
Stains & CD markers
Progesterone receptor (PR)


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Progesterone receptor
Progesterone receptor (PR)
Authors: Samantha Huether, D.O., Julie M. Jorns, M.D.
Editorial Board Members: Kristen E. Muller, D.O., Christian M. Schürch, M.D., Ph.D.
Last author update: 29 July 2024
Last staff update: 29 July 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Progesterone receptor
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Diagrams / tables | Clinical features | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Huether S, Jorns JM. Progesterone receptor (PR). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsprog.html. Accessed January 20th, 2025.
Definition / general
- Progesterone receptor (PR) gene on chromosome 11 encodes PR protein
- Member of hormone receptor family of ligand dependent transcription factors
Essential features
- Hormone receptor with roles in development, physiologic processes and reproduction
- Good prognostic factor in invasive breast carcinoma and indicator of response to hormonal treatment
- Nuclear positivity via immunohistochemical staining
Terminology
- PgR
- PR
Pathophysiology
- 3 isoforms: PRA, PRB, PRC
- PRA and PRB isoforms differ only in that PRB contains an additional 164 amino acid sequence at the N terminal end (Mol Cell Endocrinol 2012;357:18)
- PRA and PRB isoforms are detected nondiscriminately by common PR antibody clones (Ann Diagn Pathol 2018;35:21)
- PR is activated by the binding of progesterone then the complex moves to nucleus where it binds to DNA and activates transcription
- PR gene expression is regulated by ER
- Involved in regulation of genes that affect cellular proliferation and differentiation of nonreproductive tissues (i.e., normal developmental processes)
- Mediates the physiological effects of progesterone in the development of breast cancer
- Loss of expression is associated with abnormal ER signaling pathway
Diagrams / tables
Images hosted on other servers:

PR signaling
Clinical features
- Reduced immunostaining is associated with adverse histopathological and clinical features in breast carcinoma, endometrioid endometrial carcinoma and pancreatic neuroendocrine tumors (Anal Cell Pathol (Amst) 2022;2022:6412148)
