Stains & CD markers
Congo red


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Congo red
Congo red
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Debra L. Zynger, M.D.
Last author update: 28 June 2022
Last staff update: 28 June 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Congo red
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Clinical features | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) images | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Board review style question #1 | Board review style answer #1Cite this page: Molina Nunez M, Iczkowski KA. Congo red. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainscongored.html. Accessed April 1st, 2025.
Definition / general
- Congo red is a direct diazo dye used for staining amyloid in tissue sections (Biosci Rep 2019;39:BSR20181415)
- This organic compound forms complexes with the misfolded proteins deposited in amyloidosis; analysis of the emission spectra from these complexes reveals the optical reactivity under polarized light, described as apple green birefringence (Acta Biochim Pol 2019;66:39)
Essential features
- Congo red stain is the gold standard for the demonstration of amyloid in tissue sections
- Used to evaluate the presence and extent of amyloidosis in different organs
- Common diseases for Congo red stain include primary amyloidosis, amyloid light chain (AL) seen in plasma cell dyscrasias, amyloid A (AA) associated with inflammatory conditions
- 2 factors are important for Congo red amyloid reaction: the linearity of the dye molecule and the β pleated sheet configuration (Suvarna: Bancroft’s Theory and Practice of Histological Techniques, 8th Edition, 2018)
Terminology
- Also called amyloid stain
Pathophysiology
- Amyloidosis is a rare and heterogeneous group of disorders that is characterized by the deposition of abnormally folded proteins (Acta Haematol 2020;143:322)
- A key event in the development of AL amyloidosis is the change in the secondary or tertiary structure of an abnormal monoclonal light chain, which results in an unstable conformation
