
Skin nonmelanocytic tumor
Benign (nonmelanocytic) epidermal tumors or tumor-like lesions
Epidermal nevus
Editorial Board Member: Brandon Umphress, M.D.


Last author update: 7 December 2023
Last staff update: 4 February 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Epidermal nevus

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Knittel R, Ardakani NM. Epidermal nevus. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticepidermalnevus.html. Accessed April 2nd, 2025.
Definition / general
- Epidermal nevus is a developmental malformation that involves the epidermis and clinically manifests as a discrete congenital linear patch or plaque along the Blaschko lines
- Histologically characterized by a hamartomatous keratinocyte proliferation that results in epidermal papillomatosis and acanthosis with no associated adnexal structures
- Here, the term epidermal nevus is discussed within a narrow definition and does not include organoid, sebaceous, eccrine and pilar nevi
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
Essential features
- Hamartomatous proliferation of the epidermis with no associated adnexal structures, commonly presenting at birth
- Clinically presents as single to multiple coalescing small pale to dark brown plaques, occasionally markedly papillomatous or hyperkeratotic in a Blaschko linear distribution
- It is estimated that 33% of patients with epidermal nevi have other organ involvement and occurrence is associated with multiple syndromes
- Commonly caused by mosaic postzygotic activating mutations in FGFR2 / FGFR3, PIK3CA or RAS genes in the epidermis, occurring in early embryonic development
- Development of malignant neoplasms in epidermal nevi is a rare phenomenon and almost always occurs during adulthood
Terminology
- Epithelial nevus
- Essentially a synonym for epidermal nevus; though both terms are used frequently to cover hamartomas of the epidermis along with those with adnexal malformations, this page uses the term epidermal nevus to discuss nevi arising from the epidermal keratinocytes only
