
Thyroid & parathyroid
Papillary thyroid carcinoma
Other subtypes
Tall cell
Editorial Board Member: Andrey Bychkov, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 26 August 2020
Last staff update: 18 August 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Papillary carcinoma [title] tall cell variant

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Florianova L, Pusztaszeri M. Tall cell. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidtallcellvariant.html. Accessed April 2nd, 2025.
Definition / general
- Papillary thyroid carcinoma (PTC) variant characterized by presence of ≥ 30% of tall cells (2 - 3 times taller than wide) with abundant granular eosinophilic (oncocytic-like) cytoplasm and the typical nuclear changes of PTC
- Variable diagnostic criteria over time with significant interobserver variability (Thyroid 2017;27:1498)
- Often underrecognized (Thyroid 2008;18:1179, Thyroid 2007;17:655)
- First described in 1976 (Cleve Clin Q 1976;43:207)
Essential features
- The most common aggressive variant of papillary thyroid carcinoma, characterized by tall cells occupying ≥ 30% tumor and well developed papillary thyroid carcinoma nuclear features
- Usually requires more aggressive treatment and closer disease surveillance
- BRAF V600E mutation present in most cases
- Papillary thyroid carcinomas with tall cell features (≥ 10% tall cells) have worse prognosis than those without tall cells; more than 10% tall cells in a tumor should be reported in final pathology reports
Terminology
- 2017 WHO classification of tumors of endocrine organs requires ≥ 30% of tall tumor cells to define this variant
- Variable diagnostic criteria over time
- WHO 2017 (current): 2 - 3x height / width cells occupying ≥ 30% tumor
- WHO 2004 (outdated): 3x height / width cells occupying ≥ 50% tumor
- If tall cell features are > 10% but < 30%, the tumor should be designated as PTC with tall cell features (Endocr Relat Cancer 2015;22:419)
ICD coding
Epidemiology
- 5 - 10% of PTCs (World J Surg 2008;32:1535)
- Usually older age patients; exceedingly rare in the pediatric population
- F > M (Oncotarget 2016;7:40792, Thyroid 2007;17:655, Laryngoscope 2008;118:32)
Sites
- Thyroid
- Exceedingly rare at other sites, e.g. ectopic thyroid tissue in thyroglossal duct (see case reports below)
Pathophysiology
- Clonal neoplastic proliferation of thyroid follicular cells, usually with a specific driver mutation (see molecular / cytogenetics description below)
Etiology
- Sporadic in most cases
- Shared risk factors with most other variants of PTC
- Ionizing radiation and pre-existing benign thyroid disease
Clinical features
- Asymptomatic or enlarging neck mass
- May present as an incidental thyroid nodule
