

Thyroid & parathyroid
Other uncommon lesions / neoplasms
Langerhans cell histiocytosis
Editorial Board Member: Marc Pusztaszeri, M.D.


Last author update: 1 June 2021
Last staff update: 9 April 2024
Copyright: 2014-2024, PathologyOutlines.com, Inc.
PubMed Search: Langerhans cell histiocytosis thyroid
See Also: Lung, Lymph nodes, Mandible & maxilla
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Munkhdelger J, Bychkov A. Langerhans cell histiocytosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidlch.html. Accessed November 27th, 2024.
Definition / general
- Langerhans cell hystiocytosis (LCH) is a clonal neoplastic proliferation of langerin / CD1a / S100 positive dendritic cells (Langerhans-like cells)
- LCH cells initially thought to arise from the epidermal or mucosal derived Langerhans cell due to the morphologic, immunophenotypic and ultrastructural similarities; however, gene expression profiling showed that LCH cells are not derived from terminally differentiated Langerhans cells but rather share a closer kinship with dendritic cells of the bone marrow (Blood 2017;130:176)
- Thyroid involvement is rare
- 100+ morphologically verified cases published as case series and case reports
- Can occur as a primary disease or secondary involvement in systemic disease
Essential features
- Rare histiocytic neoplasm with occasional involvement of thyroid, either a part of systemic dissemination or isolated
- Proliferation of LCH cells (CD1a / S100 / langerin positive histiocytes with convoluted nuclei) on inflammatory, typically eosinophil rich background
