
Stomach
Other nonneoplastic
Gastric antral vascular ectasia
Authors: Hunter Monroe, B.S., Tony El Jabbour, M.D.
Editorial Board Member: Aaron R. Huber, D.O.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 15 February 2023
Last staff update: 15 February 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Gastric antral vascular ectasia


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Monroe H, El Jabbour T. Gastric antral vascular ectasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachantralvascularect.html. Accessed April 1st, 2025.
Definition / general
- Antral vascular malformation with dilation of superficial mucosal and submucosal blood vessels, often with associated fibrin microthrombi
Essential features
- Accounts for up to 4% of nonvariceal gastrointestinal bleeding, usually chronic with associated iron deficiency
- Histologically characterized by variable mucosal and submucosal vessel ectasia, fibrin thrombi, reactive foveolar changes and fibromuscular hyperplasia
- May present clinically as striped (watermelon stomach) form in younger males with cirrhosis of the liver, diffuse punctate (honeycomb stomach) form in older females with autoimmune disorders or nodular form
- Endoscopic ablative therapy such as argon plasma coagulation (APC) is first line treatment; antrectomy only if severe and refractory (due to high postoperative mortality rate)
- Primary differential includes portal hypertensive gastropathy, which may present with vascular ectasia but lacks fibrin thrombi
Terminology
- Linear striped type referred to as watermelon stomach
- Diffuse punctate type called honeycomb stomach
- Originally described as erosive gastritis with venocapillary ectasia by Reider in 1953
ICD coding
Epidemiology
- Accounts for up to 4% of nonvariceal upper gastrointestinal bleeding
- Exact incidence is unknown but appears to be rising due to increased awareness and the development of reliable diagnostic modalities (Gastroenterology Res 2021;14:104)
- Strong association with autoimmune disorders (up to 62%) and liver cirrhosis (up to 30%) (J Clin Gastroenterol 1992;15:256)
- F > M (Gastroenterology Res 2021;14:104)
- Female patients are associated with autoimmune disorders
- Male patients are associated with liver cirrhosis (World J Clin Cases 2022;10:6050)
- Most often presents in elderly individuals (Gastroenterology Res 2021;14:104)
- Most commonly affects Caucasians
- Low mortality rate due to increased awareness and viable treatment options (Gastroenterology Res 2021;14:104)
Sites
- Gastric antrum
- Rare extra-antral sites include gastric cardia, duodenum, jejunum and rectum (Gut 1993;34:558)
Pathophysiology
- Pathophysiology is unknown, though several theories have been proposed:
- Chronic liver dysfunction leads to increased blood concentrations of vasodilatory hormones and metabolites such as gastrin, VIP and PGE2 (World J Gastrointest Endosc 2013;5:6)
- Mechanical stress from gastric peristalsis induces prolapse, antral mucosal trauma and vessel obstruction, resulting in vascular ectasia and fibromuscular hyperplasia
- Autoimmune antibodies react with proteins that are present in the gastric mucosal and submucosal vessels
Etiology
- Unknown
Clinical features
- Endoscopic presentations:
- Striped:
- Parallel, raised or flat red (hyperemic) longitudinal stripes beginning in pylorus and extending to antrum (watermelon stomach)
- More commonly found in noncirrhotic female patients (World J Clin Cases 2022;10:6050)
- More prone to hemorrhage than diffuse punctate pattern (World J Clin Cases 2022;10:6050)
- Diffuse punctate:
- Widespread, discontinuous erythematous lesions in antrum (honeycomb stomach)
- More commonly found in cirrhotic male patients (World J Clin Cases 2022;10:6050)
- Nodular:
- Benign appearing mucosal nodules of 1 - 5 mm dimension (Dig Dis Sci 2018;63:966)
- Possible association with cirrhosis (World J Clin Cases 2022;10:6050)
- Striped:
- Most commonly presents as chronic upper GI bleeding
- Transfusion dependent iron deficiency anemia
- Melena
- Heavy acute GI bleeding may manifest as hematemesis in a minority of patients
