Stains & CD markers
CEA / CD66e


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: CEA
Related topics: General, CD66b, CD66c, CD66d, CD66f
CEA / CD66e
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Maryam Kherad Pezhouh, M.D., M.Sc.
Last author update: 6 July 2022
Last staff update: 30 May 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: CEA
Related topics: General, CD66b, CD66c, CD66d, CD66f
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Clinical features | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) images | Positive staining - normal | Positive staining - not malignant | Positive staining - malignant | Negative staining - disease | Sample pathology report | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Skorobogatko V, Umphress B. CEA / CD66e. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainscea.html. Accessed March 30th, 2025.
Definition / general
- Glycosyl phosphatidyl inositol (GPI) cell surface anchored glycoproteins that function as a ligand for various selectins
- Immunohistochemical antibodies to carcinoembryonic antigen (CEA) are either polyclonal (pCEA) or monoclonal (mCEA)
Essential features
- Usually considered an epithelial marker with expression in various adenocarcinomas
- Can highlight ductal differentiation (i.e., poroma, porocarcinoma)
- In addition to immunostaining, CEA is a nonspecific serum biomarker that can be elevated in various malignancies (e.g., colorectal cancer)
Terminology
- CEA, carcinoembryonic antigen and CEACAM5
Pathophysiology
- Normally detected in glycocalyx of fetal epithelial cells
- Acts as a paracrine factor by activating fibroblasts through STAT3 and AKT1-mTORC1 signaling pathways and promoting their transformation into cancer associated fibroblasts (Int J Cancer 2018;143:1963)
- Involved in mucosal colonization of bacteria: lipid A, a component of gram negative bacteria, may prevent the release of CEA from mucosal surfaces, facilitating bacterial colonization (Cell Mol Biol Lett 2015;20:374)
- May play a role in the metastasis of cancer cells by protecting metastatic cells from death, promoting expression of adhesion molecules and survival of malignant cells; promotes angiogenesis (Recent Pat Biotechnol 2018;12:269)
Clinical features
- Serum CEA is associated with colorectal carcinoma; preoperative levels can be associated with advanced or metastatic disease and poorer prognosis
- Postoperatively, failure of CEA to return to normal has been found to be an indicator of residual or recurrent disease (Ann Coloproctol 2019;35:294)
- Postoperative CEA levels can be useful for detecting early recurrence of lung adenocarcinoma (Korean J Thorac Cardiovasc Surg 2015;48:335)
- Serum CEA is elevated in allergic bronchopulmonary aspergillosis (ABPA) (Sci Rep 2021;11:4025)
- Increased CEA levels correlate with eosinophil levels indicating eosinophils may function to secrete CEA
- Has been reported to be elevated in patients with COVID-19 pneumonia (J Cancer Res Clin Oncol 2020;146:3385)
- Pure small cell lung cancer (SCLC) versus small cell lung cancer combined with other pathology (CSCLC): preoperative serum CEA > 6 ng/mL found more frequently in CSCLC than pure SCLC (Adv Clin Exp Med 2017;26:1091)
Interpretation
- Variable cytoplasmic or membrane enhancement (focal / diffuse, weak / strong)
- Varying intensities of circumferential staining in ductal differentiation of the skin
Uses by pathologists
- Pulmonary adenocarcinoma: monoclonal CEA can demonstrate increased specificity for lung adenocarcinoma when compared with mesothelioma (Histopathology 2006;48:223)
- CEA can help to distinguish metastatic lung adenocarcinoma (CEA+ in 53.8%, diffuse cytoplasmic staining with membrane enhancement) from mesothelioma in pleural effusions (Iran J Pathol 2019;14:122)