Interpretation
- Nuclear staining
- Evaluate percentage of tumor cell staining and staining intensity (weak, moderate or strong)
- Cytoplasmic staining or nuclear staining in < 1% of cells is considered negative
- Standardized process for initial test validation is recommended, with ongoing proficiency testing (J Clin Oncol 2010;28:2784)
- Decalcification, alternate fixatives, prolonged cold ischemia time, fixation time out of recommended range are among variables that may negatively impact expression / interpretation (J Clin Oncol 2020;38:1346)
Uses by pathologists
- In breast cancer, used as a favorable prognostic factor and to indicate response to hormonal agents, such as tamoxifen (J Clin Oncol 2020;38:1346)
- Used in combination with ER and HER2 to guide treatment options in invasive breast carcinoma
- Considered optional in ductal carcinoma in situ (DCIS) as it does not provide additional prognostic value in ER positive cases
- Rare (0.6%) cases of DCIS may be ER negative, PR positive so reflexive PR testing may be done with negative ER staining (Am J Surg 2023;225:304)
- For metastatic tumors with unknown primary, diffuse, strong positivity supports breast or gynecological origin
- May be used in combination with ER and other markers to identify breast or gynecological origin in metastatic tumors of unknown origin
Prognostic factors
- Degree of expression is linked to prognosis and therapy response in invasive breast carcinoma (Endocr Relat Cancer 2018 Jul 10 [Epub ahead of print], Clin Cancer Res 2004;10:2751)
- Expression is not linked to prognosis in DCIS, thus testing is now considered optional by CAP / ASCO (J Clin Oncol 2020;38:1346)
Microscopic (histologic) description
- Interpretation of percent and intensity (weak, moderate or strong) of nuclear staining in breast cancer (J Clin Oncol 2020;38:1346)
- < 1% is considered negative
- ≥ 1% is considered positive
Microscopic (histologic) images
Contributed by Julie M. Jorns, M.D., Andrey Bychkov, M.D., Ph.D., Leica Microsystems and
Mowafak Hamodat, M.B.Ch.B., M.Sc. (Case #125)
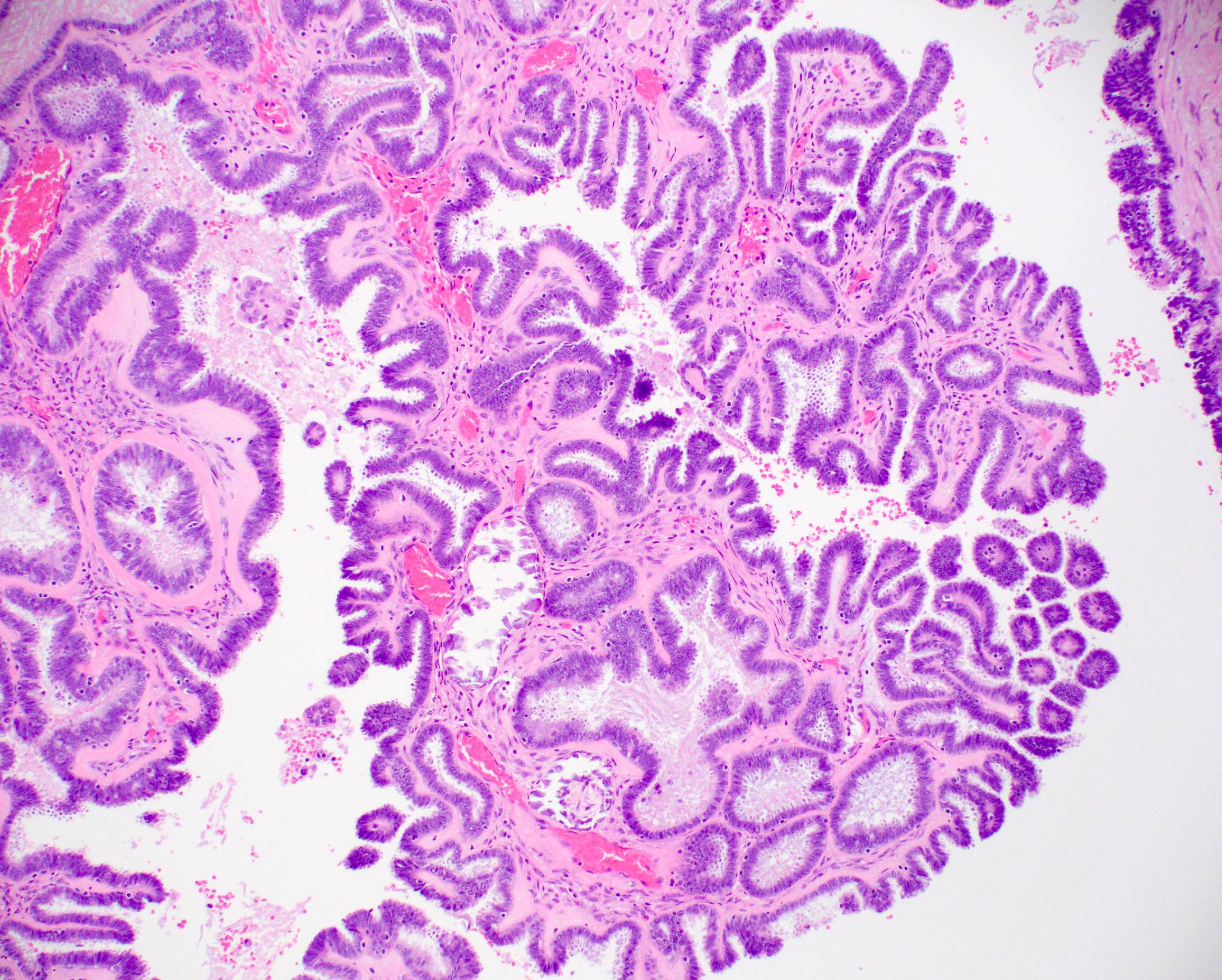

Ovary, serous borderline tumor


