

Soft tissue
Adipose tissue tumors
Liposarcoma
Atypical spindle cell / pleomorphic lipomatous tumor
Author: Borislav A. Alexiev, M.D.
Editorial Board Members: Nasir Ud Din, M.B.B.S., Farres Obeidin, M.D.

Last author update: 15 December 2022
Last staff update: 25 July 2023
Copyright: 2022-2024, PathologyOutlines.com, Inc.
PubMed Search: Atypical spindle cell / pleomorphic lipomatous tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Alexiev BA. Atypical spindle cell / pleomorphic lipomatous tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueaslt.html. Accessed December 31st, 2024.
Definition / general
- Atypical spindle cell / pleomorphic lipomatous tumor is a benign adipocytic neoplasm characterized by ill defined margins and the presence of variable proportions of mild to moderate atypical spindle cells, adipocytes, lipoblasts, pleomorphic cells, multinucleated giant cells and a myxoid or collagenous extracellular matrix
Essential features
- Variable proportions of atypical spindle cells, adipocytes, floret-like giant cells, univacuolated or multivacuolated lipoblasts, pleomorphic (multinucleated) cells and a fibromyxoid extracellular matrix with ropy collagen bundles
- RB1 is lost in a substantial subset of cases (50 - 70%), correlating with RB1 deletion (Am J Surg Pathol 2017;41:234, Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Virchows Arch 2014;465:97)
- Lack of MDM2 or CDK4 amplification
Terminology
- Atypical spindle cell lipoma
- Not recommended: spindle cell liposarcoma, fibrosarcoma-like lipomatous tumor
ICD coding
- ICD-O: 8857/0 - spindle cell lipoma
- ICD-11: 2E80 & XH4E98 - benign lipomatous neoplasm & spindle cell lipoma
Epidemiology
- Occurs predominantly in middle aged adults but can affect patients of any age (Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Am J Surg Pathol 2017;41:234)
- Slight male predominance
Sites
- Arises in the subcutis and deep somatic soft tissues and only occasionally arises in intracavitary or visceral locations
- Anatomical distribution is wide, predominating in the limbs and limb girdles
- Less common locations are the head and neck, genital area, trunk and back (Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Am J Surg Pathol 2017;41:234)
Pathophysiology
- Deletions or losses in 13q14, including RB1 and its flanking genes, have been identified in a substantial subset of cases (Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Am J Surg Pathol 2017;41:234, Int J Surg Pathol 2019;27:521, Virchows Arch 2014;465:97)
- Monosomy 7 has been reported in some cases (Am J Surg Pathol 2017;41:234)
Etiology
- Unknown
Clinical features
- Presents as a persistent or enlarging soft tissue mass
Diagnosis
- Tissue sampling is the gold standard for a definitive diagnosis; molecular testing for MDM2 / CDK4 and RB1 may be useful on biopsy
Radiology description
- Description of radiographic features of this entity is very scarce in the literature
- MRI is likely the most suitable imaging modality for the characterization of these tumors
Radiology images
Contributed by Borislav A. Alexiev, M.D.

MRI
Prognostic factors
- Has a low rate of local recurrence (10 - 15%) for incompletely removed lesions
- No documented risk for metastasis
- Most patients have an excellent prognosis if the tumor is completely excised (Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Am J Surg Pathol 2017;41:234, Int J Surg Pathol 2019;27:521, Virchows Arch 2014;465:97, J Clin Pathol 2018;71:483)
Case reports
- 31 year old woman with tumor on the ulnar side of her right hand (J Hand Surg Am 2022;47:587.e1)
- 58 year old man with enlarging painless mass at his right groin region (Cureus 2021;13:e19410)
- 63 year old man with soft tissue mass on the right ankle (Int J Surg Pathol 2019;27:521)
- 74 year old man with pedunculated cutaneous nodule (Case Rep Pathol 2021;2021:4082289)
- 74 year old man with tumors on both side of the tongue (Yonago Acta Med 2020;63:223)
Treatment
- Complete surgical excision (i.e., lesion free margin) is the appropriate treatment (Cureus 2021;13:e19410)
Clinical images
Images hosted on other servers:

Right groin region mass
Gross description
- Nonencapsulated mass with nodular or multinodular growth pattern
- Gray-yellow cut surface, without necrotic areas (Cureus 2021;13:e19410)
Gross images
Contributed by Borislav A. Alexiev, M.D.
