

Stomach
Gastritis
Russell body gastritis
Authors: Yuxin Lu, M.D., Natalya Shlyakhova, M.D.


Last author update: 1 March 2017
Last staff update: 14 June 2021
Copyright: 2017-2024, PathologyOutlines.com, Inc.
PubMed search: Russell body gastritis
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Differential diagnosisCite this page: Lu Y, Shlyakhova N. Russell body gastritis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachrussellbody.html. Accessed December 23rd, 2024.
Definition / general
- Russell body gastritis, first described in 1998, is a reactive gastric mucosal infiltration of plasma cells filled with cytoplasmic Russell bodies (Am J Hematol 2010;85:951)
- Recently recognized pseudotumoral lesion of the gastric mucosa with unknown etiology; characterized by the accumulation of numerous plasma cells containing Russell bodies (RBs) with the expression of kappa and lambda light chains (J Gastrointestin Liver Dis 2012;21:97)
- Often associated with H. pylori infection and malignancies such as lymphoplasmacytic lymphoma, plasmacytoma, signet ring cell carcinoma (Pathol Res Pract 2007;203:457, Virchows Arch 2005;446:463)
Essential features
- Russell bodies, first described by Russell in 1890, are considered to represent aggregates of immunoglobulins resulting from secretory disturbance of plasma cells