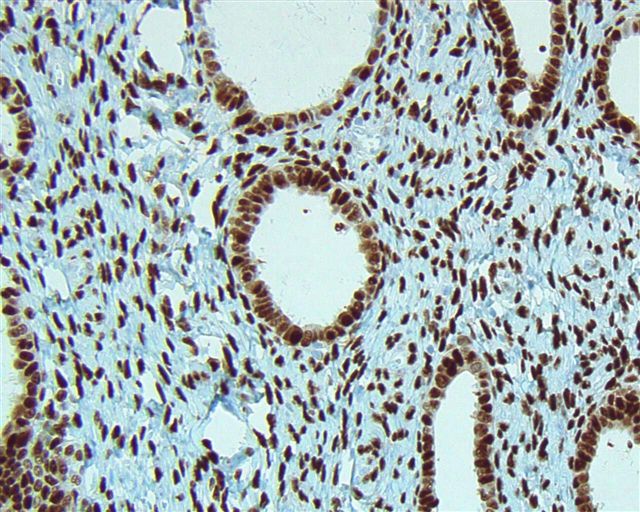
Endometrial carcinoma, endometrioid type

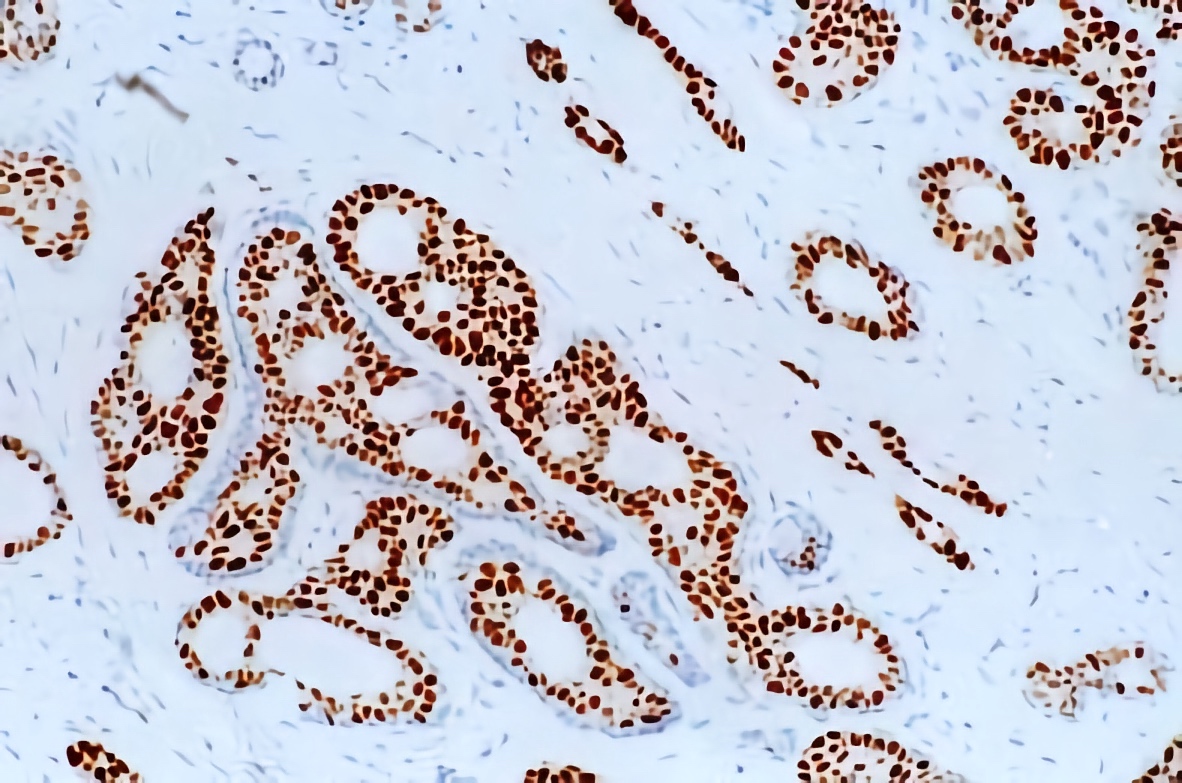
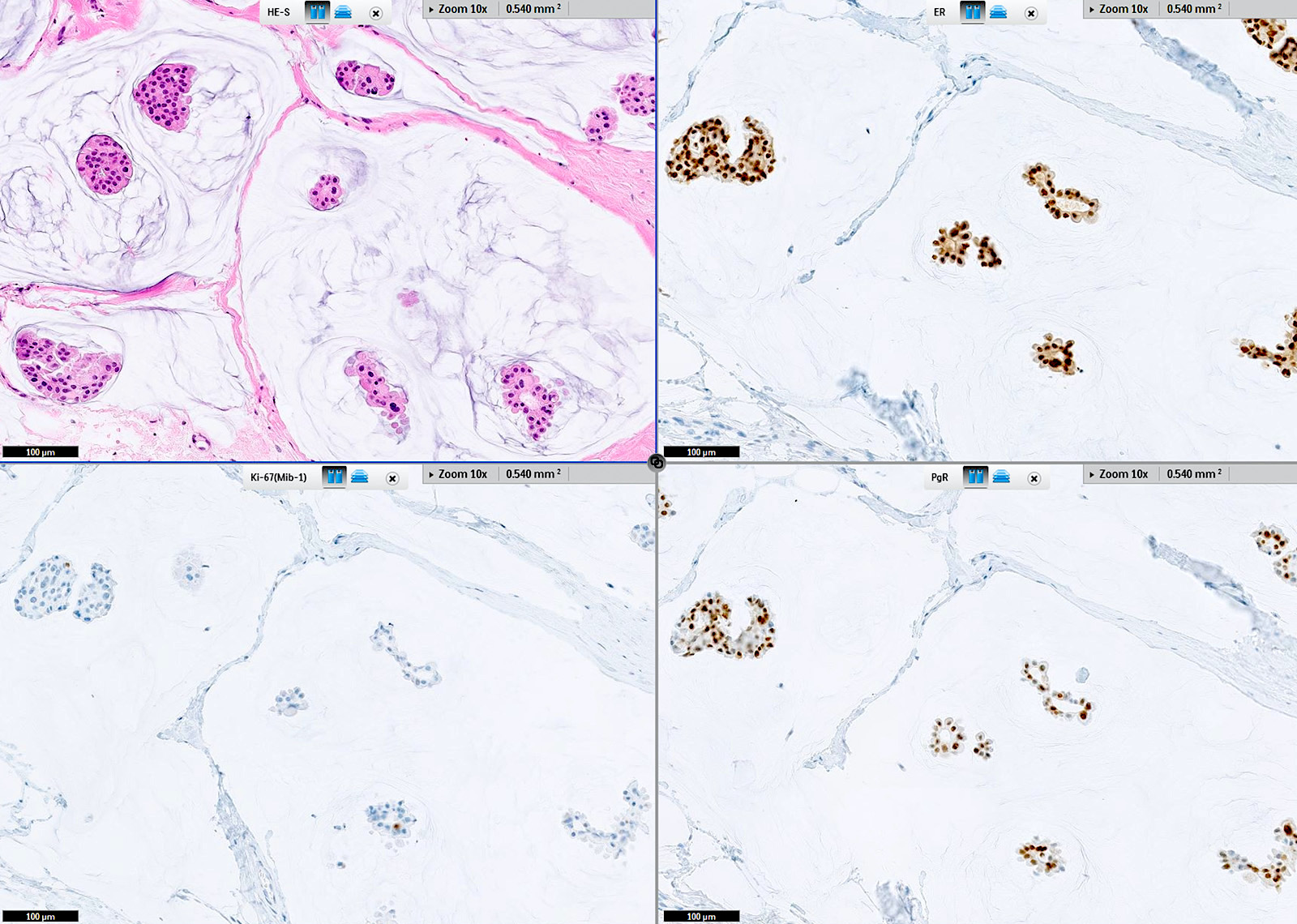
Benign breast lobule(s)
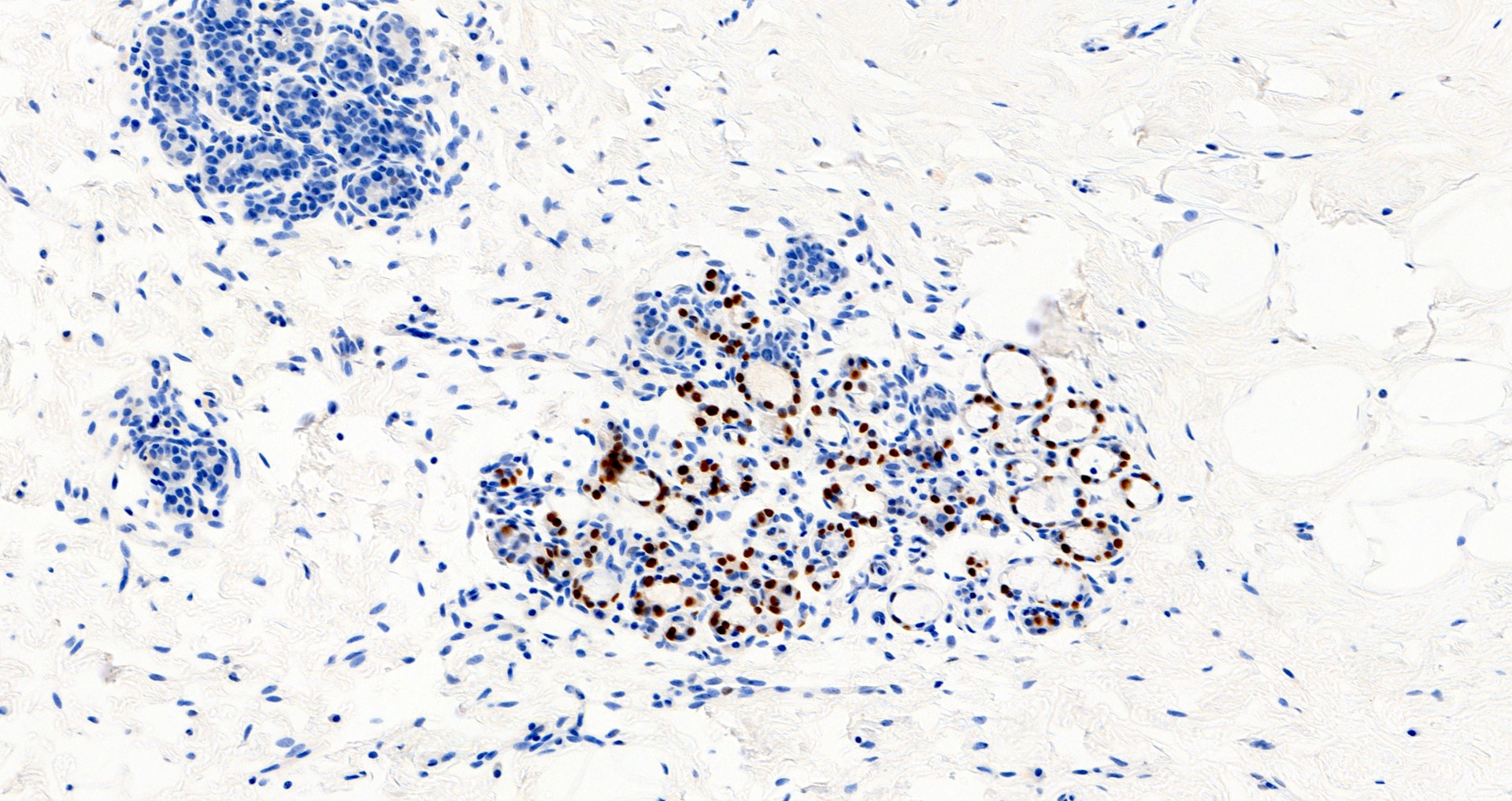
Benign breast lobule(s)

Breast and blood vessel
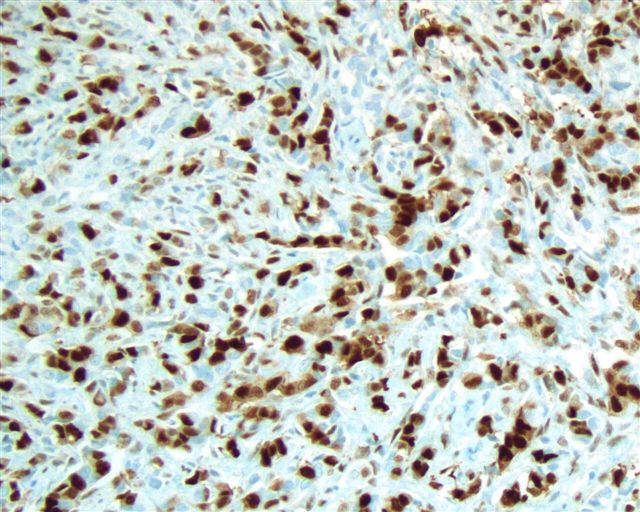
Breast, invasive ductal carcinoma
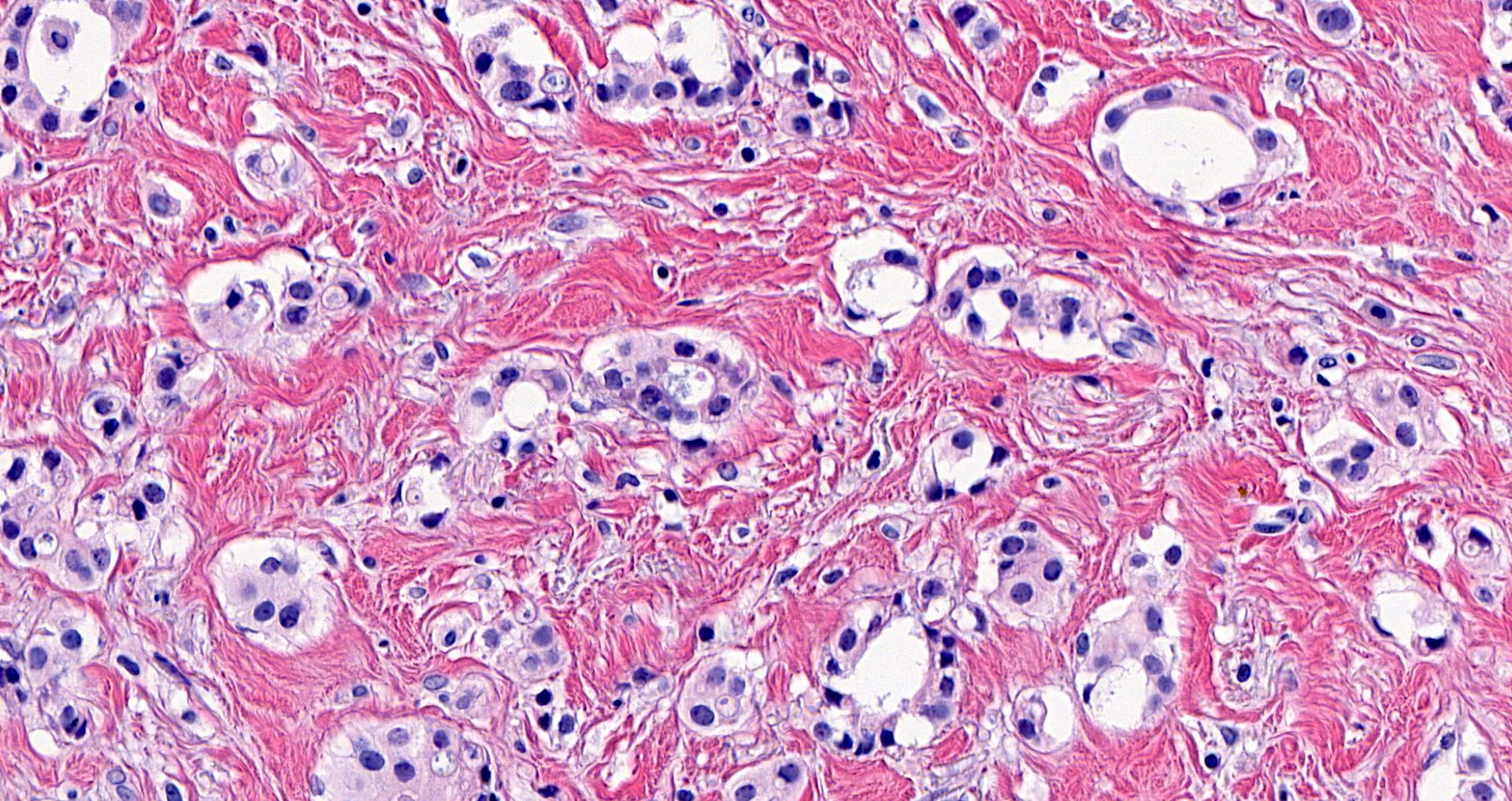
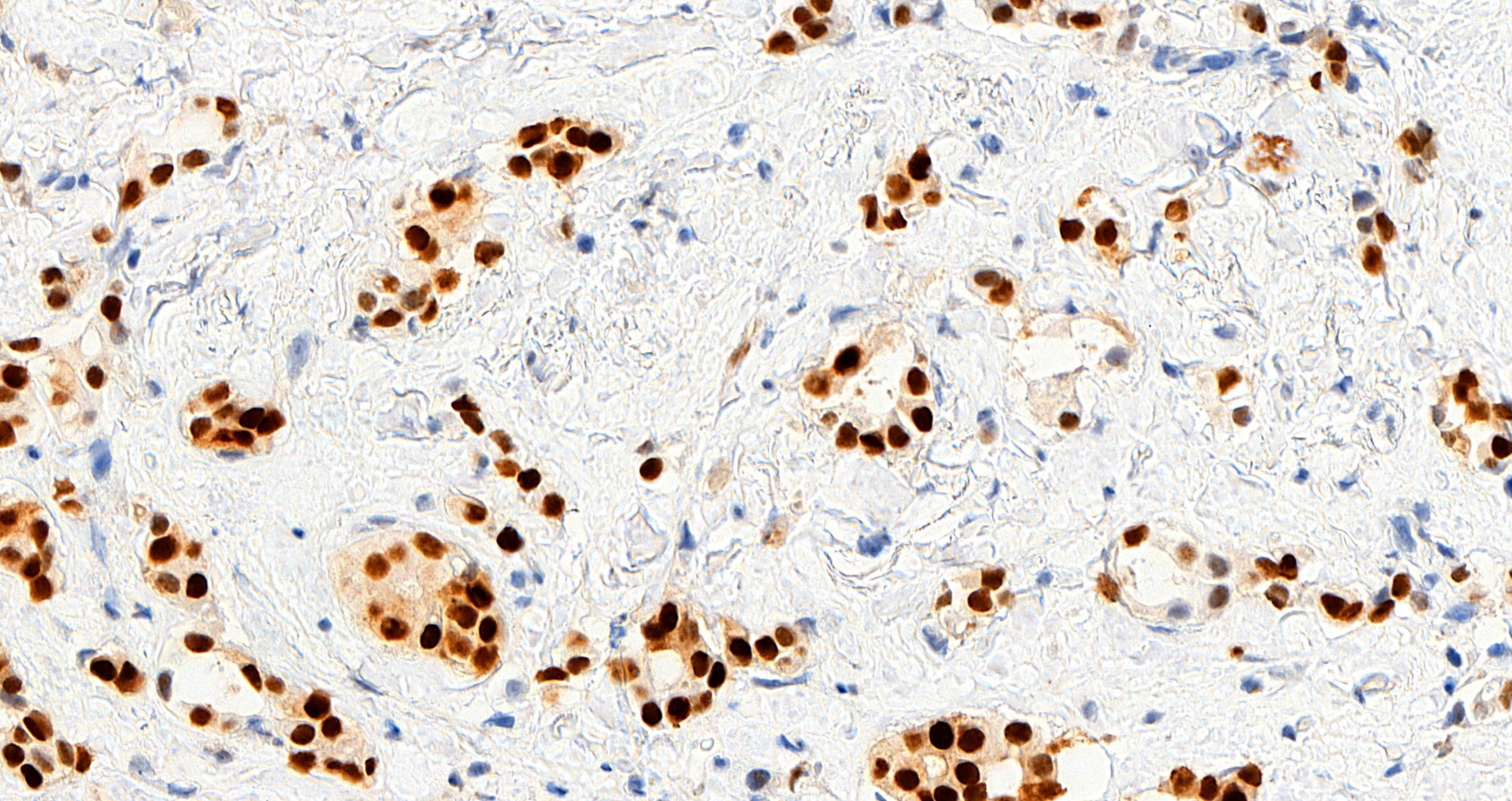
Breast, mucinous carcinoma
Cervix, metastatic breast cancer
Uterus, endometrial polyp
Virtual slides
Images hosted on other servers:

Breast, invasive ductal carcinoma, PR

Brain, angiomatous meningioma, PR
Positive staining - normal
- Breast epithelial cells, Toker cells
- Ovarian stroma
- Endocervical epithelial and stromal cells
- Islets of Langerhans of pancreas (Anal Cell Pathol (Amst) 2022;2022:6412148)
- Stromal cells of prostate (Anal Cell Pathol (Amst) 2022;2022:6412148)
- Stromal cells of seminal vesicle (Anal Cell Pathol (Amst) 2022;2022:6412148)
- Smooth muscle, including smooth muscle containing blood vessels (Circulation 1999;99:2688)
Positive staining - disease
