
Skin nonmelanocytic tumor
Fibrous, fibrohistiocytic and myofibroblastic neoplasms
Cutaneous fibroepithelial polyps
Author: Alexander Nirenberg, M.B.B.S.
Resident / Fellow Advisory Board: Caroline I. Mullins, M.D.
Editorial Board Member: Jonathan D. Ho, M.B.B.S., D.Sc.

Last author update: 24 January 2022
Last staff update: 7 November 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Fibroepithelial polyps [title]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nirenberg A. Cutaneous fibroepithelial polyps. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticfibroepithelialpolyp.html. Accessed March 31st, 2025.
Definition / general
- Benign nonepithelial tumors arising from mesodermal tissue
Essential features
- Common benign cutaneous tumor
- On eyelids, flexural areas
- F = M
- Associated with trauma, obesity, diabetes mellitus, pregnancy
Terminology
- Acrochordon, soft fibroma, fibroma molle, skin tag
ICD coding
Epidemiology
- 50+ years of age (Dermatologica 1987;174:180)
- Incidence: 46 - 64% in people > 50 years (Dermatologica 1987;174:180)
- F = M (Dermatologica 1987;174:180)
- Causal connections: obesity (Eur J Dermatol 2012;22:106)
Sites
- Eyelids
- Flexural areas: axillae, groin
- Lateral neck
- Inframammary
Pathophysiology
- Trauma → mast cell recruitment → upregulation of TNF-α → fibroblast proliferation and mitogenicity (Indian J Dermatol 2011;56:641)
- Growth factors → keratinocyte and fibroblast proliferation (Clin Cosmet Investig Dermatol 2019;12:255)
- Loss / downregulation of hamartin and tuberin (inactivating tumor suppressor proteins) (J Cutan Pathol 2004;31:383)
- Human papillomavirus (HPV) (Iran J Basic Med Sci 2012;15:840)
Etiology
- The etiology is not clear nor the same for every FEP; reported associations include:
- Trauma (Indian J Dermatol 2011;56:641)
- Diabetes mellitus, metabolic syndrome (Eur J Dermatol 2012;22:106)
- Polycystic ovary syndrome (Australas J Dermatol 2019;60:70)
- Hormonal replacement therapy (Australas J Dermatol 2019;60:70)
- Acromegaly (Acta Dermatovenerol Croat 2013;21:224)
- HPV 6 and 11 (Indian J Dermatol Venereol Leprol 2008;74:222)
- Lymphedema (APMIS 2008;116:215)
Clinical features
- Clinical appearance:
- Small soft papules, pedunculated or filiform, 2 - 5 mm, rough surface
- Pendulous fibromas can be large (several centimeters) (Australas J Dermatol 2019;60:70)
- May be multiple (Dermatologica 1987;174:180)
- Look for associated disease / physiologic states including:
- Diabetes mellitus / insulin resistance (Eur J Dermatol 2012;22:106)
- Hyperlipidemia
- Familial predisposition
- Pregnancy (J Am Acad Dermatol 1984;10:929)
- Lymphedema (APMIS 2008;116:215)
Diagnosis
- Characteristic clinical features and histopathology
Prognostic factors
- Benign
Case reports
- 19 year old woman presents with an 18 month history of a slowly enlarging and painless 20 cm vulval mass (BMJ Case Rep 2019;12:e230449)
- 23 year old woman presents with a 9 year history of a progressively enlarging vulval mass (Australas J Dermatol 2019;60:70)
- 55 year old man presents with a painless swelling on his right back (Dermatol Surg 2009;35:1804)
- 57 year old man presents with swelling of the nasal conjunctiva and a 2 year old boy presents with numerous swellings around the right lower eyelid and ocular surface (Arq Bras Oftalmol 2019;82:239)
- 63 year old man presents with a 4 month history of lower urinary tract symptoms (APMIS 2008;116:215)
Treatment
- Topical anesthetic may be used prior to procedure (Aesthetic Plast Surg 2015;39:644)
- Surgical removal / snip excision (Aesthetic Plast Surg 2015;39:644)
- Cryotherapy (Aesthetic Plast Surg 2015;39:644)
- Shave excision (Aesthetic Plast Surg 2015;39:644)
- Electrodissection (Am Fam Physician 2002;66:1259)
- Ligation (J Dermatol Surg Oncol 1994;20:151)
Clinical images
Contributed by Arvind Ranchhod, M.B.Ch.B.


Multiple skin tags
Images hosted on other servers:

Penile fibroepithelial polyp

Fibroepithelial
polyp at posterior
wall of external
auditory canal
Gross description
- Sessile or pedunculated polyp
- 2 - 5 mm to several centimeters (Australas J Dermatol 2019;60:70)
- Surface smooth or filiform
- Smaller ones may be pigmented
- Larger ones are skin colored
Gross images
Contributed by Alexander Nirenberg, M.B.B.S.

