Stains & CD markers
Cytokeratin AE1 / AE3

Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Cytokeratin AE1 / AE3
Cytokeratin AE1 / AE3
Editorial Board Members: Christian M. Schürch, M.D., Ph.D., Julie M. Jorns, M.D.
Last author update: 16 June 2022
Last staff update: 16 June 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Cytokeratin AE1 / AE3
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) images | Cytology images | Positive staining - normal | Positive staining - disease | Negative staining | Sample pathology report | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Van Bockstal MR. Cytokeratin AE1 / AE3. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsAE1AE3.html. Accessed April 3rd, 2025.
Definition / general
- Mixture of 2 different clones of anticytokeratin (CK) monoclonal antibodies (AE1 and AE3), which functions as a broad spectrum cytokeratin marker (Ann Surg Oncol 2011;18:S261)
- AE1 detects the high molecular weight cytokeratins 10, 14, 15 and 16 and the low molecular weight cytokeratin 19
- AE3 detects the high molecular weight cytokeratins 1, 2, 3, 4, 5 and 6 and the low molecular weight cytokeratins 7 and 8
- Not reactive to cytokeratins 17 and 18
Essential features
- Mixture of 2 different clones of anticytokeratin monoclonal antibodies (AE1 and AE3), which functions as a broad spectrum cytokeratin marker for cytokeratins 1 - 8, 10, 14 - 16 and 19
- Immunoreactivity is observed in epithelia and most carcinomas (i.e., tumors of epithelial origin), with cytoplasmic and membranous positivity
- Normal liver is recommended as an on slide positive external control
- CK AE1 / AE3 immunohistochemistry is used for assessment of occult lymph node metastases, residual disease after neoadjuvant therapy, invasion depth and tumor budding in multiple carcinomas
- CK AE1 / AE3 is rarely used as a standalone immunohistochemical analysis but rather as part of a panel when used to confirm or rule out epithelial nature of tumors
Terminology
- Pankeratin, broad spectrum keratin or keratin: not preferred as this can also refer to cytokeratin MNF116 and (to a lesser extent) CAM5.2
Pathophysiology
- Cytokeratins are proteins of the cytoskeletal intermediate filaments, which allow cells to cope with mechanical stress
- Type I cytokeratins are acidic and type II cytokeratins are basic, either with high or low molecular weight; acidic and basic cytokeratins often form heterodimeric pairs (Ann N Y Acad Sci 1985;455:282)
- Their expression varies throughout the tissue type and is mainly organ specific, which allows their use to identify the primary origin of a metastatic tumor (Ann N Y Acad Sci 1985;455:282, Arch Pathol Lab Med 2017;141:1014)
Interpretation
- Normal pattern in epithelium: cytoplasmic staining reaction with accentuation of the cellular membrane
- Dot-like pattern in certain tumors, such as neuroendocrine neoplasms
Uses by pathologists
- Confirm or rule out epithelial nature of tissue, tumors or components of tumors (Arch Pathol Lab Med 2017;141:1014)