- This conformational change is responsible for abnormal folding of the light chain, rich in β leaves, which assemble into monomers that stack together to form amyloid fibrils (Orphanet J Rare Dis 2012;7:54)
- Amyloid formation involves a combination of several factors, including a prolonged increase in concentration of proteins that are prone to misfolding as a result of an acquired or hereditary mutation or wild type proteins with an intrinsic propensity to misfold, or a proteolytic remodeling of a wild type protein into an amyloidogenic fragment
- Under normal conditions, misfolded proteins are promptly eliminated by the protein quality control systems; amyloidosis occurs when these systems are overwhelmed by an increased supply of misfolded proteins or when their processing capacity is reduced due to aging (Acta Haematol 2020;143:322)
- Amyloid fibril Congo red complex demonstrates green birefringence owing to the parallel alignment of dye molecules along the β pleated sheet
Clinical features
- Per the International Society of Amyloidosis, these disorders are classified as systemic or localized and as acquired or hereditary based on the pathogenesis (Amyloid 2020;27:217, J Intern Med 2021;289:268)
- Most common types are AL, AA, ATTR (amyloid transport protein transthyretin) and dialysis related amyloidosis or beta2M type (StatPearls: Amyloidosis [Accessed 19 April 2022])
- Congo red stain is mostly used for systemic or localized amyloidosis, such as AL amyloid seen in clonal proliferation plasma cell dyscrasias, AA amyloid associated with inflammatory conditions, Aβ amyloid fibrils in Alzheimer disease and TTR amyloidosis due to either familial gene mutation or wild type protein (formerly called senile amyloidosis)
- Clinical presentation is heterogeneous and the severity depends on the organ affected; most patients with AL suffer from monoclonal gammopathy of undetermined significance (Nephrol Dial Transplant 2019;34:1460)
- Cardiac involvement is most often diagnosed in patients with light chain and wild type or hereditary ATTR amyloidosis (Clin Med (Lond) 2018;18:s30)
- Amyloids can be detected in the kidney, liver, heart, central nervous system, peripheral nervous system, autonomic nervous system, skin and other organs