- Common keratinocyte nevus
- Linear epidermal nevus (Am J Dermatopathol 2014;36:430)
- Linear verrucous epidermal nevus
- Nonorganoid epidermal nevus (Dermatol Online J 2010;16:12)
Epidemiology
- Typically present at birth or develops in early childhood, with a prevalence of ~1 in 1,000 live newborns (Pediatr Dermatol 2004;21:432)
- F = M
- Secondary tumors are infrequent compared to organoid epidermal nevi (Dermatol Pract Concept 2022;12:e2022087)
- Extremely low rate of malignant transformation (Clin Exp Dermatol 2019;44:238)
- Can be associated with the following syndromes
- Schimmelpenning-Feuerstein-Mims syndrome (organoid nevi, abnormalities of the central nervous system and eyes, oral lesions and skeletal defects)
- Phakomatosis pigmentokeratotica type I (capillary malformations and epidermal nevus)
- Nevus comedonicus syndrome (ocular, skeletal and neural abnormalities, ipsilateral congenital cataract and malformations of fingers and toes) (Pediatr Dermatol 2021;38:359)
- Angora hair nevus syndrome (Angora hair nevus ocular, skeletal and neural abnormalities)
- Becker nevus syndrome (Becker nevus, poor unilateral breast or nipple development, supernumerary nipples, loss of subcutaneous fat, loss of axillary hair, musculoskeletal abnormalities)
- Proteus syndrome (overgrowth of skin and connective tissue)
- Type II segmental Cowden disease (neural defects, overgrowth of limbs and toes, polyps and nevi)
- Fibroblast growth factor receptor 3 epidermal nevus syndrome (keratinocytic epidermal nevus, acanthosis nigricans and neurological abnormalities) (J Pediatr Neurosci 2014;9:66)
- CHILD syndrome (congenital hypoplasia with ichthyosiform nevus and limb defects)
- Associated with several other less well defined epidermal nevus syndromes
- Reference: DermNet: Epidermal Naevus [Accessed 28 July 2023]
Sites
- Nearly all lesions occur on the neck, trunk and extremities