Terminology
- Not recommended / obsolete terminology:
- Morphological: eosinophilic granuloma; histiocytosis X
- Clinical: Hand-Schüller-Christian disease; Letterer-Siwe disease
ICD coding
Epidemiology
- Isolated thyroid involvement is extremely rare
- Secondary involvement is more common
- LCH incidence: 5 - 9 per million children, 1 - 2 per million adults (Blood 2020;135:1319)
- Age range: 2 months to 55 years
- Childhood onset and adult onset LCH
- Young age (< 20 years) at initial presentation in systemic disease, older age in isolated disease (Endocr Pathol 2002;13:227)
- Slight male predilection (Br J Haematol 2016;174:887)
Sites
- Thyroid involvement can be diffuse (59%) or nodular (25.8%) enlargement (Head Neck Pathol 2012;6:279)
- Main target organs in systemic LCH are bone, skin, lung and pituitary (N Engl J Med 2018;379:856)
Pathophysiology
- Not fully understood
- More than half of LCH cases have MAPK pathway alterations: either BRAF V600E or MAP2K1 (MEK1) mutations (BMC Cancer 2019;19:170, Am J Surg Pathol 2014;38:548, Pediatr Blood Cancer 2015;62:173, Eur Respir J 2020;55:1901190)
- Constitutive activation of MAPK pathway results in continuous stimulation of cell proliferation and promotes cell survival
- Hypothesis of underlying pathogenesis: interleukin 1 loop activation by Merkel cell polyomavirus infection (Cell Commun Signal 2015;13:13)
- Triple risk factor model, including cytogenetic abnormality, stress and reaction (Cell Commun Signal 2018;16:49)
Etiology
- Inflammatory myeloid neoplastic origin (Blood 2015;126:26, Adv Immunol 2013;120:127)
