
Thyroid & parathyroid
Other uncommon lesions / neoplasms
Solitary fibrous tumor
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.

Last author update: 12 May 2023
Last staff update: 16 July 2024
Copyright: 2014-2025, PathologyOutlines.com, Inc.
PubMed Search: Solitary fibrous tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nguyen TPX, Vuong HG. Solitary fibrous tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidsft.html. Accessed April 1st, 2025.
Definition / general
- Solitary fibrous tumor (SFT) of the thyroid is a fibroblastic mesenchymal neoplasm characterized by NAB2::STAT6 gene fusion
- Thyroid SFT is indistinguishable from pleural or other extrapleural solitary fibrous tumors
Essential features
- Fibroblastic tumor composed of collagen producing spindle cells arranged in a characteristic vascular pattern
- Immunohistochemical nuclear expression of STAT6 is highly sensitive and specific for the presence of the NAB2::STAT6 gene fusion product; STAT6 is a marker for confirming the diagnosis of solitary fibrous tumor
- < 10% cases of SFT of thyroid may show malignant histological features
Terminology
- Extrapleural solitary fibrous tumor
- Not recommended: hemangiopericytoma; giant cell angiofibroma; benign solitary fibrous tumor
ICD coding
Epidemiology
- Rare tumor in thyroid; < 0.1% of SFTs arise in the head and neck area (Thyroid 2010;20:435)
- M = F
- Median age: 54.4 years (28 - 88 years) (Head Neck Pathol 2019;13:597)
Sites
- Entire thyroid
Etiology
- Unknown