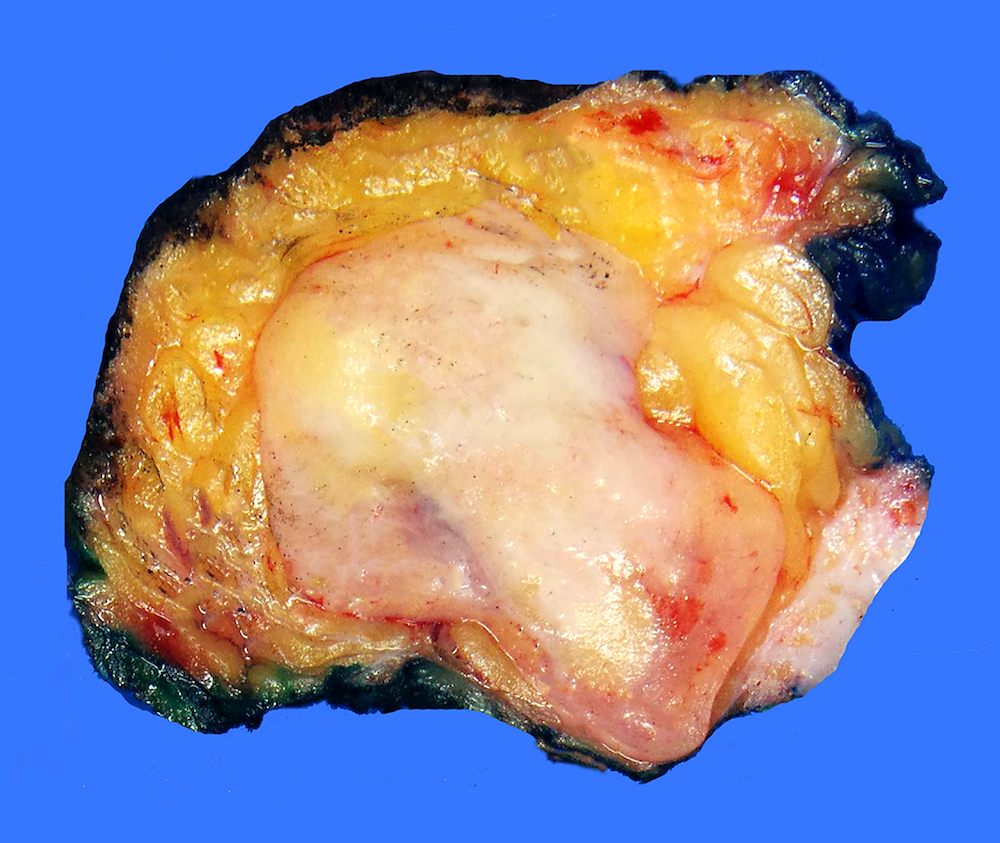
Soft tissue mass
Frozen section description
- Frozen section diagnosis is generally not recommended (Cureus 2021;13:e19410)
Microscopic (histologic) description
- Ill defined tumor margins (Pathol Int 2018;68:550, Am J Surg Pathol 2017;41:1443, Am J Surg Pathol 2017;41:234, Int J Surg Pathol 2019;27:521, Virchows Arch 2014;465:97, J Clin Pathol 2018;71:483)
- Variable proportions of mild to moderately atypical spindle cells, adipocytes, lipoblasts, floret-like multinucleated cells
- Adipocytic component has a predominantly mature morphology, with variation of adipocyte size and shape
