

Stomach
Lymphoma
Extranodal marginal zone lymphoma of mucosa associated lymphoid tissue (MALT lymphoma)
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 22 April 2021
Last staff update: 13 December 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Gastric MALT lymphoma[TI] free full text[SB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Bahceci D, Wen KW. Extranodal marginal zone lymphoma of mucosa associated lymphoid tissue (MALT lymphoma). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachMALT.html. Accessed December 26th, 2024.
Definition / general
- Extranodal lymphoma composed of morphologically heterogeneous small B cells, including marginal zone (centrocyte-like) cells, cells resembling monocytoid cells, small lymphocytes and scattered immunoblasts and centroblast-like cells (Swerdlow: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Edition, 2017)
Essential features
- Stomach is the most common site involved by MALT lymphoma
- Most gastric MALT lymphomas associated with gastritis caused by Helicobacter pylori infection
- Microscopic features: centrocyte-like cells, monocytoid cells, plasma cells, occasional large transformed lymphocytes, lymphoepithelial lesions, adjacent nonneoplastic germinal centers
- Atypical features of lymphoid infiltrate help distinguish MALT lymphoma from reactive conditions, such as H. pylori gastritis (J Clin Pathol 2007;60:361)
Terminology
- Also called MALToma
ICD coding
- ICD-10: C88.4 - Extranodal marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT lymphoma)
Epidemiology
- 7 - 8% of all B cell non-Hodgkin lymphomas (Leuk Lymphoma 2013;54:1891)
- Median age: seventh decade
- M:F = ~1:1
- Up to 50% of primary gastric lymphomas
- 85 - 90% of all GI MALT lymphomas
Sites
- Stomach (35%) is most common site of extranodal marginal zone lymphoma (Blood 2016;127:2082)
- Ocular adnexa (13%)
- Lung (9%)
- Skin (9%)
- Salivary glands (8%)
Etiology
- Related to chronic inflammatory disorders driven by infectious agents or autoimmune stimuli (Blood 2016;127:2082)
- Stomach: H. pylori associated gastritis
- H. pylori infection attracts B cells, T cells and neutrophils to the gastric mucosa; B cell proliferation is driven by reactive T cells, as well as by cytokines
- Chronic proliferative state of these B cells, as well as neutrophil mediated release of reactive oxygen species in areas of chronic inflammation, induces additional oncogenic events that eventually make lymphoproliferation independent of antigenic stimulation