- Local symptoms (dysphagia, hoarseness, stridor) may be present for more advanced cases with vocal cord paralysis or tracheal compression
- Thyroid function tests at the time of diagnosis are typically normal
Diagnosis
- Gold standard for the diagnosis of the tall cell variant is histopathologic evaluation of thyroid resection specimens
- Nevertheless, tall cell features may be recognized on fine needle aspiration cytology
Laboratory
- Persistent or recurrent disease can be monitored by serum thyroglobulin (J Clin Endocrinol Metab 2003;88:3668)
Radiology description
- Cold nodules on thyroid scanning
- Highly suspicious nodule on thyroid ultrasound in most cases
- Markedly hypoechoic solid nodule with microcalcifications and ill defined spiculated or microlobulated margins (Front Endocrinol (Lausanne) 2018;9:223, Ultrasonography 2017;36:103, J Ultrasound Med 2011;30:853)
- Extrathyroidal extension and metastatic lymph nodes are commonly seen
Radiology images
Images hosted on other servers:

Tall cell variant in 19 year old woman
Prognostic factors
- Even without extrathyroidal extension, tall cell variant was shown to have a more aggressive behavior than classic PTC independent of age, gender and tumor size (Thyroid 2007;17:655)
- Often but not always larger tumor size, more frequent extrathyroidal extension and lymph node involvement as well as a higher stage at presentation than classic PTC (Thyroid 2007;17:655, Laryngoscope 2008;118:32, Hum Pathol 2007;38:212, Oncol Lett 2017;13:3501, Oncotarget 2017;8:6222, Oncotarget 2016;7:40792)
- Higher recurrence rate, increased tumor related mortality and more frequent distant metastases compared with classic PTC (Thyroid 2007;17:655, Laryngoscope 2008;118:32, Oncol Lett 2017;13:3501, Oncotarget 2017;8:6222, Oncotarget 2016;7:40792)
- Accounts for ~20% of radioiodine refractory thyroid carcinomas (Thyroid 2008;18:1179, Cancer 2008;113:48)
- Risk of dedifferentiation into poorly differentiated or anaplastic thyroid carcinoma (tall cell PTC often seen as a component of these tumors) (Mod Pathol 1991;4:637)
- The tall cell variant of papillary microcarcinoma (< 1 cm) is also associated with aggressive features at presentation and should be differentiated from other papillary thyroid microcarcinomas (Thyroid 2013;23:1525, Thyroid 2007;17:655)
Case reports
- 40 year old woman with tall cell PTC in struma ovarii (J Cancer Res Ther 2013;9:119)
- 51 year old man with hemoptysis, shortness of breath and stridor (Case Rep Endocrinol 2017;2017:4581626)
- 62 year old man with a metastasis to the pancreas (JOP 2006;7:417)
- 72 year old man with a combined tall cell and Hürthle cell thyroid carcinoma (Arch Pathol Lab Med 2001;125:541)
- 75 year old woman with a brain metastasis at initial presentation (Head Neck Oncol 2009;1:23)
