Stains & CD markers
HMB45

Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: HMB45
HMB45
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Brandon Umphress, M.D.
Last author update: 10 July 2024
Last staff update: 10 July 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: HMB45
Table of Contents
Definition / general | Essential features | Pathophysiology | Interpretation | Uses by pathologists | Microscopic (histologic) images | Cytology images | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Maccio U. HMB45. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsHMB45.html. Accessed March 31st, 2025.
Definition / general
- Human melanoma black (HMB) antibody, developed in 1986 from an extract of melanoma cells (Am J Pathol 1986;123:195)
- Monoclonal antibody that targets the premelanosome protein gp100 (The Human Protein Atlas: PMEL [Accessed 13 June 2024])
Essential features
- Monoclonal antibody that targets gp100, a premelanosome protein
- Expressed in immature and in activated melanocytes
- Used for evaluating maturation in primary melanocytic lesions
- Usually combined with other melanocytic markers and not used alone as a screening marker for melanoma
- Typical aberrant expression in some tumors without melanocytic differentiation (angiomyolipoma, perivascular epithelioid cell tumor [PEComa], lymphangioleiomyomatosis, TFE and TFEB rearranged renal cell carcinoma)
Pathophysiology
- gp100 is a 100 kD membrane bound glycoprotein present in stage I premelanosome, stage II and nonmelanized stage III melanosomes but absent in stage IV melanosomes and melanosomes in keratinocytes (J Cutan Pathol 1991;18:432)
- Implicated in maturation of stage I premelanosome to stage II melanosome (J Biol Chem 2006;281:21198)
- Splicing variant of PMEL17 gene, located on long arm of chromosome 12 (12q13.2) (NIH: PMEL Premelanosome Protein [Homo sapiens (Human)] [Accessed 13 June 2024], Crit Rev Immunol 2010;30:387)
- Expression regulated by transcription factors of microphthalmia family (MiT) (MITF, TFE3, TFEB and TFEC) (Front Cell Dev Biol 2021;8:609683)
- MITF regulates expression of PMEL17 / gp100 in melanocytes and melanoma (Am J Pathol 2003;163:333)
- TFE and TFEB gene upregulation can lead to HMB45 positivity in tumors without melanocytic differentiation (e.g., TFE and TFEB rearranged renal cell carcinoma) (Mol Cancer Res 2017;15:1637)
- Chimeric product of fusion EWSR::ATF1 in clear cell sarcoma upregulates MITF promoter and thus gp100 expression (Cancer Cell 2006;9:473)
- gp100 is organelle specific but not lineage specific (Arch Pathol Lab Med 2007;131:1517)
Interpretation
- Cytoplasmic stain
- Stains immature melanocytes
- Gradient of maturation in benign nevus: diminution of HMB45 from surface (HMB45+, immature) toward base (HMB45-, mature) (Semin Diagn Pathol 2022;39:239)
- Typically no maturation in melanoma
Uses by pathologists
- Melanocytic marker for diagnosis of primary and metastatic melanoma (increased diagnostic accuracy in combination with other markers like SOX10, MelanA / MART1, S100, MITF, tyrosinase) (Int J Mol Sci 2022;23:5911)
- Distinction between dermal component of cutaneous nevus (negative) and cutaneous melanoma (positive) (Int J Mol Sci 2022;23:5911)
- Caution
- Benign blue nevi typically positive for HMB45
- Deep penetrating nevi often show HMB45 expression
- Halo nevi may show aberrant HMB45 expression in up to 50% of cases (J Cutan Pathol 2021;48:519)
- Desmoplastic melanomas are negative or only focally positive for HMB45
- Caution
- Evaluating sentinel lymph nodes for melanoma (Semin Diagn Pathol 2008;25:116)
- Caution: HMB45 may react with melanophages and rarely nodal nevi (Am J Surg Pathol 2001;25:1039)
- For diagnosis of melanocytic lesions usually combined with other markers (sensitivity: S100 >> MelanA > HMB45; specificity: HMB45 > MelanA >> S100) (Semin Diagn Pathol 2022;39:239)
- Distinction between melanoma with epithelioid morphology (HMB45+) and other epithelioid tumors (HMB45-) (Diagnostics (Basel) 2020;10:233)
- Distinction between melanoma in situ (HMB45+) and mammary or extramammary Paget disease (HMB45-) (Virchows Arch 1996;429:371)
- Distinction between metastasis of melanoma (HMB45+) and carcinoma (HMB45-) in panel with other markers (Hum Pathol 2004;35:217)
- Distinction between angiomyolipoma (HMB45+) and tumor with similar morphology (HMB45-) (e.g., leiomyoma or angiolipoma) (Am J Surg Pathol 2015;39:349)
- Distinction between epithelioid angiomyolipoma / epithelioid PEComa (HMB45+) and tumors with similar morphology (HMB45-) (e.g., clear cell carcinoma of the kidney and urothelial carcinoma with sarcomatoid differentiation) (Am J Surg Pathol 2001;25:65)
- Distinction between lymphangioleiomyomatosis (HMB45+) and other cystic lesions of the lung (HMB45-) (Appl Immunohistochem Mol Morphol 2022;30:108)
- Distinction between melanoma (HMB45+) in adrenal gland and adrenal cortical carcinoma (HMB45-) in combination with other markers (Medicine (Baltimore) 2017;96:e8956)
Microscopic (histologic) images
Contributed by Umberto Maccio, M.D., M.Sc., M.B.A.