- Rare sites of presentation include intraoral and the face
Pathophysiology
- Epidermal nevi typically result from a postzygotic somatic mutation in an embryotic cell
- This leads to genetic mosaicism and the phenotypic consequence of the somatic mutation depends on how early the mutation arises, with very early mutations leading to extensive epidermal nevi and organ involvement (Dermatol Online J 2010;16:12)
Clinical features
- Epidermal nevi exhibit diverse clinical patterns, which can be attributed to a variety of histological patterns
- Epidermal nevi typically present as multiple warty brown patches or plaques along the lines of Blaschko
- Epidermal nevi can form a linear or zosteriform lesion
- At puberty, lesions become thicker, more verrucous and hyperpigmented (Curr Derm Rep 2012;1:186)
- Terms for different clinical patterns
- Nevus verrucosus (verrucous epidermal nevus): localized wart-like lesions
- Nevus unius lateris: unilateral, long, linear lesions on the extremities
- Ichthyosis hystrix: large, bilateral nevi on the trunk
- En bloc movement on the wobble test (characteristic of an epidermal growth)
- Patches of discoloration with minimal scale as a presentation have been described
- Epidermal nevi measure a few millimeters to several centimeters in length
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
Diagnosis
- Usually clinically suspected and diagnosed
- Skin biopsy may be required for confirmation or assessment of neoplasms developing in the lesion
Prognostic factors
- Generally, an epidermal nevus will persist indefinitely and follow a benign course
- It is estimated that 33% of patients with epidermal nevi have other organ involvement (Indian Dermatol Online J 2015;6:37)
- Benign secondary tumors have been reported arising from epidermal nevi showing divergent differentiation (e.g., toward sweat ducts in poromas and syringocystadenoma papilliderums) (Dermatol Pract Concept 2022;12:e2022087, Am J Dermatopathol 2014;36:430)