- Additional genetic alterations can ultimately result in transformation to clinically aggressive diffuse large B cell lymphoma (Nat Rev Gastroenterol Hepatol 2010;7:336)
Clinical features
- Can be asymptomatic or cause epigastric pain, anorexia, weight loss, anemia, early satiety, occasionally fever and night sweats
- Most are low stage (stage I and II) at presentation
- 23 - 40% of patients may present with disseminated disease, involving other mucosal sites, lymph nodes or bone marrow (Blood 2000;95:802)
- > 75% of cases will regress with successful treatment for H. pylori
- Increased risk has been reported in patients with chronic hepatitis C virus (HCV) infection (Blood 2016;127:2082)
Diagnosis
- Diagnostic workup includes endoscopic findings, histology with immunohistochemistry and molecular analysis
Prognostic factors
- Indolent
- Lugano staging system: most widely accepted staging system (UpToDate: Treatment of Extranodal Marginal Zone Lymphoma of Mucosa Associated Lymphoid Tissue (MALT Lymphoma) [Accessed 10 February 2021])
- Recurrences may involve other extranodal sites
- BIRC3-MALT1 translocation is associated with H. pylori treatment resistance
- Histologic transformation, defined as an infiltration of 50% or more of large B cells, occurs in 8% of patients during the course of the disease (Mod Pathol 2013;26:182)
Case reports
