Stains & CD markers
Cytokeratin CAM 5.2


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: CAM 5.2
Cytokeratin CAM 5.2
Authors: Kemal Kösemehmetoğlu, M.D., Nat Pernick, M.D.
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Brandon Umphress, M.D.
Last author update: 16 June 2023
Last staff update: 16 June 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: CAM 5.2
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) description | Microscopic (histologic) images | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kösemehmetoğlu K. Cytokeratin CAM 5.2. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsCAM52.html. Accessed March 31st, 2025.
Definition / general
- Low molecular weight keratin that mainly reacts with human keratin proteins corresponding to Moll's peptides #7 (KRT7, 48 KD) and #8 (KRT8, 52 KD) on secretory epithelia of normal human tissue and associated adenocarcinomas
Essential features
- Low molecular weight keratin (mainly reacts with K7 and K8)
- Diffuse and strong cytoplasmic expression but some tumors show dot-like staining pattern
- Almost all glandular epithelia and adenocarcinomas are positive, whereas squamous epithelium and squamous cell carcinomas usually do not show CAM 5.2 expression
- Excellent accompaniment to pankeratin in the immunopanel to confirm or rule out the epithelial nature of tissue, tumors or components of tumors
- References: Cell 1982;31:11, J Clin Pathol 1984;37:975, Am J Pathol 1990;136:657
Terminology
- Antibody generated by using the human colorectal carcinoma cell line HT24
- Anti-CAM 5.2 reacts with the majority of epithelial tumors, including lung, liver, pancreas, GI tract, breast, genitourinary system, female reproductive organs and some endocrine organs (Cell 1982;31:11)
- Not a pankeratin but reacts with many epithelia and their neoplasms due to the abundance of K7 and K8 throughout the body
Pathophysiology
- There is controversy regarding which keratins CAM 5.2 reacts with; it was originally described as highlighting both K8 and K18 by Makin et al. but now it has been shown to react with K7 and K8, not K18 and K19 (J Clin Pathol 1984;37:975, Am J Pathol 1990;136:657)
- K7 and K8 antigens are widespread in human epithelia, especially on secretory epithelia but not on the stratified squamous epithelium
Interpretation
- Cytoplasmic staining, usually diffuse and strong
- Dot-like staining especially in neuroendocrine tumors, rhabdoid tumors, desmoplastic small round cell tumor, etc.
Uses by pathologists
- Excellent accompaniment to pankeratin in the immunopanel to confirm or rule out the epithelial nature of tissue, tumors or components of tumor
- Identifies metastatic carcinoma (especially micrometastases and isolated tumor cells) in lymph nodes but also stains reticulum cells and plasma cells, so AE1 / AE3 may be better (Int J Gynecol Cancer 2006;16:1336, Appl Immunohistochem Mol Morphol 2001;9:297, Arch Pathol Lab Med 2000;124:1310)
- Identifies metastases in bone marrow, although false positives may occur (Br J Cancer 2002;86:1047, Eur J Surg Oncol 2001;27:740)
- Identifies residual tumor post-treatment; however attention must be paid to the nature of cells, since CAM 5.2 may stain myofibroblasts and smooth muscle cells (Am J Surg Pathol 2007;31:390)
- Distinguishes metastatic carcinoma (CAM 5.2+, GFAP-) from glioblastoma (CAM 5.2-, GFAP+); saves from the pitfall of AE1 / AE3 cross reaction with glioblastoma (Arch Pathol Lab Med 1999;123:917)
- Part of a panel to distinguish uterine tumors resembling ovarian sex cord tumors (CAM 5.2+) from smooth muscle neoplasms (negative) (Mod Pathol 2006;19:17)
- Distinguishes Paget disease (CAM 5.2+) from pagetoid squamous cell carcinoma in situ (negative); used in the immune panel including BerEP4 and p63 (J Cutan Pathol 2003;30:449, Dermatopathology (Basel) 2015;2:15)
Prognostic factors
- Detection of micrometastases as a poor prognostic factor in bile duct (hilar) carcinoma, esophageal carcinoma, rectal carcinoma and stomach carcinoma (World J Gastroenterol 2006;12:2549, Ann Thorac Surg 2004;78:1161, Dis Colon Rectum 2003;46:333, Am J Surg Pathol 2005;29:1135)
- High expression in esophageal squamous cell carcinoma is associated with poor prognosis (Medicine (Baltimore) 2019;98:e17104)
Microscopic (histologic) description
- Usually strong and diffuse cytoplasmic staining in adenocarcinomas or can be dot-like, especially in neuroendocrine tumors
Microscopic (histologic) images
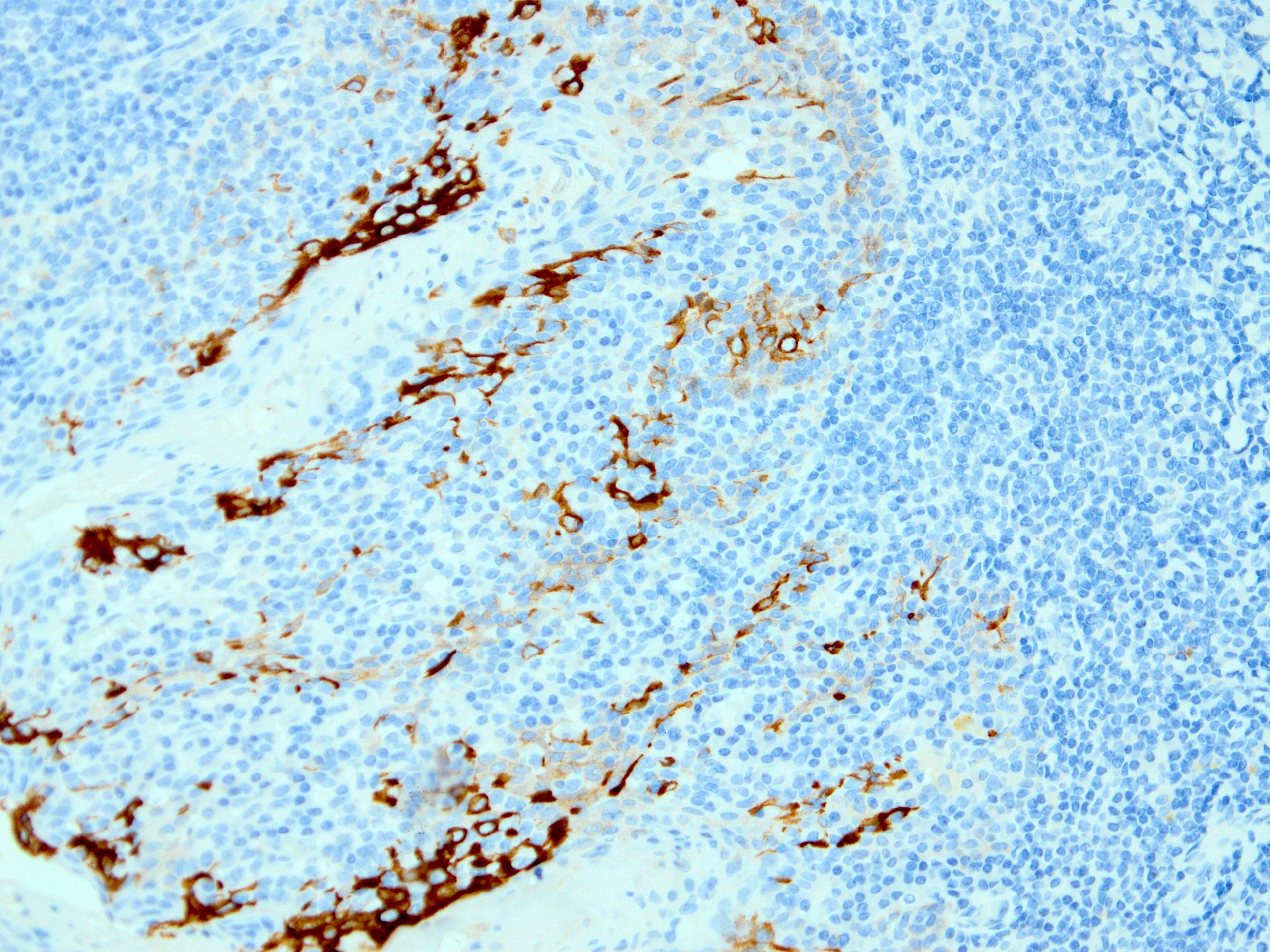
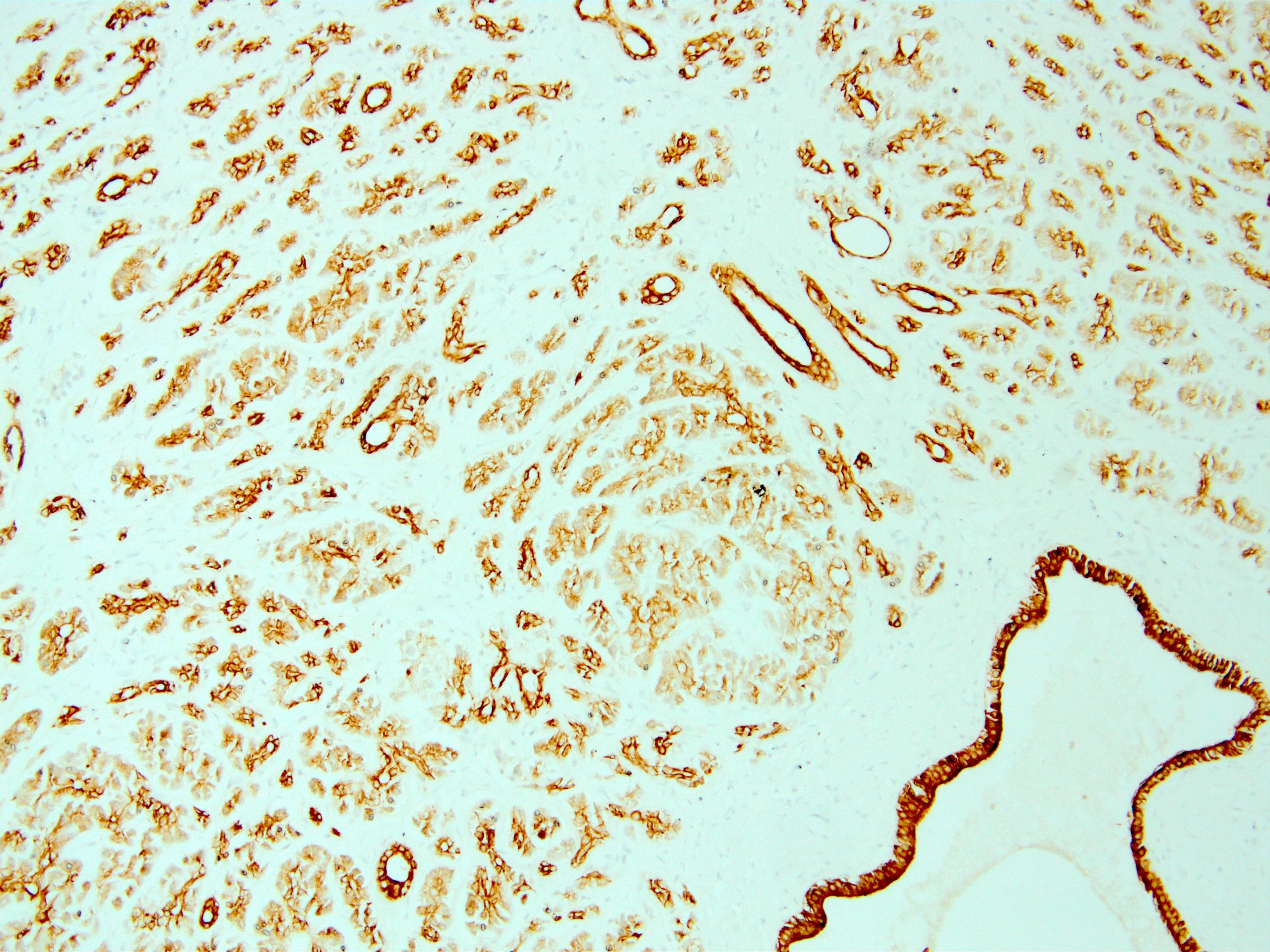
Contributed by Kemal Kösemehmetoğlu, M.D.