- Frequent BRAF and MAP2K1 mutations in LCH support neoplastic origin (Blood 2014;124:867, Blood 2014;124:3007)
- Findings suggesting inflammatory reactive origin
- Features of IL17A related inflammatory disease (Blood 2014;124:867)
- Identification of Merkel cell polyomavirus DNA in peripheral blood and tissues of LCH patients (Hum Pathol 2014;45:119)
- Most cases are sporadic but variant SMAD6 has been associated with susceptibility to LCH (Blood 2020;135:1319)
Diagrams / tables
Images hosted on other servers:


Risk factor model
Clinical features
- Diffuse enlargement or unilateral thyroid nodule
- Commonly associated with Hashimoto thyroiditis
- Presenting features of systemic LCH are variable and depend on the index organ involved: bone pain, fracture, skin rash, lymphadenopathy, diabetes insipidus and more (Blood 2020;135:1319)
Diagnosis
- Fine needle aspiration cytology aided by immunostaining
- If immunocytochemistry is not available, immunostaining in suspicious cases can be performed on core needle biopsy
- Histologic evaluation of surgical specimen, if surgery performed
- History of systemic LCH in multiorgan disease
Laboratory
- 41% euthyroid, 20% hypothyroid (BMJ Case Rep 2014;2014:bcr2014206760)
- Antithyroglobulin or antimicrosomal antibody (AMA) in cases associated with Hashimoto thyroiditis (Head Neck Pathol 2012;6:279)
Radiology description
- Cold nodule on thyroid scan
- Ultrasonography: heterogeneous or hypoechoic mixed density nodules (Int J Clin Exp Pathol 2014;7:1229)
- Nonspecific
- Increased uptake on FDG-PET
