
Soft tissue
Fibroblastic / myofibroblastic
Superficial CD34+ fibroblastic tumor
Author: Borislav A. Alexiev, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 22 October 2020
Last staff update: 9 November 2021
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Superficial CD34+ fibroblastic tumor pathology review

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Alexiev B. Superficial CD34+ fibroblastic tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuesuperficialcd34fibro.html. Accessed April 2nd, 2025.
Definition / general
- Superficial CD34+ fibroblastic tumor is a distinctive low grade neoplasm of the skin and subcutis, characterized by a fascicular proliferation of spindled cells with abundant, eosinophilic, granular to glassy cytoplasm, marked nuclear pleomorphism and low mitotic count (Mod Pathol 2014;27:294)
- Invariably express CD34 and are focally immunoreactive for keratin in close to 70% of cases (Mod Pathol 2014;27:294, Histopathology 2017;70:394)
Essential features
- Superficial location (Mod Pathol 2014;27:294)
- Spindle cells with eosinophilic granular to glassy cytoplasm
- Nuclear pleomorphism but extremely low mitotic rate (Indian J Pathol Microbiol 2018;61:421)
- Diffuse CD34 expression and frequent keratin (AE1 / AE3) immunoreactivity
Terminology
- PRDM10 rearranged soft tissue tumor
ICD coding
Epidemiology
- Fewer than 40 cases have been reported (Mod Pathol 2014;27:294, Histopathology 2017;70:394)
- Most tumors occurred in middle aged adults (median age 38 years, range 20 - 76 years) with slight male predominance (Mod Pathol 2014;27:294, Histopathology 2017;70:394)
Sites
- Tumor may occur anywhere in the body but most lesions appear on the lower limbs, particularly the thighs (Am J Dermatopathol 2020;42:68, Mod Pathol 2014;27:294, Histopathology 2017;70:394)
Etiology
- Unknown at this time
Clinical features
- Tumor typically presents as a slowly enlarging, firm, painless mass of the superficial soft tissue (J Dermatol 2016;43:934, Indian J Pathol Microbiol 2018;61:421)
Diagnosis
- Tissue sampling with microscopic examination is the gold standard for a definitive diagnosis
Radiology description
- Well marginated tumor without calcification in the subcutaneous adipose tissue on CT / MRI scans (Oncol Lett 2017;14:3395)
- Tumor demonstrates abnormal uptake on 2-(18F) fluoro-2-deoxy-D-glucose (18F-FDG) (PET) (Oncol Lett 2017;14:3395)
Radiology images
Contributed by Borislav Alexiev, M.D.

CT scan
Prognostic factors
- Indolent clinical behavior (Histopathology 2017;70:394)
- Majority of patients have no disease recurrence (Mod Pathol 2014;27:294)
- One patient had regional lymph node metastases 7 years after incomplete excision of the primary tumor (Mod Pathol 2014;27:294)
Case reports
- 18 year old man with a painless mass in the medial aspect of his right distal thigh (Oncol Lett 2017;14:3395)
- 48 year old man presented with a gradually increasing soft tissue mass in his right forearm of 2 years' duration (Indian J Pathol Microbiol 2018;61:421)
- 48 year old woman presented with a painless, slow growing, brown nodule on the left thigh (J Dermatol 2016;43:934)
- 50 year old woman presented with a four month history of a slowly enlarging, firm, painless mass at the medial aspect of her right knee below unremarkable overlying skin (Diagn Cytopathol 2016;44:926)
- 55 year old woman with a slowly enlarging mass on the ventral antebrachium (Dermatol Surg 2017;43:1489)
- 75 year old woman with no significant medical history presented with a firm erythematous asymptomatic nodule on the left posterior thigh (Dermatol Surg 2018;44:313)
Treatment
Clinical images
Images hosted on other servers:

Thigh mass
Gross description
- Firm, yellow to tan soft tissue masses with a variably gelatinous appearance (Mod Pathol 2014;27:294)
- Tumors range in size from 1 - 10 cm (Mod Pathol 2014;27:294)
Gross images
Contributed by Borislav Alexiev, M.D.
