
Skin nonmelanocytic tumor
Adnexal tumors
Sweat gland derived (apocrine & eccrine glands)
Polymorphous sweat gland carcinoma
Authors: Shira Ronen, M.D., Saul Suster, M.D.
Resident / Fellow Advisory Board: Farres Obeidin, M.D.


Last author update: 4 October 2021
Last staff update: 22 June 2023
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Polymorphous sweat gland carcinoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Clinical features | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ronen S, Suster S. Polymorphous sweat gland carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticpolysweatglandcarcinoma.html. Accessed April 2nd, 2025.
Definition / general
- First described by Suster and Wong in 1994 (Histopathology 1994;25:31)
- Uncommon, low grade, malignant adnexal tumor
Essential features
- Histologically, the lesions are characterized by a cellular proliferation showing a combination of growth patterns, including trabecular, solid, tubular, cribriform or adenoid cystic and pseudopapillary (Am J Dermatopathol 2018;40:580)
- Marked predilection for the distal extremities
Terminology
- Polymorphous sweat gland carcinoma
- Polymorphous low grade sweat gland carcinoma
- PSGC
ICD coding
- ICD-O-3 topography code: C44 - Skin
Epidemiology
- Middle aged to older patients
- No sex preference (Am J Dermatopathol 2018;40:580)
Sites
- Favors the extremities (10 cases), followed by head and neck (4 cases) and the trunk (2 cases) (J Am Acad Dermatol 2002;46:914, Ann Pathol 1996;16:442)
Clinical features
- Slow growing, skin colored, firm dermal nodule measuring 1 - 8.5 cm (Am J Dermatopathol 2018;40:580)
Case reports
- 51 year old man with a slow growing tan‐brown nodule on the left upper chest of 1 year's duration (J Cutan Pathol 2016;43:594)
- 54 year old woman with a 1 cm slow growing nodule on the elbow (J Cutan Pathol 2016;43:594)
- 56 year old man with multiple large skin nodules (J Am Acad Dermatol 2002;46:914)
- 60 year old man with a 20 - 30 mm, skin colored, mobile, firm tumor (Histopathology 2020;76:779)