- Rarely pernicious anemia (J Clin Gastroenterol 1992;15:256)
- Many clinical correlates, especially autoimmune disorders:
- Isolated Raynaud phenomenon (31%) and sclerodactyly (20%) (J Clin Gastroenterol 1992;15:256)
- Systemic sclerosis and CREST syndrome
- Up to 22.5% of affected patients may have symptomatic or asymptomatic gastric antral vascular ectasia (GAVE) (Arthritis Res Ther 2022;24:103)
- GAVE may be first symptom in up to 7.7% of patients (Arthritis Res Ther 2022;24:103)
- Additional symptoms may include calcinosis, esophageal dysmotility / dysphagia, scleroderma renal crisis and telangiectasias (Semin Arthritis Rheum 2020;50:938)
- Liver cirrhosis
- Most commonly due to nonalcoholic steatohepatitis (NASH) (Can Liver J 2019;2:84)
- Chronic renal failure (Gastroenterology Res 2021;14:104)
- Hypertension (Gastroenterology Res 2021;14:104)
- Systemic lupus erythematosus
- Sjögren syndrome
- Primary biliary cholangitis (Cureus 2022;14:e21676)
- Atrophic gastritis (J Clin Gastroenterol 1992;15:256)
- Proton pump inhibitors (Gastroenterology Res 2013;6:77)
- Bone marrow transplants (World J Gastrointest Endosc 2013;5:6)
- Chemotherapy:
- Everolimus (IJU Case Rep 2020;3:293)
- Imatinib (Clin Case Rep 2014;2:77)
Diagnosis
- Esophagogastroduodenoscopy (EGD) is gold standard for endoscopy (Semin Arthritis Rheum 2020;50:938)
- Antral biopsy may be useful to rule out portal hypertensive gastropathy if comorbid cirrhosis
- Biopsy may not exclude GAVE, as lesions may be focal
- Fecal occult blood tests
Laboratory
- Anemia
- Iron deficiency
- Anti-RNA polymerase III (RNAPIII) antibodies present in up to 71% of GAVE patients with systemic sclerosis (Semin Arthritis Rheum 2020;50:938)
- Concomitant GAVE and anti-RNAPIII is strongly correlated with scleroderma renal crisis
Radiology description
- Unreliable
- Endoscopic ultrasound (EUS):
- Hypertrophic antrum with well preserved muscularis propria (World J Gastrointest Endosc 2013;5:6)
Prognostic factors
- Exact mortality is unknown but appears to be low (Gastroenterology Res 2021;14:104)
- Recurrence rate is ~40%
- Factors associated with poorer prognosis (Gastroenterology Res 2021;14:104):
- Hemorrhage associated with higher mortality
- Mortality increases with number of comorbidities
- Hispanic status may be associated with poorer prognosis
- Higher mortality rate if refractory to endoscopic ablation
Case reports
- 70 year old man with severe asthenia, abdominal pain and anemia (Int J Surg Case Rep 2022;98:107474)
- 76 year old man with chronic symptomatic anemia and melena (J Transl Int Med 2018;6:47)
- 76 year old woman with symptomatic lupus and anemia (BMC Nephrol 2020;21:468)
Treatment
- Symptom management with blood transfusions and iron supplements
- Endoscopic ablative treatments are first line:
- Argon plasma coagulation (APC):
- Higher success rate for diffuse / punctate pattern (Ther Adv Chronic Dis 2021;12:20406223211039696)
- Associated with high risk of posttreatment recurrence
- May show better outcomes and less recurrence with addition of saline injection or polidocanol (Ther Adv Chronic Dis 2021;12:20406223211039696)
- Neodymium yttrium aluminum garnet (Nd:YAG) laser photocoagulation:
- Risk of gastric ulceration and perforation (World J Gastrointest Endosc 2013;5:6)
- Radiofrequency ablation (RFA):
- High success rate for GAVE refractory to APC
- Endoscopic band ligation
- Nitrous oxide cryoablation (United European Gastroenterol J 2018;6:1155)
- Argon plasma coagulation (APC):
- Surgery:
- Antrectomy:
- Used in only severe refractory cases due to postoperative mortality, up to 6.6% (World J Gastrointest Endosc 2013;5:6)
- Orthotopic liver transplantation (OLT):
- Variable success in cirrhotic or chronic liver disease patients (World J Hepatol 2020;12:1067)
- Antrectomy:
- Pharmacotherapy and chemotherapy are experimental and shown to be viable only in isolated case reports:
- Cyclophosphamide (Intern Med 2019;58:135)
- Estrogen and progesterone (World J Gastrointest Endosc 2013;5:6)
- Octreotide (Gastroenterology Res 2013;6:77)
Clinical images
Contributed by Tony El Jabbour, M.D.