- 32 year old man presented with epigastric pain of 6 months duration (BMC Gastroenterol 2002;2:6)
- 58 year old woman was referred with epigastric pain and 10 kg weight loss (Histopathology 1995;27:89)
- 72 year old woman presented with a 10 month history of intermittent epigastric discomfort without vomiting, anorexia or weight loss (J Clin Pathol 2002;55:548)
Treatment
- H. pylori eradication - first line therapy (Gut 2012;61:507)
- Curative in majority of gastric MALT lymphomas
- Resolution can take up to 24 months
- Some primary gastric diffuse large B cell lymphomas may also respond to antibiotic eradication therapy alone
- If H. pylori eradication therapy fails → second line therapy (Med Oncol 2010;27:291)
- Chemotherapy
- Radiation
- Surgery: only necessary if complications (perforation, obstruction, bleeding) occur
Gross description
- Large mass with or without ulcer
- Diffusely thickened gastric wall
- Polypoid lesions
Microscopic (histologic) description
- Mass lesion with the following features
- Sheets of neoplastic small lymphocytes
- Irregular / angulated nuclear contours with inconspicuous nucleoli (centrocyte-like)
- Relatively abundant pale cytoplasm (monocytoid appearance)
- Cells with plasmacytic differentiation
- Clonally related to the small lymphocytes
- ~33% of gastric lymphomas
