
Skin nonmelanocytic tumor
Adnexal tumors
Follicular derived
Trichilemmoma
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 1 November 2019
Last staff update: 13 March 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Trichilemmoma[TI] OR tricholemmoma[TI]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Turnbull N, Carr RA. Trichilemmoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocytictrichilemmoma.html. Accessed March 31st, 2025.
Definition / general
- Benign follicular tumor (Arch Dermatol 1962;86:430, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
Essential features
- Bulbous profile
- Thickened or prominent basement membrane
- CD34+ (may be focal) (Clin Exp Dermatol 2006;31:807, Am J Dermatopathol 2018;40:561)
Terminology
- Also called tricholemmoma
ICD coding
- ICD-10: D23 - other benign neoplasms of skin
Epidemiology
- Usually middle aged adults (J Cutan Pathol 1990;17:45, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
Sites
- Typically located on the head and neck
- Predilection for central face (Arch Dermatol 1973;107:866, Arch Dermatol 1978;114:286)
Pathophysiology
- Derived from the outer root sheath of the hair follicle (Arch Dermatol 1962;86:430, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
Etiology
- Has been postulated to be related to human papillomavirus, though disputed (Arch Dermatol 1978;114:286, Arch Dermatol 1984;120:859, J Cutan Pathol 1991;18:193, Br J Dermatol 2014;171:1073)
- Cowden syndrome:
- Autosomal dominant genodermatoses associated with mutation in PTEN tumor suppressor gene
- Characterized by multiple trichilemmomas, mucosal papillomas and various hamartomas
- Increased risk of carcinomas of thyroid, breast and gastrointestinal tract (J Dermatol Surg Oncol 1979;5:12, Br J Dermatol 1979;100:667, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
Clinical features
- Clinically nondescript wart-like or smooth dome shaped appearance
Diagnosis
