
Stomach
Polyps
Hyperplastic polyp
Editorial Board Member: Maryam Kherad Pezhouh, M.D., M.Sc.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 8 September 2023
Last staff update: 8 September 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Stomach hyperplastic polyp
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Aljuboori O, Garcia-Buitrago MT. Hyperplastic polyp. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachhyperplastic.html. Accessed March 28th, 2025.
Definition / general
- The second most common gastric epithelial polyp encountered during endoscopy
- Usually a solitary polyp, commonly found in gastric antrum
- Associated with autoimmune type gastritis, Helicobacter pylori gastritis, postsurgery and bile reflux gastritis (Am J Surg Pathol 2001;25:500, Am J Surg Pathol 2010;34:1591)
- Usually < 1 cm, more than 50% are < 0.5 cm; large polyps up to 12 cm can occur and mimic malignancy
- Dysplasia is more likely when > 1 cm and > 2.5 cm (Gut Liver 2009;3:271, GE Port J Gastroenterol 2021;28:328)
- Resembles other GI dysplasia, either low grade or high grade
Essential features
- Surface epithelium derived polyp
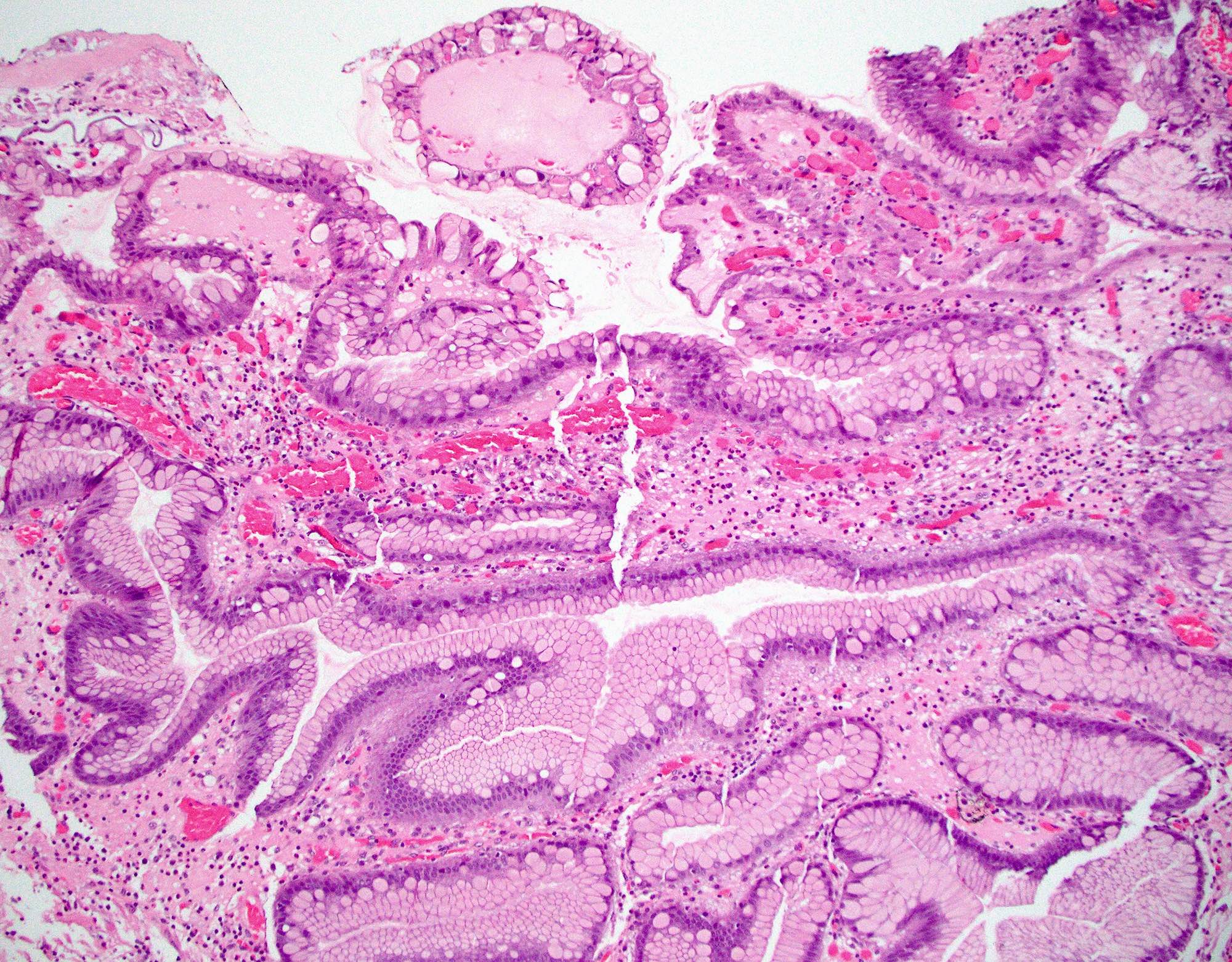
- Elongated and architecturally distorted, irregular foveolar epithelium with cystic dilatations
- Corkscrew appearance can occur
- Lamina propria shows edema, congestion, variable acute and chronic inflammation
- Smooth muscle strands can be seen extending from muscularis mucosae towards surface
- Thick walled vessels may be present towards the base of the polyp
Terminology
