
CNS nontumor
Malformations
Arnold-Chiari malformation
Author: Erdener Özer, M.D., Ph.D.

Last author update: 1 May 2016
Last staff update: 7 April 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Arnold-Chiari Malformation [title]

Table of Contents
Definition / general | Essential features | Diagrams / tables | Terminology | Epidemiology | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Treatment | Clinical images | Differential diagnosis | Additional referencesCite this page: Özer E. Arnold-Chiari malformation. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/syndromesarnoldchiari.html. Accessed March 31st, 2025.
Definition / general
- Chiari malformations, types I-IV, refer to a spectrum of congenital hindbrain abnormalities affecting the structural relationships between the brainstem, cerebellum, upper cervical cord and bony cranial base
- Hans Chiari, an Austrian pathologist, classified Chiari malformations into types I through III in 1891
- Chiari's German colleague, Julius Arnold, made additional contributions to the definition of Chiari II malformation
- Therefore the type II malformation is commonly referred to as the Arnold-Chiari malformation
- Later, other investigators added a fourth (Chiari IV) malformation
Essential features
- Scale of severity is rated I - IV with IV being the most severe
- Chiari type I malformation: elongation of one or both cerebellar tonsils, which protrude through the foramen magnum of the spinal canal and may become sclerotic; there may be associated syringomyelia or syringobulbia
- Chiari type II malformation: most common cause of congenital hydrocephalus
- Cerebellar tonsils extend far down into the spinal canal, accompanied by an elongated fourth ventricle
- There is a lumbar spina bifida with a meningomyelocele
- Hydrocephalus is associated with enlargement of the lateral and third ventricle, a paper thin tentorium and falx cerebri
- The outer surface of the cerebral hemispheres is flattened and the cortex is thinned
- The vault of the skull is large or enormous, the fontanelles are very wide and the posterior fossa is small
- Lower limb muscles show varying degrees of denervation atrophy
- Chiari type IIII malformation: further herniation of the cerebellum below the foramen magnum forming an encephalocele, in addition to spina bifida, syringomyelia and hydrocephalus
- Chiari type IV malformation: hypoplasia or aplasia of the cerebellum in addition to other features
- Conditions associated with Chiari malformation include hydrocephalus, syringomyelia, spinal curvature, tethered spinal cord syndrome and connective tissue disorders such as Ehlers-Danlos syndrome
Diagrams / tables
Contributed by Erdener Özer, M.D., Ph.D.
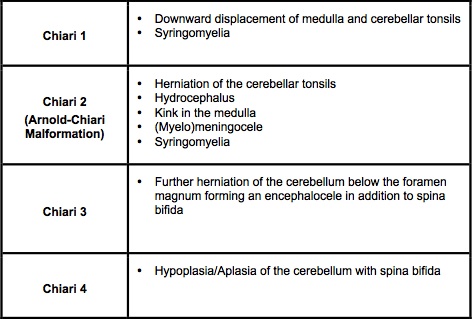
Types of Chiari malformations
Terminology
- Chiari or Chiari’s malformation
Epidemiology
- There are no population based studies on the incidence or prevalence of Chiari malformations
- From clinical series, prevalence has been estimated at 0.1 to 0.5%
- However with routine use of magnetic resonance imaging, Chiari malformation is discovered with increasing frequency
- Types III and IV are very rare (J Genet Couns 2003;12:297)
Pathophysiology
- Symptoms of Chiari type I malformation develop due to compression of medulla and upper spinal cord, compression of cerebellum or disruption of cerebrospinal fluid flow through the foramen magnum
- The pathophysiology of Chiari type II malformation is more complex; although compressive mechanisms likely play a role, additional mechanisms may be functional
Etiology
- Chiari type I:
- Based on analysis of familial aggregation, a genetic basis has been suggested due to alterations in chromosomes 9 and 15
- It may be a disorder of para-axial mesoderm, which subsequently results in formation of a small posterior fossa
- Development of the cerebellum within this small compartment results in herniation of the cerebellar tonsils (Am J Med Genet A 2006;140:2776, J Genet Couns 2003;12:297)
- Chiari type II:
- Theories must take into account its invariable association with myelomeningocele
- The "CSF loss" theory claims that escape of CSF fluid through the open placode in myelomeningocele results in an inadequate stimulus for mesenchymal condensation at the skull base
- Disordered and inadequate growth of the posterior fossa results in downward herniation of brainstem
Clinical features
- Chiari’s type I malformation is usually seen in older children and adults; type II is seen in infants and younger children
- Some patients are asymptomatic and the malformation does not interfere with activities of daily living
- Symptomatic patients often present with headaches, fatigue, muscle weakness, difficulty swallowing, vomiting, dizziness, nausea, tinnitus, impaired coordination, neck pain and speech problems
Diagnosis
- Diagnosis requires patient history, neurological examination and medical imaging
- Magnetic resonance imaging is considered the best imaging modality for Chiari malformation
- Diagnosis of Chiari type II malformation can be made prenatally through ultrasound (J Neurosurg Pediatr 2015;16:159)
Radiology description
- Neuroradiological investigation is used to rule out intracranial conditions responsible for tonsillar herniation, to evaluate the cerebellar tonsil position, the crowding of neural structures within the posterior cranial fossa and their impact on the foramen magnum (J Neurosurg Pediatr 2015;16:159)
Radiology images
Images hosted on other servers:

Sagittal FLAIR MRI scan
Treatment
- Vitamin A and folic acid supplementation in pregnancy reduces the risk of its development
- In symptomatic cases, medications may ease certain symptoms such as pain
- Surgical shunting and decompression of the foramen magnum are the only treatments which reduce the impact of hydrocephalus and the progression of damage to the central nervous system
Clinical images
Contributed by Erdener Özer, M.D., Ph.D.
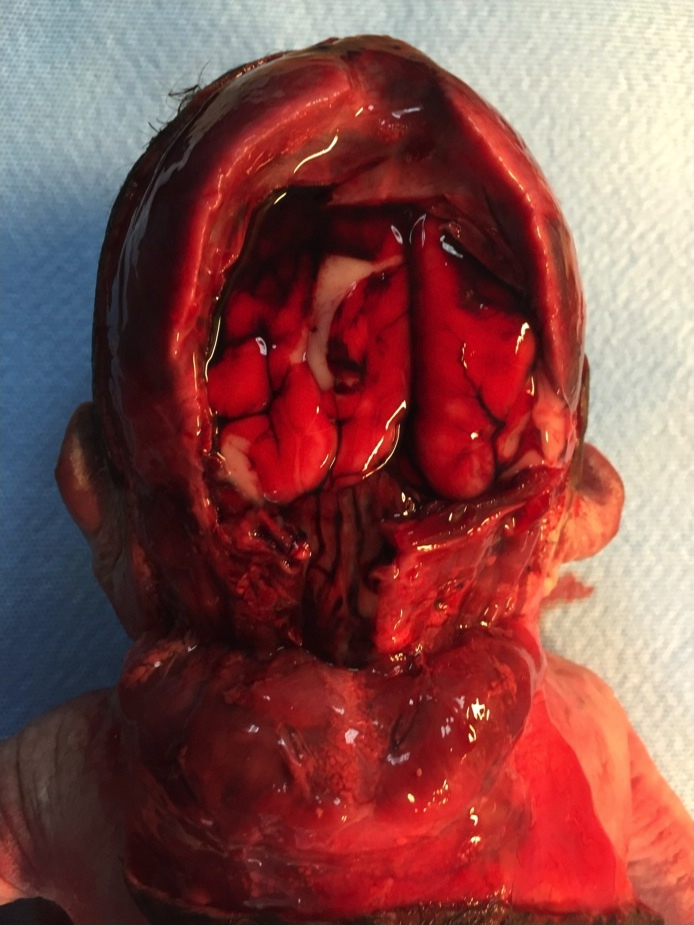
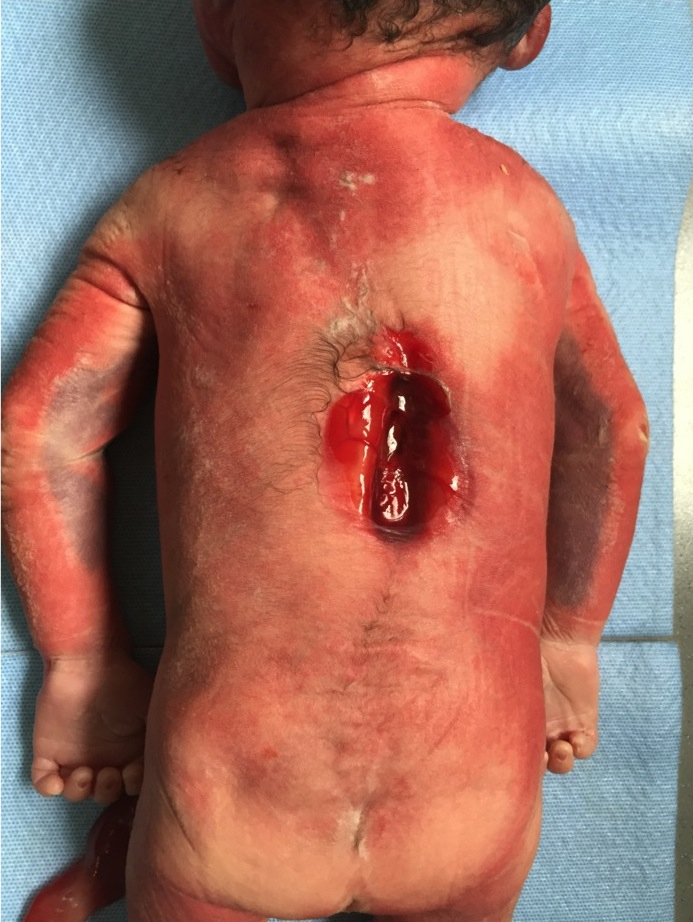
Chiari type II malformation
Differential diagnosis
- In pseudo-Chiari malformation, leaking of cerebrospinal fluid may cause displacement of the cerebellar tonsils and resemble Chiari’s type I malformation
Additional references