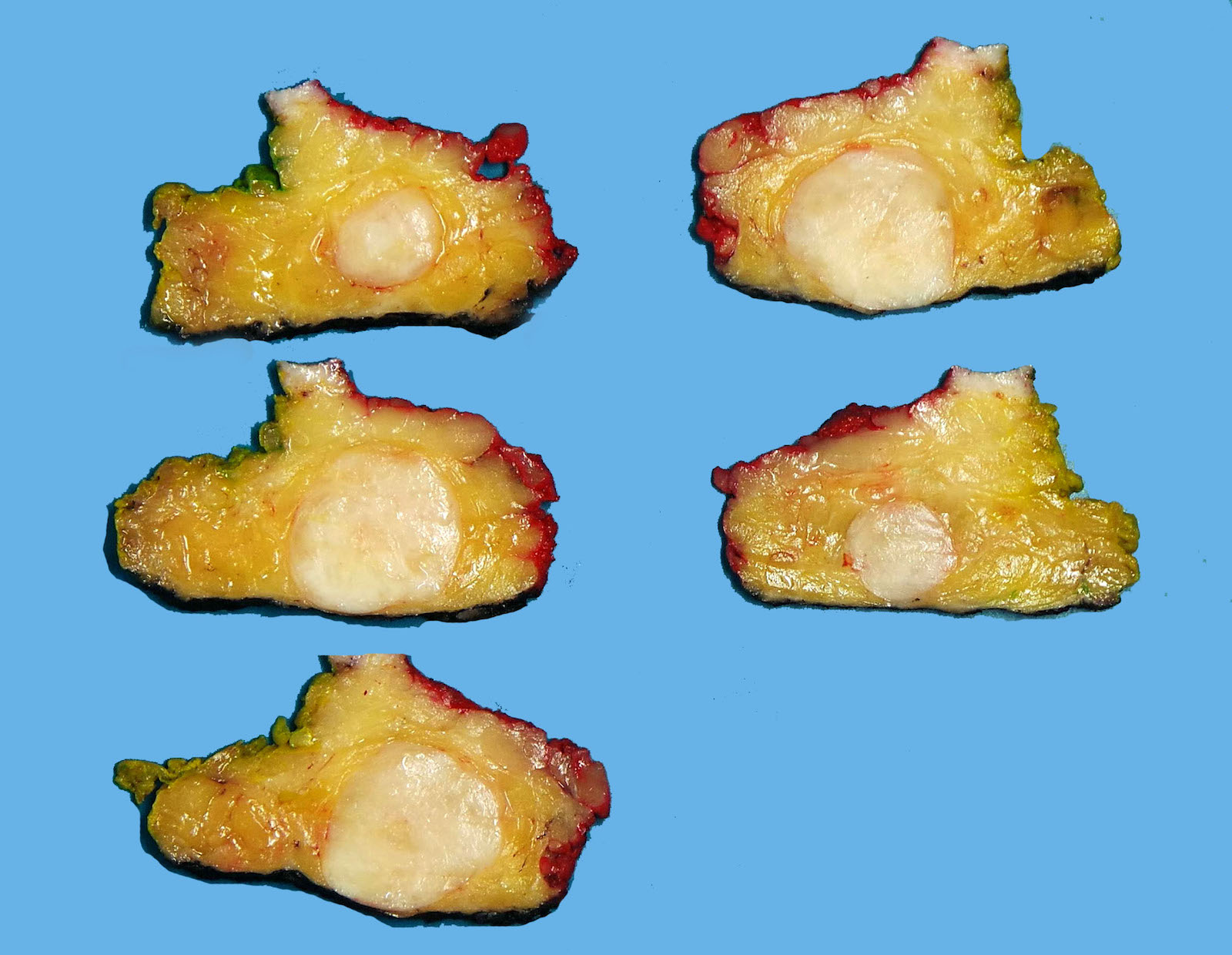
Soft tissue mass
Frozen section description
- Low grade spindle cell neoplasm with pleomorphism and low mitotic activity (Am J Dermatopathol 2020;42:68, Int J Clin Exp Pathol 2020;13:38)
Microscopic (histologic) description
- Tumor involving dermis and subcutaneous fat (Indian J Pathol Microbiol 2018;61:421)
- Generally circumscribed growth (Mod Pathol 2014;27:294)
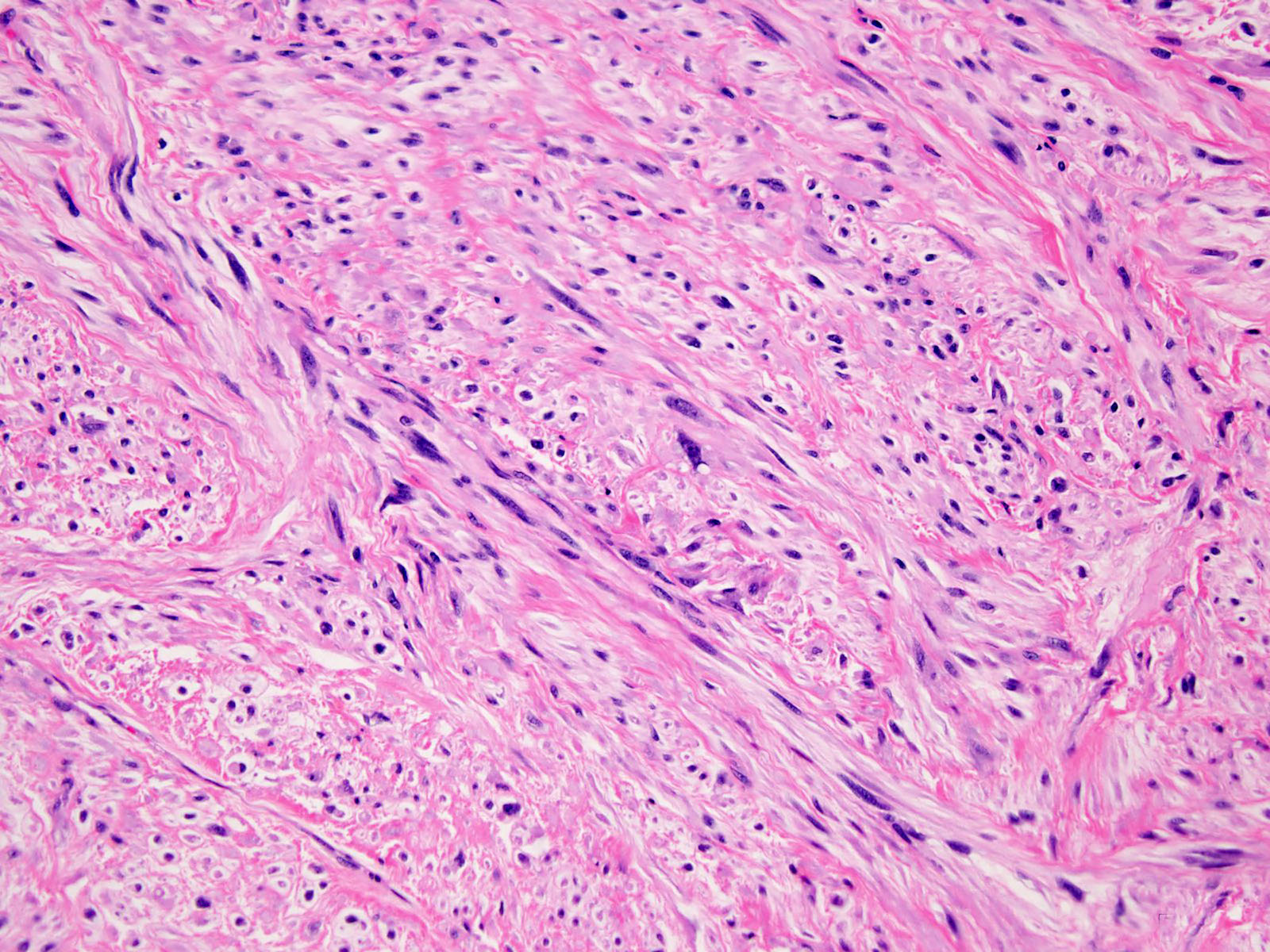
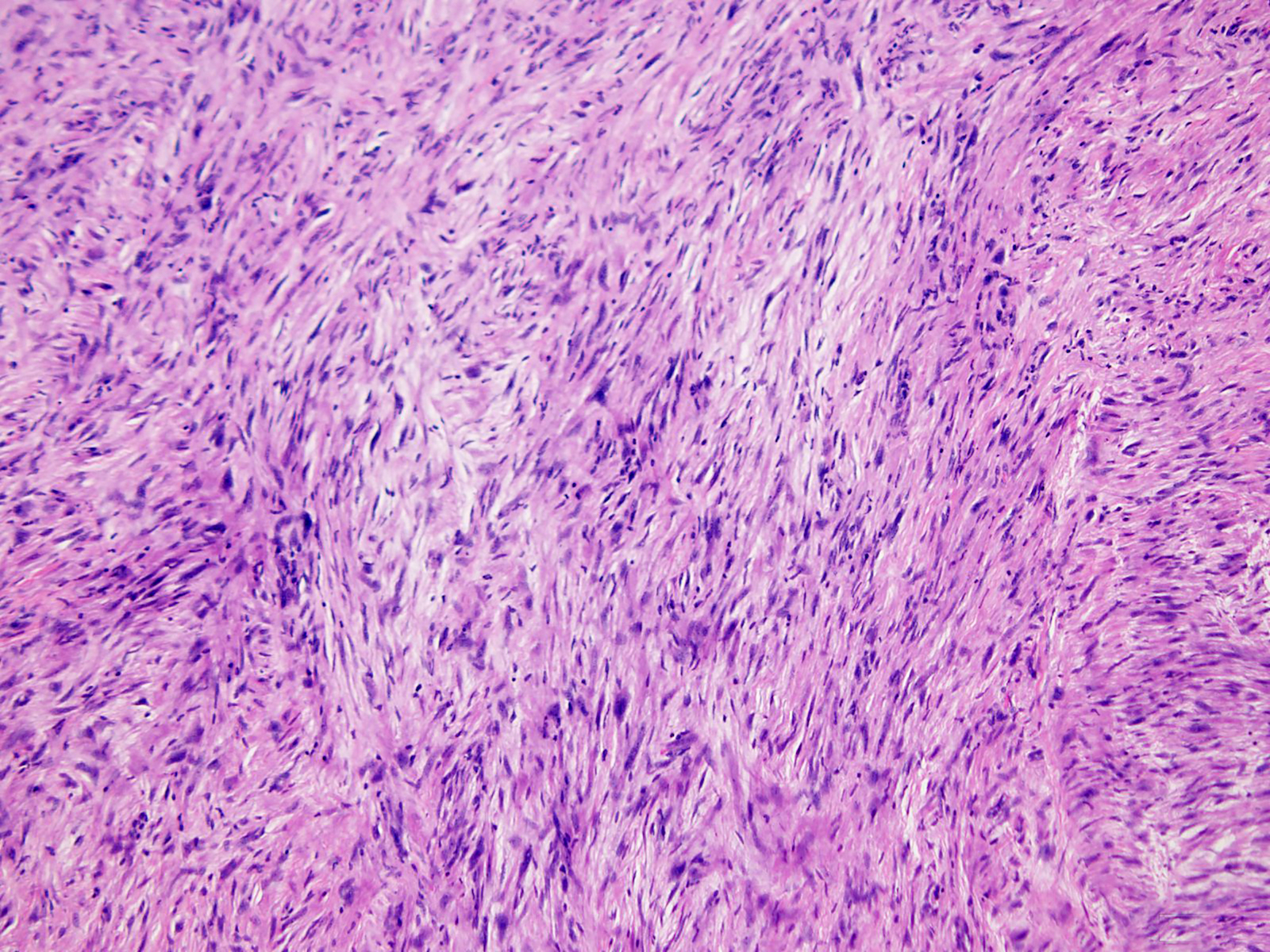
- Fascicles or sheets of epithelioid to spindle cells with abundant granular or glassy eosinophilic cytoplasm (Am J Dermatopathol 2020;42:68)
- Pleomorphic, hyperchromatic nuclei
- Intranuclear cytoplasmic pseudoinclusions (Int J Clin Exp Pathol 2020;13:38)
- Variably prominent nucleoli (Mod Pathol 2014;27:294, Indian J Pathol Microbiol 2018;61:421)
- Xanthomatous change in a subpopulation of tumor cells (Mod Pathol 2014;27:294)
- Extremely low mitotic rate (Am J Dermatopathol 2020;42:68, Int J Clin Exp Pathol 2020;13:38)
- Necrosis is uncommon (Mod Pathol 2014;27:294)
- Mixed chronic inflammatory infiltrate of lymphocytes, plasma cells, mast cells and often eosinophils (Mod Pathol 2014;27:294, Am J Surg Pathol 2019;43:504, Indian J Pathol Microbiol 2018;61:421)
- Arborizing capillary sized vasculature is frequently present (Mod Pathol 2014;27:294)
Microscopic (histologic) images
Contributed by Borislav Alexiev, M.D.