- Synonyms: regenerative polyp and hyperplasiogenous polyp (Tohoku J Exp Med 1984;142:125)
ICD coding
- ICD-10: K31.7 - polyp of stomach and duodenum
Epidemiology
- Second most common gastric polyp in adults, accounting for 17% of gastric polyps (Histopathology 2021;78:106, Am J Gastroenterol 2009;104:1524)
- This could be due to increasing use of proton pump inhibitors and detection of fundic gland polyps (World J Gastroenterol 2016;22:8883, Dig Dis Sci 2009;54:1839, Arq Gastroenterol 2007;44:14)
- Most common polyp among children, representing 42% of gastric polyps (Histopathology 2021;78:106)
- M = F; age range: 20 - 80 years, peaks in sixth and seventh decades (World J Gastroenterol 2016;22:8883)
- Usually solitary, can be multiple in 20% of cases, commonly in atrophic gastritis (Histopathology 2021;78:106, Diagn Histopathol 2021;27:75)
- If multiple, must rule out juvenile polyposis, Peutz-Jeghers or familial adenomatous polyposis (FAP) syndromes (Surg Pathol Clin 2020;13:431)
- > 50 polyps suggests gastric polyposis syndrome, an entity not well established by diagnostic criteria (J Clin Diagn Res 2012;6:1428)
- Dysplasia occurs in 2 - 19% (Int J Surg Pathol 2016;24:704, GE Port J Gastroenterol 2021;28:328)
- Risk increases with age and polyp size
- Polyps > 1 - 2.5 cm, presence of intestinal metaplasia and pedunculated in shape and age, particularly if > 50 years
- Carcinoma reported in 0.6 - 2.1% (Int J Surg Pathol 2016;24:704, GE Port J Gastroenterol 2021;28:328)
Sites
