Stains & CD markers
Tpit

Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Tpit
Tpit
Author: William McDonald, M.D.
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Brandon Umphress, M.D.
Last author update: 24 August 2022
Last staff update: 1 February 2023
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Tpit
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Diagrams / tables | Clinical features | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) images | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1Cite this page: McDonald W. Tpit. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsTpit.html. Accessed March 31st, 2025.
Definition / general
- Pituitary adenomas / pituitary neuroendocrine tumors have traditionally been classified using a combination of immunohistochemical stains for anterior pituitary hormones, including stains for prolactin, growth hormone, thyrotropin (TSH), luteinizing hormone (LH), follicle stimulating hormone (FSH), adrenocorticotropic hormone (ACTH) and the alpha subunit (ASU) of the glycoprotein hormones
- Immunostains for anterior pituitary transcription factors steroidogenic factor 1 (SF1), Pit1 and T box transcription factor (Tpit) have been shown to have higher sensitivity and specificity than hormone IHC stains and are often used in conjunction to classify pituitary adenomas
- Transcription factor Tpit drives corticotroph differentiation; IHC for Tpit is useful in identifying corticotroph adenomas
- Immunohistochemical stains for Tpit identify nonneoplastic corticotrophs within the anterior pituitary and both silent and functioning corticotroph adenomas
Essential features
- Tpit IHC shows strong nuclear staining
- Tpit is expressed within anterior pituitary gland corticotroph cells and within corticotroph adenomas
- Tpit IHC is more sensitive and specific than IHC stain for ACTH
Terminology
- T box transcription factor (Tpit)
- Gene name: T box transcription factor 19 (TBX19)
Pathophysiology
- Terminal differentiation of corticotrophs is controlled by transcription factor Tpit
- Germline mutations of TBX19 cause isolated ACTH deficiency (J Mol Endocrinol 2016;56:T99)
Diagrams / tables
Contributed by William McDonald, M.D.
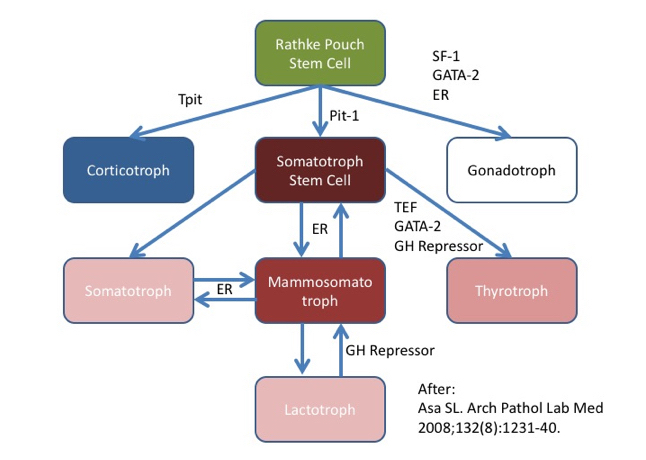
Tpit drives corticotroph lineage
Clinical features
- Most corticotroph adenomas are hormonally functional microadenomas
- Functional adenomas tend to be smaller; corticotroph macroadenomas are often hormonally silent
Interpretation
- Nuclear expression is evaluated (reactivity only in the cytoplasm is regarded as negative)
- Tpit immunoreactivity in corticotroph adenoma is typically diffuse, strong and nuclear (score 7 or 8 in the Allred scale) (Mod Pathol 1998;11:155)
- Immunoreactivity in anterior pituitary gland (nonneoplastic anterior pituitary) shows moderate to strong nuclear staining in scattered adenohypophysis cells, within occasional clusters of cells and often in grouped cells associated with the pituitary stalk (so called basophil invasion); corticotrophs are a minority population within the adenohypophysis
Uses by pathologists
- Useful for diagnosis of corticotroph adenomas (Acta Neuropathol 2017;134:675, Arch Pathol Lab Med 2017;141:104, Mod Pathol 2018;31:900)
- More sensitive than antibodies to ACTH (Arch Pathol Lab Med 2021;145:592, Acta Neuropathol 2017;134:675)
- Also present within normal anterior pituitary gland (therefore, the presence of pituitary adenoma must be confirmed on H&E stains [occasionally with the support of ancillary stains such as reticulin to assess for normal adenohypophyseal architecture])
- Often used in conjunction with other pituitary transcription factor IHC; see Pit1 and SF1 (Arch Pathol Lab Med 2021;145:592)
Prognostic factors
- Untreated Cushing disease has high morbidity and mortality, with surgery being the treatment of choice for small, functioning corticotroph adenomas (Endocr Rev 2015;36:385)
- Some subtypes of corticotroph adenoma (including Crooke cell tumors, silent corticotroph tumors and sparsely granulated corticotroph tumors) are reportedly more aggressive but available series are often small, highly biased or assembled prior to the routine use of transcription factor immunohistochemistry (Am J Surg Pathol 2003;27:1330, Int J Radiat Oncol Biol Phys 2014;90:903, Neurosurgery 2000;47:723, Front Endocrinol (Lausanne) 2021;12:672178)
Microscopic (histologic) images
Contributed by William McDonald, M.D.

