
Lymph nodes & spleen, nonlymphoma
Spleen-other nonneoplastic disorders
Immune thrombocytopenia (ITP)
Author: Rick Kapur, M.D., Ph.D., M.Sc.
Editorial Board Member: Patricia Tsang, M.D., M.B.A.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.

Last author update: 2 April 2021
Last staff update: 19 January 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Immune thrombocytopenia[TI] spleen pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kapur R. Immune thrombocytopenia (ITP). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/spleenITP.html. Accessed April 2nd, 2025.
Definition / general
- Acquired autoimmune bleeding disorder characterized by isolated thrombocytopenia (peripheral blood platelet count < 100 × 109/L) (Blood 2009;113:2386)
- Mixed cell mediated and antibody mediated: abnormal T cell responses resulting in platelet destruction primarily in the spleen, mainly due to antiplatelet autoantibodies (J Clin Med 2017;6:16)
Essential features
- Immune thrombocytopenia (ITP) is a diagnosis of exclusion with an isolated thrombocytopenia of < 100 × 109/L (Blood 2009;113:2386)
- Affected sites predominantly include skin and mucous membranes (petechiae, wet / dry purpura) and spleen (primary site of platelet clearance)
- Impairment in CD4+ T regulatory cells and dendritic cells leads to the initiation and perpetuation of ITP (Curr Opin Hematol 2020;27:423)
- Thrombocytopenia is due to IgG antiplatelet autoantibodies (principle mechanism of antibody mediated platelet phagocytosis), cytotoxic CD8+ T cells and impaired megakaryocyte function (J Clin Med 2017;6:16)
- Primary diagnostic tests include complete blood counts, peripheral blood smear and testing to exclude HIV and hepatitis C virus; antiplatelet antibody testing is among the supportive tests that may be performed (UpToDate: Immune Thrombocytopenia (ITP) in Adults - Clinical Manifestations and Diagnosis [Accessed 16 February 2021])
Terminology
- Formerly known as idiopathic thrombocytopenic purpura
ICD coding
- ICD-10: D69.3 - Immune thrombocytopenic purpura
Epidemiology
- Annual incidence: ~1 - 6 per 100,000 adults (Am J Hematol 2012;87:848)
- Prevalence: ~12 per 100,000 in adults and 8 per 100,000 in children (Am J Hematol 2012;87:848)
- Increased incidence with increasing age (Am J Hematol 2012;87:848, Br J Haematol 2009;145:235)
- Incidence: M = F when > 60 years of age
- Childhood ITP is a clinically distinct condition from adult ITP with a higher likelihood of spontaneous remission
Sites
- Skin:
- Petechiae (flat, red, discrete lesions that do not blanch under pressure), often lower legs in ambulatory patients or sacral area in recumbent patients
- Dry purpura (coalescence of petechiae, nonpalpable)
- Mucous membranes (such as oral mucosa):
- Wet purpura (hemorrhagic blisters)
- Severe bleeding:
- Affects a minority of patients (J Thromb Haemost 2015;13:457)
- Associated with marked thrombocytopenia and new diagnosis of ITP
- Extensive mucosal bleeding often present
- Intracranial hemorrhage uncommon
- Spleen: primary site of platelet clearance in most patients
- Liver, bone marrow or lymph nodes: may also be sites of platelet clearance
Pathophysiology
- Impairment in CD4+ T regulatory cells and dendritic cells leads to the initiation and perpetuation of ITP
- Decreased CD4+ CD25+ FOXP3+ T regulatory cell levels and function in patients with active disease (Curr Opin Hematol 2020;27:423)
- Also dendritic cells and myeloid derived suppressor cells have been described to be impaired in ITP (Curr Opin Hematol 2020;27:423, Blood 2016;127:1587)
- Thrombocytopenia due to:
- IgG antiplatelet autoantibodies (principle mechanism) bind to platelet surface antigens (such as glycoprotein [GP] αIIbβ3 [GPIIbIIIA] and GPIb-IX-V)
- Platelets with bound autoantibodies are subsequently recognized by macrophages bearing Fcγ receptors (FcγRs), resulting in antibody mediated platelet phagocytosis and destruction primarily in the spleen (Haematologica 2021;106:250)