- Intranuclear (Dutcher bodies) or intracytoplasmic (Russell bodies) immunoglobulin inclusions can be seen
- Nuclear polymorphism may be noted
- May see occasional transformed lymphocytes resembling centroblasts and immunoblasts
- Larger nuclei with more open chromatin and prominent nucleoli
- If solid or sheet-like proliferations of transformed cells → diffuse large B cell lymphoma (Arch Pathol Lab Med 2018;142:44)
- Lymphoepithelial lesions (specific but not sensitive)
- Infiltration of gastric glands by neoplastic lymphocytes (> 3 centrocyte-like cells causing epithelial damage)
- Residual gastric glands are separated by the neoplastic lymphocytes
- Oxyphilic change (eosinophilic degeneration) of epithelial cells
- May lead to destruction of glands
- Adjacent reactive germinal centers
- Neoplastic cell colonization may resemble follicular lymphoma
- Amyloid deposition can be seen (Am J Clin Pathol 2012;137:51)
- H. pylori gastritis associated changes can often be present in biopsies from patients
- Active or chronic inflammation
- Diffuse chronic monocytic infiltrate, microerosions, large lymphoid follicles and regenerative foveolar hyperplasia
Microscopic (histologic) images
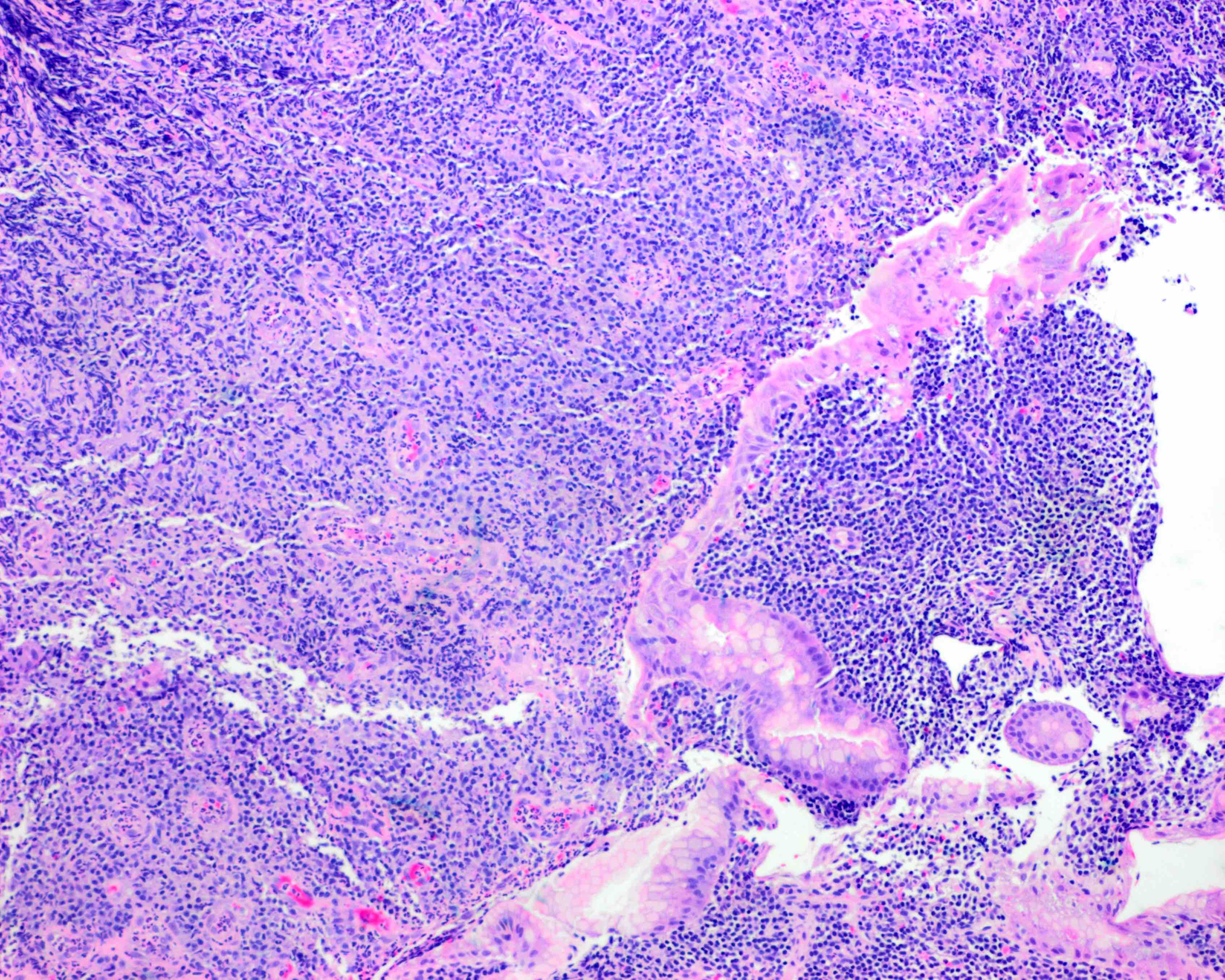
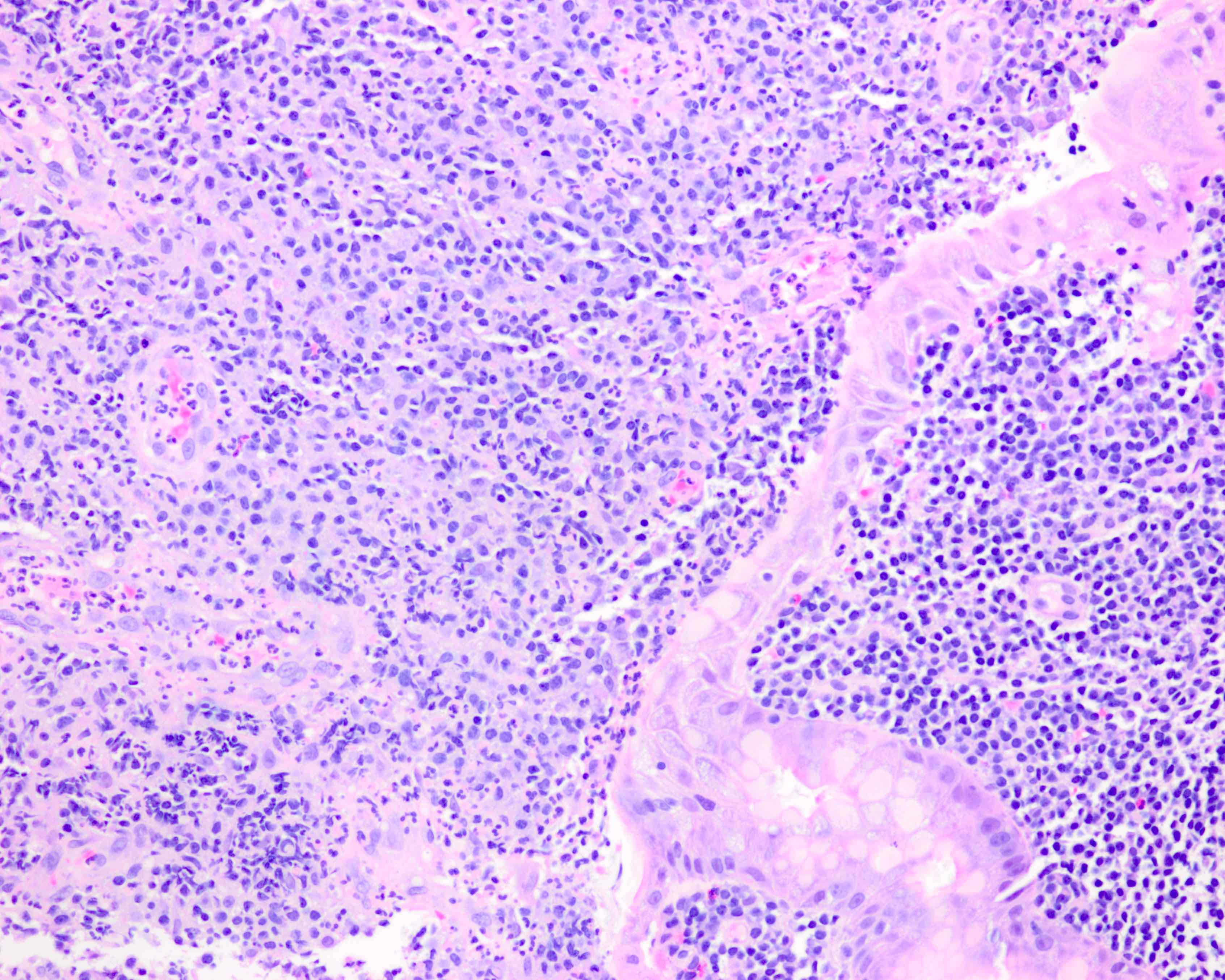
