
Testis & paratestis
Germ cell tumors
Teratoma
Authors: Christopher Dall, M.D., Debra L. Zynger, M.D.


Last author update: 14 May 2021
Last staff update: 7 August 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Testis teratoma


Table of Contents
Definition / general | Terminology | Epidemiology | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dall C, Zynger D. Teratoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testisteratoma.html. Accessed April 1st, 2025.
Definition / general
- Tumor originating from germ cells with more than one embryonic germ layer
Terminology
- Prepubertal and postpubertal teratoma: currently accepted categories of teratoma
- Either category may occur in either age group
- Teratoma with somatic type malignancy: teratoma with malignant transformation that occupies at least a 4x magnification (0.5 cm) (Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours), Fourth Edition, 2016)
- Do not divide into mature and immature as both are malignant and this nomenclature is misleading, no longer accepted and has no clinical relevance (Med Surg Urol 2014;3:1)
Epidemiology
- Teratoma is second most common germ cell tumor type in pediatrics, after yolk sac tumor (Rev Urol 2004;6:11)
- Incidence increasing, as testicular germ cell tumors are increasing (Hum Reprod 2001;16:972)
- Most commonly presents at age 25 - 35 years
- Postpubertal teratoma more frequent that prepubertal teratoma
- Pure teratomas (5%) are more rare than mixed germ cell tumors as malignant germ cells differentiate into other malignant phenotypes prior to teratoma (Med Surg Urol 2014;3:1)
- Teratoma is a component of 50% of mixed germ cell tumors (Moch:WHO Classification of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours), Fourth Edition, 2016)
Pathophysiology
- Postpubertal type associated with germ cell neoplasia in situ (GCNIS) and chromosome 12p amplification (Med Surg Urol 2014;3:1)
- Thought to arise from GCNIS
- Prepubertal is not associated with GCNIS or chromosome 12p amplification (Med Surg Urol 2014;3:1)
- Prepubertal type significantly less likely to metastasize or recur
Etiology
- Genetic component; higher incidence with family history and Caucasians (Int J Dev Biol 2013;57:201)
- Possible contribution of environmental exposures but the data is inconclusive (Arch Environ Occup Health 2006;61:87, PLoS One 2013;8:e77130)
- Animal studies have demonstrated associations with diethylstilbestrol (J Urol 1987;138:1446), other groups have hypothesized links between in utero and early life exposure to endocrine disrupting agents (J Urol 1979;122:36, Int J Androl 2008;31:275)
Clinical features
- Most commonly presents with painless swelling of the testicle (Histopathology 1988;12:491)
- Pain may be associated with hemorrhage or hematoma (Med Surg Urol 2014;3:1)
- About 1/3 of pure testicular teratomas present with advanced disease (Cancer 1995;75:2244)
- Mediastinal masses may present with cough, dyspnea or cyanosis (Histopathology 1988;12:491)
- Intracranial masses may present with headache, vomiting or visual disturbances (Histopathology 1988;12:491)
- Growing teratoma syndrome, an enlarging mass during or following chemotherapy for mixed germ cell tumor, may occur (Case Rep Urol 2014;2014:139425)
Diagnosis
- Ultrasound is used to evaluate a testicle mass
- Avoid biopsies to prevent cancer seeding
- Radical orchiectomy is initial procedure to diagnose a testicular mass in an adult
- Increasing rate of antenatal diagnoses (J Pediatr Surg 2006;41:1513)
- May use intraoperative frozen sections to guide therapy in pediatric populations
Laboratory
- In pure testicular teratomas, serum markers (b-hCG and AFP) are usually normal (Med Surg Urol 2014;3:1)
Radiology description
- Ultrasound is used to help exclude benign pathology
- Imaging may demonstrate calcifications or predominantly cystic lesions
- Computed tomography of the chest and abdomen used for staging purposes
Radiology images
Images hosted on other servers:

Testicular teratoma diagnosed in utero

Demonstrating vascularity of testicular teratoma with calcifications
Prognostic factors
- The International Germ Cell Consensus Classification guides prognosis and risk of recurrence for testicular germ cell malignancies (IGCCCG) (J Clin Oncol 1997;15:594, J Clin Oncol 2007;25:1033)
- Presence of teratoma is associated with better prognosis and therefore histologic recognition and documentation is required (Eur J Cancer 2001;37:576)
- Germ cell tumors with > 50% teratoma have fewer metastases (J Clin Oncol 1988;6:1467)
- Germ cell tumors with > 25% teratoma have less lymphovascular invasion (pT1) (Am J Clin Pathol 2016;145:341)
Case reports
- Antenatal diagnosis of teratoma in an undescended testicle (Ultrasound Obstet Gynecol 2016;47:527)
- 23 year old man with growing teratoma syndrome (Case Rep Urol 2014;2014:139425)
Treatment
- Radical orchiectomy is first line therapy for testicular mass in an adult
- Increasing rate of testis sparing surgery for prepubertal tumors (Rev Urol 2004;6:11)
- Retroperitoneal lymph node dissection and platinum based chemotherapy are adjunctive therapies for testicular germ cell tumor
- Treatment guidelines are based on postorchiectomy TNM stage (NCCN guidelines: Testicular Cancer)
- Consider sperm preservation options
Gross description
- Lobulated, with cysts of mucinous, gelatinous or serous material
Gross images
Contributed by Debra L. Zynger, M.D.