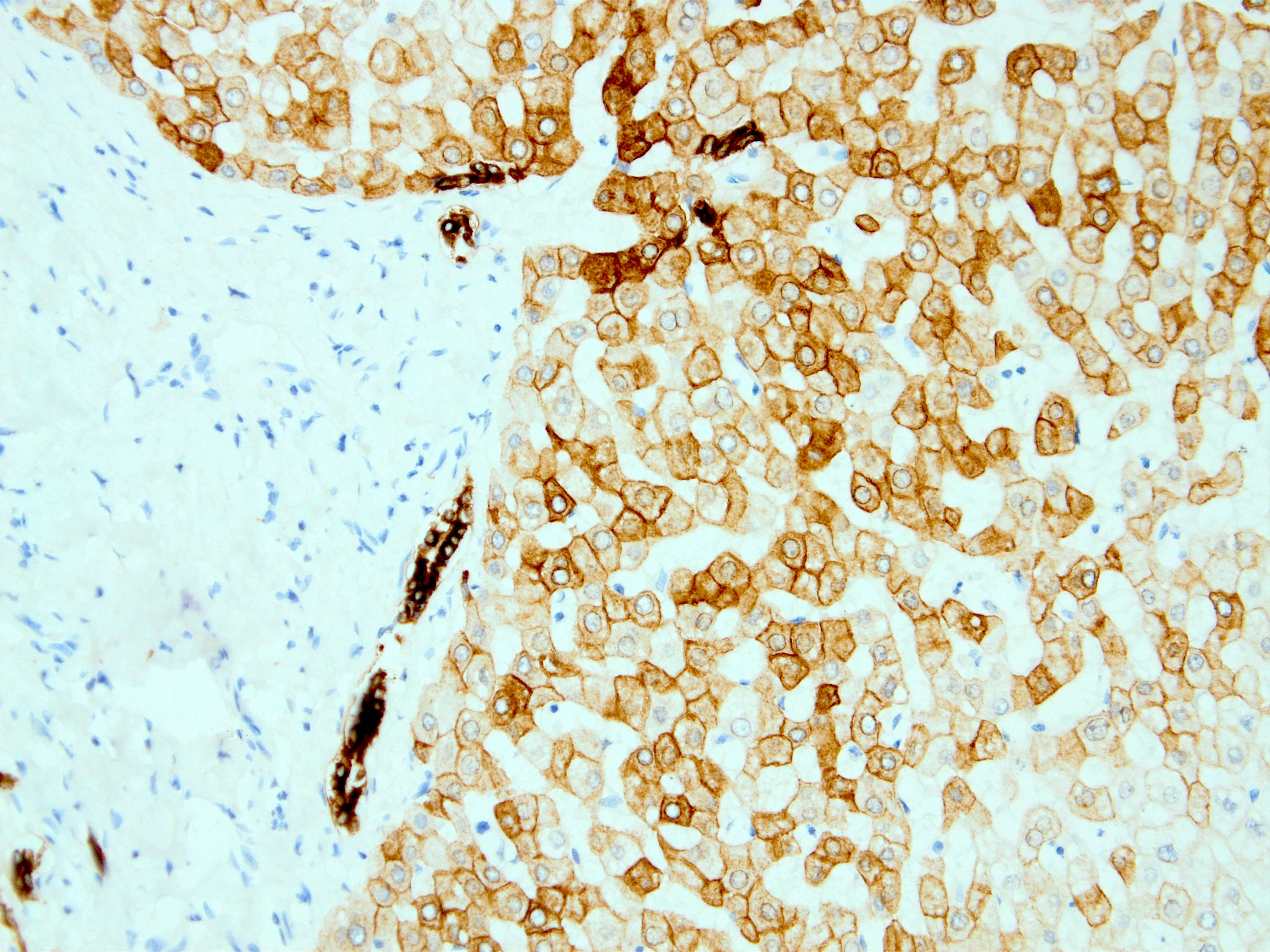
Normal liver
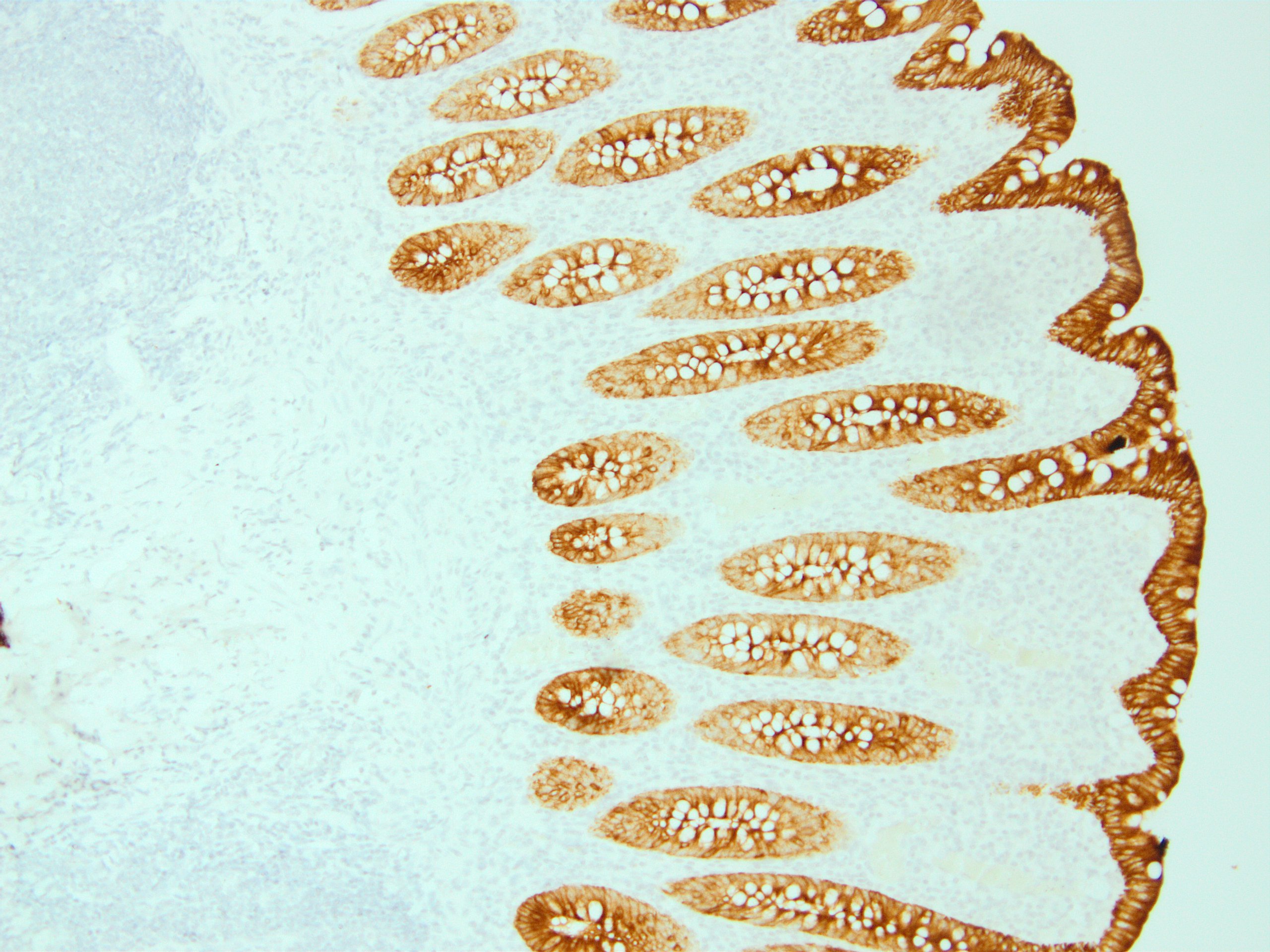
Colon mucosa
Tonsil
Pancreas
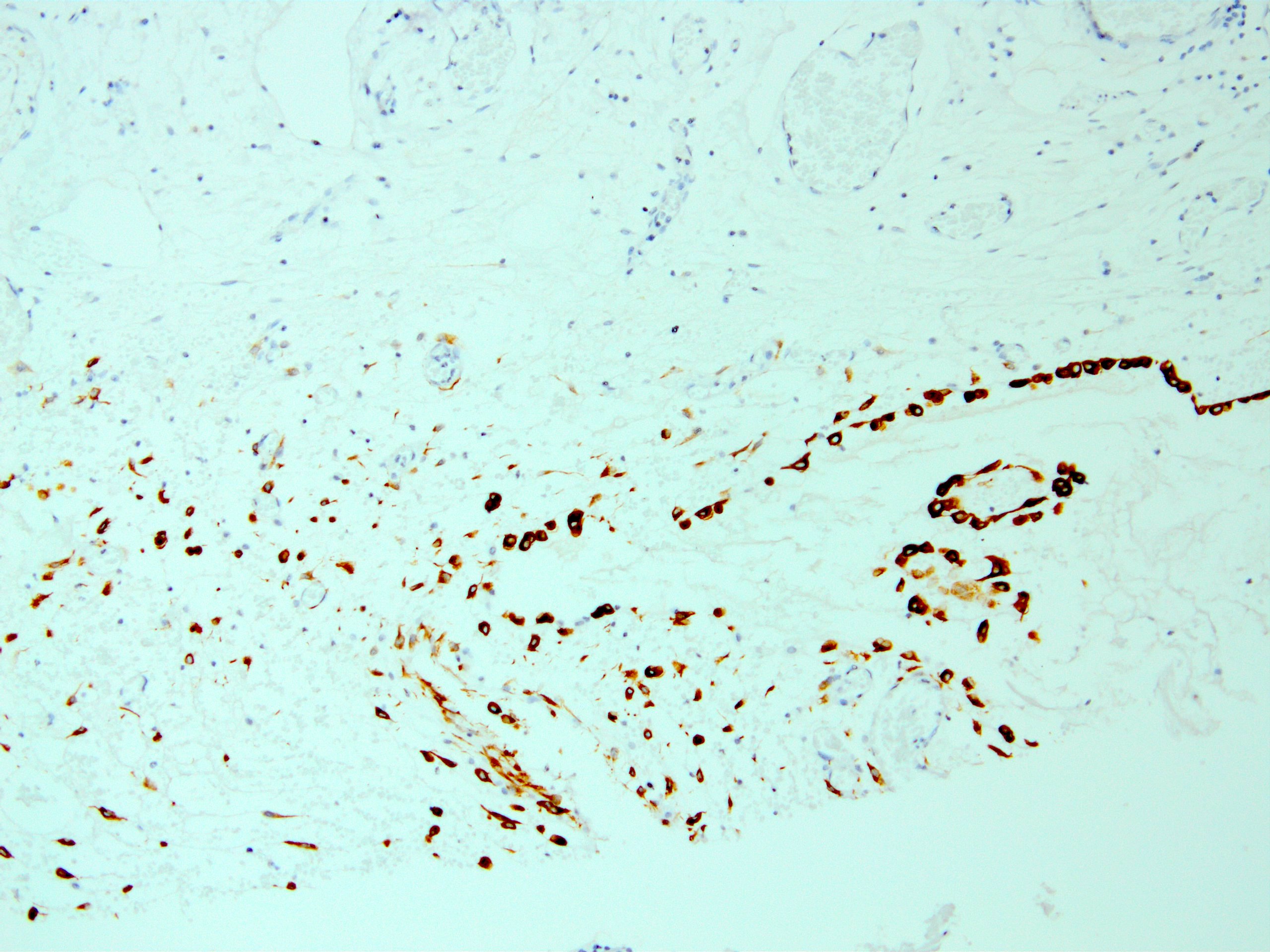
Peritoneum
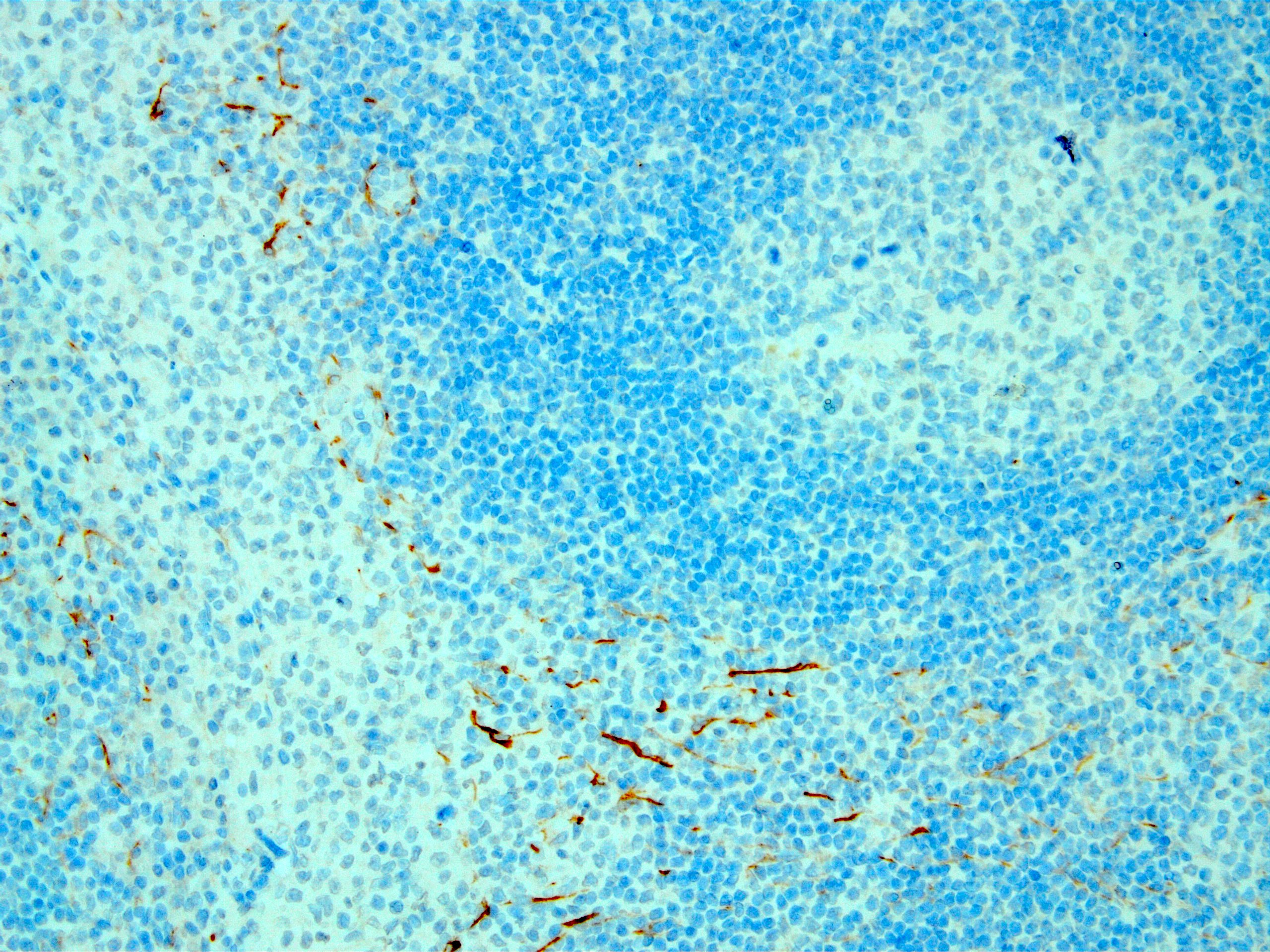
Dendritic cell staining in lymph node
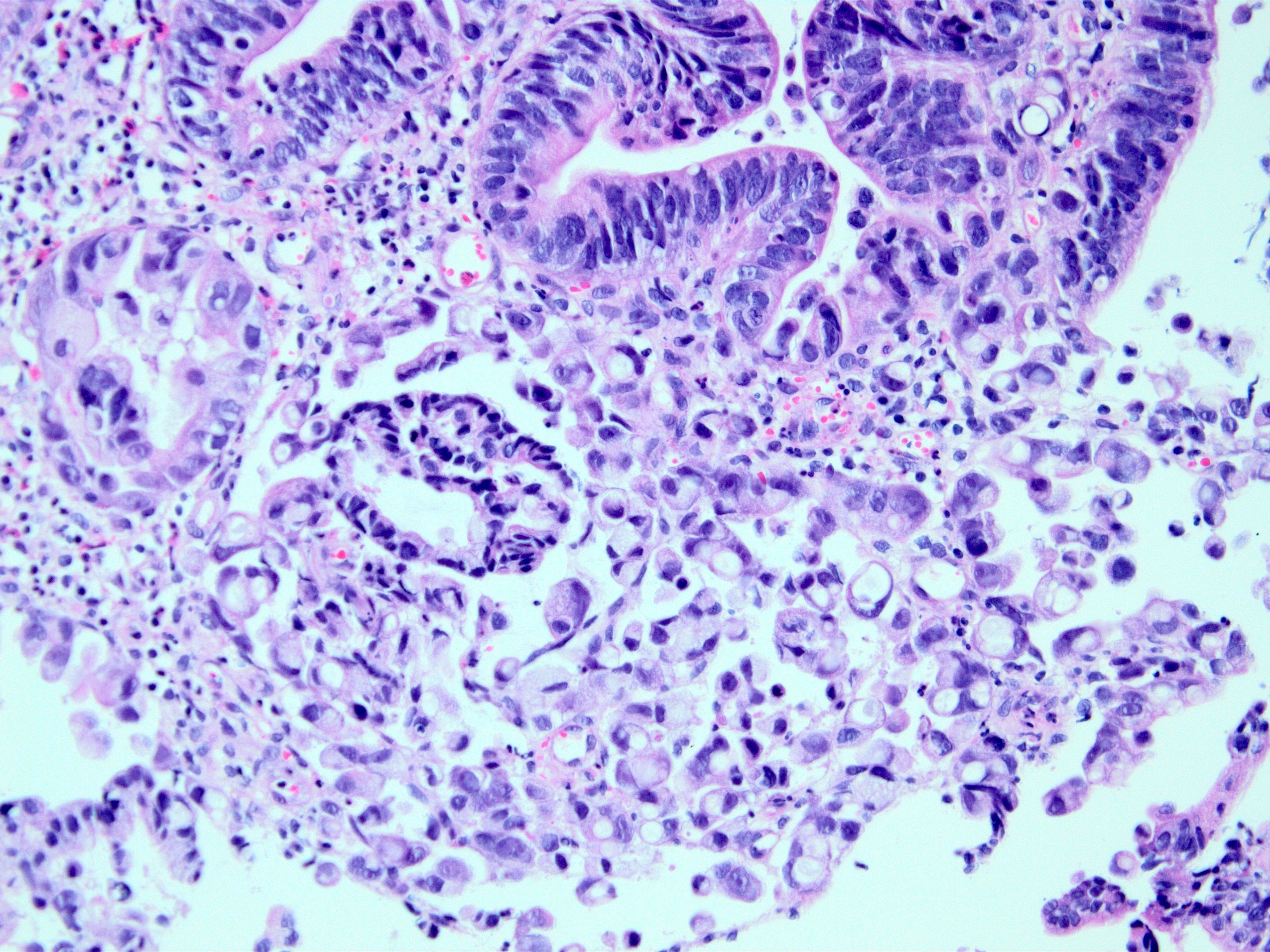
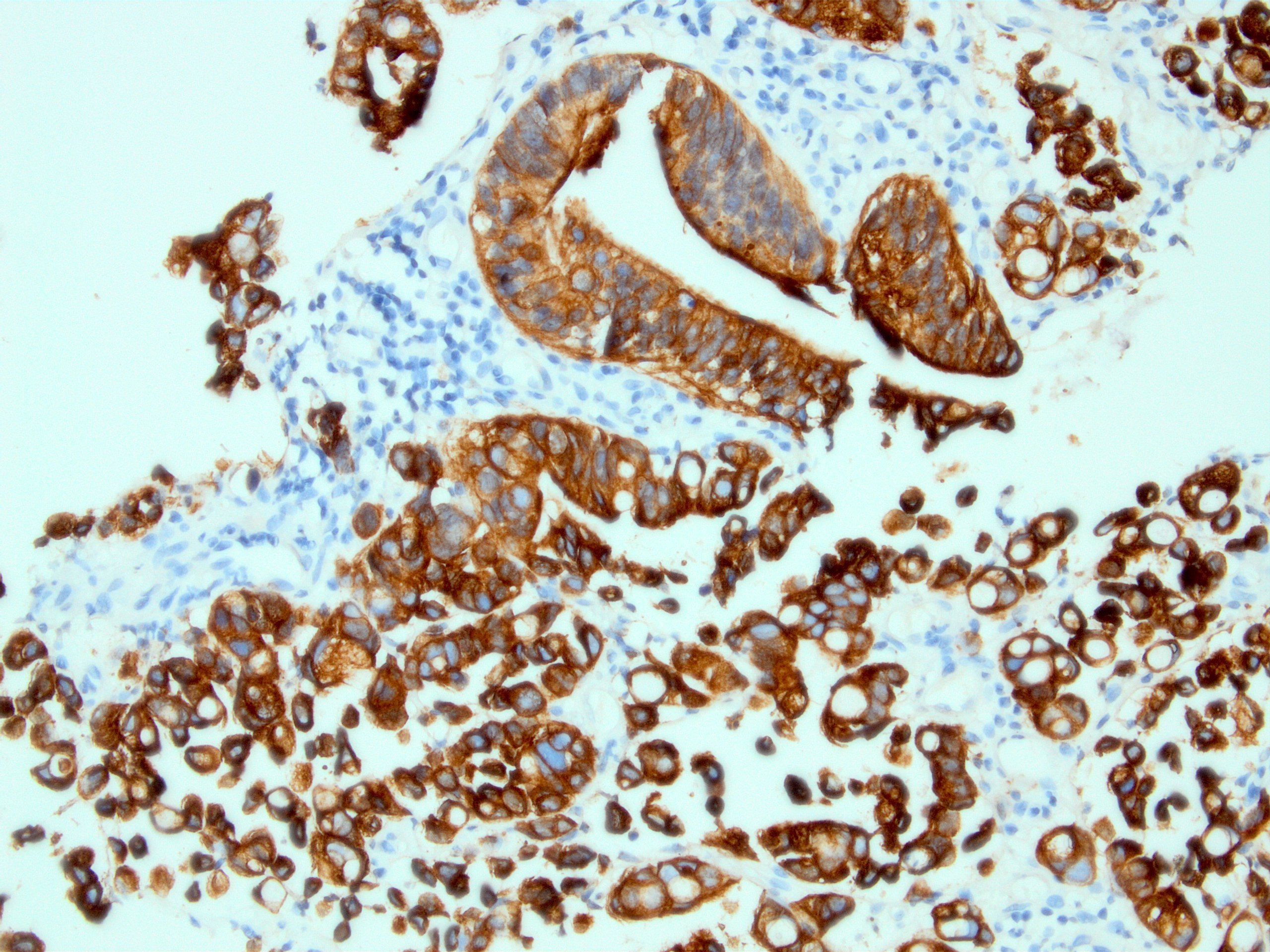
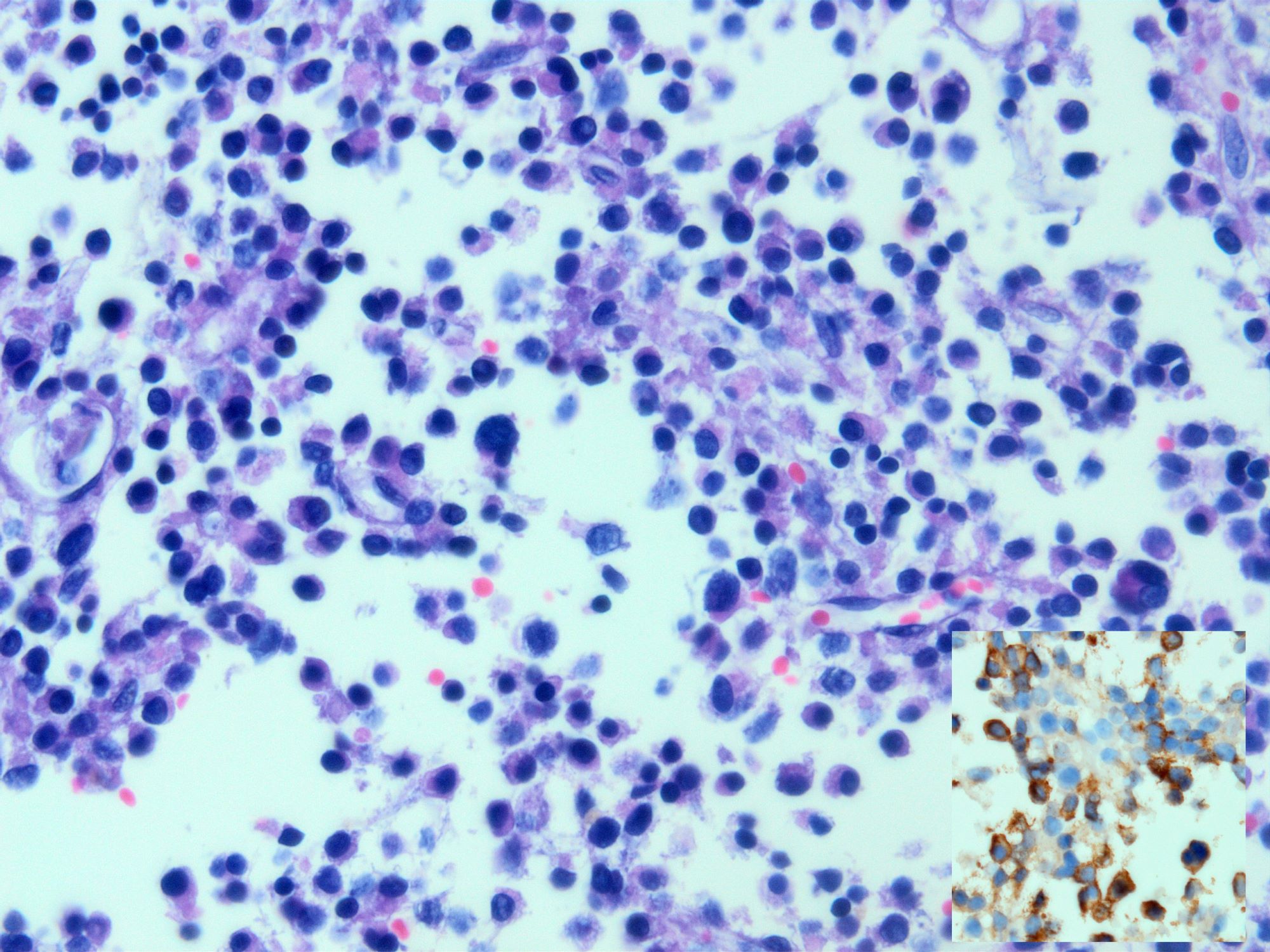
Signet ring carcinoma of stomach
Signet ring carcinoma infiltrating omentum
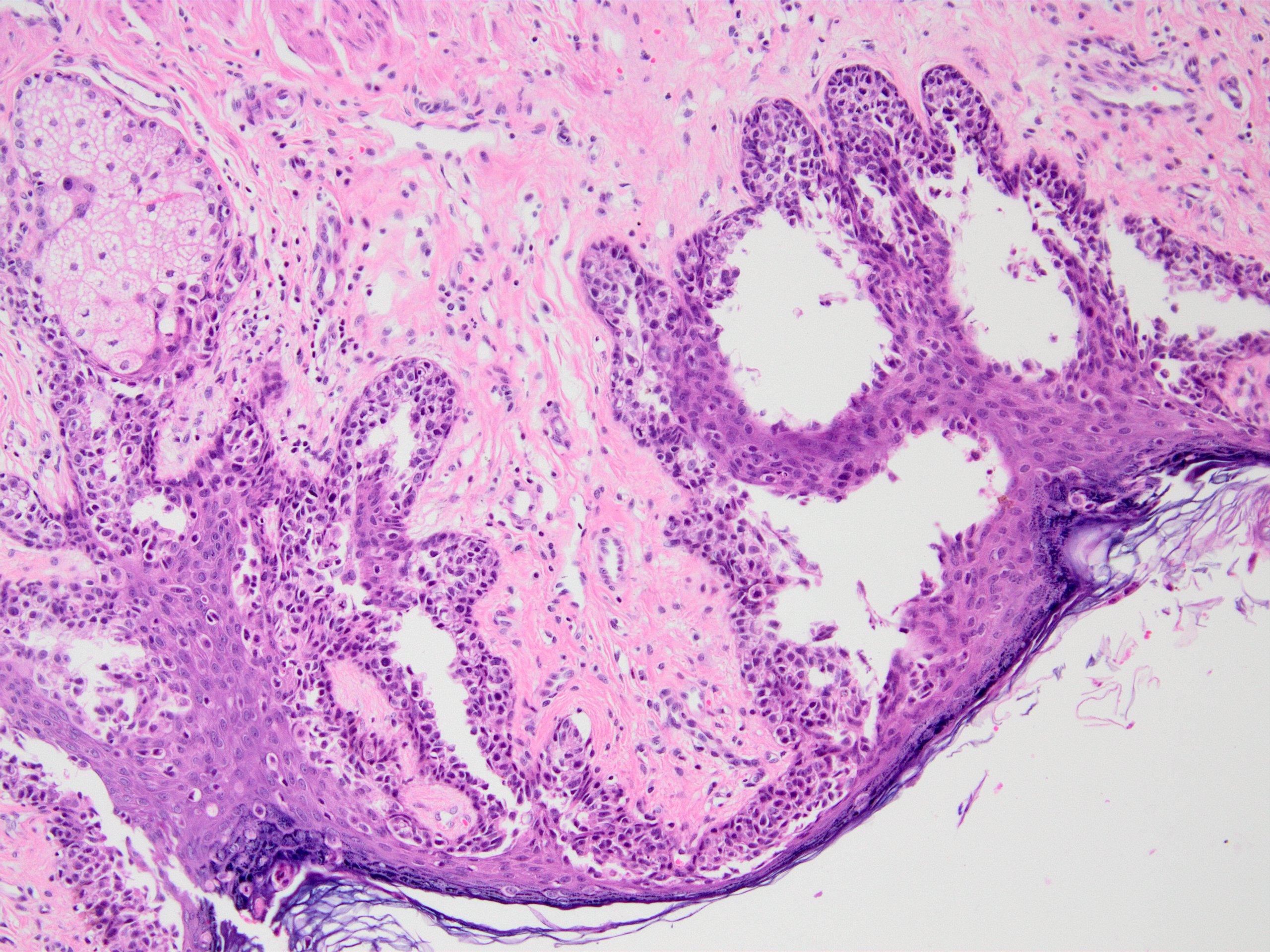
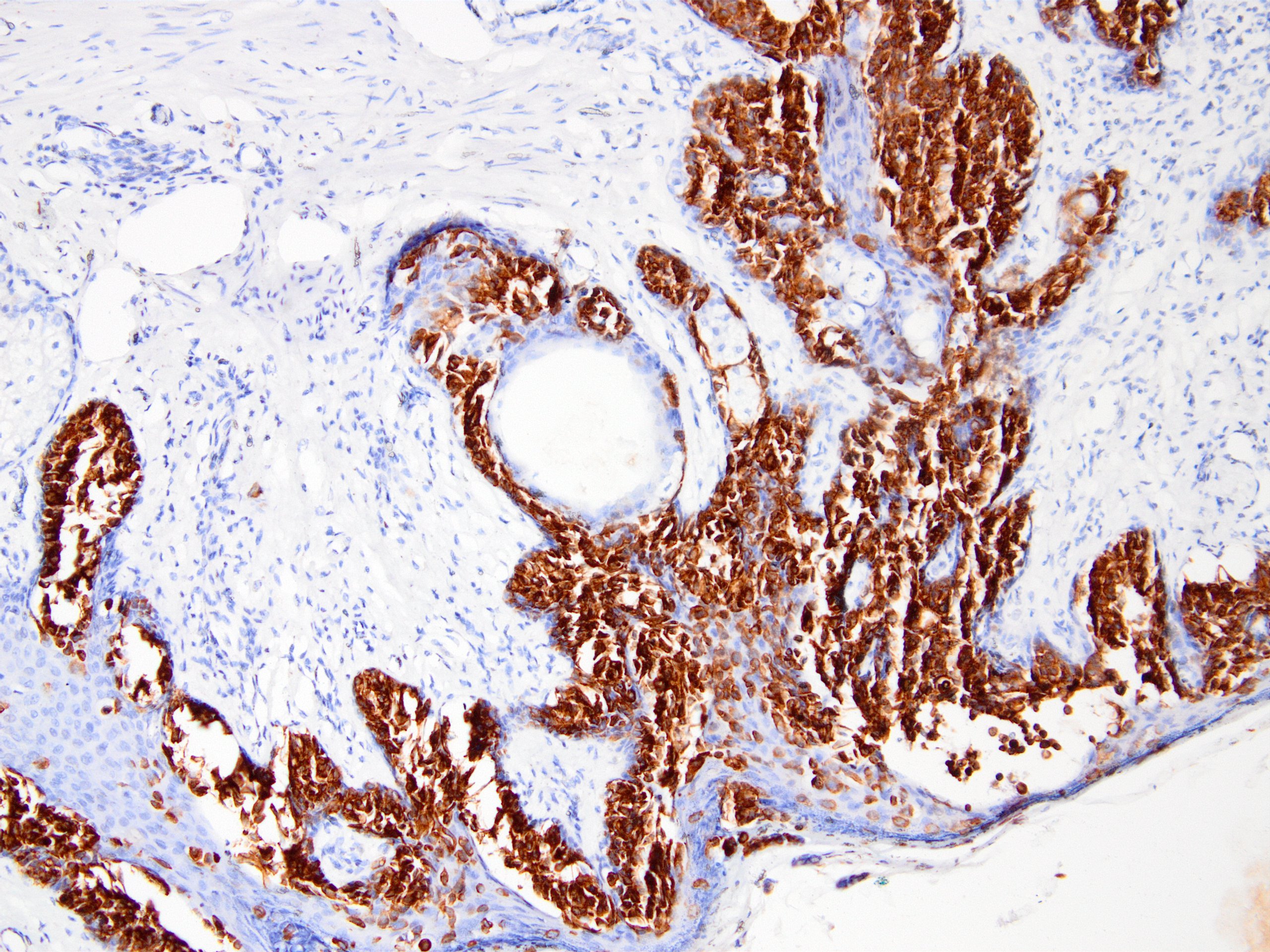
Paget disease of nipple


Nipple duct adenoma
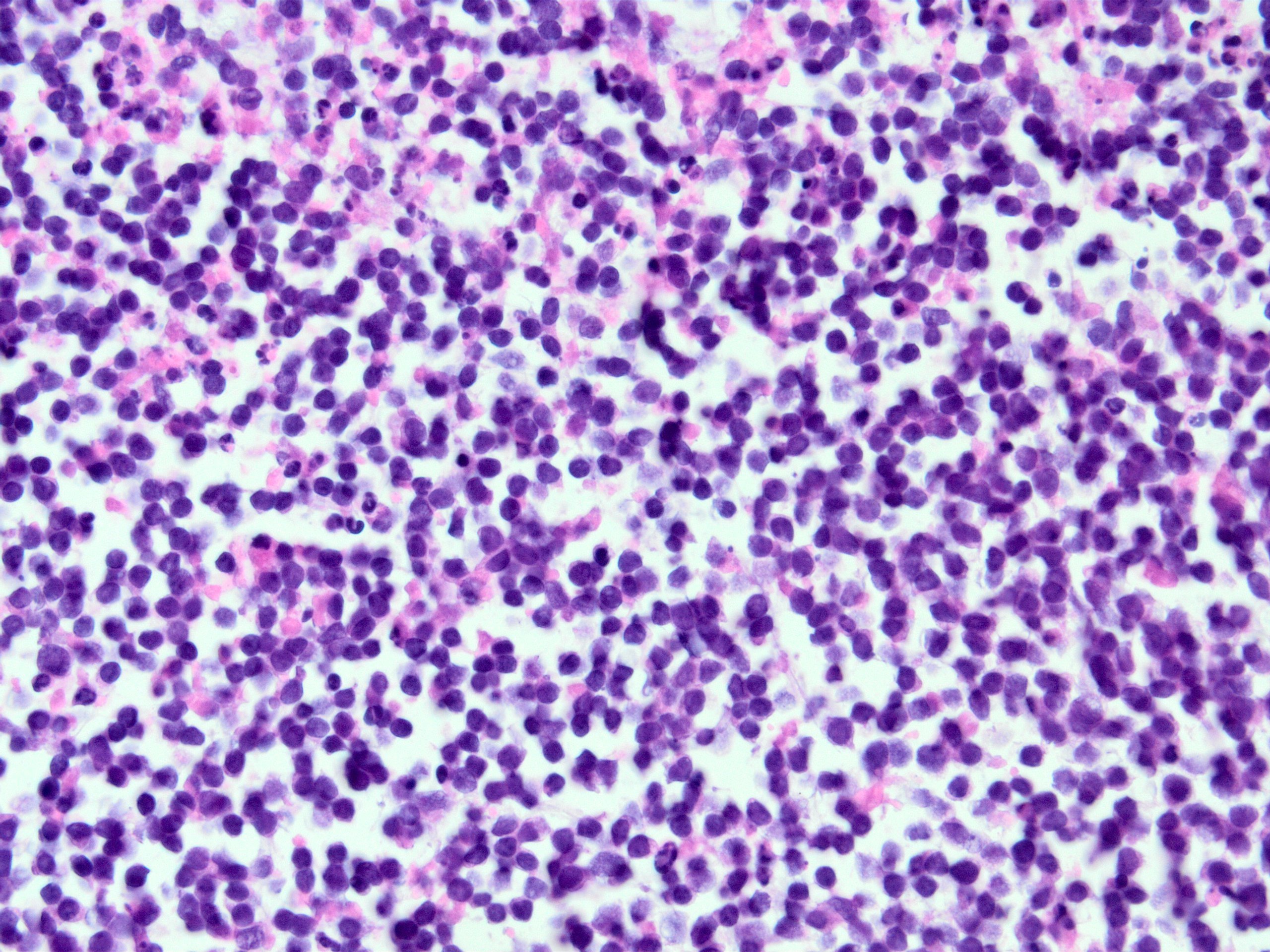
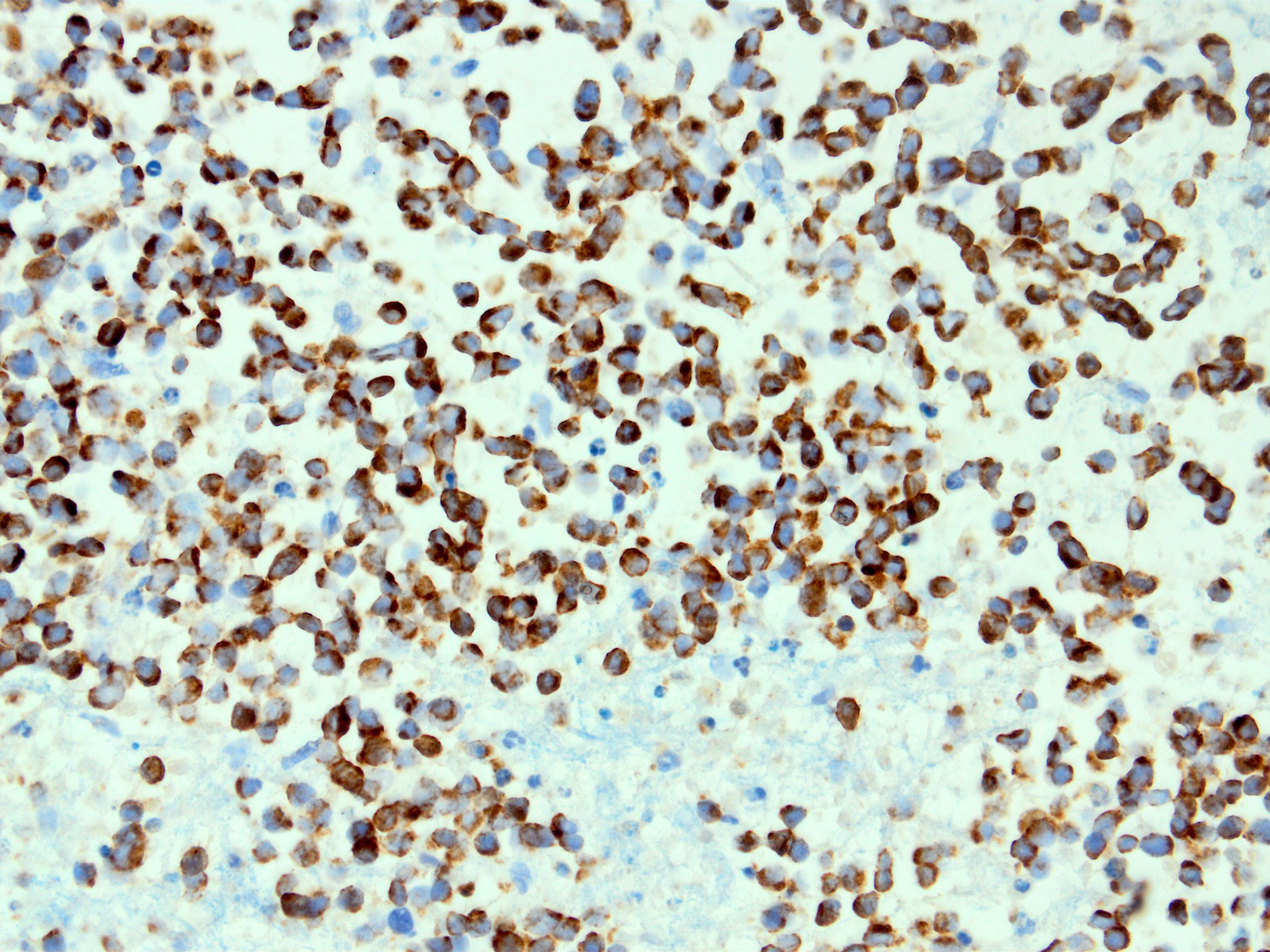
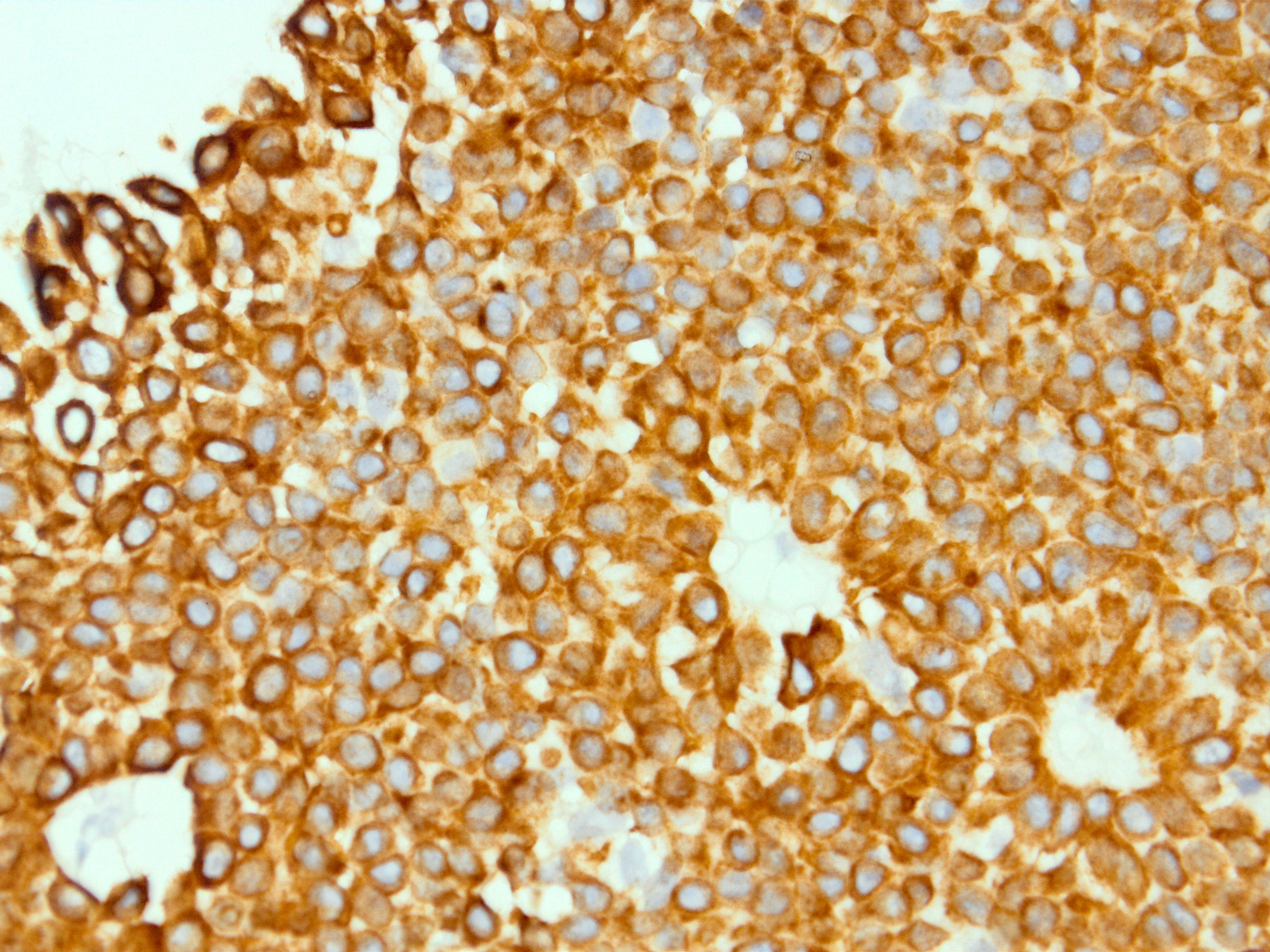
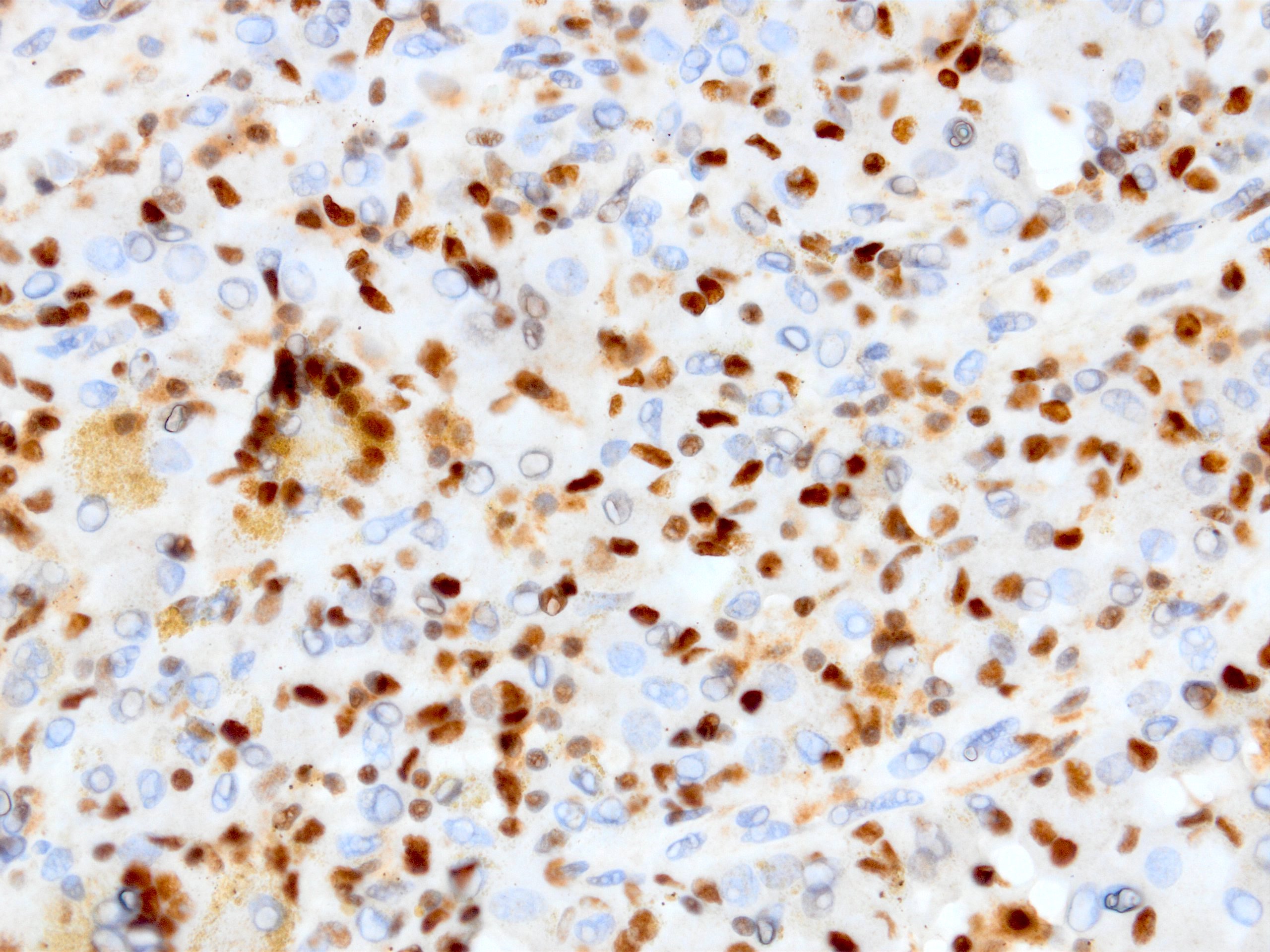
High grade neuroendocrine carcinoma
CAM 5.2 in Crooke cell adenoma

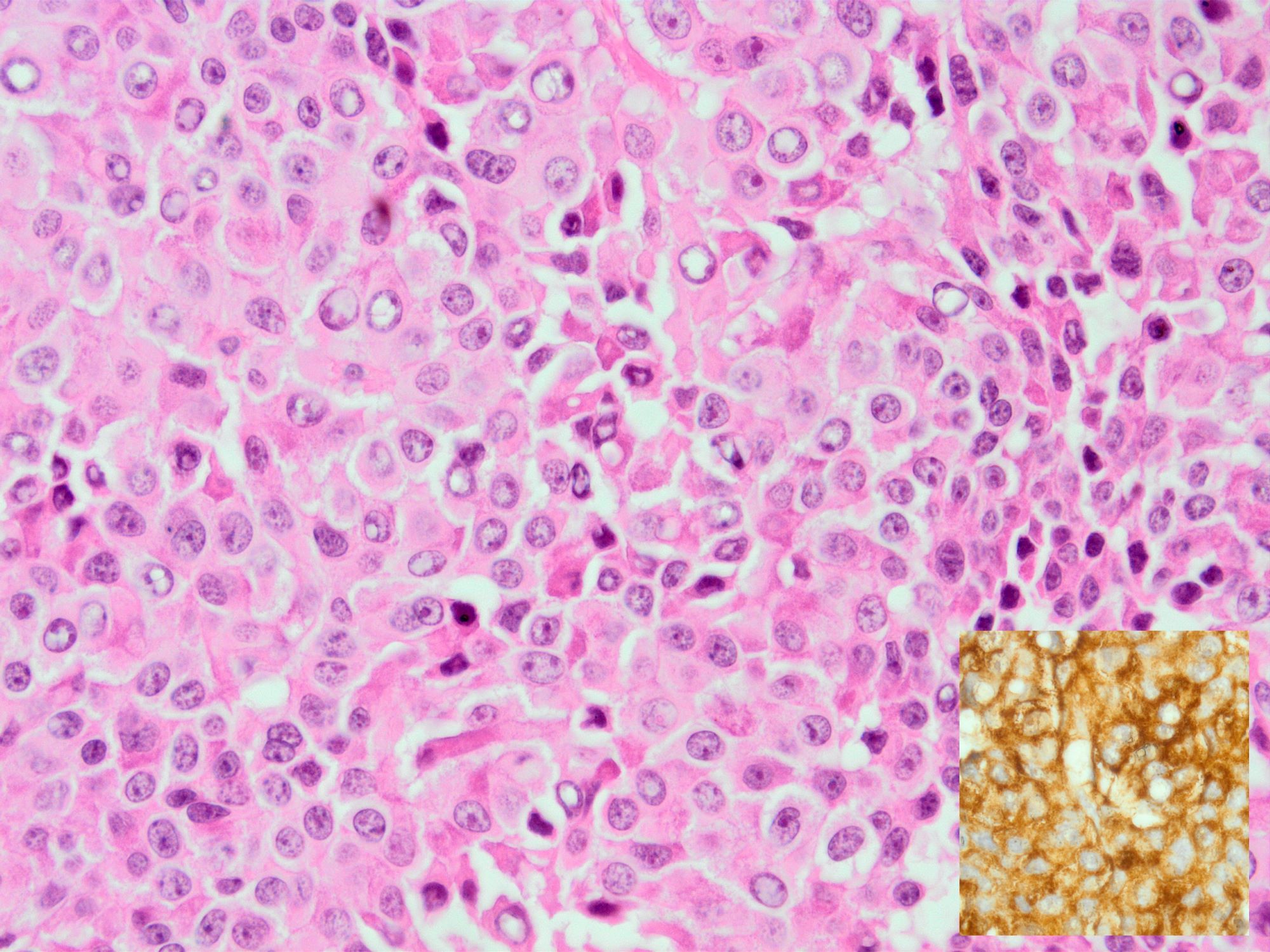
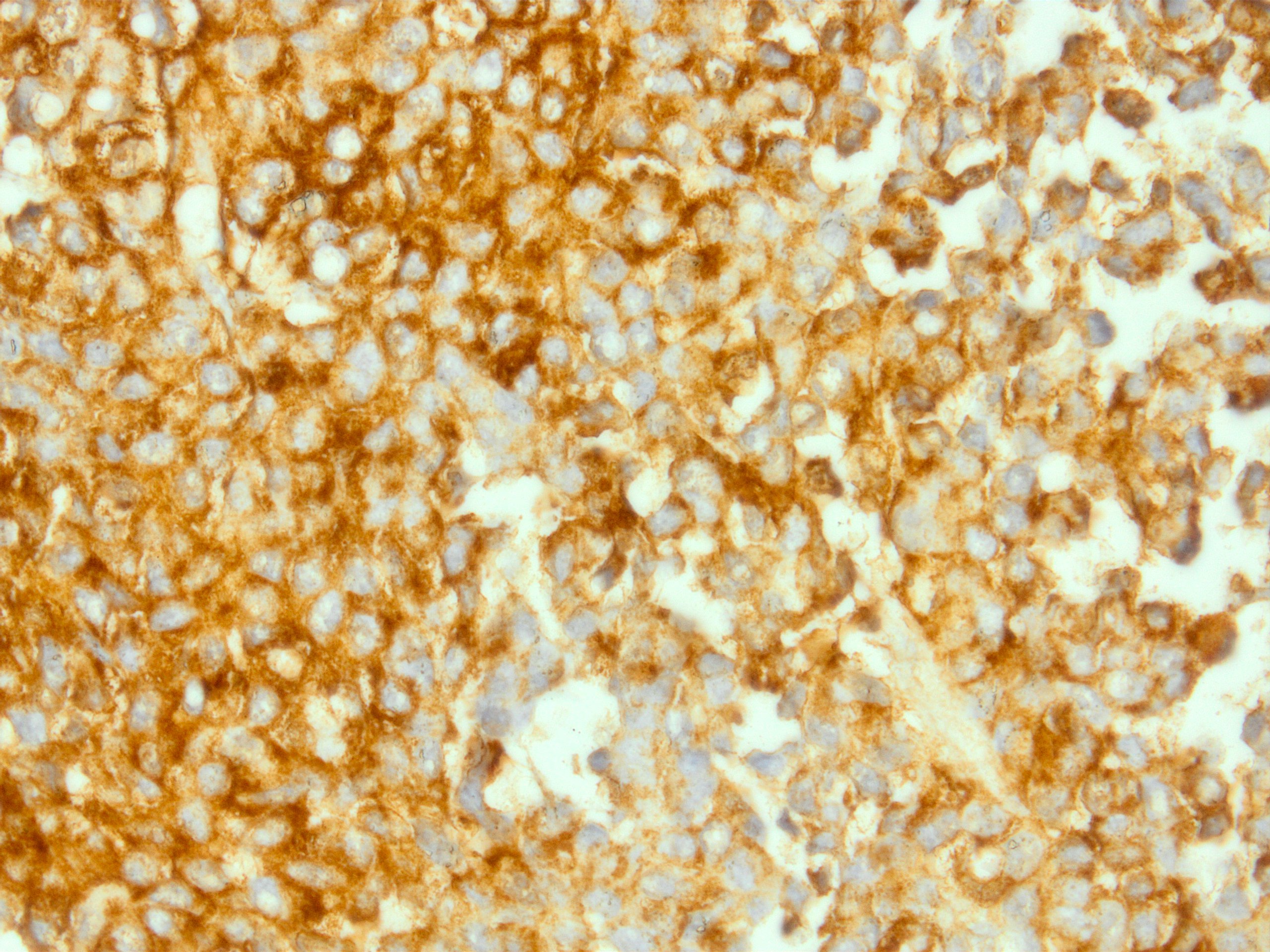
CAM 5.2 in sparsely granulated somatotroph adenoma
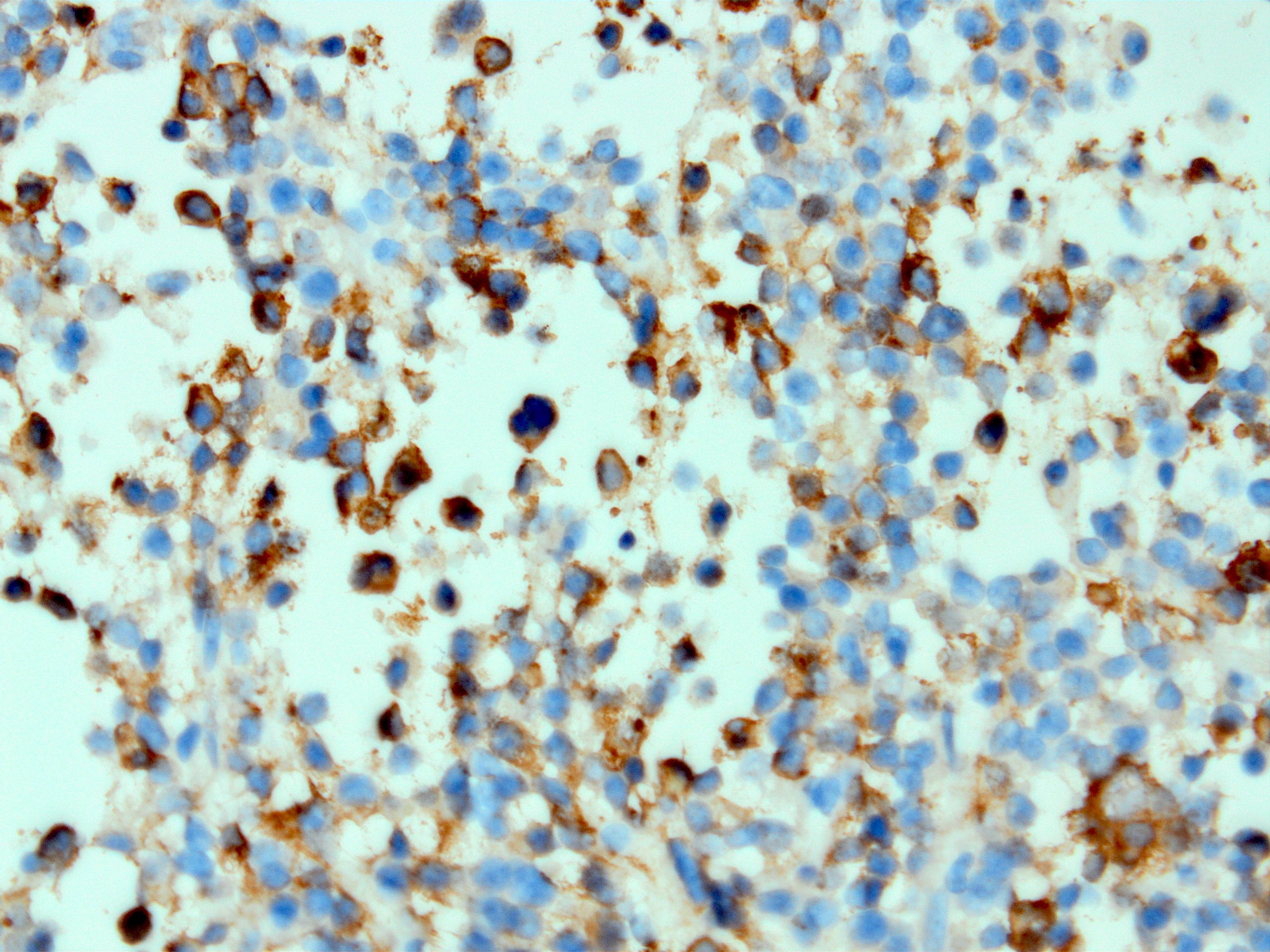
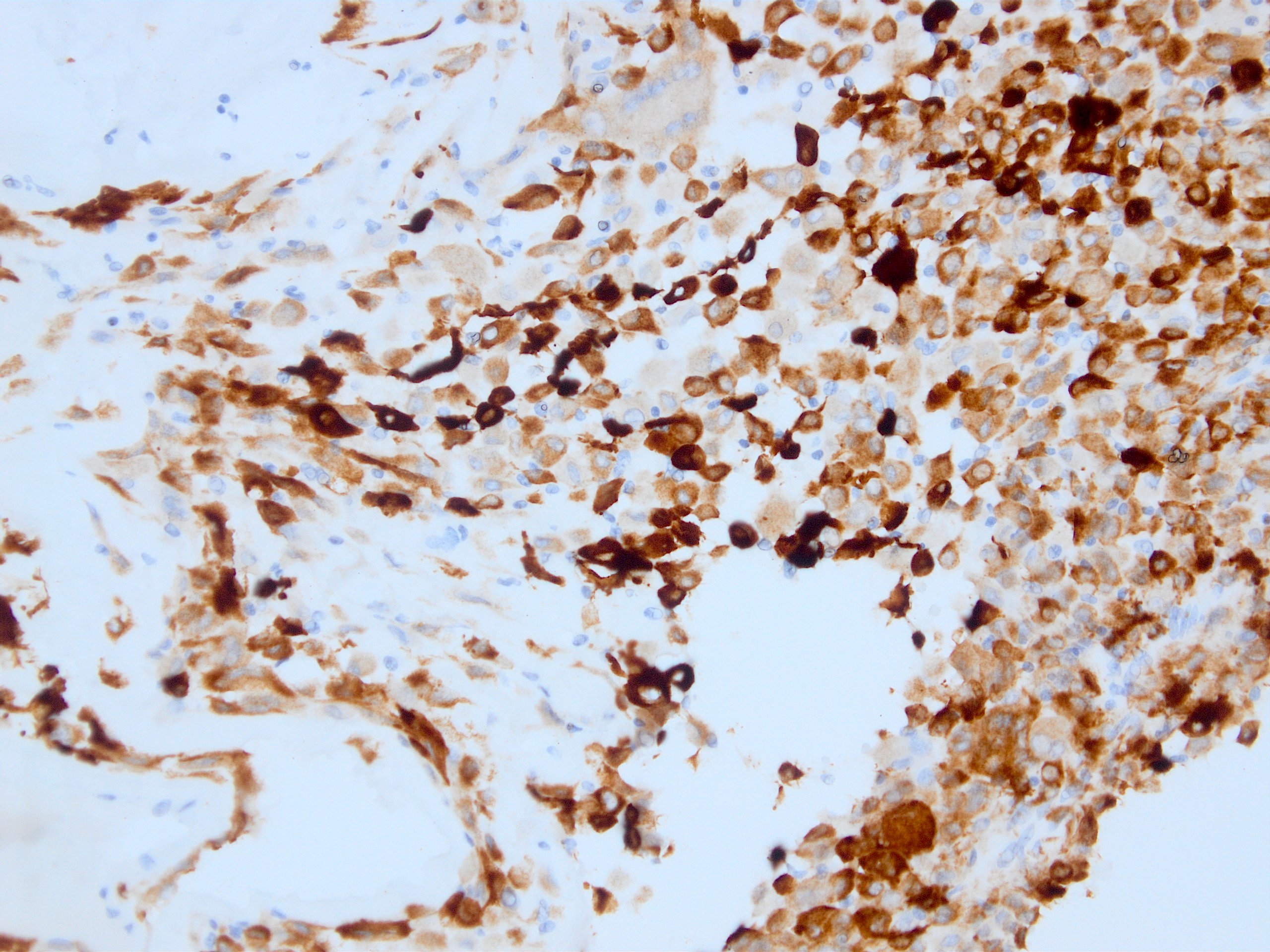
CAM 5.2 in sarcomatoid carcinoma
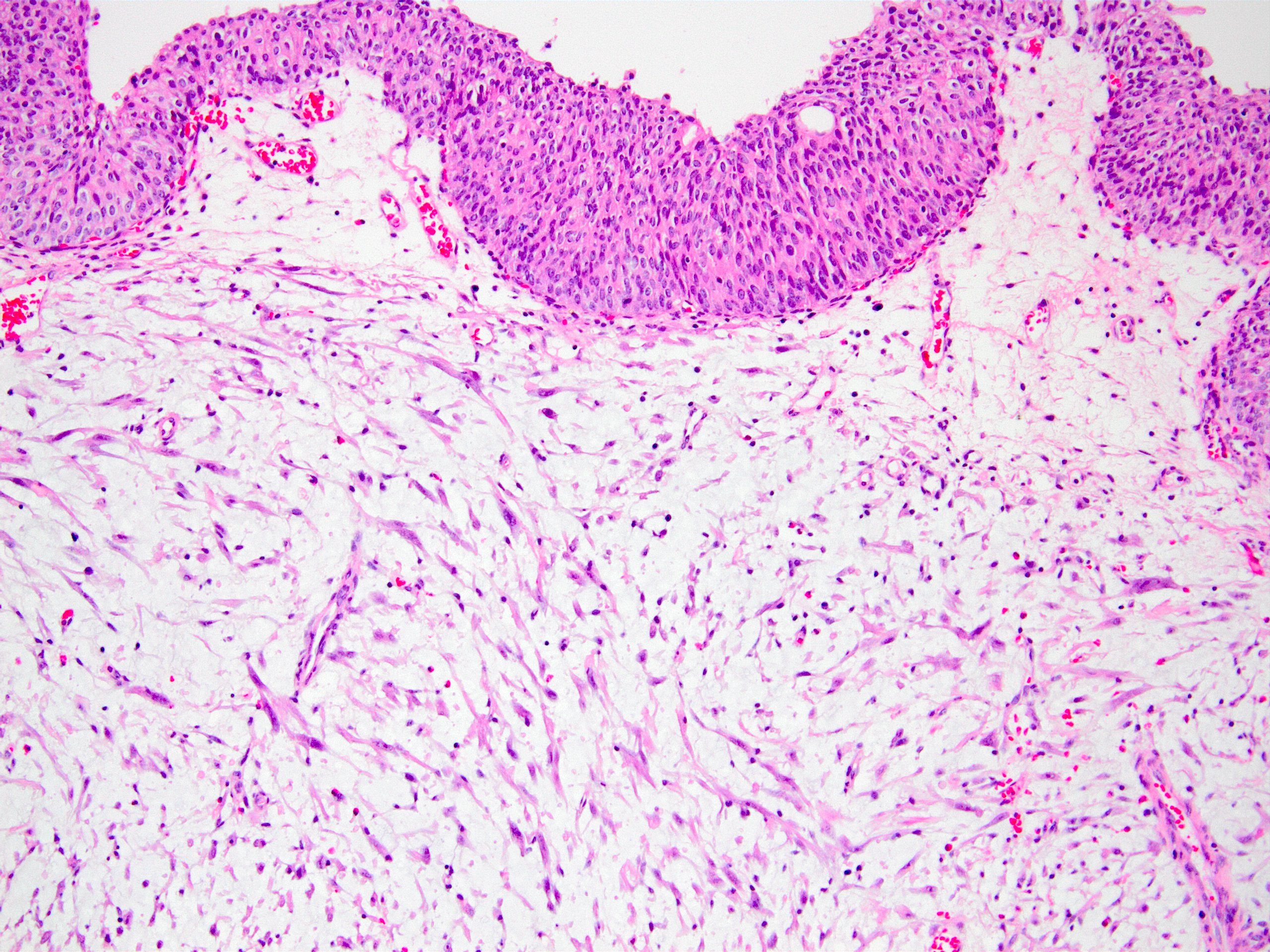
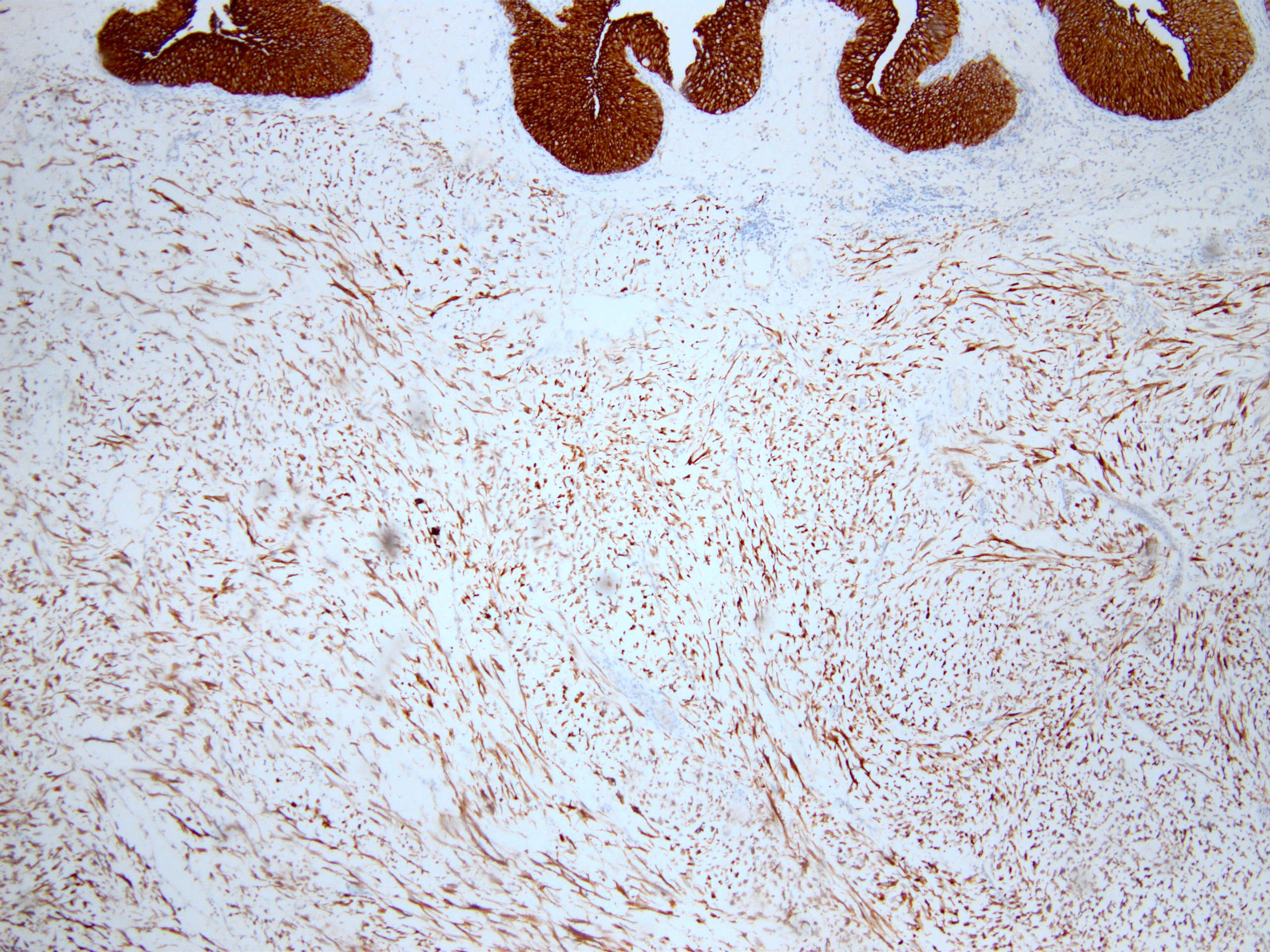
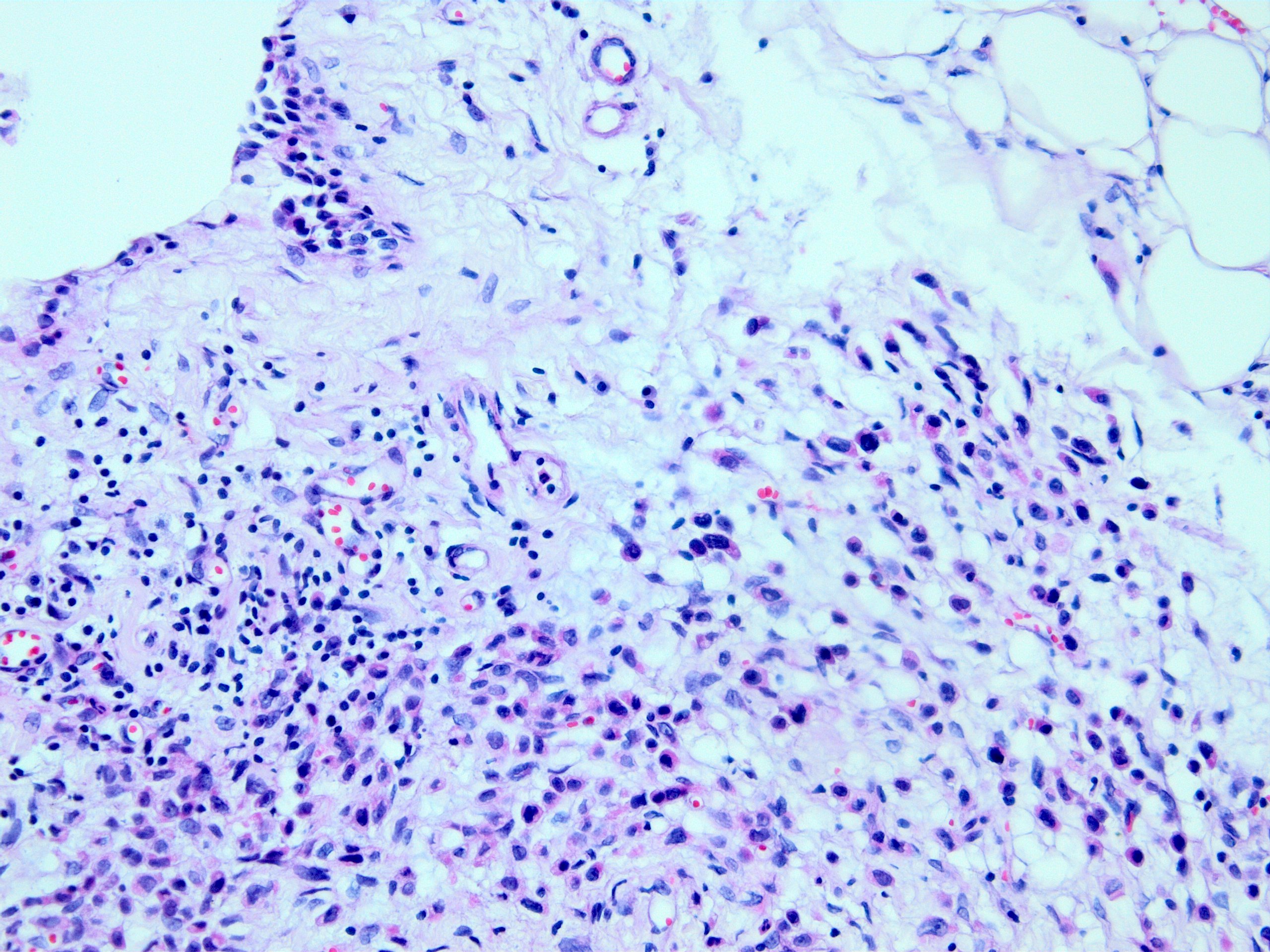
