
Testis & paratestis
Nonneoplastic lesions
Torsion
Author: Ritu Bhalla, M.D.
Resident / Fellow Advisory Board: Alcino Pires Gama, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.

Last author update: 31 August 2023
Last staff update: 31 August 2023
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Testicular torsion


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Bhalla R. Torsion. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testistorsion.html. Accessed April 1st, 2025.
Definition / general
- Twisting of the spermatic cord and its contents
- Surgical emergency
- Reference: Am Fam Physician 2013;88:835
Essential features
- Vascular congestion, edema and interstitial bleeding
- Hemorrhagic infarction of the testis
ICD coding
- ICD-10: N44.00 - torsion of testis, unspecified
Epidemiology
- Annual incidence: 3.8 per 100,000 in boys younger than 18 years
- 2 peaks of incidence: perinatal and puberty
- Up to 14% of cases occur in adults
- 12 - 21% of neonatal cases are bilateral
- References: Am Fam Physician 2013;88:835, Am J Emerg Med 2023;66:98
Sites
- Testis
Pathophysiology
- Twisting of the testicle along the spermatic cord results in reduced venous outflow and vascular congestion
- Prolonged twisting impairs arterial flow and ischemia
- Prolonged ischemia can result in necrosis
- Reference: Am J Emerg Med 2023;66:98
Etiology
- Abnormal or absent fixation of testicle and tunica vaginalis
- Tunica vaginalis contains the spermatic cord and normally adheres to the posterolateral part of the testicle
- Absent or abnormal fixation can result in twisting of the testicle, compromising the blood flow
- 2 classic anatomic forms
- Intravaginal (more common)
- Puberty and adulthood
- Abnormalities in tunica vaginalis attachment
- Bell clapper deformity: abnormally high reflection of tunica vaginalis, allowing the spermatic cord to twist inside the tunica
- Extravaginal
- Infancy and childhood
- Tunica vaginalis is not adhered to the gubernaculum
- Both the tunica vaginalis and spermatic cord are prone to torsion
- Intravaginal (more common)
- References: Am J Emerg Med 2023;66:98, J Ultrasound Med 2022;41:271
Diagrams / tables
Images hosted on other servers:

Bell clapper deformity
leading to intravaginal
testicular torsion
Clinical features
- Intravaginal
- Sudden or insidious onset of pain
- Nausea and vomiting
- Followed by swelling of the ipsilateral scrotum
- Most commonly, these symptoms occur several hours after minor trauma or physical activity
- In some instances, history of previous pain
- Extravaginal
- May be entirely asymptomatic