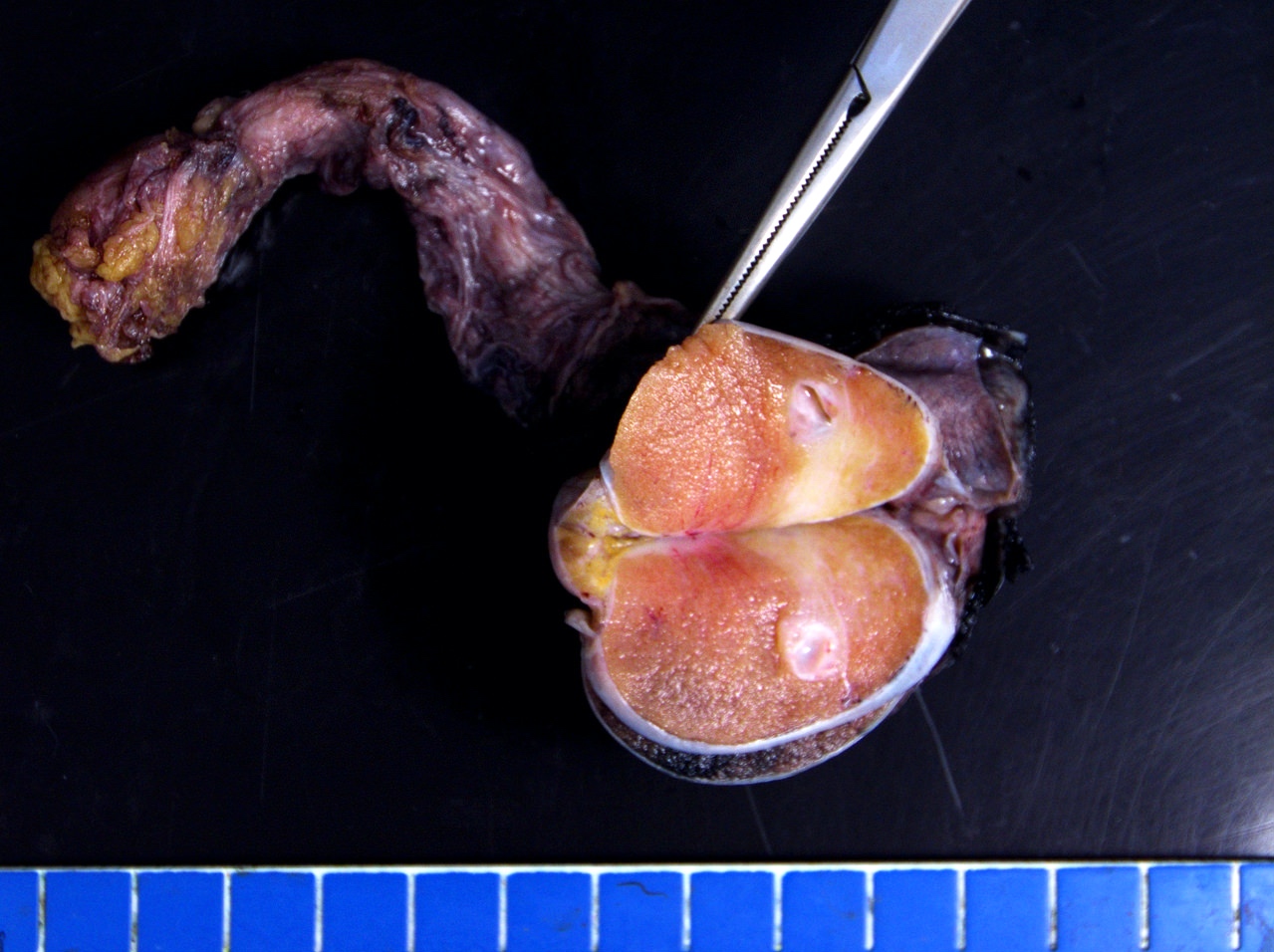

Teratoma (100%)