- 77 year old woman with tall cell PTC arising in a thyroglossal duct cyst Ann Med Surg (Lond) 2015;4:129)
- 80 year old woman with a squamous cell carcinoma arising in a tall cell PTC (J Clin Pathol 2005;58:662)
- Man with a thyroid carcinoma with mixed tall cell and columnar cell features (Am J Clin Pathol 1990;94:442)
Treatment
- Total thyroidectomy in most cases
- With or without neck lymph node dissection with or without radioiodine therapy in selected cases
- BRAF targeted therapy may be beneficial in selected advanced cases (J Endocr Soc 2017;1:285, Lancet Oncol 2016;17:e468)
Gross description
- Tend to be large (> 5 cm)
- Extrathyroidal extension may be grossly apparent
Gross images
Contributed by Andrey Bychkov, M.D., Ph.D.
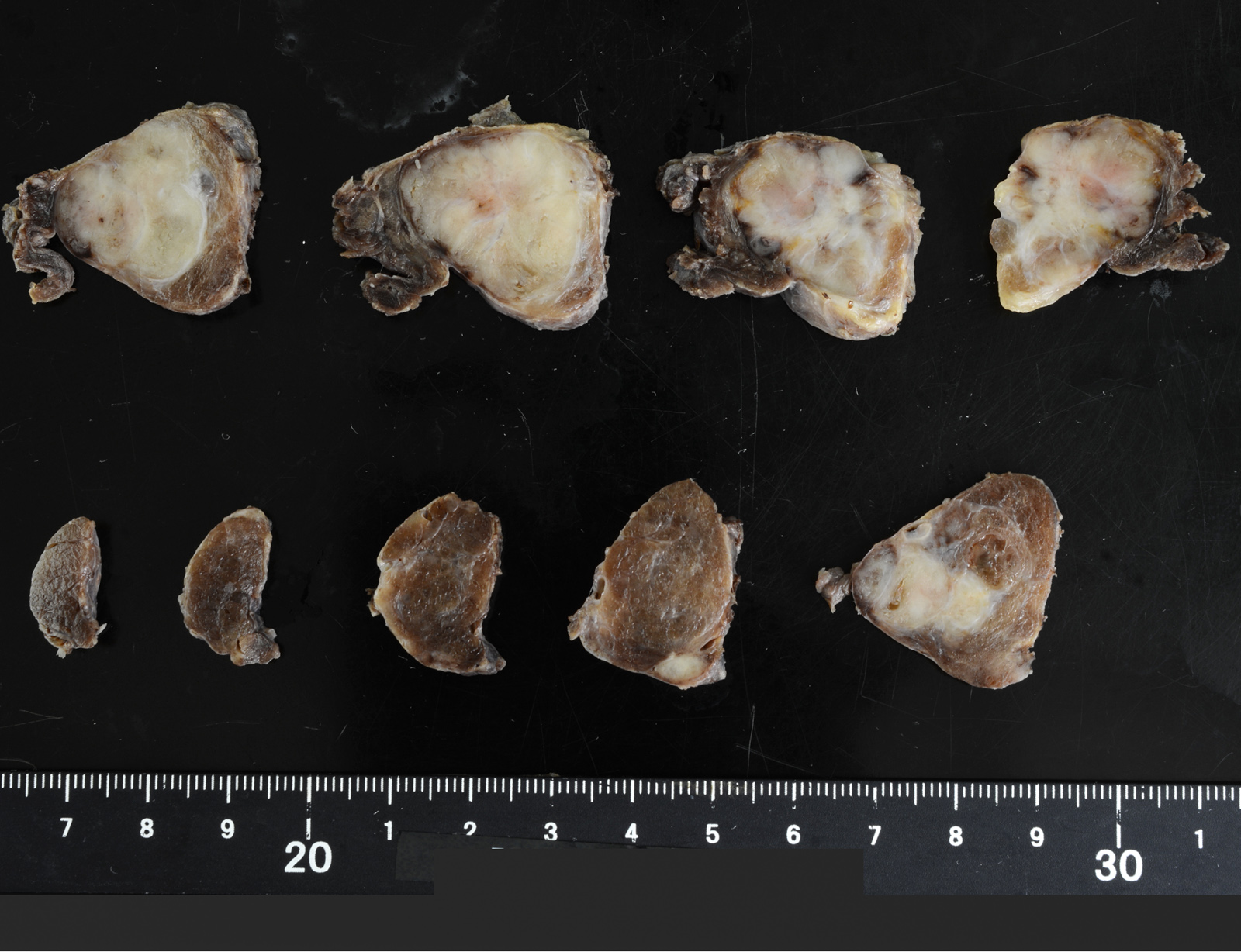
Entire lobe
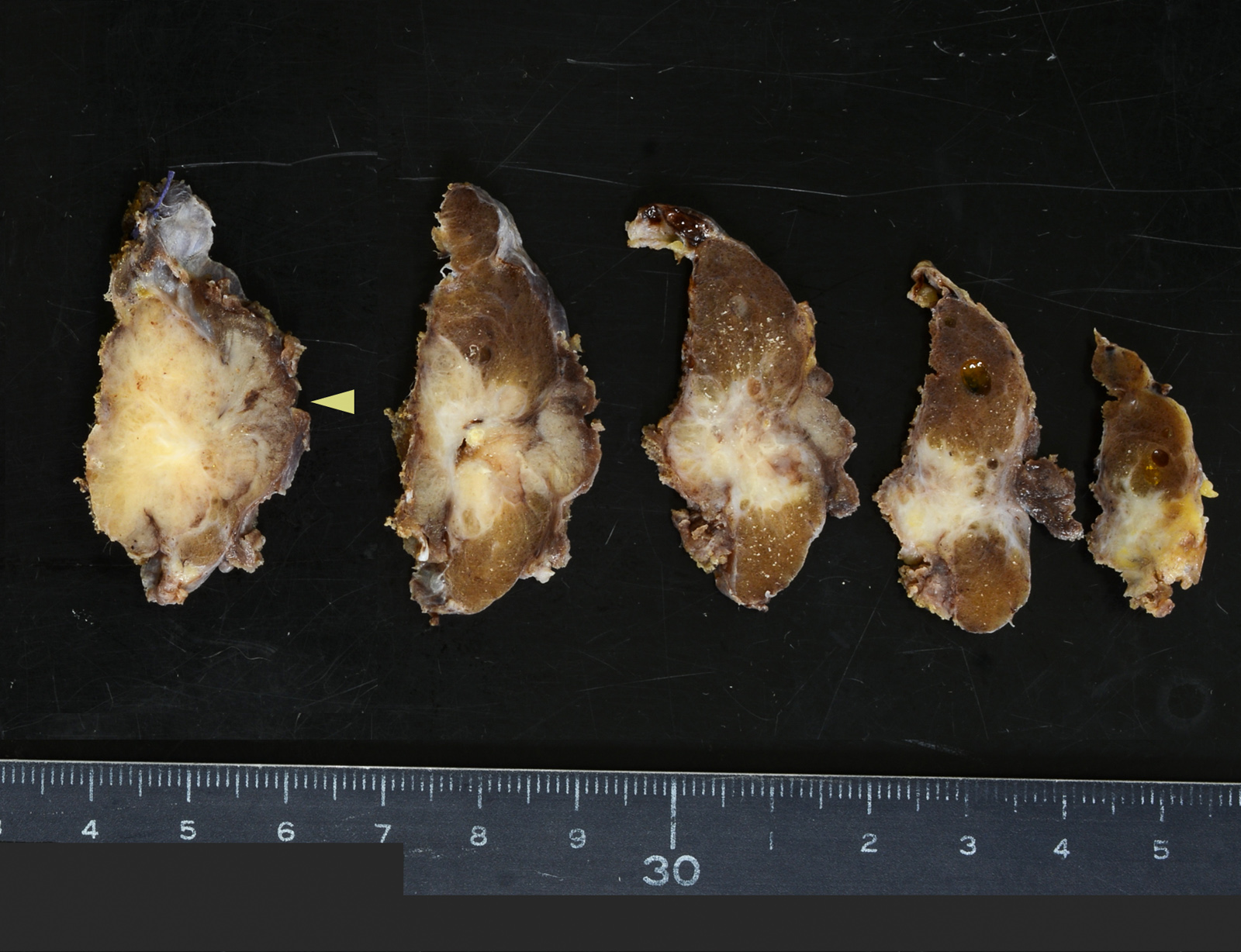
Muscular invasion
Frozen section description
- Frozen section is usually not indicated
- Standard of care is to perform preoperative fine needle aspiration to establish the diagnosis of PTC and to determine the most appropriate surgical procedure
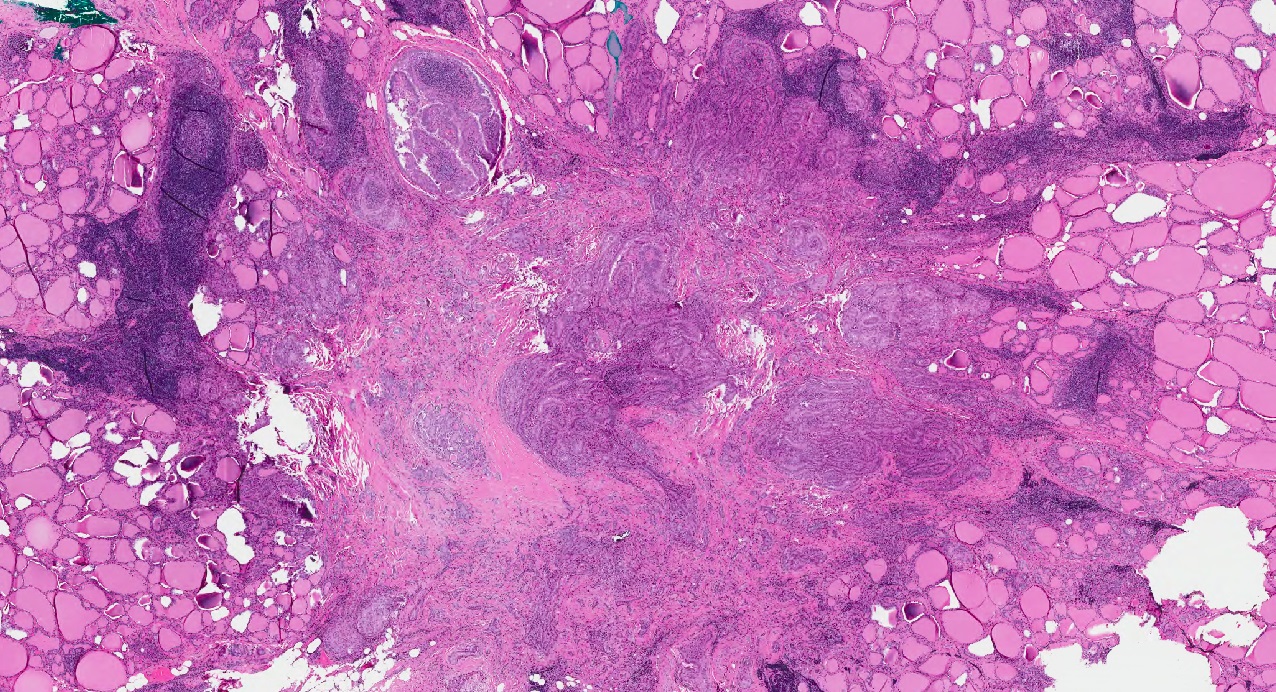
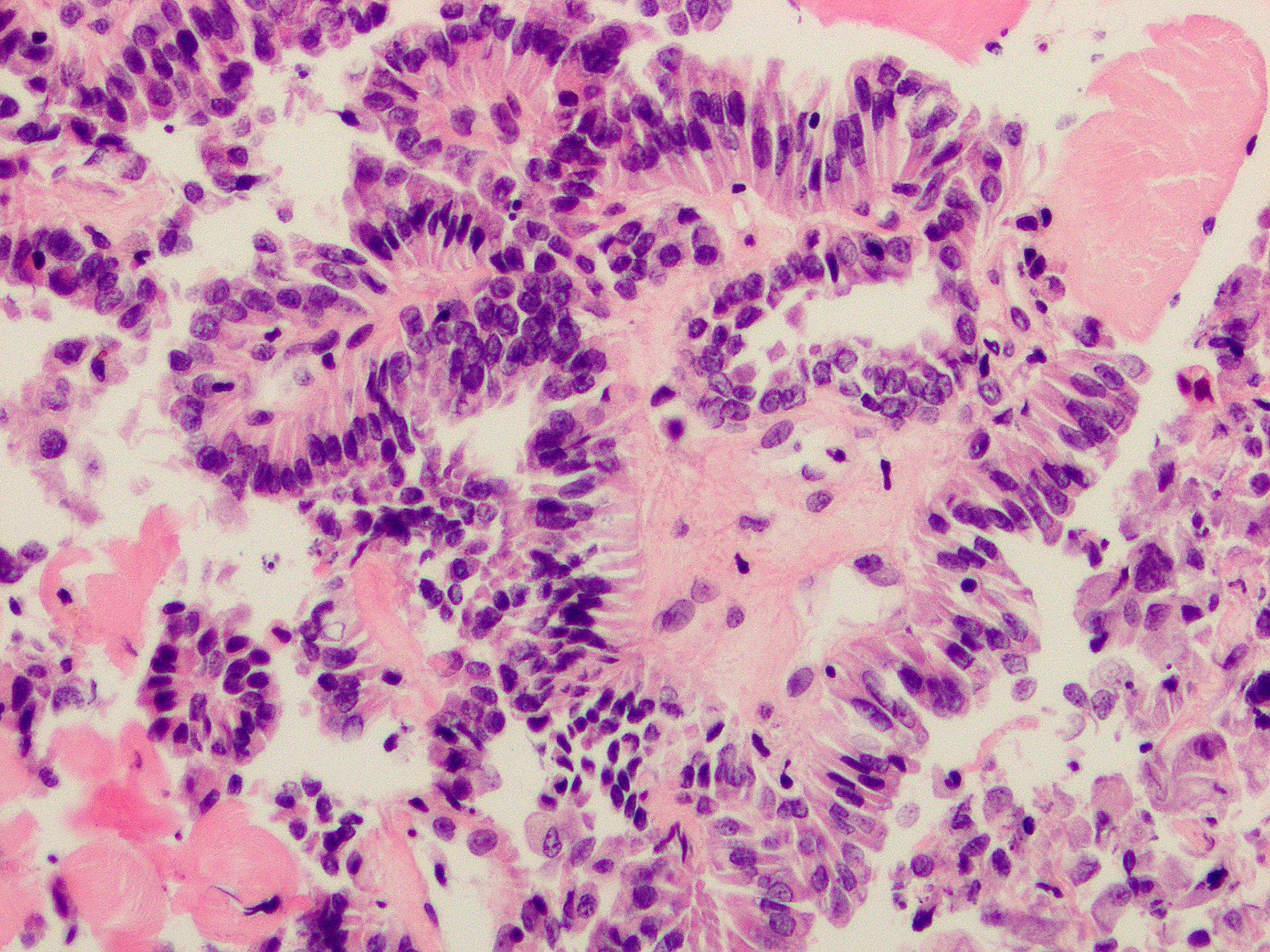
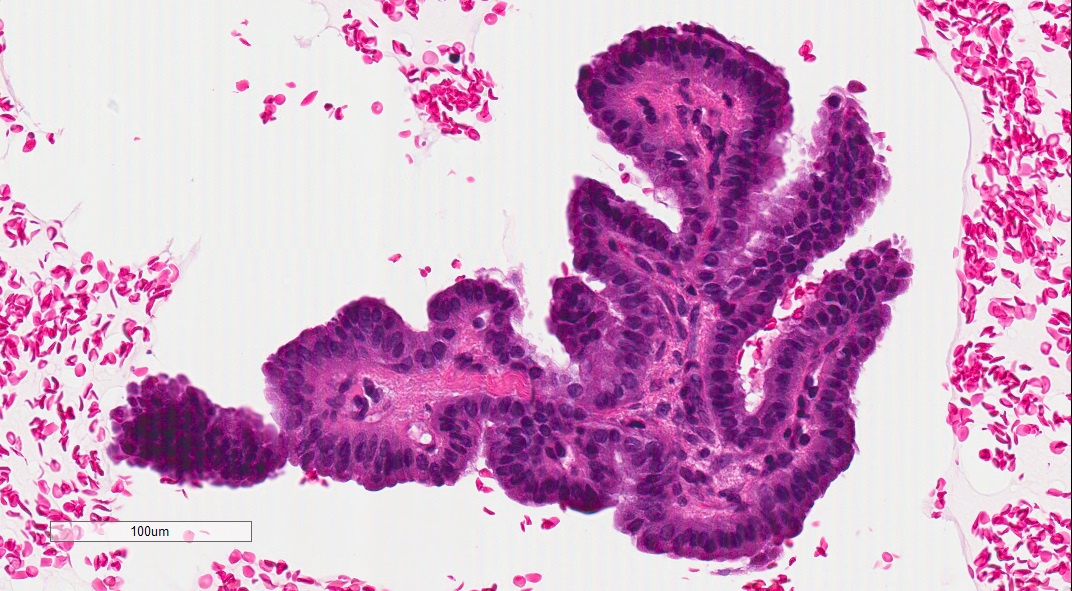
Microscopic (histologic) description
- Usually unencapsulated and infiltrative
- Growth patterns
- Papillary is the most common
- Trabecular (due to closely packed papillae) and follicular
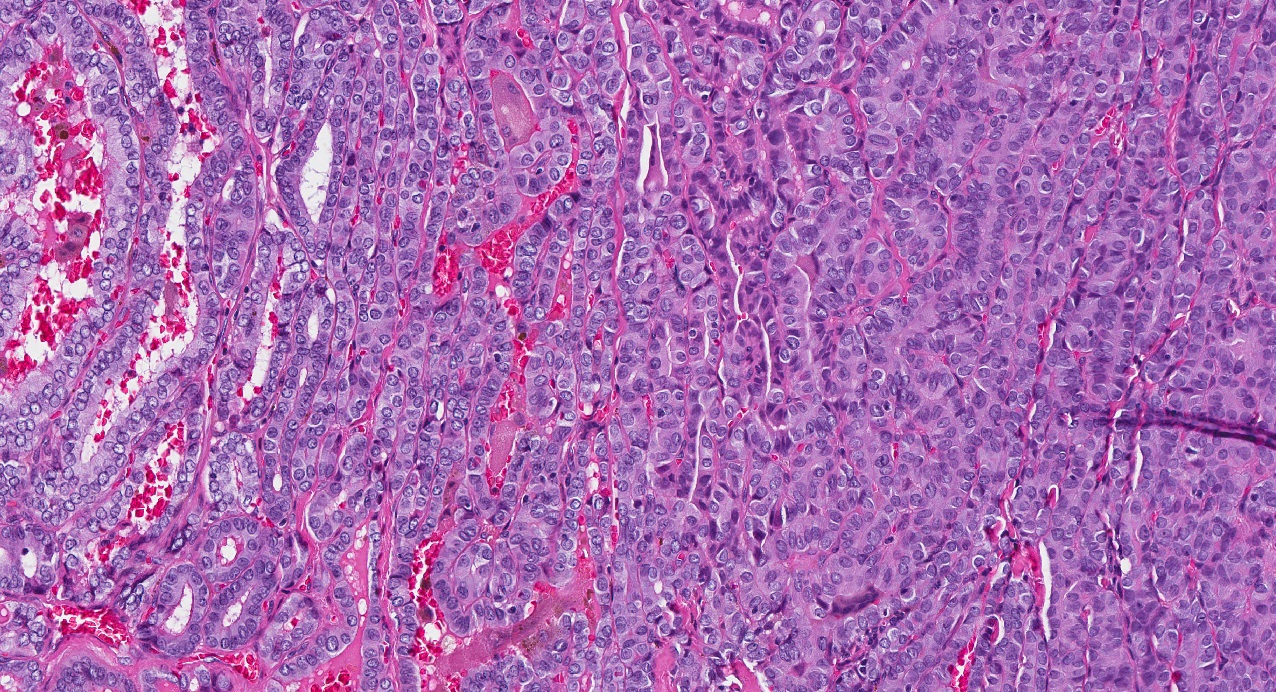
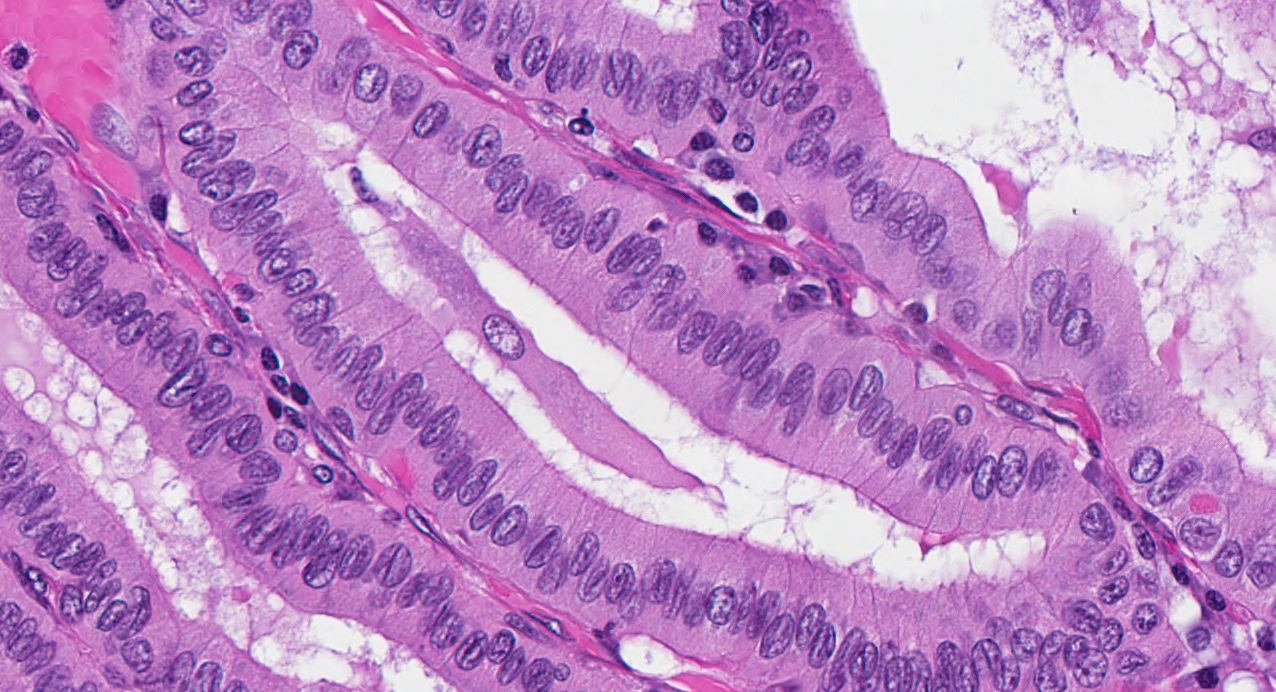
- Areas of tram track or railroad track-like appearance on lower power
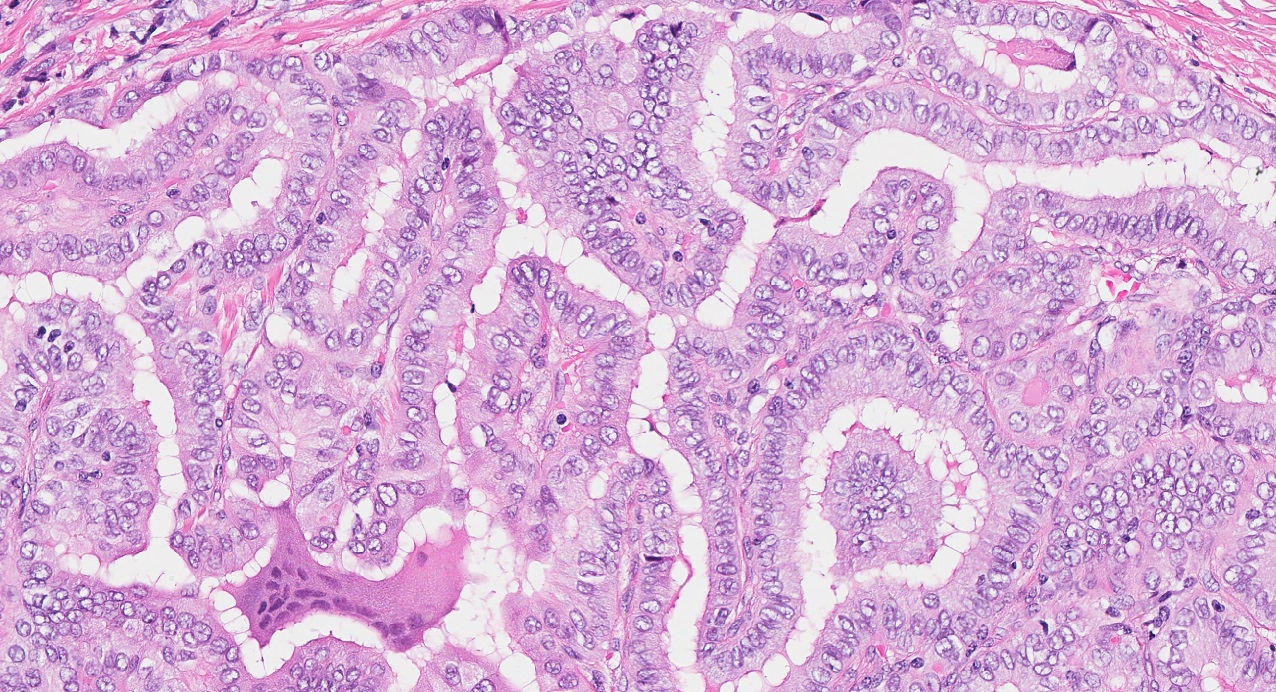
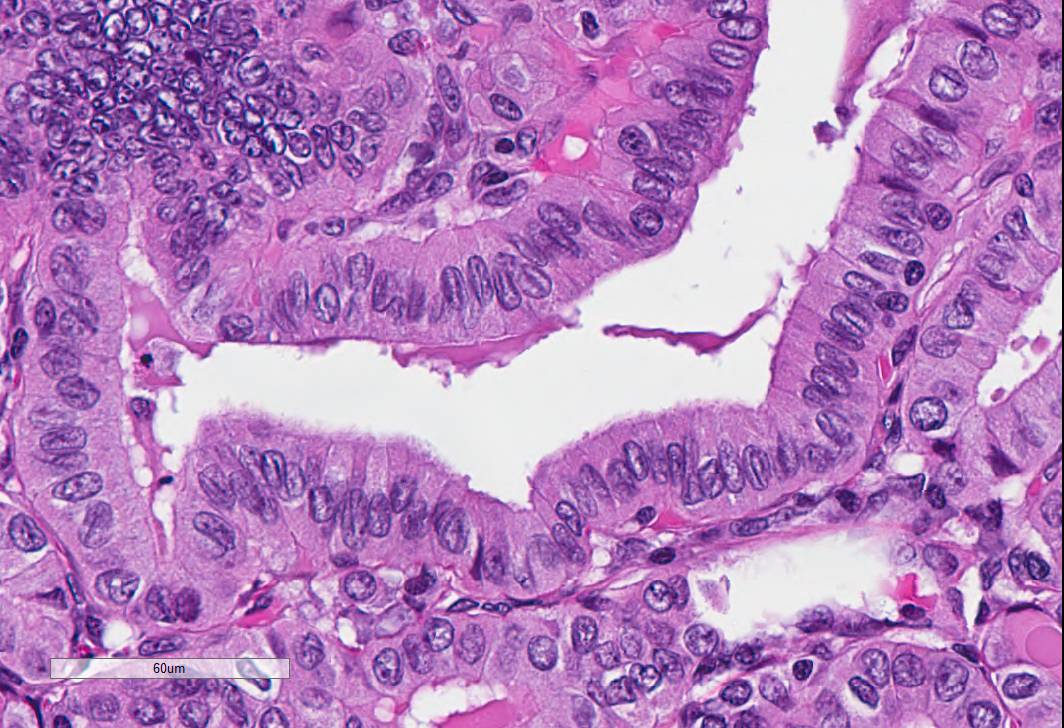
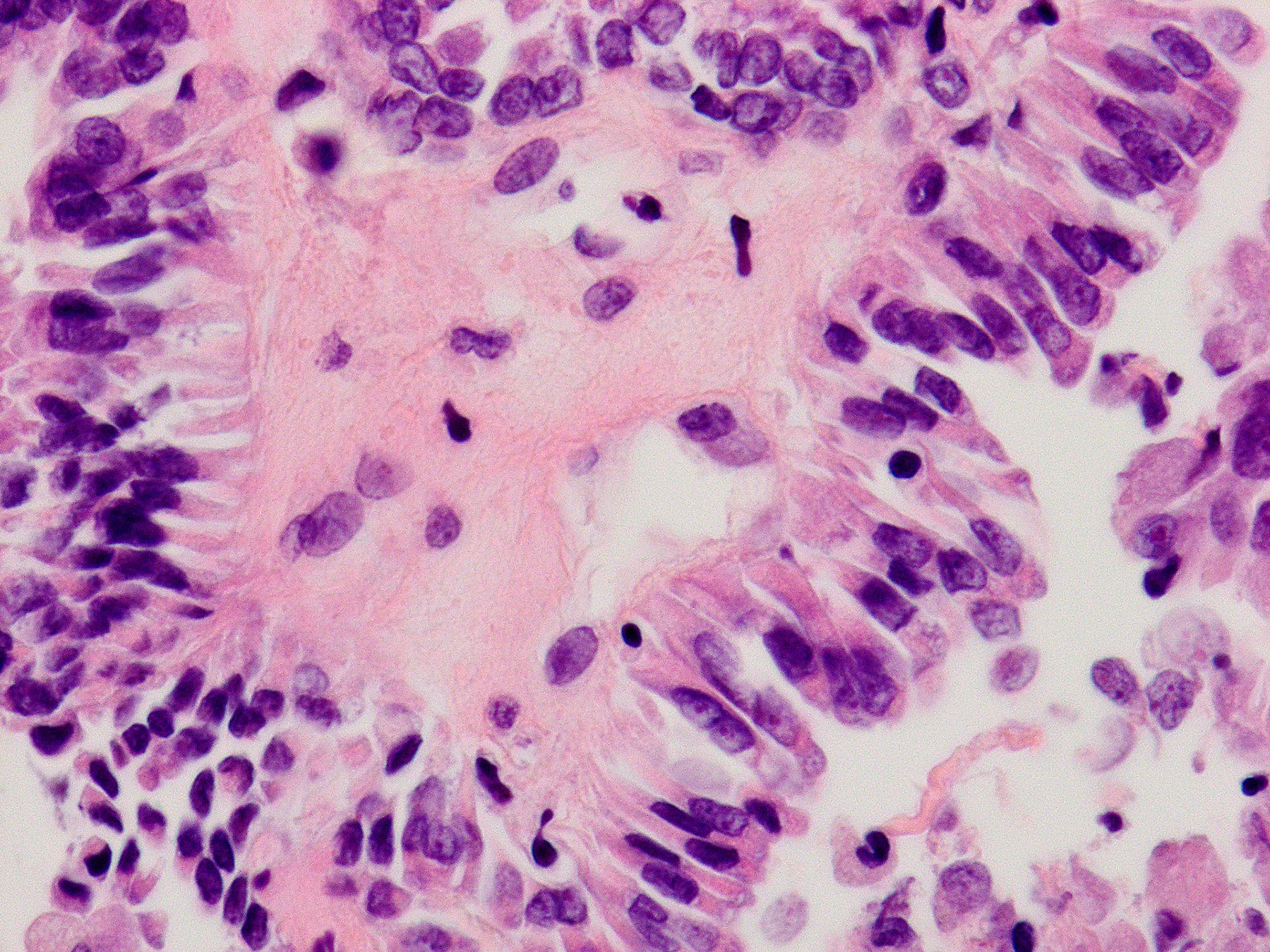
- Intricate, well formed, long papillae lined by single layer of tall columnar cells (cell height is 2 - 3 times their width)
- Depending on the plane of sectioning, cells may appear wide rather than tall
- Well developed and easily identifiable nuclear features of PTC: enlarged nuclei with numerous grooves and pseudoinclusions
- Sharply delineated cell borders with intensely eosinophilic and finely granular cytoplasm
- Tall cell features / pattern are frequently seen in the areas of extrathyroidal invasion of PTC
- Psammoma bodies uncommon
- Absent features: nuclear stratification, squamoid morules
- May exhibit prominent vascular invasion, mitotic activity
- Often found as a well differentiated component within anaplastic (undifferentiated) carcinomas and poorly differentiated thyroid carcinomas (Thyroid 2011;21:493)
- May be associated with lymphocytic thyroiditis
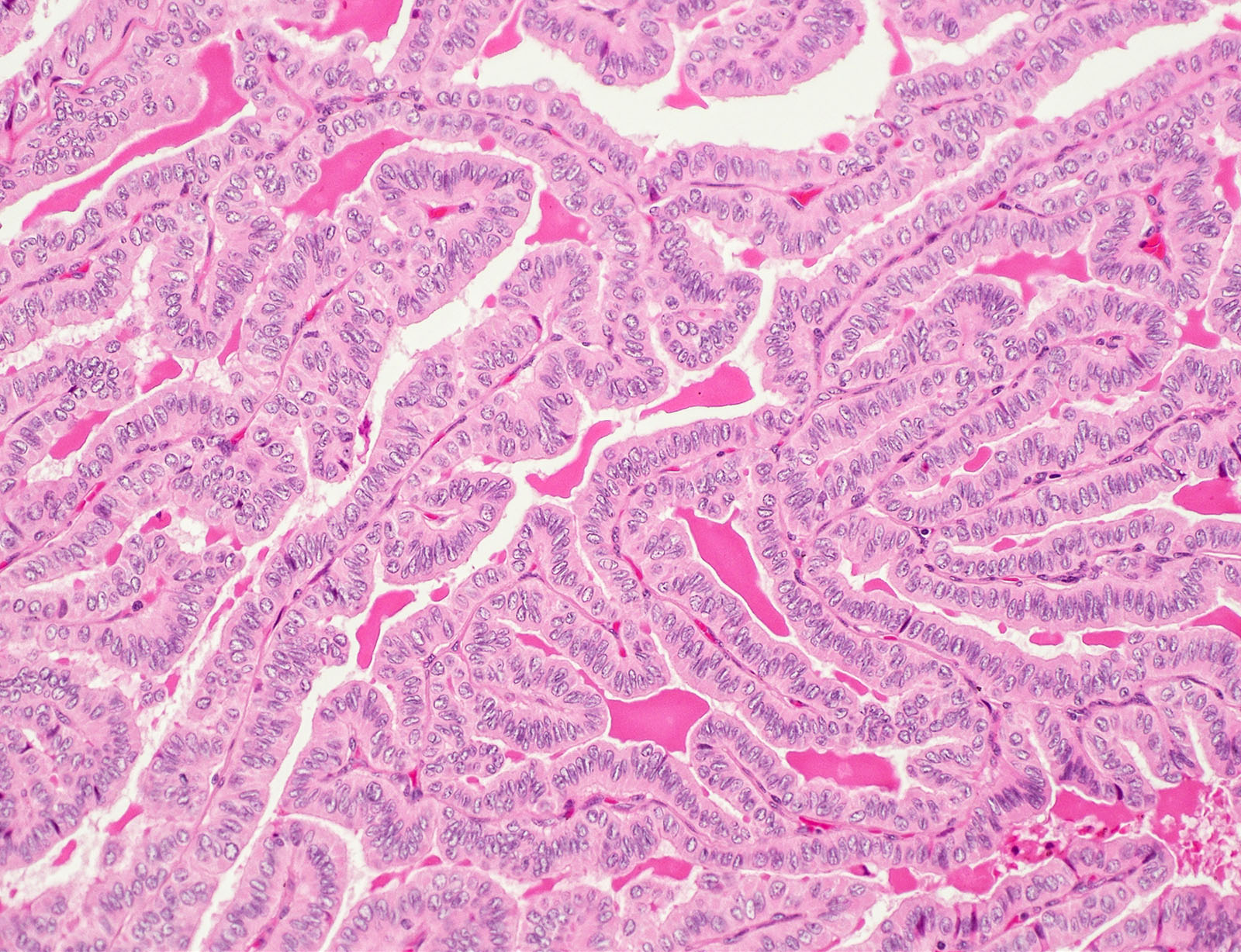
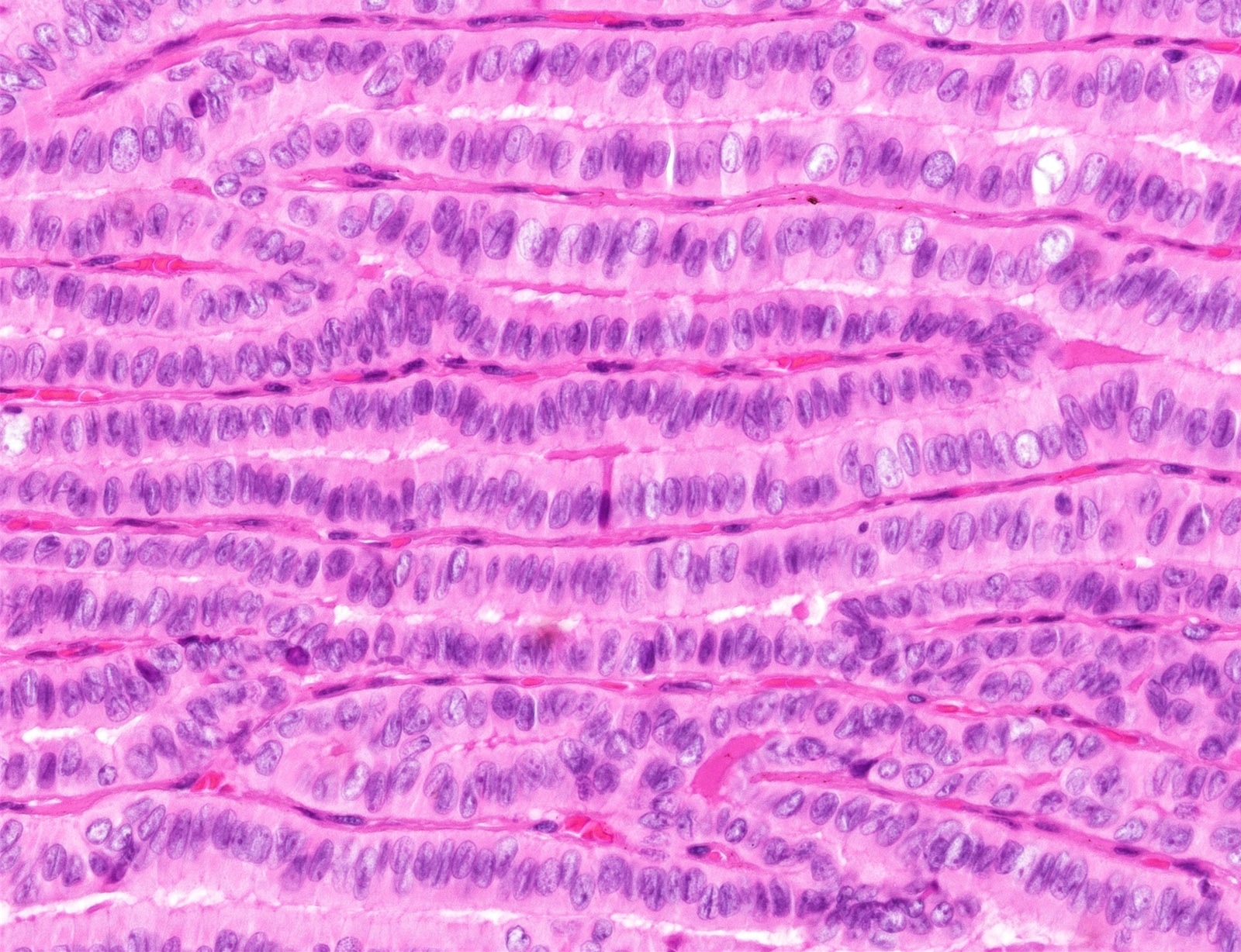
Microscopic (histologic) images
Contributed by Livia Florianova, M.D., M.Sc. and Marc Pusztaszeri, M.D.

