
Skin nonmelanocytic tumor
Carcinoma (nonadnexal)
Verrucous carcinoma
Resident / Fellow Advisory Board: Caroline I. Mullins, M.D.


Last author update: 7 March 2022
Last staff update: 22 June 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Verrucous carcinoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ireland A, Ardakani NM. Verrucous carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticverrucousscc.html. Accessed April 1st, 2025.
Definition / general
- Verrucous carcinoma is a subtype of squamous cell carcinoma that affects skin and mucosa and has characteristic slow growth and bland histological features; suspect if a longstanding verrucous lesion or cyst is unresponsive to routine treatment (Int J Surg Pathol 2017;25:438)
Essential features
- Low grade subtype of squamous cell carcinoma with good prognosis when affecting skin
- Association with human papillomavirus (HPV) DNA is rarely reported in mucosal and genital areas; may represent incidental colonization
- Association with alcohol consumption, smoking, areca nut chewing and oral microbiota has been reported in oral verrucous carcinoma
- Can arise in association with inflammatory and neoplastic conditions
- Diagnosis can be delayed due to bland histopathological features and mimicking reactive processes
- Caution should be exercised when making diagnosis in superficial or fragmented biopsies
Terminology
- Ackerman tumor, oral florid papillomatosis, papillomatosis cutis carcinoides
ICD coding
- ICD-10: C44 - subtype of squamous cell carcinoma
Epidemiology
- M > F
- Older individuals (average 50 - 70 years old); 75% of patients > 60 years old (Cancer 2001;92:110)
Sites
- Skin (e.g., wrists, fingers, nail bed, sole of the foot, ear, nose eyelid, scalp, buttocks, anorectal region, penis, vulva, shoulder, axilla, abdominal wall and lip) and oral cavity
- Most cases (90%) on the feet (Indian Dermatol Online J 2014;5:218)
- Oral cavity: also called Ackerman tumor, oral florid papillomatosis; see esophagus, larynx, oral cavity
Pathophysiology
- Carcinogens interfere with DNA replication and cause DNA single strand breaks and mutations that facilitate tumor growth (Int J Oncol 2016;49:59)
Etiology
- Chronic inflammation or irritation / repeated trauma and carcinogens, including alcohol, smoking and areca nut, particularly in the oral cavity (Int J Oncol 2016;49:59)
- Can arise in chronic inflammatory conditions, such as lichen sclerosus, burns scars, chronic ulcers or leishmaniasis and low risk HPV (Actas Dermosifiliogr 2012;103:21, JAAD Case Rep 2019;5:225, Int J Surg Pathol 2019;27:407, Acta Trop 2017;172:240, Clin Case Rep 2019;7:836)
