
Thyroid & parathyroid
Thyroid - general
Grossing
Author: Andrey Bychkov, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 2 July 2019
Last staff update: 12 September 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Gross thyroid specimens
See Also: Features to report

Table of Contents
Surgical procedures | Step by step procedure | Tips | Sections to obtain | Gross appearance of main thyroid lesions | Gross description template | Diagrams / tables | Gross images | Videos | Additional referencesCite this page: Bychkov A. Grossing. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidgrossing.html. Accessed March 27th, 2025.
Surgical procedures
- Note operation records of surgeon and clinical history; this will help guide dissection
- Diagnosis of papillary carcinoma is usually made preoperatively by fine needle aspiration
- Describe how specimen is received (fresh or fixed, intact or fragmented)
- Procedure
- Lobectomy
- Hemithyroidectomy: lobe with isthmus
- Subtotal thyroidectomy: small portion of uninvolved thyroid gland is left to preserve endocrine function
- Total thyroidectomy: entire gland
- Completion thyroidectomy: second lobe after lobectomy / hemithyroidectomy
- Each type of thyroidectomy can be accompanied by central compartment / modified radical neck dissection (removal of cervical lymph nodes)
Step by step procedure
- Measure 2 lobes and isthmus (3 dimensions) and weigh thyroid gland
- Describe shape, color, symmetry and consistency of entire specimen before cutting
- Ink if tumor is suspected
- Section transversely (or longitudinally or frontal / coronally) every 2 - 5 mm
- Describe number, size, location, encapsulation, color (fixed specimens are more grayscale than the fresh ones), secondary changes (hemorrhage, calcification, cystic) and the shortest distance to surgical margins for nodules
- Describe thyroid tissue away from tumor, other attached tissue (muscle, fat, trachea, esophagus, if any)
- Identify candidate parathyroids and lymph nodes
- Gross photos can be taken of
- Fresh specimen
- Fixed uncut specimen
- Serially sectioned specimen
- Do sampling, as per Sections to obtain below
- Keep remaining tissue in formalin until the final histopathological diagnosis is established
Tips
- Fix overnight (2 days for large nodules) in 10% buffered formalin; in addition to easier cutting, this may prevent bulging of capsule of the encapsulated nodule and artefactual nuclear atypia (Japanese Society of Thyroid Surgery: General Rules for the Description of Thyroid Cancer, 7th Edition, 2015)
- Large specimens (> 4 cm nodules) can be infiltrated with fixative using syringe (Japanese Society of Thyroid Surgery: General Rules for the Description of Thyroid Cancer, 7th Edition, 2015)
- Tumor / nodule size is best measured by sonography - refer to clinical records (Eur Thyroid J 2017;6:315)
- Chart with ultrasound mapping can be supplied
- Inking is not necessary if proper 3D mapping is done during grossing; see Sampling gross images below (Japanese Society of Thyroid Surgery: General Rules for the Description of Thyroid Cancer, 7th Edition, 2015)
- Identify and mark on gross photo upper and lower poles, medial (isthmic) side, anteriolateral and posterior surfaces
- Anatomic features can be helpful, such as pointed end (upper pole), convex (anterolateral) and concave (posterior) surfaces, attached muscle (anterior), cauterized transected surface (isthmus)
- Check orientation marks made by surgeon (sutures, clips)
- Refer to schematic drawings provided by surgeon
- Some surgeons submit a specimen oriented on a board with schematic drawing of the major neck structures; this is particularly helpful for mapping of lymph nodes (see Gross images below)
- Capsular invasion can be detected or suspected on magnification (zoom of digital photo or loupe) - use for large encapsulated nodules with a thick capsule (Japanese Society of Thyroid Surgery: General Rules for the Description of Thyroid Cancer, 7th Edition, 2015)
- If searching for microcarcinoma, slice the specimen into 2 - 3 mm sections and transilluminate them to identify discrete white spots / scars (Rosai: Tumors of the Thyroid and Parathyroid Glands, 4th Series, 2016)
- Sampling of the lower lobe with attached fibroadipose tissue may yield clinically unrecognized metastatic perithyroidal lymph nodes
- Cytologic smears can be done by fine needle aspiration from freshly submitted specimen using syringe (Kakudo: Thyroid FNA Cytology - Differential Diagnoses and Pitfalls, 2nd Edition, 2019)
Sections to obtain
- Thyroid without nodules (diffuse inflammatory lesions, i.e. Graves, Hashimoto or completion thyroidectomy):
- 3 sections from each lobe (upper, mid, lower), 1 from isthmus
- Multinodular goiter:
- 1 cassette per centimeter of the greatest dimension of the lobe
- Or 1 cassette per 5 g of tissue up to 10 per lobe and 2 for isthmus (total of 22 per case) (Nikiforov: Diagnostic Pathology and Molecular Genetics of the Thyroid, 3rd Edition, 2019)
- Focus on suspicious areas (solid, sclerotic, firm)
- Grossly infiltrative lesion (or ill defined edge), usually papillary carcinoma:
- If small, submit entire lesion
- If > 2 cm, submit 1 section per centimeter, including nearest margin and interface with normal thyroid