- It is noted, however, that a panel of markers is recommended to more reliably differentiate between these 2 tumors
- Distinguishes between hidradenomas (CEA+) and cutaneous clear cell renal cell carcinoma (CEA-) (J Cutan Pathol 2017;44:612)
- Hepatocellular carcinoma: canalicular pattern for polyclonal CEA is 50 - 90% sensitive for hepatocellular carcinoma, > 95% specific (Mod Pathol 2002;15:1279)
- Monoclonal CEA is usually negative (Hum Pathol 2002;33:1175)
- Microvillous inclusion disease of small intestine: pCEA bright apical cytoplasmic blush / staining on surface enterocytes (Ultrastruct Pathol 2010;34:327)
- Cysts (various): CEA levels > 5 ng/dL in ascites fluid are associated with malignancy (J Clin Pathol 2001;54:831)
- Fluid in cysts may be CEA+ even when benign (Mod Pathol 1998;11:1171)
Prognostic factors
- Breast carcinoma: 88.3% specific and 46.2% sensitive for diagnosis of metastatic disease (Cancer Treat Res Commun 2021;28:10040)
- Cholangiocarcinoma: elevated CEA levels associated with decreased survival (Sci Rep 2017;7:16975)
- Colorectal carcinoma: monitor serum levels to detect recurrence (Int J Biol Markers 2019;34:60)
- Elevated preoperative serum levels are a poor prognostic factor (Cancer Biomark 2016;16:245, Pol Przegl Chir 2014;86:319)
- Elevated postoperative CEA levels are associated with increased risk of recurrence especially within the 12 months following surgery (JAMA Oncol 2018;4:309)
- Caution: elevated levels also present in cirrhosis, biliary obstruction, hepatitis, inflammatory bowel disease, smokers and postsurgical bowel sequestration with mucocele (Arch Pathol Lab Med 2003;127:1376)
- Elevated levels are preoperatively associated with a worse 3 year overall survival in invasive urothelial carcinoma (Urol Oncol 2014;32:648)
- Esophageal adenocarcinoma: elevated pretreatment CEA levels are associated with early treatment failure and decreased overall survival (Am J Clin Oncol 2019;42:345)
- Extramammary Paget disease (EMPD): CEA levels predict metastasis and treatment response (Br J Dermatol 2019;181:535)
- Gallbladder carcinoma: CEA > 5 ng/mL can predict metastatic disease in anicteric patients with 80% specificity and 52% sensitivity (BMC Cancer 2020;20:826)
- Gastric carcinoma: elevated levels aid in diagnosis and are associated with lymph node metastasis (BMC Gastroenterol 2020;20:100)
- Higher values are associated with unresectable esophageal cancer; is an accurate biomarker of occult advanced disease (World J Surg 2015;39:424)
- Intraductal papillary mucinous neoplasm of pancreas: high CEA level in pancreatic juice is an independent predictor of malignant transformation within 5 years (hazard ratio 17, p = 0.02) (J Gastroenterol 2019;54:1029)
- Lung adenocarcinoma: elevated levels in nonlepidic histologic subtype associated with decreased 5 year survival (Asian Pac J Cancer Prev 2015;16:3857)
- Medullary thyroid cancer: CEA > 271 ng/mL associated with advanced tumor size, staging, metastasis to central compartment and decreased chance of biochemical cure; CEA > 500 ng/mL associated with significant mortality (J Otolaryngol Head Neck Surg 2018;47:55)
- Higher CEA levels are associated with prediction of lateral lymph node metastasis (Clin Lab Anal 2020;34:e23278)
- Pancreatic adenocarcinoma: monoclonal CEA is 92% sensitive for metastases versus 0% for bile duct adenoma (Am J Surg Pathol 2005;29:381)
- Elevated in 30 - 60% of pancreatic cancer patients and high CEA, > 5 ng/mL, is associated with decreased overall survival (Pancreatology 2016;16:859)
Microscopic (histologic) images
Contributed by Brandon Umphress, M.D. and Andrey Bychkov, M.D., Ph.D.
