

Testis & paratestis
Germ cell tumors
Teratoma-neuroendocrine tumor
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 24 November 2023
Last staff update: 24 November 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Teratoma - neuroendocrine tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Gilani SI, Jimenez RE. Teratoma-neuroendocrine tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testiscarcinoid.html. Accessed November 29th, 2024.
Definition / general
- Well differentiated neuroendocrine tumor (NET) is a low grade epithelial neoplasm with neuroendocrine differentiation
Essential features
- Primary testicular NETs can be pure (75%) or associated with teratoma (25%)
- Tumors show an insular or trabecular growth pattern with salt and pepper nuclear chromatin pattern
- Most are not associated with isochromosome 12p or germ cell neoplasia in situ (GCNIS)
Terminology
- Also known as pure NET, testicular NET, prepubertal type or postpubertal type or monodermal teratoma
- Terminology not recommended: carcinoid, atypical carcinoid, neuroendocrine carcinoma
ICD coding
- ICD-O: 8240/3 - well differentiated neuroendocrine tumor (monodermal teratoma)
- ICD-11: 2F77 & XH8DS0 - neoplasms of uncertain behavior of male genital organs & neuroendocrine tumor, NOS
Epidemiology
- Extremely rare, accounting for < 1% of all testicular neoplasms (Am J Surg Pathol 2010;34:519)
- More common in ovaries than testes (15:1)
- Mean age at presentation: 46 years (range: 10 - 83 years)
- Most cases are reported in Europe and the U.S. with fewer cases from Asia and Africa
- Metastatic neuroendocrine tumor from other sites (e.g., lung or gastrointestinal tract) to the testis has been reported
Sites
- NET in the genitourinary tract is rare and can occur in the kidney, bladder, prostate, testicle or urethra
Pathophysiology
- Arise in the setting of prepubertal teratoma (testicular NET, prepubertal type)
- 75% occur as pure NET, with the remaining 25% occurring with other teratomatous components (dermoid and epidermoid cysts) (Cancer 1978;42:2696, Am J Surg Pathol 2010;34:519, Cancer 1993;72:1726)
- Most are not associated with GCNIS or isochromosome 12p
- Rare cases of postpubertal type testicular NET have been reported (Clin Cancer Res 2008;14:1393)
Etiology
- Unknown
Clinical features
- Most commonly presents as a testicular mass or swelling, which may or may not be associated with testicular pain
- Bilateral involvement is uncommon and association with cryptorchidism is rare
- 10% of cases occur in association with hydrocele (Cancer 1993;72:1726)
- Clinical carcinoid syndrome (hot flashes, diarrhea and palpitations) has been reported in 7 - 12% of cases (Cancer 1993;72:1726, Am J Surg Pathol 2010;34:519)
