

Testis & paratestis
Sex cord stromal tumors
Sertoli cell tumor
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 10 June 2021
Last staff update: 28 March 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Testis Sertoli cell tumor[TI] full text[SB] pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kravtsov O, Mesa H. Sertoli cell tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testisSertoliNOS.html. Accessed December 22nd, 2024.
Definition / general
- Sex cord stromal tumor of testis composed of cells showing features of fetal, prepubertal, adult or atrophic Sertoli cells, at least focally
Essential features
- Second most common type of pure sex cord stromal tumor after Leydig cell tumor
- Most are small, unilateral tumors in adults and the vast majority are benign
- Characterized by tubular or cord pattern, at least focally
- Positive for SF1 and nuclear beta catenin
- Variable and inconsistent expression of calretinin, inhibin A, androgen receptor, CD56
- Negative for SALL4, OCT4 and other germ cell markers
- Poor response to therapy when metastatic
Terminology
- Androblastoma (obsolete)
Epidemiology
- < 1% of testicular tumors
- Rare before age 20; mean age 45 years
Etiology
- Risk factors: cryptorchidism, familial adenomatous polyposis (Virchows Arch 2012;461:713)
- No known environmental factors
Clinical features
- Slowly enlarging unilateral testicular mass
- Testicular discomfort, pain or incidental finding
- Hormonal manifestations very rare; more common in malignant tumors
- Exceptionally, metastases are initial manifestation
- References: Histopathology 2017;70:513, Ulbright: Tumors of the Testis and Adjacent Structures (AFIP Atlas of Tumor Pathology, Series 4), 1st Edition, 2014, Am J Surg Pathol 2015;39:1390
Diagnosis
- For suspected testicular mass, the first test is scrotal ultrasound (US) (sensitivity 95%, specificity 97%)
- If US confirms a lesion, the patient should be immediately referred to a urologist for evaluation and management
- Men 15 to 44 years old with retroperitoneal mass / metastases should undergo testicular examination and scrotal US
- Evaluate serum markers
- Biopsy of testicular tumors is in general not performed, to prevent tumor seeding
- Staging:
- In clinically stable patients, imaging may be performed before or after orchiectomy
- Imaging: computed tomography (CT) scan of the abdomen / pelvis with intravenous contrast, chest radiograph (CXR)
- Noncontrast chest CT should be performed if CXR is abnormal
- Reference: Med Clin North Am 2018;102:251
Laboratory
- Serum tumor markers:
- Beta human chorionic gonadotropin (hCG), alpha fetoprotein (AFP) should be normal and are used to exclude nonseminomatous germ cell tumors
- Lactate dehydrogenase (LDH) to assess global tumor burden
Radiology description