- Incidence of development of malignant neoplasms (e.g., basal cell carcinoma, keratoacanthoma and squamous cell carcinoma) in epidermal nevi is very rare (Case Rep Dermatol 2013;5:272)
Case reports
- 10 month old girl with epidermal nevus syndrome with a PTCH1 gene mutation and cerebral infarction (J Med Case Rep 2022;16:343)
- 22 year old woman with a keratinocytic epidermal nevus and ipsilateral breast hypoplasia (Int J Womens Dermatol 2019;5:181)
- 28 year old woman developed syringocystadenoma papilliferum and eccrine poroma in a verrucous epidermal nevus (Dermatol Pract Concept 2022;12:e2022087)
- 31 year old man with adult onset verrucous epidermal nevus overlying an implanted cardioverter defibrillator (JAAD Case Rep 2023;34:58)
Treatment
- Topical treatments (i.e., retinoic acid or 5-fluorouracil) are used to improve the cosmetic appearance of epidermal nevi by removing the keratotic surface
- Smaller lesions can be surgically excised
- Larger lesions can be treated by laser or cryotherapy
- Pulsed erbium: yttrium aluminium garnet (YAG) laser is effective and has a low incidence of scarring (Dermatol Surg 2004;30:378)
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
Clinical images
Images hosted on other servers


Verrucous epidermal nevus

Nevus unius lateris

Keratinocytic epidermal nevus

Oral linear epidermal nevus

Epidermal nevus
Gross description
- Well defined, elevated, tan verrucous linear plaque
Microscopic (histologic) description
- Epidermal nevus can show a spectrum of histological patterns with occasionally more than 1 pattern existing in a single lesion; the patterns are described below
- Common keratinocyte pattern (> 60% of cases)
- Hyperkeratosis (occasionally columns of parakeratosis)
- Irregular acanthosis
- Broad papillomatosis with flat vertical peaks
- Sharply demarcated from the adjacent normal epidermis
- Occasional focal thickening of the granular layer