- As such, usually not performed as a standalone immunohistochemical analysis but rather used as part of a panel of immunohistochemical stains to avoid misinterpretation (Arch Pathol Lab Med 2014;138:1583)
- Identification of occult tumor cells of carcinomas (either isolated tumor cells or micrometastases) in lymph nodes or bone marrow or (less common) at frozen section (Ann Surg Oncol 2020;27:4204, Am J Surg Pathol 2017;41:1212, J Clin Oncol 2003;21:3469, BMC Cancer 2012;12:403, Acta Histochem Cytochem 2011;44:133)
- Note: per current invasive breast cancer NCCN guidelines, routine cytokeratin IHC to define node involvement is not recommended in clinical decision making (NCCN: Breast Guidelines [Accessed 9 June 2022])
- Epithelial cells in lymph nodes may represent an artefact (displaced epithelium by recent biopsy) instead of true metastasis (Histopathology 2015;66:283, J Clin Oncol 2006;24:2013)
- Hyalinized cytokeratin particles without tumor cell nuclei may mimic isolated tumor cells and may cause misinterpretation (J Surg Res 2002;107:75, Hepatogastroenterology 2014;61:1235)
- Dispersed interstitial reticulum cells with dendritic / reticular pattern show weak to moderate cytoplasmic immunoreactivity (J Cutan Pathol 2016;43:1231, NordiQC: Pan Cytokeratin (CK-PAN) [Accessed 5 May 2022])
- Identification of tumor cells of epithelial origin in difficult cases in which there are few cells, there are significant cautery artifacts or there is a dense inflammatory infiltrate obscuring infiltrating cancer cells (Am J Surg Pathol 2014;38:e20)
- Identification of residual tumor cells of epithelial origin in fibrous scars or cauterized tissue of patients with prior surgical resections or after neoadjuvant chemotherapy (Urology 1997;49:721, Int J Colorectal Dis 2010;25:805)
- Keratin positive tumor cells should be distinguished from keratin positive myofibroblasts; simultaneous staining for actin may be useful (Am J Surg Pathol 2014;38:e20)
- Identification of areas of interest (hotspots) for the assessment of tumor budding on hematoxylin / eosin stained slides in colorectal cancer (Am J Clin Pathol 1991;95:137, Ann Surg 2022;275:e549, Virchows Arch 2021;479:459, Mod Pathol 2017;30:1299)
- Visualization of Mallory bodies in a variety of liver diseases, although CK8/18 might be more effective (Med Electron Microsc 2004;37:114)
- Assessment of the depth of tumor invasion (Diagn Pathol 2015;10:200, PLoS One 2020;15:e0225958)
- Establish the presence of noninvasive epithelial downgrowth after penetrating keratoplasty (Cornea 2006;25:727)
- Part of flow cytometry strategy to enrich epithelial cells in sputum (Cytometry A 2004;60:1)
- Identification of lymphoepithelial lesions in MALT lymphomas of the stomach and other sites (Respir Med Case Rep 2019;27:100826)
- Identification of trophoblastic tissue (i.e., cytotrophoblast, syncytiotrophoblast and intermediate trophoblast) in curettages of missed and habitual abortions (Am J Clin Pathol 1991;95:137)
Prognostic factors
- Micrometastases and isolated tumor cells are generally associated with poorer prognosis in many cancer types:
- Occult tumor cells are associated with poor recurrence free survival and increased risk of cancer related death in gastric cancer patients staged as pN0 (Ann Surg Oncol 2020;27:4204)