- Metastases occur via hematogenous spread to lungs, liver, bones, soft tissue, skin, heart as well as contralateral testis; however, lymphatic spread is also seen
Diagnosis
- Diagnosis of testicular NET is made based on histologic examination of the surgical resection specimen
Prognostic factors
- Primary testicular NET associated with testicular teratoma seems to have a better prognosis than pure NET
- Metastatic disease is associated with atypical features, including larger tumor size (> 7 cm), increased mitotic activity and carcinoid syndrome (Am J Surg Pathol 2010;34:519, Cancer 1993;72:1726)
Case reports
- 23 year old man with asymptomatic scrotal swelling (Arch Ital Urol Androl 2016;88:245)
- 29 year old man with scrotal swelling and pain (Tumori 2019;105:NP20)
- 34 year old man with chronic right scrotal swelling and pain (Am J Case Rep 2015;16:328)
- 44 year old man with primary testicular NET (BMC Urol 2020;20:197)
- 49 year old man with primary testicular NET presenting with carcinoid heart disease (Indian J Urol 2015;31:65)
Treatment
- Orchiectomy
- In a metastatic setting, retroperitoneal dissection and receptor targeted radiotherapy may be used; however, chemotherapy and radiotherapy are reported to provide minimal benefits
Gross description
- Well circumscribed, solid, yellow-tan to brown and ranging in size from 0.5 cm up to 11 cm (Cancer 1993;72:1726)
- Cystic changes or calcifications can be seen in association with teratomatous component
- Extratesticular growth with involvement of spermatic cord occurs uncommonly
Gross images
AFIP images

Solid tan mass
Microscopic (histologic) description
- Growth pattern
- Mostly solid nests, insular or trabecular growth patterns
- Acinar and glandular growth pattern with luminal mucin admixed with other growth patterns may be seen (Am J Surg Pathol 2010;34:519, Clin Cancer Res 2008;14:1393)
- Stroma
- Delicate fibrous or hyalinized stroma (Tumori 2019;105:NP20)
- Neoplastic cells
- Monomorphic with abundant granular eosinophilic to pale cytoplasm
- Uniform round nuclei with fine or salt and pepper chromatin (Am J Surg Pathol 2010;34:519)
- Most cases are unassociated with GCNIS (Am J Surg Pathol 2010;34:519)
- Mitotic figures, necrosis and vascular invasion are infrequently seen (Am J Surg Pathol 2010;34:519)
- Atypical features include necrosis, nuclear atypia and > 2 mitoses per 10 high power fields (HPF) (Am J Surg Pathol 2010;34:519, Am J Clin Pathol 2003;120:182)
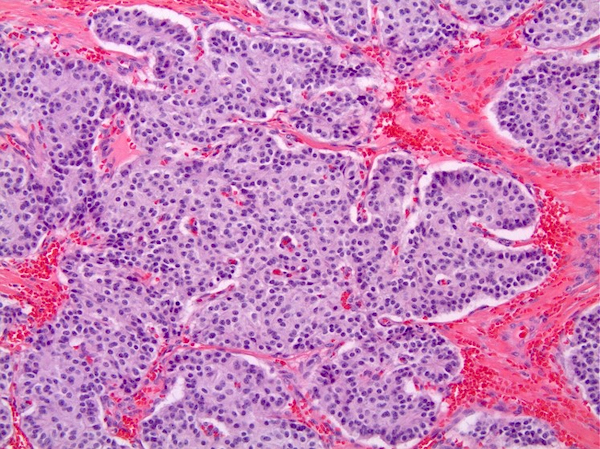
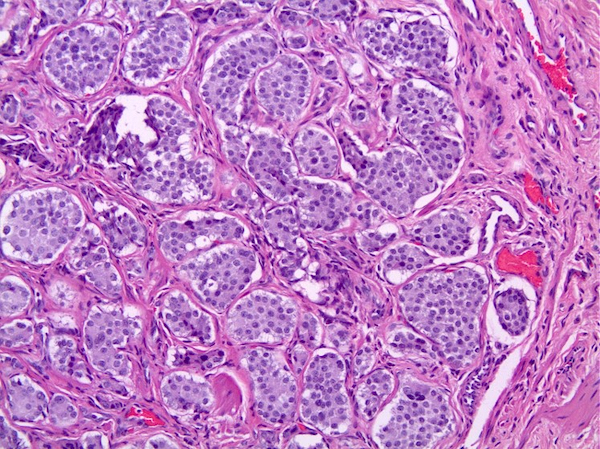
Microscopic (histologic) images
Contributed by Sounak Gupta, M.B.B.S, Ph.D. and Rafael E. Jimenez, M.D.