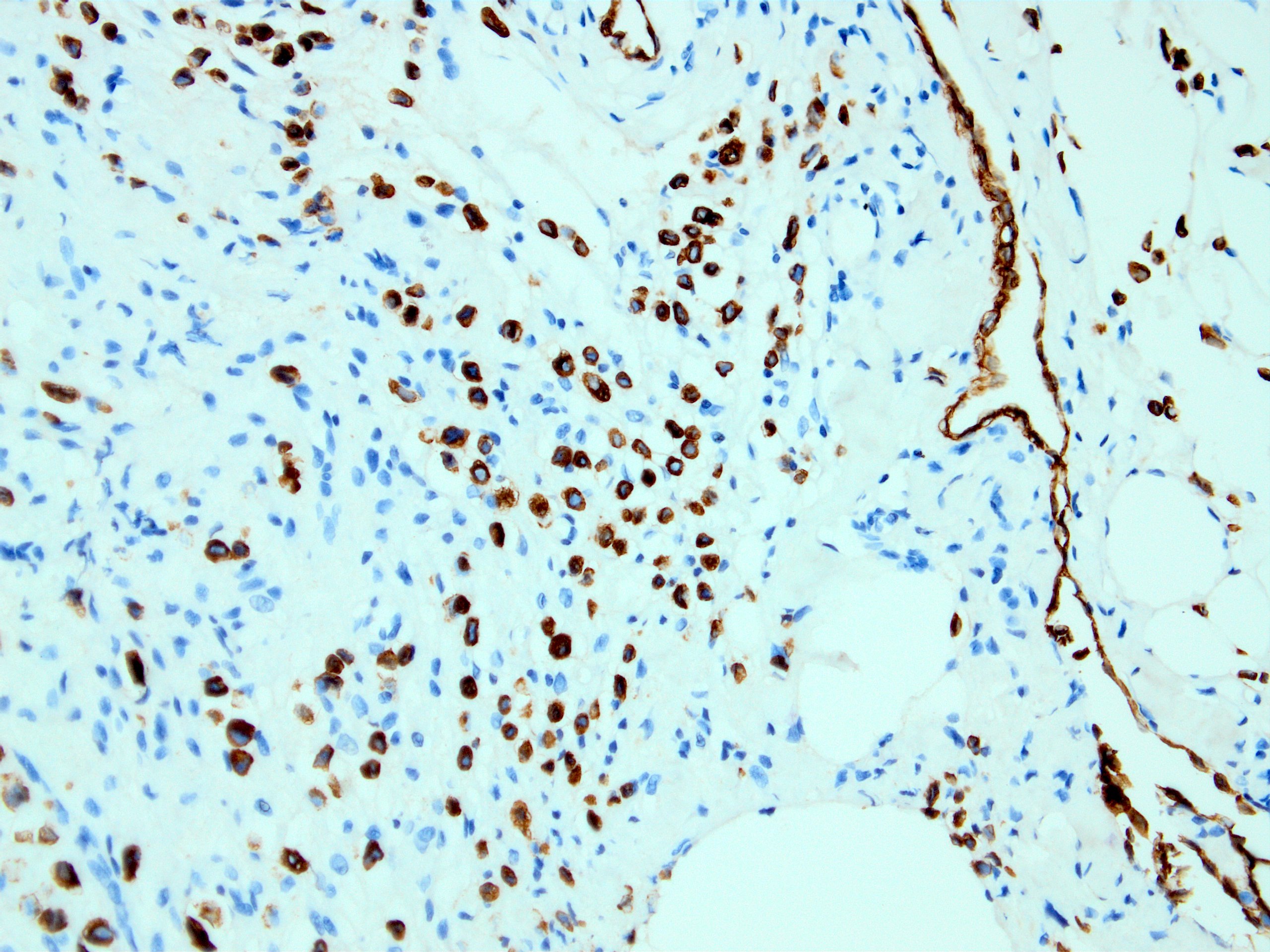
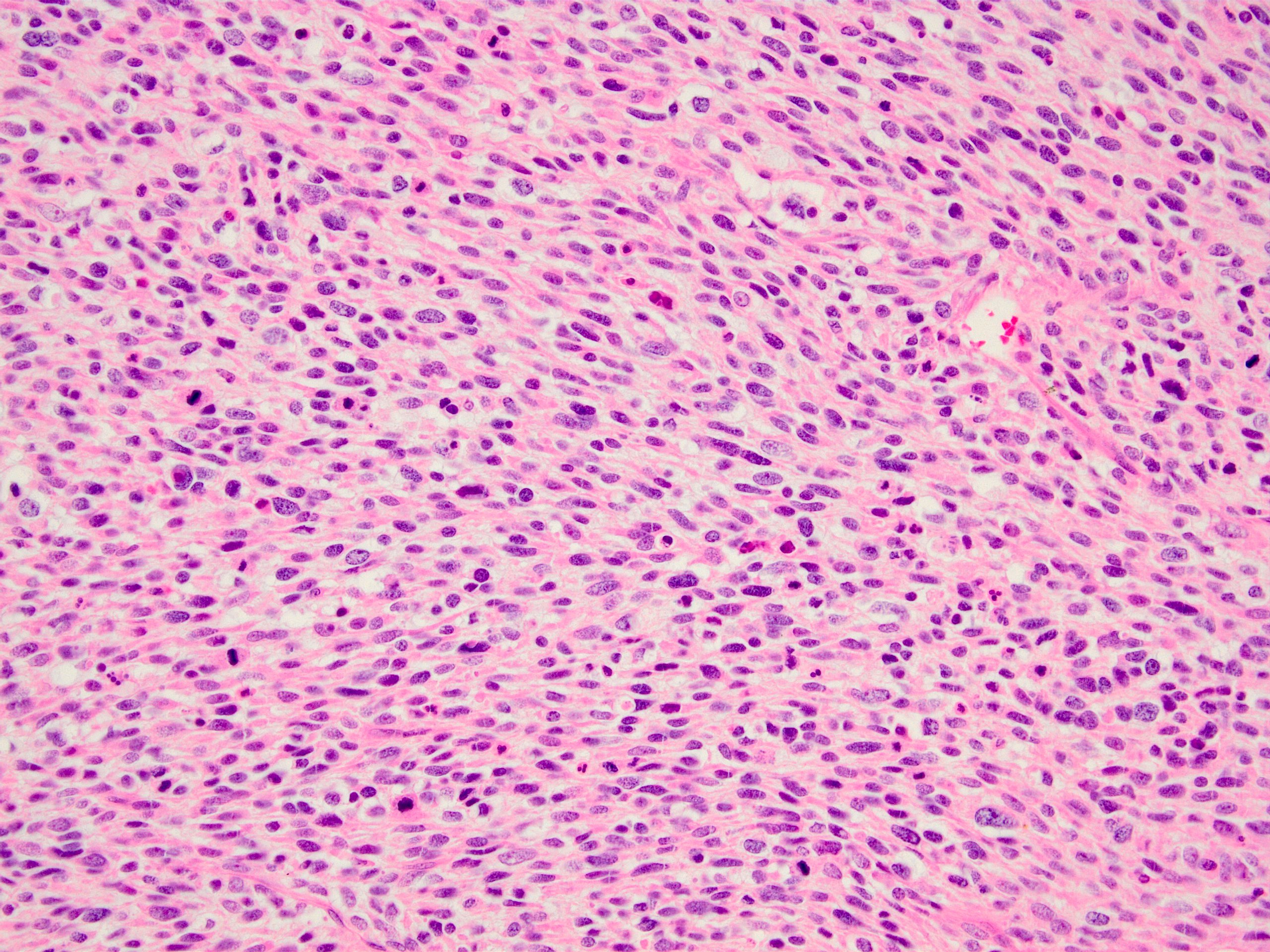
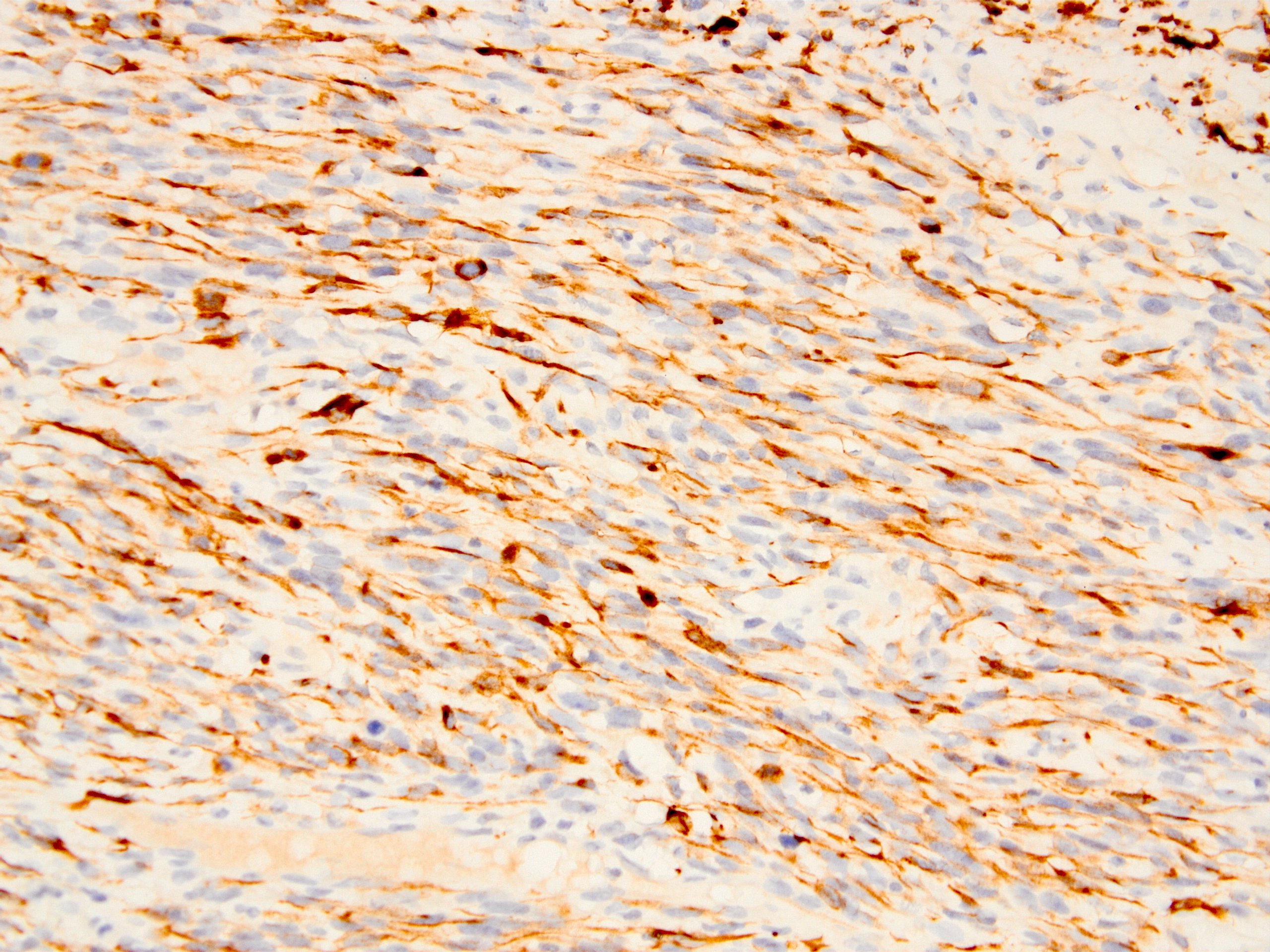
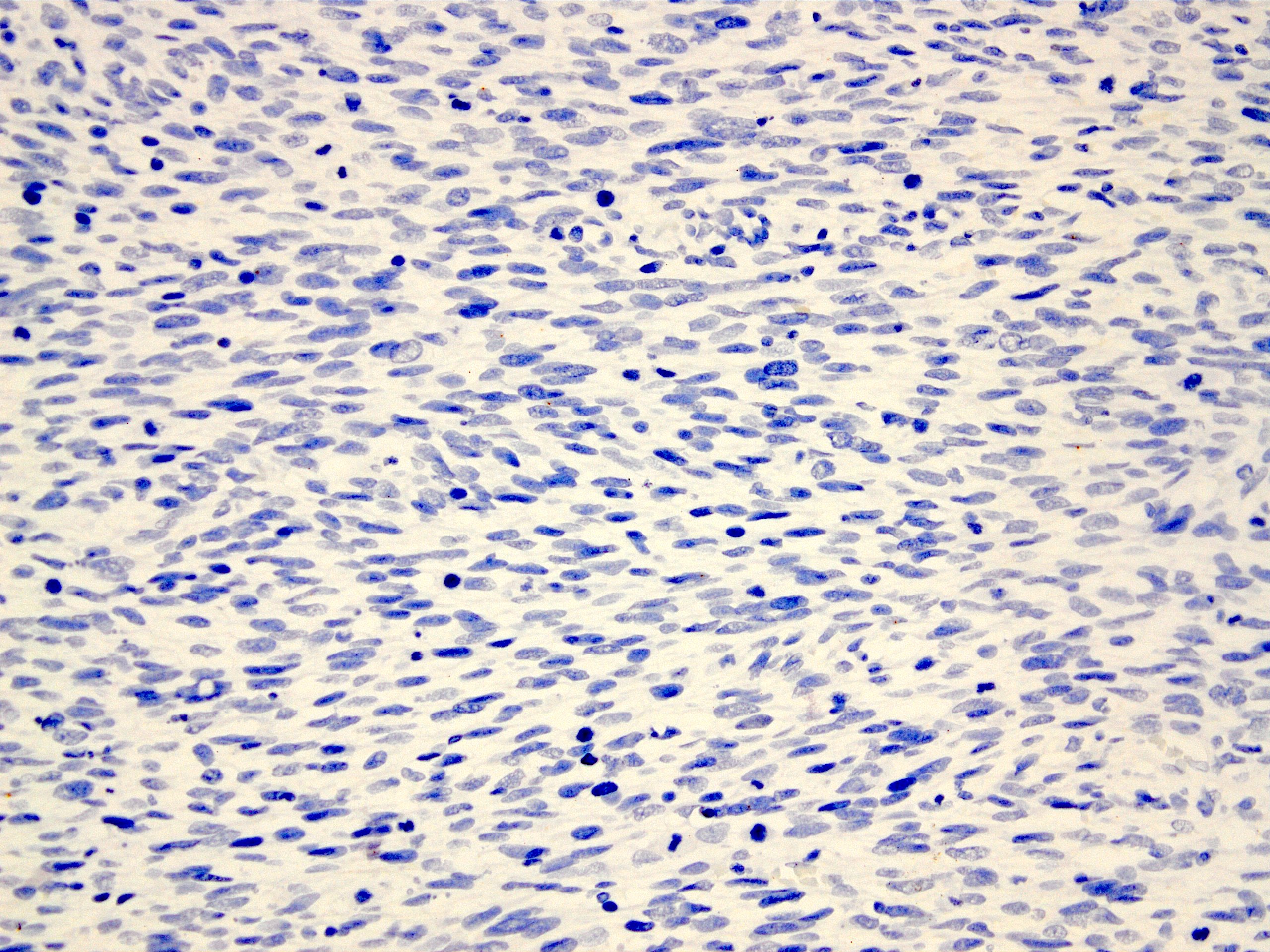
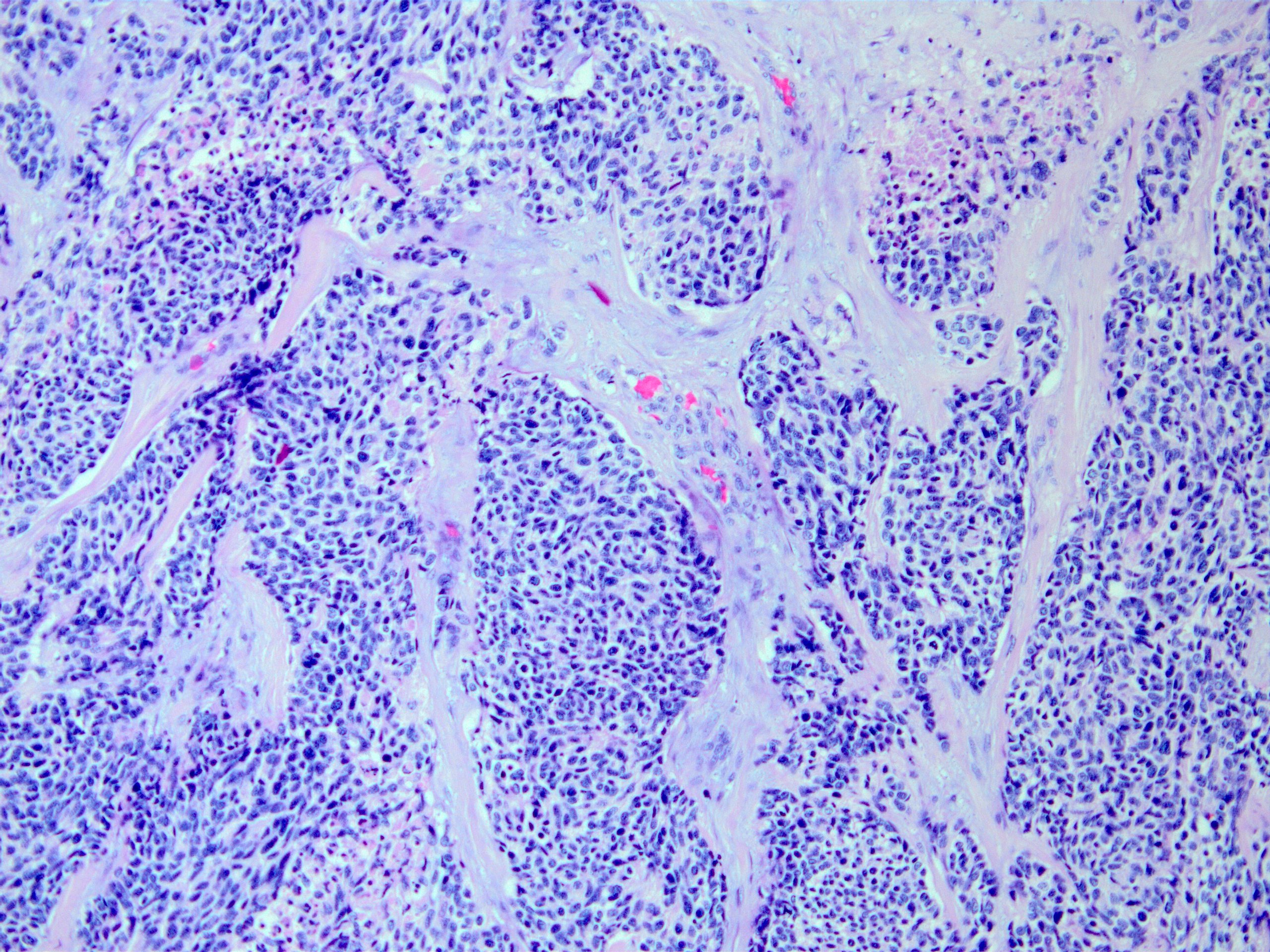
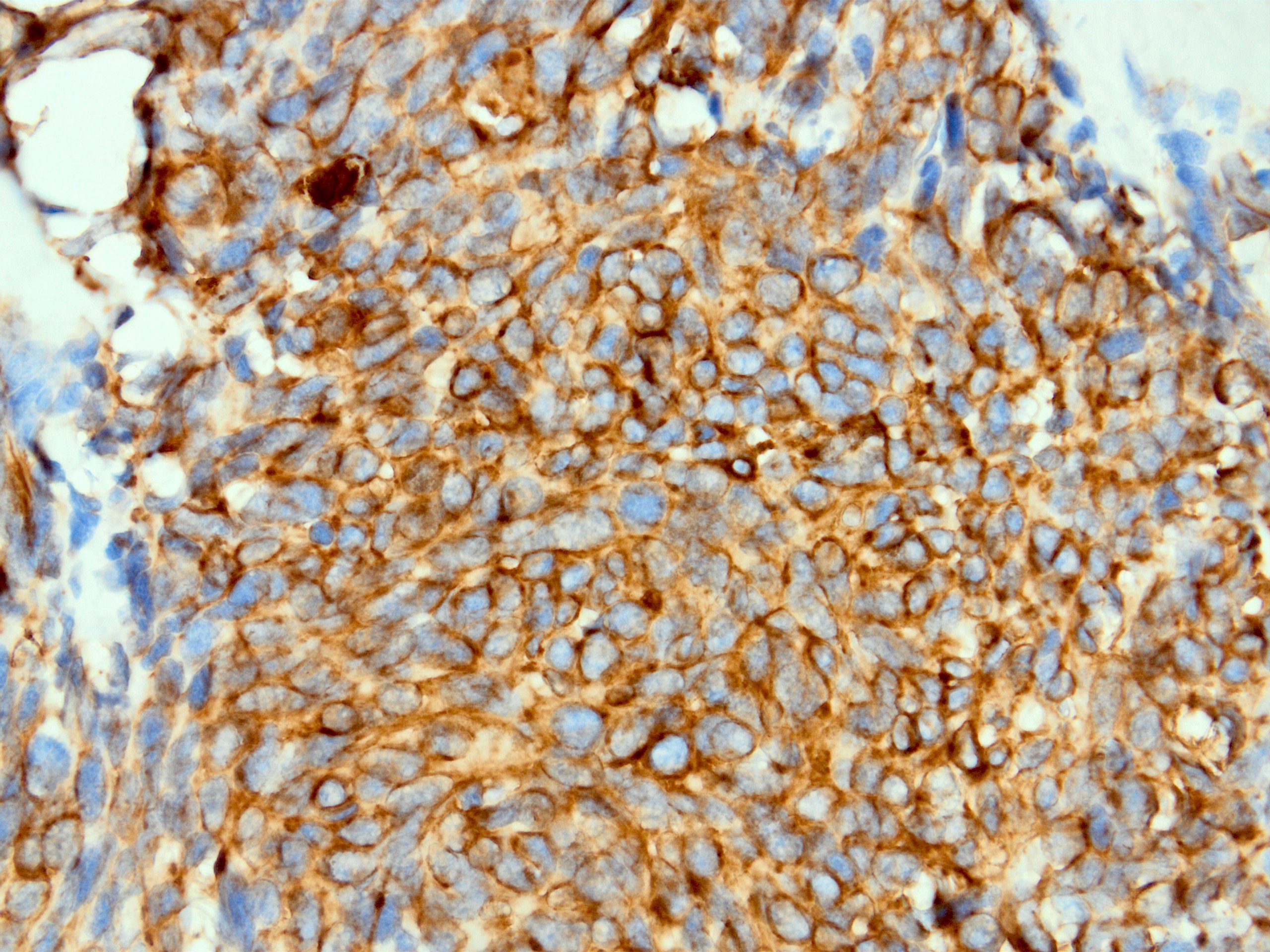
Inflammatory myofibroblastic tumor of the bladder

CAM 5.2 in epithelioid sarcoma (proximal variant)
CAM 5.2 in desmoplastic small round cell tumor
Positive staining - normal
- Secretory coils of eccrine sweat glands and apocrine glands (Dermatopathology (Basel) 2015;2:15)
- Glandular type epithelial cells, including hepatocytes and renal epithelium (Am J Surg Pathol 1988;12:187)
- Dendritic cells (J Clin Pathol 1989;42:271)
- Toker cells (Virchows Arch 2002;441:117, Histol Histopathol 2009;24:367)
- Trophoblasts (Int J Gynecol Pathol 1986;5:345)
Positive staining - disease
- Most carcinomas, including adenocarcinomas, sarcomatoid carcinoma, neuroendocrine tumors (dot-like perinuclear pattern for neuroendocine carcinomas including small cell carcinoma)
- Adrenal tumors: oncocytic adrenocortical neoplasm and pheochromocytoma (Am J Surg Pathol 1998;22:603, Am J Surg Pathol 2000;24:1552)