- Diagnosis is rarely made by clinical examination, more often made by pathologist via tissue examination revealing characteristic histological morphology
Prognostic factors
- These are benign tumors but may be a manifestation of Cowden syndrome as above (J Dermatol Surg Oncol 1979;5:12, Br J Dermatol 1979;100:667, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
Case reports
- 28 year old woman with multiple erythematous lesions over the left ankle (J Cutan Pathol 2017;44:93)
- 38, 54 and 74 year old men with nasal vestibule tumors (Head Neck Pathol 2012;6:492)
- 55 year old man with a lesion on his right upper eyelid (J Cutan Pathol 2007;34:22)
- 58 year old woman with a lesion on the scalp (An Bras Dermatol 2017;92:836)
- 78 year old man with desmoplastic histology clinically mimicking carcinoma (An Bras Dermatol 2014;89:796)
Treatment
- Not required
- Curettage or shave excision
- Excision
- Laser
Clinical images
Images hosted on other servers:

Trichilemmoma

Central ulceration
Microscopic (histologic) description
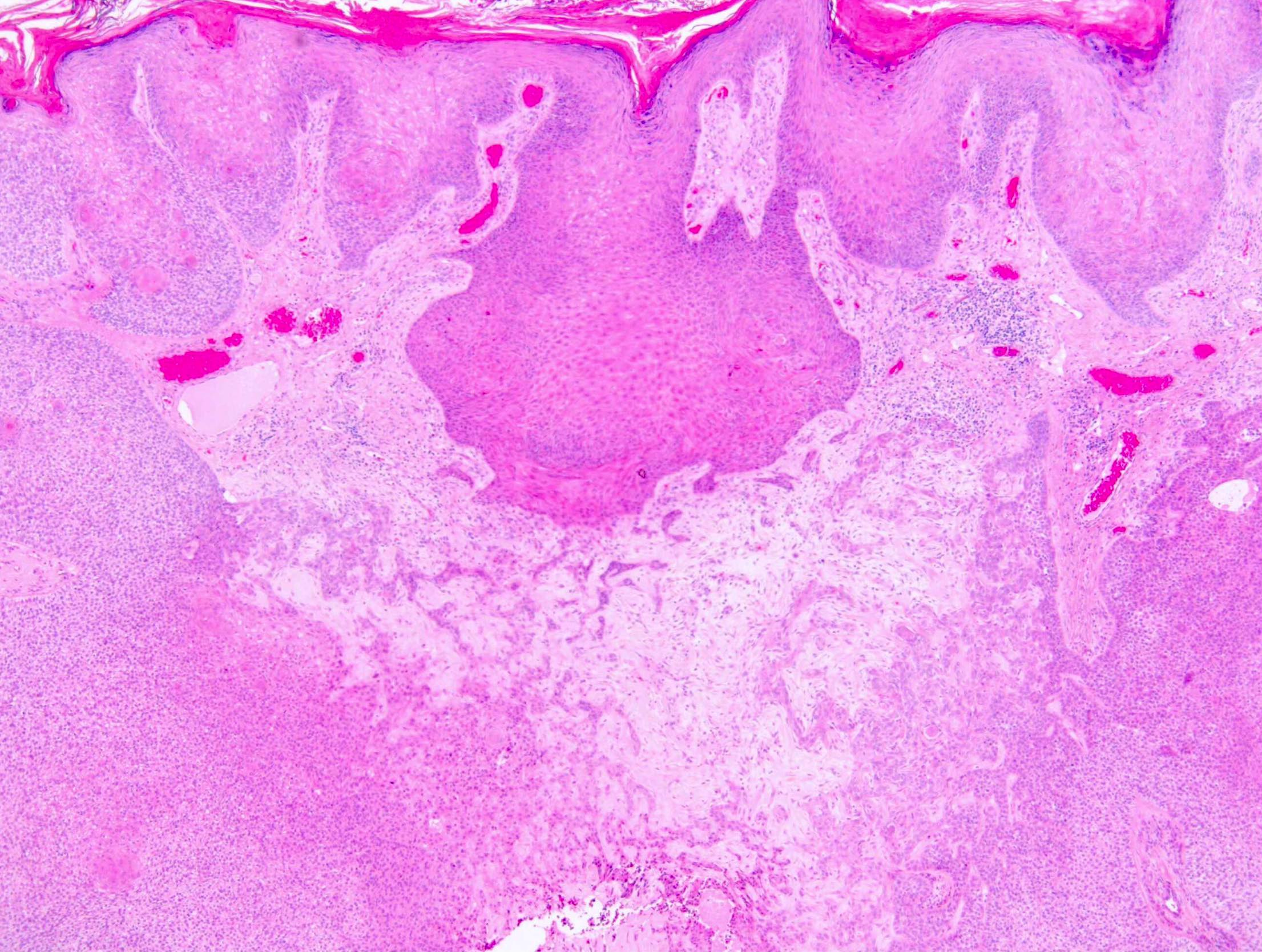
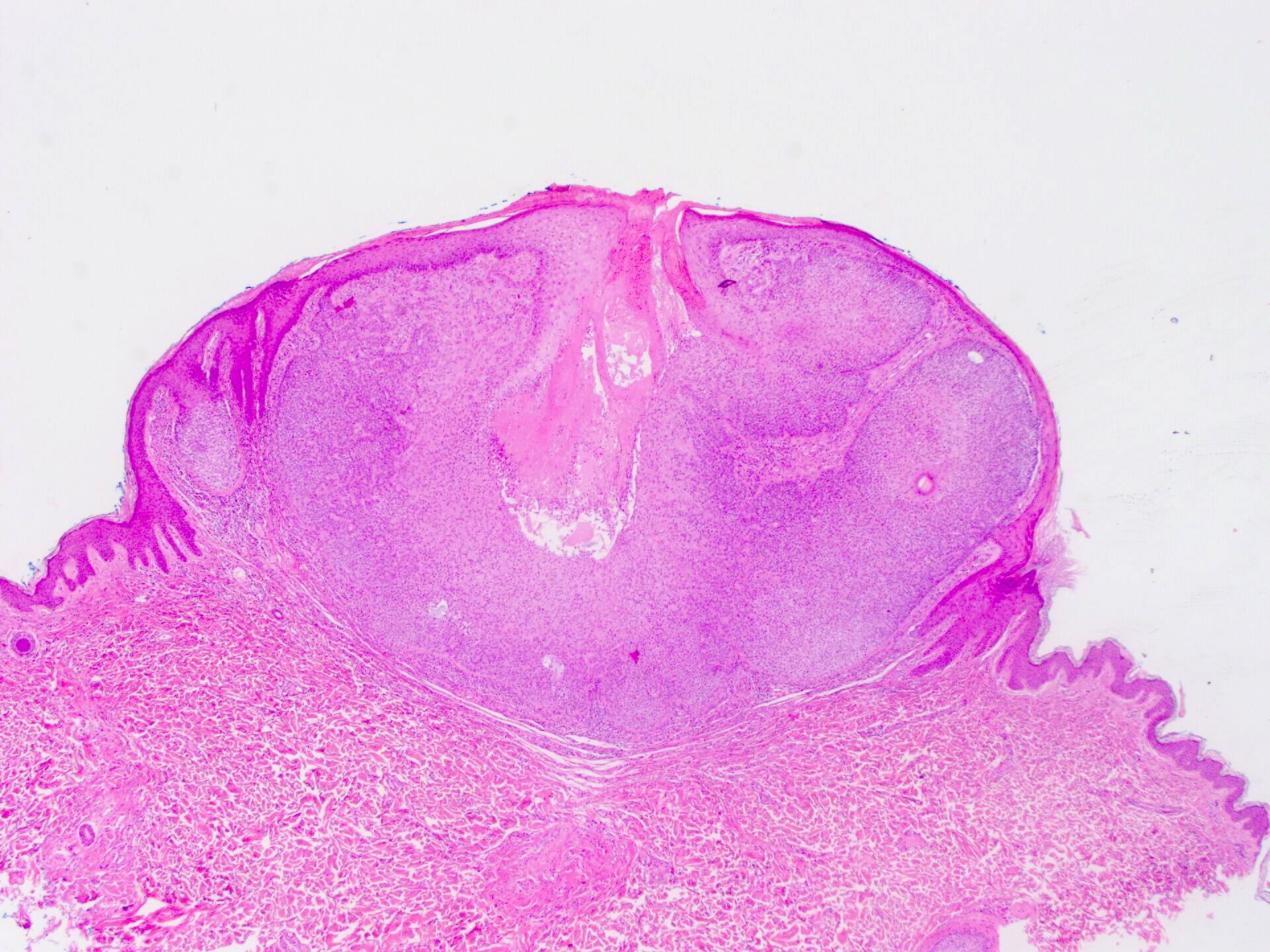
- Squamoproliferative lesion in continuity with the epidermis
- Hyperkeratosis and stromal clefting are often associated
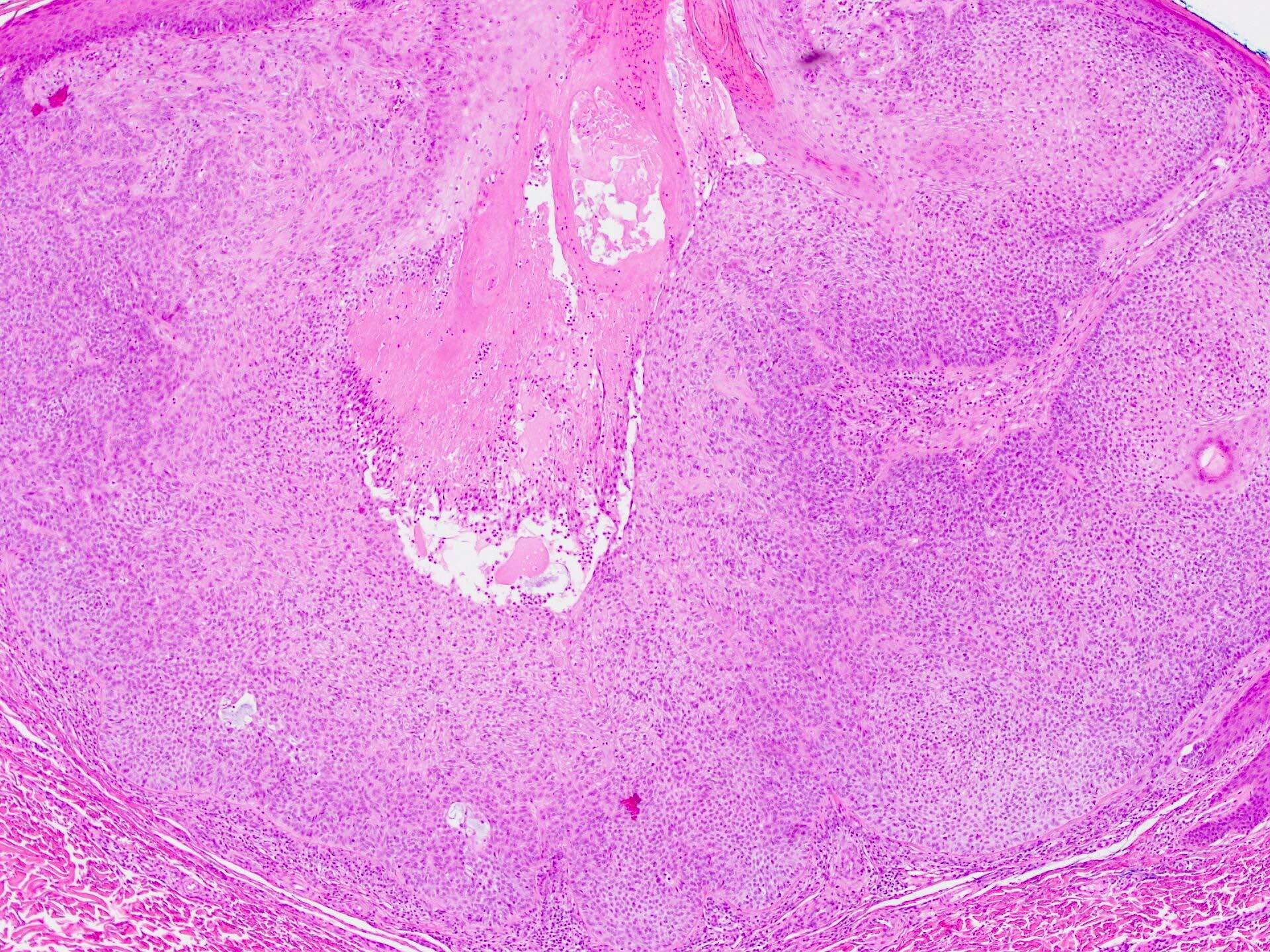
- Pale eosinophilic or clear cells
- Rounded lobular profile
- Peripheral palisade of cuboidal or columnar cells
- Clear cells (characteristic but uncommon)
- Reverse polarity of peripheral cells (characteristic but uncommon)
- Distinct basement membrane resembling the hair outer root sheath zone below the level of the follicular isthmus (Arch Dermatol 1962;86:430, Am J Dermatopathol 2018;40:561, Current Diagnostic Pathology 2007;13:273)
- Basaloid cell predominance may be seen mimicking basal cell carcinoma
- Central desmoplasia, squamous morules and mucin pools may be seen (uncommon)
Microscopic (histologic) images
Contributed by Nicholas Turnbull, M.B.Ch.B. and Richard A. Carr, M.B.Ch.B.