- Not associated with a longstanding pre-existing goiter or thyroid tumor
- Possibly primitive mesenchymal cells capable of myofibroblastic, adipose and hemangiopericytic differentiation (Nose: Diagnostic Pathology - Endocrine, 2nd Edition, 2018)
Diagrams / tables
Images hosted on other servers:

4 variable risk stratification
Clinical features
- Painless, slow growing neck mass in euthyroid patients (Nose: Diagnostic Pathology - Endocrine, 2nd Edition, 2018)
- Tumor may extend inferiorly from the thyroid gland and present as a mediastinal mass (Med J Islam Repub Iran 2014;28:51)
- Compressive symptoms and respiratory failure may occur in some rare cases (Ann Thorac Cardiovasc Surg 2014;20:427, Saudi Med J 2004;25:805)
Diagnosis
- Based on histological findings and NAB2::STAT6 gene fusion (immunohistochemical or molecular tests)
Laboratory
- Serum thyroid function tests such as thyroid stimulating hormone (TSH), triiodothyronine (T3), free thyroxine (T4) and thyroperoxidase (TPO) antibodies are normal (Endocr Pathol 2011;22:165)
Radiology description
- Ultrasonography: heterogeneous, mainly hyperechoic nodule (World J Clin Cases 2020;8:782)
- Computed tomography (CT): heterogeneous enhanced lesion (Clinical Imaging 2019;53:105)
- Magnetic resonance imaging (MRI): fibrous areas have intermediate intensity on T1 while cellular or myxoid zones present as variable hypointensity to hyperintensity on T2 (Trans Gastroenterol Hepatol 2018;3:94)
Radiology images
Images hosted on other servers:

Ultrasound: heterogeneous, hyperechoic solitary nodule

CT: heterogeneous enhanced lesion
Prognostic factors
- High mitotic index, tumor cellularity, necrosis, nuclear pleomorphism correlated with metastatic or local recurrence potential
- Difficult to predict patient's clinical course if based solely on histologic parameters (Ann Surg Oncol 2017;24:3865)
- Age ≥ 55, tumor size ≥ 10 cm, mitotic count ≥ 4/10 high power fields, tumor necrosis ≥ 10% are unfavorable prognostic factors in SFTs of all anatomic sites (Mod Pathol 2017;30:1433)
- TERT promoter mutations may be associated with a poor prognosis (Mod Pathol 2016;29:1511, Histopathology 2018;73:843)
Case reports
- 34 year old woman with enlarging thyroid mass (Arch Clin Cases 2021;8:97)
- 41 and 64 year old men with a firm, painless cervical mass (Pathol Int 2006;56:471)
- 42 year old woman with a solid nodule in her right thyroid lobe and 61 year old man with a right cervical lump (Head Neck Pathol 2008;2:231)
- 47 year old woman with a neck mass and 59 year old man with an asymptomatic neck swelling (Endocr Pathol 2011;22:165)
- 58 year old man presented with worsening respiratory symptoms (Thyroid 2010;20:435)
- 59 year old man with a large neck mass (World J Clin Cases 2020;8:782)
- 61 year old man with a slow growing thyroid mass (Diagn Cytopathol 2003;28:213)
- 68 year old man with a left cervical lump (Pathol Res Pract 2003;199:687)
- 76 year old woman with an enlarging neck mass (Diagn Cytopathol 2011;39:694)