- Hyperpigmentation of the basal keratinocytes
- Uncommonly has associated mild inflammation or perivascular lymphocytes
- Seborrheic keratosis-like pattern
- Hyperkeratosis
- Acanthosis and papillomatosis (with flattening of the lower border, Mesa sign)
- Horn pseudocysts
- Verrucoid pattern
- Hyperkeratosis (orthokeratosis and parakeratosis)
- Vacuolated cells in the granular and upper spinous layer
- Increased keratohyaline granules
- No prominent vascularity in the papillary dermis (typical of verruca vulgaris)
- Acrokeratosis verruciformis pattern
- Marked hyperkeratosis
- Acanthosis and papillomatosis with peaks resembling church spires
- Thickened granular layer
- Porokeratotic pattern
- Orthokeratosis and acanthosis are less prominent that other variants of epidermal nevus
- Parakeratotic columns (with focal occasional vacuolated keratinocytes below)
- Cornoid lamellae (with a focal absent granular layer below)
- Focal acantholytic dyskeratotic Darier disease-like pattern
- Hyperkeratosis
- Acanthosis and papillomatosis
- Acantholytic dyskeratotic cells (corps ronds) and acantholytic basophilic keratinocytes (grains) in the granular layer and spinous layers
- Scattered acantholytic spinous cells above suprabasal clefts
- Acanthosis nigricans-like pattern (Australas J Dermatol 1983;24:130)
- Hyperkeratosis
- Papillomatosis
- Mild irregular acanthosis with poorly developed rete ridges
- Hailey-Hailey disease-like pattern (Br J Dermatol 1985;112:349)
- Mild hyperkeratosis
- Papillomatosis
- Suprabasal acantholysis, similar to a dilapidated brick wall
- Rare dyskeratotic cells
- Incontinentia pigmenti-like (verrucous phase) pattern (Pediatr Dermatol 1985;3:69)
- Hyperkeratosis (vertical parakeratosis)
- Acanthosis and papillomatosis
- Thickened granular layer
- Many individual dyskeratotic cells within the epidermis
- Epidermolytic hyperkeratosis pattern (Australas J Dermatol 1983;24:130)
- Hyperkeratosis
- Acanthosis and papillomatosis
- Perinuclear vacuolization