- Plasma cells with Russell bodies can be seen in a variety of mucosal surfaces, including gastrointestinal tract in association with chronic inflammation such as H. pylori gastritis.
ICD coding
- 2017 ICD-10-CM Diagnosis Code K29.70 - Gastritis, unspecified, without bleeding
Epidemiology
- Only 39 cases involving the gastrointestinal tract have been reported in English literature, which include Russell body gastritis, duodenitis and esophagitis (Int J Surg Pathol 2015;23:667)
Sites
- Stomach, duodenum, esophagus (Int J Surg Pathol 2015;23:667)
Pathophysiology
- Russell bodies represent a cellular response to overstimulation of plasma cells, leading to the accumulation of abundant, nondegradable, condensed immunoglobulin in dilated rough endoplasmic reticulum cisternae (Int J Surg Pathol 2015;23:667)
- Considering the other cases reported in the literature, it seems as if H. pylori plays an active role in the etiology of the condition, either by promoting it or by modulating the extension of the disease locally (J Gastrointestin Liver Dis 2012;21:97)
Etiology
- Unknown (J Gastrointestin Liver Dis 2012;21:97)
Clinical features
- Asymptomatic or symptoms related to H. pylori or associated malignancy
Diagnosis
- Histology showing diffuse infiltration with plasma cell filled with Russell bodies