- Breast: fibroadenoma (stromal cells), myofibroblastoma, phyllodes tumors (epithelial cells), pseudoangiomatous stromal hyperplasia, intraductal papilloma, columnar cell lesion
- Breast carcinoma (usually well differentiated tumors, including lobular, mucinous, papillary and tubular subtypes)
- Endometrial adenocarcinoma (75 - 96%)
- Cervical carcinoma: endometrioid, minimal deviation
- Endometriosis (glands and stroma)
- Uterus: endometrial carcinoma, endometrial stromal tumors, leiomyoma, smooth muscle tumor of uncertain malignant potential (STUMP); epithelioid leiomyosarcoma (54%) (Anal Cell Pathol (Amst) 2022;2022:6412148, Am J Surg Pathol 2022;46:464)
- Ovarian tumors: endometrioid carcinoma (64.2%), ependymoma, fibromatosis (88%), granulosa cell (juvenile), mucinous borderline endocervical type, high grade serous (50%) (Gynecol Oncol 2005;96:671, Biosci Rep 2021;41:BSR20210478)
- Kidney: mixed epithelial and stromal tumor
- Liver: biliary cystadenoma (stroma), hepatic adenoma
- Lymphangioleiomyomatosis
- Soft tissue aggressive angiomyxoma, angiomyofibroblastoma, cellular angiofibroma
