
Soft tissue
Smooth muscle
Leiomyoma
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 13 December 2024
Last staff update: 13 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Leiomyoma soft tissue

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Venkatraman Ravisankar H, Warmke L. Leiomyoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueleiomyoma.html. Accessed March 31st, 2025.
Definition / general
- Leiomyoma is a benign smooth muscle neoplasm that arises in deep soft tissue of the extremities (somatic), retroperitoneum or abdominopelvic cavity
- Leiomyomas of soft tissue are very rare compared to their malignant counterpart and should be diagnosed using only the most stringent criteria
Essential features
- Smooth muscle neoplasm that arises in soft tissue
- No evidence of gynecologic origin
- No necrosis, no significant nuclear pleomorphism and virtually no mitotic activity (< 1 mitotic figure per 50 high power fields)
Epidemiology
- Rare overall
- Fourth through sixth decades of life most common
- More common in retroperitoneum / pelvis than deep somatic soft tissue
- Leiomyomas of somatic soft tissue occur primarily in middle aged adults with no sex preference (Am J Surg Pathol 1994;18:576)
- Leiomyomas of retroperitoneum and abdominopelvic cavity are much more common in women, often of perimenopausal age (Am J Surg Pathol 2001;25:1355)
Sites
- Leiomyomas of somatic soft tissue mostly occur in extremities and arise in deep subcutis or skeletal muscle (Am J Surg Pathol 2001;25:1134)
- They may also occur in the retroperitoneum, abdominal wall, omentum, mesentery and peritoneal surface
- In the inguinal region, leiomyomas may arise from the round ligament (Am J Surg Pathol 2011;35:315)
Pathophysiology