- Patient with polymorphic sweat gland adenocarcinoma (Ann Pathol 1996;16:442)
Treatment
- Complete excision with conservative margins has been recommended as the preferred modality of treatment
Microscopic (histologic) description
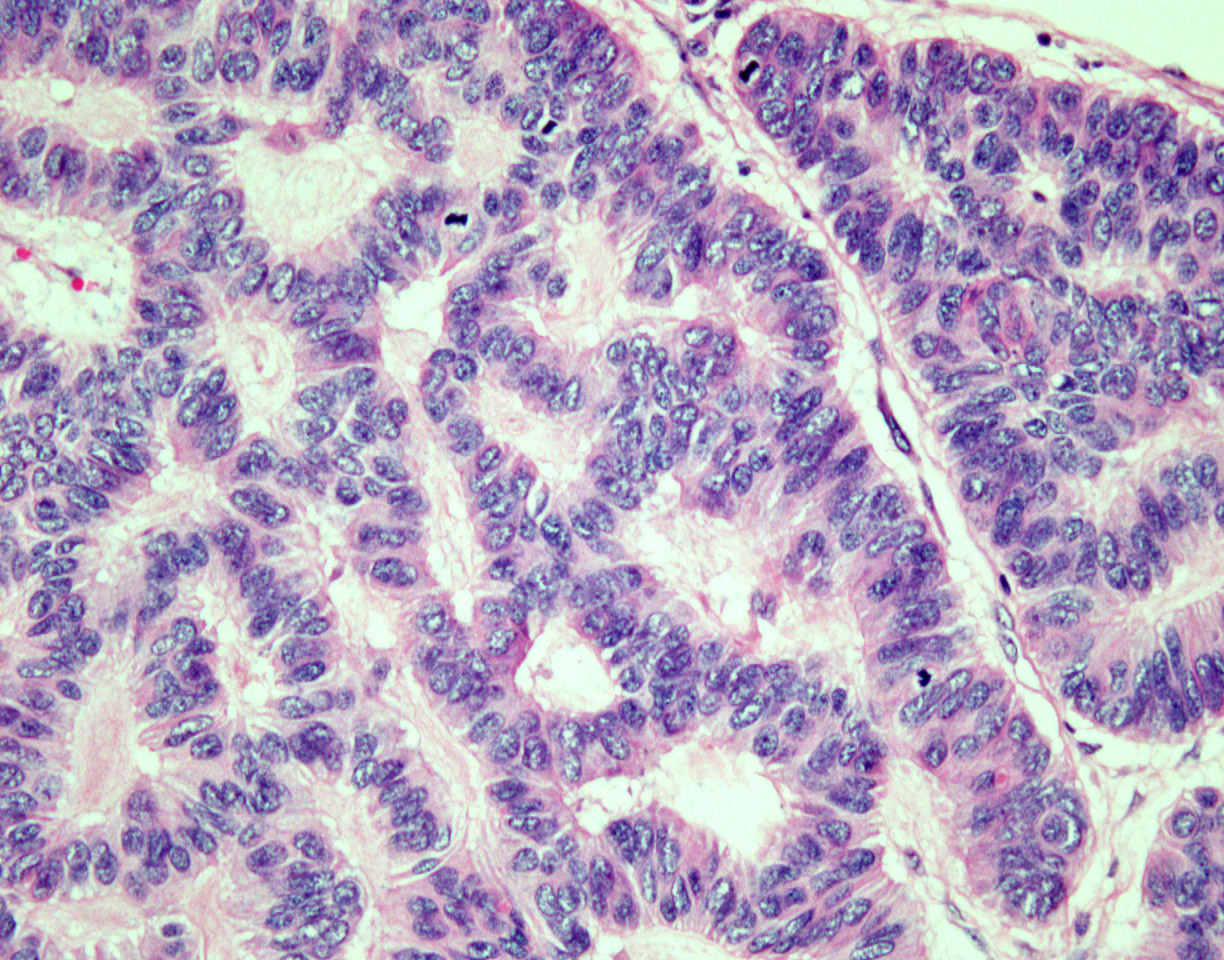
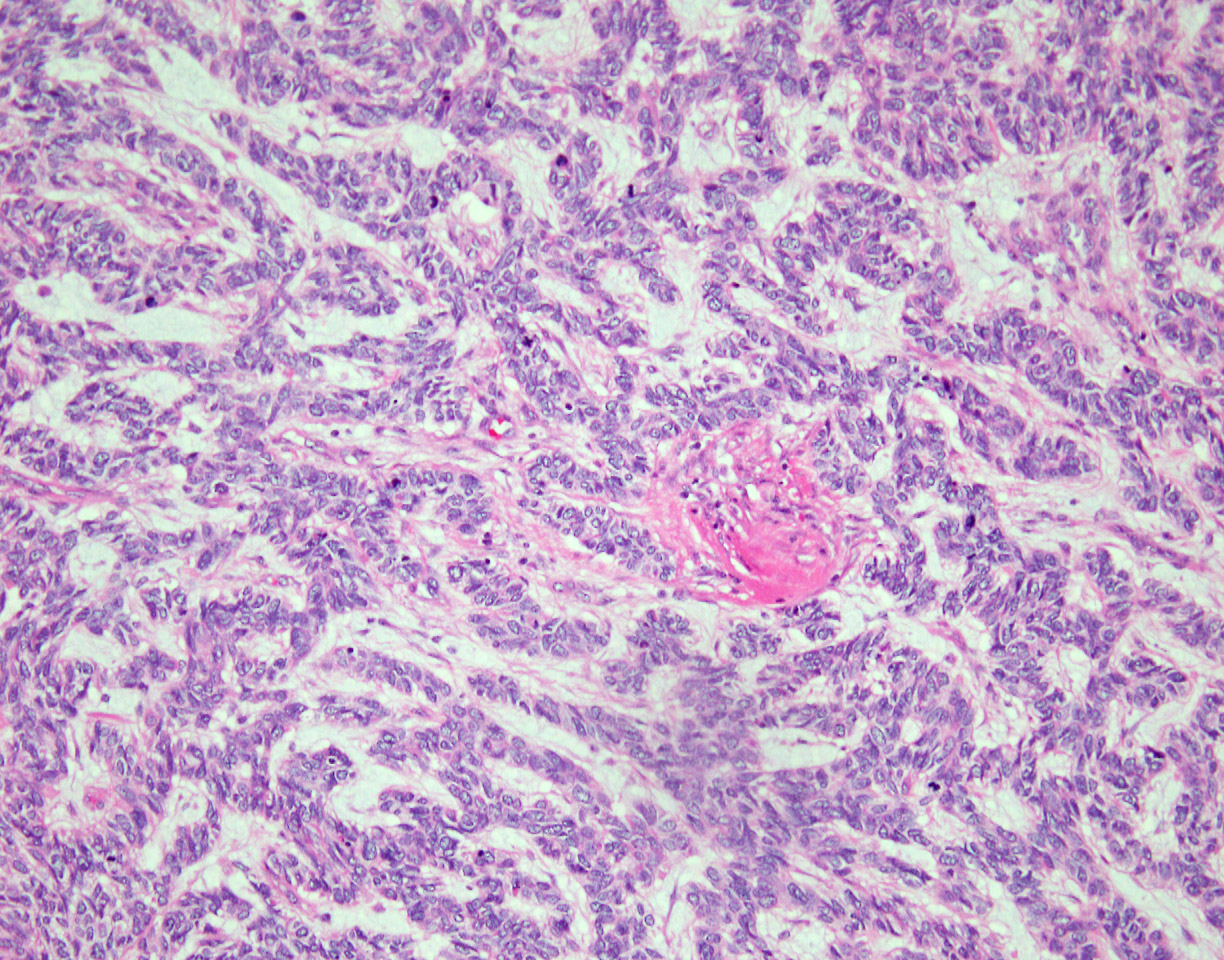
- Characterized by an admixture of multiple growth patterns within the same lesion, including trabecular, solid, tubular, cylindromatous and pseudopapillary, as well as prominent stromal changes, including hyalinization, hemorrhage, calcification and cystic changes
- Tumors grow within the dermis in a generally well demarcated, pushing border but rarely can show infiltration at the edges
- Parts of the tumor also show glandular differentiation and adnexal differentiation, such as abortive hair follicle formation and numerous squamous eddies
- Tumors are predominantly composed of large epithelioid cells with atypical nuclei and abundant eosinophilic cytoplasm
- Smaller cells with darker, angulated nuclei are scattered throughout the tumor