- Increased irregularly shaped keratohyaline granules
- Indistinct cell borders
- Inflammatory linear verrucous epidermal nevus (ILVEN), epidermal nevus with skyline basal cell layer (PENS) and nevus comedonicus are regarded as distinct entities, although they are sometimes included as histological patterns of epidermal nevus
- Reference: Am J Dermatopathol 1982;4:161
Microscopic (histologic) images
Contributed by Ronan Knittel, M.D.
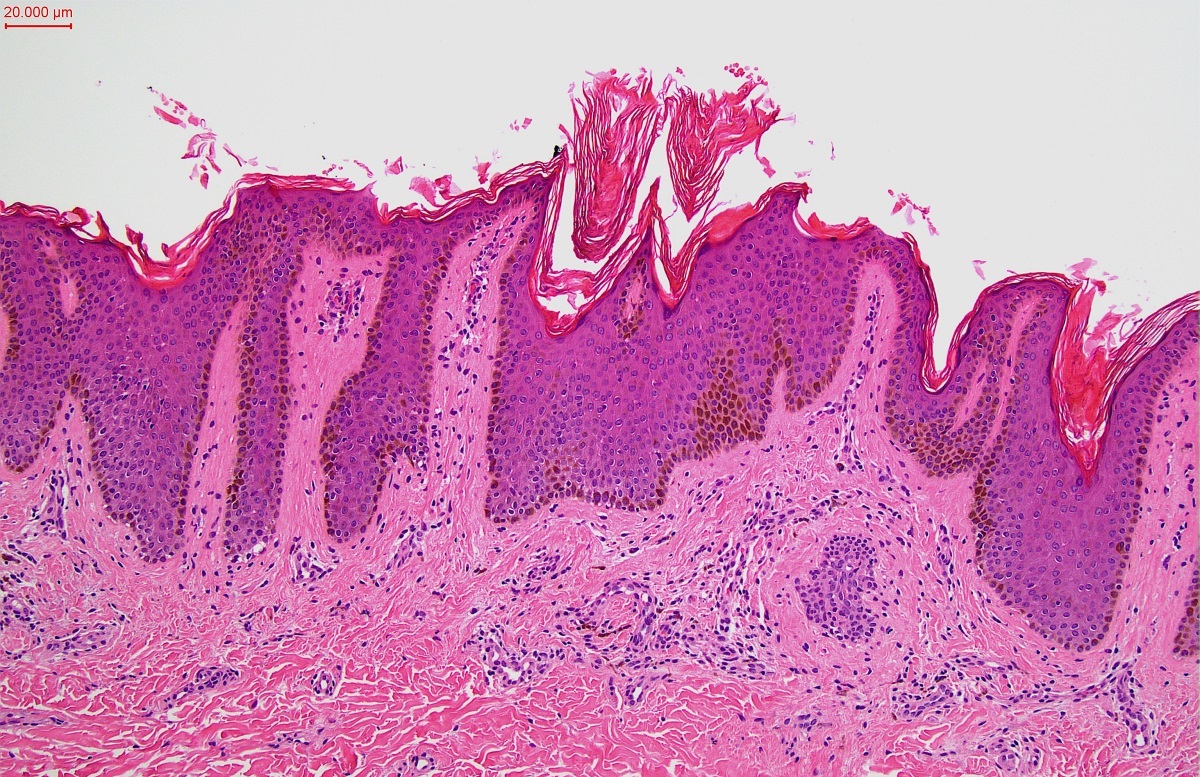
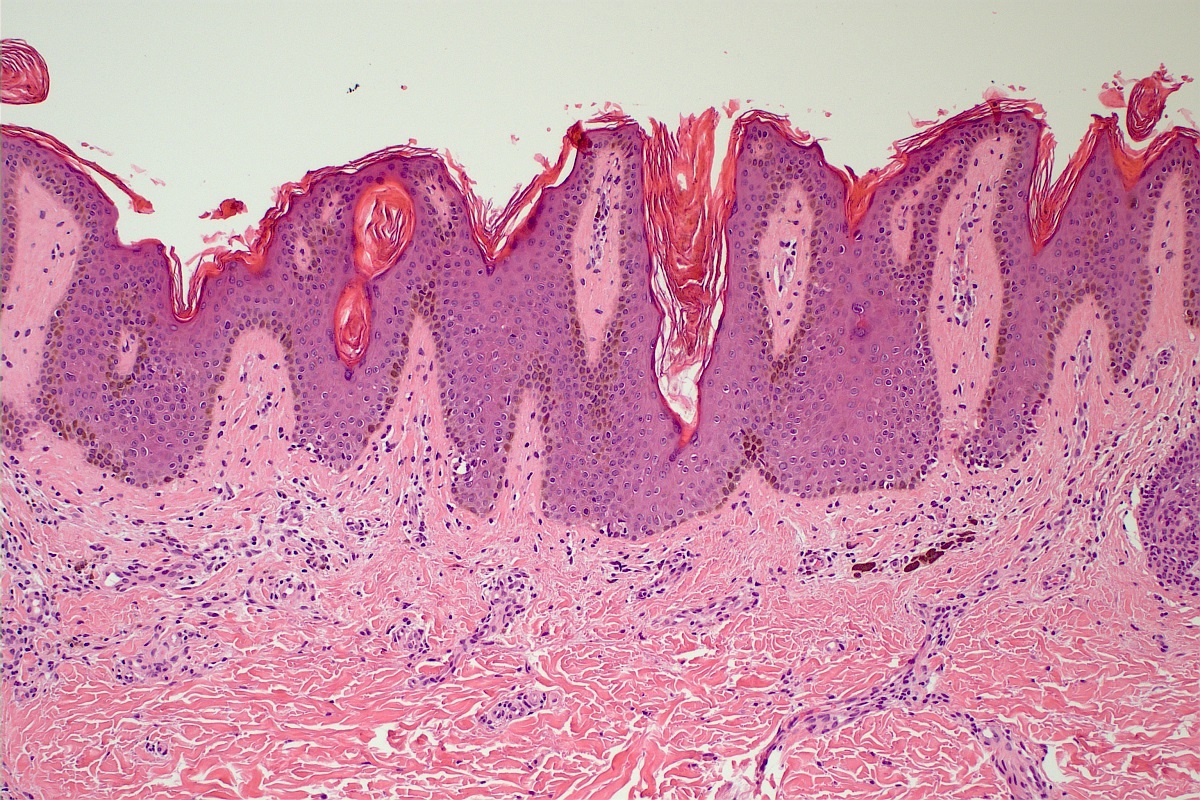
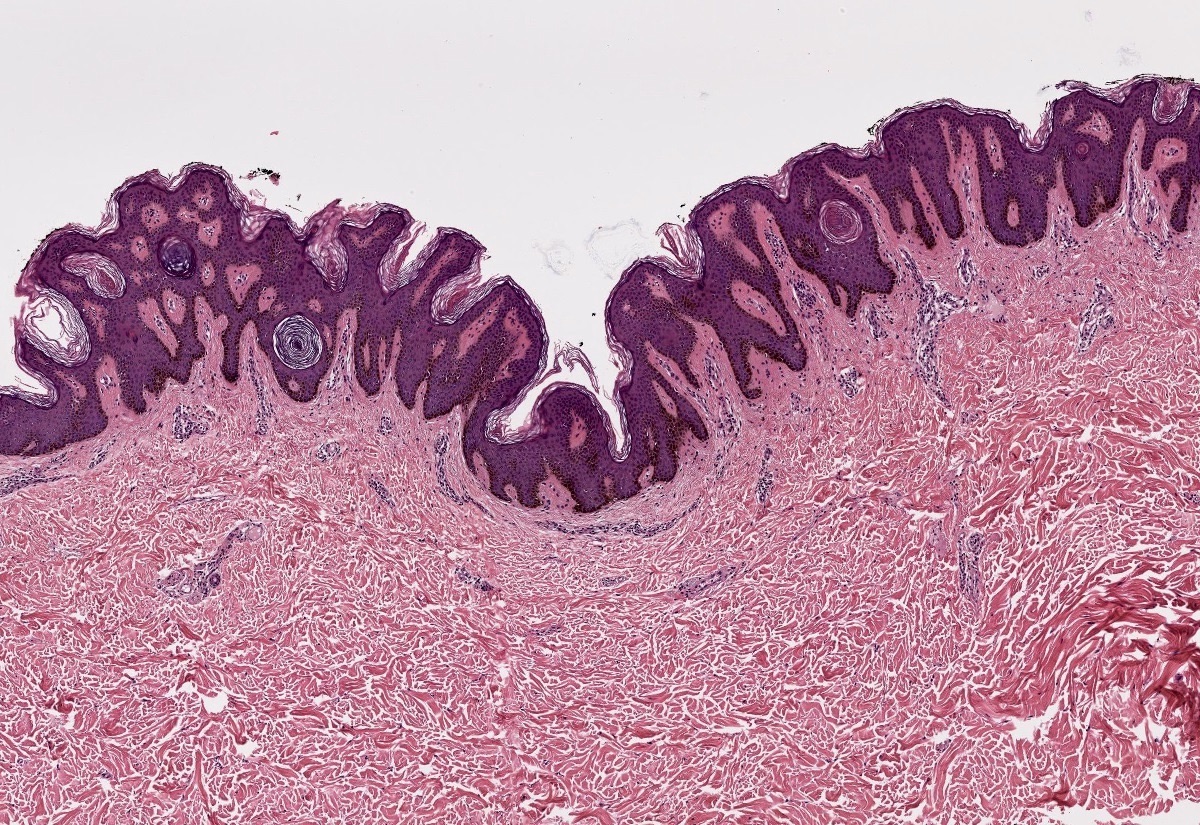
Basal hyperpigmentation
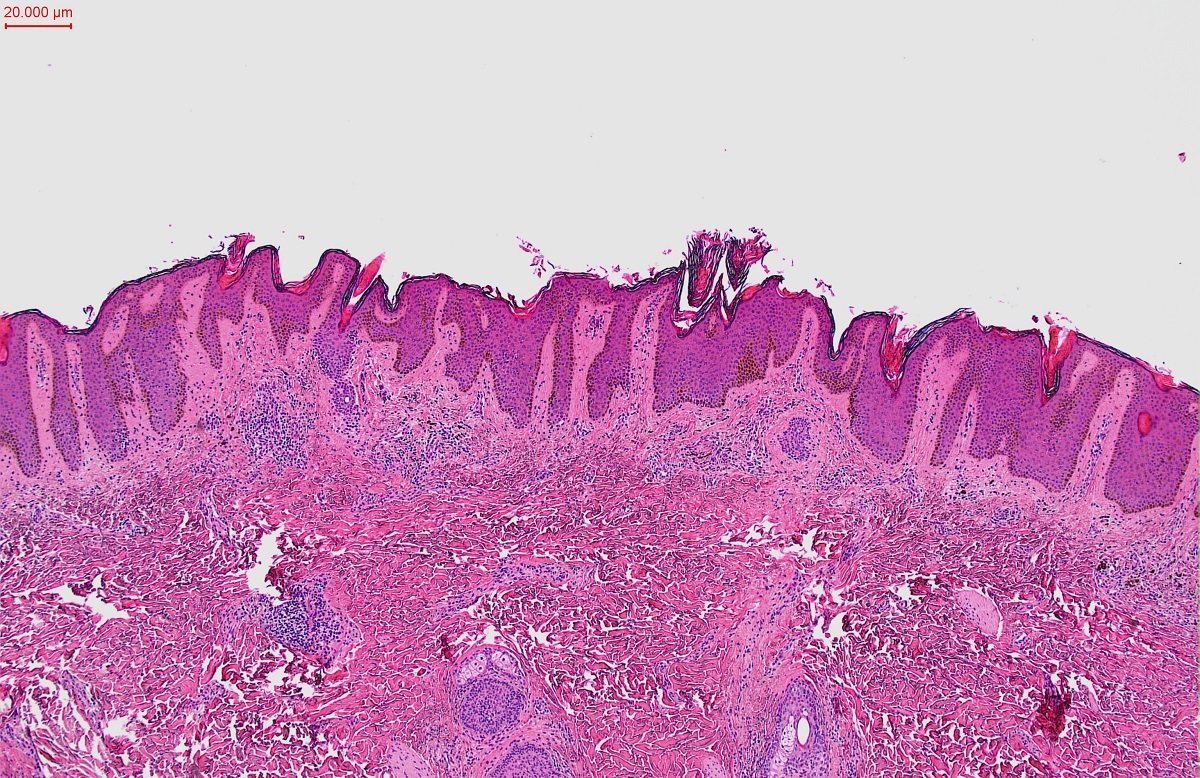
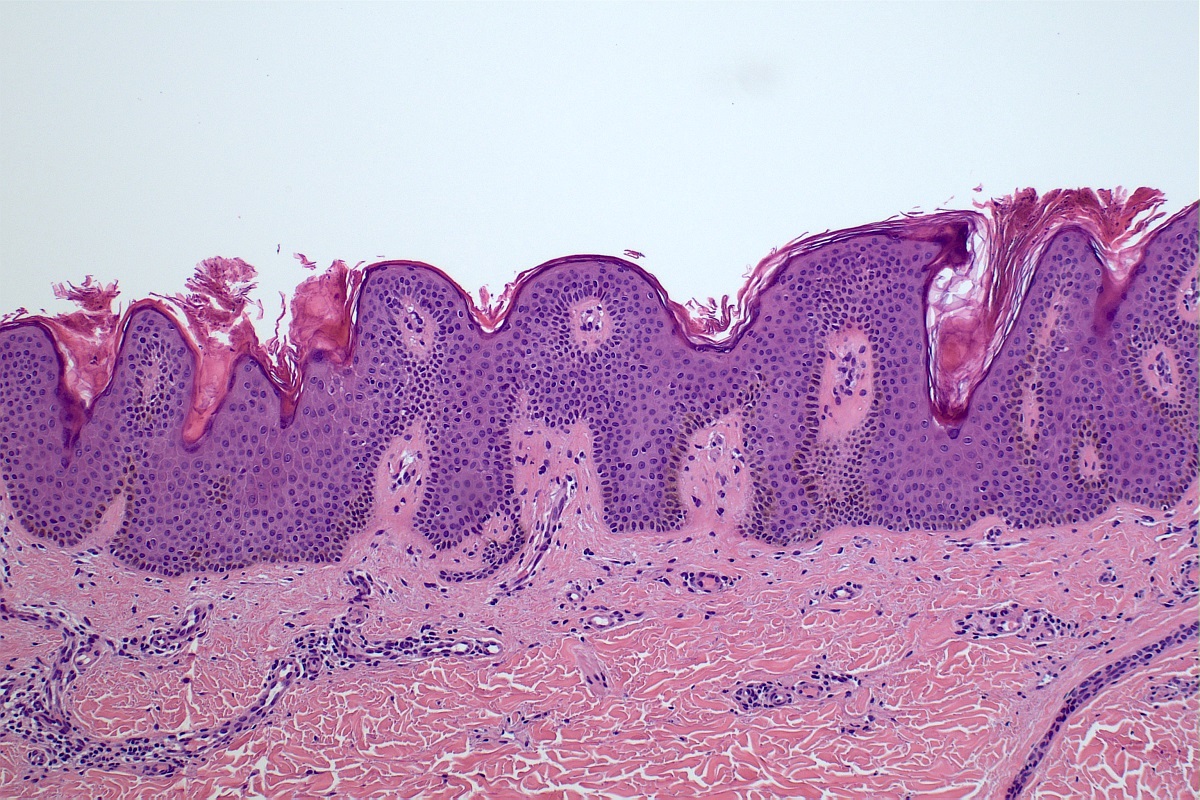
Acanthosis
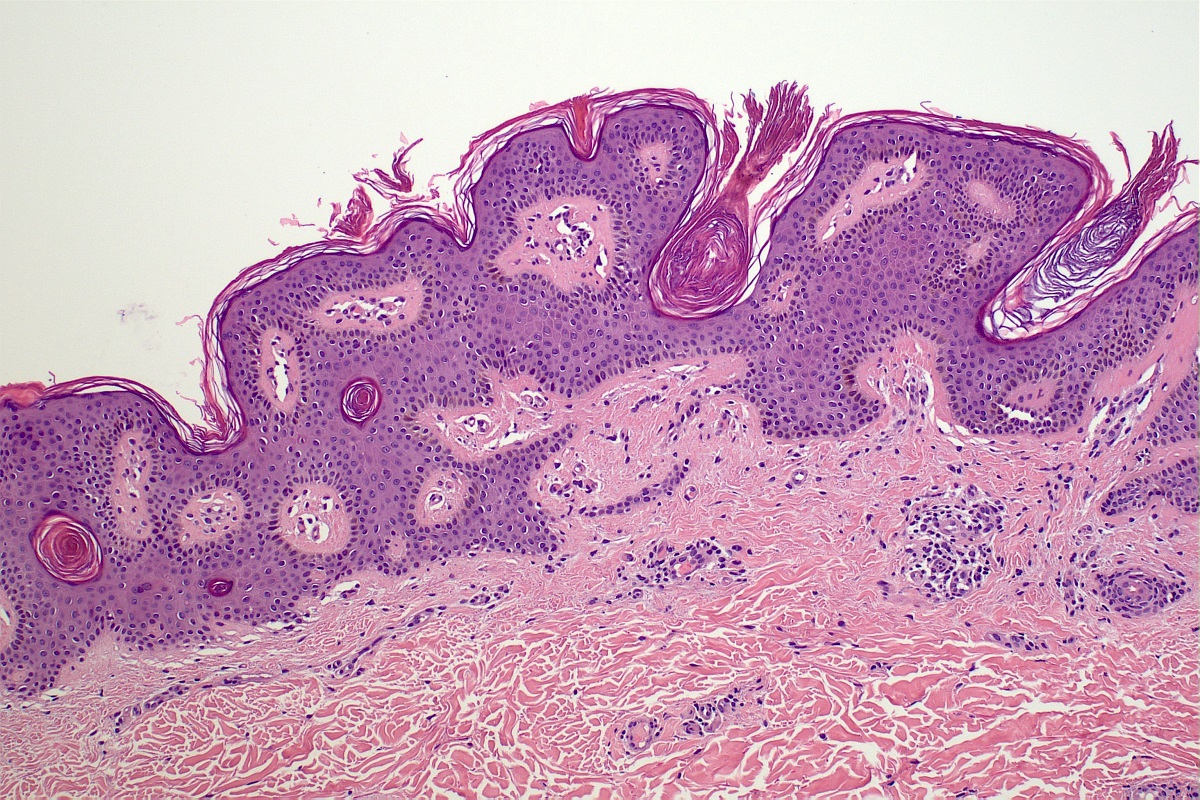
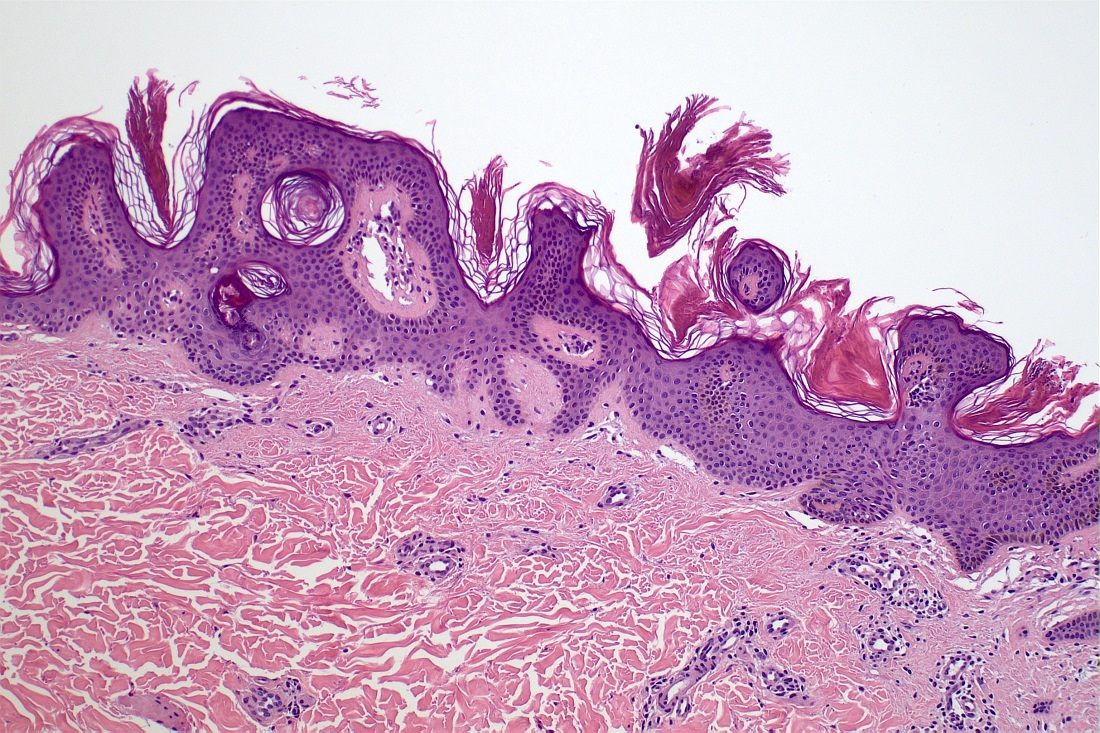
Hyperkeratosis
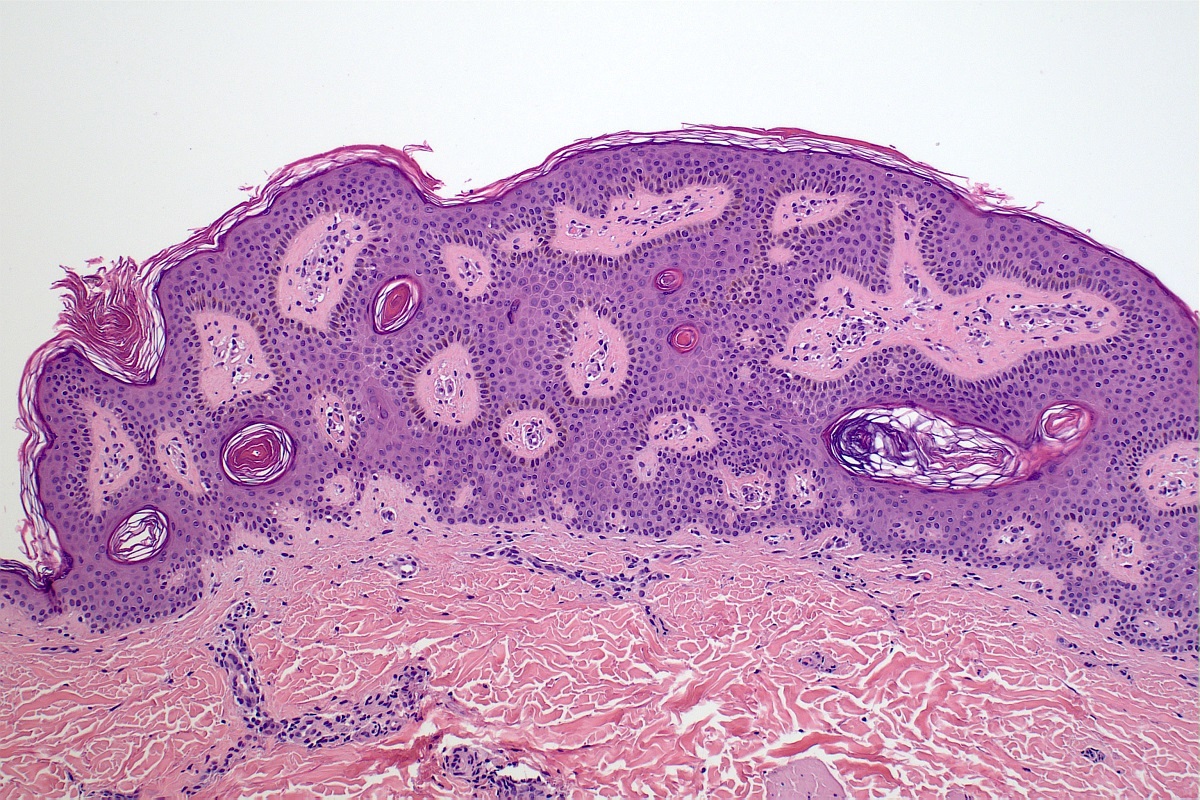
Horn pseudocysts
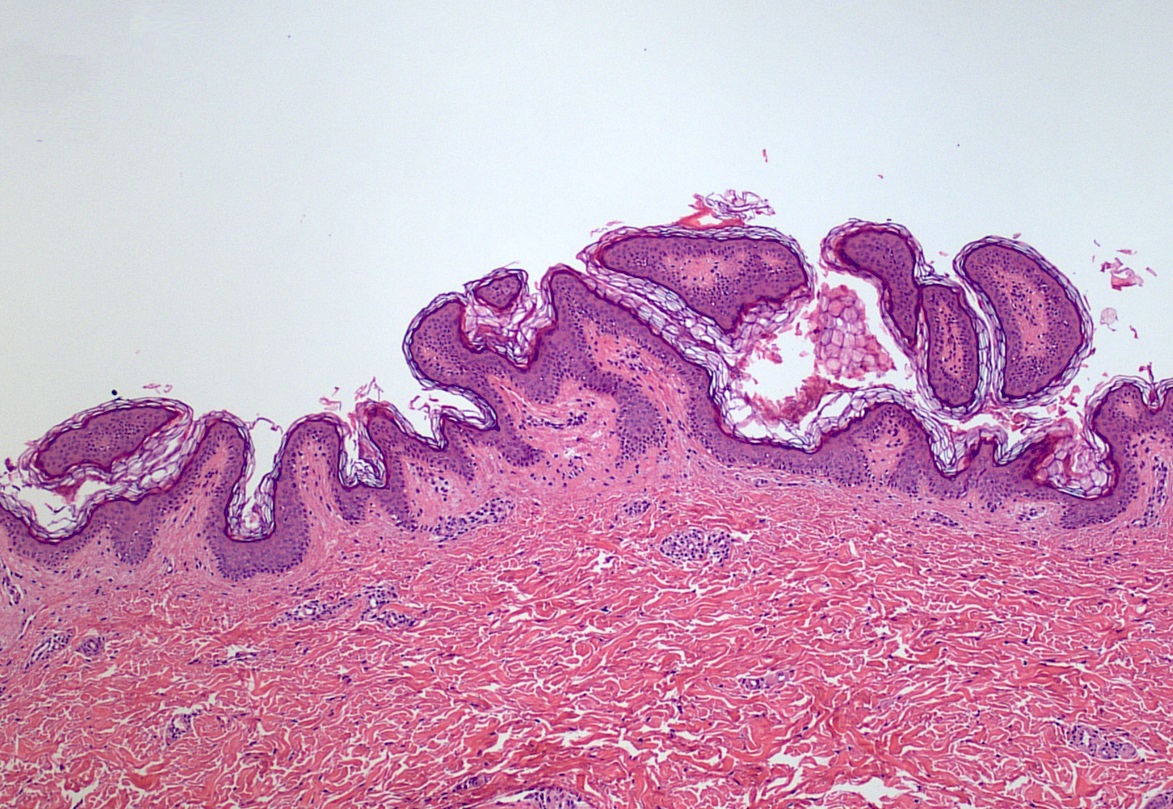
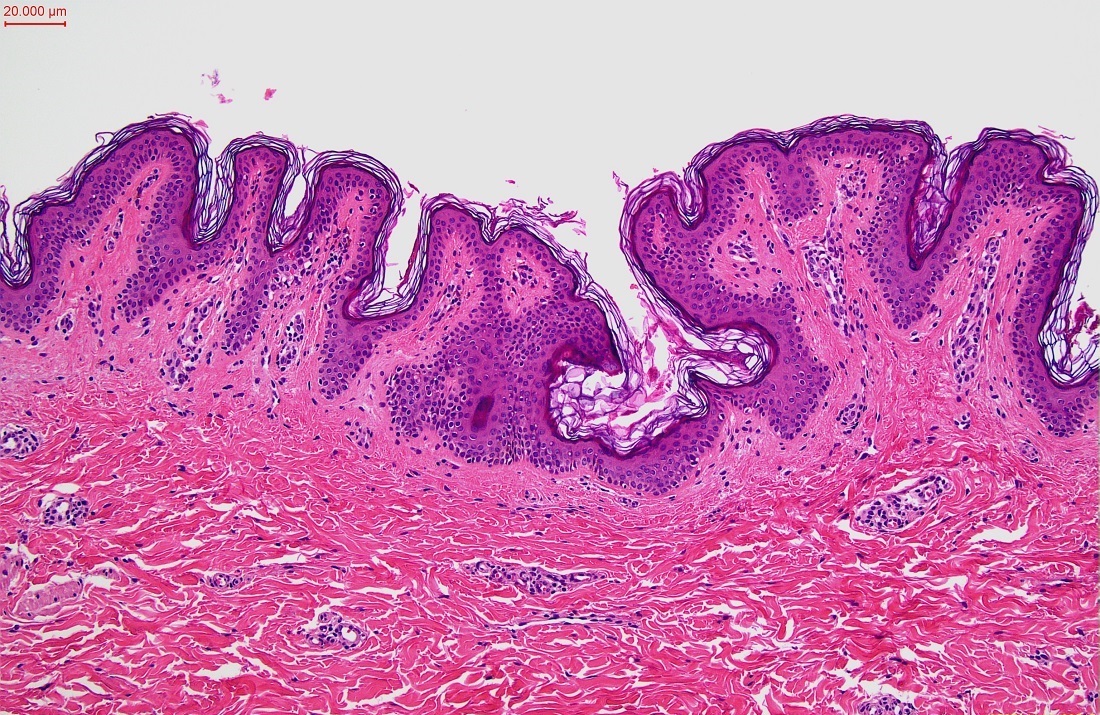
Papillomatosis
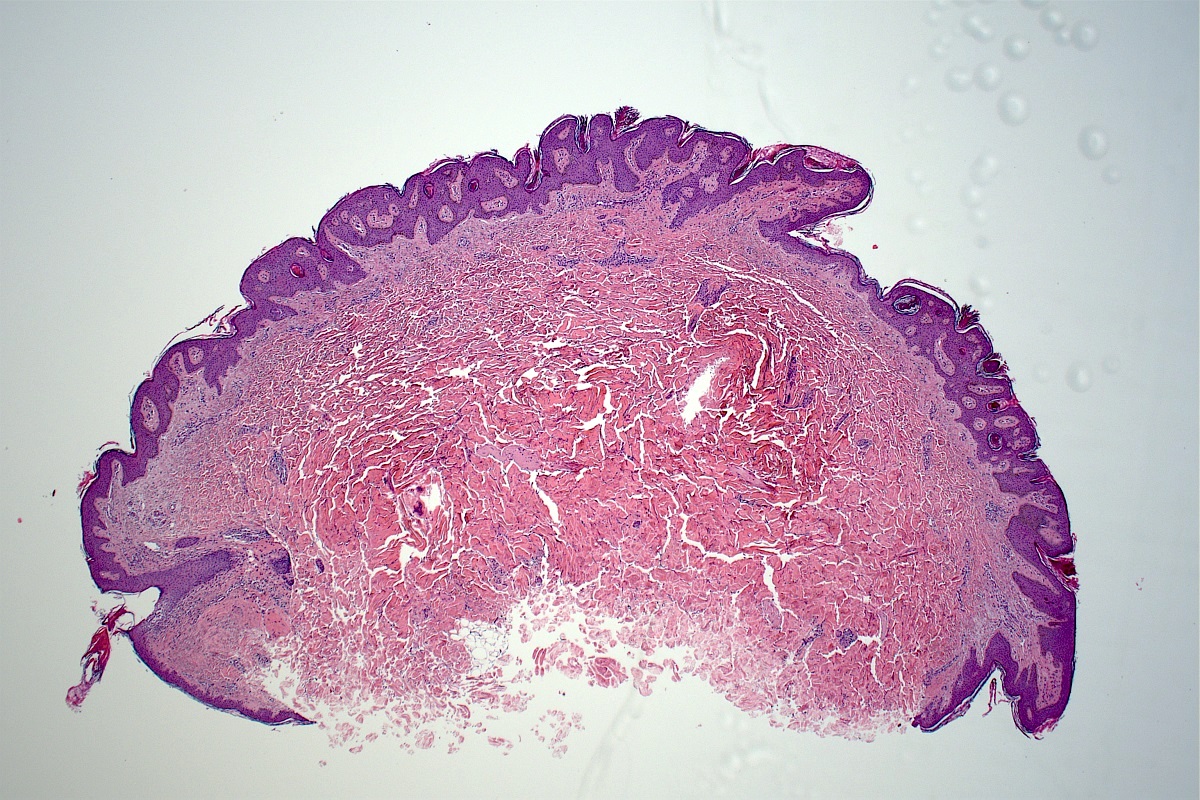
Adjacent normal epidermis
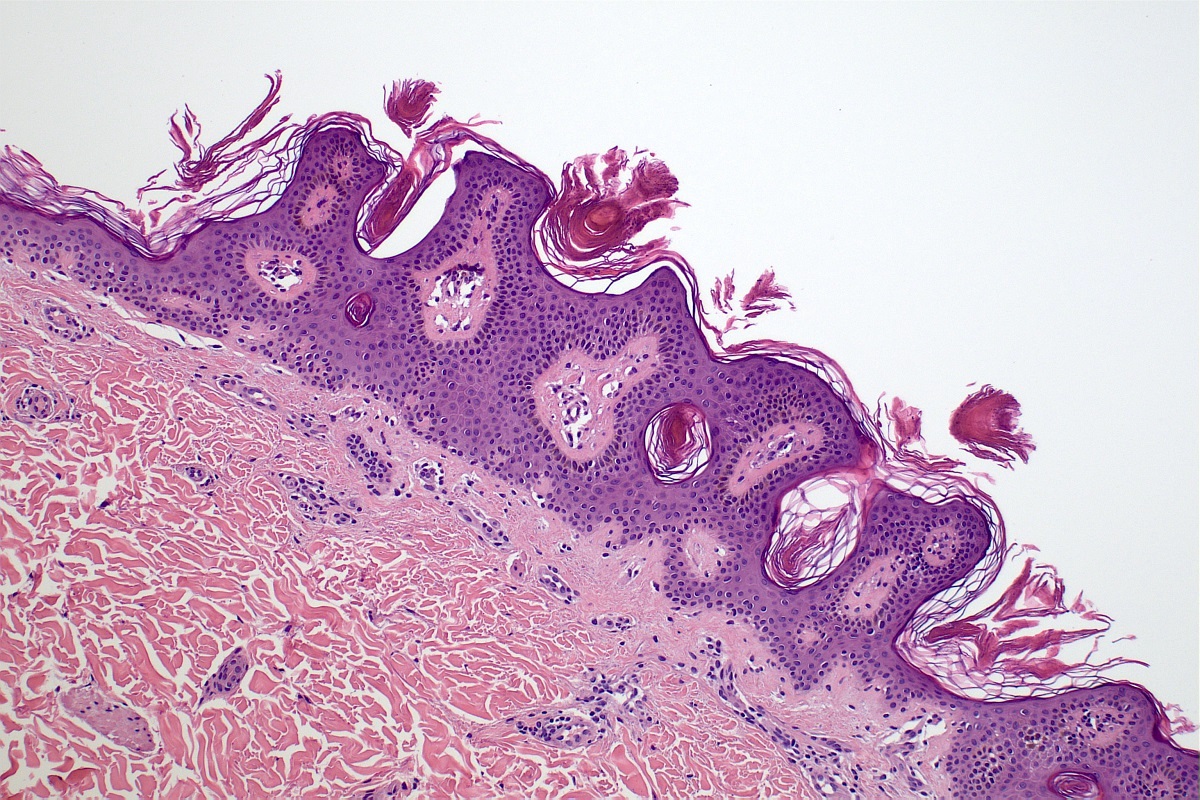
Flattened epidermal base
Virtual slides
Images hosted on other servers

Epidermal nevus
Molecular / cytogenetics description
- Typically not required for diagnosis
- 40% of epidermal nevi harbor a postzygotic activating mutation in FGFR3 and PIK3CA
- Another 40% harbor a RAS (i.e., KRAS, NRAS, HRAS) postzygotic activating mutation (typically HRAS G13R)
- Another 5 - 10% harbor an embryonic postzygotic FGFR2 activating mutation (J Invest Dermatol 2016;136:1718)
- Missense mutation c.109G>T in PTCH1 gene was detected in a patient with epidermal nevi and cerebral infarction (J Med Case Rep 2022;16:343)
Sample pathology report
- Skin, neck, excision:
- Epidermal nevus (see comment)
- Comment: Histological examination demonstrates skin to the subcutis with a lesion comprising an acanthotic and papillomatous epidermis with overlying hyperkeratosis. The underlying dermis appears unremarkable with no abnormal pilosebaceous units identified. There is no evidence of an associated neoplastic growth or malignancy in the material examined.