- Breast: benign proliferative nipple duct lesions, most breast carcinomas (CAM 5.2 is one of the least positive keratins in metaplastic carcinomas) (Am J Surg Pathol 1999;23:1349, Appl Immunohistochem Mol Morphol 2016;24:622)
- CNS: choroid plexus papilloma, malignant meningioma (75%), secretory meningioma (Histopathology 1989;15:61, Mod Pathol 2004;17:1129)
- Eye: melanoma of uvea (focal in ~66% of cases) (Am J Pathol 1992;141:169)
- Genitourinary: urothelial carcinoma, inflammatory myofibroblastic tumor of bladder (67%), negative in other inflammatory myofibroblastic tumors (J Clin Pathol 1988;41:1288, Am J Surg Pathol 2006;30:1502, Am J Surg Pathol 2011;35:135)
- Heart: cardiac myxoma with glandular elements (Ir J Med Sci 1993;162:95, Arch Pathol Lab Med 1989;113:735)
- Hypophysis: intensely positive in the densely granulated somatotroph, mammosomatotroph and plurihormonal PIT1 lineage tumors, with a predominant cytoplasmic perinuclear pattern highlighting prominent fibrous bodies in the sparsely granulated somatotroph tumors (Hum Pathol 2021;107:87)
- Liver: cholangiocellular carcinoma and hepatocellular carcinoma, Mallory bodies (Am J Surg Pathol 1988;12:187, Histopathology 1988;13:605)
