
Skin nonmelanocytic tumor
Adnexal tumors
Sweat gland derived (apocrine & eccrine glands)
Syringocystadenoma papilliferum
Authors: Mahyar Khazaeli, M.D., Kiran Motaparthi, M.D.
Editorial Board Member: Farres Obeidin, M.D.

Last author update: 10 March 2022
Last staff update: 24 January 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Syringocystadenoma papilliferum [TI] "last 5 years"[DP]

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Khazaeli M, Motaparthi K. Syringocystadenoma papilliferum. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticpapillarysyringadenoma.html. Accessed April 2nd, 2025.
Definition / general
- Benign, hamartomatous, adnexal tumor (J Clin Diagn Res 2014;8:QD03)
- Originates from the apocrine or the eccrine sweat glands (J Clin Diagn Res 2013;7:742)
Essential features
- Benign adnexal tumor, most commonly occurring in the head and neck in early childhood (J Dermatol 2004;31:939)
- Most are solitary papules but variable clinical presentation
- Macroscopic: pink, hairless plaque or nodule
- Microscopic: cystic invaginations of the infundibular epithelium extending into the dermis with a double cell layer of inner columnar and outer cuboidal cells
Terminology
- Syringocystadenoma papilliferum (SCAP), also known as papillary syringadenoma (J Clin Diagn Res 2014;8:QD03)
Epidemiology
- M = F (Indian J Dermatol Venereol Leprol 2009;75:170)
- 50% of cases present at birth or in early childhood (Onco Targets Ther 2013;6:233)
- 15 - 30% of cases develop during puberty (Onco Targets Ther 2013;6:233)
Sites
- 75% of cases are reported in the head and neck region (Indian J Dermatol Venereol Leprol 2009;75:170)
- Unusual locations: buttock, vulva and scrotum, pinna, eyelid, outer ear canal, postoperative scar, scalp, nipple, thigh, axilla, back and right lower abdomen (3 cases) (J Clin Diagn Res 2014;8:QD03)
Pathophysiology
- Benign hamartomatous adnexal tumor (J Clin Diagn Res 2014;8:QD03)
- Origin is uncertain:
- Derived from apocrine glands, eccrine glands or both:
- Immunohistochemical studies support an apocrine origin (J Clin Diagn Res 2014;8:QD03)
- Ultrastructural analysis favors an eccrine derivation (J Clin Diagn Res 2014;8:QD03)