- Cytotoxic CD8+ T cells may directly lyse platelets (Nat Med 2003;9:1123)
- Impaired megakaryocyte function resulting in impaired platelet production due to targeting by antiplatelet autoantibodies or CD8+ T cells in the bone marrow (Haematologica 2015;100:623, Blood 2008;112:1078)
Diagnosis
- ITP is a diagnosis of exclusion; an isolated thrombocytopenia is present (peripheral blood platelet count < 100 × 109/L) without anemia or leukopenia and without another apparent cause of thrombocytopenia
Laboratory
- Complete blood counts, peripheral blood smear: to confirm thrombocytopenia and to exclude platelet morphology abnormalities (e.g. lack of platelet granules or uniformly large or small platelets) suggestive of hereditary platelet disorders or myelodysplasia
- HIV and hepatitis C virus testing: may explain the thrombocytopenia and treating the underlying infection might improve the platelet count
- Additional testing for patients with suspected ITP may include:
- Helicobacter pylori testing: in case of gastrointestinal symptoms suggestive of infection due to association between ITP and H. pylori infection
- Bone marrow investigation: not required for typical presentation
- Normal or increased number of megakaryocytes
- In some patients, a shift towards younger megakaryocytes with hypolobation or lesser degrees of nuclear polyploidy and less evidence of platelet production
- Vitamin B12 and folate levels: required for hematopoiesis and their deficiency may present with mild thrombocytopenia
- Coagulation studies: to investigate and treat other potential causes of thrombocytopenia (e.g. liver disease) and bleeding (e.g. vitamin K deficiency)
- Immunologic studies (e.g. testing for antinuclear antibodies or quantitative immunoglobulin levels to identify underlying common variable immune deficiency)
- Antiplatelet antibody testing (not always detectable)
- Reference: Curr Opin Hematol 2020;27:423, UpToDate: Immune Thrombocytopenia (ITP) in Adults - Clinical Manifestations and Diagnosis [Accessed 16 February 2021]
Prognostic factors
- Adult ITP: majority stable, safe platelet count due to spontaneous remission (up to 10%) or therapy, often within first 6 months (Br J Haematol 2003;122:966)
- Childhood ITP: spontaneous remission (up to 50%) after months or even years of chronic ITP
Case reports
- 3 year old boy and girl with intravenous immunoglobulin refractory ITP receiving chemotherapy for high risk neuroblastoma (J Pediatr Hematol Oncol 2019;41:e257)
- 41 year old woman with anti-GPVI mediated ITP (Res Pract Thromb Haemost 2017;1:291)
- 48 year old man critically ill with COVID-19 (Int J Infect Dis 2020;99:269)
- 65 and 71 year old men presenting with lethal diffuse alveolar hemorrhage (Case Rep Hematol 2019;2019:5170282)
Treatment
- First line includes corticosteroids, intravenous immunoglobulin and anti-D immunoglobulin
- Subsequent treatments include rituximab, splenectomy or thrombopoietin receptor agonists
- Treatment goals: maintaining platelet counts > 20 - 30 × 109/L for at least symptomatic patients (Blood Adv 2019;3:3780)
Clinical images
Images hosted on other servers:

Petechiae or small bruise-like markings
Microscopic (histologic) description
- Splenic white pulp is prominent, with focal germinal centers and hyperplastic marginal zones
- Red pulp is cellular with histiocytes, activated lymphocytes (immunoblasts) and neutrophils
- Increased number of cordal macrophages, with phagocytosis of (apparent) antibody coated platelets
- Cords of Billroth may have a dirty appearance due to granular platelet debris both within macrophages and extracellularly
- Reference: HemaSphere: The spleen in immune thrombocytopenia [Accessed 22 February 2021]
Microscopic (histologic) images
Contributed by Julia Geyer, M.D.