- Micrometastasis is associated with worse recurrence free survival and overall survival in stage I lung adenocarcinoma (Am J Surg Pathol 2017;41:1212)
- Lymph node micrometastasis is more frequently observed in stage I lung adenocarcinoma with a micropapillary component (Am J Surg Pathol 2017;41:1212)
- Presence of micrometastases and isolated tumor cells in (early stage) breast cancer is associated with poorer disease free and overall survival; however, NSABP-32 findings support that local radiation and systemic therapy, particularly endocrine therapy, may attenuate the unfavorable effect (J Natl Cancer Inst 2010;102:410, Br J Cancer 2018;118:1529, N Engl J Med 2011;364:412)
- CK AE1 / AE3 immunohistochemistry is not recommended for routine evaluation of pelvic lymph nodes in prostate cancer patients as it does not reveal additional information to a standard hematoxylin and eosin section (Virchows Arch 2014;464:45)
- Although tumor budding is assessed in one hotspot at the invasive front (in a field measuring 0.785 mm2) of a single hematoxylin / eosin stained slide, CK AE1 / AE3 immunohistochemistry may help to identify hotspots (Virchows Arch 2021;479:459, Mod Pathol 2017;30:1299)
- Tumor budding is associated with poor prognosis in several cancer types:
- High budding in colorectal carcinoma is associated with higher tumor grade, higher TNM stage, vascular invasion and reduced survival (Mod Pathol 2013;26:295)
- Tumor budding in colorectal carcinoma is classified as follows (Mod Pathol 2017;30:1299):
- Bd1 (low budding) : 0 - 4 buds per 0.785 mm2
- Bd2 (intermediate budding) : 5 - 9 buds per 0.785 mm2
- Bd3 (high) : ≥ 10 buds per 0.785 mm2
- Tumor budding in tongue squamous cell carcinoma and colorectal carcinoma is defined as a single cancer cell or small cluster of < 5 cancer cells at the tumor's invasive front (Hum Pathol 2018;76:1, Mod Pathol 2017;30:1299)
- Tumor budding score ≥ 4 is a significant predictor of occult metastasis in cT2N0 tongue squamous cell carcinoma (Hum Pathol 2018;76:1)
- High tumor budding is associated with worse overall survival in resected esophageal adenocarcinoma (Virchows Arch 2021;478:393)
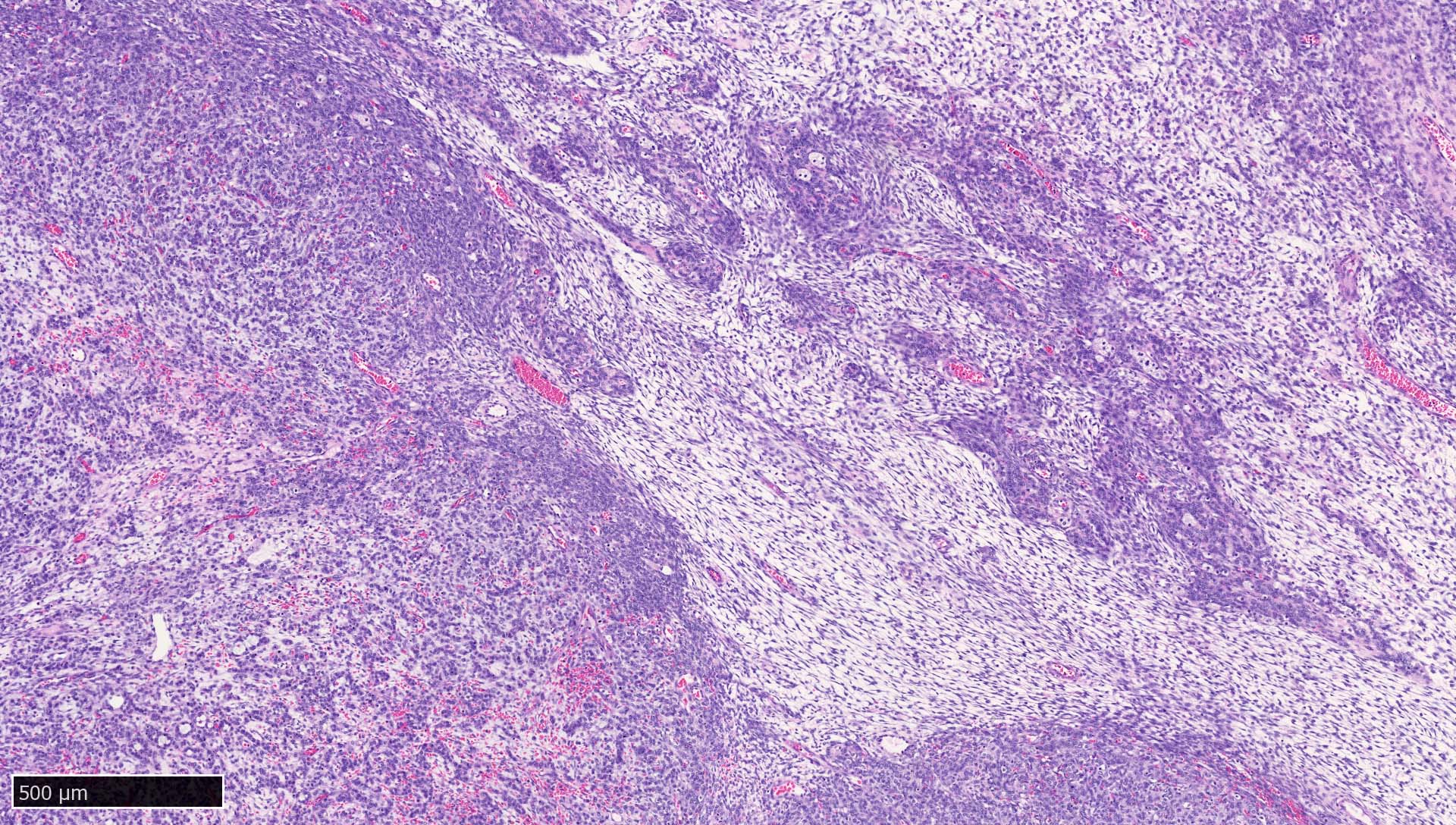
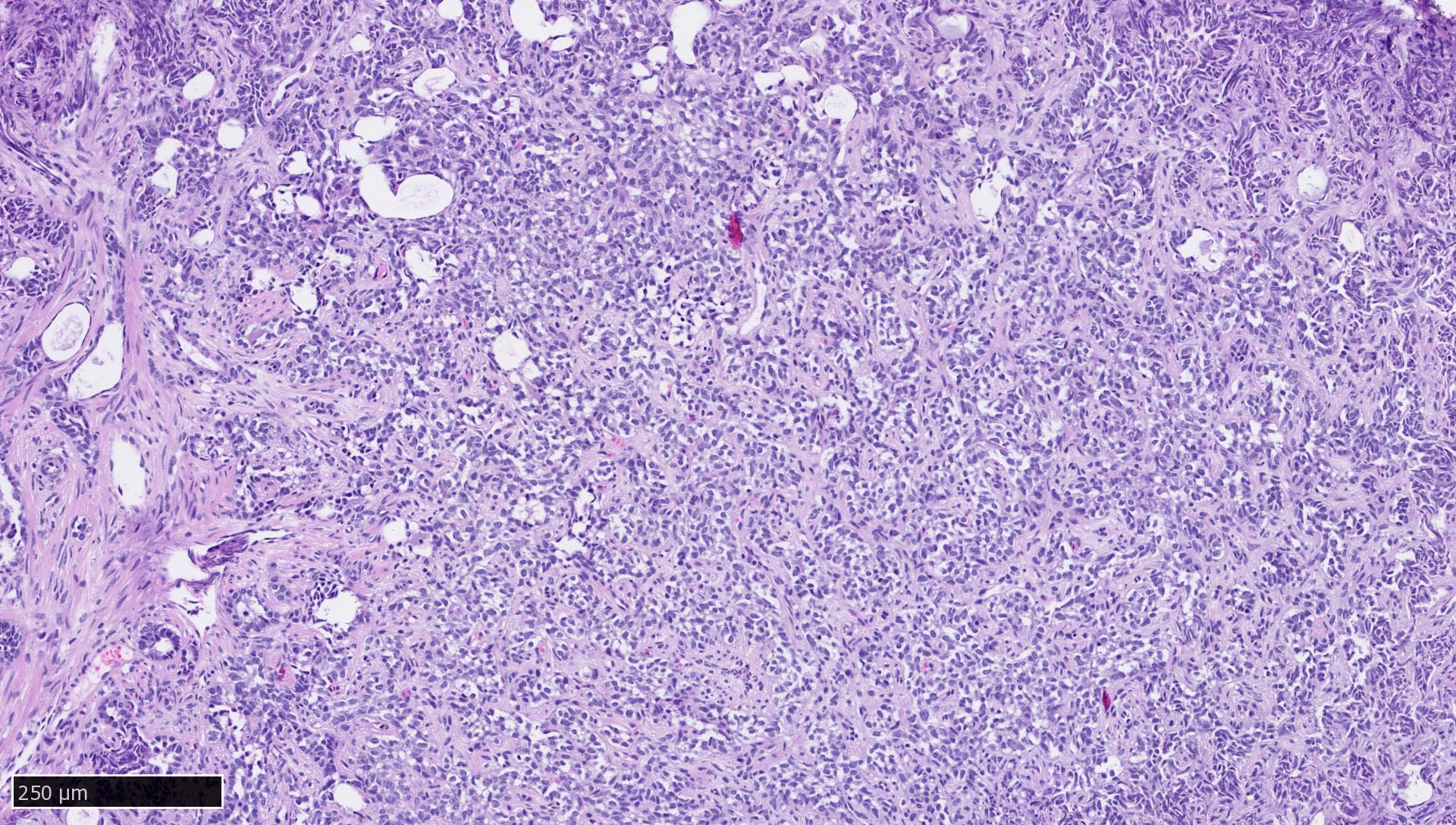
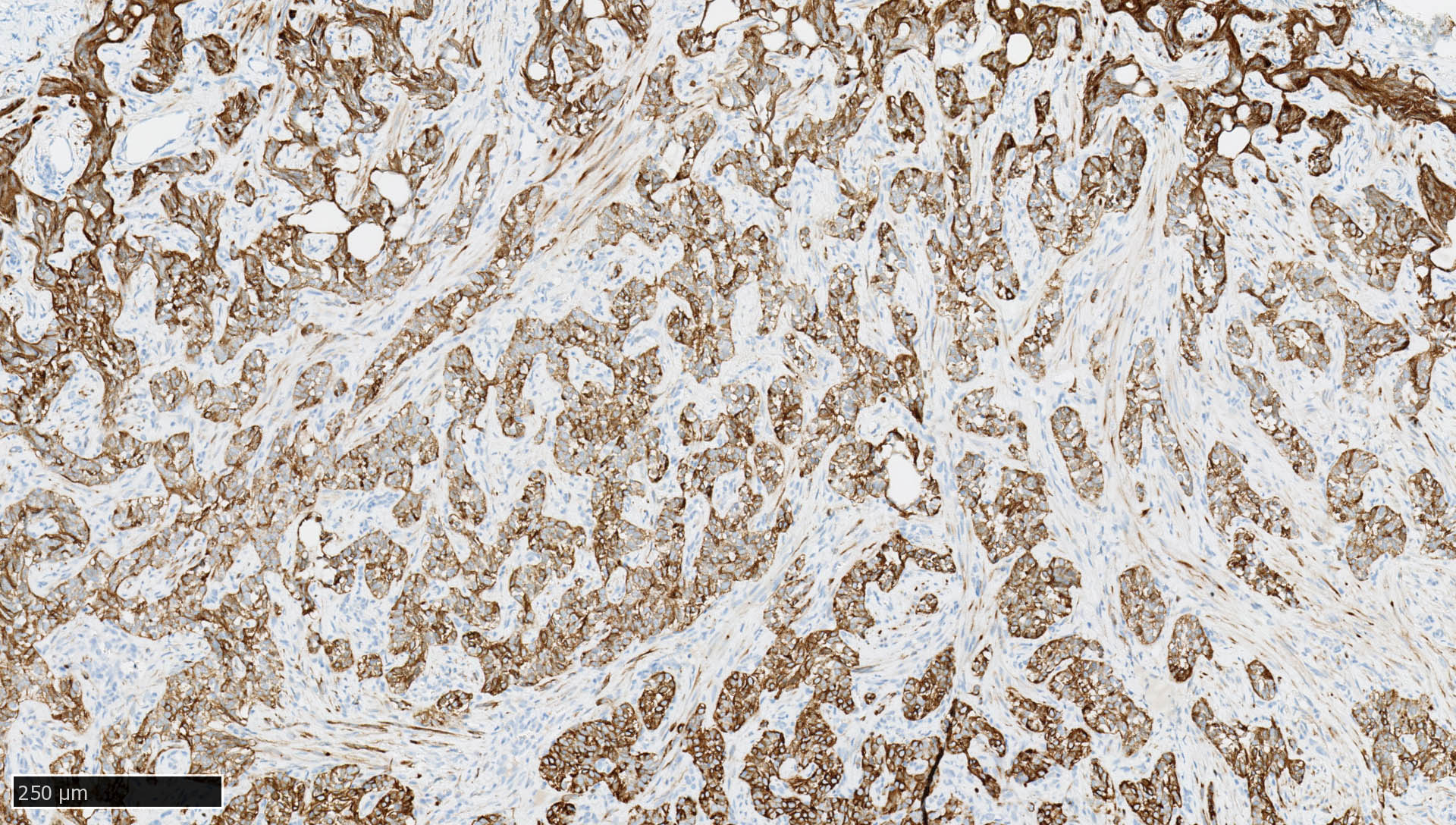
Microscopic (histologic) images
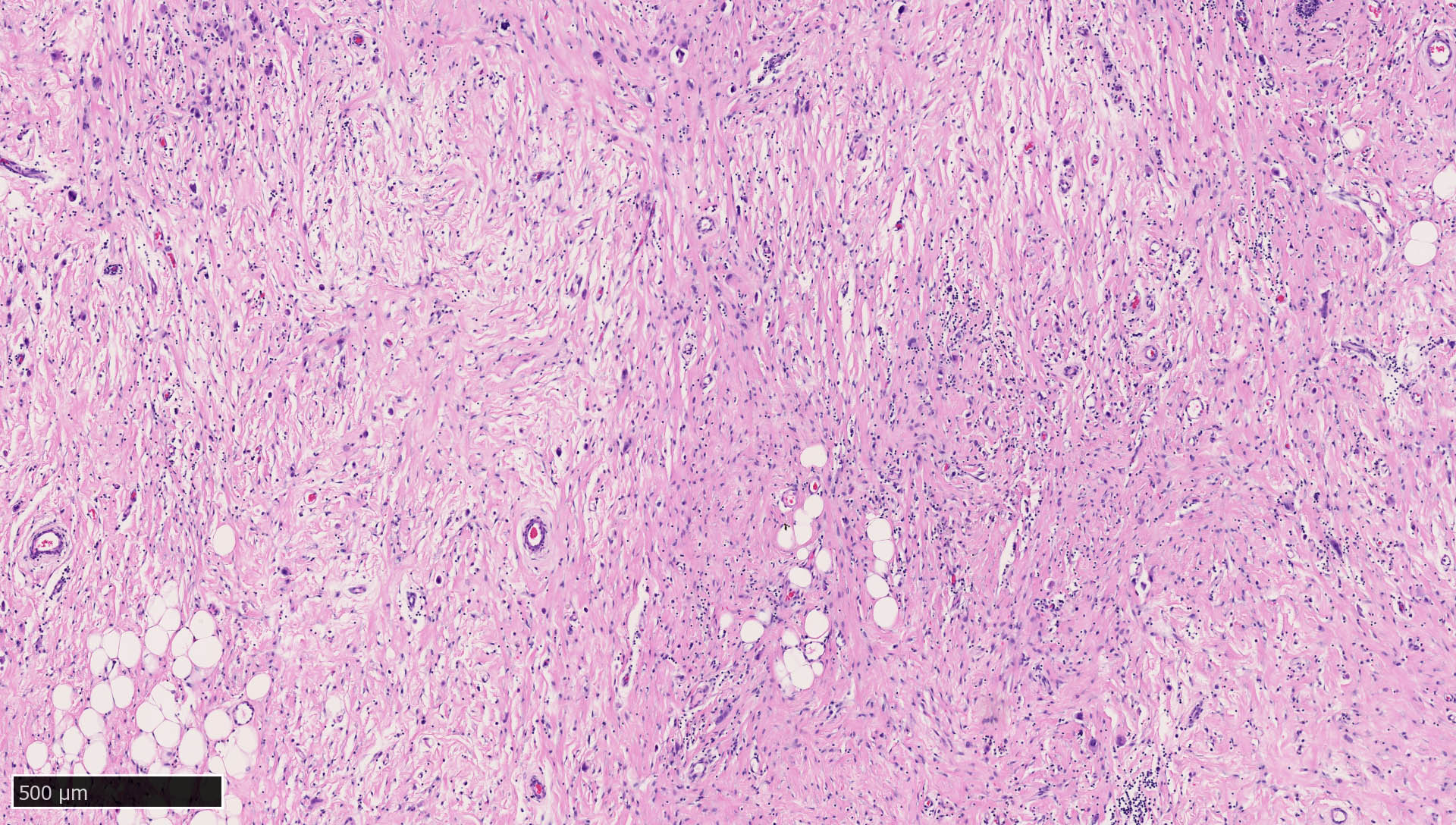
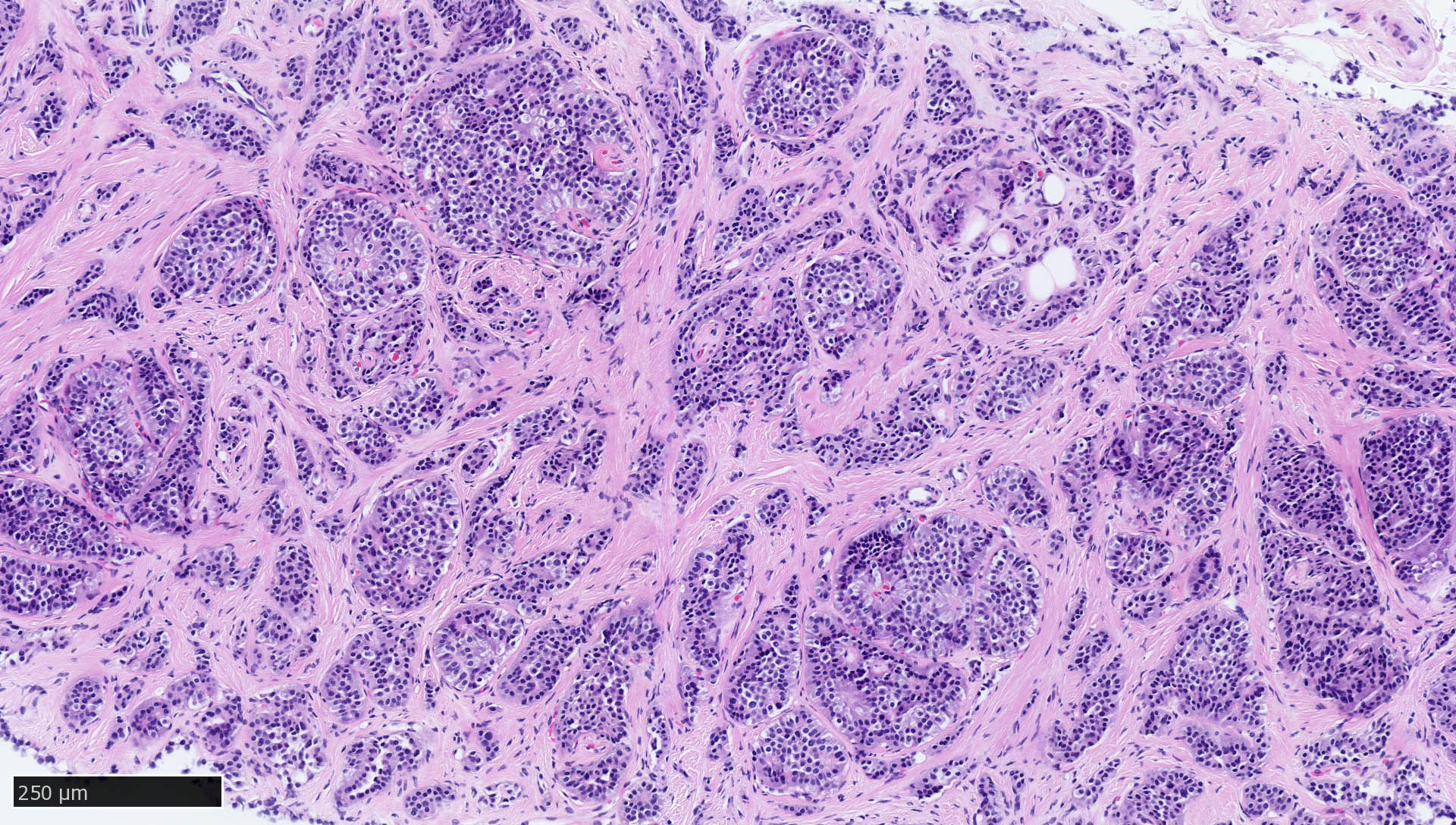
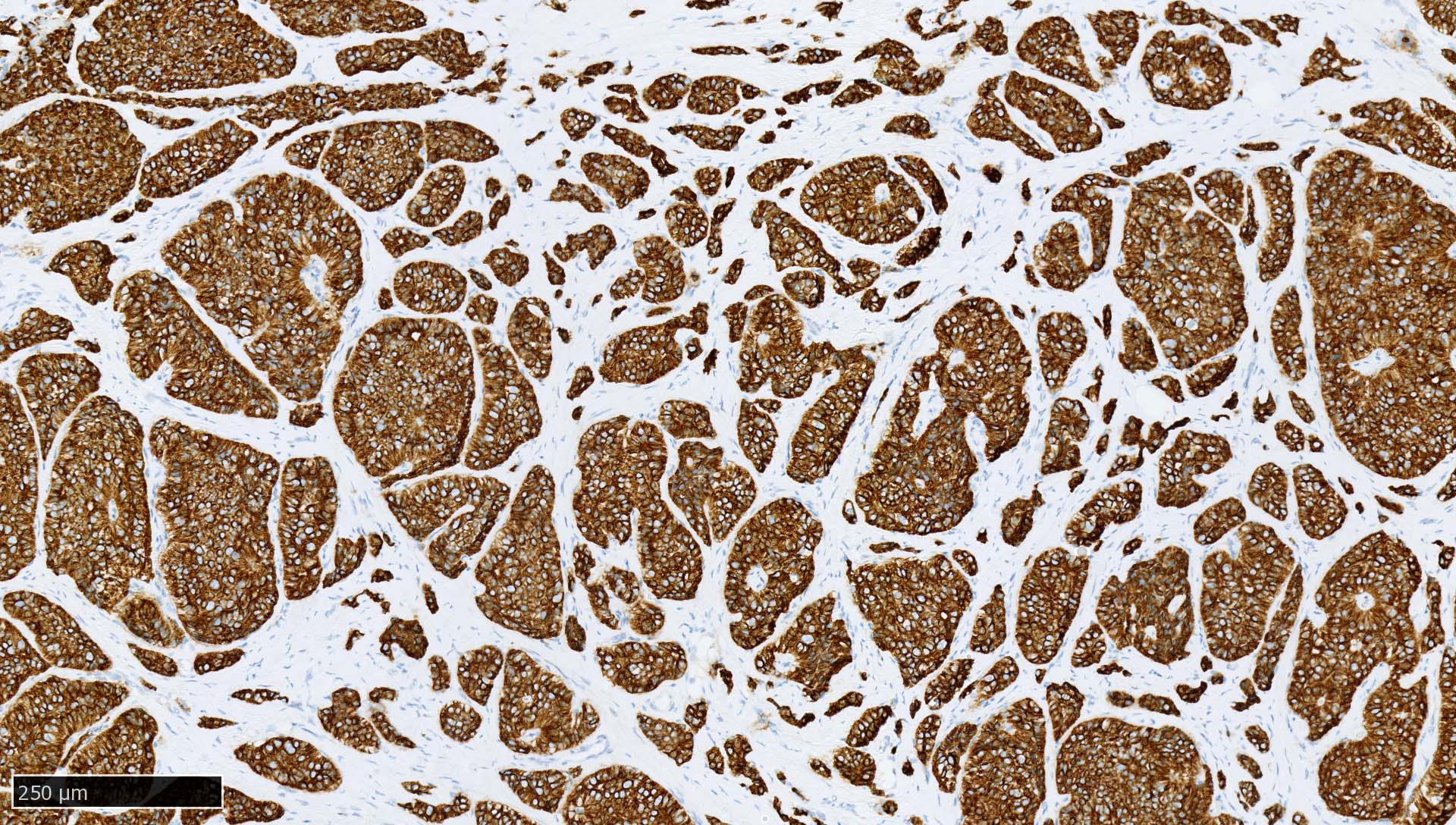
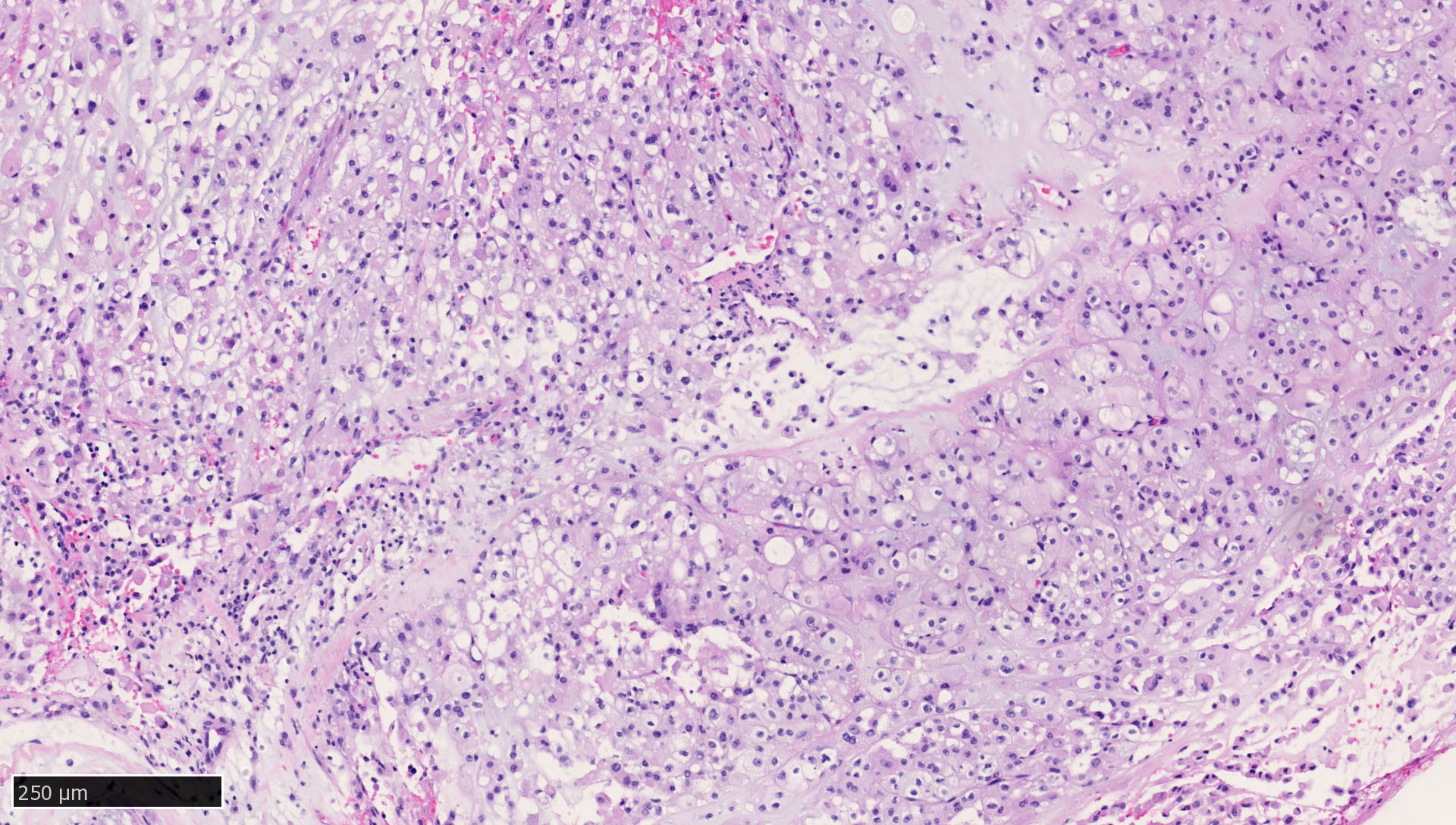
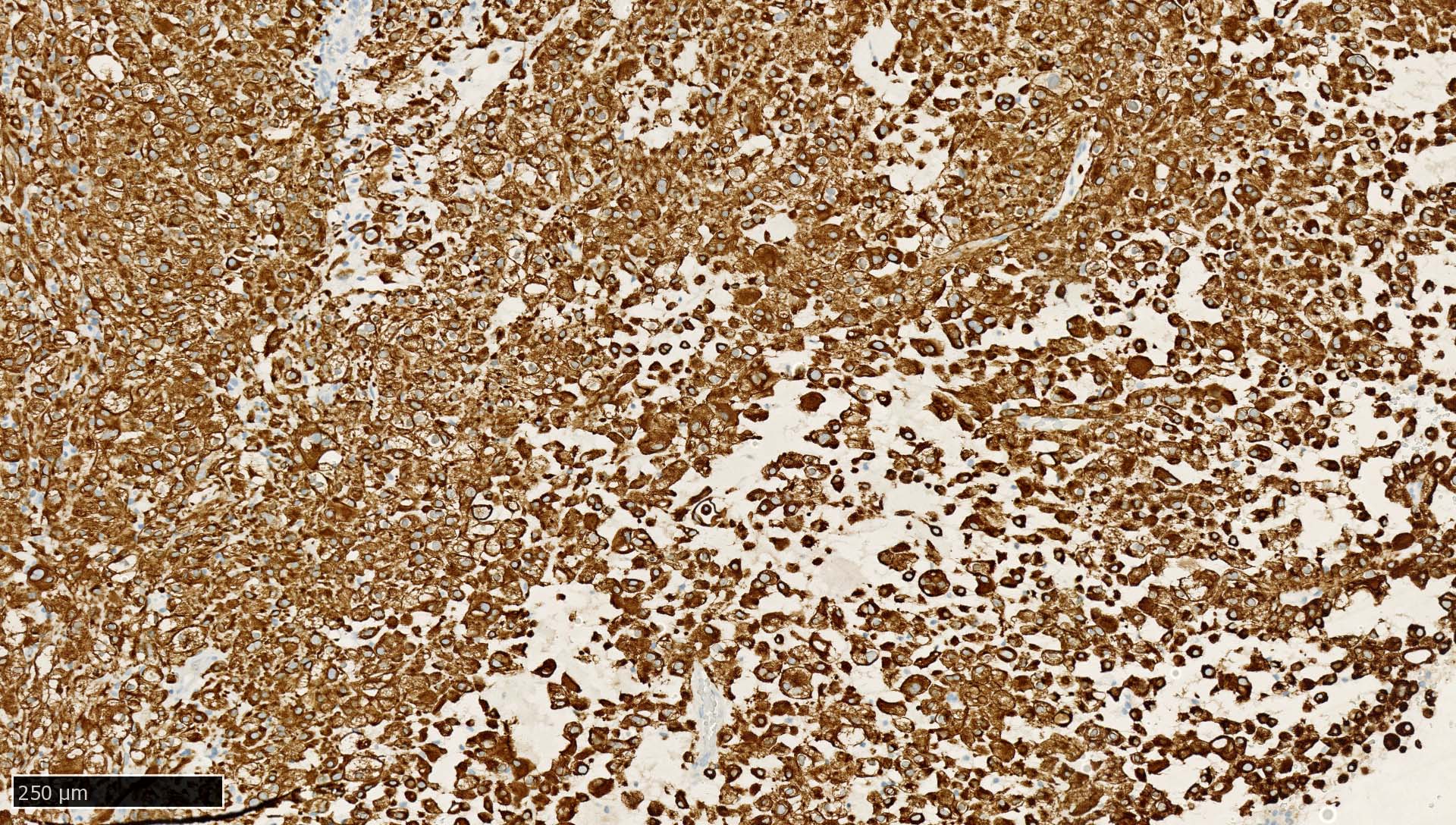
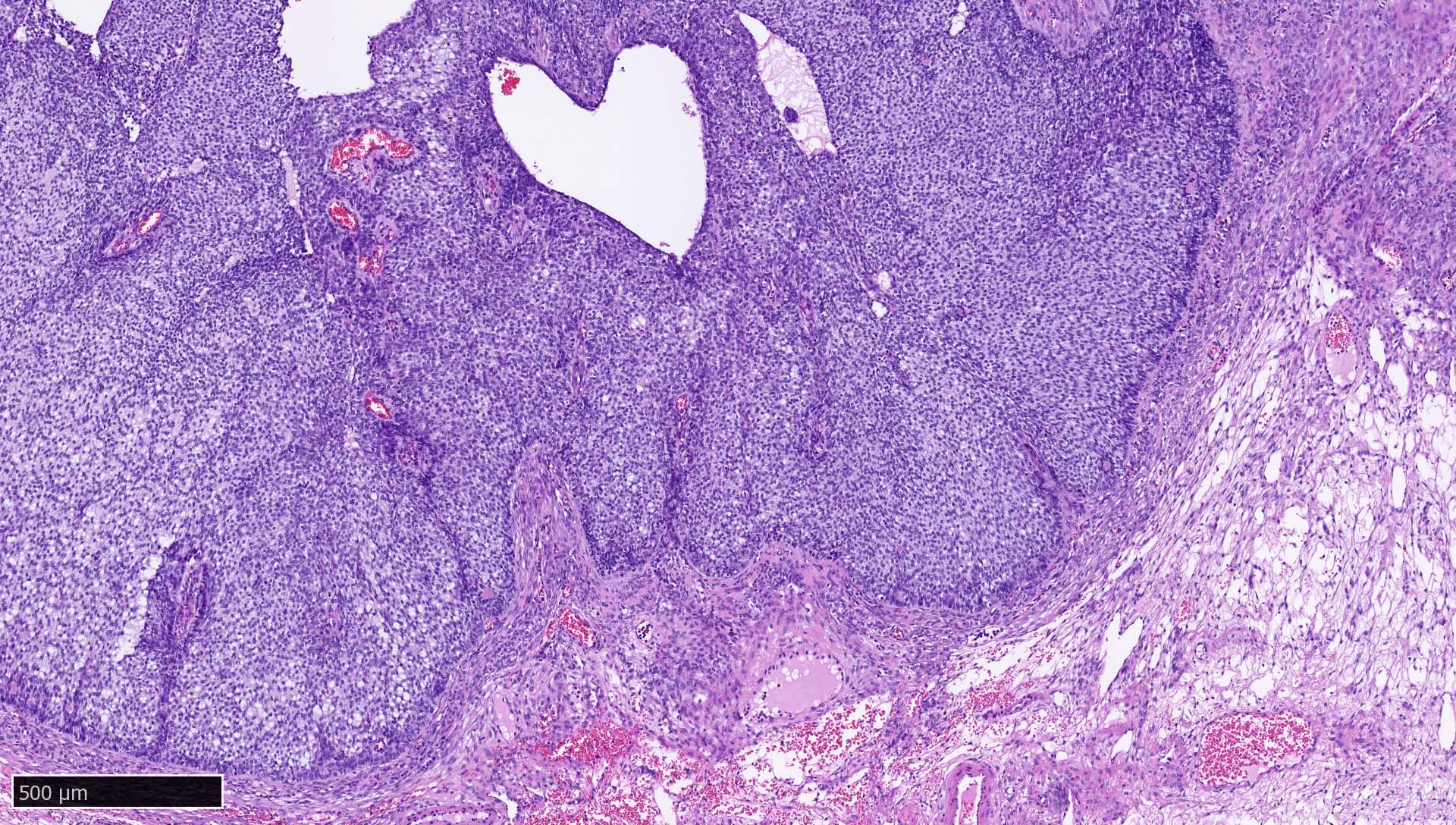
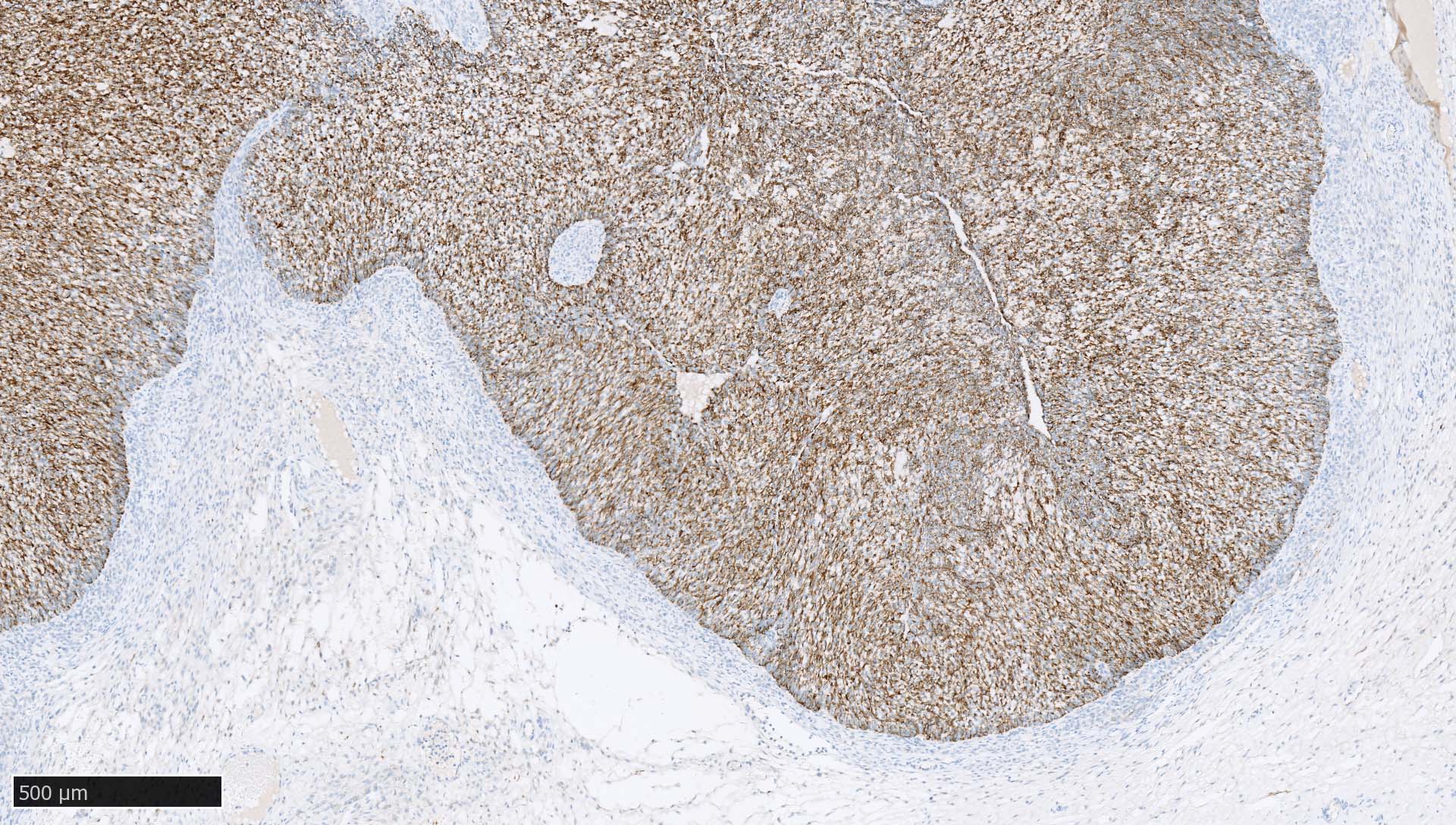
Contributed by Mieke R. Van Bockstal, M.D., Ph.D., Christine Galant, M.D., Ph.D. and Andrey Bychkov, M.D., Ph.D.
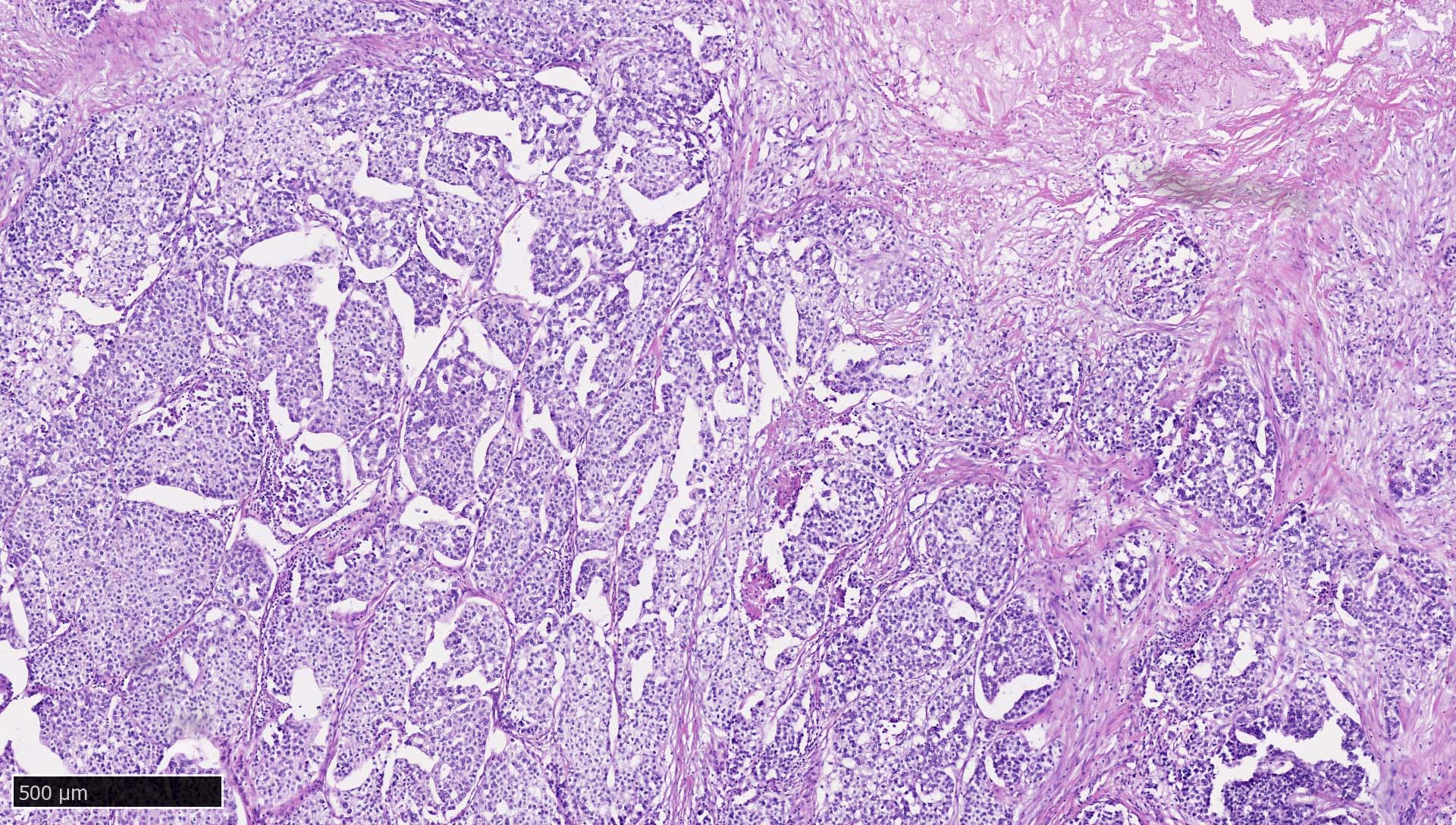
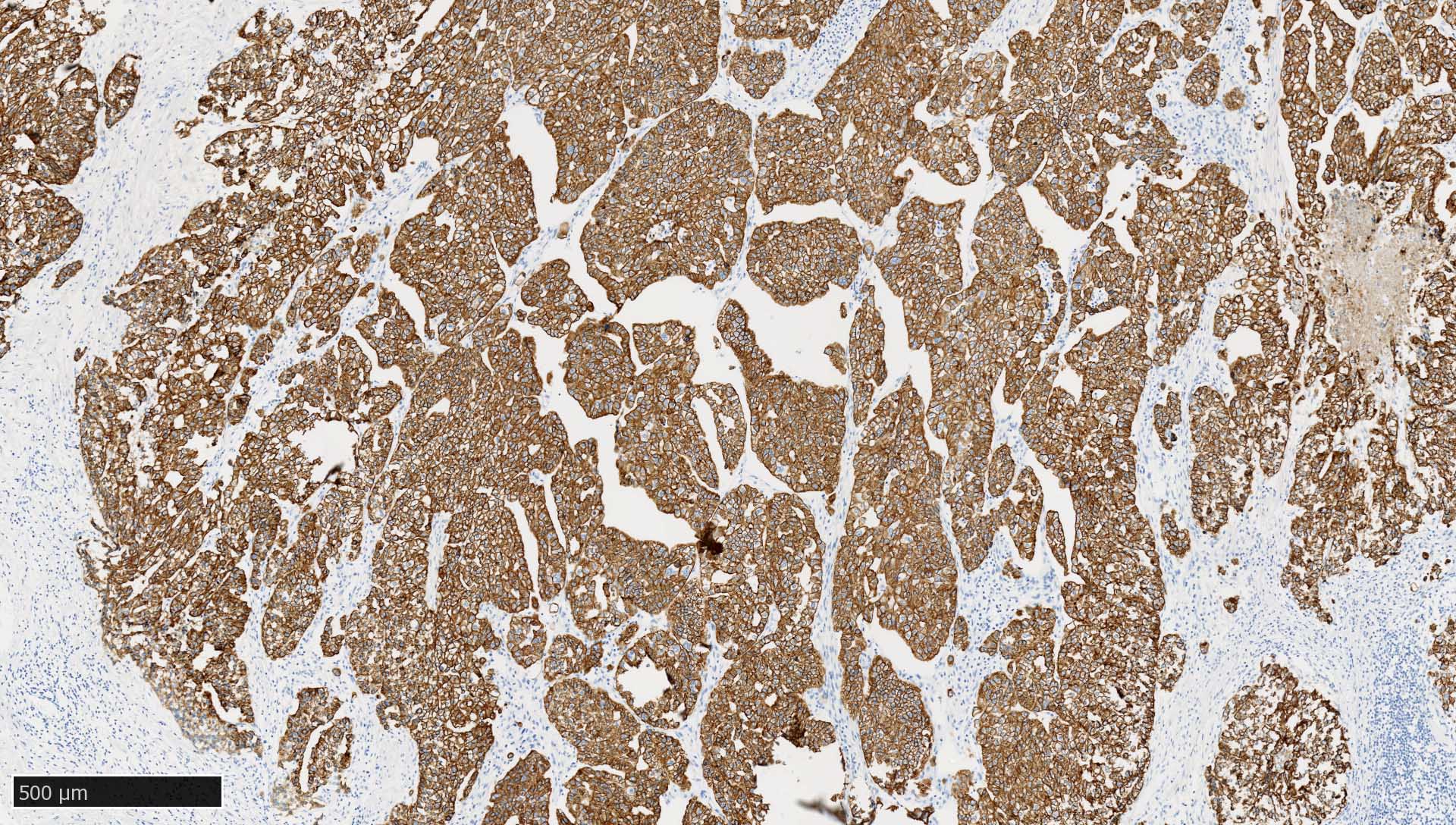
Serous carcinoma
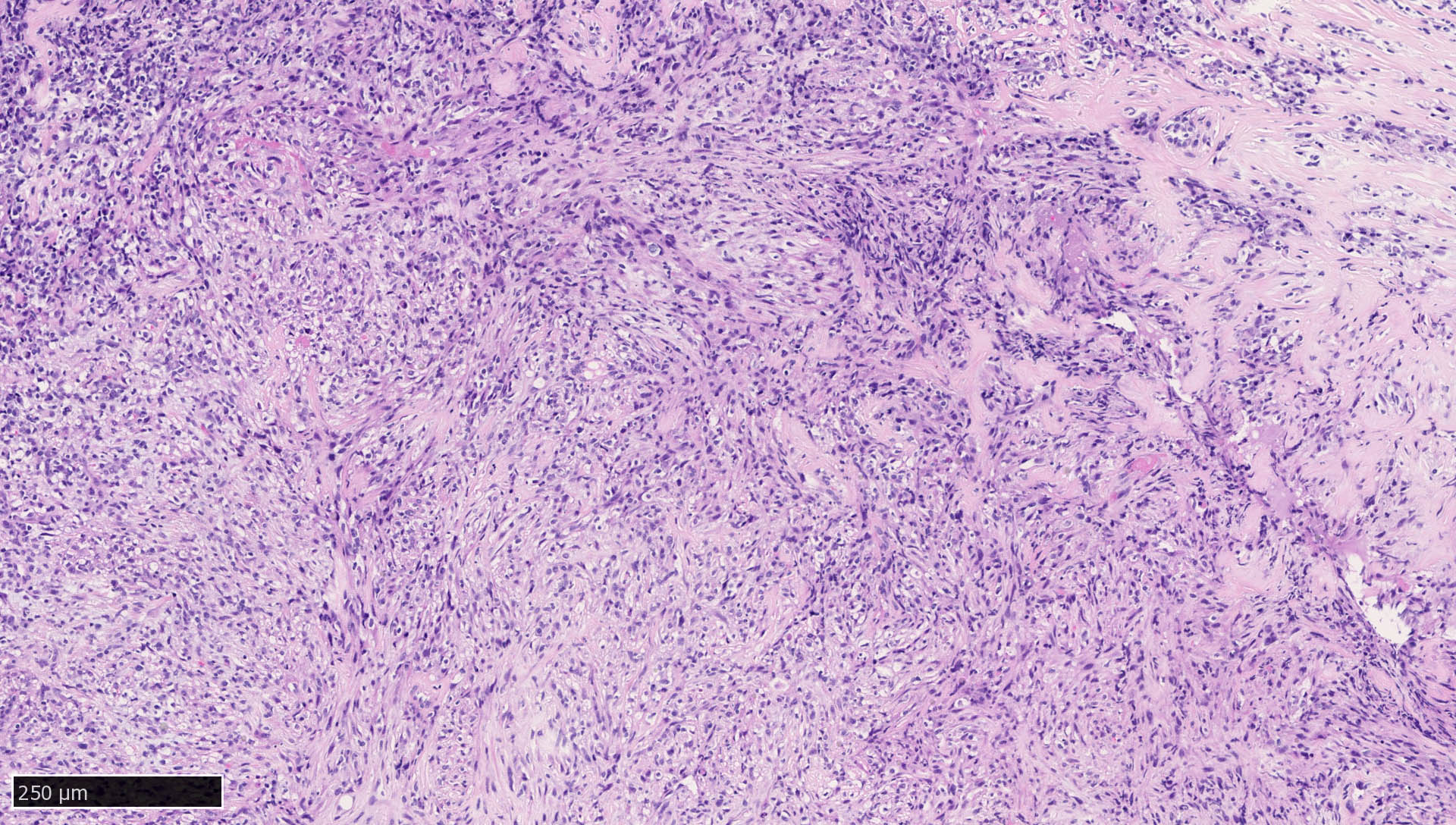
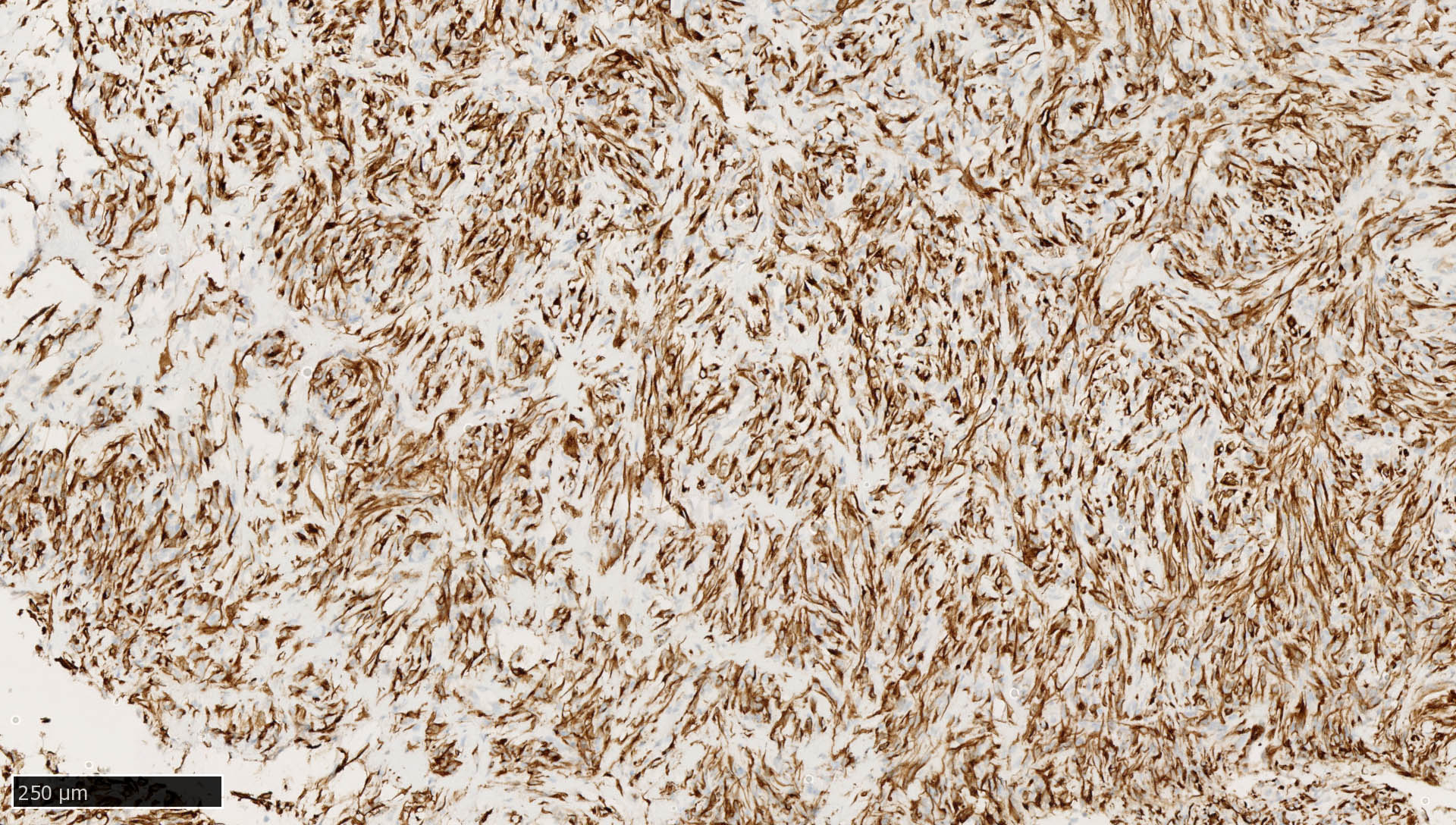
Mammary spindle cell carcinoma
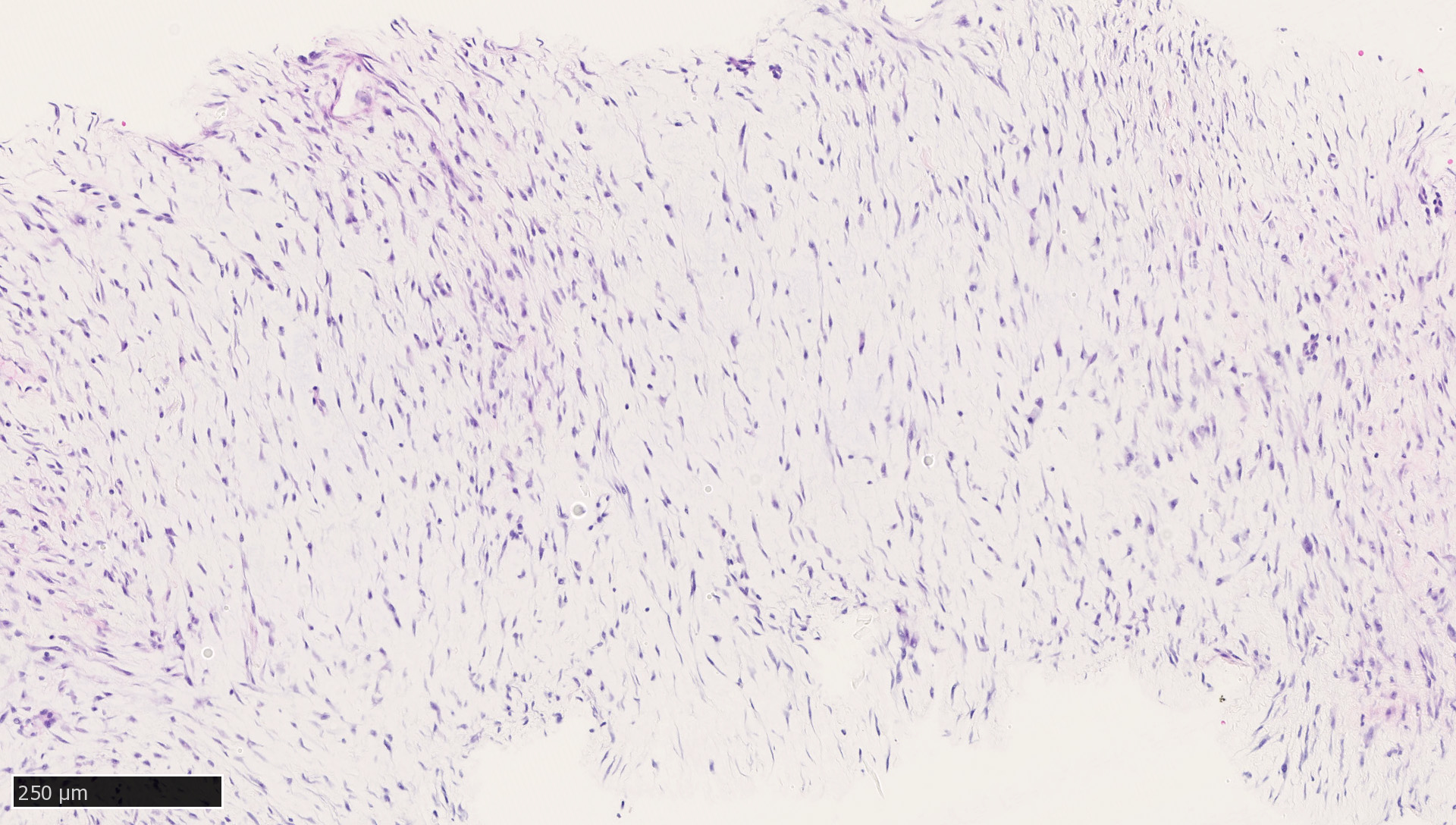

Mammary desmoid fibromatosis

Residual breast carcinoma
Ileal neuroendocrine tumor
