
Stomach
Gastritis
Lymphocytic gastritis
Authors: Matthew Morrow, M.D., Raul S. Gonzalez, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 10 December 2020
Last staff update: 27 July 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Lymphocytic gastritis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Morrow M, Gonzalez RS. Lymphocytic gastritis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachlymphocyticgastritis.html. Accessed March 31st, 2025.
Definition / general
- A pattern of gastric mucosal injury characterized by increased intraepithelial lymphocytes (> 25 per 100 epithelial cells) and increased chronic inflammatory cells in the lamina propria
Essential features
- Associated with Helicobacter pylori infection and celiac disease, among other etiologies
- Variable clinical presentation
- Uncertain pathogenesis
Terminology
- The older entity “varioliform gastritis” (endoscopic mucosal appearance of small nodules with central erosions and enlarged rugal folds) appears to represent a subset of lymphocytic gastritis (J Pathol 1989;158:19)
ICD coding
- ICD-10: K52.89 - other specified noninfective gastroenteritis and colitis
Epidemiology
- Rare, with a prevalence of < 0.3% in gastric biopsies (Odze and Goldblum: Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas, 3rd Edition, 2015)
- Presents around the sixth decade of life (Am J Surg Pathol 1999;23:153)
- No sex predilection
- Common etiologic associations include celiac disease (Am J Surg Pathol 1999;23:153)
- Also associated with HIV infection, Crohn disease, Ménétrier disease, NSAIDs and lymphocytic or collagenous colitis
- Unknown etiology in up to 20% of cases (Am J Surg Pathol 1999;23:153)
- Rare in children but seen predominately with celiac disease; may suggest a more severe disease course in this setting (Pediatr Dev Pathol 2011;14:280)
Sites
- Antral predominance or diffuse involvement may be associated with celiac disease (J Clin Pathol 1999;52:815)
- Corpus predominance may be associated with H. pylori infection (Am J Surg Pathol 1999;23:153)