- Submit other suspicious / discrete lesions
- Submit representative uninvolved thyroid, as for nonnodular thyroid above
- Single well circumscribed nodule (encapsulated or well demarcated):
- Submit entire tumor capsule and include nearest inked margins or at least 10 sections
- Submit representative central portion of tumor
- Diagnosis of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) may require submitting entire tumor, including interface and parenchyma (Mod Pathol 2017;30:810)
- Submit representative uninvolved thyroid, as for nonnodular thyroid above
- Medullary thyroid carcinoma:
- Tumor as per recommendations above
- At least 1 extra specimen each of bilateral upper mid poles (to assess for C cell hyperplasia)
- MEN syndrome, prophylactic thyroidectomy:
- Submit the entire thyroid sequentially
- Thyroidectomy for occult primary (e.g. nodal metastasis without primary on imaging, thyroglossal duct carcinoma):
- Submit the entire thyroid or at least 20 blocks
- For all procedures:
- Submit all candidate lymph nodes and parathyroids
- Can put 2 - 3 sections in each cassette
- If ancillary molecular studies needed, tissue should be sampled from the fresh / unfixed specimen
- In resource limited settings, a number of sections can be decreased:
- Up front submission of the entire periphery of encapsulated lesion may not be necessary; additional blocks can be prepared from stored specimens
- Single encapsulated nodule: 1 - 2 blocks for each centimeter of diameter (i.e. 10 blocks for a 5 cm nodule) at initial gross examination
- Multinodular goiter: 1 section per nodule up to 5 nodules in a nodular process
Gross appearance of main thyroid lesions
- Multinodular goiter:
- Asymmetrically enlarged and distorted thyroid with diffuse heterogeneous nodularity, frequent scarring, hemorrhage, calcifications and cysts
- It is often difficult to distinguish a dominant nodule
- Graves disease:
- Gland is symmetrically enlarged, beefy red and homogeneous without nodularity
- Hashimoto thyroiditis:
- Diffuse symmetric enlargement, tannish yellow on cut resembling lymph node; may appear multilobular due to parenchymal fibrosis
- Papillary thyroid carcinoma:
- White to yellow-white, sometimes cystic, often firm / sclerotic and calcified with a rim of peritumoral fibrosis; multifocality is common
- Papillary projections can be seen in cystic and encapsulated tumors
- May grossly invade the thyroid capsule and adjacent muscle
- Occult microcarcinoma may appear as a tiny pale gray scar
- Follicular neoplasm:
- Follicular adenoma: solitary, 2 - 4 cm, completely encapsulated (thin capsule), pale tan to gray mass, soft, gelatinous or fleshy
- Follicular carcinoma: similar to adenoma but larger and has a thick capsule (> 1 mm)
- Widely invasive follicular carcinoma has infiltrative border, sometimes multinodular
- Hürthle cell tumor:
- Tan-brown to mahogany brown with frequent parenchymal hemorrhage
- Medullary carcinoma:
- Located in the middle and upper third of the central portion of the lobe
- Well circumscribed but nonencapsulated, gray to yellow, with a soft and fleshy or firm and gritty consistency; often multifocal
- Anaplastic carcinoma:
- Large, firm to hard, pale gray with areas of necrosis and hemorrhage
- Because of invasive nature, is often submitted with attached adjacent tissues (muscle, trachea); recognizable thyroid may not be present
Gross description template
- Blank template (UCLA Pathology & Laboratory Medicine: Head and Neck Pathology Grossing Guidelines [Accessed 25 April 2019])
- Received [fresh / in formalin] is [intact / disrupted] [hemi / total] thyroidectomy specimen
- [Orientation if provided]
- The thyroid measures __ × __ × __ mm [add measurements for lobes, if total thyroidectomy], weight __ grams
- The capsule is [intact, ruptured, smooth] [with / without] adherent skeletal muscle
- The specimen is serially sectioned into __ levels to reveal [describe lesions including size, color, shape, encapsulation, degenerative changes, relationship to margins]
- Nodule #1 is __ × __ mm [encapsulated / well circumscribed / ill defined / infiltrative] and measures __ mm to the closest [anterior, posterior, etc.] margin / surface, [describe color, homo / heterogeneous, degenerative changes]
- Nodule #2 …
- The remaining cut surface is [red-brown, smooth, unremarkable]
- Papillary carcinoma (Lester: Manual of Surgical Pathology, 3rd Edition, 2010)
- Received fresh is a 65 g total thyroidectomy specimen consisting of right lobe (6 × 5 × 4 cm), left lobe (5 × 3 × 2.5 cm) and isthmus (2 × 1.5 × 1 cm). Anterior surface has a fragment of attached skeletal muscle. The right upper pole is oriented with a white surgical suture. On cut, there is a 4 × 3 × 2 cm ovoid white-tan firm mass with a finely granular appearance present in the right lobe and extending into the isthmus. The central portion is densely white, firm and focally calcified. The lesion is poorly circumscribed and grossly invades the thyroid capsule at the posterior plane but is 0.1 cm from the inked resection margin. The remainder of the parenchyma is red-brown and homogeneous with a single colloid filled nodule (0.5 cm) in the lower portion of the left lobe. Parathyroid glands are not recognized grossly.