- Retroperitoneal / abdominal cavity leiomyomas carry some of the same genetic changes as uterine leiomyomas (PLoS One 2015;10:e0117010)
- Genetic aberrations in HMGA2 and PLAG1 (Oncotarget 2017;8:48769)
- Mutations in MED12 have been reported in retroperitoneal leiomyomas (Mod Pathol 2013;26:743)
- KAT6B::KANSL1 and EWSR1::PBX3 fusion genes were found in retroperitoneal leiomyomas with t(10;17)(q22;q21) and t(9;22)(q33;q12) chromosomal translocations, respectively (PLoS One 2015;10:e0117010, PLoS One 2015;10:e0124288)
Etiology
- Causation of somatic leiomyomas is unknown
- The fact that > 40% of retroperitoneal leiomyomas were reported in patients who had concurrent uterine leiomyomas or had undergone previous hysterectomy for uterine leiomyomas may support a theory of multifocal origin (Hum Pathol 1989;20:80)
Clinical features
- Slow growing, painless mass
- Usually solitary
- Retroperitoneal tumors may be multiple (Am J Surg Pathol 2001;25:1134)
Diagnosis
- Intersecting fascicles of benign smooth muscle (Am J Surg Pathol 1994;18:576)
- Expression of SMA and desmin
- No necrosis, no significant nuclear pleomorphism and no / rare mitotic activity
Radiology description
- Somatic tumors often have calcification, which may be detected radiographically (Am J Surg Pathol 1994;18:576)
- Computed tomography (CT) may show mulberry-like calcifications (Pediatr Radiol 1999;29:135)
- Magnetic resonance imaging (MRI) showed signal characteristics similar to muscle on both T1 and T2 weighted sequences (Skeletal Radiol 1999;28:411)
Radiology images
Images hosted on other servers:

Retroperitoneal leiomyoma
Prognostic factors
- Benign tumor if correctly diagnosed
- No recurrence has been reported in somatic leiomyomas (Am J Surg Pathol 1994;18:576)