Pathophysiology
- Uncertain pathogenesis overall
- Due to its association with celiac disease and H. pylori, it has been proposed to be a local immune response to luminal antigens such as gliadin and Helicobacter antigens (Am J Surg Pathol 1999;23:153)
Clinical features
- Dyspepsia, abdominal pain and iron deficiency anemia have been reported but presenting symptoms are variable (Pathol Case Rev 2008;13:167)
- Predominately recurrent vomiting, epigastric pain or chronic diarrhea is seen in pediatric patients (J Pediatr 1994;124:57)
- Cases associated with endoscopic varioliform gastritis may present with weight loss and anorexia (Gut 1990;31:282)
- Cases associated with Ménétrier disease may present with protein losing enteropathy (Hum Pathol 1991;22:379)
Diagnosis
- Established by gastric biopsy
Case reports
- 2 year old child autopsy findings after presenting with hepatic failure (Ann Diagn Paed Pathol 1998;2:27)
- 47 year old woman and 57 year old man with H. pylori and associated gastric MALT lymphoma (Korean J Gastroenterol 2005;45:354)
- 63 year old man with gastric adenocarcinoma and total gastrectomy (Gut 1991;32:1565)
- 77 year old man with worsening anemia (Gastrointest Endosc 2001;54:251)
- 84 year old man with abdominal pain and varioliform gastritis seen on EGD (Ann Gastroenterol 2018;31:520)
Treatment
- Targets the underlying associated etiology
- Can spontaneously regress (Aliment Pharmacol Ther 2006;23:473)
Clinical images
Images hosted on other servers:

Varioliform gastritis:
multiple nodules with
central mucosal
atrophy / erosion
Gross description
- Small nodules with central erosions and enlarged rugal folds (“varioliform gastritis”)
- Early studies suggested this finding in 80% of cases
- Subsequent articles reported incidence of 4% to 30% (Pathol Case Rev 2008;13:167)
- Additional findings: small elevated plaques, superficial erosions, nodular appearance, thickened folds
- Unremarkable appearance in up to 50% of cases (J Clin Pathol 1995;48:939, Gut 1988;29:1258)