- Exclusion of other associated conditions
Radiology description
- Computed tomography scan may show esophageal and gastric wall thickening (Conn Med 2012;76:261)
Prognostic factors
- Although RBG is by itself a benign condition, its long term effect, such as its possible increased risk for the development of neoplasia, is unknown (J Gastrointestin Liver Dis 2012;21:97)
Case reports
- 44 year old woman with history of diabetes mellitus, post kidney and pancreas transplant (Int J Surg Pathol 2015;23:667)
- 53 year old man with localized accumulation of plasma cells containing Russell bodies (Pathol Int 1998;48:242)
- 60 year old woman with history of epigastric pain (Pathol Res Pract 2007;203:457)
- 82 year old man with Russell body gastritis associated with HIV infection (Conn Med 2012;76:261)
- Ten cases involving Russell bodies and plasma cell infiltration, seven of which are associated with H. pylori infection (J Gastrointestin Liver Dis 2012;21:97)
- Russell body esophago-gastro-duodenitis (Clin Res Hepatol Gastroenterol 2014;38:e89)
Treatment
- Treatment of H. pylori usually results in the resolution of Russel bodies in cases associated with H. pylori
Gross description
- Endoscopy reveals nonspecific congestion of the mucosa (Pathol Res Pract 2007;203:457) or multiple ulcer scars in the antrum of the stomach (Pathol Int 1998;48:242)
- Can present with erythema in the gastric body and a large, irregular, fungating, ulcerated, nearly circumferential mass at the incisura angularis of the stomach (J Gastrointestin Liver Dis 2012;21:97)
- Gastritis on endoscopy (Conn Med 2012;76:261)
Gross images
Images hosted on other servers:

Large, irregular and deep
ulcerated mass lesion
with central ulceration
at the incisura angularis
Microscopic (histologic) description
- Plasma cell infiltrates with extensive formation of Russell bodies (Mott cells) within the lamina propria of the antral mucosa