- Role of HPV is controversial as diagnostic thresholds vary but if histologic criteria are rigorously applied, low risk HPV is only rarely positive (Mod Pathol 2012;25:1354)
- Can arise in association with other lesions, including syringocystadenoma papilliferum (SCAP), congenital venous malformation and cutaneous horn (Dermatol Surg 2018;44:1144, Br J Oral Maxillofac Surg 2016;54:842, Case Rep Otolaryngol 2020;2020:7134789)
Clinical features
- Unicentric (in the skin), hyperkeratotic warty growths that are longstanding, progressive and may or may not be locally destructive
Diagnosis
- Longstanding and slow growing exophytic hyperkeratotic tumor at typical anatomical sites, such as foot and oral cavity
- Imaging evidence of deep endophytic growth with or without invasion to the bone
- Evidence of well differentiated squamous proliferation on a shave or punch biopsy in an appropriate clinical and imaging context
- Definitive diagnosis requires a deep incisional sample or excision of tumor
- Can be mistaken for benign squamous lesions on superficial biopsies (J Am Acad Dermatol 1995;32:1)
Prognostic factors
- Recurrence rate high if incompletely excised
- Recurrent tumor can be more aggressive than original, with bone and cartilage invasion and destruction
- Metastases are rarely documented, most often from oral and mucosal lesions (In Vivo 2007;21:909, Cancer 2001;92:110)