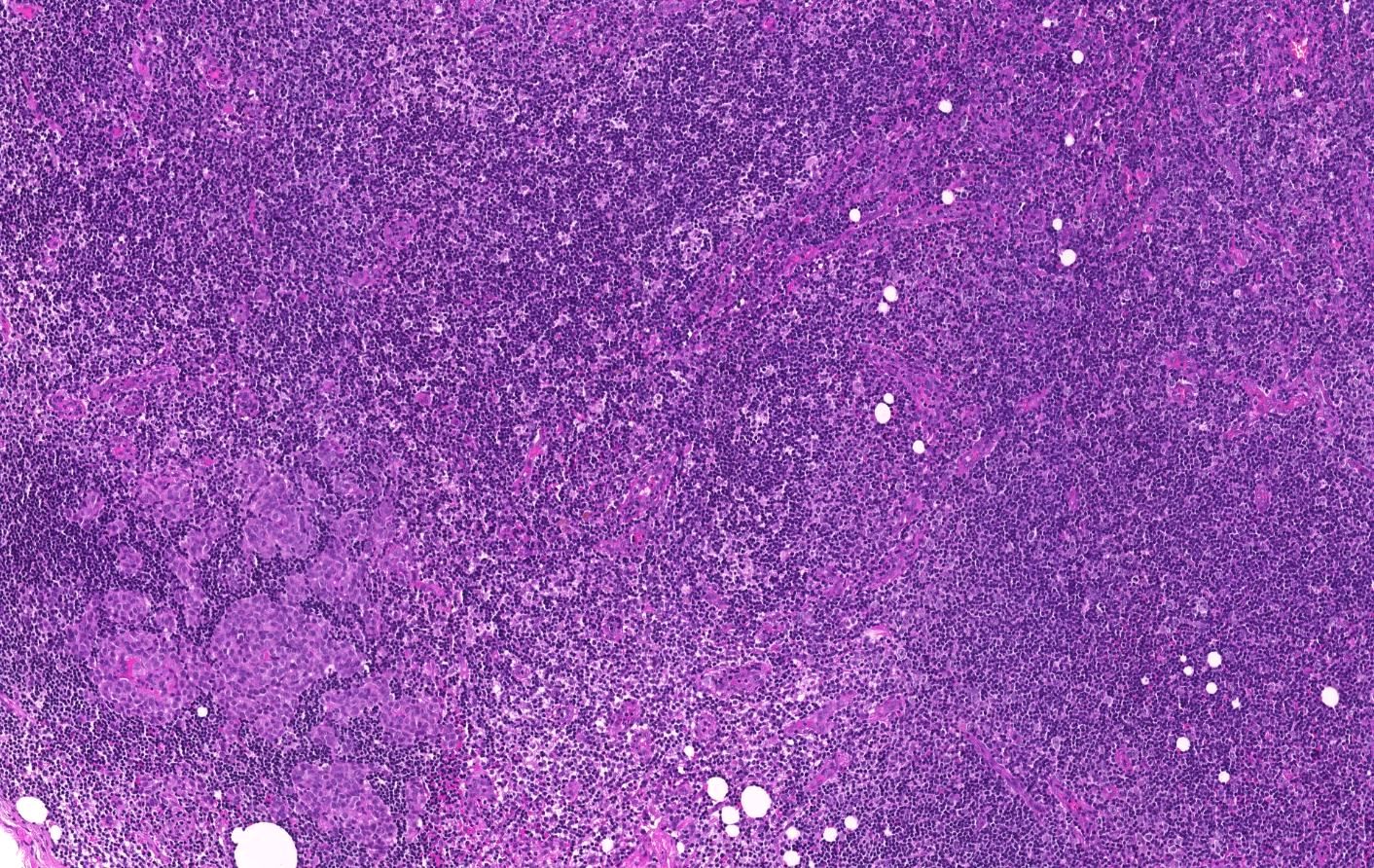
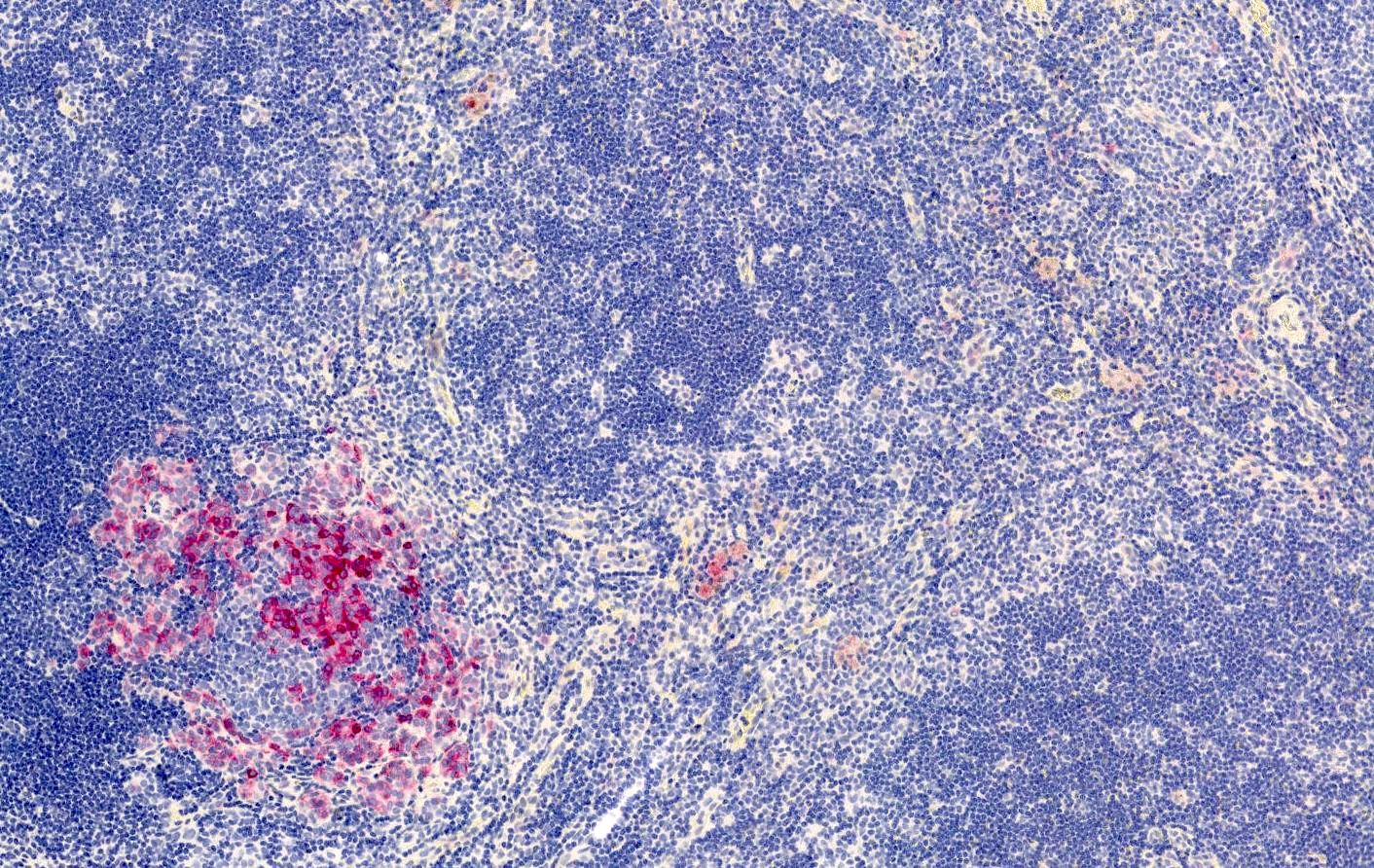
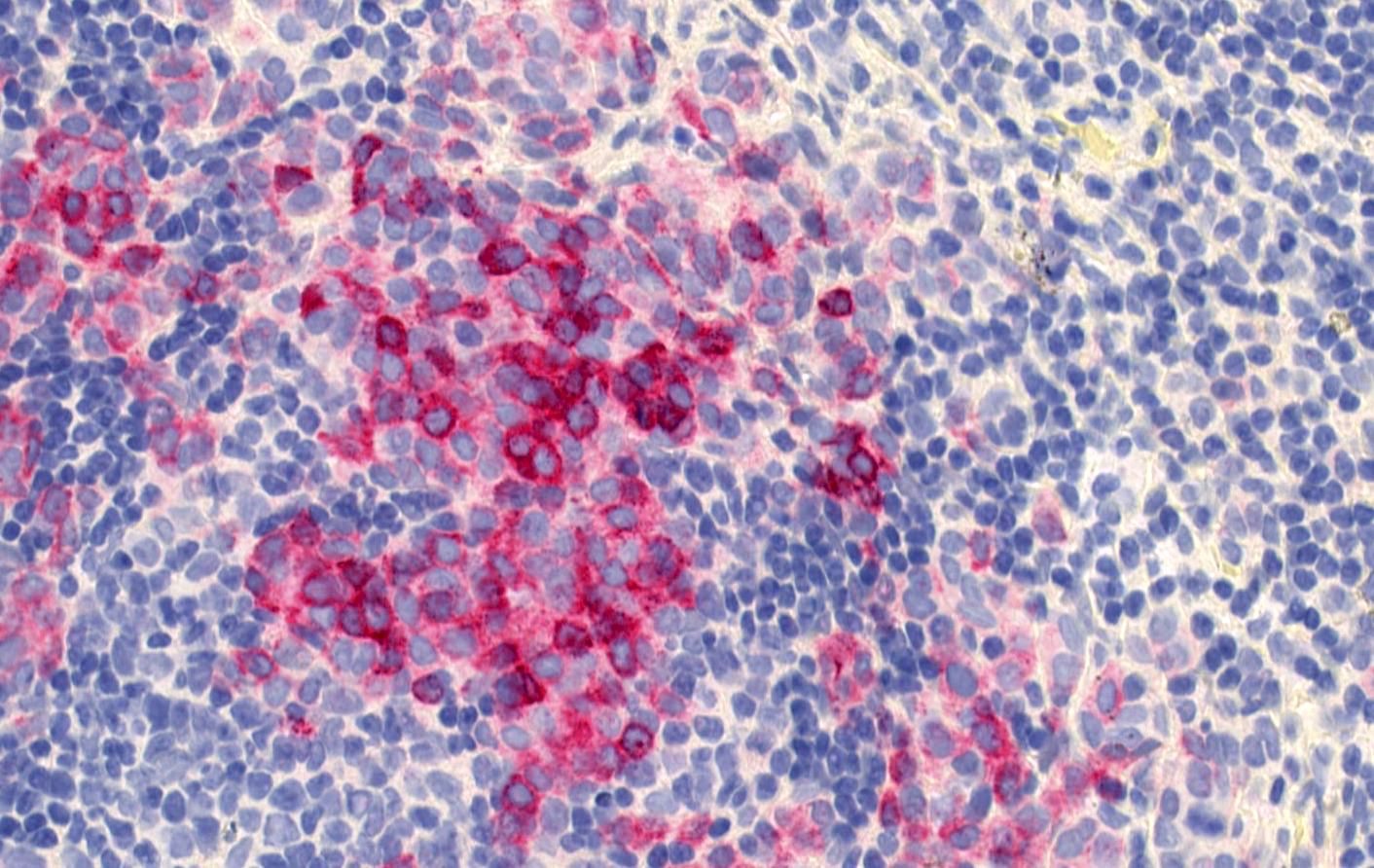
Melanoma metastasis
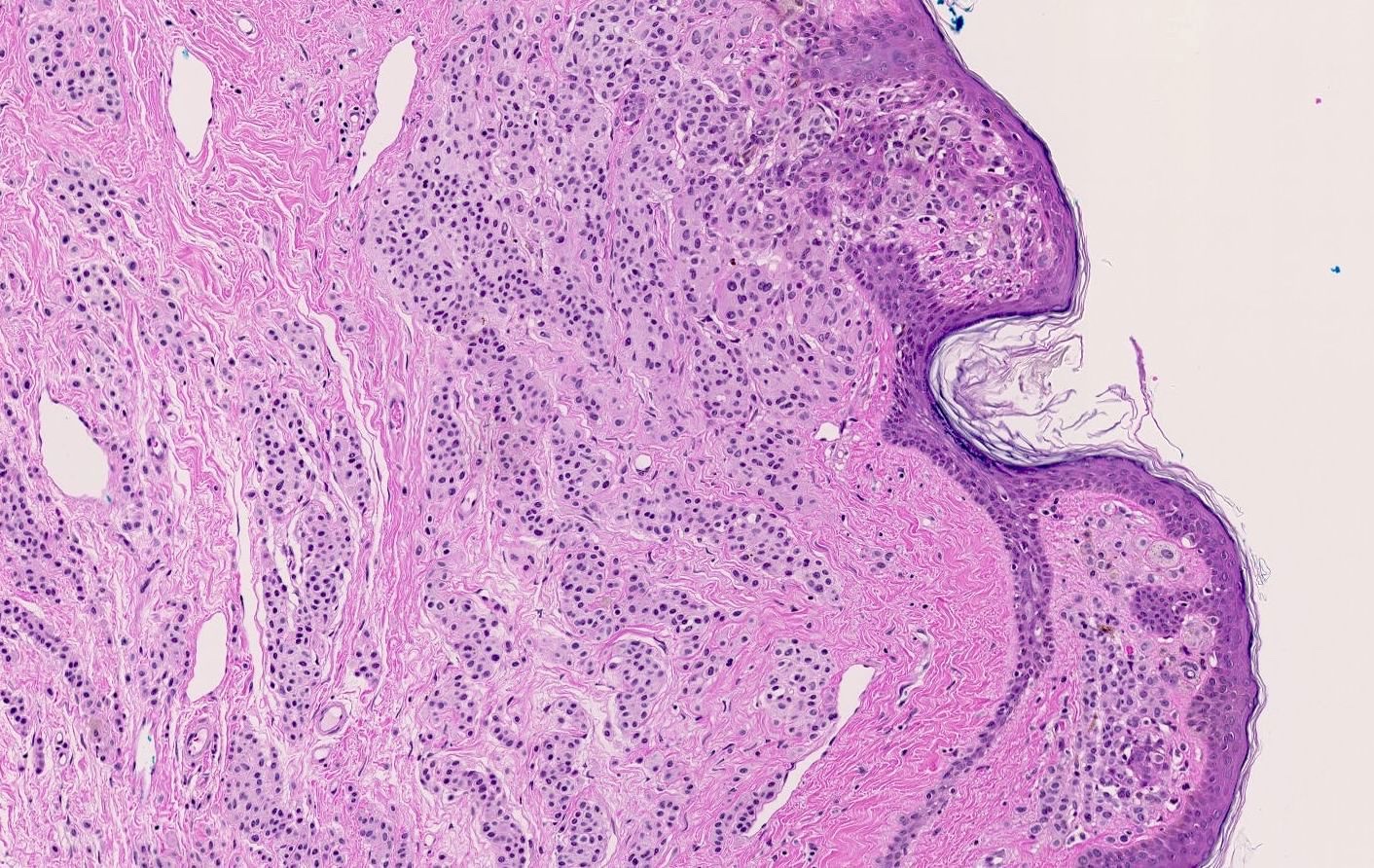
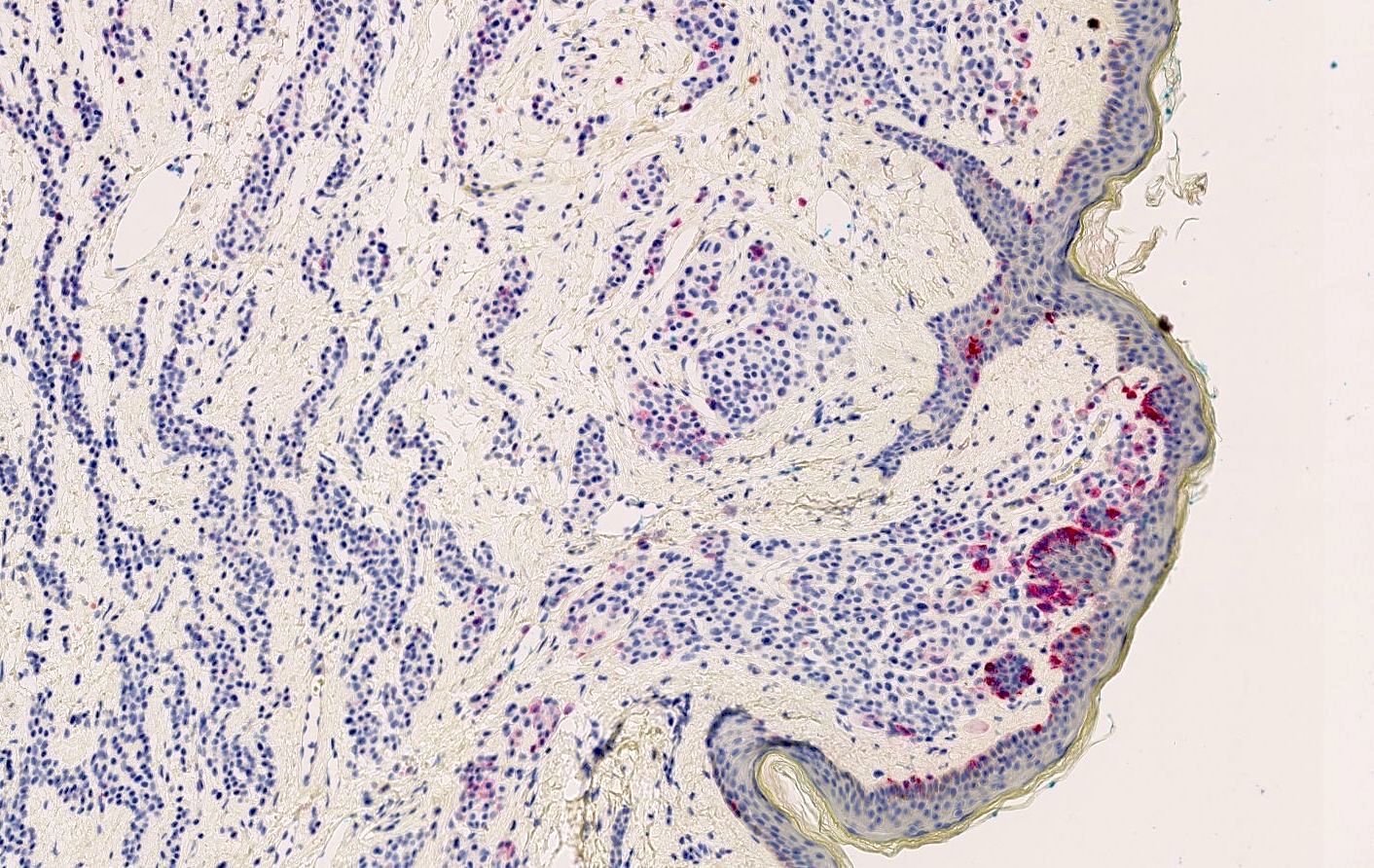
Compound nevus
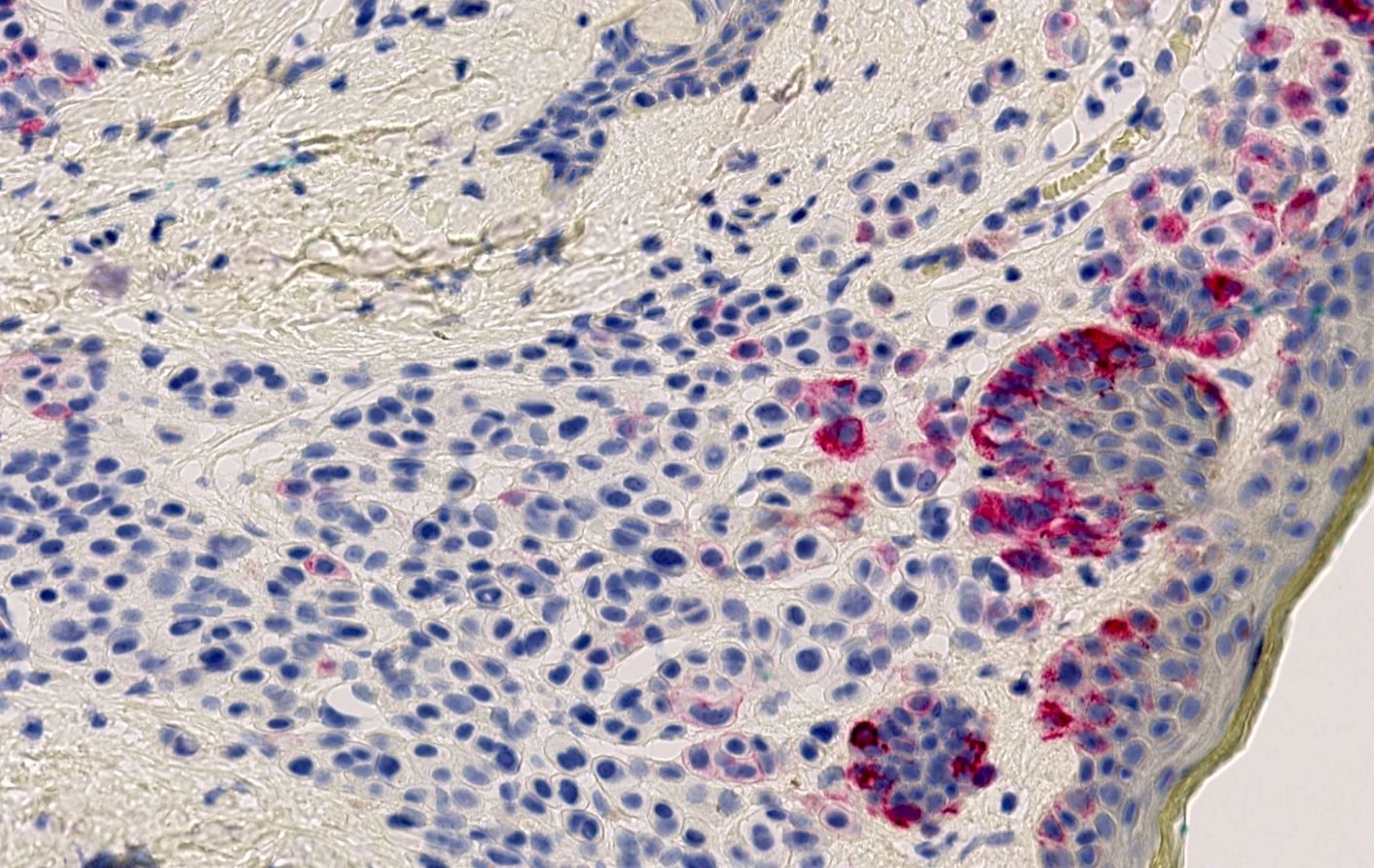
Compound nevus
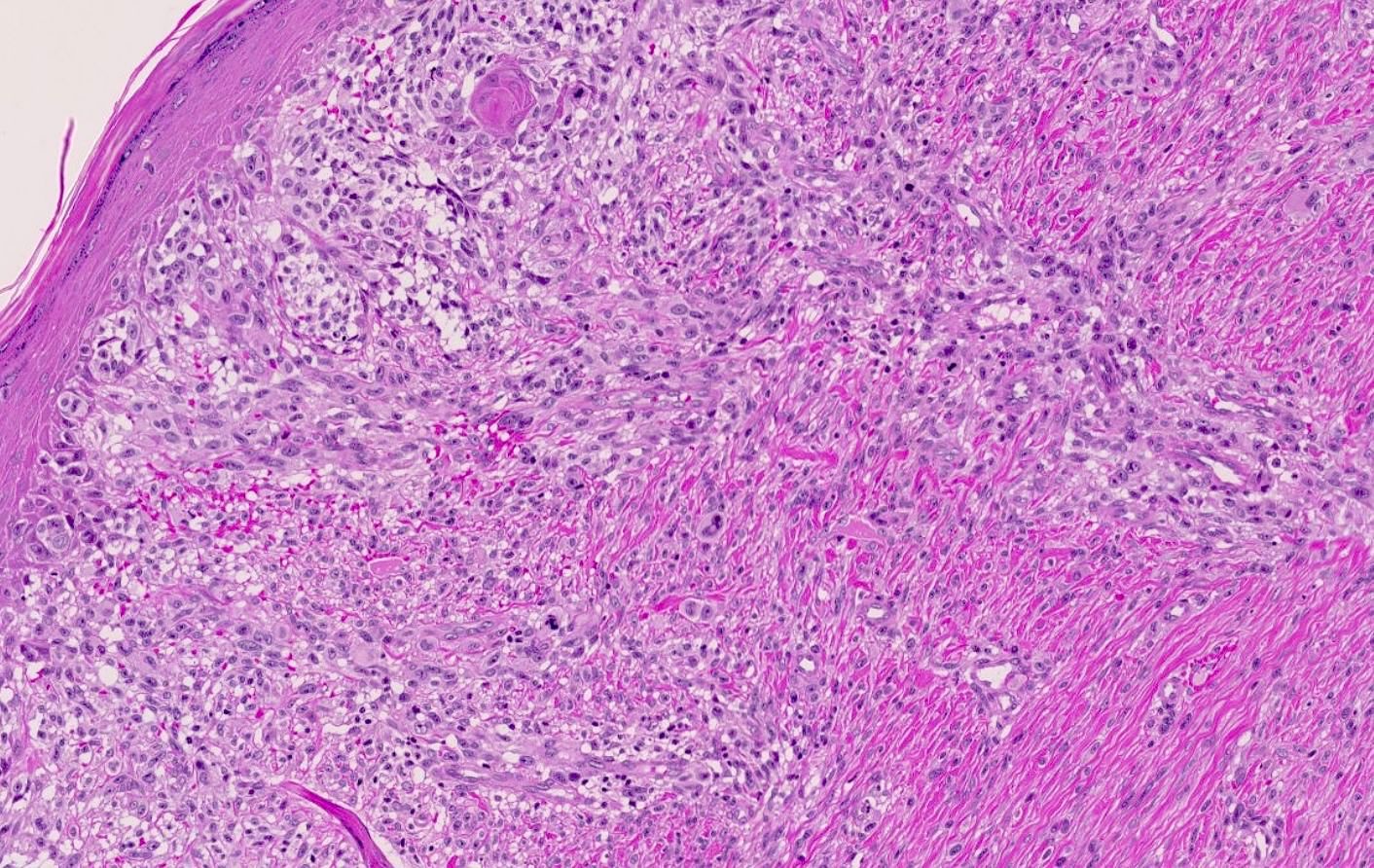
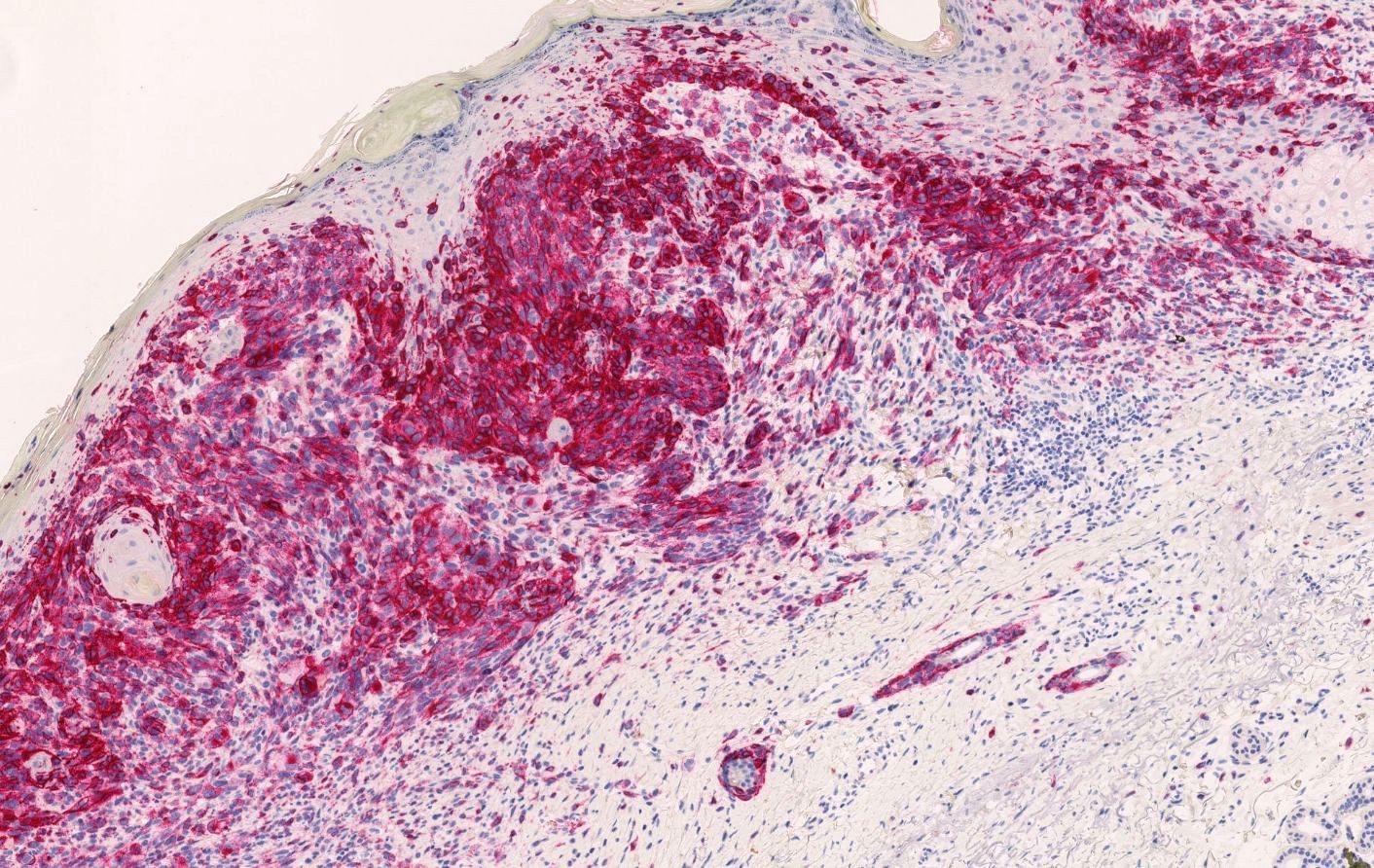
Cutaneous melanoma
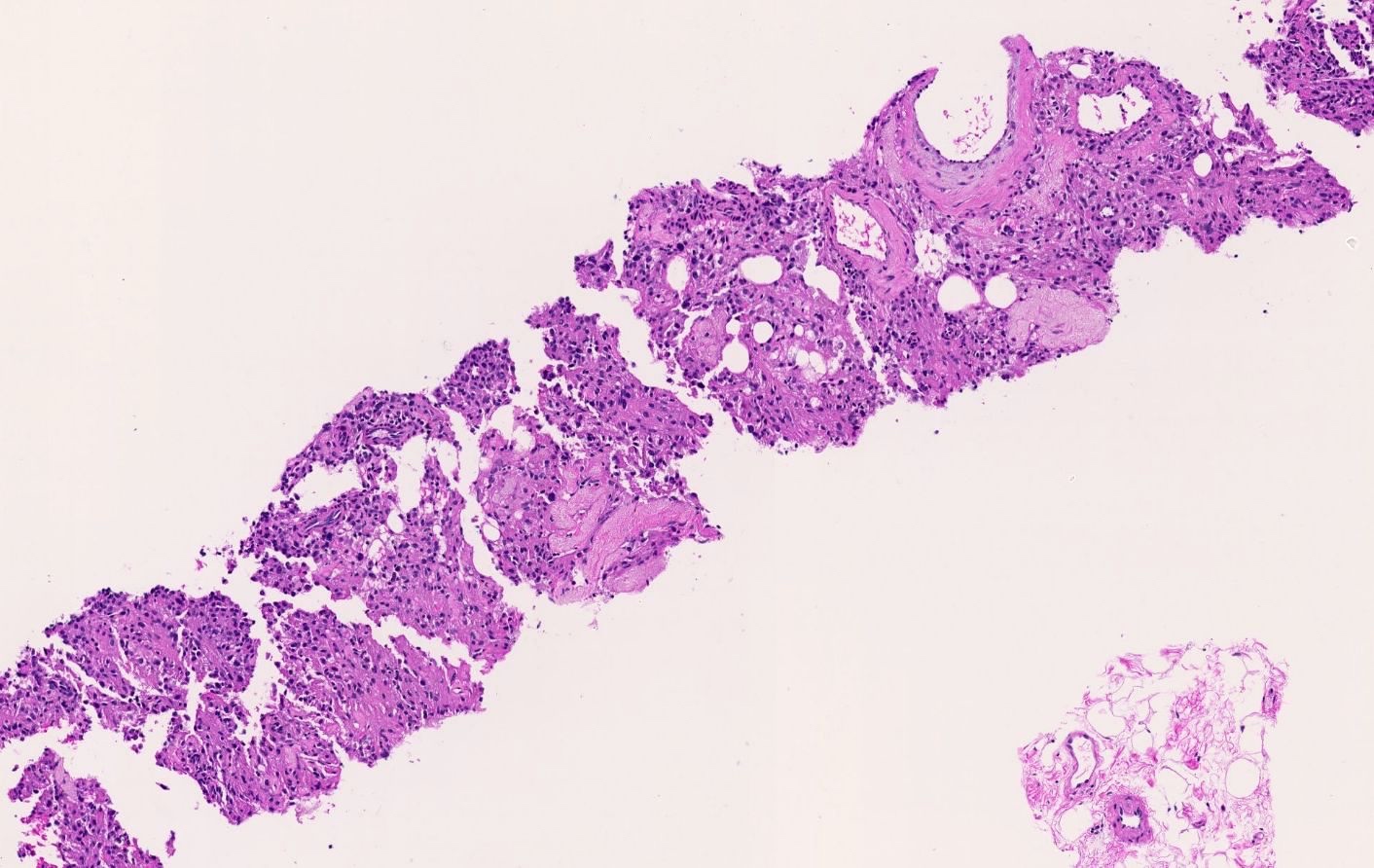
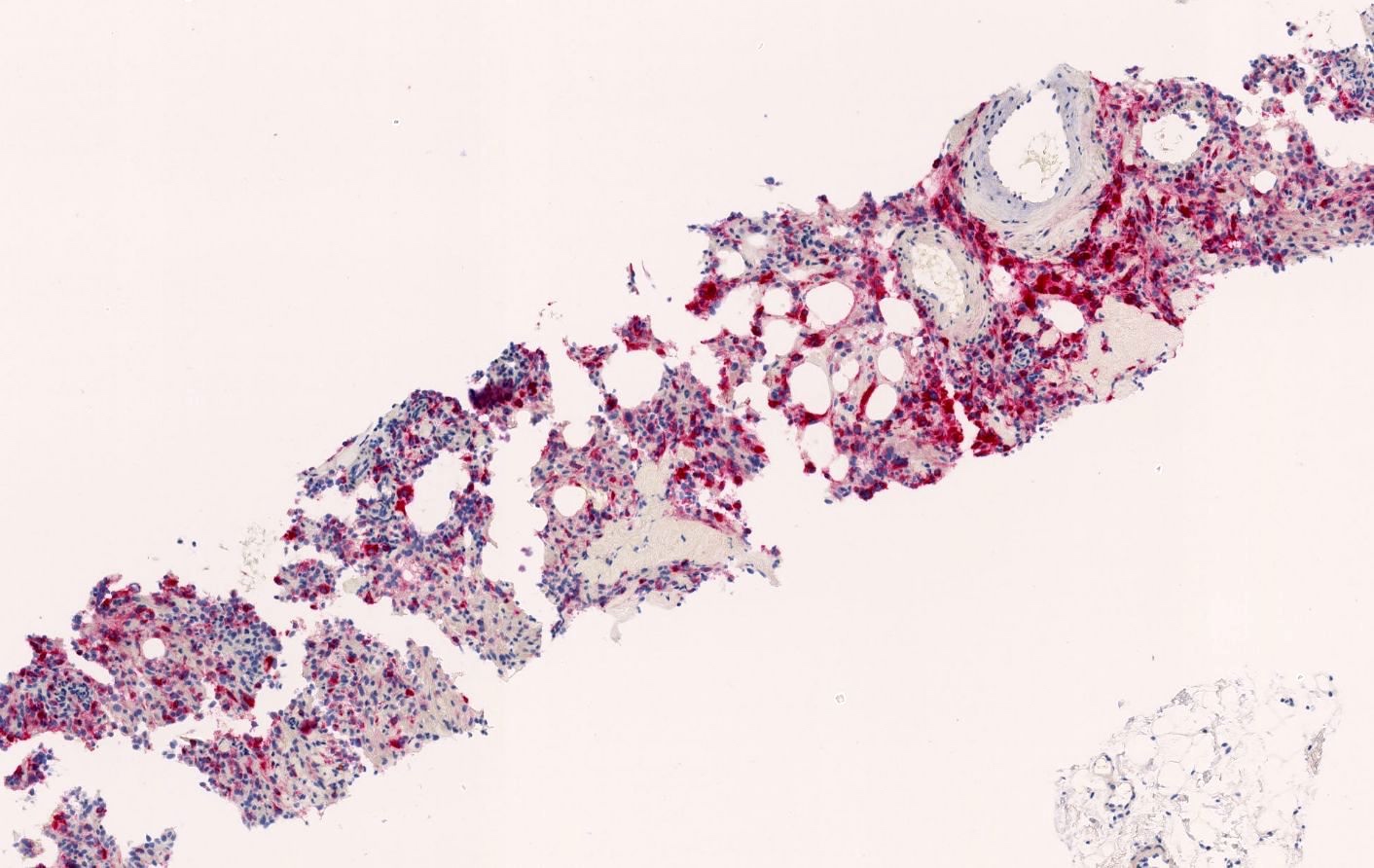
Angiomyolipoma
Cytology images
Images hosted on other servers:

Thyroid, metastatic melanoma
Positive staining - normal
- Lymph nodes: scattered mononuclear cells (Am J Surg Pathol 2000;24:1140)
- Normal fetal and neonatal melanocytes (Appl Immunohistochem 1996;4:73)
- Reactive melanocytes present in inflamed adult skin, near neoplastic lesions or scar tissue (J Cutan Pathol 1989;16:49)
Positive staining - disease
- In benign nevi: junctional nests, papillary dermal nests and nests around adnexal structures (but expression lost with increasing dermal depth, consistent with maturation) (Semin Diagn Pathol 2022;39:239)
- Aberrant dermal expression in blue nevi and in 50% of halo nevi (J Cutan Pathol 2021;48:519)
