
Thyroid & parathyroid
Thyroid cancer
Molecular pathology-practical

Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: molecular pathology thyroid cancer
See also: Basics of molecular pathology, Molecular testing in FNA

- Thyroid cancer is a genetically simple disease with a relatively low number of mutations in each tumor
- Driver mutations and gene fusions are identified in over 90% of thyroid cancers, making it one of the best molecular characterized malignancies in humans
- MAPK and PI3K-AKT are 2 main signaling pathways involved in the development of thyroid tumors
- MAPK pathway: activated through point mutations of BRAF or RAS genes and RET / PTC rearrangements; primarily involved in papillary carcinoma
- PI3K-AKT pathway: activated through point mutations in RAS, PIK3CA, AKT1 and PTEN; primarily involved in follicular carcinoma
- Simultaneous activation of both pathways becomes more frequent as the tumor grade increases
- Collectively, the most common alterations are BRAF and RAS point mutations and RET / PTC and PAX8 / PPARγ chromosomal rearrangements
- Driver gene aberrations in well differentiated thyroid cancer are mutually exclusive (median = 1 mutation per tumor)
- Dedifferentiated cancers accumulate additional genetic alterations, so called late events (median = 6 mutations per tumor)
- Chromosomal rearrangements (and resultant gene fusions) are associated with radiation
- Most somatic mutations are not thyroid specific and are commonly found in various solid cancers
- Molecular techniques are typically applied to cytological smears, formalin fixed paraffin embedded and snap frozen tissue, see details on Molecular pathology basics page
- Mutations are detected with real time PCR and DNA sequencing
- Chromosomal rearrangements are detected with FISH and RT-PCR
- Immunohistochemistry is specific for detecting mutant proteins (BRAF V600E, NRAS Q61R)
Images hosted on other servers:

Progress in identifying
mutational markers
in thyroid cancer

Gene mutations in thyroid tumors


Genomic landscape of PTC

Gene fusions in PTC

BRAF mutation and iodine uptake

BRAF V600E and tumor recurrence

TERT mutations

Drug targets in thyroid cancer
- Preoperative diagnosis of thyroid nodules with indeterminate FNA
- Potential prognostic value to predict aggressive disease
- Targeted therapy
- Follicular adenoma (FA)
- RAS 20 - 40%
- PAX8 / PPARγ 5 - 20%
- No RET / PTC translocations, BRAF V600E mutation, PTEN mutations (except germline mutations in Cowden syndrome) or PIK3CA / AKT pathway mutations
- Hyalinizing trabecular tumor
- Although early reports found RET / PTC somatic translocations with similar frequency as PTC, this was not confirmed with more robust techniques
- Absence / extreme rarity of BRAF and RAS mutations
- Follicular thyroid carcinoma (FTC)
- Mutually exclusive RAS point mutations or PAX8 / PPARγ rearrangements in 75%
- RAS 30 - 50%
- PAX8 / PPARγ 30 - 35%
- TERT 10 - 20%
- PTEN < 10%
- PIK3CA 5 - 10%
- Hürthle cell carcinoma (oncocytic variant of FTC)
- Alteration of mitochondrial DNA, including deletions, frameshift and missense point mutations
- Lower prevalence of mutations associated with nononcocytic FTC (RAS, PAX8 / PPARγ)
- GRIM19 mutations 10 - 20%
- RAS 10 - 20%
- PAX8 / PPARγ 5 - 15%, associated with follicular architecture
- TERT 15 - 20%
- TP53 up to 20%
- RET / PTC 35%, all with solid pattern of growth (based on one study)
- Papillary thyroid carcinoma (PTC)
- Mutually exclusive genetic events found in 75 - 90% cases: point mutations in BRAF and RAS, rearrangements of RET and NTRK1
- BRAF 40 - 50%
- RAS 10 - 20%
- RET / PTC 5 - 20%
- TERT 5 - 10%
- NTRK 5%
- Common PTC variants
- Classic variant: BRAF 40 - 70%, RET / PTC 5 - 40%, RAS 3 - 10%, TERT 10%, NTRK 0 - 5%
- Follicular variant: RAS 25 - 50%, PAX8 / PPARγ 5 - 30%, BRAF V600E up to 25% (invasive type), TERT 1 -10%, RET / PTC 5%, NTRK 0 - 10%, BRAF K601E < 1%
- NIFTP: RAS 30 - 45%, PAX8 / PPARγ up to 20%, THADA fusion up to 20%, EIF1AX 5%, absence of BRAF mutation and RET / PTC translocations