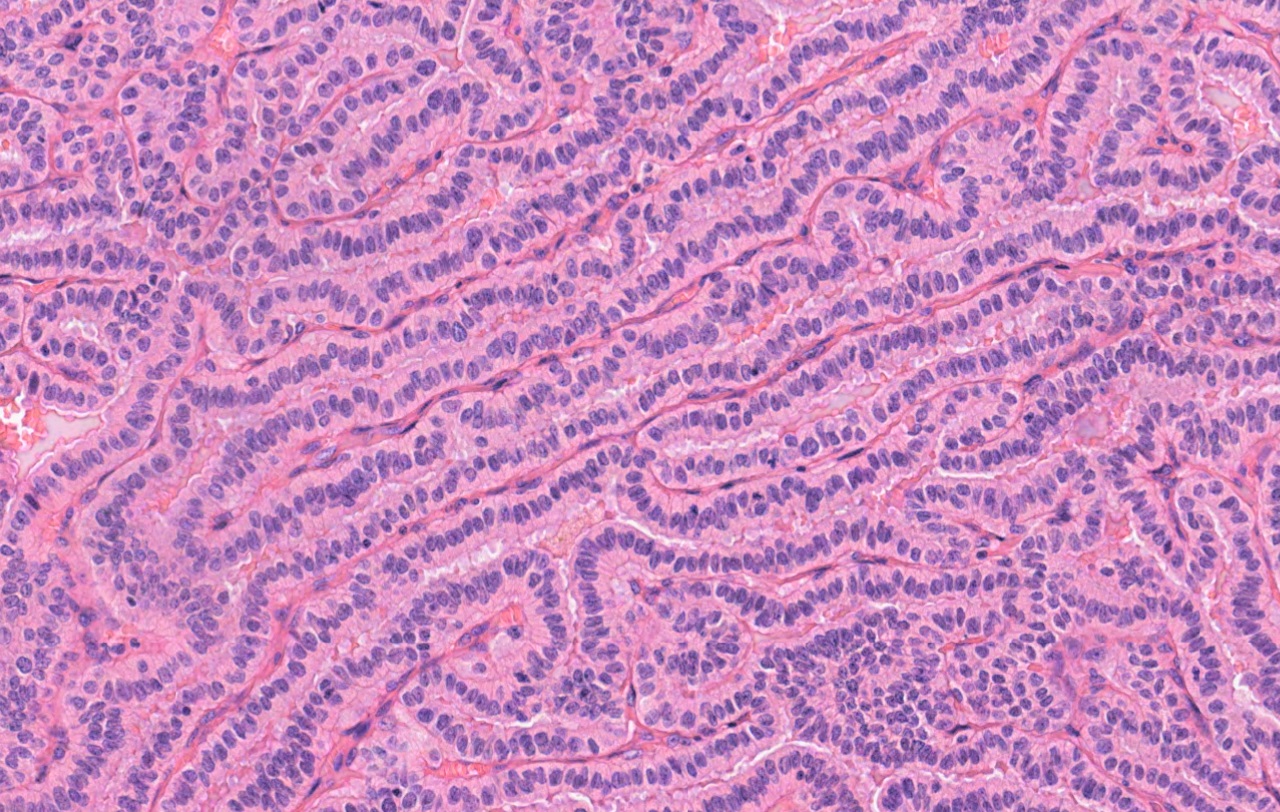
Tram track pattern
Papillary architecture
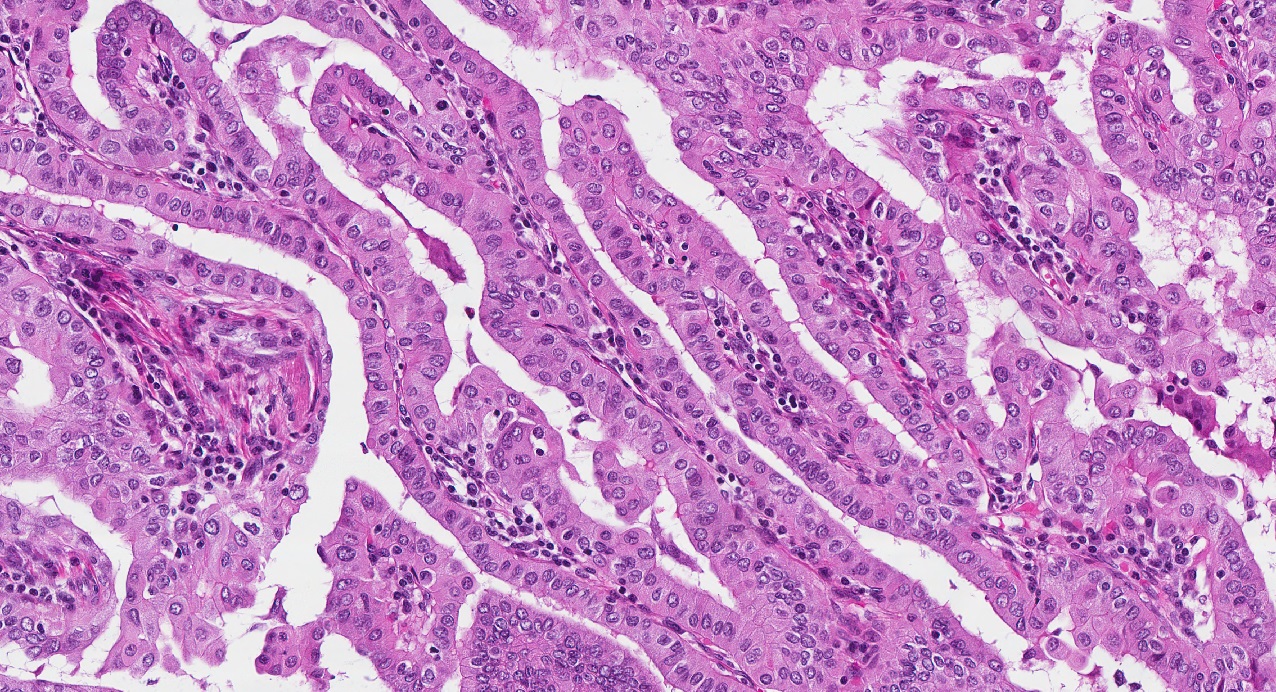
Elongated papillae
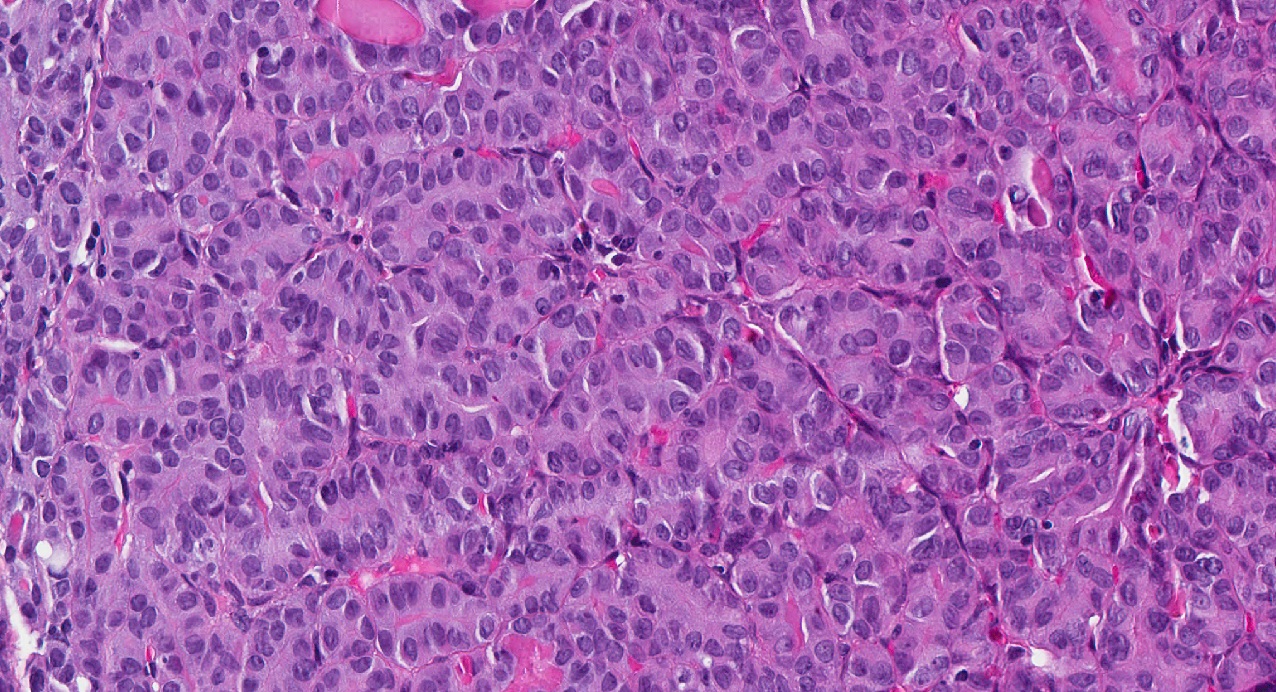
Solid architecture
Trabecular architecture
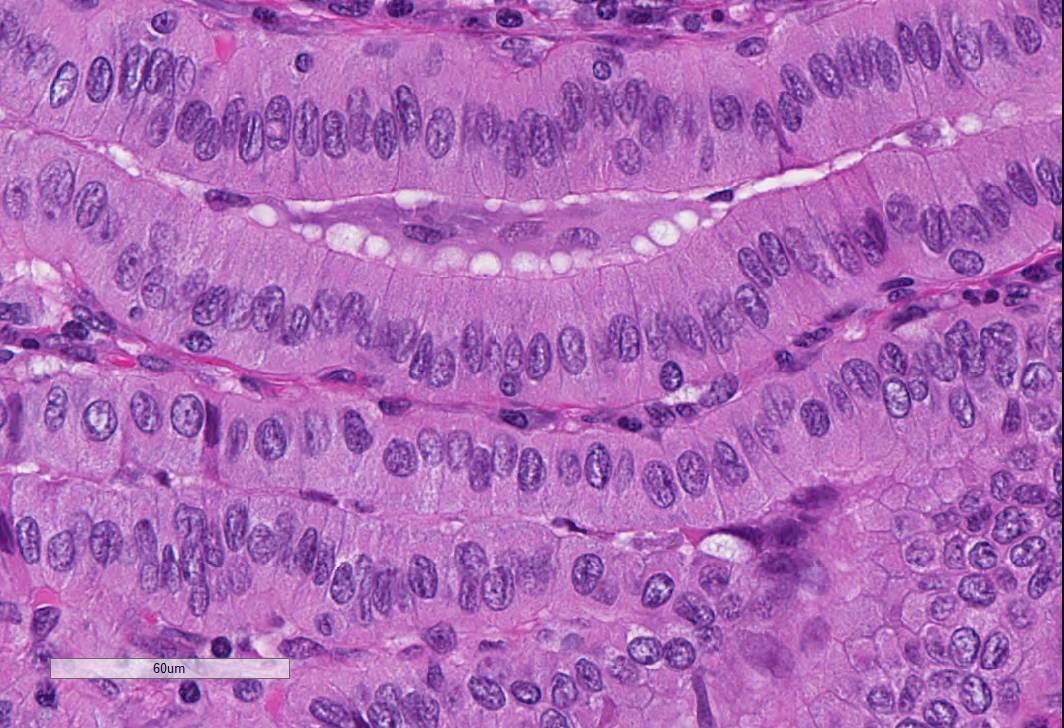
Tall cells
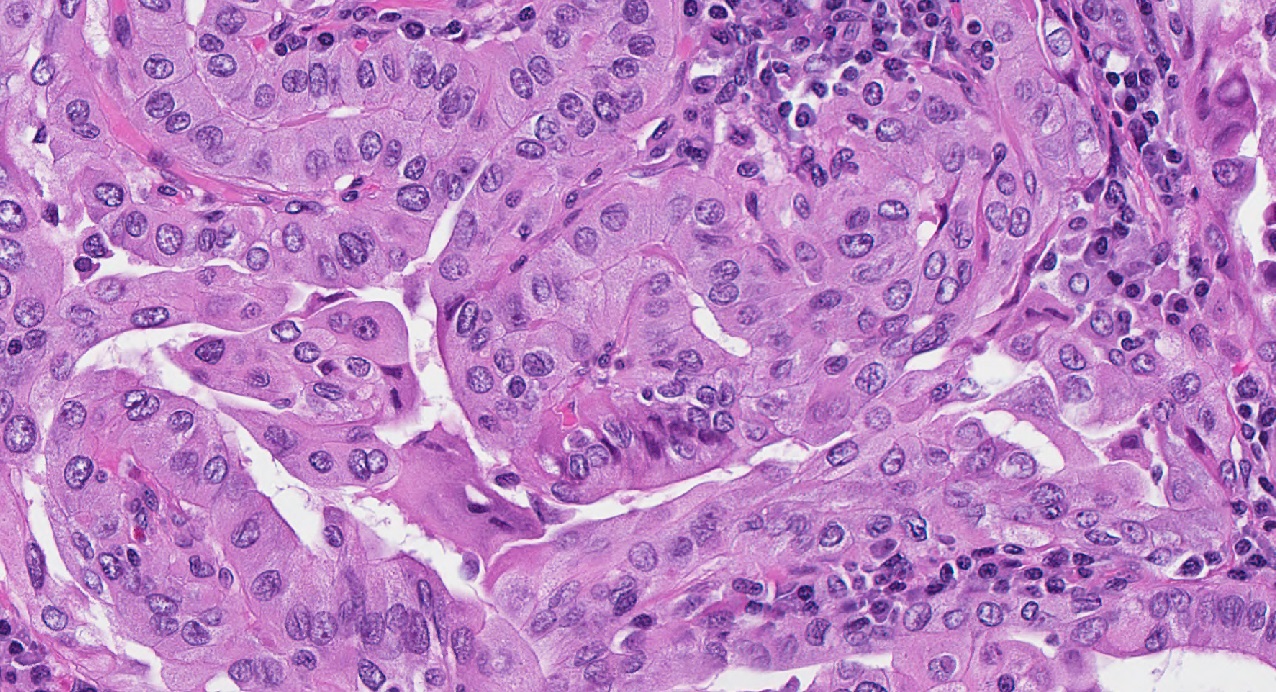
Oncocytic-like cytoplasm
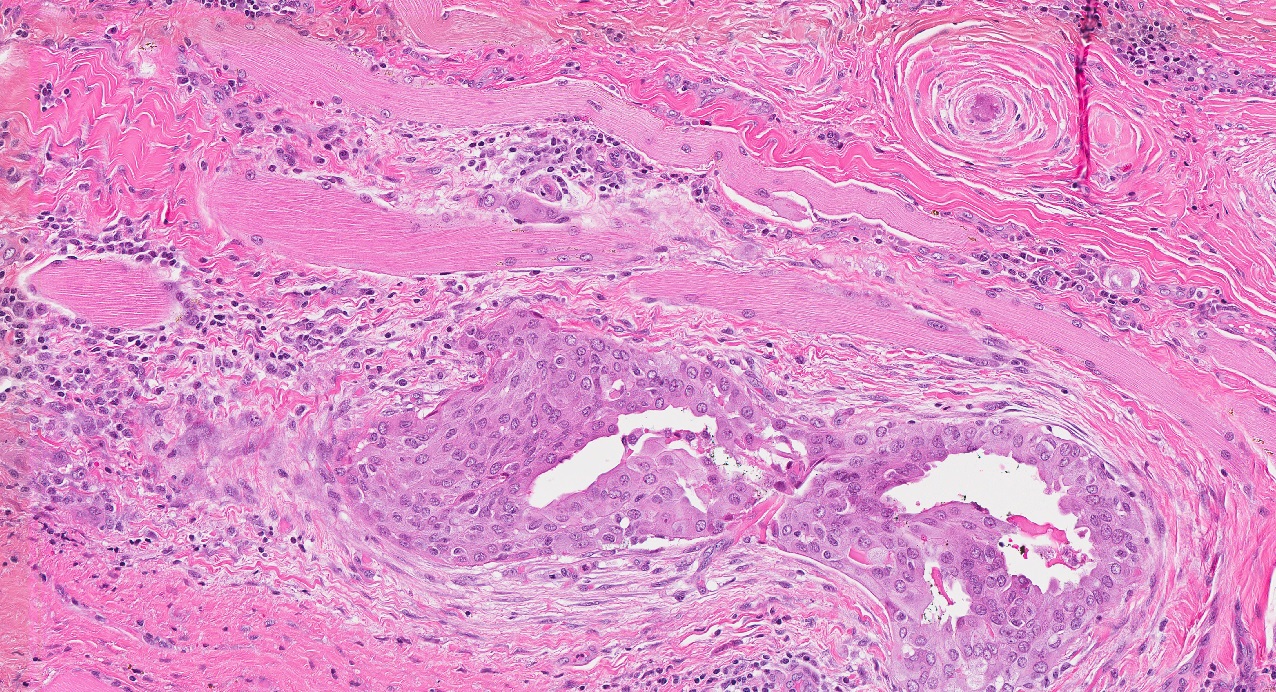
Extrathyroidal extension
Microcarcinoma with infiltrative borders
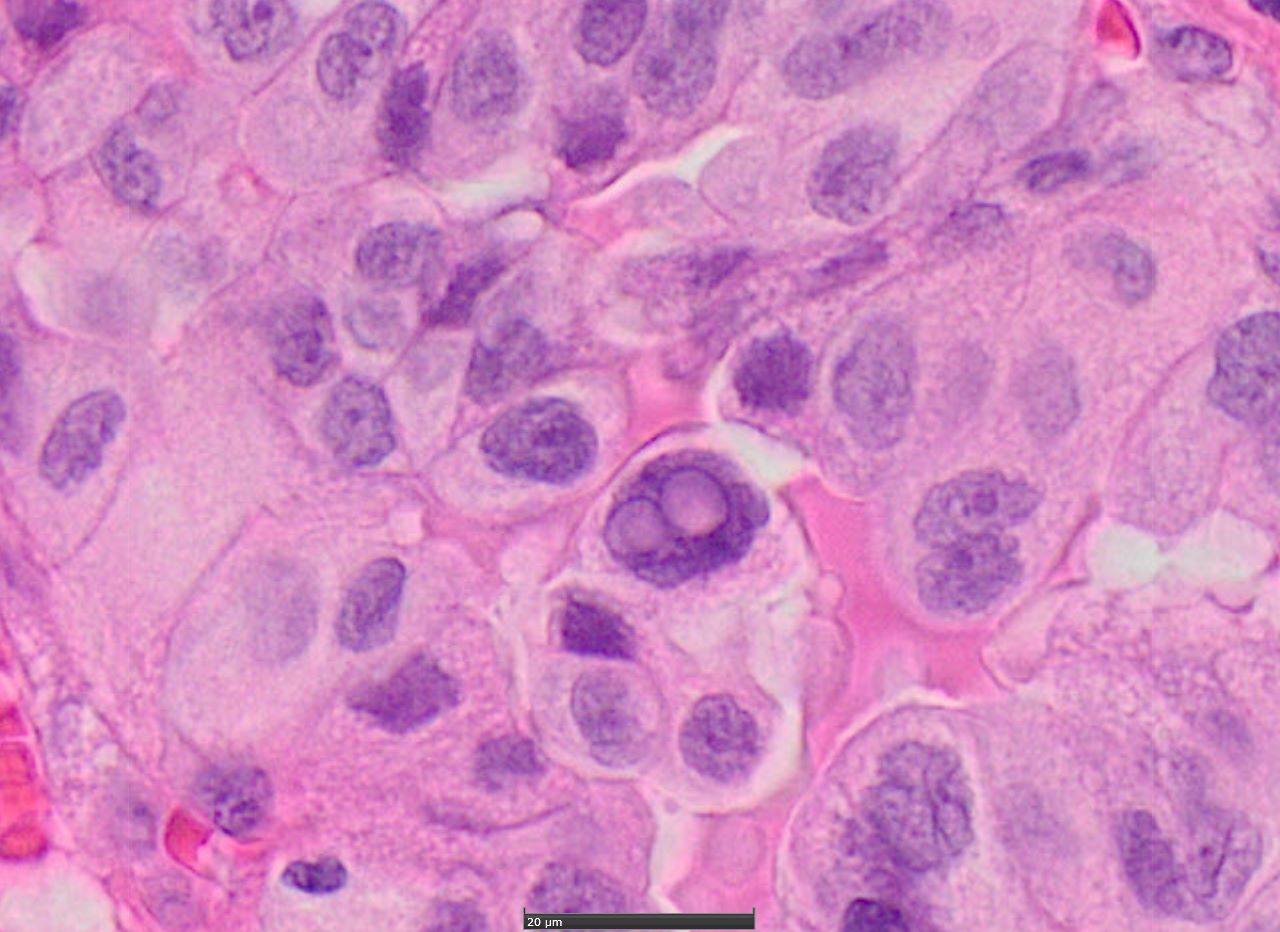
Nuclear features
HBME-1
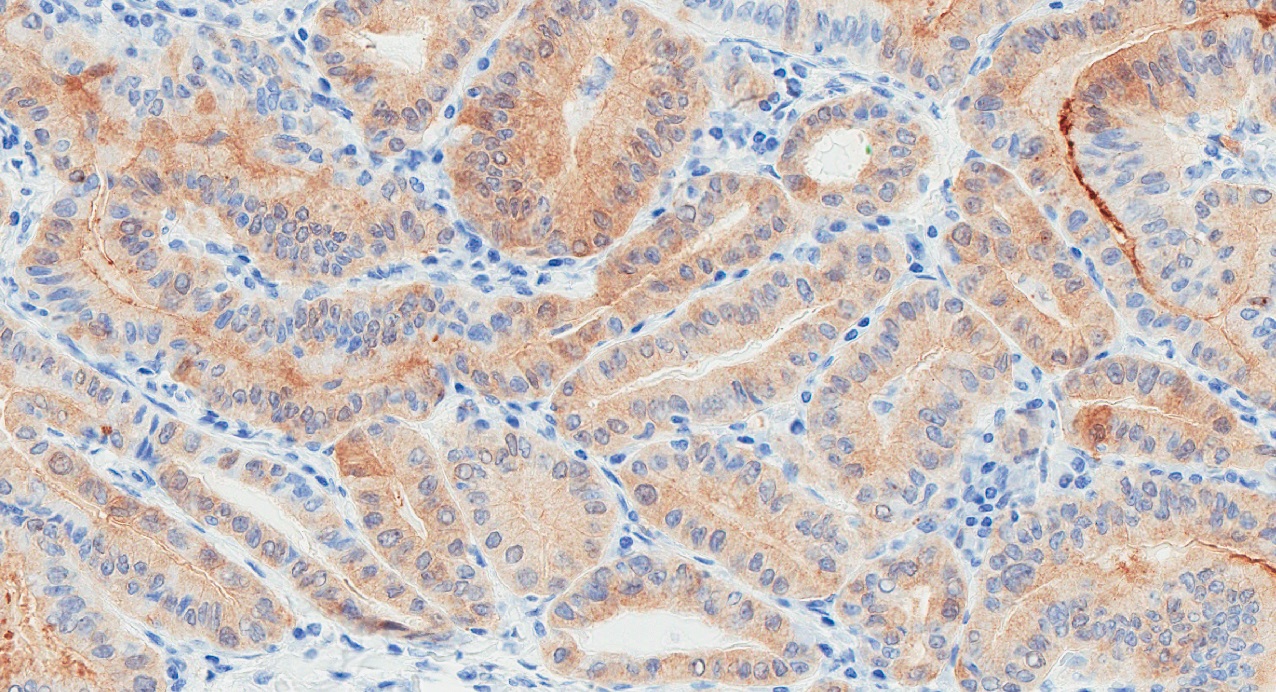
Galectin 3
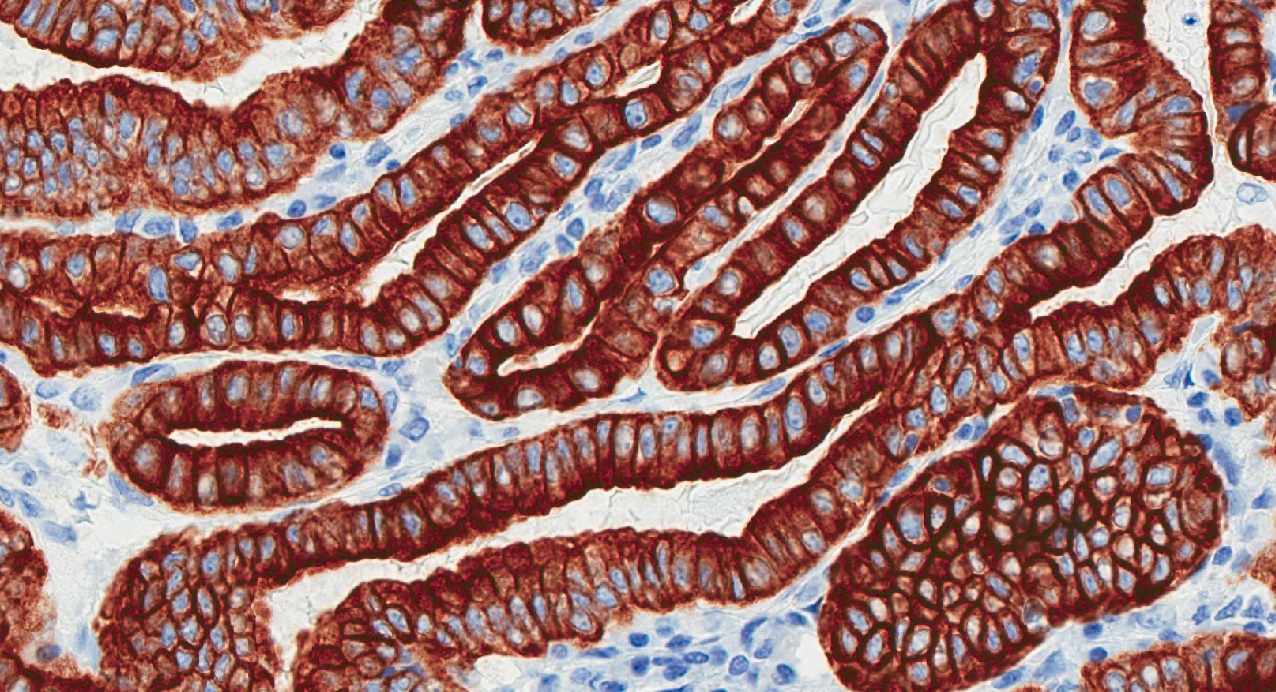
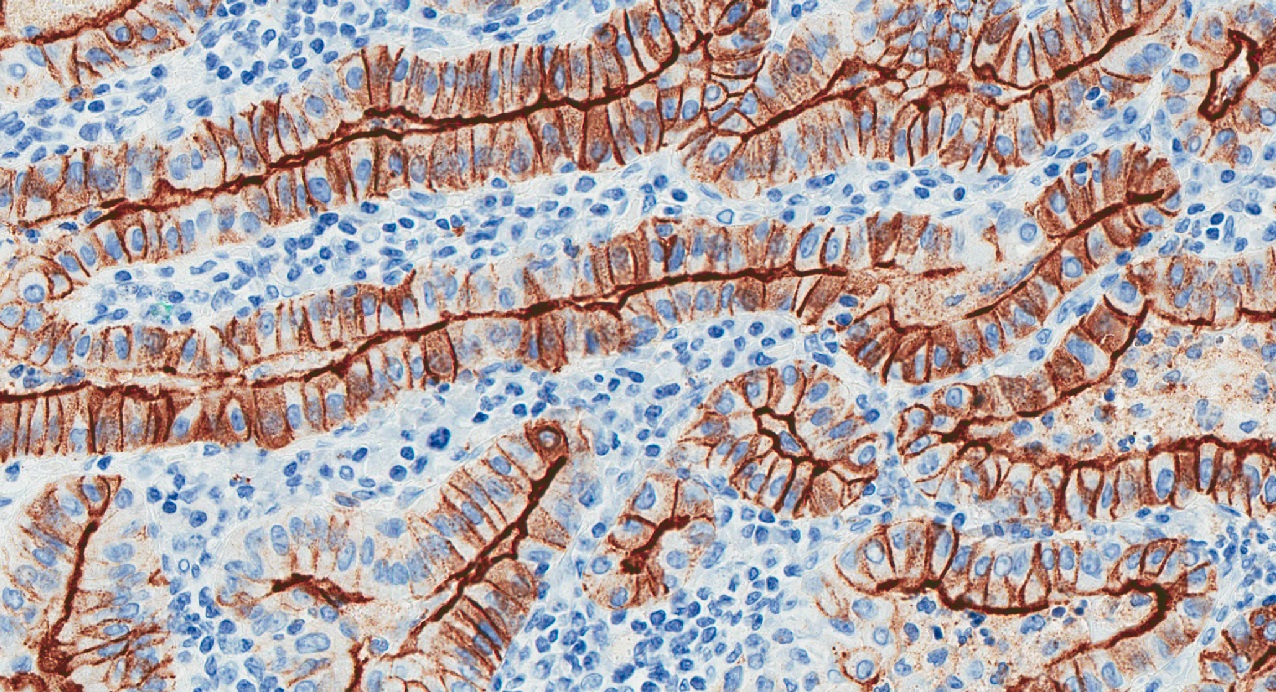
Cytokeratin 19
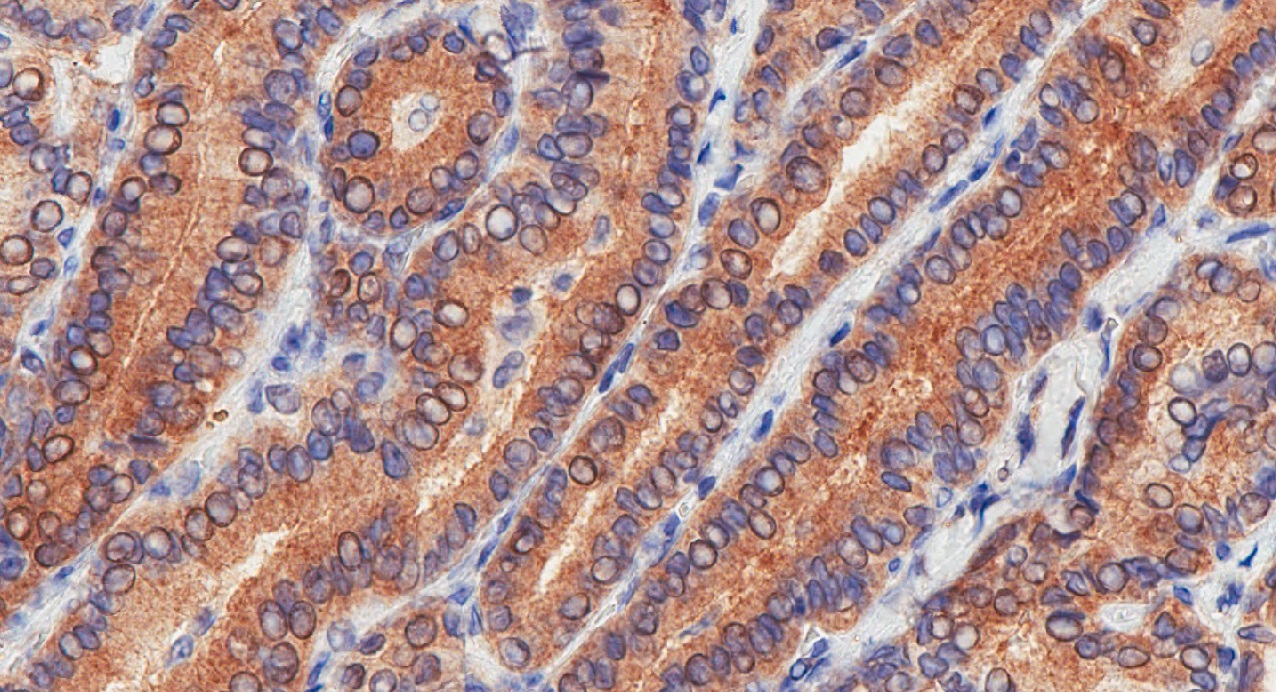
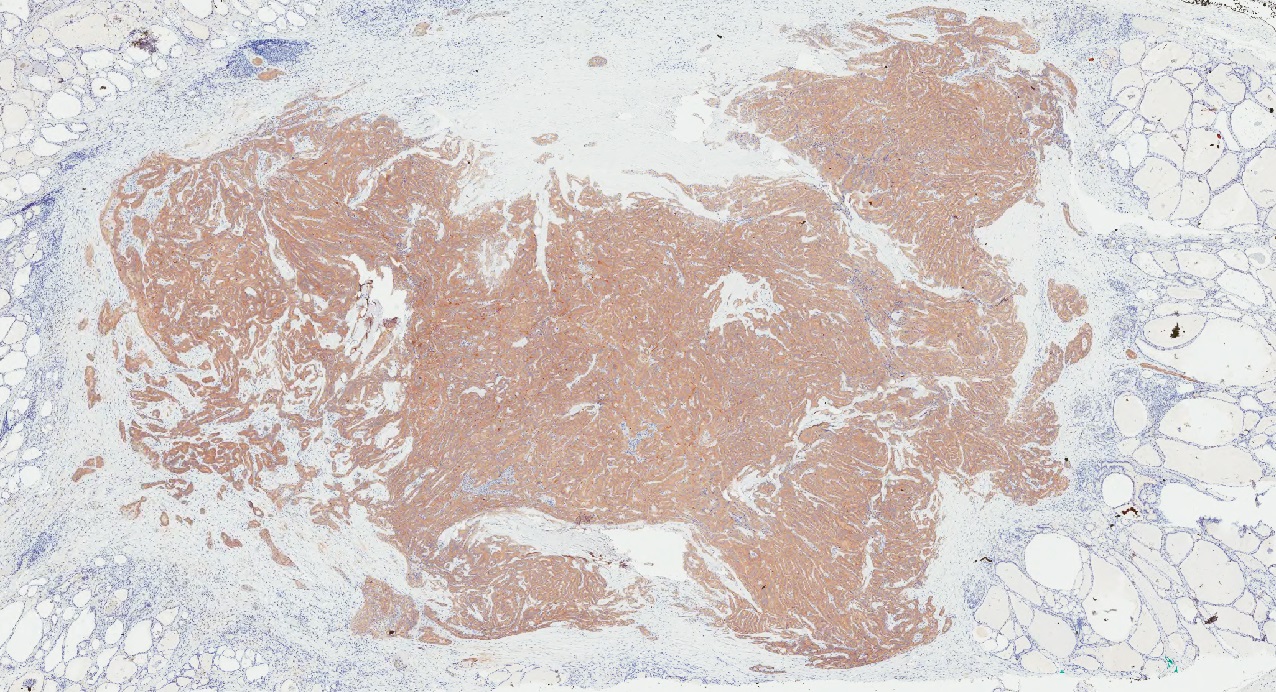
BRAF V600E
Contributed by Andrey Bychkov, M.D., Ph.D.
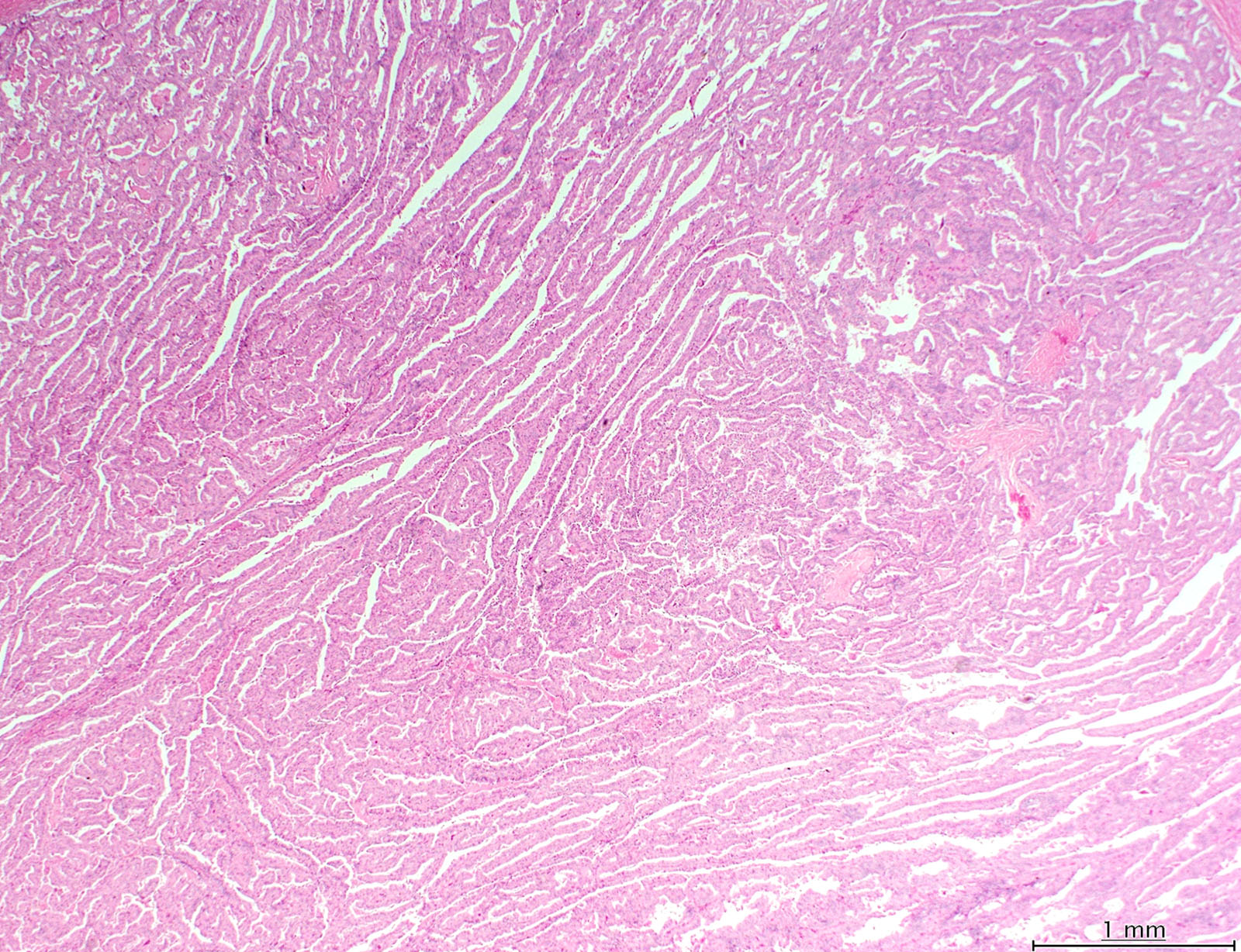
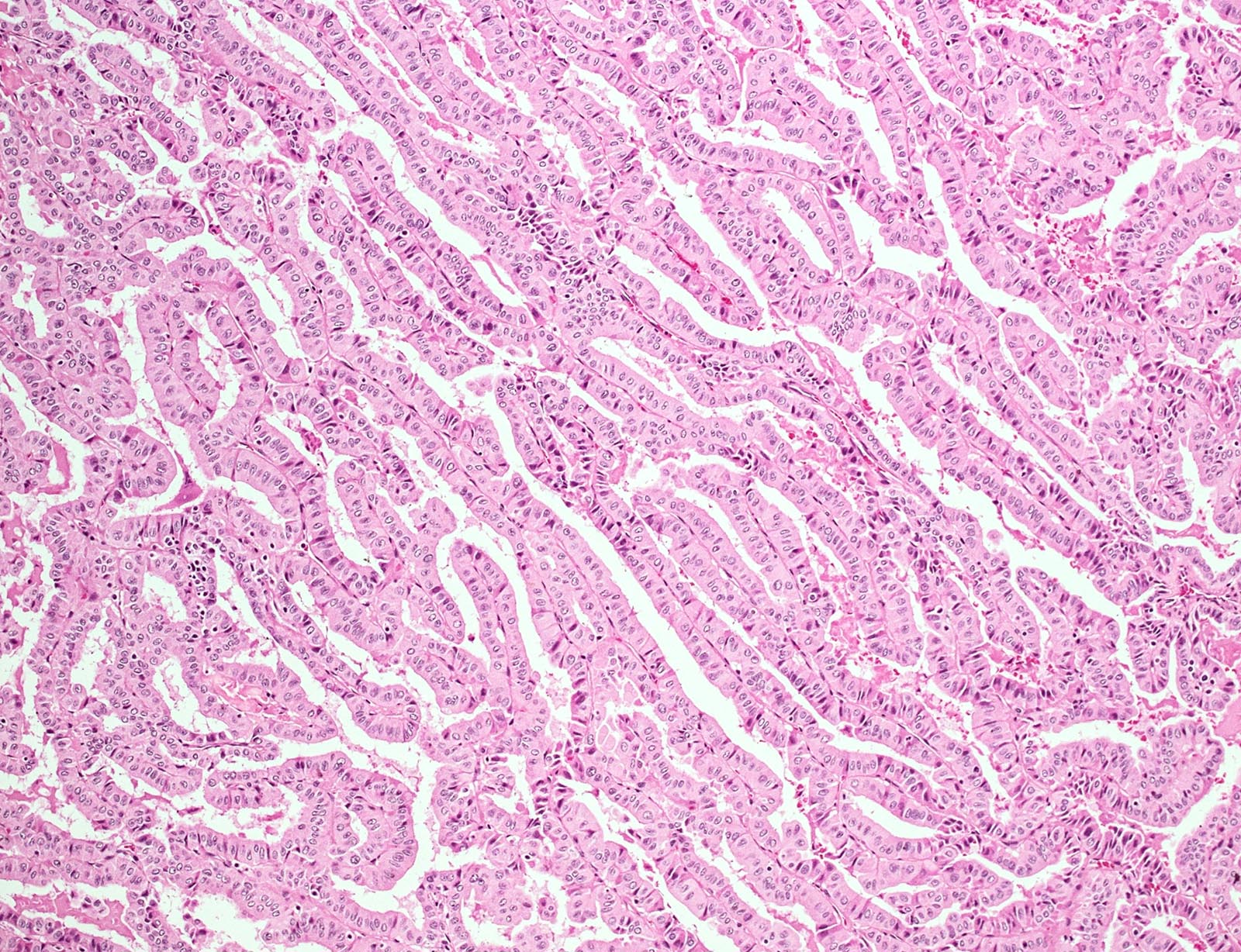
Long papillae with tall cells
Tram track pattern
Virtual slides

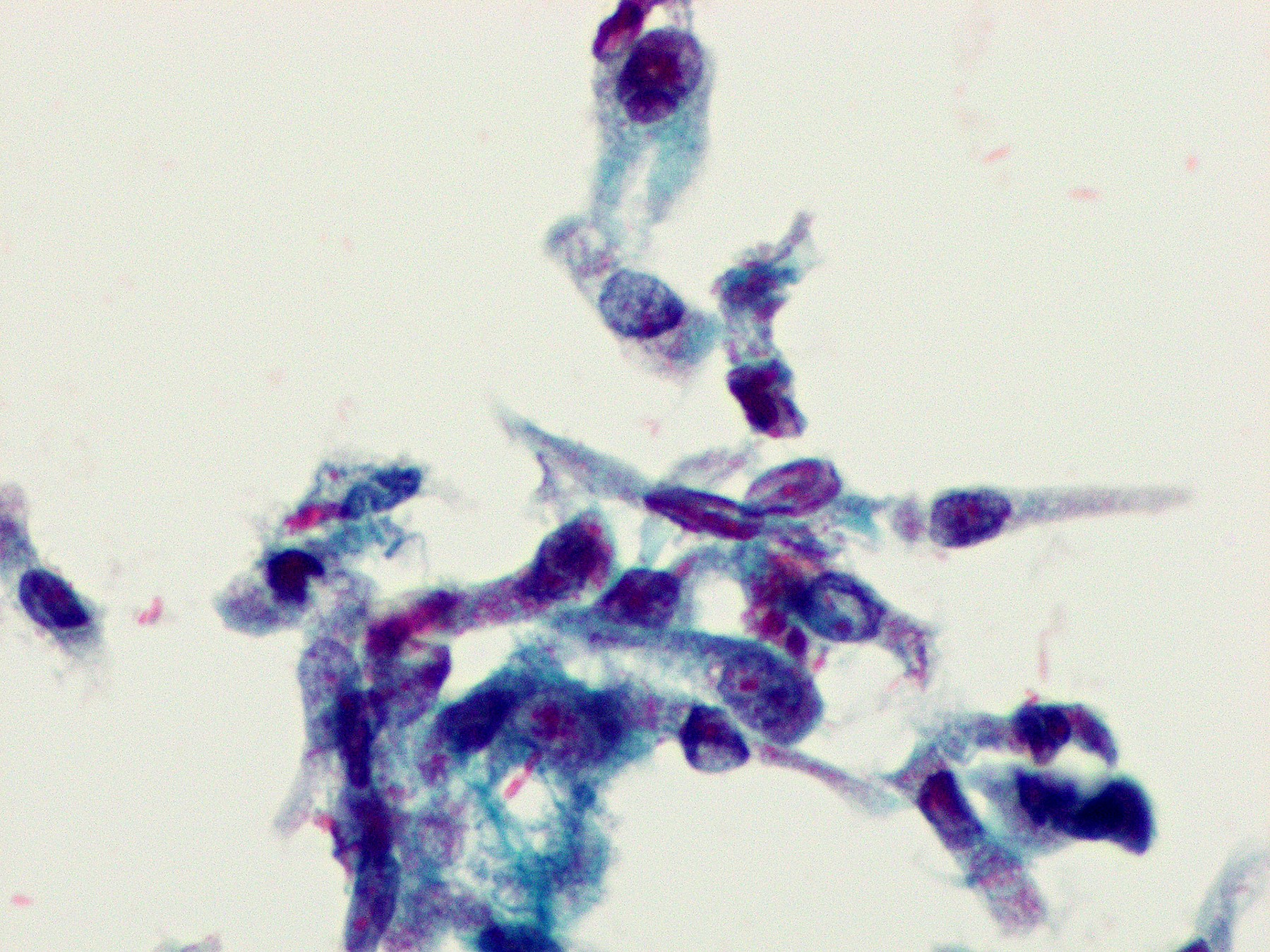
Cytology description
- Tall cell features may be recognized by cytology (see below) but a definitive diagnosis of a tall cell variant requires histologic evaluation (see definition)