- Spindling of tumor cells can be seen focally
- Mitoses are present and can vary from case to case
Microscopic (histologic) images
Contributed by Shira Ronen, M.D.
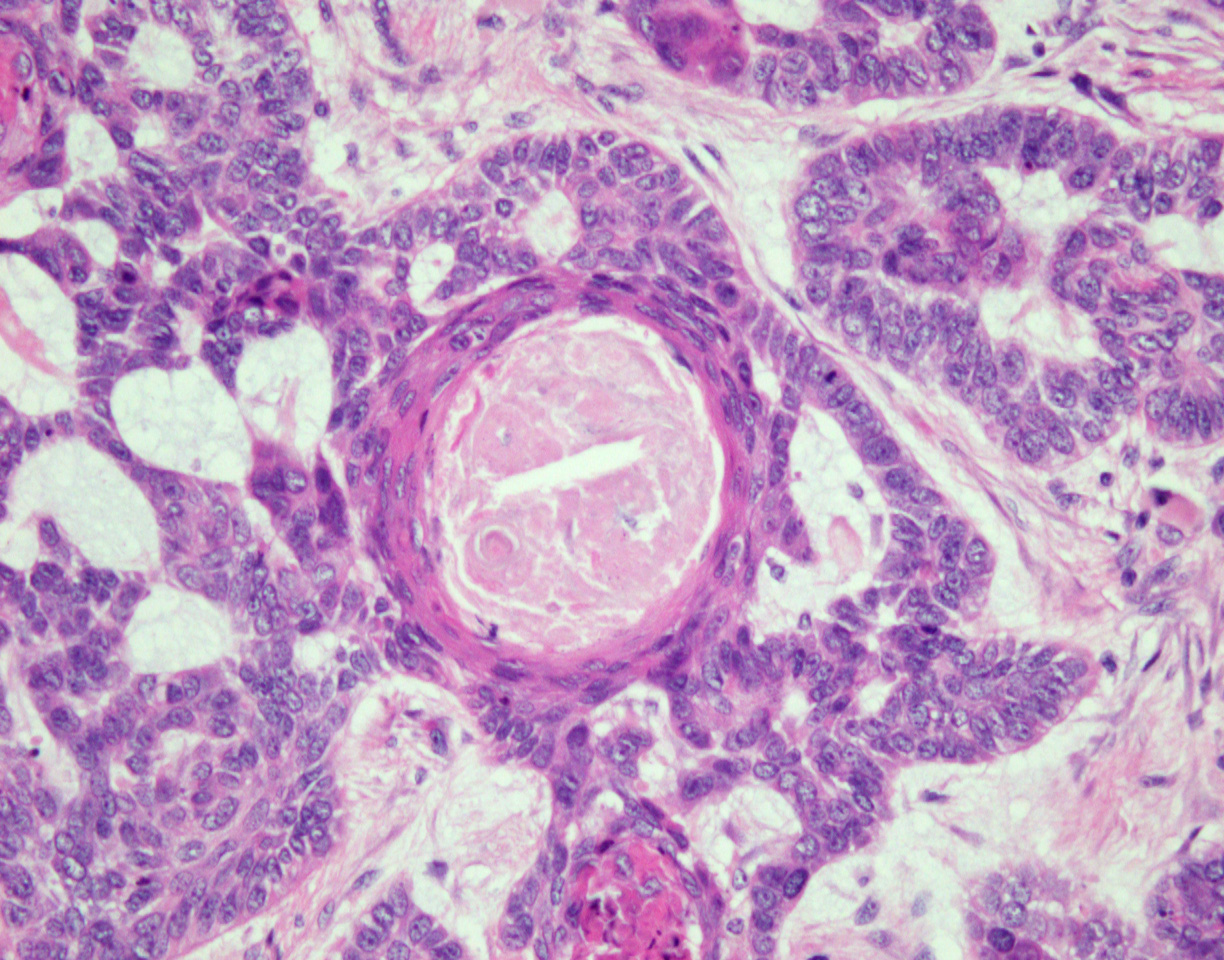
Abortive hair follicle formation
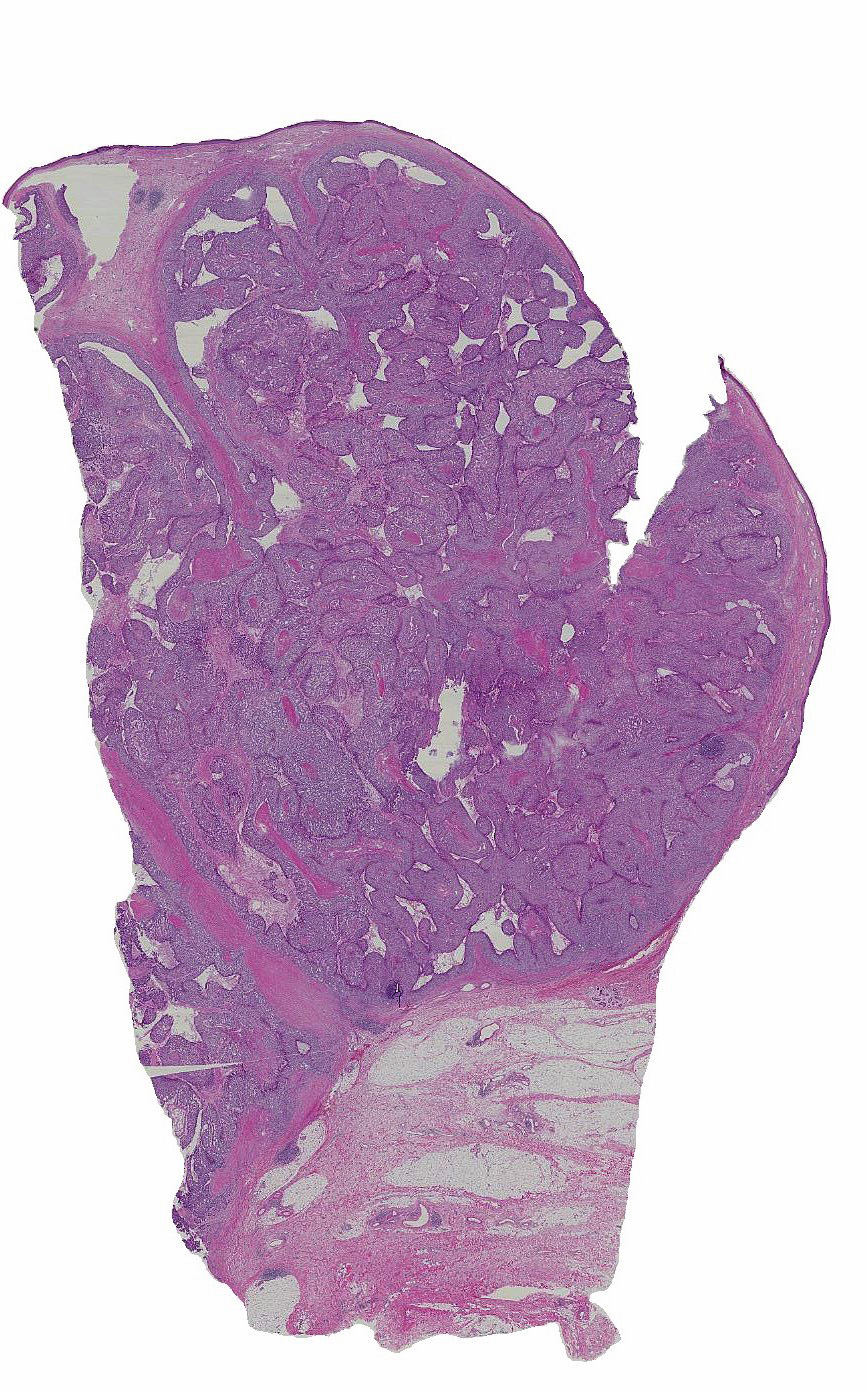
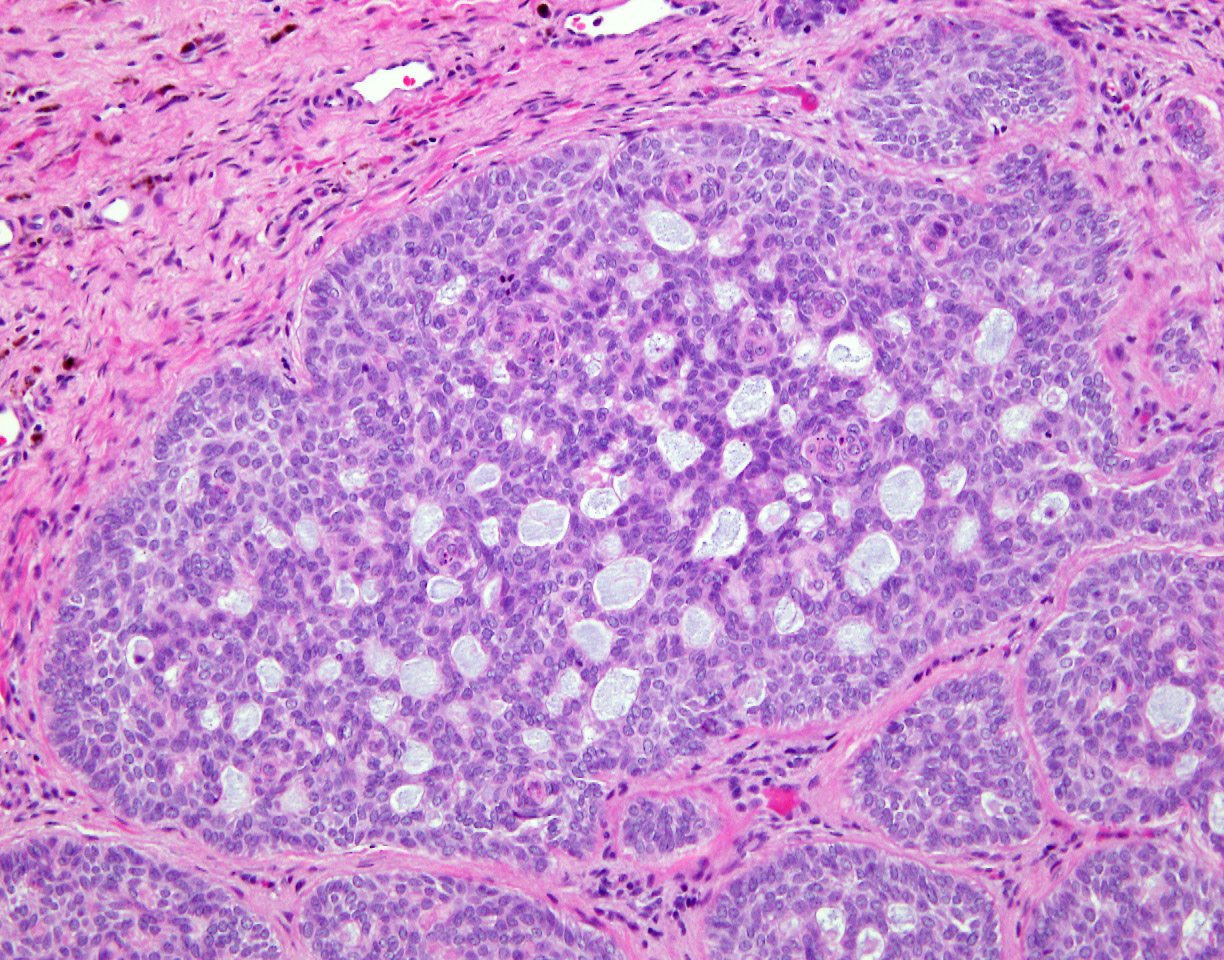
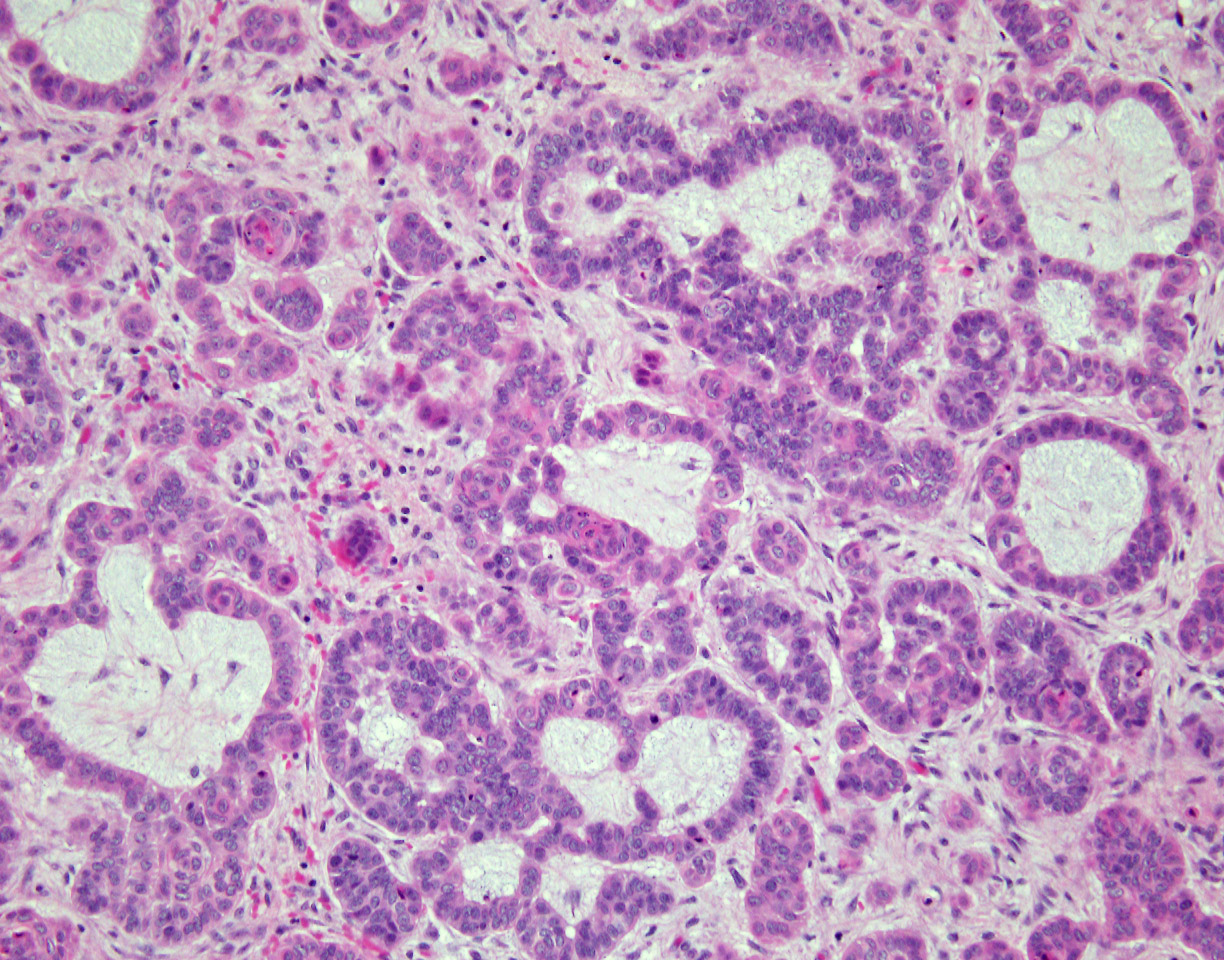
Combination of growth patterns
Combination of growth patterns
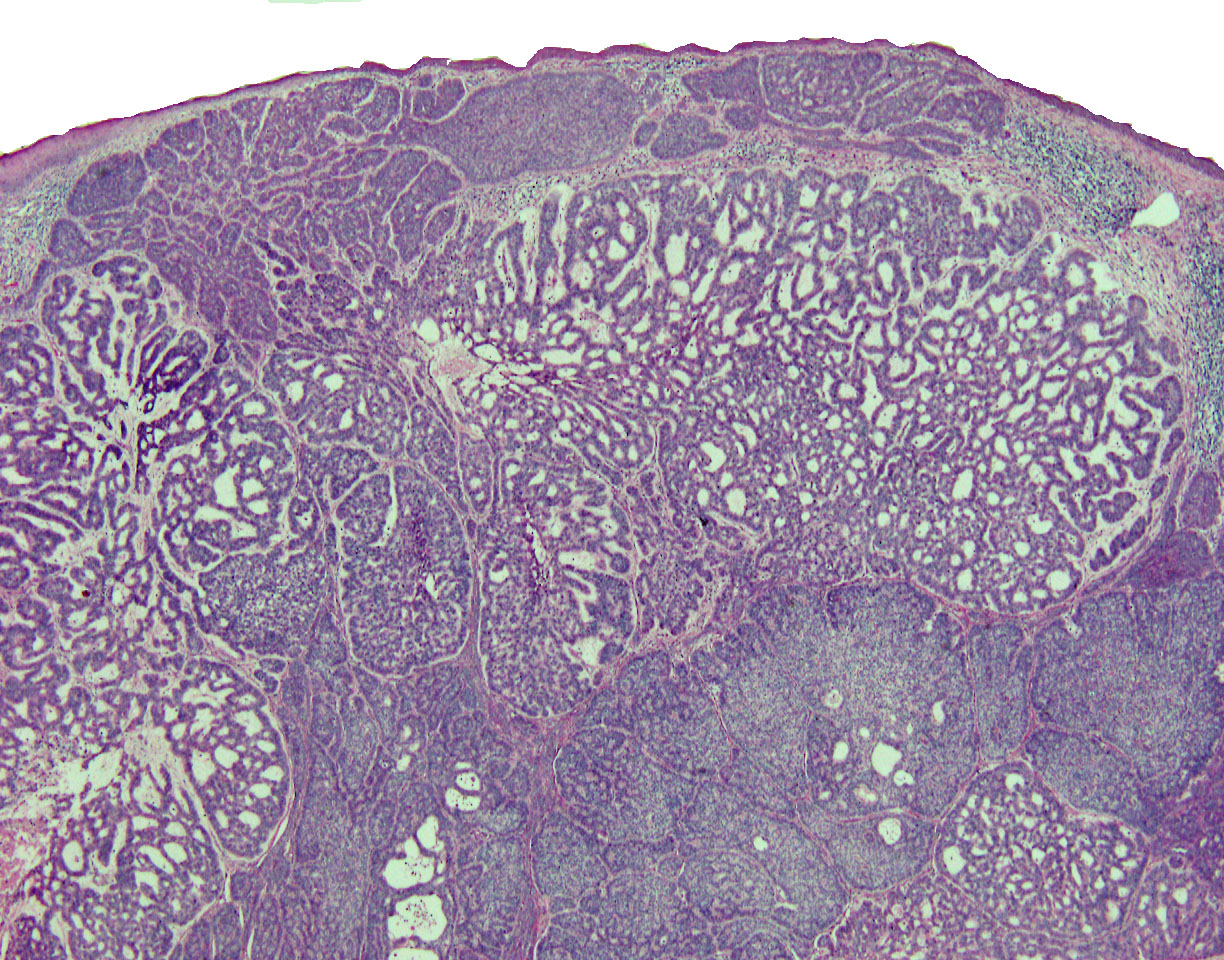
Cribriform growth pattern
Glandular differentiation
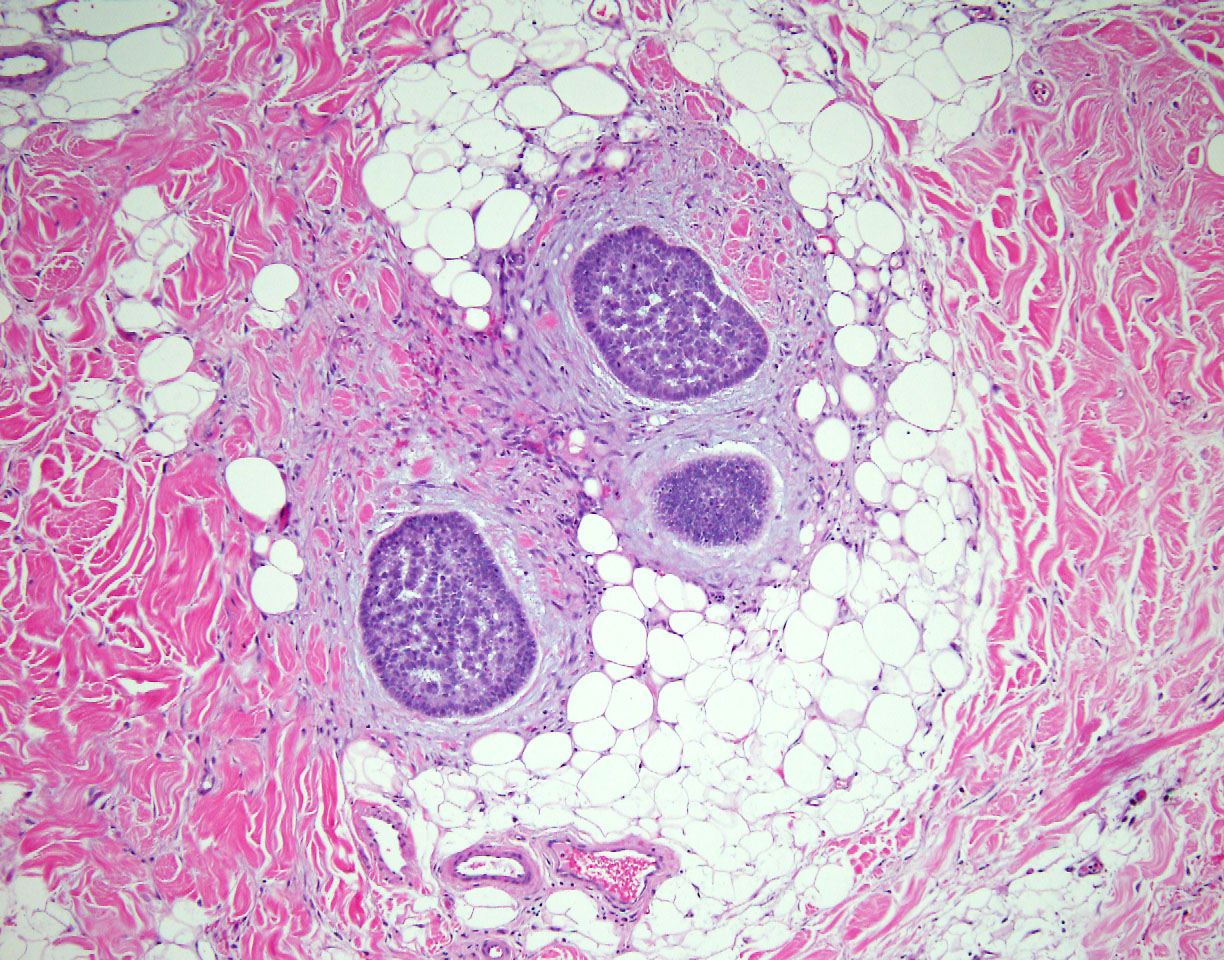
Infiltration of surrounding fibroadipose tissue
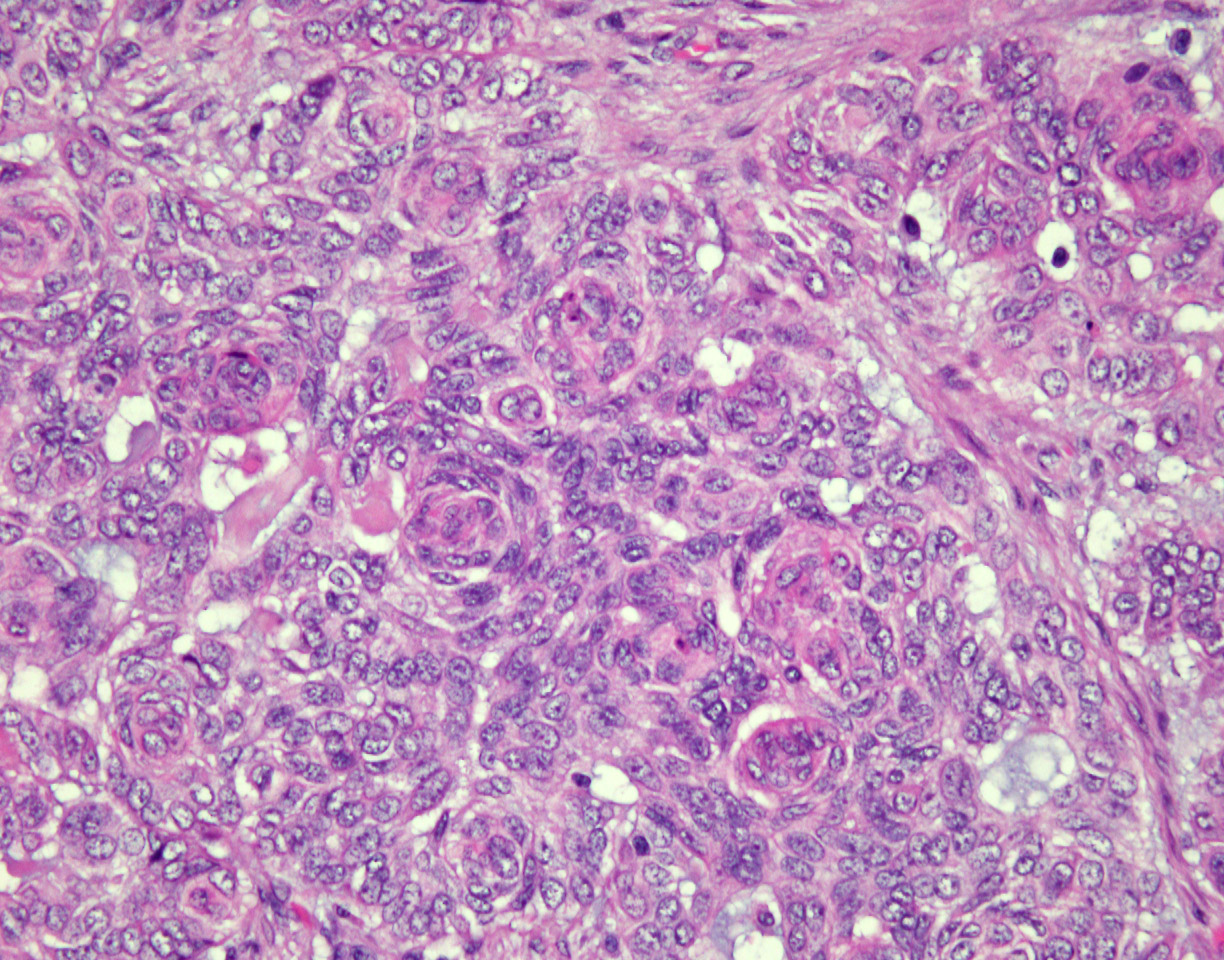
Numerous squamous eddies
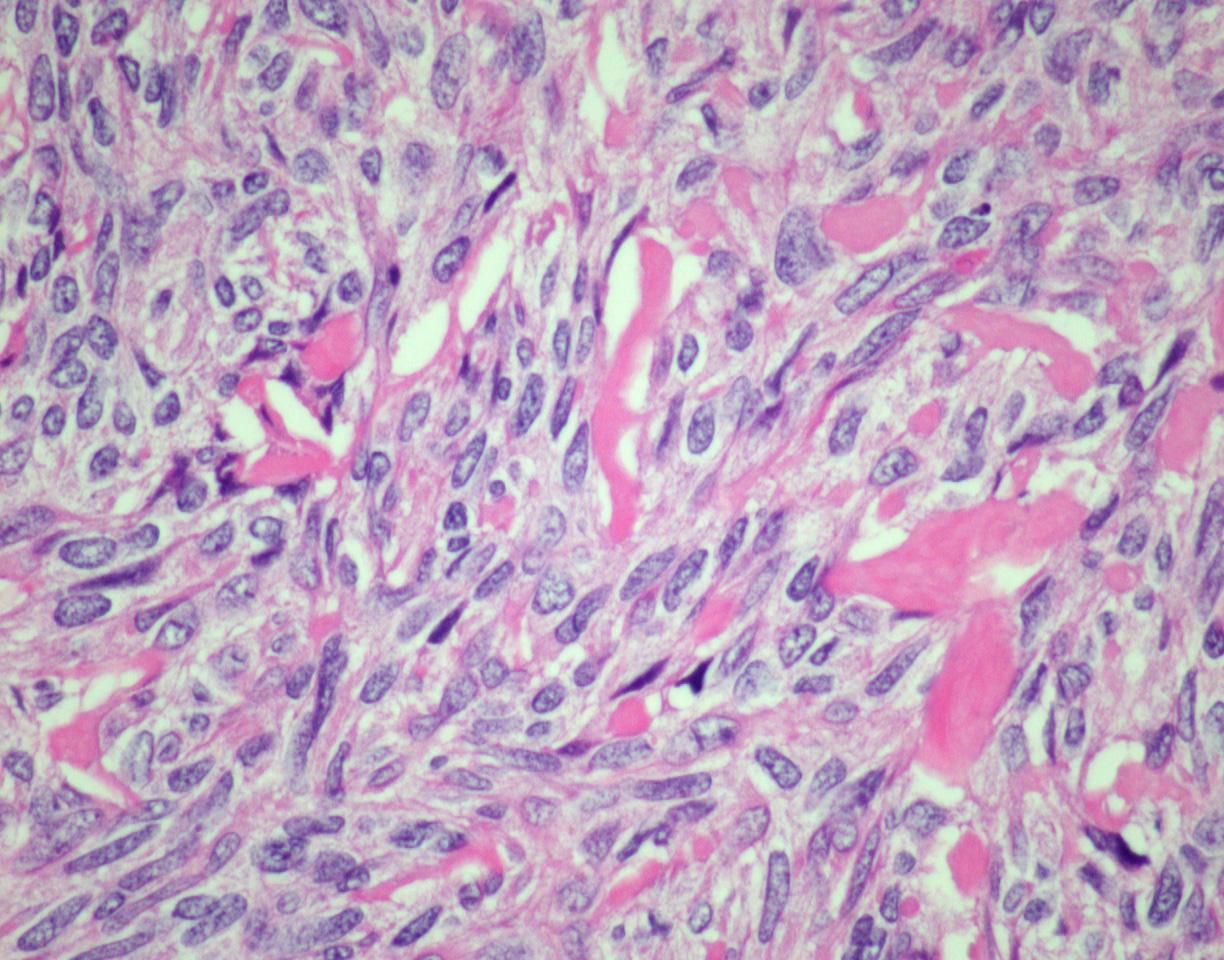
Spindle cell appearance
Trabecular growth pattern
Androgen receptor (AR)
CD56
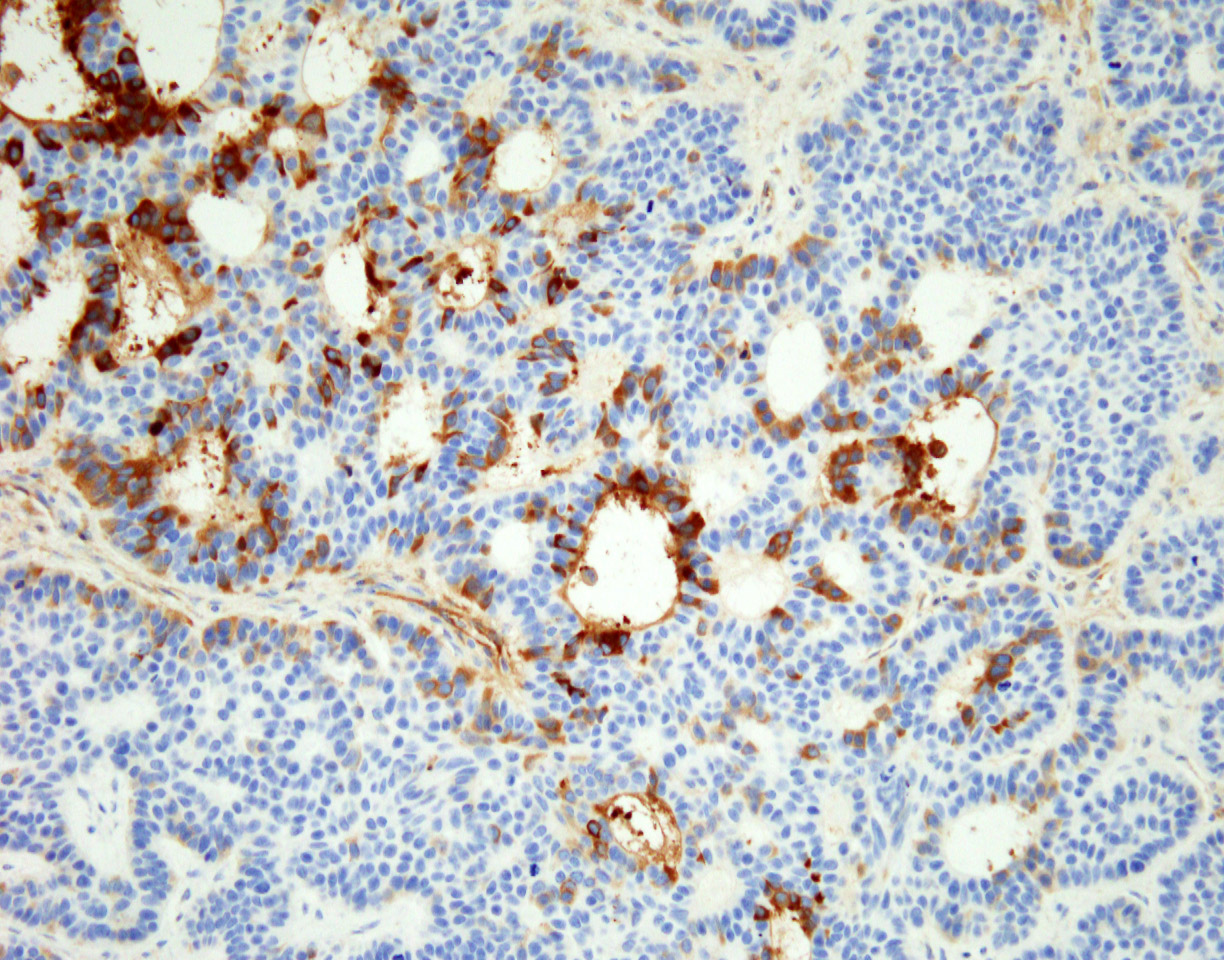
Chromogranin
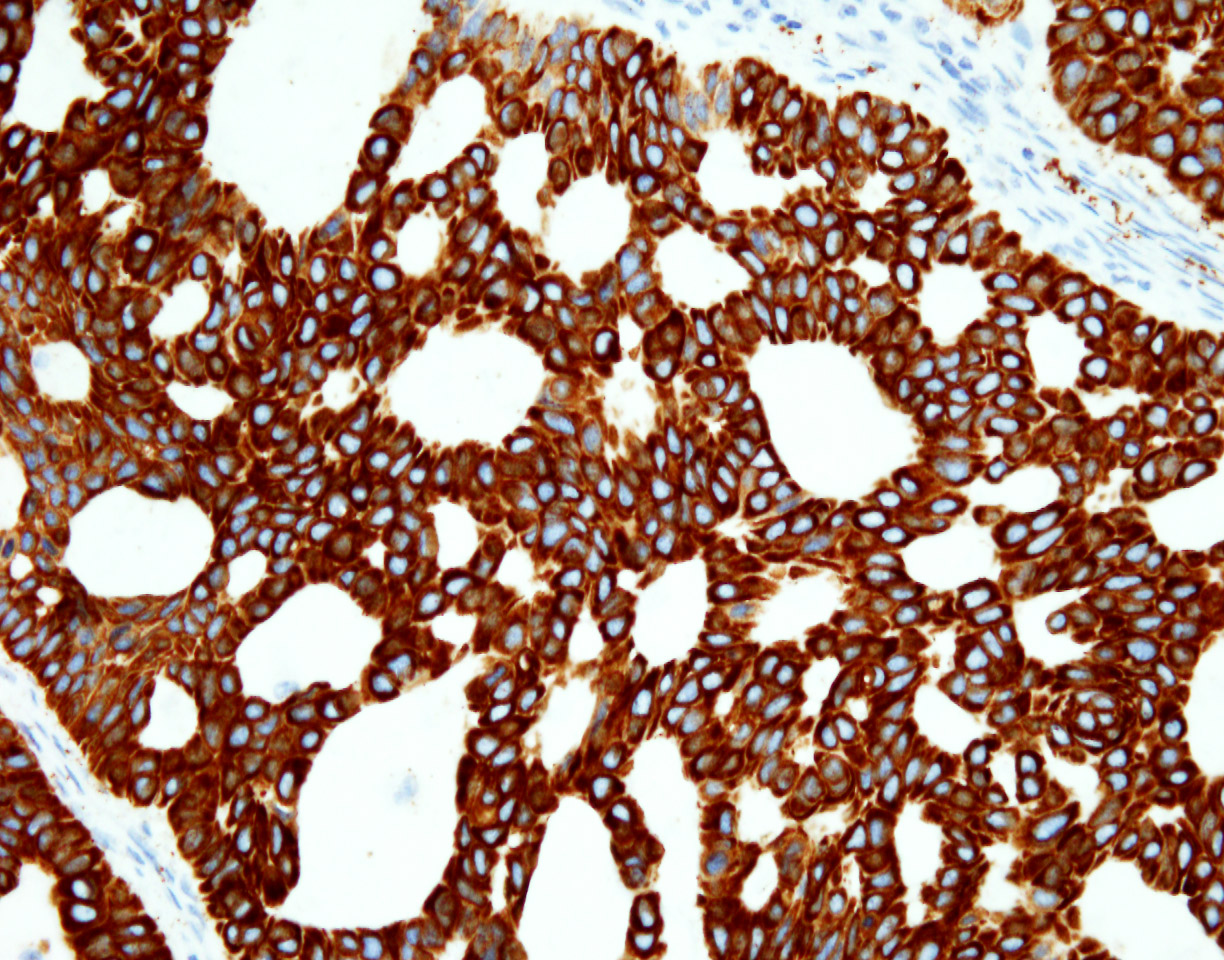
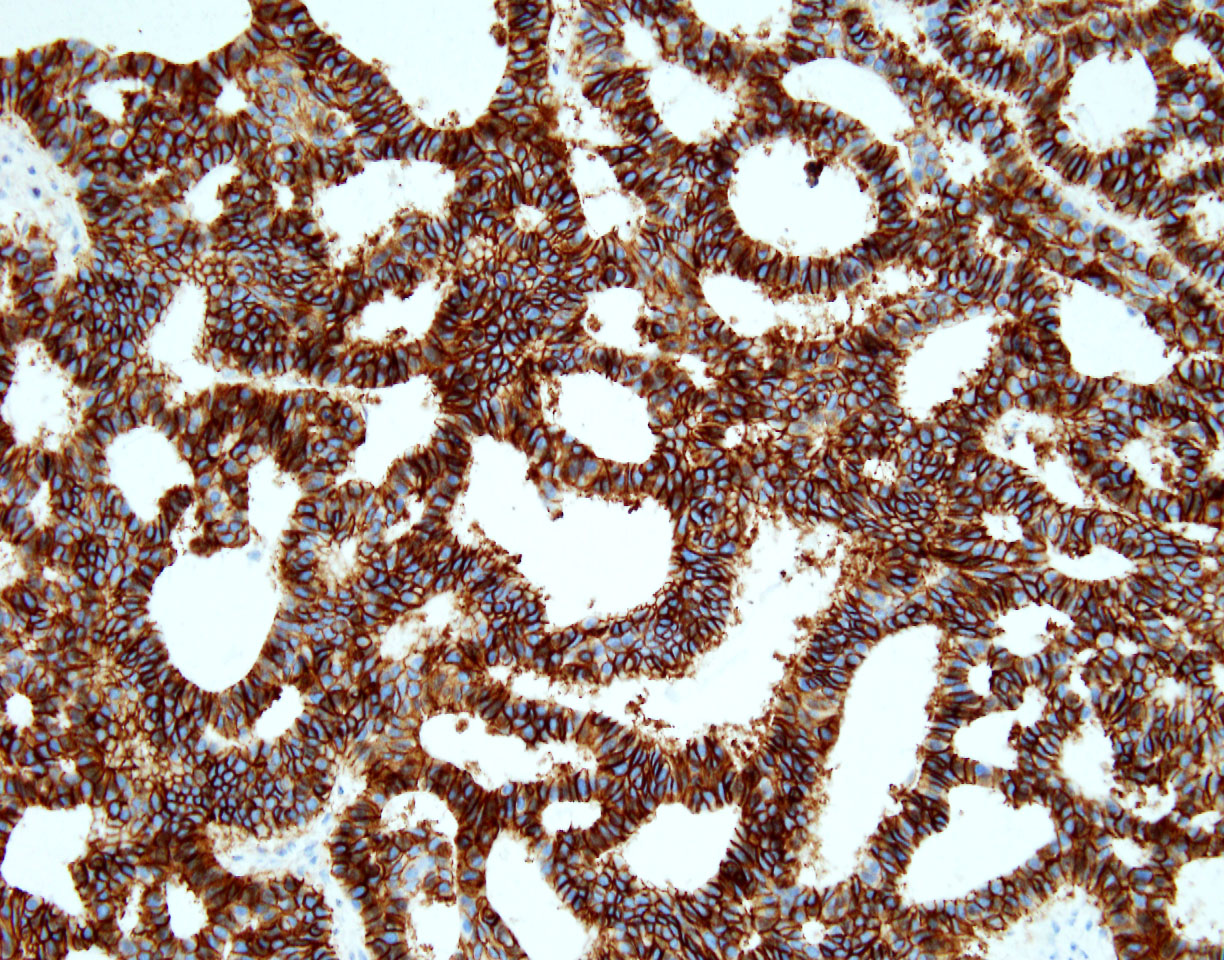
CK5/6
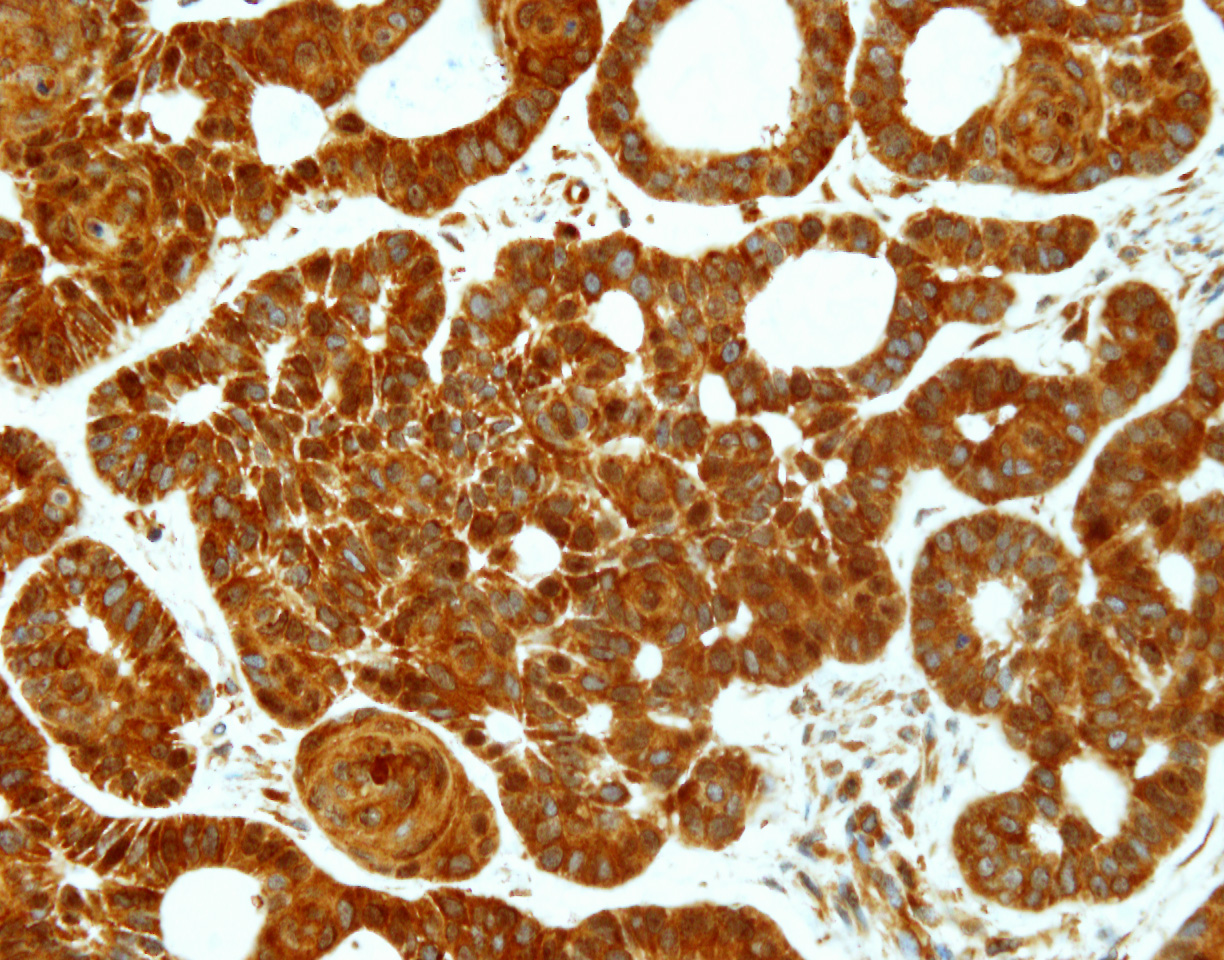
p16

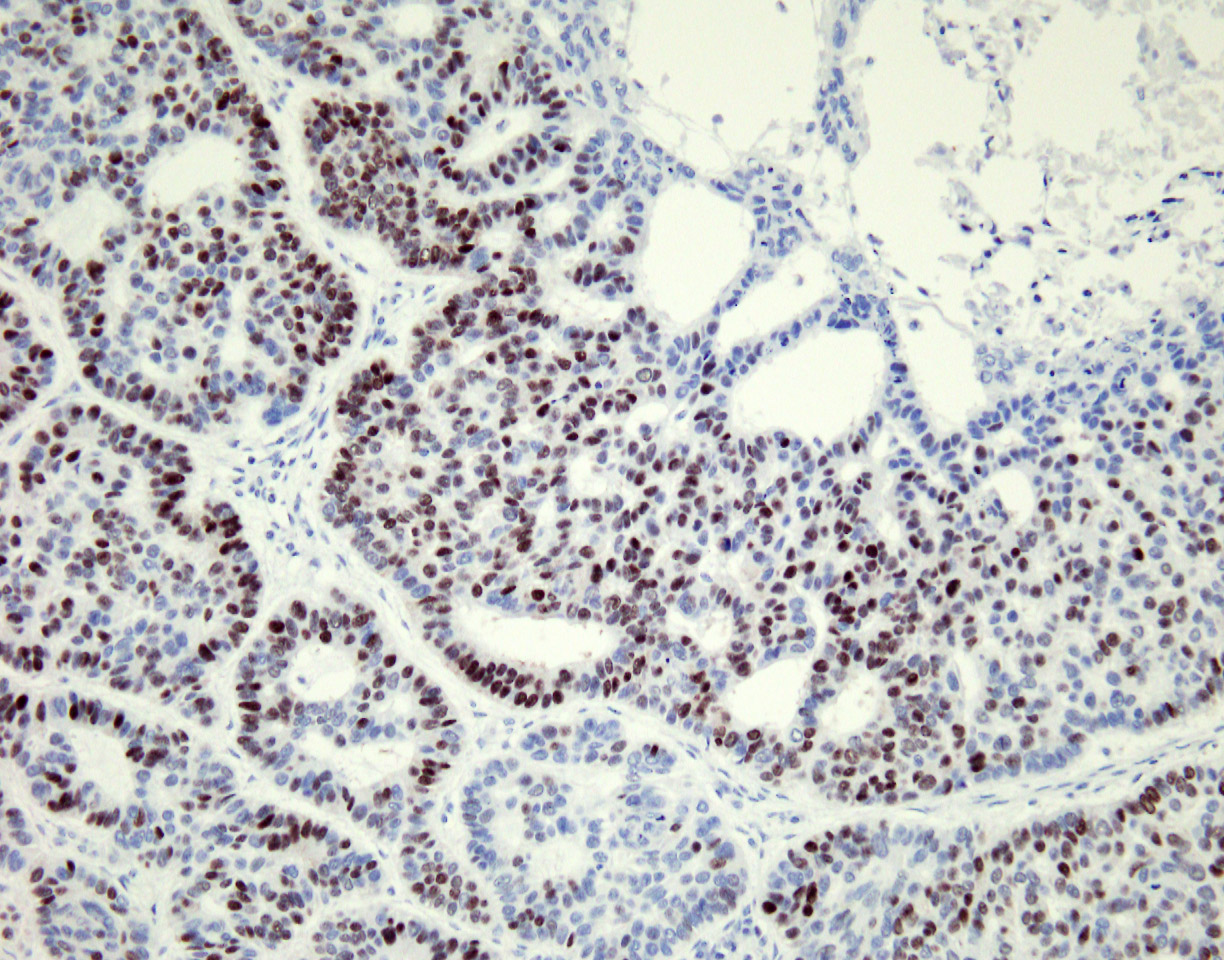