- Enlargement of draining lymph nodes is common and usually represents reactive hyperplasia secondary to inflammatory reaction to the tumor (Head Neck Surg 1982;5:29)
- Progression to aggressive squamous cell carcinoma after radiation or chemotherapy
Case reports
- 19 year old man with an ulcerated lesion on the big toe (Cutis 2019;104:E34)
- 43 year old man with a cutaneous verrucous carcinoma superimposed on chronically inflamed ileostomy site (Iran J Pathol 2018;13:285)
- 44 year old woman with uncontrolled diabetes, peripheral neuropathy and bilateral foot verrucous carcinoma (Case Rep Dermatol Med 2018;2018:4192657)
- 48 year old man with an ulcerated mass on his left middle finger (Curr Health Sci J 2019;45:235)
- 53 year old man with a verrucous plaque on his inner thigh and 95 year old woman with a brownish verrucous plaque on her right lower leg (J Nippon Med Sch 2018;85:47)
Treatment
- Surgical excision is the most common mode of treatment (J Dermatolog Treat 2021 Apr 14 [Epub ahead of print])
- Other modes: cryosurgery, carbon dioxide laser, chemotherapy, intralesional or iontophoretic methods, photodynamic therapy, systemic retinoid therapy, radiotherapy
Clinical images
Images hosted on other servers:


Finger tumors

Vulvar tumor

Heel tumor
Gross description
- Fungating, verrucous or polypoid lesions sometimes with ulceration
- May invade and destroy underlying bone
