
Thyroid & parathyroid
Other thyroid malignancies
Lymphoma
Author: Sheren Younes, M.D., Ph.D.

Last author update: 1 September 2015
Last staff update: 20 September 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: lymphoma thyroid

Table of Contents
Definition / general | Epidemiology | Clinical features | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Molecular / cytogenetics description | Differential diagnosis | Additional referencesCite this page: Younes S. Lymphoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidlymphoma.html. Accessed April 1st, 2025.
Definition / general
- Comprises 2.5% of extranodal lymphoma and 4 - 5% of thyroid malignancies
- Usually arise on top of Hashimoto thyroiditis or lymphocytic thyroiditis
- Most are diffuse large B cell lymphoma, marginal zone B cell / MALT lymphoma or mixtures of these two
- Rarely follicular cell lymphoma
- Hong Kong / Chinese cases are only rarely EBV+ (Am J Clin Pathol 1999;112:263)
- Follicular lymphoma has two subgroups:
- t(14;18) or bcl2 overexpression, usually CD10+ and WHO grade 1-2
- No t(14;18) or bcl2 overexpression, often CD10- and WHO grade 3 (Am J Surg Pathol 2009;33:22, Mod Pathol 2005;18:1471)
- Hodgkin lymphoma: very rare, favorable prognosis, female predominance (Neuroimaging Clin N Am 2003;13:371)
Epidemiology
- 75% women, usually adults or elderly (Am J Surg Pathol 2000;24:623)
Clinical features
- Rapidly growing neck mass
- Compression symptoms including dysphagia and hoarseness
- Can present with diffuse thyroid enlargement
- May be accidentally discovered
- Hypothyroid manifestations may develop
- Cold nodule
- Virtually all primary thyroid lymphomas are MALT-type arising after 20 - 30 years of lymphocytic thyroiditis in older patients (mean age 64 years)
- Sequence similarity in clonal IgH bands suggests lymphoma may arise from thyroiditis (J Clin Pathol 2008;61:438)
- Secondary involvement seen in 20% dying of generalized lymphoma, although usually does not produce clinical hypothyroidism
- Regional lymph node enlargement can be seen
- Hodgkin lymphoma: thyroid mass, cervical lymphadenopathy, patient is euthyroid but may be hypothyroid
Prognostic factors
- Overall 5 year survival is 80%
- Poor prognostic factors: diffuse B cell lymphoma subtype, perithyroidal soft tissue invasion, stage 2E or higher
- Good prognostic factors: marginal zone lymphoma subtype or stage IE
Case reports
- 19 year old woman with syncytial variant of nodular sclerosing Hodgkin lymphoma (Acta Cytol 1995;39:543)
- 22 and 29 year old women with thyroid nodule as a first manifestation of Hodgkin lymphoma (Diagn Pathol 2013;8:116)
- 32 year old man with primary T cell lymphoma of thyroid (Med Oncol 2008;25:462)
- 37 year old woman with nodular sclerosing Hodgkin lymphoma (Ann Endocrinol (Paris) 2012;73:492)
- 48 year old woman with primary thyroid lymphoma (Diagn Cytopathol 2012;40:444)
- 54 year old man with primary mediastinal large B cell lymphoma (Int J Clin Exp Pathol 2015;8:5944)
- 62 year old woman with Hodgkin lymphoma presenting as abscess in thyroid gland (Indian J Pathol Microbiol 2012;55:122)
- 65 year old woman with thyroid MALT lymphoma (Ann Thorac Surg 2015;100:700)
- 70 year old man with diffuse large B cell lymphoma of thyroid (Cytojournal 2006;3:23)
Treatment
- Often curable by radiation or chemotherapy (particularly MALT), in contrast to anaplastic carcinoma
- Surgery is rare (Eur J Surg Oncol 2008;34:576)
Gross description
- Variable sized, rubbery / soft mass
- White cut surface with fish flesh appearance
- Necrosis could be found
Gross images
AFIP images