- Mesothelial neoplasms: adenomatoid tumor, malignant mesothelioma, benign cystic mesothelioma (Am J Surg Pathol 2003;27:969, Semin Diagn Pathol 2006;23:15)
- Myofibroblasts in appendicitis and gastric ulcer (Med Mol Morphol 2006;39:209, Histol Histopathol 2006;21:697)
- Olfactory neuroblastoma (40%) (Brain Tumor Pathol 2012;29:207)
- Ovary: adenocarcinomas, dysgerminoma (19%), ependymoma (60%), female adnexal tumors of probable Wolffian origin, granulosa cell tumor adult type (33 - 50%), Sertoli cell tumor (Hum Pathol 2006;37:1015, Histopathology 2001;38:237, Am J Surg Pathol 1992;16:962)
- Prostate: adenocarcinoma neuroendocrine cells (Prostate 2006;66:1399)
- Renal cell carcinoma (Hum Pathol 1988;19:980)
- Skin: Paget disease (mammary and extramammary), Merkel cell carcinoma (J Cutan Pathol 2003;30:449, Am J Surg Pathol 1992;16:58, APMIS 1990;98:741)
- Soft tissue: alveolar rhabdomyosarcoma (52%), angiosarcoma (variable), desmoplastic round cell tumor, epithelioid sarcoma, Ewing sarcoma (20%), dot-like or membranous, pseudomyogenic hemangioendothelioma, schwannoma glandular, smooth muscle tumors (myxoid - 25%), synovial sarcoma (71%) (Mod Pathol 2008;21:795, Am J Surg Pathol 2004;28:298, Mod Pathol 2003;16:229, J Cutan Pathol 