Clinical skin tag
Microscopic (histologic) description
- Epidermis may be hyperplastic and papillomatous and may have keratotic cysts and pigment in basal epidermal keratinocytes
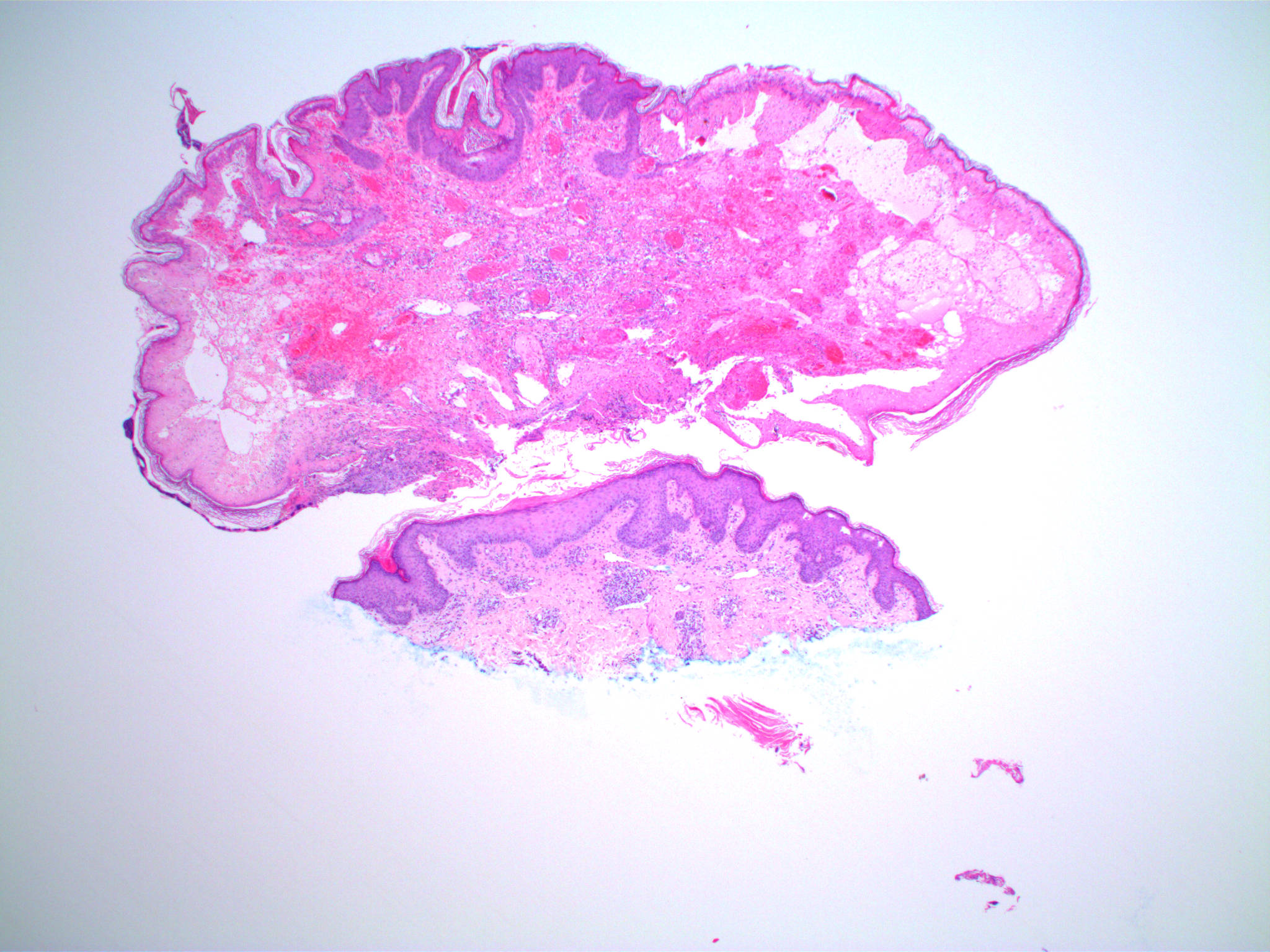
- Loose fibrocollagenous stroma, abundant vessels
- Usually no adnexa
- Variable adipose tissue in larger ones - lipofibroma
- Traumatic changes: lichen simplex chronicus, epidermal necrosis, ulceration, pagetoid dyskeratosis, lichen sclerosus-like change (Am J Dermatopathol 2006;28:478, Am J Dermatopathol 2019;41:e64)
- Pseudosarcomatous change: pleomorphic stellate stromal cells, multinucleated stromal cells, myxoid to collagenous stroma (Ann Diagn Pathol 2008;12:440)
- On IHC, the pleomorphic cells stain diffusely for vimentin; there is variable staining for CD34 and factor 13a and the cells do not stain for SMA or desmin (Ann Diagn Pathol 2008;12:440)
- Some of the lesions with pseudosarcomatous change overlap with pleomorphic fibroma
- A subset of cellular pseudosarcomatous fibroepithelial polyps occurs in the female genital tract including the vulva (Am J Surg Pathol 2000;24:231)
Microscopic (histologic) images
Contributed by Alexander Nirenberg, M.B.B.S.