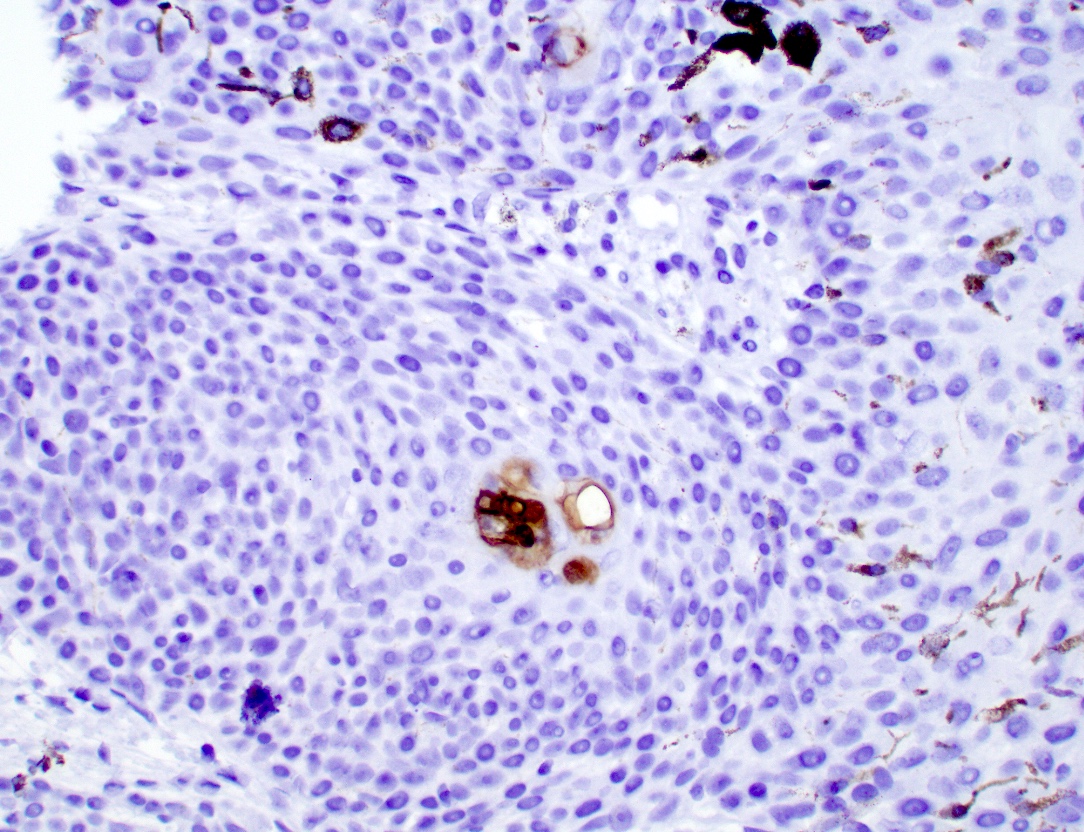

Porocarcinoma, ductal differentiation
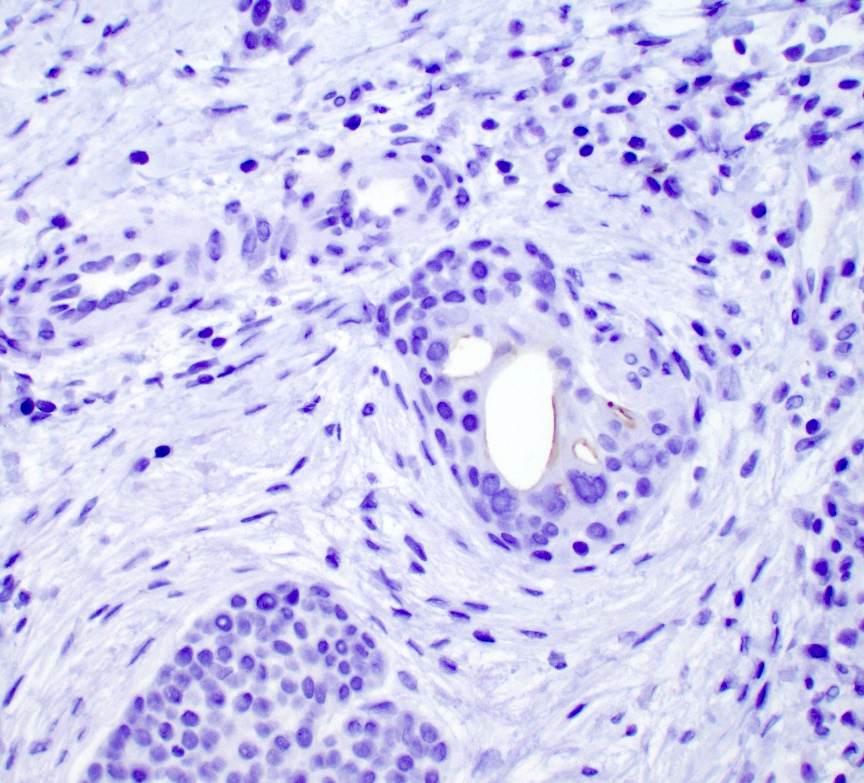
Porocarcinoma with invasion into the dermis
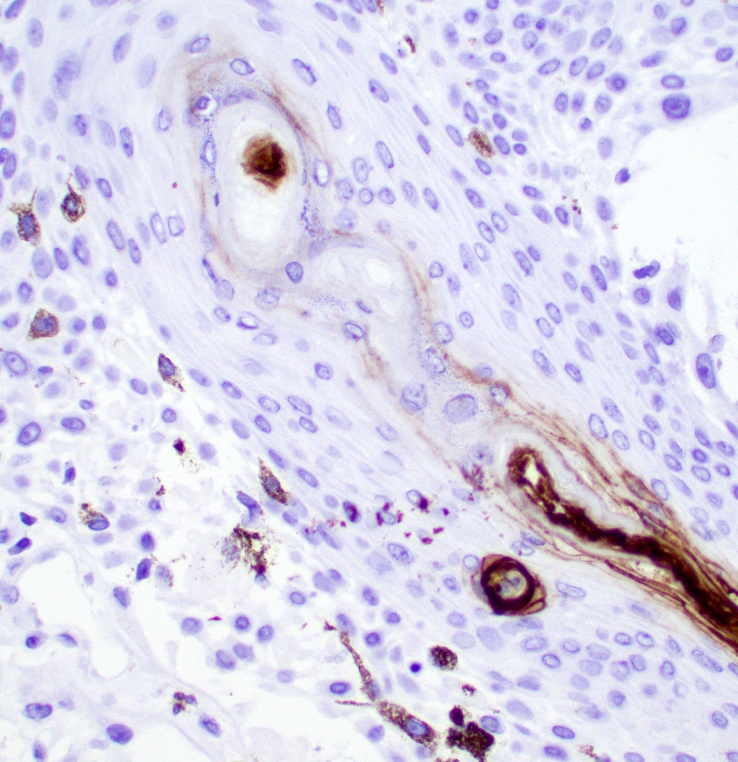
Acrosyringeal unit
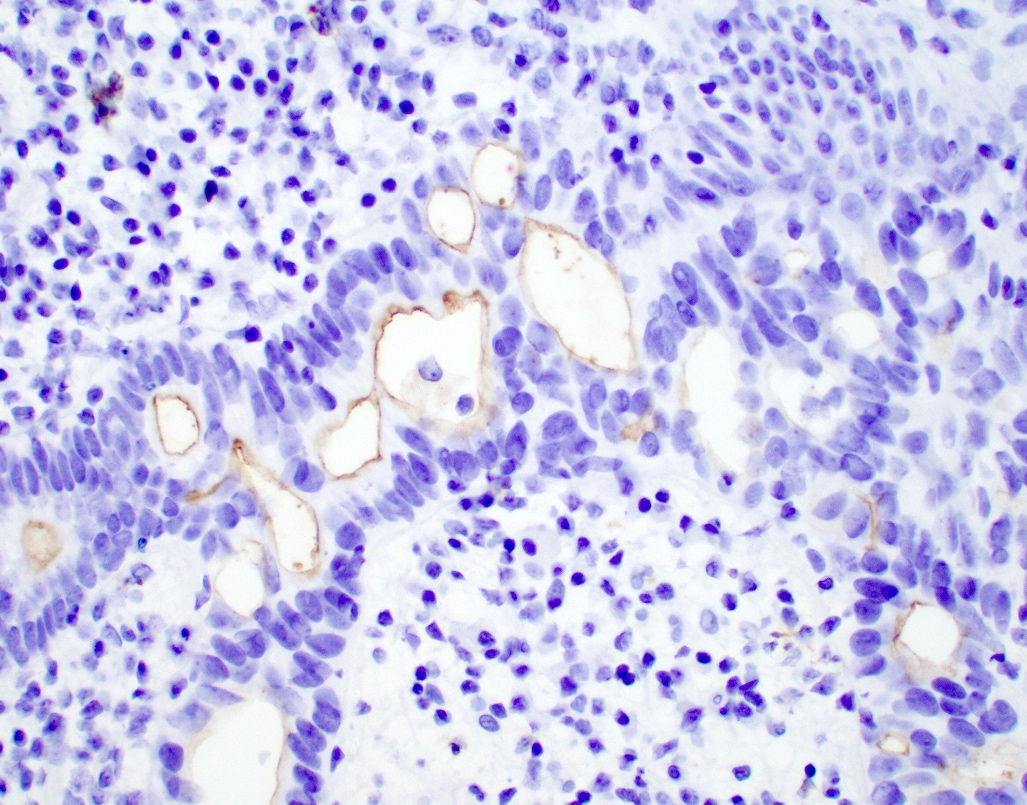
CEA expression in a poorly differentiated carcinoma
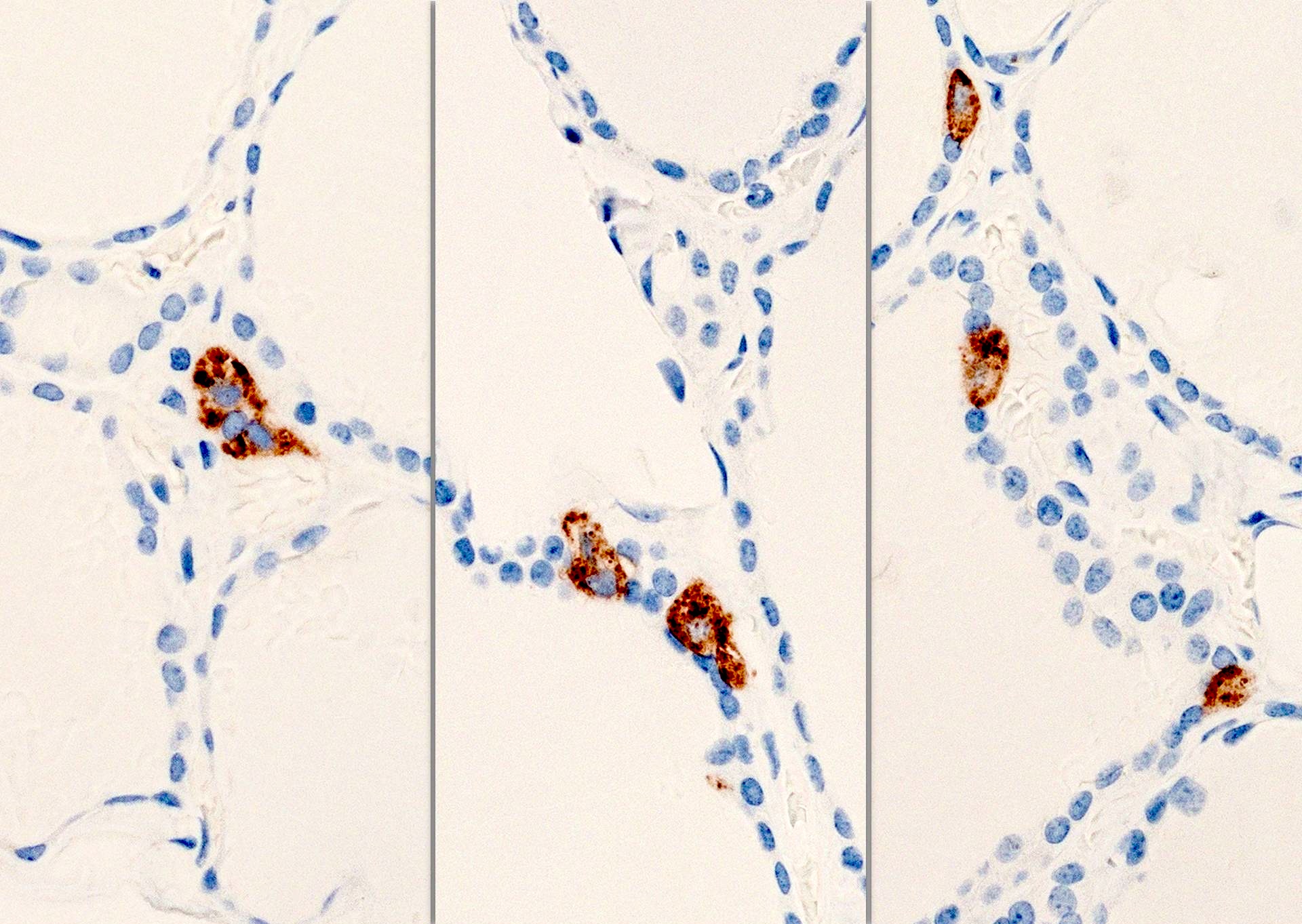
C cells in relation to thyroid follicle

Clustered C cells
Positive staining - normal
- Eccrine sweat glands
- Granulocytes and epithelial cells (apical surfaces)
- Biliary tract including gallbladder, colon (fetal), hepatocytes, prostatic secretory cells (25%) and small intestinal crypts
- Small intestinal goblet cell mucin (not intracytoplasmic), thyroid cell nests and C cells
Positive staining - not malignant
- Bizarre parosteal osteochondromatous proliferation (BPOP) (World J Surg Oncol 2016;14:35)
- Central odontogenic fibroma (focal and weak) (J Formos Med Assoc 2014;113:321)
- Chondroid syringoma (monoclonal, 53%) (G Ital Dermatol Venereol 2016;151:358)
- Clear cell papulosis (Dermatol Online J 2018;24:13030)
- Cutaneous clear cell hidradenoma (focal) (J Cutan Pathol 2016;43:702, J Cutan Pathol 2017;44:612)