- Microcarcinoma: BRAF 20 - 80%, RET / PTC rearrangements and RAS mutations can be found, TERT < 5%
- Tall cell variant: BRAF 80 - 100%, TERT 20 - 30%, RET / PTC3
- Rare PTC variants (based on small series)
- Columnar variant: BRAF 33%
- Diffuse sclerosing variant: RET / PTC rearrangement frequently found, while BRAF mutation is uncommon
- Hobnail variant: BRAF V600E mutation in most cases (50 - 80%), RET / PTC1 is much rarer (up to 20%)
- Warthin-like variant: BRAF 65%
- Cribriform-morular variant: RET / PTC rearrangements, RAS mutations and BRAF mutations not identified; germline APC or CTNNB1 mutations in familial adenomatous polyposis coli syndrome
- Poorly differentiated thyroid carcinoma (PDTC)
- TERT 30 - 40%
- RAS 20 - 40%
- BRAF 5 - 30%, higher rate if arises from PTC
- EIF1AX 10%
- Rare chromosomal translocations (RET / PTC, PAX8 / PPARγ, ALK1)
- Late genetic events are common: TP53 (10 - 40%), CTNNB1 (0 - 25%) and genes that encode effectors of the PI3K-AKT signaling pathway, including PIK3CA, AKT1 and PTEN (10 - 20% collectively)
- Anaplastic thyroid carcinoma (ATC)
- Coexisting mutations (median is 6 per case)
- TP53 50 - 80%
- TERT 30 - 50%
- RAS 20 - 50%
- BRAF 20 - 45%, especially if progress from PTC
- Less common mutations: CTNNB1 5 - 65%, PIK3CA 5 - 25%, PTEN 5 - 20%, RASAL 15%, EIF1AX 10%
- Fusions, e.g., ALK, are infrequent
- Medullary thyroid carcinoma (MTC), sporadic
- Mutually exclusive RET or RAS mutations
- RET 30 - 65%, mainly RET M918T
- RAS 25% (HRAS > KRAS)
- Medullary thyroid carcinoma (MTC), hereditary
- Germline RET mutations > 95%, with predominant RET C634A in MEN2A, and RET M918T in MEN2B syndromes, respectively
Clinically significant signatures
Diagnostic molecular signatures
- Molecular testing is widely used for preoperative triage of patients with thyroid nodules indeterminate on FNA (Bethesda III - V), see Molecular testing in FNA
- Presence of certain mutations in a sample has high sensitivity and specificity for malignancy, with recommendation for total thyroidectomy instead of diagnostic lobectomy