- Recurrence has been reported in < 10% of leiomyomas of retroperitoneum / abdominopelvic cavity (Am J Surg Pathol 2001;25:1134)
- No metastatic risk
Case reports
- 6 year old boy with calcified leiomyoma of deep soft tissue in left leg (Virchows Arch 1994;425:217)
- 14 year old girl with deep soft tissue leiomyoma of popliteal fossa (Arch Orthop Trauma Surg 2001;121:604)
- 52 year old woman with large retroperitoneal leiomyoma (J Med Case Rep 2018;12:81)
Treatment
- Simple surgical excision
Gross description
- Well circumscribed but nonencapsulated mass
- Tan-gray to white-gray nodular or lobular mass (Am J Surg Pathol 2001;25:1355)
- Rubbery texture and whorled cut surface
- No necrosis
- Wide size range (3 - 20 cm)
- Retroperitoneal tumors can reach a very large size
- Calcification not uncommon
Gross images
Images hosted on other servers:

Myxoid subcutaneous tumor
Microscopic (histologic) description
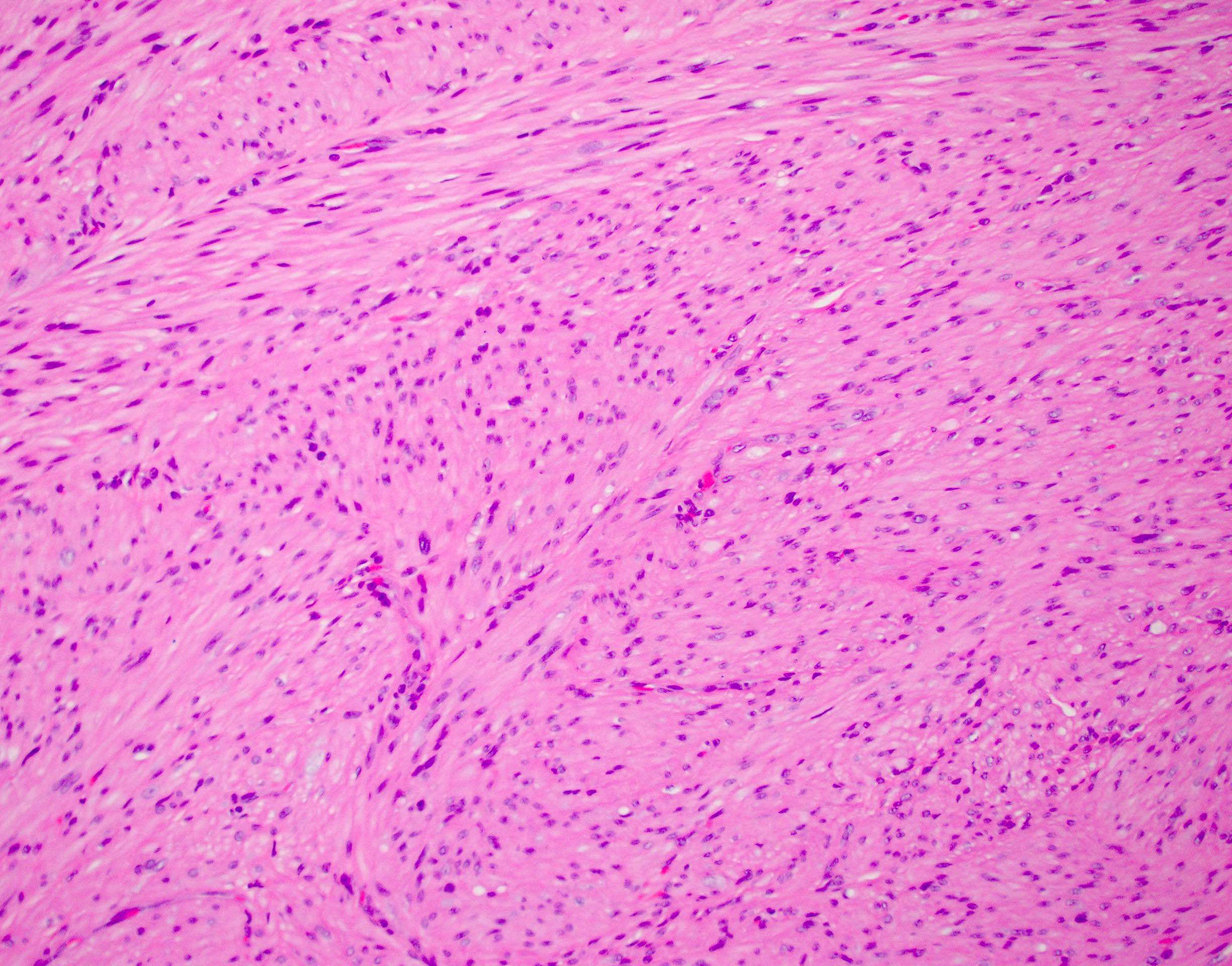
- Uniform spindle cells with abundant eosinophilic cytoplasm and blunt ended, cigar shaped nuclei
- Variable degrees of fascicular growth and different sized bundles
- No significant nuclear pleomorphism, mitotic activity or necrosis
- Focal degenerative atypia may be present
- Stromal edema may be present
- Most hypocellular with stromal hyalinization
- Fibrosis, calcification and myxoid change may be seen
- May show macrotrabecular and microtrabecular organization
- Verocay body-like formation and nuclear palisading may be seen (J Dermatol 2002;29:160)
- Focal epithelioid and clear cell change may be seen
- Mature adipose tissue occasionally present
- Scattered mast cells
Microscopic (histologic) images
Contributed by Laura Warmke, M.D. and AFIP