- Common site is gastric antrum but can occur anywhere in the stomach; recently body of the stomach has become more common due to autoimmune gastritis and the increased use of proton pump inhibitors (Am J Gastroenterol 2009;104:1524, Int J Mol Sci 2021;22:6548)
- Hyperplastic polyps in pyloric and prepyloric regions may have features of prolapse associated polyps
- Hyperplastic polyps at gastroesophageal junction are associated with Barrett esophagus in 33% of cases (Am J Surg Pathol 2011;35:1038)
Pathophysiology
- Excessive proliferation of foveolar cells lining the surface and pits accompanied by increased exfoliation in response to longstanding mucosal injury (World J Gastroenterol 2016;22:8883, Surg Pathol Clin 2020;13:431)
Etiology
- Associated with underlying gastritis
- Helicobacter pylori associated chronic gastritis (25%) (Histopathology 2021;78:106)
- Reactive gastropathy (chemicals, drugs, bile reflux) (21%) (Histopathology 2021;78:106)
- Autoimmune gastritis (12%) (World J Gastroenterol 2016;22:8883)
- Association with gastric antral vascular ectasia and cytomegalovirus gastritis has also been reported (Histopathology 2021;78:106)
- Helicobacter pylori CagA protein expression can lead to development of hyperplastic polyps (Am J Gastroenterol 2009;104:1524, Proc Natl Acad Sci USA 2008;105:1003)
- CagA can cause aberrant activation of human oncoprotein SHP2 in stomach (Proc Natl Acad Sci USA 2008;105:1003)
Clinical features
- Mean age: 65 years
- In the last decade, patients aged 45 - 59 had twice as many gastric polyps as 10 years ago (World J Gastroenterol 2016;22:8883)
- Dyspepsia, heartburn and abdominal pain; patients may have anemia due to upper gastrointestinal bleeding (Dig Dis Sci 2007;52:105)