- Diagnosis relies on the identification of the fibrillar deposits in tissues and typing of the amyloid (Kasper: Harrison's Manual of Medicine, 20th Edition, 2019)
- While biopsy on a target organ is most sensitive if amyloid is clinically suspected, a less invasive biopsy is recommended (e.g., abdominal fat) (Hum Pathol 2018;72:71)
- Emanation of new techniques of proteomic analysis such as mass spectrometry / laser microdissection, has provided greater accuracy in amyloid typing (Protoplasma 2020;257:1259)
Interpretation
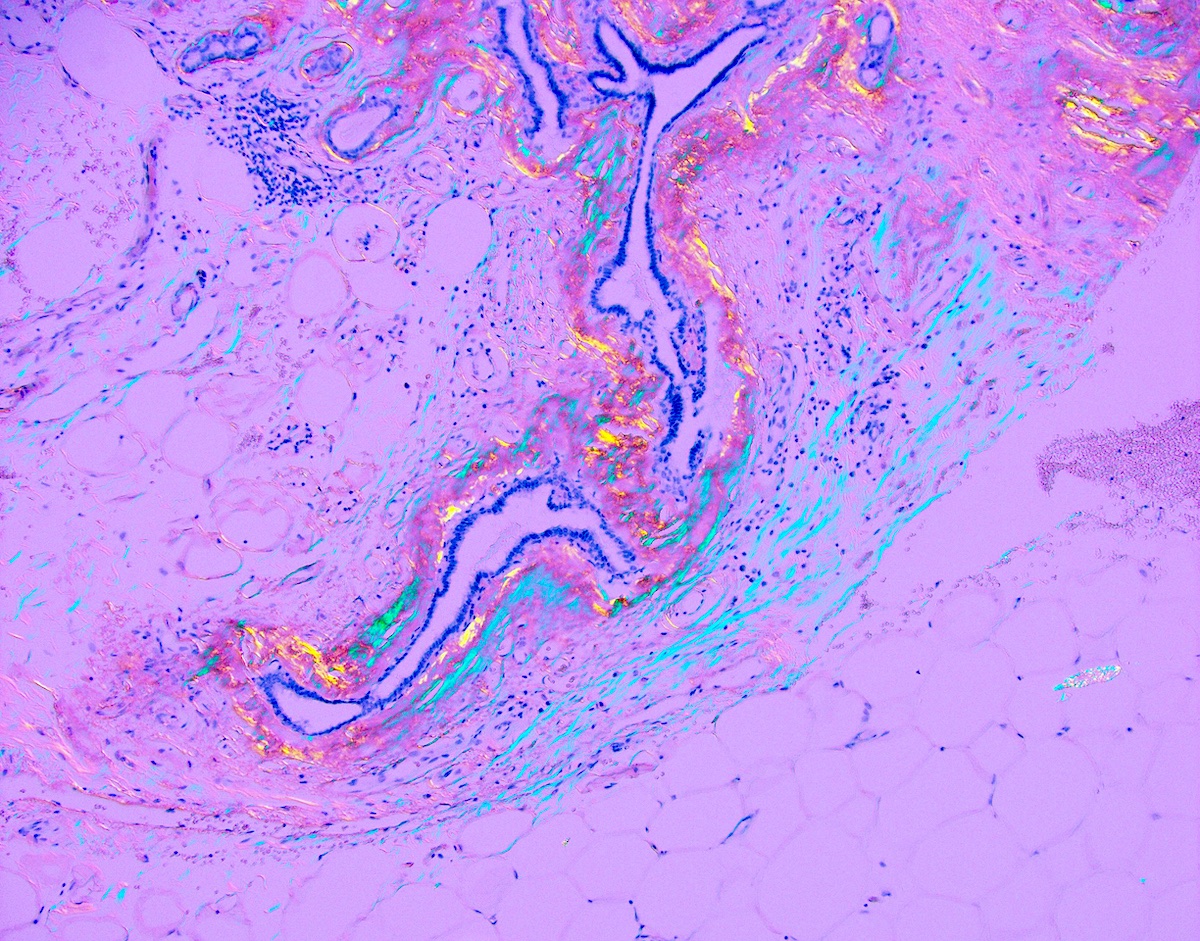
- Amyloid deposits in tissue exhibit a deep red or salmon color, whereas elastic tissue remains pale pink
- When viewed under polarized light, amyloid deposits exhibit apple green birefringence, orange-red fluorescence using Texas red filter visualized under ultraviolet light
- Thickness of the section is critical (8 - 10 μm) (Gattuso: Differential Diagnosis in Surgical Pathology, 2nd Edition, 2010)
- Rotating the slide or the polarizing filter is important for visualizing the birefringence (Diagn Pathol 2019;14:57)
- Improved sensitivity is reported when using a metallurgical polarized microscope (Diagn Pathol 2019;14:57)
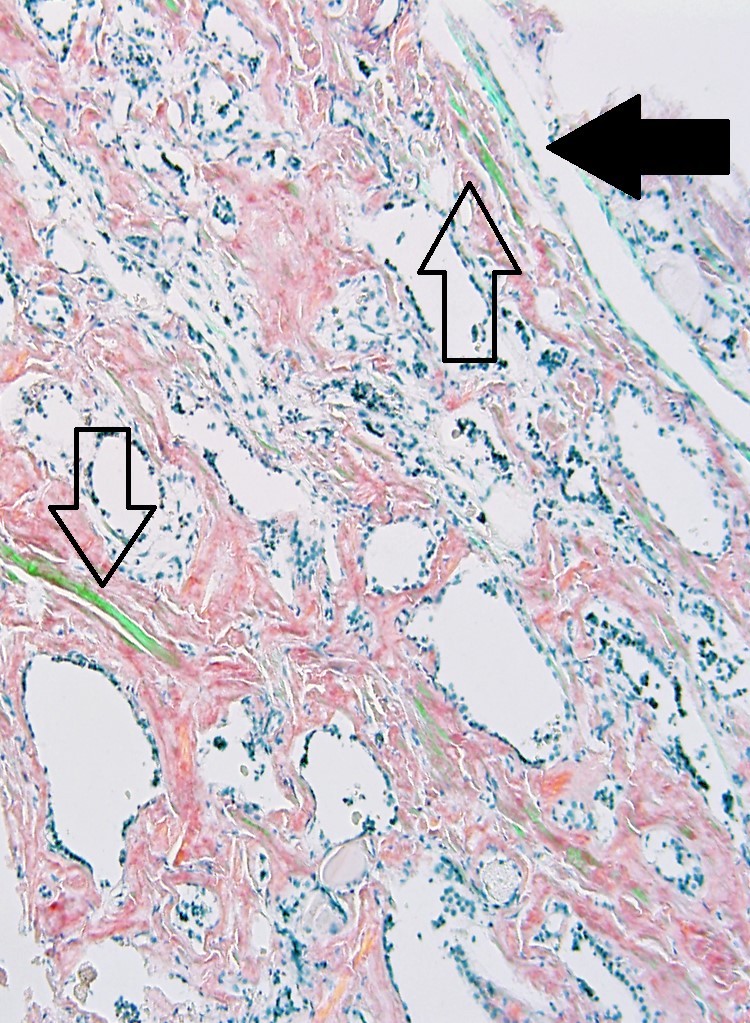
- Tissue elements such as collagen, elastin (and others) may display birefringence of varying colors that may be misinterpreted as amyloid (Hum Pathol 2014;45:1766)
- Do not mistake the blue-green of collagen for the lime green of amyloid
Uses by pathologists
- Evaluate the presence and extent of systemic or localized amyloidosis (Virchows Arch 2018;473:627)
- Evaluate the progression of multiple myeloma and other plasma cell dyscrasias (Am J Hematol 2020;95:848)
Prognostic factors
- Amyloid heart disease is the main prognostic factor with an unfavorable outcome (Future Rheumatol 2008;3:369)
- Multiple myeloma associated amyloidosis is an independent high risk prognostic factor (Ann Hematol 2009;88:59)
Microscopic (histologic) images
Contributed by Christian M. Schürch, M.D., Ph.D. and Kenneth A. Iczkowski, M.D.