Chordoma
Juvenile granulosa cell tumor

Sertoli-Leydig cell tumor
Uterine tumor resembling ovarian sex cord tumor (UTROSCT)
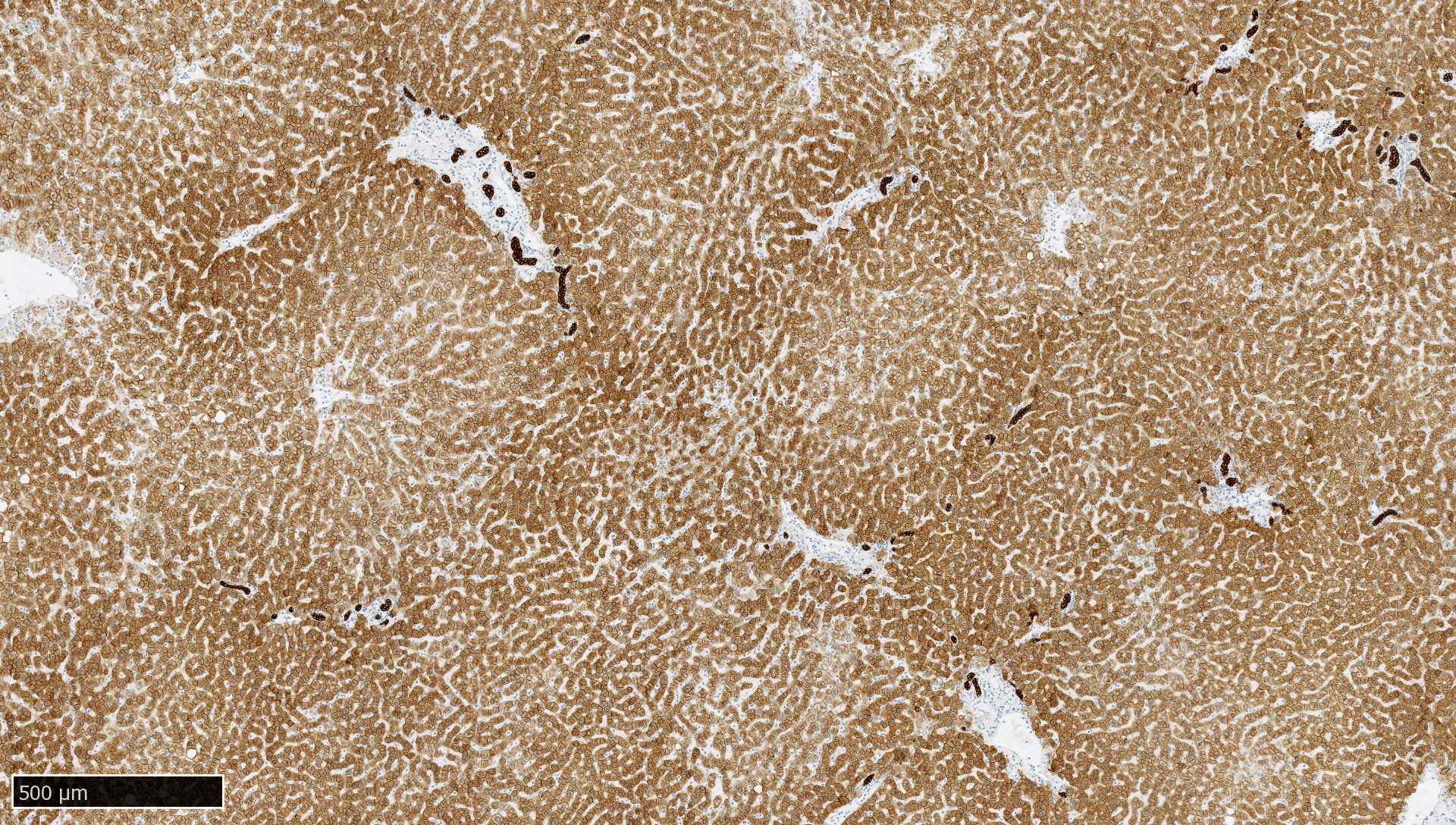
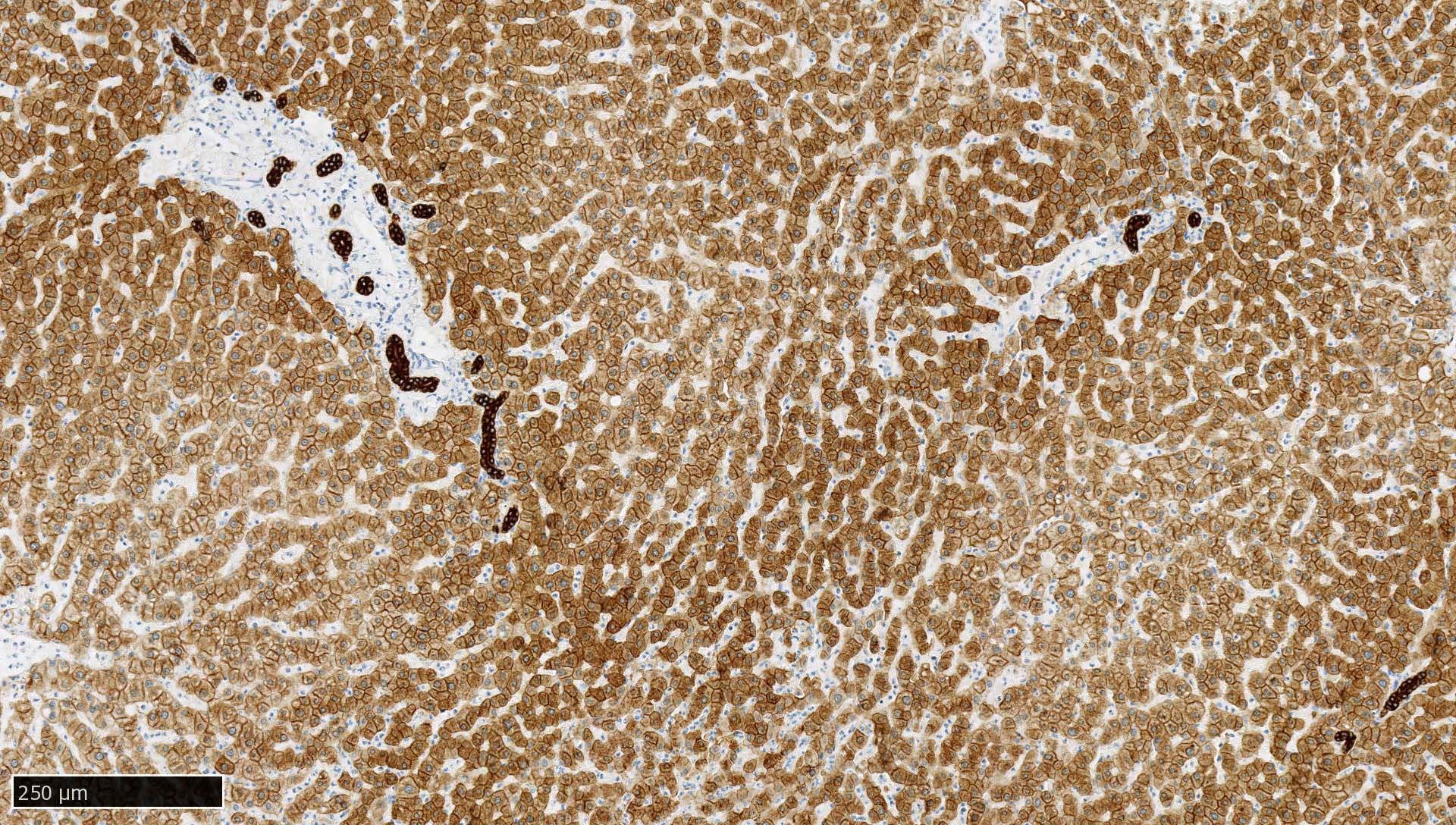
Normal liver
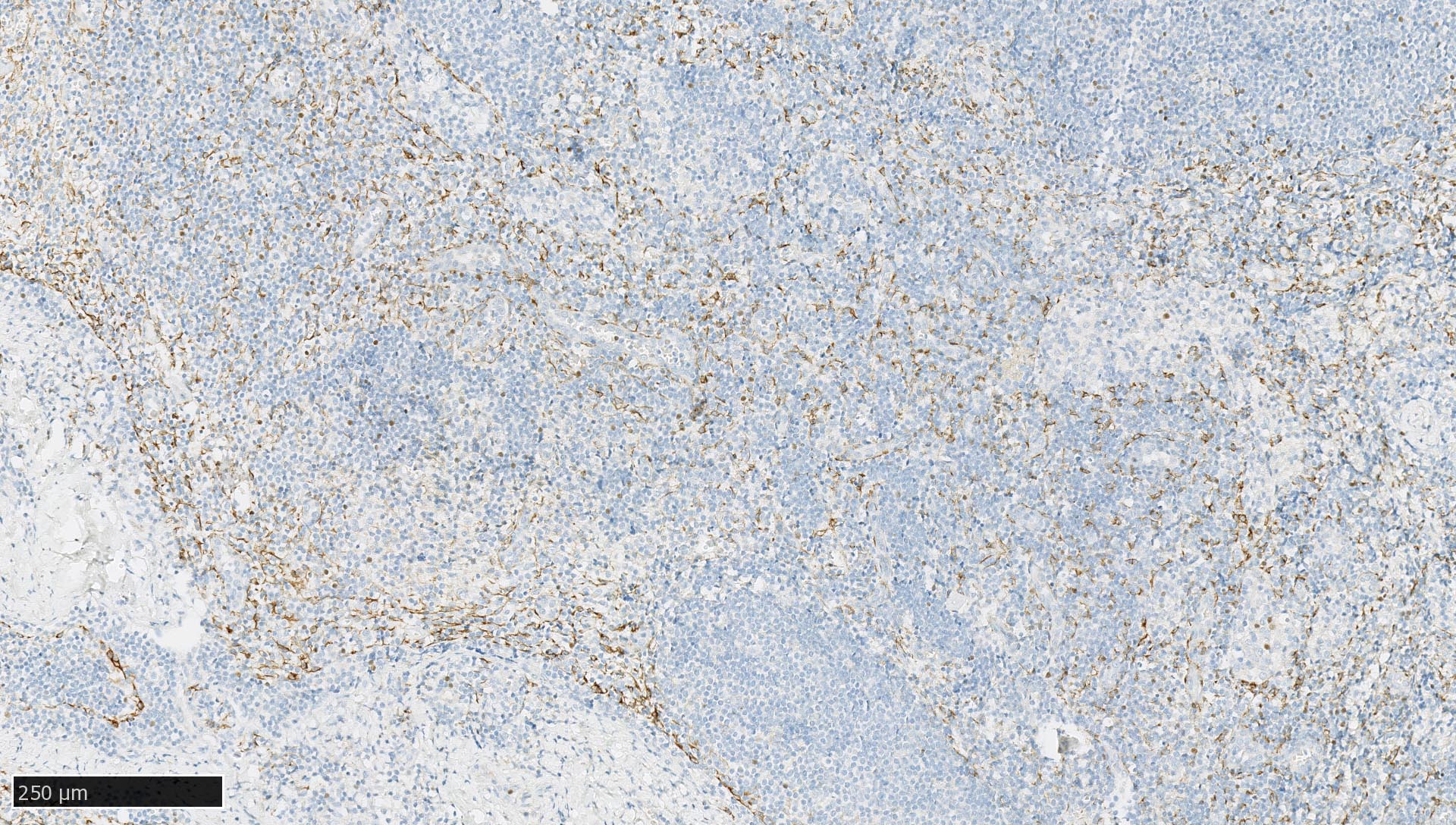
Normal lymph node
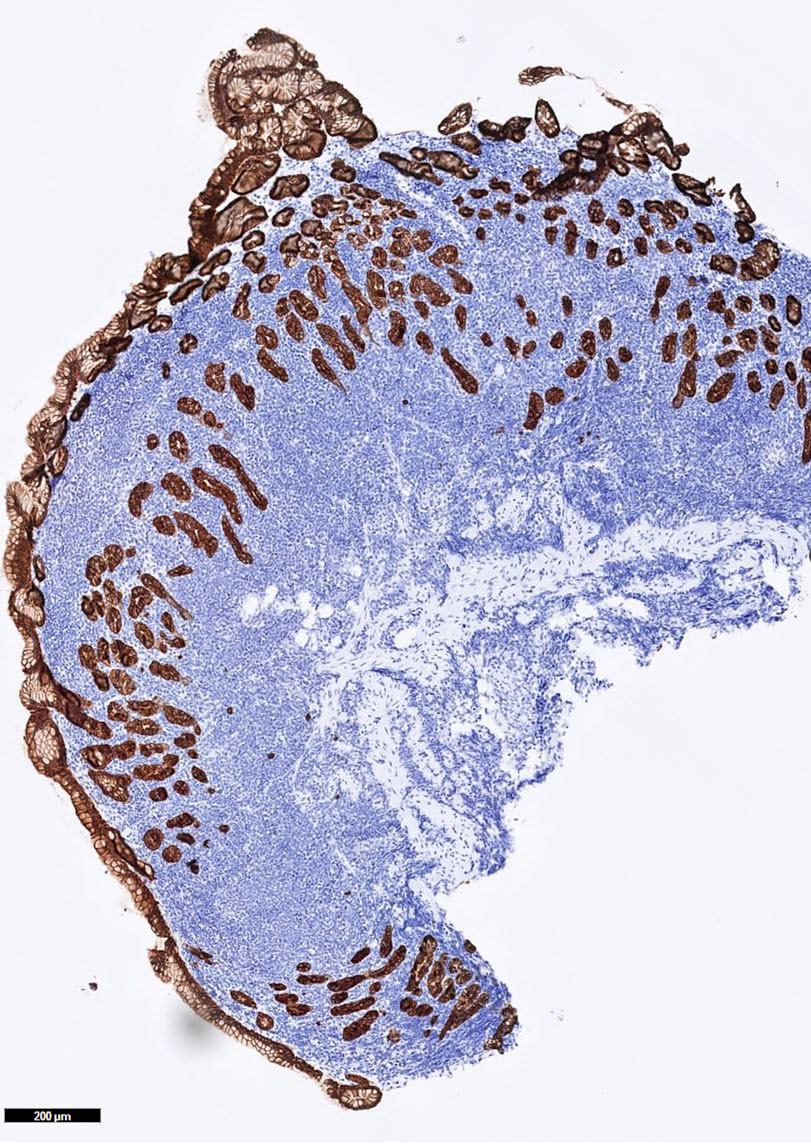
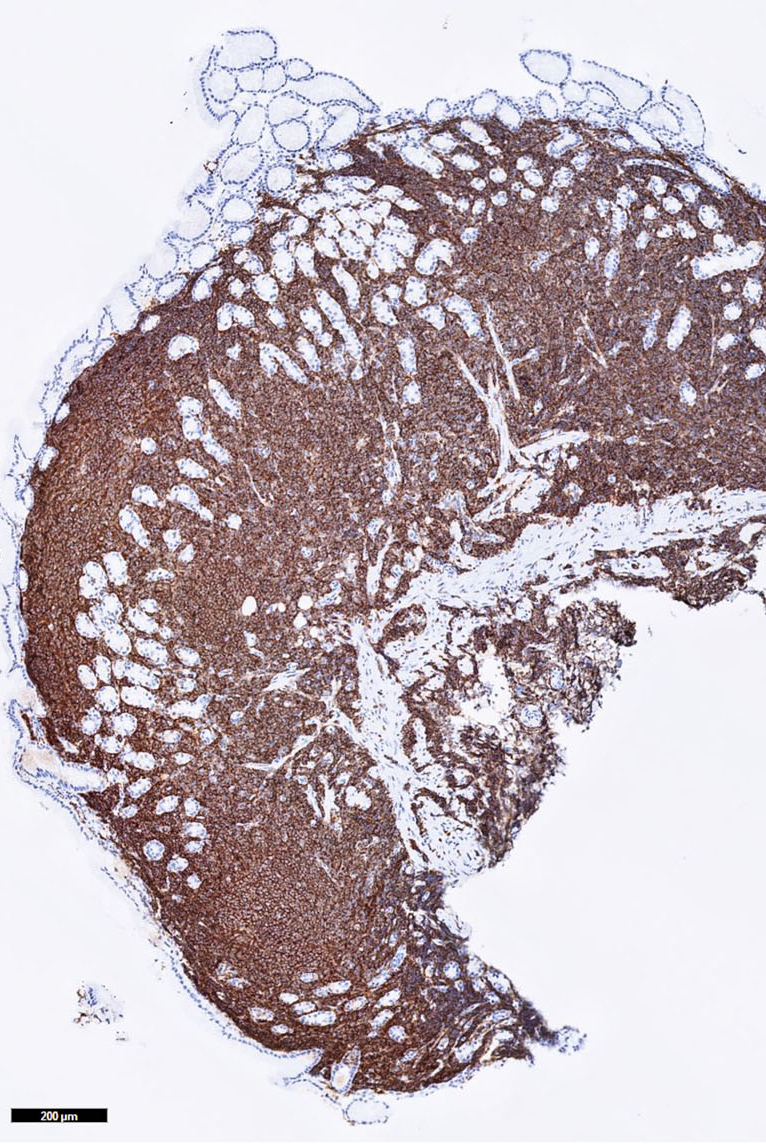
Gastric MALT lymphoma
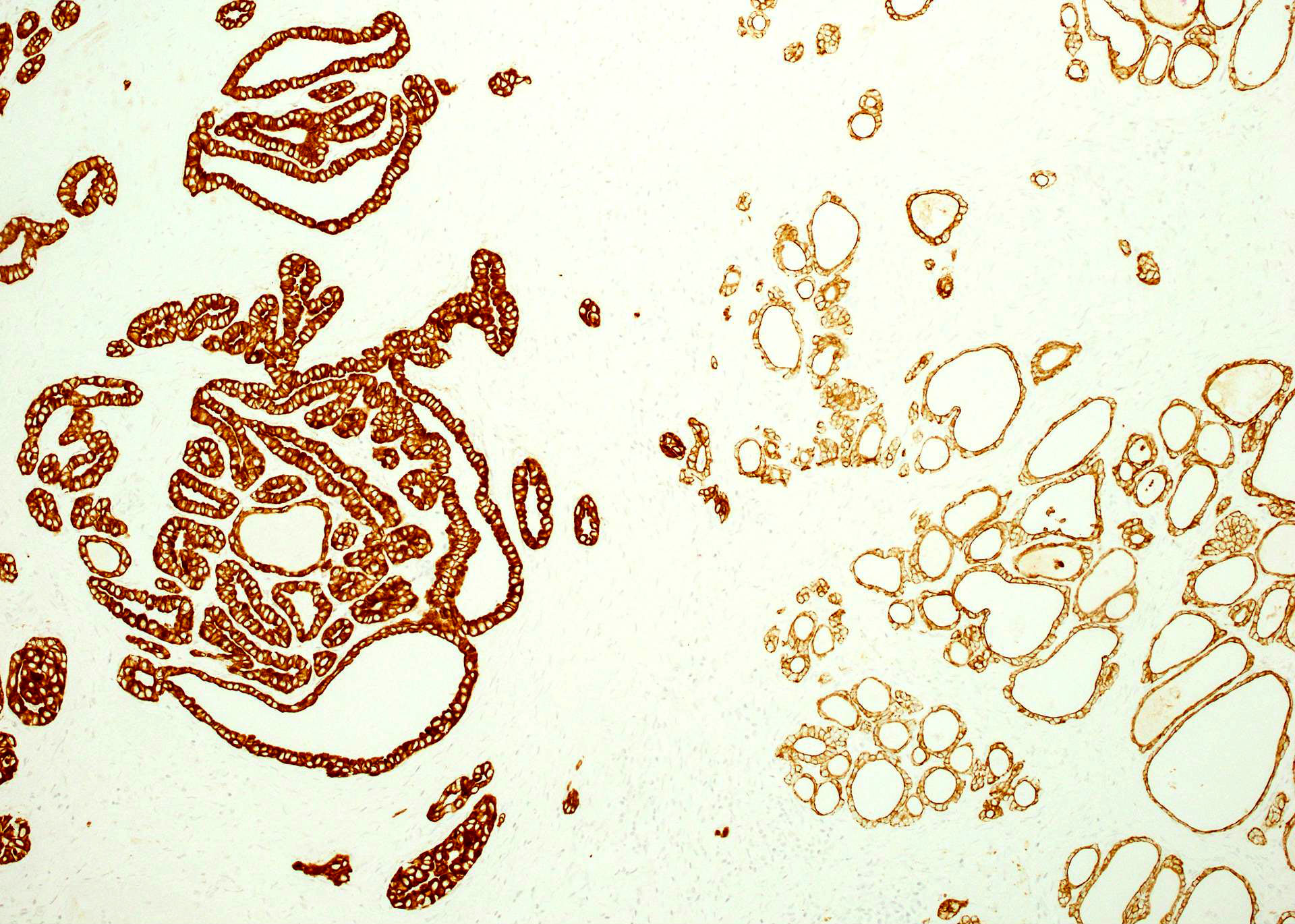
Papillary thyroid cancer
Cytology images
Images hosted on other servers:

CK AE1 / AE3 highlights reactive mesothelial cells
Positive staining - normal
- Epithelium (Arch Pathol Lab Med 2017;141:1014, J Clin Pathol 1991;44:660)
- Trophoblast (Am J Clin Pathol 1991;95:137)
- Follicular cells in the adenohypophysis (Pathol Int 2005;55:244, Hum Pathol 2021;114:1)
- Lymph nodes and lymphoid tissues: lymphocytes are negative but dispersed interstitial reticulum cells with dendritic / reticular pattern show weak to moderate cytoplasmic immunoreactivity (J Cutan Pathol 2016;43:1231, NordiQC: Pan Cytokeratin (CK-PAN) [Accessed 5 May 2022])
- Liver:
- Recommended as an on slide positive control for CK AE1 / AE3 immunohistochemistry by NordiQC (NordiQC: Pan Cytokeratin (CK-PAN) [Accessed 5 May 2022])
- Vast majority of hepatocytes show a distinct cytoplasmic staining reaction with membrane accentuation, while bile ducts display a strong cytoplasmic and membranous staining reaction (NordiQC: Pan Cytokeratin (CK-PAN) [Accessed 5 May 2022])
- Acinar gradient should be present: zone 1 hepatocytes stain more intensely and a rim of hepatocytes around terminal hepatic venules and adjacent to subhepatic veins should also stain more intensely (Virchows Arch A Pathol Anat Histopathol 1987;412:63)
Positive staining - disease
- Most carcinomas (Arch Pathol Lab Med 2017;141:1014)
- Adamantinoma-like Ewing sarcoma of the salivary glands: 100% (Am J Surg Pathol 2019;43:187)
- Adenocarcinoma of the rete testis: 100% (Am J Surg Pathol 2019;43:670)
- Adenomatoid odontogenic tumor: 100% (J Dent Sci 2021;16:7)
- Adenomatoid tumor: 100% (paratesticular), 100% (uterine), 100% (adrenal gland) (Histopathology 2000;36:109, Appl Immunohistochem Mol Morphol 2012;20:173, Am J Surg Pathol 2003;27:969)
- Anaplastic astrocytoma: 63% (Histopathology 1989;14:359)
- Anaplastic carcinoma of the pancreas with rhabdoid features: 100% (Virchows Arch 2014;465:531)
- Calcifying nested stromal and epithelial tumor of the liver: 100% (at least focal immunoreactivity) (Am J Surg Pathol 2009;33:976, Arch Pathol Lab Med 2019;143:264)
- Calcifying odontogenic cyst: 100% (J Dent Sci 2021;16:7)
- Chondroblastoma: 62% (Hum Pathol 2013;44:237)
- Chordoma: 100% (conventional chordoma), 94% (chondroid chordoma), 100% (poorly differentiated chordoma with loss of INI1) (Microsc Res Tech 1996;33:73, Ann Diagn Pathol 2021;55:151809)
- Choroid plexus carcinoma: 100% (Arq Neuropsiquiatr 2004;62:600)
- Choroid plexus papilloma: 100% (Arq Neuropsiquiatr 2004;62:600)
- Cutaneous myoepithelial neoplasms on acral sites: 100% (Am J Surg Pathol 2022 Mar 31 [Epub ahead of print])
- Cytokeratin positive interstitial reticulum cell tumor: 100% (Diagn Pathol 2020;15:121)