- Hypertrophic gastric folds has been described in cases of Ménétrier disease (Hum Pathol 1991;22:379)
Microscopic (histologic) description
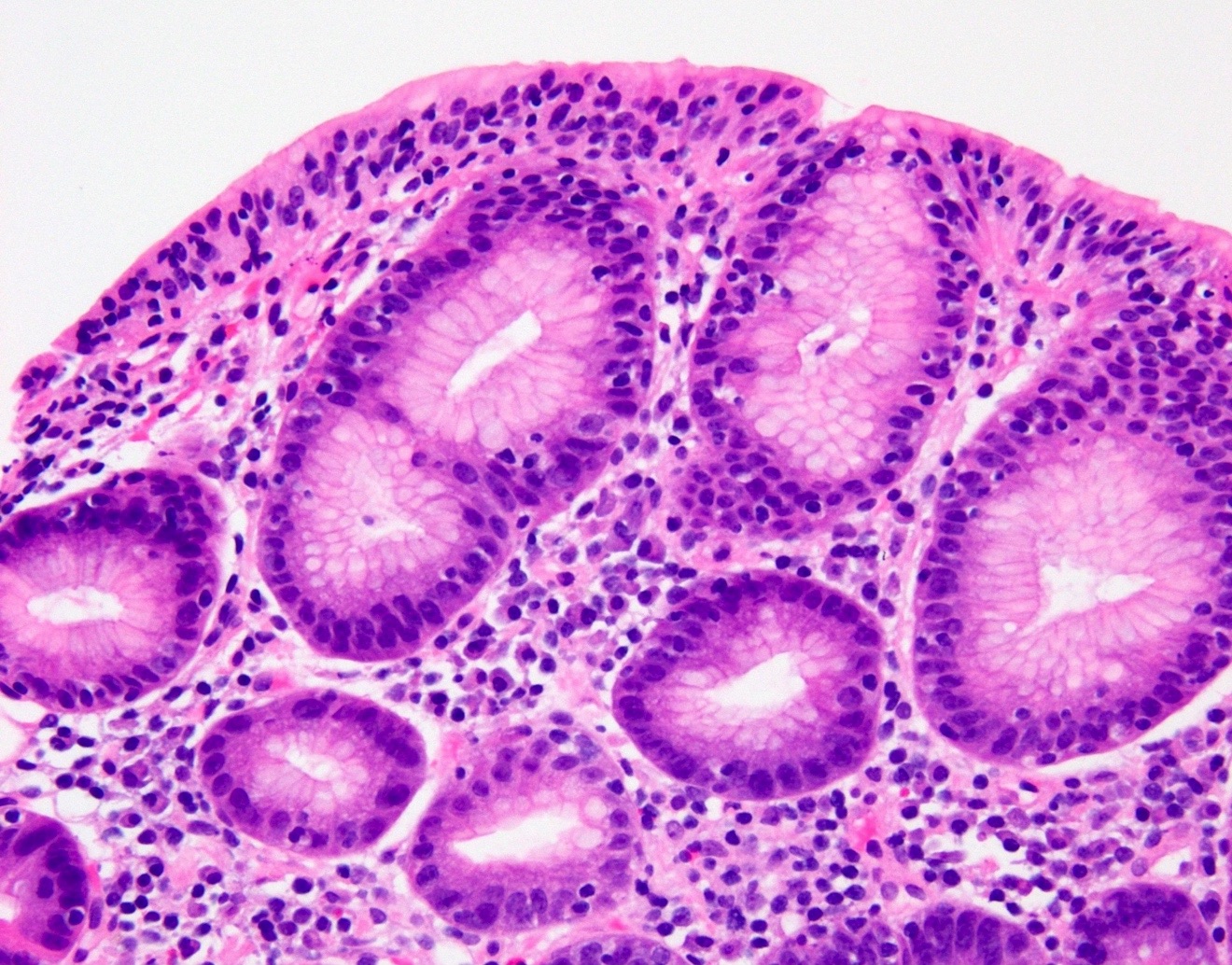
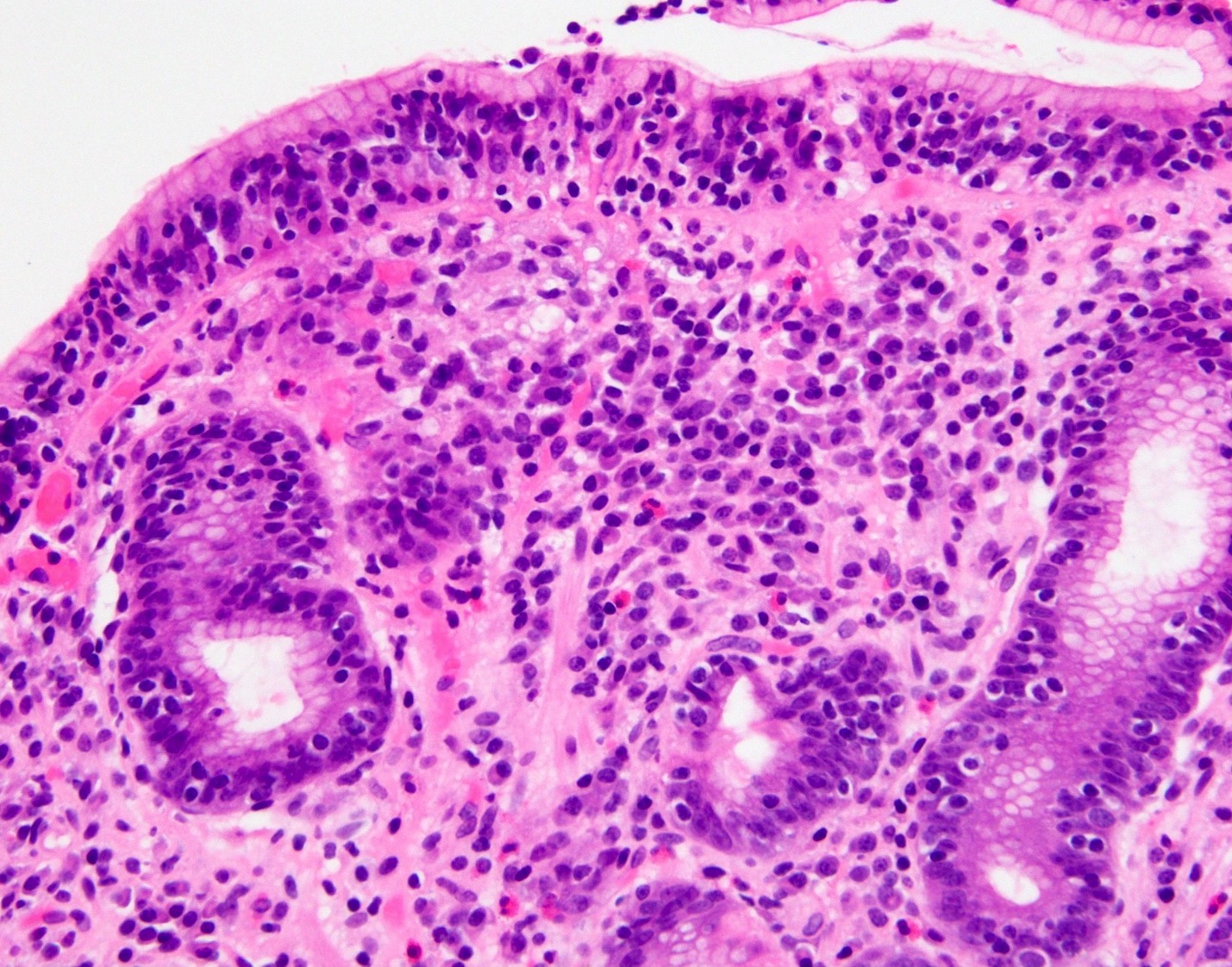
- Defined by increased gastric intraepithelial lymphocytes (> 25 per 100 epithelial cells)
- Intraepithelial lymphocytosis is typically greater in the surface epithelium
- Most cases show around 35 - 75 surface intraepithelial lymphocytes per 100 epithelial cells (Gut 1990;31:282)
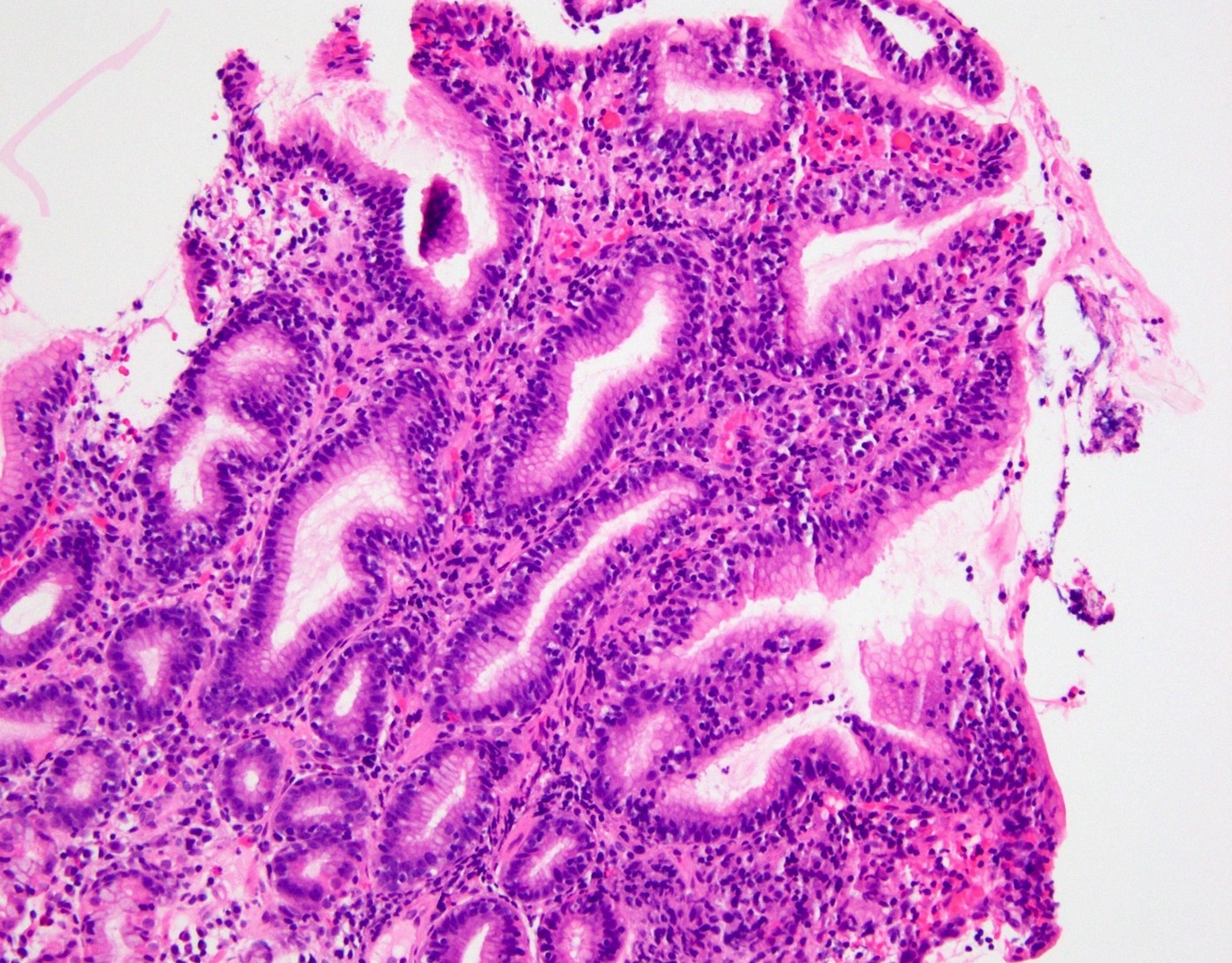
- Lymphoplasmacytic expansion of the lamina propria can be additionally seen
- Intraepithelial neutrophils may be seen, especially in the setting of H. pylori infection or mucosal erosion
- Lymphoepithelial lesions are not present
Microscopic (histologic) images
Contributed by Matthew Morrow, M.D.
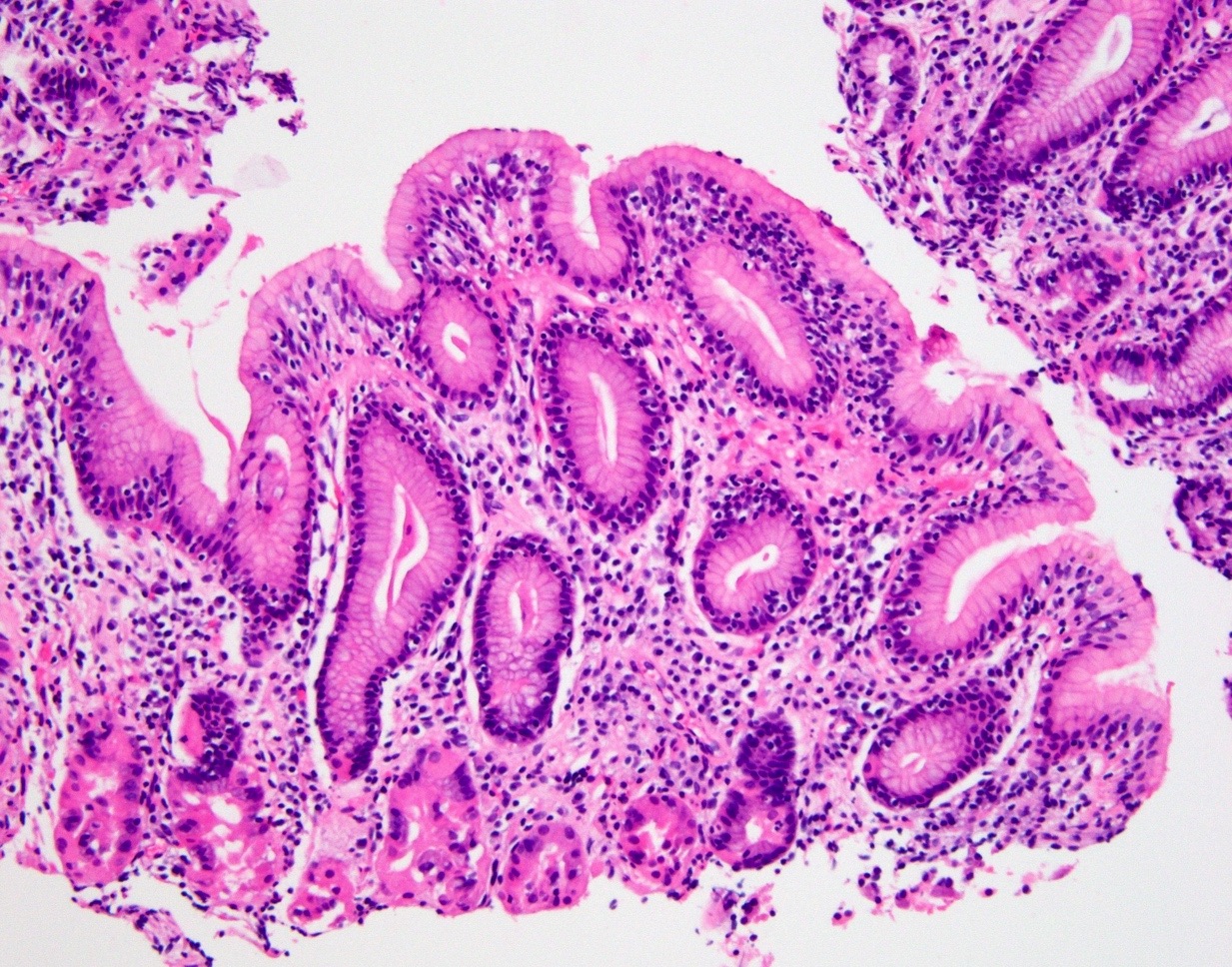
Increased intraepithelial lymphocytes
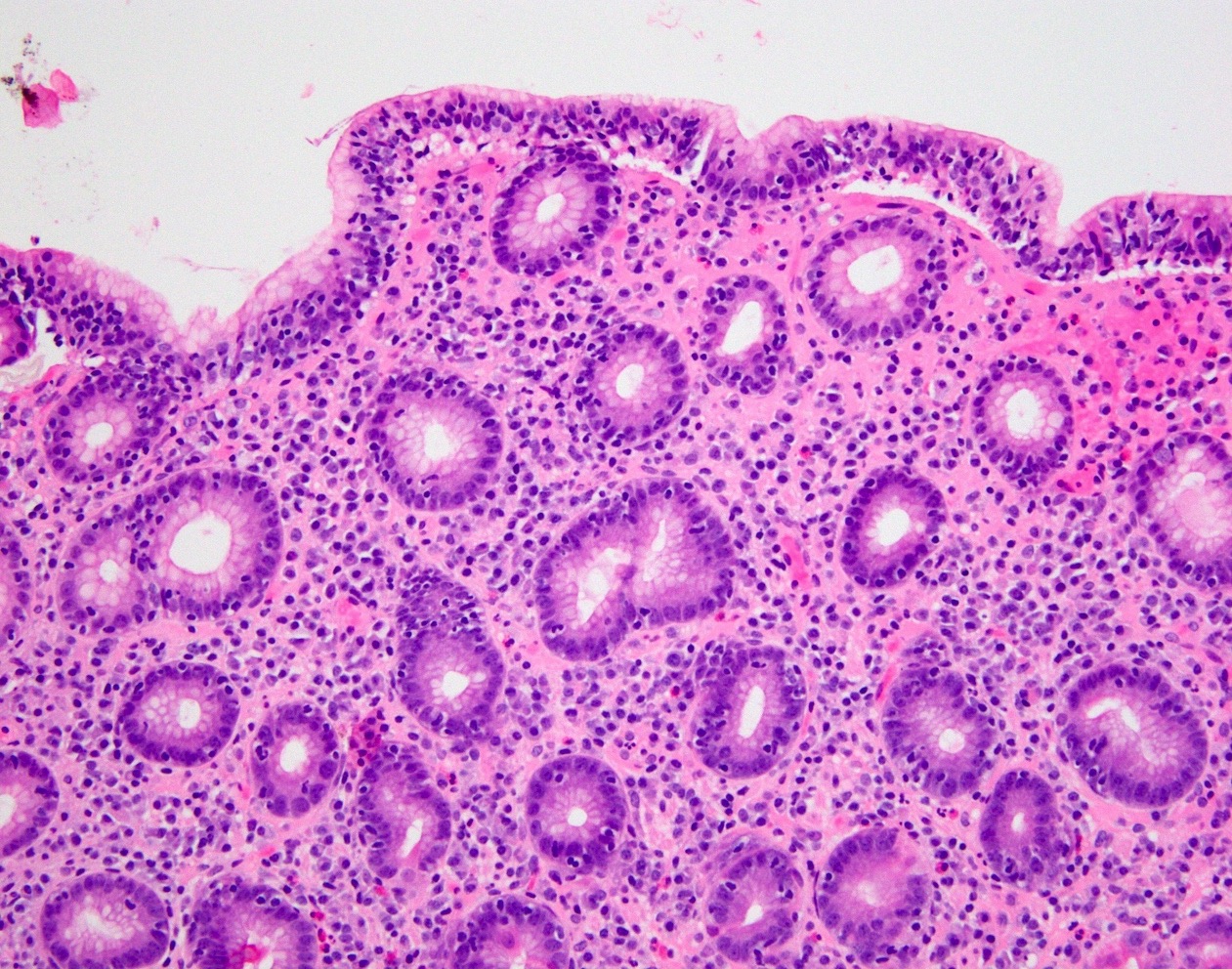
