
Soft tissue
Plexiform fibrohistiocytic tumor


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Plexiform fibrohistiocytic tumor

- Uncommon, biphasic dermal or subcutaneous mesenchymal neoplasm
- Variable mixture of fibroblasts and histiocyte-like cells in a plexiform or multinodular arrangement
- Neoplasm involving the dermis or subcutis
- Nodules of histiocytoid cells surrounded by fascicles of myofibroblastic spindle cells
- Plexiform growth pattern
- Osteoclast-like giant cells
- First described in 1988 (Am J Surg Pathol 1988;12:818)
- Abbreviations: plexiform fibrohistiocytic tumor (PFHT)
- Other name(s): plexiform fibrous histiocytoma
- ICD-O: 8835/1 - plexiform fibrohistiocytic tumor
- ICD-11: 2F7C & XH4GL1 - neoplasms of uncertain behavior of connective or other soft tissue & plexiform fibrohistiocytic tumor
- Most common in infants, children and young adults
- Rarely occurs after the age of 30 (Int J Clin Exp Pathol 2016;9:4693)
- F > M (Arch Pathol Lab Med 2007;131:1135, Ann Diagn Pathol 2007;11:313, Am J Surg Pathol 1999;23:662)
- Most common: upper extremity (40 - 50%), usually fingers, hand, wrist
- Other sites: lower extremity (9 - 20%), trunk (8 - 15%), head and neck (7 - 10%) (Case Reports Plast Surg Hand Surg 2021;8:164, Ann Diagn Pathol 2007;11:313, Am J Surg Pathol 1999;23:662, Histopathology 1991;19:503, Am J Surg Pathol 1988;12:818)