Gross images
Contributed by Amanda Ireland, M.B.B.S.

Dorsal view

Palmar view

Lateral view
Microscopic (histologic) description
- Histologically similar regardless of anatomical site
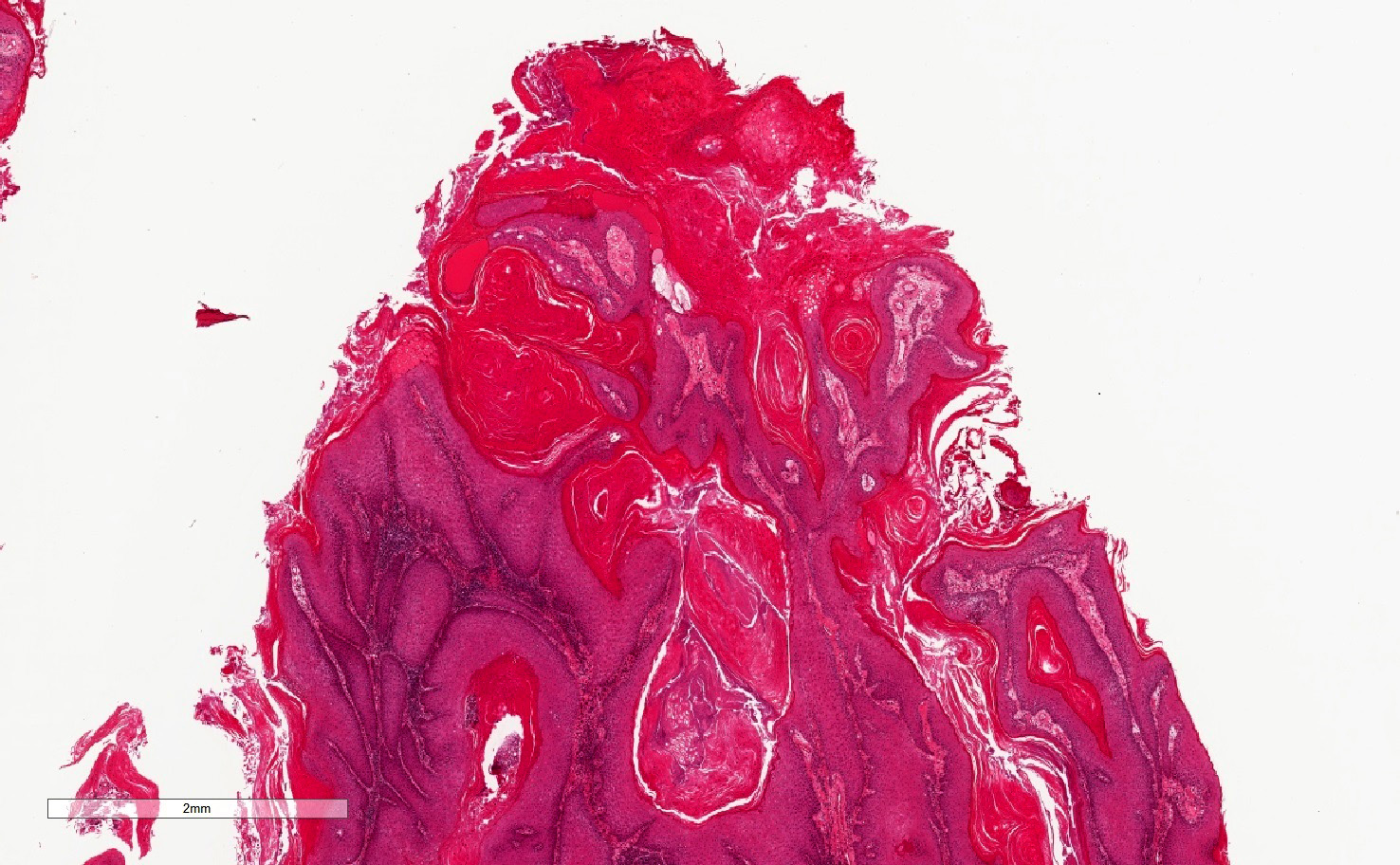
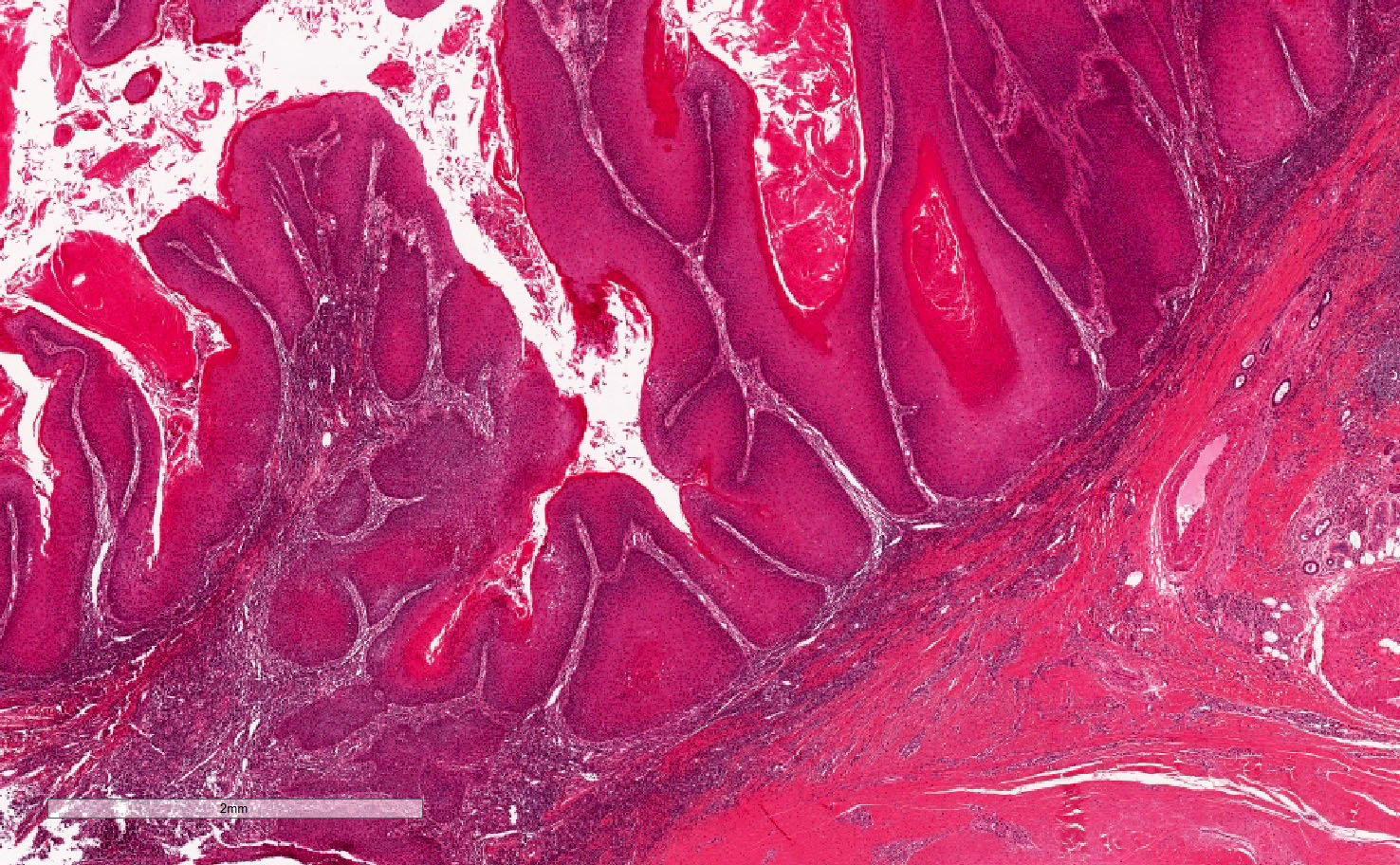
- Well differentiated squamous proliferation with exophytic and endophytic components
- Exophytic component with papillomatosis and massive hyperkeratosis, often with expanded granular layer with parakeratosis
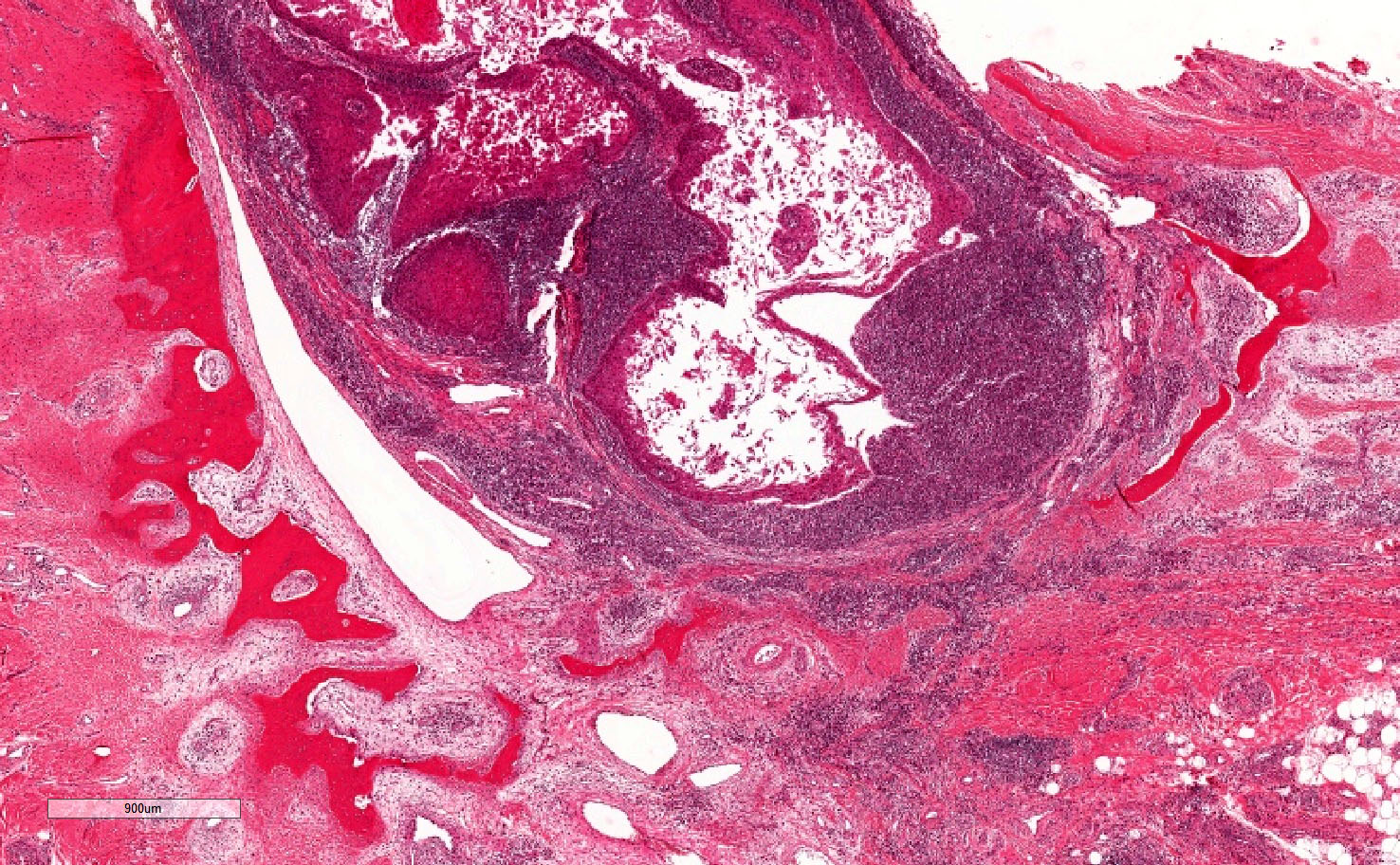
- Endophytic component with blunt projections of well differentiated squamous epithelium with deep bulbous processes and a pushing margin
- Constituent cells; large polygonal squamous cells with abundant pink cytoplasm and enlarged nuclei with minimal nuclear atypia (apart from several layers at the interface of bulbous tips)
- Often inflamed edematous stroma filled with lymphocytic cells immediately adjacent to the advancing edge
- Tissue between bulbous processes is greatly diminished with reduced vascularity
- Deeper biopsy shows broad bands of epidermal proliferation with parakeratotic centers; bases of proliferation are large and bulbous and invade deep dermis in a pushing manner (Calonje: McKee's Pathology of the Skin, 5th Edition, 2019)
Microscopic (histologic) images
Contributed by Amanda Ireland, M.B.B.S.