- Focal, mild to moderate adipocytic atypia with nuclear enlargement and chromatin coarsening can be observed
- Lipoblasts can vary from small and univacuolated or bivacuolated to larger and multivacuolated (pleomorphic)
- Bizarre, hyperchromatic, pleomorphic multinucleated cells are often scattered within the spindle cells or adipocytic components
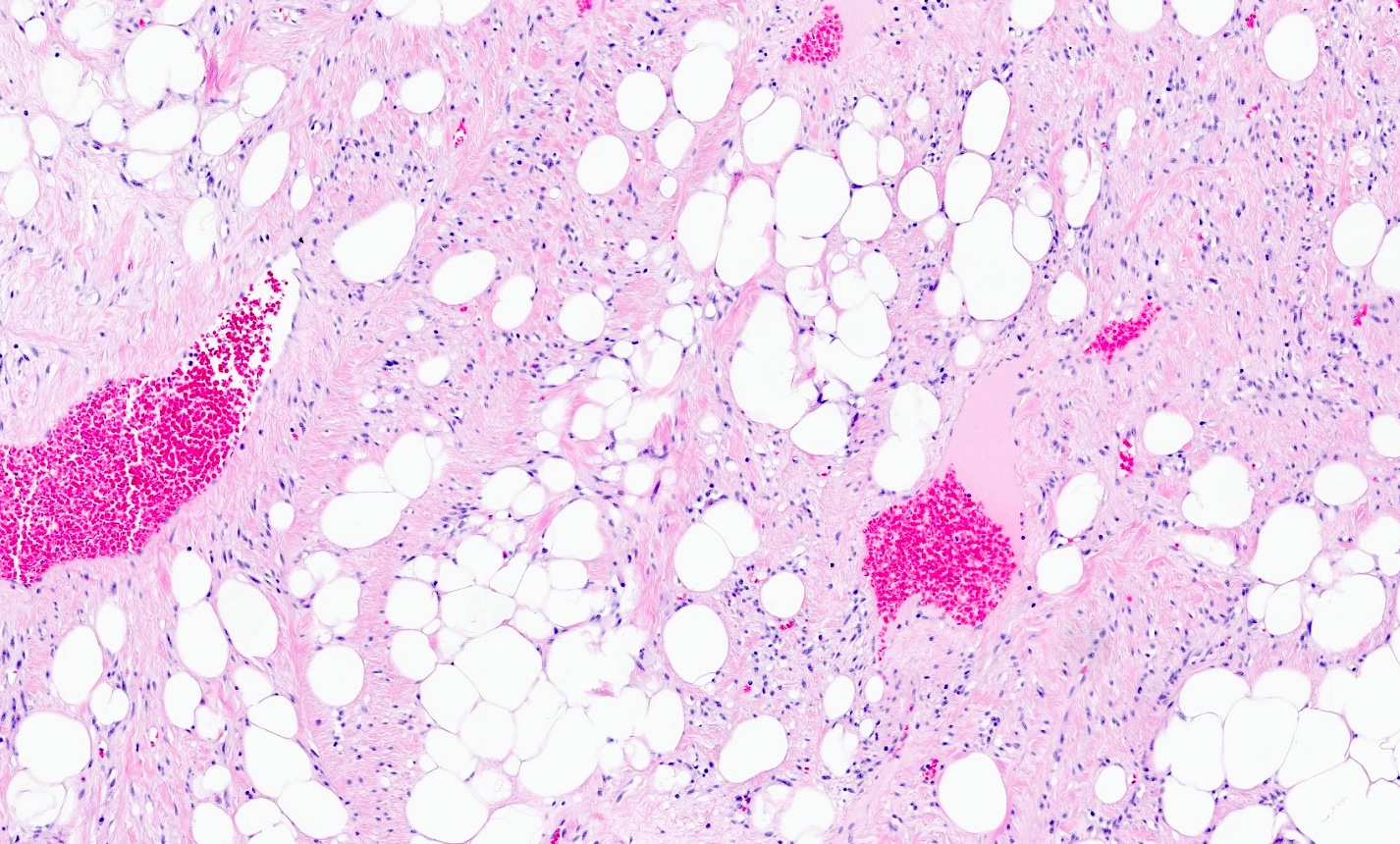
- Myxoid or collagenous extracellular matrix with ropy collagen bundles
- Mitotic figures are often present but are mostly scarce
- Tumor necrosis is absent
- Heterologous differentiation, including the presence of smooth muscle, cartilage or bone, is rarely observed
Microscopic (histologic) images
