
Soft tissue
Peripheral nerve
Other benign
Benign triton tumor / neuromuscular choristoma
Editorial Board Member: Laura Warmke, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 4 November 2024
Last staff update: 4 November 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Benign triton tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Frazzette N, Mantilla JG. Benign triton tumor / neuromuscular choristoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueneuromuscularhamartoma.html. Accessed March 31st, 2025.
Definition / general
- Rare, benign developmental lesion composed of peripheral nerve elements admixed with muscle (most often skeletal) within the endoneurium (Am J Surg Pathol 2016;40:1368)
Essential features
- Benign intraneural proliferation composed of mature peripheral nerve and interspersed muscle
- In most cases, the lesional muscle is of skeletal differentiation but can be smooth muscle (Am J Surg Pathol 2016;40:1368)
Terminology
- Benign triton tumor, neuromuscular hamartoma
- Acceptable terms according to the WHO: nerve rhabdomyoma, ectomesenchymal hamartoma
ICD coding
- ICD-10: D36.10 - benign neoplasm of peripheral nerves and autonomic nervous system, unspecified
Epidemiology
- Very rare lesion
- Usually occurs in children and adolescents, often in the first decade of life (Acta Neuropathol 2012;123:295)
- M = F
Sites
- Large nerves (e.g., sciatic) or nerve plexuses (e.g., brachial) (Surg Neurol Int 2013;4:8, J Plast Reconstr Aesthet Surg 2024;93:83)
- Cranial nerves (Childs Nerv Syst 2022;38:2055, Pediatr Dev Pathol 2014;17:400)
- Intraorbital (Eur J Ophthalmol 2022;32:NP85, J Fr Ophtalmol 2015;38:112)
Pathophysiology
- Owing to its rarity, exact pathophysiology is poorly understood
- Hypotheses include
- Incorporation of mesenchymal tissue in nerve sheaths during embryogenesis
- Aberrant differentiation of neuroectoderm into mesenchymal tissue
- Alteration of the motor end plate of muscle fibers leading to reactive proliferation of neural and skeletal tissue
- Reference: Am J Clin Pathol 1995;103:460
Etiology
- Developmental disorder
- Pathogenesis is unclear, with no known etiologic associations
Clinical features
- Fusiform enlargement of the involved nerve(s) (Neurosurgery 2021;88:804)
- Clinical presentation often includes neuropathy / plexopathy, muscular atrophy, progressive pain and secondary deformities (e.g., cavus deformity, limb undergrowth) (BMC Musculoskelet Disord 2022;23:464)
- May regress with time
- May have a direct relationship with desmoid type fibromatosis and up to 80% of patients with these lesions may develop desmoid type fibromatosis in the same area (Neurosurgery 2021;88:804, Am J Surg Pathol 2016;40:1368)
Diagnosis
- Characteristic radiologic and histologic features are sufficient for diagnosis; biopsy is discouraged in cases that are clinically and radiologically consistent, since intervention may precipitate the development of desmoid type fibromatosis (J Neurosurg 2013;119:252, Am J Surg Pathol 2016;40:1368)
Radiology description
- Characteristic magnetic resonance imaging (MRI) findings include fusiform enlargement of the affected nerve, isointense to skeletal muscle in T1 and T2 sequences (Am J Surg Pathol 2016;40:1368, J Neurosurg 2013;119:252)
- Well defined solid lesion with < 50% intralesional fat on MRI (J Neurosurg 2013;119:252)
Prognostic factors
- Local recurrence in 33%
- Most recurrent cases are associated with desmoid type fibromatosis
- 80% develop desmoid type fibromatosis in cases with long term clinical follow up
- Development of desmoid type fibromatosis may be precipitated by biopsy
- Reference: Lindberg: Diagnostic Pathology - Soft Tissue Tumors, 4th Edition, 2023
Case reports
- 3 month old girl with tumor of brachial plexus (Pediatr Dev Pathol 2021;24:213)
- 10 year old boy with tumor of trigeminal nerve (Childs Nerv Syst 2022;38:2055)
- 46 year old man with esophageal neuromuscular choristoma (BMC Gastroenterol 2022;22:180)
- 51 year old man with migraine (Cephalalgia 2012;32:171)
- 61 year old man with thyroid orbitopathy (Orbit 2010;29:168)
Treatment
- Due to rarity, gold standard treatment is not clear
- Surgical resection for symptomatic cases or tumors with mass effect
- Observation for asymptomatic cases, as an intervention may be associated with the development of desmoid type fibromatosis (J Neurosurg 2013;119:252, Am J Surg Pathol 2016;40:1368)
Gross description
- Well demarcated, elastic / firm, nodular, gray-white mass arising from or attached to nerve
Gross images
Images hosted on other servers:

Enlarged sciatic nerve
Microscopic (histologic) description
- Abundant, densely eosinophilic smooth or striated muscle fibers intercalated among Schwannian nerve fibers
Microscopic (histologic) images
Contributed by Anshu Bandhlish, M.D. and AFIP


Muscle fibers intercalated among nerve fibers
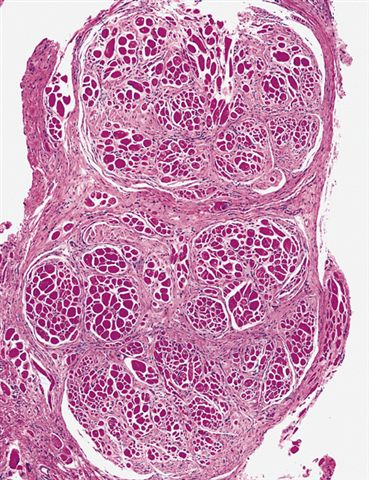
Nodules of skeletal muscle and neural elements