Normal adenohypophysis

Normal adenohypophysis
(reticulin)
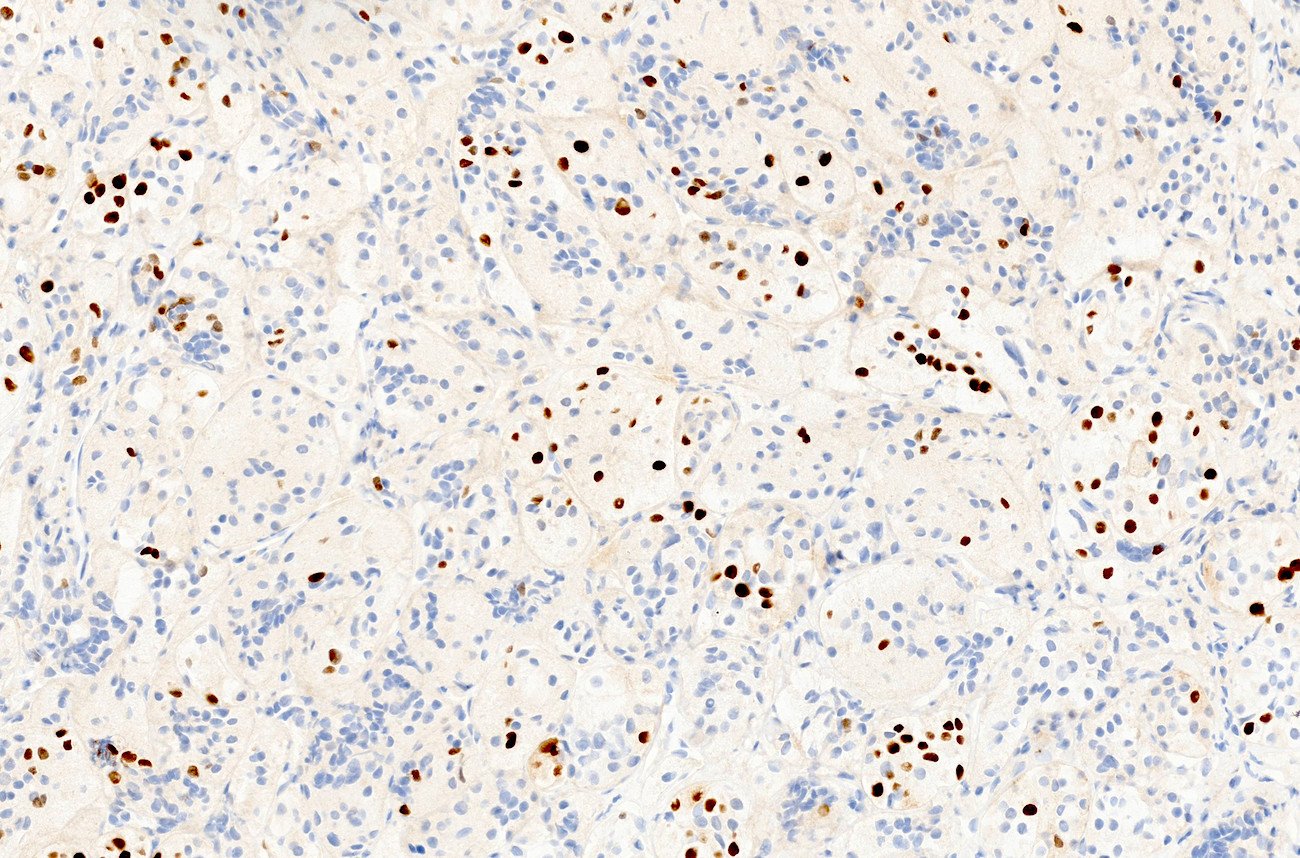
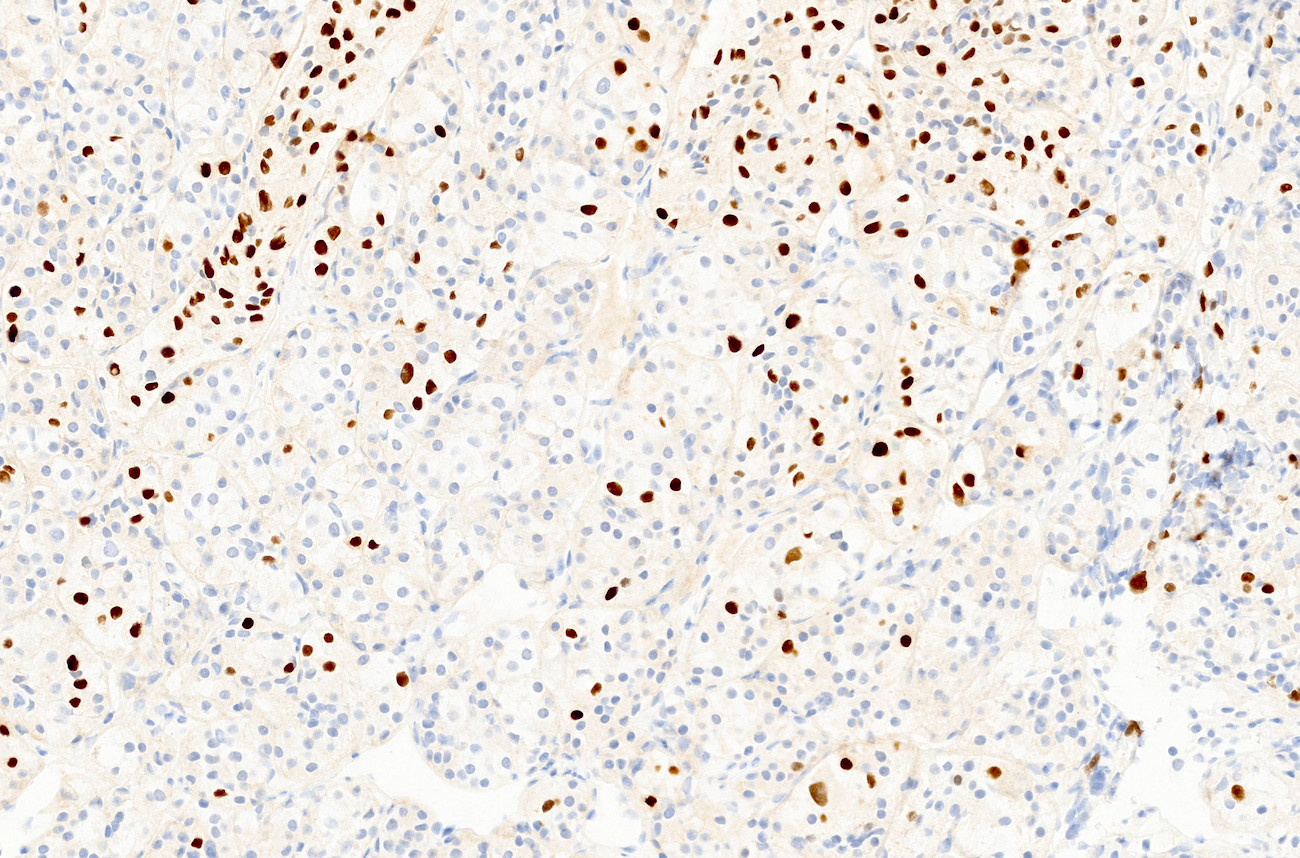
Normal adenohypophysis
(Tpit)
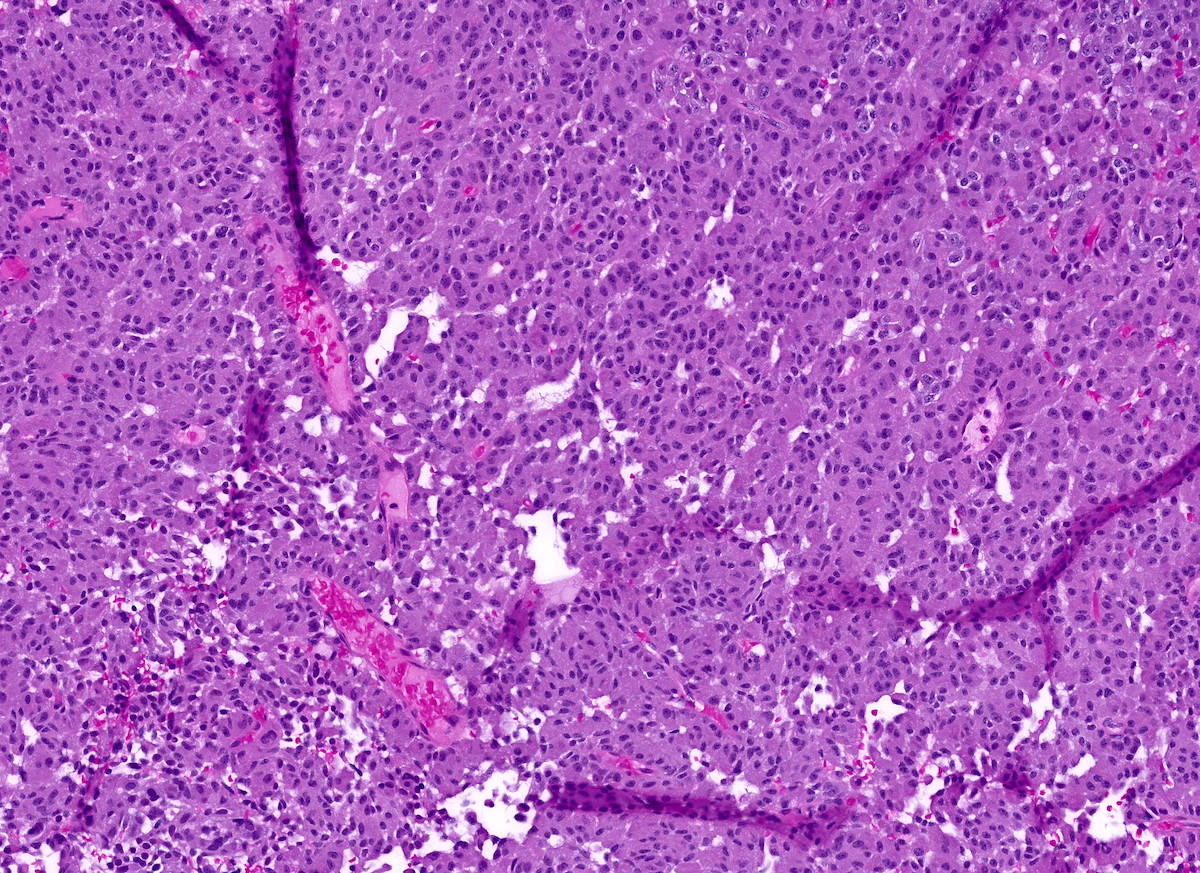
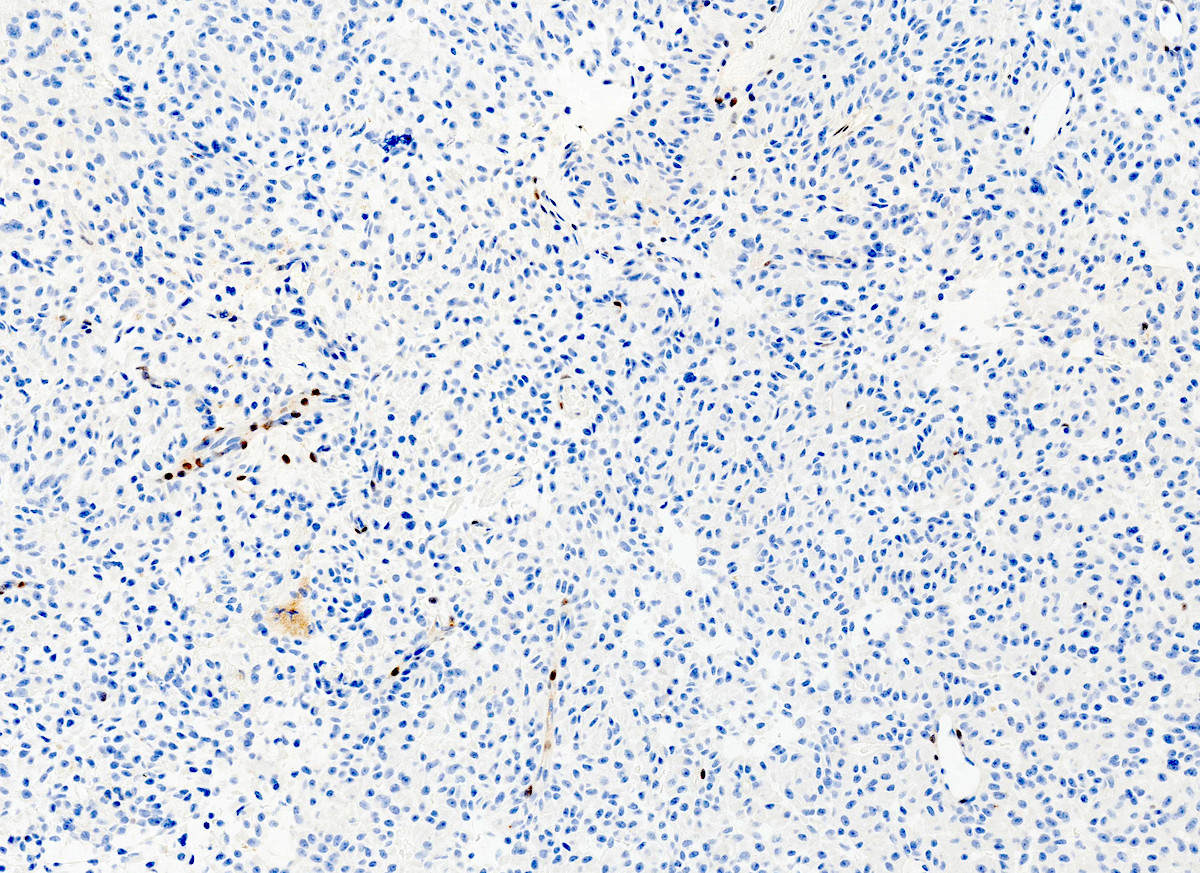
Corticotroph adenoma
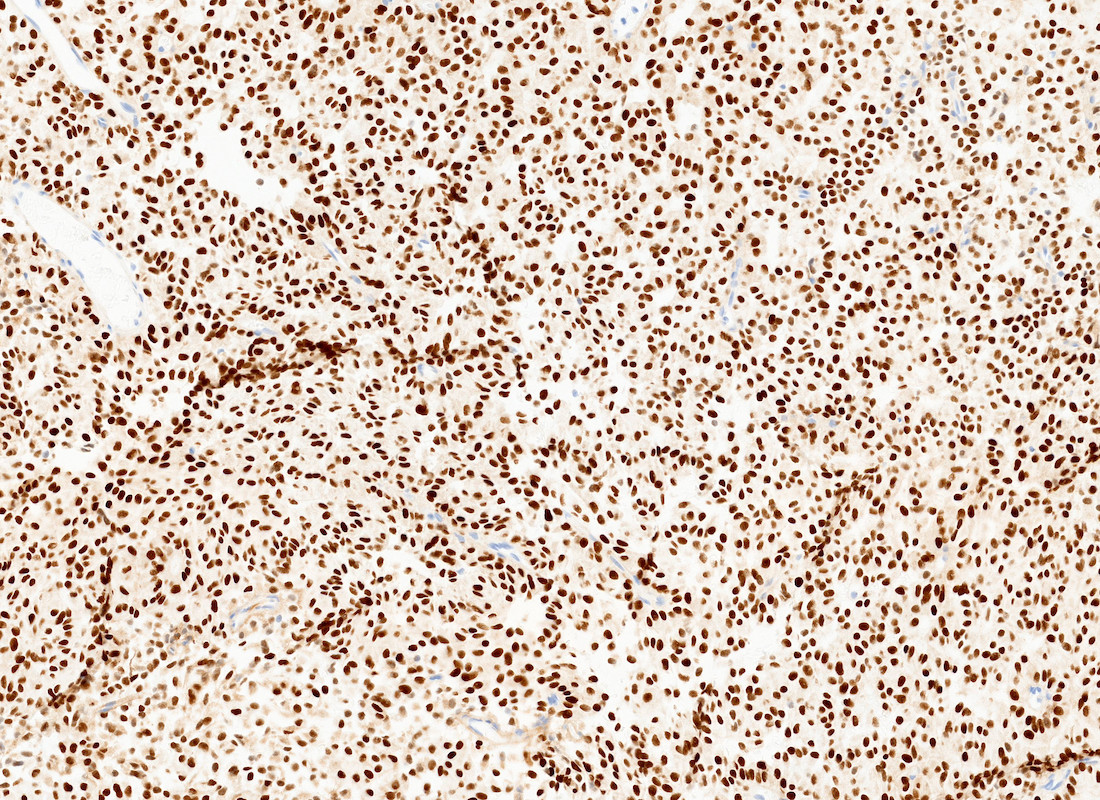
Corticotroph adenoma
(Tpit)

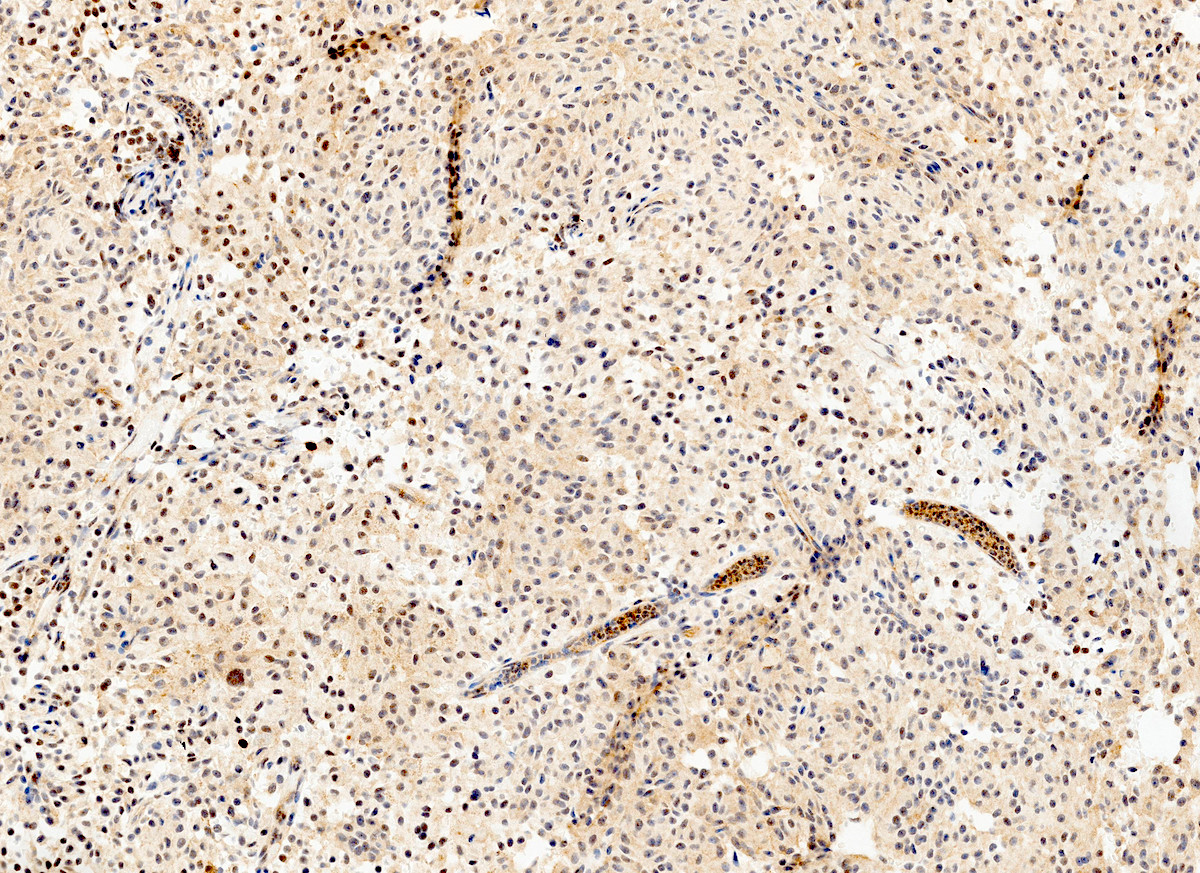
Corticotroph adenoma
(SF1)
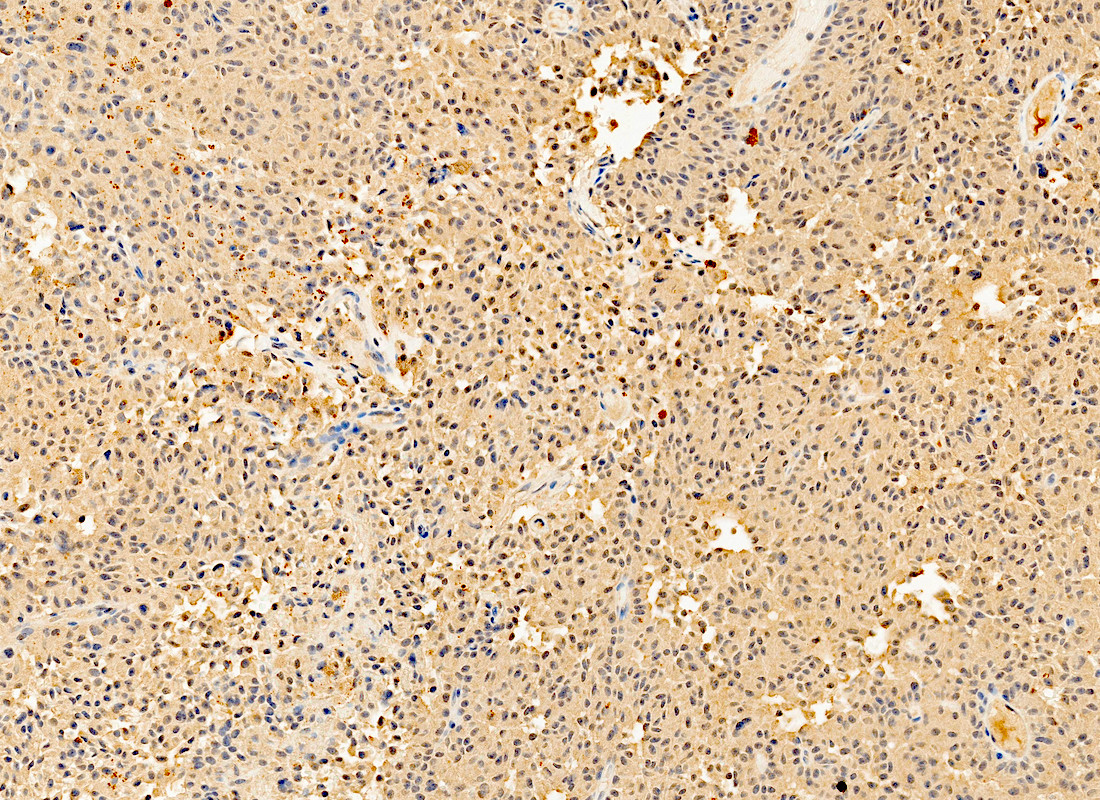
Corticotroph adenoma
(Pit1)