- BRAF V600E or RET / PTC rearrangement has virtually 100% risk of malignancy, likely to be conventional or tall cell variant PTC
- RAS, PAX8 / PPARγ or BRAF K601E confers 75 - 90% risk of cancer, most likely follicular variant PTC
- TERT, p53 or PIK3CA mutation predicts thyroid cancer (almost 100% risk), particularly advanced disease with propensity for dedifferentiation and distant metastasis
- RET M918T is associated with MTC (very high accuracy)
- Single gene testing (usually BRAF V600E) is inexpensive, and can be performed using in house facilities
- Molecular panels provide the best performance
- 4 genes (BRAF V600E, RAS, RET / PTC and PAX8 / PPARγ) are essential for any thyroid panel
- Commercially available panels include early generation (8 and 15 genes) and extended (60+ genes) panels
- Mutation / fusion panels are highly sensitive for malignancy, often having over 95% positive predictive value ("rule in" cancer), however negative result of mutation test does not always predicts benign thyroid nodule; gene expression classifiers based on mRNA expression signatures provide 95% negative predictive value ("rule out" cancer)
- Combination of rule in (mutation / fusion panel) and rule out (gene expression classifier) tests is potentially the best approach to indeterminate thyroid nodules, however its cost effectiveness is doubtful
Prognostic significance
- BRAF V600E is a marker of higher tumor recurrence and tumor related mortality in PTC patients
- These patients may benefit from more extensive initial surgery with central compartment lymph node dissection to prevent tumor recurrence
- BRAF mutation is a sensitive, but not a specific marker of tumor aggressiveness
- Most patients with BRAF V600E mutation do not have recurrent disease and overall survival remains very high in both groups of patients
- TERT promoter mutations are associated with aggressive phenotype of PTC and FTC, including high persistence / recurrence and increased mortality
- Recent studies have shown that the prognostic value of TERT mutations is significantly stronger than that of BRAF V600E
