

Stains & CD markers
Androgen receptor (AR)


Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Androgen receptor[title] breast cancer "loattrfree full text"[sb]
Androgen receptor (AR)
Authors: Gina Johnson, M.D., Monika Roychowdhury, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.
Last author update: 1 February 2018
Last staff update: 18 June 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Androgen receptor[title] breast cancer "loattrfree full text"[sb]

Table of Contents
Definition / general | Essential features | Pathophysiology | Diagnosis | Clinical features | Uses by pathologists | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive staining - normal | Positive staining - disease | Negative staining | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Johnson G, Roychowdhury M. Androgen receptor (AR). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsar.html. Accessed December 25th, 2024.
Definition / general
- Androgen receptor (AR) is a member of the superfamily of ligand responsive transcription regulators
- It functions in the nucleus where it is believed to act as a transcriptional regulator mediating the action of androgens
- 918 amino acid protein encoded by a single copy gene on X q11 - q12
Essential features
- Expressed variably by both ER / PR+ as well as ER / PR- breast cancers
- Most useful for triple negative breast cancer, luminal androgen subtype
- Detected by IHC or gene classifier (molecular testing)
- Predicts favorable prognosis in early stage disease based on current studies, some controversy exists
- Ongoing trials to study the effect of androgen receptor targeted therapy in
- AR+ triple negative breast cancer
- Hormone receptor positive metastatic breast cancer
- HER2+ metastatic breast cancer
Pathophysiology
- Expressed in two types of mammary epithelial cells:
- Metaplastic apocrine cells (lack ER / PR)
- Luminal epithelial cells (5 - 30%) (co-expressed with ER / PR)
Diagnosis
- May be detected by gene classifier or IHC
- Any nuclear IHC staining in tumor cells is considered as positive result but further subdivided into subgroups with 1 - 10% and > 10% positive staining
Clinical features
- Expressed variably depending on tumor subtype:
- ER+ breast tumors: 67 - 88%
- All molecular apocrine tumors
- 12 - 50% of ER- classic invasive ductal carcinoma
- Triple negative breast tumors: 6.6 - 75%; range due to variable cutoffs, source of antibody and methodologies, highest expression in luminal androgen receptor subtype (Breast Cancer Res Treat 2011;130:477, Clin Cancer Res 2011;17:1867, Clin Cancer Res 2013;19:5505, Clin Adv Hematol Oncol 2016;14:186)
- Predicts favorable prognosis based on some studies, however controversy exists
Uses by pathologists
- Apocrine marker
- Breast carcinoma marker helpful in determining primary site of metastases
- Paget disease marker
- Sebaceous carcinoma marker; may help differentiate from squamous cell and basal cell carcinomas (Am J Clin Pathol 2010;134:22)
Treatment
- In addition to neoadjuvant chemotherapy, patients with AR+ tumors may benefit from AR targeted therapies such as bicalutamide (AR antagonist) or enzalutamide (AR inhibitor) (ascopost: Targeting the Androgen Receptor in Breast Cancer [Accessed 8 May, 2018])
- Newer therapies are underway
Microscopic (histologic) description
- Nuclear stain in tumor cells is quantified
Microscopic (histologic) images
Contributed by Monika Roychowdhury, M.D.