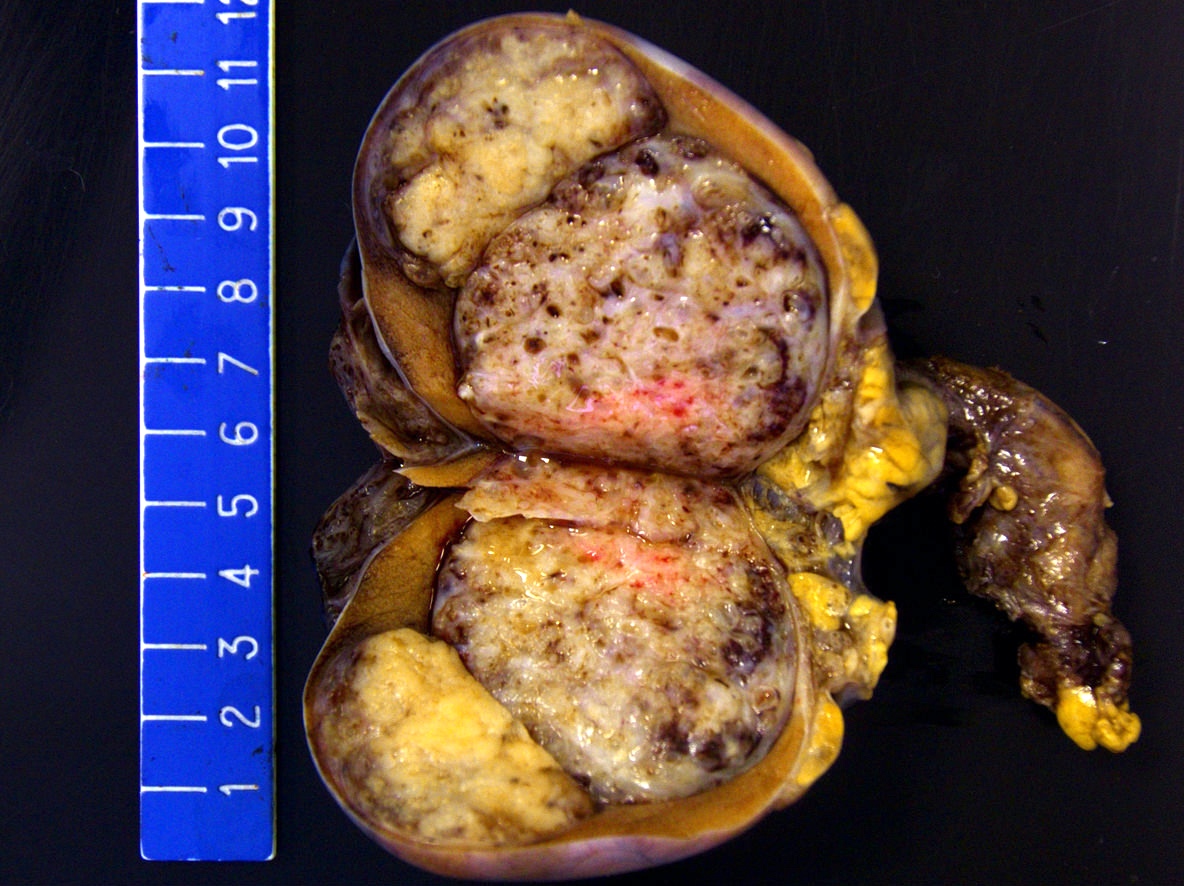

Mixed GCT
Microscopic (histologic) description
- Postpubertal type
- Recognition is important as the percentage of teratoma must be documented in orchiectomy specimens and metastatic lesions
- Demonstrate varying degrees of atypia
- Any type of tissue may be present, such as gastrointestinal glands, respiratory epithelium, cartilage, squamous epithelium with keratinization, primitive undifferentiated spindle cells, or neuroepithelium
- Will have GCNIS (Med Surg Urol 2014;3:1)
- Associated with atrophic testis with sclerosis and microliths (Ulbright: Atlas of Tumor Pathology, 4th Series - Tumors of the Testis and Adjacent Structures, First Edition, 2013)
- Prepubertal type
- More likely to have tissue arrangements mimicking organs (organoid morphology with tissue layers visible such as epithelium, lamina propria and muscularis propria) but any tissue type may be present (Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours), Fourth Edition, 2016)