- Obstructive symptoms if near pylorus or gastroesophageal junction
Diagnosis
- Histopathology
Case reports
- 55 year old woman with malignant transformation of gastric hyperplastic polyp (BMC Gastroenterol 2016;16:130)
- 60 year old man with a history of hematemesis and epigastric pain who was found to have a giant gastric hyperplastic polyp (Radiol Case Rep 2021;17:355)
- 70 year old woman with melena found to have a adenocarcinoma arising in a hyperplastic polyp (AIM Clinical Cases 2022;1:e210041)
- 75 year old man with abdominal pain and constipation found to have inverted hyperplastic polyp (Exp Ther Med 2022;25:6)
Treatment
- Management of hyperplastic polyps is determined by the size and presence or absence of dysplasia
- Endoscopic mucosal resection for polyps > 1 cm or symptomatic, with annual follow up if dysplasia is found (Histopathology 2021;78:106)
- Since dysplasia suggests background chronic mucosal injury, close follow up is needed to rule out dysplasia elsewhere in stomach (Gastroenterol Rep (Oxf) 2016;4:158)
- Eradication of H. pylori infection; 71% regress after resolution of H. pylori infection (StatPearls: Gastric Polyp [Accessed 24 August 2023], Ann Intern Med 1998;129:712, Eur J Gastroenterol Hepatol 1999;11:727)
- 50% recur after resection by endoscopy
Gross description
- Broad based polyp with smooth lobulated contour (Surg Pathol Clin 2020;13:431)
- Surface erosion may occur in large polyps
- Should be submitted entirely to rule out dysplasia or malignancy