- Sole clinical manifestation may be unilateral mass in the inguinal region or in the superior aspect of the scrotum
- Reference: Clin Radiol 1999;54:343
Diagnosis
- Imperative to rule out testicular torsion in a patient presenting with acute scrotum
- High index of suspicion on the part of the physician is needed
- Scrotal Doppler ultrasonography is the imaging study of choice (Am Fam Physician 2013;88:835)
Radiology description
- Scrotal Doppler ultrasonography
- Flow in the symptomatic testis may be absent, reduced or have abnormally high resistance
- In bell clapper deformity, testis can rotate
- Doppler ultrasound flow abnormalities can differ depending on the degree of rotation, which ranges from 180° to 270°
- Venous outflow occlusion precedes arterial inflow occlusion
- Early or partial torsion can result in areas with high resistance flow rather than absent flow owing to compromised venous outflow
- If spontaneous detorsion occurs, Doppler ultrasound flow within the involved testis may increase
- Reference: Radiographics 2020;40:529
Radiology images
Contributed by Raman Danrad, M.D.
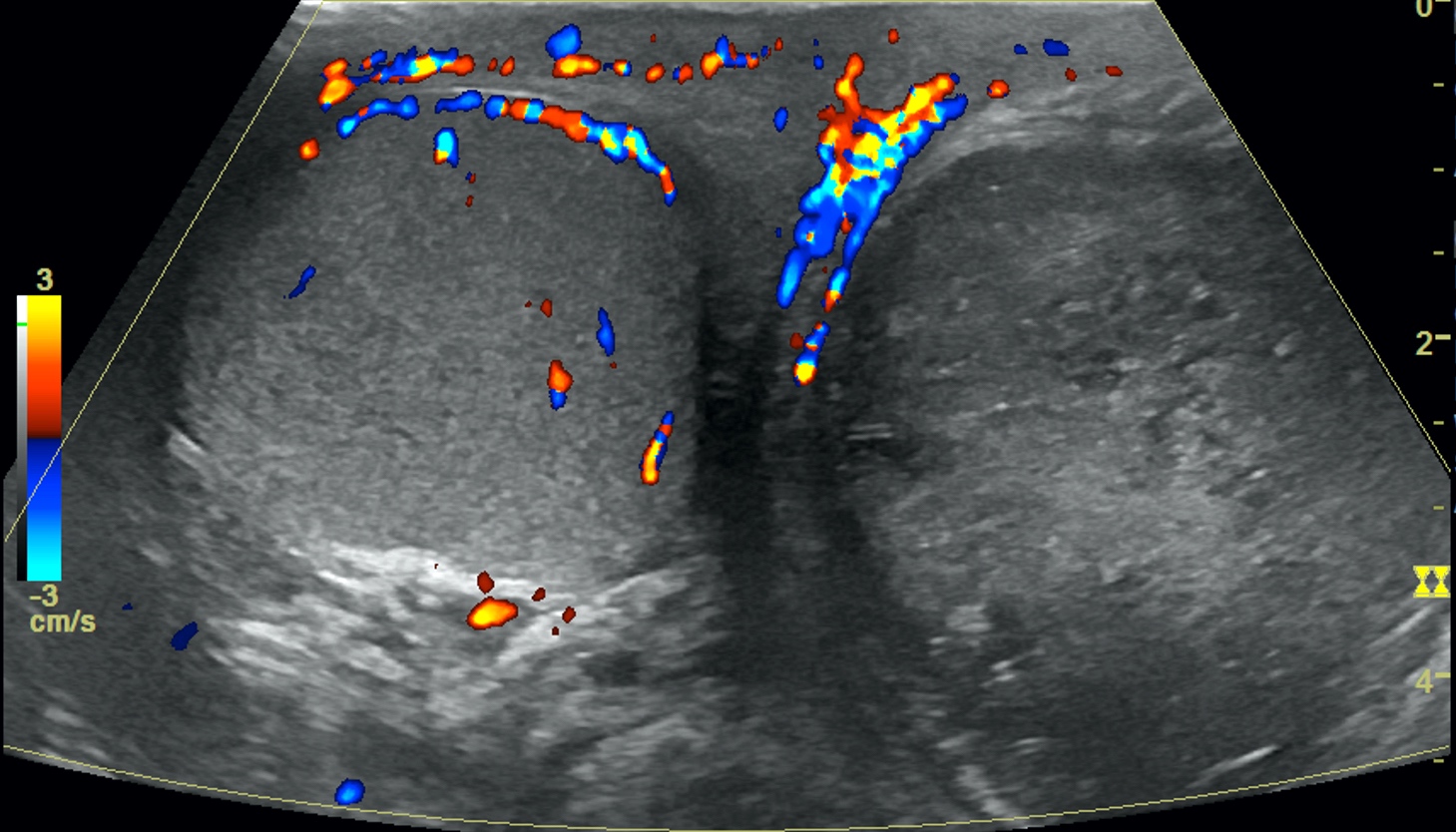
Ultrasound of bilateral testis
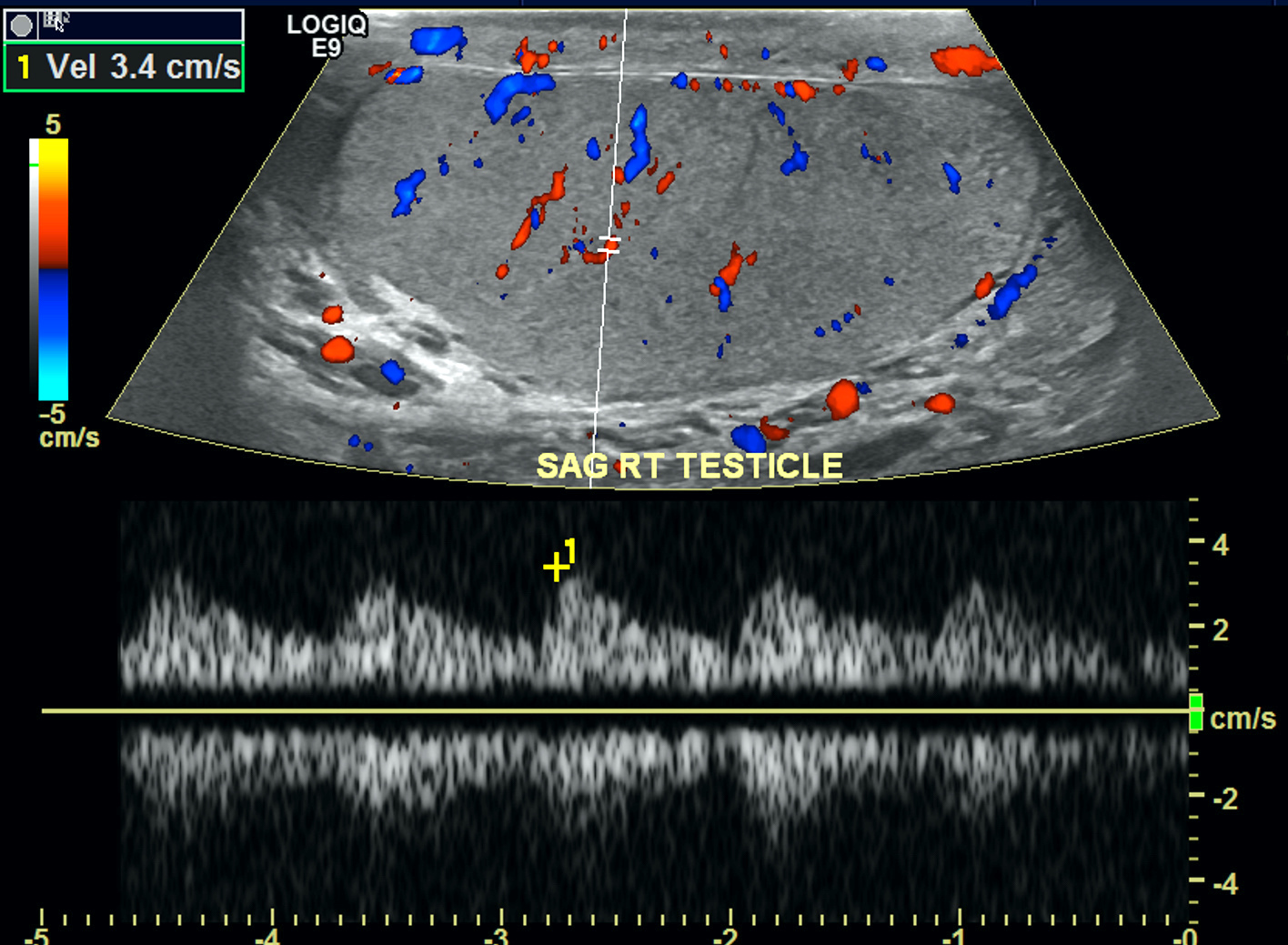
Ultrasound of right normal testis
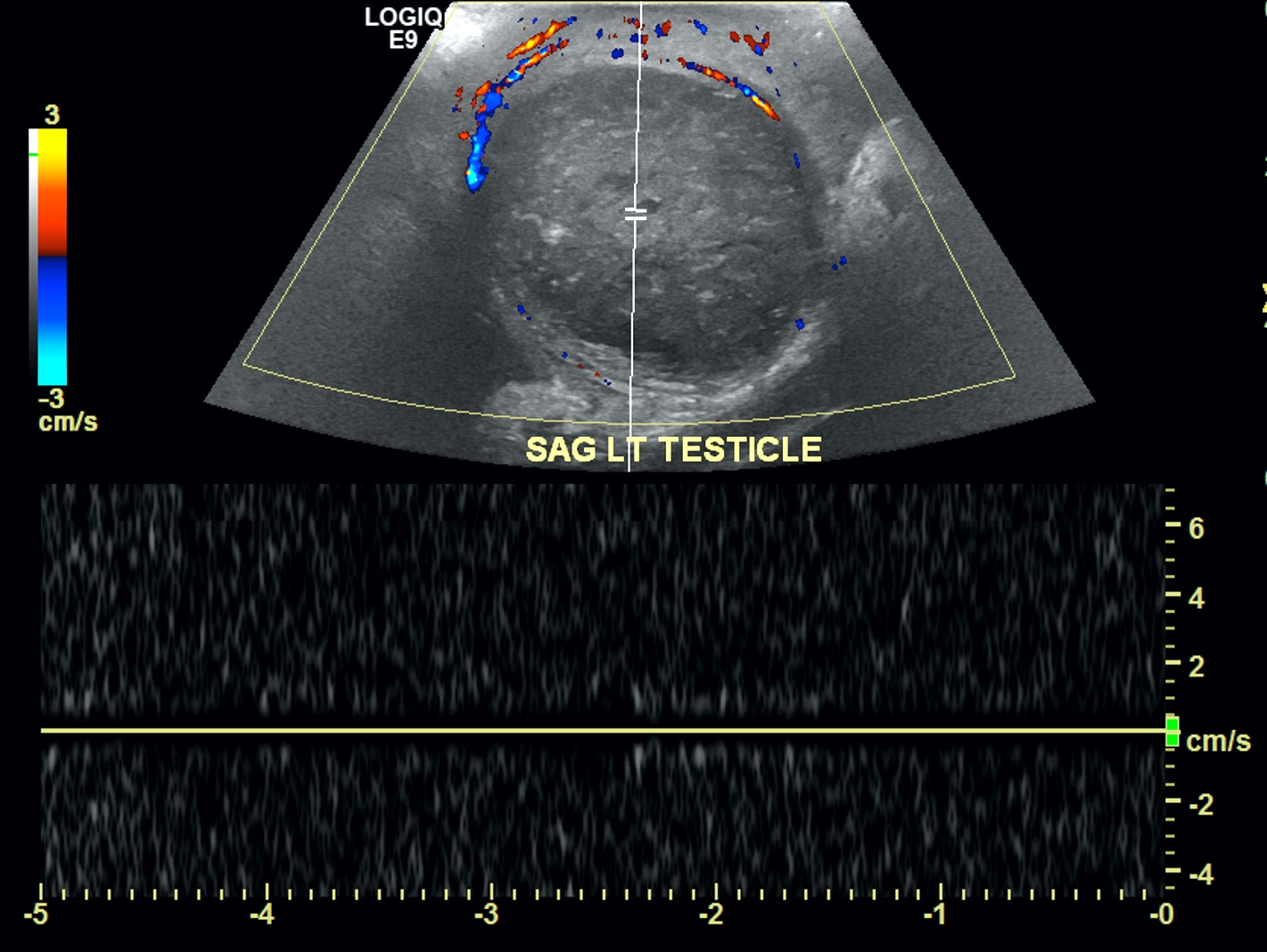