Corticotroph adenoma
(ACTH)
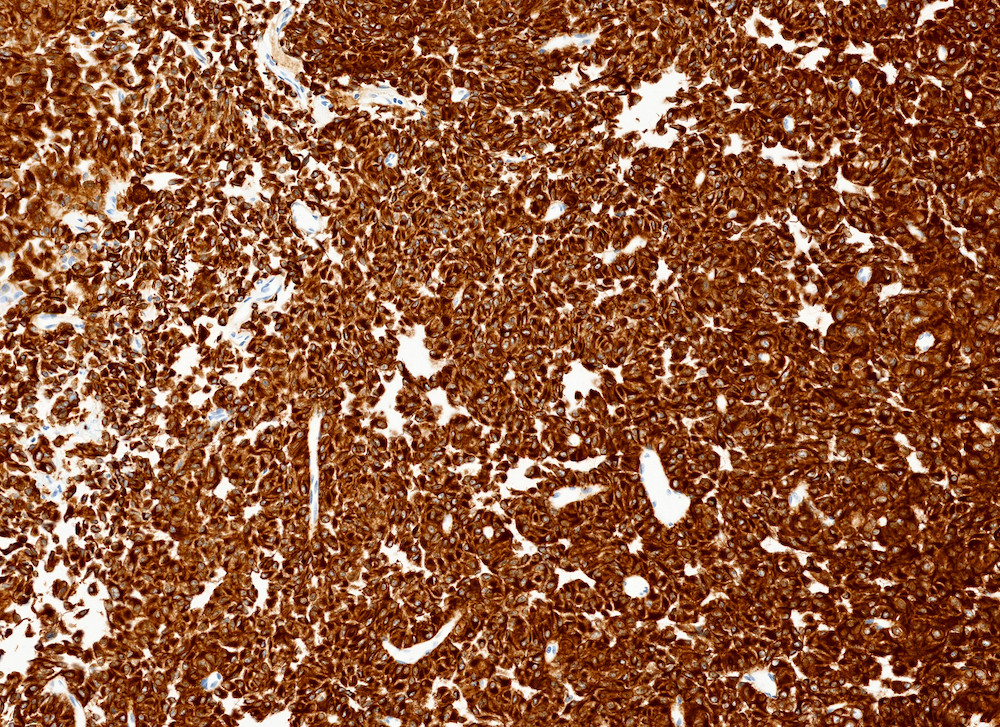
Corticotroph adenoma
(CAM5.2)
Corticotroph adenoma
(GATA3)
Positive staining - normal
- Corticotrophs within the normal anterior pituitary gland (Endocr Pathol 2020;31:330, Acta Neuropathol 2017;134:675)
Positive staining - disease
- Corticotroph pituitary adenoma (Endocr Pathol 2020;31:330, Acta Neuropathol 2017;134:675)
Negative staining
- Noncorticotroph pituitary adenomas, including those of the gonadotroph and acidophil (Pit1) lineages (Arch Pathol Lab Med 2021;145:592)