- Exact etiology and pathophysiology unknown (Virchows Arch 2022;481:739)
- Preceding trauma reported in a few cases (Arch Pathol Lab Med 2007;131:1135)
- Congenital cases identified in 2 series (Arch Pathol Lab Med 2007;131:1135)
- Unknown
- Small (1 - 3 cm, rarely larger) dermal or subcutaneous mass
- Slow growing, usually asymptomatic
- Overlying skin is usually raised and firm with ill defined borders
- Rarely: central depression, discoloration, ulceration
- Can also occur as a flattened, indurated plaque (less frequently)
- Reference: Case Reports Plast Surg Hand Surg 2021;8:164
- Combined history, physical examination, imaging (ultrasound, MRI) and pathological diagnosis
- Ultrasound: hypoechoic nodule or discrete mass with some vascularity on color Doppler
- MRI: poorly demarcated, infiltrative mass
- Can appear as a plaque-like or infiltrative lesion in the subcutaneous tissues, sometimes without a discrete mass (Skeletal Radiol 2019;48:437)
- Isointense on T1 weighted images, hyperintense on fluid sensitive images and enhancing after gadolinium administration
- Can show contact with or abutment of underlying connective tissues (tendons, muscles, bone)
Images hosted on other servers:

Poorly defined, infiltrative tumor

Plaque-like tumor

Hypoechoic nodule on ultrasound
- No well documented prognostic factors