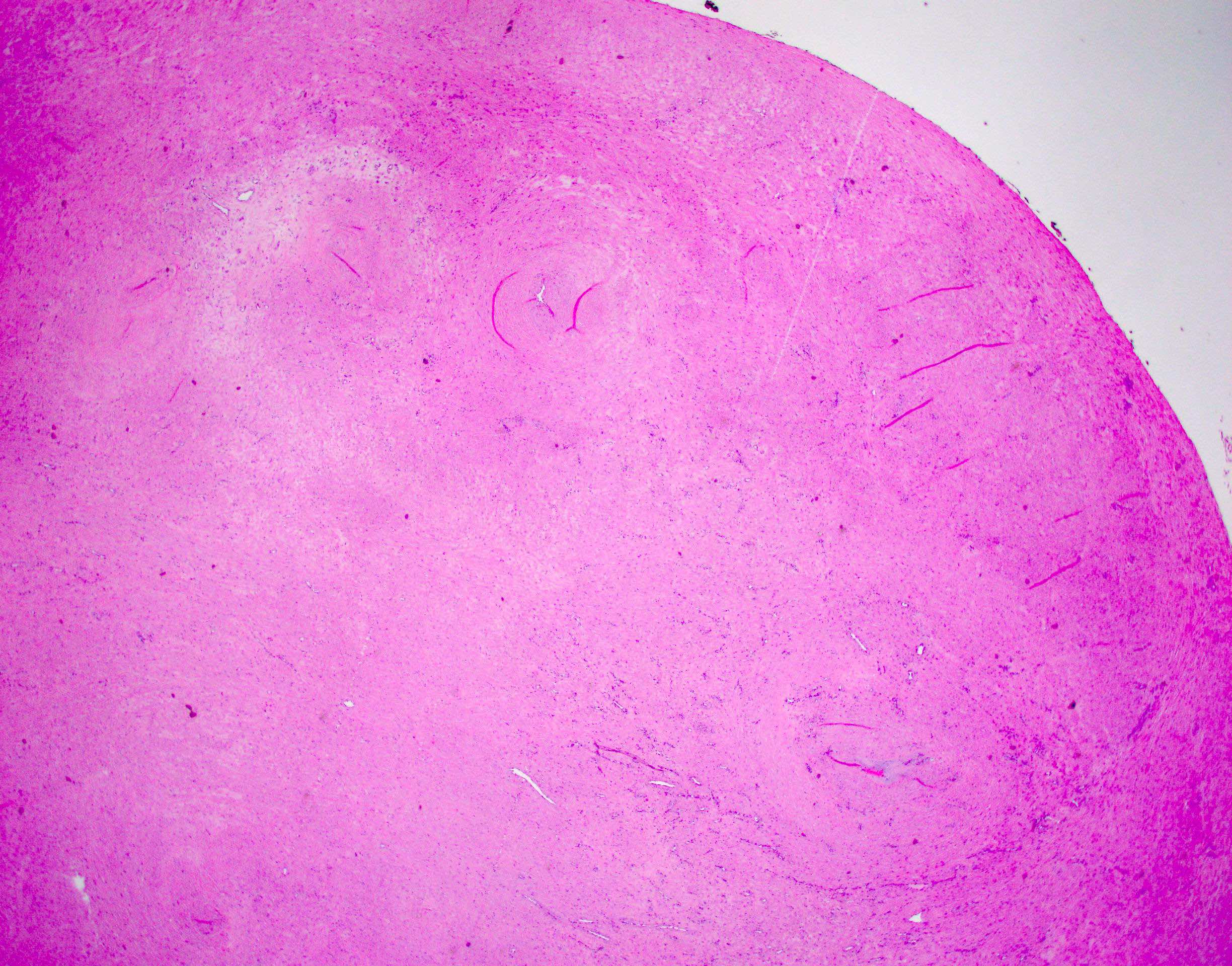
Well circumscribed mass
Eosinophilic cytoplasm
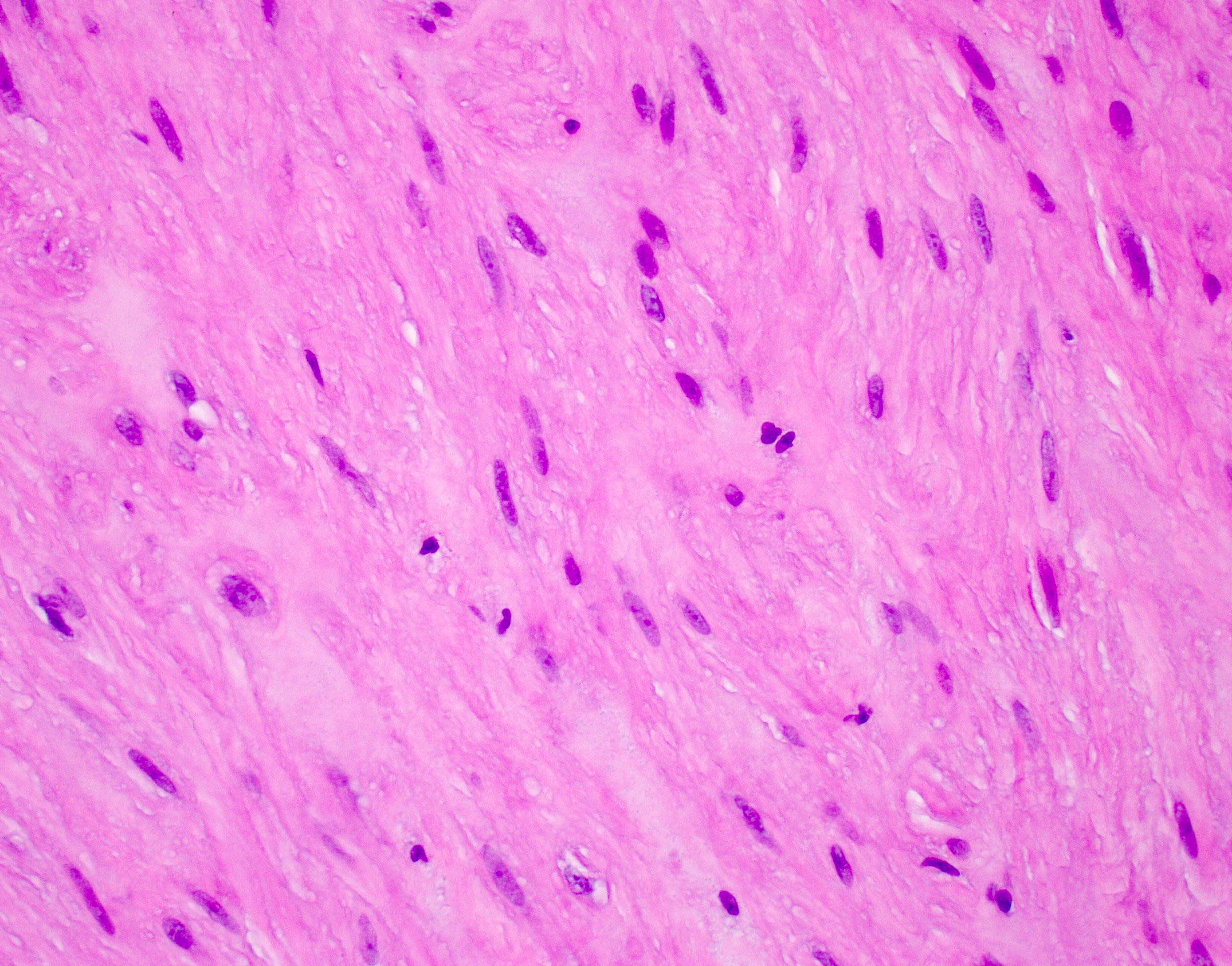
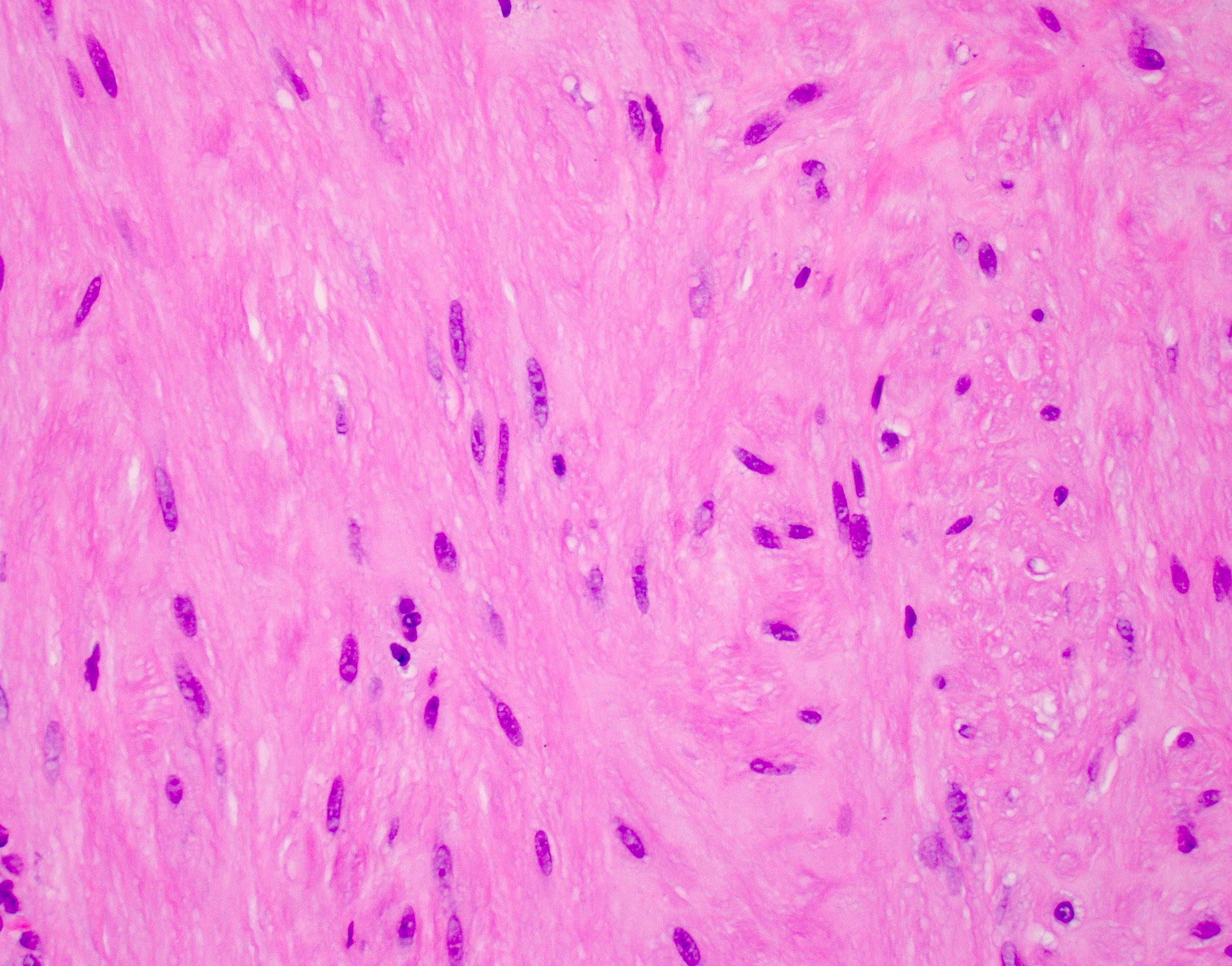
Cigar nuclei
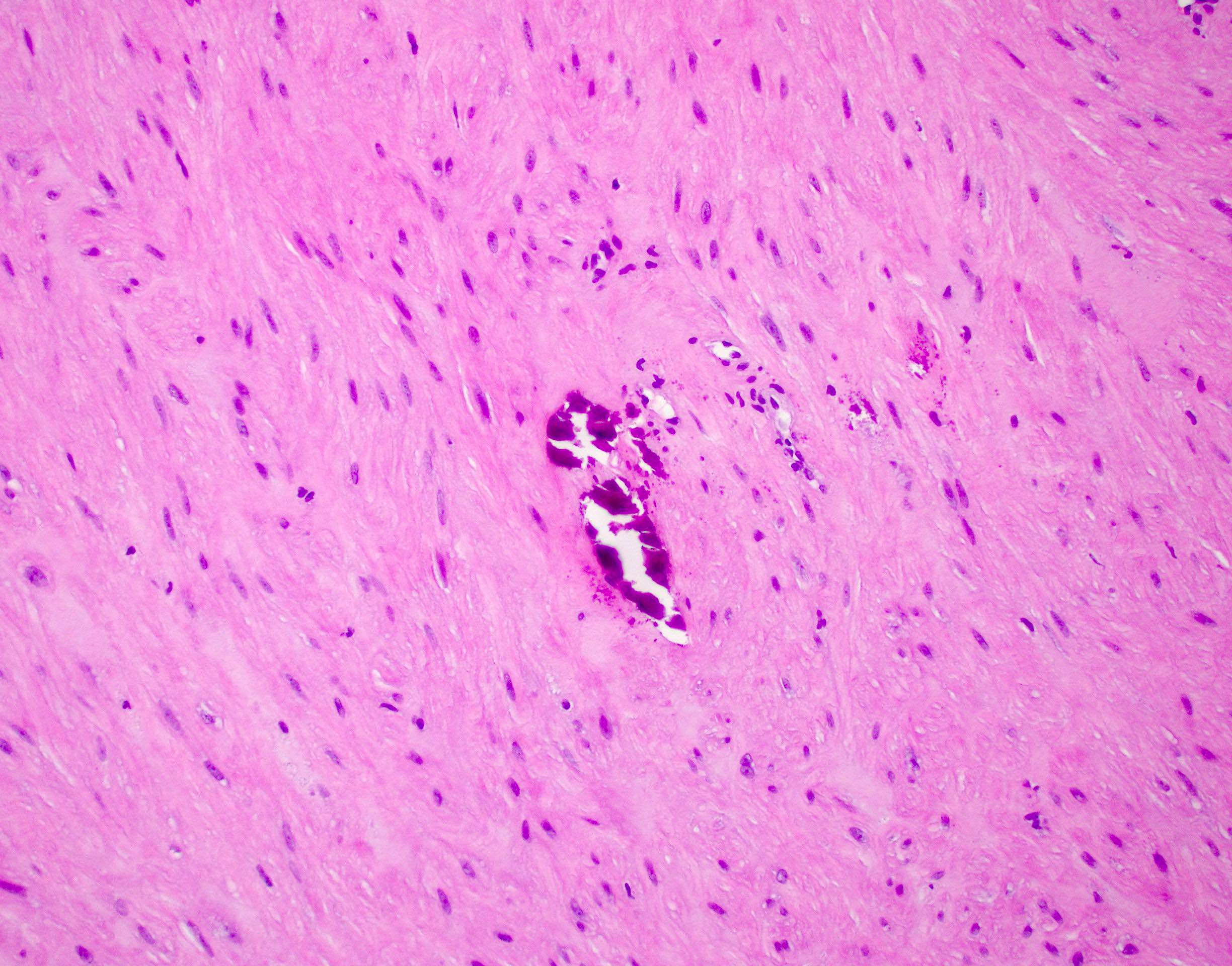
Focal calcification
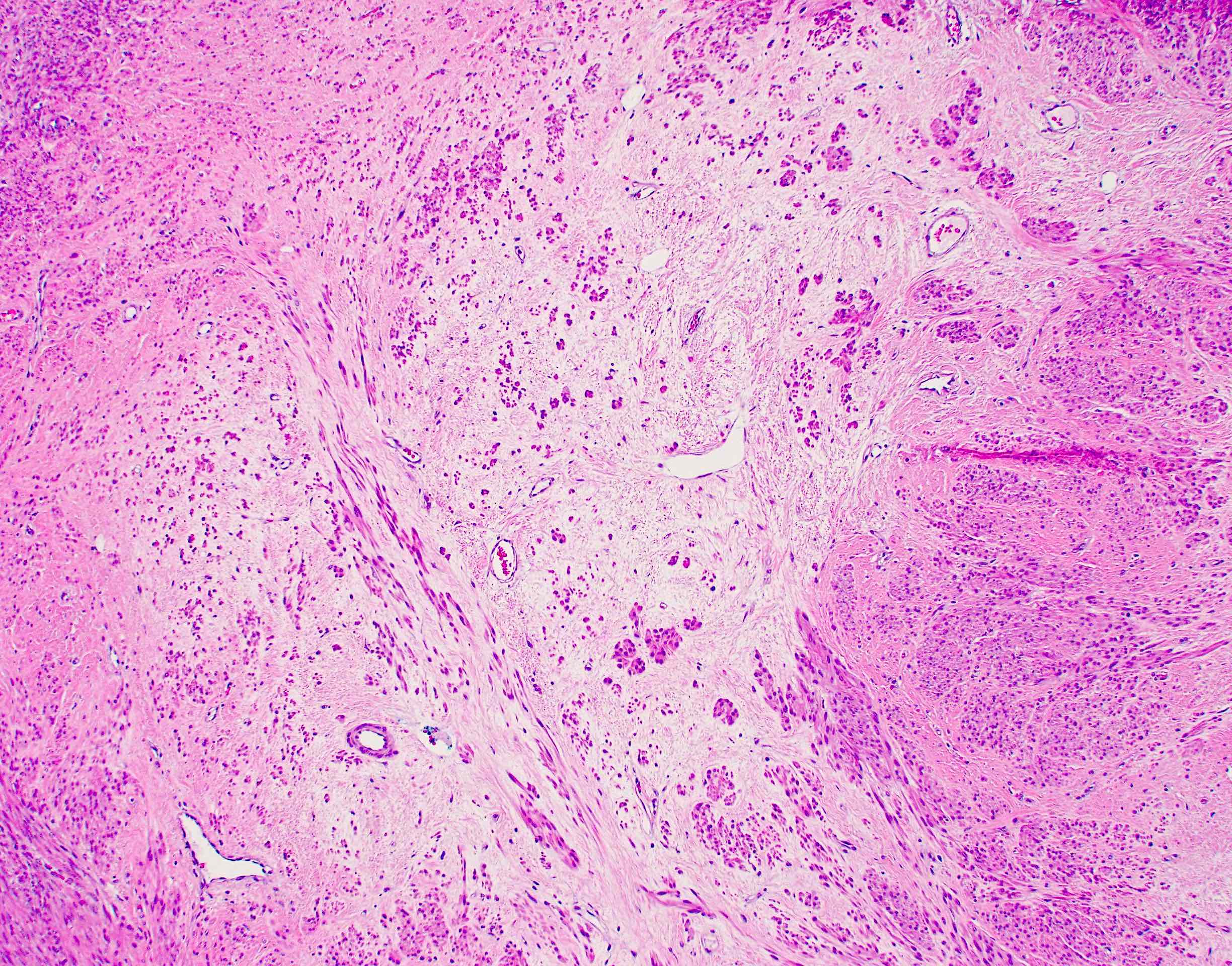
Stromal edema
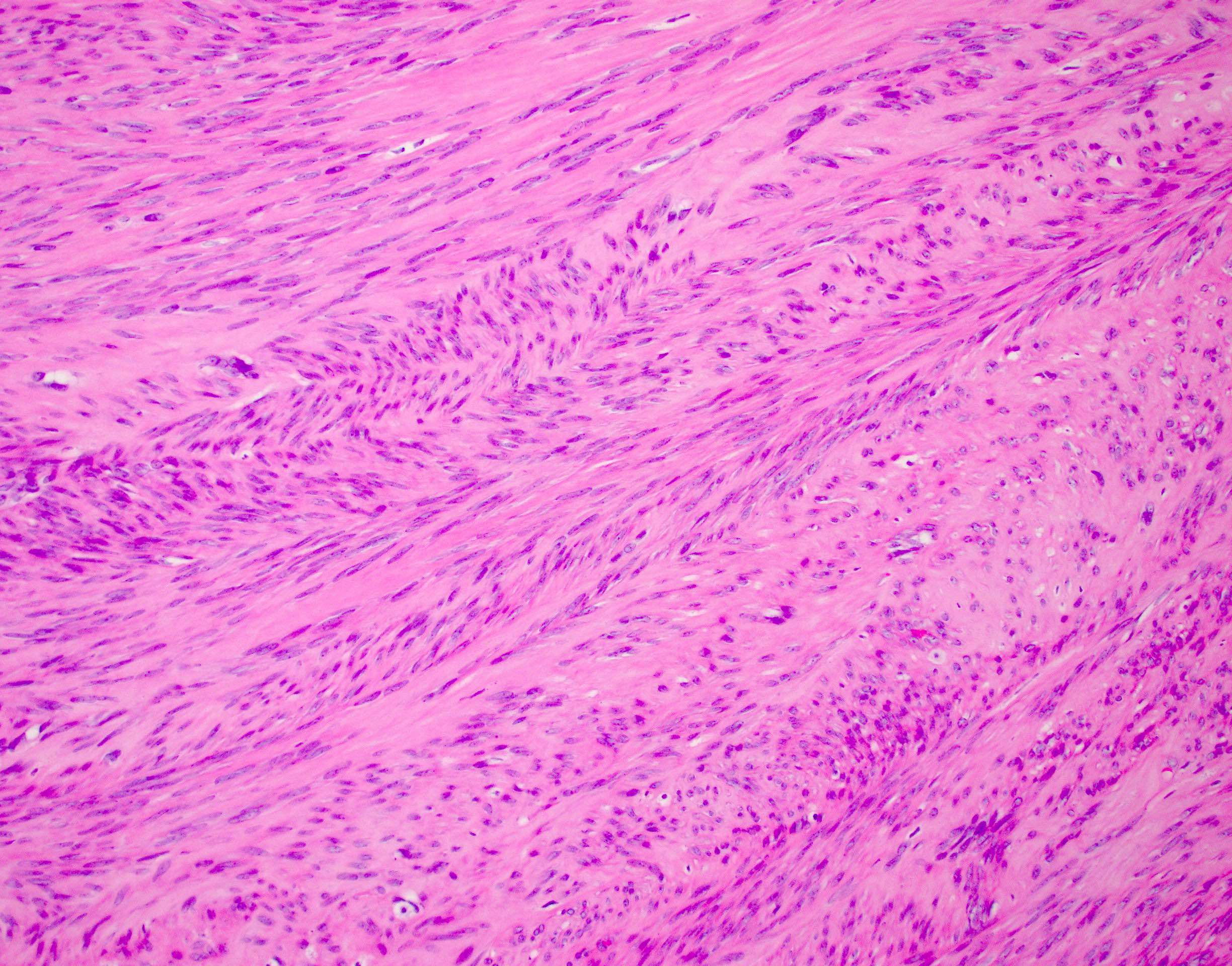
Fascicles
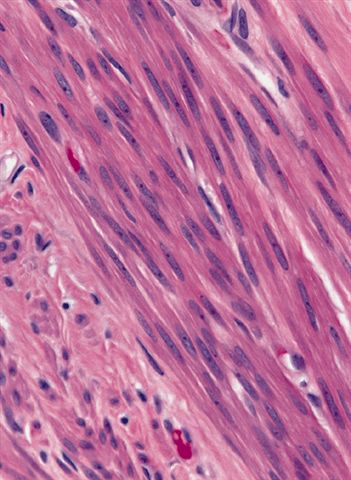
Oblong nuclei have rounded ends
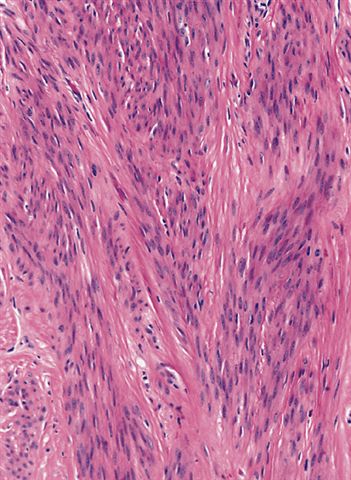
Bundles of elongate cells
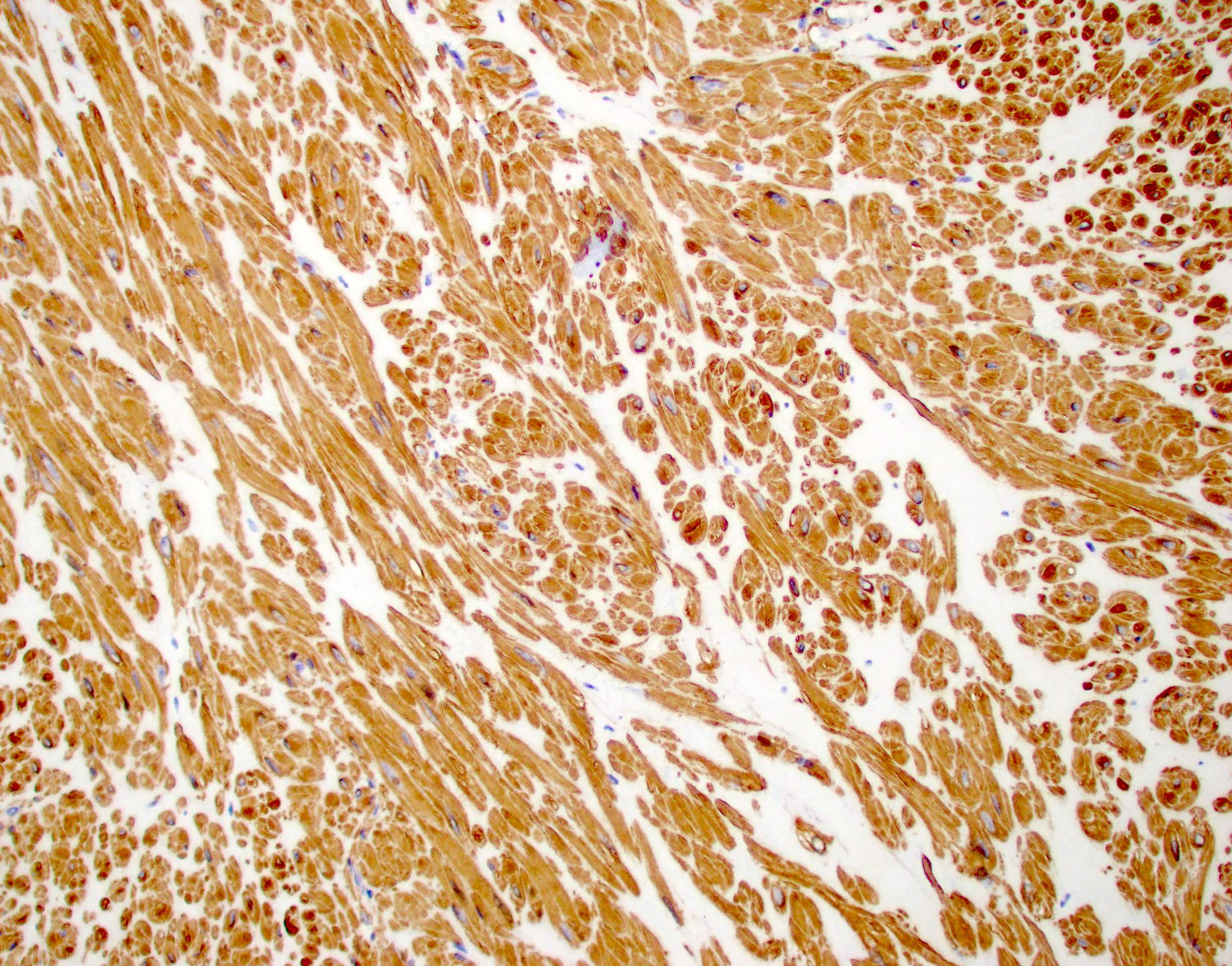
Smooth muscle actin
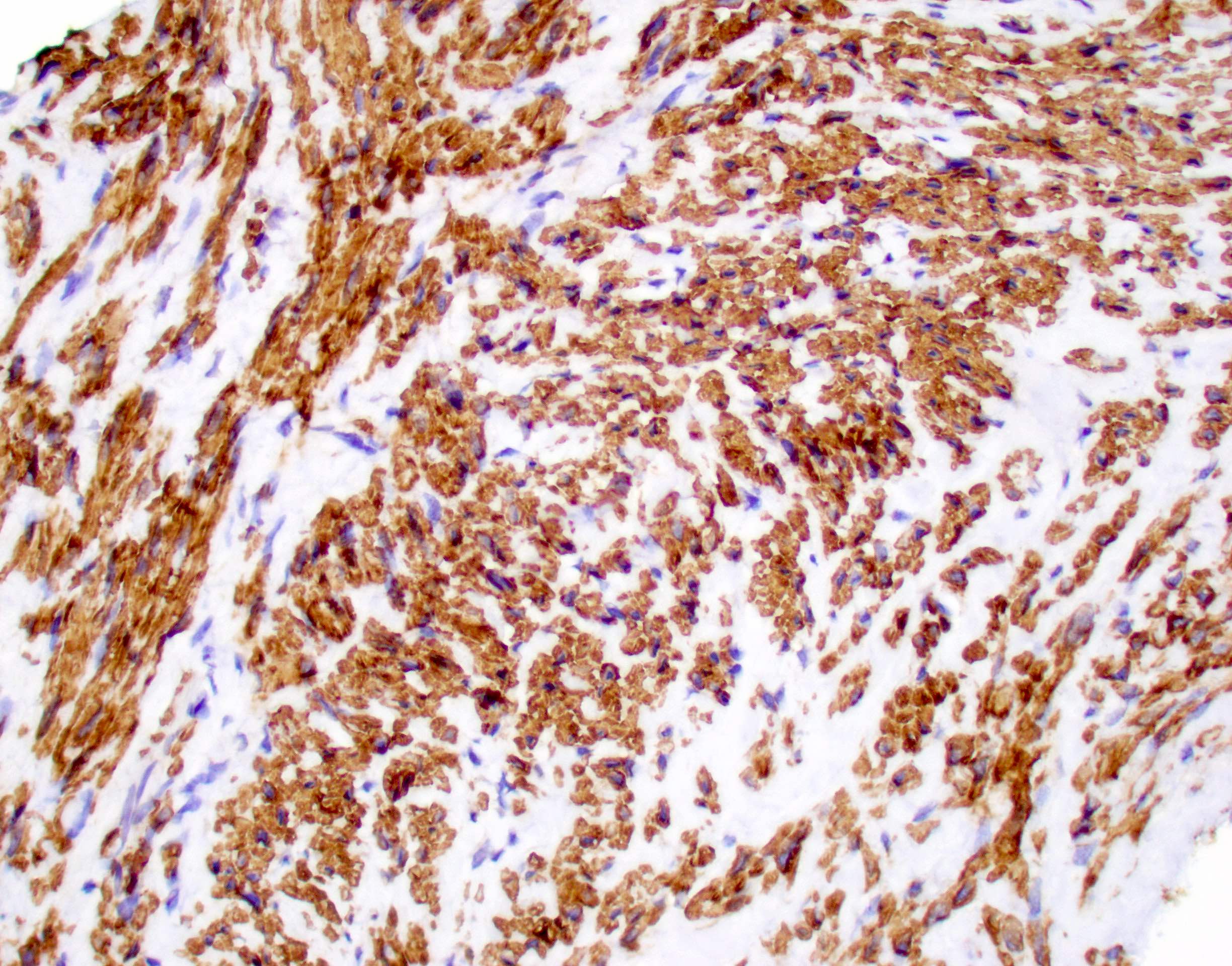
Caldesmon
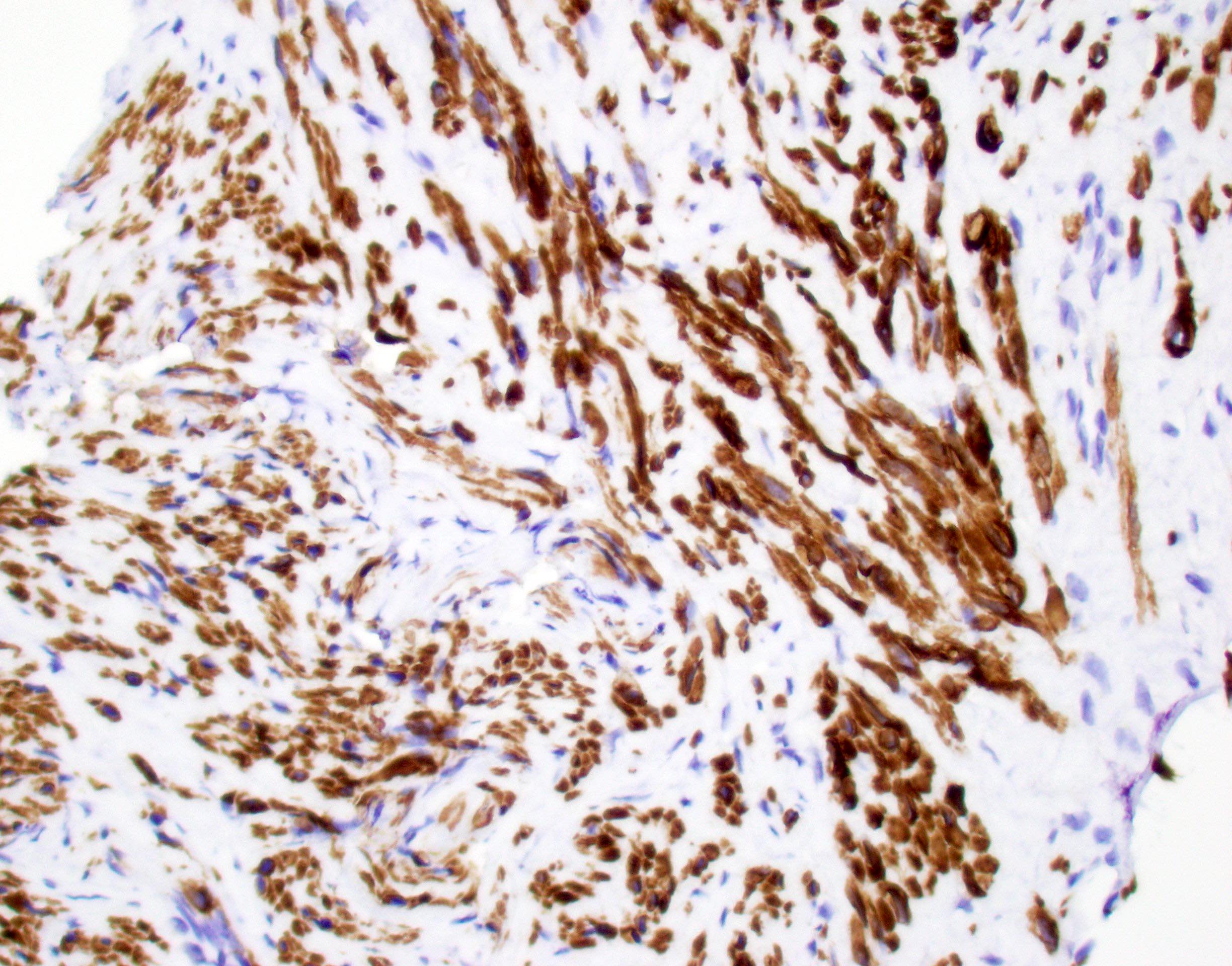
Desmin
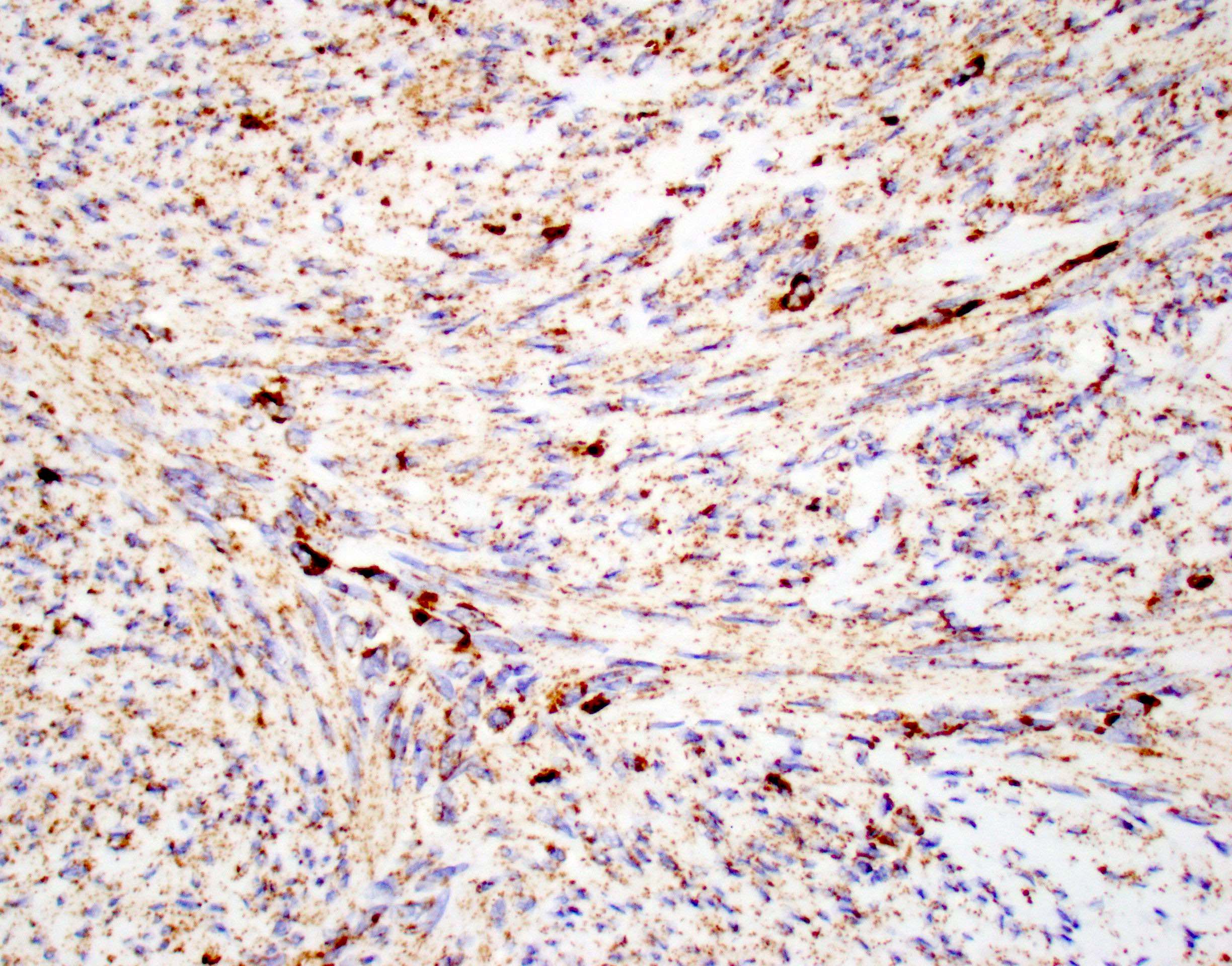
Fumarate hydratase
Virtual slides
Images hosted on other servers:

Leiomyoma with hydropic change
Cytology description
- Bland spindle cells
Cytology images
Contributed by Laura Warmke, M.D.
