissue (e.g., bone)
- Hypoechoic: darker than surrounding tissue (e.g., soft tissue versus bone)
- Isoechoic: same intensity as surrounding tissue
- Ultrasound artifacts:
- Posterior (acoustic) shadowing: strong reflectors (air) or absorbers (stones, bones) block visualization of structures beyond them in relation to the beam
- Posterior (acoustic) enhancement: anechoic structures (cysts) show brighter signals from areas beyond them in relation to the beam
- Eggshell calcification: nodules surrounded by a layer of calcium have bright anterior and posterior walls due to a reflection from the surface but posteriorly there is acoustic shadowing; this phenomenon also leads to edge artifact in which parallel dark lines extend posteriorly from the sides of nodules
- Reverberation artifact: sound waves reflect off a very reflective surface and are re-reflected from the skin, resulting in phantom images behind the target image
- Comet tail artifact: reverberation artifact from front and back of a very strong reflector / absorber (air bubble, metal fragment) - can also happen with dense colloid
- Bayonet sign:
- Due to speed propagation artifact, machines use average speed of sound to calculate depth
- If sound actually travels faster in the tissue (anechoic or hypoechoic structures), a reflector will appear closer to the transducer than its actual depth and vice versa
- Needle with its tip in a cyst or nodule with differing echogenicity from surrounding tissue will appear to have its tip bent due to this artifact, looking like a bayonet
- References: Arch Pathol Lab Med 2010;134:1541, Radiol Clin North Am 2011;49:417, Korean J Radiol 2014;15:267, Endotext: Ultrasonography of the Thyroid [Accessed 12 October 2022], Radiol Clin North Am 2020;58:1033, Radiol Clin North Am 2020;58:1041, Milas: Advanced Thyroid and Parathyroid Ultrasound, 1st Edition, 2017, Halenka: Atlas of Thyroid Ultrasonography, 1st Edition, 2017
Diagrams / tables
Contributed by Rachel Jug, M.B.B.Ch.
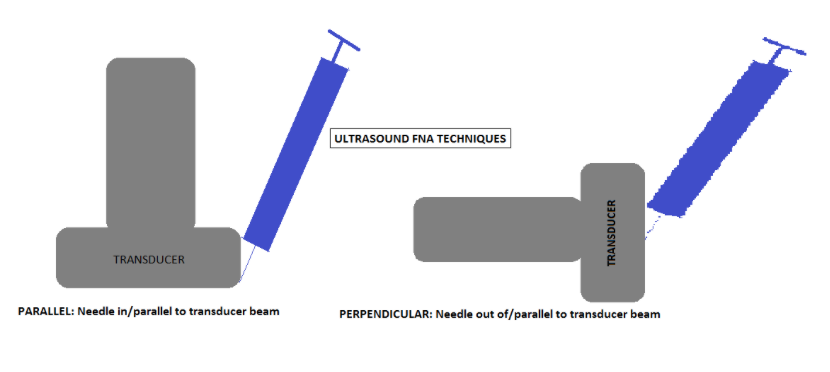
Ultrasound FNA techniques
Images hosted on other servers:

Risk of thyroid cancer

ATA algorithm for
patients with
thyroid nodules

ATA association

ACR TI-RADS chart

Comparison of systems
Typical appearances of diffuse thyroid diseases
| Thyroid disorder | Grayscale ultrasound | Color Doppler | Key features |
|---|---|---|---|
| Graves thyroiditis | Enlarged, mildly hypoechoic, heterogeneous | Markedly ↑ | Markedly hyperemic; proptosis; hyperthyroid; + antithyroid antibodies |
| Hashimoto thyroiditis | Enlarged, heterogeneous with lobular margins; hypoechoic and micronodular, septal lines | Highly variable: both ↑ and ↓ flow possible | + Antithyroid antibodies, hypothyroidism; cervical adenopathy |
| Subacute lymphocytic thyroiditis (painless) | Hypoechoic | Insufficient data | + Antithyroid antibodies; postpartum; transient |
| De Quervain thyroiditis (subacute granulomatous) | Painful patchy areas of hypoechogenicity | ↓ in the hypoechoic patch | Thyroid pain over area of hypoechogenicity; ↑ erythrocyte sedimentation rate (ESR) |
| Acute suppurative thyroiditis | Abscess or infected linear tract in the thyroid | Normal background; no flow within an abscess | Acute presentation with signs of infection and pain; ↑ ESR; possible pyriform sinus fistula |
| Riedel thyroiditis | Large hypoechoic thyroid with coarse parenchyma | Insufficient data | Large, rock hard gland; encases adjacent structures |
| Medication induced (i.e., amiodarone induced thyrotoxicosis [AIT]) | Type 1: abnormal thyroid; type 2: normal thyroid | Type 1: ↑; type 2: absent | History of current or recent amiodarone use; hyperthyroid |
| Atrophic thyroiditis | Small, hypoechoic thyroid | ↓ | + Antithyroid antibodies; usually hypothyroid |
| Radiation thyroiditis | Small, hypoechoic thyroid | Variable | Known external beam or I131 administration |
| Thyroid lymphoma | Large, ill defined, markedly hypoechoic nodules or masses with ↑ through transmission on background of Hashimoto thyroiditis | ↓ in the hypoechoic mass | Rapidly enlarging neck mass in patient with history of Hashimoto, with or without adenopathy |
| Multinodular goiter | Closely opposed or interspersed, similar appearing nodules replace parenchyma, coarse calcifications, variable cystic changes in nodules | Variable | Confluent nodules in a normal or enlarged thyroid; with or without abnormal thyroid function tests |
Sonographic features of thyroid nodules and lymph nodes
- Sonographic features of benign thyroid nodules:
- Small size (< 1 cm)
- Fluid filled
- Honeycomb morphology
- Hyperechoic (colloid nodule or focal nodular Hashimoto thyroiditis)
- Large nodules if they are predominantly cystic (cystic change accounts for > 50% of nodule)
- Sonographic features of thyroid nodules suspicious for malignancy (Diagn Cytopathol 2008;36:390, Eur J Endocrinol 2009;161:103):
- Solid oval nodules (anterior - posterior dimension: transverse dimension ratio is > 1)
- Presence of discrete coarse echogenic foci or microcalcifications
- Hypoechoic (medullary and papillary thyroid cancers)
- Thin capsules or irregular borders (suggestive of extracapsular spread)
- Intranodular vascularity
- Nodal metastases
- Sonographic features of benign lymph nodes:
- Oval shape (short axis:long axis ratio ≤ 0.5)
- Hypoechoic cortex and echoic hilum (due to adipose tissue)
- Clearly demarcated margin from surrounding tissue
- Central vascularization
- Sonographic features of lymph nodes suspicious for malignancy (Eur J Endocrinol 2009;161:103):
- Round shape (short axis:long axis ratio > 0.5)
- Echogenic heterogeneity of cortex and absent fatty hilum
- Irregular margin with surrounding tissue
- Increased or abnormally located vascularity
- Features suggestive of metastatic thyroid cancer: cystic appearance, hyperechoic punctations / calcifications
- 2015 American Thyroid Association (ATA) Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer (Thyroid 2016;26:1):
- Strongly recommends ultrasonic examination of thyroid and cervical lymph nodes if thyroid nodules; fine needle aspiration (FNA) for sampling is recommended if > 1 cm in greatest dimension and high suspicion sonographic pattern (estimates a 70 - 90% risk of malignancy), including:
- Solid hypoechoic nodule or nodule that is partially solid and hypoechoic and partially cystic with 1 or more of the following features:
- Irregular margins (infiltrative, microlobulated)
- Microcalcifications
- Oval (taller than wide) shape
- Rim calcifications with an extrusive soft tissue component
- Evidence of extrathyroidal extension
- Solid hypoechoic nodule or nodule that is partially solid and hypoechoic and partially cystic with 1 or more of the following features:
- Strongly recommends ultrasonic examination of thyroid and cervical lymph nodes if thyroid nodules; fine needle aspiration (FNA) for sampling is recommended if > 1 cm in greatest dimension and high suspicion sonographic pattern (estimates a 70 - 90% risk of malignancy), including:
Reporting systems
- American College of Radiology (ACR) Thyroid Imaging, Reporting and Data System (TI-RADS) categorizes lesions based on ultrasound features and provides recommendations for whether or not to FNA the lesion:
- Benign (TR1): no FNA
- Not suspicious (TR2): no FNA
- Mildly suspicious (TR3): FNA if ≥ 2.5 cm; follow if ≥ 1.5 cm
- Moderately suspicious (TR4): FNA if ≥ 1.5 cm; follow if ≥ 1 cm
- Highly suspicious (TR5): FNA if ≥ 1 cm; follow if ≥ 0.5 cm
- See ACR TI-RADS chart
- Modifications of TI-RADS:
- European: EU TI-RADS (Eur Thyroid J 2017;6:225)
- Korean: K TI-RADS (Korean J Radiol 2021;22:1569)
- Chinese: C TI-RADS (Endocrine 2020;70:256)
Advanced imaging approaches
- Thyroid elastography: characterizes thyroid nodules by determining hardness / stiffness; can be integrated into the conventional thyroid ultrasound (Ultraschall Med 2009;30:175)
- Stiffness measured in kPa and elasticity ratios comparing cancerous to benign tissue
- Lesions with low stiffness are considered to be benign, while stiff lesions are considered to be malignant (Diagn Interv Imaging 2013;94:535, Ultraschall Med 2009;30:175)
- Contrast enhanced ultrasound (CEUS): qualitative and quantitative approach to analyze the microvascular patterns of thyroid nodules and lymph nodes to characterize them as benign or malignant
- Method increases diagnostic accuracy of ultrasonography (J Clin Med 2021;10:4559)
Clinical features
- Indications for UGFNA:
- Nonpalpable or difficult to palpate nodules, most commonly of the thyroid
- Targeting specific areas in complex and cystic nodules, such as solid areas
- Repeat FNA, when a prior palpation guided FNA sample was insufficient (Diagn Cytopathol 2008;36:390)
- Follow up for patients postpartial or total thyroidectomy for malignancy, e.g., to sample thyroid bed (J Ultrasound Med 2013;32:1319)
- Benefits of UGFNA compared to conventional FNA alone:
- Higher rates of successful biopsy (J Clin Ultrasound 1994;22:535, Thyroid 1998;8:15, Thyroid 1998;8:283)
- Potentially lowers risk of damage to surrounding structures, which can be visualized
- Varying reports on cost effectiveness (BMC Endocr Disord 2009;9:14, Thyroid 2006;16:555)
- Efficacy of UGFNA is improved by the presence of a cytopathologist onsite, decreasing the overall inadequacy rate from 9.3% to 6% (Br J Radiol 2014;87:20130571)
- Complications and contraindications: same as conventional FNA
- Overview of procedure - focused thyroid ultrasound and biopsy:
- Image each thyroid lobe in the transverse and longitudinal planes to determine the overall appearance and locate nodules
- After completing ultrasonic assessment of the thyroid, relocate the position and measure size of the suspicious nodules
- Approaches to UGFNA relative to the transducer beam (azimuthal plane):
- For each approach, orient the needle with the bevel tip up to create the greatest reflection
- Parallel approach (in beam):
- Point the needle down, along the plane of the beam, toward the nodule
- Maintain needle and transducer in the same plane, parallel to the plane of the transducer, then advance the needle into the nodule
- Advantage: entire length of needle can be seen
- Perpendicular approach (out of beam):
- Point the needle toward the midpoint of the transducer's side (long axis)
- Perpendicular approach will result in visualization of the needle as it transversely crosses the plane of the beam at 90 degrees
- Nodule and needle point will be centered in the midpoint of the transducer's long axis
- Advantage: desirable, due to anatomy in some locations
- Disadvantage: entire length of needle is not visualized
- Needle based sample collection techniques:
- With aspiration / suction:
- 27 or 25G needle attached to a 10 cc syringe (with or without extension tubing) withdrawn so that 1 - 2 cc of negative pressure induces aspiration
- Without aspiration / nonsuction:
- 27 or 25G needle (with or without stylet; may attach open syringe) is introduced into nodule and capillary action causes uptake of cellular material into the needle
- With aspiration / suction:
- Sample preparation: same as for palpation guided FNA
Radiology description
Radiology images
Images hosted on other servers:

Calcified nodule

Complex cystic thyroid nodule

Multinodular goiter

17 year old girl with Graves disease

35 year old woman
with diffuse
Hashimoto
thyroiditis

50 year old woman
with colloid
multinodular
goiter

Hypoechoic nodule

Microcalcifications in a thyroid nodule

Intranodular vascularity in thyroid nodule

Oval shaped thyroid nodule
Case reports
- 18 year old woman with a mass in her left neck with stiffness and normal thyroid function (Medicine (Baltimore) 2021;100:e25517)
- 24 year old woman with a palpable painless mass in the left thyroid lobe (J Int Med Res 2020;48:300060520954718)
- 71 year old woman with swelling of the anterior neck and history of airway obstruction (J Ultrasound 2018;21:165)
Videos
Fine needle aspiration (FNA) biopsy techniques - Dr. Britt Marie Ljung playlist
Neck ultrasonography basics
Thyroid ultrasound course
Additional references
Board review style question #1
Which of the following sonographic features of a thyroid nodule would increase suspicion for malignancy?
- Cystic change accounting for > 50% of nodule
- Fluid filled
- Honeycomb morphology
- Hyperechoic
- Presence of discrete coarse echogenic foci or microcalcifications
Board review style answer #1
E. Presence of discrete coarse echogenic foci or microcalcifications
Comment Here
Reference: Ultrasound guided FNA
Comment Here
Reference: Ultrasound guided FNA
Board review style question #2
What is the typical appearance of chronic lymphocytic (Hashimoto) thyroiditis on a grayscale ultrasound?
- Abscess or infected linear tract in the thyroid
- Enlarged, heterogeneous with lobular margins; hypoechoic and micronodular, septal lines
- Enlarged, mildly hypoechoic, heterogeneous
- Large, ill defined, markedly hypoechoic nodules or masses
- Small, hypoechoic thyroid
Board review style answer #2
B. Enlarged, heterogeneous with lobular margins; hypoechoic and micronodular, septal lines
Comment Here
Reference: Ultrasound guided FNA
Comment Here
Reference: Ultrasound guided FNA