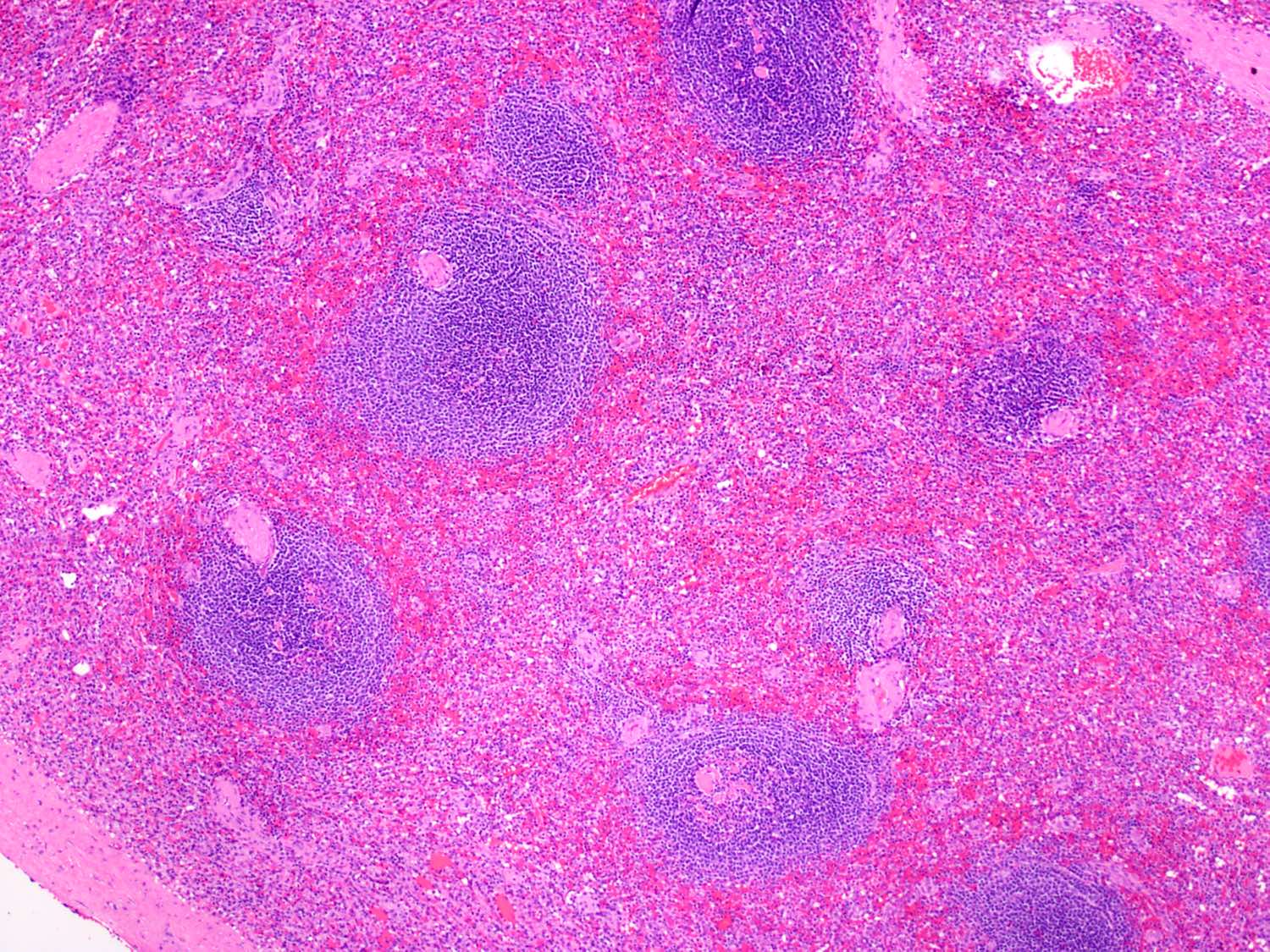
Focal germinal centers, hyperplastic marginal zones

Histiocytes, immunoblasts, neutrophils, macrophages