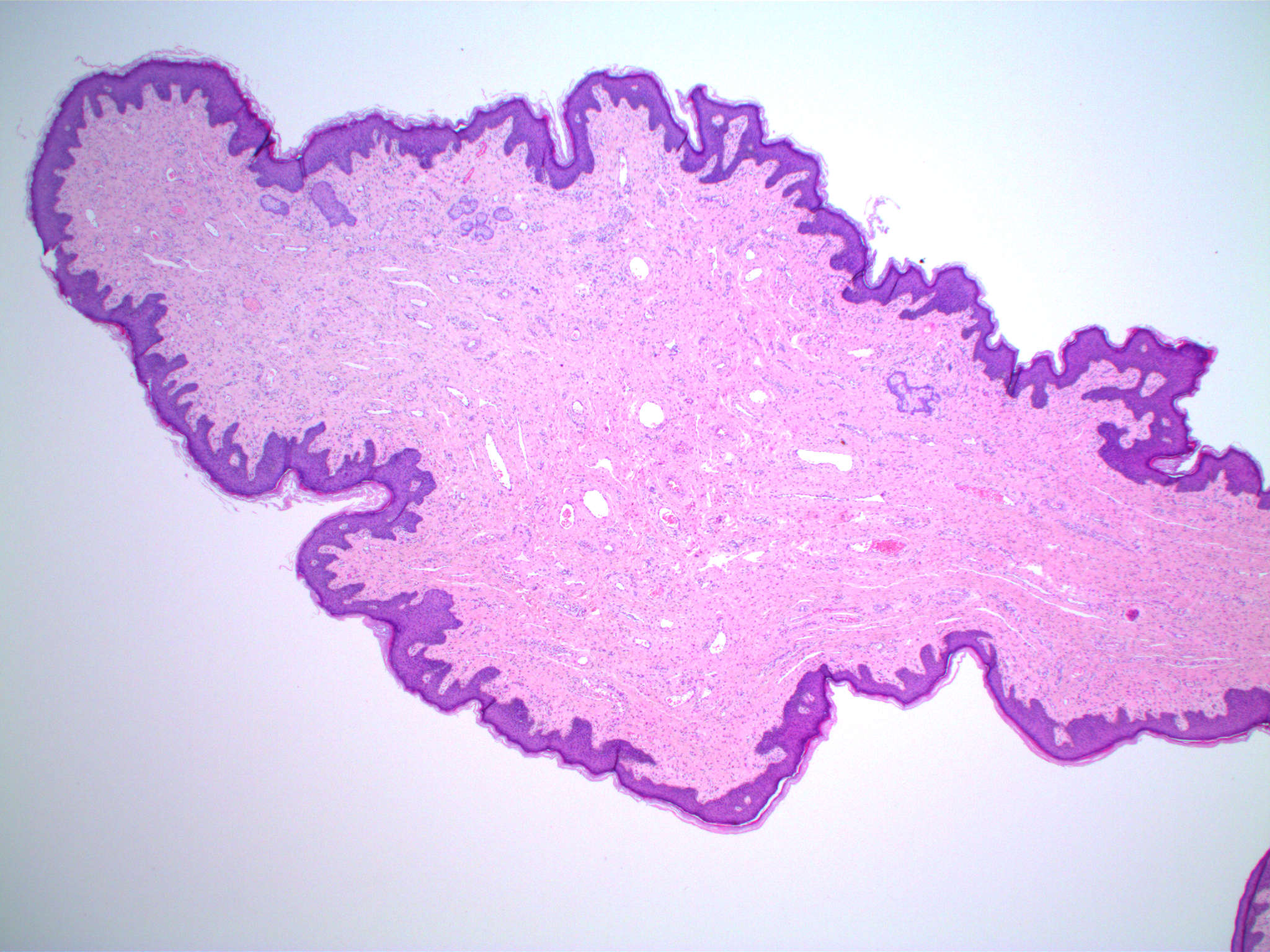
Classic features
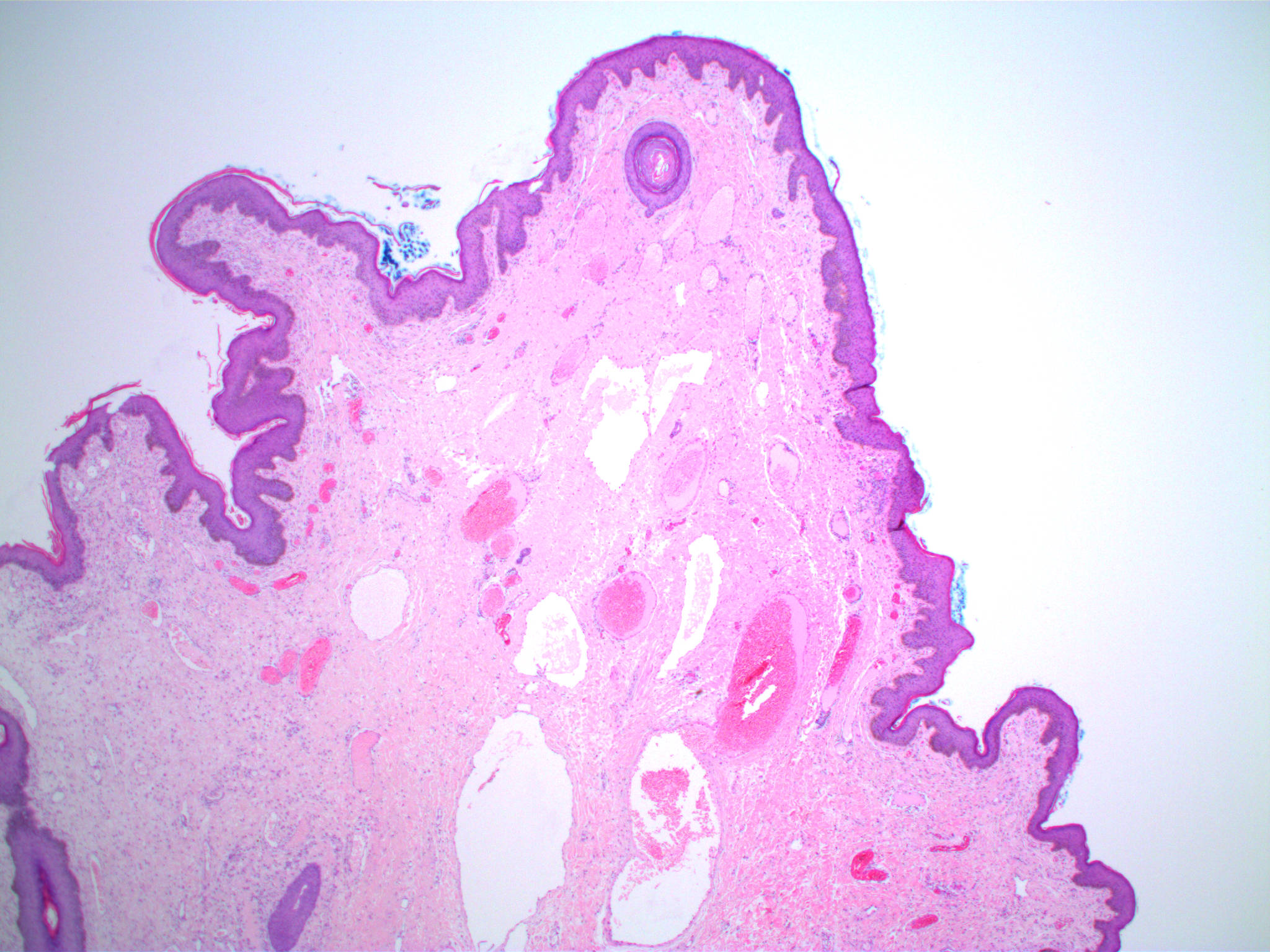
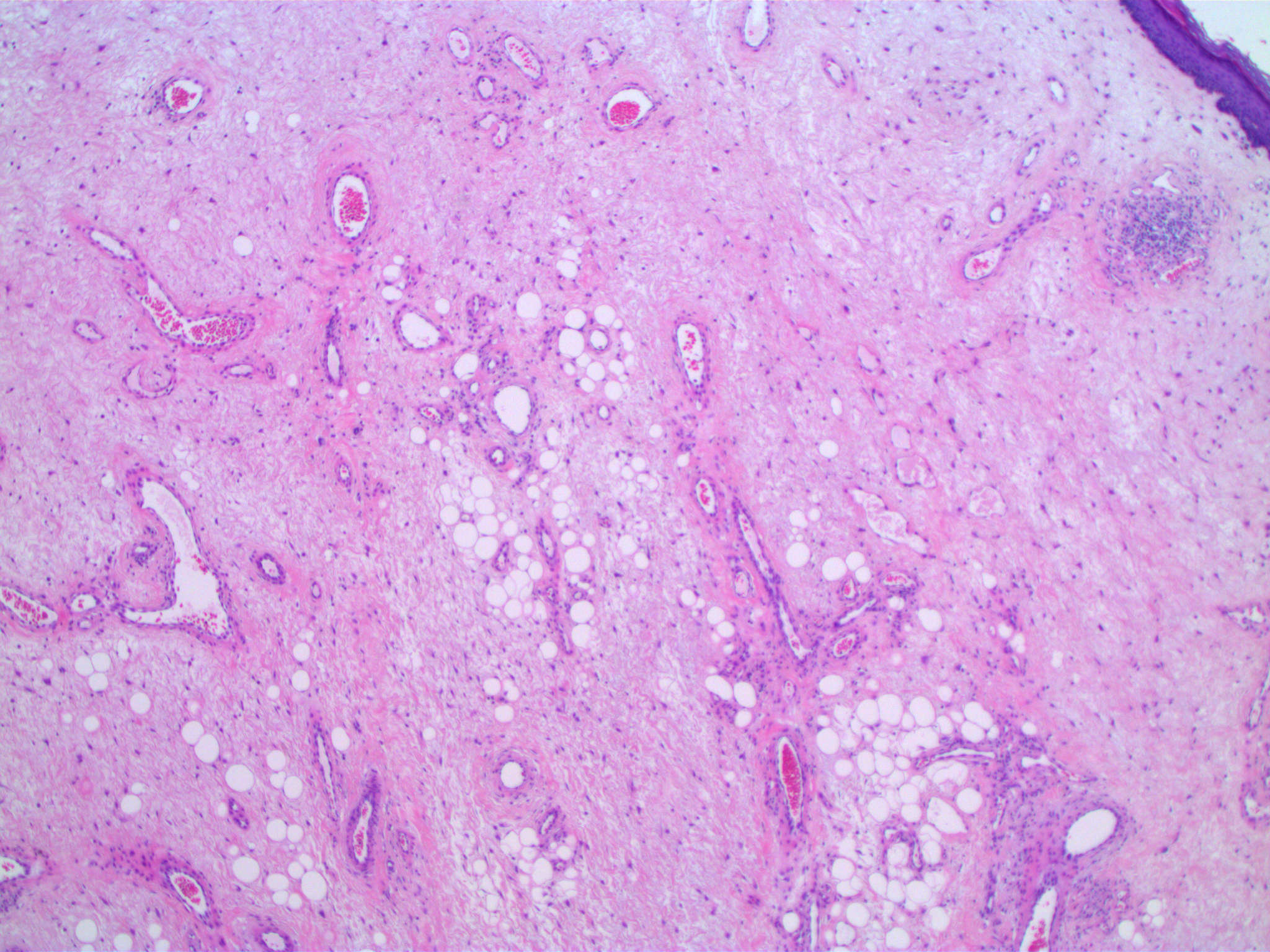
