

Thyroid & parathyroid
Hyperplasia / goiter
C cell hyperplasia
Last author update: 1 August 2017
Last staff update: 16 August 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: "C cell hyperplasia" thyroid


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Satturwar S, Ally Z. C cell hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidccell.html. Accessed December 26th, 2024.
Definition / general
- Variously defined as at least 50 immunostained C cells per low power of x100 (Endocr Pathol 2001;12:365) and more than 50 calcitonin positive cells in three low power fields of x100 (Mod Pathol 2003;16:756)
- Neoplastic CCH is diagnosed as a separate form of CCH, when intrafollicular or nodular C cells with nuclear pleomorphism are seen on H&E, and are morphologically distinct from follicular cells
- Estimated on at least 2 sections taken from the junction of the middle and upper thirds of the thyroid lobes which can be grossly recognized by the presence of prominent vessels
Essential features
- Neoplastic CCH can be diagnosed by routine H&E stains, but reactive CCH requires calcitonin staining
- Calcitonin levels may be elevated in both reactive and neoplastic CCH
ICD coding
- E07.0
Epidemiology
- Reactive CCH commonly occurs in adults (at autopsy, 41% of men and 15% of women, J Clin Endocrinol Metab 1997;82:42)
- Women with elevated basal calcitonin and CCH have almost 100% risk of developing medullary thyroid carcinoma versus 31% of men, who may have C cell hyperplasia only (Mod Pathol 2003;16:756, Endocr Relat Cancer 2009;16:243)
Sites
- Upper 2/3 of both thyroid lobes
Clinical features
- C Cell hyperplasia is classified as:
- Reactive or physiologic CCH
- May be seen in neonates and elderly subjects
- Twice as common in men as in women
- Associated with prolonged hypercalcemia, hyperparathyroidism, hypergastrinemia, Hashimoto thyroiditis, follicular thyroid neoplasm and nodular or diffuse hyperplastic goiter
- Neoplastic C cell hyperplasia or carcinoma in situ / intraepithelial neoplasia
- Has genetic and kinetic characteristics consistent with a malignant C cell lesion, including a family history of thyroid cancer or MEN 2A or 2B (J Clin Endocrinol Metab 2001;86:3948)
- Precursor lesion of sporadic and familial medullary carcinoma
- Caused by mutation of RET oncogene
- Bilateral and multifocal tiny nodules in thyroid visualized by ultrasound
- Mildly increased calcitonin levels
- Reactive or physiologic CCH
Diagnosis
- Suspected in cases of elevated calcitonin levels and fine needle aspiration cytology; diagnosis on histology from thyroidectomy for definitive diagnosis
Laboratory
- Mildly elevated calcitonin levels: routine screening of serum calcitonin in patients with nodular goiter demonstrated abnormal values in 4.5% and all of the abnormal cases had MTC or CCH (Am J Surg Pathol 1998;22:722)
Radiology description