- Combination of BRAF V600E mutation with TERT, AKT1, PIK3CA or TP53 mutations predicts more aggressive tumor behavior
- Patients with BRAF and TERT mutations alone had recurrence rates of 25% and 50%, respectively, whereas patients with both mutations had a recurrence rate of 70%
- With a high rate of targetable ("druggable") molecular abnormalities in thyroid cancer, genotyping has diagnostic and possibly therapeutic relevance
- Patients who may benefit from targeted therapy
- Radioiodine resistant differentiated thyroid cancer (metastatic PTC or FTC)
- PDTC, ATC
- MTC
- The most studied drugs are tyrosine kinase inhibitors (TKI, or MKI, multikinase inhibitors)
- MKIs block various cell surface (growth factor receptor) and intracellular (members of MAPK signaling) kinases
- Inhibition of VEGF (vascular endothelial growth factor) mediated pathways contributes to the antiangiogenic effect of MKI
- Currently, 4 kinase inhibitors are approved for treatment of differentiated thyroid cancer and MTC
- Sorafenib, an inhibitor of VEGFR1, VEGFR2, VEGFR3, RET (including RET / PTC), RAF (including BRAF V600E), and PDGFRβ (platelet derived growth factor receptor β)
- Lenvatinib blocks VEGF receptors 1, 2 and 3, FGF receptors 1 - 4, PDGFRα, RET and KIT
- Vandetanib (VEGFR2, RET, EGFR) and Cabozantinib (VEGFR2, RET, MET) are approved in the USA and EU for treatment of MTC
- MKI treatment is not curative, and patients eventually develop resistance
- Other targeted therapies currently in clinical trials:
- Selective BRAF inhibitors (Vemurafenib, Dabrafenib)
- PPARγ agonists
- ALK inhibitors (Crizotinib)
- Highly selective mTOR inhibitors
- PTEN modulators
- NTRK inhibitors
- Immune checkpoint blockade (anti-CTLA4, anti-PD1, and anti-PDL1)
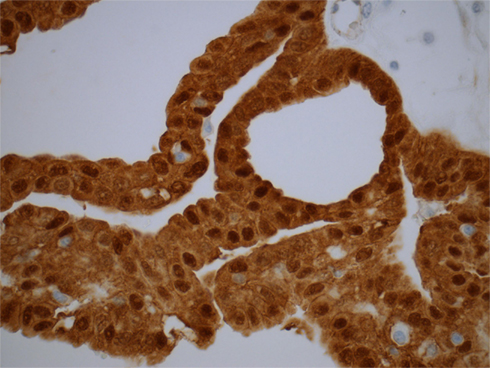
Contributed by Andrey Bychkov, M.D., Ph.D.
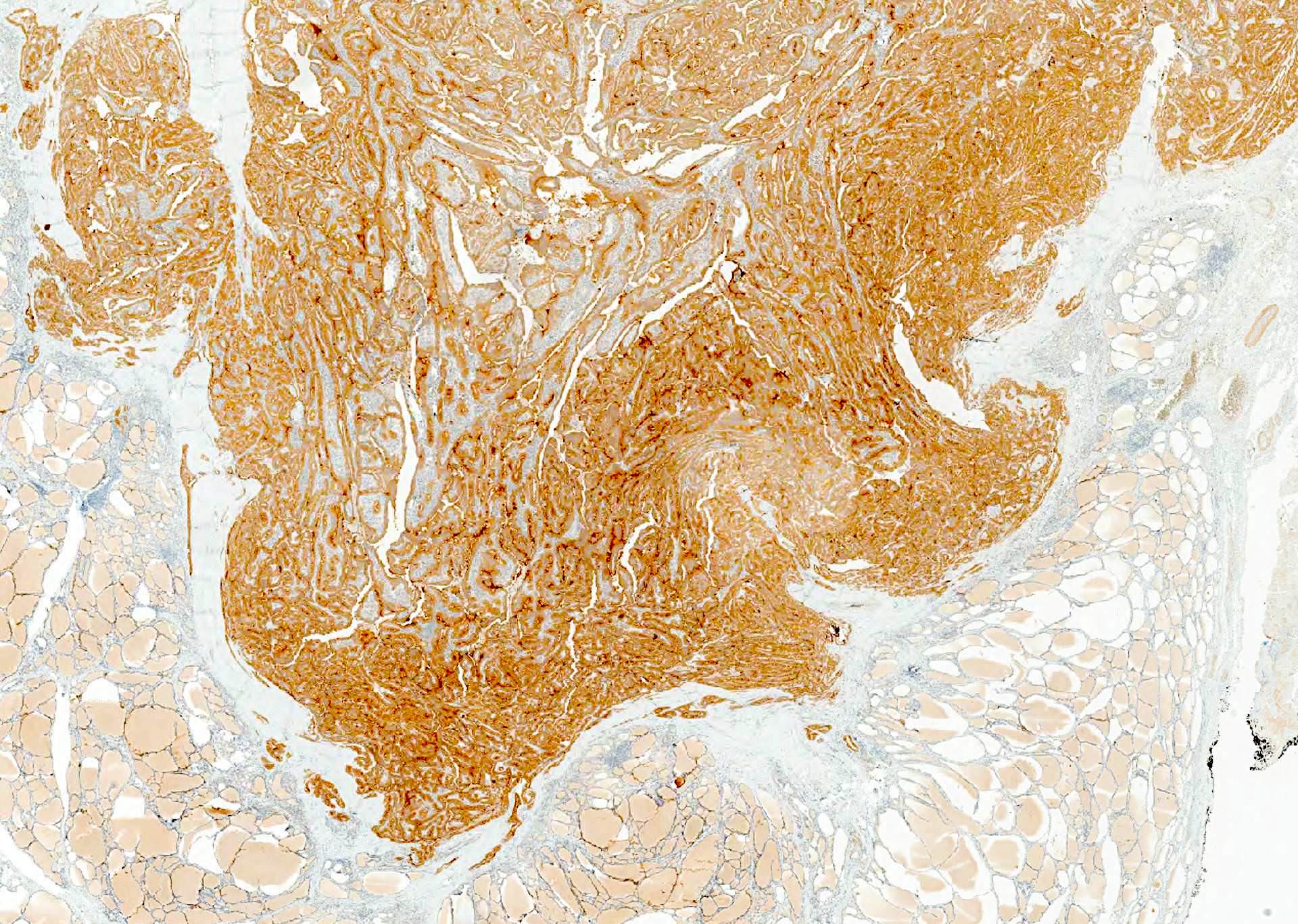
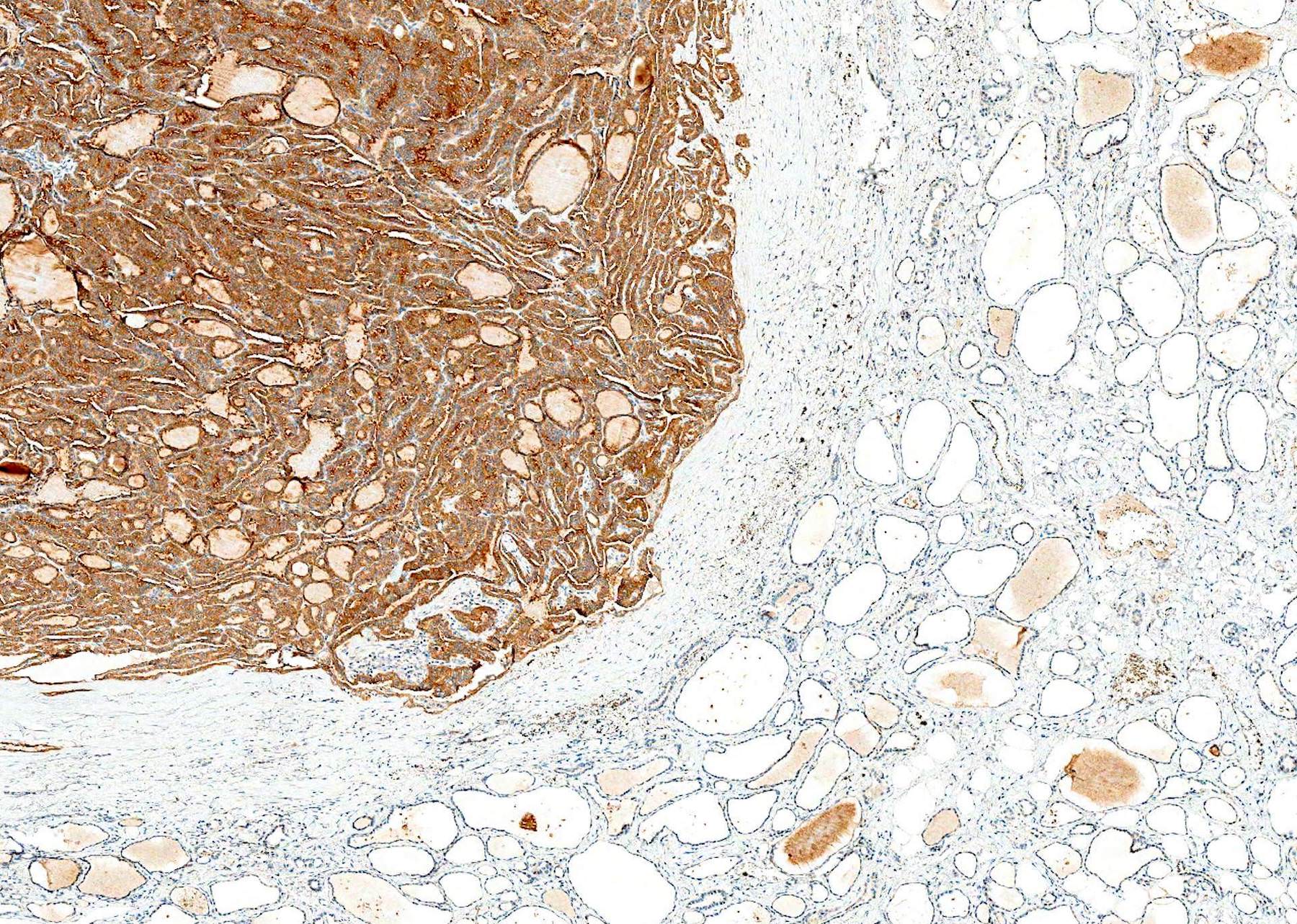
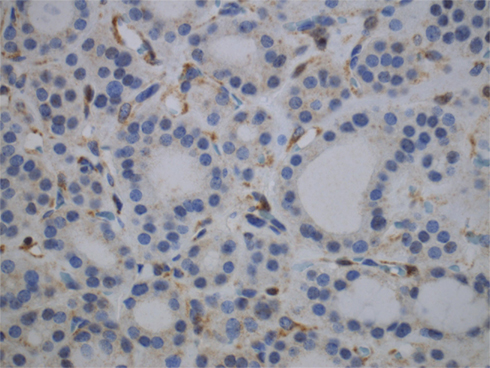
V600E mutant protein is diffusely expressed in tumor / cancer, but not normal tissue

