
Soft tissue
So called fibrohistiocytic
Giant cell tumor of soft tissue
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 3 September 2021
Last staff update: 21 August 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Giant cell tumor of soft tissue

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dehner C, Dehner LP. Giant cell tumor of soft tissue. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuegct.html. Accessed March 31st, 2025.
Definition / general
- Tumor of low malignant potential that is considered the soft tissue analog of giant cell tumor of bone (Mod Pathol 1999;12:894)
Essential features
- Giant cell tumor of soft tissue (GCT-ST) is morphologically identical to giant cell tumor of bone
- Tumor of low grade malignant potential, which is cured by complete surgical resection
- Lacks mutations in the H3F3A gene, which makes it distinct from giant cell tumor of bone
Terminology
- Soft tissue giant cell tumor of low malignant potential
- Giant cell tumor of soft parts
- Extraskeletal giant cell tumor, osteoclastoma of soft tissue (not recommended or commonly used)
ICD coding
Epidemiology
- Rare benign neoplasm, exact incidence unknown
- M = F
- Age average ~40 years (range: 1 - 86 years)
- Can be associated with Paget disease of bone (Diagn Cytopathol 1998;19:352)
Sites
- Arms, hand and thighs are most common sites (Mod Pathol 1999;12:894)
- May develop in superficial or deep soft tissue
- May present multifocal
Clinical features
- Painless mass
Diagnosis
- Indistinguishable from giant cell tumor of bone in the absence of radiology or clinical information
Radiology description
- Soft tissue mass
- Mineralization in some cases
- May present as cystic lesion with internal nodules; nonspecific soft tissue changes adjacent
- Reference: BJR Case Rep 2020;6:20200012
Radiology images
Images hosted on other servers:

T1 and T2 weighted images
Prognostic factors
- Conservative surgical resection with negative margins is curative in the majority of cases
- Local recurrence rate ~6 - 10%
- Lymph node metastasis and distant metastasis very uncommon
- Single cases of malignant GCT-ST with metastases have been reported (Am J Surg Pathol 2000;24:248, Am J Surg Pathol 2000;24:386)