- Eccrine angiomatous hamartoma, eccrine portion (Zhonghua Bing Li Xue Za Zhi 2016;45:467)
- Glandular cardiac myxoma (Indian J Pathol Microbiol 2017;60:319)
- Pulmonary ciliated muconodular papillary tumor (CMPT) (J Cardiothorac Surg 2019;14:143)
- Vaginal adenosis, gastric type (67%) (Am J Surg Pathol 2018;42:958)
- Vulvar interstitial / enteric heterotopia (Int J Gynecol Pathol 2014;33:258)
Positive staining - malignant
- Bile duct tumors (benign or malignant)
- Bladder adenocarcinoma and benign tumors
- Breast ductal carcinoma
- Carcinoma showing thymus-like differentiation of the thyroid (CASTLE) (Am J Surg Pathol 2006;30:994)
- Cervical adenocarcinoma (Arch Pathol Lab Med 2003;127:1586)
- Cholangiocarcinoma (monoclonal and polyclonal, cytoplasmic and luminal but not canalicular pattern)
- Colorectal carcinoma (almost all, throughout cell surface)
- Cutaneous apocrine carcinoma (diffuse) (Diagn Pathol 2015;10:64)
- Endocrine mucin producing sweat gland carcinoma (EMPSGC) (polyclonal) (Int J Dermatol 2014;53:1228)
- Gastric type adenocarcinoma