Diffuse cytoplasmic staining
Images hosted on other servers:


ALK fusions

β-catenin (nuclear) in cribriform-morular PTC associated with FAP syndrome

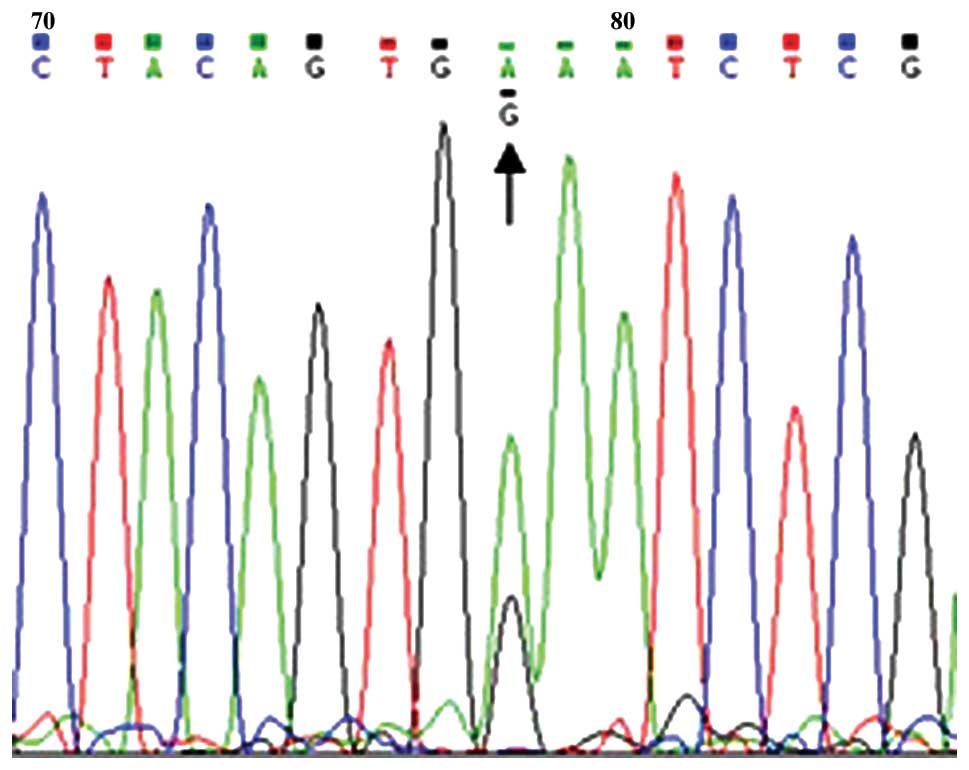
BRAF V600E (sequencing)