- Cytokeratin positive malignant tumor in the abdomen with EWSR1 / FUS::CREB fusion: 100% (Am J Surg Pathol 2022;46:134)
- Embryonal carcinoma (Arch Pathol Lab Med 2015;139:39, Am J Surg Pathol 2009;33:1293, Hum Pathol 2006;37:662)
- Ependymoma: 98% (Appl Immunohistochem Mol Morphol 2000;8:25)
- Epididymal papillary cystadenoma: 100% (Arch Pathol Lab Med 2010;134:630)
- Epithelioid hemangioendothelioma of the liver: 67% (Ann Diagn Pathol 2020;49:151589)
- Epitheloid sarcoma: 93% (Am J Surg Pathol 2013;37:1580)
- Ewing sarcoma of the uterine cervix: 50% (Am J Surg Pathol 2021;45:523)
- Female adnexal tumor of probable Wolffian origin: 100% (Arch Pathol Lab Med 2022;146:166)
- Glioblastoma multiforme: 97% (Pathol Oncol Res 2015;21:817)
- Granulosa cell tumor (GCT) - cystic: 57% (focal and patchy expression) (Arch Pathol Lab Med 2022 Mar 30 [Epub ahead of print])
- Granulosa cell tumor (GCT) - juvenile: 100% (Mod Pathol 2003;16:584)
- Hepatoblastoma: 100% (Pediatr Dev Pathol 2006;9:196)
- High grade oncocytic renal tumor: 100% (Virchows Arch 2018;473:725)
- Leiomyosarcoma of bone: 57% (Virchows Arch 2012;461:561)
- Lymphoepithelioma-like carcinoma of the upper urinary tract: 100% (Virchows Arch 2017;470:703)
- Malignant meningioma: 75% (Mod Pathol 2004;17:1129)
- Mesothelioma - sarcomatoid: 100% (Int J Surg Pathol 2021;29:820)
- Mesothelioma - epithelioid: 100% (Pathol Int 2007;57:190)
- Metaplastic carcinoma of the breast: 100% (fibromatosis-like spindle cell carcinoma), 98% (matrix producing carcinoma), 88% (squamous cell carcinoma), 83 - 100% (low grade adenosquamous carcinoma), 80% (spindle cell carcinoma) (Histopathology 2017;70:975)
- Myoepithelioma-like sarcoma: 50% (Virchows Arch 2012;461:561)
- Nonconventional papillary thyroid carcinoma with pleomorphic tumor giant cells: 100% (Virchows Arch 2010;456:661)
- Odontoma - complex and compound: 100% (J Dent Sci 2021;16:7)
- Papillary renal neoplasm with reverse polarity: 100% (Am J Surg Pathol 2019;43:1099)
- Paratesticular fibrous pseudotumor: 54% (Am J Surg Pathol 2010;34:569)
- Pituitary neuroendocrine tumors (PitNET) (Hum Pathol 2021;107:87)
- Polymorphous sweat gland carcinoma: 100% (Am J Dermatopathol 2018;40:580)
- Poorly differentiated nonkeratinizing squamous cell carcinoma of the thymus: 100% (Am J Surg Pathol 2018;42:1224)
- Pseudomyogenic hemangioendothelioma (Acta Dermatovenerol Alp Pannonica Adriat 2018;27:225, Pathologica 2018;110:96)
- Reactive nodular fibrous pseudotumor: 86% (Int J Surg Pathol 2004;12:365)
- Retroperitoneal schwannoma: 69% (Mod Pathol 2006;19:115)
- Rhabdoid and undifferentiated phenotype in renal cell carcinoma: 94% (variable intensity and extent) (Am J Surg Pathol 2017;41:253)
- Sertoli-Leydig cell tumor of the ovary: 100% (Mod Pathol 2003;16:584)
- Sex cord tumor with annular tubules (SCTAT): 66% (Mod Pathol 2003;16:584)
- Small cell carcinoma of hypercalcemic type: 60% (usually focally positive) (Histopathology 2017;70:1147, Int J Gynecol Pathol 2004;23:330)
- STK11 adnexal tumor: 93% (Am J Surg Pathol 2021;45:1061)