Case reports
- 18 year old woman with a mediastinal mass (World J Surg Oncol 2017;15:137)
- 28 year old man with a painless mass in the spinal muscle of the neck (N Am J Med Sci 2009;1:319)
- 41 year old woman with a left neck mass (Ear Nose Throat J 2019;98:165)
- 73 year old woman with a left thigh lesion (J Cutan Pathol 2009;36 Suppl 1:20)
Treatment
- Surgical resection is curative
Clinical images
Images hosted on other servers:

54 year old man

Firm, polypoid nodule
Gross description
- Up to 10 cm, usually dermis or subcutis, 30% are below superficial fascia
- Well circumscribed, nodular, fleshy, red-brown-gray, gritty at periphery due to calcification
Gross images
Images hosted on other servers:

Gross specimen of GCT-ST
Microscopic (histologic) description
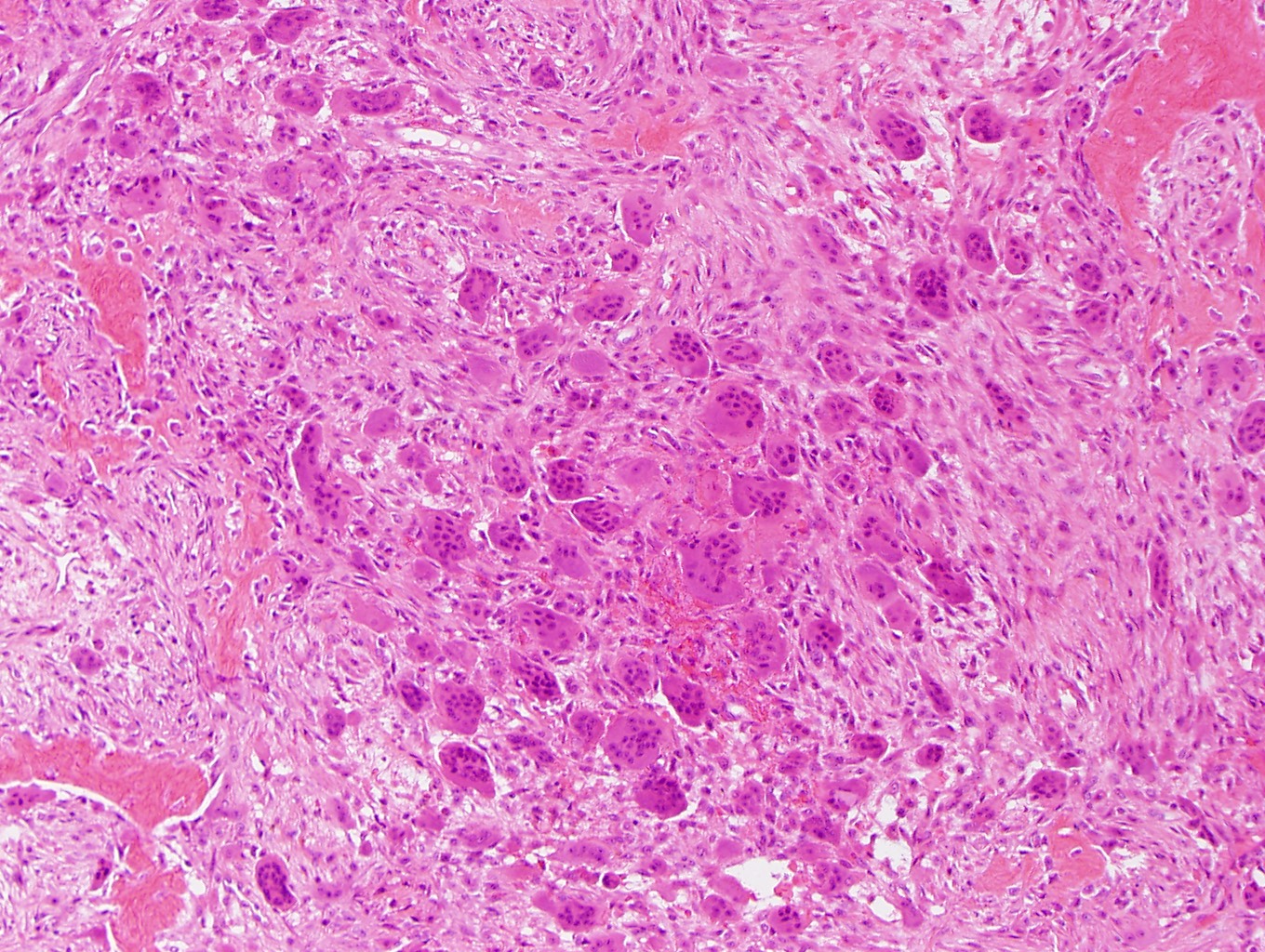
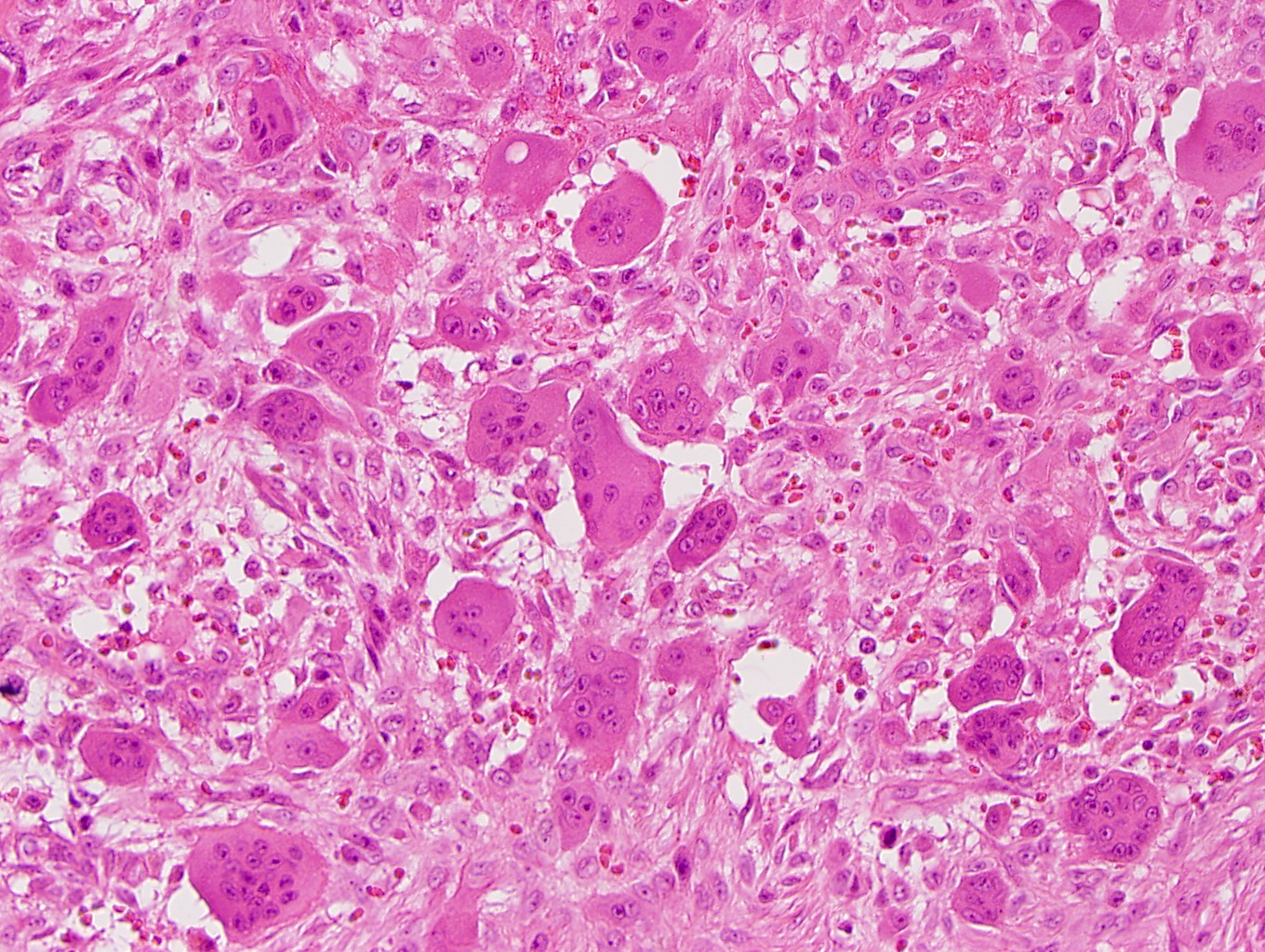
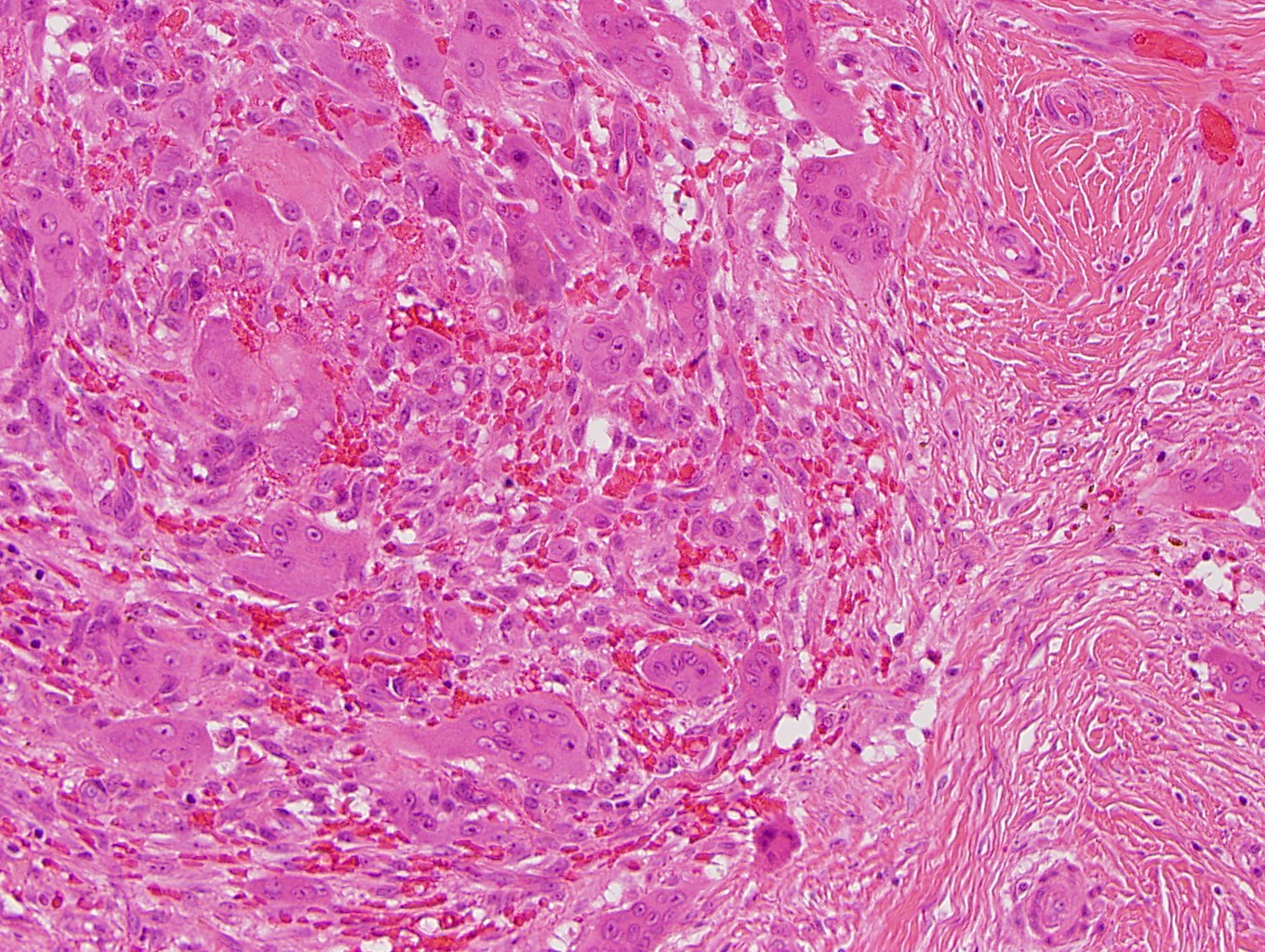
- Tumors present as multinodular lesions diffusely infiltrating soft tissue
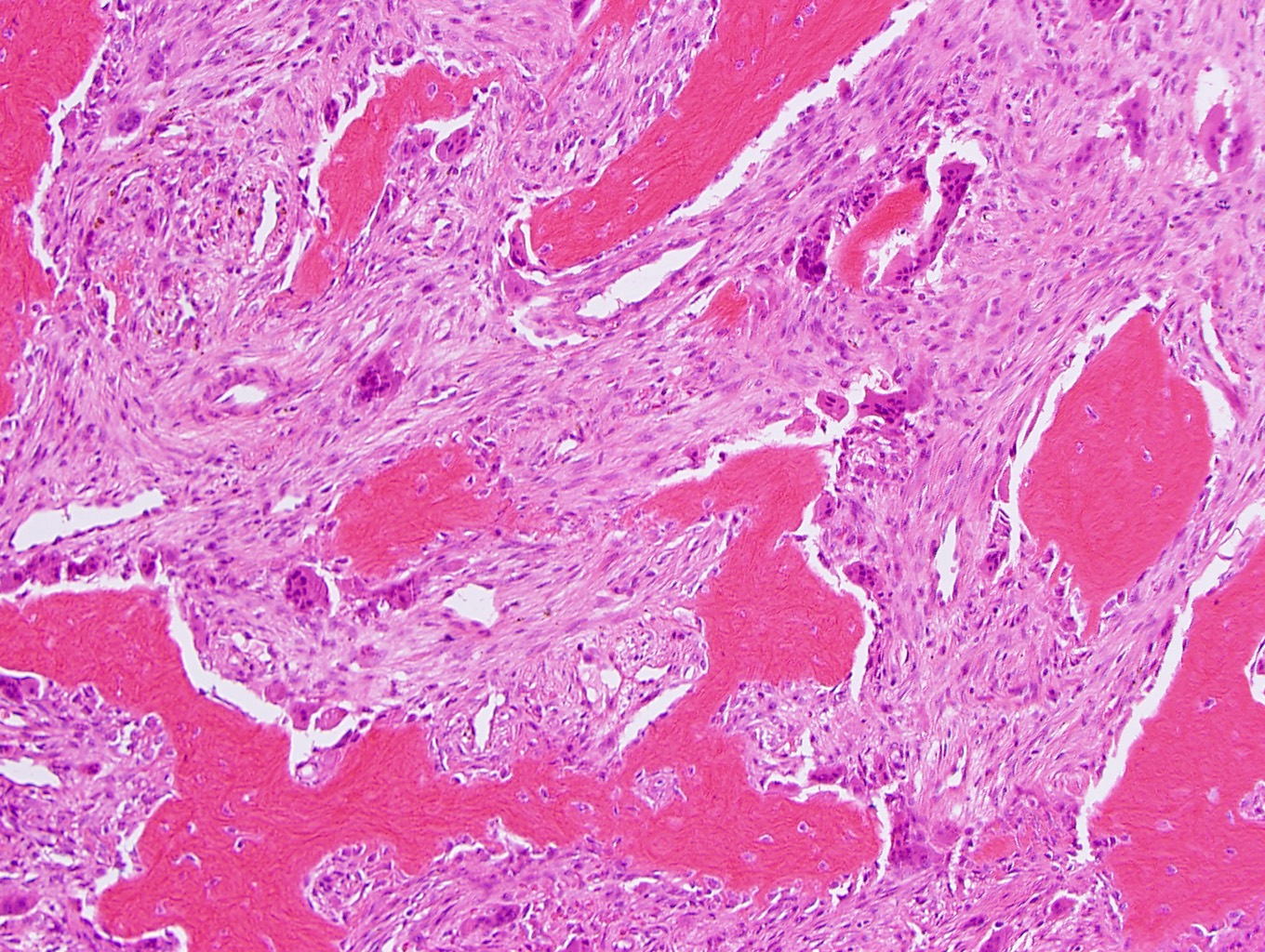