Exophytic / endophytic squamous proliferation
Superficial aspect
Deep aspect
Pushing margins
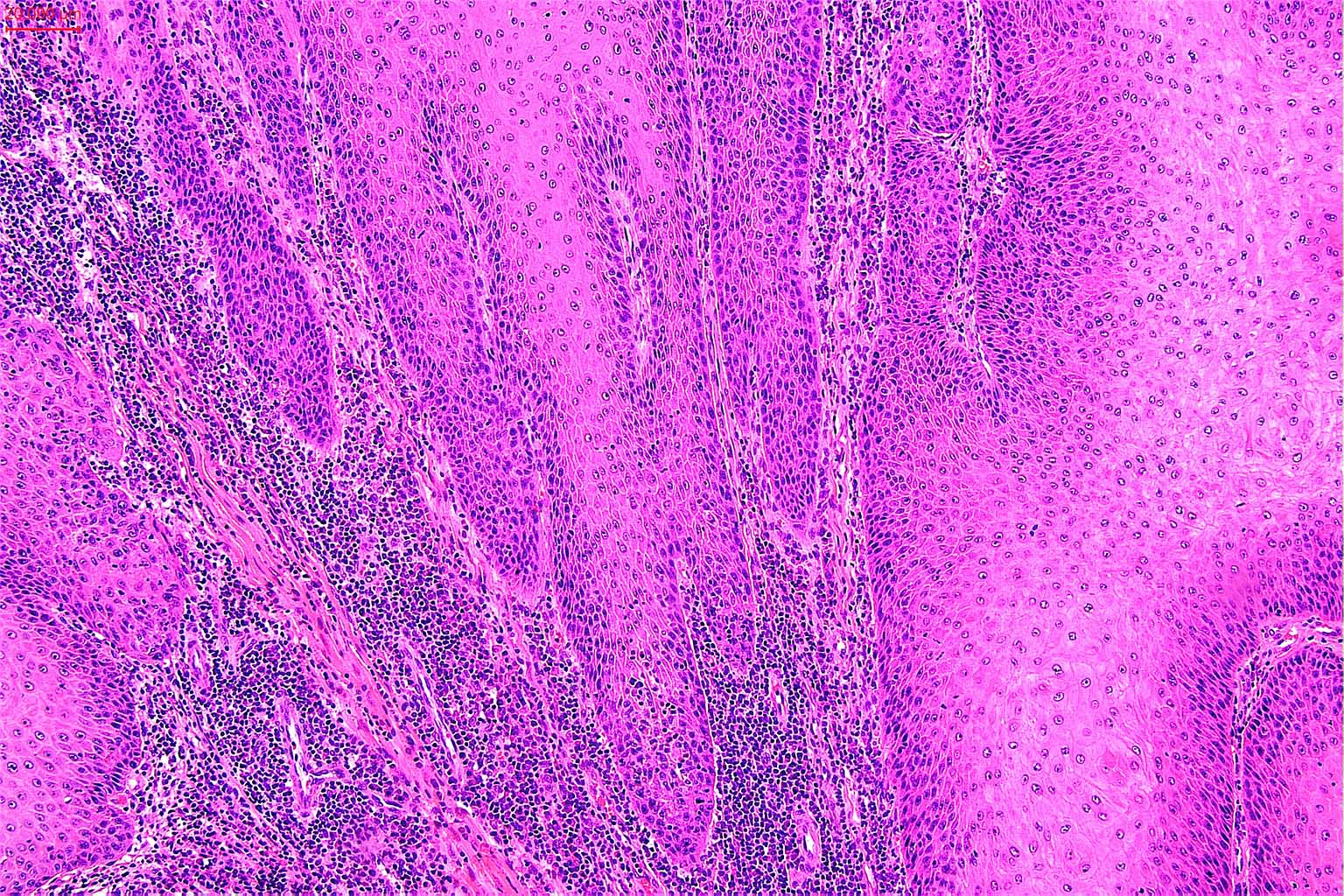
Tumor stromal interface
Virtual slides
Images hosted on other servers:


Verrucous carcinoma, skin

Verrucous carcinoma in wart

Verrucous carcinoma, vulva
Molecular / cytogenetics description
- Association with somatic HRAS, PIK3CA and BRAF mutations and less commonly PTEN, EGFR and GNAS mutations has been described in vulva in a spectrum of lesions from verrucous carcinoma to differentiated vulvar intraepithelial dysplasia (Mod Pathol 2020;33:2011, J Cutan Pathol 2020;47:12, Int J Gynecol Pathol 2021;40:391)
Sample pathology report
- Skin, excision:
- Verrucous carcinoma, clear of the margins (see comment)
- Comment: Microscopic examination reveals a well differentiated squamous proliferation characterized by an acanthotic squamous epithelium with exophytic papillary processes with overlying hyperkeratosis and parakeratosis. There is also an associated endophytic component composed of deeply penetrating bulbous processes with pushing borders. The keratinocytes are well differentiated with abundant glassy cytoplasm and enlarged nuclei. Mitoses are rare and there is no tumor necrosis. The superficial dermis shows a band-like lymphocytic inflammation. There is no lymphovascular or perineural invasion. The tumor is well clear of the resection margins.