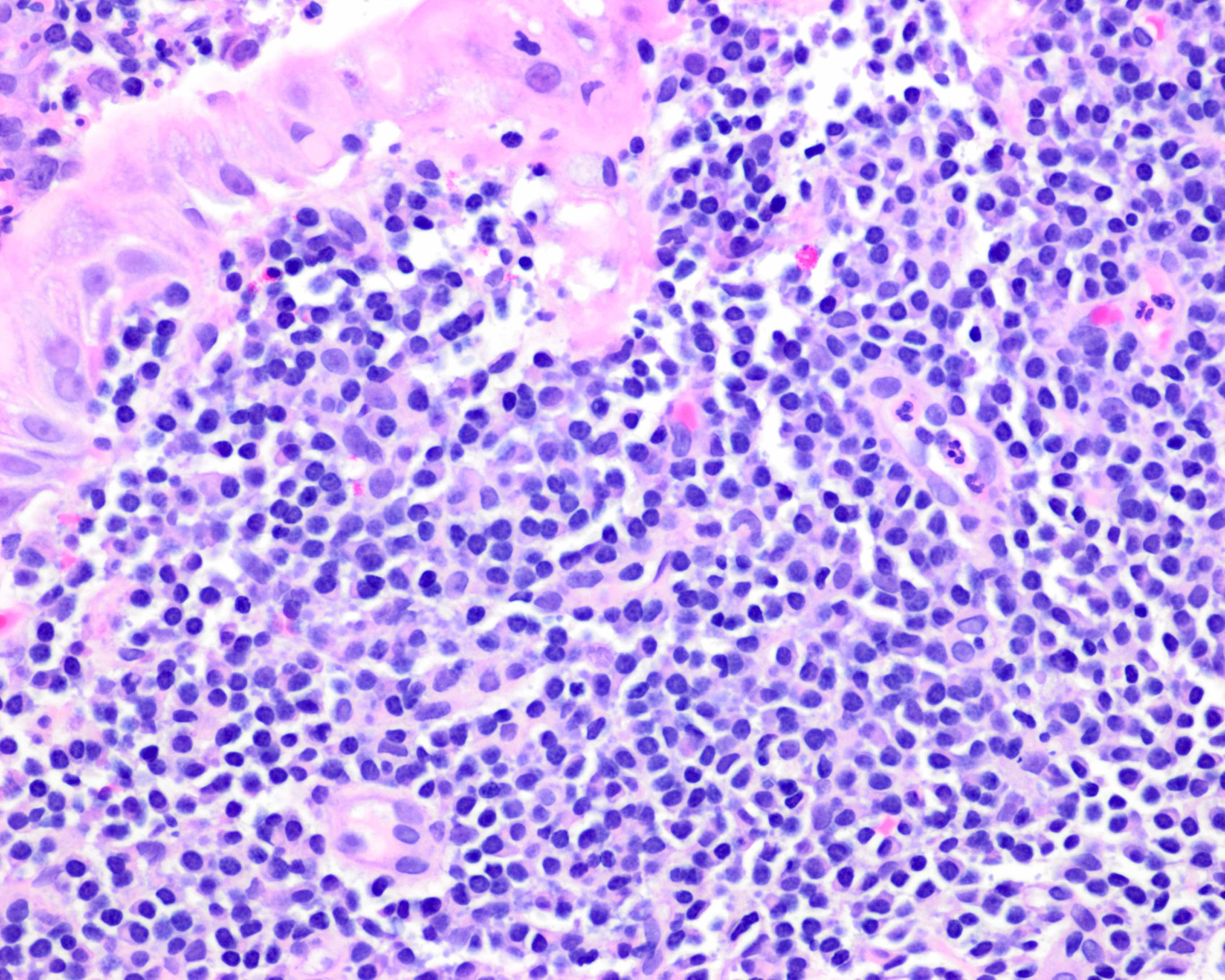
Contributed by Kwun Wah Wen, M.D., Ph.D.
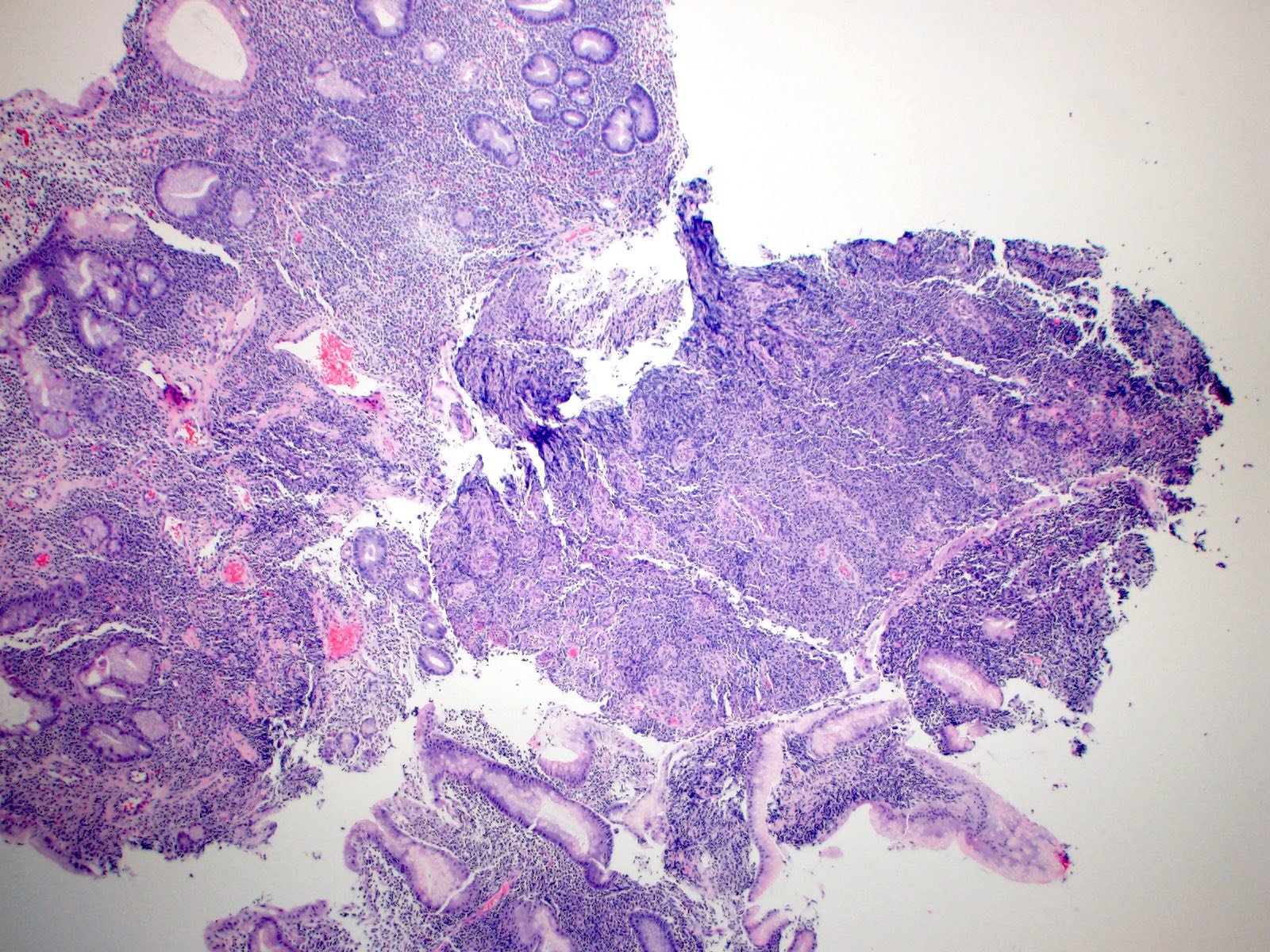
Dense lymphoplasmacytic infiltrate
Destruction of gastric glands
Focus of active inflammation
Marked plasmacytic differentiation
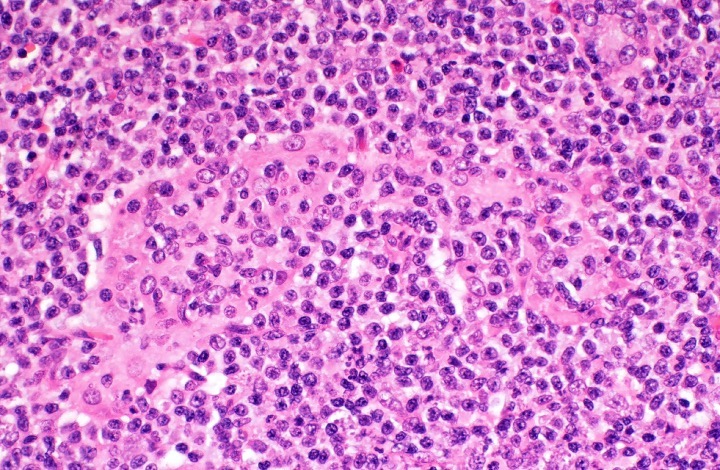
Lymphoepithelial lesion
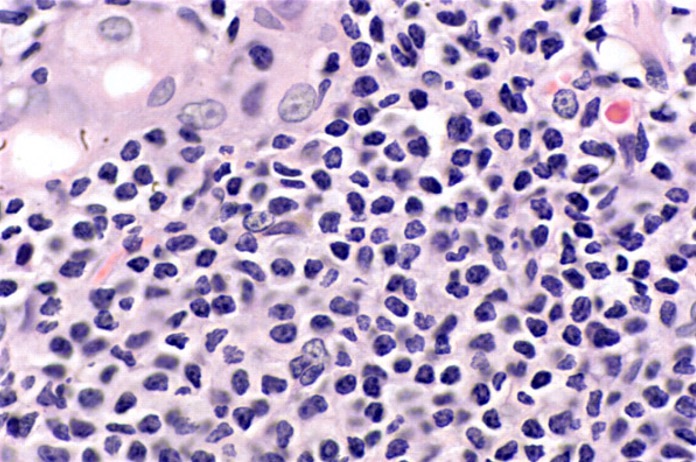
Cytologic features of lymphoma cells
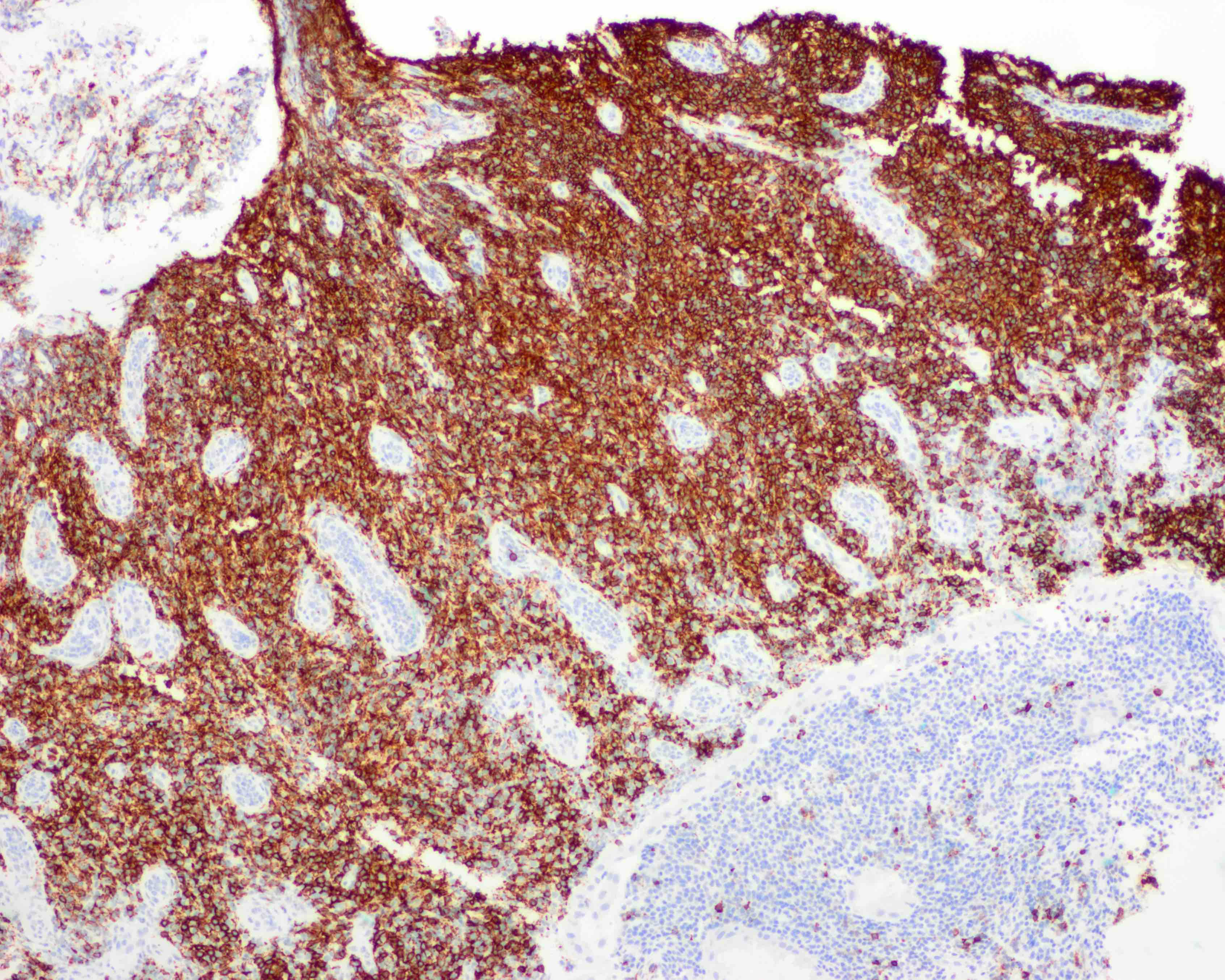
Diffusely positive for CD20
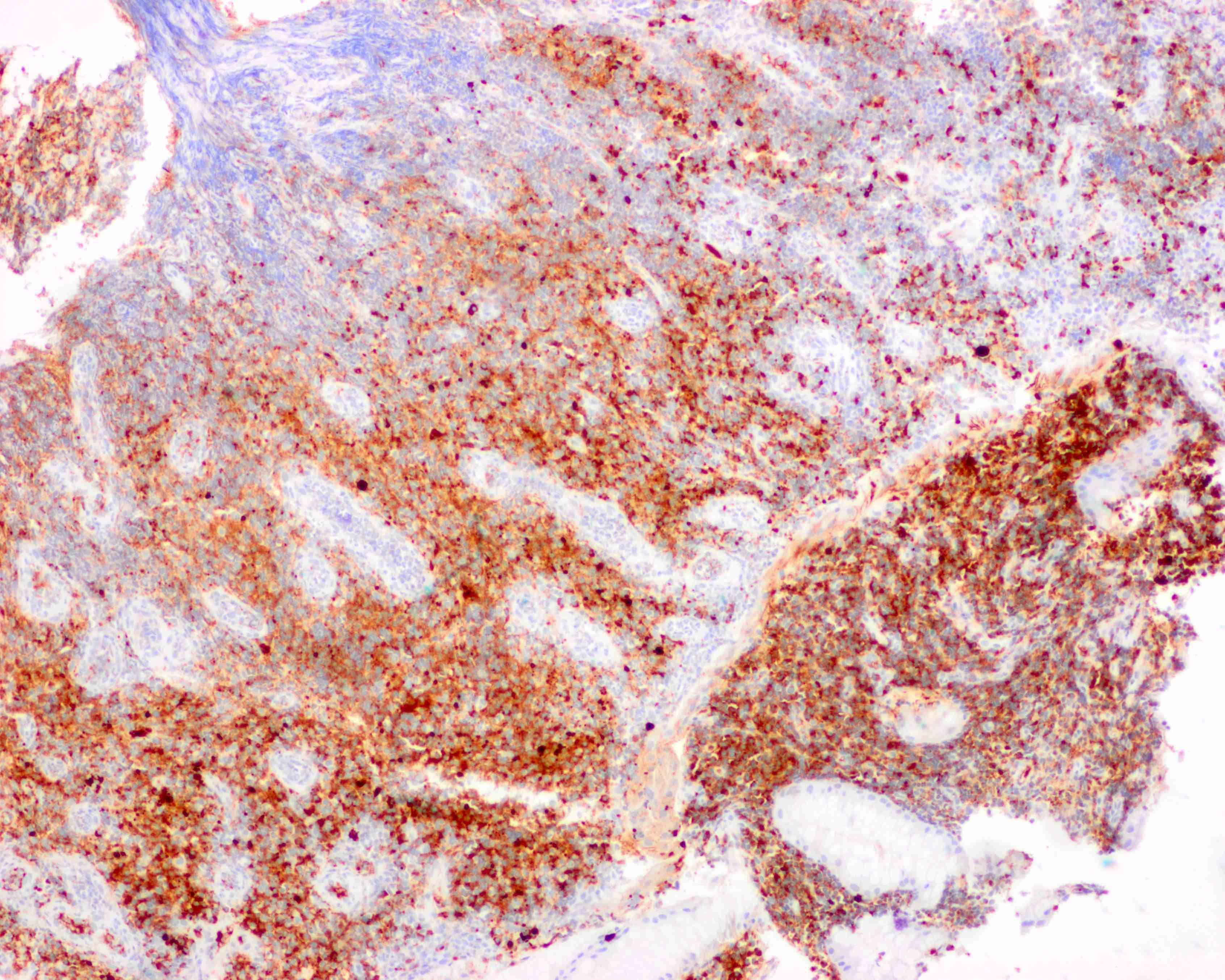
Numerous kappa restricted cells (κ:λ = > 8:1)
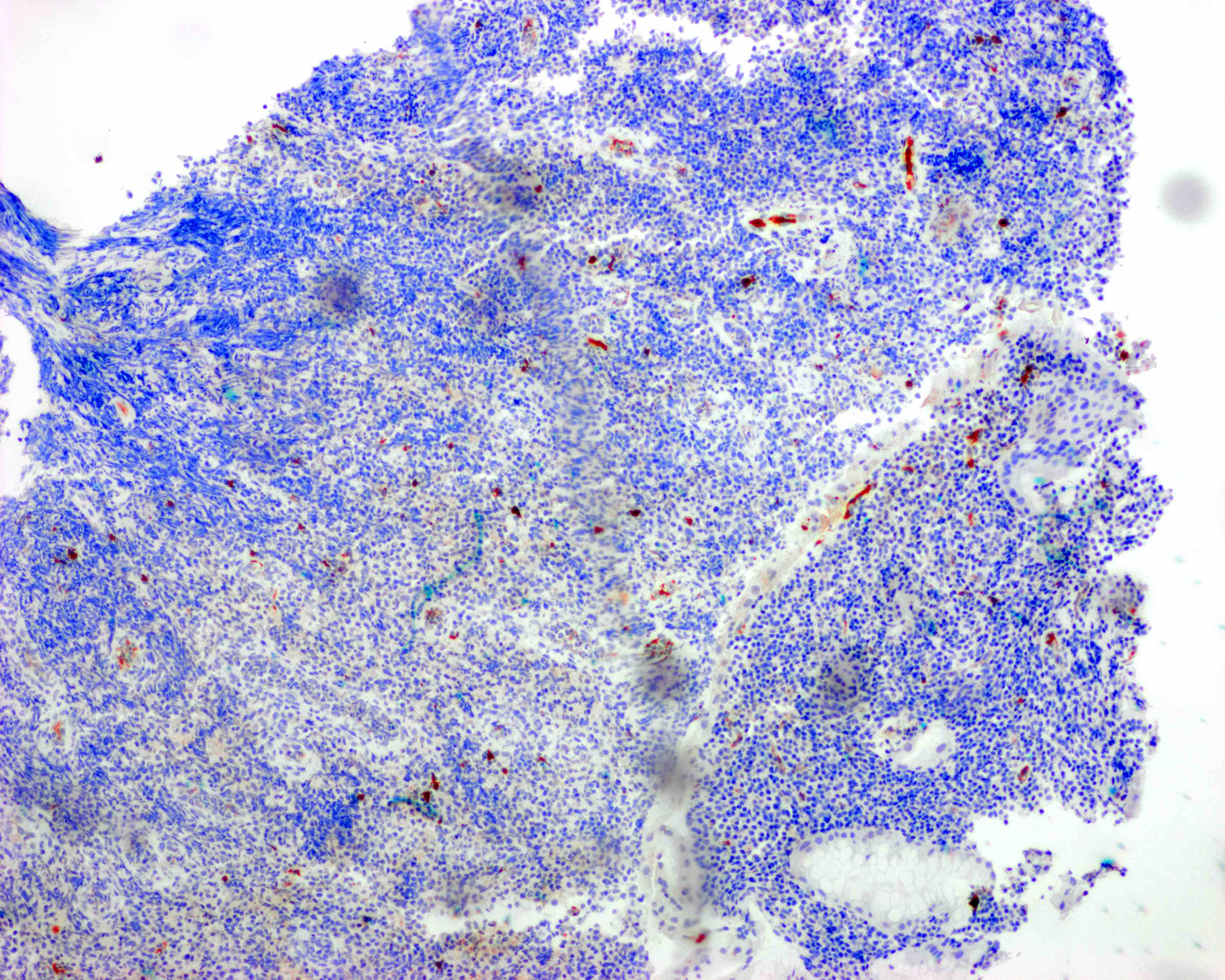
Rare lambda positive cells (κ:λ = > 8:1)

Low proliferative index
Positive stains
- Neoplastic cells of MALT lymphoma: CD19, CD20, CD22, CD79a, CD43 variable, BCL2 (Arch Pathol Lab Med 2018;142:44)
- Kappa / lambda: can be useful to demonstrate light chain restriction (especially if there are abundant neoplastic plasma cells)
- Staining for CD21, CD23 and CD35 typically reveals disrupted and occasionally expanded meshwork of intermixed follicular dendritic cells, which may help to recognize colonized follicles
- Keratin: can accentuate lymphoepithelial lesions
- Congo red: can highlight amyloid deposition present in a subset of cases
- MNDA staining: MALT (61 - 75%) versus follicular (< 10%) lymphoma (Am J Clin Pathol 2019;151:337)