- Tumor nodules consist of a mix of bland, round to oval mononuclear cells, spindle cells and multinucleated giant cells of osteoclast type
- Spindle cells may be arranged in a storiform or fascicular pattern
- Tumors commonly have a peripheral rim of metaplastic bone that may extend to the center
- Hemorrhage and cystic areas, consistent with secondary aneurysmal bone cyst-like changes, are commonly appreciated
- Significant atypia will exclude this diagnosis, however, mitotic activity is commonly seen and may be brisk
- Vascular invasion is seen in up to 50% of cases (Mod Pathol 1999;12:894)
- Necrosis is uncommon
Microscopic (histologic) images
Contributed by Carina Dehner, M.D., Ph.D.
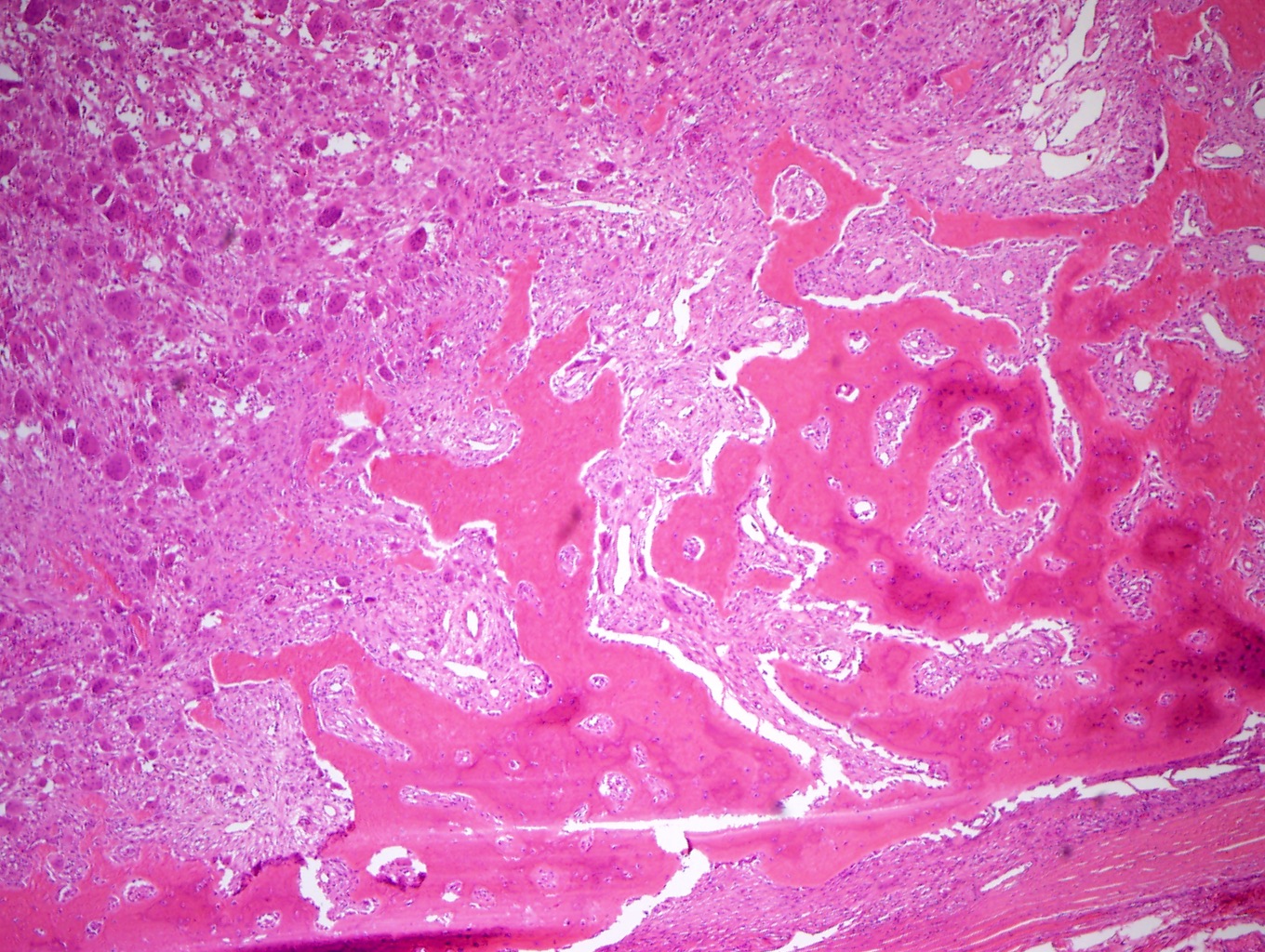
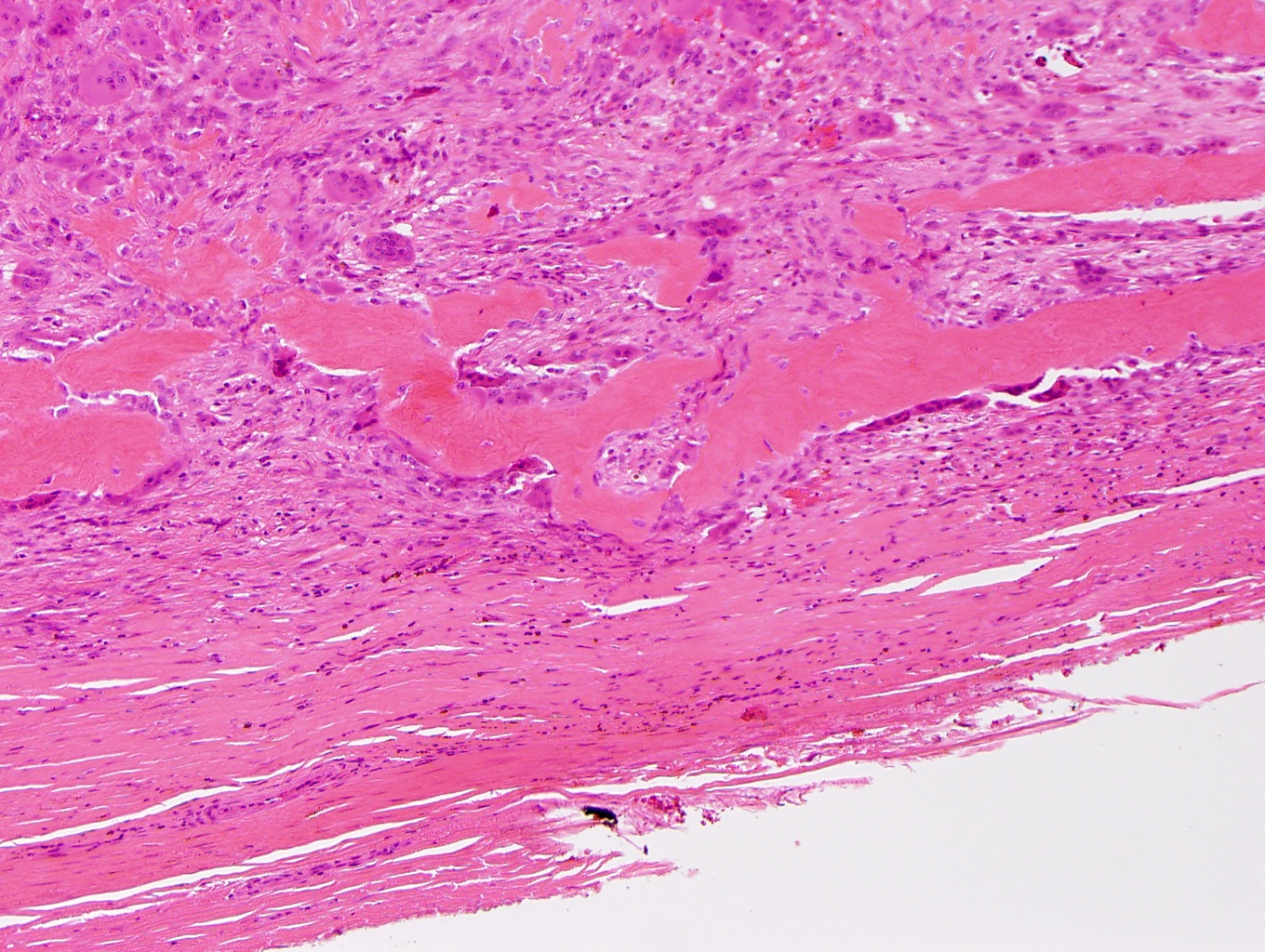
Well circumscribed lesion
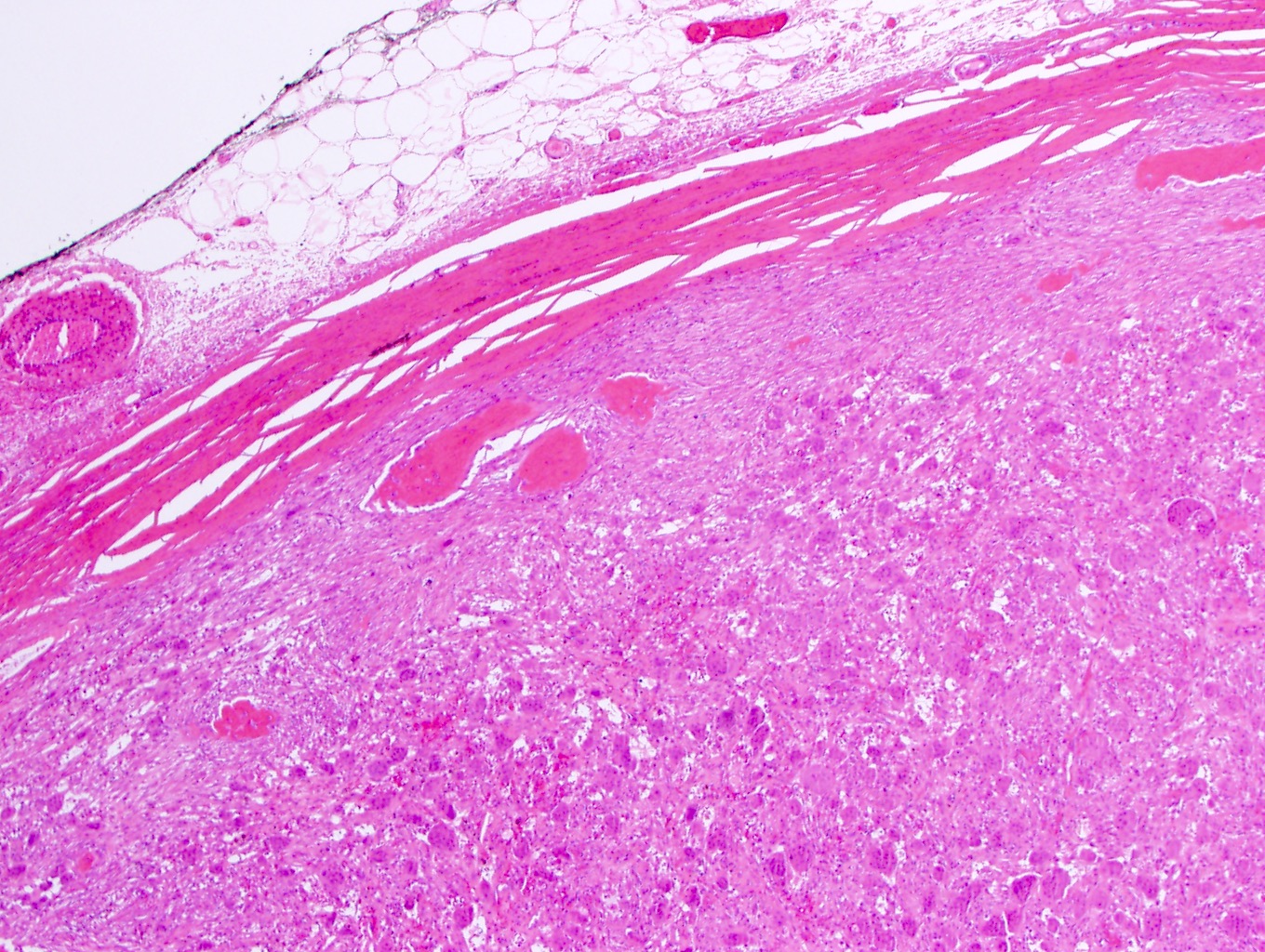
Subcutaneous lesion

Minimal atypia
Spindling of cells
Giant, mononuclear and spindle cells
Mononuclear cells

Epithelioid cells
Lobulated lesion
Cytology description
- Mononuclear stromal cells have oval to spindle shaped nuclei with ill defined cytoplasm lacking significant atypia