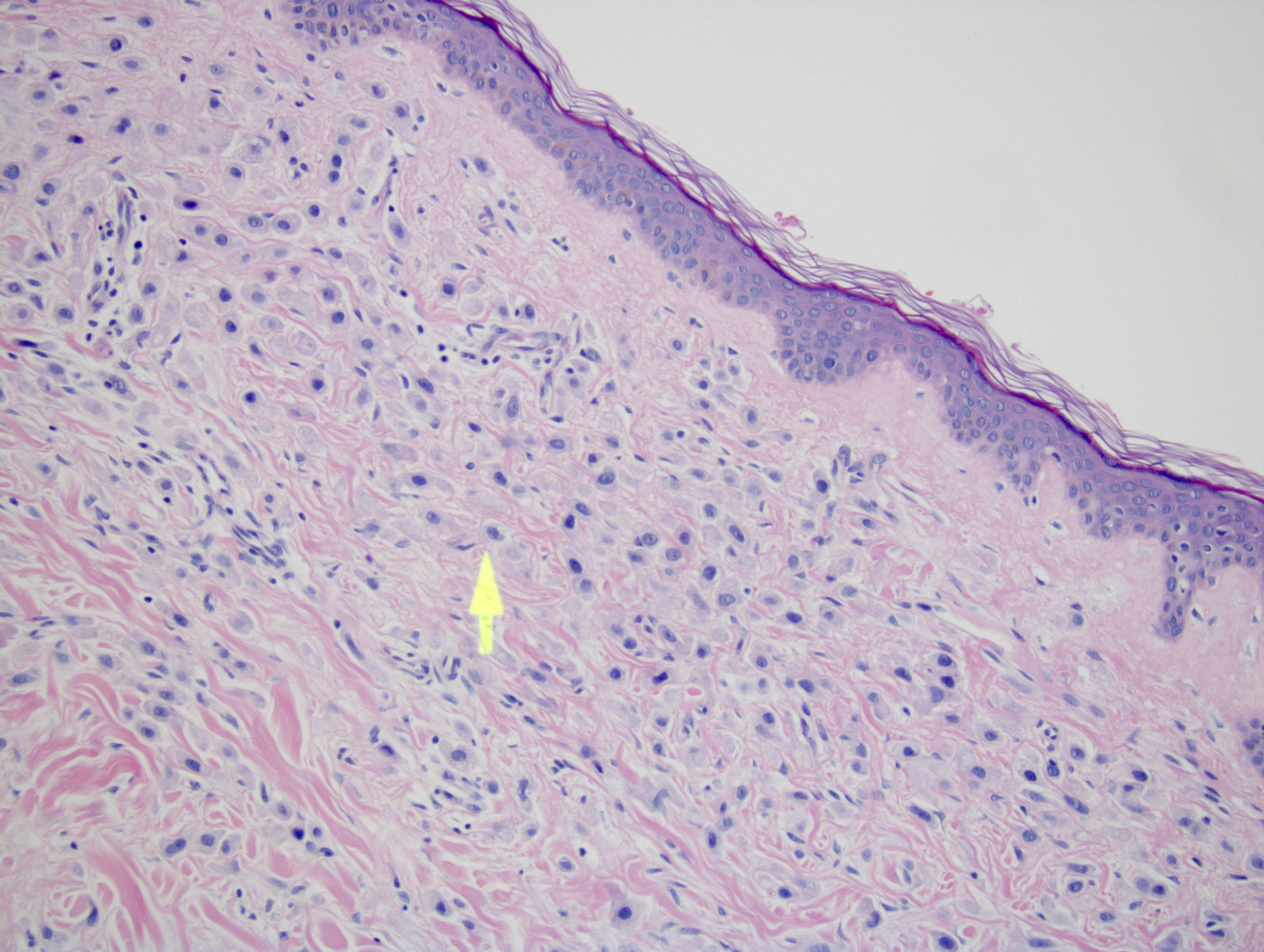
Skin metastatic breast carcinoma 20x
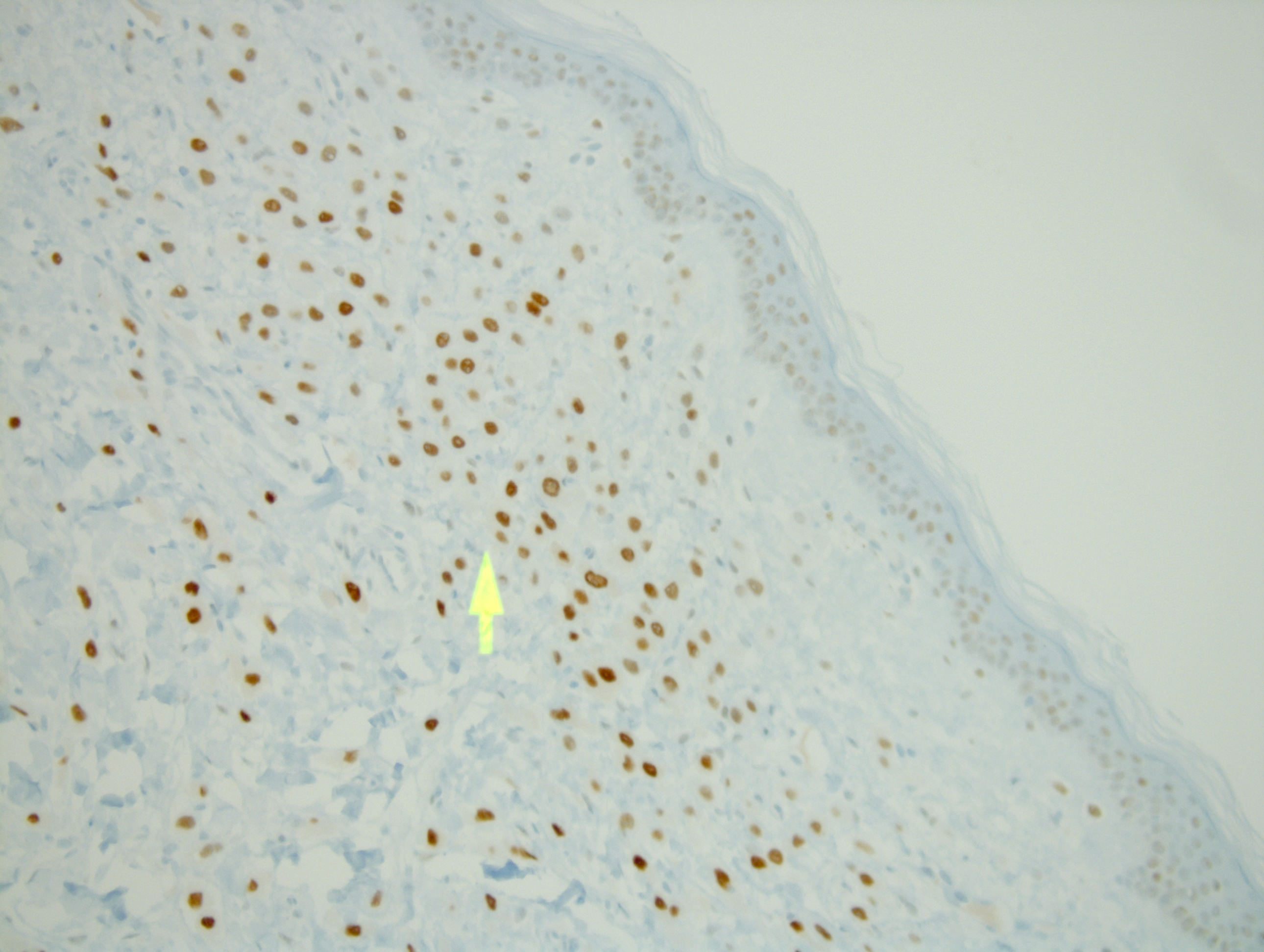
Androgen receptor
in metastatic breast
carcinoma 20x
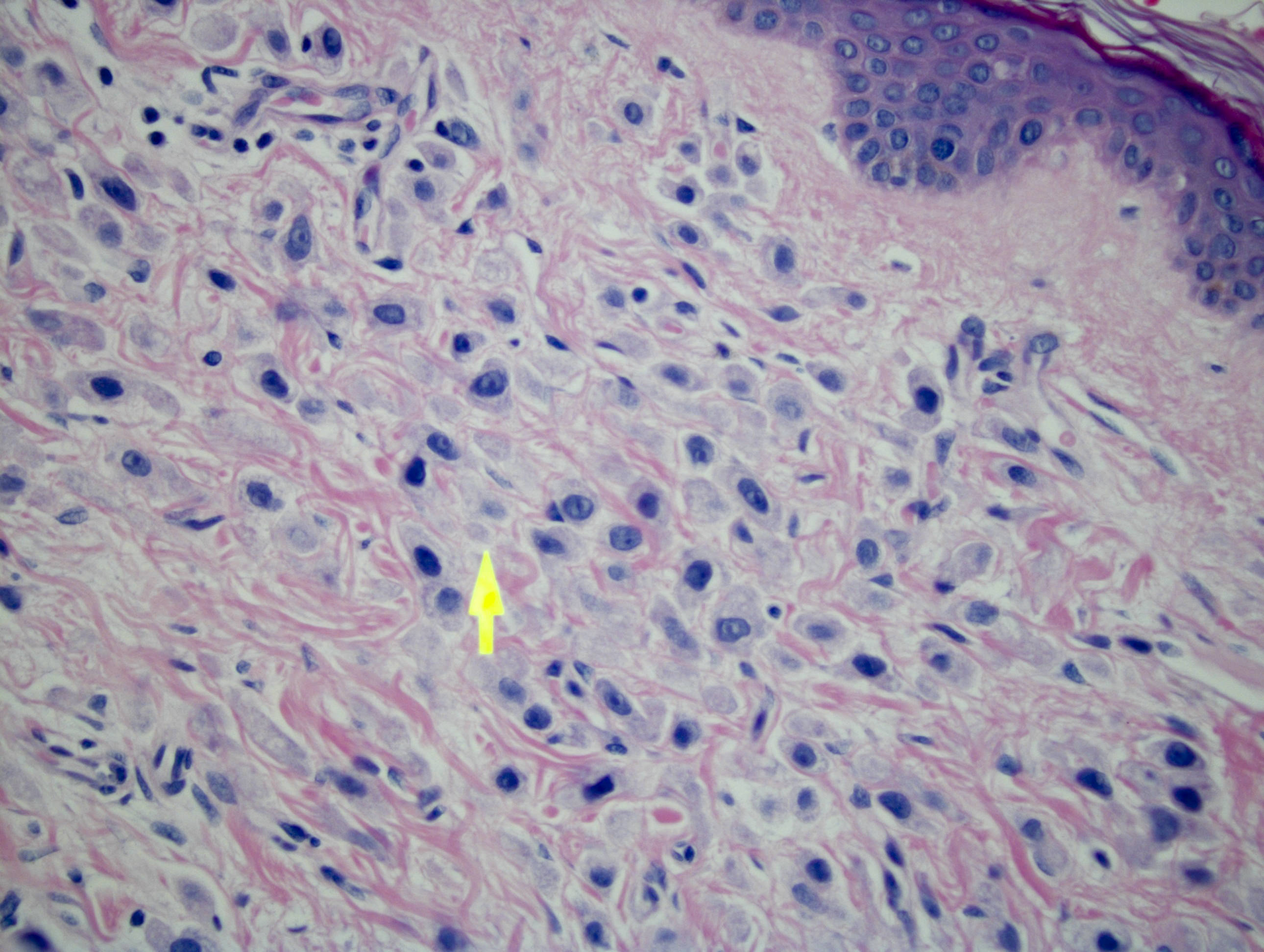
Skin metastatic breast carcinoma 40x
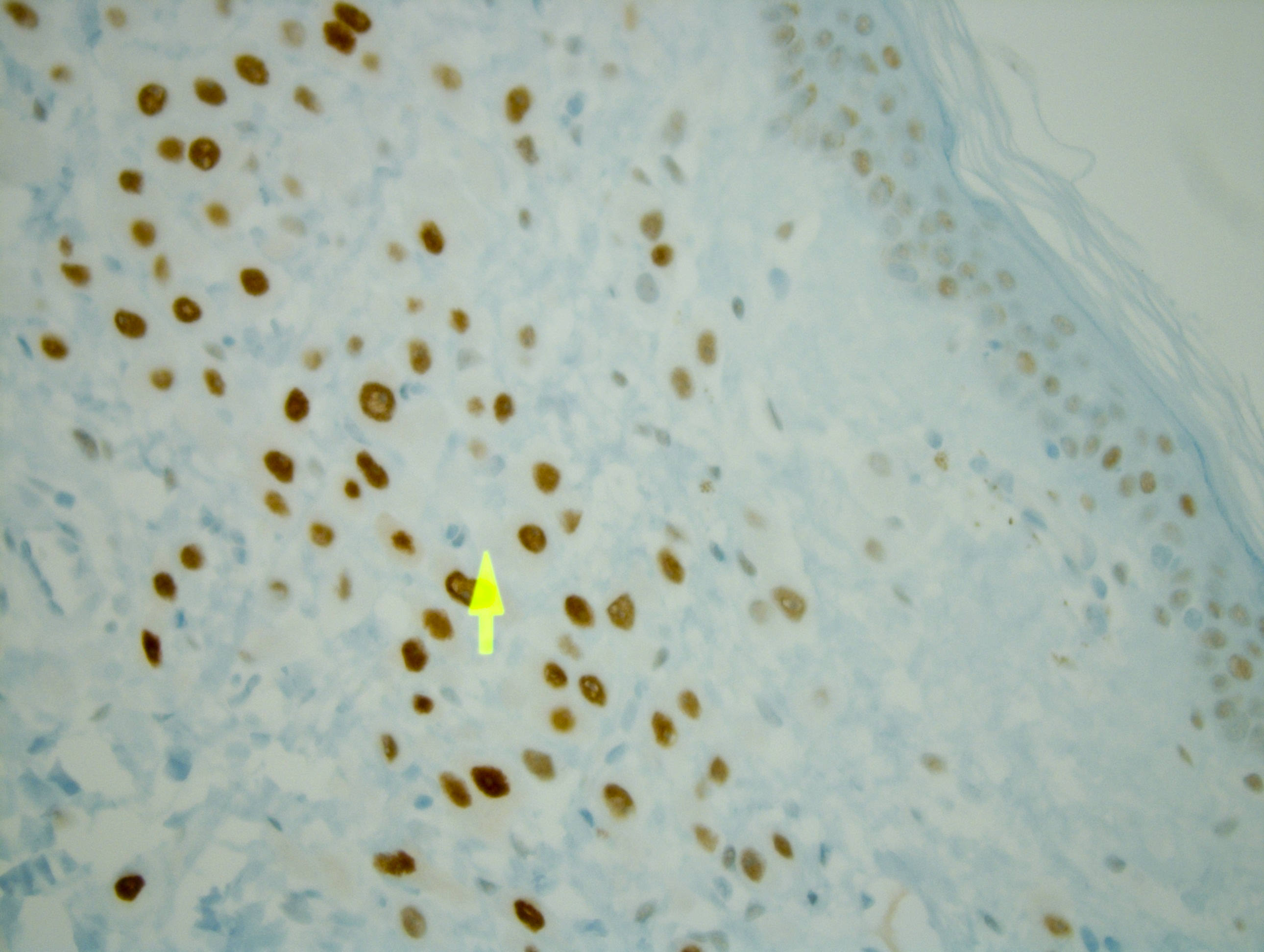
Androgen receptor
in metastatic breast
carcinoma 40x
Case #214
Salivary gland AR-
low grade cribriform
cystadenocarcinoma
Images hosted on other servers:

Breast: apocrine DCIS

Breast: apocrine metaplasia

Prostate carcinoma
metastatic to bone
Positive staining - normal
- Skin apocrine and sebaceous glands (J Invest Dermatol 1991;97:264), prostate basal cells (J Steroid Biochem Mol Biol 1992;41:693)