- Hair follicles may be seen (not in postpubertal type)
- No cytologic atypia, GCNIS or necrosis; minimal mitoses (Ulbright: Atlas of Tumor Pathology, 4th Series - Tumors of the Testis and Adjacent Structures, First Edition, 2013)
- Teratoma with somatic type malignancy
- Sarcoma is most prevalent somatic type malignancy but other tumor types occur, including adenocarcinoma, squamous cell carcinoma and primitive neuroectodermal tumor (PNET) (Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours), Fourth Edition, 2016, J Urol 1998;159:133, Ulbright: Atlas of Tumor Pathology, 4th Series - Tumors of the Testis and Adjacent Structures, First Edition, 2013)
Microscopic (histologic) images
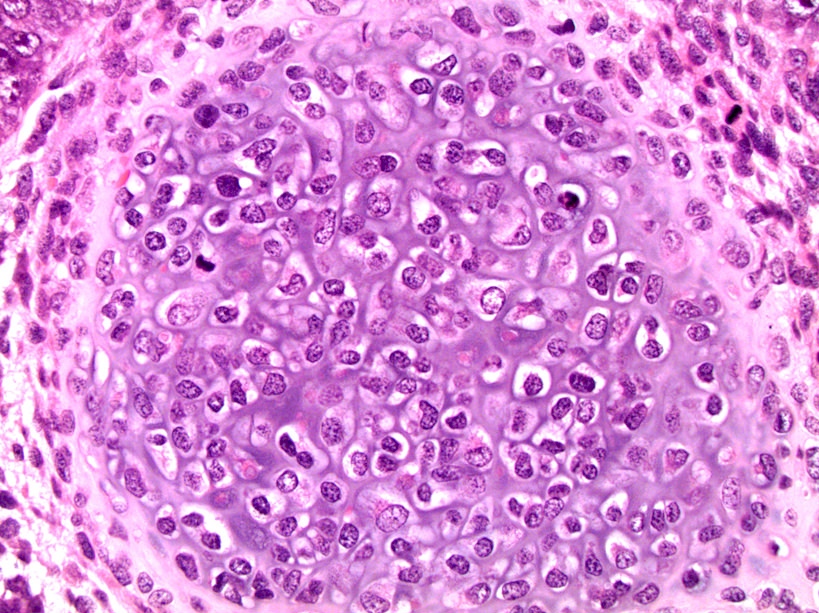
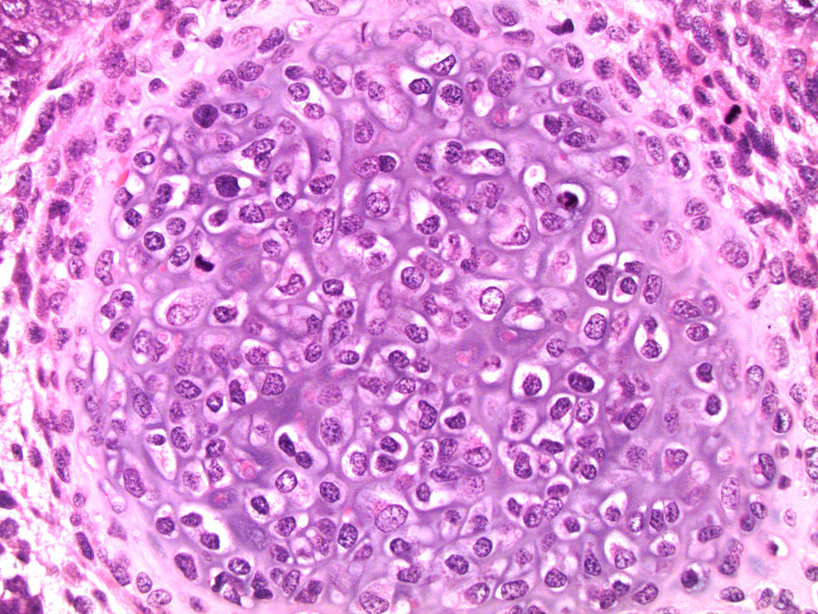
Contributed by Debra L. Zynger, M.D.
Cartilage surrounded by mitotically active spindle cells