- Overall prognosis is good after complete excision (J Clin Diagn Res 2022;16:ED01)
- High local recurrence rate after incomplete excision
- Rare cases of lymph node and distant metastasis have been reported (Am J Surg Pathol 1988;12:818, Am J Surg Pathol 1997;21:469, Am J Surg Pathol 1999;23:662)
- Newborn boy with a painful congenital ulcerated plaque on left foot (Pediatr Dermatol 2018;35:e360)
- 4 year old boy with a foot nodule since birth (Case Reports Plast Surg Hand Surg 2021;8:164)
- 9 year old boy with a slow growing, painless mass lesion in the left back region (Case Rep Pathol 2013;2013:547372)
- 12 year old girl with a lesion on the back of her hand (Actas Dermosifiliogr 2022;113:821)
- 23 year old woman with a nodular lesion in vulva (Rev Bras Cancerol 2021;67:e141269)
- 40 year old woman with a central neck mass clinically mimicking a thyroglossal duct cyst (Head Neck Pathol 2020;14:262)
- 45 year old woman with a lesion in the right popliteal fossa; tumor showed myxoid changes (Case Rep Pathol 2017;2017:5370894)
- 46 year old woman with tumor involving frontal region of head with underlying frontal bone invasion (J Clin Diagn Res 2022;16:ED01)
- Complete surgical resection with wider margins to prevent local recurrence
- High local recurrence rate (Arch Pathol Lab Med 2007;131:1135)
- Long term follow up is recommended to detect nodal or pulmonary metastasis