- Hepatoblastoma (polyclonal antibody, canalicular pattern, particularly in fetal subtype)
- Hepatocellular carcinoma (polyclonal CEA, canalicular pattern, 90%) (Hum Pathol 2005;36:1226)
- Hepatoid adenocarcinoma of the lung (monoclonal, 60%) (Mod Pathol 2014;27:535)
- Lung adenocarcinoma
- Lung squamous cell carcinoma (nonkeratinizing, 77%) (Mod Pathol 2006;19:417)
- Medullary thyroid carcinoma (91%) (Hum Pathol 2017;65:217)
- Microcystic adnexal carcinoma, solid variant (focal) (J Cutan Pathol 2018;45:897)
- Mixed adenoneuroendocrine carcinoma (MANEC), exocrine portion (Int J Clin Exp Pathol 2018;11:1499, Surg Case Rep 2016;2:133, Int J Clin Exp Pathol 2014;7:6395)
- Ovarian mucinous tumors including carcinoma (92%) (Am J Clin Pathol 2001;116:246)
- Pancreatic, metastatic (monoclonal, 92%) (Am J Surg Pathol 2005;29:381)
- Paget disease (breast, vulva, scrotum)
- Pancreatic adenocarcinoma (including foamy gland variant and lining of cysts) (Am J Surg Pathol 2000;24:493, Mod Pathol 2005;18:1157)
- Penile clear cell carcinoma (Am J Surg Pathol 2004;28:1513)
- Porocarcinoma (focal, luminal) (J Cutan Pathol 2016;43:219)