- Neoplastic CCH: tiny nodules in upper 2/3 of both lobes of thyroid
Prognostic factors
- Reactive CCH: good prognosis since it has no premalignant potential or RET mutation
- Neoplastic CCH: premalignant and progresses to medullary thyroid cancer over time
Case reports
- 58 year old man with bilateral C cell hyperplasia and chronic lymphocytic thyroiditis (Am J Surg Pathol 1991;15:599)
Treatment
- Total thyroidectomy, particularly if familial history or RET mutation positive
- Isthmus preserving total bilobectomy: rationale for this procedure is that C cells derived from the ultimobranchial body migrating into the thyroid do not reach isthmus region and are distributed along the vertical axes of the thyroid lobes
- Remnant of isthmus can, over time, compensate for loss of thyroid, especially in children (World J Surg 2006;30:860)
Gross description
- Neoplastic CCH may have 1 - 2 mm nodules in upper 2/3 of thyroid lobes
- Reactive CCH does not have distinct gross lesion apart from that associated with the underlying pathology
Microscopic (histologic) description
- Increased C cells
- 3 architectural patterns: (Cancer 1996;77:750)
- Focal (segmental proliferation of C cells within thyroid follicles)
- Diffuse (circumferential intrafollicular collars pushing the follicular cells into the lumen)
- Nodular (clusters of C cells completely replacing the follicle)
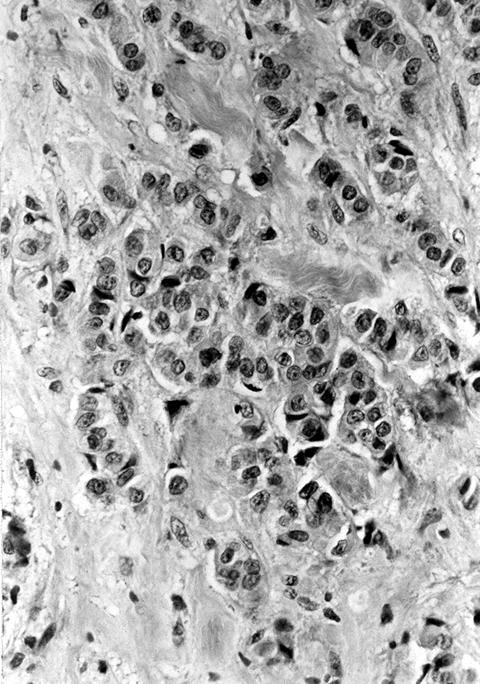