BRAF V600E (MALDI-TOF)
BRAF K601E

BRAF V600E / VE1
KRAS mutations
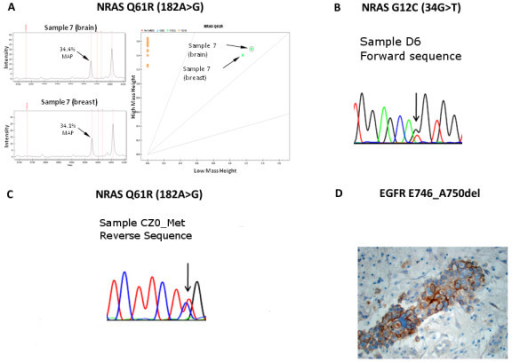
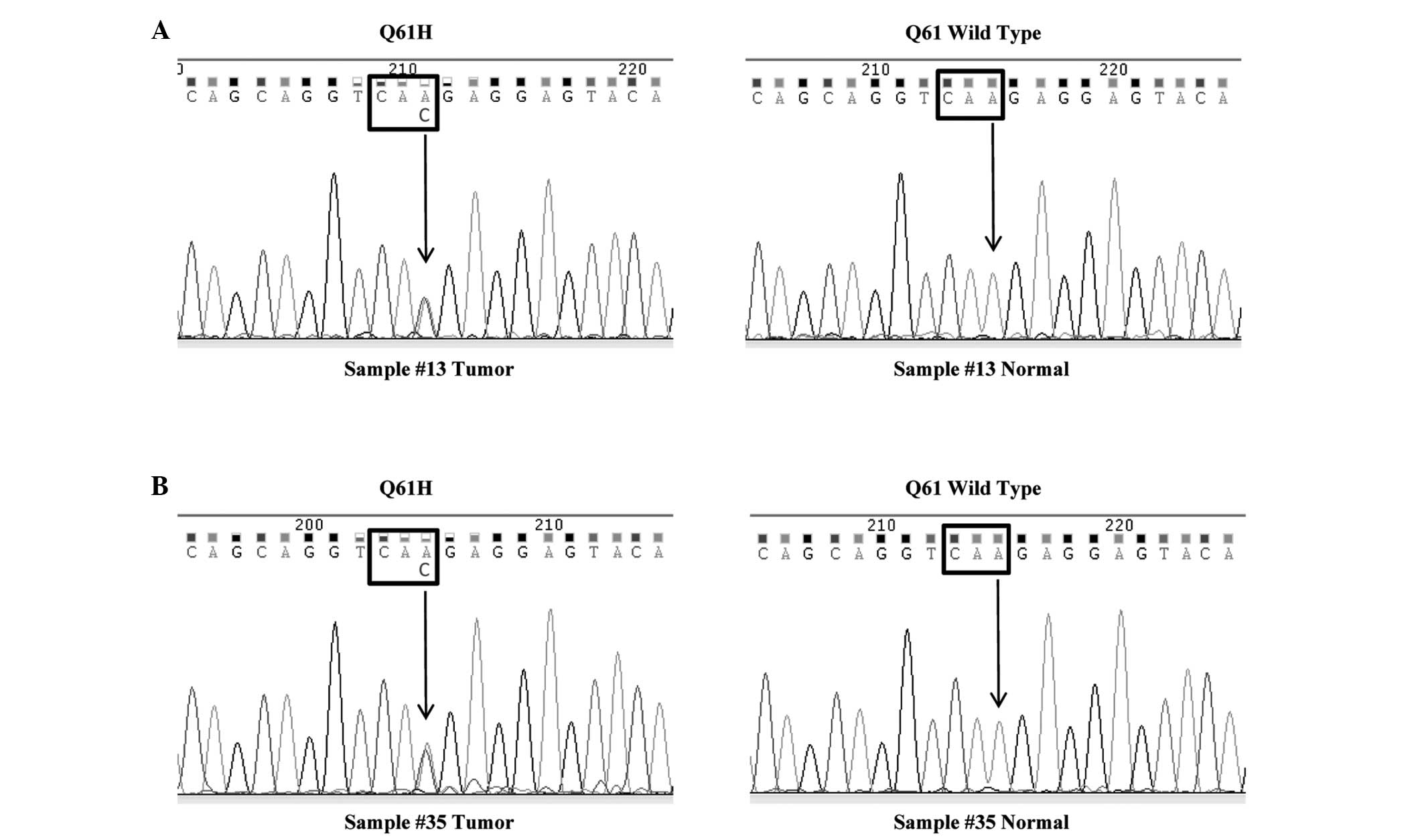
NRAS mutations (sequencing)

NRAS mutations (pyrosequencing)

PPARγ IHC in FTC (A)