Diffuse large cell lymphoma: fish flesh cut surface

Hodgkin lymphoma:
nodular sclerosing
subtype
Microscopic (histologic) description
- Varies by histologic type
- Diffuse large B cell lymphoma:
- Diffuse infiltrate destroying thyroid follicles
- Large cells with moderate amphophilic cytoplasm, vesicular nuclei, prominent nucleoli
- Bizarre cells may be seen
- MALT lymphoma:
- Infiltration of thyroid epithelium creates lymphoepithelial lesions (lymphocytes "stuff" glandular lumina, Arch Pathol Lab Med 2007;131:1673)
- May have background lymphocytic thyroiditis
- Follicular lymphoma:
- Usually prominent follicular pattern with prominent interfollicular neoplastic infiltrate, lymphoepithelial lesions are common
- May arise on top of thyroiditis
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D.
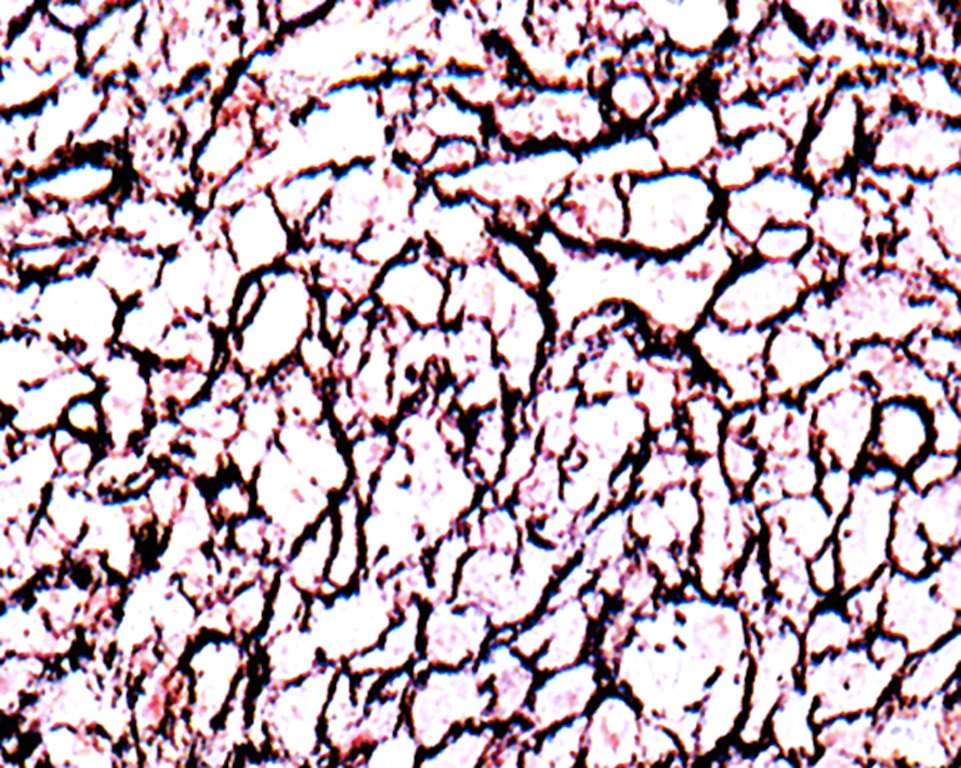
Large cell type, reticulin stain
AFIP images
Diffuse large B cell lymphoma:

Tumor cells

Follicle in lower right

Fibrous bands

Tumor cells are CD45 (LCA)+

Keratin, thyroglobulin
Hodgkin lymphoma:

Nodular sclerosing subtype
Follicular lymphoma:

Residual thyroid follicles
Images hosted on other servers:

Large pleomorphic cells

Hodgkin lymphoma: nodular sclerosis type

Hodgkin lymphoma: CD30+

Follicular lymphoma: morphology

Follicular lymphoma: negative for bcl2 and IGH-BCL2

Follicular lymphoma: positive for bcl2 and IGH-BCL2
Cytology description
- Monotonous population of large atypical lymphoid cells (scant cytoplasm, finely granular chromatin, prominent nucleoli), lymphoglandular bodies present (cytoplasmic fragmentation), karyorrhexis (Cytojournal 2005;2:21)
- MALT features: see Acta Cytol 2015;59:26
- May be misdiagnosed as lymphocytic thyroiditis
- Hodgkin lymphoma: some atypical cells, may have marked fibrosis
Cytology images
Contributed by Ayana Suzuki, C.T. and Mark R. Wick, M.D.