- Solitary fibrous tumor
- Meningioma (fibrous, myxoid and secretory) (39 - 88%) (Front Oncol 2021;11:611218)
- Pancreas: solid pseudopapillary neoplasm (63%)
Negative staining
- Breast: apocrine metaplasia and carcinomas, microglandular adenosis, myoepithelium and myoepithelial tumors, cylindroma, fibromatosis
- Breast carcinomas - various (triple negative, including adenosquamous, basal-like, BRCA1 related, medullary, mucinous cystadenocarcinoma, metaplastic; also lipid rich)
- Endocervical adenocarcinoma
- Ovary: clear cell carcinoma, Leydig cell tumor, Sertoli cell tumor, steroid cell tumor
- Salivary gland intraductal and other carcinomas
- Uterus: serous carcinoma, endometrial clear cell carcinoma (Anal Cell Pathol (Amst) 2022;2022:6412148)
Sample pathology report
- Left breast, 3 o'clock, 3 cm from the nipple, core biopsy:
- Invasive ductal carcinoma, preliminary modified Bloom Richardson (Nottingham) grade 1 (2+1+1) (see comment)
- Comment: immunohistochemical stains show invasive carcinoma to be
- Estrogen receptor (91 - 100%, strong) positive
- Progesterone receptor (91 - 100%, strong) positive
- HER2 / neu (1+) negative for overexpression
- Controls are appropriate
Additional references
Board review style question #1
A middle aged woman presents with a 1 cm breast mass detected on breast imaging screening. Progesterone receptor staining is shown. How should this immunohistochemical stain be interpreted?
- Low positive, good prognosis
- Low positive, poor prognosis
- Negative, poor prognosis
- Positive, good prognosis
- Positive, poor prognosis
Board review style answer #1
D. Positive, good prognosis. Answer D is correct because positive PR expression is associated with a better prognosis than negative expression in invasive ductal breast carcinomas. Answer E incorrect because the biopsy of the breast mass shows a low grade invasive ductal carcinoma with diffuse, strong PR positivity, which is a favorable prognostic feature. Answers A, B and C are incorrect because the carcinoma is not low positive (1 - 10%, a category currently used for ER but not PR) or negative (< 1%) for PR.
Comment Here
Reference: Progesterone receptor (PR)
Comment Here
Reference: Progesterone receptor (PR)