- Ultrasound: solitary hypoechoic lesion; not helpful in distinguishing from germ cell tumors
Radiology images
Images hosted on other servers:

Hypoechoic lesion
Prognostic factors
- Vast majority are benign, ~ 5% cases are malignant
- Tumors with sclerosis > 50% almost invariably benign (Am J Surg Pathol 2014;38:510)
- Features associated with malignancy: extratesticular spread, size > 5 cm, lymphovascular invasion, high grade cytological atypia, tumor necrosis, mitotic index > 5/10 high power fields (Am J Surg Pathol 1998;22:709)
- Very rarely tumors without malignant histology metastasize
Case reports
- 23 year old man with small, solid, well demarcated intraparenchymal tumor (Case #18)
- 23 year old man with sclerosing Sertoli cell tumor (Rev Urol 2014;16:191)
- 34 year old man with familial adenomatous polyposis and bilateral Sertoli cell tumors (Virchows Arch 2012;461:713)
- 13 examples of malignant Sertoli cell tumors (Am J Surg Pathol 2002;26:541)
Treatment
- Orchiectomy (total or partial) is treatment of choice
- Retroperitoneal lymph node dissection for malignant Sertoli cell tumors
- No specific therapy; poor response to chemotherapy or radiotherapy
- Reference: Med Clin North Am 2018;102:251
Gross description
- Cut surface usually homogenous white or yellowish
- Cystic component present in ~ 30% of cases (Am J Surg Pathol 1998;22:709)
- Benign: well circumscribed, most between 2 - 5 cm (Am J Surg Pathol 2014;38:510)