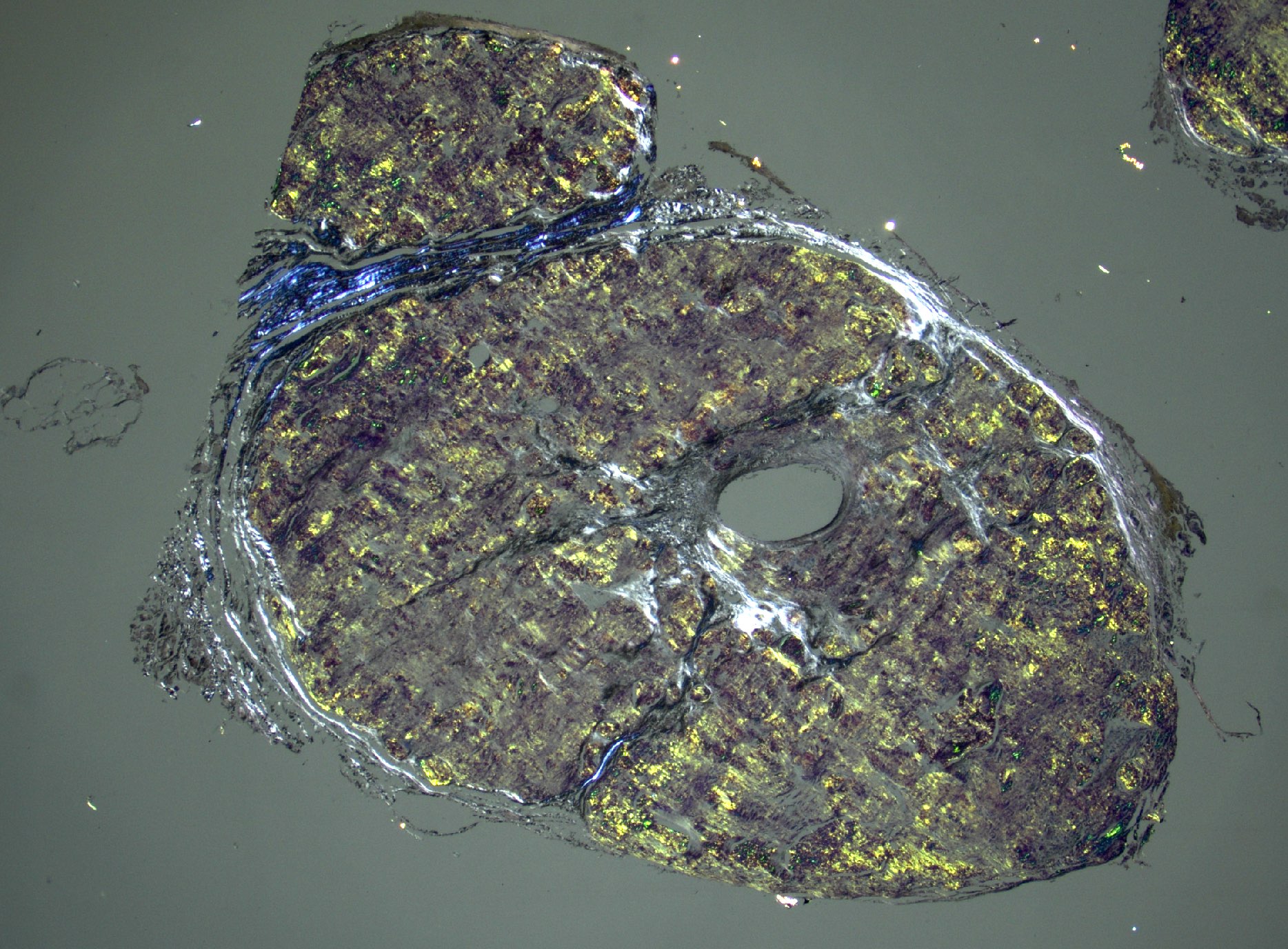

Amyloidosis

Transthyretin amyloidosis
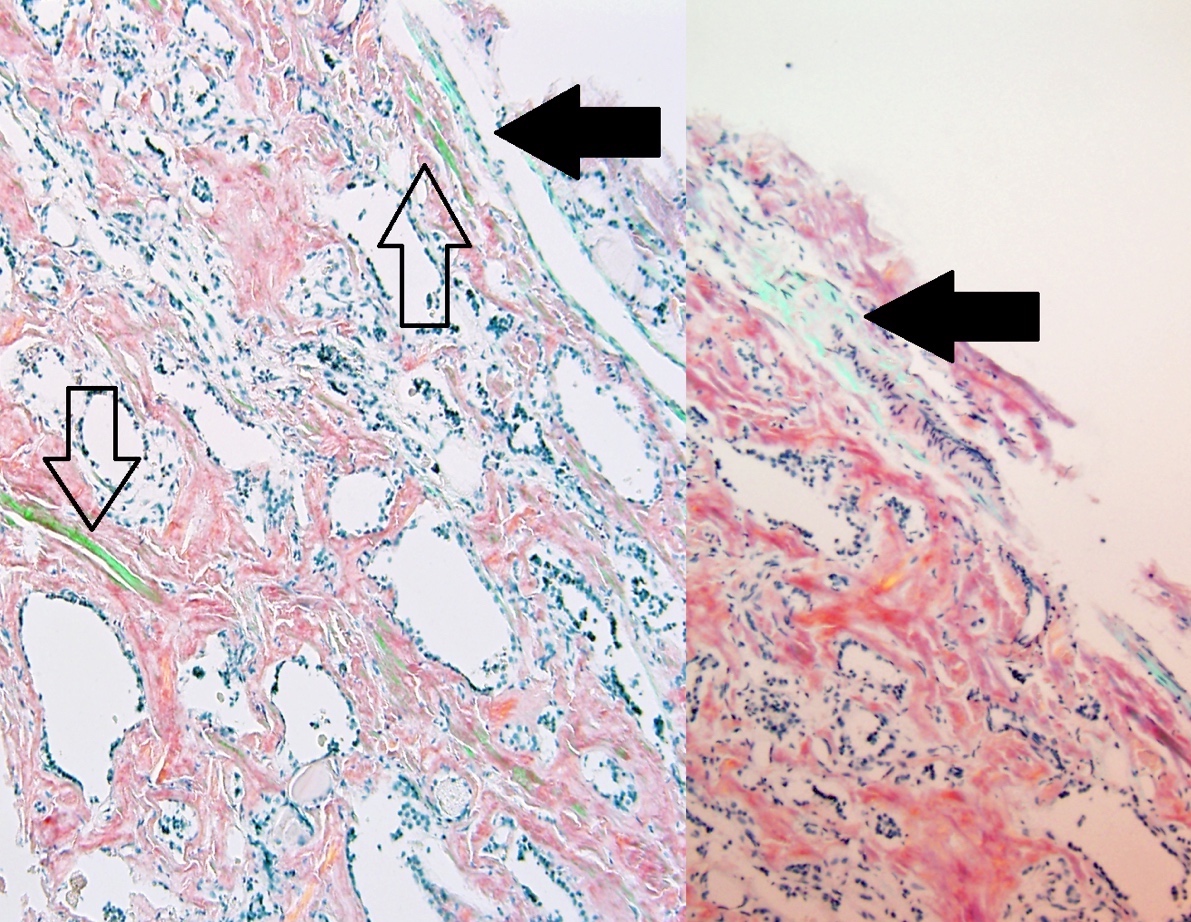
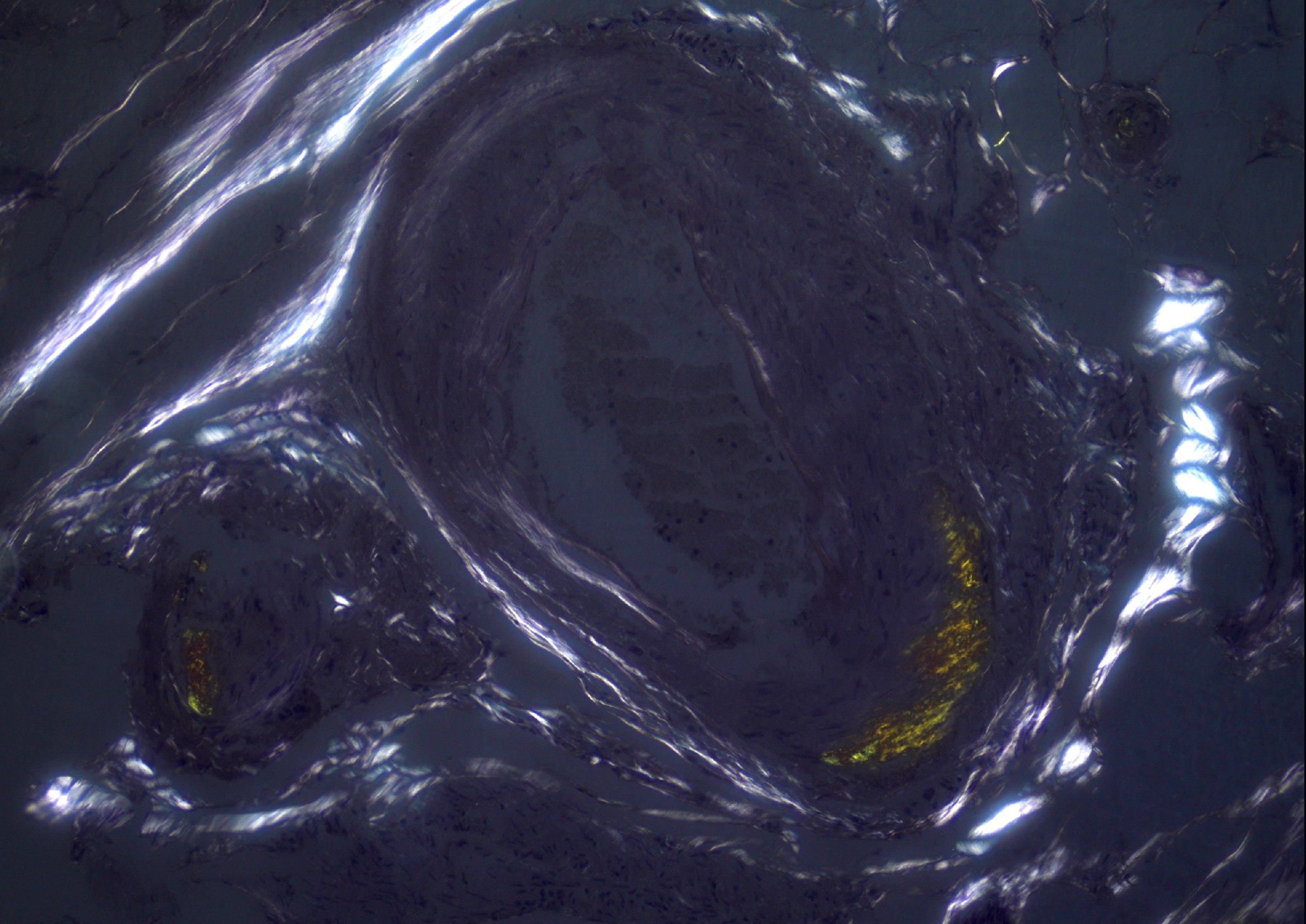
Distinguishing the correct color
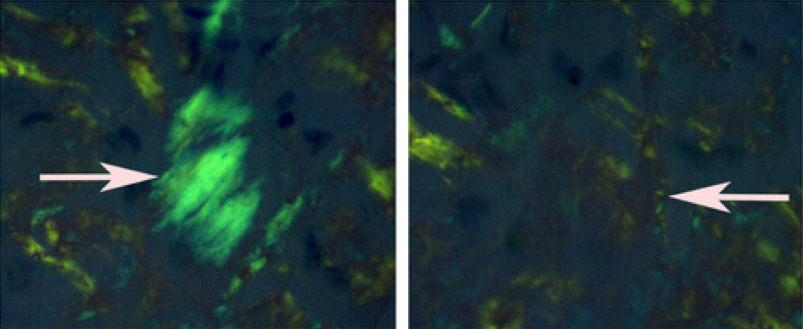
Rotation to visualize Congo red

Optimized AL amyloid imaging
Breast amyloidosis
Positive staining - normal
- None
Positive staining - disease
- Primary systemic amyloidosis
- Breast (BMC Surg 2016;16:62)
- Central nervous system (J Clin Neurosci 2006;13:159)
- Heart (Rev Assoc Med Bras 2018;64:787)
- Kidney (J Int Med Res 2019;47:1778, Am J Kidney Dis 2019;74:276)
- Liver (J Int Med Res 2019;47:1778)
- Muscle (Muscle Nerve 1995;18:1016)
- Nerve, gastrointestinal tract, lung and soft tissue (Am J Hematol 2005;79:319)
- Salivary gland (Otolaryngol Head Neck Surg 2006;135:471)
- Skin (J Clin Diagn Res 2017;11:WC01)
- Spleen (Eur J Case Rep Intern Med 2018;5:0001010)
- Stomach (Case Rep Gastroenterol 2018;12:317)