- Early male and female fetal gonads (Hum Reprod 2004;19:1659)
- Also oral mucosa
Positive staining - disease
- Breast: apocrine metaplasia (100%, J Clin Pathol 1999;52:838) apocrine DCIS (J Clin Pathol 2002;55:14) apocrine carcinoma (Jpn J Clin Oncol 2012;42:375, Case Rep Pathol 2013;2013:170918), cystic hypersecretory DCIS (Histopathology 2005;46:43), high grade DCIS, high grade invasive breast carcinoma (primary and metastatic), mammary and extramammary Paget disease (Mod Pathol 2005;18:1283), PASH spindle cells (Int J Clin Exp Pathol 2009;3:87), sebaceous carcinoma, tall cell-like tumors (Int J Surg Pathol 2006;14:79)
- Associated with better prognosis in all types of breast cancer, and better overall survival in ER+ tumors (PLoS One 2013;8:e82650)
- Nasal cavity: nasopharyngeal angiofibroma (75%, Mod Pathol 1998;11:1122, stromal cells in 38% Am J Clin Pathol 2006;125:832)
- Ovary: serous tumors (50%), Sertoli-Leydig tumor (Hum Pathol 1997;28:1206), ovarian surface epithelium (higher AR staining in patients with cervical squamous cell carcinoma, J Ovarian Res 2013;6:85)
- Salivary glands: giant cell tumor, salivary duct carcinomas (Am J Clin Pathol 2003;119:801)
- Skin: Paget disease, sebaceous carcinoma (Am J Clin Pathol 2010;134:22)
- Soft tissue: desmoid tumor (53%, Tohoku J Exp Med 2006;210:189), spindle cell lipoma in men and most women (Arch Pathol Lab Med 2008;132:81)
- Uterus: adenosarcoma (35%), endometrial polyp with atypical features, endometrial stromal nodule, endometrium in polycystic ovarian syndrome. (Biol Reprod 2002;66:297), leiomyosarcoma (variable, Cancer 2004;101:1455, Tumour Biol 2011;32:451)
Negative staining
- Neuroendocrine cells
- Adenomatoid tumor, BRCA1 breast carcinoma, breast fibromatosis (Arch Pathol Lab Med 2000;124:276)
Additional references
Board review style question #1
Androgen receptor testing is most useful in:
- ER+, PR+, HER2+ breast tumor
- ER+, PR+, HER2- breast tumor
- ER-, PR-, HER2+ breast tumor
- ER-, PR-, HER2- breast tumor
Board review style answer #1