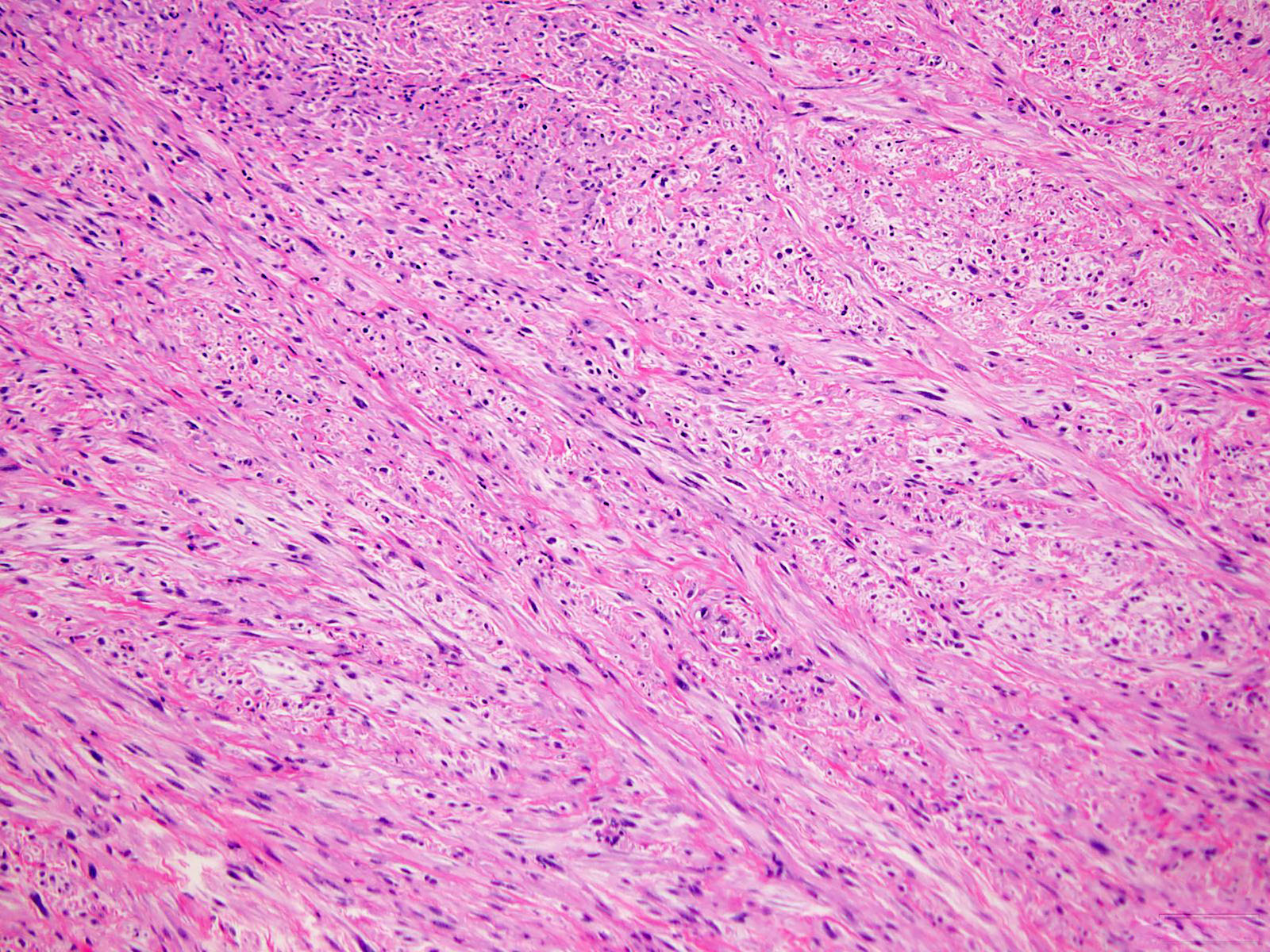
Spindle cells

Chronic inflammation
Fascicular growth pattern
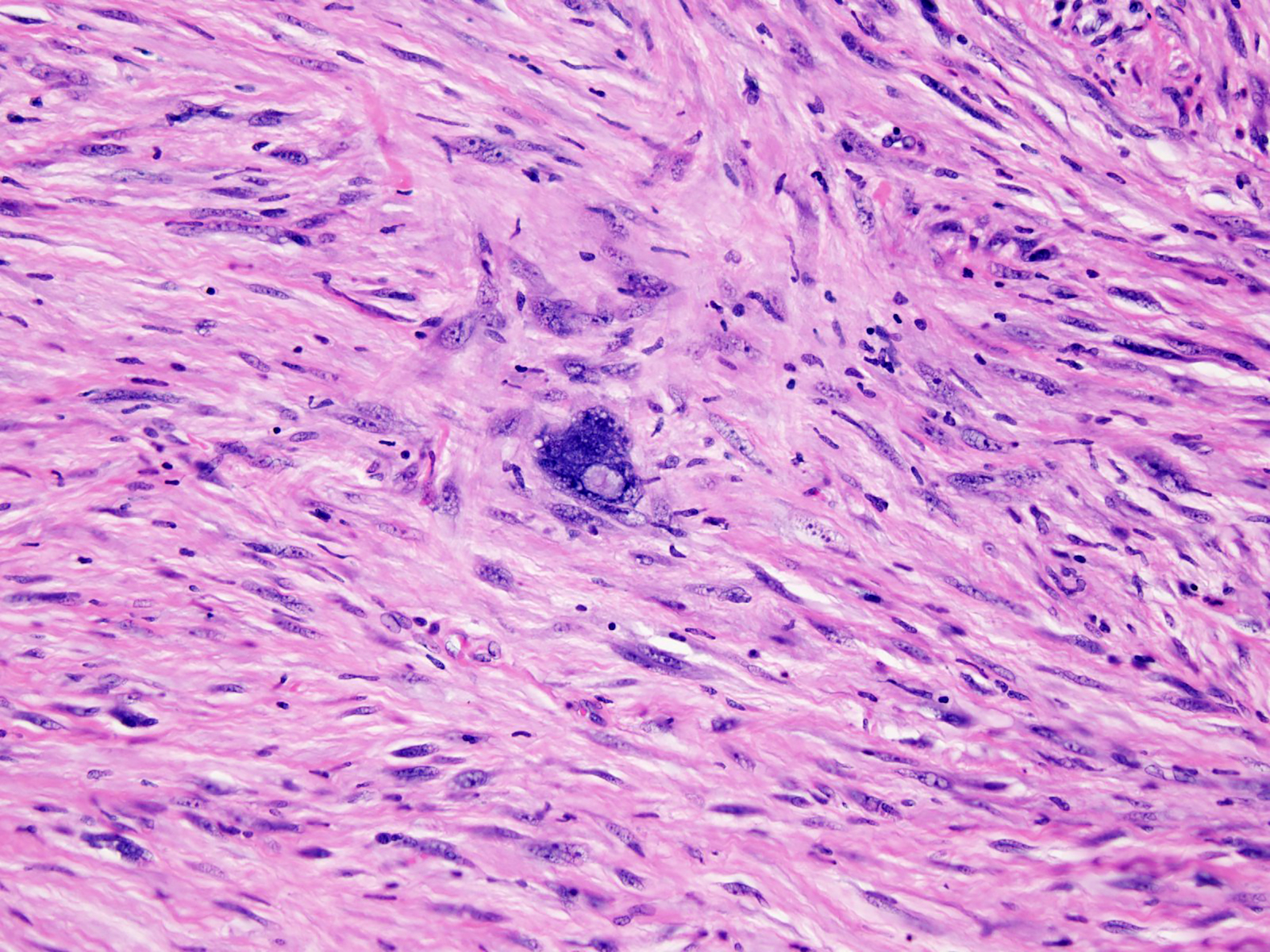
Pleomorphic nuclei
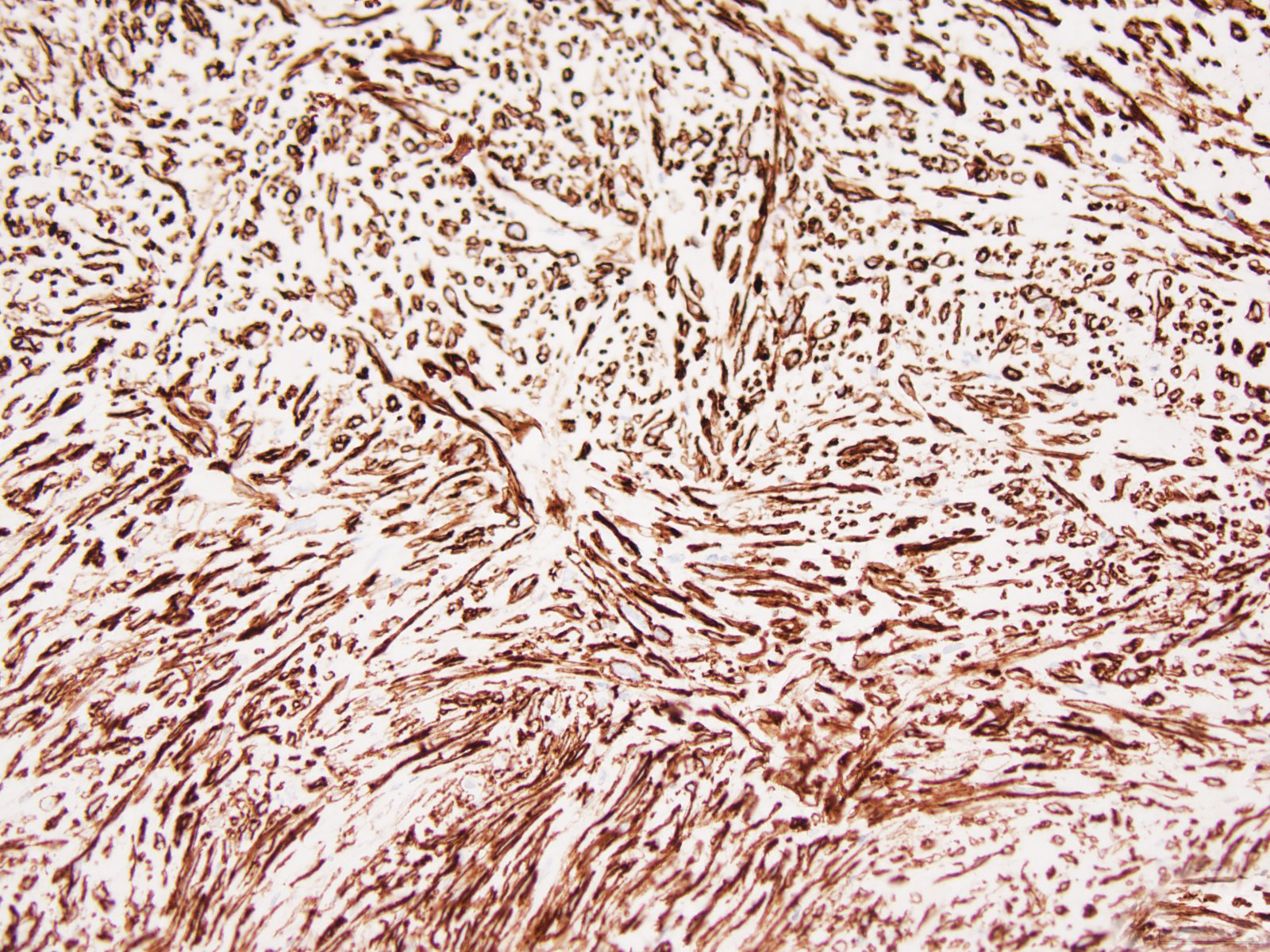
CD34
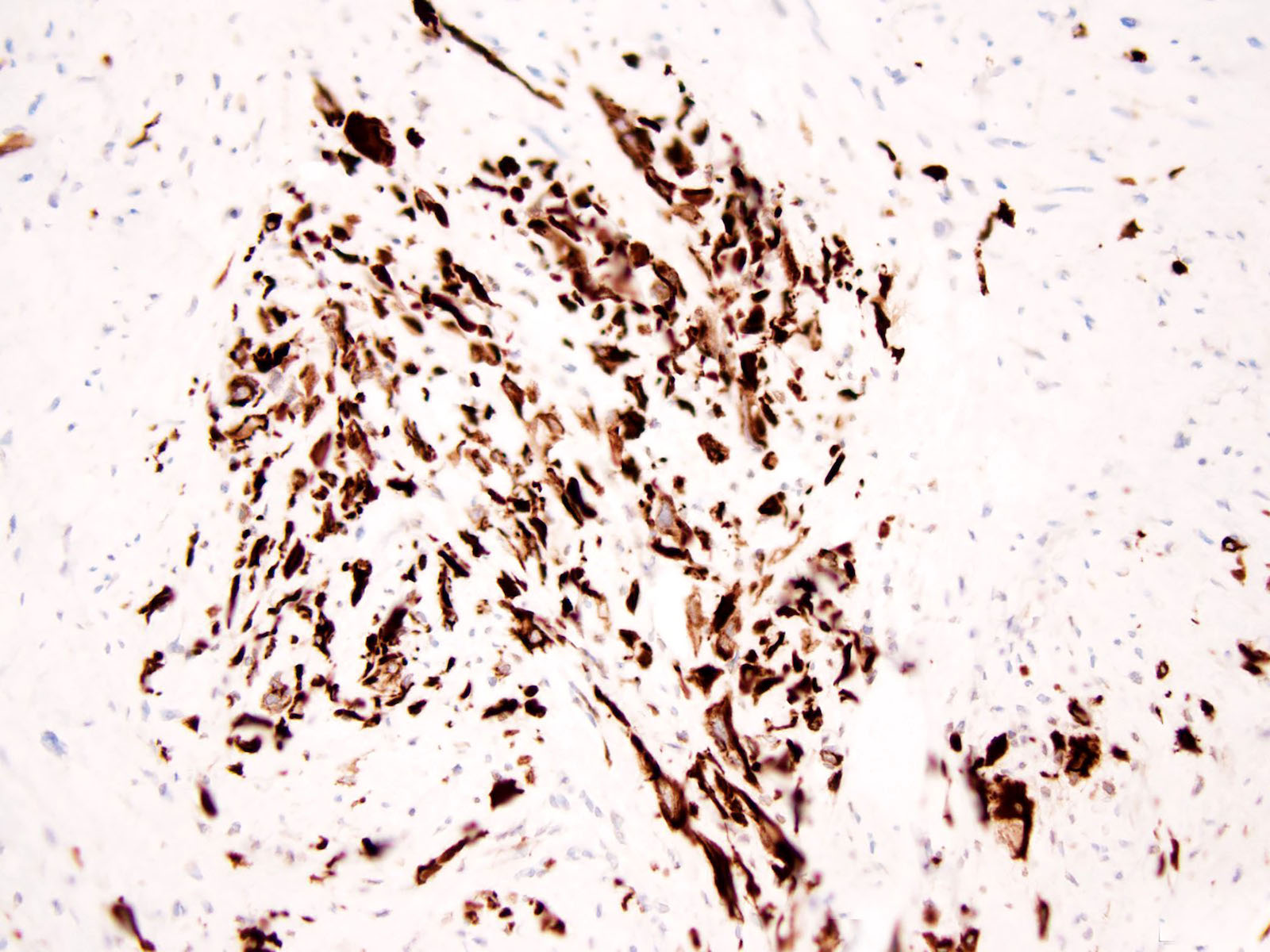
AE1 / AE3
Cytology description
- Cellular specimen composed of mostly spindle cells, arranged singly and in clusters in the background of fragments of collagenized stroma (Diagn Cytopathol 2016;44:926)
- Numerous spindle cells with tapered nuclei and elongated cytoplasmic processes admixed with scattered large pleomorphic cells with enlarged plump nuclei, irregular nuclear contours and bizarre shapes (Diagn Cytopathol 2016;44:926)
Positive stains
- CD34 (Mod Pathol 2014;27:294, Histopathology 2017;70:394, Am J Dermatopathol 2020;42:68)
- Cytokeratin, at least focal (Mod Pathol 2014;27:294, Am J Dermatopathol 2020;42:68)