- Malignant: > 5 cm, poor circumscription, extratesticular extension, necrosis, hemorrhage
Gross images
Images hosted on other servers:

Tumor in lower pole
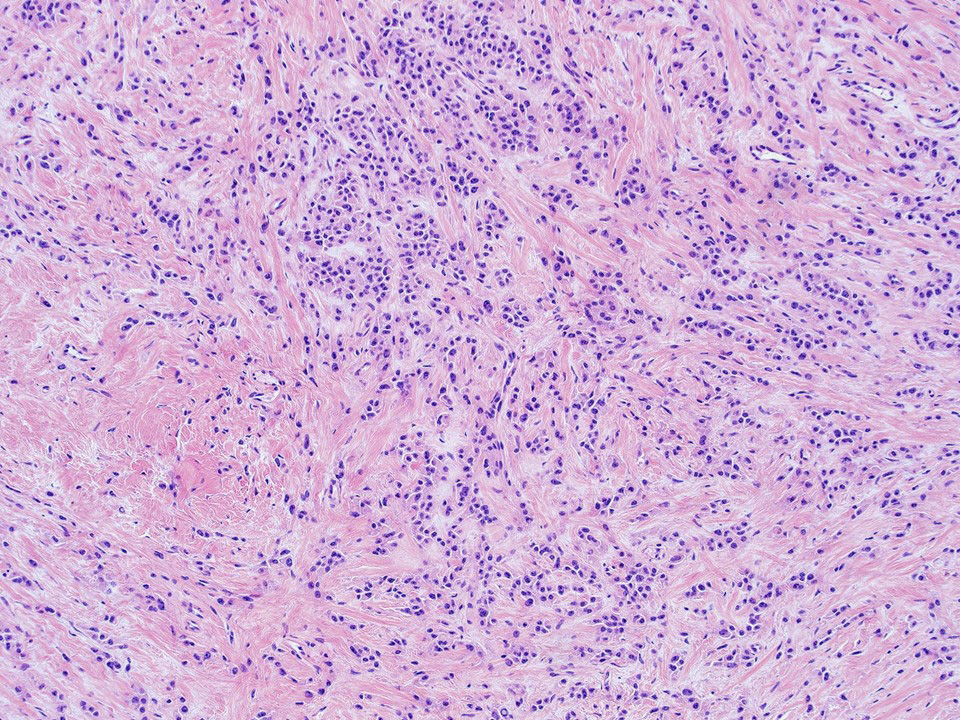
Microscopic (histologic) description
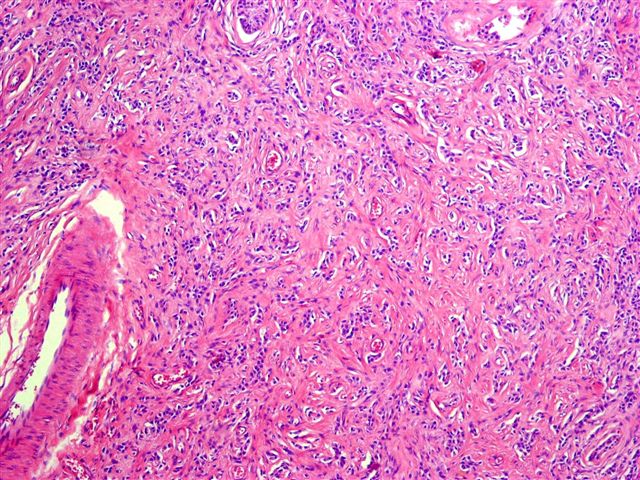
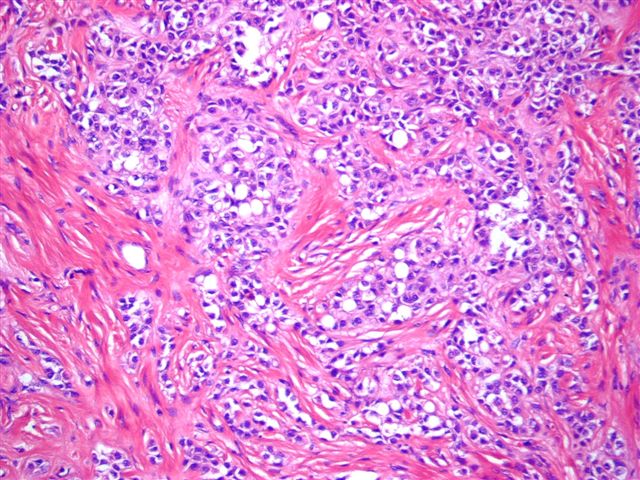
- Architecture: tubular (lumen), cords (no lumen), tubulopapillary present at least focally
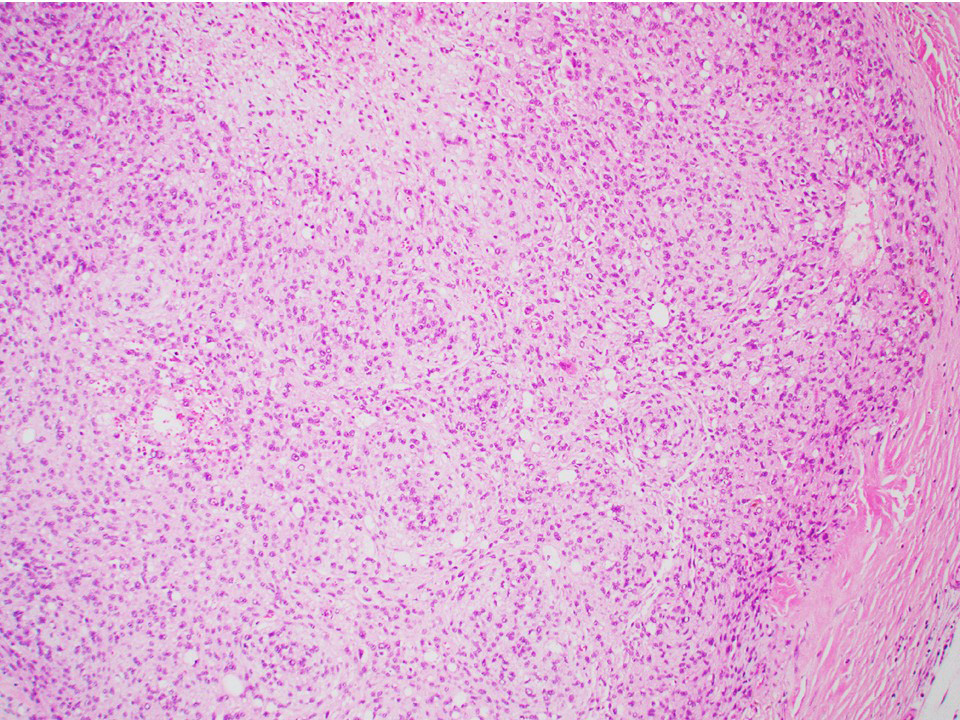
- Other patterns: macro or microcystic, nested, trabecular, whorled, solid, retiform, pseudopapillary; most tumors show mixed patterns
- Nuclei: bland, uniform, round to ovoid in benign tumors; small hyperchromatic or large with prominent nucleoli in malignant tumors
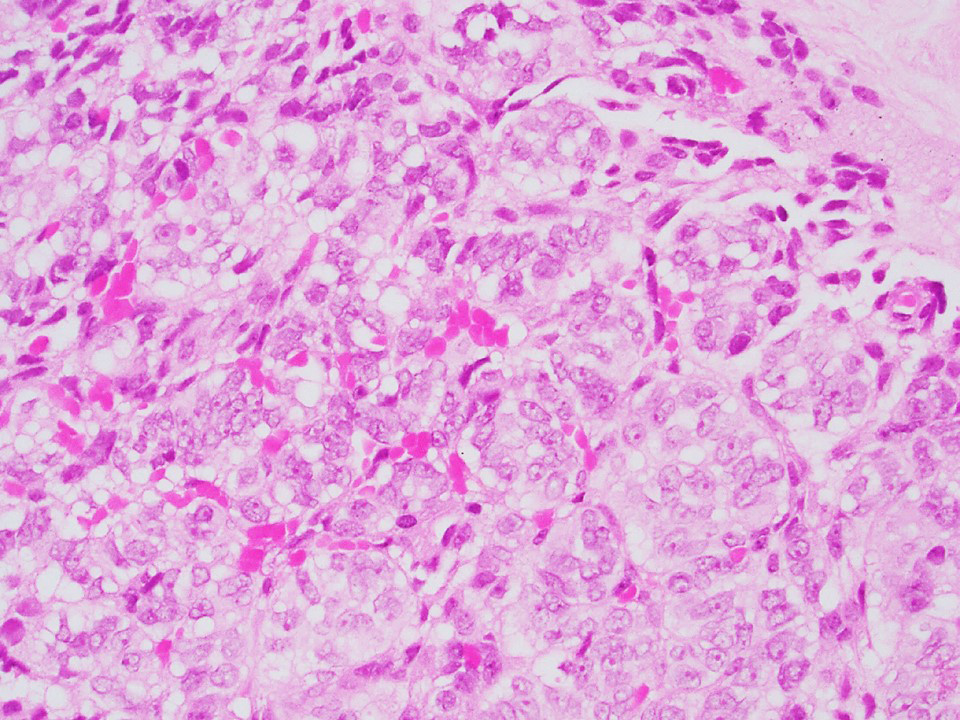
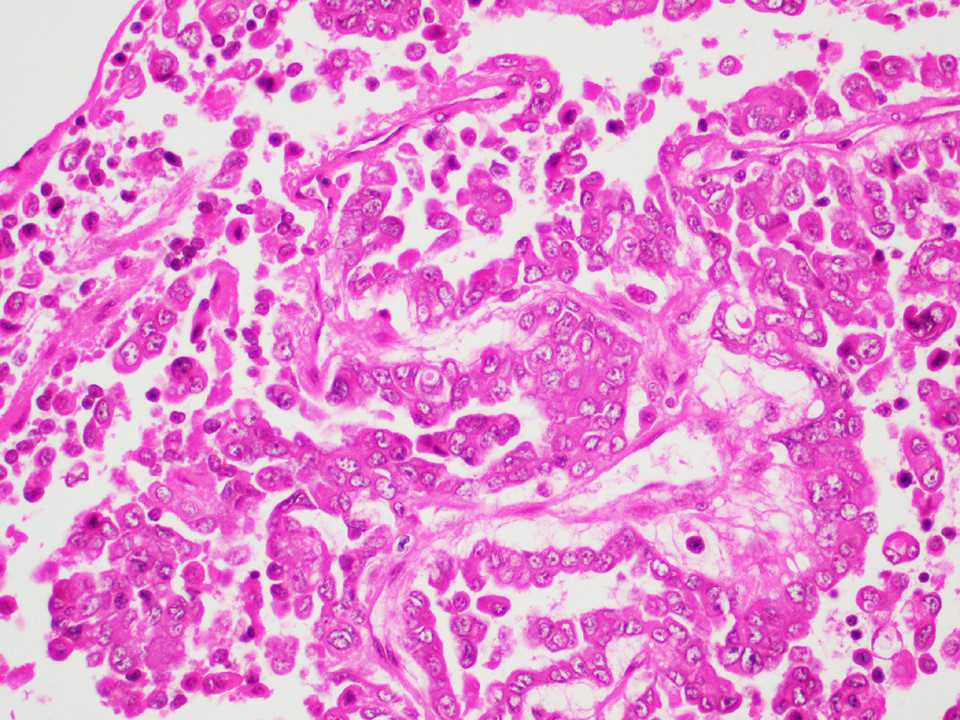
- Cytoplasm: usually clear and abundant but extremely variable, ranging from scant, foamy, eosinophilic to markedly lipidized; hyaline globules are common
- Stroma: variable, basement membrane-like material around tubules, sclerotic, myxoid, edematous, angiomatous
- If sclerosis > 50% → sclerotic variant (now considered subtype of Sertoli cell tumor, NOS)
- Inflammatory cells usually absent, rarely prominent
- References: Histopathology 2017;70:513, Ulbright: Tumors of the Testis and Adjacent Structures (AFIP Atlas of Tumor Pathology, Series 4), 1st Edition, 2014, Am J Surg Pathol 2015;39:1390