- C cells are pale staining, polygonal or spindle shaped, with abundant clear to fine granular cytoplasm and round / oval vesicular nuclei; they are located within the follicular basement membrane, do not extend through defects in follicular basal lamina, do not infiltrate thyroid interstitium
- Unlike reactive CCH, neoplastic CCH is associated with cytologic atypia and hence recognizable on H & E
Reactive CCH criteria:
- Not evident on routine H & E staining
- Cytologically bland C cells are similar to follicular cells and histiocytes
- Need immunohistochemical staining for calcitonin to identify C cells
Neoplastic CCH criteria:
- Often bilateral
- Can be readily identified by routine H & E staining and does not require calcitonin staining
- Cells with mild to moderate atypia and nuclear pleomorphism resembling medullary thyroid carcinoma cells
- Progresses from focal to diffuse and nodular hyperplasia to medullary thyroid carcinoma in situ
- Can use PAS or anticollagen IV antibodies to highlight follicular basement membrane and distinguish cells within follicles (noninvasive) from those outside follicles (invasive)
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D.

Various images
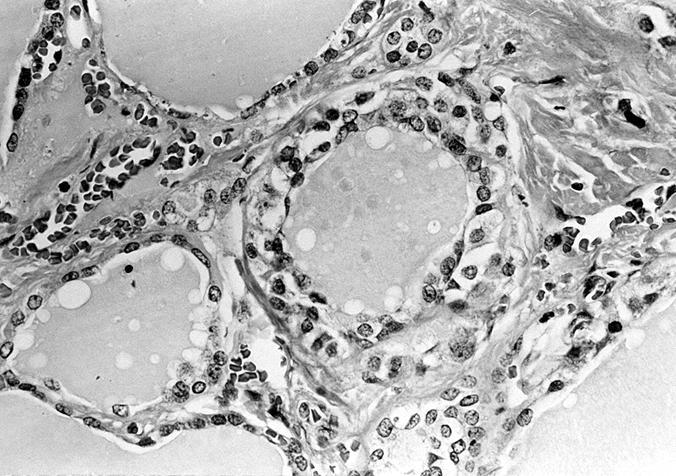
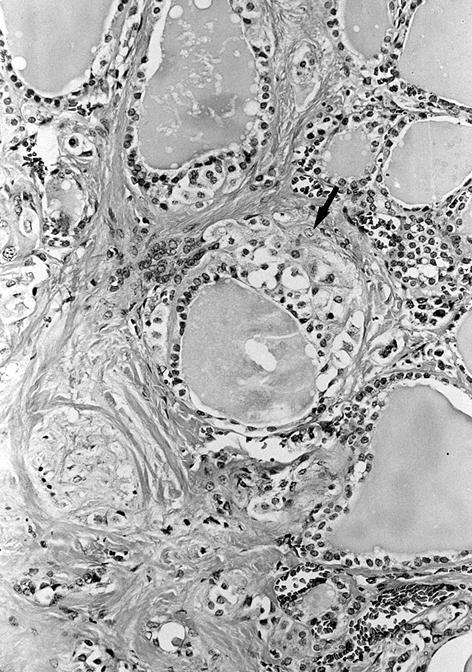
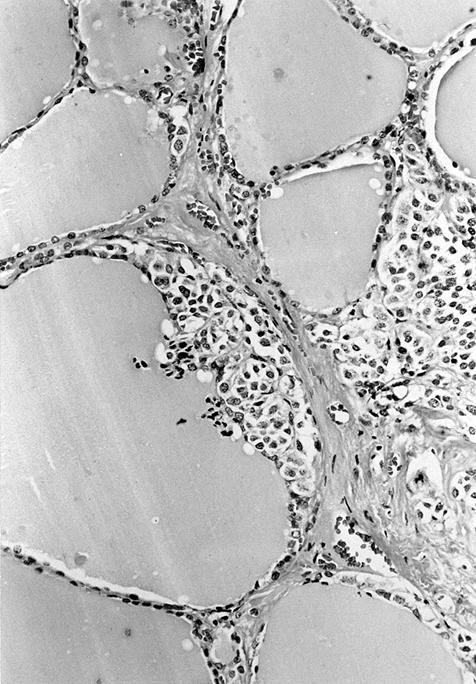
AFIP images
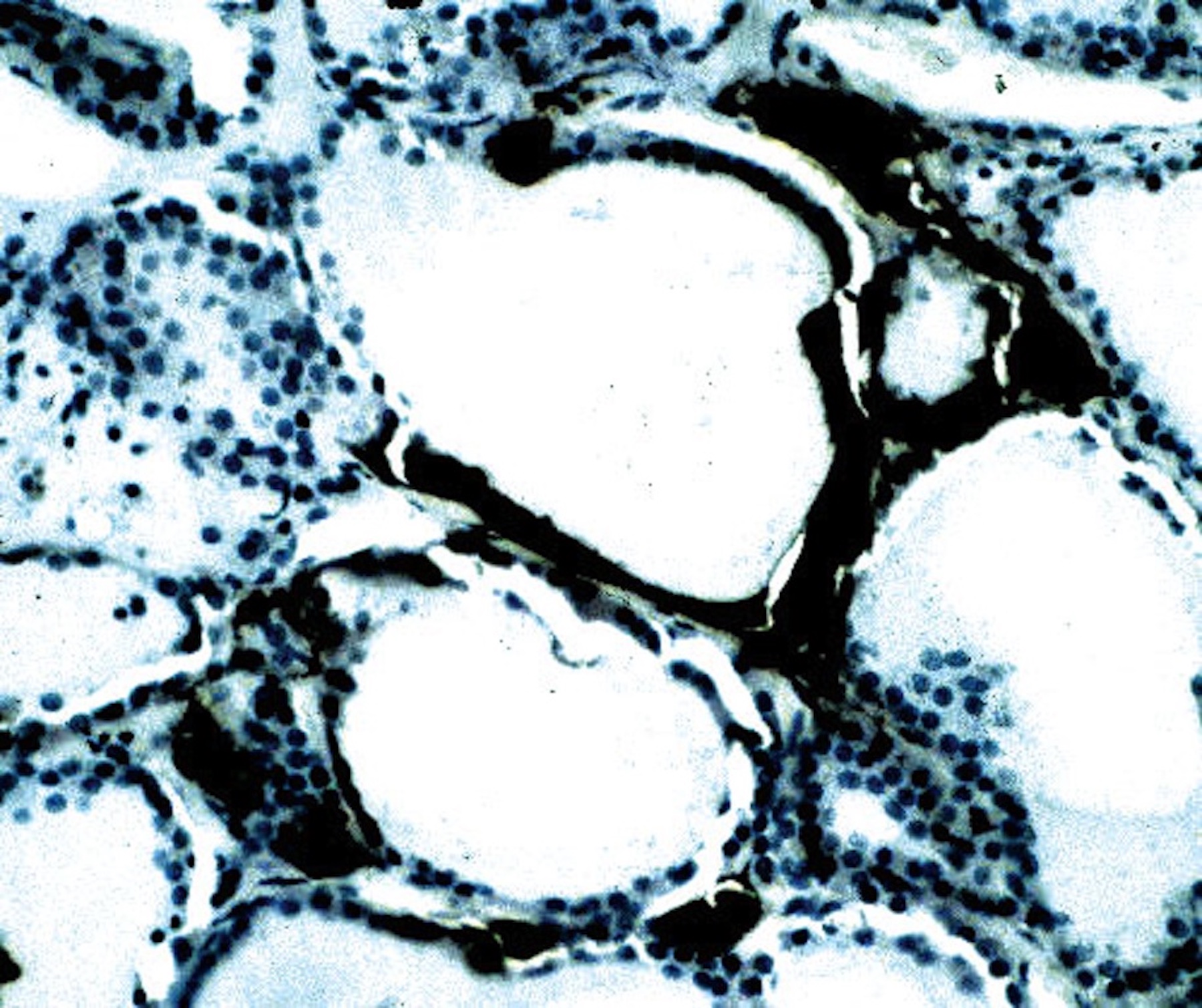
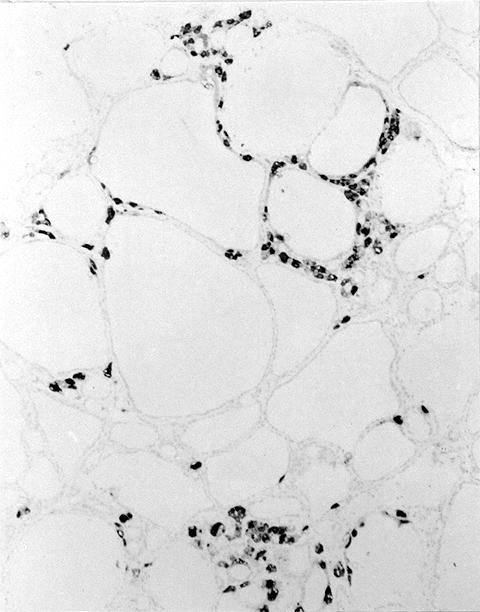
Calcitonin staining:
C cells highlighted
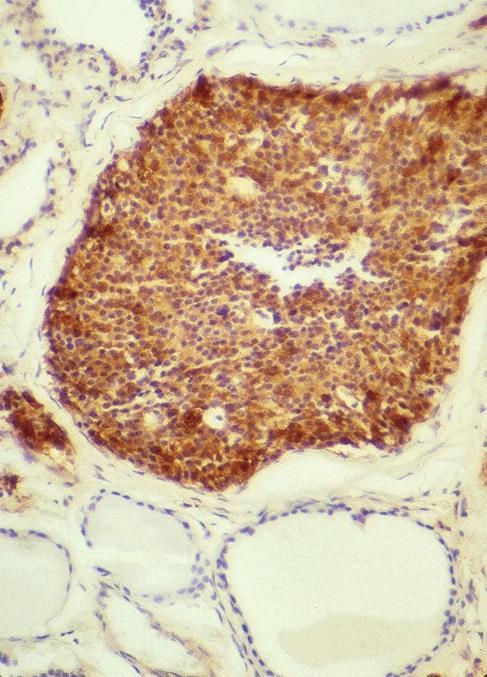
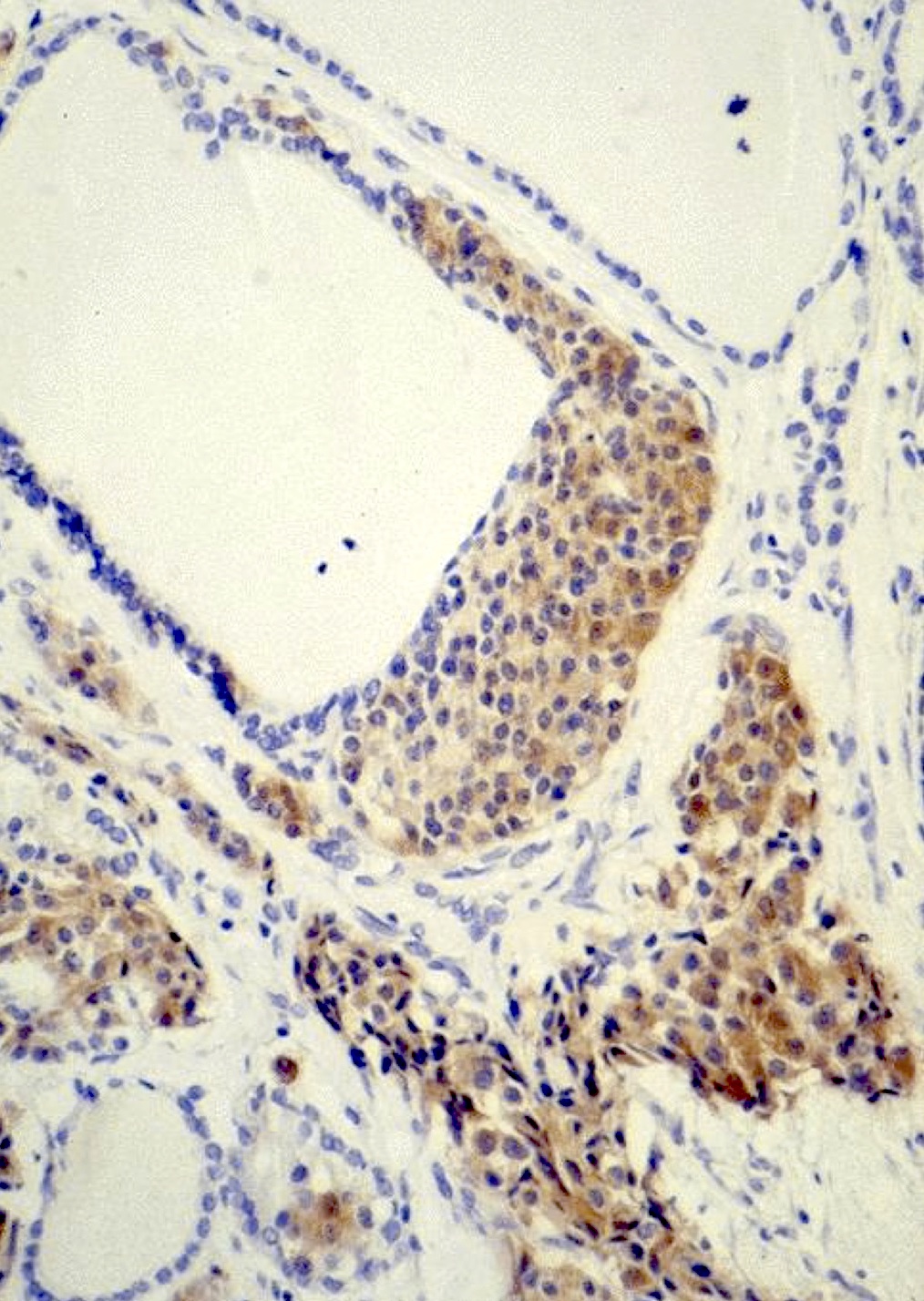
Nodular CCH
C cells adjacent to follicular carcinoma
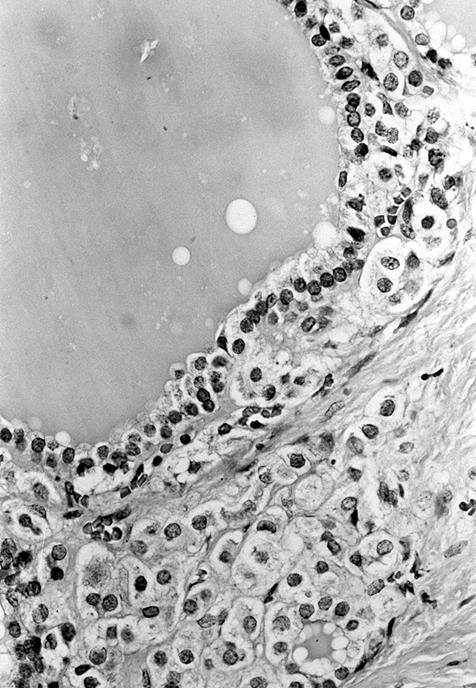
MEN2A patients:
Circumferential proliferation
Focal proliferation of C cells
Eccentric intrafollicular proliferation
MEN2A patients with early medullary carcinoma:
Group of C cells extends into interstitium
Images hosted on other servers:

Calcitonin staining, C cells form ring around follicle

Associated with nodular goiter

MEN2A patient

High power
Cytology description
- Scant bimodal cell population of benign follicular cells and larger calcitonin positive cells (Acta Cytol 1998;42:963)
Positive stains
- Calcitonin
- Also calcitonin gene related peptide, CEA, chromogranin, synaptophysin and neuron specific enolase (NSE), NCAM/CD56 (NCAM/CD56) (neoplastic cases)
- Also ER-beta (neoplastic cases, Virchows Arch 2007;450:433)
Negative stains
- Thyroglobulin, neural cell adhesion molecular (reactive cases), galectin3 (Clin Endocrinol (Oxf) 2002;57:813)
Electron microscopy description
- Proliferation of C cells within follicular basement membrane adjacent to luminal colloid; two main types of secretory granules (containing calcitonin)
- Prominent rough endoplasmic reticulum
Molecular / cytogenetics description
- RET mutation in neoplastic (Ann Endocrinol (Paris) 2006;67:190) but not in reactive CCH (J Mol Diagn 2007;9:214)