- WNT activated deep penetrating / plexiform melanocytoma (deep penetrating nevus) (Biology (Basel) 2022;11:460)
- Atypical Spitz nevus (variable or diminished stain in the dermis) (Front Oncol 2022;12:889223)
- Primary melanomas (sensitivity 70 - 95%) (J Cutan Pathol 2008;35:433, J Pers Med 2023;13:898)
- Spitz melanoma (common deep staining of the dermis) (Front Oncol 2022;12:889223)
- Metastatic melanomas (sensitivity 58 - 95%) (Hum Pathol 2004;35:217, J Pers Med 2023;13:898)
- Primary diffuse leptomeningeal melanomatosis (PDLM) (Surg Neurol Int 2014;5:147)
- Meningeal melanocytoma and melanoma (J Neurooncol 2016;127:279)
- TFE3 and TFEB rearranged renal cell carcinoma (Genes Chromosomes Cancer 2022;61:219, Biomedicines 2023;11:245)
- Angiomyolipoma (Arch Pathol Lab Med 2007;131:122, Pathology 2021;53:129)
- PEComa (Ann Diagn Pathol 2015;19:359)
- Lymphangioleiomyomatosis (85%) (Appl Immunohistochem Mol Morphol 2022;30:108)
- Tumors of tuberous sclerosis complex (angiomyolipoma, lymphangioleiomyomatosis, cardiac rhabdomyoma but not subependymal giant cell astrocytoma, see Negative staining) (Mod Pathol 1997;10:952)
- Malignant melanotic nerve sheath tumor (100%) (Am J Surg Pathol 2014;38:94)
- Melanotic schwannoma (Arch Pathol Lab Med 2018;142:1517)