- Encapsulated solitary nodule (follicular adenoma, noninvasive follicular thyroid neoplasm with papillary-like nuclear features [NIFTP], follicular carcinoma)
- Received in the fresh state is a specimen identified as left hemithyroidectomy (left lobe with isthmus). A black suture is present at the isthmusectomy margin. The specimen weighs 35 g and measures 65 × 40 × 30 mm. The outer surface is smooth and the consistency is homogeneously firm. An ill defined bulging is noted in the lower pole of the left lobe. No parathyroid glands or lymph nodes are identified. Parallel longitudinal sections of the specimen reveal a round nodule in the lower lobe measuring 25 mm in greatest diameter. It is entirely surrounded by a very thin fibrous capsule that shows no gross evidence of invasion. The cut surface of the nodule is solid, slightly bulging and tan, with punctate areas of fresh hemorrhage. The capsule of the nodule is 5 mm distant from the thyroid capsule in anterior and posterior planes and 12 mm distant from the surgical margin at the isthmus. The rest of the thyroid shows no gross abnormalities.
Diagrams / tables
Images hosted on other servers:



Ink color scheme



How to serially section
Gross images
Contributed by Andrey Bychkov, M.D., Ph.D.
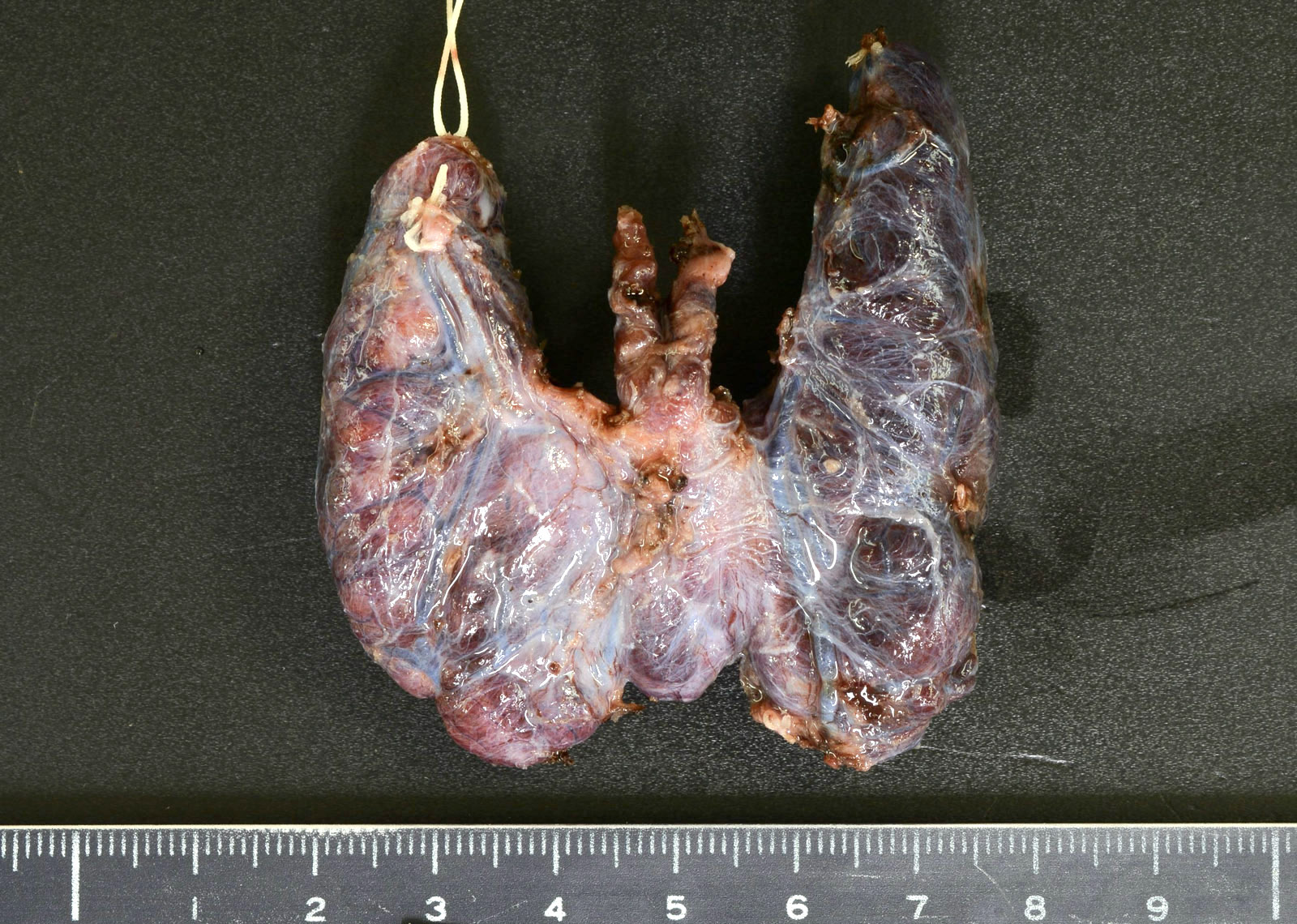