Microscopic (histologic) description
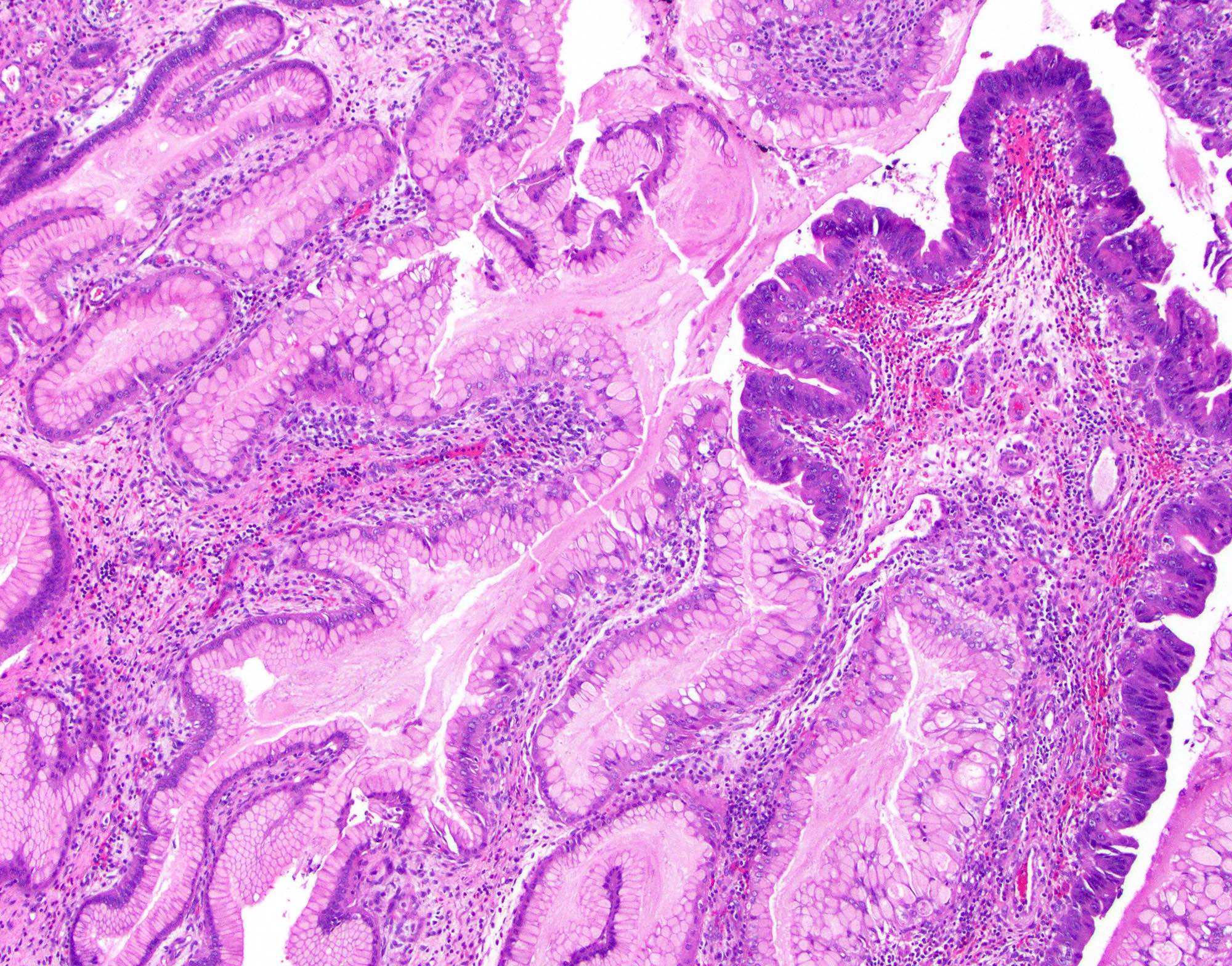
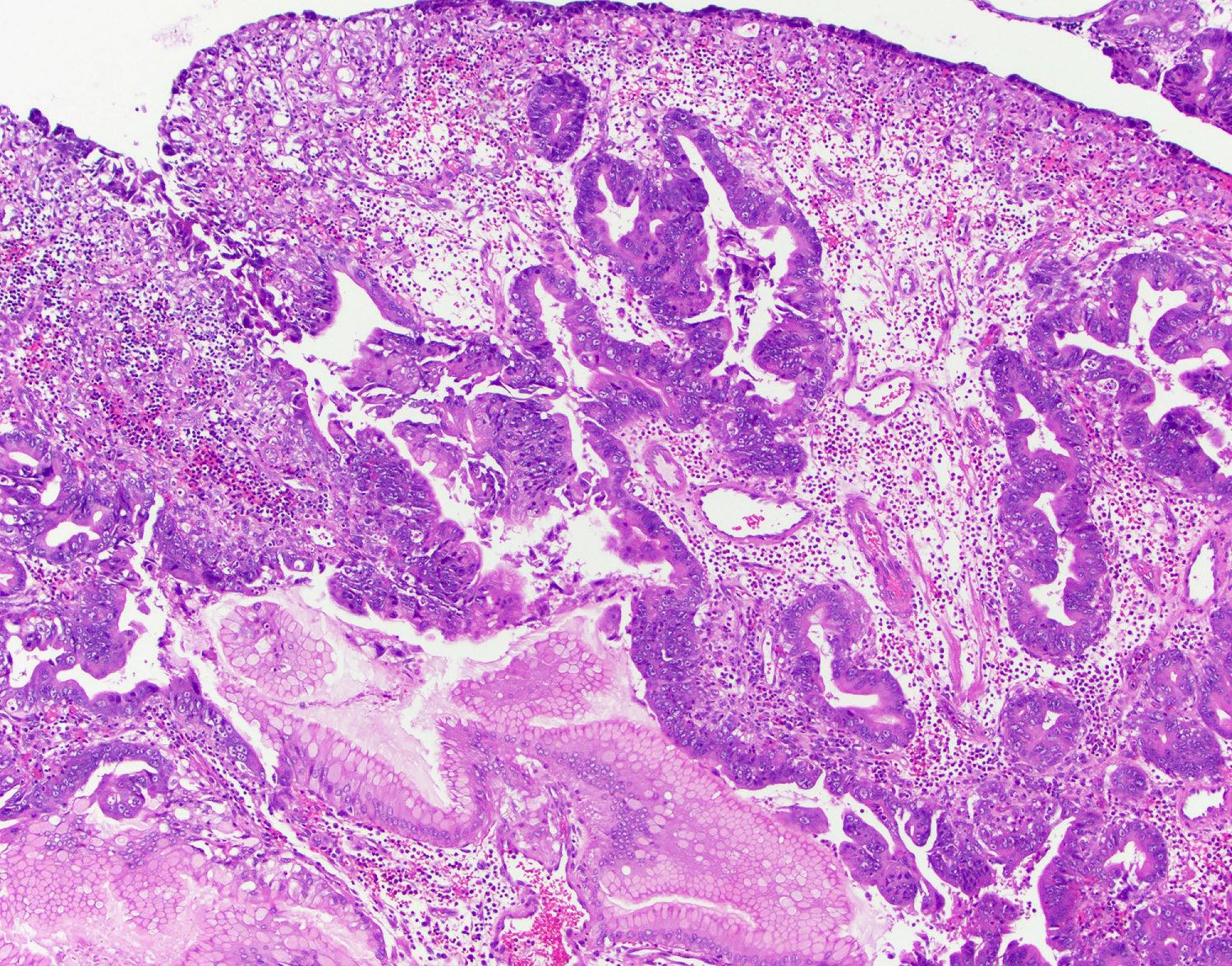
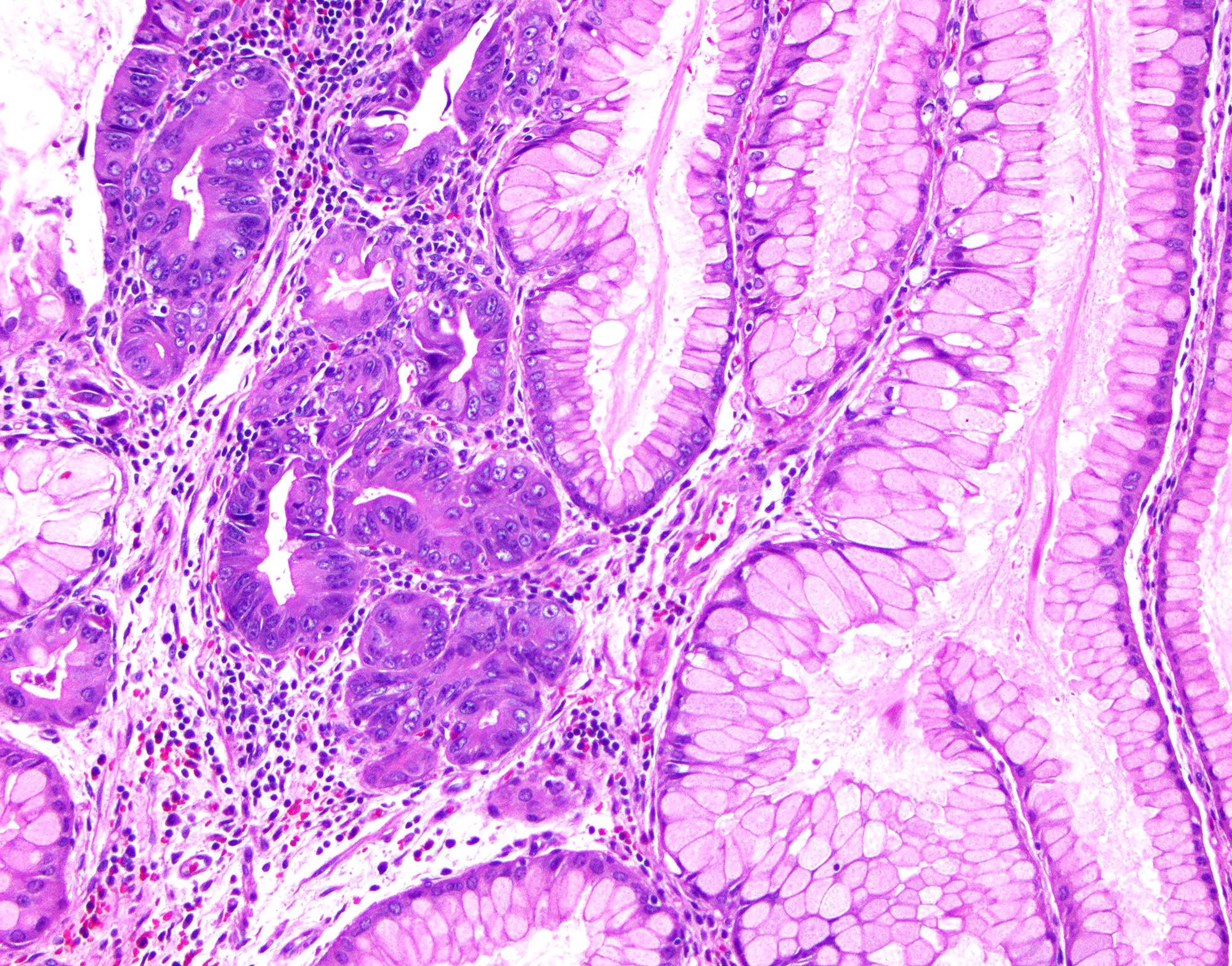
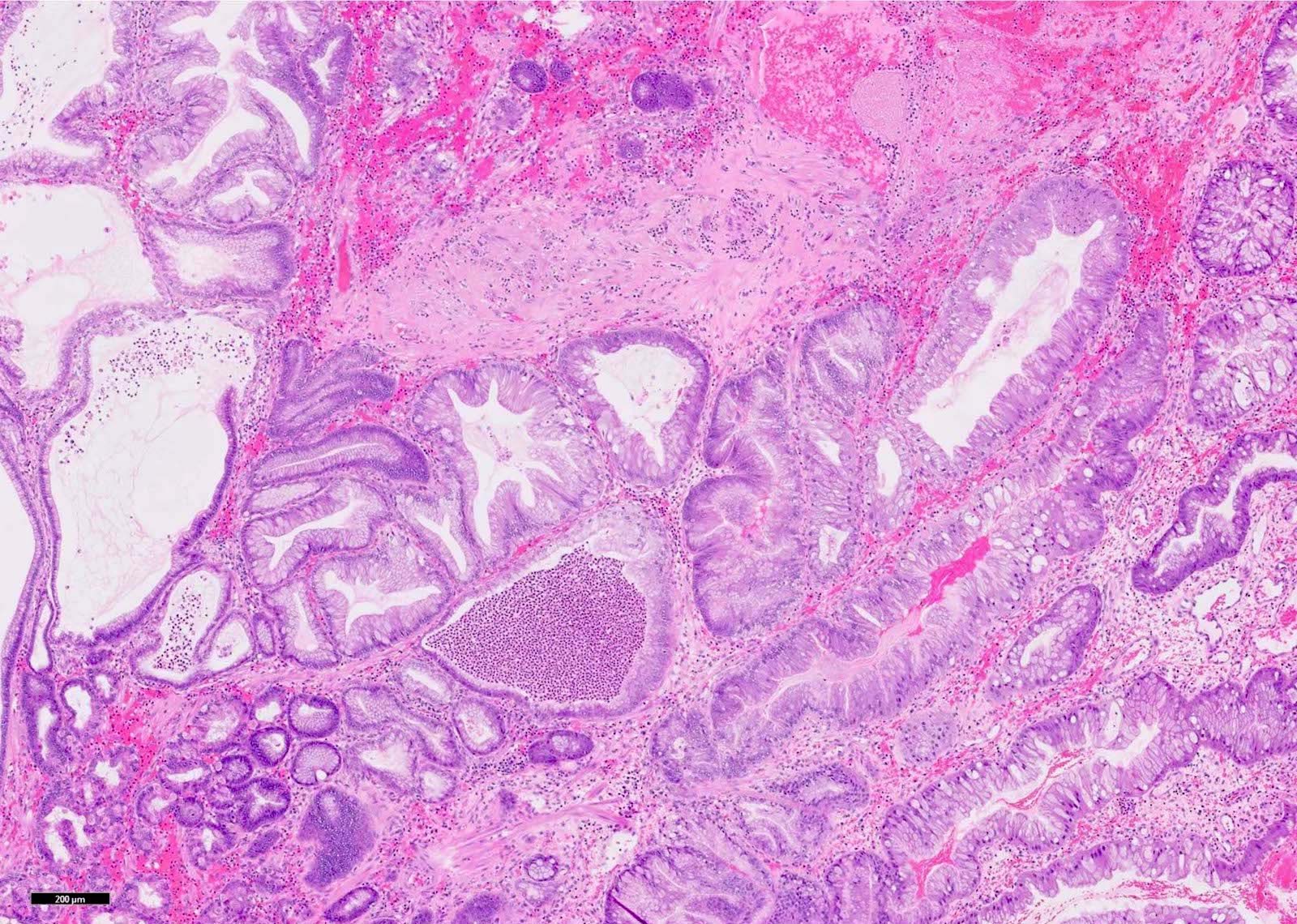
- Elongated, architecturally distorted, irregular pits with outpouchings, cystic dilation and papillary formation
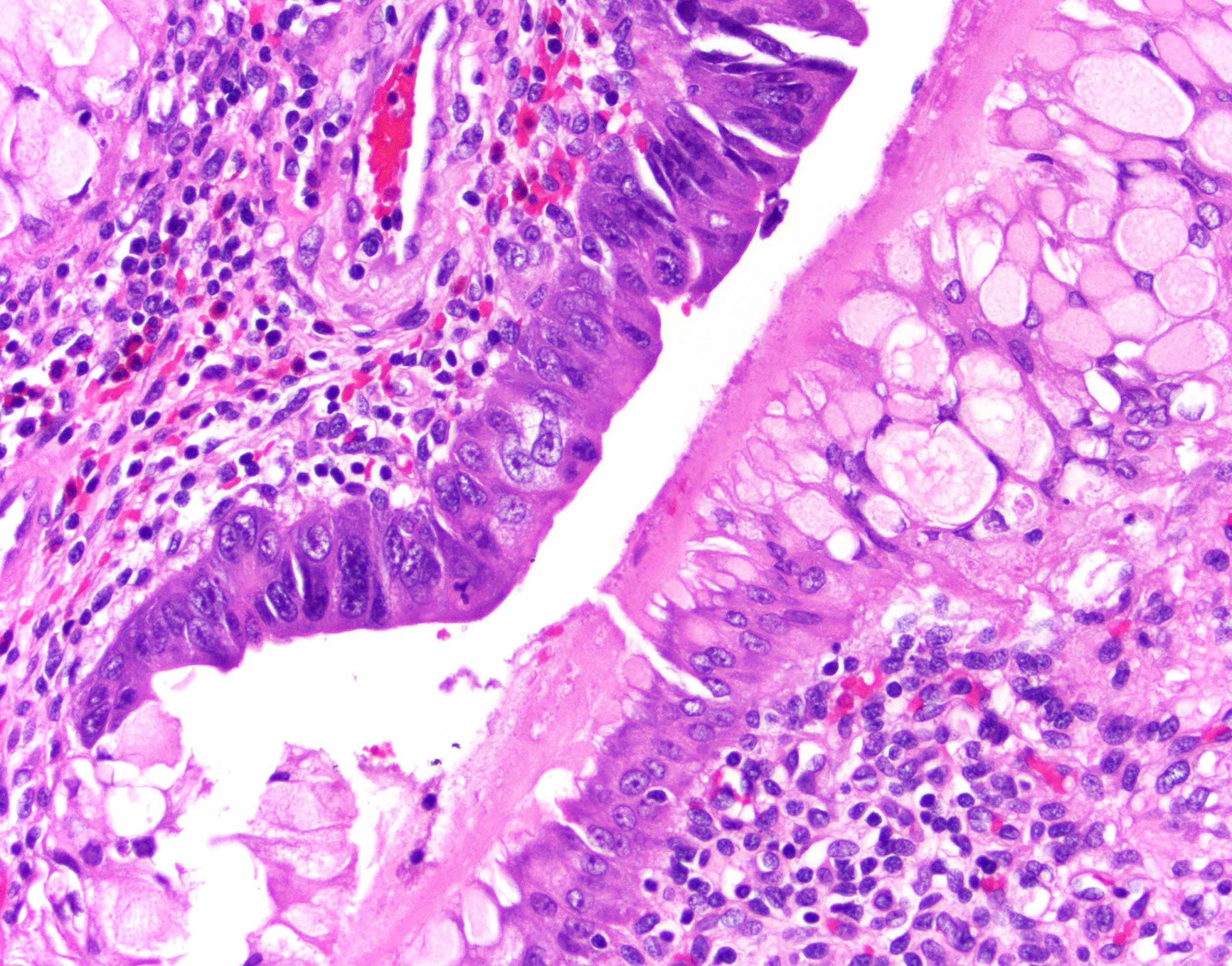
- Foveolar epithelium with apical neutral mucin cap
- Can show overt hypertrophic features with the formation of clustered pseudogoblet cells or even pseudo-signet ring cells, especially in damaged areas
- Edematous lamina propria with lymphocytes, plasma cells and eosinophils
- Erosion areas can also show neutrophils
- Helicobacter pylori associated polyps: more likely show lymphoplasmacytic inflammation in lamina propria and neutrophils in the epithelium (Int J Surg Pathol 2016;24:704)
- Smooth muscle strands can extend from muscularis mucosae to the surface
- Thick walled blood vessels can be seen at the base
- Intestinal metaplasia can be seen
- Regenerative epithelial changes with focal mucin depletion, prominent nucleoli and hyperchromasia
- Ulcerated areas can display increased mitotic activity in epithelium and granulation tissue with reactive fibroblasts and endothelial cells
- Dysplasia is rare (4%); may be intestinal, foveolar or mixed (Histopathology 2021;78:106)
- High grade dysplasia: complex architecture with cribriform formation or budding, back to back arrangement of glands
Microscopic (histologic) images
Contributed by Monica T. Garcia-Buitrago, M.D., Omar Aljuboori, M.B.B.S. and Andrey Bychkov, M.D., Ph.D.