- May arise from pluripotent stem cells (J Clin Diagn Res 2014;8:QD03)
- Derived from apocrine glands, eccrine glands or both:
- During puberty, may increase in size and develop a crusted and papillomatous texture (Br J Dermatol 2000;142:543)
- Although benign, co-occurrence of basal cell carcinoma, verrucous carcinoma metastatic adenocarcinoma and ductal carcinoma may be observed (Onco Targets Ther 2013;6:233, OrphaNet: Syringocystadenoma Papilliferum [Accessed 5 November 2021])
Etiology
- Often observed in association with other benign adnexal neoplasms, such as nevus sebaceus (8 - 19% of patients), apocrine nevus, tubular apocrine adenoma, apocrine hidrocystoma, apocrine cystadenoma and clear cell syringoma (Pathologica 2006;98:178)
Clinical features
- Measures between 1 - 3 cm and < 4 cm in diameter (J Clin Diagn Res 2013;7:742)
- Variable clinical presentation:
- Solitary papule
- Linear arrangement of several papules (Onco Targets Ther 2013;6:233)
- Most patients present with solitary lesions in the head and neck region at birth or in early childhood (J Clin Diagn Res 2014;8:QD03)
- Variable presentations:
- Warty plaques on the head and neck (J Clin Diagn Res 2014;8:QD03)
- Papule or a smooth hairless plaque on the scalp and forehead (Indian J Dermatol Venereol Leprol 2009;75:170)
- Often in the setting of nevus sebaceus (J Clin Diagn Res 2014;8:QD03)
- Nodular or verrucous transformation is noted at puberty (Indian J Dermatol Venereol Leprol 2009;75:170)
- Multiple lesions are rarely seen and those that arise outside the head and neck region are even more uncommon (J Clin Diagn Res 2014;8:QD03)
- With increasing size:
- More prominent papillary configuration develops (Onco Targets Ther 2013;6:233)
- Surface can develop hemorrhagic crust (Onco Targets Ther 2013;6:233)
Diagnosis
- Skin biopsy
Case reports
- 6 year old boy with progressive growth lesion on left flank (An Bras Dermatol 2020;95:112)
- 25 year old man with a 10 year history of an asymptomatic, slowly growing skin lesion on face (Case Rep Dermatol 2019;11:36)
- 45 year old woman with a right supraclavicular lesion since childhood (J Nippon Med Sch 2017;84:79)
- 56 year old woman with a swelling lesion on right temporal scalp (Malays J Pathol 2019;41:47)