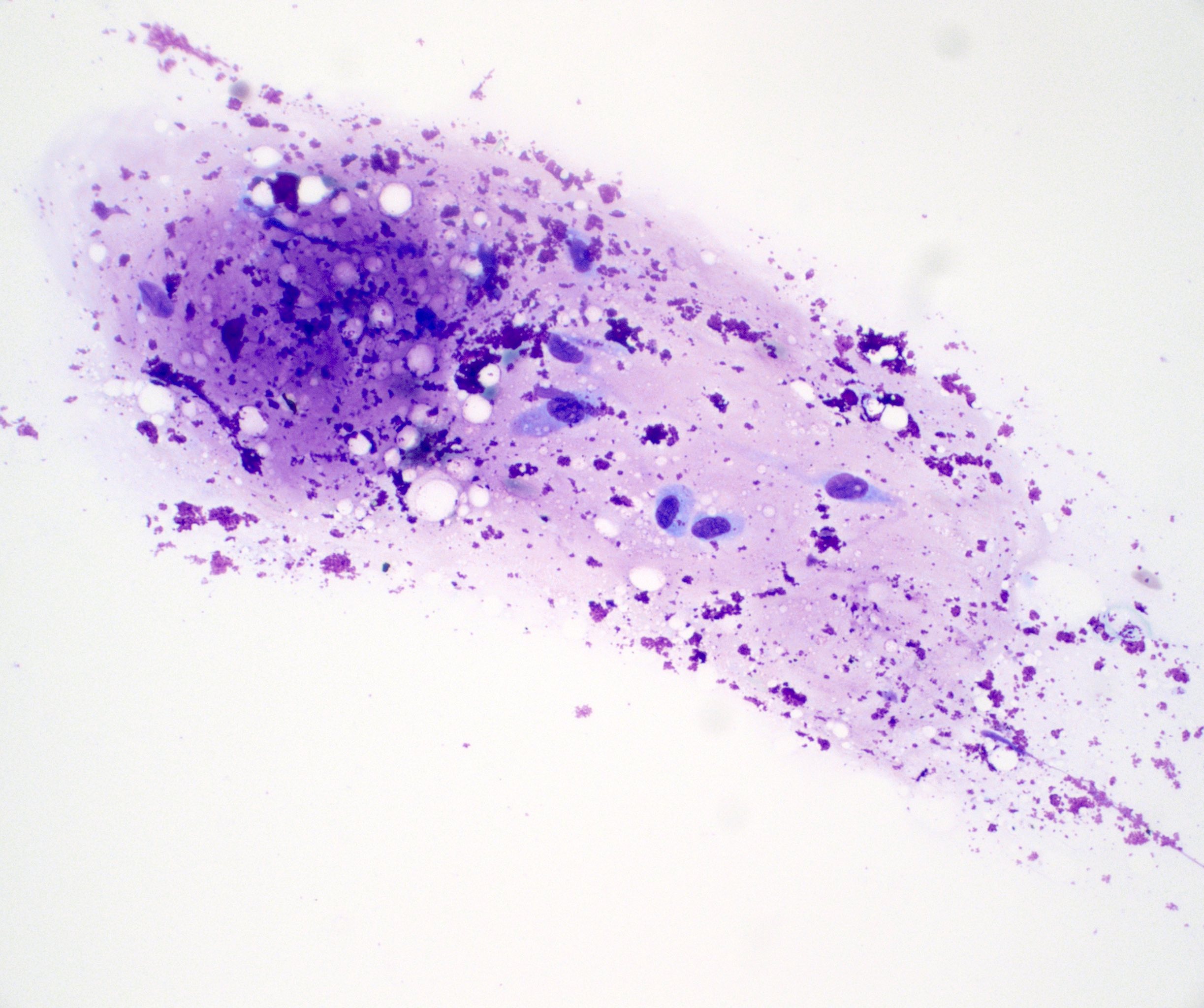
Touch prep
Positive stains
- Smooth muscle actin (SMA)
- Muscle specific actin (MSA)
- Desmin (may be lacking in tumors of vascular origin) (Am J Surg Pathol 1994;18:576)
- h-caldesmon
- Masson trichrome (highlights myofibrils in red)
- ER, PR and WT1 (often expressed in retroperitoneal or abdominopelvic tumors in women, rare in deep somatic tumors)
- Subset may show focal keratin / EMA expression
Negative stains
- Fumarate hydratase (intact without loss of expression)
- EBER ISH
- HMB45
- MelanA
- S100 protein (Am J Surg Pathol 2001;25:1355)
- SOX10
- DOG1
- CD117
Electron microscopy description
- Cells are characterized by clusters of mitochondria, rough endoplasmic reticulum and free ribosomes
- Cytoplasm (sarcoplasm) is filled with myofilaments oriented parallel to the long axis of the cell
- Abundant actin myofilaments present (Acta Ophthalmol Scand 1997;75:470)
Molecular / cytogenetics description
- Genetic heterogeneity
- Mutations in MED12 gene are typically present in pelvic and retroperitoneal leiomyomas (Hum Pathol 2014;45:65)
- HMGA2 and PLAG1 gene aberrations
- Retroperitoneal leiomyoma with EWSR1::PBX3 fusion and KAT6B::KANSL1 fusion has been described (PLoS One 2015;10:e0124288, PLoS One 2015;10:e0117010)
Videos
Myofibroblasts versus smooth muscle
Sample pathology report
- Soft tissue, mass, excision:
- Leiomyoma (see comment)
- Comment: Sections show a well circumscribed mass composed of bland spindle cells with abundant eosinophilic cytoplasm and blunt, cigar shaped nuclei. No necrosis, no mitotic activity and no significant cytologic atypia is identified. Immunohistochemical stains show that the lesional cells are positive for SMA, caldesmon and desmin, while they are negative for S100 protein, HMB45 and DOG1. These results support the above diagnosis. All control slides are stained appropriately.
Differential diagnosis
- Cutaneous leiomyoma (leiomyoma cutis):
- Arises from pilar arrector muscle
- Multiple lesions may be associated with hereditary leiomyomatosis and renal cell cancer syndrome (HLRCC or Reed syndrome) secondary to germline mutation in fumarate hydratase gene
- Angioleiomyoma:
- Painful, subcutaneous lesions
- Numerous thick walled vessels
- PEComa:
- Gastrointestinal stromal tumor (GIST):
- Cellular schwannoma:
- EBV associated smooth muscle tumor:
- Typically occurs in immunocompromised patients
- Positive for EBER ISH
- Smooth muscle tumor of uncertain malignant potential (STUMP):
- Well differentiated smooth muscle tumor
- No atypia and no necrosis
- 1 - 5 mitotic figures per 50 high power fields (HPF) in deep somatic soft tissue (or retroperitoneal / abdominopelvic tumors in men)
- 5 - 10 mitotic figures per 50 HPF in retroperitoneal / abdominopelvic tumors in women
- Leiomyosarcoma:
- More common in deep soft tissue than leiomyoma
- Infiltrative growth pattern
- Necrosis or nuclear pleomorphism present
- More than minimal nuclear pleomorphism and mitotic activity
- If no nuclear pleomorphism or necrosis, > 5 mitotic figures per 50 HPF in deep somatic soft tissue (or retroperitoneal / abdominopelvic tumors in men) and > 10 mitotic figures per 50 HPF in retroperitoneal / abdominopelvic tumors in women
Additional references
Board review style question #1
Which of the following immunohistochemical profiles is most consistent with a leiomyoma of deep soft tissue?
- Desmin+ and MyoD1+
- Desmin+ and SOX10+
- SMA+ and desmin+
- SMA+ and HMB45+
Board review style answer #1
C. SMA+ and desmin+. Leiomyomas frequently show expression of SMA and desmin, which is compatible with smooth muscle differentiation. Answer D is incorrect because it is typically seen in PEComas, which demonstrate immunohistochemical expression of both myogenic and melanocytic markers. Answer A is incorrect because it is seen in tumors with skeletal muscle differentiation, such as rhabdomyoma or rhabdomyosarcoma. Answer B is incorrect because it could be seen in a malignant peripheral nerve sheath tumor (MPNST) with rhabdomyosarcomatous differentiation (malignant triton tumor) among others. SOX10 should be negative in leiomyomas.
Comment Here
Reference: Leiomyoma
Comment Here
Reference: Leiomyoma
Board review style question #2
Which of the following is allowed in a leiomyoma of deep soft tissue?
- < 1 mitotic figure per 50 high power fields (HPF)
- Infiltrative borders
- Necrosis
- Nuclear pleomorphism
Board review style answer #2
A. < 1 mitotic figure per 50 HPF. Leiomyoma of soft tissue is very rare and strict criteria must be followed when making the diagnosis, as malignant smooth muscle tumors are more commonly encountered in deep soft tissue. Answers B - D are incorrect because necrosis, significant nuclear pleomorphism and infiltrative borders are not allowed. Virtually no or very rare mitotic activity (< 1 mitotic figure per 50 HPF) may be seen.
Comment Here
Reference: Leiomyoma
Comment Here
Reference: Leiomyoma