Radiology images
Images hosted on other servers:

Ultrasound

MRI

FDG-PET
Prognostic factors
- Excellent prognosis in rare cases with isolated thyroid disease
- ≥ 99% survival for unifocal (single organ) disease
- Up to 20% mortality for patients with organ dysfunction (Blood 2020;135:1319)
- 66% mortality for young children with multisystem involvement who do not respond to therapy (J Pediatr 2001;138:728, Med Pediatr Oncol 2002;39:581, Med Pediatr Oncol 2001;37:108)
- High risk factors: involvement of the bone marrow, liver, lung (Med Pediatr Oncol 2002;39:581, Med Pediatr Oncol 2001;37:108)
- Patient age is less important than extent of disease (Med Pediatr Oncol 2002;39:581, Med Pediatr Oncol 2001;37:108)
Case reports
- 5 month old girl with isolated LCH of thyroid (Eur J Pediatr 2007;166:1151)
- 18 year old man with LCH goiter (Endocr J 2012;59:47)
- 19 year old woman with LCH involving thyroid and parathyroid (Mod Pathol 2001;14:111)
- 27 year old woman with thyroid LCH and papillary thyroid carcinoma involving cervical lymph nodes (Gland Surg 2016;5:537)
- 29 year old woman with thyroid involvement in systemic LCH with EBV infection (Head Neck Pathol 2020 Nov 2 [Epub ahead of print])
- 35 year old woman with thyroid LCH diagnosed on FNA cytology (Head Neck Pathol 2015;9:496)
- 36 year old woman with synchronous papillary thyroid carcinoma and LCH with BRAF mutation (BMC Cancer 2019;19:170)
- 41 year old man with systemic LCH involving endocrine organs (Medicine (Baltimore) 2018;97:e11215)
- 44 year old woman with solitary LCH of the thyroid (Head Neck Pathol 2012;6:279)