- 78 year old man with a right cervical mass (Med Mol Morphol 2014;47:117)
Treatment
- Total thyroidectomy or lobectomy (Laryngoscope 2009;119:2306, Med Mol Morphol 2014;47:117)
- Roles of chemotherapy or radiation therapy are controversial (Diagn Cytopathol 2011;39:694)
- Close follow up after surgery seems to be the most commonly used approach
Gross description
- Well circumscribed mass
- Relatively large (5 - 10 cm)
- White to gray-brown color, usually solid, sometimes with cystic spaces (Head Neck Pathol 2019;13:597)
Gross images
Images hosted on other servers:

Solid, well circumscribed white nodule

Encapsulated, tan-pink to tan-white mass
Microscopic (histologic) description
- Similar to SFT of any other organ
- Usually unencapsulated
- Proliferation of spindled cells with alternating hypo and hypercellular areas
- Tumor cells are spindled with elongated, slender nuclei surrounded by scant cytoplasm; nuclear chromatin is delicate, fine to vesicular
- Patternless architecture interspersed with loosely to densely collagenized or myxoid stroma
- Highly vascular, with dilated, branching, hyalinized staghorn-like (hemangiopericytoma-like), thin walled vessels
- Infiltration by inflammatory cells (mainly mast cells) can be seen
- Mitoses and nuclear atypia are rare; necrosis is absent or rare
- Uncommon: cysts, myxoid change, lipomatous features (Thompson: Diagnostic Pathology - Head and Neck, 2nd Edition, 2016)