Sample pathology report
- Sella turcica, resection:
- Pituitary adenoma (pituitary neuroendocrine tumor), corticotroph type (see comment)
- Comment: This tumor shows diffuse nuclear immunoreactivity for Tpit and no immunoreactivity for SF1 or Pit1. Moderate ACTH immunoreactivity is observed, as is diffuse, strong staining for PAS and immunoreactivity for low molecular cytokeratin CAM5.2, supporting the impression. In the context of a microadenoma with clinical signs and symptoms of Cushing disease, this is a corticotroph adenoma (densely granulated subtype).
- Clinical information (mandatory to include): The patient presented with a 6 month history of central obesity, diabetes mellitus, hypertension and thin skin with striae; magnetic resonance imaging showed a 4 mm hypoenhancing mass within the pituitary gland.
- Available preoperative endocrine testing (also mandatory): Midnight salivary cortisol levels were elevated; tests for prolactin, TSH, free T4 and IGF1 were normal.
Additional references
Board review style question #1

A 48 year old woman presents with bitemporal vision loss. MRI reveals a 2.5 cm sellar and suprasellar tumor, which compresses the optic chiasm. No signs or symptoms or Cushing disease or other hormone excess are present clinically. Transphenoidal resection confirms pituitary adenoma by H&E stains. The adenoma shows immunohistochemical staining as illustrated above. How is this adenoma best classified?
- Corticotroph adenoma
- Gonadotroph adenoma
- Null cell adenoma
- Prolactinoma
Board review style answer #1
A. Corticotroph adenoma. This clinically silent corticotroph adenoma became symptomatic when it compressed the optic apparatus, a common presentation for large pituitary macroadenomas. Strong, diffuse nuclear immunoreactivity for Tpit, along with characteristically pale immunoreactivity for ACTH and strong, diffuse cytoplasmic staining for CAM5.2 support the diagnosis. Gonadotroph adenomas (answer B), while often presenting in similar fashion as clinically nonfunctioning macroadenoma, would have SF1 immunoreactivity and lack staining for Tpit. Null cell adenoma (answer C) by definition lacks hormone or transcription factor immunostaining. Prolactinoma (answer D) would also lack Tpit staining and would show strong nuclear immunoreactivity for transcription factor Pit1.
Comment Here
Reference: Tpit
Comment Here
Reference: Tpit