Treatment
- Surgical excision for isolated disease
- Combination chemotherapy for systemic disease (Head Neck Pathol 2012;6:279, N Engl J Med 2018;379:856)
Gross description
- Focal of diffuse involvement
- Variable sized nodules
- Similar to other noncystic thyroid nodules
Microscopic (histologic) description
- Nodular or diffuse proliferation of LCH cells
- LCH cells characteristic of disease are histiocytoid cells recognized by their grooved, convoluted, indented or lobed nuclei (Arch Pathol Lab Med 2015;139:1211, Thyroid 2001;11:697, Mod Pathol 1996;9:145)
- Nuclear appearance is often described as resembling coffee beans, horseshoes or kidneys
- Nuclear atypia is absent or minimal
- Mitoses variable, not correlated with aggressiveness
- Cytoplasm is moderately abundant and slightly eosinophilic
- Unlike epidermal Langerhans cells, LCH cells are oval in shape and devoid of dendritic cell processes
- Typical background includes eosinophils with a variable amount of neutrophils, lymphocytes and occasional multinucleated giant cells
- Rarely, eosinophilic abscesses may be formed
- Temporal trend
- In early lesions, LCH cells predominate, along with eosinophils and neutrophils
- In late lesions, the LCH cells are decreased in number, with more foamy macrophages and increased fibrosis
- In most cases, at least some LCH cells can be found
- Effacement of the surrounding thyroid parenchyma due to infiltration of thyroid follicles by LCH cells
- Chronic lymphocytic thyroiditis is common