- Tall / polygonal cells whose height is 2 - 3 times their width (Diagn Cytopathol 2019;47:452)
- Well defined granular eosinophilic or dense cytoplasm
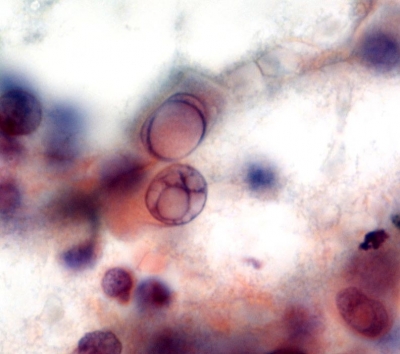
- Nuclei with grooves and pseudoinclusions which can resemble soap bubbles due to multiple pseudoinclusions in the same nucleus (Diagn Cytopathol 2002;27:143, Diagn Cytopathol 2019;47:452)
- Palisaded arrangement and solid clusters
- Cells at the periphery of clusters show a tapering cytoplasmic tail to the outside (cytoplasmic elongation or tadpole cell-like)
- Individual detached cells may show a spindle-like shape or tombstone appearance (both luminal and basal cell borders are horizontal) (Diagn Cytopathol 2019;47:452)
- Lymphocytes may also be present (Acta Cytol 2004;48:325, Diagn Cytopathol 2019;47:452)
Cytology images
Contributed by Papanicolaou Society and the Bethesda System for Reporting Thyroid Cytopathology, Manon Auger, M.D., C.M., Livia Florianova, M.D., M.Sc. and Marc Pusztaszeri, M.D.

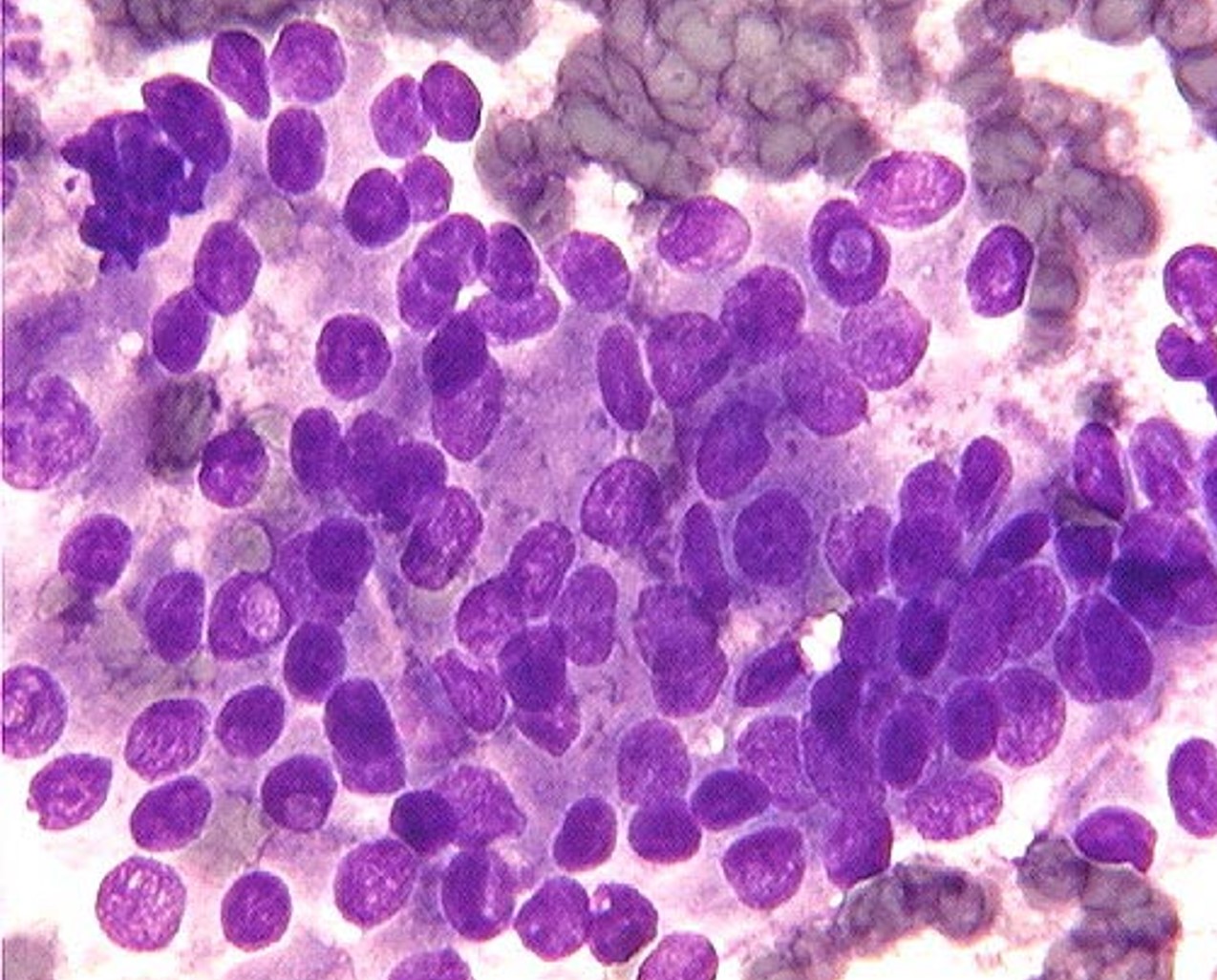
Giemsa
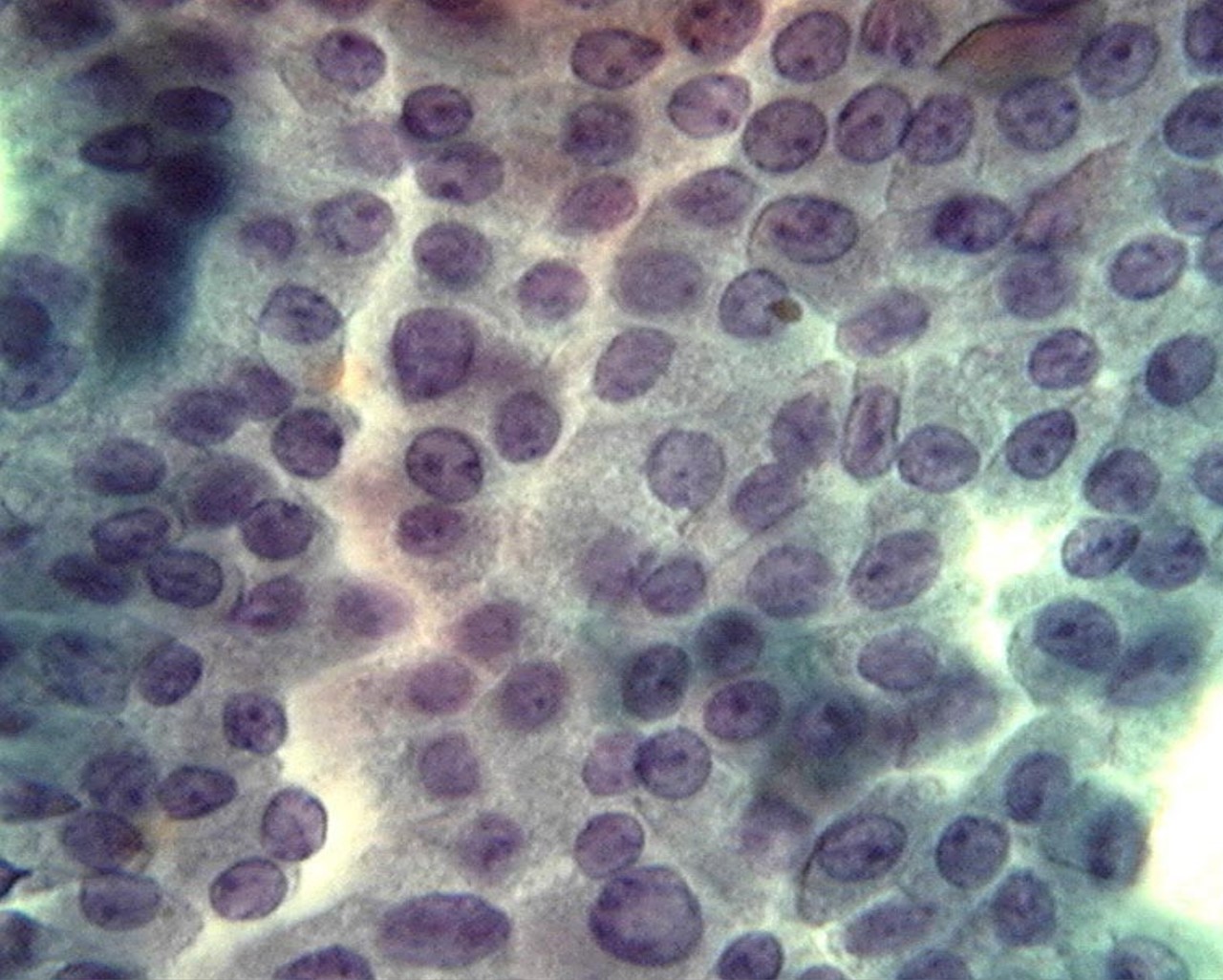
Papanicolaou
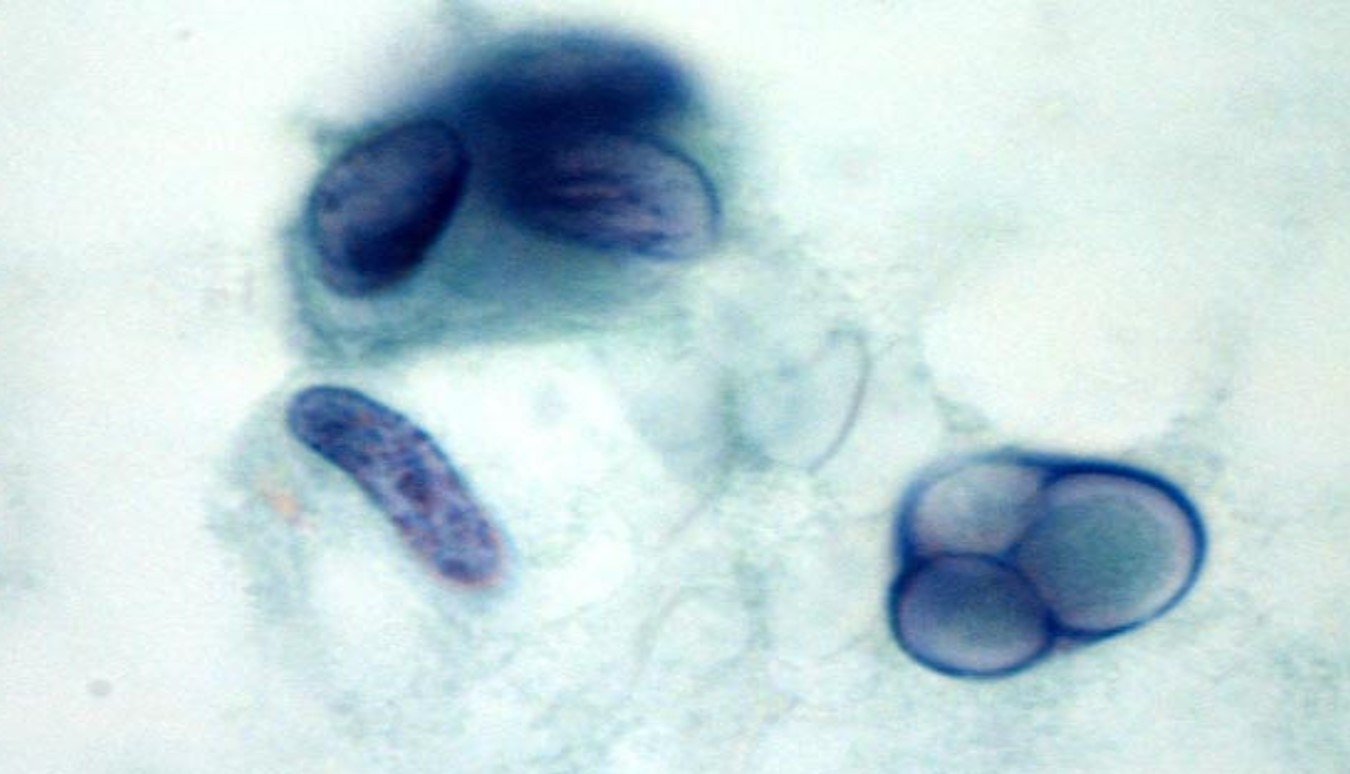
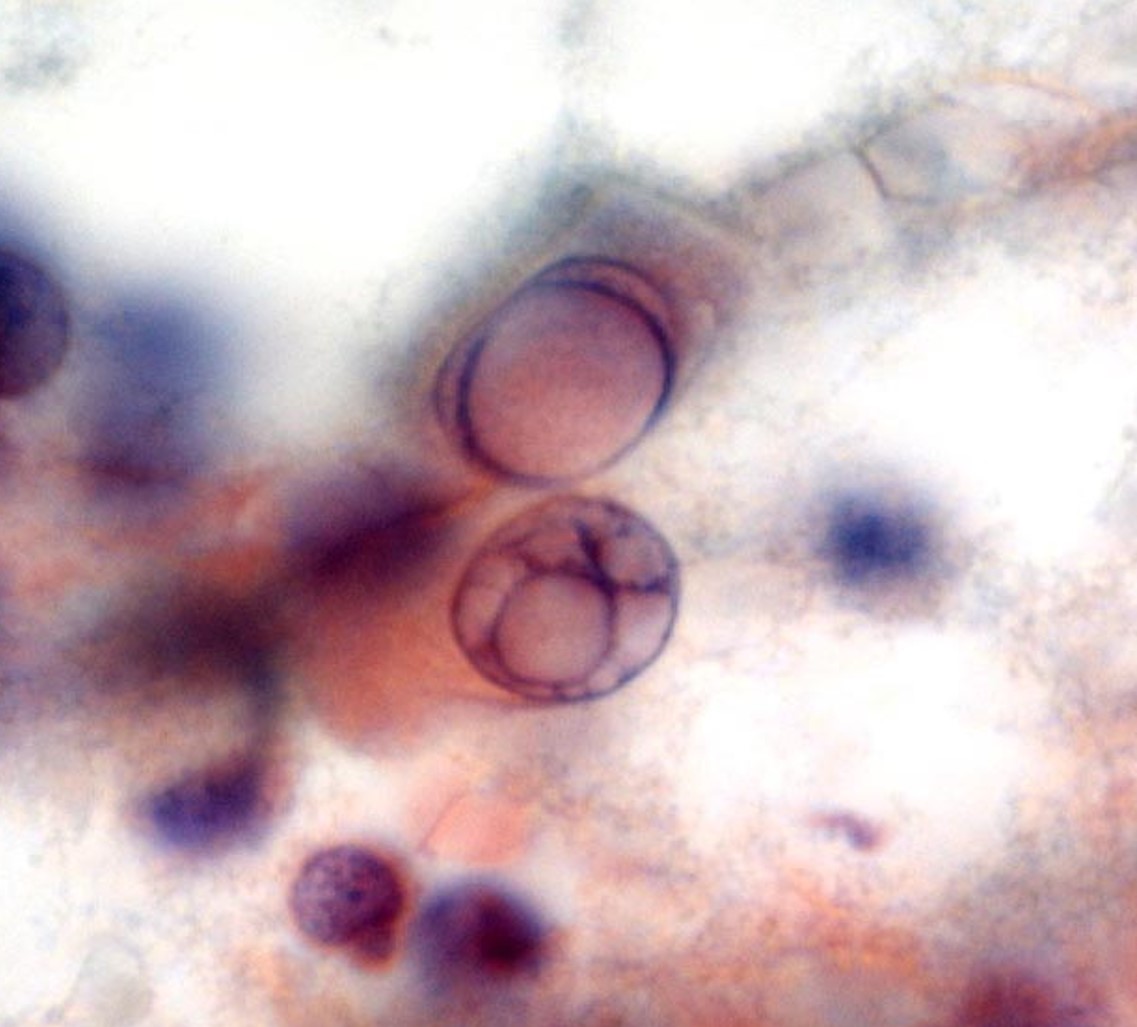