- Pigmented (melanotic) neurofibroma (90%) and in a variable proportion of nonpigmented neurofibromas (Am J Surg Pathol 2000;24:331, Am J Surg Pathol 2013;37:1182)
- Clear cell sarcoma (85%) (Cancers (Basel) 2023;15:3584, Dermatol Res Pract 2012;2012:984096)
- Melanotic neuroectodermal tumor of infancy (StatPearls: Melanotic Neuroectodermal Tumor of Infancy [Accessed 13 June 2024], J Oral Maxillofac Pathol 2019;23:134)
Negative staining
- Adult / resting melanocytes (J Cutan Pathol 1989;16:49)
- Dermal component of benign nevi (Semin Diagn Pathol 2022;39:239)
- Desmoplastic melanoma (J Eur Acad Dermatol Venereol 2021;35:1290)
- Undifferentiated / dedifferentiated melanoma (Am J Surg Pathol 2016;40:181)
- Adrenal cortical carcinoma (Medicine (Baltimore) 2017;96:e8956)
- Atypical fibroxanthoma (only one case reported to be positive) (J Cutan Pathol 2011;38:954, Am J Dermatopathol 2021;43:e218)
- Granular cell tumor (Am J Dermatopathol 2007;29:22)
- Epithelioid sarcoma (Am J Surg Pathol 1997;21:130)
- Angiolipoma (World J Gastroenterol 2007;13:467)
- Clear cell renal cell carcinoma (Cancers (Basel) 2020;12:602)
- Low grade oncocytic tumor of the kidney (LOT) (Virchows Arch 2022;480:999)
- Subependymal giant cell astrocytoma (SEGA) (Mod Pathol 1997;10:313)