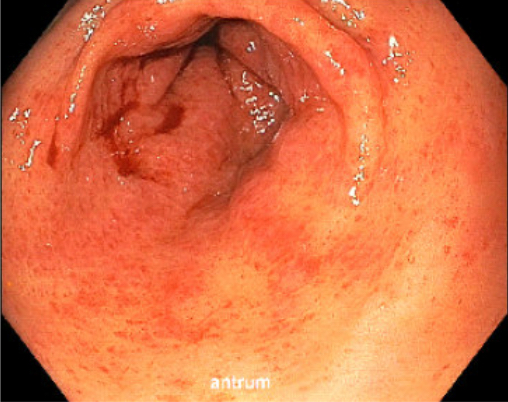
Diffuse punctate pattern
Images hosted on other servers:

Striped pattern

Diffuse punctate pattern

Nodular pattern
Microscopic (histologic) description
- Dilated mucosal capillaries
- Reactive foveolar changes
- Intravascular fibrin thrombi
- May have higher prevalence in nodular and striped forms (Dig Dis Sci 2018;63:966)
- Fibromuscular hyperplasia of lamina propria
- Fibrohyalinosis (perivascular hyalinization)
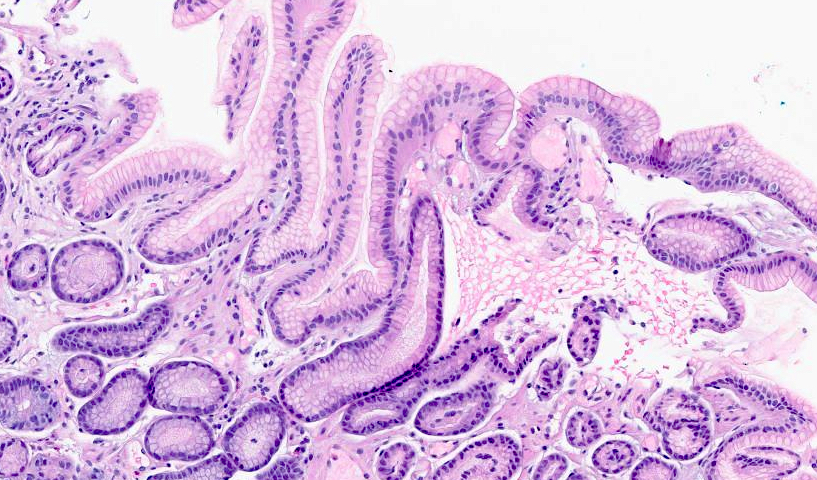
Microscopic (histologic) images
Contributed by Hwajeong (Jenny) Lee, M.D.

Antrum with reactive changes
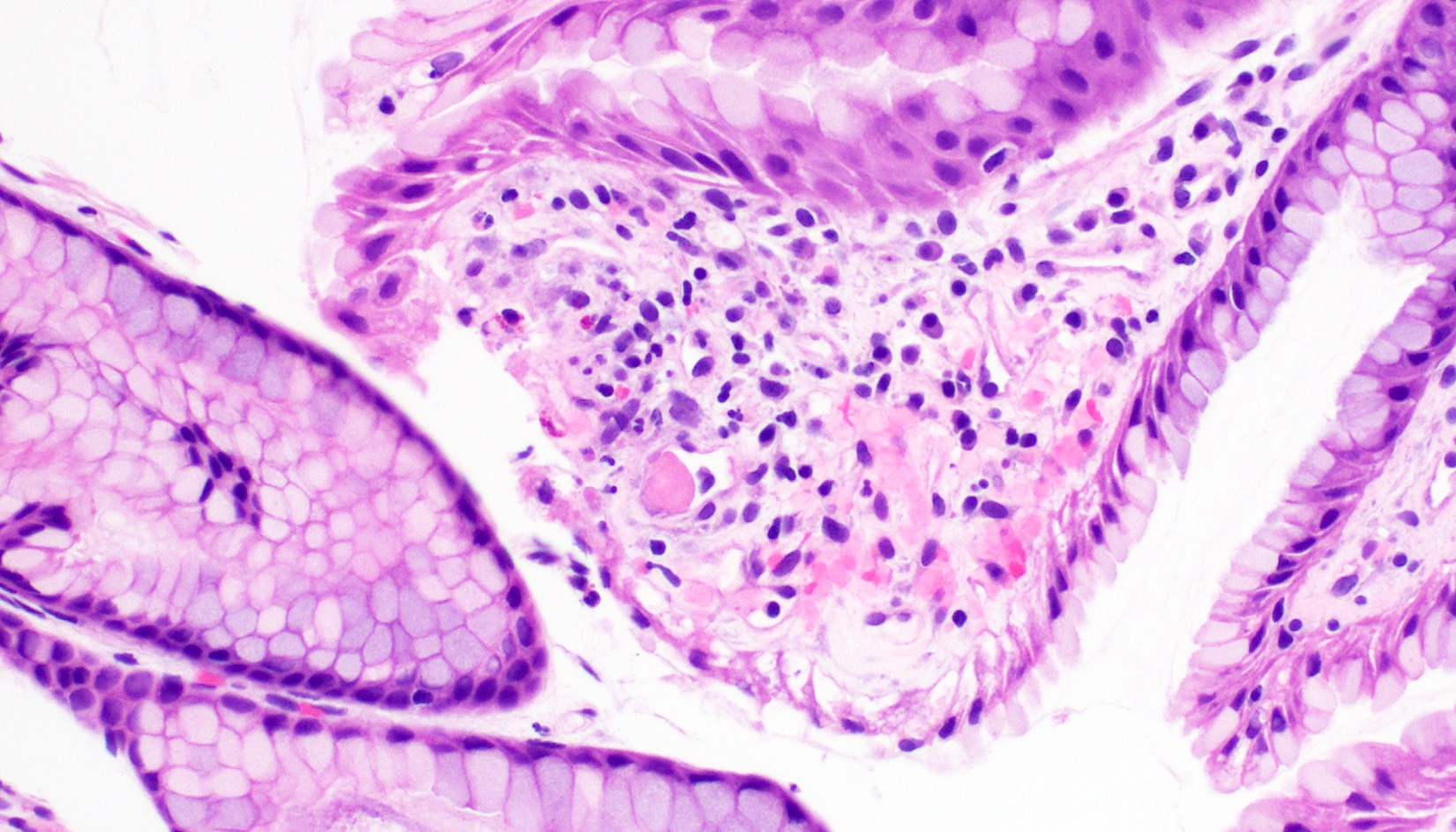
Fibrin thrombus
Videos
Histopathology of gastric antral vascular ectasia
Sample pathology report
- Antrum, biopsy:
- Gastric antral mucosa with vascular dilation in the lamina propria with extravasation of red blood cells and rare fibrin thrombi (see comment)
- Comment: These features could be seen in gastric antral vascular ectasia (GAVE) and portal hypertensive gastropathy. Correlation with the clinical history and endoscopic aspect of the mucosa at the site of the biopsy are necessary to establish the diagnosis.
Differential diagnosis
- Portal hypertensive gastropathy (World J Gastrointest Endosc 2013;5:6):
- May present with vascular ectasia
- Affects gastric fundus and corpus
- Endoscopically presents with mosaic red point lesions, cherry red spots or black-brown spots
- Lacks fibrin microthrombi
- Responds to portal hypertensive therapies (beta blockers, portocaval shunt, etc.)
- Telangiectasia:
- Presents with mucosal capillary ectasia
- Association with hemodialysis, medication side effects or Osler-Weber-Rendu syndrome
- Reactive gastropathy:
- Appears with similar, if identical, reactive foveolar changes
- May contain mucosal capillary ectasia
- Typically lacks fibrin microthrombi
- Hyperplastic polyps:
- May mimic nodular GAVE on endoscopy
- Contains elongated, cystically dilated foveolar epithelium
- More prominent inflammation in lamina propria
Board review style question #1
The microphotograph above demonstrates a section obtained from a biopsy of the gastric antrum in a 71 year old woman presenting with chronic melena and iron deficiency anemia. Which of the following is true of this patient's disease?
- Antrectomy is associated with the most favorable postoperative outcomes
- Endoscopic ablative treatments such as argon plasma coagulation are first line
- It typically presents as acute heavy upper gastrointestinal bleeding
- On endoscopy, it usually presents as parallel red stripes in patients with comorbid cirrhosis
Board review style answer #1
B. Endoscopic ablative treatments such as argon plasma coagulation are first line
Comment Here
Reference: Gastric antral vascular ectasia
Comment Here
Reference: Gastric antral vascular ectasia
Board review style question #2
Which of the following is true of both gastric antral vascular ectasia (GAVE) and portal hypertensive gastropathy?
- Dilated mucosal capillaries are routinely present on histology
- Endoscopically presents as mosaic red point lesions and black-brown spots
- Histologically characterized by intravascular fibrin thrombi
- Responsive to antihypertensive therapies such as beta blockers
Board review style answer #2
A. Dilated mucosal capillaries are routinely present on histology
Comment Here
Reference: Gastric antral vascular ectasia
Comment Here
Reference: Gastric antral vascular ectasia