Images hosted on other servers:

Firm nodule on finger

Nodule with infiltrative borders
- White-gray tumor, averaging 1 - 3 cm in size (range: 0.3 - 8.5 cm) (Patterson: Weedon's Skin Pathology, 5th Edition, 2020)
- Firm consistency
Images hosted on other servers:

Globular, firm, white mass
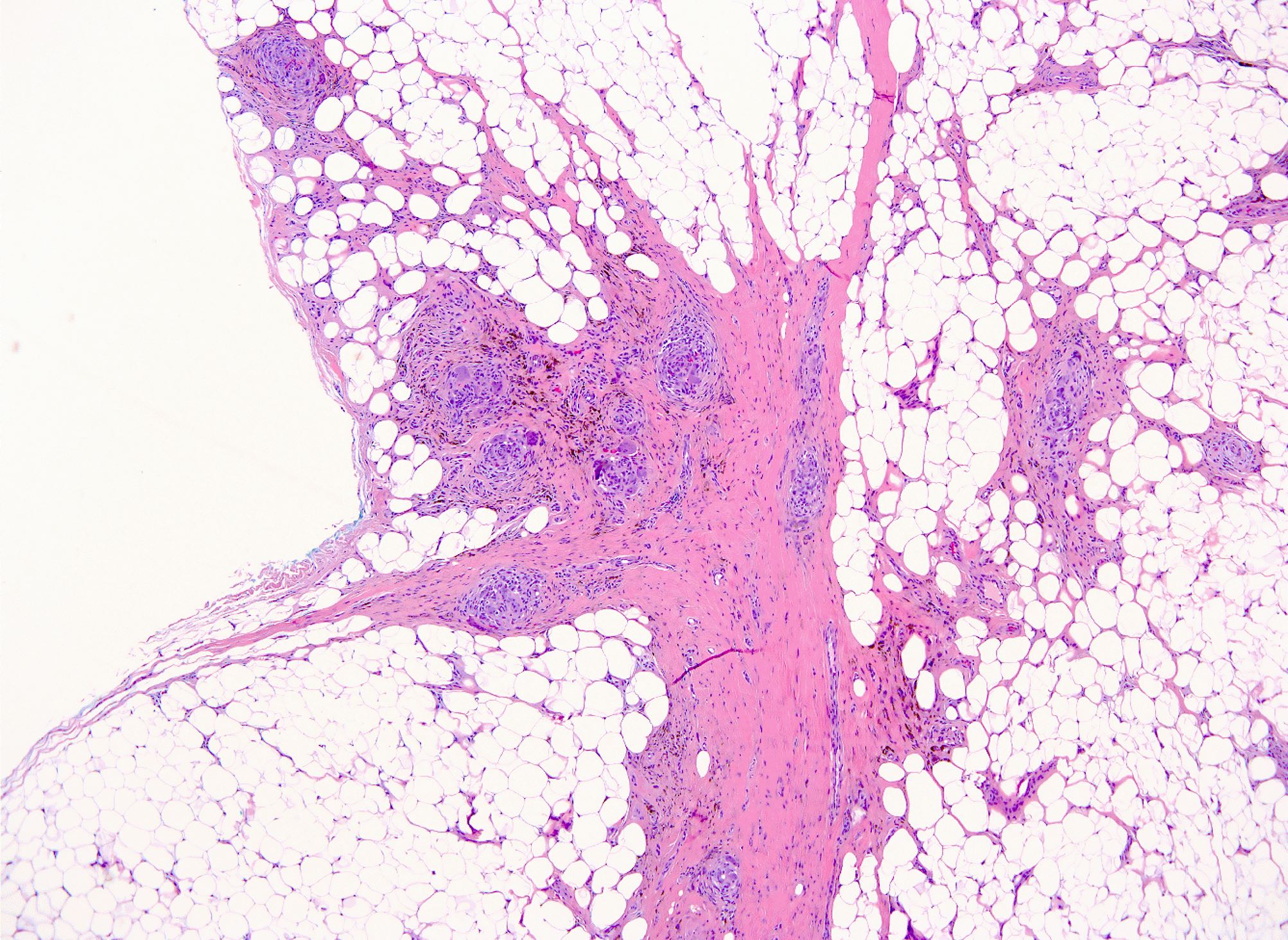
- Centered on dermal / subcutaneous junction
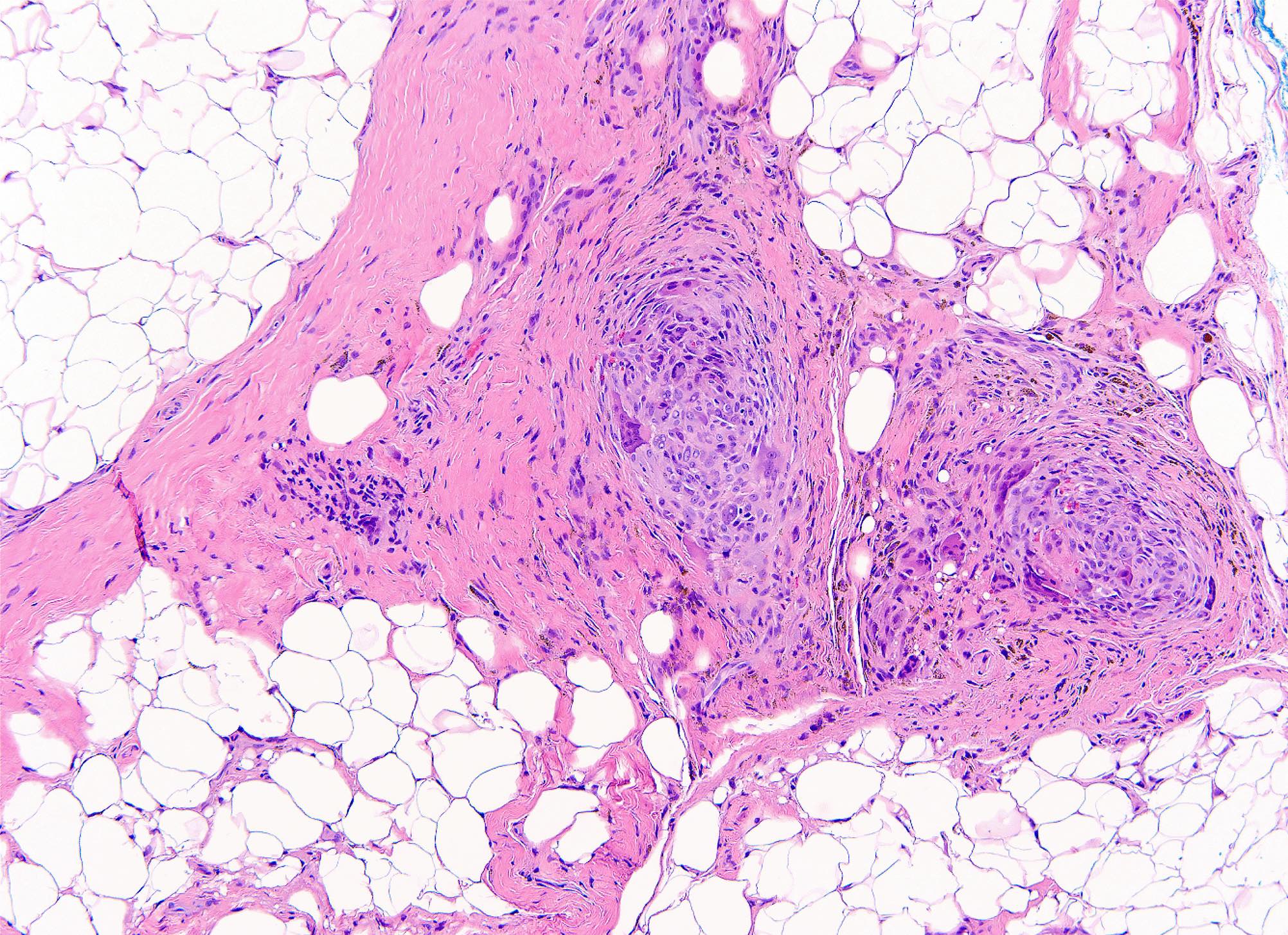
- Multinodular and plexiform architecture, can often be infiltrative
- Normal overlying epidermis (usually)
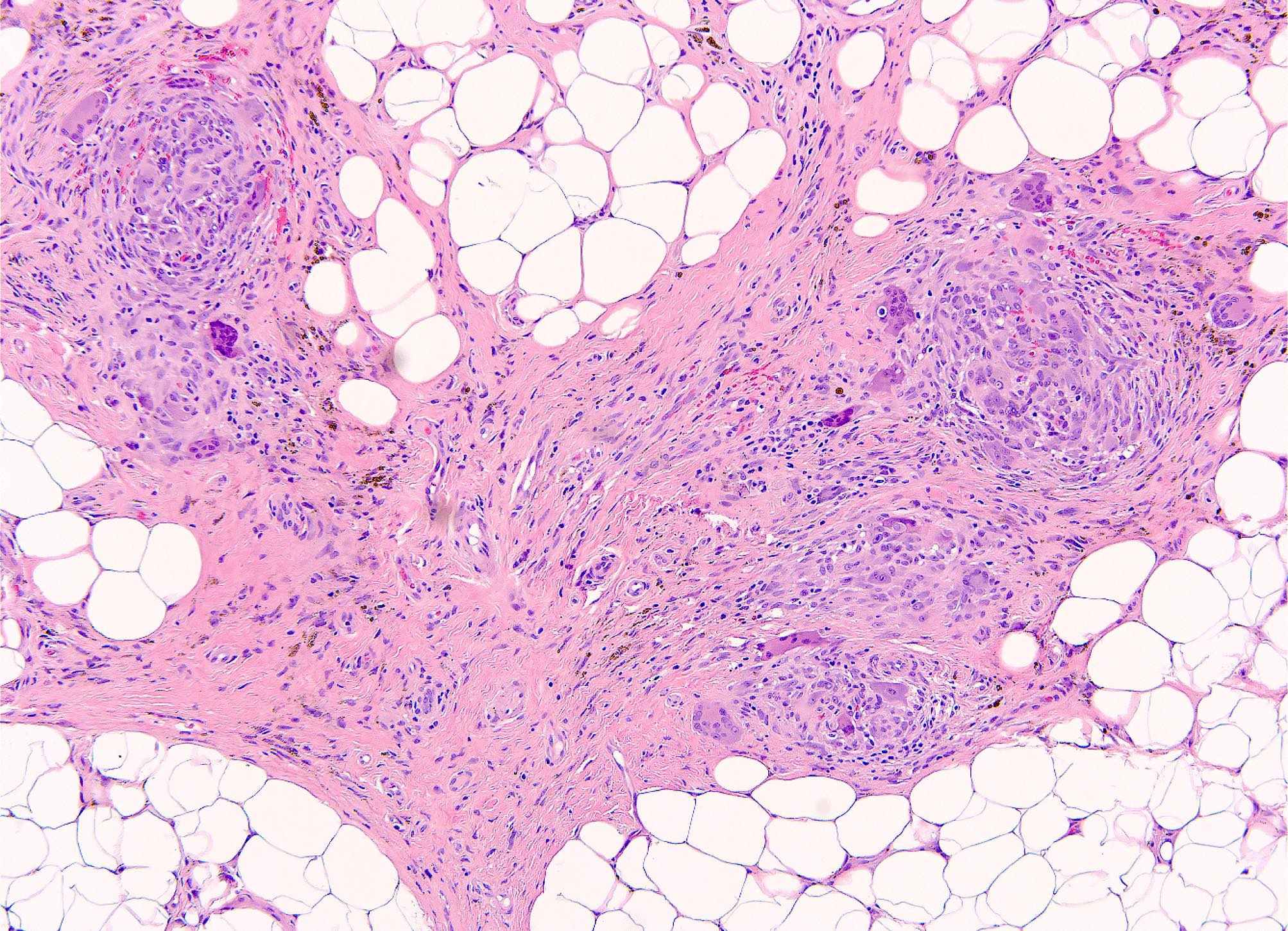
- Mixture of fascicles of spindle cells and nodular aggregates of histiocytoid cells in variable proportion
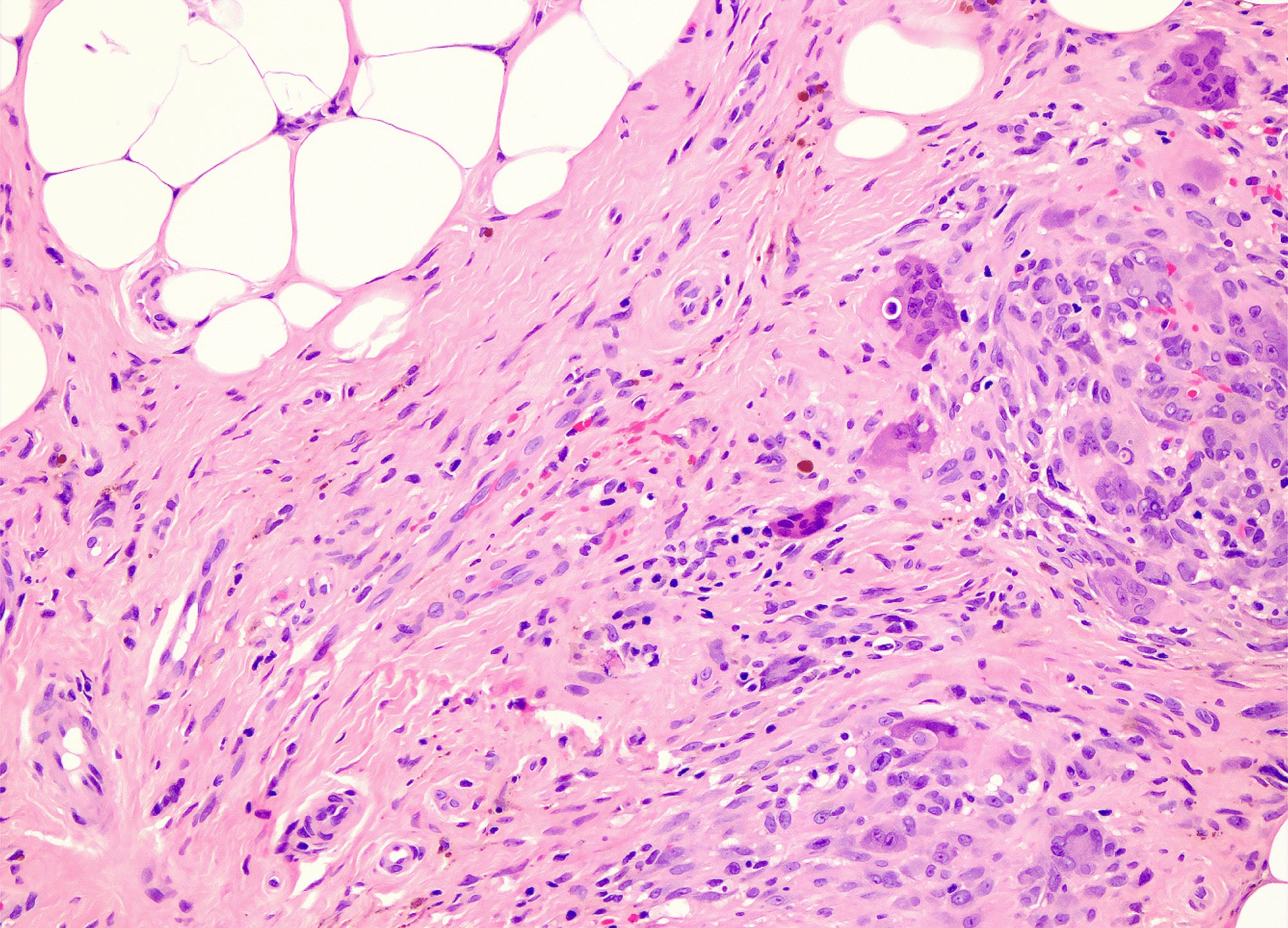
- Fascicles of uniform, eosinophilic (myo)fibroblasts
- Nodules of histiocytoid cells, often with osteoclast-like giant cells
- No atypia or pleomorphism
- Low mitotic count (usually 0 - 2 mitotic figures [MF]/10 high power fields [HPF]), no necrosis
- Stroma can show hyalinization or myxoid change; rarely metaplastic bone formation
- Microhemorrhage and hemosiderin deposition can occur
- Invasion into underlying skeletal muscle can occur
- Vascular invasion in ~20% of cases (Fletcher: Diagnostic Histopathology of Tumors, 5th Edition, 2020)
- Variants: fibroblastic, histiocytic, mixed (Am J Surg Pathol 1999;23:662, Ann Diagn Pathol 2007;11:313)