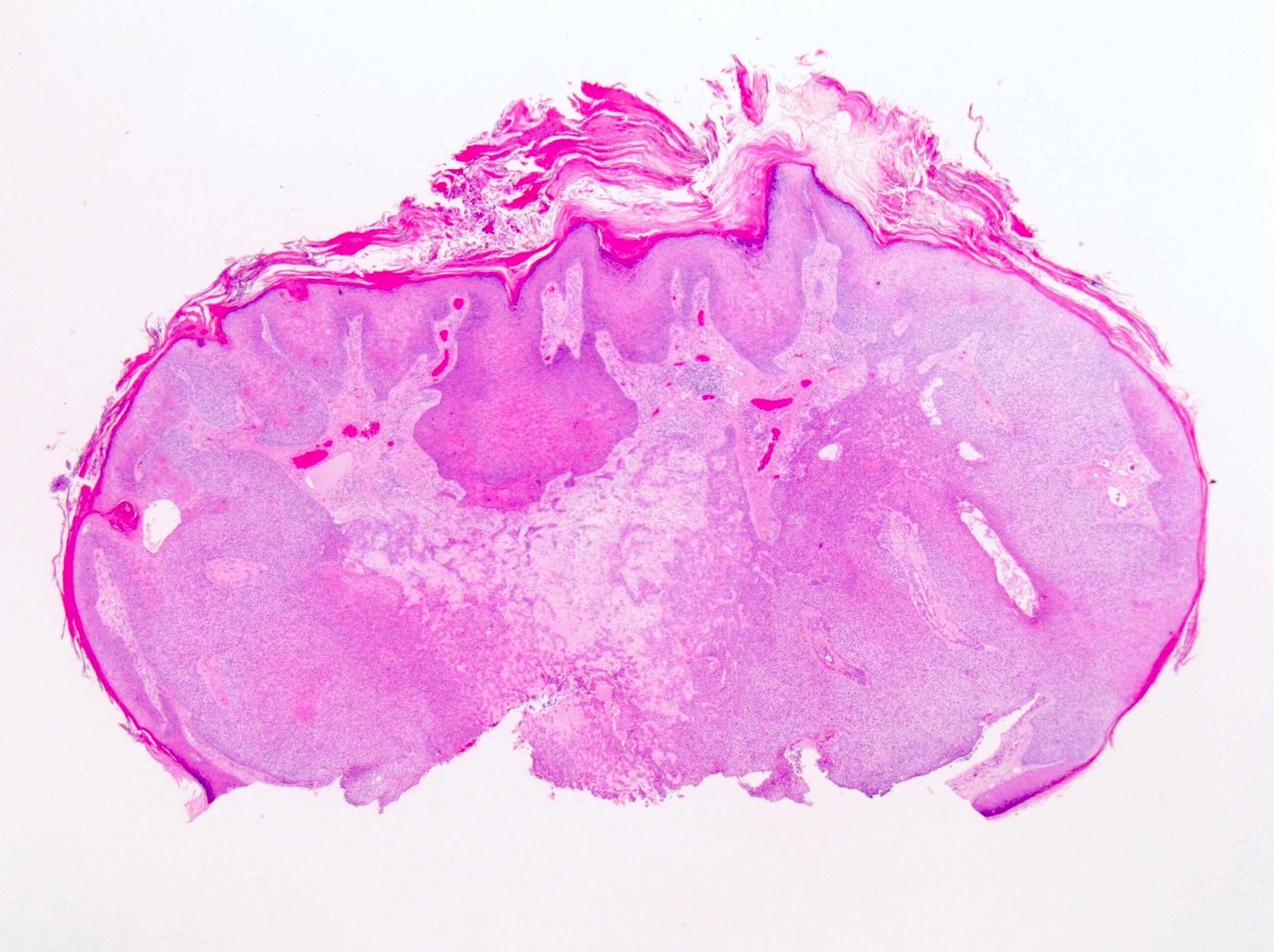
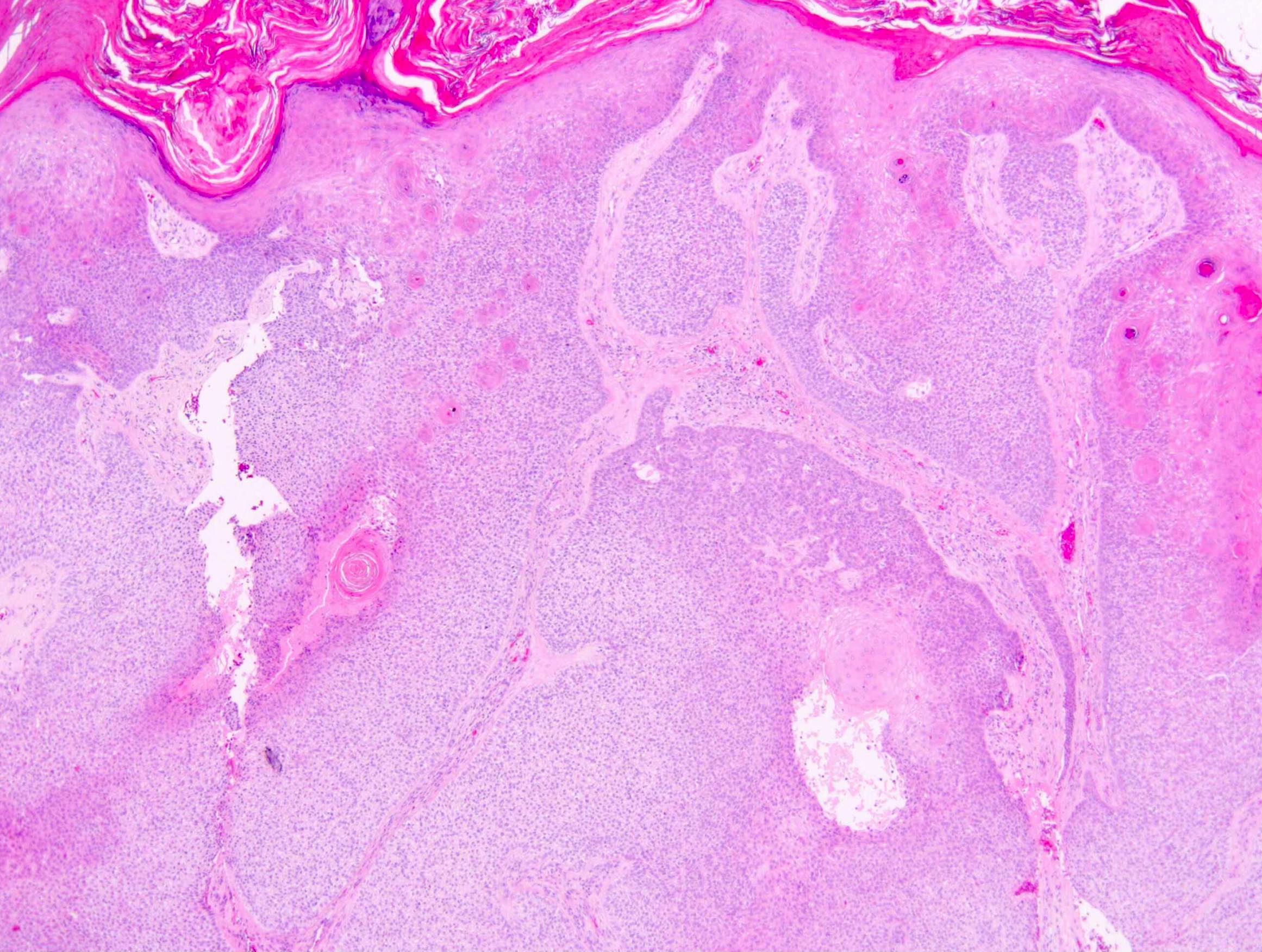
Bulbous basaloid tumor
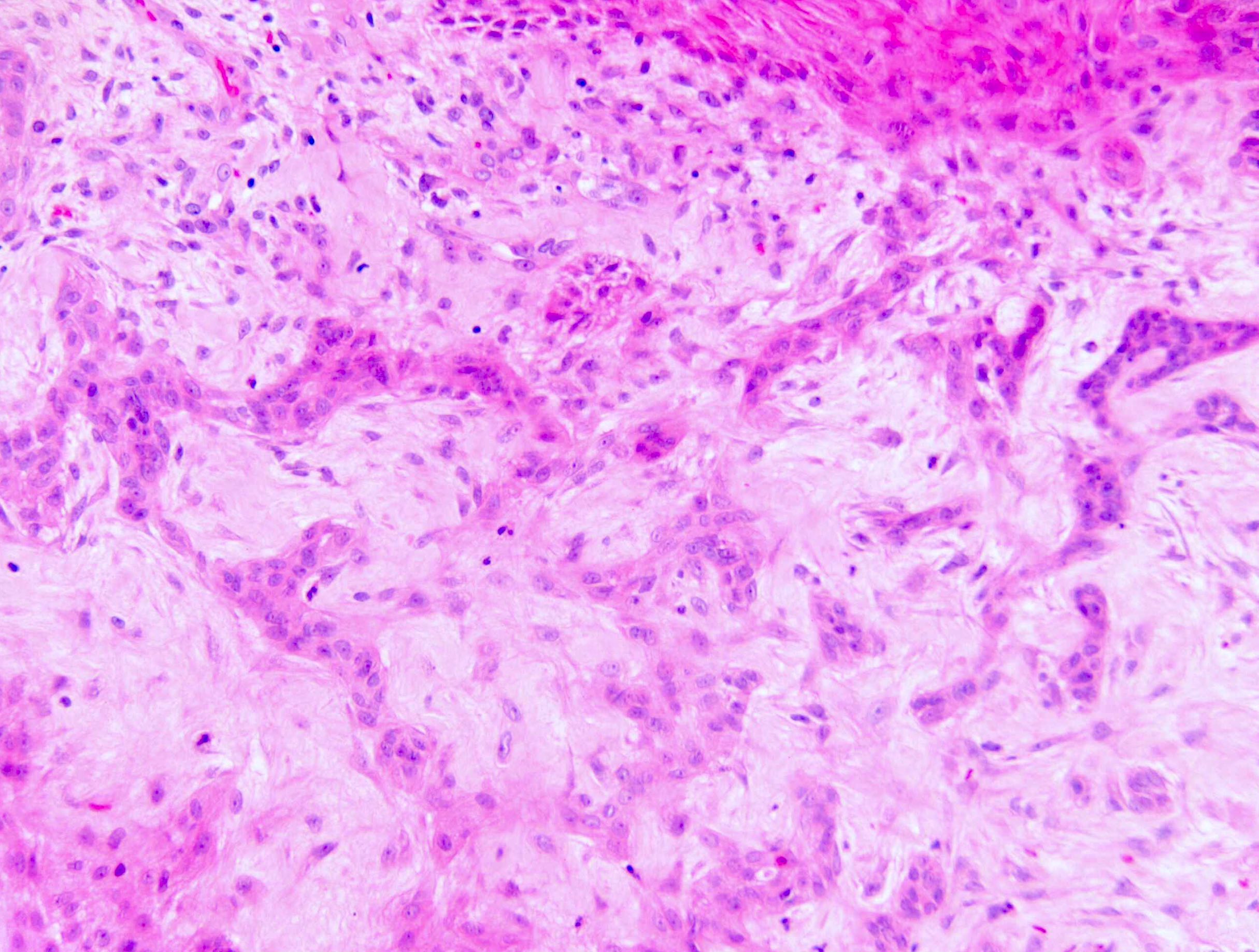
Desmoplasia
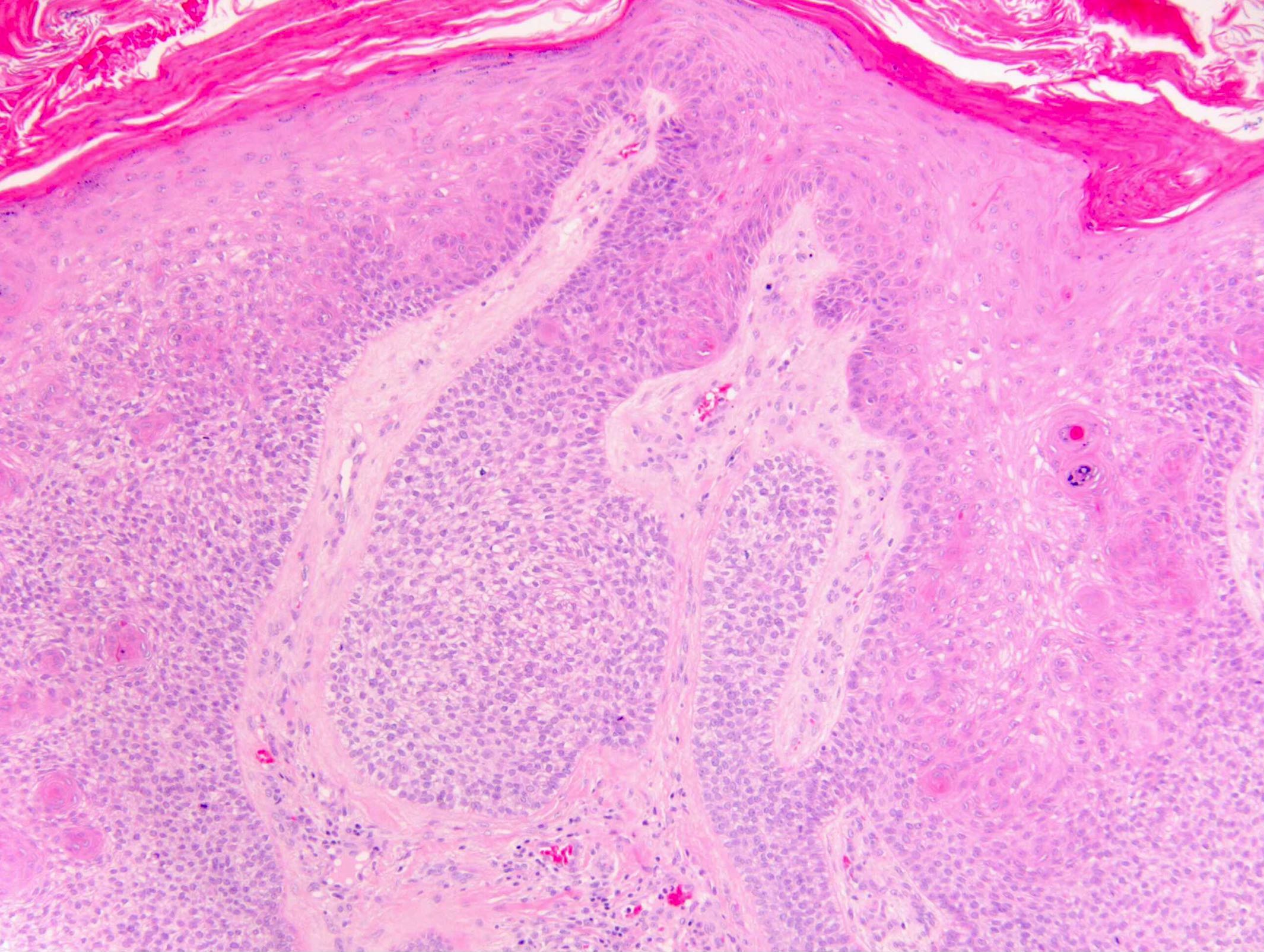

Area composed of clear cells
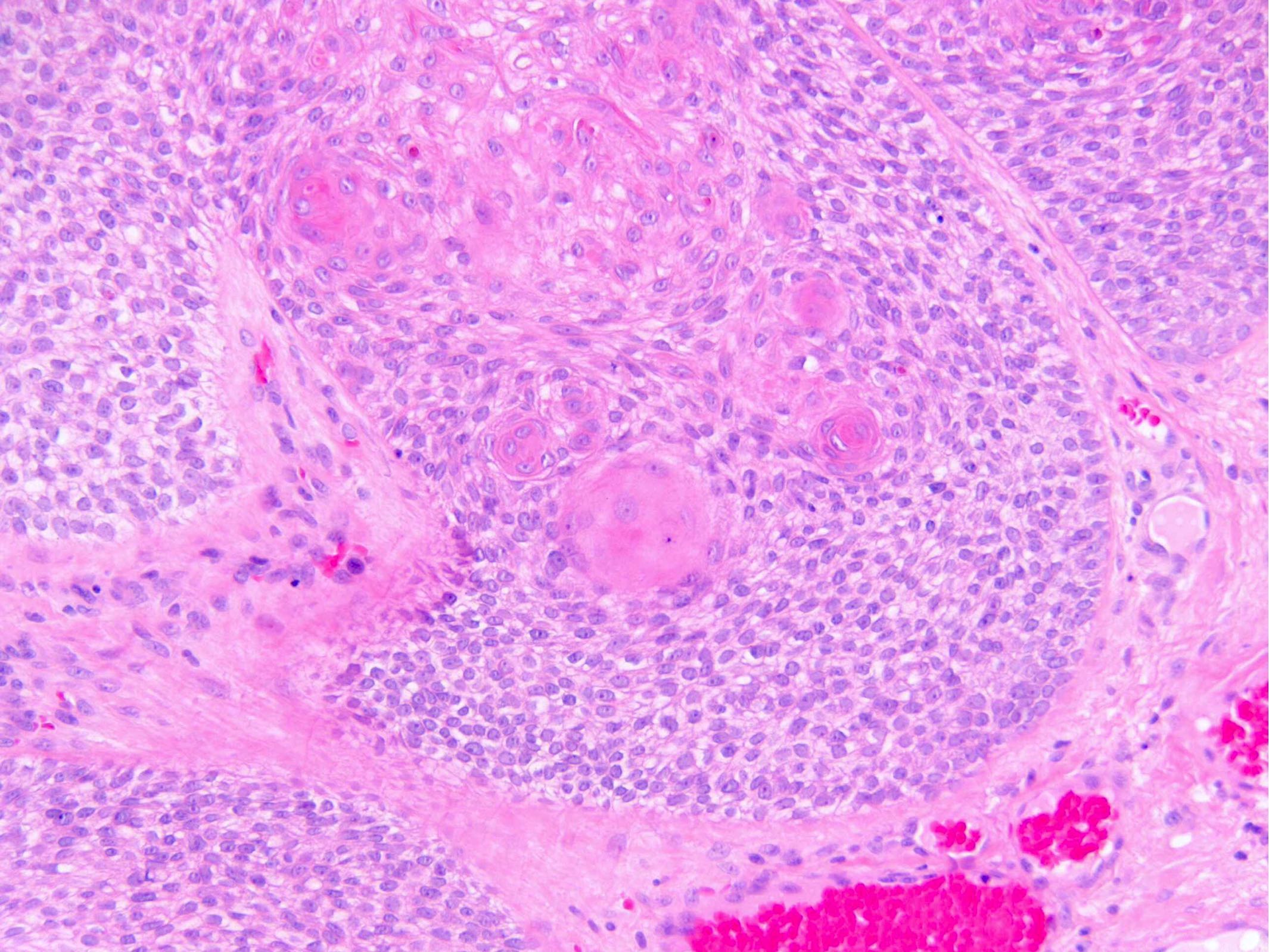
Squamous morules and mucinous pools
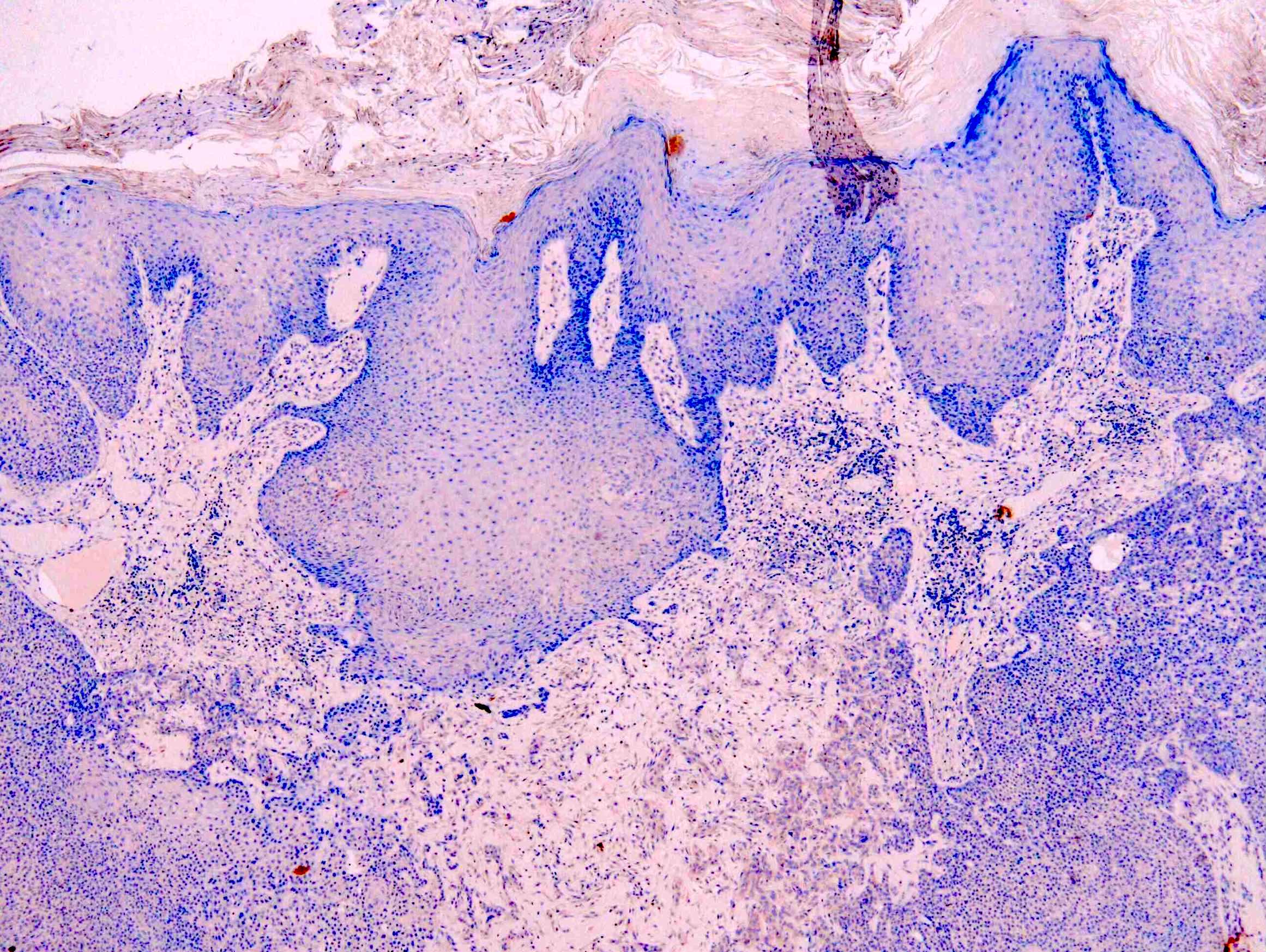
BerEP4
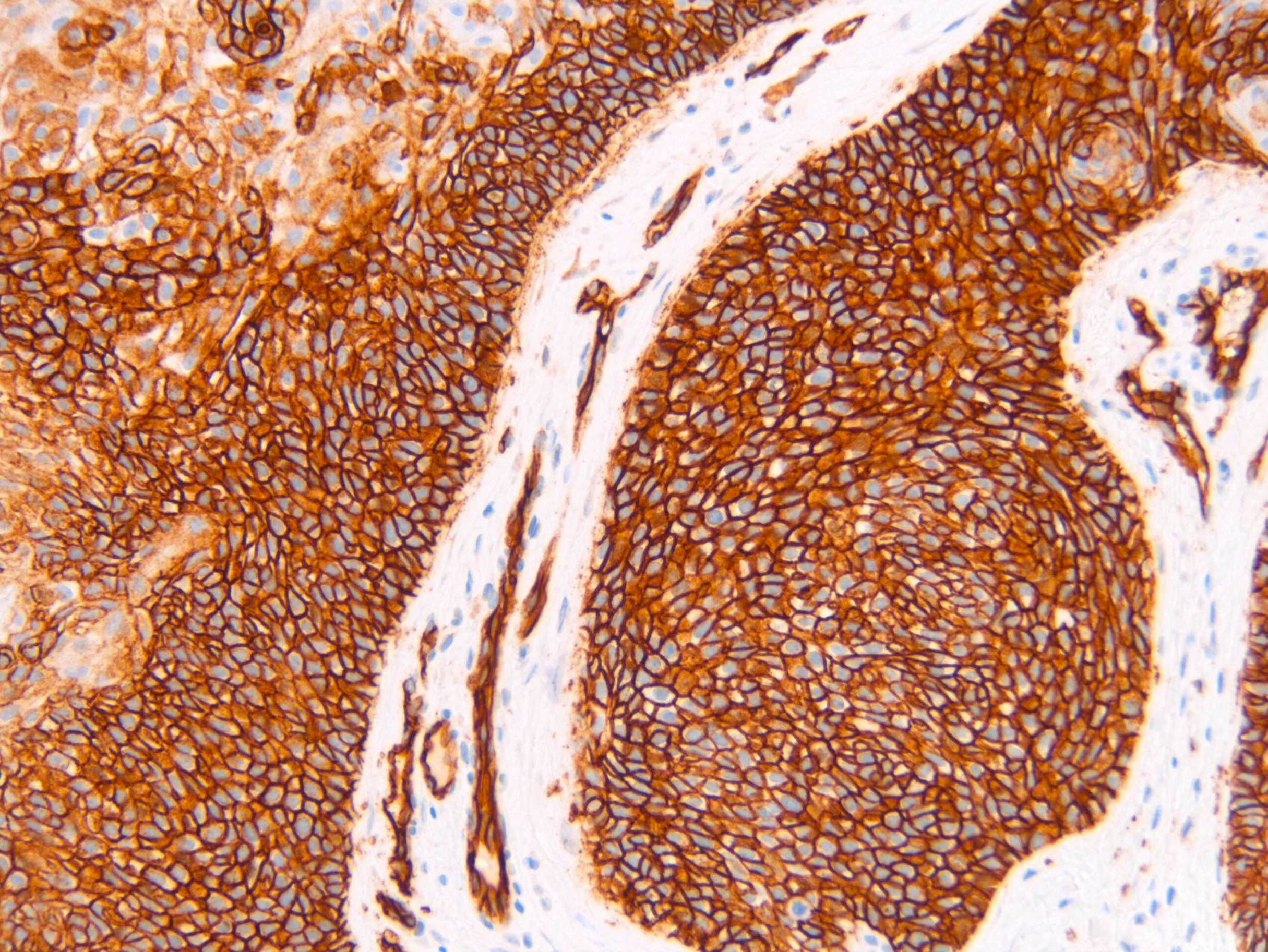
EMA
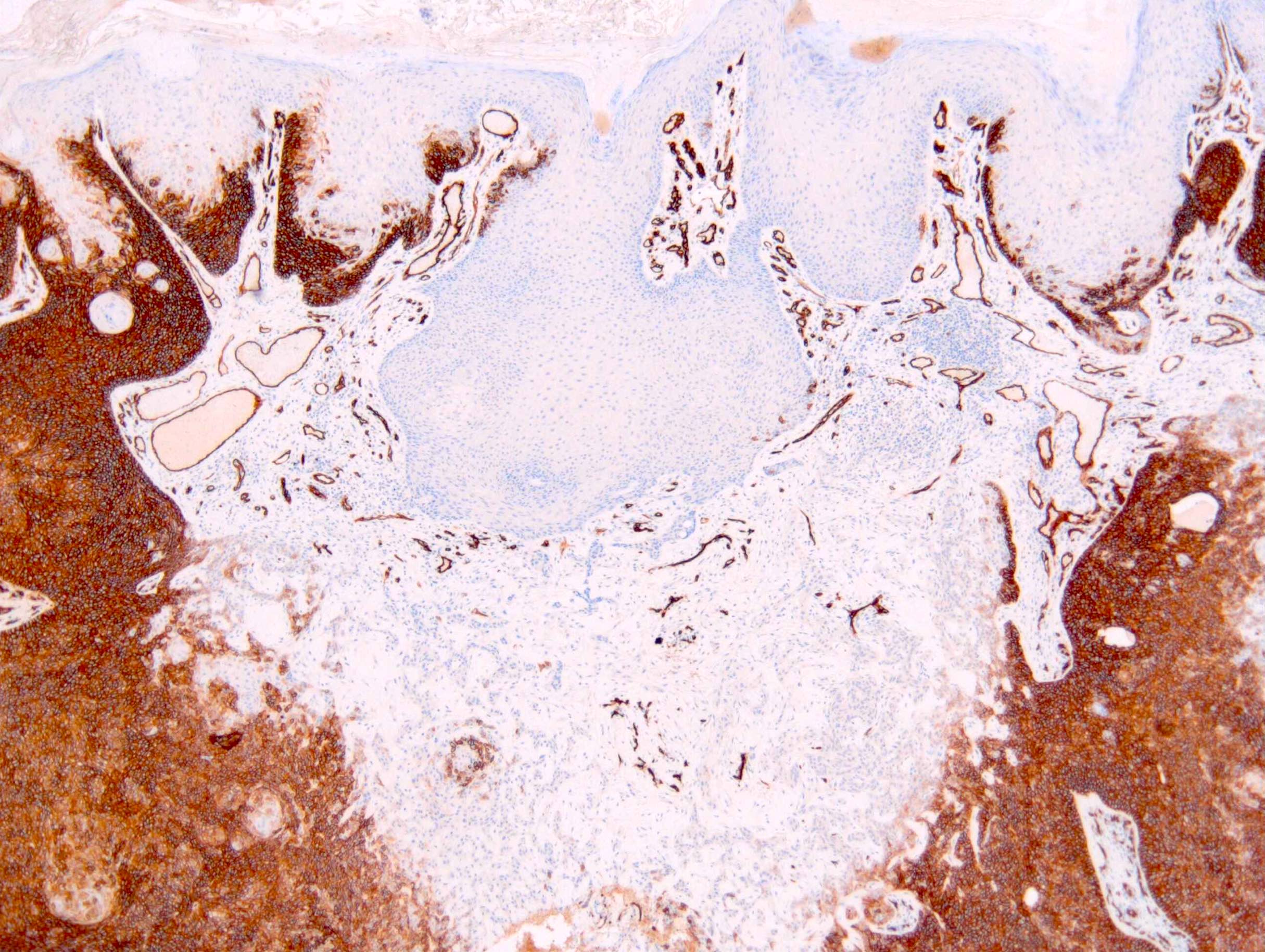
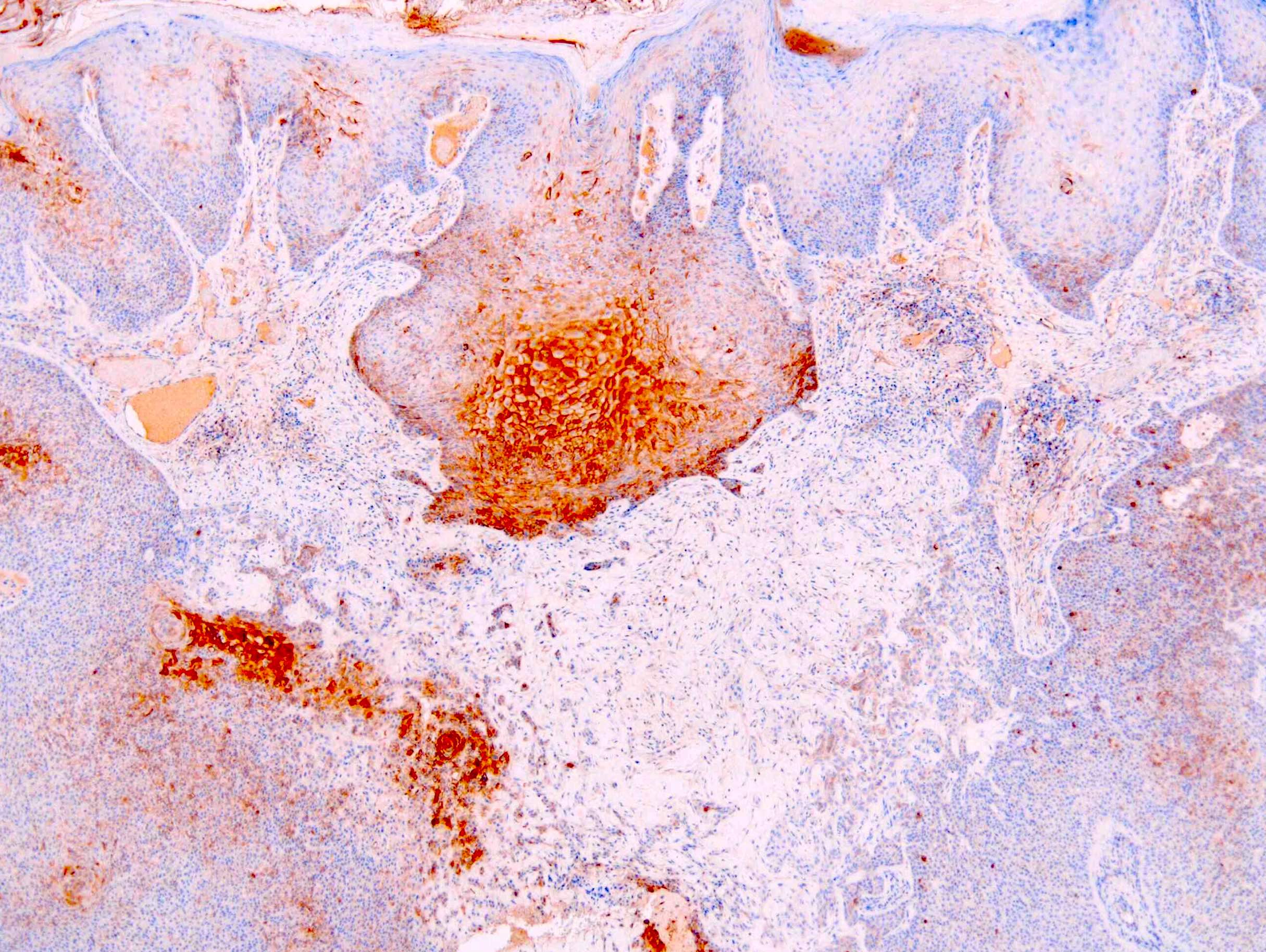
CD34
Positive stains
- CD34: may be very focal and require multiple sections to find (Am J Dermatopathol 2018;40:561)
Negative stains