- PRDM10 nuclear positivity (Am J Surg Pathol 2019;43:504)
- INI1 / SMARCB1 expression retained (Mod Pathol 2014;27:294)
Negative stains
- Desmin (Mod Pathol 2014;27:294)
- Alpha smooth muscle actin (Mod Pathol 2014;27:294)
- S100 (Mod Pathol 2014;27:294)
- ERG (Mod Pathol 2014;27:294)
- FLI1 (Mod Pathol 2014;27:294)
- CD99 (Int J Clin Exp Pathol 2020;13:38)
- ALK1 (Int J Clin Exp Pathol 2020;13:38)
- BCL2 (Int J Clin Exp Pathol 2020;13:38)
- p53 (Mod Pathol 2014;27:294)
Electron microscopy description
- Spindle to oval shaped cells without intercellular junctions (Oncol Lett 2017;14:3395)
- Irregular or convoluted nuclei with abundant euchromatin prominent nucleoli (Oncol Lett 2017;14:3395)
- Abundant rough endoplasmic reticulum, mitochondria, lysosomes, ribosomal aggregates and aggregated lipid globules (Oncol Lett 2017;14:3395)
Electron microscopy images
Images hosted on other servers:

Lipid globules
Molecular / cytogenetics description
- PRDM10 rearrangements in 3 of 7 tumors (Am J Surg Pathol 2019;43:504)
- t(2;5)(q31;q31) translocation in 1 tumor (Am J Surg Pathol 2019;43:504, Oncol Lett 2017;14:3395)
- Negative fluorescence in situ hybridization studies for TGFBR3 or MGEA5 (Mod Pathol 2014;27:294)
Molecular / cytogenetics images
Images hosted on other servers:

t(2;5)
Sample pathology report
- Thigh, mass, excision:
- Superficial CD34+ fibroblastic tumor (see comment)
- Comment: Microscopic sections show a circumscribed tumor in the dermis and subcutaneous fat composed of spindle cells containing moderate to abundant glassy eosinophilic cytoplasm, vesicular nuclei with distinct nucleoli and intranuclear pseudoinclusions, along with interspersed pleomorphic giant cells. Tumor cells are arranged in fascicular or sheet-like patterns. Neither necrosis nor mitotic activity is identified. Also present is a chronic inflammatory infiltrate of lymphocytes, plasma cells, mast cells and eosinophils.
- Immunohistochemically, neoplastic cells show diffuse and strong expression of CD34 and focal staining of cytokeratin while are negative for myogenin, S100 and STAT6. INI1 is preserved. Fluorescence in situ hybridization studies for TGFBR3 and MGEA5 are negative.
- This constellation of morphological, immunohistochemical and molecular features strongly supports the diagnosis of superficial CD34+ fibroblastic tumor. It is a distinctive low grade neoplasm of the skin and subcutis. The majority of patients have no disease recurrence.