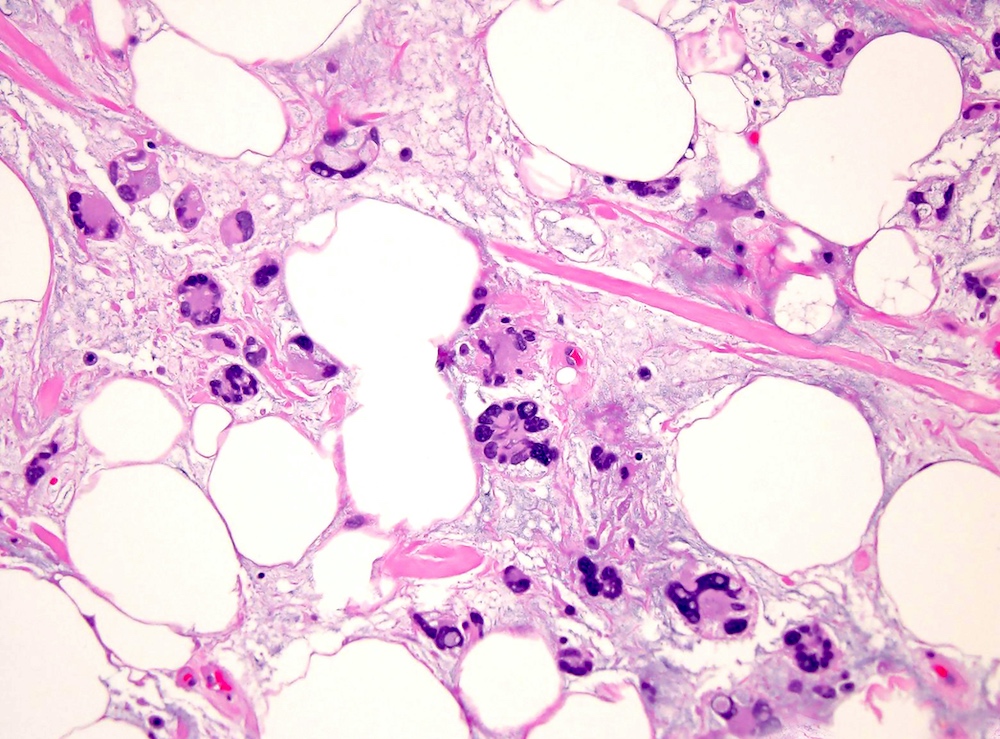
Contributed by Borislav A. Alexiev, M.D. and Farres Obeidin, M.D.
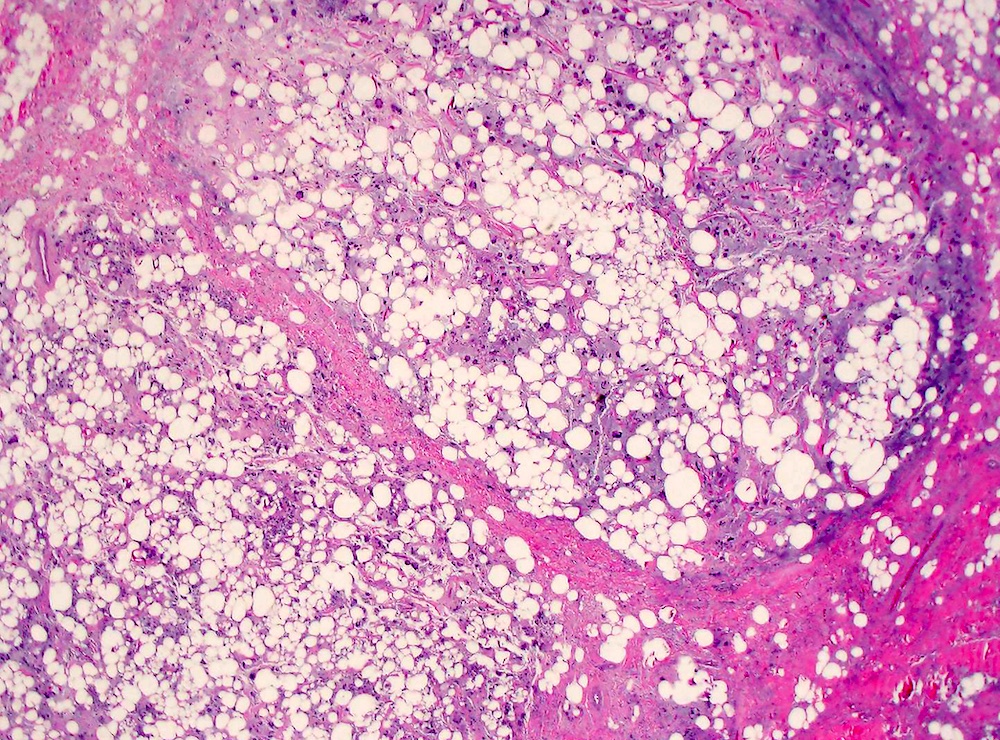
Adipocytic neoplasm
Pleomorphic lipoma-like morphology
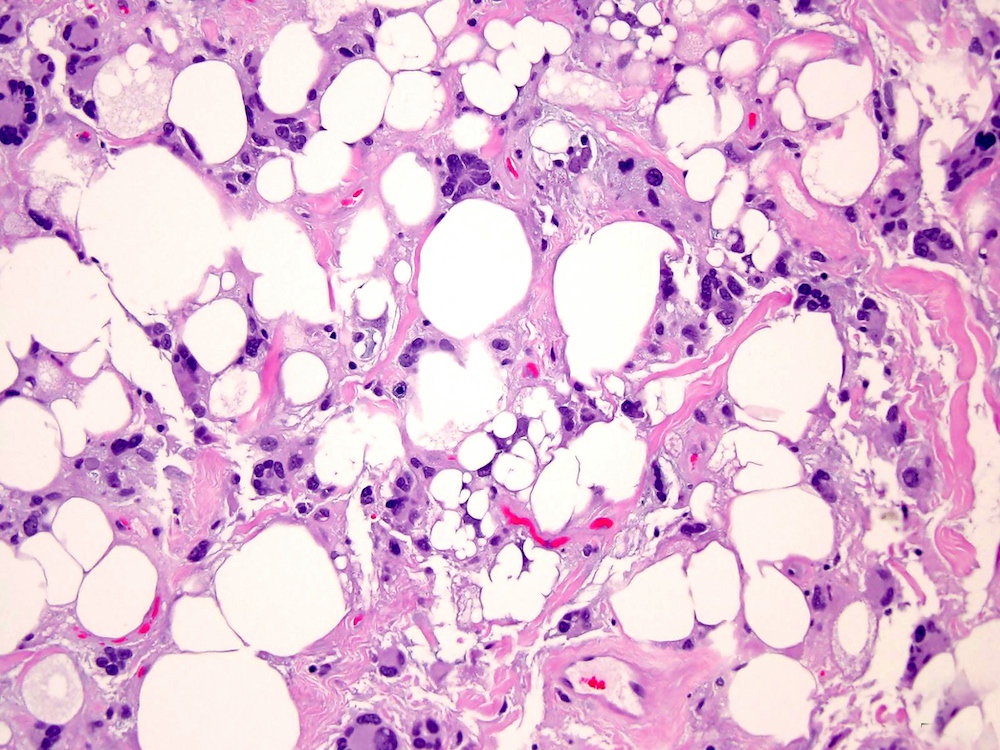
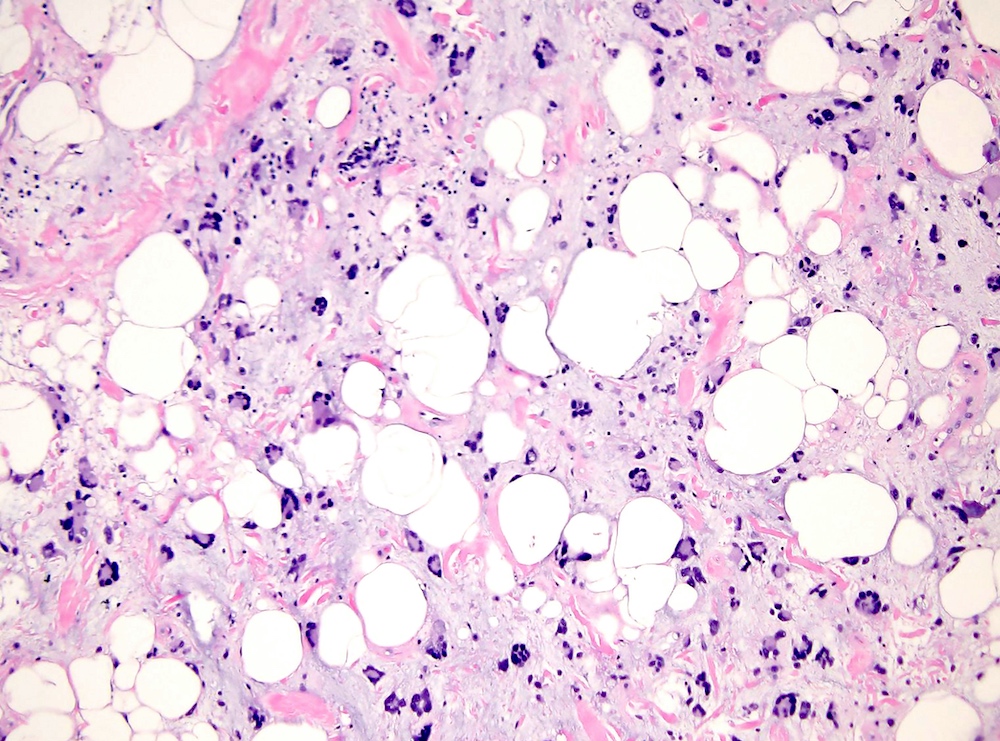
Atypical lipoblasts
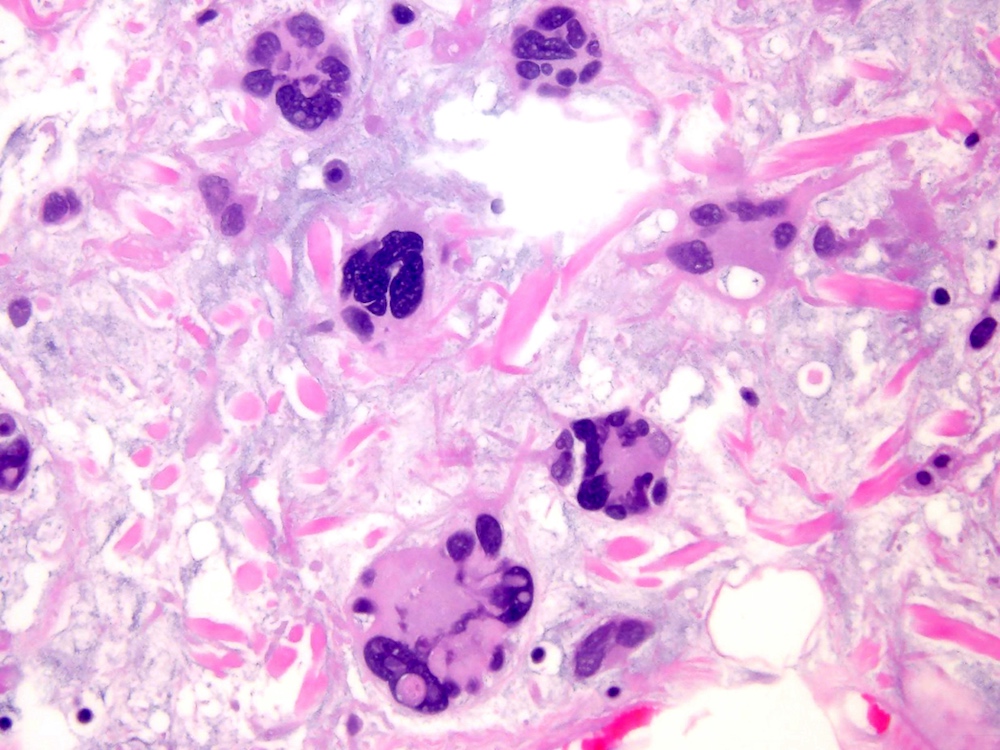
Pleomorphic multinucleated cells
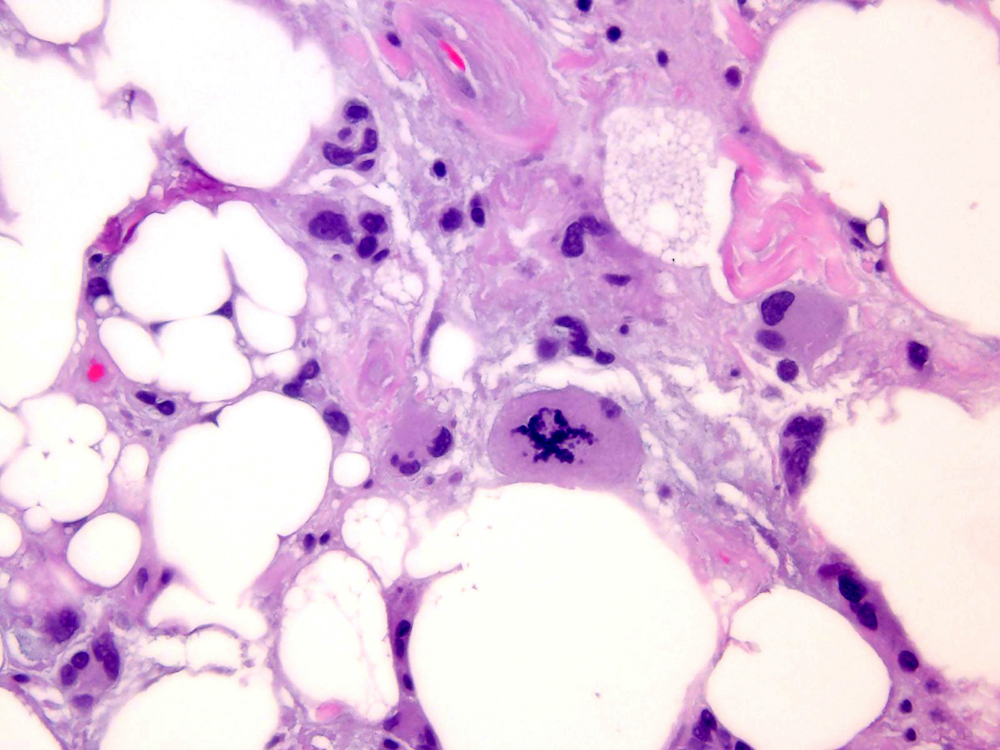
Atypical mitosis
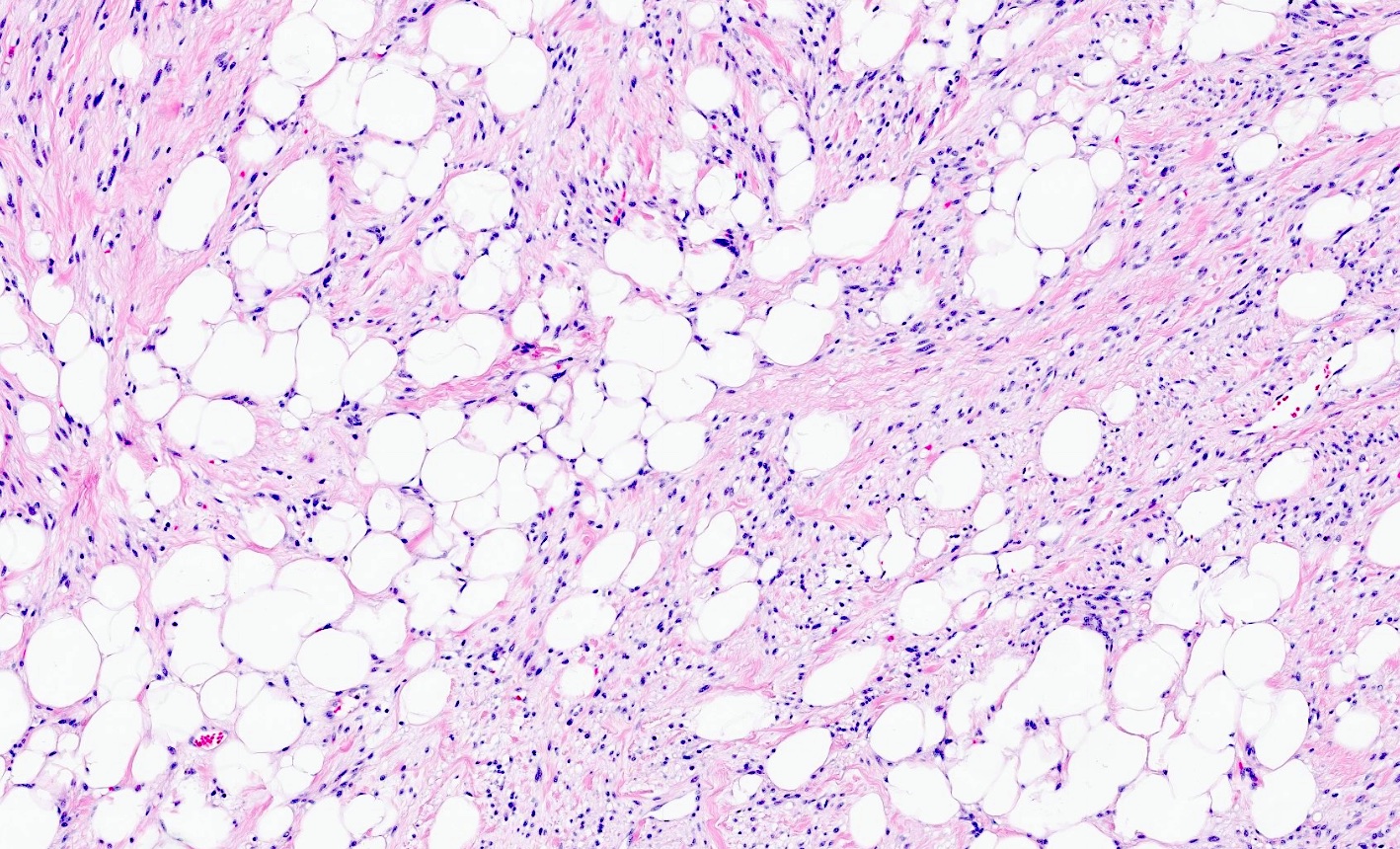
Variation in adipocyte size

Mild to moderate cytologic atypia

Cellular areas
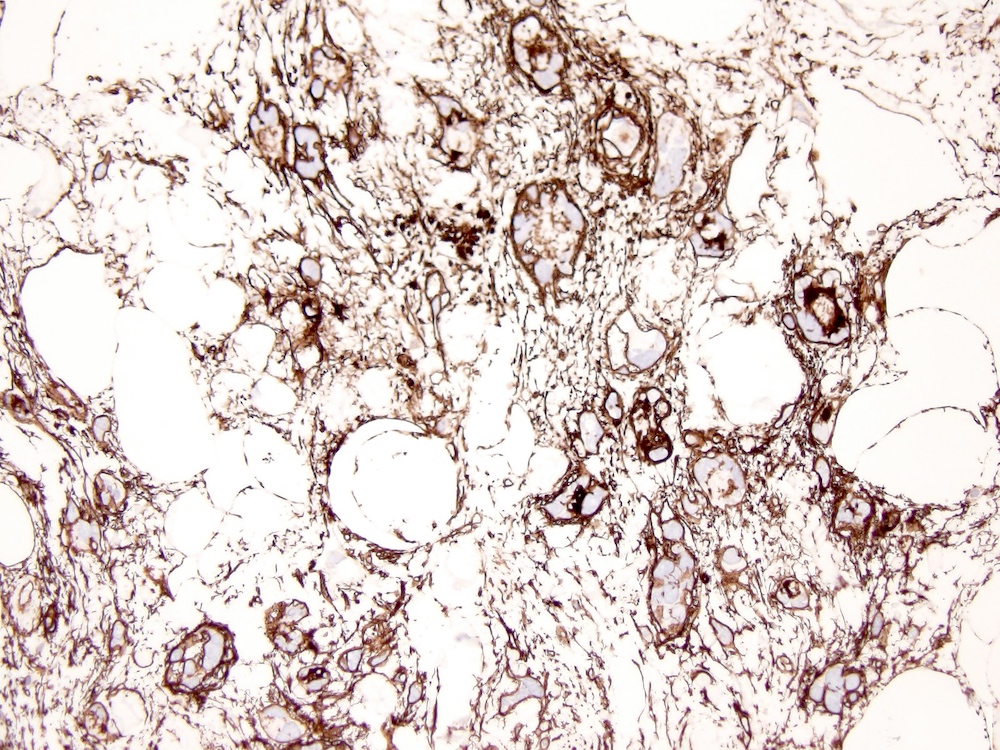
CD34
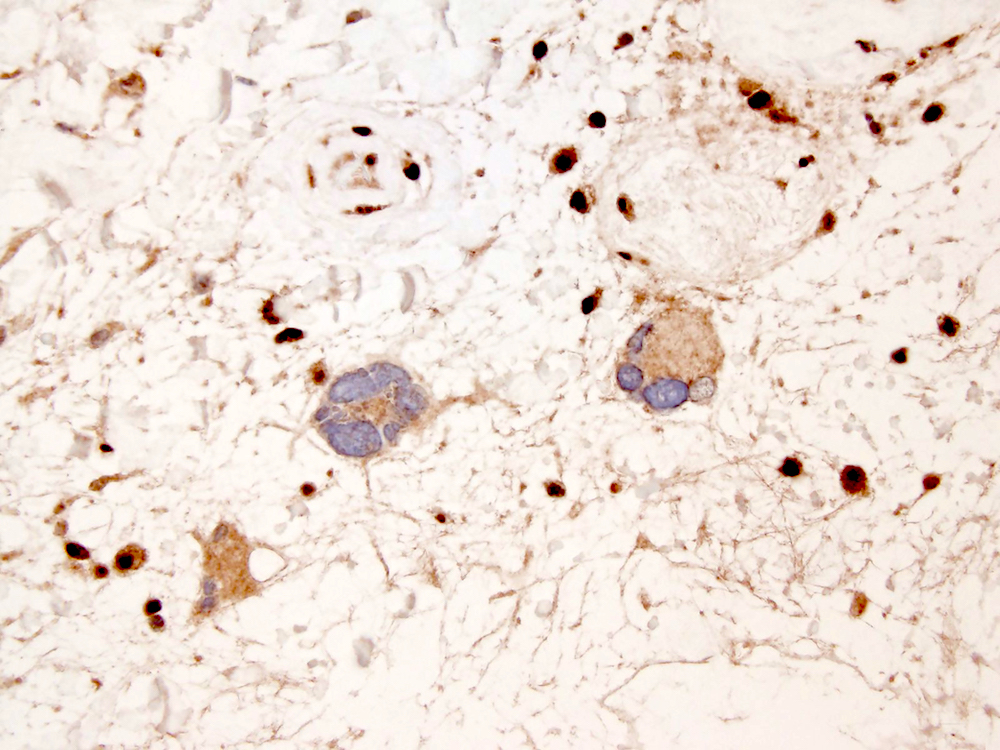
RB1
Cytology description