Microscopic (histologic) images
Contributed by Thomas Ulbright, M.D. and Case #18
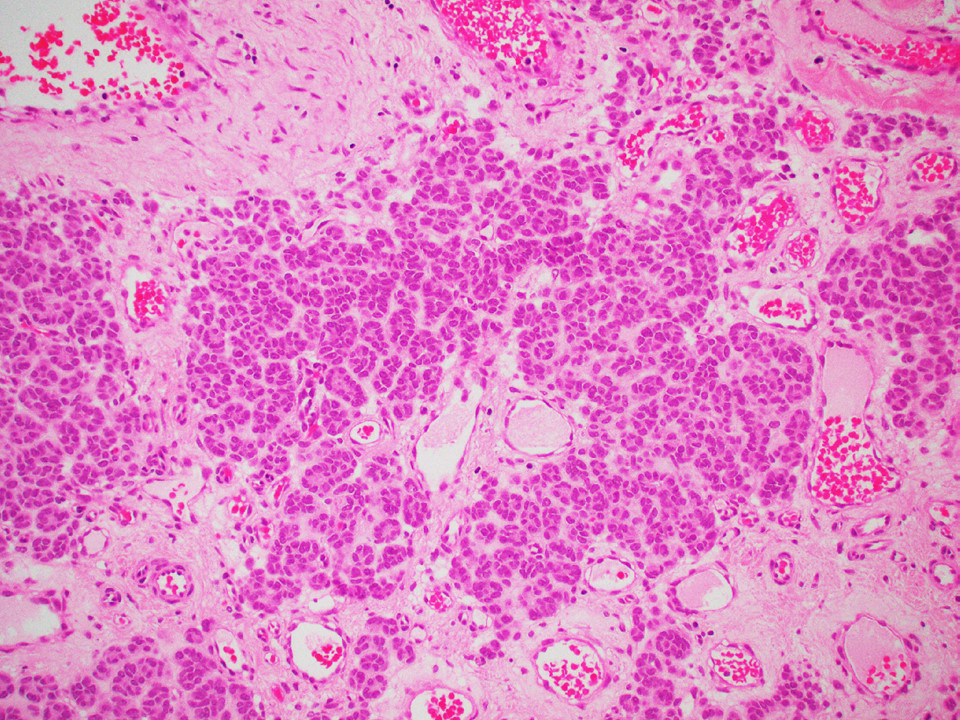
Architectural patterns
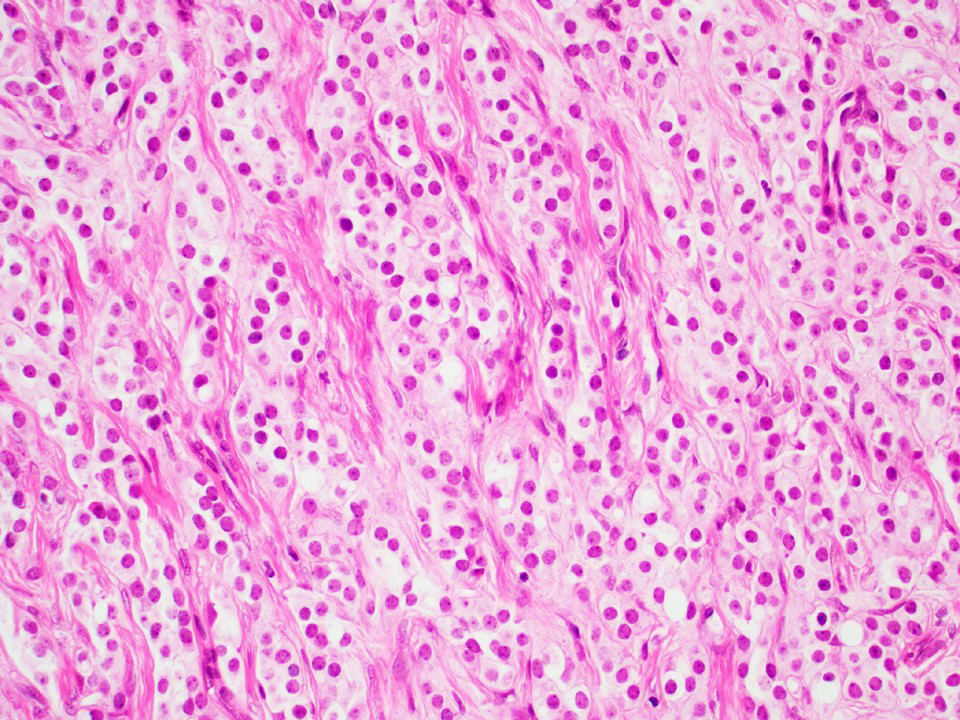
Cords
Tubules
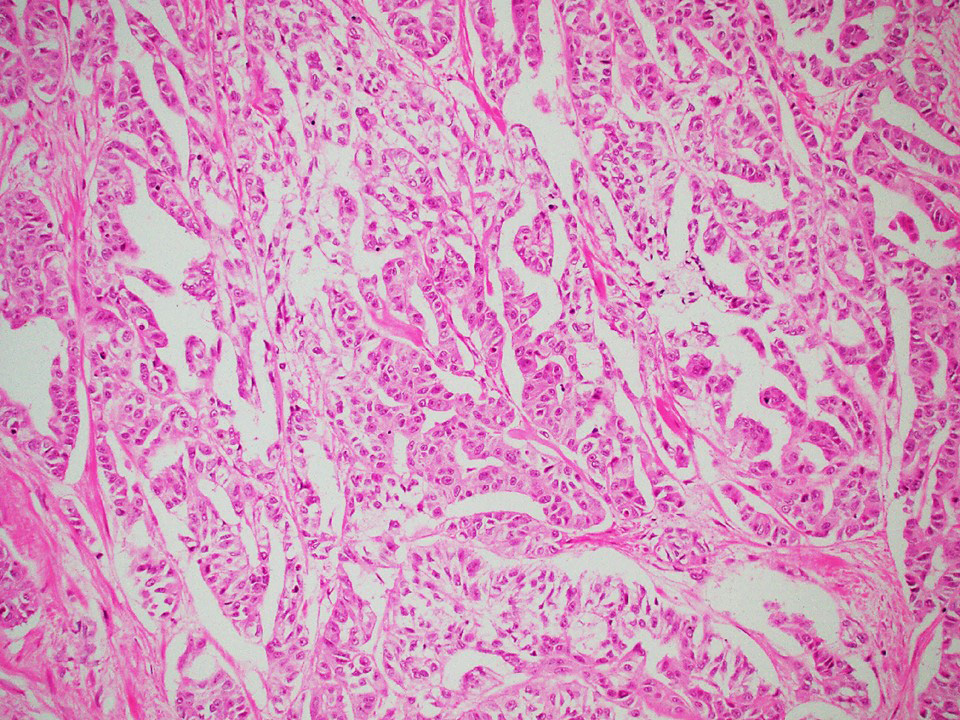
Tubopapillary
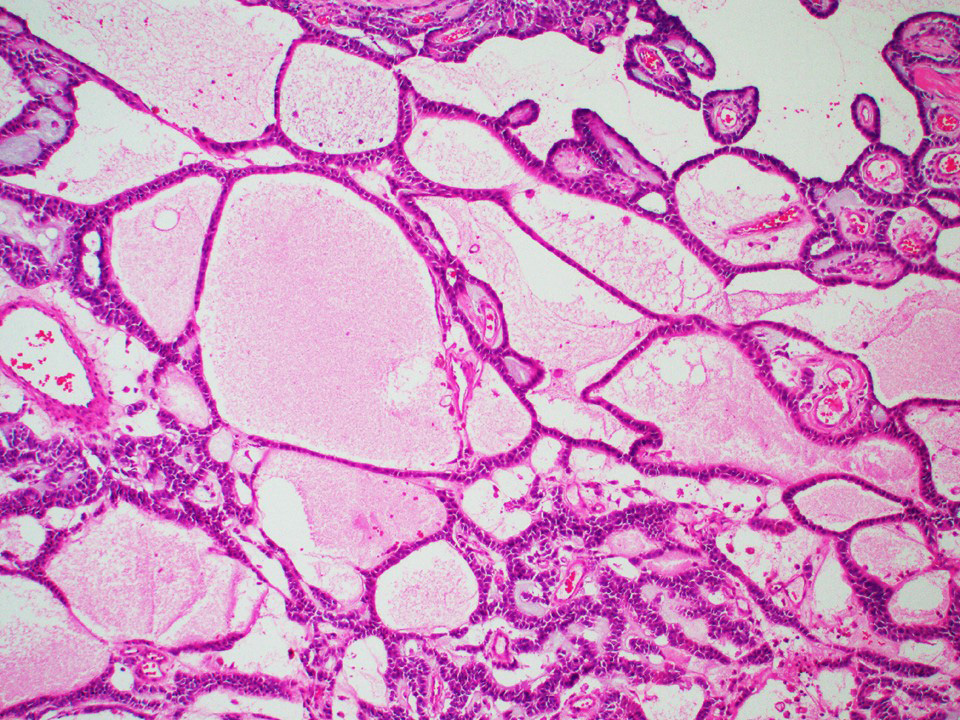
Macrocystic
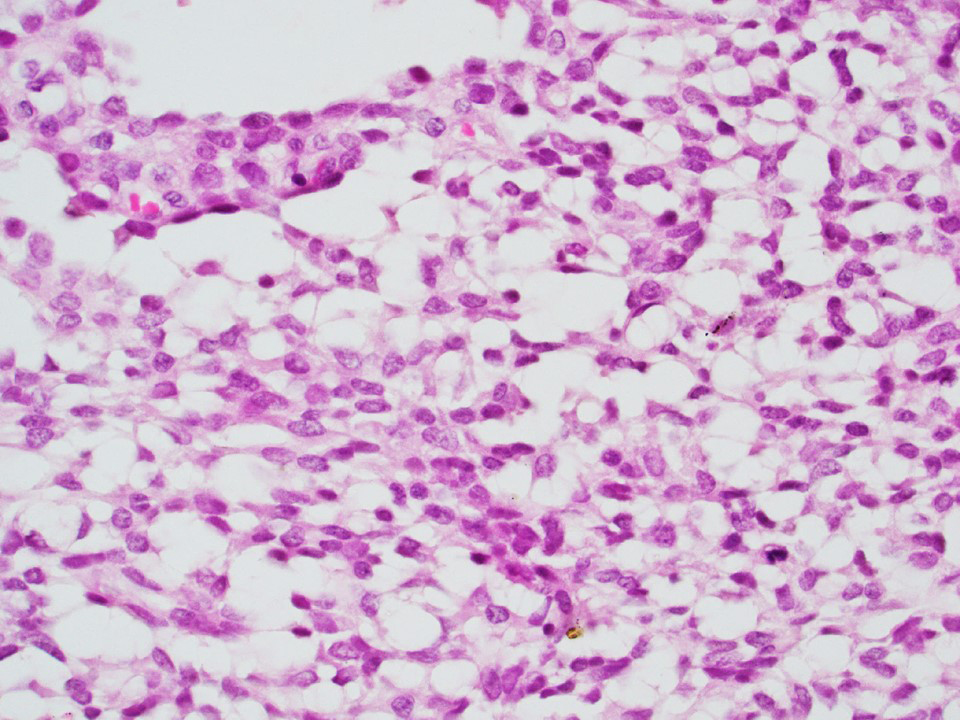
Microcystic
Architectural patterns
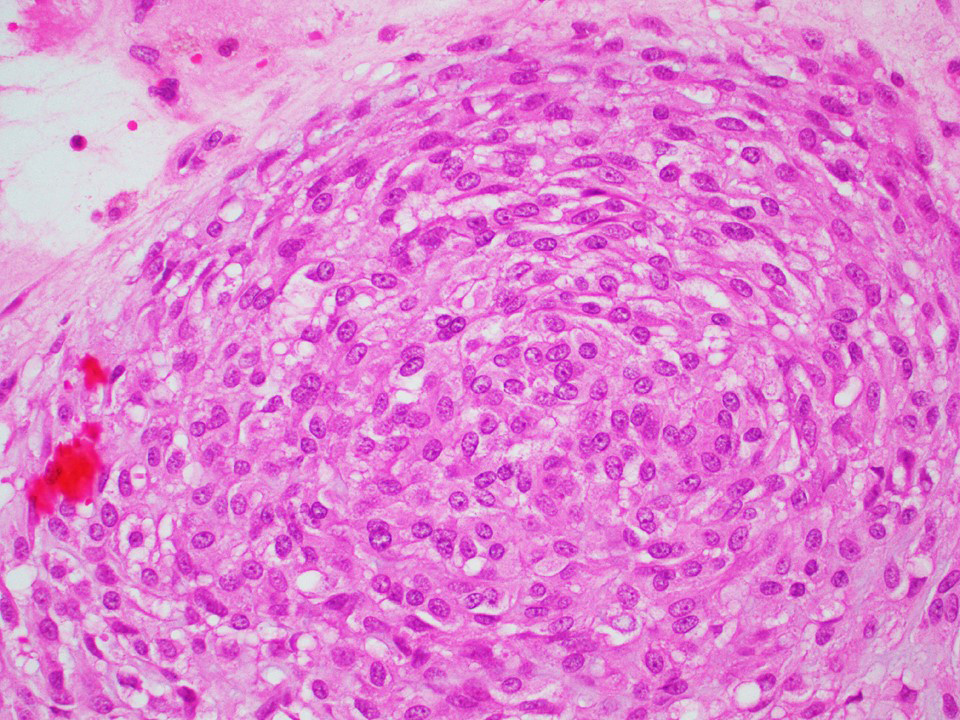
Whorled
Trabecular
Sclerosing Sertoli cell tumor

Various images
Cells
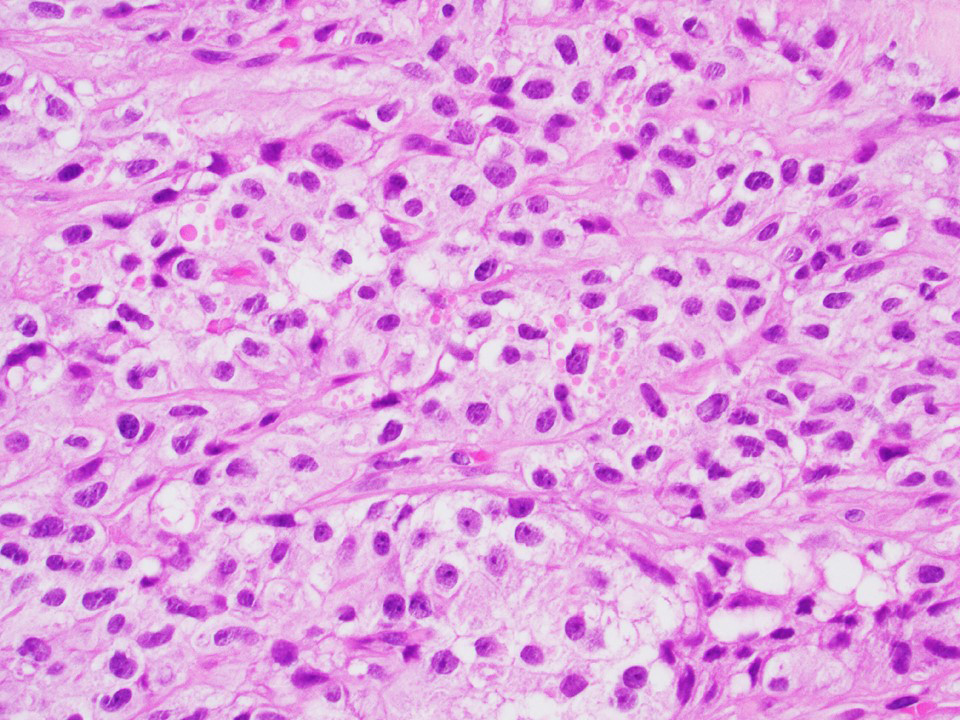
Abundant clear cytoplasm (most common)
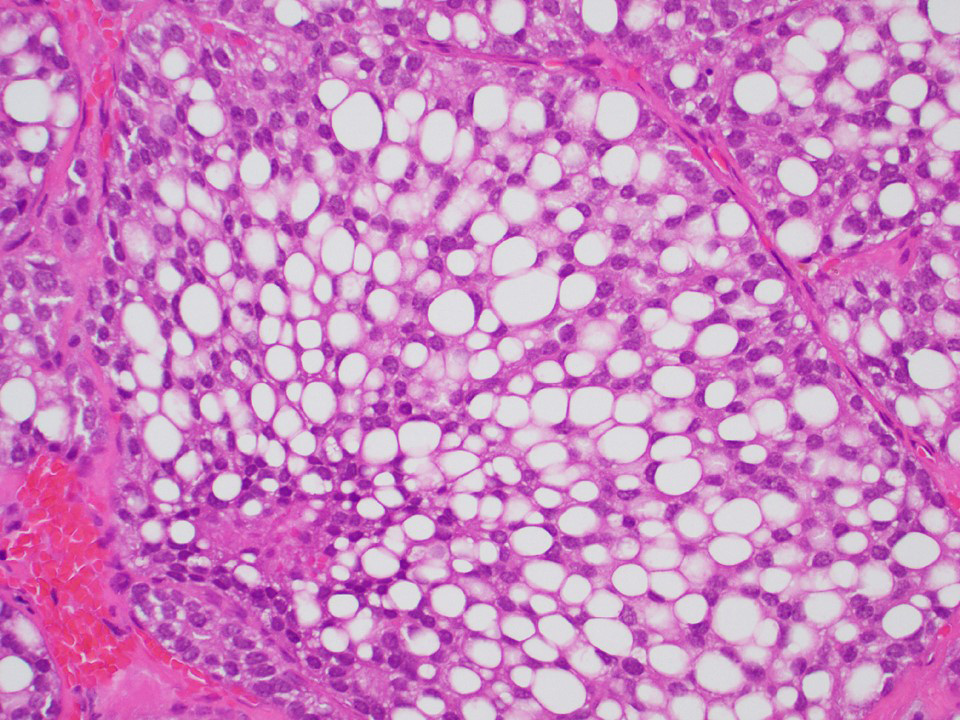
Heavily lipidized
Malignant
Marked cytologic atypia
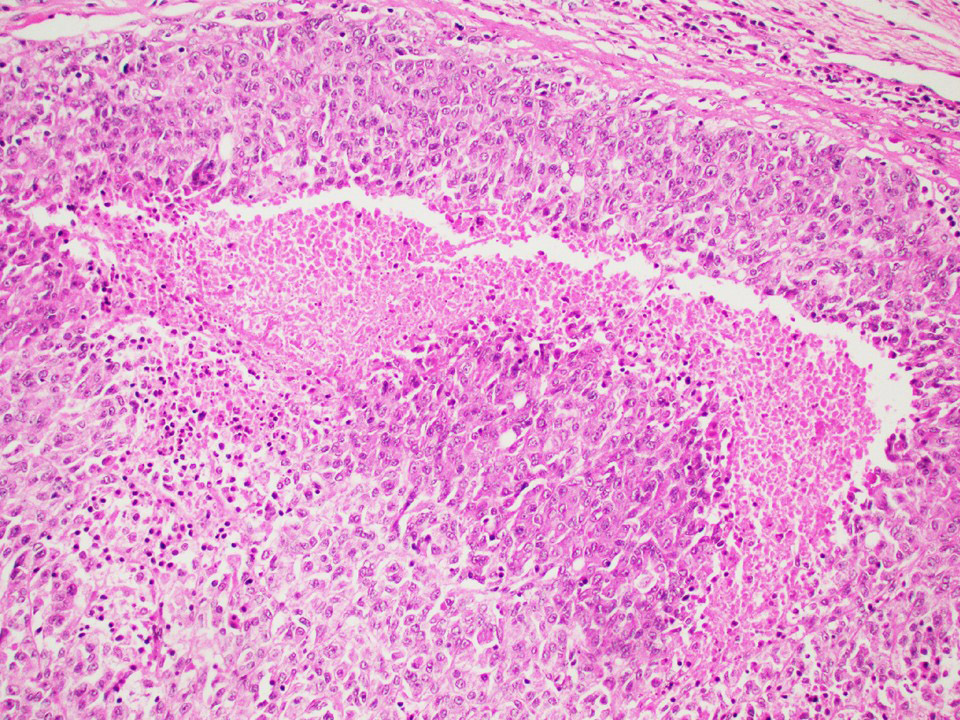
Tumor necrosis
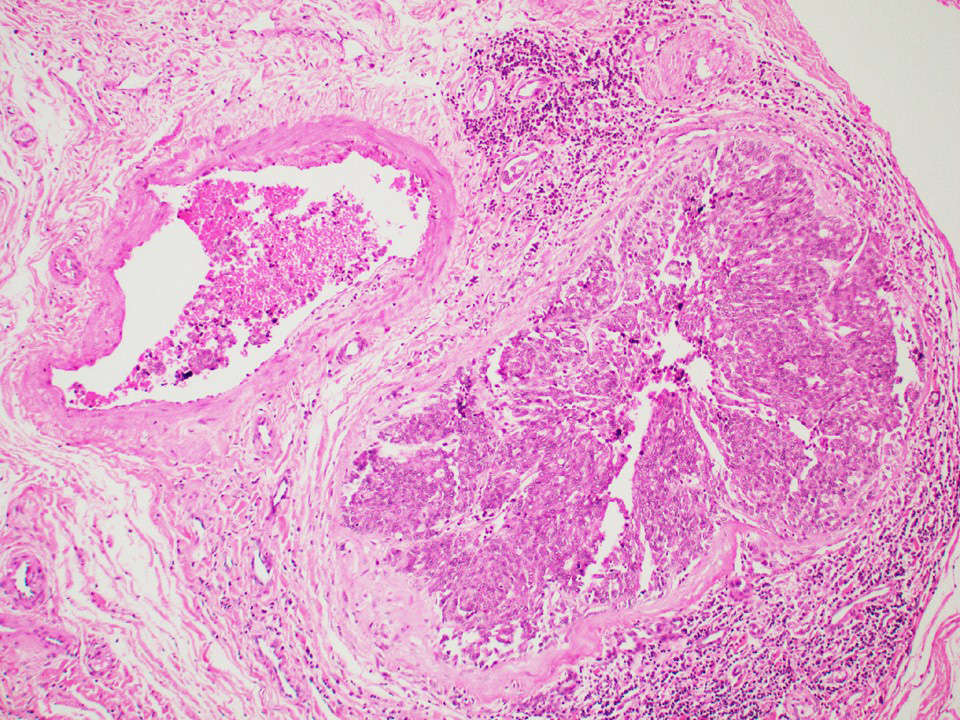
Lymphovascular invasion
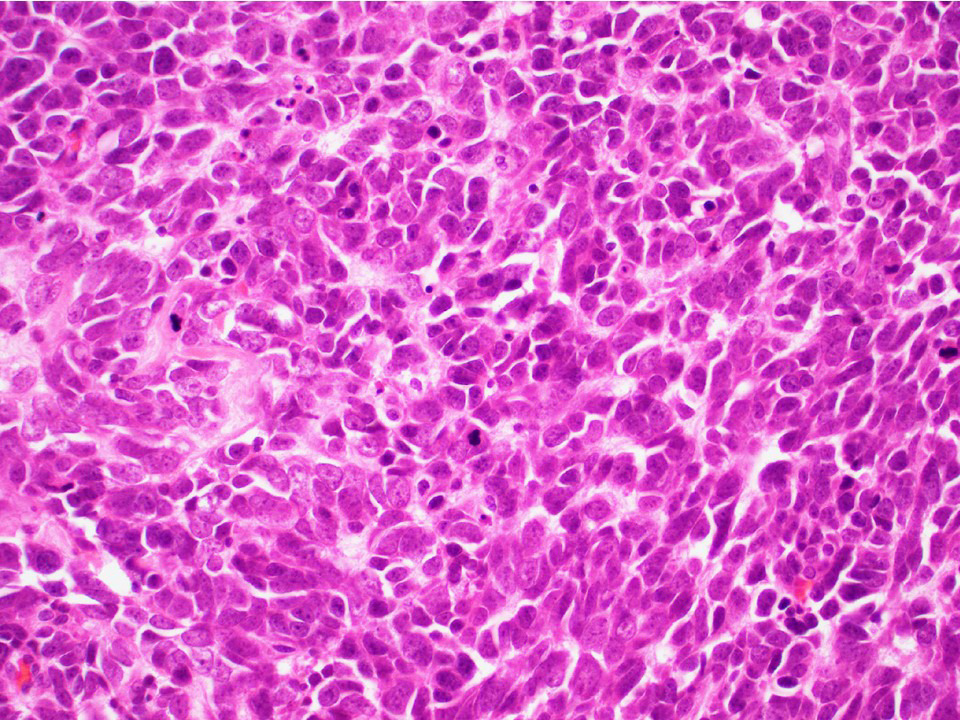
High N/C ratio,
increased
mitotic / apoptotic
activity
Cytology description
- Cytologic samples are from metastatic (malignant) Sertoli cell tumors
- Aspirates show branching tubules, microacinar and papillary groups
- Numerous individual cells are present in the background
- Cells are small, ovoid to plasmacytoid, relatively uniform
- Nuclei show smooth cell membranes and granular chromatin pattern
- Malignancy evident by nuclear overlap, discordant large nuclei and mitotic activity
- Aspirates resemble neuroendocrine tumors or well differentiated adenocarcinomas