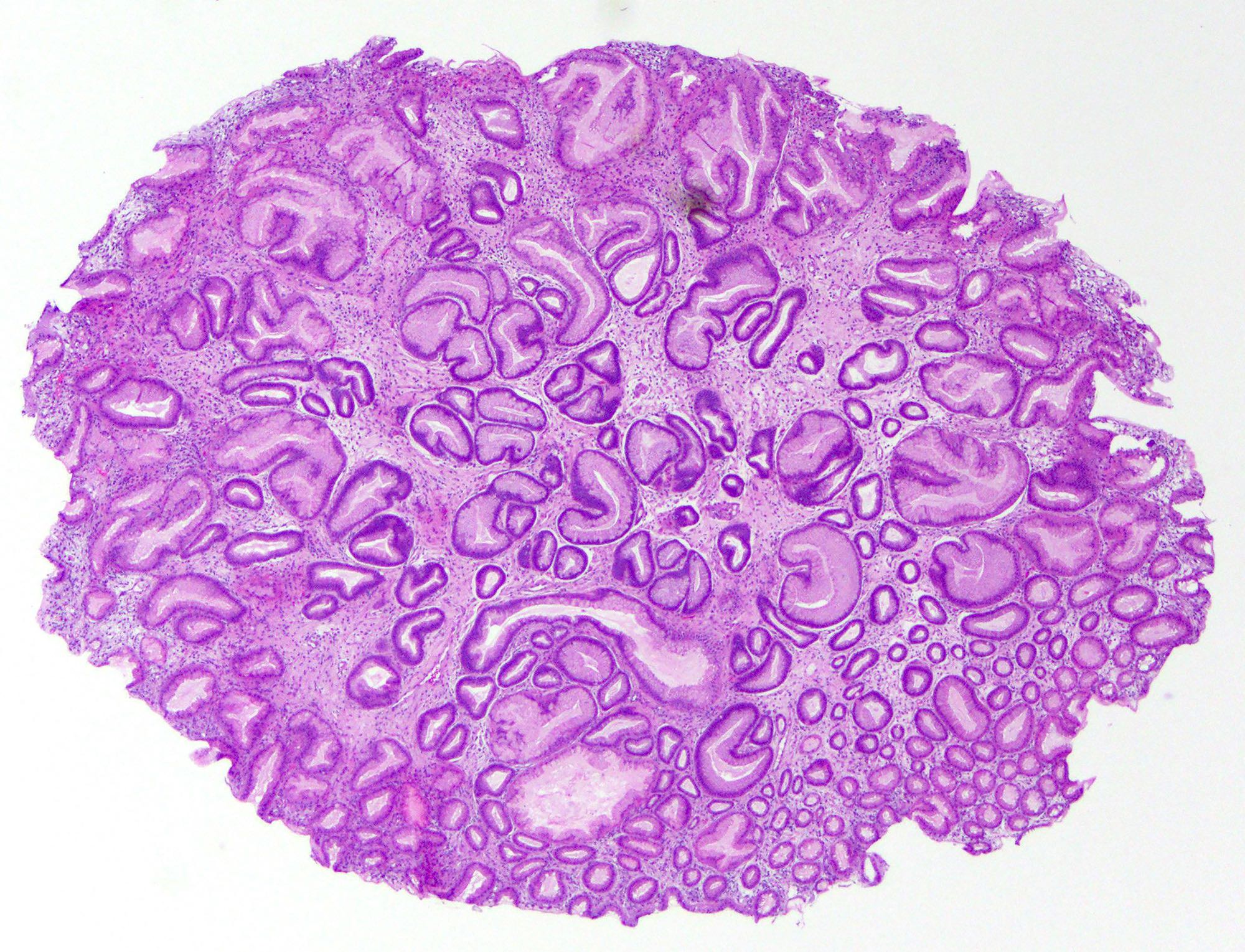
Dilated gastric pits
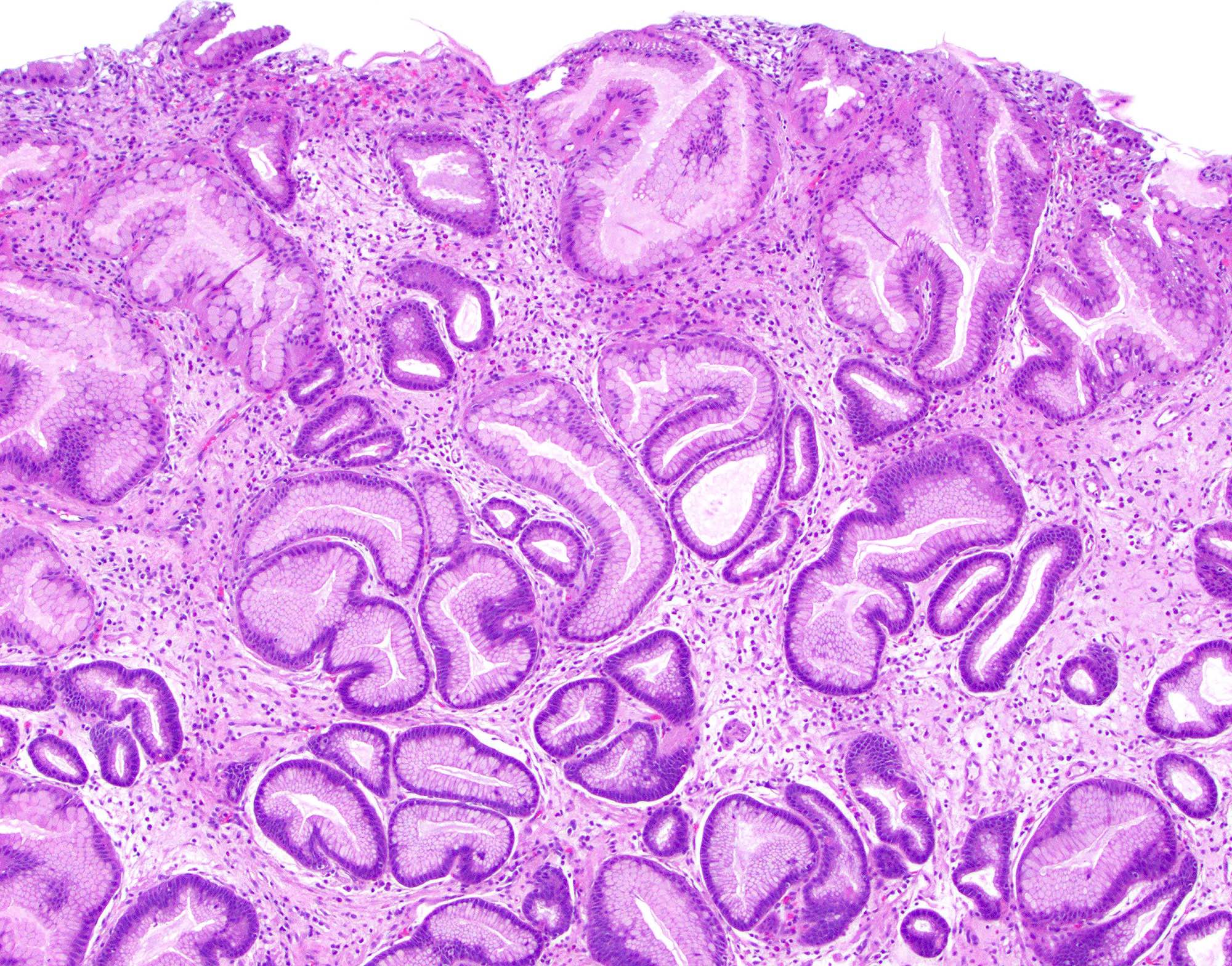
Tortuous gastric pits
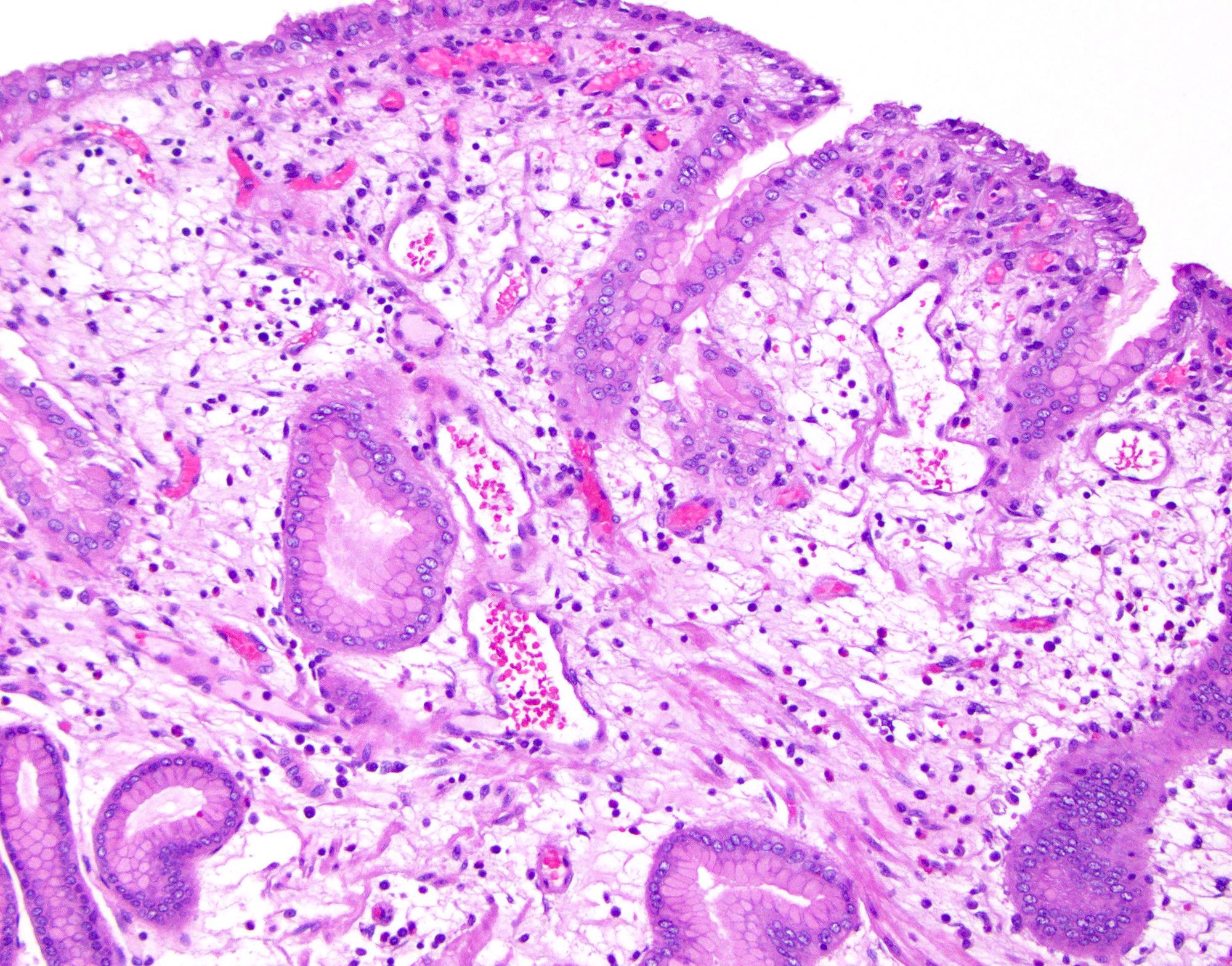
Edematous lamina propria
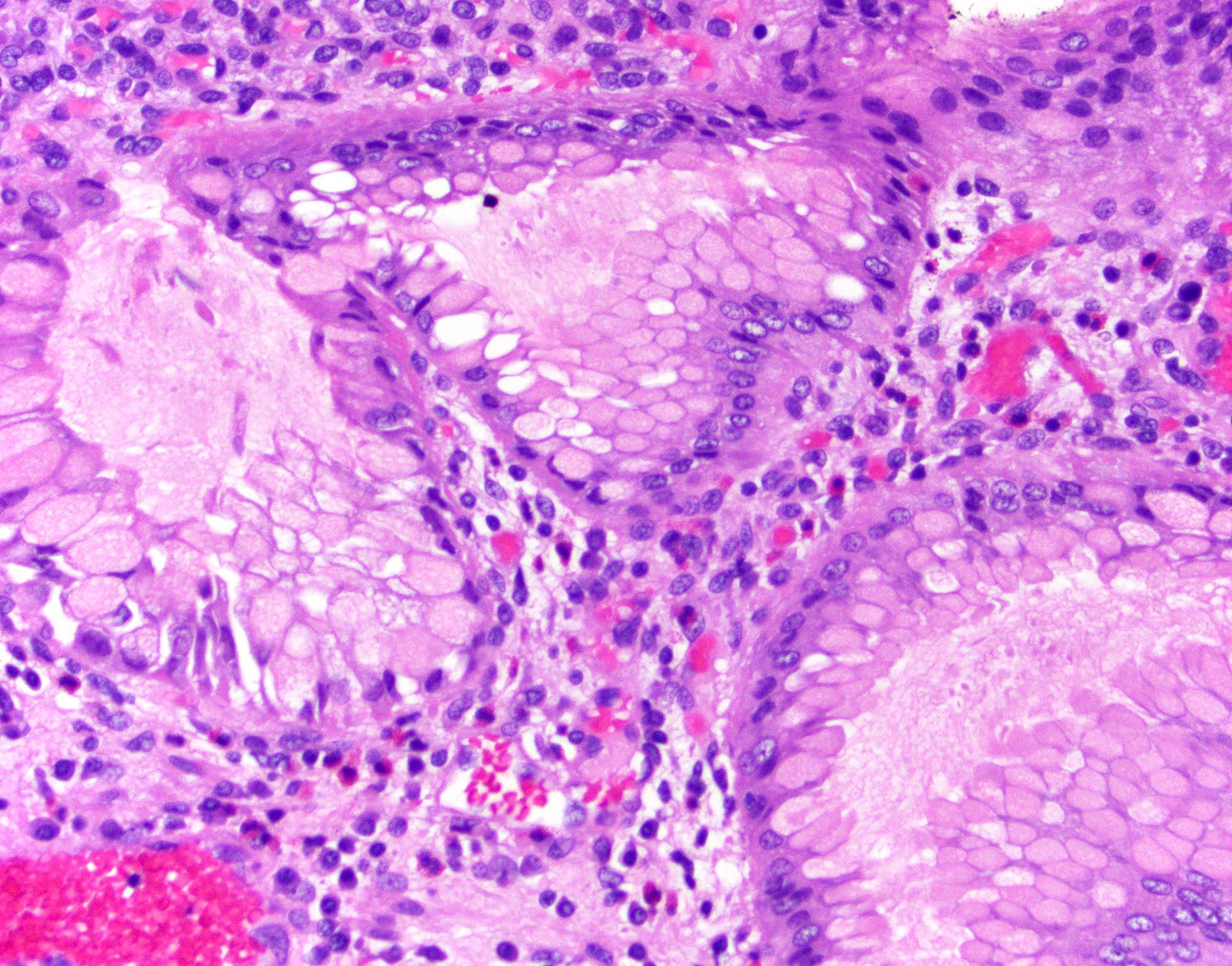
Pseudogoblet cells
Dysplasia
Dysplastic polyp
Dysplasia
Adenocarcinoma

Polypoid lesion

Hemorrhagic and ulcerated
Cystic hyperplastic glands
Molecular / cytogenetics description
- Genetic alterations identified in large dysplastic hyperplastic polyps, including loss of MGMT expression, APC or CTNNB1 and TP53; less frequently KRAS or BRAF alterations (Virchows Arch 2019;475:383, Exp Mol Pathol 2015;99:468)
Sample pathology report
- Stomach, esophagogastroduodenoscopy:
- Gastric hyperplastic polyp (see comment)
- Comment: Large gastric hyperplastic polyps typically arise in a background of damaged mucosa and are frequently associated with Helicobacter pylori or autoimmune gastritis. Follow up sampling of the flat mucosa from both the antrum and body / fundus in such patients may provide information on the setting in which the polyp has arisen.
Differential diagnosis
- Polypoid gastritis:
- Normal architecture, no smooth muscle wisps
- Polypoid foveolar hyperplasia:
- No cystic dilation, no smooth muscle wisps
- Gastritis cystica profunda:
- Entrapped, distorted, dilated glands in muscularis
- Fundic gland polyp:
- Distorted glands and cysts lined by parietal and chief cells