Differential diagnosis
- Myxoinflammatory fibroblastic sarcoma:
- Multilobulated architecture with prominent paucicellular myxoid zones (Am J Dermatopathol 2020;42:68)
- Increased mitotic activity or atypical mitotic figures (Am J Surg Pathol 2014;38:1)
- t(1;10)(p22;q24) TGFBR3 / MGEA5 translocation (Arch Pathol Lab Med 2019;143:212)
- D2-40 (86%), CD34 (50%), keratin(s) (33%) (Am J Surg Pathol 2014;38:1)
- Myxofibrosarcoma:
- Myxoid multinodular growth pattern
- Curvilinear thin walled blood vessels
- Perivascular tumor cell condensation
- Increased mitotic activity (Am J Dermatopathol 2020;42:68)
- CD34 focally expressed (Mod Pathol 2017;30:1698)
- Lack of expression for cytokeratin (Mod Pathol 2017;30:1698)
- Dermatofibrosarcoma protuberans:
- Cytologically bland, lacking pleomorphism (Mod Pathol 2014;27:294)
- Several variants: pigmented (Bednar tumor), myxoid, myoid, granular cell, sclerotic, atrophic, giant cell fibroblastoma and DFSP with fibrosarcomatous areas (Semin Diagn Pathol 2013;30:13)
- Loss of CD34 expression in fibrosarcomatous areas (Mod Pathol 2014;27:294)
- Lack of expression for cytokeratin (Oncol Lett 2016;11:661)
- Specific translocation t(17;22)(q22;q13) with COL1A1-PDGFB fusion transcripts (Ann Diagn Pathol 2016;25:64)
- Undifferentiated pleomorphic sarcoma:
- Great majority occur in subfascial location (Mod Pathol 2014;27:294)
- Typically a high grade lesion (Clin Cancer Res 2015;21:864)
- No identifiable line of differentiation
- High mitotic rate (Am J Dermatopathol 2020;42:68)
- Necrosis is common
- Lacks diffuse CD34 expression (Mod Pathol 2014;27:294)
- Epithelioid sarcoma:
- Granuloma-like pattern, conventional type (Am J Surg Pathol 1997;21:130, Cancer 1970;26:1029)
- Rhabdoid features, marked cytologic atypia, proximal type (Am J Surg Pathol 1997;21:130)
- High mitotic rate (Am J Surg Pathol 1997;21:130)
- Necrosis is common
- Loss of INI1 / SMARCB1 expression (Adv Anat Pathol 2016;23:41)
- Pleomorphic hyalinizing angiectatic tumor:
- Hemosiderin rich spindle cell proliferation (Am J Surg Pathol 2004;28:1417)
- Ecstatic blood vessels surrounded by perivascular hyaline material (Am J Surg Pathol 1996;20:21)
- Lacks keratin expression (Mod Pathol 2014;27:294)
- t(1;10)(p22;q24) TGFBR3 / MGEA5 translocation (Arch Pathol Lab Med 2019;143:212)
- Malignant granular cell tumor:
- Mitotic figures and tumor necrosis (Case Rep Pathol 2019;2019:9576487)
- S100+ (Am J Dermatopathol 2020;42:68)
- CD68+ (Case Rep Pathol 2019;2019:9576487)
- TFE3+ (Hum Pathol 2014;45:1039)
- Lacks CD34 and keratin expression (Mod Pathol 2014;27:294, Case Rep Pathol 2019;2019:9576487)
- Solitary fibrous tumor:
- Irregular fascicles of spindled cells, staghorn-like blood vessels and variable amounts of collagen (Am J Surg Pathol 2018;42:778)
- CD99 and BCL2+ (J Dermatol 2019;46:267)
- STAT6+ (Am J Surg Pathol 2018;42:778)
- Keratin expression in dedifferentiated solitary fibrous tumor (Int J Surg Pathol 2018;26:423)
- Low grade fibromyxoid sarcoma:
- Bland spindle cells with small, angulated nuclei and scant, wispy cytoplasm (Ann Diagn Pathol 2017;28:60, Int J Clin Exp Pathol 2018;11:5860)
- Whorled growth pattern with abrupt transition from myxoid to fibrous areas (Ann Diagn Pathol 2017;28:60)
- Giant rosettes may be observed in tumors with variant morphology
- MUC4+ (Ann Diagn Pathol 2017;28:60)
- CD34- (Int J Clin Exp Pathol 2018;11:5860)
- Recurrent (7;16)(q34;p11) translocation, resulting in FUS-CREB3L2 fusion gene (Ann Diagn Pathol 2017;28:60)
Additional references
Board review style question #1
A 29 year old man presented with a left thigh mass. Hematoxylin eosin stains demonstrate a circumscribed tumor in the dermis and subcutaneous fat composed of spindle cells containing moderate to abundant glassy eosinophilic cytoplasm, vesicular nuclei with distinct nucleoli and intranuclear pseudoinclusions, along with interspersed pleomorphic giant cells. Tumor cells are arranged in fascicular or sheet-like patterns. Neither necrosis nor mitotic activity is identified. Immunohistochemical stains for CD34 and keratin AE1 / AE3 are positive in tumor cells while all of the following are negative: MUC4, SMA, Desmin, S100 and STAT6. INI1 is retained. Which of the following is most likely the correct diagnosis?
- Epithelioid sarcoma
- Low grade fibromyxoid sarcoma
- Myxofibrosarcoma
- Solitary fibrous tumor
- Superficial CD34+ fibroblastic tumor
Board review style answer #1
E. Superficial CD34+ fibroblastic tumor
Comment Here
Reference: Superficial CD34+ fibroblastic tumor
Comment Here
Reference: Superficial CD34+ fibroblastic tumor
Board review style question #2
Which of the following is true about superficial CD34+ fibroblastic tumor?
- High recurrence rate
- INI1 / SMARCB1 expression is lost
- Tumor is negative for keratin
- Tumor is positive for TGFBR3 / MGEA5 translocation
- Tumor is positive for PRDM10
Board review style answer #2