Gastrointestinal epithelium

Squamous epithelium

Cellular mesenchyme
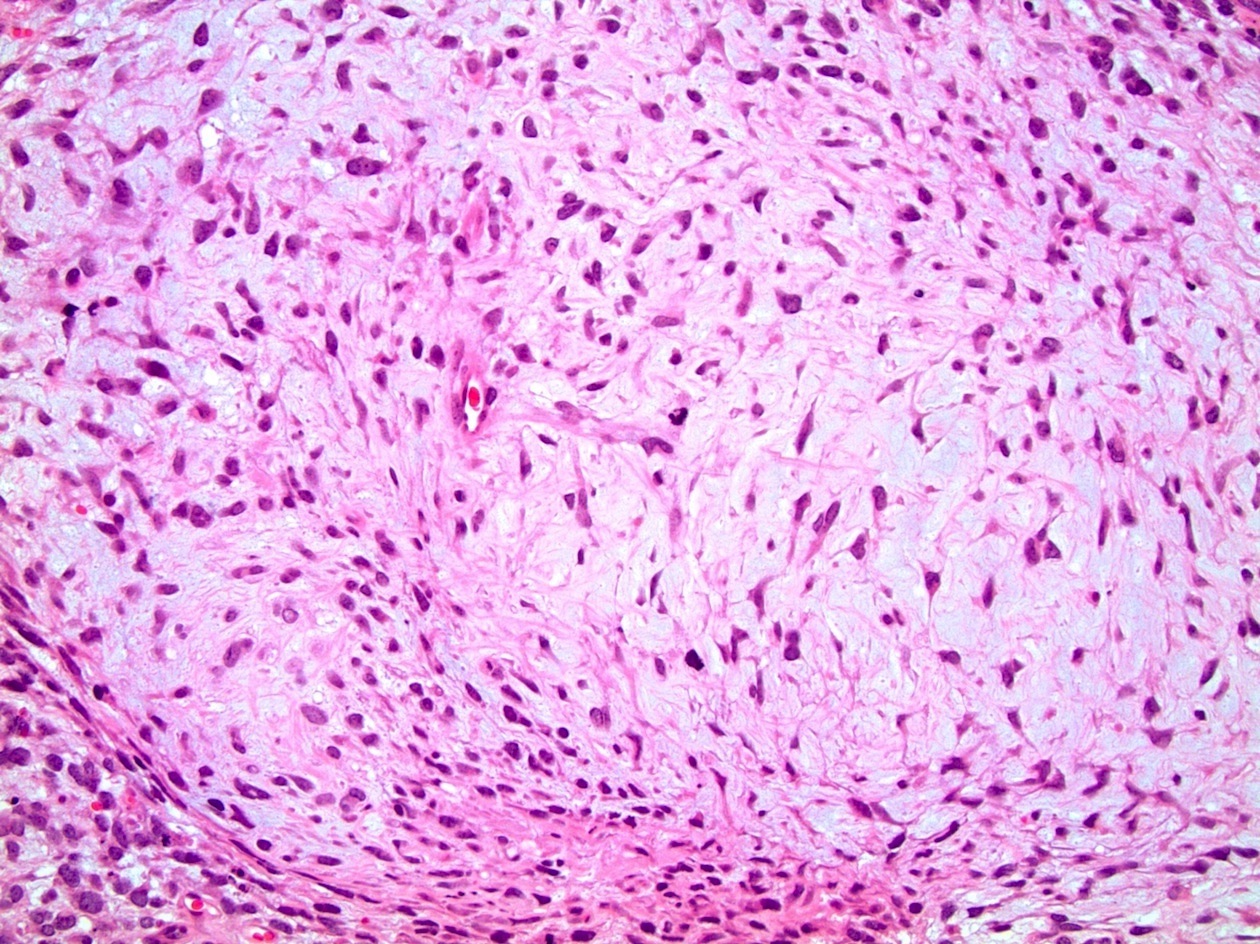
Loose mesenchyme

Neuroectoderm
Molecular / cytogenetics description
- 12p amplification present in postpubertal teratomas and teratomas with somatic type malignancy (Arch Pathol Lab Med 2012;136:435, Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours), Fourth Edition, 2016)
Sample pathology report
- Right testicle, radical orchiectomy:
- Mixed germ cell tumor, teratoma (55%), seminoma (20%), embryonal carcinoma (10%), yolk sac tumor (10%) and choriocarcinoma (5%) types (see synoptic report)
Differential diagnosis
- Dermoid cyst:
- Squamous epithelium, hair follicles / sebaceous glands
- May have adjacent lipogranulomas but no other embryonic germ cell types
- Lacks GCNIS and cytologic atypia (Arch Pathol Lab Med 2012;136:435)
- Epidermoid cyst:
- Nonneoplastic squamous epithelium producing keratin with lamellar targetoid appearance
- No other embryonic germ cell types
- Lacks GCNIS and cytologic atypia (Arch Pathol Lab Med 2012;136:435)
- Sarcoma:
- Can mimic teratoma with sarcoma as somatic type malignancy
- Lacks GCNIS and other germ cell tumor components
- Yolk sac tumor:
Board review style question #1
A 27 year old man presents with a painless enlarging testicular mass. He undergoes appropriate workup and orchiectomy confirms diagnosis of a pure postpubertal teratoma. Which of the following is likely to be true?
- AFP is likely elevated
- Cytogenetic analysis will reveal chromosomal abnormalities
- Few mitotic figures will be identified microscopically
- Hair follicles are likely to be seen microscopically
- He has a poor prognosis
Board review style answer #1
Board review style question #2
A 37 year old woman gives birth to a male baby who is diagnosed with an undescended testicle. Further workup reveals a large intra abdominal mass, which is resected. Pathology is consistent with a pure teratoma. Which of the following is most likely present on microscopic examination?
- Adjacent areas of germ cell neoplasia in situ
- Areas with organoid morphology
- Many mitotic figures and cytologic atypia
- Sarcomatous elements
- Significant areas of testicular tubular atrophy
Board review style answer #2