Soap bubble nuclear pseudoinclusions
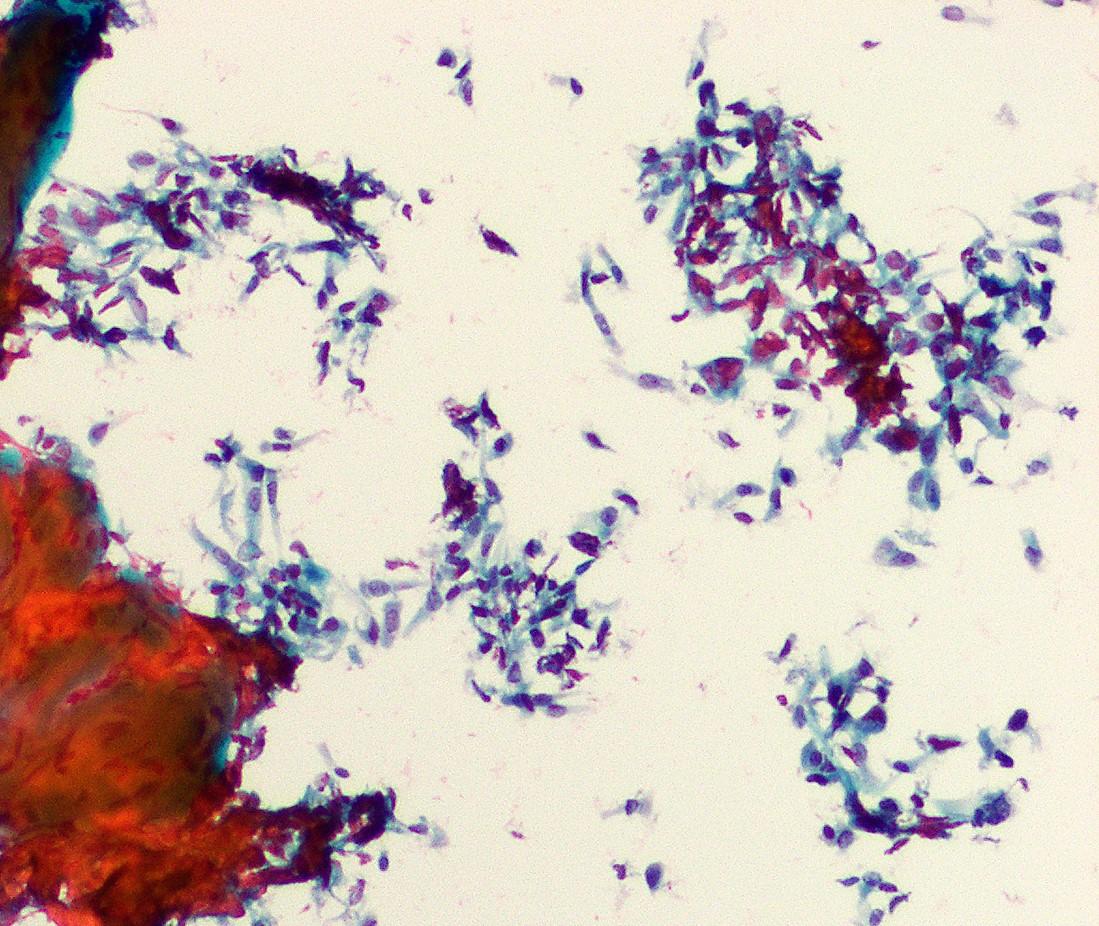
Tall cells
Papillae (cell block)
Tall cells (cell block)
Positive stains
- Thyroid specific: Thyroglobulin, TTF1, PAX8
- Cytokeratins: CK19, broad spectrum cytokeratins (AE1 / AE3)
- HBME, galectin3
- BRAF V600E by mutation specific antibody (VE1)
- May be positive for napsin A (DDx with metastatic lung carcinoma) (Hum Pathol 2010;41:20, Endocr Pathol 2020;31:39)
Negative stains
Electron microscopy description
- Intranuclear cytoplasmic inclusions and abundant mitochondria in cytoplasm (Ultrastruct Pathol 1985;8:131)
Molecular / cytogenetics description
- Highest mutation density (DNA copy number alterations) of all PTC variants (Cell 2014;159:676)
- BRAF V600E mutation in ~80% of cases (Oncogene 2004;23:7436, Endocr Relat Cancer 2005;12:245, J Clin Endocrinol Metab 2003;88:5399)
- Higher frequency of TERT promoter mutations than in classic PTC (5 - 30% versus 10%) (Endocr Relat Cancer 2013;20:60)
- RAS mutations have not been identified
Videos
High grade and poorly differentiated and anaplastic thyroid carcinoma
Ultrasound of tall cell variant of PTC
Sample pathology report