- Osteoclast type giant cells are evenly distributed throughout the lesion with bland, vesicular nuclei
- Reference: J Cytol 2009;26:33
Cytology images
Images hosted on other servers:

Multinucleated giant cells
Positive stains
- Vimentin, SMA, CD68, p63 in mononuclear cells
- Osteoclast type giant cells positive for tartrate resistant acid phosphatase (TRAP), TRAIL, RANKL and osteoprotegerin (Hum Pathol 2005;36:945)
Negative stains
- CD45, S100 protein, desmin, lysozyme, SATB2 (different than GCT of bone), H3.3 G34W (Histopathology 2017;71:453, Mod Pathol 1999;12:894)
Molecular / cytogenetics description
- Lacking somatic mutations of the H3F3A gene separating GCT-ST from their bone counterpart (Mod Pathol 2017;30:728, Histopathology 2017;71:453)
Sample pathology report
- Soft tissue, left arm, excision:
- Giant cell tumor of soft tissue, 3.5 cm, involving dermis and subcutis (see comment)
- Comment: Provided hematoxylin and eosin stained sections show a well circumscribed, multinodular tumor composed of sheets of evenly distributed, multinucleated giant cells of osteoclast type. The latter are intervened by abundant mononuclear cells, some of which show spindling. Immunohistochemical studies (single stain antibody procedure with adequate controls) show that tumor cells are positive for SMA (patchy) and CD68, while negative for S100 protein, CD45 and desmin. An immunohistochemical study for H3K34W is negative, ruling out a metastasis of giant cell tumor primary to the bone. Morphologic and immunohistochemical studies support the diagnosis of giant cell tumor of soft tissue.
Differential diagnosis
- Giant cell tumor of bone:
- If a tumor with this morphology presents in the subcutaneous tissue, giant cell tumor of soft tissue should be considered; consider molecular testing
- Tenosynovial giant cell tumor, localized type:
- Located near tendons, more prominent hyalinization of stroma
- Xanthomatous cells, siderophages and lymphocytes are commonly admixed with the population of osteoclast type giant cells and mononuclear and spindle cells
- Giant cell rich variants of undifferentiated pleomorphic sarcoma:
- Striking atypia, atypical mitotic figures and necrosis
- Malignant melanoma with osteoclast-like giant cells:
- Can have different morphological features (spindle cell, nodular, desmoplastic or pleomorphic cells with admixed giant cells), may have pigment
- Leiomyosarcoma with osteoclast-like giant cells:
- May present as cellular spindle cell lesion with osteoclast type giant cells
- However, the spindle cell component will usually express SMA, desmin and caldesmon and lack the peripheral shell of bone (Zhonghua Bing Li Xue Za Zhi 2011;40:363)
- Keratin positive giant cell rich tumor of soft tissue:
- Shows a predilection for younger, female patients
- Demonstrates a fibrous pseudocapsule with a lymphoid cuff
- Contains a variable number of mononuclear, presumed to be epithelial, cells that express keratin
- Lacks the peripheral shell of metaplastic bone
- Harbors a HMGA2::NCOR2 fusion (Surg Pathol Clin 8 August 2023[Epub ahead of print])
Additional references
Board review style question #1
The tumor shown in the image above presented as a subcutaneous mass in the arm. What is the diagnosis?
- Giant cell tumor of bone
- Giant cell tumor of soft tissue
- Tenosynovial giant cell tumor, localized type
- Undifferentiated pleomorphic sarcoma
Board review style answer #1
B. Giant cell tumor of soft tissue presents as subcutaneous lesion rather than a bone lesion (therefore, A is wrong). It has a peripheral shell of metaplastic bone (which distinguishes it from C) and is not as atypical as D.
Comment Here
Reference: Giant cell tumor of soft tissue
Comment Here
Reference: Giant cell tumor of soft tissue
Board review style question #2
What genetic aberration may be helpful to distinguish primary giant cell tumor of soft tissue from a metastasis of a giant cell tumor of bone?
- Lack of a mutation in H3F3A
- Presence of a mutation in H3F3A
- Presence of a mutation in CSF1
- Presence of a mutation in H3K36M
Board review style answer #2
A. H3F3A mutations can be found in giant cell tumor of bone but not in giant cell tumor of soft tissue. CSF1 is the molecular feature of tenosynovial giant cell tumor and H3K36M is the mutation found in chondroblastoma.
Comment Here
Reference: Giant cell tumor of soft tissue
Comment Here
Reference: Giant cell tumor of soft tissue