- Fibroblastic
- Fascicles of spindled (myo)fibroblasts
- Plexiform to infiltrative growth pattern
- Ray-like extensions into subcutaneous tissue
- Chronic inflammation
- Histiocytic
- Mononuclear histiocytoid cells
- Multinodular growth
- Multinucleated osteoclast-like giant cells
- Mixed
- Nodules of histiocytoid cells separated by fascicles of spindle cells
- Fibroblastic
Contributed by Carina Dehner, M.D., Ph.D. and AFIP
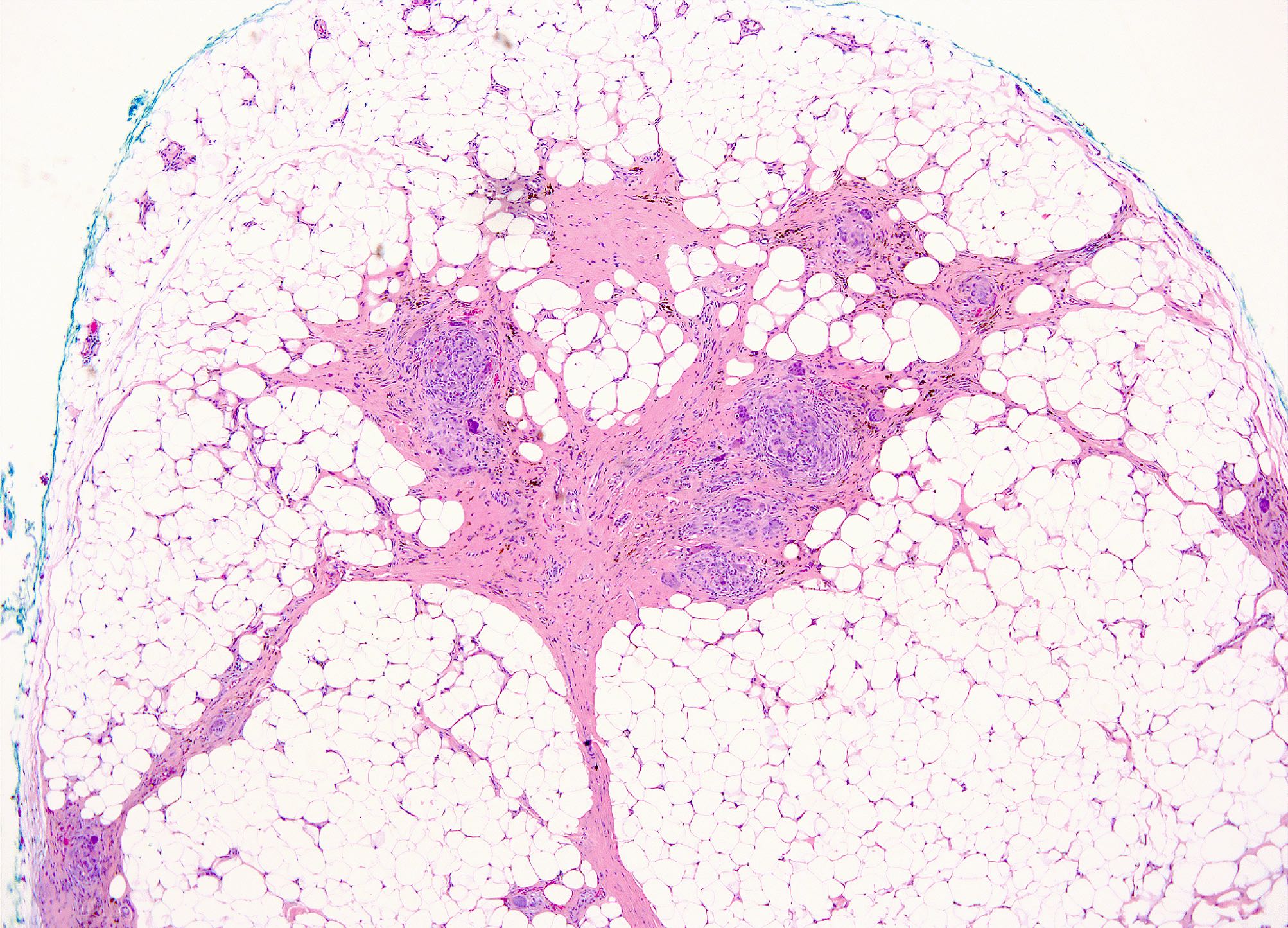
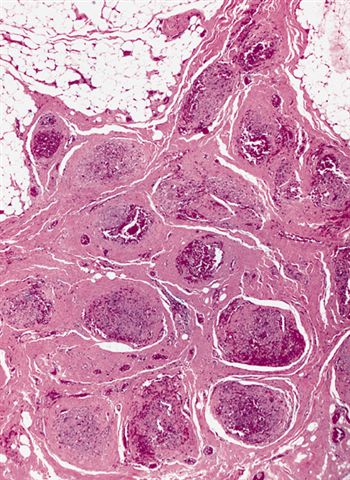
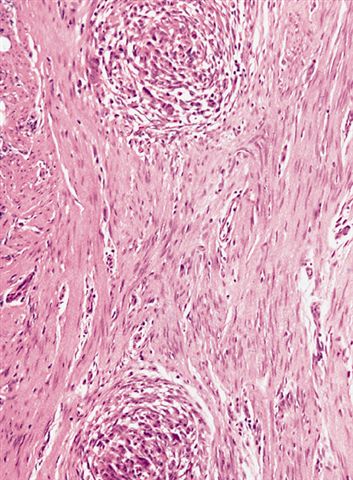
Nodular and plexiform growth
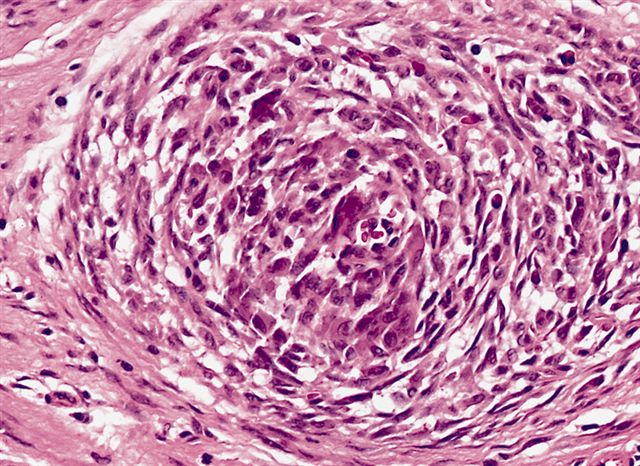
Lack of pleomorphism or mitoses
Subcutaneous mass
Infiltrative growth pattern
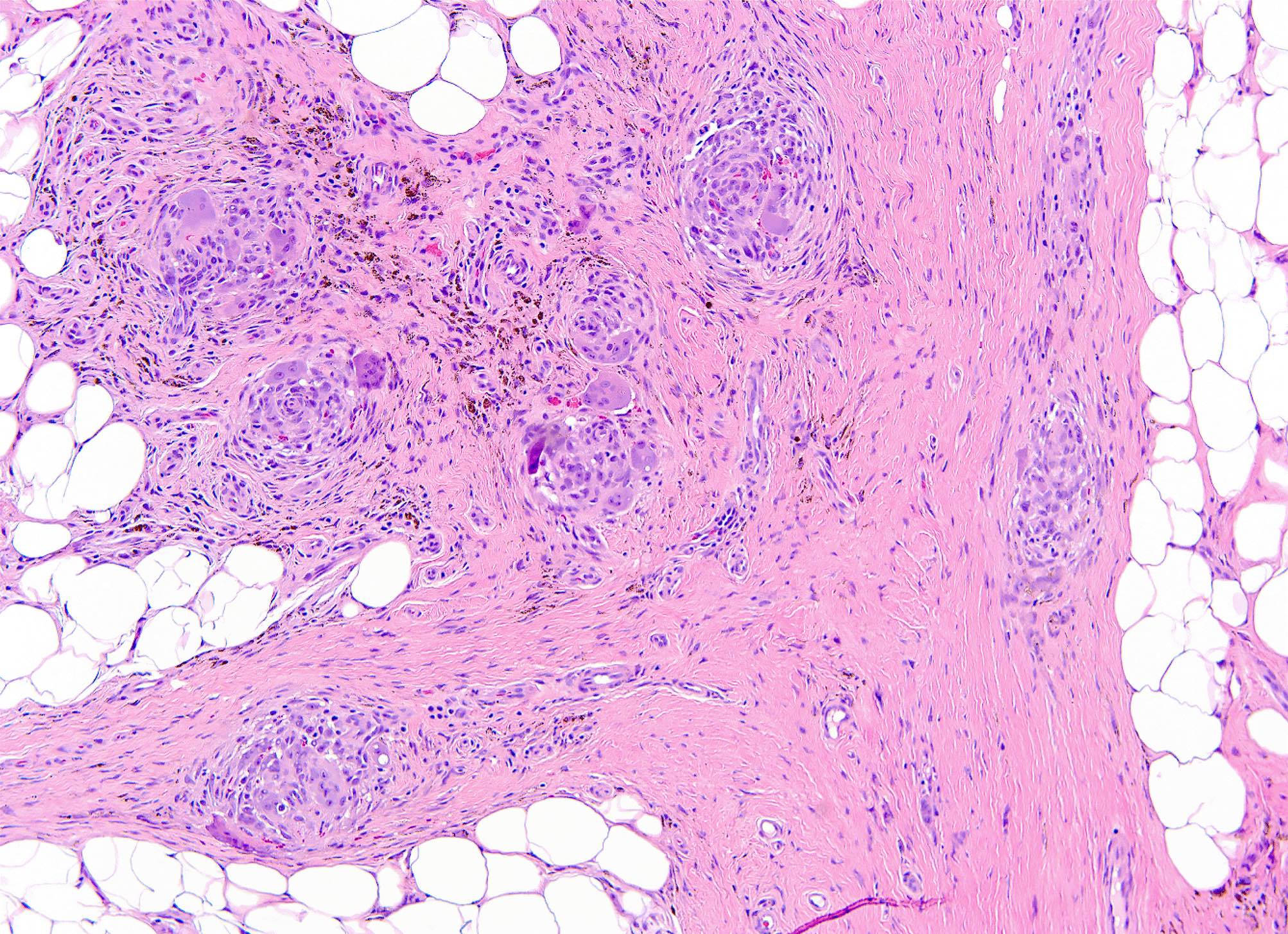
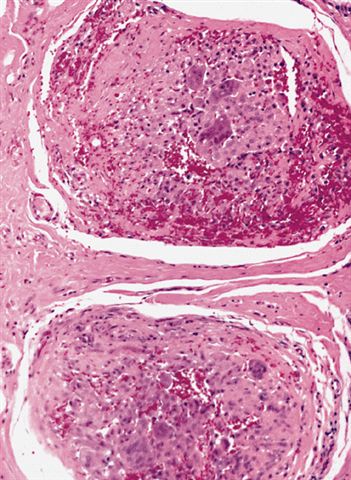
Nodules of histiocytoid cells
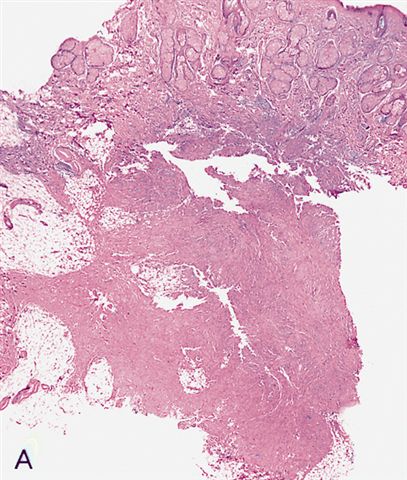
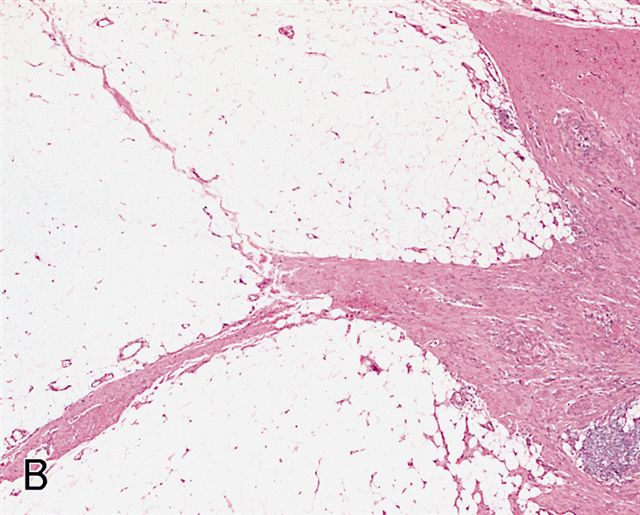
Subcutaneous proliferation of bland fibrous tissue
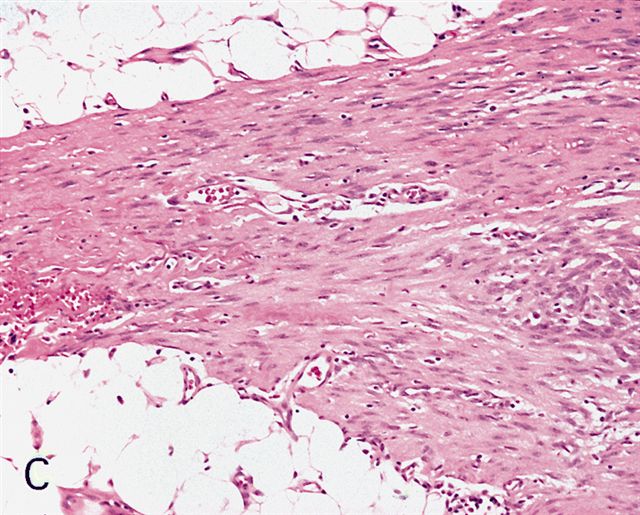
Subcutaneous proliferation of bland fibrous tissue
Nodules of histiocyte-like cells
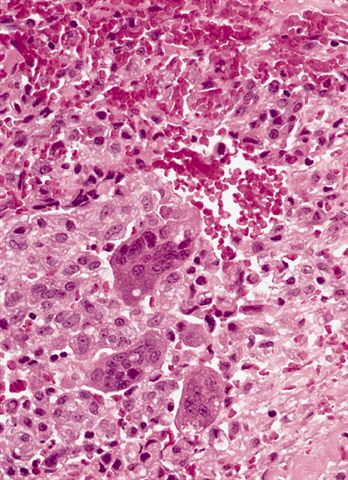
Histiocyte-like cells
Cells with elongated nuclei
Tumor with nodules and fibrous tissue
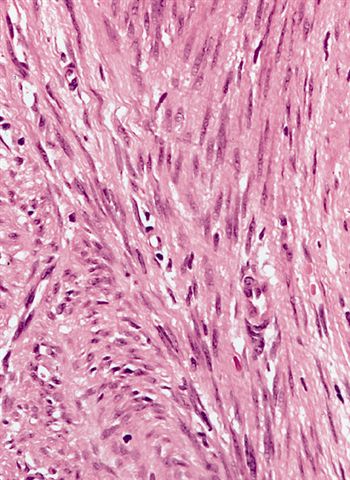
Resemblance to desmoid fibromatosis
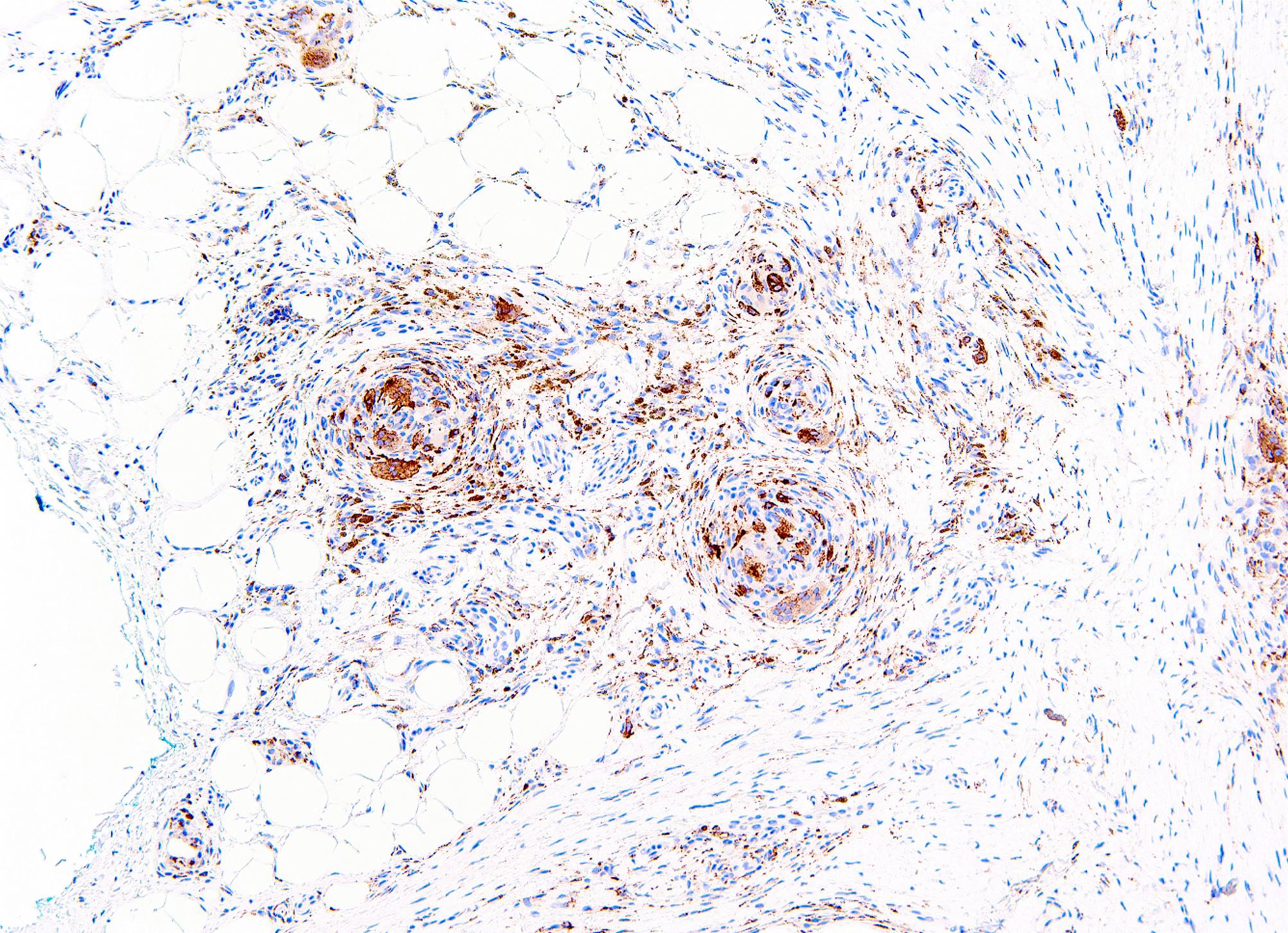
CD68 IHC