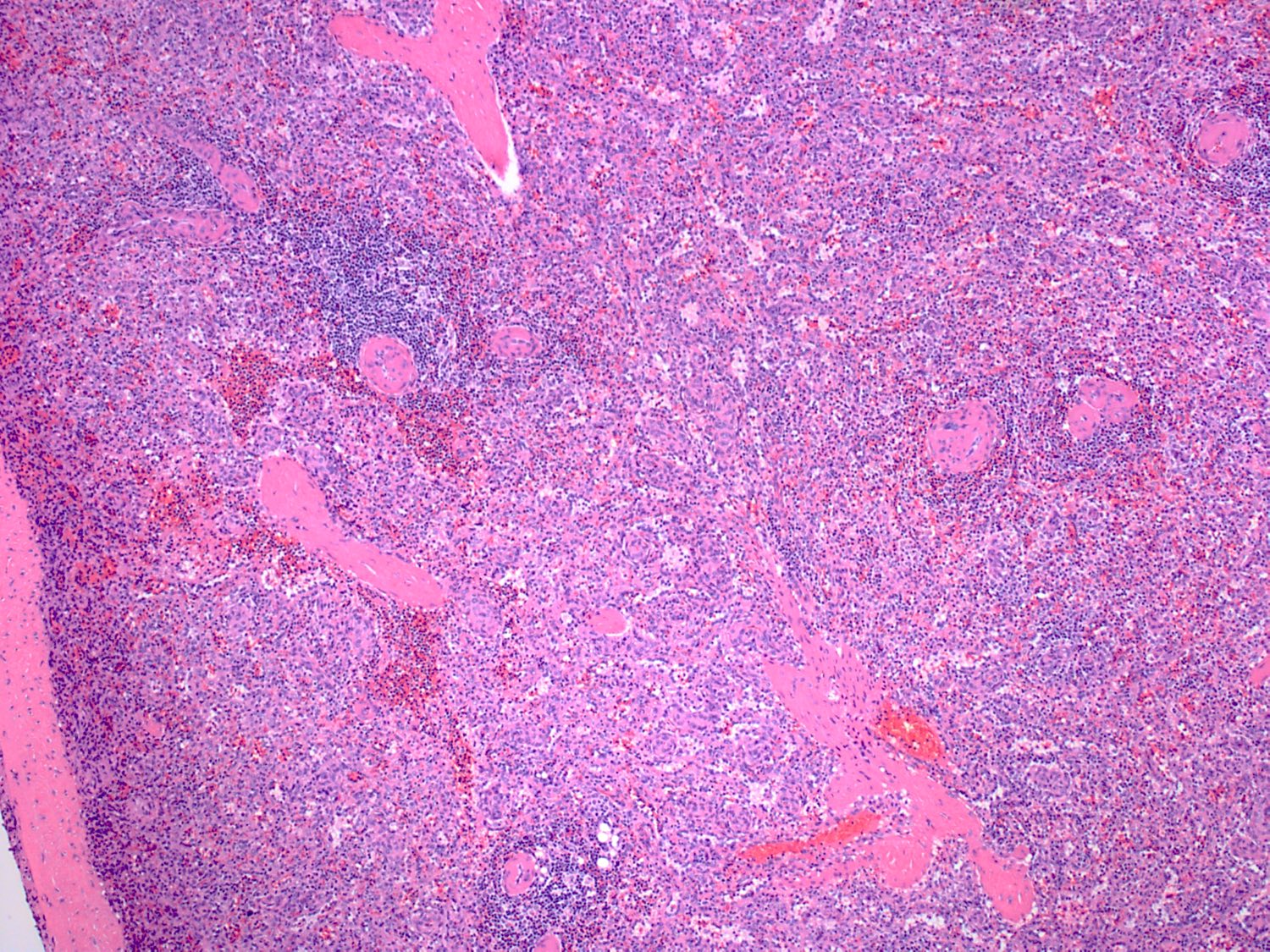
Expanded red pulp, atrophic white pulp
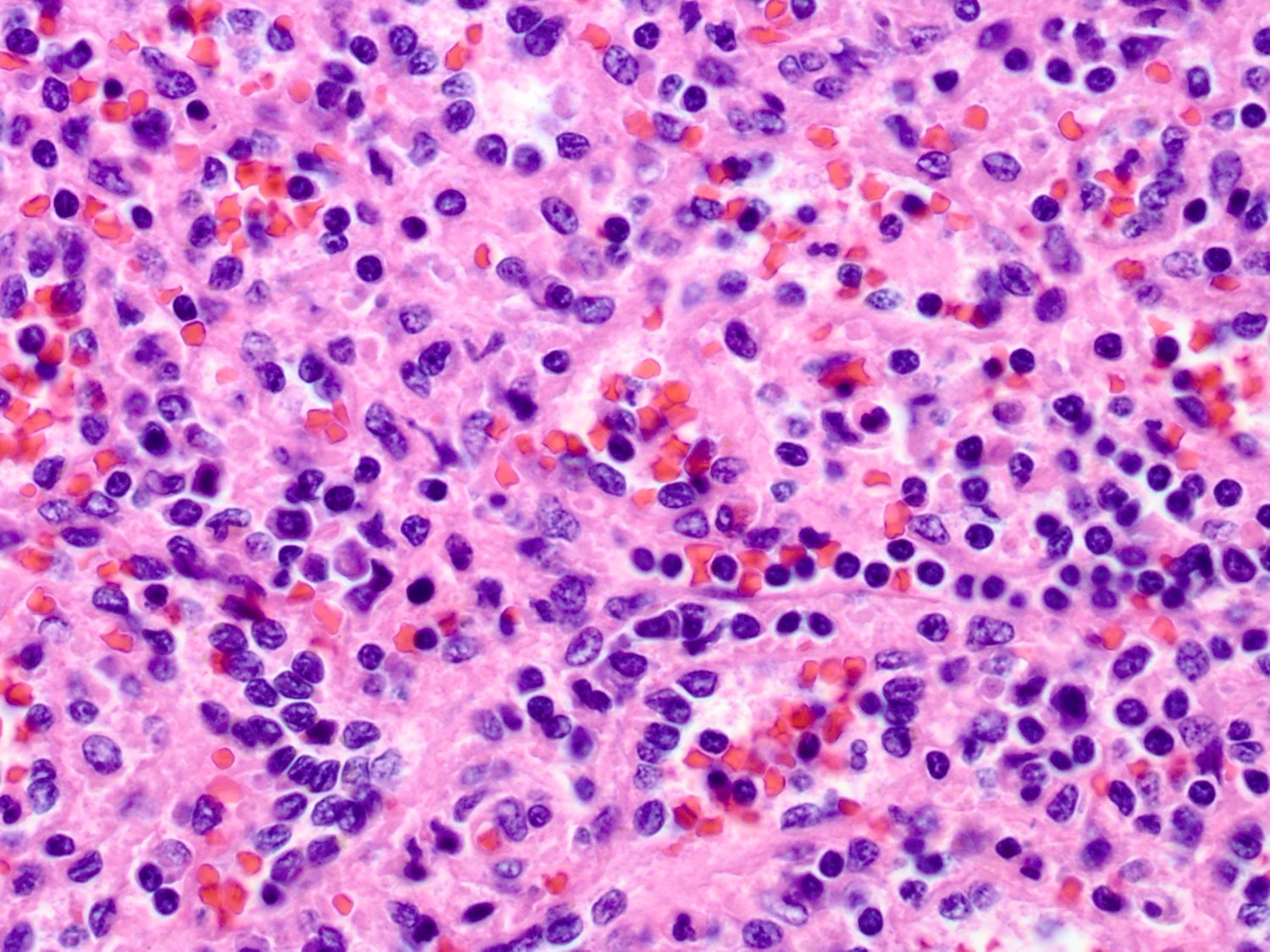
Cordal macrophages, phagocytosing platelets
Sample pathology report
- ITP is a clinical diagnosis of exclusion, typically not based primarily on a pathology specimen.