- 64 year old man with a growing mass on left occipital scalp (Case Rep Pathol 2019;2019:1783758)
Treatment
- Surgical excision (J Cutan Aesthet Surg 2016;9:204)
Clinical images
Images hosted on other servers:

Posterior cranium, exophytic mass

Rose colored papule, left flank

Erythematous plaque, central crustation

Papillomatous exophytic, temporal scalp
Gross description
- Macroscopic:
- Skin colored to pink, hairless, firm plaque of grouped nodules or as a solitary nodule
- Verrucous, papillary, hyperkeratotic, moist or fleshy excrescences have also been described (Onco Targets Ther 2013;6:233)
- Some tumors may show central umbilication through which small fistulae may discharge fluid (Onco Targets Ther 2013;6:233)
- Mature lesions:
- Clusters of pinkish brown nodules (Onco Targets Ther 2013;6:233)
- 2 - 10 mm in diameter (Onco Targets Ther 2013;6:233)
- Occasional central opening (Onco Targets Ther 2013;6:233)
- Skin colored to pink, hairless, firm plaque of grouped nodules or as a solitary nodule
Microscopic (histologic) description
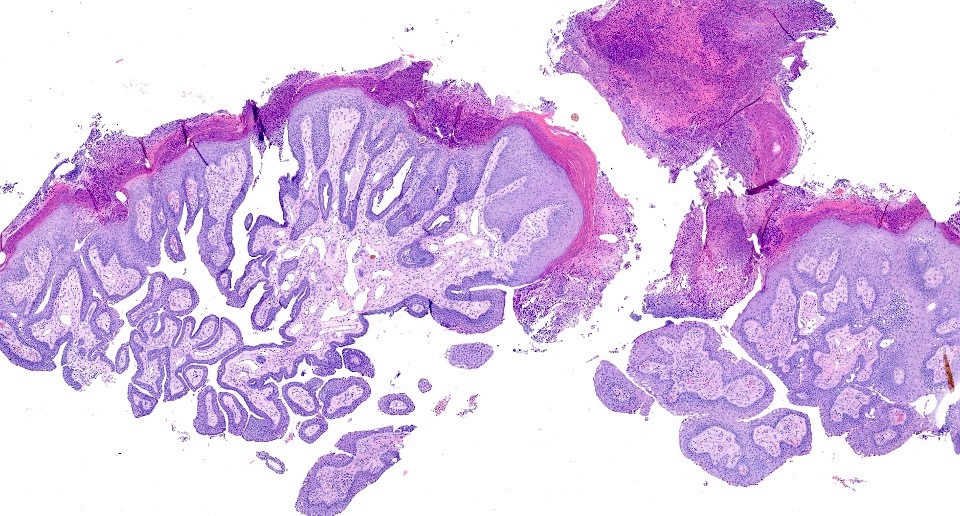
- Cystic invaginations of the infundibular epithelium projecting into the dermis, covered by a double cell layer (An Bras Dermatol 2017;92:721, J Clin Diagn Res 2014;8:QD03):
- Innermost layer is composed of columnar cells with decapitation secretion
- Outermost layer is composed of cuboidal cells with papillary projections
- Verrucous (papillomatous) epidermal hyperplasia with hyperkeratosis and hypergranulosis (Pathologica 2006;98:178)
- Exoendophytic configuration with a gradual transition from stratified squamous epithelium at the epidermal surface to a bilayered ductal epithelium (Pathologica 2006;98:178)
- Papillary fronds extend upward from the base and plasma cells are common in the stroma of each frond (Pathologica 2006;98:178)
- Many irregular duct-like structures and cystic spaces (Pathologica 2006;98:178)
- Ducts, containing papillary processes and lined by 2 epithelial cell layers, connect to the surface (Indian J Dermatol Venereol Leprol 2009;75:170)
- Exoendophytic architecture, verrucous epidermal hyperplasia, sometimes pseudoepitheliomatous hyperplasia and connection of glands to epidermis (An Bras Dermatol 2017;92:721)
