
Soft tissue
Fibroblastic / myofibroblastic
Fibrosarcoma
Infantile fibrosarcoma
Authors: Patrick Azar, M.D., Laura Warmke, M.D.
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 6 December 2024
Last staff update: 6 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Infantile fibrosarcoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Azar P, Warmke L. Infantile fibrosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuefibrosarcomainfantile.html. Accessed March 30th, 2025.
Definition / general
- Fibroblastic tumor, most commonly occurring in infancy
- Locally aggressive but infrequently metastasizes
- Characterized by ETV6::NTRK3 fusion or other fusions leading to oncogenic activation of tyrosine kinase signaling
Essential features
- Occurs in infants and young children
- Primitive ovoid / round cell or spindle cell tumor arranged in sheets or fascicles with hemangiopericytoma (HPC)-like vessels
- ETV6::NTRK3 fusion or other fusions / activating alterations of receptor tyrosine kinase pathway genes (e.g., NTRK1, NTRK2, NTRK3, RET, MET, BRAF)
Terminology
- Congenital fibrosarcoma
- Cellular congenital mesoblastic nephroma (analogous tumor in kidney)
ICD coding
- ICD-O: 8814/3 - infantile fibrosarcoma
- ICD-11: 2B5F.2 & XH7BC6 - sarcoma, not elsewhere classified of other specified sites & infantile fibrosarcoma
Epidemiology
- Congenital or tends to arise in the first 2 years of life
- Median age is 3 - 4 months (Cancer 1976;38:729)
- Majority (75%) occur during the first year of life
- < 10% occur in older children and adults (Am J Surg Pathol 2018;42:28)
- Slight male predominance
Sites
- Most commonly involves the superficial and deep soft tissues of the extremities
- Less commonly occurs on trunk and in head and neck region
- Intra-abdominal, retroperitoneal and visceral sites have been reported (Cancer 1976;38:729, Fetal Pediatr Pathol 2011;30:329)
- Analogous tumors in the kidney are designated as cellular congenital mesoblastic nephroma (Cancer Res 1998;58:5046, Nat Commun 2018;9:2378)
Pathophysiology
- Oncogenesis is through the activation of kinase signaling, most commonly from in frame gene fusions or less frequently, through activating mutations (Nat Commun 2018;9:2378)
- Most frequent genetic alteration is the ETV6::NTRK3 gene fusion resulting from the t(12;15)(p13;q25) chromosomal translocation
- Other NTRK3 fusion partners have been reported, including EML4::NTRK3 fusions (Mod Pathol 2018;31:463)
- Alternative fusions have been described involving other tyrosine kinase genes, including NTRK1, NTRK2, RET, MET and RAF1 (Am J Surg Pathol 2019;43:374, Am J Surg Pathol 2018;42:28)
- BRAF fusions, complex deletions and point mutations have been described (Am J Surg Pathol 2018;42:28, Nat Commun 2018;9:2378)
Etiology
- Unknown
Clinical features
- Large solitary neoplasm
- Typically presents as a painless mass or exophytic nodule
- Rapid growth may occur (Cancer 1976;38:729)
- Overlying skin may be ulcerated
- Dilated vessels and hemorrhage may be present, resembling a vascular tumor (Pediatr Dermatol 2006;23:330, Pediatr Radiol 2014;44:1124)
Diagnosis
- Biopsy and histological examination are necessary for definitive diagnosis
Radiology description
- Variable findings on multiple imaging modalities
- Large soft tissue mass
- May show osseous erosion
- Ultrasound
- Often the first imaging method used for palpable soft tissue masses
- Solid to complex with solid and cystic components
- Variable echogenicity
- Hypervascularity is seen in the majority of cases, which can lead to being misdiagnosed as vascular malformation (Clin Radiol 2022;77:e532)
- Magnetic resonance imaging (MRI)
- Solid and cystic with heterogeneous intensity and enhancement
- Highly cellular component makes it hyperintense on T2 weighted scans
- Isointense on T1 weighted imaging relative to skeletal muscle
- Heterogeneous enhancement with well defined margins
- Hemorrhagic components and necrosis are more common in larger masses (Radiographics 2016;36:1195)
- Calcifications and osseous involvement are rare
Radiology images
Images hosted on other servers:

3 month old boy with right arm mass

4 month old boy with calf mass
Prognostic factors
- Overall favorable prognosis with treatment
- Locally aggressive, infrequently metastatic tumor
- With surgery or cytotoxic chemotherapy, the 10 year overall survival rate is ~90% (Cancer 1976;38:729)
- Spontaneous regression is rare but has been reported
- Local recurrence rates range from 20 to 40%
- Subset of patients (8 - 15%) develop metastasis (Am J Surg Pathol 2019;43:435)
- Mortality ranges from 5 to 25%
Case reports
- Newborn girl presented with a rapidly enlarging perineal mass discovered on prenatal ultrasonography (BMC Pediatr 2023;23:327)
- 25 day old boy presented with a large, hypervascular abdominal wall mass (Radiol Case Rep 2024;19:3176)
- 6 month old boy presented with an enlarging tongue mass (Cureus 2023;15:e49586)
- 2 year old boy presented with a mass in the distal radius (J Orthop Case Rep 2023;13:58)
Treatment
- Complete excision with tumor free margins may be difficult
- Combined chemotherapy and surgery
- Targeted tyrosine kinase inhibitor therapies may be used
- Larotrectinib has been shown to help successfully treat tumors with NTRK fusions (Pediatr Blood Cancer 2020;67:e28330, Cancer Discov 2015;5:1049)
Gross description
- Size of the tumor varies, ranging from 10 to > 150 mm
- Poorly circumscribed tumor, infiltrating into the surrounding soft tissue
- Subset have a thin, fibrous pseudocapsule (Cancer 1977;40:1711, Am J Surg Pathol 2019;43:435)
- Firm, gray-white cut surface
- Hemorrhagic and necrotic foci are often present
Gross images
Contributed by Sadia Sayeed, M.D. and AFIP

Focal ulceration

Amputation

Amputation with ulceration

Solid and cystic

Heterogeneous cut surface
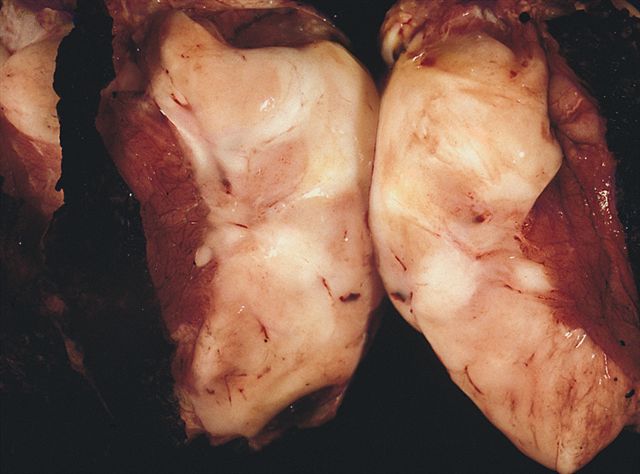
Fleshy white
mass similar
to adult
fibrosarcoma
Microscopic (histologic) description
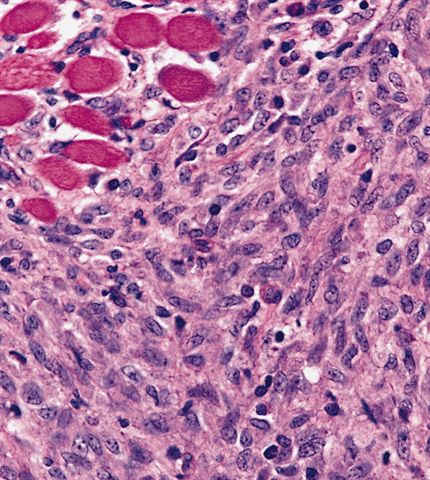
- Cellular neoplasm composed of primitive, immature tumor cells
- Plump, spindled, immature appearing fibroblastic tumor cells arranged in short fascicles
- Usually very little cellular pleomorphism
- Scattered chronic inflammatory cells, especially lymphocytes, interspersed between tumor cells
- Prominent chronic inflammation may be present (Cancer 1976;38:729)
- Often has prominent ectatic or hemangiopericytoma-like vasculature
- Background stroma may be myxoid or collagenous
- Subset of cases may have decreased cellularity mimicking a benign lesion (Pediatr Dev Pathol 2012;15:127)
- Mitotic counts range widely with no atypical mitotic forms (Cancer 1976;38:729)
- Areas of tumor necrosis or hemorrhage are frequent
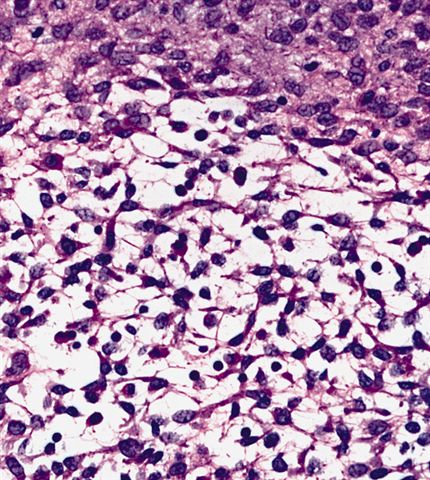
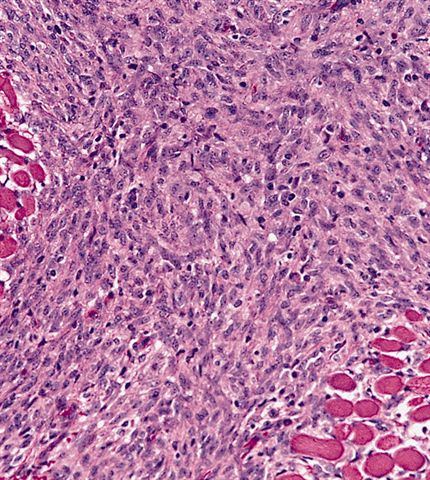
Microscopic (histologic) images
Contributed by Jessica L. Davis, M.D. and AFIP