- High mitotic index (> 4 mitoses per 10 high power fields); hypercellularity, nuclear atypia; hemorrhage and necrosis are suggestive of malignant transformation (Am J Surg Pathol 1998;22:1501)
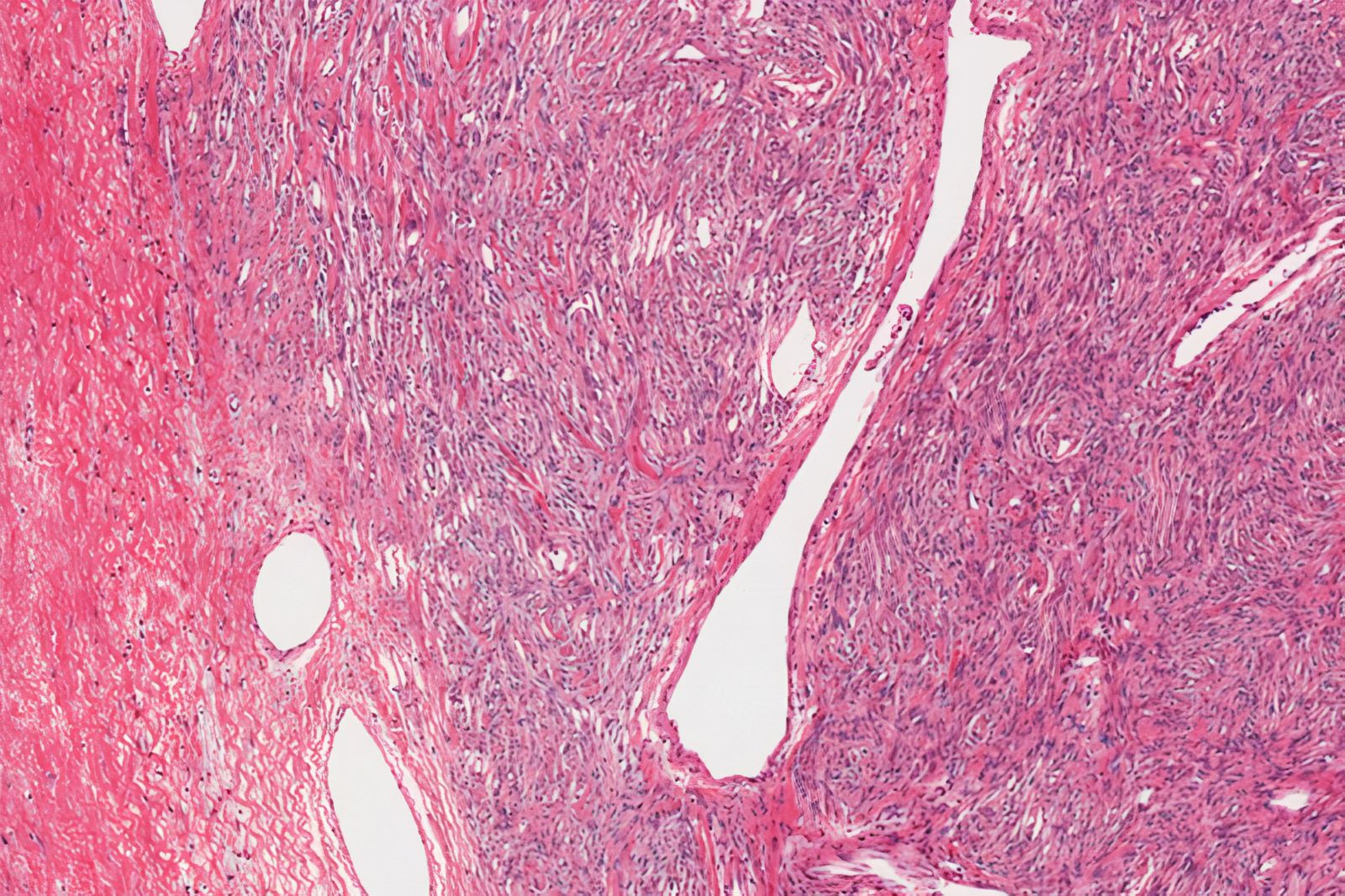
Microscopic (histologic) images
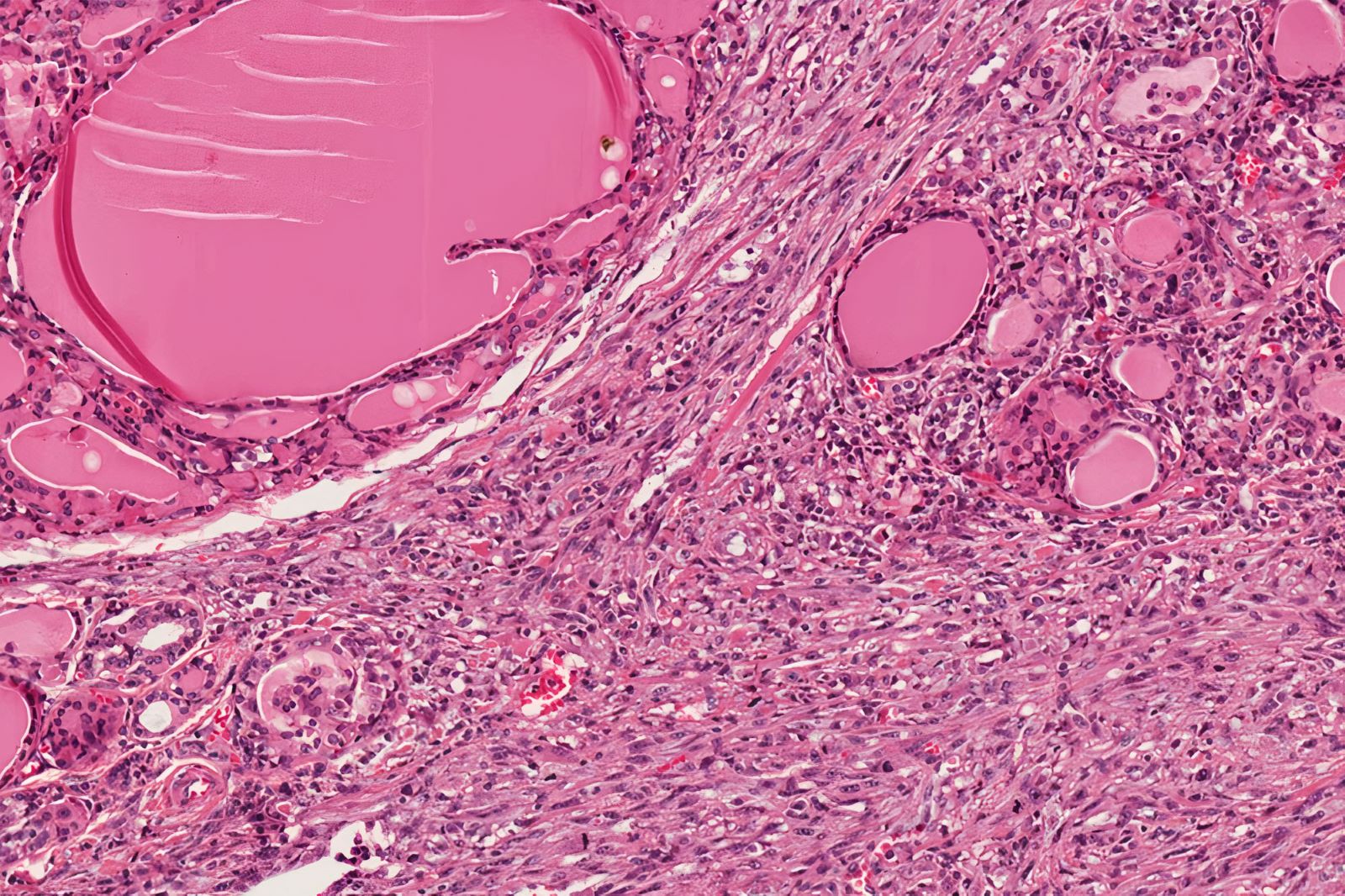
Contributed by Truong Phan Xuan Nguyen, M.D.
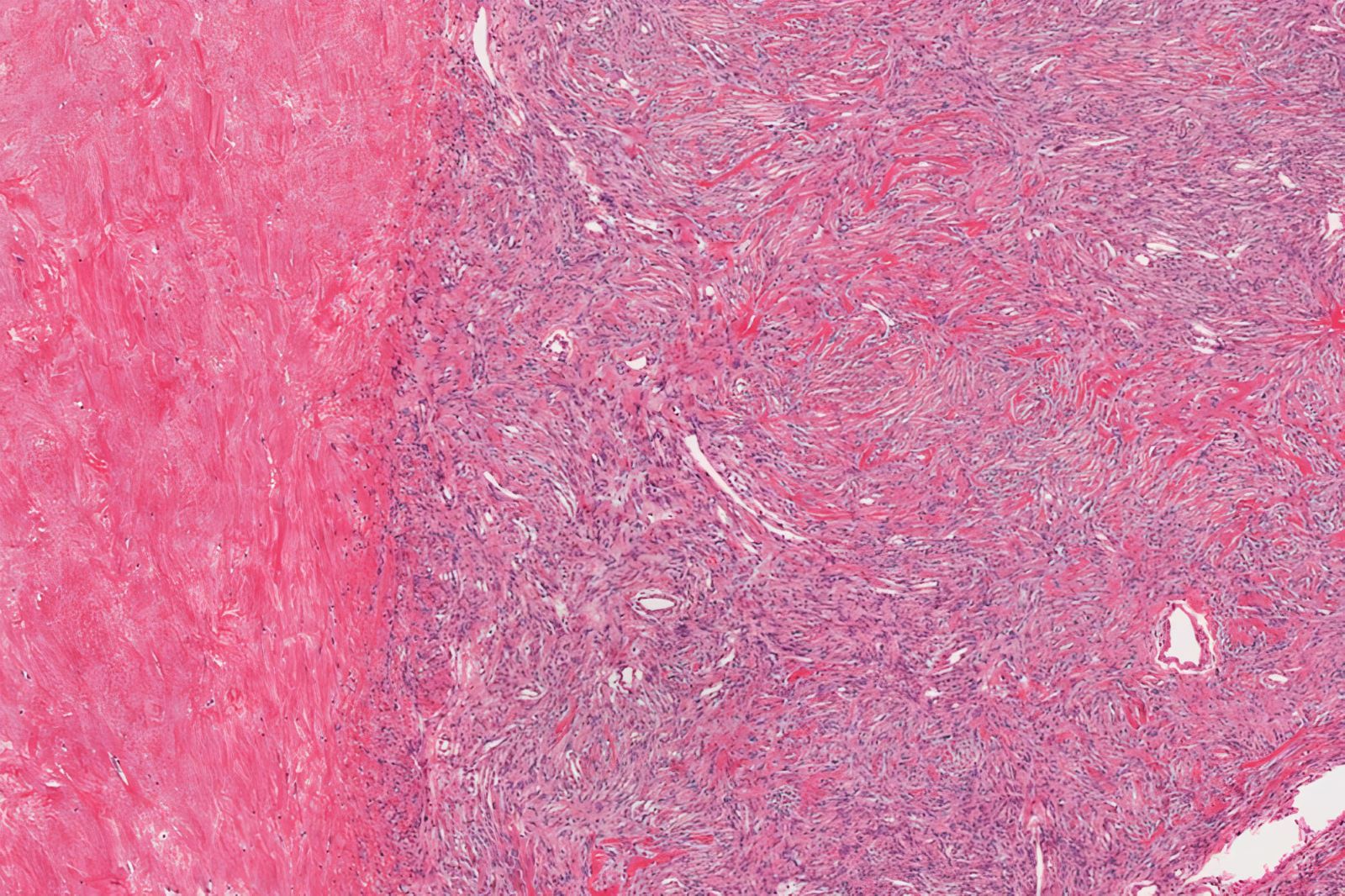
Well defined border
Entrapped thyroid follicles
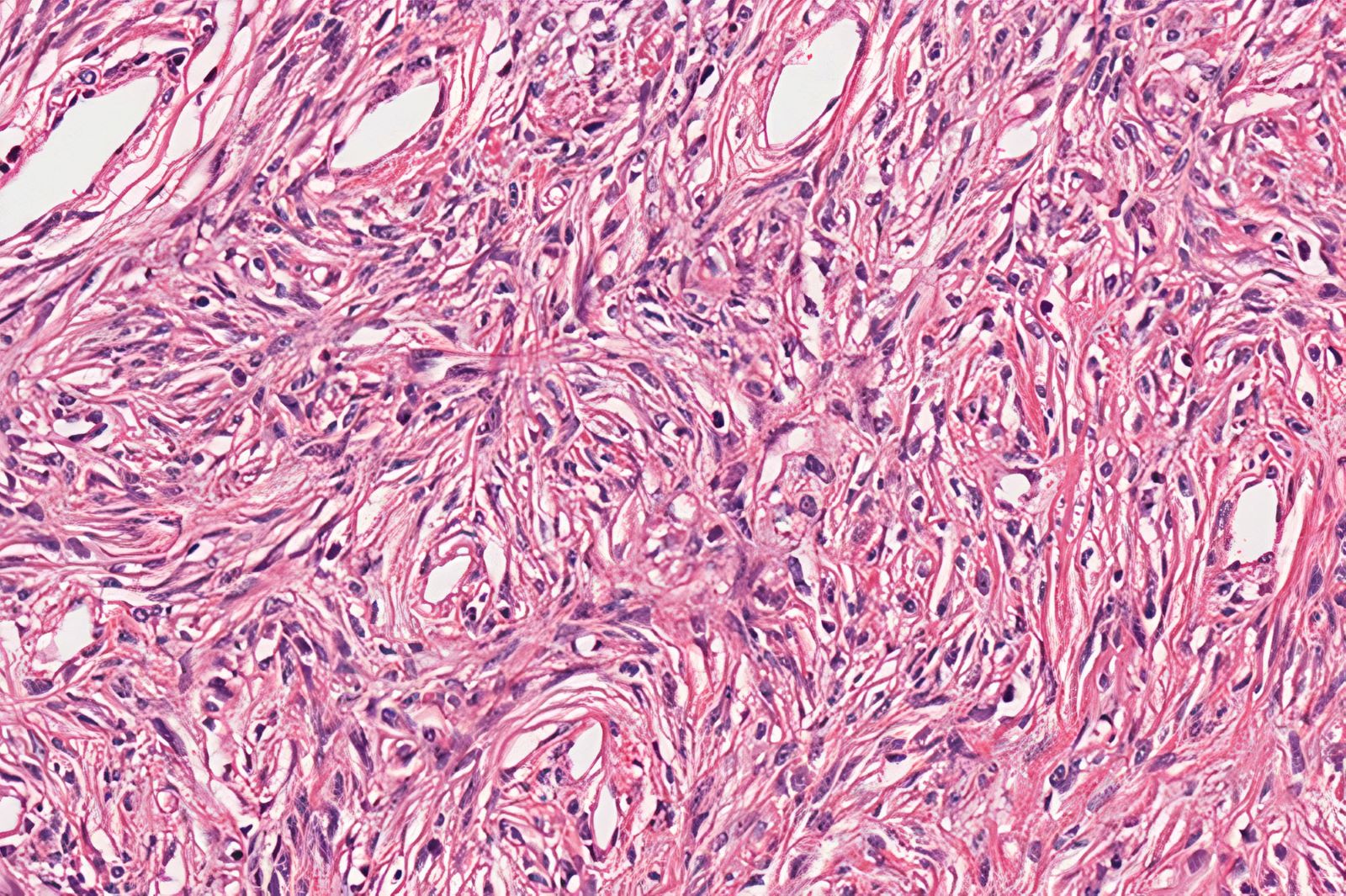
Patternless proliferation of spindled cells
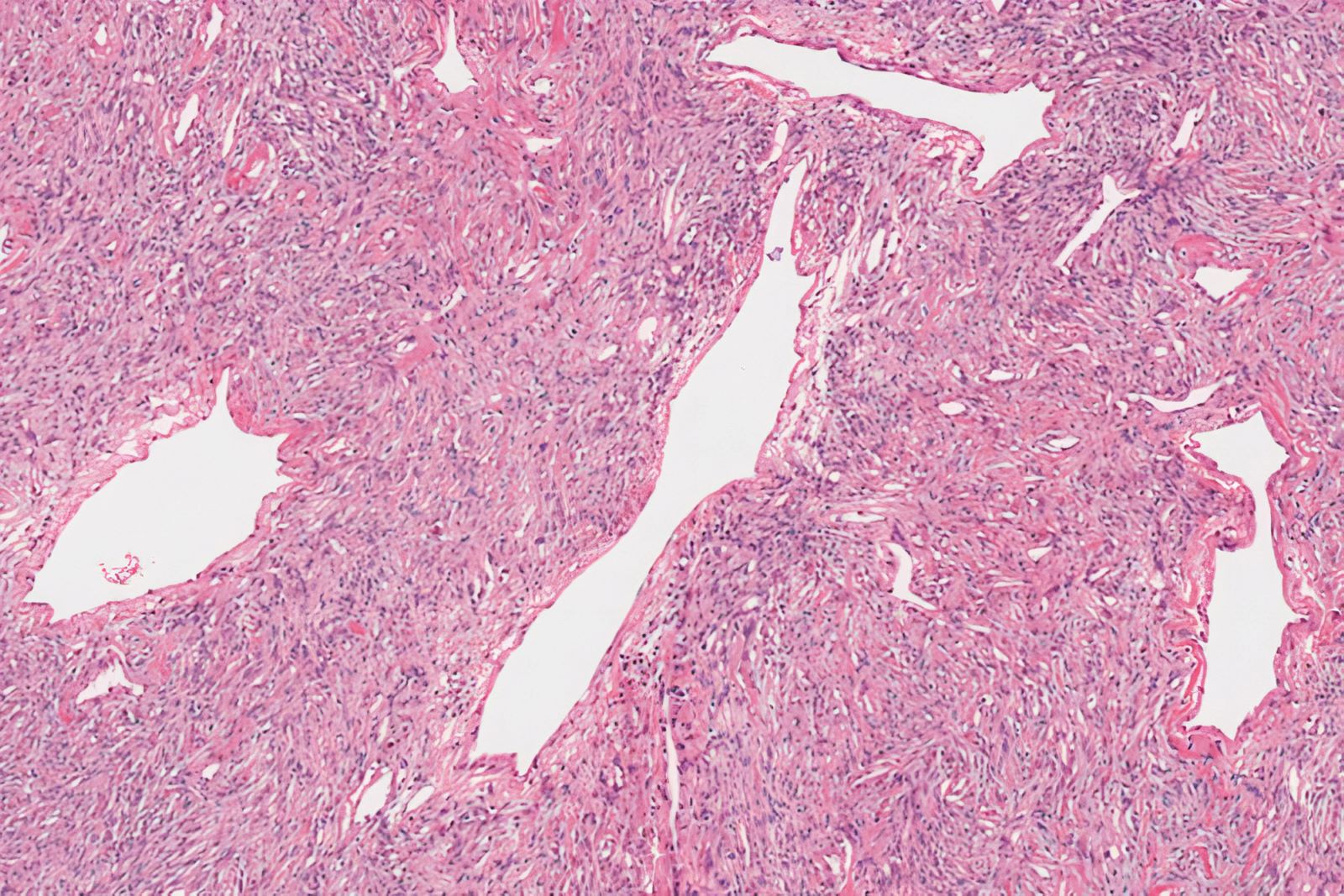
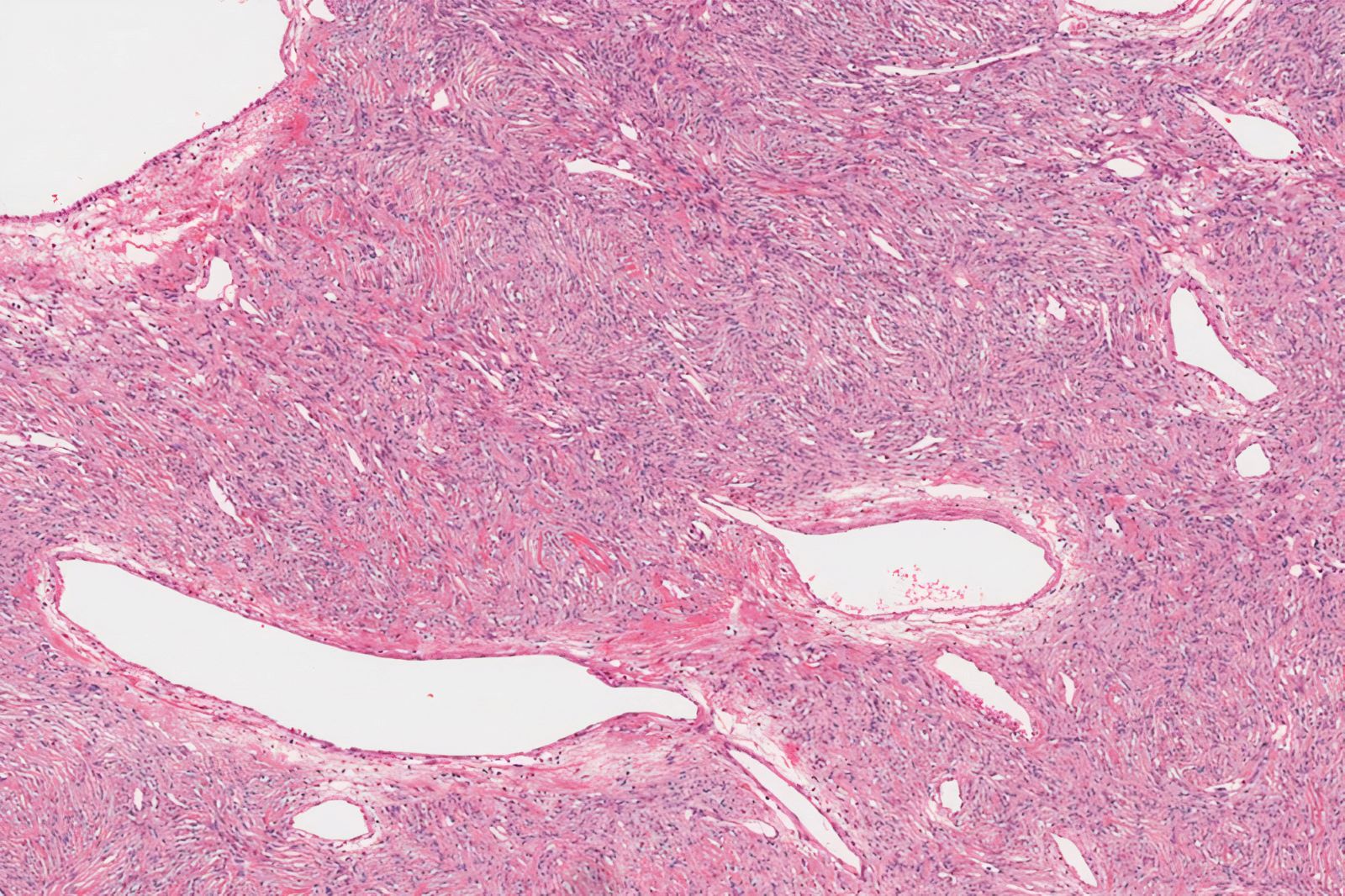
Staghorn-like vessels
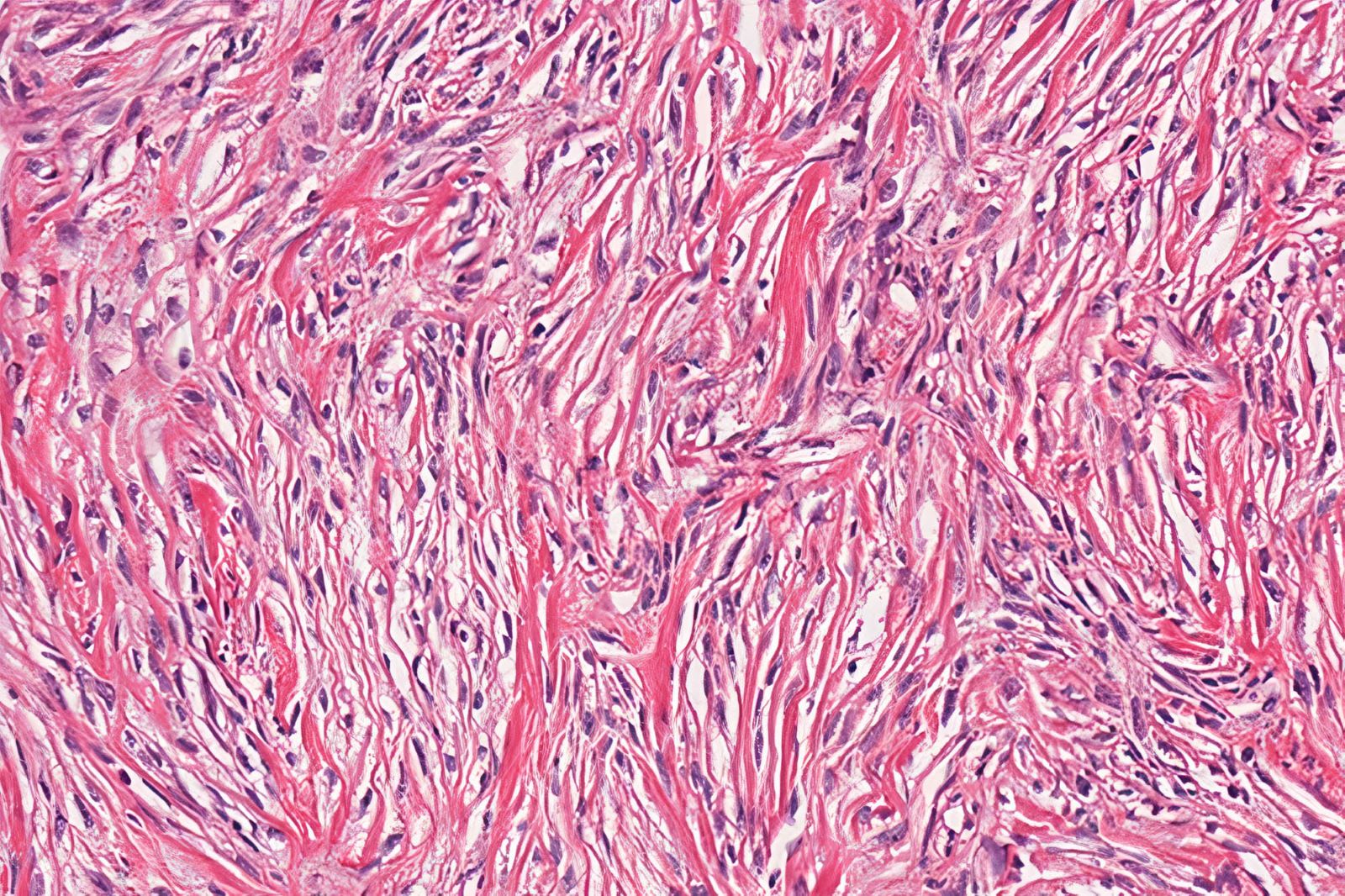
Collagenous stroma
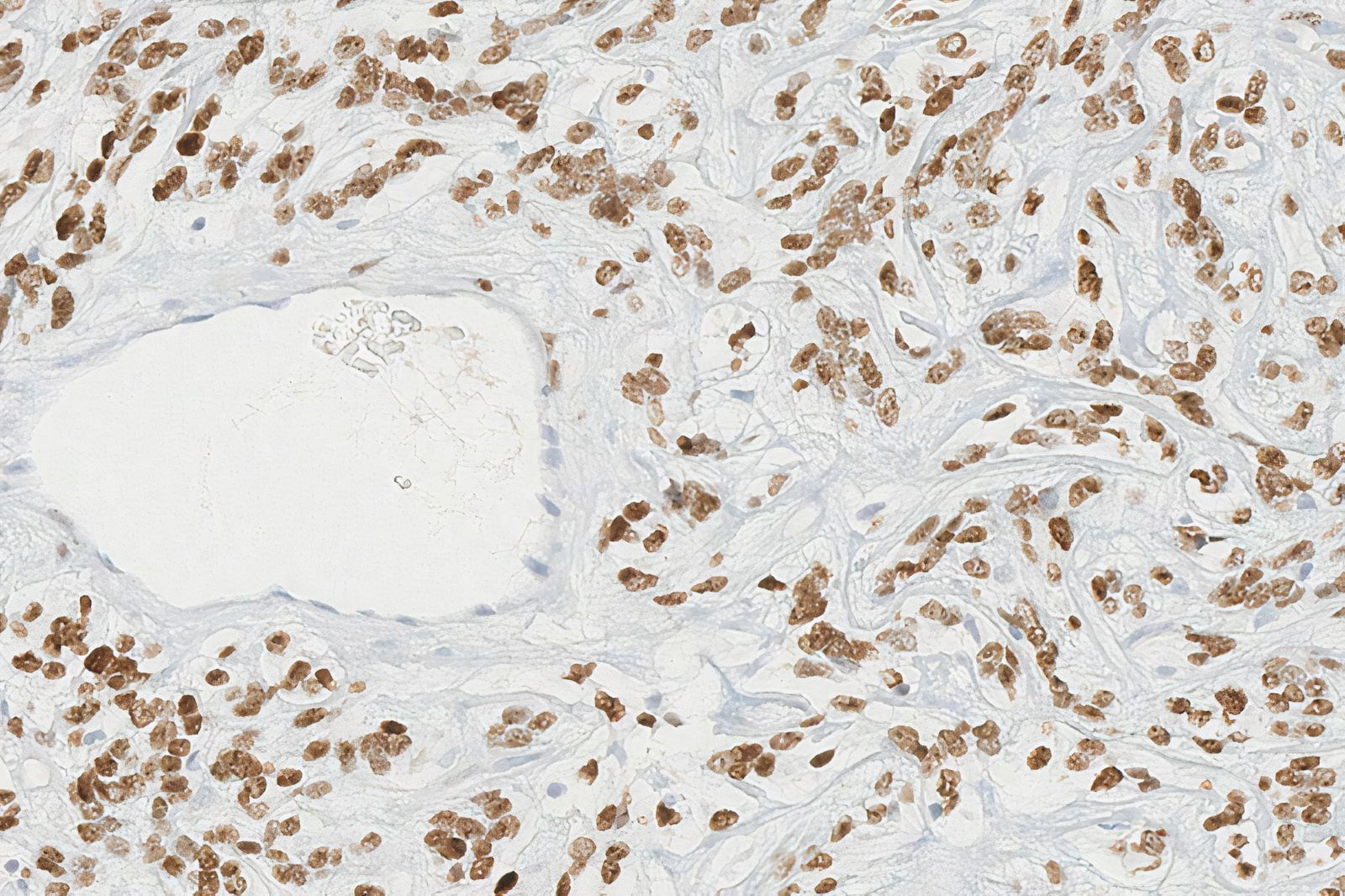
STAT6
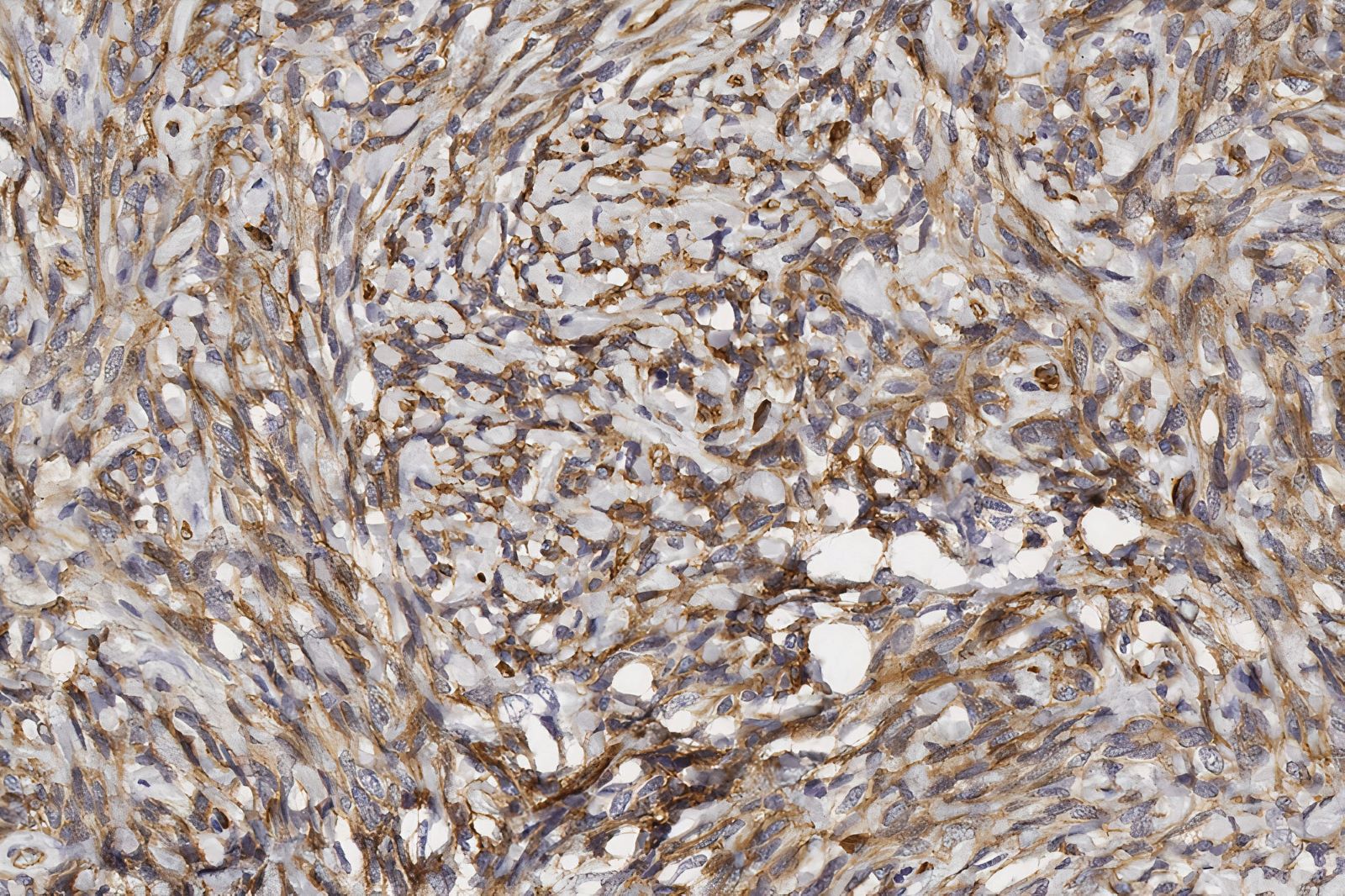
CD34
Virtual slides
Images hosted on other servers:


Solitary fibrous tumor of thyroid
Cytology description
- Smears contain loosely cohesive clusters around blood vessels or dispersed cells with bare nuclei; the cells are oval, elongated or rounded with thin cytoplasm and eosinophilic collagenous stroma (Virchows Arch 2023 Apr 20 [Epub ahead of print])
- Adjacent follicular epithelium often shows features compatible with atypia of undetermined significance or follicular lesions of undetermined significance (Diagn Cytopathol 2003;28:213, Med Mol Morphol 2014;47:117)
- Liquid based cytology specimens show only dispersed monomorphic spindle cells with bland nuclear features (Virchows Arch 2023 Apr 20 [Epub ahead of print])
Cytology images
Images hosted on other servers:

Scattered spindle-like cells with fusiform nuclei