Differential diagnosis
- ITP is a diagnosis of exclusion; an isolated thrombocytopenia is present (peripheral blood platelet count < 100 × 109/L) without anemia or leukopenia and without another apparent cause of thrombocytopenia such as:
- Drug induced thrombocytopenia, including heparin induced thrombocytopenia
- Infections
- Liver disease
and hypersplenism - Microangiopathic processes
- Hereditary thrombocytopenia
- Myelodysplastic syndromes and other acquired bone marrow disorders
Board review style question #1
A previously healthy 38 year old woman comes to the physician because of petechiae and bruising on her arms and legs for 3 weeks. CBC shows a platelet count of 15 × 109/L as the sole abnormality. What should be the next step for the physician?
- A bone marrow aspirate should be conducted to investigate megakaryocytes for confirmation of diagnosis of ITP
- Other causes of thrombocytopenia should be excluded first to confirm the diagnosis of ITP
- Patient should be started on corticosteroids for treatment of ITP
- Patient should be tested for the presence of antiplatelet autoantibodies to confirm the diagnosis of ITP
Board review style answer #1
B. Other causes of thrombocytopenia should be ruled out first, which includes hereditary platelet disorders, HIV and hepatitis C virus infection.
Bone marrow investigation is not required in cases of typical presentation. It could be supportive as in some ITP patients a shift towards younger megakaryocytes with lesser degrees of nuclear polyploidy and less evidence of platelet production may be seen (answer A). Before considering any treatments for ITP, the diagnosis of ITP should be confirmed first. ITP is a diagnosis of exclusion. An isolated thrombocytopenia should be present (peripheral blood platelet count < 100 × 109/L) without anemia or leukopenia and without another apparent cause of thrombocytopenia (answer C). The presence of antiplatelet autoantibodies could be supportive but is not required for the diagnosis of ITP. These autoantibodies are also not always detectable (answer D).
Comment Here
Reference: Immune thrombocytopenia
Bone marrow investigation is not required in cases of typical presentation. It could be supportive as in some ITP patients a shift towards younger megakaryocytes with lesser degrees of nuclear polyploidy and less evidence of platelet production may be seen (answer A). Before considering any treatments for ITP, the diagnosis of ITP should be confirmed first. ITP is a diagnosis of exclusion. An isolated thrombocytopenia should be present (peripheral blood platelet count < 100 × 109/L) without anemia or leukopenia and without another apparent cause of thrombocytopenia (answer C). The presence of antiplatelet autoantibodies could be supportive but is not required for the diagnosis of ITP. These autoantibodies are also not always detectable (answer D).
Comment Here
Reference: Immune thrombocytopenia
Board review style question #2
Which of the following is true regarding the bleeding disorder ITP?
- Certain drugs can trigger the onset of ITP
- Cytotoxic CD8+ T cells may play a pathogenetic role in platelet breakdown
- Platelet breakdown occurs predominantly in the bone marrow
- CD4+ CD25+ FOXP3+ T regulatory cells levels are increased in number and function in active disease
Board review style answer #2
B. Not only antiplatelet autoantibodies but also cytotoxic CD8+ T cells can be responsible for the platelet destruction.
When drugs trigger the onset of ITP, the diagnosis is drug induced thrombocytopenia, which should always be considered in the differential diagnosis of ITP (answer A). While the spleen is the primary site for platelet destruction, platelet clearance can also occur in liver, bone marrow or lymph nodes. ITP may still (re)occur after splenectomy (answer C). There is an impairment in CD4+ T regulatory cells which leads to the initiation and perpetuation of ITP, so CD4+ CD25+ FOXP3+ T regulatory cells are decreased in number and function in patients with active disease (answer D) (Curr Opin Hematol 2020;27:423).
Comment Here
Reference: Immune thrombocytopenia
When drugs trigger the onset of ITP, the diagnosis is drug induced thrombocytopenia, which should always be considered in the differential diagnosis of ITP (answer A). While the spleen is the primary site for platelet destruction, platelet clearance can also occur in liver, bone marrow or lymph nodes. ITP may still (re)occur after splenectomy (answer C). There is an impairment in CD4+ T regulatory cells which leads to the initiation and perpetuation of ITP, so CD4+ CD25+ FOXP3+ T regulatory cells are decreased in number and function in patients with active disease (answer D) (Curr Opin Hematol 2020;27:423).
Comment Here
Reference: Immune thrombocytopenia