Differential diagnosis
- Nevus sebaceus (of Jadassohn):
- Clinically often presents as a single yellow patch of alopecia on the scalp
- Histologically similar epidermal changes, though with additional sebaceous gland alterations and ectopic dilated apocrine glands
- Seborrheic keratosis:
- Unusual diagnosis in children / young adults
- Histologically similar, though more likely to have pseudohorn cysts, squamous eddies and compact basaloid cells
- Verruca vulgaris:
- Papillomatosis, hypergranulosis and hyperparakeratosis
- Elongated rete ridges with inward bending at the edge of the lesion
- Intracorneal hemorrhage and ectatic capillaries
- Koilocytes may be seen
- Acanthosis nigricans:
- Usually found in flexural areas of the body, particularly the axilla
- Associated with an underlying metabolic disorder or malignancy
- Usually, lesser degrees of hyperkeratosis and papillomatosis
- Inflammatory linear verrucous epidermal nevus:
- Alternating orthokeratosis and parakeratosis
- Psoriasiform epidermal hyperplasia
- Prominent granular layer underlies the orthokeratosis while the epidermis under the parakeratosis lacks a granular layer
- Mild perivascular lymphocytic infiltrate in the upper dermis
- Nevus with skyline basal cell layer (PENS):
- Mild orthohyperkeratosis, slight papillomatosis and broad acanthosis
- Distinctly palisaded basilar layer with a widened space separating this layer from the overlying spinous layer keratinocytes
- Confluent and reticulated papillomatosis (CARP) (of Gougerot and Carteaud):
- Clinically confluent patches or plaques centrally with a reticular pattern peripherally around the upper trunk, neck and axillae
- Usually, lesser degrees of hyperkeratosis and papillomatosis
- Acanthosis is present in the base of the papillae
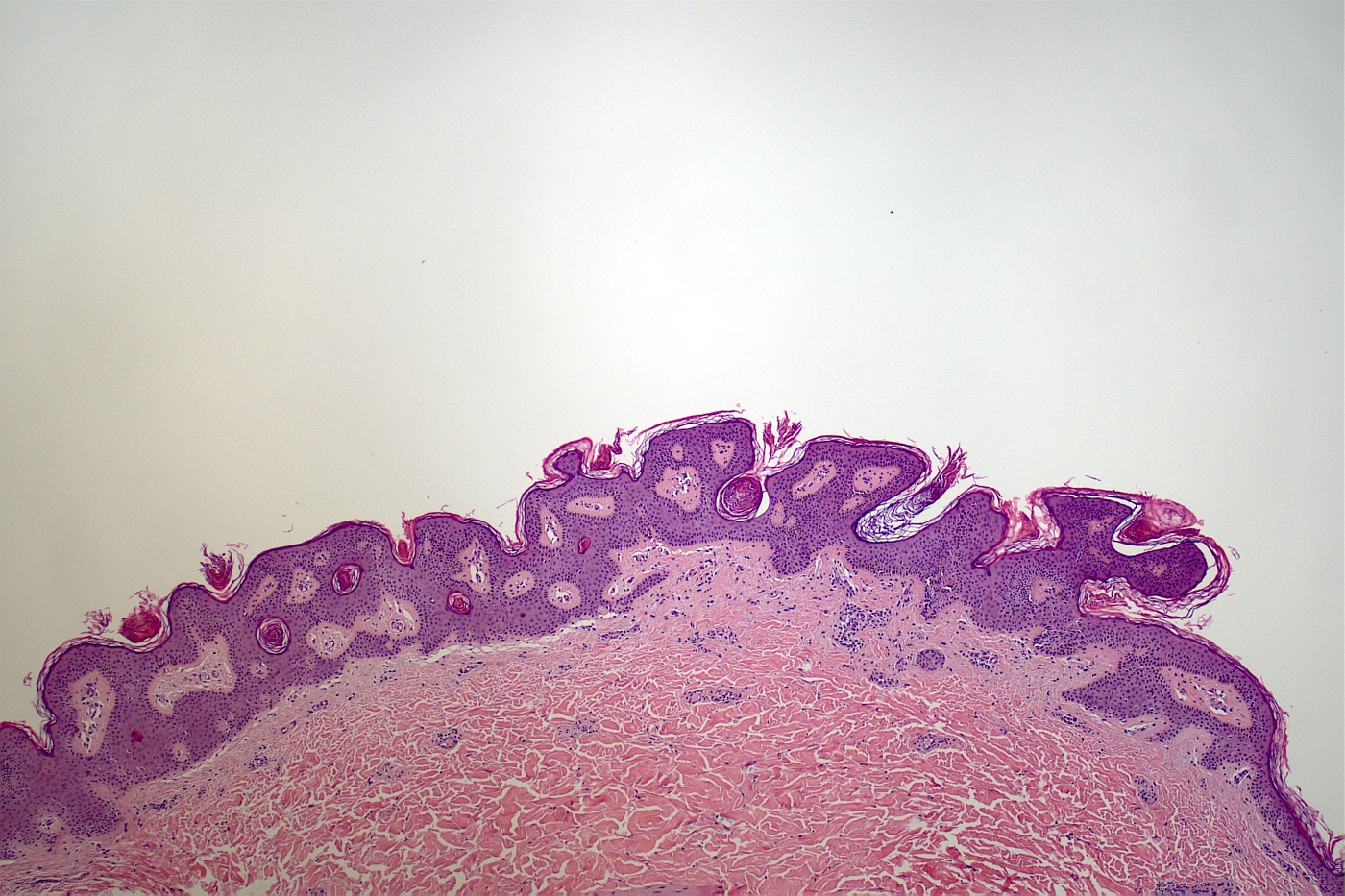
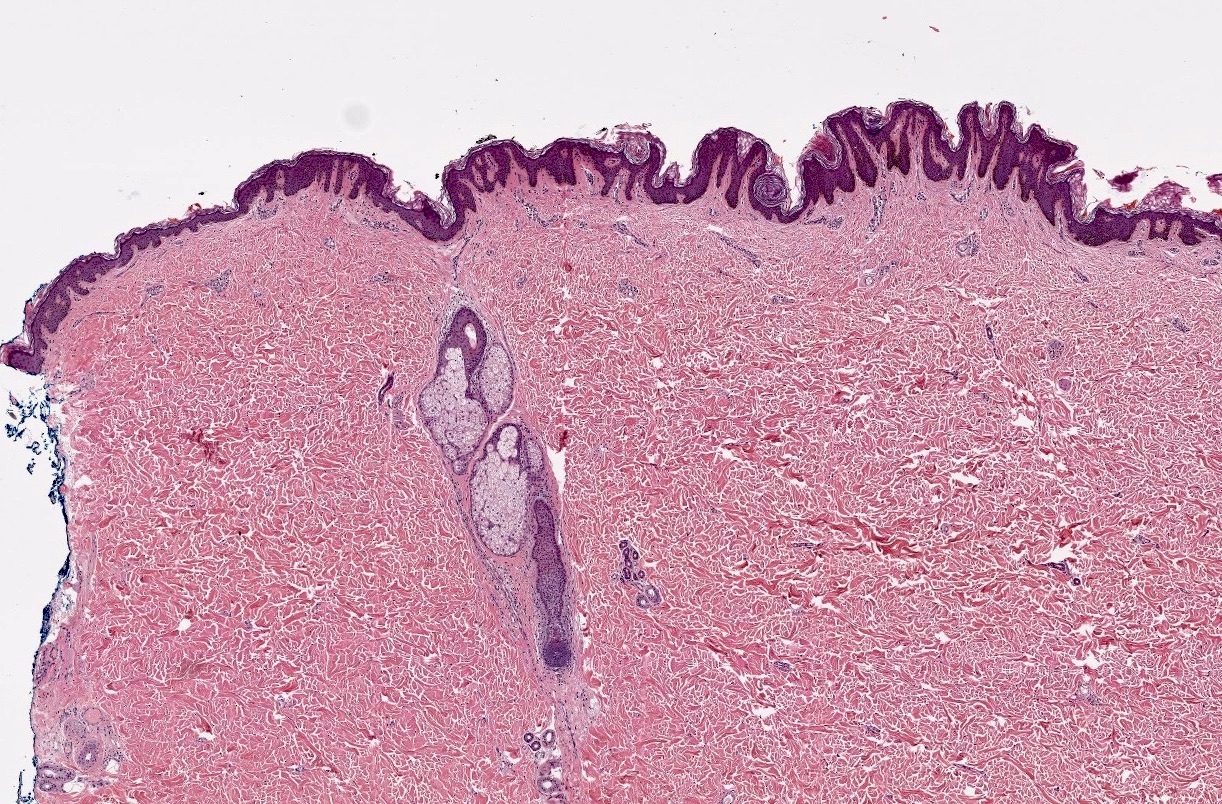