Sample pathology report
- Skin, right side of nose, punch biopsy:
- Trichilemmoma (see comment)
- Comment: This is a benign tumor. Multiple trichilemmomas may be associated with Cowden syndrome. Clinical correlation advised or specialist dermatology assessment should be considered if clinically indicated.
- Microscopic description: A folliculocentric tumor with bulbous profile and stromal clefting is seen in the dermis with connection to the epidermis. The tumor is composed of basaloid cells and cells with clear cytoplasm. Peripheral palisading and a thickened basement membrane is noted. The overlying epidermis demonstrates hyperkeratosis. No dysplasia is seen.
Differential diagnosis
- Inverted follicular keratosis:
- Characterized by small basaloid cells and tight squamous eddies
- Viral wart (verruca):
- May be indistinguishable but typically demonstrates peripheral in turning of the rete ridges, marked hyperkeratosis, with columns of parakeratosis overlying the papillomatous projections
- Blood is often seen with the tips of parakeratosis
- Basal cell carcinoma:
- May have similar silhouette, in particular to the basaloid variant trichilemmoma
- Artifactual clefting with mucin within the space, in contrast to the stromal clefting of a benign follicular tumor, is seen
- Mitotic activity is usually obvious
- BerEP4 is strong and diffuse (unless superficial or eroded)
- CD34 is negative
- Squamous cell carcinoma:
- In particular the follicular variant may be confused with trichilemmoma
- Has cellular pleomorphism, brisk and abnormal mitotic activity and invasive borders
- Lack CD34 expression
- Trichilemmal carcinoma:
- Considered the malignant counterpart of trichilemmoma
- It is very rare
- Distinction is made by cellular pleomorphism
- Brisk and abnormal mitotic activity
- Usually lack CD34 expression
Additional references
Board review style question #1
Which of the following is true of trichilemmomas?
- Are a cutaneous marker of internal malignancy
- Are found predominantly on the trunk and acral sites
- Are typically present in children
- Multiple trichilemmomas are pathognomonic of Cowden syndrome
Board review style answer #1
D. Multiple trichilemmomas are pathognomonic of Cowden syndrome
Comment Here
Reference: Trichilemmoma
Comment Here
Reference: Trichilemmoma
Board review style question #2
A 30 year old man had a punch biopsy of a forehead papule which was possible basal cell carcinoma based on appearance.
With respect to the pictographs above
With respect to the pictographs above
- Any focal BerEP4 stain positivity confirms this as a basaloid trichilemmoma
- CD34 staining may be very focal and require careful sectioning to demonstrate
- Mucin and atypia distinguish this lesion as a follicular squamous cell carcinoma
- Presence of clear cells can distinguish basaloid trichilemmoma from basal cell carcinoma
Board review style answer #2
B. This is a trichilemmoma. CD34 staining may be very focal and require careful sectioning to demonstrate.
Comment Here
Reference: Trichilemmoma
Comment Here
Reference: Trichilemmoma