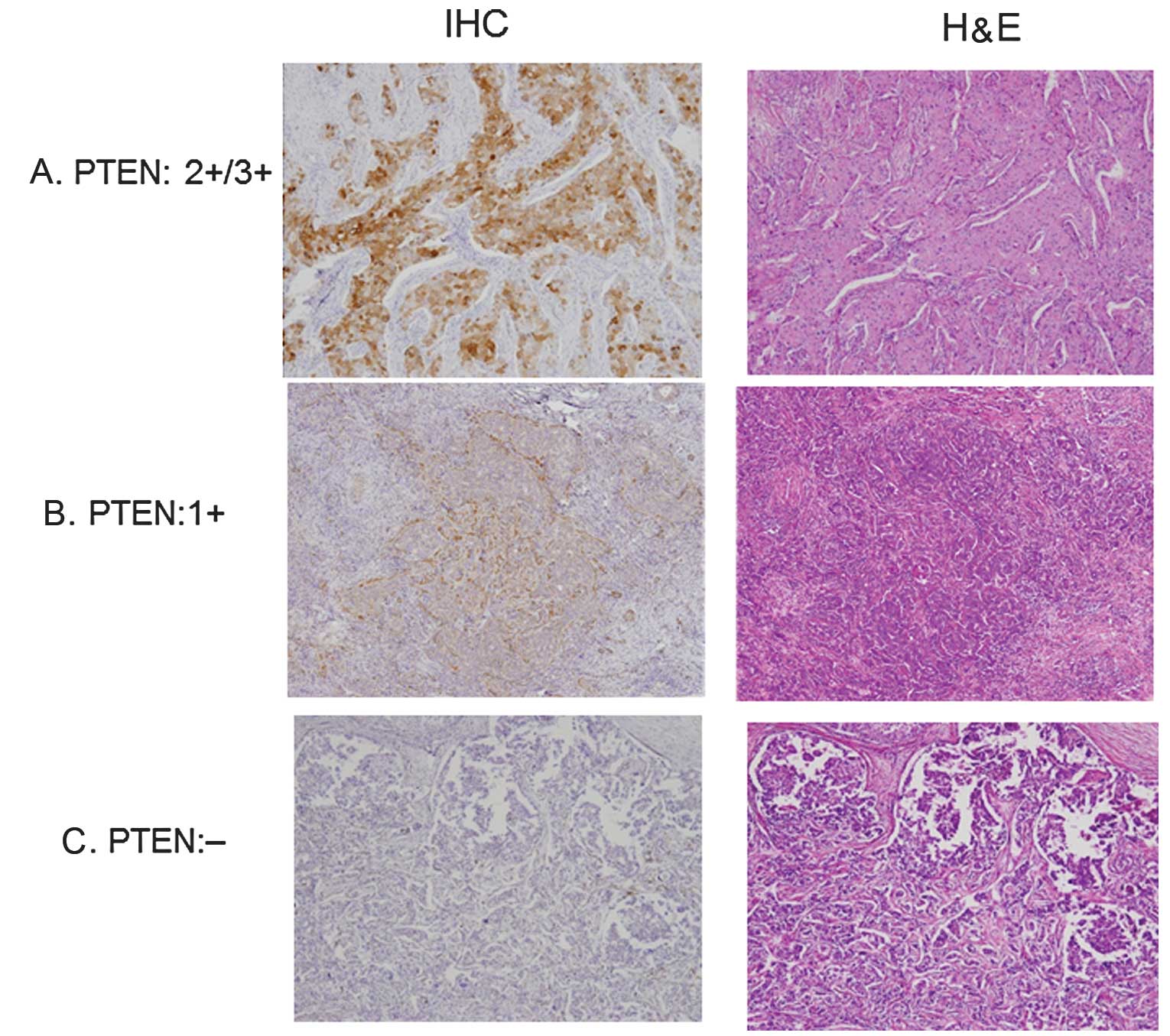
PTEN IHC (A - C)
PTEN loss in Cowden syndrome
PTEN evaluation (breast cancer)
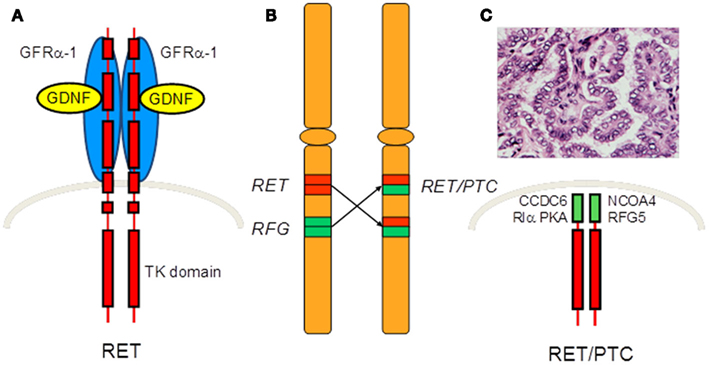
RET / PTC rearrangements

TERT promoter mutations
Molecular influence in thyroid cancer (2014)
Biomarkers in thyroid cancer (2015)
Drugs in development for refractory thyroid cancer (2015)
Molecular targeted therapeutics for medullary thyroid cancer (2015)
- Articles: Nat Rev Cancer 2013;13:184, Crit Rev Oncol Hematol 2014;90:233, Endocr Relat Cancer 2014;21:T301, Cell 2014;159:676, Ann Endocrinol (Paris) 2015;76:1S8, Nat Rev Dis Primers 2015;1:15077
- Books: Nikiforov: Diagnostic Pathology and Molecular Genetics of the Thyroid, 2nd ed, 2012, Wenig: Atlas of Head and Neck Pathology, 3rd ed, 2015
- Other: CAP: Protocol for the Examination of Specimens From Patients With Carcinomas of the Thyroid Gland