Positive stains
- STAT6
- The most sensitive and specific marker for establishing a diagnosis of SFT (Am J Clin Pathol 2015;143:672, Pathology 2014;46:389)
- Strong nuclear expression reflects underlying STAT6 gene fusion
- CD34, CD99, BCL2: not specific
- Actin, EMA may be focal
Negative stains
- Thyroid specific markers: TTF1, thyroglobulin, calcitonin
- Cytokeratins
- Desmin, CD31, CD117, S100
Molecular / cytogenetics description
- Multiple NAB2::STAT6 gene fusion variants detected by whole exome sequencing and RT-PCR (Am J Pathol 2014;184:1209)
- Due to the proximity of the 2 genes on chromosome 12, NAB2::STAT6 gene fusion may be missed by fluorescence in situ (J Clin Pathol 2017;70:508)
- Moderate to strong and diffuse immunohistochemistry expression of STAT6 correlated with the NAB2::STAT6 gene fusion (Pathol Res Pract 2017;213:1404)
Molecular / cytogenetics images
Images hosted on other servers:

NAB2::STAT6 gene fusion variants
Sample pathology report
- Thyroid, completion thyroidectomy:
- Solitary fibrous tumor of thyroid, 35 mm, margins of resection are uninvolved (see comment)
- Comment: The histological sections show a well circumscribed mass made of moderately cellular spindle cells in a collagenous stroma with prominent dilated staghorn type vasculature. No mitosis or necrosis is seen. Benign thyroid parenchyma is uninvolved and compressed at periphery of the tumor. Immunohistochemistry studies show that the tumor cells are positive for STAT6, CD34 and BCL2 