2003;30:242, Am J Surg Pathol 2000;24:410, Ann Diagn Pathol 2019;41:116, Hum Pathol 2018;71:126, Br J Dermatol 2001;145:834, Dermatopathology (Basel) 2019;6:206, Histopathology 1987;11:477, Histopathology 1987;11:487, Am J Surg Pathol 2000;24:927, Histopathology 1986;10:1315)
- Squamous cell carcinoma (SCC): variable, negative in vulvar squamous cell carcinoma, 17% in cutaneous squamous cell carcinoma, mainly pagetoid pattern; however, frequently positive in effusion cytology (Int J Gynecol Pathol 1991;10:341, J Cutan Pathol 2013;40:646, Semin Diagn Pathol 2006;23:15)
- Testis: all germ cell tumors with lesser extent in seminomas, more frequent in mediastinal seminomas than testicular seminomas, seminoma with atypia (Am J Clin Pathol 2000;113:583, Hum Pathol 1998;29:737, Am J Surg Pathol 2008;32:146, Int J Surg Pathol 2002;10:23)
- Thymoma, epithelial component (J Clin Pathol 1988;41:1297)
- Trophoblastic tumors (Int J Gynecol Pathol 1986;5:345)
- Uterus: endometrial stromal sarcoma (variable staining in most cases) (Hum Pathol 2008;39:1459, Appl Immunohistochem Mol Morphol 2019;27:466)
Negative staining
- CNS: glioblastoma, most meningiomas, supratentorial primitive neuroectodermal tumor (Arch Pathol Lab Med 1999;123:917)