Ultrasound of left torsed testis
Case reports
- 13 year old boy with torsion of biolobed testis (Can Urol Assoc J 2010;4:E67)
- 15 year old boy with testicular cavernous hemangioma associated with testicular torsion (Int J Surg Case Rep 2018;49:247)
- 16 year old boy with torsion of right undescended testis (Urol Case Rep 2023;50:102480)
- 57 year old man presented with 9 day history of testicular pain following lawnmowing (J Am Coll Emerg Physicians Open 2021;2:e12545)
Treatment
- Prompt restoration of blood flow is critical in cases of testicular torsion
- Typically, there is a 4 - 8 hour window before significant ischemic damage occurs
- Viability of testicle is difficult to predict, hence emergent surgical management is indicated
- Reported testicular salvage rates are 90 - 100% if surgical exploration is performed within 6 hours of symptom onset
- Orchiectomy is performed if the affected testicle appears grossly necrotic or nonviable
- If the affected testicle is deemed viable, orchiopexy with a permanent suture should be performed to permanently fix the testicle within the scrotum
- Contralateral orchiopexy should be performed regardless of the viability of the affected testicle
- Reference: Am Fam Physician 2013;88:835
Clinical images
Images hosted on other servers:

Twisting of spermatic cord
Gross description
- Depends on the degree of torsion and the time lapse since onset of symptoms
- Dark red testis with smooth external surface and solid consistency
Gross images
Images hosted on other servers:

Smooth external surface of torsed testis

Dark red hemorrhagic cut surface
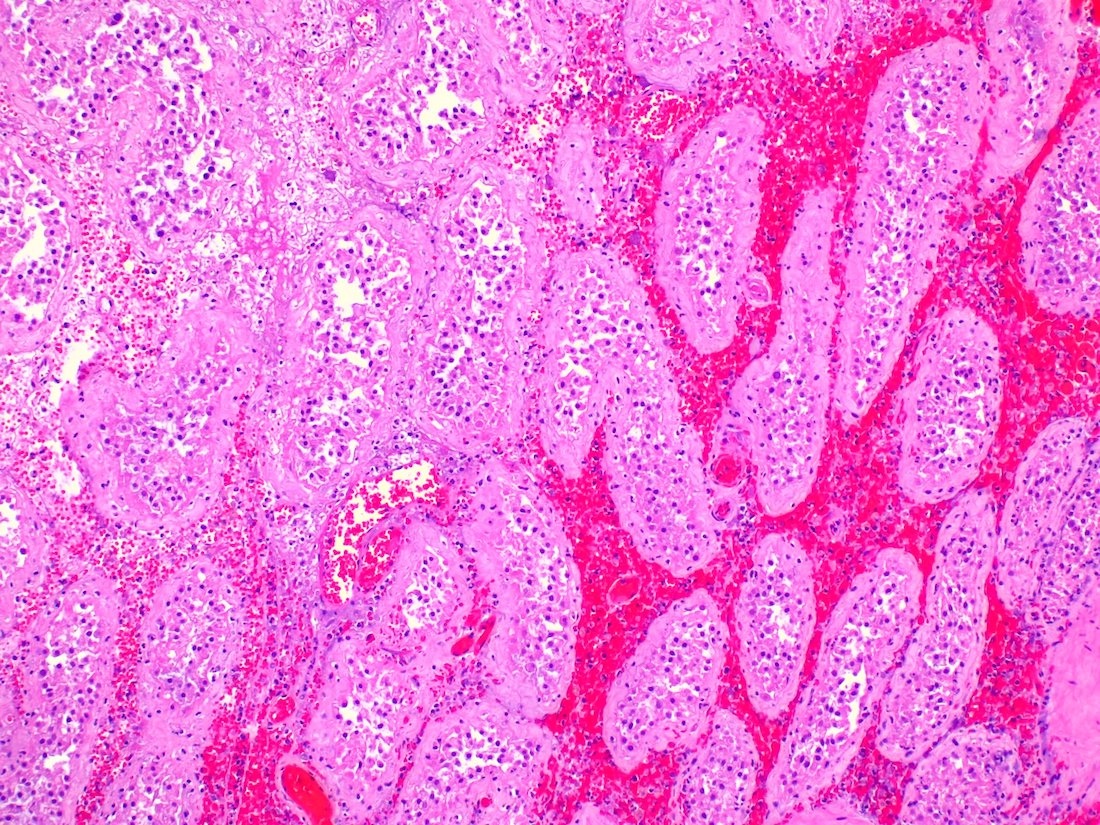
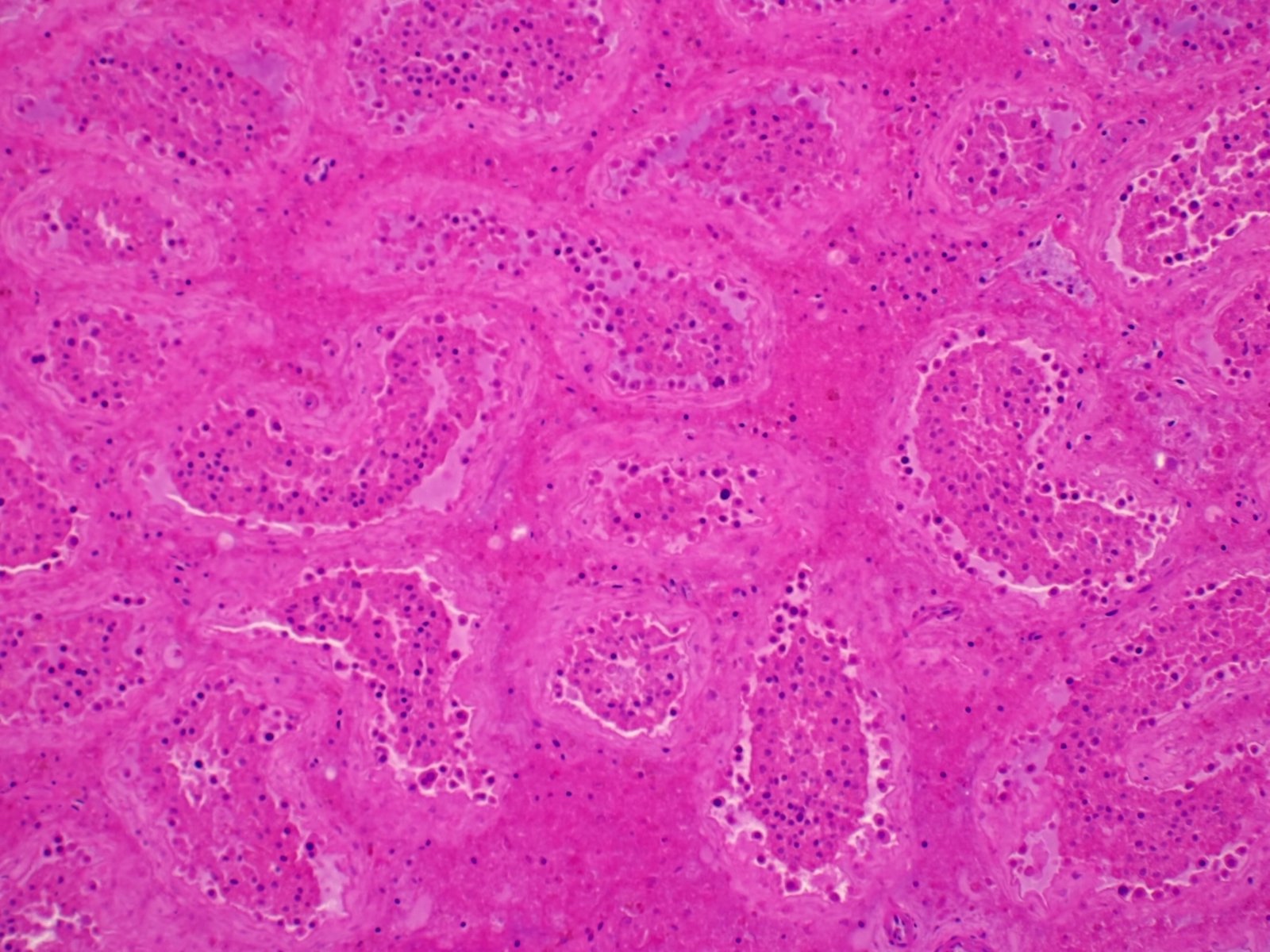
Microscopic (histologic) description
- Edema, congestion and interstitial hemorrhage with venous outflow obstruction
- Early conservation of germ cells, which later disappear
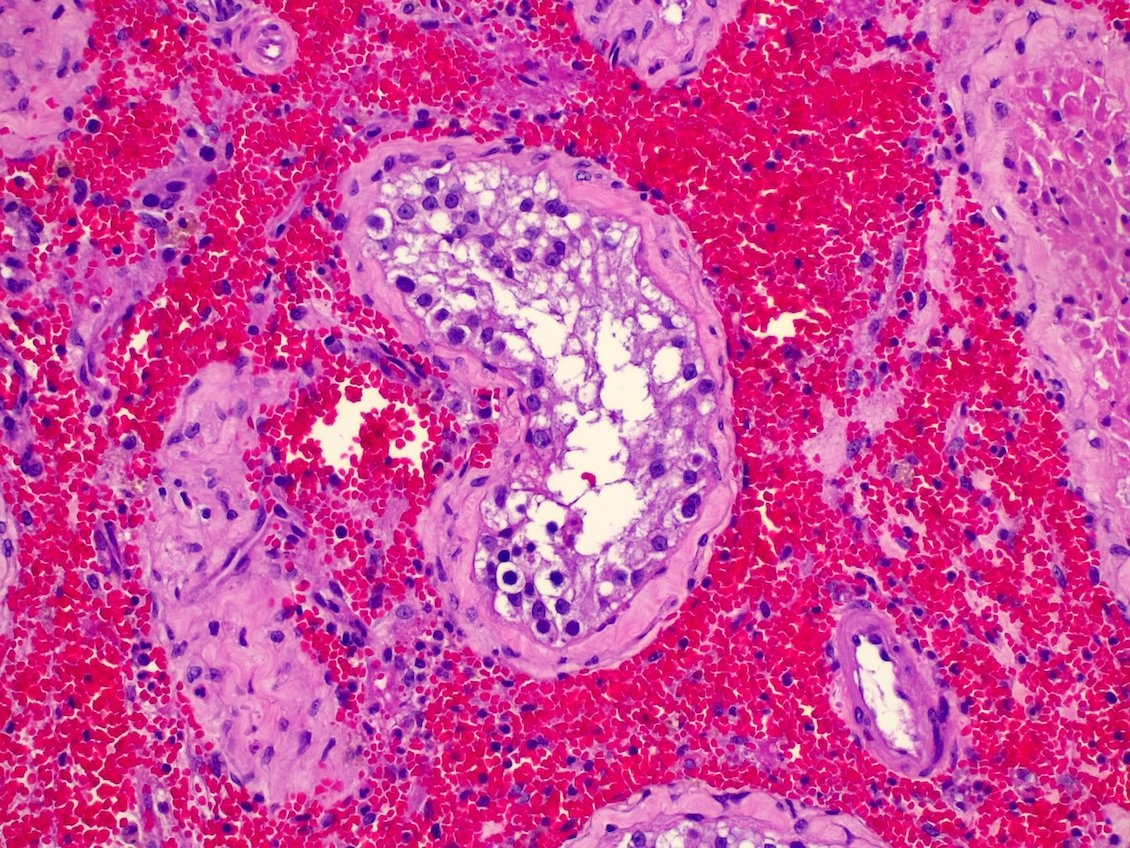
- Initial phase (< 6 hours): dilatation of seminiferous tubules with sloughing of germ cells and vacuolization of Sertoli cells
- Followed by pronounced hemorrhage and sloughing of all germ cells
- Necrosis of the seminiferous epithelium
- Hemorrhagic infarction of testicle
- References: Maclennan: Urologic Surgical Pathology, 4th Edition, 2019, Amin: Urological Pathology, 1st Edition, 2014
Microscopic (histologic) images
Contributed by Ritu Bhalla, M.D.
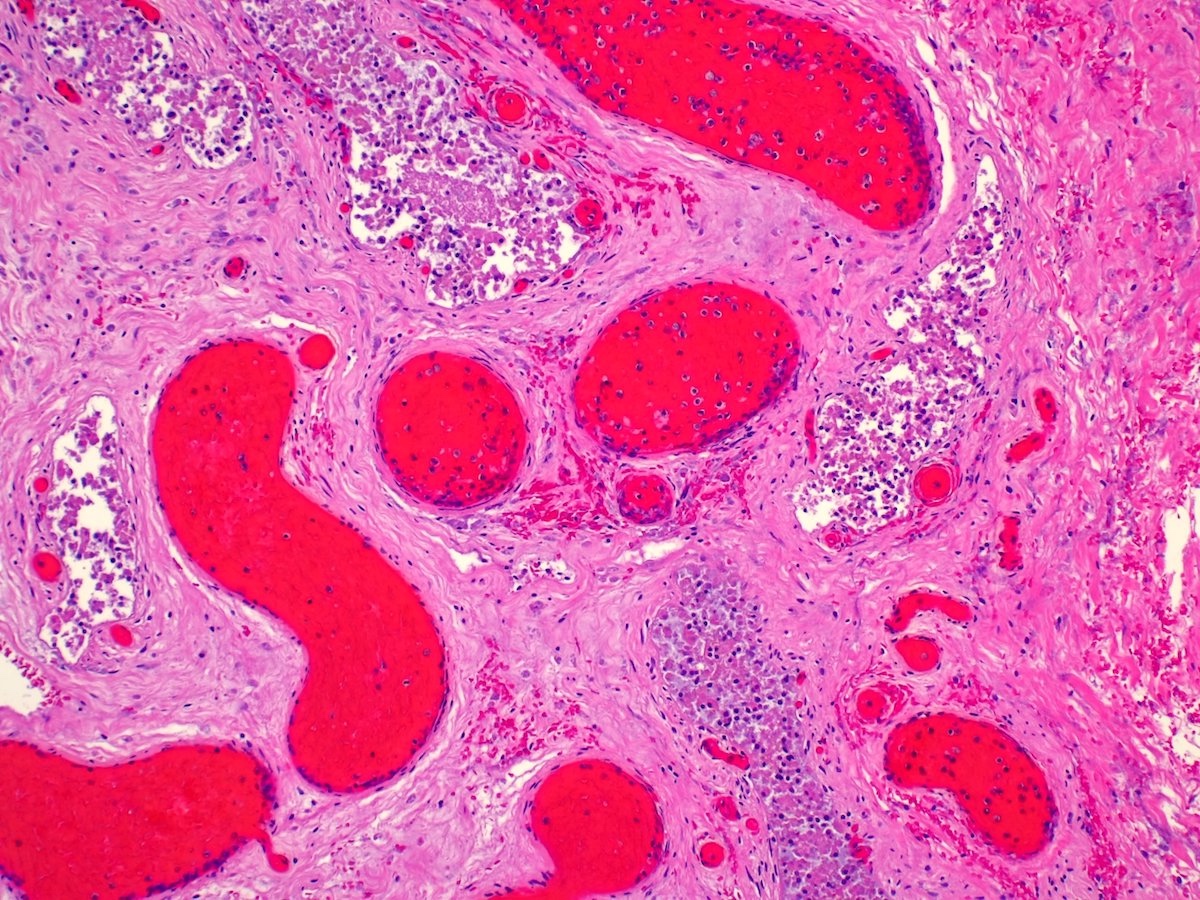
Congestion
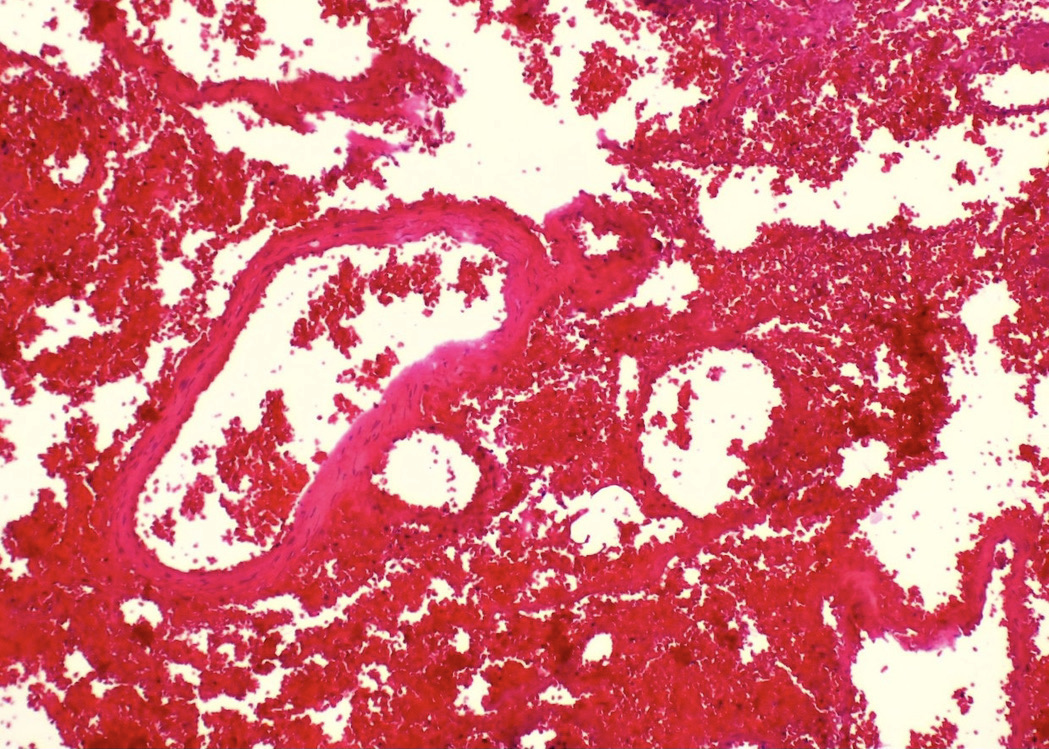
Hilar hemorrhage
Sloughing of cells
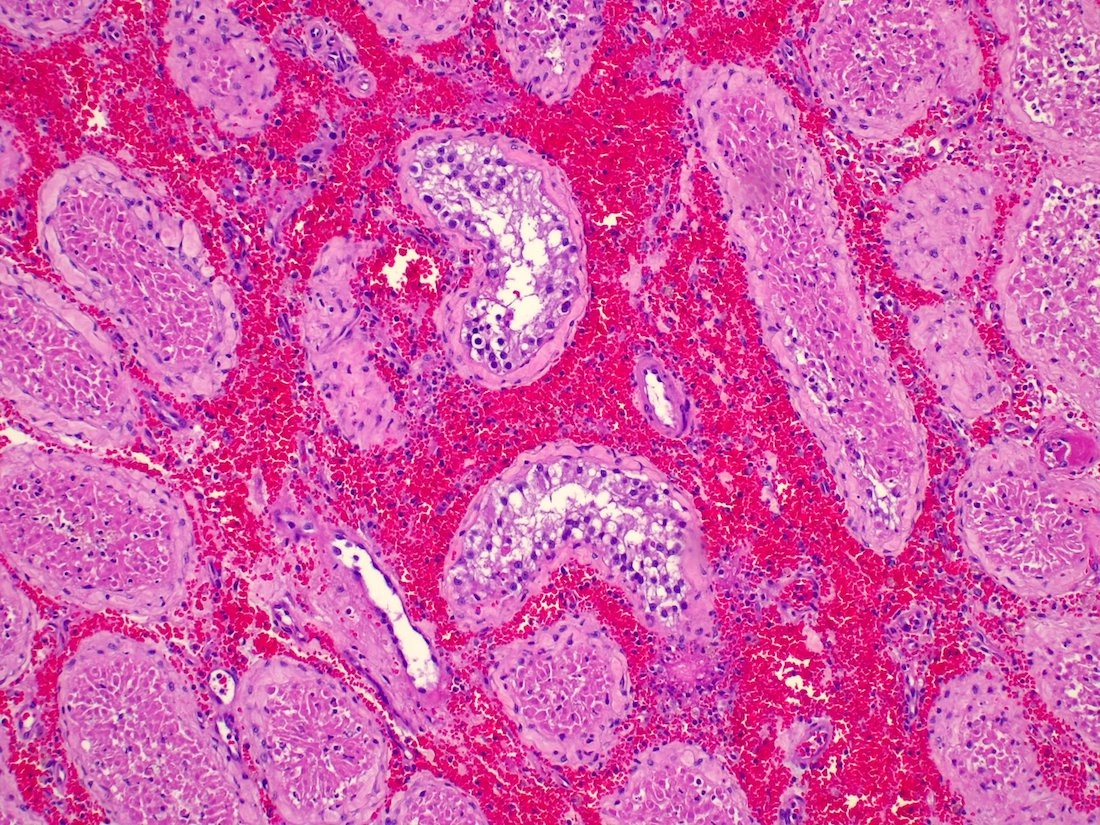
Interstitial hemorrhage
Residual germ cells
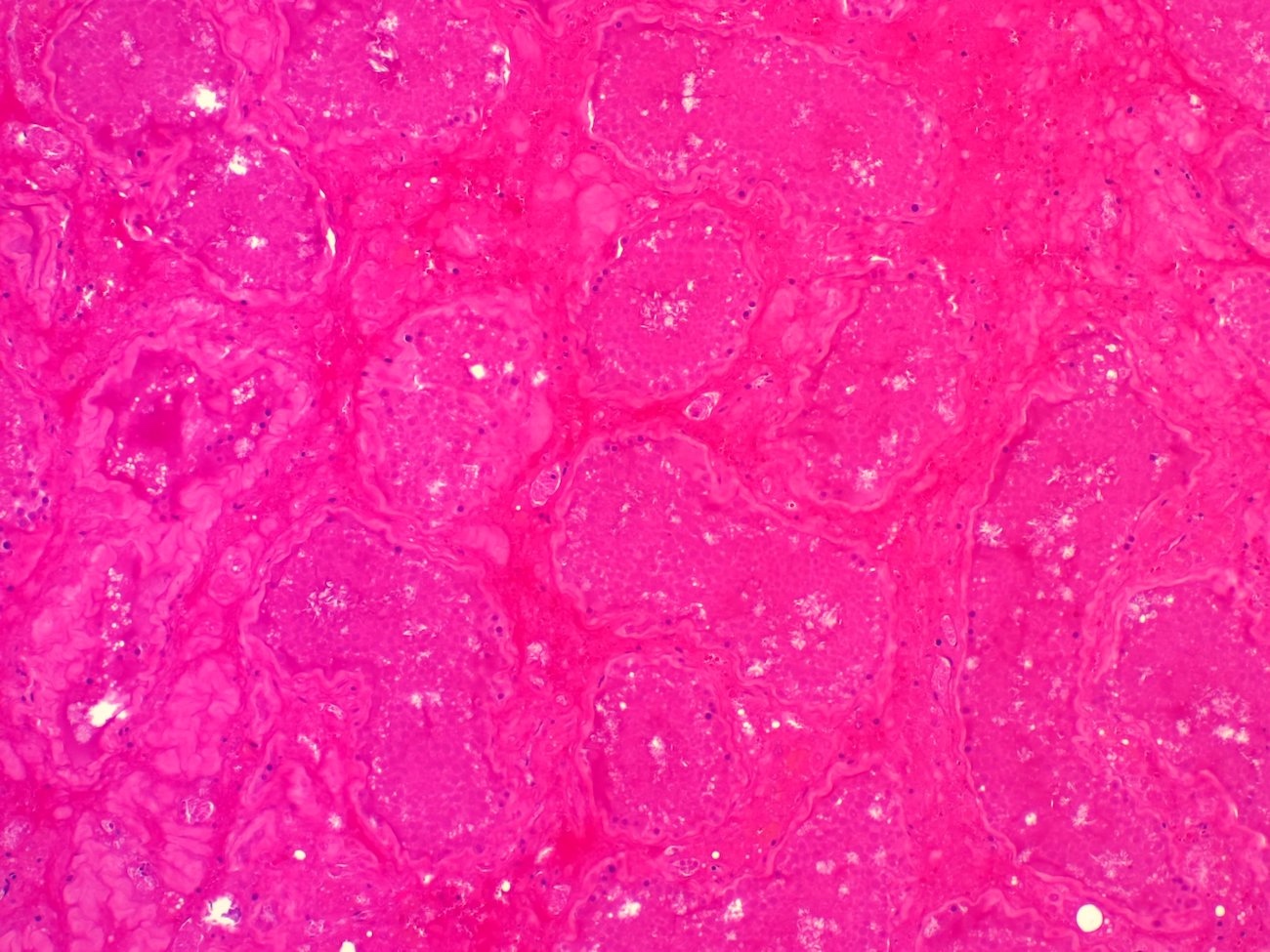