Prominent vascular stroma
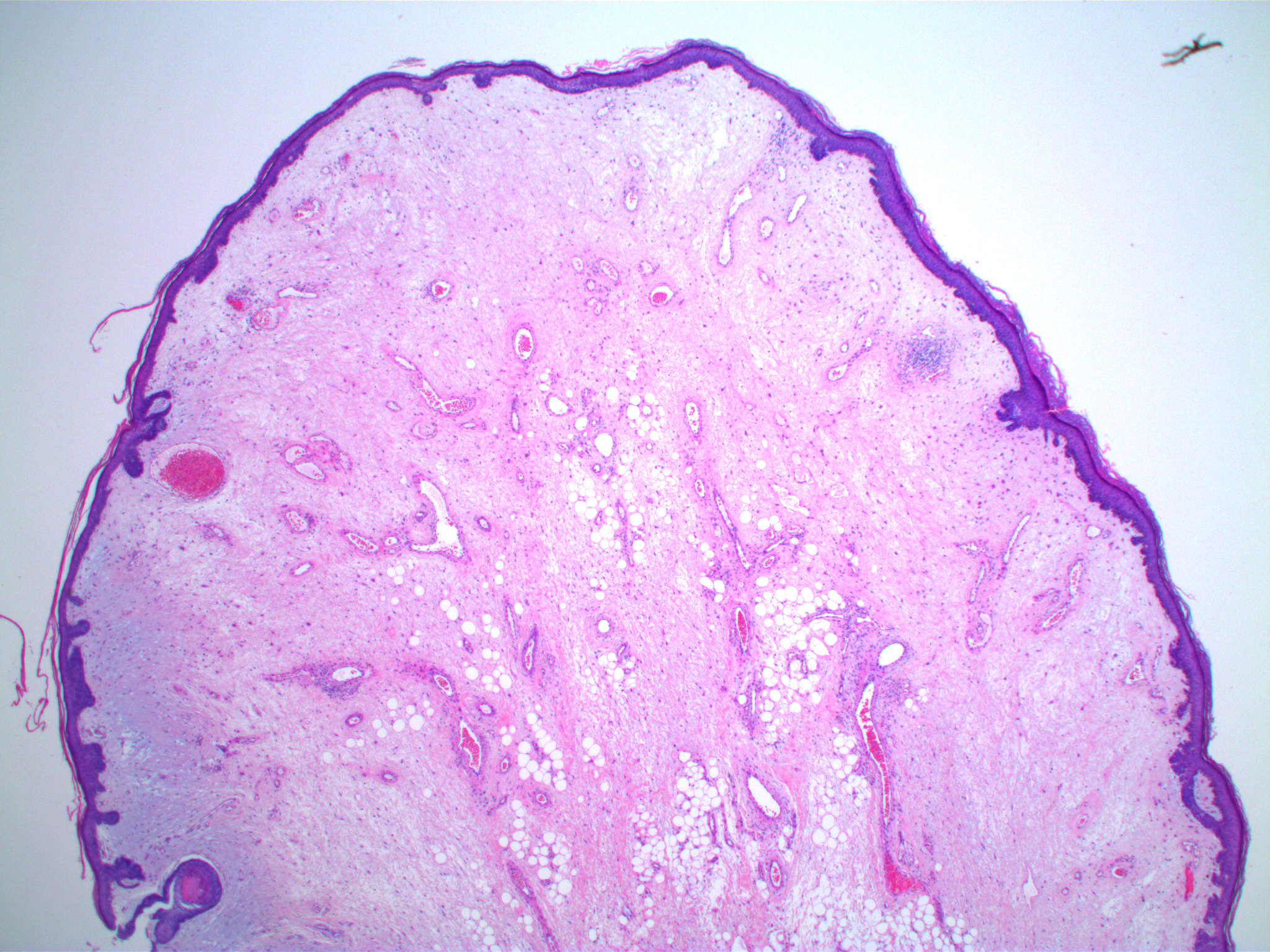
Stromal edema
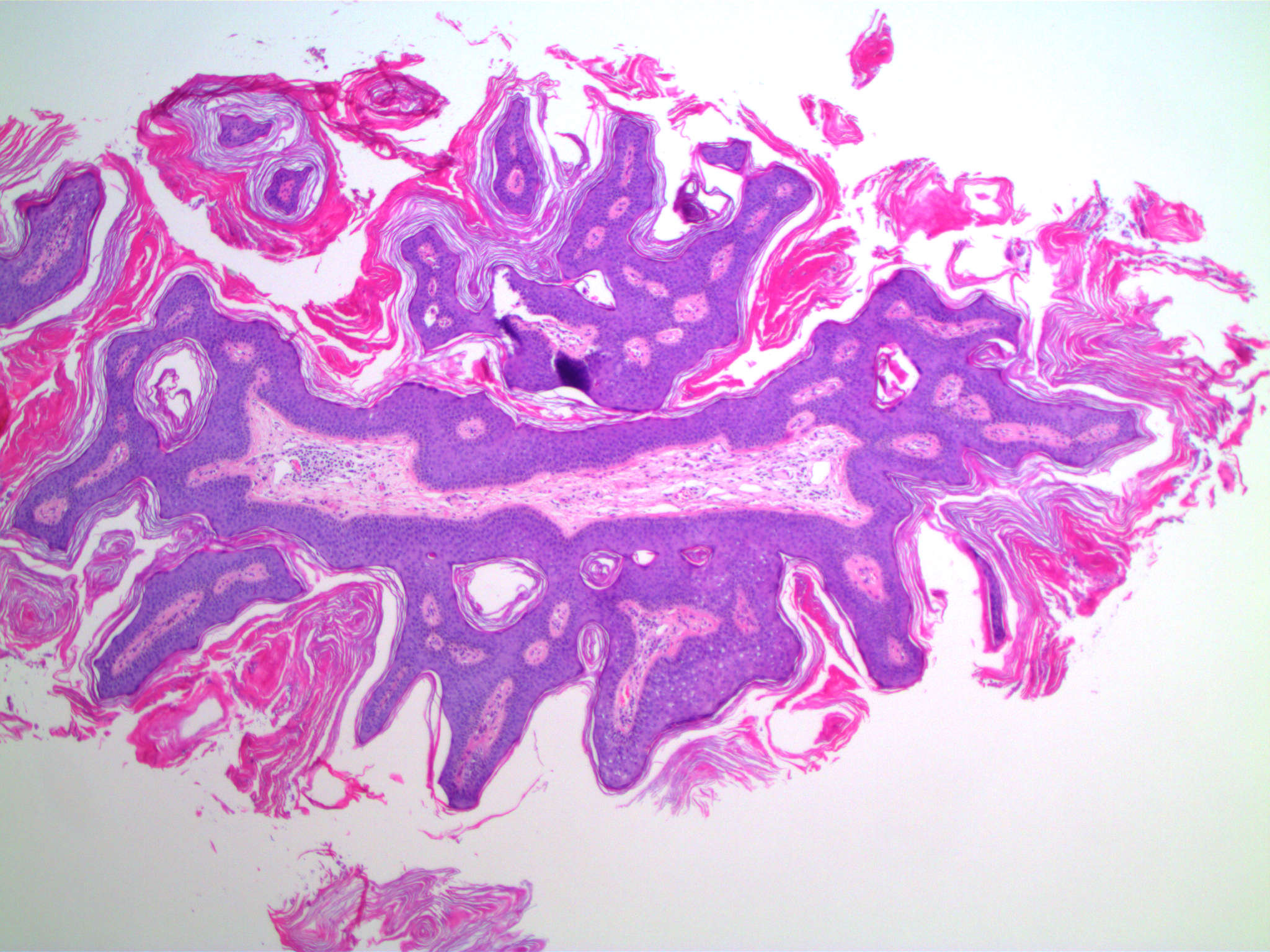
Epidermal hyperplasia