- Intracytoplasmic inclusions, homogeneous, mainly round to oval, which push the nucleus toward the periphery
Microscopic (histologic) images
Case #410
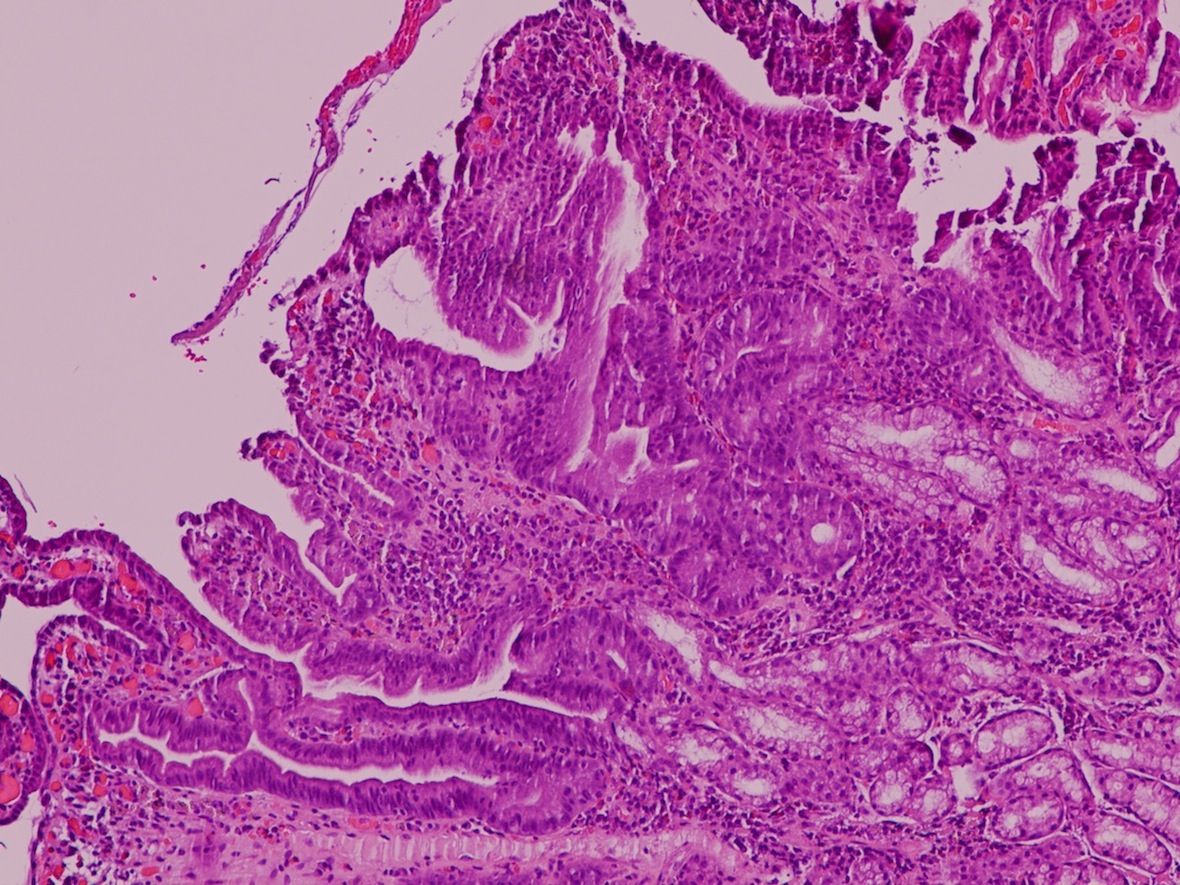

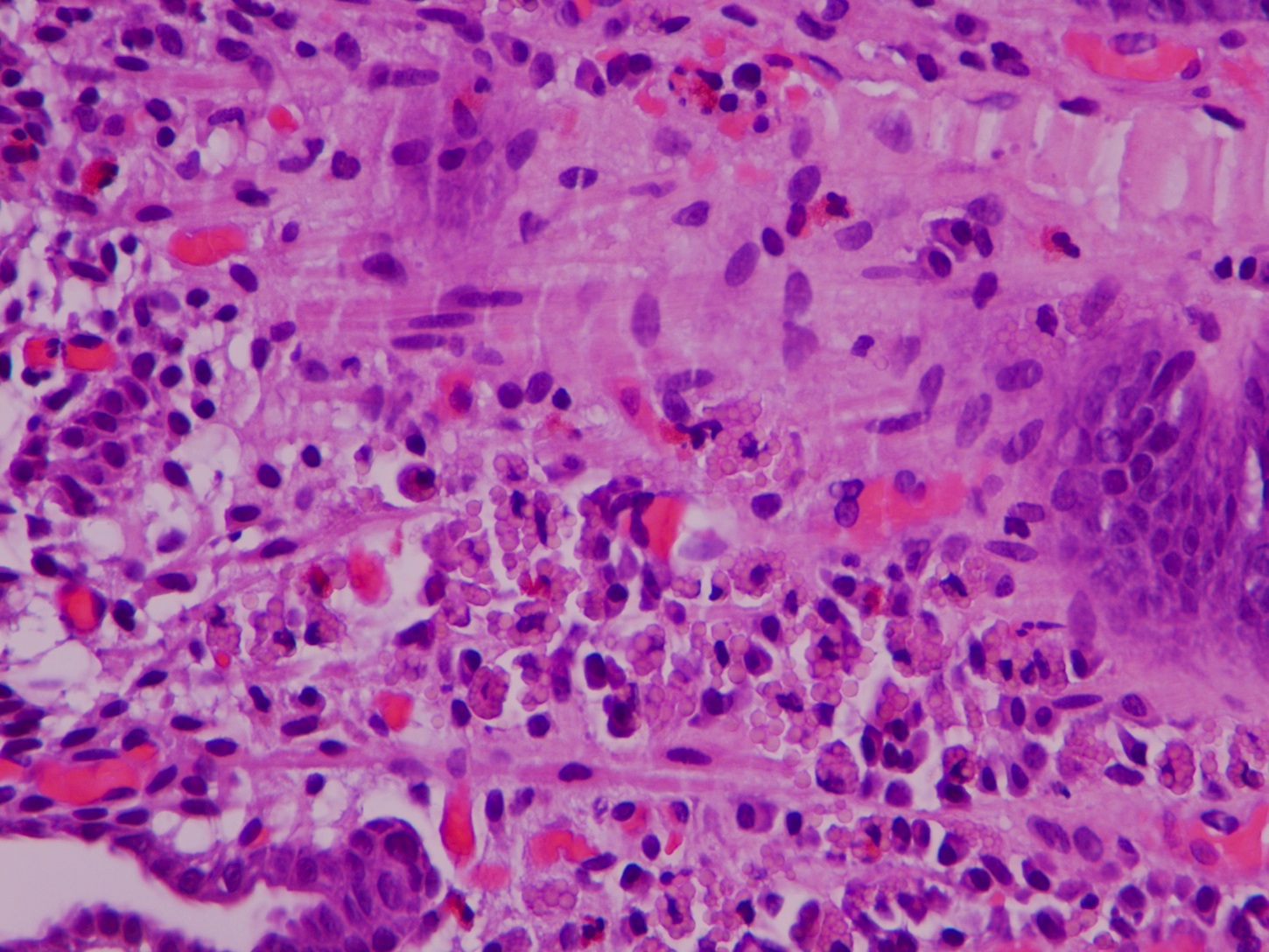
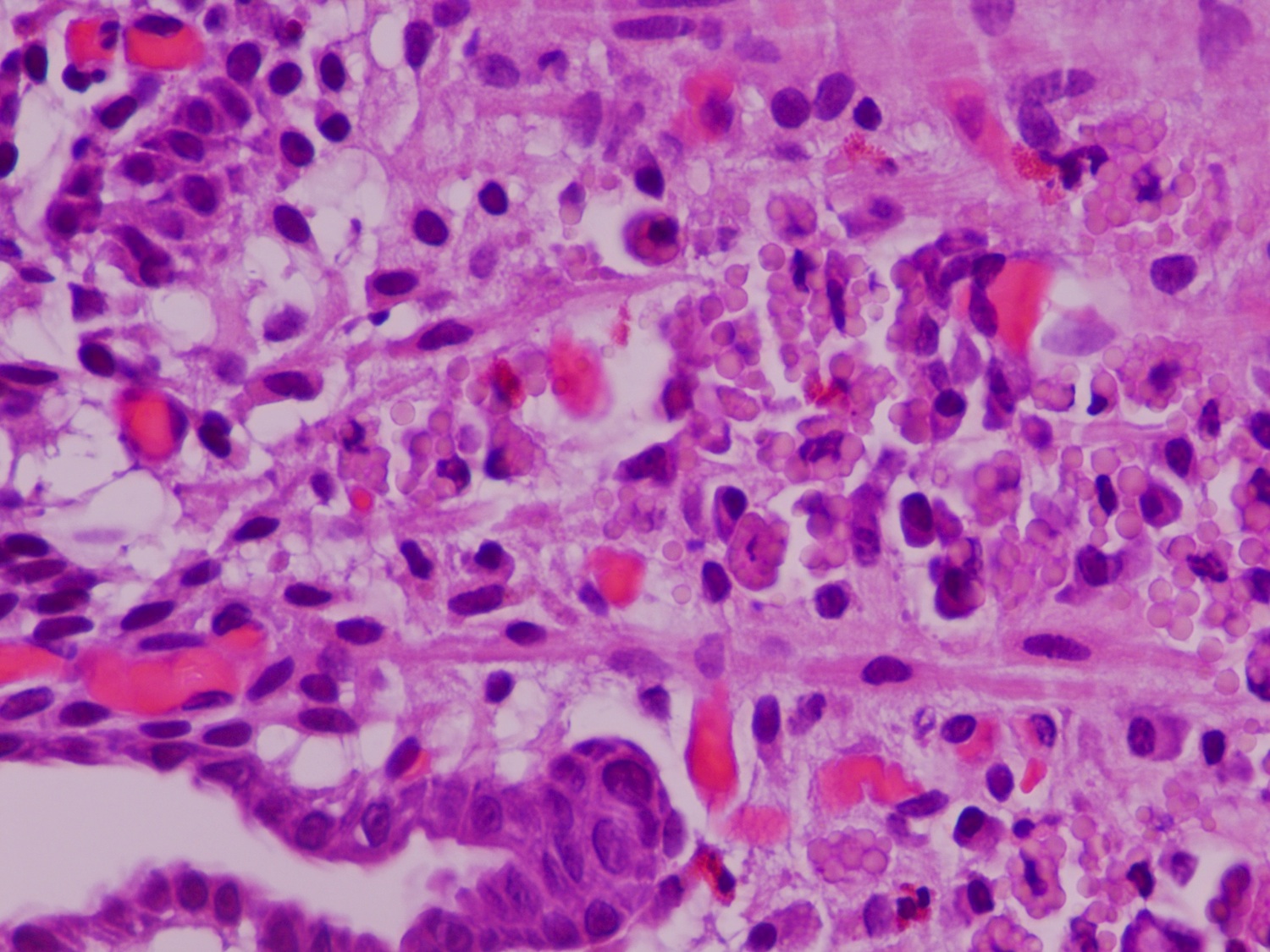
H&E
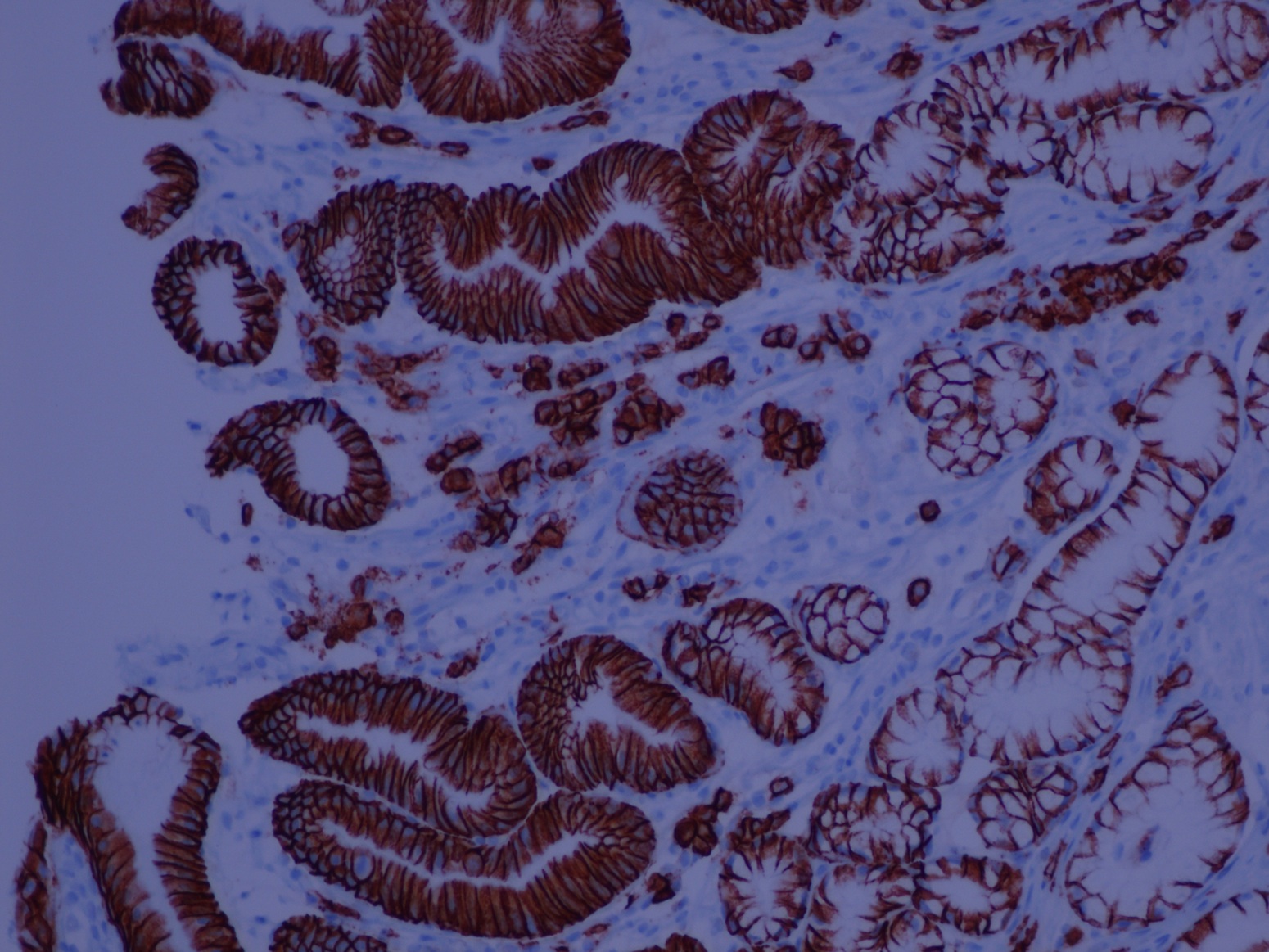
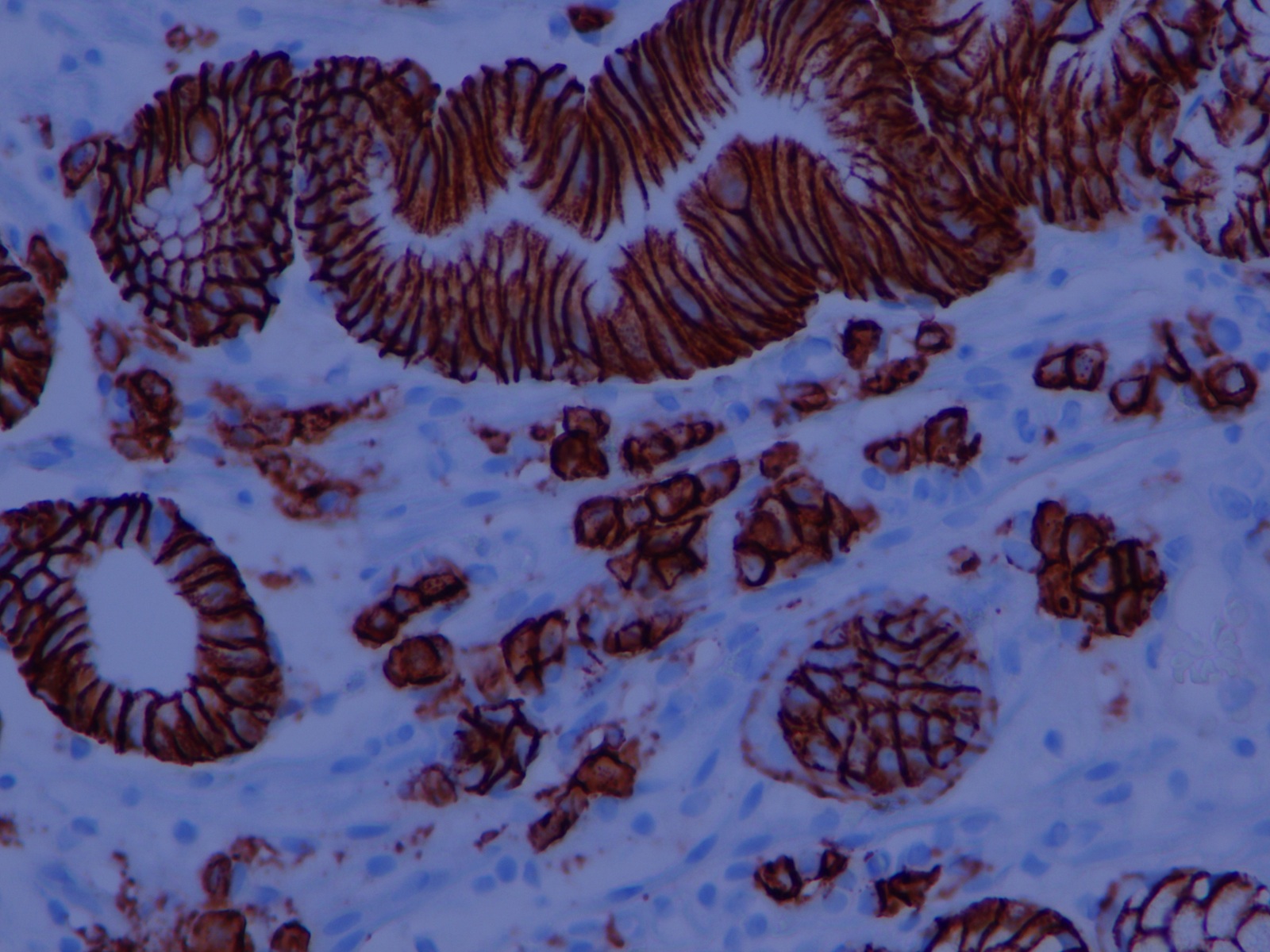
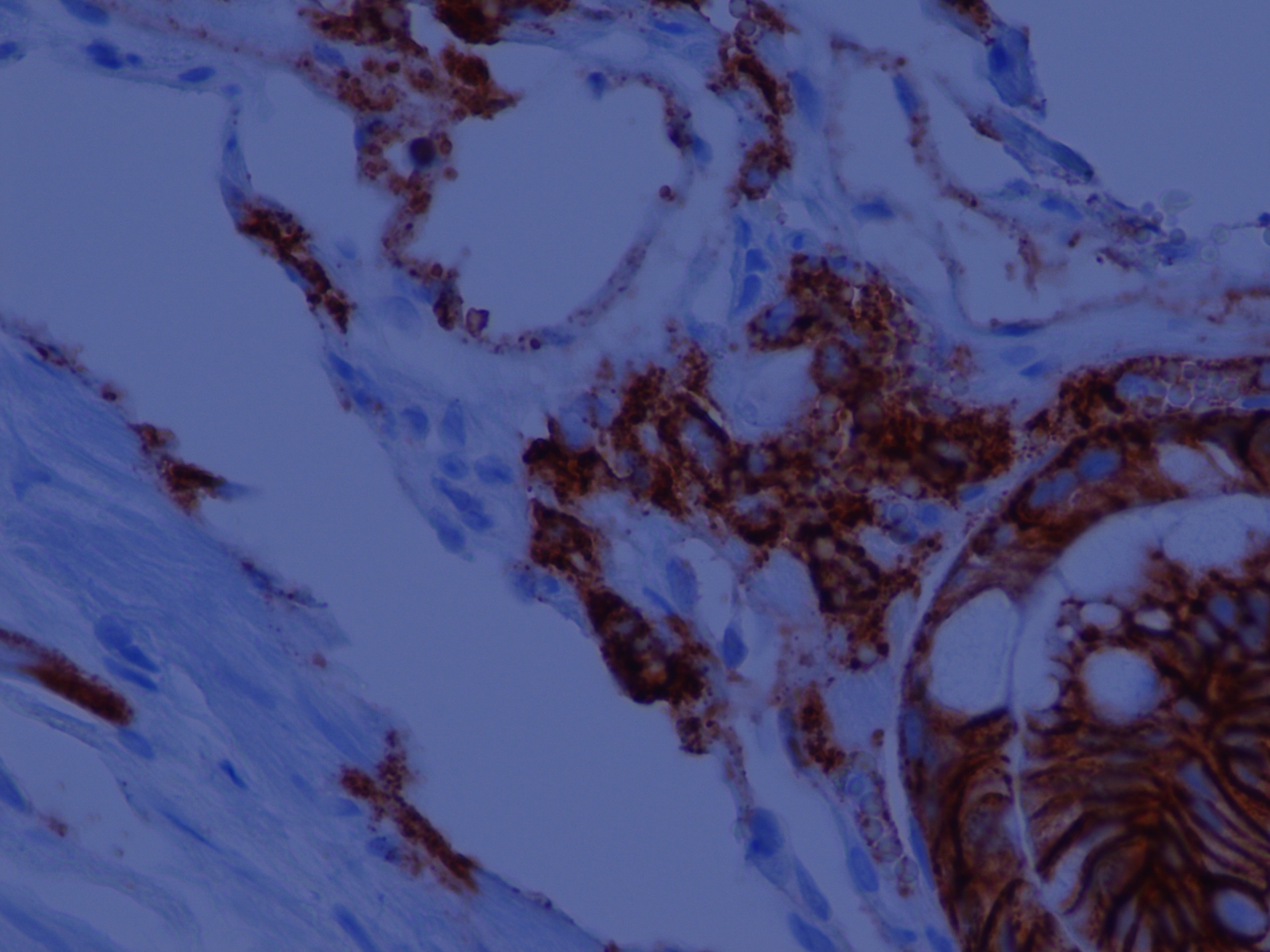
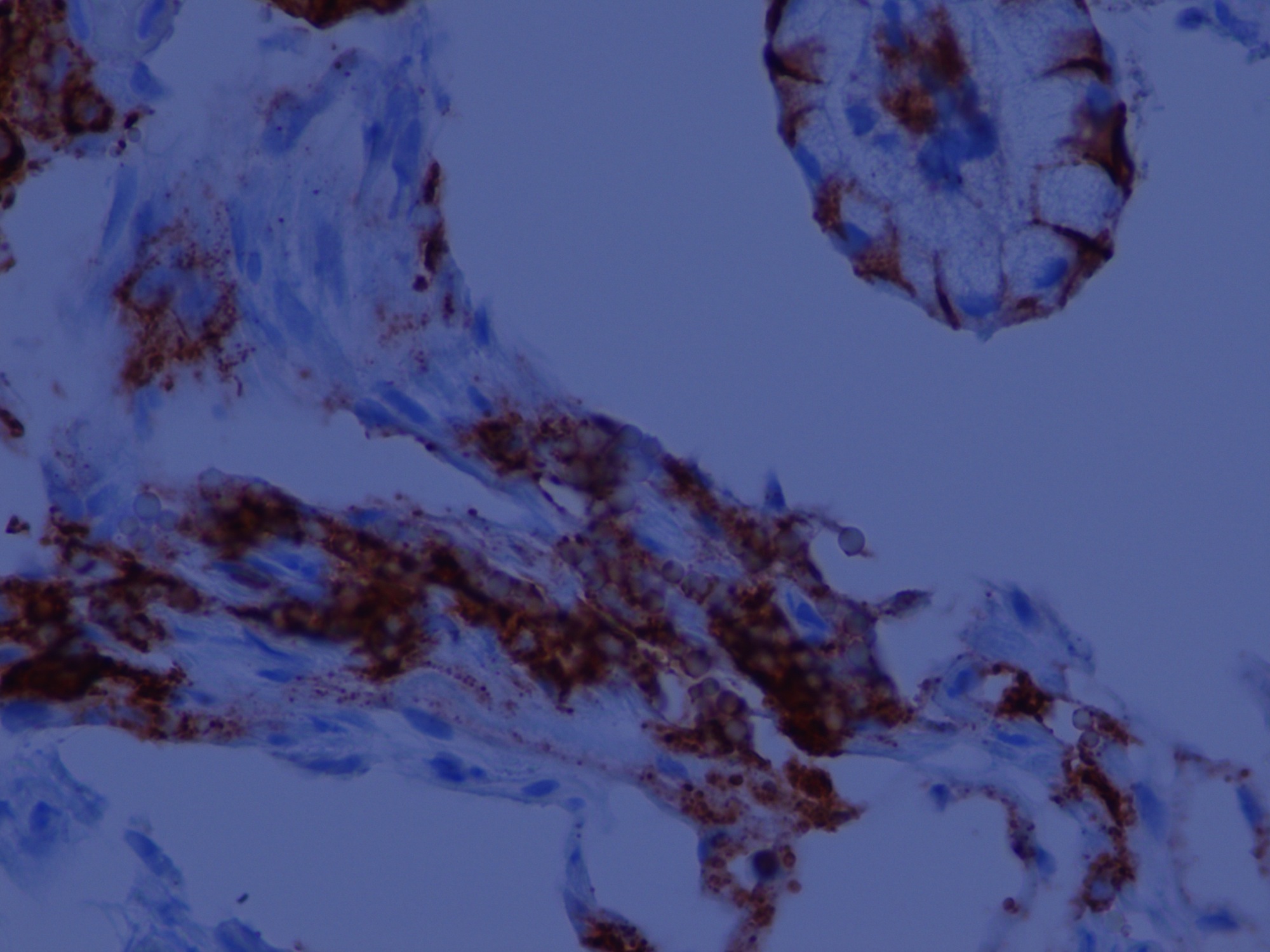
Positive for CD138 stain
Positive stains
- PAS positive; react to antibodies against polytypic light chains, CD79a and antiplasma cell antibody (Pathol Res Pract 2007;203:457)
Negative stains
Differential diagnosis