Infarcted tubules
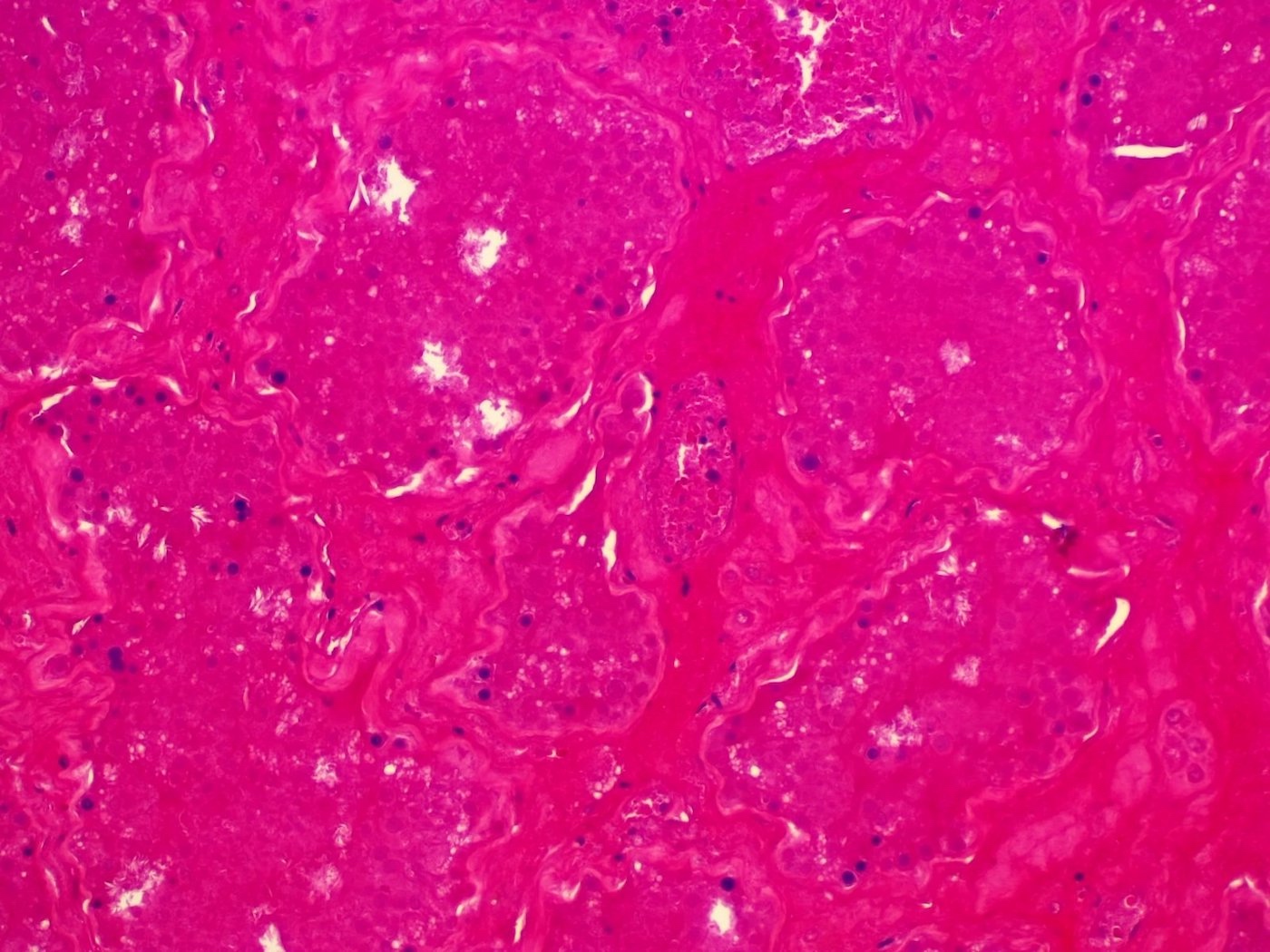
Necrotic parenchyma
Sample pathology report
- Testicle, left, orchiectomy:
- Testicular parenchyma with hemorrhagic infarction, consistent with testicular torsion
Differential diagnosis
- Systemic vasculitides:
- Can present in 1 of 2 patterns
- Polyarteritis nodosa pattern
- Fibrinoid necrosis of medium sized arteries
- Dense transmural neutrophilic infiltrates
- Testicular infarct and hemorrhage
- Granulomatosis with polyangiitis pattern
- Destructive granulomatous vascular inflammation
- Polyarteritis nodosa pattern
- Can present in 1 of 2 patterns
- Germ cell neoplasia in situ (GCNIS):
- Presence of undifferentiated germ cells within seminiferous tubules; the cells possess
- Large, hyperchromatic nuclei, with 1 - 2 prominent nucleoli
- Clear cytoplasm
- Spermatogenesis is usually absent
- Thickened peritubular basement membrane
- OCT 3/4 positive
- Presence of undifferentiated germ cells within seminiferous tubules; the cells possess
- Regressed germ cell tumor:
- Vascularized fibrotic scar with inflammation
- Surrounding hyalinized or atrophic seminiferous tubules
- Psammomatous calcifications
- Residual germ cell neoplasm or GCNIS may be present
- Choriocarcinoma:
- Hemorrhage and necrosis surrounded by cytotrophoblasts and syncytiotrophoblasts