- Synovial sarcoma: 50% (focal reactivity); 100% in biphasic synovial sarcomas (Virchows Arch 2017;471:799, Mod Pathol 2005;18:40, J Neuropathol Exp Neurol 2017;76:289)
- Testicular Sertoli cell tumor: 64% (Mod Pathol 1998;11:774)
- TFE3 gene fusion associated renal cell carcinoma: 71% (Am J Surg Pathol 2020;44:1450)
- Thymoma: 100% (atypical thymomas with squamoid and spindle cell features), 100% (type A thymoma), biphasic expression in metaplastic thymoma and type AB thymoma (Mod Pathol 2022 Feb 10 [Epub ahead of print], Virchows Arch 2014;464:725)
- Undifferentiated / dedifferentiated urothelial carcinoma of the urinary tract: 100% (Virchows Arch 2016;469:321)
- Xanthogranulomatous epithelial tumor: 100% (Mod Pathol 2020;33:1889)
- Yolk sac tumor: 100% (also 100% in testicular sarcomatoid yolk sac tumors after chemotherapy) (Am J Surg Pathol 2012;36:360, Am J Surg Pathol 2022;46:309, Am J Surg Pathol 2015;39:251)
Negative staining
- Adrenocortical carcinoma: 84% negative (Hum Pathol 2015;46:1799)
- Adult granulosa cell tumors: 65% negative (Mod Pathol 2003;16:584)
- Aggressive angiomyxoma: 72% negative (Virchows Arch 2005;446:157)
- Angiosarcoma: 97 - 100% negative (up to 31% positive in hepatic angiosarcoma) (Arch Pathol Lab Med 2007;131:288, Am J Surg Pathol 2013;37:1580, Ann Diagn Pathol 2020;49:151589)
- Atypical fibroxanthoma: 100% negative (Australas J Dermatol 2020;61:e22)
- Benign meningioma: 100% negative (Mod Pathol 2004;17:1129)
- Chondrosarcoma: 100% negative (but up to 60% positive in clear cell chondrosarcoma) (Hum Pathol 2013;44:237, Neuroendocrinology 2020;110:836)
- Chordoid meningioma: 100% negative (J Neurooncol 2010;99:41)
- Clear cell sarcoma of soft tissue: 97% negative (Am J Surg Pathol 2008;32:452)
- Endometrial stromal sarcoma: 76% negative (Mod Pathol 2005;18:40)
- Epithelioid angiosarcoma of the bladder: 66% negative (Am J Surg Pathol 2015;39:1377)
- Ewing sarcoma family of tumors / PNET: 81% negative (Virchows Arch 2011;459:409, Am J Surg Pathol 2000;24:410)
- Gliosarcoma: 100% negative (J Neuropathol Exp Neurol 2017;76:289)
- Hemangioblastoma: 94 - 97% negative (Am J Surg Pathol 2008;32:1051, J Neuropathol Exp Neurol 2017;76:289)
- Hepatocellular carcinoma: 72% negative (Arch Pathol Lab Med 2014;138:1583)
- Melanoma: 55% negative (epithelioid melanoma), 73% negative (spindle cell / desmoplastic melanoma) (Mod Pathol 2015;28:1033)
- Meningioma: 94% negative (J Neuropathol Exp Neurol 2017;76:289)
- Malignant peripheral nerve sheath tumor (MPNST): 50 - 100% negative (J Neuropathol Exp Neurol 2017;76:289, Am J Clin Pathol 1999;112:641)
- Myofibroblastic-like sarcoma: 63% (Virchows Arch 2012;461:561)
- Myxofibrosarcoma: 100% negative (Virchows Arch 2012;461:561)
- Neurofibroma: 100% negative (J Neuropathol Exp Neurol 2017;76:289)
- Nodular fasciitis: 91% negative (Am J Surg Pathol 2012;36:1404)
- Oncocytic adrenocortical neoplasm: 62% negative (Hum Pathol 2011;42:489)
- Ovarian fibroma: 80% negative (Mod Pathol 2003;16:584)
- Ovarian thecoma and fibrothecoma: 100% negative (Mod Pathol 2003;16:584)
- Paraganglioma: 98% negative (Hum Pathol 2019;93:16)
- Peripheral schwannoma: 100% negative (Mod Pathol 2006;19:115)