Board review style question #1
A 3 month old boy presents with a linear plaque on the neck along the lines of Blaschko. The image above is seen on histological examination. What is the most likely diagnosis?
- Acanthosis nigricans
- Epidermal nevus
- Nevus sebaceus (of Jadassohn)
- Seborrheic keratosis
- Verruca vulgaris
Board review style answer #1
B. Epidermal nevus. This clinical history and histology is classic for an epidermal nevus. Answer D is incorrect because though the histology raises the possibility of seborrheic keratosis, the clinical history rules it out. Answer A is incorrect because the clinical history rules out acanthosis nigricans. Answer C is incorrect because the histology shows there are no abnormal adnexal structures. Answer E is incorrect because there is no hemorrhage, parakeratosis or prominent vascularity in the papillary dermis.
Comment Here
Reference: Epidermal nevus
Comment Here
Reference: Epidermal nevus
Board review style question #2
What is the most likely molecular alteration in an epidermal nevus?
- Germline activating mutation in FGFR3
- Germline inactivating mutation in FGFR3
- Postzygotic activating mutation in FGFR3
- Postzygotic inactivating mutation in FGFR3
- Somatic activating mutation in FGFR3 after birth
Board review style answer #2
C. Postzygotic activating mutation in FGFR3 is one of the most common molecular alterations observed in epidermal nevus. Answer D is incorrect because an inactivating mutation of FGFR3 would potentially have a different consequence. Answer A is incorrect because epidermal nevi result from postzygotic and not germline mutations in FGFR3 gene. Answer B is incorrect because epidermal nevi result from postzygotic (and not germline) and activating mutations in FGFR3 gene. Answer E is incorrect because an epidermal nevus essentially arises from a postzygotic activating mutation in FGFR3 gene.
Comment Here
Reference: Epidermal nevus
Comment Here
Reference: Epidermal nevus