- Lymphoma:
- Clonal population of lymphoid cells
- Reference: Am J Surg Pathol 2014;38:34
Board review style question #1
A 14 year old boy presents to emergency room with severe left sided testicular pain associated with nausea and vomiting. A Doppler ultrasound shows loss in blood flow in the affected testis. Subsequent orchiectomy reveals red-tan, smooth surfaced testis, with microscopic appearance as seen in the image above. Which of the following can be seen in this condition?
- Clonal population of lymphoid cells
- Elevated alpha fetoprotein (AFP) levels
- Hemorrhage surrounded by trophoblastic cells
- Initial preservation of germ cells
- Undifferentiated malignant cells within seminiferous tubules
Board review style answer #1
D. Initial preservation of germ cells. The patient's presentation, including imaging and pathology, is diagnostic of testicular torsion. Testicular infarct following torsion is initially associated with conservation of germ cells; however, as congestion and hemorrhage increase, these cells slough into the lumens of seminiferous tubules and ultimately the entire tubule undergoes necrosis. Answer C is incorrect because hemorrhage surrounded by trophoblastic cells is typically observed in choriocarcinoma. Answer E is incorrect because germ cell neoplasia in situ (GCNIS) is associated with undifferentiated malignant cells within seminiferous tubules. Answer A is incorrect because clonal population of lymphocytes is seen in lymphoma. Answer B is incorrect because although AFP can be elevated in several conditions, including yolk sac tumor and teratoma, it is usually not elevated in torsion.
Comment Here
Reference: Torsion
Comment Here
Reference: Torsion
Board review style question #2
Which of the following is the most common cause of testicular torsion?
- Bell clapper deformity
- Choriocarcinoma
- Cryptorchidism
- Mumps orchitis
- Varicocele
Board review style answer #2
A. Bell clapper deformity is the most frequent cause of testicular torsion. Tunica vaginalis is normally attached to the testis posterolaterally. In this anomaly, the attachment is abnormally high, which allows the spermatic cord to twist itself within the tunica vaginalis, resulting in testicular torsion. Answer C is incorrect because cryptorchidism may also be associated with torsion but not as frequently as bell clapper deformity. Answers B, D and E are incorrect because varicocele, mumps orchitis and choriocarcinoma are typically not associated with testicular torsion.
Comment Here
Reference: Torsion
Comment Here
Reference: Torsion