- Description of cytologic features of this entity is very scarce in the literature
Positive stains
Negative stains
- Loss of nuclear RB1 expression (57%)
- MDM2 and CDK4 are never coexpressed; weak or focal expression of MDM2 (2% positive) or CDK4 (12% positive) can rarely be seen (Am J Surg Pathol 2021;45:1282)
- Variable expression of desmin (23% positive)
- Reference: Am J Surg Pathol 2017;41:234
Molecular / cytogenetics description
- Deletions or losses in 13q14, including RB1, have been identified in a significant subset of cases (Histol Histopathol 2020;35:769)
- Consistent absence of MDM2 or CDK4 amplification (Histol Histopathol 2020;35:769)
- Chromosome 12 polysomy (MDM2/CEP12 ratio of < 2.0 with > 2 signals of both probes) (unpublished author observation)
Molecular / cytogenetics images
Contributed by Xinyan Lu, M.D.
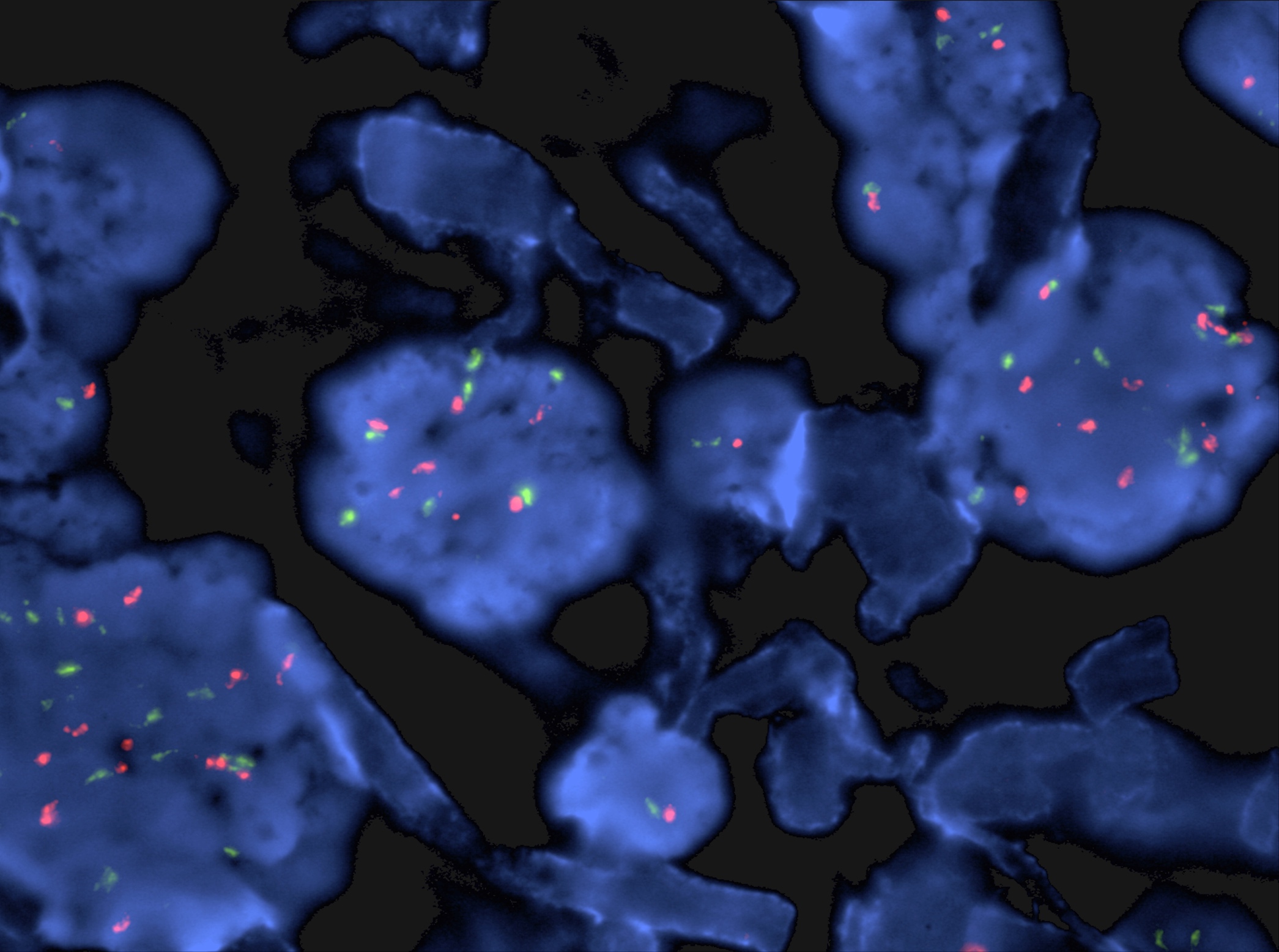
MDM2 FISH
Sample pathology report
- Abdominal mass, excision:
- Atypical spindle cell / pleomorphic lipomatous tumor, 3.2 cm in greatest dimension (see comment)
- Tumor extends to the inked soft tissue margin
- Comment: Tumor consists of poorly marginated proliferation of mild to moderately atypical spindle cells, adipocytes, lipoblasts and floret-like giant cells set in a fibromyxoid stroma with ropy collagen. The adipocytic component shows variation in adipocytic size and scattered nuclear atypia. Frequent univacuolated and multivacuolated (pleomorphic) lipoblasts are seen. Bizarre, hyperchromatic and pleomorphic multinucleated cells are scattered within the spindle cell and adipocytic components. Mitotic figures are present (2 mitoses/10 high power fields) but tumor necrosis is absent. By immunohistochemistry, tumor cells stain positive for CD34 and S100 (focal) and show loss of RB1 expression. The findings support the above diagnosis. Atypical spindle cell / pleomorphic lipomatous tumor has a low rate of local recurrence for incompletely excised lesions. There is no documented risk for metastasis.