DLBCL
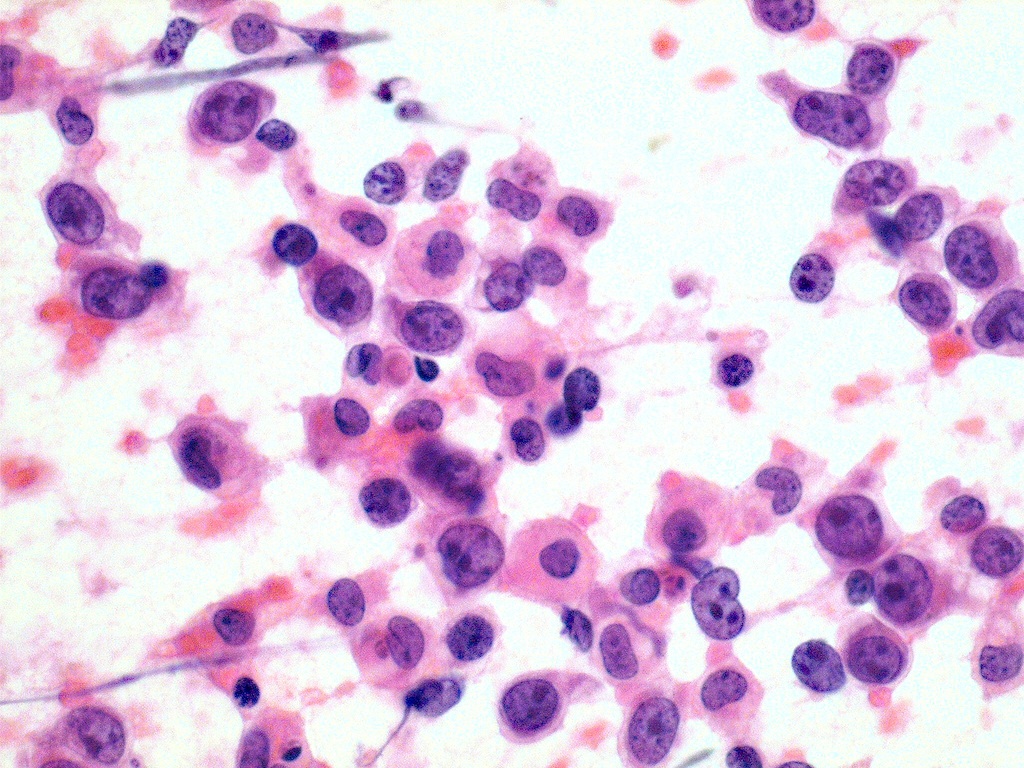
Large cell type
Images hosted on other servers:

Intermediate grade lymphoma

MALT lymphoma

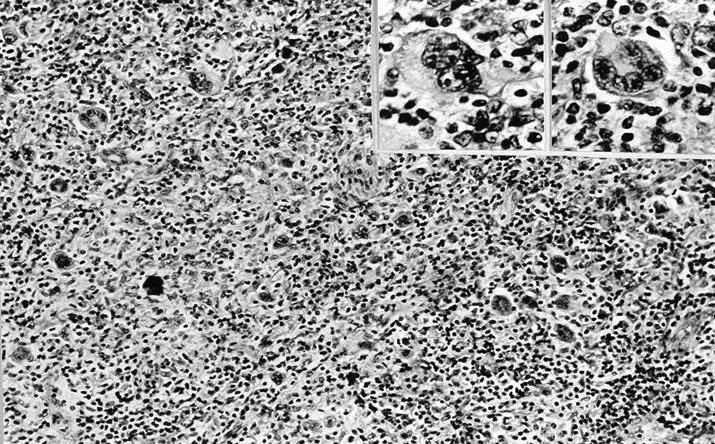
Hodgkin lymphoma: Reed-Sternberg cell
Diffuse large B cell lymphoma:

Large and irregular lymphoid cells

Misdiagnosed as anaplastic carcinoma

High grade lymphoma

CD45 / LCA+, CD20+, keratin-
Positive stains
- CD20 and keratin highlight lymphoepithelial lesions
- Thyroglobulin stains entrapped follicular epithelium
- Also CD45
Molecular / cytogenetics description
- t(11;18) is not present in thyroid MALT lymphomas (Mod Pathol 2006;19:1578)
Differential diagnosis
- Anaplastic carcinoma
- Insular carcinoma
- Small cell variant of medullary carcinoma
- Thyroiditis (Hashimoto or lymphocytic):
- Diagnosis of lymphoma is supported by the presence of a dense clonal proliferation of lymphoid cells, lymphoepithelial lesions and CD20 positivity (Acta Cytol 2012;56:352)
- Undifferentiated carcinoma (Eur Radiol 2016;26:1031)
Additional references