- Testis (Urology 2002;59:201)
- Tongue and eyelid (Clin Chim Acta 2019;494:112)
- Amyloidosis associated with multiple myeloma
- Bone marrow (Ann Hematol 2010;89:469)
- Heart (Rev Med Panama 1994;19:147)
- Joint (Q J Med 1981;50:417)
- Kidney (Recenti Prog Med 1994;85:123)
- Lung (BMC Cancer 2018;18:802)
- Muscle (Int J Hematol 2012;95:716)
- Skin (Oncol Lett 2016;11:3617)
- Stomach (Case Rep Gastrointest Med 2015;2015:320120)
- Thyroid (Arch Pathol Lab Med 1990;114:429)
- Tongue (J Oral Pathol 1988;17:554)
- Secondary systemic amyloidosis
- Kidney in celiac disease (ACG Case Rep J 2018;5:e24)
- Kidney in long term inflammatory disorder (Rheum Dis Clin North Am 2018;44:585)
- Kidney in systemic lupus erythematosus (Hum Pathol 1981;12:853)
- Kidneys, retroperitoneal lymphoma mass, blood vessels and adrenal glands in non-Hodgkin lymphoma (Hum Pathol 2004;35:1041)
- Secondary corneal amyloidosis in keratoconus (Cornea 2011;30:716)