- Neoplastic cells can extend beyond thyroid capsule and occasionally spread to cervical lymph nodes (Case Rep Pathol 2014;2014:184237)
- Thyroid carcinoma may coexist and even collide with LCH (Endocr Pathol 2010;21:274, Case Rep Pathol 2014;2014:184237)
Microscopic (histologic) images
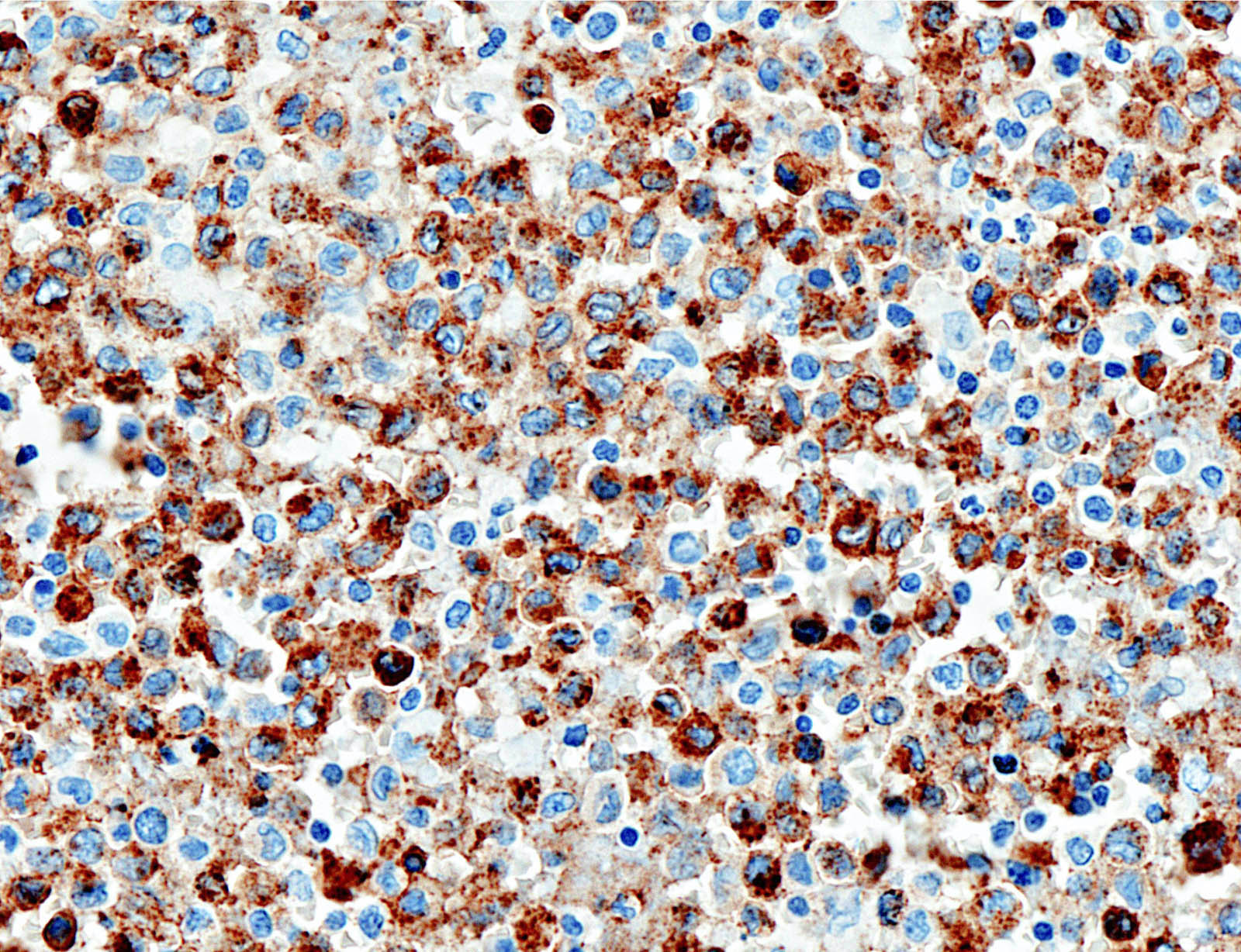
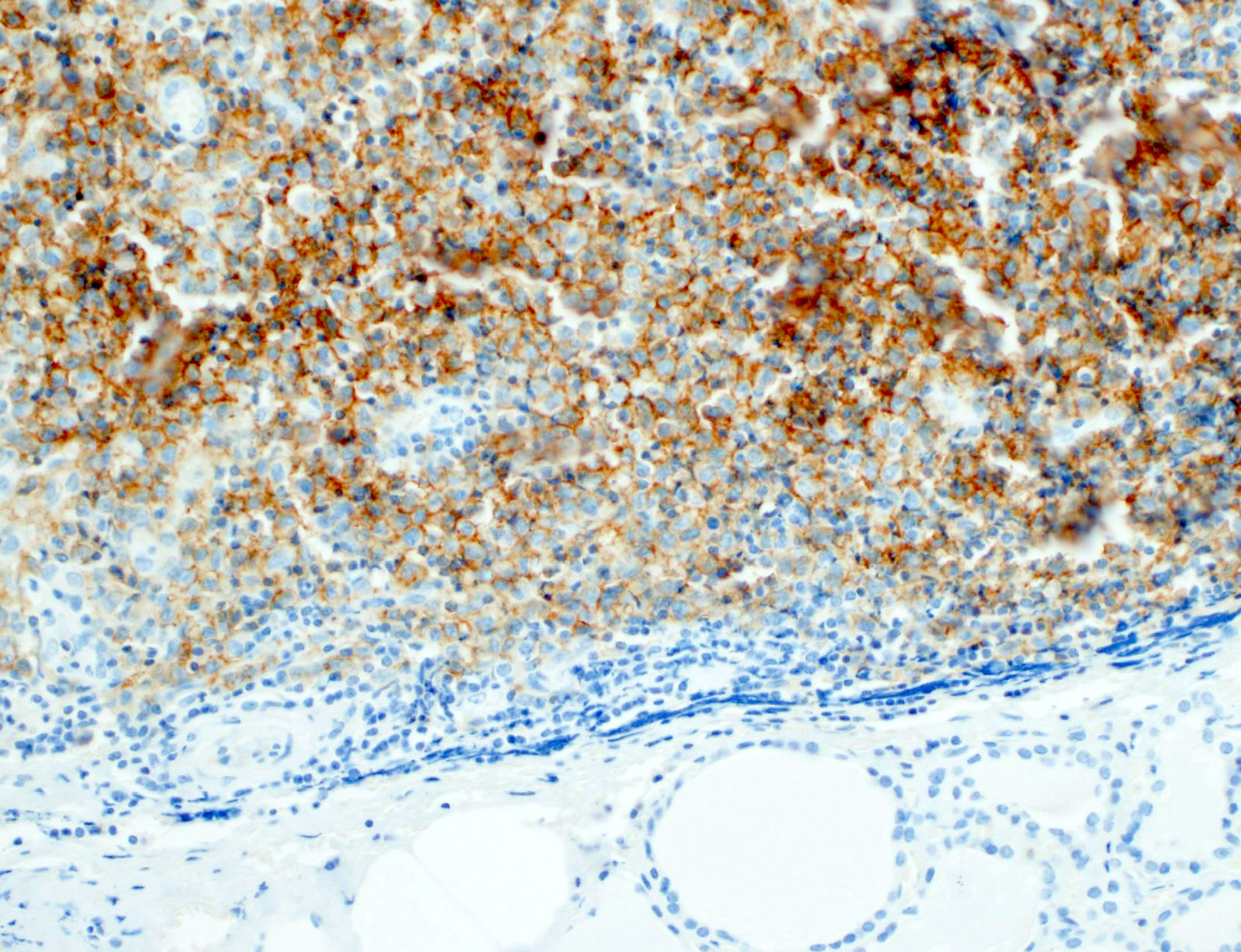
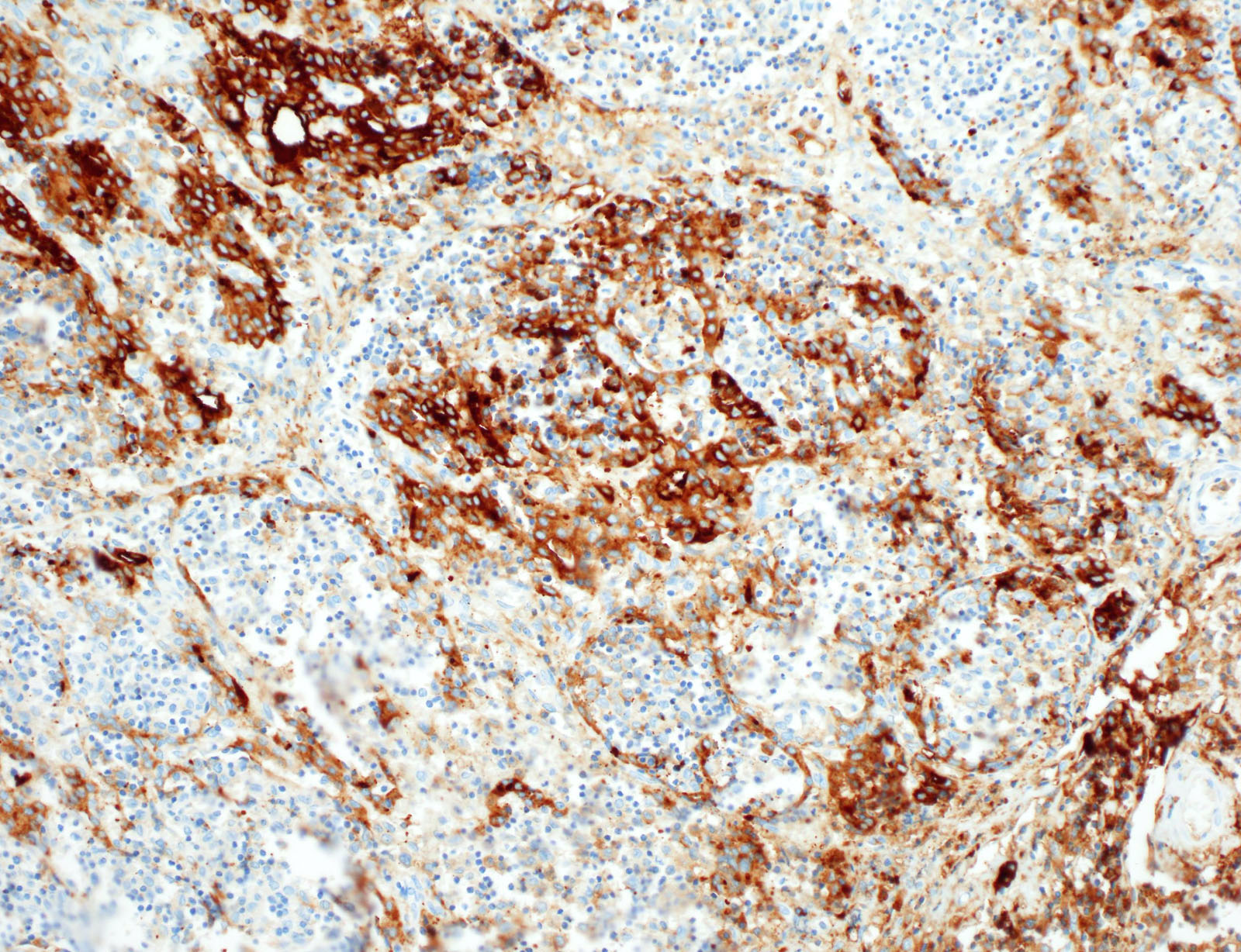
Contributed by Somboon Keelawat, M.D. and Jijgee Munkhdelger, M.D., Ph.D.
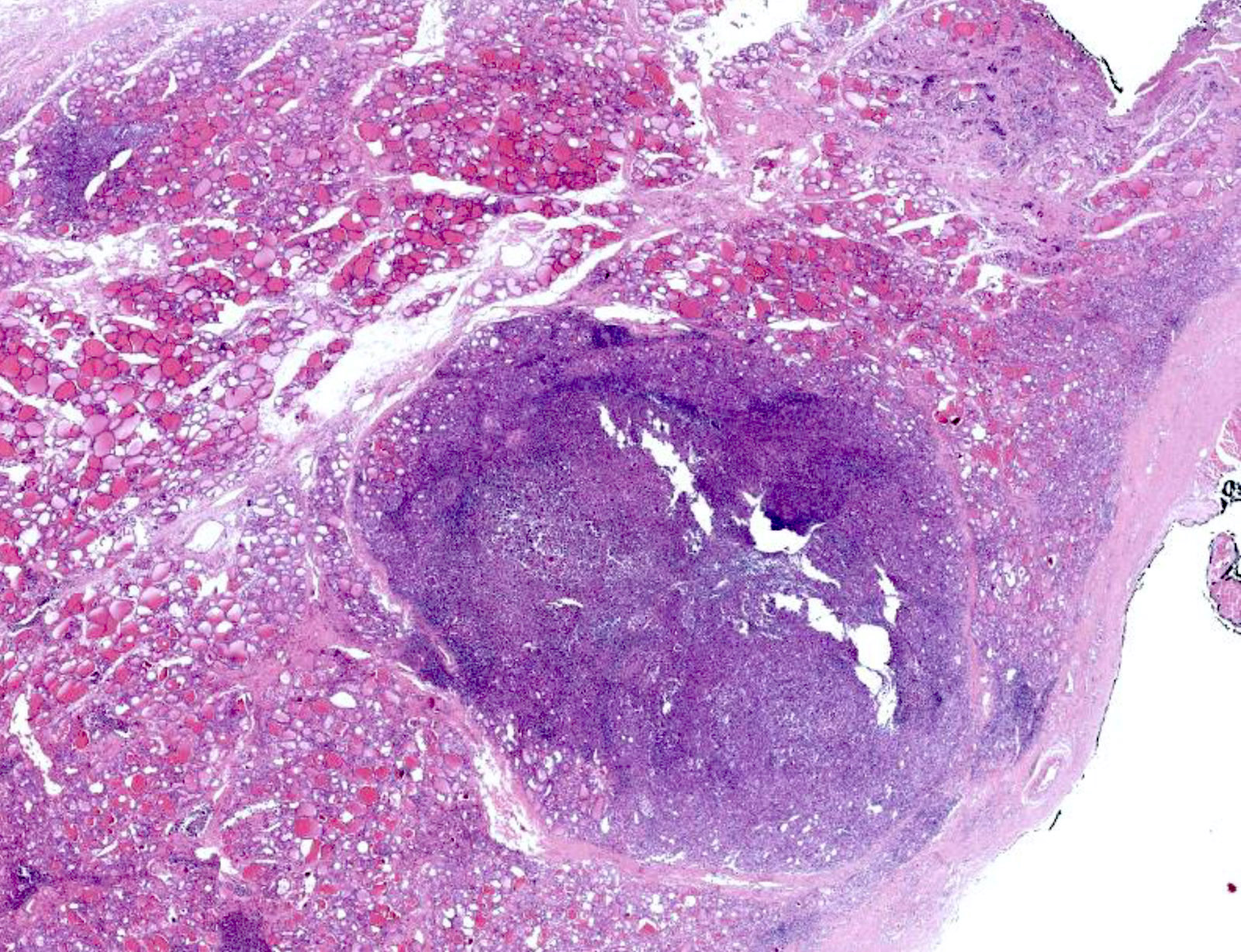
Discrete nodule
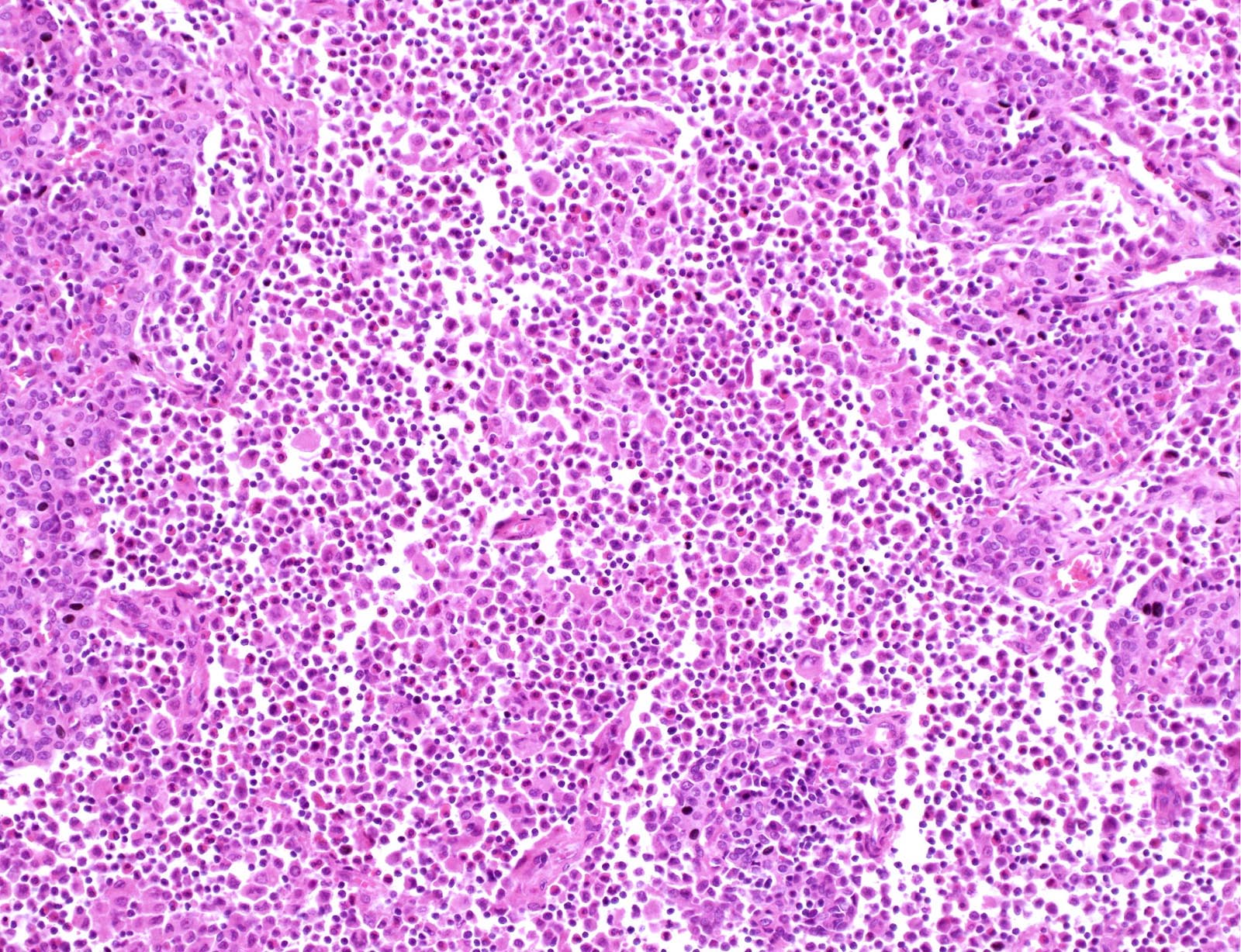
Eosinophils
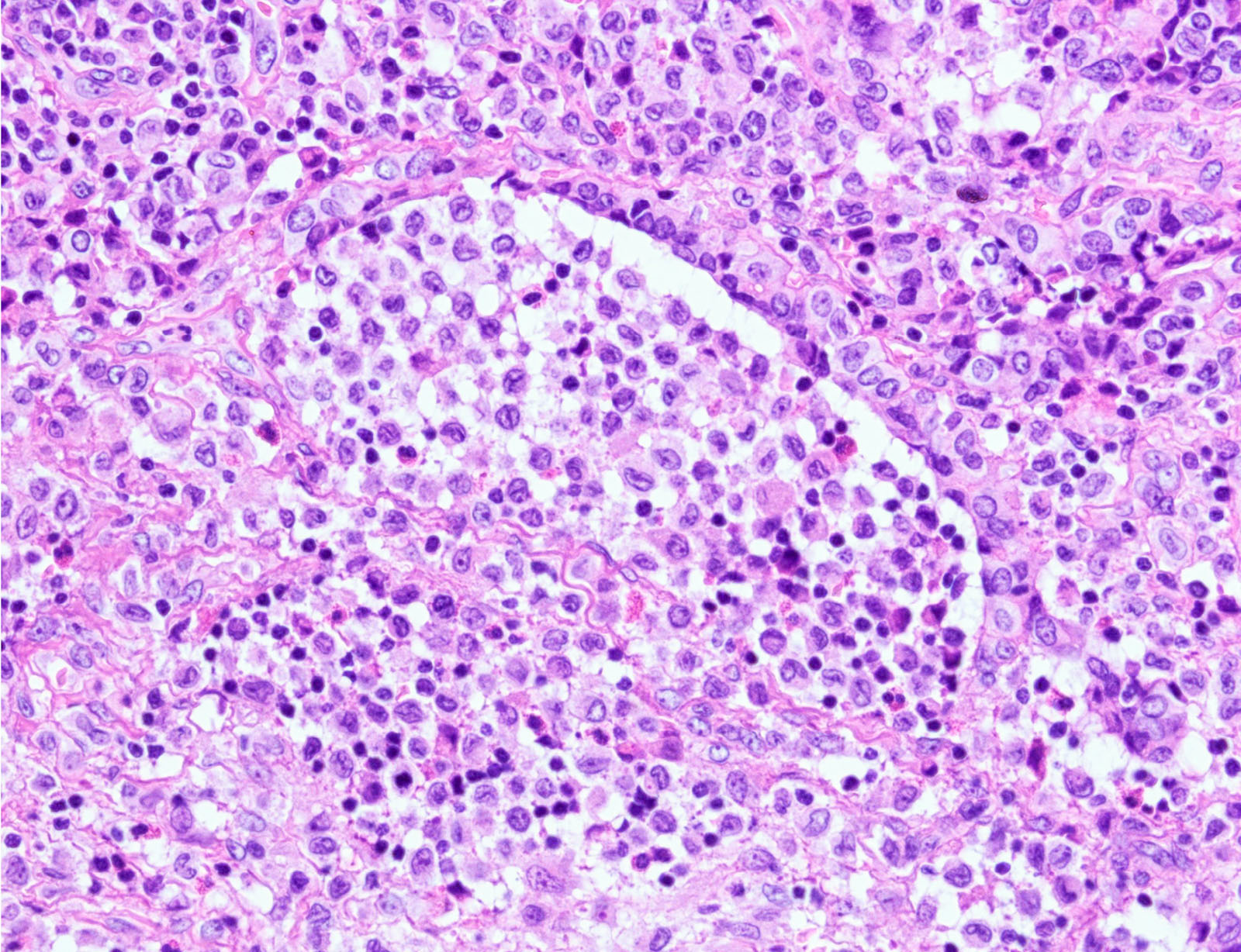
Follicular stuffing
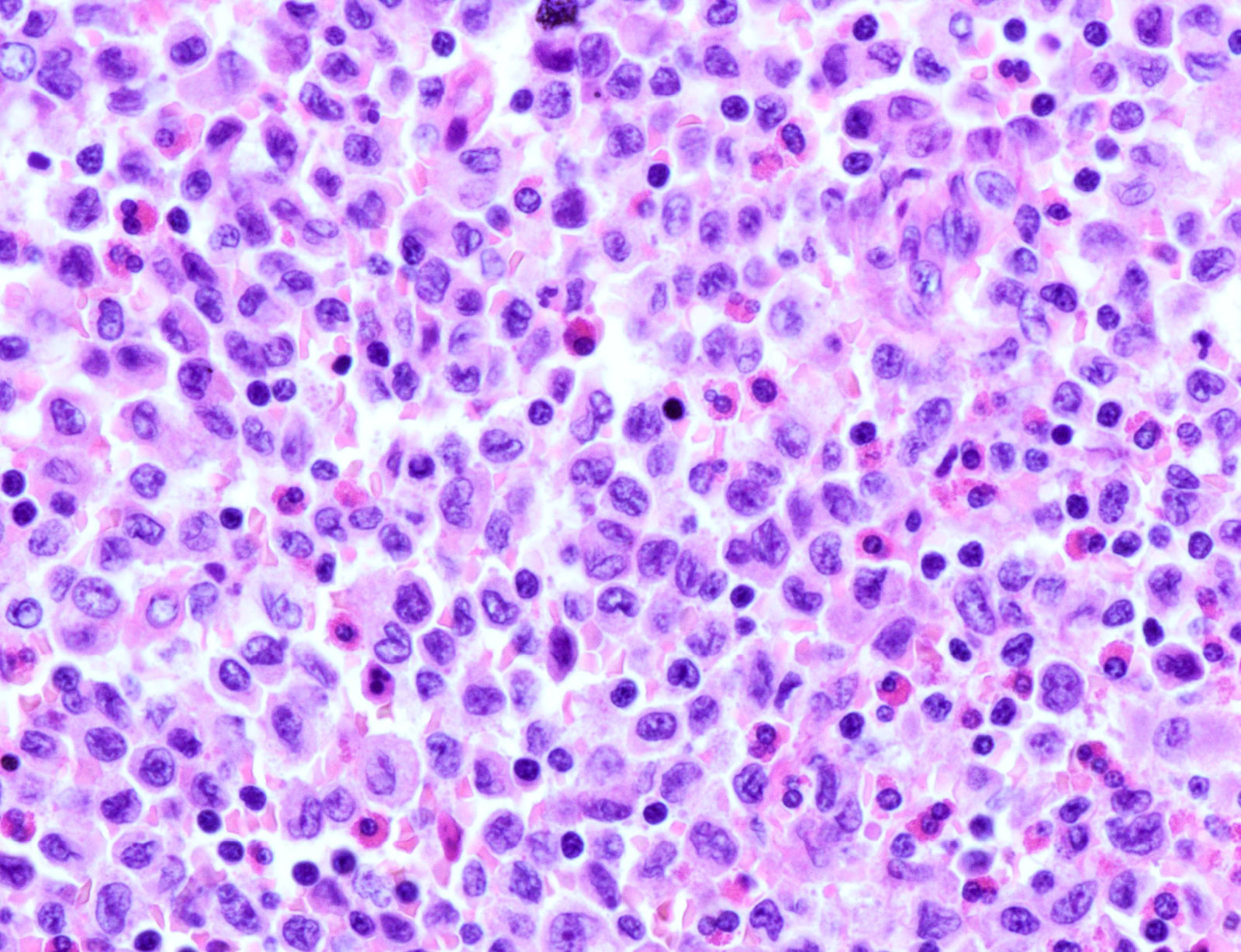
LCH cells
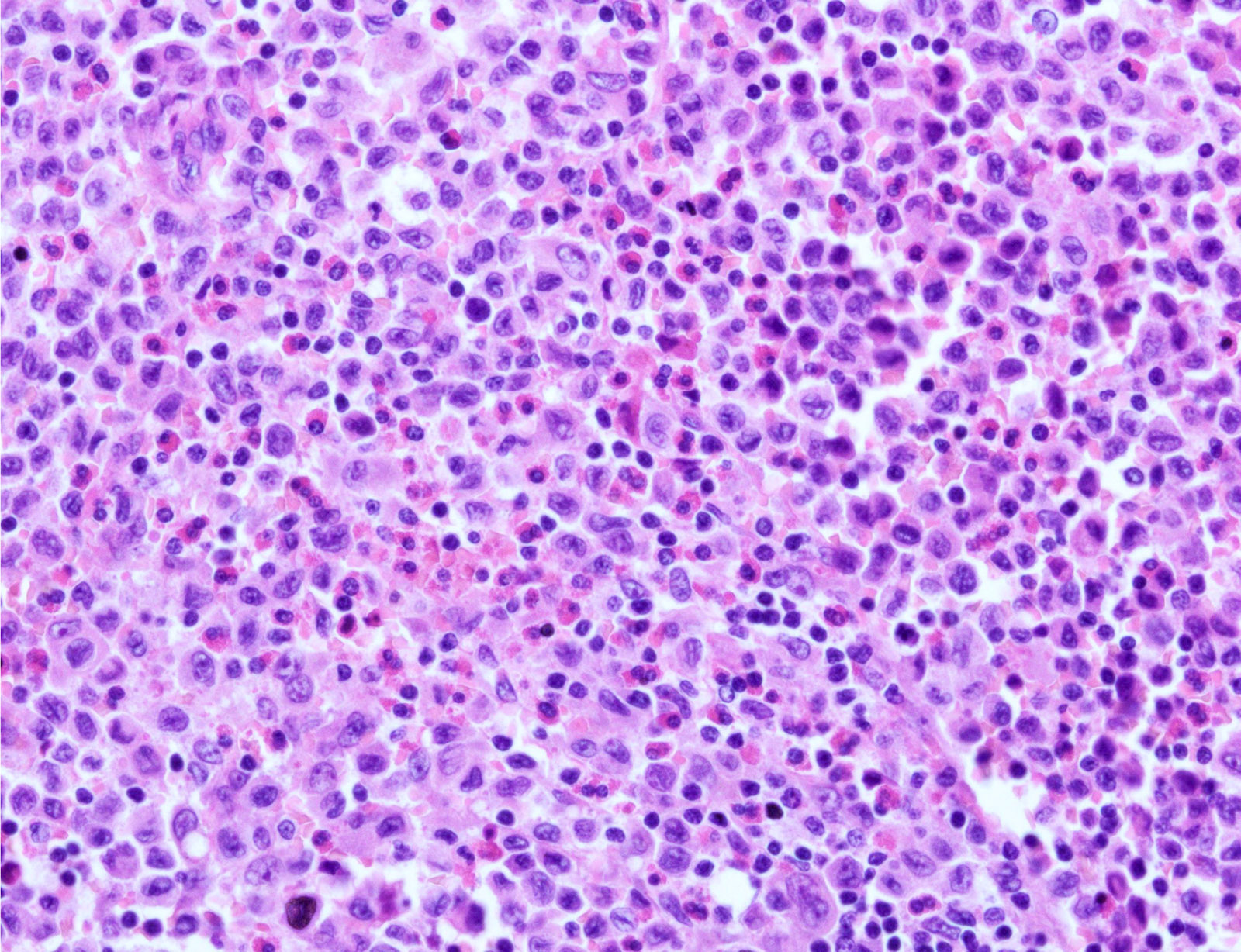
LCH cells and eosinophils
Langerin
CD1a
Thyroglobulin
Virtual slides
Images hosted on other servers:

Thyroid LCH
Cytology description
- Variably cellular smears
- Aggregates or isolated histiocytoid LCH cells with grooved / contorted nuclei and moderate amount of pale cytoplasm (Acta Cytol 2015;59:418)
- Inflammatory background with variable amount of eosinophils (occasional Charcot-Leyden crystals), scattered small lymphocytes, foamy histiocytes and multinucleated giant cells (Acta Cytol 2013;57:406)
- FNA samples lack follicular cells and background colloid (Acta Cytol 2017;61:96, Cancer Cytopathol 2021 Jan 25 [Epub ahead of print])
Cytology images
Images hosted on other servers:


FNA smear

S100 and CD1a
Positive stains
- CD1a, S100, langerin (Blood 2001;97:1241, BMJ Case Rep 2014;2014:bcr2014206760)
- CD1a or combination CD1a / S100 is most commonly used