- Ménétrier disease:
- Affects gastric body only; foveolar hyperplasia, atrophy of glands, adjacent epithelium normal
- Cronkhite-Canada syndrome:
- Affects entire stomach; foveolar hyperplasia, atrophy of glands, adjacent epithelium shows atrophy of glands and microcystic change
- Juvenile polyposis:
- Adjacent mucosa is normal as opposed to hyperplastic polyp, which often has chronic gastritis
- Peutz-Jeghers polyposis:
- Autosomal dominant inherited disorder with multiple hamartomatous polyps and mucocutaneous hyperpigmentation
- Pyloric adenoma:
- Closely packed tubular glands lined by cuboidal to low columnar epithelium with ground glass cytoplasm, bland nuclei and no well formed apical mucin cap
- Inflammatory fibroid polyp:
- Submucosal lesion composed of spindle and stellate stromal cells
- Dysplasia must be differentiated from regenerative change:
- Dysplasia is present at the surface; regenerative change shows surface maturation and atypia like changes only in the proliferative zones, not at the surface
- Dysplasia is typically abrupt
- Dysplasia has architecturally complex patterns (cribriform, budding and branching)
- Dysplasia has nuclear pleomorphism, elongation and hyperchromasia without prominent nucleoli
- Regenerative epithelium shows gradual change, lacks complex patterns, has hyperchromasia but with ovoid nuclei and prominent nucleoli
Board review style question #1