Orientation of specimen by surgeon
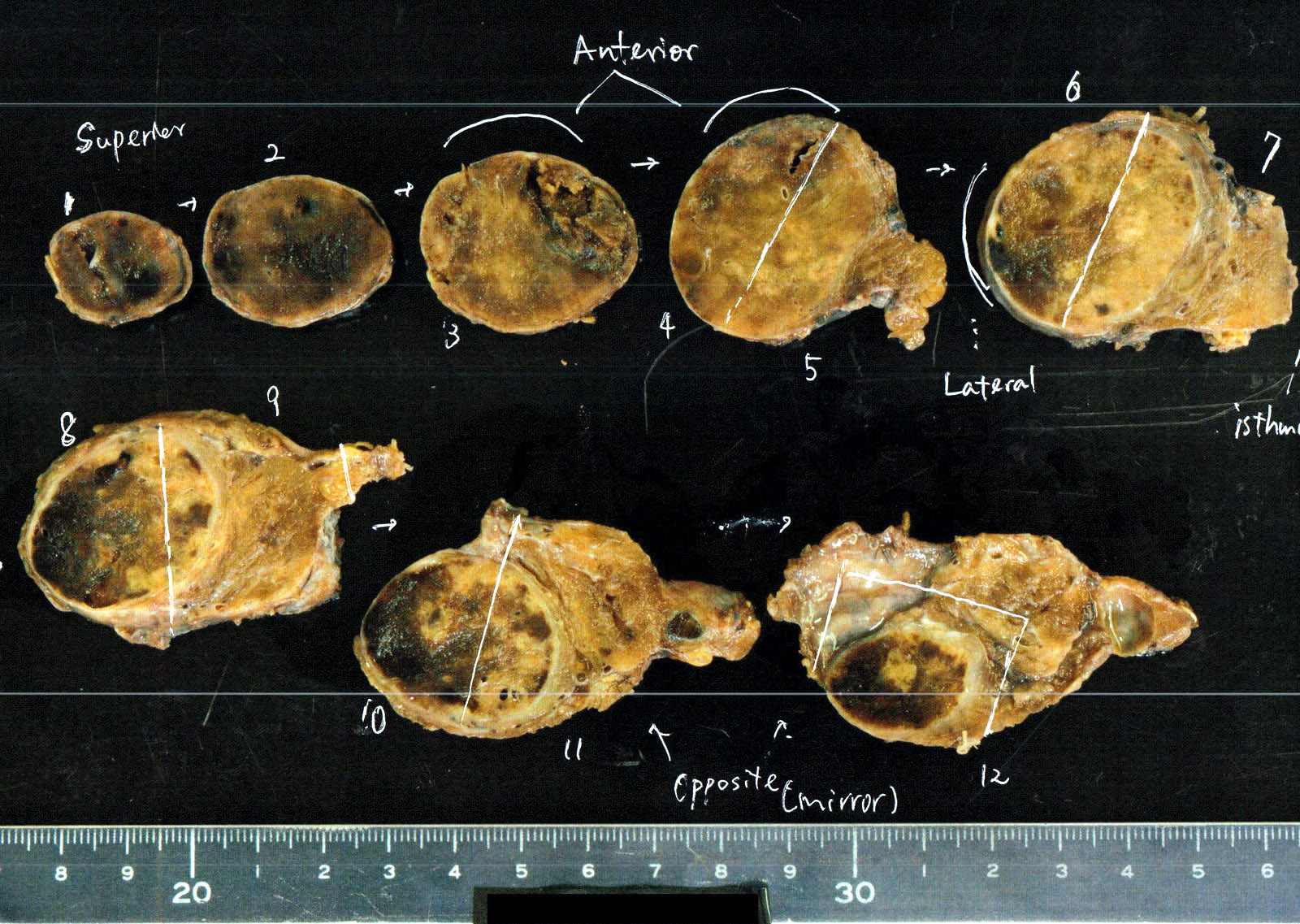
Sampling encapsulated lesion
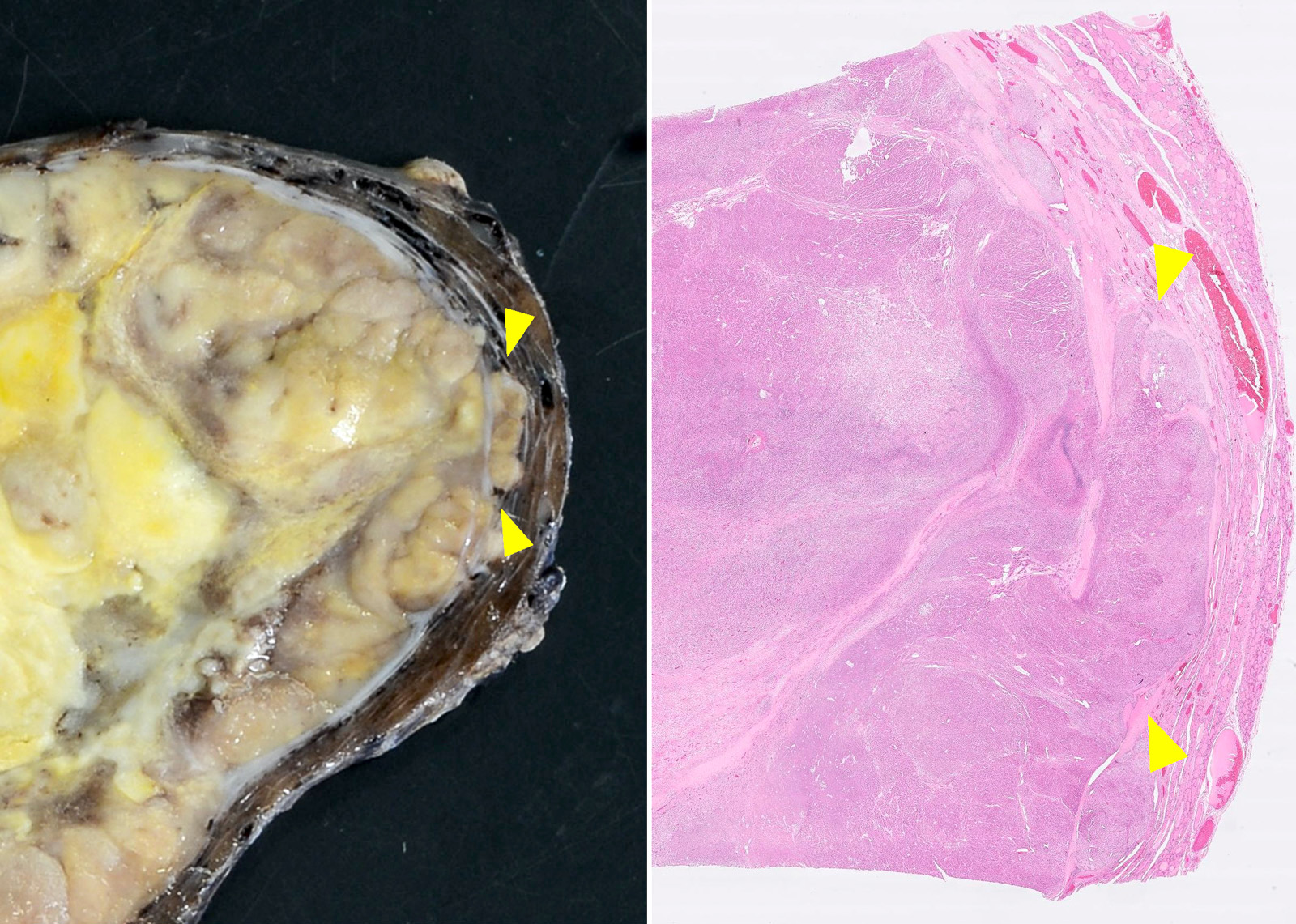
Detecting capsular invasion
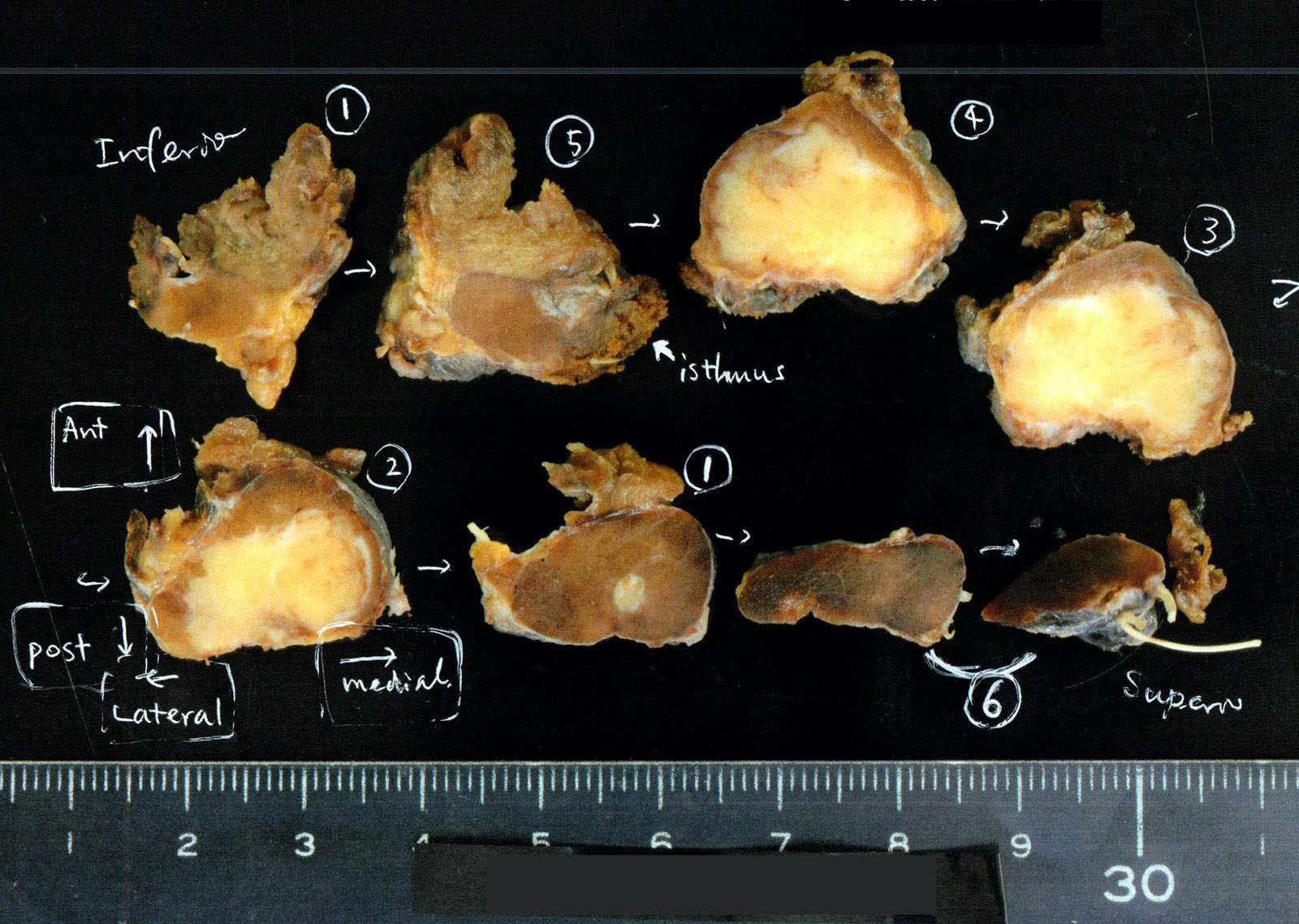
Sampling papillary carcinoma
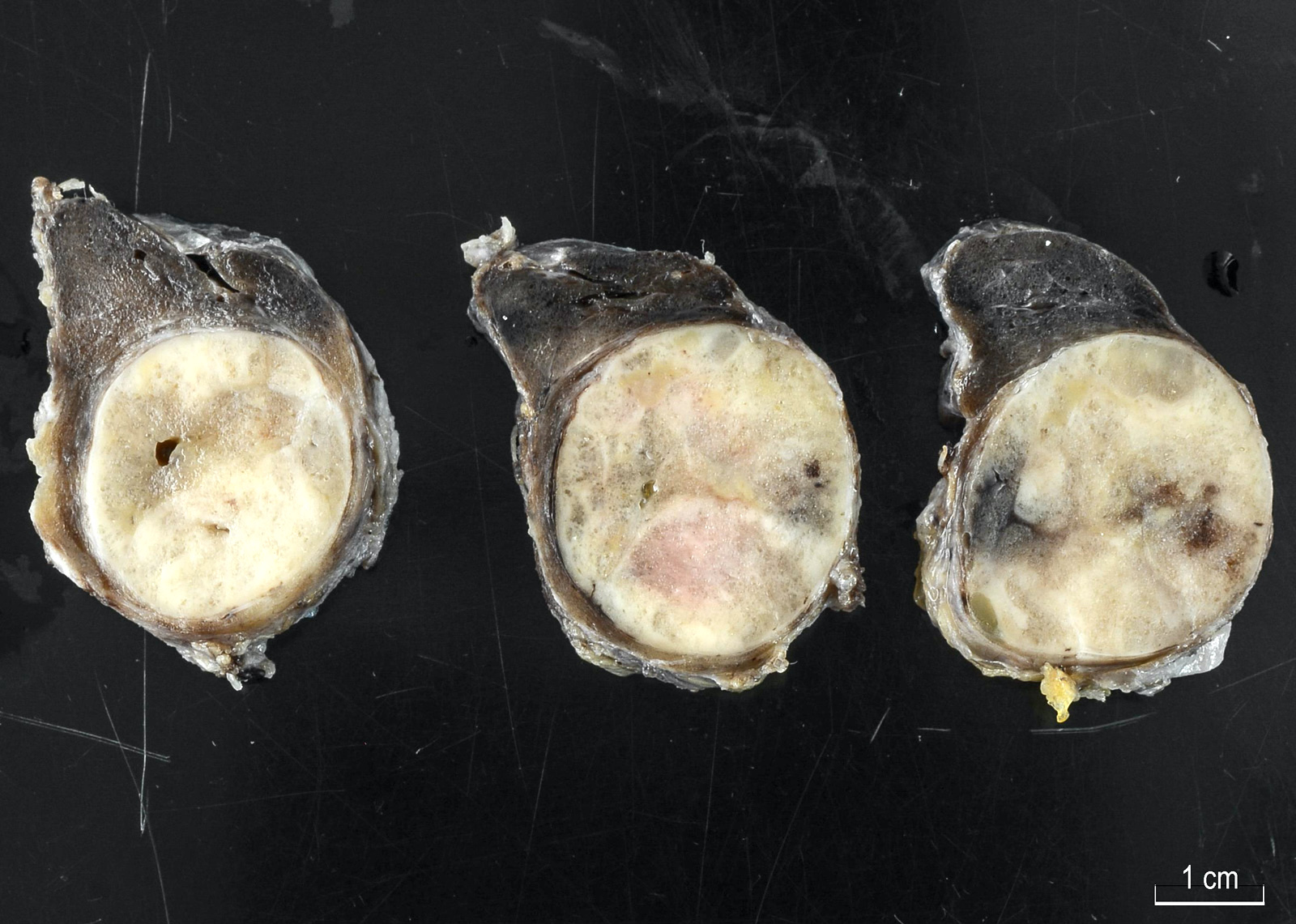
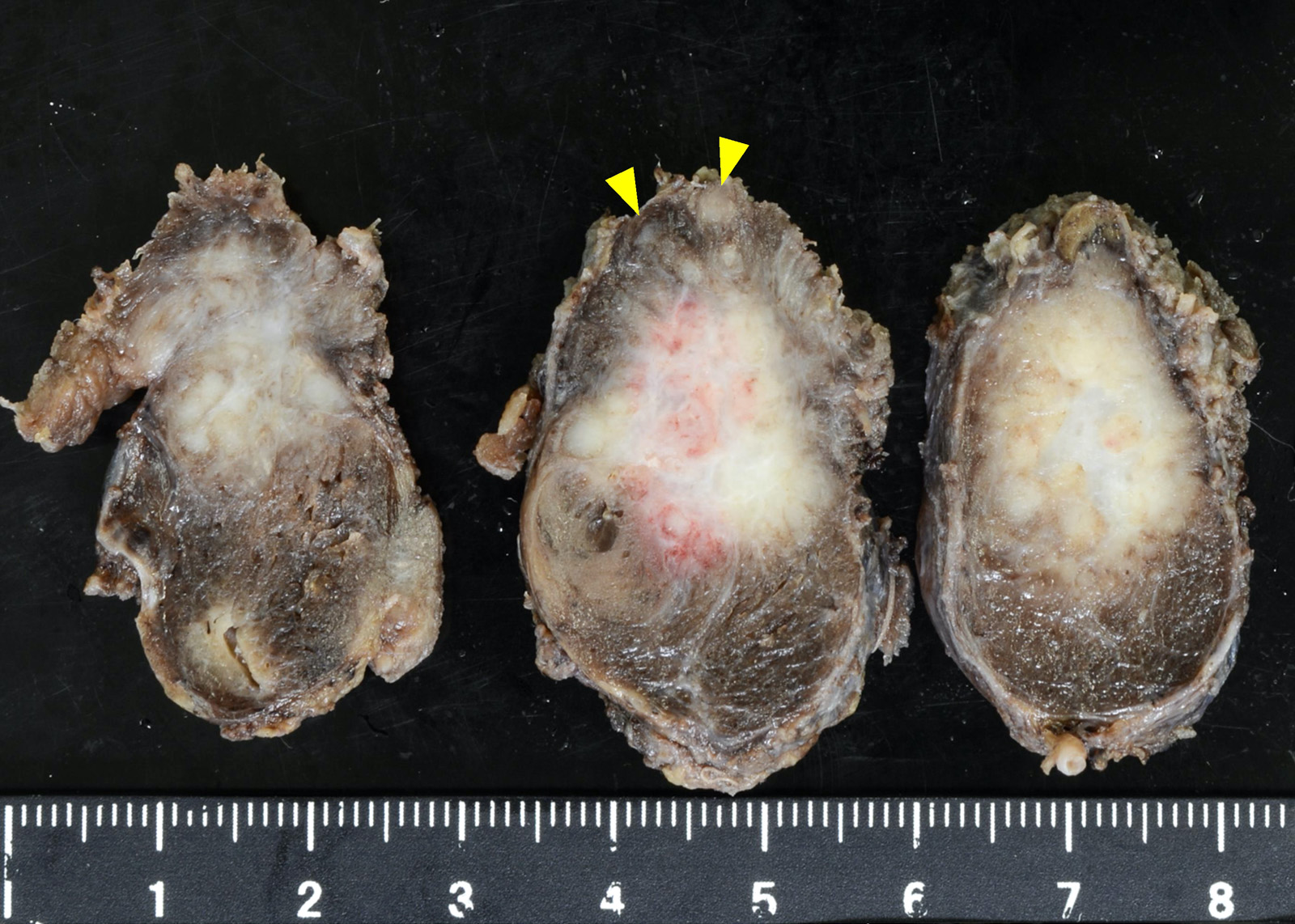