- References: Histopathology 2017;70:513, Ulbright: Tumors of the Testis and Adjacent Structures (AFIP Atlas of Tumor Pathology, Series 4), 1st Edition, 2014, Am J Surg Pathol 2015;39:1390
Cytology images
Contributed by Indiana University School of Medicine
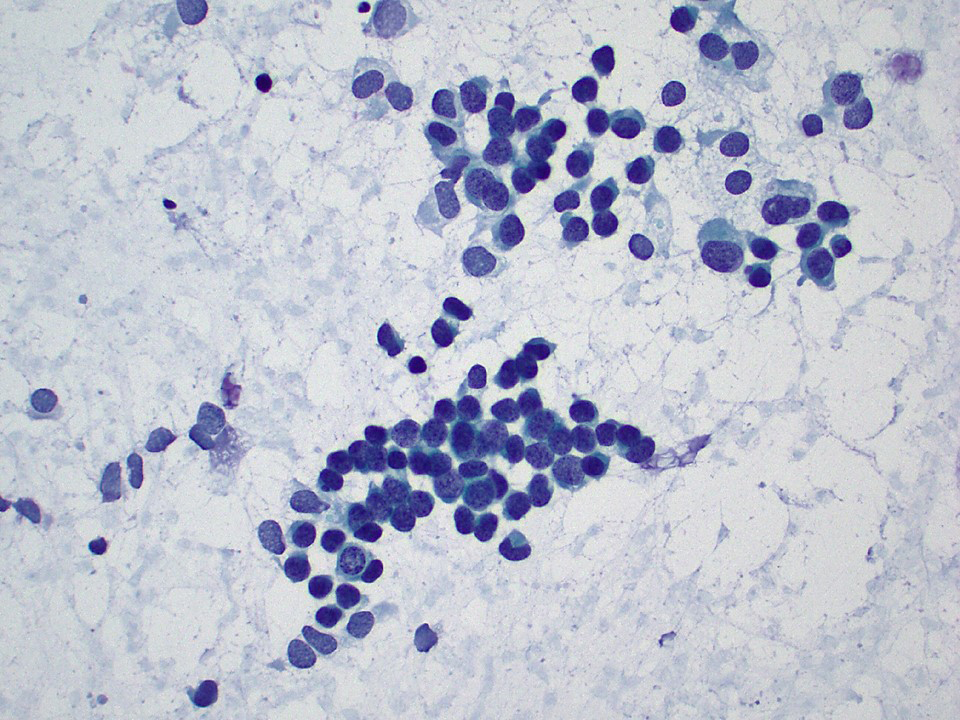
Tubular formations, monotonous small cells (Pap)

Papillary groups and discohesive cells (Pap)
Positive stains
- Consistent markers: SF1, nuclear beta catenin
- Inconsistent markers: calretinin, inhibin A, cytokeratins, MelanA, WT1, CD99, SOX9, vimentin, CD56, chromogranin, synaptophysin, nestin, PAX2, PAX8, androgen receptor (Am J Surg Pathol 2015;39:1390, Hum Pathol 2017;68:99, Hum Pathol 2017;61:181)
Electron microscopy description
- Prominent Golgi complex, variable smooth endoplasmic reticulum, lipid droplets, glycogen
- Cells interconnected by desmosomes, peripheral basement membrane
- References: Histopathology 2017;70:513, Ulbright: Tumors of the Testis and Adjacent Structures (AFIP Atlas of Tumor Pathology, Series 4), 1st Edition, 2014, Am J Surg Pathol 2015;39:1390
Molecular / cytogenetics description
- CTNNB1 gene mutations (Am J Surg Pathol 2014;38:66)
- Negative for isochromosome 12p
- Cytogenetics: gains of X chromosome (~ 40% cases), loss of chromosomes 2 and 19 (less common) (Virchows Arch 2007;450:425)
Sample pathology report
- Left testis, orchiectomy:
- Sertoli cell tumor, not otherwise specified (see comment and synoptic report)
- Comment: The morphologic features are diagnostic of Sertoli cell tumor, not otherwise specified. No features of malignancy are identified in this tumor (i.e. extratesticular spread, size > 5 cm, high grade cytologic atypia, > 5 mitotic figures per 10 high power fields, necrosis or lymphovascular invasion).
Differential diagnosis
- Rete testis adenoma:
- Located at the rete testis
- Strong diffuse positivity for PAX2, PAX8 and pankeratin
- Adenomatoid tumor:
- Paratesticular location
- Uniformly positive mesothelial markers: pankeratin, CK7, WT1, CK5/6, calretinin
- Negative for SF1 or nuclear beta catenin
- Leydig cell tumor:
- Abundant eosinophilic cytoplasm, absent tubules / cords
- Consistent strong expression of calretinin, inhibin A, SF1
- Negative beta catenin (Am J Surg Pathol 2015;39:1390)
- Yolk sac tumor:
- Positive for SALL4, glypican 3, alpha fetoprotein, pankeratin
- Negative for OCT4, SF1, nuclear beta catenin, inhibin A, calretinin
- Seminoma:
- Positive for SALL4, OCT4, KIT, D2-40, PLAP
- Negative for SF1, nuclear beta catenin, inhibin A, calretinin
- Juvenile granulosa cell tumor:
- Most common in infants; 90% occur before age 10
- Follicles with mucicarmine+ basophilic or eosinophilic secretions
- Variable solid pattern, frequent brisk mitotic / apoptotic activity