- Background features of nevus sebaceus may be observed (An Bras Dermatol 2017;92:721)
Microscopic (histologic) images
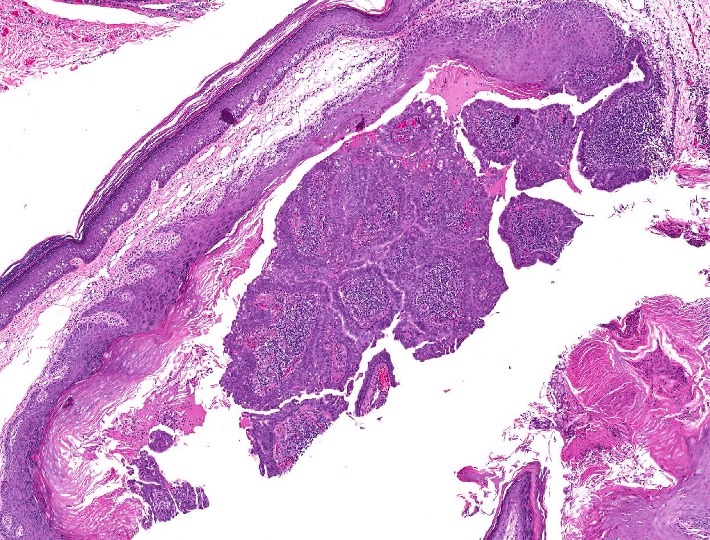
Contributed by Kiran Motaparthi, M.D.
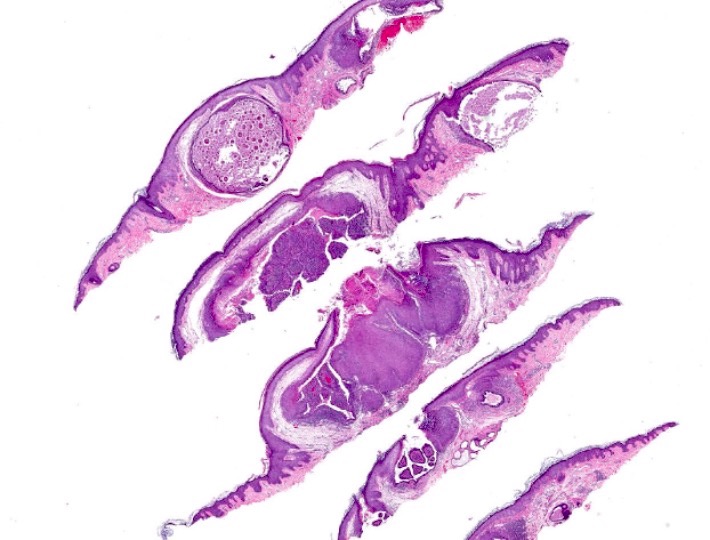
Glandular proliferation
Cystic proliferation

Glands with epidermal connection

Glands with double layer
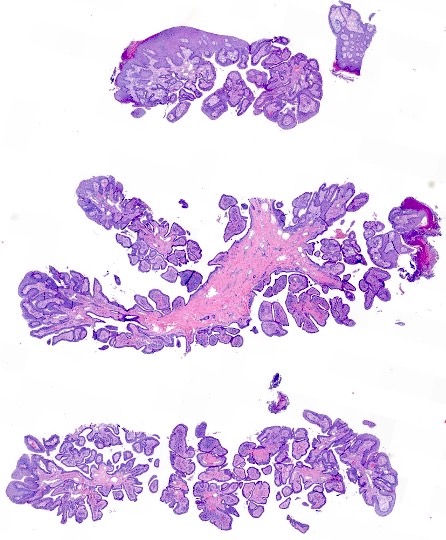
Glands forming papillae
Cystic and papillary appearance glands
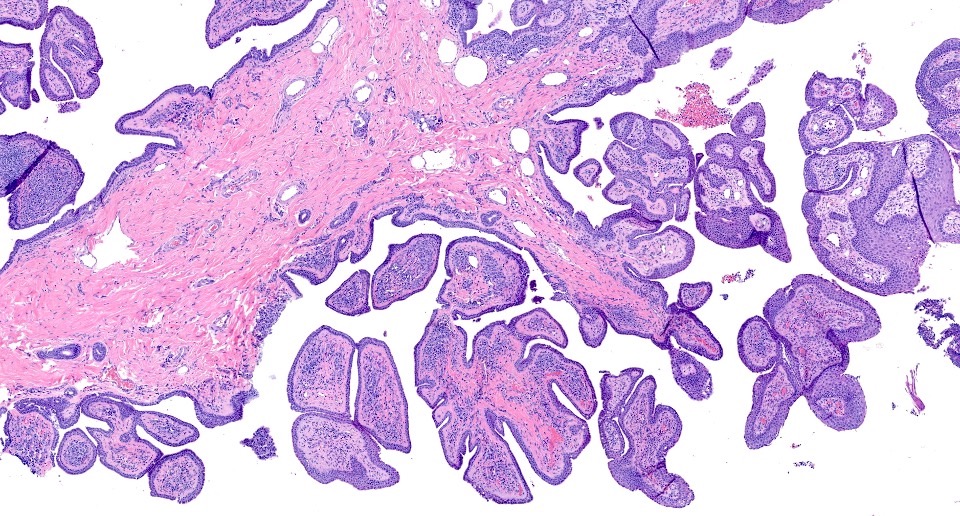
Papillary architecture
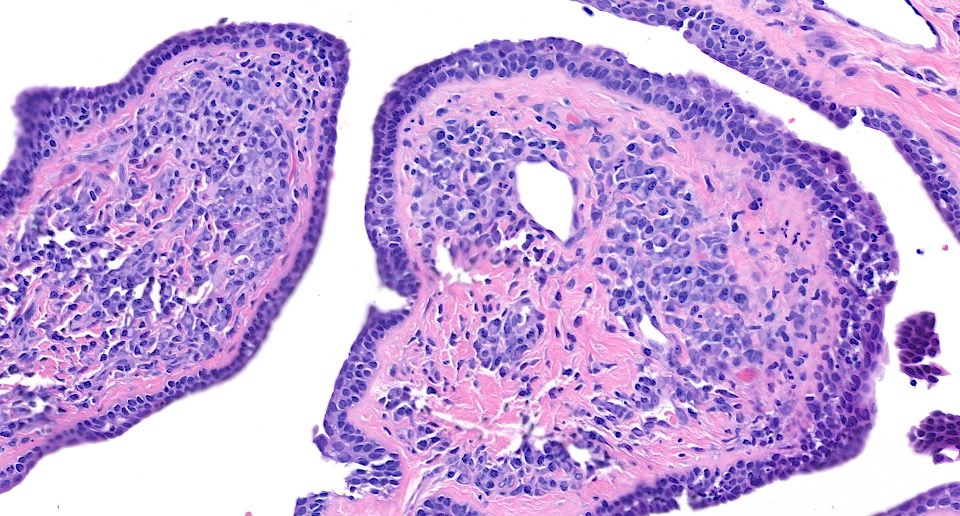
Double layer epithelium
Positive stains
- IHC may help in favoring eccrine or apocrine lineage but is not required for diagnosis (Indian J Dermatol 2013;58:409)
- Positive stains:
- CEA, AE1 / AE3 and EMA highlight ductal epithelium (Indian J Dermatol 2013;58:409)
- Luminal columnar cells:
- Positive for CK7 (Br J Dermatol 2002;147:936)
- > 70% positive for CK19 (Br J Dermatol 2002;147:936)
- CK1, CK5, CK8, CK10, CK14: heterogeneous expression (Br J Dermatol 2002;147:936)
- Basal cuboidal cells:
- Almost constantly express CK1, CK5, CK7, CK8, CK10, CK14 (Br J Dermatol 2002;147:936)
- Basal tumor cells express CK19 and vimentin heterogeneously and alpha smooth muscle actin focally (Br J Dermatol 2002;147:936)
- Positive for SMA, CK5/6 and p63, consistent with myoepithelial differentiation
Molecular / cytogenetics description
- Some cases have mutations in:
- Patched gene (PTCH) (Indian J Dermatol 2013;58:409)
- p16 tumor suppressor gene (Indian J Dermatol 2013;58:409)
Sample pathology report
- Scalp, biopsy:
- Syringocystadenoma papilliferum (see comment)
- Comment: Several cystic invaginations arise from a papillomatous epidermis. These invaginations demonstrate papillae lined by 2 rows of cuboidal to columnar epithelial cells, with oval nuclei and a pale eosinophilic cytoplasm. The deep dermis contains tubular glands with apocrine decapitation secretion. The stroma contains a dense mononuclear infiltrate, which is comprised predominantly of plasma cells.
Differential diagnosis
- Hidradenoma papilliferum:
- Almost exclusively occurs in the anogenital region of women; diagnosis outside of this site should be exceptional (J Clin Diagn Res 2014;8:QD03)