and negative for TTF1, thyroglobulin, calcitonin, cytokeratins, desmin and S100. The overall findings favor a solitary fibrous tumor, likely thyroid primary. According to the 2017 risk stratification criteria by Demicco et. al., this should be classified as a low risk solitary fibrous tumor.
Differential diagnosis
- Post-fine needle aspiration spindle cell nodules:
- Localized phenomenon adjacent to fine needle aspirated thyroid nodule with hemosiderin, extravasated erythrocytes, reactive vascular pattern
- Follicular thyroid adenoma with prominent spindle cells:
- Lacks collagen while showing colloid production (Int J Clin Exp Pathol 2012;5:143)
- Positive: cytokeratins, TTF1, thyroglobulin
- Hyalinizing trabecular tumor:
- Smooth muscle tumors:
- Riedel thyroiditis:
- Schwannoma:
- Antoni A and B areas, wavy nuclei and tapered cells
- Positive: S100
- Medullary thyroid carcinoma:
- Medullary thyroid carcinoma of spindle cell variant may be similar morphologically to SFT
- Positive: chromogranin, calcitonin, TTF1, cytokeratins
- Presence of amyloid
- Spindle epithelial tumor with thymus-like differentiation:
- Biphasic pattern: spindled epithelial cells merge into glandular structures
- Rare monomorphic variant can have spindle cells or glandular only
- Young patients
- Positive: 34 beta E12, CK7
- Negative: CD34
- Paucicellular variant of anaplastic thyroid carcinoma:
- Acellular or necrotic fibrous tissue with hypocellular foci of mildly atypical spindle cells obliterating large blood vessels