- Non-small cell lung cancer (NSCLC, positive in < 1% of cases) (Diagn Pathol 2018;13:68)
- Metaplastic breast carcinoma and ductal carcinoma, no special type (NST) with melanotic pattern (focal positive only in isolated cases) (Mod Pathol 1997;10:592, Am J Clin Pathol 1989;92:491)
- Mammary Paget disease (positive only in isolated cases) (J Am Acad Dermatol 2011;65:247)
- Malignant lymphoma (positive only in one isolated case) (Arch Pathol Lab Med 1991;115:826)
- Malignant peripheral nerve sheath tumor (other than melanotic) (Histopathology 2018;73:969)
- Alveolar soft part sarcoma (only one isolated case with focal positivity) (Am J Clin Pathol 1990;93:32, Am J Surg Pathol 2017;41:622)
- Epithelioid fibrous histiocytoma (Diagnostics (Basel) 2020;10:233)
- Myoepithelioma / myoepithelial carcinoma (Diagnostics (Basel) 2020;10:233)
- Cutaneous carcinomas (squamous cell, basal cell and Merkel cells) (Diagnostics (Basel) 2020;10:233)
- Pheochromocytoma (chief cells can be positive in 33% of cases) (Arch Pathol Lab Med 1992;116:151)
- Uterine leiomyosarcoma (can be focally positive in 36% of cases) (Am J Surg Pathol 2007;31:95)
Sample pathology report
- Lymph node, biopsy:
- Metastatic melanoma involving one lymph node (1/1) (see comment)