Epidermoid cyst and NET

Retraction artifact
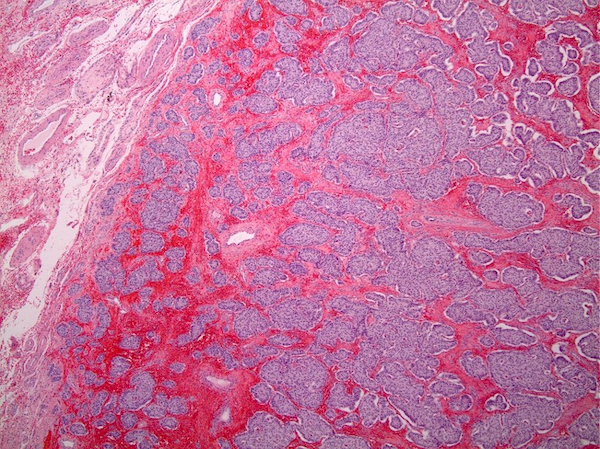
Multiple solid nests
Insular growth pattern
Nests of tumor cells
Cytology description
- Isolated or sheets of neoplastic cells with granular cytoplasm, uniform round nuclei and uniformly distributed fine nuclear chromatin
Positive stains
- Cytokeratins, synaptophysin, chromogranin A and CD56 are mostly positive (Cancer 1993;72:1726, Oncol Lett 2015;9:2017)
- Substance P, gastrin, VIP and neurofilaments are less frequently expressed (Am J Clin Pathol 1982;78:860)
Negative stains
- OCT 3/4, CD30, KIT, TTF1, SF1, SOX2, alpha inhibin and CDX2 (Clin Cancer Res 2008;14:1393)
Electron microscopy description
- Pleomorphic to more regular round to oval neurosecretory granules
Molecular / cytogenetics description
- DNA ploidy studies show a near diploid profile (Cancer 1993;72:1726)
- As most cases are not associated with GCNIS, they do not show isochromosome 12p or numerical aberrations in the X chromosome, which are commonly seen in GCNIS derived germ cell tumors
- In rare cases, assessment of isochromosome 12p may be indicated if the postpubertal type is suspected
Videos
Testicular NET
Sample pathology report
- Testis and spermatic cord, left, radical orchiectomy:
- Testicular well differentiated neuroendocrine tumor, prepubertal type (monodermal teratoma) and epidermoid cyst (see comment)
- Comment: No germ cell neoplasia in situ (GCNIS) is identified in the background seminiferous tubules.
Differential diagnosis
- Metastatic neuroendocrine tumor to testis:
- Usually presents with bilateral involvement, multifocality, vascular invasion and extratesticular localization
- Sertoli cell tumor:
- Lacks prominent cytoplasmic granularity and salt and pepper pattern of nuclear chromatin
- Expresses alpha inhibin, calretinin, SF1 and beta catenin (nuclear) and sometimes chromogranin and synaptophysin
- Granulosa cell tumor:
- Neoplastic cells have scant cytoplasm, elongated nuclei with nuclear grooves
- No expression of synaptophysin or chromogranin
Additional references
Board review style question #1
A 35 year old man underwent a left radical orchiectomy that demonstrated a 4.0 cm cystic mass (see image). No serological markers (alpha fetoprotein [AFP], beta human chorionic gonadotropin [beta hCG] or lactate dehydrogenase [LDH]) were elevated. Regarding this entity, which of the following statements is true?
- CDX2 is usually positive in testicular neuroendocrine tumor
- Cystic changes can be seen with teratomatous components
- Cytokeratins are usually negative in testicular neuroendocrine tumor
- Glandular growth pattern is not observed
- These tumors are mostly found in association with germ cell neoplasia in situ (GCNIS) / isochromosome 12p
Board review style answer #1
B. Cystic changes can be seen with teratomatous components. Primary testicular neuroendocrine tumor (NET) can occur as pure NET (75%) or in association with testicular teratoma (25%). Cystic changes in these lesions can be seen with teratomatous components. Answer D is incorrect because these tumors mostly exhibit an insular or trabecular growth pattern that can be intermixed with glandular / acinar structures with luminal mucin. Answer E is incorrect because most of these cases are not associated with GCNIS and do not show isochromosome 12p or numerical aberrations in the X chromosome, which are commonly seen in GCNIS derived germ cell tumors. Answers C and A are incorrect because testicular NET expresses cytokeratins and is negative for CDX2.
Comment Here
Reference: Teratoma - neuroendocrine tumor
Comment Here
Reference: Teratoma - neuroendocrine tumor