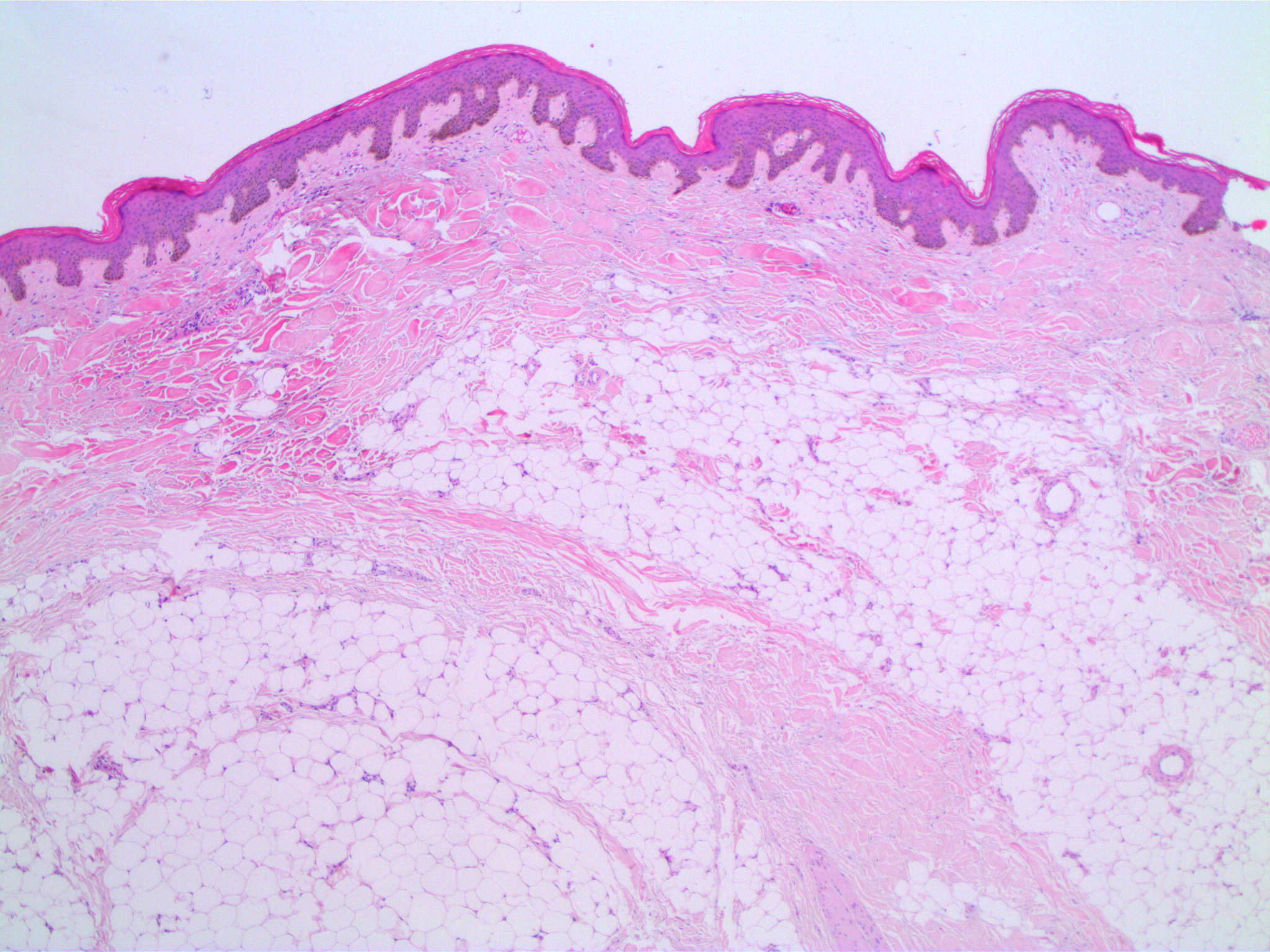
Adipose tissue
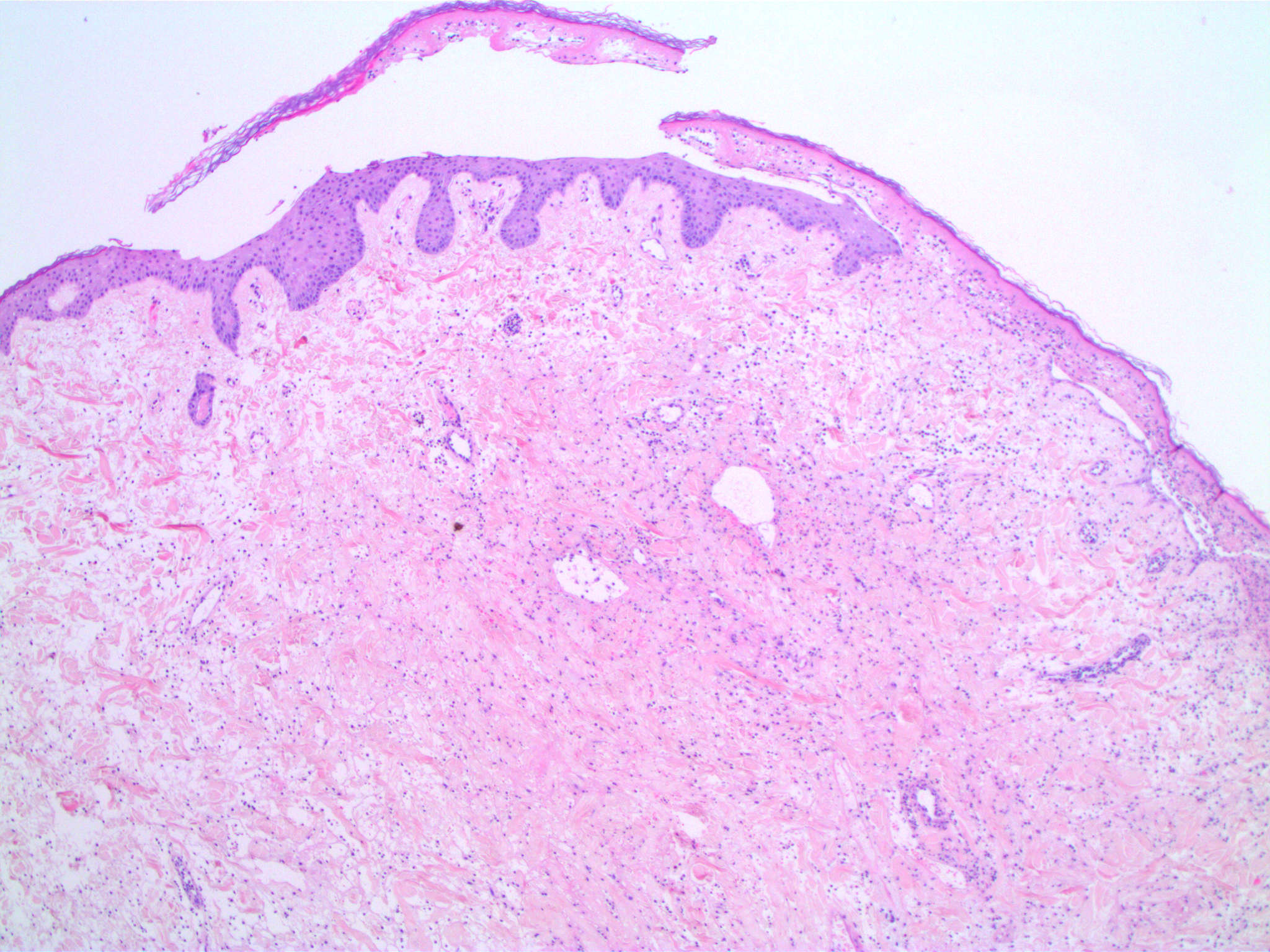
Trauma / inflammation
Sample pathology report
- Left neck, shave biopsy:
- Fibroepithelial polyp / acrochordon (see comment)
- Comment: A polyp covered by mildly acanthotic epidermis with mild hyperkeratosis. There is a mildly cellular fibrovascular core with scattered dilated small thin walled vessels and a sparse lymphocytic infiltrate. Dysplasia or malignancy is not seen.