Fascicles and nerve fibers

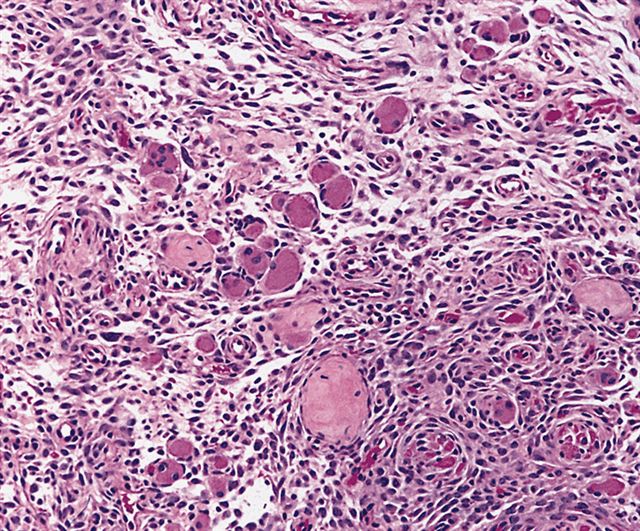
Haphazardly distributed skeletal muscle and nerve fibers

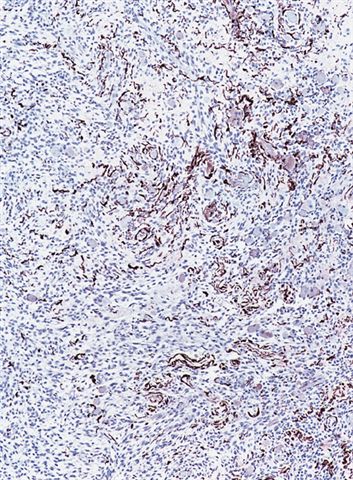
Nerve fibers are S100+
Positive stains
- Nuclear reactivity for beta catenin in both components
- Skeletal muscle component: desmin, muscle specific actin, myogenin (focal), MyoD1 (rare)
- Neural component: S100, neurofilament
- References: Childs Nerv Syst 2022;38:2055, J Neurosurg Case Lessons 2024;7:CASE23517, BMC Gastroenterol 2022;22:180
Molecular / cytogenetics description
- Most cases have point mutations in CTNNB1 (p.S45F, p.T41) (J Neuropathol Exp Neurol 2021;80:1068, Am J Surg Pathol 2016;40:1368)
Sample pathology report
- Brachial plexus, mass; biopsy:
- Neuromuscular choristoma (see comment)
- Comment: Sections demonstrate intercalated dense muscle fibers and Schwannian nerve fibers without significant atypia in either population. Overall, this represents a benign process most consistent with neuromuscular choristoma (benign triton tumor).
Differential diagnosis
- Embryonal rhabdomyosarcoma:
- Fetal rhabdomyoma:
- Benign lesion composed of skeletal muscle and immature mesenchymal cells
- Lacks expression of nerve sheath markers
- Lacks nuclear expression of beta catenin
- Malignant peripheral tumor with heterologous rhabdomyosarcomatous elements (malignant triton tumor):
- Aggressive sarcoma; most cases have high grade morphologic features
- Patchy expression of nerve sheath markers, myogenic markers in areas of rhabdomyosarcomatous differentiation
- Lacks nuclear expression of beta catenin
- Lipomatosis of nerve (fibrolipomatous hamartoma):
- Presence of fibroadipose tissue
- Infiltrative morphology (versus intercalated morphology seen in neuromuscular choristoma)
- Desmoid type fibromatosis:
- Monomorphic tumor population (versus dual muscular and neural morphology seen in neuromuscular choristoma)
- Absence of neural tissue (S100, neurofilament negative)
- Desmin is typically negative or only focally positive
Additional references
Board review style question #1
A 5 year old boy presents with a suspected neuromuscular choristoma (benign triton tumor). Immunohistochemical analysis is performed on the biopsy specimen. Which of the following immunohistochemical stains is most likely to be positive in this tumor?
- Beta catenin
- CD31
- CD45
- HM45
- Smooth muscle actin (SMA)
Board review style answer #1
A. Beta catenin. Neuromuscular choristoma has a characteristic immunophenotype, with a combined expression of nerve sheath and myogenic markers, as well as nuclear expression of beta catenin, which is associated with point mutations in CTNNB1 in the majority of cases. Answers B, C, D and E are incorrect because none of these other markers are typically expressed in neuromuscular choristoma.
Comment Here
Reference: Benign triton tumor / neuromuscular choristoma
Comment Here
Reference: Benign triton tumor / neuromuscular choristoma
Board review style question #2
Which of the following is a known complication associated with surgical treatment for neuromuscular choristoma?
- Desmoid type fibromatosis
- Keloid scar
- Malignant transformation
- Postoperative hematoma
- Tumor embolism
Board review style answer #2
A. Desmoid type fibromatosis. The development of desmoid type fibromatosis is a well known complication of surgical intervention (including biopsy) in neuromuscular choristoma. For this reason, it is preferred to observe these lesions if they are asymptomatic. Given the presence of beta catenin point mutations in these lesions, they are considered to share a similar pathogenesis. Answers D and B are incorrect because the development of hematoma and keloid scar are potential complications of surgical procedures but not specific to these tumors. Answer E is incorrect because tumor embolism is not a described complication of neuromuscular choristoma. Answer C is incorrect because malignant transformation has not been described in these lesions.
Comment Here
Reference: Benign triton tumor / neuromuscular choristoma
Comment Here
Reference: Benign triton tumor / neuromuscular choristoma