Spindle cell neoplasm

HPC-like vessels

Primitive spindle cells

Cellular spindle cell neoplasm

Lymphocytes

Fascicular growth

Fascicular growth with HPC-like vessels

EML4::NTRK3 fusion

Fibromatosis-like areas
Myxoid area
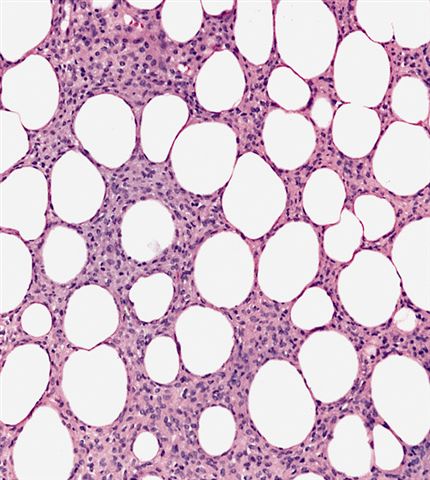
Infiltration of fat
Infiltration of muscle
Spindle cells
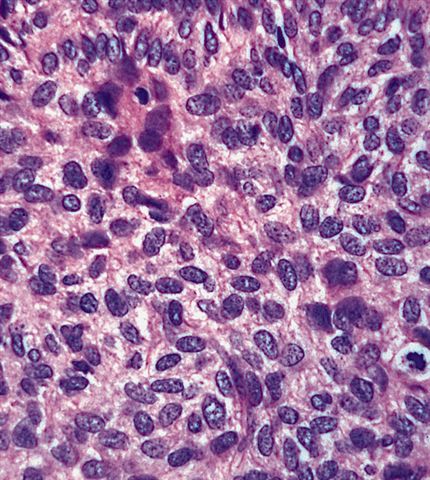
Plump cells

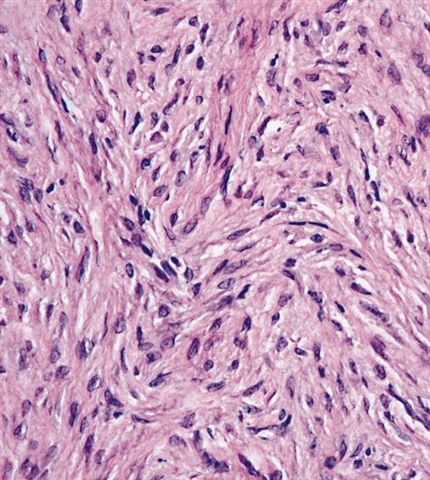
Less cellular tumor that overlaps with infantile fibromatosis

Pan-TRK
Virtual slides
Images hosted on other servers:

Infantile fibrosarcoma
Positive stains
- Pan-TRK in tumors harboring NTRK gene rearrangements, nuclear staining in lesions with NTRK3 fusions and cytoplasmic staining in lesions with NTRK1 and NTRK2 fusions (Histopathology 2018;73:634)
- SMA (variable)
- S100 protein (variable)
- CD34 (variable)
Negative stains
- Desmin (rarely positive)
- MyoD1
- Myogenin
- CK cocktail
Electron microscopy description
- Features of fibroblasts and myofibroblasts (Adv Anat Pathol 2004;11:190)
- Large tumor cell nuclei
- Dilated rough endoplasmic reticulum
- Abundant lysosomes
Molecular / cytogenetics description
- Gene fusions or activating alterations involving receptor tyrosine kinase or downstream effector molecules (Am J Surg Pathol 2000;24:937)
- Most cases contain chromosomal translocation t(12;15)(p13;q26), corresponding to an NTRK3::ETV6 gene fusion
- Other NTRK3 fusion partners have been reported (e.g., EML4::NTRK3)
- Alternate fusions involving other tyrosine kinase genes have been reported with a variety of fusion partners (e.g., NTRK1, NTRK2, MET, RET, BRAF)
Videos
Fibrosarcoma and herringbone pattern
Sample pathology report
- Soft tissue, right arm, mass, excision:
- Infantile fibrosarcoma (see comment)
- Comment: Sections show a highly cellular neoplasm composed of monotonous, primitive spindle cells with a fascicular growth pattern and scattered hemangiopericytoma-like vessels. Numerous mitotic figures and focal areas of necrosis are present. Immunohistochemical stains show that the tumor cells are positive for vimentin and pan-TRK, while they are negative for CK cocktail, S100 protein and desmin. Additional molecular testing revealed a NTRK3::ETV6 fusion, supporting the above diagnosis.
Differential diagnosis
- Desmoid fibromatosis:
- Bland spindle cell proliferation
- Low proliferative activity
- Nuclear expression of beta catenin
- May be associated with familial adenomatosis polyposis (Gardner syndrome)
- Infantile myofibroma / myofibromatosis:
- Biphasic growth
- Mature spindled myogenic tumor cells
- Immature ovoid tumor cells with numerous vessels
- Immunohistochemical expression of actins
- Recurrent PDGFRB alterations
- Do not metastasize to distant sites
- May occur as solitary tumors or multiple tumors with or without visceral involvement
- Congenital / infantile spindle cell rhabdomyosarcoma:
- Scattered rhabdomyoblasts
- Focal expression of desmin and myogenin
- Gene fusions involving VGLL2, SRF, TEAD1, NCOA2 and CITED2 (Genes Chromosomes Cancer 2013;52:538, Am J Surg Pathol 2016;40:224)
- In older children, spindle cell rhabdomyosarcoma may have a MYOD1 p.L122R point mutation
- Inflammatory myofibroblastic tumor:
- Occurs most often in viscera and deep soft tissue
- Myxoid stromal changes are usually present
- Prominent inflammatory infiltrate with lymphocytes and plasma cells
- Immunohistochemical expression of ALK in 40 - 60% of cases
- Some patients develop a constitutional inflammatory syndrome including fever, malaise, weight loss and anemia
- Low grade myofibroblastic sarcoma:
- Usually occurs in adults
- Diffuse infiltration of preexisting structures
- Tumor necrosis is usually absent
- Predilection for head and neck sites
Additional references
Board review style question #1
Which of the following gene fusions is most commonly seen in infantile fibrosarcoma and corresponds to a t(12;15)(p13;q26) chromosomal translocation?
- COL1A1::PDGFB
- EWSR1::ATF1
- NTRK3::ETV6
- SS18::SSX
Board review style answer #1
C. NTRK3::ETV6. NTRK3::ETV6 gene fusions are most commonly seen in infantile fibrosarcoma and correspond to the t(12;15)(p13;q26) chromosomal translocation. Answer A is incorrect because COL1A1::PDGFB fusions are associated with dermatofibrosarcoma protuberans (DFSP). Answer D is incorrect because SS18::SSX fusions are seen in synovial sarcoma. Answer B is incorrect because EWSR1::ATF1 fusions may be seen in clear cell sarcoma of soft tissue.
Comment Here
Reference: Fibrosarcoma-infantile
Comment Here
Reference: Fibrosarcoma-infantile
Board review style question #2
Which of the following tumors occurs in the kidney and is analogous to infantile fibrosarcoma, having the identical gene fusion and histologic morphology?
- Cellular congenital mesoblastic nephroma
- Cellular infantile fibromatosis
- Infantile myofibroma
- Spindle cell rhabdomyosarcoma
Board review style answer #2
A. Cellular congenital mesoblastic nephroma. Cellular congenital mesoblastic nephroma is analogous to infantile fibrosarcoma, occurs in the kidney and has the identical gene fusion. Answers B, C and D are incorrect because infantile myofibroma, cellular infantile fibromatosis and spindle cell rhabdomyosarcoma are all not analogous to infantile fibrosarcoma and do not carry the same fusion.
Comment Here
Reference: Fibrosarcoma-infantile
Comment Here
Reference: Fibrosarcoma-infantile