- IRTA1 antibody: potential MALT specific antibody
Negative stains
- CD5, CD10 (rarely can be positive), BCL6, BCL1 / cyclin D1 (rules out mantle cell lymphoma) (Arch Pathol Lab Med 2018;142:44)
Molecular / cytogenetics description
- PCR can help confirm clonally rearranged immunoglobulin genes in challenging cases (those that show no aberrant expression of CD43 and BCL2)
- t(11;18)(q21;q21): BIRC3 (API2)-MALT1 (6 - 26%) (Haematologica 2019;104:e558)
- Associated with resistance to H. pylori eradication therapy
- t(14;18)(q32;q21): IGH-MALT1 (1 - 5%)
- t(1;14)(p22:q32): BCL10-IGH (not seen in gastric cases)
- t(3;14)(p13;q32): FOXP1-IGH (not seen in gastric cases)
- Trisomy 3 (11%)
- Trisomy 18 (6%)
- TNFAIP3 deletion / hypermethylation
- Point mutations in Ig genes
Molecular / cytogenetics images
Images hosted on other servers:

t(11;18)(q21;q21) translocation
Sample pathology report
- Gastric ulcers, biopsy:
- Extranodal marginal zone lymphoma (MALT lymphoma) (see comment)
- Comment: H&E sections of the biopsy show patchy involvement by a dense and atypical lymphoplasmacytic infiltrate with lymphoepithelial lesions. The background stomach shows chronic active gastritis. No carcinoma, dysplasia, Helicobacter organisms or intestinal metaplasia is present.