- Comment: The submitted biopsy material shows fragments of lymph node tissue with infiltration by discohesive epithelioid neoplastic cells exhibiting marked cytological atypia, high mitotic activity and the presence of widespread necrosis. Their immunohistochemical profile demonstrates strong and diffuse positivity for HMB45, SOX10, S100 and MelanA and negativity for AE1 / AE3 (by positive internal control), consistent with the diagnosis of melanoma.
Additional references
Board review style question #1
Which statement about HMB45 is correct?
- HMB45 can be used as marker alone to diagnose a melanoma in metastatic setting
- HMB45 combined with other makers (e.g., S100) can be helpful in diagnosing melanoma
- In nonneoplastic tissues, HMB45 expression is limited only to fetal or neonatal melanocytes
- Melanocytic lesion with HMB45+ dermal component is always consistent with melanoma
Board review style answer #1
B. HMB45 combined with other makers (e.g., S100) can be helpful in diagnosing melanoma. HMB45 is a relatively specific marker but should be combined with other markers for diagnosing a melanoma. Answer D is incorrect because other melanocytic lesions (e.g., blue nevi) can be positive for HMB45. Answer A is incorrect because HMB45 alone is neither sensitive nor specific for melanoma (i.e., melanomas can be negative for HMB45 and other tumors such as PEComas can be positive for HMB45). Answer C is incorrect because HMB45 can be also expressed in reactive melanocytes (e.g., in case of inflammatory skin disorders).
Comment Here
Reference: HMB45
Comment Here
Reference: HMB45
Board review style question #2
A renal tumor shows a mixed morphology with mature adipose tissue, epithelioid cells and thick walled vessels. Immunohistochemistry for HMB45 is shown in figure above. SMA is also positive, whereas AE1 / AE3, PAX8 and CAIX are negative (not shown). Which is the most likely diagnosis?
- Adrenal cortical carcinoma
- Angiomyolipoma
- Clear cell renal cell carcinoma
- Metastatic melanoma
Board review style answer #2
B. Angiomyolipoma. The morphology is consistent with a tumor with 3 components without atypia, mitotic activity or necrosis, which in this anatomic location is suggestive of angiomyolipoma. Immunohistochemistry for HMB45 is positive, which combined with the immunohistochemical profile provided above is diagnostic for angiomyolipoma. Answer D is incorrect because the morphology described is not typical for melanoma and HMB45 alone is not specific for melanoma as it can be expressed in other tumors. Answer C is incorrect because although some renal cell carcinomas (e.g., TFE and TFEB rearranged renal cell carcinoma) can express HMB45, clear cell carcinomas are typically negative for HMB45 and express PAX8 and CAIX. Answer A is incorrect because adrenal cortical carcinomas are typically negative for HMB45, although they express MelanA.
Comment Here
Reference: HMB45
Comment Here
Reference: HMB45
Board review style question #3
Which of the following tumors is typically positive for HMB45?
- Angiolipoma
- Desmoplastic melanoma
- Oncocytoma
- TFE rearranged renal cell carcinoma
Board review style answer #3
D. TFE rearranged renal cell carcinoma. Rearrangements of genes of the MiT family (MITF, TFE, TFEB) lead typically to overexpression of premelanosome protein gp100, resulting in positivity for HMB45. Answer B is incorrect because desmoplastic melanomas are most commonly negative for HMB45. Answer C is incorrect because HMB45 is typically negative in oncocytic tumors of the kidney. Answer A is incorrect because HMB45 is typically positive in angiomyolipoma but not in angiolipoma.
Comment Here
Reference: HMB45
Comment Here
Reference: HMB45