- Phyllodes tumor of the breast: 100% negative (benign and borderline phyllodes tumors), 79% negative (malignant phyllodes tumors) (Int J Surg Pathol 2018;26:232, Histopathology 1989;14:141)
- Plasmacytoma / multiple myeloma: 64% negative (occasional positivity can occur in up to 36%) (Int J Surg Pathol 2018;26:232, Histopathology 1989;14:141)
- Proliferative fasciitis: 54% negative (Am J Surg Pathol 2012;36:1404)
- Renal epithelioid angiomyolipoma: 100% negative (Sci Rep 2015;5:10030)
- Solitary fibrous tumor (SFT): 89 - 95% negative (Am J Surg Pathol 2012;36:1404, J Neuropathol Exp Neurol 2017;76:289)
- Spindle cell sarcoma, NOS: 100% negative (Virchows Arch 2012;461:561)
- Testicular Leydig cell tumor: 58% negative (Mod Pathol 1998;11:774)
- Undifferentiated pleomorphic sarcoma: 72% negative (Virchows Arch 2012;461:561)
- Well differentiated astrocytoma: 60 - 78% (Histopathology 1989;14:359, Indian J Pathol Microbiol 2007;50:478)
- YAP1::TFE3 fused hemangioendothelioma: 80% negative (Mod Pathol 2021;34:2211)
Sample pathology report
- Immunohistochemical analysis for cytokeratin AE1 / AE3, performed on an automated slide stainer (brand name):
- The tissue sample shows no / focal / diffuse* dot-like / cytoplasmic / membrane* staining with weak / moderate / strong* intensity.
- External on slide tissue control (liver - in accordance with the NordiQC recommendations): positive
- * Select the appropriate option
- Biopsy, left breast (external superior quadrant):
- Desmoid fibromatosis of the breast, with presence of an APC gene mutation (see comment)
- Number of biopsies: 2
- Maximum length of the biopsy: 14 mm
- Lesion type / histological description: Both biopsies show a spindle cell proliferation with fascicular architecture. In one of these biopsies, diffuse infiltration of the fatty stroma is observed. The spindle cells are bland, elongated and slender, with a pale slightly eosinophilic cytoplasm. They are surrounded by a densely collagenous stroma. There is no overt cytonuclear atypia, no clear nucleoli and no nuclear hyperchromasia. There are < 1 mitosis per 10 high power fields.
- Presence of calcifications: no
- Immunohistochemistry and discussion: Immunohistochemical stains for p63, cytokeratin AE1 / AE3, cytokeratin 8/18 and cytokeratin 34betaE12 are negative, which excludes a low grade fibromatosis-like metaplastic breast carcinoma. Immunohistochemical stains for SOX10 and S100 are negative, which excludes a neurofibroma. There is no immunoreactivity for desmin, which excludes a leiomyoma. Immunohistochemistry for CD34 is negative, which excludes a myofibroblastoma and PASH with fascicular architecture. The spindle cells show cytoplasmic immunoreactivity for SMA and beta catenin. There is no nuclear expression of beta catenin.
- Molecular analysis and discussion: FISH analysis did not show USP6 rearrangement, which excludes a nodular fasciitis. Next generation sequencing of the tumor sample did not show any mutations in the CTNNB1 gene but revealed a c.4626_4645del; p.(Lys1543Argfs*9) mutation in the APC gene, with a variant allele frequency of 52%.