Gross appearance of main thyroid lesions: follicular adenoma and papillary carcinoma
Images hosted on other servers:

Orientation of specimen by surgeon
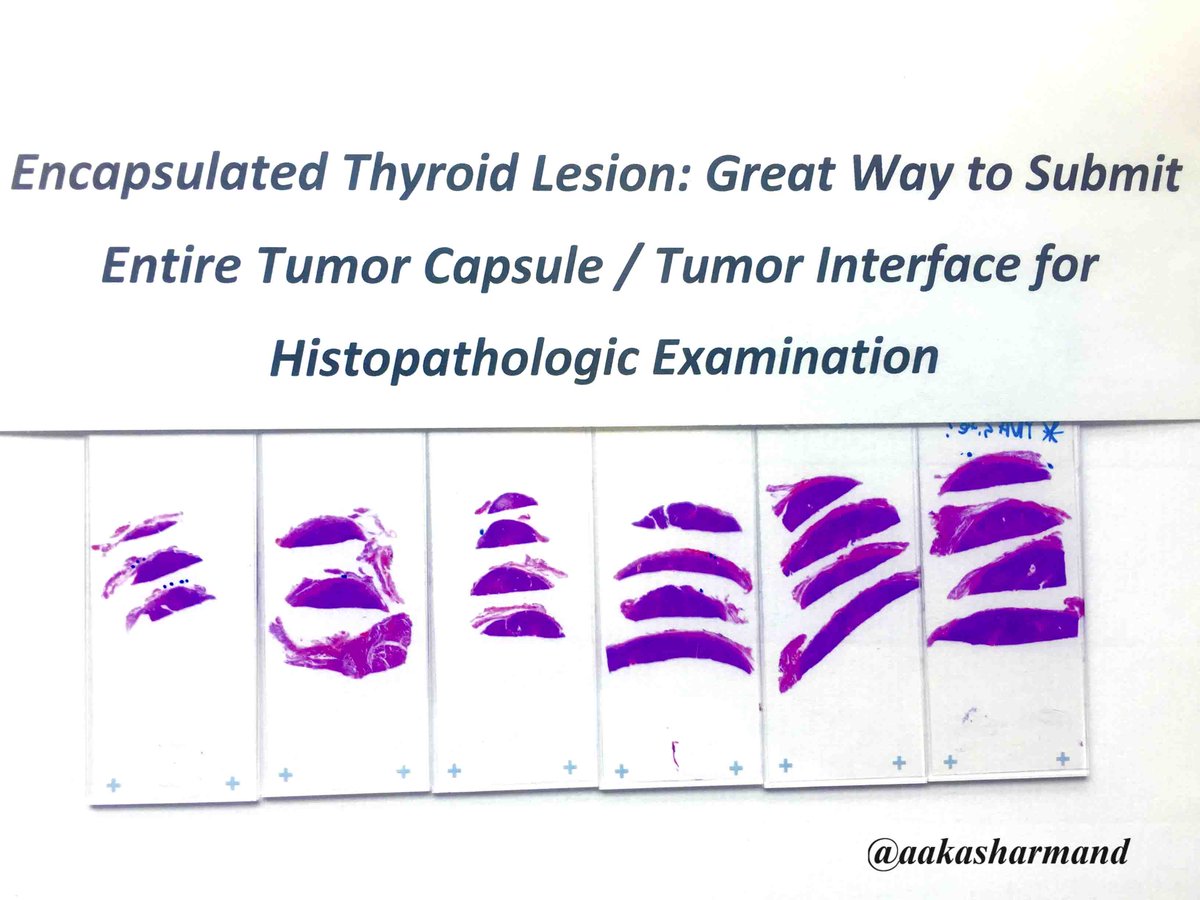
Sampling encapsulated lesion
Videos
Grossing by Weill Cornell
Grossing by Gross Cutting Room
Additional references