Increased intraepithelial lymphocytes, expanded lamina propria
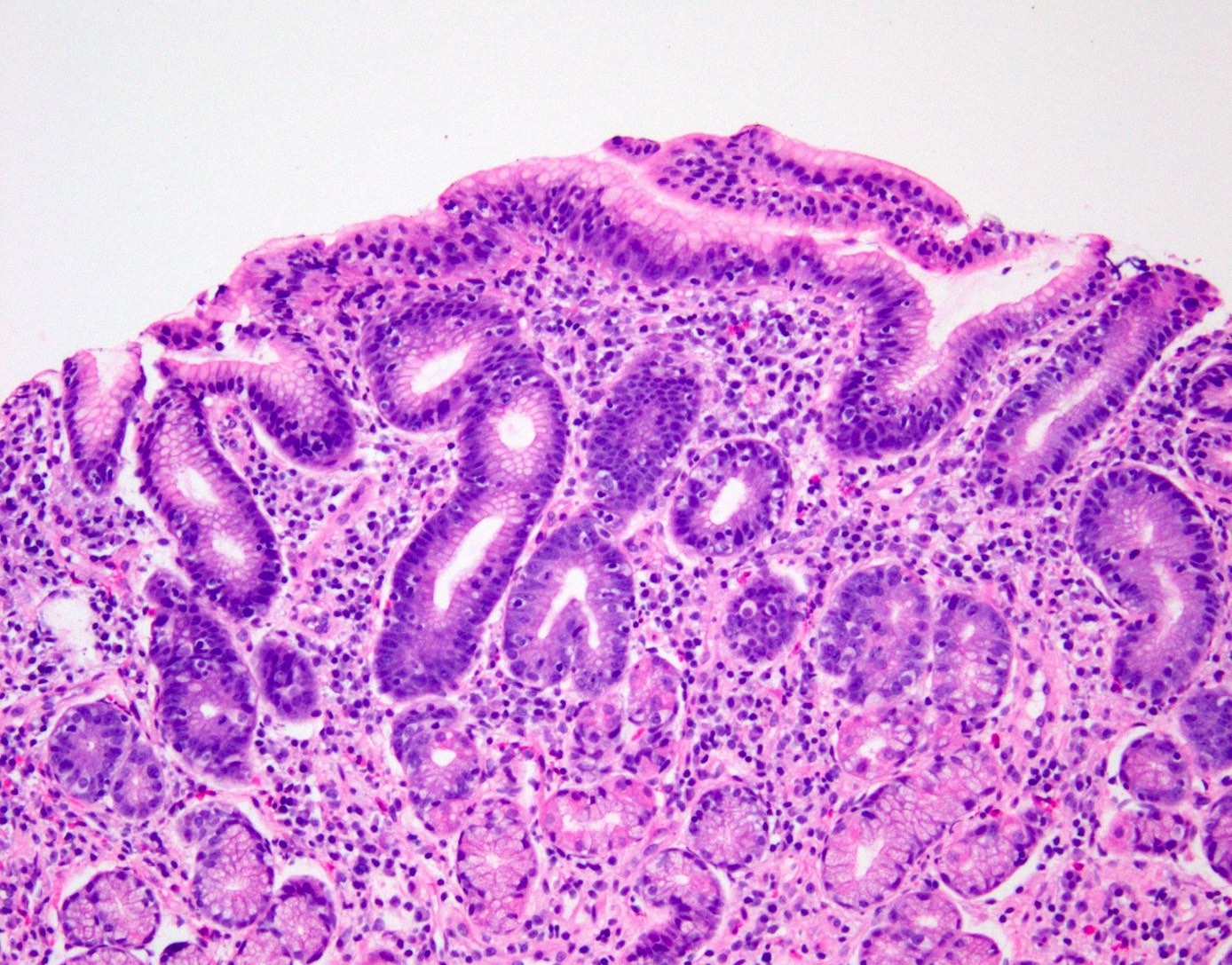
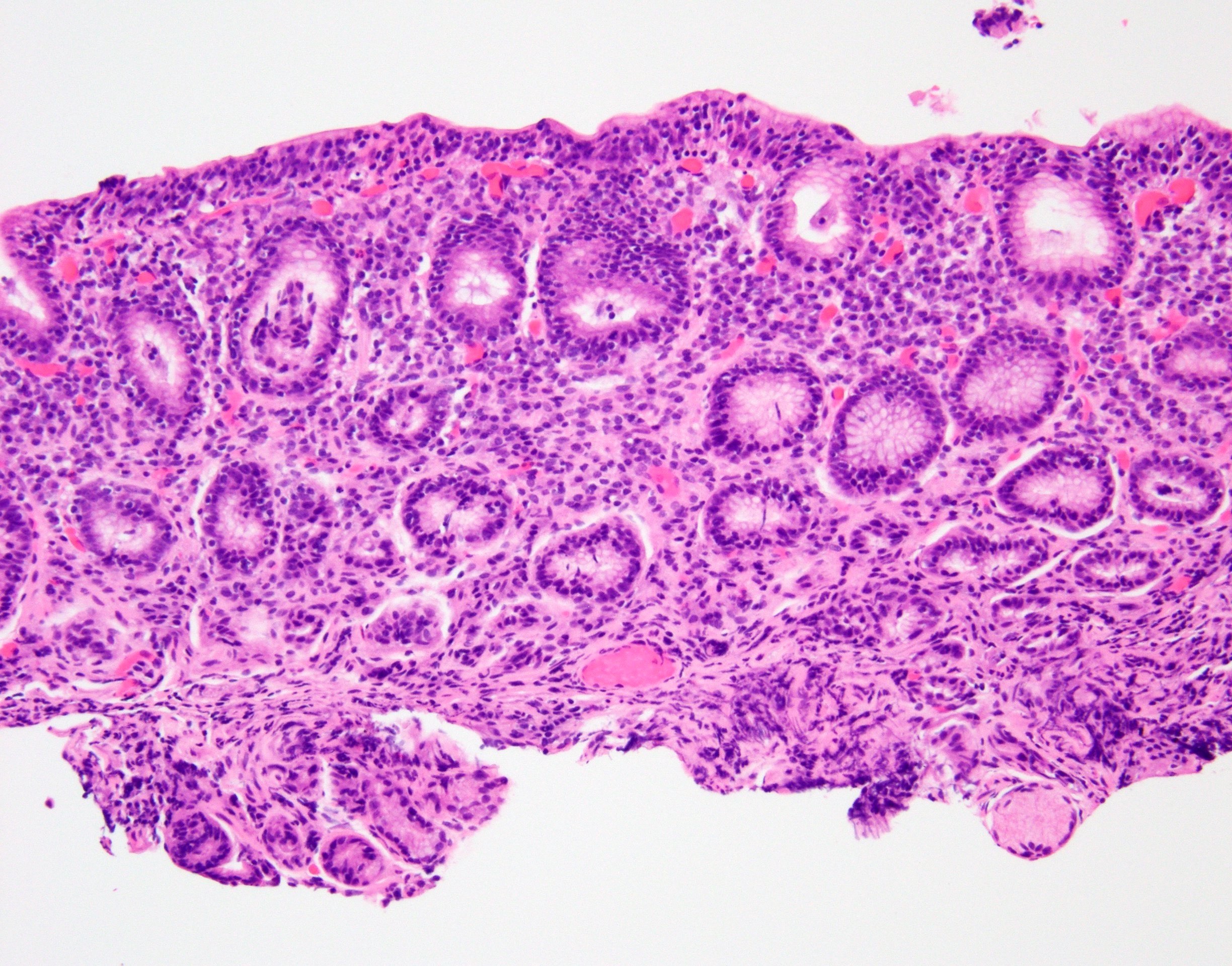
Biopsy from area of nodular gastric mucosa
Contributed by @RaulSGonzalezMD on Twitter
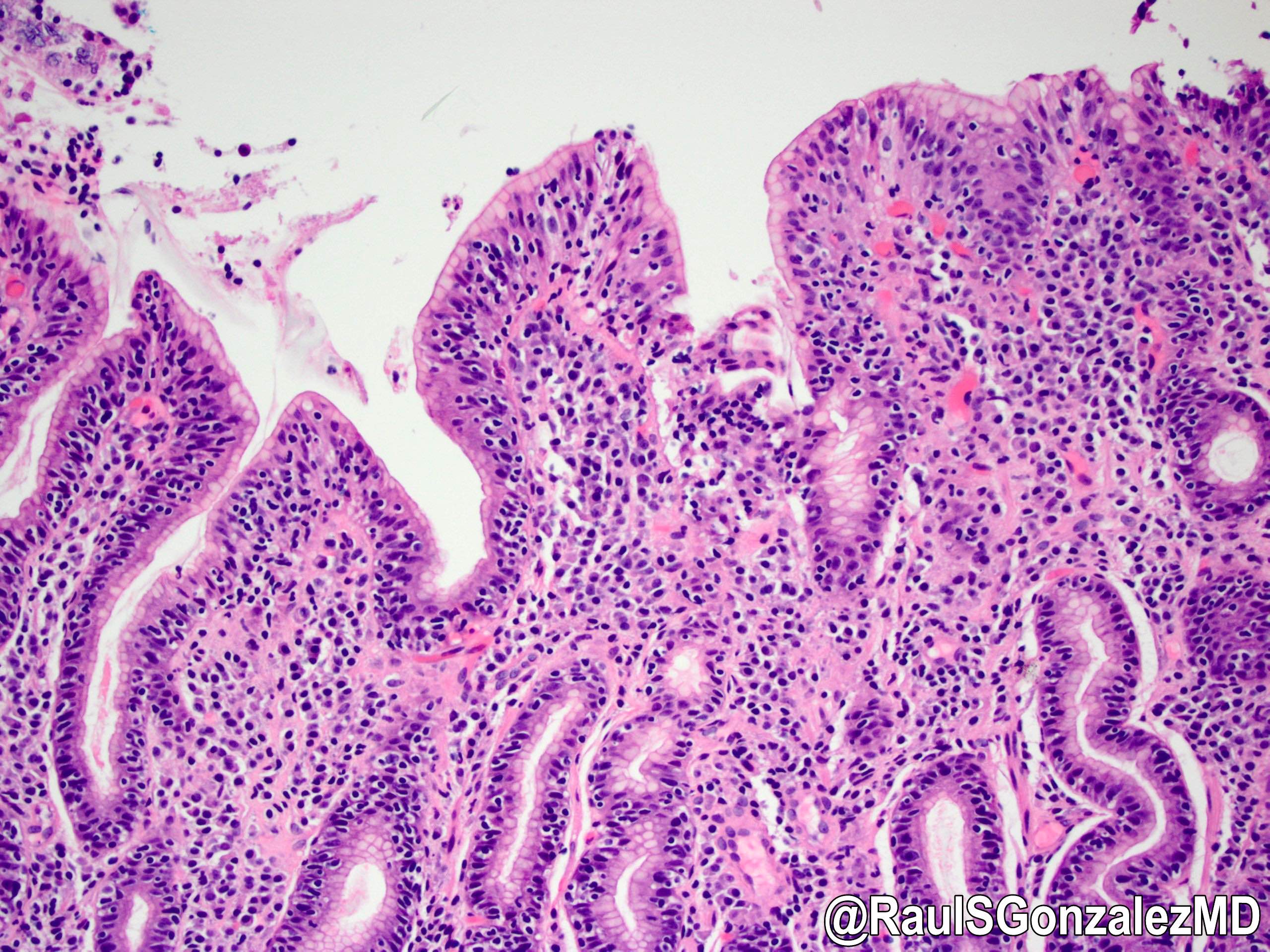
Lymphocytic gastritis
Sample pathology report
- Stomach, biopsy:
- Corpus and antral mucosa with chronic inactive gastritis with increased intraepithelial lymphocytes (see comment)
- Immunostain for Helicobacter species is negative
- Comment: The finding of intraepithelial lymphocytosis is consistent with lymphocytic gastritis, which may be associated with celiac disease, H. pylori gastritis, viral infection, Crohn disease, certain medications and other etiologies
Differential diagnosis
- Gastric lymphoma
- Often causes a mass lesion, unlike lymphocytic gastritis
- Patchy increased intraepithelial lymphocytes can be seen in MALT lymphoma (Korean J Pathol 2007;41:289)
- Lymphocytes in MALT lymphoma are CD20+ B cells