- Unlike syringocystadenoma papilliferum, there is no epidermal connection (it hides in the dermis) (J Clin Diagn Res 2014;8:QD03)
- Dermal nodule that consists of arborizing ducts that produce maze-like patterns (J Clin Diagn Res 2014;8:QD03)
- Papillary eccrine adenoma:
- Composed of multiple, dermal, dilated, duct-like spaces containing papillary projections (J Clin Diagn Res 2014;8:QD03)
- No exoendophytic architecture, glands appear cystic, no epidermal connection and lacks plasmacellular stroma
- Warty dyskeratoma:
- Exoendophytic architecture and verrucous epidermal hyperplasia but lacks ductal epithelium
- Lined by elongated dermal papillae with suprabasilar acantholysis of keratinocytes, some of which are dyskeratotic (J Clin Diagn Res 2014;8:QD03)
- Tubular apocrine adenoma:
- Predominantly cuboidal and columnar cells with or without secretions (J Cytol 2015;32:130)
- No epidermal connection
- Glands contain papillary projections and form cysts
- Syringocystadenocarcinoma papilliferum (J Korean Med Sci 2007;22:762):
- Nipple adenoma (and variant erosive adenomatosis of the nipple):
- Anatomic site permits differentiation
Board review style question #1
A 38 year old man presents with a verrucous nodule on the scalp, present for the past 12 years. Representative histopathology is shown in the above image. Which of the following statements is correct?
- More common in adulthood
- Represents a malignant adnexal tumor
- Subset of tumors have loss of heterozygosity for PTCH or p16
- Usually does not communicate with surface epithelium
Board review style answer #1
C. Subset of tumors have loss of heterozygosity for PTCH or p16
Comment Here
Reference: Syringocystadenoma papilliferum
Comment Here
Reference: Syringocystadenoma papilliferum
Board review style question #2
An 8 year old girl presents with a slowly growing, 3 cm, erythematous nodule with smooth surface on the left labium majus, present since birth. A biopsy is performed (see above image). Which of the following is most associated with this tumor?
- Basal cell carcinoma
- Merkel cell carcinoma
- Nevus sebaceus
- Squamous cell carcinoma
Board review style answer #2