- Thyroid, left lobe, fine needle aspiration:
- Satisfactory for evaluation
- Malignant (Bethesda diagnostic category VI)
- Papillary thyroid carcinoma, favor tall cell variant
- Thyroid, left lobe, left hemithyroidectomy:
- Papillary thyroid carcinoma, classic type with tall cell features (20%) (see synoptic report)
- Thyroid, total thyroidectomy:
- Papillary thyroid carcinoma, tall cell variant (see synoptic report)
Differential diagnosis
- Other papillary thyroid carcinoma variants:
- Classic variant with tall cell features:
- < 30% of tall cell component
- Columnar cell variant:
- Nuclear stratification, rare nuclear pseudoinclusions, absence of eosinophilic cytoplasm and distinct cell borders
- Often CDX2 positive
- Warthin-like variant:
- Dense lymphocytic infiltration within vascular cores of stroma, rarely infiltrative
- Oncocytic variant:
- No or only rare tall cells, lack of distinct cell borders, prominent nucleoli
- Classic variant with tall cell features:
- Breast tall cell carcinoma with reversed polarity (very rare):
- Focal positivity for GATA3, GCDFP-15 and mammaglobin
- TTF1, thyroglobulin and BRAF V600E consistently negative (Mod Pathol 2018;31:1367, Am J Surg Pathol 2017;41:887, Histopathology 2018;73:339)
Board review style question #1
Which of the following statements concerning the tall cell variant of papillary thyroid carcinoma is correct?
- It usually has an indolent clinical course
- Most cases are associated with a RAS mutation
- Patients are usually older adults
- The tumor is positive for TTF1, synaptophysin and calcitonin
- Tumor cells are stratified and only focal areas show characteristic papillary thyroid carcinoma nuclear features
Board review style answer #1
Board review style question #2
Which of the following diagnostic features are associated with the tall cell variant of papillary thyroid carcinoma?
- A dense lymphocytic infiltration of tumor stroma
- Cells with granular eosinophilic cytoplasm and nuclei with a soap bubble appearance on cytology
- Focal positivity for GATA3
- Infrequent nuclear grooves and pseudoinclusions
- High nucleus to cytoplasm ratio
Board review style answer #2
B. Cells with granular eosinophilic cytoplasm and nuclei with a soap bubble appearance on cytology
Comment Here
Reference: Papillary carcinoma, tall cell variant
Comment Here
Reference: Papillary carcinoma, tall cell variant