- Consistent expression of inhibin A, calretinin, FOXL2
- Large cell calcifying Sertoli cell tumor:
- Large epithelioid cells, lamellated calcifications
- Associated with Carney complex
- Sertoli cell nodule (Pick adenoma):
- Small size, multifocal, monotonous tubular / cord architecture, associated with androgen insensitivity syndrome and cryptorchidism
Additional references
Board review style question #1
A 60 year old man presents with a 1.1 cm mass in the left testis. The tumor is positive for SF1, nuclear beta catenin, androgen receptor, variable for inhibin A and calretinin and negative for SALL4. What is the most likely diagnosis?
- Adenomatoid tumor
- Seminoma
- Sertoli cell tumor, NOS
- Yolk sac tumor
Board review style answer #1
Board review style question #2
What is the characteristic immunoprofile of a testicular Sertoli cell tumor, NOS?
- Positive for SF1, calretinin, chromogranin, synaptophysin; negative for SALL4 and beta catenin
- Positive for SALL4; negative for SF1, inhibin A and calretinin
- Positive for SF1, calretinin, inhibin A, beta catenin (nuclear); negative for SALL4, chromogranin, synaptophysin
- Positive for CD45; negative for SF1, inhibin A and SALL4
Board review style answer #2
C. Positive for SF1, calretinin, inhibin A, beta catenin (nuclear); negative for SALL4, chromogranin, synaptophysin
Comment Here
Reference: Sertoli cell, NOS
Comment Here
Reference: Sertoli cell, NOS