Differential diagnosis
- Giant condyloma / Buschke-Löwenstein tumor:
- Histologically identical but detection of low risk HPV (6 and 11) by PCR indicates a giant condyloma (Histopathology 2017;70:938)
- Verrucae (warts):
- Distinction difficult in superficial biopsies
- Warts often have well formed lateral collarets, a significantly expanded granular layer with coarse basophilic keratohyalin granules and no deeply extending bulbous processes
- Pseudoepitheliomatous epidermal hyperplasia (PEH):
- Distinction is difficult in superficial biopsies
- PEH is more superficial, extends horizontally with at most a focal, limited deep, bulbous growth
- Verrucous psoriasis:
- Regular acanthosis and Munro microabscesses
- If there is considerable traumatization and pseudoepitheliomatous hyperplasia, clinical correlation and history of psoriasis is key (JAAD Case Rep 2019;5:723)
- Fungal / protozoal / mycobacterial infection with extensive pseudoepitheliomatous hyperplasia:
- Look for organisms in the dermis with or without special stains
- Keratoacanthoma:
- Often more endophytic growth with a central cavity / crater filled with keratin
- May contain intraepidermal neutrophilic microabscesses
- May show signs of regression / atrophy, surface undulation and stromal fibrosis and inflammation
- Usually does not extend beyond eccrine glands
- Squamous cell carcinoma (conventional and nonverrucous subtypes):
- Depending on differentiation, often shows variable degrees of cytologic atypia, mitotic activity and infiltrative growth, at least focally
- Distinction from a well differentiated conventional SCC is difficult; however, the latter is usually less exophytic
- Carcinoma cuniculatum / epithelioma cuniculatum:
- Well differentiated squamous carcinoma that presents on the plantar foot
- No significant verrucous or exophytic growth
- Surface is flat with infiltrative growth of sinus tracts (J Cutan Pathol 2012;39:1083)
Differential diagnosis of verruciform tumors (adapted from figure 12.215 on page 534 of Calonje: McKee's Pathology of the Skin, 5th Edition, 2019)
| Papillae | Viral cytoplasmic effect | Lower border | HPV status | |
| Verrucous carcinoma | Thin and elongated - usually without fibrovascular core | Absent | Bulbous | Often negative |
| Giant condyloma | Fibrovascular cores | Focal, mainly superficial | Bulbous | Low risk HPV |
| Warty carcinoma | Various shapes with thick cores | Diffuse | Irregular | High risk HPV |
| Papillary carcinoma | Complex | Absent | Irregular | Negative |
Additional references
Board review style question #1
Which statement is applicable to the tumor depicted in the image shown above?
- Enlargement of draining lymph nodes commonly occurs
- Initial rapid growth often followed by regression
- Poorly differentiated and aggressive squamous neoplasm with bulbous processes
- Recurrence with local destructive growth is common following a complete surgical excision
Board review style answer #1
Board review style question #2
Which of the following options best describes the histological features of verrucous carcinoma?
- Exophytic and endophytic growth of bland appearing squamous epithelium with deep pushing borders
- Exophytic verrucous growth of squamous epithelium commonly with koilocytosis change
- Exophytic verrucous growth of squamous epithelium with high mitotic activity and necrosis
- Well differentiated squamous neoplasm with mainly endophytic infiltrative growth
Board review style answer #2
A. Exophytic and endophytic growth of bland appearing squamous epithelium with deep pushing borders
Comment Here
Reference: Verrucous carcinoma
Comment Here
Reference: Verrucous carcinoma