- Tongue in long term hemodialysis (Spec Care Dentist 2018;38:434)
- Medullary thyroid carcinoma (Acta Cytol 1992;36:137)
- Alzheimer disease (Uversky: Bio-nanoimaging - Protein Misfolding and Aggregation, 1st Edition, 2014)
- Amyloid tumor of the breast (Surg Case Rep 2019;5:31)
- Amyloid tumor of the parotid gland (Oral Surg Oral Med Oral Pathol 1988;66:466)
- Amyloid insulin bodies at an insulin injection site (Am J Dermatopathol 2018;40:527)
- Lumbar epidural amyloidoma (Neurosurgery 2005;57:E196)
Negative staining
- Hyalinizing trabecular adenoma of the thyroid gland (Am J Surg Pathol 1987;11:583)
- Fibrillary glomerulonephritis (Kidney Int 2003;63:1450)
- Primary central nervous system nonamyloidogenic light chain deposition disease (Int J Surg Pathol 2017;25:755)
- Cardiac fibrosis due to infarct or multiple infarctions
Sample pathology report
- Heart, endomyocardium, biopsies:
- Polarizable material evident by Congo red stain, consistent with amyloid protein
Board review style question #1
Which of the following lesions should be negative for Congo red?
- Bone marrow in a patient with multiple myeloma
- Hyalinizing trabecular adenoma of the thyroid gland
- Kidney in a patient with systemic lupus erythematosus
- Liver in a patient with systemic light chain amyloidosis
- Medullary thyroid carcinoma
Board review style answer #1
B. Hyalinizing trabecular adenoma of the thyroid gland. Typical features of hyalinizing trabecular adenoma of the thyroid gland include oval and elongated nuclei, perinucleolar vacuoles, acidophilic nuclear inclusions, fine nuclear grooving and infrequent mitotic figures. Perivascular hyaline fibrosis and cell degeneration can mimic amyloid but these tumors are Congo red negative (Am J Surg Pathol 1987;11:583).
Comment Here
Reference: Congo red
Comment Here
Reference: Congo red