- Langerin (CD207) is a prototypic marker immunolocalized in Birbeck granules but less widely used
- VE1 immunostaining (anti-BRAF V600E) correlates with the mutation status of BRAF (Am J Surg Pathol 2014;38:548)
- Ki67 variable, of no significance
Negative stains
- Thyroid specific: TTF1, PAX8, thyroglobulin
- Cytokeratins
- Most B cell and T cell lineage markers
Electron microscopy description
- Birbeck granules are characteristic cytoplasmic inclusions (Blood 2020;135:1319)
- Rod to flask to tennis racket shaped
- 200 - 400 nm long x 33 nm wide
- Zipper-like appearance due to a median striated line
- Electron microscopy is less often used today
- Replaced by immunostains
- Birbeck granules present in a variable percentage of LCH cells
Electron microscopy images
Images hosted on other servers:


Birbeck granules
Molecular / cytogenetics description
- BRAF V600E mutation in about 50% (Am J Surg Pathol 2014;38:548, Hum Pathol (N Y) 2019;17:200302)
- MAP2K1 (MEK1) in about half of remaining cases
Sample pathology report
- Thyroid gland, total thyroidectomy:
- Histiocytic proliferation with eosinophil rich inflammatory background, consistent with Langerhans cell histiocytosis (see comment)
- Comment: The immunohistochemical stains are positive for CD1a / S100 and negative for thyroglobulin in the histiocytes. These findings support the above diagnosis. Clinical correlation (history, systemic involvement) is recommended.
Differential diagnosis
- Other histiocytic disorders / Rosai-Dorfman disease:
- Lymphocytic thyroiditis:
- No LCH cells, no eosinophils
- Granulomatous thyroiditis:
- Well formed granulomas
- No LCH cells, no eosinophils
- Lymphoma:
- Monotonous population of large atypical lymphoid cells
- Lymphoepithelial lesion
- Anaplastic carcinoma:
- Greater degree of pleomorphism
- Necrosis
- No inflammatory background
- Medullary thyroid carcinoma:
- Positive for calcitonin, CEA
- Papillary thyroid carcinoma:
- Positive for cytokeratin, thyroglobulin, TTF1
| Differential diagnosis of thyroid LCH | |||
| Entity | Potential pitfall | Morphological hallmark | IHC profile |
| Rosai-Dorfman disease | Histiocytic origin; S100+ | Histiocytes with emperipolesis | CD1a-, CD207- |
| Lymphoma | Lymphocyte rich neoplasm | Monotonous proliferation of atypical lymphoid cells | B or T lineage markers+; CD1a-, CD207- |
| Papillary thyroid carcinoma | Grooved and indented nuclei; BRAF mutation | Papillary and follicular patterned epithelial tumor | TTF1 / Tg+; LCH immunophenotype- |
| Hashimoto thyroiditis | Lymphocyte rich background obscuring LCH cells | Lymphocytic infiltration | LCH immunophenotype- |
| Anaplastic thyroid carcinoma | Unusual morphology | Marked pleomorphism | LCH immunophenotype- |
Additional references
Board review style question #1
What is a widely used IHC marker for Langerhans cell histiocytosis?
- CD1a
- CD20
- Cytokeratin
- Thyroglobulin
- TTF1
Board review style answer #1
Board review style question #2
What is the most common molecular alteration in Langerhans cell histiocytosis?
- BRAF V600E mutation
- EGFR mutation
- RAS family mutations
- TERT promoter mutation
- TP53 mutation
Board review style answer #2