Differential diagnosis
- Nodular CCH versus microinvasive medullary carcinoma:
- PAS or anti collagen IV antibodies to highlight follicular basement membrane and distinguish neoplastic CCH cells within follicles (noninvasive) from those outside follicles (invasive / microinvasive medullary thyroid carcinoma)
- Stromal sclerosis in microcarcinoma
- Ongoing debate of lower limit for microinvasive medullary carcinoma and upper limit of nodular CCH
- Solid cell nests including squamous metaplasia (associated with thyroiditis), parathyroid nests, thymic remnants, nests of thyroid follicular cells with tangential sectioning (cytoplasm not clear)
Additional references
Board review style question #1
- Which of the following statements are not true of C cell hyperplasia?
- C cells are found along the entire longitudinal axis of the thyroid lobe
- Neoplastic C cell hyperplasia can be detected in H&E stains
- Patients with a thyroid mass and hypercalcinemia may have something other than MTC
- Reactive and neoplastic C cell hyperplasia are biologically and morphologically distinct
- RET mutation distinguishes neoplastic from reactive C cell hyperplasia
Board review style answer #1
A. C cells are not found along the entire longitudinal axis of the thyroid lobe, since only the upper two thirds of the thyroid lobes are populated by C cells.
Comment Here
Reference: C cell hyperplasia
Comment Here
Reference: C cell hyperplasia