- Melanoma: usually; however, uveal tumors are CAM 5.2+ (Histopathology 1986;10:1315, Int J Dermatol 2003;42:123, Am J Surg Pathol 1997;21:1196)
- Most sarcomas: exceptions indicated above
- Squamous epithelium
Sample pathology report
- Omentum, biopsy:
- Adenocarcinoma, signet ring cell type (see comment)
- Comment: Histologic sections show a small number of signet ring-like discohesive and monotonous cells highlighted by CAM 5.2 and mucicarmine.
Board review style question #1
Which one of the following diagnoses is expected to show dot-like staining with CAM 5.2?
- Malignant mesothelioma
- Paget disease of nipple
- Sarcomatoid carcinoma
- Signet ring carcinoma
- Sparsely granulated hypophyseal adenoma
Board review style answer #1
E. Sparsely granulated hypophyseal adenoma. Sparsely granulated somatotroph tumors have distinct fibrous bodies that appear as pale spherical inclusions on H&E staining and stain strongly with CAM 5.2 and CK18 antibodies as well as AE1 / AE3. There is a growing evidence that sparsely granulated somatotroph adenomas are larger, more common in younger female patients and are more proliferative and infiltrative (Endotext: Pathology and Pathogenesis of Pituitary Adenomas and Other Sellar Lesions [Accessed 5 January 2023]).
Comment Here
Reference: Cytokeratin CAM 5.2
Comment Here
Reference: Cytokeratin CAM 5.2
Board review style question #2
A 30 year old male nonsmoker with hematuria has undergone transurethral resection. The bladder mass invades the muscularis propria (not shown); histological morphology and CAM 5.2 expression are shown above. Which antibody should be requested to reach the correct diagnosis of inflammatory myofibroblastic tumor?
- ALK
- Desmin
- DOG1
- GATA3
- Pankeratin
Board review style answer #2
A. ALK. Keratin expression is a common finding in inflammatory myofibroblastic tumor of bladder. In this morphological setting characterized by spindle cells with inflammatory background, ALK expression along with SMA in myofibroblastic staining pattern will lead to the correct diagnosis of inflammatory myofibroblastic tumor. Here, the diagnosis of sarcomatoid carcinoma is a major pitfall given the abundant keratin expression and infiltrative pattern (Am J Surg Pathol 2006;30:1502).
Comment Here
Reference: Cytokeratin CAM 5.2
Comment Here
Reference: Cytokeratin CAM 5.2