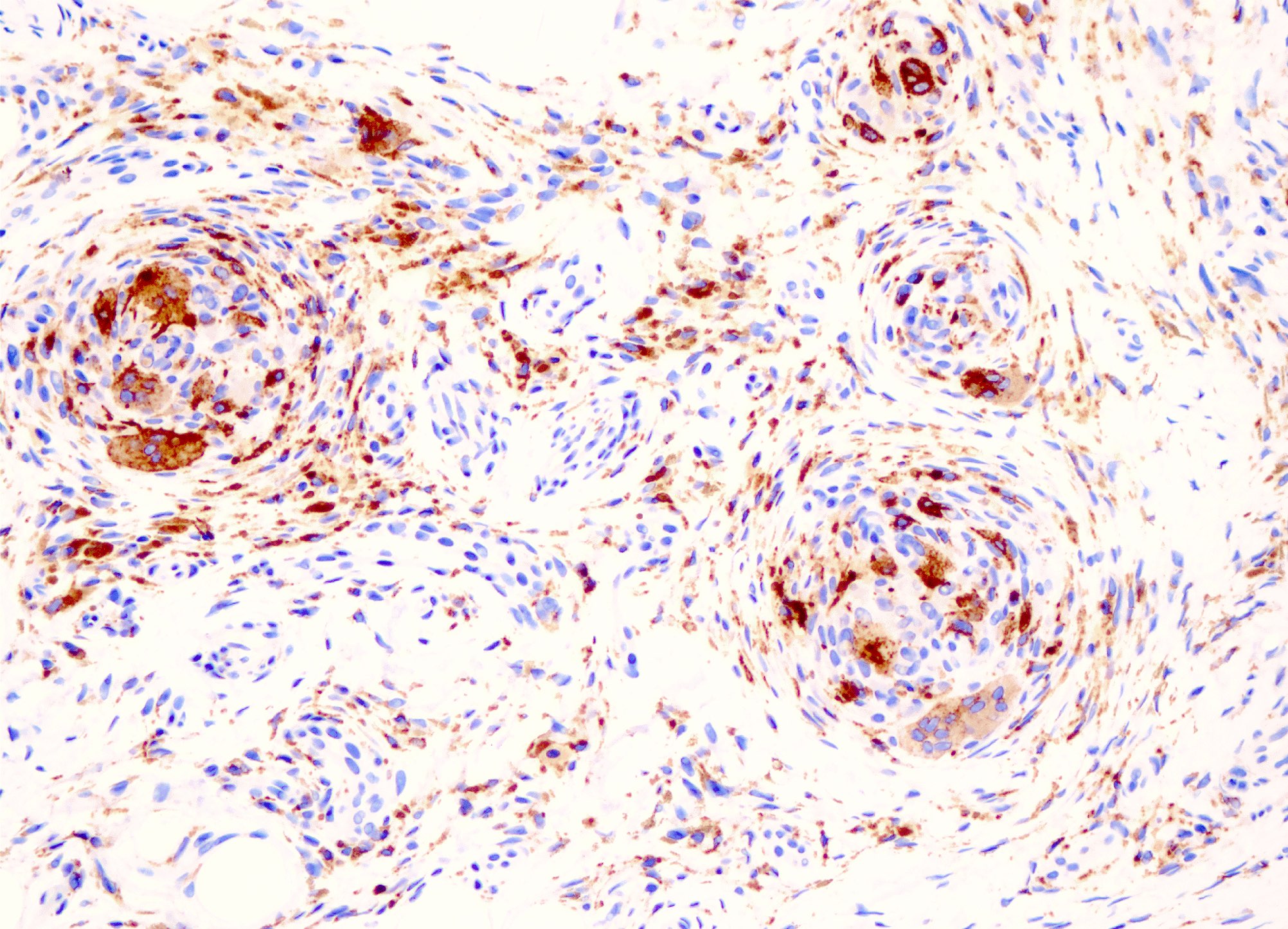
CD68 IHC
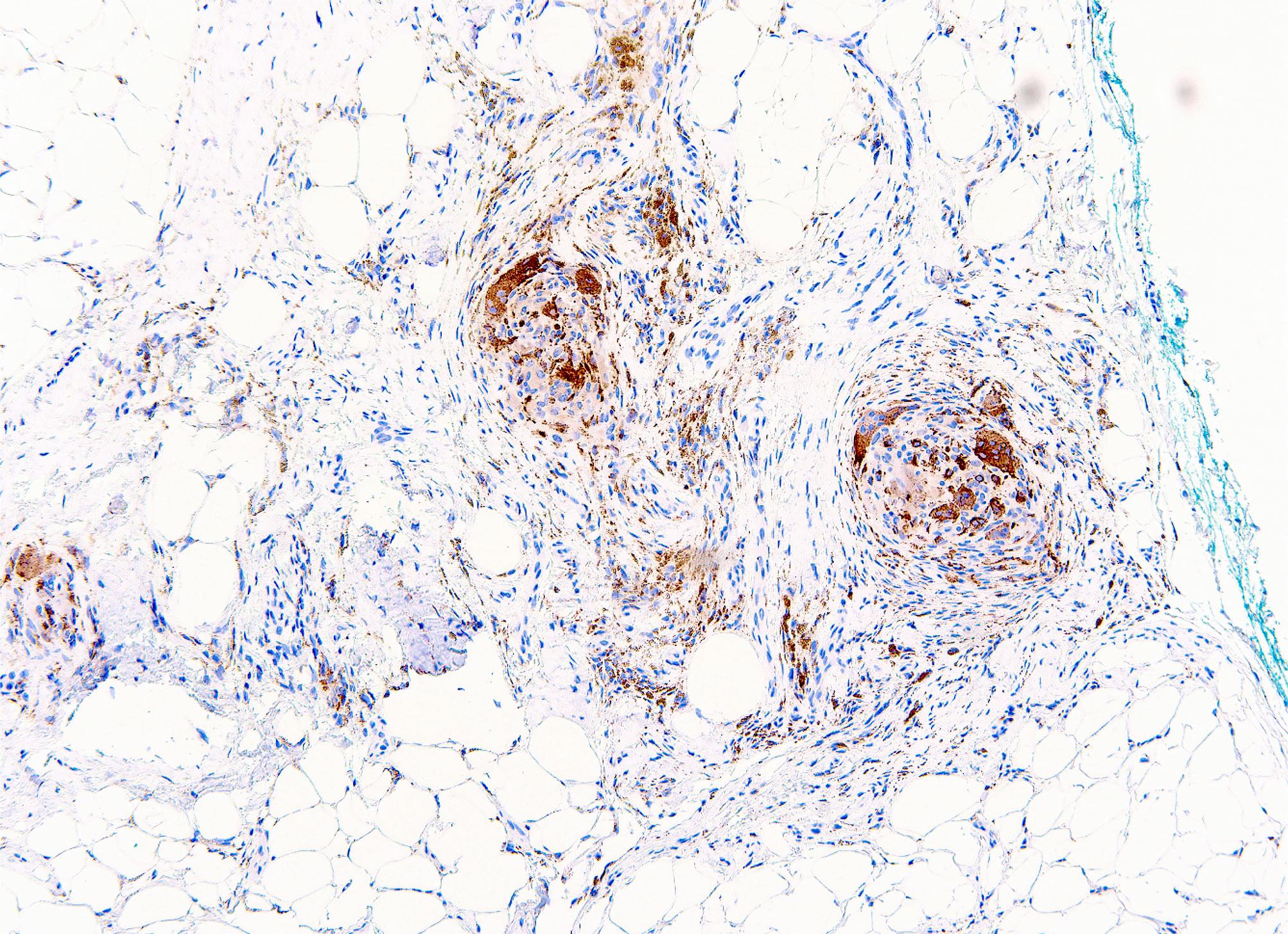
CD68 IHC
Images hosted on other servers:

Plaque-like lesion (back)
- Plump fibroblastic spindle cells and histiocytoid cells
- Scattered multinucleated osteoclast-like giant cells (Arch Pathol Lab Med 2007;131:1135)
- No significant pleomorphism (Head Neck Pathol 2020;14:262)
- Fine, granular myxoid background
Images hosted on other servers:

Plump histiocytoid cells
- Tumor cells have features of myofibroblasts and histiocyte-like cells (Pathol Res Pract 1992;188:350)
- Myofibroblast-like cells have abundant thin cytoplasmic filaments associated with dense bodies (Histopathology 1991;19:503, Pathol Res Pract 1992;188:350)
- Histiocyte-like cells have lysosomes and multiple filopodia (Pathol Res Pract 1992;188:350)
- Specific chromosomal abnormalities have not been identified
- So far, no specific molecular aberrations have been identified (Virchows Arch 2022;481:739)
- CSF1 chromogenic in situ hybridization (CISH) shows null cell population (Virchows Arch 2022;481:739)
Plexiform fibrohistiocytic tumor (case 3) by Dr. Melanie Bourgeau
Kaposiform hemangioendothelioma, plexiform fibrohistiocytic tumor, etc. by Dr. Jerad Gardner
- Soft tissue, right small finger, excision:
- Fibrohistiocytic neoplasm involving adipose tissue, consistent with plexiform fibrohistiocytic neoplasm, extends to inked tissue edges (see comment)