Differential diagnosis
- Spindle cell / pleomorphic lipoma:
- Atypical multivacuolated lipoblasts and atypical mitoses are not compatible with the diagnosis of spindle cell / pleomorphic lipoma (Hum Pathol 2018;74:188)
- Chromosome 12 polysomy (MDM2/CEP12 ratio of < 2.0 with > 2 signals of both probes) in 89% of cases (Mod Pathol 2008;21:943)
- Atypical lipomatous tumor / well differentiated liposarcoma:
- Variation in adipocytic size associated with nuclear atypia
- Scattered hyperchromatic atypical stromal cells and hyperchromatic bizarre stromal cells
- Varying number of lipoblasts (from many to none)
- Fibrillary collagenous stroma
- Detection of MDM2 or CDK4 amplification serves to distinguish atypical lipomatous tumors / well differentiated liposarcoma from benign adipose tumors and malignant mimickers (Am J Surg Pathol 2007;31:1476)
- RB1 expression is retained
- Dedifferentiated liposarcoma:
- Abrupt or gradual transition from atypical lipomatous tumor / well differentiated liposarcoma to spindle cell or pleomorphic nonlipogenic (rarely lipogenic) tumor of low or high grade (Virchows Arch 2020;476:455)
- Detection of MDM2 amplification is helpful to distinguish dedifferentiated liposarcoma from benign and malignant mimickers in the appropriate clinical context
- RB1 expression is retained
- Pleomorphic liposarcoma:
- Despite some overlapping morphologic, immunohistochemical and genetic features between atypical pleomorphic lipomatous tumor (APLT) and pleomorphic liposarcoma (PLS) (for example: infiltration, pleomorphism including pleomorphic lipoblasts, and loss of RB1), PLS can be differentiated from APLT by a higher degree of pleomorphism, high mitotic activity and tumor necrosis (Am J Surg Pathol 2017;41:1443)
- Presence of a pleomorphic lipoma-like component demonstrating floret-like multinucleated cells and ropy collagen is a defining feature of APLT, not present in PLS (Am J Surg Pathol 2017;41:1443)
- Pleomorphic lipoblasts in the background of a high grade, usually pleomorphic, undifferentiated sarcoma (Histopathology 2014;64:38)
- Almost half of the cases contain focal areas similar to intermediate or high grade myxofibrosarcoma associated with pleomorphic lipoblasts (Am J Surg Pathol 2002;26:601, Am J Surg Pathol 2004;28:1257)
- Epithelioid morphology is seen in about 25% of cases
- Necrosis is present in the majority of cases
- Amplification of MDM2 or CDK4 is absent
- Strong and diffuse CD34 expression is absent
Board review style question #1
Which of the following is true about atypical spindle cell / pleomorphic lipomatous tumor?
- High recurrence rate
- Loss of RB1 expression is observed in 50 - 70% of cases
- MDM2 amplification is almost always present
- Most common locations are head and neck and genital area
- Risk for dedifferentiation
Board review style answer #1
B. Loss of RB1 expression is observed in 50 - 70% of cases
Comment Here
Reference: Atypical spindle cell / pleomorphic lipomatous tumor
Comment Here
Reference: Atypical spindle cell / pleomorphic lipomatous tumor
Board review style question #2
A 56 year old man presented with a left thigh mass. Histologically, the tumor was characterized by ill defined margins and the presence of mild to moderately atypical spindle cells, mature adipocytes, univacuolated and multivacuolated (pleomorphic) lipoblasts and multinucleated floret-like cells set in a myxoid stroma with ropy collagen. Bizarre, hyperchromatic and pleomorphic multinucleated cells were scattered within the spindle cell and adipocytic components. Occasional mitotic figures, including 1 atypical mitosis, were identified. No tumor necrosis was seen. On immunohistochemistry, the tumor was positive for CD34 and S100 and showed loss of RB1.
Which of the following is most likely the correct diagnosis?
- Atypical lipomatous tumor / well differentiated liposarcoma
- Atypical spindle cell / pleomorphic lipomatous tumor
- Dedifferentiated liposarcoma
- Pleomorphic liposarcoma
- Spindle cell / pleomorphic lipoma
Board review style answer #2
B. Atypical spindle cell / pleomorphic lipomatous tumor
Comment Here
Reference: Atypical spindle cell / pleomorphic lipomatous tumor
Comment Here
Reference: Atypical spindle cell / pleomorphic lipomatous tumor