p63
Positive stains
- Strong positivity for cytokeratin AE1 / AE3, CK5/6, p40, p63 and p16 (Am J Dermatopathol 2018;40:580)
- MIB1 proliferation index is very high
- Focal expression of the neuroendocrine markers CD56 and chromogranin
Negative stains
- Negative for CD117, CEA, S100, vimentin, EMA, DOG1, estrogen receptor, progesterone receptor, synaptophysin, SMA, HBME-1 and mammaglobin (Am J Dermatopathol 2018;40:580)
Molecular / cytogenetics description
- Negative for MYB-NFIB fusion
Sample pathology report
- Neck mass, excision:
- Polymorphous sweat gland carcinoma (see comment)
- Comment: Sections show a relatively well demarcated tumor involving the dermis without a connection to the epidermis. The tumor shows multiple growth patterns including solid, trabecular, tubular and focal cribriform. Prominent hemorrhage, cystic changes and calcifications are seen. The cells are mostly epithelioid with prominent nucleoli and eosinophilic cytoplasm. Scattered mitotic figures are also observed. There is no evidence of significant cytologic atypia or necrosis. Overall, in the absence of a known or occult primary malignancy, the tumor is most consistent with a polymorphous sweat gland carcinoma. A clinical workup to exclude the possibility of metastasis, as clinically indicated, is recommended.
Differential diagnosis
- Adenoid cystic carcinoma (ACC) (Am J Dermatopathol 1986;8:2):
- ACC is characterized by monomorphic basaloid cells, which are arranged in tubules, elongated nests and cords
- There are typically numerous cystic and ductular spaces with a prominent cribriform pattern
- In comparison, polymorphous sweat gland carcinoma is characterized by striking variegation of histologic growth patterns, including glandular, trabecular, solid, cylindromatous and cribriform areas within the same tumor mass
- MYB overexpression
- Consistently expresses EMA
- Positive for CD117, CEA, S100 and vimentin
- Basal cell carcinoma (Am J Dermatopathol 1986;8:2):
- Retains striking peripheral nuclear palisading and stromal retraction
- Metastases from internal malignancies:
- Benign and malignant adnexal neoplasm, such as ductal eccrine carcinoma, microcystic carcinoma and papillary digital eccrine carcinoma:
- Key difference is the striking variegation of histologic growth patterns seen in polymorphous sweat gland carcinoma that would not be seen in other adnexal neoplasms
Board review style question #1
Which of the following statements is true about polymorphic sweat gland adenocarcinoma?
- It is characterized by an admixture of multiple growth patterns within the same lesion
- The most common location is the abdomen
- The tumor is common
- This tumor shows MYB-NFIB fusion
- It is a fast growing tumor
Board review style answer #1
A. It is characterized by an admixture of multiple growth patterns within the same lesion. The other answer choices are incorrect, since the tumor is shown to favor the extremities (choice B), the tumor is uncommon and only a few case reports and case series have been described (choice C), polymorphic sweat gland adenocarcinoma is negative for the MYB-NFIB fusion (choice D) and it is a slow growing, skin colored, firm dermal nodule (choice E).
Comment Here
Reference: Polymorphous sweat gland carcinoma
Comment Here
Reference: Polymorphous sweat gland carcinoma
Board review style question #2
Which of the following immunohistochemical stains will show strong diffuse positivity in polymorphic sweat gland adenocarcinoma?
- CD117 and CEA
- p63 and p16
- Vimentin and cytokeratin AE1 / AE3
- Chromogranin and S100
- DOG1 and p40
Board review style answer #2
B. p63 and p16. The other answer choices are incorrect, since CD117 and CEA are negative (choice A), vimentin is negative within this entity, while cytokeratin AE1 / AE3 shows strong diffuse positivity (choice C), chromogranin stain shows focal expression, while S100 is negative within the tumor (choice D) and DOG1 is negative within this entity, while p40 shows strong diffuse positivity (choice E).
Comment Here
Reference: Polymorphous sweat gland carcinoma
Comment Here
Reference: Polymorphous sweat gland carcinoma