- Comment: Sections show a neoplasm composed of a mix of nodules containing epithelioid histiocytes with scattered osteoclast type giant cells and fascicles of spindled fibroblastic cells involving adipose tissue. The cytomorphology of the tumor cells is bland without significantly increased mitotic activity or nuclear pleomorphism. Immunohistochemical stains show that the histiocytes are positive for CD68, while S100, MITF and keratin AE1 / AE3 are negative. CD34 is patchy positive. Given that the tumor extends to the inked tissue edges, a narrow re-excision to obtain clear margins and to reduce the risk of local recurrence could be considered.
- Cellular neurothekeoma:
- Epithelioid to spindled cells arranged in nests divided by dense fibrous septa
- Myxoid change is common
- Nuclear pleomorphism (25%)
- Mitotic activity is common, can have atypical mitoses
- Osteoclastic or Touton multinucleated giant cells
- Podoplanin positive
- CD63 (NKI-C3), PGP9.5 and MITF positive
- Dermatofibroma:
- Older patients
- No nodules of histiocytoid cells
- No osteoclast-like giant cells
- No plexiform extensions of fibrous tissue
- Giant cell tumor of soft tissue:
- Prominent nodules with abundant osteoclast-like giant cells
- No infiltrative spindle cell component
- Peripheral shell or rim of woven bone (~50%)