- Primary extramammary Paget disease (EMPD) (Int J Clin Exp Pathol 2019;12:3426)
- Secretory meningioma
- Seromucinous carcinoma of the ovary (Am J Surg Pathol 2015;39:983)
- Sweat gland tumors including carcinoma (73%) (Arch Pathol Lab Med 2001;125:498)
- Thyroid medullary carcinoma
- Villoglandular adenocarcinoma of the cervix (Indian J Pathol Microbiol 2018;61:549)
Negative staining - disease
- Clear cell carcinoma of the Bartholin gland (Rom J Morphol Embryol 2018;59:1233)
- Endometriosis
- Leydig cell tumor of the testes (Zhonghua Nan Ke Xue 2016;22:442)
- Melanoma
- Mesothelioma (Indian J Cancer 2018;55:190)
- Including testis (Am J Surg Pathol 2006;30:1)
- Papillary cystadenoma of the epididymis (Zhonghua Nan Ke Xue 2015;21:157)
- Prostate adenocarcinoma (usually) (Am J Clin Pathol 2002;117:471)
- Renal cell carcinoma
- Respiratory epithelial adenomatoid hamartoma (REAH) (Diagn Pathol 2014;9:70)
- Thyroid carcinoma (other than medullary)
Sample pathology report
- Leg, right anterior, excisional biopsy:
- Porocarcinoma (see comment)
- Comment: Histologic sections demonstrate an infiltrating tumor extending into the deep dermis, characterized by significant pleomorphism with areas of ductal formation in a background of hyalinized to desmoplastic stroma. CEA and EMA highlight foci of ductal differentiation, while BerEP4 and MelanA are negative within the lesional cells of interest. The morphologic and immunophenotypic findings are most consistent with a porocarcinoma.
Board review style question #1
Serum CEA levels could be useful for monitoring recurrence of which disease state?
- Basal cell carcinoma
- Colorectal carcinoma
- Leiomyosarcoma
- Melanoma
Board review style answer #1
B. Colorectal carcinoma. Serum CEA levels can be elevated in colorectal carcinoma and can be useful in detecting possible recurrence.
Comment Here
Reference: CEA / CD66e
Comment Here
Reference: CEA / CD66e
Board review style question #2
Board review style answer #2
D. Porocarcinoma. CEA immunostaining can highlight the presence of ductal formation, aiding in the diagnosis of porocarcinoma. Answers A - C are incorrect because melanoma, mesothelioma and papillary thyroid carcinoma typically do not express CEA.
Comment Here
Reference: CEA / CD66e
Comment Here
Reference: CEA / CD66e