- Lymphoma may display an infiltrative pattern with lymphoepithelial lesions and architectural distortion
- Cytologic atypia may be present
- Helicobacter pylori gastritis
- Curved slender bacteria present in the superficial mucus layer and along the surface of gastric epithelial cells
- Neutrophils and germinal centers may be seen
- Chronic gastritis, such as mononuclear expansion of the lamina propria seen in lymphocytic gastritis, should prompt scrutiny for Helicobacter organisms
- Helicobacter immunostain, Giemsa and silver stains highlight organisms
Additional references
Board review style question #1
- The image above is from an antral biopsy from a 9 year old boy. What additional histological finding is most likely to be present in this patient?
- Increased intraepithelial eosinophils with eosinophilic microabscesses in the upper esophagus
- Curved bacteria rods present in the superficial mucus layer of the stomach
- Duodenal increased intraepithelial lymphocytes, crypt hyperplasia and villous blunting
- Duodenal villous blunting, crypt hyperplasia and focal surface epithelial “tufting”
Board review style answer #1
C. Lymphocytic gastritis is most commonly seen in a background of celiac disease in children (intraepithelial lymphocytes, crypt hyperplasia and villous blunting in the duodenum) and may portend a more severe disease course. Helicobacter infection (choice B) would be more likely in an adult patient.
Comment Here
Reference: Lymphocytic gastritis
Comment Here
Reference: Lymphocytic gastritis
Board review style question #2
Aside from increased intraepithelial lymphocytes, what other histologic feature in the stomach is commonly described in lymphocytic gastritis?
- Lymphoepithelial lesions
- Lymphoplasmacytic expansion of the lamina propria
- Loss of parietal cells
- Increased subepithelial collagen deposition
Board review style answer #2
B. Lymphoplasmacytic expansion of the lamina propria is also commonly seen in lymphocytic gastritis.
Comment Here
Reference: Lymphocytic gastritis
Comment Here
Reference: Lymphocytic gastritis