- Frequent mitoses
- Fibromatosis:
- No nodules of histiocytoid and osteoclast-like giant cells
- Characteristic stromal vasculature
- Nuclear beta catenin positive
- Low grade myofibroblastic sarcoma:
- Predominantly adults
- Frequently in head and neck region
- Arises in deep subcutaneous tissue or skeletal muscle
- Diffusely infiltrative, often with checkerboard pattern
- At least focal mild to moderate atypia (enlarged nuclei, hyperchromasia)
- SMA positive / myofibroblastic immunophenotype
- Nodular fasciitis:
- Small, rapidly growing, well circumscribed
- Myxoid stroma, especially in early stages
- No multinodular or plexiform growth
- MYH9::USP6 fusion
- Fibrous hamartoma of infancy:
- Predominantly infants
- Common in axilla
- Foci of immature mesenchymal tissue, myxoid stroma
- Pilar leiomyoma:
- Neurofibroma:
- No distinct nodule formation
- S100 positive
A 19 year old man presented with a 2 cm painless nodule on his right index finger. What is the diagnosis?
- Cellular neurothekeoma
- Fibromatosis
- Giant cell tumor of soft tissue
- Plexiform fibrohistiocytic tumor
- Schwannoma
Comment Here
Reference: Plexiform fibrohistiocytic tumor
- Brisk mitotic activity
- Characteristic vasculature
- Involvement of epidermis
- Multinucleated giant cells
- Nuclear pleomorphism
Comment Here
Reference: Plexiform fibrohistiocytic tumor