- Comment: APC gene mutations are commonly observed in breast desmoid fibromatosis and might either be somatic or germline (Am J Surg Pathol 2020;44:1266).
- Recommendation: These findings are to be correlated with the clinical history and family history of the patient, as a germline APC mutation (Gardner / familial adenomatous polyposis syndrome) should be excluded.
Board review style question #1
Which of the following tissues is the best choice as a positive on slide control for cytokeratin AE1 / AE3 immunohistochemistry?
- Adrenal gland
- Appendix
- Gastric mucosa
- Liver
- Placenta
Board review style answer #1
D. Liver. The liver shows strong, distinct cytoplasmic immunoreactivity of all bile ductal epithelial cells, as well as at least moderate cytoplasmic staining of the majority of hepatocytes. Hepatocytes show membrane accentuation. A low expressor (such as hepatocytes) is required to enable the detection of a slightly failing immunohistochemical staining reaction (resulting in insufficient intensity in low expressors), as strong expressors (such as most epithelia) will still present with an intense cytoplasmic staining.
Comment Here
Reference: Cytokeratin AE1 / AE3
Comment Here
Reference: Cytokeratin AE1 / AE3
Board review style question #2
Which of the following tumors is predominantly positive for cytokeratin AE1 / AE3?
- Adrenocortical carcinoma
- Aggressive angiomyxoma
- Benign meningioma
- Paraganglioma
- STK11 adnexal tumor
Board review style answer #2
E. STK11 adnexal tumor. 93% of STK11 adnexal tumors present at least some immunoreactivity for CK AE1 / AE3, whereas 72% of aggressive angiomyxomas are negative for CK AE1 / AE3. Nearly all benign meningiomas, 84% of adrenocortical carcinomas and 98% of paragangliomas do not present any immunoreactivity for CK AE1 / AE3.
Comment Here
Reference: Cytokeratin AE1 / AE3
Comment Here
Reference: Cytokeratin AE1 / AE3
Board review style question #3
This tissue was stained for cytokeratin AE1 / AE3. Which is the correct statement?
- The protocol of this immunohistochemical stain should be revised as lymphoid tissue should not show any immunoreactivity for cytokeratin AE1 / AE3
- This axillary lymph node contains isolated tumor cells from an invasive lobular carcinoma of the breast
- This axillary lymph node shows weak to moderate cytoplasmic staining in interstitial reticulum cells with dendritic / reticular pattern
- This immunohistochemical staining pattern is compatible with a nodal histiocytic sarcoma
Board review style answer #3
C. This axillary lymph node shows weak to moderate cytoplasmic staining in interstitial reticulum cells with dendritic / reticular pattern. The tissue shown in the photograph is a normal lymph node. A weak to moderate cytoplasmic staining reaction in the interstitial reticulum cells of a lymph node is normal and therefore the protocol of this stain should not be revised. Normal liver is a better external control tissue than a lymph node, as it contains both low and high expressors of CK AE1 / AE3.
Comment Here
Reference: Cytokeratin AE1 / AE3
Comment Here
Reference: Cytokeratin AE1 / AE3