Which Helicobacter pylori protein is associated with a role in the development of gastric neoplasia?
- CagA
- PAR1
- SHP2
- SRC
Board review style answer #1
A. CagA. CagA in Helicobacter pylori can cause aberrant activation of SHP2, a human oncoprotein, in the stomach (Proc Natl Acad Sci USA 2008;105:1003). Answer B is incorrect because PAR1 is a human kinase inhibited by CagA. Answer C is incorrect because SHP2 is a human oncoprotein, not a Helicobacter pylori protein. Answer D is incorrect because SRC is a human tyrosine kinase that mediates CagA phosphorylation and cytoskeletal rearrangements.
Comment Here
Reference: Hyperplastic polyp
Comment Here
Reference: Hyperplastic polyp
Board review style question #2
Which of the following polyps is seen in this picture?
- Fundic gland polyp
- Hyperplastic polyp
- Polypoid foveolar hyperplasia
- Polypoid gastritis
Board review style answer #2
B. Hyperplastic polyp. Gastric polyp showing elongated, tortuous and dilated gastric pits and edematous lamina propria (Surg Pathol Clin 2020;13:431). Answer A is incorrect because the polyp shows dilated pits lined by foveolar epithelium, not oxyntic epithelium. Answer C is incorrect because the polyp shows cystically dilated pits. Answer D is incorrect because the polyp has abnormal architecture and does not show predominant plasmacytic and neutrophilic inflammation.
Comment Here
Reference: Hyperplastic polyp
Comment Here
Reference: Hyperplastic polyp