- Positive: cytokeratins, EMA, p53
Additional references
Board review style question #1
A 50 year old woman presented with a 4.5 cm, well circumscribed, firm mass in the right lobe of thyroid. Histologic sections showed ovoid to spindled cells arranged haphazardly around prominent thin walled, hyalinized, dilated staghorn type vasculature (see image above). Which of the following is the diagnosis of this thyroid tumor?
- Medullary carcinoma
- Riedel thyroiditis
- Solitary fibrous tumor
- Spindle epithelial tumor with thymus-like differentiation
- Anaplastic thyroid carcinoma, paucicellular variant
Board review style answer #1
C. Solitary fibrous tumor. This case has gross appearance and histological features consistent with solitary fibrous tumor of thyroid. Differential diagnosis includes other thyroid tumors with the spindle cell pattern.
Comment Here
Reference: Solitary fibrous tumor
Comment Here
Reference: Solitary fibrous tumor
Board review style question #2
Which of the following is the most sensitive and specific immunohistochemical marker for solitary fibrous tumor of the thyroid?
- CD34
- Cytokeratin CAM 5.2
- STAT6
- Thyroglobulin
- TTF1
Board review style answer #2
C. STAT6. STAT6 is a highly sensitive and specific marker for the presence of the NAB2::STAT6 gene fusion product, which is identified to be the pathognomonic molecular aberration in solitary fibrous tumor.
Comment Here
Reference: Solitary fibrous tumor
Comment Here
Reference: Solitary fibrous tumor