- Immunostains were performed and evaluated with the following results:
- CD3: Highlights background small reactive T cells.
- CD20: Highlights diffuse sheets of neoplastic B cells in some fragments.
- CD21: Highlights rare residual dendritic cell meshworks underlying one lymphoid follicle.
- Kappa: Highlights B cells and plasma cells with kappa restriction (kappa:lambda ratio > 8:1).
- Lambda: Highlights a rare subset of B cells and plasma cells (kappa:lambda ratio > 8:1).
- H. pylori: Negative.
- CD5: Negative in B cells; positive in background T cells.
- CD10: Negative in B cells.
- CD43: Negative in B cells; positive in T cells.
- BCL1: Negative for mantle cell lymphoma.
- BCL2: Positive in B cells and T cells.
- CD23: Negative in B cells.
- Ki67: Low proliferative index.
- AE1 / AE3: Negative for carcinoma.
- The above findings support the interpretation of extranodal marginal zone lymphoma in the stomach.
Differential diagnosis
- Severe H. pylori gastritis / reactive lymphoid hyperplasia:
- No clonal B cell populations demonstrated by light chain restriction
- No sheets of monocytoid or monomorphous cell populations
- No abnormal plasma cells with nuclear irregularities
- No lymphoepithelioid lesions
- CLL / SLL:
- Mantle cell lymphoma:
- Lymphocytes intermediate in size with irregular contours
- Stains: CD5+, cyclin D1 / BCL1+, SOX11+
- Follicular lymphoma:
- Reactive germinal centers colonized by MALT can mimic follicular lymphoma (Surg Pathol Clin 2017;10:1021)
- Stains: CD10+, BCL6+, BCL2 variable
- Lymphoplasmacytic lymphoma:
- Histologic and immunohistochemical features overlap; monocytoid B cells and centrocyte-like neoplastic cells are more common in gastric MALToma
- MYD88 L265P mutation, serum protein study
- Russell body gastritis (J Clin Pathol 2006;59:1316):
- Polyclonal immunoreactive pattern to immunoglobulin light chains
Board review style question #1
You are asked to consult on a 55 year old patient with mucosa associated lymphoid tissue (MALT) lymphoma of the stomach. She is H. pylori positive. PET-CT does not show any other evidence of disease outside the stomach. The lesion is 5 - 6 cm and confined to fundus. A bone marrow biopsy is negative. Which of the following statements about MALT lymphoma is true?
- Combination chemotherapy is used as the first curative approach
- Gastric MALT may progress into diffuse large B cell lymphoma
- H. pylori infection is associated with gastric MALT in a minority of cases
- Most patients present with multi-organ involvement
Board review style answer #1
B. Gastric MALT may progress into diffuse large B cell lymphoma
Comment Here
Reference: MALT lymphoma
Comment Here
Reference: MALT lymphoma
Board review style question #2
Which cytogenetic / molecular abnormality of gastric MALT lymphoma is associated with resistance to H. pylori antibiotic treatment?
- t(11;18)(q21;q21): BIRC3-MALT1
- t(14;18)(q32;q21): IGH-MALT1
- TNFAIP3 deletion / hypermethylation
- Trisomy 3
Board review style answer #2
Board review style question #3
Which of the following is true regarding MALT lymphoma of the stomach?
- Evidence of H. pylori infection should only be sought in the presence of symptoms, such as dyspepsia, bloating, nausea
- Lymphomas with sheets of large cells should be diagnosed as high grade MALT lymphoma
- Neoplastic lymphocytes are positive for CD5 and cyclin D1
- Neoplastic lymphocytes ranging from small lymphocytic to monocytoid cells infiltrating into epithelial structures are characteristic for gastric MALT lymphoma
Board review style answer #3
D. Neoplastic lymphocytes ranging from small lymphocytic to monocytoid cells infiltrating into epithelial structures are characteristic for gastric MALT lymphoma
Comment Here
Reference: MALT lymphoma
Comment Here
Reference: MALT lymphoma