Differential diagnosis
- Polypoid / papillary variants of:
- Seborrheic keratosis (Arch Dermatol 1996;132:1459):
- Generally lacks the fibrovascular core of a fibroepithelial polyp
- Dermatosis papulosa nigra:
- Considered to be a seborrheic keratosis; however, it has a well developed fibrous stroma
- It is a clinically distinct entity (Clin Dermatol 2017;35:491)
- Verruca vulgaris / squamous cell papilloma (Australas J Dermatol 2019;60:70):
- Epidermal papillomatosis with coarse hypergranulosis
- May have koilocytosis
- Hyperkeratosis with columns of parakeratosis
- Melanocytic nevus (Arch Dermatol 1996;132:1459):
- Melanocytic proliferation within the polyp
- Commonly intradermal or compound
- Neurofibroma (Australas J Dermatol 2019;60:70):
- Cellular stromal proliferation of spindle cells with wavy nuclei
- Mast cells within the lesion
- Hemangioma and pyogenic granuloma (Arch Dermatol 1996;132:1459):
- Large number of vessels in the stroma
- Fibroepithelial tumor of Pinkus:
- Thin anastomosing strands of basaloid or squamous keratinocytes projecting downward from the epidermis in a fenestrated pattern
- Abundant fibrous stroma (Am J Dermatopathol 2005;27:149)
- Polypoid trichodiscomas and fibrofolliculomas in Birt-Hogg-Dubé syndrome:
- Infundibular structures in the stroma (Am J Dermatopathol 1999;21:369)
- Accessory tragus:
- Most commonly preauricular
- Vellus hairs, eccrine glands, adipose tissue and cartilage in the stroma (J Am Acad Dermatol 2007;56:AB54)
- Supernumerary digit:
- Congenital
- Increased peripheral nerves in the stroma (Arch Dermatol 1973;108:223)
- Acquired digital fibrokeratoma:
- Acral skin
- Marked epidermal acanthosis and hyperkeratosis
- Thickened stromal collagen parallel to the long axis of the lesion (J Am Acad Dermatol 1985;12:816)
- Seborrheic keratosis (Arch Dermatol 1996;132:1459):
Board review style question #1
A 62 year old woman presents with multiple lesions on the neck (shown above) with pathological diagnosis of fibroepithelial polyps, NOS. Which clinical association should you consider?
- Anorexia
- Birt-Hogg-Dubé syndrome
- Diabetes mellitus
- Dysplastic nevus syndrome
- Neurofibromatosis
Board review style answer #1
C. Diabetes mellitus. Skin tags may be associated with diabetes mellitus / metabolic syndrome as well as obesity. The other listed conditions have not been shown to have increased incidence of fibroepithelial polyps but may have other cutaneous polypoid lesions. Birt-Hogg-Dubé syndrome was initially reported as having increased incidence of skin tags, however, the lesions are polypoid trichodiscomas and fibrofolliculomas.
Comment Here
Reference: Cutaneous fibroepithelial polyps
Comment Here
Reference: Cutaneous fibroepithelial polyps
Board review style question #2
A clinician excises a skin tag from the groin of a 73 year old woman (microscopic image shown above). The best diagnosis is
- Cutaneous myxoma
- Neurofibroma
- Pseudosarcomatous fibroepithelial polyp
- Pyogenic granuloma
- Traumatized fibroepithelial polyp
Board review style answer #2
E. Traumatized fibroepithelial polyp. This is a fibroepithelial polyp with features of trauma, including an area of epidermal necrosis, stromal edema and stromal inflammatory cells. The stroma is loose and has low cellularity of mesenchymal cells, unlike a neurofibroma. The stroma is edematous rather than myxoid. It lacks the pleomorphic stellate and multinucleated stromal cells of a pseudosarcomatous fibroepithelial polyp. The lesion has dilated vessels, however, it lacks the lobular proliferation of capillaries that characterizes a pyogenic granuloma.
Comment Here
Reference: Cutaneous fibroepithelial polyps
Comment Here
Reference: Cutaneous fibroepithelial polyps
